112 4 1232.full
User Manual: 112-4
Open the PDF directly: View PDF ![]() .
.
Page Count: 6

Evening use of light-emitting eReaders negatively
affects sleep, circadian timing, and
next-morning alertness
Anne-Marie Chang
a,b,1,2
, Daniel Aeschbach
a,b,c
, Jeanne F. Duffy
a,b
, and Charles A. Czeisler
a,b
a
Division of Sleep and Circadian Disorders, Departments of Medicine and Neurology, Brigham and Women’s Hospital, Boston, MA 02115;
b
Division of Sleep
Medicine, Harvard Medical School, Boston, MA 02115; and
c
Institute of Aerospace Medicine, German Aerospace Center, 51147 Cologne, Germany
Edited by Joseph S. Takahashi, Howard Hughes Medical Institute, University of Texas Southwestern Medical Center, Dallas, TX, and approved November 26,
2014 (received for review September 24, 2014)
In the past 50 y, there has been a decline in average sleep duration
and quality, with adverse consequences on general health. A
representative survey of 1,508 American adults recently revealed
that 90% of Americans used some type of electronics at least
a few nights per week within 1 h before bedtime. Mounting
evidence from countries around the world shows the negative
impact of such technology use on sleep. This negative impact on
sleep may be due to the short-wavelength–enriched light emitted
by these electronic devices, given that artificial-light exposure has
been shown experimentally to produce alerting effects, suppress
melatonin, and phase-shift the biological clock. A few reports have
shown that these devices suppress melatonin levels, but little is
known about the effects on circadian phase or the following sleep
episode, exposing a substantial gap in our knowledge of how this
increasingly popular technology affects sleep. Here we compare
the biological effects of reading an electronic book on a light-emit-
ting device (LE-eBook) with reading a printed book in the hours
before bedtime. Participants reading an LE-eBook took longer to
fall asleep and had reduced evening sleepiness, reduced melatonin
secretion, later timing of their circadian clock, and reduced next-
morning alertness than when reading a printed book. These results
demonstrate that evening exposure to an LE-eBook phase-delays
the circadian clock, acutely suppresses melatonin, and has important
implications for understanding the impact of such technologies on
sleep, performance, health, and safety.
sleep
|
chronobiology
|
phase-shifting
|
digital media
|
electronics
The use of electronic devices for reading, communication, and
entertainment has greatly increased in recent years. Greater
portability, convenience, and ease of access to reading materials
in electronic form add to the popularity of these devices. The use
of light-emitting devices immediately before bedtime is a con-
cern because light is the most potent environmental signal that
impacts the human circadian clock and may therefore play a role
in perpetuating sleep deficiency (1). The circadian-timing system
synchronizes numerous internal physiological and biochemical
processes, including the daily rhythm of sleep propensity (2), to
external environmental time cues. For optimal sleep duration
and quality, the timing of the sleep episode must be appropri-
ately aligned with the timing of the circadian clock. In humans,
exposure to light in the evening and early part of the night, even
at low intensity, suppresses the release of the sleep-facilitating
hormone melatonin (3–5) and shifts the circadian clock to a later
time (3, 6), both of which make it more difficult to fall asleep at
night. Light exposure in the biological evening/night also acutely
increases alertness (7, 8), but not much is known about its impact
on alertness the following day. Here we present results from a
randomized study comparing the effects of reading before bed-
time using a light-emitting eReader (LE-eBook) with reading a
printed book by reflected light. We examined circadian timing and
suppression of melatonin, polysomnographic (PSG) recordings of
sleep, and subjective and objective measures of sleepiness both in
the evening while reading and the following morning.
Results
Twelve healthy young adults (mean ±SD: 24.92 ±2.87 y; six
women) completed a 14-d inpatient protocol. The randomized,
crossover design (shown in Fig. 1) consisted of two conditions:
(i) reading an LE-eBook in otherwise very dim room light for
∼4 h before bedtime for five consecutive evenings, and (ii)
reading a printed book in the same very dim room light for ∼4h
before bedtime for five consecutive evenings. All participants
completed both reading conditions but were randomized to the
order. Hourly blood samples were collected during portions of
Significance
The use of light-emitting electronic devices for reading, com-
munication, and entertainment has greatly increased recently.
We found that the use of these devices before bedtime pro-
longs the time it takes to fall asleep, delays the circadian clock,
suppresses levels of the sleep-promoting hormone melatonin,
reduces the amount and delays the timing of REM sleep, and
reduces alertness the following morning. Use of light-emitting
devices immediately before bedtime also increases alertness at
that time, which may lead users to delay bedtime at home. Overall,
we found that the use of portable light-emitting devices immedi-
ately before bedtime has biological effects that may perpetuate
sleep deficiency and disrupt circadian rhythms, both of which can
have adverse impacts on performance, health, and safety.
Author contributions: A.-M.C., J.F.D., and C.A.C. designed research; A.-M.C. performed
research; A.-M.C. and D.A. analyzed data; and A.-M.C. and C.A.C. wrote the paper.
Conflict of interest statement: Dr. Czeisler has received consulting fees from or served as
a paid member of scientific advisory boards for: Boston Celtics; Boston Red Sox; Citgo Inc.;
Cleveland Browns; Merck; Novartis; Purdue Pharma LP; Quest Diagnostics, Inc.; Teva
Pharmaceuticals Industries Ltd.; Valero Inc.; Vanda Pharmaceuticals, Inc. Dr. Czeisler
currently owns an equity interest in Lifetrac, Inc.; Somnus Therapeutics, Inc.; Vanda Phar-
maceuticals, Inc., and between October 2012 and October 2013, Apple, Inc. and Microsoft,
Inc. Dr. Czeisler received royalties from McGraw Hill, Penguin Press/Houghton Mifflin
Harcourt, and Philips Respironics, Inc. and has received grants and research support from
Cephalon Inc., National Football League Charities, Philips Respironics, ResMed Founda-
tion, San Francisco Bar Pilots and Sysco. Dr. Czeisler is the incumbent of an endowed
professorship provided to Harvard University by Cephalon, Inc. and holds a number of
process patents in the field of sleep/circadian rhythms (e.g., photic resetting of the human
circadian pacemaker). Since 1985, Dr. Czeisler has also served as an expert witness on
various legal cases related to sleep and/or circadian rhythms, including matters involving
Bombardier, Inc.; Delta Airlines; FedEx; Greyhound; Michael Jackson’s mother and chil-
dren; Purdue Pharma, L.P.; United Parcel Service and the United States of America.
This article is a PNAS Direct Submission.
Freely available online through the PNAS open access option.
See Commentary on page 946.
1
Present address: Department of Biobehavioral Health, Pennsylvania State University,
University Park, PA 16802.
