2 . Boston Scienti c, Master Brand DFU Template 8.2677in x 11.6929in A4, 92238519A) eDFU, MB, LOTUS Edge Valve System, EN, 50473081-01D Black (K) ≥E ≤5.0
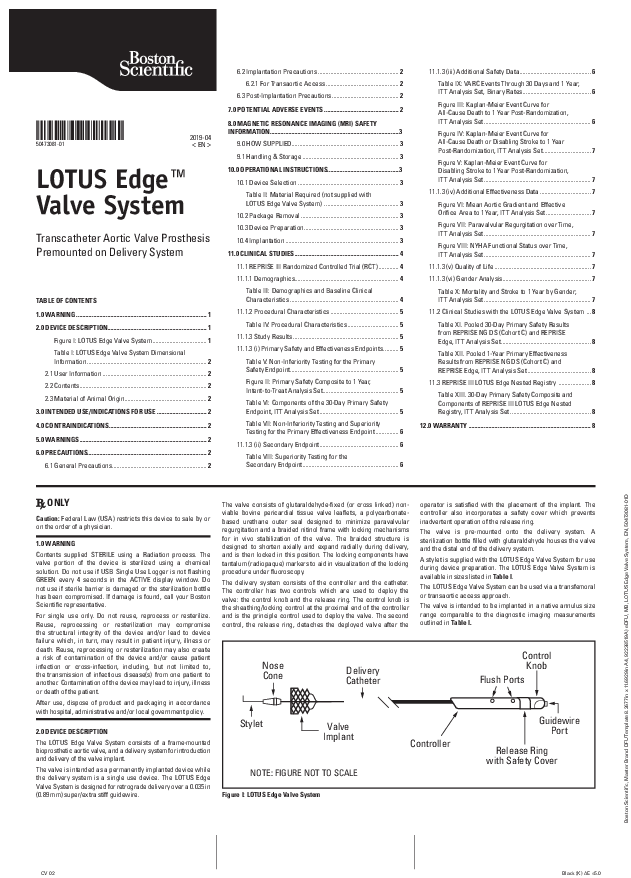
50473081-01 2019-04 < EN > LOTUS EdgeTM Valve System Transcatheter Aortic Valve Prosthesis Premounted on Delivery System TABLE OF CONTENTS 1.0 WARNING .................................................................................... 1 2.0 DEVICE DESCRIPTION................................................................1 Figure I: LOTUS Edge Valve System ................................... 1 Table I: LOTUS Edge Valve System Dimensional Information ............................................................................. 2 2.1 User Information ................................................................... 2 2.2 Contents..................................................................................2 2.3 Material of Animal Origin.....................................................2 3.0 INTENDED USE/INDICATIONS FOR USE ................................2 4.0 CONTRAINDICATIONS...............................................................2 5.0 WARNINGS..................................................................................2 6.0 PRECAUTIONS.............................................................................2 6.1 General Precautions.............................................................2 6.2 Implantation Precautions .................................................... 2 6.2.1 For Transaortic Access ............................................... 2 6.3 Post-Implantation Precautions........................................... 2 7.0 POTENTIAL ADVERSE EVENTS ................................................ 2 8.0 MAGNETIC RESONANCE IMAGING (MRI) SAFETY INFORMATION................................................................................... 3 9.0 HOW SUPPLIED..................................................................... 3 9.1 Handling & Storage .............................................................. 3 10.0 OPERATIONAL INSTRUCTIONS..............................................3 10.1 Device Selection ................................................................. 3 Table II: Material Required (not supplied with LOTUS Edge Valve System) ................................................ 3 10.2 Package Removal ............................................................... 3 10.3 Device Preparation............................................................. 3 10.4 Implantation ......................................................................... 3 11.0 CLINICAL STUDIES ................................................................... 4 11.1 REPRISE III Randomized Controlled Trial (RCT) ............. 4 11.1.1 Demographics................................................................... 4 Table III: Demographics and Baseline Clinical Characteristics ...................................................................... 4 11.1.2 Procedural Characteristics ............................................ 5 Table IV: Procedural Characteristics ................................. 5 11.1.3 Study Results .................................................................... 5 11.1.3 (i) Primary Safety and Effectiveness Endpoints.......... 5 Table V: Non-Inferiority Testing for the Primary Safety Endpoint...................................................................... 5 Figure II: Primary Safety Composite to 1 Year, Intent-to-Treat Analysis Set................................................. 5 Table VI: Components of the 30-Day Primary Safety Endpoint, ITT Analysis Set ................................................... 5 Table VII: Non-Inferiority Testing and Superiority Testing for the Primary Effectiveness Endpoint ............... 6 11.1.3 (ii) Secondary Endpoint................................................... 6 Table VIII: Superiority Testing for the Secondary Endpoint.............................................................. 6 11.1.3 (iii) Additional Safety Data.............................................. 6 Table IX: VARC Events Through 30 Days and 1 Year; ITT Analysis Set, Binary Rates............................................ 6 Figure III: Kaplan-Meier Event Curve for All-Cause Death to 1 Year Post-Randomization, ITT Analysis Set..................................................................... 6 Figure IV: Kaplan-Meier Event Curve for All-Cause Death or Disabling Stroke to 1 Year Post-Randomization, ITT Analysis Set............................... 7 Figure V: Kaplan-Meier Event Curve for Disabling Stroke to 1 Year Post-Randomization, ITT Analysis Set..................................................................... 7 11.1.3 (iv) Additional Effectiveness Data ................................. 7 Figure VI: Mean Aortic Gradient and Effective Orifice Area to 1 Year, ITT Analysis Set ............................. 7 Figure VII: Paravalvular Regurgitation over Time, ITT Analysis Set..................................................................... 7 Figure VIII: NYHA Functional Status over Time, ITT Analysis Set..................................................................... 7 11.1.3 (v) Quality of Life .............................................................. 7 11.1.3 (vi) Gender Analysis......................................................... 7 Table X: Mortality and Stroke to 1 Year by Gender; ITT Analysis Set..................................................................... 7 11.2 Clinical Studies with the LOTUS Edge Valve System ... 8 Table XI. Pooled 30-Day Primary Safety Results from REPRISE NG DS (Cohort C) and REPRISE Edge, ITT Analysis Set.......................................................... 8 Table XII. Pooled 1-Year Primary Effectiveness Results from REPRISE NG DS (Cohort C) and REPRISE Edge, ITT Analysis Set ......................................... 8 11.3 REPRISE III LOTUS Edge Nested Registry ..................... 8 Table XIII. 30-Day Primary Safety Composite and Components of REPRISE III LOTUS Edge Nested Registry, ITT Analysis Set .................................................... 8 12.0 WARRANTY ............................................................................... 8 ONLY Caution: Federal Law (USA) restricts this device to sale by or on the order of a physician. 1.0 WARNING Contents supplied STERILE using a Radiation process. The valve portion of the device is sterilized using a chemical solution. Do not use if USB Single Use Logger is not flashing GREEN every 4 seconds in the ACTIVE display window. Do not use if sterile barrier is damaged or the sterilization bottle has been compromised. If damage is found, call your Boston Scientific representative. For single use only. Do not reuse, reprocess or resterilize. Reuse, reprocessing or resterilization may compromise the structural integrity of the device and/or lead to device failure which, in turn, may result in patient injury, illness or death. Reuse, reprocessing or resterilization may also create a risk of contamination of the device and/or cause patient infection or cross-infection, including, but not limited to, the transmission of infectious disease(s) from one patient to another. Contamination of the device may lead to injury, illness or death of the patient. After use, dispose of product and packaging in accordance with hospital, administrative and/or local government policy. 