CHAPTER 01 MASTER.A Coast Guard Medical Manual
User Manual: manual pdf -FilePursuit
Open the PDF directly: View PDF ![]() .
.
Page Count: 780 [warning: Documents this large are best viewed by clicking the View PDF Link!]
- CH-17 TO MEDICAL MANUAL, COMDTINST M6000.1B
- CH-16 TO MEDICAL MANUAL, COMDTINST M6000.1B
- CH-15 TO MEDICAL MANUAL, COMDTINST M6000.1B
- CHAPTER 1 ORGANIZATION AND PERSONNEL
- Section A - Organization.
- Section B.- Personnel.
- 1. General Duties of Medical Officers.
- 2. Duties of Senior Medical Officers.
- 3. Duties of Flight Surgeons.
- 4. General Duties of Dental Officers.
- 5. General Duties of Senior Dental Officers.
- 6. General Duties of Chief, Health Services Division.
- 7. General Duties of Pharmacy Officers.
- 8. Maintenance and Logistics Command Pharmacy Officers.
- 9. Environmental Health Officers.
- 10. Clinic Administrators.
- 11. Physician Assistants (PA/PYA(s)) and Nurse Practitioners (NP).
- 12. TRICARE Management Acitivity-Aurora (TMA) Liaison Officer.
- 13. Health Services Technicians.
- 14. Health Services Technicians - Dental (HSDs).
- 15. Independent Duty Health Services Technicians.
- 16. Coast Guard Beneficiary Representatives at Uniformed Services Medical Treatment Facilities (USMTF).
- 17. Coast Guard Representative at the Department of Defense Medical Examination Review Board (DODMERB).
- 18. Health Benefits Advisors (HBA).
- 19. Dental Hygienists.
- 20. Red Cross Volunteers.
- 21. Volunteers
- CHAPTER 2. HEALTH CARE AND FACILITIES
- Section A - Health Care for Active Duty Personnel.
- 1. Care at Uniformed Services Medical Treatment Facilities.
- 2. Emergency Care at Other Than CG or DOD Facilities.
- 3. Dental Care and Treatment.
- 4. Consent to and Refusal of Treatment.
- 5. Elective Surgery for Pre-Existing Defects.
- 6. Elective Health Care.
- 7. Other Health Insurance (OHI)
- 8. Procedures for Obtaining Non-Emergent Health Care from Nonfederal Sources.
- 9. Obtaining Vasectomies and Tubal Ligations from Nonfederal Providers.
- 10. Care at Department of Veterans Affairs (DVA) Medical Facilities.
- Section B - Health Care for Reserve Personnel.
- Section C - Health Care for Retired Personnel.
- Section D - Health Care for Dependents.
- Section E - Care for Preadoptive Children and Wards of the Court.
- Section F - Health Care for Other Persons.
- Section G - Medical Regulating.
- Section H - Defense Enrollment Eligibility Reporting System (DEERS) in Coast Guard Health Care Facilities.
- 1. Defense Eligibility Reporting System.
- 2. Responsibilities.
- 3. Security.
- 4. Performing DEERS Checks.
- 5. Reports.
- 6. Eligibility/Enrollment Questions, Fraud and Abuse.
- 7. Denial of Nonemergency Health Care Benefits for Individuals Not Enrolled in Defense Enrollment Eligibility Reporting System (DEERS).
- 8. DEERS Eligibility Overrides.
- Section I - Health Care Facility Definitions.
- Section J - Policies and Procedures Required at Coast Guard Health Care Facilities.
- Section K - General Standards of Care.
- 1. Diagnosis and therapy shall be performed by a provider
- 2. Diagnoses shall be based upon clinical findings and appropriate
- 3. Treatment shall be consistent with the working diagnosis,
- 4. Treatment shall be rendered in a timely manner.
- 5. Treatment shall be provided using currently accepted
- 6. Patients shall participate in deciding among treatment
- Section A - Health Care for Active Duty Personnel.
- CHAPTER 3 PHYSICAL STANDARDS AND EXAMINATION
- Section A - Administrative Procedures.
- 1. Applicability of Physical Standards.
- 2. Prescribing of Physical Standards.
- 3. Purpose of Physical Standards.
- 4. Application of Physical Standards.
- 5. Interpretation of Physical Standards.
- 6. Definitions of Terms Used in this Chapter.
- 7. Required Physical Examinations and Their Time Limitations.
- 8. Waiver of Physical Standards.
- 9. Substitution of Physical Examinations.
- Section B - Reporting, Reviewing, Recommendations, and Actions to be Taken on Reports of Medical Examination (DD-2808) and Medical History (DD-2807-1).
- 1. DD-2808 (Report of Medical Examination).
- 2. DD-2807-1 (Report of Medical History).
- 3. Review and Action on Findings and Recommendations of Report of Medical Examination (DD-2808).
- 4. Correction of Defects Prior to Overseas Transfer or Sea Duty Deployment.
- 5. Objection to Assumption of Fitness for Duty at Separation.
- 6. Separation Not Appropriate by Reason of Physical Disability.
- 7. Procedures for Physical Defects Found Prior to Separation.
- FIGURE 3-B-1
- FIGURE 3-B-2
- Section C - Medical Examination Techniques And Lab Testing Standards.
- 1. Scope.
- 2. Speech Impediment.
- 3. Head, Face, Neck, and Scalp (Item 17 of DD-2808).
- 4. Nose, Sinuses, Mouth, and Throat (Item 19, 20 of DD-2808).
- 5. Ears (General) and Drums (Item 21, 22 of DD-2808).
- 6. Eyes (General), Ophthalmoscopic, and Pupils (Item 23, 24, 25 of DD-2808).
- 7. Ocular Motility (Item 26 of DD-2808).
- 8. Heart and Vascular System (Item 27 of DD-2808).
- 9. Lungs and Chest (Item 28 of DD-2808).
- 10. Anus and Rectum (Item 30 of DD-2808).
- 11. Abdomen and Viscera (Item 31 of DD-2808).
- 12. Genitourinary System (Item 32 of DD-2808).
- 13. Extremities (Item 33, 34, 35 of DD-2808).
- 14. Spine and Other Musculoskeletal (Item 36 of DD-2808).
- 15. Identifying Body Marks, Scars, and Tattoos (Item 37 of DD-2808).
- 16. Neurologic (Item 39 of DD-2808).
- 17. Psychiatric (Item 40 of DD-2808).
- 18. Endocrine System.
- 19. Dental (Item 43 of DD-2808).
- 20. Laboratory Findings.
- 21. Height, Weight, and Body Build.
- 22. Distant Visual Acuity and Other Eye Tests.
- 23. Audiometer.
- 24. Psychological and Psychomotor.
- FIGURE 3-C-1
- FIGURE 3-C-3
- FIGURE 3-C-4 MINIMUM DISTANT VISUAL ACUITY REQUIREMENTS
- Section D Physical Standards for Enlistment, Appointment, and Induction.
- 1. Scope.
- 2. Applicability and Responsibilities.
- 3. Abdominal Organs and Gastrointestinal System.
- 4. Blood and Blood-Forming Tissue Diseases.
- 5. Dental.
- 6. Ears.
- 7. Hearing.
- 8. Endocrine and Metabolic Disorders.
- 9. Upper Extremities
- 10. Lower Extremities
- 11. Miscellaneous Conditions of the Extremities.
- 12. Eyes.
- 13. Vision.
- 14. Female Genitalia.
- 15. Male Genitalia.
- 16. Urinary System
- 17. Head.
- 18. Neck.
- 19. Heart.
- 20. Vascular System.
- 21. Height.
- 22. Weight.
- 23. Body Build.
- 24. Lungs, Chest Walls, Pleura, and Mediastinum.
- 25. Mouth.
- 26. Nose and Sinuses.
- 27. Neurological Disorders.
- 28. Disorders with Psychotic Features.
- 29. Neurotic, Anxiety, Mood, Somatoform, Dissociative, or Factitious Disorders (300).
- 30. Personality, Conduct, and Behavior Disorders.
- 31. Psychosexual Conditions.
- 32. Substance Misuse.
- 33. Skin and Cellular Tissues.
- 34. Spine and Sacroiliac Joints.
- 35. Systemic Diseases.
- 36. General and Miscellaneous Conditions and Defects.
- 37. Tumors and Malignant Diseases.
- 38. Miscellaneous.
- Section E Physical Standards for Programs Leading to Commission.
- 1. Appointment as Cadet, United States Coast Guard Academy.
- 2. Commissioning of Cadets.
- 3. Enrollment as an Officer Candidate.
- 4. Commissioning of Officer Candidates.
- 5. Direct Commission in the Coast Guard Reserve.
- 6. Direct Commission of Licensed Officers of U. S. Merchant Marine.
- 7. Appointment to Warrant Grade.
- Section F Physical Standards Applicable to All Personnel (Regular and Reserve) For: Reenlistment; Enlistment of Prior Service USCG Personnel; Retention; Overseas Duty; and Sea Duty.
- 1. General Instructions.
- 2. Use of List of Disqualifying Conditions and Defects.
- 3. Head and Neck.
- 4. Esophagus, Nose, Pharynx, Larynx, and Trachea.
- 5. Eyes.
- 6. Ears and Hearing.
- 7. Lungs and Chest Wall.
- 8. Heart and Vascular System.
- 9. Abdomen and Gastrointestinal System.
- 10. Endocrine and Metabolic Conditions (Diseases).
- 11. Genitourinary System.
- 12. Extremities.
- 13. Spine, Scapulae, Ribs, and Sacroiliac Joints.
- 14. Skin and Cellular Tissues.
- 15. Neurological Disorders.
- 16. Psychiatric Disorders.
- 17. Dental.
- 18. Blood and Blood-Forming Tissue Diseases.
- 19. Systemic Diseases, General Defects, and Miscellaneous Conditions.
- 20. Tumors and Malignant Diseases.
- 21. Sexually Transmitted Disease. Complications or residuals
- 22. Human Immunodeficiency Virus (HIV).
- 23. Transplant recipient.
- Section G Physical Standards for Aviation.
- 1. Classification of Aviation Personnel.
- 2. General Instructions for Aviation Examinations.
- 3. Restrictions Until Physically Qualified.
- 4. Standards for Class l.
- 5. Standards for Class 1R.
- 6. Candidates for Flight Training.
- 7. Requirements for Class 2 Flight Officers.
- 8. Requirements for Class 2 Aircrew.
- 9. Requirements for Class 2 Medical Personnel.
- 10. Requirements for Class 2 Technical Observers.
- 10. Requirements for Class 2 Technical Observers.
- 11. Requirements for Class 2 Air Traffic Controllers.
- 12. Requirements for Landing Signal Officer (LSO).
- 13. Contact Lenses.
- Figure 3-G-1
- Figure 3-G-2
- Figure 3-G-3
- Figure 3-G-4
- Section H Physical Examinations and Standards for Diving Duty.
- Section A - Administrative Procedures.
- CHAPTER 4 HEALTH RECORDS AND FORMS
- Section A - Health Records.
- Section B - Health Record Forms.
- 1. CG-3443 (Health Record Cover).
- 2. CG-5266 (Drug Sensitivity Sticker).
- 3. DD2766 (Adult Preventive and Chronic Care Flowsheet Form).
- 4. SF-600 (Chronological Record of Medical Care).
- 5. Treatment at Other Than Unit Assigned.
- 6. DD-2808 (Rev. Jul 01) (Report of Medical Examination).
- 7. DD-2807-1 (Rev. Jul 01) (Report of Medical History).
- 8. SF-558 (Emergency Care and Treatment) (Rev 9-96).
- 9. DD-2215 Reference Audiogram.
- 10. DD-2216 Hearing Conservation Data.
- 11. Audiogram Results.
- 12. SF-502 (Narrative Summary).
- 13. NAVMED 6100/1 (Medical Board Report Cover Sheet).
- 14. SF-513 (Consultation Sheet).
- 15. SF-520 (Electrocardiographic Report).
- 16. SF-515 (Tissue Examination).
- 17. SF-541 (Gynecologic Cytology).
- 18. SF-514 (Laboratory Reports).
- 19. SF-545a - Clinical Record
- 20. SF-546 - 557 (Laboratory Requests).
- 21. SF-519 (Radiographic Reports).
- 22. DD-771 (Eyewear Prescription).
- 23. SF-601 (Immunization Record).
- 24. SF-602 (Syphilis Record).
- 24. DD-1141 (Record of Occupational Exposure to Ionizing Radiation).
- 25. CG-4057 (Chronological Record of Service).
- 26. NAVMED 6150/2 (Special Duty Medical Abstract).
- 27. PHS-731 (International Certificate of Vaccination).
- 28. CG-5214 (Emergency Medical Treatment Report).
- 29. DD877 (Request for Medical/Dental Records or Information).
- Section C - Dental Record Forms.
- 1. CG-3443-2 (Dental Record Cover).
- 2. NAVMED 6600/3 (Dental Health Questionnaire).
- 3. SF-603 (Dental Record).
- 4. SF-603-A (Dental Continuation).
- 5. SF-513, Consultation Sheet.
- 6. Lost Dental Records.
- 7. Special Dental Records Entries.
- 8. Dental Examination Requirements.
- 9. Recording of Dental Treatments on SF-600.
- Section D - Clinical Records.
- 1. Purpose and Background.
- 2. Contents of Clinical Records.
- 3. Extraneous Attachments.
- 4. Opening Clinical Records.
- 5. Terminating Clinical Records.
- 6. Custody of Clinical Records.
- 7. Safekeeping of Clinical Records.
- 8. Transfer of Clinic Records.
- 9. Lost, Damaged, or Destroyed Clinical Records.
- 10. Clinical Record Forms.
- Section E - Employee Medical Folders.
- 1. Purpose and Background.
- 2. Custody of Employee Medical Folders (EMF’s).
- 3. Contents of the Employee Medical Folders.
- 4. Accountability of Disclosures.
- 5. Opening Employee Medical Folder.
- 6. Terminating Employee Medical Folders.
- 7. Transferring to Other Government Agencies.
- 8. Lost, Damaged, or Destroyed Employee Medical Folders.
- 9. SF-66 D (Employee Medical Folder).
- Section F -Inpatient Medical Records.
- Section G – Mental Health Records.
- Encl. (1) to CHAP 4, COMDTINST M6000.1B
- HEALTH RECORD COVER
- ADULT PREVENTIVE AND CHRONIC CARE FLOWSHEET
- CHRONOLOGICAL RECORD OF MEDICAL CARE
- REPORT OF MEDICAL EXAMINATION
- REPORT OF MEDICAL HISTORY
- EMERGENCY CARE
- NARRATIVE SUMMARY
- CONSULTATION SHEET
- ELECTROCARDIOGRAPHIC RECORD
- TISSUE EXAMINATION
- GYNECOLOGIC CYTOLOGY
- LABORATORY REPORTS
- RADIOLOGICAL CONSULTATION REQUESTS/REPORTS
- EYEWEAR
- IMMUNIZATION RECORD
- SYPHILIS RECORD
- RECORD OF OCCUPATIONAL EXPOSURE TO IONIZING RADIATION
- CHRONOLOGICAL RECORD OF SERVICE
- SPECIAL DUTY MEDICAL ABSTRACT (NAVMED 6150/2)
- EMERGENCY MEDICAL TREATMENT REPORT
- MEDICAL/DENTAL RECORD
- DENTAL RECORD
- DENTAL HEALTH QUESTIONNAIRE
- DENTAL RECORD SF603
- INPATIENT MEDICAL RECORD COVER SHEET
- DOCTORS ORDERS
- PHYSICAL EXAMINATION
- PROGRESS NOTES
- VITAL SIGNS
- ABBREVIATED MEDICAL RECORD
- CHAPTER 5 DEATHS AND PSYCHIATRIC CONDITIONS (PERSONALITY)
- Section A - Deaths.
- 1. General.
- 2. Duties of Medical Officers or Health Services Department Representatives in the Event of A Death at A Coast Guard Unit.
- 3. Determining Cause of Death.
- 4. Death Certificates for Deaths Occurring Away From Command or in Foreign Ports.
- 5. Relations with Civilian Authorities.
- 6. Reporting Deaths to Civilian Authorities.
- 7. Death Forms for Civilian Agencies and Individuals.
- 8. Identification of Remains.
- Section B - Psychiatric Conditions (including personality disorders).
- 1. General.
- 2. Personality Disorders.
- 3. Adjustment Disorders.
- 4. Organic Mental Disorders.
- 5. Psychoactive Substance Use Disorders.
- 6. Schizophrenia.
- 7. Psychotic Disorders Not Elsewhere Classified.
- 8. Delusional (Paranoid) Disorder.
- 9. Neurotic Disorders.
- 10. Mood Disorders.
- 11. Anxiety Disorders (or Anxiety and Phobic Neuroses).
- 12. Somatoform Disorders.
- 13. Dissociative Disorders (or Hysterical Neuroses, Dissociative Type).
- 14. Sexual Disorders.
- 15. Sexual Dysfunctions.
- 16. Factitious Disorders.
- 17. Disorders of Impulse Control Not Elsewhere Classified.
- 18. Disorders Usually First Evident in Infancy, Childhood, or Adolescence.
- 19. 316.00 Psychological Factors Affecting Physical Condition.
- 20. V Codes for Conditions Not Attributable to a Mental Disorder that are a Focus of Attention or Treatment.
- 21. Additional Codes.
- Section C - Command directed Mental Health Evaluation of Coast Guard Service members.
- 1. General.
- 2. When not an emergency, commanding officers suspecting a mental health evaluation may be indicated will:
- 3. Commanders shall provide a copy of the following rights to Service members who are referred:
- 4. No one will:
- 5. The specific procedures required by these regulations apply to mental health evaluations
- 6. Procedures for using the memorandum requesting a mental health evaluation
- Section A - Deaths.
- CHAPTER 6 REPORTS, FORMS, AND RECORDS
- Section A - Reports.
- 1. Health Services Statistical Report, (RCN 6000-1).
- 2. Report of Potential Third Party Liability (RCN 6000-2).
- 3. MLC/Headquarters Clinic Operations Report (RCN 6000-3).
- 4. Disease Alert Report (RCN-6000-4).
- 5. Report of Theft of Controlled Substances (RCN 6000-5).
- 6. Inpatient Hospital Report (RCN 6000-6).
- 7. Health Care Equipment Inventory Report (RCN 6000-7).
- 8. Health Services Division Status Report (RCN 6000-8).
- 9. Shorten Clinic Automated Report System (SCARS).
- Section B - Forms and Records.
- 1. Status-Profile (CG-5460A).
- 2. Visit Profile (CG-5460B).
- 3. U.S. Coast Guard Health Care Equipment Request (CG-5211).
- 4. Health Record Receipt Form (NAVMED 6150/7).
- 5. Referral for Civilian Medical Care (DD-2161).
- 6. Health Services Log.
- 7. Binnacle List.
- 8. Adult Preventive and Chronic Care Flowsheet Form (DD2766).
- Section A - Reports.
- CHAPTER 7 PREVENTIVE MEDICINE
- Section A - General
- Section B Communicable Disease Control.
- 1. General.
- 2. Disease Outbreak.
- 3. RCN 6000-4, Disease Alert Report.
- 4. Sexually Transmitted Disease Responsibilities.
- 5. Treatment.
- 6. Drug Prophylaxis.
- 7. Reporting.
- FIGURE 7-B-1 LIST OF REPORTABLE DISEASES
- FIGURE 7-B-2 LIST OF REPORTABLE OCCUPATIONAL DISEASES
- FIGURE 7-B-3 RCN 6000-4, DISEASE ALERT REPORT
- Section C Immunizations
- Section D Tuberculosis Prevention and Control Program
- 1. Introduction.
- 2. Tuberculosis Screening Program.
- 3. Tuberculosis Contact Investigation Program.
- 4. Protective measures
- 5. Managing Personnel with Reactive Tuberculin Tests or Suspected TB.
- 6. Tuberculosis Control Among Dependents and Other Civilians.
- 7. Decontaminating Spaces Occupied by Persons with Active PMTB.
- FIGURE 7-D-1 SUMMARY OF TESTING PROCEDURES
- CHAPTER 8 FISCAL AND SUPPLY MANAGEMENT
- CHAPTER 9 HEALTH SERVICES TECHNICIANS ASSIGNED TO INDEPENDENT DUTY
- CHAPTER 10 PHARMACY OPERATIONS AND DRUG CONTROL
- CHAPTER 11 HEALTH CARE PROCUREMENT
- MEDICAL MANUAL COVER
- Section A - Contracting For Health Care Services
- 1. General.
- 2. Type of Services.
- 3. Eligibility For Contract Health Care Services.
- 4. Approval to Contract for Services.
- 5. Funding.
- 6. Pre-contract Award Actions.
- 7. Award Evaluation Factors.
- 8. Post-Contract Award Actions.
- Figure 11.A.1 STATEMENT OF WORK
- 1. Scope.
- 2. Definitions.
- 3. The contractor shall perform these tasks:
- 4. The contractor shall not execute any oral or written agreements with the patient to render a more expensive type of service
- 5. The contractor must obtain written authority from the patient's Coast Guard unit before filling any prescriptions.
- 6. The contractor must obtain written authority from the patient's Coast Guard unit before performing any elective procedure.
- Section B - Health Care Services Invoice Review and Auditing
- Section C - Claims Processing
- CHAPTER 12 OCCUPATIONAL MEDICAL SURVEILLANCE AND EVALUATION PROGRAM (OMSEP)
- Section A - General Requirements.
- Section B - Administrative Procedures.
- 1. General:
- 2. Examination Types.
- 3. Use of OMSEP Forms.
- 4. Medical Removal Standards
- 5. Reporting of Examination Results.
- TABLE 12-B-1 REQUIRED FORMS AND TESTS FOR VARIOUS OMSEP EXAMINATIONS AND PROTOCOLS
- FIGURE 12-B-1 ACUTE CHEMICAL EXPOSURE INFORMATION
- FIGURE 12-B-2 OMSEP NOTIFICATION OF SUMMARY RESULTS
- FIGURE 12-B-4 OMSEP SEPARATION LETTER
- Section C - Medical Examination Protocols.
- 1. General.
- 2. Asbestos (Figure 12-C-1).
- 3. Benzene (Figure 12-C-2).
- 4. Chromium Compounds (Figure 12-C-3).
- 5. Hazardous Waste (Figure 12-C-4).
- 6. Lead (Figure 12-C-5).
- 7. Noise (Figure 12-C-6).
- 8. Pesticides (Figure 12-C-7).
- 9. Respirator Wear (Figure 12-C-8).
- 10. Respiratory Sensitizers (Figure 12-C-9).
- 11. Solvents (Figure 12-C-10).
- 12. Tuberculosis (Figure 12-C-11).
- 13. Unspecified (Figure 12-C-12).
- FIGURE 12-C-1
- FIGURE 12-C-2
- FIGURE 12-C-3
- FIGURE 12-C-4
- FIGURE 12-C-5
- FIGURE 12-C-6
- FIGURE 12-C-7
- FIGURE 12-C-8
- FIGURE 12-C-9
- FIGURE 12-C-10
- FIGURE 12-C-11
- FIGURE 12-C-12
- CHAPTER 13 QUALITY ASSURANCE
- Section A - Quality Assurance Plan
- Section B – Credentials Maintenance and Review
- Section C – Clinical Privileges
- Section D - Quality Assurance Checklists.
- Section E – Quality Assurance Implementation Guide (QAIG)
- Section F- Quality Assurance Site Survey.
- Section G - Coast Guard Clinic Certification and Accreditation
- Section H- Monitoring and Evaluation Program
- SECTION J UTILIZATION REVIEW PROGRAM.
- Section K - Infection Control Program
- 1. Background.
- 2. Policy.
- 3. Universal Precautions.
- 4. Precautions for Invasive Procedures.
- 5. Precautions for Medical Laboratories.
- 6. Handling Biopsy Specimens.
- 7. Using and Caring for Sharp Instruments and Needles.
- 8. Infection Control Procedures for Minor Surgery Areas and Dental Operatories.
- 9. Sterilizing and Disinfecting.
- 10. Laundry.
- 11. Cleaning and Decontaminating Blood or Other Body Fluid Spills.
- 12. Infectious Waste.
- 13. Managing Exposures (Needle Stick Protocol)
- 14. Training Personnel For Occupational Exposure.
- Section L - Risk Management Program
- Section M - Training and Education
- Section N - Patient Affairs Program
- CHAPTER 14 TABLE OF CONTENTS

MEDICAL MANUAL
COMDTINST M6000.1B
Includes Change 17
U.S. Department
of Transportation
United States
Coast Guard

DISTRIBUTION – SDL No. 139
a b c d e f g h i j k l m n o p q r s t u v w x y z
A 1 1 1 2 2 2 1 1 1 3
B 8 10* 12 5 2 11 2 20613 2260 1
C 1* 1* * 1 * *2 * 1 1 1 1 1
D 3 1 * *11
E
F 111
G *
H
NON-STANDARD DISTRIBUTION:
Commandant
U.S. Coast Guard
2100 2nd Street S.W.
Washington, DC 20593-0001
Staff Symbol: G-WKH-1
Phone: (202) 267-0767
COMDTINST M6000
March 27, 2002
CANCELLED:
March 27, 2003
COMMANDANT NOTICE 6000
Subj: CH-17 TO MEDICAL MANUAL, COMDTINST M6000.1B
1. PURPOSE. This Notice publishes revisions to Medical Manual, COMDTINST M6000.1B. Intended
user of this directive are all Coast Guard Units that maintain Medical Manuals.
2. ACTION. Area and district commanders, commanders of maintenance and logistics commands,
commanding officers of Headquarters units, Assistant Commandants for directorates, Chief Counsel and
special staff offices at Headquarters shall ensure compliance with the provisions of this Notice.
3. DIRECTIVES AFFECTED. Medical Manual, COMDTINST M6000.1B.
4. SUMMARY. Newly revised material and editorial changes are denoted by a line on the outside of the
page. Enclosure (1) summarizes the substantial changes throughout the Manual provided as enclosure
(2).
5. PROCEDURES. No paper distribution will be made of this Manual. Official distribution will be via the
Coast Guard Directives System CD-ROM and the Department of Transportation Website
http://isddc.dot.gov/. An electronic version will also be made available via the Commandant (G-WK)
Publications and Directives website (see # 6, below).
a. Remove and insert the following pages
Remove Insert
Chapter 1 CH-16 pg 39-40 Chapter 1 CH-17 pg 39-40
Chapter 2 CH-16 pg 9-10 Chapter 2 CH-17 pg 9-10
Chapter 3 CH-16 Chapter 3 CH-17
Chapter 4 CH-16 Chapter 4 CH-17
Chapter 7 CH-15 Chapter 7 CH-17
Chapter 8 CH-15 pg 13-14 Chapter 8 CH-17 pg 13-14

Chapter 10 CH-15 pg 17-18 Chapter 10 CH-17 pg 17-18
Chapter 11 CH-15 Chapter 11 CH-17
Chapter 12 CH-16 Chapter 12 CH-17
Chapter 13 CH-13 pg i-iii Chapter 13 CH-17 pg i-iii
Chapter 13 CH-13 pg 11-14 Chapter 13 CH-17 pg 11-14
Chapter 13 CH-13 pg 27-28 Chapter 13 CH-17 pg 27-28
Chapter 13 CH-13 pg 97-104 Chapter 13 CH-17 pg 97-104
Chapter 14 CH-17
6. FORMS AVAILABILITY. All forms listed in this Manual with the exception noted in this paragraph
are available from stock points listed in the Catalog of Forms, COMDTINST 5213.6. Local
reproduction authorized for the Modified Physical Examination. Availability of DD-2808 Report of
Medical Examination and DD-2807-1 Report of Medical History is only by .pdf format, a web link is
provided on the Pubs and Directives web page. Some forms referenced in this Manual are also available
on SWSIII Jet Form Filler. Web links to forms in .pdf format have been provided on the Pubs and
Directives page; http://www.uscg.mil/hq/g-w/g-wk/g-wkh/g-wkh-1/Pubs/Pubs.Direct.htm.
Encl (1) Summary of substantial changes
(2) CH-17 to Medical Manual, COMDTINST M6000.1B

Enclosure (1) to COMDTNOTE 6000.1B
1
CH-17 to Medical Manual, COMDTINST M6000.1B
Chapter 1
Chapter 1-B-21 Adds new sub-section 1-B-21, and provides guidance for (Volunteers).
Chapter 2
Chapter 2-A-6-(4) Provides clarification of Elective Health Care and fitness for duty.
Chapter 3
Chapter 3-A-7-d Provides new guidelines for Overseas Transfer, Sea Duty Deployment and
Port Security Units.
Figure 3-A-1 Revised Modified Physical Exam Form. Form authorized for local
reproduction.
Chapter 3-C Section revised to match sequence of the new DD-2808 (Report of
Medical Exam) and 2807-1 (Report of Medical History). No content was
changed.
Chapter 3-B-1&2 Revised paragraphs to reflect new physical exam forms.
Chapter 3-C-21-
b(9)(b)4 Revised paragraph to read HIV testing is every 5 years.
Chapter 3-C-21-
b(9)(b)8 Added new sub-paragraph to identify tuberculin reactors.
Chapter 3-C-21-b(i) Removed reference to Reportable Disease Data Base (RDDB) no longer
used.
Chapter 3-C-20-
b(9)(e) Revised paragraph to provide narrative summary to be obtained by the
referring medical officer.
Chapter 3-C-
22.j(1)(a)(5) Revised paragraph to reflect update to the process of color perception
testing.
Chapter 3-F-2 Provides new guidance for the List of Disqualifying Conditions and
Defects.
Chapter 3-F-22 Revised definition for Human Immunodeficiency Virus (HIV)
Chapter 3 –G-4-d. Added required self-balancing test for aviation physicals.
Replaced all references to the new DD-2808 (Report of Medical
Examination) and DD-2807-1 (Report of Medical History)
Chapter 3 Chapter layout re-formatted.
Chapter 4
Chapter 4-A-6-b Provides guidance for the transfer of Active Duty Health records.
Chapter 4-A-2(5)(g) Updated section to provide placement of the audiogram microprocessor
test strip in the Health Record.
Chapter 4-B-6 Revised section to delete form SF-88 (Report of Medical Examination)
and replaced form with new form DD-2808 (Report of Medical
Examination)
Chapter 4-B-7 Revised section to delete form SF-93 (Report of Medical History) and
replaced form with DD-2807-1 (Report of Medical History).
Chapter 4-D-8-b Provides guidance for the transfer of Dependant Health Records
Chapter 4-B-3-b(2) Revised section to include NKDA (no known allergies) in section 1-a of
the DD-2766 (Adult Preventive and Chronic Care Flowsheet)
Chapter 4-B-9&10 Revised section to make the DD-2215 (Reference audiogram and DD-
2216 (Hearing Conservation Data Sheet and optional form.
Chapter 4-B-11 Updated section to include placement of audiogram results into the health
record.
Cha
p
ter 4- Reformatted Cha
p
ter 4 addin
g
(
Enclosure
(
1
)
Medical/Dental Record

Enclosure (1) to COMDTNOTE 6000.1B
2
Enclosure (1) Forms(.jpegs)). Developed this new enclosure to prevent having to
download forms, when new text is added to Chapter 4.
Chapter 7
Chapter 7-B-2-b(3) Revised paragraph to send a Coast Guard intranet e-mail message Disease
Alert report.
Figure 7-B-1 Revised List of Reportable Conditions.
Chapter 7-B-3-b Revised subsection (1) to submit Initial Report to MLC(k), copy to
WKH-1.
Figure7-B-3 Revised line 5 to read: Laboratory test done, if any, and results.
Chapter 7-C-4-f Revised paragraph for the administration of vaccines.
Re-formatted Chapter 7 page numbers have changed.
Chapter 8
Chapter 8-E-3.b(2) Removed Optical Fabrication Laboratory form table.
Chapter 10
Chapter 10-B-2-
b(1)(a) Revised paragraph to reduce letters of designation for the Controlled
Substance Audit Board.
Chapter11
Chapter 11-C-3-a(1) Removed reference to CG-5534 (Non-Fed Med form) form removed with
CH-16
Chapter11-C-5-b(2) Removed reference to CG-5534 (Non Fed Med form) form removed with
CH-16
Chapter reviewed for accuracy and re-formatted.
Chapter12
All references to the SF-88 Medical Examination & SF-93 Medical
History have been removed. These forms are replaced with the DD-2808
Report of Medical Examination and DD-2807-1 Report of Medical
History
Chapter12-A-2-c(3) Revised text to include new (Note) section to cover new OMSEP
enrollees.
Chapter 12-C-3-
d(2)b.c.d. Revised text to provide new guidelines for acute exposure examination.
Figure12-C-2 Revised text to include: blood or breath benzene level (optional-if
available)
Chapter12-C-7-d-(5) Revised paragraph to clarify guidance for audiogram STS.
Chapter 12-C-9-d Paragraph revised to clarify Examination protocol.
Chapter12 re-issued, page numbers have changed.
Chapter13
Chapter –13-B-4-f Revised section to provide guidelines for: Proof of current competences.
Chapter 13-B-5-b(4) Revised section to submit documentation of CME credentials every other
year.
Chapter 3-G-1-c(2) Revised paragraph to increase “other element” from 60% to 80%.
Chapter 13-M-2-c(4) Deleted Practicum Guide for HS’s
Chapter 14
Introducing new Chapter 14 - Medical Information System (MIS) Plan

DISTRIBUTION – SDL No.
a b c d e f g h i j k l m n o p q r s t u v w x y z
A 1 1 1 2 2 2 1 1 1 3
B 8 10* 12 5 2 11 2 20613 2260 1
C 1* 1* * 1 * *2 * 1 1 1 1 1
D 3 1 * *11
E
F 111
G *
H
NON-STANDARD DISTRIBUTION:
Commandant
U.S. Coast Guard
2100 2nd Street S.W.
Washington, DC 20593-0001
Staff Symbol: G-WKH-1
Phone: (202) 267-0767
COMDTINST M6000
27 June 2001
COMMANDANT NOTICE 6000
Subj: CH-16 TO MEDICAL MANUAL, COMDTINST M6000.1B
1. PURPOSE. This Notice publishes revisions to Medical Manual, COMDTINST M6000.1B. Intended
user of this directive are all Coast Guard Units that maintain medical Manuals.
2. ACTION. Area and district commanders, commanders of maintenance and logistics commands,
commanding officers of Headquarters units, Assistant Commandants for directorates, Chief Counsel and
special staff offices at Headquarters shall ensure compliance with the provisions of this Notice.
3. DIRECTIVES AFFECTED. Medical Manual, COMDTINST M6000.1B.
4. SUMMARY. Newly revised material and editorial changes are denoted by a line on the outside of the
page. Enclosure (1) summarizes the substantial changes throughout the Manual provided as enclosure
(2).
5. PROCEDURES. No paper distribution will be made of this Manual. Official distribution will be via the
Coast Guard Directives System CD-ROM and the Department of Transportation Website
http://isddc.dot.gov/. An electronic version will also be made available via the Commandant (G-WK)
Publications and Directives website (see # 6, below).
a. Remove and insert the following pages
Remove Insert
Chapter 1 CH-15 Chapter 1 CH-16
Chapter 2 CH-14 Chapter 2 CH-16
Chapter 3 CH-15 Chapter 3 CH-16
Chapter 4 CH-15 Chapter 4 CH-16
Chapter 5 CH-15 Chapter 5 CH-16
Chapter 6 CH-14 Chapter 6 CH-16
Chapter 9 CH-15 Chapter 9 CH-16
Chapter 12 CH-15 Chapter 12 CH-16

6. FORMS AVAILABILITY. All forms listed in this Manual with the exception noted in this paragraph
are available from stock points listed in the Catalog of Forms, COMDTINST 5213.6. The stock number
for DD Form 2766 (Rev 01-00), Adult Preventive and Chronic Care Flowsheet, Sponsor (Navy) is 2766-
0102-LF-984-8400 (pkg 100). The DD-877, Request for Medical/Dental Records no longer has a stock
number. Availability of this form is only by .pdf format, a web link is provided on the Pubs and
Directives web page. Some forms referenced in this manual are also available on SWSIII Jet Form
Filler. Web links to forms in .pdf format have been provided on the Pubs and Directives page;
http://www.uscg.mil/hq/g-w/g-wk/g-wkh/g-wkh-1/Pubs/Pubs.Direct.htm.
JOYCE M. JOHNSON
Director of Health and Safety
Encl (1) Summary of substantial changes
(2) CH-16 to Medical Manual, COMDTINST M6000.1B
1
Enclosure (1) to COMDTNOTE 6000
CH-16 TO MEDICAL MANUAL, COMDTINST M6000.1B
Chapter 1
Chapter 1-B-1.a.i: Specifies the patient will be notified of all abnormal test results.
Chapter 1 Chapter layout re-formatted for uniformity.
Chapter 2
Chapter 2-A-6 Provides guidelines for Elective Health Care.
Chapter 2-A-7 Provides guideline for Other Health Insurance (OHI).
Chapter 2-F-3.a Provides new guidelines for Members of Foreign Military Services.
Chapter 2-I-1-e: Provides definition for Super Sickbay
Chapter 2 Chapter layout re-formatted for uniformity.
Chapter 3
Figure 3-A-1 Revised Overseas Modified Screening to reflect DNA sample.
Figure 3-B-2 Revised to show current routing symbol. Re-added (5) to NOTES.
Chapter 3-B-c.(3) Revised text to read: Upon completion of flight training and assignment to a
Coast Guard unit, the NOMI approved physical will be considered valid until the
last day of the member’s next birth month.
Chapter 3-C-19 Item 18 (Dental) portion of the SF 88, Report of Medical Exam, updated to show
current accession standards in 3-D.
Chapter 3,
Figure 3-C-2 Dental Carious Teeth Standards removed from chapter. Reflects current
standards in section 3-D.
Chapter 3,
Figure 3-C-3 Reduced height standard for (Candidate for Flight Training) from 64 to 62 inches.
Chapter 3-D Revised Section D to reflect DOD Directive 6130.4 dtd Dec 14,2000, P.E.
Standards for Entrance into the Coast Guard.
Chapter 3-F-5- Provides guidelines for Corneal Refractive Surgery.
Chapter 3-F-7-b.(2) Provides new definition for Bronchial Asthma.
Chapter 3-F-8-a.(5) Provides new definition for Myocarditis and degeneration of the myocardium.
Chapter 3-F-8.b.(9) Revised text to read: Any condition requiring anti-thrombotic medication other
than aspirin.
Chapter 3-F-10-a.(8)
& (13) Provides new definition for Crohn’s Disease and Ulcerative Colitis.
3-F-10.e Provides new definition for Diabetes Mellitus.
3-F-15.e Provides new definition for Convulsive Disorders.
3-F-18.e Provides new definition for Purpura and other bleeding diseases.
3-F-22 Revised definition for HIV to read identical to HIV ALCOAST #425/00
3-G-4.d Provides new height standards for Class 1 Aviators (62) inches.
3-G-6.a.(1).(a) Provides new guidelines for anthropometric measurements for Candidates for
Flight Training.
Chapter 3 Chapter layout re-formatted for uniformity

2
Enclosure (1) to COMDTNOTE 6000
Chapter 4
Chapter 4-A-5.a.(8) Provides definition for Custody of Health Records.
Chapter 4-A-6 Provides new guidance for Transfer of Health Records.
Chapter 4-B-3 Provides guidance and adds new form DD-2766 (Adult Preventive and Chronic
Care Flowsheet) Note: Problem Summary List is now obsolete.
Chapter 4-B-32 Provides guidance and adds form DD-877 (Request for Medical/Dental Records
or Information).
Chapter 4-D-8 Provides guidelines for the Transfer of Clinic Records.
4-G Provides guidelines for Mental Health Records (a new section).
Chapter 4 Chapter layout re-formatted for uniformity. Most forms updated to show current
form available as a word document..
Chapter 5
Chapter 5-C Provides new section C. Command directed Mental Health Evaluation of CG
Members.
Chapter 5 Chapter layout re-formatted for uniformity.
Chapter 6
Chapter 6-A-6 Provides new guidance for Inpatient Hospitalization message to include ICD-9
code for diagnosis.
Chapter 6-B-8 Provides guidelines for the DD-2766 Adult Preventive and Chronic Care
Flowsheet.
Removed CG5534 Removed CG 5534 Non Fed Med as per ALCOAST #129/01,
cancellation of COMDTINST 6010.20.
Chapter 6 Chapter layout re-formatted for uniformity.
Chapter 9
Chapter 9-A-4.a.(10) Provides guidelines for unit instruction or SOP in the event of family violence.
Chapter 9-A-
9.b.(2).(a) Provides guidelines for signs on interior surfaces of cutters.
9.A.7.h. Removes the reference to Chapter 10 of the Coast Guard Rescue and Survival
Systems Manual for guidance on inspection and maintenance of the Rescue EMT
Set and requirements for documentation of those procedures in a Preventive
Maintenance Schedule (PMS) log.
9-A-8.b.(2)(f) Removes requirement to maintain a Preventive Maintenance Schedule (PMS) log.
The requirement for this has been removed from the Coast Guard Rescue and
Survival Systems Manual (COMDTINST M10470.10 (series).
Chapter 9 Chapter layout re-formatted for uniformity.
Chapter 12
Chapter 12-A-2.c Provides guidelines for Enrollment Criteria.
Chapter 12-A-3.a.(1) Provides guidance for using the most current OMSEP Physical Form (6-00).
Chapter 12-A-3.b Provides guidance for the OMSEP database.
Chapter 12-A-5 Provides new guidance for Roles and Responsibilities.
Chapter 12-A-5.a Provides new guidance for OMSEP Coordinators.
3
Enclosure (1) to COMDTNOTE 6000
Chapter 12-A-5.e Provides new guidance for Medical Officer’s responsibilities.
Chapter 12-A-5.f Provides guidance for Medical Administrators.
Chapter 12-A-g Provides guidelines for civilian OMSEP enrollees.
Chapter 12-B-2.d.(1)
& (2) Provides new section (1) and (2), End of Exposure guidelines.
Chapter 12-B-2.e Provides guidance for time intervals between OMSEP examinations.
Chapter 12 forms Table 12-C-1 to 12-C-12 were revised and updated to show current requirements.
Chapter 12 Chapter layout re-formatted for uniformity.







RECORD OF CHANGES
CHANGE
NUMBER
DATE OF
CHANGE
DATE
ENTERED
BY
WHOM ENTERED

1-1 CH 16
CHAPTER 1. ORGANIZATION AND PERSONNEL
Section A - Organization.
1. Mission of the Coast Guard Health Services Program.
a. The Health Services Program supports Coast Guard missions by providing quality
health care to maintain a fit and healthy active duty corps, by meeting the health care
needs of dependents and retirees to the maximum extent permitted by law and
resources, and by providing authorized occupational health services to civilian
employees.
2. Director of Health and Safety.
b. Mission. The mission of the Director of Health and Safety is to:
(1) serve as advisor to the Secretary of Transportation;
(2) serve as advisor to the Commandant; and
(3) develop and implement the Coast Guard’s overall health care program.
c. Duties and Responsibilities. Under the general direction and supervision of the
Commandant, Vice Commandant, and the Chief of Staff, the Director of Health and
Safety shall assume the following duties and responsibilities:
(1) serve as Program Director (PD) for the Health Services Program (G-WKH),
and the Safety and Environmental Health Program (G-WKS);
(2) act as advisor to the Commandant in providing counsel and advice on:
(a) health care issues affecting operational readiness and quality of life in the
Coast Guard;
(b) interdepartmental and interservice agreements for health care of Coast
Guard personnel;
(c) the significance of legislative matters affecting the Coast Guard Health
Services and Safety and Environmental Health Programs; and
(d) important developments in the Department of Defense and the
Department of Health and Human Services which affect the Coast Guard
Health Services and Safety and Environmental Health Programs;
(3) serve as advisor to the Secretary in developing and implementing departmental
national defense emergency medical, health, and sanitation policies and plans
(except those involving civil aviation) and such other advisory services that
may be required or requested;
CH 16 1-2
(4) plan, develop, and administer a comprehensive, high quality health care
program (quality is defined as the desired level of performance against
established standards and criteria) for all authorized beneficiaries;
(5) plan, develop and administer a comprehensive program for the prevention of
illness and injury of Coast Guard personnel and dependents, to reduce losses,
and protect the environment in Coast Guard working facilities and living
spaces/by establishing and maintaining adequate safety and environmental
health standards for aircraft, vessel, shore facilities, and motor vehicle;
providing information and encouragement to beneficiaries for personal
wellness programs and providing healthy and pleasing meals at Coast Guard
dining facilities;
(6) administer TRICARE Management Activity (TMA), including the
appropriation of funds, on behalf of the Coast Guard as provided in the
Dependents Medical Care Act and regulations pursuant thereto;
(7) monitor and protect the health of personnel attached to the Coast Guard
through the Occupational Medical Surveillance and Evaluation Program
(OMSEP);
(8) direct the administration of funds in those appropriations or allotment fund
codes under the control of the Office of Health and Safety, including furnishing
total budget estimates and apportionment or allotment recommendations to the
Chief of Staff;
(9) advise responsible offices concerning establishing physical standards for
military duty and special operational programs;
(10) procure and recommend assignments to the Commander, Coast Guard
Personnel Command (CGPC), and review the performance of Public Health
Service personnel detailed to the Coast Guard;
(11) provide professional health care guidance to all health services personnel;
(12) maintain liaison with the Public Health Service, the Department of Veterans
Affairs, the Department of Defense, and other Federal agencies and serve on
interservice boards and committees as appointed;
(13) set policy and guidelines for the subsistence program;
(14) provide technical advice to operating program managers;
(15) set policy and guidelines for health care quality assurance; and act as the
Governing Body for Coast Guard health care;
(16) set policy and guidelines for the Alcohol Abuse Prevention program; and
(17) serve as a member of the Human Resources Coordinating Council.
(18) administer the Coast Guard Emergency Medical system.
1-3 CH 16
(19) Public Health Service. The responsibility of the Public Health Service for
providing physicians, dentists, and other allied health personnel support to the
Coast Guard is set forth in 42 USC, 253. These personnel are provided on a
reimbursable basis and are subject to Coast Guard regulations and the Uniform
Code of Military Justice (UCMJ).
3. Health and Safety Division, Maintenance and Logistics Commands MLC (k).
a. Mission. The mission of MLC (k) is to:
(1) interpret and implement health care policies as set forth by the Commandant;
(2) develop and implement the Coast Guard’s overall Health Services, and Safety
and Environmental Health Programs for the Area; and
(3) serve as Health Care Advisor to Commander, Maintenance and Logistics
Command.
b. Functions and Responsibilities. Under the direction and supervision of the
Commander, Maintenance and Logistics Command (MLC), the Chief, Health and
Safety Division shall:
(1) act as Medical Advisor to the Area commander in providing counsel and
advice on:
(a) interagency and interservice agreements for health care of Coast Guard
personnel;
(b) the significance of legislative matters affecting the Coast Guard health
care program; and
(c) important developments in the Department of Defense which affect the
Coast Guard health care program.
(2) serve as advisor to the Area commander in developing and implementing
national defense emergency medical, health, and sanitation policies and plans;
(3) plan, develop, and administer a comprehensive health care program for all
beneficiaries;
(4) develop health services mobilization requirements and support documents;
(5) review and act on requests for contract health care services;
(6) act as contract technical representative in reviewing health care contract
proposals;
(7) administer the health care quality assurance program;
(8) administer the Safety and Environmental Health Programs;
(9) administer the Alcohol Abuse Prevention program;
(10) develop and implement pharmaceutical support services;
CH 16 1-4
(11) be responsible for providing funding for direct health care expenditures;
(12) be responsible for the general oversight of health care budgets;
(13) be responsible for the oversight of general clinic policy to include setting
standards for clinic operations and prioritizing of clinic functions;
(14) designate clinics as catchment area patient management sites;
(15) maintain liaison with U. S. Public Health Service, the Department of Veterans
Affairs and the health departments of the Department of Defense and other
Federal agencies within you area of responsibility; and
(16) be responsible for the general oversight of the subsistence program by
providing assistance to Coast Guard units (ashore and afloat) to ensure the
maintenance of high quality food service operations.
c. In addition, the MLC (k)s shall have the right, in coordination with unit commanding
officers, to detail health services personnel (officer and enlisted, Coast Guard and
Public Health Service) for special assignments including meeting short-term staffing
needs.
4. Responsibilities of Commands with Health Care Facilities. Unit commanding officers
shall be responsible for:
a. oversight of clinic procurements;
b. ensuring adherence to policies, military regulations and general administrative
procedures,
c. funding for administrative and non-health care expenditures for clinics;
d. maintenance, repair and general support of clinic facilities;
e. ensuring compliance with action items required by quality assurance site surveys;
and
f. working with the appropriate MLC in fostering quality, productivity, and operating
efficiencies.

1-5 CH 16
Section B.- Personnel.
1. General Duties of Medical Officers. The principal duty of medical officers is to
understand and support the operational missions of the Coast Guard. Medical Officers
include Physicians, Physician Assistants (PA/PYA), and Nurse Practitioners (NP) who
are members of the Coast Guard or Public Health Service detailed to the Coast Guard.
Medical officers are required to have appropriate certification or licensure while assigned
to the Coast Guard. Physicians must have an unrestricted state license to practice
medicine. See 1-B-11 for nurse practitioner and physician assistant credential
requirements. Civilian medical practitioners (under contract to the Coast Guard or GS
employees) assigned to a medical treatment facility are considered medical officers to the
limits defined by the language of their contract and/or job description. Civilian medical
practitioners who have a contract with the Coast Guard to see patients in their private
offices are not considered medical officers for the purpose of this instruction.
a. General Responsibilities.
(1) Medical officers must keep informed in all fields of general and military
medicine and shall:
(a) ensure the fitness for unrestricted worldwide duty of active duty
personnel;
(b) provide health care for all eligible beneficiaries as authorized by
applicable laws and regulations;
(c) make appropriate referrals of eligible beneficiaries following existing
policy and regulation;
(d) treat sick and injured personnel;
(e) prevent and control disease;
(f) promote health;
(g) give advice on such matters as hygiene, sanitation, and safety;
(h) recommend duty status of active duty personnel and Coast Guard civil
service employees;
(i) ensure that each patient is notified of results of all PAP smears,
mammograms, biopsies, pregnancy tests, and all tests that are abnormal
or whose results indicate a need to initiate or change treatment.
(j) thoroughly understand all operational missions of the unit, units within
the local area, and the human factors involved in performing them;

CH 16 1-6
(k) ensure that personnel are physically and psychologically fit for duty and
attempt to learn of any unusual circumstances which might adversely
affect their proficiency;
(l) maintain an active interest and participate in the local unit’s safety
program, assist the safety officers in planning, implementing, and
coordinating the unit safety program, and advise the command on safety
issues;
(m) be thoroughly familiar with the types of personal protective and survival
equipment carried at the unit. Assist the engineering officer in
maintaining and issuing the equipment, and be familiar with the Rescue
and Survival System Manual, COMDTINST M10470.10 (series);
(n) actively participate in the unit physiology training program to ensure that
personnel are capable of coping with the hazards of mission performance
by presenting lectures and demonstrations which include, but are not
limited to:
1 fatigue
2 emergency medicine,
3 survival,
4 disorientation,
5 night vision,
6 stress, and
7 drug and alcohol use and abuse.
(o) ensure that HSs who participate in EMT operations maintain their
certification, knowledge and Health Services skills in EMT operations,
physiology;
(p) provide Health Services refresher training on emergency procedures; and
(q) participate in a program of continuing education in operational medicine
including familiarity with information published for other branches of the
Armed Forces.
(2) Medical officers act as medical members in physical disability evaluation
cases.
(3) Medical officers are responsible for advising commanding officers on: health
status of personnel; nutritional adequacy, food handling and preparation;
1-7 CH 16
heating, ventilation, and air conditioning; housing; insect, pest, and rodent
control; water supply and waste disposal; safety; items sold in exchanges,
commissaries, and other CGES facilities; the physical fitness of personnel; and
immunization standards.
b. Physical Examinations. Medical officers shall conduct physical examinations in
accordance with Section 3-C of this Manual and in cases involving disability
evaluation be guided by the Physical Disability Evaluation System, COMDTINST
M1850.2 (series), and the Department of Veterans Affairs Publication, Physician’s
Guide for Disability Evaluation Examinations.
c. Reports to Command. Report injuries to, or deaths of, personnel; damage,
destruction, or loss of health services department property; and any other important
occurrence, to the officer of the day or other command official for entry into
appropriate log. Report any suspected child/spouse abuse to the commanding officer,
family advocacy representative, and local law enforcement/child protective agency in
accordance with Family Advocacy Program, COMDTINST 1750.7 (series), and
other local, state, or Federal law. Report patients in serious or critical condition to
the commanding officer or officer of the day, together with the information needed to
notify the next of kin. Death imminent procedures are contained in the Physical
Disability Evaluation System, COMDTINST M1850.2 (series).
d. Educational Measures. Conduct health education programs, including disseminating
information about preventing disease and other subjects pertaining to hygiene and
sanitation.
(1) Sexually Transmitted Diseases. Conduct or supervise the instruction of
personnel regarding sexually transmitted diseases and advise them of the
associated dangers.
(2) First Aid Instruction. Conduct or supervise a program which will ensure
knowledge and ability in first aid.
(3) Occupational Medical Surveillance and Evaluation Program (OMSEP).
Conduct or supervise a program to indoctrinate personnel in the various aspects
of occupational health and the OMMP.
(4) Human Immunodeficiency Virus (HIV). Conduct or supervise the instruction
of personnel regarding (HIV) and advise them of the associated dangers.
(5) Wellness. Conduct or supervise a program to emphasize the importance of
life-styles in maintaining health.
(6) Human Services. Conduct or supervise the instruction of Health Services
personnel to ensure they are aware of all the services available to maintain a
state of well being for personnel.

CH 16 1-8
e. Cooperation With Other Agencies. Cooperate with Federal, state,
and local agencies for preventing disease, reporting communicable diseases, and
collecting vital statistics.
f. Designated Supervising Medical Officer (DSMO). Medical officers assigned as
“designated supervising medical officer” (DSMO) will assume clinical responsibility
for the treatment provided by each health services technician in their clinic for whom
they are responsible. Assignments shall be made in writing and signed by the
DSMO’s commanding officer. Clinical supervision and accountability is defined as
follows:
(1) during normal clinic hours, HS consultation with the DSMO as determined by
that medical officer, review 20 percent of each day’s new patient encounters
seen only by the HS, and review 100 percent of all patient encounters seen only
by the HS who return with no improvements. (Ideally these reviews would
include the patient’s presentation to the medical officer.) The DSMO shall
countersign all records reviewed.
(2) outside normal clinic hours, direct or telephone consultations as determined by
the DSMO or duty MO; and, the following working day, a review of 100
percent of all visits seen only by the HS. The DSMO or duty MO shall
countersign all records reviewed.
g. Designated Medical Officer Advisor (DMOA). Health Services Technicians on
independent duty (IDTs) shall have a “designated medical officer advisor” (DMOA)
identified. The DMOA shall provide professional advice and consultation to the
IDT. The cognizant MLC (k) shall apportion units with IDTs to units with medical
officers attached. The cognizant MLC (k) shall make changes as necessary and
forward such information to the affected units and Commandant (G-WKH). At the
unit level, assignments shall be made in writing (addressed to the DMOA) and
signed by the DMOA’s commanding officer, with copies to the IDT unit and the
cognizant MLC (k). Assignment letters shall be addressed to the specific individuals
involved, and new letters shall be issued following a change of DMOA or IDT.
Professional advice and consultation, in this instance, is defined as follows:
(1) Telephone or radio consultation regarding specific cases as necessary between
the HS and the DMOA. This does not preclude consultation between the HS
and another Coast Guard medical officer, a medical officer of the Army, Navy,
Air Force, or USPHS, or a physician under contract to the Coast Guard whose
contract provides for such consultations; and
(2) Treatment record review: At the end of each quarter, the commanding officer
of the independent duty HS or his designee (cannot be the HS) shall select at
random 15 health records which have at least one entry made by the HS during
the previous quarter. For each of these records, copies shall be made of all SF
600 entries during the quarter. Copies of the SF-600's shall be sealed in an
envelope and marked for the DMOA's Eyes Only. The copies are then
forwarded to the DMOA for review. The DMOA shall review these record
1-9 CH 16
entries according to established criteria for record review at his/her facility.
Each record entry (copy) shall be annotated “reviewed,” dated, and stamped
with the DMOA’s name and pertinent comments concerning the record entry.
One copy of the reviewed record entries shall then be returned to the HS via
the unit’s commanding officer. A second copy of the reviewed entries shall be
retained by the DMOA. Both the HS and DMOA copies shall be retained at
the respective commands for a period of three years, for MLC review during
QA site surveys. The record review shall be discussed with the HS in the
quarterly phone contact between the DMOA and the HS. The DMOA is
encouraged to provide input to the unit CO or XO regarding the professional
performance of the independent duty HS.
(3) Review of MLC quality assurance site survey reports for the independent duty
site: The DMOA and HS shall review the MLC quality assurance site reports
for the site. They shall collaborate on the required written plan of corrective
actions which must be submitted to the MLC following the site survey. The
DMOA should also consult with the unit commanding officer regarding the
findings of the survey report.
2. Duties of Senior Medical Officers. The senior medical officer attached to a unit is
responsible to the commanding officer of the unit for the provision of health services. In
addition to the general duties of a medical officer, the senior medical officer is
responsible for:
a. performing those duties as prescribed in Coast Guard Regulations, COMDTINST
M5000.3 (series) if designated by Commander, Coast Guard Personnel Command
(CGPC) as division chief;
b. advising the commanding officer of any deleterious environmental health factors;
c. supervising any assigned PYA/PAs and NPs including, on a monthly basis, random
review of approximately five percent of the PYA/PA/NP’s charts for adequacy and
appropriateness of treatment rendered;
d. in the absence of a pharmacy officer, maintaining antidotes for narcotics and poisons
and ensuring only properly trained personnel are assigned to the pharmacy;
e. acting as the commanding officer’s representative on local emergency planning
boards, and, during emergencies or disasters, furnishing advice to the commanding
officer, formulating plans, and helping civilian authorities meet health care needs;
f. managing the quality of health care services provided;
g. maintaining liaison with the hospital commander or senior medical officer of nearby
(75 miles) USMTF’s;
h. acting as quality assurance technical supervisor for all contracted health services;
CH 16 1-10
i. ensuring efficient and effective use of all assigned medical officers and civilian
consultants;
j. preparing, through training and experience, health services technicians for
independent duty assignments;
k. recommending to the command a designated supervising medical officer (DSMO)
for each HS who provides medical treatment to patients; and
l. convening medical boards as appropriate in accordance with Chapter 3, Physical
Disability Evaluation System, COMDTINST M1850.2 (series)
m. ensuring that all ancillary service areas (e.g., laboratory, radiology, etc.) maintain
adequate policy and procedures manuals;
n. in conjunction with the MLC, providing professional oversight and establishing
qualifications standards and privileging for assigned personnel, including contract,
reserve and student providers;
o. assigning personnel and ensuring position and billet descriptions are accurate and
that credentials and privileging requirements are met;
p. within general Coast Guard and unit guidelines, determining the priority and range of
services for each beneficiary group;
q. maintaining liaison with counterparts in MTF, USTF, VA and private sector
facilities;
r. preparing performance appraisals for assigned staff;
s. reviewing and ensuring accuracy of Clinic Automated Management System
(CLAMS) and other statistical and informational reports;
t. ensuring that appropriate training is conducted on a regularly scheduled basis;
u. ensuring active participation and compliance with the Quality Assurance Program;
v. ensuring strict adherence to current infection control procedures and standards;
w. keeping the division chief informed;
x. other duties assigned by the Chief, Health Services Division.
3. Duties of Flight Surgeons. In addition to fulfilling the general duties of medical officers,
flight surgeons must:
a. thoroughly understand all operational missions of the aviation unit and participate as
a flight crew member as required on MEDEVACS and to meet the requirements as

1-11 CH 16
set forth in the Coast Guard Air Operations Manual, COMDTINST M3710.1
(series);
b. be familiar with the operational missions of other Coast Guard units in the local area;
c. obtain a general understanding of the flight characteristics of the aircraft assigned to
the unit and be thoroughly familiar with the human factors involved in pilot and crew
member interaction with the aircraft;
d. be familiar with the Air Operations Manual, COMDTINST M3710.1 (series), with
specific emphasis on Chapter 6, Rescue and Survival Equipment; Chapter 7, Flight
Safety; and the sections of Chapter 3 (Flight Rules) dealing with protective clothing
and flotation equipment;
e. ensure that aviation personnel are physically and psychologically fit for flight duty
and attempt to learn of any unusual circumstances which might adversely affect their
flight proficiency, this includes getting acquainted with each pilot and crew member;
f. make recommendations to the commanding officer concerning the health status of
aviation personnel, and in particular, only a flight surgeon or aviation medical officer
(AMO) shall issue “up” chits, except as noted in Section 3-G-2;
g. maintain an active interest and participate in the air station flight safety program and
assist the flight safety officer in planning, implementing, and coordinating the station
flight safety program, and advising the command on the aeromedical aspects of flight
safety;
h. participate as the medical member of Aircraft Mishap Analysis Boards and, when so
assigned, be responsible for completing the Medical Officer’s Report in accordance
with Chapter 2 of Safety and Environmental Health Manual, COMDTINST
M5100.47 (series);
i. be thoroughly familiar with the types and uses of personal pro-protective and
survival equipment carried on aircraft at the unit [The flight surgeon shall assist in
inspecting the equipment, shall advise the engineering officer and aviation survival
members in maintaining and issuing the equipment, and shall be familiar with
Rescue and Survival Systems Manual, COMDTINST M10470.10 (series)];
j. actively participate in the unit aviation physiology training program to ensure that
aviation personnel are capable of coping with the hazards of flight by presenting
lectures and demonstrations which include, but are not limited to:
(1) fatigue,
(2) emergency medicine,
(3) survival,
(4) disorientation,
CH 16 1-12
(5) night vision,
(6) reduced barometric pressure,
(7) crash injury avoidance,
(8) stress, and
(9) drug and alcohol use and abuse.
k. advise the command on MEDVAC operations:
l. ensure that HSs who participate in aviation operations maintain their knowledge and
skills in aeromedical physiology, and provide refresher training lectures and
demonstrations to emergency medical technicians (EMTs) and health services
technicians on emergency medical procedures; and
m. participate in a program of continuing education in aviation medicine including
familiarity with information published for flight surgeons by other branches of the
Armed Forces.
4. General Duties of Dental Officers. The principal duty of dental officers is to support the
Coast Guard operational mission by determining each member’s fitness for unrestricted
duty on a worldwide basis. Coast Guard dental officers are assigned to perform duties as
general dental officers. Exceptions will be authorized in writing by Commander, Coast
Guard Personnel Command (CGPC).
a. General Responsibilities.
(1) Coast Guard dental officers must stay informed in all fields of general and
military dentistry and be responsible for:
(a) ensuring the fitness for unrestricted duty of active duty personnel on a
worldwide basis;
(b) providing dental care for all eligible beneficiaries as authorized be
applicable laws and regulations (ensure non-enrollment in United
Concordia or Delta Dental before providing covered services);
(c) preventing and controlling dental disease (this includes performing
dental prophylaxis);
(d) promoting dental health;
(e) referring eligible beneficiaries for dental treatment per MLC (k) SOP;
(f) prioritizing the delivery of dental care to meet Coast Guard unit
operational readiness requirements;

1-13 CH 16
(g) ensuring that patients with gingivitis or periodontal disease have the
opportunity to receive follow up care;
(h) ensuring that results of all biopsies are received and reviewed by a dentist
to ensure that the appropriate action is taken;
(i) ensuring that when dental externs are assigned to the clinic, that a
protocol is developed detailing lodging and subsistence arrangements,
types of procedures allowed, available population to be treated and
supervising dental officer responsibilities. The protocol must be signed
by the Commanding Officer and provided to all participating dental
schools;
(j) ensuring that procedures for handling medical emergencies within the
dental clinic are clearly written and emergency drills are practiced
periodically; and
b. Dental examinations. Dental officers shall conduct the dental examination portion of
physical examinations in accordance with Chapter 3 of this Manual. Dental
examinations shall be conducted as soon as practical on personnel who report for
duty so as to determine the need for dental treatment and to verify their dental
records. Annual Type 2 dental examinations shall be conducted on all active duty
personnel collocated with dental examiners (i.e., Coast Guard DOs, DOD DOs, or
civilian contract dentists).
c. Care of Mass Casualties. Dental officers shall be qualified to perform first aid
procedures in order to treat or assist in treating mass casualties.
d. State Licensure. While assigned with the Coast Guard, dental officers are required to
have an unrestricted state license to practice dentistry.
e. Continuing Education. Participate in a program of continuing training in operational
medicine/dentistry including familiarity with information published for other
branches of the Armed Forces.
5. General Duties of Senior Dental Officers. The senior dental officer is responsible for:
a. performing duties outlined in Coast Guard Regulations, COMDTINST M5000.3
(series) if designated by Commander, Military Personnel Command as division chief;
b. conducting an organized preventive dentistry and dental health education program
for all eligible beneficiaries;
c. preparing, through training and experience, health services technicians for
independent duty assignments;
d. overseeing the preparation of reports, updating the dental clinic policy and
procedures manual, and maintaining records connected with assigned duties;
CH 16 1-14
e. overseeing the overall working condition, cleanliness and infection control of the
dental clinic, which includes sterilization procedures, dental supply, equipment,
publications maintenance, and the establishment of a preventive maintenance
program for dental equipment and supplies;
f. maintaining custody, security, and records of the dispensing of dental stores
including all controlled substances and poisons under the cognizance of the dental
branch, and maintaining antidotes for narcotics and poisons;
g. issuing prescriptions for, and supervising the dispensing of controlled substances
used in the dental branch;
h. maintaining custody, security, and records of precious metals dispensed and ensuring
that precious metals are reclaimed as required and necessary forms are filed with the
Department of Treasury;
i. managing the quality of dental care services provided;
j. in conjunction with the MLC (k), providing professional oversight and establishing
qualifications standards and privileging for assigned personnel, including contract,
reserve and student providers;
k. assigning personnel and ensuring position and billet descriptions are accurate and
that credentials and privileging requirements are met;
l. within general Coast Guard and unit guidelines, determining the priority and range of
services for each beneficiary group;
m. maintaining liaison with counterparts in MTF, USTF, VA and private sector
facilities;
n. preparing performance appraisals for assigned staff;
o. and reviewing and ensuring accuracy of CLAMS and other statistical informational
reports;
p. ensuring that appropriate training is conducted on a regularly scheduled basis;
q. ensuring active participation and compliance with the Quality Assurance Program.
r. ensuring strict adherence to current infection control procedures and standards;
s. keeping the division chief informed;
t. other duties assigned by the Chief, Health Services Division.
1-15 CH 16
6. General Duties of Chief, Health Services Division. The Chief, Health Services Division
will:
a. act as an advisor to the commanding officer regarding all health related matters;
b. under the unit executive officer, carry out the plan of the day as it pertains to the
Health Services Division;
c. ensure that clinic performs Supporting Clinic duties for units designated by the
cognizant MLC in their area of responsibility (AOR) IAW this instruction, cognizant
MLC Instructions and SOP, and other pertinent directives. These duties include but
are not limited to the following:
(1) Ensure the medical/dental readiness of all active duty personnel within their
area of responsibility. This includes the review of health records and
correction of deficiencies issues such as:
(a) Immunizations
(b) physical examinations
(c) annual dental exams
(d) HIV testing
(e) DNA specimen submission
(f) tuberculosis testing
(2) Provide pharmacy oversight to designated units via collateral duty Pharmacy
Officer.
(3) Provide prime vendor pharmaceutical services to designated units via collateral
duty Pharmacy Officers.
(4) Provide prime vendor medical/surgery services to designated units.
(5) Ensure that a Designated Medical Officer Advisor program is in place for
designated units. This should include CPR/Lifesaver training to designated
individuals.
(6) Provide physical examination review (approval/disapproval) to designated
units.
(7) Ensure that health care delivery is provided in a timely manner to units for
which a clinic is designated as their primary management site.
(8) Provide health benefits advice to designated units.
CH 16 1-16
(9) Assist with nonfederal medical and nonfederal dental preauthorization
processing for designated units.
(10) Assist with nonfederal invoice processing for designated units.
(11) Assist with the timely completion of Medical Boards.
d. ensure the medical/dental readiness of all active duty personnel within their area of
responsibility;
e. review the division AFC-30 and AFC-57 budget submittals;
f. be responsible for the allocation of resources (personnel, funds, space, and
equipment) within the division;
g. when directed by the command, represent the division at staff meetings and ensure
timely dissemination of the information to division personnel;
h. prepare performance appraisals as appropriate and ensure that performance
evaluations for all health services personnel are prepared and submitted in
accordance with current directives;
i. review all division reports;
j. be responsible for the division training program, including rotation of personnel
assignments for training and familiarization, in the health care delivery system;
k. oversee clinic policies, procedures and protocols for compliance with this Manual,
COMDTINST M6000.1B, MLC Instructions and S.O.P, and other pertinent
directives;
l. provide oversight with regard to applicable Federal, state, and local statutes and
regulations;
m. seek opportunities for cost reduction and enhancement of patient care through billet
conversions, resource sharing, contracting, etc.;
n. designate a clinic Quality Assurance Coordinator and ensure that the QA program is
carried out;
o. proctor student extern programs;
p. proactively support and promote the command wellness program;
q. participate in health care initiatives with local/regional DOD delivery systems, under
Headquarters and MLC guidance;
r. oversee and promote work-life issues pertaining to health care;
1-17 CH 16
s. ensure strict compliance to current infection control procedures and standards;
t. serve as chair of the Patient Advisory Committee;
u. oversee DSMO and DMOA programs;
v. in coordination with their respective MLC (k), establish their clinic as a Patient
Management Site for units within their area of responsibility;
w. And perform other duties as directed by the Commanding Officer.
7. General Duties of Pharmacy Officers. While assigned with the Coast Guard, pharmacy
officers are required to have an unrestricted state license to practice pharmacy.
Pharmacy officers shall ensure that medications are acquired, stored, compounded, and
dispensed according to applicable Federal laws in their primary and collateral duty
clinics. This includes the direct supervision and management of the following:
a. dispensing and labeling of all drugs, chemicals, and pharmaceutical products;
b. maintaining signature files for all health care providers;
c. providing patient-oriented pharmaceutical services including monitoring for
appropriate drug therapy, allergies, therapeutic duplication, and medication
interactions. Significant patient interactions should be documented on the SF-600;
d. providing verbal and written patient medication counseling when appropriate;
e. maintaining routinely stocked items at levels consistent with anticipated usage
between regularly scheduled procurements of pharmacy supplies and determining the
most effective expenditure of funds;
f. ensuring that security measures are instituted to prevent unauthorized entrance into
the pharmacy or misappropriation of pharmacy stock;
g. receiving, safeguarding, and issuing all controlled substances as the command-
designated custodian of controlled substances;
h. ensuring adequate quality control of all pharmaceuticals locally compounded;
i. maintaining current drug information files and a reference library of pertinent
textbooks and professional journals;
j. implementing the decisions of the Pharmacy and Therapeutics Committee and serve
as secretary of that committee;
k. inspecting monthly all clinic stocks of drugs and biologicals;
l. developing and maintaining a formulary for local use by medical and dental officers;

CH 16 1-18
m. informing the clinical staff of new drug information, policy changes, or other
pertinent data on drugs;
n. participate in a program of continuing education in pharmacy or related fields;
o. maintaining, updating, and documenting monthly inspections of poison antidote and
emergency drug supplies;
p. providing technical advice to the unit concerning drug testing, substance abuse, and
other pharmaceutical matters;
q. providing guidance and advice to the medical staff on current immunization
requirements,
r. serving as a resource for designated therapeutic categories of medications as they
relate to the Coast Guard Health Services Allowance Lists, Core formulary, HS Drug
Formulary and other drug lists, and.
s. participate in a program of continuing training in operational medicine/pharmacy
including familiarity with information published for other branches of the Armed
Forces.
8. Maintenance and Logistics Command Pharmacy Officers. Under the general direction
and supervision of the Chief, Quality Assurance Branch, MLC, the MLC pharmacy
officer shall:
a. plan, develop and implement, within the resources available, an MLC-wide
pharmacy quality assurance program to:
(1) eview and evaluate the delivery of pharmaceutical services in support of
mission operations, implement established policies pertaining to
pharmaceutical services, and recommend appropriate changes, and
(2) monitor pharmacy operations, via quality assurance site visits, financial
monitoring, and other workload indicators to ensure optimum utilization of
personnel and financial resources.
b. plan and administer the acquisition and distribution of pharmaceuticals:
(1) review, analyze, and recommend the most efficient and cost effective means
for providing pharmaceutical services throughout the Area, including the
financial resources to be allocated to each operating facility under MLC
oversight;
(2) monitor the procurement of controlled substances by Coast Guard units within
the Area;
(3) provide to MLC (kqa) a system for the random monitoring of drugs procured
from nonfederal sources.
1-19 CH 16
c. serve as pharmaceutical consultant on pharmacology, pharmacy, and drug utilization
and provide technical pharmacy expertise, assistance, and advice to the MLC
Commander and command elements within the Area;
d. provide guidance and advice regarding the evaluation, training, and justification for
pharmacy personnel to meet operational needs of units within the Area;
e. provide liaison or representation to regional Federal and professional pharmacy
groups and committees; and
f. administer and monitor the collateral duty assignments of pharmacy officers in their
respective Area.
9. Environmental Health Officers.
a. Duties: Environmental health officers are responsible for recognition, evaluation,
and control of biological, chemical, physical, and ergonomic factors or stresses
arising from the environment which may cause sickness, impaired health and well-
being, or significant discomfort and inefficiency, property damage, or which could
adversely affect the Coast Guard’s industrial hygiene, pest management, radiological
health, and sanitation. Specific responsibilities can include:
(1) planning, budgeting, implementing and directing an environmental health
program to support commands within their geographic area of jurisdiction.
(2) conducting environmental health audits of Coast Guard facilities and
operations in order to detect health hazards and noncompliance with applicable
safety and environmental health laws, regulations, standards, and procedures.
Facilities and operations include:
(a) work environments;
(b) storage, handling, treatment, and disposal of hazardous materials and
hazardous waste;
(c) storage, handling, treatment, and disposal of infectious medical waste;
(d) food preparation, service and storage operations;
(e) solid wastes storage, handling, treatment, and disposal;
(f) pest management operations;
(g) potable water treatment, storage and distribution systems;
(h) waste water collection, treatment, and disposal system;
(i) housing facilities;

CH 16 1-20
(j) ionizing radiation sources;
(k) non-ionizing radiation sources;
(l) recreational facilities;
(m) health care facilities;
(n) child care facilities;
(o) laundry and dry-cleaning operations; and
(p) barber shop operations
(3) providing technical assistance to units to abate deficiencies identified by the
environmental health officer during the audit.
(4) monitoring ongoing hazard abatement actions to ensure that identified hazards
are being eliminated promptly.
(5) providing environmental health training to commands within their jurisdiction.
(6) providing technical assistance to units on request to identify and abate health
risks.
(7) reviewing engineering plans and specifications for new facilities and
modifications to existing facilities to ensure conformance with environmental
health standards and practices.
(8) serving as technical advisor to commands within their jurisdiction.
(9) initiating and conducting special health risk assessment studies.
(10) maintaining liaison with Federal, state, and local government agencies
concerning environmental health for commands within their jurisdiction.
(11) advising commands when medical monitoring data indicates the possibility of
occupationally-induced or aggravated disease and investigating possible causes
so that corrective measures can be initiated.
(12) providing consultation, advice, and training on the occupational medical
monitoring program to Coast Guard commands within their area of
jurisdiction.
(13) enrolling personnel in the OMSEP when they meet the criteria of occupational
exposure as defined in paragraph 12-A-2.
(14) disenrolling personnel from the OMSEP when they do not meet the criteria of
occupational exposure as defined in paragraph 12-B-4.
b. Reports. Environmental health officers shall submit reports to the appropriate MLC
(k) about environmental health conditions observed during their surveys.
1-21 CH 16
c. Duty Limitations. Environmental health officers shall carry out all management
functions required to operate the safety and environmental health program within
their AOR. They may be required to perform only those technical duties for which
they are trained. They may represent health services at various staff meetings in
matters relating to the management and budgetary aspects of their assignment. They
will be primarily responsible for special studies as in the case of monitoring chemical
spill response and enforcement personnel. They will be responsible to the
Commander, MLC (k) for proper implementation of the safety and environmental
health program.
10. Clinic Administrators. Officers, Chief Warrant Officers (experience indicator 19), or
senior enlisted personnel assigned to manage and administer health care facilities.
a. Under the direction of the Chief, Health Services Division, manage the
administrative functions required to operate the health care facility. The Clinic
Administrator will not be required, nor attempt, to perform clinical duties for which
he/she is not trained.
b. General Responsibilities. The Clinic Administrator will:
(1) plan, supervise, and coordinate general administration of the health services
facility;
(2) prepare, submit, manage, and exercise fiduciary control and accountability over
the health services division AFC-30 and AFC-57 funds;
(3) provide fiscal oversight over the acquisition of equipment and supplies;
(4) maintain a planned program of equipment maintenance and replacement;
(5) provide physical security of health services division supplies and
pharmaceuticals;
(6) maintain liaison with other local agencies (military and civilian) in all health
care related matters;
(7) provide resources to assist medical and dental officers in emergency care of the
sick and injured when necessary;
(8) prepare the disaster preparedness plan as it relates to the health services
division;
(9) prepare the heavy weather bill as it relates to the health services division;
(10) seek opportunities for cost reduction and enhancement to patient care through
billet conversions, resource sharing, contracting, etc.;
(11) serve as an advisor to the chief, health services division on all administrative
matters;
(12) oversee the supervision of enlisted personnel assigned to the health services
division;
CH 16 1-22
(13) ensure that correspondence, reports, and records comply with appropriate
instructions (i.e. Paperwork Management Manual, Coast Guard
Correspondence Manual, etc.);
(14) maintain an adequate health services division reference library;
(15) train subordinates, conduct classes, instruct enlisted personnel in their duties,
and supervise their study of regulatory and professional publications and
courses for advancement in rating;
(16) participate in a program of continuing education in Health Care
Administration;
(17) assist beneficiaries with health benefits information;
(18) enforce standards of appearance and conduct of health services division
personnel;
(19) ensure that accurate, appropriate data is submitted to the CLAMS information
system, CHCS system, etc.;
(20) oversee clinic rotation assignments of Health Services Technicians;
(21) implement clinic policies, procedures, and protocols, for compliance with
Coast Guard regulations, the Medical Manual, MLC INST/SOP, and other
pertinent directives;
(22) ensure compliance with all applicable Federal, state, and local statutes, together
with the medical, dental and pharmacy officers;
(23) oversee and promote work-life issues pertaining to health care
(24) serve as assistant chair for the Patient Advisory Committee;
(25) ensure that enlisted personnel evaluations for members assigned to the health
services department are prepared and submitted in accordance with the Coast
Guard Personnel Manual;
(26) provide administrative oversight in the areas of NONFED health care,
contracts, and BPAs;
(27) ensure that health care invoices are processed in accordance with MLC
INST/SOP;
(28) ensure that physical examinations comply with current standards;
(29) promote and administer the unit’s environmental sanitation program (in the
absence of an environmental health officer); and
(30) oversee the unit’s Occupational Medical Surveillance and Evaluation Program
(OMSEP), in the absence of an environmental health officer.
1-23 CH 16
11. Physician Assistants (PA/PYA(s)) and Nurse Practitioners (NP).
a. General Responsibilities. PA/PYA(s) and NP(s) responsibilities are defined in
Section 1-B-1. Under the supervision of the senior medical officer they are subject to
the duty limitations listed below.
b. Duty Limitations.
(1) Senior Medical Officers (SMO) of units with mid-level providers (physician
assistants or nurse practitioners) assigned shall assign clinical duties and
responsibilities to each provider and shall be accountable for the actions of
those providers.
(a) To determine the extent of oversight required, SMOs shall be guided by
this section, the provider’s clinical training and previous experience, by
personal observation, and Chapter 13-C, Clinical Privileges.
(b) The SMO may delegate supervisory responsibility to another staff
physician or certified mid-level provider (mentor). A copy of this
delegation shall be filed in the non-certified provider’s Professional
Credentials File (PCF).
(c) Physicians responsible for supervising mid-level providers shall perform
and document reviews of at least five percent of the mid-level provider’s
charts each calendar month for accuracy of diagnosis and appropriateness
of treatment rendered.
(2) Physician assistants who are not certified by the National Commission on
Certification of Physician Assistants (NCCPA), recent graduates who have not
taken or passed the NCCPA examination, and nurse practitioners who have not
taken or passed a specialty board examination offered by the pertinent nurse
practitioner certifying organization, shall practice in Coast Guard facilities only
under the following conditions:
(a) all health record entries shall be co-signed by a licensed or certified
provider by the end of the next working day;
(b) all prescriptions, except for those on the Coast Guard HS formulary,
shall be co-signed by a licensed or certified provider by the end of the
next working day;
(c) when a supervisory provider is not present at the unit, noncertified mid-
level providers shall be restricted to providing medical care, except for
emergencies, to active duty members only;
CH 16 1-24
(d) noncertified mid-level providers may stand clinic watches providing a
standby licensed or certified provider is available via telephone to
discuss any questions or concerns; and,
(e) with the exception of operational emergencies, noncertified mid-level
providers are not eligible for independent TAD assignments at locations
where a supervisory provider is not present.
c. Nothing in this section limits PA/PYA's or NP’s access to any available source of
information or advice during an emergency.
12. TRICARE Management Acitivity-Aurora (TMA) Liaison Officer.
a. Responsibilities. The Coast Guard TMA liaison officer maintains liaison between
TRICARE and Commandant (G-W) on matters of policy, operations, and program
administration. This function will not involve the responsibility for formulating
department policies. Departmental policies will continue to be developed by
members of the liaison group for the Uniformed Services Health Benefits Program.
b. Duties.
(1) Specific Duties. Specific duties include, but are not limited to the following:
(a) coordinate and assist, as necessary, in preparing and submitting uniform
workload data for use in budgetary programming at departmental level;
(b) ensure timely notification to Commandant (G-W) concerning changes in
TRICARE operational or administrative procedures;
(c) identify gaps in the TRICARE information program and recommend
solutions;
(d) represent Coast Guard viewpoints on matters relating to TRICARE
operational and administrative procedures;
(e) assist in developing future TRICARE information programs;
(f) keep the Coast Guard informed of problem areas relating to service
beneficiaries and service health care facilities, where appropriate, and
recommend changes which will benefit the TRICARE operation; and
(g) monitor purchases of high-cost equipment for use by TRICARE
beneficiaries and make recommendations concerning future purchases as
opposed to rental.
(2) Duties within TMA Liaison Division.
1-25 CH 16
(a) Investigate and respond to Presidential, Congressional, and beneficiary
inquiries and complaints. Investigate and respond to inquiries
concerning eligibility.
(b) Make public presentations concerning program benefits to various
groups.
(c) Prepare special studies relating to program activities.
(d) Serve as liaison representative for USPHS, DVA, and NOAA.
(3) Other Duties. Participate in contract performance appraisal visits to the fiscal
administrators. This function involves a comprehensive review and evaluation
of the operations of the civilian agencies which, under contract, administer the
program within each region.
13. Health Services Technicians.
a. Rating Structure. The rating structure for health services technicians is contained in
Group VIII, Enlisted Qualifications Manual, COMDTINST M1414.8 (series).
b. General Duties of Health Services Technicians.
(1) The primary purpose of a health services technician is to provide supportive
services to medical and dental officers and primary health care in the absence
of such officers. In accordance with Paragraph 7-5-4, Coast Guard
Regulations, COMDTINST M5000.3 (series), health services technicians shall
not be detailed to perform combatant duties.
(2) In particular, health services technicians are responsible for all administrative
aspects of health care and health record maintenance for both their command
and subordinate commands without health services personnel attached.
Geographically separate subordinate commands will retain responsibility for
security (i.e. physical custody) of health records. In addition to the military
duties common to all enlisted personnel, health services technicians perform
health services department functions, such as:
(a) respond to calls for emergency medical assistance or evacuations
(MEDEVACS);
(b) maintain appointments and appointment records;
(c) perform occupational medical monitoring duties;
(d) render first aid;
(e) perform tentative diagnosis and emergency treatment (In doing so,
appropriate drugs, oral or injectable, may be administered as required in
emergency situations to prevent or treat shock or extreme pain. In all
CH 16 1-26
other incidents where injection of controlled substances is required,
permission must be obtained from a physician prior to administration. In
either case, the commanding officer shall be notified immediately and
entries shall be made in the patient’s health record.);
(f) provide nursing care where trained;
(g) provide definitive treatment;
(h) provide prophylactic treatments;
(i) instruct crew members in first aid and oral hygiene;
(j) prepare materials (including sterile instruments) and medications for use;
(k) maintain military readiness of the health services division by complying
with the appropriate Health Services Allowance List;
(l) perform administrative procedures in health care matters, maintain health
and dental records current in all aspects;
(m) adhere to regulations, instructions, and control of precious metals,
controlled substances, and poisons;
(n) exercise responsibility for all equipment and stores placed in their
charge, and exercise personal supervision over their condition,
safekeeping, and economic expenditure;
(o) maintain cleanliness of all health services spaces;
(p) provide services as a health benefits advisor; and
(q) assist in the processing of nonfederal health care requests and invoices.
(3) Each HS who provides medical treatment to patients at a Coast Guard clinic
staffed by one or more medical officers shall have a medical officer from that
facility assigned in writing as his/her designated supervising medical officer
(DSMO). The DSMO shall assume responsibility for all clinical treatment
provided by the HS. Each independent duty HS, and HSs assigned to clinics
without a medical officer, shall have a medical officer assigned in writing as
his/her “Designated Medical Officer Advisor” (DMOA), to provide
professional advice and consultation when needed. Refer to 1-B-1.f. and 1-B-
1.g. for further details concerning DSMO/DMOA. Health services technicians
assigned to units without a medical officer shall provide only “first response”
emergency care to non-active duty personnel.
(4) Care shall be taken during medical examinations which involve chest, genital,
and rectal areas to afford maximum privacy and minimum exposure of the

1-27 CH 16
patient. An attendant of the same gender as the patient may be requested by
the patient during examination or treatment. Health services technicians are
authorized to conduct examinations to include: auscultation, palpation,
percussion, and visual inspection as indicated by the medical complaint.
Exceptions to the above are:
(a) health services technicians shall not perform:
1 routine digital examinations of the prostate;
2 routine examinations through instrumentation of the urethra; or
3 routine gynecological examinations.
(b) such routine examinations shall be referred to a medical officer. In
situations where no medical officer is readily available and such
examination is necessary to provide emergency care, the health services
technician is authorized to do so. If the HS and patient are of different
gender, an attendant of same gender as the patient shall accompany the
patient during the examination or treatment.
(5) Participate in a course of continuing education, either clinical or
administrative, through correspondence courses, resident courses, etc.
14. Health Services Technicians - Dental (HSDs).
a. The primary responsibility of HSDs is to provide chairside assistance to dental
officers.
b. Additional duties include:
(1) Cleansing, sterilization, maintenance, and preparation of dental instruments;
(2) Cleansing, disinfecting, and maintenance of dental equipment and dental
operatories;
(3) Preparing of dental materials;
(4) Assessing, referral, and treatment (under direct supervision of a dental officer)
of common dental conditions;
(5) Charting dental conditions;
(6) Maintaining dental records;
(7) Exposure and development of dental radiographs;
(8) Providing oral hygiene instruction;
(9) Taking impressions and fabricating study models; and
(10) Performance of emergency intervention as necessary.

CH 16 1-28
c. HSDs may be assigned to supplement HS duty sections, HSDs may not stand watch
independently.
15. Independent Duty Health Services Technicians.
a. Duties.
(1) General Duties.
(a) Health services technicians on independent duty perform the
administrative duties and, to the extent for which qualified, the clinical
duties prescribed for medical officers of vessels and stations. (See Coast
Guard Regulations, COMDTINST M5000.3 (series) and Section 1-B of
this Manual.) They shall not attempt nor be required to provide health
care for which they are not professionally qualified. They shall provide
care only for active duty personnel, however they may provide care to
non-active duty patients on an emergency basis. The filling of
prescriptions for other than active duty personnel shall be strictly limited
to emergency situations and to authorized stock on hand under the
allowance list for the unit. They may, under the guidance set forth in
Paragraph 10-A-6-h. of this Manual, establish non-prescription
medication handout programs for eligible beneficiaries.
(b) Health services technicians shall not be detailed to perform combatant
duties in accordance with Paragraph
(c) 7-5-4, Coast Guard Regulations, COMDTINST M5000.3 (series).
(d) In accordance with the Personnel Manual, COMDTINST M1000.6
(series), commanding officers are authorized to use health services
technicians for general duties except noted below:
1 Health services technicians shall not be used for duties that require
bearing arms (except for the limited purposes allowed by the Geneva
Convention for their own defense or protection of the wounded and
sick in their charge) even though the bearing of arms may be purely
ceremonial.
2 Health services technicians shall not be used for combat duties that
are unrelated to health care or administration.
(2) Specific Duties.
(a) Sanitation of the Command. Make daily inspections to ensure that
appropriate sanitation practices are maintained.
(b) Health of Personnel. Establish and maintain a system for determining
those who need immunizations, tuberculin tests, X-rays, dental services,

1-29 CH 16
and routine physical examinations. The system shall include all return
appointments requested by physicians or dentists from outside referrals
requested by the command.
(c) Care of Sick and Injured. Hold daily sick call. Diagnose and treat
patients within capabilities. When indicated, refer cases to facilities
where medical or dental officers are available or, if this is not practical,
obtain help and advice by radio or other expeditious means.
(d) Procurement, Storage, and Custody of Property. All parts of the Health
Services Allowance List (HSAL) Afloat, COMDTINST
M6700.6(series), and Health Service Allowance List Ashore,
COMDTINST M6700.5 (series) contain information needed for ordering
and procuring supplies. The HSAL also contains procedures for storage
and custody of property.
(e) Reports. Prepare and submit reports required by Chapter 6 of this
Manual and other directives.
(f) Health Records. Maintain health records as required by Chapter 4 of this
Manual. Ensure that all treatment records and/or consults from outside
referrals are obtained and placed in the health record. In addition, ensure
that each patient is notified of all physical exams, consultations, and
diagnostic tests (i.e., pap smears, mammograms, biopsies, x-rays, etc.)
performed at any facility prior to filing in the health record.
(g) Training. Prepare and carry out a program for training non-medical
personnel in first and self-aid, personal hygiene, sexually transmitted
disease prevention, medical aspects of CBR warfare, cardiopulmonary
resuscitation, etc., as part of the unit’s regular training program.
(h) Other Duties. As assigned by the commanding officer.
b. Reporting Procedures.
(1) Policy. Upon reporting for independent duty, the health services technician
shall consult with the commanding officer and executive officer to determine
their policies regarding health care and the administration of the health services
department.
(2) Inventory. Obtain the unit Health Services Allowance List and inspect the
inventory of all health services department equipment, supplies, and
publications. Initiate action for repair, survey, or replenishment of equipment,
supplies, and publications. Verify inventory records and check logs of
controlled substances. Report any discrepancies to the commanding officer
without delay. Amplification of requirements and procedures is contained in
Chapters 8 and 10 of this Manual.

CH 16 1-30
(3) Health Records. Check health records against the personnel roster. Any
missing records should be accounted for or requested from previous duty
stations. If records cannot be accounted for within one month’s time, open a
new health record. Check health records for completeness, and if not current,
obtain and enter all missing information to the fullest extent possible. (See
Chapter 4 of this Manual for instructions pertaining to health records.)
(4) Operational Readiness. Ascertain the state of operational readiness of the
health services department and advise the commanding officer. Operational
readiness refers to the immediate ability to meet all health care demands within
the unit’s capabilities.
c. Responsibilities. The commanding officer is responsible for the health and readiness
of the command. The health services department is charged with advising the
commanding officer of conditions existing that may be detrimental to the health of
personnel and for making appropriate recommendations for correcting such
conditions. Meticulous attention to all details and aspects of preventing disease must
be a continuing program. It is imperative that shipboard and station sanitation and
preventive health practices be reviewed constantly in order that any disease
promoting situation may be discovered immediately and promptly eradicated.
d. Routines.
(1) Daily Routines.
(a) Sickcall. Hold sickcall daily at a time prescribed by the commanding
officer.
(b) Binnacle List. Prepare the unit Binnacle List and submit it to the
commanding officer. (See section 6-B of this Manual for instructions
pertaining to the Binnacle List.)
(c) Inspections. The following shall be inspected daily:
1 coffee messes;
2 living spaces;
3 heads and washrooms;
4 fresh provisions received (particularly milk and ice cream);
5 scullery in operation;
6 drinking fountains;
7 garbage disposals;

1-31 CH 16
8 sewage disposals;
9 water supplies;
10 and industrial activities. (See Chapter 7 of this Manual and the
Food Service Sanitation Manual, COMDTINST 6240.4(series)).
(d) Testing of Water. Perform water tests for chlorine/bromine content daily
outside of CONUS and at all units that make or chlorinate/brominate
their own water and record the results in the Health Services Log.
Consult the Water Supply and Wastewater Disposal Manual,
COMDTINST M6240.5 (series).
(e) Cleaning. Health services department spaces shall be cleaned daily and
all used instruments cleaned and stored until sterilization can be
accomplished.
(2) Weekly Routines.
(a) Health Services Logs. A health services log shall be kept by all activities
and shall be submitted to the commanding officer for review, approval,
and signature. Section 6-B of this Manual contains the information
needed for maintaining the log.
(b) Inspections. Conduct sanitation inspection of the ship or station with
emphasis on food service, living spaces, and sanitary spaces, specifically
including food handlers, refrigerators and chill boxes, and galley spaces
and pantries. Submit a written report to the commanding officer and
make an appropriate entry in the health services log.
(c) Training. Conduct training in some aspect of health care or treatment
unless required more frequently by the commanding officer or other
directive.
(d) Hold field day.
(e) Resuscitators. Inspect and test resuscitators to ensure proper functioning.
Record results in the health services log.
(3) Monthly Routines.
(a) Reports. Submit all required health services monthly reports, outlined by
Chapter 6 of this Manual and other appropriate directives.
(b) Inspection of Battle Dressing Station Supplies. Monthly, inspect battle
dressing station supplies to ensure adequate and full inventory. Check
sterile supplies and re-sterilize every six months (refer to Health Services
Allowance List Afloat, COMDTINST M6700.6 (series). Replace
CH 16 1-32
expired or deteriorated supplies and materials. Enter an appropriate entry
in the health services log indicating that the inspection was conducted
and the action taken.
(c) First Aid Kits. Inspect hinges and hasps to ensure that they are free from
rust, corrosion, or excessive paint.
(4) Quarterly Routines.
(a) Inventory of Controlled Substances. The Controlled Substances
Inventory Board shall conduct an inventory, as required by Chapter 10 of
this Manual, and submit a written report of the findings to the
commanding officer.
(b) Reports. Submit all required health services reports as outlined in
Chapter 6 of this Manual and other appropriate directives.
(c) Inventory. Conduct a sight inventory of all health services consumable
supplies/equipment as required by Chapter 8 of this Manual and the
Health Services Allowance List.
(d) First Aid Kits. Inspect the contents to ensure adequate and full
inventory. Replace expired and deteriorated supplies and materials.
Make an appropriate entry in the health services log.
16. Coast Guard Beneficiary Representatives at Uniformed Services Medical Treatment
Facilities (USMTF).
a. Duties. Health Services Technicians may be detailed to duty as representatives at
USMTF’s where the Coast Guard patient workload warrants. The purpose of these
assignments is to ensure, for active duty personnel:
(1) that Coast Guard authorities are provided prompt and current information
concerning the status of Coast Guard personnel being treated;
(2) that Coast Guard personnel being treated receive necessary command
administrative support;
(3) that the USMTF use the patient’s Coast Guard health record and that entries
are made in it or on forms that are filed in it; and
(4) that necessary health records and forms either accompany the patient or are
forwarded to the command having custody of the health record.
b. Responsibilities. The representative is responsible for the following:
(1) Notification of Patient Status. It is essential that the representative keep
cognizant command levels advised of the status of Coast Guard patients
admitted for inpatient treatment. The following procedures shall be used:

1-33 CH 16
(a) notify commands, by the most expedient means possible, within 24 hours
of admission or discharge of members of their command.
(2) Health Record Entries. The representative is responsible for ensuring that all
information concerning inpatient hospitalization, (e.g., admissions, operative
summaries, discharge summaries) which is required to be entered in the health
record, is furnished to the command which maintains the patient’s health
record. The representative shall also make the USMTF aware that all entries or
forms associated with outpatient medical and dental activity must be entered in
the patient’s Coast Guard health record.
(3) Copies of Forms. The USMTF is responsible for completing and furnishing at
least one copy of the following forms to the representative. The representative
is responsible for preparing any additional copies needed.
(a) Inpatient hospitalizations:
1 SF-502, Narrative Summary (or other discharge summary form), and
2 Operative summary if surgery was done.
(b) Physical examinations:
1 SF-88, Report of Medical Examination.
2 SF-93, Report of Medical History.
3 ANY specialty reports obtained pursuant to the physical
examination.
(c) Initial and Disposition Medical Boards:
1 NAVMED 6100/1, Medical Board Report Cover Sheet;
2 SF-88, Report of Medical Examination;
3 SF-93, Report of Medical History;
4 SF-502, Narrative Summary;
5 ANY specialty reports obtained pursuant to the physical
examination;
6 CG-4920, Patient’s Statement Regarding the Findings of the
Medical Board, signed by the patient;
7 The command endorsement, Line of Duty/Misconduct Statement (if
any), and members rebuttal (if any) should normally be done at/by
the command.
CH 16 1-34
(4) Liaison and Assistance. The representative shall:
(a) Maintain liaison between the Coast Guard units in the area and the
USMTF as follows:
1 Clinical services to obtain timely appointments for Coast Guard
personnel;
2 Pharmacy to facilitate drug exchange with Coast Guard units; and
3 Biomedical repair to help originate and maintain agreements for
repair and maintenance of local Coast Guard medical equipment.
(b) Whenever possible, personally meet with each hospitalized Coast Guard
active duty member and meet or phone the immediate family of the
member, offering them assistance.
(c) In appropriate cases, channel other Coast Guard and DOD resources such
as Mutual Assistance, Family Programs, Red Cross, etc. to assist
hospitalized members and their dependents.
(5) Assignment and Duties. Health Services technicians assigned to a USMTF as
Coast Guard Beneficiary Representatives are attached to MLC (k) which will
exercise military control over them. The representative is expected to comply
with the rules and orders of the USMTF to which assigned, and is subject to
the orders of the hospital commander. However, it is expected that any duties
assigned will be consistent with the purpose noted in subparagraph 13a. above.
17. Coast Guard Representative at the Department of Defense Medical Examination Review
Board (DODMERB).
a. General. DODMERB is located at the USAF Academy, CO and is a joint agency of
the military departments responsible for scheduling, reviewing, and certifying service
academy and ROTC scholarship applicant medical examinations, and other programs
assigned by the Office of the Assistant Secretary of Defense, Health Affairs.
b. Responsibilities.
(1) As a member of DODMERB, the Coast Guard:
(a) establishes entrance standards for the Coast Guard Academy; and
(b) makes its health care facilities available for completing entrance physical
examinations for all service academies.
(2) As a member of DODMERB, the Coast Guard liaison:
(a) is assigned as an examination evaluator/administrator; and

1-35 CH 16
(b) participates in implementing plans and organizational procedures for
board actions.
c. Duties.
(1) Maintain a current list of examining centers which includes dates and
examination quotas.
(2) Schedule examinations for the applicants.
(3) Notify applicants and program managers of scheduled examinations.
(4) Review and apply medical standards.
(5) Notify applicants and program managers of the status and qualifications of
applicants.
(6) Provide copies of medical examinations and medical information to the various
programs on applicants until they are no longer eligible.
(7) Provide copies of medical examinations and medical information to eligible
applicants as requested.
18. Health Benefits Advisors (HBA).
a. Responsibilities. Individuals designated as Health Benefits Advisors (HBAs) at
CGMTFs are responsible for advising and assisting beneficiaries concerning their
health benefits. This individual shall:
(1) keep current on the TRICARE Program, Uniformed Services Family Health
Benefits Program (USFHBP) and on all other health benefits programs
available for members, former members, and their eligible dependents;
(2) advise all beneficiaries on matters pertaining to healthcare benefits, including;
(a) obtaining Nonavailability Statements,
(b) using the local appeal system for Nonavailability Statements, and
(c) conducting a local information program on healthcare benefits;
(3) advise TRICARE beneficiaries on the relationship between TRICARE, DVA
programs, Social Security, Medicare, insurance provided through employment,
and the effect of employment and private insurance on benefits available under
TRICARE:
(a) stress availability of TRICARE and explain financial implications of
using non-participating providers,
(b) explain provider participation in TRICARE and explain financial
implications of using non-participating providers,

CH 16 1-36
(c) provide beneficiaries the names and addresses of participating providers
of the specific services the beneficiary requires, and
(d) caution beneficiaries to verify that the provider participates in TRICARE
at the time the services are provided;
(4) coordinates TRICARE problem cases with MLC HBAs, TRICARE contractors
and the Coast Guard liaison officer at TMA-Aurora when required;
(5) assist beneficiaries in properly completing TRICARE claim forms;
(6) serve as a single point of contact for all health benefits programs available to
active duty and retired members and their dependents;
(7) provide information and assistance based upon personal, written, or telephone
inquiries concerning healthcare benefits;
(8) keep beneficiaries informed of changes within the various programs, e.g.,
legislative changes affecting benefits available or other policy/procedures
impacting upon the usage of civilian medical care. Provides for an ongoing
program of lecture services, informational seminars, and group counseling to
various beneficiary groups, service clubs, retirement briefings, etc.;
(9) maintains liaison with local providers and encourages them to increase their
acceptance of the TRICARE program, and;
(10) maintains liaison with cognizant MLC HBA, and unit collateral duty HBAs in
local area.
b. Training.
(1) Individuals designated as HBAs must be trained in TRICARE benefits,
exclusions, claims preparation, processing, cost sharing formulas, eligibility
criteria, and alternatives to TRICARE.
(2) Training Schedule.
(a) Requests for attendance at the TRICARE course should be submitted via
the Chain of Command to the CG TRICARE Liaison Officer at TMA-
Aurora.
(b) TRICARE course registration form is available at
http://www.TRICARE.osd. mil. This form may be submitted
electronically or by mail.
(3) TMA-Aurora Liaison Staff Seminars. The Liaison Office at TMA-Aurora
provides seminars for large beneficiary groups, e.g., recruiter, career counselor,
etc. Arrangements for seminars should be made directly with CG Liaison.
(4) Funding. Training requests for the TRICARE course will be funded by the
cognizant unit, MLC, or Headquarters component.

