593458 Uk Kisqali Therapy Management Guide Digital 2018 V3.1
User Manual:
Open the PDF directly: View PDF ![]() .
.
Page Count: 13

Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard.
Adverse events should also be reported to Novartis Pharmaceuticals UK Ltd on 01276 698370,
at medinfo.uk@novartis.com or online through the patient safety information tool at https://psi.novartis.com
KISQALI® (ribociclib)
Optimising treatment
for your patients
KISQALI in combination with an aromatase inhibitor is indicated for the treatment of
postmenopausal women with HR+/HER2- locally advanced or metastatic breast cancer
as initial endocrine-based therapy.1
HR+/HER- = Hormone-receptor-positive and human epidermal growth factor receptor 2-negative.
Prescribing Information can be found on pages 22 and 23 of this document.
This medicinal product is subject
to additional monitoring.
THERAPY
MANAGEMENT
GUIDE

2 3
KISQALI is a CDK4/6 inhibitor for first-line HR+/HER2- locally advanced or metastatic breast
cancer treatment.1
This guide provides information for healthcare professionals about how to use KISQALI,
detailing posology, how to monitor patients, and how to manage important adverse events.
INDICATION1
KISQALI in combination with an aromatase inhibitor is indicated for the treatment of
postmenopausal women with HR+/HER2- locally advanced or metastatic breast cancer as
initial endocrine-based therapy.
MECHANISM OF ACTION1
KISQALI is a selective inhibitor of CDK4/6, which play a crucial role in signalling pathways
that lead to cell cycle progression and cellular proliferation.
KISQALI works with an aromatase inhibitor (e.g. letrozole) to induce G1 arrest and delay
disease progression.1
Introduction
CDK4/6 = cyclin-dependent kinases 4 and 6; ER = oestrogen receptor; G1 = gap phase 1.
Contents
CONTENTS ..........................................................................................................................PAGE
DOSING AND ADMINISTRATION ...................................................................4
Pharmaceutical form .................................................................................................................4
Starting dose ...............................................................................................................................4
Dosing schedule ..........................................................................................................................5
Method of administration .........................................................................................................5
DOSE MODIFICATIONS ................................................................................. 6
MONITORING ................................................................................................ 7
AE PROFILE ................................................................................................. 8
MANAGING NEUTROPENIA .........................................................................10
Clinical incidence .......................................................................................................................10
Neutropenia management algorithm .................................................................................... 11
MANAGING HEPATOBILIARY TOXICITY ......................................................12
Clinical incidence .......................................................................................................................12
ALT/AST management algorithm ..........................................................................................13
MANAGING QT PROLONGATION ..................................................................14
Clinical incidence .......................................................................................................................14
QT prolongation management algorithm ............................................................................15
GENERAL AE MANAGEMENT ......................................................................16
Clinical incidence .......................................................................................................................16
General AE management algorithm .....................................................................................16
OTHER SPECIAL WARNINGS AND PRECAUTIONS .......................................18
Effects during pregnancy and lactation, and on fertility .................................................18
Critical visceral disease ............................................................................................................18
Soya lecithin ...............................................................................................................................18
INTERACTIONS: EFFECTS ON KISQALI BY OTHER PRODUCTS ...................19
Strong CYP3A4 inhibitors .......................................................................................................19
Strong CYP3A4 inducers .........................................................................................................19
INTERACTIONS: EFFECTS ON OTHER PRODUCTS BY KISQALI ..................20
CYP3A4 substrates ..................................................................................................................20
Substances that are substrates of transporters ...............................................................20
ANTICIPATED INTERACTIONS ....................................................................21
Medicinal products that may prolong the QT interval ......................................................21
KISQALI PRESCRIBING INFORMATION....................................................... 22
2
11
3
4
5
6
7
9
9
10
10
ANDROGEN
OESTROGEN
ER
CYCLIN D1
CDK4/6
AROMATASE
AROMATASE
INHIBITOR
KISQALI
8
3
1
4 5
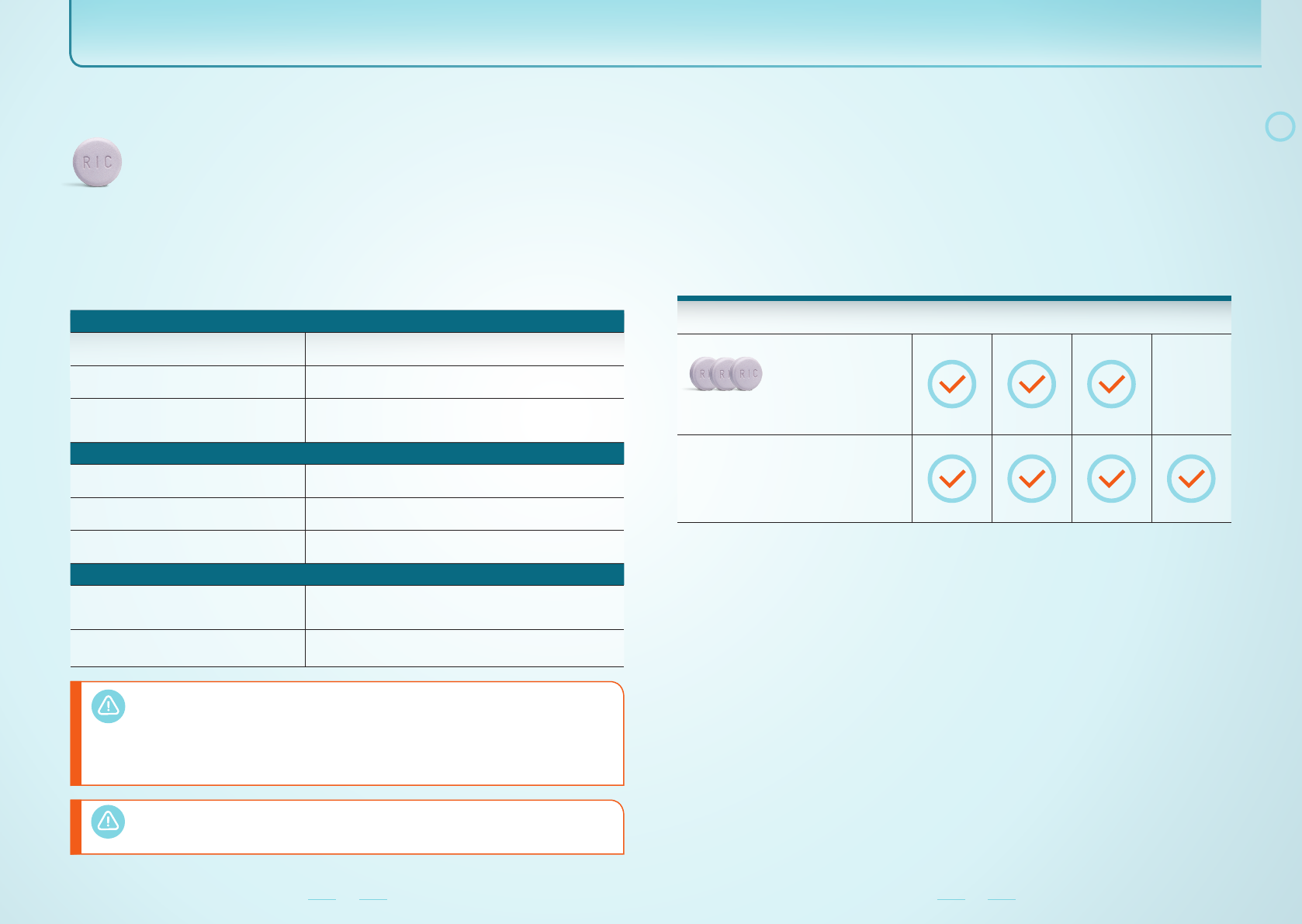
PHARMACEUTICAL FORM1
KISQALI is available as 200 mg film-coated tablets.
