Organization Philips Medical Alarms MP60/70/80/90 Reduction Bring Down The Noise
User Manual: Philips Medical Alarms MP60/70/80/90
Open the PDF directly: View PDF ![]() .
.
Page Count: 13
- 37_Alarms_Reduction(1)
- 37_Alarms_Reduction_alarm_agreement
- 37_Alarms_Reduction_Alarm_Management_Plastic_Card
- 37_Alarms_Reduction_ALARMS_MANAGEMENT_SELF_LEARNING_5_2014
- 37_Alarms_Reduction_Alarms_Management_Self_Learning_Tech_Version
- 37_Alarms_Reduction_Copy_of_New_Apollo_Pager_Quick_Ref_Guide
- 37_Alarms_Reduction_HCU_IMC_ICU_Alarms_Checklist_5_2014
Organization: Northwest Hospital
Solution Title: Alarms Reduction – Bring Down the Noise!
Project Description:
The Problem: Staff desensitization to clinical alarms has become a growing concern.
Desensitization places patients at unnecessary risk when potentially actionable and life
threatening alarms are missed. Customization of clinical alarms is a key strategy in
enhancing staff awareness of alarms yet this practice has not been embedded or culturally
accepted in our organization. Additionally, patient complaints about alarm noise leads to
deterioration of patient satisfaction.
Identification: Two sentinel events, within the past 3 years, and previous work on our
Heart Care Unit (HCU) related to alarms spurred us to convene a workgroup in
December 2013. Leadership identified alarm management as a priority and charged the
group to proactively address the Joint Commission Sentinel Event Alert. Since the start of
our work, alarm management has become a National Patient Safety Goal.
Baseline Data: We collected alarm data in 2012 and 2013 which revealed >40,000
alarms in a week period of time across the telemetry units. HCAHPS scores and patient
survey comments related to Quietness of the Hospital were less than favorable at the start
of our work.
Goals:
Hardwire alarm customization of alarms on telemetry units
Reduce alarms paged out to the Emergin Pager system by 30% across all
telemetry units
Reduce noise and patient complaints of noise
Process: The workgroup convened as an interprofessional hospital wide group to evaluate and
prioritize alarms to manage as well as facilitate an action plan to address identified opportunities.
Membership included representation from all telemetry nursing units, education, clinical
engineering, quality improvement, risk management, respiratory therapy, as well as a physician
champion. The group is chaired by a Clinical Nurse Specialist (CNS).
Solution: Educated and competency validated the staff on the monitors and alarm customization.
Identified and addressed equipment operational barriers and issues. Smart Alarms were
deactivated on HCU to improve interference of nursing customization. Evaluated alarm default
settings and parameters in preparation for adjustments to ensure alarms are actionable.
Monitored noise levels and patient comments related to Quietness of the Hospital.
Measurable Outcomes: No sentinel events related to alarm management in over 1 year. There
was a reduction in the number of pages/alarms by 65% in a 9 month period. We also noted
improvement in HCAHPS scores related to the question “Quietness of the Hospital”.
Sustainability: Addition of alarm customization and familiarity in unit orientation. Competency
validation will be on-going. There will be auditing to ensure nursing is reviewing and
customizing alarms. The current workgroup will be maintained to continue to work on reducing
the alarms and address any future issues that may arise.
Role of Collaboration and Leadership: Leadership was very supportive about and engaged in
our endeavors. Since alarm management is a priority focus for Northwest Hospital we initiated a
Failure Modes Effectiveness Analysis (FMEA) to additionally document our work. All data and
progress is reported out to Nursing Quality, the Patient Safety Committee and our
Multidisciplinary PI committee.
Committee members worked collaboratively to identify priority alarms, alert. This included
identification of important alarms, alerting clinical engineering of issues, create meaningful
education, review and development of policies, and validating staff competencies. The members
of this workgroup are true champions of alarm management and vital to the success of the
initiative.
