4008 ACRIN SIM V2 01022014
User Manual: 4008
Open the PDF directly: View PDF ![]() .
.
Page Count: 27
Version: Finalv.2
Date:02January2014
SiteImagingManual
ACRIN PA 4008
ArterialStiffnessandWaveReflectionsasDeterminantsof
RegressionofLeftVentricularHypertrophyandFibrosisAssessed
withCardiacMRIafterAorticValveReplacementforSevere
AorticStenosis

ACRINPA4008SiteImagingManual
Final02January2014 pg.1of18
TableofContents
LetterofIntroduction…..…………………………………………………………………………………………………………..………..……….……...3
ACRINPA4008StudySchema……………………………………………………………………………………………………………………………...4
1.0OVERVIEWOFIMAGINGREQUIREMENTS…………………………………………………………………………………………….….5
2.0STUDYOBJECTIVES/SPECIFICAIMS………………………………………………………………………………………….…………….…5
2.1StudyOverview…………………………………………………………………………………………………………….……………..5
2.2PrimaryHypothesis…………………………………………………………………………………………………………..…….…..6
3.0SCANNERQUALIFICATION…………………………………………………………………………………………………………………….…6
3.1QualificationReview…………………………………………………………………………………………………………………..7
3.2VolunteerRe‐scanning………………………………………………………………………………………………………….…...7
3.3QualifyingImageSubmission……………………………………………………………….…………………………………….8
4.0ParticipantEligibility……………………………………………………………………………………………………………………………....9
4.1InclusionCriteria……………………………………………………………………………………………………..…………………9
4.2ExclusionCriteria………………………………………………………………………………………………………………..……..9
5.0ParticipantScheduling……………………………………………………………………………………………………………………….….10
6.0ParticipantPreparationforMRIImaging………………………………………………………………………………………….……10
7.0ContrastAgentAdministration…………………………………………………………………………………………………….………..10
8.0MRIStandardizedImageAcquisitionProtocol……………………………………………………………………………………....11
9.0ArterialTonometry……………………………………………………………………………………………………………………………..…17
10.0ImageSubmission………………………………………………………………………………………………………………………………...17
10.1TRIAD…………………………………………………………………………………………………………………………………….…..17
10.2ImageTransmittalWorksheet(ITW)…………………………………………………………………………………….……17
11.0ImageQualityControl(QC)………………………………………………………………………………………………………………..….18
11.1ACRINCoreLaboratoryQualityControlTechnicalReview…..…………………………………………..…………18
11.2ImageDataQueries……………………………………………………..…………………………………………………..……….18
12.0ImagingForms……………………………………………………………………………………………………………………………………...18
References………………………………………………………………………..……………………………………………………………………………….19
APPENDIXI:Phase‐ContrastImageAcquisitionInstructions
ACRINPA4008SiteImagingManual
Final02January2014 pg.2of18
HistoryofRevisions:
02‐Jan‐2014RevisionstoreflectAmendment3oftheProtocol.Editsmadetoeligibility
criteriaandprotocolspecificparameters.

ACRINPA4008SiteImagingManual
Final02January2014 pg.3of18
LetterofIntroduction
DearImagingStaff,
ThisSiteImagingManualcontainstheimageacquisitioninstructionsfortheACRINPA4008trial:“
ArterialStiffnessandWaveReflectionsasDeterminantsofRegressionofLeftVentricular
HypertrophyandFibrosisAssessedwithCardiacMRIAfterAorticValveReplacementforSevere
AorticStenosis.”
Tosuccessfullymeetthestudyobjectives,itiscriticalthattheCardiacMRIimagedatasetsareacquired
accordingtotheimagingprotocoldetailedinthismanual.
QualityControl(QC)reviewoftheimageswillbeperformedbytheACRImagingCoreLaboratory.This
reviewwillbeperformedinatimelyfashion,aspartofACRINstandardoperatingprocedures.Ifany
protocoldeviationsortechnicalissuesareidentifiedduringthereview,anACRCoreLabImaging
Technologistwillcontactyoursitetoprovidefeedbackexpeditiously.Thiswillallowyoursitetomake
anynecessaryadjustmentsearlyintheconductofthestudy.
TheACRINPA4008ImagingTeamwishestothankyouinadvanceforyourdiligenceinadheringtothe
proceduresdescribedinthismanualtoensuretheintegrityoftheimagedatacollectedforthestudy.
PleasedonothesitatetocontacttheACRINPA4008ImagingTechnologist(seecontactinformation
below)ifyouhaveanyquestions.
Sincerely,
DenaFlamini
ACRINPA4008ImagingAnalyst
AmericanCollegeofRadiology
1818MarketStreet‐Suite1600
Philadelphia,PA19103
Phone:(215)940‐8880
Fax:(215)923‐1737
www.acrin.org
Dflamini@acr.org
ACRINPA4008SiteImagingManual
Final02January2014 pg.4of18
ACRINPA4008StudySchema
3WeeksPriortoAVR
MRIScan1:
Gad‐EnhancedCardiacMRI
ArterialTonometry
6‐MonthsPost‐AVR(±2weeks)
MRIScan2:
Gad‐EnhancedCardiacMRI
6‐MinuteWalkTest
ArterialTonometry
AorticValveReplacement:
(AVR)InstitutionalStandard
PracticeWithin8WeeksAfter
Enrollment
Day#0
Eligibility/Enrollment
ACRINPA4008SiteImagingManual
Final02January2014 pg.5of18
1.0 OverviewofImagingRequirements
Qualification
Submitpriortositeactivation(foreachscanner):
ProtocolSpecificApplication(PSA);
Submissionofoneprotocolspecificqualificationexam
TRIADInstallation
Shouldbeinstalledpriortostudyparticipantenrollmentforsecure,
electronicsubmissionofimagingtoACRIN.
TimePointsforTrial
Examinations
MRIScan1:(Within3weekspriortoAVR)
o Gad‐EnhancedCardiacMRIandArterialTonometry
MRIScan2:(6monthspostAVRsurgery)
o Gad‐EnhancedCardiacMRI,6‐MinuteWalkTest,andArterial
Tonometry
ImageSubmission
ACRINPA4008imagingshouldbesubmittedelectronicallytotheACR
ImagingCoreLabviaTRIAD.Allimagingshouldbesubmittedwithin48hours
afteracquisitionandshouldincludeanImageTransmittalWorksheet(ITW).
DataQueriesACRINwillissuequeries,asneeded,basedonQCreviewofimaging.
GeneralTrialRequirements:
1.5TSiemensMRIscanner
InstitutionalexpertiseincardiacMRI(establishedcardiacMRIprogram)
Sitemustbeabletoutilizeaphased‐arraycoil
Sitemustbeabletoutilizeapowerinjector
Thesitemustbeabletosubmit(1)protocolspecificqualifyingexamination
SitemustsubmitalltrialexamstoACRINwithin48hoursafteracquisition
NOTE: ItmaybehelpfultokeepacopyofthisManualintheimagingdepartment,soall
technologistsinvolvedintheimageacquisitionofACRINPA4008areprivytotheprotocol‐required
imagingspecifications.
2.0 StudyObjectivesandSpecificAims
2.1 StudyOverview
ACRINPA4008SiteImagingManual
Final02January2014 pg.6of18
ACRINPA4008isamulti‐institutionalprojecttoprospectivelyevaluatepotentialdeterminants
oftheregression(improvement)ofLVhypertrophyandfibrosisassessedbycardiacMRIbefore
andafterAVRforsevereaorticstenosis.Atotalof80eligibleparticipantswilljointhestudy
fromACRIN‐qualifiedinstitutionswiththerequiredtechnology.Potentialparticipantswillbe
scheduledtoundergoAVRforseveresymptomaticaorticstenosiswithin8weeksafter
enrollment.Agadolinium‐enhancedcardiacMRIscan,alongwitharterialpulsewaverecordings
andnovelnon‐contrastmyocardialtissuecharacterizationsequences(T1rhomapping),willbe
performedwithin3weeksbeforetheAVRandrepeatedapproximately6monthsafterAVR.
ThesedatawillbeusedtoassessLVmass,LVmyocardialfibrosis,arterialstiffness,andwave
reflections.Additionalproceduresinthestudywillincludearterialtonometrymeasurements,
medicalhistoryreview,bloodcollection,aquality‐of‐lifequestionnaireanda6‐minutewalk
test.