Diameter: 11.1 mm.
STARTING DOSE1
The recommended starting dose is 600 mg/day (3 x 200 mg tablets).
•A reduced starting dose may be required for special populations.
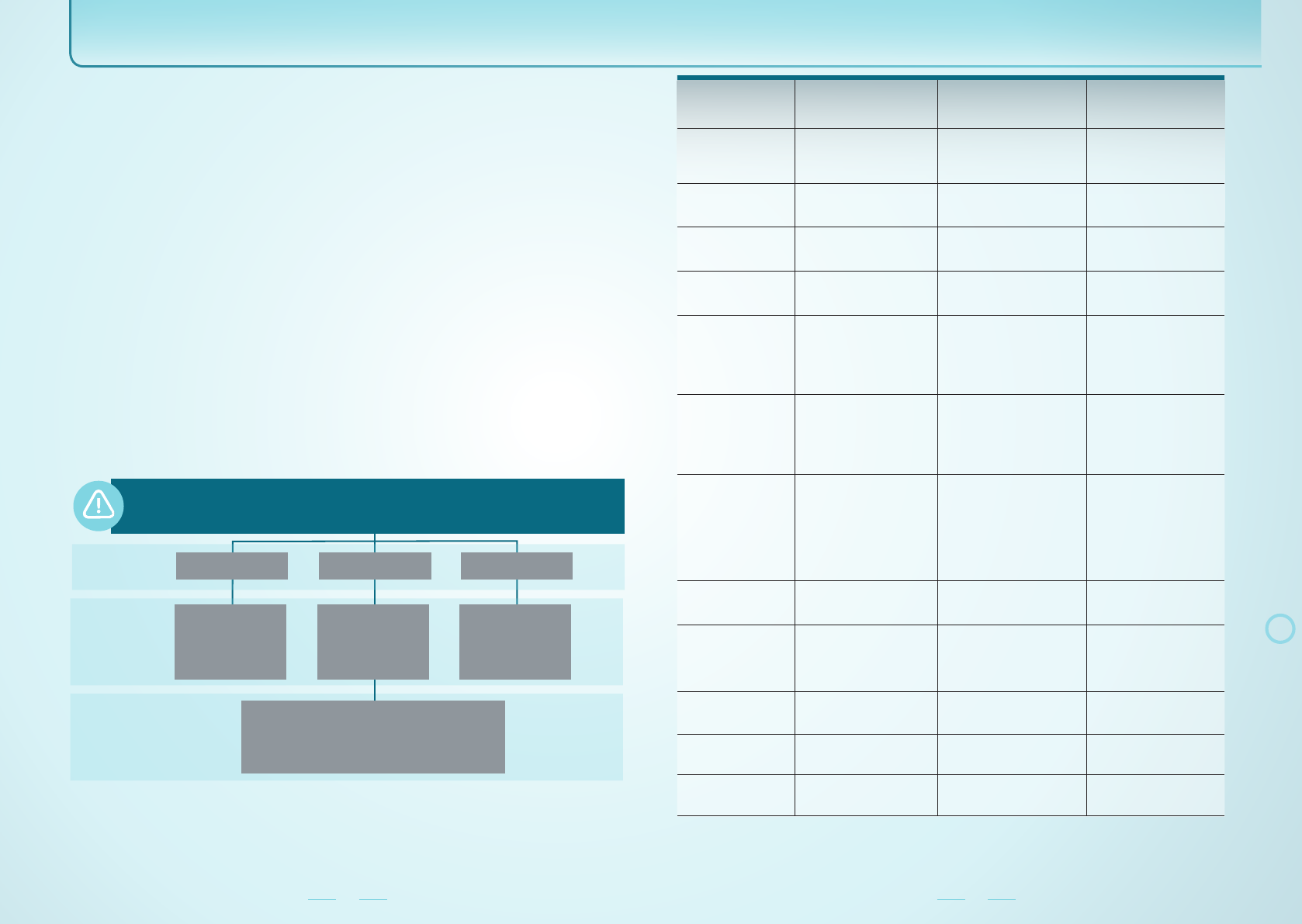
RECOMMENDED STARTING DOSES OF KISQALI FOR SPECIAL POPULATIONS1
RENAL IMPAIRMENT
MILD
(eGFR 60 to <90 ml/min/1.73 m2)No dose adjustment required.
MODERATE
(eGFR 30 to <60 ml/min/1.73 m2)No dose adjustment required.
SEVERE
(eGFR <30 ml/min/1.73 m2)
Caution should be used in patients with severe renal
impairment with close monitoring of signs of toxicity as there
is no experience with KISQALI in this population.
HEPATIC IMPAIRMENT
MILD
(Child–Pugh class A) No dose adjustment required.
MODERATE
(Child–Pugh class B) The recommended starting dose is 400 mg/day.
SEVERE
(Child–Pugh class C) The recommended starting dose is 400 mg/day.
PAEDIATRIC AND ELDERLY POPULATIONS
PAEDIATRIC POPULATION
(aged <18 years)
The safety and efficacy of KISQALI in children and
adolescents aged below 18 years have not been established
as no data are available.
ELDERLY
(aged >65 years) No dose adjustment required.
Dosing and administration
eGFR = estimated glomerular filtration rate; QTc = Corrected QT interval.