Innovation: Frontline staff was the driving force behind creating a safer environment. This was
innovative in the sense that we had active participation from many disciplines that collaborated
to produce a significant reduction in the number of alarms. Their involvement in developing
education and advocating for customization of alarms was crucial to the success of this project.
Empowering front line staff to support the change was innovative for Northwest Hospital. Staff
felt that they made a difference in how they work and patient safety.
Related Tools and Resources:
Northwest Hospital Developed Tools –
Education Packets
Commitment to addressing alarms “agreement” with nurses
Competency Assessment Tool
Badge Tags
Super users/ unit champions

Evidence Based Resources –
AACN, (2013). NTI ActionPak: strategies for managing alarm fatigue.
Retrieved from:
http://www.aacn.org/dm/practice/actionpakdetail.aspx?itemid=28337&learn=true
Allen, J.S., Hileman, K., & Ward, A. (2013). Safety innovations: Simple solutions
for improving patient safety in cardiac monitoring – Eight critical elements to
monitor alarm competency. AAMI Foundation. Healthcare Technology Safety
Insititute.
Graham, K.C. & Cvach, M., (2010). Monitor alarm fatigue: Standardizing use of
physiological monitors decreasing nuisance alarms. American Journal of Critical
Care (19) 28-34. Doi:10.4037/ajcc2010651
IntelliVue Patient Monitor Instructions for Use Manual (MP 20/30, MP 40/50,
MP60/70/80/90 Release G.0 with Software Revision G.0x.xx) Philips:Germany.
Pennsylvania Patient Safety Authority. (2008) Alarm interventions during
medical telemetry monitoring: a failure mode and effects analysis. PA Patient
Safety Advisory Supplementary Review
Contact Person: Meredith Stein, JD, MSN, RN, CCNS
Clinical Nurse Specialist Critical Care, Heart Care Unit, Observation, ED
merstein@lifebridgehealth.org
410-521-2200 x50098

Alarm Management Contract
Employee’s Name: ________________________________Clock # ___________
Employee Signature: ______________________________ Date:_______________
Responding to all types of alarms and pages is essential to patient care. I am aware
of how to address alarms in a timely manner and will follow up with any questions I
may have. If any concerns or questions arise related to care of a patient in response
to telemetry monitoring, I will follow up immediately with the leadership team,
charge nurse or medical staff. In addition, I am aware that responding to all red
alarms, regardless of my patient assignment is an expectation.
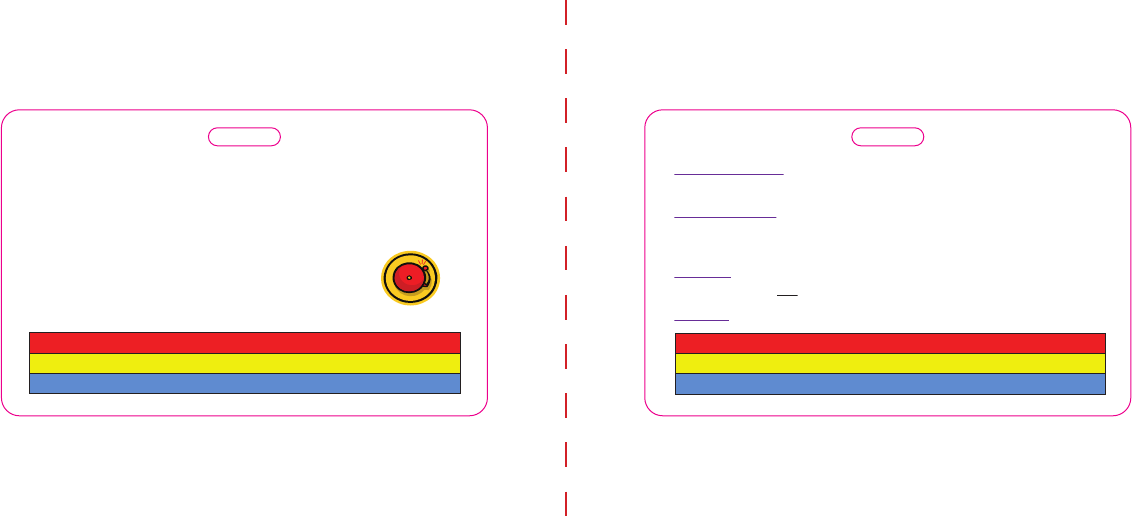
Front Back
ALARM MANAGEMENT
A -- Assess paent monitoring needs
L -- Learn paent baseline
A -- Adjust/Customize Alarms
A -- Acknowledge Alarms as they go off
R -- Readjust/Reassess Q4 and PRN
M -- Manage the paent, not Alarms!
