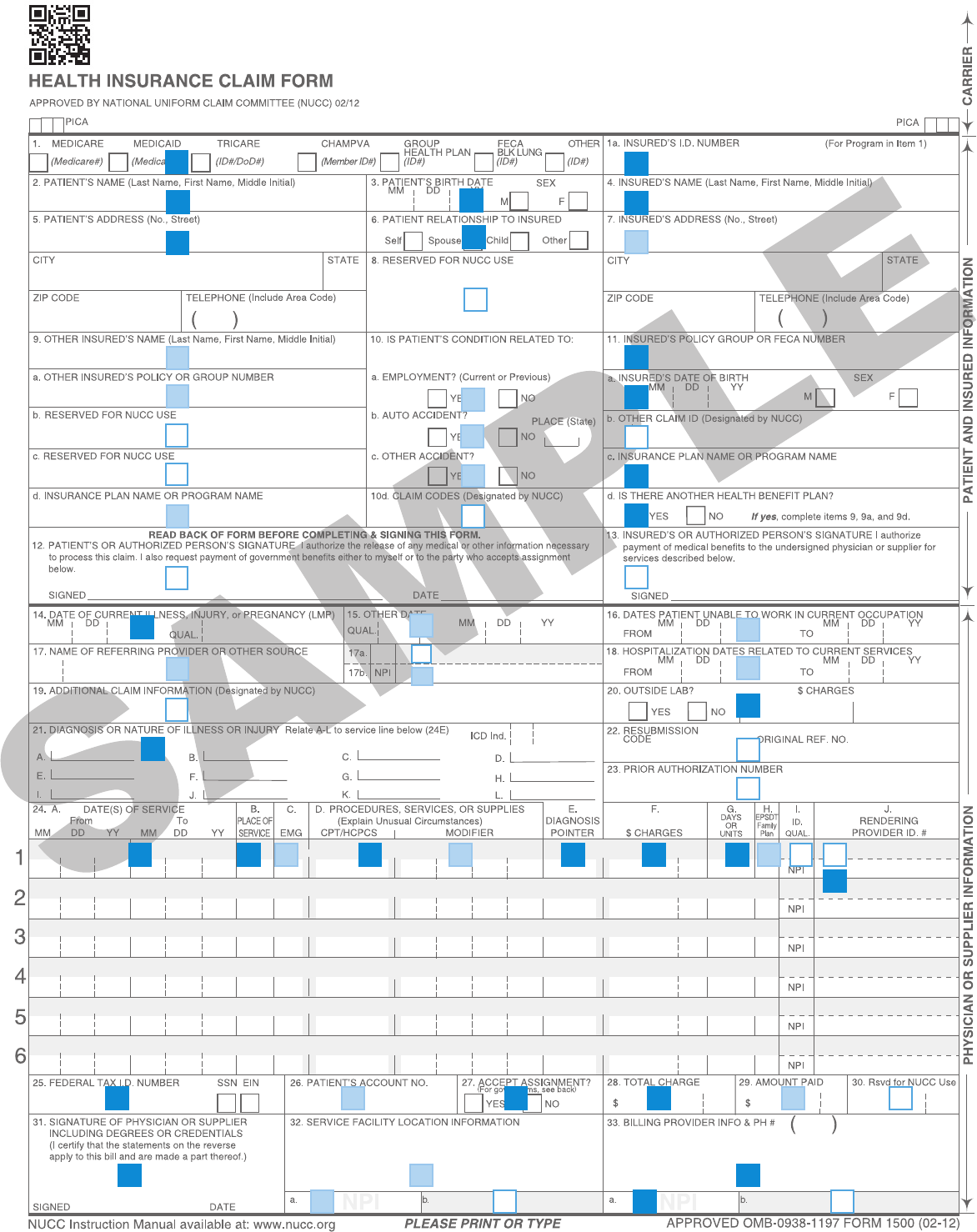
CMS 1500 Billing Guide
User Manual:
Open the PDF directly: View PDF ![]() .
.