2.2 PrimaryHypothesis
Studyhypothesesincludethatarterialstiffnessandarterialwavereflectionsareassociatedwith
alesspronouncedreductionofLVmassandfibrosisandwithagreaterdegreeofresidual
fibrosisandhypertrophydespitecorrectionofaorticstenosisviaAVR.Researchersexpectto
demonstratethatarterialstiffnessandwavereflectionsareimportantdeterminantsofresidual
leftventricularhypertrophyandfibrosis(adverseprognosticmarkersassessedwithcardiac
MRI)afteraorticvalvereplacement.Thiswouldidentifyanovel,potentiallytreatable
mechanismthatcouldbetargetedwiththerapyinfuturestudiesandcanbeassessedby
cardiacimagingstudies.
Importantly,thevalueofT1rhoimagingwillbeassessedtoevaluateitsvalueindetectingthe
degreeofmyocardialfibrosisatbaselineanddegreeofreductionafterAVR,usingpost‐
gadoliniumT1‐mappingasareferencemethod.ResearchersexpecttovalidateT1rho,anovel
MRIimagingmethodthatdoesnotrequiregadoliniumcontrast,asatechniqueforthe
assessmentofmyocardialfibrosis.Thiswouldallowformyocardialfibrosis(animportant
abnormalitythatneedstobeassessedinseveralcardiacconditions)tobeimagedwithoutthe
useofgadoliniumcontrast,whichiscontraindicatedinmanypatientswhohaveadvanced
kidneyimpairment.
3.0 ScannerQualification
ParticipationintheACRINPA4008trialrequiresthatallsitesadheretotheprotocolspecificcardiac
MRIparametersdetailedinthismanual.Theuseofstandardimagingguidelinesisanessential
componentofclinicaltrialsinwhichimagingplaysacentralroleintheresearchendpoints.Thisisof
particularimportanceinmulticentertrialswhereequipment,personnel,andimagingacquisition
protocolscanvarysignificantly.Thus,theuseofstandardizedimagingguidelineshelpscontrolthe
inter‐andintra‐variabilityinherentinmulticenterimagingtrials.

ACRINPA4008SiteImagingManual
Final02January2014 pg.7of18
Thepurposeofanyimagingqualificationprocessistohelpensurethetrialimagingisofhighquality
andperformedperthetrial‐standardizedacquisitionprotocol.ToparticipateintheACRINPA4008
trial,eachsitemustqualifybyfirstscanning(1)volunteerutilizingtheACRINPA4008scanning
protocolparameters(withoutaninjectionofgadoliniumcontrast).Thesubmissionofaqualifying
examprovidesanopportunitytoevaluatecompliancewithsampleimagingacquisitionprotocols
priortoparticipantrecruitmentandactualtrial‐specificprotocols.
ThequalifyingexamwillbereviewedbytheACRImagingCoreLabforbothprotocolcomplianceand
imagequality;approvalofthequalificationexamisrequiredpriortoACRINPA4008siteactivation.
Suboptimalimagequalityand/orimagingnotperformedperthetrial‐standardizedprotocolcan
resultinexclusionoftheimagingexam(s)and/ortheentirecasefromanalysis.Therefore,routineQC
andstrictadherencetotheACRINPA4008imageacquisitionprotocolareofgreatimportance,and
siteswillbeaskedtore‐scanavolunteershouldtherebeanysubstantivechangesinhardwareor
softwaretothescannerduringtheconductofthetrial.
3.1 QualificationReview
Thequalifyingexamwillbeevaluatedforimagequality(e.g.artifacts,distortion,andsignal‐
to‐noise)andcompliancewiththeprotocolspecificcardiacMRIparameters.AnACRImaging
CoreLabImagingTechnologistwillnotifythesiteoftheresultsofthequalifyingreviewviae‐
mail.E‐maildocumentationwillincludeyoursite’sStudyCoordinator(SC),sitePI,andlead
technologisttoinformthesiteteamwhetherthequalifyingexamhasbeenapproved.Ifthe
qualifyingexamisnotapproved,requiredcorrectionsforrescanningwillbeincludedinthee‐
mail.
NOTE:Approvalofthequalifyingexamismandatorypriortoyoursiteregisteringa
participantontotheACRINPA4008trial.
3.2 VolunteerRe‐scanning
Iftheinitialqualifyingexamisnotapproved,are‐scanofavolunteerwillberequireduntil
parametersforapprovalaremetforsitequalification.Uponapprovalofthequalifyingexam,
noadditionalrequalificationisrequiredunlessoneofthefollowingconditionsoccurs:
a. Newscannerbeingintroduced.
b. Majorchangestothequalifiedscanner.Amajorchangeinscannerhardwareor
softwareoccursduringthecourseofthestudy.Thiswouldincludemajorsoftware
upgrades(i.e.,asoftwareupgradethatresultinanewsoftwareprimaryversion
number)andchangestothecoilsystem,gradientsystems,orRFamplifier.Periodic
minorupdatestoexistingsoftwareversionsarenotconsideredmajorchanges.
ACRINPA4008SiteImagingManual
Final02January2014 pg.8of18
3.3 QualifyingImageSubmission
AllqualifyingexamsinDICOMformataretobesenttotheACRImagingCoreLabonCompact
Disc(CD)orDVD.
Pleaselabelthedisk,inpermanentmarker,withthefollowinginformation:
SiteName
TrialName:ACRINPA4008
DateofImaging(DD‐MMM‐YYY)
Forquestionsrelatedtoscannerqualification,pleasesendanemailto:
imagearchive@acr.org.Enter“ACRINPA4008ScannerQualification”inthesubjectline.
ShipAllQualificationImagingto:
AmericanCollegeofRadiology
1818MarketSt.,Suite1600
Philadelphia,PA19103
Attn:ACRINPA4008ScannerQualification

ACRINPA4008SiteImagingManual
Final02January2014 pg.9of18
4.0 ParticipantEligibility
4.1 InclusionCriteria
18yearsofageorolder
Severesymptomaticaorticstenosis(estimatedaorticvalvearea<1cm2)
PlannedforAVRprocedurewithin8weeksafterenrollment
AbletohaveacardiacMRIwithin3weekspriortoAVR
AbletotoleratecardiacMRIimagingwithgadoliniumcontrast
Willingandabletoprovideawritteninformedconsent
4.2 ExclusionCriteria
KnownLVejectionfraction<50%
Previousaorticvalvereplacement
Plannedadditionalvalverepair/replacement
Infectiveendocarditis
Moderateorsevereaorticvalveregurgitation
Rhythmotherthansinusrhythm(i.e.,atrialfibrillation)
Unstableanginainthepreviousmonth
Pre‐operativeestimatedglomerularfiltrationrate(eGFR)<45mL/min/1.73m²ofbody
surfacearea
Presenceofabicuspidaorticvalve,whichisassociatedwithanintrinsicaortopathy
thatmayaffectarterialloadinitsownright
Restingheartrate>120beatsperminute,systolicbloodpressure>180mmHg,or
diastolicbloodpressure>100mmHg
Pregnancyorintenttobecomepregnant
Unwillingnessofthepatienttosigntheconsentform
5.0 ParticipantScheduling
Participantswillundergotwo1.5TcardiacMRIstudiesforthetrial.MRISCAN1mustbecompleted
within(3)weekspriortoAVRandMRIScan2mustbecompleted(6)monthspostAVR.
ACRINPA4008SiteImagingManual
Final02January2014 pg.10of18
6.0 ParticipantPreparationforMRIImaging
Preparetheparticipantaccordingtolocalstandardpractice,includinganypre‐treatmentfor
severeclaustrophobiaoranxiety.
Confirmrenalfunctionsufficiencypriortoimaging;eGFRmustbe>30mL/min/1.73m²ofbody
surfacearea.
Iftheparticipanthassmoked,orhadfood,alcoholorcaffeinatedbeverageswithinfour(4)
hourspriortotesting,theMRIscanforthestudywillneedtoberescheduled.
Iftheparticipanthastakenashort‐actingnitratewithinfour(4)hourspriortotesting,theMRI
scanforthestudywillneedtoberescheduled
NOTE:aninclusioncriterionforthetrialisthepresenceofeGFR>45mL/min/1.73m²ofbody
surfacearea.ThisistominimizethepossibilityofeGFRdroppingto<30mL/min/1.73m²bythe
timeofthe2nd(final)MRI6monthspost‐AVR.ShouldasubjectdemonstrateaeGFR<30
mL/min/1.73m²atthetimeofthefinalMRI(6‐monthspost‐AVR),thesubjectshouldundergo
theMRIbutcontrastadministration,perfusionimaging,anddelayedenhancementinversion
recoverysequencesshouldnotbeperformed.Inthisinstance,variousotherMRImeasurements
willstillbeusefulforsomestudyend‐points(forinstance,LVmass).