E -- Evaluate the issues
D -- Document when appropriate
Red – high priority, potenally life threatening
Yellow
–
arrhythmia/parameter violaon
Blue – inoperable
Red Examples: V-Tach, Asystole
Yellow Example: “Irregular” alarms on a paent with afib
Blue Example: “Leads off”
Silencing Alarms – Check paent first, then silence. Silencing the alarm
tells the monitor that you have acknowledged the alarm
Pausing Alarms (Available ICU/ED/PACU/IR/CL ONLY) – prevents the
monitor from indicang any paent alarm. This pauses alarms for 1-3
minutes. Press the key again to switch on alarm indicaon.
Suspend (Available Tele areas ONLY) – suspends alarms for 10 minutes.
Per policy should not be set for >10min.
Standby – Monitoring is suspended, paent data is retained.

MSS 5/14
Alarms Management Self-Learning
Why Alarms Management (AACN, 2013) --
As acute and critical care nurses, we know firsthand how noisy the health care environment can be. Add in the multitude
of audible and visual alarms, and the environment becomes even more chaotic. With an overwhelming number of alarms,
it is not surprising that, at some point, alarm fatigue sets in. Unfortunately, this desensitization and fatigue can contribute
to unintended patient consequences and even death. The following are evidence based practices to help reduce the
alarms that result from our ECG Monitoring whether at the bedside or at a central monitor. Please use these to be part of
the solution.
EKG Electrode Skin Prep
o ECG electrodes should be changed daily to reduce artifact (AACN, 2013)
o Date and time pads
o Remove excessive hair with clippers, not razors
o Prep the skin by vigorously washing the area with soap and water, allow to completely dry before applying the
leads
o Do not use alcohol for skin preparation as it can dry out the skin
o Open packages will promote drying out of the gel so it is best to use a fresh package or apply gel directly to the dry
lead’s center
o When changing one ECG electrode, change them all.
o Limit monitoring interruption time during bathing by removing leads only long enough to prep the skin and change
them
o Respiratory leads are the white (RA) and red leads (LL). If they are applied incorrectly, the monitor can’t analyze
the patient’s breathing.
Monitoring Leads
o The Philips monitor defaults to monitoring in Lead II and V1
o If the QRS complex is not 2x the amplitude of the P and T waves, a different monitoring lead should be selected
(otherwise you may experience the misery of double counting)
o To change the lead:
Select the HR numeric to open the “Setup ECG” menu
Use the arrow keys to scroll down to “Primary Lead”
Select the lead from the 7 lead choices that you want to use for primary lead
Repeat the steps to select secondary lead
Select “Analysis Mode” to select Multi-lead or Single-lead
Arrhythmia Alarms
o “All Alarms on” is the default. The monitor will resume default settings for each new admission
o Blue/INOPs – conditions that cause monitoring to be interrupted.
Leads off
o Yellow – a lower priority patient alarm or an alarm specific to arrhythmia or parameter related conditions
Yellow alarms should not be turned off unless provider is aware of the arrhythmia.