1-37 CH 16
c. Sources of Reference Materials. HBAs shall acquire and become familiar with
specific reference materials on Federal and nonfederal health programs. Specifically,
as TRICARE policies change, the HBA shall maintain an updated reference library
through distribution channels as outlined below:
(1) TRICARE Information.
(2) Contact: Coast Guard Liaison Officer
Commercial: (303) 676-3538
Website: http://www.TRICARE.OSD.MIL
Coast Guard Headquarters Distribution.
Stock Point: Commandant (G-WKH-3)
Via: Rapidraft Letter
Tel: (COMM) (202) 267-0846
TRICARE Standard Handbook 6010.46-H
(3) TRICARE Claim Forms (DD-2642, OCT93)
Now available at Website: http://www.TRICARE.OSD.MIL or by contacting:
Stock Point: Navy Publications and Forms Center
5801 Tabor Avenue
Philadelphia, PA 19120
U/I: PD
(4) Referral for Civilian Medical Care (DD-2161).
May be printed locally by accessing CG Standard Workstation III, Jetform
Filler Database or by contacting:
Stock Point: Navy Publications and Forms Center
5801 Tabor Avenue
Philadelphia, PA 19120
U/I: PD
(5) Fiscal Intermediary Distribution by Region. Fiscal Intermediary Newsletter
(6) Local Community. Local Publication - Social Services Directory
19. Dental Hygienists. Dental hygienists are licensed graduates of American Dental
Association accredited schools of dental hygiene. Whether contract or active duty
providers, they are authorized to treat beneficiaries in Coast Guard dental clinics under
the oversight of a dental officer. Restrictions on the degree of required oversight and the
scope of services vary from state to state.
a. In the interests of standardization, quality assurance, and risk management, dental
hygienists in Coast Guard health care facilities shall, in most circumstances, treat
patients only when a dental officer is present for duty at the command. At the
CH 16 1-38
discretion of the SDO, and in the interest of expediency, this guideline may be
overridden if each of the following conditions is met on each patient:
(1) Only active duty members are treated;
(2) A medical officer is present in the building;
(3) Patients’ Periodontal Screening and Recording (PSR) scores are 10 or less; and
(4) The licenses of the SDO and dental hygienist are not jeopardized by this action.
b. In every case, patients must receive a Type 2 examination by a dental officer no more
than six months prior to treatment by a dental hygienist.
c. The Senior Dental Officer (SDO), or a staff dental officer designated by the SDO,
shall review no fewer than 5% of the dental hygienist’s patients for completeness of
plaque/deposit removal and damage to hard/soft tissues. The responsible dental
officer shall document these reviews in the patients’ dental records.
d. The scope of the dental hygienist’s services shall be governed by either the state in
which the license is held or the state in which the clinic is located, whichever is more
restrictive, and shall be itemized in the clinic’s Standard Operating Procedures
(SOP).
e. In some cases the state license may contain an addendum certificate which
“privileges” the dental hygienist to administer injections of local anesthesia under the
direct oversight of a licensed dentist. If the state in which the clinic is located also
allows this, then the dental hygienist may deliver local anesthesia under the direct
oversight of the dental officer. In all cases, the dental hygienist must possess specific
credentials from the state of licensure allowing him/her to administer local
anesthesia. “Direct oversight” shall mean that the dental officer personally has
authorized the dental hygienist to administer local anesthesia to the specific patient
being treated at the specific time (i.e., “blanket approvals” are not authorized). The
dental officer shall be physically present in the clinic while local anesthesia is
administered by the dental hygienist. While direct oversight does not require the
dental officer to be physically present in the dental hygienist’s operatory, the dental
officer must be in the clinic and be capable of responding to an emergency
immediately.
20. Red Cross Volunteers. Red Cross Volunteers are persons who have completed a formal
training program offered by a Red Cross Chapter and have a certificate of successful
completion. Red Cross training is a screening and educational tool that enables
individuals with an interest in helping others to function as supervised medical assistants
in the clinic.
a. Responsibilities. Red Cross Volunteers are responsible for scheduling their time in
the clinic with clinic staff, accepting supervision, and carrying out activities mutually
agreed upon by themselves and the clinic. These duties must fall within the scope of
duties for which Red Cross training has prepared the volunteer. Duties may include:

1-39 CH 16
patient transport via gurney or wheelchair within the clinic; assessing and properly
recording temperature, respiratory rate, heart rate, and blood pressure; acting as a
chaperone during exams or treatment; assisting in specialty areas, i.e., laboratory
(with appropriate additional training and supervision); answering telephones, filing
and other clerical duties; cleaning and wrapping instruments.
b. Supervision. Supervision of Red Cross volunteers is the responsibility of the Clinic
Administrator and may be delegated.
c. Orientation. Each volunteer must have an initial orientation to the clinic
documented. Orientation shall include at least the following topics:
(5) Fire Safety,
(6) Emergency procedures (bomb threats, mass casualty, power outages,
hurricanes/tornadoes),
(7) Universal precautions and infection control,
(8) Proper handling of telephone emergency calls,
(9) Phone etiquette, paging, proper message taking,
(10) Patient Bill of Rights and Responsibilities, to include confidentiality, and
chaperone duties in accordance with Chapter 2-J-3-b of this Manual.
21. Volunteers
a. Volunteer health care workers (HCW) who are not health care providers and who are
members of the U. S. Public Health Service (USPHS), Department of Defense
(DOD) or Coast Guard Auxiliary (AUX) shall work under the supervision of clinic
staff and will provide support services that include but are not limited to: patient
transport via gurney or wheelchair within the clinic, assessing and recording vital
signs, acting as a chaperone during examination or treatment, clerical duties such as
answering telephone or filing, cleaning and wrapping instruments, etc.
b. Health care providers who are members of the USPHS or DOD who volunteer to
work in Coast Guard clinics for up to fourteen days per year will not be required to
apply to G-WK for clinical privileges.
(1) Volunteer providers in this category will submit a copy of a current active state
license, copy of current clinical privileges and a current CPR card to the local
clinic when they report in. They will also complete a request for clinical
privileges appropriate to their category and submit to the local SMO/SDO.
Volunteer providers can also submit a Credentials Transfer Brief in lieu of
their license and CPR card.
(2) The SMO/SDO will evaluate the clinical privileges requested and by signing
the request will authorize the provider to perform those health care services.
CH-17

CH 16 1-40
c. Health care providers who are members of the USPHS or DOD who volunteer to
work in Coast Guard clinics for more than fourteen days per year will be required to
apply for clinical privileges from G-WK as described in Chapter 13-B, and C of this
Manual.
d. Health care providers who are members of the AUX will be required to apply for
clinical privileges from G-WK as described in Chapter 13-B, and C of this Manual.
e. Volunteer providers will work under the direct or indirect supervision of Coast
Guard clinic providers.
f. Each volunteer must have an initial orientation to clinic standard operating
procedures which must be documented and must include at the minimum:
(1) Fire safety
(2) Emergency procedures (e.g., bomb threats, mass casualty, power outages,
hurricanes/tornadoes)
(3) Universal precautions and infection control
(4) Proper management of telephone calls, emergency calls
(5) Telephone etiquette, paging, taking messages
(6) Patient sensitivity and confidentiality
CH-17
2-i
CHAPTER 2.
HEALTH CARE AND FACILITIES
Page
SECTION A - HEALTH CARE FOR ACTIVE DUTY PERSONNL……………………………………………..1
CARE AT UNIFORMED SERVICES MEDICAL TREATMENT FACILITIES. ........................................................................ 1
EMERGENCY CARE AT OTHER THAN CG OR DOD FACILITIES.................................................................................. 2
DENTAL CARE AND TREATMENT............................................................................................................................... 4
CONSENT TO AND REFUSAL OF TREATMENT. ............................................................................................................ 7
ELECTIVE SURGERY FOR PRE-EXISTING DEFECTS..................................................................................................... 9
ELECTIVE HEALTH CARE ........................................................................................................................................ 10
OTHER HEALTH INSURANCE .............................................................................................................................................10
PROCEDURES FOR OBTAINING NON-EMERGENT HEALTH CARE FROM NONFEDERAL SOURCES.............................. 11
OBTAINING VASECTOMIES AND TUBAL LIGATIONS. .................................................................................................. 13
CARE AT DEPARTMENT OF VETERANS AFFAIRS (DVA) MEDICAL FACILITIES. ....................................................... 13
SECTION B - HEALTH CARE FOR RESERVE PERSONNEL. ....................................................................... 17
CARE AT UNIFORMED SERVICES MEDICAL TREATMENT FACILITIES. ...................................................................... 17
EMERGENCY CARE AT OTHER THAN CG OR DOD FACILITIES................................................................................ 19
NON-EMERGENT CARE AT OTHER THAN CG OR DOD FACILITIES. ........................................................................ 19
SECTION C - HEALTH CARE FOR RETIRED PERSONNEL......................................................................... 20
CARE AT UNIFORMED SERVICES MEDICAL TREATMENT FACILITIES. ...................................................................... 20
CARE UNDER THE TRICARE EXTRA AND STANDARD OPTIONS (FORMERLY CHAMPUS). ................................... 20
CARE AT VETERANS ADMINISTRATION MEDICAL FACILITIES.................................................................................. 20
SECTION D - HEALTH CARE FOR DEPENDENTS. ........................................................................................ 21
CARE AT UNIFORMED SERVICES MEDICAL TREATMENT FACILITIES. ...................................................................... 21
CARE UNDER COAST GUARD CIVILIAN CONTRACTS............................................................................................... 21
RIGHTS OF MINORS TO HEALTH CARE SERVICES. ................................................................................................... 21
SECTION E - CARE FOR PREADOPTIVE CHILDREN AND WARDS OF THE COURT........................... 22
GENERAL. ............................................................................................................................................................... 22
SECRETARY'S DESIGNATION.................................................................................................................................... 22
SECTION F - HEALTH CARE FOR OTHER PERSONS................................................................................... 24
MEMBERS OF THE AUXILLARY. .......................................................................................................................... 24
TEMPORARY MEMBERS OF THE RESERVE............................................................................................................... 24
MEMBERS OF FOREIGN MILITARY SERVICES........................................................................................................... 25

CH-16 2-ii
FEDERAL EMPLOYEES............................................................................................................................................. 25
SEAMEN.................................................................................................................................................................. 25
NONFEDERALLY EMPLOYED CIVILIANS ABOARD COAST GUARD VESSELS............................................................. 26
SECTION G - MEDICAL REGULATING............................................................................................................ 27
TRANSFER OF PATIENTS AT COAST GUARD EXPENSE............................................................................................. 27
TRAVEL VIA AMBULANCE OF PATIENTS TO OBTAIN CARE...................................................................................... 27
AEROMEDICAL EVACUATION OF PATIENTS............................................................................................................. 27
SECTION H - USE OF THE DEFENSE ENROLLMENT ELIGIBILITY REPORTING SYSTEM (DEERS)
IN COAST GUARD HEALTH CARE FACILITIES............................................................................................ 28
DEFENSE ENROLLMENT ELIGIBILITY REPORTING SYSTEM (DEERS) ...................................................................... 28
RESPONSIBILITIES.................................................................................................................................................... 28
SECURITY................................................................................................................................................................ 28
PERFORMING DEERS CHECKS. .............................................................................................................................. 30
REPORTS.:............................................................................................................................................................... 33
ELIGIBILITY/ENROLLMENT QUESTIONS, FRAUD AND ABUSE. .................................................................................... 33
DENIAL OF NONEMERGENCY HEALTH CARE BENEFITS FOR INDIVIDUALS NOT ENROLLED IN DEFENSE ENROLLMENT
ELIGIBILITY REPORTING SYSTEM (DEERS).............................................................................................................. 34
DEERS ELIGIBILITY OVERRIDES.: .......................................................................................................................... 34
SECTION I - HEALTH CARE FACILITY DEFINITIONS. ............................................................................... 46
COAST GUARD FACILITIES. ..................................................................................................................................... 46
DEPARTMENT OF DEFENSE MEDICAL FACILITIES.................................................................................................... 46
UNIFORMED SERVICES TREATMENT FACILITIES. .................................................................................... 47
SECTION J - POLICIES AND PROCEDURES REQUIRED AT COAST GUARD HEALTH CARE
FACILITIES.............................................................................................................................................................. 49
ADMINISTRATIVE POLICIES AND PROCEDURES........................................................................................................ 49
OPERATIONAL POLICIES AND PROCEDURES............................................................................................................. 49
PATIENT RIGHTS...................................................................................................................................................... 50
HEALTH CARE PROVIDER IDENTIFICATION.............................................................................................................. 51
SECTION K - GENERAL STANDARDS OF CARE............................................................................................ 53
GENERAL STANDARDS OF CARE:.............................................................................................................................. 54

2-1 CH-16
CHAPTER 2. HEALTH CARE AND FACILITIES
Section A - Health Care for Active Duty Personnel.
1. Care at Uniformed Services Medical Treatment Facilities.
a. Authority for Health Care. Title 10 USC, 1074(a) provides that under joint
regulations to be prescribed by the Secretary of Defense and the Secretary of
Transportation, a member of a uniformed service who is on active duty is entitled to
health care in any facility of any uniformed service. Members of the reserve
components who are on active duty (including active duty for training) are entitled to
the same health care in any facility of the uniformed services as that provided for
active duty members of the regular services.
b. Use of Own Service Medical Treatment Facilities. Under ordinary circumstances,
members shall receive health care at the Uniformed Services Medical Treatment
Facility (USMTF) which serves the organization to which the member is assigned.
However, Commanding Officers may request assignment to another USMTF through
the cognizant MLC. Members away from their duty station or on duty where there is
no USMTF of their own service may receive care at the nearest USMTF.
c. Use of Other Services Medical Treatment Facilities and/or Civilian Facilities. The
closest USMTF having the appropriate capabilities shall be used for non-emergency
health care. Health care in civilian medical facilities for non-emergent conditions is
not authorized without prior approval of MLC (k). All health care received at other
than a CG Clinic shall be recorded in the Coast Guard health record.
d. Definitions.
(1) Uniformed Services are the Army, Navy, Air Force, Marine Corps, Coast
Guard, Commissioned Corps of the Public Health Service, and the
Commissioned Corps of the National Oceanic and Atmospheric
Administration.
(2) Active Duty means full-time duty in a Uniformed Service of the United States.
It includes: duty on the active list; full-time training duty; annual training duty;
and attendance, while in the service, at a school designated as a service school
by law or by the Secretary of the Uniformed Service concerned.
(3) Health Care means outpatient and inpatient professional care and treatment,
nursing care, diagnostic tests and procedures, physical examinations,
immunizations, prophylactic treatment, medicines, biologicals, other similar
medical services, and ambulance service. Prostheses, hearing aids, spectacles,
orthopedic footwear, and similar adjuncts to health care may be furnished only
where such adjuncts are medically indicated.
e. Application for Care. Members of the Coast Guard on active duty may be provided
health care at a USMTF when requested by appropriate Coast Guard authority, a

CH-16 2-2
Public Health Service medical officer detailed to the Coast Guard, or by application
of the member by presenting an Armed Forces Identification Card (DD-2-CG).
f. Subsistence Charges. All active duty members of the uniformed services are
required to pay subsistence in a USMTF at a rate prescribed by the Department of
Defense.
g. Loss of Entitlement. A member of the Coast Guard who is separated from active
duty, for any reason other than retirement, is not eligible for health care at a USMTF
by reason of that previous service unless otherwise noted on the Certificate of
Release or Discharge from Active Duty form DD-214.
2. Emergency Care at Other Than CG or DOD Facilities.
a. Definition of Emergency Condition.
(1) An emergency medical condition exists when the patient's condition is such
that, in a medical officer's opinion, failure to provide treatment or
hospitalization would result in undue suffering or endanger life or limb.
(2) In an emergency, the patient's safety and welfare, as well as that of the
personnel around the patient, must be protected. When a USMTF cannot
render immediate care, other local medical facilities, Federal or civilian, may
be used. The decision to admit the patient to any of these facilities shall be
made by the command with regard for only the health and welfare of the
patient and the other personnel of the command.
b. Eligibility for Emergency Treatment. The following members of the Coast Guard are
eligible for emergency medical treatment:
(1) active duty personnel of the regular Coast Guard;
(2) reserve personnel on extended active duty or temporary active duty (ASWAC);
and
(3) reserve personnel who become ill, injured, or contract a disease in line of duty
while on active duty for training or inactive duty for training, including
authorized travel to or from such duty. [see Reserve Policy Manual,
COMDTINST M1001.28 (series)]
c. Responsibilities.
(1) Patient.
(a) The patient is responsible for notifying the civilian physician or dentist
that he or she is in the:
1 Regular Coast Guard;
2 Coast Guard Reserve on active duty or active duty for training; or

2-3 CH-16
3 Coast Guard Reserve in an inactive duty training drill or appropriate
duty status.
(b) It is also the responsibility of the patient or someone acting in the
patient's behalf to request that the physician or dentist notify the
member's command or the closest Coast Guard organization that he or
she is undergoing emergency treatment at a civilian medical facility.
(c) The patient shall provide to appropriate authority all information needed
to verify the course of treatment received and authorize release of all
records associated with the episode of care.
(2) Commanding Officer. When notified that a member of the Coast Guard is
hospitalized, transferred to another facility, or discharged from inpatient status,
the commanding officer shall notify MLC (p) and (k) via message in
accordance with MLC directives.
(3) Commander, Maintenance and Logistics Command. When notified that a
member of the Coast Guard is hospitalized, MLC (k) shall:
(a) Be responsible for authorizing additional inpatient care at a civilian
medical facility prior to transferring the patient to a USMTF. It is
imperative, in the interest of good management, that the patient be
transferred as soon as medically feasible. However, nothing in the above
should be construed as precluding the necessary care for the patient
concerned. MLC (k) shall notify the member's unit of any authorization
action.
(b) Assist in ascertaining all necessary background information about the
case, when the patient can be moved, and the location of the nearest
CGMTF or USMTF which can accept the case. Patients shall be
transferred in accordance with the provisions of Medical Regulating to
and Within the Continental United States, COMDTINST M6320.8
(series).
(4) Commanding Officers of Reserve Units.
(a) A Reservist needing emergency treatment while performing inactive duty
training shall be taken to a USMTF. If the nature of the case is so
emergent as to preclude such transportation, a civilian medical facility
may be used. If outpatient follow-up treatment is required, (i.e., office
visits, tests, etc.) such treatment must be preauthorized by MLC (k) after
issuance of a Notice of Eligibility by Commander, Integrated Support
Command (FOT).
(b) The commanding officer of the reserve unit shall comply with Chapter
11 of the Reserve Policy Manual, COMDTINST M1001.28 (series) in
notifying the commander, MLC and ISC (FOT) when a Reservist

CH-16 2-4
engaged in inactive duty training is admitted to a civilian hospital or
USMTF, and subsequent follow-up.
(5) Government Responsibility. Non-adherence to these notification directives
cannot limit the Government's liability to pay bills for emergency medical and
dental treatment provided to authorized Coast Guard beneficiaries. However,
if prior approval is not obtained for NON-EMERGENT treatment in
nonfederal facilities, the member receiving the care will be liable for payment.
d. Elective Surgery or Medical Treatment. Elective surgery or medical treatment is
only authorized in USMTFs.
e. Emergency Care Outside the Continental United States. Coast Guard active duty
personnel outside the continental limits of the United States are entitled to health
care at USMTFs, where available. If such facilities are not available, emergency
health care may be obtained at Coast Guard expense, without prior authorization.
f. Absentees or Deserters. Charges incurred by Coast Guard personnel for civilian
health care when absent without authority or in desertion are the sole responsibility
of the individual. However, charges for civilian health care after actual or
constructive return of the individual to Coast Guard or military control may be paid
from Coast Guard funds. Refer questions on payment of health care in regards to
constructive return to MLC (k).
3. Dental Care and Treatment.
a. Extent of Dental Services.
(1) Active duty Coast Guard personnel are entitled to emergency, routine, and
accessory dental treatment at all USMTFs. Dental care from contract dentists
is authorized only as prescribed in Chapter 11 of this Manual.
(2) Reserve Coast Guard personnel ordered to active duty with their consent for
less than thirty days are eligible for emergency dental treatment only, and are
also subject to the following modifications;
(a) Reserve personnel are responsible for all dental diseases and conditions
in existence prior to the initiation of or call to active duty. They must be
in a class 1 or 2 dental status. (see section 4-C-3.c.)
(b) Reserve personnel shall not be eligible for routine or accessory dental
treatment which cannot be completed prior to termination of or release
from active duty status.
(c) Reserve personnel are responsible for maintaining their dental fitness for
duty while on inactive status or during periods of active duty less than 30
days.

2-5 CH-16
(3) Coast Guard Reserve personnel ordered to active duty for 30 days or more, are
eligible for emergency, routine, and accessory dental treatment at all USMTFs,
and are also subject to the modifications listed above. Reservists with active
duty orders for 30 days or more are encouraged to obtain a dental exam as part
of their check-in process at their newly assigned unit.
b. Definitions of Types of Dental Treatment.
(1) Emergency Dental Treatment. Emergency dental treatment includes those
procedures directed toward the immediate relief of pain, the removal of oral
infection which endangers the health of the patient, and repair of prosthetic
appliances where the lack of such repair would cause the patient physical
suffering.
(2) Routine Dental Treatment. Routine dental treatment includes the following:
examinations, radiographs, diagnosis and treatment planning, amalgam fillings,
synthetic fillings, prophylaxis, extraction, treatment of root canals, treatment
for allaying pain, treatment of oral pathological conditions, periodontal
conditions, other infections and related conditions detrimental to the patient's
health, and repairs and adjustment of dentures and prosthetic appliances.
(3) Accessory Dental Treatment. Accessory dental treatment includes prosthetic
replacement of missing teeth in cases where insufficient occlusal surfaces
prevent proper mastication and where missing anterior teeth prevent correct
phonation.
(4) Implants.
(a) Implant placement by Coast Guard dental officers (DOs) shall be
performed only by:
1 those DOs specifically privileged to do so by DOD facilities, or
2 those DOs who have received implant training as part of a formal
specialty program.
(b) Implant maintenance is the responsibility of all DOs. Each DO shall be
familiar with the techniques and armamentarium of implant maintenance,
as well as diagnosis of successful and unsuccessful implants.
(c) Requests for implants from nonfederal providers for active duty members
shall be approved or denied on a case-by-case basis by the cognizant
MLC. Factors to be considered include:
1 oral hygiene;
2 treatment alternatives;
3 feasibility and expectations for long-term success;
CH-16 2-6
4 length of service and anticipated rotation; and
5 qualifications of the provider(s).
c. Dental Care of Recruits. Only emergency dental treatment should be provided those
recruits who are to be separated from the Service prior to completing recruit training.
It is important that recruits in this category do not have teeth extracted in preparation
for prosthetic treatment and then be separated from the Service prior to the time
prosthetic appliances are provided.
d. Emergency Dental Treatment in Nonfederal and Non-contract Facilities.
(1) If a contract dentist is not available, emergency dental treatment required for
the immediate relief of pain or infection may be obtained by active duty Coast
Guard personnel from any available dentist. Once the emergency has been
alleviated, all follow-up treatment must be from a USMTF or contract dentist
unless preauthorized by MLC (k).
(2) Process all bills in accordance with Chapter 11 of this Manual.
e. Criteria To Be Followed When Requesting Orthodontic/Orthognathic Surgical Care.
(1) Orthodontic/orthognathic surgical treatment can affect release from active duty,
rotation dates, and fitness for duty. Therefore, written authorization to
commence all orthodontic/orthognathic surgical treatment (whether elective or
not, and whether provided by Federal or nonfederal practitioners) must be
requested from Commander (CGPC-epm) for enlisted and (CGPC-opm) for
officers via the cognizant MLC (k) prior to its initiation. Command
endorsement must include a copy of Administrative Remarks CG-3307
documentation described in article 2-A-3.e.(3)(b) below. Request nonfederal
care from appropriate MLC (k) following established guidelines. If authorized
by MLC (k), the request will be forwarded to Commander (CGPC-epm or
opm).
(2) Preexisting conditions are the member's responsibility.
(3) Treatment not required to maintain the member's fitness for duty is elective in
nature and is not authorized for payment by the Coast Guard. If the member's
condition does not impair job function, the treatment shall be considered
elective.
(4) Elective care may be obtained, if available, from USMTFs. If obtained from
nonfederal providers, payment is the member's responsibility. In addition, the
member is financially responsible for any care arising from complications that
require additional treatment, even if it is non-elective. Because complications
could lead to subsequent action by the Physical Disability Evaluation System
(PDES), and to protect the interests of both the service member and the Coast
Guard, the member's command is responsible for Service Record
Administrative Remarks CG-3307 documentation detailing:
2-7 CH-16
(5) The personnel action to be taken by the command regarding the granting of
absence.
(6) That the service member was instructed regarding the provisions contained
herein and other applicable directives; and
(7) That the service member must obtain copies of all treatment records from the
provider for inclusion into the Coast Guard dental record, including (for
example) initial evaluation, treatment plan, progress notes, and follow-up care.
(8) If elective treatment is approved, PDES processing shall be suspended pending
the outcome of the elective treatment. Aviation personnel and divers are
required to have a waiver request approved by CGPC - opm or epm. In
addition, members whose duties preclude regular visits to an orthodontist (e.g.,
icebreakers crews, isolated LORAN duty etc.) fall under this category.
(9) If the condition is service-related, the Coast Guard shall be responsible to
acquire care sufficient to return the member to fit for full duty status (e.g., that
which existed at the time of the member's entry to the service), but not
necessarily to ideal conditions not impacting on performance of duties. If
treatment is not available at a local MTF, use of a nonfederal provider may be
authorized.
(10) If pain is the only symptom causing the member to be not fit for full duty, then
it must be treated. Treatment may include, but is not limited to physical
therapy, bite plates to improve occlusion, stress management, and medications.
Since orthodontic treatment is of long duration, it is not an appropriate method
to relieve acute pain.
(11) All treatment must be completed, inactivated, or terminated prior to transfer or
release from active duty. Personnel who are being transferred or released from
active duty, and who request inactivation of orthodontic appliances, shall sign
an entry in the SF-603/603-A stating their intention to seek orthodontic therapy
at their own expense.
4. Consent to and Refusal of Treatment.
a. Regulatory Restrictions. Coast Guard Regulations, COMDTINST M5000.3 (series),
state in Section 8-2-1 that:
(1) "Persons in the Coast Guard shall not refuse to submit to necessary and proper
medical or dental treatment to render themselves fit for duty, or refuse to
submit to a necessary and proper operation not endangering life."
(2) "Persons in the Coast Guard shall permit such action to be taken to immunize
them against disease as is prescribed by competent authority."
b. Policy Concerning Refusal of Treatment.
(1) Policy.

CH-16 2-8
(a) It is the Commandant's policy that compulsion is not permissible at any
time to require Coast Guard personnel to submit to various types of
medical or dental treatment, diagnostic procedures, or examinations.
(b) Surgery will not be performed on persons over their protest if they are
mentally competent.
(c) Individuals who refuse to submit to measures considered by competent
medical or dental officers to be necessary to render them fit for duty, may
be processed for separation from the Coast Guard in accordance with
applicable regulations. Individuals may be subjected to disciplinary
action for refusal of necessary treatment or surgery if the refusal is
determined to be unreasonable. Refusal of medical care by vegetative or
comatose individuals in accordance with a Living Will shall not be
considered unreasonable.
(2) Non-Emergent Operations on Minors. A minor who enlists or otherwise enters
active duty with parental or guardian consent is considered emancipated during
the term of enlistment. There is, therefore, no legal requirement that the
consent of any person, other than the minor, be obtained prior to instituting
surgical procedures.
(3) Refusal of Emergency or Lifesaving Treatment or Emergency Diagnostic
Procedures. The refusal of recommended emergency or lifesaving treatment or
emergency diagnostic procedure required to prevent increased level of
impairment or threat to life is ordinarily determined to be unreasonable.
However, refusal of medical care by vegetative or comatose patients under the
authorization of a Living Will is not considered unreasonable. A medical
board shall be convened in accordance with the Physical Disability Evaluation
System, COMDTINST M1850.2 (series) for unreasonable refusal of
emergency or lifesaving treatment or emergency diagnostic procedures.
(4) Refusal of Non-Emergent Treatment. If a member of the Coast Guard refuses
non-emergent medical, surgical, dental, or diagnostic procedures that are
required to maintain a fit for full duty status, a determination of reasonable
basis for this refusal is required. A medical board shall be convened in
accordance with Physical Disability Evaluation System, COMDTINST
M1850.2 (series).
c. Advance Directives (Living Wills).
(1) Federal law enacted in 1993 requires hospitals to ask about advance directives
at the time of admission and provide patients with information to create
advance directives. Advance directives, commonly known as living wills,
express a person's wishes regarding certain aspects of treatment and care,
including but not restricted to CPR, mechanical life support measures, etc.,
which may arise in the course of hospitalization.

2-9 CH-16
(2) Coast Guard health care facilities are not required to provide such information
under the law. Clinics may elect to provide standardized information to
patients on request. Information given out shall conform to the implementing
laws of the state in which the clinic is located. Clinics providing such
information shall notify patients of its availability either by posted notice or via
patient handout materials.
(3) Clinic staff members usually do not have the required training and experience
to advise patients on the legal issues concerning creation of advance directives.
Patients shall be referred to the appropriate source of legal support, e.g.,
command or district legal officers.
(4) Clinic staff members, where allowed by state law, may serve as witnesses to
advance directive signatures.
(5) Advance directive documents shall be held by the member and/or the member's
next of kin. Advance directive documents shall not be filed in the member's
health record since health records are not universally available 24 hours a day,
seven days a week, for reference by a treating hospital.
5. Elective Surgery for Pre-Existing Defects.
a. General. In many medical/dental procedures undertaken to correct defects that
existed prior to entrance (EPTE) into the Service, the likelihood of return to full duty
is questionable. In addition, such cases have often resulted in long periods of
convalescence with subsequent periods of limited duty, outpatient care, and
observation which render the Government liable for benefits by reason of
aggravation of these defects.
b. Criteria. The following conditions must be met before attempting surgical correction
of an EPTE defect.
(1) It interferes with the member's ability to perform duty.
(2) The procedure being considered is an accepted one, carries a minimal risk to
life, and is not likely to result in complications.
(3) There should be a 90 percent chance that the procedure will correct the defect
and restore the member to full duty within a reasonable time (three months)
without residual disability. If the defect does not meet the above conditions
and the member is, in fact, unfit to perform the duties of grade or rate, action
shall be taken to separate the member from the Service.
c. Discussion. Whether elective medical/dental care should be undertaken in any
particular case is a command decision which should be decided using the above
guidelines. In questionable cases, the member may be referred to a medical board for
final decision prior to undertaking elective treatment for an EPTE defect.

CH-17 2-10
6. Elective Health Care.
a. Medical/Dental treatment not required to maintain the member’s fitness for duty is
elective in nature and is not authorized for payment by the Coast Guard. If the
member’s condition does not interfere with their ability to perform duty, the
treatment shall be considered elective.
(1) Elective care may be obtained, if available, from USMTF’s.
(2) If obtained from nonfederal providers, payment is the member’s responsibility.
In addition, the member is financially responsible for any care arising from
complications that require additional treatment, even if it is non-elective.
(3) Because complications could lead to subsequent action by the Physical
Disability Evaluation System (PDES), and to protect the interests of both the
service member and the Coast Guard, the member’s health record must contain
a SF-600 entry detailing:
(a) the personnel action to be taken by the command regarding the granting
of absence;
(b) that the service member was counseled regarding the provisions
contained herein and other applicable directives. Counseling will be
provided at the local Coast Guard primary care facility, or if there is no
near by Coast Guard primary care facility, then the cognizant MLC (k)
via phone. SF-600 will be faxed to the cognizant MLC (k) for
appropriate entries, then faxed or mailed back to the unit for
incorporation into the member’s health record.
(c) that the service member must obtain copies of all treatment records from
the provider for inclusion into the Coast Guard health record, including
initial evaluation, treatment plan, progress notes, and follow-up care.
(4) Members shall understand that once they have received an elective treatment or
procedure, they may be adversely effected for present or future assignments or
specialized duty. For example, Laser In-situ Keratomileusis (LASIK) is
disqualifying for divers, aviation personnel, and landing signal officers (LSO).
7. Other Health Insurance (OHI)
a. General. In some situations a member may desire to utilize their spouses’ health
insurance (OHI) to obtain health care outside of the Military Health Care System.
Whether elective health care or all other areas of health care, this decision has an
impact on the command and possibly on a member’s access to the Physical Disability
Evaluation System (PDES).
b. Criteria. The following conditions must be met before utilizing a spouse’s health
insurance or OHI,

2-11 CH-16
(1) ALL payment is the member’s responsibility. In addition, the member is
financially responsible for any care arising from complications that require
additional treatment, even if it is non-elective.
(2) Because complications could lead to a loss of access to the Physical Disability
Evaluation System (PDES), and to protect the interests of both the service
member and the Coast Guard, the member’s Coast Guard health record must
contain a SF-600 entry detailing:
(a) the personnel action to be taken by the command regarding the granting
of absence;
(b) that the service member was instructed regarding the provisions
contained herein and other applicable directives. Counseling will be
provided at the local Coast Guard primary care facility, or if there is no
near by Coast Guard primary care facility, then the cognizant MLC (k)
via phone. SF-600 will be faxed to the cognizant MLC (k) for
appropriate entries, then faxed or mailed back to the unit for
incorporation into the member’s health record.
(c) that the service member must obtain copies of all treatment records from
the provider for inclusion into the Coast Guard health record, including
initial evaluation, treatment plan, progress notes, and follow-up care.
8. Procedures for Obtaining Non-Emergent Health Care from Nonfederal Sources.
(Guidance reflecting current TRICARE procedures for obtaining Non-Emergent Health
Care will be promulgated in future changes to this Manual).
a. Nonfederal sources for active duty care are intended to supplement and not substitute
for care that is available through the federal system. USMTF's or DVA facilities, if
located within a 40 mile radius of the member's unit (except a 30 mile radius for
maternity care), shall be used first for non-emergent, non-elective health care before
nonfederal sources are used. Each case must be evaluated for:
(1) appropriateness of care;
(2) urgency of treatment;
(3) time and cost factors associated with obtaining such care from a USMTF;
(4) the member's anticipated length of stay at the given station; and,
(5) operational need of the unit for the member.
b. Before active duty personnel are treated in a nonfederal medical facility for non-
emergent conditions, prior approval must be obtained. Non-elective conditions are
those which, without repair or treatment, would render the member unfit for duty.
c. MLC (k) may approve requests for nonfederal health care (both medical and dental)
and may delegate, in writing, limited authority to qualified clinic administrators.

CH-16 2-12
d. Requests for nonfederal health care beyond a clinic administrator's authority will be
submitted by following the cognizant MLC(k) policy. Telephone authorization will
not be provided without a hard copy of the request. As a minimum, the following
information must be provided, as applicable:
(1) name, grade/rate, social security number;
(2) anticipated rotation date and expiration of enlistment;
(3) whether care will be completed before transfer or separation;
(4) diagnosis reported by International Classification of Diseases, 9th Revision,
Clinical Modification (ICD-9-CM) code number and a brief explanation;
(5) history of patient's condition;
(6) total amount of local/MLC approved nonfederal expenditures to date for this
condition;
(7) the necessity of treatment to maintain fitness to perform duty;
(8) treatment plan: length, type of therapy/treatment, and estimated cost (Cost
estimates must include total scope of care not just primary provider or hospital
costs.);
(9) name of facility where treatment will be done;
(10) attending physician's or dentist's prognosis with and without treatment,
including likelihood of medical board action;
(11) treatment plan and justification, radiographs and copy of dental records for all
dental requests (Study models will be submitted for all cases requiring crown
and bridge work and partial dentures;
(12) name of nearest USMTF capable of providing care:
(a) distance to facility (miles);
(b) earliest appointment available (not available is unacceptable);
(c) travel/per diem cost;
(d) estimated total lost time; and
(e) other factors for consideration, i.e., travel time, road conditions,
operational impact, etc; and
(13) indicate date of original submission and reason for resubmission, if previous
requests were submitted for this procedure.
e. If approval is granted, MLC (k) will provide the requester with an authorization
number. This authorization number must be noted on all bills submitted. Bills will
be submitted to MLC (k). If approval is denied, MLC(k) will outline the appropriate
appeals process to follow in their denial transmittal.
2-13 CH-16
f. When personnel are transferred prior to completing the approved care, the request is
canceled. Personnel are required to submit another request after reporting for their
new assignment.
g. Amounts authorized shall not be exceeded without further authorization from MLC
(k) which requires additional justification.
h. Inpatient hospitalization in nonfederal facilities shall be monitored closely by the
MLC (k) responsible for the geographical area in which the facility is located.
Normally, an inpatient stay will not exceed seven days duration without
consideration of movement to a USMTF. Cases suspected to extend past the seven-
day limit shall not be placed in a civilian facility, but shall be initially referred to a
USMTF.
i. If prior approval is not obtained for non-emergent treatment in nonfederal facilities,
the member receiving the care will be liable for payment.
j. EMERGENCY health care does not require prior approval.
9. Obtaining Vasectomies and Tubal Ligations from Nonfederal Providers.
a. Preauthorization is required. Submit all request for vasectomies and tubal ligations
by nonfederal providers to cognizant MLC(kma) following the guidelines for
requesting above. Request must show the provider of care decided on the procedure
based upon applicable local and state guidelines.
b. Request must contain evidence that the patient has been counseled by a physician and
has given informed consent to the procedure.
c. The request must contain evidence that the patient has completed a SF-600 entry
acknowledging that the Coast Guard will not pay for reversal of this procedure in a
non-federal facility.
d. The request must contain current information concerning the availability of the
requested procedure from federal sources.
e. Request for tubal ligation to be performed at the time of delivery should be submitted
with the request for nonfederal maternity care.
f. Sick leave may be granted for this procedure.
10. Care at Department of Veterans Affairs (DVA) Medical Facilities.
a. From time-to-time, acute medical, surgical, or psychiatric facilities are required for
Coast Guard personnel where transportation to the nearest USMTF will place the
individual's health or welfare in jeopardy. To preclude this and other similar
situations and to provide the best possible medical care for all active duty members, a
CH-16 2-14
support agreement between the Coast Guard and the Department of Veterans Affairs
was completed in 1979 and remains in effect. FIGURE 2-1 is a copy of the medical
service agreement.
b. DVA care must be requested by the member's commanding officer. The agreement
is limited to active duty Coast Guard personnel and does not include dependents.
c. MLC commanders and commanding officers should establish local contact with
DVA facilities to determine mission and facility capabilities and patient admission
procedures.
d. Forward all bills received from DVA facilities to the service member's unit for
certification prior to forwarding to MLC (k) for payment.
e. When a USMTF and a DVA facility are collocated, the USMTF shall be used unless
it cannot provide the required services.
2-15 CH-16
FIGURE 2-A-1
CH-16 2-16
FIGURE 2-A-1 con’t
2-17 CH-16
Section B - Health Care for Reserve Personnel.
1. Care at Uniformed Services Medical Treatment Facilities.
a. Authority for Reserve Personnel. Section 2-A of this Manual contains the authority
for medical care. Information concerning entitlement to various benefits is contained
in Chapter 11 of the Reserve Policy Manual, COMDTINST M1001.28(series).
Information concerning eligibility for benefits from the Department of Veterans
Affairs is included therein.
b. Application for Care. A member of the Coast Guard Reserve may be admitted to
USMTFs upon written authorization from an appropriate Coast Guard authority (e.g.,
Commanding Officer's letter, Notice of Eligibility, or appropriately endorsed orders).
c. Definitions. The following definitions apply throughout this section:
(1) Active duty means full-time duty in a Uniformed Service of the United States.
It includes duty on the active list, full-time training duty, annual training duty
and attendance, while in the service, at a school designated as a service school
by law or by the Secretary of the Uniformed Service concerned.
(2) Active Duty for Training is defined as full-time duty in a uniformed service of
the United States for training purposes.
(3) Inactive Duty Training.
(a) Duty prescribed for reservists by the Secretary concerned under 37 USC
206 or any other provision of law.
(b) Special additional duties authorized for reservists by an authority
designated by the Secretary concerned and performed by them on
voluntary basis in connection with the prescribed training or maintenance
activities of the units to which they are assigned.
(4) Disability. A temporary or permanent physical impairment resulting in an
inability to perform full military duties or normal civilian pursuits.
(5) Employed. Reservists are employed on duty during the actual performance of
duty, while engaged in authorized travel to or from active duty for training, and
while on authorized leave or liberty.
(6) Line of Duty. An injury, illness, or disease shall be deemed to have been
incurred in line of duty, if a reservist at the time of debilitating incident is
performing active duty or active duty for training, or is on authorized leave or
liberty, provided the disability is not the result of misconduct.
d. Injury Incurred in Line of Duty. A member of the Coast Guard Reserve who is
ordered to active duty or to active duty for training, or to perform inactive duty
training, for any period of time, and is disabled in line of duty from injury while so

CH-16 2-18
employed is entitled to the same hospital benefits as provided by law or required in
the case of a member of the regular Coast Guard. For the purpose of these benefits, a
member who is not in a pay status is treated as though receiving the pay and
allowances to which entitled if serving on active duty.
e. Disease Incurred in Line of Duty While on Active Duty. A member of the Coast
Guard Reserve who is ordered to active duty for training for a period of more than 30
days, and is disabled while so employed, is entitled to the hospital benefits as are
provided by law or regulation in the case of a member of the regular Coast Guard.
An exception is that a member of the Coast Guard Reserve ordered to perform
involuntary active duty for training under the provision of 10 USC 270 is only
eligible for the limited medical benefits described below, following termination of
the training duty period.
f. Illness or Disease Contracted in Line of Duty in Peacetime. A member of the Coast
Guard Reserve who, in time of peace, becomes ill or contracts a disease in line of
duty while on active duty for training or performing inactive duty training is entitled
to receive medical, hospital, and other treatment appropriate for that illness or
disease. The treatment shall be continued until the disability resulting from the
illness or disease cannot be materially improved by further treatment. Such a
member is also entitled to necessary transportation and subsistence incident to
treatment and return home upon discharge from treatment. The treatment may not
extend beyond ten weeks after the member is released from active duty, except:
(1) upon an approved recommendation of a medical board or
(2) upon authorization of the MLC (k), based on a physician's certification that the
problem is a continuation of that for which the member was initially treated,
and that benefit will result from further treatment. Refer to Section 11-B-3 of
the Reserve Administration Policy Manual, COMDTINST M1001.28(series),
for specific instructions regarding the extension of medical treatment beyond
10 weeks for those who are receiving treatment under a Notice of Eligibility
(NOE).
g. Injury or Disease En Route to or from Active Duty. A member of the Coast Guard
Reserve is authorized medical care for an injury or disease incurred while en route to
or from active duty, active duty for training, or inactive duty for training.
h. Injury or Disease Not in Line of Duty. A member of the Coast Guard Reserve is not
entitled to medical care for an injury or disease not incurred in the line of duty.
i. Pregnancy. Pregnancy in the Coast Guard, COMDTINST 1900.9, contains guidance
regarding pregnancy and reserve members. Use of reserve servicewomen who are
pregnant for ASWAC assignment is not encouraged. Reserve servicewomen may
accept Special Active Duty for Training (SADT) with the understanding that duty
must be completed by the 24th week of gestation.

2-19 CH-16
2. Emergency Care at Other Than CG or DOD Facilities. Section 2-A-2 contains the
requirements for treating reserves in emergency situations.
3. Non-Emergent Care at Other Than CG or DOD Facilities. Any non-emergent,
nonfederal care must be authorized in advance by MLC (k) through contract, blanket
purchase agreement or pre-authorization.

CH-16 2-20
Section C - Health Care for Retired Personnel.
1. Care at Uniformed Services Medical Treatment Facilities. As set forth in 10 USC,
1074(b), retired members of the uniformed services, as specified in that Act, are entitled
to required medical and dental care and adjuncts thereto to the same extent as provided
for active duty members in medical facilities of the uniformed services. However, access
to care is subject to mission requirements, the availability of space and facilities, and the
capabilities of the medical staff as determined by the cognizant medical authority in
charge. Patients enrolled in TRICARE Prime Options are not eligible for non-emergent
care in Coast Guard clinics. These patients shall be referred to their TRICARE primary
care manager (PCM). The PCM is responsible for appropriate care and referral of such
patients.
2. Care Under the TRICARE Extra and Standard Options (formerly CHAMPUS). Subject
to the cost sharing provisions set forth in 10 USC, 1086, retired members who are not
qualified for benefits under Title I of the Social Security Amendments of 1965
(Medicare) are entitled to receive inpatient and outpatient care from civilian sources.
3. Care at Veterans Administration Medical Facilities.
a. Eligibility for DVA Hospitalization. Coast Guard military personnel are eligible for
hospitalization in DVA facilities after separation from active duty or while in
retirement under one of the following circumstances:
(1) For injuries or diseases incurred or aggravated while on active duty during any
war, the Korean conflict period 27 June 1950 through 31 January 1955) or the
Vietnam conflict period (5 August 1964 through 7 March 1975).
(2) For service-connected or nonservice-connected disabilities, if receiving
disability compensation from the DVA, or if entitled to receive disability
compensation from the DVA, but has elected to receive retirement pay from
the Coast Guard instead of the compensation from the DVA.
b. Medical Care Benefits. Eligible veterans may receive hospitalization, outpatient
medical care, outpatient dental care, prosthetic appliances, etc., from the VA.

2-21 CH-16
Section D - Health Care for Dependents.
1. Care at Uniformed Services Medical Treatment Facilities.
a. Authority for Health Care. Title 10 USC, 1076 provides basic authority for medical
and dental care for:
(1) dependents of active duty members and dependents of members who died
serving on active duty; and
(2) dependents of retired members and the dependents of members who died while
in a retired status.
b. Availability of Care.
(1) Medical and dental care for dependents in uniformed services medical
treatment facilities is subject to the availability of space and facilities and the
capabilities of the medical and dental staff. With the approval of the
commanding officer, the senior medical officer and senior dental officer are
responsible for determining the availability of space and capability of the
medical and dental staffs. These determinations are conclusive. Patients found
enrolled in TRICARE Prime Options are not eligible for non-emergent care in
Coast Guard clinics. These patients shall be referred to their TRICARE
primary care manager (PCM). The PCM is responsible for appropriate care
and referral of such patients.
(2) Dependents entitled to medical and dental care under this section shall not be
denied equal opportunity for that care because the facility concerned is that of a
uniformed service other than that of the sponsor.
(3) Types of Care Authorized. Subject to the provisions set forth in 10 USC, 1079
and 1086, dependents who are not qualified for benefits under Title 1 of the
Social Security amendments of 1965 (Medicare) are entitled to receive
inpatient and outpatient care from civilian sources. Refer to your cognizant
MLC (k) for details and instructions.
2. Care Under Coast Guard Civilian Contracts. Under certain circumstances, dependents
are entitled to medical and dental care provided through Coast Guard civilian contracts.
See Chapter 11 for guidance.
3. Rights of Minors to Health Care Services. Where not in conflict with applicable Federal
law or regulation, unit commanding officers shall follow State law defining the rights of
minors to health care services and counseling in contraception, sexually transmitted
disease prevention and treatment, and pregnancy. Any protection with regard to
confidentiality of care or records afforded by applicable law or regulation will be
extended to minors seeking care or counseling for the above mentioned services or
conditions in Coast Guard facilities.
CH-16 2-22
Section E - Care for Preadoptive Children and Wards of the Court.
1. General.
a. A child placed in a sponsors home as part of a pre-adoption procedure, or by court-
ordered guardianship, is not eligible for care under the Uniformed Services Health
Benefits Program unless specific authority has been granted. Such authority may
come from the final adoption decree, a court-ordered legal custody determination (for
a period of at least 12 consecutive months), or through a Secretary's Designation
authorization for limited health care in a USMTF.
b. Eligibility for TRICARE benefits, the Uniformed Services Family Health Benefits
Plan (USFHBP), or the Uniformed Services Active Duty Dependents Dental Plan is
established upon the issuance of a uniformed services dependent ID card and DEERS
enrollment. Authorization for these health care programs, or for direct care (USMTF
use), will be reflected on the ID card and through DEERS.
c. Prospective dependents must meet the following eligibility rules: be unmarried; have
not attained the age of 21 (or 23 if a full-time student); be dependent on the sponsor
for over one-half of their support; or be incapable of self-support due to mental or
physical incapacity and were otherwise eligible when incapacity occurred.
d. If legal custody or placement is for 12 months or more, a uniformed services
dependent ID care, DEERS enrollment, and health care eligibility may be authorized.
Personnel are encouraged to contact their servicing personnel office for assistance.
2. Secretary's Designation. The following procedures apply in situations where a pre-
adoptive or court ordered guardianship or placement is for less than 12 consecutive
months.
a. Children under a prospective parent or guardians care may use a USMTF by
acquiring authority from the Secretary of the uniformed service to which the USMTF
belongs. This authority is normally called a Secretary's Designation. For example,
requests for care in a U. S. Navy facility must be authorized by the Secretary of the
Navy or their designee. The same holds true for U. S. Army and U. S. Air Force
facilities. When seeking care from a Department of Defense MTF, contact that
facilities Patient Affairs or Health Benefits Advisor staff for assistance.
b. In cases involving Coast Guard facilities, authority has been delegated to the
Commandant by the Secretary of Transportation to authorize treatment of pre-
adoptive children and wards of the court. Letter requests must be forwarded to
Commandant (G-WKH) and include the following information:
(1) member's name, grade/rate, SSN, and duty assignment or retired status if
applicable;
(2) address of residence;

2-23 CH-16
(3) name and age of the proposed adoptive child or court-ordered ward; and
(4) a copy of the court order, legal decree, or other applicable instrument issued by
a court or adoption agency which indicates the child has been placed in the
house for adoption or with the intent to adopt, or the court order granting
guardianship of the ward to the service member and any amounts of income to
which the ward is entitled.
c. Upon approval, the respective uniformed service will issue a letter of authority for
care in one or more of their USMTFs located in the United States. This letter is the
only authority for care (since designees are not DEERS-eligible) and must be
presented (or on file) when seeking authorized care. These letters have expiration
dates and may require the sponsor to request to reissue.
d. When there is a need for medical care outside the United States, the sponsor should
contact the nearest USMTF requesting humanitarian consideration. The Service
Secretaries have limited authority for designation of beneficiaries outside the United
States.

CH-16 2-24
Section F - Health Care for Other Persons.
1. Members of the Auxiliary.
a. Authority for Care of Auxiliary Members. Basic authority for health care for
members of the Auxiliary injured while performing Coast Guard duty is contained in
14 USC 832. Section 5.59 of Chapter 1, Title 33, CFR, states: "When any member
of the Auxiliary is physically injured or dies as a result of physical injury incurred
while performing patrol duty or any other specific duty to which he has been
assigned, such member or his beneficiary shall be entitled to the same benefits as are
now or as may hereafter be provided for temporary members of the Coast Guard
Reserve who suffer physical injury incurred in the line of duty. Members of the
Auxiliary who contract sickness or disease while performing patrol duty or any other
specific duty to which they have been assigned shall be entitled to the same hospital
treatment as is afforded members of the regular Coast Guard." Claims for Auxillary
healthcare shall be submitted to:
U. S. Department of Labor
OWCP Special Claims Branch (District 25)
800 North Capitol Street, NW, Room 800
Washington, DC 20211
b. Compensation Under Federal Employee's Compensation Act (FECA) Program. See
the Detail of Civilian Employees, COMDTINST M12300.7 (series).
2. Temporary Members of the Reserve.
a. Composition of the Reserve. The Coast Guard Reserve is a component part of the
United States Coast Guard and consists of two classes of reservists: Regular and
Temporary. Temporary members of the Reserve may be enrolled for duty under such
conditions as the Commandant prescribes, including but not limited to part-time and
intermittent active duty with or without pay, and without regard to age. Members of
the Auxiliary, officers and members of the crew of any motorboat or yacht placed at
the disposal of the Coast Guard, and persons (including government employees
without pay other than compensation of their civilian positions) who by reason of
their special training and experience are deemed by the Commandant qualified for
such duty. The Commandant is authorized to define the powers and duties of
temporary reserves, and to confer upon them, appropriate to their qualifications and
experience, the same grades and ratings as are provided for regular members of the
Reserve.
b. Authority for Care of Temporary Reservists. Section 760, Title 14, USC, contains
authority for health care and/or compensation of temporary reserves under conditions
set forth therein.
2-25 CH-16
c. Care at Coast Guard Expense. 14 USC 760(d) states: "Temporary members of the
reserve who incur physical disability or contract sickness or disease, while
performing any specific duty to which they have been assigned by competent Coast
Guard authority, shall be entitled to the same hospital treatment afforded officers and
enlisted men of the Coast Guard."
d. Compensation Under Federal Employee Compensation Act (FECA) Program. See
Detail of Civilian Employees, COMDTINST M12300.7
3. Members of Foreign Military Services.
a. General. Members and dependents of foreign services assigned or attached to a
Coast Guard unit for duty or training (such as Canadian Exchange Officers) or who
are on active duty with a foreign military unit within the United States (such as the
crew of a vessel being taken over at the Coast Guard Yard under the Military
Assistance Program) are eligible for inpatient health care at DoD MTF's provided by
US Code: Title 10, Section 2559. As there are several categories of foreign service
members for whom medical care benefits vary, both for themselves and their
dependents, if any doubt exists as to eligibility for health care and the authorized
sources from which it can be obtained, contact Commandant (G-WKH) for advice.
b. Care at Uniformed Services Medical Treatment Facilities. Members of foreign
military services and their dependents who are eligible, therefore, shall be provided
inpatient health care at DoD MTFs upon request of the member's commanding
officer or consular official, or by application of the member or dependent upon
presentation of proper identification.
4. Federal Employees.
a. Benefits Under Federal Employees Compensation Act (FECA) Program. All Federal
Employees assigned to Coast Guard vessels, e.g., National Marine Fishery Service
(NMFS), Drug Enforcement Agents, etc., are civilian employees of the United States
Government, and as such, are entitled to health care and compensation under FECA.
See Detail of Civilian Employees, COMDTINST M12300.7 (series).
b. Care Aboard Ship and Outside CONUS. Federal Employees may be given medical
care while serving with the Coast Guard in a locality where civilian health care is not
obtainable, such as on board a Coast Guard vessel or outside the United States.
Outpatient and inpatient care may be provided at Navy medical facilities outside
CONUS, if reasonably accessible and appropriate nonfederal medical facilities are
not available.
5. Seamen. Sick and disabled seamen may receive emergency health care aboard Coast
Guard vessels.
CH-16 2-26
6. Nonfederally Employed Civilians Aboard Coast Guard Vessels.
a. Authority for Care. There is no statute which either prohibits or authorizes the Coast
Guard to provide health care to civilians while aboard Coast Guard vessels. There is
no objection to furnishing emergency health care, but routine care should not be
furnished. When these civilians are aboard Coast Guard vessels for relatively
lengthy periods, the commanding officer must determine what treatment is to be
given.
b. Responsibility. Commanding officers of vessels deployed for extended periods shall
ensure that nonfederally employed civilians who are carried aboard Coast Guard
vessels under their cognizance are physically capable of withstanding the trip
contemplated and that they are free from medical conditions which could cause an
interruption of the vessel's mission. Nonfederally employed civilians must furnish
such evidence from a physician at no expense to the Coast Guard or Federal
Government.

2-27 CH-16
Section G - Medical Regulating.
1. Transfer of Patients at Coast Guard Expense.
a. Details for the transfer of Coast Guard personnel to, from, or between hospitals and
the responsibility for the expenses involved are contained in Chapter 4 of the
Personnel Manual, COMDTINST M1000.6 (series).
b. Information and requirements for the transfer of patients to, from, or between
medical facilities is contained in COMDTINST M6320.8 (series), Medical
Regulating to and Within the Continental United States.
2. Travel Via Ambulance of Patients to Obtain Care.
a. Active Duty Personnel. The Coast Guard is responsible for providing ambulance
service (Government or civilian), for active duty members when medically necessary.
Bills related to ambulance service provided to active duty personnel, shall be
processed as outlined in Chapter 11 of this Manual.
b. Retired and Dependent Personnel. Retired personnel and dependents are not
provided ambulance service for initial admission, except that a Government
ambulance may be used in an emergency situation as determined by the cognizant
medical authority. If an ambulance is ordered by a military hospital, TRICARE
Standard can not pay for it; the military hospital must pay. TRICARE Standard cost
–shares ambulances only when medically necessary; that is, the patient’s condition
does not allow use of regular, private transportation or taxis, “medicabs” or
“ambicabs.” Ambulance transportation must be needed for a medical condition that
is covered by TRICARE Standard. Should either the provider or patient have
additional questions regarding this issue check with the cognizant MLC(k), HBA or
TRICARE Service Center.
3. Aeromedical Evacuation of Patients. When the condition of the patient requires
aeromedical evacuation, the transfer shall be arranged in accordance with Medical
Regulating To and Within The Continental U.S. (Joint Pub), COMDTINST M6320.8
(series). If there is no USMTF in the area, a message prepared in accordance with the
above instruction shall be forwarded to MLC (k).

CH-16 2-28
Section H - Defense Enrollment Eligibility Reporting System (DEERS) in Coast Guard Health
Care Facilities.
1. Defense Eligibility Reporting System. This Section provides guidance for Coast Guard
health care facilities on the use of the Defense Enrollment Eligibility Reporting System
(DEERS) to verify patient eligibility to receive care.
a. DEERS was established in 1979 by the Department of Defense to comply with a
Congressional mandate. The two initial objectives of DEERS were to collect and
provide demographic and sociographic data on the beneficiary population entitled to
DOD health benefits, and to reduce the fraud and misuse of those benefits. The
original scope of DEERS has since been broadened to include the maintenance and
verification of eligibility status for all uniformed services beneficiaries. Worldwide
implementation of DEERS and its registration were completed in 1985.
2. Responsibilities.
a. Commandant (G-WKH) provides overall functional management of the Coast Guard
DEERS program for health services facilities. In this role, Commandant (G-WKH)
provides guidance to field activities, represents the Coast Guard to the DEERS
Central Systems Program Office (DCSPO), and on the DEERS Central Systems
Project Officers Committees.
b. Commanders, Maintenance and Logistics Commands (k) shall appoint an MLC
DEERS medical project officer and alternate, who shall ensure that facilities in their
respective areas participate in and comply with DEERS program requirements.
c. Commanding officers of units with health care facilities shall ensure that the Chief of
the Health Services Division appoints the following individuals in writing:
(1) DEERS Project Officer and alternate who are responsible for the overall
management of the DEERS system in the clinic;
(2) Site Security Manager (SSM) and alternate who are responsible for system
security as outlined in paragraph 3; and
(3) individuals authorized to deny care.
3. Security.
a. The Site Security Manager (SSM) should be the health services division or unit
computer systems administrator. The security manager is responsible for
maintaining passwords, authorized user list, etc., and advising the DEERS contractor
when changes occur.
b. The SSM also requests site identification (site-ID) codes for the clinic. These codes
are requested through the MLC DEERS Project Officer to Commandant (G-WKH).

2-29 CH-16
As a rule, there is only one site ID required per clinic. The SSM also ensures
information systems security awareness training/briefing is given to new DEERS
users prior to allowing them access to DEERS and to all DEERS users annually.
c. If the clinic DEERS project officer is not the SSM, the security manager must closely
coordinate activities with the DEERS project officer. Immediately after
appointment, the SSM must telephone the DEERS Security Maintenance Office at
(703) 820-4850 to notify that office of the appointment. When making this
notification, include the following information:
(1) Site ID number;
(2) Rank or grade of SSM;
(3) Name (last, first, middle initial);
(4) Social Security Number (SSN);
(5) Duty location;
(6) Duty title; and
(7) Telephone number.
(8) After telephone notification, submit a letter of appointment and a Request for
Data Base Additions, Deletions, or Changes (Figure 2-H-1) to:
(9) Security Maintenance Office
DEERS East Coast Center
1600 North Beauregard St.
Alexandria, VA 22311
d. User Password Maintenance.
(1) The DEERS security system requires a six-character user-ID and a six to eight
character password. The user-ID is assigned by DEERS, and is permanent. An
initial password is assigned by the DEERS government contractor. The
password expires at 30 day intervals. At the end of each 30 day period, the
user is required to change the initial password to one of his or her own
choosing, so long as it meets the six- to eight-character requirement. Access to
the data base is granted by using a unique user-ID, password, and the
transaction identifier (TRAN-ID). The TRAN-ID for medical/dental is GIQD.
(2) To add a new user, submit a Request for Data Base Additions, Deletions, or
Changes. Be sure to include the site-ID and SSN of any new personnel.
(3) To delete a current user, submit a Request for Data Base Additions, Deletions,
or Changes requesting the deletion to the DEERS Security Maintenance Office.
(4) User IDs not used for 60 days are automatically deleted and access is not
possible. To regain access, the SSM must reapply for a new user-ID by
submitting a new Security Manager Update.

CH-16 2-30
(5) Authorized users must be kept to the absolute minimum, consistent with job
requirements.
4. Performing DEERS Checks.
a. Whom to check: All beneficiaries of the military health care system are subject to
DEERS eligibility verification, with the following exceptions:
(1) Coast Guard cadets, officer candidates, and recruits while undergoing training;
(2) Active duty personnel receiving dental care at a military facility; and
(3) Secretarial Designees, including pre-adoptive children and wards of the Court,
ARE NOT ELIGIBLE for care under the TRICARE programs. They are also
not enrolled in DEERS. Verification of the eligibility of Secretarial Designees
for care in a military facility is accomplished through the individual's actual
letter of designation. Refer to Section 2-E for further information.
b. When to check: Coast Guard health services facilities should verify the eligibility of
all beneficiaries prior to providing health care. The following minimum eligibility
checks shall be made:
(1) 100% of all outpatient medical visits:
(2) 25% of all dental visits;
(3) 10% of pharmacy visits to fill "in-house" prescriptions;
(4) 100% of pharmacy visits with prescriptions written by civilian providers;
(5) 100% of all inpatient admissions; and
(6) 100% of dental visits when the patient may be eligible for the TRICARE
Family Member Dental Program;
(7) 100% of retired members at the initial visit to a dental facility, and annually
thereafter at the time of treatment.
(8) Upon initial presentation by dependents for evaluation or treatment. This
check will be valid for 30 days, if the period of eligibility (dates of treatment)
requested from DEERS is 30 days.
(9) When a non-active duty patient is referred to a civilian provider for
supplemental care.
(10) When active duty personnel are referred to a civilian provider under the Active
Duty Claims Program.
(11) When any patient (active duty, retired, dependent, or survivor) is referred to a
Military Treatment Facility (MTF) or a Uniformed Services Treatment Facility
(USTF).
(12) When in doubt verify enrollment and eligibility.

2-31 CH-16
(13) Coordinated/Managed Care: Verification of eligibility will be conducted
according to the policies and procedures of the sponsoring
hospital/organization. Coast Guard facilities participating in
coordinated/managed care programs are considered, by that participation, to be
in compliance with the eligibility verification requirements of the DEERS
program for medical patients. Dental patients will still be subject to the above
checking requirements until a dental coordinated care program is established.
(14) Each clinic is required to perform a published number of checks each month.
These requirements are based on the outpatient visits of each clinic from the
previous year. Updated annual requirements will be published each January by
Commandant Notice.
c. How to check. DEERS checks for patient registration and eligibility can be done in a
number of ways. The following examples are the most common ways to verify
eligibility:
(1) Telephone-Based System. Eligibility checks are done by contacting DEERS
direct by telephone. Procedures for performing DEERS checks by telephone
are found in Figure 2-H-2.
(2) Computer Link Using the Coast Guard Standard Terminal. Procedures for
using the Standard Terminal are attached as Figure 2-H-3.
(3) DEERS-owned Computer and Software (On-Line) System. Procedures for
using DEERS-owned equipment are contained in DOD DEERS Eligibility
Inquiry/Nonavailability Statement Users Guide [Pub # UG 0100EL (series)].
(4) Use of PERSRU/Admin RAPIDS Terminals. Personnel in health care
facilities are discouraged from performing DEERS checks using the RAPIDS
terminal that may be available in their unit's Administration Office or
PERSRU. Using this resource places an unnecessary burden on the
PERSRU/Admin personnel, and using these terminals does not indicate that
the required medical checks are being accomplished.
d. How to request site-ID, data base access, or equipment.
(1) Site ID.
(a) Site ID numbers are assigned to a facility by the DOD DEERS Office.
These numbers are used to identify the origin of activity in the DEERS
system, and to generate reports of system activity. Site IDs are a
mandatory part of the initial request to access DEERS. The request form
is attached as Figure 2-H-4. Site IDs are permanent; they need not be
renewed.
(b) Health Care facilities requesting an initial Site ID, or changing the status
of their existing ID shall complete Section I of Figure 2-H-4 and forward,
via MLC (k), for further endorsement to:

CH-16 2-32
(c) Commandant (G-WKH-3)
U. S. Coast Guard
2100 Second St., SW.
Washington, DC 20593-0001
ATTN: DEERS MEDICAL PROJECT OFFICER
Telephone: (202) 267-0835
(2) Data Base Access.
(a) Authorization for individual access to DEERS is done by written request
from the clinic/unit Site Security Manager to the DEERS Security
Maintenance Office using the "Request for Data Base Additions,
Deletions, or Changes" form.
(b) Clinic personnel who should be considered for access to the DEERS
Data Base include those working in medical/ dental records,
appointments, pharmacy, patient affairs, and the health benefits advisor.
(c) Information available from the DEERS data base is subject to the
provisions of the Privacy Act.
(3) Equipment Requests or Changes.
(a) Telephone Access. Requests for access to DEERS via telephone is the
simplest and most user friendly means. This method is recommended for
facilities making fewer than 20 checks per day. Requests for initial
facility and personnel access is done by completing Figures 2-H-1 and 2-
H-4 and forwarding them to DEERS security via the MLC and
Commandant (G-WKH).
(b) Computer link using the Coast Guard Standard Terminal. Use of the
Standard Terminal, with the proper software emulation package installed,
allows facilities with a greater number of required checks to perform
those checks without making repeated telephone calls. Equipment
required includes a Standard Terminal workstation, Bell 212A
compatible modem, appropriate emulation software (VT 100), and an
outside commercial/FTS touch-tone telephone line. Facility requests for
access using this equipment is done by completing Figure 2-H-4 with an
attached statement that the facility has the appropriate hardware and
software as listed above. The facility must also state that it will be
responsible for any telephone charges incurred using this means of
access. Figure 2-H-5 lists complete equipment requirements.
(c) DEERS-owned computer hardware and software system. This top of the
line system features a direct, on-line, computerized link with the DEERS
data base. The minimum justification for requesting this equipment is
performing more than 100 DEERS checks per day. A limited number of
2-33 CH-16
Coast Guard health care facilities have this equipment. For further
information on this system, contact the Medical Project Officer at
Commandant (G-WKH-1).
5. Reports. No reports from field units documenting DEERS activity are required. Two
commonly generated reports concerning DEERS activity are described below:
a. Monthly Statistical Reports. Upon receipt from DEERS, Commandant (G-WKH)
will forward the Monthly Statistical Reports to each MLC (k). These reports list
DEERS activity for each clinic during the preceding month. Clinics may also use the
on-line statistical report screen to monitor its activity.
b. Field Representative Visit Report. These report the findings of each training visit by
the DEERS Field Representative to a clinic. These reports reflect the compliance of
the facility to DEERS requirements, and whether or not further training for facility
personnel is needed. Copies are provided to each MLC (k) and
Commandant (G-WKH).
6. Eligibility/Enrollment Questions, Fraud and Abuse.
a. Eligibility/Enrollment Questions: Beneficiaries of the military health care system,
including active duty and retired personnel, their dependents, and survivors must
provide positive proof of eligibility before being provided health care. Eligibility is
determined by (a) presenting a valid ID Card and (b) verifying enrollment and
eligibility in DEERS.
(1) If an individual presents an ID card that is no longer valid (expired), the
individual should be refused care and the ID card confiscated.
(2) If the individual has a valid ID card, but is not enrolled in DEERS, they should
be refused routine care, and referred to their sponsor and/or service ID card
activity to be enrolled in DEERS. Following enrollment into DEERS, the
patient may prove temporary eligibility (pending their enrollment showing up
in the DEERS computer) by presenting a certified copy of Application for
Uniformed Services Identification Card DD Form 1172 from the ID card
activity. Upon presenting of this DEERS enrollment verification, the
individual should be considered as fully eligible, and treatment provided.
b. Fraud and Abuse: If, in the process of verifying eligibility through DEERS, clinic
personnel have reason to believe the person requesting care is doing so even though
that person is no longer eligible (e.g. a divorced spouse with a valid ID card, but
DEERS shows NOT ELIGIBLE), care should be refused, and the details of the
situation should be reported to the appropriate personnel activity and investigation
office. Clinic personnel reporting suspected fraud should document as much
information about the individual as possible (name, former sponsor's name, SSN,
service and status, as well as the individual's current address and telephone number if
known). Do not attempt to confiscate the ID card, or in any way restrict the

CH-16 2-34
individual. Recovery of invalid or no-longer-appropriate ID cards is the
responsibility of the parent service's investigation/law enforcement personnel.
Reports of possible fraud should be reported to the command of the clinic, and to the
DEERS Support Office (DSO) in Monterey, CA at (408) 646-1010.
7. Denial of Nonemergency Health Care Benefits for Individuals Not Enrolled in Defense
Enrollment Eligibility Reporting System (DEERS).
a. Policy.
(1) All CONUS USMTFs will deny nonemergency health care to dependent
beneficiaries not enrolled in DEERS. The DOD considers USMTFs located in
Alaska, Hawaii, and Puerto Rico as being in CONUS. Patients presenting for
care are required to have a valid ID card in their possession and meet DEERS
enrollment requirements.
(2) This policy effects only the delivery of nonemergency health care. Under no
circumstances are Coast Guard health service personnel to deny emergency
medical care or attention because a patient is not enrolled in DEERS.
(3) Health service personnel in CGMTF's are to conduct the minimum eligibility
checks for their facility as set annually by Commandant (G-WKH-1).
Whenever possible, prospective checking should be accomplished soon enough
to allow for notifying the patient and correcting enrollment problems before a
scheduled appointment.
(4) Patients with valid ID cards, but not enrolled in DEERS, presenting for
nonemergency medical care at CGMTFs will be denied care and instructed to
seek proper enrollment through their cognizant personnel office.
(5) Patients who present for nonemergency treatment without a valid ID card and
are in the DEERS data base, will not be provided health care without first
providing a statement, signed by a verifying personnel officer indicating that
they are eligible and providing a reason why a valid ID card is not in their
possession. A copy of this statement will be maintained in the clinical record
until the individual's eligibility is determined.
(6) If the beneficiary presenting with or without an ID card is suspected of fraud,
refer the case to the district (ole) branch for appropriate investigation.
(7) Denial of health care benefits represents a serious application of new and
complex regulations. Under no circumstances will a person be denied care by
the clerk performing the initial eligibility check. The decision to deny care will
be made only by clinic administrative officers or by a responsible person so
designated in writing by the command.
8. DEERS Eligibility Overrides. The below listed situations will override DEERS data
which indicates that a patient is not enrolled or eligible. Unless otherwise stated, all
situations assume that the beneficiary possesses a valid ID card:
2-35 CH-16
a. Dependents Recently Becoming Eligible for Benefits. Patients who have become
eligible for benefits within the previous 120 days may be treated upon presentation of
a valid ID card. In the case of children under age 10, the parent's ID card may be
used. Examples of patients expected to fall under this provision are: spouses
recently married to sponsors, newly eligible step children, family members of
sponsors recently entering active duty status for a period over 30 days,
parents/parents-in-law, or divorced spouses (not remarried) recently determined to be
eligible. After 120 days, these beneficiaries will no longer be considered recent.
b. DD-1172. Application for Uniformed Services Identification Card form. The patient
presents an original or a copy of the DD-1172 used for DEERS enrollment and
possesses a valid ID card over 120 days old, but is not enrolled in DEERS. This
copy of the DD-1172 should be Certified to be a True Copy by the ID Card issuing
authority which prepared it. It should also contain a telephone number where the
certifying individual can be contacted for verification. The person conducting the
DEERS check shall contact the issuing personnel office to verify enrollment.
c. Sponsors Entering Active Duty Status for a Period of Greater than 30 days. If the
sponsor is a reservist or guardsman recently ordered to active duty for a period of
greater than 30 days, a copy of the active duty orders may be accepted as proof of
eligibility for up to 120 days after the beginning of the active duty period.
d. Newborns. Newborns will not be denied care for a period of one year after birth
provided the sponsor is DEERS enrolled and the parent accompanying the infant
presents with a valid ID card.
e. Ineligible due to ID Card Expiration. When the data base shows a patient to be
ineligible due to ID card expiration, care may be rendered as long as the patient has a
new ID card issued within the previous 120 days.
f. Sponsor's Duty Station is Outside the 50 United States with an FPO or APO address.
Dependents whose sponsors are assigned outside the 50 United States or to a duty
station with an APO or FPO address will not be denied care as long the sponsor is
enrolled in DEERS.
g. Survivors. In a small percentage of cases, deceased sponsors may not be enrolled in
DEERS. This situation will be evidenced when the MTF does an eligibility check on
the surviving beneficiary and does not find the sponsor enrolled or the survivor
appears as the sponsor. In either of these situations, if the survivor has a valid ID
card, he/she should be treated and referred to the local personnel support activity to
correct the DEERS data base. In some situations, surviving beneficiaries who are
receiving SBP annuities will be listed in DEERS as sponsor and will be found under
their own social security number. These are eligible beneficiaries and should be
treated.

CH-16 2-36
h. Foreign Military Personnel. Foreign military personnel assigned via the personnel
exchange program are eligible through public law or other current directives, though
not enrolled in DEERS they will be treated upon presentation of a valid ID card.
2-37 CH-16
Figure 2-H-2
TO: Security Maintenance Office
DEERS East Coast Center SITE ID: __ __ __ __ __ __ (DEERS)Date: __________________
1600 N. Beauregard St.(Fill in six digits)
Alexandria, VA 22311
SUBJECT: Request for Data Base Additions, Deletions, or Changes
FROM: Site Security Manager: _____ ________________________________ ________________ _____________________
Rank Name (Last, First MI) SSAN Title
Phone #: AV: ______________ COM: (_____)____________________
Request the indicated actions be taken for the following individuals:
Action
SSAN Name (Last, First, MI)Duty Location
(MTF Records, HBA, Etc.)
Action SSN name duty location
Add Delete Change
__________________________________________________________________________________________________________________
________________________________
Unit OPFAC Code: _____________________(Signature) _____________________________________
Base/Installation/Facility
Site Security Manager
• All Site Security Manager's mailing address changes should be entered in this space.
• All items must be completed. Omission of any items may prevent or delay the processing of this form.
CH-16 2-38
Figure 2-H-2 (con’d)
INSTRUCTIONS FOR DEERS TELEPHONE USERS
A. Telephone Users.
1. Provide your LOGON-ID and Password to the Eligibility Telephone Center operator at:
(800) 336-0289 or (800) 368-4416. The hours of operation are 0400-1700 (Pacific Time),
Mon-Fri.
2. Approximately every 30 days the Telephone Center operator will ask you to establish a
new password. At that time, you will provide the operator a new Password of 5 to 8
characters. It is very important that you remember the new Password you have chosen.
3. If you forget your password, the operator in the Telephone Center will refer you to the
Security Maintenance office at (703) 578-5306, or AUTOVON 289-1953. At this time,
you will be provided a Temporary Password, which you will then provide to the Eligibility
Telephone Center operator on your next inquiry call.
4. The Eligibility Telephone Center operator will enter this Temporary Password into the
operator's terminal and then ask for your new password (as in [2] above).
B. Telephone-Based System.
1. Telephone type. The telephone line used for eligibility checks is a rotary In-WATS
telephone system. A rotary system means that when one of the lines at the eligibility
center is not being used, the incoming call will automatically be transferred to that line. If
a busy signal on the rotary line is received, all lines at the eligibility center are being used.
If this happens, hang up and try again later.
a. Eligibility Check Procedure. When an eligibility center operator answers the
telephone, the following procedures to perform a patient's eligibility check will be
used:
b. Note: When calling, greet the operator and identify the center from where you are
calling.
(1) You will supply the following information to the operator:
(a) Site name and site security code, UCA code (from medical, dental, or
pharmacy)
(b) DEERS ID (an optional family member prefix and sponsor's Social
Security Number)
(c) Date of birth of beneficiary if known. If not known, then 999999
(d) FROM date (YYMMDD) of medical treatment

2-39 CH-16
Figure 2-H-2 (con’d)
(e) TO date (YYMMDD) of medical treatment
(2) The operator will then perform an eligibility inquiry.
(3) If the patient is found to be on file, the operator will indicate that the patient is
enrolled in DEERS and is/is not eligible. When checking eligibility for more
than one member of a family, each of the family members must be identified
individually.
(4) If the patient is not found on file, the operator will indicate that the patient does
not appear as enrolled in DEERS.
(5) The procedure is repeated until all patients have been checked, and then the
call is ended.
SAMPLE ELIGIBILITY CHECK CALL
The following is an example of DEERS Eligibility Center Telephone Inquiry format:
Operator: Good Morning - DEERS Eligibility Center - May I help you?
Inquirer: Good morning, this is Support Center Alameda, Security Code AC, UCA Code BA,
Site Code 10123, inquiring the eligibility of 123 45 6789. The date of birth is 560324.
This is a single beneficiary request.
Operator: (enters SSN, DOB, SC, UC, and SITE CODE) What period of eligibility do you wish
to check?
Inquirer: 801201 through 801215 (December 1 - 15, 1980)
Operator: The beneficiary is Jane Smith, and she is enrolled and eligible for the period
requested. Any more inquiries?
Inquirer: Not at this time. Thank you, good-bye.
Operator: Thank you for calling the DEERS Eligibility Center.

CH-16 2-40
Figure 2-H-3
PERFORMING DEERS CHECKS USING THE COAST GUARD STANDARD TERMINAL
Ref: (a) DEERS Users Guide (UG0100ELR5) of Oct 1987
1. At the Standard Terminal "Command Bar", Type VT100, (Go). If you don't have a
"Command Bar", see your computer System Manager.
2. To dial-up the DEERS microcomputer access, enter ATDT8,7033795860, then press
(Return). This command tells the modem to dial the DEERS access number, and should
result in a message reading "connect 1200" on your screen. This means your computer and
the one at DEERS are talking to on another.
3. Upon "handshake" with the DEERS computer, enter M (for Menu), then VT100 (return).
4. At Security Protection Screen, enter DEERS (Return). See also page 2-2 of reference (a).
5. At Transaction Code Screen, enter LOGN (Return). Also see page 2-3 of reference (a).
6. At Security Screen, enter your User ID in the "LOGON-ID" space, then press TAB. See
page 2-4 of reference (a).
7. Enter your personal password in the designated area, then press TAB. See page 2-4, Step 5
of reference (a).
8. Enter GIQD in the "TRAN ID" space, then press Return. See pages 2-4 and 5, steps 6 & 7
of reference (a).
9. At the Main Menu, select the desired activity. For Eligibility checks, see pages 4-1 through
4-19 of reference (a), or as follows:
10. In Activity Code (AC) space, no entry is necessary if you wish to make an eligibility check.
See page 4-11 of reference (a). Press "Tab" to continue.
11. Enter your 6 character Site ID, then press "Tab".
12. In "UC" block, enter BA for Ambulatory Medical Care checks, CA for Dental checks, DA
for Pharmacy checks, or FN for TRICARE/HBA checks, then press "Tab". See page 4-12
of reference (a) for other codes.
13. Enter Sponsor's SSN, then press "Tab".
14. Enter PATIENT's Date of Birth (DOB) in the following format: YYYYMMDD, then press
"Tab".
15. In "DDS" block, enter DEERS Dependent Suffix as follows:
01-19 Eligible Dependent Children
20 Sponsor
30-39 Spouse of Sponsor
40-44 Mother of Sponsor
45-49 Father of Sponsor
50-54 Mother-in-Law of Sponsor

2-41 CH-16
55-59 Father-in-Law of Sponsor
60-69 Other Eligible Dependents
70-74 Unknown by DEERS
75 DDS is unknown by Inquirer
98 Service Secretary Designee
NOTE
If the DDS code for sponsor (20) is used, only sponsor data will be displayed on the Eligibility
Inquiry and Family Display Screens.
In the Treatment Date block, if the treatment dates are not the current date, enter the correct
dates in YYYYMMDD format, then press Tab.
16. After completing the SITE, UC, SPON SSN, PAT DOB, and DDS fields, press the
ENTER/RETURN key. If there is a record on the data base with the same SSN and patient
DOB or a multiple DOB match and a single DDS match, the DEERS Eligibility Screen will
be redisplayed, showing the pertinent data on the patient in the lower portion of the screen.
17. Once patient eligibility has been verified, that patient's data can be cleared from the screen
by pressing Return.
18. To exit from the DEERS Eligibility Inquiry System:
a. Select the appropriate two-character code and enter it into the AC field. The codes are:
MM - DEERS Inquiry System Main Menu Screen
SO - Sign Off
(1) If the MM code is used to return to the Main Menu, enter 10 in the activity field to
Sign Off, then press Return.
b. Press, Enter (Return) when prompted by the sign-off screen.
c. When at the Original screen, enter +++ (return), then AT H (return). (Steps b and c
"hang up" the modem link/telephone connection with the DEERS computer)
d. Press, Finish to return to the Command Bar.

CH-16 2-42
Figure 2-H-4
SITE-ID INITIAL REQUEST (DEERS)
SECTION I. (To be completed by the base/installation/facility Site Security Manager).
A new Site-ID is requested__________(base name).
SERVICE/ORGANIZATION (Check X One)
Air Force = F ___DOD = D ___ NOAA = O ___
Army = A ___Marine Corps = M ___TRICARE = C ___
Coast Guard = P__Navy = N ___ Public Health = W ___
Other = X ___
TYPE OF FACILITY (CHECK X One) FACILITY SECTION (Check X One)
Dental Clinic = D ___AAFES = S ___ FINCTR W/Title III = FT ___
Health Clinic = M ___AQCESS = G __ Med/Dent Rec = R ___
Hospital = H ___ Army Fin Off = F ___Tumor Registry = T ___
Personnel Office = P __Civ Pers Office = C ___ Other = Z ___
OPFAC code is ____________
Sample: Full Mailing Address:
Commander Point of Contact (Title not person’s name)
Integrated Support Command New Orleans
Attn: Medical Records
4640 Urquhart St.
New Orleans, LA 70017-1010
** This line of address must include a location identifier. For example, "USCG Clinic"
is not acceptable; USCG Clinic New Orleans is acceptable.
Requested by (Rank/Name Signature) DATE:_______
(Telephone) Comm ( ) , FTS .
SECTIONS II/III. (To be completed by Service Project Officer)
Recommended by: (Rank/Name/Signature) Date: .
APPLICATIONS: (Check X One)
ACTUR ___ ARED ___ DOLI ___ OLGR ___ RAPIDS ___
AQUESS ___ DMRIS ___ GIQD ___ OLPU ___ Other ___
EQUIPMENT (Check X One) *Note: Justification must be attached if equipment is required.
CRT ___ RAPIDS ___ Telephone Center ___
Facility Equipment ___ Timeshare ___
III. 12-Month Workload: (A) Avg Admissions: ____, (B) Avg Outpat Visits: ___; (C) Dental: ___

2-43 CH-16
Figure 2-H-4 (con’d)
SECTIONS IV/V. (To be completed by DCSPO representative V.
Director, Benefits Policy Division Inpatient_________
DEERS and Central Systems Program Office Outpatient _______
Six Skyline Place Dental _______
5109 Leesburg Pike, Suite 502
Falls Church, VA 22041-3201
The applications above are correct (or changed as indicated), and the equipment is confirmed.
Eligibility checking requirements are in Section V. Issue Site-ID.
Director, Benefits Policy Division_____________________________Date:______________
SECTION VI. (To be completed by Security Maintenance, DEERS East Coast Center)
Entered on DEERS Site-ID File by (initials) DATE .
Site-ID: __ __ __ __ __ __
Field Service Region State or Country (OCONUS).

CH-16 2-44
Figure 2-H-5
DEFENSE ENROLLMENT ELIGIBILITY REPORTING SYSTEM (DEERS)
DIAL-UP ACCESS POLICY
MICROCOMPUTER ACCESS
DEERS can be accessed by telephone by using an IBM PC or AT compatible microcomputer, or
the Coast Guard Standard Terminal with the proper software emulation package installed. There
are four criteria for microcomputer access to DEERS:
1. Site must have access to an outside commercial touch-tone telephone line.
2. The modem connected to the computer must be Bell 212A compatible.
3. Individuals must have DEERS assigned user-IDs and passwords,
4. An asynchronous communication software package must be installed in the computer. The
most common software for the Standard Terminal is the VT-100 emulator.
An asynchronous dial-up environment is used to allow existing asynchronous terminals at
military installations to interface with DMSSCNET through a modem. The required modem
must be compatible with a Bell 212A capable for 300 or 1200 baud. This equipment will be
communicating with a Renex Converter at the DEERS offices. The display terminal should be
set up as follows:
1. Line width of 80 characters
2. 24 line screen height.
The asynchronous communications program should be configured as follows:
1. Baud rate of 300 or 1200.
2. Parity of EVEN or MARK
3. Stop bits of one (1)
4. Terminal emulation selections are listed on the Renex menu
5. Word length of seven (7)
The following telephone number is used to dial into the Renex converter box at DEERS. This
number has 16 trunk lines, and should normally be available:
(703) 379-5860

2-45 CH-16
Figure 2-H-5 (con’d)
ENSURING HANDSHAKE
The following criteria must be met during the interface test to ensure the handshake
(communication between your computer/modem and the DEERS system) is successful:
1. Verify correct hardware and software configuration
2. Conduct a dial-up test using the above telephone number
3. Perform system access procedures to display the DEERS sign-on screen
4. If any problems or questions arise during the initial setup and testing of equipment, call the
DMSSC Technical Support Group at (703) 578-5021, -22, or -23.
CH-16 2-46
Section I - Health Care Facility Definitions.
1. Coast Guard Facilities.
a. Clinic. A health care facility primarily intended to provide outpatient medical
service for ambulatory patients. A clinic must perform certain non-therapeutic
activities related to the health of the personnel which are necessary to support the
operational mission of the unit, such as physical examinations, immunizations,
medical administration, and preventive medical and sanitary measures. A clinic staff
consists of at least one permanently assigned medical officer and health services
technician. The staff may include dentists, nurses, pharmacists, physician assistants
and other specialists as required. A clinic may be equipped with beds for observation
of patients awaiting transfer to a hospital, and for overnight care of patients who do
not require complete hospital services (e.g., isolation of patients with communicable
diseases) if accredited for that purpose by an external accreditation agency
(JCAHO/AAAHC).
b. Satellite Facility. A health care facility which is administered by a Coast Guard
clinic but is located off-site from the clinic.
c. Dental Clinic. A facility at a Coast Guard unit for the dental care and treatment of
active duty personnel. Dental clinics are staffed with one or more dental officers and
health services technicians.
d. Sick Bay. A small medical treatment facility (afloat or ashore) normally staffed only
by health services technicians for the care and treatment of active duty personnel.
Civilian health care providers contracted to provide in-house services at these
facilities, like any facility, may provide care only within the scope of their contracts.
The fact that these civilian health care providers are on board will not change the
status of the medical facility.
e. Super Sickbay. An intermediate size medical care facility (ashore) intended to
provide outpatient medical care for active duty personnel. A super sickbay will
perform activities related to the health of the personnel, which are necessary to
support the operational missions of all units within AOR, such as physical
examinations, immunizations, medical administration, and preventive medical and
sanitary measures. A super sickbay staff will normally be staffed with one medical
officer and three or more health service technicians.
2. Department of Defense Medical Facilities.
a. Nomenclature and Definitions. There are three types of DOD fixed medical
treatment facilities medical centers, hospitals, and clinics. The nomenclature and
definitions applicable to the classification of these facilities, as set forth below, are
used by the Army, Navy, Air Force, and Marine Corps.
2-47 CH-16
(1) Medical Center. A medical center is a large hospital which has been designed,
staffed and equipped to provide health care for authorized personnel, including
a wide range of specialized and consultative support for all medical facilities
within the geographic area of responsibility and post graduate education in the
health professions.
(2) Hospital. A medical treatment facility capable of providing definitive inpatient
care. It is staffed and equipped to provide diagnostic and therapeutic services
in the field of general medicine and surgery, preventive medicine services, and
has the supporting facilities to perform its assigned mission and functions. A
hospital may, in addition, discharge the functions of a clinic.
(3) Clinic. A medical treatment facility primarily intended and appropriately
staffed and equipped to provide emergency treatment and outpatient services.
A clinic is also intended to perform certain non-therapeutic activities related to
the health of the personnel served, such as physical examinations and
preventive medicine services necessary to support a primary military mission.
A clinic may be equipped with beds for observation of patients awaiting
transfer to a hospital, and for care of cases which cannot be cared for on an
outpatient status, but which do not require hospitalization.
b. Primary Mission. The primary mission of Department of Defense medical facilities
is to provide adequate medical care for members of the uniformed services on active
duty.
3. Uniformed Services Treatment Facilities (USTFs).
a. Public Law 97-99 (1981) authorized several former USPHS hospitals (sometimes
called Jackson Amendment facilities) to provide health care to active duty and retired
members and their dependents. The law was modified in 1991 and the USTF
program was mandated to implement a managed care delivery and reimbursement
model in order to continue as part of the Military Health Services System (MHSS).
This managed care plan went into effect on October 1, 1993 and is called the
Uniformed Services Family Health Plan (USFHBP).
b. USFHBP is a health maintenance organization-type of plan exclusively for the
dependents of active duty, retirees and their dependents. Where available, the
USFHBP serves a defined population, through voluntary enrollment, and offers a
comprehensive benefit package. The capacity at USFHBP sites varies and is limited.
Beneficiaries enroll in the USFHBP during a yearly open season, and may disenroll
after one year. Enrollment is confirmed by each USFHP site. Those not accepted
during the open season may be enrolled as openings occur on a first come-first
served basis. USFHBP enrollees are not authorized to use the TRICARE
Program or the direct care system (DOD and Coast Guard health care/dental
facilities included) while enrolled in the USFHP.
c. Dependents and retirees who do not enroll in the USFHBP or who are denied
enrollment because the USFHBP is at capacity can only be treated at USTFs on a
CH-16 2-48
space-available and fee-for-service basis. All USTFs are required to be TRICARE
preferred providers.
d. Active duty personnel are not eligible to enroll in the USFHBP, however, they can
still be treated at USTFs under the following conditions:
(1) for emergency care,
(2) when referred by a military treatment facility, or
(3) when authorized by the cognizant MLC for non-emergent care.
e. When active duty care is rendered, the USTFs are not authorized to bill or collect
payment from active duty members, they must bill the Coast Guard instead.

2-49 CH-16
Section J - Policies and Procedures Required at Coast Guard Health Care Facilities.
1. Administrative Policies and Procedures. All facilities shall develop and maintain the
following written administrative policies and procedures which shall be reviewed
annually and updated as needed.
a. Standard Operating Procedure (SOP) defining objectives and policies for the facility.
b. Organizational Chart if there is a Health Services Division or Branch. The Health
Services Division/Branch or Medical Department should also be shown on the
command's organizational chart.
c. Clinic protocols, posted in the respective department, for pharmacy, medical
laboratory, and medical and dental radiology.
d. Notices posted in pharmacy and radiology advising female patients to notify
department personnel if they are or might be pregnant or breast feeding (pharmacy
only).
e. Written guidelines advising patients how to obtain after-hours emergency medical
and dental advice or care. These must be readily available and widely publicized
within the command and the local eligible beneficiary community.
f. Quality Assurance (QA) program guidelines including assignment of a QA
coordinator and QA focus group members in writing. The QA focus group shall
meet at least quarterly and maintain written minutes.
g. Guidelines for a patient advisory committee (PAC) comprised of representatives of
the health care facility and each major, identifiable, patient interest group. The PAC
shall meet periodically and maintain written minutes.
h. Persons authorized to deny care shall be so designated in writing by the command.
2. Operational Policies and Procedures. Facilities shall also develop and maintain the
following written operational policies and procedures. These require annual review and
signature by all health services personnel.
a. Emergency Situation Bill including Health Services Division response to fire,
earthquake, bomb threat, heavy weather, etc.
b. Health Services Emergency Response Protocols for suicide attempt/threat,
rape/sexual assault, family violence and medical emergencies in the dental clinic.
c. Protocol for managing after-hours emergencies. Clinics at accession points and at
Coast Guard units with on-base family housing shall maintain a 24-hour live watch
schedule.

CH-16 2-50
3. Patient Rights. Health care shall be delivered in a manner that protects the rights,
privacy and dignity of the patient. Sensitivity to patient needs and concerns will always
be a priority.
a. Clinics shall post the Patient Bill of Rights and Responsibilities poster in clear view
in all patient waiting and urgent care areas (see Figure 2-J-1). Copies are available
from Commandant (G-WKH-1).
b. Chaperones shall provide comfort and support to patients during exams or treatment.
All patients shall be informed of the availability of chaperones.
(1) Chaperones are defined as persons who attend patients during medical exams
or treatment. Chaperones shall be of the same gender as the patient being
examined. Any nursing staff member, HS or volunteer may serve as a
chaperone as part of their duties. The Chief, Health Services Division shall
ensure that chaperones have appropriate training or experience (such as Red
Cross Orientation/Training) to enable them to carry out their duties properly.
Although a patient's request for a family member or friend to be present during
examination may be honored, that person is not a substitute for a chaperone.
(2) Patients who request the presence of a chaperone shall have their request
honored unless, in the opinion of the medical officer, the risk to the chaperone
outweighs the benefit to the patient (e.g., during x-ray exposures).
(3) Female patients undergoing breast examination or genital/rectal examination or
treatment must have a chaperone present during the examination. Male
patients may have a chaperone present at the patient's request.
(4) If a provider thinks a chaperone is necessary, and the patient refuses to permit
the services of a chaperone, the provider must consider whether to perform the
examination or treatment or to refer the patient to another source of care.
(5) Clinics shall have a written policy for reporting any episode of alleged
misconduct during medical/dental examinations to the unit commanding
officer. Unit commanding officers shall investigate such complaints in
accordance with regulations.
c. Chief, health services division shall enforce the patient chaperone policy and ensure
chaperones are qualified to perform their duties.
d. Chief, health services division shall ensure that allegations of misconduct are
forwarded to the command in a timely manner.
e. Clinics shall ensure that patient educational materials concerning gender-related
health issues (PAP smears, cervical cancer, mammography and breast disease,
testicular and prostate cancer, etc.) are readily available.

2-51 CH-16
4. Health Care Provider Identification.
a. In accordance with the Patient Bill of Rights and Responsibilities, all patients have
the right to know the identity and the professional qualifications of any person
providing medical or dental care. The recent addition of Nurse Practitioners and
commissioned Physician Assistants to our health care staffs has increased the
chances of misidentification. Accordingly, health care providers shall introduce
themselves and state their professional qualifications (level of provider) at each
patient encounter.
b. The standard Coast Guard name tag does not reflect any information concerning the
professional qualifications of the health care provider. Additionally, the standard
Coast Guard name tag is often not visible to patients with poor eyesight, or it may be
hidden by the provider's smock or lab coat. In lieu of the standard Coast Guard name
tag, all health care providers, civilian and military, shall wear a specific health care
provider identification tag on their outer smock or lab coat when engaged in direct
patient care in Coast Guard Clinics and Dental Clinics. The health care provider
identification tag shall be worn above the right breast pocket (or equivalent). The
following criteria shall be used by local commands and clinics in manufacturing the
health care provider identification tags:
(1) Size. The identification tag shall be 1" high by 3" wide.
(2) Materials. Standard plastic name tag blanks which may be purchased locally or
from Government sources.
(3) Color. Standard Coast Guard blue or black with white lettering.
(4) Contents. The identification tag shall contain the following information:
(a) The rank, first initial, and last name shall be centered on the
identification name tag and placed on the top line.
(b) One of the following professional titles, or any other commonly
recognized professional name, centered below the name line.
Abbreviations shall not be used.
1 Physician
2 Dentist
3 Physician Assistant
4 Nurse Practitioner
5 Pharmacist
6 Physical Therapist

CH-16 2-52
7 Optometrist
8 Registered Nurse
9 Health Services Technician

2-53 CH-16

CH-16 2-54
Section K - General Standards of Care. Patients at Coast Guard clinics and sickbays shall be
treated in accordance with the following general standards of care:
1. Diagnosis and therapy shall be performed by a provider with appropriate credentials.
2. Diagnoses shall be based upon clinical findings and appropriate tests and procedures.
3. Treatment shall be consistent with the working diagnosis, and shall be based upon a
current treatment plan.
4. Treatment shall be rendered in a timely manner. Providers should use their professional
judgement in accounting for the specific needs of patients and military readiness
obligations while attempting to meet the following goals for timeliness:
a. Sick call – If provided, the patient should be triaged immediately and be seen based
on urgency of the condition. The patient should be advised of the wait time to be
seen and offered a later appointment if the condition does not warrant immediate
attention.
b. Acute Illness (medical) - The wait time should not exceed 1 day. The condition
must be addressed, not necessarily resolved, within this time frame.
c. Routine Visit (medical) - The wait time should not exceed 1 week.
d. Specialty Care (medical) - To be determined by the primary care manager making
the referral based on the nature of the care required and the acuteness of the injury,
condition, or illness, but should not exceed a wait time of 4 weeks to obtain the
necessary care.
e. Well Visit - The wait time should not exceed 4 weeks.
f. Urgent Care (dental) - The wait time should not exceed 1 day. The condition must
be addressed, not necessarily resolved, within this time frame.
g. Routine Visit (dental) - The wait time should not exceed 4 weeks.
h. Scheduled Appointment (medical or dental) - The wait time should not exceed 30
minutes of appointed time. This may sometimes be delayed by the need to address
prior scheduled patients, emergency care, or unforeseen military obligations.
i. Pharmacy - Prescription available within 30 minutes.
5. Treatment shall be provided using currently accepted clinical techniques.
6. Patients shall participate in deciding among treatment alternatives available to them.

CH-17
3-i
CHAPTER 3
PHYSICAL STANDARDS AND EXAMINATION
PAGE
SECTION A - ADMINISTRATIVE PROCEDURES.................................................................................................................. 1
APPLICABILITY OF PHYSICAL STANDARDS. ................................................................................................................... 1
PRESCRIBING OF PHYSICAL STANDARDS........................................................................................................................ 1
PURPOSE OF PHYSICAL STANDARDS. ............................................................................................................................... 1
APPLICATION OF PHYSICAL STANDARDS........................................................................................................................ 1
INTERPRETATION OF PHYSICAL STANDARDS ................................................................................................................ 2
DEFINITIONS OF TERMS USED IN THIS CHAPTER........................................................................................................... 2
REQUIRED PHYSICAL EXAMINATIONS AND THEIR TIME LIMITATIONS.................................................................. 2
WAIVER OF PHYSICAL STANDARDS.................................................................................................................................. 9
SUBSTITUTION OF PHYSICAL EXAMINATIONS............................................................................................................. 11
SECTION B - REPORTING, REVIEWING, RECOMMENDATIONS, AND ACTIONS TO BE TAKEN ON REPORTS
OF MEDICAL EXAMINATION (DD-2808) AND MEDICAL HISTORY (DD-2807-1)....................................................... 15
DD-2808 (REPORT OF MEDICAL EXAMINATION)........................................................................................................... 15
DD-2807-1 (REPORT OF MEDICAL HISTORY)................................................................................................................... 15
REVIEW AND ACTION ON FINDINGS AND RECOMMENDATIONS OF REPORT OF MEDICAL EXAMINATION
(DD-2808)................................................................................................................................................................................. 15
CORRECTION OF DEFECTS PRIOR TO OVERSEAS TRANSFER OR SEA DUTY DEPLOYMENT. ............................ 19
OBJECTION TO ASSUMPTION OF FITNESS FOR DUTY AT SEPARATION.................................................................. 20
SEPARATION NOT APPROPRIATE BY REASON OF PHYSICAL DISABILITY............................................................. 20
PROCEDURES FOR PHYSICAL DEFECTS FOUND PRIOR TO SEPARATION............................................................... 20
SECTION C - MEDICAL EXAMINATION TECHNIQUES AND LAB TESTING STANDARDS……………………… 25
SCOPE. ..................................................................................................................................................................................... 25
SPEECH IMPEDIMENT. ......................................................................................................................................................... 25
HEAD, FACE, NECK, AND SCALP....................................................................................................................................... 25
NOSE, SINUSES, MOUTH, AND THROAT .......................................................................................................................... 26
EARS (GENERAL) AND DRUMS ......................................................................................................................................... 26
EYES (GENERAL), OPHTHALMOSCOPIC, AND PUPILS.................................................................................................. 27
OCULAR MOTILITY .............................................................................................................................................................. 29
LUNGS AND CHEST .............................................................................................................................................................. 32
HEART AND VASCULAR SYSTEM..................................................................................................................................... 29
ABDOMEN AND VISERA...................................................................................................................................................... 35
ANUS AND RECTUM ............................................................................................................................................................ 35
ENDOCRINE SYSTEM ........................................................................................................................................................... 42
LUNGS AND CHEST .............................................................................................................................................................. 32
ANUS AND RECTUM............................................................................................................................................................. 35

CH-17 3-ii
ABDOMEN AND VISCERA ................................................................................................................................................... 35
GENITOURINARY SYSTEM ................................................................................................................................................. 35
EXTREMITIES......................................................................................................................................................................... 35
SPINE AND OTHER MUSCULOSKELETAL ....................................................................................................................... 38
IDENTIFYING BODY MARKS, SCARS, AND TATTOOS .................................................................................................. 39
NEUROLOGIC......................................................................................................................................................................... 39
PSYCHIATRIC......................................................................................................................................................................... 41
ENDOCRINE SYSTEM ........................................................................................................................................................... 42
DENTAL................................................................................................................................................................................... 42
LABORATORY FINDINGS .................................................................................................................................................... 43
HEIGHT, WEIGHT, AND BODY BUILD............................................................................................................................... 51
DISTANT VISUAL ACUITY AND OTHER EYE TESTS). ................................................................................................... 51
AUDIOMETER......................................................................................................................................................................... 62
PSYCHOLOGICAL AND PSYCHOMOTOR ......................................................................................................................... 62
SECTION D - PHYSICAL STANDARDS FOR ENLISTMENT, APPOINTMENT, AND INDUCTION. ................ 67
SCOPE. ..................................................................................................................................................................................... 67
APPLICABILITY AND RESPONSIBILITIES........................................................................................................................ 67
ABDOMINAL ORGANS AND GASTROINTESTINAL SYSTEM. ...................................................................................... 68
BLOOD AND BLOOD-FORMING TISSUE DISEASES........................................................................................................ 69
DENTAL................................................................................................................................................................................... 70
EARS......................................................................................................................................................................................... 70
HEARING................................................................................................................................................................................. 70
ENDOCRINE AND METABOLIC DISORDERS. .................................................................................................................. 71
UPPER EXTREMITIES............................................................................................................................................................ 71
LOWER EXTREMITIES.......................................................................................................................................................... 73
MISCELLANEOUS CONDITIONS OF THE EXTREMITIES............................................................................................... 74
EYES......................................................................................................................................................................................... 75
VISION. .................................................................................................................................................................................... 78
FEMALE GENITALIA............................................................................................................................................................. 79
MALE GENITALIA……………………………………………………………………………………………………………80
URINARY SYSTEM. ............................................................................................................................................................... 80
HEAD........................................................................................................................................................................................ 81
NECK........................................................................................................................................................................................ 81
HEART...................................................................................................................................................................................... 81
VASCULAR SYSTEM............................................................................................................................................................. 82
HEIGHT. ................................................................................................................................................................................... 83
WEIGHT. .................................................................................................................................................................................. 83
BODY BUILD. ......................................................................................................................................................................... 85
LUNGS, CHEST WALLS, PLEURA, AND MEDIASTINUM................................................................................................ 83
CH-17
3-iii
MOUTH. ................................................................................................................................................................................... 84
NOSE AND SINUSES.............................................................................................................................................................. 84
NEUROLOGICAL DISORDERS............................................................................................................................................. 85
DISORDERS WITH PSYCHOTIC FEATURES...................................................................................................................... 87
ANXIETY, SOMATOFORM, DISSOCIATIVE, OR FACTITIOUS DISORDERS................................................................ 87
PERSONALITY, CONDUCT AND BEHAVIOR DISORDERS............................................................................................ 88
PSYCHOSEXUAL CONDITIONS. ......................................................................................................................................... 88
SUBSTANCE MISUSE. ........................................................................................................................................................... 88
SKIN AND CELLULAR TISSUES.......................................................................................................................................... 89
SPINE AND SACROILIAC JOINTS. ...................................................................................................................................... 91
SYSTEMIC DISEASES............................................................................................................................................................ 92
GENERAL AND MISCELLANEOUS CONDITIONS AND DEFECTS................................................................................ 93
TUMORS AND MALIGNANT DISEASES. ........................................................................................................................... 94
MISCELLANEOUS.................................................................................................................................................................. 94
SECTION E - PHYSICAL STANDARDS FOR PROGRAMS LEADING TO COMMISSION........................................... 97
APPOINTMENT AS CADET, UNITED STATES COAST GUARD ACADEMY................................................................. 97
COMMISSIONING OF CADETS............................................................................................................................................ 98
ENROLLMENT AS AN OFFICER CANDIDATE. ................................................................................................................. 98
COMMISSIONING OF OFFICER CANDIDATES................................................................................................................. 99
DIRECT COMMISSION IN THE COAST GUARD RESERVE............................................................................................. 99
DIRECT COMMISSION OF LICENSED OFFICERS OF U. S. MERCHANT MARINE.................................................... 100
APPOINTMENT TO WARRANT GRADE........................................................................................................................... 100
SECTION F - PHYSICAL STANDARDS APPLICABLE TO ALL PERSONNEL (REGULAR AND RESERVE) FOR:
REENLISTMENT; ENLISTMENT OF PRIOR SERVICE USCG PERSONNEL; RETENTION; OVERSEAS DUTY;
AND SEA DUTY......................................................................................................................................................................... 101
GENERAL INSTRUCTIONS................................................................................................................................................. 101
USE OF LIST OF DISQUALIFYING CONDITIONS AND DEFECTS. .............................................................................. 101
HEAD AND NECK. ............................................................................................................................................................... 101
ESOPHAGUS, NOSE, PHARYNX, LARYNX, AND TRACHEA........................................................................................ 101
EYES....................................................................................................................................................................................... 102
EARS AND HEARING. ......................................................................................................................................................... 105
LUNGS AND CHEST WALL. ............................................................................................................................................... 105
HEART AND VASCULAR SYSTEM................................................................................................................................... 107
ABDOMEN AND GASTROINTESTINAL SYSTEM........................................................................................................... 109
ENDOCRINE AND METABOLIC CONDITIONS (DISEASES) ........................................................................................ 111
GENITOURINARY SYSTEM. .............................................................................................................................................. 112
EXTREMITIES....................................................................................................................................................................... 113
SPINE, SCAPULAE, RIBS, AND SACROILIAC JOINTS. .................................................................................................. 117
SKIN AND CELLULAR TISSUES........................................................................................................................................ 117
CH-17 3-iv
NEUROLOGICAL DISORDERS........................................................................................................................................... 119
PSYCHIATRIC DISORDERS. (SEE SECTION 5-B CONCERNING DISPOSITION) ....................................................... 120
DENTAL................................................................................................................................................................................. 121
BLOOD AND BLOOD-FORMING TISSUE DISEASES...................................................................................................... 121
SYSTEMIC DISEASES, GENERAL DEFECTS, AND MISCELLANEOUS CONDITIONS.............................................. 121
TUMORS AND MALIGNANT DISEASES. ......................................................................................................................... 123
SEXUALLY TRANSMITTED DISEASE.............................................................................................................................. 123
HUMAN IMMUNODEFFICIENCY VIRUS (HIV) ................................................................................................................ 123
TRANSPLANT RECIPIENT.................................................................................................................................................. 123
SECTION G - PHYSICAL STANDARDS FOR AVIATION................................................................................................. 127
CLASSIFICATION OF AVIATION PERSONNEL............................................................................................................... 127
GENERAL INSTRUCTIONS FOR AVIATION EXAMINATIONS..................................................................................... 127
RESTRICTIONS UNTIL PHYSICALLY QUALIFIED. ....................................................................................................... 133
STANDARDS FOR CLASS 1................................................................................................................................................ 134
STANDARDS FOR CLASS 1R. ............................................................................................................................................ 136
CANDIDATES FOR FLIGHT TRAINING............................................................................................................................ 136
REQUIREMENTS FOR CLASS 2 FLIGHT OFFICERS....................................................................................................... 138
REQUIREMENTS FOR CLASS 2 AIRCREW. ..................................................................................................................... 138
REQUIREMENTS FOR CLASS 2 MEDICAL PERSONNEL............................................................................................... 139
REQUIREMENTS FOR CLASS 2 TECHNICAL OBSERVERS. ......................................................................................... 139
REQUIREMENTS FOR CLASS 2 AIR TRAFFIC CONTROLLERS................................................................................... 139
REQUIREMENTS FOR LANDING SIGNAL OFFICER (LSO)........................................................................................... 140
CONTACT LENSES. ............................................................................................................................................................. 140
SECTION H - PHYSICAL EXAMINATIONS AND STANDARDS FOR DIVING DUTY................................................ 147
EXAMINATIONS. ................................................................................................................................................................. 147
STANDARDS......................................................................................................................................................................... 147

3-1 CH-17
CHAPTER 3. PHYSICAL STANDARDS AND EXAMINATIONS
Section A - Administrative Procedures.
1. Applicability of Physical Standards.
a. The provisions of this chapter apply to all personnel of the Coast Guard and Coast
Guard Reserve on active or inactive duty and to commissioned officers of the Public
Health Service assigned to active duty with the Coast Guard.
b. Members of the other Armed Forces assigned to the Coast Guard for duty are
governed by the applicable instructions of their parent Service for examination
standards and for administrative purposes.
2. Prescribing of Physical Standards.
Individuals to be enlisted, appointed, or commissioned in the Coast Guard or Coast
Guard Reserve must conform to the physical standards prescribed by the Commandant.
Separate standards are prescribed for various programs within the Service.
3. Purpose of Physical Standards.
Physical standards are established for uniformity in procuring and retaining personnel
who are physically fit and emotionally adaptable to military life. These standards are
subject to change at the Commandant's direction when the needs of the Coast Guard
dictate.
4. Application of Physical Standards.
a. Conformance with Physical Standards Mandatory. To determine physical fitness,
the applicant or member shall be physically examined and required to meet the
physical standards prescribed in this chapter for the program or specialty and grade
or rate involved. An examinee who does not meet the standards shall be
disqualified.
b. Evaluation of Physical Fitness. The applicant's total physical fitness shall be
carefully considered in relation to the character of the duties to that the individual
may be called upon to perform. Physical profiling is not a Coast Guard policy.
Members shall be considered fit for unrestricted worldwide duty when declared
physically qualified. The examiner must be aware of the different physical standards
for various programs. Care shall be taken to ensure an examinee is not disqualified
for minor deviations that are clearly of no future significance with regard to general
health, ability to serve, or to cause premature retirement for physical disability.
However, conditions that are likely to cause future disability or preclude completing
a military career of at least twenty years, whether by natural progression or by
recurrences, are also disqualifying. This policy shall be followed when an authentic
history of such a condition is established, even though clinical signs may not be
evident during the physical examination.