2.0 DEVICE DESCRIPTION The LOTUS Edge Valve System consists of a frame-mounted bioprosthetic aortic valve, and a delivery system for introduction and delivery of the valve implant. The valve is intended as a permanently implanted device while the delivery system is a single use device. The LOTUS Edge Valve System is designed for retrograde delivery over a 0.035 in (0.89 mm) super/extra stiff guidewire. The valve consists of glutaraldehyde-fixed (or cross linked) nonviable bovine pericardial tissue valve leaflets, a polycarbonatebased urethane outer seal designed to minimize paravalvular regurgitation and a braided nitinol frame with locking mechanisms for in vivo stabilization of the valve. The braided structure is designed to shorten axially and expand radially during delivery, and is then locked in this position. The locking components have tantalum (radiopaque) markers to aid in visualization of the locking procedure under fluoroscopy. The delivery system consists of the controller and the catheter. The controller has two controls which are used to deploy the valve: the control knob and the release ring. The control knob is the sheathing/locking control at the proximal end of the controller and is the principle control used to deploy the valve. The second control, the release ring, detaches the deployed valve after the operator is satisfied with the placement of the implant. The controller also incorporates a safety cover which prevents inadvertent operation of the release ring. The valve is pre-mounted onto the delivery system. A sterilization bottle filled with glutaraldehyde houses the valve and the distal end of the delivery system. A stylet is supplied with the LOTUS Edge Valve System for use during device preparation. The LOTUS Edge Valve System is available in sizes listed in Table I. The LOTUS Edge Valve System can be used via a transfemoral or transaortic access approach. The valve is intended to be implanted in a native annulus size range comparable to the diagnostic imaging measurements outlined in Table I. Nose Cone Delivery Catheter Control Knob Flush Ports Stylet Valve Implant NOTE: FIGURE NOT TO SCALE Figure I: LOTUS Edge Valve System Controller Guidewire Port Release Ring with Safety Cover Boston Scientific, Master Brand DFUTemplate 8.2677in x 11.6929in A4, 92238519A) eDFU, MB, LOTUS Edge Valve System, EN, 50473081-01D CV 02 Black (K) E 5.0 Table I: LOTUS EdgeTM Valve System Dimensional Information Transfemoral Access Transaortic Access Valve Delivery Catheter Aortic Annulus Femoral Artery Diameter Ascending Aorta Size Frame Height Outer Diameter Nominal Length Diameter With iSLEEVETM Introducer Set With LotusTM Introducer Set Access Site to Basal Plane Distance 23 mm 25 mm 19 mm 7.2 mm 114 mm 20 mm & 23 mm 23 mm & 25 mm 5.9 mm 6.5 mm 6.0 cm 27 mm 7.4 mm 115 mm 25 mm & 27 mm Available imaging modalities provide important information on the anatomy of the aortic valve complex and should be used in a complementary fashion to select proper valve size. Valve sizing may vary slightly from the above chart based on such information. 2.1 User Information The LOTUS Edge Valve System should only be used by physicians who have undergone training on the implantation of this device. Patient treatment should be determined in consultation with the Heart Team. 2.2 Contents One (1) LOTUS Edge Valve System One (1) Stylet 2.3 Material of Animal Origin Non-viable bovine pericardial tissue valve leaflets 3.0 INTENDED USE/INDICATIONS FOR USE The LOTUS Edge Valve System is indicated for relief of aortic stenosis in patients with symptomatic heart disease due to severe native calcific aortic stenosis (aortic valve area [AVA] of 1.0 cm2 or index of 0.6 cm2/m2) who are judged by a heart team, including a cardiac surgeon, to be at high or greater risk for open surgical therapy (i.e., predicted risk of surgical mortality 8% at 30 days, based on the Society of Thoracic Surgeons (STS) risk score and other clinical comorbidities unmeasured by the STS risk calculator). 4.0 CONTRAINDICATIONS · Non-calcified aortic annulus. · Active systemic infection, sepsis or endocarditis. · Known hypersensitivity to contrast agents that cannot be adequately pre-medicated, or has known hypersensitivity or contraindication to aspirin, thienopyridines, heparin, nickel, titanium, tantalum, bovine-derived materials or polyurethanes. · Severe arterial tortuosity or calcification that would prevent safe placement of the introducer sheath. 5.0 WARNINGS · Valve implantation should only be performed in a facility where emergency aortic valve surgery is available. · Do not attempt to place the valve if patient's annulus is outside of the dimensions specified in Table I. Patient prosthesis mismatch, valve migration or embolization may lead to severe patient compromise, additional procedures or death. · Valve leaflets should be kept hydrated at all times and should not be exposed to solutions other than the shipping solution and sterile physiological saline rinsing solution. · Do not perform more than one full resheathe as it may impact valve hemodynamic performance and/or valve durability. · Throughout the procedure, do not use excessive force while turning either the control knob or the release ring as it may adversely impact the delivery system. · Once the valve has been released, do not attempt to reposition or extract the implant using the delivery system as it may adversely impact valve hemodynamic performance and/or result in vascular or myocardial trauma. 6.0 PRECAUTIONS 6.1 General Precautions · Device implantation should only be performed by physicians who have completed training with the LOTUS Edge Valve System. · The sterile package of the LOTUS Edge Valve System should be inspected prior to use. If sterility or integrity of the package is compromised, device should not be used. · Use device only if you see a GREEN light flash every 4 seconds in the ACTIVE display window on the USB Single Use Logger located on the face side of the product carton. · Prepare the device following the "Device Preparation" instructions in the "OPERATIONAL INSTRUCTIONS" section. · Administer periprocedural antiplatelet and/or anticoagulant therapy at the discretion of the physician consistent with the local standard-of-care. · Safety, effectiveness and durability have not been established for valve-in-valve procedures. The safety and effectiveness of the LOTUS Edge Valve System has not been established in patients with the following characteristics/comorbidities: · Congenital unicuspid or congenital bicuspid aortic valve · Severe ventricular dysfunction with left ventricular ejection fraction <20% · Hypertrophic obstructive cardiomyopathy · Echocardiographic evidence of intracardiac mass, thrombus, or vegetation · Blood dyscrasias defined as: leukopenia (WBC < 1000 cells/mm3), acute anemia (Hgb < 9 g/ dL), thrombocytopenia (platelet count < 50,000 cells/mm3), history of bleeding diathesis or coagulopathy · Pre-existing prosthetic heart valve or prosthetic ring in any position · Any considerations for coronary artery obstruction · End-stage renal disease or has GFR <20 (based on Cockcroft-Gault formula) · Severe (4+) aortic, tricuspid, or mitral regurgitation · Mixed aortic valve disease (aortic stenosis and aortic regurgitation with predominant aortic regurgitation > 3+) 6.2 Implantation Precautions · Perform balloon aortic valvuloplasty (BAV) with an appropriately sized balloon prior to delivery of the valve to the aortic annulus at the discretion of the implanting physician. · Partial resheathing (and subsequent unsheathing) can be performed an unlimited number of times during any phase of the procedure prior to valve release. Valve may be completely resheathed (past the post markers) once during the procedure at any phase prior to valve release. If a second full resheathing becomes necessary, exchange the device. 