COSMED Srl K4B2T-USA TELEMETRY UNIT User Manual III
COSMED Srl TELEMETRY UNIT Users Manual III
UserManual.wiki
>
COSMED Srl
>
K4B2T-USA User Manual
>
Users Manual III
Contents
1.
Users Manual I
2.
Users Manual II
3.
Users Manual III
Users Manual III
Navigation menu
Upload a User Manual
Namespaces
Wiki Guide
HTML
PDF
Info
Views
User Manual
Discussion / Help
Navigation
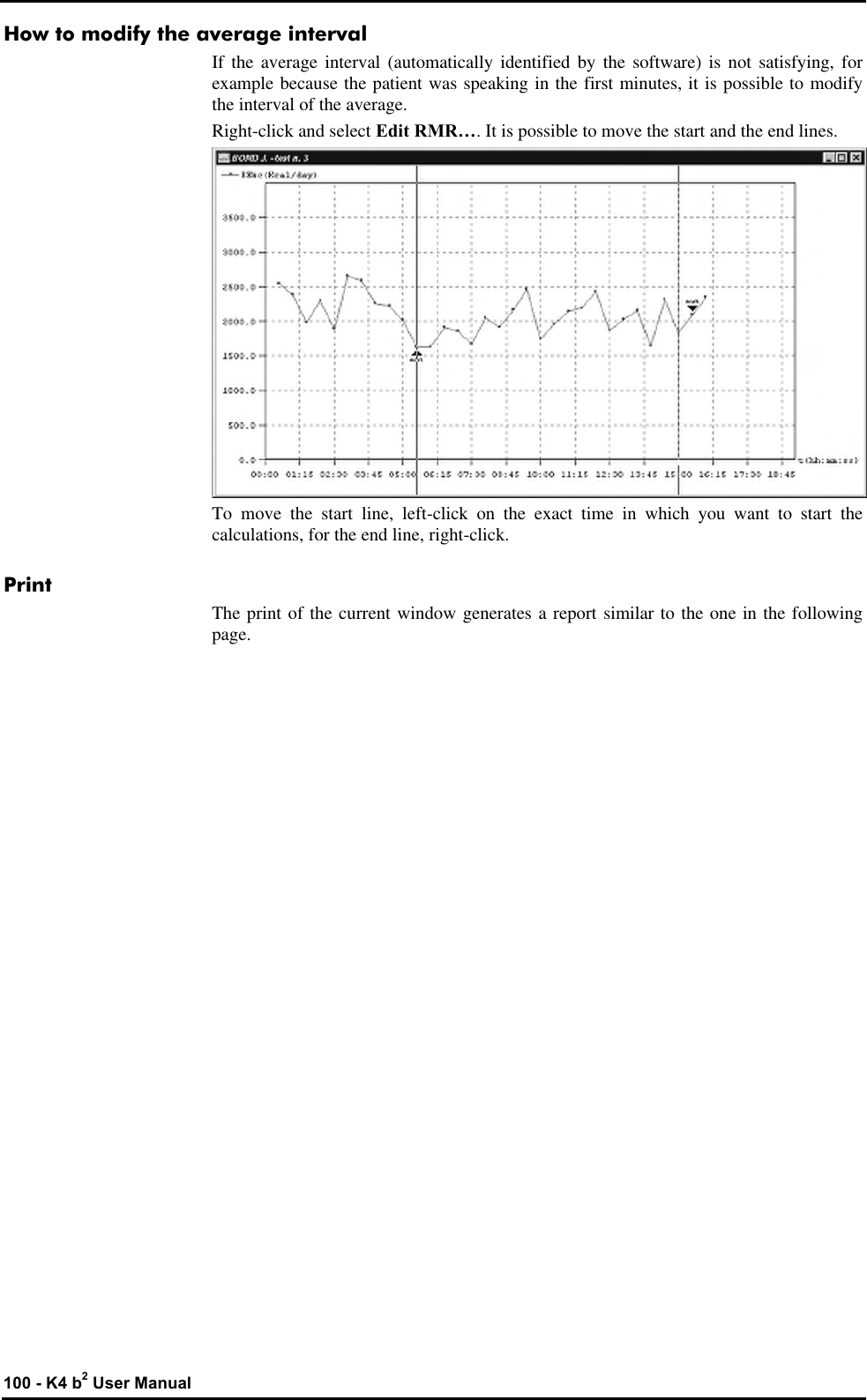
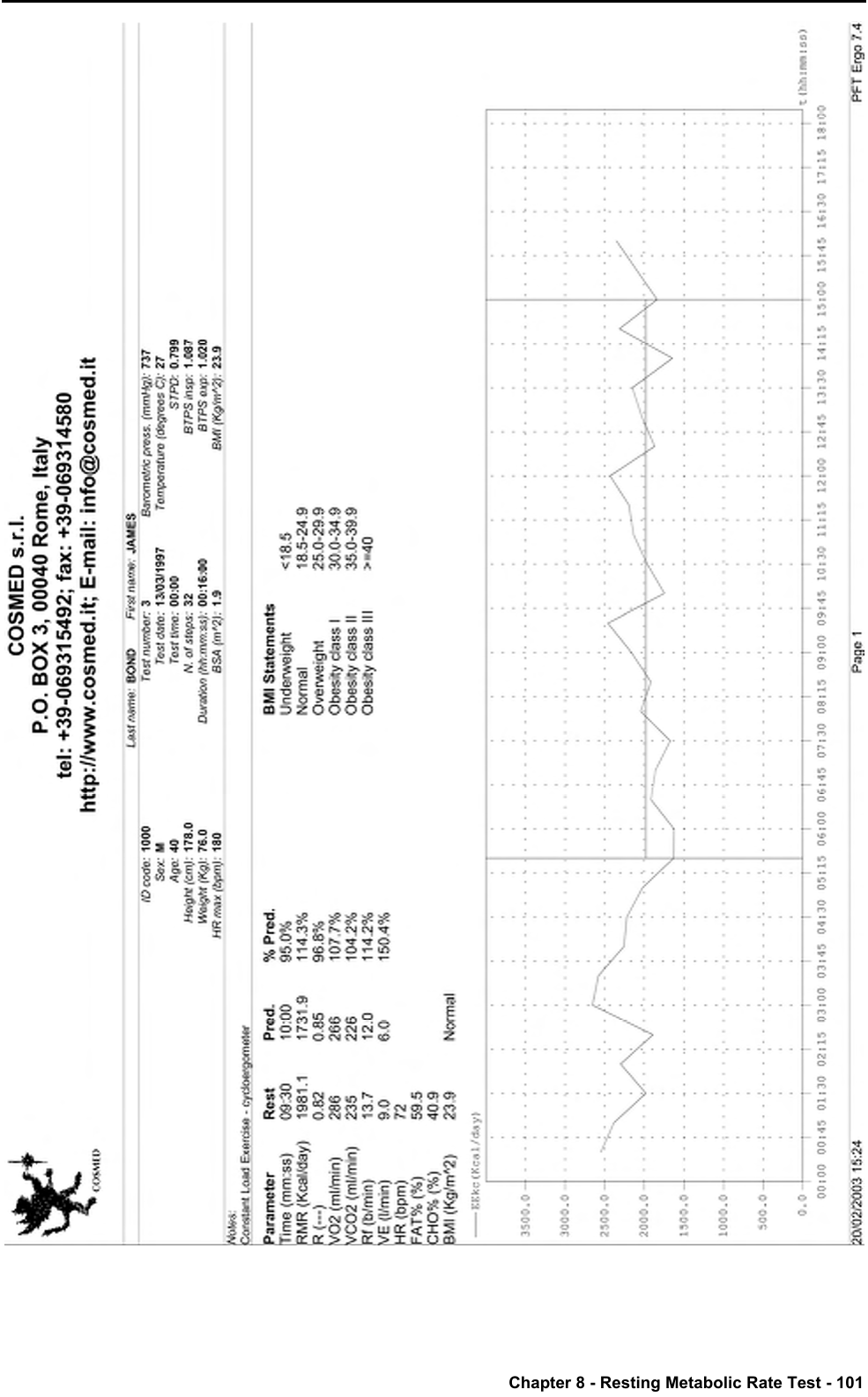
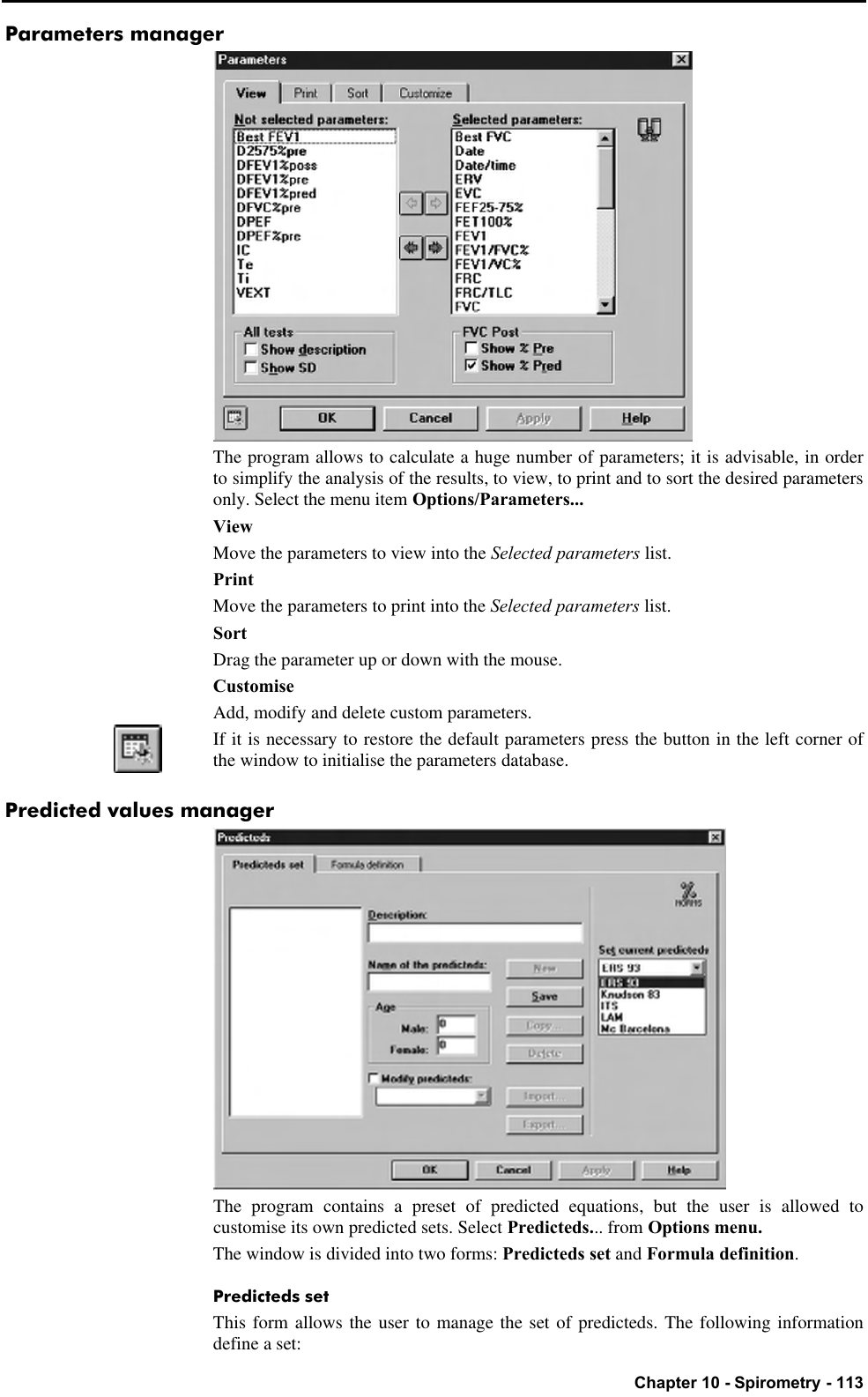
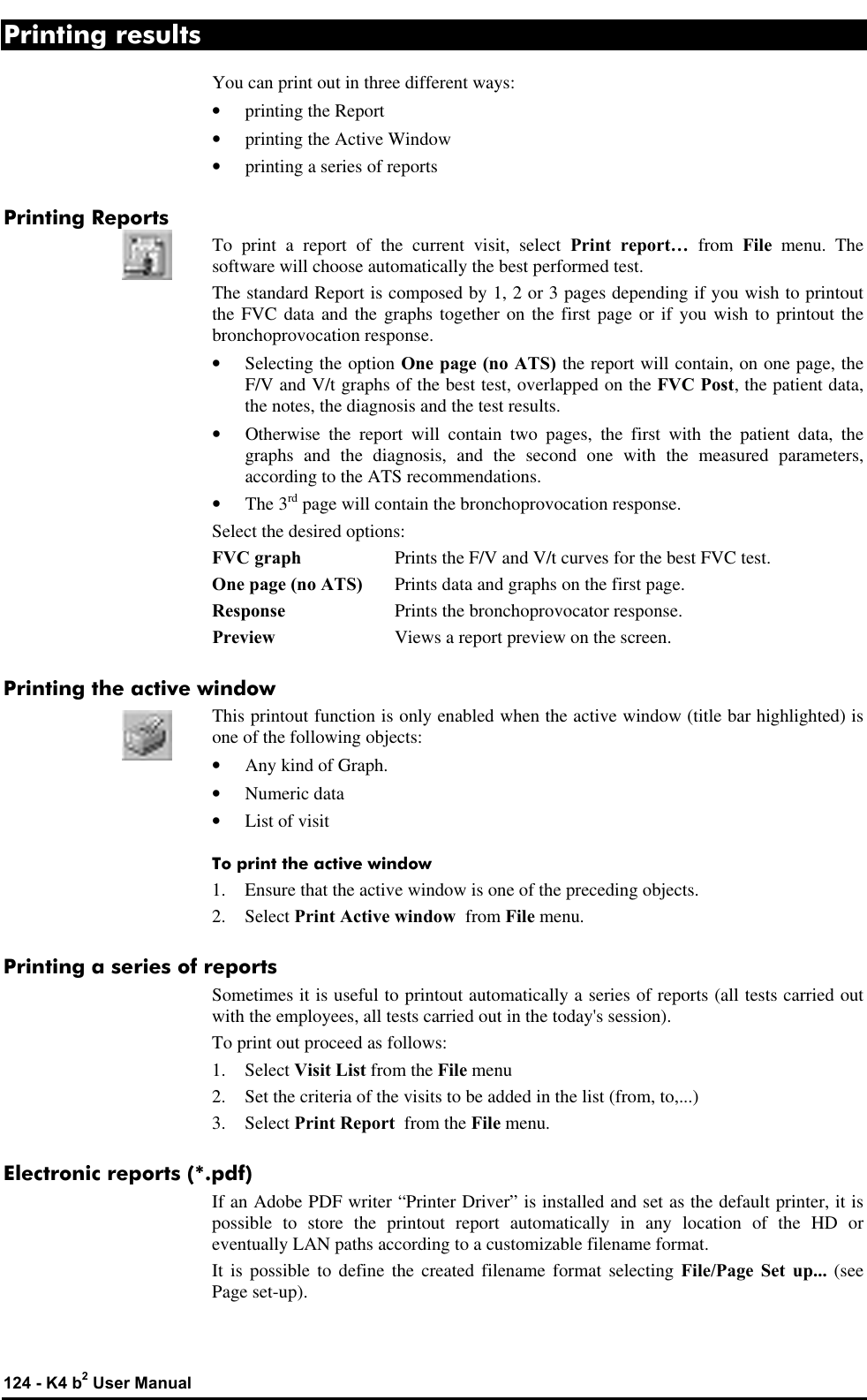
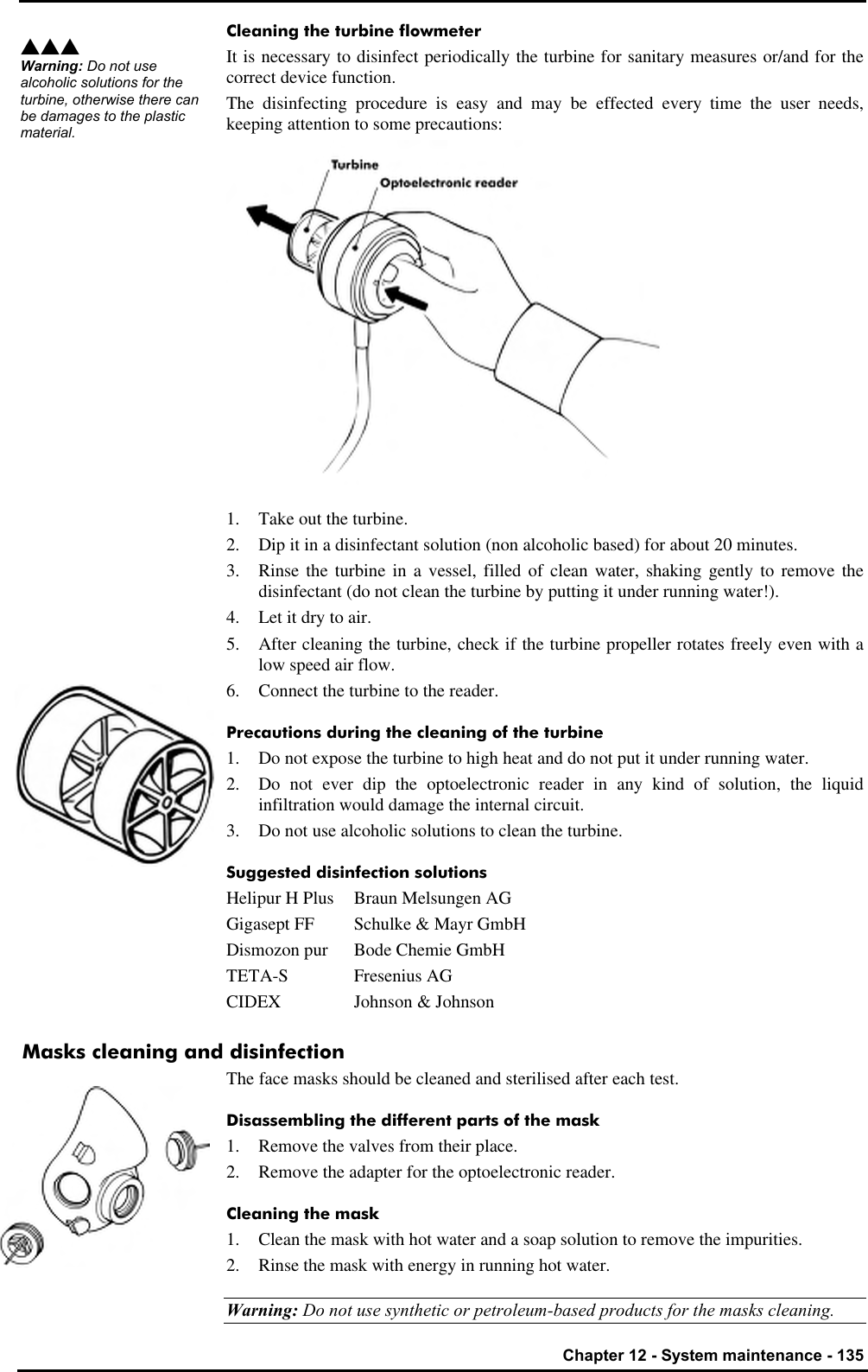
![96 - K4 b2 User Manual Metabolism Metabolism can be understood as the conversion by the human body between food and accumulated fat into energy. The energy is used by the body to maintain constant temperature , to move and to make all the organ function. Measure of metabolism is: calories (cal). Total Metabolic Rate The total metabolic rate are the total calories that the human body needs in order to actuate the daily functional activities. Resting Metabolic Rate (RMR) Resting Metabolic Rate represents the calories that the vital organs need to properly operate at rest ( heart , brain , lungs , liver , kidneys etc.) . RMR represents between 60 % and 75 % of the human ‘s total metabolism. Importance to measure RMR A knowledge of the RMR is very helpful in order to understand the nutritional needs and to