Page Count: 3
R
S
R
RR
R
R
R
S
S
S
S
S
R
R
R
R R R
R
R
R
R R
R
SR
S
S
S
S
R
R
R
R
S
S
R
S
R
S
S
S
R
NR
NR
NR
NR
NR
NR
NR
NR
NR NR
NR NR
S
S
NR
NR
NR
NR
1. TYPE OF HEALTH INSURANCE COVERAGE R
Select “Other”
1A. INSURED ID NUMBER R
Enter the subscriber’s identification number
2. PATIENT’S NAME R Last name, First name, Middle initial
Enter the patient’s last name, first name and middle initial.
3. PATIENT’S BIRTH DATE/SEX R
Enter the patient’s date of birth using the eight-digit date format (MM/DD/CCYY).
Next, select the patient’s gender.
4. INSURED’S NAME R Last name, First name, Middle initial
Enter the insured’s last name, first name and middle initial.
5. PATIENT’S ADDRESS/TELEPHONE NUMBER R
Enter the patient’s permanent mailing address and telephone number.
6. PATIENT’S RELATIONSHIP TO THE INSURED R
Select the appropriate box for patient’s relationship to the insured person.
7. INSURED’S ADDRESS/TELEPHONE NUMBER S
Enter the insured person’s permanent mailing address (complete if different from the patient’s address)
8. RESERVED FOR NUCC USE NR
9. OTHER INSURED’S NAME S
Enter the other insured person’s last name, first name and middle initial. When the patient has other
insurance coverage, you will need to complete fields 9a through 9d. This information is necessary to
coordinate benefits with other insurance companies.
9A. OTHER INSURED’S POLICY OR GROUP NUMBER S
Enter the other insured person’s policy or group number.
9B. RESERVED FOR NUCC USE NR
Enter the other insured person’s date of birth in an eight-digit date format (MM/DD/CCYY).
9C. RESERVED FOR NUCC USE NR
Enter the other insured person’s employer or school name.
9D. INSURANCE PLAN NAME OR PROGRAM NAME S
Enter the name of the other insured person’s insurance plan or program name.
10A-D. IS PATIENT’S CONDITION RELATED TO:
For 10a – 10d, required status is contingent upon a definitive “Yes” or “No” answer. If you are unsure,
leave blank.
10A. Select whether the patient’s condition is related to employment. S
10B. Select whether the patient’s condition is related to an auto accident and enter the state in which the
accident occurred. Use two-character abbreviation, i.e. IL. S
10C. Select whether the patient’s condition is related to any other type of accident. S
10D. CLAIM CODES (DESIGNATED BY NUCC) NR
11. INSURED’S POLICY GROUP OR FECA NUMBER
Enter the subscriber’s ID number again.
11A. INSURED’S DATE OF BIRTH, SEX R
Enter the subscriber’s date of birth using the eight-digit date format (MM/DD/CCYY) and
select the subscriber’s gender.
11B. OTHER CLAIM ID (DESIGNATED BY NUCC) NR
Enter the subscriber’s employer or school name.
11C. INSURANCE PLAN NAME OR PROGRAM NAME R
Enter the subscriber’s insurance plan name (PCU or RMA or UC)
11D. IS THERE ANOTHER HEALTH INSURANCE BENEFIT PLAN R
Select whether there is another health insurance plan. Remember, if there is another health
insurance plan, you will need to complete fields 9, 9a, and 9d. This information is necessary to
coordinate benefits with other insurance companies.
12. PATIENT OR AUTHORIZED PERSON’S SIGNATURE NR
13. INSURED OR AUTHORIZED PERSON’S SIGNATURE NR
14. DATE OF CURRENT ILLNESS, INJURY, OR PREGNANCY (LMP) R
Enter the date using an eight-digit date format (MM/DD/CCYY).
15. OTHER DATE S
Enter the date using an eight-digit date format (MM/DD/CCYY).
16. DATES PATIENT UNABLE TO WORK IN CURRENT OCCUPATION S
Enter the date using an eight-digit date format (MM/DD/CCYY).
17. NAME OF REFERRING PROVIDER OR OTHER SOURCE S
Enter the referring, ordering or supervising provider’s first name, middle initial, last name and
credentials. This field is required only if there is a referring, ordering or supervising provider.
