STATE AGENCY ACTION REPORT 59C 2 10138
User Manual: 59C-2
Open the PDF directly: View PDF ![]() .
.
Page Count: 79
STATE AGENCY ACTION REPORT
ON APPLICATION FOR CERTIFICATE OF NEED
A. PROJECT IDENTIFICATION
1. Applicant/CON Action Number
Landmark Hospital of Southwest Florida, LLC/CON #10137
240 South Mount Auburn Road
Cape Girardeau, Missouri 63701
Authorized Representative: Dr. William Kapp
(573) 331-8040
Kindred Hospitals East, LLC/CON #10138
680 South Fourth Street
Louisville, Kentucky 40202
Authorized Representative: Bud Wurdock
(502) 596-7718
2. Service District
District 8
B. PUBLIC HEARING
A public hearing was not held or requested with regard to the
establishment of the proposed long-term care hospitals in District 8.
However, letters of support were submitted as follows:
Landmark Hospital of Southwest Florida, LLC (CON #10137)
submitted one letter of support for the project. The letter was dated
March 9, 2012 from Dr. Allen Weiss, President and CEO of the NCH
Healthcare System. Dr. Weiss states that he can, “confidently state [that]
patients, their families, physicians and the entire community would be
better served by having an excellent local long-term acute care (LTAC)
facility such as Landmark.” He indicates that some of the 35,000 yearly
discharges from the NCH Healthcare System would benefit by long-term
acute care. Dr. Weiss adds that “Currently, patients too ill for

CON Action Numbers: 10137 & 10138
2
skilled nursing care are either kept as inpatients which is a misuse of
valuable resources or shipped to facilities outside our area.” He notes
that this change of venue can be risky for patients and inconvenient to
their families.
Dr. Weiss states that the proposed facility will help “keep our objective
quality moving in the correct direction [and] assist the local economy on
our journey to be a medical tourist attraction”. He cites that one in eight
inpatients at NCH come from outside southwest Florida, “the lower east
coast, the original colonies and the 1-75 corridors along with other
areas”. Dr. Weiss maintains that, “having additional excellent
capabilities along the continuum of health care such as Landmark will
accelerate our progress”.
He states that the proposed facility and NCH plan to share and
collaborate whenever, “it makes sense in caring for patients”. Dr. Weiss
indicates that a seamless local transfer from inpatient ICU to a nearby
LTAC with the same physicians caring for the patient will surely improve
care. He states that NCH and the proposed facility will explore services
that can be shared to take advantage of economies of scale to best
compete efficiently in a global economy.
Kindred Hospitals East, LLC (CON #10138) submitted 143
unduplicated letters of support for the project (CON application #10138,
Tab 4). One hundred and thirty-six letters were dated between March 6,
and March 30, 2012. Seven letters were not dated. One hundred and
forty were form letters. Thirteen of these form letters were missing
information in the blanks provided.
Letters from local physicians include Dr. Richard J. Juda, Director of
Critical Care Medicine at Physicians Regional Medical Center, who writes
that there is an urgent need for a long-term care facility for the residents
of Collier County because the current options, “are leading to increased
morbidity hence worsening outcomes.” Dr. Juda states that, “Over the
past four-and-a-half years I have been caring for the critically ill in
Southwest Florida [and] I have referred over 150 long-stay patients for
long-term acute care who refused the transfer…due to geography and
transportation difficulties.” Citing the lack of a facility in the Naples/Fort
Myers area, Dr. Juda writes that there is an increased morbidity and
mortality in the area. He emphasizes that he has had “patients walk out
of Kindred who years ago would be committed to long-term institutional

CON Action Numbers: 10137 & 10138
3
care for the rest of their lives” and that the proposed facility, “with its
high caliber of patient care also decreases health care costs for not only
the patient but the community it services.”
Dr. Imtiaz Ahmad from the Allergy Sleep & Lung Care PA states that as a
pulmonary and critical care specialist, he “desperately needs” a facility to
transfer ventilator dependent patients that is closer to Lee County. Dr.
Ahmad elaborates by stating, “Over the past eight years of my practice in
Lee County, I have transferred a large number of patients who require
long-term ventilator care. However, not having a facility nearby,
certainly delayed providing appropriate care to hasten early recovery.”
Dr. Robert P. Casola of Wound and Limb Restoration Center of
Southwest Florida states, “The extensive population at this point
demands that there be a facility for long-term care of certain individuals
that may need certain type of reconstruction, ventilator support and
long-term rehabilitation. Currently, there is no facility in this area that
offers the unique services that we find at Kindred Hospital.” Dr. Casola
cites that currently, “I have a large volume of patients who after initial
treatment and stabilization require the extensive long-term services and
the expertise that is provided for them in the St. Petersburg area with the
Kindred Hospital Facility.” The importance of proper follow-up and
postoperative and interventional services for patients is noted by Dr.
Casola. He states that, “Kindred Facilities offer a well-known means of
ensuring proper follow-up as well as excellent patient care for these
individuals.”
The applicant’s 140 form letters had three formats. One letter cites:
The growing population of the area, in particular the senior
population will benefit from the proposed services.
Kindred Healthcare has a long-standing history of responding to the
hospital and health care needs of the residents throughout Florida.
The location of the proposed facility will enhance service, offer
patients continuity of care and provide easy access.
This letter was signed by 16 members of the Hospitalist Group of
Southwest Florida, four members of Pulmonary Consultants of
Southwest Florida, 18 members of the Physicians Regional Healthcare
System, 18 members of the Fort Myers Republican Women’s Club and 17
members of the Fort Myers and North Fort Myers community. Jorge
Aguilera, Deputy Chief of EMS with the North Naples Fire Control &
Rescue District added that “Currently, our resident’s only option is to
travel a long distance in order to obtain Kindred’s high caliber care”.

CON Action Numbers: 10137 & 10138
4
The second form letter restates the above language and adds:
In my practice, I have seen ___ long-stay patients who would have
benefited from the care provided at a long term care hospital if one
were available in the Naples/Ft. Myers area. However, these patients
rarely go to other existing long-term care facilities in Florida because
of distance, reluctance to change physicians or medical instability
that made transport difficult.
This letter was signed by 10 members of Pulmonary Disease Associates,
P.A., three physicians with the Gulf Coast Cardiothoracic and Vascular
Surgeons group, eight members of the NCH Healthcare Group,
Pulmonary & Critical Care Medicine, one physician with Gulf Coast
Medical Center and one physician’s assistant with Physicians Regional
Healthcare System. The NCH Healthcare Group had added “@ 100-long
stay patients per year” in the blank, eight left it blank and none of the
others were specific adding “many”, one adding “65”, one “>50” and one
“50”. Todd Lupton, CEO of Physicians Regional Healthcare System,
signed this letter changing from “In my practice, I have seen” to state “As
a Health Care System CEO, I am all too familiar with scores of long stay
patients….”
The third form letter indicates that the writer is a registered nurse or
caseworker (one in the case worker count struck case worker and added
social worker) who is “compelled to write and ask that you grant”
approval to the project, stating that:
The additional beds will directly affect the medical care received by
patients at my hospital.
A most challenging aspect of my job is to arrange for continued
inpatient care for patients who need a wide range of health services.
This process is difficult due to reimbursement issues and the
dwindling number of facilities willing to accept medically complex
patients.
I can identify ___ long-stay patients who would have benefited from
the care provided at a long term care hospital if one were available in
the Naples/Ft. Myers area. However, these patients rarely go to other
existing long-term care facilities in Florida because of distance,
reluctance to change physicians or medical instability that made
transport difficult.
I am familiar with Kindred hospitals and their high level of care and
service to their patients.

CON Action Numbers: 10137 & 10138
5
This letter was signed by eight case managers with Physicians Regional
Healthcare who could identify “many” and “multi” long-stay patients who
would have benefited from LTCH care. Twenty two were signed by
registered nurses with Physicians Regional Healthcare, one who
identified “43”, two “4” and one “2” long-stay patients, 13 inserted “many
or multi” and five left the insert blank. Eleven of these were submitted
by registered nurses with Gulf Coast Medical Center, one who could
identify “100’s”, three “15”, one “10” and six indicated that
“many/countless/numerous” patients who would benefit from LTCH
services. One of the RNs with Physicians Regional also provided one of
these indicating that she worked at NCH & NCHO and could identify
“>25” at these facilities.
C. PROJECT SUMMARY
Landmark Hospital of Southwest Florida, LLC (CON #10137),
affiliated with Landmark Hospitals and Landmark Holdings of Missouri,
LLC that operates four long-term care hospitals (LTCHs) nationwide,
proposes to establish a long-term care hospital of 50 beds in District 8,
Collier County. The proposed facility will have all private patient rooms,
including a 10-bed ICU. The applicant did not include potential sites for
the proposed facility.
The proposed hospital involves 56,809 gross square feet (GSF) of new
construction. Total project cost per bed is $442,496. Total construction
cost is estimated to be $13,480,000 and total project cost is
$22,124,800.
As a condition of approval, the applicant proposes to provide 2.54
percent of the facility’s total annual patient days to charity. Landmark
also stated its willingness to accept any and all conditions placed on the
award of the certificate of need based on statements contained within
CON application #10137.
Kindred Hospitals East, LLC (CON #10138), a subsidiary of Kindred
Healthcare, Inc. and licensee/operator of 31 LTCHs, 10 in the state of
Florida, proposes to establish a 40-bed LTCH to be located in Collier
County, District 8. The proposed facility will have all private patient
rooms, including a 10-bed ICU. The applicant did not include potential
sites for the proposed facility.
Kindred Healthcare Inc. is the parent corporation of the applicant and is
one of the largest providers of post-acute health services in the United
States, including 121 LTCHs.

CON Action Numbers: 10137 & 10138
6
The proposed hospital involves 56,581 GSF of new construction. Total
cost per bed is $873,033. Total construction cost is estimated to be
$17,075,774 and total project cost is $34,921,329.
As a condition of approval, the applicant agrees to a combined provision
of two percent of the facility’s total annual patient days to Medicaid and
charity care patients.
D. REVIEW PROCEDURE
The evaluation process is structured by the certificate of need review
criteria found in Section 408.035, Florida Statutes; and applicable rules
of the State of Florida, Chapters 59C-1 and 59C-2, Florida
Administrative Code. These criteria form the basis for the goals of the
review process. The goals represent desirable outcomes to be attained by
successful applicants who demonstrate an overall compliance with the
criteria. Analysis of an applicant's capability to undertake the proposed
project successfully is conducted by evaluating the responses and data
provided in the application, and independent information gathered by the
reviewer.
Applications are analyzed to identify strengths and weaknesses in each
proposal. If more than one application is submitted for the same type of
project in the same district, applications are comparatively reviewed to
determine which applicant best meets the review criteria.
Chapter 59C-1.010 (3) (b), Florida Administrative Code, prohibits any
amendments once an application has been deemed complete. The
burden of proof to entitlement of a certificate rests with the applicant.
As such, the applicant is responsible for the representations in the
application. This is attested to as part of the application in the
Certification of the Applicant.
As part of the fact-finding, the consultant, Marisol Novak analyzed the
application with consultation from Financial Analysts, Derron Hillman
and Everett “Butch” Broussard, who evaluated the financial data, and
Said Baniahmad of the Office of Plans and Construction, who reviewed
the application for conformance with the architectural criteria.

CON Action Numbers: 10137 & 10138
7
E. CONFORMITY OF PROJECT WITH REVIEW CRITERIA
The following indicate the level of conformity of the proposed project with
the criteria and application content requirements found in Florida
Statutes, Sections 408.035 and 408.037; and applicable rules of the
State of Florida, Chapter 59C-1 and 59C-2, Florida Administrative Code.
1. Fixed Need Pool
a. Does the project proposed respond to need as published by a fixed
need pool? ss. 408.035(1)(a), Florida Statutes and Ch. 59C-1.008(2),
Florida Administrative Code.
Need is not published by the Agency for LTCH beds. It is the applicant’s
responsibility to demonstrate need.
An LTCH is defined as a hospital licensed under Chapter 395, Florida
Statutes, which meets the requirements of Title 42, subpart B, paragraph
412.23(e), Code of Federal Regulations; the provider must have an
agreement under Part 489 and the facility must have an average
Medicare inpatient length of stay of greater than 25 days.
In addition to meeting the condition of participation applicable to acute
care hospitals, as of 2007
1
, LTCHs are now required to:
Have a patient review process that screens patients both before
admission and regularly throughout their stay to ensure
appropriateness of admission and continued stay, although the law
does not specify the patient criteria to be used to determine
appropriateness.
Have active physician involvement with patients during their
treatment, with physician on-site availability on a daily basis to review
patient progress and consulting physicians on call and capable of
being at the patient’s side within a period of time determined by the
Secretary.
Have interdisciplinary treatment teams of health care professionals,
including physicians, to prepare and carry out individualized
treatment plans for each patient.
MedPAC is a commission that makes recommendations to Congress and
the Secretary of the federal Department of Health and Human Services
(DHHS) regarding reimbursement for long-term hospital services.
1
As part of the Medicare, Medicaid and SCHIP Extension Act of 2007.

CON Action Numbers: 10137 & 10138
8
Medicare is the primary payer for LTCH services—in 2010, Medicare
spent $5.2 billion on care furnished in an estimated 412 LTCHs
nationwide.
2
Under the current reimbursement system, Medicare
reimburses LTCHs prospective per discharge rates based primarily on the
patient’s diagnosis and the facility’s wage index.
LTCHs furnish care to patients with clinically complex problems, such as
multiple acute or chronic conditions, which need hospital-level care for
relatively extended periods. The highest single LTCH diagnostic related
group [DRG] was respiratory system diagnosis with ventilator support for
96 or more hours in fiscal year 2010. According to MedPAC, over the
past decade, there has been marked growth in the number and the share
of critically ill patients transferred from acute care hospitals to LTCHs.
The commission states that patients who can be appropriately treated in
settings of lower acuity should not be admitted to LTCHs—because the
cost of care in LTCHs is so high. However, it was noted by MedPAC that
LTCH care may have value for very sick patients. While research has
shown that Medicare pays more for patients using LTCHs than for
similar patients in other settings, payment differences were not
statistically significant when LTCH care was targeted to the most severely
ill patients.
The commission cites that not all cases in LTCHs are high severity. In
2010, about 13 percent of LTCH cases were of minor or moderate
severity, as measured by all patient refined DRGs. MedPAC states that
LTCHs with the smallest shares of high-severity cases are far more likely
to be located in rural areas (20 percent vs. five percent of all LTCHs) and
are somewhat more likely to be not-for-profit (28 percent vs. 19 percent
for all LTCHs).
MedPAC determined in its 2012 review, that Medicare accounts for about
two-thirds of LTCH discharges. The commission determined that
between 2005 and 2008, growth in cost per case outpaced that for
payments. After Congress provided temporary relief from some payment
regulations that would have constrained payments, payments per case
climbed 6.4 percent between 2008 and 2009. Payment growth slowed to
two percent between 2009 and 2010. In 2010, the Medicare margin for
LTCHs was 6.4 percent and estimates LTCHs’ aggregate Medicare margin
will be 4.8 percent in 2012. It was also noted in the 2012 report that
Medicare payments increased faster than costs between 2009 and 2010,
resulting in an aggregate 2010 Medicare margin of 6.4 percent. Medicare
margins increase for all types of LTCHs in 2010 except nonprofits. After
2
According to the MedPAC Report to the Congress: Medicare Payment Policy, March 2012.

CON Action Numbers: 10137 & 10138
9
its study, the commission concluded that LTCHs could accommodate the
cost of caring for Medicare beneficiaries in 2013 without an update to the
payment rate.
Unlike most other health care facilities, LTCHs do not submit quality
data to the Centers for Medicare and Medicaid Services (CMS). In the
absence of this data, MedPAC uses unadjusted aggregate trends in rates
of in-facility mortality, mortality within 30 days of discharge and
readmissions from LTCHs to acute care hospitals. It should be noted
that the Patient Protection and Affordable Care Act of 2010 mandates
that CMS implement a pay-for-reporting program for LTCHs by 2014.
A panel assembled by the commission suggested that CMS begin with a
starter set of 10 to 12 measures based on those the LTCHs already use
for internal quality monitoring. These panelists did warn that careful
attention is needed in the creation of these measures so as not to create
incentives for providers to avoid admitting certain types of cases. The
commission states that the quality measures developed for LTCHs must
be comparable to those used in other post-acute settings. MedPAC
considers a pay-for-reporting program to be a first step toward pay for
performance.
The commission has recommended that CMS develop patient and facility
criteria that could be used to define LTCHs and ensure that patients
admitted to such facilities were medically complex and had a good
chance of improvement. MedPAC states that the development of these
criteria has proven difficult as research has been unable to clearly
distinguish LTCH patients from the medically complex patients receiving
care in acute care hospitals and some skilled nursing facilities. In its
March 2011 report, MedPAC stated its long-standing concern about the
nature of services furnished by LTCHs and the possibility that acute care
hospitals discharging patients to LTCHs may be unbundling services
paid for under the acute care hospital prospective payment system (PPS).
There have been several provisions related to long-term care hospitals
passed from 2007-2010
3
. These include:
A moratorium on new LTCHs and new beds in existing facilities until
December 29, 2012.
3
These provisions are part of the Medicare, Medicaid and SCHIP Extension Act of 2007 subsequently
amended in the American Recovery and Reinvestment Act of 2009 and the Patient Protection and
Affordable Care Act of 2010.

CON Action Numbers: 10137 & 10138
10
Currently the Secretary of the Department of Health and Human
Services is prohibited from applying the 25 percent rule to
freestanding LTCHs before cost-reporting periods beginning on
July 1, 2012.
4
The current rolled-back implementation of the 25
percent rule for hospitals within hospitals and satellites, limits the
proportion of Medicare patients who can be admitted from a hospital
within a hospital or a satellite’s host hospital during a cost-reporting
period to not more than 50 percent and holding it at this level until
October 1, 2012.
The Secretary is prohibited from further reducing payments for LTCH
cases with the shortest lengths of stay until December 29, 2012.
The Secretary is prohibited from applying any budget-neutrality
adjustment to the current LTCH prospective payment system until
December 29, 2012.
The requirement that the Secretary conduct a study on the use of
LTCH facilities and patient criteria to determine medical necessity and
appropriateness of admission to and continued stay at LTCHs. This
study was due to the Congress in July 2009, as of March 2011 it is
still pending.
CMS is required to implement a pay-for-reporting program for LTCHs
by 2014. The program should require LTCHs to report a specified list
of quality measures—to be determined by CMS—each year in order to
receive a full update to Medicare payment rates in the ensuing year.
An annual update to the LTCH standard rate shall be reduced by a
quarter of a percentage point in 2010 and by half of a percentage
point in 2011. For rate years 2012-2019, any update shall be
reduced by the specified productivity adjustment.
Despite the moratorium imposed in July 2007 on new LTCHs and new
beds in existing LTCHs, the number of LTCHs filing Medicare cost reports
increased 6.1 percent between 2008 and 2010—with almost all the
growth taking place in 2009. MedPAC found that beneficiaries’ use of
services suggests that access has not been a problem since the
moratorium was imposed. Controlling for the number of fee-for-service
beneficiaries, the commission found that the number of LTCH cases rose
3.5 percent between 2009 and 2010—suggesting that access to care
increased during this period.
4
CMS established a 25 percent rule in fiscal year 2005 that uses payment adjustments to limit the
percentage of Medicare patients who are admitted from a hospital within a hospital or satellite’s host
hospital and paid for at full LTCH payment rates.

CON Action Numbers: 10137 & 10138
11
It is noted in the March 2012 MedPAC report that LTCHs are not
distributed evenly across the nation. Some areas have many LTCHs and
others have none. The commission concludes that the absence of LTCHs
in many areas of the country suggests that medically complex patients
can be treated appropriately in other settings—making it difficult to
assess the need for LTCH care and, therefore, the adequacy of supply. In
fact, MedPAC’s analysis of LTCH claims from 2010 found that average
case mix for LTCH admissions is lower in communities with the highest
use of LTCHs compared with communities with the lowest use of LTCHs.
The commission states that these findings suggest that an oversupply of
LTCH beds in a market may result in admissions to LTCHs of less
complex cases that could appropriately be treated in less costly settings.
Additionally, the commission questions the clustering of LTCHs in
certain markets as LTCHs are supposed to be serving unusually sick
patients, a relatively rare occurrence. MedPAC states that an oversupply
of LTCH beds in a market may result in admission to LTCHs of less
complex cases that could be appropriately treated in other, less costly
settings. The commission also cites that there is little evidence that
patient outcomes in LTCHs are superior to those achieved in other
settings.
In a report prepared for CMS, Kennell and Associates stated that the
most commonly used definition of medically complex patients was
proposed by Nierman and Nelson.
5
This stated that the chronically
critically ill patient exhibited metabolic, endocrine, physiologic and
immunologic abnormalities that resulted in profound debilitation and
often ongoing respiratory failure, abnormalities that slowed or precluded
recovery from a wide range of acute forms of medical, surgical and
neurologic critical illness. On this definition’s basis, Kennell suggested
the following as specific attributes of medically complex patients:
Prolonged mechanical ventilation
Multiple organ failure
Multiple or chronic comorbidities (such as coronary artery disease,
chronic obstructive pulmonary disease, stroke, diabetes and renal
failure)
Multiple community-acquired or hospital-acquired infections or ulcers
5
Determining medical necessity and appropriateness of care for Medicare long-term care hospitals was
prepared under contract to the Centers for Medicare and Medicaid Services in 2010 by Kennell and
Associates, Inc.

