10 Journey Handout Tenth Mile And Course Evaluation
User Manual: 10-Journey-handout-Tenth-Mile-and-course-evaluation
Open the PDF directly: View PDF ![]() .
.
Page Count: 9
Parent Child Journey
An Individualized Approach to Raising Your Challenging Child
by Dan Shapiro, MD
Tenth Mile: Weaknesses, Strengths, and Independence
(followed by course evaluation)
Realistic expectations
Don’t expect too much
Don’t expect too little
Do assessment before intervention
Do not think “can versus can’t”; do think “easy versus difficult”
Do not confuse inconsistency with inability
Do break it down
Don’t underestimate the importance of patience and hard work
Do consider response to intervention
Do promote self-awareness and self-responsibility
Do not just focus on weaknesses; do nurture strengths
Accommodations versus interventions
Acceptance versus development
Dependence versus independence
Public versus private
Inconsistency versus Consistency
Alternatives versus persistence
504 versus IEP
Empathy and common sense versus expertise and science
Identify the biggest remaining factors
2

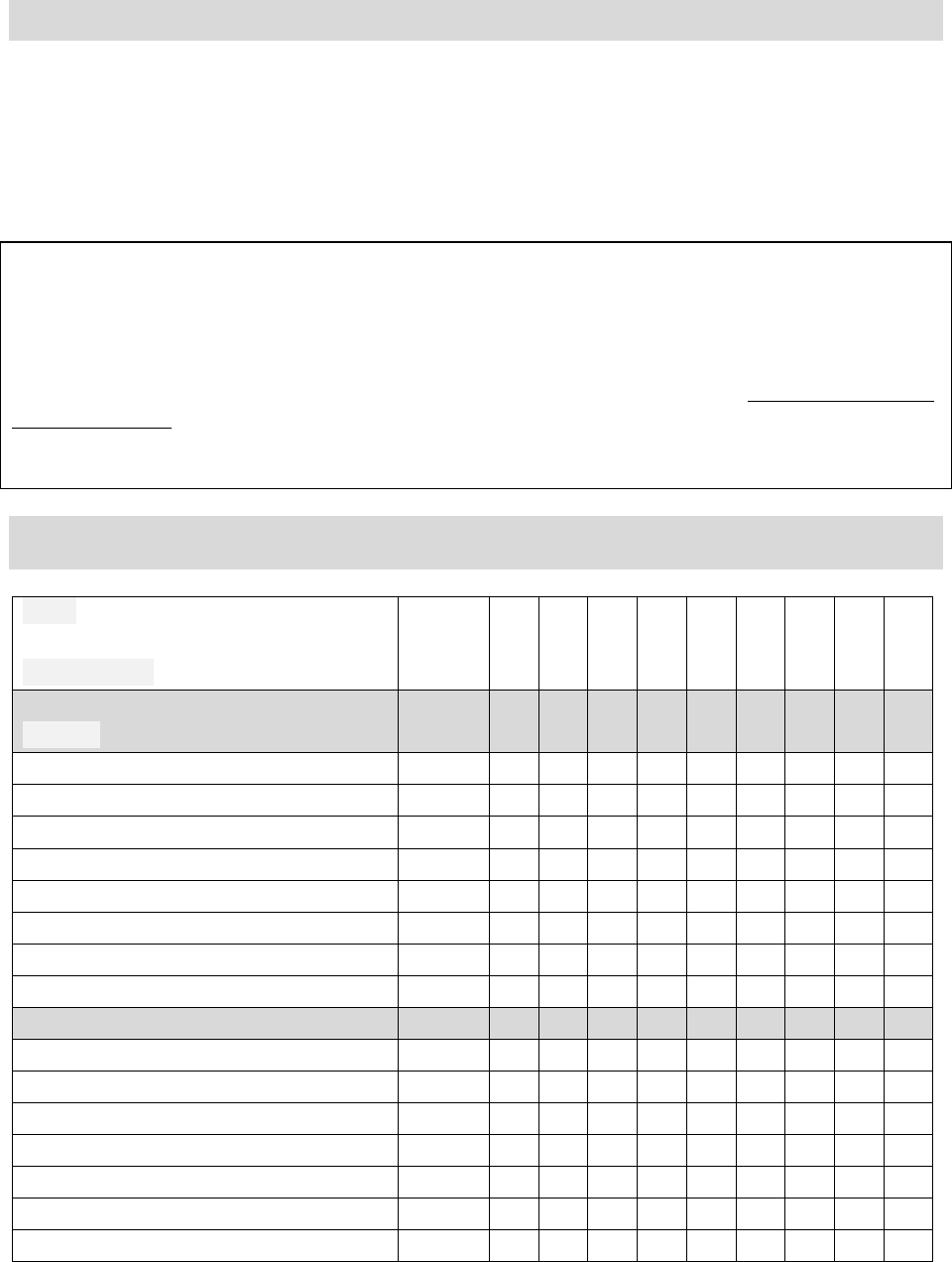
Relative Impact Scale
Rate each facet: 0, insignificant (no big deal); 1, causes a minor degree of impairment (little deal);
2, causes a moderate degree of impairment (medium deal); 3, causes a severe degree of impairment (bid deal)
Gander facet Relative impact 0–3
Temperament
Motor activity level
Impulsivity
Attention span
Initial reaction
Adaptability
Intensity of reaction
Usual mood
Regularity / predictability
Sensory
Hearing speech
Hearing noise
Vision
Taste
Smell
Light touch
Deep touch
Movement / body position in space
Internal body awareness / Physical symptoms
Skill
Fine motor
Handwriting
Gross motor
Speaking
Listening
Writing
Reading
Understanding spatial relations
Visual arts
Music
Math
Time awareness