6.2.1 For Transaortic Access · Throughout the procedure, ensure the introducer sheath remains 1 cm to 2 cm below the aortotomy site. · If repositioning is required, ensure the catheter tip remains distal to the introducer sheath tip. 6.3 Post-Implantation Precautions · Use caution when removing the delivery system. Seat the nosecone in the catheter tip prior to withdrawal through the introducer sheath. 7.0 POTENTIAL ADVERSE EVENTS Adverse events (in alphabetical order) potentially associated with transcatheter aortic valve implantation (including standard cardiac catheterization, BAV and the use of anesthesia) as well as additional risks related to the use of the LOTUS Edge Valve System are listed below. · Abnormal lab values (including electrolyte imbalance) · Access site complications (including arteriovenous (AV) fistula, hematoma or lymphatic problems) · Allergic reaction (including to medications, anesthesia, contrast, or device materials, including nickel, titanium, tantalum, bovine-derived materials or polyurethanes) · Anemia · Angina · Arrhythmia or new conduction system injury (including need for pacemaker insertion) · Bleeding or hemorrhage (possibly requiring transfusion or additional procedure) · Cardiac arrest · Cardiac failure/low cardiac output · Cerebrovascular accident, stroke, transient ischemic attack or cerebral infarction including asymptomatic neuroimaging findings · Coronary obstruction · Death · Device misplacement, migration or embolization · Emboli (including air, tissue, thrombus or device materials) · Endocarditis · Fever or inflammation · Heart failure · Hemodynamic instability or shock · Hemolysis and/or hemolytic anemia · Hypertension/hypotension · Infection (local and/or systemic) · Mitral valve insufficiency · Myocardial infarction · Myocardial or valvular injury (including perforation or rupture) · Nerve injury or neurologic deficits (including encephalopathy) · Pain · Pericardial effusion or tamponade · Peripheral ischemia or infarction · Permanent disability · Pleural effusion · Pulmonary edema · Renal insufficiency or failure 2 Boston Scientific, Master Brand DFUTemplate 8.2677in x 11.6929in A4, 92238519A) eDFU, MB, LOTUS Edge Valve System, EN, 50473081-01D Black (K) E 5.0 · Respiratory insufficiency or failure · Restenosis (including pannus formation) · Valve dysfunction, deterioration or failure · Valve or device thrombosis · Valvular stenosis or regurgitation (central or paravalvular) · Vessel injury (including spasm, trauma, dissection, perforation, rupture, pseudoaneurysm or arteriovenous fistula). As a result of these adverse events, the subject may require medical, percutaneous or surgical intervention, including re-operation and replacement of the valve. These events may lead to fatal outcomes. 8.0 MAGNETIC RESONANCE IMAGING (MRI) SAFETY INFORMATION Magnetic Resonance MR Conditional Non-clinical testing has demonstrated that the LOTUS EdgeTM Valve is MR Conditional. A patient with this device can be safely scanned in an MR system meeting the following conditions: · Static magnetic field of 1.5 or 3.0 tesla · Maximum spatial field gradient of 9,900 gauss/cm (99 T/m) or less · Maximum MR system reported, whole body averaged specific absorption rate (SAR) of 2 W/kg (Normal Operating Mode) Under the scan conditions defined above, the LOTUS Edge Valve is expected to produce a maximum temperature rise of 1.5°C after 15 minutes of continuous scanning. In non-clinical testing, the image artifact caused by the device extends as far as 10.4 mm from the LOTUS Edge Valve frame when imaged with a gradient echo pulse sequence and a 3 Tesla MR System. 9.0 HOW SUPPLIED The LOTUS Edge Valve System is supplied sterile and intended for single use only. The LOTUS Edge Valve System is sterilized by irradiation. The bioprosthetic valve portion of the device is sterilized and fixed using a chemical solution. The LOTUS Edge Valve System is non-pyrogenic. A USB Single Use Logger is located on the face side of the product carton and must be flashing GREEN every 4 seconds in the ACTIVE display window. If not, do not use the device as it may impact valve hemodynamic performance. The USB Single Use Logger should be disposed of in accordance with local / regional requirements for electronic equipment. Do not use if USB Single Use Logger is not flashing GREEN every 4 seconds in the ACTIVE display window. Do not use if package is opened or damaged. Do not use if labeling is incomplete or illegible. 9.1 Handling & Storage Store at 25 °C (77 °F); excursions permitted from 15 °C - 30 °C (59 °F - 86 °F). Device shipping conditions must be maintained between 2 °C - 40 °C (35.6 °F - 104 °F). Use products prior to the "Use By" date on package label. 10.0 OPERATIONAL INSTRUCTIONS 10.1 Device Selection Select valve per sizing instruction in Table I. Table II: Material Required (not supplied with LOTUS Edge Valve System) Item Devices and accessories required for valvuloplasty (valvuloplasty balloons, guidewire, introducer, inflation device) Introducer For Transfemoral access: 15F iSLEEVETM or LotusTM Introducer Set - Large For Transaortic Access: Minimum 22F ( 7.33 mm) Introducer Sheath Guidewire Safari2 ® Guidewire or 0.035 in (0.89 mm) super/extra stiff guidewire with a minimum length of 275 cm 1.0 liter or larger rinsing bowls 500 ml bowls 2.0 liter or larger chemical waste container 1.0 liter sterile physiological saline 0.9% 30 ml syringe Waste bag Timer Quantity 1 each 1 1 2 2 1 3 2 1 1 10.2 Package Removal 1. A USB Single Use Logger is located in the face side of the product carton and must be flashing GREEN every 4 seconds in the ACTIVE display window. Note: Use device only if you see a GREEN light flash every 4 seconds in the ACTIVE display window on the USB Single Use Logger. Do not use if there is no light or it is flashing red in the HI or LO panels. Replace device. 2. Remove device from box. Inspect pouch for damage or signs of leakage. Note: If damage or leakage is noted, do not use. Replace device. 3. Open pouch (chevron (^) seal end) and transfer tray containing device to sterile field. Inspect tray for damage or leakage. Note: If damage or leakage is noted, do not use. Replace device. 4. To remove the Tray Lid from the Tray base, hold the base at the locations marked "HOLD" and separate the Tray lid by lifting from the locations marked "LIFT". 5. Remove the stylet and place it in the second rinse bowl. 10.3 Device Preparation Note: Device preparation should only be performed by persons who have completed relevant training with the LOTUS Edge Valve System. 1. Drain glutaraldehyde from sterilization bottle into a waste container. 2. Remove all three luer caps (distal, proximal and guidewire). 3. Attach a sterile syringe filled with a minimum of 15 ml sterile physiological saline to the guidewire port and flush glutaraldehyde from the system. Repeat for the proximal flush port. 4. Loosen the sterilization bottle from the white cap by holding the white cap and rotating the bottle clockwise. Remove the valve from the bottle. Unscrew the small cap and push the white cap and smaller components back along the catheter. Moisten the inside of the white cap with physiological saline to help slide the components back. 5. Inspect valve and delivery system for defects. Ensure leaflets are kept moist. If damage is noted, do not use. Replace device. 6. Turn the control knob counterclockwise and confirm that the valve locks. Locking should occur before a "click" has been heard or felt. Continue rotating until it comes to a hard stop. 7. Unlock valve by turning the control knob clockwise. Unlocking should occur after a "click" has been heard or felt. Continue rotating until the distal flush port starts to move. 8. Submerge valve in a rinse bowl filled with a minimum of 500 ml sterile physiological saline. Hold the distal end of the catheter and agitate the valve in the rinse bowl of sterile physiological saline for a minimum of sixty (60) seconds. Keep valve submerged. 