SamesizeandplacementoftheintravenouscatheterisrecommendedforbothMRIscans.
Optimally,eachparticipantshouldreceiveanintravenouscatheterwithagaugenosmaller
than20gauge.
Theparticipantwillbeplacedsupineinthemagnet;armsatsideareacceptable.Thephased‐
arraycoilshouldbeplacedandtheparticipantshouldbelocalizedperinstitutionalstandard
practice.
Initiateimaging…
7.0 ContrastAgentAdministration
Eachparticipantshouldreceiveanintravenouscatheternosmallerthan20gauge
MultiHanceshouldbeadministeredinadynamicfashionwithapowerinjectoratbothtime
points.
Forthedynamicsequence,MultiHanceshouldbeadministeredintravenouslyatadoseof0.15
mmol/kgofbodyweightandrateof2ml/second,followedbya20mlsalineflush.
Thetype,amount,rateofinjection,andsite/gaugeofIVshouldcomplywiththestudy
guidelinesandshouldbedocumentedbythetechnologistontheMRIAssessmentform.
ACRINPA4008SiteImagingManual
Final02January2014 pg.11of18
NOTE:KeepinmindthatthesamedoseandrateofMultiHance,samearm,andsamerateof
contrastadministrationshouldbemaintainedforbothMRIScan1and2.
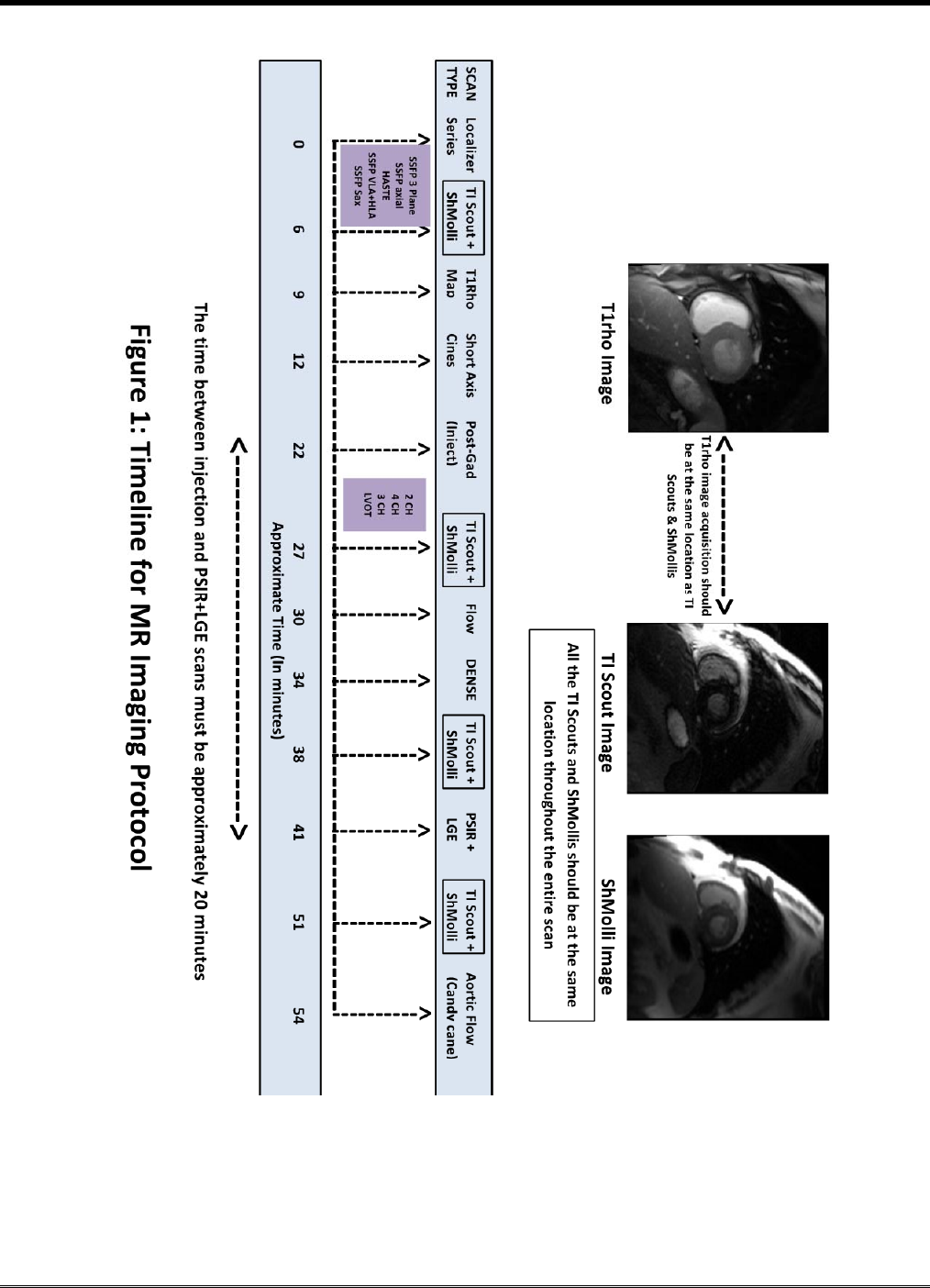
8.0 MRIStandardizedImageAcquisitionProtocol
BothMRIScan1and2ACRINPA4008imagingprotocolwillincludea:
LocalizerSeries
o 3‐planelocalizersSSFP(BHexpiration)
o AxialthoracicsingleshotaxialscoutSSFT(Non‐BH)
o HASTEthoracicFatsat(fromlowernecktobelowcosto‐phrenicangles)(Non‐BH)
o Double‐obliquelong‐axisLVplane,e.gpseudoVLAandHLAviewsSSFP(pseudoscout)
(BH‐expiration)
o ShortaxisLVplanesfrombasetoapex(pseudoscout)(BH‐expiration)
PRE‐GADAcquisitions:
TI‐ScoutLook‐Lockerinversionrecoveryacquisitionofamid‐ventricularshort‐axisLVview.
Therewillbebothalongandashortbreath‐holdTIScoutimageacquisition.NOTE:All
subsequentmid‐ventricularshortaxisviewsshouldbedoneatthislevel.Approximatelyten
imagesneedtobeacquiredsequentiallyatincreasinginversiontimes.
Note:Askthepatienttodohisbesttoholdhis/herbreathonthelongbreathhold,lettingthem
knowitwilllikelybedifficultandiftheyhaveto,lettheairoutoftheirlungsslowlybeforethey
breath.Iftheyareunabletoholdtheirbreathforthelongbreathholdsequence,itisvery
importanttheydotheirbesttoholditontheshortbreathholdsequence.
o RecommendedParameters:
Increasinginversiontimes:approximately50to1,000ms
Slicethickness:6mm
Baseresolution:192
Phaseresolution:50%
SH‐MOLLIacquisitionofT1maps(mid‐ventricularshort‐axisview,samesliceastheTI‐scout)
usingsingle‐shot,modifiedLook‐Lockerinversionrecoverysequence.(BH‐expiration)
o RecommendedParameters:
Slicethickness:6mm
Baseresolution:192
Phaseresolution:81%
PartialFourier:6/8

ACRINPA4008SiteImagingManual
Final02January2014 pg.12of18
T1RhoMAPAcquisitionT1rhomyocardialmaps(mid‐ventricularshort‐axisview,samesliceas
TImapabove)usingvariousspin‐locktimesinordertoreconstructT1rhomaps.Therewillbe
bothalongandashortbreath‐holdT1RhoMAPimageacquisition.(BH‐expiration).
o RecommendedParameters:
Variousspin‐locktimes:10‐50ms
Slicethickness:8mm
MultiHanceInjection:0.15mmol/kgofbodyweightatarateof2ml/second,followedbya20
mlsalineflush.Beforeinjection,setupturboflashdynamicperfusionsequence,shortaxis,at
thesamelocationastheTIscout.Justbeforeinjection,starttheperfusionsequenceandthen
injectcontrast.Donotchangeanyparameters.