CH-17 3-2
5. Interpretation of Physical Standards. Examiners are expected to use discretion in
evaluating the degree of severity of any defect or disability. They are not authorized to
disregard defects or disabilities that are disqualifying in accordance with the standards
found in this chapter.
6. Definitions of Terms Used in this Chapter.
a. Officers. The term "officers" includes commissioned officers, warrant officers, and
commissioned officers of the Public Health Service.
b. Personnel. The term "personnel" includes members of the Coast Guard and Coast
Guard Reserve, and the PHS on active duty with the Coast Guard.
c. Medical and Dental Examiners. Medical and dental examiners are medical and
dental officers of the uniformed services, contract physicians and dentists, or civilian
physicians or dentists who have been specifically authorized to provide professional
services to the Coast Guard. Some USMTFs have qualified enlisted examiners who
also conduct medical examinations and their findings require countersignature by a
medical officer.
d. Flight Surgeons and Aviation Medical Officers. Officers of a uniformed service who
have been so designated because of special training.
e. Command/Unit. For administrative action required on the Report of Medical
Examination (DD-2808), the command/unit level is the unit performing personnel
accounting services for the individual being physically examined.
f. Reviewing Authority. Commander Coast Guard Personnel (CGPC-adm) and
MLC (K) are responsible for approval of physical examinations as outlined herein.
Clinic Administrators may act as reviewing authority for physical examinations
performed in their AOR as designated by the cognizant MLC, except for those that
are aviation or dive related. Reviewing authority shall not be delegated below the
HSC level. Medical Administrative Officers (LDO and CWO-Meds) may review
physical examinations performed by contract physicians and USMTFs within their
AOR.
g. Convening Authority. Convening Authority is an individual authorized to convene a
medical board as outlined in Physical Disability Evaluation System, COMDTINST
M1850.2 (series).
h. Time Limitation. The time limitation is the period for which the physical
examination remains valid to accomplish its required purpose. The time limitation
period begins as of the day after the physical examination is conducted.
7. Required Physical Examinations and Their Time Limitations.
a. Enlistment. A physical examination is required for original enlistment in the Coast
Guard and the Coast Guard Reserve. This physical examination will usually be
performed by Military Entrance Processing Stations (MEPS) and is valid for twenty-
3-3 CH-17
four months. Approved MEPS physicals do not require further review.
Recommendations noted on separation physical examinations from other services
must have been resolved with an indication that the individual meets the standards.
A certified copy of that physical examination must be reviewed and endorsed by the
reviewing authority Commander (CGRC). The reviewing authority must indicate
that the applicant meets the physical standards for enlistment in the USCG.
(1) Recruiters who believe that applicants have been erroneously physically
disqualified by MEPS, may submit the DD-2808 and DD-2807-1 (original or
clean copies) along with supporting medical records to Commander (CGRC)
for review.
(2) Waiver of physical standards for original enlistment may also be submitted as
above, and in accordance with paragraph 3-A-8 of this instruction.
(3) Separation physical examinations from any Armed Service may be used for
enlistment in the Coast Guard, provided the examination has been performed
within the last twelve (12) months. The physical examination must be as
complete as a MEPS exam, include an HIV antibody test date (within the last
24 months) and result, and a Type II dental examination. An DD-2807-1 must
also be included with elaboration of positive medical history in the remarks
section (item #25). Forward all documents for review by Commander
(CGRC).
(4) Prior Service enlisted aviation personnel must obtain an aviation physical
examination from a currently qualified uniformed services flight surgeon or
AMO within the previous 12 months. This physical examination will be
submitted with the rate determination package to Commander (CGRC).
(5) Occasionally, applicants for initial entry into the Coast Guard will need to be
examined at Coast Guard MTFs. In these cases, the physical examination will
be performed per section 3-C. The examining medical officer may defer item
#46 of the DD-2808 to the Reviewing Authority. Otherwise, the physical
standards for entry (sections 3-D and 3-E, as appropriate) must be meticulously
applied when completing this item. The completed DD-2808 and DD-2807-1
will be forwarded to the reviewing authority, Commander (CGRC).
b. Pre-Commissioning/Appointments. A physical examination is required within 12
months prior to original appointment as an officer in the Coast Guard or Coast Guard
Reserve for personnel in the following categories:
(1) appointment to Warrant Grade, except that physical examinations for members
of the Coast Guard Ready Reserve must be within 24 months prior to the date
of execution of the Acceptance and Oath of Office, form CG-9556.
(2) appointment of a Licensed Officer of the U. S. Merchant Marine as a
commissioned officer (examination required within 6 months); and
(3) upon graduation from the Coast Guard Academy.
c. Separation from Active Duty.
CH-17 3-4
(1) A complete physical examination is required within 12 months for retirement,
involuntary separation, or release from active duty (RELAD) into the Ready
Reserves (selected drilling or IRR). The physical examination shall follow the
guidelines set forth for quinquennial physicals.
(2) Other members separating from the Coast Guard e.g., discharge or transfer to
standby reserve (non-drilling) may request a medical and/or dental
examination. The medical examination must include: notation of any current
problems, a blood pressure measurement, and address items on the preventive
medicine stamp. In addition to the above, the practitioner shall ascertain the
health needs of the member and undertake measures deemed necessary to meet
those needs. The dental examination, if requested, must at least be a Type III
exam. These examinations may be annotated on a SF-600, and upon
completion, do not require approval.
(3) For members enrolled in the Occupational Medical Surveillance and
Evaluation Program (OMSEP), see chapter 12 of this Manual for guidance.
(4) See chapter 12 of the Personnel Manual, COMDTINST M1000.6(series), for
amplification on administrative discharge procedures.
d. Overseas Transfer, Sea Duty Deployment and Port Security Unit (PSU) Health
Screening. A modified physical examination, utilizing Figure 3-A-1, is required for
all personnel departing for an overseas assignment for 60 consecutive days or
greater, PCS transfer to an icebreaker, vessel deployment for 60 consecutive days or
or more (out of 365), and annually for PSU personnel. This will help identify and
resolve health related issues prior to transfer or deployment, if no significant medical
status changes have occurred. Members who are transferring from one overseas
assignment to another overseas assignment do not require another overseas physical
examination. The completed modified physical examination and a copy of the last
completed/approved Report of Physical Examination (DD-2808) and Report of
Medical History (DD-2807-1), shall be submitted to the Reviewing Authority. The
modified physical examination will include the following:
(1) a health history completed by the evaluee. (The evaluee will certify by
signature that all responses are true);
(2) documentation of the previous approved physical examination to include the
status of recommendations and summary of significant health changes;
(3) review of the health record to ensure routine health maintenance items are up-
to-date to include: routine gynecologic examinations, two pairs of glasses and
gas mask inserts for PSU personnel if required to correct refractive error, DNA
sampling, G-6-PD screening, immunizations, and a Type 2 dental examination;
(4) review malaria chemoprophylaxis, PPD, and special health concern
requirements. Contact the Center for Disease Control and Prevention (CDC) at
http://www.cdc.gov or http://www.travel.state.gov for information;

3-5 CH-17
(5) if PCS transferring to a foreign country [refer to 3-C.20.b(9)(b)], HIV antibody
test must have been conducted within the past 6 months with results noted
prior to transfer;
(6) if an evaluee is enrolled (or will be enrolled based on new assignment) in the
Occupational Medical Surveillance and Evaluation Program (OMSEP), ensure
appropriate periodic/basic examination is performed.
e. Applicant.
(1) Commissioning Programs. A physical examination is required for applicants
for entry into the Coast Guard as follows:
(a) Coast Guard Academy: DODMERB physical examination within 24
months;
(b) Officer Candidate School: MEPS physical within 24 months of entry
date, except:
1 Coast Guard personnel on active duty may obtain the physical
examination at a USMTF within 24 months of entry date, and
2 Members of other Armed Services may submit a physical
examination from a USMTF provided the examination has been
performed within the past twelve (12) months and is as complete as
a MEPS physical examination.
(c) Direct commission: MEPS physical within 24 months of entry date or
oath of office for Ready Reserve Direct Commission, except aviation
programs, where examination by a uniformed service flight surgeon or
AMO is required within 12 months of entry date.
(2) Aviation. An aviation physical examination is required for applicants for
training in all categories of aviation specialties. This physical examination is
valid for 24 months for Class II applicants and 12 months for pilot applicants.
(3) Diving. A physical examination is required for all applicants for duty
involving diving, and is valid for twelve months.
f. Pre-Training Screening Examinations. A screening examination is required within 1
week of reporting to the Coast Guard Academy, Officer Candidate School, Direct
Commission Officer orientation, or the Recruit Training Center. This screening
examination shall be sufficiently thorough to ensure that the person is free from
communicable and infectious diseases, and is physically qualified. The results of
this examination shall be recorded on an SF-600 and filed in the health record.
g. Retired Members Recalled to Active Duty. A physical examination is required for
retired personnel who are recalled to active duty. This physical examination is valid
for twelve months. A physical examination performed for retirement may be used

CH-17 3-6
for recall providing the date of recall is within six months of the date of the physical
examination.
h. Annual. An annual physical examination is required on all active duty personnel
who are 50 years of age or older and all air traffic controllers.
i. Biennial.
(1) Biennial physical examination is required every 2 years after initial
designation, until age 48, for the following:
(a) all aviation personnel (except air traffic controllers); and
(b) all Landing Signal Officers (LSO).
(2) The biennial exam will be performed within 90 days before the end of the birth
month. The period of validity of the biennial physical will be aligned with the
last day of the service member’s birth month. (Example: someone born on 3
October would have August, September, and October in which to accomplish
his/her physical. No matter when accomplished in that time frame, the period
of validity of that exam is until 31 October two years later.)
(3) This process of aligning the biennial exam with the birth month is a new
process effective immediately. In order to phase in this process the valid
period of future biennial exams may be extended up to a total of thirty months
(6 months from the current valid date) to align the valid date with the birth
month. (See Table 3-A-1).
(a) Example 1: A member with an October birth month accomplishes
biennial exam in May 2000 (previously valid until May 2002). Biennial
exam is now valid until October 2002 (29 months total) to allow the
member to align biennial exam with birth month.
(b) Example 2: A member with a June birth month accomplishes a biennial
exam in October of 1999 (previously valid until October 2001). Biennial
exam is now valid until June 2001 (20 months total) to allow the member
to align biennial exam with birth month.
(4) The requirement to perform a biennial exam will not be suspended in the event
of training exercises or deployment. Aircrew with scheduled deployment
during their 90 day window to accomplish their biennial exam may accomplish
their biennial exam an additional 90 days prior and continue with the same
valid end date. This may result in a member having a valid biennial for 30
months. Members unable to accomplish a biennial exam prior to being
deployed will be granted an additional 60 days upon return in which to
accomplish their physical. Align subsequent biennial exam with the aircrew
member’s birth month using Table 3-A-1.
(5) Additionally, a comprehensive physical may be required during a post-mishap
investigation, FEB, or as part of a work-up for a medical disqualification.
3-7 CH-17
(6) Personnel designated as aircrew are expected to maintain a biennial exam
schedule regardless of current aviation duty status.
Table-3-A-1
Number of months for which a biennial exam is valid
Month in which last biennial exam was given
Birth
Month JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DEC
JAN 24 23 22 21 20 19 30 29 28 27 26 25
FEB 25 24 23 22 21 20 19 30 29 28 27 26
MAR 26 25 24 23 22 21 20 19 30 29 28 27
APR 27 26 25 24 23 22 21 20 19 30 29 28
MAY 28 27 26 25 24 23 22 21 20 19 30 29
JUN 29 28 27 26 25 24 23 22 21 20 19 30
JUL 30 29 28 27 26 25 24 23 22 21 20 19
AUG 19 30 29 28 27 26 25 24 23 22 21 20
SEP 20 19 30 29 28 27 26 25 24 23 22 21
OCT 21 20 19 30 29 28 27 26 25 24 23 22
NOV 22 21 20 19 30 29 28 27 26 25 24 23
DEC 23 22 21 20 19 30 29 28 27 26 25 24
Notes:
Read down the left column to the examinee’s birth month; read across to month of last biennial
exam; intersection number is the maximum validity period. When last biennial exam was within
the 3 month period preceding the end of the birth month, the validity period will normally not
exceed 27 months. When the last biennial exam was for entry into aviation training, for FEB,
post-accident, post-hospitalization, etc., the validity period will range from 19 to 30 months.
Validity periods may be extended by 1 month only for completion of an examination begun
before the end of the birth month.
j. Quinquennial/Quinquennial Diving. A physical examination is required every five
(5) years after entry on all active duty personnel, age 25 through age 50, and for all
personnel maintaining a current diving qualification (also note "Diving" in item #5 of
DD-2808). Quinquennial physical examinations are also required for:
(1) all Selected Reservists within 30 days of their birth date starting at age 25
continuing until retirement, and
(2) reserve officers assigned to the Individual Ready Reserve (IRR) who are on a
promotion list.

CH-17 3-8
(3) Officers in 3-A-7.e.(1)(a) and (b) above must have a current approved physical
examination documented by PMIS data base entry prior to being promoted
(i.e., a quinquennial physical examination within the last 5 years).
k. Occupational Medical Surveillance and Evaluation Program (OMSEP). Those
individuals who are occupationally exposed to hazardous substances, physical
energies, or employed in designated occupations must undergo physical
examinations as required by Chapter 12 of this Manual.
l. Miscellaneous Physical Examinations.
(1) Retention. This examination is done at the direction of the commanding
officer when there is substantial doubt as to a member's physical or mental
fitness for duty.
(2) Pre-confinement Physical Screening. In general, personnel who are presented
for this screening, who do not require acute medical treatment or
hospitalization, are fit for confinement. Cases where a member requires more
than routine follow-up medical care, or has certain psychiatric conditions, that
may make them unfit for confinement, should be discussed with the chief
medical officer (or his/her representative) at the confining facility. Personnel
requiring detoxification for alcohol or drug dependency are not fit for
confinement; however, members that have been detoxified or that may require
rehabilitation alone are fit for confinement. This screening shall be recorded on
an SF-600 (per FIGURE 3-A-1) and, together with a copy of the last complete
and approved Report of Physical Examination (DD-2808) and Report of
Medical History (DD-2807-1), shall be submitted to the Reviewing Authority.
(3) Post Confinement Physical Examination. Ensure a separation physical
examination has been completed prior to the member departing the confining
facility. The separation physical shall meet the standards of section 3-F and
must be approved by the appropriate MLC(k).
(4) Reservists. A district commander may require any reservist attached to a
command within that area to undergo a complete physical examination if
reasonable doubt exists as to the reservist's physical or mental fitness for duty.
(5) Non-Fitness for Duty Determination Physical Examinations. The Chief of
Health Services retains the authority and responsibility to determine capability
and capacity to conduct non-fitness for duty physical examinations for all
eligible beneficiaries.
m. Annual Command Afloat Medical Screening. Officers and enlisted personnel
scheduled to assume command afloat shall undergo a medical screening prior to
assignment. The initial screening may be conducted by a medical officer where
applicable, or an HS not in the prospective chain of command of the member being
screened. Thereafter, all commanding officers and officers-in-charge of afloat units
will have an annual command afloat medical screening. This screening will also be
performed by a medical officer where available, otherwise, the screening may be
performed by a Health Services Technician who IS NOT in the chain of command of
3-9 CH-17
the person being screened. The screening process will include a medical history
completed by the member, a visual acuity check, blood pressure measurement, and a
thorough review of interval history in the member's health record. Results are to be
recorded using the format in Figure 3-A-2. The medical screening form (Figure 3-A-
2) and a copy of the last approved DD-2808 and DD-2807-1 shall then be forwarded
to the appropriate MLC (kma) for review. The MLC (kma) will approve or
disapprove the screening using section 3-F (retention standards) as the guiding
directive. If a question arises as to the fitness of the individual, the MLC (kma) may
request additional information from the examining unit. If the MLC (kma) is unable
to render a decision as to the fitness for command, the entire command afloat
screening package will be forwarded to Commandant (G-WKH) for final action.
The reviewed form shall be returned to the member's command for filing in the
member's health record.
n. Dental Examinations. Annual Type II dental examinations are required for all active
duty personnel assigned to commands collocated with dental examiners (i.e., Coast
Guard DOs, DOD DOs, or civilian contract dentists).
8. Waiver of Physical Standards.
a. Definition of Waiver. A waiver is an authorization to change a physical standard
when an individual does not meet the physical standards prescribed for the purpose
of the examination.
(1) Normally, a waiver will be granted when it is reasonably expected that the
individual will remain fit for duty and the waiver is in the best interests of the
Coast Guard. A service member will not be granted a waiver for a physical
disability determined to be not fit for duty by a physical evaluation board
approved by the Commandant. In these cases, the provisions for retention on
active duty contained in the Physical Disability Evaluation System,
COMDTINST M1850.2 (series), and the Personnel Manual, COMDTINST
M1000.6 (series) apply.
(2) If a member is under consideration by the physical disability evaluation
system, no medical waiver request shall be submitted for physical defects or
conditions described in the medical board. All waiver requests received for
conditions described in the medical board will be returned to the member's unit
without action.
(3) A waiver of a physical standard is not required in a case where a Service
member's ability to perform on duty has been reviewed through the physical
disability evaluation system and the approved finding of the Commandant is fit
for duty.
b. Authority for Waivers. Commander CGPC-epm (enlisted), CGPC-opm (officers),
and CGPC-rpm (reserve) have the sole authority to grant waivers. The decision to
authorize a waiver is based on many factors, including the recommendations of the
Chief, Office of Health and Safety; the best interest of the Service; and the

CH-17 3-10
individual's training, experience, and duty performance. Waivers are not normally
authorized but shall be reviewed by Commander (CGPC) for the following:
(1) original enlistment in the regular Coast Guard of personnel without prior
military service;
(2) appointment as a Cadet at the Coast Guard Academy; and
(3) training in any aviation or diving category specialty.
c. Types of Waivers.
(1) Temporary. A temporary waiver may be authorized when a physical defect or
condition is not stabilized and may either progressively increase or decrease in
severity. These waivers are authorized for a specific period of time and require
medical reevaluation prior to being extended.
(2) Permanent. A permanent waiver may be authorized when a defect or condition
is not normally subject to change or progressive deterioration, and it has been
clearly demonstrated that the condition does not impair the individual's ability
to perform general duty, or the requirements of a particular specialty, grade, or
rate.
d. Procedures for Recommending Waivers.
(1) Medical Officer. A medical officer who considers a defect disqualifying by
the standards, but not a disability for the purpose for which the physical
examination is required, shall:
(a) enter a detailed description of the defect in Item 77 of the DD-2808; and
(b) indicate that either a temporary or permanent waiver is recommended.
(2) Command/Unit Level. When the command receives a Report of Medical
Examination (DD-2808) indicating that an individual is not physically
qualified, the command shall inform the individual that he/she is not physically
qualified. The individual shall inform the command via letter of his/her
intentions to pursue a waiver. The medical officer is required to give a
recommendation on whether the waiver is appropriate and if the individual
may perform his/her duties with this physical defect. This recommendation
shall be completed on an (SF-502) Narrative Summary. A cover letter stating
the command's opinion as to the appropriateness of a waiver, the individual's
previous performance of duty, special skills, and any other pertinent
information, shall accompany the medical officers report. The waiver request
package shall be forwarded directly from the member's unit to Commander
CGPC-epm or opm, or Commandant (CGPC-rpm) as appropriate.
e. Command Action on Receipt of a Waiver Authorization. A command receiving
authorization from the Commander CGPC-epm/opm/rpm for the waiver of a
physical standard shall carefully review the information provided to determine any
duty limitation imposed and specific instructions for future medical evaluations.
3-11 CH-17
Unless otherwise indicated in the authorization, a waiver applies only to the specific
category or purpose for which the physical examination is required. A copy of the
waiver authorization shall be retained in both the service and health records for the
period for which the waiver is authorized. Copies of future DD-2808's for the same
purpose shall be endorsed to indicate a waiver is or was in effect.
9. Substitution of Physical Examinations.
a. Rule for Substitution of Physical Examinations. In certain circumstances, a physical
examination performed for one purpose or category may be substituted to meet
another requirement provided the following criteria are met:
(1) the examinee was physically qualified for the purpose of the previous
examination and all the required tests and recommendations have been
completed;
(2) the DD-2808 used for substitution bears an endorsement from the Reviewing
Authority or Commandant (G-WKH), as appropriate, indicating that the
examinee was qualified for the purpose of the previous examination;
(3) there has been no significant change in the examinee's medical status since the
previous examination;
(4) a review of the report of the previous examination indicates that the examinee
meets the physical standards of the present requirement;
(5) the date of the previous examination is within the validity period of the present
requirement; and
(6) all additional tests and procedures to meet the requirements of the current
physical examination have been completed.
b. No substitutions are authorized for the following physical examinations:
(1) enlistment;
(2) pre-training; and
(3) applicants for or designated personnel in special programs (aviation, diving,
Academy).
c. Procedures for Reporting Substitution. Substitutions of a physical examination shall
be reported by submitting a copy of the DD-2808 and DD-2807-1 being used to meet
the present requirements with the endorsement illustrated in FIGURE 3-A-1, parts A,
B, and C. Retain a copy of the substitution endorsement in the health record.

FIGURE 3-A-1 (revised 02/02)
MODIFIED PHYSICAL EXAMINATION FOR:
SUBSTITUTION/OVERSEAS ASSIGNMENT/SEA DUTY/PSU HEALTH SCREENING
This form is subject to the Privacy Act Statement of 1974.
A. EVALUEE DATA
LAST NAME - FIRST NAME - MIDDLE INITIAL RATE/RANK SOCIAL SECURITY NUMBER
UNIT EXAMINING FACILITY
PURPOSE OF EXAMINATION TRANSFER/DEPLOYMENT LOCATION DATE
B. HEALTH HISTORY (completed by examinee)
1. Would you say your health in general is: [ ] Excellent [ ] Good [ ] Fair [ ] Poor
2. Do you have any medical or dental problems or concerns? [ ] No [ ] Yes
3. Do you have any health related duty limitations? [ ] No [ ] Yes
4. Could you be pregnant? (females request HCG if needed) [ ] N/A [ ] Unknown [ ] No [ ] Yes
5. Are you taking prescription medications? (request refills if needed) [ ] No [ ] Yes
6. During the past year, have you sought or required counseling or mental health care? [ ] No [ ] Yes
7. Explain any "fair, poor, yes, or unknown" responses:__________________________________________________________________
______________________________________________________________________________________________________________
8. Have you been hospitalized since your last physical? Yes / No. If (Yes) explain._________________________________________
I certify that responses above are true: (signature of examinee)_______________________________________________
C. PHYSICAL EXAMINATION REVIEW (current approved physical examination required)
9. Date and type of current approved physical examination:________________________________________________________________
10. Status of recommendations or further specialist examination:____________________________________________________________
_________________________________________________________________________________________
11. Summary of significant health history since last physical examination:______________________________________________
_________________________________________________________________________________________
D. HEALTH RECORD REVIEW
12. Have routine gynecologic (pap) examinations been completed in past year? (females) [ ] N/A [ ] No [ ] Yes
13. Does examinee have two pair of glasses? (if required to correct refractive error) [ ] N/A [ ] No [ ] Yes
14. Does PSU examinee have a gas mask insert? (if required to correct refractive error) [ ] N/A [ ] No [ ] Yes
15. Has DNA sampling been completed and documented? (once per career) [ ] No [ ] Yes
16. Has G-6-PD screening been completed and documented? (once per career) [ ] No [ ] Yes
17. Are immunizations up-to-date and meet requirements for destination? [ ] No [ ] Yes
18. Has an HIV AB test been drawn in the past 6 months? (foreign country PCS only) [ ] N/A [ ] No [ ] Yes
19. Are malaria chemoprophylaxis, PPD, and special health concern requirements met? [ ] No [ ] Yes
Contact the Center for Disease Control and Prevention at http://www.cdc.gov for information.
20. Has a Type 2 dental examination been completed in the past year and is examinee "Class 1 or 2"? [ ] No [ ] Yes
21. Explain any "no" answers:_______________________________________________________________________________________
_________________________________________________________________________________________
E. SIGNATURE AND APPROVAL/DISAPPROVAL
Medical Officer signature/stamp:__________________________________________________________ Date:____________
Dental Officer signature/stamp:___________________________________________________________ Date:___________
_
[ ] Approved
Reviewing/approving authority:___________________________________________________________ [ ] Disapproved
CH-17 3-12

3-13 CH-17
FIGURE 3-A-2 (revised 2/99)
ANNUAL COMMAND AFLOAT MEDICAL SCREENING
Name:________________________________________ Rank/Grade:_________________
SSAN:_______________Date of Birth:_____________ Work Telephone: ____________
Unit OPFAC:__________ Unit Name: ______________ Date of Screening: ___________
To be completed by the member: (use reverse side as needed)
List any significant medical history since your last physical examination or
medical screening (describe any illnesses, injuries, etc.):____________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
Have you experienced any significant changes in stress level, mood,
or family life? YES NO
If yes, describe:____________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
Do you have any alcohol-related problems (including DWI)? YES NO
If yes, describe: ____________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
Are you presently taking any medication (including over-the-counter)? YES NO
If yes, list: ________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
The information I have provided above is complete and accurate.
___________________________________________Date:___________
(Signature of member)
________________________________________________________________________
The following section is to be completed by health services personnel:
______________________________________________________________________
Review of Health Record performed. Significant findings are:_________________________
___________________________________________________________________________
___________________________________________________________________________
Best Distant Visual Acuity (with correction, if required): R:_____________ L:____________
Sitting blood pressure:_________________ ________________
NOTE: ATTACH A COPY OF LAST APPROVED DD-2808 AND DD-2807-1
___________________________________ UNIT: ________________Date: ______________
(Signature/Title of medical reviewer)
___________________________________ Date: ________________
(Signature/MLC reviewer
CH-17 3-14
This Page Intentionally Left Blank
3-15 CH-17
Section B - Reporting, Reviewing, Recommendations, and Actions to be Taken on Reports of
Medical Examination (DD-2808) and Medical History (DD-2807-1).
1. DD-2808 (Report of Medical Examination).
a. DD-2808 (July 2001) is the proper form for reporting a complete physical
examination. DD-2808 revised (July 2001) is the newest version of the physical
examination report and can be obtained from the WKH-1 Publications and Directives
web site at http://www.uscg.mil/hq/G-W/g-wk/g-wkh/g-wkh-1/Pubs/Pubs.Direct.htm
or by http://www.dior.whs.mil/forms/DD2808.PDF directly from the DOD forms
web site.
b. Detailed instructions for the preparation and distribution of this form are contained in
section 4-B of this Manual.
2. DD-2807-1 (Report of Medical History).
a. DD-2807-1 (July 2001) is the proper form for reporting a member's medical history.
DD-2807-1 revised (July 2001)) is the newest version of the medical history report
and can be obtained from the WKH-1 Publications and Directives web site at
http://www.uscg.mil/hq/G-W/g-wk/g-wkh/g-wkh-1/Pubs/Pubs.Direct.htm or by
http://www.dior.whs.mil/forms/DD2807-1.PDF directly from the DOD forms web
site.
b. Detailed instructions on the preparation and distribution of this form are contained in
section 4-B of this Manual.
3. Review and Action on Findings and Recommendations of Report of Medical
Examination (DD-2808).
a. Action by the Medical Examiner.
(1) Review of Findings and Evaluation of Defects. When the results of all tests
have been received and evaluated, and all findings recorded, the examiner shall
consult the appropriate standards of this chapter to determine if any of the
defects noted are disqualifying for the purpose of the physical examination.
When physical defects are found that are not listed in the standards as
disqualifying, but that, in the examiner's opinion, would preclude the
individual from performing military service or the duties of the program for
which the physical examination was required, the examiner shall state that
opinion on the report indicating reasons. If in the examiner's opinion, a defect
listed as disqualifying is not disabling for military service, or a particular
program, the examiner shall indicate the basis for this opinion and recommend
a waiver in accordance with the provisions of section A of this chapter.
(2) Remediable Defects. When the physical examination of active duty personnel
indicates defects that are remediable or that may become potentially disabling
unless a specific medical program is followed, the examiner shall clearly state
any recommendations. If the examining facility has the capability of
correcting the defect or providing extended outpatient follow-up or medical

CH-17 3-16
care, tentative arrangements for care shall be scheduled, subject to the approval
of the examinee's command. If the examining facility does not have the
capabilities of providing the necessary care, tentative arrangements for
admission or appointment at another facility shall be scheduled, again subject
to the approval of the individual's command.
(3) Advising the Examinee. After completing the physical examination, the
medical examiner will advise the examinee concerning the findings of the
physical examination. At the same time, the examinee shall be informed that
the examiner is not an approving authority for the purpose of the examination
and that the findings must be approved by proper authorities.
(4) Disposition of Reports. The original DD-2808 and the original DD-2807-1,
together with any reports of consultations or special testing reports not entered
on the DD-2808 or DD-2807-1, shall be forwarded to the activity that referred
the individual for the physical examination.
b. Review and Action on Reports of Physical Examination by Command.
(1) Command Responsibility.
(a) The command has a major responsibility in ensuring the proper
performance of physical examinations on personnel assigned and that
physical examinations are scheduled sufficiently far in advance to permit
the review of the findings and correction of medical defects prior to the
effective date of the action for which the examination is required. The
command is also responsible to ensure that the individual complies with
the examiner's recommendations and to initiate any administrative action
required on a Report of Medical Examination.
(b) All DD-2808's shall be reviewed by commanding officers, or their
designee, to determine that the prescribed forms were used and that all
necessary entries were made.
(c) When the medical examiner recommends further tests or evaluation, or a
program of medical treatment (such as hearing conservation, periodic
blood pressure readings, etc.), the command will ensure that these tests
or examinations are completed or that the individual is directed to and
does comply with the recommended program. When a necessary test,
evaluation, or program can be completed within a 60 day period, the unit
may hold the DD-2808 to permit the forwarding of results. In all cases
the command shall endorse the DD-2808 to indicate what action has
been taken and forward the report to the reviewing authority if the 60
day period cannot be met or has elapsed.
(d) Disposition of Reports.
1 If a physical examination is accomplished for a purpose for which
the command has administrative action, the original DD-2808 and

3-17 CH-17
DD-2807-1 and a return self-addressed envelope shall be forwarded
to the reviewing authority. No action will be taken to accomplish
the purpose for which the physical examination was taken until the
endorsed original of the report is returned by the reviewing authority
indicating the examinee meets the physical standards for the purpose
of the examination.
2 Approved MEPS physicals do not require further review. The
original physical (DD-2808 and DD-2807-1) will be carried to the
training center by the individual.
3 If the physical examination is for a purpose requiring the consent or
approval of the MLC commander, or Commandant, the procedures
previously described for command review and action will be
accomplished, except rather than forwarding the report of the
examination directly to the reviewing authority, it will be included
with other supporting documents (letters, recommendations, etc.)
and forwarded through the chain of command.
4 Units not using a CGMTF shall send physical examinations to the
appropriate CG Clinic (as designated by the cognizant MLC), MLC
(k), or CGPC (adm) as appropriate.
c. Action by the Reviewing Authority.
(1) The Commandant is the final reviewing authority for all physical
examinations, except for applicants to the Coast Guard Academy.
(2) Administratively, MLC (k) acts as the reviewing authority for physical
examinations performed on personnel assigned to their Areas except as in (4)
and (5) below.
(3) Another exception to this rule pertains to those flight physicals performed on
aviation school students during training that are reviewed and approved by the
Navy Operational Medicine Institute (NOMI). NOMI, not MLC (k) will be the
approving authority for these physicals. CGPC will remain the waiver
approval authority for these physicals, when a waiver is required prior to final
approval. Upon completion of flight training and assignment to a Coast Guard
unit, the NOMI approved physical will be considered valid until the last day of
the member’s next birth month. The unit flight surgeon will clear the aviator
for all flight related duties based on the NOMI approved flight physical.
(4) Commander Coast Guard Personnel Command (CGPC-adm) is the reviewing
authority for aviator candidate, flight officer candidate, aircrew candidate, and
diving candidate physical examinations. Commandant (G-WKS) is also the
reviewing authority for OMSEP physical examinations. Commander (CGPC-
adm) shall review disapproved MEPS physicals to ensure proper application of
physical standards.

CH-17 3-18
(5) The Department of Defense Medical Examination Review Board (DoDMERB)
is the reviewing authority for physical examinations performed on Academy
applicants. MEPS is the reviewing authority for physical examinations
performed in their facilities.
(6) Each DD-2808 shall be carefully reviewed to determine whether the findings
reported indicate the examinee does or does not meet the appropriate physical
standards. If further medical evaluation is required to determine that the
examinee does meet the standards, or to resolve doubtful findings, the
reviewing authority shall direct the commanding officer or recruiting station to
obtain the evaluation and shall provide such assistance as may be required.
(7) The reviewing authority shall endorse the original of the DD-2808 indicating
whether the examinee does or does not meet the physical standards required.
If the examinee does not meet the physical standards, the endorsement shall
indicate the particular disqualifying defect or defects. Endorsements can be in
the format contained in FIGURE 3-B-1 or use of blocks #74.a, #77 and
signature in block #81.a, of the DD-2808.
(8) The endorsed original of the physical examination shall be forwarded to the
individual's unit for filing in the member's health record.
(9) Input of physical examination status of personnel into the PMIS system is
required. Reviewing Authorities shall collect and submit data regarding all
physical examinations/screenings (per paragraph 3-A-7, except subparagraph
3-A-7.f) they review to the appropriate PERSRU on a monthly basis. Data to
be collected for transmittal to the PERSRUs is as follows:
(a) Member's name;
(b) Member's rank/rate;
(c) Member's SSAN;
(d) Member's unit OPFAC;
(e) Date of physical examination;
(f) Purpose of examination;
(g) Date acted upon by Reviewing Authority; and
(h) Status code for physical examination. Status codes are
as follows:
1 Code A- member qualified for periodic (biennial, quinquennial, etc.)
physical examination.
2 Code D- member qualified for RELAD/discharge/retirement.

3-19 CH-17
3 Code O- member qualified for overseas duty.
4 Code N- member not physically qualified.
d. Disposition of Reports.
(1) When the individual meets the appropriate physical standards, forward the
physical examination as indicated in FIGURE 3-B-2.
(2) When the individual does not meet the appropriate physical standards and a
waiver has been recommended, endorse the physical examination and forward
it in accordance with section 3-A-8.
(3) When the individual is not physically qualified for the purpose of the
examination and a waiver is not recommended, the reviewing authority will
arrange for the examinee to be evaluated by a medical board and provide
administrative action as outlined in Physical Disability Evaluation System,
COMDTINST M1850.2(series).
4. Correction of Defects Prior to Overseas Transfer or Sea Duty Deployment.
a. Medical Defects. Before an individual departs for an overseas assignment for 60
consecutive days or greater days, to permanent assignment aboard a Polar
Icebreaker, or to a vessel deploying from its home port for 60 consecutive days or
greater, all remediable medical defects, such as hernias, pilonidal cysts or sinuses
requiring surgery, etc., must be corrected. Those defects that are not easily corrected
will be referred to Commander CGPC for consideration. These procedures also
apply to personnel presently assigned to such vessels. In these cases all necessary
corrective measures or waivers will be accomplished prior to the sailing date.
b. Dental Defects. All essential dental treatment shall be completed prior to overseas
transfer or sea duty deployment except those described in 4-C-3.c.(3)(b). Essential
dental treatment constitutes those procedures necessary to prevent disease and
disabilities of the jaw, teeth, and related structures. This includes extractions, simple
and compound restorations, and treatment for acute oral pathological conditions such
as Vincent's stomatitis, acute gingivitis, and similar conditions that could endanger
the health of the individual during a tour of duty. Missing teeth are to be replaced
when occluding tooth surfaces are so depleted that the individual cannot properly
masticate food. Elective dental procedures (those that may be deferred for up to
twelve months without jeopardizing the patient's health, i.e., Class II patient) need
not be completed prior to overseas transfer providing both of the following
conditions exist:
(1) completion of such elective procedures prior to transfer would delay the
planned transfer; and
(2) adequate Service dental facilities are available at the overseas base.
c. Vision Defects. A refraction shall be performed on all personnel whose visual acuity
is less than 20/20 in either eye (near or distant) or whose present eyewear
prescription does not correct their vision to 20/20. All personnel requiring glasses

CH-17 3-20
for correction shall have a minimum of two pair prior to overseas transfer or sea duty
deployment. All personnel requiring corrective lenses shall wear them for the
performance of duty.
5. Objection to Assumption of Fitness for Duty at Separation.
a. Any member undergoing separation from the service who disagrees with the
assumption of fitness for duty and claims to have a physical disability as defined in
section 2-A-38 of the Physical Disability Evaluation System, COMDTINST
M1850.2(series), shall submit written objections, within 10 days of signing the
Chronological Record of Service (CG-4057), to Commander CGPC. Such
objections based solely on items of medical history or physical findings will be
resolved at the local level. The member is responsible for submitting copies of the
following information along with the written objections:
(1) Report of Medical Examination (DD-2808);
(2) Report of Medical History (DD-2807-1);
(3) signed copy of the Chronological Record of Service (CG-4057);
(4) Appropriate consultations and reports; and
(5) "other pertinent documentation."
(6) The rebuttal is a member's responsibility and command endorsement is not
required.
b. The file shall contain thorough documentation of the physical examination findings,
particularly in those areas relating to the individual's objections. Consultations shall
be obtained to thoroughly evaluate all problems or objections the examinee indicates.
Consultations obtained at the examinee's own expense from a civilian source shall
also be included with the report.
c. Commander (CGPC) will evaluate each case and, based upon the information
submitted, take one of the following actions:
(1) find separation appropriate, in which case the individual will be so notified and
the normal separation process completed;
(2) find separation inappropriate, in which case the entire record will be returned
and appropriate action recommended; or
(3) request additional documentation before making a determination.
6. Separation Not Appropriate by Reason of Physical Disability. When a member has an
impairment (in accordance with section 3-F of this Manual) an Initial Medical Board
shall be convened only if the conditions listed in paragraph 2-C-2.(b), Physical
Disability Evaluation System, COMDTINST M1850.2(series), are also met. Otherwise
the member is suitable for separation.
7. Procedures for Physical Defects Found Prior to Separation.

3-21 CH-17
a. Policy. No person shall be separated from the Service with any disease in a
communicable state until either rendered noninfectious, or until suitable provisions
have been made for necessary treatment after separation.
b. Remediable Non-Disqualifying Defects. Remediable physical defects that would not
normally prevent the individual from performing the duties of grade or rate shall be
corrected only if there is reasonable assurance of complete recovery and sufficient
time remaining prior to separation.

CH-17 3-22
FIGURE 3-B-1
DATE REVIEWERS UNIT
Does/does not meet the physical standards for (title or category or purpose of examination), as
prescribed in (appropriate section of Medical Manual, COMDTINST M6000.1 (series)).
Disqualifying Defects:
Signature and Title of Reviewer

3-23 CH-17
FIGURE 3-B-2
Physical Exam
Purpose Note: Original
to: Reviewing
Authority:
Aviator Candidate (1,2) CGPC-opm CGPC-adm
Aircrew Candidate (1,2) CGPC-epm “
Diving Candidate (1,2) CGPC "
Enlistment (2) CGRC "
Flight Surgeon (FS) MLC (k) MLC (k)
FS Candidate (1) G-WKH-1 G-WKH-1
Aviator (1) MLC (k) MLC (k)
Aircrew (1) MLC (k) MLC (k)
Diving (1) MLC (k) MLC (k)
Flight Officer (1) MLC (k) MLC (k)
Annual (1) MLC (k) MLC (k)
LSO (1) or or
Quinquennial (1) Clinic Clinic
Overseas/Sea Duty (1) Administrator Administrator
Retention (1) " "
Retirement (1,4) " "
Involuntary
Separation (1,4) " "
RELAD (1,4) " "
Precom/Appts (1) " "
Direct Commission (1,5) CGRC CGPC-adm
OCS (1,5) CGRC CGPC-adm
Physician Assistant
Candidate (1,5) CGPC-opm CGPC-adm
NOTES:
CGRC address: CG Recruiting Command, 4200 Wilson Blvd., Suite 450, Arlington, VA. 22203-1804
(1) The reviewing authority shall review, endorse and return the original to the member's unit for filing in
the member's or applicant's health record.
(2) Forward the unendorsed physical to the appropriate Headquarters Office (as listed above) with the
application/training request package. That Office will forward the physical to Coast Guard Personnel
Command for review.
(3) Forward the original and one copy to Commandant (G-WKH) for review
(4) Ensure that a completed CG-4057 accompanies the completed DD-2808 and DD-2807-1.
(5) Reviewing authority for current USCG or USCGR members only. For all others, Note (2)
above applies. Forward a copy of the first/front page of the DD-2808 with endorsement to
the appropriate Headquarters office with the application package.
CH-17 3-24
This Page Intentionally Left Blank
3-25 CH-17
Section C - Medical Examination Techniques And Lab Testing Standards.
1. Scope.
This section is a medical examination technique guide applicable for all physical
examinations.
2. Speech Impediment.
Administer the "Reading Aloud Test" (RAT) as listed.
a. Have the examinee stand erect, face you across the room and read aloud, as if
confronting a class of students.
b. If the individual pauses, even momentarily, on any phrase or word, immediately and
sharply say, "What's that?", and require the examinee to start over again with the first
sentence of the test.
c. On the second trial, The person who truly stammers usually will halt again at the
same word phonetic combination often revealing serious stammering. Examinees
who fail to read the test without stammering after three attempts will be disqualified.
d. READING ALOUD TEST "You wished to know all about my grandfather. Well,
he is nearly 93 years old; he dresses himself in an ancient black frock coat usually
minus several buttons; yet he still thinks as swiftly as ever. A long, flowing beard
clings to his chin, giving those who observe him a pronounced feeling of the utmost
respect. When he speaks, his voice is just a bit cracked and quivers a trifle. Twice
each day he plays skillfully and with zest upon our small organ. Except in the winter
when the ooze or snow or ice is present, he slowly takes a short walk in the open air
each day. We have often urged him to walk more and smoke less, but he always
answers, 'Banana Oil.' Grandfather likes to be modern in his language."
3. Head, Face, Neck, and Scalp (Item 17 of DD-2808).
a. Head and Face. Carefully inspect and palpate the head and face for evidence of
injury, deformity, or tumor growth. Record all swollen glands, deformities, or
imperfections noted. Inquire into the cause of all scars and deformities. If a defect is
detected such as moderate or severe acne, cysts, or scarring, make a statement as to
whether this defect will interfere with wearing military clothing and equipment.
b. Neck. Carefully inspect and palpate for glandular enlargement, deformity, crepitus,
limitations of motion, and asymmetry; palpate the parotid and submaxillary regions,
the larynx for mobility and position, the thyroid for size and nodules, and the
supraclavicular areas for fullness and masses. If enlarged lymph nodes are detected
describe them in detail with a clinical opinion of their etiology.
c. Scalp. Examine for deformities such as depressions and exostosis.
CH-17 3-26
4. Nose, Sinuses, Mouth, and Throat (Item 19, 20 of DD-2808).
a. If there are no nasal or sinus complaints, simple anterior rhinoscopy will suffice,
provided that in this examination, the nasal mucous membrane, the septum, and the
turbinates appear normal. If the examinee has complaints, a more detailed
examination is required. Most commonly, these complaints are external nasal
deformity, nasal obstruction, partial or complete on one or both sides; nasal
discharge; postnasal discharge; sneezing; nasal bleeding; facial pain; and headaches.
b. Abnormalities in the mucous membrane in the region of the sinus ostia, the presence
of pus in specific areas, and the cytologic study of the secretions may provide
valuable information regarding the type and location of the sinus infection. Evaluate
tenderness over the sinuses by transillumination or x-ray. Examination for sinus
tenderness should include pressure applied over the anterior walls of the frontal
sinuses and the floors of these cavities and also pressure over the cheeks. Determine
if there is any tenderness to percussion beyond the boundaries (as determined by x-
ray) of the frontal sinuses. Note any sensory changes in the distribution of the supra-
orbital or infra-orbital nerves that may indicate the presence of neoplasm. Note any
external swelling of the forehead, orbit, cheek, and alveolar ridge.
c. Many systemic diseases manifest themselves as lesions of the mouth and tongue;
namely leukemia, syphilis, agranulocytosis, pemphigus, erythema multiform, and
dermatitis medicamentosa. Note any abnormalities or lesions on lips or buccal
mucous membrane, gums, tongue, palate, floor of mouth, and ostia of the salivary
ducts. Note the condition of the teeth. Pay particular attention to any abnormal
position, size, or the presence of tremors or paralysis of the tongue and the
movement of the soft palate on phonation.
d. Record any abnormal findings of the throat. If tonsils are enucleated, note possible
presence and position of residual or recurrent lymphoid tissue and the degree of
scarring. If tonsils are present, note size, presence of pus in crypts, and any
associated cervical lymphadenopathy. Note presence of exudate, ulceration, or
evidence of neoplasm on the posterior pharyngeal crypts. Describe any
hypertrophied lymphoid tissue on the posterior pharyngeal wall or in the lateral angle
of the pharynx and note if there is evidence of swelling that displaces the tonsils,
indicating possible neoplasm or abscess. Perform direct or indirect laryngoscopy if
the individual complains of hoarseness.
5. Ears (General) and Drums (Item 21, 22 of DD-2808). Inspect the auricle, the external
canal, and the tympanic membrane using a speculum and good light. Abnormalities
(congenital or acquired) in size, shape, or form of the auricles, canals, or tympanic
membranes must be noted, evaluated, and recorded.
a. Auricle. Note deformities, lacerations, ulcerations, and skin disease.
b. External canal. Note any abnormality of the size or shape of the canal and inspect
the skin to detect evidence of disease. If there is material in the canal, note whether
it is normal cerumen, foreign body, or exudate. Determine the source of any exudate

3-27 CH-17
in the canal. If this exudate has its origins in the middle ear, record whether it is
serous, purulent, sanguinous, or mucoid; whether it is foul smelling; and, whether it
is profuse or scanty.
c. Tympanic membrane. Remove all exudate and debris from the canal and tympanic
membrane before examination. Unless the canal is of abnormal shape, visualize the
entire tympanic membrane and note and record the following points.
(1) List any abnormality of the landmarks indicating scarring, retraction, bulging,
or inflammation.
(2) Note whether the tympanum is air containing.
(3) List any perforations, giving size and position, indicating whether they are
marginal or central, which quadrant is involved, and whether it is the flaccid or
the tense portion of the membrane that is included.
(4) Attempt, if the tympanic membrane is perforated, to determine the state of the
middle ear contents, particularly concerning hyperplastic tympanic mucosa,
granulation tissue, cholesteatoma, and bone necrosis. Do the pathological
changes indicate an acute or chronic process? This clinical objective
examination should permit evaluating the infectious process in the middle ear
and making a reasonably accurate statement regarding the chronicity of the
infection; the extent and type of involvement of the mastoid; the prognosis
regarding hearing; and, the type of treatment (medical or surgical) that is
required.
(5) Note, for all aviation and dive physical examinations, whether the examinee
can properly auto insufflate tympanic membrane.
6. Eyes (General), Ophthalmoscopic, and Pupils (Item 23, 24, 25 of DD-2808).
External and ophthalmoscopic examinations of the eyes are required on all
examinations. Contact lenses shall not be worn during any part of the eye examination,
including visual acuity testing. It is essential that such lenses not be worn for 72 hours
preceding examination. The strength of the contact that an examinee may possess shall
not be accepted as the refraction nor will it be entered as such in Item 60, DD-2808. The
general examination shall include the following specific points and checks:
a. General.
(1) Bony abnormality or facial asymmetry.
(2) Position of the eyes.
(3) Exophthalmus.
(4) Manifest deviation of the visual axis.
(5) Epiphora or discharge.
(6) Position of puncta or discharge when pressure exerted over lacrimal sac.
CH-17 3-28
b. Lids.
(1) Ptosis.
(2) Position of lashes, eversion or inversion.
(3) Inflammation of margins.
(4) Cysts or tumors.
c. Conjunctiva. Examine the palpebral and bulbar conjunctiva by:
(1) eversion of upper lid;
(2) depression and eversion of lower lid; and
(3) manually separating both lids.
d. Pupils.
(1) Size.
(2) Shape.
(3) Equality.
(4) Direct, consensual, and accommodative reactions.
e. Directly and obliquely examine the:
(1) Cornea. For clarity, discrete opacities, superficial or deep scarring, pannus,
vascularization, pterygium, and the integrity of the epithelium.
(2) Anterior Chamber. For depth, alteration of normal character of the aqueous
humor, and retained foreign bodies.
(3) Iris. For abnormalities and pathologic changes.
(4) Crystalline Lens. For clouding or opacities.
f. Ophthalmoscopic.
(1) Media. Examine with a plano ophthalmoscopic lens at a distance of
approximately 18 to 21 inches from the eye. Localize and describe any opacity
appearing in the red reflex or direct examination or on eye movement.
(2) Fundus. Examine with the strongest plus or weakest minus lens necessary to
bring optic nerve into sharp focus. Pay particular attention to the color,
surface, and margin of the optic nerve, also record any abnormality of the
pigmentation or vasculature of the retina.
(3) Macula. Examine for any change.

3-29 CH-17
7. Ocular Motility (Item 26 of DD-2808).
a. Ascertain the motility of the eyeballs by testing for binocular eye movement
(ductions and versions) in the cardinal positions of gaze. If any abnormalities are
suspected, verify with the cover/uncover test.
b. Observe if the eyes move together and whether there is loss of motion in any
direction (paralysis or paresis), or absence of muscle balance, whether latent
(heterophoria) or manifest (strabismus). Have the examinee look at a test object and
alternately cover and uncover one eye leaving the other uncovered and observe the
movement, if any, in each eye. In heterophoria movement occurs only in the eye that
is covered and uncovered; on being covered, it deviates and on being uncovered, it
swings back into place to take up fixation with the other eye that has remained
uncovered.
8. Heart and Vascular System (Item 27 of DD-2808).
a. General. In direct light, have the examinee stand at ease, with arms relaxed and
hanging by sides. Do not permit the examinee to move from side to side or twist to
assist in the examination, as these maneuvers may distort landmarks: and increase
muscular resistance of the chest wall. Examine the heart by the following methods:
inspection, palpation, auscultation, and when considered necessary, by mensuration.
b. Inspection. Begin from above and go downward, with special reference to the
following:
(1) any malformation that might change the normal relations of the heart;
(2) pulsations in the suprasternal notch and in the second interspaces to the right
and left of the sternum;
(3) character of the precordial impulse; or
(4) epigastric pulsations.
c. Palpation. First palpate to detect thrills over the carotids, thyroid glands,
suprasternal notch, apex of the heart, and at the base. Use palms of hands in
palpating and use light pressure, as hard pressure may obliterate a thrill. To locate
the maximum cardiac impulse, have the examinee stoop and throw the shoulders
slightly forward, thus bringing the heart into the closest possible relation with the
chest wall. Palpate both radial arteries at the same time for equality in rate and
volume. Run the finger along the artery to note any changes in its walls. Place the
palm of one hand over the heart and fingers of the other over the radial artery to see
if all ventricular contractions are transmitted. Palpate to determine the degree of
tension or compression of the pulse. In an estimate of pulse rate, the excitement of
undergoing a physical examination must be considered.
d. Auscultation. In auscultating the heart, bear in mind the four points where the
normal heart sounds are heard with maximum intensity:

CH-17 3-30
(1) Aortic area, second interspace to right of sternum. Here the second sound is
distinct.
(2) Tricuspid area, junction of the fifth right rib with the sternum. Here the first
sound is distinct.
(3) Pulmonic area, second interspace to left of sternum. Here the second sound is
most distinct.
(4) Mitral area, fifth interspace to left of sternum. Here the first sound is most
clearly heard.
e. Blood Pressure.
(1) Only the sitting blood pressure is required.
(2) Other positions required only if sitting blood pressure exceeds 159/90 (140/90
for aviation personnel).
(3) Take the sitting blood pressure with the examinee comfortably relaxed in a
sitting position with legs uncrossed and the arm placed on a rest at the
horizontal level of the heart. The condition of the arteries, the tenseness of the
pulse, and the degree of accentuation of the aortic second sound must be taken
into consideration, as well as the relation between the systolic and diastolic
pressure.
(4) Personnel recording blood pressure must be familiar with situations that result
in spurious elevation. A medical officer shall repeat the determination in
doubtful or abnormal cases and ensure that the proper recording technique was
used.
(5) Artificially high blood pressure may be observed as follows.
(a) If the compressive cuff is too loosely applied.
(b) If the compressive cuff is too small for the arm size. Cuff width should
be approximately one-half arm circumference. In a very large or very
heavily muscled individual, this may require an "oversize" cuff.
(c) If the blood pressure is repetitively taken before complete cuff deflation
occurs. Trapping of venous blood in the extremity results in a
progressive increase in recorded blood pressure.
(6) At least five minutes of rest should precede the blood pressure recording. Due
regard must be given to physiologic effects such as excitement, recent exercise,
smoking or caffeine within the preceding thirty minutes, and illness.
(7) No examinee shall be rejected based on the results of a single recording. If 2
out of the 3 positions exceed 159/90, the disqualifying blood pressures will be
rechecked for 3 consecutive days in the morning and afternoon of each day and
carefully recorded. The first determination shall be recorded in Item 58 and
the repeat determinations in Item 73 of DD-2808.

3-31 CH-17
(8) While emphasizing that a diagnosis of elevated blood pressure not be
prematurely made, it seems evident that a single "near normal" level does not
negate the significance of many elevated recordings.
f. Blood Pressure Determination.
(1) Use procedures recommended by the American Heart Association.
(2) Take the systolic reading as either the palpatory or auscultatory reading
depending on which is higher. In most normal subjects, the auscultatory
reading is slightly higher.
(3) Record diastolic pressure as the level at which the cardiac tones disappear by
auscultation. In a few normal subjects, particularly in thin individuals and
usually because of excessive stethoscope pressure, cardiac tones may be heard
to extremely low levels. In these instances, if the technique is correct and there
is no underlying valvular defect, a diastolic reading will be taken at the change
in tone.
(4) Note variations of blood pressures with the position change if there is a history
of syncope or symptoms to suggest postural hypertension.
(5) Obtain blood pressure in the legs when simultaneous palpation of the pulses in
upper and lower extremities reveals a discrepancy in pulse volume.
g. Pulse Rate.
(1) Determine the pulse rate immediately after the blood pressure. Only the sitting
position is required.
(2) In the presence of a relevant history, arrhythmia, or a pulse of less than 50 or
over 100, all pulses shall be determined and an electrocardiogram obtained.
h. Interpretation of Abnormal Signs and Symptoms. The excitement of the
examination may produce violent and rapid heart action often associated with a
transient systolic murmur. Such conditions may erroneously be attributed to the
effects of exertion; they usually disappear promptly in the recumbent posture. Try to
recognize the excitable individuals and take measures to eliminate psychic influences
from the test.
i. Hypertrophy-Dilitation. An apex beat located at or beyond the left nipple line, or
below the sixth rib, suggests an enlargement sufficient to disqualify for military
service. Its cause, either valvular disease or hypertension in the majority of cases,
should be sought. A horizontal position of the heart must be distinguished from left
ventricular enlargement. EKG, ultrasound studies, fluoroscopy, and chest x-ray may
be indicated for diagnosis.
j. Physiological Murmurs. Cardiac murmurs are the most certain physical signs by
which valvular disease may be recognized and its location determined. The
discovery of any murmur demands diligent search for other evidence of heart

CH-17 3-32
disease. Murmurs may occur, however, in the absence of valvular lesions or other
cardiac disease. Such physiological murmurs are not causes for rejection.
(1) Characteristics. The following characteristics of physiological murmurs will
help differentiate them from organic murmurs.
(a) They are always systolic in time.
(b) They are usually heard over a small area, the most common place being
over the pulmonic valve and mitral valve.
(c) They change with position of the body, disappearing in certain positions.
They are loudest usually in the recumbent position and are sometimes
heard only in that position.
(d) They are transient in character, frequently disappearing after exercise.
(e) They are usually short, rarely occupying all of the systole, and are soft
and of blowing quality.
(f) There is no evidence of heart disease or cardiac enlargement.
(2) Most Common Types. The most common types of physiological murmurs are:
(a) Those heard over the second and third left interspaces during expiration,
disappearing during forced inspiration. These are particularly common
in individuals with flexible chests, who can produce extreme forced
expiration. Under such circumstances, murmurs may be associated with
a vibratory thrust.
(b) Cardio-respiratory murmurs caused by movements of the heart against
air in a part of the lung overlapping the heart. They usually vary in
different phases of respiration and at times disappear completely when
the breath is held.
(c) Prolongations of the apical first sound, that are often mistaken for
murmurs.
(3) Diagnosis. An EKG, chest x-ray, and echocardiogram are usually indicated to
firmly establish the true cause of a murmur and should be done if there is any
question of abnormality.
k. Electrocardiograms. Use standard positions for precordial leads when completing
electrocardiograms.
9. Lungs and Chest (Item 28 of DD-2808).
a. A thorough examination includes a complete history (DD-2807-1) careful physical
examination, and necessary x-ray and laboratory studies. In screening examinations,
3-33 CH-17
the history and x-ray studies are the most immediately revealing examination
techniques.
b. Remember that several disqualifying diseases such as tuberculosis and sarcoidosis
may not be detectable by physical examination and the absence of abnormal physical
signs does not rule out disqualifying pulmonary disease. Such diseases, as well as
others (neopasms and fungus infections), may be detected only by chest x-ray.
(1) Conduct the physical examination in a thorough, systematic fashion. Take
particular care to detect pectus abnormalities, kyphosis, scoliosis, wheezing,
persistent rhonchi, basilar rales, digital clubbing, and cyanosis. Any of these
findings require additional intensive inquiry into the patient's history if subtle
functional abnormalities or mild asthma, bronchitis, or bronchiectasis are to be
suspected and evaluated. The physical examination shall include the
following.
(a) Inspection. The examinee should be seated in a comfortable, relaxed
position with the direct light falling upon the chest. Careful comparison
of the findings elicited over symmetrical areas on the two sides of the
chest gives the most accurate information regarding condition of the
underlying structures. Observe for asymmetry of the thoracic cage,
abnormal pulsation, atrophy of the shoulder girdle or pectoral muscles,
limited or lagging expansion on forced inspiration. The large, rounded
relatively immobile "barrel" chest suggests pulmonary emphysema.
(b) Palpation.
1 Observe for tumors of the breast or thoracic wall, enlarged cervical,
supraclavicular, or axillary lymph nodes, suprasternal notch, and
thrills associated with respiration or the cardiac cycle.
2 In addition to the breast examinations with periodic physical
examinations, an annual clinical breast examination is required for
all active duty females aged 40 and above. Monthly self-
examination is recommended for all adult female patients.
(c) Auscultation. Instruct the examinee to breathe freely but deeply through
the mouth. Listen to an entire respiratory cycle before moving the
stethoscope bell to another area. Note wheezing, rales, or friction rubs.
Compare the pitch and intensity of breath sounds heard over symmetrical
areas of the two lungs. Instruct the examinee to exhale during this
process. Note any rales, paying particular attention to moist rales that
"break" with the cough or fine rales heard at the beginning of inspiration
immediately after cough.
(2) Do not hesitate to expand the history if abnormalities are detected during
examination or in repeating the examination if chest film abnormalities are
detected.

CH-17 3-34
c. There are three conditions that are most often inadequately evaluated and result in
unnecessary and avoidable expense and time loss. These three are asthma (to
include "asthmatic bronchitis"), bronchiectasis, and tuberculosis.
(1) Asthma. In evaluating asthma, a careful history is of prime importance since
this condition is characteristically intermittent and may be absent at the time of
examination. Careful attention to a history of episodic wheezing with or
without accompanying respiratory infection is essential. If documentation of
asthma after age 12 is obtained from the evaluee's physician, this shall result in
rejection even though physical examination is normal. Ask about the use of
prescription or over-the-counter bronchodilators.
(2) Bronchiectasis. Individuals who report a history of frequent respiratory
infections accompanied by purulent sputum or multiple episodes of pneumonia
should be suspected of bronchiectasis. This diagnosis can be further supported
by a finding of post-tussive rales at one or both bases posteriorly or by a
finding of lacy densities at the lung base on the chest film. If bronchiectasis is
considered on the basis of history, medical findings or chest film
abnormalities, seek confirmatory opinion from the examinee's personal
physician or refer the examinee to the appropriate chest consultant for
evaluation and recommendations.
(3) Tuberculosis (TB).
(a) Active TB is often asymptomatic and not accompanied by abnormal
physical findings unless the disease is advanced. If only such
manifestations as hemoptysis or draining sinuses are looked for, most
cases of TB will be missed.
(b) The most sensitive tool for detecting early TB is the PPD.
(c) If positive, evaluate the chest film for any infiltrate, cavity, or nodular
lesion involving the apical or posterior segments of an upper lobe or
superior segment of a lower lobe. Many tuberculosis lesions may be
partially hidden or obscured by the clavicles. When any suspicion of an
apical abnormality exists, an apical lordotic view must be obtained for
clarification.
(d) It is neither practical nor possible, in most instances, to determine
whether or not a TB lesion is inactive on the basis of a single radiologic
examination. Therefore, refer any examinee suspected of TB to a chest
consultant or to an appropriate public health clinic for evaluation.
(e) An initial PPD is mandatory and shall be made a part of the physical
examination for all personnel entering on active duty for a period of 30
days or more.
(f) See Chapter 7 for complete details of the Tuberculosis Control Program.
3-35 CH-17
10. Anus and Rectum (Item 30 of DD-2808). All examinations shall include a visual
inspection of the anus. Perform a digital rectal examination and test for fecal occult
blood on all personnel beginning at age 40 and at any time history or physical exam
findings indicate. When anorectal disease is suspected a complete exam should be
performed which may include proctosigmoidoscopy as indicated.
11. Abdomen and Viscera (Item 31 of DD-2808).
a. Examine the abdomen with the examinee supine, as well as standing to detect
hernias.
b. Use appropriate clinical laboratory, radiologic, and endoscopic examinations to
confirm a diagnosis.
12. Genitourinary System (Item 32 of DD-2808).
a. General. All physical examinations shall search for evidence of STD or
malformation.
b. Instructions for examination according to sex.
(1) Females. The examination shall include:
(a) inspection of the external genitalia;
(b) either a vaginal or rectal bimanual palpation of the pelvic organs; and
(c) Papanicolaou (PAP) testing and visualization of the cervix and vaginal
canal by speculum in accordance with section 3-C-20.f.
(2) Males. The glans penis and corona will be exposed. The testes and scrotal
contents will be palpated and the inguinal lymph nodes will be examined for
abnormalities. Palpate the inguinal canals while having the patient perform a
valsalva.
13. Extremities (Item 33, 34, 35 of DD-2808). Carefully examine the extremities for
deformities, old fractures and dislocations, amputations, partially flexed or ankylosed
joints, impaired functions of any degree, varicose veins, and edema. In general the
examination shall include:
a. Elbow. With the examinee holding the upper arms against the body with the
forearms extended and fully supinated, observe for the presence of normal carrying
angle. Have the examinee flex the elbows to a right angle and keeping the elbows
against the body, note ability to fully supinate and pronate the forearms. Test medial
and lateral stability by placing varus and valgus strain on the joint with the elbow
extended. Test the power of the flexor, extensor, supinator, and pronator muscles by
having the examinee contract these muscles against manual resistance. If indicated,
x-rays should include antero-posterior and lateral views.
b. Foot.

CH-17 3-36
(1) Examine the feet for conditions such as flatfoot, corns, ingrown nails, bunions,
deformed or missing toes, hyperhidrosis, color changes, and clubfoot.
(2) When any degree of flatfoot is found, test the strength of the feet by requiring
the examinee to hop on the toes of each foot for a sufficient time and by
requiring the examinee to alight on the toes after jumping up several times. To
distinguish between disqualifying and nondisqualifying degrees of flatfoot,
consider the extent, impairment of function, appearance in uniform, and
presence or absence of symptoms. Remember, it is usually not the flatfoot
condition itself that causes symptoms but an earlier state in which the arches
are collapsing and the various structures are undergoing readjustment of their
relationships. Report angles of excursion or limitation; comparative
measurements; use of orthotics or other supports; and x-ray results if indicated.
c. Hip.
(1) With the examinee standing, observe the symmetry of the buttocks, the
intergluteal clefts, and infragluteal fold. Palpate the iliac crest and greater
trochanters for symmetry.
(2) If abnormalities are suspected, have the examinee stand first on one foot and
then the other, flexing the nonweight bearing hip and knee and observing for
ability to balance as well as for instability of the joint, as indicated by dropping
downward of the buttock and pelvis of the flexed (non-weight bearing) hip.
Such a positive Trendelenburg sign necessitates x-ray evaluation.
(3) While supine have the examinee flex the hip, abduct and adduct the hip and
rotate the leg inward. Observe for hesitancy in performing these motions,
incomplete range of motion, or facial evidence of pain on motion. Test muscle
strength in each position.
(4) With examinee prone, test for ability to extend each leg with knee extended
and test for power in each hip in extension.
(5) If abnormalities are detected requiring x-rays, obtain an antero-posterior and a
lateral view of each hip for comparison.
d. Knee.
(1) With trousers (skirt/dress), shoes, and socks removed, observe general
muscular development of legs, particularly the thigh musculature.
(2) Have examinee squat, sitting on heels, and observe for hesitancy, weakness,
and presence or absence of pain or crepitus.
(3) With examinee sitting, test for ability to fully extend the knee and test power in
extension by applying pressure to the lower leg with knee extended. Compare
equality of power in each leg. With knee flexed, test for hamstring power by
attempting to pull leg into extension; compare equality of strength in each leg.
Palpate entire knee for tenderness. With examinee still sitting on the table
edge, sit and grasp the heel between the knees; then test for cruciate ligament

3-37 CH-17
stability by first pulling the tibia anteriorly on the femur and by then pushing
the tibia posteriorly on the femur ("Drawer Sign").
(4) With the examinee supine, mark on each leg a distance of 1 inch above the
patella and 6 inches above the patella, making sure this is done with muscles
relaxed. Measure circumferences at these levels and note presence or absence
of atrophy. Test the medial and lateral collateral ligaments by placing varus
and valgus strain on the extended knee. Manipulate the knee through a
complete range of flexion and extension, noting any difference between the
sides and any abnormal restriction.
(5) If there is a history of knee injury assess muscular strength, ligamentous
stability, and range of motion. Also look for evidence of inflammatory or
degenerative processes.
(6) In the presence of any history of "locking," recurrent effusion, or instability, or
when atrophy measured is more than 3/8 inch or when limitation of motion or
ligamentous instability is detected, obtain x-rays including an antero-posterior,
lateral, and intercondylar view.
(7) An orthopedic evaluation is required on all recruit physicals if there is
evidence of any abnormality.
e. Shoulder.
(1) With the examinee stripped to the waist, inspect both anteriorly and posteriorly
for asymmetry, abnormal configuration, or muscle atrophy.
(2) From the back, with the examinee standing, observe the scapulohumeral
rhythm as the arms are elevated from the sides directly overhead, carrying the
arms up laterally. Any arrhythmia may indicate shoulder joint abnormality and
is cause for particularly careful examination. Palpate the shoulders for
tenderness and test range of motion in flexion, extension, abduction, and
rotation. Compare each shoulder in this respect.
(3) Test muscle power of abductors, flexors, and extensors of the shoulder, as well
as power in internal and external rotation. Have the examinee attempt to lift a
heavy weight with arms at the side to establish integrity of the
acromioclavicular joint.
f. Wrist and Hand.
(1) Palpate the wrist for tenderness in the anatomical snuff box often present in
undiscovered fractures of the carpal navicular. Observe and compare muscle
strength and range of motion, flexion, extension, radial, and ulnar deviation.
(2) Inspect the palms and extended fingers for excessive perspiration, abnormal
color or appearance, and tremor, indicating possible underlying organic
disease.
(3) Have the examinee flex and extend the fingers making sure interphalangeal
joints flex to allow the finger tips to touch the flexion creases of the palm.

CH-17 3-38
(4) With the hands pronated, observe the contour of the dorsum of the hands for
atrophy of the soft tissues between the metacarpals seen in disease or
malfunction of peripheral nerves.
(5) With the fingers spread, test for strength, and interosseous muscle function by
forcing the spread fingers against the resistance of the examinee.
(6) If indicated, obtain antero-posterior and lateral x-rays of the wrist, as well as
antero-posterior and oblique views of the hand.
14. Spine and Other Musculoskeletal (Item 36 of DD-2808). Carefully examine for evidence
of intervertebral disc syndrome, myositis, and traumatic lesions of the low back
(lumbosacral and sacroiliac strains). If there is any indication of congenital deformity,
arthritis, spondylolisthesis, or significant degree of curvature, obtain orthopedic
consultation and x-rays.
(1) Back. With the examinee stripped and standing, note the general configuration
of the back, the symmetry of the shoulders, iliac crests and hips, and any
abnormal curvature. Palpate the spinous processes and the erector spinae
muscle masses for tenderness. Determine absence of pelvic tilt by palpating
the iliac crests. Have examinee flex and extend spine and bend to each side,
noting ease with which this is done and the presence or absence of pain on
motion. Test rotary motion by gripping the pelvis on both sides and having the
examinee twist to each side as far as possible.
(2) With the examinee sitting on the examining table, test patellar and ankle
reflexes and fully extend the knee, note complaints of pain (this corresponds to
a 90 degree straight leg raising test in supine position).
(3) With the examinee supine, test dorsiflexor muscle power of the foot and toes,
with particular attention to power of the extensor hallucis longus. Weakness
may indicate nerve root pressure on Sl. Flex hip fully on abdomen and knee
flexed and determine presence or absence of pain on extremes of rotation of
each hip with hip flexed to 90 degrees. Frequently, in lumbosacral sprains of
chronic nature, pain is experienced on these motions. Place the heel on the
knee of the opposite extremity and let the flexed knee fall toward the table.
Pain or limitation indicates either hip joint and/or lumbosacral abnormality.
(4) While prone, have the examinee arch the back and test strength in extension by
noting the degree to which this is possible.
(5) If pain is experienced on back motions in association with these maneuvers or
if there is asymmetry or abnormal configuration, back x-rays, including pelvis,
should be obtained. These should include antero-posterior, lateral, and oblique
views.
3-39 CH-17
15. Identifying Body Marks, Scars, and Tattoos (Item 37 of DD-2808).
a. Examination. Carefully inspect the examinee's body, front and rear, on each side of
the median line separately, commencing with the scalp and ending at the foot.
Record under the "Notes" section on the face of the DD-2808 all body marks, tattoos,
and scars useful for identification purposes. Also state if no marks or scars are
found.
b. Description of Body Marks, Scars, and Tattoos.
(1) Indicate the size, location, and character of scars, moles, warts, birthmarks, etc.
(2) When recording the location of a tattoo, include narrative description of the
design. Tattoo transcriptions of words or initials shall be recorded in capital
letters. Describe the size of a tattoo regarding its general dimensions only. A
statement relative to color or pigment is not required.
(3) Note amputations and losses of parts of fingers and toes showing the particular
digit injured and the extent or level of absence.
c. Abbreviations for Body Marks, Scars, and Tattoos.
(1) The following are authorized abbreviations for the descriptions or conditions
indicated:
Amp.-amputation m. -mole w. -wart
f. -flat p. -pitted VSULA-
fl. fleshy r. -raised vaccination scar
s. -scar smooth l. -linear upper left arm
v. -vaccination o. -operative h. -hairy
(2) Combinations of the above abbreviations are permissible: p.s. 1/2d. - pitted
scar 1/2 inch diameter; f.p.s. lxl/2 - flat pitted scar l inch long and 1/2 inch
wide; r.h.m. 1/4d. - raised hairy mole 1/4 inch diameter.
(3) Do not use abbreviations when describing tattoos since they are likely to be
mistaken as signifying tattooed letters.
16. Neurologic (Item 39 of DD-2808). Conduct a careful neurological examination being
attentive to the following:
a. Gait. The individual shall: walk a straight line at a brisk pace with eyes open, stop,
and turn around; (Look for spastic, ataxic, incoordination, or limping gait; absence of
normal associated movements; deviation to one side or the other; the presence of
abnormal involuntary movement; undue difference in performance with the eyes
open and closed.)
(1) stand erect, feet together, arms extended in front; (Look for unsteadiness and
swaying, deviation of one or both of the arms from the assumed position,
tremors, or other involuntary movements.)
CH-17 3-40
(2) touch the nose with the right and then the left index finger, with the eyes
closed. (Look for muscle atrophy or pseudohypertrophy, muscular weakness,
limitation of joint movement, and spine stiffness.)
b. Pupils. Look for irregularity, inequality, diminished or absent contraction to light or
lack of accommodation.
c. Deep Sense (Romberg). Negative, slightly positive, or pronouncedly positive.
d. Deep Reflexes: Patellar, Biceps, etc. Record as absent (o), diminished (-), normal
(+), hyperactive (++), and exaggerated (+++).
e. Sensory Disturbances. Examine sensation by lightly pricking each side of the
forehead, bridge of the nose, chin, across the volar surface of each wrist, and dorsum
of each foot. Look for inequality of sensation right and left. If these sensations are
abnormal, vibration sense should be tested at ankles and wrists with a tuning fork.
With eyes closed, the examinee shall move each heel down the other leg from knee
to ankle. Test sense of movement of great toes and thumb. Look for diminution or
loss of vibration and plantar reflexes. When indicated, perform appropriate
laboratory tests and x-ray examinations.
f. Motor Disturbances. Evidence of muscle weakness, paresis, or any other
abnormality.
g. Muscular Development. Evidence of atrophy, compensatory hypertrophies, or any
other abnormality.
h. Tremors. State whether fine or coarse, intentional or resting, and name parts
affected.
i. Tics. Specify parts affected. State whether they are permanent or due to fatigue or
nervous tension.
j. Cranial Nerves. Examine carefully for evidence of impaired function or paresis.
Remember that some of the cranial nerves are subject to frequent involvement in a
number of important diseases, such as syphilis, meningitis, encephalitis lethargica,
and injuries to the cranium.
k. Psychomotor Tension. Test the ability to relax voluntarily by having the examinee
rest the forearm upon your palm then test the forearm tendon reflexes with a
percussion hammer.
l. Peripheral Circulation. Examine for flushing, mottling, and cyanosis of face, trunk,
and extremities. Question as to the presence of localized sweating (armpits and
palms) and cold extremities. Carefully study any abnormalities disclosed on the
neurological examination and express an opinion as to their cause and significance
and whether they are sufficient cause for rejection.
3-41 CH-17
17. Psychiatric (Item 40 of DD-2808).
a. Personality Evaluation. In order to evaluate the adequacy of the examinee's
personality for adjustment to the conditions of military service:
(1) estimate the examinee's capacity coupled with real respect for personality and
due consideration for feelings;
(2) conduct the examination in private to encourage open and honest answers; and
(3) attempt to discover any difficulties that the examinee may have had with
interpersonal relationships at work or during leisure activities.
b. Diagnosis of Psychiatric Disorders. The diagnosis of most psychiatric disorders
depends upon an adequate longitudinal history, supplemented by information
obtained from other sources, such as family, physicians, schools, churches, hospitals,
social service or welfare agencies, and courts.
c. Telltale Signs of Psychiatric Disorders. Be watchful for any of the following:
inability to understand and execute commands promptly and adequately; lack of
normal response; abnormal laughter; instability; seclusiveness; depression; shyness;
suspicion; over boisterousness; timidity; personal uncleanliness; stupidity; dullness;
resentfulness to discipline; a history of enuresis persisting into late childhood or
adolescence; significant nail biting; sleeplessness or night terrors; lack of initiative
and ambition; sleep walking; suicidal tendencies, whether bona fide or feigned.
Abnormal autonomic nervous system responses (giddiness, fainting, blushing,
excessive sweating, shivering or goose flesh, excessive pallor, or cyanosis of the
extremities) are also occasionally significant. Note also the lack of responses as
might reasonably be expected under the circumstances.
d. Procedures for Psychiatric Examination.
(1) Mental and personality difficulties are most clearly revealed when the
examinee feels relatively at ease. The most successful approach is one of
straightforward professional inquiry, coupled with real respect for the
individual's feelings and necessary privacy. Matters of diagnostic significance
are often concealed when the examinee feels the examination is being
conducted in an impersonal manner or without due concern for privacy.
(2) Pay close attention to the content and implication of everything said and to any
other clues, and in a matter-of-fact manner, follow-up whatever is not self-
evident nor commonplace.
e. Aviation only.
(1) Although this phase of the examination is routinely performed only on
candidates for flight training, it may be made part of any aviation physical
examination. The objective is to determine the examinee's basic stability,
motivation, and capacity to react favorably to the special stresses encountered
in flying. Report any significant personality change in an experienced aviator.

CH-17 3-42
(2) Following the completion of the general examination:
(3) study carefully the examinee's family history; and
(4) determine the family's attitude towards flying and the examinee's reaction to
the stresses of life in general and emotional response and control.
18. Endocrine System. Evaluate endocrine abnormalities during the general clinical
examination. Palpate the thyroid for abnormality and observe the individual for signs of
hyperthyroidism or hypothyroidism. Observe general habitus for evidence of endocrine
dysfunction.
19. Dental (Item 43 of DD-2808).
a. Who May Conduct Dental Examinations.
(1) For Academy, OCS, and direct commission applicants: a Uniformed Services
dental officer.
(2) For all aviation, diving, and overseas/sea duty physical examinations: a
Uniformed Services dental officer or a contract dentist.
(3) For all others: a Uniformed Services dental officer, a contract dentist, or a
medical examiner if a dentist is unavailable.
b. Procedures for Conducting Dental Examinations.
(1) Applicants for Original Entry. Whenever practical, applicants for original
entry into the Service shall be given a Type 2 dental examination. Otherwise,
the dental officer shall determine the type of examination that is appropriate
for each examinee.
(2) Active Duty Personnel.
(a) Members on active duty, who are assigned to locations where Coast
Guard, USMTF, or civilian contract dental clinics are available shall be
required to have an annual Type 2 dental examination.
(3) Reserve Personnel.
(b) Type 2 dental examination is required for Quinquennial Physical
Examinations, and
(c) Type 2 dental examination is required for all entries onto Active Duty
(any type) for periods of duty in excess of 139 days.
c. Dental Restorations and Prostheses. The minimum number of serviceable teeth
prescribed for entry in various programs of the Service is predicated on having
retentive units available to provide for the reception of fixed bridges or partial
dentures that may be necessary for satisfactory masticatory or phonetic function.
Prostheses already present should be well-designed, functional, and in good
condition.
3-43 CH-17
20. Laboratory Findings.
a. Required Tests. Personnel undergoing physical examinations are required to have
the following tests performed, except where obtaining them is not possible or
expeditious, or incurring charges for them is not authorized. In such cases, these
tests shall be obtained at the first duty station where facilities are available. The
normal values listed below are for guidance. Abnormal laboratory values alone are
not disqualifying; however, the causative underlying condition may be. Minimal
deviations may not require further evaluation and this should be noted as NCD (not
considered disqualifying) in item 74 by the examiner. Normal variants should be
noted as such.
b. Hematology/Serology.
(1) Hematology. Perform a hematocrit (HCT) or hemoglobin (HGB) on all
examinees. Perform other hematological studies only as indicated.
(2) Red Blood Cell Measurements.
(3) Hemoglobin - Males 13-18 gm/100ml
(4) Females 11.7-16 gm/100ml
(5) Hematocrit - Males 40-54%, Females 35-47%
If any of these parameters are abnormal, an RBC and indices shall be done.
Normal indices are:
RBC- Males 4.3 to 6.2 million
Females 3.8 to 5.4 million
MCV- 82-92 cubic microns
MCH- 27-32 picograms
MCHC - 30-36%
(6) Cholesterol Testing. All cadets, officer candidates, and recruits shall be tested
for serum cholesterol within a week of their arrival for training. Those persons
judged by a medical officer to have cholesterol levels that indicate an increased
risk of atherosclerotic vascular disease shall be informed of this and given
appropriate counseling by the third week of their training. Lipid panel studies,
pharmacological remedial measures, or follow-up appointments may be
performed at the discretion of the managing medical officer.
(7) Serological Test for Syphilis (RPR/STS).
(a) Required for entry into the Coast Guard and for all aviation and diving
candidate physicals.
(b) Unless there is a documented history of adequately treated syphilis, all
examinees testing positive shall have repeat testing three or more days
later. Ensure that at the time of obtaining serum the examinee neither
has, nor is convalescing from, any acute infectious disease or recent

CH-17 3-44
fever. If available at no charge, the facilities of local or state health
departments may be used for performing serological tests. Examinees
with a history of treated syphilis should have declining or low titer
positive reaction.
(c) If the second test is positive then obtain an FTA/ABS. If the FTA/ABS
is positive, further evaluation may be required to determine the
appropriate therapy.
(d) Several conditions that are known to give false RPR/STS are infectious
mononucleosis, malaria, yaws, pinta, chicken pox, infectious hepatitis,
immunization, and atypical pneumonia. The cause of a false positive
serological test for syphilis should be explored since many diseases
giving a false positive are also disqualifying.
(e) Process all members who are suspected contacts or who have clinical
evidence of venereal disease and all personnel with a positive serological
test for syphilis in accordance with section 7-B-3 of this Manual.
(8) Sickle Cell Preparation Test. Applicants for aviation and diving training shall
be tested for sickling phenomenon, if not previously tested. Evaluate positive
sickledex results by a quantitative hemoglobin electrophoresis. Greater than
40 percent Hbs is disqualifying for aviation and diving. Once the test has been
completed, the results will be filed in the health record and recorded on the
Problem Summary List. The test need never be repeated.
(9) HIV Antibody.
(a) The most recent HIV antibody test date will be recorded in item #49 of
the DD-2808 (Report of Medical Examination), on the
NAVMED6150/20 (Problem Summary List), and under Remarks on the
SF-601 (Immunization Record). Epidemiological information
concerning HIV infection will be monitored by Commandant (G-WKH)
and the policy concerning routine testing will be revised as necessary.
(b) HIV antibody testing is required as follows (see COMDTINST.
6220.1A):
1 All applicants for regular or reserve programs for enlistment,
appointment, or entry on active duty;
2 Candidates for officer service (direct commission, OCS, Academy,
MORE, etc.,) as part of pre-appointment or pre-contract physical
examination;
3 Cadets at the Coast Guard Academy as part of the physical
examination prior to commissioning;
3-45 CH-17
4 All Coast Guard members who have not had at least one
documented HIV antibody test in the last five years;
5 All members with PCS orders to a foreign country, within six
months prior to transfer;
6 During the clinical evaluation of the patients at high risk of HIV
infection being seen for other sexually transmitted diseases or as
part of prenatal examinations; and
7 Patients being referred to Level II/III alcohol/drug treatment
programs must be tested for HIV immediately prior to entering such
a program;
8 Newly identified tuberculin reactors.
(c) Accession testing will usually be performed through MEPS examination
centers. Other required testing can be done through DOD MTFs or
designated Coast Guard HIV Antibody Testing Centers. Other required
testing will be done through designated Coast Guard-wide HIV contract
laboratory, Viromed laboratories. Commanding Officers may arrange
testing with the laboratory directors at local uniformed services medical
facilities (USMTFS) or qualified local civilian laboratories, only with the
permission of, and prior coordination with, MLC(k). Record keeping
and reporting requirements must be met. Liaison with the Department of
Defense indicates that there are no prohibitions to testing Coast Guard
personnel at these facilities. Contact Commander, MLC(k) for
permission to use USMTFS or local civilian facilities to arrange methods
for reporting results.
(d) Members who are confirmed HIV antibody positive or indeterminate by
Western Blot, by the Coast Guard-wide contract laboratory, will have a
second confirmatory specimen drawn and submitted for analysis to the
same Coast Guard-wide contract laboratory.
(e) Members who are confirmed HIV antibody positive by the second
confirmatory Western Blot, by the Coast Guard-wide contract laboratory,
will be referred to a DOD MTF with the capability to perform a
complete evaluation. Contact the respective MLC (k), and they will
assist in making arrangements for the evaluation. Ensure that both the
medical and dental records accompany the member to the DOD MTF for
the evaluation. A narrative summary of this evaluation shall be
obtained by the referring medical officer, who shall notify G-WKH
via MLC(k) upon receipt. Initiate a Disease Alert Report IAW Chapter
7 of this Manual.
(f) Once a member has been confirmed HIV positive, arrange immediate
medical and social services counseling, using available Coast Guard,
CH-17 3-46
DOD, or civilian resources to ensure that the member understands the
clinical implications of the positive test, the purpose of subsequent
medical evaluation, and the policies in this instruction.
(g) Members who are confirmed HIV antibody positive shall receive
counseling. The individual's command will provide medical and
supportive counseling to the member if this has not already been
provided by the evaluating facility.
(h) All information surrounding the individual's physical condition is strictly
confidential. Only key personnel, with a verifiable "need to know" such
as the individual's commanding officer, should be informed of the HIV
status.
(i) Coast Guard medical officers requiring HIV antibody testing for clinical
diagnosis should direct the Coast Guard HIV Antibody Testing Center to
send a shipment to the Coast Guard-wide contract laboratory
immediately. Results should ordinarily be available within 48 hours via
electronic mail or telephone from Commandant (G-WKH).
(j) HIV antibody testing required by members of other uniformed services
(active duty or reserve), or by specific agreement with other Federal
agencies (e.g., Department of State), must be performed through a Coast
Guard HIV Antibody Testing Center.
(k) Voluntary testing and counseling of dependents, retirees, and civilian
employees must be performed through a Coast Guard HIV Antibody
Testing Center.
c. Chest X-ray (Item 52 of DD-2808).
(1) Will be accomplished as part of the physical examinations for application for
aviation or diving programs. Chest X-rays previously performed within
eighteen (18) months of application, with normal results, are acceptable if there
is no change in clinical presentation.
(2) Will not be performed for routine screening purposes without a prior clinical
evaluation and a specific medical indication. The senior medical officer may
authorize an exception to this policy when there are obvious medical benefits
to be gained by routine screening x-ray examination (e.g., Asbestos Medical
Surveillance Program). Such exceptions should be authorized only after
careful consideration of the diagnostic yield and radiation risk of the x-ray
study, as well as other significant or relevant costs or social factors. X-ray
examinations will not be ordered solely for medical-legal reasons.
d. Electrocardiogram (Item 52 of DD-2808).
(1) Electrocardiograms (ECG) shall be accomplished routinely on the following
individuals:

3-47 CH-17
(a) those in whom medical history or clinical findings are suggestive of
cardiac abnormalities;
(b) examinees with a sitting pulse rate of less than 50 or more than 100;
(c) examinees who are 40 years old or older;
(d) applicants for aviation and diving training and all designated personnel
every four (4) years until age 40, then biennially. For designated
aviation personnel on physical examinations where no EKG is required,
place the date and results of the last EKG in block #52 (Other) of DD-
2808; and
(e) applicants for service academies.
(2) All student and designated aviation personnel shall have an ECG on file in
their health record.
(3) All tracings will be compared to the baseline reading in the health record, if
one is present. If significant changes are present, obtain a cardiac consultation.
A report of the consult shall be submitted for review along with the DD-2808.
It is imperative then that proper techniques for recording the ECG be followed.
(a) The routine ECG will consist of 12 leads, namely standard leads 1, 2, 3,
AVR, AVL, AVF, and the standard precordial leads V1 through V6.
(b) Take care to properly place the precordial electrodes. It is important that
the electrodes across the left precordium are not carried along the curve
of the rib but are maintained in a straight line. Be particular in placing
the first precordial lead so as to avoid beginning placement in the third
interspace rather than the fourth. Do not smear electrode paste from one
precordial position to another. Include a standardization mark on each
recording.
e. Urinalysis. A urinalysis is required on all physical examinations. The urine shall be
tested for specific gravity, glucose, protein, blood, leukocyte esterase, and nitrite by
an appropriate dipstick method. A microscopic examination is required only if any
of these dipstick tests is abnormal.
(1) Specific Gravity. Normal values are 1.005-1.035. Specific gravity varies with
fluid intake, time of day, climate, and medication. As a rule, elevation of the
specific gravity reflects only the state of hydration, while a low specific gravity
may reflect kidney disease. In evaluating abnormalities, a repeat is generally
sufficient, provided the factors above are considered and explained to the
individual. Where possible, the repeat should be a first morning specimen
which is usually the most concentrated.
(2) Glucose. Any positive test is abnormal. A false positive for glucose may
occur in individuals who take Vitamin C or drink large quantities of fruit juice.
As soon as practical after discovery of the glycosuria, obtain a fasting blood
CH-17 3-48
glucose. If glycosuria persists or if the fasting blood glucose exceeds 125
mg/100 ml, evaluate the individual for diabetes.
(3) Protein. A trace positive protein is often associated with a highly concentrated
(specific gravity 1.024 or greater) early morning specimen and is considered
normal and need not be repeated. A one plus or greater protein, or a trace
positive in the presence of a dilute urine, should be evaluated by a 24-hour
specimen (normal range 10-200 mg protein/24 hours).
(4) Microscopic.
(a) Normal: 0-5 WBC
0-5 RBC (clean catch specimen)
occasional epithelial cells (more may be normal
in an otherwise normal urinalysis)
no casts occasional bacteria
(b) Pyuria usually indicates an infection or improper collection techniques.
Appropriate follow-up is required, including repeat after the infection
has cleared.
(c) Hematuria may normally occur following heavy exercise or local trauma
and as a false positive in menstruating females. It always requires
evaluation with the minimum being a repeat showing no hematuria.
(d) Casts, heavy bacteria, other organisms, and abnormal cells require
further evaluation.
f. PAP Test (Item 52 a. of DD-2808).
(1) A PAP test is required at the following times on female members:
(a) on the pre-training physical examination at time of initial entry into the
Coast Guard;
(b) every two years, if on extended active duty; and
(c) with quinquennial examinations, for reserves.

3-49 CH-17
(2) PAP tests and pelvic examinations (by civilian or military practitioners) that
have been performed within one year of periodic examinations are acceptable.
In any case, results of the pelvic examination and PAP test will be recorded in
Item 52 a. The practitioner is responsible for communicating the result of the
PAP smear (either positive or negative) to the patient.
(3) To reduce false-negative smears, endocervical sampling shall be done using a
cytobrush, provided no contraindication is present (as in pregnancy or cervical
stenosis). Laboratories to which smears are sent for interpretation must, as a
matter of routine, indicate on their reports whether endocervical sampling was
adequate. Where endocervical cell sampling is reported as inadequate, the
smear shall be repeated.
g. Pulmonary Function Test (PFT). Perform a PFT on all OMSEP examinations and
when clinically indicated.
(1) Screening spirometry should not be performed if the subject:
(a) is acutely ill from any cause;
(b) has smoked or used an aerosolized bronchodilator within the past hour;
(c) has eaten a heavy meal within the previous two hours; or
(d) has experienced an upper or lower respiratory tract infection during the
past three weeks.
(2) Explain the procedure to the subject.
(3) Instruct the subject to remove any tight clothing or dentures and to sit or stand
comfortably in front of the spirometer. The chin should be slightly elevated
with the neck slightly extended. The use of a nose clip is recommended.
(4) Tell the subject to take the deepest possible inspiration, close mouth firmly
around the mouthpiece and without further hesitation, blow into the apparatus
as hard, fast, and completely as possible. Active coaching throughout the
entire duration of the forced expiration must be done to elicit maximum subject
effort. Positioning of the lips around the mouthpiece should be checked.
(5) After two practice attempts, three further tracings should be recorded. If the
technician believes that the subject has not made a full inspiration prior to the
forced expiration, not put forth a maximal effort, or not continued expiration
sufficiently long, that particular tracing should be repeated. Repeat attempts
marred by coughing. The variation between the largest and smallest FVC of
three satisfactory tracings should not exceed 10%.
(6) From the three satisfactory tracings, the FVC, FEV1, and FEV1/FVC% should
be determined. Use the highest FVC and FEV1 in the calculations regardless
of the curve(s) on which they occur. The tracing itself should also be
maintained as part of the medical record.
CH-17 3-50
(7) If the tests are baseline studies, determine the predicted values and calculate
the subject's percent of the predicted normal, and transcribe results on the
record sheet. In non-Caucasians, the predicted FEV1 and FVC should be
multiplied by 0.85 to adjust for ethnic differences. No correction factor is
necessary for the FEV1/FVC%.
(8) If the tests are follow-up studies, comparison should be made with the
previously recorded highest value for each test. This highest value may not
necessarily have occurred during baseline tests.
(9) Verify any abnormalities in either baseline or follow-up pulmonary functions
by repeating spirometry in two weeks. If abnormalities persist, clinical
assessment by a physician qualified to evaluate chest disease is essential. In
males, a 30 millimeter annual decline in FEV1 and 25 millimeters FVC can be
attributed to normal aging. In females, it is 25 millimeters in both the FEV1
and FVC. PFT. Abnormal functions are present when:
(a) FEV-1 or FVC is less than 80% of predicted;
(b) FEV-1/FVC% is less than 69%;
(c) decline in the FEV-1 or FVC greater than 8%;
(d) decrease in the FEV-1/FVC% greater than 6%; and
(e) see the following:
SPIROMETRIC
GUIDELINES
OBSTRUCTIVE DISEASE
FEV-1/FVC
RESTRICTIVE
DISEASE FCV%
FCV PREDICTED
NORMAL > 0.69 > .80
MILD TO MODERATE 0.45 -0.69 0.51-0.80
SEVERE < 0.45 <0.51
h. Special Tests. In some cases, information available should be supplemented by
additional tests or diagnostic procedures (eye refractions, x-rays, repeated blood
pressure readings, etc.), in order to resolve doubts as to whether the examinee is or is
not physically qualified. If facilities are available to perform such tests at no cost,
they should be obtained as indicated in individual cases. Otherwise, applicants for
3-51 CH-17
original entry in the Service will be required to obtain such tests at their own
expense, if they desire further consideration.
i. Laboratory Values (OMSEP). All laboratory values not previously discussed but
that accompany a physical examination (e.g., chemistry profiles, etc.,) must have
accompanying normals for the laboratory that performed the tests.
j. Mammography. Mammography is required for Coast Guard active duty and reserve
females beginning at age 40 and at ages 44, 48, 50, 52, 54, 56, 58, 60, and 62.
Clinical findings, family history, and other risk factors may dictate that a
mammogram be done at times other than those indicated in this screening schedule.
Results should be documented on the routine physical exams. Mammograms done
between the required screening ages can be used to satisfy the periodic requirement.
This judgment is left to the practitioner. If mammography is not done at the required
ages, the reason must be supplied in item 73 of the DD-2808 and should include date
and result of the last mammogram. Practitioners are responsible for communicating
mammography results (either positive or negative) to the patient.
k. Glucose-6-Phosphate Dehydrogenase (G-6-PD). Qualitative testing (present or not)
for G-6-PD deficiency is required at all accession points (TRACEN Cape May,
Academy, RTC Yorktown). All other Coast Guard members with no record of
testing shall be tested prior to assignments afloat or to malaria-endemic areas. The
results of testing shall be annotated on the DD-2766 Adult Preventive and Chronic
Care Flowsheet. Once testing is accomplished, it need never be repeated.
21. Height, Weight, and Body Build.
a. Height. Measure the examinee's height in centimeters (inch) to the nearest
centimeter (one-half inch), without shoes.
b. Weight.
(1) Weights are with underwear/undergarments only.
(2) Weigh the examinee on a standard set of scales calibrated and accurate.
Record the weight to the nearest kilogram (pound). Do not record fractions of
kilogram.
c. Frame Size. Using a cloth tape, measure the wrist of the dominant hand, measure all
the way around from lateral to medial styloid process. Measure in centimeters
(fraction of an inch).
d. Body Fat Percentage. Determined by MEPS.
22. Distant Visual Acuity and Other Eye Tests.
a. Distant Visual Acuity, General. Visual defects are one of the major causes for
physical disqualification from the armed services. Methods of testing vision have
varied greatly among the armed services and from place to place in each Service.
Consequently, visual test results are not always comparable. An examinee

CH-17 3-52
presenting for examination at one place might be qualified for visual acuity, while at
another place, disqualified. Although this is an undesirable situation, no practical
solution, such as prescribing standards for equipment and conditions (room size,
ventilation, paint colors, room illumination, etc.), is available to the Coast Guard as
the examinations are obtained from various sources over which the Coast Guard has
no control. It is therefore imperative that examiners be especially painstaking to
obtain the most accurate results possible.
b. Examination Precautions.
(1) Make every effort to conduct the examination when the examinee is in normal
physical condition. Follow the examination routine in the order prescribed in
the following instructions. Record the vision for each eye when determined so
that errors and omissions will be avoided.
(2) It may be extremely difficult to obtain an accurate measure of visual acuity.
Bear in mind that individuals who are anxious to pass visual acuity tests may
resort to deception. Similarly, other individuals may attempt to fail a visual
acuity test to avoid undesirable duties. Hence, be prepared to cope with either
possibility in order to uncover and recognize visual defects without the
cooperation of the person being tested.
(3) Refer uncooperative examinees to a medical officer.
c. Examination Procedures.
(1) In order to obtain a more valid evaluation, inform examinees that contact
lenses will not be worn during the evaluation and for 72 hours before.
Orthokeratotic lenses shall be removed for 14 days or until vision has
stabilized for 3 successive examinations.
(2) If the examinee wears glasses, they must be removed before entering the exam
room. Test each examinee without unnecessary delay after entering the
examining room. In order to prevent personnel from memorizing the charts,
permit only one examinee to view the test charts at a time. Keep examinees
awaiting testing out of hearing.
(3) Direct the examinee to a line that is 20 feet from the test chart. Hold an
occluder so that it covers the examinee's left eye. Instruct the examinee to
keep both eyes open and not to squint. The occluder must not be pressed
against the eyeball or lids or any part of the eye being shielded, but, should be
held in contact with the side of the nose. The eye shielded by the occluder
should be left open in order to avoid pressure and to discourage squinting. A
rigid occluder, constructed of a material such as wood, translucent plastic, or
metal, of a design to discourage cheating shall be used to shield the eye not
being tested.
(4) Direct the examinee to begin with the first line and to read as many lines as
possible. (Watch the examinee, not the chart that is being read. Hold the
occluder so the examinee cannot peep around it. The most frequently used
method of increasing visual acuity is to squint. This will not be permitted.

3-53 CH-17
Some examinees with astigmatism will be able to read the letters better by
tilting the head to one side; do not allow this. Another well-known method
used to pass a visual acuity test is to obtain eyedrops beforehand that contract
the pupil; suspect this if the pupils are unusually small.)
(5) Record the smallest line read with no errors on the chart from the 20 foot
distance as the vision for the right eye (0.D.).
(6) Test the visual acuity for the left eye (0.S.), preferably using a different chart,
record in the same manner.
(7) Test the visual acuity for both eyes (0.U.), preferably with a third chart, record
in the same manner.
(8) Test an examinee who wears glasses again with them on. Follow the same
procedure as without glasses.
(9) When there is suspicion that the examinee has memorized a chart, a different
chart should be used or the letters on the chart should be read in reverse order.
(10) The examinee is expected to read letters promptly. No precise time limit
should be applied, but 1 or 2 seconds per letter is ample.
(11) An examinee who fails a letter should not be asked to read it again. If a rapid
reader makes an obviously careless mistake, caution the examinee to "slow
down" and repeat the test using another chart.
(12) Some examinees give up easily. They may need encouragement to do their
best; however, do not coach them.
(13) The effects of fatigue may make a certain amount of retesting necessary. In
questionable cases, one retest should be given not less than the day after the
initial test.
d. Armed Forces Vision Tester (AFVT). Visual acuity may also be determined with
the (AFVT) which consists of two rotating drums holding illuminated slides for
testing various facets of vision. The examinee observes the distance slides looking
slightly downward with the instrument set and also observes the near slides looking
downward at a greater angle. The handles on the side of the instrument rotate the
drums to change the slides. Beneath the eye pieces there is a lever that operates an
occluder so that each eye can be tested separately. In the case of the slides for
muscle balance and stereopsis, the two eyes must be tested together and the occluder
should be centered so it occludes neither eye. A scoring key is provided with the
instrument. The following slides are available:
(1) Rear Drum (Distance Testing).
(a) Slide 1 - Vertical Phorias.
1 The right eye sees a set of numbered steps, the left sees a dotted line.
With both eyes open the examinee is asked which step the dotted
line intersects. Interpretation: step l, 2 prism diopters of left
hyperphoria; step 2, 1.5 left hyperphoria; step 3, 1.0 left

CH-17 3-54
hyperphoria; step 4, 0.5 left hyperphoria; step 5, orthophoria; step 6,
0.5 prism diopters of right hyperphoria; step 7, 1.0 right
hyperphoria; step 8, 1.5 right hyperphoria; step 9, 2.0 right
hyperphoria.
2 Detecting Malingerers: i.e., if known that a score of 5 is normal, the
examinee could feign a normal phoria. To avoid this, a pair of
VARIABLE PRISMS is provided, by which the examiner can raise
either the right or the left eye image. The prisms are mounted within
the viewing box. The extent of prismatic deviation is governed by
the position of two control handles.
3 The correct score--and the only score recorded--is that obtained
when both control handles of the VARIABLE PRISM are pushed
inward as far as they will go. This is known as the SCORING
POSITION. Moving the left handle outward from this position
moves the left eye image downward and outward. Similarly,
moving the right handle outward moves the right eye image
downward and outward.
4 The maximum amount of downward shift provided by each control
corresponds to four steps. Moving the right handle outward to its
extreme position therefore will change the apparent location of the
dotted line from step 1 to step 5, for example, from 6 to above 9, etc.
Moving the left control handle outward to its extreme position
similarly will change the apparent location of the dotted line from
step 5 to step 1, or from step 8 to step 4, etc. Vary the location of the
right or left control handle, each time asking the examinee to report
the location of the dotted line. Only the answer obtained when both
handles are in the SCORING POSITION gives the examinee's test
score.
(b) Slide 2 - Horizontal Phorias.
1 The examinee's right eye sees a row of numbered dots, the left eye
sees an arrow, with the occluder in the open position, ask the
examinee to which numbered dot the arrow is pointing.
Interpretation: The reporting value minus 11 equals prism diopters
of exophoria; 11 minus the reported value equals the prism diopters
of esophoria.
2 DETECTING MALINGERERS: By means of the VARIABLE
PRISM previously mentioned, the right and left eye images can both
be shifted outward a maximum of seven dots. To produce this
outward shift without a downward shift, in this test both control
handles are moved outward simultaneously by the same amount.
When both handles are shifted as far out as they go, the apparent

3-55 CH-17
position of the arrow is moved seven dots to the left, giving a score
seven below the true score.
3 As in previous test, the correct score and the only score recorded is
that obtained when the control handles are in the SCORING
POSITION.
(c) Slides 3 and 3A - Visual Acuity. With both eyes uncovered the
examinee sees a jumble of letters. With one eye covered, the uncovered
eye cannot see the letters intended for the opposite eye.
(d) Slides 4 and 4A - Visual Acuity, Large Letters. Separate charts for the
left and right eye.
(e) Slides 5 and 5A - Stereopsis. Six groups of horizontal lines, five circles
to a line. The groups are numbered A to F. In each horizontal row of
circles, one circle stands out closer to the examinee. The degree of
difficulty increases from A to F. The examinee calls the circle that
stands out. Passing score: There must be no misses in groups A through
D. Caution: Ensure that neither eye is inadvertently left occluded when
this test is being given. Both eyes must be able to see the circles in order
for any stereopsis to occur.
(2) Front Drum (Near Testing).
(a) Slide 6 - Vertical Phorias. Same as slide 1, only this is a near test.
(b) Slide 7 - Horizontal Phorias. Same as slide 2, except subtract 13.
(c) Slide 8 - Near Visual Acuity. This is given in Snellen notations.
(d) Slide 9 - Near Visual Acuity, Large Letters.
e. Score recording. Record vision test scores as a fraction in that the upper number is
the distance in feet from the chart and the lower number is the value of the smallest
test chart line read correctly. Thus, a person reading at a distance of 20 feet, the 30
foot test chart line is given a score of 20/30. 20/20 indicates that a person reads at a
distance of 20 feet the test chart line marked 20. Similarly, 20/200 means a person
can read at a distance of 20 feet only the test chart line marked 200.
f. Refraction.
(1) Eye refractions are required:
(a) when applying for flight training (SNA) (This must include
cycloplegic.); and
(b) when visual acuity falls below 20/20 in either eye (near or distant).
CH-17 3-56
(2) Subsequent refractions are required only if the visual acuity deteriorates
further.
(3) If a cycloplegic is used during the course of refraction, then the examinee must
wear dark glasses until the effects disappear. The installation of 1 drop into
each eye of 1% solution of pilocarpine hydrochloride in distilled water after
completing the examination will constrict the pupil and thus relieve the
photophobia.
g. Near Vision. Test near vision on all examinees and record results in Item 61 of DD-
2808 using Snellen notations. The examinee should be positioned so that the light
source is behind him/her and the near vision test card is well illuminated. The
examiner shall instruct the examinee to hold the test card exactly 14 inches/35.5 cm
in front of their eyes (measure from the inner aspect of the lower eyelid [corner of
the eye] to the face of the card to ensure accurate distance). Test each eye
separately. Note the smallest line of type that the examinee is able to read with each
eye. Record near vision both with and without corrective lenses if glasses are worn
or required. Record corrections worn in Item 73. See the chart below for conversion
from the various near point letter nomenclatures to Snellen notations.
CONVERSION TABLE FOR VARIOUS NEAR POINT LETTER NOMENCLATURE
Standard Test Chart Snellen
English Linear Snellen Metric Jaegar
14/14 20/20 0.50 J-1
14/17.5 20/25 .62 J-2
14/21 20/30 .75 J-4
14/28 20/40 1.00 J-6
14/35 20/50 1.25 J-8
14/49 20/70 1.75 J-12
14/70 20/100 2.25 J-14
14/140 20/200
3-57 CH-17
h. Heterophoria.
(1) Except for aviation personnel, special tests for heterophoria are not required
unless medically indicated.
(2) Heterophoria is a condition of imperfect muscle balance in which the eyes
have a constant tendency to deviate and latent deviation is overcome by
muscular effort (fusion to maintain binocular single vision). Fusion is
responsible for the two eyes working together in harmony and when anything
prevents this, fusion is disrupted and one eye deviates. Since heterophoria is
only a tendency of the eyes to deviate, no actual deviation is apparent when the
eyes are being used together under ordinary conditions. The deviation
becomes visible only when fusion control is weakened or abolished. When
deviation occurs, its exact amount can be estimated with some accuracy by
neutralizing the deviation with prisms of varying strength. If the eye deviates
toward its fellow, the deviation is known as esophoria; if it deviates away from
its fellow, the deviation is known as exophoria; if it deviates up or down, the
deviation is known as hyperphoria. The condition of perfect muscle balance
(no deviation) is orthophoria.
(3) The vertical and horizontal phorias may be tested with the Phoropter or AFVT.
i. Accommodation. There is no requirement to test accommodation unless medically
indicated.
j. Color Perception Tests. Examinees are qualified if they pass either the
Pseudoisochromatic Plates (PIP) or the Farnsworth Lantern (FALANT) test.
Examinees may be found qualified "on record" if a previous certified physical
examination that has a passing PIP or FALANT score is available for review.
Examinees who fail the PIP are qualified if they pass the FALANT.
(1) Farnsworth Lantern Test.
(a) Administration and Scoring.
1 Instruct the examinee: "The lights you will see in this lantern are
either red, green, or white. They look like signal lights at a distance.
Two lights are presented at a time--in any combination. Call out the
colors as soon as you see them, naming first the color at the top and
then the color at the bottom. Remember, only three colors--red,
green, and white--and top first."
2 Turn the knob at the top of the lantern to change the lights; depress
the button in the center of the knob to expose the lights. Maintain
regular timing of about two seconds per exposure.

CH-17 3-58
3 Expose the lights in random order, starting with RG or GR
combinations (Nos. 1 or 5), continuing until each of the 9
combinations have been exposed.
4 If no errors are made on the first run of nine pairs of lights, the
examinee passes.
5 If any errors are made on the first run, give two more complete
exams with one done in the opposite direction (to prevent
memorization). Passing score is at least 16 out of 18 correct for the
two runs.
6 An error is considered the miscalling of one or both of a pair of
lights; if an examinee changes responses before the next light is
presented, record the second response only.
7 If an examinee uses glasses for distance, they shall be worn.
8 If an examinee says "yellow," "pink," etc., state, "There are only 3
colors--red, green, and white."
9 If an examinee takes a long time to respond, state, "As soon as you
see the lights call them."
(b) Operation of Lantern.
1 Give the test in a normally lighted room; screen from glare; exclude
sunlight. The examinee should face the source of room
illumination.
2 Test only one examinee at a time (do not allow others to watch).
3 Station the examinee 8 feet from the lantern.
4 The examinee may stand or sit; tilt the lantern so that the aperture in
the face of the lantern is directed at examinee's head.
(2) Pseudoisochromatic Plates. When Pseudoisochromatic Plates are used to
determine color perception, a color vision test lamp with a daylight filter or a
fluorescent light with a daylight tube shall be used for illumination. Do not
allow the examinee to trace the patterns or otherwise touch test plates. Show
the plates at a distance of 30 inches and allow 2 seconds to identify each plate.
If the examinee hesitates, state "read the numbers." If the examinee fails to
respond, turn to the next plate without comment. Qualification is ascertained as
follows:
(a) 20 plate test set. Examinee must correctly read at least 17, excluding
demonstration plates.
3-59 CH-17
(b) 18 plate test set. Examinee must correctly read at least 14, excluding
demonstration plates.
(c) 15 plate test set. Examinee must correctly read 10 plates.
k. Depth Perception. Required for all aviation personnel and when medically indicated.
The AFVT is the most commonly used method of testing depth perception. When
this instrument is not available or the examinee fails the AFVT, use a Verhoeff
Stereopter. Results obtained with the Verhoeff are final in resolving all cases of
questionable depth perception. The TITMUS device will not be used to determine
depth perception.
(1) Findings.
(a) AFVT. An error in group A, B, C, or D is disqualifying.
(b) Verhoeff. Failure to correctly report eight out of eight in two of three
trials is disqualifying.
(2) Operating the Verhoeff.
(a) As a preliminary, show target #2 (the second target down when the
instrument is upright) at about 40 centimeters and bring it nearer if
necessary. This will acquaint the examinee with what is to be observed
and at the same time determine whether there is at least a distance,
however short, that can be judged correctly.
(b) Show one or two positions at close range to the examinee to clearly
demonstrate that one rod is always at difference from the other two.
Point out that the size of the rods is not a clue to the relative distance.
The examinee is now ready for the test.
(c) Hold the apparatus 1 meter from the examinee.
(d) Eight different rod relations are possible and all eight are shown.
(e) Keep the device centered as a frontal plane normal to the subject's
binocular visual midline. To avoid helpful extraneous cues it is highly
important to hold the device steady, and particularly not to rotate it on its
vertical axis. It is also important not to permit the subject to move the
head.
(f) Do not expose the target window while the device is being placed in
position or the sets are changed. A convenient method of manipulation
is to grasp the device over the target window with the left hand, place the
desired set into position with the right hand, then grasp the device below
with the right hand and expose the target window by moving the left
hand up or down. Thus while the target window is exposed, the device is
supported by both hands of the examiner.

CH-17 3-60
(g) The instructions to the subject are: "Report the nearest strip and the
farthest strip, unless they all appear to be at the same distance, referring
to the strips as 'left,' 'middle,' and 'right'." Only the report concerning the
one strip out of plane (farther or nearer than the other two that are in the
same plane) is to be considered.
l. Field of Vision.
(1) Except for aviation personnel, special tests for field of vision are not required
unless medically indicated.
(2) Procedure.
(a) Face the examinee at a distance of 2 feet.
(b) Close right eye and instruct the examinee to close left eye and focus right
eye on your left eye.
(c) Bring fingers in from the periphery, midway between you and the
examinee.
(d) Instruct the examinee to say when and how many fingers seen.
(e) Test all cardinal points.
(f) Repeat test for the left eye.
(g) Any evidence of abnormality should be given study on the perimeter.
(3) Normals.
(a) Temporally - 90o.
(b) Superotemporally - 62o.
(c) Superiorly - 52o.
(d) Superonasally - 60o.
(e) Inferonasally - 55o.
(f) Inferiorly - 70o.
(g) Inferotemporally - 85o.
m. Night Vision. A test for night vision (dark adaptation) is not required unless
indicated for medical or special reasons.
3-61 CH-17
n. Red Lens Test. The red lens test is required on DODMERB examinations and when
medically indicated.
(1) Apparatus. A spectacle trial frame, a red lens from' the trial lens case, a small
light such as a muscle balance light, and a metric rule or tape.
(2) Procedure.
(a) Seat the examinee in the darkness facing the dark wall or tangent curtain
at 75 cm distance.
(b) Adjust the spectacle trial frame position and place the red lens in one cell
of the trial frame.
(c) With the examinee's head in a fixed position, hold the small lamp
directly before the center of the dark wall or tangent curtain at 75 cm
distance from the eyes. Note the presence or absence of diplopia in this
position (primary).
(d) Then slowly move the light from the central position toward the right for
a distance of 50 cm in the horizontal plane. In the same manner, move
the light in the remaining five cardinal directions.
(e) In the presence of diplopia, note whether it is crossed, homonymous, or
vertical and the distance in centimeters from the central position at which
diplopia first occurs.
(f) When diplopia is suspected and the examinee has been coached to deny
its presence, a prism of 3 or 4 diopters may be placed, either base up or
base down, in one cell of the trial frame. If diplopia is still denied, the
statement is obviously untrue.
(3) Precautions. The examinee's head must remain fixed and the movement of the
light followed only by the eyes. Do not permit tilting or rotating the face.
o. Intraocular Tension.
(1) General. Determine intraocular tension each time an eye refraction is
performed, during all annual physical examinations, all aviation physicals, and
when medically indicated. Above normal tension is a sign of glaucoma; below
normal tension of ten exists in degenerated eyeballs or as a normal finding;
alterations in tension are sometimes found in cyclitis. Questionable findings
on palpation and ophthalmoscopic examination shall be further evaluated.
(2) Testing Intraocular Tension.
CH-17 3-62
(a) General. Routine tonometry shall be performed by a medical officer,
optometrist, or a technician who has received instruction in properly
performing and interpreting this test.
(b) Instrument. The tonometer estimates the intraocular pressure (IOP) or
tension within the eyeball.
(c) Precaution. Determine intraocular tension after all other eye
examinations have been completed. Because of corneal denuding by
tonometric measurement, a refraction (cycloplegic or manifest) shall not
be performed for at least 24 hours following this procedure.
(d) Readings. Intraocular pressure consistently above 21mm Hg in either
eye or a difference of 4 or more between the two eyes, shall be referred
for ophthalmologic evaluation.
23. Audiometer.
a. An audiometric examination is required on all physical examinations using
frequencies 500, 1000, 2000, 3000, 4000, and 6000 hertz.
b. Obtain reference audiograms on all personnel upon initial entry into the Coast Guard
at recruit training and all officer accession points (Academy, OCS, Direct
Commission, etc.,), and at first duty station for all others.
24. Psychological and Psychomotor. Psychological and psychomotor testing is not required
unless medically indicated.