Planning, organization, and implementation
Social skills
Life Stresses
Physical health, environment, school placement
Who ya gonna call?
For motor activity level, impulsivity, attention span:
o Medication: pediatrician, child psychiatrist, developmental-behavioral pediatrician
o Behavior therapy: behavior analyst, psychologist, social worker
For initial reaction, adaptability, intensity of reaction, usual mood, regularity/ predictability:
o Cognitive-behavioral therapy: psychologist, social worker, behavior analyst
o Medication: child psychiatrist, developmental-behavioral pediatrician
For sensory differences:
o Occupational therapist, psychologist, behavior analyst
For fine motor, handwriting:
o Occupational therapist
For gross motor:
o Physical therapist, sports therapist, occupational therapist
For language; speaking, listening, writing, reading:
o Speech-language therapist, teacher, tutor
For understanding spatial relations, visual arts:
o Art teacher / therapist
For music:
o Music teacher / therapist
For math:
o Math teacher / tutor
For time awareness, planning, organization and implementation:
o Speech-language therapist, executive skills coach, teacher / tutor
For social skills:
o Individual, group or parent-centered therapy: psychologist, speech-language therapist,
social worker, developmental consultant
For physical health, environmental /life-stresses, school placement:
o Social worker, primary care or specialist physician, psychologist, marriage counselor,
special education consultant
For care coordination: pediatrician, school counselor, or many of the specialists listed above.
Ideally, the case manager is someone with broad developmental expertise and deep familiarity
with local resources. Obviously, he or she needs to know your child well and earn your trust.
An increasing number of communities have “navigators” who assume this role.