9. Repeat rinse with fresh sterile physiological saline for a second time. Keep valve submerged in sterile physiological saline. 10. Following the second rinse, carefully insert entire sheathing stylet through the lumen in the nosecone and resubmerge valve. 11. With valve submerged but the catheter not submerged, flush a minimum of 15 ml of sterile physiological saline through both the distal and proximal flush ports. 12. With valve and catheter tip submerged, flush a minimum of 15 ml of sterile physiological saline through both the distal and proximal flush ports. Gently agitate the valve in sterile physiological saline until trapped bubbles on the leaflets are removed. NOTE: Do not proceed to the next steps until the guidewire is across the annulus. 13. While submerged, fully sheathe the valve to the nosecone by turning the control knob clockwise. Crimp the valve as per device preparation training to ensure smooth transition into the catheter. 14. Seat the nosecone appropriately. Carefully remove the stylet and flush the guidewire lumen with a minimum of 30 ml of sterile physiological saline, and until no air bubbles are noticed. Carefully remove both sterilization bottle caps from the catheter. 10.4 Implantation Caution: Device implantation should only be performed by physicians who have completed relevant training with the LOTUS Edge Valve System. 1. Introduce the introducer sheath into the access artery per the instructions provided with the device. 2. If implanting physician elects to perform BAV, it should be performed on the native aortic valve following standard techniques using an appropriately sized balloon to ensure complete expansion of the prosthetic valve. NOTE: Prior to performing BAV, ensure that device has been prepared per Device Preparation instructions. 3. Backload the delivery catheter onto a 0.035 in (0.89 mm) super/extra stiff guidewire, maintaining proper guidewire positioning across the native valve and into the ventricle. NOTE: The wire should be managed throughout the procedure to prevent vascular or ventricular damage. 4. Advance the delivery system over the guidewire. Verify nosecone seating prior to proceeding. 5. Advance the delivery system through the introducer. While advancing, activate the hydrophilic coating on the outer catheter with sterile physiological saline. 6. Using fluoroscopy, advance the system in the descending aorta and around the aortic arch. While advancing, ensure the central marker is oriented towards the greater curvature of the anatomy. Use an orthogonal view to ensure best visualization. Carefully cross the aortic valve annulus. NOTE: The risk of vascular trauma during tracking can be reduced by maintaining the marker position toward the greater curvature as it traverses the aortic arch. 3 Boston Scientific, Master Brand DFUTemplate 8.2677in x 11.6929in A4, 92238519A) eDFU, MB, LOTUS Edge Valve System, EN, 50473081-01D Black (K) E 5.0 NOTE: If the catheter kinks during tracking, the valve and delivery system must be removed and replaced. 7. Deploy the valve by turning the control knob counterclockwise. Position the valve at the intended location. NOTE: Typically, the final implant has approximately 4 mm of the braid frame below the level of the annulus. 8. Pause and fluoroscopically confirm the valve is locked (i.e. that there is no gap between the buckle and post markers on all three locking mechanisms). Continue to turn the control knob counterclockwise until a click has been felt and it reaches a hard stop. NOTE: An assessment of Post Top and Buckle rotational alignment prior to locking, along with assessment of uniform gap closure during locking, is necessary. Failure to assess appropriately may result in procedural complications. NOTE: An orthogonal view is necessary to confirm locking. Failure to assess appropriately may result in deployment of an unlocked valve. NOTE: If a click occurs prior to visually confirming the valve is locked, turn the control knob in a clockwise direction until another click is heard. Then attempt to lock again slowly. WARNING: If the valve cannot lock or unlock, attempt to resheathe with clockwise rotations on the blue control knob to remove the valve and delivery system. If valve cannot be resheathed consider surgical intervention. 9. Assess coronary flow, valve location, function and size. If repositioning is desired, turn the control knob in a clockwise direction to unlock and then until the valve is partially or fully sheathed to allow repositioning. Once repositioned, fully redeploy the valve by turning the control knob counterclockwise until it locks, clicks and then reaches a hard stop. NOTE: If repositioning higher, perform a partial resheathe. If repositioning lower, a full resheathe (past the post markers) may be necessary. NOTE: Partial resheathing (and subsequent unsheathing) can be performed an unlimited number of times during any phase of the procedure prior to valve release. Valve may be completely resheathed (past the post markers) once during the procedure at any phase prior to valve release. If a second full resheathing becomes necessary, replace device. NOTE: If there is concern about the valve being under-sized, a tug test can be performed to assess for anchoring. NOTE: In cases of severe waist, assess valve hemodynamics, consider repositioning or downsizing. 10. Confirm valve position and function prior to release. 11. To release the valve, slide open the safety cover. Slowly rotate the release ring clockwise until the first set of lines (pause sign) on the controller and the release ring are aligned. Pause and confirm valve is locked and functioning properly. NOTE: This is the last point at which the valve can be removed. 12. Once final valve assessment is complete, resume the release ring rotation in the same direction (clockwise), and observe the 3 fingers detaching from the valve. 13. Continue rotating until a hard stop is felt, ensuring the second set of lines on the controller and release ring are aligned (i.e. the collars are removed from the valve frame). Apply slight pull on the catheter to disengage the sheathing aids from the valve. NOTE: If resheathing is initiated prior to disengagement of the sheathing aids, valve embolization can occur. 14. Rotate the control knob clockwise to resheathe the delivery system. Retract the delivery system into the ascending aorta. Continue to rotate the control knob clockwise to seat the nosecone into the catheter tip and then carefully retrieve the delivery system from the body through the introducer. NOTE: Seat the nosecone properly to ensure smooth withdrawal. 