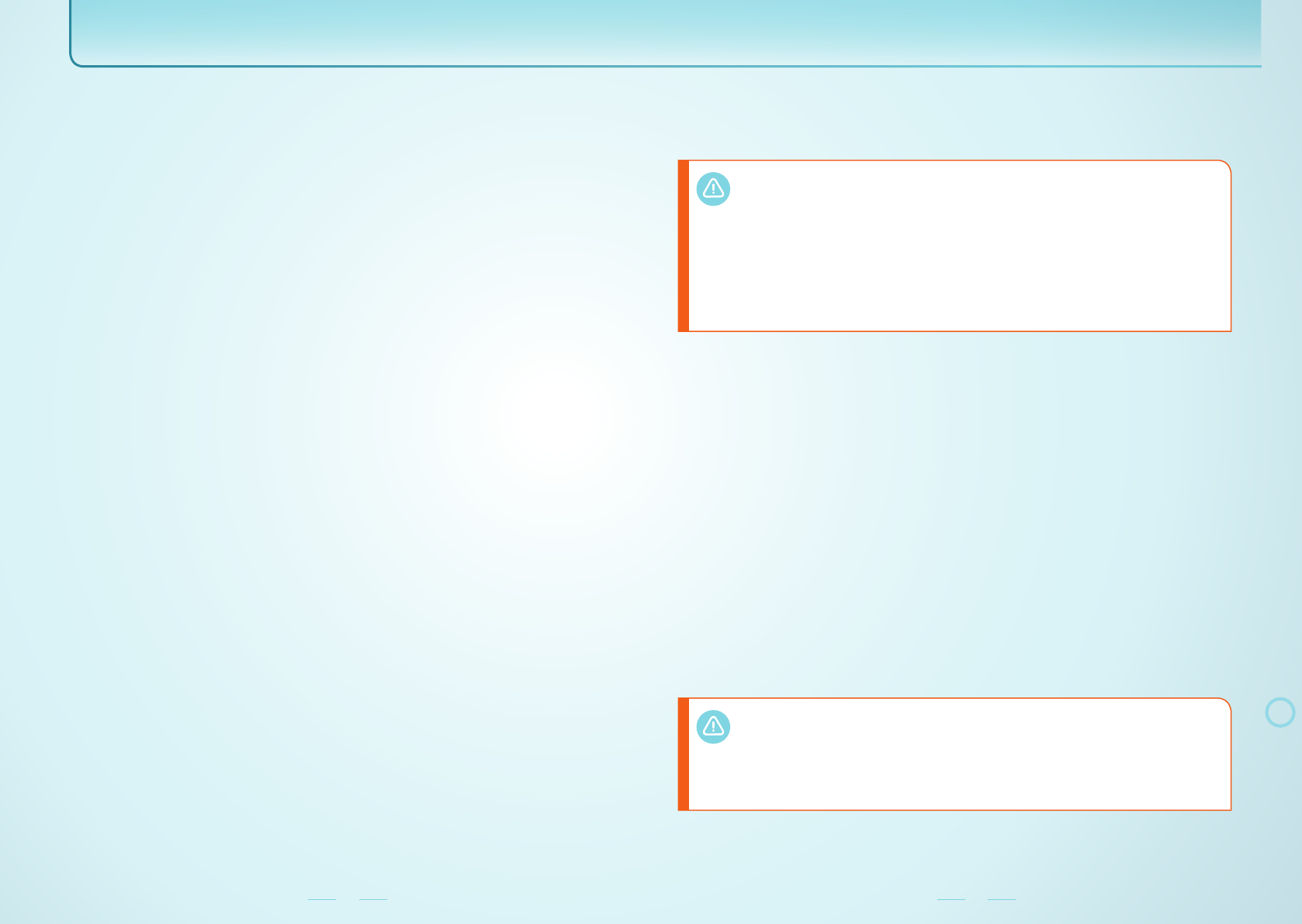
DOSING SCHEDULE1
KISQALI should be taken as part of a 28-day treatment cycle comprising a once-daily dose
of KISQALI for 21 consecutive days followed by 7 consecutive days off treatment. Treatment
with KISQALI should be continued as long as the patient is deriving clinical benefit from
therapy or until unacceptable toxicity occurs.
KISQALI should be used together with 2.5 mg letrozole or another aromatase inhibitor. The
aromatase inhibitor should be taken orally once daily continuously throughout the 28-day
cycle. Please refer to the Summary of Product Characteristics of the aromatase inhibitor for
additional details.
RECOMMENDED DOSING SCHEDULE FOR KISQALI (28-DAY CYCLE)1
WEEK 1 WEEK 2 WEEK 3 WEEK 4
KISQALI
600 mg (3 x 200 mg tablets) once daily for
21 consecutive days followed by 7 days off
treatment.
AROMATASE INHIBITOR
(e.g. 2.5 mg letrozole)
Once daily continuously throughout the
28-day cycle. Please see the Summary of
Product Characteristics for the aromatase
inhibitor for details.
Patients should take their dose at approximately the same time each day, preferably in the
morning. If the patient vomits after taking a dose or misses a dose, an additional dose should
not be taken that day. The next prescribed dose should be taken at the usual time.
METHOD OF ADMINISTRATION1
KISQALI should be taken orally once daily with or without food. KISQALI tablets should be
swallowed whole and should not be chewed, crushed or split prior to swallowing. No tablet
should be ingested if it is broken, cracked or otherwise not intact.
KISQALI can be administered with or without food, but patients should be instructed to avoid
pomegranates, pomegranate juice, grapefruit and grapefruit juice. These are known to inhibit
CYP3A4 enzymes and may increase the exposure to Kisqali.1
The use of KISQALI should be avoided in patients who already have or who are at significant
risk of developing QTc prolongation. These include patients with the following:
•long QT syndrome;
•uncontrolled or significant cardiac disease, including recent myocardial infarction,
congestive heart failure, unstable angina and bradyarrhythmias;
•electrolyte abnormalities.
A reduced dose of KISQALI may be required when strong CYP3A4 inhibitors are
concomitantly administered.
Dose adjustments with strong CYP3A4 inhibitors are detailed on page 19 of this guide.
2
6 7
Dose modifications
DOSE MODIFICATIONS
Management of severe or intolerable adverse events may require temporary dose
interruption, reduction or discontinuation of KISQALI.1
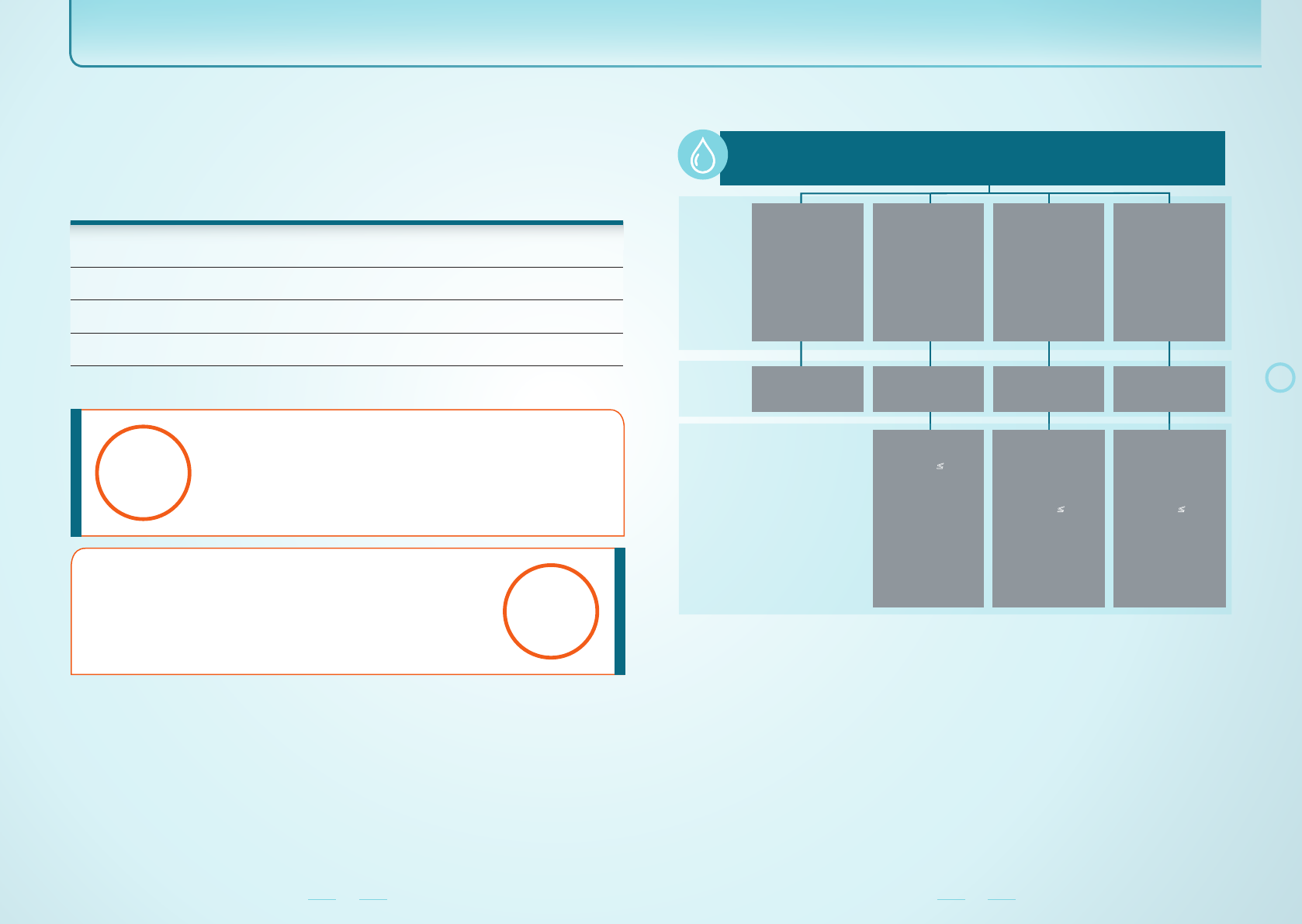
RECOMMENDED STEPWISE DOSE MODIFICATIONS1
RECOMMENDED
STARTING DOSE
FIRST
DOSE REDUCTION
SECOND
DOSE REDUCTION
600 mg/day
(3 x 200 mg tablets) ›
400 mg/day
(2 x 200 mg tablets) ›
200 mg/day
(1 x 200 mg tablet)
If further dose reduction below 200 mg/day is required, the treatment should be
permanently discontinued.