properly manage it. Measure of the rest metabolic rate with indirect calorimetry Energy expenditure can be measured directly by putting a person in a calorimeter and measuring the amount of heat produced by the body mass. This is expensive and very impractical in the clinical setting. Energy expenditure can be measured indirectly with a metabolic cart by analysis of respired gases (usually expired) to derive volume of air passing through the lungs, the amount of oxygen extracted from it (i.e., oxygen uptake VO2) and the amount of carbon dioxide, as a by-product of metabolism, expelled to atmosphere (CO2 output – VCO2). With these measurements the resting energy expenditure (RMR) and respiratory quotient (RQ) can be calculated. The RQ represents the ratio of carbon dioxide exhaled to the amount of oxygen consumed by the individual. RQ is useful in interpreting the results of the RMR. The abbreviated Weir equation is probably the most common calculation of RMR. Abbreviated Weir equation: RMR = [3.9 (VO2) + 1.1 (VCO2)] 1.44 How to perform a RMR test For best results, when having a REE done, there are certain conditions that need to be controlled and others that just require documenting at the time of the test. During the test the individual is interfaced with a metabolic measurement system by means of a facemask. A mouthpiece with a nose clip is also sometimes used, but it may create overly stressful conditions to a subject (patient). Important considerations or conditions to improve the RMR measurement: • No food for at least 12 hours and no smoke for at least 2 hours before the test. • Maintain quiet surroundings when the test is in progress and normal temperature. The individual should not move arms or legs during the test. • Medications taken should be noted, such as stimulants or depressants. • The first 5 minutes of acquisition should be discarded by the computation of RMR • Steady state should be achieved, which would be identified clinically by the following criteria: 5 minute period when average minute VO2 and VCO2 changes by less than 10%, average RQ changes by less than 5% • Stable interpretable measurements should be obtained in a 15 to 20 minute test. • Renal failure patients requiring hemodialysis should not be tested during dialysis therapy.](https://usermanual.wiki/COSMED-Srl/K4B2T-USA.Users-Manual-III/User-Guide-568599-Page-2.png)
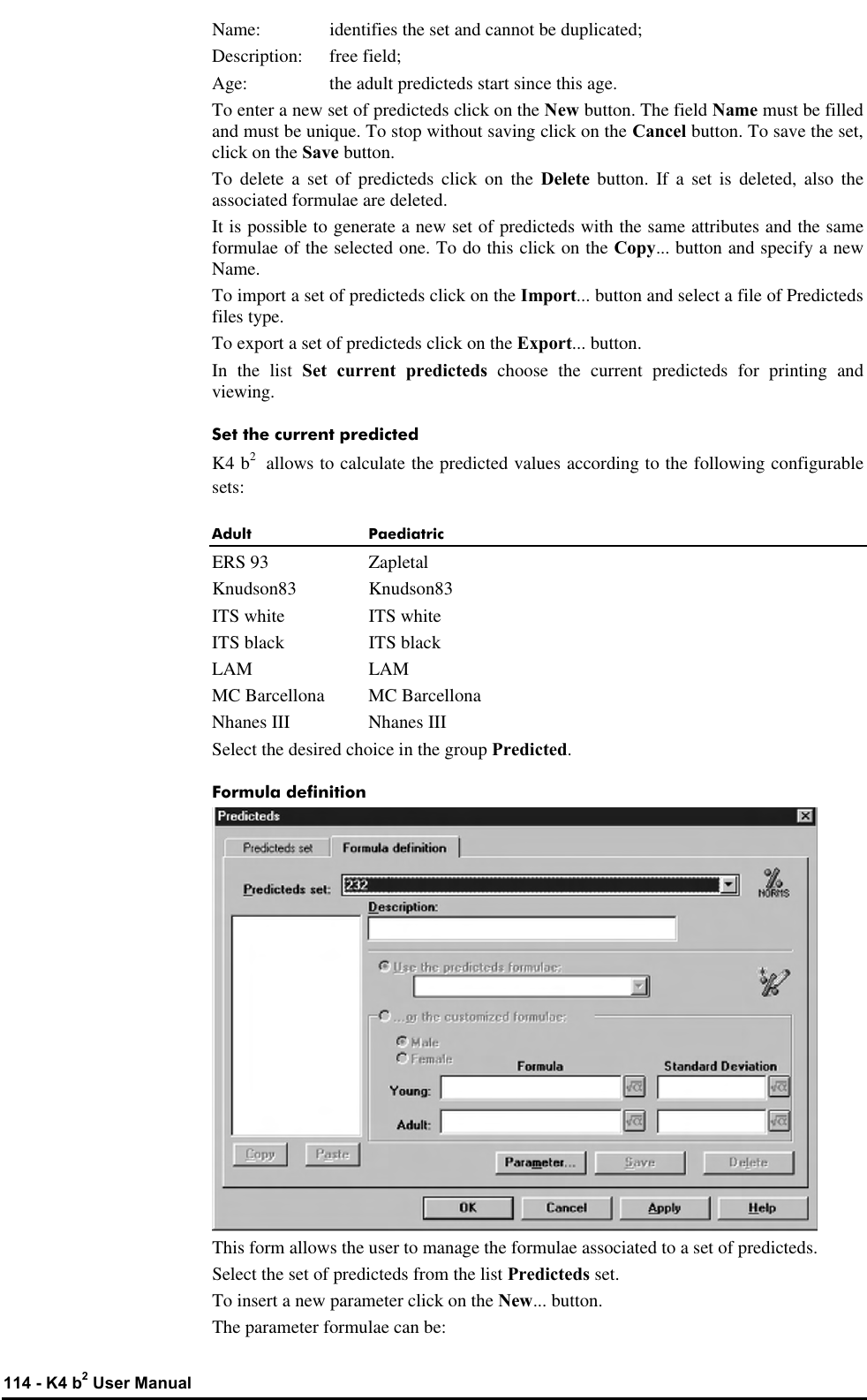
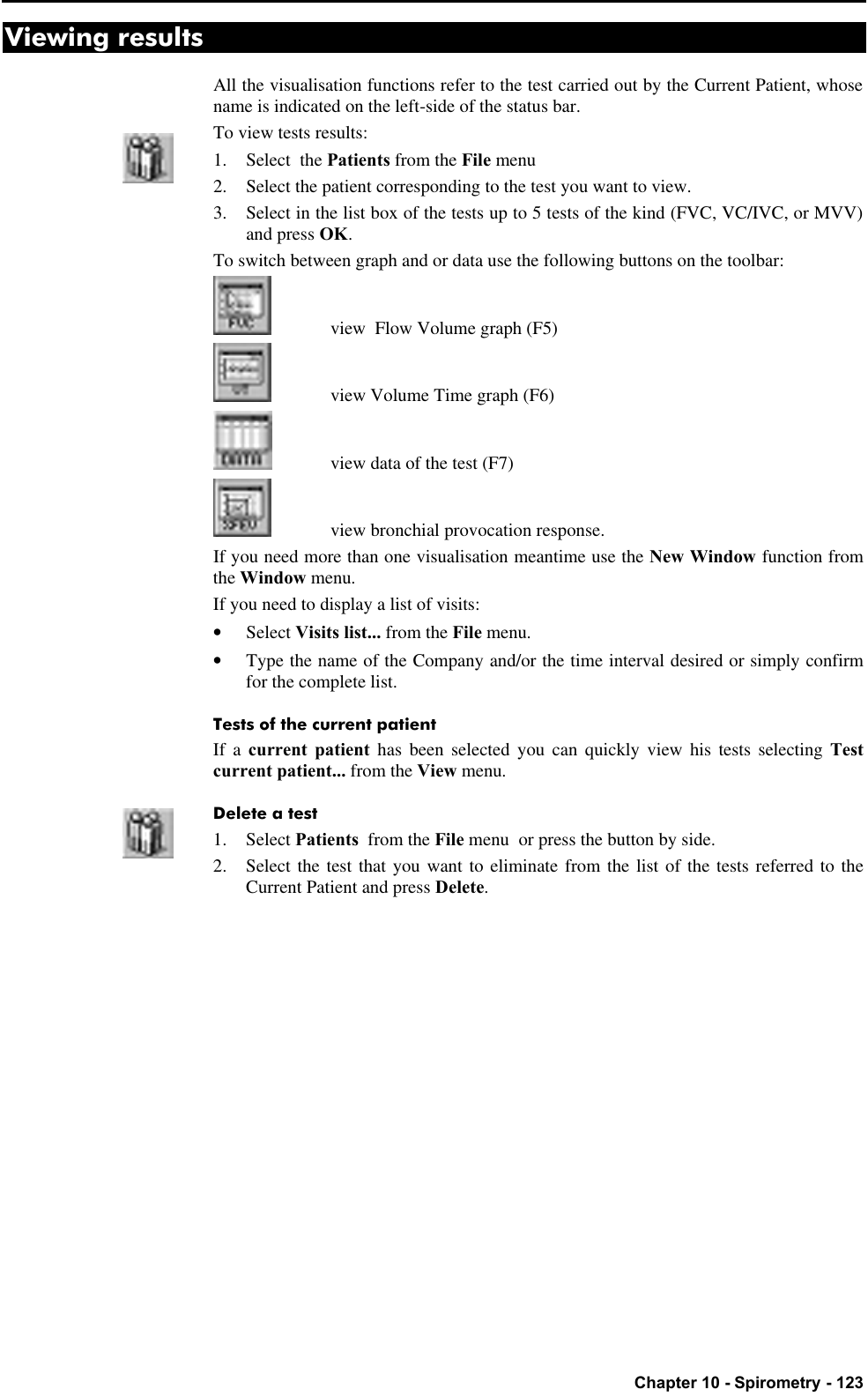
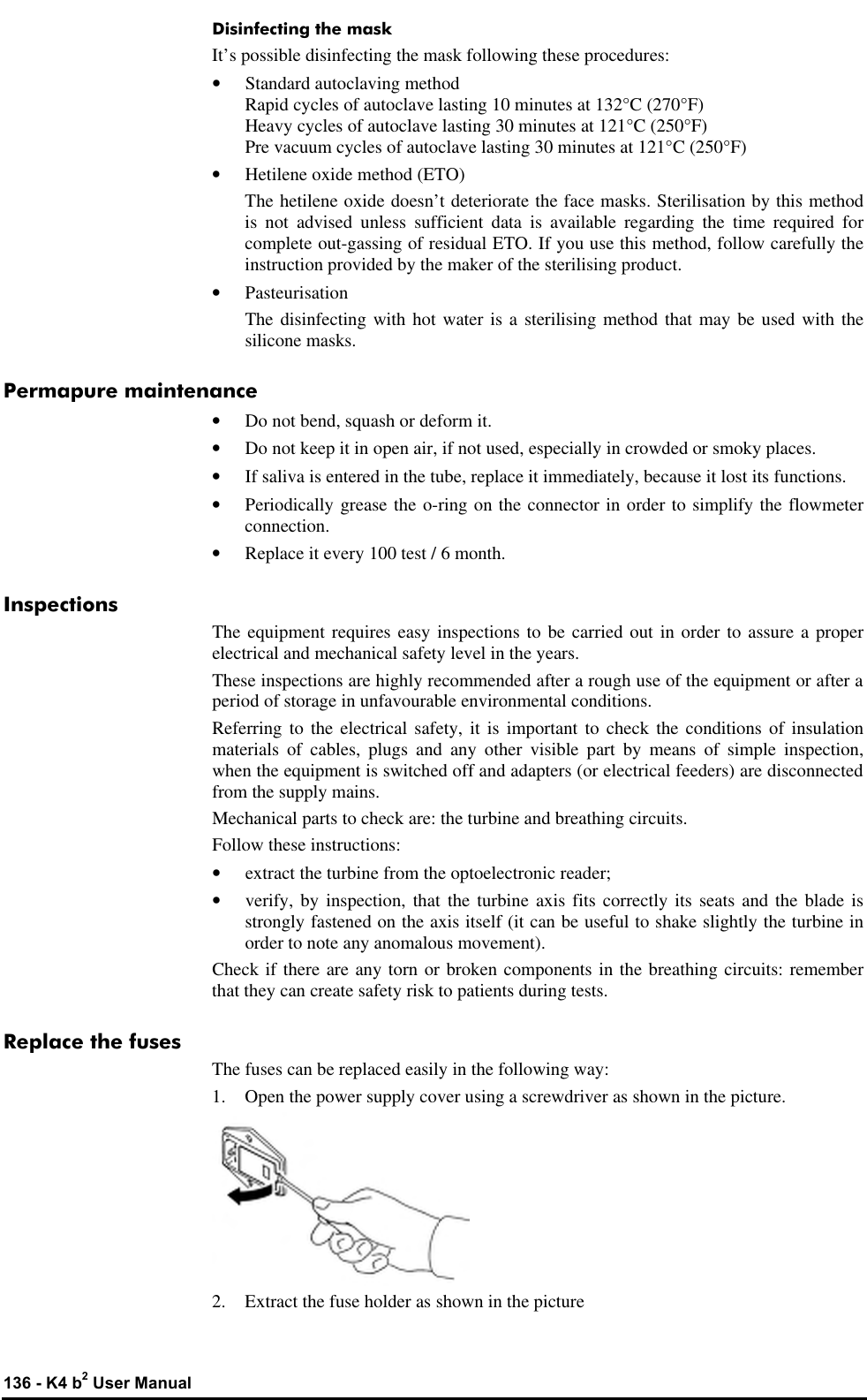
![110 - K4 b2 User Manual Performing the test In this chapter it is supposed that the user is able to: • perform an exercise test • create exercise protocols • view, edit and print tests If this is not the case, please read the Exercise testing chapter. To perform a sub-maximal