11.0 CLINICAL STUDIES 11.1 REPRISE III Randomized Controlled Trial (RCT) Primary Objective: The primary objective of the REPRISE III RCT was to evaluate the safety and effectiveness of the LotusTM Valve System for transcatheter aortic valve replacement (TAVR) in symptomatic patients with calcific, severe native aortic stenosis who are considered at extreme or high risk for surgical valve replacement. The Lotus Valve System studied in the REPRISE III RCT is the early iteration of the LOTUS EdgeTM Valve System. The LOTUS Edge Valve System represents a modification to the Lotus Valve System to improve flexibility and deliverability, and to reduce the profile of the delivery system. Additionally, Depth GuardTM Technology was incorporated to minimize the depth the frame travels into the left ventricular outflow tract. While the delivery system was modified to make LOTUS Edge more flexible than its predecessor, the valve component is essentially the same as that of the Lotus Valve System with additional radiopaque tantalum markers on the buckle and post components of the locking mechanism to aid in visualization of the locking procedure under fluoroscopy. Design: The REPRISE III clinical study is a prospective, multicenter, randomized (2:1), controlled trial designed to evaluate the safety and effectiveness of the Lotus Valve System for transcatheter aortic valve replacement in symptomatic patients with calcific, severe native aortic stenosis. Patients had documented calcified severe native aortic stenosis with an initial aortic valve area (AVA) of 1.0 cm2 (or AVA index of 0.6 cm2/m2) and a mean pressure gradient 40 mmHg or a jet velocity 4 m/s, were NYHA Functional Class II, and were determined by a heart team to be at high or extreme risk for surgery (predicted operative mortality or serious, irreversible morbidity risk 15% or 50%, respectively). Based on pre-procedure diagnostic imaging, patients had a documented aortic annulus size of 20 mm and 27 mm. Patients were randomized 2:1 to the Lotus Valve System (23 mm, 25 mm, and 27 mm valve sizes) or a commercially available CoreValve® Valve (26 mm, 29 mm, and 31 mm valve sizes). A center was allowed to use CoreValve® Evolut® R Valve System with the aforementioned size matrix if the center no longer had access to CoreValve Valve. The primary safety endpoint was the composite of all-cause mortality, stroke, life-threatening and major bleeding events, stage 2 or 3 acute kidney injury, or major vascular complications at 30 days. The primary effectiveness endpoint was the composite of all-cause mortality, disabling stroke, and moderate or greater paravalvular regurgitation (PVR, based on independent core lab assessment) at 1 year. The secondary endpoint was the core-lab determined rate of moderate or greater PVR at 1 year. A total of 912 patients (607 Lotus, 305 CoreValve) were randomized and enrolled at 55 sites in Australia, Canada, Europe and the United States. Follow-up includes clinical assessments at discharge or 7 days post-procedure (whichever comes first), 30 days, 6 months, 1 year, and then annually for 5 years post-procedure. Enrolled patients who did not receive a study valve (Lotus or CoreValve) were followed for 1 year. The study is now considered complete with regard to the primary endpoint. The following data summarize the results from the REPRISE III RCT. 11.1.1 Demographics Table III presents demographics and baseline clinical characteristics for the Intention-to-Treat (ITT) analysis set. The two cohorts were well-balanced. Overall, mean age was around 83 years and about half of the patients were female. The proportion of patients considered at extreme surgical risk was similar between the 2 groups. Table III: Demographics and Baseline Clinical Characteristics Variable LotusTM (N=607) CoreValve® (N=305) Age at time of consent (years) 82.8 ± 7.1 (607) 82.9 ± 7.6 (305) Female 50.1% (304/607) 52.1% (159/305) Overall Risk Assessments Extreme risk 23.1% (140/607) 21.6% (66/305) High risk 76.9% (467/607) 78.4% (239/305) EuroSCORE 2011 (%) 6.4 ± 5.5 (605) 6.4 ± 5.5 (304) STS Score (%) 6.7 ± 4.0 (607) 6.9 ± 4.1 (305) STS Score 8 31.0% (188/607) 29.5% (90/305) STS Score < 8 69.0% (419/607) 70.5% (215/305) Porcelain aorta 4.5% (19/419) 3.3% (7/215) Severe pulmonary hypertension 8.1% (34/419) 8.4% (18/215) Orthopedic disease 18.6% (78/419) 12.6% (27/215) Neuromuscular disease 1.4% (6/419) 2.3% (5/215) Prior chest radiation therapy 4.1% (17/419) 3.7% (8/215) Hostile chest 4.1% (17/419) 4.7% (10/215) Severe lung disease 15.3% (64/419) 14.0% (30/215) CABG at risk with re-operation 16.0% (67/419) 20.0% (43/215) Childs Class A or B liver disease 1.7% (7/419) 1.9% (4/215) Frailty 72.6% (304/419) 70.7% (152/215) Age 90 years 10.0% (42/419) 12.6% (27/215) Other 4.1% (17/419) 7.0% (15/215) General Medical History Diabetes mellitus (medically treated) 30.9% (187/606) 32.6% (99/304) History of hyperlipidemia (medically treated) 74.6% (453/607) 75.7% (230/304) History of hypertension 91.8% (557/607) 93.8% (286/305) History of peripheral vascular disease 31.1% (187/602) 25.7% (78/304) History of dialysis dependent renal failure 0.2% (1/603) 1.3% (4/305) COPD - Supplemental oxygen dependent 6.5% (39/599) 6.3% (19/303) Cardiac History History of coronary artery disease 71.5% (433/606) 73.4% (224/305) History of myocardial infarction 18.3% (109/597) 19.0% (58/305) History of congestive heart failure 77.0% (463/601) 79.8% (241/302) History of percutaneous coronary intervention 33.1% (201/607) 32.5% (99/305) History of coronary artery bypass graft surgery 23.6% (143/606) 23.3% (71/305) 4 Boston Scientific, Master Brand DFUTemplate 8.2677in x 11.6929in A4, 92238519A) eDFU, MB, LOTUS Edge Valve System, EN, 50473081-01D Black (K) E 5.0 Cumulative Event Rate Primary Safety Endpoint Boston Scientific, Master Brand DFUTemplate 8.2677in x 11.6929in A4, 92238519A) eDFU, MB, LOTUS Edge Valve System, EN, 50473081-01D Table III: Demographics and Baseline Clinical Characteristics Variable LotusTM (N=607) CoreValve® (N=305) History of atrial fibrillation 35.1% (213/606) 31.6% (96/304) History of atrial flutter 4.9% (29/594) 6.7% (20/300) Prior pacemaker implant 17.8% (108/607) 19.0% (58/305) NYHA functional class Class I 0.0% (0/607) 0.0% (0/305) Class II 28.7% (174/607) 32.1% (98/305) Class III 63.6% (386/607) 61.0% (186/305) Class IV 7.7% (47/607) 6.9% (21/305) Neurological History History of transient ischemic attack 8.3% (50/601) 7.9% (24/303) History of cerebrovascular accident 11.3% (68/603) 14.5% (44/304) Cognitive and Daily Living Assessments Mini-cognitive assessment for dementia score 3.6 ± 1.4 (599) 3.7 ± 1.4 (304) Katz Index Activities of Daily Living score 5.6 ± 0.9 (605) 5.6 ± 1.0 (305) Strength and Balance Assessments Use of wheelchair 5.8% (35/606) 4.9% (15/305) Gait speed average to walk 5 meters (seconds) 8.7 ± 5.2 (565) 8.7 ± 4.2 (285) Falls in the past 6 months 0.4 ± 1.1 (604) 0.5 ± 1.8 (304) Maximal grip strength average (kg) 21.1 ± 10.1 (605) 20.4 ± 9.7 (303) Echocardiographic Findings Aortic valve area (cm2) 0.69 ± 0.19 (541) 0.70 ± 0.19 (280) Mean aortic valve gradient (mmHg) 44.64 ± 13.35 (575) 43.85 ± 12.31 (294) Doppler velocity index 0.22 ± 0.05 (553) 0.23 ± 0.05 (292) Values are presented as mean ± standard deviation (n) or % (count/sample size) Abbreviations: CABG = Coronary Artery Bypass Graft; COPD = Chronic Obstructive Pulmonary Disease; NYHA = New York Heart Association; STS = Society of Thoracic Surgeons 11.1.2 Procedural Characteristics Procedural characteristics are shown in Table IV Table IV: Procedural Characteristics Measure Lotus (N=607) Time from randomization to procedure (days) 13.0 ± 17.7 (596) Total procedure time (min) 86.8 ± 41.8 (596) Total time with study introducer (min) 50.4 ± 24.1 (595) Total time with study valve delivery system (min) 23.8 ± 17.6 (595) Total fluoroscopy time (min) 27.1 ± 10.8 (595) Total contrast used for procedure (cc) 110.6 ± 62.3 (593) Post-dilation 1.5% (9/596) TEE used during implant procedure 59.2% (353/596) Successful vascular access, delivery and deployment of the study valve system, and successful retrieval of the delivery system 97.8% (583/596) Conversion to open heart surgery 0.7% (4/596) Unplanned use of cardiopulmonary bypass 0.7% (4/596) Values are presented as mean ± standard deviation (n) or % (count/sample size) Abbreviation: TEE = Transesophageal Echocardiography CoreValve (N=305) 13.0 ± 12.6 (301) 76.7 ± 40.6 (299) 44.9 ± 36.9 (297) 15.0 ± 17.0 (298) 22.2 ± 12.2 (299) 120.9 ± 64.6 (299) 31.2% (94/301) 55.7% (167/300) 99.0% (297/300) 0.7% (2/300) 1.0% (3/300) 11.1.3 Study Results 11.1.3 (i) Primary Safety and Effectiveness Endpoints Primary Safety Endpoint The primary safety endpoint was the composite of all-cause mortality, stroke, life-threatening and major bleeding events, stage 2 or 3 acute kidney injury, or major vascular complications at 30 days. The primary analysis set for the primary safety endpoint is the implanted analysis set, which includes all patients who signed an informed consent form, were enrolled in the trial, and were implanted with the assigned, randomized study device. The non-inferiority hypothesis for the primary safety endpoint was met because in the implanted analysis set the rate for the Lotus group (20.3%) was non-inferior to the rate for the CoreValve group (17.2%). Non-inferiority was concluded because the one-sided upper 97.5% confidence bound on the difference between treatment groups was less than the non-inferiority margin of 10.5% with a P value < 0.025 (P = 0.0027). Results were similar for the ITT analysis set. Table V: Non-Inferiority Testing for the Primary Safety Endpoint Analysis Set Lotus CoreValve Difference [95% CI] One-sided 97.5% UCB a NonInferiority Margin One-sided P value b Implanted (N=874) (N=577) 20.3% (117/576) (N=297) 17.2% (51/297) 3.1% [-2.3%, 8.5%] 8.32% 10.5% 0.0027 Intentto-Treat (N=912) (N=607) 19.0% (114/601) (N=305) 16.2% (49/303) 2.8% [-2.4%, 8.0%] 7.75% 10.5% 0.0011 Rates are presented as % (count/sample size) a: Farrington-Manning upper confidence bound; b: P value is from the Farrington-Manning test and based on the standard normal distribution Abbreviations: CI = Confidence Interval; UCB = Upper Confidence Bound Figure II shows that the safety composite of all-cause mortality, stroke, life-threatening and major bleeding events, stage 2 or 3 acute kidney injury, and major vascular complications was not different between the 2 treatment groups to 1 year. 40% 35% 30% 25% 20% 15% 10% 5% 0% 0 30 Number at Risk Lotus CoreValve 607 485 305 253 Lotus CoreValve 60 90 120 456 233 (30.7% - Lotus 30.2% - CoreValve) 150 180 210 240 270 300 330 360 390 Days Since Randomization 438 419 334 215 207 165 Figure II: Primary Safety Composite to 1 Year, Intent-to-Treat Analysis Set Cumulative event rate ± 1.5 standard error Table VI shows that the components of the 30-day primary safety endpoint were similar between the two treatment groups. Table VI: Components of the 30-Day Primary Safety Endpoint, ITT Analysis Set Outcome Lotus (N=607) CoreValve (N=305) All-cause mortality 2.5% (15/601) 2.3% (7/303) Stroke 4.8% (29/601) 4.3% (13/303) Disabling 2.0% (12/601) 3.3% (10/303) Life-threatening or disabling bleeding 8.0% (48/601) 5.0% (15/303) Major bleeding 4.8% (29/601) 5.9% (18/303) Major vascular complications 7.0% (42/601) 5.3% (16/303) Acute kidney injury 2.5% (15/601) 3.6% (11/303) Values are presented as % (count/sample size) Primary Effectiveness Endpoint The primary effectiveness endpoint is the composite of all-cause mortality, disabling stroke, and moderate or greater PVR (based on independent core lab assessment) at 1 year. The primary hypothesis of the primary effectiveness endpoint was that Lotus Valve is non-inferior to CoreValve Valve when tested using the implanted analysis set. The non-inferiority hypothesis for the primary effectiveness endpoint was met because in the implanted analysis set the rate for the Lotus group (15.4%) was non-inferior to the rate for the CoreValve group (25.5%). Non-inferiority was concluded because the one-sided upper 97.5% confidence bound on the difference between treatment groups (Lotus minus CoreValve; -4.41%) was less than the non-inferiority margin of 9.5% with a P value < 0.025 (P < 0.0001). According to the pre-specified statistical analysis plan, a test for superiority of Lotus compared to CoreValve for the primary effectiveness endpoint was to be performed if the Lotus rate was below the CoreValve rate, non-inferiority was shown for the primary safety and primary effectiveness endpoints, and superiority was shown for the secondary endpoint. The primary analysis set for superiority testing of the primary effectiveness endpoint was the ITT analysis set. Lotus was found to be non-inferior and also superior to CoreValve for the primary effectiveness endpoint. Table VII shows the results of the non-inferiority and superiority testing for the primary effectiveness endpoint. Lotus was found to be non-inferior and also superior to CoreValve for the primary effectiveness endpoint. 5 Black (K) E 5.0 Table VII: Non-Inferiority Testing and Superiority Testing for the Primary Effectiveness Endpoint Analysis Set LotusTM CoreValve® Difference [95%CI] One-sided 97.5% UCB a NonInferiority Margin P value b NonInferiority Superiority ITT (N=912) (N=607) 15.8% (82/520) (N=305) 26.0% (68/262) -10.2% [-16.3%, -4.0%] -4.54% 9.5% < 0.0001 0.0006 Implanted (N=874) (N=577) 15.4% (78/506) (N=297) 25.5% (66/259) -10.1% [-16.2%, -3.9%] -4.41% 9.5% < 0.0001 0.0007 Rates are presented as % (count/sample size). a: Farrington-Manning upper confidence bound b: P value is from the Farrington-Manning test and is based on the standard normal distribution for the noninferiority testing and from the chi-square test for the superiority testing. 11.1.3 (ii) Secondary Endpoint The secondary endpoint was the core-lab determined rate of moderate or greater PVR at 1 year. The primary analysis set for superiority testing of the secondary endpoint was the ITT analysis set. The secondary endpoint was met because in the ITT analysis set the rate of core-lab determined moderate or greater PVR for the Lotus group (0.9%) was superior to the rate for the CoreValve group (6.9%, P < 0.0001). Table VIII: Superiority Testing for the Secondary Endpoint Analysis Set Lotus CoreValve Intent-to-Treat (N=912) (N=607) 0.9% (4/452) (N=305) 6.9% (15/216) Implanted (N=874) (N=577) 0.9% (4/443) (N=297) 6.9% (15/216) Rates are presented as % (count/sample size). a: P value is from the chi-square test for the superiority testing. Difference [95% CI] P value a -6.1% [-9.6%, -2.6%] < 0.0001 -6.0% [-9.5%, -2.5%] < 0.0001 11.1.3 (iii) Additional Safety Data Table IX shows binary rates of CEC-adjudicated, VARC-defined events occurring from randomization to 30 days and 1 year in the ITT analysis set. Table IX: VARC Events Through 30 Days and 1 Year; ITT Analysis Set, Binary Rates Outcome 30 Days Lotus (N=607) CoreValve (N=305) 1 Year Lotus (N=607) CoreValve (N=305) All-cause mortality 2.5% (15/601) 2.3% (7/303) 11.9% (70/587) 13.5% (40/297) Cardiovascular 2.3% (14/601) 2.3% (7/303) 7.7% (45/587) 9.8% (29/297) Non-cardiovascular 0.2% (1/601) 0.0% (0/303) 4.3% (25/587) 3.7% (11/297) Stroke 4.8% (29/601) 4.3% (13/303) 7.0% (41/587) 9.4% (28/297) Disabling 2.0% (12/601) 3.3% (10/303) 3.6% (21/587) 7.1% (21/297) Ischemic 1.8% (11/601) 3.3% (10/303) 2.9% (17/587) 6.4% (19/297) Hemorrhagic 0.2% (1/601) 0.0% (0/303) 0.7% (4/587) 0.3% (1/297) Undetermined 0.0% (0/601) 0.0% (0/303) 0.2% (1/587) 0.3% (1/297) Non-disabling 2.8% (17/601) 1.0% (3/303) 3.6% (21/587) 2.4% (7/297) Ischemic 2.3% (14/601) 1.0% (3/303) 3.1% (18/587) 2.4% (7/297) Hemorrhagic 0.2% (1/601) 0.0% (0/303) 0.2% (1/587) 0.0% (0/297) Undetermined 0.3% (2/601) 0.0% (0/303) 0.3% (2/587) 0.0% (0/297) All-cause mortality or disabling stroke 4.0% (24/601) 5.3% (16/303) 13.3% (78/587) 17.8% (53/297) Cardiac death or disabling stroke 3.8% (23/601) 5.3% (16/303) 9.5% (56/587) 14.8% (44/297) Major vascular complications 7.0% (42/601) 5.3% (16/303) 7.7% (45/587) 6.1% (18/297) Access site related 