POST‐GADAcquisitions:
Sequentialcontiguousshort‐axiscinescoveringtheLVfrombasetotheapexwiththe
useofbreath‐holdcinesteadystatefreeprecessionsequence(SSFP).1.QueSaxslice.
2.Hit“SCAN,”DONOTuse“APPEND”3.Presscontrol‐3or4toshiftby1slicetoward
theapex4.RepeatuntilfullLVcoverage.Note1:Control‐4or3shiftsbackwards
towardsthebase.Note2:Ifpoorquality(breathing,artifactsetc.)repeatscanAND
discardthepoorqualityimage(fromthelocaldatabase).(BH‐expiration)
o RecommendedParameters:
TR:28ms
TE:1.18ms,
Phases:30
Slicethickness:8mm
Interslicedistance:0mm
Matrix:192x192
IPAT:3or2(thefastestthecoilswillallowwithanacceptableimage)
SSFPCinelong‐axisplanes(2‐,4‐,3‐chamberviewsandLVOT)
o RecommendedParameters:
TR:30.6ms
TE:1.3ms
Phases:30
Slicethickness:8mm

ACRINPA4008SiteImagingManual
Final02January2014 pg.13of18
Matrix:192x192
IPAT:3or2(thefastestthecoilwillallowwithanacceptableimage)
TI‐ScoutLook‐Lockerinversionrecoveryofamid‐ventricularshort‐axisLVview(same
parameters,plane,andfieldofviewasinpre‐contrastacquisition).Thissequenceallowsfor
measurementofaveragemyocardialT1time
o RecommendedParameters:
Approximately10imagesacquiredsequentiallyatincreasinginversiontimes
(approximately50to1,000ms).
SH‐MOLLIacquisitionofT1mapsofamid‐ventricularshort‐axisLVview(sameparameters,
plane,andfieldofviewasinpre‐contrastacquisition)usinganECG‐gatedsingle‐shotmodified
Look‐Lockerinversionrecovery(sh‐MOLLI)sequence
Flow3chamberphasecontrastRtoLANDAtoP(twoseparateacquisitionswiththeONLY
changethedirectionoftheVENC)
o RecommendedParameters:
TR:35.15ms
TE:3.14ms
Slicethickness:5.5mm
BaseResolution:256
PhaseResolution:50%
IPAT:2
Flipangle:10degrees
Venc:130
FlowMode:SingleDirection
DENSEAcquisitionsofdisplacement‐encodedsequencesinamid‐ventricularshortaxis(same
slicepositionasallothersinglesliceSaximages)anda4‐chamberview
o RecommendedParameters:
Slicethickness:8mm
Matrix:112x112

ACRINPA4008SiteImagingManual
Final02January2014 pg.14of18
TI‐ScoutLook‐Lockerinversionrecoveryofamid‐ventricularshort‐axisLVview(same
parameters,plane,andfieldofviewasinpre‐contrastacquisition).Thissequenceallowsfor
measurementofaveragemyocardialT1time.
o RecommendedParameters:
Approximately10imagesacquiredsequentiallyatincreasinginversiontimes
(approximately50to1,000ms).
SH‐MOLLIacquisitionofT1mapsofamid‐ventricularshort‐axisLVview(sameparameters,
plane,andfieldofviewasinpre‐contrastacquisition)usinganECG‐gatedsingle‐shotmodified
Look‐Lockerinversionrecovery(sh‐MOLLI)sequence
TRUEFISPPSIRsingle‐shotSSFPphase‐sensitiveinversion‐recoveryacquisitionwithaninversion
timeprescribedtonullthemyocardialsignalapproximately20minutesafterthe
administrationofgadoliniumperformedincontiguousshort‐axisviews(copyprescriptionfrom
shortaxiscine).Thiswillbedonein2breathholdsalthoughcanbechangedifneeded.
o RecommendedParameters:
Slicethickness:8mm
Baseresolution:160
Phaseresolution:75%.
TURBOFLASHsegmentedphase‐sensitiveinversion‐recoveryacquisitionwithaninversiontime
prescribedtonullthemyocardialsignalimmediatelyaftertheSSFPsingle‐shortinversion
recoveryacquisition.1short‐axisslice(sameslicepositionasallothersinglesliceSax
images).Ifthereisbreathingartifact,pleaserepeattheacquisitionuntilahigh‐qualityimage
isobtained.
o RecommendedParameters:
Slicethickness:8mm
Baseresolution:256
Phaseresolution:75%.
TI‐ScoutLook‐Lockerinversionrecoveryofamid‐ventricularshort‐axisLVview(same
parameters,plane,andfieldofviewasinpre‐contrastacquisition).Thissequenceallowsfor
measurementofaveragemyocardialT1time
o RecommendedParameters:
Approximately10imagesacquiredsequentiallyatincreasinginversiontimes
(approximately50to1,000ms)

ACRINPA4008SiteImagingManual
Final02January2014 pg.15of18
SH‐MOLLIacquisitionofT1mapsofamid‐ventricularshort‐axisLVview(sameparameters,
plane,andfieldofviewasinpre‐contrastacquisition)usinganECG‐gatedsingle‐shotmodified
Look‐Lockerinversionrecovery(sh‐MOLLI)sequence
CANDY‐CANE/VENCIMAGINGFORTONOMETRYCOMPARISON
In‐planephase‐contrastacquisitionsinthe“candy‐cane”aorticview,tovisualizein‐planeflow
fordeterminationofaorticpulsewavevelocityfollowedbyshort‐axisaorticSFPcine
acquisitionsandthrough‐planeproximalaorticphase‐contrastacquisitions(whichwillbeused
formeasurementofvolumeflow).
NOTE:SeeAppendixIfordetailedphase‐contrastimageacquisitioninstructions
ACRINPA4008SiteImagingManual
Final02January2014 pg.16of18
ACRINPA4008SiteImagingManual
Final02January2014 pg.17of18
9.0 ArterialTonometry
ApplanationtonometryshouldbeperformedimmediatelyaftertheMRIscan(inwhichphasecontrast
acquisitionsofaorticflowareacquired).Thetonometryprocedureshouldbeperformedwith
prohibitionsonsmoking,meals,andalcohol,andbeveragescontainingcaffeineforthefour(4)hours
beforemeasurements,andbeveragescontainingcaffeinefor24hoursbeforemeasurements.The
high‐fidelityMillartonometerwillbeusedtorecordbrachialandradialarterywaveformsfromthe
wristofthedominantarm.
Fordetailedprocedures,seetheArterialTonometryStandardOperatingProcedures,availableonline
atwww.acrin.org/4008_imagingmaterials.aspx
10.0 ImageSubmission
10.1 TRIAD
AlltrialexamswillbesubmittedtoACRCoreLaboratoryviaTRIAD.TRIADisasoftware
applicationthatACRINprovidesforinstallationonasite’sPC.Oneorseveralcomputersof
choicewithintheinstitutional“firewall”andontheinstitutionalnetworkmaybeequippedwith
TRIADsoftware;internetaccessisalsorequired.TheTRIADapplicationcanthenbeconfigured
asaDICOMdestinationoneitherscanner(s)and/orPACSsystemfordirectnetworktransferof
studyrelatedimagesintotheTRIADdirectory.Whenproperlyconfigured,theTRIADsoftware
anonymizes,encrypts,andperformsalosslesscompressionoftheimagesbeforetheyare
transferredtotheACRINimagearchiveinPhiladelphia.
Onceequipment‐readinesshasbeendetermined,imagingpersonnelfromACRINwill
coordinateinstallationandtrainingforthesoftware.
TocontactTRIADSupportcall:215‐940‐8820oremailTRIAD‐Support@acr.org
10.2 ImageTransmittalWorksheet(ITW)
Allimagingshouldbesubmittedwithin48hoursafteracquisitionandshouldincludeanImage
TransmittalWorksheet(ITW).AnImageTransmittalWorksheet(ITW)isusedduringtheexam
QCreviewtoverifyacompletetransferofimagedatahasbeensubmittedtotheACRImaging
CoreLab.
ACRINPA4008SiteImagingManual
Final02January2014 pg.18of18
11.0 ImageQualityControl(QC)
11.1 ACRINCoreLaboratoryQualityControlTechnicalReview
UponreceiptoftheimagesattheACRImagingCoreLab,aninitialQCreviewwillbeconducted
byaqualifiedACRINImagingTechnologist.TheACRINImagingTechnologistwillcheckfor
missingimages/sequences,appropriateimageanonymization,completeanatomicalcoverage
oftheheart,adherenceofallsequencestoimagingprotocol,andabsenceofimageartifact.