17A. OTHER ID# NR
Not required, reserved for taxonomy code (preceded by “ZZ” qualifier).
17B. NPI # S
Enter the 10-digit NPI number of the referring, ordering or supervising provider.
18. HOSPITAL DATES RELATED TO CURRENT SERVICES S
Enter the hospital dates using an eight-digit date format (MM/DD/CCYY).
19. ADDITIONAL CLAIM INFORMATION (DESIGNATED BY NUCC) NR
20. OUTSIDE LAB/CHARGES R
Select “Yes” or “No” to indicate if the claim includes charges for lab services performed outside
of the physician’s office. If “Yes,” enter the total charges.
21. DIAGNOSIS OR NATURE OF ILLNESS OR INJURY R
Enter the ICD-9-CM codes. The primary diagnosis should be entered first, followed by other
diagnoses if applicable. Up to three additional ICD-9-CM codes can be entered.
22. RESUBMISSION NR
23. PRIOR AUTHORIZATION NUMBER NR
24. SHADED AREA – SUPPLEMENTAL INFORMATION –
The shaded area of field 24a - 24h was created to accommodate supplemental information, i.e., Anesthesia.
For more information, see the National Uniform Claim Committee’s website at www.nucc.org.
24A. DATE(S) OF SERVICE R
Enter the dates of service using an eight-digit date format (MM/DD/CCYY).
24B. PLACE OF SERVICE R
Enter the appropriate two-digit Place of Service code.
24C. EMG S
If this service was an emergency, enter “Y” for “Yes,” or leave blank if “No”.
24D. PROCEDURES, SERVICES, OR SUPPLIES R
Enter the CPT or HCPCS code for the procedures, services or supplies, and enter a modifier if applicable.
24E. DIAGNOSIS POINTER R
Enter the appropriate ICD-9-CM diagnosis code or codes for each procedure performed. Enter one
code per line of service.
24F. CHARGES R
Enter the charge for each line of service. Do not include discounts.
24G. DAYS OR UNITS R
Enter the number of days or units for each line of service.
24H. EPSDT/FAMILY PLAN S
If applicable, enter the appropriate Early and Periodic Screening, Diagnosis and Treatment (EPSDT)
code or family planning (FP) code.
24I. ID QUALIFIER - SHADED FIELD NR
Not required, reserved for taxonomy code qualifier, “ZZ.”
24J. RENDERING PROVIDER ID. #
SHADED FIELD
NR
Not required, reserved for taxonomy code.
NON-SHADED FIELD R
Enter the performing provider’s 10-digit NPI number in the non-shaded area.
25. FEDERAL TAX ID NUMBER R
Enter the Federal Tax ID Number for the provider of service. Select the appropriate field for SSN or EIN.
26. PATIENT ACCOUNT NUMBER S
Enter account number assigned to the patient, if applicable.
27. ACCEPT ASSIGNMENT R
Select “Yes” if the provider should be paid, or select “No” if the patient should be paid.
28. TOTAL CHARGE R
Enter the total charge for all services (total of all charges in 24f).
29. AMOUNT PAID S
Enter any amount paid by the patient only. Do not enter any amount by Medicare or other insurance.
30. RSVD FOR NUCC USE NR
Enter the difference, if any, between the total charge and the amount paid.
31. SIGNATURE OF PHYSICIAN OR SUPPLIER INCLUDE DEGREES OR CREDENTIALS R
The claim must be signed by the physician/supplier or an authorized representative. The form must also
be dated, using an eight-digit date format (MM/DD/CCYY).
32. SERVICE FACILITY LOCATION INFORMATION S
Enter the location where the services were rendered. The provider of service must identify the
supplier’s information when billing for purchased diagnostic tests.
Note: Per the NUCC Instruction Manual, Field 32 is required if Field 20 is checked “yes.”
For more information, see the National Uniform Claim Committee’s website at www.nucc.org.
32A. NPI S
Enter the 10-digit NPI number of the service facility location.