test, follow these instructions: 1. Create a proper protocol (procedural guidelines for several sub-maximal testing protocols are provided in [ACSM’s Guidelines for Exercise Testing and Prescription, 6th Edition Philadelphia: Williams&Wilkins, 2000:22-29]). 2. Start an exercise test. 3. Perform the test as it were a maximal exercise test, ending it when the heart rate reaches the 85% of the Hrmax, or it happens an event listed in the section Test termination. 4. Display a VO2/Kg vs. HR plot 5. Right-click on the graph and select VO2 submax from the pop-up menu. If the predicted HR max (calculated as 220-age) is not suitable for the patient tested, it is possible to edit the HR max value from the View/Information… page. An example of testing protocol An example of protocol is reported here. The YMCA cycle ergometry protocol is defined as follows. 1st step: workload 150 kgm/min 2nd step: if the HR at the end of the 1st step is: <80 80-89 90-100 >100 set the workload at (kgm/min) 750 600 450 300 3rd step: if the HR at the end of the 2nd step is: <80 80-89 90-100 >100 set the workload at (kgm/min) 900 750 600 450 4th step: if the HR at the end of the 3rd step is: <80 80-89 90-100 >100 set the workload at (kgm/min) 1050 900 750 600](https://usermanual.wiki/COSMED-Srl/K4B2T-USA.Users-Manual-III/User-Guide-568599-Page-16.png)
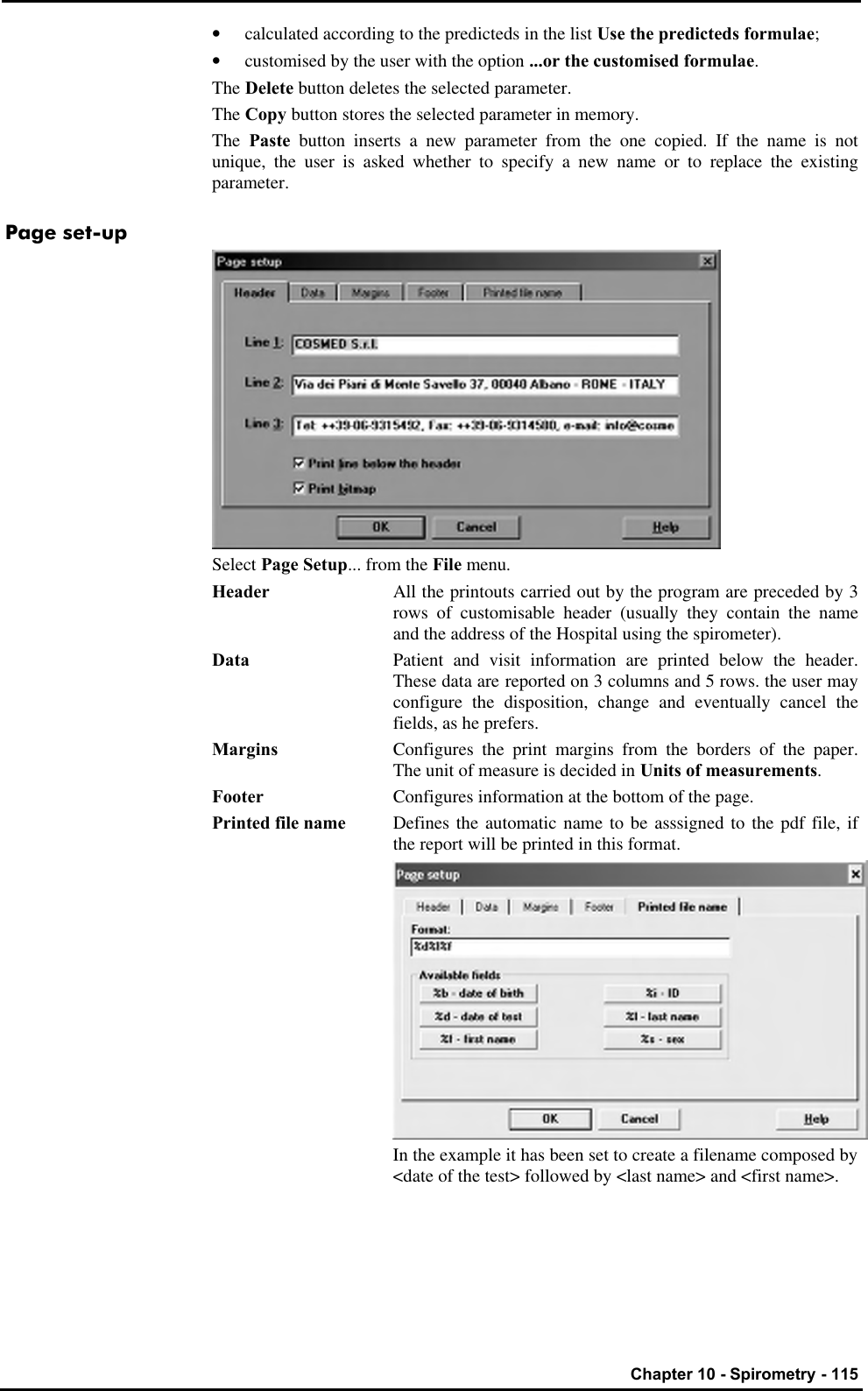