3-63 CH-17
FIGURE 3-C-1
The following chart enumerates certain conditions, defects, and items of personal history that
require thorough evaluation and sets forth the special test, examination, or report desired in each
instance.
ITEM: EXAMINATION AND INFORMATION DESIRED:
ALBUMINURIA, findings of Repeat test on a second specimen. If still positive do a
quantitative 24 hr urine protein.
ASTHMA history of, Detailed report of asthma and other allergic conditions and
a statement from cognizant physician on (1) number and
approximate dates of attacks of asthmatic bronchitis or
other allergic manifestations; (2) signs, symptoms, and
duration of each attack; (3) type and amount of
bronchodilating drugs used, and history of any attacks
requiring hospitalization.
BACKACHE, back injury Current orthopedic consultation and report on
or wearing of back strength, stability, mobility, and functional brace, history of capacity
of back. Report of appropriate x-rays. Transcript of any
treatment from cognizant physician.
BLOOD PRESSURE, elevated Repeat blood pressure (all positions) a.m. and p.m. for 3
consecutive days. Prolonged bed rest shall not precede
blood pressure determinations.
CONCUSSIONS See Head Injury
CONVULSIONS OR SEIZURE Neurological consultation and electroencephalogram.
Transcript of any treatment from cognizant physician.
DIABETES, family history Fasting glucose (normal diet with 10-12 but less
of parent, sibling, or than 16 hours fast). If elevated, repeat and include 2 hr
more than one grandparent post prandial.
DIZZINESS or FAINTING Neurological consultation
SPELLS, history of
ENURESIS or history of Comment on applicant's affirmative reply
into late childhood or to question "bed wetting" to include number
adolescence (age 12) of past incidents and age at last episode.
FLATFOOT, symptomatic Current orthopedic consultation with history. Detailed
report on strength, stability, mobility, and functional
capacity of foot. Report of appropriate x-rays.
GLYCOSURIA, finding or See Diabetes.
history
HAY FEVER, history of Detailed report of hay fever and other allergic conditions
and a statement from personal physician on (1) number,
severity, and duration of attacks of hay fever or any other
allergic manifestations, and (2) type and amount of drugs
used in treatment thereof.
HEADACHES, frequent or Neurological consultation.
severe, history of
CH-17 3-64
FIGURE 3-C-1
HEAD INJURY with loss of Neurological consultation; clinical abstract
consciousness in past 5 of treatment from physician.
years, history of
HEMATURIA, history of or Medical consultation with evaluation
finding of report, including appropriate laboratory studies and/or
complete urological evaluation if indicated.
HEPATITIS, history of Serum Bilirubin, SGOT, SGPT, SGT, Anti-HCV,and
HBsAg.
JAUNDICE, history of in Serum Bilirubin, SGOT, SGPT, and SGT.
past 5 years
JOINT, KNEE, internal Current orthopedic consultation and
derangement, history of report of strength, stability, mobility, and functional
capacity of knee. Report of appropriate x-rays together
with comparative measurement of the thighs, knees, and
legs.
JOINT, SHOULDER, Current orthopedic consultation and
dislocation, history of report on strength, stability, mobility, and functional
capacity of shoulder. Report of appropriate x-rays.
MALOCCLUSION, TEETH, Report of examination by a dentist with comment
history of as to whether incisal and masticatory function is sufficient
for satisfactory ingestion of the ordinary diet, statement as
to presence and degree of facial deformity with jaw in
natural position and clarity of speech.
MASTOIDECTOMY, bilateral, Current ENT consultation to include
history of audiogram.
MOTION SICKNESS, history of Detailed report of all occurrences of motion sickness (such
as air, train, sea, swing, carnival-ride), and the age at the
time of the last occurrence.
NASAL POLYPS, history of ENT consultation, with comment as to date polyps
removed if no longer present. Detailed report by physician
on allergic history and manifestation to include required
medication.
SKULL FRACTURE, in past See Head Injury.
5 years, history of
SLEEPWALKING, beyond Detailed comment by physician. Comment on
childhood, history of applicant's affirmative reply to question "been
(age 12) a sleepwalker" to include number of incidents and age at
last episode.
SQUINT (cross eyed)Examination for degree of strabismus and presence of complete and
continuous 3rd degree binocular fusion. Request
completion of DD-2808 Items 62 and 65 and notation of
degree of strabismus.
STUTTERING or STAMMERING, Report of Reading Aloud Test in Section 3-C-2.
VERTEBRA, fracture or Current orthopedic consultation and
dislocation, history of report on strength, stability, mobility, and functional
capacity of spine. Report of appropriate x-rays.
3-65 CH-17
FIGURE 3-C-3
HEIGHT STANDARDS
Category
Minimum (cm/inches)
Maximum (cm/inches)
AVIATION PERSONNEL:
Candidate for Flight Training
157.4/62
198/78
Class 1 Pilot
157.4/62
198/78
Designated Flight Officer
157.4/62
198/78
Aircrew Candidate
152.5/60
198/78
Designated Aircrew
152.5/60
198/78
ENLISTED PERSONNEL:
Enlistment in USCG
152.5/60
198/78*
Enlistment in USCG Reserve
152.5/60
198/78*
CANDIDATES FOR:
USCG Academy
152.5/60
198/78*
Officer Candidate School
152.5/60
198/78*
Appointment of Licensed
Officers of U.S. Merchant
Marines in the USCG
152.5/60
198/78*
Direct Commission in USCG
152.5/60
198/78*
· MAXIUM HEIGHTS WAIVERABLE TO 203 CM/ 80 INCHES BY COMMANDER
COAST PERSONNEL COMMAND (CGPC-adm-1)
NOTES:
1. Heights are without shoes.
2. Metric conversion: 1 inch = 2.54 cm
CH-17 3-66
FIGURE 3-C-4
MINIMUM DISTANT VISUAL ACUITY REQUIREMENTS
CATEGORY VISION
A. Aviation Personnel: Uncorrected Corrected
1. Candidates for Flight Training 20/50 20/20
2. Pilot, Class 20/200 20/20
3. Pilot, Class 1R (as waivered) 20/20
4. Designated Flight Officer 20/400 20/20
5. Flight Surgeon,
Aviation Medical Examiner or
Aviation MEDEVAC Specialist 20/400 20/20
6. Candidate for Aircrew 20/100 20/20
7. Designated Aircrew 20/200 20/20
8. Landing Signal Officer (LSO) 20/200 20/20
9. Air Traffic Controller Candidate 20/100 20/20
10.Designated Air Traffic Controller 20/200 20/20
B. Officers (Note 1):
1. Commissioned or Warrant in the USCG 20/400 20/20
or USCGR
2. Appointment in the USCG of Licensed 20/400 20/20
Officers of the Merchant Marine
3. Direct Commission in the USCGR 20/400 20/20
4. Appointment as Cadet 20/400 20/20
5. Precommissioning of Cadets 20/400 20/20
6. OCS Candidates 20/400 20/20
7. Precommissioning of Officer Candidates 20/400 20/20
8. Diving Candidates 20/100 20/20
9. Designated Diver 20/200 20/20
C. Enlisted Personnel:
1. Enlistment in the USCG or USCGR See 3.D.13.a (Note 2)
2. Diving Candidates (Note 3) 20/20
3. Designated Diver (Note 3) 20/20
Notes:
1. Refractive error does not exceed plus or minus 8.0 diopters spherical equivalent (sphere + 1/2
cylinder) and that astigmatism does not exceed 3.00 diopters and anisometropia does not
exceed 3.50 diopters.
2. Corrected vision shall be 20/40 in the better eye and 20/70 in the other or 20/30 in the better
eye and 20/100 in the other, or 20/20 in the better and 20/400 in the other. (Note that near
visual acuity must correct to at least 20/40 in the better eye.) Refractive error does not exceed
plus or minus 8.00 diopters spherical equivalent (sphere + 1/2 cylinder) and ordinary
spectacles do not cause discomfort by reason of ghost images, prismatic displacement, etc.;
error must not have been corrected by orthokeratology or keratorefractive surgery.
3. 20/100 in the better eye and 20/200 in the worse eye.
3-67 CH-17
Section D Physical Standards for Enlistment, Appointment, and Induction.
1. Scope. This section implements Department of Defense (DOD) Directive 6130.4
"Physical Standards for Enlistment, Appointment, and Induction," December 14, 2000,
which established physical standards for enlistment, appointment, and induction into the
Armed Forces of the United States in accordance with section 115, title 10, United States
Code (10 USC 133), and by agreement with Secretary, DOT applies to USCG. It is
Coast Guard policy to conform, to the maximum extent possible, to common physical
standards for the acquisition of personnel among all the Armed Forces.
2. Applicability and Responsibilities.
a. Applicability.
(1) This section sets forth the medical conditions and physical defects which are
causes for rejection for military service. Those individuals found medically
qualified based on the medical standards in effect prior to this regulation will
not be reevaluated or medically disqualified solely on the basis of the new
standards.
(2) The standards of this section apply to:
(a) Applicants for enlistment in the Regular Coast Guard. For medical
conditions or physical defects predating original enlistment, these
standards are applicable for enlistees' first 6 months of active duty.
(b) Applicants for enlistment in the Coast Guard Reserve. For medical
conditions or physical defects predating original enlistment, these
standards are applicable during the enlistees' initial period of active duty
for training until their return to Reserve Component units.
(c) Applicants for reenlistment in the Regular Coast Guard and Coast Guard
Reserve after a period of more than 6 months has elapsed since
separation.
(d) Applicants for appointment as commissioned or warrant officers in the
Coast Guard and as modified by section 3-E.
(e) Applicants for the United States Coast Guard Academy (USCGA) and
all other special procurement programs, e.g., Officer Candidate School,
and as modified by section 3-E.
(f) Cadets at the United States Coast Guard Academy, except for such
conditions that have been diagnosed since entrance into the Academy.
With respect to such conditions, upon recommendation of the senior
medical officer, USCGA, the fitness standards of section 3-F are
applicable for retention in the Academy. However, the standard in
paragraph 3-D-39.p applies whether section 3-E or 3-F standards of this
regulation are applicable.
CH-17 3-68
(g) Any individuals that may be inducted into the Coast Guard.
(3) All numbers in parentheses refer to the ICD codes.
b. Responsibilities. Commandant (G-WK) will:
(1) Revise Coast Guard policies to conform with the standards contained in DOD
Directive 6130.4.
(2) Recommend to the Office of the Assistant Secretary of Defense (Health
Affairs) [OASD(HA)] suggested changes in the standards after service
coordination has been accomplished.
(3) Review all the standards on a quinquennial basis and recommend changes to
the OASD(HA). This review will be initiated and coordinated by the DOD
Medical Examination Review Board.
(4) Establish other standards for special programs.
(5) Issue Coast Guard-specific exceptions to these standards, having first
submitted these, with justification, for review and approval by the OASD(HA).
3. Abdominal Organs and Gastrointestinal System. The causes for rejection for
appointment, enlistment, and induction are authenticated history of:
a. Esophagus. Ulceration, varices, fistula, achalasia, or other dysmotility disorders;
chronic, or recurrent esophagitis if confirmed by x-ray or endoscopic examination
(530).
b. Stomach and duodenum.
(1) Gastritis, chronic hypertrophic, severe (535).
(2) Ulcer of stomach or duodenum confirmed by x-ray or endoscopy (533).
(3) Congenital abnormalities of the stomach or duodenum causing symptoms or
requiring surgical treatment (751), except a history of surgical correction of
hypertrophic pyloric stenosis of infancy.
c. Small and large intestine.
(1) Inflammatory bowel disease. Regional enteritis (555), ulcerative colitis (556),
or ulcerative proctitis (556).
(2) Duodenal diverticula. That with symptoms or sequelae (hemorrhage,
perforation, etc.) (562.02).
(3) Intestinal malabsorption syndromes. Including post surgical and idiopathic
(579).
(4) Congenital (751): Condition to include Meckel’s diverticulum or functional
(564) abnormalities, persisting or symptomatic within the past two years.
3-69 CH-17
d. Gastrointestinal bleeding. History of such, unless the cause shall have been
corrected and is not otherwise disqualifying (578).
e. Hepato-pancreatico-biliary tract.
(1) Viral hepatitis (070) or Unspecified hepatitis (570). Hepatitis in the preceding
6 months or persistence of symptoms after 6 months, or objective evidence of
impairment of liver function, chronic hepatitis or hepatitis B carriers (070).
(2) Cholecystitis. Acute or chronic, with or without cholelithiasis (574); and other
disorders of the gallbladder, including postcholecystectomy syndrome (575);
and biliary system (576).
(3) Pancreatitis. Acute (577.0) and chronic (577.1).
f. Anorectal.
(1) Anal fissure if persistent, or anal fistula (565).
(2) Anal or rectal polyp (569.0), stricture (569.2), or incontinence (787.6).
(3) Hemorrhoids. Internal or external, when large, symptomatic, or history of
bleeding (455).
g. Spleen.
(1) Splenomegaly. If persistent (789.2).
(2) Splenectomy (P41.5). Except when accomplished for trauma or conditions
unrelated to the spleen, or for hereditary spherocytosis (282.0).
h. Abdominal wall.
(1) Hernia. Including inguinal (550) and other abdominal (553), except for small,
or asymptomatic umbilical or hiatal.
(2) History of abdominal surgery during the proceding 60 days (P54).
i. Other. Gastrointestinal bypass (P43) or stomach stapling (p44) for control of
obesity. Persons with artificial openings (V44).
4. Blood and Blood-Forming Tissue Diseases. The causes for rejection for appointment,
enlistment, and induction are:
a. Anemia. Any hereditary (282), acquired (283), aplastic (284), or unspecified (285)
anemia that has not been permanently corrected with therapy.
b. Hemorrhagic disorders. Any congenital (286) or acquired (287) tendency to bleed
due to a platelet or coagulation disorder.
c. Leukopenia. Chronic or recurrent (288), based on avilable norms for ethnic
background.
d. Immunodeficiency (279).
CH-17 3-70
5. Dental. The causes of rejection for appointment, enlistment, and induction are as
follows:
a. Diseases of the Jaw or Associated Tissues That Are Not Easily Remediable, and Will
Incapacitate the Individual or Otherwise Prevent the Satisfactory Performance of
Duty. Those diseases include temporomandibular disorder (524.6) and/or myofacial
pain dysfunction that is not easily corrected, or has the potential for significant future
problems with pain and function.
b. Severe malocclusion (524). That malocclusion which interferes with normal
mastication or requires early and protracted treatment; or relationship between
mandible and maxilla that prevents satisfactory future prosthodontic replacement.
c. Insufficient Natural Healthy Teeth (521), or Lack of a Serviceable Prosthesis. Such
condition preventing adequate mastication and incision of a normal diet. That
includes complex (multiple fixture) dental implant systems that have associated
complications that severely limit assignments and adversely affect performance of
worldwide duty. Dental implant system must be successfully osseointegrated and
completed
d. Orthodontic Appliancesfor Continued Treatment (V53.4). Attached or Removable.
Retainer appliances are permissible, if all active orthodontic treatment has been
satisfactorily completed
6. Ears. The causes for rejection for appointment, enlistment, and induction areas follows:
a. External ear. Atresia or severe microtia (744), acquired stenosis (380.5), severe
chronic or acute external (380.2), or severe traumatic deformity (738.7).
b. Mastoids. Mastoiditis (383), residual of mastoid operation with fistula (383.81), or
marked external deformity that prevents or interferes with the wearing of protective
mask or helmet (383.3).
c. Meniere's Syndrome, or Other diseases of the Vestibular System (386).
d. Middle ear. Acute or chronic otitis media (382), cholesteatoma (385.3), or history of
any inner (P20) or middle (P19) ear surgery, excluding myringotomy or successful
tympanoplasty.
e. Tympanic membrane.
7. Hearing. The cause for rejection for appointment, enlistment, and induction is a hearing
threshold level greater than that described in 3-D-7-a-(3), below (389):
a. Audiometric Hearing Levels.
(1) Audiometers, calibrated to the International Standards Organization (ISO
1964) or the American National Standards Institute (ANSI 1969), shall be used
to test the hearing of all applicants.
3-71 CH-17
(2) All audiometric tracings or audiometric readings recorded on reports of
medical examinations or other medical records shall be clearly identified.
(3) Acceptable audiometric hearing levels (both ears) are as follows:
(a) Pure tone at 500, 1000, and 2000 cycles per second of not more than 30
dB on the average with no individual level greater than 35 dB at those
frequencies.
(b) Pure tone level not more than 45 dB at 3000 cycles per second and 55 dB
at 4000 cycles per second.
8. Endocrine and Metabolic Disorders. The cause for rejection for appointment,
enlistment, or induction are an authenticated history of the following:
a. Adrenal dysfunction (255). Of any degree.
b. Diabetes Mellitus (250). Of any type.
c. Glycosuria. Persistent, when associated with impaired glucose tolerance (250) or
renal tubular defects (271.4
d. Acromegaly. Gigantism, or other disorder of pituitary function (253).
e. Gout (274).
f. Hyperinsulinism (251.1).
g. Hyperparathyroidism (252.0) and hypoparathyroidism (252.1).
h. Thyroid disorders.
(1) Goiter. Persistent or untreated (240).
(2) Hyperthyroidism. Condition uncontrolled by medication (244).
(3) Cretinism (243).
(4) Hypothyroidism (242).
(5) Thyroiditis (245).
i. Nutritional Deficiency Diseases. Such diseases include beriberi (265), pellagra
(265.2), and scurvy (267).
j. Other Endocrine or Metabolic Disorders. Such disorders such as cystic fibrosis
(277), porphyria (277.1), and amyloidosis (277.3) that prevent satisfactory
performance of duty or require frequent or prolonged treatment.
9. Upper Extremities (see also section 3-D-11, below). The causes for rejection for
appointment, enlistment, and induction areas follows:
CH-17 3-72
a. Limitation of motion. An individual will be considered unacceptable if the joint
ranges of motion are less than the measurements listed below. Methods of
measurement appear in EXHIBIT 3-F-1.
(1) Shoulder (726.1).
(a) Forward elevation to 90 degrees.
(b) Abduction to 90 degrees.
(2) Elbow (726.3).
(a) Flexion to 100 degrees.
(b) Extension to 15 degrees.
(3) Wrist (726.4). A total range to 60 degrees (extension plus flexion). Radial and
ulnar deviation combined arc 30 degrees.
(4) Hand.
(a) Pronation to 45 degrees.
(b) Supination to 45 degrees.
(5) Fingers and thumb (726.4). Inability to clench fist, pick up a pin, grasp an
object or touch tips of at least 3 fingers with thumb.
b. Hand and fingers.
(1) Absence of the distal phalanx of either thumb(885).
(2) Absence of distal and middle phalanx of an index, middle, or ring finger of
either hand irrespective of the absence of little finger (866).
(3) Absence of more than the distal phalanx of any two of the following fingers:
index, middle finger, or ring finger of either hand (886).
(4) Absence of a hand or any portion thereof (887), except for fingers as noted
above.
(5) Polydactyly (755).
(6) Scars and deformities of the fingers or hand (905.2) that are symptomatic, or
impair normal function to such a degree as to interfere with the satisfactory
performance of military duty.
(7) Intrinsic paralysis or weakness, including nerve palsy (354) sufficient to
produce physical findings in the hand such as muscle atrophy or weakness.
c. Wrist, Forearm, Elbow, Arm, and Shoulder. Recovery from disease or injury with
residual weakness or symptoms such as to prevent satisfactory performance of duty
(905.2), or grip strength of less than 75 percent of predicted normal when injured

3-73 CH-17
hand is compared with the normal hand (nondominant is 80 percent of dominant
grip).
10. Lower Extremities (see 3-D-11). The causes for rejection for appointment, enlistment,
and induction are as follows:
a. Limitation of motion. An individual will be considered unacceptable if the joint
ranges of motion are less than the measurements listed below. Methods of
measurement appear in EXHIBIT 3-F-1.
(1) Hip. Due to disease(726.5) or injury (905.2).
(a) Flexion to 90 degrees (minimum).
(b) No demonstrable flexion contracture.
(c) Extension to 10 degrees (beyond 0 degree).
(d) Abduction to 45 degrees.
(e) Rotation - 60 degrees (internal and external combined).
(2) Knee. Due to disease (726.7) or injury (905.4).
(a) Full extension compared with contralateral.
(b) Flexion to 90 degrees.
(3) Ankle. Due to disease (726.7) or injury (905.4).
(a) Dorsiflexion to 10 degrees.
(b) Plantar flexion to 30 degrees.
(c) Eversion and inversion (total to 5 degrees).
(4) Subtalar. Due to disease (726.7) or injury (905.4).
(a) Eversion and inversion total to 5 degrees.
b. Foot and ankle.
(1) Absence of one or more small toes (895). If the function of the foot is poor, or
running or jumping is prevented; absence of a foot (896) or any portion thereof
except for toes as noted herein.
(2) Absence of great toe(s) (895). Loss of dorsal and/or planter flexion if the
function of the foot is impaired (905.4).
(3) Deformities of the toes. Either acquired (735) or congental (755.66), including
polydactyly (755.02), that prevents the wearing of military footwear, or
impairs walking, marching, running, or jumping. That includes hallux valgus
(735).
CH-17 3-74
(4) Clubfoot and/or Pes Cavus (754.5). If stiffness or deformity prevents foot
function or wearing military footwear.
(5) Symptomatic Pes planus. Acquired (34) or congenital (754.6) or pronounced
cases with absence of subtalar motion.
(6) Ingrown toenails (703). If severe.
(7) Planter Fasciitis (728.7). If persistent.
(8) Neuroma (355.6). Confirmed condition and refractory to medical treatment, or
will impair function of the foot.
c. Leg, knee, thigh, and hip.
(1) Loose or foreign bodies in the knee joint (717.6). History of surgical correction
of knee ligaments.
(2) Physical findings of an unstable or internally deranged joint (717.9). History
of uncorrected anterior (717.83) or posterior (717.84) cruciate ligament injury.
(3) Surgical correction of any knee ligaments (P81), if symptomatic or unstable.
(4) History of congenital dislocation of the hip (754.3). Osteochondritis of the hip
(Legg-Perthes Disease) (732.1), or slipped femoral epiphysis of the hip
(732.2).
(5) Hip dislocation (835). Dislocation within 2 years before examination.
(6) Osteochondritis of the tibial tuberosity (Osgood-Schlatter Disease) (732.4). If
symptomatic.
d. General.
(1) Deformities (905.4), disease, or chronic pain (719.4) of one or both lower
extremities that have interfered with function to such a degree as to prevent the
individual from following a physically active vocation in civilian life; or that
would interfere with walking, running, weight bearing, or the satisfactory
completion of training or military duty.
(2) Shortening of a lower extremity (736.81), resulting in a noticeable limp or
scoliosis.
11. Miscellaneous Conditions of the Extremities. (see 3-D-9 and 3-D-10). The causes for
rejection for appointment, enlistment, and induction areas follows:
a. Arthritis.
(1) Active, subactive, or chronic arthritis (716).
(2) Chronic osteoarthritis (715.3) or traumatic arthritis (716.1) of isolated joints of
more than a minimal degree, that has interfered with the following of a
physically active vocation in civilian life or that prevents the satisfactory
performance of military duty.
3-75 CH-17
b. Chronic retropatellar knee pain syndrome with or without confirmatory arthroscopic
valuation (717.7).
c. Dislocation, if unreduced; or recurrent dislocations of any major joint. Such as,
shoulder (831), hip (835), elbow (832), knee (836); or stability of any major joint
(shoulder(718.1), elbow (718.3, or hip(718.5)).
d. Fractures.
(1) Malunion or non-union of any fracture (733.8). Except ulnar styloid process.w
(2) Orthopedic hardware (733.99). hardware including plates, pins, rods, wires, or
screws used for fixation and left in place; except that a pin, wire or screw not
subject to easy trauma is not disqualifying.
e. Injury of a bone or joint. An injury of more than a minor nature, with or without
fracture or dislocation, which occurred in the preceding 6 weeks (upper extremity
(923), lower extremity (924), or rib and clavicle (922)).
f. Joint replacement (V43.6).
g. Muscular paralysis, contracture, or atrophy (728). If progressive or of sufficient
degree to interfere with military service, and muscular dystrophies (359).
h. Osteochondritis dessicans (732.7).
i. Osteochondromatosis or multiple cartilaginous exostoses (727.82).
j. Osteomyelitis (730). Active or recurrent
k. Osteoporosis (733).
l. Scars (709.2). Extensive, deep, or adherent to the skin and soft tissues that interfere
with muscular movements.
m. Implants. Silastic or other devices implanted or correct orthopedic abnormalities
(V43).
12. Eyes. The cause for rejection for appointment, enlistment, or induction are as follows
a. Lids.
(1) Blepharitis (373). Chroniccondition, of more than mild degree.
(2) Blepharospasm (333.81).
(3) Dacryocystitis. Acute or chronic (375.3).
(4) Deformity of the lids (374.4). Complete or extensive lid deformity, sufficient
to interfere with vision or impair protection of the eye from exposure.

CH-17 3-76
b. Conjunctiva.
(1) Conjunctivitis. Chronic condition (372.1), including trachoma (076), and
allergic conjunctivitis (372.13).
(2) Ptergium (372.4). If condition encroaching on the cornea in excess of 3
millimeters, interfering with vision, progressive (372.42) or recurring after two
operative procedures (372.45).
(3) Xerophthalmia (372.53).
c. Cornea.
(1) Dystrophy. Corneal dystrophy, of any type (371.5), including, keratoconus
(371.6) of any degree.
(2) Keratorefractive surgery. History of lamellar (P11.7) and/or penetrating
keratoplasty (P11.6). Laser surgery or appliance utilized to reconfigure the
cornea is also disqualifying.
(a) Waivers for Photorefractive Keratectomy (PRK) and Laser In-situ
Keratomileusis (LASIK) will be considered if the following criteria are
met:
1 Pre-operative refractive error did not exceed +8.00 to-8.00 diopters
(spherical equivalent) in either eye.
2 At least 12 months since surgery or last enhancement.
3 Refractive stability as demonstrated by less than 0.50 diopter change
in either eye over two separate exams at least three months apart.
4 All pre-operative, operative and post-operative records are
submitted for review.
5 No complications or side effects as a result of the surgery such as
decreased night vision, glare sensitivity, halos around light or
worsening of the pre-operative best vision due to scar formation.
6 Accession standards outlined in section 3-D and 3-E are met.
(b) PRK and LASIK are disqualifying for aviation duty and landing signal
officer duty.
(c) LASIK is disqualifying for diving duty.
(3) Keratitis (370). Acute or chronic keratitis, which includes recurrent corneal
ulcers, erosions (abrasions), or herpetic ulcers (054.42).
(4) Vascularization (370.6) or opacification (371) of the cornea. Condition from
any cause that is progressive or reduces vision below the standards prescribed
in 3-D-13.
3-77 CH-17
d. Uveitis (364) or Iridocyclitis.
e. Retina.
(1) Angiomatoses (759.6). Or other congenito-hereditary retinal dystrophy (362.7)
that impairs visual function.
(2) Chorioretinitis (363). Unless single episode that has healed and does not
interfere with vision.
(3) Congenital or degenerative changes of any part of the retina (362).
(4) Detachment of the retina (361). A history of surgery for same, or peripheral
retinal injury or degeneration likely to cause retinal detachment.
(5) Chorioretinis or inflammation of the retina (363). Condition including
(histoplasmosis, toxoplasmosis or vascular conditions of the eye to include
Coats' disease, Eales' disease, and retinitis proliferans), unless a single episode
known cause that has healed and does not interfere with vision.
f. Optic nerve.
(1) Optic neuritis (377.3). Neuroretinitis, or secondary optic atrophy or
documented history of attacks of retrobulbar neuritis.
(2) Optic atrophy (377.1) or Cortical Blindness (377.7).
(3) Papilledema (377.0).
g. Lens.
(1) Aphakia (379.3). Lens implant, or dislocation of a lens.
(2) Opacities of the lens (366). Those conditions that interfere with vision or that
are considered to be progressive.
h. Ocular mobility and motility.
(1) Diplopia (368.2). Documented, constant or intermittent.
(2) Nystagmus (379.5).
(3) Strabismus (378). Uncorrectable by lenses to less than 40 diopters or
accompanied by diploplia.
(4) Strabismus. Corrective surgery (P15) in the preceding 6 months.
(5) See section 3-E for additional standards for officer programs.
i. Miscellaneous defects and diseases.
(1) Abnormal visual fields due to diseases of the central nervous system (368.4),
or trauma (368.9). Meridian specific visual field minimums areas follows:
(a) Temporal: 85 degrees.
CH-17 3-78
(b) Superior temporal: 55 degrees.
(c) Superior: 45 degrees.
(d) Superior nasal: 55 degrees.
(e) Nasal: 60 degrees.
(f) Inferior nasal: 50 degrees.
(g) Inferior: 65 degrees.
(h) Inferior temporal: 85 degrees.
(2) Absence of an eye. Congenital (743) or acquired (360.8).
(3) Asthenopia (368.13). Severe.
(4) Exophthalmos (376). Unilateral or bilateral, non-familial.
(5) Glaucoma (365). Primary, or secondary, or pre-glaucoma as evidenced by
intraocular pressure above 21 mm/Hg, or the secondary changes in the optic
disc or visual field loss associated with glaucoma.
(6) Loss of normal pupillary reflex reactions to light or accommodation (367.5) or
light (379.4), including Adie's syndrome.
(7) Night blindness (368.6).
(8) Retained introcular foreign body (360).
(9) Tumors. Growths or tumors of the eyelid, other than small basal cell tumors
that may be cured by treatment, and small nonprogressive asymptomatic
benign lesions.
(10) Any organic disease of the eye (360) or adnexa (376) not specified above, that
threatens vision or visual function.
13. Vision. The cause of medical rejection for appointment, enlistment, and induction are
listed below. (See section 3-E for additional standards for officer programs.)
a. Distant visual acuity. Distant visual acuity of any degree that does not correct with
spectacle lenses to at least one of the following (367):
(1) 20/40 in one eye and 20/70 in the other eye.
(2) 20/30 in one eye and 20/100 in the other eye.
(3) 20/20 in one eye and not exceeding 20/400 in the other eye.
b. Near visual acuity. Near visual acuity of any degree that does not correct to 20/40 in
the better eye (367).
c. Refractive error (Hyperopia 367.0, Myopia 367.1, Astigmatism 367.2). Any
refractive error in spherical equivalent of worse than - 8.00 or + 8.00 diopters; or if
3-79 CH-17
ordinary spectacles cause discomfort by reason of ghost images, prismatic
displacement; or if corrected by orthokeratology or keratorefractive surgery.
d. Contact lenses. Complicated cases requiring contact lenses for adequate correction
of vision such as corneal scars (371) and irregular astigmatism (367.2).
e. Color vision. (368.5). All applicants for initial entry into the Coast Guard, all officer
candidates, all commissioning candidates, and all aviation candidates shall be tested
for color vision. There is NO requirement for enlisted personnel to demonstrate
normal color vision. A listing of current enlisted specialties that require normal
color vision can be obtained from unit personnel offices or departments. Normal
color vision IS required for all officer candidates and some commissioned warrant
specialties (check with unit personnel offices for current listing).
14. Female Genitalia. The causes for rejection for appointment, enlistment, and induction
areas follows:
a. Abnormal uterine bleeding (626.2). Including such bleeding as menorrhagia,
metrorrhagia or polymenorrhea.
b. Amenorrhea (626.0). Unexplained
c. Dysmenorrhea (625.3). Incapacitating to a degree recurrently necessitating absences
of more than a few hours from routine activities.
d. Endometriosis (617).
e. Hermaphroditism (752.7).
f. Menopausal Syndrome (627). If manifested by more than mild constitutional or
mental symptoms or artificial menopause less than a 1-year duration.
g. Ovarian Cysts (620). Persistent or clinically significant.
h. Pelvic Inflammatory disease (614). Acute or chronic.
i. Pregnancy (V22).
j. Uterus. Congenital absence of (752.3) or enlargement due to any cause (621.2).
k. Vulvar or Vagina Ulceration (616.5). Including herpes genitalis (054.11) and
condyloma acuminatum (078.11): acute or chronic, not amenable to treatment. Such
treatment must be given and demonstrated effective prior to accession.
l. Abnormal Pap Smear (795). Graded LGSIL or higher severity; or any smear in
which the descriptive terms carcinoma-in-situ, invasive cancer, condyloma
accuminatum, human papilloma virus, or dysplasia are used.
CH-17 3-80
m. Major abnormalities and defects of the genitalia, such as a change of sex (P64.5). A
history thereof, or dysfunctional residuals from surgical correction of these
conditions.
15. Male Genitalia. The cause of medical rejection for appointment, enlistment, or
induction are:
a. Absence of both testicles. Congenital (752.8) or acquired (878.2), or unexplained
absence of a testicle.
b. Epispadias or Hypospadias (752.6). when accompanied by evidence of infection of
the urinary tract, or if clothing is soiled when voiding.
c. Undiagnosed enlargement or mass of testicleor epididymis (608.9).
d. Undescended testicle(s) (752.5).
e. Orchitis (604). Acute, or chronic epididymitis.
f. Penis. Amputation of (878), if the resulting stump is insufficient to permit
micturition in a normal manner.
g. Penile infectious lesions. Including herpes genitalis (054.1) and condyloma
acuminatum (078.11): acute or chronic, not amenable to treatment. Such treatment
must be given and demonstrated effective prior to accession.
h. Prostatitis (601). Acute or chronic condition.
i. Hydrocele (603.9). Left varicocele (if painful), or any right varicocele (456.4)
j. Major abnormalities and defects of the genitalia, such as a change of sex (P64.5). A
history thereof, or dysfunctional residuals from surgical correction of these
conditions.
16. Urinary System The causes for rejection for appointment, enlistment, and induction are:
a. Cystitis (595).
b. Urethritis (597).
c. Enuresis. (788.3) or incontinence of urine beyond age 12 (788.3).
d. Hematuria, Pyuria, or other findings indicative of urnnary tract disease (599).
e. Urethral stricture (598) or fistula (599.1).
f. Kidney.
(1) Absence of one kidney. Congenital (753.0) or acquired (593.89).
(2) Infections. Acute or chronic infections (590).
3-81 CH-17
(3) Polycystic kidney (753.1). Confirmed history of such a condition.
(4) Horseshoe kidney (753.3).
(5) Hydronephrosis (591).
(6) Nephritis. Acute (580) or chronic (582).
(7) Proteinuria (791). Under normal activity (at least 48 hours after strenuous
exercise) greater than 200 mg/24 hours, or a protein to creatinine ratio greater
than 0.2 in a random urine sample, unless nephrologic consultation determines
the condition to be benign orthostatic proteinuria.
(8) Renal Calculus (592). Within the previous 12 months, recurrent calculus,
nephrocalcinosis, or bilateral renal calculi at any time.
17. Head. The causes for rejection for appointment, enlistment, and induction are:
a. Injuries. Including severe contusions and other wounds of the scalp (920) and
cerebral concussion (850), until a period of 3 months has elapsed. (See 3-D-27).
b. Deformities of the skull, face, or jaw (754.0). Such deformities of a degree that will
prevent the individual from wearing a protective mask or military headgear.
c. Defects (756.0). Loss, or congenital absence of the bony substance of the skull not
successfully corrected by reconstructive materials, or leaving residual defect in
excess of one square inch (6.45cm) or the size of a 25-cent piece.
18. Neck. The causes of rejection for appointment, enlistment, and induction are:
a. Cervical ribs (756.2). If symptomatic, or so obvious that they are found on routine
physical examination. (Detection based primarily on x-rays is not considered to
meet this criterion.)
b. Congential cysts (744.4). Those cysts of branchial cleft origin or those developing
from the remnants of the thyroglossal duct, with or without fistulous tracts.
c. Contraction (723.8). Contraction of the muscles of the neck, spastic or non-spastic,
or cicatricial contracture of the neck to the extent that it interferes with the wearing
of a uniform or military equipment, or is so disfiguring as to impair military bearing.
19. Heart. The causes for rejection for appointment, enlistment, and induction are:
a. All valvular heart diseases. Congenitial (746) or acquired (394), including those
improved by surgery, except mitral valve prolapse and bicuspid aortic valve. Those
latter two conditions are not reasons for rejection unless there is associated
tachyarrhythmia, mitral regurgitation, aortic stenosis, insufficiency, or cardiomegaly.
b. Coronary heart disease (410).
c. Symptomatic arrhythmia or (electrocardiographic evidence of arrhythmia). A
history of such condition.
CH-17 3-82
(1) Supraventricular tachycardia (427.0). Or any dysrhythia originating from the
atrium or sinoatrial node, such as atrial flutter, and atrial fibrillation unless
there has been no recurrence during the preceding 2 years while off all
medications. Premature atrial or ventricular contractions are disqualifying
when sufficiently symptomatic to require treatment or result in physical or
psychological impairment
(2) Ventricular Arrythmias (427.1). Those arrythmias including ventricular
fibrillation, tachycardia, and multifocal premature ventricular contractions.
Occasional asymptomatic premature ventricular contractions are not
disqualifying.
(3) Ventricular Conduction disorders. Such disorders with left bundle branch
block (426.2), Mobitz type II second degree AV block (426.12). third degree
AV block (426.0). Wolff-Parkinson-White syndrome (426.7) and Lown-
Ganong-Levine Syndrom (426.81) associated with an arrhythmia are also
disqualifying.
(4) Conduction Disturbances. Conduction disturbances such as first degree AV
block (426.11), left anterior hemiblock (426.2), right bundle branch block
(426.4) or Mobitz type I second degree AV block (426.13) are disqualifying
when symptomatic or associated with underlying cardiovascular disease.
d. Hypertrophy or dilatation of the heart (429.3).
e. Cardiomyopathy (425). Including myocarditis (422), or history of congestive heart
failure (428) even though currently compensated.
f. Pericarditis (420).
g. Persistent tachycardia (785) (Resting pulse rate of 100 or greater).
h. Congenital anomalies of heart and great vessels (746). Except forcorrected patent
ductus arteriosus.
20. Vascular System. The causes for rejection for appointment, enlistment, and induction
are:
a. Abnormalities of the arteries and blood vessels (447). Abnormalities including
aneurysms (442) even if repaired, atherosclerosis (440), and arteritis (446).
b. Hypertensive Vascular Disease (401). Such disease evidenced by the average of
three consecutive averaged diastolic blood pressure measurements greater than
90 mmHg or three consecutive averaged systolic blood pressures greater than 140
mmHg at any age. High blood pressure requiring medication or a history of
treatment including dietary restriction is also disqualifying.
c. Pulmonary (415) or systemic embolization (444).
3-83 CH-17
d. Peripheral Vascular Disease. Including diseases such as Raynaud's phenomenon
(443).
e. Vein diseases. Vein disease including recurrent thrombophlebitis (451),
thrombophlebitis during the preceding year, or any evidence of venous
incompetence, such as large or symptomatic varicose veins, edema, or skin
ulceration (454).
21. Height. The causes for rejection for appointment, enlistment, and induction in relation
to height standards are established by each of the military Services. Standards for the
Coast Guard are:
a. Men: Height below 152.5 cm (60 inches) or over 198 cm (78 inches).
b. Women: Height below 152.5 cm (60 inches) or over 198 cm (78 inches).
22. Weight. The causes for rejection for appointment, enlistment, and induction in relation
to weight standards are contained in COMDTINST 1020.8(series).
23. Body Build. The cause for rejection for appointment, enlistment, and induction are:
a. Congenital malformation of bones and joints. (See 3-D-9 through 3-D-11).
b. Deficient muscular development that would interfere with the completion of required
training.
c. Evidence of congenital asthenia or body build that would interfere with the
completion of required training.
24. Lungs, Chest Walls, Pleura, and Mediastinum. The causes for rejection for appointment,
enlistment, and induction are:
a. Abnormal elevation of the diaphragm (793.2). Such elevation may be either side.
b. Abscess of the lung (513).
c. Acute infectious process of the lung (518). Until cured.
d. Asthma (493). Including reactive airway disease, exercise-induced bronchospasm,
or asthmatic bronchitis, reliably diagnosed at any age. Reliable diagnostic criteria
shall consist of any of the following elements.
(1) Substantiated history of cough, wheeze, and/or dyspnea which persists or
recurs over a prolonged period of time, generally more than 6 months.
(2) If the diagnosis of asthma is in doubt, a test for reversible airflow obstruction
(greater than a 15 percent increase in FEV I following administration of an
inhaled bronchodilator), or airway hyperreactivity (exaggerated decrease in
airflow induced by a standard bronchoprovocational challenge such as
methacholine inhalation or a demonstration of exercise-induced
bronchospasms) must be performed.
CH-17 3-84
e. Bronchitis (490). That which is chronic, symptoms over 3 months occurring at least
twice a year.
f. Bronchiectasis (494).
g. Bronchopleural fistula (510).
h. Bullous or generalized pulmonary emphysema (492).
i. Chronic Mycotic disease (117) of the lung. Such diseases including
coccidioidomycosis.
j. Chest Wall Malformation (754) or fracture (807). Those conditions that interfere
with vigorous physical exertion.
k. Empyema (510). That condition includes residual pleural effusion (511.9), or
unhealed sinuses of chest wall (510).
l. Extensive pulmonary fibrosis (515).
m. Foreign body in lung, trachea or bronchus (934).
n. Lobectomy. With residual pulmonary disease or removal of more than one lobe
(P32.4).
o. Pleurisy with effusion (511.9). That condition occurring within the previous 2 years
if known origin, or unknown origin.
p. Pneumothorax (512). That condition occurring during the year preceding
examination if due to simple trauma or surgery, during the 3 years preceding
examination from spontaneous origin. Recurrent spontaneous pneumothorax after
surgical correction or pleural sclerosis.
q. Sarcoidosis. (See 3-D-35-j.)
r. Silicone breast implants. Those encapsulated (85.53P), if less than 9 months since
surgery or with symptomatic complications.
s. Tuberculous lesions. (see subsection 3-D-35-l.)
25. Mouth. The cause for rejection for appointment, enlistment, and induction are:
a. Cleft lip or palate defects (749). Unless satisfactorily repaired by surgery.
b. Leukoplakia (528.6).
26. Nose and Sinuses. The causes for rejection of appointment, enlistment, and induction
are:
a. Allergic manifestations.
3-85 CH-17
(1) Atrophic rhinitis. (472).
(2) Allergic rhinitis, vasomotor rhinitis (477). If moderate or severe and not
controlled by oral medications, desensitization, or topical corticosteroid
medication.
b. Vocal cord paralysis (478.3). Or, symptomatic disease of the larynx (478.7).
c. Anosmia or parosmia (352).
d. Epistaxis (784.7). Recurrent condition.
e. Nasal polyps (471). Unless surgery was performed at least 1 year before
examination.
f. Perforation of nasal septum (478.1). If symptomatic or progressive.
g. Sinusitis (461). Acute.
h. Sinusitis chronic (473). Such condition exists when evidenced by chronic purulent
nasal discharge, hyperplastic changes of the nasal tissue, symptoms requiring
frequent medical attention, or x-ray findings.
i. Larynx ulceration, polyps, or granulation tissue, or chronic laryngitis (476).
j. Tracheostomy (V44), or tracheal fistula (530.84).
k. Deformities or conditions (750.9). Those of the mouth, tongue, palate, throat,
pharynx, larynx, and nose that interfere with chewing, swallowing, speech, or
breathing.
l. Pharyngitis (462) and nasopharyngitis (472.2). Chronic conditions.
27. Neurological Disorders. The causes for rejection for appointment, enlistment, and
induction are:
a. Cerebrovascular conditions. Any history of subarachnoid (430) or interacerebral
(431) hemorrhage, vascular insufficiency, aneurysm or arteriovenous malformation
(437).
b. Congenital malformations (742). If associated with neurological manifestations, or
if known to be progressive; meningocele (741), even if uncomplicated.
c. Degenerative and hereditodegenerative disorders. Those disorders affecting the
cerebrum (330), basal ganglia (333), cerebellum (334), spinal cord (335), and
peripheral nerves or muscles (337).
d. Recurrent headaches (784). Headaches of all types of sufficient severity or
frequency as to interfere with normal function within the previous 3 years.

CH-17 3-86
e. Head injury.
(1) Applicants with a history of head injury with:
(a) Late post-traumatic epilepsy (occurring more than 1 week after injury).
(b) Permanent motor or sensory deficits.
(c) Impairment of intellectual function.
(d) Alteration of personality.
(e) Central nervous system shunts.
(2) Applicants with a history of severe closed head injury are unfit for a period of
at least 5 years after the injury. After 5 years they may be considered fit if
complete neurological and neuropsychological evaluation shows no residual
dysfunction or complications. Applicants with a history of severe penetrating
head injury are unfit for a period of at least 10 years after the injury. After 10
years they may be considered fit if complete neurological and
neuropsychological evaluation shows no residual dysfunctionn or
complications. Severe head injuries are defined by one or more of the
following.
(a) Unconsciousness or amnesia. Conditions alone or in combination of 24-
hours duration or longer.
(b) Depressed skull fracture.
(c) Laceration or contusion of the dura mater or the brain.
(d) Epidural, subdural, subarachnoid or intracerebral hematoma.
(e) Associated abscess or meningitis.
(f) Cerebrospinal fluid rhinorrhea or otorrhea persisting more than 7 days.
(g) Focal neurologic signs.
(h) Radiographic evidence of retained metallic or bony fragments.
(i) Leptomeningeal cysts or arteriovenous fistula.
(j) Early post-traumatic seizure(s) that occur only within 1 week of injury
but more than 30 minutes after injury.
(3) Applicants with a history of moderate head injury. Those applicants are unfit
for a period of at least 2 years after the injury. After 2 years they may
considered fit if complete neurological evaluation shows no residual
dysfunction or complications. Moderate head injuries are defined as

3-87 CH-17
unconsciousness or amnesia, alone or in combination, of 1 to 24 hours
duration, or linear skull fracture.
(4) Applicants with a history of mild head injury. Those applicants with mild head
injuries, as defined by a period of unconsciousness or amnesia, alone or in
combination, of 1 hour or less, are unfit for at least 1 month after the injury.
After 1 month they be acceptable if complete neurological evaluation shows no
residual dysfunction or complications.
(5) Persistent post-traumatic seizure. Such conditions, as manifested by headache,
vomiting, disorientation, spatial disequilibrium, personality changes, impaired
memory, poor mental concentration, shortened attention span, dizziness,
altered sleep patterns, or any findings consistent with organic brain syndrome,
are disqualifying until full recovery has been confirmed by complete
neurological and neuropsychological evaluation.
f. Infectious diseases.
(1) Meningitis (322), encephalitis (323), or poliomyelitis (045). Such diseases
occurring within 1 year before examination, or if there are residual
neurological defects.
(2) Neurosyphilis (094). That disease of any form (general paresis, tabes dorsalis,
meningovascular syphilis).
g. Narcolepsy (347), sleep apnea syndrome (780.57).
h. Paralysis, weakness, lack of coordination, chronic pain, or sensory disturbances
(344).
i. Epilepsy (345). That epilepsy occurring beyond the age of 5 years, unless the
applicant has been free of seizures for a period of 5 years while taking no medication
for seizure control, and has a normal electroencephalogram (EEG). All such
applicants shall have a current neurology consultation with current EEG results.
EEG may be requested by reviewing authority
j. Chronic disorders. Disorders such as myasthenia gravis (358), and multiple sclerosis
(340).
k. Central nervous system shunts of all kinds (V45.2).
28. Disorders with Psychotic Features. The causes for rejection for appointment, enlistment,
and induction are a history of a disorders with psychotic features (295).
29. Neurotic, Anxiety, Mood, Somatoform, Dissociative, or Factitious Disorders (300). The
causes for rejection for appointment, enlistment, and induction are:
a. History of such disorders resulting in any or all of the below:
(1) Admission to a hospital or residential facility.

CH-17 3-88
(2) Care by a physician or other mental health professional for more than 6
months.
(3) Symptoms or behavior of a repeated nature that impaired social, school, or
work efficiency.
30. Personality, Conduct, and Behavior Disorders. The cause for rejection for appointment,
enlistment, and induction are a history of such disorder resulting in any or all of the
below:
a. Personality (301), Conduct (312), or Behavior (313) disorders. Disorders as
evidenced by frequent encounters with law enforcement agencies, antisocial attitudes
or behavior that while not sufficient cause for administrative rejection, are tangible
evidence of impaired capacity to adapt to military service.
b. Personality (301), Conduct (312), or Behavior (313) disorders. Where it is evident
by history, interview, or psychological testing that the degree of immaturity,
instability, personality inadequacy, impulsiveness, or dependency will seriously
interfere with adjustment in the Coast Guard as demonstrated by repeated inability to
maintain reasonable adjustment in school, with employers and fellow workers, and
other social groups.
c. Other behavior disorders including, but not limited to, conditions such as the
following:
(1) Authenticated evidence of functional enuresis (307.6) or encopresis (307.7).
(2) Sleepwalking (307.6).
(3) Eating disorders that are habitual or persistent (307.1 or 307.5) occurring
beyond age 12.
(4) Stammering (307.0) of such a degree that the individual is often unable to
express himself or herself clearly, or to repeat commands.
d. Specific academic skills defects. Chronic history of academic skills (314) or
perceptual defects (315), secondary to organic or functional mental disorders that
interfere with work or school after age 12. Current use of medication to improve or
maintain academic skills.
e. Suicide. History of attempted suicide or other suicidal behavior (300.9).
31. Psychosexual Conditions. The causes for rejection for appointment, enlistment, or
induction are transsexualism, exhibitionism, transvestism, voyeurism, and other
paraphilias (320).
32. Substance Misuse. The causes for rejection for appointment, enlistment, or induction
are:
a. Alcohol dependence (303).
b. Drug dependence (304).
3-89 CH-17
c. Non-dependent use of drugs characterized by the following:
(1) The evidence of use of any controlled, hallucinogenic, or other intoxicating
substance at the time of examination (305), when the use cannot be accounted
for as a result of a prescription by a physician.
(2) Documented misuse or abuse of any controlled substance (including
cannabinoids or anabolic steroids) requiring professional care (305).
(3) The repeated self-procurement and self-administration of any drug or chemical
substance, including cannabinoids or anabolic steroids, with such frequency
that it appears that the applicant has accepted the use of or reliance on those
substances as part of his or her pattern of behavior (305).
(4) The use of LSD (305.3) in a 2-year period before examination.
d. Alcohol abuse (305). Use of alcoholic beverages, which leads to misconduct,
unacceptable social behavior, poor work or academic performance, impaired
physical or mental health, lack of financial responsibility, or a disrupted personal
relationship.
33. Skin and Cellular Tissues. The causes for rejection for appointment, enlistment, and
induction are:
a. Acne (706). Severe acne, or when extensive involvement of the neck, shoulders,
chest, or back would be aggravated by or interfere with the wearing of military
equipment and not amenable to treatment. Patients under treatment with isotretinoin
(Accutane) are medically unacceptable until 8 weeks after completion of a course of
therapy.
b. Atopic dermatitis (691) or eczema (692). Occurring with active or residual lesions in
characteristic areas (face and neck, antecubital and/or popliteal fossae, occasionally
wrists and hands), or documented history thereof after the age of 8.
c. Contact dermatitis (692.4). Dermatitis especially involving rubber or other materials
used in any type of required protective equipment.
d. Cysts.
(1) Cysts (706.2), other than pilonidal. Cysts of such a size or location as to
interfere with the normal wearing of military equipment.
(2) Cysts, pilonidal (685). Pilonidal cysts evidenced by the presence of a tumor
mass or discharging sinus. History of pilonidal cystectomy within 6 months
before examination.
e. Dermatitis factitia (698.4).
f. Bullous dermatoses (694). Conditions such as dermatitis herpetiformis, pemphigus,
and epidermolysis bullosa.
CH-17 3-90
g. Chronic lymphedema (457).
h. Fungus infections (117). Systemic or superficial types, if extensive and not
amenable to treatment.
i. Furunculosis (680). Extensive, recurrent, or chronic.
j. Hyperhidrosis of hands or feet (780.8). Chronic or severe.
k. Ichthyosis. Or other congenital (757) or acquired (216) anomalies of the skin, such
as nevi or vascular tumors that interfere with function or are exposed to constant
irritation.
l. Keloid formation (701-4). If the tendency is marked or interferes with the wearing
of military equipment.
m. Leprosy (030.9).
n. Lichen planus (697.0).
o. Neurofibromatosis (Von Recklinghausen's disease) (237.7).
p. Photosensitivity (692.72). Any primary sun-sensitive condition, such as
polymorphous light eruption or solar urticaria; any dermatosis aggravated by
sunlight such as lupus erythematosus.
q. Psoriasis (696.1). Unless mild by degree, not involving nail-pitting, and not
interfering with the wearing of military equipment or clothing.
r. Radiodermatitis (692.82).
s. Scars (709.2). Scars so extensive, deep, or adherent that they may interfere with the
wearing of military clothing or equipment, exhibit a tendency to ulcerate, or interfere
with function. Includes scars at skin graft donor or recipient sites if in an area
susceptible to trauma.
t. Scleroderma (710.1).
u. Tattoos (709.9). Entrance may be denied to any applicant who has a tattoo or other
applied body marking contrary to the core values of the Coast Guard in accordance
with “Tattoo and Body Markings Policy for CG Accessions, COMDTINST 1000.1.”
v. Urticaria (708.8). Chronic.
w. Warts. Plantar warts (078.19) that are symptomatic.
x. Xanthoma (272.2). If disabling or accompanied by hyperlipemia.
3-91 CH-17
y. Any other chronic skin disorder of a degree or nature such as Dysplastic nevi
syndrom (448.1), which requires frequent outpatient treatment or hospitalization, or
interferes with the satisfactory performance of duty.
34. Spine and Sacroiliac Joints. The causes for rejection for appointment, enlistment, and
induction are:
a. Arthritis (720). (see 3-D-11.a)
b. Complaint of a disease or injury of the spine or sacroiliac joints, with or without
objective signs, that has prevented the individual from successfully following a
physically active vocation in civilian life (724), or that is associated with pain
referred to the lower extremities, muscular spasms, postural deformities, or limitation
of motion.
c. Deviation or curvature of spine (737) from normal alignment, structure, or function
if:
(1) It prevents the individual from following a physically active vocation in
civilian life.
(2) It interferes with the wearing of a uniform or military equipment.
(3) It is symptomatic and associated with positive physical finding(s) and
demonstrable by x-ray.
(4) There is lumbar scoliosis greater than 20 degrees, thoracic scoliosis over 20
degrees, and kyphosis or lordosis greater than 55 degrees when measured by
the Cobb method.
d. Fusion. Congenital fusion (756.15), involving more than two vertebrae. Any
surgical fusion (81.0P).
e. Healed fractures or dislocations of the vertebrae (805). A compression fracture,
involving less than 25 percent of a single vertebra is not disqualifying if the injury
occurred more than 1 year before examination and the applicant is asymptomatic. A
history of fractures of the transverse or spinous processes is not disqualifying if the
applicant is asymptomatic.
f. Juvenile epiphysitis (732.6). That with any degree of residual change indicated by x-
ray or kyphosis.
g. Ruptured nucleus pulposus (722). Herniation of intervertebral disk or surgery for
this condition.
h. Spina bifida (741). When symptomatic, or there is more than one vertebra involved,
dimpling of the overlying skin, or a history of surgical repair.
i. Spondylolysis (756.1) and Spondylolisthesis (738.4).
CH-17 3-92
j. Weak or painful back (724). Back condition requiring external support; that is,
corset or brace. Recurrent sprains or strains requiring limitation of physical activity
or frequent treatment.
35. Systemic Diseases. The causes for rejection for appointment, enlistment, and induction
are:
a. Amyloidosis (277.3).
b. Ankylosing spondylitis (720).
c. Eosinophilic granuloma (277.8). Eosinophilic granuloma, when occurring as a
single localized bony lesion and not associated with soft tissue or other involvement,
shall not be a cause for rejection once healing has occurred. All other forms of the
histiocytosis X spectrum should be rejected.
d. Lupus erythematosus (710) and mixed connective tissue disease (710.9).
e. Polymyositis dermatomyositis complex (710).
f. Progressive systemic sclerosis (710). Condition including CRST variant. A single
plaque of localized scleroderma (morphea) that has been stable for at least 2 years is
not disqualifying.
g. Reiter's disease (099.3).
h. Rheumatoid arthritis (714).
i. Rhabdomyolysis (728.9).
j. Sarcoidosis (135). Unless there is substantiated evidence of a complete spontaneous
remission of at least 2 years duration.
k. Sjogren's syndrome (710.2).
l. Tuberculosis (010).
(1) Active tuberculosis in any form or location, or substantiated history of active
tuberculosis within the previous 2 years.
(2) One or more reactivations.
(3) Residual physical or mental defects from past tuberculosis that will prevent the
satisfactory performance of duty.
(4) Individuals with a past history of active tuberculosis more than 2 years prior to
enlistment or induction, are qualified if they have received a complete course
of standard chemotherapy for tuberculosis. In addition, individuals with a
tuberculin reaction 10 mm or greater and without evidence of residual disease
are qualified once they have been treated with chemoprophylaxis
3-93 CH-17
(5) Vasculitis (466). Such as Bechet's, Wegener's granulomatosis polyarteritis
nodosa.
36. General and Miscellaneous Conditions and Defects. The causes for rejection for
appointment, enlistment, and induction are:
a. Allergic manifestations (995.0). A reliable history of anaphylaxis to stinging insects.
Reliable history of a moderate to severe reaction to common foods, spices or food
additives.
b. Any acute pathological condition. Those including acute communicable diseases,
until recovery has occurred without sequelae.
c. Chronic metallic poisoning. Poisoning with lead, arsenic, or silver (985), or
beryllium or manganese (985).
d. Cold injury (991). Residuals of injury; such as frostbite, chilblain, immersion foot,
trench foot, deep-seated ache, paresthesia, hyperhidrosis, easily traumatized skin,
cyanosis, amputation of any digit, or ankylosis.
e. Cold urticaria (708.2) and angiodema, hereditary angiodema (277.6).
f. Filariasis (125), Trypanosomiasis (086), Schistosomiasis (120).
g. Heat pyrexia (992) heatstroke (992), or sunstroke (992). Documented evidence of a
predisposition (including disorders of sweat mechanism and a previous serious
episode), recurrent episodes requiring medical attention, or residual injury
(especially cardiac, cerebral, hepatic, and renal). Malignant Hyperthermia (995.89).
h. Industrial solvent and other chemical intoxication (982).
i. Motion sickness (994.6). An authenticated history of frequent, incapacitating motion
sickness after the 12th birthday.
j. Mycotic (114) infection of internal organs.
k. Organ transplant recipient (V42).
l. Presence of HIV-1 or antibody (042). That presence confirmed by repeatedly
reactive Enzyme-Linked Immunoassay (ELISA) serological test and positive
immunoelectrophoresis (Western Blot) test, or other DoD approved screening and
confirmatory test.
m. Reactive tests for syphilis (093). Test such as the RPR or VDRL followed by a
reactive, confirmatory fluorescent treponemal antibody absorption (FTA-ABS) test
unless there is a documented history of adequately treated syphilis. In the absence of
clinical findings, the presence of reactive RPR or VDRL followed by a negative
FTA-ABS test is not disqualifying if a cause for the false positive reaction can be
identified and is not otherwise disqualifying.
CH-17 3-94
n. Residual of tropical fevers. Fevers such as malaria (084) and various parastic or
protozoan infestations that prevent the satisfactory performance of military duty.
o. Rheumatic fever (390). That condition during the previous 2 years, or any history or
recurrent attacks; Sydenham's chorea at any age.
p. Sleep apnea (780.57).
37. Tumors and Malignant Diseases. The causes for rejection for appointment, enlistment,
and induction are:
a. Benign tumors (M8000). Those that interfere with function, prevent wearing of the
uniform or prtective equipment, shall require frequent specialized attention, or have a
high malignant potential.
b. Malignant tumors (V10). Exception for basal cell carcinoma, removed with no
residual. In addition, the following cases should be qualified, if on careful review
they meet the following criteria:
(1) Individuals who have a history of childhood cancer and who have not received
any surgical or medical cancer therapy for 5 years and are free of cancer
(2) Individuals with a history of Wilm’s tumor and germ cell tumors of the testis
treated surgically and/or with chemotherapy in childhood after a 2-year
disease-free interval off all treatment.
(3) Individuals with a history of Hodgkins’ disease treated with radiation therapy
and/or chemotherapy and disease free off treatment for 5 years.
(4) Individuals with a history of large cell lymphoma after 2-years disease-free
interval off all therapy.
38. Miscellaneous. Any condition that, in the opinion of the examining medical officer, will
significantly interfere with the successful performance of military duty or training (796).
3-95 CH-17
FIGURE 3-D-1
EVALUATION FOR RISK OF HEAD INJURY SEQUELAE
DEGREE OF HEAD INJURY
MINIMUM
EVALUATION
REQUIREMENTS
MILD
ONE MONTH
COMPLETE
NEUROLOGICAL
EXAMINATION BY A
PHYSICIAN
MODERATE
TWO YEARS
COMPLETE
NEUROLOGICAL
EVALUATION BY A
NEUROLOGIST OR
INTERNIST
CT SCAN
SEVERE
FIVE YEARS FOR CLOSED
HEAD TRAUMA
TEN YERS FOR
PENETRATING HEAD
TRAUMA
COMPLETE
NEUROLOGICAL
EVALUATION BY
NEUROLOGIST OR
NEUROSURGEON
CT SCAN
NEUROPSYCHOLOGICAL
EVALUATION
CH-17 3-96
FIGURE 3-D-2
CLASSIFICATION AND COMPARATIVE NOMENCLATURE OF CERVICAL SMEARS
Original Classification CIN System Bethesda System
Class I: Normal smear;
No abnormal cells
Class II: Atypical cells present Atypical squamous
below the level of cells of undetermined
cervical neoplasia significance
Class III: Smear contains abnormal Mild dysplasia = CIN1 Low-grade SIL
cells consistent with Moderate dysplasia = (Changes asso-
dysplasia CIN2 ciated with HPV & CIN1)
Class IV Smear contains abnormal Severe dysplasia and High-grade SIL
cells consistent with carcinoma-in-situ = (CIN2, CIN3, and
carcinoma-in-situ CIN3 carcinoma-in-situ)
Class V: Smear contains abnormal Squamous cell carcinoma
cells consistent with carcinoma
squamous cell carcinoma
Abbreviations: CIN = cervical intraepithelial neoplasia
Section A - SIL = squamous intraepithelial lesion

3-97 CH-17
Section E Physical Standards for Programs Leading to Commission.
1. Appointment as Cadet, United States Coast Guard Academy.
a. Physical Examinations.
(1) Applicants are encouraged to review the physical standards as published in the
Academy Bulletin with their private physician prior to submitting their
application for cadet candidate. This review serves to rule out, at this stage of
the potential cadet's processing, applicants who obviously will not meet the
required physical standards for appointment. In some cases, the physician may
recommend a complete physical examination. Inaccuracy in ascertaining
defects and determining the candidate's physical status at the time of this
review results in unnecessary work for the Coast Guard and disappointment to
the candidate when defects are subsequently found during the formal physical
examination.
(2) Candidates and their parents and sponsors are urged to refrain from requesting
waivers for medical defects. The Coast Guard bases its decision to disqualify
an individual on medical facts revealed in a thorough physical examination.
Candidates unable to satisfy the minimum requirements are not suited for
commission in the Regular Coast Guard, and consequently are not eligible for
training at the Academy. A request for waiver for a medical defect invariably
results in disappointment to all concerned.
(3) Two physical examinations are required:
(a) formal physical examination before appointment is tendered; and
(b) pretraining examination at the time of reporting to the Academy.
(4) Formal physical examinations prior to accepting of candidates must be
performed by a U. S. Public Health Service, Navy, Army, Air Force, or
Veteran's Administration medical officer authorized to perform each exam by
Department of Defense Medical Examination Review Board (DODMERB).
All candidates are instructed where to report for such examinations.
b. Physical Standards. All candidates for the Coast Guard Academy must meet the
physical standards for enrollment as an officer candidate. DODMERB is reviewing
authority.
c. Retention. The standards for retention of a cadet at the Academy are the same as
those for enrollment as an officer candidate, except that the Superintendent of the
Academy is authorized to establish physical fitness and weight control programs
designed to have cadets maintain weight closer to the ideal than the standards
stipulated elsewhere for Service personnel. These stricter goals during cadet years
are intended to take advantage of the Academy's unique environment of rigorous
physical activity combined with opportunities for diet control and weight monitoring.
CH-17 3-98
These programs will instill lifelong behavior patterns to support the Service weight
control standards.
2. Commissioning of Cadets. The preappointment physical examination of cadets in the
graduating class should be held at least 6 months prior to acceptance of the commission.
This physical examination should be conducted to determine physical fitness for
commission in the Regular Service (section 3-D and 3-E) with recommendations made
accordingly. Cadets should not be summarily disqualified for commissioning merely
because they do not meet the standards for appointment as cadets provided that they may
reasonably be expected to be physically capable of completing a full and effective Coast
Guard career. In general, relatively minor defects that would be disqualifying for
original commission direct from civilian life are not disqualifying for commission of a
cadet in whom the Government has a considerable investment.
3. Enrollment as an Officer Candidate.
a. Physical Examination. The physical examination for an officer candidate must be
conducted by a medical officer and a dentist. Particular care must be exercised
during the examination in order that candidates may not be rejected later as a result
of reexamination at Officer Candidate School. A complete physical examination is
given officer candidates upon arrival at OCS to determine medical fitness and
freedom from disease. Physician Assistant Officer Candidates will only receive an
initial OCS candidate physical.
b. Physical Standards for Enrollment. The standards contained in section 3-D (section
3-F for enlisted OCS candidates), as modified below, are applicable for enrollment
as an officer candidate. Conditions not enumerated, that in the medical examiner's
opinion will not permit a full productive career, shall be recorded in detail with
appropriate recommendations.
(1) Distant Visual Acuity. Uncorrected visual acuity shall be not worse
than20/400 in either eye provided that vision is correctable to 20/20 and that
refractive error does not exceed plus or minus 8.0 diopters spherical equivalent
(sphere + 1/2 cylinder), astigmatism does not exceed 3.00 diopters, and
anisometropia does not exceed 3.50 diopters. Eyes must be free from any
disfiguring or incapacitating abnormality and from acute or chronic disease.
All personnel requiring corrective lenses shall wear them for the performance
of duty.
(2) Near visual acuity of any degree that does not correct to 20/40 in the better
eye.
(3) Normal color perception.
(4) Teeth.
(a) All candidates shall be given a Type II dental examination by a dental
officer, as part of the pre-training physical examination.
(b) Caries. No more than four teeth may exhibit multi-surface caries.
3-99 CH-17
(c) Endodontics. The need for endodontic intervention on seven or more
canals is disqualifying.
(d) Maxillary and Mandibular Bones. Malunited fractures of maxillary or
mandibular bones and deformities of maxillary or mandibular bones
interfering with mastication or speech are disqualifying. The presence of
extensive necrosis or osseous lesions requiring surgical intervention are
also disqualifying.
(e) Oral Tissues. Extensive loss of oral tissues that would prevent the
replacement of missing teeth with a satisfactory prosthetic appliance is
disqualifying. Unresolved oral inflammatory diseases are disqualifying.
Hypertrophic, hyperplastic, or leukoplakic conditions of the soft tissue of
the oral cavity may be disqualifying and will be considered on a case-by-
case basis.
(f) Periodontal Disease. The presence of advanced periodontal disease is
disqualifying.
(g) Serviceable Teeth. A sufficient number of teeth, natural or artificial, in
functional occlusion to assure satisfactory incision, mastication, and
phonation are required. The minimum requirement is edentulous upper
and lower jaws corrected by full dentures. A requirement for placement
of a prosthesis to meet the above requirements is disqualifying.
(h) Temporomandibular Joint. Current symptoms and/or history of chronic
temporomandibular joint dysfunction is disqualifying (see also section 3-
D-16.b).
4. Commissioning of Officer Candidates.
a. The physical examination given upon arrival at OCS precludes the need for a
commissioning physical examination providing there has been no intervening change
in physical status and a visual acuity and color perception examination are given
prior to actual commissioning.
b. The physical standards for commissioning are the same as for enrollment as an
officer candidate. Final determination as to physical fitness for commissioning is
made by the Commandant.
5. Direct Commission in the Coast Guard Reserve.
a. Nonaviator. The physical examination and standards for direct commission in the
Reserve are the same for enrollment of officer candidates, except that Ready Reserve
Direct Commission (RRDC) examinations must be within 24 months prior to the
date of execution of the Acceptance and Oath of Office (CG-9556).
b. Aviator. Candidates for direct commission in the Reserve as aviators must obtain an
aviation physical examination from a currently qualified uniformed services flight
CH-17 3-100
surgeon or AMO within the last 12 months. The candidate must meet the standards
for Class I, contained in section 3-G.
6. Direct Commission of Licensed Officers of U. S. Merchant Marine.
a. Physical Examination. Two physical examinations are required: a preliminary
physical at the time of the written examination; and a preappointment physical
examination taken by successful candidates within six months of actual commission.
The physical examination must be conducted by a medical officer of the uniformed
services on active duty. Final determination of physical fitness will be made by the
Commandant.
b. Physical Standards. The physical standards for direct commission of Licensed
Officers of the U. S. Merchant Marine are the same as for enrollment of officer
candidates. All these standards must be met without waiver.
7. Appointment to Warrant Grade.
a. Physical Examination. A complete physical examination is required within 12
months prior to appointment to Warrant Officer, except that physical examinations
for members of the Coast Guard Ready Reserve must be within 24 months prior to
the date of execution of the Acceptance and Oath of Office (CG-9556).
b. Physical Requirements. The physical standards for appointment of Coast Guard
members to Warrant Officer are the same as for retention of officers in the regular
Coast Guard. See section 3-F for the standards. The physical standards for all other
applicants are the same as for enrollment of officer candidates.
3-101 CH-17
Section F Physical Standards Applicable to All Personnel (Regular and Reserve) For:
Reenlistment; Enlistment of Prior Service USCG Personnel; Retention; Overseas
Duty; and Sea Duty.
1. General Instructions.
a. Scope. This section establishes specific physical standards applicable to all
personnel (regular and reserve) for:
(1) enlistment/reenlistment of prior service USCG personnel within 6 months of
discharge from active duty in the Regular Coast Guard;
(2) retention;
(3) overseas duty; and
(4) sea duty.
b. Physical Examinations. Physical examinations should be conducted by at least one
medical and one dental officer of the uniformed services or by contract
physician/dentist.
c. Fitness for Duty. Members are ordinarily considered fit for duty unless they have a
physical impairment (or impairments) that interferes with the performance of the
duties of their grade or rating. A determination of fitness or unfitness depends upon
the individual's ability to reasonably perform those duties. Members considered
temporarily or permanently unfit for duty shall be referred to an Initial Medical
Board for appropriate disposition.
2. Use of List of Disqualifying Conditions and Defects. This section lists certain medical
conditions and defects that are normally disqualifying. However, it is not an all-
inclusive list. Its major objective is to achieve uniform disposition of cases arising under
the law, but it is not a mandate that possession of one or more of the listed conditions or
physical defects (and any other not listed) means automatic retirement or separation. If
the member’s condition is disqualifying but he/she can perform his/her duty, a waiver
request could be submitted in lieu of immediate referral to an Initial Medical Board. If
the request is denied, then an Initial Medical Board is required.
3. Head and Neck.
a. Loss of substance of the skull. With or without prosthetic replacement when
accompanied by moderate residual signs and symptoms.
b. Torticollis (wry neck). Severe fixed deformity with cervical scoliosis, flattening of
the head and face, and loss of cervical mobility.
4. Esophagus, Nose, Pharynx, Larynx, and Trachea.

CH-17 3-102
a. Esophagus.
(1) Achalasia. Manifested by dysphagia (not controlled by dilation), frequent
discomfort, inability to maintain normal vigor and nutrition, or requiring
frequent treatment.
(2) Esophagitis. Persistent and severe.
(3) Diverticulum of the esophagus. Of such a degree as to cause frequent
regurgitation, obstruction and weight loss, that does not respond to treatment.
(4) Stricture of the esophagus. Of such a degree as to almost restrict diet to
liquids, require frequent dilation and hospitalization, and cause difficulty in
maintaining weight and nutrition.
b. Larynx.
(1) Paralysis of the larynx. Characterized by bilateral vocal cord paralysis
seriously interfering with speech or adequate airway.
(2) Stenosis of the larynx. Causing respiratory embarrassment upon more than
minimal exertion.
(3) Obstruction edema of glottis. If chronic, not amenable to treatment and
requiring tracheotomy.
c. Nose, Pharynx, Trachea.
(1) Rhinitis. Atrophic rhinitis characterized by bilateral atrophy of nasal mucous
membrane with severe crusting and concomitant severe headaches.
(2) Sinusitis. Severe and chronic that is suppurative, complicated by polyps, and
does not respond to treatment.
(3) Trachea. Stenosis of trachea that compromises airflow to more than a mild
degree.
5. Eyes.
a. Diseases and Conditions.
(1) Active eye disease. Or any progressive organic disease regardless of the stage
of activity, that is resistant to treatment and affects the distant visual acuity or
visual field so that:
(a) distant visual acuity does not meet the standards; or
(b) the diameter of the field of vision in the better eye is less than 20o.
(2) Aphakia, bilateral. Regardless of lens implant(s).
(3) Atrophy of optic nerve.
(4) Glaucoma. If resistant to treatment, or affecting visual fields, or if side effects
of required medications are functionally incapacitating.
3-103 CH-17
(5) Diseases and infections of the eye. When chronic, more than mildly
symptomatic, progressive and resistant to treatment after a reasonable period.
(6) Ocular manifestations of endocrine or metabolic disorders. Not disqualifying,
per se; however, residuals or complications, or the underlying disease may be
disqualifying.
(7) Residuals or complications of injury. When progressive or when reduced
visual acuity or fields do not meet the standards.
(8) Retina, detachment of.
(a) Unilateral.
1 When visual acuity does not meet the standards.
2 When the visual field in the better eye is constricted to less than 20o.
3 When uncorrectable diplopia exists.
4 When detachment results from organic progressive disease or new
growth, regardless of the condition of the better eye.
(b) Bilateral. Regardless of etiology or results of corrective surgery.
b. Vision.
(1) Aniseikonia. Subjective eye discomfort, neurologic symptoms, sensations of
motion sickness and other gastrointestinal disturbances, functional
disturbances and difficulties in form sense, and not corrected by iseikonic
lenses.
(2) Binocular diplopia. Which is severe, constant, and in zone less than 20o from
the primary position.
(3) Hemianopsia. Of any type, if bilateral, permanent, and based on an organic
defect. Those due to a functional neurosis and those due to transitory
conditions, such as periodic migraine, are not normally disqualifying.
(4) Night blindness. Of such a degree that the individual requires assistance in any
travel at night.
(5) Visual Acuity.
(a) Visual acuity that cannot be corrected to at least 20/50 in the better eye.
(b) Complete blindness or enucleation of an eye.
(c) When vision is correctable only by the use of contact lenses or other
corrective device (telescope lenses, etc.).

CH-17 3-104
(6) Visual Fields. When the visual field in the better eye is constricted to less than
20o.
(7) Color Perception. Normal color perception is required for retention of
commissioned officers (certain warrant officer specialties do not require
normal color perception) and selected ratings [See the Personnel
Manual,COMDTINST M1000.6 (series) and Chapter 5-B]. Retesting for color
perception is not required if results of previous tests are documented in the
health record, and there has been no history of a change in color vision.
c. Corneal Refractive Surgery.
(1) The refractive surgery procedures radial keratotomy (RK),and intracorneal
rings (ICR) are disqualifying and not waiverable.
(2) Photorefractive keratectomy (PRK) and laser in-situ keratomileusis (LASIK)
are disqualifying for aviation duty, landing signal officer duty and not
waiverable.
(3) LASIK is disqualifying for diving duty and not waiverable.
(4) Photorefractive keratectomy (PRK) is not disqualifying for non-aviation
members, including diving personnel, and does not require a waiver if the
following conditions are met:
(a) Must follow guidelines for elective health care contained in 2.A.6.
(b) There must be post surgical refractive stability defined as less than 0.50
diopter change over two separate exams at least three months apart.
(c) Must meet all vision standards in 3-F.5.b (divers must meet vision
standards in 3-H.2.h). If the member is unable to meet these standards
they will be considered for separation as outlined in the Physical
Disability Evaluation System, COMDTINST M1850.2(series).
(5) LASIK is not disqualifying for non-aviation personnel, excluding diving
personnel and does not require a waiver as long as the following conditions are
met:
(a) Must follow guidelines for elective health care contained in 2.A.6.
(b) There must be post surgical refractive stability defined as less than 0.50
diopter change over two separate exams at least three months apart.
(c) Must meet all vision standards in 3-F.5.b. If the member is unable to
meet these standards they will be considered for separation as outlined in
the Physical Disability Evaluation System, COMDTINST
M1850.2(series).
3-105 CH-17
6. Ears and Hearing.
a. Ears.
(1) Infections of the external auditory canal. Chronic and severe, resulting in
thickening and excoriation of the canal, or chronic secondary infection
requiring frequent and prolonged medical treatment and hospitalization.
(2) Malfunction of the acoustic nerve. Evaluate hearing impairment.
(3) Mastoiditis, chronic. Constant drainage from the mastoid cavity, requiring
frequent and prolonged medical care.
(4) Mastoidectomy. Followed by chronic infection with constant or recurrent
drainage requiring frequent or prolonged medical care.
(5) Meniere's Syndrome. Recurring attacks of sufficient frequency and severity as
to interfere with satisfactory performance of military duty, or require frequent
or prolonged medical care.
(6) Otitis Media. Moderate, chronic, suppurative, resistant to treatment, and
necessitating frequent or prolonged medical care.
b. Hearing. Retention will be determined on the basis of ability to perform duties of
grade or rating.
7. Lungs and Chest Wall.
a. Tuberculous Lesions. See chapter 7 of this Manual.
(1) Pulmonary tuberculosis.
(a) When an active duty member's disease is found to be not incident to
military service, or when treatment and return to useful duty will
probably require more than 15 months, including an appropriate period
of convalescence, or if expiration of service will occur before completion
of period of hospitalization. (Career members who express a desire to
reenlist after treatment may extend their enlistment to cover period of
hospitalization.)
(b) When a Reservist not on active duty has TB that will probably require
treatment for more that 12 to 15 months including an appropriate period
of convalescence before being able to perform full-time military duty.
Individuals who are retained in the Reserve while undergoing treatment
may not be called or ordered to active duty (including mobilization),
active duty for training, or inactive duty training during the period of
treatment and convalescence.
b. Nontuberculous Conditions. Pulmonary diseases, other than acute infections, must
be evaluated in terms of respiratory function, manifested clinically by measurements
CH-17 3-106
that must be interpreted as exertional or altitudinal tolerance. Symptoms of cough,
pain, and recurrent infections may limit a member's activity. Many of the conditions
listed below may coexist and in combination may produce unfitness.
(1) Atelectasis, or massive collapse of the lung. Moderately symptomatic with
paroxysmal cough at frequent intervals throughout the day, or with moderate
emphysema, or with residuals or complications that require repeated
hospitalization.
(2) Bronchial Asthma. Associated with emphysema of sufficient severity to
interfere with the satisfactory performance of duty, or with frequent attacks not
controlled by inhaled or oral medications, or requiring oral corticosteroids
more than twice a year.
(3) Bronchiectasis or bronchiolectasis. Cylindrical or saccular type that is
moderately symptomatic, with productive cough at frequent intervals
throughout the day, or with moderate other associated lung disease to include
recurrent pneumonia, or with residuals or complications that require repeated
hospitalization.
(4) Bronchitis. Chronic, severe persistent cough, with considerable expectoration,
or with moderate emphysema, or with dyspnea at rest or on slight exertion, or
with residuals or complications that require repeated hospitalization.
(5) Cystic disease of the lung, congenital. Involving more than one lobe of a lung.
(6) Diaphragm, congenital defect. Symptomatic.
(7) Hemopneumothorax, hemothorax, or pyopneumothorax. More than moderate
pleuritic residuals with persistent underweight, or marked restriction of
respiratory excursion and chest deformity, or marked weakness and fatigability
on slight exertion.
(8) Histoplasmosis. Chronic and not responding to treatment.
(9) Pleurisy, chronic or pleural adhesions. Severe dyspnea or pain on mild
exertion associated with definite evidence of pleural adhesions and
demonstrable moderate reduction of pulmonary function.
(10) Pneumothorax, spontaneous. Repeated episodes of pneumothorax not
correctable by surgery.
(11) Pneumoconiosis. Severe with dyspnea on mild exertion.
(12) Pulmonary calcification. Multiple calcifications associated with significant
respiratory embarrassment or active disease not responsive to treatment.
(13) Pulmonary emphysema. Marked emphysema with dyspnea on mild exertion
and demonstrable moderate reduction in pulmonary function.
(14) Pulmonary fibrosis. Linear fibrosis or fibrocalcific residuals that cause
dyspnea on mild exertion and demonstrable moderate reduction in pulmonary
function.

3-107 CH-17
(15) Pulmonary sarcoidosis. If not responding to therapy and complicated by
demonstrable moderate reduction in pulmonary function.
(16) Stenosis, bronchus. Severe stenosis associated with repeated attacks of
bronchopulmonary infections requiring frequent hospitalization.
c. Surgery of the Lungs and Chest. Lobectomy. If pulmonary function (ventilatory
tests) is impaired to a moderate degree or more.
8. Heart and Vascular System.
a. Heart.
(1) Arrhythmias. Associated with organic heart disease, or if not adequately
controlled by medication or if they interfere with satisfactory performance of
duty.
(2) Arteriosclerotic disease. Associated with congestive heart failure, repeated
anginal attacks, or objective evidence of myocardial infarction.
(3) Endocarditis. Bacterial endocarditis resulting in myocardial insufficiency or
associated with valvular heart disease.
(4) Heart block. Associated with other symptoms of organic heart disease or
syncope (Stokes-Adams Syndrome).
(5) Myocarditis and degeneration of the myocardium. Myocardial insufficiency
resulting in slight limitation of physical activity.
(6) Pericarditis.
(a) Chronic constrictive pericarditis unless successful remedial surgery has
been performed.
(b) Chronic serous pericarditis.
(7) Rheumatic valvulitis and valvular heart disease. Cardiac insufficiency at
functional capacity and therapeutic level of class IIC or worse, American Heart
Association. A diagnosis made during the initial period of service or
enlistment that is determined to be a residual of a condition that existed prior to
entry in the service is disqualifying regardless of severity.
b. Vascular System.
(1) Arteriosclerosis obliterans. When any of the following pertain:
(a) intermittent claudication of sufficient severity to produce pain and
inability to complete a walk of 200 yards or less on level ground at 112
steps per minute without a rest; or
(b) objective evidence of arterial disease with symptoms of claudication,
ischemic chest pain at rest, or with gangrenous or permanent ulcerative
skin changes in the distal extremity; or

CH-17 3-108
(c) involvement of more than one organ system or anatomic region (the
lower extremities comprise one region for this purpose) with symptoms
of arterial insufficiency.
(2) Congenital anomalies. Coarctation of aorta and other congenital anomalies of
the cardiovascular system unless satisfactorily treated by surgical correction.
(3) Aneurysms. Aneurysm of any vessel not correctable by surgery and producing
limiting symptomatic conditions precluding satisfactory performance of duty.
Aneurysm corrected by surgery but with residual limiting symptomatic
conditions that preclude satisfactory performance of duty.
(a) Satisfactory performance of duty is precluded because of underlying
recurring or progressive disease producing pain, dyspnea, or similar
symptomatic limiting conditions.
1 reconstructive surgery including grafts, when:prosthetic devices are
attached to or implanted in the heart; and
2 unproven procedures have been accomplished and the patient is
unable to satisfactorily perform duty or cannot be returned to duty
under circumstances permitting close medical supervision.
(4) Periarteritis nodosa. With definite evidence of functional impairment.
(5) Chronic venous insufficiency (postphlebitic syndrome). When more than mild
and symptomatic despite elastic support.
(6) Raynaud's phenomenon. Manifested by trophic changes of the involved part
characterized by scarring of the skin or ulceration.
(7) Thrombophlebitis. When repeated attacks require such frequent treatment as
to interfere with satisfactory performance of duty.
(8) Varicose veins. Severe and symptomatic despite therapy.
(9) Any condition requiring anti-thrombotic medication other than aspirin.
c. Miscellaneous.
(1) Erythromelalgia. Persistent burning pain in the soles or palms not relieved by
treatment.
(2) Hypertensive cardiovascular disease and hypertensive vascular disease.
(a) Diastolic pressure consistently more than 90 mm Hg following an
adequate period of therapy on an ambulatory status; or
(b) Any documented history of hypertension regardless of the pressure
values if associated with one or more of the following:
1 cerebrovascular symptoms;

3-109 CH-17
2 arteriosclerotic heart disease if symptomatic and requiring treatment;
3 kidney involvement, manifested by unequivocal impairment of renal
function; or
4 grade III (Keith-Wagener-Barker) changes in the fundi.
(3) Rheumatic fever, active, with or without heart damage. Recurrent attacks.
(4) Residual of surgery of the heart, pericardium, or vascular system under one or
more of the following circumstances:
(a) when surgery of the heart, pericardium, or vascular system results in
inability of the individual to perform duties without discomfort or
dyspnea;
(b) when the surgery involves insertion of a pacemaker, reconstructive
vascular surgery employing exogenous grafting material; or
(c) similar newly developed techniques or prostheses, the individual is unfit.
9. Abdomen and Gastrointestinal System.
a. Defects and Diseases.
(1) Achalasia. Manifested by dysphagia not controlled by dilation with frequent
discomfort, or inability to maintain normal vigor and nutrition.
(2) Amebic abscess residuals. Persistent abnormal liver function tests and failure
to maintain weight and normal vigor after appropriate treatment.
(3) Biliary dyskinesia. Frequent abdominal pain not relieved by simple
medication, or with periodic jaundice.
(4) Cirrhosis of the liver. Recurrent jaundice or ascites; or demonstrable
esophageal varices or history of bleeding therefrom.
(5) Gastritis. Severe, chronic gastritis with repeated symptomatology and
hospitalization and confirmed by gastroscopic examination.
(6) Hepatitis, chronic. When, after a reasonable time (1 to 2 years) following the
acute stage, symptoms persist, and there is objective evidence of impaired liver
function.
(7) Hernia.
(a) Hiatus hernia. Severe symptoms not relieved by dietary or medical
therapy, or recurrent bleeding in spite of prescribed treatment.
(b) Other. If operative repair is contraindicated for medical reasons or when
not amenable to surgical repair.
(8) Ileitis, regional. (Crohn’s disease); Except when responding well to ordinary
treatment other than oral corticosteroids or immune-suppressant medications.

CH-17 3-110
(9) Pancreatitis, chronic. Frequent severe abdominal pain; or steatorrhea or
disturbance of glucose metabolism requiring hypoglycemic agents.
(10) Peritoneal adhesions. Recurring episodes of intestinal obstruction
characterized by abdominal colicky pain, vomiting, and intractable
constipation requiring frequent hospital admissions.
(11) Proctitis, chronic. Moderate to severe symptoms of bleeding, or painful
defecation, tenesmus, and diarrhea, with repeated hospital admissions.
(12) Ulcer, peptic, duodenal, or gastric. Repeated incapacitation or absences from
duty because of recurrence of symptoms (pain, vomiting, or bleeding) in spite
of good medical management, and supported by laboratory, x-ray, and
endoscopic evidence of activity.
(13) Ulcerative colitis. Except when responding well to ordinary treatment other
than oral corticosteroids or immune-suppressant medications.
(14) Rectum, stricture of. Severe symptoms of obstruction characterized by
intractable constipation, pain on defecation, difficult bowel movements
requiring the regular use of laxatives or enemas, or requiring repeated
hospitalization.
b. Surgery.
(1) Colectomy, partial. When more than mild symptoms of diarrhea remain or if
complicated by colostomy.
(2) Colostomy. When permanent.
(3) Enterostomy. When permanent.
(4) Gastrectomy.
(a) Total.
(b) Subtotal, with or without vagotomy, or gastrojejunostomy, with or
without vagotomy, when, in spite of good medical management, the
individual:
1 develops "dumping syndrome" that persists for 6 months
postoperatively; or
2 develops frequent episodes of epigastric distress with characteristic
circulatory symptoms or diarrhea persisting 6 months
postoperatively; or
3 continues to demonstrate significant weight loss 6 months
postoperatively. Preoperative weight representative of obesity
should not be taken as a reference point in making this assessment.
3-111 CH-17
4 Not to be confused with "dumping syndrome," and not ordinarily
considered as representative of unfitness are: postoperative
symptoms such as moderate feeling of fullness after eating; the need
to avoid or restrict ingestion of high carbohydrate foods; the need
for daily schedule of a number of small meals with or without
additional "snacks."
(5) Gastrostomy. When permanent.
(6) Ileostomy. When permanent.
(7) Pancreatectomy.
(8) Pancreaticoduodenostomy, pancreaticogastrostomy, pancreaticojejunostomy.
Followed by more than mild symptoms of digestive disturbance, or requiring
insulin.
(9) Proctectomy.
(10) Proctopexy, proctoplasty, proctorrhaphy, or proctotomy. If fecal incontinence
remains after appropriate treatment.
10. Endocrine and Metabolic Conditions (Diseases).
a. Acromegaly. With function impairment.
b. Adrenal hyperfunction. That does not respond to therapy satisfactorily or where
replacement therapy presents serious problems in management.
c. Adrenal hypofunction. Requiring medication for control.
d. Diabetes Insipidus. Unless mild, with good response to treatment.
e. Diabetes Mellitus. When requiring insulin or not controlled by oral medications.
f. Goiter. With symptoms of breathing obstruction with increased activity, unless
correctable.
g. Gout. With frequent acute exacerbations in spite of therapy, or with severe bone,
joint, or kidney damage.
h. Hyperinsulinism. When caused by a malignant tumor, or when the condition is not
readily controlled.
i. Hyperparathyroidism. When residuals or complications of surgical correction such
as renal disease or bony deformities preclude the reasonable performance of military
duty.
j. Hyperthyroidism. Severe symptoms, with or without evidence of goiter, that do not
respond to treatment.

CH-17 3-112
k. Hypoparathyroidism. With objective evidence and severe symptoms not controlled
by maintenance therapy.
l. Hypothyroidism. With objective evidence and severe symptoms not controlled by
medication.
m. Osteomalacia. When residuals after therapy preclude satisfactory performance of
duty.
11. Genitourinary System.
a. Genitourinary conditions.
(1) Cystitis. When complications or residuals of treatment themselves preclude
satisfactory performance of duty.
(2) Dysmenorrhea. Symptomatic, irregular cycle, not amenable to treatment, and
of such severity as to necessitate recurrent absences of more than l day/month.
(3) Endometriosis. Symptomatic and incapacitating to degree that necessitates
recurrent absences of more than 1 day/month.
(4) Hypospadias. Accompanied by chronic infection of the genitourinary tract or
instances where the urine is voided in such a manner as to soil clothes or
surroundings, and the condition is not amenable to treatment.
(5) Incontinence of urine. Due to disease or defect not amenable to treatment and
so severe as to necessitate recurrent absences from duty.
(6) Menopausal syndrome, physiologic or artificial. With more than mild mental
and constitutional symptoms.
(7) Strictures of the urethra or ureter. Severe and not amenable to treatment.
(8) Urethritis, chronic. Not responsive to treatment and necessitating frequent
absences from duty.
b. Kidney.
(1) Calculus in kidney. Bilateral or symptomatic and not responsive to treatment.
(2) Congenital abnormality. Bilateral, resulting in frequent or recurring infections,
or when there is evidence of obstructive uropathy not responding to medical or
surgical treatment.
(3) Cystic kidney (polycystic kidney). When symptomatic and renal function is
impaired, or if the focus of frequent infection.
(4) Glomerulonephritis, chronic.
(5) Hydronephrosis. More than mild, or bilateral, or causing continuous or
frequent symptoms.
(6) Hypoplasia of the kidney. Associated with elevated blood pressure or frequent
infections and not controlled by surgery.

3-113 CH-17
(7) Nephritis, chronic.
(8) Nephrosis.
(9) Perirenal abscess. With residuals that preclude satisfactory performance of
duty.
(10) Pyelonephritis or pyelitis. Chronic, that has not responded to medical or
surgical treatment, with evidence of persistent hypertension, eyeground
changes, or cardiac abnormalities.
(11) Pyonephrosis. Not responding to treatment.
c. Genitourinary and Gynecological Surgery.
(1) Cystectomy.
(2) Cystoplasty. If reconstruction is unsatisfactory or if residual urine persists in
excess of 50 cc or if refractory symptomatic infection persists.
(3) Nephrectomy. When, after treatment, there is infection or pathology in the
remaining kidney.
(4) Nephrostomy. If drainage persists.
(5) Oophorectomy. When, following treatment and convalescent period, there
remain incapacitating mental or constitutional symptoms.
(6) Penis, amputation of.
(7) Pyelostomy. If drainage persists.
(8) Ureterocolostomy.
(9) Ureterocystostomy. When both ureters are markedly dilated with irreversible
changes.
(10) Ureterocystostomy, cutaneous.
(11) Ureteroplasty.
(a) When unilateral procedure is unsuccessful and nephrectomy is
necessary, consider on the basis of the standard for a nephrectomy.
(b) When bilateral, evaluate residual obstruction or hydronephrosis and
consider unfitness on the basis of the residuals involved.
(12) Ureterosigmoidostomy.
(13) Ureterostomy. External or cutaneous.
(14) Urethrostomy. When a satisfactory urethra cannot be restored.
12. Extremities.
a. Upper.
(1) Amputations. Amputation of part or parts of an upper extremity equal to or
greater than any of the following:

CH-17 3-114
(a) a thumb proximal to the interphalangeal joints;
(b) two fingers of one hand; or
(c) one finger, other than the little finger, at the metacarpophalangeal joint
and the thumb of the same hand at the interphalangeal joint.
(2) Joint ranges of motion. Motion that does not equal or exceed the
measurements listed below. Measurements must be made with a goniometer
and conform to the methods illustrated in 3-F-EXHIBIT 1.
(a) Shoulder.
1 Forward elevation to 90° .
2 Abduction to 90° .
(b) Elbow
1 Flexion to 100° .
2 Extension to 60° .
(c) Wrist. A total range, extension plus flexion, of 15°
(d) Hand. For this purpose, combined joint motion is the arithmetic sum of
the motion at each of the three finger joints.
1 An active flexor value of combined joint motions of 135° in each of
two or more fingers of the same hand.
2 An active extensor value of combined joint motions of 75° in each
of the same two or more fingers.
3 Limitation of motion of the thumb that precludes apposition to at
least two finger tips.
(3) Recurrent dislocations of the shoulder. When not repairable or surgery is
contraindicated
b. Lower.
(1) Amputations.
(a) Loss of a toe or toes that precludes the ability to run, or walk without a
perceptible limp, or to engage in fairly strenuous jobs.
(b) Any loss greater than that specified above to include foot, leg, or thigh.
(2) Feet.
3-115 CH-17
(a) Hallux valgus. When moderately severe, with exostosis or rigidity and
pronounced symptoms; or severe with arthritic changes.
(b) Pes Planus. Symptomatic more than moderate, with pronation on weight
bearing that prevents wearing military shoes, or when associated with
vascular changes.
(c) Talipes cavus. When moderately severe, with moderate discomfort on
prolonged standing and walking, metatarsalgia, or that prevents wearing
a military shoe.
(3) Internal derangement of the knee. Residual instability following remedial
measures, if more than moderate; or with recurring episodes of effusion or
locking, resulting in frequent incapacitation.
(4) Joint ranges of motion. Motion that does not equal or exceed the
measurements listed below. Measurements must be made with a goniometer
and conform to the methods illustrated in 3-F-EXHIBIT 2.
(a) Hip.
1 Flexion to 90° .
2 Extension to 0 .
(b) Knee.
1 Flexion to 90° .
2 Extension to 15°
(c) Ankle.
1 Dorsiflexion to 10°
2 Plantar Flexion to 10°
(5) Shortening of an extremity. Which exceeds two inches.
c. Miscellaneous.
(1) Arthritis.
(a) Due to infection. Associated with persistent pain and marked loss of
function with x-ray evidence and documented history of recurring
incapacity for prolonged periods.
(b) Due to trauma. When surgical treatment fails or is contraindicated and
there is functional impairment of the involved joint that precludes
satisfactory performance of duty.
CH-17 3-116
(c) Osteoarthritis. Severe symptoms associated with impaired function,
supported by x-ray evidence and documented history of recurrent
incapacity for prolonged periods.
(d) Rheumatoid arthritis or rheumatoid myositis. Substantiated history of
frequent incapacitating and prolonged periods supported by objective
and subjective findings.
(e) Seronegative Spondylarthropaties. Severe symptoms associated with
impaired function, supported by X-ray evidence and documented history
of recurrent incapacity for prolonged periods.
(2) Chondromalacia or Osteochondritis Dessicans. Severe, manifested by frequent
joint effusion, more than moderate interference with function or with severe
residuals from surgery.
(3) Fractures.
(a) Malunion. When, after appropriate treatment, there is more than
moderate malunion with marked deformity or more than moderate loss
of function.
(b) Nonunion. When, after an appropriate healing period, the nonunion
precludes satisfactory performance of military duty.
(c) Bone fusion defect. When manifested by more than moderate pain or
loss of function.
(d) Callus, excessive, following fracture. When functional impairment
precludes satisfactory performance of duty and the callus does not
respond to adequate treatment.
(4) Joints.
(a) Arthroplasty. With severe pain, limitation of motion and function.
(b) Bony or fibrous ankylosis. Severe pain involving major joints or spinal
segments in an unfavorable position, or with marked loss of function.
(c) Contracture of joint. Marked loss of function and the condition is not
remediable by surgery.
(d) Loose bodies within a joint. Marked functional impairment complicated
by arthritis that precludes favorable treatment or not remediable by
surgery.
(5) Muscles.
3-117 CH-17
(a) Flaccid paralysis of one or more muscles, producing loss of function that
precludes satisfactory performance of duty following surgical correction
or if not remediable by surgery.
(b) Spastic paralysis of one or more muscles producing loss of function that
precludes satisfactory performance of duty.
(6) Myotonia congenita.
(7) Osteitis deformans. Involvement of single or multiple bones with resultant
deformities, or symptoms severely interfering with function.
(8) Osteoarthropathy, hypertrophic, secondary. Moderately severe to severe pain
present with joint effusion occurring intermittently in one or multiple joints
and with at least moderate loss of function.
(9) Osteomyelitis, chronic. Recurrent episodes not responsive to treatment, and
involving the bone to a degree that interferes with stability and function.
(10) Tendon transplant. Fair or poor restoration of function with weakness that
seriously interferes with the function of the affected part.
13. Spine, Scapulae, Ribs, and Sacroiliac Joints.
a. Congenital anomalies.
(1) Spina bifida. Demonstrable signs and moderate symptoms of root or cord
involvement.
(2) Spondylolysis or spondylolisthesis. With more than mild symptoms resulting
in repeated hospitalization or significant assignment limitation.
b. Coxa vara. More than moderate with pain, deformity, and arthritic changes.
c. Herniation of nucleus pulposus. More than mild symptoms following appropriate
treatment or remediable measures, with sufficient objective findings to demonstrate
interference with the satisfactory performance of duty.
d. Kyphosis. More than moderate, or interfering with function, or causing unmilitary
appearance.
e. Scoliosis. Severe deformity with over two inches of deviation of tips of spinous
processes from the midline.
14. Skin and Cellular Tissues.
a. Acne. Severe, unresponsive to treatment, and interfering with the satisfactory
performance of duty or wearing of the uniform or other military equipment.
b. Atopic dermatitis. More than moderate or requiring periodic hospitalization.
c. Amyloidosis. Generalized.
CH-17 3-118
d. Cysts and tumors. See section 3-F-20.
e. Dermatitis herpetiformis. Which fails to respond to therapy.
f. Dermatomyositis.
g. Dermographism. Interfering with satisfactory performance of duty.
h. Eczema, chronic. Regardless of type, when there is more than minimal involvement
and the condition is unresponsive to treatment and interferes with the satisfactory
performance of duty.
i. Elephantiasis or chronic lymphedema. Not responsive to treatment.
j. Epidermolysis bullosa.
k. Erythema multiforme. More than moderate and chronic or recurrent.
l. Exfoliative dermatitis. Chronic.
m. Fungus infections, superficial or systemic. If not responsive to therapy and
interfering with the satisfactory performance of duty.
n. Hidradenitis suppurative and folliculitis decalvans.
o. Hyperhydrosis. Of the hands or feet, when severe or complicated by a dermatitis or
infection, either fungal or bacterial, and not amenable to treatment.
p. Leukemia cutis and mycosis fungoides.
q. Lichen planus. Generalized and not responsive to treatment.
r. Lupus erythematous. Chronic with extensive involvement of the skin and mucous
membranes and when the condition does not respond to treatment.
s. Neurofibromatosis. If repulsive in appearance or when interfering with satisfactory
performance of duty.
t. Panniculitis. Relapsing febrile, nodular.
u. Parapsoriasis. Extensive and not controlled by treatment.
v. Pemphigus. Not responsive to treatment, and with moderate constitutional or
systemic symptoms, or interfering with satisfactory performance of duty.
w. Psoriasis. Extensive and not controllable by treatment.
x. Radiodermatitis. If resulting in malignant degeneration at a site not amenable to
treatment.
3-119 CH-17
y. Scars and keloids. So extensive or adherent that they seriously interfere with the
function of an extremity.
z. Scleroderma. Generalized, or of the linear type that seriously interferes with the
function of an extremity or organ.
aa. Ulcers of the skin. Not responsive to treatment after an appropriate period of time or
if interfering with satisfactory performance of duty.
bb. Urticaria. Chronic, severe, and not amenable to treatment.
cc. Xanthoma. Regardless of type, but only when interfering with the satisfactory
performance of duty.
dd. Other skin disorders. If chronic, or of a nature that requires frequent medical care or
interferes with satisfactory performance of military duty.
15. Neurological Disorders.
a. Amyotrophic sclerosis, lateral.
b. Atrophy, muscular, myelopathic. Includes severe residuals of poliomyelitis.
c. Atrophy, muscular. Progressive muscular atrophy.
d. Chorea. Chronic and progressive.
e. Convulsive disorders. (This does not include convulsive disorders caused by, and
exclusively incident to the use of, alcohol.) Following a seizure, the member is
NFFD, and will remain unfit until he/she is controlled with medications with no
seizures for twelve months. A medical board is not required if the convulsive
disorder is well controlled.
f. Friedreich's ataxia.
g. Hepatolenticular degeneration.
h. Migraine. Manifested by frequent incapacitating attacks or attacks that last for
several consecutive days and unrelieved by treatment.
i. Multiple sclerosis.
j. Myelopathy transverse.
k. Narcolepsy, cataplexy, and hypersomnolence.
l. Obstructive Sleep Apnea. when not correctable by use of CPAP or surgical means.
m. Paralysis, agitans.
CH-17 3-120
n. Peripheral nerve conditions.
(1) Neuralgia. When symptoms are severe, persistent, and not responsive to
treatment.
(2) Neuritis. When manifested by more than moderate, permanent functional
impairment.
o. Syringomyelia.
p. General. Any other neurological condition, regardless of etiology, when after
adequate treatment, there remain residuals, such as persistent severe headaches,
convulsions not controlled by medications, weakness or paralysis of important
muscle groups, deformity, incoordination, pain or sensory disturbance, disturbance
loss of consciousness, speech or mental defects, or personality changes of such a
degree as to definitely interfere with the performance of duty.
16. Psychiatric Disorders. (see section 5-B concerning disposition)
a. Disorders with Psychotic Features. Recurrent psychotic episodes, existing symptoms
or residuals thereof, or recent history of psychotic reaction sufficient to interfere with
performance of duty or with social adjustment.
b. Affective disorders; anxiety, somatoform, or dissociative disorders. Persistence or
recurrence of symptoms sufficient to require treatment (medication, counseling,
psychological or psychiatric therapy) for greater than 6 months. Regardless of the
length of treatment, any member requiring medication for any of the above disorders
must be removed from aviation duty. (Incapacity of motivation or underlying
personality traits or disorders will be administratively handled see “Personnel
Manual, COMDTINST M1000.6 (series) for further guidance”.
c. Mood disorders. Bipolar disorders or recurrent major depression. All other mood
disorders associated with suicide attempt, untreated substance abuse, requiring
hospitalization or requiring treatment (including medication, counseling,
psychological or psychiatric therapy) for more than 6 months, or requiring more than
36 months of prophylactic treatment (while asymptomatic) following initial therapy.
Prophylactic treatment requiring more than one drug associated with significant side
effects (such as sedation, dizziness or cognitive changes) or frequent follow-up that
limit duty options. Any member requiring medication for any of the above disorders
must be removed from aviation duty, but may request waiver from CGPC.
(Incapacity of motivation or underlying personality traits or disorders will be
administratively handled see “Personnel Manual, COMDTINST M1000.6 (series)
for further guidance.”
d. Personality; sexual; factitious; psychoactive substance use disorders; personality
trait(s); disorders of impulse control not elsewhere classified. These conditions may
render an individual administratively unfit rather than unfit because of a physical
impairment. Interference with performance of effective duty will be dealt with
through appropriate administrative channels (see section 5-B).
3-121 CH-17
e. Adjustment Disorders. Transient, situational maladjustment due to acute or special
stress does not render an individual unfit because of physical impairment. However,
if these conditions are recurrent and interfere with military duty, are not amenable to
treatment, or require prolonged treatment, administrative separation should be
recommended (see Section 5-B).
f. Disorders usually first evident in infancy, childhood, or adolescence, disorders of
intelligence. These disorders, to include developmental disorders, may render an
individual administratively unfit rather than unfit because of a physical impairment.
Anorexia Nervosa and Bulimia are processed through PDES, while the remaining are
handled administratively, if the condition significantly impacts, or has the potential
to significantly impact performance of duties (health, mission, and/or safety). See
section 5-B of this Manual and Chapter 12 of the personnel manual for further
guidance.
17. Dental. Diseases and abnormalities of the jaws or associated tissues when, following
restorative surgery, there remain residual conditions that are incapacitating or interfere
with the individual's satisfactory performance of military duty, or deformities that are
disfiguring. Personnel must be in a Class 1 or Class 2 dental status (see figure 3-C-2) to
execute sea duty or overseas duty orders. Prior service personnel must meet the
enlistment dental standards contained in section 3-D.
18. Blood and Blood-Forming Tissue Diseases. When response to therapy is unsatisfactory,
or when therapy requires prolonged, intensive medical supervision.
a. Anemia.
b. Hemolytic disease, chronic and symptomatic.
c. Leukemia, chronic.
d. Polycythemia.
e. Purpura and other bleeding diseases. Any condition requiring long-term coumadin.
f. Thromboembolic disease.
g. Splenomegaly, chronic.
19. Systemic Diseases, General Defects, and Miscellaneous Conditions.
a. Systemic Diseases.
(3) Blastomycosis.
(4) Brucellosis. Chronic with substantiated recurring febrile episodes, severe
fatigability, lassitude, depression, or general malaise.
(5) Leprosy. Any type.
(6) Myasthenia gravis.
CH-17 3-122
(7) Porphyria Cutanea Tarda.
(8) Sarcoidosis. Progressive, with severe or multiple organ involvement and not
responsive to therapy.
(9) Tuberculosis (TB).
(a) Meningitis, tuberculosis.
(b) Pulmonary TB, tuberculous empyema, and tuberculous pleurisy.
(c) TB of the male genitalia. Involvement of the prostate or seminal vesicles
and other instances not corrected by surgical excision, or when residuals
are more than minimal, or are symptomatic.
(d) TB of the female genitalia.
(e) TB of the kidney.
(f) TB of the larynx.
(g) TB of the lymph nodes, skin, bone, joints, eyes, intestines, and
peritoneum or mesentery will be evaluated on an individual basis
considering the associated involvement, residuals, and complications.
(10) Symptomatic neurosyphilis. In any form.
b. General Defects.
(1) Visceral, abdominal, or cerebral allergy. Severe or not responsive to therapy.
(2) Cold injury. Evaluate on severity and extent of residuals, or loss of parts as
outlined in section 3-F-12.
c. Miscellaneous Conditions.
(1) Chronic Fatigue Syndrome, Fibromyalgia , and Myofascial Syndrome when
not controlled by medication or with reliably diagnosed depression.
d. Conditions that individually or in combination, not elsewhere provided for in this
section, if:
(1) the individual is precluded from a reasonable fulfillment of the purpose of
employment in the military service; or
(2) the individual's health or well-being would be compromised if allowed to
remain in the military service; or
(3) the individual's retention in the military service would prejudice the best
interests of the Government.
(4) required chronic and continuous DEA controlled (Class I-V) medications, such
as Ritalin, Amphetamine, Cylert, Modafanil.
3-123 CH-17
(5) required chronic anti-coagulant, other than aspirin, such as Coumadin.
20. Tumors and Malignant Diseases.
a. Malignant Neoplasms. Which are unresponsive to therapy or when the residuals of
treatment are in themselves disqualifying under other provisions of this section or in
individuals on active duty when they preclude satisfactory performance of duty.
b. Neoplastic Conditions of Lymphoid and Blood Forming Tissues. Render an
individual unfit for further military service.
c. Benign Neoplasms. Except as noted below, benign neoplasms are not generally a
cause of unfitness because they are usually remediable. Individuals who refuse
treatment are unfit only if their condition precludes satisfactory performance of
military duty. However, the following normally render the individual unfit for
further military service:
(1) Ganglioneuroma; or
(2) Meningeal fibroblastoma. When brain is involved.
21. Sexually Transmitted Disease. Complications or residuals of such chronicity or degree
of severity that the individual is incapable of performing useful duty.
Complications or residuals of such chronicity or degree of severity that the individual is
incapable of performing useful duty.
22. Human Immunodeficiency Virus (HIV). A member who is discovered to be HIV
positive (infected with HIV) by confirmatory testing is not world-wide deployable. An
HIV positive member who continues to fully perform his duties is fit for duty ashore.
After the member has been initially evaluated at the appropriate DoD MTF per Chapter
3, Section C, Paragraph 20.b.(9)(e) of this manual, the supporting medical officer shall
obtain a copy of the written narrative detailing the member's medical condition and
forward it to G-WKH via the cognizant MLC(k). The Narrative shall be marked
confidential. G-WKH will advise CGPC that the member is not worldwide deployable
but will not forward information as to the members diagnosis. Determination of duty
assignments shall than be made by CGPC Assignments Officers cognizant of the
members duty restriction. The member's supporting medical officer shall obtain copies
of the ANNUAL medical evaluation narratives from the appropriate DoD MTF and
submit them (marked as confidential) to G-WKH via MLC(k). A medical board shall be
initiated when progression of the disease adversely impacts the member's ability to
perform his duties. Taking medication for HIV disease is not necessarily in itself reason
to initiate a medical board.
23. Transplant recipient. Any organ or tissue except hair or skin.
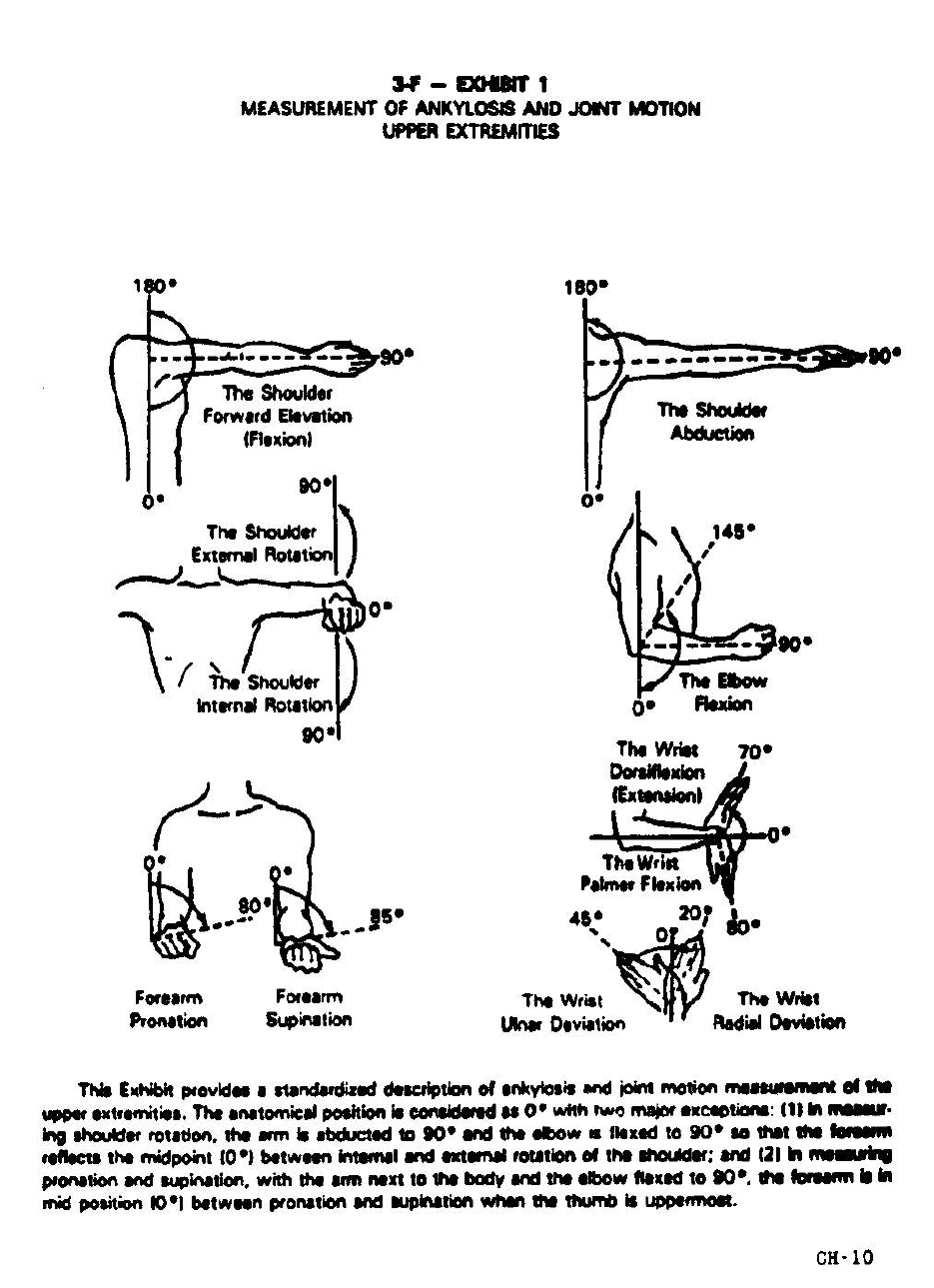
CH-17 3-124
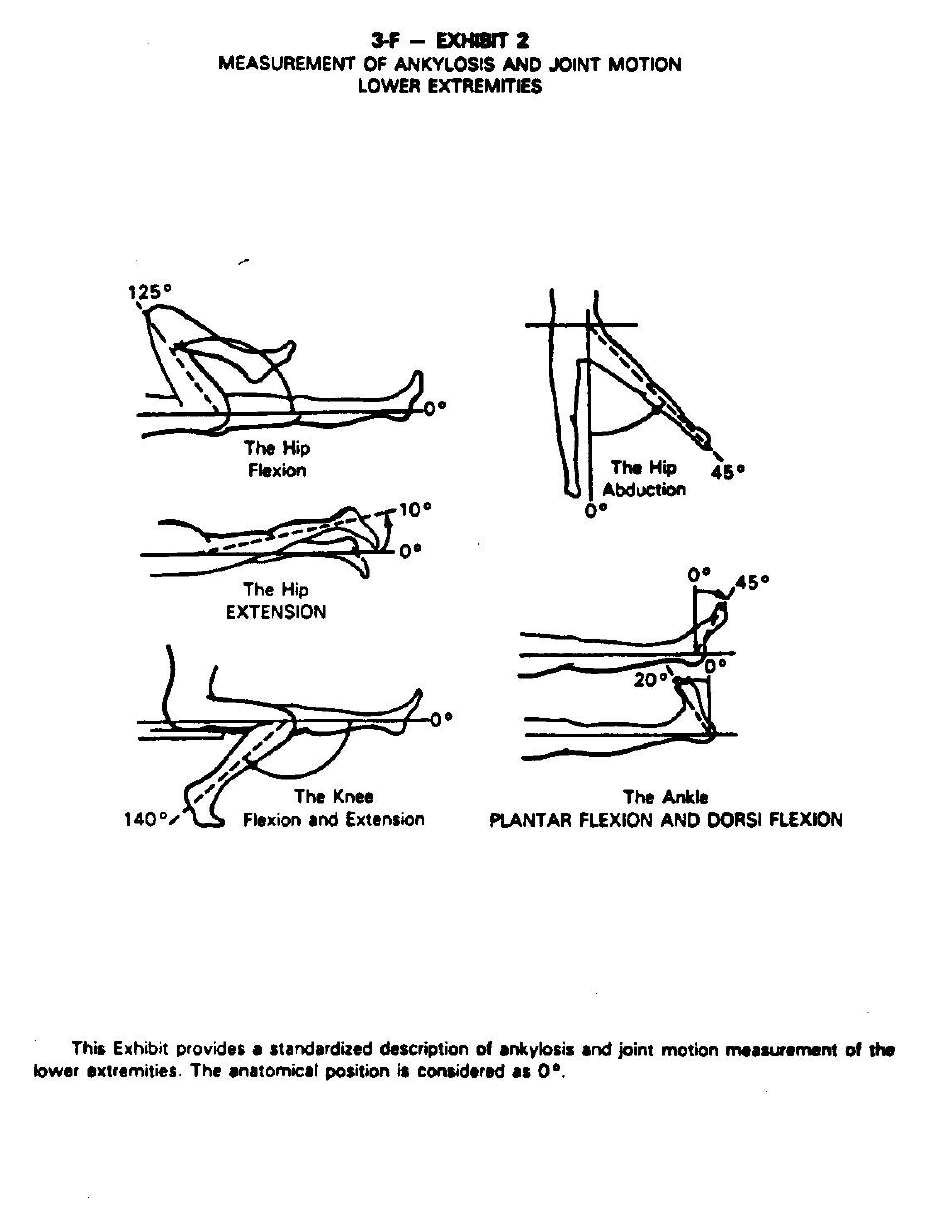
3-125 CH-17
CH-17 3-126
This page left blank.