The science of choosing specific interventions
Seek out objective experts
Do not trust just one source or one study
Don’t speculate, experiment
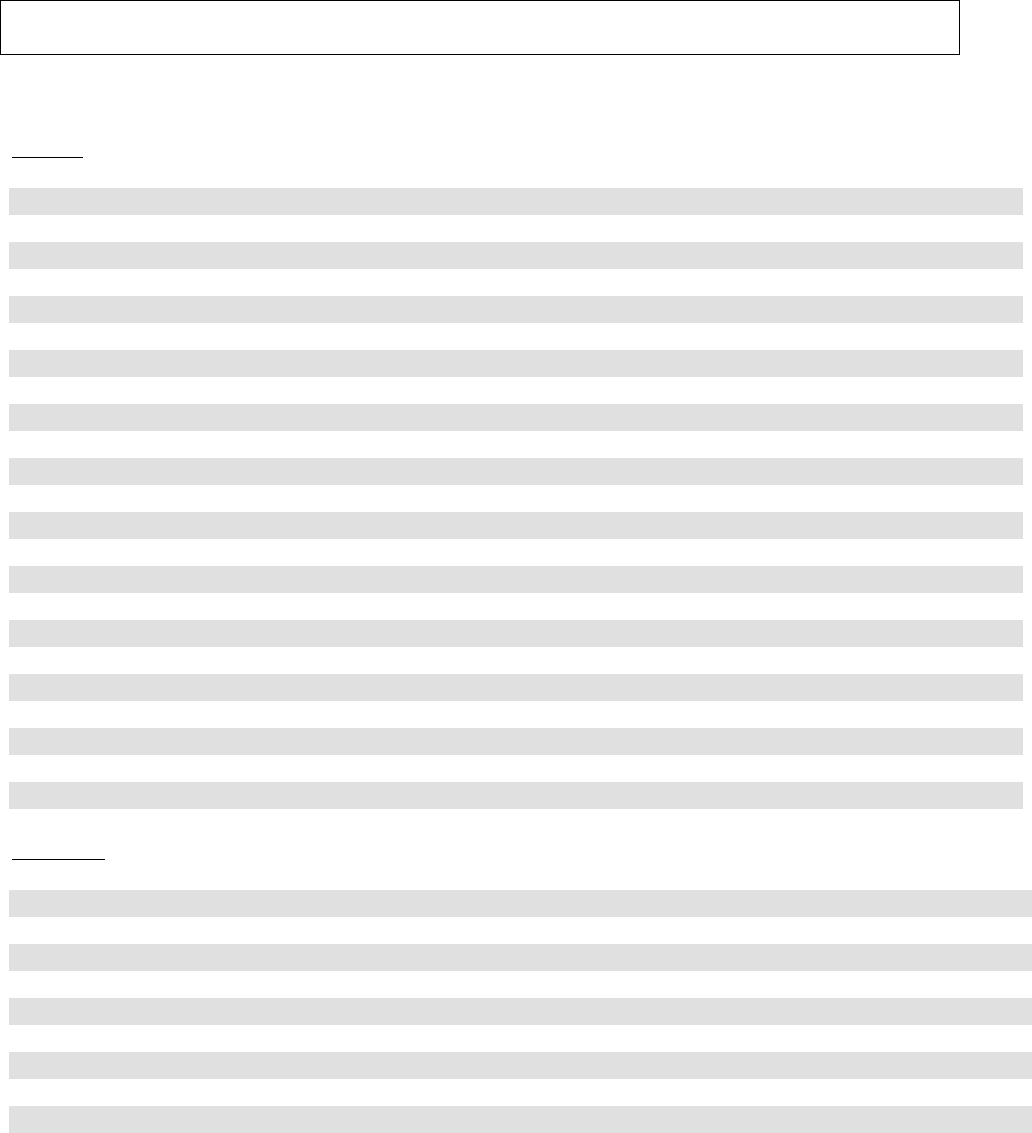
TREATMENT TRIAL FORM for: __________________________________
Child’s name: ______________________Grade: ___________ Year: _______
Person completing this form: _____________Relation to child: _________________
Usual observation time: mornings / afternoons / evenings / weekdays / weekends (circle)
Observations will be recorded every: day / week / month (circle)
Dear Parents, Teachers, and Child:
Thank you very much for your help. It is so important to conduct this trial in a careful and controlled fashion. Please
complete the table below. If you were not able to make observations for a period, leave that column blank. In addition
to these numbers, your written comments are very helpful. On the back, please record the date and provide general
impressions, including the following: Were there any problems with the intervention? Were there any benefits? Give
details. If you have any questions or concerns, please call. After each set of observations, please copy / e-mail
/ fax and send to:
Thank you.
During the observation period, how big were these problems?
0 = no problem, 1 = little problem, 2 = medium problem, 3 = big problem
Goal:
Intervention:
Baseline
DATE
Targets
Possible Side Effects
Feel free customize this form to fit your child’s target symptoms, the chosen intervention,
observation intervals, and the possible side effects.
