12 FHC Deliverable 4 3 1 Reporting Plan To Guide The Development And Use Of Ky HDT
User Manual:
Open the PDF directly: View PDF ![]() .
.
Page Count: 11

Kentucky Health Data Trust Initiative
Creating the Reporting Plan: a Process to Guide the
Development and Use of the KyHDT
Deliverable 4.3.1
Prepared for the Kentucky Health Data Trust
Interagency Governance Workgroup
Freedman HealthCare
July 27, 2015
© Freedman HealthCare, 2015 Page 1 of 9
REPORTING PLAN OVERVIEW
A Reporting Plan outlines how information from the KyHDT will be disseminated, and defines – at a high
level – the format, frequency, and level of detail of all expected outputs. The Reporting Plan reflects the
priorities of the database’s primary users by laying out a reporting strategy targeted towards their
specific use cases. The KyHDT team should engage all Data Trust stakeholders in developing the
Reporting Plan, as it allows interested parties to reach consensus on the end goals for the Data Trust.
Creating a Reporting Plan early in the Data Trust planning process, with buy-in from all stakeholders,
drives subsequent development and implementation.
The Reporting Plan contains information about
1. Establishing the KyHDT vision
2. Defining use cases
3. Identifying the primary audiences for different reports and data products
4. Prioritizing use cases
5. Determining the reporting mechanism
The purpose of this document is to guide the Kentucky Cabinet for Health and Family Services (CHFS)
through these five steps and set the stage for its development of a KyHDT Reporting Plan. The following
sections summarize key findings from Freedman HealthCare’s discussions with KyHDT project
leadership, representatives from participating CHFS agencies, and external stakeholders from the
commercial payer community.
STEP 1: ESTABLISHING THE VISION
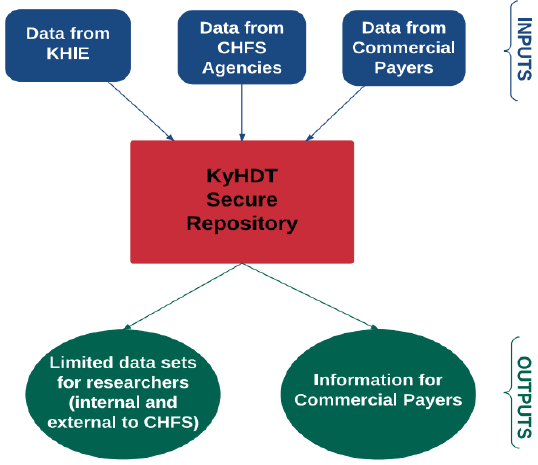
Figure 1: Data Flow through the KyHDT
The KyHDT initiative has tremendous
potential to benefit a range of users both
internal and external to CHFS. The
Cabinet’s overall vision for the KyHDT is to
collect public health information from CHFS
agencies, clinical records from the
Kentucky Health Information Exchange
(KHIE), and claims data from commercial
payers in one integrated database. Linking
data from across the spectrum of state
agencies, clinical providers, and
commercial payers will better equip CHFS
and other public and private health entities
to measure progress in meeting established
goals, identify health disparities and needs,
and add value to ongoing health care
initiatives.
As depicted in Figure 1, the KyHDT will be a centralized, secure repository within CHFS that houses data
from a range of internal and external sources. Encrypted data files from CHFS agencies, KHIE, and

© Freedman HealthCare, 2015 Page 2 of 9
commercial payers will flow into the KyHDT, where a team of
data experts will validate the data and assign a master patient
identifier (MPI) to all datasets. Using Business Intelligence tools
and other analytic resources, the KyHDT team will then produce
custom reports and limited data sets for internal (CHFS) and
external (non-CHFS) researchers. In addition, the KyHDT will feed
clinical information (i.e. medical record data) to each commercial
payer for the individuals in that payer’s member pool. In the
diagram above, the blue boxes represent data flowing into the
KyHDT, while the green boxes show the enhanced, integrated
information that the KyHDT produces.