Incaseswhereimagesetsarejudgedtobesuboptimal(“technicallyinadequate”),thetrialPI
willbeinformed,andareplacementparticipantwillbeaccruedfromparticipatinginstitution.
11.2 ImageDataQueries
IfitisfoundduringtheQCreviewthatthesubmittedexamhasmissingdataordoesnotfollow
theprotocolguidelines,detailedinthismanual,anImagingTechnologistwillissueaqueryto
thesiteSC.Sitesareexpectedtoresolvedataqueriesexpeditiously.Queriesnotresolved
within7businessdayswillbesenttotheACRINPA4008trialteamforadditionalfollow‐up.
12.0 ImagingForms
Thereare(2)imagingformsthatmustbecompletedandsubmittedforeachimagingtimepoint:
ImageTransmittalWorksheet(ITW)
MRIAssessmentForm
Itisrecommendedthateachoftheaboveformsbemadeavailable,inhardcopyformat,forthe
ImagingTechnologiststocompleteduringtheimageacquisitionwhentherequestedinformationon
theseformsismostreadilyavailable.

AppendixI
Phase‐ContrastImage
AcquisitionInstructions
ACRINPA4008:SiteImagingManual AppendixI
Phase‐ContrastImageAcquisitionInstructionsPage2of622May2013
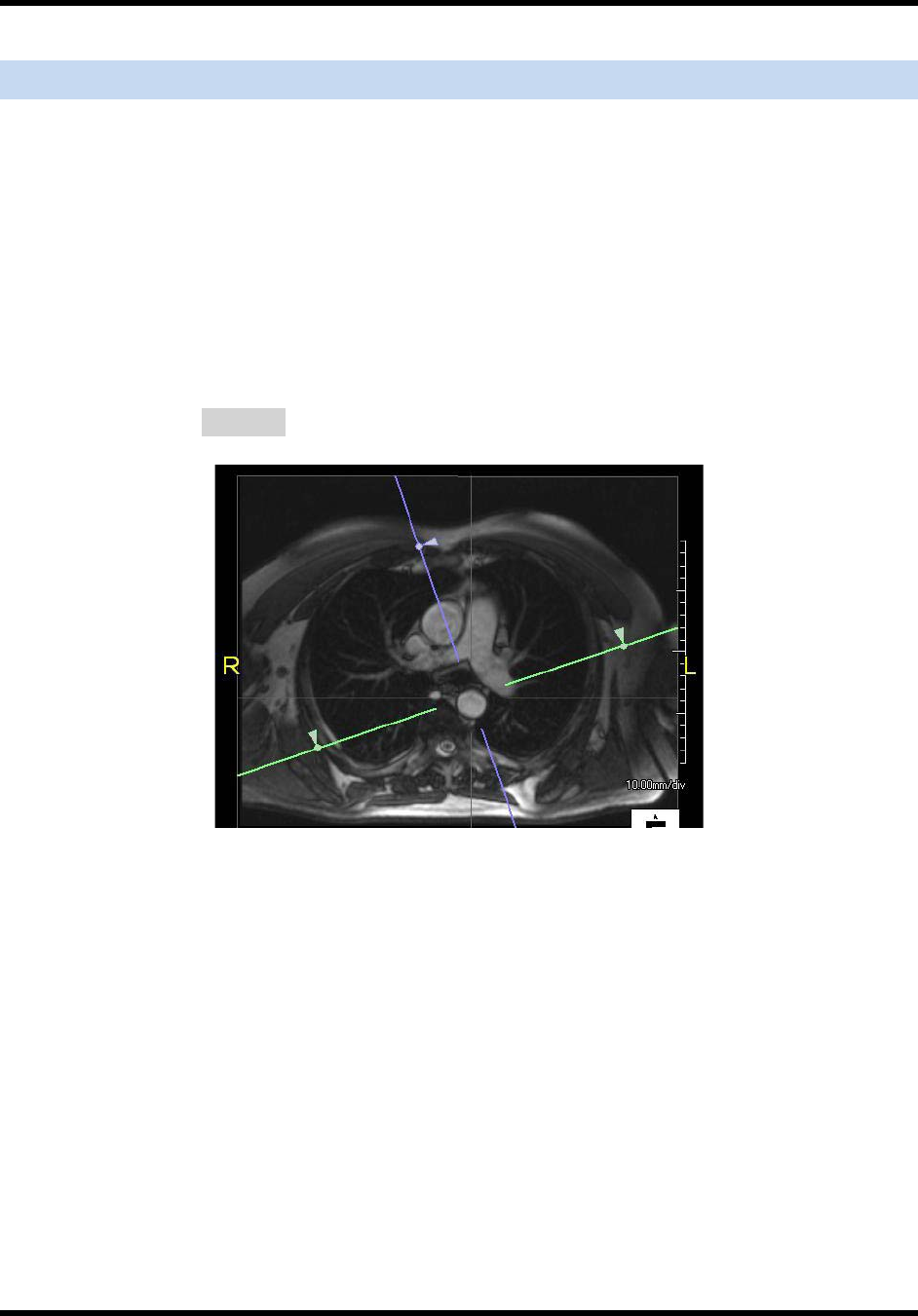
IdentifyingandPrescribingtheCandyCaneView
Usingtheaxialstackasa3Dscoutvolume,prescribeaplanethatshowsthethoracic
aortainitslongaxis(“candycane”view,asshownbelow).
Thisplaneshouldbeprescribedsothatitvisualizesaslargeasegmentofthethoracic