4.7% (28/601) 3.3% (10/303) 5.1% (30/587) 3.7% (11/297) Not access site related 2.5% (15/601) 2.0% (6/303) 2.7% (16/587) 2.4% (7/297) New PPM implanted 29.1% (175/601) 15.8% (48/303) 34.2% (201/587) 18.5% (55/297) No prior PPM 35.5% (175/493) 19.6% (48/245) 41.4% (201/485) 23.0% (55/239) Bleeding 12.8% (77/601) 10.9% (33/303) 18.1% (106/587) 17.8% (53/297) Life-threatening or disabling 8.0% (48/601) 5.0% (15/303) 9.9% (58/587) 9.8% (29/297) Major 4.8% (29/601) 5.9% (18/303) 8.3% (49/587) 8.4% (25/297) Myocardial infarction 0.7% (4/601) 1.3% (4/303) 3.2% (19/587) 4.4% (13/297) Peri-procedural MI 0.5% (3/601) 1.0% (3/303) 0.5% (3/587) 1.3% (4/297) Spontaneous MI 0.2% (1/601) 0.3% (1/303) 2.7% (16/587) 3.4% (10/297) Acute kidney injury 2.5% (15/601) 3.6% (11/303) 2.6% (15/587) 3.7% (11/297) Table IX: VARC Events Through 30 Days and 1 Year; ITT Analysis Set, Binary Rates Outcome 30 Days Lotus (N=607) CoreValve (N=305) 1 Year Lotus (N=607) CoreValve (N=305) Stage 2 1.0% (6/601) 1.3% (4/303) 1.0% (6/587) 1.3% (4/297) Stage 3 1.5% (9/601) 2.3% (7/303) 1.5% (9/587) 2.4% (7/297) Repeat procedure for valverelated dysfunction 0.0% (0/601) 1.0% (3/303) 0.2% (1/587) 2.0% (6/297) TAVR 0.0% (0/601) 0.7% (2/303) 0.0% (0/587) 1.7% (5/297) Valvuloplasty 0.0% (0/601) 0.0% (0/303) 0.0% (0/587) 0.0% (0/297) SAVR 0.0% (0/601) 0.0% (0/303) 0.2% (1/587) 0.0% (0/297) Other 0.0% (0/601) 0.3% (1/303) 0.0% (0/587) 0.3% (1/297) Hospitalization 1.7% (10/601) 3.0% (9/303) 11.2% (66/587) 13.8% (41/297) New onset atrial fibrillation/flutter 5.8% (35/601) 4.3% (13/303) 6.6% (39/587) 4.7% (14/297) Atrial fibrillation 5.8% (35/601) 4.3% (13/303) 6.6% (39/587) 4.7% (14/297) Atrial flutter 0.0% (0/601) 0.0% (0/303) 0.0% (0/587) 0.0% (0/297) Coronary obstruction 0.2% (1/601) 0.3% (1/303) 0.2% (1/587) 0.7% (2/297) Cardiac tamponade 2.5% (15/601) 1.0% (3/303) 2.6% (15/587) 1.3% (4/297) Prosthetic aortic valve malpositioning 0.0% (0/601) 2.6% (8/303) 0.0% (0/587) 2.7% (8/297) Valve migration 0.0% (0/601) 0.7% (2/303) 0.0% (0/587) 0.7% (2/297) Valve embolization 0.0% (0/601) 2.0% (6/303) 0.0% (0/587) 2.0% (6/297) Ectopic valve deployment 0.0% (0/601) 0.3% (1/303) 0.0% (0/587) 0.3% (1/297) TAV-in-TAV deployment 0.0% (0/601) 3.0% (9/303) 0.0% (0/587) 3.7% (11/297) Prosthetic aortic valve thrombosis 0.0% (0/601) 0.0% (0/303) 1.5% (9/587) 0.0% (0/297) Prosthetic aortic valve endocarditis 0.2% (1/601) 0.0% (0/303) 0.7% (4/587) 0.0% (0/297) Values are presented as % (count/sample size). Abbreviations: CEC = Clinical Events Committee; VARC = Valve Academic Research Consortium MI = Myocardial Infarction; PPM = Permanent Pacemaker SAVR = Surgical Aortic Valve Replacement; TAV = Transcatheter Aortic Valve TAVR = Transcatheter Aortic Valve Replacement Time-to-event event curves (Kaplan-Meier analysis) to 1 year for all-cause death, all-cause death or disabling stroke, and disabling stroke are shown below for the ITT analysis set. The estimated event rate for all-cause death to 1 year was similar for the 2 cohorts (11.9% for Lotus and 13.7% for CoreValve). The combined outcome of all-cause death or disabling stroke to 1 year was 13.2% for Lotus compared to 17.9% for CoreValve. The estimated rate for disabling stroke to 1 year was 3.6% for Lotus compared to 7.3% for CoreValve. 25% Lotus 20% CoreValve 15% 13.7% 11.9% 10% 5% 0% 0 30 60 90 120 150 180 210 240 270 300 330 360 390 Number at Risk Days Since Randomization Lotus 607 596 581 560 541 481 CoreValve 305 302 292 281 266 238 Figure III: Kaplan-Meier Event Curve for All-Cause Death to 1 Year Post-Randomization, ITT Analysis Set Cumulative event rate ± 1.5 standard error 6 Cumulative Event Rate - All-Cause Death Boston Scientific, Master Brand DFUTemplate 8.2677in x 11.6929in A4, 92238519A) eDFU, MB, LOTUS Edge Valve System, EN, 50473081-01D Black (K) E 5.0 Cumulative Event Rate All-Cause Death or Disabling Stroke 25% LotusTM 20% CoreValve® 15% 10% 17.9% 13.2% 5% 0% 0 30 60 90 120 150 180 210 240 270 300 330 360 390 Number at Risk Days Since Randomization Lotus 607 591 572 550 534 474 CoreValve 305 299 284 269 253 226 Figure IV: Kaplan-Meier Event Curve for All-Cause Death or Disabling Stroke to 1 Year PostRandomization, ITT Analysis Set Cumulative event rate ± 1.5 standard error Cumulative Event Rate - Disabling Stroke 25% Lotus 20% CoreValve 15% 10% 7.3% 5% 3.6% 0% 0 30 60 90 120 150 180 210 240 270 300 330 360 390 Number at Risk Days Since Randomization Lotus 607 588 565 545 529 469 CoreValve 305 297 280 265 252 222 Figure V: Kaplan-Meier Event Curve for Disabling Stroke to 1 Year Post-Randomization, ITT Analysis Set Cumulative event rate ± 1.5 standard error 11.1.3 (iv) Additional Effectiveness Data Figure VI shows that Mean Aortic Gradient improved in both cohorts from baseline to discharge and remained low out to 1 year. Mean Effective Orifice Area (EOA) improved in both cohorts from baseline to discharge and remained high at 1 year. Effective Orifce Area (cm²) CoreValve Lotus 100 Mean Aortic Gradient (mmHg) 80 Lotus 60 44.6±13.4 43.9±12.3 CoreValve 40 0.70±0.19 20 0.69±0.19 0 Baseline Gradient Lotus (N) 575 CoreValve (N) 294 EOA Lotus (N) 541 CoreValve (N) 280 1.96±0.52 1.98±0.51 1.65±0.47 1.59±0.45 12.2±5.2 8.2±4.0 12.0±6.1 7.3±3.4 Discharge 564 281 510 247 30 Days 544 261 506 238 1.74±0.55 1.46±0.46 11.9±5.2 7.9±4.3 6 Months 485 234 440 210 2 1.69±0.52 1.6 1.49±0.45 1.2 0.8 12.3±5.8 7.9±3.5 0.4 0 1 Year 462 219 420 199 Figure VI: Mean Aortic Gradient and Effective Orifice Area to 1 Year, ITT Analysis Set Values are mean ± standard deviation Paravalvular aortic regurgitation over time is illustrated in Figure VII. At discharge, 87.4% of evaluable patients in the Lotus cohort had no or trace PVR compared to 47.4% in the CoreValve cohort. At 30 days, 88.1% of evaluable patients in the Lotus group had no or trace PVR compared to 41.3% in the CoreValve group. At 1 year, 87.6% of evaluable patients in the Lotus cohort had no or trace PVR compared to 51.0% in the CoreValve cohort. There was no severe PVR in either cohort at any time. 100% 80% 60% KEY: 0.4 12.3 11.0 None 3.8 48.9 Trace Mild 0.2 0.4 11.4 11.4 Moderate 7.5 51.2 Moderate-Severe 0.9 1.0 11.5 6.4 5.9 41.7 Percent of Evaluable Echocardiograms 87.4 40% 18.8 76.4 88.1 76.7 15.5 81.7 87.6 11.3 47.4 51.0 20% 41.3 39.7 28.6 25.8 0% Lotus CoreValve (N=529) (N=266) Discharge Lotus (N=511) CoreValve (N=252) 30 Days Figure VII: Paravalvular Regurgitation over Time, ITT Analysis Set Lotus (N=443) CoreValve (N=204) 1 Year Figure VII shows results from evaluable echocardiograms that were gradable. NYHA functional status of patients from baseline to 1 year is shown in Figure VIII While all patients were classified as NYHA Class II, III, or IV at baseline, the majority in both cohorts were Class I or II at 30 days and 1 year. 100% 80% Evaluable Subjects 60% 40% 91% 88% 90% 91% 20% 29% 32% 0% Lotus CoreValve (N=607) (N=305) Baseline Lotus CoreValve (N=556) (N=276) 30 Days Lotus CoreValve (N=477) (N=226) 1 Year Figure VIII: NYHA Functional Status over Time, ITT Analysis Set 11.1.3 (v) Quality of Life Health status was evaluated using the SF-12 Quality of Life questionnaire and Kansas City Cardiomyopathy Questionnaire (KCCQ). SF-12 Among assessed patients in the Lotus cohort, the mean SF-12 physical summary score improved from 31.9 ± 9.0 at baseline to 37.0 ± 9.8 at 30 days and remained high at 1 year (36.9 ± 10.6). The mental health summary score improved from 49.6 ± 11.6 to 52.9 ± 10.9 at 30 days and was 53.6 ± 9.7 at 1 year. Similar results were seen in the CoreValve cohort. KCCQ Among assessed patients in the Lotus cohort, the overall summary score improved from 51.9 ± 23.5 at baseline to 73.0 ± 21.3 at 30 days and remained high at 1 year (74.9 ± 21.0). The clinical summary score improved from 55.2 ± 23.3 to 73.1 ± 21.4 at 30 days and was 73.1 ± 21.3 at 1 year. Similar results were seen in the CoreValve cohort. 