Dose modifications for specific adverse events are detailed on pages 10–17 of this guide.
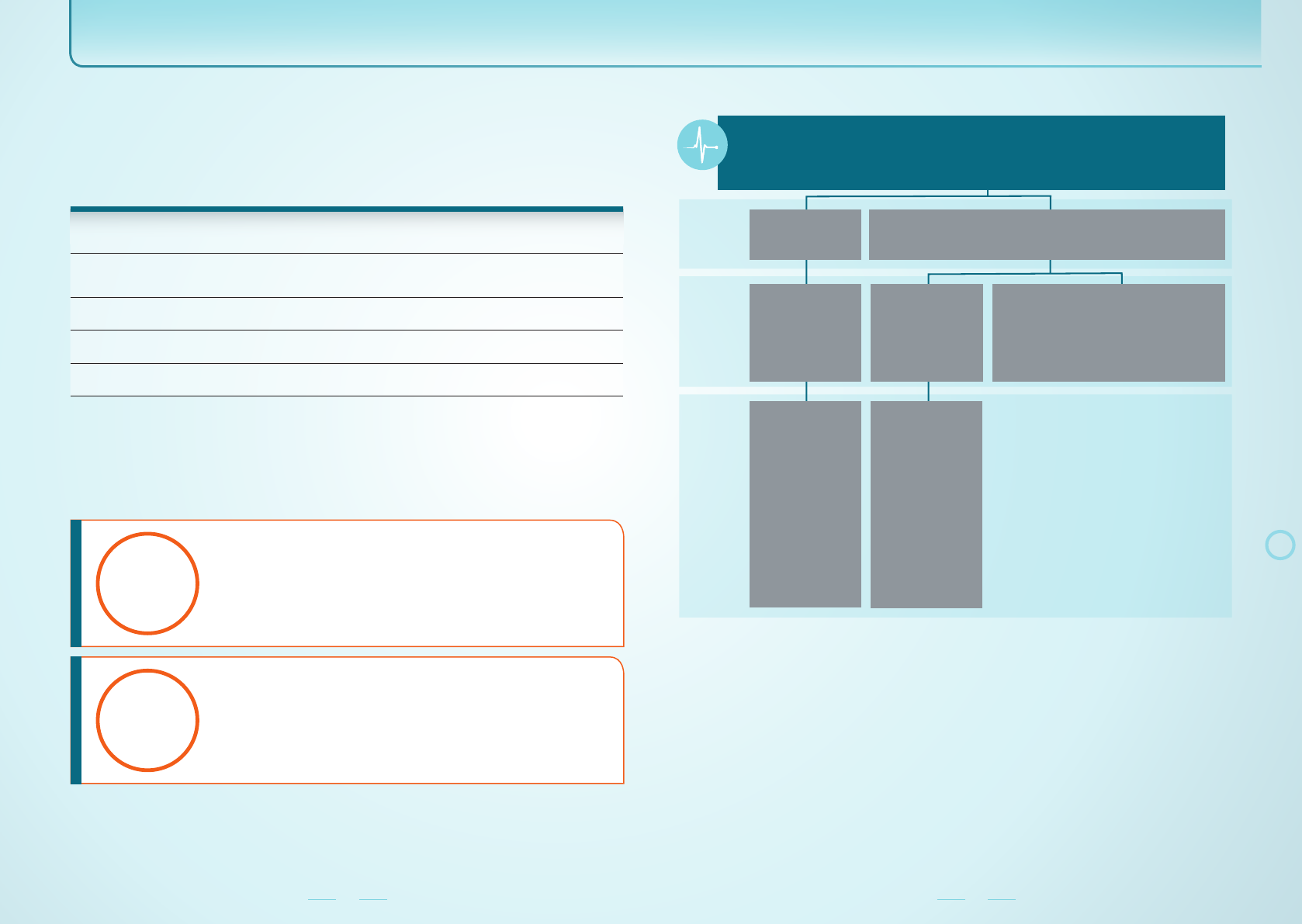
MONITORING
It is recommended that certain blood tests and an ECG assessment be performed prior to and
during treatment with KISQALI.1
RECOMMENDED MONITORING SCHEDULE1
CYCLE 1 CYCLE 2 CYCLES 3–6 THEREAFTER
BLOOD
FBC
LFTs Test prior to initiation. Day 14 Days 1 and 14 Day 1 of each
cycle
As clinically
indicated
Electrolytes
Test prior to initiation.
Correct any
abnormalities before
initiating treatment
with KISQALI.
Day 1 Day 1 Day 1 of each
cycle
As clinically
indicated
CARDIAC
ECG
Test prior to initiation.
KISQALI should only
be initiated in patients
with QTcF <450 msec.
Day 14 Day 1 As clinically
indicated
As clinically
indicated
•More frequent monitoring is recommended in the event of liver enzyme elevations
at grade ≥2 or QTcF prolongation during treatment.
As a result of monitoring, adverse events which require dose modification may be identified.
Dose modifications for specific adverse events are detailed on pages 10–17 of this guide.
ECG = electrocardiogram; FBC = full blood count; LFT = liver function test;
QTcF = QT interval corrected using Fridericia’s formula.
Monitoring
3

8 9
Adverse events profile
Frequencies of adverse events with KISQALI reported in MONALEESA-2, a Phase III clinical
study, are listed below. Frequencies are defined as: very common (≥1/10); common (≥1/100 to
<1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); and very rare (<1/10,000).1
FREQUENCIES OF ADVERSE EVENTS OBSERVED WITH KISQALI IN MONALEESA-21
AE FREQUENCY
Infections and infestations
Urinary tract infection Very common
Blood and lymphatic system disorders
Neutropenia Very common
Leukopenia Very common
Anaemia Very common
Lymphopenia Very common
Thrombocytopenia Common
Febrile neutropenia Common
Metabolism and nutrition disorders
Decreased appetite Very common
Hypocalcaemia Common
Hypokalaemia Common
Hypophosphataemia Common
Nervous system disorders
Headache Very common
Insomnia Very common
Eye disorders
Lacrimation increased Common
Dry eye Common
Cardiac disorders
Syncope Common
Respiratory, thoracic and mediastinal disorders
Dyspnoea Very common
Epistaxis Common
AE FREQUENCY
Gastrointestinal disorders
Nausea Very common
Diarrhoea Very common
Vomiting Very common
Constipation Very common
Stomatitis Very common
Abdominal pain Very common
Dysgeusia Common
Dyspepsia Common
Hepatobiliary disorders
Hepatotoxicity* Common
Skin and subcutaneous tissue disorders
Alopecia Very common
Rash†Very common
Pruritus Very common
Erythema Common
Musculoskeletal and connective tissue disorders
Back pain Very common
General disorders and administration site conditions
Fatigue Very common
Peripheral oedema Very common
Asthenia Very common
Pyrexia Very common
Investigations
Abnormal liver function tests‡Very common
Blood creatinine increased Common
Weight decreased Common
Electrocardiogram QT prolonged Common
*
Hepatotoxicity: hepatocellular injury, drug induced liver injury, hepatotoxicity, hepatic failure (single non-fatal case),
autoimmune hepatitis (single case).