Step 2: DEFINING DATA USES
Defining clear and specific data uses is the next critical step in developing the KyHDT Reporting Plan.
Understanding what types of information stakeholders (including those internal and external to the
State) wish to receive from the KyHDT, and how they will use this information, will help CHFS clarify
what data to collect, and what outputs to produce. Figure 2 below shows some of the potential reports
that the KyHDT could produce to benefit a range of users both internal and external to CHFS
This section presents a selection of potential
data uses for the KyHDT, based on conversations
with internal and external KY stakeholders as
well as common uses in other APCD states. CHFS
and its partners should review this list and
confirm that these uses align with their goals
and objectives for the KyHDT.
2a. Use Cases Based on Existing CHFS Data
Sources
Through preliminary conversations with CHFS
agencies, KyHDT project leaders have identified
several existing data sources for the KyHDT
within CHFS. For the purposes of the KyHDT
project, characteristics of an existing data source
include the following:
It is currently collected and stored in a data warehouse
It is controlled by a Cabinet agency
Figure 2: Potential KyHDT Reports
DRAFT VISION STATEMENT FOR THE KENTUCKY HEALTH DATA TRUST
The Kentucky Health Data Trust is a collaborative public-private initiative that aims to provide timely,
comprehensive health care data to improve health quality, value and outcomes for all Kentuckians. The Data
Trust will act as a neutral resource for all users and seek to disseminate useful information according to all
applicable laws and the terms of data use agreements.
What Users Want:
Critical Requirements for the KyHDT
Timely
Credible
Protective of privacy
Protective of trade secrets
Appropriately accessible
Affordable
Holistic
Builds over time
© Freedman HealthCare, 2015 Page 3 of 9
It contains person-level information
In general, data elements support cross-file linkages, preferably at the person level
The table below lists the existing data sources within CHFS that can be linked within the KyHDT.
Agency
Available Data
Department of Medicaid Services (DMS)
Medicaid claims, enrollment, member, provider
data
Department for Behavioral Health, Development,
and Intellectual Disabilities (DBHDID)
Utilization data from Community Mental Health
Centers (CMHC) and mental health facilities
Office of the Inspector General (OIG)
Controlled substance prescriptions through the
Kentucky All Schedule Prescription Electronic
Report (KASPER)
Department for Public Health (DPH)
Vital Statistics data (birth, death, marriage, and
divorce certificates)
Kentucky Health Benefits Exchange (KHBE)
Exchange enrollment data
Office of Health Policy (OHP)
De-identified hospital/ED discharge data
Potential options for linking these existing datasets include the following:
1. KASPER person-level data aligned with Medicaid enrollment files
The State’s KASPER system records prescription drug dispensing for narcotics and other controlled
substances. Information about Medicaid patients can be cross-referenced to their patient information,
including conditions and diagnoses. Such information could generate notices to MCOs, primary care
clinicians and care managers for purposes of outreach and health monitoring. This information could
also be linked to person level records for households with records of children in residence.
Possible Outputs:
Referral to medical or behavioral health care management
Outreach to clinicians treating flagged individuals
Dashboards showing areas with high match rates, type of prescription and other match/no
match information
Data/reports for prescription drug overdose prevention education (all clinicians or subset of
Medicaid clinicians in geographic areas of interest).
2. KASPER prescription data compared to Medicaid claims data to monitor Medicaid prescription drug
patterns
Prescription drug data is typically timelier than medical services claims, and may indicate emerging or
exacerbated conditions. Continuous and interrupted patterns are one indication that further patient
engagement may be required.
Possible Outputs:
Medication compliance patterns for individuals with chronic conditions, including behavioral
health medication continuity.
Information for primary care practices about patient medication activity.
Alerts regarding medication interactions identified through claims data.
Percentage of Medicaid prescriptions filled at out of state and bordering locations.
© Freedman HealthCare, 2015 Page 4 of 9
Assessment of whether controlled substances prescriptions for Medicaid enrollees are paid out
of pocket rather than by Medicaid.