For example, the “irregular” alarm should be turned off for a patient with known and current atrial
fibrillation.
o Red – a high priority alarm that is potentially life threatening
The patient should be visualized before silencing the alarm
This alarm is dramatic, long and continuous
MSS 5/14
Acknowledging Alarms –
o Silencing Alarms – Check the patient first, then silence. Silencing the alarm tells the monitor that you have
acknowledged the alarm
o Pausing Alarms (ICU/ED/PACU/IR/CL ONLY) – prevents the monitor from indicating any patient alarm. This
pauses alarms for 1-3 minutes (setting can be changed). Press the key again to switch on alarm indication.
o Suspend (Tele areas ONLY) – suspends alarms for 10 minutes. Per policy should not be set for >10min.
o Standby – Monitoring is suspended, patient data is retained.
Alarm Limits
o To reduce alarm fatigue, alarms should be customized for the patient
o An Alarm limit is a Nursing Tool to be used to alert you of changes that you want to be aware of when you are not
with your patient.
Ask yourself, “When do I want to be notified for an arrhythmia or vital sign change?”
Example: Mrs. Smith has a baseline HR of 49. She is asymptomatic at this rate. The Provider is aware. To
prevent the lower HR alarm from continuously alarming, decrease the lower HR limit to 45.
Telemetry Strip Analysis
o Strips should be interpreted and documented every 12 hours (minimum), when there is a change in patient
condition and upon initiation, discontinuation, and resumption of care.
Acute care -- Analysis includes HR. rhythm, and RN signature
Critical Care – Analysis includes HR, rhythm, PR, QRS, and QT intervals, and RN signature
Alarm Review
o Review alarm histories every 4 hours from the Central Monitor -- to view all alarms missed and customize alarms.
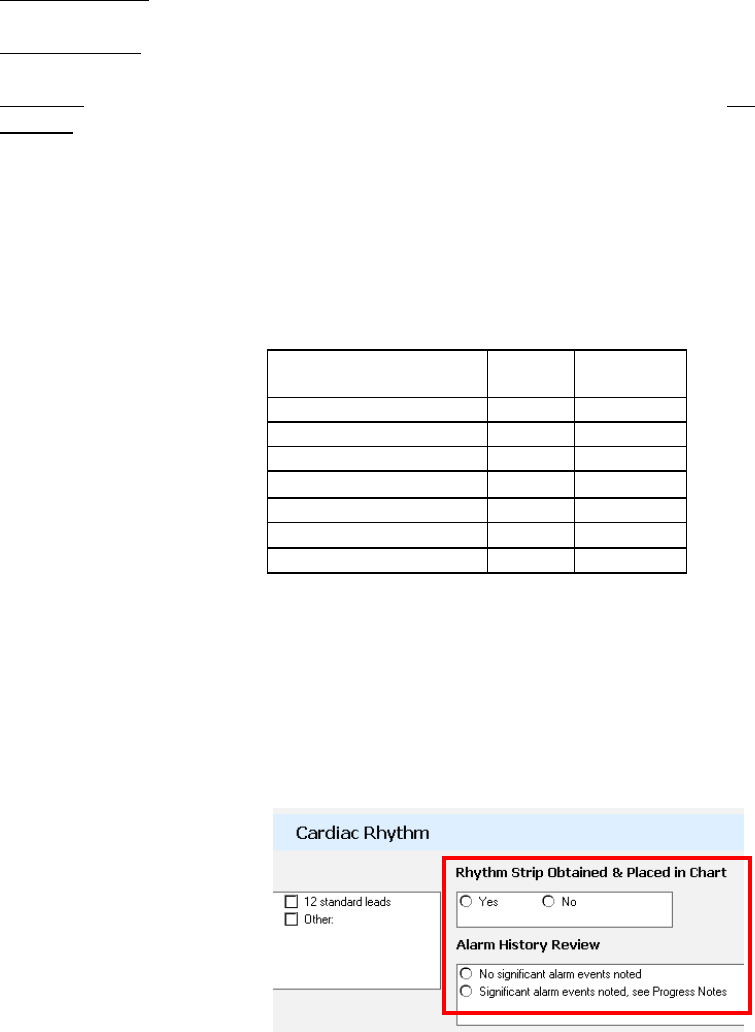
Document in the Adult Assessment under Cardiac Rhythm:
o Remember; notify Provider for changes in rhythm. Print, interpret, and place the strip in the Interdisciplinary Notes.