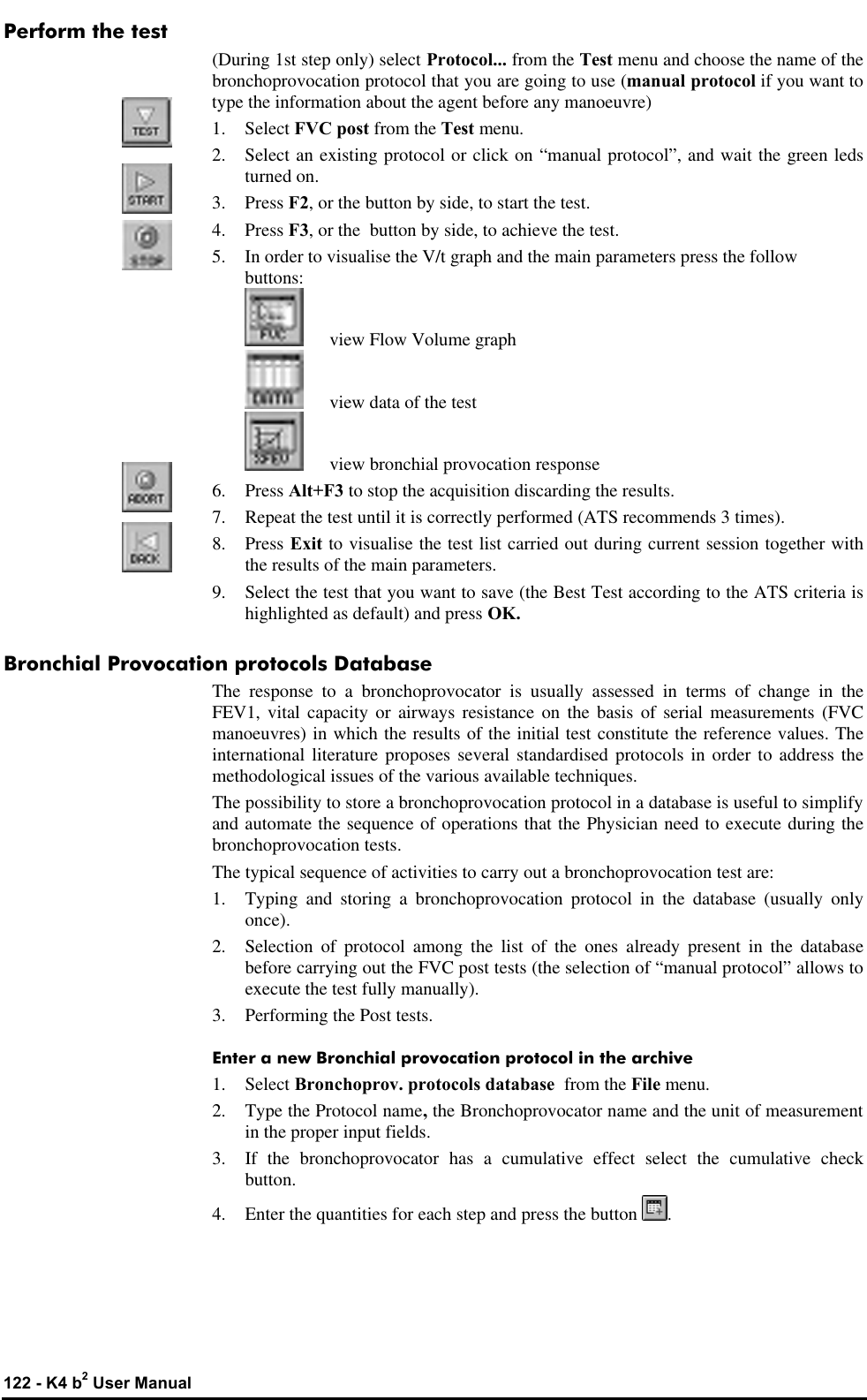
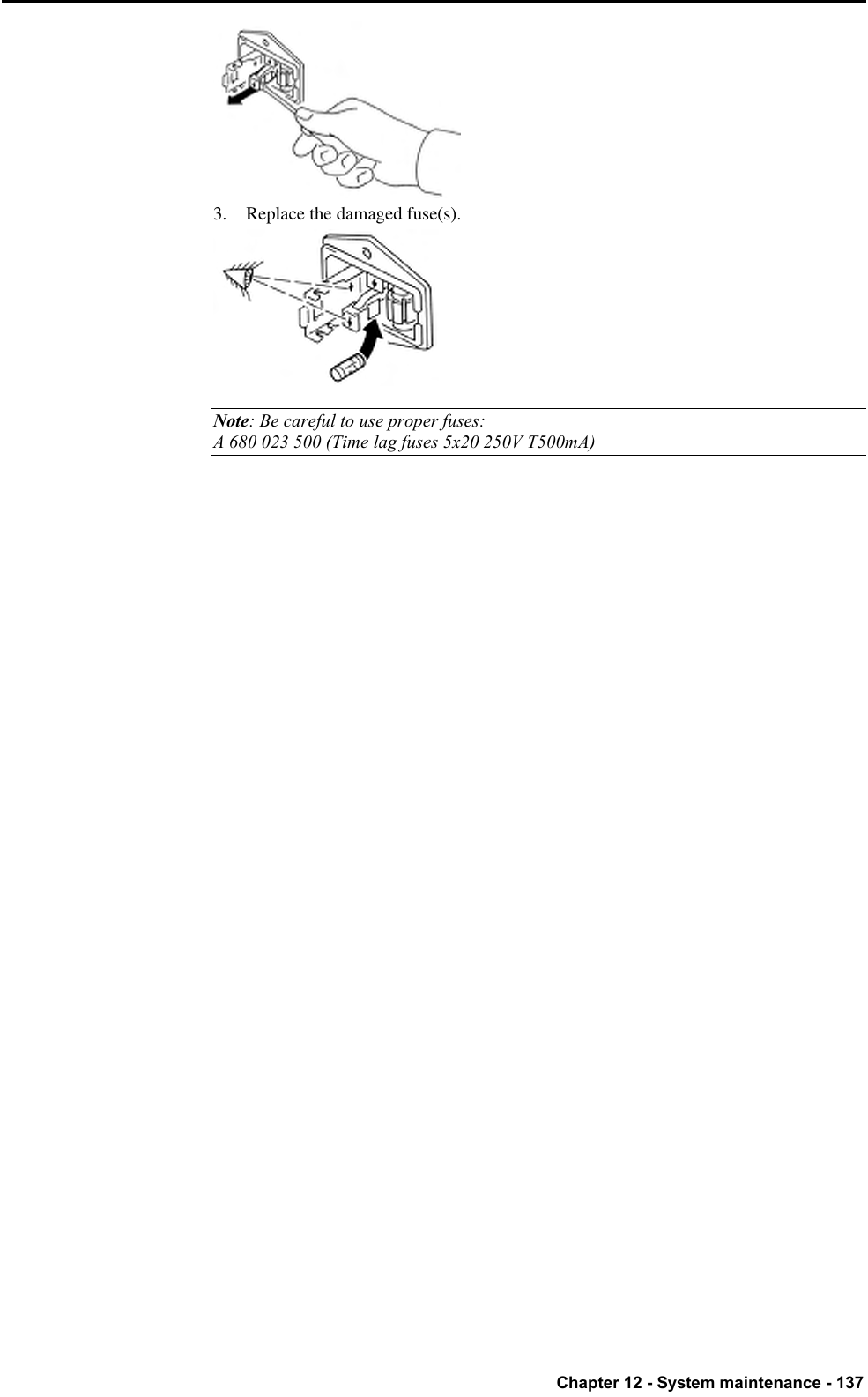
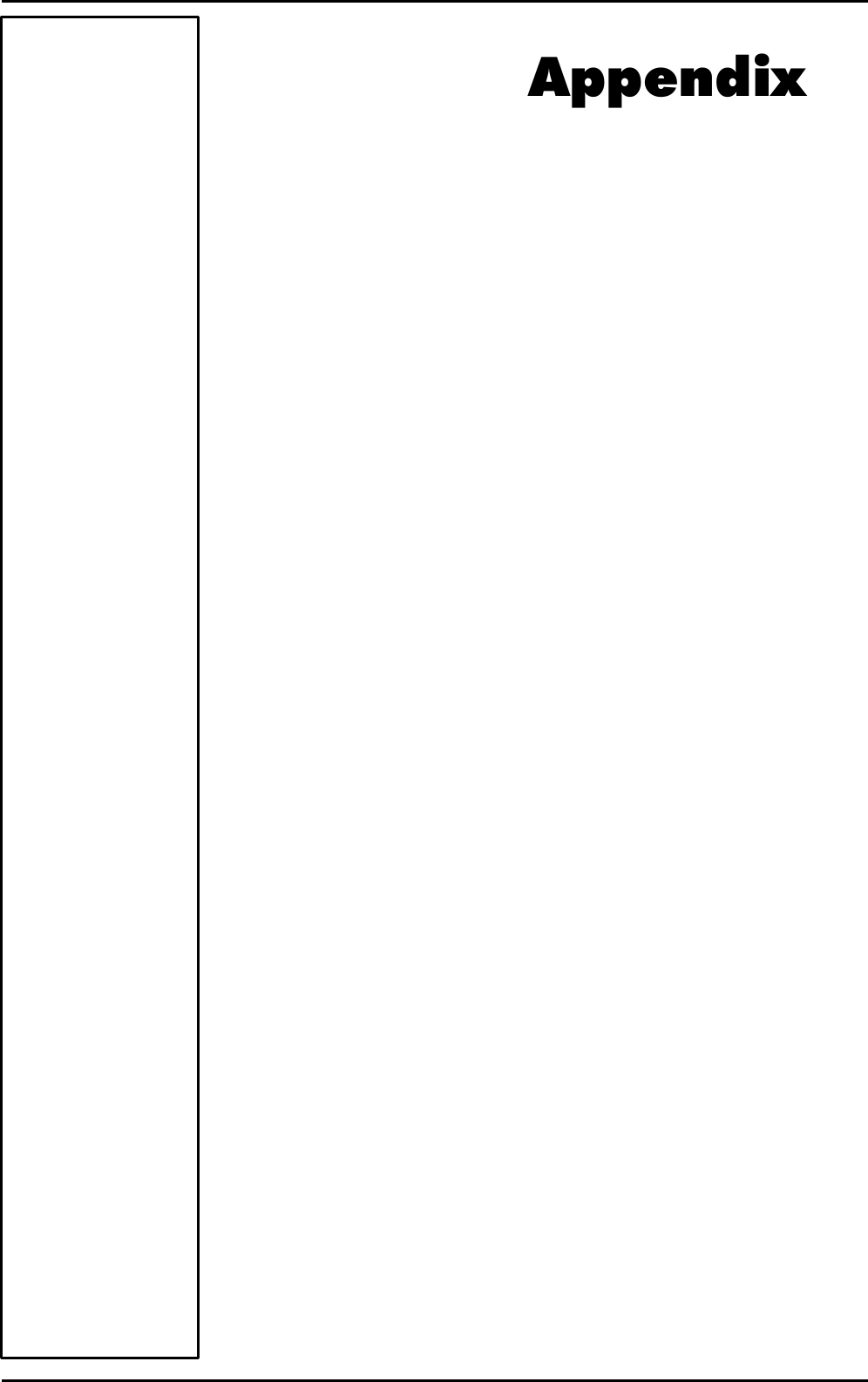
![Chapter 10 - Spirometry - 121 Bronchial Provocation Test Bronchodilator test Bronchodilators are administered routinely in the b2 laboratory to determine whether airflow obstruction is reversible. Bronchodilators increase airway calibre by relaxing airway smooth muscle. The test consists of comparing results between the reference FVC (FVC PRE) and the FVC POST performed after the administration of the drug. Increasing value of 13-15% of FEV1, respect to the basal value (FVC Pre) is considered as a reversible condition. Main parameters are the following: DFEV1%pre Change of FEV1 as a percentage of test PRE DFVC%pre Change of FVC as a percentage of test PRE DPEF%pre Change of PEF as a percentage of test PRE Some authors states that the above mentioned parameters are too dependent from the FVC Pre, hence latest reference (ERS93, [A comparison of six different ways of expressing the bronchodilating response in asthma and COPD; reproducibility and dependence of pre bronchodilator FEV1: E. Dompeling, C.P. van Schayck et Al; ERJ 1992, 5, 975-981]) recommend the following parameters: DFEV1%pred Change of FVC as a percentage of predicted value DFEV1%poss Change of FEV1 as a percentage of “possible value” Methacholine and Histamine Bronchial provocation Tests The most