2
To whom correspondence should be addressed. Email: amchang@psu.edu.
This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.
1073/pnas.1418490112/-/DCSupplemental.
1232–1237
|
PNAS
|
January 27, 2015
|
vol. 112
|
no. 4 www.pnas.org/cgi/doi/10.1073/pnas.1418490112
the study for assessment of plasma melatonin concentrations.
Sleep latency (i.e., interval between lights-out and the timing of
sleep onset) was assessed from PSG recordings on the fourth and
fifth nights of each condition. In addition, we assessed total sleep
time (TST), sleep efficiency (the percentage of time in bed spent
asleep), and the time spent in each sleep stage. Participants rated
their sleepiness using a computerized Karolinska Sleepiness Scale
(KSS) (9) every evening and morning, and waking electroen-
cephalogram (EEG) measures were recorded on two evenings and
two mornings of each reading condition. More detailed methods
are described in Materials and Methods.
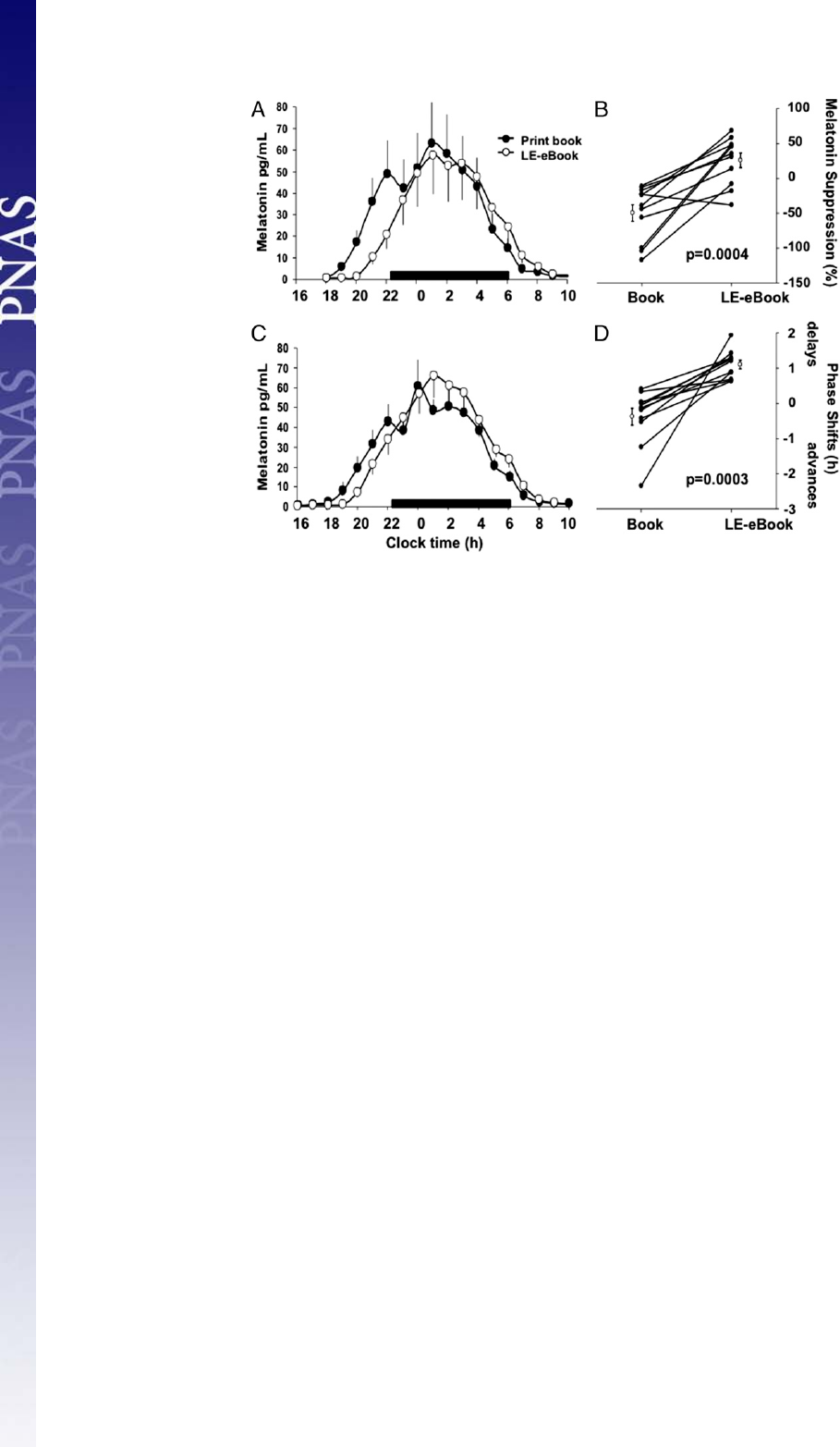
LE-eBook Effects on Levels and Circadian Timing of Melatonin. The
LE-e-book condition suppressed evening levels of melatonin by
55.12 ±20.12%, whereas the print-book condition showed no
suppression (−18.77 ±39.57%) as measured during the fifth
night (P<0.001; Fig. 2 Aand B). Dim light melatonin onset
was >1.5 h later on the day following the LE-eBook condition
(22:31 ±0:42) than in the print-book condition (21:01 ±0:49;
P<0.001; Fig. 2 Cand D).
