470 4389 Consumer Directed Attendant Care (CDAC) Daily Service Record
User Manual: 4389
Open the PDF directly: View PDF ![]() .
.
Page Count: 2
470-4389 (Rev. 11/09)
Iowa Department of Human Services
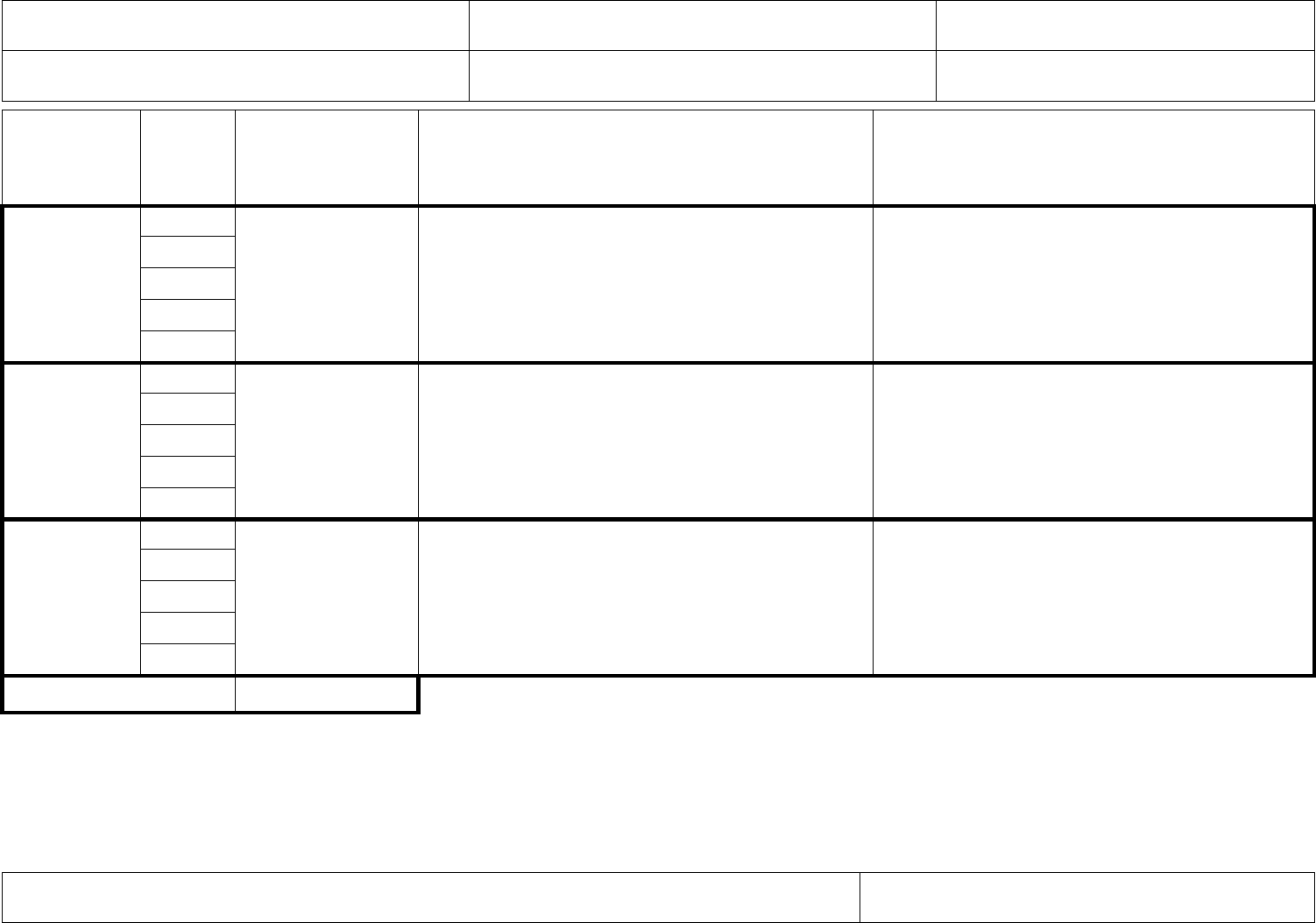
Consumer-Directed Attendant Care (CDAC) Daily Service Record
1. Provider name (first, middle initial, last)
2. Agency name (If an agency)
3. Daily date of service (month, day, year)
4. Consumer name (first, middle initial, last)
5. Consumer’s Medicaid ID number
6. Location(s) where service was given
7. Time I
was with the
consumer
(circle am/pm)
8.
