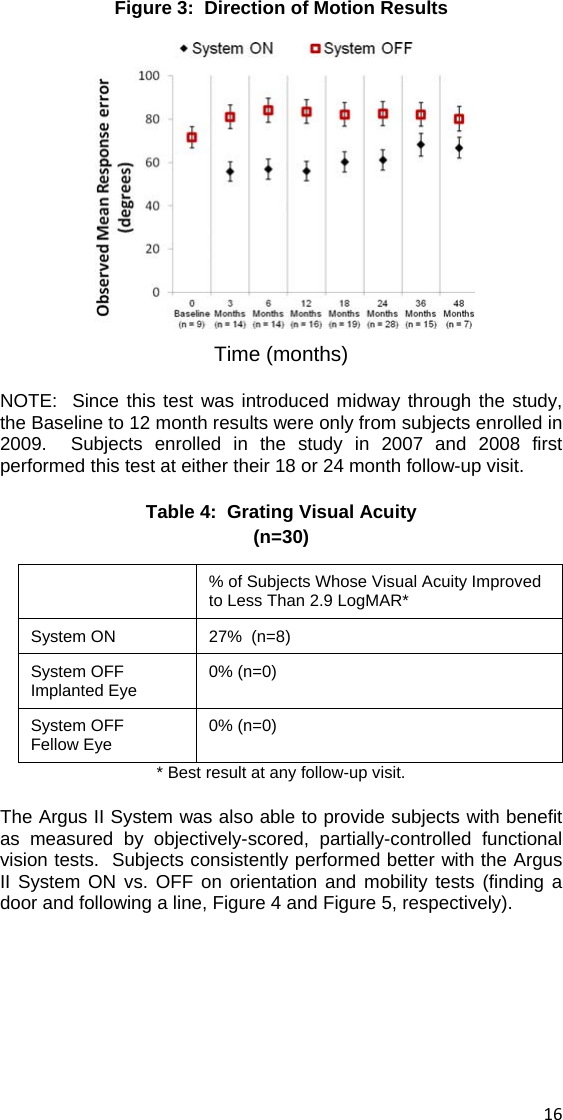
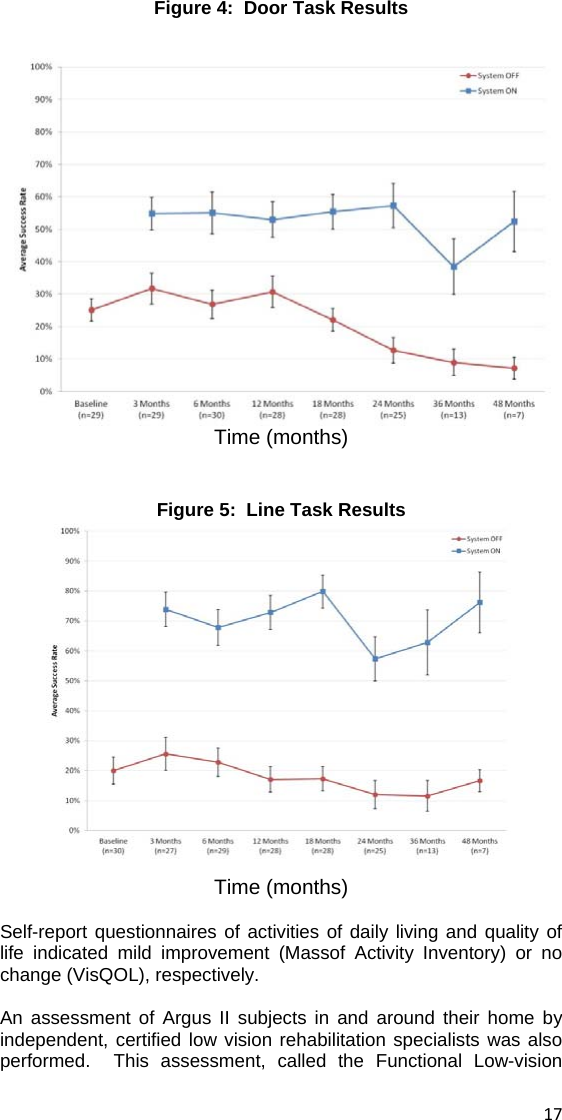
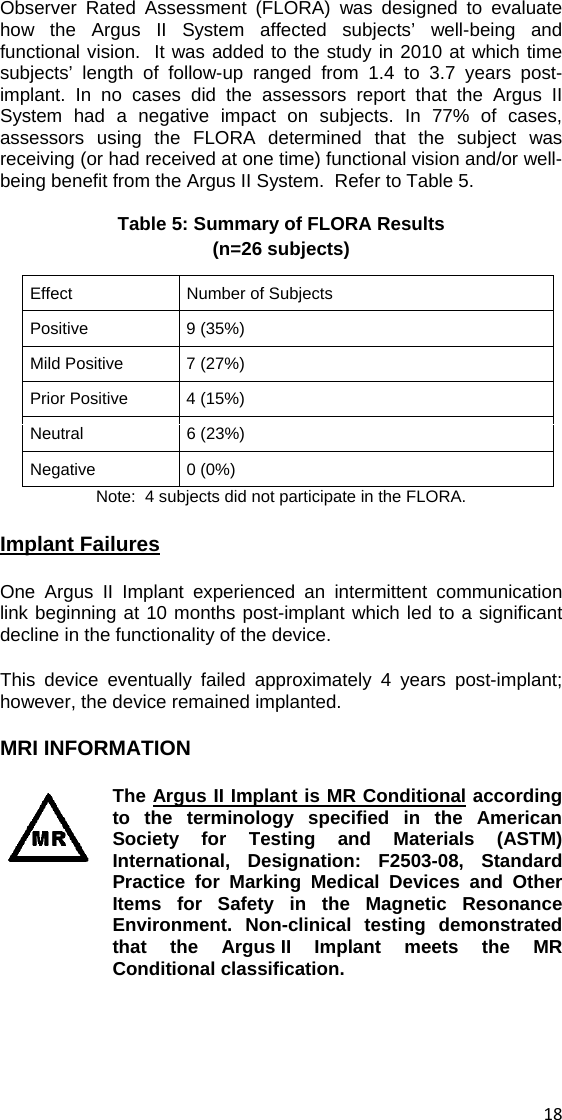
Second Sight Medical A01 Argus II Retinal Prosthesis System User Manual Doctors Users Manual
Second Sight Medical Products, Inc. Argus II Retinal Prosthesis System Doctors Users Manual
Contents
- 1. Doctors Users Manual
- 2. Patient Users Manual
Doctors Users Manual
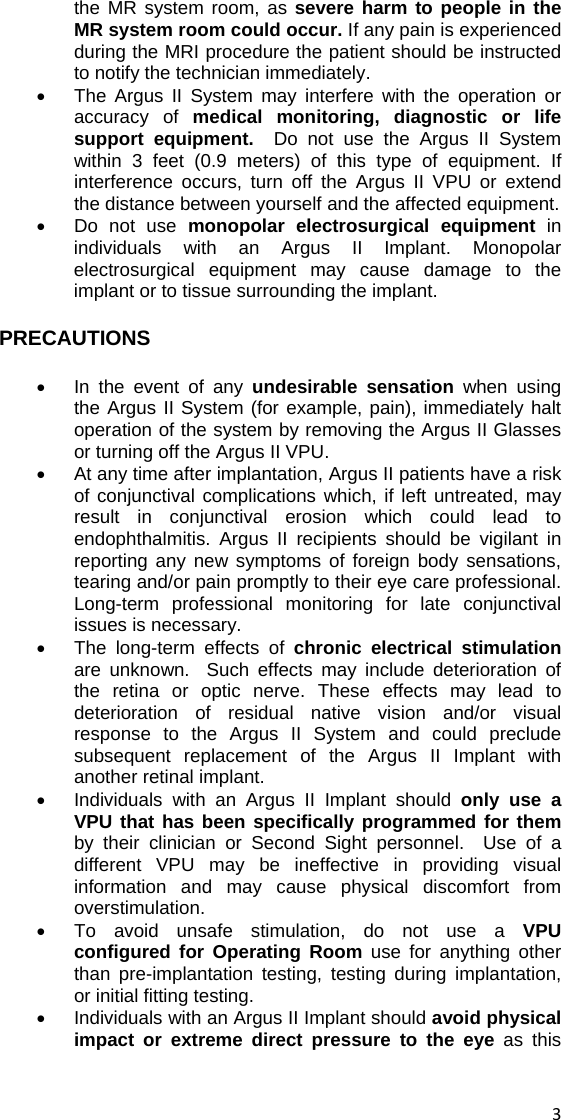