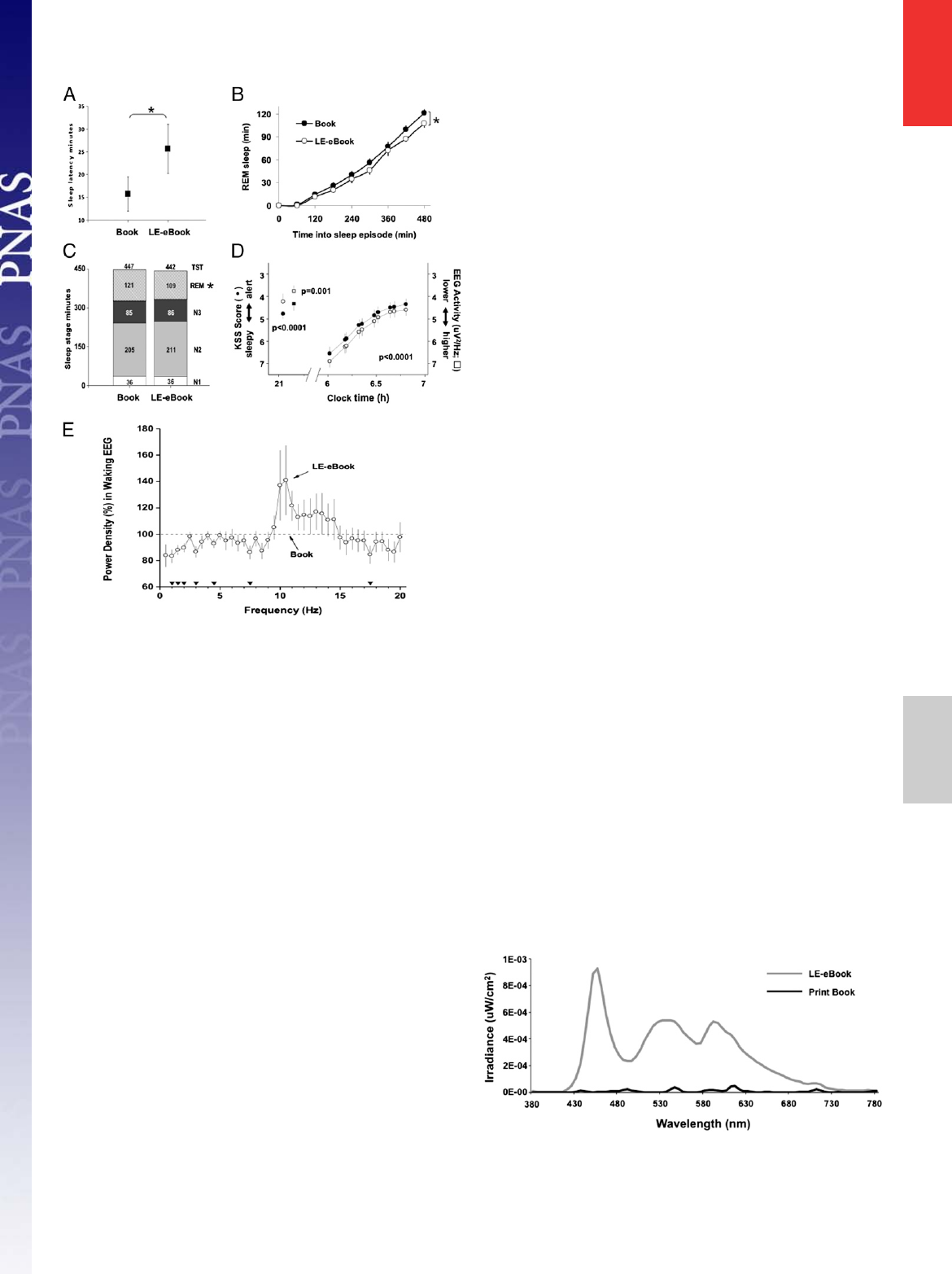
Impact of Reading Condition on Sleep. In the LE-eBook condition,
participants averaged nearly 10 minlongertofallasleepthaninthe
print-book condition (mean ±SD, 25.65 ±18.78 min vs. 15.75 ±
13.09 min; P=0.009; mixed model; Fig. 3A). Participants also had
significantly less rapid eye movement (REM) sleep following the
LE-eBook condition (109.04 ±26.25 min vs. 120.86 ±25.32 min in
the print-book condition; P=0.03; Fig. 3 Band C), reflecting
a lower average rate of accumulation of REM sleep during sleep
(Fig. 3B). There was no difference between conditions in TST, sleep
efficiency, or the duration of non-REM sleep (stages 1–3; Fig. 3C)
in the sleep episode, which were scheduled for eight hours each.
Effects on Acute Evening Alertness and Morning Sleepiness. Reading
the LE-eBook was associated with decreased sleepiness in the
evening. An hour before bedtime, study participants rated
themselves as less sleepy (P<0.01; Fig. 3D), and their EEG
showed less power within the delta/theta frequency range (1.0–
7.5 Hz; Fig. 3 Dand E) in the LE-eBook condition. The fol-
lowing morning, however, the results for self-reported sleepiness
were reversed, with participants feeling sleepier the morning
after reading an LE-eBook the prior evening (P<0.001; Fig.
3D). Furthermore, not only did they awaken feeling sleepier, it
took them hours longer to fully “wake up”and attain the same
level of alertness than in the printed book condition.
Many eReaders Emit Short-Wavelength Light. Full spectral profiles
for the LE-eBook used by the study participants in the current
study and for the incident reflected light in the print book con-
ditions are shown in Fig. 4. Table 1 displays the illuminance
measures (cyanopic, melanopic, rhodopic, chloropic, and eryth-
ropic lux in comparison with photopic lux) for both the LE-eBook
and the reflected light of the print book, using the recently pro-
posed light measurement strategy that takes into account non–
image-forming retinal responses to light (see Methods). Light
readings for the LE-eBook as well as from several light-emitting
and non–light-emitting eReaders and other electronic devices are
shown in Table S1. Light from the LE-eBook is short-wavelength–
enriched, with a peak at 452 nm in the blue light range, compared
with broad-spectrum light (white light), with a peak at 612 nm. As
shown in Table S1, measurements from several other light-
emitting devices are also enriched for short-wavelength light.
Discussion
We found that, compared with reading a printed book in reflected
light, reading a LE-eBook in the hours before bedtime decreased
subjective sleepiness, decreased EEG delta/theta activity, and
suppressed the late evening rise of pineal melatonin secretion
during the time that the book was being read. We also found that,
compared with reading a printed book, reading an LE-eBook in
the hours before bedtime lengthened sleep latency; delayed the
phase of the endogenous circadian pacemaker that drives the
timing of daily rhythms of melatonin secretion, sleep propensity,
and REM sleep propensity; and impaired morning alertness.
These results indicate that reading an LE-eBook in the hours
before bedtime likely has unintended biological consequences
that may adversely impact performance, health, and safety. The
results of this study are of particular concern, given recent evi-
dence linking chronic suppression of melatonin secretion by
nocturnal light exposure with the increased risk of breast, co-
lorectal, and advanced prostate cancer associated with night-shift
work (for review, see ref. 10), which has now been classified as
a probable carcinogen by the World Health Organization (11, 12).
Moreover, the observation that the endogenous circadian mela-
tonin phase was 1.5 h later when reading an LE-eBook compared
with reading from a printed book suggests that using a light-
emitting device in the hours before bedtime is likely to increase
the risk of delayed sleep-phase disorder and sleep onset insomnia
(13), especially among individuals living in society who self-select
their bedtimes and wake times. Induction of such misalignment of
circadian phase is likely to lead to chronic sleep deficiency (1).