†Rash: rash, rash maculopapular.
‡Abnormal liver function tests: alanine aminotransferase increased, aspartate aminotransferase increased,
blood bilirubin increased.AE = adverse event
For a full list of adverse events, please consult the Summary of Product Characteristics
for KISQALI.
4
10 11
Managing neutropenia
CLINICAL INCIDENCE1
Neutropenia is a very common adverse event associated with KISQALI treatment (occurring
at a frequency of ≥1/10 patients), and was the most frequently reported adverse event in
MONALEESA-2.
NEUTROPENIA* EVENTS REPORTED IN PATIENTS RECEIVING
KISQALI (N=334) IN MONALEESA-21
EVENT†PROPORTION OF PATIENTS WITH
AT LEAST ONE EVENT (%)
Neutropenia at any grade 74 . 3
Neutropenia at grade 3 or 4 59.6
Febrile neutropenia 1.5
TIME TO ONSET AND IMPROVEMENT OF NEUTROPENIA IN MONALEESA-21
*Decrease in neutrophil count, based on laboratory findings.
†
Grading according to Common Terminology Criteria for Adverse Events (CTCAE) Version 4.032:
grade 3 neutropenia: ANC 500 to 1000/mm3; grade 4 neutropenia: ANC <500/mm3.
ANC = absolute neutrophil count.
NEUTROPENIA MANAGEMENT ALGORITHM1
Full blood counts should be performed before initiating with KISQALI.
After initiation of KISQALI, full blood count should be monitored every 2 weeks for the first
2 cycles, at the beginning of each of the subsequent 4 cycles, then as clinically indicated.
ANC 1000/mm3
to ≤LLN
(Grades 1 or 2*)
ANC
500–1000/mm3
(Grade 3*)
Grade 3*
neutropenia with a
single fever
>38.3°C [or >38°C
for more than
1 hour and/or
concurrent
infection]
(Grade 3* febrile
neutropenia)
ANC <500/mm3
(Grade 4*)
Clinical
description
Dose
modification
No dose
adjustment is
required.
Dose interruption
until recovery to
grade ≤2.
Dose interruption
until recovery to
grade ≤2.
Dose interruption
until recovery to
grade ≤2.
If neutropenia
improves to
grade ≤2:
Resume KISQALI
at the same dose
level.
If toxicity recurs at
grade 3:
Dose interruption
until recovery to
grade ≤2, then
resume KISQALI
and reduce by one
dose level.
If neutropenia
improves to
grade ≤2:
Resume KISQALI
and reduce by one
dose level.
If neutropenia
improves to
grade ≤2:
Resume KISQALI
and reduce by one
dose level.
Follow-up
If dose reduction below 200 mg/day is required, the treatment should be permanently
discontinued.
*Grading according to Common Terminology Criteria for Adverse Events (CTCAE) Version 4.03.2
LLN = lower limit of normal.
Among the patients who had
grade 2, 3 or 4† neutropenia,
the median time to onset was 16 days.
The median time to improvement of grade ≥3†
events with KISQALI (to grade <3) was 15 days
following treatment interruption and/or
reduction and/or discontinuation.
16
days
15
days
5

12 13
Managing hepatobiliary toxicity
CLINICAL INCIDENCE1
Hepatobiliary toxicity events* are a common adverse event associated with KISQALI
treatment, (occurring at a frequency of ≥1/100 patients, but <1/10 patients). Abnormal liver
function tests are a very common adverse event (occurring at a frequency of ≥1/10 patients).
HEPATOBILIARY TOXICITY EVENTS REPORTED IN PATIENTS RECEIVING KISQALI
(N=334) IN MONALEESA-21
EVENT†PROPORTION OF PATIENTS WITH
AT LEAST ONE EVENT (%)
Any hepatobiliary toxicity event
At any grade
At grade 3 or 4
24.0
11.4
ALT elevations at grade 3 or 4 10.2
AST elevations at grade 3 or 4 6.9
Concurrent elevations in ALT or AST >3 x ULN and total bilirubin >2 x ULN, with normal
alkaline phosphatase, in the absence of cholestasis occurred in 4 (1.2%) patients receiving
KISQALI in MONALEESA-2, all of whom recovered to normal levels within 154 days after
treatment with KISQALI was discontinued.
TIME TO ONSET AND IMPROVEMENT OF LIVER ENZYME ELEVATIONS IN
MONALEESA-2 AND A PHASE IB STUDY OF KISQALI PLUS LETROZOLE1
Based on the severity of the transaminase elevations, treatment with KISQALI may have to be
interrupted, reduced or discontinued as described on the page opposite. In MONALEESA-2,
discontinuation of KISQALI due to abnormal liver function tests or hepatotoxicity occurred in
3.0% and 0.6% of patients respectively.
Recommendations for patients who have grade ≥3 ALT/AST elevation at baseline have not
been established.
Page 12 footnotes:
*Hepatotoxicity included hepatocellular injury, drug-induced liver injury, hepatotoxicity, hepatic failure (of which there was
a single non-fatal case) and autoimmune hepatitis (of which there was a single case).
†Grading according to Common Terminology Criteria for Adverse Events (CTCAE) Version 4.032:
grade 3 ALT/AST elevation: >5–20 x ULN; grade 3 ALT/AST elevation: >20 x ULN.
ULN = upper limit of normal.
ALT/AST MANAGEMENT ALGORITHM1
Liver function tests should be performed before initiating treatment with KISQALI.
After initiation, liver function tests should be performed every 2 weeks for the first 2 cycles,
at the beginning of each of the subsequent 4 cycles, then as clinically indicated.
If grade ≥2 abnormalities are noted, more frequent monitoring is recommended.
No dose
adjustment is
required.
>ULN to 3 x ULN
(Grade 1*)
If grade 2 at
baseline:
No dose
adjustment is
required.
>3-5 x ULN
(Grade 2*)
If grade <2 at
baseline:
Dose
interruption
until recovery
to ≤ baseline
grade.
If ALT/AST
elevations improve
to ≤ baseline grade:
Resume KISQALI
at the same dose
level.
If toxicity recurs at
grade 2:
Resume KISQALI
and reduce by one
dose level.
If ALT/AST
elevations improve
to ≤ baseline grade:
Resume KISQALI
and reduce by one
dose level.
If toxicity recurs at
grade 3:
Discontinue
KISQALI.
Dose
interruption of
KISQALI until
recovery to ≤
baseline grade.
>5-20 x ULN
(Grade 3*)
Discontinue
KISQALI.
>20 x ULN
(Grade 4*)
Clinical
description
Dose
modifications
for ALT and/or
AST elevations
from baseline,
without
increase in
total bilirubin
above 2 x ULN
Follow-up
If patients develop ALT and/or AST >3 x ULN along with total bilirubin >2 x ULN
irrespective of baseline grade, discontinue KISQALI.
