ℹ️ Document Conversion Notice:
This page was converted from the original file for easier reading. Diagrams/images may appear only in the original PDF below.
File info: application/pdf · 1 pages · 4.78MB
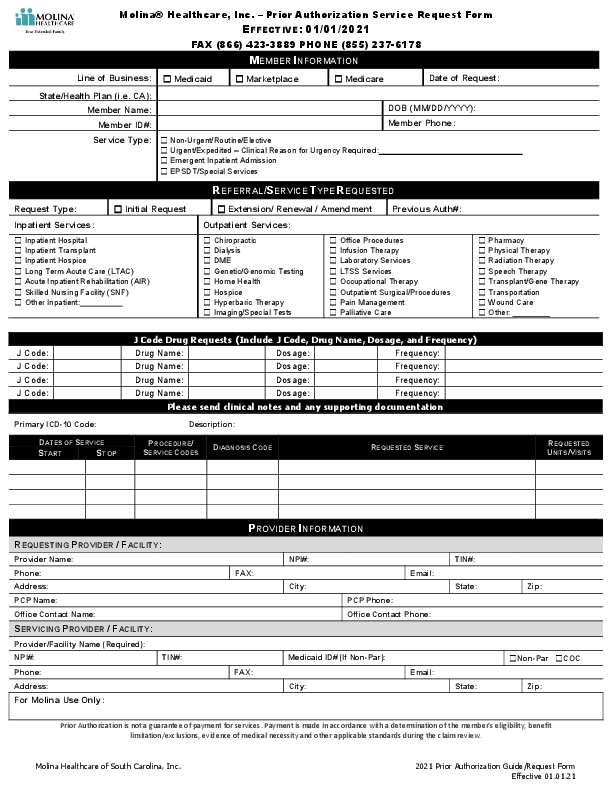
Molina Healthcare Prior Authorization Service Request Form
Effective Date: 01/01/2021
Contact: FAX (866) 423-3889 | PHONE (855) 237-6178
MEMBER INFORMATION
Line of Business:[ ] Medicaid[ ] Marketplace[ ] Medicare
Service Type:[ ] Non-Urgent/Routine/Elective[ ] Urgent/Expedited - Clinical Reason for Urgency Required[ ] Emergent Inpatient Admission[ ] EPSDT/Special Services
REFERRAL/SERVICE TYPE REQUESTED
Request Type:[ ] Initial Request[ ] Extension / Renewal / Amendment
Inpatient Services:[ ] Inpatient Hospital[ ] Inpatient Transplant[ ] Inpatient Hospice[ ] Long Term Acute Care (LTAC)[ ] Acute Inpatient Rehabilitation (AIR)[ ] Skilled Nursing Facility (SNF)[ ] Other Inpatient:
Outpatient Services:
[ ] Chiropractic[ ] Dialysis[ ] DME[ ] Genetic/Genomic Testing[ ] Home Health[ ] Hospice[ ] Hyperbaric Therapy[ ] Imaging/Special Tests
[ ] Office Procedures[ ] Infusion Therapy[ ] Laboratory Services[ ] LTSS Services[ ] Occupational Therapy[ ] Outpatient Surgical/Procedures[ ] Pain Management[ ] Palliative Care
[ ] Pharmacy[ ] Physical Therapy[ ] Radiation Therapy[ ] Speech Therapy[ ] Transplant/Gene Therapy[ ] Transportation[ ] Wound Care[ ] Other:
J Code Drug Requests
Include J Code, Drug Name, Dosage, and Frequency
| J Code | Drug Name | Dosage | Frequency |
|---|---|---|---|
[ ] Please send clinical notes and any supporting documentation
Primary ICD-10 Code
DATES OF SERVICE
| START | STOP | PROCEDURE/ SERVICE CODES | DIAGNOSIS CODE | REQUESTED SERVICE | REQUESTED UNITS/VISITS |
|---|---|---|---|---|---|
PROVIDER INFORMATION
Requesting Provider / Facility
Servicing Provider / Facility
[ ] Non-Par[ ] COC
For Molina Use Only
This section is for internal use by Molina Healthcare.
Prior Authorization is not a guarantee of payment for services. Payment is made in accordance with a determination of the member's eligibility, benefit limitation/exclusions, evidence of medical necessity and other applicable standards during the claim review.
Full PDF Document

If the inline viewer fails, it will open the original document in compatibility mode automatically. You can also open the file directly.