3. Medicaid data linked to DPH Vital Statistics data
Possible Outputs:
Provider profiling and mortality rates by state, county, and provider – e.g. assess 30-day
mortality after date of admission for a defined set of medical conditions (such as heart bypass
surgery, stroke, heart attack, pneumonia, suicide, or overdose).
Trends in incidence, hospitalization, or mortality due to a particular condition.
Rate of delivery by cesarean section among Medicaid beneficiaries by county, facility, and
provider.
Prevalence of substance addiction among neonates at birth.
4. OHP Hospital Discharge and Emergency Department data aligned with DPH Vital Statistics death
data
Possible Outputs:
Top 10 admission diagnoses or ED presentations for patients who did not survive
Range of charges for admissions aligned with dates of death
5. Other topics:
Portrait of Medicaid service utilization prior to dual eligibility: Align Medicaid and Medicare
enrollee information; look back at Medicare service utilization for prediction of dual eligibility.
Health outcomes measurement for stroke and diabetes: Link Medicaid or Medicare clinical data
to disease registries.
2b. Use Cases Incorporating CHFS Data Sources Expected in 2016
The table below shows the agency datasets that CHFS expects will be available in 2016. Projects listed in
this section build upon the analysis and linking efforts mentioned above and require more complex
analytic processes, modeling tools and alignment across more than two files.
Agency
Expected in 2016
Department for Behavioral Health, Development,
and Intellectual Disabilities (DBHDID)
Integrated behavioral health/physical health
outcomes data
Department for Public Health (DPH)
Lab data and disease registries
Potential options for leveraging these additional datasets include the following:
1. Create new flags in KHIE to feed data to CHFS agencies and/or directly to the KyHDT
ED visits
BH diagnoses
Substance abuse (SA)

© Freedman HealthCare, 2015 Page 5 of 9
2. Align new DPH lab database and Medicaid data
Track diabetes (uncontrolled or undiagnosed), kidney function (identifying early stage renal
disease), cholesterol, communicable diseases, and Hepatitis C in the Medicaid population for
improved care management and targeted interventions
3. Use the MPID in Release 5 to develop cross-programs utilization portrait
Develop cross-agency total cost of care and analysis of state-funded service use.
Analyze service outcomes.
Potential data sources include: Medicaid eligibility and claims data; DBHDID; SNAP; TANF;
KASPER; OHP KHA discharge data; KHIE clinical data
4. Implement a predictive modeling tool based on claims data.
Analytic opportunities include:
Identify the predictive cost per member per quarter for the Medicaid population
o Map the geographic distribution of “healthiest” Medicaid populations
o Evaluate against self-reported illness burden (BRFSS) and disease registries.
o Identify patterns of service utilization to assess gaps in care
o Explore clinical service delivery models in operation that point to better care.