o Select “Patient Window”
Select “Alarm Review” (the 120 most recent alarms display here)
Click on the “Tabular Display” Box
“All alarms” should be pre-selected from the drop-down box. This includes all yellow and red alarms.
Click on alarm to see the strip.
Select “Record” to print a strip
**Always -- Inform and educate patients and families about
alarms and what each alarm means. **
Vital Sign Alarms
Default
Monitor
Capability
Heart Rate Low
50
15-95
Heart Rate High
120
65-300
NBP Systolic Low
90
30-155
NBP Systolic High
160
95-270
SPO2 low
92
50-99
Resp Rate High
30
0-100
Resp Rate Low
8
0-100

Alarms Management Self-Learning (Tech)
EKG Electrode Skin Prep
o ECG electrodes should be changed daily to reduce artifact (AACN, 2013)
o Date and time pads
o Remove excessive hair with clippers, not razors
o Prep the skin by vigorously washing the area with soap and water, allow to completely dry before applying
the leads
o Do not use alcohol for skin preparation as it can dry out the skin
o Open packages will promote drying out of the gel so it is best to use a fresh package or apply gel directly to
the dry lead’s center
o When changing one ECG electrode, change them all.
o Limit monitoring interruption time during bathing by removing leads only long enough to prep the skin and
change them
o Respiratory leads are the white (RA) and red leads (LL). If they are applied incorrectly, the monitor can’t
analyze the patient’s breathing.
Monitoring
o On Telemetry Units –
o New patients get new batteries in the tele boxes
o Check the monitors for the bars in the battery symbol, if there is one bar replace the