CON Action Numbers: 10137 & 10138
12
The commission notes that it is important that potential patients that are
identified as medically complex should also be likely to benefit from a
LTCH program, as some of the most severely ill medically complex
patients are too sick for LTCH care or because their prognosis for
improvement is so poor. MedPAC states that other options may be better
suited to these patient’s needs and may cost Medicare less.
In this comparative batch review, the two co-batched applicants have
each described their respective patient populations as “medically
complex” and indicated they were high acuity patients. As noted by
MedPAC, some portion of LTCH patients nationwide can be described in
the way the co-batched applicants have described their respective patient
populations, while others are of a lesser acuity level and could be treated
in another post-acute care setting. As discussed below, it is the burden
of any CON applicant applying outside of a state published fixed need
pool to define its patient population and base need projections on that
defined patient population. If, as here, the applicant proposes to serve a
medically complex, largely medically unstable, high acuity patient
population, then need projections should clearly identify that population
and the medically complex and unstable high acuity population should
be the only target.
Medicare is identified by each co-batched applicant as its primary payer.
Unlike what is used by CMS for other post-acute care providers, CMS
does not have an accepted assessment tool for LTCH services and
government evaluators have found some portion of LTCH admissions do
not meet the patient profile described by both the co-batched applicants
as the population it intends to serve. Of interest in this review is
MedPAC’s note that two large LTCH chains own slightly more than half of
all LTCHs. One of these large LTCH chains is identified in the report as--
Kindred Healthcare. This is one of the co-batched applicants in this
review cycle.
Given the above, it is important that the determination of specific clinical
complexity and clinical instability along with severity of conditions and
multi-morbidities of patients being served in LTCHs be identified and
that the establishment of a LTCH does not represent a more costly and
possibly duplicative post-acute care option. It is further important that
appropriate staff be identified and that sufficient patient volume based
on need for services be demonstrated.
CON Action Numbers: 10137 & 10138
13
b. Determination of Need.
In the absence of agency policy regarding long-term care hospital beds
and services, Chapter 59C-1.008 (2)(e), Florida Administrative Code,
provides a needs assessment methodology which must include, at a
minimum, consideration of the following topics, except where they are
inconsistent with the applicable statutory or rule criteria:
a. Population demographics and dynamics;
b. Availability, utilization and quality of like services in the district,
subdistrict or both;
c. Medical treatment trends; and
d. Market conditions.
The existence of unmet need will not be based solely on the absence of a
health service, health care facility, or beds in the district, subdistrict,
region or proposed service area.
At present, there are 24 LTCHs with 1,398 beds licensed to operate in
the State of Florida. There are an additional 168 approved, but not yet
licensed LTCH beds representing four facilities in two districts.
The following table illustrates the distribution of approved, but not yet
licensed LTCH beds in Florida.
Florida Approved-Not Yet Licensed Long-Term Care Hospital Beds
Hospital
District
Beds
Select Specialty Hospital - Lee, Inc. (CON #9715)
8
60
MJHS LTAC, LLC (CON #10092)
11
24
Select Specialty Hospital - Miami (NF #0700002)
11
24
Select Specialty Hospital - Dade, Inc. (CON #9892)
11
60
Total
168
Source: Florida Hospital Bed Need Projections & Service Utilization by District published 01/20/2012.
Note: Promise Healthcare, Inc., acquired all outstanding shares of Select Specialty Hospital-Lee, Inc. and
Select Specialty Hospital-Dade, Inc. and is the sole shareholder of these entities.
As shown in the table above, there are 168 approved, but not yet licensed
LTCH beds. However, MJHS LTAC, LLC (CON #10092) was terminated
effective March 14, 2012. The 60 beds approved in District 8 are to be
located in a new Lee County LTCH that will be owned and operated by
Promise of Lee.
6
6
On March 31, 2008, Promise Healthcare, Inc. acquired all of the outstanding shares of Select
Specialty Hospital—Lee, Inc. becoming the sole shareholder of the Select entity.
CON Action Numbers: 10137 & 10138
14
The average occupancy of the operational programs reporting utilization
was 62.47 percent for the July 2010-June 2011 reporting period. LTCH
programs in operation for the total 12-month reporting period, ranged in
occupancy from a low occupancy rate of 35.65 percent for Kindred
Hospital Melbourne (District 7) to a high of 92.21 percent for Select
Specialty Hospital-Miami (District 11). The following chart shows
statewide occupancy by year for the past five years.
Statewide LTCH Occupancy
12 Month Reporting Periods Ended
June 30, 2007-2011
Time Period
Occupancy Rate
Total Patient Days
July 2006-June 2007
65.73%
211,802
July 2007-June 2008
62.73%
239,987
July 2008-June 2009
58.70%
265,528
July 2009-June 2010
62.64%
293,303
July 2010-June 2011
62.47%
309,658
Source: Florida Hospital Bed Need Projections & Service Utilization by District published in January 2008-2012.
The service area for LTCH services is the district, not the county or any
one geographic section or part of a county, or even necessarily a cluster
of counties. One facility currently serves this district and one is
approved to serve this district. HealthSouth Ridgelake Hospital in
Sarasota County has 40 licensed LTCH beds with a 71.29 percent
occupancy for July 2010-June 2011.
7
CON #9715, Select Specialty
Hospital of Lee, Inc. is approved to construct a 60-bed LTCH in Lee
County that is not yet under construction.
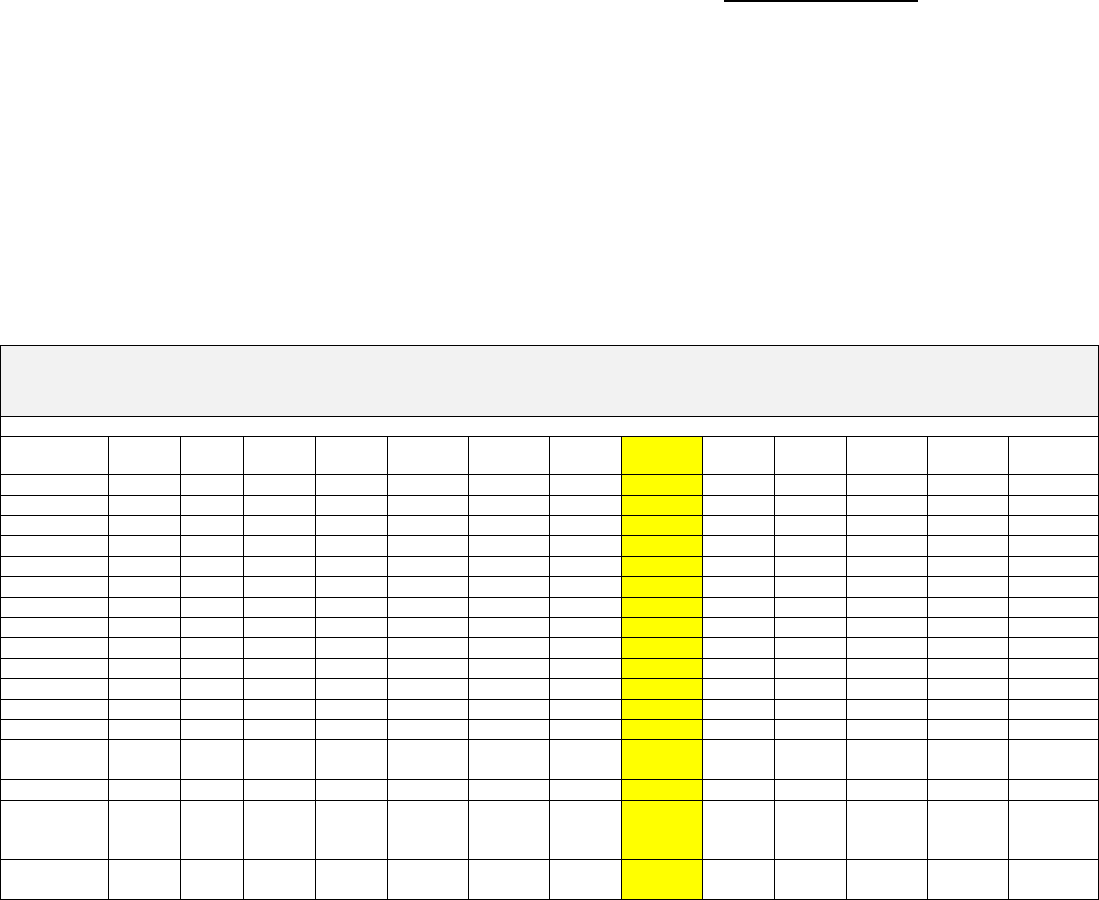
The chart below illustrates the number of LTCH discharges of District 8
residents (age 18+) July 1, 2010 through June 30, 2011.
7
This facility changed ownership as of August 1, 2011, and is now licensed as Complex Care Hospital
At Ridgelake.

CON Action Numbers: 10137 & 10138
15
LTCH District 8 Resident Discharges
Age 18+
July 1, 2010 through June 30, 2011
Facility Name
Charlotte
Collier
DeSoto
Glades
Hendry
Lee
Sarasota
Total
District 8
Discharges
Percentage
of
facilities’
total
Discharges
HealthSouth
Ridgelake Hospital
40
9
9
39
140
237
57.66%
Kindred Hospital-
Bay Area-St
Petersburg
5
14
1
38
11
69
18.11%
Kindred Hospital-
South Florida-
Hollywood
6
2
2
10
1.31%
Select Specialty
Hospital-Palm
Beach
1
2
7
10
1.82%
Kindred Hospital
The Palm Beaches
1
6
7
1.72%
Kindred Hospital-
Bay Area-Tampa
1
2
2
5
1.36%
Kindred Hospital-
Central Tampa
1
2
1
1
5
1.00%
Kindred Hospital
Melbourne
3
3
1.15%
Kindred Hospital-
South Florida-Coral
Gables
1
2
3
0.53%
Florida Hospital at
Connerton Long
Term Acute Care
Hospital
1
1
2
0.37%
Kindred Hospital-
North Florida
1
1
0.17%
Select Specialty
Hospital-Miami
1
1
0.16%
Select Specialty
Hospital
Jacksonville
1
1
0.13%
TOTAL
46
35
13
2
16
90
152
354
Source: Florida Center for Health Information and Policy Analysis hospital discharge data.
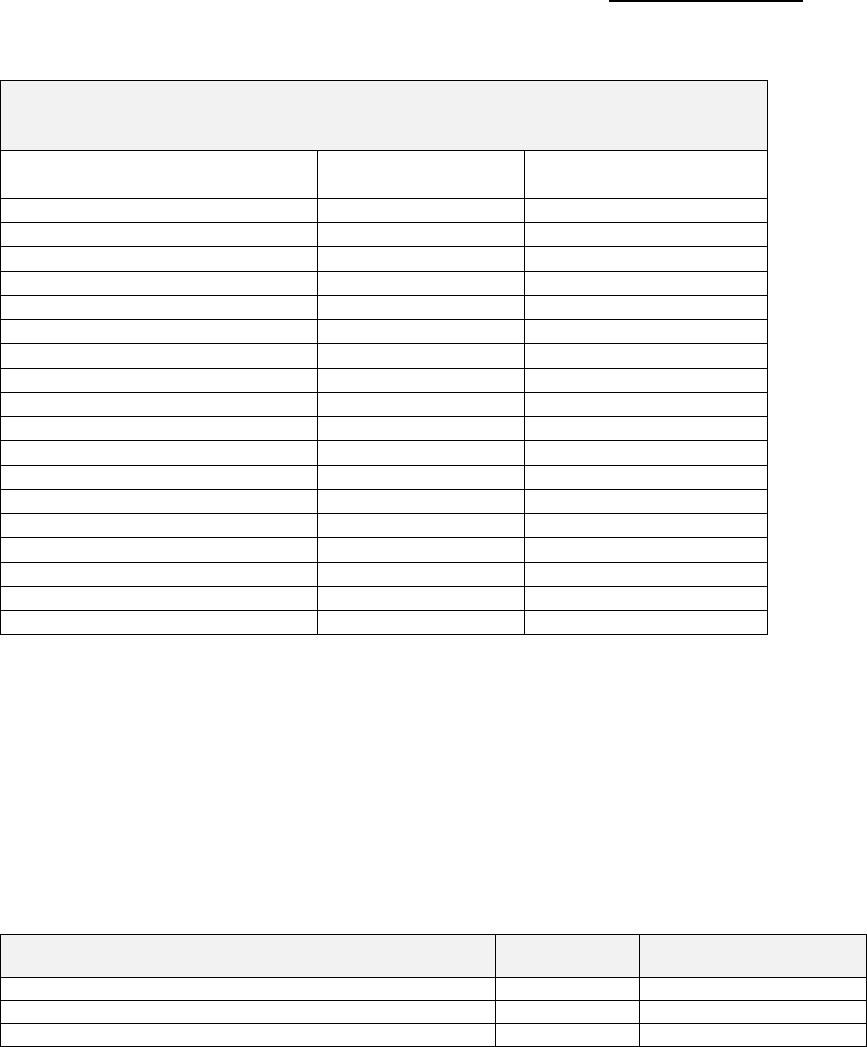
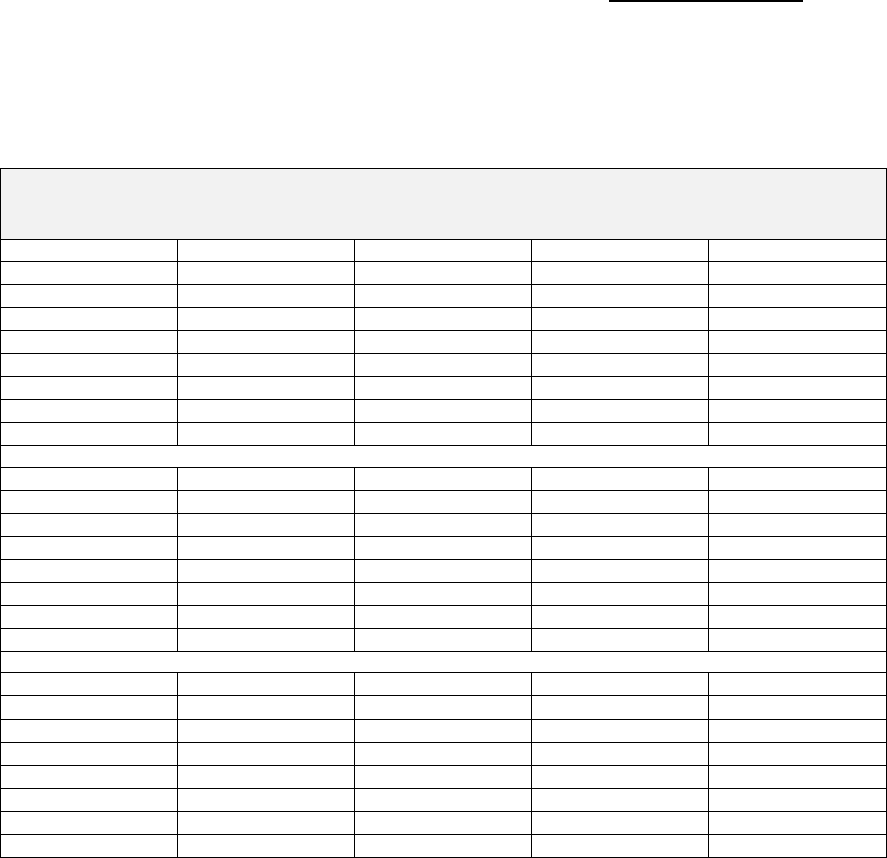
The chart below illustrates the number of LTCH discharges at the single
LTCH facility currently operating in District 8 for July 1, 2010 through
June 1, 2011 by county of origin.
CON Action Numbers: 10137 & 10138
16
HealthSouth Ridgelake Hospital Discharges*
Patients Age 18+
July 1, 2010 through June 30, 2011
County of Residence
Health Planning
District
Number of
Admissions
Alachua
3
1
Charlotte
8
40
Citrus
3
1
Collier
8
9
DeSoto
8
9
Hamilton
3
1
Hardee
6
2
Highlands
6
21
Hillsborough
6
19
Lake
3
1
Lee
8
39
Manatee
6
110
Okeechobee
9
1
Pinellas
5
5
Polk
6
1
Sarasota
8
140
Unknown/Out of State
11
Total
411
Source: Florida Center for Health Information and Policy Analysis hospital discharge data.
* This facility changed ownership and is licensed as Complex Care Hospital at Ridgelake
effective August 1, 2011.
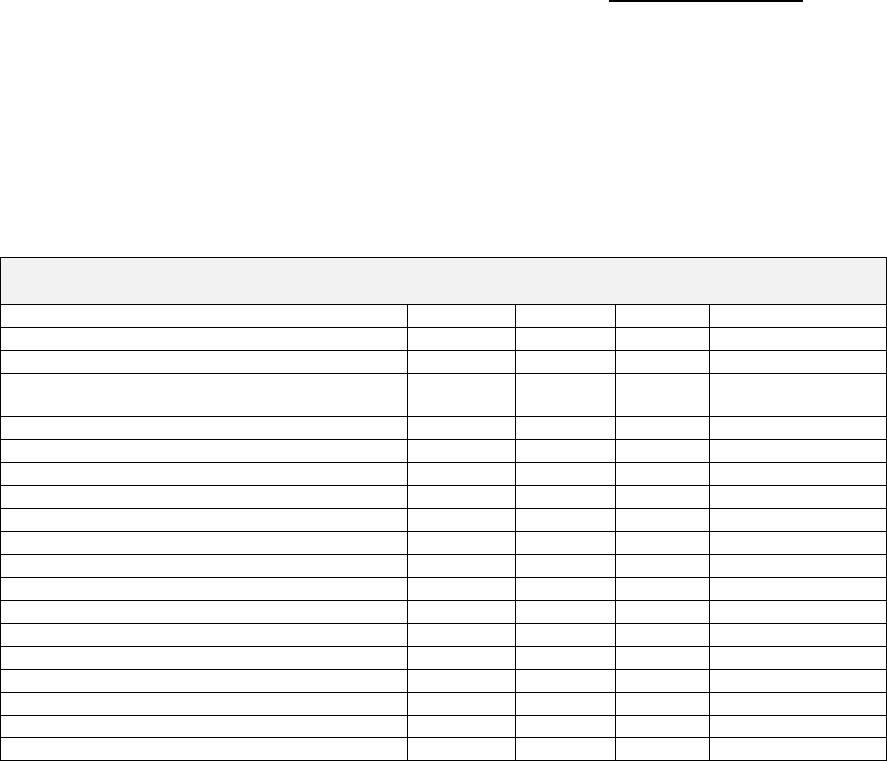
The current bed complement with the average occupancy of acute care
hospital and other forms of post-acute care (substitute care options when
LTCH services are not desired or available) in District 8 is presented as
follows:
Acute Care and Post-Acute Care Providers
District 8 Beds and Utilization
July 2010-June 2011
Facility Type
Total Beds
District 8
Percent Occupancy
Acute Care
4,055
55.16%
Comprehensive Medical Rehabilitation
260
63.61%
Skilled Care Community Nursing Homes
7,008
82.24%
Source: Florida Hospital Bed Need Projections & Service Utilization by District published January 20, 2012 &
Florida Nursing Home Utilization by District & Subdistrict July 2010-June 2011 published September 30, 2011.
As previously noted, LTCHs are designed to treat patients with medical
conditions requiring extended hospital-level services, for a period of at
least 25 days on average. The applicants state that their proposals will
provide LTCH services to patients with complex and medically unstable
conditions that cannot be adequately addressed in licensed acute care
beds, CMR, SNFs or home health care in the service planning area (in
whole or in part). However, despite claims that proposals are for

CON Action Numbers: 10137 & 10138
17
medically complex/unstable and multiple co-morbidity high acuity
patients, neither co-batched applicant demonstrated through existing
data-driven evidence that this patient population and their families:
were unable to locate and access needed LTCHs outside of District 8
burdened the existing District 8 acute care resources through
extended acute care stays by quantifying the number of patients so
impacting the existing acute care facilities; or
received inappropriate care that lead to measurably poorer health care
outcomes, a reported rate of re-admission or a mortality rate higher
than is characteristic in this select population.
No objectively measurable, data-driven and case-specific evidence was
provided to show harm or poor health care outcomes as a result of the
treatment alternatives selected.
As noted at the beginning of this section and pursuant to section
59C-1.008 (2) (e) 3., Florida Administrative Code, the existence of unmet
need will not be based solely on the absence of a health service, health
care facility, or beds in the district, subdistrict, region or proposed
service area. Despite projections to the contrary, is it more likely that
the CON approved LTCH in District 8 will serve a larger area than
proposed in their CON application. This is expected because of CMS
stated plans to reform post-acute care based on MedPAC
recommendations over the past several years that were discussed in
detail above.
Discussions of the applicants’ need analysis follows.
Landmark Hospital of Southwest Florida, LLC (CON #10137) states
that it will provide intensive recovery services for those transferred from
acute care hospitals, whose conditions are not appropriate for post-acute
placement. The major programs that the hospital will provide are
characterized as:
Pulmonary and Mechanical Ventilator Management
Complex Wound Care
Hemodialysis and Infectious Disease Treatment
The applicant maintains that all of the above broad programs involve a
variety of clinical professionals engaged in restorative and rehabilitative
services. Twenty-four hour physician coverage is provided to ensure that
changes in a patient’s condition can be addressed quickly. Among the
most frequent physician collaborators are cardiologists and
pulmonologists as well as orthopedists and endocrinologists.

CON Action Numbers: 10137 & 10138
18
Landmark states that it provides 24-hour chaplain services to meet the
spiritual needs of patients and their families. Additional supportive
therapies are provided as well, including pet and music therapy.
The applicant notes it is aware of the federal moratorium on the
construction of new long-term care hospitals and bed additions to
existing long-term care hospitals. Landmark states that the proposed
facility is based on the presumption that the moratorium will sunset on
December 28, 2012. The applicant bases this presumption on its
understanding that the purpose of the moratorium was to provide time
for federal policy makers to study LTCHs further and develop
recommendations regarding changes to current practices.
Landmark indicates that it is actively pursuing options outside of the
moratorium to contain costs within its profession association, Acute
Long Term Care Hospital Association. The applicant asserts that it is an
advocate for implementing changes that would attain cost containment
objectives allowing the expiration of the moratorium. Specifically
creating distinctions so that LTCHs serve the most severely ill and
eliminating providers who do not provide the intensity of care/focus to
complex, severely ill patients. Examples include:
Need for admission reflects clinical indicators based on current
practice standards that include procedures provided by a registered
nurse certified in critical care
The patient’s care requires involvement of one or more specialist or
subspecialist
Stressing direct admission from an acute care hospital’s intensive
care unit as the source of admission
Attending physician’s determination that the patient’s condition is
complex and that skilled nursing and comprehensive rehabilitation
are ruled out as are other post-acute options. The LTCH option
should remain an acute, not a post-acute care option.
The applicant states that in the event that the U.S. Congress extends the
moratorium, Landmark understands that the federal moratorium will not
permit the Agency for Health Care Administration to extend its CON
termination date, should it have a valid CON. Landmark would do one of
two things in the above situation:

CON Action Numbers: 10137 & 10138
19
1. Proceed in accordance with project completion forecast to open the
hospital as of January 1, 2015, working under the assumption
that the moratorium would sunset by that time. This choice
clearly makes Landmark bear all risk and makes Landmark
responsible for any future outcome.
2. Return the CON and re-apply in a later batching cycle under the
resumption that a future termination date would accommodate the
federal action with respect to the moratorium. Landmark
understands that such an action would require demonstrated
entitlement to a certificate of need and that the Agency for Health
Care Administration would not be bound, influenced or otherwise
enjoined to issue one to Landmark.
Landmark maintains that no prediction on the federal moratorium can
be certain but it remains optimistic that LTCHs are important additions
to the continuum of care and will remain necessary. The number of
LTCH patients—highly complex, multiple systems involved and medically
intensive—will not diminish but will grow. The applicant contends that it
is the LTCH, one that evolves, adapts and adopts protocols/technologies
that achieve treatment effectiveness and cost-containment that will meet
the needs of these patients.
The applicant states that there is one LTCH in District 8, Complex Care
Hospital at Ridgelake (an affiliate of Lifecare Hospitals) with a reported
occupancy rate of 78 percent in CY 2010.
8
In addition, there is one
approved LTCH project in District 8, Select Medical Corporation of Lee
County whose assets were acquired by Promise Hospital of Lee, Inc. This
project is pending and has approval for 60 beds LTCH in Lee County
through CON #9715 issued December 14, 2007. The applicant notes
that this project has not commenced construction and Promise continues
to request and receive extensions on this CON. Landmark states that
there is sufficient need for the proposed facility in addition to the Promise
approved CON.
Landmarks cites that the statewide ratio of LTCH admission to acute
care hospital admissions is 0.5 percent. District 8 and 10 are tied for the
lowest ratio with 0.2 according and District 2 has the highest ratio with
0.9 percent, according to the applicant.
8
This hospital was formerly known as HealthSouth Ridgelake Hospital (an affiliate of HealthSouth) and
had a 77.61 percent occupancy rate in CY 2010.

CON Action Numbers: 10137 & 10138
20
The applicant states that there were 172,954 acute care discharges in
District 8 during April 1, 2010 through March 31, 2011, but just 365
patients were admitted to LTCHs. Using the statewide 0.5 percent ratio,
District 8 should have had at least 865 LTCH admissions. Landmark
contends that this indicates a lack of access and availability of services
for 500 persons. The applicant uses an estimated average length of stay
of 30 days to produce 15,000 LTCH inpatient days—or an average daily
census (ADC) of 41 persons throughout District 8 without access.
Landmark contends that in Florida, the wider availability of beds
corresponded with increased use of LTCHs across the district. The
applicant uses historical data, linear regression and trend line analysis
to establish that beds have to be available and when they are, these beds
are used. The applicant maintains that there is clear reduced access to
LTCH services in District 8 as demonstrated by patterns of use by county
residents. In addition, the discharge rate from LTCHs for patient origin
place District 8 last among the 11 health care districts. The reviewer
notes that the applicant does not document that the current providers
are not serving the long-term care needs of District 8 patients.
Population Estimates and Dynamics
The applicant presents the Major Diagnostic Category (MDC) and
counties of residence for patients aged 15 and older who were admitted
at HealthSouth Ridgelake Hospital during April 1, 2010 through March
31, 2011.
9
Landmark then used January 2011 population estimates to
calculate the use rate per 1,000 persons aged 15 years and older by their
counties of residence. The applicant says that the data shows a lack of
uniform access, which can be expected, given the location of the only
LTCH in the district. Landmark contends this data confirms reduced
access to LTCH services for residents within District 8 and being treated
within the district—Lee County residents have the lowest access,
followed by Charlotte and Collier County residents.
10
See the table
below.
9
At the time of the data reported, the LTCH had not changed ownership yet.
10
The applicant’s data shows that Hendry County residents have the lowest calculated rate, followed
by Collier then Lee County residents.