The decreased sleepiness before bedtime and longer sleep
latency we observed in the LE-eBook condition is likely due to
both an acute alerting effect of light and a delay of the circadian
timing system. Suppression of melatonin by exposure to evening
light may be an underlying mechanism by which light acutely
increases alertness, as seen in the present study and in previous
reports (14–19). Other studies, however, have not found a re-
lationship between alertness and melatonin levels during light
exposure (20, 21) or have shown changes in alertness induced by
light exposure during the day, when melatonin levels are at low
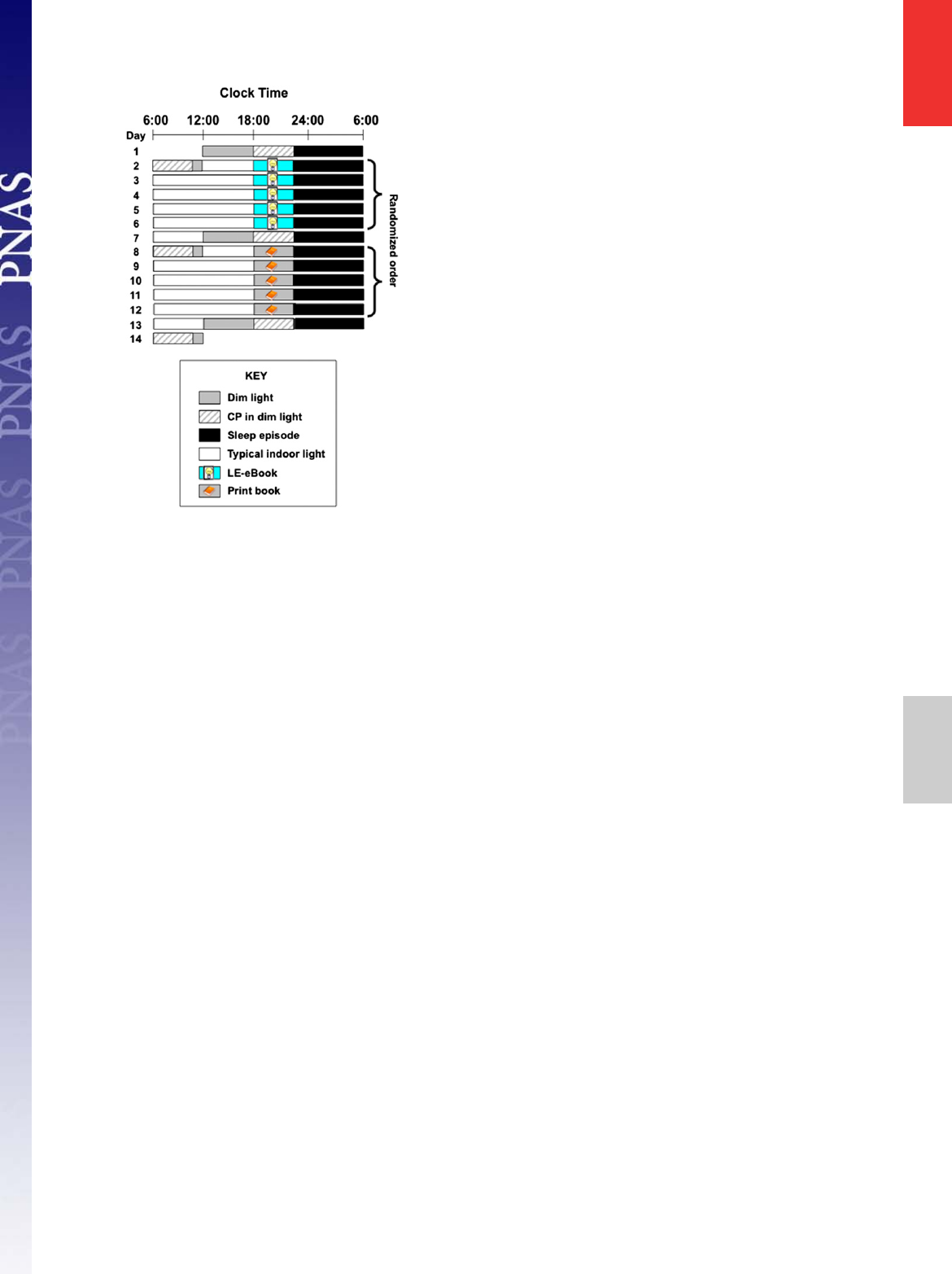
Fig. 1. Representative raster plot of the 14-d study protocol. Black bars
indicate the 10:00 PM–6:00 AM sleep episode in darkness. Gray bars denote
dim room light (∼3 lx of white light in the angle of gaze; Materials and
Methods), and white bars denote typical indoor room light (∼90 lx in the
angle of gaze). Striped bars show the constant posture (CP) procedures.
Reading sessions are marked either by the LE-eBook or the print-book and
symbols. Participants were randomized to the order of reading condition.
Ambient room light level for all reading sessions was dim (∼3 lx).
Chang et al. PNAS
|
January 27, 2015
|
vol. 112
|
no. 4
|
1233
PHYSIOLOGY SEE COMMENTARY
or undetectable levels (22–24). The circadian-phase delay, as
marked by the endogenous melatonin rhythm, probably also
contributed to the delay of sleep onset that occurred after study
participants were reading the LE-eBook. The significant differ-
ence in sleep latency occurred even though the scheduled bedtime
was fixed at 10:00 PM each night during the study protocol to
ensure an 8-h sleep opportunity in bed. Thus, these results likely
underestimate the impact that use of these devices in the hours
before bedtime has on self-selected sleep timing and duration.
The effects of the LE-eBook on sleepiness the following
morning, however, cannot be due to the acute effects of light
observed the previous evening. Individuals were sleepier the
morning after reading in the LE-eBook condition than after
reading a printed book the evening before; however, the light
levels in the morning were identical for both reading conditions.
Therefore, the difference in morning sleepiness between the
conditions is most likely due to differences in the prior sleep
episode and/or the circadian-phase delay. Indeed, it did take
longer for participants to fall asleep after the LE-eBook condi-
tion, but there was no difference in average sleep duration and
the magnitude of the difference in sleep latency is unlikely to
account for the effect on alertness observed 8 h later. The dif-
ference in REM sleep between the conditions may have con-
tributed to the difference in morning sleepiness ratings. Given
that the majority of REM sleep occurs in the latter portion of the
sleep episode (25) (i.e., closer to wake time), participants had
significantly less REM sleep in the LE-eBook condition. Because
most spontaneous awakenings occur out of REM sleep (26, 27),
this reduction in REM sleep in the LE-eBook condition may
have also impacted sleepiness upon awakening. The significant
phase delay after the LE-eBook condition suggests that the
evening light from the LE-eBook phase delayed the circadian
clock, delaying the nadir of the circadian rhythm of sleep pro-
pensity (2) and thereby resulting in a robust, albeit indirect, effect
on morning sleepiness. A phase delay of the circadian clock is
consistent with the slower rise in the rate of accumulation of REM
sleep. The change in the timing of REM sleep likely represents
a delay in the circadian rhythm of REM sleep propensity, which is
temporally coincident with the sleep propensity rhythm (25).