How to do a treatment trial:
1. Choose a goal
2. Choose an intervention strategy
3. Establish baseline measures for targets and possible side effects
4. Establish observation intervals
5. Observe
6. Evaluate and reevaluate
a. promising:
b. disappointing or even harmful
c. inconclusive
Homework for the Tenth Mile
1. Assign each facet of the Gander a number that reflects its potential for ongoing negative
impact. Can these areas of need be successfully accommodated? Which facets of your child’s
profile require intervention most? Consult an expert. Review the science. Consider all
possible benefits and side effects. Set up a well-controlled treatment trial.
2. Assign each facet of the Gander a number that reflects its potential for positive impact. Be
sure to give your child regular opportunities to enhance these natural skills and pursue these
passions.
3. Parent Child Journey trial for behavior management: What about the effectiveness of the
interventions recommended in this program? If you used circles on the precourse Behavioral
Topography Survey, you could use triangles to indicate your postcourse ratings. Did your 2s
and 3s come down to 1s and 2s? Did your 1s and 2s come down to 0s and 1s? In this way,
you can use your Behavioral Topography Survey as a treatment trial rating form for this
course.
4. Please complete the course evaluation that follows. Thanks!
Behavioral Topography Survey
Name: _____________________________ Date: ____________ Rater: _____________
Circle (pre-course) and triangle (post-course) ratings:
0, no problem; 1, little problem; 2, medium problem; 3, big problem
Problem Situations
HOME
0 1 2 3 Getting ready to go in the morning
0 1 2 3 Transitioning into the car
0 1 2 3 Riding in the car
0 1 2 3 Arriving home
0 1 2 3 Transitioning out of the car
0 1 2 3 Mealtime (circle: before, during, after)
0 1 2 3 Playing with other children
0 1 2 3 While using electronic devices (which ones? ____________ )
0 1 2 3 When asked to stop using electronic devices
0 1 2 3 During unstructured free time
0 1 2 3 When visitors come over
0 1 2 3 When visiting others
0 1 2 3 In public places (which one(s)? ______________________)
0 1 2 3 With adult(s) (which one(s)? _________________________)
0 1 2 3 With sibling(s) (which one(s)? _______________________)
0 1 2 3 With babysitter(s) (which one(s)? ________________)
0 1 2 3 Homework (circle: starting, during, finishing)
0 1 2 3 Doing chores (which one(s)? __________________)
0 1 2 3 Getting ready for bed (washing, bathing, teeth-brushing, etc.)
0 1 2 3 Getting into bed
0 1 2 3 Falling asleep
0 1 2 3 Staying asleep
0 1 2 3 Other: ___________________________________________
0 1 2 3 Other: ___________________________________________
SCHOOL
0 1 2 3 Arriving at school
0 1 2 3 During class (Which one? __________________________ )