11.1.3 (vi) Gender Analysis A total of 449 male patients (49.2%) were enrolled in the ITT analysis set; 303 were randomized to Lotus and 146 were randomized to CoreValve. There were 463 female patients (50.8%) in the ITT analysis set; 304 were in the Lotus arm and 159 were in the CoreValve arm. Table X shows mortality and stroke rates in male and female patients at 1 year. Table X: Mortality and Stroke to 1 Year by Gender; ITT Analysis Set Outcome Male Patients Lotus (N=303) CoreValve (N=146) Female Patients Lotus (N=304) CoreValve (N=159) All-cause mortality Cardiovascular 11.5% (34/295) 14.8% (21/142) 12.3% (36/292) 12.3% (19/155) 8.1% (24/295) 12.0% (17/142) 7.2% (21/292) 7.7% (12/155) Non-cardiovascular 3.4% (10/295) 2.8% (4/142) 5.1% (15/292) 4.5% (7/155) Stroke 6.1% (18/295) 9.2% (13/142) 7.9% (23/292) 9.7% (15/155) Disabling 2.7% (8/295) 7.7% (11/142) 4.5% (13/292) 6.5% (10/155) Non-disabling 3.4% (10/295) 1.4% (2/142) 3.8% (11/292) 3.2% (5/155) All-cause mortality or disabling stroke 12.9% (38/295) 18.3% (26/142) 13.7% (40/292) 17.4% (27/155) Values are % (count/sample size) 7 Boston Scientific, Master Brand DFUTemplate 8.2677in x 11.6929in A4, 92238519A) eDFU, MB, LOTUS Edge Valve System, EN, 50473081-01D Black (K) E 5.0 11.2 Clinical Studies with the LOTUS EdgeTM Valve System The LOTUS Edge Valve System is a design iteration of the LotusTM Valve System which was modified to improve flexibility and deliverability, to reduce the profile of the delivery system, and to minimize how deep the valve frame travels into the left ventricular outflow tract with the Depth GuardTM technology. The valve component is essentially the same but with additional radiopaque tantalum markers to aid in visualization of the locking procedure under fluoroscopy. The REPRISE NG DS (Cohort C) and REPRISE Edge studies evaluated the LOTUS Edge Valve System to confirm its acute performance and safety when used with the LotusTM or iSLEEVETM Introducer Set for TAVR in symptomatic subjects with severe calcific aortic valve stenosis who were at high risk for surgical aortic valve replacement (SAVR). Both studies have the same overall study design (prospective, single-arm study), inclusion and exclusion criteria and assessments, and both studies use the same CEC and core laboratories (echocardiography, angiography and computed tomography/X-ray). There were 21 subjects enrolled in REPRISE NG DS Cohort C at 2 centers in Australia and 15 subjects enrolled in REPRISE EDGE at 3 European centers to evaluate the same LOTUS Edge design. Table XI and Table XII show the pooled primary safety and effectiveness composite results and their components (defined similarly as in REPRISE III RCT) from both studies (N=36). Table XI. Pooled 30-Day Primary Safety Results from REPRISE NG DS (Cohort C) and REPRISE Edge, ITT Analysis Set Outcome Primary Safety Composite All-cause mortality All Stroke Disabling Life-threatening or Disabling bleeding Major bleeding Major vascular Complications Acute kidney injury 30 Days REPRISE NGDS (Cohort C) and REPRISE Edge (N=36) 22.2% (8/36) 0.0% (0/36) 5.6% (2/36) 5.6% (2/36) 5.6% (2/36) 13.9% (5/36) 13.9% (5/36) 0.0% (0/36) 12.0 WARRANTY Boston Scientific Corporation (BSC) warrants that reasonable care has been used in the design and manufacture of this instrument. This warranty is in lieu of and excludes all other warranties not expressly set forth herein, whether express or implied by operation of law or otherwise, including, but not limited to, any implied warranties of merchantability or fitness for a particular purpose. Handling, storage, cleaning and sterilization of this instrument as well as other factors relating to the patient, diagnosis, treatment, surgical procedures and other matters beyond BSC's control directly affect the instrument and the results obtained from its use. BSC's obligation under this warranty is limited to the repair or replacement of this instrument and BSC shall not be liable for any incidental or consequential loss, damage or expense directly or indirectly arising from the use of this instrument. BSC neither assumes, nor authorizes any other person to assume for it, any other or additional liability or responsibility in connection with this instrument. BSC assumes no liability with respect to instruments reused, reprocessed or resterilized and makes no warranties, express or implied, including but not limited to merchantability or fitness for a particular purpose, with respect to such instruments. CoreValve is a registered trademark of Medtronic CV Luxembourg S.a.r.l. Evolut is a registered trademark of Medtronic, Inc. Table XII. Pooled 1-Year Primary Effectiveness Results from REPRISE NG DS (Cohort C) and REPRISE Edge, ITT Analysis Set Outcome 1 Year REPRISE NGDS (Cohort C) and REPRISE Edge (N=36) Primary Effectiveness Composite 5.7% (2/35) All-cause mortality 0.0% (0/36) Disabling stroke 5.6% (2/36) Moderate or greater PVR 0.0% (0/34) 11.3 REPRISE III LOTUS Edge Nested Registry Additional design modifications were made to the LOTUS Edge Valve System to improve deliverability and deployment. This modified version of the device was studied in the REPRISE III LOTUS Edge Nested Registry. Primary Objective: The objective of the REPRISE III LOTUS Edge Nested Registry is to confirm performance of the LOTUS Edge Valve implantation procedure with the LOTUS Edge delivery system. Design: The REPRISE III LOTUS Edge Nested Registry is a prospective, single-arm, multicenter study designed to evaluate the safety and performance of the LOTUS Edge Valve System for TAVR. Inclusion criteria and patient eligibility requirements are the same as for the RCT. A total of 50 subjects were enrolled at 4 centers in the US and Australia. Study Results: Table XIII shows LOTUS Edge Nested Registry clinical outcomes at 30 days for the components of the RCT primary composite safety endpoint. Table XIII. 30-Day Primary Safety Composite and Components of REPRISE III LOTUS Edge Nested Registry, ITT Analysis Set Outcome 30 Days REPRISE III LOTUS Edge Nested Registry (N=50) Primary Safety Composite 14.3% (7/49) All-cause mortality Stroke 0.0% (0/49) 4.1% (2/49) Disabling 2.0% (1/49) Life-threatening or disabling bleeding Major bleeding 4.1% (2/49) 6.1% (3/49) Major vascular complications 6.1% (3/49) Acute kidney injury 4.1% (2/49) 8 Boston Scientific, Master Brand DFUTemplate 8.2677in x 11.6929in A4, 92238519A) eDFU, MB, LOTUS Edge Valve System, EN, 50473081-01D Black (K) E 5.0 CV 02 Brazil BRA Local Contact Para informações de contato da Boston Scientifc do Brasil Ltda, por favor, acesse o link www.bostonscientifc.com/bra EC REP EU Authorized Representative Boston Scientifc Limited Ballybrit Business Park Galway IRELAND AUS Australian Sponsor Address Boston Scientifc (Australia) Pty Ltd PO Box 332 BOTANY NSW 1455 Australia Free Phone 1800 676 133 Free Fax 1800 836 666 ARG Argentina Local Contact Para obtener información de contacto de Boston Scientifc Argentina SA, por favor, acceda al link www.bostonscientifc.com/arg Legal Manufacturer Boston Scientifc Corporation 300 Boston Scientifc Way Marlborough, MA 01752 USA USA Customer Service 888-272-1001 Do not use if package is damaged. Recyclable Package © 2019 Boston Scientific Corporation or its affiliates. All rights reserved. Black (K) E 5.0 Boston Scientific, Master Brand DFUTemplate 8.2677in x 11.6929in A4, 92238519A) eDFU, MB, LOTUS Edge Valve System, EN, 50473081-01DAdobe InDesign CC 13.1 (Windows) Adobe PDF Library 15.0