The spectral composition of the light emitted by the LE-eBook
may explain why the magnitude of the melatonin-suppressing
and phase-shifting response observed was greater than would be
predicted for this moderately low level of light (3). In humans,
exposure to short-wavelength monochromatic light in the even-
ing has been shown to induce greater circadian and alerting
responses than exposure to the same number of photons of
longer-wavelength monochromatic light (17–19, 28–34), even
though the shorter-wavelength light may have a much lower il-
luminance level when measured in photopic lux (35). For this
reason, it has recently been proposed that lux is an inappropriate
measure for estimation of the impact of light on melatonin
suppression, circadian-phase shifting, and other non–image-
forming effects of retinal light exposure (35).
This study had a number of limitations. First, melatonin sup-
pression was assessed on the fifth and final evening of each
reading condition. Although it is likely that the phase shift in the
LE-eBook condition had already occurred by this time, melato-
nin suppression was calculated by using the shifted area under
the curve (AUC) from the following evening and thus should
control for any phase shift. Therefore, the greater suppression
seen was not due to an effect of a delayed phase in the LE-eBook
condition. Second, the duration of the evening reading sessions
were 4 h long. However, given that the average teenager in the
United States spends 7.5 h per day engaged in recreational
media plus time spent on homework—which both occur in the
late afternoon/evening, including the hour before bedtime (36),
and which both involve exposure to light-emitting screens (e.g.,
LE eReaders, computers, televisions, tablets, smartphones, video
game consoles, etc.)—the 4-h exposure interval used in this study is
likely in the range of screen time exposure experienced by millions
of Americans each evening. Third, in the present study, the
LE-eBook was set to maximum brightness throughout the 4-h
Fig. 2. Melatonin suppression (Aand B) and phase shifting (Cand D) during and after the LE-eBook and print book reading conditions. (A) Average
waveforms of melatonin (±SEM) during the fifth night of each reading condition. The black bar denotes the scheduled sleep episode (22:00–06:00). (B)
Percent suppression for each condition for each participant (filled symbols) and group average (±SEM; open symbols). (C) Average waveforms of melatonin
(±SEM) on the evening/night after each reading condition. (D) Average phase shift of melatonin onset for each condition for each participant (filled symbols)
and group average (±SEM; open symbols). The main effect of Condition was significant (P<0.05, mixed model).
1234
|
www.pnas.org/cgi/doi/10.1073/pnas.1418490112 Chang et al.
reading session, whereas, by comparison, the print-book condi-
tion consisted of reflected exposure to very dim light. However,
a number of newer models of light-emitting devices are even
brighter than those used in this study. Moreover, in this study, the
LE-eBook reader was held at a fixed distance (30–45 cm) from the
eye, further from the eye than many people might have chosen
(therefore reducing retinal light exposure), particularly for users
of smaller devices who may hold the smaller screens closer to the
eyes. Lastly, although the short-wavelength light from the LE-
eBook may have been responsible for the effects reported here,
this study did not include a light-emitting device with longer
wavelength for comparison, so our findings may be due to the
difference in irradiance level rather than spectral composition.
This study demonstrates that use of a light-emitting electronic
device in the hours before bedtime can have significant impact
on sleep, alertness, and the circadian clock. The 10-min-shorter
sleep latency after the print-book condition compared with sleep
latency after the LE-eBook condition is similar to the effect size
of eszopiclone treatment on sleep latency in patients with pri-
mary insomnia (37). Our findings provide evidence that the
electric light to which we are exposed between dusk and bedtime
has profound biological effects. Because technology use in the
hours before bedtime is most prevalent in children and adoles-
cents (36), physiological studies on the impact of such light ex-
posure on both learning and development are needed. Further
investigation of the physiological and medical effects of elec-
tronic devices is warranted, because the acute responses to the
short-wavelength–enriched light emitted by them may have
longer-term health consequences than previously considered.
Materials and Methods
Informed written consent was obtained from study participants before enroll-
ment in the study. The protocol was approved by the Partners Human Research
Committee, and all procedures were conducted according to the Declaration of
Helsinki. Study participants were compensated for their participation.
Study Participants and Screening Procedures. Twelve young healthy adults
completed the 14-d in-patient study protocol (six females and six males; mean
age ±SD: 24.92 ±2.87). Potential participants were extensively screened for
physical and psychological health, which included questionnaires, laboratory
tests, physical examination, EKG, eye examination, and psychological in-
terview to determine suitability for participation in the study. Participants
with chronic medical or psychological conditions or sleep disorders and those
taking prescription medications were excluded from study. History of night
work or shift work in the prior 3 y and travel across more than one time zone
in the previous 3 mo was also exclusionary. The presence of any eye or vision
abnormality or the inability to read in dim light without the use of corrective
lenses was exclusionary. Participants were instructed to refrain from use of
medications, drugs, alcohol, nicotine, or caffeinated products for 3 wk be-
fore admission, which was verified by toxicological testing upon admission
to the laboratory. Participants were also required to maintain a fixed 8-h
sleep schedule (10:00 PM to 6:00 AM), to complete a daily sleep/wake log,
and to call in their bedtimes and wake times every day during this 3-wk
interval. This sleep schedule was verified by wrist actigraphy (Actiwatch-L;
Philips/Respironics) during the week before admission.
Study Protocol. Participants lived in a private room in the Intensive Physio-
logical Monitoring Unit of the Center for Clinical Investigation of Brigham
and Women’s Hospital during the 14-d protocol. They were scheduled to
sleep on the identical fixed 8-h sleep schedule (10:00 PM to 6:00 AM) they
maintained for 3 wk before admission. The randomized, crossover protocol
design consisted of two conditions: (i) reading an LE-eBook (iPad; Apple Inc.,
Cupertino, CA) in otherwise very dim room light for ∼4 h before bedtime for
five consecutive evenings, and (ii) reading printed books in the same very
dim room light for ∼4 h before bedtime for five consecutive evenings
(Fig. 1). Primary outcome measures included sleep latency, timing and
amount of melatonin secretion, and self-reported ratings and EEG measures
of sleepiness/alertness. On three occasions (days 1, 7, and 13) participants
completed constant posture (CP) procedures for 4 h before and 4 h after the
8-h sleep episode.
