Peripheral Vascular Diagnostic and Intervention Coding Sheet
File info: application/pdf · 2 pages · 197.22KB
Peripheral Vascular Diagnostic and Intervention Coding Sheet
Medtronic Controlled
Medtronic, Controlled
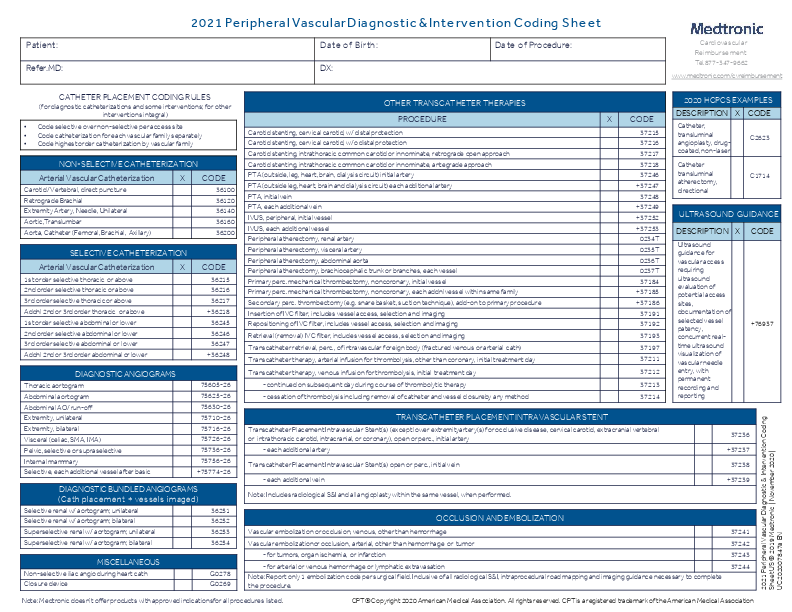
Note: Includes radiological S&I and all angioplasty within the same vessel, when performed. 2020 HCPCS EXAMPLES. DESCRIPTION X CODE. Catheter, transluminal.
Primary. Add-on: 37220 - iliac, unilateral,transluminal angioplasty (TLA) 37222 - iliac each addtl. Ipsilateral; TLA (se in conjunction withu 37220, 37221)
Full PDF Document

If the inline viewer fails, it will open the original document in compatibility mode automatically. You can also open the file directly.
Extracted Text
Patient: Refer.MD: 2021 Peripheral VascularDiagnostic &Intervention Coding Sheet Date of Birth: Date of Procedure: DX: Cardiovascular Reimbursement Tel.877-347-9662 www.medtronic.com/cvreimbursement CATHETER PLACEMENT CODING RULES (for diagnostic catheterizations and some interventions; for other interventions integral) � Code selective over non-selective per access site � Code catheterization for each vascular family separately � Code highest order catheterization by vascular family NON-SELECTIVE CATHETERIZATION Arterial Vascular Catheterization Carotid/ Vertebral, direct puncture Retrograde Brachial Extremity Artery, Needle, Unilateral Aortic,Translumbar Aorta, Catheter (Femoral, Brachial, Axillary) X CODE 36100 36120 36140 36160 36200 SELECTIVE CATHETERIZATION Arterial Vascular Catheterization X 1st order selective thoracic or above 2nd order selective thoracic or above 3rd order selective thoracic or above Addnl 2nd or 3rd order thoracic or above 1st order selective abdominal or lower 2nd order selective abdominal or lower 3rd order selective abdominal or lower Addnl 2nd or 3rd order abdominal or lower CODE 36215 36216 36217 +36218 36245 36246 36247 +36248 DIAGNOSTIC ANGIOGRAMS Thoracic aortogram Abdominal aortogram Abdominal AO/ run-off Extremity, unilateral Extremity, bilateral Visceral (celiac, SMA, IMA) Pelvic, selective or supraselective Internal mammary Selective, each additional vessel after basic 75605-26 75625-26 75630-26 75710-26 75716-26 75726-26 75736-26 75756-26 +75774-26 DIAGNOSTIC BUNDLED ANGIOGRAMS (Cath placement + vessels imaged) Selective renal w/ aortogram; unilateral Selective renal w/ aortogram; bilateral Superselective renal w/ aortogram; unilateral Superselective renal w/ aortogram; bilateral 36251 36252 36253 36254 MISCELLANEOUS Non-selective iliac angio during heart cath Closure device G0278 G0269 OTHER TRANSCATHETER THERAPIES PROCEDURE Carotid stenting, cervical carotid, w/ distal protection Carotid stenting, cervical carotid, w/o distal protection Carotid stenting, intrathoracic common carotid or innominate, retrograde open approach Carotid stenting, intrathoracic common carotid or innominate, antegrade approach PTA (outside, leg, heart, brain, dialysis circuit) initial artery PTA (outside leg, heart, brain and dialysis circuit) each additional artery PTA, initial vein PTA, each additional vein IVUS, peripheral, initial vessel IVUS, each additional vessel Peripheral atherectomy, renal artery Peripheral atherectomy, visceral artery Peripheral atherectomy, abdominal aorta Peripheral atherectomy, brachiocephalic trunk or branches, each vessel Primary perc. mechanical thrombectomy, noncoronary, initial vessel Primary perc. mechanical thrombectomy, noncoronary, each addnl vessel within same family Secondary perc. thrombectomy (e.g. snare basket, suction technique), add-on to primary procedure Insertion of IVC filter, includes vessel access, selection and imaging Repositioning of IVC filter, includes vessel access, selection and imaging Retrieval (removal) IVC filter, includes vessel access, selection and imaging Transcatheter retrieval, perc., of