CON Action Numbers: 10137 & 10138
21
Patients Aged 15 Years and Older by County of Residence in District 8*
Treated at HealthSouth Ridgelake Hospital
April 1, 2010 through March 31, 2011
MDC
Charlotte
Collier
Desoto
Hendry
Lee
Sarasota
All
Other
Total
00-MDC Not Assigned
2
4
6
01-Nervous System
1
1
2
04-Respiratory System
28
7
8
1
39
80
108
271
05-Circulatory System
1
2
3
06-Digestive System
2
1
4
9
16
07-Hepatobiliary System/Pancreas
2
1
1
4
08-Musculoskeletal/Conn Tissue
1
1
9
6
17
09-Skin, Subcutaneous Tissue & Breast
1
3
3
3
10
11-Kidney & Urinary Tract
1
6
1
8
17-Myeloproliferative & Neoplasm
1
1
18-Infectious & Parasitic Diseases
4
2
1
1
28
23
59
21-Injury, Poisonings & Toxic Effects
1
3
2
6
23-Factors Influencing Health Status
2
1
4
7
25-Human Immunodeficiency Virus
1
1
TOTAL
41
10
12
1
45
142
160
411
Percent of Total
10.0%
2.4%
2.9%
0.2%
10.9%
34.5%
38.9%
100%
Population 1/2011
146,893
278,548
28,062
30,993
517,353
341,732
Rate/1,000 persons age 15+
0.279
0.036
0.428
0.032
0.087
0.416
Source: CON application #10137, page 1-9.
*Glades is not included above as no residents of that county were treated at this hospital.
Landmark maintains that it is an indication that HealthSouth Ridgelake
Hospital is not functioning as an accessible district resource because the
residents of all District 8 counties with the exception of Sarasota
comprise only 26 percent of the cases treated at this LTCH. The
applicant presents data on access for District 8 residents to LTCH
services located anywhere in Florida resulting in the fact that the
residents in the more southern counties of District 8 do not find the
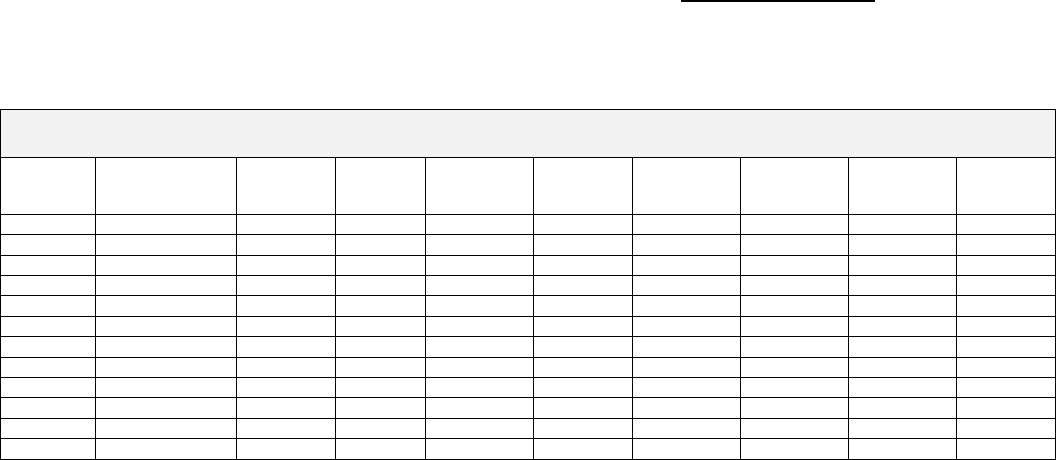
Sarasota LTCH accessible. See the table below.
Patients Aged 15 Years and Older by County of Residence in District 8
Treated at any LTCH in Florida
April 1, 2010 through March 31, 2011
MDC
Charlotte
Collier
Desoto
Glades
Hendry
Lee
Sarasota
Total
00-MDC Not Assigned
3
1
1
1
3
5
14
01-Nervous System
1
2
3
03-Ear, Nose, Mouth & Throat
1
1
2
04-Respiratory System
32
25
10
1
9
77
85
239
05-Circulatory System
2
2
4
06-Digestive System
2
1
1
4
8
07-Hepatobiliary System/Pancreas
1
1
2
1
5
08-Musculoskeletal/Conn Tissue
1
1
9
11
09-Skin, Subcutaneous Tissue & Breast
1
3
4
8
10-Endocrine, Nutritional & Metabolic
1
2
3
11-Kidney & Urinary Tract
1
6
7
17-Myeloproliferative & Neoplasm
1
1
18-Infectious & Parasitic Diseases
5
3
1
1
8
30
48
21-Injury, Poisonings & Toxic Effects
1
1
3
5
23-Factors Influencing Health Status
2
2
1
5
25-Human Immunodeficiency Virus
2
2
TOTAL
48
33
15
2
16
98
153
365
Percent of Total
13.2%
9.0%
4.1%
0.5%
4.4%
26.8%
41.9%
100%
Source: CON application #10137, page 1-11.
CON Action Numbers: 10137 & 10138
22
Landmark asserts that the hospital discharge data demonstrates that the
District 8 resident outmigration to receive LTCH care is large, 114
persons or over 30 percent, clearly demonstrating reduced access to
LTCH services within the district. The applicant presents data showing
where District 8 residents received LTCH services during the 12 month
period ending March 31, 2011, in the table below.
LTCH Services Utilized by District 8 Residents, Age 15 Years and Older
April 1, 2010 through March 31, 2011
Hospital
Cases
Percent
ALOS
HealthSouth Ridgelake Hospital
251
68.8%
26.6
Out-Migration Destinations
Cases
Percent
ALOS
% Out Migr
n=114
Kindred Hospital-Bay Area (St Pete)
72
19.7%
46.7
63.2%
Kindred Hospital-Bay Area (Tampa)
7
1.9%
24.3
6.1%
Kindred Hospital-Central Florida
2
0.5%
21.5
1.8%
Kindred Hospital-North Florida
1
0.3%
22.0
0.9%
Kindred Hospital-S FL-Coral Gables
1
0.3%
27.0
0.9%
Kindred Hospital-S FL-Ft Lauderdale
1
0.3%
29.0
0.9%
Kindred Hospital Melbourne
1
0.3%
30.0
0.9%
Kindred Hospital Palm Beaches
7
1.9%
57.1
6.1%
Select Specialty Hospital Palm Beach
9
2.5%
16.2
7.9%
Select Specialty Hospital Miami
1
0.3%
23.0
0.9%
Sister Emmanuel Hospital Continuing Care
1
0.3%
55.0
0.9%
Specialty Hospital Jacksonville
1
0.3%
23.0
0.9%
UCH LTACH at Connerton
1
0.3%
40.0
0.9%
Sum of Out-Migration
114
NA
42.0
100.0%
Grand Total
365
100.0%
31.4
Source: CON application #10137, page 1-12.
The applicant poses two possible explanations for the out-migration of
residents:
Too few beds exist (40), so that when a bed is needed it is not
available given the facility’s occupancy rate (above 75 percent)
At 40 beds, the current LTCH is constrained by what types of
conditions it can treat.
Regardless of the reason for the high out-migration, Landmark contends
that its occurrence establishes that LTCH services are not uniformly
available within the district with some residents without access to a
different degree than other residents of District 8.
Landmark notes that the majority of District 8 out-migration was to
District 6 at Kindred Hospital-Bay Area (72 of 114 patients, 63 percent).
The average length of stay (ALOS) for these patients was 46.7 days,
indicating that these were complex cases with high acuity. The applicant
cites that this facility has 82 beds and a CY 2010 occupancy rate of 55.4
CON Action Numbers: 10137 & 10138
23
percent, indicating capacity exists to accommodate a request for a bed
when needed. The District 8 LTCH facility had an ALOS of 26.6,
indicating less acuity.
The applicant states that the out-migration data demonstrates that one
hospital in District 8 with 40 beds cannot meet the complex needs of
persons within the district as reflected in the length of stay. This out-
migration pattern for District 8 differs from the experience of most health
planning districts. See the table below.
Out-Migration for LTCH Services for Health Planning Districts in Florida
Residents Aged 15 Years and Older
April 1, 2010-March 31, 2011
Number of LTCH Cases Based on Patients’ District of Residence
Hospital
District
1
2
3
4
5
6
7
8
9
10
11
UNK
TOTAL
1
563
3
3
1
1
54
625
2
17
557
3
2
1
1
116
697
3
1
3
497
35
4
5
5
5
1
12
568
4
1
1
119
1,072
2
2
11
2
2
165
1,377
5
1
1
70
2
720
324
2
73
2
2
34
1,231
6
1
27
4
54
699
53
9
1
1
1
15
865
7
1
1
55
35
1
89
740
1
17
1
15
956
8
2
4
141
251
1
12
411
9
1
3
3
16
811
15
2
26
877
10
1
1
1
1
3
1
10
26
799
446
24
1,313
11
1
1
3
4
27
1,438
12
1,486
TOTAL
584
568
777
1,151
787
1,267
818
365
871
844
1,889
485
10,406
ALOS
26.2
28.3
27.7
29.6
32.3
32.0
29.8
31.4
30.6
31.3
28.5
# Out-
Migration
21
11
280
79
67
568
78
114
60
45
451
Percent
3.6%
1.9%
36%
6.9%
8.5%
44.8%
9.5%
31.2%
6.9%
5.3%
23.9%
ALOS
within the
District
25.7
27.3
27.5
29.2
31.5
36.3
27.9
26.6
30.8
31.8
27.4
ALOS Out-
Migration
37.5
82.3
28.1
34.2
40.8
26.6
47.8
42.0
28.7
22.8
31.7
Source: CON application #10137, page 1-14.
Landmark states that according to the data above, District 8 ranks last
in terms of the number of persons treated in LTCH facilities. The
applicant also cites that District 8 residents experienced the third longest
ALOS at 31.4 days—longer lengths of stay reflect both higher severity
and increased age.
The applicant notes that only two districts had higher ALOS for residents
that out-migrated for LTCH services than District 8 residents. The 114
District 8 cases that out-migrated for LTCH care had an ALOS of 42.0
days compared to patients that remained in District 8 for LTCH care with
an ALOS of 26.6 days. Landmarks states that this data demonstrates
that the current capability within District 8 is not sufficient in size or in
complexity of care. Therefore, the applicant asserts, the proposed facility
would markedly enhance access and availability of care.
CON Action Numbers: 10137 & 10138
24
Landmark presents population estimates by county for District 8. See
the table below.
Population Estimates for Counties of District 8
Age 65 Years and Older
2012 and 2015-2017 (first three years of operation)*
County
January 2012
January 2015
January 2016
January 2017
Charlotte
148,085
155,344
157,711
160,009
Collier
281,944
303,090
310,451
317,615
DeSoto
28,041
28,969
29,289
29,574
Glades
9,611
9,846
9,903
9,957
Hendry
31,046
32,335
32,795
33,221
Lee
526,307
571,746
587,300
602,528
Sarasota
344,806
362,674
368,680
374,656
Total
1,369,840
1,464,004
1,496,129
1,527,560
Net Increase from the Previous Year
Charlotte
1,192
2,530
2,367
2,298
Collier
3,396
7,623
7,361
7,164
DeSoto
-21
340
320
285
Glades
35
77
57
54
Hendry
53
471
460
426
Lee
8,954
16,034
15,554
15,228
Sarasota
3,074
6,306
6,006
5,976
Total
16,683
33,381
32,125
31,431
Percent Increase from the Previous Year
Charlotte
0.8%
1.7%
1.5%
1.5%
Collier
1.2%
2.6%
2.4%
2.3%
DeSoto
-0.1%
1.2%
1.1%
1.0%
Glades
0.4%
0.8%
0.6%
0.5%
Hendry
0.2%
1.5%
1.4%
1.3%
Lee
1.7%
2.9%
2.7%
2.6%
Sarasota
0.9%
1.8%
1.7%
1.6%
Total
1.2%
2.3%
2.2%
2.1%
Source: CON application #10137, page 1-17.
*Applicant included first three years of operation as the proposed facility will not be profitable until year three.
Landmark next presents population estimates by District 8 county for
the age cohort 65 years of age and older. This data shows large gains
and much higher proportionate increases above the rate for the district.
Patient 65 years and older comprise 70 percent of LTCH cases and
population growth in that age cohort creates demand for care. These
population estimates show that growth will continue, further
exacerbating the disparity in access and availability of LTCH services in
District 8 with just one 40-bed hospital. See the table below.

CON Action Numbers: 10137 & 10138
25
Population Estimates for Counties of District 8
Age 65 Years and Older
2012 and 2015-2017 (first three years of operation)
County
January 2012
January 2015
January 2016
January 2017
Charlotte
57,859
62,062
63,752
65,536
Collier
83,949
93,766
97,511
101,353
DeSoto
6,480
6,993
7,176
7,353
Glades
2,165
2,280
2,323
2,370
Hendry
4,451
4,847
4,972
5,084
Lee
155,833
176,668
184,353
192,205
Sarasota
127,797
139,828
144,446
149,286
Total
438,534
486,444
504,533
523,187
Net Increase from the Previous Year
Charlotte
900
1,459
1,690
1,784
Collier
2,093
3,500
3,745
3,842
DeSoto
92
181
183
177
Glades
26
38
43
47
Hendry
75
141
125
112
Lee
4,880
7,434
7,685
7,852
Sarasota
2,847
4,198
4,618
4,840
Total
10,913
16,951
18,089
18,654
Percent Increase from the Previous Year
Charlotte
1.6%
2.4%
2.7%
2.8%
Collier
2.6%
3.9%
4.0%
3.9%
DeSoto
1.4%
2.7%
2.6%
2.5%
Glades
1.2%
1.7%
1.9%
2.0%
Hendry
1.7%
3.0%
2.6%
2.3%
Lee
3.2%
4.4%
4.3%
4.3%
Sarasota
2.3%
3.1%
3.3%
3.4%
Total
2.6%
3.6%
3.7%
3.7%
Percent of Total Population that are Persons Aged 65 Years and Older
Charlotte
39.1%
40.0%
40.4%
41.0%
Collier
29.8%
30.9%
31.4%
31.9%
DeSoto
23.1%
24.1%
24.5%
24.9%
Glades
22.5%
23.2%
23.5%
23.8%
Hendry
14.3%
15.0%
15.2%
15.3%
Lee
29.6%
30.9%
31.4%
31.9%
Sarasota
37.1%
38.6%
39.2%
39.8%
Total
32.0%
33.2%
33.7%
34.2%
Source: CON application 10137, pages 1-17 and 1-18.
Availability, Utilization and Quality of Like Services in District 8
Landmark provides the use rate per 1,000 persons of LTCH services,
inside or outside of the district, demonstrating a low use rate—the lowest
of all health planning districts. See the table below.
CON Action Numbers: 10137 & 10138
26
Use Rates for LTCH Services for Ages 15+ and 65+ for Health Planning Districts of Residence
April 1, 2010-March 31, 2011
District
15+
Pop.
Rate/
1,000
# LTCH
Beds
# LTCH
Beds/
100,000
Dischg/
Bed
65+
Pop.
Rate/
1,000
# LTCH
Beds/
100,000
Dischg/
Bed
1
581,199
1.0048
54
9.3
10.8
98,966
3.8195
54.5642
7.0000
2
610,606
0.9302
59
9.7
9.6
98,966
3.8599
59.6164
6.4746
3
1,374,792
0.5652
75
5.5
10.4
373,599
1.2982
20.0750
6.4667
4
1,616,085
0.7122
187
11.6
6.2
314,039
2.5092
59.5467
4.2139
5
1,151,309
0.6836
180
15.6
4.4
306,540
1.6703
58.7199
2.8444
6
1,795,640
0.7056
175
9.7
7.2
370,376
2.1897
47.2493
4.6343
7
1,907,606
0.4288
135
7.1
6.1
308,427
1.5855
43.7705
3.6222
8
1,353,157
0.2697
40
3.0
9.1
427,621
0.5987
9.3541
6.4000
9
1,570,633
0.5546
130
8.3
6.7
430,205
1.4737
30.2182
4.8769
10
1,404,154
0.6011
194
13.8
4.4
253,599
2.4369
76.4987
3.1856
11
2,057,175
0.9182
129
6.3
14.6
371,058
4.3848
34.7655
12.6124
TOTAL
15,422,356
0.6747
1,358
8.8
7.7
3,361,577
2.1707
40.3977
5.3733
Source: CON application #10137, page 1-19.
The applicant cites that District 8’s use rate of 0.2697 per 1,000 persons
is more than one and one half times lower than the next lowest in
District 7—if District 8 had the same use rate as District 7 then it would
have 580 instead of 365 admissions. Landmark contends that use-rate
is one component in District 8’s under-service, the other variable is bed
supply. District 8 has the lowest bed supply of all health planning
districts. The applicant maintains that this data demonstrates that
District 8 residents do not have similar access to LTCH services as those
who reside in other districts. The reviewer notes that the applicant does
not provide documentation that District 8 and Collier County residents
are unable to access long-term care services.
Landmark employs the statewide use rate and bed supply based on the
elderly age cohort resulting in an estimate for LTCH services in District 8
of 928 admissions and a bed supply of 172.
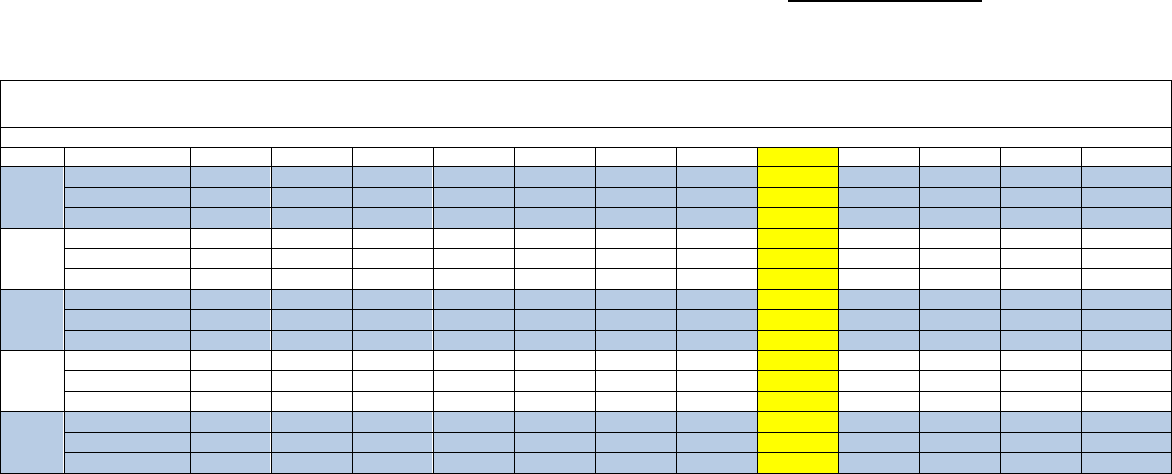
The applicant provided the following information to show the occupancy
rates of LTCH beds for the most recent five calendar years by each of the
11 health planning districts. See the table below.
CON Action Numbers: 10137 & 10138
27
Pattern of Utilization of LTCHs in all Health Planning Districts
CY 2006-2010
Health Planning District
CY
Factor
1
2
3
4
5
6
7
8
9
10
11
State
2006
# of Lic Beds
0
59
75
187
82
175
75
40
0
194
129
1,016
Patient Days
0
9,115
7,593
42,207
19,561
37,234
14,178
9,838
0
44,208
40,614
224,548
Occupancy
0.0%
60.8%
63.6%
64.3%
65.4%
58.3%
97.1%
67.4%
0.0%
62.4%
87.2%
66.2%
2007
# of Lic Beds
54
59
75
187
130
175
75
40
60
194
129
1,178
Patient Days
837
11,094
9,181
44,828
20,711
38,475
19,533
10,147
305
43,870
41,006
239,987
Occupancy
11.7%
54.7%
46.0%
65.5%
58.5%
60.1%
71.2%
69.3%
4.4%
61.8%
86.9%
62.7%
2008
# of Lic Beds
54
59
75
187
130
175
75
40
130
194
129
1,248
Patient Days
3,617
13,808
12,304
44,668
21,731
34,638
21,970
9,054
2,437
43,109
41,708
249,044
Occupancy
21.1%
63.9%
44.8%
65.3%
49.1%
54.1%
80.0%
62.0%
8.8%
60.7%
88.3%
57.8%
2009
# of Lic Beds
54
59
75
187
180
175
135
40
130
194
129
1,358
Patient Days
10,863
17,160
14,326
42,960
24,703
34,564
21,198
10,176
18,493
44,041
42,243
280,727
Occupancy
55.1%
79.7%
52.3%
62.9%
52.1%
54.1%
72.5%
69.7%
39.0%
62.2%
89.7%
61.4%
2010
# of Lic Beds
54
59
75
187
180
175
135
40
130
194
129
1,358
Patient Days
14,770
18,394
14,514
42,407
36,606
33,045
24,889
11,331
26,616
43,054
41,621
307,247
Occupancy
74.9%
85.4%
53.0%
62.1%
55.7%
51.7%
50.5%
77.6%
56.1%
60.8%
88.4%
62.0%
Source: CON application #10137, page 1-21.
Landmark states that the statewide occupancy rate of 62 percent for
calendar year 2010, below the planning standard of 75 percent appears
to indicate an available capacity of approximately 500 beds. The
reviewer notes that the Agency does not have a planning standard of
occupancy for LTCHs. This planning standard was established by
Landmark. The applicant contends that this can be a misleading
assumption as the ALOS for patients in a LTCH varies considerably
typically on the high side. Data shows that the ALOS for CY 2010 was
30 days and the median was 29.7 days with a standard deviation of 3.1
days. For the one LTCH in District 8 the ALOS for CY 2010 was 31.8.
Therefore Landmark contends that occupancy in this type of extended
stay service may not the best measure of available capacity.
The applicant indicates that location does influence use along with the
number of beds available. Regionalization of LTCH services is difficult in
practice, asserts Landmark, because of the generally advanced age and
serious conditions of the patients admitted. The applicant cites that
residents in Sarasota, the county where the LTCH is located in District 8,
had the highest access. Patients may decline LTCH admission if distance
and time to travel are perceived as too great resulting in some negative
consequences, such as:
If the patient is a Medicare beneficiary, the hospital will be
reimbursed an outlier payment if the patient remains in an acute care
hospital. This is insufficient to cover the cost of care, creating a loss
for the hospital.

CON Action Numbers: 10137 & 10138
28
Remaining in a hospital may not be the most effective and efficient
use of resources for a patient that is appropriate for LTCH admission.
Generally such patients remain in intensive care, with the result that
this resource may not afford the necessary access to rehabilitative
and restorative therapies as frequently or of a duration that would
otherwise be provided in a less restrictive, intensive care room.
A single acute care hospital generally has too few such patients to
have a critical mass that would support a dedicated unit and staff to
care for them. Each hospital, with such cases, disproportionately
creates expenses which, if all such patients were located together,
could be reduced through enhanced efficiency.
A few LTCH appropriate patients at one hospital means that expertise
and treatment protocols for the LTCH patient may not be the most
effective or efficient to produce the same results in the same time
period that an LTCH can achieve. For highly complex patients that
already present needs for expensive staff and other resources, the
LTCH is the preferred environment of care.
Landmark notes that there is local interest in having Landmark as a
LTCH provider, emphasizing need for LTCH services in light of current
limited access to residents of Collier County. The applicant cites Dr.
Allen Weiss’, President and CEO of NCH Healthcare, letter of support.
The applicant states that the sole provider of LTCH services in District 8,
Complex Care Hospital at Ridgelake, received The Joint Commission
accreditation and Gold Seal Approval. All of the LTCH hospitals who
treated District 8 residents that out-migrated for care also attained The
Joint Commission accreditation and Gold Seal Award.
Landmark states that its current LTCH facilities have The Joint
Commission accreditation and Gold Seal Approval. The applicant
maintains that the proposed project will be at the same high level as the
current Landmark Hospitals and those others that provide care to
residents of District 8. Landmark states that the proposed project will
assure the community standard of care for highly complex, seriously ill
patients will persist.
Medical Treatment Trends
The applicant indicates that treatment for seriously ill persons remains a
focus as data continues to show that the largest proportion of the
Medicare budget is spent on persons in the last year of life. Landmark
identifies three approaches that define the health care system:

CON Action Numbers: 10137 & 10138
29
Prevention of chronic illness and debilitation
Intervention to delay the onset of chronic conditions or to manage
them when identified
Treatment in settings that create efficiencies and economies.
Landmark states that the LTCH has emerged as another treatment
location for highly complex, multiple system failures or involvements
following episodic hospitalization. The role of the LTCH is to accept
patients whose conditions meet medical necessity for acute admission
whose recovery will require a mix of therapies and treatments over time.
By accepting transfers from many hospitals, the LTCH has a critical
mass of patients and staff that can operate more efficiently.
The applicant states that LTCHs are under study as their numbers
increase. This research questions the amount of saving that can be
achieved mixed with the expected high mortality rate of LTCH patients,
given their advanced age and complications. Landmark cites two such
studies, Long-term Acute Care Hospitalization After Critical Illness and
Post-ICU Mechanical Ventilation at 23 Long-Term Care Hospitals. The first
study did not produce clear results, “whether these hospitals
meaningfully improve outcomes for either patient group [reference most
severely ill versus less severely ill] is unknown” but do point out that
incentives exist to transfer severely ill patient to free up intensive care
beds.
11
The second study found that more than half of the ventilator-
dependent survivors of catastrophic illness were transferred from the ICU
were successfully weaned in the LTCH setting.
12
Landmark provides Florida data for LTCHs’ discharge disposition for all
cases, not those on mechanical ventilation. See the table below.
11
Long-term Acute Care Hospitalization After Critical Illness (Kahn, Benson et al. JAMA; 20103030(22);
2253-2259).
12
Post-ICU Mechanical Ventilation at 23 Long-Term Care Hospitals (Scheinhorn, Hassenpflug et al.
Chest; 131 (1), January 2007).
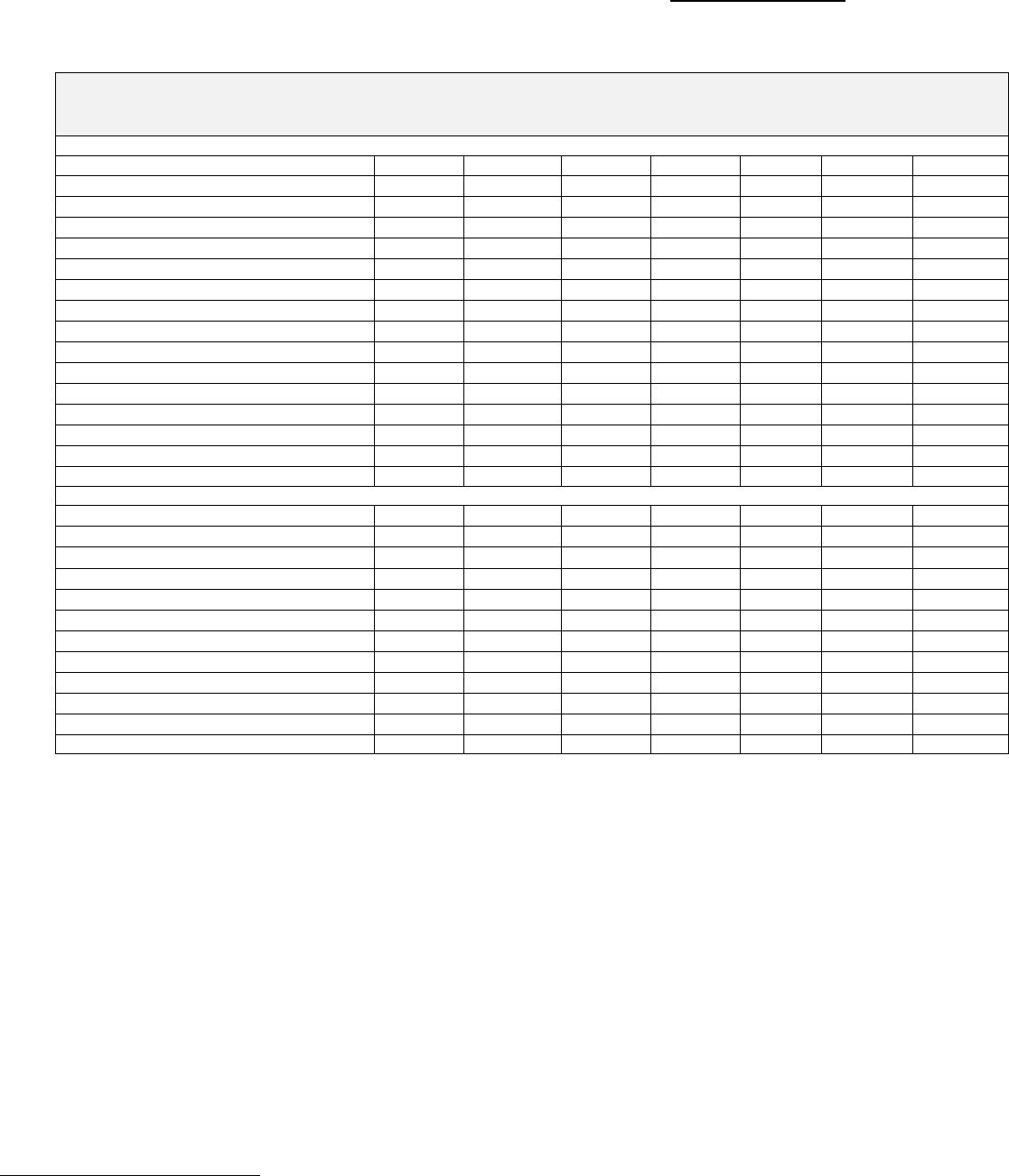
CON Action Numbers: 10137 & 10138
30
LTCH Patient Discharge Disposition
Florida and District 8
April 1, 2010-March 31, 2011
Statewide Age Cohort
Discharge Status
15-24
25-44
45-64
65-74
75+
Total
Percent
01-Discharged Home
10
66
179
107
92
454
4.4%
02-DC to short term general hospital
13
59
406
422
449
1,349
13.0%
03-DC to Medicare SNF
12
118
826
1,028
1,650
3,634
34.9%
04-DC to intermediate care facility
1
4
5
17
27
0.3%
05-DC to cancer/children’s facility
1
1
1
3
0.0%
06-DC to home health care
16
148
520
462
498
1,644
15.8%
07-Left AMA
2
15
17
14
20
68
0.7%
20-Deceased
3
34
319
562
1,129
2,047
19.7%
50-DC to Hospice home
1
22
35
83
141
1.4%
51-DC to Hospice facility
6
63
104
255
428
4.1%
62-DC to inpatient rehab facility
9
42
177
161
145
534
5.1%
63-DC to Medicare cert LTC hospital
4
12
12
22
50
0.5%
65-DC to Psych hospital/unit
2
1
1
4
0.0%
10-DC to another type not in list
2
7
14
23
0.2%
Total
65
494
2,550
2,921
4,376
10,406
100.0%
District 8 Age Cohort
01-Discharge Home
1
4
1
1
7
1.9%
02-DC to short term general hospital
1
24
19
23
67
18.4%
03-DC to Medicare SNF
3
7
27
37
43
117
32.1%
06-DC to home health care
8
11
8
27
7.4%
07-Left AMA
1
1
0.3%
20-Deceased
1
2
25
32
60
16.4%
50-DC to Hospice home
1
1
0.3%
51-DC to Hospice facility
2
2
3
7
1.9%
62-DC to inpatient rehab facility
1
3
21
21
12
58
5.9%
63-DC to Medicare cert LTC hospital
3
3
0.8%
70-DC to another type not in list
2
5
10
17
4.7%
Total
4
13
92
121
135
365
100.0%
Source: CON application #10137, page 1-28.
Another national comprehensive study discussed by the applicant, Long-
Term Care Hospital Payment System Monitoring and Evaluation, Phase II
Report, identifies that DRG 475, Respiratory System Diagnosis with
Ventilator Support, is the most common admission at LTCHs.
13
The
second most frequent admission was DRG 249, After Care
Musculoskeletal System & Connective Tissue. Landmark presents the
top 25 DRGs treated at Florida LTCHs, pointing out that the Florida
experience departs from the national findings. See the table below.
13
Long-Term Care Hospital Payment System Monitoring and Evaluation, Phase II Report (Gage,
Pilkauskas et al., RTI International, CMS Contract NO. 500-00-0024-TO#20, January 2007: RIT
Project Number 07964.020).
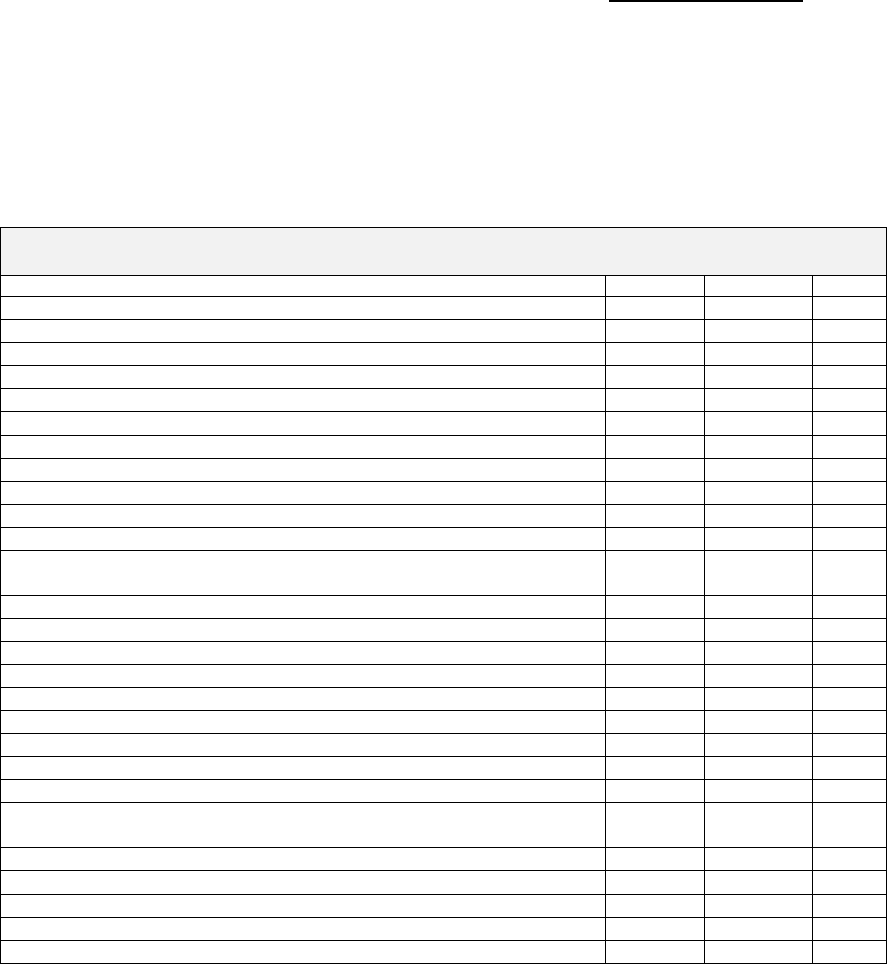
CON Action Numbers: 10137 & 10138
31
The applicant states that the applicability to Florida’s LTCHs with respect
to some national findings demonstrates how discrepant the provisions of
LTCH services are within the nation. Landmark contends that clearly,
the implications for costs, margins and payment rates with such
variability can raise concern.
Top 25 DRGs Treated at Florida LTCHs with ALOS
April 1, 2010-March 31, 2011
DRG
Cases
Percent
ALOS
Grand Total
10,406
100.0%
29.7
Respiratory System Diagnosis with Ventilator Support 96+ Hours
2,079
20.0%
40.6
Pulmonary Edema & Respiratory Failure
1,325
12.7%
21.0
Septicemia or Severe Sepsis without MV 96 Hours with MCC
493
4.7%
21.3
Respiratory System Diagnosis with Ventilator Support <96 Hours
350
3.4%
14.4
Respiratory Infections & Inflammations with MCC
292
2.8%
21.9
Aftercare with CC/MCC
226
2.2%
20.7
Other Respiratory System O.R. Procedures with MCC
223
2.1%
66.0
Septicemia or Severe Sepsis with MV 96+ Hours
223
2.1%
40.5
Skin Ulcers with MCC
192
1.8%
26.4
Chronic Obstructive Pulmonary Disease with MCC
180
1.7%
18.9
Trach with MV 96+ Hours or PDX EXC Face, Mouth & Neck
without Major O.R.
164
1.6%
63.3
Postoperative & Post-Traumatic Infections with MCC
158
1.5%
24.7
Osteomyelitis with MCC
154
1.5%
28.4
Respiratory Infections & Inflammations with CC
133
1.3%
18.9
Complications of Treatment with MCC
130
1.2%
33.2
Renal Failure with MCC
126
1.2%
23.6
Skin Ulcers with CC
125
1.2%
22.7
Infectious & Parasitic Diseases with O.R. Procedure with MCC
122
1.2%
55.9
Simple Pneumonia & Pleurisy with MCC
117
1.1%
18.5
Other Circulatory System Diagnoses w MCC
115
1.1%
23.3
Extensive O.R. Procedure Unrelated to Principal Diagnosis with
MCC
115
1.1%
72.4
Skin Graft and/or Debrid for Skin Ulcer or Cellulitis with MCC
105
1.0%
43.8
Chronic Obstructive Pulmonary Disease W CC
103
1.0%
15.8
Heart Failure & Shock with MCC
97
0.9%
20.9
Aftercare, Musculoskeletal System & Connective Tissue with MCC
88
0.8%
24.3
Subtotal
7,432
71.4%
31.3
Source: CON application #10137, page 1-30.
Landmark states that residents from District 8 needing LTCH services
follow a similar pattern as above of clinical conditions.

CON Action Numbers: 10137 & 10138
32
The above mentioned study, Long-Term Care Hospital Payment System
Monitoring and Evaluation, Phase II Report, mentions that because all
LTCHs must be licensed as acute hospitals in the state in which they
operate it is difficult to determine levels of care associated with LTCH
admissions.
14
This study did develop recommendations for identifying
patients appropriate for admission to LTCHs.
15
These are as follows:
The primary diagnosis must be medical, not physical functioning or
psychiatric.
The cases must be medically complex, defined broadly to include
conditions with severe medical complications, co-morbidities, or
system failures and together represent a complicated, severely ill
patient.
Require LTCHs to discharge those not having diagnostic procedures or
improving with treatment.
Develop criteria to measure medical severity for hospital admission.
Develop a Technical Advisory Group (TAG) composed of physicians
who treat medically complex patients to develop a set of criteria and
measures.
Collect data and analyze it.
Require LTCHs to collect and submit functional impairment measures
as well as physiologic measures on all patients receiving physical,
occupational or speech/language pathology services.
Landmark states that LTCHs in Florida strive to be the place for severely
ill, medically complex patients. A mix of therapies and services are
offered, the conditions admitted are life-threatening and life-limiting,
with 70 percent over age 65. The applicant indicates that within these
parameters, Florida LTCHs operate in concert with the recommendations
of the abovementioned report.
Landmark states that the proposed facility for Collier County will direct
care to the most severely ill patients, with most receiving mechanical
ventilation. The applicant’s goal is to wean patients from the ventilator.
To achieve its goal, Landmark adopts the latest in advances that have
demonstrated success. Landmark contends there is sufficient need for
the Lee County 60-bed LTCH and its project.
14
Since the study was published, medical severity is now a feature in the DRG schema as a parameter
to distinguish cases in the future.
15
Tables of Characteristics were presented in Section 6, “Recommendations of the Report”.

CON Action Numbers: 10137 & 10138
33
The applicant maintains that it provides 24-hour physician coverage--
unusual in the LTCH industry and a higher standard of care. Landmark
also accommodates clinical research and internships.
Many protocols and patient care standard of practice evolve over time for
the severely ill with life-threatening conditions. Landmark maintains
that its staff participates in techniques and studies which advance from
research and improve the practice of care in the hospital. Current areas
on interest include, but are not limited to the following:
Techniques and new applications of research in wound care, recently
adopting the use of platelet-rich plasma therapy in place of negative-
pressure wound therapy.
Implementation of the InTouch Health ® RP-7 robot, which is
controlled by a board-certified physician that makes rounds. The
robot is not a substitute for doctors, but allows staff to interface with
a live board-certified physician for routine issues after hours with the
on-call physician available for emergencies.
Investigation into the implementation of the Electronic Health Record.
Interface technology allows the physician to have the record convert
basics for billing, and also access the latest information regarding
standards of practice and “diagnostic trees” for treatment.
Landmark states that innovation that enhances the ability to efficiently
manage severe cases improves the provision of care and allows staff to be
effective in applying treatments timely, appropriately and consistently.
The applicant strives to be among the first to use technologies as both
clinical staff extenders and cost-containment modalities.
Market Conditions
The applicant notes that the development of LTCHs gained momentum
and mushroomed in the late 1990s and into the new millennium.
Florida’s development was slowed, in part due to the certificate of need
requirements and due to the definition of the LTCH as regional service
with a geographical boundary, the health planning district.
Landmark cites that federal initiatives also slowed the development of
LTCHs, these include:
The development and refinement of LTCH-DRG prospective payment
rates.

CON Action Numbers: 10137 & 10138
34
The concept of a hospital within a hospital, permitting an acute care
hospital to lease a floor or area of the hospital to a LTCH and the
subsequent refinements and limitations on the hospital within a
hospital to restrict admissions from the host hospital, requirement of
complete separation of ownership and medical staffs and limitations
on the services purchased from the host hospital.
Enactment of a three-year moratorium, beginning December 29,
2007, on enrolling any new LTCHs, creating LTCH satellite hospitals
or adding LTCH beds. This moratorium was extended by the
Affordable Care Act from December 29, 2010 to December 29, 2012.
The applicant states that since the moratorium has been in place, federal
spending on LTCHs has been flat. The industry’s rapid growth from
fewer than 10 hospitals in the 1980s to treating 200,000 patients a year
(with 130,000 of those being Medicare beneficiaries)—Medicare costs are
estimated to be $4.8 billion in 2010, up from $400 million in 1993.
Landmark states that profit margins on Medicare in LTCHs are about six
percent, on the other side at general acute care hospitals, the losses on
Medicare patients run about six percent. The applicant notes that Dr.
Christopher Cox, an associate professor of critical care medicine at Duke
University, states that Medicare reimbursement rules encourage the
development of LTCHs, receiving payment on the basis of diagnosis
rather than the cost of care.
Landmark asserts that the direction that policy makers will pursue in
the future direction of LTCHs is cost of care. For example, LTCH
appropriate patients who remain in the acute care setting create loss as
the Medicare outlier payment is insufficient to cover the cost of care.
Hospitals therefore incur losses since Medicare does not cover the full
cost of care. The applicant cites Post-ICU Mechanical Ventilation at 23
Long-Term Care Hospitals again, noting the authors’ assumptions that
the weaning from mechanical ventilation as part of the cost of care in the
LTCH would be far less than it would be in the ICUs at acute care
hospitals. Landmark contends that this illustrates the economy of care
afforded by the LTCHs.
The applicant states that what providers charge differs from costs as well
as from what payers will reimburse under negotiated rates. Medicare is
the primary payer for LTCH services with commercial insurers a distant
second. Landmark notes that charges vary by payers and variations
exist in the charge per day. See the table below.
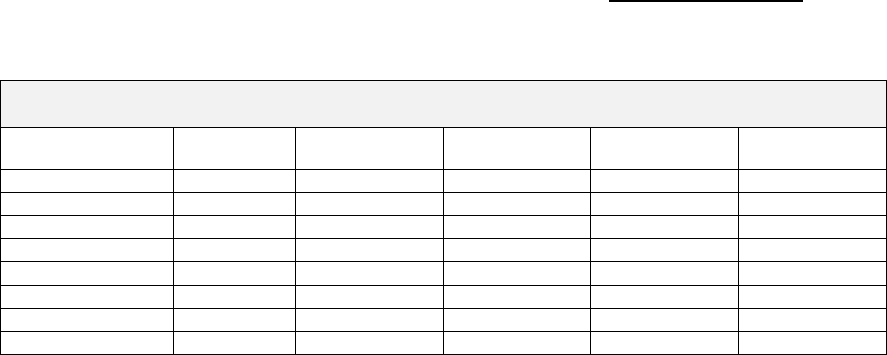
CON Action Numbers: 10137 & 10138
35
Charges Statewide by Payer for LTCHs
April 1, 2010 to March 31, 2011
Payer
Cases
Percent
ALOS
Total
Charge/Case
Total
Charge/Day
Charity
49
0.5%
34.9
$172,167
$4,939
Commercial
2,396
230%
35.5
$186,776
$5,266
Government
13
0.1%
42.0
$204,841
$4,877
Medicaid
149
1.4%
36.6
$161,982
$4,424
Medicare
7,632
73.3%
26.8
$120,178
$4,489
Self/Other
125
1.2%
80.0
$490,277
$6,128
Workers Comp
42
0.4%
43.9
$179,873
$4,095
Grand Total
10,406
100.0%
29.7
$141,148
$4,756
Source: CON application #10137, page 1-37.
The reviewer notes that the above table represents charges statewide.
Based on the Florida Hospital Uniform Reporting System (FHURS) 2010
Actual Reports, the breakdown for actual payments to LTCHs is as
follows: Medicare 79.5 percent, Medicaid 1.8 percent, HMO-PPO 14.9
percent, commercial insurance 2.4 percent and charity 1.4 percent.
Landmark indicates that information available from the CMS website
reported that in 2010 Medicare spent $5.2 billion on LTCHs with
134,700 cases at an average payment of $38,600. The standardized cost
per discharge was $26,600 and $36,251, respectively for high-margin
and low-margin profitable LTCHs. Medicare payment per discharge was
$38, 557 for high profit-margin, LTCHs and $38,137 per discharge for
the low-profit margin LTCHs. Within the high-profit margin LTCHs, 90
percent were for-profit compared to 64 percent for-profit LTCHs in the
low-profit margin group.
The applicant reviewed the available data for Florida LTCHs for 2009 on
the Group 12, Long-Term Care Hospitals. Landmark notes that the
mean standard cost per adjusted admission across all payers was
$35,619-higher than that reported for the high margin LTCHs and just
slightly higher than that reported for the low margin hospitals. The
applicant identifies that Florida’s mean cost per adjusted admission is
much higher at admission, $45,724, than is the Medicare cost per
discharge in either group. Landmark states that Florida’s LTCHs do
treat a higher intensity, severely ill patient group with multiple
complexities—it follows that the costs would be higher. See the table
below.
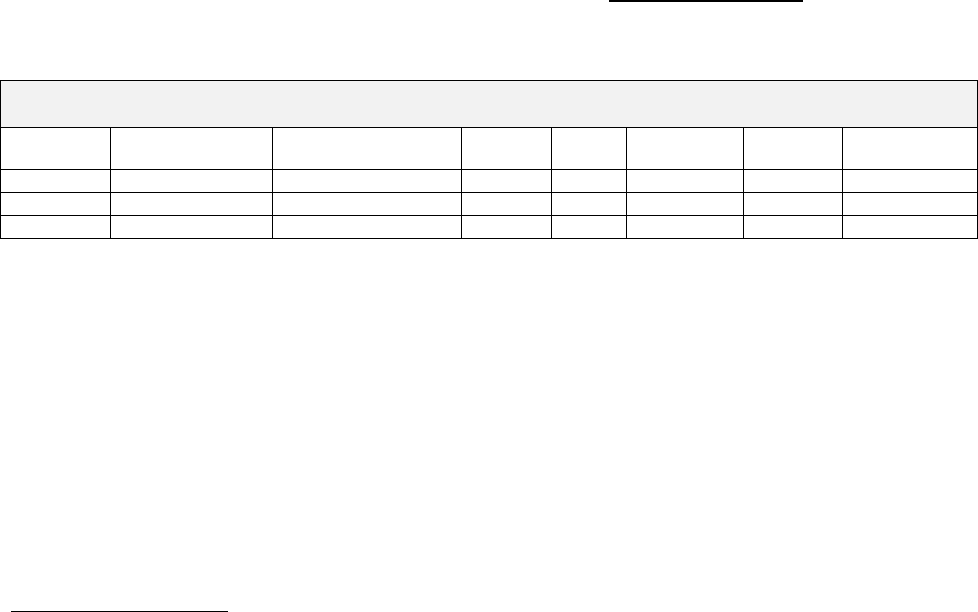
CON Action Numbers: 10137 & 10138
36
Florida LTCH Reported Costs
Calendar Year 2009
Standard
Cost/Adj Adm.
Cost/Adj. Admits
Bed
Size
ADC
Medicaid
& Charity
ALOS
LTCH Case
Mix
Mean
$35,619
$45,724
62.4
38.8
2.94%
30
1.2813
Median
$33,634
$45,764
57.0
36.09
2.53%
29.7
1.2992
S.D.
6.121
8.688
26.6
15.94
1.80%
3.1
0.1334
Source: CON application #10137, page 1-38.
Landmark states that the federal government did make downward
adjustments in payments to LTCHs as a cost-controlling mechanism.
The LTCH PPS federal rate for FY 2011 is $39,599.95, effective after
October 1, 2010—reflecting a downward adjustment as contained in the
Affordable Care Act. The applicant cites other adjustments: MS-LTC-
DRG Grouper version 28 (up from 27), a fixed loss amount of $18,785,
the labor share of 75.271 percent and cost to charge ratio (CCR) ceiling
of 1.231. Landmark contends that greater risk for costs is placed on
LTCHs with these changes.
Bed Need Analysis
The applicant states that several methods were applied to forecast the
demand expected for LTCH services in District 8. The first method was
the use rate—discharges per 1,000 persons aged 15 and older.
Landmark applies the statewide average and statewide median rates to
future population estimates for District 8 to gauge demand for LTCH
services. The statewide average and median were figured using
previously introduced information on LTCH services by persons aged 15
and older, rates of use discussed earlier in the application and on page
24 of this State Action Agency Report. The applicant provides the
statewide use rate applied to District 8 population estimates for years
2015 to 2018 to forecast the cases, patient days, ADC and beds needs at
the 75 percent occupancy standard. See the table below.
CON Action Numbers: 10137 & 10138
37
Forecasted LTCH Cases per Year Using the Statewide Use Rate
District 8 Future Population Estimates
Ages 15 Years and Older
January 2015-January 2018
Number of Cases
Statewide Use Rate of .6747/1,000 Persons
County
January 2015
January 2016
January 2017
January 2018
Charlotte
105
106
108
109
Collier
204
209
214
219
DeSoto
20
20
20
20
Glades
7
7
7
7
Hendry
22
22
22
23
Lee
386
396
407
417
Sarasota
245
249
253
257
District 8
988
1,009
1,031
1,051
Number of Patient Days
Statewide Use Rate, ALOS=29.7
County
January 2015
January 2016
January 2017
January 2018
Charlotte
3,113
3,160
3,206
3,251
Collier
6,073
6,221
6,365
6,505
DeSoto
580
587
593
598
Glades
197
198
200
201
Hendry
648
657
666
674
Lee
11,457
11,769
12,074
12,373
Sarasota
7,267
7,388
7,508
7,627
District 8
29,337
29,980
30,610
31,228
Average Daily Census
County
January 2015
January 2016
January 2017
January 2018
Charlotte
9
9
9
9
Collier
17
17
17
18
DeSoto
2
2
2
2
Glades
1
1
1
1
Hendry
2
2
2
2
Lee
31
32
33
34
Sarasota
20
20
21
21
District 8
80
82
84
86
Beds Needed at 75% Occupancy Standard
County
January 2015
January 2016
January 2017
January 2018
Charlotte
11
12
12
12
Collier
22
23
23
24
DeSoto
2
2
2
2
Glades
1
1
1
1
Hendry
2
2
2
2
Lee
42
43
44
45
Sarasota
27
27
27
28
District 8
107
110
112
114
Source: CON application #10137, pages 1-40 and 1-41.
Landmark notes that looking at the results for the two southernmost
counties—Collier and Lee—a demand of 64 beds is generated by January
2015. The applicant provides identical information using the median
(District 5’s use rate) instead of the statewide use rate. See the table
below.
CON Action Numbers: 10137 & 10138
38
Forecasted LTCH Cases per Year Using the Median Use Rate
District 8 Future Population Estimates
Ages 15 Years and Older
January 2015-January 2018
Number of Cases
District 5 Use Rate, .6836/1,000 Persons
County
January 2015
January 2016
January 2017
January 2018
Charlotte
106
108
109
111
Collier
207
212
217
222
DeSoto
20
20
20
20
Glades
7
7
7
7
Hendry
22
22
23
23
Lee
391
401
412
422
Sarasota
248
252
256
260
District 8
1,001
1,023
1,044
1,065
Number of Patient Days
District 5 Use Rate, ALOS=32.3
County
January 2015
January 2016
January 2017
January 2018
Charlotte
3,430
3,482
3,533
3,583
Collier
6,692
6,855
7,013
7,168
DeSoto
640
647
653
659
Glades
217
219
220
221
Hendry
714
724
734
742
Lee
12,624
12,968
13,304
13,634
Sarasota
8,008
8,141
8,273
8,404
District 8
32,326
33,035
33,729
34,410
Average Daily Census
County
January 2015
January 2016
January 2017
January 2018
Charlotte
9
10
10
10
Collier
18
19
19
20
DeSoto
2
2
2
2
Glades
1
1
1
1
Hendry
2
2
2
2
Lee
35
36
36
37
Sarasota
22
22
23
23
District 8
89
91
92
94
Beds Needed at 75% Occupancy Standard
County
January 2015
January 2016
January 2017
January 2018
Charlotte
13
13
13
13
Collier
24
25
26
26
DeSoto
2
2
2
2
Glades
1
1
1
1
Hendry
3
3
3
3
Lee
46
47
49
50
Sarasota
29
30
30
31
District 8
107
110
112
114
Source: CON application #10137, pages 1-42 and 1-43.
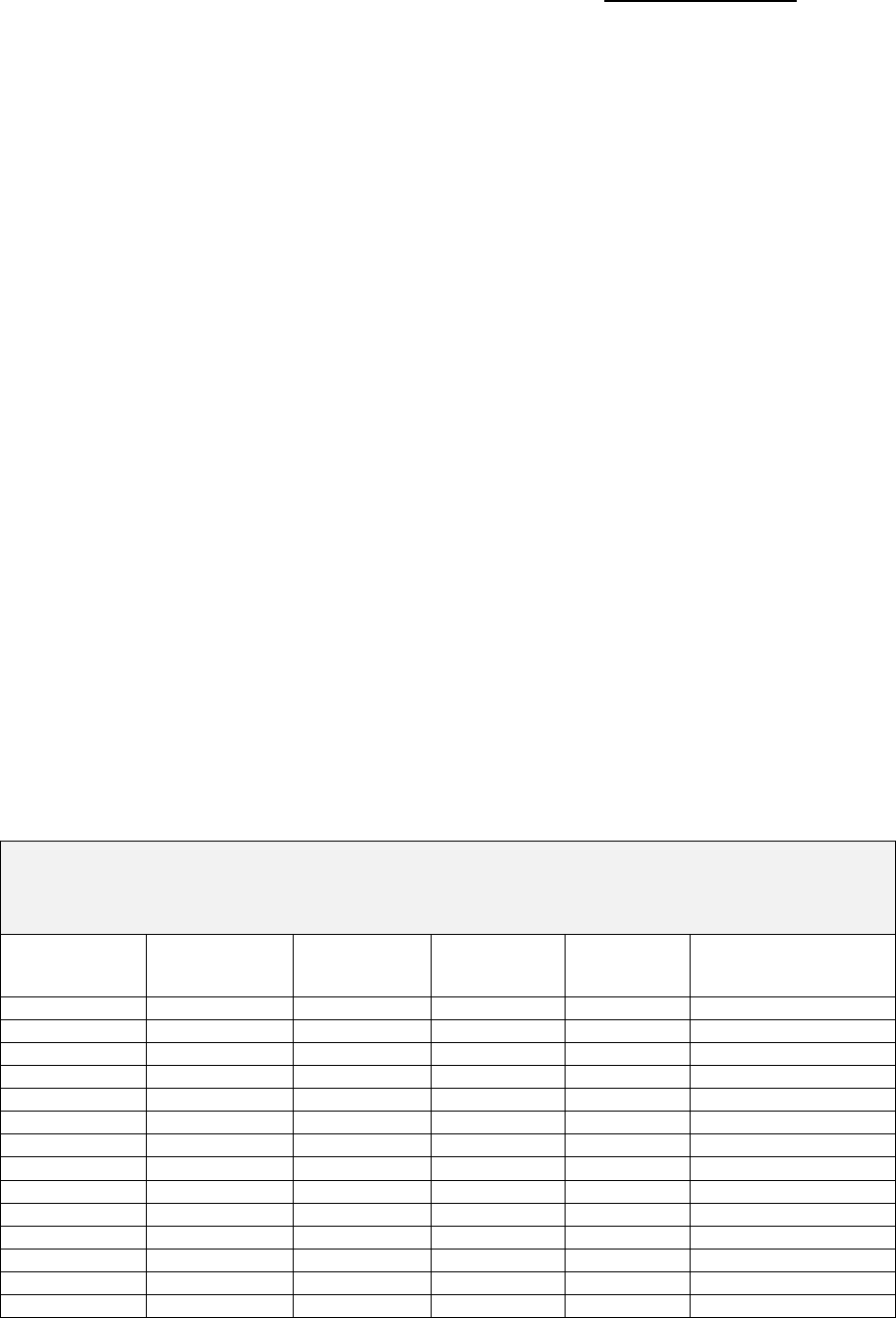
CON Action Numbers: 10137 & 10138
39
The applicant maintains that using the District 5 median use rate the
ADC estimates for District 8 increase by nine persons over the average
daily census when using the statewide use rate. Landmark contends
that employing the statewide (average) or District 5 (median) use rate to
approximate demand is realistic given that the District 8 rate is so far
below the rest of the districts’ experience. The applicant indicates that
the above data confirms the following points:
The current number of LTCH beds in District 8 (40 beds) is too few to
meet demand.
By January 2015, modeling indicates that at least 107 to 118 beds
are needed to achieve some parity with the rest of the health care
planning districts with respect to access to the service.
Over the period 2015 to 2018 demand increases, roughly adding
approximately two to three beds a year, just to remain at an
occupancy standard of 75 percent. Therefore, the demand persists
and the current LTCH is already above 75 percent, insufficient under
either use rate.
Landmark contends that with this health care service, supply is integral
to demand—unless the supply exists, no service can be delivered. The
applicant maintains that as the supply increases so does use because
providers become aware of the options. Landmark provides data
applying each health care planning district’s bed rate to the population
estimate for persons aged 15 and above for January 2015. See the table
below.
Bed Supply Forecast for District 8 Based on Each Health Planning District’s Bed to
Population Ratio Applied to
January 2015 Population Estimates for
District 8
Apply the
District Bed
Rate of…
LTCH Beds
Forecasted
for District 8
Less
Licensed
LTCH Beds
Less
Approved
LTCH Beds
Net Beds
Needed for
District 8
Net Beds Needed @
75% Occupancy*
District 5
229
40
60
129
172
District 10
202
40
60
102
136
District 4
169
40
60
69
93
District 6
143
40
60
43
57
District 2
141
40
60
41
55
District 1
136
40
60
36
48
District 9
121
40
60
21
28
District 7
104
40
60
4
5
District 11
92
40
60
-8
-11
District 3
80
40
60
-20
-27
District 8
43
40
60
-57
-76
State
129
40
60
29
39
Median
136
40
60
36
48
Average
133
40
60
33
44
Source: CON application #10137, page 1-44.
*Note: The applicant chose this occupancy standard.