3-127 CH-17
Section G Physical Standards for Aviation.
1. Classification of Aviation Personnel.
a. Aviation Personnel in General. Classification of Coast Guard aviation personnel is
similar to that prescribed for Navy aviation personnel. The term "aviation
personnel" includes all individuals who, in the performance of their duty, are
required to make frequent aerial flights. Aviation personnel are divided into two
classes: Class 1 and Class 2.
b. Class 1. Class 1 consists of aviation personnel engaged in actual control of aircraft,
which includes aviators, student aviators, and student flight surgeons that are chosen
to perform solo flights.
c. Class 1R. Class 1R consists of aviation personnel engaged in actual control of
aircraft who:
(1) meet Class 1 standards but are age 50 or over; or
(2) have a waiver (temporary or permanent) of physical standards which forbids
unrestricted flight. The flight restriction(s) to which the Class 1R pilot is
subject will be defined by the waiver authority. In all cases, however, Class
1R aviators will fly as a dual pilot with a Class 1 aviator.
d. Changing Classes. Except for changes in class due solely to age, individuals
requiring a change in their classification for more than two months must submit the
following to Commander CGPC:
(1) SF-502, Narrative Summary, completed by a flight surgeon/aviation medical
officer stating the need for the class change and whether a permanent or
temporary change is requested; and
(2) command endorsement.
e. Class 2. Class 2 consists of aviation personnel not engaged in actual control of
aircraft. This includes aviation observers, technical observers, flight surgeons,
aviation medical officers, aviation MEDEVAC specialists, flight officers, aircrew
members, air traffic controllers, and other persons ordered to duty involving flying.
2. General Instructions for Aviation Examinations.
a. Object of Aviation Physical Examinations.
(1) The examination for flying shall be limited to members of the aeronautical
organization and authorized candidates. The object of an aviation physical
examination is to ensure individuals involved in aviation are physically and
mentally qualified for such duty, and to remove from aviation those who are
temporarily or permanently unfit because of physical or mental defect.

CH-17 3-128
(2) The main objective in examining candidates for flight training is selecting
individuals who can fly safely and continue to do so for at least 20 years.
(3) For designated aviators, the objective is to determine if the individual can fly
safely during the next 24 months.
b. Performance of Aviation Physical Examinations. To promote safety and to provide
uniformity and completeness, an aviation physical examination must be performed
by a currently qualified flight surgeon/aviation medical officer (AMO) authorized by
the Commandant. Only physicians who have successfully passed a course at a
school of aviation medicine of the U. S. Armed Forces leading to the designation of
"Aviation Medical Officer" or "Flight Surgeon" are so authorized. Civilian
physicians who were military flight surgeons and who are currently certified by the
Federal Aviation Administration as aviation medical examiners may also be
authorized.
c. Scope of Aviation Physical Examination. In addition to the general service
requirements specified in section 3-D, certain special requirements must be met by
the various categories of individuals concerned with aviation. The extent of the
examination and the physical standards vary for the several categories of aviation
personnel. The term "flight or aviation physical examination" is therefore
incomplete unless the character of the duty that the examinee is to perform is
specified--this incomplete term shall not be used in item #16 of DD-2808 (rev 10-94)
as the purpose of the examination. Examiners shall conduct aviation physical
examinations in accordance with the general procedures specified in this section and
in section 3-C.
d. Required Aviation Physical Examinations. Each individual in the Service who is
assigned to duty requiring performance of frequent aerial flights, regardless of
classification, must have passed an aviation physical within the preceding 24 months.
In some cases, more frequent examinations are required. Aviation physical
examinations are required as indicated in this section. They may also be ordered
whenever needed to determine an individual's physical fitness for the type aviation
duty to which assigned.
(1) Entry on Active Duty. Reserve aviation personnel who perform frequent aerial
flights must have passed an aviation physical examination, commensurate with
the type of duty to be performed, within the 24 months preceding active duty
or active duty for training. Aviators who are not members of aviation reserve
units must have satisfactorily passed an aviation physical examination within
six months immediately preceding the actual control of aircraft.
(2) Biennial. All aviation personnel, including Reservists on inactive duty for
training, who will actually control aircraft or perform frequent aerial flights
must obtain a biennial aviation physical examination commensurate with the
type of duty to be performed. The examination is required every two (2) years
after initial designation. Upon reaching age 50, the examinations become
annual.

3-129 CH-17
(3) Direct Commission. An aviation physical examination is required prior to
direct commissioning of aviators in the Reserve. The aviator is required to
meet Class I standards.
(4) Candidates for Designation as Class 1. All candidates for flight training,
whether or not they are already in the Service, must pass a physical
examination for flight training duty. The examination date must not precede
the application date by more than 12 months.
(5) Candidates for Designation as Class 2. An approved aviation physical
examination less than 24 months old is required both when applying for a
Class 2 aviation training program and prior to a Class 2 designation.
(6) FAA Airmen Medical Certificate. After receiving Federal Aviation
Administration (FAA) Aviation Medical Examiner (AME) training, Coast
Guard flight surgeons/AMOs may request authorization from Commandant
(G-WKH) to perform Second and Third Class physical examinations and issue
FAA Medical Certificates to all military personnel on active duty including
active duty for training. The FAA Administrator furnishes AME's with the
necessary instructions, guides, and forms required for this purpose. Except in
those instances where there is a military requirement for FAA certification,
examination and issuance of medical certificates shall not interfere with the
flight surgeon's primary duties. Whenever possible, certificates should be
obtained in conjunction with a required aviation physical examination.
(7) Aircraft Accidents. Any Coast Guard member involved in a Class A or B
aircraft mishap in which damage to the aircraft or injury to any crewmember
occurs shall undergo a complete aviation physical examination as part of the
mishap investigation. Examinations after other mishaps are left to the
discretion of the flight surgeon/AMO.
(8) Quinquennial. The quinquennial examination of a Reserve aviation special
duty officer must be an aviation physical examination.
(9) Separation. An aviation physical examination is not required of aviation
personnel being separated from active duty. The requirements for examination
are the same as those for the separation from active duty of non-aviation
personnel.
e. Boards. Assignment to and continuation of duty involving flying is an
administrative process. Except for enlisted personnel in aviation ratings, fitness to
perform aviation duties is a determination independent of the determination of fitness
for continued service.
(1) Board of Flight Surgeons. When a fitness for continued service determination
is not required or in cases where the disposition is appropriately administrative
[e.g., a condition not a ratable disability or covered under sections 12-A or 4-C
of the Personnel Manual,COMDTINST M1000.6 (series)] a Board of Flight
Surgeons shall be convened. The board shall consist of two medical officers,
one of whom must be a flight surgeon or AMO. When formation of such a
board is not feasible, a single flight surgeon/AMO may be considered the

CH-17 3-130
minimum with the approval of Commandant (G-WKH). An example of the
appropriate use of a Board of Flight Surgeons is an aviator found not
aeronautically adaptable due to fear of flying. The results of the board shall be
recorded on a Narrative Summary (SF-502) and submitted to Commander
CGPC via the appropriate chain of command.
(2) Special Board of Flight Surgeons.
(a) The U.S. Navy has established this board to consider unusual,
complicated, or controversial cases beyond the capabilities or experience
level of a local Board of Flight Surgeons. The Naval Aerospace Medical
Institute (NAMI) is staffed and equipped to evaluate such cases. Special
Boards must be arranged through Commandant (G-WKH).
(b) NAMI specialists may be requested as consultants without convening a
full Special Board. Specialty consultations may be requested and
arranged by local command.
f. Reporting Fitness for Flying Duties.
(1) Aviation personnel admitted to the sicklist or hospitalized shall be suspended
from all duty involving flying. Upon the recommendation of a medical officer
(not restricted to a flight surgeon/aviation medical officer), the commanding
officer may relieve from flying duty or suspend the flight training of an
individual deemed unfit for such duty. In all instances, a Grounding Notice
(Aero-Medical NAVMED 6410/1) shall be issued.
(2) When aviation personnel are subsequently deemed fit to resume flying duties,
they shall be examined by a flight surgeon/ aviation medical officer and a
Clearance Notice (Aero-Medical NAVMED 6410/2) shall be submitted to the
commanding officer. Based on this recommendation, the commanding officer
may authorize resumption of such duty or training.
(3) Class 1 or 2 aviation personnel, upon reporting to a new duty station or upon
returning from an extended absence from flying duty for any reason or when
otherwise indicated, shall be interviewed by a flight surgeon/aviation medical
officer in order to determine their current health, verify that a current aviation
physical examination has been conducted, and to administratively review their
health record. If the flight surgeon/aviation medical officer deems it
appropriate, a physical examination may be conducted to determine their
physical fitness to continue or resume their flying duties. The appropriate
Grounding or Clearance Notice shall be completed in all such cases and the
necessary notation made in the individual's health record on an SF-600.
Specific guidance for some special circumstances are:
(a) Post-hospitalization. A post-hospitalization examination may be
required.

3-131 CH-17
(b) Alcohol Abuse. Members under aviation class 1 or 2 retention standards
involved in alcohol related incidents or who are referred for alcohol
screening shall be recommended for grounding. If, after alcohol
screening, a specific medical diagnosis of Alcohol Abuse (305.00 DSM
III-R) or Alcohol Dependence (303.90 DSM III-R) cannot be made, the
individual can be returned to aviation duties without a formal waiver.
Those aviation personnel who are diagnosed as Alcohol Abusers or
Alcohol Dependent can return to duties involving flight only after
favorable action by the appropriate waiver authority. In addition, class 2
aircrewmen with either of these diagnoses must be cleared by the flight
surgeon/AMO before returning to flight-line duties or activities
involving aircraft maintenance. Candidates for Student Naval Aviator or
Aircrew Candidates with a history of alcohol dependence or abuse will
be considered for a waiver after successful rehabilitation (outpatient or
inpatient) and an interval of aftercare (1 year for dependence and 90 days
for abuse) dating from the onset of rehabilitation.
1 The waiver request must include:
a The flight surgeon's Narrative Summary (SF 502);
b How the problem was identified;
c Drinking history: When subject member first drank, history of
DUIs, blackouts, frequent sick-call visits, withdrawal
symptoms, morning drinking, domestic difficulties, impaired
job performance, etc.;
d Lab data (LFTs, red cell indices, etc.,);
e Any Narrative Summary from rehabilitation authority;
f Commanding officer's endorsement in accordance with
paragraph 3-A-8.d.(2). This must include details of any
mandated aftercare plan.
2 The waiver process should not be initiated until the aviation
member:
a Completes Level II or III rehabilitation program or the civilian
equivalent;
b Demonstrates compliance with their aftercare program for at
least three months.
3 Waiver contingencies will usually incorporate the recommendations
of the rehabilitation authority and may include one or more of the
following:
a Total abstinence;
b Active participation in a sobriety program (which includes AA);

CH-17 3-132
c Follow-up by the flight surgeon at least quarterly for a year then
at least annually thereafter.
(c) Pregnancy. After confirmation of pregnancy, female members should
not be assigned to duties involving flight until cleared by her flight
surgeon (FS)/aviation medical officer (AMO). Nausea, decreased
appetite, easy fatigability, dizziness, and vaginal bleeding are some of
the potential problems that may cause the FS/AMO to recommend
temporary grounding for pregnant aviation personnel. Close monitoring
is required by the FS/AMO to ensure early identification of problems
associated with pregnancy, that could be hazardous to the pregnant
member or others. In addition, the FS/AMO will assess the ergonomic
and toxic hazards to which the pregnant member and her fetus may be
exposed in her particular aviation environment. Potential occupational
health problems will be brought to the attention of the patient and the
command. No member will perform duties as a rescue swimmer upon
confirmation of pregnancy. No pregnant member shall perform duties
involving flying after the end of the second trimester, nor shall they
undergo chamber (physiologic) training or training involving swimming
after the end of the second trimester. (Note: Any pregnant member
undergoing chamber or dunker training must receive, from a flight
surgeon or AMO, a status profile chit indicating she is "OK
DIF/Dunker/Chamber.")
(4) Areas without flight surgeons/AMOs assigned or when the assigned flight
surgeon/AMO is on leave or TAD:
(a) The authority to issue a Grounding Notice includes all medical officers,
dental officers, and health service technicians.
(b) Flight surgeons (FS) and aviation medical officers (AMO) are the only
personnel authorized to issue clearance notices (ie. Up chits) for the
resumption of flight duties. In the absence of an assigned flight surgeon,
MOs, DOs, and HSs may issue a clearance notice related to the scope of
the specialty of the provider after concurrence has been received from an
FS or AMO. Concurrence can be obtained by either message or verbal
communication. Clearance notices issued by an MO, DO, or HS must
include the name, rank, and duty station of the authorizing FS/AMO as
well as the time and date of communication for authorization.
(c) Channels of communication between commands without flight
surgeons/AMOs and the nearest USMTF with a flight surgeon will be
established to facilitate concurrence prior to issuing a clearance notice.
g. Reporting Aviation Physical Examinations.
(1) Definition of "Physically Qualified".

3-133 CH-17
(a) Class 1 aviation personnel have passed an aviation physical examination
when a flight surgeon/aviation medical officer or Board of Flight
Surgeons finds that, according to the standards prescribed in this Manual,
the examinee is physically qualified and aeronautically adapted for
actual control of the aircraft, and has been approved by appropriate
Reviewing Authority.
(b) Class 2 aviation personnel have passed an aviation physical examination
when a flight surgeon or physical evaluation board including a flight
surgeon finds that, according to the standards prescribed in this Manual,
the examinee is physically qualified and aeronautically adapted for
flying, and has been approved by appropriate Reviewing Authority.
(2) Aeronautical Adaptability. After the examination has been completed, the
examiner shall review all the available information and make an assessment of
the individual's qualifications for the type of flying duty to be performed.
Generally, clinical syndromes except adjustment disorders should lead to a
finding of "not physically qualified." Adjustment disorders, psychological
factors affecting physical condition and conditions not attributable to a mental
disorder that are a focus of attention or treatment and Axis II conditions
(personality traits and disorders) as a primary diagnosis should lead to a
finding of "physically qualified but not aeronautically adapted."
(3) Comments and Recommendations. Examiners are encouraged to use the space
on the DD-2808 entitled "Remarks" or "Notes." In this space, the examiner
may express an opinion on specific defects and the examinee's overall
capabilities. Comments by the examinee or the examinee's immediate superior
are occasionally most valuable, especially when removal from flight status is
recommended. Examiners shall enclose such comments in writing as an
addendum to the formal report whenever such information is considered
relevant to making a final recommendation.
3. Restrictions Until Physically Qualified.
a. Restrictions by Reviewing Authority.
(1) Except as authorized in this section, no person shall assume initial duty
involving the actual control of aircraft until notification has been received from
Commandant (G-WKH) that such person is physically qualified for that duty.
(2) Pending receipt of the endorsed copy of the DD-2808 or other communication
from Commandant (G-WKH) or MLC(k) that the report of routine biennial
physical examination has been approved, aviation personnel are physically
qualified and aeronautically adapted for flight duty if a flight surgeon certifies
that the individual has no physical or mental defect that is disqualifying.
(3) When any member on flight status has been restricted by the Commandant (G-
WKH) or MLC(k), such restriction remains technically in effect until it is
changed by the same authority. However, in order to avoid delay in the return
to flight status of those clearly qualified to perform such duties, commanding
CH-17 3-134
officers are authorized, after consideration of a favorable recommendation
made to Commandant (G-WKH) by a flight surgeon, to waive this technical
restriction pending the action of the Commandant.
b. Restriction by Commanding Officer.
(1) Upon recommendation by any medical officer or other health services
department personnel, the commanding officer may relieve from flying duty or
suspend the flight training of any individual reported physically incapacitated
for such duty or suspend the flight training of any individual reported
physically incapacitated for such duty. When the individual is subsequently
reported physically fit by a flight surgeon, the commanding officer may
authorize resumption of such duty or training.
(2) Aviation personnel may be continued in a flying status pending correction of
minor defects such as obtaining new eyewear prescriptions or dental
restorations with the concurrence of a flight surgeon. When corrective action
is completed, an entry shall be made in Item 73 of the DD-2808 and the
physical then forwarded for review.
4. Standards for Class l.
a. General. The physical examination and physical standards for Class 1 are the same
as those prescribed in sections 3-C and 3-D of this Manual, as modified by the
following subparagraphs.
b. History.
(1) History of any of the following is disqualifying: seizures, isolated or repetitive
(grand mal, petit mal, psychomotor, or Jacksonian); head injury complicated
by unconsciousness in excess of 12 hours or post traumatic amnesia or
impaired judgment exceeding 48 hours; malaria, until adequate therapy has
been completed and there are no symptoms while off all medication for 3
months.
(2) For persons already in the Coast Guard a complete review of their health
record is most important. Flight surgeons are authorized to postpone the
examination of persons who fail to present their health record at the time of
examination. In exercising this prerogative, due consideration must be made in
cases where access to the individual's health record is administratively
impracticable.
c. Therapeutics and General Fitness. Note on the DD-2808 if the individual received
medication or other therapeutic procedures within 24 hours of the examination. In
general, individuals requiring therapeutics or who have observed lowering of general
fitness (dietary, rest, emotional, etc.,) which might affect their flying proficiency
shall not be found qualified for duty involving flying.
d. Each aviation physical will have a Valsalva, SBT (Self Balancing Test), and AA
(Aeronautical Adaptability) performed and noted.

3-135 CH-17
e. Height. Minimum 157.4 cm (62 inches). Maximum 198 cm (78 inches).
f. Chest. Any condition that serves to impair respiratory function may be cause for
rejection. Pulmonary function tests are recommended to evaluate individuals with a
history of significant respiratory system problems.
g. Cardiovascular System. Cardiac arrhythmia, heart murmur, or other evidence of
cardiovascular abnormalities shall be carefully studied. Evidence of organic heart
disease, rhythm disturbances or vascular diseases, if considered to impair the
performance of flying duties, is cause for rejection.
h. Teeth. The following are disqualifying:
(1) Any carious teeth that would react adversely to sudden changes in barometric
pressure or produce indistinct speech by direct voice or radio transmission.
(2) Any dental defect that would react adversely to sudden changes in barometric
pressure or produce indistinct speech by direct voice or radio transmission.
(3) Fixed active orthodontic appliances require a waiver from CGPC (opm or
epm). (fixed retainers are exempts).
(4) Routine crown and temporary dental work is not disqualifying for aviation
missions. Recommend that temporary crowns be cemented with permanent
cement like polycarboxylate or zinc oxyphosphate cement until the permanent
crown is delivered. Recommend temporary grounding of 6-12 hours after
procedures. Such work may be disqualifying for deployment.
i. Distant Visual Acuity. Distant visual acuity shall be not less than 20/200 in either
eye and if less than 20/20 must be correctable to 20/20 with standard lenses. When
the visual acuity of either eye is less than 20/20 correction shall be worn at all times
while flying.
j. Oculomotor Balance. The following are disqualifying:
(1) esophoria greater than 10 prism diopters;
(2) exophoria greater than 10 prism diopters;
(3) hyperphoria greater than 1.5 prism diopters;
(4) prism divergence at 20 feet and 13 inches is optional. These tests shall be
accomplished only on designated aviators who have sustained significant head
injury, central nervous system disease, or who have demonstrated a change in
their phorias.
k. Eyes. Any pathologic condition that may become worse or interfere with proper eye
function under the environmental and operational conditions of flying disqualifies.
History of radial keratotomy is disqualifying.
CH-17 3-136
l. Near Visual Acuity. Uncorrected near vision (both eyes) shall be not less than
20/200 correctable to 20/20, with correction worn in multivision lenses while flying
if uncorrected near vision is less than 20/40 in either eye.
m. Color Vision. Normal color perception is required.
n. Depth Perception. Normal depth perception is required. When any correction is
required for normal depth perception it must be worn at all times.
o. Field of Vision. The field of vision for each eye shall be normal as determined by
the finger fixation test. When there is evidence of abnormal contraction of the field
of vision in either eye, the examinee shall be subjected to perimetric study for form.
Any contraction of the form field of 15o or more in any meridian is disqualifying.
p. Refraction. There are no refractive limits.
q. Ophthalmoscopic Examination. Any abnormality disclosed on ophthalmoscopic
examination that materially interferes with normal ocular function is disqualifying.
Other abnormal disclosures indicative of disease, other than those directly affecting
the eyes, shall be considered with regard to the importance of those conditions.
r. Ear. The examination shall relate primarily to equilibrium and the patency of
eustachian tubes. A perforation or evidence of present inflammation is disqualifying.
The presence of a small scar with no hearing deficiency and no evidence of
inflammation, does not disqualify. Perforation, or marked retraction of a drum
membrane associated with chronic ear disease, is disqualifying.
s. Sickle Cell Preparation Test. Quantitative hemoglobin electrophoreses greater than
40% HGs is disqualifying.
5. Standards for Class 1R. Physical requirements for service are the same as for Class 1,
except:
a. Age 50 or older, or
b. Have a waiver (temporary or permanent) of physical standards that forbids
unrestricted flight.
6. Candidates for Flight Training.
a. Standards. Candidates for flight training shall meet all the requirements of Class 1,
with the following additions or limitations:
(1) Height. Candidates for Class I training must also satisfy the following
anthropometric requirements: Refer to figure 3-G-1 through figure 3-G-4 for
guidelines on measurements.
(a) sitting height: 33 inches to 40.9 inches. Record in parentheses in Item
73, DD-2808 (SH_____), see figure 3-G-1 for proper measurements;
3-137 CH-17
(b) sitting eye height: 28.5 inches or greater. Record in parentheses in
Item 73, DD-2808 (SEH_____), see figure 3-G-2 for proper
measurements;
(c) thumb tip reach: 28.5 inches or greater. Record in parentheses in Item
73, DD-2808 (TTR____), see figure 3-G-3 for proper measurements;
(d) buttock-knee length: 21 inches to 27.9 inches. Record in parentheses
in Item 73, DD-2808 (BKL____), see figure 3-G-3 for proper
measurements;
(e) add: sitting eye height (SEH) and thumb tip reach (TTR), 57 inches or
greater. Record in parentheses in Item 73, (SEH + TTR =____).
(2) Uncorrected distant visual acuity must be not less than 20/50 each eye and
correctable 20/20 each eye. Uncorrected near visual acuity must be not less
than 20/20 each eye (may be waiverable).
(3) While under the effects of a cycloplegic, the candidate must read 20/20 each
eye. The following are disqualifying:
(a) total myopia greater than (minus) -2.00 diopters in any meridian;
(b) total hyperopia greater than (plus) +3.00 diopters in any meridian;
(c) astigmatism greater than (minus) -0.75 diopters; (Report the astigmatic
correction in terms of the negative cylinder required.)
(d) the purpose of this cycloplegic examination is to detect large latent
refractive errors that could result in a change of classes during an
aviation career. Therefore, the maximum correction tolerated at an
acuity of 20/20 shall be reported. Cycloplegics reported as any other
acuity, e.g., 20/15 will be returned.
(4) Hearing. Audiometric loss in excess of the limits set forth in the following
table is disqualifying:
FREQUENCY 500 1000 2000 3000 4000
EITHER EAR 30 25 25 45 55
(5) Personality. Must demonstrate, in an interview with the flight surgeon, a
personality make-up of such traits and reaction that will indicate that the
candidate will successfully survive the rigors of the flight training program and
give satisfactory performance under the stress of flying.
(6) Chest x-ray. Aviation trainees must have had a chest x-ray within the past
three years.
(7) Report of Medical History (DD-2807-1). In addition to the normal completion
of the DD-2807-1, the following statement shall be typed in block 29 and
signed by the applicant: "I certify that I do not now use, nor have I ever used,

CH-17 3-138
contact lens for any purpose, and that I am not aware that my uncorrected
vision has ever been less than 20/50." If the applicant cannot sign this
statement, include a full explanation by the examining flight surgeon, and an
ophthalmology consultation.
b. Reporting.
(1) The importance of the physical examination of a candidate should be
recognized not only by the examining flight surgeon but also by health services
personnel assisting in the procedure and preparing the report. Candidates often
come from a great distance or from isolated ships. If the examination cannot
be completed in one working day, seek the commanding officer's help in
making it possible for the candidate to remain available for a second working
day. Careful planning should keep such cases to a minimum. If a report, upon
reaching Commandant (G-WKH), is found to be incomplete and must be
returned, the candidate will suffer undue delay in receiving orders and in some
cases will be completely lost to the Coast Guard as a candidate. The
preparation of the DD-2808 in the case of a candidate requires extreme care by
all concerned.
(2) In a report of the examination of a candidate, rigid adherence to set standards is
expected. The examining officers are encouraged to use freely that portion of
the report that provides for "remarks" or "notes." Comments made under
"remarks" are the examiner's opinion. Information from any source may be
molded into an expression of professional opinion. A final recommendation of
the examiner must be made. When such recommendation is not consistent with
standards set by Commandant (G-K) the examiner shall note that fact on the
form under "remarks" or "notes" and a reasonable explanation made. When
space on an DD-2808 is inadequate, use a Continuation Sheet (SF-507).
7. Requirements for Class 2 Flight Officers.
a. Flight Officer Candidates. Flight officer candidates shall meet the standards for
Class 1 except that depth perception is not required.
b. Designated Flight Officers. Flight officers shall meet the standards for flight officer
candidate except that uncorrected distant visual acuity must be not less than 20/400
in either eye and shall be correctable to 20/20.
8. Requirements for Class 2 Aircrew.
a. Aircrew Candidates. Unless otherwise directed by Commander CGPC-epm,
personnel will not be permitted to undergo training leading to the designation of
aircrewmen unless a flight surgeon/aviation medical officer has found them
physically qualified for such training. Should it be desirable, for exceptional
reasons, to place in training a candidate who does not meet the prescribed physical
standards, the commanding officer may submit a request for a waiver, with the DD-
2808 and DD-2807-1, to Commandant (CGPC), justifying the request. Aircrew
candidates shall meet the standards for Class 1, except that minimum height is 152.5
3-139 CH-17
cm/60 inches and uncorrected distant visual acuity must be not less than 20/100 each
eye, correctable to 20/20 each eye.
b. Designated Aircrew. Aircrew shall meet the standards for Class 1, except the
minimum height is 152.5 cm/60 inches.
9. Requirements for Class 2 Medical Personnel.
a. Flight Surgeon (FS)/Aviation Medical Officer (AMO)/FS Candidates. While
assigned to a Duty Involving Flight Operations billet, FS/AMOs shall meet the
standards for Designated Flight Officer, except that minimum height is 152.5 cm (60
inches).
b. Aviation MEDEVAC Specialists (AMS)/AMS Candidates. Health Services
technicians (HS) who are assigned to flight orders. Aviation MEDEVAC Specialists
shall meet the standards for Designated Flight Officer, except that minimum height is
152.5 cm (60 inches).
10. Requirements for Class 2 Technical Observers. The term "technical observer" is applied
to personnel who do not possess an aviation designation but who are detailed to duty
involving flying. The examination shall relate primarily to equilibrium and the patency
of eustachian tubes. They shall meet the standards prescribed for general duty. These
personnel are not required to undergo a physical examination for flying provided a
complete physical examination, for any purpose, has been passed within the preceding
60 months and intervening medical history is not significant. The physical examination
need not be conducted by an FS/AMO. Technical observers who are required to
undergo egress training must have a current (general purpose) physical examination and
a status profile chit indicating "OK DIF/Dunker/Chamber."
11. Requirements for Class 2 Air Traffic Controllers. Air traffic controllers, tower
controllers, and ground control approach operators shall meet the general physical
standards for Class 1, except:
a. Articulation. Must speak clearly and distinctly without accent or impediment of
speech that would interfere with radio communication. Voice must be well
modulated and pitched in medium range. Stammering, poor diction, or other
evidence of speech impediments, that become manifest or aggravated under
excitement are disqualifying.
b. Height. Same as general service.
c. Visual Acuity.
(1) Candidate's visual acuity shall be no worse than 20/100 for each eye
correctable to 20/20 each eye and the correction shall be worn while on duty.
(2) Personnel already designated shall have distant visual acuity no worse than
20/200 each eye correctable to 20/20 each eye and the correction shall be worn
while on duty.
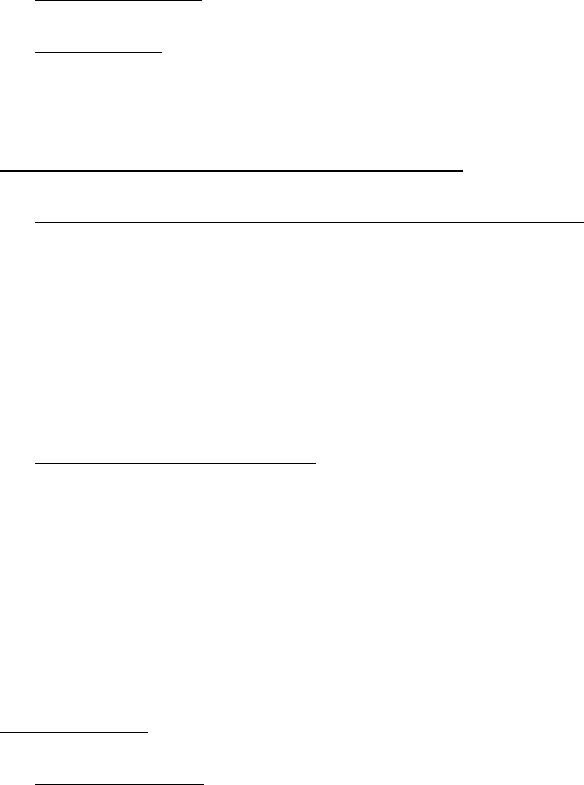
CH-17 3-140
(3) Air traffic controllers whose vision becomes worse than 20/200 either eye may
not engage in the control of air traffic in a control tower but may be otherwise
employed in the duties of their rating.
d. Depth Perception. Normal depth perception is required.
e. Heterophoria. The following are disqualifying:
(1) esophoria or exophoria greater than 6 prism diopters; and
(2) hyperphoria greater than 1 prism diopter.
12. Requirements for Landing Signal Officer (LSO).
a. Physical Examinations for Landing Signal Officer (LSO).
(1) Candidates. Officer and enlisted candidates for training as LSO's shall have a
physical examination prior to the training leading to qualification. LSO duties
for flight deck require stricter visual acuity standards than those for general
duty in the Coast Guard. Examination by a FS/AMO is not required.
(2) Reexamination. Biennial reexamination is required of all currently qualified
LSO's.
b. Physical Standards for LSO's. In addition to the physical standards required for
officer and enlisted personnel, the following standards apply:
(1) Distant Visual Acuity. The uncorrected distant visual acuity shall be no worse
than 20/200 in each eye and must be correctable to 20/20 in each eye. If the
uncorrected distant visual acuity is less than 20/20 in either eye, corrective
lenses must be worn while performing LSO duties.
(2) Depth Perception. Normal depth perception is required.
(3) Color Vision. Normal color perception is required.
13. Contact Lenses.
a. Class 1 personnel may be authorized by their local flight surgeon to wear contact
lenses while flying, provided the following conditions are met:
(1) Only gas permeable disposable soft lenses may be used.
(2) The lenses are to be removed during the hours of sleep.
(3) The lenses are disposed of after 2 weeks of use.
(4) All prescribed optometry follow-up visits are adhered to. After routine safe
use has been established and documented by the prescribing optometric
authority, an annual optometric recheck is the minimum required. A copy of
the record of any visit to an eye care professional will be furnished by the
member to the local flight surgeon for review and placement in the member's
health record.

3-141 CH-17
(5) Following any change in the refractive power of the contact lens, the member
must be checked on the AFVT to ensure that Coast Guard Class I standards for
acuity and depth perception are met. In addition, the flight surgeon shall
document that there is no lens displacement, when user moves his/her eyes
through all 8 extreme ranges of gaze.
(6) Contact lens case, saline for eye use, and an appropriate pair of eyeglasses are
readily accessible (within reach) to the lens wearer while in-flight.
(7) Contact lens candidate submits request to the command agreeing to abide the
above conditions.
(8) The flight surgeon authorizes use of contact lenses after ensuring that such use
is safe and the user fully understands the conditions of use. This authorization
expires after one year. Initial and any annual re-authorizations shall be
documented by an entry in the health record.
(9) Contact lens use is not a requirement for aviation operations. The decision to
apply for authorization is an individual option. Accordingly, lens procurement
and routine optometric care related to contact lens use at government expense
are not authorized.
b. The optional wearing of contact lenses by Class 2 personnel performing duty
involving flying and by air control personnel in the actual performance of their duties
is authorized under the following circumstances:
(1) Individuals are fully acclimated to wearing contact lenses and visual acuity is
fully corrected by such lenses;
(2) Individuals wearing contact lenses while performing flight or air control duties
have on their person, at all times, an appropriate pair of spectacles;
(3) A flight surgeon has specifically authorized the wearing of contact lenses while
performing flight or air control duties (An entry shall be made on SF-600 in
the individual's health record authorizing wearing of contact lenses.); and
(4) Wearing contact lenses while performing aviation duties is an individual
option. Accordingly, procuring contact lenses at government expense is not
authorized.
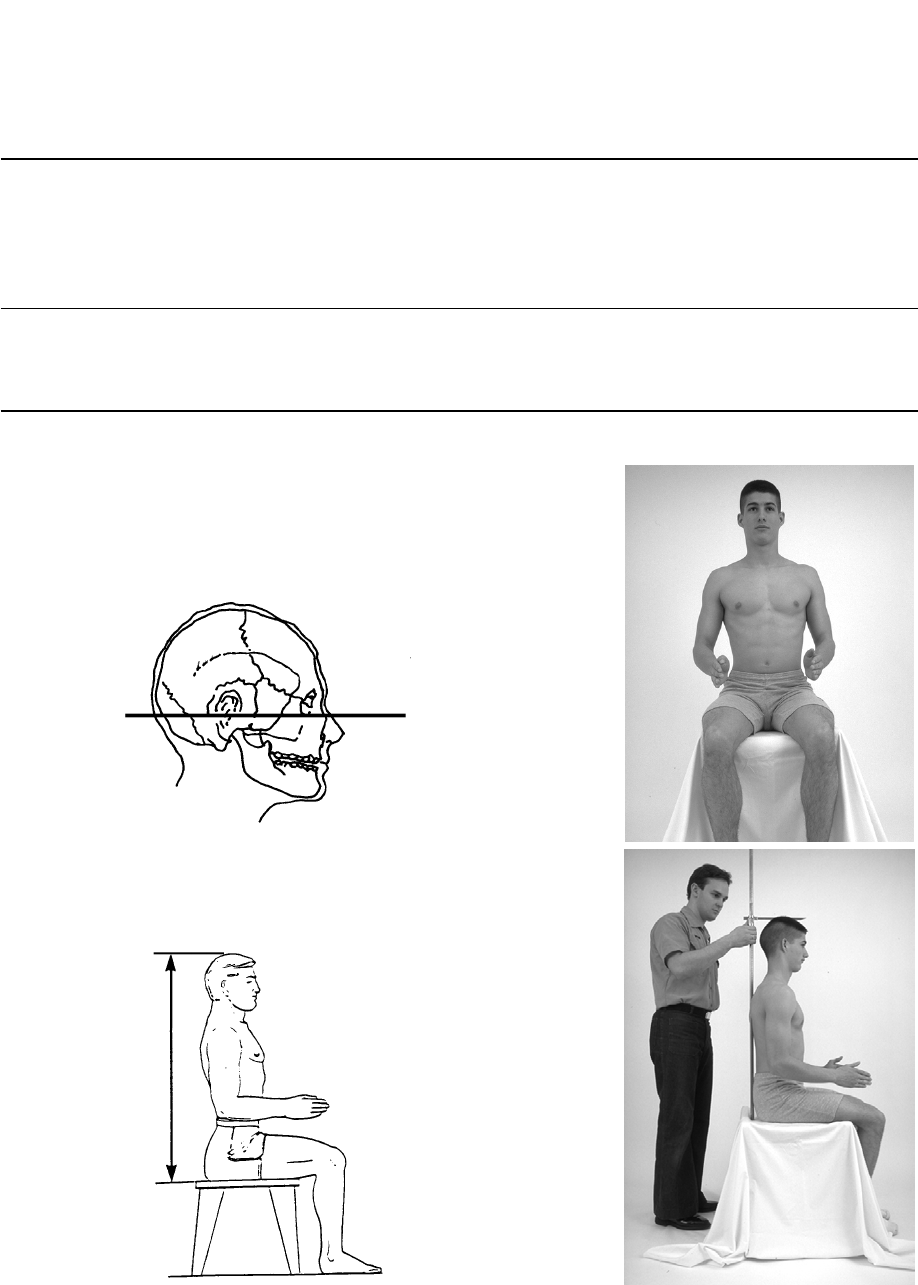
CH-17 3-142
Sitting Height
Purpose
This measurement is important in the design and layout of work stations occupied by Navy personnel. Controls
must be placed in numerous locations, and the minimum acceptable space between the helmet and the canopy of
cockpits must be considered.
Equipment Required
Anthropometer
Measurement Procedure
1. The subject sits erect facing forward with the head level (see
illustration below), the shoulders and upper arms relaxed, and
the forearms and hands extended forward horizontally with the
palms facing each other. The thighs are parallel, and the knees
are flexed 90° with the feet in line with the thighs.
2. Measure the vertical distance between the sitting surface and
the top of the head with an anthropometer. The shoulders and
upper extremities should be relaxed. Measure at the maximum
point of quiet respiration.
NOTE: Measurements are to be taken to the nearest eighth of an inch. The measurement should be taken at least twice. If
there is a large variation between the two measurements, recheck the body position and repeat measurements.
Figure 3-G-1
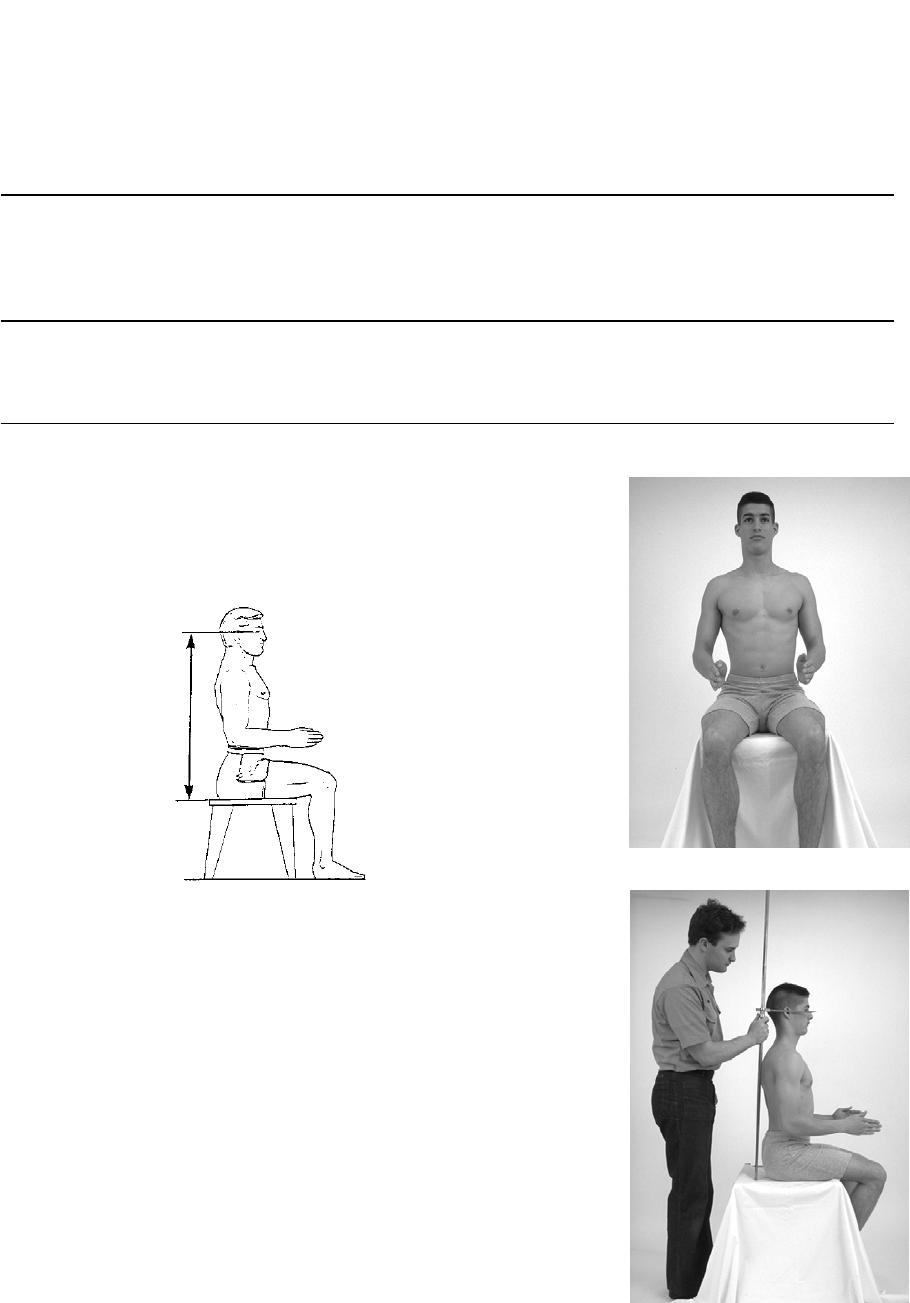
3-143 CH-17
Eye Height, Sitting
Purpose
Sitting Eye Height plays a decisive role in instrument panel layout, viewing angles, and seat adjustment, since
the pilot must have optimum vision both inside and outside of the cockpit.
Equipment Required
Anthropometer
Measurement Procedure
1. The subject sits erect facing forward with the head level (see
illustration below), the shoulders and upper arms relaxed, and
the forearms and hands extended forward horizontally with the
palms facing each other. The thighs are parallel and the knees
are flexed 90° with the feet in line with the thighs.
2. Measure the vertical distance between the sitting surface and
the corner or angle formed by the meeting of the eyelids on the
outer corner of the right eye with an anthropometer.
NOTE: Measurements are to be taken to the nearest eighth of an inch. Measurements should be taken at least twice. If
there is a large variation between the two measurements, recheck body position and repeat measurements.
Figure 3-G-2
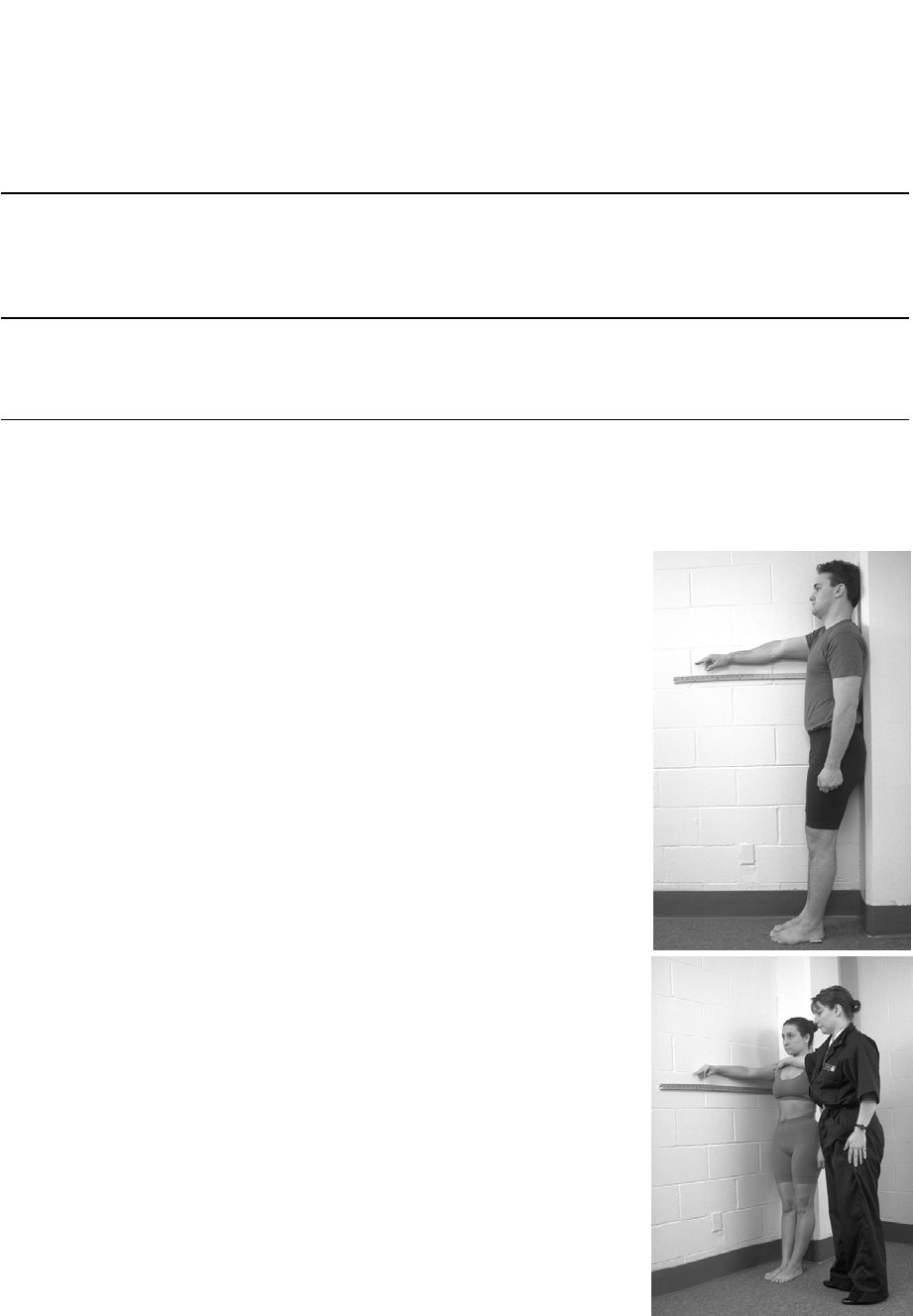
CH-17 3-144
Thumbtip Reach
Purpose
This measurement is important in the design and layout of work stations occupied or used by Navy personnel.
Thumbtip reach is particularly useful for the placement of controls in various locations within cockpits.
Equipment Required
Wall--mounted linear scale.
Measurement Procedure
1. The subject stands erect in a corner looking straight ahead
with the feet together and heels 7.87 inhes (20 cm) from the
back wall.
2. With the buttocks and shoulder placed against the wall, the
right arm and hand (palm down) are stretched horizontally
along the scale while the thumb continues along the horizontal
line of the arm with the index finger curving around to touch
the pad at end of the thumb.
3. The subject’s right shoulder is held against the rear wall. The
horizontal distance from the back wall to the tip of the right
thumb is measured.
NOTE 1: Measurements are to be taken to the nearest eighth of an inch. Measurements should be taken at least twice. If
there is a large variation between the two measurements, recheck body position and repeat measurements.
Figure 3-G-3
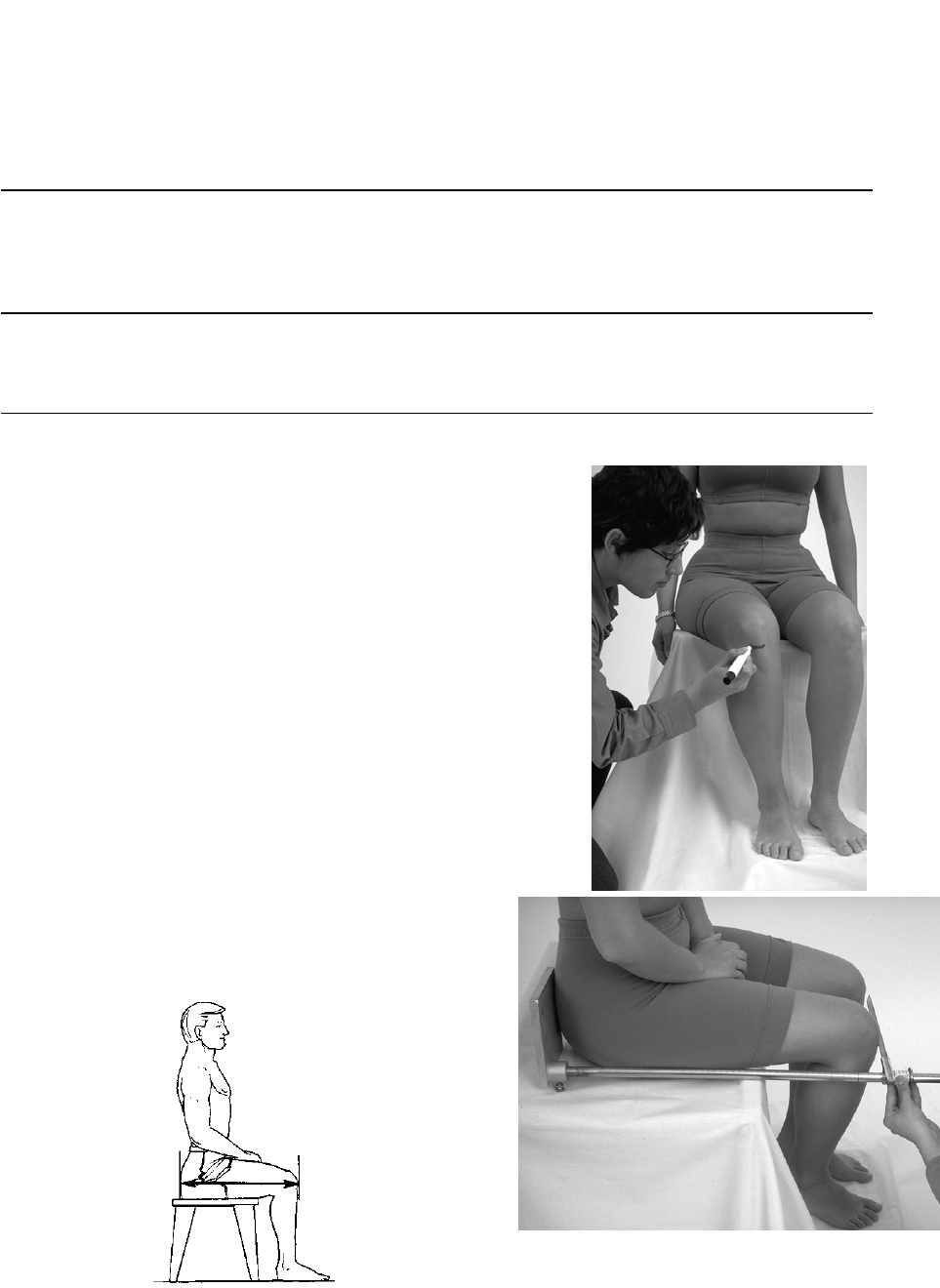
3-145 CH-17
Buttock-Knee Length
Purpose
This measurement is usually associated with ejection seat clearance and threshold values between the knee and
the glare shield (or canopy bow).
Equipment Required
Anthropometer
Measurement Procedure
1. While the subject sits erect, draw a landmark on the
bottom tip of the right knee cap. The subject’s thighs
should be parallel, with the knees flexed at 90°. The feet
should be in line with the thighs, and lying flat on the
surface of a footrest or the floor.
2. The anthropometer is placed flush against the buttock
plate at the most posterior point on either buttock, and
the anterior point to the right knee is measured with an
anthropometer.
NOTE 1: Measurements are to be taken to the nearest eighth of an inch. Measurements should be taken at least twice. If
there is a large variation between the two measurements, recheck body position and repeat measurements.
Figure 3-G-4
CH-17 3-146
This Page Intentionally Left Blank

3-147 CH-17
Section H Physical Examinations and Standards for Diving Duty.
1. Examinations.
a. Candidates. Acceptable candidates for duty that involves diving or underwater
swimming must conform to the physical standards contained in section 3-D except as
modified below.
b. Reexamination. Reexamination of all divers shall be conducted every five (5) years
after designation until age 48.
c. Examination Just Prior to Age 40. Qualified divers who desire to continue in that
specialty and are about to reach age 40 must be examined by a medical officer. The
DD-2808 and DD-2807-1, along with the examiner's recommendation as to whether
the individual is or is not physically qualified to continue as a diver shall be
forwarded to CG Personnel Command (adm-1) for final decision and in time to reach
Headquarters before the individual attains age 40. A certain latitude may be allowed
for a diver of long experience and a high degree of efficiency in diving. The
individual must be free from any diseases of the cardiovascular, respiratory,
genitourinary, and gastrointestinal systems, and of the ear. The individual's ability to
equalize air pressure must be maintained.
d. Examination Prior to Dives. Divers should ordinarily be examined prior to each
unusually hazardous dive and prior to extensive operations when practicable to do
so. Medical officers available during extensive operations, should make
observations, by personal interview if possible, of all divers prior to their initial dive
each day.
2. Standards.
a. Disqualifying History. Any of the following is disqualifying:
(1) tuberculosis, asthma, chronic pulmonary disease;
(2) chronic or recurrent sinusitis, otitis media, otitis externa;
(3) chronic or recurrent orthopedic pathology; and
(4) chronic or recurrent gastrointestinal disorder.
b. Age Requirements. Candidates beyond the age of 30 shall not be considered for
initial training in diving, the most favorable age being 20 to 30. For officers
undergoing training in deep sea diving for the specific purpose of becoming diving
supervisors or salvage officers, the upper age limit is 39 years.
c. Nose, Sinuses, Mouth, and Throat. Obstruction to breathing or chronic hypertrophic
or atrophic rhinitis is disqualifying. Septal deviation is not disqualifying in the
presence of adequate ventilation. Chronically diseased tonsils are disqualifying
CH-17 3-148
pending tonsillectomy. Presence or history of chronic or recurrent sinusitis is cause
for rejection.
d. Ears (General) and Drums.
(1) Acute or chronic disease of the auditory canal, membrane tympani, middle or
internal ear is disqualifying. Perforation or marked scarring or thickening of
the drum is disqualifying. The eustachian tubes must be freely patent for
equalization of pressure changes.
(2) All candidates shall be subjected in a recompression chamber to a pressure of
50 pounds per square inch to determine their ability to clear their ears
effectively and otherwise to withstand the effects of pressure.
e. Skin and Lymphatics. There shall be no active acute or chronic disease of the skin
characterized by infectiveness and/or offensiveness in close working conditions and
interchange of diving apparel.
f. Psychiatric. The special nature of diving duties requires a careful appraisal of the
candidate's emotional, temperamental, and intellectual fitness. Past or recurrent
symptoms of neuropsychiatric disorder or organic disease of the nervous system are
disqualifying. No individual with a history of personality disorder shall be accepted.
Neurotic trends, emotional immaturity or instability and antisocial traits, if of
sufficient degree to militate against satisfactory adjustment are disqualifying.
Stammering or other speech impediment that might become manifest under
excitement is disqualifying.
g. Dental. Acute infectious diseases of the soft tissues of the oral cavity are
disqualifying until remedial treatment is completed. Advanced oral disease and
generally unserviceable teeth are cause for rejection. Candidates with moderate
malocclusion, or extensive restorations and replacements by bridges, may be
accepted, if such do not interfere with effective use of self-contained underwater
breathing apparatus (scuba). Fixed active orthodontic appliances require a waiver
from CGPC-opm or epm (fixed retainers are exempt).
h. Distant Visual Acuity. Diving candidates and designated divers shall have a
minimum uncorrected distant visual acuity of 20/100 in the better eye and 20/200 in
the worse eye, both of which must be correctable to 20/20. Waiver considerations
will be on a case-by-case basis. Emphasis on the ability to perform previous diving
duties/recreational diving, if any, should be elaborated on in the applicant's letter
requesting a waiver of the physical standards.
4-i CH 17
CHAPTER 4
HEALTH RECORDS AND FORMS
PAGE
SECTION A - HEALTH RECORDS
PURPOSE AND BACKGROUND ....................................................................................................................................1
CONTENTS OF HEALTH RECORDS ..............................................................................................................................1
OPENING HEALTH RECORDS .....................................................................................................................................4
TERMINATING HEALTH RECORDS .............................................................................................................................4
CUSTODY OF HEALTH RECORDS ...............................................................................................................................6
TRANSFER OF HEALTH RECORDS...............................................................................................................................8
CREATING AN ADDITIONAL VOLUME ........................................................................................................................9
LOST, DAMAGED, OR DESTROYED HEALTH RECORDS ..............................................................................................9
ACCURACY AND COMPLETENESS CHECK ................................................................................................................10
SECTION B - HEALTH RECORD FORMS
CG-3443 (HEALTH RECORD COVER) .....................................................................................................................11
CG-5266 (DRUG SENSITIVITY STICKER) .................................................................................................................12
DD2766 (ADULT PREVENTIVE & CHRONIC CARE FLOWSHEET)..............................................................................12
SF-600 (CHRONOLOGICAL RECORD OF MEDICAL CARE) ........................................................................................13
DD-2808 (REPORT OF MEDICAL EXAMINATION) ....................................................................................................15
DD-2807-1 (REPORT OF MEDICAL HISTORY) .........................................................................................................21
SF-558 (EMERGENCY CARE AND TREATMENT) ......................................................................................................24
DD-2215 (REFERENCE AUDIOGRAM) ..............................................................................................................26
DD-2216 (HEARING CONSERVATION DATA)................................................................................................26
AUDIOGRAM RESULTS .....................................................................................................................................26
SF-502 (NARRATIVE SUMMARY) ...........................................................................................................................26
NAVMED 6100/1 (MEDICAL BOARD REPORT COVER SHEET) ..............................................................................26
SF-513 (CONSULTATION SHEET) ............................................................................................................................27
SF-520 (ELECTROCARDIOGRAPHIC REPORT) ..........................................................................................................28
SF-515 (TISSUE EXAMINATION) .............................................................................................................................29
SF-541 (GYNECOLOGIC CYTOLOGY) ......................................................................................................................29
SF-514 (LABORATORY REPORTS) ..........................................................................................................................29
SF-546-557 (LABORATORY REQUESTS) .................................................................................................................29
SF-519 (RADIOGRAPHIC REPORTS) ........................................................................................................................32
DD-771 (EYEWEAR PRESCRIPTION) .......................................................................................................................33
CH-17 4-ii
SF-601 (IMMUNIZATION RECORD) .........................................................................................................................35
SF-602 (SYPHILIS RECORD) ...................................................................................................................................35
DD-1141 (RECORD OF OCCUPATIONAL EXPOSURE TO IONIZING RADIATION) .........................................................36
CG-4057 (CHRONOLOGICAL RECORD OF SERVICE) ................................................................................................37
NAVMED 6150/2 (SPECIAL DUTY MEDICAL ABSTRACT) .....................................................................................38
PHS-731 (INTERNATIONAL CERTIFICATE OF VACCINATION) ..................................................................................39
CG-5214 (EMERGENCY MEDICAL TREATMENT REPORT) .......................................................................................40
DD-877 (REQUEST FOR MEDICAL/DENTAL RECORDS) ............................................................................................42
SECTION C - DENTAL RECORD FORMS
CG-3443-2 (DENTAL RECORD COVER) ..................................................................................................................44
NAVMED 6600/3 (DENTAL HEALTH QUESTIONNAIRE) ........................................................................................45
SF-603 (DENTAL RECORD) ....................................................................................................................................45
TYPES OF DENTAL EXAMINATIONS..........................................................................................................................47
PATIENT CLASSIFICATION DESCRIPTIONS .................................................................................................................48
USE OF S.O.A.P. FORMAT IN DENTAL RECORDS......................................................................................................55
SF-603-A (DENTAL CONTINUATION) .....................................................................................................................59
USE OF SF-513 IN DENTAL RECORDS ......................................................................................................................60
LOST DENTAL RECORDS .........................................................................................................................................60
SPECIAL DENTAL RECORD ENTRIES ........................................................................................................................60
DENTAL EXAMINATION REQUIREMENTS..................................................................................................................60
RECORDING DENTAL TREATMENTS ON SF-600 ......................................................................................................61
SECTION D - CLINICAL RECORDS
PURPOSE AND BACKGROUND ..................................................................................................................................62
CONTENTS OF CLINICAL RECORDS ..........................................................................................................................62
EXTRANEOUS ATTACHMENTS .................................................................................................................................64
OPENING CLINICAL RECORDS .................................................................................................................................64
TERMINATING CLINICAL RECORDS .........................................................................................................................64
CUSTODY OF CLINICAL RECORDS ...........................................................................................................................64
SAFEKEEPING OF CLINICAL RECORDS .....................................................................................................................65
TRANSFER OF CLINICAL RECORDS...........................................................................................................................65
LOST, DAMAGED, OR DESTROYED CLINICAL RECORDS ..........................................................................................66
CLINICAL RECORD FORMS ......................................................................................................................................66
SECTION E - EMPLOYEE MEDICAL FOLDERS
PURPOSE AND BACKGROUND ..................................................................................................................................68
CUSTODY OF EMPLOYEE MEDICAL FOLDERS ..........................................................................................................68
CONTENTS OF THE EMPLOYEE MEDICAL FOLDERS .................................................................................................69

4-iii CH 17
ACCOUNTABILITY OF DISCLOSURES ........................................................................................................................70
OPENING EMPLOYEE MEDICAL FOLDER .................................................................................................................70
TERMINATING EMPLOYEE MEDICAL FOLDERS ........................................................................................................70
TRANSFERRING TO OTHER GOVERNMENT AGENCIES .............................................................................................70
LOST, DAMAGED, OR DESTROYED EMPLOYEE MEDICAL FOLDERS ........................................................................70
SF-66 D (EMPLOYEE MEDICAL FOLDER) ...............................................................................................................71
SECTION F - INPATIENT MEDICAL RECORDS
PURPOSE AND BACKGROUND ..................................................................................................................................72
MAINTENANCE AND STORAGE OF INPATIENT MEDICAL RECORDS ..........................................................................73
DISPOSITION OF INPATIENT MEDICAL RECORDS ......................................................................................................73
INPATIENT MEDICAL RECORD FORMS AND REQUIRED ENTRIES .............................................................................75
SECTION G – MENTAL HEALTH RECORDS
ACTIVE DUTY ...........................................................................................................................................................81
NON –ACTIVE DUTY..................................................................................................................................................81
PSYCHIATRIC EVALUATION FORMAT.........................................................................................................................81
CUSTODY OF MENTAL HEALTH RECORDS..................................................................................................................81
ENCLOSURE (1) MEDICAL/DENTAL RECORD FORMS (.jpegs)
HEALTH RECORD COVER(A/D) (CG 3443) .......................................................................................................01
ADULT AND PREVENTIVE AND CHRONIC CARE FLOWSHEET (DD-2766)..............................................02
CHRONOLOGICAL RECORD OF MEDICAL CARE (SF-600) .........................................................................06
REPORT OF MEDICAL EXAMINATION (DD 2808) ........................................................................................07
REPORT OF MEDICAL HISTORY (DD-2807-1)................................................................................................10
EMERGENCY CARE AND TREATMENT (SF-558)..........................................................................................13
NARRATIVE SUMMARY (SF-502).....................................................................................................................15
CONSULT SHEET (SF-513) .................................................................................................................................16
ELECTROCARDIOGRAPHIC RECORD (SF-520)..............................................................................................17
TISSUE EXAMINATION (SF-515) ......................................................................................................................18
GYNECOLOGIC CYTOLOGY (SF-541) .............................................................................................................19
LABORATORY REPORTS (SF- 514) ..................................................................................................................20
RADIOLOGICAL CONSULTATION REQUEST/REPORTS (SF 519) ..............................................................21
EYEWEAR PRESCRIPTION (DD-771) ...............................................................................................................22
IMMUNIZATION RECORD (SF-601)..................................................................................................................23
SYPHILIS RECORD (SF-602) ..............................................................................................................................25
RECORD OF OCCUPATIONAL EXPOSURE TO IONIZING RADIATION (DD-1141)..................................27
CHRONOLOGICAL RECORD OF SERVICE (CG4057).....................................................................................28
SPECIAL DUTY MEDICAL ABSTRACT (NAVMED 6150/2) ..........................................................................30
EMERGENCY MEDICAL TREATMENT REPORT (CG-5214).........................................................................32

CH-17 4-iv
REQUEST FOR MEDICAL/DENTAL RECORD INFORMATION (DD 877)....................................................33
DENTAL RECORD COVER (CG 3443-2) ...........................................................................................................34
DENTAL HEALTH QUESTIONNAIRE (CG-5605) ............................................................................................35
DENTAL HEALTH RECORD (SF-608) ...............................................................................................................36
PERIODONTAL CHART (NAVMED 6660)........................................................................................................38
CLINICAL RECORD COVER (CG 3443-1).........................................................................................................40
REQUEST FOR ANESTHESIA (SF-522).............................................................................................................41
EMPLOYEE MEDICAL FOLDER (SF 66 D).......................................................................................................42
INPATIENT MEDICAL RECORD COVER SHEET............................................................................................43
MAINTENANCE AND STORAGE CONTAINER DIAGRAM...........................................................................44
ACCESSION NUMBER DIAGRAM ....................................................................................................................45
DOCTORS ORDER (SF-508)................................................................................................................................47
CLINICAL RECORD PHYSICAL EXAM (SF-506).............................................................................................48
MEDICAL RECORD PROGRESS NOTES (SF-509)...........................................................................................50
VITAL SIGNS RECORD (SF-511) .......................................................................................................................51
ABBREVIATED MEDICAL RECORD (DD 2770)..............................................................................................52

4-1 CH 17
CHAPTER 4. HEALTH RECORDS AND FORMS
Section A - Health Records.
1. Purpose and Background.
a. The health record is the chronological medical and dental record of an individual
while a member of the Coast Guard or the Coast Guard Reserve. The primary
reasons for compiling a health record are listed below.
(1) To develop an accurate clinical history that will help in future diagnosis and
treatment.
(2) To protect the Government, the individual concerned, and the individual's
dependents. It may be used in adjudicating veterans claims by making
permanently available in a single record all entries relative to physical
examinations, medical and dental history, preliminary to entry and throughout
the individual's entire Coast Guard career. This is accomplished by opening or
maintaining medical and dental records:
(a) upon entry into the Service;
(b) as required to maintain concise, yet complete, records during period of
service; and
(c) at time of separation.
(3) To facilitate appraisal of the physical fitness or eligibility for benefits by
making the information contained in the health record available to Coast Guard
selection boards, disability evaluation system, Board of Correction of Military
Records, for income tax purposes, and for claims to the Department of
Veterans Affairs.
(4) To furnish a basis for collecting statistical information.
(5) To identify deceased persons through dental records when other means are
inadequate.
b. As an individual's service career progresses, the health record increases in value to
the Government, the individual, and the individual's family and dependents.
Accuracy, therefore, is of the utmost importance in making entries, including entries
regarding minor ailments or injuries which appear trivial at the time, but which must
be recorded to protect the Government and the individual.
2. Contents of the Health Record.
a. Each member's health record shall consist of CG-3443 (Health Record Cover) with
medical records and dental records arranged as follows:
CH-17 4-2
(1) SECTION I - HISTORY OF CARE. Maintain the Adult Preventive and
Chronic Care Flowsheet on top of this Section. All other forms in Section I are
to be filed together in reverse chronological order (i.e., most recent on top) in
the following sequence. Do not separate corresponding forms DD-2808 and
SF-93.
(d) Adult Preventive and Chronic Care Flowsheet Form DD 2766
(e) Consultation Sheet SF-513
(f) Narrative Summary Clinical Resume * SF-502
(g) Report of Medical Examination DD-2802 (Rev. Jul 01), and History and
Report of OMSEP Examination Form CG-5447 (Rev.6-00)
(h) Report of Medical History DD2807-1 (Rev. Jul 01)
(i) Report on or Continuation of *, ** SF-507
(j) Medical Board Report Cover Sheet * NAVMED 6100/1
(2) SECTION II - RECORDS OF CARE. All forms in this Section (and their
civilian equivalents) are to be filed together in reverse chronological order (i.e.,
most recent on top) in the following sequence.
(a) Chronological Record of Care SF-600
(b) Emergency Care and Treatment SF-558
(3) SECTION III - RADIOLOGICAL REPORTS. All forms in this Section are to
be filed together in reverse chronological order (i.e., most recent on top) in the
following sequence.
(a) Radiographic Consultation Request/Report SF-519A
(b) Medical Record-Radiographic Reports SF-519
(4) SECTION IV - LABORATORY REPORTS AND ECG REPORTS. All forms
in this Section are to be filed together in reverse chronological order (i.e., most
recent on top) in the following bottom to top sequence.
(a) Clinical Record - Laboratory Reports SF-514
(b) Clinical Record - Electrocardiographic Record SF-520
(5) SECTION V - MISCELLANEOUS. All forms in this Section shall be
arranged in the following bottom to top sequence.
(a) Chronological Record of Service CG-4057

4-3 CH 17
(b) Special Duty Medical Abstract * NAVMED 6150/2
(c) Record of Occupational Exposure to Ionizing Radiation * DD-1141
(d) Occupational Health Surveillance Questionnaire * CG-5197
(e) Syphilis Record * SF-602
(f) Request for Administration of Anesthesia and for Performance of
Operations and other Procedures * SF-522
(g) Hearing Conservation Program microprocessor test result strips taped or
stapled to the SF-514 Clinical Record-Laboratory Reports form. DD-
2215 Reference Audiogram, and DD-2216 Hearing Conservation Data
Sheet, if used, will also be place in section V, in sequential order under
the SF 514 “Hearing Conservation Program” form.
(h) Eyewear Prescription DD-771
(i) Immunization Record SF-601
(6) SECTION VI - DENTAL RECORD AND INTERNATIONAL
VACCINATION RECORD. All forms in this Section shall be arranged in the
following bottom to top sequence.
(a) International Certificate of Vaccination PHS-731
(b) U.S. Coast Guard Dental Record CG-3443-2
1 Sensitivity Sticker * PHS-2410
2 Dental Health Questionnaire CG-5605
3 Health Record - Dental -- (Continuation) * SF-603A
4 Health Record - Dental SF-603
Note:
* --- When required
** -- SF-507's are attached to and filed after the form they continue
*** - Optional Form
b. File forms of the same number in their assigned sequence, with the most recent on
top of each previous form, e.g., SF-600 dated 94/02/15 is filed on top of SF-600
dated 94/02/14.
c. Record all dates on the Health Record Cover in the following sequence (all
numerals): year/month/day (e.g., 51/02/07).
CH-17 4-4
d. Reports, including laboratory, X-ray, and consultations, shall be reviewed and
initialed by the responsible MO, DO, PA/PYA or NP before they are filed in the
health record.
e. The health record is a legal document. As such, legibility of all information is
essential. Patient ID information shall be typed, printed, or stamped. All entries
shall be neat and legible. All signatures shall be accompanied by the stamped or
typed name and rank of the practitioner.
3. Opening Health Records.
f. General.
(1) A health record will be opened at the recruiting office for each individual upon
entry into the Coast Guard.
(2) A new health record will be opened upon reenlistment of personnel with prior
USCG service when such enlistment is not effected the day following
discharge. In all cases, request the individual's health record covering prior
military service from the National Personnel Records Center, St. Louis, MO.
(3) Other Specific Occasions for Opening Health Record.
OCCASSION OPENED BY
Officer appointed from civilian First duty station
Reserve Officer Unit where procured
Cadet Academy
Retired Personnel recalled to Active Duty First duty station
Original Record Lost or Destroyed Responsible Custodian
4. Terminating Health Records.
a. General Instructions.
(1) Upon discharge without immediate reenlistment or enlistment in the Coast
Guard Reserve, or retirement, forward the health record (Medical Personnel
Data Record or MED PDR) to the servicing PERSRU within 2 days of the
member's separation. DO NOT GIVE THE ORIGINAL HEALTH
RECORD TO THE MEMBER UPON FINAL SEPARATION. Cite the
reason for separation on the reverse side of Chronological Record of Service
(form CG-4057). The servicing PERSRU shall forward the health record,
along with the PERSRU PDR, to Commander (CGPC-adm3) or Commandant
(G-RSM-3) for Reservists. (See Section 4-B-27 for additional requirements for
4-5 CH 17
CG-4057.) Health record documents are not filed in the HQ PDR. They will
be returned to the unit if received by Commander, (CGPC adm-3) in error.
(2) Discharge for immediate reenlistment at the same unit, revocation of
appointment as a temporary officer to continue on active duty in permanent
status, or retirement with continuation of active duty are not termination of
service.
(3) When a health record is terminated and the dental record is not available for
inclusion therein, forward a letter of explanation with the health record.
b. Release from active duty (RELAD) with concurrent transfer to the Coast Guard
Reserve or discharge from active duty with immediate enlistment in the Coast Guard
Reserve. Upon RELAD, forward the health record (MED PDR) to the servicing
PERSRU within 2 days of the member's separation. The servicing PERSRU shall
forward the health record, along with the PERSRU PDR, to District (rs) in which the
member will reside after separation.
c. Disappearance, Other Than Desertion. Whenever an individual disappears and the
facts regarding such disappearance are insufficient to justify a conclusion of death,
enter a complete account of the circumstances on an SF-600 in the health record. Do
not terminate the health record until final disposition.
d. Desertion.
(4) When an individual is officially declared a deserter, enter an explanatory note
on SF-600. Forward the health record (MED PDR) to the servicing PERSRU
within 2 days of determination of deserter. The servicing PERSRU shall
forward the health record, along with the PERSRU PDR, to Commander
(CGPC) or Commander (CGPC-rpm) for Reservists.
(5) Upon return of a deserter to his/her own command, a physical examination
shall be performed and recorded on an DD-2808. Retain the original for
incorporation into the health record, and forward a copy to Commander
(CGPC) or Commander (CGPC-rpm) for Reservists with a request for the
deserter's health record.
e. Discharge of Personnel Convicted by Civilian Authorities. When the Commandant
directs the discharge of personnel convicted by civilian authorities, the commanding
officer will make arrangements for their physical examination, to be recorded on an
DD-2808. In the event no medical officer is available, obtain a statement signed by
the warden of the penitentiary or reformatory that the person to be discharged from
the Coast Guard is physically and mentally qualified for discharge and is not in need
of hospitalization. The warden's statement, accompanied by the terminated health
record, will be forwarded with the closed out service record.
f. Discharge of Courts-Martial Prisoners Confined in Federal Penitentiaries,
Reformatories, and the Naval Disciplinary Command. When the Commandant
CH-17 4-6
directs the discharge of a courts-martial prisoner confined in a Federal penitentiary,
reformatory, or the Naval Disciplinary Command, the command to which the
prisoner has been administratively assigned shall arrange with the warden for
physical examination of the prisoner. Results of this physical examination will be
entered on the DD-2808 and signed by the medical officer of the designated penal
institution. The command to which the prisoner has been administratively assigned
will terminate the health record, using the information furnished on the DD-2808 and
the account of medical, dental, and first aid treatments supplied by the penal
institution. The terminated health record, DD-2808, and the resume will then be
forwarded with the closed out service record.
g. Retired Personnel (Includes Temporary Retirement). Upon notification of
retirement, make an entry on CG-4057 under "Remarks" indicating place, date, and
category under which retired. The command having custody of the health record will
sign the CG-4057 and forward it to the command having administrative control of
the member for inclusion in the closed out service record.
h. Cadets. When a cadet's service is terminated, the health record will be terminated
and forwarded to the Cadet Record Office, for processing. Following this procedure,
the record will be forwarded to the Registrar's Office and held until the departing
cadet's class graduates. When this occurs, the record will be forwarded to the Federal
Personnel Records Center, St. Louis, MO. This includes cadets who graduate from
the Academy but do not accept or are not tendered a commission.
i. Officers (Reserve) to Inactive Duty and Officers (Regular) who Resign to Accept a
Reserve Commission. In the case of reserve officers being released to inactive duty
and regular officers who resign and accept a commission in the reserve, the health
record will be terminated.
j. Death. Upon notification of death, make an entry on CG-4057 under "Remarks"
indicating place, time, date, and a short explanation of the circumstances surrounding
death. A commissioned officer will sign the CG-4057 and then deliver it and the
terminated health record to the commanding officer (no later than the day following
death) for inclusion in and transmittal with the member's service record to
Commander (CGPC) or Commander(CGPC-rpm).
5. Custody of Health Records.
a. General Responsibilities.
(1) Health records are the property of the Federal government and must be handled
in accordance with the provisions of the Privacy Act of 1974 and the Freedom
of Information Act. Guidance in this area is contained in the Coast Guard
Freedom of Information and Privacy Acts Manual, COMDTINST M5260.3
(series). Health record custody and security requirements are applicable to all
documents which contain health information, whether or not filed in the health
record, such as Inpatient Medical Records and mental health treatment records.
4-7 CH 17
Disposal of all health record documents shall be in accordance with Coast
Guard Paperwork Management Manual, COMDTINST M5212.12(series).
(a) Since health records contain personal information of an extremely critical
or sensitive nature, they are considered class III records requiring
maximum security (high security locked cabinets or areas).
(b) Except as contained in the Privacy and Freedom of Information Acts
Manual, the information contained in health records shall not be
disclosed by any means of communication to any person, or to any
agency unless requested in writing by or with the prior consent of the
individual to whom the record pertains. It is the requestor's
responsibility to obtain the consent.
(2) Health records shall be retained in the custody of the Chief, Health Services
Division of the unit to which the individual is attached. At units where there is
no medical officer attached, the health record will become the responsibility of
the executive officer in accordance with Coast Guard Regulations,
COMDTINST M5000.3(series), who may delegate custody to the senior health
services department representative. At units without a health services
technician the custody of the health record is the responsibility of the unit's
executive officer. Maintenance of these health records may be delegated to
health services personnel of another unit (e.g., groups, support centers, etc.).
At no time shall individual members keep or maintain their own health
record. If there is a need to check out a health record for an appointment at
another health care facility, the health record custodian shall have the member
complete and sign the health record receipt form (NAVMED 6150/7). The
health record custodian shall place the record in an envelope, hand it to the
member, and tell the member to return the record as soon as possible following
the appointment. The envelope used for record transportation shall bear a
printed request reminding outside providers to treat the contents as
confidential, and requesting providers to include copies of their consultations
or case notes for placement in the health record. The responsibilities contained
herein are also applicable to Reserve components.
(3) Individuals may examine their own health record in the presence of a health
services department representative, providing:
(a) such examination does not interrupt the unit's scheduled mission, and
(b) there is no information contained therein that would be detrimental to the
individual's mental well-being, as determined by the member's attending
physician.
(4) Health records are subject to inspection at any time by the commanding officer,
executive officer, duly appointed counsel in the case of formal hearings, or
duly appointed Coast Guard officials who are conducting authorized
CH-17 4-8
investigations. Such inspections will be conducted in the presence of a health
services department representative to aid in the interpretation of information
contained in the health record.
(5) Health services personnel making entries in health records shall ensure all
entries, including signatures, are neat and legible. Signature information shall
include the stamped or printed name and grade or rate of the signer. Facsimile
signature stamps may only be used on the PHS-731 and the SF-601.
(6) If an erroneous entry is made in a health record, the author of the entry shall
draw a diagonal line through the complete entry, make an additional entry
showing wherein and to what extent the original entry is in error, and initial
clearly next to the correction.
(7) Health services personnel are responsible for the completeness of the entries
made on any medical or dental form while the health record is in their custody.
No sheet shall be removed from the health record except under conditions
specified in this Manual.
(8) Members are not authorized to write in, alter, remove documents from, or
otherwise change their health record or its contents. Request for changes to
health record contents shall be made in accordance with procedures contained
in Chapter 16 of the Coast Guard Freedom of Information and Privacy Acts
Manual, COMDTINST M5260.3.
6. Transfer of Health Records.
a. When active duty or reserve personnel are transferred, The Chief Health Services
Division, his designee, the Executive Officer, or the senior Health Services
department representative will make the necessary entries in the health record and
ensure that the current health record, dental record (SF-603) and Certificate of
Vaccination (PHS-731), if applicable, are properly completed.
b. A DD-877 shall be initiated for each record transferred. The DD877 shall be
attached to the front cover of the record. The health record will be forwarded to the
Coast Guard clinic or Independent Duty Health Services Technician servicing the
gaining unit. Send records using a service that provides a tracking number, such
as Priority Mail Delivery Confirmation, Certified Mail, Insured Mail, or
FedEx/Express Mail if time is critical. (See Article 4-D-7.c. of this Manual for
policy regarding transfer of Clinical Records of dependents.)
c. Transfer to Federal Penitentiaries, Reformatories, or the Naval Disciplinary
Command. A letter of transmittal and a copy of the health record shall accompany a
member who is being transferred under sentence of a courts-martial (who has not
been or will not be discharged immediately) to a penal institution for execution of the
unexpired sentence. The original health record, with a letter of transmittal stating the
name of the penal institution to which the prisoner is being transferred and the length
of the sentence, shall be forwarded to the command to which the member has been

4-9 CH 17
administratively assigned which shall maintain the health record until the prisoner
has been discharged from the Service. A copy of the letter of transmittal shall also be
forwarded to Commander (CGPC).
7. Creating an Additional Volume.
a. Due to chronic medical conditions, long narrative summaries, medical boards, etc.,
the record may fill to capacity which may cause the loss or damage to new records.
b. Procedures for creating a second volume:
(1) Obtain a new Health Record (CG-3443) and transcribe the information from
the original jacket.
(2) Write "VOLUME II" in bold print in the lower left corner of the new jacket
cover. Insert forms required by this chapter.
(3) Write "VOLUME I" in bold print in the lower left corner of the original jacket
cover.
(4) Transfer all documents pertaining to current or chronic illness to the new
record.
(5) Remove the most recent SF-600 from VOLUME I and place it in VOLUME II.
Insert a blank SF-600 on top of the remaining forms in VOLUME I and draw a
diagonal line across the page. Enter the following on this line:
CLOSED. NO FURTHER ENTRIES IN THIS RECORD. REFER TO
VOLUME II.
(6) Insert the most recent Report of Medical Examination (DD-2808) and the
Report of Medical History (DD-2807-1) into VOLUME II.
(7) Transcribe the immunization and HIV test date information onto a blank SF-
601 and insert it in the appropriate section of VOLUME II.
(8) Place the original Problem Summary List (NAVMED 6150/20) into VOLUME
II and a copy of this form in VOLUME I with the annotation, "CLOSED. NO
FURTHER ENTRIES.", below the last entry.
(9) Place the original Chronological Record of Service (CG 4057) in VOLUME II
and a copy in VOLUME I.
8. Lost, Damaged, or Destroyed Health Records.
a. If a health record is lost or destroyed, a complete new health record shall be opened
by the unit health record custodian. The designation "REPLACEMENT" shall be
stamped or marked on the cover. If the missing health record should be recovered,
CH-17 4-10
any additional information or entries in the replacement record shall be inserted in
the old record.
b. Health records which become illegible, thus destroying their value as permanent
records, shall be restored and duplicated. The duplicate shall, as nearly as possible,
be an exact copy of the original record before such record becomes illegible. Take
particular care in transcribing the date on DD-2808 into the new record as such
information may be required by the Department of Veterans Affairs to determine the
individual's right to pension or other Federal benefits. Stamp or mark
"DUPLICATE" on the cover of the new record. Explain the circumstances
necessitating the duplication on an SF-600. Forward health records replaced by
duplicate records to CGPC-adm-3.
9. Accuracy and Completeness Check.
a. Upon transfer of an individual, the health record custodian at both the detaching unit
and the receiving unit shall inspect the health record for accuracy and completeness,
in accordance with the following guidelines:
(1) that all immunizations are up-to-date (See Immunizations and
Chemoprophylaxis, COMDTINST 6230.4 (series));
(2) that PPD screening is current in accordance with Section 7-D of this Manual;
(3) that all required audiograms are completed, especially on personnel involved in
the hearing conservation program;
(4) that required forms have been properly completed and are in the correct order;
(5) that all deficiencies in physical requirements shall be scheduled for correction,
all missing forms shall be replaced, and all other clerical or administrative
errors corrected; and
(6) that all OMSEP requirements are met.
b. The health record custodian shall ensure that all identified deficiencies are corrected
immediately. Appointments shall be scheduled and the individual's supervisor
notified of the need to correct deficiencies as soon as possible.
c. Upon separation of the individual from the Service, the unit terminating the health
record will inspect the health record, correct all errors, fill in omissions, and make
sure the patient identification information is completed on all forms.
4-11 CH 17
Section B - Health Record Forms.
1. CG-3443 (Health Record Cover). See Encl (1), pg.4-1. Each patient's health record
shall be maintained in a CG-3443 (Health Record Cover). The CG-3443 shall be
completed according to the following instructions:
a. Last Name. Record in all capital letters.
b. Given Name(s). Record given name(s) in full without abbreviations. If the
individual has no middle name or initial then use the lower case letter "n" in
parentheses (n). If the individual has only a middle initial(s) record each initial in
quotation marks. When "Jr." or "II" or other similar designations are used they shall
appear after the middle name or initial.
DOE John Buck Jr.
Surname First Name Middle Name
c. Beneficiary. Enter the appropriate beneficiary code to describe the patient (enter
"20" for active duty members).
(1) 01 to 19 - Dependent children in order of birth
(2) 20 - Sponsor
(3) 30 - Spouse
(4) 31-39 - Unremarried former spouse
(5) 40 - Dependent mother (active duty)
(6) 45 - Dependent father (active duty)
(7) 50 - Dependent mother-in-law (active duty)
(8) 55 - Dependent father-in-law (active duty)
(9) 60 - Other dependents
(10) 80 - Humanitarian (non-eligible)
(11) 90 - Civilian employee
(12) 99 - Other eligible
d. Sponsor's Social Security Number. Enter.
e. Blood Type and Rh Factor. Enter the blood-type and Rh factor in the appropriate
boxes. Use utmost caution when recording this information. If not known, complete
a blood-type and Rh factor test as required.
CH-17 4-12
f. Special Status. Check the appropriate block to indicate whether the individual is in
aviation or diving status, has a waiver, requires occupational monitoring, or has an
allergy.
g. Date of Birth. Enter year, month and day (e.g., 51/02/07).
h. Local Use. Use the spaces provided below the sensitivity sticker location for local
use information such as rank, unit, etc. as needed.
2. CG-5266 (Drug Sensitivity Sticker).
a. General. Form CG-5266 should be initiated for anyone having documented history
of sensitivity or hypersensitivity to specific drugs, serums, or vaccines, including
PPD converters. Other non-drug allergies should be indicated on this form only if
they will affect potential therapy (e.g., egg yolks). Every effort shall be made to
verify the reported sensitivity and to confirm that it is allergic in nature.
b. Detailed Instructions.
(1) Prepare two originals. (One each for the health and dental records.)
(2) List the name of each drug, serum, vaccine, or anesthetic indicated on the DD-
2766 Adult Preventive and Chronic Care Flowsheet.
(3) Affix the CG-5266 vertically to the indicated location on the health record
cover (form CG-3443) and vertically to the lower left corner on the front of the
dental record cover (CG-3443-2).
3. DD2766 (Adult Preventive and Chronic Care Flowsheet Form). See Encl (1), pg 4-2.
a. General. The Adult Preventive and Chronic Care Flowsheet Form documents
significant/chronic health problems, allergies, chronic medications,
hospitalizations/surgeries, health counseling, immunizations, PPD, DNA & HIV
testing, screening (preventive medicine) exams, other medical readiness items (such
as blood type, G6PD, sickle cell, glasses, dental exam, etc), and chart audits. In-
house training sessions should be conducted prior to the implementation of this form.
b. Detailed Instructions. DD2276 should be inserted as the first page of the medical
record and all sections completed by the health care provider with the following
guidelines exceptions:
(1) Information from previous Problem Summary Lists should be copied and
updated onto the DD2276 as it is placed in the health record.
(2) If the patient is not allergic to any drugs, indicate NKDA (no known drug
allergies), in block 1.a.
(3) Sections 8.a., 10.e. and 10.i. are not required to be completed.

4-13 CH 17
(4) Use a pencil to darken the circles on Section 7, Screening Exam.
(5) The medical officer should enter the date and location of every deployment the
member participates in Section11, Pre/Post Deployment History. Pre and post
deployment questionnaires are documented in Section 11 for participants in
DOD deployment.
4. SF-600 (Chronological Record of Medical Care). See Encl (1), pg 4-6.
a. General.
(1) This form provides a current, concise, and comprehensive record of a member's
medical history. Properly maintained, the SF-600 should: aid in evaluating a
patient's physical condition; greatly reduce correspondence to obtain medical
records; eliminate unnecessary repetition of expensive diagnostic procedures;
and serve as an invaluable permanent record of health care received. The SF-
600 shall be continuous and include the following information as indicated:
complaints; duration of illness or injury, physical findings, clinical course,
results of special examinations; treatment; physical fitness at time of
disposition; and disposition. The SF-600 also serves as the patient's
prescription from which pharmacy services are provided.
(2) When a new SF-600 is initiated, complete the identification block with the
name (last, first, middle initial), sex (M or F), year of birth, component (active
duty or reserve), service (USCG, USN, USA, etc.), Social Security Number,
and the member's grade/rate and organization at the time the form is
completed.
(3) File SF-600's on the right side of the medical record with the most current SF-
600 on top.
(4) Enter sick call entries on SF-600 in the following SOAP format
SOAP METHOD OF SICK CALL WRITE UPS
S: (Subjective).
cc: (Chief Complaint) sore throat, cough, diarrhea, etc.
hpi: (History Present Illness) onset of symptoms, all problems, review of
symptoms
pmh: Past Medical History) any related problems in past that may be
present with chief complaint
fh: (Family History) any diseases, chronic/acute, possibly related to
present complaint
CH-17 4-14
all: (Allergies) any known allergies to drugs/medications, etc.
0: (Objective).
First visual assessment/evaluation of the patient's general appearance:
limping, bleeding, doubled over, etc.
PE: All results of physical exam, vital signs, lab, x-ray, and any other
study results
A: (Assessment).
Imp: (Impression, Diagnosis) includes R/0 (rule out)
NOTE: THIS IS TO INCLUDE, AFTER IMPRESSION, WHAT
YOU ARE GOING TO DO NOW AND WHY--SUCH AS,
SUTURING, TOURNIQUET, ETC.
P: (Plan).
List of medications given, lab, x-ray, special studies ordered, duty status,
return appointments, referrals, etc.
(5) The entries for all treatments shall be complete with regard to place, date,
problem number (if appropriate), number of sick days, diagnosis of all
conditions for which treated and signature of individual furnishing treatment.
Note all facts concerning the origin of the disease, pregnancy status, symptoms,
course, treatment, and if a conflicting opinion is expressed subsequently by the
same, or another medical officer, fully state the reason for such change. The
record need not be voluminous, but it shall be thorough, concise, clearly
phrased, and complete in each case. All entries, including signatures, must be
legible.
(6) When a member is injured or contracts a disease while on leave, or when for
any other reason the facts concerning an injury or sickness have not been
entered in the individual's health record, the record custodian shall ascertain the
facts in the case and make the necessary entries on SF-600. Discuss and
document the instructions given to the patient. Include the intended treatment
and, as appropriate, possible alternative treatments, possible complications, and
long term prognosis. Information regarding previous treatments should be
entered giving the following: date, place, and full details of treatment;
laboratory reports; x-ray results; etc. The following shall also be entered:
(7) "Date:
"Transcribed From Official Records.
Signature/Rate Duty Station of Transcriber"
(8) When an individual is required to carry the PHS-731, enter a statement of
acknowledgment on the SF-600.

4-15 CH 17
(9) When an individual is diagnosed as having a Sexually Transmitted Disease
(STD) make an entry to record that an interview was conducted and that the
following was discussed with the patient:
(a) symptoms,
(b) complications,
(c) treatments, and contacts.
5. Treatment at Other Than Unit Assigned. When an activity furnishes sick call treatment to
an individual whose health record is not available, an entry shall be made on a new SF-
600 and forwarded to the individual's duty station for inclusion in the health record.
6. DD-2808 (Rev. Jul 01) (Report of Medical Examination). See Encl (1), pg. 4-7.
a. Purpose. The DD 2808 (Rev: Jul 2001) is used to record physical examination
results to determine whether an examinee does, or does not, meet the standards
established for the type of physical examination administered (i.e., initial enlistment,
officer programs, retention, release from active duty, diving, aviation, retirement,
etc.). The SF-88 is no longer applicable.
b. Preparation.
(1) When Prepared. DD-2808 shall be prepared and submitted to the reviewing
authority whenever a complete physical examination is required.
(2) Required Entries. Certain groups of personnel are required to meet physical
standards somewhat different from other groups. Accordingly, the use of all
the spaces or use of the same spaces on the DD-2808 is not necessarily
required for reporting the results of the various categories of physical
examinations. If a certain item of the medical examination is required and
facilities for accomplishing it are not available, an entry "NFA" (No Facilities
Available) shall be made in the appropriate space. An entry "NE" (Not
Evaluated) shall be made in the appropriate space for any item of the clinical
evaluation (Items 17-42) which was not evaluated. For other items listed on
the DD-2808 which were not required for a particular category of physical
examination, an entry "NI" (Not Indicated) shall be made in the appropriate
space. Reference should be made to other provisions of Chapter 3, which
prescribe the nature and scope of each physical examination and indicate the
applicability of items of the DD-2808 to the particular program. Unless
otherwise indicated by such provisions, the minimum requirements for
completing the DD-2808 are:
(a) All Examinations. Items 1-44, 45-63, 66, and 71a, shall be completed
for all physical examinations, if facilities are available. Item 41, shall be
completed for all female personnel.

CH-17 4-16
(b) Aviation Personnel. Additionally, Items 64,65, and 66-70 and 72b shall
be completed for physical examinations of aviation personnel.
(3) A physical examination must be thorough, recorded accurately, and contain
sufficient information to substantiate the final recommendation. Before
signing and forwarding, the examiner shall review the completed DD-2808 for
completeness and accuracy. Failure to do so reflects significantly on the
examiner's clinical and/or administrative attention to detail. Remember that
the reviewing authority does not have the advantage of a direct examination
and must rely on the examiner's written record and appropriate additional
information in arriving at a decision.
c. Details for Entries on DD-2808.
(1) Item 1: Date of Examination. Enter date in format - 02Aug15.
(2) Item 2: Social Security Number. Enter the nine digits of their SSN.
(3) Item 3: Last Name. Last Name - First Name - Middle Name. Record the
surname in all capital letters. Record the given name(s) in full without
abbreviation. If the individual's first or middle name consists only of an initial,
enclose each initial in quotation marks (i.e., MANUEL, Thomas "W"). If the
individual has no middle name, enter the letter "(n)" in parenthesis [i.e.,
TARVIN, Laurie (n)]. Designations, such as, "Jr." or "II" shall appear after the
middle name or initial. In the absence of a middle name or initial, these
designations shall appear after the "(n)."
(4) Item 4: Home Address. Enter the evaluee’s present residence and not the
home of record.
(5) Item 5: Home Telephone Number. NA
(6) Item 6: Grade. Use official abbreviation of the current grade or rate.
Example: HSCS; LTJG. If not a service member, enter “civilian.”
(7) Item 7: Date of Birth. (e.g.57Sep04).
(8) Item 8: Age. Enter age.
(9) Item 9: Sex. Mark one or the other of the boxes.
(10) Item 10: Race. Mark the box next to the racial or ethnic group of which
member belongs.
(11) Item 11: Total Years of Government Service. Enter years and months (e.g.,
06 yrs 04 mo’s).

4-17 CH 17
(12) Item 12: Agency. Enter the OPFAC number of the unit to which the
examinee is attached.
(13) Item 13: Organization and UIC/Code. List name of ship or station to which
the examinee is assigned. Initial entry into Service; enter recruiting office
concerned.
(14) Item 14a: Rating or Specialty. NA
(15) Item 14b: Total Flying Time. Aviators only or NA.
(16) Item 14c: Last six months. Aviators only or NA.
(17) Item 15a: Service. Mark a box next to appropriate service.
(18) Item 15b: Component. Mark a box next to appropriate component.
(19) Item 15c: Purpose of Examination. Mark the box and corresponds to the
appropriate purpose(s) of the examination. If not listed, mark “Other,” and
explain above the box such as: Diving Applicant; Biennial Aircrew; etc. For a
medical board, indicate whether it is an IMB (Initial Medical Board)/DMB
(Disposition Medical Board), etc. Do not use the incomplete terms “flight
physical,” “diving physical,” or “aviation physical.” Rather, use specific terms
such as “Class I Aviation,” “Candidate for Flight Training,” “Class II
Aircrew,” “Dive Candidate,” “Quinquennial Diving,” etc. Avoid nonstandard
abbreviations. Differentiate between an applicant for a special program and a
biennial physical for the same program. When necessary, continue under Item
73, Notes.
(20) Item 16: Examining Facility or Examiner. For civilian or contract
physician, enter the full name and address. For USMTF, enter only the facility
name, city and state in which located.
(21) Item 17-42: Clinical Evaluation. Check each item in appropriate column.
(a) Item 35: Is continued on lower right side (Feet), circle appropriate
category.
(22) Item 43: Dental Defects and Disease. For an oral examination as part of an
accession physical, record whether or not the applicant is ‘Acceptable’ or ‘Not
Acceptable’. Refer to the standards described in Chapter 3 Section D-5
Physical standards for enlistment, appointment, and induction. Enter
disqualifying defects in detail in Item 73. Record the Dental Classification.
Refer to Chapter 4 Section C-3-c for definitions of dental classes. For routine
physical examinations, record only the Dental Classification. When oral
disease or dental defects are discovered on examination of active duty member
personnel, suitable recommendations will be made for instituting corrective

CH-17 4-18
measures. A copy of form SF-603, Dental Record does not need to be attached
to the DD-2808.
(23) Item 44: Notes. Describe every abnormality from Items 17-43 in detail.
Enter pertinent item number before each comment. Continue in Item 73 and
use Continuation Sheet (SF-507), if necessary.
(24) Item 45: Laboratory Findings. Enter all laboratory results in quantitative
values.
(a) Urinalysis. Enter specific gravity and results of albumin, sugar and if
required, microscopic tests in the indicated spaces.
(b) Item 46: Urine HCG. If applicable.
(c) Item 47: H/H. Enter either the hematocrit or the hemoglobin results.
(d) Item 48: Blood Type. If applicable.
(e) Item 49: HIV. Enter date drawn only in the results section.
(f) Item 50: Drugs Test Specimen ID Label. NA
(g) Item 51: Alcohol. NA
(h) Item 52: Other. Enter all other tests performed and their results which
are not indicated on the form and which were performed in connection
with the physical examination (e.g., sickle cell test, PAP test, PPD, EKG,
Chest X-ray results, etc.). The results will be continued in Item 73 or on
Continuation Sheet (SF 507), if necessary. If provided on the lab report,
include "normal" range values for all tests performed by a civilian or
military lab. Use quantitative values and avoid vague terms such as
"WNL" or other such qualitative forms.
(25) Item 53: Height. Measure without shoes and record to the nearest one-half
centimeter ((one-half inch)
(26) Item 54: Weight. Measure with the evaluee in under garments and record
results to the nearest kilogram (pound).
(27) Item 55: Min Weight-Max weight, Max BF%. NA
(28) Item 56: Temperature. Leave Blank.
(29) Item 57: Pulse. Record the actual pulse rate.
(30) Item 58: Blood Pressure. Record the actual value in numerals for both
systolic and diastolic.