aortaaspossible.
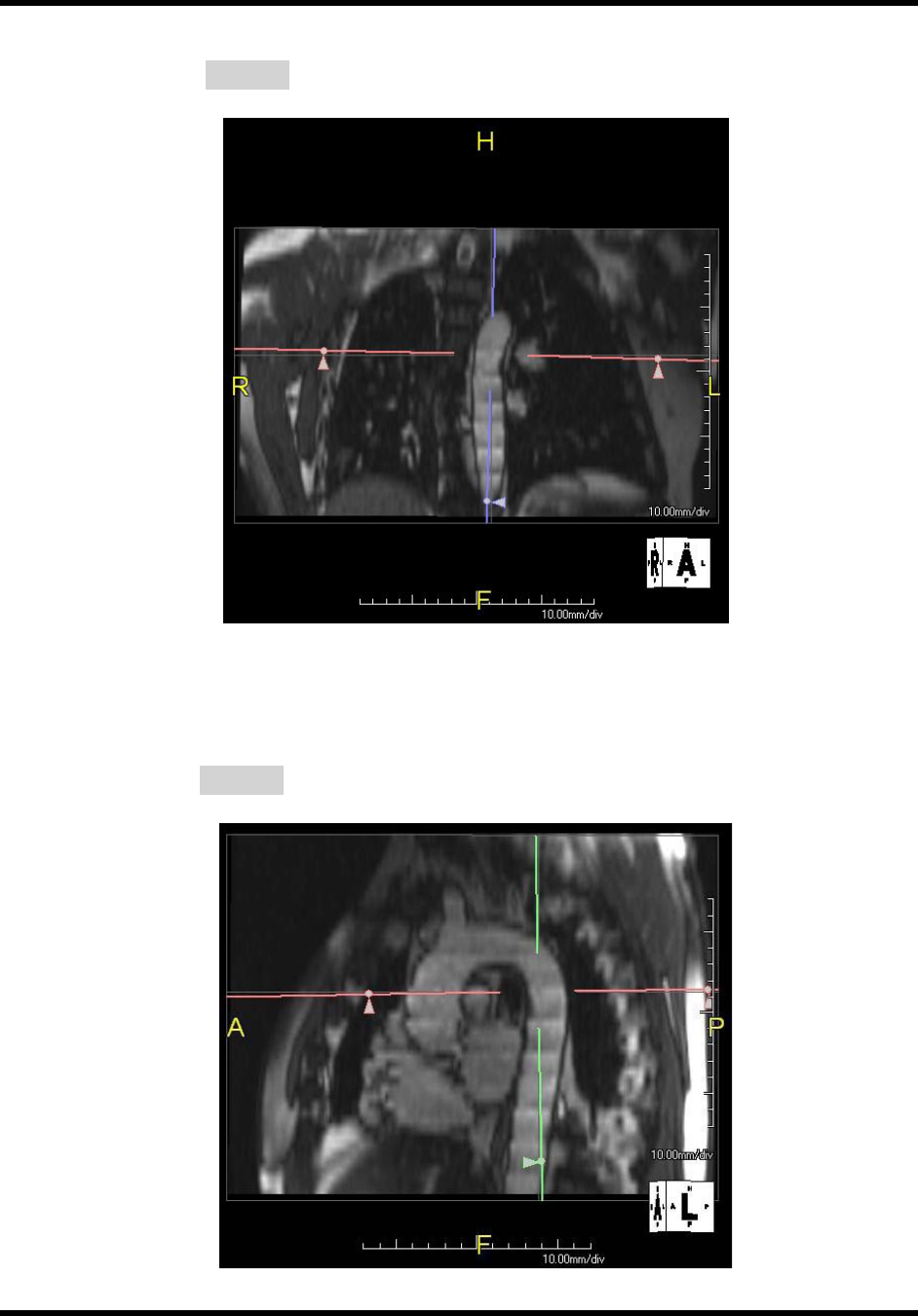
Inordertoprescribethisplaneproperly,findtheaxiallocalizerviewthatshowsthe
ascendinganddescendingaortaatthelevelofthepulmonaryarterybifurcationand
prescribeaplanethatpassesthroughthecenterofboththeascendinganddescending
aorta(purpleplaneinFigure1below):
Figure1:
Then,usingtheaxiallocalizerstackviewedin3Dmode,usethecoronalplane
reconstructiontoidentifythedescendingthoracicaortaandmakesuretheplanegoes
throughthemiddleofthelumenforaslongasegmentaspossible(purpleplanein
Figure2below).Usually,thisrequiresslightcounter‐clockrotationoftheplane
ACRINPA4008:SiteImagingManual AppendixI
Phase‐ContrastImageAcquisitionInstructionsPage3of622May2013
Figure2:
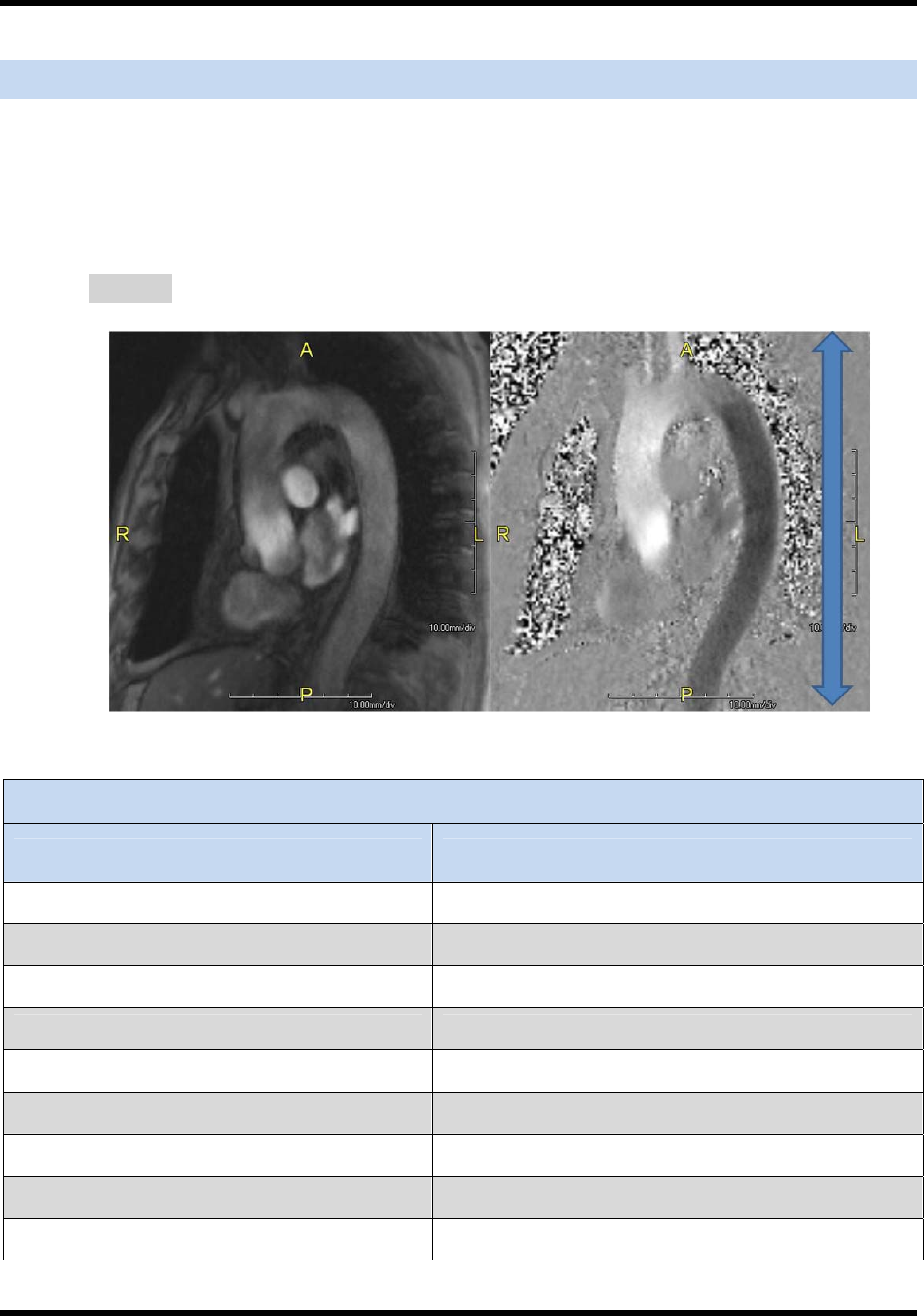
Finally,“finetune”theplanetovisualizeaslargeasegmentoftheaortaaspossible.As
seeninFigure3below.
Figure3:
ACRINPA4008:SiteImagingManual AppendixI
Phase‐ContrastImageAcquisitionInstructionsPage4of622May2013
CandyCaneView:ExecutionDetailsandParameterRecommendations
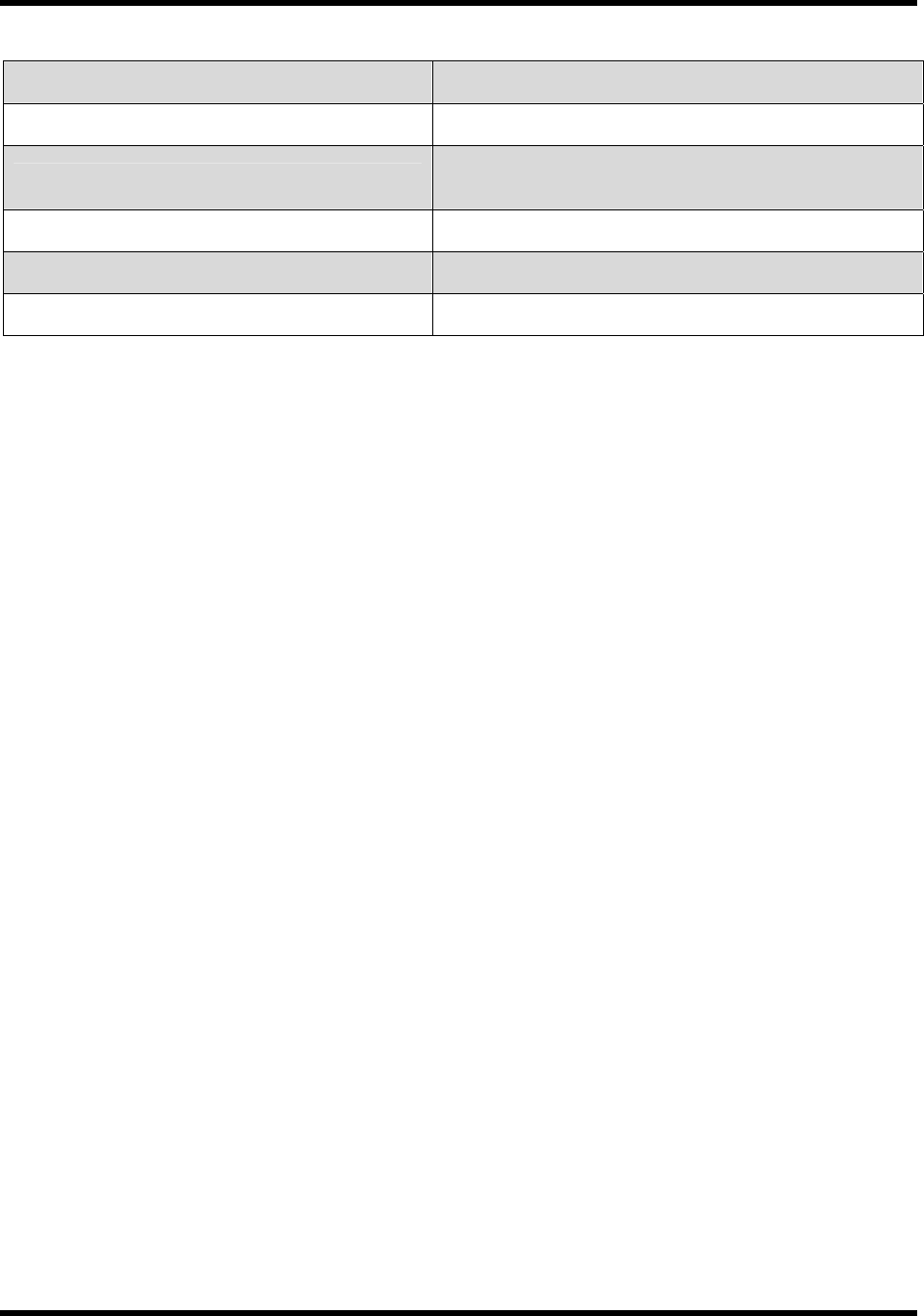
Oncethisplaneisidentified,aphase‐contrastsequencewithin‐planephaseencoding
fromheadtofootwillbeacquired.Thevelocity‐encodingdirectionisrepresentedby
thebluearrowbelowinFigure4.