common indication for performing methacholine and histamine bronchial challenges is to diagnose hyperresponsive airways. Some patients demonstrate normal baseline pulmonary function despite complaints of “tightness” wheezing, cough, and a little or not response to bronchoconstrictor. Other patients demonstrate spirometric improvement after use of bronchoconstrictor have diurnal variation in peak flows. In this groups aerosolised bronchial challenges are used to confirm a diagnosis of Asthma. We can summarise the use of the test as follows: 1. Diagnose asthma 2. Confirm a diagnosis of asthma 3. Document the severity of hyperresponsivness 4. Follow changes in hyperresponsivness When patients with hyperresponsive airways inhale certain pharmacologic agents (i.e. Methacholine or histamine) the airways respond by constricting. Test consists of executing repeated FVC following the pharmacologic agents inhalation according to an established protocol. The fall of the FEV1 parameter is used to calculate the bronchial hyperresponsivness. The most important parameter is the PD20 that is amount of drug (mg/ml) that causes a reduction of 20% of the FEV1 respect the basal value (without drug). Main parameters are: P10 Dose that causes a 10% fall of FEV1. P15 Dose that causes a 15% fall of FEV1. P20 Dose that causes a 20% fall of FEV1. The representative plot is the Dose/response curve, showing the percentage variation of FEV1 versus the Drug dose in logarithmic scale. The program assumes as the baseline test the best FVC pre carried out during the today’s visit. You can change the reference pre test editing the Post test. The name of the drug, its quantity and its unit of measurement, can be typed immediately before any FVC post manoeuvre (manual protocol) or can be stored in a database of bronchoprovocation (File/Bronchial Provocation protocols Database…). sss Note: Read carefully the contraindications in Chapter 1.](https://usermanual.wiki/COSMED-Srl/K4B2T-USA.Users-Manual-III/User-Guide-568599-Page-27.png)
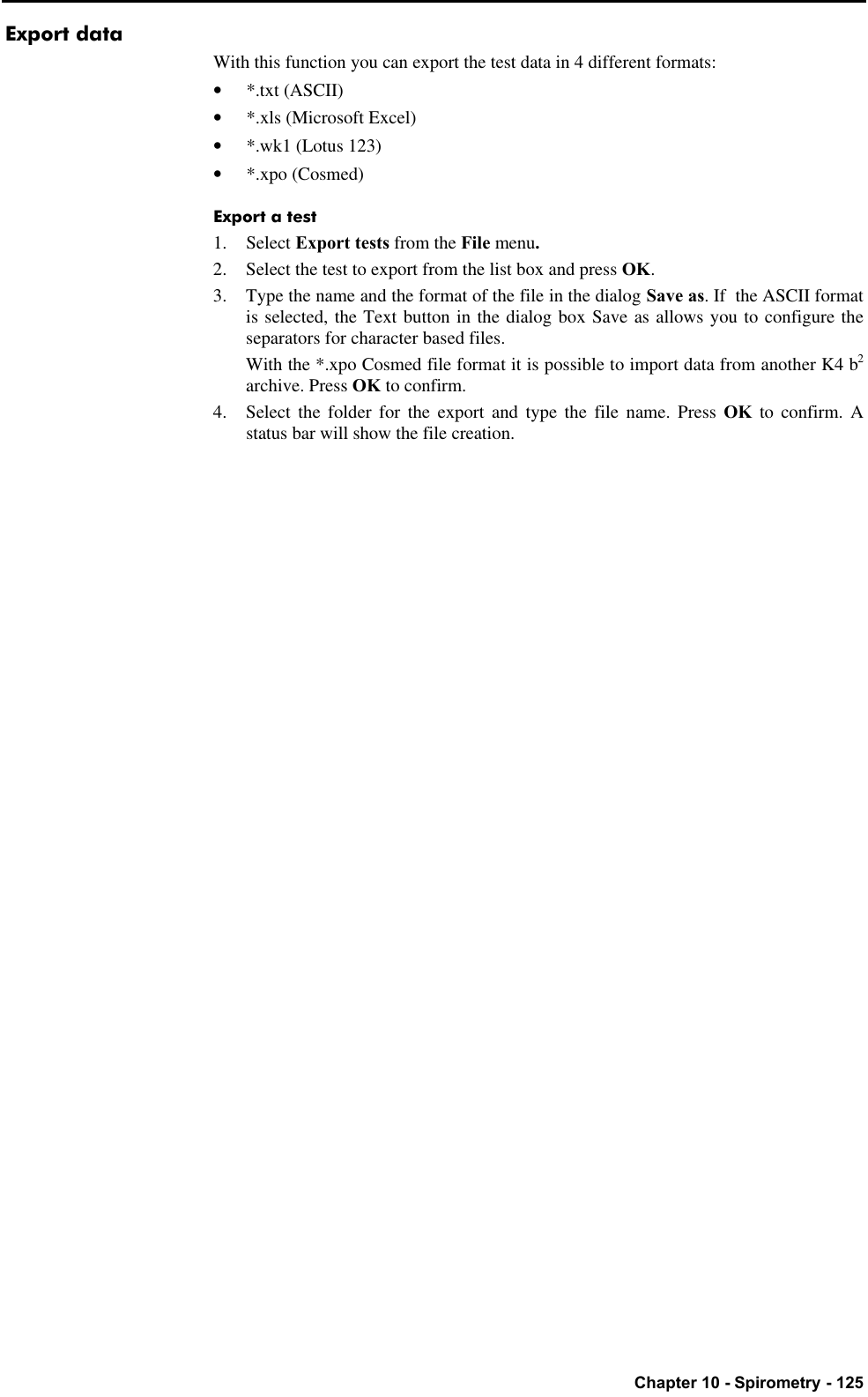



![Chapter 13 - Appendix - 149 References Gas Exchange References [“On line computer analysis and breath by breath graphical display of exercise function tests.”; Beaver, Wasserman, Whipp, JAP , 34(1):128-132, 1973] [“Measurement and analysis of gas exchange during exercise using a programmable calculator”; Sue, Hansen, Blais, Wasserman, JAP, 49(3), 1980:456-461] [“Principles of exercise testing and interpretation, 2° edition”; Wasserman et Al, 1994] [“Clinical Exercise Testing, 3rd edition”, Jones 1988] ERS task force on standardization of clinical exercise testing. “Clinical exercise testing with reference to lung disease: indications, standardization and interpretation