CON Action Numbers: 10137 & 10138
40
The applicant contends that the data above clearly shows the
discrepancies in the availability of LTCH beds. District 5’s beds rate
when applied to District 8 forecasted population results in a gross bed
need of 229 LTCH beds, while the current bed rate for District 8
produces a gross need of 43. Landmark maintains that knowing District
8’s use and bed rates are the lowest among the districts, the results in
the net beds needs at 75 percent occupancy standard column reflects
marked variability. The applicant concludes that looking at the last
three rows in the above table—the state, median and average bed rates
return a final need for District 8 of 39, 48 or 44 beds beyond the number
of licensed and approved LTCH beds. Landmark stated that the
proposed 50-bed facility is within these parameters.
Landmark tested the accuracy of its bed analysis with a regression
equation. Using the equation y=b=mx yielded 9,846 patient days that a
50-bed LTCH would return based on the state’s historical experience
among LTCHs in the 11 health planning districts.
16
The applicant then
performed a linear trend line using the same historical data, returning
10,738.17 LTCH patient days. Both of these equations, Landmark
maintains, indicate the reasonableness of the 50 beds proposed.
The applicant forecasts approximately 9,100 patient days in the second
year of operations. From historical data, the 9,100 forecasted patient
days would generate 62 LTCH beds, based on the regression formula.
Using a linear trend line, a calculation of 81.20982 LTCH beds were
generated using 9,100 patient days—indicating that the statewide
experience with patient days would produce a higher expected number of
beds. Landmark explains this phenomenon by the fact that the
statewide numbers of LTCH beds are associated with lower numbers of
patient days.
Landmark asserts that the above data confirms that the 50 LTCH beds
sought are within reasonable parameters and reflect the statewide
experience among the 11 health planning districts. The result of
increasing the number of beds within District 8 improves access and
availability making the district in closer parity with the others.
16
In this equation, “y” is the predicted value, “b” is the intercept, “m” is the slope and “x” is the known
variable from which “y” will be calculated.
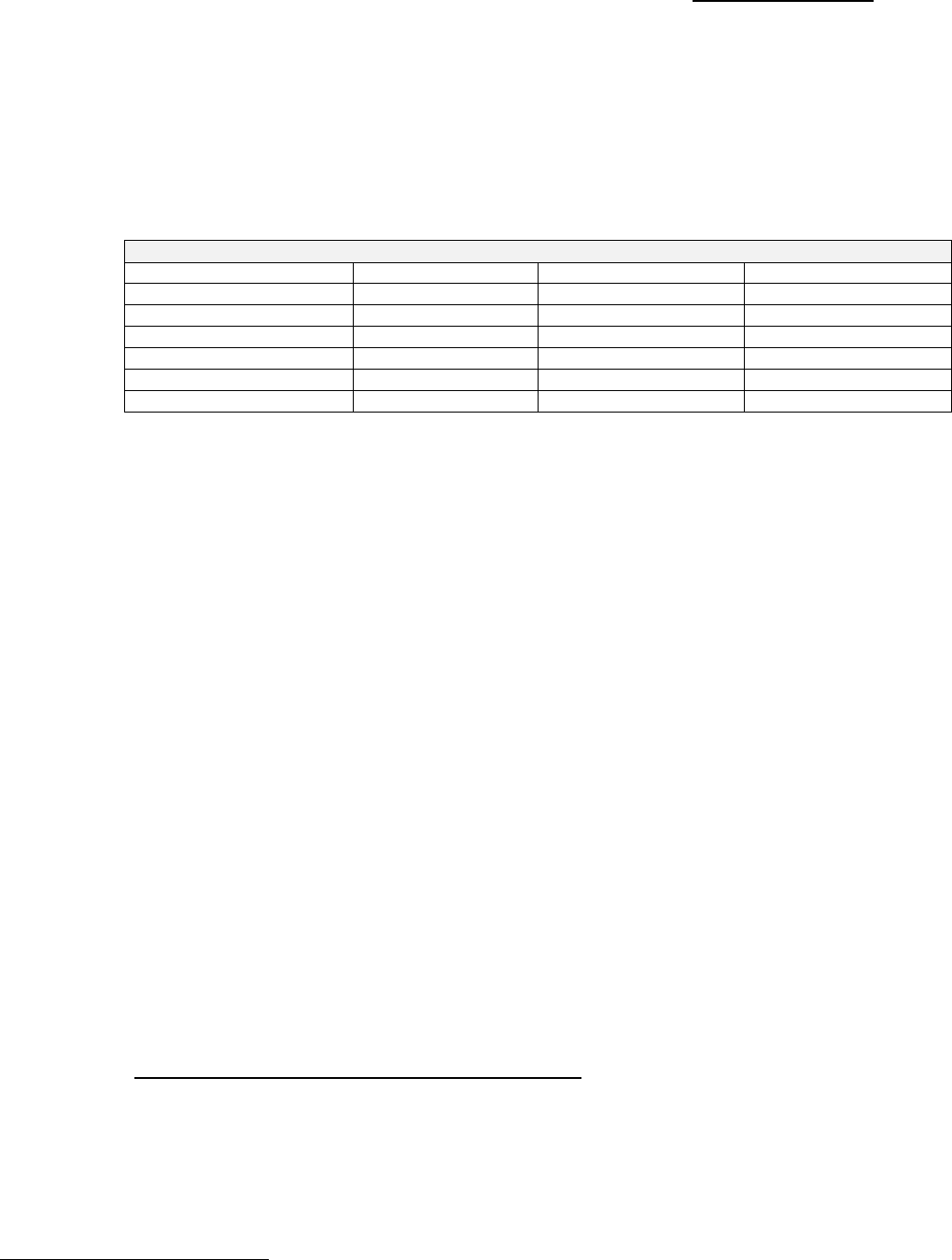
CON Action Numbers: 10137 & 10138
41
The applicant states that it used the District 5 use rate, as it represents
the calculated median experience and could be considered conservative.
This rate was applied to forecasted population estimates for those aged
15 years and older in District 8 for the calendar year 2015-2017 to
generate the gross numbers of LTCH cases. The applicant then assumed
a market share.
Utilization Forecast for Landmark Hospital of Southwest Florida
Factor
Year 1: CY 2015
Year 2: CY 2016
Year 3: CY 2017
Gross Cases, District 8
1,001
1,023
1,044
Market Share
17%
27%
40%
Hospital Cases
170
283
427
Occupancy
30%
50%
74%
ALOS
32
32
32
ADC
15
25
37
Source: CON application #10137, page 1-48.
Landmark cites Governor Rick Scott’s mandate to create and sustain
jobs in Florida noting the Creation and Economic Growth Agenda he
signed into law on March 28, 2012. The applicant asserts that the
proposed project will create jobs. Landmark states that there are 142
FTEs associated with the proposed project with an average salary with
benefits of about $65,000 a year.
17
Most of these jobs are in professional
and technical fields. Landmark indicates that the impact of the proposed
project would be $9.2 million in rough terms added to the local economy
in the form of permanent jobs.
The applicant maintains that the proposed project will also employ
trades and journeymen. Steven’s Construction Company in Collier
County estimate an average daily work force of 51 throughout a year at
2,080 hours/man at an average wage of $45 per hour. This results in an
estimate of $4.5 million in wages to workers. Landmark estimates a total
of $850,613 in permits, impact fees and other costs paid to Collier
County and the City of Naples government. The applicant states that the
indirect workforce associated with the hospital will also increase jobs in
the area.
Kindred Hospitals East, LLC (CON #10138):
Population Demographics and Dynamics
Kindred states that Collier County, the primary service area (PSA),
contains a population of 236,484 with 87,409 (37 percent) age 65+. The
population is expected to increase 11 percent in the next five years and
the 65+ population is expected to have a 17 percent increase over the
same time period. The applicant identifies Lee and Hendry County as
the secondary service area for the proposed facility and cites a current
17
The applicant’s Schedule 6 year three projections actually show 141 FTEs for the project.
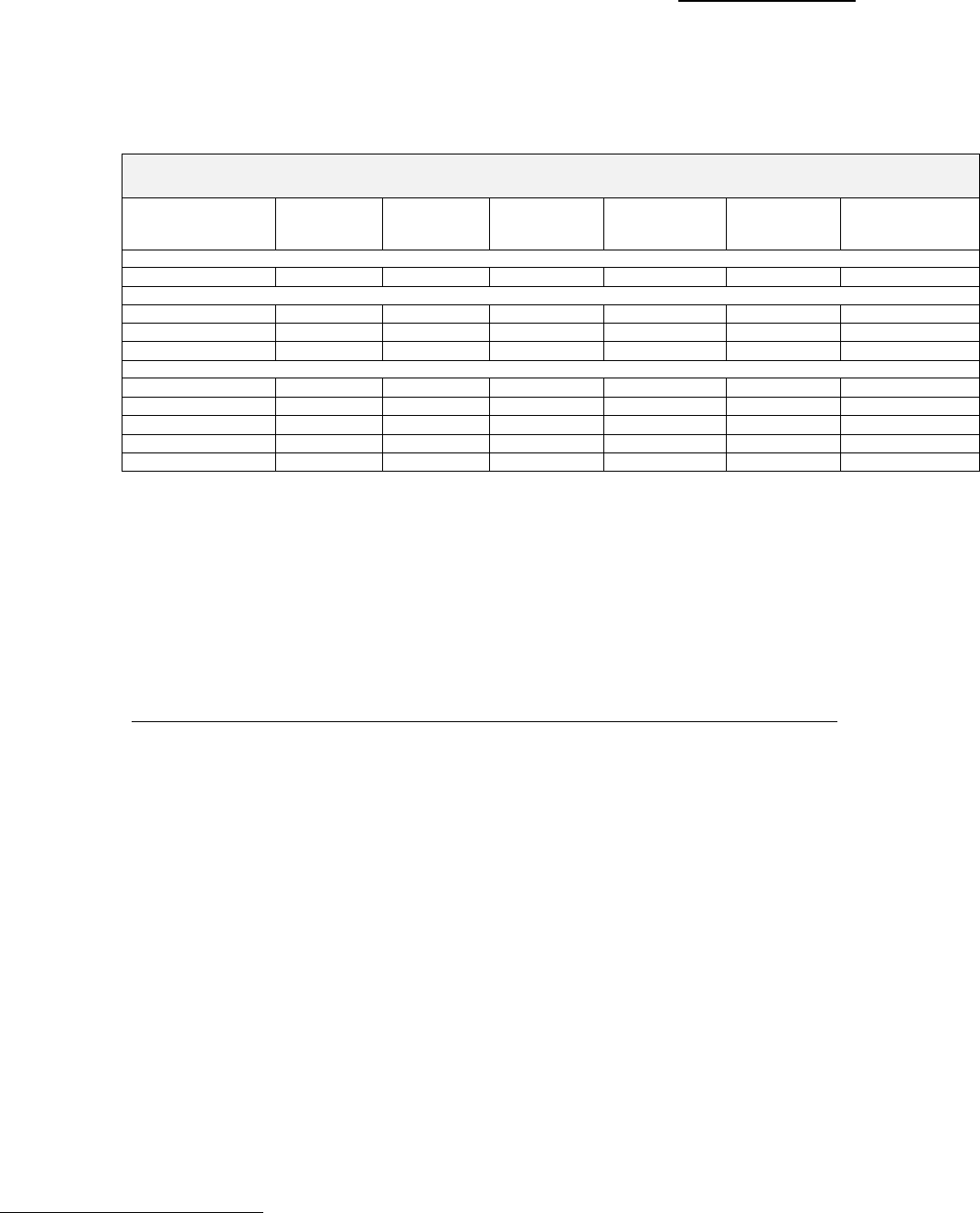
CON Action Numbers: 10137 & 10138
42
65+ population of 241,412 (24 percent of total population) that is
expected to increase to 286,370 (19 percent) over the next five years. See
the table below.
Population Estimates for Primary, Secondary and District Area
2012 and 2017
County
1/1/2012
Total
Population
1/1/2017
Total
Population
Total
Population
% Change
1/1/2012
65+
Population
1/1/2017
65+
Population
Total
65+Population
% Change
Primary Service Area
Collier
326,484
363,068
11.2%
87,409
102,304
17.0%
Secondary Service Area
Lee
633,147
726,611
14.8%
149,378
178,691
19.6%
Hendry
38,859
40,874
5.2%
4,625
5,375
16.2%
Service Area Total
998,490
1,130,553
13.2%
241,412
286,370
18.6%
Remaining District 8 Counties
Charlotte
161,143
170,827
6.0%
55,421
60,909
9.9%
DeSoto
34,711
36,836
6.1%
6,273
6,955
10.9%
Glades
12,828
14,122
10.1%
2,797
3,278
17.2%
Sarasota
383,289
409,298
6.8%
120,874
136,027
12.5%
District 8 Total
1,590,461
1,761,636
10.8%
426,777
493,539
15.6%
Source: CON application #10138, page 4.
The applicant contends that with the increase in the senior population,
the financial and capacity burdens on short-term hospitals from long-
term patients will continue to increase. Kindred asserts that the need for
long-term care hospital services in Collier County will exceed the
capabilities of existing LTCH facilities in the district thereby creating a
substantial unmet need in the delivery of health care in District 8.
Availability, Utilization and Quality of Like Services in the District
Kindred states that only one LTCH exists in District 8, Complex Care
Hospital at Ridgelake, a 40-bed LTCH in Sarasota County with an
average 12-month occupancy of over 71 percent.
The applicant indicates that Complex Care Hospital at Ridgelake is
approximately two hours away from the southern portion of the district.
Kindred states that this necessitates traveling long distances for
extended periods of time for patients, their families and physicians
causing a great burden. The applicant maintains that a patient’s
interaction with family and their own physician is significant to the
rehabilitation process and denying it can damage that patient’s quality of
care.
Kindred states that it demonstrates in its bed need analysis that the
existing facility in Sarasota and the approved 60-bed facility in Lee
County do not have sufficient capacity to meet the current need nor the
increasing need for LTCH services.
18
The applicant maintains that the
18
Kindred’s bed need analysis on page 13-14 of CON application #10138 states that there is an unmet
need of 43 LTCH beds in the District in 2017.

CON Action Numbers: 10137 & 10138
43
proposed facility in Collier County will significantly improve the
availability of needed LTCH services to residents of District 8. The
reviewer notes that the applicant does not provide documentation that
District 8 or Collier County residents are unable to obtain long-term care
services.
The applicant maintains that short-term acute care hospitals are not the
ideal setting for the treatment of medically complex patients for two
reasons:
LTCH appropriate patients reduce the short-term hospital’s ability to
care for acute patients admitted from the emergency room that need
intensive care services.
The cost to provide care to medically-complex patients is higher than
caring for these patients in a long-term care hospital.
19
Kindred asserts that comprehensive medical rehabilitation facilities are
not an appropriate option for treating LTCH patients because they
cannot withstand three or more hours of therapy a day and are not
stable enough to be managed by a physician whose specialty is physical
medicine. Neither is a SNF, the applicant states, an appropriate setting
for LTCH patients as these facilities are restricted to serving less
medically complex cases with more stable patients.
The applicant provides a table to illustrate the difference in services
offered in LTCHs, rehabilitation hospitals and SNFs.
19
Kindred cites page 11 of a Quality and Social Responsibility Report published annually by Kindred
and included in Appendix of CON application #10138.