intravascular foreign body (fractured venous or arterial cath) Transcatheter therapy, arterial infusion for thrombolysis, other than coronary, initial treatment day Transcatheter therapy, venous infusion for thrombolysis, initial treatment day - continued on subsequent day during course of thrombolytic therapy - cessation of thrombolysis including removal of catheter and vessel closureby any method X CODE 37215 37216 37217 37218 37246 +37247 37248 +37249 +37252 +37253 0234T 0235T 0236T 0237T 37184 +37185 +37186 37191 37192 37193 37197 37211 37212 37213 37214 TRANSCATHETER PLACEMENT INTRAVASCULAR STENT Transcatheter Placement Intravascular Stent(s) (except lower extremityartery(s) for occlusive disease, cervical carotid, extracranial vertebral or intrathoracic carotid, intracranial, or coronary), open or perc., initial artery - each additional artery Transcatheter Placement Intravascular Stent(s) open or perc., initial vein - each additional vein Note: Includes radiological S&I and all angioplasty within the same vessel, when performed. 2020 HCPCS EXAMPLES DESCRIPTION X CODE Catheter, transluminal angioplasty, drugcoated, non-laser C2623 Catheter transluminal atherectomy, directional C1714 ULTRASOUND GUIDANCE DESCRIPTION X Ultrasound guidance for vascular access requiring ultrasound evaluation of potential access sites, documentation of selected vessel patency, concurrent realtime ultrasound visualization of vascular needle entry, with permanent recording and reporting CODE +76937 37236 +37237 37238 +37239 OCCLUSION AND EMBOLIZATION Vascular embolization or occlusion, venous, other than hemorrhage Vascular embolizationor occlusion, arterial, other than hemorrhage or tumor - for tumors, organ ischemia, or infarction - for arterial or venous hemorrhage or lymphatic extravasation Note: Report only 1 embolization code per surgical field. Inclusive of all radiological S&I, intraprocedural road mapping and imaging guidance necessary to complete the procedure. 37241 37242 37243 37244 Note: Medtronic doesn't offer products with approved indicationsfor all procedures listed. CPT� Copyright 2020 American Medical Association. All rights reserved. CPT is a registered trademark of the American Medical Association 2021 Peripheral Vascular Diagnostic & Intervention Coding Sheet US � 2019 Medtronic | November 2020 | UC202007847a EN Medtronic does not represent or guarantee that this information is complete, accurate, or applicable to any particular patient or third-party payor. The final decision of billing for any service must be made by the health care provider. Healthcare providers should consult with their own advisors regarding coding, coverage, and payment. CPT� is a trademark of the American Medical Association. UC202007847 EN �2020 Medtronic. All rights reserved. Medtronic, Medtronic logo and Further, Together are trademarks of Medtronic. All other brands are trademarks of a Medtronic company. For distribution in the USA only. 11/2020. NORMAL CAROTID ANATOMY +36228 +36227 36226 36224 36225 36223 36222 36221 DIAGNOSTIC BUNDLED CAROTID ANGIOGRAMS (Cath placement + Vessels imaged) Selective catheterization of each intracranial branch of internal carotid or vertebral, unilat., with selected vessel angiography (use w/ 36224 or 36226) Selective catheterization of external carotid, unilat., with external carotid angiography + (all vessels imaged (use w/ 36222, 36223 or 36224) Selective catheterization of vertebral, unilat., with vertebral angiography + (all vessels) imaged Selective catheterization of internal carotid, unilat., with intracranial carotid angiography + (all vessels) imaged Selective catheterization of subclavian or innominate, unilat., with vertebral angiography + (all vessels imaged) Selective catheterization of common carotid or innominate, unilat., with intracranial carotid