battery.
o If you see “__ LEAD OFF” , replace the specified lead
o Telemetry Certified Techs –
o Be mindful of the monitors and acknowledge alarms as appropriate.
Care of the Telemetry Transmitters:
o TRANSMITTERS ARE NOT WATERPROOF
o Clean the Transmitters with the orange top PDI Sani-Cloth Bleach Wipes ONLY.
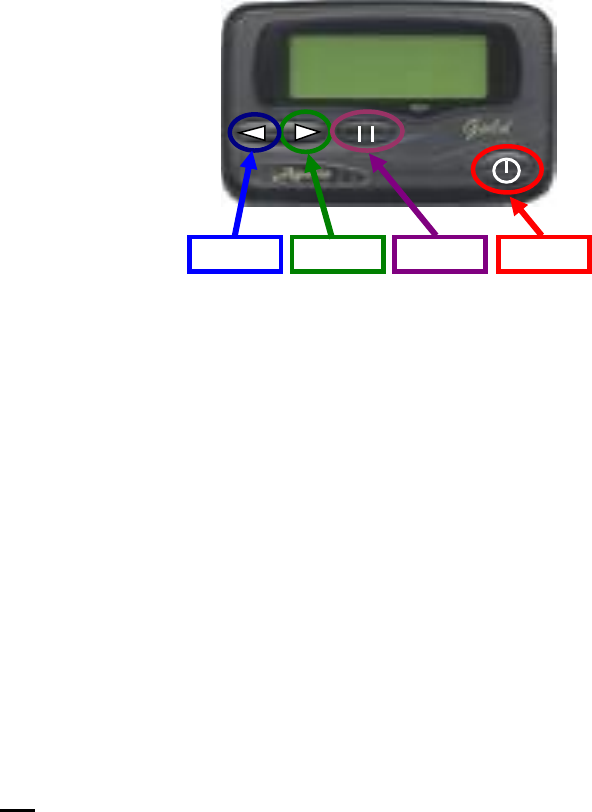
Apollo Gold Pager Quick Reference Guide
Button 1 Button 2 Button 3 Button 4
3) Press Button 3 to enable time set
4) Press Button 3 to change each set of flashing digits, while using Button 2 to move the cursor
3) Press Button 4 to activate the time and date changes
3) Press Button 2 to turn off the pager
Turning Pager On:
1) Press and hold Button 4 until it beeps to turn on the pager
Setting Time/Date:
1) Press Button 3 until UP OR ESCAPE shows on the screen
2) Press Button 1 to scroll to SET TIME
* Please Note: If any messages are not read, the pager will periodically vibrate/beep
3) Release Button 4 and then quickly press it again to confirm delete
2) Press and hold Button 4 for about 2 seconds until DELETE ? comes up on the screen
1) Follow steps 1 - 4 under Reading Old Messages
Deleting One Message:
4) Press Button 1 to scroll through and read your messages
3) Press Button 4 to pull up the last message
Reading Messages:
1) When the pager alerts you that there is a message, press Button 4 to stop the vibrate/beep
2) Press Button 4 to read through the message
Reading Old Messages:
2) A Flashing 5 in the upper left screen indicates there is an unread message
1) Press Button 4 to turn on or wake up your pager
Deleting All Messages:
3) Press Button 3 to confirm