CON Action Numbers: 10137 & 10138
44
LTCH Comparison to Rehab Hospitals and SNFs
LTCH
Rehab Hospital
SNFs
License
Acute hospital
Rehabilitation hospital
Skilled nursing facility
Medicare Certification
Long-term hospital
Rehabilitation hospital
Skilled nursing facility
Admitting Criteria
Meets acute criteria
75% falls into case
mix groups for rehab
Meets chronic care
criteria
Length of Stay
Minimum 25 days
Kindred ALOS 28
Typically 12-18
Typically Medicare 25-
35 days
Physician Involvement
Care directed by
multiple medical sub
specialties; daily visits
Care directed by
physical medicine
physician
Physician visits
weekly/monthly
Manage Critically Ill
Patients
Yes; telemetry
monitoring,
intravenous pressors,
dialysis
No
No
Patient
Characteristics
Typically after illness
from respiratory
disease, stroke or
infection; many
concurrent illnesses
Typically after knee,
hip or back surgery
Frequently requires
therapy services to
increase mobility
Vent Weaning
Vent weaning-major
focus; established
programs
Rare but vent weaning
possible in facilities
with vent program
Primarily
maintenance rather
than weaning
Respiratory Therapy
24 hours/ 7 days
in-house
Yes
No
No
Rehab Therapy
Approximately one
hour per patient day
Three hours per
patients day in at
least two disciplines
Approximately 1.5
hours per patient day
in at least two
disciplines
Source: CON application #10138, page 7.
Kindred states that the proposed facility’s goal is to resolve or stabilize
the patient’s multiple problems at the same time as they are receiving
rehabilitative services and then ultimately discharge them to a lower level
setting such as a skilled nursing facility, rehabilitation hospital or home.
Medical Treatment Trends
The applicant states that it treats the very sickest patients who require
the most intensive and life-saving medical interventions. These patients
have three to six concurrent active diagnoses and have suffered an acute
episode on top of several chronic illnesses. Kindred uses patient
screening to evaluate the appropriateness of patients, dictating that long-
term acute care is comparable to a traditional acute hospital level of care
and address each patient’s needs for high intensity of services because of
an intense severity of illness.
Kindred contends that the predominance of LTCHs throughout the
country is due in part to the following factors:

CON Action Numbers: 10137 & 10138
45
Federal recognition of the special role that LTCHs play in the health
care continuum as reflected in the separate certification category for
LTCHs and their separate reimbursement system.
The increasing need of short-term hospitals for discharge options for
their medically-complex long-term patients. This need has especially
grown since federal reimbursement changes made it financially
unfeasible for most nursing facilities to provide care to ventilator
patients and other high-acuity patients.
Increasing awareness and understanding of LTCH by physicians,
hospital discharge planners and other medical professionals—
especially a greater understanding of the benefits that LTCHs provide
to their medically complex patients.
The applicant asserts that the given inadequate supply of long-term care
hospital beds in District 8 creates financial losses for short-term
hospitals and limits the level of care that patients care receive. Kindred
maintains that its facilities are a cost-effective means of providing the
most appropriate, high quality services to the medically complex patient.
Kindred provides a detailed listing of the services it currently provides to
LTCH patients on pages 8-10 of CON application #10139, these include:
Respiratory services
IV services
Surgical services
Neurological services
Skin services
Renal services
Cardiac services
Additional services
The applicant states that Kindred hospitals employ aggressive therapy on
various fronts to improve patient outcomes as well as the psychosocial
needs of patients and families. Kindred maintains that the types of
medical conditions that necessitate long-term hospitalization are those
that warrant hospital level services but do not heal rapidly or repair
quickly. The applicant asserts that it has developed the expertise to
successfully care for the catastrophically ill, medically complex patient
outside of the traditional intensive care unit.
Kindred states that its ICU services are a vital part of the service offering
at the proposed facility that ensures patients receive the highest-quality,
most clinically appropriate care for medically-complex conditions. The
reviewer notes that the architectural review for this proposed facility
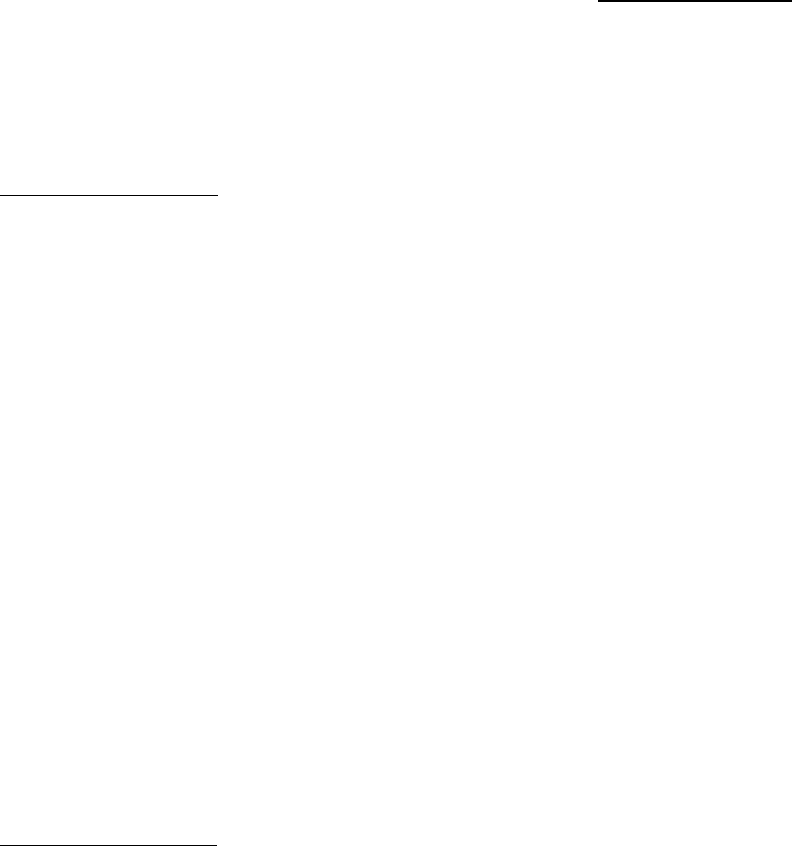
CON Action Numbers: 10137 & 10138
46
found the ICU patient bedroom clearance requirements insufficient to
meet the minimum clearances—a significant impact on the proposed
facility.
Market Conditions
The applicant indicates that the need for LTCH services in District 8 far
exceeds the current supply of long-term care hospital beds. Kindred
notes that the only LTCH in District 8 is approximately two hours away
from the southern portion of the district and contends that physicians in
the southern area of the district are not able to access the LTCH
continuum of care. The reviewer notes that the applicant does not
provide documentation regarding lack of access to long-term care for
District 8 and Collier County residents.
Kindred cites the letters of support included in Appendix 4 of CON
application #10138 as further documentation of the need for a Kindred
LTCH in Collier County. The applicant submitted 143 unduplicated
letters of support for the project, 140 letters were form letters. These
letters represented a number of health care providers including:
physicians, nurses, case managers and other therapists.
Kindred contends that the previously discussed population increase in
Collier County will result in greater demand for LTCH services. The
proposed facility will increase the availability of these services and ease
the burden of travel on patients, families and physicians.
Bed Need Analysis
Kindred estimated long-term bed need based on the acute care
discharges and days occurring to residents of the service area. The
applicant analyzed individual-level patient discharge data for the 12
months ending September 2011 for all hospitals in the State of Florida.
Kindred used this information to identify the number of actual short-
term acute care hospital patients and patient days which could be served
by the proposed long-term hospital.
The applicant used three patient characteristics in this analysis:
Diagnosis
Age
Length of Stay.

CON Action Numbers: 10137 & 10138
47
Kindred considered patients to be appropriate for long-term hospital care
if they are:
Residents of Collier, Lee or Hendry County
Eighteen years of age or older
Not assigned to an omitted Diagnosis Related Group (DRG)
Have a short-term hospital length of stay that exceeds their DRG-
specific national geometric mean length of stay by at least 16 days
(referral period [four days] + LTCH minimum length of stay [12 days]).
The applicant states that it estimates that during the 12 months ending
September 2011, there were approximately 20,147 potential long-term
care hospital days provided in the 10 short-term acute care hospitals in
Collier, Lee and Hendry Counties. Kindred maintains that an additional
3,096 potential long-term care hospital days were produced by service
area residents treated in short-term acute care hospitals elsewhere in
Florida. This results in a potential long-term care hospital average daily
census for District 8 to 64.
Kindred states that 150 residents of the service area received LTCH
hospital services elsewhere in the state of Florida—despite the significant
distance and cost involved—producing 5,041 long-term care hospital
days. The applicant contends that it is reasonable to assume that the
identified patients would return to the service area for LTCH care if such
a facility existed there. This results in a potential long-term care hospital
ADC of 14.
The applicant cites the expected 13.2 percent population growth in the
service area over the next five years and applies it the current potential
ADC, this results in a potential long-term care hospital ADC of 10.
Kindred then applies the long-term hospital target occupancy of 85
percent to the potential long-term care hospital bed need for CY 2017
equaling 103 beds. Subtracting the already approved LTCH project in
Lee County for 60 beds, the applicant produces an estimated net bed
need in CY 2017 of 43 beds. See the table below.
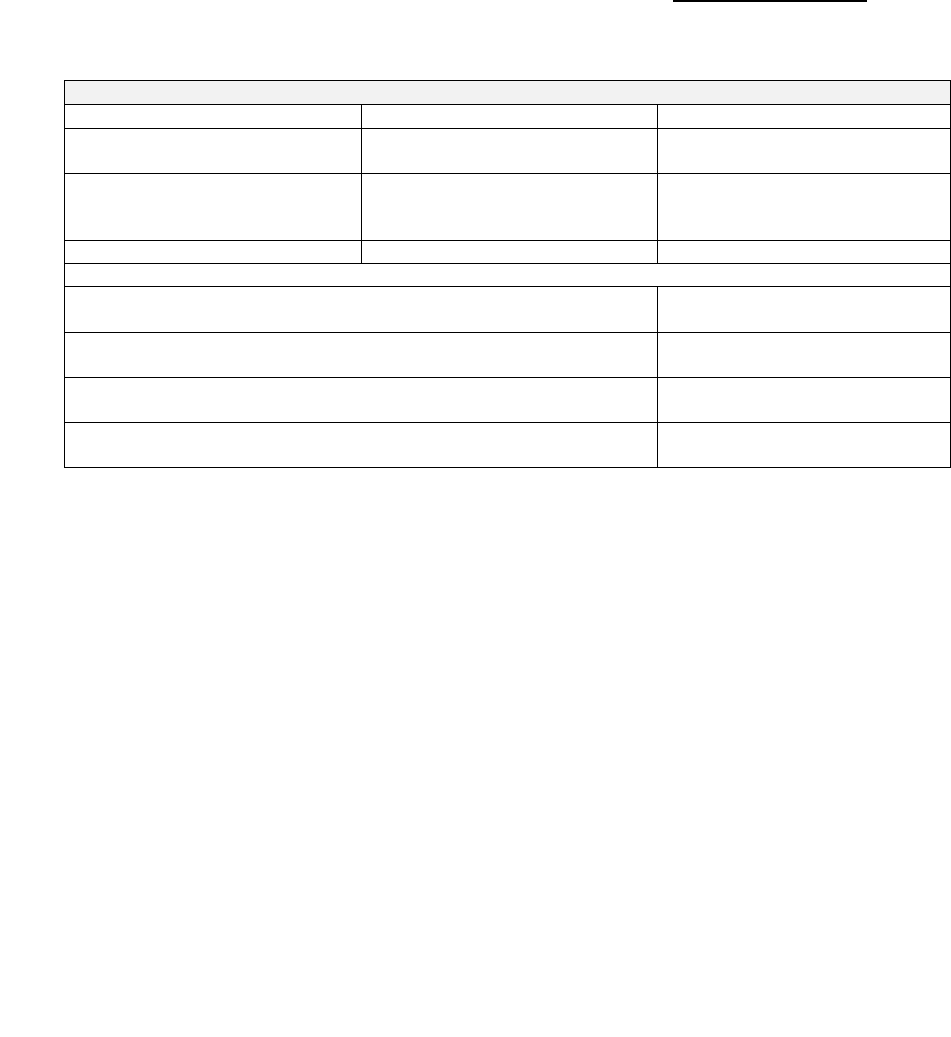
CON Action Numbers: 10137 & 10138
48
Bed Need Analysis Chart
Potential Hospital Days
Potential ADC
Current patients in short-term
acute care hospitals
23,243
64
Current patients seeking LTCH
care outside Collier, Lee or
Hendry County
5,041
14
Total
28, 284
78
The expected population growth for the service area of 13.2%
multiplied by total potential ADC from above
10
Added to total potential ADC from above for CY 2017 potential
ADC
88
CY 2017 potential ADC divided by target long-term care hospital
occupancy of 85%
103 beds
Subtract 60 potential LTCH beds for CON-approved project in
Lee County
43 LTCH bed need in Collier,
Lee and Hendry Counties
Source: CON reviewer based on information in the narrative on pages 13-14 of CON application #10138.
Kindred concludes that by using reasonable assumptions and actual
discharge data for the residents of Collier, Lee and Hendry Counties, the
above analysis clearly demonstrates that there is more than sufficient
need to justify and support the 40-bed long-term care hospital proposed
by herein.
2. Agency Rule Criteria
The Agency does not currently have adopted preferences or Rule criteria
relating to LTCHs.
3. Statutory Review Criteria
a. Is need for the project evidenced by the availability, quality of care,
efficiency, accessibility, and extent of utilization of existing health
care facilities and health services in the applicant’s service area?
ss. 408.035(1)(a) and (b), Florida Statutes.
There is one licensed LTCH with 40 licensed beds and one CON approved
LTCH with 60 approved beds in District 8. The licensed LTCH, Complex
Care Hospital at Ridgelake, had an occupancy level of 71.29 percent in
the 12-month period ending June 2011. The 60-bed CON approved
LTCH is not under construction at this time.
Landmark Hospital of Southwest Florida, LLC (CON #10137) states
that, as discussed in the need analysis, District 8 ranked last with
respect to:

CON Action Numbers: 10137 & 10138
49
The discharge rate to LTCHs
The number of LTCH beds
The number of LTCH beds per 1,000 persons aged 15 and older
The discharges per LTCH bed
With respect to benchmarking using the elderly population.
The applicant also asserts that reduced availability of LTCH services in
District 8 was associated with reduced access.
Landmark uses other rates to further illustrate the lack of availability
within District 8. Using the statewide average rate of 40.3977 for “beds
per 100,000 population”, the applicant yielded 173 LTCH beds to attain
parity with the state for District 8. Therefore, Landmark concludes that
too few LTCH beds exist in District 8 and that more are required to
assure better availability of LTCH services. The applicant maintains that
the proposed 50-bed facility is within the conservative parameters to
improve availability.
The applicant states that the severities of LTCH patients’ conditions
require attention to the quality of offered services in light of the
possibility of mortality. The central issue is where to place patients in an
environment that houses a critical mass of patients to make treatment
less costly and maximize limited health care dollars. Therefore, the
applicant concludes that accreditation with The Joint Commission and
Gold Seal approval is important to ensuring the best care occurs.
Landmark makes and continues to make this a condition of operation.
Landmark maintains that one of the many distinguishing features that it
will bring to the state is the use of the InTouch Health ® robot, which
extends the ability of the on-call physician to engage interactively in real
time with patients or staff. The applicant states that it is also evaluating
a nuanced platform that uses the iPad to create an electronic health
record.
Landmark contends that only 40 LTCH beds in District 8 are a barrier for
residents in the southern-most parts of the district as these beds are
located in Sarasota County. These beds are too distant to be a
reasonable referral and placement for residents in Lee and Collier
County. Landmark indicates that travel distances to LTCH services are
problematic for both the patient as well as the patient’s friends and
family. Travel for family and friends raise concern for a variety of
reasons, including:

CON Action Numbers: 10137 & 10138
50
Elderly persons traveling by car over distances when tired, or making
frequent trips (perhaps in peak times) increases the probability of
accidents.
Stress on the family as time is required to travel—the greater the
distance, the more time is required. The desire to see the family
member also may create stress to accommodate work schedules, time
out and visitation with the hospitalized family member.
Increased costs to the family for travel and loss of wages if leave is
required to be taken without pay.
The applicant maintains that the transport of LTCH patients over
distance can pose problems even with emergency vehicles due to the
unstable nature of the patients. Additionally, the source of a majority of
LTCH patients’ are transferred directly from acute care hospitals by
medical transport. Landmark asserts that using medical transports,
specifically if emergency vehicles provide it, take the vehicles away from
the county—making them unavailable for a period of time until the
vehicles return. This creates greater stress on the existing system to
cover transports locally. The reviewer notes that the applicant does not
provide documentation of any current logistical issue within Collier
County as regards to emergency transportation.
Landmark also states that in certain months of the year as well as
certain times of the day, traveling in District 8 can take much longer
between points of service due to traffic congestion. The impact of traffic
congestion would be negative of transporting fragile, unstable patients.
Given that the LTCH patient has high acuity, the applicant states that
the probability of mortality is also greater. The fragility of the patients’
condition increases the stress on family to visit and participate in the
care and comfort thereby making geographic accessibility an important
variable. Landmark contends that a LTCH within closer proximity to
Collier County is justified and would have a positive impact toward
improving access further. The applicant maintains that the approved
60-bed facility by Promise Hospital of Lee, Inc. will be located in Lee
County, further improving access to the District 8 population. Landmark
contends there is sufficient need for the Lee County LTCH and its
project.
Landmark indicates that Medicare is the major payer for LTCH patients
since 70 percent of patients are 65 years of age and older. The applicant
contends that statewide 73 percent of Florida’s LTCH cases’ care is
reimbursed by Medicare, with commercial insurers at 23.3 percent. See
the table below.
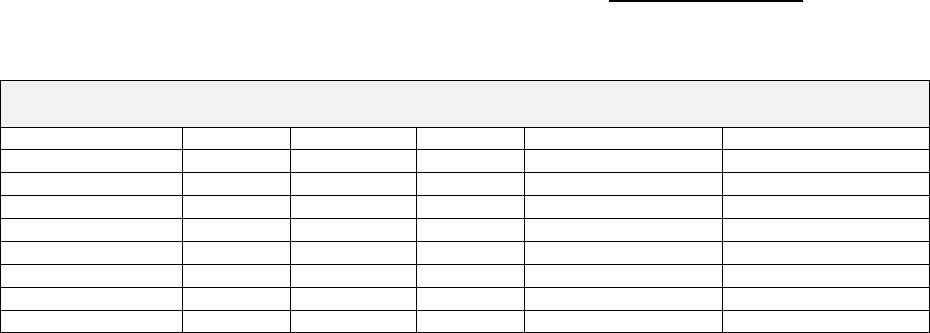
CON Action Numbers: 10137 & 10138
51
Charges Statewide by Payer for LTCHs
April 1, 2010 to March 31, 2011
Payer
Cases
Percent
ALOS
Total Charge/Case
Total Charge/Day
Charity
49
0.5%
34.9
$172,167
$4,939
Commercial
2,396
23.0%
35.5
$186,776
$5,266
Government
13
0.1%
42.0
$204,841
$4,877
Medicaid
149
1.4%
36.6
$161,982
$4,424
Medicare
7,632
73.3%
26.8
$120,178
$4,489
Self/Other
125
1.2%
80.0
$490,277
$6,128
Workers Comp
42
0.4%
43.9
$179,873
$4,095
Grand Total
10,406
100.0%
29.7
$141,148
$4,756
Source: CON application #10137, page 3-7.
The reviewer notes that the above table represents charges statewide.
Based on the Florida Hospital Uniform Reporting System (FHURS) 2010
Actual Reports, the breakdown for actual payments to LTCHs is as
follows: Medicare 79.5 percent, Medicaid 1.8 percent, HMO-PPO 14.9
percent, commercial insurance 2.4 percent and charity 1.4 percent.
The applicant maintains that Medicare drives policies on reimbursement
and the MS-LTCH-DRGs are dominant in creating the parameter for
payment that commercial insurers (which include managed care options)
adopt. Landmark contends that since federal policies require that LTCHs
be licensed as acute care hospitals in the state in which they operate and
that MS-LTCH-DRGs drive payment—financial access in large part will
be based upon the age and clinical factors for ensuring admission. The
applicant notes that financial penalties are imposed for short-stays and
readmissions, therefore the prevailing practice is to follow Medicare
eligibility and payment requirements to their fullest.
Kindred Hospitals East, LLC (CON #10138) contends that the proposed
facility will increase availability and accessibility, improve efficiency of
the services and enhance the overall quality of the continuum of care in
District 8.
The applicant maintains that the current LTCH facility in Sarasota
County is approximately two hours away from the southern portion of
the district causing a burden on patients, families and patient’s
physicians. Kindred states that denying a patient geographic
accessibility to interaction with family and physicians can be damaging
to the patient’s quality of care. The applicant contends that even with
the construction of Promise of Lee’s 60 CON-approved LTCH beds, there
is an estimated net bed need of 43 beds in District 8.

CON Action Numbers: 10137 & 10138
52
Kindred maintains that short-term acute care facilities, SNFs and other
subacute providers are not appropriate settings for long-term care
hospital patients. The applicant contends that its long-term care
facilities don’t compete but complement the existing health care
providers. Kindred states that the proposed facility will work with local
providers to offer a continuum of care within the community.
The applicant states that the proposed facility will improve efficiency of
services as it works with area providers to integrate a continuum of care
to promote efficient use of area resources and placement of patients in
the most appropriate setting. Kindred maintains that the establishment
of the proposed facility will promote efficient access to area residents
needing long-term hospital services.
Kindred cites its larger health care company stating that the proposed
facility will have improved efficiency because it will be able to utilize
centralized services at the corporate office such as purchasing, project
management, clinical/quality management, medical records and many
other services. This results in significant cost savings to the facility and
to patients.
b. Does the applicant have a history of providing quality of care? Has
the applicant demonstrated the ability to provide quality care?
ss. 408.035(1) (c), Florida Statutes.
Landmark Hospital of Southwest Florida, LLC (CON #10137) states
that it is an affiliate of Landmark Holdings of Missouri, LLC an operator
of LTCHs through affiliates. The applicant includes two articles citing
Landmark Hospital of Joplin’s ability to continue operations during a
blizzard and a multiple-vortex tornado due to successful disaster
planning and preparations.
The applicant maintains that all established affiliates of Landmark
Hospitals are accredited by The Joint Commission with commendation.
The proposed facility will follow the same pattern and engage in the same
preparations to achieve this distinction. Landmark asserts that practice
patterns are established to ensure the highest clinical standards in
nursing, clinical and medical care. The applicant states that corporate-
wide performance benchmarks and standards are enforced through a
continuous quality improvement system.

CON Action Numbers: 10137 & 10138
53
Landmark states that it strives to improve quality and outcomes through
the implementation of procedures and technologies. Some recent
developments that make staff more effective and enhance patient’s
outcomes include:
Techniques and new applications of research in wound care, adopting
the use of platelet-rich plasma therapy in place of negative-pressure
wound therapy.
Implementation of the InTouch Health ® RP-7 robot, which is
controlled by a board-certified physician that makes rounds. The
robot is not a substitute for doctors, but allows staff to interface with
a live board-certified physician for routine issues after hours with the
on-call physician available for emergencies.
Investigation into the implementation of the Electronic Health Record.
Interface technology allows the physician to have the record convert
basics for billing, and also access the latest information regarding
standards of practice and “diagnostic trees” for treatment.
The applicant states that it will deploy a range of innovations to allow
staff to become more effective in patient care and management, and as
an outcome, contain health care costs.
Landmark states that it selected Hunton Brady Architects to design the
proposed facility as this firm has forward-thinking designs in health care.
The proposed facility will be similar to Hunton Brady’s Florida Hospital
at Wesley Chapel, utilizing an arc design. This design affords greater
patient privacy and creates a “back of the house” access capability that
also enhances patient privacy. The design has all private rooms with
handicap accessible bathroom situated close to the bed and sleep-in
accommodations for families. Landmark notes that the footwall is
designed for future communication equipment that will allow patients to
have access to family members and other information.
The applicant indicates that Landmark’s response to the Joplin, Missouri
tornado and blizzard demonstrates its disaster planning and adequate
follow-through that creates a safe and secure environment. Landmark
indicates that this proposed environment of care includes structures that
support social interaction and socialization, the practice of self-
determination and choice while allowing for a variety of options in
treatment and daily routines.

CON Action Numbers: 10137 & 10138
54
Landmark states that it uses the collaborative care quality of care model,
based upon a multidisciplinary team approach. The applicant will
develop detailed care plans using an integrated medical record, so that
each member of the multidisciplinary team will have access to the work
of other professionals.
Pre-admission screenings and admission determinations, notes the
applicant, are made based upon pre-set criteria and guidelines for the
provision of long-term care. InterQual criteria is used to determine the
appropriateness of patient admission and continued hospital stay.
Landmark asserts that daily physician rounds are required. The six
major InterQual subsets treated by the applicant are:
Ventilator weaning
Respiratory complex
Other medically complex
Infectious diseases
Wound/skin
Cardiovascular/peripheral vascular.
Landmark indicates that a plan of care is initiated for each patient within
24 hours of admission and within the first week of admission the
transdisciplinary care team will meet formally to incorporate evaluations
of various disciplines and further develop the plan. Patients and their
families are offered opportunities to attend transdisciplinary team
conferences or family conferences during treatment at the hospital.
Landmark states that upon discharge patients are provided the
opportunity to choose continuum of care placement or services. When
home is the possible discharge destination, information is gathered
regarding the home environment and conducting home evaluations.
Landmark maintains that the quality improvement process involves
leaders of all levels of the organization to establish priorities for
performance improvement with the governing board retaining the
ultimate authority. Priorities for this plan include patient health
outcomes and high-volume, high-risk and/or problem-prone processes.
The hospital collects data on the following measures:
Performance improvement priorities
Operative or other procedures
Adverse events related to using moderate sedation
The use of blood and blood components

CON Action Numbers: 10137 & 10138
55
All reported and confirmed transfusion reactions
The results of resuscitation
Significant medication errors
Significant adverse drug reactions
Patient perceptions of the safety and quality of care, treatment and
services (including pain management).
The applicant states that Landmark hospitals utilize clinical practice and
evidence-based guidelines when designing or improving processes.
Annually, Landmark hospitals provide governance with written reports
on items such as the following:
All system or process failures
Number and type of sentinel events
Whether the patients and the families were informed of the event
All actions taken to improve safety (proactive and in response to
actual occurrence)
The determined number of distinct improvement projects to be
conducted
The results of the analyses related to adequacy of staffing.
Landmark also has organizational education requirements,
environmental safety activities, surveillance activities, emergency
management activities and infection control activities as part of its
performance improvement plan.
The applicant maintains that the structure, function, activities and
accomplishments of the performance improvement plan are reviewed at
least annually to assure that the program is achieving its objectives, is
demonstrating impact and is consistent with federal/state regulations as
well as The Joint Commission requirements. The reappraisal process
takes into account evidence of substantial impact and other internal and
external information reflecting the plan’s effectiveness.
Landmark hospitals have adopted benchmarks that are used in the
industry to measure performance as well as factors that are followed to
ensure that care meets standards. The applicant uses a performance
improvement dashboard to track quality improvement and safety
indicators. Landmark includes the 2011 performance improvement
dashboard for Landmark Hospital of Athens beginning on page 4-13 of
CON application #10137. Extracts from it appear below:

CON Action Numbers: 10137 & 10138
56
Ventilator Weaning Rate 86%
Catheter Associated UTI Rate (goal: <4) 0.79
Central Line Infection Rate 0.7
Ventilator Acquired Pneumonia Rate 1.7
Wound Volume Healing Rate 75%
Percent Discharged Home 11.9%
Percent Discharge Home w/Home Health 31.8%
The applicant contends that the above information reflects its ability to
deliver the highest quality of services in the clinical and medical
management of patients in the long-term care hospital. Landmark states
that it demonstrates consistency with and conformity to the statutory
criterion to provided quality care.
Kindred Hospitals East, LLC (CON #10138) states that it is committed
to providing high quality patient care and outstanding customer service.
The applicant maintains that it is driven by its commitment to its
mission and values. Kindred states that its management philosophy is
simple, “focus on people, on quality and customer service, and our
business results will follow.”
The applicant indicates that all Kindred LTCHs are accredited by the
Joint Commission, meet all conditions of participations for the Medicare
program as overseen by the National Centers for Medicare and Medicaid
Services and are licensed and inspected by state regulatory authorities.
Kindred states that it has operated LTCHs in Florida for 20 years
demonstrating a long history of providing high quality long-term acute
care services throughout the state.
Kindred includes its annual Quality and Social Responsibility Report in
Appendix 3 of CON application #10139. This report outlines the
company’s continued commitment to improving person-centered care
coordination. The applicant states that in 2011, Kindred’s long-term
acute care hospitals continued to outperform national benchmarks in
many key quality indicators while caring for sicker patients. Kindred
maintains that its performance has resulted in decreased length of stay,
fewer readmissions to general acute care hospitals and more patients
going home sooner at a lower cost to the health care system.
Kindred has 10 licensed LTCHs in Florida with a total of 745 licensed
beds. Agency data obtained April 19, 2012 indicates that Kindred
affiliated hospitals had 29 substantiated complaints during the previous
36 months. A single complaint can encompass multiple complaint
categories. The table below has these listed by complaint categories.
CON Action Numbers: 10137 & 10138
57
Kindred Substantiated Complaint Categories in the Past 36 Months
Complaint Category
Number Substantiated
Nursing Services
18
Quality of Care/Treatment
14
Resident/Patient/Client Assessment
7
Infection Control
4
Plan of Care
2
Admission, Transfer & Discharge Rights
2
Administration/Personnel
1
Restraints/Seclusion General
1
Physical Environment
1
Unqualified Personnel
1
Source: Agency for Health Care Administration complaint records.
c. What resources, including health manpower, management
personnel, and funds for capital and operating expenditures, are
available for project accomplishment and operation? ss. 408.035
(1)(d), Florida Statutes.
Landmark Hospital of Southwest Florida, LLC (CON #10137) is a
development stage enterprise. The audited financial statements of the
applicant for the period ending January 31, 2012 were analyzed for the
purpose of evaluating the applicant’s ability to provide operational
funding necessary to implement the project. The applicant indicated that
Carter Validis Mission Critical REIT (REIT) and Medistar Corporation of
Houston Texas will finance the construction of the hospital, own the
hospital and lease it to the applicant.
Capital Requirements:
The applicant indicates on Schedule 2 capital projects totaling $22.1
million which includes this project.
Available Capital:
The applicant indicates on Schedule 3 that funding for the project will be
provided by the REIT. The REIT provided no proof of available funding.
As of January 31, 2012, the applicant had $2.1 million in working
capital, and a $2.6 million line of credit from Montgomery Bank for
working capital, as well as a $1.8 million line of credit for equipment
purchases.
Staffing:
See the table below.
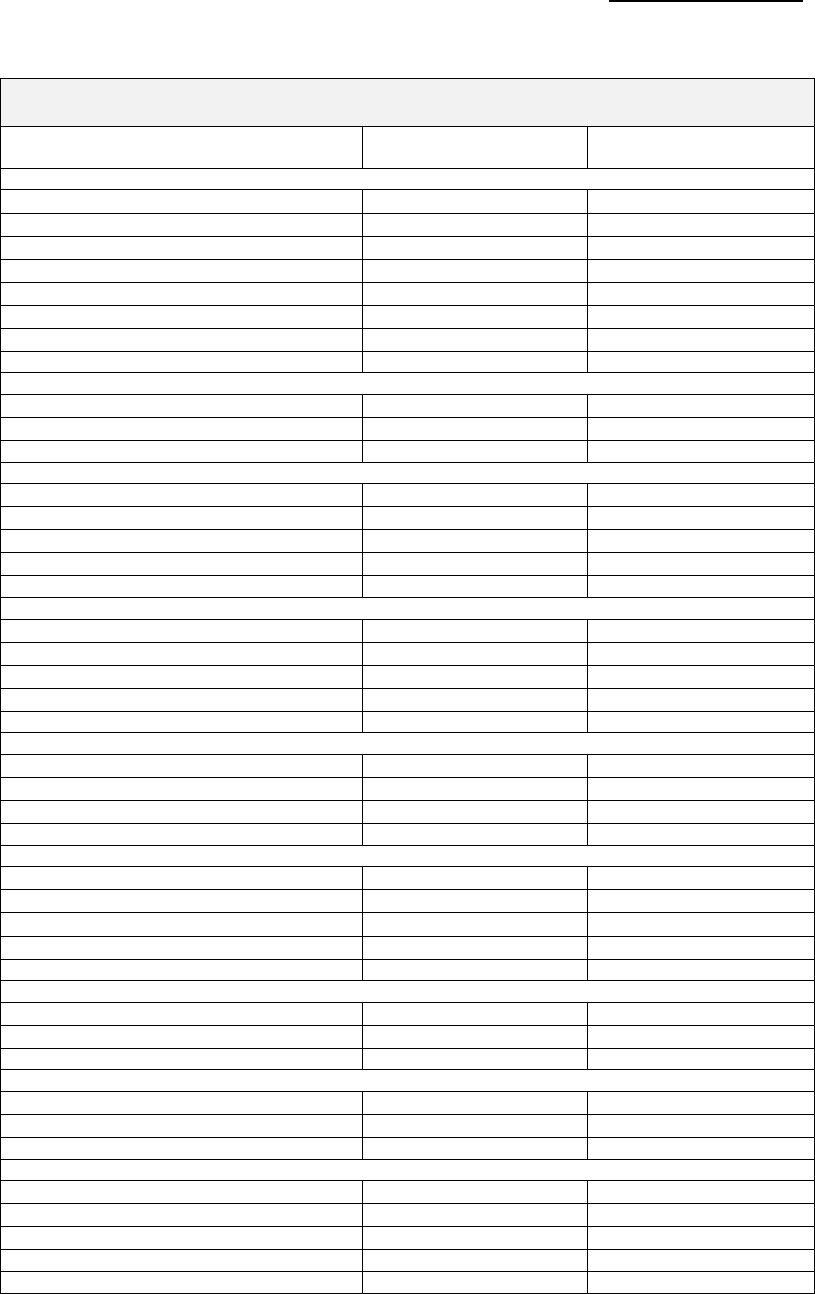
CON Action Numbers: 10137 & 10138
58
Landmark Hospital of Southwest Florida, LLC
Staffing Patterns for Year One and Year Two of Operations
Year One FTEs
Ending 12/31/2015
Year Two FTEs
Ending 12/31/2016
Administration
Chief Executive Officer
1.0
1.0
Chief Clinical Officer
1.0
1.0
Director of Quality
1.0
1.0
Director of Human Resources
1.0
1.0
Business Office Liaison
1.0
1.0
Director of HIM
1.0
1.0
HIM Assistant
1.0
1.0
TOTAL
7.0
7.0
Physicians
Medical Director
1.0
1.0
Hospitalist
2.0
4.0
Total
3.0
5.0
Nursing
RNs
26.0
40.0
Nurse Manager
--
1.0
Nurses Aides
6.0
10.0
Wound Care Nurse
1.0
1.0
TOTAL
33.0
52.0
Ancillary
Physical Therapist
1.0
1.0
Speech Therapist
--
1.0
Occupational Therapist
--
1.0
Respiratory Therapist
6.0
10.0
TOTAL
7.0
18.1
Dietary
Dietary Supervisor
1.0
1.0
Cooks
1.0
1.0
Dietary Aides
1.0
2.0
TOTAL
3.0
4.0
Social Services
Social Service Director
1.0
1.0
Activity Director
1.0
1.0
Activities Assistant
1.0
2.0
Other
--
--
Total
3.0
4.0
Housekeeping
Housekeeping Supervision
1.0
1.0
Housekeepers
3.0
5.0
Total
4.0
6.0
Other
Respiratory Manager
1.0
1.0
Clinical Educator
1.0
1.0
Total
2.0
2.0
Plant Maintenance
Maintenance Supervisor
1.0
1.0
Maintenance Assistance
1.0
2.0
Other: Security
3.0
4.0
TOTAL
5.0
7.0
GRAND TOTAL
68.0
100.0
Source: CON application #10138, Schedule 6.

CON Action Numbers: 10137 & 10138
59
The applicant notes that staffing patterns and the number of FTEs are
based on the historical experience of management.
Conclusion:
Funding for this project and the capital budget is entirely dependent on a
third party’s ability to fund the construction of the hospital. It is the
applicant’s plan to lease the land and buildings from the third party.
Kindred Hospitals East, LLC (CON #10138): The audited financial
statements of the applicant were reviewed for the period ending
December 31, 2011, for the purpose of evaluating the applicant’s ability
to provide the capital and operational funding necessary to implement
the project. The applicant indicated that its parent company, Kindred
Healthcare, Inc. (parent), would provide funding for this project.
Therefore, we have also evaluated the parent’s December 31, 2011, 10-K
to evaluate the parent’s ability to fund the project.
Short-Term Position - Applicant:
The applicant’s current ratio of 2.2 is slightly above average and
indicates current assets are approximately 2.2 times current liabilities, a
good position. The working capital (current assets less current liabilities)
of $77.0 million is a measure of excess liquidity that could be used to
fund capital projects. The ratio of cash flow to current liabilities of 0.2 is
well below average and a weak position which may indicate difficulties in
securing future debt. Overall, the applicant has an adequate short-term
position (See Table 1).
Short-Term Position – Parent:
The parent’s current ratio of 1.5 is slightly below average and indicates
current assets are approximately 1.5 times current liabilities, an
adequate position. The working capital (current assets less current
liabilities) of $384.4 million is a measure of excess liquidity and is
sufficient to cover the capital budget multiple times. The ratio of cash
flow to current liabilities of 0.2 is well below average and a weak position.
Overall, the parent has an adequate short-term position. (See Table 1).
Long-Term Position—Applicant:
The ratio of long-term debt to net assets of 0.0 is well below average and
indicates the applicant has equity to acquire future debt financing
against if necessary, a good position (apparently all long-term debt is
held by the parent). The ratio of cash flow to assets of 5.1 percent is
below average and a weak position. The most recent year the applicant
reported a net operating loss of $40,099,916, which resulted in a
negative 6.1 percent operating margin, a weak position. Overall, the
applicant has a moderately weak long-term position. (See Table 1).

CON Action Numbers: 10137 & 10138
60
Long-Term Position – Parent:
The ratio of long-term debt to net assets of 1.5 is above average and
indicates that long-term debt exceeds equity, a weak position. The ratio
of cash flow to assets of 3.7 percent is below average and a weak
position. The most recent year had revenues in excess of expenses of
negative $53.5 million, which resulted in a negative 1.0 percent operating
margin. Overall, the parent has a weak long-term position. (See Table 1)
TABLE 1
Kindred Hospitals East, LLC (Applicant)
Kindred Healthcare, Inc. (Parent)
Applicant
Parent
12/31/11
12/31/11
Current Assets (CA)
$140,798,848
$1,233,282,000
Cash and Current Investment
$220,308
$41,561,000
Total Assets (TA)
$279,715,108
$4,138,493,000
Current Liabilities (CL)
$63,772,299
$848,923,000
Total Liabilities (TL)
$67,968,453
$2,817,952,000
Net Assets (NA)
$211,746,655
$1,320,541,000
Total Revenues (TR)
$659,072,439
$5,521,763,000
Interest Expense (Int)
$9,693,120
$80,919,000
Excess of Revenues Over Expenses (ER)
($40,068,948)
($53,481,000)
Cash Flow from Operations (CFO)
$14,213,871
$153,706,000
Working Capital
$77,026,549
$384,359,000
FINANCIAL RATIOS
Applicant
Parent
12/31/11
12/31/11
Current Ratio (CA/CL)
2.2
1.5
Cash Flow to Current Liabilities (CFO/CL)
0.2
0.2
Long-Term Debt to Net Assets (TL-CL/NA)
0.0
1.5
Times Interest Earned (ER+Int/Int)
1.0
0.3
Net Assets to Total Assets (NA/TA)
75.7%
31.9%
Operating Margin (ER/TR)
-6.1%
-1.0%
Return on Assets (ER/TA)
0.0%
-1.3%
Operating Cash Flow to Assets (CFO/TA)
5.1%
3.7%
CON Action Numbers: 10137 & 10138
61
Capital Requirements:
Schedule 2 indicates total capital projects of $50,928,366, which
includes the CON subject to this review.
Available Capital:
While the applicant is an on-going corporation, it states on Schedule 3,
funding for this project will be operating cash flows from the applicant’s
parent company, Kindred Healthcare, Inc.
In support of its ability to fund the project, the applicant provided a letter
of financial commitment from the parent company and a copy of Kindred
Healthcare, Inc.’s 10-k filing with the Securities and Exchange
Commission. According to the audit, the parent has working capital
available of $384.4 million and cash flow from operations of $153.7
million. Staff has been notified that that the architectural plans for the
hospital as filed must undergo significant modifications to be acceptable.
The effect on cost and scheduling is unknown and it is unclear if a
material change in cost would impact the applicant’s decision to go
forward. However, the parent could fund a six fold increase in the
capital budget through working capital alone and therefore, would likely
be able to fund this project even if the cost increased materially.
Staffing:
See the table below.

CON Action Numbers: 10137 & 10138
62
Year One FTEs
Ending 12/31/2015
Year Two FTEs
Ending 12/31/2016
Administration
Administrator
1.0
1.0
Chief Clinical Officer
1.0
1.0
Director of Human Resources
1.0
1.0
Controller
1.0
1.0
Secretary/Admin Assistants
2.0
2.0
Other: Accounting, Case
Management, Purchasing, et al
17.0
21.0
TOTAL
23.0
27.0
Physicians
Medical Director
Contracted Service
Contracted Service
Nursing
RNs
11.0
22.9
LPNs
3.2
6.8
Nurses Aides
5.9
12.6
Wound Care
0.7
1.4
Nurse Administrators
7.0
9.0
Other: Non-productive time
1.8
3.8
TOTAL
29.6
56.5
Ancillary
Respiratory Therapist
5.9
12.0
Other: Non-productive time
0.5
1.1
Other: Pharmacy, Radiation,
Laboratory, Dialysis
3.0
5.0
TOTAL
9.4
18.1
Dietary
Dietary Supervisor
1.0
1.0
Dietician
1.0
2.0
Cooks
2.0
2.0
Dietary Aides
2.0
3.0
TOTAL
6.0
8.0
Housekeeping
Housekeeping Supervision
Contracted Service
Contracted Service
Housekeepers
Contracted Service
Contracted Service
Laundry
Laundry Supervisor
Contracted Service
Contracted Service
Laundry Aides
Contracted Service
Contracted Service
Plant Maintenance
Director of Plant Operations
1.0
1.0
Maintenance Assistant
1.0
1.0
TOTAL
2.0
2.0
GRAND TOTAL
70.0
111.5*
Source: CON application #10138, Schedule 6.
*This number totals 111.6.
The applicant notes that the majority of FTEs required by the
implementation of the proposed project are direct care givers consisting
of a mix of RNs, LPNs and CNAs based on hours per patient day basis.
Non-clinical and clinical staffing levels, wage rates and compensation
were based upon similar factors at Kindred Hospital Bay Area-St.
Petersburg, a similar Kindred hospital.

CON Action Numbers: 10137 & 10138
63
Kindred states that there will be physical, rehab and occupational
therapists working in the hospital but that these will technically be
employees of RehabCare Services Division, an operating diving of Kindred
Healthcare. Therefore, this is a contracted service.
Conclusion:
Funding for this project and the entire capital budget should be available
as needed.
d. What is the immediate and long-term financial feasibility of the
proposal? ss. 408.035(1)(f), Florida Statutes.
A comparison of the applicant’s estimates to the control group values
provides for an objective evaluation of financial feasibility, (the likelihood
that the services can be provided under the parameters and conditions
contained in Schedules 7 and 8), and efficiency, (the degree of economies
achievable through the skill and management of the applicant). In
general, projections that approximate the median are the most desirable,
and balance the opposing forces of feasibility and efficiency. In other
words, as estimates approach the highest in the group, it is more likely
that the project is feasible, because fewer economies must be realized to
achieve the desired outcome.
Conversely, as estimates approach the lowest in the group, it is less
likely that the project is feasible, because a much higher level of
economies must be realized to achieve the desired outcome. These
relationships hold true for a constant intensity of service through the
relevant range of outcomes. As these relationships go beyond the
relevant range of outcomes, revenues and expenses may, either, go
beyond what the market will tolerate, or may decrease to levels where
activities are no longer sustainable.
It should be noted that currently, a moratorium exists on new LTCH
beds. The Affordable Care Act extended the moratorium (with few
exceptions) from December 28, 2010 until December 28, 2012. These
provisions of the Act are scheduled to sunset at that time. If the
moratorium is once again extended then these projects will not be
permitted to go forward and thus not be feasible.
Landmark Hospital of Southwest Florida, LLC (CON #10137):
Projected net revenue and expenses of the applicant will be compared to
hospitals in the Long Term Acute Care Group (Group 12). An intensity
factor of 1.0774 was calculated for the applicant by taking the projected
average length of stay indicated and dividing it by the weighted average
length of stay for the peer group. This methodology is used to adjust the

CON Action Numbers: 10137 & 10138
64
group values to reflect the intensity of the patient as measured by length
of stay. Per diem rates are projected to increase by an average of 3.1
percent per year. Inflation adjustments were based on the new CMS
Market Basket, 4th Quarter, 2011.
Gross revenues, net revenues, and costs were obtained from Schedules 7
and 8 in the financial portion of the application and compared to the
control group as a calculated amount per adjusted patient day. For the
total hospital comparison, we used the applicant’s historic adjustment
factor for patient days.
Projected net revenue per adjusted patient day (NRAPD) of $1,737 in year
one and $1,784 in year two is between the control group median and
highest values of $1,416 and $1,885 in year one and $1,459 and $1,941
in year two. With net revenues falling between the median and highest
level, the facility is expected to consume health care resources in
proportion to the services provided. (See Table 1).
Anticipated costs per adjusted patient day (CAPD) of $2,191 in year one
and $1,889 in year two is between the control group median and highest
values of $1,378 and $2,929 in year one and $1,420 and $3,017 in year
two. With projected cost falling between the median and highest level,
the facility is expected to spend on health care in proportion to the
services provided. Costs appear to be reasonable. (See Table 2). The
applicant is projecting a decrease in CAPD between year one and year
two of $302, or 13.8 percent. It should be noted that this application is
for a new facility. The first year of operation has a below average
occupancy rate. The low occupancy rate decreases economies of scale
and as the occupancy rate increases, CAPD would be expected to
decrease.
The year two projected operating loss for the hospital of $963,600
computes to an operating margin per adjusted patient day of a negative
$105 or a negative 5.9 percent which is between the control group lowest
and median values of a negative $1,208 and $9. The applicant projects
being profitable by year three. The year three projected operating income
for the hospital of $1,179,431 computes to an operating margin per
adjusted patient day of $87 or 4.9 percent which is between the control
group median and highest values of $9 and $189. Operating income
appears reasonable. (See Table 2).
CON Action Numbers: 10137 & 10138
65
TABLE 1
Landmark Hospital of Southwest Florida, LLC
CON #10137
Dec-16
YEAR 2
VALUES ADJUSTED
2010 DATA Peer Group 12
YEAR 2
ACTIVITY
FOR INFLATION
ACTIVITY
PER DAY
Highest
Median
Lowest
ROUTINE SERVICES
16,735,704
1,830
2,617
1,386
513
INPATIENT AMBULATORY
0
0
11
0
0
INPATIENT SURGERY
0
0
0
0
0
INPATIENT ANCILLARY SERVICES
0
0
5,504
3,527
1,375
OUTPATIENT SERVICES
0
0
7
0
0
TOTAL PATIENT SERVICES REV.
16,735,704
1,830
7,437
5,013
1,888
OTHER OPERATING REVENUE
0
0
13
3
0
TOTAL REVENUE
16,735,704
1,830
7,442
5,017
1,889
DEDUCTIONS FROM REVENUE
425,304
47
0
0
0
NET REVENUES
16,310,400
1,784
1,941
1,459
693
EXPENSES
ROUTINE
4,243,000
464
694
408
182
ANCILLARY
5,448,000
596
505
374
224
AMBULATORY
0
0
0
0
0
TOTAL PATIENT CARE COST
9,691,000
1,060
0
0
0
ADMIN. AND OVERHEAD
3,616,000
395
0
0
0
PROPERTY
3,967,000
434
0
0
0
TOTAL OVERHEAD EXPENSE
7,583,000
829
2,108
693
281
OTHER OPERATING EXPENSE
0
0
0
0
0
TOTAL EXPENSES
17,274,000
1,889
3,017
1,420
687
OPERATING INCOME
-963,600
-105
189
9
-1,208
-5.9%
PATIENT DAYS
9,143
ADJUSTED PATIENT DAYS
9,143
TOTAL BED DAYS AVAILABLE
18,250
VALUES NOT ADJUSTED
ADJ. FACTOR
1.0000
FOR INFLATION
TOTAL NUMBER OF BEDS
50
Highest
Median
Lowest
PERCENT OCCUPANCY
50.10%
91.7%
61.8%
19.2%
PAYER TYPE
PATIENT DAYS
% TOTAL
SELF PAY
232
2.5%
MEDICAID
0
0.0%
7.2%
1.5%
0.0%
MEDICAID HMO
314
3.4%
MEDICARE
6,312
69.0%
88.5%
61.1%
48.6%
MEDICARE HMO
0
0.0%
INSURANCE
2,146
23.5%
HMO/PPO
0
0.0%
49.4%
34.6%
1.3%
OTHER
139
1.5%
TOTAL
9,143
100%
CON Action Numbers: 10137 & 10138
66
TABLE 2
Landmark Hospital of Southwest Florida, LLC
CON #10137
Dec-17
YEAR 3
VALUES ADJUSTED
2010 DATA Peer Group 12
YEAR 3
ACTIVITY
FOR INFLATION
ACTIVITY
PER DAY
Highest
Median
Lowest
ROUTINE SERVICES
24,893,121
1,837
2,696
1,427
529
INPATIENT AMBULATORY
2,918
0
12
0
0
INPATIENT SURGERY
0
0
0
0
0
INPATIENT ANCILLARY SERVICES
0
0
5,669
3,633
1,416
OUTPATIENT SERVICES
0
0
7
0
0
TOTAL PATIENT SERVICES REV.
24,896,039
1,837
7,660
5,164
1,945
OTHER OPERATING REVENUE
0
0
14
3
0
TOTAL REVENUE
24,896,039
1,837
7,666
5,168
1,946
DEDUCTIONS FROM REVENUE
632,608
47
0
0
0
NET REVENUES
24,263,431
1,791
2,000
1,502
713
EXPENSES
ROUTINE
6,476,000
478
715
421
187
ANCILLARY
7,945,000
586
521
385
231
AMBULATORY
0
0
0
0
0
TOTAL PATIENT CARE COST
14,421,000
1,064
0
0
0
ADMIN. AND OVERHEAD
4,621,000
341
0
0
0
PROPERTY
4,042,000
298
0
0
0
TOTAL OVERHEAD EXPENSE
8,663,000
639
2,172
714
289
OTHER OPERATING EXPENSE
0
0
0
0
0
TOTAL EXPENSES
23,084,000
1,704
3,107
1,462
707
OPERATING INCOME
1,179,431
87
189
9
-1,208
4.9%
PATIENT DAYS
13,549
ADJUSTED PATIENT DAYS
13,549
TOTAL BED DAYS AVAILABLE
18,250
VALUES NOT ADJUSTED
ADJ. FACTOR
1.0000
FOR INFLATION
TOTAL NUMBER OF BEDS
50
Highest
Median
Lowest
PERCENT OCCUPANCY
74.24%
91.7%
61.8%
19.2%
PAYER TYPE
PATIENT DAYS
% TOTAL
SELF PAY
344
2.5%
MEDICAID
0
0.0%
7.2%
1.5%
0.0%
MEDICAID HMO
465
3.4%
MEDICARE
9,353
69.0%
88.5%
61.1%
48.6%
MEDICARE HMO
0
0.0%
INSURANCE
3,180
23.5%
HMO/PPO
0
0.0%
49.4%
34.6%
1.3%
OTHER
207
1.5%
TOTAL
13,549
100%