Figure4:
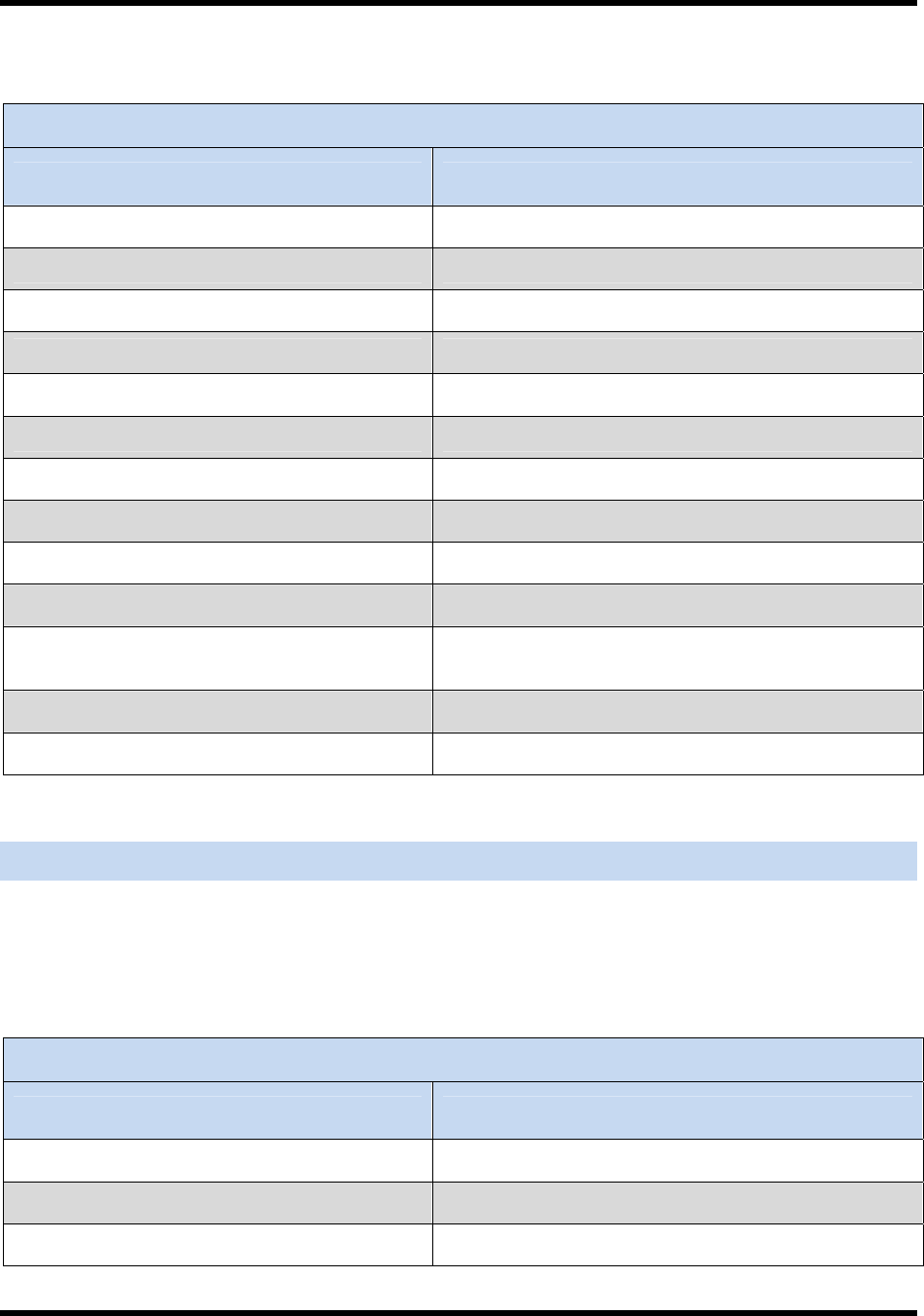
Table1:CandyCaneViewParameterRecommendations
ParameterValue
Sequencetype FLASH
TR minimized(~10ms)
TE 3.2ms
Segments 1
Flipangle 30
Fieldofview ~340x340
Imagematrix 256x256
Slicethickness 8mm
Numberofslices 1
ACRINPA4008:SiteImagingManual AppendixI
Phase‐ContrastImageAcquisitionInstructionsPage5of622May2013
Gating Retrospective
Numberofaverages 2
VENC 130cm/sec
**prescribedad‐hoctoavoidaliasing**
Numberofphases maximized(accordingtoheartrate)
BreathingType Free‐breathing
Bandwidth 31KHz
ACRINPA4008:SiteImagingManual AppendixI
Phase‐ContrastImageAcquisitionInstructionsPage6of622May2013
ShortAxisCineExecutionDetailsandParameterRecommendations
One‐sliceSSFP(trueFISP)cine
Theimagingplaneshouldbeprescribedimmediatelyabovethetopleveloftheright
pulmonaryartery,orslightlyabove,toavoidthehigh‐velocityflowclosetotheaortic
valve.
Thesagittalscoutviewandthecandy‐caneviewshouldbeusedtoprescribethisplane.
Theplaneshouldbeperpendiculartothelongaxisoftheaorta.