Turning Pager Off: (Do not take out the battery)
1) Press Button 3 until UP OR ESCAPE shows on the screen
2) Press Button 1 to scroll to PAGER OFF
* Please Note: Only messages that have been read will be deleted
2) Press Button 2 to scroll to DELETE ALL
1) Press Button 3 until UP OR ESCAPE shows on the screen
3) Press Button 3 to confirm
3) Press Button 2 to Delete all Messages

Apollo Gold Pager Quick Reference Guide
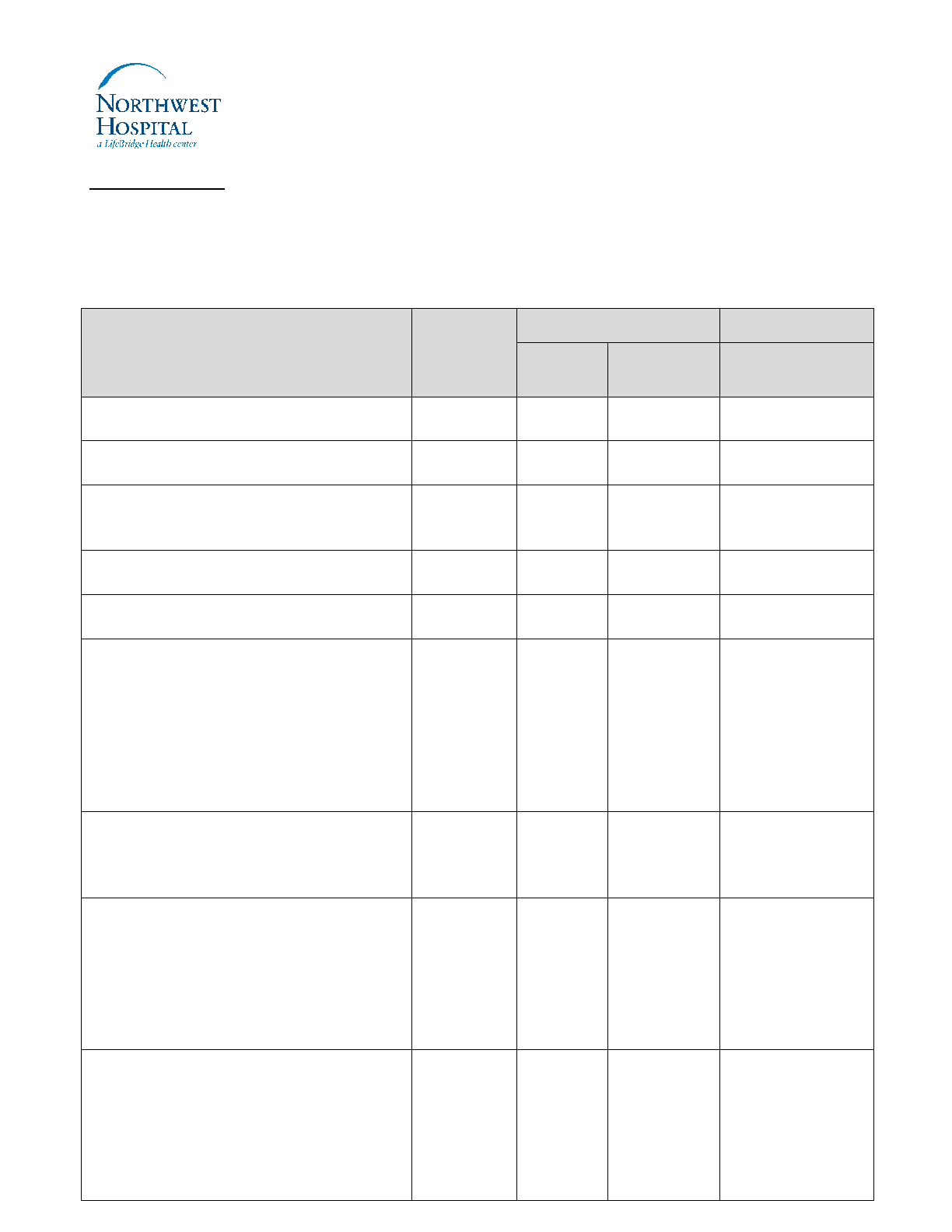
COMPETENCY: IntelliVue Patient Monitor (HCU/IMC/ICU)
Employee’s Name: _________________________ Clock # ______________ Unit: __________
□ Initial Education □Recurring Validation
Validation Method Key: B = Bedside Observation, C = Chart Documentation, D= Demonstration,
E = Education Provided, V = Verbalizes
Performance Criteria
Validation
Method
Performance Criteria
Comments
Met
(initials/
date)
Unmet
(Initials/date)
1. States how to admit and discharge
a patient
2. Associates the patient through
CareAware (ICU)
3. Ensures transport monitor seated
correctly behind bedside monitor
(ICU)
4. Pairs the MP30 (when applicable)
5. Identifies patient’s current rate and
rhythm
6. Reviews/Adjusts settings for each
patient
a. Selects best lead for ECG tracing
b. Turns pacing on
c. Adjusts HR alarm
d. Adjust thresholds or turn off
arrhythmia alarms based on
history of patient rhythm
7. Discuss the 3 levels of alarms:
a. Red
b. Yellow
c. INOPs (Blue)
8. Understands difference between
the following and states when to
use each:
a. Silence
b. Pause
c. Suspend
d. Standby
9. Check battery life and change if
needed (HCU/IMC).
a. A new patient needs a new
battery.