Fig. 3. Sleep and sleepiness/alertness measures during and after the print-
book and LE-eBook reading conditions. (A) Mean (±SEM) sleep latency to
stage N2 in minutes for each reading condition. *P=0.009, mixed model. (B)
Mean (±SEM) accumulation of REM across 8-h sleep episode for each con-
dition. *P=0.029. (C) Mean duration (in minutes) of sleep stages N1 (white),
N2 (light gray), N3 (dark gray), and REM (patterned), and total sleep time
(TST; numbers at top of bar) for each reading condition. *P=0.029. (D)
Mean (±SEM) alertness ratings (circles) during and on the morning after each
reading condition with respect to clock hour. Mean delta/theta activity in
the waking EEG, power density in the 1.0–7.5 Hz range (squares), that was
derived from C3/M2 during the fourth and fifth reading sessions of each
condition is also shown. (E) Power density in the waking EEG during the
LE-eBook condition (open circles) expressed as a percentage of the printed-
book condition (100%; dashed line). Two-way mixed-model ANOVA on
log-transformed absolute power densities per 0.5-Hz was significant for
condition (P<0.04). Filled triangles at the bottom indicate EEG frequency
bins for which the difference between conditions was significant (P<0.05,
post hoc paired ttests).
Fig. 4. Spectral radiometric profile of the LE-eBook device (gray) and in-
cident light reflected by the printed book (black). The peak irradiance for
the LE-eBook eReader is ∼450 nm and for the reflected light is 612 nm.
Chang et al. PNAS
|
January 27, 2015
|
vol. 112
|
no. 4
|
1235
PHYSIOLOGY SEE COMMENTARY

Reading Sessions and Lighting Conditions. A total of 10 reading sessions—5in
the LE-eBook condition and 5 in the printed book condition—were sched-
uled during the 14-d study. Participants were randomized to the order of
reading condition. Reading sessions began at 6:00 PM and ended at 10:00
PM just before bedtime, with a 15-min “break”scheduled at 8:45–9:00 PM.
For the first ∼3 h portion of the reading session (6:00–8:45 PM) participants
read while seated in a fixed location in the room. During the break, they
were allowed to stop reading and do other activities (walk around the room,
prepare for bed, etc.) until 9:00 PM, when they resumed the reading session.
For this last hour, participants read while seated in bed. During LE-eBook
reading sessions, the light-emitting device was set to maximum brightness
and placed in a stand that held it at a fixed angle. This stand was placed on
a table directly in front of the individual at a 30- to 45-cm distance from their
eyes. Participants were allowed to turn pages on the LE-eBook, but were
asked not to hold it while reading or make any adjustments to the settings.
During the printed book reading sessions, participants were allowed to hold
the book at any desired distance from their eyes. Participants selected their
own reading materials and supplied their own printed books. There were
two requirements regarding reading material in either electronic or printed
form: (i) it had to consist of printed text on the page (no pictures, illus-
trations, graphic novels, magazines, puzzles, etc.); and (ii) it had to be con-
sidered “pleasure”or “leisure”reading (no textbooks, reference books, or
coursework). A technician was present for all reading sessions to coordinate
and administer the reading session, ensure compliance of the participants,
and collect and record the light measurements.
Light readings were recorded during all reading sessions at multiple times:
at the beginning, at the end, and at 1 h intervals during the reading sessions.
Illuminance was measured by using an IL1400 radiometer/powermeter with
a SEL-033/Y/W detector (International Light, Inc., Peabody, MA) with the
sensor placed next to the participant’s eye and pointed at the LE-eBook or
printed book. For the LE-eBook reading condition, the distance between the
participant and the LE-eBook in the stand was adjusted (e.g., moved closer
or farther) if the light reading measured outside of the range of 30–50
photopic lux in the angle of gaze so that the light measurement was
maintained within range.
Ambient room lighting during the study was from ceiling-mounted 4100K
fluorescent lamps (Philips Lighting, Eindhoven, The Netherlands). During
reading sessions, CP, and upon waking, the room light was ∼0.0048 W/m
2
at
137 cm from the floor in the vertical plane with a maximum <0.025 W/m
2
at
187 cm from the floor in the horizontal plane anywhere in the room. During
the rest of the waking episodes, participants were in typical indoor room
lighting of ∼0.23 W/m
2
at 137 cm from the floor in the vertical plane, with
a maximum of 0.48 W/m
2
at 187 cm from the floor in the horizontal plane
anywhere in the room. During all scheduled sleep episodes, participants
were in darkness.
Radiometric light measurements of electronic devices were conducted in
the same light conditions and at the same distance (30–45 cm) as during the
reading sessions (described above). The irradiance output in the range of
380–780 nm at 4-nm intervals was converted to 1-nm intervals for calculation
of the human retinal photopigment illuminance measures (cyanopic, mela-
nopic, rhodopic, chloropic, and erythropic lux) (35).
CP Procedures. CP procedures occurred on day 1 (baseline) and on days 7 and
13, after the five consecutive nights of each reading condition for the as-
sessment of circadian phase of the melatonin rhythm. Participants remained
in bed in a semirecumbent posture with minimal activity for 4 h before and
4 h after the 8-h sleep episode. Room temperature and dim light conditions
remained constant during the CP; participants were in darkness fully
recumbent during the sleep episode.
Plasma Melatonin. Hourly blood samples were collected via an indwelling
forearm IV catheter during portions of the protocol for measurement of
melatonin levels. Samples were collected and then frozen (−80 °C) for
subsequent assay. Plasma melatonin samples were assayed (SolidPhase Inc.,
Portland, ME) using the BÜHLMANN Melatonin Radio-immunoassay (ALPCO
Diagnostics, Salem, NH), which has a functional sensitivity of 0.9 pg/mL and an
analytical sensitivity of 0.3 pg/mL, an intraassay precision of 7.9–8.2%, and
interassay precision of 11.7%.
Melatonin suppression was determined by using the AUC (by trapezoidal
method) during the 4-h reading session on the fifth night of each reading
condition and comparing it to the AUC during the corresponding 4-h time
window during the CP 24 h following the reading session. Circadian phase of
the dim light melatonin onset (DLMO) was calculated as the time at which levels
of melatonin rose above 25% of the peak-to-trough amplitude of a three-
harmonic waveform fitted to the 24-h melatonin data from the CP (38, 39).
Phase shifts were calculated as the difference between the DLMO from the
CP after the five-night reading condition and the DLMO from the CP before
the reading condition (i.e., shift =DLMO from day 13 –DLMO from day 7).
Because of missing blood samples during the fifth night of one reading
session, one study participant was excluded from analysis of melatonin
suppression. Another participant was excluded from analysis of DLMO timing
due to missing blood samples during one of the CPs. Therefore, melatonin
suppression and phase were each determined in 11 participants.