0 1 2 3 In school hallways / bathrooms
0 1 2 3 Recess at school
0 1 2 3 Lunch at school
0 1 2 3 School field trips
0 1 2 3 With adult (Name: ________________________________)
0 1 2 3 Pickup at school
0 1 2 3 School bus
0 1 2 3 Other: __________________________________________
0 1 2 3 Other: __________________________________________
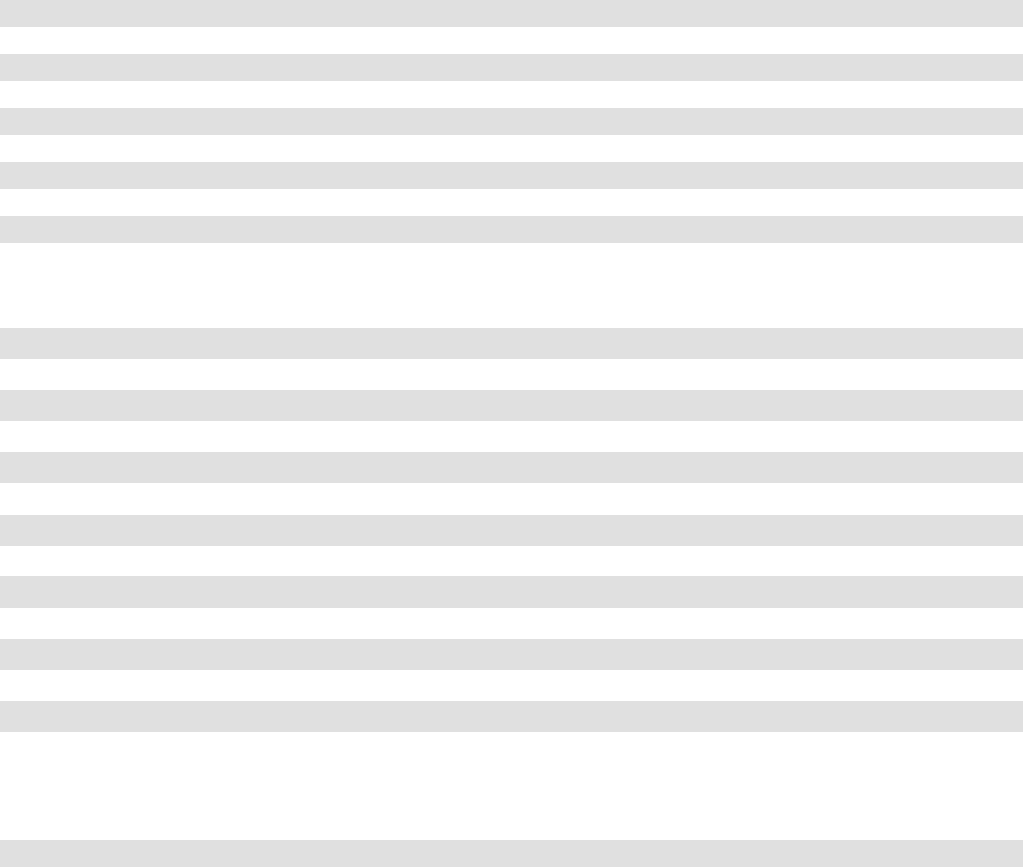
COMMUNITY
0 1 2 3 Grocery store
0 1 2 3 Eating out
0 1 2 3 House of worship
0 1 2 3 Shopping
0 1 2 3 Neighborhood playground
0 1 2 3 Festivals
0 1 2 3 Outdoor events
0 1 2 3 Indoor events (concerts, movies, etc.)
0 1 2 3 Other: ___________________________________________
0 1 2 3 Other: ___________________________________________
Problem Behaviors
0 1 2 3 Actively defies / refuses to comply
0 1 2 3 Loses temper
0 1 2 3 Argues with adults
0 1 2 3 Deliberately annoys people
0 1 2 3 Blames others for his or her mistakes or misbehaviors
0 1 2 3 Is touchy or easily annoyed by others
0 1 2 3 Is angry or resentful
0 1 2 3 Is spiteful or vindictive
0 1 2 3 Bullies, threatens, or intimidates others
0 1 2 3 Initiates physical fights
0 1 2 3 Lies / “cons”
0 1 2 3 Skips school
0 1 2 3 Is physically cruel to people or animals
0 1 2 3 Has stolen items of nontrivial value
0 1 2 3 Deliberately destroys other’s property
Other problem behaviors and situations:
0 1 2 3 ________________________________________________
0 1 2 3 ________________________________________________

Parent Child Journey Course evaluation
date: ______________________________
location: __________________________
instructor: _________________________
Thanks for your feedback.
1. On the Behavioral Topography Survey, compare ratings from pre-course baseline (circles) against
post-course follow-up (triangles). Having completed this ten-week program, would you say that
your child’s problem behaviors and problem situations have improved?
__ not at all (0%) Comments:
__ a little bit (10-25%)
__ medium (25-50%)
__ a lot (greater than 50%)
2. How do you think you did implementing the strategies presented?
__ not well Comments:
__ ok
__ well
__ very well
3. As a result of this course, how do you feel about yourself as a parent and your relationship with
your child?
__ worse Comments:
__ no different
__ a little better
__ medium better
__ a lot better
4. What was most useful about this course?
5. What was least useful about this course?
6. What would you change?
7. Please grade the program: A=excellent, B=good, C=OK, D=weak, F=failed
Course organization and content: ___
Instructor presentations: ___
Physical setting/ comfort: ___
Web site handouts ___
Dr. Shapiro’s book ___
Overall satisfaction with the program: ___
8. Other comments:
Thank you for your feedback. Most of all, thank you for your participation. I hope that this program has
been helpful. Good luck to you and your family.