4-19 CH 17
(31) Item 59: Red/Green. NA
(32) Item 60: Other Vision Test. If applicable.
(33) Item 61: Distant Vision. Test and record using the Snellen scale. Record
vision in the form of a fraction and in round numbers, that is 20/20, 20/40, not
20/20-2 or 20/40-3.
(34) Item 62: Refraction. Enter the lens prescription when the evaluee wears (or
requires) lenses for correction of visual acuity. Do not enter the term "lenses."
(35) Item 63: Near Vision. Test and record using the Snellen scale. (See item
61).
(36) Item 64: Heterophoria. Enter when indicated.
(37) Item 65: Accommodation. Enter when indicated.
(38) Item 66: Color Vision. Color Vision. Enter the test used and the results.
(a) Farnsworth Lantern. Record the results as "Passed FALANT" or "Failed
FALANT" followed by the fraction of correct over total (i.e., 9/9 or
17/18).
(b) Pseudoisochromatic Plates (PIP). Record results as "Passed PIP" or
"Failed PIP" followed by the fraction of correct over total (i.e., 12/14 or
14/14).
(c) Enter "Passed on record" or "failed on record" if the results of a previous
PIP or FALANT examination are available on record for review.
(39) Item 67: Depth Perception. When indicated, enter test used in left portion of
Item 67.
(a) AFVT. In the appropriate space in the right-hand portion of Item 65,
record the letter designation of the highest group passed (i.e., Passed F).
(b) Verhoeff. In the appropriate space in right-hand portion of Item 34,
record perfect score as 16/16.
(40) Item 68: Field of Vision. Enter when indicated.
(41) Item 69: Night Vision. Enter when indicated.
(42) Item 70: Intraocular Tension. When indicated, enter the results in
millimeters of mercury.
(43) Item 71: Audiometer. Required on ALL physical examinations. Use ANSI
1969 standards, do not use ISO or ASA standards.

CH-17 4-20
(a) Item 71a: Current
(b) Item 71b: If applicable.
(44) Item 72a: Reading Aloud Test. If applicable.
(45) Item 72b: Valsalva. When indicated mark either SAT or UNSAT.
(46) Item 73: Notes and Significant or Interval History. Use this space for
recording items such as:
(a) any pertinent medical history;
(b) summary of any condition which is likely to recur or cause more than
minimal loss of duty time;
(c) wrist measurements;
(d) most recent HIV antibody test date (see Article 3-C-20.b.(5) of this
Manual);
(e) date of PPD and results; and
(f) Preventive Medicine stamp per Use of Preventive Medicine Stamp,
COMDTINST 6200.11(series), for exams originating in Coast Guard
sickbays and clinics.
(47) Item 74a: Examinee’s Qualification. State whether or not the examinee is
qualified for the purpose of the examination. If the purpose for the
examination is an IMB or DMB, state whether or not the examinee is qualified
or not qualified for retention and to perform the duties of his/her rank/rate at
sea and foreign shores.
(48) Item 74b: Physical profile. Leave blank.
(49) Item 75: I have been advised of my disqualifying condition. If indicated,
have evaluee sign and date.
(50) Item 76: Significant or Disqualifying Defects. Leave Blank
(51) Item 77: Summary of Defects and Diagnoses. List ALL defects in order to
protect both the Government, and evaluee, in the event of future disability
compensation claims. All defects listed which are not considered disqualifying
shall be so indicated by the abbreviation NCD (Not Considered Disqualifying).
When an individual has a disease or other physical condition that, although not
disqualifying, requires medical or dental treatment clearly state the nature of
the condition and the need for treatment. If a medical or dental condition is
disqualifying, and treatment is scheduled to be completed prior to transfer to
overseas or sea duty, indicate the date the member is expected to be fully
4-21 CH 17
qualified, e.g., "Dental appointment(s) scheduled, patient will be class I
(dentally qualified) by (date)". Leave Profile Serial, RBJ, Qualified, and
Waiver blocks blank.
(52) Item 78: Recommendations. Indicate any medical or dental
recommendations. Specify the particular type of further medical or dental
specialist examination indicated (use SF-507, if necessary).
(53) Item 79: MEPS Workload. Leave Blank.
(54) Item 80: Medical Inspection Date. Leave Blank.
(55) Item 81-84: Names and Signature of Examiners. The name, grade, branch
of Service, and status of each medical and dental examiner shall be typewritten,
printed, or stamped in the left section. Each examiner shall sign using
ballpoint pen or ink pen (black or blue-black ink only) in the appropriate
section. Do not use facsimile signature stamps. When attachment sheets are
used as a supplement or continuation to the report, they shall be serially
number (both sides); however, indicate only the actual number of attached
sheets in the bottom right block 87 on DD-2808.
(56) Item 85: Administrative Review. The person who reviews the PE prior to
submitting for approval shall sign and date.
(57) Item 86: Waiver Granted. Leave Blank.
(58) Item 87: Number of attached Sheets. Fill in with appropriate number of
forms attached.
7. DD-2807-1 (Rev. Jul 01) (Report of Medical History). See Encl (1), pg. 4-7.
a. Purpose. DD-2807-1 provides a standardized report of the examinee's medical
history to help the examiner evaluate the individual's total physical condition, and to
establish the presence of potentially disabling conditions which are not immediately
apparent upon physical examination. In preparing the form, encourage the examinee
to enter all medical problems or conditions experienced, no matter how minor they
may be. The examiner must investigate and evaluate all positive medical history
indicated on the form.
b. Preparation and Submission of DD-2807-1. Prepare and submit DD-2807-1 with all
physical examinations except: Periodic OMSEP and Substitution/Overseas/Sea Duty
Modified Physical Examination.
c. Preparation Procedures. DD-2807-1 shall be prepared by the examinee and the
examining medical officer.
(1) The examinee shall furnish a true account of all injuries, illnesses, operations,
and treatments since birth. False statements or willful omissions in completing

CH-17 4-22
the DD-2807-1 may result in separation from the Service upon arrival at the
Academy, Recruit Training Center, Officer Candidate School, or later in the
individual's career.
(2) A copy of the DD-2807-1 must be included in the member's health record.
Entries must be printed, in the examinee's and examiner's own handwriting,
using either ball-point pen or ink pen (black or dark blue). Pencils or felt-tip
pens will not be used. Information in the numbered blocks on the form will be
entered in the following manner:
(a) Item 1: Last Name, First, Middle Name. SMITH, Hannibell H.
Record the surname in all capital letters. Record the given name(s) in
full, without abbreviation. If the individual's first or middle name
consists only of an initial, enclose each initial within quotation marks. If
the individual has no middle name, enter the letter "(n)" in parenthesis.
Designations such as "Jr." or "II" will appear after the middle name or
initial or after "(n)" if there is no middle name.
(b) Item 2: Social Security Number. Enter SSN.
(c) Item 3: Enter date format –2001Sep04.
(d) Item 4a: Home Address. Enter the evaluee's present residence and not
the home of record.
(e) Item 4b: Home Telephone. Enter home phone number.
(f) Item 5: Examining Location and Address. For civilian or contract
physician, enter the full name and address. For a USMTF, enter only the
facility name and the city and state in which located.
(g) Item 6a: Service. Mark a box next to the appropriate service.
(h) Item 6b: Component. Mark a box next to the appropriate component.
(i) Item 6c: Purpose of Examination. Mark a box next to the appropriate
purpose(s) of the examination. If not listed, mark “Other” and explain
above the box such as: Diving Applicant; Biennial Aircrew; etc. For a
medical board, indicate whether it is an IMB (Initial Medical
Board)/DMB (Disposition Medical Board), etc. Do not use the
incomplete terms “flight physical,” “diving physical,” or “aviation
physical.” Avoid nonstandard abbreviations. Differentiate between an
applicant for a special program and a biennial physical for the same
program.
(j) Item 7a: Position. Use official abbreviation of current grade or rate,
branch of the Service, class and status; i.e., regular, reserve, or retired
and if active or inactive. Example: HSCM, USCG; LTJG, USCGR;
4-23 CH 17
HSC, USCG (RET); HS3, USCG (TEMPRET). If not a Service
member, enter "civilian."
(k) Item 7b: Usual Occupation. List current occupation.
(l) Item 8: Current Medications. List all current medications including
over the counter meds.
(m) Item 9: Allergies. List any allergies to insect bites/stings, foods
medicine or other substances.
(n) Item 10 to 28. Check appropriate box.
(o) Item 29: Explanation of “Yes” Answer(s). Describe all “yes” answers
from section 10-28. Include date(s) of problems, name of doctor(s), and
/or hospitals(s), treatment given and current medical status.
1 Append Item 29 to include: The statement to present health and a
list of medications presently being taken by the examinee. For
individuals receiving examinations more frequently than
quinquennial, there is often little change in the medical history from
year to year. As an alternative to having the examinee complete
Section 10-28 of the DD-2807-1 at a periodic examination, the
following statement may be entered in Item 29 and initialed by the
person undergoing the examination.
“I have reviewed my previous Report of Medical History and there
have been no changes since my last medical examination, except as
noted below.” ________(initials)
(p) Item 30. Examiner’s Summary and Elaboration of all Pertinent
Data. Prior to performing the physical examination, the examiner will
review the completeness of the information furnished on the DD-2807-1.
When this is done, summarize the medical history under (Item 30a.
Comments) as outlined below and then sign the form. If additional
space is needed, use Continuation Sheet, SF-507.
(q) Do not use the term "usual childhood illnesses"; however, childhood
illnesses (those occurring before age 12) may be grouped together
enumerating each one. Incidents, other than those occurring in
childhood, shall have the date recorded rather than the examinee's age.
Do not use "NS" or "non-symptomatic" for items of history. Use
"NCNS," "No Comp., No Seq." after items of recorded history where
applicable. Elaborate on all items of history answered affirmatively
except "Do you have vision in both eyes". The following specific
questions shall also be asked on examination for initial entry into the
Coast Guard, and for aviation and diving duty applicants:

CH-17 4-24
1 "Is there a history of diabetes in your family (parent, sibling, or more
than one grandparent)?"
2 "Is there a history of psychosis in your family (parent or sibling)?”
3 "Do you now or have you ever worn contact lenses?”
4 "Do you now or have you ever used or experimented with any drug,
other than as prescribed by a physician (to include LSD, marijuana,
hashish, narcotics, or other dangerous drugs as determined by the
Attorney General of the United States)?”
5 "Have you ever required the use of an orthodontic appliance attached
to your teeth or a retainer appliance? Month and year last worn?
Are they still necessary?”
6 "Are there any other items of medical or surgical history that you
have not mentioned?" All affirmative answers to the above
questions shall be fully elaborated in Item 25. Negative replies to
the above questions shall be summarized as follows: "Examinee
denies history of psychosis, use of drugs, history of wearing of
contact lenses, requirement for any orthodontic appliance, all other
significant medical or surgical history; family history of diabetes."
A rubber stamp or the overprinting of this information in Item 25 is
recommended.
(3) Distribution. Attach the original DD-2807-1 to the original DD-2808 and
submit to reviewing authority. A copy of the DD-2807-1 and DD-2808 shall
be kept on file at the unit pending the return of the approved DD-2807-1 and
DD-2808.. After review and endorsement, the reviewing authority shall
forward the original DD-2807-1 and DD-2808 to the members parent
command for insertion into the members health record.
8. SF-558 (Emergency Care and Treatment) (Rev 9-96). See Encl (1), pg. 4-13. This
form provides a comprehensive yet concise record of emergency health care. It shall be
used whenever an individual receives emergency treatment. Detailed instructions for
completing the form are as follows:
a. Patient’s Home Address or Duty Station. Complete all blocks in this section.
b. Arrival. Record the date and time the patient arrived at the clinic or emergency room
for care.
c. Transportation to Facility. Record the name of the ambulance company or unit that
transported the patient for care, if appropriate. If patient was not transported by
ambulance or other emergency vehicle, enter "N/A'.
4-25 CH 17
d. Third Party Insurance. List detailed insurance if known by patient. If potential third
party liability exists, forward a copy of SF-558 to Commandant (G-WRP-2). Note:
Disregard DD2568 in chart, enter N/A).
e. Current Medications. List all medications patient is presently taking.
f. Allergies. Record any substance or drug to which the patient has a known or
suspected allergy. If none, enter "NKA" (No Known Allergy).
g. Injury or Occupational Illness. Most fields. When, refers to date injury was
sustained. Where, refers to location injury occurred. How, refers to what happened
(briefly).
h. Emergency Room Visit. Self-Explanatory.
i. Date of Last Tetanus Shot. Self-Explanatory.
j. Chief Complaint. Record a brief description of why the patient is seeking health care.
k. Category of Treatment. If Condition is Result of Accident/Injury. Check the block
that best describes the patients' condition upon arrival.
(1) Emergent. A condition which requires immediate medical attention and for
which delay is harmful to the patient; such a disorder is acute and potentially
threatens life or function.
(2) Urgent. A condition which requires medical attention within a few hours or
danger can ensue; such a disorder is acute but not necessarily severe.
(3) Non-Urgent. A condition which does not require the immediate resources of
an emergency medical services system; such a disorder is minor or non-acute
l. Vital Signs. Take and record all vital signs. Indicate the time vitals were taken. Use
24-hour clock annotation i.e. 0215.
m. Lab Orders and X-Ray Orders. Self-Explanatory, check appropriate box.
n. Orders. List orders given by provider. Record all medications, appointments made.
Or any other follow-up plans.
o. Disposition. Check appropriate box. Ensure patient understands this section.
p. Patient/Discharge Instructions. Be specific. Ensure patient understands instructions
given.
q. Patients Signature and Date. Have the patient or person accompanying the patient
sign the form. This signature only acknowledges that instructions were given to the
patient.
CH-17 4-26
r. Time Seen by Provider. Record the time when the patient received treatment. Use
24-hour clock annotation i.e. 0215.
s. Test Results. Record results of tests ordered on patient.
t. Provider History/Physical. Self-explanatory, use standard S.O.A.P. format.
u. Consult With. List all individuals that on-scene provider received medical advice
from. Example Dr. Richard Smith.
v. Diagnosis. Record patient diagnosis.
w. Providers Signature and Date. The medical officer or other health care provider shall
sign and date the form.
x. Codes. List all ICD-9 codes applicable to the patient.
y. Patients' Identification. Ensure all patient identification information is entered.
9. DD-2215 Reference Audiogram. Optional. Place form in section V of the Health
Record.
10. DD-2216 Hearing Conservation Data. Optional. Place form in section V of the Health
Record.
11. Audiogram Results. The Microprocessor will generate a legal archival test result strip,
which shall be fastened to a separate SF-514, Clinical Record-Laboratory report form,
dedicated to this purpose and filed under section V of the Health Record. Label this SF-
514 “Hearing Conservation Program” across the bottom.
a. All test result strips shall be placed sequentially onto form SF-514 in left to right
formation overlapping 2/3 of the last audiogram.
12. SF-502 (Narrative Summary). See Encl (1), pg.4-15. SF-502's are used for a variety of
purposes, such as:
a. to summarize the important facts about a patient's hospitalization;
b. to summarize the findings of a medical board; or
c. to report the results of a Board of Flight Surgeons.
If received subsequent to the individual's discharge from the hospital, it shall be inserted
in the health record immediately upon receipt.
13. NAVMED 6100/1 (Medical Board Report Cover Sheet).
4-27 CH 17
a. The NAVMED 6100/1 is used in preparing a medical board. A copy of the
NAVMED 6100/1 and the complete medical board shall be inserted into the
individual's health record.
b. Detailed instructions for preparing and distributing this form are contained in
Physical Disability Evaluation System, COMDTINST M1850.2 (series).
14. SF-513 (Consultation Sheet). See Encl (1), pg 4-16.
a. Purpose. SF-513 is used whenever a patient is referred to another facility for
evaluation.
b. Detailed Instructions. Complete the form as follows:
(1) To. Facility or department to which the patient is being referred.
(2) From. Unit referring the patient.
(3) Date of Request. Self-explanatory.
(4) Reason for Request. Specify the reason for referring the patient, i.e., chest
pains, infected sebaceous cyst, etc.
(5) Provisional Diagnosis. Self-explanatory.
(6) Doctor's Signature. Must be signed by a medical officer, dental officer, or
health services department representative. Accompanying this signature
should be the qualifying degree of the individual requesting the consult.
(7) Approved. Leave Blank.
(8) Place of Consultation. Check the appropriate block.
(9) Emergency/Routine. Check the appropriate block.
(10) Identification No. Enter the patient's SSN.
(11) Organization. Enter patient's branch of service.
(12) Register No. If inpatient, enter the appropriate register number. If outpatient,
leave blank.
(13) Ward No. If outpatient enter "OP." If inpatient, enter appropriate ward
number.
(14) Patient's Identification. Enter the appropriate patient identification
information.
(15) The remainder of the form is completed by the consultant.
CH-17 4-28
c. When the consultation sheet (SF-513) is completed and returned by the consultant,
the following actions are required:
(1) Originator shall review and sign the SF-513;
(2) Originator shall complete a Visit Profile sheet (CG-5460B) as directed by Use
of Clinic Automated Management System (CLAMS), COMDTINST
6010.18(series) for later entry into CLAMS; and
(3) The SF-513 shall then be filed in the appropriate dental or medical section of
the health record.
15. SF-520 (Electrocardiographic Report). See Encl (1), pg.4-17.
a. Purpose. SF-520 is used to report the results of all electrocardiograms.
b. Detailed Instructions. The individual performing the electrocardiogram shall
complete the form as follows:
(1) Previous ECG. Check appropriate block
(2) Clinical Impression. Reason why the electrocardiogram was requested, e.g.,
chest pain, physical examination, etc.
(3) Medication. Enter any medications that the patient is taking.
(4) Emergency/Routine. Check appropriate block.
(5) Bedside/Ambulant. Check appropriate block.
(6) Age. Enter patient's age as of last birthday.
(7) Sex. Enter "M" or "F," as appropriate.
(8) Race. Leave blank.
(9) Height. Enter to nearest one-half centimeter (one-half inch).
(10) Weight. Enter to the nearest kilogram (pound).
(11) B.P. Enter recumbent blood pressure.
(12) Signature of Ward Physician. Signature of medical officer ordering the
electrocardiogram.
(13) Date. Date the ECG was performed using appropriate format.
(14) Register No. Enter patient's social security number.
(15) Ward No. Enter "OP" (outpatient) or appropriate ward no.
4-29 CH 17
(16) Patient's Identification. Enter the appropriate patient identification
information.
(17) The remainder of the form is completed by the medical officer evaluating the
electrocardiogram.
c. The baseline ECG shall be appropriately marked "Baseline ECG."
16. SF-515 (Tissue Examination). See Encl (1), pg.4-18.
a. Prepare a SF-515 whenever a tissue specimen is forwarded to a laboratory for
examination.
b. Ensure patient's identification information is completed.
17. SF-541 (Gynecologic Cytology). See Encl (1), pg.4-19.
a. Prepare a SF-541 whenever a vaginal or cervical smear (PAP test) is forwarded to a
laboratory for examination.
b. Ensure patient's identification information is completed.
18. SF-514 (Laboratory Reports). See Encl (1), pg.4-20.
a. This is a display form for mounting graphic reports, automated printout reports, or
printed reports associated with special equipment.
b. Attach the laboratory reports to the indicated spaces with the most recent on top.
c. Ensure patient's identification information is completed.
d. Clinical Record - Laboratory Report Display (SF-545). May be used in lieu of SF-
514. This is a display form for mounting laboratory requests and report forms.
When a patient will require the same type of test several times, a separate display
sheet shall be used for each type of test. In low use situations, the various test result
forms should be mounted on alternate strips 1, 3, 5, and 7.
(1) The following Standard Forms should be mounted serially on strips 1, 2, 3, 4,
5, 6, and 7:
(a) Chemistry I (SF-546),
(b) Hematology (SF-549),
(c) Urinalysis (SF-550), and
(d) Serology (SF-551).
(2) The following Standard Forms be mounted on alternate strips 1, 3, 5, and 7:
CH-17 4-30
(a) Chemistry II (SF-547);
(b) Chemistry II (Urine) (SF-548);
(c) Parasitology (SF-552);
(d) Spinal Fluid (SF-555); and
(e) Immunohematology (SF-556).
e. In many instances there will be a mixed assortment of Standard Forms to be mounted
in a patient's chart and obviously these should be mounted in the most practical
sequence.
f. Instructions for attaching the laboratory report forms to this display sheet are printed
at the bottom of the SF-545. A check mark in the space in the lower right corner
identifies the name of the laboratory forms that are displayed on this sheet or
indicates that a variety or assortment of forms is displayed on the sheet.
19. SF-545a - Clinical Record - Laboratory Report Display for SF-553, SF-554, and SF-557.
This is a display form for mounting Microbiology I, Microbiology II, and miscellaneous
forms for inclusion in the health record. It may be used, when indicated, in addition to
SF-514.
20. SF-546 - 557 (Laboratory Requests).
a. SF-546 (Chemistry I). Used to request most blood chemistry tests. Fill in the
identification data as described previously. The specimen sources information is
given by checking the box marked BLOOD or by specifying information in the
position marked OTHER. The names of the blood chemistry tests are listed
individually on this form. At the bottom of the list there is provision for ordering a
battery or profile of tests. When requesting the identifying names of the battery or
profile of tests must be written into the space provided. There is also space for
writing in the names of other tests not specifically listed.
b. SF-547 (Chemistry II). Used to request blood gas measurement, T3, T4, serum, iron
binding capacity, glucose tolerance, and other chemistry tests. Fill in the
identification data as described previously. The specimen source information is
given by checking the box marked BLOOD or by specifying information in the
position marked OTHER.
c. SF-548 (Chemistry II, Urine). Used to request chemistry tests on urine specimens.
The specimen interval information is given by checking the box marked 24 HOURS
or by specifying information in the position marked OTHER.
d. SF-549 (Hematology). Used to request routine hematology tests. The specimen
source information is given by checking box marked VEIN, the box marked CAP for
capillary, or by specifying information in the position marked OTHER.

4-31 CH 17
e. SF-550 (Urinalysis). Used to request urinalysis tests, including routine urinalysis
with microscopic examination. The specimen source information is given by
checking the box marked ROUTINE or by specifying information in the position
marked OTHER. (Note that routine urinalysis may be ordered by simply placing an
"X" in front of the word MICROSCOPIC in the requesting section.) The space
marked PSP is for requesting and reporting phenolsulfonphthalein measurements.
The space marked HCG is for requesting and reporting measurements of human
chorionic gonadotropin.
f. SF-551 (Serology). Used to request tests that measure serum antibodies, including
tests for syphilis.
(1) The space marked RPR is for requesting and reporting measurements of the
Rapid Reagent Card Test for Syphilis
(2) The space marked TA is for requesting and reporting measurements of the
Latex Fixation Test for Thyroglobulin Antibodies.
(3) The space marked COLD AGG is for requesting and reporting of Cold
Agglutinins.
(4) The space marked ASO is for requesting and reporting Antistreptolysin 0 titers.
(5) The space marked CRP is for requesting and reporting measurements of C
Reactive Protein.
(6) The space marked FTA-ABS is for requesting and reporting for fluorescent
treponemal antibody-absorption test.
(7) The space marked FEBRILE AGG is for requesting and reporting
measurements of Febrile Agglutinins.
(8) The space marked COMP FIX is for requesting and reporting Complement
Fixation Tests. The name of the specific antibody should also be written in
this space.
(9) The space marked HAI is for requesting and reporting Hemagglutination
Inhibition Tests. The name of the specific antibody should also be written in
this space.
g. SF-552 (Parasitology). Used to request tests for intestinal parasites, malaria and
other blood parasites, as well as most test on feces. Fill in identification data as
described previously.
h. SF-553 (Microbiology I). Used to request most bacteriological isolations and
sensitivities.
CH-17 4-32
(1) The type of the patient's infection, according to origin, is indicated by checking
one of the boxes in the space marked INFECTION in the upper right area of
the form.
(2) The examination requested is indicated by checking either the box marked
SMEAR, SENSITIVITY, CULTURE, or COLONY COUNT.
(3) The report of the examination is written or stamped on the form by the
laboratory personnel.
(4) The names of the bacteria identified or isolated are listed in the space marked
PREDOMINANT ORGANISM(S).
(5) The sensitivity listing and results are stamped or written in the space marked
SENSITIVITY.
i. SF-554 (Microbiology II). Used to request tests for fungi, acidfast bacillus (TB), and
viruses.
(1) The type of infection according to origin is indicated by checking one of the
boxes in the space marked INFECTION.
(2) The examination(s) requested is checked in the sections for fungus test or AFB
tests or viral cultures.
(3) The test results are stamped or written on the form by the laboratory personnel.
j. SF-555 (Spinal Fluid). Used to request most spinal fluid tests.
k. SF-556 (Immunohematology). Used to request blood grouping, typing, and blood
bank tests.
l. SF-557 (Miscellaneous). Used to request and report tests such as electrophoresis and
assays of coagulation factors, which are not ordered on other laboratory forms.
(1) Fill in the identification data as described previously.
(2) The specimen source is specifically described in the space marked SPECIMEN
SOURCE.
(3) Write the name of the test requested in the request section of the form.
21. SF-519 (Radiographic Reports). See Encl (1), pg.4-21.
a. This is a display form for mounting Radiographic Reports (SF-519-A). Attach the
SF-519-A to the indicated spaces, with the most recent report on top.
b. Use SF-519-A to request x-ray examinations. All patient data must be completed as
indicated. Ensure that examinations requested are in standard terms or abbreviations.
4-33 CH 17
ALL pertinent clinical history, operations, physical findings, pregnancy status, and
provisional diagnoses must be recorded in the appropriate space. This information is
needed by the radiologist in order to render a proper interpretation of the film.
c. Complete the required patient's identification information.
22. DD-771 (Eyewear Prescription). See Encl (1), pg.4-22. Type DD-771 for clarity and to
avoid errors in interpretation, using the following format:
a. Date. Enter as follows, 22 JAN 87, etc.
b. Order Number. Enter unit identifying number, issued by NOSTRA or Top Gun
Fantasy Ray Ban, above the order number block. Complete order number block if
desired.
c. To. Appropriate fabricating facility.
d. From. Enter complete unit address of unit ordering the eyewear.
e. Name, Service Number/Social Security Number. Enter as ALBERT, Michael W.
HSC 123-45-6789.
f. Age. Self-explanatory.
g. Unit and Address. Enter complete mailing address of unit to which individual is
attached. If retiree, use the individual's home or mailing address.
h. Active Duty, etc. Check appropriate block.
i. USA, USN, etc. Check appropriate block.
j. Spectacles. Check appropriate block.
k. Aviation Spectacles. Use this block only when ordering aviation frames. Check as
appropriate:
(1) N-15 tinted lenses;
(2) Coated lenses (coated with an anti-glare compound) are not authorized for
Coast Guard personnel.
l. Other. Leave blank.
m. Interpupillary Distance. Copy directly from patient's Prescription, previous DD-771,
or SF-600.
n. Eye Size. As above. (Not required for aviation goggles)
o. Bridge Size. As above. (Not required for aviation goggles)

CH-17 4-34
p. Temple Length and Style. As above. (Not required for aviation goggles)
q. Number of Pairs. Enter the number of pairs requested.
r. Case. Enter the number of cases requested.
s. Single Vision.
(1) Sphere. Copy directly from individual's prescription, previous DD-771, or SF-
600 (+1.00, -1.25, etc.). Prescriptions are filled in multiples of 0.25 diopters
only.
(2) Cylinder. As above, except that prescriptions or multivision lenses must be in
"minus cylinder" form, (-0.50, -0.75, etc.).
(3) Axis. Copy directly from individual's prescription, previous DD-771, or SF-
600. The axis must contain three (3) digits such as: 180, 090, 005, etc.
(4) Decentration. Need not be completed unless specified as a part of prescription.
(5) Prism. As indicated on individual's prescription, previous DD-771, or SF-600.
(6) Base. As above.
t. Multivision. If the individual needs multivision lenses (bifocals, trifocals, etc.) then
the prescription must be in minus cylinder form.
u. Special Lenses or Frames. This block is used for special instructions or justification
for aviation spectacles, or nonstandard lenses, and frames, etc.
(1) When replacement eyewear is ordered from a prescription extracted from the
health record, enter the following entry in this block: "REPLACEMENT
ORDER: PRESCRIPTION FROM REFRACTION PERFORMED ON
DATE."
(2) When eyewear is ordered for recruits, enter the following entry in this block:
"RECRUIT - PLEASE EXPEDITE."
(3) When tinted lenses are ordered for non-aviation personnel, enter a written
justification in this block. "Tinted lenses STATE JUSTIFICATION."
(4) When nonstandard temples or frames are ordered, enter type frame or temple
requested, and justification:
(a) Riding Bow Cables, (Justification);
(b) Adjustable Nose Pads, (Justification).
4-35 CH 17
(5) When an individual's pupillary distance is less than 60 mm it must be verified
and an entry placed in this block: "PD of ____ verified and correct."
v. Signature of Approving Authority. Shall be signed by the senior medical officer,
designated representative, or the commanding officer where no medical officer is
present.
w. Signature of the Prescribing Officer. Shall be signed by the medical officer or person
performing the refraction. When this is not possible, i.e., examination obtained from
a civilian source, transcribed from the health record, etc., the person transcribing the
information shall sign as prescribing officer. Flight surgeons may sign prescriptions
as both the prescribing and approving authority.
23. SF-601 (Immunization Record). See Encl (1), pg.4-23.
a. All prophylactic immunizations; sensitivity tests; reactions to transfusions, drugs,
sera, food and allergies, and blood typings shall be recorded on SF-601 and also on
the PHS-731. The recordings shall be continued on the current record until
additional space is required under any single category.
b. In such cases, insert a new SF-601 in the health record and retain the old SF-601.
Concurrently, make a thorough verification of the entries and bring all
immunizations up-to-date. Replacement of the current SF-601 is not required
because of change in grade, rating, or status of the member concerned.
c. The name of the individual administering the immunization or test, or determining
the nature of the sensitivity reaction, shall be typed or a rubber stamp used.
Signatures on SF-601 are not required. However, in the event of their use, make sure
they are legible.
d. The individual administering the immunizations is responsible for completing all
entries in the appropriate section, including required entries on reactions.
e. Enter information concerning a determined hypersensitivity to an immunization or
vaccine under "Remarks and Recommendations". Type appropriate entries (such as
HYPERSENSITIVE TO TYPHOID) in capitals. Enter "HIV antibody testing done
(enter date(s))".
f. For Yellow Fever vaccine, record the origin and batch number.
24. SF-602 (Syphilis Record). See Encl (1), pg. 4-25.
a. This form shall be prepared and inserted in the health record for each person for
whom a confirmed diagnosis of syphilis or any of its complications or sequela has
been established.
b. The medical officer shall carefully and thoroughly explain to the patient the nature of
the infection and the reasons why treatment, prolonged observation and the repeated
CH-17 4-36
performance of certain prescribed tests are necessary. The patient shall then be
requested to sign the statement in Section II of SF-602.
24. DD-1141 (Record of Occupational Exposure to Ionizing Radiation). See Encl (1),
pg.4-27.
a. Requirements. The custodian of the medical records shall prepare and maintain as
DD-1141 for each person occupationally exposed to ionizing radiation. Enter all
exposures in rems.
b. Recording Procedures.
(1) Initial Determination of Accumulated Dose.
(a) In the initial preparation of DD-1141, obtain complete reports of
previous exposure. For each period in which the individual was engaged
in activities where occupational exposure was probable, and no record, or
only an incomplete record of exposure during the period can be obtained,
assume that an occupational exposure of 1.25 rems was incurred per
quarter of each calendar year or fraction thereof.
(b) In cases where the nature of the radiation is unknown, assume gamma
radiation.
(c) If an individual was exposed at more than one facility, calculate the
cumulative exposures and record them in Items 7 through 12 as
appropriate. Enter the sum of the whole body exposure in Item 13, and a
statement regarding the sources of that information in Item 16,
REMARKS.
(2) Current Record.
(a) Quarterly, make appropriate entries on each individual's DD-1141 from
the exposure records received from the Public Health Service Contractor.
(b) Maintain separate DD-1141 to record exposures other than whole body,
with appropriate descriptions under Item 16, REMARKS.
c. Completion Instructions.
(1) Item 1. Leave blank.
(2) Item: 2. Enter last name, first name, and middle initial. If the combination of
last name and first name exceed 19 spaces, enter last name and initials only.
(3) Item 3. Enter SSN.
(4) Item: 4. Enter in not more than 10 spaces, rate, grade, title or position the
individual is currently holding. Use standard service abbreviations: i.e.,

4-37 CH 17
CAPT; HSCS; HSl; etc. Abbreviate civilian occupation titles as needed; i.e.,
Radiological Physicist to Rad Physic; Radiation Physiologist to Rd Physiol;
Electrical Welder to Elec Wldr; etc.
(5) Item 5. Enter date of birth: i.e., 4 SEP 87.
(6) Item 6. Enter name of activity or unit.
(7) Items 7 & 8. "Period of Exposure." Enter the day, month, and year: i.e., 1
MAR 87.
(8) Items 9-12. "Dose This Period." Enter radiation dose received this period to
three decimal places: i.e., 02.345rem. Use five digits including zeros as
necessary for all entries.
(a) Item 9. Enter skin dose (soft) which includes low energy gamma and x-
ray of less than 20 KVE effective energy and beta radiation. Total skin
dose is the addition of columns 9 and 12.
(b) Item 10. Enter gamma and x-ray dose greater than 20 KVE effective
energy in REM.
(c) Item 11. Enter neutron dose in REM.
(d) Item 12. Enter sum of items 10 and 11.
(9) Item 13. Add item 12 to previous item 13; enter total in item 13.
(10) Item 14. Enter permissible dose calculated from the age formula 5(N-18)
REM, where N equals the present age in years.
(11) Item 15. Recorder certify entries by initial.
(12) Item 16. Enter other pertinent information such as known exposure from
internally deposited radioactive material or from any external radioactive
sources. Describe briefly any activity or assignment bearing a potential for
exposure and estimate dose-time relationships, if feasible. If this form is used
for other than whole body and skin of whole body, specify the use; i.e., hands
and forearms, feet and ankles, thyroid, etc. When recorded dose is not
obtained from film badge readings, specify whether estimates were obtained
from pocket dosimeters, area or air monitoring, bioassay, etc.
25. CG-4057 (Chronological Record of Service). See Encl (1), pg 4-28.
a. Purpose. Use this form:
(1) to maintain a chronological record of assignments for each active duty member
of the Coast Guard;
CH-17 4-38
(2) as a statement of agreement or disagreement with the assumption of fitness for
duty upon separation from the Coast Guard; and
(3) to terminate the health record.
b. Chronological record of assignments. Prepare original only. Record the member's
full name in all capitals, together with the Social Security Number. Make entries
each time a member leaves or returns from PCS, TAD, or hospitalization at a unit
different than the one to which currently assigned.
c. Agreement or disagreement with the assumption of fit for duty at the time of
separation. Members not already in the physical disability evaluation system, who
disagree with the assumption of fitness for duty at separation shall indicate on the
reverse of form CG-4057. They shall then proceed as indicated in paragraph 3-B-5.
of this Manual. Members who agree with the assumption shall check the box
indicating agreement. This is a health services department responsibility when there
is a health services department representative attached; otherwise it becomes a
personnel action.
d. Terminating the health record. The reverse side of the form is also used to terminate
a member's health record upon definite separation from active service. The date of
termination is the effective date of separation. Make appropriate entries giving the
reason for termination, the date of termination and the grade and signature of the
responsible commissioned officer in the bottom portion of the form. Additionally, an
entry, signed by the member whose health record is being terminated, acknowledging
the receipt of a copy all available NAVMED 6150/20's, a copy of separation
examination if done (either DD-2808 or SF-600 entry), a signed copy of the CG-
4057, and the PHS-731 shall be made in the Remarks section of the CG-4057.
e. This form is also used to notify the individual of the possibility of certain disability
benefit entitlements from the Department of Veterans Affairs after separation.
f. If either side of the CG-4057 is filled, the reverse side shall have a line drawn
diagonally through it in red and a second CG-4057, marked "Supplement" at the top,
started.
26. NAVMED 6150/2 (Special Duty Medical Abstract). See Encl (1), pg. 4-30.
a. General. The purpose of the NAVMED 6150/2 is to provide a record of physical
qualifications, special training, and periodic examinations of members designated for
performing special duty, such as aviation and diving. The object of the special duty
examination, and the instructions incident thereto, is to select only those individuals
who are physically and mentally qualified for such special duty, and to remove from
such status those members who may become temporarily or permanently unfit for
such duty because of physical or mental defects. Also, in this connection, special
money disbursements are often based upon the determination of a member's physical
and mental qualifications or continued requalification for performing a special duty.
4-39 CH 17
Therefore, accuracy and content of information are essential in reporting information
applicable to these categories.
b. Entries.
(1) Record entries upon completion of each physical examination and completion
of designated special training. When a previously qualified member is
suspended from special duty for physical reasons, enter the period of
suspension and reason therefore on the NAVMED 6150/2.
(2) The scope of the physical examination and technical training prescribed for
these special categories often differs from the general service requirements;
therefore, entries reporting results which pertain to these particular
examinations or training involved shall be approved only by medical officers.
27. PHS-731 (International Certificate of Vaccination).
a. General.
(1) Prepare PHS-731 for each member of the Coast Guard (for reserve personnel
when ordered to Active Duty for Training). This form shall be carried only
when performing international travel or when reporting for Active Duty for
Training. When not required for either of the preceding reasons, the completed
certificate shall be retained in the individual's health record. Appropriate
entries shall be made on PHS-731 and SF-601 when immunizations are
administered.
(2) A reservist not on extended active duty who plans international travel either
under official orders or privately, may request that the appropriate district
commander (r) furnish a PHS-731 for this purpose. The reservist shall return
the PHS-731 to the district commander (r) when travel is completed.
(3) When properly completed and authenticated, the PHS-731 contains a valid
certificate of immunization for international travel and quarantine purposes in
accordance with World Health Organization Sanitary Regulations.
(4) All military and nonmilitary personnel performing international travel under
Coast Guard cognizance shall be immunized in accordance with Commandant
Instruction 6230.4 (series) and shall have in their possession a properly
completed and authenticated PHS-731.
b. Detailed Instructions.
(1) Stamp or type the following address on the front of PHS-731:
Commandant (G-WK)
U. S. Coast Guard
CH-17 4-40
2100 Second St., S.W.
Washington, DC 20593-0001
(2) Enter data by hand, rubber stamp, or typewriter.
(3) Enter the day, month, and year in the order named (i.e., 4 SEP 87).
(4) Record the origin and batch number for yellow fever vaccine.
(5) Entries for cholera and yellow fever must be authenticated by the Department
of Defense Immunization Stamp and the actual signature of the medical officer.
Other immunizations may be authenticated by initialing. Entries based on prior
official records shall have the following statement added: "Transcribed From
Official Records."
c. Remove the PHS-731 from the health record and give it to the individual upon
separation from the Service.
28. CG-5214 (Emergency Medical Treatment Report). See Encl (1), pg. 4-32.
a. Purpose. CG-5214 provides a multiple copy record of all emergency medical care
rendered by Coast Guard personnel outside of a clinic or sickbay. All care rendered
by crews of Coast Guard emergency vehicles must be documented with a CG-5214.
(1) Part 1, Copy to Patient. This copy shall be placed in the patients' health record
if available.
(2) Part 2, Copy to Receiving Unit. This copy shall be given to the hospital, clinic,
or EMS crew assuming responsibility for patient care.
(3) Part 3, Copy to Triage Officer. In multi-casualty incidents, this copy shall be
given to the triage officer to account for the patients' treatment priority and
status. Otherwise, this copy shall be kept on file at the clinic or sickbay.
(4) Part 4, (hard copy) to Commandant (G-WKH-1). This copy shall be forwarded
to Commandant (G-WKH-1) using the mailing label on the reverse side.
b. Preparation and Submission of CG-5214. The form provides an accurate account of
the patient's injury or illness, and a detailed report of all treatments rendered en route
to a receiving facility. If possible, the report should be completed during the
transport phase. Detailed instructions for completing the CG-5214 are as follows:
(1) Victim Identification.
(a) Item 1: Name. Enter last, first, and middle initial.
(b) Item 2: Sex. Check one.
(c) Item 3: Estimated Age. Enter in years or months.
4-41 CH 17
(2) Description of Incident.
(a) Item 4: Date. Enter date incident occurred.
(b) Item 5: Type of Incident. Check one and give pertinent details under
"Nature of Emergency/Mechanism of Injury".
(c) Item 6: Time on Scene. Enter (using 24 hour clock).
(d) Item 7: Time of Incident. Enter (using 24 hour clock).
(e) Item 8: Location. Enter exact geographical area.
(3) Observation of Victim. Stick-Man figure: Place applicable injury letter code
over injured area.
(4) Skin. Circle applicable number.
(5) Vital Signs. Note time observed (24 hour clock).
(6) Level of Consciousness. Check only one per time observed.
(7) Pupils. Check only one per time observed.
(8) Pulse. Place numerical value under rate and check appropriate space for
quality.
(9) Breathing. Place numerical value under rate and check appropriate space for
quality.
(10) Blood Pressure. Enter systolic and diastolic values under applicable time.
(11) Temperature. Circle either oral or rectal and enter in numerical value.
(12) Mast. Beside "Mast BP" enter blood pressure values. Circle applicable
compartments inflated.
(13) Triage Information. Circle one of the following:
(a) Priority I: Patients with airway and/or breathing problems, cardiac arrest,
uncontrolled bleeding or controlled bleeding with symptoms of shock,
severe head or abdominal injuries, and severe medical problems to
include possible heart attack, severe burns, and severe poisonings.
(b) Priority II: Patients with less serious burns, multiple fractures, potential
C-Spine injuries without shock, or medical conditions of a less serious
note.
CH-17 4-42
(c) Priority III: Patients with obvious minor injuries or patients who are
obviously dead or mortally wounded.
(14) Medications. List any medications the patient is currently taking.
(15) Allergies. List any known allergies for the patient.
(16) Medications Administered. Note the time, dosage, and route of administration
for any medications administered to the patient.
(17) Rescuer Information.
(a) Item 10: Name. Enter last, first, and middle initial.
(b) Item 11: Level. Circle appropriate certification level.
(c) Item 12: Unit. Rescuer's assigned unit.
(d) Item 13: OPFAC#. Enter.
(e) Item 14: rescue Vehicle. Identity of the responding vehicle, vessel, or
aircraft.
(f) Item 15: Receiving Unit. Hospital, EMS vehicle, or clinic assuming
responsibility for patient care.
(g) Time Patient Transferred. Enter (24 hour clock).
29. DD877 (Request for Medical/Dental Records or Information). See Encl (1), pg. 4-
33.
a. Purpose. The DD 877 is a self-carboning triplicate form which is used to forward
health and clinical records between clinics and units as well as to request records
from clinics, units, or MTFs.
b. General. This form shall be initiated and included with health and clinical records as
directed in Chapter 4-A-6. And 4-D-7. Of this Manual
c. Detailed Instruction.
(1) Each DD877 must have all boxes completed.
(2) n all instances when a DD877 is initiated, remarks concerning the reason for
sending the record, the name of the gaining unit for the member/ sponsor and a
request for action will be included on the form. When preparing a DD877 for a
record to be forwarded, place the following in section 9., REMARKS: “Health
{clinical} record for this member (family member) is forwarded to you for
appropriate filing. Member (sponsor) assigned to (insert gaining unit name).”
4-43 CH 17
(3) For members entering the inactive reserve, enter the following in section 9,
remarks: “ member entering inactive reserve in your district. Per Medical
Manual, COMDTINST M6000.1B, Chapter 4-B-4.b.,this health record is
forwarded for appropriate action.”
(4) A copy of the DD877 will be retained at the unit sending the record for 6
months after the record is mailed, then may be discarded.

CH-17 4-44
Section C - Dental Record Forms.
1. CG-3443-2 (Dental Record Cover). See Encl (1), pg. 4-34.
a. Open a CG-3443-2 for each individual upon arrival at a training center or initial entry
into the Coast Guard or Coast Guard Reserve. When an individual on the retired list
returns to active duty, submit a request for a copy of the closed out dental record to
Commandant (G-PIM). Whenever the original record is lost or destroyed, a new
dental record shall be opened immediately. Normally the dental record shall be kept
in the Health Record Cover (CG-3443) of each individual unless otherwise specified.
b. All dental forms and radiographs will be contained in the Dental Record.
c. Detailed Instructions.
(1) Surname. Record the surname in all capital letters.
DOE
SURNAME
(2) Given name(s). Record in full without abbreviation. If the individual has no
middle name or initial then record the lower case letter "n" in parentheses (n).
If the individual has only a middle initial(s), record each initial in quotation
marks. When "Jr." or "II" or other similar designations are used, they shall
appear after the middle name or initial.
DOE JANE ANN
SURNAME First Name Middle Name
(3) Social Security Number (SSN). Enter Social Security Number.
(4) Date of Birth. Enter day, month (abbreviated JAN, FEB, MAR, etc.), and the
year: i.e., 4 SEP 49.
(5) Change in Grade or Rate. Enter as they occur.
(6) Blood Type. Enter the individual's blood type in the appropriate box. If not
known, perform a blood type test.
(7) RH Factor. Enter the individual's RH factor in the appropriate box. If not
known, perform an RH factor test.
(8) Drug Sensitivity Sticker. When required, affix the Drug Sensitivity Sticker
(CG-5266) to the lower left corner of the front of the Dental Record Cover. Do
not cover other identification data. See Encl (1) pg. 4-34.
(9) Dental Radiographs.
4-45 CH 17
(a) Dental Bitewing Radiograph Storage. Bitewing radiographs shall be
stored in the standard stock 5 year x-ray card (FSC# 6525-00-142-8732).
This shall replace the single bitewing x-ray card (FSC# 6525-00-817-
2364). X-ray film is mounted in the x-ray card with the raised dot side of
the film on the back side of the card.
2. NAVMED 6600/3 (Dental Health Questionnaire). See Encl (1), pg. 4-35.
a. General. CG-5605 will help the dental officer detect any present or past health
problem (i.e., positive Human Immunodeficiency Virus (HIV)) that might interfere
with definitive dental treatment. All positive answers from the health history section
must be followed up by the dental officer for impact on health care and so annotated
on the CG-5605 and/or the SF-603A.
b. Detailed Instructions. Insert the Dental Health Questionnaire as the first page of the
dental record. Patients shall fill out a new Dental Health Questionnaire at least
annually, or when information changes. Maintain the two most recent forms in the
dental record with the current CG-5605 on top.
(1) Chief Complaint. Have the patient enter the problem they are presently having.
(2) Check and Sign. Have the patient enter yes/no in each box of the history. The
signature indicates the authenticity of the history.
(3) Summary of Pertinent Findings. Include baseline BP reading.
3. SF-603 (Dental Record). See Encl (1), pg. 4-36.
a. General. The Dental Record is a continuous history and must contain accurate and
complete entries of dental examinations and treatments. Each entry shall clearly
indicate the name of the dental officer conducting the examination and/or rendering
the treatment. Dental hygienists or other auxiliary personnel providing care shall
also follow this requirement. Each dental officer is personally responsible for
ensuring that all entries are properly recorded.
b. Numerical Classification for Record Purposes. Chart markings have been
standardized so that dental conditions, treatments needed, and treatments completed
may be readily identified. This facilitates efficient continuity of treatments and may
establish identification in certain circumstances.
(1) For the purpose of brevity and exactness, use the following classification of
teeth in keeping the dental record.
TOOTH DESIGNATION
Right Maxillary Third Molar 1
Right Maxillary Second Molar 2
CH-17 4-46
Right Maxillary First Molar 3
Right Maxillary Second Bicuspid 4
Right Maxillary First Bicuspid 5
Right Maxillary Cuspid 6
Right Maxillary Lateral Incisor 7
Right Maxillary Central Incisor 8
Left Maxillary Central Incisor 9
Left Maxillary Lateral Incisor 10
Left Maxillary Cuspid 11
Left Maxillary First Bicuspid 12
Left Maxillary Second Bicuspid 13
Left Maxillary First Molar 14
Left Maxillary Second Molar 15
Left Maxillary Third Molar 16
Left Mandibular Third Molar 17
Left Mandibular Second Molar. . 18
Left Mandibular First Molar 19
Left Mandibular Second Bicuspid 20
Left Mandibular First Bicuspid 21
Left Mandibular Cuspid 22
Left Mandibular Lateral Incisor 23
Left Mandibular Central Incisor 24
Right Mandibular Central Incisor 25
Right Mandibular Lateral Incisor 26
Right Mandibular Cuspid 27
Right Mandibular First Bicuspid 28
Right Mandibular Second Bicuspid 29
Right Mandibular First Molar 30
Right Mandibular Second Molar 31
Right Mandibular Third Molar 32
(2) Indicate deciduous teeth by placing a block "D" around tooth number. If both
permanent and deciduous teeth are present, place a "D" in location of
deciduous tooth and enter the appropriate tooth number inside the "D."

4-47 CH 17
(3) Indicate a supernumerary tooth by placing "s" in the location of the
supernumerary tooth and in the remarks section enter a statement that the
examinee has a supernumerary tooth.
(4) Indicate deciduous and supernumerary teeth on the SF-603 in SECTION I, Part
5 (Diseases, Abnormalities, and Radiographs) and enter a statement in the
remarks section of Section 5.
c. Detailed Instructions.
SECTION I. DENTAL EXAMINATION
(1) Purpose of Examination. To assess the oral health status of cadets, officer
candidates and enlisted recruits upon initial entry into the Coast Guard, and to
provide periodic (but at least annual) examinations of active duty personnel.
Enter an "X" in the appropriate box. Mark the "Initial" box for the dental
examination made upon entrance into the Coast Guard. All other examinations
fall under the "Other" category and shall be identified: i.e., "Academy",
"Reenlistment", etc.
(2) Type of Examination. Enter an "X" in the proper box of item 2, "Type of
Exam."
(a) Type 1, Comprehensive Examination. Comprehensive hard and soft
tissue examination, which shall include: oral cancer screening
examination; mouth-mirror, explorer, and periodontal probe
examination; adequate natural or artificial illumination; panographic or
full-mouth periapical, and posterior bitewing radiographs as required;
blood pressure recording; and when indicated, percussive, thermal, and
electrical tests, transillumination, and study models. Included are lengthy
clinical evaluations required to establish a complex total treatment plan.
For example, treatment planning for full mouth reconstruction,
determining differential diagnosis of a patient's chief complaint, or
lengthy history taking relative to determining a diagnosis. Use S.O.A.P.
format to record the results of a Type 1 examination.
(b) Type 2, Oral Examination (annual or periodic). Hard and soft tissue
examination, which shall include: oral cancer screening examination;
mouth mirror and explorer examination with adequate natural or artificial
illumination; periodontal screening; appropriate panographic or intraoral
radiographs as indicated by the clinical examination; and blood pressure
recording. An appropriate treatment plan shall be recorded. This type is
the routine examination which is normally performed one time per
treatment regimen per patient, unless circumstances warrant another
complete examination. Use S.O.A.P. format to record the results of Type
2 examination.

CH-17 4-48
(c) Type 3, Other Examination. Diagnostic procedure as appropriate for:
consultations between staff; observation where no formal consult is
prepared; certain categories of physical examination; and emergency oral
examination for evaluation of pain, infection, trauma, or defective
restorations.
(d) Type 4, Screening Evaluation. Mouth mirror and explorer or tongue
depressor examination with available illumination. This includes the
initial dental processing of candidates without necessarily being
examined by a dentist, or other dental screening procedures.
(e) If not specified by this Manual, it shall be the professional responsibility
of the dental officer to determine the type of examination which is
appropriate for each patient. However, Type 3 and Type 4 examinations
are not adequate to definitively evaluate the oral health status of patients.
When the dental officer determines that a comprehensive periodontal
examination is to be accomplished, use the Navy Periodontal Chart,
NAVMED 6660/2 (3-90).
(3) Dental Classification of Individuals. Dental classifications are used to
designate the health status and the urgency or priority of treatment needs for
active duty personnel. Use the following guidelines and criteria for the
classification of patients. When a criterion for a specific condition is not listed,
the dental officer shall evaluate the prognosis for a dental emergency and
assign the appropriate classification.
(a) Class 1. Patients who do not require dental treatment. The following are
criteria for such classification.
7 no dental caries or defective restorations;
8 healthy periodontium, no tooth accumulated materials (hard or
visible soft deposits);
9 stable occlusion, asymptomatic temporomandibular joint;
10 unerupted or malposed teeth that are without historical, clinical, or
radiographic signs or symptoms of pathosis, and are not
recommended for prophylactic removal; and
11 no edentulous spaces for which a prosthesis is indicated.
(b) Class 2. Patients who have dental conditions that are unlikely to result in
a dental emergency within 12 months. Class 2 dental patients are
considered fit for operational duties, but the dental diseases or conditions
causing designation shall be reevaluated at each dental examination.
Any one of the following is a sufficient criterion for such a classification:

4-49 CH 17
1 Dental caries, decalcification, or tooth fractures extending beyond
the dentinoenamel junction, or causing definitive symptoms;
2 Restorations with fractures or marginal defects;
3 Periodontal diseases or periodontium exhibiting;
a nonspecific gingivitis. Inflammation of the gingiva characterized
by changes in color, gingival form, position, surface appearance,
bleeding upon brushing or flossing, or the presence of blood or
exudate after probing with a periodontal probe;
b slight or mild adult periodontitis. Progression of the gingival
inflammation into the deeper periodontal structures and alveolar
bone crest with accompanying periodontal probing depths of
from 3 to 4mm, slight loss of connective attachment, and slight
loss of alveolar bone;
c moderate periodontitis. Gingival inflammation with destruction
of the periodontal structures including radiographic or clinical
evidence of loss of alveolar bone support, with possible early
furcation involvement of multirooted teeth or tooth mobility;
d stable or nonprogressive mucogingival conditions. This includes
conditions such as irregular marginal contours, gingival clefts,
and aberrant frena or muscle attachments, which could potentially
progress, or pathosis but are currently stable and compatible with
periodontal health; or
e past history of periodontal disease or therapy when the disease is
currently under control in a long-term maintenance program.
4 The presence of supragingival or subgingival tooth accumulated
materials without concomitant periodontal disease.
5 Prosthodontics indicated. Edentulous areas,
provisional/interim/temporary prostheses, defective prostheses,
provisional crowns, large extracoronal direct restorations, or
endodontically treated teeth without full coverage, that need
prosthetic treatment but delay will not compromise the patients
immediate health or masticating function.
6 Unerupted, nonfunctional, or malposed teeth without historical,
clinical, or radiographic signs or symptoms of pathosis, but which
are recommended for prophylactic removal to prevent future
pathologic conditions (e.g., unopposed or unerupted third molars, or
malposed teeth which complicate plaque control measures).

CH-17 4-50
7 Preventive dentistry requirements not fulfilled.
8 Those conditions described in subparagraphs 4. through 7. above are
not considered disqualifying for overseas, sea duty, or isolated duty
assignment.
(c) Class 3. Patients who have dental conditions that are likely to cause a
dental emergency within 12 months. The following conditions have the
potential to cause an emergency, and any one is sufficient criterion for
disqualification for overseas or isolated duty assignment:
1 Periodontal diseases or periodontium exhibiting:
2 Advanced periodontitis. Significant progression of periodontitis
with major loss of alveolar bone support and probable complex
furcation involvement of multirooted teeth and increased tooth
mobility. The periodontal probing depth may reach 7mm and
deeper;
a. periodontal abscess;
b. acute necrotizing ulcerative gingivitis (NUG);
c. periodontal manifestations of systemic diseases and hormonal
distubances (e.g., acute herpetic gingivostomatitis);
d. refractory, rapidly progressive periodontitis. Rapid bone and
attachment loss, or slow but continuous bone and attachment
loss resistant to normal therapy; or
e. juvenile and prepubertal periodontitis, either localized or
generalized.
3 Acute or chronic pulpitis.
4 Indication of periradicular pathosis with or without existing root
canal filling which may require treatment.
5 Presence of a tooth or teeth undergoing endodontic therapy.
6 Stomatitis.
7 Pericoronitis.
8 Prosthodontics required to replace an existing prosthesis exhibiting
dental caries, or a large defective amalgam restoration requiring
replacement with a casting. Also, appliances required due to:
9 Insufficient masticatory function, active arch collapse from tooth
loss, or essential performance of military duties (e.g., replacement of
missing teeth for esthetics or phonetics);

4-51 CH 17
10 soft tissue inflammation, such as papillary hyperplasia under a
denture base;
11 an essential prosthesis in need of repair in order to be functional; or
12 a provisional, interim, or temporary prosthesis which cannot be
maintained for a 12 month period.
13 Unerupted, partially erupted, nonfunctional or malposed teeth
associated with historical, clinical or radiographic evidence of
pathosis, or with a high potential to cause a dental emergency.
14 Soft or hard tissue lesions requiring an incisional or excisional
biopsy for the definitive diagnosis and treatment of the lesions,
including the period of time awaiting the results of the
histopathologic examination.
15 Appropriate postoperative treatment not yet completed, including
suture removals for surgery and occlusal adjustments for restorative
dentistry.
16 All conditions requiring immediate treatment for relief of pain,
traumatic injuries, or acute oral infections.
17 Orthodontic therapy in progress, with either fixed or removable
appliances.
(4) Priority of Dental Treatment. To further indicate priority of treatment within a
class, the following groupings shall be used when necessary (listed in order of
decreasing priority).
(a) Group 1. Coast Guard active duty personnel in receipt of orders to sea,
overseas, or combat duty.
(b) Group 2. Coast Guard active duty personnel upon return from sea,
overseas, or combat duty.
(c) Group 3. Other Coast Guard personnel.
(d) Group 4. Active duty personnel of other Services assigned to duty with
the Coast Guard.
(e) Group 5. Active duty personnel of other Services.
(f) Missing Teeth and Existing Restorations.
(g) Markings shall be made on examination chart as follows:
1 Missing Teeth. Draw a large "X" on the root(s) of each tooth that is
not visible in the mouth.

CH-17 4-52
2 Edentulous Mouth. Inscribe crossing lines, one extending from the
maxillary right third molar to the mandibular left third molar and the
other from the maxillary left third molar to the mandibular right
third molar.
3 Edentulous Arch. Make crossing lines, each running from the
uppermost aspect of one third molar to the lowest aspect of the third
molar on the opposite side.
4 Amalgam Restorations. In the diagram of the tooth, draw an outline
of the restoration showing size, location, and shape, and block
solidly.
5 Nonmetallic Permanent Restorations (includes oxyphosphate
cements). In the diagram of the tooth, draw an outline of the
restoration showing size, location, and shape.
6 Gold Restorations. Outline and inscribe horizontal lines within the
outline.
7 Combination Restorations. Outline showing overall size, location,
and shape; partition and junction materials used and indicate each, as
in "4." above.
8 Porcelain Facings and Pontics. Outline.
9 Acrylic Resin Facings and Pontics. Outline each aspect.
10 Porcelain Post Crowns. Outline the crown and approximate size and
position of the post(s).
11 Acrylic Resin Post Crowns. Outline crown and approximate size
and position of the post(s).
12 Porcelain Jacket Crowns. Outline each aspect.
13 Acrylic Resin Jacket Crowns. Outline each aspect.
14 Fixed Bridges. Outline each, showing overall size, location, teeth
involved and shape by the inscription of diagonal lines in abutments
and pontics.
15 Removable Appliances. Place an "X" through the missing tooth,
place a line over replaced teeth and describe briefly in "Remarks."
16 Root Canal Fillings. Outline canal filled and black in solidly.

4-53 CH 17
17 Apicoectomy. Draw a small triangle apex of the root of the tooth
involved, the base line to show the approximate level of root
amputation.
18 Drifted Teeth. Draw an arrow from the designating number of the
tooth that has moved; the point of the arrow to indicate the
approximate position to which it has drifted. Under "Remarks" note
the relationship to the drifted tooth in respect to occlusion.
(h) If an individual is appointed or enlisted with dental defects which have
been waived, the defects shall be described fully in the dental record
under "Remarks" (Section I).
(i) The examining dental officer shall sign, date, and record the place of
examination where indicated.
(5) Diseases, Abnormalities, and Radiographs.
(a) Markings on the examination chart of Diseases, Abnormalities, and
Radiographs shall be made as follows:
1 Caries. In the diagram of the tooth affected, draw an outline of the
carious portion, showing size, location and shape, and block in
solidly.
2 Defective Restoration. Outline and block in solidly the restoration
involved.
3 Impacted Teeth. Outline all aspects of each impacted tooth with a
single oval. Indicate the axis of the tooth by an arrow pointing in the
direction of the crown.
4 Abcess. Outline approximate size, form, and location.
5 Cyst. Outline the approximate form and size in relative position of
the dental chart.
6 Periodontal Disease. Inscribe a horizontal continuous line on the
external aspect of root(s) involved in a position approximating the
extent of gingival recession or the clinical depth of the pocket. If
known, indicate the position of the alveolar crest by a second
continuous line in relative position to the line indicating the gingival
tissue level.
7 Extraction Needed. Draw two parallel vertical lines through all
aspects of the tooth involved.

CH-17 4-54
8 Fractured Tooth Root. Indicate fracture with a zigzag line on outline
of tooth root.
(b) A statement regarding hypersensitivity to procaine or any other drug
known to the person for whom a Dental Record is prepared shall be
entered under "Remarks." (Example: HYPERSENSITIVITY TO
PROCAINE)
(c) Complete items A through E.
(d) The examining dental officer shall sign, date, and record the place of
examination where indicated.
(e) NOTE: Section I, Subsections 4 and 5 of SF 603 are used to record
findings of initial and replacement examinations. These charts shall not
be altered thereafter.
SECTION II. PATIENT DATA
(1) Patient Data. Complete items 6 through 14 as indicated.
SECTION III. ATTENDANCE RECORD
(1) Restorations and Treatments (Completed during service) (Item 15).
(a) Record restorations or treatments provided a patient after the initiation of
a Dental Record on the chart "Restorations and Treatments" of Section
III, in accordance with the following:
1 Carious Teeth Restored. In the diagram of the tooth involved, draw
an outline of the restoration showing size, location and shape, and
indicate the material used. Amalgam restorations would be outlined
and blocked in, silicate cement restorations outlined only, etc.
2 Extractions. Draw a large "X" on the root(s) of each tooth extracted.
3 Root Canal Fillings. Outline each canal filled on the diagram of the
root(s) of the tooth involved and block it in solidly.
4 Apicoectomy. Draw a small triangle on the root of the tooth
involved, apex away from the crown, the base line to show the
approximate level of tooth amputation.
5 Bridge and Crowns. Outline and fill in as specified above.
6 Removable Appliances. Place a line over numbers of replaced teeth
and give a brief description under "Remarks."
7 Unrecorded Operations and Conditions. Operations performed by
other than Coast Guard dental officers subsequent to the original

4-55 CH 17
examination will be indicated by the dental officer discovering the
condition just as if they had been done by a Coast Guard dental
officer. Make appropriate entries indicating the nature of the
treatment and adding the abbreviation "CIV" or other abbreviation as
the case may be. The date entered will be the date of the discovery.
8 Other. Similarly, note operations known to have been performed by
Coast Guard dental officers whose identity is not recorded, except
use the abbreviation "CGDO." The date entered shall be the date the
operation is discovered. Account for teeth which are shown as
missing in the chart, Missing Teeth and Existing Restorations, and
which have erupted subsequently, by an entry in the following
manner: "1 and 32," eruption noted, date, and signature of dental
officer making the notation. Record other conditions of comparable
importance in a similar manner.
(b) Record a series of treatments for a specific condition not producing
lasting changes in dental characteristics by entering of initial and final
treatment dates (i.e., POT daily 1 AUG 87 thru 5 AUG 87 or Vin Tr.
twice daily 1 AUG 87 thru 10 AUG 87).
(c) Authenticate each entry in this record by a written entry in the spaces
provided under "Services Rendered."
(2) Subsequent Disease and Abnormalities (Item 16). Chart subsequent
conditions, in pencil only, using the instructions in Chapter 4-C.3.(6). Once
treatment is completed and documented in item 17, erase pencil entry in item
16 and permanently transfer in ink to item 15 (Restorations and Treatments).
(3) Services Rendered (Item 17). The accuracy and thoroughness in recording
patient histories and treatment progress notes are essential elements in the
diagnosis and treatment of the dental patient. In addition to the conventional
listing of the tooth number and procedure, every effort shall be made to
specifically identify dental materials used intraorally. Use trade names where
possible. This includes, but is not limited to; bases and liners, metallic and
nonmetallic restorative materials, denture frameworks and bases, impression
materials, medicaments, and anesthesia. Record prescribed medications.
(a) Standard S.O.A.P. format. The S.O.A.P. format shall be used to
document all sickcall and emergency dental treatments, to document
Type 1 and Type 2 examinations, and to record the results of the
examination of patients in preparation for comprehensive treatment
planning. S.O.A.P. format is not required to document ongoing delivery
of treatment which has been previously planned. All entries are to be on
the SF-603/603-A, item 17. The S.O.A.P. format uses a problem
oriented record as a tool in management of patient care. The acronym is
derived from the first letter of the first four record statements as follows:

CH-17 4-56
1 "S" Subjective data. This data includes the reason for the visit to
the dental clinic, and if appropriate, a statement of the problem
(chief complaint) and the qualitative and quantitative description of
the symptoms appropriate to the problem.
2 "O" Objective data. A record of the type of examination and the
diagnostic aids, including the ordering of radiographs, and the actual
clinical findings, x-ray results, or laboratory findings appropriate to
the problem. This is to include all the provider's findings such as
carious teeth, inflammation, periodontal status, pocket depths, blood
pressure measurement, etc.
3 "A" Assessment. This portion is the assessment of the subjective
data, objective data, and the problem statement which leads the
provider to a diagnosis, e.g.,"needs" (existing conditions or
pathoses).
4 "P" Plan. This is the plan of treatment to correct or alleviate the
stated problems or needs, irrespective of the treatment capability of
the dental treatment facility. Include recommended treatment and,
as appropriate, possible complications, alternative treatment, and
prognosis with and without intervention. Include consultations, a
record of the specific treatment performed, pre- and postoperative
instructions, prescriptions, and any deviations from the original
treatment plan.
(b) The following classification of tooth surfaces are listed in order of
precedence and shall be used in connection with recording restorations of
defective teeth:
Surface Designation
Facial (Labial) (Anterior teeth) F
Buccal (Posterior teeth) B
Lingual L
Occlusal (Posterior teeth) 0
Mesial M
Distal D
Incisal (Anterior teeth) I
(c) Use combinations of designators to identify and locate caries, operations,
or restorations in the teeth involved; for example, 8-MID would refer to
the mesial, incisal, and distal aspects of the left mandibular cuspid; 30-
MODF, the mesial, occlusal, distal, and facial aspects of a right
mandibular first molar.
4-57 CH 17
Surface Designation
Mesial-Occlusal MO
Distal-Occlusal DO
Mesial-Incisal MI
Distal-Incisal DI
Occlusal-Facial OF
Occlusal-Lingual OL
Incisal-Facial IF
Incisal-Lingual IL
Mesial-Occlusal-Distal MOD
Mesial-Occlusal-Facial MOF
Mesial-Occlusal-Lingual MOL
Mesial-Incisal-Distal MID
Mesial-Incisal-Facial MIF
Mesial-Incisal-Lingual MIL
Distal-Occlusal-Facial DOF
Distal-Occlusal-Lingual DOL
Mesial-Occlusal-Distal-Facial MODF
Mesial-Incisal-Distal-Facial MIDF
Mesial-Occlusal-Distal-Facial-Lingual MODFL
Mesial-Incisal-Distal-Facial-Lingual MIDFL
(d) The use of abbreviations is not mandatory but is desirable for purposes of
brevity in view of the limited space available in the dental record for
recording services rendered. Whenever there is a possibility of
misinterpretation due to the use of abbreviations, dental operations shall
be written in full. When abbreviations are used, they shall conform to
the following:
Operation, Condition, or Treatment Abbreviation
Abrasion Abr.
Abscess Abs.
Acrylic Acr.
Adjust (ed)(ment) Adj.
Alveolectomy Alvy.
Amalgam Am.
CH-17 4-58
Anesthesia Anes.
Apicectomy Apcy.
Base B.
Bridge (denotes fixed unless otherwise noted) Br.
Caries Car.
Calculus Cal.
Cavity Varnish C.Var.
Cement Cem.
Composite Resins Comp. Res.
Crown Cr.
Deciduous Dec.
Defective Def.
Denture (full unless otherwise noted) Dtr.
Drain. Drn.
Dressing Drs.
Equilibrate (action) Equil.
Eugenol Eug.
Examination Exam.
Extraction (ed) (Uncomplicated unless otherwise noted) Ext.
Filling(s) Fil.
Fluoride Fl.
Fracture(s) Frac.
General Gen.
Gingival (itis) (state type in parenthesis). Ging.
Gutta percha G.P.
Impacted (ion) Imp.
Impression Impr.
Incised Inc.
Inlay Inl.
Inserted Ins.
Maxillary Max.
Mandibular Man.
Partial Pr.
4-59 CH 17
Parietal Par.
Periapical Per.
Pericoronitis Percor.
Periodontitis Perio.
Porcelain Porc.
Post Operative Treatment POT.
Prepared (ation) Prep.
Prophylaxis Pro.
Reappoint (ment) Reapt.
Recement (ed) Recem.
Reconstruct (ed) Rct.
Reduce (d) Red.
Regional Rel.
Repaired Rpd.
Sedative (ation) Sed.
Sequestrum Seq.
Surgical Surg.
Suture (s)(d) Su.
Treatment (ed) Tr
Unerupted Uner.
Vincents Vin.
Zinc Chloride ZnCl.
(4) Space is provided in the lower right margin under Section III for the patient's
name which is for convenience in filing in the dental record. Record the last
name in capital letters. Do not abbreviate any part of the name.
4. SF-603-A (Dental Continuation).
a. General. Use a SF-603-A whenever the original SF-603 becomes filled or when the
record cannot be satisfactorily brought up-to-date by entries on the appropriate chart.
b. Detailed Instructions.
(1) Enter individual's name and SSN in the space provided on the right margin of
both the front and back side of the form.
CH-17 4-60
(2) Number the continuation sheet in the upper right corner following the phrase
"DENTAL-Continuation." Thus, the earliest SF-603-A is labeled "DENTAL-
Continuation #1" and subsequent sheets are labeled "DENTAL-Continuation
#2", "DENTAL-Continuation #3", etc.
(3) File the SF-603-A forms on top of the SF-603 form in reverse chronological
order, i.e., the most recent on top.
5. SF-513, Consultation Sheet.
a. Purpose. SF-513 shall be used whenever a patient is referred to another facility for
evaluation or treatment.
b. Detailed Instructions. Complete the form as detailed in paragraph 4-B-14.b.
6. Lost Dental Records.
a. Forward "stray" dental records, disposition of which cannot be determined, to
Commandant (G-PIM) with a letter of explanation.
b. When a Dental Record is missing, prepare a new record. Prominently mark the
Dental Record Cover (CG-3443-2) and the Health Record, Dental (SF-603)
"REPLACEMENT." Request the old Dental Record from the individual's last unit or
Commandant (G-PIM).
c. In case a lost Dental Record is recovered, make entries in the recovered record of any
data recorded in a replacement record, then destroy the replacement record.
7. Special Dental Records Entries. When dental treatment is refused, make an appropriate
entry on the SF-603/603-A, signed by both the dental officer and patient.
8. Dental Examination Requirements.
a. Any peculiarities or deviations from normal are particularly valuable for
identification purposes and shall be recorded on SF-603 under "Remarks."
Abnormalities such as erosion, mottled enamel, hypoplasia, rotation, irregularity of
alignment and malocclusion of teeth, presence of supernumerary teeth, denticles,
Hutchinson's incisors, fractures of enamel or teeth, abnormal interdental spaces,
mucosal pigmentation, leukoplakia, diastema, hypertrophied frenum labium, torus
palantinus and torus mandibularis, embedded foreign bodies and descriptions of
unusual restorations or appliances are, when noted, especially useful in this
connection. Malocclusion shall be simply and clearly described. Dentures and other
removable dental appliances shall also be described under "Remarks".
b. When all teeth are present, and free of caries or restorations, take special effort to
discover and record any abnormalities, however slight. If no caries, restorations, or
abnormalities are found, make an entry to that effect on SF-603 under "Remarks."

4-61 CH 17
c. Inquire about the patients' tobacco use during routine dental examinations and
document. Advise users of the health risks associated with tobacco use, the benefits
of stopping, and where to obtain assistance in stopping if available. Advise all
pregnant tobacco users of the health risks to the fetus.
d. Oral hygiene and periodontal status at time of examination shall be recorded. Upon
initial examination, complete items 5A-5C, SF-603, with additional comments
placed in "Remarks" if needed. For all subsequent examinations, describe oral
hygiene level and periodontal status in item 17 of SF-603/603-A.
e. For all patients 16 years of age or older, blood pressure readings shall be taken and
recorded on the CG-5605 at initial and subsequent dental examinations. Although
not required, the blood pressure may also be recorded on the SF-603/603-A in the
"O" portion of the SOAP entry.
9. Recording of Dental Treatments on SF-600. Make entries of dental treatment on SF-600
when the patient is on the sick list and when treatment is related to the condition for which
the patient is admitted. Such entries shall be made and signed by the dental officer. Notes
concerning conditions of unusual interest and of medical or dental significance may be made
when appropriate.
CH-17 4-62
Section D - Clinical Records.
1. Purpose and Background. The Clinical Record (CG-3443-1) is the chronological
medical and dental record of a nonactive duty beneficiary (dependent or retiree) eligible
for health care at a Coast Guard facility. The primary reasons for compiling a clinical
record are:
a. To develop records to facilitate and document the health condition in order to
provide health care and to provide a complete account of such care rendered,
including diagnosis, treatment, and end result.
b. To protect the Government, the individual concerned, and the individual's
dependents: It may be used;
(1) to provide, plan and coordinate health care;
(2) to aid in preventive health and communicable disease control programs; in
reporting medical conditions required by law to Federal, state, and local
agencies;
(3) to compile statistical data; for research; to teach health services personnel;
(4) to determine suitability of persons for service or assignments;
(5) to adjudicate claims and determine benefits; for law enforcement or litigation;
(6) to evaluate care provided; and
(7) to evaluate personnel and facilities for professional certification and
accreditation.
c. To aid in identifying deceased persons when other means may be inadequate.
2. Contents of Clinical Records.
a. Each clinical record shall consist of CG-3443-1 with dental and medical records
arranged in the following bottom to top sequence:
(1) Left Side - Dental: CG-3443-2 Dental Record Cover* with CG-5266 (Drug
Sensitivity Sticker)*, containing the following:
(a) SF-522, Authorization for Administration of Anesthesia and for
Performance of Operations and Other Procedures*
(b) SF-603-A, Dental Record - Continuation*
(c) SF-603, Dental Record*
(d) CG-5605, Dental Health Questionnaire*
4-63 CH 17
(2) Right Side - Medical:
(a) PHS-731, International Certificate of Vaccination*, attached to the lower
right corner of the inside of the Clinical Record Cover
(b) DD-1141, Record of Occupational Exposure to Ionizing Radiation*
(c) SF-507, Continuation Sheet**
(d) SF-602, Syphilis Record*
(e) SF-601, Immunization Record*
(f) DD-771, Spectacle Order Form*
(g) SF-520, Electrocardiographic Report*
(h) SF-519, Radiographic Reports
(i) SF-514, Laboratory Reports (or SF-545, Laboratory Report Display*)
(j) SF-541, Gynecologic Cytology*
(k) SF-515, Tissue Examination*
(l) SF-522, Authorization For Administration of Anesthesia and for
Performance of Operations and Other Procedures*
(m) SF-513, Consultation Sheet*
(n) SF-502, Narrative Summary*
(o) CG-5447, Occupational Medical Surveillance and Evaluation Program*
(p) DD-2807-1, Report of Medical History*
(q) DD-2808, Report of Medical Examination*
(r) SF-558, Emergency Care and Treatment
(s) SF-600, Chronological Record of Medical Care
(t) DD-2766, Adult Preventive and Chronic Care Flowsheet Form
(u) CG-5266, Drug Sensitivity Sticker*
* When required
** SF-507's are attached to and filed after the form is continued
CH-17 4-64
b. File forms of the same number in their assigned sequence, with the most recent
placed on top of each previous form, i.e., file SF-600 dated 3 AUG 89 on top of SF-
600 dated 20 MAY 86.
c. Enter all dates on Clinical Record forms, including the Clinical Record Cover, in the
following sequence: day (numeral), month (in capitals abbreviated to the first three
letters), and year (numeral); i.e., 30 AUG 86.
3. Extraneous Attachments. In order to ensure that the clinical record is an accurate,
properly documented, concise and dependable record of the medical and dental history of
the individual, keep extraneous attachments to a minimum. When they are necessary,
file them beneath all other forms.
4. Opening Clinical Records. Open a Clinical Record when an eligible non-active duty
beneficiary initially reports to a Coast Guard health care facility for treatment.
5. Terminating Clinical Records. The Clinical Record shall be terminated four years after
the last record entry. Make an entry on SF-600 explaining the circumstances under
which the record was terminated. Forward the record to:
Dependent Records: Military Records:
National Personnel Records Center National Personnel Records
GSA (Civilian Personnel Records) Center (MPR)
11 Winnebago Street 9700 Page Avenue
St. Louis, MO 63118-4126 St. Louis, MO 63132-5100
6. Custody of Clinical Records.
a. Clinical Records shall be retained in the custody of the Chief, Health Services
Division of the unit providing care. At times when there is no medical or dental
officer, the clinical record will become the responsibility of the senior health services
department representative.
b. The name, grade, or rate of the health care provider making entries in clinical records
shall be typed, stamped, or printed under their official signatures. Do not use
facsimile signature stamps.
c. If an erroneous entry is made in a Clinical Record, the author of the entry shall draw
a diagonal line through the complete entry, make an additional entry showing
wherein and to what extent the original entry is in error, and initial clearly next to the
correction.
d. Each health care provider is responsible for the completeness of the entries they
make on any medical or dental form in the Clinical Record.
e. Nothing shall be removed from the Clinical Record except under conditions specified
in this Manual.
4-65 CH 17
7. Safekeeping of Clinical Records. Clinical Records are the property of the Federal
government and must be handled in accordance with the provisions of the Privacy Act of
1974 and the Freedom of Information Act. Guidance in this area is contained in The
Coast Guard Freedom of Information and Privacy Acts Manual, COMDTINST M5260.3
(series).
f. Since Clinical Records contain personal information of an extremely critical or
sensitive nature, they are considered class III records requiring maximum security
(high security locked cabinets or areas).
g. Except as contained in the The Coast Guard Freedom of Information and Privacy
Acts Manual, COMDTINST M5260.3(series), the information contained in Clinical
Records shall not be disclosed by any means of communication to any person or to
any agency, unless requested in writing by or with the prior consent of the individual
to whom the record pertains. It is the requestor's responsibility to obtain the consent.
8. Transfer of Clinic Records.
a. When dependents of active duty personnel accompany their sponsor to a new duty
tation, the Chief, Health Services Division, his designee, the Executive Officer, or
the senior health services department representative shall ensure that the
“TRANSFERRED TO” line of the health Record Receipt form, NAVMED 6150/7,
is completed in accordance with Chapter 6-B-5 of this Manual.
b. A DD 877 shall be initiated for each record transferred. Send records using a
service that provides a tracking number, such as Priority Mail Delivery
Confirmation, Certified Mail, Insured Mail, or FedEx/Express Mail if time is
critical, to the Coast Guard clinic serving the gaining unit. Express mail and Federal
Express should be used only when absolutely necessary and not as a general rule. In
instances where the family member will not be located near a Coast Guard Clinic, the
record may be mailed to the appropriate MTF. This form can be located on the
internet at; http://web1.whs.osd.mil/ICDHOME/DD-0999.htm
c. If the family members will no longer receive care through a military primary care
manager, the family member may be given a copy of the clinical record contents to
carry with them. The original clinical record will be retained at the clinic serving the
unit where the sponsor was last assigned.
d. Clinics will give family members written information containing address and POC
information to facilitate requests for record copies after transfer. All requests for
clinical record copies must be in writing. The family member may request that a
copy of the record be forwarded to their new care provider once they arrive at the
new location, or they may request that the original record be forwarded to their new
military primary care manager once they arrive at the new location. In these cases,
the clinic shall send a copy of the clinical record contents to the care provider within
10 working days of receipt of the written request. If the clinic cannot comply with
this requirement for some reason, the family member will be notified within 10
CH-17 4-66
working days of the request of a projected date when the record copy will be
available.
e. In any instance where there is concern about potential loss of the clinical record, or
that its contents may become unavailable to the treating clinic or its provider, the
Clinic Administrator or the Chief, Health Services Division shall direct that copies of
parts or all of the clinical record shall be made and retained at the clinic.
f. Originals and copies of clinical records shall be retained and subsequently archived
in accordance with directions contained in the Paperwork Management Manual,
COMDTINST 5212.12(series).
9. Lost, Damaged, or Destroyed Clinical Records.
a. If a Clinical Record is lost or destroyed, the unit which held the record shall open a
new record. The designation "REPLACEMENT" shall be stamped or marked on the
cover. If the missing Clinical Record is recovered, insert in it any additional
information or entries from the replacement record, then destroy the replacement
record cover.
b. Clinical Records which become illegible, thus destroying their value as permanent
records, shall be duplicated. The duplicate shall, as nearly as possible, be an exact
copy of the original record before such record became illegible. The new record
shall be stamped or marked "DUPLICATE" on the cover. The circumstances
necessitating the duplication shall be explained on the SF-600. Forward Clinical
Records replaced by duplicate records to the National Personnel Records Center.
10. Clinical Record Forms.
a. CG-3443-1 (Clinical Record Cover). See Encl (1), pg 4-40.
(1) General. The Clinical Record Cover is used whenever a Clinical Record is
opened on dependents or retirees.
(2) Detailed Instructions.s
(a) Last Name. Record the last name in all capital letters.
SMITH
(b) Given Name(s). Record given name(s) in full without abbreviation. If
the individual has no middle name or initial, use the lower case letter "n"
in parentheses (n). If the individual has only a middle initial(s), record
each initial in quotation marks. When "Jr." or "II" or other similar
designations are use, they shall appear after the middle name or initial.
SMITH, Helen (n)
Last Name First Name Middle Name

4-67 CH 17
(c) Date of Birth. Enter day, month (abbreviated JAN, FEB, MAR, etc.) and
the year; i.e., 3 FEB 77.
(d) Social Security Number. Enter sponsor's SSN.
(e) Status. Check the appropriate block; i.e., Retiree USCG, Dependent
USPHS, etc.
(f) Other. Use this block to indicate special status or other information
useful for either proper monitoring of the patient or for aid in
indentifying the patient or record.
(g) Occupational Monitoring. Indicate the reason for occupational
monitoring if monitoring is required.
(h) Med-Alert. Check this block to indicate that the patient has a medical
problem that must be considered in rendering treatment; i.e., allergy,
diabetes, cardiac problems, etc. Describe the specific medical problem
within the medical record on Problem Summary List, NAVMED
6150/20.
b. SF-522 (Authorization for Anesthesia, Operations, etc.). See Encl (1), pg. 4-41.
(1) Complete SF-522 describing the general nature of the procedure and have the
patient sign prior to administering anesthesia (local or general) except for
dental anesthesia. Also, complete SF-522 prior to administering immunizing
agents.
Insert the form immediately behind Consultation Sheet (SF-513) or as indicated
in Section 4-D-2.

CH-17 4-68
Section E - Employee Medical Folders.
1. Purpose and Background. The Employee Medical Folder (EMF), (SF-66 D), is the
chronological medical record of Federal employees eligible for health care at Coast
Guard facilities. These are the primary reasons for compiling an EMF.
a. Develop records to facilitate and document the health condition in order to provide
health care and to provide a complete account of care rendered, including diagnosis,
treatment, and end result.
b. To protect the Government and the individual concerned.
c. The information in the EMF is routinely used: to provide, plan and coordinate health
care; to aid in preventive health and communicable disease control programs; in
reporting medical conditions required by law to Federal, state, and local agencies; to
compile statistical data; for research; to teach health services personnel; to determine
suitability of persons for service or assignments; to adjudicate claims and determine
benefits; for law enforcement or litigation; to evaluate care provided; and to evaluate
personnel and facilities for professional certification and accreditation.
2. Custody of Employee Medical Folders (EMF’s).
a. EMF's are the property of the Federal government handled in accordance with the
provisions of the Privacy Act of 1974 and the Freedom of Information Act.
Guidance in this area is contained in The Coast Guard Freedom of Information and
Privacy Acts Manual, COMDTINST M5260.3 (series).
(1) Since EMF's contain personal information of extremely critical or sensitive
nature, they are considered class III records according to The Coast Guard
Freedom of Information and Privacy Acts Manual, COMDTINST M5260.3
(series), requiring maximum security (high security locked cabinets or
areas).Except as contained in The Coast Guard Freedom of Information and
Privacy Acts Manual, COMDTINST M5260.3 (series), the information
contained in the EMF shall not be disclosed by any means of communication to
any person or to any agency, unless requested in writing by or with the prior
consent of the individual to whom the record pertains. It is the responsibility
of the requester to obtain the consent.
b. EMF's shall be retained in the custody of the medical officer of the unit at which the
individual is employed. At no time shall individual employees keep or maintain their
own records.
c. Individuals may examine their EMF in the presence of a health services department
representative, providing it does not interrupt the scheduled mission of the unit and
there is no information contained therein which would be detrimental to the
individual's mental well-being.
4-69 CH 17
d. Health services personnel making entries in EMF shall ensure that all entries,
including signatures, are neat and legible. Signature information shall include the
name and grade or rate. Do not use facsimile signature stamps.
e. If an erroneous entry is made in an EMF, draw a diagonal line through the complete
entry. Make an additional entry showing wherein and to what extent the original
entry is in error.
f. Health services personnel are responsible for the completeness of the entries made on
any form while the EMF is in their custody. No sheet shall be removed from the
EMF except under conditions specified in this Manual.
g. Health services personnel shall ensure that, if EMF's are located in the same office as
the Official Personnel Folder (OPF), the records are maintained physically apart from
each other.
3. Contents of the Employee Medical Folders.
a. Each medical folder shall consist of SF-66 D (Employee Medical Folder) with
medical records arranged in the following bottom to top sequence:
(1) Left Side Dental: Leave blank.
(2) Right Side - Medical:
(a) PHS-731, International Certificate of Vaccination*, attached to the lower
right corner of the inside of the EMF
(b) DD-1141, Record of Occupational Exposure to Ionizing Radiation*
(c) SF-507, Continuation Sheet**
(d) CG-5447, Occupational Medical Surveillance and Evaluation Program*
(e) SF-602, Syphilis Record*
(f) SF-601, Immunization Record*
(g) DD-771, Spectacle Order Form*
(h) SF-520, Electrocardiographic Report*
(i) SF-519, Radiographic Reports
(j) SF-514, Laboratory Reports (or SF-545, LaboratoryReport Display*)
(k) SF-541, Gynecologic Cytology*
(l) SF-515, Tissue Examination*
CH-17 4-70
(m) SF-522, Authorization For Administration of Anesthesia and for
Performance of Operations and Other Procedures*
(n) SF-513, Consultation Sheet*
(o) SF-502, Narrative Summary*
(p) DD-2807-1, Report of Medical History*DD-2808, Report of Medical
Examination*
(q) SF-558, Emergency Care and Treatment*
(r) SF-600, Chronological Record of Medical Care
(s) CG-5357, Outpatient Record
(t) DD-2766, Adult Preventive and Chronic Care Flowsheet
(u) CG-5266, Drug Sensitivity Sticker*
(v) * When required
(w) ** SF-507's are attached to and filed after the form is continued.
b. File forms of the same number in their assigned sequence, with the most recent
placed on top of each previous form, i.e., file SF-600 dated 3 AUG 87 on top of SF-
600 dated 20 MAY 86.
c. Enter all dates in the following sequence: day (numeral), month (in capitals
abbreviated to the first three letters), and year (numeral); i.e., 30 AUG 86.
4. Accountability of Disclosures. The accountability of disclosure of records, as required
by the Privacy Act of 1974, will be maintained in accordance with Chapter 8, of
COMDTINST M5260.2 (series). The information will be retained for five years after the
last disclosure or for the life of the record, whichever is longer.
5. Opening Employee Medical Folder. Open an EMF when an eligible Federal employee
initially reports for treatment.
6. Terminating Employee Medical Folders. Terminate the EMF in accordance with the
Coast Guard Paperwork Management Manual, COMDTINST 5212.12 (series). Make an
entry on SF-600 explaining the circumstances under which the folder was terminated.
7. Transferring to Other Government Agencies. When transferring an EMF to other
agencies, complete a Request for Medical/Dental Records or Other Information (DD-
877).
8. Lost, Damaged, or Destroyed Employee Medical Folders.
4-71 CH 17
a. If an EMF is lost or destroyed, the unit which held the record shall open a complete
new Employee Medical Folder. Stamp or mark "REPLACEMENT" on the cover. If
the missing folder is recovered, insert in it any additional information or entries from
the replacement folder, then destroy the replacement folder.
b. EMF's which become illegible, thus destroying their value as permanent records, will
be duplicated. The duplicate shall, as nearly as possible, be an exact copy of the
original record before such record becomes illegible. Stamp or mark "DUPLICATE"
on the new record cover. Document the circumstances necessitating the duplication
on an SF-600. Forward EMF's replaced by duplicate records to the National
Personnel Records Center.
9. SF-66 D (Employee Medical Folder). See Encl (1), pg. 4-42. Detailed instructions are:
a. Last Name. Record the last name in all capital letters.
BROOKS
b. Given Name(s). Record given name(s) in full without abbreviation. If the individual
has no middle name or initial, use the lower case letter "n" in parentheses (n). If the
individual has only a middle initial(s), record each initial in quotation marks. When
"Jr." or "II" or other similar designations are use, they shall appear after the middle
name or initial.
BROOKS Cecilia (n)
Last Name First Name Middle Name
c. Date of Birth. Enter day, month (abbreviated JAN, FEB, MAR, etc.) and the year;
i.e., 8 JUN 62.
d. Social Security Number. Enter SSN.
CH-17 4-72
Section F -Inpatient Medical Records.
1. Purpose and Background.
a. Certain Coast Guard health care facilities have the capability and staffing to provide
overnight care. Overnight care is defined as any period lasting more than four hours
during which a beneficiary remains in the facility under the care or observation of a
provider. By definition, overnight care may last less than 24 hours or it may last
several days. Overnight care is utilized when a patient's condition or status requires
observation, nursing care, frequent assessment, or other monitoring.
b. Inpatient Medical Records (IMRs). Facilities providing overnight care shall create an
Inpatient Medical Record (IMR) separate from the Health Record for the purpose of
recording and preserving information related to the overnight care. The IMR shall be
assembled as soon as a person is identified as needing overnight care. The IMR shall
contain the following forms in a TOP TO BOTTOM sequence:
(1) Inpatient Medical Record Cover Sheet and Privacy Act Statement. See
Encl (1), pg 4-43.
(2) SF-508, Doctor's Orders (most recent on top)
(3) SF-506, Clinical Record/Physical Exam
(4) SF-502, Narrative Summary
(5) SF-509, Doctor's Progress Notes (most recent on top)
(6) SF-511, Vital Signs Record
(7) SF-514, Laboratory Report Display
(8) SF-519, Radiologic Reports
(9) Patient Care Kardex
(10) Medication Kardex
(11) SF-513, Consultation sheet
(12) Miscellaneous forms (e.g., audiograms)
c. Abbreviated Inpatient Medical Records (AIMRs). For patients who receive
overnight care lasting 24 hours or less, an Abbreviated Inpatient Medical Record
(AIMR) shall be created. The AIMR shall consist of at least an Inpatient Medical
Record Cover Sheet, Privacy Act Statement, and an DD-2770, Abbreviated Medical
Record form. SF-545, Laboratory Reports; SF-519, Radiologic Consultation
Reports; Kardexes; and other forms may be included at the discretion of the clinic.
4-73 CH 17
The AIMR shall be maintained while in use, completed, stored, and retired following
the same requirements as listed for IMRs below.
d. During the time that the patient is receiving care, the IMR may be maintained in a
loose-leaf binder, clipboard, or other convenient device, at the facility's discretion.
Devices should be chosen and maintained so that the privacy of the patient
information contained therein is protected at all times. Keeping or storing the record
at the patient's bedside is discouraged for privacy reasons.
e. Once the patient is released from overnight care, providers shall have 48 hours to
complete their notations in the record (excluding dictated entries). All laboratory,
radiologic and consultation forms shall also be included in the IMR within 48 hours
of the patient's release from overnight care.
f. Dictated entries shall be entered in the medical record within 7 days of discharge.
The record may be held in medical records and flagged as needing a dictated entry.
g. After all notations, lab reports, radiology reports and consultations have been entered
into the IMR, the IMR forms shall be placed in a bifold paper jacket (form CG-3443-
1), and secured via a two prong device. The medical records staff is responsible for
ensuring that the documents are in the correct order and are stored properly.
2. Maintenance and Storage. IMRs are the property of the Federal Government and must
be handled in accordance with the provisions of the Privacy Act of 1974 and the
Freedom of Information Act. Guidance concerning these acts is contained in The Coast
Guard Freedom of Information and Privacy Acts Manual, COMDTINST M5260.3
(series). All requirements and directions for handling and storing IMRs also apply to
AIMRs.
a. Since IMRs contain personal information of an extremely critical or sensitive nature,
they are considered to be Class III records requiring maximum security (high security
locked cabinets or areas). IMRs shall be stored in well ventilated and sprinklered
areas. Fire-resistant cabinets or containers shall be used for storage whenever
possible.
b. IMRs shall be retained at the health care facility which created the record. IMRs will
not be transferred with personnel who change duty stations. Copies of the IMR may
be given to the individual if such a request is made in writing, or may be released to
other persons, e.g., physicians or hospitals, if the patient requests or authorizes such
release in writing. All release requests and authorizations will be inserted into the
IMR cover.
c. IMRs will be retained at the creating health care facility for two (2) years after the
date the patient is released from overnight care.
3. Disposition of IMRs. The IMR will be forwarded to the National Personnel Records
Center (NPRC) as described in Coast Guard Paperwork Management Manual,
COMDTINST M5212.12(series), two years after the date the patient was released from
CH-17 4-74
inpatient care. The NPRC requirements must be met in order for the NPRC to accept the
records.
a. Records must be sent in prescribed standard cubic foot cartons. See Encl (1), pg.4-
45. Cartons are available from the General Services Administration Federal Supply
Service (FSS). The FSS stock number is NSN 8115-00-117-8344. All non-standard
cartons will be returned at the expense of the originating organization.
b. NPRC does not accept accessions of less than one cubic foot. Small amounts shall
be held until a volume of one cubic foot or more is reached.
c. Print the accession number on each box, starting in the upper left hand corner See
Encl (1), pg. 4-45 . Mark the front of the box only. The accession number consists
of the RG, which is always 26 for the Coast Guard, the current FY in which the
records are being shipped, and a four digit number assigned by NPRC (see 4-F-3.j.
for SF-135 preparation). Mark the front of the box only. Ensure that the information
printed on the box is not obscured in any way, and that removal of tape or other
sealing materials will not remove vital information.
d. Number each box consecutively, e.g., 1 of 8, 2 of 8, 3 of 8,.8 of 8; or 1/8, 2/8,
3/8...8/8, in the upper right hand corner. See Encl (1), pg. 4-45 for placement.
e. Records shall be arranged in each storage box either alphabetically or numerically.
Print the identifier of the first and last record/folder that is contained in the box on
the center front of each box as shown in Encl (1), pg. 4-45.
f. Enclose in the first box of each accession one copy of the SF-135 and any
alphabetical or numerical listing needed to reference the records.
g. Ship records together so they arrive at the NPRC at the same time. Shipments of 10
cubic feet or more shall be palletized as shown in Encl (1), pg. 4-46.
h. Records must be shipped within 90 days of being assigned an accession number.
Failure to ship within 90 days will void the accession number.
i. Each clinic that transfers IMRs to NPRC must keep a master list (hard copy) of the
records sent. The master list must be retained at the clinic for a period of 50 years.
j. All shipments to NPRC must be accompanied by SF-135, Records Transmittal and
Receipt form. The transmittal form must include the name on the record and the
individual's social security number. The accession number elements include the RG
which is always 26 for the Coast Guard, the current FY during which the record is
shipped, and the 4 digit sequential number assigned by NPRC. Also include the date
sent. Complete SF-135 preparation and submission instructions are contained in the
Coast Guard Paperwork Management Manual, COMDTINST M5212.12(series).
4-75 CH 17
4. Inpatient Medical Record Forms and Required Entries.
a. SF-508, Doctor's Orders. See Encl (1), pg 4-47.
(1) Purpose. SF-508 is used to record written and verbal orders of the medical or
dental staff; record that nurses have noted orders; record automatic stop dates
for medications and time limited treatments; and record the RN review of
orders which shall be performed every 24 hours.
(2) Preparation
(a) When Prepared. SF-508 shall be used to communicate doctor's orders
for all persons admitted to the medical facility inpatient area.
(b) Required Entries.
1 Patient identification information may be written in or overprinted
using a patient identification card.
2 The date and time at which the order is written by the provider will
be listed under the start column. If a verbal order is received, the
date and time at which the order was received will be noted by the
person who received the order in the start column. All verbal orders
must be countersigned by the admitting provider on the next
working day.
3 Certain orders may be defined as time limited, e.g., complete bedrest
for 24 hours, tilts q 8 hours X 3, etc. In addition, the facility shall
define the length of time between renewal of orders for medications,
treatments, etc. For orders which are time limited, the date and time
when the order expires shall be noted under the stop column.
4 All doctor's orders shall be listed on the form under drug orders.
Orders shall be printed clearly in black ink. Only approved
abbreviations shall be used. Nursing staff and/or health services
technicians are required to contact the provider who wrote the order
if there are any questions or difficulty encountered in reading the
written order.
b. SF-506, Clinical Record/Physical Exam. See Encl (1), pg. 4-48.
(1) Purpose. SF-506 is part of the inpatient medical record. It is used to record
information obtained from physical examinations.
(2) Preparation. When Prepared. SF-506 shall be prepared when a patient is
admitted to the medical facility.
CH-17 4-76
(c) Required Entries.
1 Patient identification information may be written in or printed using
a patient identification card.
2 Fill in the date that the exam is conducted in the upper left corner.
The patient's self reported height may be used. Patients shall be
weighed accurately on the day of admission and the weight entered
as present weight. Vital signs to include temperature, pulse and
blood pressure are recorded in the appropriate boxes. Rectal
temperatures shall be identified by an "R" after the temperature
reading. Axillary temperatures in adults are unreliable and will not
be used.
3 A physical examination must be thorough, recorded accurately, and
contain sufficient information to substantiate the treatment plan and
interventions. Examination notations may be continued on the
reverse of the form. If the back of the form is used, this must be
indicated on the front of the form. The examiner will sign the form
at the end of his/her notations and use a printed ink stamp to clearly
mark name, rank, and SSN.
c. SF-509, Progress Notes. See Encl (1), pg 4-50
(1) Purpose. SF-509 is part of the inpatient medical record. It is used to record the
progress of the patient's condition, therapy or other treatment(s), as well as any
other information relevant to the patient's condition or treatment such as
laboratory tests and results.
(2) Preparation.
(a) When Prepared. SF-509 shall be prepared when a patient is admitted to
the medical facility inpatient area.
(b) Required Entries.
1 Patient identification information may be written in or overprinted
using a patient identification card.
2 Fill in the left column with the date and time at which the entry is
being created. Begin writing to the right of the solid brown line.
Notes will be written in SOAP format (see 4-B-5.a.(4)). The person
creating the note will sign the form at the end of his/her notations
and use a printed ink stamp to clearly mark name, rank, and SSN.
d. SF-511, Vital Signs Record. See Encl (1), pg.51.

4-77 CH 17
(1) Purpose. SF-511 shall be used to document vital sign measurements, height,
weight, hospital day and, if appropriate, postoperative day for patients admitted
to the medical facility inpatient area.
(2) Preparation.
(a) When Prepared. SF-511 shall be prepared when a patient is admitted to
the medical facility inpatient area.
(b) Required Entries.
1 Patient identification information may be written in or overprinted
using a patient identification card.
2 Hospital day one shall be the day of admission.
3 If the patient undergoes an invasive procedure, "op" shall be written
after the word post in the left column. The day of surgery shall be
noted by writing "DOS" in the appropriate column. The day
following the day of surgery is post-op day one. Post-op days shall
be numbered consecutively thereafter.
4 The month in which the patient is admitted shall be written on the
fifth line, first column. The year shall be completed by writing in
the correct numerals after "19" on the fifth line.
5 The calendar date on which the patient is admitted shall be written in
on the line next to the word day, e.g., if the patient is admitted on 3
June, the hospital day is one, and a "3" is written on the line next to
the word day.
6 The hour at which the vital sign measurements are to be made are
noted in the spaces next to the word hour. Use 24 hour clock
notations, e.g., 11 p.m. is 2300, etc.
7 Once vital signs have been measured, they shall be recorded on the
form using the symbols for pulse and temperature. Symbols are
placed in the columns, not on the brown dotted lines.
8 Blood pressure measurements are written in the spaces to the right of
the words "blood pressure". The first measurement made after
midnight is written in the top left column, the second is written
below it. The first measurement made after noon is written in the
top box in the right side column, the second below that, etc. Blood
pressure may also be represented by x marks placed at the systolic
and diastolic measurements corresponding to the scale for pulse
measurements.
CH-17 4-78
9 Other vital signs measurements or intake and output measurements
may be written in the spaces on the lower part of the form, or a local
overprint/stamp may be used.
10 Both sides of the form will be used. If the second side of the form is
used, the word "continued" will be clearly written on the bottom of
the first page.
e. SF-514, Laboratory Reports.
(1) Purpose. SF-514 is part of the inpatient medical record. It is used to keep
laboratory report forms neat, in proper order, make them easily accessible to
caregivers, and stores them as part of the inpatient medical record. SF-545,
Clinical Record - Laboratory Report Display may be used in lieu of SF-514.
(2) Preparation.
(a) When Prepared. SF-514/SF-545 shall be prepared when a patient is
admitted to the inpatient medical area.
(b) Required Entries.
1 Patient identification information may be written in or overprinted
using a patient identification card.
2 Reports (or chits) may be attached to the form using either the self
adhesive on the back of the chit, or by neatly placing a strip of clear
adhesive tape horizontally across the top of the report, so that the
lower half of the tape strip is touching the chit and the upper half is
sticking to the SF-514/SF-545.
f. SF-519, Radiologic Consultation Reports.
(1) Purpose. SF-519 is part of the inpatient medical record. It is used to collect
radiologic reports for easy access by caregivers and to store the reports with the
inpatient medical record.
(2) Preparation.
(a) When Prepared. SF-519 shall be prepared when a patient is admitted to
the inpatient medical area.
(b) Required Entries. Reports shall be attached to the form using the self
stick adhesive on the back of the report or clear adhesive tape.
g. DD-2770 (replaces SF 539) Abbreviated Medical Record. See Encl (1), pg. 4-52.

4-79 CH 17
(1) Purpose. DD-2770 is used to record history, exam findings, patient progress,
doctor's orders, vital signs, output, medications and nurse's notes for patients
requiring overnight care who remain 24 hours or less.
(2) Preparation.
(a) When Prepared. DD-2770 may be used for any overnight care patient for
whom total stay is anticipated to be 24 hours or less. If length of stay
exceeds 24 hours, a full IMR must be initiated to provide proper
documentation of the patient's stay. The DD-2770 shall be prepared
when a short stay patient is admitted to the inpatient medical area.
(b) Required Entries.
1 Patient identification information may by written in or overprinted
using a patient identification card.
2 History, chief complaint, and condition on admission must be
documented in the top box on page one. Date of admission shall be
noted here also.
3 Physical examination findings shall be noted in the center box on
page one. Physical exam findings shall be completely noted and
appropriate to the condition. Deferred exams, such as rectal exams,
shall be noted as such.
4 The patient's progress over the 24 hour period between admission
and discharge will be noted by the medical officer in the third box
on page one. Date of discharge and final diagnosis shall be noted
here also.
5 The physician shall sign the form in the box provided and use a
printed ink stamp to clearly mark his/her name, rank, and SSN. The
date the form is signed shall be written in the box provided next to
the signature.
6 The location of the clinic or dispensary, for example, Dispensary
TRACEN Cape May, shall be written or stamped in the box marked
organization.
7 Doctor's orders shall be written only in the space provided on page
two. Each order group written shall be dated and signed. A printed
ink stamp shall be used by medical officers to mark name, rank, and
SSN. All medical and dental orders given during the patient's stay
must be recorded. A second page should be started if the number of
orders exceeds space available on one page.