Sleep and Wake Recordings. PSG was recorded during the final two sleep epi-
sodes and for several hours before and after the sleep episode of each reading
condition for a total of four PSG recordings per study participant. Surface
electrodes were applied to specific locations on the face and scalp to record the
EEG (F3/M2, F4/M1, C3/M2, C4/M1, O1/M2, O2/M1), and the left and right
electrooculogram, and the submental electromyogram. The data were collected
by using the Vitaport-3 system (TEMEC Instruments B.V., Kerkrade, The Neth-
erlands). Signals were sampled at 256 Hz, low-pass filtered, and stored at 128 Hz.
For sleep recordings, data were scored in 30-s epochs according to standard
criteria (40). Sleep measures included latency to sleep onset (time from lights
off until the first occurrence of stage N2), TST, sleep efficiency (ratio of TST/
the time spent in bed), wake after sleep onset, and time spent in each stage
of sleep (N1, N2, N3, and REM). Wake recordings were scored in 30-s epochs
to verify wakefulness and identify any unintentional episodes of sleep.
Waking EEG recordings collected during the 3-min KDT were also quantified
by spectral analysis. They were first inspected visually to identify and remove
2-s epochs contaminated by artifacts such as eye blinks and eye or body
movements. The data were then subjected to a Fast Fourier Transform
procedure, and power spectra were calculated for 2-s epochs over the fre-
quency range of 0.5–20.0 Hz in 0.5-Hz bins.
Subjective and Objective Measures of Sleepiness/Alertness. Subjective sleepi-
ness was measured with a computer-administered KSS. The KSS is a 9-point
Likert scale with all numbers having valid point values, but only the odd numbers
have descriptions: 1 representing “extremely alert,”3representing“alert,”
5representing“neither alert nor sleepy,”and 9 representing “extremely
sleepy”(9, 41). Study participants completed the KSS each evening ∼1hbefore
bedtime and several times each morning: within 1–5 min after scheduled wake
time and then every 4–10 min for 1 h after wake time. Participants typically
completed the KSS in <30 s, and the computer screen was set to a dim light
level of <8lx(0.025W/m
2
) from the participants’eye in the angle of gaze.
Participants also completed the Karolinska Drowsiness Test (KDT; ref. 9)
(3 min eyes open) during which they were instructed to relax, keep eyes open,
and maintain a fixed gaze on a black dot in front of them while avoiding any
movements or frequent blinking. The KDT allowed for waking EEG recording
under standardized and reproducible conditions where artifacts from move-
ment were minimized.
Table 1. Photopic illuminance and human retinal photopigment-weighted illuminance
measures from the LE-eBook device and light reflected by the printed book
Device Photopic lux Cyanopic lux Melanopic lux Rhodopic lux Chloropic lux Erythropic lux
Print book* 0.91 0.45 0.65 0.68 0.81 0.92
LE-eBook 31.73 31.64 31.03 31.68 31.84 30.69
Radiometric light readings were taken in the same dim background room light conditions and from the same
distance (38–40 cm). The LE-eBook was set to the maximum brightness setting.
*Illuminance in the printed book condition was measured from the ambient room light emitted by the ceiling
fixtures and reflected by the book, using the recently proposed light measurement strategy that takes into
account non–image-forming retinal responses to light (see Methods).
1236
|
www.pnas.org/cgi/doi/10.1073/pnas.1418490112 Chang et al.

Statistical Analysis. Statistical analyses were performed by using SAS (Version
9.2; SAS Institute, Cary, NC). We compared sleep and circadian measures
between reading conditions using a mixed model analysis with factors Con-
dition (LE-eBook or printed book), Order, and their Interaction (Condition X
Order). Mixed model was also used for comparing KSS score and EEG power
with factors Condition,Order,Time (repeated measures in the first hour after
awakening), and the Interaction (Condition XTime). Post hoc paired Student
ttests were used for comparisons between conditions for subjective and
objective measures of sleepiness. Pvalues <0.05 were considered significant.
ACKNOWLEDGMENTS. We thank the study participants, the staff of the
Brigham and Women’s Hospital Center for Clinical Investigation [part of the
Harvard Catalyst Clinical and Translational Science Center (CTSC)], the staffs
of the Division of Sleep Medicine Sleep and EEG Core and Chronobiology
Core, Dayna Bradstreet for significant contributions to recruitment and con-
duct of the study, and Michael Herf and Robert Lucas, Ph.D. for assistance
with the spectral light analysis. We also thank Wei Wang, Ph.D. for assis-
tance with statistical analysis supported by the Harvard Catalyst CTSC
[National Center for Research Resources (NCRR) and the National Center
for Advancing Translational Sciences, National Institutes of Health (NIH)
Award UL1 RR025758 and financial contributions from the Brigham and
Women’s Hospital (BWH), Harvard University, and its other affiliated aca-
demic health care centers]. This work was supported by NIH Grant
R01HL077453. The inpatient studies were conducted in the Harvard CTSC,
supported by NCRR Grant UL1 RR025758. A-M.C. was supported in part by
NIH Grant K01HL115458. D.A. was supported in part by the German Aero-
space Center. J.F.D. was supported in part by NIH Grant R01HL094654. C.A.C.
was supported in part by NASA NNX10AF47G and the National Space Bio-
medical Research Institute through NASA NCC 9-58.
1. Czeisler CA (2013) Perspective: Casting light on sleep deficiency. Nature 497(7450):
S13.
2. Dijk DJ, Czeisler CA (1995) Contribution of the circadian pacemaker and the sleep
homeostat to sleep propensity, sleep structure, electroencephalographic slow waves,
and sleep spindle activity in humans. J Neurosci 15(5 Pt 1):3526–3538.
3. Zeitzer JM, Dijk DJ, Kronauer R, Brown E, Czeisler C (2000) Sensitivity of the human
circadian pacemaker to nocturnal light: Melatonin phase resetting and suppression.
J Physiol 526(Pt 3):695–702.
4. McIntyre IM, Norman TR, Burrows GD, Armstrong SM (1989) Human melatonin sup-
pression by light is intensity dependent. J Pineal Res 6(2):149–156.
5. Brainard GC, et al. (1988) Dose-response relationship between light irradiance and the
suppression of plasma melatonin in human volunteers. Brain Res 454(1-2):212–218.
6. Khalsa SBS, Jewett ME, Cajochen C, Czeisler CA (2003) A phase response curve to
single bright light pulses in human subjects. J Physiol 549(Pt 3):945–952.
7. Cajochen C, Zeitzer JM, Czeisler CA, Dijk DJ (2000) Dose-response relationship for light
intensity and ocular and electroencephalographic correlates of human alertness.
Behav Brain Res 115(1):75–83.