angiography + (all vessels) imaged (including extracranial when performed) Selective catheterization of common carotid or innominate, unilat., with extracranial carotid angiography + (all vessels) Non-selective thoracic catheterization with cervicocerebral angiography of all extra- and intracranial vessels imaged, uni- or bilateral (do not report w/36222-36226) MODERATE SEDATION RULES Moderate sedation codes are based on the documented physician face- to-face time beginning when the patient is administered sedation and ends when the patient no longer requires physician monitoring. or when the physician leaves the room. Moderate Sedation Codes MD performing svc initial 15 min. intra-svctime; < 5 years old 99151 MD performingsvc initial 15 min. intra- svc time;>5 yrs old + each addtl 15min. intraservicetime MD not performing service initial 15 minutes intra- service time; < 5 years old MD not performing service initial 15 minutes intra- service time; > 5 yearsold + each addtl 15min. intra-service time 99152 +99153 99155 99156 +99157 ILIAC FEMORAL/ POPLITEAL LOWER EXTREMITY ANATOMY LOWER EXTREMITY INTERVENTIONS CommonIliac(R) InternalIliac (Hypogastric) DeepIliac Crcumfexli External Iliac Com onIliac(L) MiddleSacral InternalIliac (Hypogastric) DeepIliac Circumflex External Iliac Superficial IliacCircumflex Medial Femoral Circumflex Lateral Femoral Circumflex Profunda Femoris Perforating Inferior Eplgastric Com on Femoral External Pudendal MedialFemoral Circumflex Superficial Femoral Superficial IliacCircumflex Medial Femoral Circumflex Lateral Femoral Circumflex Profunda Femoris Perforating SuperiorLateral Genicular InteriorLateral Genicular Anterior Tibial Peroneal Lateral Anterior Maleolar SuperiorMedial Genicular Popliteal Inferior Medial Genicular Posterior Tibial Medial Anterior Maleolar SuperiorLateral Genicular InteriorLateral Genicular Anterior Tibial Peroneal Lateral Anterior Maleolar ILIAC TERRITORY Primary 37220 - iliac, unilateral, transluminal angioplasty (TLA) 37221 - iliac, unilateral, transluminal stent(s), includes TLA when performed 0238T* - iliac atherectomy (emerging tech code, no RVUs) Add-on +37222 - iliac each addtl. Ipsilateral; TLA (use in conjunction with 37220, 37221) +37223 � iliac each addtl. Ipsilateral; stent(s) includes TLA when performed (use in conjunction with 37221) FEMORAL/ POPLITEAL TERRITORY 37224 - femoral/popliteal, unilateral, transluminal angioplasty (TLA) 37226 - femoral/popliteal, unilateral, transluminal stent(s), includes TLA when performed 37225 - femoral/popliteal, unilateral, atherectomy, includes TLA when performed 37227 - femoral/popliteal, unilateral, atherectomy + stent(s), includes TLA when performed TIBIAL/ PERONEAL TERRITORY 37228 � tib/per, unilateral, transluminal angioplasty (TLA) 37230 � tib/per, unilateral, transluminal stent(s), includes TLA when performed 37229 - tib/per, unilateral, atherectomy, includes TLA when performed There are no add-on codes for additional vessels treated because only 1 service is reported when 2 lesions are treated in this territory. Report the most complex service (e.g. use 37227 if a stent is placed for 1 lesion and an atherectomy is performed on 2nd lesion). +37232 � tib/per, unilateral, each addl; TLA (use w/ 37228-37231) +37234 � tib/per, unilateral, each addl; stent(s), includes TLA when performed +37233 � tib/per, unilateral, each addl; atherectomy, includes TLA when performed 37231 � tib/per, unilateral, atherectomy + stent(s), includes TLA when +37235 � tib/per,unilateral, each addl; atherectomy + stent(s), includes TLA when Dorsalis Pedis performed performed Note: Medtronic doesn't offer products with approved indicationsfor all procedures listed. CPT� Copyright 2020 American Medical Association. All rights reserved. CPT is a registered trademark of the American Medical Association TIBIAL/ PERONEAL