CON Action Numbers: 10137 & 10138
67
Conclusion:
Assuming that the REIT has adequate funding for the land acquisition
and construction of the facility and that the LTCH bed moratorium is not
extended, this project appears to be financially feasible.
Kindred Hospitals East, LLC (CON #10138): The applicant will be
compared to hospitals in the Long Term Acute Care Group (Group 12).
An intensity factor for comparative purposes of 1.1246 was calculated
based on the ratio of average length of stay for all Kindred long-term care
hospitals in the group, to the weighted average length of stay for the
group as a whole. We used the existing Kindred hospitals average length
of stay as a proxy for the applicant since average length of stay for this
project was not included in the application. This methodology is used to
adjust the group values to reflect the intensity of the patient as measured
by length of stay. Per diem rates are projected to increase by an average
of 3.1 percent per year. Inflation adjustments were based on the new
CMS Market Basket, 4nd Quarter, 2011.
Gross revenues, net revenues, and costs were obtained from Schedules 7
and 8 in the financial portion of the application and compared to the
control group as a calculated amount per adjusted patient day.
Projected net revenue per adjusted patient day (NRAPD) of $1,572 in year
one and $1,765 in year two falls between the control group median and
highest values of $1,475 and $1,952 in year one, and $1,519 and $2,011
in year two, respectively. With net revenues falling between the median
and highest level, the facility is expected to consume health care
resources in proportion to the services provided. (See Table 2).
Anticipated costs per adjusted patient day (CAPD) of $2,708 in year one
and $1,755 in year two is between the control group median and highest
values of $1,439 and $3,057 in year one and $1,482 and $3,149 in year
two. With projected cost between the median and highest value in the
control group in year one, costs appear reasonable (See Table 2). The
applicant is projecting a decreased CAPD between year one and year two
from $2,708 to $1,755, or 35.2 percent. It should be noted that this
application is for a new facility. The first year of operation has a below
average occupancy rate. The low occupancy rate decreases economies of
scale and as the occupancy rate increases, CAPD would be expected to
decrease.
The year two projected operating income for the project of $94,701
computes to an operating margin per adjusted patient day of $9, or 0.5
percent, which equals the control group’s median value of $9. With a
CON Action Numbers: 10137 & 10138
68
projected operating margin equaling the median value in the control
group, the operating margin appears reasonable and efficient.
TABLE 2
Kindred Hospitals East
CON #10138
Dec-16
YEAR 2
VALUES ADJUSTED
2010 DATA Peer Group 12
YEAR 2
ACTIVITY
FOR INFLATION
ACTIVITY
PER DAY
Highest
Median
Lowest
ROUTINE SERVICES
93,389,262
9,050
2,732
1,446
536
INPATIENT AMBULATORY
0
0
12
0
0
INPATIENT SURGERY
0
0
0
0
0
INPATIENT ANCILLARY SERVICES (P)
0
0
5,745
3,681
1,435
OUTPATIENT SERVICES (Q)
0
0
8
0
0
TOTAL PATIENT SERVICES REV. (R)
93,389,262
9,050
7,762
5,233
1,971
OTHER OPERATING REVENUE
0
0
14
3
0
TOTAL REVENUE
93,389,262
9,050
7,768
5,237
1,972
DEDUCTIONS FROM REVENUE
75,179,980
7,286
0
0
0
NET REVENUES
18,209,282
1,765
2,011
1,519
723
EXPENSES
ROUTINE
3,780,710
366
719
426
190
ANCILLARY
4,430,264
429
523
390
234
AMBULATORY
0
0
0
0
0
TOTAL PATIENT CARE COST
8,210,974
796
0
0
0
ADMIN. AND OVERHEAD
6,631,658
643
0
0
0
PROPERTY
3,271,949
317
0
0
0
TOTAL OVERHEAD EXPENSE (V)
9,903,607
960
2,201
723
293
OTHER OPERATING EXPENSE
0
0
0
0
0
TOTAL EXPENSES
18,114,581
1,755
3,149
1,482
723
OPERATING INCOME
94,701
9
189
9
-1,208
0.5%
PATIENT DAYS
10,319
ADJUSTED PATIENT DAYS
10,319
TOTAL BED DAYS AVAILABLE
14,600
VALUES NOT ADJUSTED
ADJ. FACTOR
1.0000
FOR INFLATION
TOTAL NUMBER OF BEDS
40
Highest
Median
Lowest
PERCENT OCCUPANCY
70.68%
91.7%
61.8%
19.2%
PAYER TYPE
PATIENT DAYS
% TOTAL
SELF PAY
0
0.0%
MEDICAID (BA)
107
1.0%
7.2%
1.5%
0.0%
MEDICAID HMO
0
0.0%
MEDICARE (AW)
6,007
58.2%
88.5%
61.1%
48.6%
MEDICARE HMO
2,182
21.1%
INSURANCE
1,911
18.5%
HMO/PPO (BF)
0
0.0%
49.4%
34.6%
1.3%
OTHER
112
1.1%
TOTAL
10,319
100%
CON Action Numbers: 10137 & 10138
69
Conclusion:
Assuming the applicant will be able to obtain funding for the project, the
40-bed LTCH appears to be financially feasible.
e. Will the proposal foster competition to promote quality and cost-
effectiveness? ss. 408.035 (1)(e), Florida Statutes.
Currently, a moratorium exists on new LTCH beds. The Affordable Care
Act extended the moratorium (with few exceptions) from December 28,
2010 until December 28, 2012. These provisions of the Act are
scheduled to sunset at that time. If the moratorium is once again
extended (and assuming the CON is granted), the applicants will have to
commence construction of the facility with hopes that the moratorium
will be lifted by completion date or forfeit the CON and re-apply if and
when the moratorium is lifted.
Competition to promote quality and cost effectiveness is driven primarily
by the best combination of high quality and fair price. Competition
forces entities to ultimately increase quality and reduce charges/cost in
order to remain viable in the market. The health care industry has
several factors that limit the impact competition has to promote quality
and cost-effectiveness. These factors include a disconnect between the
payer and the end user of health care services as well as a lack of
consumer friendly quality measures and information. These factors
make it difficult to measure the impact this project will have on
competition to promote quality and cost effectiveness. However, we can
measure the potential for competition to exist in a couple of areas.
Landmark Hospital of Southwest Florida, LLC (CON #10137):
Provider-Based Competition:
The applicant is applying to establish a new 50-bed long-term care
hospital in District 8. There is one existing long-term care hospital in
District 8 with a total of 40 long-term care beds. In addition, CON #9715
was granted for a 60-bed LTCH in Lee County. This CON was granted in
2007 and is still active. Therefore, this project would over double the
number of active beds and be a 50 percent increase in the approved beds
in the area.
Price-Based Competition:
The impact of the price of services on consumer choice is limited to the
payer type. Most consumers do not pay directly for hospital services.
Rather, they are covered by a third party payer. The impact of price-
based competition would be limited to third party payers that negotiate

CON Action Numbers: 10137 & 10138
70
price for services, namely managed care organizations. Therefore, price
competition is limited to the share of patient days that are under
managed care plans. The applicant is projecting 23.5 percent of patient
days from managed care payers with 72.4 percent of patient days
expected to come from fixed price government payer sources (Medicare
and Medicaid) (Table 2).
Conclusion:
The potential for provider based competition will increase. However,
price-based competition will likely be limited.
Kindred Hospitals East, LLC (CON #10138):
Provider-Based Competition:
The applicant is applying to establish a new 40-bed long-term care
hospital in District 8. There is one existing long-term care hospital in
District 8 with a total of 40 long-term care beds. In addition, CON #9715
was granted for a 60-bed LTCH in Lee County. This CON was granted in
2007 and is still active.
Therefore, this project would double the number of active beds and be a
40 percent increase in the approved beds in the area.
Currently, a moratorium exists on new LTCH beds. The Affordable Care
Act extended the moratorium (with few exceptions) from 12/28/2010
until 12/28/2012. These provisions of the Act are scheduled to sunset
at that time. If the Act is once again extended (and assuming the CON is
granted), the applicant will have to commence construction of the facility
with hopes that the moratorium will be lifted by completion date or forfeit
the CON and re-apply if and when the moratorium is lifted.
Price-Based Competition:
The impact of the price of services on consumer choice is limited to the
payer type. Most consumers do not pay directly for hospital services.
Rather, they are covered by a third party payer. The impact of price-
based competition would be limited to third party payers that negotiate
price for services, namely managed care organizations. Therefore, price
competition is limited to the share of patient days that are under
managed care plans. The applicant is projecting 18.5 percent of patient
days from managed care payers with 80.3 percent of patient days
expected to come from fixed price government payer sources (Medicare
and Medicaid) (Table 2).

CON Action Numbers: 10137 & 10138
71
f. Are the proposed costs and methods of construction reasonable? Do
they comply with statutory and rule requirements? ss. 408.035 (1)
(h), Florida Statutes; Ch. 59A-3 or 59A-4, Florida Administrative
Code.
The architectural reviews of the applications shall not be construed as
in-depth efforts to determine complete compliance with all applicable
codes and standards. The final responsibility for facility compliance
ultimately rests with the owner.
Landmark Hospital of Southwest Florida, LLC (CON #10137): The
50-bed freestanding LTCH will be designed as a three story building of
FBC Type IA and NFPA Type I (443). Both construction types are
suitable for the proposed facility. According to the narrative the building
will be fully sprinklered.
All of the 50-bed LTCH patient rooms are private and exceed the
minimum size requirements for new hospitals. Each patient room has a
private toilet room with a lavatory and a shower. It appears that all of
the new patient rooms have been made handicapped accessible. The
patient support spaces appear to meet all of the space requirements of
the current edition of the Florida Building Code (FBC).
According to the application and the submitted plans, this new hospital
will consist of a 30-bed medical/surgical unit, a 10-bed critical care unit
(CCU) and a 10-bed ICU--all located on level two. The plan provides all
the required support spaces, such as nurse stations, soiled utility, clean
utility, nourishment room, medication room, staff lounge/locker and
toilets. All of these spaces appear to be adequately sized and positioned
within the unit. There is also a speech therapy room and multi-purpose
room, located on this level.
Plans show two isolation rooms in the ICU unit. There is no indication of
an isolation room in the medical/surgical unit; a minimum of one
isolation room is needed to be in compliance with the guidelines for
design and construction of health care facilities.
The operating suite contains one operating room, a three-bed post
anesthesia care unit and a control/nursing station. All other supporting
service elements appear to be provided for in this operating suite.

CON Action Numbers: 10137 & 10138
72
In addition, all of the supporting service areas such as physical therapy,
emergency, a small lab, CT scan room, administration, medical records,
dining, dietary, maintenance, storage, other spaces and utilities as
required by the required codes have all been provided for a functional
facility.
According to the plans and the application, the entire building will
comply with all new codes and standards including the hurricane
provisions of the FBC, Chapter 4, and Section 419.4 including onsite
water storage, and protection of all utilities.
The cost estimated for the construction of the new LTCH appears to be
reasonable in comparison to similar projects. The time schedule for
construction, from the time of building permit to final inspection, seems
reasonable. The project is well designed and should meet or exceed code
requirements.
Although the area of ICU patient rooms is adequate some design
modification is needed to provide the required head clearance.
Additional exit for the dining room is required to be in compliance with
Florida Building Code.
The plans submitted with this application were schematic in detail with
the expectation that they will necessarily be revised and refined during
the design development (preliminary) and contract document stages.
Kindred Hospitals East, LLC (CON #10138): The 40-bed freestanding
long-term care hospital will be designed as a three-story building. The
application does not specify construction types for the facility nor the
minimum codes and standards that will apply. The disaster
preparedness requirement must be a key criteria in selecting a site,
building design and construction.
All 40-bed LTCH patient rooms including the 10-bed ICU unit are private
and appear to exceed the minimum size requirements for new hospitals.
Each of the patient rooms, except the ICU rooms, have private toilet
rooms with a lavatory and a shower. It appears that all of the new bed
rooms are meant to be made handicapped accessible. The plans do not
designate required isolation rooms.
According to the application and the submitted plan, this new hospital
will consist of two patient (second and third) floors with a 10-bed ICU on
the third floor. Both nursing units will be supported from large
centralized nursing stations.

CON Action Numbers: 10137 & 10138
73
The ICU unit contains 10 beds, none of which appear to meet the
minimum clearances. Additionally, toilets have not been separated from
patient rooms as required by the guidelines for design and construction
of health care facilities. The plan provides all the required support
spaces, such as soiled utility, clean utility, nourishment room and
medication room. All of these spaces appear to be adequately sized and
positioned within the unit.
There are supporting service areas on the first floor such as
administration, dietary, maintenance, storage, pharmacy, therapy,
radiology and other support spaces have been provided. The insufficient
information provided on the plan makes it impossible for the reviewer to
tell if the supporting service spaces will meet all of the space
requirements of the current edition of the required codes.
The applicant provides no information regarding building materials,
structural, finish, and mechanical/electrical systems. The plans
submitted with this application do not indicate smoke
compartmentalization and are not to scale as required by Schedule 9
item #6.
Compared to similar projects, the proposed cost estimate for the
construction of Kindred’s new LTCH is considerably high. The time
schedule for construction, from the time of building permit to final
inspection, is reasonable.
The ICU patient bedroom clearance requirements would have a
significant impact on the proposed facility.
Additional information regarding construction type,
compartmentalization and separation of hazardous areas is needed to
make a determination of code compliance.
g. Does the applicant have a history of providing health services to
Medicaid patients and the medically indigent? Does the applicant
propose to provide health services to Medicaid patients and the
medically indigent? ss. 408.035 (1)(i), Florida Statutes.
According to the 2010 Hospital Financial Data Report, reporting the most
recent data available, LTCHs in the state averaged 1.8 percent Medicaid
patient days and 1.4 percent charity patient days.
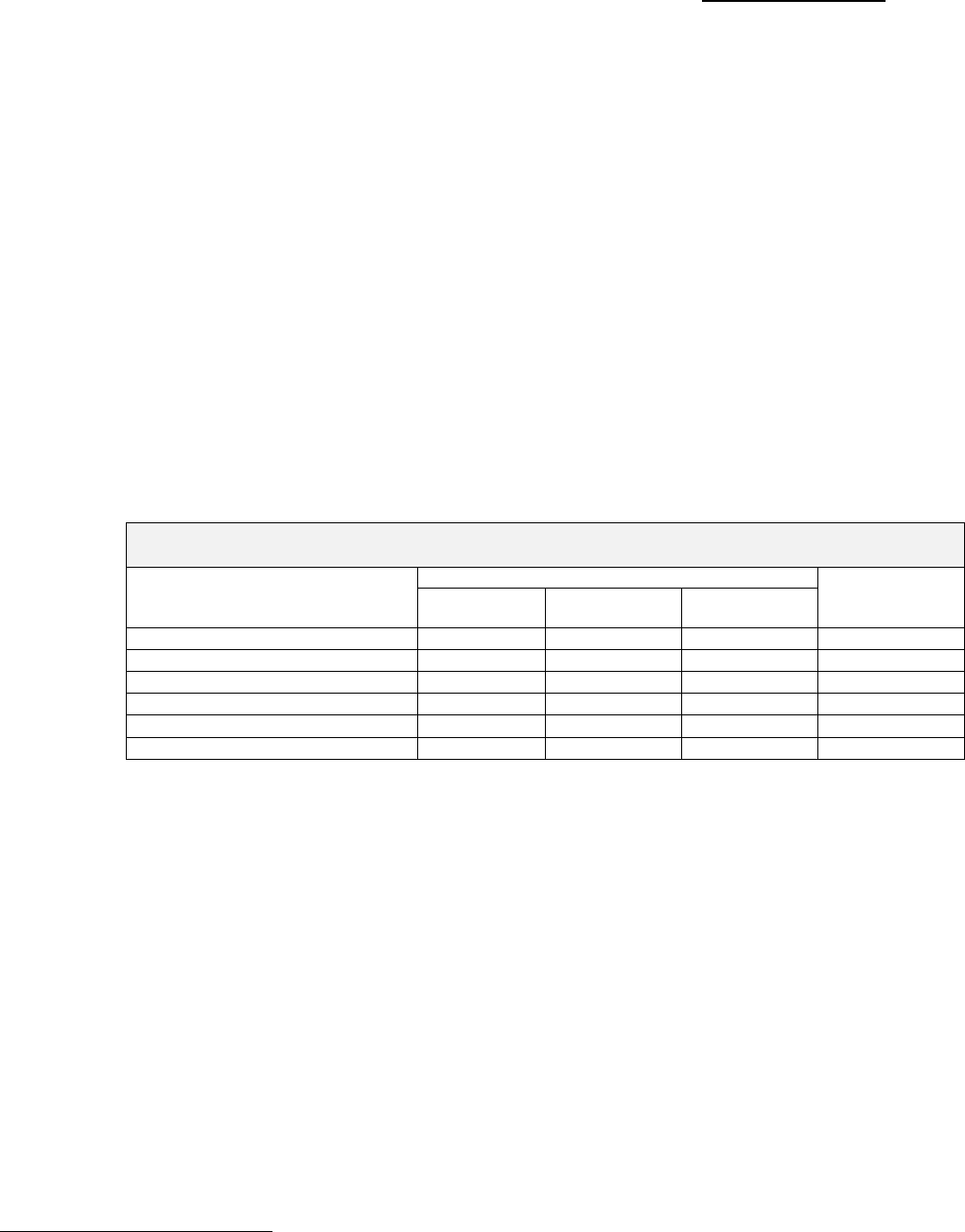
CON Action Numbers: 10137 & 10138
74
Landmark Hospital of Southwest Florida, LLC (CON #10137) states
that it was created recently and that the projections for the proposed
facility are based both on the Florida experience as well as the experience
of other Landmark Hospital’s affiliates.
The applicant indicates that the 2012 Long Term Care Group financial
data reported in the Agency’s FY 2009 Hospital Financial Data publication
shows a mean of 2.94 percent and median of 2.53 percent for Medicaid
and Charity Care—with a standard deviation of 1.8 percent. Landmark
maintains that the proposed facility will exceed the statewide experience.
The reviewer notes that the FY 2010 Hospital Financial Data shows a
mean of 3.2 percent and median of 3.4 percent for Medicaid, Medicaid
HMO and charity care.
Landmark provides projected patient days by payer for the first three
years of operation. See the table below.
Projected Patient Days by Payer for Landmark’s Proposed LTCH
January 2015-December 2017
Payer
Patient Days
Distribution
of Days
Year One
(2015)
Year Two
(2016)
Year Three
(2017)
Medicare
3,929
6,312
9,353
69.03%
Medicaid/HMO
195
314
465
3.43%
Commercial Insurance
1,336
2,146
3,180
23.47%
Self-Pay/Charity
145
232
344
2.54%
Other
87
139
207
1.53%
Total
5,692
9,144
13,549
100.00%
Source: CON application #10137, page 9-1.
The applicant states that it is willing to condition approval of CON
#10137 on the projected 2.54 percent charity care. However, Landmark
states that the combined charity and Medicaid percentage projection is
5.97 percent—above the LTCH group mean and median. The applicant
concludes by stating that the approval of this application assures access
to long-term acute care services for Medicaid patients as well as the
medically indigent.
Kindred Hospitals East, LLC (CON #10138) states that it has a history
of providing health services to Medicaid patients and the medically
indigent. The applicant indicates that six of nine (see footnote below)
Kindred LTCHs in Florida exceeded the median Medicaid and charity
percentage of 3.39 percent.
20
Kindred commits to provide a combined
20
The reviewer notes that the FY 2010 Hospital Financial Data shows a median of 3.4 percent for
Medicaid, Medicaid HMO and charity care. Five of 10 Florida Kindred facilities exceeded the median.
One met this median. Four Kindred facilities did not.
CON Action Numbers: 10137 & 10138
75
two percent Medicaid and charity days showing its dedication to continue
its focus on providing high quality medical care to such patients who
many not otherwise have access to this care.
The applicant states that charity days occur after a patient has
exhausted both Medicare and Medicaid benefits. Kindred maintains that
the proposed facility in Collier County will continue to care for patients
after their Medicare and Medicaid benefits expire—as the number of
Medicaid patients increases, the likelihood of charity care days will also
increase. The proposed facility will not discriminate or deny any
individual access to care or services regardless of his/her ability to pay.
Below are Kindred’s projected patient days by payer for the first two
years of operation. See the table below.
Projected Patient Days by Payer for Kindred’s Proposed LTCH
January 2015-December 2016
Payer
Patient Days
Percent of Days
Year One
(2015)
Year Two
(2016)
Year One
(2015)
Year Two
(2016)
Corrected
Year Two
Percentages*
Medicare/Medicare HMO
3,824
8,189
79.5%
170.1%
79.4%
Medicaid
45
107
0.9%
1.0%
1.0%
Commercial Insurance
890
1,911
18.5%
39.7%
18.5%
Charity Care
55
112
1.1%
1.1%
1.1%
Total
4,814
10,319
100.0%
211.9%
100.0%
Source: CON application #10138 Schedule 7A.
*Kindred’s Schedule 7A showed the percentages in the year two percent of days column. The reviewer
corrected these to reflect a percentage out of one hundred.
F. SUMMARY
Landmark Hospital of Southwest Florida, LLC (CON #10137) proposes
to establish a 50-bed long-term care hospital in District 8, Collier
County. The applicant did not include potential sites for the proposed
facility.
The proposed hospital involves 56,809 GSF of new construction. Total
project cost per bed is $442,496. Total construction cost is estimated to
be $13,480,000 and total project cost is $22,124,800.
As a condition of approval, the applicant agrees to provide a minimum of
2.54 percent of the facility’s total annual patient days to charity.
Kindred Hospitals East, LLC (CON #10138) proposes to establish a 40-
bed LTCH to be located in Collier County, District 8. The applicant did
not include potential sites for the proposed facility.

CON Action Numbers: 10137 & 10138
76
The proposed hospital involves 56,581 GSF of new construction. Total
cost per bed is $873,033. Total construction cost is estimated to be
$17,075,774 and total project cost is $34,921,329.
As a condition of approval, the applicant agrees to provide a minimum of
two percent of the facility’s total annual patient days to Medicaid and
charity care patients combined.
After weighing and balancing all applicable review criteria, the primary
issues are summarized below:
Need:
Need is not published by the Agency for long-term care hospital beds. It
is the applicant's responsibility to demonstrate need.
Neither applicant demonstrated objectively measurable and fact-based
evidence to show that patients were unable to access needed services or
were harmed or their health care outcomes were worsened as a result of
their chosen treatment regimen.
Landmark Hospital of Southwest Florida, LLC (CON #10137)
concludes that the state, median and average bed rates return a final
need for District 8 of 39, 48 or 44 beds beyond the number of licensed
and approved LTCH beds.
The applicant maintains that the result of increasing the number of beds
within District 8 improves access and availability making the district in
closer parity with the others. Landmark states that there is clear
reduced access to LTCH services in District 8 as demonstrated by
patterns of use by county residents.
Landmark indicates that data show that patients 65 years and older
comprise 70 percent of LTCH cases and population growth in that age
cohort creates demand for care. These population estimates show that
growth will continue, further exacerbating the disparity in access and
availability of LTCH services in District 8 with just one 40-bed hospital.
Kindred Hospitals East, LLC (CON #10138) contends that as result of
the increase in the senior population, the financial and capacity burdens
on short-term hospitals from long-term patients will continue to
increase. Kindred asserts that the need for long-term care hospital
(LTCH) services in Collier County will exceed the capabilities of existing
LTCH facilities in the district thereby creating a substantial unmet need
in the delivery of health care in District 8.

CON Action Numbers: 10137 & 10138
77
The applicant asserts that the inadequate supply of long-term care
hospital beds in District 8 creates financial losses for short-term
hospitals and limits the level of care that patients receive. Kindred
maintains that its facilities are a cost-effective means of providing the
most appropriate, high quality services to the medically complex patient.
Kindred projects a net LTCH bed need in CY 2017 of 43 beds.
Quality of Care:
Landmark Hospital of Southwest Florida, LLC (CON #10137) states
that it is an affiliate of Landmark Holdings of Missouri, LLC an operator
of LTCHs through affiliates. The applicant provides a reasonable
description of its quality of care mechanisms.
Kindred Hospitals East, LLC (CON #10138) states that it has operated
LTCHs in Florida for 20 years demonstrating a long history of providing
high quality long-term acute care services throughout the state.
Kindred has 10 licensed LTCHs in Florida with a total of 745 licensed
beds. Agency data obtained April 19, 2012 indicates that Kindred
affiliated hospitals had 29 substantiated complaints during the previous
36 months.
Cost/Financial Analysis
Landmark Hospital of Southwest Florida, LLC (CON #10137):
Funding for this project and the capital budget is entirely dependent on a
third party’s ability to fund the construction of the hospital. It is the
applicant’s plan to lease the land and buildings from the third party.
Assuming that the REIT, the third party, has adequate funding for the
land acquisition and construction of the facility and that the LTCH bed
moratorium is not extended; this project appears to be financially
feasible.
Kindred Hospitals East, LLC (CON #10138) Funding for this project
and the entire capital budget should be available as needed.
Assuming the applicant will be able to obtain funding for the project and
that the LTCH moratorium is not extended, this project appears to be
financially feasible.

CON Action Numbers: 10137 & 10138
78
Architectural Analysis:
Landmark Hospital of Southwest Florida, LLC (CON #10137): This
new hospital will be designed as a three-story building of FBC Type IA
and NFPA Type I (443)—both suitable for the proposed facility. The
building will be fully sprinklered.
According to the plans and the application, the entire building will
comply with all new codes and standards including the hurricane
provisions of the FBC, Chapter 4, and Section 419.4 including onsite
water storage, and protection of all utilities.
The cost estimated for the construction of the new LTCH appears to be
reasonable in comparison to similar projects. The time schedule for
construction, from the time of building permit to final inspection, seems
reasonable. The project is well designed and should meet or exceed code
requirements.
Kindred Hospitals East, LLC (CON #10138): The application does not
specify construction types for the facility nor the minimum codes and
standards that will apply. The disaster preparedness requirement must
be a key criteria in selecting a site, building design and construction.
Compared to similar projects, the proposed cost estimate for the
construction of the proposed new LTCH is considerably high. The time
schedule for construction, from the time of building permit to final
inspection, is reasonable.
The ICU unit contains 10 beds, none of which appear to meet the
minimum clearances. Additionally, toilets have not been separated from
patient rooms as required by the guidelines for design and construction
of health care facilities. The ICU patient bedroom clearance
requirements would have a significant impact on the proposed facility.
Additional information regarding construction type,
compartmentalization and separation of hazardous areas is needed to
make a determination of code compliance.
G. RECOMMENDATION
Deny CON #10137 and CON #10138.
CON Action Numbers: 10137 & 10138
79
AUTHORIZATION FOR AGENCY ACTION
Authorized representatives of the Agency for Healthcare Administration
adopted the recommendation contained herein and released the State
Agency Action Report.
DATE:
James B. McLemore
Health Services and Facilities Consultant Supervisor
Certificate of Need
Jeffrey N. Gregg, Director
Florida Center for Health Information and Policy Analysis