8. Cajochen C (2007) Alerting effects of light. Sleep Med Rev 11(6):453–464.
9. Åkerstedt T, Gillberg M (1990) Subjective and objective sleepiness in the active in-
dividual. Int J Neurosci 52(1–2):29–37.
10. Costa G, Haus E, Stevens R (2010) Shift work and cancer - considerations on rationale,
mechanisms, and epidemiology. Scand J Work Environ Health 36(2):163–179.
11. Straif K, et al. (2007) Carcinogenicity of shift-work, painting, and fire-fighting. Lancet
Oncol 8(12):1065–1066.
12. Erren TC (2010) Shift work, cancer and “white-box”epidemiology: Association and
causation. Epidemiol Perspect Innov 7:11.
13. Dijk DJ (2013) Why do we sleep so late? J Sleep Res 22(6):605–606.
14. Perrin F, et al. (2004) Nonvisual responses to light exposure in the human brain during
the circadian night. Curr Biol 14(20):1842–1846.
15. Figueiro MG, Bullough JD, Bierman A, Fay CR, Rea MS (2007) On light as an alerting
stimulus at night. Acta Neurobiol Exp (Wars) 67(2):171–178.
16. Revell VL, Barrett DC, Schlangen LJ, Skene DJ (2010) Predicting human nocturnal
nonvisual responses to monochromatic and polychromatic light with a melanopsin
photosensitivity function. Chronobiol Int 27(9–10):1762–1777.
17. Chellappa SL, et al. (2011) Non-visual effects of light on melatonin, alertness and
cognitive performance: Can blue-enriched light keep us alert? PLoS ONE 6(1):e16429.
18. Cajochen C, et al. (2011) Evening exposure to a light-emitting diodes (LED)-backlit
computer screen affects circadian physiology and cognitive performance. J Appl
Physiol (1985) 110(5):1432–1438.
19. Cajochen C, et al. (2005) High sensitivity of human melatonin, alertness, thermo-
regulation, and heart rate to short wavelength light. J Clin Endocrinol Metab 90(3):
1311–1316.
20. Dollins AB, Lynch HJ, Wurtman RJ, Deng MH, Lieberman HR (1993) Effects of illumi-
nation on human nocturnal serum melatonin levels and performance. Physiol Behav
53(1):153–160.
21. Chang AM, Scheer FA, Czeisler CA, Aeschbach D (2013) Direct effects of light on
alertness, vigilance, and the waking electroencephalogram in humans depend on
prior light history. Sleep 36(8):1239–1246.
22. Phipps-Nelson J, Redman JR, Dijk DJ, Rajaratnam SM (2003) Daytime exposure to
bright light, as compared to dim light, decreases sleepiness and improves psycho-
motor vigilance performance. Sleep 26(6):695–700.
23. Rüger M, Gordijn MC, Beersma DG, de Vries B, Daan S (2006) Time-of-day-dependent
effects of bright light exposure on human psychophysiology: Comparison of daytime
and nighttime exposure. Am J Physiol Regul Integr Comp Physiol 290(5):R1413–R1420.
24. Vandewalle G, et al. (2006) Daytime light exposure dynamically enhances brain re-
sponses. Curr Biol 16(16):1616–1621.
25. Czeisler CA, Zimmerman JC, Ronda JM, Moore-Ede MC, Weitzman ED (1980) Timing
of REM sleep is coupled to the circadian rhythm of body temperature in man. Sleep
2(3):329–346.
26. Czeisler CA, Weitzman Ed, Moore-Ede MC, Zimmerman JC, Knauer RS (1980) Human
sleep: Its duration and organization depend on its circadian phase. Science 210(4475):
1264–1267.
27. Weitzman ED, Czeisler CA, Zimmerman JC, Ronda JM (1980) The timing of REM sleep
and its relation to spontaneous awakening during temporal isolation in man. Sleep
Res 9:280.
28. Wood B, Rea MS, Plitnick B, Figueiro MG (2013) Light level and duration of exposure
determine the impact of self-luminous tablets on melatonin suppression. Appl Ergon
44(2):237–240.
29. Brainard GC, et al. (2001) Action spectrum for melatonin regulation in humans: Evi-
dence for a novel circadian photoreceptor. J Neurosci 21(16):6405–6412.
30. Thapan K, Arendt J, Skene DJ (2001) An action spectrum for melatonin suppression:
Evidence for a novel non-rod, non-cone photoreceptor system in humans. J Physiol
535(Pt 1):261–267.
31. Lockley SW, Brainard GC, Czeisler CA (2003) High sensitivity of the human circadian
melatonin rhythm to resetting by short wavelength light. J Clin Endocrinol Metab
88(9):4502–4505.
32. Lockley SW, et al. (2006) Short-wavelength sensitivity for the direct effects of light on
alertness, vigilance, and the waking electroencephalogram in humans. Sleep 29(2):
161–168.
33. Münch M, et al. (2006) Wavelength-dependent effects of evening light exposure on
sleep architecture and sleep EEG power density in men. Am J Physiol Regul Integr
Comp Physiol 290(5):R1421–R1428.
34. Santhi N, et al. (2012) The spectral composition of evening light and individual dif-
ferences in the suppression of melatonin and delay of sleep in humans. J Pineal Res
53(1):47–59.
35. Lucas RJ, et al. (2014) Measuring and using light in the melanopsin age. Trends
Neurosci 37(1):1–9.
36. Gradisar M, et al. (2013) The sleep and technology use of Americans: Findings from
the National Sleep Foundation’s 2011 Sleep in America poll. J Clin Sleep Med 9(12):
1291–1299.
37. Krystal AD, et al. (2012) Eszopiclone treatment for insomnia: Effect size comparisons
in patients with primary insomnia and insomnia with medical and psychiatric co-
morbidity. Prim Care Companion CNS Disord 14(4).
38. Wright HR, Lack LC (2001) Effect of light wavelength on suppression and phase delay
of the melatonin rhythm. Chronobiol Int 18(5):801–808.
39. Klerman EB, Gershengorn HB, Duffy JF, Kronauer RE (2002) Comparisons of the
variability of three markers of the human circadian pacemaker. J Biol Rhythms 17(2):
181–193.
40. Iber C, Ancoli-Israel S, Chesson A, Quan SF (2007) The AASM Manual for the Scoring of
Sleep and Associated Events: Rules, Terminology and Technical Specifications (American
Academy of Sleep Medicine, Westchester, IL).
41. Gillberg M, Kecklund G, Åkerstedt T (1994) Relations between performance and
subjective ratings of sleepiness during a night awake. Sleep 17(3):236–241.
Chang et al. PNAS
|
January 27, 2015
|
vol. 112
|
no. 4
|
1237
PHYSIOLOGY SEE COMMENTARY