Service
Code
9. Actual hours
of CDAC services
(list time worked
and being billed)
10. Description of the services
I performed for the consumer
11. Describe the consumer’s response
to services provided in box 10.
Start Time
___:___
am pm
End Time
___:___
am pm
Start Time
___:___
am pm
End Time
___:___
am pm
Start Time
___:___
am pm
End Time
___:___
am pm
12. Total hours
Service codes from CDAC Service Agreement. Choose from the list below. Enter the code in the “Service code” box 8 to show the service you provided.
Non-Skilled Services: N1 – Dressing
N5 – Transferring, ambulation, mobility
N9 – Assistance in the workplace
N2 – Bathing, grooming, personal hygiene
N6 – Essential housekeeping
N10 – Communication
N3 – Meal preparation & feeding
N7 – Minor wound care
N11 – Essential transportation
N4 – Toileting
N8 – Financial and scheduling assistance
N12 – Medication assistance
Skilled Services: S1 – Tube feedings
S5 – Respiratory care
S9 – Care of medical conditions
S2 – Intravenous therapy assistance
S6 – Care of decubiti and other areas
S10 – Post-surgical nurse delegated activities
S3 – Parenteral injections
S7 – Rehabilitation services
S11 – Monitoring reactions to medication
S4 – Catheterizations
S8 – Colostomy care
S12 – Prepare/monitor therapeutic diets
S13 – Recording and reporting of changes in vital signs to the nurse or therapist
13. Provider’s Signature
14. Date
470-4389 (Rev. 11/09)
This form is to record the services you provide. It is required that you fill out one of these forms every day that you provide services. Your billings may
be audited and if you do not have this form to support what you billed and were paid for, you may have to repay the Medicaid program. This form will be
used as the record for what you have done. Make sure that the form is filled out COMPLETELY.
This form must be maintained during the time that the member is receiving services and a minimum of five years from the last claim
submission date, even if you are no longer providing services.
You should use the form as a tool to keep a record of what you do. You provide very important care to your consumer. Part of your role is also to
monitor how your consumer is doing. Is the customer safe at home? Is the customer’s health getting worse? Is there anything going on to be
concerned about? Use this record to keep track of how your consumer does every day. Over time you might see a pattern. Contact the consumer’s
case manager if you are concerned regarding these services.
Directions: Fill out this form every time you provide services to your consumer. The CDAC Agreement (form 470-3372) lists the services you are
authorized to provide. After you finish performing the service, fill out this form. If you need more space to enter your information, you may use another
form for the same date of service. If you use more than one form for a date of service, you must still complete all of the fields on the other forms,
including the required signatures. Use a new form for each shift. This form must be completed in English.
Box by box instructions:
1. Provider name: Enter your name – first, middle initial, and last name.
2. Agency name (if an agency): If you are an agency waiver provider, enter the agency name.
3. Daily date of service: Enter the month, day, and year on which the service took place. It is required that you fill out a CDAC Daily Service
Record form every day that you provide service.
4. Consumer name: Enter the name of the person you are providing services for – first name, middle initial, and last name.
5. Consumer’s Medicaid ID number: Enter the Medicaid ID number of the person you are providing services for.
6. Location(s) where service was given: Enter the places where you performed the service. For example: home, work, school, etc.
7. Time I was with the consumer: Enter the time you began and ended each shift. You do not need to enter start and end times every time you
perform a service (toileting, meal preparation, etc.). You will enter one start time and one end time to make a record of your shift. Make sure to
use am/pm.
8. Service codes: Enter the service code (found in the list at the bottom of the page) that corresponds to the service you provided. These codes
must match what you have been approved to perform in your CDAC Agreement. You may have several codes in this field.
9. Actual hours of CDAC services: Enter the hours and minutes you actually provided for the service code you entered in box 8. (Note: The
amount of time entered in box 9 may be less than the full span of time entered in box 7.)
10. Description of the services I performed for the consumer: Explain what you did for the member.
11. Describe the consumer’s response to services provided in box 10 and any changes you saw with the consumer or service.
12. Total hours: Enter the number of hours you provided for the approved CDAC services described on the form. If you need to use more than one
form, only put the total number of hours provided for each separate form.
13. Provider’s signature: The actual provider of service.
14. Date: Enter the date of service on which the form was signed. This date should match the date of service entered in box 3.