If dose reduction below 200 mg/day is required, the treatment should be permanently
discontinued.
*Grading according to Common Terminology Criteria for Adverse Events (CTCAE) Version 4.03.2
The majority (83.8%) of grade 3 or 4† ALT/
AST elevation events occurred within the first
6 months of treatment. Among the patients
who had grade 3 or 4† ALT/AST elevation, the
median time to onset was 57 days.
57
days
The median time to improvement
(to grade ≤2) was 24 days.
24
days
6
14 15
Managing QT prolongation
CLINICAL INCIDENCE1
QT prolongation is a common adverse event associated with KISQALI treatment (occurring at
a frequency of ≥1/100 patients, but fewer than 1/10 patients).
QT INTERVAL PROLONGATION REPORTED IN PATIENTS RECEIVING KISQALI
(N=334) IN MONALEESA-21
EVENT PROPORTION OF PATIENTS WITH
AT LEAST ONE EVENT (%)
Any QT interval prolongation
(including ECG QT prolonged
and syncope)
7. 5
QTcF interval >500 msec 0.3
QTcF interval >480 msec 3.3
QTcF increase >60 msec
from baseline 2.7
7.5% of patients had at least one event of QT interval prolongation (including ECG QT
prolonged and syncope) with KISQALI. There were no reported cases of torsade de pointes.
Dose interruptions/adjustments due to ECG QT prolongation and syncope were reported in
0.9% of patients who were receiving KISQALI.
TIME TO ONSET OF QT INTERVAL PROLONGATION IN MONALEESA-21,3
QTcF interval prolongation >480 msec with
KISQALI mostly occurred within the first 4 weeks
of treatment.
4
weeks
Amongst the patients who had QTcF prolongation
>480 msec, the median time to onset was
15 days, and these changes were reversible with
dose interruption and/or dose reduction.
15
days
Based on the severity of QT interval prolongation, treatment with KISQALI may have to be
interrupted, reduced or discontinued as described on the page opposite.
QT PROLONGATION MANAGEMENT ALGORITHM1
ECG should be assessed before initiating treatment. Treatment with KISQALI should be
initiated only in patients with QTcF values <450 msec. After initiation, ECG should be
repeated at approximately day 14 of the first cycle and at the beginning of the second cycle,
then as clinically indicated. In case of QTcF prolongation during treatment, more frequent
ECG monitoring is recommended.
ECGs with QTcF
>480 msec
Dose interruption
until recovery to
<481 msec
If QTcF is greater
than 500 msec on at
least two separate
ECGs:
Interrupt KISQALI
until QTcF is
<481 msec
If QTcF improves to
<481 msec:
Resume KISQALI
at the same dose
level.
If QTcF
prolongation recurs
at ≥481 msec:
Dose interruption
until QTcF improves
to <481 msec and
then resume
KISQALI and
reduce by one dose
level.
If QTcF improves to
<481 msec:
Resume KISQALI
and reduce by one
dose level.
ECGs with QTcF >500 msec
If QTcF interval prolongation to greater than
500 msec or greater than 60 msec change
from baseline occurs
in combination with
torsade de pointes or polymorphic
ventricular tachycardia or signs/symptoms of
serious arrhythmia:
Permanently discontinue KISQALI.
Clinical
description
Dose
modification
Follow-up
If dose reduction below 200 mg/day is required, the treatment should be permanently
discontinued.
7
16 17
General adverse events management
CLINICAL INCIDENCE1
The most common adverse events of any grade (reported in ≥20% of patients) for which the
frequency for KISQALI plus letrozole exceeds the frequency for placebo plus letrozole were:
•neutropenia
•leukopenia
•headache
•back pain
•nausea
•fatigue
•diarrhoea
•vomiting
•constipation
•alopecia
•rash
The most common adverse events at grade 3 or 4 (reported in ≥2% of patients) for which the
frequency for KISQALI plus letrozole exceeds the frequency for placebo plus letrozole were:
•neutropenia
•leukopenia
•abnormal liver
function test
•lymphopenia
•hypophosphataemia
•vomiting
•nausea
•fatigue
•back pain
Management of severe or intolerable adverse events with KISQALI may require temporary
dose interruption, reduction or discontinuation, as described on the page opposite.
GENERAL ADVERSE EVENTS MANAGEMENT ALGORITHM1
No dose adjustment
is required.
Initiate appropriate
medical therapy
and monitor as
clinically indicated.
Dose interruption
until recovery to
grade ≤1.
Discontinue
KISQALI.
Dose
modification
If AE improves to grade ≤1:
Resume KISQALI at the same dose level.
If toxicity recurs at grade 3:
Resume KISQALI and reduce by one dose level.
Follow-up
Management of severe or intolerable adverse events with KISQALI may require temporary dose
interruption, reduction or discontinuation.
Grade 1 or 2* Grade 3* Grade 4*
Clinical
description
If dose reduction below 200 mg/day is required, the treatment should be permanently
discontinued.
*Grading according to Common Terminology Criteria for Adverse Events (CTCAE) Version 4.03.2
*Grading according to Common Terminology Criteria for Adverse Events (CTCAE) Version 4.03.2
ADL = activities of daily living; BSA = body surface area; LLN = lower limit of normal; N/A = grade is not available;
TPN = total parenteral nutrition.
AE GRADES 1 & 2 GRADE 3 GRADE 4
Vomiting 1–5 episodes separated by
5 minutes) in 24 hours
≥6 episodes (separated
by 5 minutes) in 24 hours;
tube feeding, TPN or
hospitalisation indicated
Life-threatening
consequences; urgent
intervention indicated
Headache Mild or moderate pain;
limiting instrumental ADL
Severe pain;
limiting self-care ADL N/A
Back pain Mild or moderate pain;
limiting instrumental ADL
Severe pain;
limiting self-care ADL N/A
Fatigue
Fatigue relieved by rest, or
fatigue not relieved by rest;
limiting instrumental ADL
Fatigue not relieved by rest,
limiting self-care ADL N/A
Nausea
Loss of appetite without
alteration in eating habits,
or oral intake decreased
without significant weight
loss, dehydration or
malnutrition
Inadequate oral caloric or
fluid intake; tube feeding,
TPN, or hospitalisation
indicated
N/A
Diarrhoea
Increase of <7 stools per
day over baseline; mild
to moderate increase in
ostomy output compared
to baseline
Increase of ≥7 stools per day
over baseline; incontinence;
hospitalisation indicated;
severe increase in ostomy
output compared to baseline;
limiting self-care ADL
Life-threatening
consequences; urgent
intervention indicated
Constipation
Occasional or intermittent
symptoms; occasional use
of stool softeners, laxatives,
dietary modification, or
enema, or Persistent
symptoms with regular use
of laxatives or enemas;
limiting instrumental ADL
Obstipation with manual
evacuation indicated;
limiting self-care ADL
Life-threatening
consequences; urgent
intervention indicated
Alopecia
Any hair loss that is
abnormal for that
individual
N/A N/A
Rash
(maculopapular)
Macules/papules covering
<30% BSA with or without
symptoms (e.g. pruritus,
burning, tightness); limiting
instrumental ADL
Macules/papules covering
>30% BSA with or without
associated symptoms;
limiting self-care ADL
N/A
Hypophosphataemia <LLN to 2.0 mg/dL;
<LLN to 0.6 mmol/L
<2.0–1.0 mg/dL;
<0.6–0.3 mmol/L
<1.0 mg/dL;
<0.3 mmol/L; life-
threatening consequences
Leukopenia <LLN to 2000/mm3;
<LLN to 2.0 x 109/L
<2000–1000/mm3;
<2.0–1.0 x 109/L <1000/mm3; <1.0 x 109/L
Lymphopenia <LLN to 500/mm3;
<LLN to 0.5 x 109/L
<500–200/mm3;
<0.5–0.2 x 109/L <200/mm3; <0.2 x 109/L
Adapted from Common Terminology Criteria for Adverse Events (CTCAE) Version 4.03.2
8
18 19
Interactions: effects on KISQALI by other products
EFFECTS DURING PREGNANCY AND LACTATION, AND ON FERTILITY
KISQALI is indicated for use in postmenopausal women, but please note the following
effects of its active ingredient during pregnancy and lactation and on fertility.