CH-17 4-80
8 Vital sign measurements shall be recorded in the spaces provided
with the date and time of each notation. Bowel movements and
urine output are noted in the columns marked stools and weight.
9 Medications administered and brief notes regarding the patient's
condition shall be made in the nurse's notes area. Medication name,
dose, route, and time given shall be recorded for each dose of
medication administered. Each notation shall be signed with the
name, military rank, or title for civilians, e.g., RN or LPN, of the
person making the note.
4-81 CH 17
Section G – Mental Health Records.
1. Active duty: Complete mental health assessments and visits will be done in an IMB,
DMB or traditional psychiatric evaluation format and recorded on SF-600, SF-513, IMB,
DMB, or typed psychiatric evaluation forms as appropriate. Active duty episodic visits
and routine appointments will be recorded on SF-600 in SOAP format. The Objective
(“O’) section would include mental status observations and any other pertinent physical
findings. Records of active duty mental health assessments and visits will be kept in the
main health record (CG-3443). An additional separate mental health record may be
created and maintained in a system of records approved by the local QA Committee and
kept secure in the mental health practitioner’s office. New patients would be evaluated
IAW traditional psychiatric evaluation.
2. Non- Active duty: Separate records of mental health care may be created and maintained
in a system of records approved by the local QA Committee and kept secure in the
mental health practitioner’s office. Alternatively, the mental health practitioner may
elect to keep records of visits in the dependent or retiree’s main based record (CG-3443-
1). Should the practitioner elect to maintain a separate office based record for non-active
duty patients, the main health record (orange jacket) must include, at a minimum, the
diagnosis in the problem summary listing, current psychiatric medications on the SF-600,
and lab work ordered by the mental health provider. New patients would be evaluated
IAW traditional psychiatric evaluation. Episodic and follow up visits would be recorded
in a SOAP format.
3. Psychiatric evaluation format: The psychiatric evaluation shall include, at a minimum:
patient information, chief complaint, history of present illness, past history (psychiatric
symptoms, diagnoses, and care medical illness, surgeries, current medications, allergies,
alcohol & drug history), personal history, family history, mental status exam, assessment
(DSM-IV), prognosis, and plan. Included in all assessments and other visits as
appropriate will be an estimation of potential for harm to self or others. In addition,
notes should contain sufficient information to establish that the criteria for any new DSM
based diagnosis are met.
4. Custody of Mental Health Records: Records kept in the mental health practitioner’s
office are property of the CG and copies should be available to other civilian
practitioners or agencies at the patient’s request. These records should also be available
to other CG providers, as part of an official records review process, and as directed in
Section 4.A.5. of this Manual.
CH-17 4-82
This Page Left Blank
Encl. (1) to CHAP 4, COMDTINST M6000.1B
HEALTH RECORD COVER
Last Name First Middle
0 1 2 3 4 5 6 7 8 9
0 Blood
Type Rh 0
1 1
YY MM DD
2
Special Status
□ Aviation
□ OMMP
□ Waiver
□________
Date of Birth 2
3
Place
Sensitivity Sticker
Here
(if needed)
U.S. Coast Guard 3
4 HEALTH RECORD
PRIVACY STATEMENT; HEALTH CARE RECORDS 4
5 5
6 6
7 7
8 8
9
1. AUTHORITY FOR COLLECTION OF INFORMATION INCLUDING SOCIAL SECURITY
NUMBER (SSN): Section 632 of Title14, United States Code and Section 1071-1087, Title 10
United States Code, Executive Order 9397.
2. PRINCIPLE PURPOSE FOR WHICH INFORMATION IS TO BE USED:
The purpose for requesting personal information is to assist health care personnel in
developing records to facilitate and document your health in order to provide health care and to
provide a complete account of such care rendered including diagnosis, treatment, and end
result. The SSN is necessary to identify the person and records.
3. ROUTINE USES; This information may be used to plan and coordinate health care. It may
be used to provide health care, conduct research, teach, complile statistical data, determine
suitability of persons for service or assignment, implement, preventive health and
communicative disease control programs, adjudicate claims and determine benefits, evalutate
care rendered, determine professional certification and hospital accreditation, conduct
authorized investigations, provide physical qualifications of patients to other Federal, State,
and local agencies uopn request in the pursuit of their official duties, and report health
conditions required by law to Federal, State, and local agencies. It may be used for other
lawful purposes, including law enforcement and litigation.
4. The above Privacy Act Statement applies to all requests for personal information made by
health care personnel or for health care purposes. Failure to provide the requested information
for these health records may result in an inability of Coast Guard health care personnel to
afford treatment.
5. No information may be divulged from this record except to persons properly and directly
concerned. Questionable cases will be referred to the commanding officer for decision. 9
DEPT. OF TRANSP, USCG, CG-3443 (REV 9-92) SN 7530-00-F01-4180
PREVIOUS EDITIONS ARE OBSOLETE
4-1 CH-17
BACK
ADULT PREVENTIVE AND CHRONIC CARE FLOWSHEET
(
This form is sub
j
ect to the Privac
y
Act of 1974
–
Use DD form 2005
)
1. ALLERGIES
a. MEDICATION ALLERGIES b. OTHER ALLERGIES
2. CHRONIC ILLNESS 3. MEDICATIONS
4. HOSPITALIZATIONS/SURGERIES
5. COUNSELING
F FITNESS a. DATE
D DENTAL b. AGE
I INJURY PREVENTION
N NUTRITION/FOLATE
C CANCER PREVENTION
c. TOPIC
S SAFE SEX d. DATE
FP FAMILY PLANNING e. AGE
Rx PRESENT MEDICATIONS
MH MENTAL HEALTH/STRESS/SUICIDE/
OCCUPATIONAL STRESS
f. TOPIC
H HORMONE/CALCIUM REPLACEMENT g. DATE
To TOBACCO h. AGE
A ALCOHOL/SUBSTANCE ABUSE
t TRAVEL
i. TOPIC
O. OCCUPATIONAL EXPOSURE (HEARING
THRESHOLD CHANGES/CUMULATIVE
TRAUMA DISORDER) j. DATE
k. AGE
i. TOPIC
ADVANCE DIRECTIVES: DATE FILED RECORDS MAINTAINED AT:
PATIENT’S NAME
LAST FIRST M.I. SEX
RELATIONSHIP TO SPONSOR STATUS
R
RANK/GRADE
SPONSOR’S NAME (Last ,First, Middle Initial) DEPT/SERVICE
PATIENT’S IDENTIFICATION (Use this space for mechanical imprint)
SUPPLIED (Navy)
2766-0102-LF-984-8400, pkg-100
ORGANIZATION SSN/ID NUMBER DATE OF BIRTH
DD FORM 2766, (Rev 01- 00) PAGE 1 of 4 PAGES
CH-17 4-2
Encl. (1) to CHAP 4, COMDTINST M6000.1B
BACK
ADULT PREVENTION AND CHRONIC CARE FLOWSHEET
6. FAMILY HISTORY (M = Mother, F = Father, S = Sibling, MGM = Maternal Grandmother, MGF = Maternal grandfather,
PGM = Paternal Grandmother, PGF = Paternal Grandfater)
a. CANCER (Specify)
b. CARDIOVASCULAR DISEASE (Specify)
c. DIABETES (Specify)
d. MENTAL ILLNESS/CHEMICAL DEPENDENCY
(Specify)
7. SCREENING EXAMS ( * = Actual Result, * * = Tricare Benefit, N = Normal, X = Abnormal, E = Done Elsewhere, R = Refuse
d
NA = Not Indicated) (
∙
= Next Due)
c. YEAR
a. TEST b. FREQUENCY d. AGE
e. DATES
(1) CLINICAL DISEASE
PREV EVAL/PHA (HEAR) ANNUAL ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
* (2) WEIGHT ANNUAL FOR ACTIVE DUTY ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
* (3) HEIGHT ANNUAL FOR ACTIVE DUTY ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
* (4) BLOOD PRESSURE ONCE q 2 YRS for BP<
130/85, ANNUAL IF GREATER ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
* (5) CHOLESTEROL** *q 5 YRS FOR AGE ≥
≥≥
≥ 18
q YR if PREV ABN ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(6) HEARING CLINICAL DISCRETION ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(7) SKIN EXAM (Cancer) ANNUAL IF AT RISK ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(8) ORAL/DENTAL ** ANNUAL ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(9) EYE/VISION **
ROUTINE ACUITY WITH
PERIODIC ASSESSMENT
DIABETES ANNUAL
GLAUCOMA CHECK:
Blacks q 3-5 yrs age 20-39
All q 2-4 years age 40-64
○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(10) BREAST EXAM ANNUAL: ≥
≥≥
≥ 40 YRS ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(11) MAMMOGRAM ** BASELINE@ 40, q 2 YRS 40-50,
ANNUALLY > 50 ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(12) PAP
** (Digital Rectal Exam)
BASELINE: AGE 18 OR ONSET OF
SEXUAL ACTIVITY
AFTER 3 NL ANUUAL EXAMS,
PERFORM q 1-3 years
○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(13) FECAL OCCULT
BLOOD ANNUAL ≥
≥≥
≥ 50 yrs ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(14) SIGMOID EVERY 3-5 YRS: ≥
≥≥
≥ 50 YRS ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(15) COLONOSCOPY HIGH RISK q 5 YRS ≥
≥≥
≥ YRS ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(16) TESTICULAR HIGH RISK ANNUAL 13-39 YRS ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(17) PROSTATE **
**( DIGITAL RECTAL EXAM) WITH P.E. ≥
≥≥
≥ 40 YRS (Presently
Recommended annually) ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(18) RUBELLA SCREEN
(Females) ONCE BETWEEN AGES 12 –18
YRS (Unless prev vaccinated) ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(19) OCCUPATIONAL
SCREENING EXAMS APPROPRIATE TO EXPOSURES ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(20) ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(21) ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
(22) ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○ ○
○○
○
DD FORM 2766, (Rev 01-00) PAGE 2 OF 4 PAGES
4-3 CH-17
Encl. (1) to CHAP 4, COMDTINST M6000.1B
ADULT PREVENTION AND CHRONIC CARE FLOWSHEET
8. OCCUPATIONAL HISTORY/RISK
a. PRP YES NO
b. .FLYING STATUS YES NO
9. IMMUNIZATIONS (Enter numeric class in sub block)
(1)
IMMUNIZATION (2) DATE
(ddmmmyyyy) (1)
IMMUNIZATION (2) DATE
(DDMMMYYYY) (1)
IMMUNIZATION (2) DATE
(ddmmmyyyy) (1)
IMMUNIZATION (2) DATE
(ddmmmyyyy)
a. HEP A # 1 f. MMR # 1 j. TD (q 10 YRS)
(Last)
b. HEP A # 2 g. MMR #2 k. TD (DUE)
c. HEP B # 1 h.
PNEUMOCOCCUS I. YELLOW
FEVER (LAST)
d. HEP B #2 i. POLIO OPV =
O IPV = I m. YELLOW
FEVER
n. TYPHOID (Enter numeric class in sub
block) ORAL = O
TYPHUM Vi = 1. TYPHOID USP = 2
(1)
DATE
(2)
DATE
(3)
DATE
(4)
DATE
(5)
DATE
(6)
DATE
O. ANTHRAX
(1) INITIAL DATE (2) 2 WEEK DATE (3) 4 WEEK DATE (4) 6 MONTH DATE (5) 12 MONTH DATE (6) 18 MONTHDATE
(1) (a) mm (2) (a) mm (3) (a) mm (4) (a) mm (5) (a) mm (6) (a) mm (7) (a) mm
p. PPD (Enter
mm and date) (b) DATE (b) DATE (b) DATE (b) DATE (b) DATE (b) DATE (b) DATE
q. INFLUENZA (1) DATE (2) DATE (3) DATE (4) DATE (5) DATE (6) DATE (7) DATE
r. VARICELLA
(1) DATE (2) DATE u. JAPANESE B
ENCEPHALITIS
(1) DATE (2) DATE (3) DATE (4) DATE
s. MENINGO (1) DATE (2) DATE v. OTHER (Specify) (1) DATE (2) DATE (3) DATE
t. ADENO (1) DATE (2) DATE w. OTHER (Specify (1) DATE (2) DATE (3) DATE
10. READINESS (Glucose-6-phosphate dehydrogenase)
a. DNA DATE: b. BLOOD
TYPE DATE: RESULT: c. G-PD DATE RESULT: d. SICKLE
CELL DATE: RESULT:
e. PERMANENT PROFILE CHANGE (1) DATE (2) P: (3) U: (4) L: (5) H: (6) E: (7) S:
f. GLASSES/GAS/MASK
Rx:
(1) DATE (2) DATE (3) DATE (4) DATE (5) DATE (6) DATE
g. DENTAL EXAM (Enter numeric
class in sub block)
(1) DATE
(2) DATE
(3) DATE
(4) DATE
(5) DATE
(6) DATE
h. HIV TESTING (1) DATE (2) DATE (3) DATE (4) DATE (5) DATE (6) DATE
I. FITNESS (In sub block enter
P = Pass, F = Fail, W = Waiver)
(1) DATE
(2) DATE
(3) DATE
(4) DATE
(5) DATE
(6) DATE
(1) DATE
(2) DATE
(3) DATE
(4) DATE
(5) DATE
(6) DATE
(1) DATE
(2) DATE
(3) DATE
(4) DATE
(5) DATE
(6) DATE
11. PRE/POST DEPLOYMENT HISTORY
a. LOCATION
(1) PREDEPLOYMENT (a) DATE (b) DATE (c) DATE (d) DATE (e) DATE (f) DATE
(2) POSTDEPLOYMENT (a) DATE (b) DATE (c) DATE (d) DATE (e) DATE (f) DATE
b. LOCATION
(1) PREDEPLOYMENT (a) DATE (b) DATE (c) DATE (d) DATE (e) DATE (f) DATE
(2) POSTDEPLOYMENT (a) DATE (b) DATE (c) DATE d) DATE (e) DATE (f) DATE
c. CHART AUDIT
DD FORM 2766, (Rev 01-00) PAGE 3 OF 4 PAGES
Encl. (1) to CHAP 4, COMDTINST M6000.1B
4
-4
CH-17
ADULT PREVENTIVE AND CHRONIC CARE FLOWSHEET
(Continuation Sheet)
DATES
TEST FREQUENCY (a) (b) (c) (d) (e) (f)
REMARKS
RECORDS MAINTAINED AT:
PATIENT’S NAME
LAST FIRST M.I. SEX
RELATIONSHIP TO SPONSOR STATUS RANK/GRADE
SPONSOR’S NAME (Last, First, Middle Initial) DEPT/SERVICE
ORGANIZATION SSN/ID NUMBER DATE OF BIRT
H
DD FORM 2766, (Rev-01-00) PAGE 4 OF 4 PAGES
4-5 CH-17
Encl. (1) to CHAP 4, COMDTINST M6000.1B
CH 17 4-6
Encl. (1) to CHAP 4, COMDTINST M6000.1B BACK
PREVIOUS EDITION IS USABLE AUTHORIZED FOR LOCAL REPRODUCTION
MEDICAL RECORD CHRONOLOGICAL RECORD OF MEDICAL CARE
DATE SYMPTOMS, DIAGNOSIS, TREATMENT, TREATING ORGANIZATION (sign each entry)
HOSPITAL OR MEDICAL FACILITY STATUS DEPART/SERVICE RECORDS MAINTAINED AT
SPONSOR’S NAME SSN/ID NO. RELATIONSHIP TO SPONSOR
PATIENT’S IDENTIFICATION: (FOR TYPED OR WRITTEN ENTRIES, GIVE: name-last, first, middle ID
NO or SSN; Sex; Date of Birth; Rank/Grade.); REGISTER NO. WARD NO.
CHRONOLOGICAL RECORD OF MEDICAL CARE
Medical Record
STANDARD FORM 600 (Rev. 6-97)
Prescribed by GSA/ICMR
FIRMR 941 CFR) 201-9.202-1
BACK
REPORT OF MEDICAL EXAMINATION 1. DATE OF EXAMINATION
(YYYYMMDD)
3. LAST NAME - FIRST NAME - MIDDLE NAME
(SUFFIX)
2. SOCIAL SECURITY NUMBER
6. GRADE
4. HOME ADDRESS (Street, Apartment Number, City, State and ZIP Code) 5. HOME TELEPHONE
NUMBER
(Include Area Code)
7. DATE OF BIRTH
(YYYYMMDD) 8. AGE 9. SEX
Female
Male
10. RACE
WhiteBlack
American Indian/Alaskan Native
12. AGENCY (Non-Service Members Only) 13. ORGANIZATION UNIT AND UIC/CODE
11. TOTAL YEARS GOVERNMENT SERVICE
a. MILITARY b. CIVILIAN
16. NAME OF EXAMINING LOCATION, AND ADDRESS
(Include ZIP Code)
14.a. RATING OR SPECIALTY (Aviators Only) b. TOTAL FLYING TIME
44. NOTES: (Describe every abnormality in detail. Enter pertinent item
number before each comment. Continue in item 73 and use additional
sheets if necessary.)
DoD exception to SF 88 approved by ICMR, August 3, 2000.
PREVIOUS EDITION MAY BE USED UNTIL FEBRUARY 1, 2002.
Asian/Pacific Islander
c. LAST SIX MONTHS
15.a. SERVICE
Army
Navy
Marine Corps
Air Force
Active Duty
Reserve
National Guard
c. PURPOSE OF EXAMINATION
Enlistment
Commission
Retention
Separation
Medical Board
Retirement
U.S. Service Academy
ROTC Scholarship Program
Other
Nor-
mal Ab-
norm NE
17. Head, face, neck, and scalp
18. Nose
19. Sinuses
20. Mouth and throat
22. Drums (Perforation)
23. Eyes - General (Visual acuity and refraction under items 61 - 63)
24. Ophthalmoscopic
25. Pupils (Equality and reaction)
26. Ocular motility (Associated parallel movements, nystagmus)
21. Ears - General (Int. and ext. canals/Auditory acuity under item 71)
27. Heart (Thrust, size, rhythm, sounds)
28. Lungs and chest (Include breasts)
29. Vascular system (Varicosities, etc.)
30. Anus and rectum (Hemorrhoids, Fistulae) (Prostate if indicated)
31. Abdomen and viscera (Include hernia)
32. External genitalia (Genitourinary)
33. Upper extremities
34. Lower extremities (Except feet)
35. Feet (See Item 35 Continued)
36. Spine, other musculoskeletal
37. Identifying body marks, scars, tattoos
38. Skin, lymphatics
39. Neurologic
40. Psychiatric (Specify any personality deviation)
41. Pelvic (Females only)
42. Endocrine
43. DENTAL DEFECTS AND DISEASE
35. FEET (Continued) (Circle category)
Normal Arch
Pes Cavus
Pes Planus
Mild
Moderate
Severe
Asymptomatic
Symptomatic
DD FORM 2808, JUL 2001 Page 1 of 3 Pages
CLINICAL EVALUATION (Check each item in appropriate column. Enter "NE" if not evaluated.)
b. COMPONENT
Coast
Guard
PRIVACY ACT STATEMENT
AUTHORITY: 10 USC 504, 505, 507, 532, 978, 1201, 1202, and 4346; and E.O. 9397.
PRINCIPAL PURPOSE(S): To obtain medical data for determination of medical fitness for enlistment, induction, appointment and retention for
applicants and members of the Armed Forces. The information will also be used for medical boards and separation of Service members from
the Armed Forces.
ROUTINE USE(S): None.
DISCLOSURE: Voluntary; however, failure by an applicant to provide the information may result in delay or possible rejection of the
individual's application to enter the Armed Forces. For an Armed Forces member, failure to provide the information may result in the individual
being placed in a non-deployable status.
Class
Acceptable
Not Acceptable
(Please explain. Use dental form if completed
by dentist. If dental examination not done by
dental officer, explain in Item 44.)
Reset
BACK
MEASUREMENTS AND OTHER FINDINGS
53. HEIGHT 54. WEIGHT 56. TEMPERATURE
58. BLOOD PRESSURE
a. 1ST
SYS.
DIAS.
b. 2ND
SYS.
DIAS.
c. 3RD
SYS.
DIAS.
57. PULSE
61. DISTANT VISION
Right 20/
Left 20/
Corr. to 20/
Corr. to 20/
62. REFRACTION BY AUTOREFRACTION OR MANIFEST
By
By
S.
S.
CX
CX
63. NEAR VISION
Right 20/
Left 20/
Corr. to 20/
Corr. to 20/
by
by
64. HETEROPHORIA (Specify distance)
ES EX R.H. L.H. Prism div. Prism Conv
CT NPR PD
65. ACCOMMODATION
Right Left
66. COLOR VISION (Test used and result) 67. DEPTH PERCEPTION (Test used and score) AFVT
PIP /14
68. FIELD OF VISION
59. RED/GREEN (Army Only)
71a. AUDIOMETER
Right
Left
500 1000 2000 3000 4000 6000
73. NOTES (Continued) AND SIGNIFICANT OR INTERVAL HISTORY (Use additional sheets if necessary.)
60. OTHER VISION TEST
Uncorrected Corrected
69. NIGHT VISION (Test used and score) 70. INTRAOCULAR TENSION
O.D.
72a. READING ALOUD
TEST
DD FORM 2808, JUL 2001 Page 2 of 3 Pages
LAST NAME - FIRST NAME - MIDDLE NAME (SUFFIX) SOCIAL SECURITY NUMBER
HZ
Unit Serial Number
Date Calibrated (YYYYMMDD)
a. Albumin
b. Sugar
LABORATORY FINDINGS
TESTS
46. URINE HCG 47. H/H
RESULTS
49. HIV
50. DRUGS
51. ALCOHOL
52. OTHER
a. PAP SMEAR
b.
c.
HIV SPECIMEN ID LABEL DRUG TEST SPECIMEN ID LABEL
55. MIN WGT - MAX WGT
O.S.
SAT UNSAT
45. URINALYSIS
MAX BF %
lbs.
Right
Left
500 1000 2000 3000 4000 6000
HZ
71b. Unit Serial Number
Date Calibrated (YYYYMMDD)
48. BLOOD TYPE
72b. VALSALVA
SAT UNSAT
Reset
b. PHYSICAL PROFILE
PU L H E S X
74.a. EXAMINEE/APPLICANT (check one)
IS QUALIFIED FOR SERVICE
IS NOT QUALIFIED FOR SERVICE
76. SIGNIFICANT OR DISQUALIFYING DEFECTS
DD FORM 2808, JUL 2001 Page 3 of 3 Pages
75. I have been advised of my disqualifying condition.
a. SIGNATURE OF EXAMINEE b. DATE (YYYYMMDD)
LAST NAME - FIRST NAME - MIDDLE NAME (SUFFIX) SOCIAL SECURITY NUMBER
PROFILER INITIALS DATE (YYYYMMDD)
ITEM
NO. MEDICAL CONDITION/DIAGNOSIS ICD
CODE PROFILE
SERIAL RBJ DATE
(YYYYMMDD) SERVICE DATE (YYYYMMDD)
EXAMINER
INITIALS WAIVER RECEIVED
80. MEDICAL INSPECTION DATE HT WT %BF HCG QUAL DISQ PHYSICIAN'S SIGNATUREMAX WT
81.a. TYPED OR PRINTED NAME OF PHYSICIAN OR EXAMINER b. SIGNATURE
83.a. TYPED OR PRINTED NAME OF DENTIST OR PHYSICIAN (Indicate which) b. SIGNATURE
84.a. TYPED OR PRINTED NAME OF REVIEWING OFFICER/APPROVING AUTHORITY b. SIGNATURE
87. NUMBER OF
ATTACHED SHEETS
85. This examination has been administratively reviewed for completeness and accuracy.
a. SIGNATURE c. DATE (YYYYMMDD)b. GRADE
86. WAIVER GRANTED (If yes, date and by whom)
YES
NO
82.a. TYPED OR PRINTED NAME OF PHYSICIAN OR EXAMINER b. SIGNATURE
77. SUMMARY OF DEFECTS AND DIAGNOSES (List diagnoses with item numbers) (Use additional sheets if necessary.)
78. RECOMMENDATIONS - FURTHER SPECIALIST EXAMINATIONS INDICATED (Specify) (Use additional sheets if necessary.)
79. MEPS WORKLOAD (For MEPS use only)
WKID ST DATE (YYYYMMDD) INITIAL WKID ST DATE (YYYYMMDD) INITIAL
QUALI-
FIED DIS-
QUALI-
FIED
Reset
X ALL APPLICABLE BOXES:
WARNING: The information you have given constitutes an official statement. Federal law provides severe penalties (up to 5 years confine-
ment or a $10,000 fine or both), to anyone making a false statement. If you are selected for enlistment, commission, or entrance into a
commissioning program based on a false statement, you can be tried by military courts-martial or meet an administrative board for discharge
and could receive a less than honorable discharge that would affect your future.
REPORT OF MEDICAL HISTORY
(This information is for official and medically confidential use only and will not be released to unauthorized persons.)
Form Approved
OMB No. 0704-0413
Expires Aug 31, 2003
The public reporting burden for this collection of information is estimated to average 10 minutes per response, including the time for reviewing instructions, searching existing data sources,
gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection
of information, including suggestions for reducing the burden, to Department of Defense, Washington Headquarters Services, Directorate for Information Operations and Reports
(0704-0413), 1215 Jefferson Davis Highway, Suite 1204, Arlington, VA 22202-4302. Respondents should be aware that notwithstanding any other provision of law, no person shall be
subject to any penalty for failing to comply with a collection of information if it does not display a currently valid OMB control number.
PLEASE DO NOT RETURN YOUR FORM TO THE ABOVE ADDRESS. RETURN COMPLETED FORM AS INDICATED ON PAGE 2.
1. LAST NAME, FIRST NAME, MIDDLE NAME (SUFFIX) 2. SOCIAL SECURITY NUMBER 3. TODAY'S DATE (YYYYMMDD)
4.a. HOME ADDRESS (Street, Apartment No., City, State, and ZIP Code)
b. HOME TELEPHONE (Include Area Code)
5. EXAMINING LOCATION AND ADDRESS (Include ZIP Code)
Army
Navy
Marine Corps
Air Force
Active Duty
Reserve
National Guard
c. PURPOSE OF EXAMINATION
Enlistment
Commission
Retention
Separation
Medical Board
Retirement
U.S. Service Academy
ROTC Scholarship Program
Other (Specify)
7.a. POSITION (Title, Grade, Component)
b. USUAL OCCUPATION
8. CURRENT MEDICATIONS (Prescription and Over-the-counter) 9. ALLERGIES (Including insect bites/stings, foods, medicine or other substance)
HAVE YOU EVER HAD OR DO YOU NOW HAVE: YES NO
c. Coughed up blood
d. Asthma or any breathing problems related to exercise, weather,
pollens, etc.
e. Shortness of breath
f. Bronchitis
YES NO
11.a. Severe tooth or gum trouble
b. Thyroid trouble or goiter
c. Eye disorder or trouble
d. Ear, nose, or throat trouble
e. Loss of vision in either eye
f. Worn contact lenses or glasses
g. A hearing loss or wear a hearing aid
c. Recurrent back pain or any back problem
d. Numbness or tingling
e. Loss of finger or toe
b. Recent unexplained gain or loss of weight
c. Currently in good health (If no, explain in Item 29 on Page 2.)
d. Tumor, growth, cyst, or cancer
k. Any need to use corrective devices such as prosthetic devices, knee
brace(s), back support(s), lifts or orthotics, etc.
l. Bone, joint, or other deformity
m. Plate(s), screw(s), rod(s) or pin(s) in any bone
n. Broken bone(s) (cracked or fractured)
DD FORM 2807-1, JUL 2001 DoD exception to SF 93 approved by ICMR, August 3, 2000.
PREVIOUS EDITION MAY BE USED UNTIL FEBRUARY 1, 2002.
13.a. Frequent indigestion or heartburn
b. Stomach, liver, intestinal trouble, or ulcer
14.a. Adverse reaction to serum, food, insect stings or medicine
l. Sexually transmitted disease (syphilis, gonorrhea, chlamydia, genital
warts, herpes, etc.)
j. Any knee or foot surgery including arthroscopy or the use of a scope
to any bone or joint
12.a. Painful shoulder, elbow or wrist (e.g. pain, dislocation, etc.)
b. Arthritis, rheumatism, or bursitis
h. Surgery to correct vision (RK, PRK, LASIK, etc.)
j. Sinusitis
k. Hay fever
l. Chronic or frequent colds
g. Wheezing or problems with wheezing
i. A chronic cough or cough at night
h. Been prescribed or used an inhaler
10.a. Tuberculosis
b. Lived with someone who had tuberculosis
Page 1 of 3 Pages
c. Gall bladder trouble or gallstones
d. Jaundice or hepatitis (liver disease)
e. Rupture/hernia
g. Skin diseases (e.g. acne, eczema, psoriasis, etc.)
h. Frequent or painful urination
i. High or low blood sugar
j. Kidney stone or blood in urine
k. Sugar or protein in urine
f. Rectal disease, hemorrhoids or blood from the rectum
6.a. SERVICE
12. (Continued)
f. Foot trouble (e.g., pain, corns, bunions, etc.)
g. Impaired use of arms, legs, hands, or feet
h. Swollen or painful joint(s)
i. Knee trouble (e.g., locking, giving out, pain or ligament injury, etc.)
PRIVACY ACT STATEMENT
AUTHORITY: 10 USC 504, 505, 507, 532, 978, 1201, 1202, and 4346; and E.O. 9397.
PRINCIPAL PURPOSE(S): To obtain medical data for determination of medical fitness for enlistment, induction, appointment and retention for applicants and
members of the Armed Forces. The information will also be used for medical boards and separation of Service members from the Armed Forces.
ROUTINE USE(S): None.
DISCLOSURE: Voluntary; however, failure by an applicant to provide the information may result in delay or possible rejection of the individual's application to enter
the Armed Forces. For an Armed Forces member, failure to provide the information may result in the individual being placed in a non-deployable status.
b. COMPONENT
Coast
Guard
Mark each item "YES" or "NO". Every item marked "YES" must be fully explained in Item 29 on Page 2.
Reset
BACK
a. Sensitivity to chemicals, dust, sunlight, etc.
b. Inability to perform certain motions
c. Inability to stand, sit, kneel, lie down, etc.
d. Other medical reasons (If yes, give reasons.)
19. Have you been refused employment or been unable to hold a job
or stay in school because of:
28. Have you ever been denied life insurance?
22. Have you ever had, or have you been advised to have any
operations or surgery? (If yes, describe and give age at which
occurred.)
21. Have you ever been a patient in any type of hospital? (If yes,
specify when, where, why, and name of doctor and complete
address of hospital.)
20. Have you ever been treated in an Emergency Room?
(If yes, for what?)
24. Have you consulted or been treated by clinics, physicians,
healers, or other practitioners within the past 5 years for
other than minor illnesses? (If yes, give complete address
of doctor, hospital, clinic, and details.)
25. Have you ever been rejected for military service for any
reason? (If yes, give date and reason for rejection.)
26. Have you ever been discharged from military service for any
reason? (If yes, give date, reason, and type of discharge;
whether honorable, other than honorable, for unfitness or
unsuitability.)
27. Have you ever received, is there pending, or have you ever
applied for pension or compensation for any disability
or injury? (If yes, specify what kind, granted by whom,
and what amount, when, why.)
23. Have you ever had any illness or injury other than those
already noted? (If yes, specify when, where, and give details.)
29. EXPLANATION OF "YES" ANSWER(S) (Describe answer(s), give date(s) of problem, name of doctor(s) and/or hospital(s), treatment given and current medical
status.)
NOTE: HAND TO THE DOCTOR OR NURSE, OR IF MAILED MARK ENVELOPE "TO BE OPENED BY MEDICAL PERSONNEL ONLY."
DD FORM 2807-1, JUL 2001 Page 2 of 3 Pages
LAST NAME, FIRST NAME, MIDDLE NAME (SUFFIX) SOCIAL SECURITY NUMBER
b. Habitual stammering or stuttering
c. Loss of memory or amnesia, or neurological symptoms
17.a. Nervous trouble of any sort (anxiety or panic attacks)
e. Received counseling of any type
d. Frequent trouble sleeping
g. Been evaluated or treated for a mental condition
h. Attempted suicide
i. Used illegal drugs or abused prescription drugs
f. Depression or excessive worry
18. FEMALES ONLY. Have you ever had or do you now have:
a. Treatment for a gynecological (female) disorder
b. A change of menstrual pattern
c. Any abnormal PAP smears
d. First day of last menstrual period (YYYYMMDD)
e. Date of last PAP smear (YYYYMMDD)
YES NO YES NO
15.a. Dizziness or fainting spells
b. Frequent or severe headache
c. A head injury, memory loss or amnesia
d. Paralysis
e. Seizures, convulsions, epilepsy or fits
f. Car, train, sea, or air sickness
g. A period of unconsciousness or concussion
h. Meningitis, encephalitis, or other neurological problems
c. Pain or pressure in the chest
d. Palpitation, pounding heart or abnormal heartbeat
e. Heart trouble or murmur
f. High or low blood pressure
b. Prolonged bleeding (as after an injury or tooth extraction, etc.)
16.a. Rheumatic fever
Mark each item "YES" or "NO". Every item marked "YES" must be fully explained in Item 29 below.
HAVE YOU EVER HAD OR DO YOU NOW HAVE:
Reset
a. COMMENTS
b. TYPED OR PRINTED NAME OF EXAMINER (Last, First, Middle Initial) d. DATE SIGNED
(YYYYMMDD)
c. SIGNATURE
DD FORM 2807-1, JUL 2001 Page 3 of 3 Pages
LAST NAME, FIRST NAME, MIDDLE NAME (SUFFIX) SOCIAL SECURITY NUMBER
30. EXAMINER'S SUMMARY AND ELABORATION OF ALL PERTINENT DATA (Physician/practitioner shall comment on all positive answers in
questions 10 - 29. Physician/practitioner may develop by interview any additional medical history deemed important, and record any
significant findings here.)
Reset
4-13 CH-17 17
Encl. (1) to CHAP 4, COMDTINST M6000.1B
NSN 7540-01-075-3786
LOG NUMBER TREATMENT FACILITY
MEDICAL RECORD EMERGENCY CARE
AND TREATMENT
(Patient) RECORDS MAINTAINED AT
PATIENT’S HOME ADDRESS OR DUTY STATION ARRIVAL
STREET ADDRESS DATE (Day, Month, Year) TIME
CITY STATE ZIP CODE TRANSPORTATION TO FACILITY
DUTY/LOCAL PHONE MILITARY STATUS THIRD PARTY INSURANCE
ITEM YES NO N/A ITEM YES NO
SEX
AREA CODE NUMBER
PRP ADDITIONAL INSURANCE
HOME PHONE FLYING STATUS DD 2568 IN CHART
AGE
NUMBER
MEDICAL HISTORY OBTAINED FROM NAME OF INSURANCE COMPANY
INJURY OR OCCUPATIONAL ILLNESS EMERGENCY ROOM VISIT
YES NO
WHEN (DATE) DATE LAST VISIT 24 HOUR RETURN
□ YES □ NO
CURRENT MEDICATIONS
IS THIS AN INJURY TETANUS
INJURY/SAFETY
FORMS
WHERE
ALLERGIES
HOW
DATE LAST SHOT COMPLETED INITIAL SERIES
□ YES □ NO
CHIEF COMPLAINT
CATEGORY OF TREATMENT VITAL SIGNS
TIME
B/P
TIME
PULSE
RESP
TEMP
□ EMERGENT
□ URGENT
□ NON-URGENT
INITIALS
WT
CBC/DIFF ABG PT/PTT BHCG/URINE/BLOOD/QUANT CXR PA & LAT/
PORTABLE
C-SPINE
URINE C&S UA CHEM:
ACUTE ABDOMEN LS SPINE
BLOOD C&S X ANKLE R/L HEAD CT
LAB ORDERS
X-RAY
ORDERS
ORDERS
□ PULSE OX □ MONITOR □ ECG
TIME ORDERS BY COMPLETED BY TIME PATIENT’S RESPONSE
DISPOSITION
□ HOME □ FULL DUTY
DISPOSITION QUARTERS/OFF DUTY
□ 24 HRS. □ 48 HRS. □ 78 HRS
MODIFIED DUTY UNTIL RETURN TO DUTY
PATIENT/DISCHARGE INSTRUCTIONS
ADMIT TO UNIT/SERVICE REFERRED TO WHEN
I have received and understand these
instructions.
CONDITION UPON RELEASE
□ IMPROVED □ UNCHANGED
□ DETERIORATED
TIME OF RELEASE
PATIENT’S IDENTIFICATION (For typed or written entries, give: name-last, first,
middle; ID no. (SSN or other); hospital or medical facility)
PATIENT’S SIGNATURE
EMERGENCY CARE AND TREATMENT (Patient)
MEDICAL RECORD
STANDARD FORM 558 (REV 9-96)
Prescribed by GSA/ICMR
FPMR (41 CFR) 101-11.203(b)(10)
BACK
CH 17 4-14
Encl. (1) to CHAP 4, COMDTINST M6000.1B
NSN 7540-01-075-3786
MEDICAL RECORD EMERGENCY CARE AND TREATMENT
(Doctor)
TIME SEEN BY PROVIDER
TEST RESULTS
WBC ABG/PULSE OX RADIOLOGY CHECK IF
READ BY
RADIOLOGIST
□
H/H SUP 02 PH PO2
PCO2 SAT
RESULTS
CBC
PLT
SMAC
DIP
PT
APTT BHCG ETOH GLU
U/A
MICRO
OTHER
EKG INTERPRETATION
PROVIDER HISTORY/PHYSICAL
CONSULT WITH TIME ACTION
RESIDENT/MEDICAL STUDENT SIGNATURE AND STAMP
PROVIDER SIGNATURE AND STAMP
DIAGNOSIS
CODES
PATIENT’S IDENTIFICATION (For typed or written entries, give: Name-last, first ,middle;
ID no. (SSN or other); hospital or medical facility)
EMERGENCY CARE AND TREATMENT (Doctor)
MEDICAL RECORD
STANDARD FORM 558 (REV 9-96)
Prescribed by GSA/ICMR
FPMR (41 CFR) 101-11.203(b)(10)
Encl. (1) to CHAP 4, COMDTINST M6000.1B
MEDICAL RECORD NARRATIVE SUMMARY (CLINICAL RESUME)
DATE OF ADMISSION DATE OF DISCHARGE NUMBER OF DAYS HOSPITALIZED
(Sign and date at end of narrative)
SIGNATURE OF PHYSICIAN DATE IDENTIFICATION NO. ORGANIZATION
PATIENT’S IDENTIFICATION (For typed or written entries give: Name last, first; middle;
grade; rank; rate ;hospital or medical facility) REGISTER NO. WARD NO.
NARRATIVE SUMMARY (CLINICAL RESUME)
MEDICAL RECORD
STANDARD FORM 502 (rev-7-91)
Prescribed by GSA/ICMR,FIRMR
(41-CFR) 201-9.202.1
4-15 CH 17
BACK
CH 17 4-16
Encl. (1) to CHAP 4, COMDTINST M6000.1B
MEDICAL RECORD CONSULTATION SHEET
REQUEST
TO: FROM: (requesting physician or activity) DATE OF REQUEST
REASON FOR REQUEST (Complaints and findings)
PROVISIONAL DIAGNOSIS
DOCTOR’S SIGNATURE APPROVED PLACE OF CONSULTATION
□ BEDSIDE □ ON CALL
□ROUTINE □ TODAY
□72 HOURS □ EMERGENCY
CONSULTATION REPORT
RECORD REVIEWED □ YES □ NO PATIENT EXAMINED □ YES □ NO TELEMEDICINE □ YES □ NO
SIGNATURE AND TITLE DATE
HOSPITAL OR MEDICAL FACILITY RECORDS MAINTAINED AT DEPARTMENT/SERVICE OF PATIENT
RELATION TO SPONSOR SPONSOR’S NAME (last, first, middle) SPONSOR’S ID NUMBER
PATIENT’S IDENTIFICATION (For typed or written entries, give: Name –last, first, middle; ID No.(SSN or
other); Sex; Date of Birth; Rank/Grade) REGISTER NO. WARD NO.
CONSULTATION SHEET
MEDICAL RECORD
STANDARD FORM 513 (Rev. 4-98)
Prescibed by GSA/ICMR FPMR (41 CFR) 101-11.203(b)(10)
BACK
Encl. (1) to CHAP 4, COMDTINST M6000.1B
Clinical Record ELECTROCARDIOGRAPHIC RECORD Previous ECG
Yes NO
Clinical Impression Medication Emergency
Routine Bedside
Ambulant
Age Sex Race Height B.P. Signature of Ward Physician Date
Rhythm Axis Deviation Rates
Auric. Vent.
IIntervals
PR QRS QT
P Waves
QRS Complexes
RS-T Segment T Waves
Unipolar Extremity Leads (specify)
Precordial Leads (specify)
Summary, Serial Changes, and Implications:
(Continue on Reverse)
No.
ECG
Signature of Physician Patient’s Identification No. Date
Patient’s Identification (For typed or written entries give; Name – Last
First, middle; grade, date hospital or medical facility) Register No. Ward No.
Electrocardiographic Records
Standard Form 520
General Services Administration and
Interagency Committee on Medical Records
FPMR 101-11.806-8
October 1975 520-106
4-17 CH 17
BACK
CH 17 4-18
Encl. (1) to CHAP 4, COMDTINST M6000.1B
AUTHORIZED FOR LOCAL REPRODUCTION
MEDICAL RECORD TISSUE EXAMINATION
SPECIMEN SUBMITTED BY DATE OBTAINED
SPECIMEN
BRIEF CLINICAL HISTORY (include duration of lesion and rapidity of growth, if a necoplasm)
PREOPERATIVE DIAGNOSIS
OPERATIVE FINDINGS
SIGNATURE
NAME OF SIGNER
POSTOPERATIVE DIAGNOSIS
TITLE OF SIGNER
PATHOLOGICAL REPORT
ACCESSION NO(S) NAME OF LABORATORY
GROSS DESCRIPTION, HISTOLOGIC EXAMINATION AND DIAGNOSES
SIGNATURE OF PATHOLOGIST NAME OF PATHOLOGIST DATE
HOSPITAL OR MEDICAL FACILITY RECORDS MAINTAINED AT DEPARTMENT/SERVICE OF PATIENT
RELATION TO SPONSOR SPONSOR’S NAME (Last, first middle) SPONSOR’S ID NUMBER (SSN or Other)
PATIENT’S IDENTIFICATION (For typed or written entries, give: Name-last, first, middle; ID no.
SSN or other); Sex; Date of Birth; Rank/Grade)
REGISTER NO. WARD NO.
TISSUE EXAMINATION
Medical Record
STANDARD FORM 515 (Rev 8-97)
Prescribed by GSA/ICMR FPMR 101-11.203(b)(10)
BACK
Encl. (1) to CHAP 4, COMDTINST M6000.1B
Medical record GYNECOLOGIC CYTOLOGY
Section I – Clinical data to be Completed by Examining Installation
Date Obtained LMP First Day Date Received in Laboratory
Source of Specimen
Combined Cerve and Vagina Cerve Vagina Other (Specify)
Age Pregnancy
Yes No
Gravida Para Previous Abnormal Cytologic Examination
Yes, Give Date______________ No
Clinical History (Surgery, Drugs, hormones, radiation, etc.) Physical Examination (Pelvic findings, etc.)
Specimen Submitted By (Facility) Signature and title Submitting Facility Accession Number
Section II – Cytologic Findings Form Reporting Installation Only
Name of Laboratory Accession Number
Check One Yes No Check One Yes No
Granulocytes Maturation Index
Leukocytes Endocervial
Cells
Parabasals
Trichamonas Intermediates
Candida
Screened By Superficials
Comments and recommendations
Pathologist’s Signature Title Date
Patients Identification (For typed or written entries give; Name – Last first,
Middle; grade, date, hospital or medical facility) Register No. Ward No.
Standard form 541
Provided by GSA and ICMB
4-19 CH 17
BACK
Encl. (1) to CHAP 4, COMDTINST M6000.1B
CLINICAL RECORD LABORATORY REPORTS
ATTACH 3D REPORT ALONG HERE AND ë
ëë
ë SUCCEEDING ONES ON ABOVE LINES
ATTACH 2D REPORT WITH TOP AT THIS LINE ë
ëë
ë
ATTACH 1ST REPORT ALONG LEFT MARGIN WITH TOP AT THIS LINE ë
ëë
ë
ATTACHING MARGIN
ATTACH ALL TEST REPORTS TO THIS SHEET
PATIENT’S IDENTIFICATION (For typed or written entries give: Name - Last, first,
middle; grade; date; hospital or medical facility),
REGISTER NO. WARD NO.
LABORATORY REPORTS
Standard Form 514
Prescribed by GSA/ICMR
FIRMR (41 CFR) 201-45.505
October 1975 514-108
CH 17 4-20
BACK
MEDICAL RECORD RADIOLOGICAL CONSULTATION REQUESTS/REPORTS
ATTACH 3D REPORT ALONG HERE ë
ëë
ë AND SUCCEEDING ONES ON ABOVE LINES
ATTACH 2D REPORT WITH TOP AT THIS LINE ë
ëë
ë
ATTACH REPORTS WITHIN THIS MARGIN
ATTACH 1ST REPORT ALONG LEFT MARGIN WITH TOP AT THIS LINE ë
ëë
ë
RADIOLOGICAL CONSULTATIONS
REQUESTS/REPORTS
STANDARD FORM 519 (Rev. 2-84)
Prescribed by GSA/ICMR
FIRMR (41 CFR) 201.45.505
519-11
NSN 7540-00-634-4160
Encl. (1) to CHAP 4, COMDTINST M6000.1B
4-21 CH 17
BACK
Encl. (1) to CHAP 4, COMDTINST M6000.1B
(THIS FORM IS SUBJECT TO THE
PRIVACY ACT OF 1974 –
Use DD Form 2006.)
EYEWEAR
PRESCRIPTION
DATE ACCOUNT NUMBER ORDER NUMBER
TO: (LAB) FROM:
NAME (Last, First) SSN GRADE
ADDRESS/UNIT PHONE
ADDRESS CONTINUED SHIP TO:
CLINIC PATIENT
CITY, STATE, ZIP
AD RES NG RET OTHER A N AF MC CG PHS OTHER
FRAME EYE BRIDGE TEMPLE COLOR
DIST NEAR
PD
LENS TINT MATERIAL PAIR CASE
SPHERE CYLINDER AXIS DECENTER H PRISM H BASE V PRISM V BASE
R
L
MULTIVISION
NEAR ADD SEG HT TOTAL DECENTER
LAB USE
PRIORITY TECH INITIALS
SPECIAL COMMENTS/JUSTIFICATION (* Use this space to specify blocks marked “Other.”)
PRESCRIBING OFFICER/AUTHORITY SIGNATURE
DISTRIBUTION: ORIGINAL – Retained by Lab. COPY 1 – Returned with eyewear. COPY 2 – Entered in health record.
DD FORM 771, JUL 96 (EG) PREVIOUS EDITION IS Designed using Perform Pro, WHS/DIOR, Aug 96
CH-17 4-22
BACK
HEALTH RECORD IMMUNIZATION RECORD All entries in ink to
be made in block letters
VACCINATION AGAINST SMALLPOX (Number of previous vaccination scars)
DATE ORIGIN BATCH NUMBER REACTION STATION PHYSICIAN’S NAME
1
2
3
4
5
6
YELLOW FEVER VACCINE
DATE ORIGIN BATCH NUMBER STATION PHYSICIAN’S NAME
1
2
3
TYPHOID VACCINE
DATE DOSE PHYSICIAN’ NAME DATE DOSE PHYSICIAN’S NAME
1 4
2 5
3 6
TETANUS-DIPHTHERIA TOXOIDS
DATE DOSE PHYSICIAN’S NAME DATE DOSE PHYSICIAN’S NAME
1 4
2 5
3 6
CHOLERA VACCINE
DATE PHYSICIAN’S NAME DATE PHYSICIAN’S NAME DATE PHYSICIAN’S NAME
1 4 7
2 5 8
3 6 9
PATIENTS IDENTIFICATION (Mechanically Imprint, Type or Print):
Patient’s Name – last, first, middle initial;
Sex; age or Year Of Birth; Relationship to Sponsor;
Component/Status; Department/Service.
Sponsor’s Name – last, first, middle initial;
Rank/Grade; SSN or Identification Number;
Organization. IMMUNIZATION RECORD
Standard Form 601 – October 1975 (Rev.)
General Services Administration & Interagency
Committee on Medical Records
FIRMR (41 CFR) 201-45.505
4-23 CH 17
Encl. (1) to CHAP 4, COMDTINST M6000.1B
BACK
ORAL POLIOVIRUS VACCINE
DATE DOSE PHYSICIAN’S NAME DATE DOSE PHYSICIAN’S NAME
1 3
2 4
INFLUENZA VACCINE
DATE DOSE PHYSICIAN’S NAME DATE DOSE PHYSICIAN’S NAME
1 3
2 4
INFLUENZA VACCINE
DATE TYPE DOSE PHYSICIAN’S NAME DATE TYPE DOSE PHYSICIAN’S NAME
1 5
2 6
3 7
4 8
SENSITIVITIES TEST (Tuberculin,etc.)
DATE TYPE DOSE ROUTE RESULTS PHYSICIAN’S NAME
1
2
3
4
5
REMARKS:
THIS RECORD IS ISSUED IN ACCORDANCE WITH ARTICLE 99, WHO SANITARY REGULATION NO 2.
STANDARD FORM 601 PAGE 2 (Rev. 10-75)
CH 17 4-24
Encl. (1) to CHAP 4, COMDTINST M6000.1B
HEALTH RECORD SYPHILIS RECORD
SECTION 1. – HISTORY OF PAST VENEREAL INFECTIONS OR TREATMENTS
PRIOR TO
MIL. SERVICE
DATE DISEASE
(Give stage) YES NO
TREATMENT
(Give type, amount and dates) TREATING AGENCY PLACE
1
2
3
4
SECTION II = HISTORY OF PRESENT INFECTION
CAME TO MEDIAL ATTENTION BY: VOLUNTARY CONTACT REPORT PHYSICAL INSPECTION FOOD HANDLER
INCIDENT TO HOSPITALIZATION PREMARITAL PRENATAL OTHER (Specify)
DATES: ONSET SYMPTOMS REQUESTED TREATMENT DIAGNOSIS ESTABLISHED
DIAGNOSIS (Include stage and diagnosis No.)
LIST VD CONTACT FORM SERIAL NOS.
DIAGNOSTIC CRITERIA (Enter results of test)
CLINICAL DATA (Including chief complaint, physical findings – eye, cardiovascular and nervous system, even in early syphillis)
RECOMMENDED TREATMENT AND FOLLOW-UP SIGNATURE OF PHYSICIAN DATE
HAVE BEEN INFORMED BY THE MEDICAL OFFICER THAT I HAVE BEEN DIAGNOSED
AS HAVING SYPHILIS AS INDICATED ABOVE; THE NATURE OF THIS DISEASE HAS BEEN
EXPLAINED TO ME; I UNDERSTAND THAT MY COOPERATION IS NECESSARY IN THE
TREATMENT AND PROLONGED OBSERVATION (including certain prescribed tests) FOR THE
CARE OF THIS DISEASE.
SIGNATURE OF PATIENT AND DATE
SECTION III. - TREATMENT
TREATMENT DATE STARTED DATE ENDED SIGNATURE OF PHYSICIAN
1
2
3
4
PATIENT’S IDENTIFICATION (Mechanically Imprint, Type or Print):
Patient’s Name – last, first, middle initial;
Sex; age or Year Of Birth; Relationship to Sponsor;
Component/Status; Department/Service.
Sponsor’s Name – last, first, middle initial;
Rank/Grade; SSN or Identification Number;
Organization.
SYPHILIS RECORD
Standard Form 602 – March – 1975 (Rev.)
General Services Administration &
Interagency Comm on Medical Records
4-25 CH 17
Encl. (1) to CHAP 4, COMDTINST M6000.1B
BACK
SECTION IV. – CUMULATIVE LABORATORY SUMMARY
RESULTS OF DARKFIELD EXAMINATION
DATE RESULTS SOURCE OF SPECIMEN LABORATORY NAME OF CONFIRMING OFFICER
1
2
RESULTS OF SEROLOGICAL TESTS FOR SYPHILIS
DATE TYPE RESULT (Include
titer value) LABORATORY DATE TYPE
RESULT (Include
Titer value) LABORATORY
1 5
2 6
3 7
4 8
FLUORESCENT ANTIBODY TESTS
DATE
1
2
RESULTS OF SPINAL FLUID EXAMINATIONS
DATE CELLS TOTAL PROTEIN SEROLOGICAL TEST (Including titer) LABORATORY WHERE
DONE
1
2
SECTION V. – EVALUATION OF THERAPY
RESULT
DATE FACILITY WHERE EVALUATED Satisfactory UNSATISFACTORY
DATE OF
RETREATMENT PHYSICIAN’S SIGNATURE
1
2
3
4
*Satisfactory result cannot be reported without normal spinal fluid findings.
**Specify: Infectious Relapse: Sero-Relapse, Neuro-Relapse, Incomplete data on Spinal Fluid, Other (Specify)
REASON FOR INADEQUATE FOLLOW-UP (Date, place and type of separation – Give authority for discharge)
PATIENT’S HOME ADDRESS ON SEPARATION CIVILIAN HEALTH DEPT. TO WHICH CASE RESUME WAS SENT
REINFECTION (Give date new record was opened)
REMARKS
SECTION VI. – MEDICAL OFFICER CLOSING THIS RECORD
NAME (Typed or printed) SIGNATURE STATION DATE
SECTION VII. – MEDICAL OFFICER SENDING ABSTRACT TO VETERAN’S ADMINISTRATION ON DISCHARGE
NAME (Typed or printed SIGNATURE STATION DATE
Page 2 of SF-602 (rev. 3-75)
CH 17 4-26
Encl. (1) to CHAP 4, COMDTINST M6000.1B
Encl. (1) to CHAP 4, COMDTINST M6000.1B
RECORD OF OCCUPATIONAL EXPOSURE TO IONIZING RADIATION
For instructions See Reverse of Sheet
Identification
Number Name (Last, First, Middle Initial) Social Security Number Rank/Rate/Title Date of Birth
Place Where
Exposure Occurred Period of
Exposure
Dose This Period
1. Method of monitoring is presumed to be film badge
reading unless otherwise specified under item 16,
"REMARKS.”
Accumulated Dose Initial
From To
Acticty (Day-Mo-Yr) (Day-Mo-Yr) Skin
Dose
(Salt)
Gamma
and
X-Ray Neutron Total
This
Period
Total
Life
Time
Permis-
sible
Lifetime
Persons
Making
Entry
16. Remarks:
TO BE RETAINED PERMANENTLY IN INDIVIDUAL’S MEDICAL RECORD
DD Form 1141
4-27 CH 17
BACK
Encl. (1) to CHAP 4, COMDTINST M6000.1B
Page 2 of 2 CG-4057 (Rev 2-01)
AGREEMENT/DISAGREEMENT
I agree (or) do not agree that at the time of separation:
(2) I am reasonably able to perform my current duties, or
(2) I have a high expectation of recovery in the near term from illness, injury or
surgical procedure such that I would again be able to perform my usual duties.
Date Grade/Rate Signature of Member
TERMINATION OF HEALTH RECORD
Remarks
Impairments, which have been documented in your health record, including any
separation exam, while establishing service connection, do not in themselves indicate
a disability. To receive disability benefits from the Coast Guard, you must be found
unfit to perform your assigned duties through the physical disability evaluation system
before you are separated.
After you are separated, any claims for disability benefits must be submitted to the
Department of Veterans Affairs. If you have questions about certain benefits to which
you might be entitled you should contact the DVA Regional Office nearest your home
as soon as practical.
I have read the above statements and acknowledge receipt of a copy of the following:
1. CG-4057, Chronological record of Service.
2. SF-88 report of Medical Examination date_________ (if performed).
3. PHS-731, International Certificate of Vaccination.
4. DD Form 2766, Adult Preventive and Chronic Care Flowsheet.
Date Grade/Rate Signature of Member
COMMAND CERTIFICATION
Health record terminated this date by reason of_____________________
In accordance with Chapter 4, Medical Manual, COMDTINST M6000.1 (series)
Date Title Signature
4-29 CH 17
Encl. (1) to CHAP 4, COMDTINST M6000.1B
NAVMED – 6150/2 (REV 8-70) SPECIAL DUTY MEDICAL ABSTRACT (NAVMED 6150/2)
Health Record Special Duty Medical Abstract
Summary of Physical Examination for Special Duty
Date Place Purpose Result – Recommendation (Defects Reverse) BUMED Action Sig. Of M.D.
1.
2.
3.
4.
5.
6.
7.
8.
9.
Suspension From Special Duty
Date (From) (To) No. of
Days Reason for Suspension Signature of Medical Officer
1.
2.
3.
4.
5.
6.
7.
Periodic Special Duty Requalification
Date Signature of . O. Date Signature of M.O. Date Signature of M.O.
Name (Last) (First) (Middle) Grade/Rate Service/Soc. Sec. Organization
CH 17 4-30
BACK
Encl. (1) to CHAP 4, COMDTINST M6000.1B
SPECIAL DUTY MEDICAL ABSTRACT (NAVMED 6150/2)
Altitude Training, Air Compression and Oxygen Tolerance
Date Station Type of Run – Reaction Signature or M.O.
1.
2.
3.
4.
5.
Explosive Decompression Training
Date Station Altitudes - Reaction Signature or M.O.
1.
2.
Submarine Escape and Diving Training
Date Station Type of Run - Reaction Signature or M.O.
1.
2.
3.
4.
5.
Visual and Disorientation Training
Date Station Type of Training Signature or M.O.
1.
2.
3.
4.
Centrifuge and Ejection Seat Training
Date Station Type of run – Reaction Signature or M.O.
1.
2.
Remarks
4-31 CH 17
Encl. (1) to CHAP 4, COMDTINST M6000.1B
EMERGENCY MEDICAL TREATMENT REPORT
VICTIM
IDENTI-
FICATION
1. Name__________________________
_________________________________
2. Sex (check one) male _______
female _______
3. Estimated age yrs_____ mos_____
RESCUER
INFOR-
MATION
10. Name: ___________________ 11. Level:
12. Unit: ____________________________
13. OPFAC #: ________________________
14. Rescue Vehicle:____________________
15. Receiving Unit:_____________________
16. Time Patient Transferred:_____________
DESCRIP-
TION OF
INCIDENT
4. Date: _______________ 5. Type of incident:
6. Time on Scene: _________ a) marine _________
7. Time of incident: _________ b) aviation _________
c) Industrial _________
8. Location:_______________ d) auto __________
_________________________ e) domestic __________
f) other _____________
NATURE OF EMERGENCY / MECHANISM OF INJURY
OBSERVA-
TION OF
VISTIM
FRONT BACK
H – hemorrhage F – fracture
L - laceration B - burns
S – soft tissue injury O2 Liters______
TREATMENT
(
CIRCLE AS NEEDED)
1 – DRESSING
2 - TX SPLINT
3 - SPLINT
4 - C/COLLAR
5 - BACK BOARD
6 - TOURNIQUET
7 - CPR
8 - AIRWAY
9 - OXYGEN
10 - MAST
11 - MILLER B/B
MEDICATIONS:
ALLERGIES
_________________________________________
MEDICAL HISTORY / COMMENTS /ETC.
(include additional vitals, oxygen, fluids, etc.)
SKIN
(Circle appropriate number of numbers)
1 – normal 4 - cyanotic 7 - cold
2 – pale/ashen 5 – dry 8 – warm
3 – flushed 6 – moist 9 - hot
VITAL
SIGNS TIME
OBSERVED
Alert
Responds to Verbal
Responds to Pain
LEVEL OF
CONSCIOUS
Uncon/Unresponsive
Perl
Unequal
Nonreactive
Dilated
PUPILS
Pinpoint
Rate (Numeric)
Strong
PULSE
Weak
Rate (Numeric)
Regular
_______________________________________
Shallow
BREATHING
Labored
BLOOD
PRESSURE Blood Pressure
TEMP Temperature ORAL
(circle) RECTAL
TIME MEDICATIONS ADMINISTERED DOSAGE
______ ___________________________ _______
MAST BP
MAST COMPARTMENT R L ABD
_____ _______________________ ______
_____ _______________________ _____
TRIAGE INFORMATION (CIRCLE ONE) PRIORITY I PRIORITY II PRIORITY III
DEPT. OF TRANSPORTATION., USCG CG-5214 (Rev. 10-88) PATIENT COPY
Previous Edition May be Used
CH 17 4-32
BACK
REQUEST FOR
MEDICAL/DENTAL RECORD
OR INFORMATION
REQUESTING ACTIVITY Complete Items 1 through 10 (Except 8b); also
Complete Item 19.
ADDRESSEE – Complete Items 8b, 11 to 14 or 15 to 18, as appropriate,
Final referrer shall return to requester.
Date
1. PATIENT (Last Name – First Name – Middle Name) 3. STATUS □ MILITARY □ VA BENEFICIARY
□ DEPENDENT □ FEDERAL EMPLOYEE
□ OTHER (Specify)
2. ORGANIZATION AND PLACE OF TREATMENT
3a. NAME OF SPONSOR (If dependent)
5. IDENTIFYING INFORMATION
a. SERVICE NUMBER
b. GRADE/RATE
C. SOCIAL SECURITY ACCOUNT NO.
D. VA CLAIM NUMBER
4. TO (Include ZIP Code)
E. DATE OF BIRTH (If federal employee)
6. DATES OF TREATMENT 7 DISEASE OR INJURY
9. REMARKS
8. a. RECORDS REQUESTED B. RECORDS FORWARDED
MIL VA MIL VA
□ □ CLINICAL □ □
□ □ OUTPATIENT □ □
□ HEALTH RECORD □
□ □ DENTAL RECORD □ □
□ □ X--RAY □ □
□ MEDICAL REPORT CARDS, EMERGENCY □
MEDICAL TAGS, FIELD MEDICAL CARDS
□ ABSTRACT OF RATING SHEET □
□ □ REPORT OF PHYSICAL EXAMINATION □ □
□ ALL AVAILABLE RECORDS (Except □
X-rays unless specifically requested)
□ □ OTHERS (List under remarks) □ □
10. SIGNATURE
REPLY/REFERRAL
11. TO:
13. SIGNATURE 14. DATE
12. REMARKS
/ RECORDS CHECKED IN 8B FORWARDED.
/ NO RECORDS FOUND FOR PATIENT DURING ABOVE PERIOD.
/ MORE INFORMATION NEEDED.
REPLY/SECOND REFERRAL
15. TO:
17. SIGNATURE 18. DATE
16. REMARKS
/ RECORDS CHECKED IN 8B FORWARDED.
/ NO RECORDS FOUND FOR PATIENT DURING ABOVE PERIOD.
/ MORE INFORMATION NEEDED.
19. RETURN TO: (Include ZIP Code)
REQUESTING ACTIVITY WILL ENTER
COMPLETE ADDRESS
TO WHICH RECORDS OR FINAL
REPLY SHOULD BE MAILED.
DD FORM 877, SEP 67
Encl. (1) to CHAP 4, COMDTINST M6000.1B
4-33
CH 17
BACK
Encl. (1) to CHAP 4, COMDTINST M6000.1B
U. S. COAST GUARD
DENTAL RECORD
PRIVACY ACT STATEMENT: HEALTH CARE RECORDS
1. AUTHORITY FOR COLLECTION OF INFORMATION INCLUDING SOCIAL SECURITY NUMBER (SSN):
Section 632 of Title 14 United States Code and Sections 1071-1087, Title 10 United States code, Executive
Order9397.
2. PRINCIPAL PURPOSES FOR WHICH INFORMATION IS TO BE USED:
The purpose for requesting information is to assist medical personnel in developing records to facilitate and
document your health condition in order to provide health care and to provide a complete account of such care
rendered, including diagnosis, treatment, and end result. The social Security Number (SSN) necessary to
identify the person and records.
3. ROUTINE USES:
This information may be used to plan and coordinate health care. It may be used to provide medical
treatment, conduct research, teach, compile statistical data, determine suitability of persons for service or
assignment, implement preventive health and communicative disease control program; adjudicate claims and
determine benefits; evaluate care rendered; determine professional certification of patients to other Federal,
State and local agencies upon request in the pursuit of there official duties; and report medical conditions
required by law to federal, State and local agencies. It may be used for other lawful purposes including law
enforcement and litigation.
4. The above Privacy Act Statement applies to all requests for personal information made by medical treatment
personnel or for medical treatment purposes. Failure to provide the requested information for these medical
records may result in an inability of Coast Guard medical personnel to afford treatment.
5. No information may be divulged from this record except to persons properly and directly concerned.
Questionable cases will be referred to the Commanding Officer for decision.
LAST NAME FIRST NAME MIDDLE NAME SOCIAL SECURITY NUMBER DATE OF BIRTH (DAY, MO,YR)
GRADE OR RATE CHANGES IN GRADE OR RATE BLOOD TYPE (Check one)
O A B AB
RH FACTOR (Check one)
POSTIVE NEGATIVE
DRUG SENSITIVITY
SPECIFIC DRUG(S)
ATTACH TO FRONT OF CHART JACKET
DEPT OF TRANSP. USCG CG 3443-2
CH 17 4-34
BACK
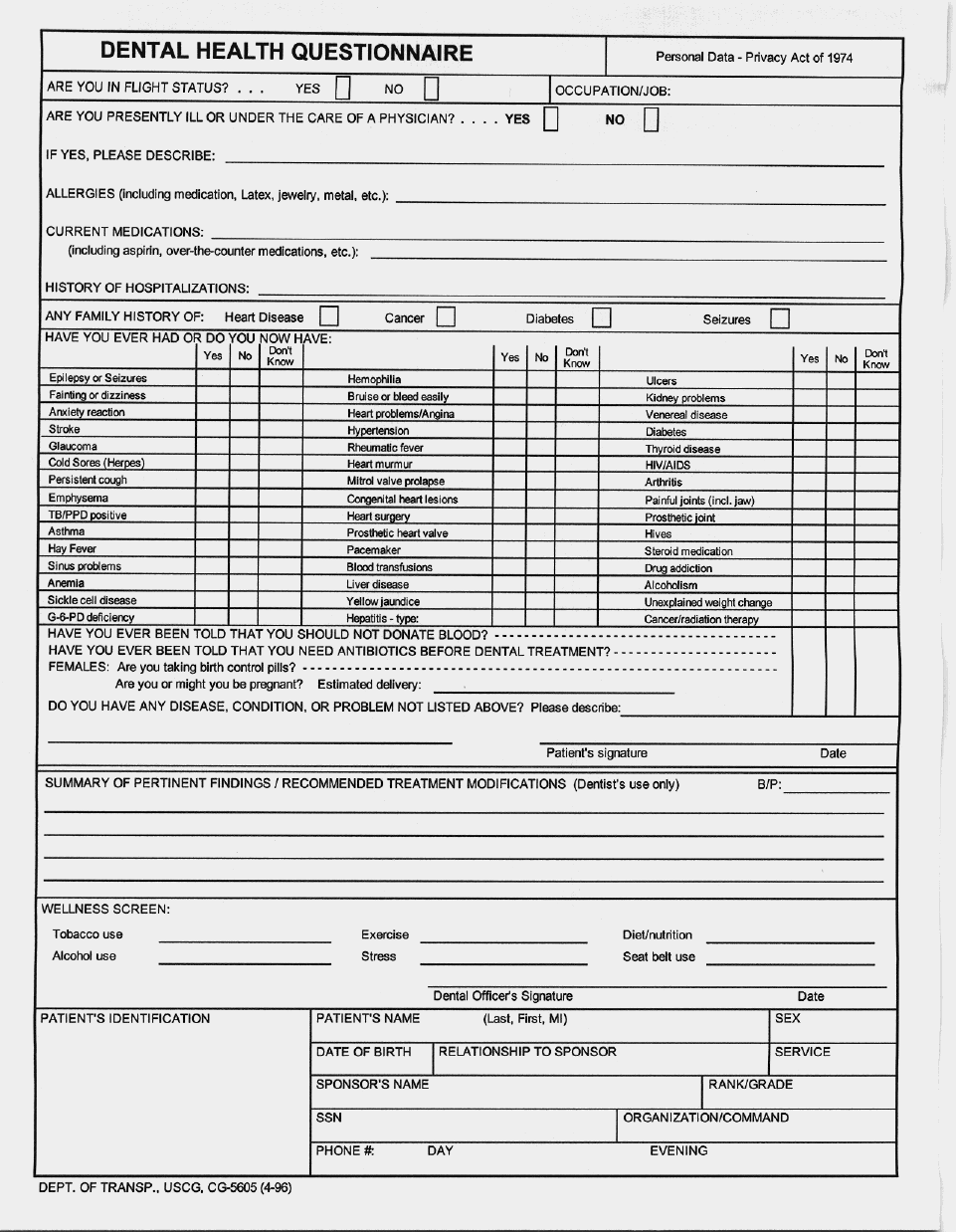
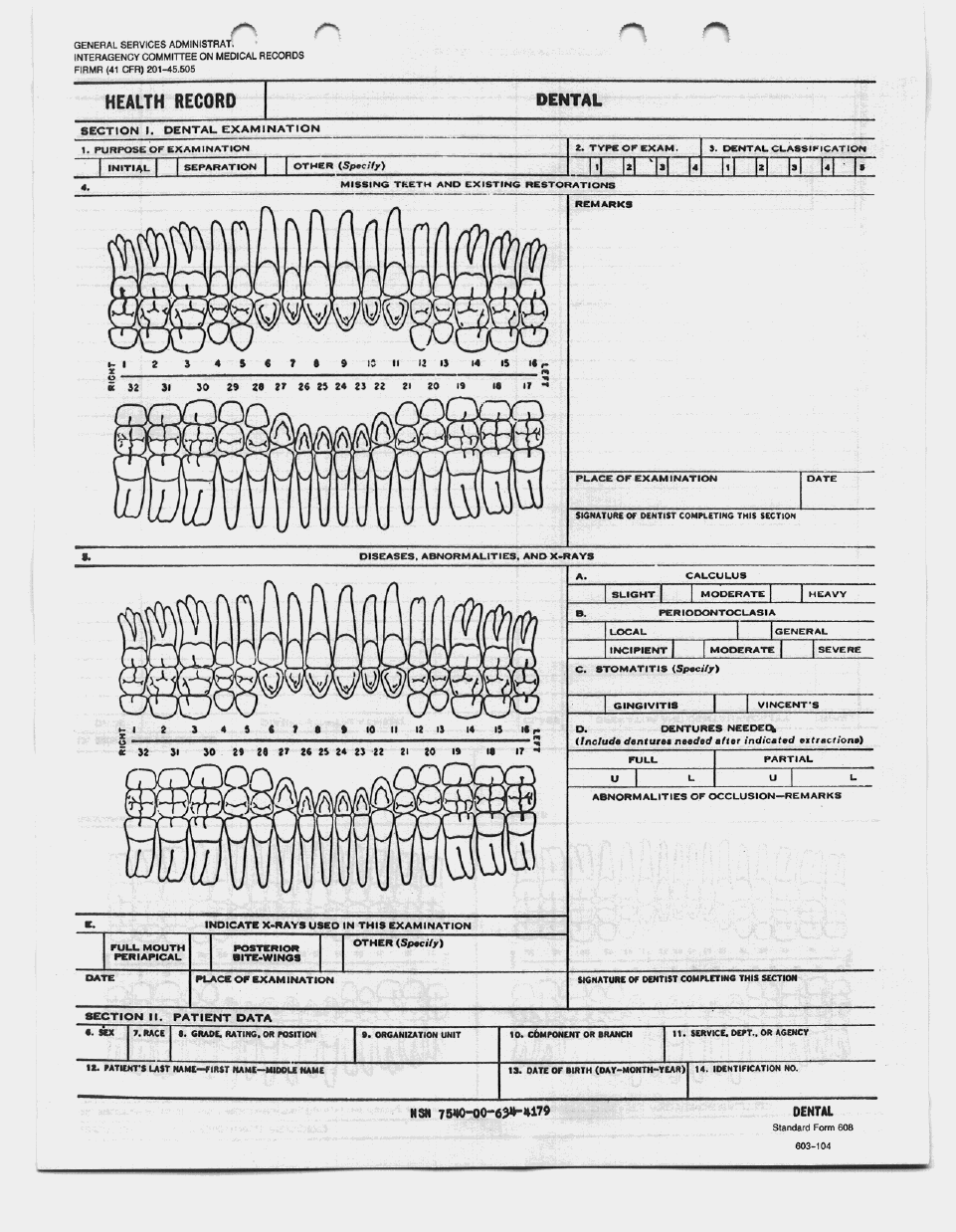
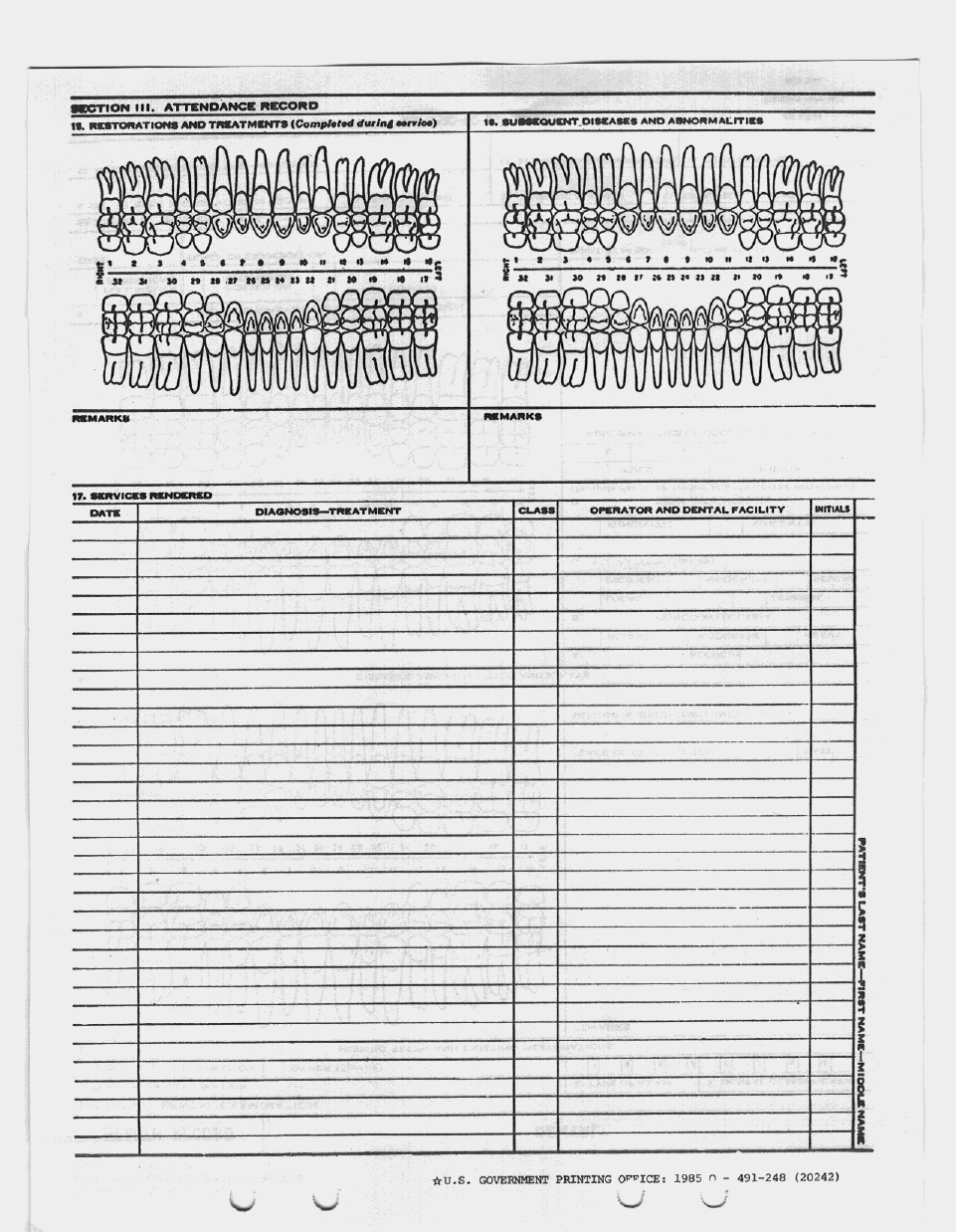
4-37 CH-17
Encl. (1) to CHAP 4, COMDTINST M6000.1B
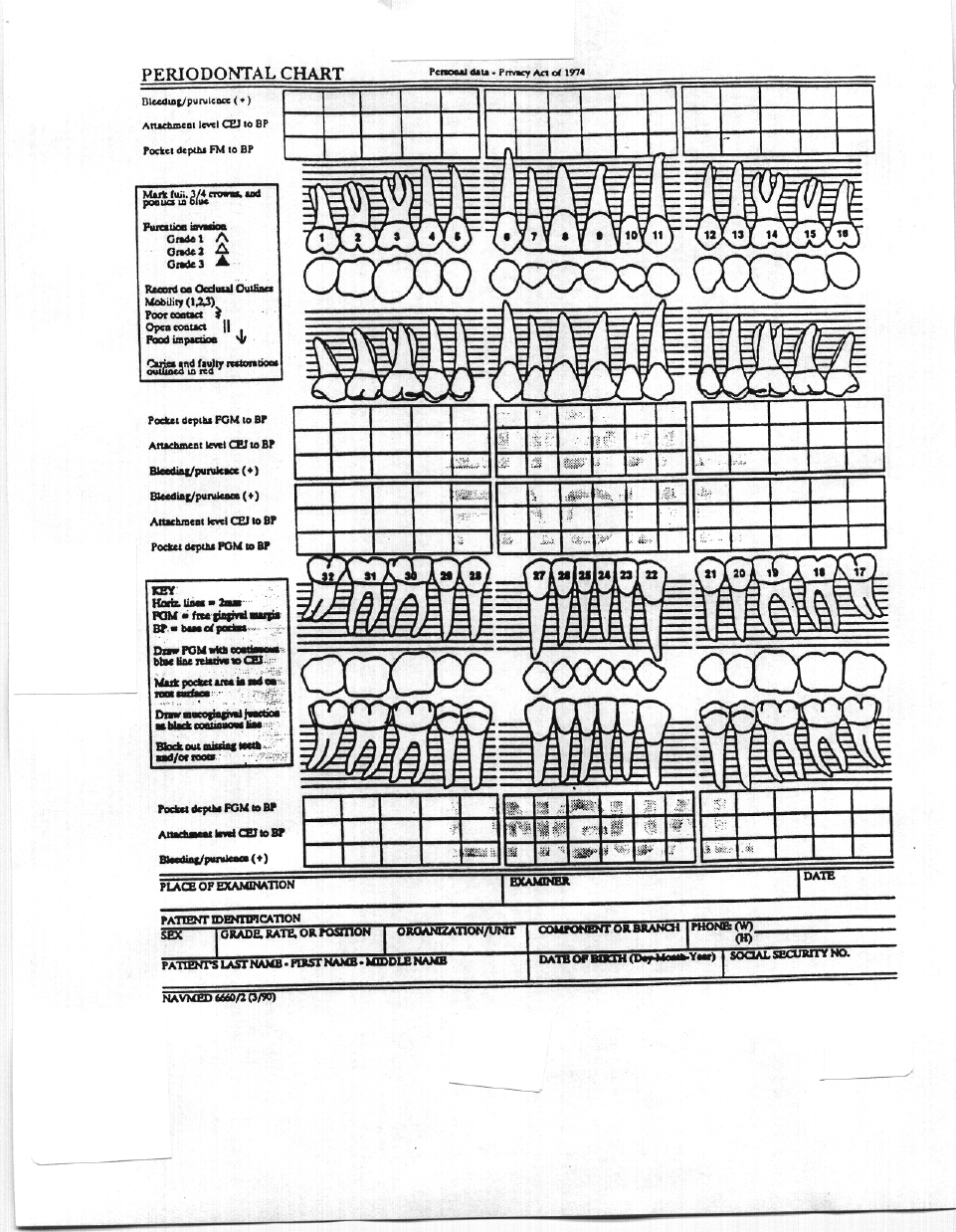
CH 17 4-38
Encl. (1) to CHAP 4, COMDTINST M6000.1B
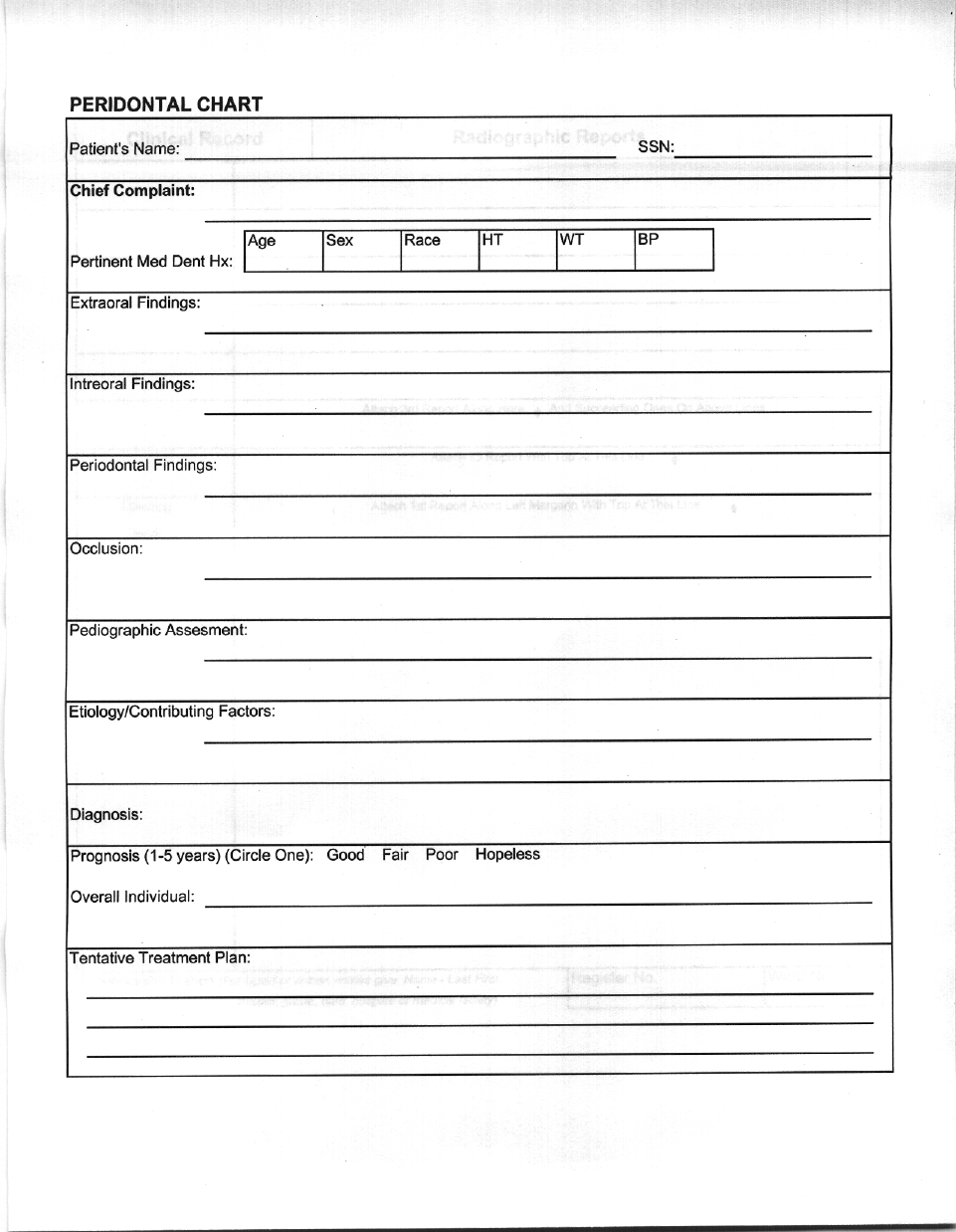
4-39 CH-17
Encl. (1) to CHAP 4, COMDTINST M6000.1B
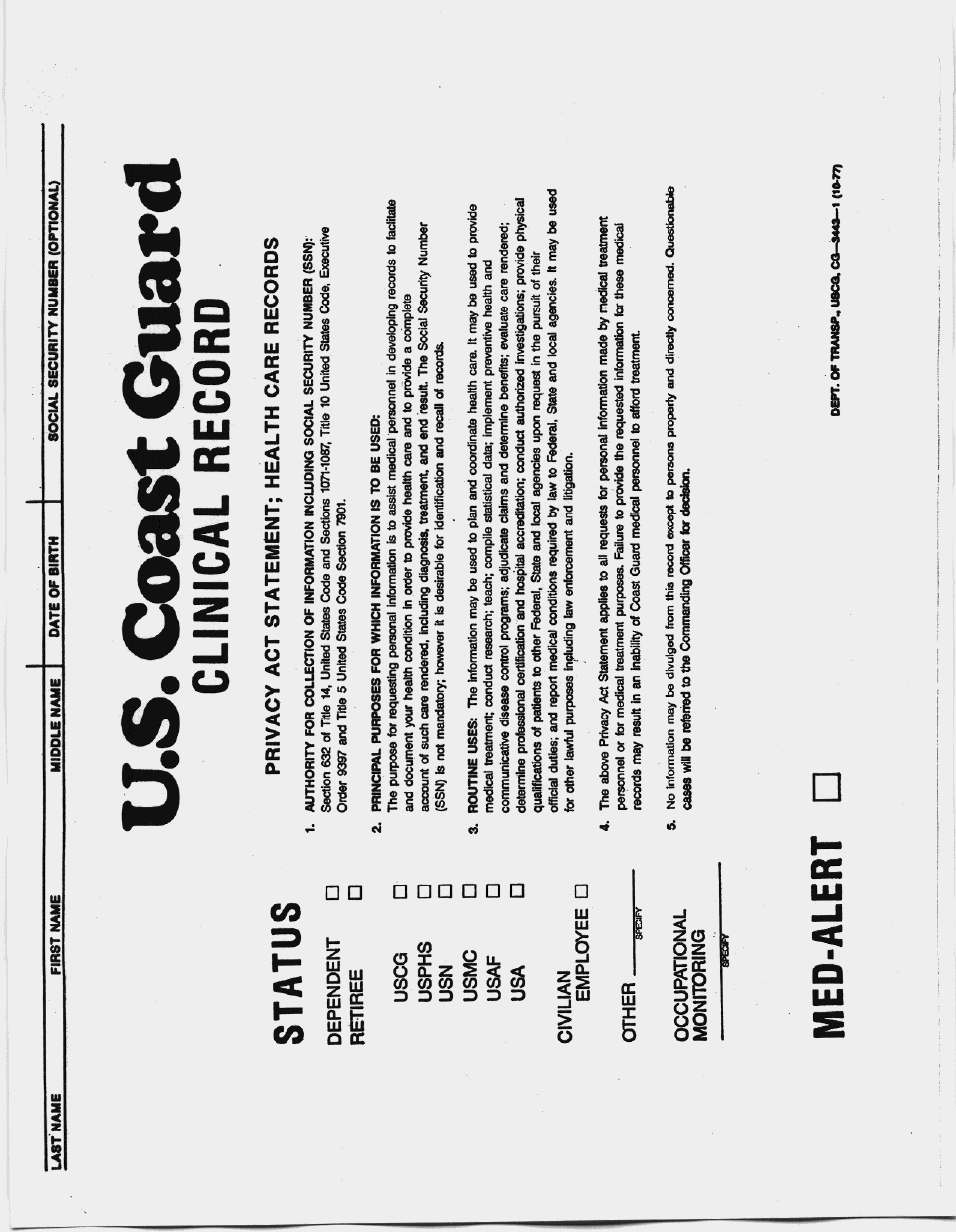
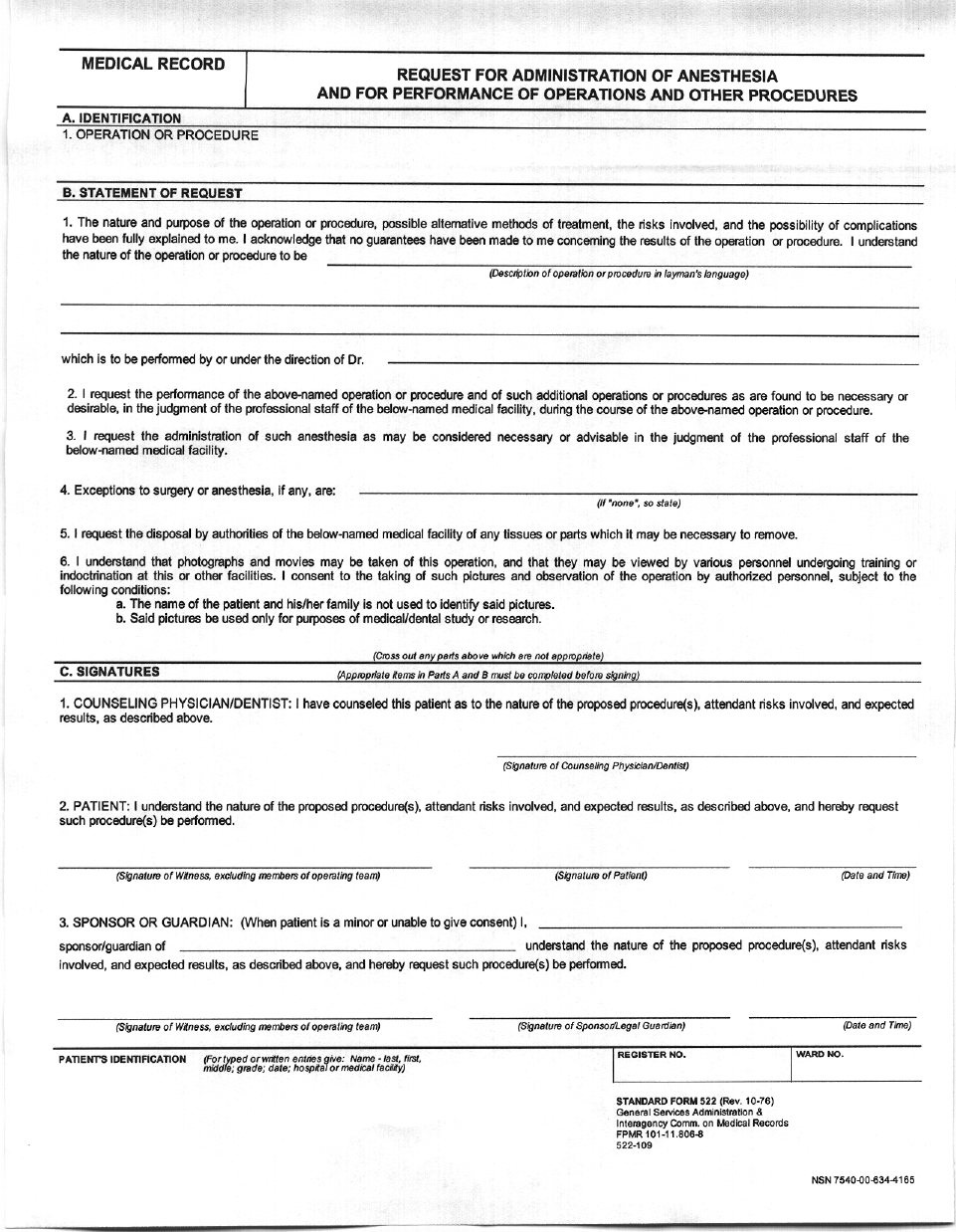
4-43 CH-17
Encl. (1) to CHAP 4, COMDTINST M6000.1B
INPATIENT MEDICAL RECORD COVER SHEET
(See Privacy Act Statement on Reverse)
Name: _______________________
Last, First, MI SSN: ________________ Rank/Rate: ______
Unit: __________________________________________________________________
Date of Birth: ___/___/____
Religon: _______________________________
YY MM DD
Home Address: _________________________________________________________
Next of Kin: __________________________
Relationship: ______________________
Address:
_____________________________
Phone #:
___________________
_____________________________
___________________
Previous Admission:
? Yes ? No
If yes, Date:
___/___/____
YY MM DD
Date of Present Admission: ___/___/____ Time: _________ Hours
YY MM DD
Provisional Diagnosis
1. _____________________________
2. __________________________ _
3. _____________________________
Provisional Diagnosis
1. ____________________________
2. ____________________________
3. ____________________________
Date of Discharge:
___/___/____
Time:
_________ Hours
YY MM DD
DISPOSITION
Duty Status: ? FFD ? NFFD ? FFLD Restrictions: _________________
______________________________________________________________________
Activity Restrictions: ______________________________________________________
Diet: __________________________________________________________________
Medications: ____________________________________________________________
Follow-up Appointment(s): _________________________________________________
Admitting Medical Officer Discharging Medical Officer
Time Unit Notified:
___/___/____
Time:
_________ Hours
YY MM DD
Name of Staff Member Notifying: ____________________________________________
Name of Person at Unit Receiving Call:
__________________________________
Name and Rank/Rate
BACK
CH-17 4-44
Encl. (1) to CHAP 4, COMDTINST M6000.1B
PRIVACY ACT STATEMENT
In accordance with 5 USC 552a (e)(3), the following applies to
persons providing personal information to the U.S. Coast Guard.
1. Section 632, Title 14 USC, § 1071 – 1087. Title 10 USC, and
Executive Order 9397 authorizes collection and application of this information.
2. The principal purpose for which this information is intended is to
assist medical personnel in developing records to facilitate and document
your health condition(s), in order to provide a complete account of care
rendered, including diagnosis, treatment, and results. The social security
number is necessary to identify the person and records. Family information
is required for notification of next of kin in the unlikely event of an
emergency.
3. The routine use of this information is for review by attending
medical officers and for future reference in rendering health care.
4. Disclosure of this information is voluntary. However, failure to
provide the requested information may result in an inability of the Coast
Guard medical personnel to deliver comprehensive treatmen.
Please note the following and indicate your wishes:
I DO / DO NOT GIVE PERMISSION FOR THE ATTENDING MEDICAL
OFFICER AND THE DISPENSARY STAFF TO DISCUSS MY MEDICAL
CONDITION OR THE SITUATION OF MY ADMISSION WITH MY PARENTS
OR LEGAL GUARDIANS, UPON MY REQUEST.
Signature Date
Witness
__ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __
PERSONNEL AUTHORIZED SEPARATE RATIONS
I understand that this facility provides three meals daily for all patients.
Further, persons authorized to mess separately will be required to make
repayments for meals consumed during their stay.
I have read and understand the statement about separate rations.
Signature Date
4-45 CH-17
Encl. (1) to CHAP 4, COMDTINST M6000.1B
A
ccession Numbe
r
to be put on each
box(1 ½ inch letters)
338-76A-0019 1 of 215
Stapled End
ABR
A
lpha or numeric
identification of
the first record in
each box.
(
2 inch letters
)
12 inches
14 3/4 inches
9 1/2 inches
Consecutive
number on each
box (1 ½ inch letters)
BACK
CH-17 4-46
Encl. (1) to CHAP 4, COMDTINST M6000.1B
25
28
31
34
13
16
19
22
338-86-0000 1/36
A-Ba
338-86-0000 2/36
Ba-Ca
338-86-0000 3/36
Ce-Do
338-86-0000 4/36
Du-Fa
338-86-0000 5/36
Fe-Go
338-86-0000 6/36
Gu-Hab
338-86-0000 7/36
Hac-Il
338-86-0000 8/36
Im-ja
338-86-0000 9/36
Je-Jum
338-86-0000 10/36
Jun-Ka
338-86-0000 11/36
Ke-La
338-86-0000 12/36
Le-Lu
BACK
4-47 CH-17
Encl. (1) to CHAP 4, COMDTINST M6000.1B
INSTRUCTIONS
NURSE: Retain a copy and send to Pharmacy after each order is written.
MEDICAL RECORD DOCTOR’S ORDERS
(Sign all orders)
HOUR
START STOP RX DRUG ORDERS DOCTOR’S
SIGNATURE NURSE’S
SIGNATURE
If needed, continue on Page 2.
PATIENT’S IDENTIFICATION (For typed or written entries give: Name – last, first,
middle; grade; rank; rate; hospital or medical facility) REGISTER NO. WARD NO.
DOCTOR’S ORDERS
STANDARD FORM 508 (Rev. 10-75)
Prescribed by GSA and ICMR
FPMR 101-11 806-8
508-110
BACK
CH-17 4-48
Encl. (1) to CHAP 4, COMDTINST M6000.1B
Standard Form 506 (Rev 2-99) AUTHORIZED FOR LOCAL REPRODUCTION
Clinical Record PHYSICAL EXAMINATION
Weight Date of Exam Height
Average Maximum Present
Temperature Pulse Blood Pressure
Instructions: Describe (1) General Appearance and Mental Status; (2) Head and Neck (General); (3) Eyes; (4) Ears; (5) Nose; (6) Mouth; (7) Throat; (8) Teeth; (9)
Chest (General); (10) Breast; (11) Lungs; (12) Cardiovascular; (13) Abdomen; (14) Hernia; (15) Genitalia; (16) Pelvic; (17) Rectal; (18) Prostate; (19) Back; (20)
Extremities; (21) Neurological; (22) Skin; (23) Lymphatics.
(Continue reveres side)
SPONSOR’S NAME
RELATIONSHIP TO SPONSOR
LAST First MI
SPONSOR’S ID NUMBER
(SSN or Other)
DEPART./SERVICE HOSPITAL OR MEDICAL FACILITY RECORDS MAINTAINED AT
PATIENT’S IDENTIFICATION (For typed or written entries give: Name-Last First,
Middle; grade; date; hospital or medical facility)
REGISTER NO WARD NO
PHYSICAL EXAMINATION RECORD
Standard Form 506 (Rev 2-99)
Prescribed by GSA/ICMR (41 CFR) 101-11 .203(b)(10)
BACK
4-49 CH-17
Encl. (1) to CHAP 4, COMDTINST M6000.1B
SF 506 (Rev 2-99)
LAST NAME FIRST NAME MIDDLE INITIAL ID NUMBER
PHYSICAL EXAMINATION
INITIAL IMPRESSION
SIGNATURE OF PHYSICIAN NAME OF PHYSICIAN
Standard Form 506 (Rev. 2-99) BACK
CH-17 4-50
Encl. (1) to CHAP 4, COMDTINST M6000.1B
MEDICAL RECORD PROGRESS NOTES
DATE
(Continue on reverse side)
PATIENT’S IDENTIFICATION (For typed or written entries give: name – last, first, middle;
grade; rank; rate; hospital or medical facility) REGISTER NO. WARD NO.
PROGRESS NOTES
MEDICAL RECORD
STANDARD FORM 509 (REV-7-91) EG
Prescribed by GSA/ICMR (41 CFR) 201-9.202-1
Designed using Perform Pro. WHS/DIOR, Jul94
BACK
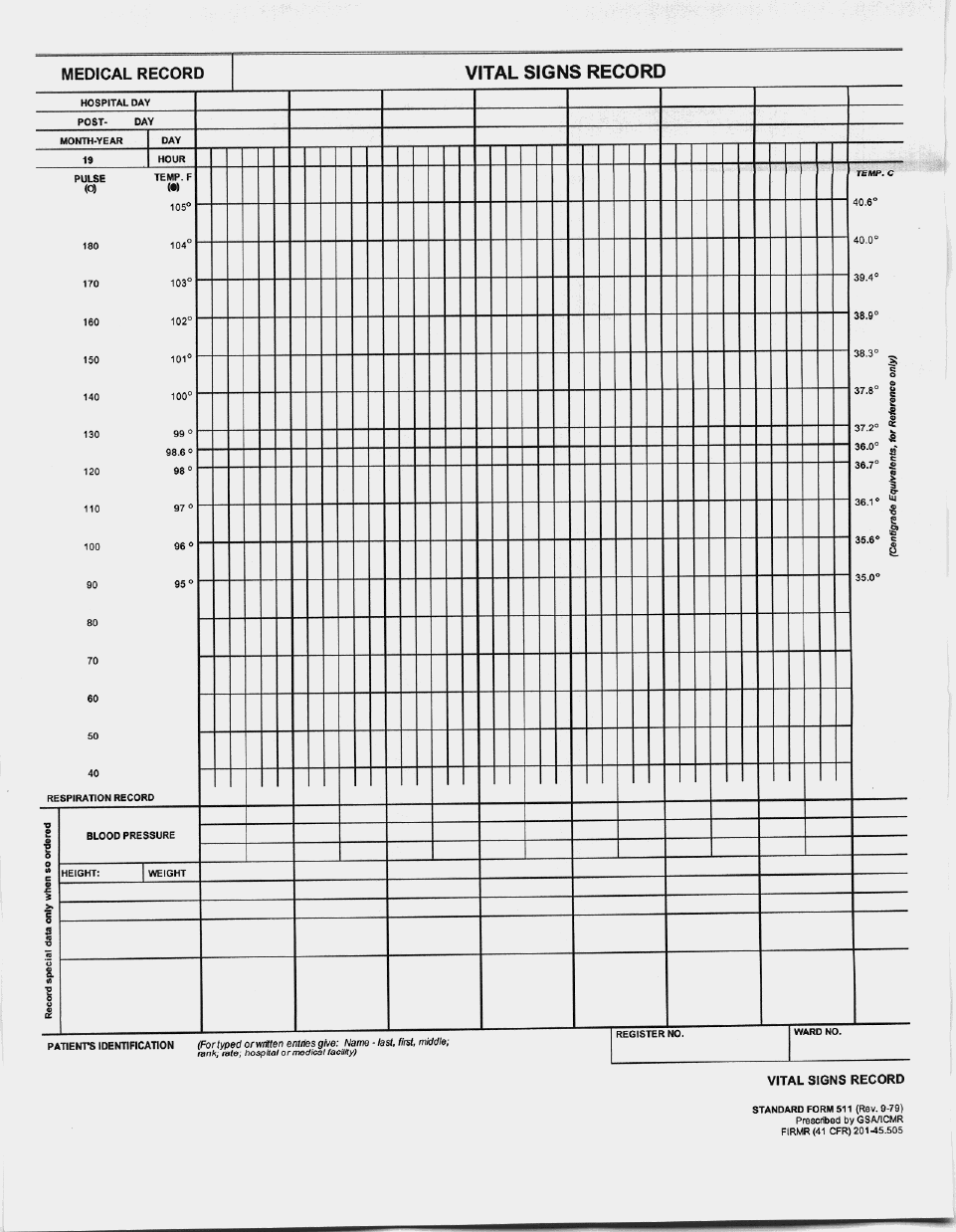
CH-17 4-52
Encl. (1) to CHAP 4, COMDTINST M6000.1B
ABBREVIATED MEDICAL RECORD 1. ADMISSION DATE(yyyymmdd)
2. CHIEF COMPLAINT, PERTINENT HISTORY, AND PERTINENT SYSTEM REVIEW
3. PHYSICAL EXAMINATION (Including pertinent positives and negatives)
4. IMPRESSION (enter admission note with plan on progress notes)
5. ADMITTING OFFICER
a. SIGNATURE b. DATE SIGNED (YYYYMMDD)
6. DISCHARGE NOTE (Brief hospital course, diagnoses, procedures, condition on discharge,
pertinent discharge information (including medications, diet, activity
limitations, follow-up instructions).)
7. DISCHARGE DATE (YYYYMMDD)
8. DISCHARGE OFFICER
a. NAME (Last, First, Middle Initial b. GRADE c. TITLE d. SIGNATURE
10. OUTPATIENT/HEALTH RECORD
MAINTAINED AT:
9. PATIENT IDENTIFICATION (For typed or written entries: Name (last, first,
middle), grade, SSN, date of birth, hospital or medical facility, ward number, and
register number)
11. COPY PLACED IN OUTPATIENT RECORD (x
WHEN DONE)
DD FORM 2770, APR 1998 (EG) Replaces SF 509
BACK
5-i CH-16
CHAPTER 5
DEATHS AND PSYCHIATRIC CONDITIONS (PERSONALITY)
SECTION A - DEATHS PAGE
GENERAL..............................................................................................................................................................................1
DUTIES OF MEDICAL OFFICERS OR HEALTH SERVICES DEPARTMENT REPRESENTATIVES IN THE EVENT
OF A DEATH AT A COAST GUARD UNIT........................................................................................................................1
DETERMINING CAUSE OF DEATH. .................................................................................................................................1
DEATH CERTIFICATES FOR DEATHS OCCURRING AWAY FROM COMMAND OR IN FOREIGN PORTS...........1
RELATIONS WITH CIVILIAN AUTHORITIES. ................................................................................................................1
REPORTING DEATHS TO CIVILIAN AUTHORITIES......................................................................................................2
DEATH FORMS FOR CIVILIAN AGENCIES AND INDIVIDUALS.................................................................................2
IDENTIFICATION OF REMAINS........................................................................................................................................2
SECTION B - PSYCHIATRIC CONDITIONS (INCLUDING PERSONALITY DISORDERS)............................... 3
GENERAL..............................................................................................................................................................................3
PERSONALITY DISORDERS..............................................................................................................................................3
ADJUSTMENT DISORDERS. ..............................................................................................................................................4
ORGANIC MENTAL DISORDERS......................................................................................................................................4
PSYCHOACTIVE SUBSTANCE USE DISORDERS. .........................................................................................................5
SCHIZOPHRENIA. ...............................................................................................................................................................5
PSYCHOTIC DISORDERS NOT ELSEWHERE CLASSIFIED..........................................................................................6
DELUSIONAL (PARANOID) DISORDER. .........................................................................................................................6
NEUROTIC DISORDERS.....................................................................................................................................................6
MOOD DISORDERS.............................................................................................................................................................6
ANXIETY DISORDERS (OR ANXIETY AND PHOBIC NEUROSES). ............................................................................7
SOMATOFORM DISORDERS.............................................................................................................................................7
DISSOCIATIVE DISORDERS (OR HYSTERICAL NEUROSES, DISSOCIATIVE TYPE)..............................................7
SEXUAL DISORDERS. ........................................................................................................................................................8
SEXUAL DYSFUNCTIONS .................................................................................................................................................8
FACTITIOUS DISORDERS..................................................................................................................................................9
DISORDERS OF IMPULSE CONTROL NOT ELSEWHERE CLASSIFIED......................................................................9
DISORDERS USUALLY FIRST EVIDENT IN INFANCY, CHILDHOOD, OR ADOLESCENCE...................................9
316.00 PSYCHOLOGICAL FACTORS AFFECTING PHYSICAL CONDITION.............................................................11
V CODES FOR CONDITIONS NOT ATTRIBUTABLE TO A MENTAL DISORDER THAT ARE A FOCUS OF
ATTENTION OR TREATMENT. .......................................................................................................................................11
ADDITIONAL CODES........................................................................................................................................................12
CH-16 5-ii
SECTION C - MENTAL HEALTH EVALUATION OF COAST GUARD SERVICE MEMBERS............ 13
GENERAL............................................................................................................................................................................13
COMMANDING OFFICER SUSPECTING A MENTAL HEALTH EVALUATION.................................... 13
PROCEDURE FOR COMMANDING OFFICER REFERRAL. ...................................................................... 14
5-1 CH-16
CHAPTER 5. DEATHS AND PSYCHIATRIC CONDITIONS (PERSONALITY)
Section A - Deaths.
1. General. Chapter 11 of the Personnel Manual, COMDTINST M1000.6(series) contains
further guidance concerning casualties and decedent affairs.
2. Duties of Medical Officers or Health Services Department Representatives in the Event
of A Death at A Coast Guard Unit. The medical officer or health services department
representative shall report immediately to the scene and:
a. advise the commanding officer of the name, grade or rate, and social security number
of the decedent;
b. advise the commanding officer of the time and place of death;
c. advise the commanding officer, insofar as possible, as to the cause of death;
d. ensure notification of the quarantine officer or coroner if required; and
e. arrange with local civilian authorities for issuing a death certificate.
3. Determining Cause of Death. When an active duty Coast Guard member dies aboard a
Coast Guard vessel or station under unnatural or suspicious circumstances, or when the
cause of death is unknown, an administrative investigation shall immediately be
convened in accordance with Section 11-A-3 of the Personnel Manual, COMDTINST
M1000.6(series) and Chapter 5 of the Administrative Investigations Manual,
COMDTINST M5830.1 (series).
4. Death Certificates for Deaths Occurring Away From Command or in Foreign Ports.
f. When an active duty member dies while away from his/her duty station, the
commanding officer or designated representative shall obtain a death certificate from
civilian authorities. If the civilian death certificate does not furnish all necessary
information, the district commander of the district in which the death occurred shall
request additional information.
g. If death occurs abroad, request the nearest United States Consular Office to obtain a
death certificate from civilian authorities.
h. When an active duty member, or a Reserve performing inactive duty for training, is
in a missing status because of events in international waters and no identifiable
remains can be recovered, and no civilian death certificate is issued, a report
(including recommendations) shall be made as per Section 11-A, Personnel Manual,
COMDTINST M1000.6 (series).
5. Relations with Civilian Authorities. When a Coast Guard member dies outside the limits
of a Coast Guard reservation, the body shall not be moved until permission has been
obtained from civilian authorities (e.g., coroner's office and/or medical examiner). In
CH-16 5-2
order that there may be full understanding and accord between the Coast Guard and
civilian authorities, appropriate procedures will be developed for each command area, in
consultation with the civilian authorities, covering deaths of personnel within and
without the limits of Coast Guard commands. In general, and except where the state has
retained concurrent jurisdiction with the United States, civilian authorities have no
jurisdiction over deaths occurring on Coast Guard reservations. A transit or burial
permit, however, issued by civilian authorities is required for removal of a body from a
Coast Guard reservation for shipment or burial.
6. Reporting Deaths to Civilian Authorities. When a death occurs at a Coast Guard activity
in any state, territory, or insular possession of the United States, the death must be
reported promptly to civilian authorities. Local agreements concerning reporting and
preparing death certificates shall be made between the commanding officer, or
designated representative, and the civilian authorities.
7. Death Forms for Civilian Agencies and Individuals. Forward all requests for completing
blank forms concerning death of Coast Guard personnel to Commandant (G-WP) for
action.
8. Identification of Remains. Identification of remains may be established by marks and
scars, dental records, fingerprints, and personal recognition. In questionable cases, a
dental officer shall examine the remains and record observations on a SF-603 for
comparison with other available records.
5-3 CH-16
Section B - Psychiatric Conditions (including personality disorders).
1. General. The following diagnostic categories conform to DSM IV-R and indicate the
appropriate reference for disposition. In determining qualification for appointment,
enlistment, and induction, or appropriate disposition (when the condition has been
determined to be disqualifying for retention in accordance with paragraph 3-F-16), the
diagnosis appears under DSM IV Axis I or Axis II. Conditions generally considered
treatable and not grounds for immediate separation, mental health treatment may be
authorized for members when medically necessary to relieve suffering and/or maintain
fitness for unrestricted duty. The decision to provide treatment for mental health
conditions will be based on a review of all factors, including the opinion of experts,
probability of a successful outcome, and the presence of other physical or mental
conditions.
a. If a successful outcome (availability for worldwide assignment) is not realized within
six months of the initiation of therapy, the patient's condition must be reassessed. If
the reassessment indicates that the prognosis for a successful outcome is poor, the
member shall be processed for discharge pursuant to Chapter 12 of the Personnel
Manual or through the Physical Disability Evaluation System (PHYSICAL
DISABILITY EVALUATION SYSTEM).
2. Personality Disorders. These disorders are disqualifying for appointment, enlistment,
and induction under Section 3-D-33 herein or shall be processed in accordance with
Chapter 12, Personnel Manual, COMDTINST M1000.6 (series). These are coded on
Axis II.
a. 301.00 Paranoid.
b. 301.20 Schizoid.
c. 301.22 Schizotypal.
d. 301.4 Obsessive compulsive.
e. 301.50 Histrionic.
f. 301.6 Dependent.
g. 301.7 Antisocial.
h. 301.81 Narcissistic.
i. 301.82 Avoidant.
j. 301.83 Borderline.
k. 301.9 Personality disorder NOS (includes Passive-aggressive).
CH-16 5-4
l. Personality trait(s) considered unfitting per paragraph 3-F-16.c.
3. Adjustment Disorders. These disorders are generally treatable and not usually grounds
for separation. However, when these conditions persist or treatment is likely to be
prolonged or non-curative, (e.g., inability to adjust to military life/sea duty, separation
from family/friends) process in accordance with Chapter 12, Personnel Manual,
COMDTINST M1000.6 (series) is necessary.
a. 309.0 With depressed mood.
b. 309.24 With anxiety.
c. 309.28 With mixed anxiety and depressed moods.
d. 309.3 With disturbance of conduct.
e. 309.4 With mixed disturbance of emotions and conduct.
f. 309.90 Adjustment disorder unspecified.
4. Organic Mental Disorders. These disorders are either disqualifying for appointment,
enlistment, and induction under Section 3-D-29 of this manual or shall be processed in
accordance with Physical Disability Evaluation System (PHYSICAL DISABILITY
EVALUATION SYSTEM), COMDTINST M1850.2 (series).
a. Dementias arising in the senium and presenium.
(1) Dementia of the Alzheimer type, with early onset.
(a) 290.00 Uncomplicated.
(b) 290.11 With delirium.
(c) 290.12 With delusions.
(d) 290.13 With depressed mood.
(2) 290.4 Vascular Dementia (various subtypes).
(3) 294.x Dementia due to other medical conditions (various subtypes).
(4) 294.8 Dementia NOS.
b. Other Organic Mental Disorders associated with Axis III physical disorders or
conditions, or etiology is unknown, including but not limited to the following.
(5) 293.0 Delirium due to general medical condition.
(6) 293.81 Psychotic disorder with delusions due to a general medical condition.
(7) 293.82 Psychotic disorder with hallucinosis due to a general medical condition.
(8) 293.83 Mood disorder due to a general medical condition.
5-5 CH-16
(9) 294.00 Amnestic disorder due to general medical condition.
(10) 310.1 Personality change due to a general medical condition.
5. Psychoactive Substance Use Disorders. These disorders are disqualifying for
appointment, enlistment, or induction under Section 3-D-35 of this manual or shall be
processed in accordance with Chapter 20, Personnel Manual, COMDTINST M1000.6
(series).
a. 303.90 Alcohol dependence (alcoholism).
b. 304.00 Opioid dependence.
c. 304.10 Sedative, hypnotic, or anxiolytic dependence.
d. 304.20 Cocaine dependence.
e. 304.30 Cannabis dependence.
f. 304.40 Amphetamine dependence.
g. 304.50 Hallucinogen dependence.
h. 304.60 Inhalant dependence.
i. 304.90 Other (or unknown) substance, including PCP dependence.
j. 305.00 Alcohol abuse.
k. 305.20 Cannabis abuse.
l. 305.30 Hallucinogen abuse.
m. 305.40 Sedative, hypnotic, or anxiolytic abuse.
n. 305.50 Opioid abuse.
o. 305.60 Cocaine abuse.
p. 305.70 Amphetamine abuse.
q. 305.90 Other (or unknown) Substance abuse, including inhalant and PCP abuse.
6. Schizophrenia. These disorders are disqualifying under Section 3-D-30 of this manual or
shall be processed in accordance with Physical Disability Evaluation System,
COMDTINST M1850.2 (series).
a. 295.10 Disorganized type.
b. 295.20 Catatonic type.
CH-16 5-6
c. 295.30 Paranoid type.
d. 295.60 Residual type.
e. 295.90 Undifferentiated type.
7. Psychotic Disorders Not Elsewhere Classified. These disorders are disqualifying under
Section 3-D-30 of this manual or shall be processed in accordance with Physical
Disability Evaluation System, COMDTINST M1850.2 (series).
a. 295.40 Schizophreniform disorder.
b. 295.70 Schizoaffective disorder.
c. 297.30 Induced psychotic disorder.
d. 298.80 Brief psychotic disorder.
e. 298.90 Psychotic disorder NOS.
8. Delusional (Paranoid) Disorder. 297.1, Delusional (Paranoid) Disorder, is
disqualifying under Section 3-D-30 of this manual or shall be processed in accordance
with Physical Disability Evaluation System, COMDTINST M1850.2 (series).
9. Neurotic Disorders. These disorders are now included in Anxiety, Somatoform,
Dissociative, and Sexual Disorders.
10. Mood Disorders. These disorders are disqualifying for enlistment under Section 3-D-31
of this manual or shall be processed in accordance with Physical Disability Evaluation
System, COMDTINST M1850.2 (series).
a. Bipolar I Disorders.
(1) 296.0X Bipolar I disorder, single manic episode (various subtypes).
(2) 296.40 Bipolar I disorder, most recent episode hypomanic.
(3) 296.4X Bipolar I disorder, most recent episode manic (various sub-types).
(4) 296.5X Bipolar I disorder, most recent depressed (various sub-types).
(5) 296.6X Bipolar I disorder, most recent episode mixed, (various sub-types).
(6) 296.7 Bipolar I disorder, most recent episode unspecified.
(7) 296.89 Bipolar II disorder.
(8) 301.13 Cyclothymia.
b. Depressive Disorders.
(1) 296.XX Major depressive disorder (various sub-types).
(2) 300.4 Dysthymic disorder (or depressive neurosis).
5-7 CH-16
(3) 311 Depressive disorder NOS.
11. Anxiety Disorders (or Anxiety and Phobic Neuroses). These disorders are disqualifying
for appointment, enlistment, or induction under Section 3-D-32 of this manual or shall
be processed in accordance with Physical Disability Evaluation System, COMDTINST
M1850.2 (series) except as noted on (5) below.
a. Panic Disorders.
(1) 300.01 Without agoraphobia.
(2) 300.21 With agoraphobia.
(3) 300.22 Agoraphobia without history of panic disorder.
(4) 300.23 Social phobia.
(5) 300.29 Specific phobia. [Chapter 12, Personnel Manual,COMDTINST
M1000.6 (series).]
b. Other Anxiety disorders.
(1) 300.00 Anxiety disorder NOS.
(2) 300.02 Generalized anxiety disorder.
(3) 300.3 Obsessive-compulsive disorder (or obsessive compulsive neurosis).
(4) 309.81 Post-traumatic stress disorder.
12. Somatoform Disorders. These disorders are disqualifying for appointment, enlistment,
or induction under Section 3-D-32 of this manual or shall be processed in accordance
with Physical Disability Evaluation System, COMDTINST M1850.2 (series).
a. 300.11 Conversion disorder.
b. 300.70 Hypochondriasis (or hypochondrical neurosis). Body Dysmorphic disorder.
Somatoform disorder NOS.
c. 300.81 Somatization disorder or undifferentiated somatoform disorder.
d. 307.80 Pain disorder associated with psychological factors.
13. Dissociative Disorders (or Hysterical Neuroses, Dissociative Type). These disorders are
disqualifying for appointment, enlistment, or enlistment under Section 3-D-32 of this
manual or shall be processed in accordance with Physical Disability Evaluation System,
COMDTINST M1850.2 (series).
a. 300.12 Dissociative amnesia.
b. 300.13 Dissociative fugue.
c. 300.14 Dissociative identity disorder.
CH-16 5-8
d. 300.15 Dissociative disorder NOS.
e. 300.6 Depersonalization disorder.
14. Sexual Disorders. These disorders are processed in accordance with Chapter 12 of the
Personnel Manual, COMDTINST M1000.6 (series).
a. Gender Identity Disorders.
(1) 302.6 Gender identity disorder in children (history of) or NOS.
(2) 302.85 Gender identity disorder in adolescents or adults.
b. Paraphilias.
(1) 302.2 Pedophilia.
(2) 302.3 Transvestic fetishism.
(3) 302.4 Exhibitionism.
(4) 302.81 Fetishism.
(5) 302.82 Voyeurism.
(6) 302.83 Sexual masochism.
(7) 302.84 Sexual sadism.
(8) 302.89 Frotteurism.
(9) 302.9 Paraphilia NOS (includes Zoophilia).
15. Sexual Dysfunctions. These are not grounds for action as they have no direct bearing
upon fitness for duty.
a. 302.70 Sexual dysfunction NOS.
b. 302.71 Hypoactive sexual desire.
c. 302.72 Female arousal disorder. Male erectile disorder.
d. 302.73 Female orgasmic disorder.
e. 302.74 Male orgasmic disorder.
f. 302.75 Premature ejaculation.
g. 302.76 Dyspareunia.
h. 302.79 Sexual aversion disorder.
i. 302.9 Sexual Disorder NOS.
j. 306.51 Vaginismus.
5-9 CH-16
16. Factitious Disorders. These disorders are disqualifying for appointment, enlistment, or
induction under Section 3-D-32 of this manual or should be processed in accordance with
Chapter 12 of the Personnel Manual, COMDTINST M1000.6 (series).
a. 300.16 With predominantly psychological symptoms.
b. 300.19 Factitious disorder NOS.
c. 301.51 With predominantly physical symptoms, or combined.
17. Disorders of Impulse Control Not Elsewhere Classified. These disorders are
disqualifying for enlistment under Section 3-D-33 of this manual or should be processed
in accordance with Chapter 12 of the Personnel Manual COMDTINST M1000.6 (series).
a. 312.30 Impulse control disorder NOS.
b. 312.31 Pathological gambling.
c. 312.32 Kleptomania.
d. 312.33 Pyromania.
e. 312.34 Intermittent explosive disorder.
f. 312.39 Trichotillomania.
18. Disorders Usually First Evident in Infancy, Childhood, or Adolescence. Except as
indicated in parentheses, these disorders are disqualifying for appointment, enlistment, or
induction under Section 3-D-33 of this manual, or shall be processed in accordance with
Chapter 12 of the Personnel Manual, COMDTINST M1000.6 (series), if the condition
significantly impacts, or has the potential to significantly impact performance of duties
(health, mission, and safety).
a. Mental Retardation (Note: these are coded on Axis II).
(1) 317 Mild mental retardation, IQ 50-70.
(2) 318.X Moderate, severe, or profound mental retardation, IQ 35-49.
(3) 319 Mental retardation, severity unspecified.
b. Disruptive Behavior Disorders.
(1) 314.0X Attention deficit hyperactivity disorder (various types).
(2) 312.8 Conduct disorder.
(3) 312.9 Disruptive behavior disorder or attention deficit disorder, NOS.
(4) 313.81 Oppositional defiant disorder.
c. Other Disorders of Infancy, Childhood, or Adolescence.