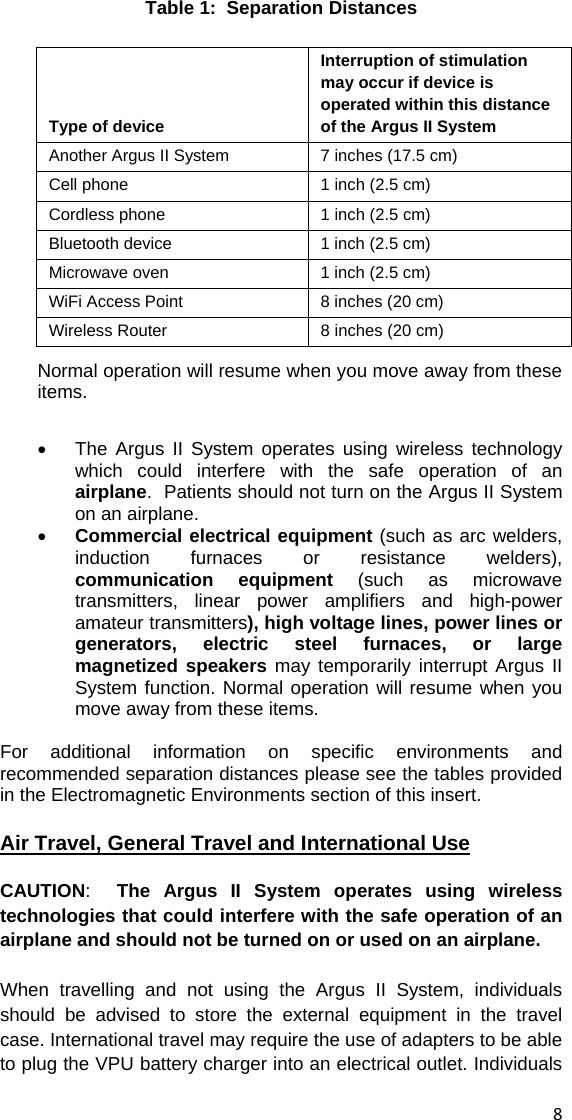
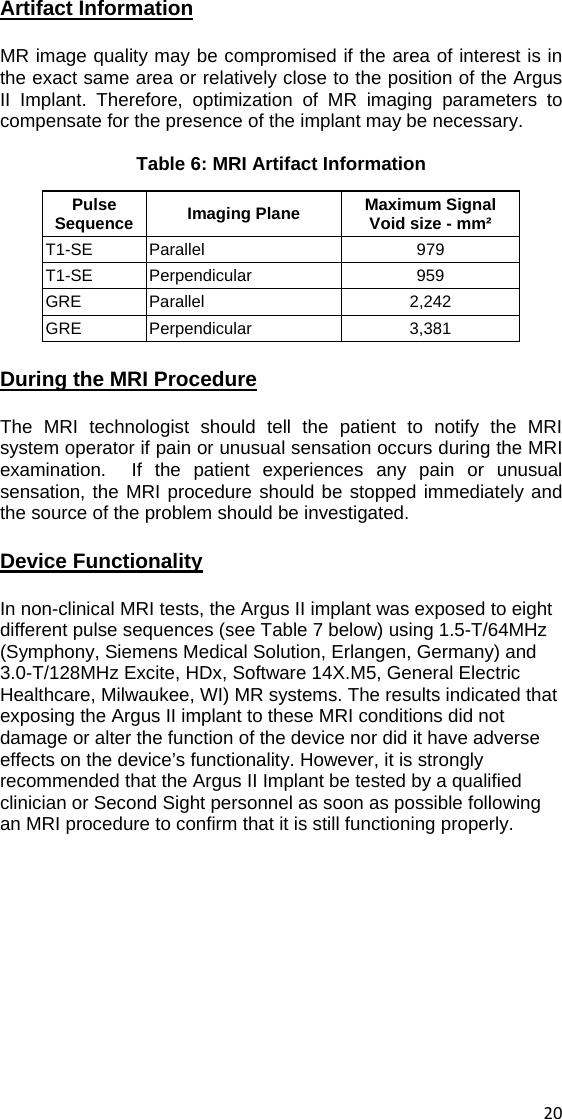
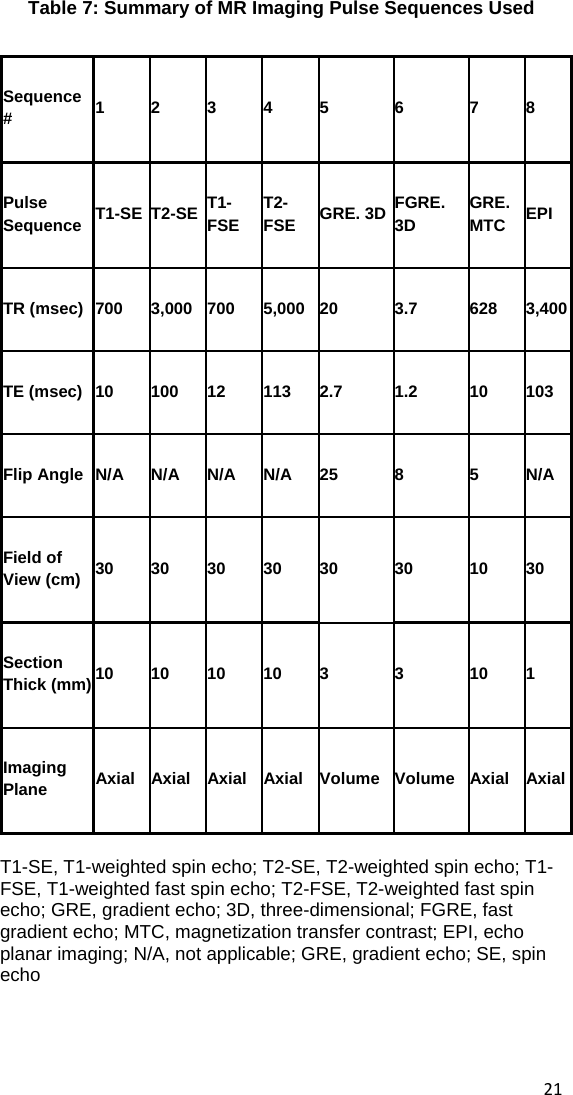
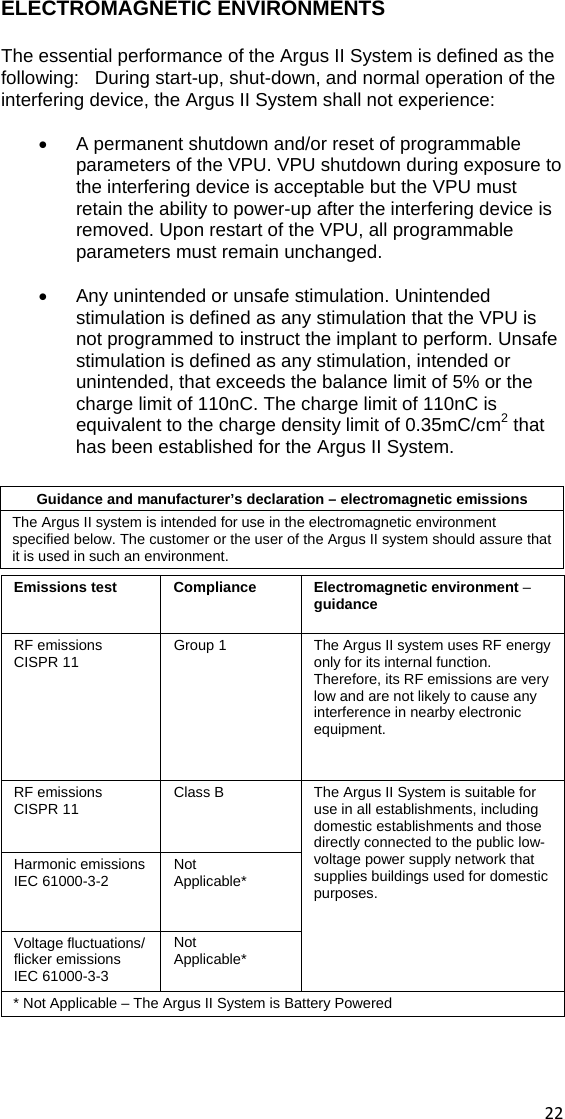
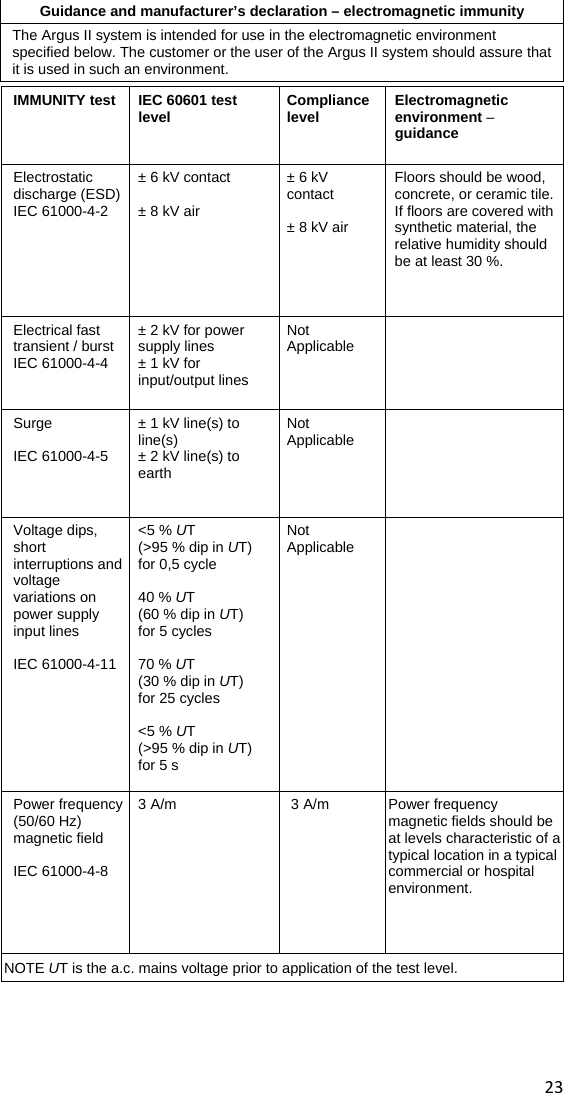
![Recommended separation distances between portable and mobile RF communications equipment and the Argus II system The Argus II system is intended for use in an electromagnetic environment in which radiated RF disturbances are controlled. The customer or the user of the Argus II system can help prevent electromagnetic interference by maintaining a minimum distance between portable and mobile RF communications equipment (transmitters) and the Argus II System as recommended below, according to the maximum output power of the communications equipment. Rated maximum output power of transmitter (W) Separation distance according to frequency of transmitter (m) 150 kHz to 80 MHz d = [ 3.5] PV180 MHz to 800 MHz d = [ 3.5] PE1800 MHz to 2.5 GHz d = [ 7 ] PE10.01 0.0117 0.0117 0.0233 0.1 0.117 0.117 0.233 1 1.17 1.17 2.33 10 11.7 11.7 23.3 100 117 117 233 For transmitters rated at a maximum output power not listed above, the recommended separation distance d in meters (m) can be estimated using the equation applicable to the frequency of the transmitter, where P is the maximum output power rating of the transmitter in watts (W) according to the transmitter manufacturer. NOTE 1 At 80 MHz and 800 Hz, the separation distance for the higher frequency range applies. NOTE 2 These guidelines may not apply in all situations. Electromagnetic propagation is affected by absorption and reflection from structures, objects, and people. 25 ](https://usermanual.wiki/Second-Sight-Medical/A01.Doctors-Users-Manual/User-Guide-2132836-Page-31.png)