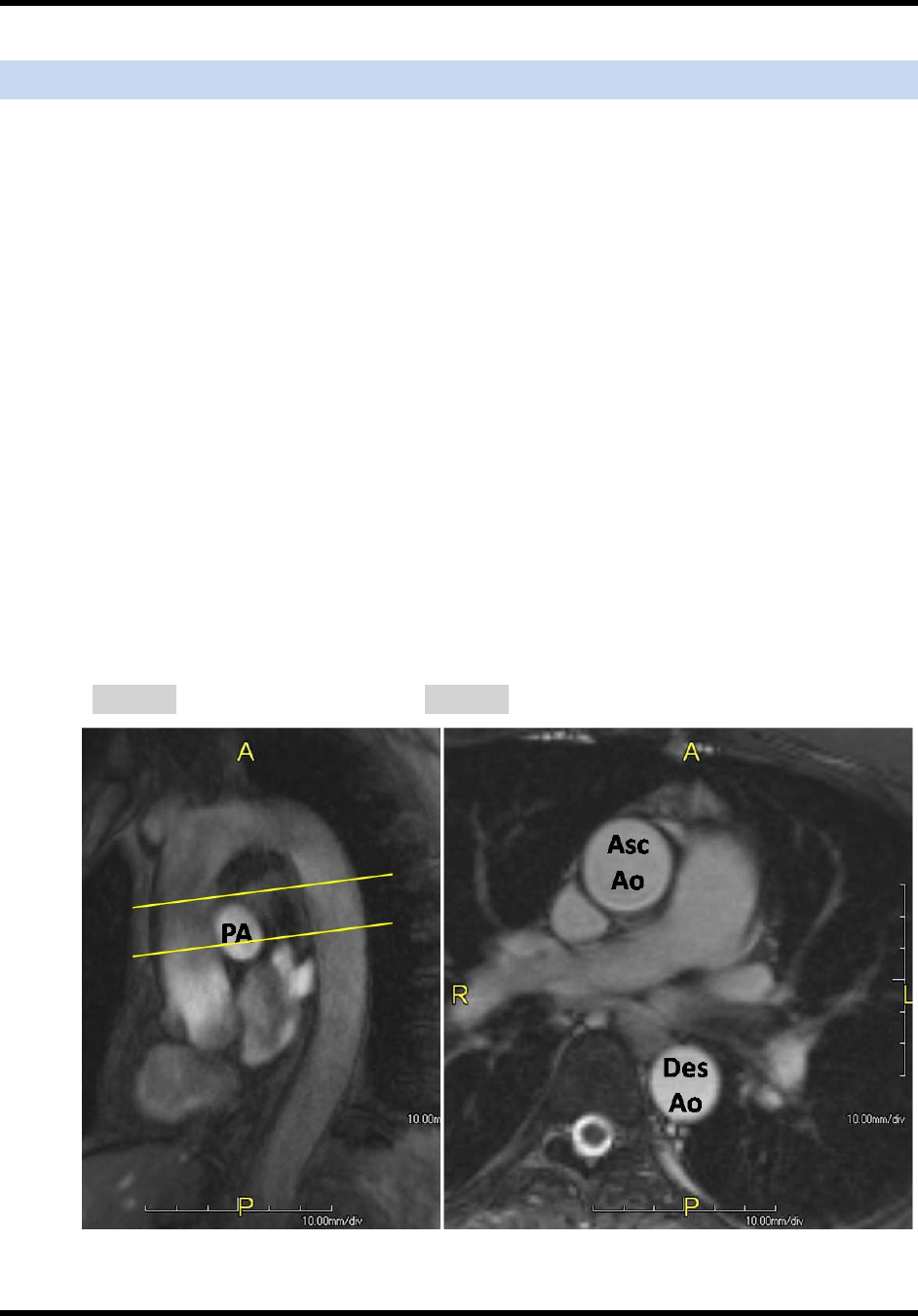
Thegoalistoacquiretheascendinganddescendingthoracicaortaas2“circles”(See
Figure6below).
Insomesubjects,thearchliesimmediatelycranialtotherightpulmonaryarteryand
thereforeitisnecessarytoprescribetheplaneatthelevelof(ratherthanabove)the
pulmonaryartery.
AnapproximaterangeofacceptableprescriptionplanesisshownbelowinFigure5
(spacebetweenyellowlines),althoughparticularlyinsubjectspre‐aorticvalve
replacement,the“higherisbetter”sincehighvelocityflowfromthevalvejetisbest
avoided.
Figure5:Figure6:
ACRINPA4008:SiteImagingManual AppendixI
Phase‐ContrastImageAcquisitionInstructionsPage7of622May2013
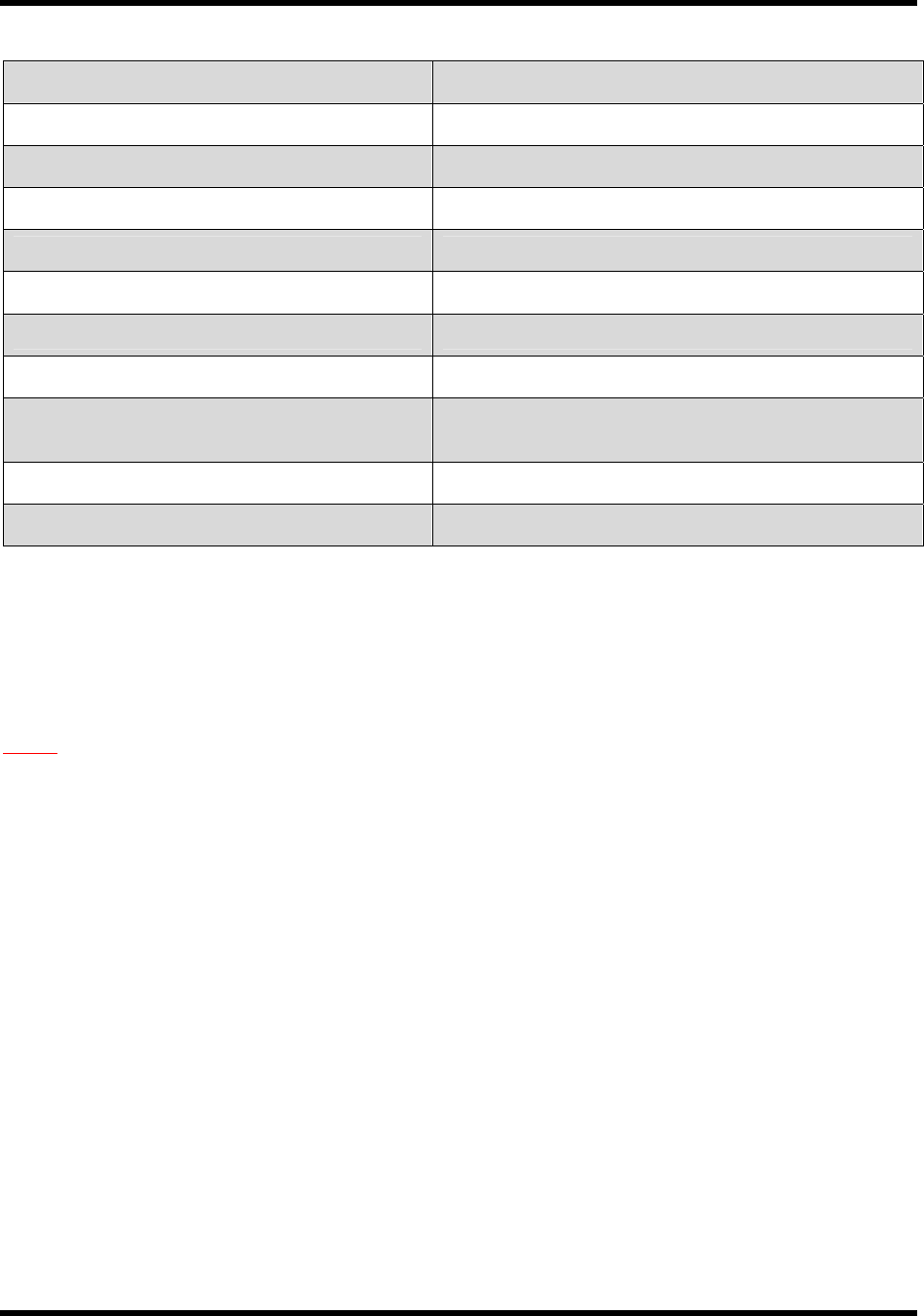
Table2:ShortAxisCineParameterRecommendations
ParameterValue
SequenceType SSFP(TrueFISP)
TR <3.8ms
TE Minimized
FlipAngle 70
FieldofView 360x360
ImageMatrix 256x256
SliceThickness 8mm
NumberofSlices 1
PartialFourier Off
NumberofPhases 30
ParallelImaging(optional)GRAPPA
AccelerationFactor:2
Gating ECGRetrospective
BreathingType Breath‐hold≤15seconds
AorticAxialCineExecutionDetailsandParameterRecommendations
Aorticaxialoneslicephase‐contrastcinebrightblood,non‐breath‐holdsequence.
ThesliceshouldbepositionedatexactlythesamelevelastheSSFPsequenceinthe
previoussection
Table3:AorticAxialCineParameterRecommendations
ParameterValue
Sequencetype FLASH
TR ~10msec(minimized)
TE 3.2ms
ACRINPA4008:SiteImagingManual AppendixI
Phase‐ContrastImageAcquisitionInstructionsPage8of622May2013
Segments 1
Flipangle 30
Fieldofview ~340x340
Imagematrix 256x256
Slicethickness 8mm
Numberofslices 1
Gating Retrospective
Numberofaverages 2
VENC 130cm/sec
**prescribedad‐hoctoavoidaliasing**
Numberofphases maximized(accordingtoheartrate)
BreathingType Free‐breathing
NOTE:PleasecarefullyreviewdetailsinSection6:ParticipantPreparationandSection8:
StandardizedImageAcquisitioninoftheSiteImagingManualasthisimagingprotocolmayor
maynotalignwithyourinstitution’sstandardprotocol.