b. Replace battery when
there is one bar noted on
screen
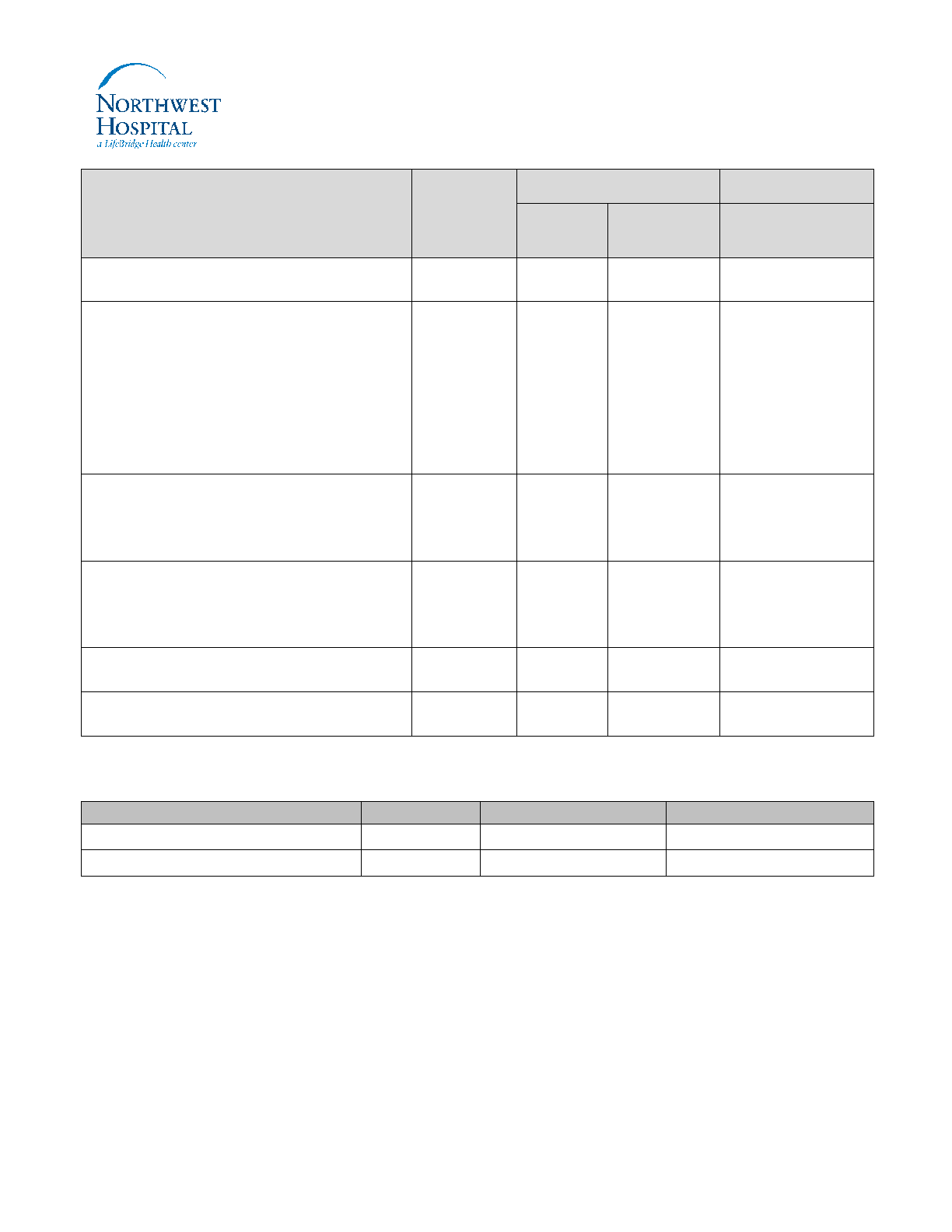
Performance Criteria
Validation
Method
Performance Criteria
Comments
Met
(initials/
date)
Unmet
(Initials/date)
10. States process for monitoring
patient off unit
11. Describe the best practice skin
prep for electrode placement
a. change electrodes daily,
date and time pads
b. Vigorously clean skin
with soap and water
c. when changing one
electrode, change them all
12. Limit monitoring interruption time
during bathing. Remove leads only
long enough to prep the skin and
change.
13. Print rhythm strip once a shift (and
prn with change in rhythm or
condition), places in patient chart
and interprets rhythm
14. Review alarm history every 4
hours and documents
15. Identifies medications or lab
values that can alter rate or rhythm
Employee Signature: ______________________________________ Date: __________________________
Validator’s Name ( Please Print)
Title
Signature
Date