2c. Use Cases with Commercial Claims Data
CHFS’s vision for the KyHDT also includes bringing in claims data from external payers, including the
following entities:
Commercial fully-insured plans
Commercial self-insured plans
Kentucky Employee Health Plan (KEHP)
Medicare
Kentucky universities
Adding claims (medical, pharmacy, and dental), enrollment, member, and provider data to the KyHDT
presents a wealth of additional use cases for CHFS. For example, CHFS can leverage these data in the
following ways:
Use Case
Examples
Population Health
Identify social determinants of health and geographic variations of
disease prevalence
Understand the state of health care access and quality at the
population level
Policy Research
Compare KY data/trends to regional and national benchmarks
Evaluate the effectiveness/impact of CHFS programs
Data-Driven Decision
Support
Demonstrate ROI for CHFS programs to inform legislate or policy
decisions
Measure the state’s existing population health goals, and set new
goals
Understand which preventive services predict better outcomes for
Kentuckians
Study the utilization, care patterns, and outcomes of individuals
enrolled in HDHPs as compared to those in HMO/PPO plans
© Freedman HealthCare, 2015 Page 6 of 9
Medicaid Program
Support
Track and assess “churn” from Medicaid to private coverage
Market Insight
Assess physician reimbursement trends
Understand provider utilization, payment, and performance
Develop a robust patient sample across multiple carriers to
determine provider quality
Perform risk-adjusted comparisons of providers and practices
Identify the predicative cost per member per quarter for the
commercial population
Support value-based insurance product design specific to Kentuckian
health care delivery
Assess the relationship between having a primary care provider and
ED use
Evaluate the impact of out-of-pocket expenditures on plan selection
and patient utilization
Publicly-Available
Purchaser Reports
Provide consumers with health care cost and quality information to
inform decision-making
Identify the expected cost of name-brand vs. generic drugs
Evaluate the effectiveness of employer wellness programs
Compare cost and utilization patterns for self-insured plans to the
statewide commercially insured population
2d. Use Cases for External Stakeholders
In addition to offering a range of potential use cases for CHFS agencies, the KyHDT will benefit external
stakeholders as well. For example, commercial payers who contribute claims data to the KyHDT may be
interested in using data derived from the KyHDT in the following ways:
Use Case
Examples
Population Health
Research
Use all payer claims data to increase the patient sample size for
research studies, by looking at patient populations across multiple
carriers rather than just one.
Access HIE, Vital Statistics, and registry data to explore new research
topics.
Use Medicaid and Medicare cost data to compare public vs. private
health care costs.
Care Management
Use chronic condition data to expedite the development of a care
management plan.
Use historical claims data to understand the history of care for new
members – including what services they’ve utilized, where they were
seeking care (provider and location), their past insurance coverage
status, etc.
Cost Trends Analysis
Access the entire claims history of new members to perform true cost
trending over time.
Use historical claims data to assess churn within the commercial
market (e.g. plan shopping) and determine its effect on cost
increases.

© Freedman HealthCare, 2015 Page 7 of 9
Business Development
and Improvement
Gain insights for expanding business to new geographic areas and
network development by using all payer data to help identify
utilization trends in those areas.
Improve policies and procedures based on a fuller picture of how a
population is utilizing services.
Data Elements that commercial payers would like to see in a Health Data Trust include:
Patient identifiers (particularly, but not only, when a patient has opted into data sharing for a
research project)
Medicare and Medicaid data
Multiple years of data
Operational considerations that commercial payers would like to see include:
Standardized format for providing data
No cost for payers to obtain data
Any cost data reported out or released represents at least three payers, with no one payer holding
more than 50% of the market share
Step 3: IDENTIFYING THE PRIMARY AUDIENCE
As evidenced by the above section, the KyHDT offers a range of benefits for many types of audiences.
Potential users include:
State agencies
Academic researchers
Hospital systems
Primary care providers
Community hospitals
Commercial health plans
State employee payers
Federal agencies
Third party administrators
Pharmaceutical companies
Employers
Public consumers/private citizens
Non-profits
Advocacy groups
Public health organizations
Legislators
When developing the reporting strategy, CHFS must decide who the target audience of the KyHDT will
be. It may be state agencies to inform research, programs and policies. It may be public consumers to
drive informed health care decision-making. It may be private or academic research groups to expand
population health research at the state, regional, or national level. The primary audience for an APCD
varies from state to state, and drives each state’s individual Reporting Plan.
Identifying the KyHDT’s primary user group, or groups, is essential for focusing CHFS’s planning efforts.
All priority use cases and outputs should focus first and foremost on meeting the priority needs of that
© Freedman HealthCare, 2015 Page 8 of 9
audience. This does not mean that the KyHDT cannot also benefit secondary and tertiary audiences and
provide helpful information for those users; rather, it allows CHFS to focus its development efforts and
implement a phased approach to KyHDT reporting.
Based on conversations with CHFS project leadership, a current assumption is that the primary audience
for the KyHDT is CHFS, and that participating CHFS agencies (DMS, DPH, DBHDID, OHP, and KHBE) would
be the primary users. Secondary audiences include public universities and commercial payers. However,
CHFS should confirm whether this assumption is correct.