Pregnancy status should be verified prior to starting treatment with KISQALI.
Based on findings in animals, KISQALI can cause foetal harm when administered to a
pregnant woman.
CRITICAL VISCERAL DISEASE
The efficacy and safety of KISQALI have not been studied in patients with critical
visceral disease.
SOYA LECITHIN
KISQALI contains soya lecithin. Patients who are hypersensitive to peanut or soya should
not take KISQALI.
Other special warnings and precautions
KISQALI is primarily metabolised by CYP3A4. Therefore, medicinal products that can
influence CYP3A4 enzyme activity may alter the pharmacokinetics of KISQALI.
STRONG CYP3A4 INHIBITORS1
The concomitant use of strong CYP3A4 inhibitors, including but not limited to the following,
must be avoided:
•Clarithromycin
•Indinavir
•Itraconazole
•Ketoconazole
•Lopinavir
•Ritonavir
•Nefazodone
•Nelfinavir
•Posaconazole
•Saquinavir
•Telaprevir
•Telithromycin
•Verapamil
•Voriconazole
Alternative concomitant medicinal products with less potential to inhibit CYP3A4 should be
considered and patients should be monitored for adverse events.
•If co-administration of KISQALI with a strong CYP3A4 inhibitor cannot be avoided, the
dose of KISQALI should be reduced to 400 mg; however, there are no clinical data with
this dose adjustment.
•In patients who have had their dose reduced to 400 mg and in whom initiation of
co-administration of a strong CYP3A4 inhibitor cannot be avoided, the dose should be
further reduced to 200 mg. In patients who have had their dose reduced to 200 mg and
in whom initiation of co-administration of a strong CYP3A4 inhibitor cannot be avoided,
KISQALI treatment should be interrupted.
•Due to inter-patient variability, the recommended dose adjustments may not be optimal
in all patients; therefore, close monitoring for adverse events is recommended. In the
event of toxicity related to KISQALI, the dose should be modified or treatment should be
interrupted until toxicity is resolved. If the strong inhibitor is discontinued, the KISQALI
dose should be resumed (after at least five half-lives of the CYP3A4 inhibitor) at the
dose used prior to the initiation of the strong CYP3A4 inhibitor.
•Patients should be instructed to avoid pomegranates, pomegranate juice, grapefruit
and grapefruit juice. These are known to inhibit CYP3A4 enzymes and may increase the
exposure to KISQALI.
STRONG CYP3A4 INDUCERS1
The concomitant use of strong CYP3A4 inducers, including but not limited to the following,
should be avoided:
•Phenytoin
•Rifampin
•Carbamazepine
•St John’s wort (Hypericum perforatum)
Alternative concomitant medicinal products with no or minimal potential to induce CYP3A4
should be considered and patients should be monitored for adverse events.
For a full list of potential interactions, please consult the Summary of Product
Characteristics for KISQALI.
9
20 21
Interactions: effects on other products by KISQALI Anticipated interactions
CYP3A4 SUBSTRATES1
KISQALI is a moderate to strong CYP3A4 inhibitor and may interact with medicinal substrates
that are metabolised via CYP3A4, which can lead to increased serum concentrations of the
concomitantly used medicinal product.
Caution is recommended when KISQALI is administered with sensitive CYP3A4 substrates
with a narrow therapeutic index. The dose of a sensitive CYP3A4 substrate with a narrow
therapeutic index, including but not limited to the following, may need to be reduced as
KISQALI can increase their exposure:
•Alfentanil
•Ciclosporin
•Everolimus
•Fentanyl
•Sirolimus
•Tacrolimus
Concomitant administration of KISQALI at the 600 mg dose with the following CYP3A4
substrates should be avoided:
•Alfuzosin
•Amiodarone
•Cisapride
•Pimozide
•Quinidine
•Ergotamine
•Dihydroergotamine
•Quetiapine
•Lovastatin
•Simvastatin
•Sildenafil
•Midazolam
•Triazolam
When KISQALI is co-administered with other medicinal products, the Summary of Product
Characteristics of the other medicinal product must be consulted for the recommendations
regarding co-administration with CYP3A4 inhibitors.
SUBSTANCES THAT ARE SUBSTRATES OF TRANSPORTERS1
KISQALI has a potential to inhibit the activities of drug transporters P-gp, BCRP,
OATP1B1/1B3, OCT1, OCT2, MATE1 and BSEP.
Caution and monitoring for toxicity are advised during concomitant treatment with sensitive
substrates of these transporters which exhibit a narrow therapeutic index, including but not
limited to the following:
•Digoxin
•Pitavastatin
•Pravastatin
•Rosuvastatin
•Metformin
MEDICINAL PRODUCTS THAT MAY PROLONG THE QT INTERVAL1
Co-administration of KISQALI with anti-arrhythmic medicinal products with a known
potential to prolong the QT interval, including, but not limited to, the following, should
be avoided:
•Amiodarone
•Disopyramide
•Procainamide
•Quinidine
•Sotalol
Co-administration of KISQALI with other medicinal products with a known potential to
prolong the QT interval, including but not limited to the following, should be avoided:
•Chloroquine
•Halofantrine
•Clarithromycin
•Haloperidol
•Methadone
•Moxifloxacin
•Bepridil
•Pimozide
• Intravenous ondansetron
For a full list of potential interactions, please consult the Summary of Product
Characteristics for KISQALI.
10

22 23
PRESCRIBING INFORMATION
Kisqali® (ribociclib succinate)
(Please refer to the SmPC before prescribing
Kisqali)
Presentation: Film-coated tablet containing
ribociclib succinate, equivalent to 200 mg
ribociclib. Indication: Kisqali, in combination
with an aromatase inhibitor, is indicated for
the treatment of postmenopausal women
with hormone receptor (HR)-positive, human
epidermal growth factor receptor 2 (HER2)-
negative locally advanced or metastatic breast
cancer as initial endocrine-based therapy.
Dosage: The recommended dose is 600 mg once
daily; taken orally with or without food at the
same time every day for 21 days, followed by 7
days off treatment, resulting in a complete cycle
of 28 days. The treatment should be continued
as long as the patient is deriving clinical benefit
from therapy or until unacceptable toxicity
occurs. Kisqali should be used together with
2.5 mg letrozole or another aromatase inhibitor
(AI). The AI should be taken orally once daily
continuously throughout the 28-day cycle. If the
patient vomits after taking the dose or misses
a dose, an additional dose should not be taken.