strategies.” J. Roca, B. Whipp, S. Anderson, R. Casaburi, J.E. Cotes, P. Palange…., ERJ 1997; 10: 2662-2689. Indirect calorimetry [“Energy Expenditure and Fuel Selection in Biological Systems: The Theory and Practice of Calculations Based on Indirect Calorimetry and Tracer Methods”: M. Elia, G. Livesey, World Rev. Nutr. Diet. Basel, Karger, 1992, vol 70, pp 68-131.] [“Nutritional Assessment in Critical Care, A Training Handbook”: Donald C. Zavala] Spirometry ATS ’94: “Standardization of Spirometry: 1994 Update”, American J. Respiratory Critical Care Medicine, Vol. 152, 1107-1136; 1995 ERS ’93: “Standardised Lung Function Testing: Official Statement of the European Respiratory Society”, The European Respiratory Journal Volume 6, Supplement 16, March ” Lung function", J.E. Cotes, Blackwell scientific publications "Guidelines for Clinical Exercises Testing Laboratories", I.L. Pina, G.J. Balady, P. Hanson, A.J. Labovitz, D.W. Madonna, J. Myers. American Heart Association. 1995; 91, 912. Sub-maximal testing [“Cardiorespiratory Assessment of Apparently Healthy Populations”, Timothy R. McConnell, in ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription, 4th Edition, pp. 361-366] [Franklin BA, ed. ACSM’s Guidelines for Exercise Testing and Prescription, 6th Edition Philadelphia: Williams&Wilkins, 2000:22-29]](https://usermanual.wiki/COSMED-Srl/K4B2T-USA.Users-Manual-III/User-Guide-568599-Page-55.png)