STEP 4: PRIORITIZING DATA USES
As previously discussed, the KyHDT holds tremendous potential for CHFS and its internal and external
stakeholders. However, the KyHDT cannot meet all of these use cases overnight. CHFS should design a
realistic, phased approach for implementing the KyHDT and producing outputs that fulfill these use
cases, based on the target audience and its specific business needs.
To do so, CHFS should rank the use cases in terms of priority, and articulate which ones it will focus on
first, second, and third. Prioritizing the use cases will help define the key reporting goals for the KyHDT.
“Priority” can be defined by various criteria, including:
Availability of the data source(s)
Level of urgency (e.g. ability to meet a critical business need)
Implementation/production cost
Implementation timeframe
Level of effort
Benefit/Impact for internal vs. external users
CHFS and its stakeholders should develop prioritization criteria for KyHDT use cases and assign weights
to each to determine which criteria are most meaningful for the KyHDT project. They should then
evaluate each use case against these weighted criteria to rank them in order of priority. This priority
ranking will help determine the data collection, analysis, and reporting goals for the KyHDT. CHFS should
then group the prioritized use cases into three buckets (highest, medium, and lowest priority), and plan
three phases of KyHDT implementation to focus on those specific use cases in the short, medium, and
long term. Phase 1 will focus its data collection, analysis, and reporting efforts on meeting the highest
priority use cases; Phases 2 and 3 will follow based on time and resource availability.
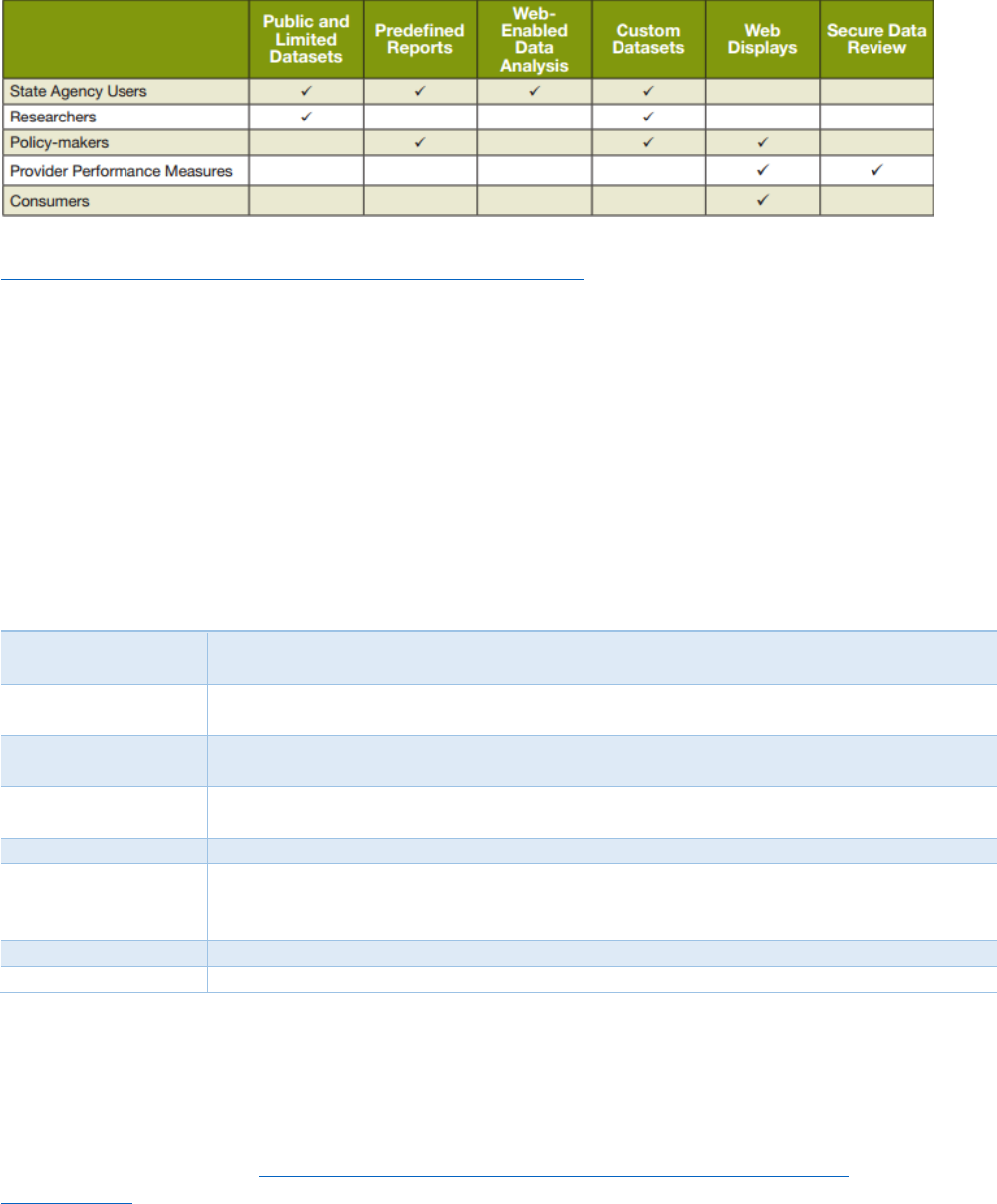
STEP 5: DETERMINING THE DATA DELIVERY MECHANISM
After CHFS and the KyHDT stakeholders prioritize use cases, they should determine the mechanism(s)
through which priority users can access the data. Table 1 provides examples of the various options for
data delivery that APCDs use, based on the category of users.
© Freedman HealthCare, 2015 Page 9 of 9
Table 1: Options for APCD Data Dissemination
Reference: Table 1: Common Data Dissemination Strategies. Realizing the Potential of All-Payer Claims Databases: Creating the