The next prescribing dose should be taken at the
usual time. Dose Modification: Management of
severe or intolerable adverse drug reactions may
require temporary dose interruption, reduction
or discontinuation of Kisqali (See Special
Warnings & Precautions). Dose reduction should
be achieved by decrements of 200 mg daily. If
further dose reduction below 200 mg/day is
required, the treatment should be permanently
discontinued. Full blood counts (FBC) should
be performed before and after initiating Kisqali
treatment. FBC should be monitored every
2 weeks for the first 2 cycles, at the beginning
of each of the subsequent 4 cycles, then as
clinically indicated. For neutropenia, no dose
modifications required for grade 1 or 2. For grade
3, interrupt the dose until recovery to grade ≤2,
then resume at same dose level. If toxicity recurs
at grade 3, interrupt the dose until recovery,
then resume Kisqali and reduce by 1 dose level.
For grade 3 febrile neutropenia interrupt the
dose until recovery to grade ≤2, resume Kisqali
and reduce by 1 dose level. For grade 4 interrupt
the dose until recovery to grade ≤2, resume
Kisqali and reduce by 1 dose level. Liver function
tests (LFTs) should be performed before and
after initiating Kisqali treatment. LFTs should be
performed every 2 weeks for the first 2 cycles,
at the beginning of each of the subsequent
4 cycles, then as clinically indicated. If
grade ≤2 abnormalities are noted, more frequent
monitoring is recommended. No dose adjustment
is required for grade 1. For grade 2: if baseline at
grade <2, interrupt until recovery to ≤ baseline
grade, then resume Kisqali at same dose, and if
grade 2 recurs, resume Kisqali at next lower dose
level; if baseline at grade 2, no dose interruption.
For grade 3: interrupt Kisqali until recovery
to ≤ baseline grade then resume at next lower
dose level. If grade 3 recurs, discontinue Kisqali.
For grade 4: discontinue Kisqali. If patients
develop ALT and/or AST >3xULN along with total
bilirubin >2xULN irrespective of baseline grade,
discontinue Kisqali. ECG should be assessed
before and after initiating treatment with Kisqali.
ECG should be repeated at approximately day 14
of the first cycle and at the beginning of the
second cycle, then as clinically indicated. In
case of QTcF prolongation during treatment,
more frequent ECG monitoring is recommended.
ECGs with QTcF >480 msec the dose should be
interrupted. If the QTcF resolves to <481 msec,
resume the treatment at same dose level and if
QTcF >481 msec recurs, interrupt the dose until
QTcF resolves to <481 and then resume Kisqali
at the next lower dose level. If QTcF >500 msec
on at least 2 separate ECGs, interrupt Kisqali
until QTcF <481 msec then resume Kisqali at next
lower dose level. If QTcF >500 msec or >60 msec
change from baseline occurs in combination with
torsade de pointes or polymorphic ventricular
tachycardia or signs/symptoms of serious
arrhythmia, permanently discontinue Kisqali. For
other toxicities no dose adjustment required for
grade 1 or 2, initiate appropriate medical therapy
and monitor as clinically indicated. For grade 3,
interrupt until recovery to grade ≤1, then resume
Kisqali at the same dose. If grade 3 recurs, resume
Kisqali at the next lower dose level. For grade 4,
discontinue Kisqali. Concomitant use of strong
CYP3A4 inhibitors should be avoided and an
alternative concomitant medicinal product with
less potential to inhibit CYP3A4 inhibition should
be considered. If patients must be given a strong
CYP3A4 inhibitor concomitantly with ribociclib,
the Kisqali dose should be reduced to 400 mg
once daily. Contraindications: Hypersensitivity
to the active substance or to peanut, soya or
any other listed excipients. Special Warnings
and Precautions: Critical Visceral Disease: The
efficacy and safety of ribociclib have not been
studied in patients with critical visceral disease.
Neutropenia Based on the severity of the
neutropenia, Kisqali treatment may have to be
interrupted, reduced or discontinued. QT Interval
prolongation: Treatment with Kisqali should
be initiated only in patients with QTcF values
less than 450 msec. Appropriate monitoring
of serum electrolytes (including potassium,
calcium, phosphorus and magnesium) should
be performed before initiating treatment, at
the beginning of the first 6 cycles and then as
clinically indicated. Any abnormality should
be corrected before initiating treatment with
Kisqali. The use of Kisqali with medicinal products
known to prolong QTc interval and/or strong
CYP3A4 inhibitors should be avoided as this
may lead to clinically meaningful prolongation
of the QTcF interval. Kisqali should be avoided
in patients with long QT syndrome, significant
cardiac disease and electrolyte abnormalities.
Hepatobiliary toxicity, CYP3A4 substrates, soya
lecithin: see other sections. Based on findings in
animals, ribociclib can cause foetal harm when
administered to a pregnant woman. Kisqali may
have a minor influence on the ability to drive
and use machinery; patients should be cautious
in case they experience fatigue. Undesirable
Effects: Very common: abdominal pain,
abnormal liver function tests (ALT, AST & blood
bilirubin increased), alopecia, anaemia, asthenia,
back pain, constipation, decreased appetite,
diarrhoea, dyspnoea, fatigue, headache,
insomnia, leukopenia, lymphopenia, nausea,
neutropenia, peripheral oedema, pruritus,
pyrexia, rash, stomatitis, urinary tract infection
and vomiting. Common: decreased weight, dry
eye, dysgeusia, dyspepsia, electrocardiogram
QT prolonged, epistaxis, erythema, febrile
neutropenia, hepatotoxicity, hypocalcaemia,
hypokalaemia, hypophosphataemia, increased
lacrimation, increased blood creatinine, syncope
and thrombocytopenia. Interactions: Ribociclib
is primarily metabolised by CYP3A4. Medicinal
products that can influence CYP3A4 enzyme
activity may alter the pharmacokinetics of
ribociclib. Ribociclib is a moderate to strong
CYP3A4 inhibitor and may interact with
medicinal substrates that are metabolised
via CYP3A4, which can lead to increased
serum concentrations of the concomitantly
used medicinal product. Co-administration of
Kisqali with medicinal products with a known
potential to prolong the QT interval such as
anti-arrhythmic medicinal products and other
medicinal products that are known to prolong
the QT interval should be avoided. Please refer
to the SmPC for other possible interactions.
Basic NHS Cost: 21 tablets = £983.33, 42 tablets
= £1,966.67, 63 tablets = £2,950.00.
Marketing Authorisation (MA) Holder:
Novartis Europharm Ltd, Frimley Business Park,
Camberley, GU16 7SR, UK.
MA Number: EU/1/17/1221/001-012
Legal category: POM
Further information is available from Novartis
Pharmaceuticals UK Ltd, Frimley Business Park,
Frimley, Camberley, Surrey, GU16 7SR, UK. Tel:
01276 692255.
Date of Preparation: July 2017
KIS17-C022
Adverse events should be reported. Reporting
forms and information can be found at
www.mhra.gov.uk/yellowcard.
Adverse events should also be reported to
Novartis on 01276 698370, at
medinfo.uk@novartis.com or online through the
patient safety information tool at
https://psi.novartis.com
Prescribing information
11

July 2018
©2018 Novartis KIS17-C010c(1)
References:
1. KISQALI Summary of Product Characteristics.
2. US Department of Health and Human Services. Common terminology criteria for adverse events (CTCAE) version
4.03. 2010. Available at: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010–06–14_QuickReference_5x7.pdf
(Accessed July 2017).
3. Hortobagyi GN, Stemmer SM, Burris HA, et al. Ribociclib as first-line therapy for HR-positive, advanced breast cancer.
NEJM. 2016; 375(18); 1738–1748.