32B. OTHER ID# NR
Not required, reserved for taxonomy code (preceded by “ZZ” qualifier).
33. BILLING PROVIDER INFO AND PH# R
Enter the information of the billing provider or supplier to be paid for services.
33A. NPI R
Enter the 10-digit NPI number of the billing provider.
33B. OTHER ID # NR
Not required, reserved for taxonomy code (preceded by “ZZ” qualifier).
R REQUIRED
S SITUATIONAL --- ONLY IF APPROPRIATE TO THIS CLAIM
NR NOT REQUIRED/NOT USED
KEY
Complete all required fields. Make certain to enter the
following identifying information:
• Put the insured’s alpha prefix and identification number
in Field 1a.
• Put the insured’s policy group number in Field 11.
•Put the physician or supplier’s billing name, address,
ZIP code, telephone number and NPI number in Field 33.
The information required to file electronic claims is the same as for paper
claims but there are major advantages to submitting electronic claims
versus paper claims:
• You will reduce your overhead, electronically submitted
claims can save hours of clerical time.
• You have better control and accuracy. Electronic claims
are entered in the BCBSIL’s system just the way they leave
your office.
• You know when your claims are received because your
office receives special reports detailing which claims were
accepted. If there is a problem with your claim, you can
correct it before the claim is processed.
To obtain more information on electronic claim filing,
call 800-746-4614 or log on to bcbsil.com.
CODES DEFINITIONS
01 Pharmacy
02 Unassigned
03 School
04 Homeless Shelter
05 Indian Health Service Free-standing Facility
06 Indian Health Service Provider-based Facility
07 Tribal 638 Free-standing Facility
08 Tribal 638 Provider-based Facility
09 Prison Correctional Facility
10 Unassigned
11 Office
12 Home
13 Assisted Living Facility
14 Group Home
15 Mobile Unit
16 Temporary Lodging
17 Walk-in Retail Health Clinic
18 Place of Employment-Worksite
19 Unassigned
20 Urgent Care Facility
21 Inpatient Hospital
22 Outpatient Hospital
23 Emergency Room Hospital
24 Ambulatory Surgical Center
25 Birthing Center
26 Military Treatment Facility
27-30 Unassigned
31 Skilled Nursing Facility
32 Nursing Facility
33 Custodial Care Facility
34 Hospice
35-40 Unassigned
41 Ambulance (Land)
42 Ambulance (Air or Water)
43-48 Unassigned
49 Independent Clinic
50 Federally Qualified Health Center
51 Inpatient Psychiatric Facility
52 Psychiatric Facility Partial Hospitalization
53 Community Mental Health Center
54 Intermediate Care Facility/Mentally Retarded
55 Residential Substance Abuse Treatment Center
56 Psychiatric Residential Treatment Center
57 Non-residential Substance Abuse Treatment Facility
58-59 Unassigned
60 Mass Immunization Center
61 Comprehensive Inpatient Rehabilitation Facility
62 Comprehensive Outpatient Rehabilitation Facility
63-64 Unassigned
65 End-Stage Renal Disease Treatment Facility
66-70 Unassigned
71 Public Health Clinic
72 Rural Health Clinic
73-80 Unassigned
81 Independent Laboratory
82-98 Unassigned
99 Other Place of Service
Place of Service Codes
Reminders
The following are types of supplemental information that can be entered
in the shaded areas of Item Number 24:
• Narrative description of unspecified codes
• National Drug Codes (NDC) for drugs
•Contract rate
•Tooth numbers and areas of the oral cavity
The following qualifiers are to be used when reporting these services.
ZZ Narrative description of unspecified code
N4 National Drug Codes (NDC)
CTR Contract rate
JP Universal/National Tooth Designation System
JO ANSI/ADA/ISO Specification No. 3950-1984 Dentistry Designation
System for Tooth and Areas of the Oral Cavity
For additional information for reporting NDC units, see the
National Uniform Claim Committee’s website at www.nucc.org.
Instructions and Examples of
Supplemental Information in
Item Number 24
Note: For more information on Place of Service Codes, see the National
Uniform Claim Committee’s website at www.nucc.org.