Reporting Plan. January 2014. Prepared by Freedman HealthCare for the Robert Wood Johnson Foundation. Available at:
http://www.rwjf.org/content/dam/farm/reports/issue_briefs/2014/rwjf409989.
For each expected output, CHFS should define, at a high-level, the format and frequency of the report.
Defining this high-level Reporting Plan should be a collaborative process with all stakeholders and will
help establish consensus and stakeholder buy-in on the “end goals” for the KyHDT.
CONCLUSION
By completing the five steps outlined above, CHFS and its partners will be able to define a high-level
Reporting Plan for the KyHDT. Having this Plan in place will drive all subsequent elements of the KyHDT
“roadmap” for building and implementing the APCD. Table 2 below provides a brief summary of the key
elements of this Roadmap that CHFS should address:
Table 2: Key Elements of the KyHDT Roadmap
Area
Planned CHFS Activities
Governance
Establish a public-private governance structure
Create new or amend existing data use agreements
Clinical Data
Roll out the Master Patient Identifier
Build out lab and imaging data capture
Claims Data
Work with payers to define claims data collection
Build out KyHDT data intake and quality control
Data Processing
Create standard data tables
Apply analytic and business intelligence tools to integrate and analyze the data
Reporting
Define the data access/reporting options
Operations
Document privacy and security procedures
Develop data access protocols
Support data use request process
Sustainability
Explore options for data service fees
Public Messaging
Communicate the KyHDT’s uses, benefits, and security protections to the public
In conclusion, the Reporting Plan is the critical first step in implementing this Roadmap. It will provide
CHFS the opportunity to clearly articulate the ultimate goals of the KyHDT initiative and align all
development activities under a shared vision.
For more information on lessons learned for APCD Reporting Plans, as well as case studies from other
APCD states, please refer to: Realizing the Potential of All-Payer Claims Databases: Creating the
Reporting Plan (January 2014), prepared by Freedman HealthCare for the Robert Wood Johnson
Foundation.
© Freedman HealthCare, 2015 Page 10 of 9