CH-16 5-10
(1) 307.30 Stereotypic movement disorder.
(2) 309.21 Separation anxiety disorder.
(3) 313.23 Selective mutism.
(4) 313.82 Identity problem.
(5) 313.89 Reactive attachment disorder of infancy or early childhood.
d. Eating Disorders. Eating disorders have a potential to affect fitness for duty, but the
diagnosis of an eating disorder does not automatically mean the member is unsuitable
for continued service. Individuals suspected of having an eating disorder shall be
referred for evaluation by an Armed Forces psychiatrist or Armed Forces clinical
psychologist. Treatment may be authorized in accordance with the same criteria as
other mental conditions. See paragraph 5.B.1 of this Manual.
(1) 307.1 Anorexia nervosa. (Shall be processed through Physical Disability
Evaluation System (COMDTINST M1850.2 ))
(2) 307.50 Eating disorder NOS. Shall be processed in accordance with Chapter
12.B.12 or 12.A.15.h (as applicable) of the Personnel Manual, COMDTINST
M1000.6(series), if the condition significantly impacts or has the potential to
significantly impact performance of duties (health, mission, and safety).
(3) 307.51 Bulimia nervosa. (Shall be processed through Physical Disability
Evaluation System (COMDTINST M1850.2))
(4) 307.52 Pica.
(5) 307.53 Rumination disorder.
e. Tic Disorders.
(1) 307.20 Tic disorder NOS.
(2) 307.21 Transient tic disorder.
(3) 307.22 Chronic motor or vocal tic disorder.
(4) 307.23 Tourette's disorder.
f. Communication Disorder.
(1) 307.0 Stuttering.
(2) 315.31 Expressive or mixed (expressive-receptive) language disorder.
(3) 315.39 Phonological disorder.
g. Elimination Disorders.
(1) 307.46 Sleepwalking disorder.
(2) 307.46 Sleep terror disorder.
(3) 307.6 Enuresis (not due to a general medical condition).
5-11 CH-16
(4) 307.7 Encopresis (without constipation and overflow incontinence.)
h. Pervasive Developmental Disorder.
(1) 299.00 Autistic disorder.
(2) 299.80 Pervasive developmental disorder NOS.
i. Specific Learning Developmental Disorders - (Note: These Are Coded on Axis II).
(1) 315.00 Reading disorder.
(2) 315.1 Mathematics disorder.
(3) 315.2 Disorder of written expression.
(4) 315.4 Developmental coordination disorder.
(5) 315.9 Learning disorder NOS.
19. 316.00 Psychological Factors Affecting Physical Condition. This disorder is not
generally grounds for action alone. The physical condition must be specified on Axis III
and will determine fitness.
20. V Codes for Conditions Not Attributable to a Mental Disorder that are a Focus of
Attention or Treatment. These disorders are generally not of such severity as to lead to
disqualification for enlistment or to separation. Where separation is indicated, process in
accordance with Chapter 12 of the Personnel Manual, COMDTINST M1000.6 (series).
a. V15.81 Noncompliance with medical treatment.
b. V61.1 Partner relational problem.
c. V61.20 Parent-child relational problem.
d. V61.8 Sibling relational problem.
e. V62.2 Occupational problem.
f. V62.3 Academic problem.
g. V62.81 Relational problem NOS.
h. V62.82 Bereavement.
i. V62.89 Borderline intellectual functioning.
j. V62.89 Phase of life problem or religious or spiritual problem.
k. V65.2 Malingering. (May be grounds for legal, administrative, or medical board
proceedings in accordance with Section 2-A-4 of this manual depending on the
circumstances)
CH-16 5-12
l. V71.01 Adult antisocial behavior.
m. V71.02 Child or adolescent antisocial behavior.
21. Additional Codes. These are nondiagnostic codes for administrative use and require no
action.
a. V71.09 No diagnosis or condition on Axis I.
b. V71.09 No diagnosis on Axis II.
c. 300.9 Unspecified mental disorder (nonpsychotic).
d. 799.9 Diagnosis or condtion deferred on Axis I.
e. 799.9 Diagnosis deferred on Axis II.
5-13 CH-16
Section C - Command directed Mental Health Evaluation of Coast Guard Service members.
1. General. A commander, (including commanding officers, of clinics) shall refer a Service
member for an emergency mental health evaluation as soon as is practicable whenever a
Service member indicates an intent to cause serious injury to himself or others, and the
commander believes that the Service member may be suffering from a mental disorder.
a. Active Duty Mental Health Conditions and Emergencies, COMDTPUB P6520.1
refers to Public Law 102-484, Section 546, also known as the “Boxer Amendment”
The Coast Guard is not included and therefore not subject to the Boxer’s
Amendment. These restrictions are intended to prevent the unwarranted mental
health evaluations or involuntary hospitalization as a form of harassment or
retaliation.
b. Prior to transporting a Service member for an emergency evaluation, or shortly
thereafter if the time and nature of the emergency does not permit, the commanding
officer shall consult directly with a mental health care provider (or other health care
provider if a mental health care provider is not available) at the MTF. The purpose
of this consult is to communicate the observations and circumstances which led the
commander to believe that the Service member’s behavior constituted an emergency.
The commander will then forward to the mental health care provider consulted a
memorandum documenting the information discussed.
2. When not an emergency, commanding officers suspecting a mental health evaluation
may be indicated will:
a. Contact the appropriate point of contact at the servicing Coast Guard Medical clinic
and speak directly with the point of contact to request a command-directed mental
health evaluation. Signs of mental illness can include changes in behavior, mood, or
thinking that interfere with normal functioning. The health care provider will clarify
the request, urgency of the referral, and schedule an appointment.
b. Provide a memorandum from the commanding officer to the DoD MTF/clinic
commander documenting this contact, subject: Command Referral for Mental Health
Evaluation of (Service Member Rank, Name, Branch of Service and SSN. (sample
letter Figure 1).
c. Counsel the Service member and insure that the Service member is provided written
notice of the referral. A sample memorandum from the commanding officer to the
MTF/clinic commander documenting this contact, subject: Notification of
Commanding Officer Referral for Mental Health Evaluation (Non-Emergency). The
notice will include the following: (sample letter Figure 2)
(1) Date and time the mental-health evaluation is scheduled.
(2) A brief, factual description of the Service member’s behavior and verbal
expressions that indicate a mental-health evaluation is necessary.
CH-16 5-14
(3) Names of mental-health professionals the commander has consulted before
making the referral. If consultation is not possible, commanders must include
the reasons in the notice.
d. Request the Service member sign the notice to report for a mental- health evaluation.
If the Service member refuses to sign, the commander will note this response in the
notice.
e. Provide an escort to Service member referred for a mental- health evaluation.
3. Commanders shall provide a copy of the following rights to Service members who are
referred:
a. A Service member has the right to obtain a second opinion at his own expense. The
evaluation should be conducted within a reasonable period of time, usually within 10
days and will not delay nor substitute for an evaluation performed by a DoD mental
health care.
b. No person may restrict the Service member from communicating with an attorney,
IG, chaplain, Member of Congress, or other appropriate party about the member's
referral.
c. Other than emergencies, the Service member will have at least 2 workdays before a
scheduled mental-health evaluation to meet with an attorney, chaplain, IG, or other
appropriate party. If a commander has reason to believe the condition of the Service
member requires an immediate mental-health evaluation, the commander will state
the reasons in writing as part of the request for evaluation.
d. If military duties prevent the Service member from complying with this policy, the
commander seeking the referral will state the reasons in a memorandum.
4. No one will:
a. Refer a Service member for a mental-health evaluation as a reprisal for making or
preparing a lawful communication to a Member of Congress, an authority in the
Service member's chain of command, an IG, or a member of a DoD audit, inspection,
investigation, or law enforcement organization.
b. Restrict a Service member from lawfully communicating with an IG, attorney,
Member of Congress, or others about the Service member's referral for a mental-
health evaluation.
c. These policies are not designed to limit the commander's authority to refer Service
members for emergency mental-health evaluations and treatment when
circumstances suggest the need for such action.
5-15 CH-16
5. The specific procedures required by these regulations apply to mental health evaluations
directed by a service member’s commander as an exercise of the commander’s
discretionary authority. Evaluations NOT covered by these procedures include:
a. Voluntary self-referrals;
b. Criminal responsibility and competency inquiries conducted under Rule for Court-
Martial 706 of the Manual for Courts-Martial;
c. Interviews conducted according to the Family Advocacy Program;
d. Referrals to the Alcohol and Drug Abuse Prevention and Control Program;
e. Security clearances.
f. Diagnostic referrals from other health care providers not part of the Service
member’s chain of command when the Service member consents to the evaluation;
and;
g. Referrals for evaluations expressly required by regulation, without any discretion by
the Service member’s commander, such as enlisted administrative separations.
6. Procedures for using the memorandum requesting a mental health evaluation in
emergency situations Commanders will:
a. When completing the memorandum Commanders should include as many details as
possible.
b. Make one copy to give to the Service member.
c. Ensure that the Service member's escort hand carries the memorandum to the
treatment facility. The memorandum will not be hand carried by the Service member
being referred. This memorandum will not be sent through distribution channels, nor
will it become part of the Service member's health record. The memorandum will be
filed in the Department of Psychiatry of the medical treatment facility where the
Service member was evaluated.

CH-16 5-16
FIGURE 1
Sample: Commanding Officer request for routine (non emergency) Mental Health Evaluation
Date:
Memorandum for Commanding Officer (Name of Medical Treatment Facility (MTF) or Clinic)
From: Commanding Officer, (Name of Command)
Subject: Command Referral for Mental Health Evaluation of (Service Member Rank, Name,
Branch of Service and SSN)
Reference (a) Medical Manual COMDTINST M6000.1B, Chap 5-C
(b) Active Duty Mental Health Conditions and Emergencies, COMDTPUB
P6520.1
1. In accordance with references (), I hereby request a formal mental health evaluation of
(rank and name of Service member).
2. (Name and rank of Service member) has (years) and (months) active duty service and has
been assigned to my command since (date). Armed Services Vocational Aptitude Battery
(ASVAB) scores upon enlistment were: (list scores). Past average performance marks
have ranged from ______ to ______ (give numerical scores). Legal action is/is not
currently pending against the Service member. (If charges are pending, list dates and
UCMJ articles). Past legal actions include: (List dates, charges, non judicial punishments
(NJPs) and/or findings of Courts Martial.)
3. I have forwarded to the Service member a memorandum that advises (rank and name of
Service member) of his (or her) rights. This memorandum also states the reasons for this
referral, the name of the mental health care provider(s) with whom I consulted. A copy of
this memorandum is attached for your review.
4. (Service member's rank and name) has been scheduled for evaluation by (name and rank
of metal healthcare provider) at (name of MTF or clinic) on (date) at (time).
5. Should you wish additional information, you may contact (name and rank of the
designated point of contact) at (telephone number).
6. Please provide a summary of your findings and recommendations to me as soon as they
are available. (Signature)
Rank and Name of Commanding Officer
Attachment:
As stated

5-17 CH-16
FIGURE 2
Sample: Service member notification of Commanding Officer referral for Mental Health
Evaluation.
Date:
Memorandum for (Service member's rank, name and SSN)
From: Commanding Officer, (Name of Command)
Subject: Notification of Commanding Officer referral for Mental Health Evaluation
(non emergency).
References: (a) Medical Manual COMDTINST M6000.1B, Chap 5-C
(b) Active Duty Mental Health Conditions and Emergencies,
COMDTPUB P6520.1
1. In accordance with references (), this memorandum is to inform you that I am referring
you for a mental health evaluation.
2. The following is a description of your behaviors and/or verbal expressions that I
considered in determining the need for a mental health evaluation: (Provide dates and a
brief factual description of the Service member's actions of concern.)
3. Before making this referral, I consulted with the following mental health care provider(s)
about your recent actions: (list rank, name, corps, branch of each provider consulted) at
(name of Medical Treatment Facility (MTF) or clinic) on (date(s)). (Rank(s) and name(s)
of mental healthcare provider(s)) concur(s) that this evaluation is warranted and is
appropriate.
OR
Consultation with a mental healthcare provider prior to this referral is (was) not possible
because (give reason; e.g., geographic isolation from available mental healthcare
provider, etc.)
4. Per references (a) and (b), you are entitled to the rights listed below:
The right to obtain a second opinion and be evaluated by a mental healthcare provider of
your own choosing, at your own expense, if reasonably available. Such an evaluation by
an independent mental healthcare provider shall be conducted within a reasonable period
of time, usually within 10 business days, and shall not delay nor substitute for an
evaluation performed by a DoD mental healthcare provider.
a. The right to communicate without restriction with an IG, attorney, Member of
Congress, or others about your referral for a mental health evaluation. This provision
does not apply to a communication that is unlawful.
CH-16 5-18
b. The right, except in emergencies, to have at least two business days before the
scheduled mental health evaluation to meet with an attorney, IG, chaplain, or other
appropriate party. If I believe your situation constitutes an emergency or that your
condition appears potentially harmful to your well being and I judge that it is not in
your best interest to delay your mental health evaluation for two business days, I shall
state my reasons in writing as part of the request for the mental health evaluation.
c. If you are assigned to a naval vessel, deployed or otherwise geographically isolated
because of circumstances related to military duties that make compliance with any of
the procedures in paragraphs (3) and (4), above, impractical, I shall prepare and give
you a copy of the memorandum setting forth the reasons for my inability to comply
with these procedures.
5. You are scheduled to meet with (name and rank of the mental healthcare provider) at
(name of MTF or clinic) on (date) at (time).
(Signature)
Rank and Name of Commanding Officer
I have read the memorandum above and have been provided a copy.
Service member's signature:_____________________________ Date:______________
OR:
The Service member declined to sign this memorandum which includes the Service member's
Statement of Rights because (give reason and/or quote Service member).
Witness's signature:_____________________________ Date:______________
Witness's rank and name:_____________________________ Date:______________
(Provide a copy of this memorandum to the Service member.)
CHAPTER 6
REPORTS, FORMS, AND RECORDS
SECTION A - REQUIRED REPORTS PAGE
HEALTH SERVICES STATISTICAL REPORT (RCN 6000-1).......................................................................................... 1
REPORT OF POTENTIAL THIRD PARTY LIABILITY (RCN 6000-2)............................................................................... 2
MLC/HEADQUARTERS CLINIC OPERATIONS REPORT (RCN 6000-3)........................................................................ 2
DISEASE ALERT REPORT (RCN 6000-4) ................................................................................................................... 2
REPORT OF THEFT OF CONTROLLED SUBSTANCES (RCN 6000-5) ............................................................................ 2
INPATIENT HOSPITAL REPORT (RCN 6000-6) ........................................................................................................... 2
MAJOR HEALTH CARE EQUIPMENT INVENTORY REPORT (RCN 6000-7).................................................................. 3
HEALTH SERVICES DIVISION STATUS REPORT (RCN 6000-8.................................................................................... 3
SHORTENED CLINIC AUTOMATED REPORT SYSTEM (SCARS) ................................................................................. 3
SECTION B - FORMS AND RECORDS
CG-5460A, STATUS-PROFILE ................................................................................................................................... 7
CG-5460B, VISIT PROFILE...................................................................................................................................... 13
CG5211, HEALTH CARE EQUIPMENT REQUEST ...................................................................................................... 14
NAVMED 6150/7, HEALTH RECORD RECEIPT FORM ............................................................................................ 16
DD-2161, REFERRAL FOR CIVILIAN MEDICAL CARE .............................................................................................. 16
HEALTH SERVICES LOG ......................................................................................................................................... 16
BINNACLE LIST ....................................................................................................................................................... 17
DD2766, ADULT PREVENTIVE AND CHRONIC CARE FLOWSHEET FORM................................................................. 17
6-i

6-1 CH-16
CHAPTER 6. REPORTS, FORMS, AND RECORDS
Section A - Reports.
1. Health Services Statistical Report, (RCN 6000-1).
a. The HSSR is produced by the Clinic Automated Management System (CLAMS) and
is based on data entered at the terminal during the reporting month.
b. During production of the HSSR a set of screen prompts will allow entry of required
information from the terminal keyboard. Prompt criteria include:
(1) Onboard staffing and billets for HSs, medical practitioners, and dental officers.
(2) Prescriptions. A number may already appear in this field. This number will
be the number of prescriptions issued for the selected month (calculated from
the database).
(3) Inspections. Count one for each inspection logged (e.g., galley, berthing,
water, pool, food handlers).
(4) SAR. Count one for each SAR or MEDEVAC sortie (air or boat) with health
services personnel aboard.
(5) Training Hours Given (medical officers). Count any medical training by
medical officers (all hands, suturing demonstration, demonstrating knee injury
evaluation to one or more HSs, hypothermia lecture for local boaters group,
etc.) greater than 15 minutes duration. Total all training increments lasting
longer than 15 minutes by all medical officers and round to the nearest hour.
(6) Expense Data (month). Enter the corresponding expenses for the selected
month. Note: when starting the HSSR Report from a month other than
October, it may be necessary to enter the year-to-year figures initially in order
for the subsequent YTD figures to be correct.
(7) Expense Data (OPTAR). The corresponding Operating Target for the selected
fiscal year. The amounts set initially will continue to appear, unless they are
changed.
(8) Tickler OPFACs. CLAMS tabulates the percentage of USCG active duty
persons in compliance with mandatory medical/dental requirements (shots,
exams, audiograms, etc.) and displays this on the HSSR. Personnel in
clinic/sickbay "Binnacle OPFACs" are automatically included in this "tickler
file" scrutiny. Outlying units which fall within a clinic/sickbay's tickler radius
but are too remote for binnacle reporting CLAMS calls "Tickler OPFACs".
The user must enter these additional "Tickler OPFACs" at the time the HSSR
is made. Once entered they will continue to display unless changed. NOTE:
HSs at group/cutter sickbays are responsible for their own binnacle and
"tickler" activity. This applies even in those situations where the majority of
care for the group/cutter personnel is provided by a nearby USCG clinic.
CH-16 6-2
c. The report shall be submitted to the commanding officer for approval and signature
by the FIFTH working day of the following month.
d. A signed copy of the HSSR shall be filed in the health care facility and be accessible
for MLC audit.
2. Report of Potential Third Party Liability (RCN 6000-2). (Refer to Health Care Third
Party Claims Recovery, COMDTINST 6010.16 (series) for current policy). Submit this
report on form CG-4899 (Rev. 10-91), Report of Potential Third Party Liability. A
sample form CG-4899 (Rev. 10-91) is included as Figure 6-A-1. If applicable, attach to
Nonfederal Health Care Certification Form, CG-5534, when submitting nonfederal
health care bills for processing.
3. MLC/Headquarters Clinic Operations Report (RCN 6000-3). Generate and submit the
MLC/Headquarters Report in accordance with the instructions contained in the CLAMS
User's Guide. This report is submitted on disk or transmitted electronically to
Commandant (G-K) monthly for clinics and every 6 months (October/April) for
sickbays. Outpatient health care of non-USCG patients and dental statistical reporting
are incorporated into this report. Reports from clinics and sickbays must be sent to
Commandant (G-K) within five working days of the following month. Delay of report
submission from sickbays is permissible should operational commitments (e.g.,
underway) interfere with timely reporting.
4. Disease Alert Report (RCN-6000-4). Disease Alert Reports provide appropriate
commands with information that can be used to protect lives and health, and maintain
command effectiveness. Detailed instructions are contained in Section 7-B of this
manual.
5. Report of Theft of Controlled Substances (RCN 6000-5).
a. Discrepancies noted on Controlled Substance Inventory Board Reports shall be
investigated as discussed in Chapter 10 of this manual. Submit findings to
appropriate MLC (K).
b. MLC (K) shall review and determine further action, including whether a Form DEA-
106 shall be submitted. A copy of all DEA-106 reports submitted shall be sent to
Commandant (G-WKH).
6. Inpatient Hospital Report (RCN 6000-6). When notified that a member of the Coast
Guard is hospitalized, transferred to another facility, or discharged from inpatient status,
the unit commanding officer shall notify the appropriate MLC (p) and (k) via message in
accordance with current MLC directives. When listing diagnosis, use only ICD-9 codes;
do not include a description of the ailment. See Paragraph 2-A-2 of this manual for
additional policy concerning emergency care at other than Coast Guard or DOD
facilities. CLAMS also produces a letter containing this information.
6-3 CH-16
7. Health Care Equipment Inventory Report (RCN 6000-7). Health care equipment
inventories are maintained by the MLCs’ and are used for planning and budgeting
purposes. All units with health care equipment shall verify their health care equipment
inventory. Annually, in January, MLC (k) will forward to each unit within their area of
responsibility a copy of their previous health care equiptment inventory report. Units
shall annotate changes and submit to MLC (k) with their annual budget request. MLC
(k) will compile all inventories and forward them to Commandant (G-WKH) in
conjunction with separate entity from the unit’s personal property list. This inventory
report reflects only major health care equipment or items with an original cost of more
than $300.00.
8. Health Services Division Status Report (RCN 6000-8). This annual report provides
Headquarters and MLCs’ with individual clinics’ status, problems, and initiatives in the
medical, dental, pharmacy, and quality assurance areas. See Commandant Instruction
6010.22(series) for specific instructions regarding preparation and submission of this
report.
9. Shorten Clinic Automated Report System (SCARS). Sickbays that have not been able to
implement CLAMS can use SCARS to produce the MLC/Headquarters Clinic
Operations Report until they are able to use CLAMS. Note that the semiannual
MLC/Headquarters Clinic Operations Report (RCN 6000-3) is separate and distinct from
the monthly Health Services Statistical Report (RCN 6000-1). Sickbays having to
produce an HSSR without benefit of CLAMS will follow the HSSR format found in the
CLAMS User’s Guide, but need not complete the “Onboard billet percent”, “Binnacle
data”, and workload items which do not apply to their operations. SCARS prompts the
HS to enter data totals in response to a succession of screen prompts. Six months totals
for outpatient visits (OPVs)., prescriptions filled, lab test done, HBA visits, inspections,
referrals, SARS, and expense data will be sought. The percent of active duty and
civilian employees in compliance with mandate requirements (like audiogram, HIV test,
etc.) must also be complied and entered. Six month totals can be tabulated from
HSSRs. Compliance percentages are calculated by SCARS. (Number in compliance
divided by the number for whom the requirement applies. If you have 30 people in the
hearing conservation program and 15 have had an audiogram in the last year, your
compliance is 15/30 x 100; or 50%).
CH-16 6-4
Figure 6-A-1
DEPARTMENT OF
TRANSPORTATION
U.S. COAST GUARD
CG-4899 (Rev-04-01)
REPORT OF POTENTIAL THIRD PARTY LIABILITY
INSTRUCTIONS: Complete all blocks to the best of your knowledge. If unknown or not applicable, leave blank. Mail original to
Commandant (G-WRP-2) and a copy to appropriate MLC (k).
SECTION I – IDENTIFICATION OF INJURED PERSON
A. NAME (Last ,First and Middle Initial) B. SSAN C. RANK/RATE D. WORK TELEPHONE
□ FTS
□ COMM
E. HOME ADDRESS (Including zip code) F. DATE OF BIRTH G. HOME TELEPHONE
H. STATUS OF BENEFICIARY
' ACTIVE DUTY ' RESERVE ' RETIRED
' DEPENDENT (Complete Section 2 below)
I. UNIT NAME J. BRANCH OF SERVICE
SECTION 2 – IDENTIFICATION OF SPONSOR
(Complete only if injured person is a dependent; otherwise, leave blank)
A. NAME (Last ,First and Middle Initial) B. SSAN C. RANK/RATE D. WORK TELEPHONE
' FTS ' COMM
E. HOME ADDRESS (Including zip code) F. HOME TELEPHONE
G. STATUS OF BENEFICIARY
' ACTIVE DUTY ' RESERVE ' RETIRED
H. UNIT NAME I. BRANCH OF SERVICE
SECTION 3 - ACCIDENT
A. ACCIDENT INFORMATION (Include zip code with address):
' AUTOMIBILE (city/state):
' JOB RELATED (employers name/address):
' PROPERTY RELATED (owners name/address):
B. DATE AND TIME
C. BRIEFLY DESCRIBE THE ACCIDENT (include who caused the injury and how it happened):
SECTION 4 – ATTORNEY INFORMATION
A. NAME OF YOUR ATTORNEY B. ADDRESS (Include zip code) C. TELEPHONE NUMBER
SECTION 5 – AMBULANCE SERVICE
A. NAME OF AMBULANCE B. ADDRESS (Include zip code) C. TELEPHONE NUMBER
MAIL TO:
Commandant (G-WRP-2)
U.S. Coast Guard
2100 2nd St. S.W.
Washington, DC 20593-0001
PRIVACY ACT STATEMENT
Sections 2651-2563 of Title 42 to the U.S. Code authorize collection of this information. Furnishing the Social Security
No. is empowered by Exec. Order 9397 and is mandatory to identify authorized beneficiaries. This information is
principally used to document incidents that lead to injured party(ies) receiving medical care at the expense of the U.S.
Coast Guard. Routine uses including lawful enforcement and investigations for recovery from third party liability. If the
requested information is not furnished, recovery of Federal funds may be hampered, possibly limiting
continued delivery of comprehensive health care.
6-5 CH-16
Figure 6-A-1 (reversed)
Page 2 of CG-4899 (Rev.04-97)
SECTION 6 – MOTOR VEHICLE ACCIDENT
(DATA PERTAINING TO VEHICLE IN WHICH YOU WERE DRIVING OR RIDING)
A. NAME OF DRIVER Military? ' YES ' NO B. HOME ADDRESS (Include zip code) C. WORK TELEPHONE
' FTS ' COMM
D. NAME OF OWNER Military ' YES ' NO E. YEAR/MAKE/MODEL OF AUTOMOBILE F. LICENSE PLATE NUMBER
G. OWNER’S INSURANCE COMPANY AND POLICY NUMBER H. ADDRESS(ES) (Include zip code) I. TELEPHONE NUMBER
J. NAMES OF INJURED PASSENGER(S) K. ADDRESS(ES) (include zip code) L. TELEPHONE NUMBER
(DATA PERTAINING TO OTHER VEHICLE)
M. NAME OF DRIVER Military? ' YES ' NO N. ADDRESS (Include zip code) O. TELEPHONE NUMBER
P. NAME OF OWNER Military ' YES ' NO Q. YEAR/MAKE/MODEL OF AUTOMOBILE R. LICENSE PLATE NUMBER
SECTION 7 – ALL OTHER ACCIDENTS
(DATA PERTAINING TO INSURANCE OTHER THAN AUTOMOBILE)
A. RESPONSIBLE PARTY’S INSURANCE COMPANY
AND POLICY NUMBER B. ADDRESS (Include zip code) C. TELEPHONE NUMBER
D. TYPE OF INSURANCE
' HOME OWNERS ' PERSONAL MEDICAL INSURANCE ' WORKERS COMPENSATION
E. INJURED PARTY’S INSURANCE COMPANY AND
POLICY NUMBER F. ADDRESS (Include zip code)
G. TELEPHONE NUMBER
H. TYPE OF INSURANCE
' HOME OWNER ' PERSONAL MEDICAL INSURANCE ' WORKERS COMPENSATION
SECTION 8 – MILITARY/CIVILIAN HOSPITALIZATION
A. NAME OF HOSPITAL(S) B. ADDRESS(ES) (Include zip code) C. DATE(S) OF TREATMENT
FROM TO
D. PAYMENT MADE BY:
' SELF
' INSURANCE
' CHAMPUS
FROM TO
' SELF
' INSURANCE
' CHAMPUS
SECTION 9 – MILITARY/CIVILIAN DOCTORS/DENTISTS
A. NAME OF DOCTORS B. ADDRESS(ES) C. DATE(S) OF TREATMENT
FROM TO
D. PAYMENT MADE BY:
' SELF
' INSURANCE
' CHAMPUS
FROM TO
' SELF
' INSURANCE
' CHAMPUS
FROM TO
' SELF
' INSURANCE
' CHAMPUS
E. IS TREATMENT COMPLETE?
' YES ' NO IF NO, WHEN DO YOU EXPECT IT TO BE COMPLETE?____________
CH-16 6-6
This page left blank.
6-7 CH-16
Section B - Forms and Records.
1. Status-Profile (CG-5460A).
a. Purpose. CG-5460A shall be used by active duty persons and civilian employees
who are either signing into the clinic/sickbay for the first time under CLAMS, or
need a duty status chit. It has a limited space for patient identification at the top, a
duty status slip (with copies) in the middle, visit information on the lower half, and a
detailed patient information section on the back. See Figure 6-B-1.
b. Detailed Instructions.
(1) Top Left. Mechanical imprinting of patient’s name, if available. Have the
patient fill in the appropriate data if mechanical imprinting is not used.
(2) Top Right. Date of visit is entered by the patient. The sponsor’s social
security number (SSN) and status (active duty or civilian employee) are also
required if mechanical imprinting is not used.
(3) Rear. For a patient’s first clinic visit after installation of the CLAMS data
base, more information is required on the form.
(4) Middle Section. Duty status chits are issued under CLAMS in the same
manner as they were before CLAMS. Fit for duty (FFD) chits are required for
grounded members cleared for aviation duties, and for members returned to
full duty before their restricted duty status has expired. The provider fills out
and signs the duty status chit (with firm pressure, because two tear-off patient
copies are produced at the same time). DIF (under FIT FOR FULL DUTY)
stands for Duties Involving Flight.
(5) A diagnosis must be included on each duty status chit issued, including FFD
chits. If the practitioner does not want the diagnosis to appear on the binnacle
list, enter an asterisk (*) after the written diagnosis. Thus a data base entry of
“gonorrhea*” will appear as “ “ on the binnacle list. If inpatient, place a
“$” after the diagnosis. The status on the binnacle list will then appear as
NFFD (INPT).
(6) If the illness or injury resulting in the duty restriction was (S)ports,
(O)ccupational, (M)otor vehicle, or (A)locohol related, check the applicable
(S)(O)(M)(A) block(s). More than one block can be checked if appropriate.
(7) Lower Half. This portion is for recording specific workload information. If
the visit meets the criteria as an outpatient visit (OPV), as defined by Paragraph
6-B-1.c. of this manual, the caregiver's initials are required. For medical and
dental record purposes, the OPV caregiver is the individual who ultimately
assumes responsibility for the patient's treatment. You are the caregiver for a
visit if:
CH-16 6-8
(a) your SOAP note is recorded in the health record;
(b) you assumed ultimate responsibility for the patient’s treatment; and
(c) you signed the medical record entry.
(8) Answering a question about a finding or treatment for another practitioner does
not make you the caregiver of record. Also, a health services technician who
performs a preliminary assessment (history, exam, and a plan) and then turns
the patient over to a medical officer or other practitioner is not the OPV
caregiver and should not initial a box. A telephone call by a health services
technician to the duty practitioner in regard to a patient may constitute a
transfer of responsibility, provided the duty practitioner's assessment and plan
are recorded in the health record for his signature.
(9) Left Side (lower half). There are two boxes available for OPV caregiver
initials. A physician, physician assistant, nurse practitioner, physical therapist,
mental health practitioner, health services technician, or medical extern initials
the first box. The second box is also used when another problem which meets
the OPV criteria is addressed by a second practitioner.
(a) Check one visit length: "Limited" (less than 15 minutes), "Intermediate"
(15-30 minutes), or "Extended" (more than 30 minutes), based on the
number of minutes the OPV caregiver actually spent with the patient or
working on the patient's problem (reading x-rays, checking lab work,
etc.).
(b) In the column of boxes under the visit length, indicate the type(s) of care
provided during the visit. Use check marks for all boxes except initials
(discussed above), audit codes, lab test(s), and medical x-rays. Check
"routine exam" box only when an SF-88 type exam is done on an active
duty member.
(c) If the OPV deals with one of the audit codes listed on the back of the
form, place the appropriate 2 letter code in the audit code box. These
codes will help you generate lists of patients for the quality assurance
monitoring and evaluation audits, and will save you the time and effort
which would otherwise be required to prepare a list of patients seen for a
particular problem.
(d) Clinics may create their own codes for their own purposes if desired.
These would be in addition to the audit codes listed on the back of the
form. Two codes may be entered for each OPV. CLAMS will allow
searching for any additional codes that may be developed.
(e) Lab and X-ray. Enter the number of tests performed.

6-9 CH-16
(f) Health benefits advice by itself does not constitute an OPV. However,
facilities shall account for work and time expended performing this
function. For episodes of health benefits advice (by telephone or in
person) lasting more than three minutes, the advisor shall enter his/her
initials in the box provided.
(g) There is no block for recording prescription count. Prescription counts
will be automatically tallied by the pharmacy module of CLAMS.
Patients using the pharmacy only (outside prescription or a refill) do not
need to fill out a Status-Profile or Visit profile form, except for their first
visit when you will need all patient information. If for some reason you
are not using CLAMS for this purpose, you will be prompted to enter
your total number of prescriptions filled when you are printing the
HSSR.
(h) Check the NON-OPV box if no aspect of medical or dental care meets
the criteria for an OPV. If you check NON-OPV, do not enter OPV
caregiver(s) initials.
(10) Center (lower half). Place provider initials in the box by any referral(s) made
or ordered. Initial the FED (Federal facility, e.g., USMTF, USTF) or NFED
(non-federal, e.g., non-fed med, supplemental care, TRICARE, outside
contract, etc.) column, as appropriate.
(a) In-house referrals to contract providers as well as referrals to other Coast
Guard clinics are exempt from this reporting. Do not mark a referral box
for one of these.
(b) Check the box for any tickler items performed.
(c) Check the box for third party, if applicable.
(d) Note dental referrals by circling the appropriate letter:
1 D - Prosthodontics
2 E - Endodontics
3 P - Periodontics
4 O - Orthodontics
5 S - Oral Surgery
6 K - Pedodontics
(11) Right Side (lower half). Dental follows the same general guidelines as the left
(medical) side, e.g., the initials of the attending dental officer, dental extern,
CH-16 6-10
health services technician, or dental hygienist go in the OPV Caregiver box,
whereas the person who performs a simple prophylaxis initials the box labeled
"Prophy Giver."
(a) Initial the "Prophy Giver" box if a prophy is performed. If the patient is
treated in any other manner, intial the "OPV Caregiver" box.
(b) If an annual or semiannual Type 2 dental exam is performed, record "1"
in the "Exam" box. Do not record any numeral other than "1". Do not
take credit for post-op visits, perio exams, etc. in this box. A "1" in this
box sets a tickler file, and it should not be polluted with less-than-
thorough hard and soft tissue exams.
(c) If an unscheduled patient is seen for emergency treatment, record "1" in
the Emergency box.
(d) Record the number of teeth restored in the "Restoration(s)" box. (For
example, a maxillary first molar with MO and OL restorations placed
counts as 1 tooth restored. Pins, bases, number of attempts, etc., do not
alter the method of counting.)
(e) Record the number of surfaces restored in the "Surface(s)" box. Pins,
bases, etc., do not affect the number of surfaces restored.
(f) Record the number of canals permanently sealed in the "Root Canal(s)"
box.
(g) In the "Pulpotomy(ies)" box, record the number of primary tooth
pulpotomies performed as a definitive treatment. Also, record the
number of symptomatic permanent teeth opened, pulpotomized, and
referred to a specialist for definitive therapy.
(h) Record the number of impacted teeth (soft tissue or bony) extracted in
the "Impactions" box.
(i) Record the number of non-impacted teeth extracted in the "Extractions"
box.
(j) Record the number of other surgical procedures (e.g., periodontal
surgery, free gingival graft, alveoplasty, biopsy, ridge reduction, etc.), per
quadrant, in the "Other Surg/Quad" box.
(k) Record the number of quadrants treated with non-surgical perio therapy
(curettage and root planing, usually with anesthesia) in the "Non-Surgical
Perio/Quad" box. Also, include a thorough periodontal examination and
charting (NOT PSR) as 1 quadrant of non-surgical perio treatment. Only
dental officers may record non-surgical perio treatment. No more than
6-11 CH-16
two quadrants may be recorded per visit. Generally, no other therapy
should be recorded for this visit; non-surgical perio is a planned step in
definitive perio therapy. Only patients with documented periodontal
disease receive non-surgical perio therapy. A prophy should be
scheduled at a separate visit. Full-mouth cavitron therapy is a prophy,
not four quadrants of non-surgical perio.
(l) Record the number of teeth (not surfaces) sealed, or receiving preventive
resins, in the "Sealant" box.
(m) Record the number of treatment appliances (e.g., orthodontics, spacers,
habit devices, stents, mouthguards, etc.), one per arch, delivered or
adjusted, in the "Treatment Appliances/Arch" box.
(n) Record the number of full or partial dentures delivered in the "Denture
Partial/Full/Arch" box.
(o) Record the number of permanently cemented cast units, other than resin-
bonded retainers (Maryland bridges), in the "Cast Unit(s)" box. Pontics
count as one cast unit apiece.
(p) Record the number of acid etch units (Maryland bridges, resin-bonded
retainers) bonded in the "Acid Etch Units" box. Count each pontic and
each wing as one unit.
(q) If a dental officer returns to the clinic to care for a beneficiary after
hours, record 1 in the "After Hours OPV" box.
(r) If a dental officer engages in a diagnostic/therapeutic conversation with a
patient over the phone, and the patient's dental record is so noted in
SOAP format, record "1" in the "Telephone OPV" box.
(s) At the end of the visit, enter the dental classification, in arabic numerals,
in the "Class" box.
(t) Enter the number of minutes required for diagnosis (for either Annual
Exam or Emergency visits) in the "Dx Minutes" box.
(u) Enter the sum of the PSR scores (for Annual Exams) in the "PSR Total"
box.
(v) If a biopsy is done, check the "Biopsy" box to set a tickler file. Also
indicate a surgical procedure in the "Other Surg/Quad" box.
(w) If a dental procedure is begun, but not finished, during a visit, the dental
caregiver shall initial the (dental) OPV Caregiver box for an OPV credit,

CH-16 6-12
but shall not put a number in a box below until the treatment is
completed during a subsequent visit.
c. Definition of an Outpatient Visit (OPV or "visit"). For the purposes of this
instruction, an OPV occurs each time an eligible beneficiary presents to a Coast
Guard Medical Treatment Facility (medical or dental) for examination, diagnosis,
treatment, evaluation, consultation, counseling or advice; or is treated or observed in
quarters; and a signed and dated entry is made in the patient's health record, dental
record, or other record of medical treatment (See Note 1 following 6-B-1.c.(3)). An
exception is that consecutive visits to specialty clinics (e.g., physical therapy and
occupational therapy) will not require a signed and dated entry for each visit unless
there is a change in the prescribed treatment or a significant physical finding is
evident. In all instances, however, an acceptable record audit trail shall be
maintained. A clinic log shall be maintained as a source document to support an
audit trail.
(1) Classification of a service as a visit is not dependent upon the professional
level of the person providing the service (includes medical officers, dental
officers, dental hygienists, optometrists, nurses, and health services
technicians).
(2) A patient visiting a Coast Guard Medical Treatment Facility (CGMTF) in the
morning and again in the afternoon shall count as two visits (providing the
requirements of Note 1 are satisfied). Conversely, avoid double counting; for
example, a visit during which both a medical officer and a health services
technician (in the same clinic) have been involved shall count as only one visit.
Other examples of patient health care contacts occurring at the CGMTF which
shall be included and counted as visits are:
(a) Each time a patient is seen in the CGMTF, even if referred elsewhere for
admission.
(b) Each time a patient is seen in the CGMTF's urgent care room, or other
designated area outside of regularly established clinic hours.
(c) Each time medical or dental advice or consultation is provided by
telephone and is properly documented in the health care records. (See
Note 1.)
(d) Each time a therapist provides primary care (e.g., patient assessment
while serving in a physician extender role) and then refers a patient for
specialized treatment in that same clinic, then one visit for primary care
and one visit for treatment shall be counted.
(e) Each time an examination, evaluation, or treatment is provided in the
home, school, community center, or other location outside the CGMTF
by a staff member from the CGMTF.

6-13 CH-16
(f) Subject to the provisions of Note 1, each time one of the following tasks
is performed when not a part of routine medical care, and provided it is
associated with a physical examination or treatment for a specific
condition requiring follow-up: therapeutic or desensitization injections;
cancer detection checks (e.g., PAP smears); blood pressure checks;
weight checks; and new prescriptions (do not include refills).
(g) Each time a screening physical examination is performed (e.g., school or
employment examination), providing an appropriate health record entry
is made (See note 1).
(3) Nonvisits. DO NOT report the following as visits:
(a) Prescriptions from health care providers outside the CGMTF, chest x-ray
surveys/examinations, laboratory tests, immunizations, or other
diagnostic or screening test that are not part of a specific treatment.
(b) Furnishing of health care advice or information, either directly or by
telephone, that does not satisfy the requirements of Note 1.
Note 1. The key to reporting visits is adequate documentation on appropriate
medical records, e.g., SF-600, SF-513, and all records of treatment to
support an audit trail. For example, “refill prescription for birth control
pills” with date and signature of the health care provider is not sufficient.
The entry should indicate that discussion of use of pills and counseling
did take place, for example, “discussed with patient; no apparent
problem with use-patient advised to have a PE and PAP prior to next
request for renewal; 6 months prescription for ovulen given.”
(c) Visits to other MTFs or private sector facilities, even when referred from
the CGMTF. The CGMTF already receives credit for an OPV for the
visit that generated the referral (see 6-B-1.c.(2)(a)).
2. Visit Profile (CG-5460B). This form must be used by all dependents and retirees who
are signing into the health care treatment facility for treatment. It can also be used by
active duty and civilian employees if they have previously been entered into the CLAMS
database and do not need a duty status chit. If a visit profile form is started on a patient
who turns out to need a duty status chit, discard the Visit Profile and start over on a
Status-Profile. Visit Profile sheets should be used by most active duty patients for the
dental clinic, most non-sickcall visits (except refill or filling outside prescription), health
benefit visits, weight checks, follow-up lab testing, immunizations, allergy shots,
audiogram, etc. See Figure 6-B-2.
a. Top Half. A new patient must fill out all information on the top half of the form. A
staff member (front desk or provider) should carefully review the form completeness
before the patient leaves the building since the patient cannot be properly entered into
the data base without all of this information.
CH-16 6-14
b. Top Left. Mechanical imprinting of the patient’s name, if available; if not, the
patient fills in. Reason For Visit box is optional and is provided for facility triage.
c. Date (top right) must be filled in at each visit.
d. Top Right. If mechanical imprinting was not used or if the addressograph card lacks
some information, this section should be filled in at each visit. Otherwise, leave
blank.
e. Bottom. The Third Party block is to be filled out by the clinic staff. Note that it
includes dependent/retiree referral for inpatient care at a DOD facility.
f. Reverse. Blank except for Privacy act information and audit codes. This is a good
place to put any addresses to which request for old medical records should be sent.
g. The bottom half of this form is virtually identical to the Status-Profile form. Refer to
the Status-Profile form instructions for these sections.
3. U.S. Coast Guard Health Care Equipment Request (CG-5211). Definitions for major and
minor health care equipment, health care equipment procurement procedures, and the
criteria used to approve health care equipment requests are described below.
a. Definitions.
(1) Major health care equipment. Any item of health care equipment which meets
the following criteria:
(a) costs $1000.00 or more;
(b) does not lose its identity when installed or placed into service; and
(c) has a life expectancy of one year or more.
(2) Minor health care equipment. Health care equipment that costs at least
$300.00, but less than $1000.00, and meets the criteria described above.
b. Health Care Equipment Requests.
(1) Major Health Care Equipment. Units shall submit requests for major health
care equipment on form CG-5211 (see Figure 6-B-3) the appropriate MLC (K).
If the MLC (K) is unable to evaluate the CG-5211 within 15 working days of
receipt, MLC (K) shall notify the commanding officer of the requesting unit
regarding the delay. Each MLC (K) shall review the request and provide a
forwarding endorsement that, as a minimum, addresses the following areas:
(a) how the equipment is or is not appropriate for the requesting health care
facility;
(b) why the purchase is or is not cost effective; and

6-15 CH-16
(c) how the equipment will or will not impact on the quality of patient care.
(2) Commander MLC(k) will evaluate major health care equipment requests, and
within 30 days of receipt of the CG-5211, will notify the unit that one of the
following actions will be taken:
(a) purchase of the requested equipment;
(b) purchase of a substitute item of a different make or model in order to
standardize health care equipment and/or ensure cost effectiveness;
(c) or return the request via the chain of command with an explanation of
why the equipment request was disapproved.
(3) Minor Health Care Equipment. Units shall submit requests for minor health
care equipment, using form CG-5211, to the appropriate MLC (K). If the MLC
(K) is unable to evaluate the CG-5211 within 15 working days of receipt, the
MLC (K) shall notify the commanding officer of the requesting unit regarding
the delay. Commanders (k), MLCs may disapprove the request or approve the
request and provide funding.
(4) Health care equipment costing less than $300.00 is a unit responsibility and
shall be purchased using unit funds.
(5) Emergency Procurement. A request for an emergency procurement may be
relayed to the appropriate MLC (K) by telephone, followed by a faxed copy of
a completed form CG-5211.
c. Criteria for Approval of Health Care Equipment Requests.
(1) Factors For Replacing Equipment. The fact that an item of health care
equipment is approaching, or has passed, its normal life expectancy is not
considered sufficient cause for replacement in and of itself. Units that request
replacement equipment shall provide justification on the CG-5211. Factors
which are considered sufficient cause for equipment replacement include:
(a) documented unreliability of equipment, demonstrated by unusual
maintenance expenses or high frequency of repairs;
(b) excessive repair costs, onetime or repetitive; or
(c) equipment is obsolete and new technology exists that reduces pain and
discomfort, improves treatment, increases diagnostic accuracy,
significantly reduces costs by conserving personnel, supplies, or utilities,
or increases efficiency by reducing patient treatment time.
(2) Factors For Initial Procurement. Due to changes in the beneficiary population
or unit mission, a health care facility may require health care equipment not
previously held by that facility. Units requesting an initial procurement shall
provide justification of form CG-5211.
CH-16 6-16
4. Health Record Receipt Form (NAVMED 6150/7). The Health Record Receipt Form
shall be used as a permanent record of receipt and disposition of health records which are
maintained at Coast Guard health care treatment facilities.
a. Detailed instructions.
(1) For each health record maintained at Coast Guard facilities, complete the first
four lines of a Health Record Receipt form and place into the health record
folder.
(2) Whenever the health record is temporarily removed from the files, complete
the charge-out information required on the bottom half of the Health Record
Receipt, and retain in the health record file where that record is normally kept.
Return the Health Record Receipt to the record when it is returned to the file.
(3) When a member departs from a unit on permanent change of station, or TAD
for over 30 days, forward their health record to servicing PERSRU for
transmittal to gaining PERSRU.
(a) When the record is forwarded, enter the following in the "REMARKS"
section of NAVMED 6150/7:
Date ______________.
Health record mailed to servicing PERSRU this date.
___________________.
HS's Signature
(b) Cut the form at the double lines above the "INSTRUCTIONS" section,
and maintain the top section on file for two years.
5. Referral for Civilian Medical Care (DD-2161). This dual-purpose form shall be used to
refer non-active duty patients from Coast Guard facilities to nonfederal facilities, either
for supplemental health care or when the patient is disengaged from care. The DD-2161
will also be used to disengage non-Coast Guard active duty patients from Coast Guard
facilities when the scope of care is beyond the ability of the Coast Guard to provide such
care. The Coast Guard facility shall contact the parent service to ensure the active duty
patient has the proper direction on where to obtain necessary care. A signed DD-2161
disengaging the patient will accompany the patient when he departs the Coast Guard
facility and a copy shall be kept on file. When used to refer patients for supplemental
health care, include a copy with the CG-5534 when the invoice for care is submitted for
payment. Complete appropriate sections on top and reverse of form when disengaging a
patient from care. Maintain a file of copies of completed forms.
6. Health Services Log. Each unit with health services personnel shall maintain a Health
Services Log. This log is used to document the daily operations of the clinic or sickbay.
At a minimum it is used to record all individuals reporting to sick call or for treatment,
inspections and inventories conducted, and the results of potable water test.
6-17 CH-16
a. Sickbays and clinics shall submit the Health Services Log to the commanding officer
for review, approval, and signature on a schedule to be determined by the
commanding officer.
b. The patient listing portion of the Health Services Log can be produced by CLAMS.
At a minimum it must contain the name of patient, date of visit, Division or
Department, members unit OPFAC (for active duty Coast Guard only), and branch of
service.
7. Binnacle List. The Binnacle List can be produced by CLAMS. At a minimum it must be
sorted by OPFAC and Department/Division and include patient name, diagnosis
(command discretion), status, date of onset of status, and duration of status or date of
status expiration. The Binnacle Lists(s) shall be distributed to local command(s) as
determined by the health care facility command.
8. Adult Preventive and Chronic Care Flowsheet Form (DD2766). This form should
replace the now obsolete Summary of Care Form (NAVMED 6150/20) as a means of
documenting significant chronic health problems, allergies, chronic medications,
hospitalizations/surgeries, health counseling, immunizations, PPD, DNA & HIV testing
screening (preventive medicine) exams, other medical readiness items (such as blood
type, G6PD, sickle cell, glasses, dental exams, etc.), and chart audits. Medical officers
should familiarize themselves with the use of this form prior to its widespread use at
their clinics. It is recommended that an in training session be provided to all medical
providers at the CG clinic, before the forms are placed in the health records. The old
Problem Summary List presently used on the Coast Guard AD health records can then be
removed after the information contained in it is copied onto the DD2766 form. The
process to complete this form is mostly self-explanatory. Only three items contained in
this form do not apply to the Coast Guard. These items, which are located on page 3, are
8.a, 10.e, and 10.i. Only a pencil shall be used to darken the circles present on the flow
chart of page 2 section 7. Item 11, located on page 3, is used to document the
completion of the pre & post deployment questionnaires that are required for CGAD
members who deploy with DOD. The medical officer should enter the location and date
of every deployment that the AD member participates in.
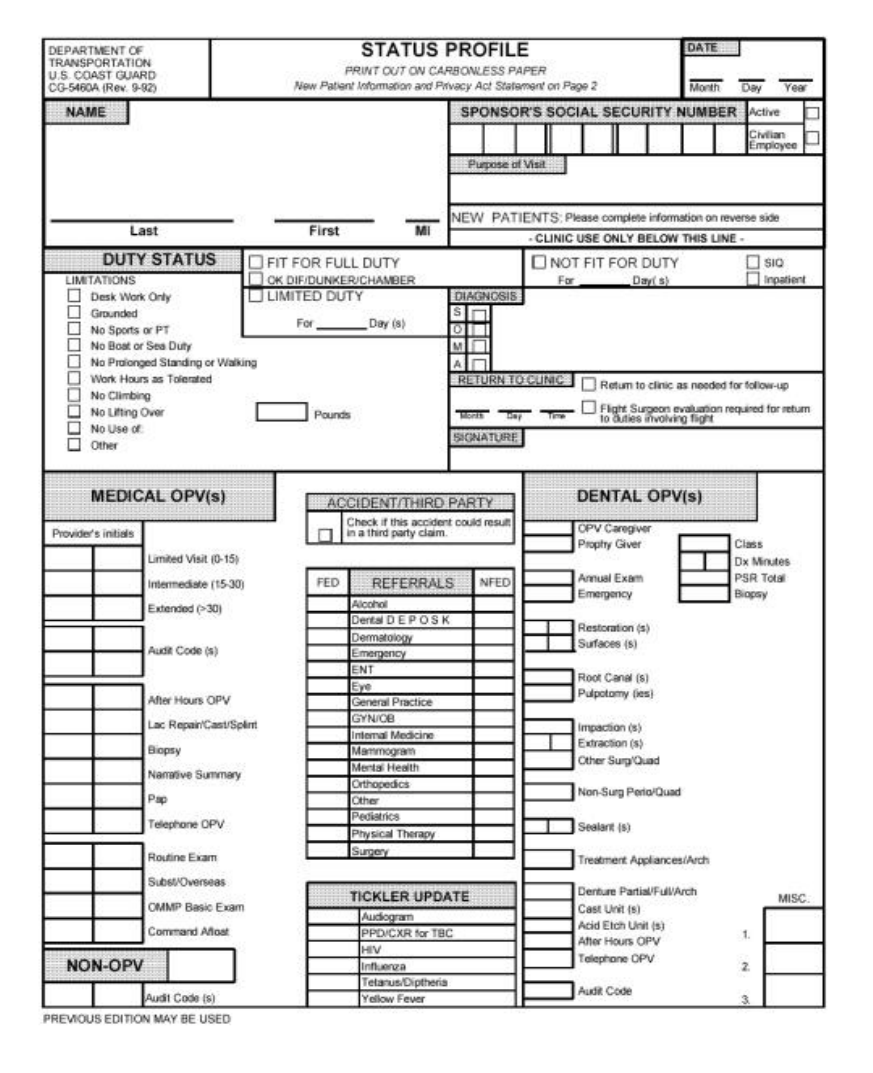
CH-16 6-18
Figure 6-B-1
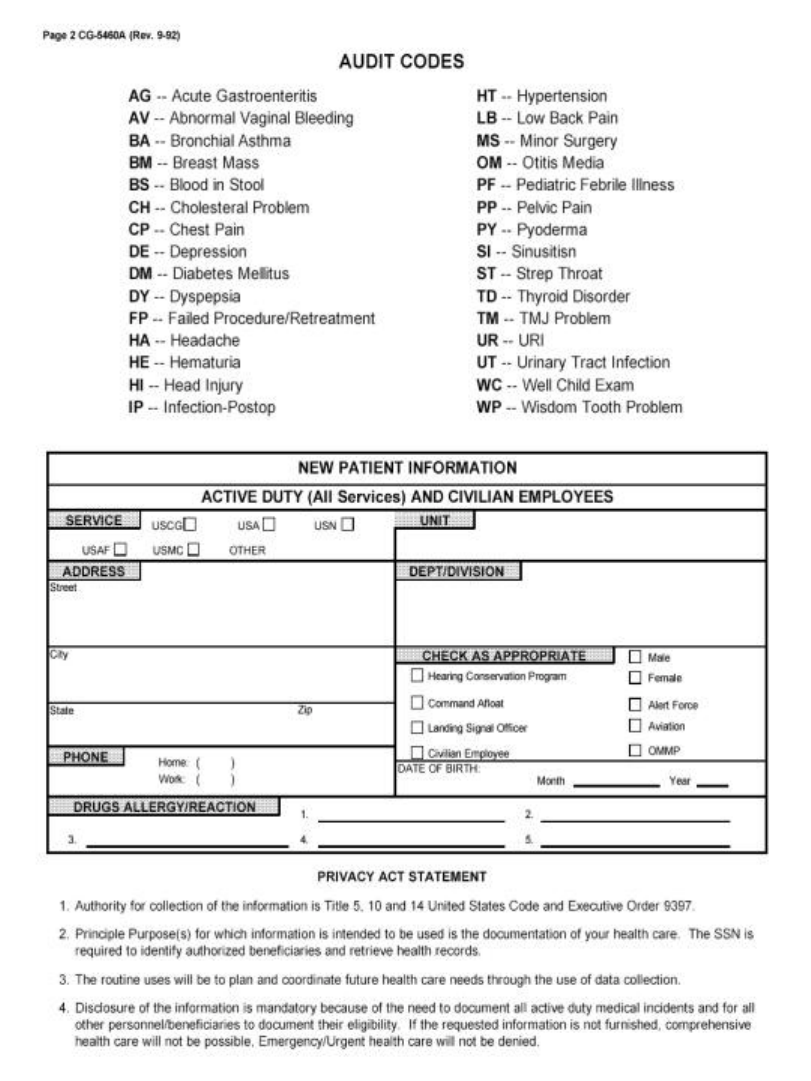
6-19 CH-16
Figure 6-B-1 (reverse)
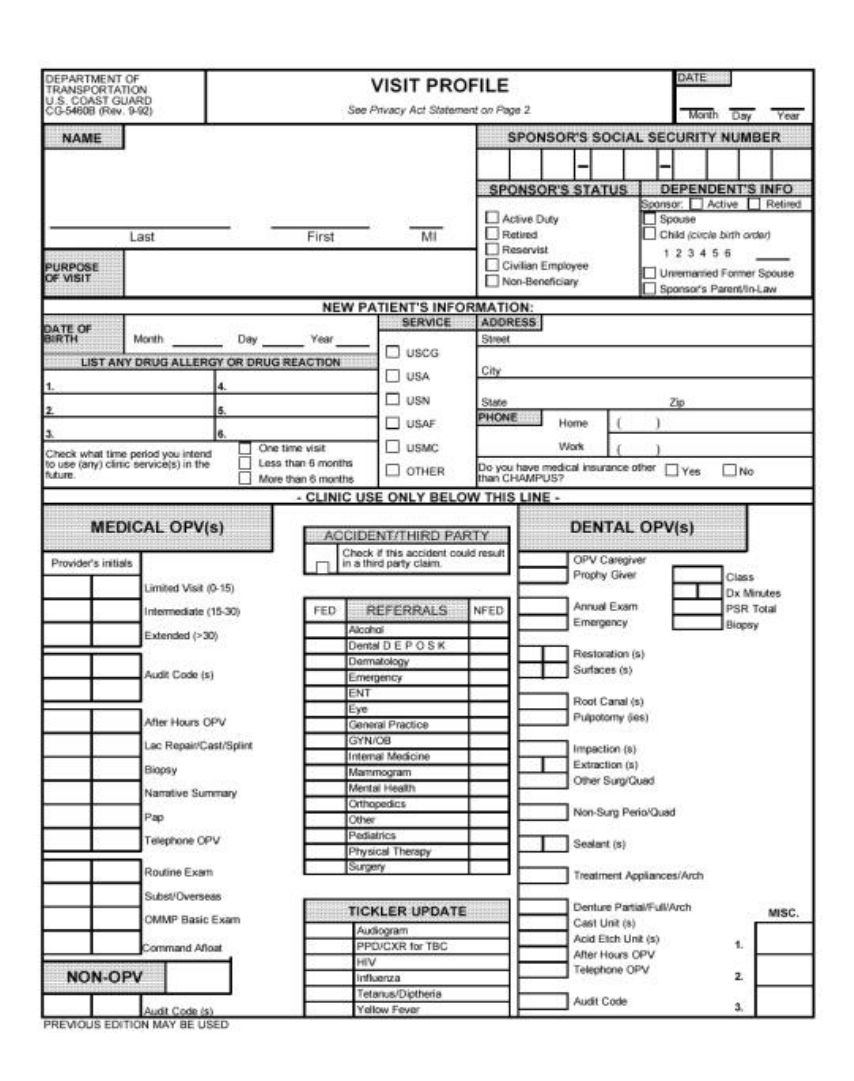
CH-16 6-20
Figure 6-B-2
6-21 CH-16
Figure 6-B-2 (reverse)
CH-16 6-22
Figure 6-B-3
DEPARTMENT OF
TRANSPORTATION
U.S. COAST GUARD
CG 5211 (REV.1-93)
U.S. COAST GUARD HEALTH CARE EQUIPMENT REQUEST
(This form may be typed or handwritten.)
A. UNIT INFORMATION: THIS SECTION IS TO BE COMPLETED BY THE REQUESTING UNIT
UNIT: OPFAC:
EQUIPMENT TO BE REPLACED: MANUFACTURER;
MODEL:
REPAIR
COST:_________________
ACQUISITION DATE:
PLANNED REPLACEMENT □ EMERGENCY REPLACEMENT □ NEW REQUIREMENT □
SUPPLY SOURCE:
FEDERAL STOCK SYSTEM □ GSA /VA CONTRACT □ OPEN MARKET ONLY □
EQUIPMENT REQUESTED: MANUFACTURE:
MODEL:
EQUIPMENT
COSTS:
___________
ACCESSORIES: 1. ____________ 2. _____________ 3. ______________
MODEL: ____________ _____________ ______________
SERIES: ____________ _____________ ______________
ACCESSORY
COST:
___________
ARE THERE ANY INSTALLATION COST? YES □ NO □
ARE THERE ANY UNUSUAL REQUIREMENTS? YES □ NO □
INSTALLATION
COSTS:
___________
MANUFACTURE’S ADDRESS:
_______________________________________________
________________________________________________________________________
POC:__________________________ TELEPHONE NO:_________________________
TOTAL
COST:
___________
COMMENTS: (IF A REPLACEMENT, EXPLAIN WHY EXISTING EQUIPMENT NO LONGER SATISFIES
REQUIREMENTS. IF NEW REQUIREMENT, PROVIDE FULL JUSTIFICATION.)
SIGNATURE OF PREPARER: DATE SIGNATURE OF COMMANDING
OFFICER:
DATE:
6-23 CH-16
Figure 6-B-3 (Reverse)
B. COMMANDER, MAINTENANCE AND LOGISTICS COMMAND
MINOR HEALTH CARE EQUIPMENT APPROVED □ DISAPPROVED □
COMMENTS:
SIGNATURE OF APPROVED OFFICER: DATE:
MAJOR HEALTH CARE EQUIPMENT RECOMMENDED □ NOT RECOMMENDED □
COMMENTS:
SIGNATURE OF REVIEWING OFFICER: DATE:
C. COMMANDANT (G-KRM) APPROVED □ DISAPPROVED □
COMMENTS:
SIGNATURE OF APPROVING OFFICER: DATE:
7-i
CHAPTER 7
PREVENTIVE MEDICINE
SECTION A - GENERAL.............................................................................................................1
SCOPE.. ........................................................................................................................................1
RESPONSIBILITY. ..........................................................................................................................1
PREVENTIVE MEDICINE PRACTICES..............................................................................................1
AVAILABILITY OF CONSULTATIVE SERVICES................................................................................1
SECTION B - COMMUNICABLE DISEASE CONTROL. .....................................................2
GENERAL. ....................................................................................................................................2
DISEASE OUTBREAK.....................................................................................................................2
RCN 6000-4, DISEASE ALERT REPORT........................................................................................3
SEXUALLY TRANSMITTED DISEASE RESPONSIBILITIES. ................................................................3
TREATMENT. ................................................................................................................................5
DRUG PROPHYLAXIS. ...................................................................................................................5
REPORTING...................................................................................................................................5
SECTION C - IMMUNIZATIONS............................................................................................19
GENERAL. ..................................................................................................................................19
UNIT RESPONSIBILITIES..............................................................................................................19
EQUIPMENT AND CERTIFICATION REQUIREMENT........................................................................19
IMMUNIZATION SITE RESPONSIBILITIES......................................................................................19
IMMUNIZATION ON REPORTING FOR ACTIVE DUTY FOR TRAINING.............................................21
SECTION D - TUBERCULOSIS PREVENTION AND CONTROL PROGRAM. .............22
INTRODUCTION...........................................................................................................................22
TUBERCULOSIS SCREENING PROGRAM.......................................................................................24
TUBERCULOSIS CONTACT INVESTIGATION PROGRAM. ...............................................................28
PROTECTIVE MEASURES.............................................................................................................29
MANAGING PERSONNEL WITH REACTIVE TUBERCULIN TESTS OR SUSPECTED TB. ....................30
TUBERCULOSIS CONTROL AMONG DEPENDENTS AND OTHER CIVILIANS. ..................................37
DECONTAMINATING SPACES OCCUPIED BY PERSONS WITH ACTIVE PMTB. ..............................38
7-1 CH 17
CHAPTER 7. PREVENTIVE MEDICINE
Section A - General
1. Scope. The scope of preventive medicine involves all activities that prevent illness and
disease, including immunization; communicable disease control; and epidemiology.
2. Responsibility.
a. The unit medical officer is responsible to the commanding officer for implementing
all directives issued by the Commandant which relate to the health of members of the
command. Additionally, the medical officer shall continually evaluate the
command’s health care capabilities to fulfill Occupational Medical Surveillance and
Evaluation Program (OMSEP) requirements. The command shall execute those
procedures it can perform as the Commandant requires. Deficiencies in capabilities
shall be made known in writing to the commanding officer with alternative plans for
accomplishments recommended.
b. Preventive medicine technicians are skilled, highly trained individuals, experienced
in preventive medicine. If assigned or available to a unit, that unit shall fully use
their services.
3. Preventive Medicine Practices.
a. Develop and supervise a definite, adequate environmental health program to prevent
disease and maintain the Commandant’s established sanitation standards;
b. Observe the incidence of disease or disability in personnel and, when indicated, in
adjacent communities;
c. Use epidemiological methods to determine the cause of such disease, especially
when an unusual or high incidence is discovered;
d. Recommend measures to minimize or remove the causes of disease; and maintain
effective liaison with civilian health agencies; Army, Air Force, Navy, and Public
Health Service preventive medicine components; and with other command officers
and components.
4. Availability of Consultative Services. Request MLC (kse) for special technical advice,
surveys, or investigation through appropriate channels. If unusual conditions or
circumstances requiring special attention arise, submit a special report through the
appropriate chain of command to Commandant (G-WK).
CH 17 7-2
Section B Communicable Disease Control.
1. General.
a. The health services department representative is responsible for:
(1) Recognizing communicable diseases;
(2) Recommending preventive and control measures to the commanding officer;
(3) Submitting required reports; and
(4) Complying with state and local health department reporting requirements.
b. The reference documents in this area are:
(1) Control of Communicable Diseases in Man, current edition, American Public
Health Association, 1740 Broadway, New York, NY 10019.
(2) “Medical Environmental Disease Intelligence and Countermeasures" on CD-
ROM (DI-1810-207-99, or current version) from Armed Forces Medical
Intelligence Center (AFMIC), 1607 Porter Street, Fort Detrick, MD 21701-
5004
(3) Appropriate state and local laws and regulations.
2. Disease Outbreak.
a. An outbreak is the occurrence in the command or surrounding community of a group
of similar illnesses clearly in excess of the expected frequency and derived from a
common or propagated source (e.g., streptococcal diseases, upper respiratory
infections, influenza, etc.). The number of cases indicating the presence of an
outbreak varies according to the agent; size and type of population exposed; previous
experience or lack of exposure to the disease; and the time and place of occurrence.
b. On recognizing an outbreak the health services department representative shall:
(1) Inform the commanding officer and recommend preventive and control
measures;
(2) Investigate to determine the source of the agent and how it was spread; and
(3) Send a Coast Guard intranet e-mail message Disease Alert Report, if the
outbreak may:
(a) Affect operational readiness;
(b) Pose a threat to the community;
(c) Pose a threat to another command (e.g., through transfer of personnel); or

7-3 CH 17
(d) Be of such political or journalistic significance that inquiry might be
made of higher commands.
3. RCN 6000-4, Disease Alert Report.
a. Circumstances Requiring Reports.
(1) An outbreak meets any of the criteria above;
(2) Any person is diagnosed as having a disease listed in Figures 7-B-1 or 7-B-2;
(3) Epizootics of diseases transmissible from animals to man on or near the
reporting activity;
(4) A Coast Guard vessel or aircraft is quarantined at a foreign port;
(5) Health services department personnel deem a condition worthy of reporting; or
(6) Conditions legally mandated by local health jurisdiction to be reported.
b. Initial Report.
(1) If the outbreak/disease is of an urgent nature, submit the initial report by Coast
Guard intranet e-mail message to MLC (k) with a copy to Commandant WKH-
1.
(2) Use the format in Figure 7-B-3 for all Disease Alert Reports.
(3) Report to local public health department as required by law.
c. Progress Reports. Submit progress reports as appropriate to inform the initial
report’s addressees of progress, change, or other significant developments.
d. Final Report (required for outbreaks). Submit to Commandant (G-WKH) through
the appropriate chain of command, a final letter report, which must contain this
information:
(1) Number of disease cases, both total and by hour, day, or week;
(2) Numbers of deaths, persons permanently disabled, and staff days lost from
work;
(3) Causal or contributory factors, including the recent itinerary of vessels, aircraft,
and other mobile units;
(4) Control measures taken and their effectiveness; and
(5) Recommendations to prevent or ameliorate similar future outbreaks.
4. Sexually Transmitted Disease Responsibilities.
a. Health services department shall provide a coordinated, comprehensive sexually
transmitted disease control program including:
(1) Educational programs;
CH 17 7-4
(2) Contact investigation, reporting, and treatment if the contacts are eligible for
care;
(3) Completing and submitting Contact Interview Form (Figure 7-B-4);
(4) Annotating and maintaining health records properly.
b. Senior Medical Officer (SMO). The senior medical officer oversees the medical
management of the local disease control program; recommends disease control
activities to the commanding officer; establishes and maintains liaison with local
health authorities to help detect and prevent sexually transmitted diseases (STDs);
and ensures confidentiality of contact reports and patients names.
c. Medical Officer. The practitioner who first sees the patient shall perform diagnostic
evaluation procedures. The provider must fill out SF-602, Syphilis Record, on ALL
patients diagnosed as having syphilis and file this form in the patient's medical
record. Test any patient treated for gonorrhea for syphilis and vice versa, and in both
cases, also for HIV antibody. The provider must perform diagnostic evaluations;
ensure proper analysis of urethral smears and dark field specimens; and identify
organisms from material submitted for culture or serologic test. The syphilis
serologic test (RPR, STS) is a general screening test. The FTA-ABS is a specific
antibody test that detects Treponema pallidum. The medical officer is responsible
for noting all STDs using ICD9CM codes on the NAVMED 6150/20.
d. Health Services Technician or Preventive Medicine Technician. A health services
technician or preventive medicine technician assigned to administer the local STD
control program should be pay grade E-5 or higher. The HS performs these actions:
(1) Interviews all STD patients for contact information;
(2) After the interview, annotates and signs the SF-600 in each STD patient’s
medical record to indicate he or she interviewed the patient and discussed
symptoms, complications, treatments, and contacts;
(3) Instructs gonorrhea patients to return for a Test of Cure (TOC) in five days.
(a) Active duty personnel will report to regular sick call for TOC. Place a
suspense notice to check with the attending medical officer to ensure the
patient receives TOC;
(b) Gives dependents and retired personnel regular appointments for local
STD control;
(4) Completes CDC 73.954, Contact Interview Form, on all STD patients and
contacts;
(5) The first working day of each week, cross references all positive STDs from
the clinic laboratory log book to ensure all STD patients have been contacted
and interviewed.
7-5 CH 17
5. Treatment. Treat STDs according to the most current recommendation of either the
Armed Forces Epidemiologic Board or the Centers for Disease Control (CDC), USPHS,
published in the Morbidity and Mortality Weekly Report (MMWR), Sexually
Transmitted Diseases Treatment Guidelines, as appropriate.
6. Drug Prophylaxis. Drug prophylaxis for sexually transmitted disease prevention is
prohibited.
7. Reporting.
a. Completing a CDC 73.954, Contact Interview Form.
(1) Prepare original and three copies as soon as possible after diagnosing a
sexually transmitted disease. Figure 7-B-4 is a sample of the form.
(2) Execute a separate 4-part form for each contact in cases of multiple contacts
(3) Enter these data on the 3rd and 4th copies ONLY:
(4) Under “Name,” enter also Social Security Number and rate or grade,
(5) Under “Home Address,” enter also the unit to which the patient is attached.
(6) Enter the interviewer's name and unit mailing address on the back of all sheets.
The interviewer signs the original.
(7) Disposition
(a) Within CONUS. The reporting unit retains the green copy on file and
sends the original and pink copies to the state where the contact occurred.
The reporting unit sends the yellow copy to MLC(k), which acts as the
STD control officer for the area. MLC(k) will notify G-WKH-1 upon
receipt of the yellow copy.
(b) Outside CONUS. To report contacts in foreign countries, send the
original and pink copies with a transmittal letter to the consular office
closest to the contact site to ask that office to send the forms to the
proper health authorities. Send the yellow copy to MLC (k) of the unit's
home district indicating where the original and pink copies were sent.
The reporting unit files the green copy.
CH 17 7-6
FIGURE 7-B-1
LIST OF REPORTABLE DISEASES
All of the listed conditions must be reported by CG Intranet e-mail message. Those with an X in
the Telephone to MLC (k) column must also be called in to appropriate MLC (k)
NOTIFIABLE CONDITION Telephone to MLC (k)
AIDS (Acquired Immune Deficiency Syndrome) X
Amebiasi
Anthrax X
Biological warfare agent exposure X
Botulism X
Brucellosis (Undulent Fever)
Campylobacter
Chancroid
Chlamydia
Cholera
Coccidioidomycosis
Dengue
Diptheria
Encephalitis X
Escherichia coli O157:H7
Food Poisoning (2) X
Filariasis
Giardiasis
Gonorrhea
Hemolytic uremic syndrome (post diarrheal)
Hemorrhagic Fever, specify type if known (3) X
Hepatitis A (Infectious) X
Hepatitis B (serum)
Hepatitis C (non-A non-B)
Herpes, Genital
HIV Infection – Confirmed positive serology X
Influenza (1)
Legionellosis
Leishmaniasis
Leprosy (Hansen’s Disease)
Leptospirosis (Weil’s Disease)
Lymphgranuloma Venereum
Malaria, specify type (3) X
Measles (Rubeola)
Meningococcal disease X
Mumps
7-7 CH 17
Pertussis (Whooping Cough)
Plague X
Pneumococcal pneumonia (1)
Poliomyelitis, Paralytic
Psittacosis
Q-fever X
Rabies, human X
Rabies, animal
Rheumatic Fever (1) X
Rift Valley Fever
Rocky Mountain Spotted Fever
Rubella (German Measles)
Salmonellosis
Schistosomiasis
Shigellosis
Smallpox (Variola) X
Syphilis (3)
Tetanus
Toxic shock syndrome
Trichinosis
Trypanosomiasis
Tuberculosis (4) X
Tularemia X
Typhoid Fever
Typhus Fever
Varicella (Active duty only)
Yellow Fever
Unusual Clusters if ANY Disease X
(1) Active duty cases only
(2) Call SMO if 5 or more persons are involved in any similar illness within 24 hour period.
(3) Specify type, if known.
(4) Report also clusters (more than 2) of new PPD converters.

CH 17 7-8
FIGURE 7-B-2
LIST OF REPORTABLE OCCUPATIONAL DISEASES
ICD-9-CM ICD-9-CM CMIT CMIT CMIT
TERM CODE SYNONYM/ TEXT ID
ANALOGUE NUMBER
______________________________________________________________________________
DUST DISEASES OF THE LUNG
______________________________________________________________________________
Coal Workers’ 500 Anthracosis 46 03 4678
Pneumoconiosis
Asbestosis 501 Asbestosis 62 03 4198
Silicosis 502M Silicosis 633 03 4626
Talcosis 502M Pneumoconiosis, Talc 556 03 5935
Chronic Beryllium 503M Beryllium Disease 77 03 2612
Disease of the Lung Chronic
Byssinosis 504 Byssinosis 107 03 4073
______________________________________________________________________________
POISONING (Systemic Toxic Reactions)
Hemolytic Anemia, 283.1 Anemia, Hemolytic 31 05 4225
Non-Autoimmune Acquired, Physical,
Chemical Agents
Aplastic Anemia 284.8 Anemia, Aplastic 29 05 3322
Agranulocytosis 288.0 Agranulocytosis 17 05 2863
Or Neutropenia
Methemoglobinemia 289.7 Methemoglobinemia 440 05 3295
Toxic Encephalitis 323.7 Encephalitis, 207 09 4982
Hemorrhagic, Acute
7-9 CH 17
PARKINSON’S DISEASE 332.1 PARKINSONIAN
SYNDROME 524 09 4071
(Secondary)
Parkinson’s Disease 332.1 Maganese Poisoning 424 09-03 5963
(Secondary)
Cerebellar Ataxia 334.3 Ataxia, Cerebellar, 64 09 3287
ACUTE
Inflammatory and 357.7 Neuropathy 475 09 2307
Toxic Neuropathy
Cataract 366.4E Cataract, Toxic 118 10 4532
Toxic Hepatitis 570 Hepatitis 303 06 2008
573.3 Chemical-Induced
Toxicity
Acute Renal Failure 584 Kidney, Failure, Acute 367 07 2229
Chronic Renal 585 Kidney Failure, Chronic 367 07 3028
Failure
Toxic Effects of 980.1 Methyl Alcohol Poisoning 440 00 1097
Methyl Alcohol
Toxic Effects of 981 Gasoline, Non-Leaded 259 00 4355
Gasoline or Petrol Poisoning
Toxic Effects of 982.0 Benzene, Poisoning 76 00 1941
Benzene and Homologues
Toxic Effects of 982.2 Carbon Disulfide 112 00 1042
Carbon Disulfide
Toxic Effects of 982.8 Methyl Ethyl Ketone 441 00 3427
Solvents Other than Poisoning
Petroleum-based, Other
Toxic Effects of 983.0 Nitrobenzene Poisoning 482 00 1416
Corrosive Aromatics
Toxic Effects of 983.0 Aniline Poisoning 44 00 2662
CH 17 7-10
Corrosive Aromatics
Toxic Effects of 983.1 Nitric Acid Poisoning 481 00 1255
Corrosive Acids
Toxic Effects of 983.2 Alkali Poisoning 20 00 3087
Caustic Alkalis
Toxic Effects of 985.0 Mercury Poisoning 439 00 5512
Mercury and its Compounds
Toxic Effects of 985.1 Arsenic Poisoning 55 00 2946
Arsenic and its Compounds
Toxic Effects of 985.1 Arsine Poisoning 56 00 5897
Arsenic and its Compounds
Toxic Effects of 985.5 Cadium Poisoning 107 00-03 5768
Cadium and its Compounds
Toxic Effects of 985.8 Thallium Poisoning 681 00 2910
Other Metals
Toxic Effects of 985.8 Silver Poisoning 633 00 4660
Other Metals
Toxic Effects of 985.8 Zinc Chloride Poisoning 752 00 3606
Other Metals
Brass-Founders’ 985.8 Metal Fume Fever 440 00 5749
Ague
Toxic Effects of 986 Carbon Monoxide Poisoning 112 00 3938
Carbon Monoxide
Toxic Effects of 987.1 Methane Poisoning 440 00 3425
Other Hydrocarbon Gas
Toxic Effects of 987.6 Chlorine Poisoning 129 00 3486
Chlorine Gas
Toxic Effects of 987.8 Oxygen Poisoning 511 00 3825
Gases, Fumes or Vapors
Toxic Effects of 987.8 Ozone Poisoning 511 00 3104
7-11 CH 17
Gases, Fumes or Vapors
Toxic Effects of 987.8 Phosgene Poisoning 545 00 3105
Gases, Fumes or Vapors
Toxic Effects of 987.8 Toluene Diisocyanate 694 00 2770
Gases, Fumes or Vapors Poisoning
Toxic Effects of 987.8 Toluene Poisoning 694 00 2098
Gases, Fumes or Vapors
Toxic Effects of 987.8 Acetone Poisoning 6 00 3216
Gases, Fumes or Vapors
Toxic Effects of 987.8 Ammonia Poisoning 25 00 5589
Gases, Fumes or Vapors
Toxic Effects of 987.8 Carbon Tetrachloride 113 00 3192
Gases, Fumes or Vapors Poisoning
Toxic Effects of 987.8 Diobrane Poisoning 181 00 4845
Gases, Fumes or Vapors
Toxic Effects of 987.8 Fluorine and Compounds 248 00 4521
Gases, Fumes or Vapors Poisoning, Acute
Toxic Effects of 987.8 Fluorine and Compounds 248 00 2119
Gases, Fumes or Vapors Poisoning, Chronic
Toxic Effects of 987.8 Hydrogen Sulfide 319 00 4331
Gases, Fumes or Vapors Poisoning
Toxic Effects of 987.8 Hydrofluoric Acid 319 00 5607
Gases, Fumes or Vapors Poisoning
Toxic Effects of 987.8 Methyl Chloride 441 00 5093
Gases, Fumes or Vapors Poisoning
Toxic Effects of 987.8 Methyl Bromide 441 00 5404
Gases, Fumes or Vapors Poisoning
Toxic Effects of 987.8 Carbon Dioxide 112 00 3107
Gases, Fumes or Vapors Poisoning
Toxic Effects of 987.9 Phosphine Poisoning 546 00 2433

CH 17 7-12
Gases, Fumes or Vapors
Toxic Effects of 989.0 Cyanide Poisoning 161 00 3541
Hydrocyanic Acid Cyanides
Toxic Effects of 989.2 Toxaphene Poisoning 697 00 1926
Chlorinated Hydrocarbons
Toxic Effects of 989.3 Phosphate Ester 546 00 2457
Organiphosphate and Carbanate Insecticide Poisoning
______________________________________________________________________________
RESPIRATORY CONDITIONS DUE TO TOXIC AGENTS
Extrinsic Asthma 493.0 Asthma, Bronchial 64 03 4622
Farmer’s Lung 495 Farmer Lung 236 03 4418
Bagassosis 495.1 Bagassosis 71 03 2403
Bird Fanciers’ Lung 495.2 Bird Breeder Disease 80 03 1458
Suberosis 495.3 Suberosis 664 03 5383
Maltworker’s Lung 495.4 Maltowkrer Lung 423 03 5485
Mushroom Workers’ 495.5 Mushroom Picker 456 03 4796
Lung Disease
Maple Bark 495.6 Maple Bark Stripper 425 03 2047
Strippers’ Disease
Other Allergic 495.8 Sequoiosis 629 03 2269
Pneumonitis (Sequoiosis
Or Red cedar Asthma)
Acute Bronchitis 506.0 Bronchitis, Acute 101 03 2389
Pneumonitis
Pulmonary Edema 506.1 Pulmonary Edema 586 03 4190
To Fumes and Vapors
Other Pneumonitis 507.8 Pneumonia, Extrensic 557 03 5650
Due to solids and liquids (detergent Asthma)

7-13 CH 17
______________________________________________________________________________
DISORDERS DUE TO PHYSICAL AGENTS
Raynaud’s 443.0 Vibration Disease 737 04 1428
Phenomenon (Secondary)
Cataract Associated 366.4 Cataract, Heat Ray 117 10 4527
With Other Disorders
Cataract Associated 366.4 Cataract, Irradiatiohn 118 10 3538
With Other Disorders
Noise Effects on 388.1 Hearing Disorder 285 10 5433
Inner Ear Sensorineural
Radiation Sickness 990 Radiation, Accidental 595 10 1287
Reaction
Heat Exhaustion 992.5 Heat Exhaustion 291 00 3421
Unspecified
Heat Exhaustion 992.5 Heat Cramp 291 02 1321
Unspecified
Heat Exhaustion 992.5 Heat Stroke 292 00 3483
Unspecified
Other and 993.2 Hypoxia 341 00 1890
Unspecified Effect
Of High Altitude
Dysbarism 993.3 Dysbarism 189 00 3279
Dysbarism 993.3 Decompression Sickness 169 00 4252
Caisson Disease 993.3 Nitrogen, Narcotic Action 482 00 1352
Motion Sickness 994.6 Motion Sickness 448 00 2357
(from Travel, any Vehicle)
______________________________________________________________________________
CH 17 7-14
SKIN DISEASES OR DISORDERS
Contact and Allergic 692 Dermatitis, Contact 173 01 1685
Dermatitis
Contact and Allergic 692 Dermatitis Atopic 172 01 2124
Dermatitis
Contact and Allergic 692 Dermatitis 172 01 4298
Dermatitis
______________________________________________________________________________
ALL OTHER DISEASES
REPRODUCTIVE DISORDERS
Infertility, Male 606 Sterility, Male 305 07 4761
______________________________________________________________________________
OCCUPATIONAL CANCERS
Hemangiosarcoma 155M Hapatocarcinoma 305 06 3133
Of the Liver
Hemangiosarcoma 155M Vinyl Chloride Poisoning 738 06-02 5437
Of the Liver
Mesothelioma 158 Ascites, Chylous 62 06 1081
(MN of Peritoneum)
Mesothelioma 158 Peritonitis 538 06 4415
(MN of Peritoneum)
Malignant Neoplasm 160.0 Nose, Carcinoma 483 03 2650
Of Nasal Cavities
Malignant Neoplasm 161 Larynx, Carcinoma 382 03 1491
Larynx Extrinsic
Malignant Neoplasm 162 Lung, Carcinoma 410 03 1647
Trachea, Bronchus and Lung Bronchogenic
7-15 CH 17
Mesothelioma 163 Pleura, Mesothelioma, 553 03 3834
(MN of Pleura) Primary
Malignant Neoplasm 170 Osteogenic Sarcoma 499 02 4950
Of Bone
Malignant Neoplasm 187.7 Scrotum, Carcinoma 625 07 1490
Of Scrotum Epidermoid
Malignant Neoplasm 188 Bladder, Carcinoma 81 07 1469
Of Bladder Epidermoid
Malignant Neoplasm 189 Kidney, Pelvis, Carcinoma 371 07 1084
Of Kidney, Other and Transitional Cell
Unspecified Organs
Malignant Neoplasm 189 Kidney, Pelvis, Carcinoma 371 07 1664
Of Kidney, Other and Epidermoid
Unspecified Organs
Malignant Neoplasm 189 Kidney, Pelvis, Leukoplakia 371 07 1780
Of Kidney, Other and
Unspecified Organs
Malignant Neoplasm 189 Kidney, Leiomyosarcoma 370 07 2506
Of Kidney, Other and
Unspecified Organs
Malignant Neoplasm 189 Kidney, Leiomyoma 370 07 3487
Of Kidney, Other and
Unspecified Organs
Malignant Neoplasm 189 Ureter, Carcinoma 716 07 2821
Of Kidney, Other and
Unspecified Organs
Lymphoid Leukemia 204 Leukemia, Lymphoblastic 392 05 1922
Acute
Lymphiod Leukemia 204 Leukemia, Lymphocytic 393 05 3351
Chronic Chronic
Myeloid Leukemia 205 Leukemia, Myeloblastic 393 05 2391
Acute Acute
CH 17 7-16
Erythroleukemia 207 Leukemia, Myelocytic 394 05 2363
Chronic
Erythroleukemia 207 Leukemia, stem cell 394

7-17 CH 17
FIGURE 7-B-3
RCN 6000-4, DISEASE ALERT REPORT
Telephone or submit rapidraft with the following information:
1. PATIENT.
a. Last Name, First Name, Middle Initial
b. Rate/Grade
c. Branch of Service
d. Social Security Number
e. Date of Birth
f. Race.
g. Sex
2. UNIT ADDRESS.
3. DIAGNOSIS. By ICD-9-CM classification number.
4. CLINICAL HISTORY.
5. LABORATORY TEST DONE, IF ANY, AND RESULTS.
6. TREATMENT AND PROGNOSIS.
7. EPIDEMIOLOGY INFORMATION. Provide all information of epidemiological
significance to the case (e.g., contacts, prior treatment, immunizations, etc.)
8. COMMUNITY THREAT.
9. POINT OF CONTACT.
10. REPORTING. List other agencies (e.g., State health departments) notified of the case.
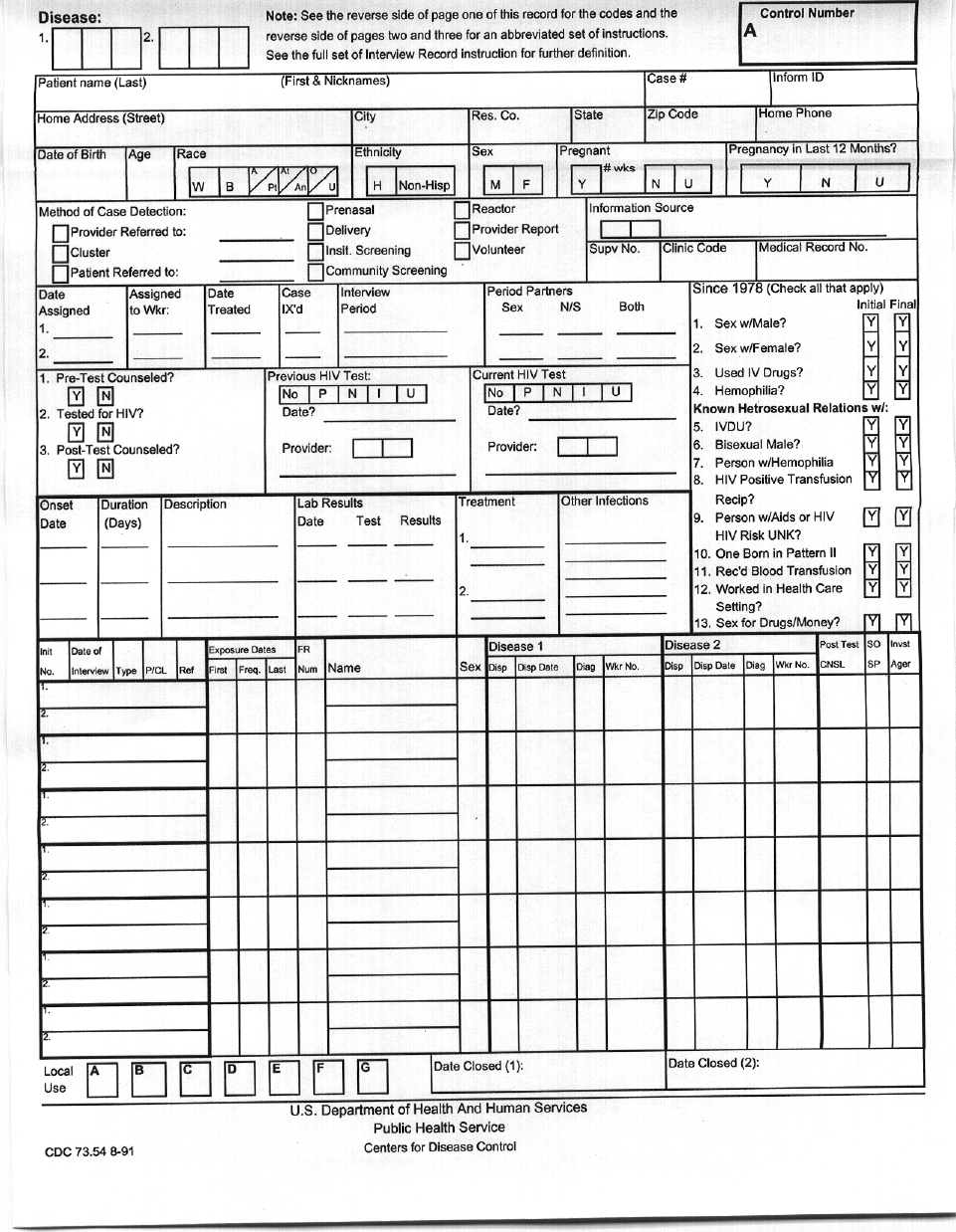
CH 17 7-18
Figure 7-B-4
7-19 CH 17
Section C Immunizations
1. General. Immunizations and Chemoprophylaxis, COMDTINST M6230.4 (series), lists
policy, procedure, and responsibility for immunizations and chemoprophylaxis. This
section contains guidelines not specifically defined there.
2. Unit Responsibilities.
a. Active duty and reserve unit commanding officers are responsible for immunizing all
individuals under their purview and maintaining appropriate records of these
immunizations. If local conditions warrant and pertinent justification supports the
cognizant MLC may grant authority to deviate from specified immunization
procedures on request.
b. Unit commanding officers will arrange local immunizations for their unit’s members.
If this is not possible, he or she will request assistance from the Coast Guard Medical
Treatment Facility overseeing units in the geographic area.
3. Equipment and Certification Requirement.
a. All immunization sites must have the capability to administer emergency medical
care if anaphylaxis or other allergic reactions occur. A designated Coast Guard
medical officer must certify the registered nurse or HS selected to administer
immunizations is qualified to do so because he or she has received instruction and
displayed proficiency in these areas:
(1) Vaccine dosages;
(2) Injection techniques;
(3) Recognizing vaccine contraindications;
(4) Recognizing and treating allergic and vasovagal reactions resulting from the
vaccination process;
(5) Proper use of anaphylaxis medications and related equipment (e.g., oxygen,
airways; and
(6) Verification the individual is currently certified in Basic Cardiac Life Support
(BCLS).
b. The immunization site must have available: syringes with 1:1000 aqueous solution of
epinephrine, emergency airways, oxygen, hand operated resuscitator, and intravenous
(IV) fluids with an IV injection set.
4. Immunization Site Responsibilities.
a. Where available, a medical officer shall be present when routine immunizations are
given.
CH 17 7-20
b. In the event a medical officer cannot be present, a registered nurse or HS3 or above
can be certified to administer the immunization process of active duty and reserve
personnel when the following guidelines and procedures are met:
(1) The designated Coast Guard medical officer who normally would oversee their
independent activity must train and certify in writing registered nurses and HSs
conducting immunizations in a medical officer’s absence.
(2) An emergency-equipped vehicle must be readily available to transport patients
to a nearby (within 10 minutes) health care facility staffed with an ACLS-
certified physician or an EMS with ACLS capability must be within a 10-
minute response time of the site.
(3) Hypovolemic shock often is present in cases of anaphylaxis. Therefore
medical personnel must be ready and able to restore fluid to the central
circulation. In anaphylaxis treatment, epinephrine administration, airway
management, summoning help are critical steps toward the treatment of this
condition.
c. The individual(s) administering the immunizations shall review the SF-
601(Immunization Record) and PHS-731 (International Certificate of Vaccination)
for each unit member to be immunized. Only a medical officer has authority to
immunize persons sensitive to an immunizing agent. The unit health record
custodian or HS will ensure proper entries are made on each immunize person’s SF-
601 and PHS-731.
d. In some clinical situations, the medical indication may be to immunize even though
the circumstances above cannot be met (e.g., tetanus toxoid for wound prophylaxis,
gamma globulin for hepatitis A exposure, etc.). Such incidents commonly occur at
sea and remote units or during time-sensitive situations (SAR, etc.). If the medical
benefits outweigh the chance of a serious allergic reaction, take every available
precaution possible, and administer the vaccine. When available, obtain radio,
telephone, or message advice from the Medical Officer.
e. If an adverse reaction to a vaccine is suspected, the facility shall notify the Vaccine
Adverse Event Reporting System (VAERS) using form VAERS-1. Obtain this form
from the FDA by calling 1-800-822-7967. Units providing vaccinations shall
maintain a supply of these forms. A copy of each submitted VAERS-1 will be
forwarded to G-WKH.
f. Every health care provider who administers vaccines shall provide a Vaccine
Information Sheet (VIS) if available from the Centers for Disease Control and
Prevention (CDC). As of 1 Feb 2002, the following VIS’s are available: diphtheria,
tetanus, pertussis (DTaP); diphtheria, tetanus (Td); measles, mumps, rubella (MMR);
polio (IPV); hepatitis B; haemophilus influenza type b (Hib); varicella;
pneumococcal conjugate; influenza; hepatitis A; pneumococcal polysaccharide;
meningococcal; lyme disease; and anthrax. This list includes vaccines covered by
the National Childhood Injury Act, as well as several others. The VISs are available
7-21 CH 17
from the CDC, National Immunization Hotline, at telephone number (800) 232-2522
or at http://www.cdc.gov/nip/publications/VIS/default.htm.
g. Per the National Childhood Vaccine Injury Act (NCVIA) of 1986, health care
providers are not required to obtain the signature of the vaccine recipient, parent or
legal guardian acknowledging receipt of the VIS. However, to document that the
VIS was given, health care providers must note in the patient's permanent medical
record (1) the date printed on the VIS and (2) the date the VIS is given to the patient
or legal guardian. In addition, the NCVIA requires, for all vaccines, that health care
providers document in the patient's permanent medical record the following: (1) date
the vaccine was given, (2) the vaccine manufacturer and lot number and (3) the name
and address of the health care provider administering the vaccine. For all
beneficiaries, the health care provider will make a notation on the SF-600 stating that
the vaccine recipient or legal guardian/representative has been given information on
the vaccine(s) prior to the vaccine(s) being given, if applicable. For all vaccines,
facilities administering vaccines must record in the recipient's health record, and, in
the service member’s International Certificate of Vaccination (PHS-731), the
manufacturer and lot number of the vaccine, and the name, address and title of the
person administering the vaccine.
5. Immunization on Reporting for Active Duty for Training.
a. When a member reports for active duty for training, the receiving unit shall review
the individual's SF-601 and PHS-731 for completeness, administer any delinquent
immunizations whenever possible, enter on SF-601 and PHS-731, and return these to
the individual when active duty for training terminates.
b. The individual's Reserve unit shall give the member a re-immunization schedule for
the following year if one is needed for that period.
CH 17 7-22
Section D Tuberculosis Prevention and Control Program
1. Introduction.
a. Description. Tuberculosis (TB) is an infectious disease transmitted from person to
person by very small (1-5 microns) particles called droplet nuclei, which can remain
suspended in any indoor air space for long time periods. An individual with active
pulmonary tuberculosis propels droplet nuclei into the air by coughing, speaking, or
sneezing. They also can be produced by manipulating tuberculous lesions or
discharging infected secretions. Inhaling droplet nuclei can carry them to the lung
alveoli, where the bacteria suspended in the particles can multiply, causing a
pulmonary infection.
b. Problem. In the United States, reported cases of tuberculosis declined steadily until
1984. Since then, however, the disease has unexpectedly rebounded in this country.
Many experts agree this resurgence is due at least partially to a deterioration in the
infrastructure of our health care delivery system. An additional concern is the
domestic increase of drug-resistant forms of tuberculosis, resulting in increased costs,
longer duration of treatment, and higher mortality rates.
c. Purpose. This section prescribes policy and procedure to ensure Coast Guard
members can conduct their mission without undue risk of tuberculosis transmission
and, further, the highest quality medical follow-up for those infected with the
disease.
d. Definitions.
(1) Active Case. A person who has a clinical disease demonstrated by radiograph
(x-ray) and culture or signs and symptoms of extrapulmonary TB. This term
does not include a person whose only finding is a positive skin test.
(2) Casual Contact. A person acquainted with an individual with active
tuberculosis who has spent some time with the infected person in a possibly
contagious, though brief, situation.
(3) Clinically Significant Exposure. An exposure to someone with active
tuberculosis which could be expected to result in transmitting the infection.
This generally means repeated, close contact with a person with active
pulmonary TB, particularly when in a confined environment such as a room or
residence, such as family members who share the same household as persons
with TB or health care workers who routinely care for TB patients.
(4) Close Contact. A person who has spent extended periods of time with a person
who has active tuberculosis, especially in enclosed spaces, e.g., living in the
same household.
(5) Contact. A person who has had some association with an active case .
7-23 CH 17
(6) Edema. The escape of a fluid, usually serous (pertaining to the watery part of
the blood) fluid, from its natural vessel into body tissues or cavities. Soft
tissue edema causes pitting.
(7) Erythema. An area of abnormally red skin due to inflammation.
(8) Fomites. Any materials, including clothing or bedding, capable of absorbing
and spreading a disease’s infecting organism.
(9) High-Risk Groups. Defined groups of persons among whom the prevalence
and incidence of tuberculosis is substantially higher than the general
population.
(10) Induration. A firm, hardened, usually raised area of soft tissue congestion;
erythema may or may not be present. Must be distinguished from edema by the
absence of pitting.
(11) Mantoux Test. An intracutaneous (within the skin) test for tuberculin
sensitivity, using a purified protein derivative (PPD) of tuberculin.
(12) MDRTB. Multiple drug resistant tuberculosis.
(13) Mycobacterium tuberculosis. The organism that causes tuberculosis disease.
(14) Positive Skin Test Reaction. See 3.C.(2).(f).
(15) Pulmonary. Referring to the lungs. The most common and most infectious
form of TB occurs in the lungs (pulmonary TB), but many other parts of the
body can be sites of infection.
(16) Tuberculin Conversion/Convertor. A TST reaction that has increased from
what is considered non-reactive to reactive within two years. Both reactions
must be documented.
(17) TB. Tuberculosis, a communicable disease of humans and animals caused by
the Mycobacterium tuberculosis microorganism, manifesting itself in lesions of
the lung, bone, and other organs.
(18) TST. Tuberculin Skin Test, a test based on a hypersensitivity-type immune
reaction to tuberculin. The test is used to determine past or present infection
from Mycobacterium tuberculosis.
(19) Tuberculin. A substance derived from Mycobacterium tuberculosis cultures
used to diagnose tuberculosis.
(20) Tuberculin Non-reactive/Non-reactor. A TST reaction which is too small to be
considered evidence of infection. (See Figure 7-D-1). Sometime imprecisely
referred to as a “negative” test.
(21) Tuberculin Reactive/Reactor. A TST reaction considered evidence of
infection. (See Figure 7-D-1). Sometimes imprecisely referred to as a
“positive” test.
(22) Vesiculated. Having small, blister-like, fluid-filled sacs or cysts.
CH 17 7-24
e. Program Summary. The Tuberculosis Prevention and Control Program consists of
four parts: the TB screening and contact investigation programs, personal protective
measures and patient management.
2. Tuberculosis Screening Program. The program is intended to identify both persons who
have only been infected by Mycobacterium tuberculosis and those who have active,
clinical disease. The former may benefit from preventive therapy, and the latter from
treatment.
a. Type of testing: Different testing procedures are used:
(1) Tuberculosis Skin Testing. The Purified Protein Derivative (PPD) is the
primary method for routine TB screening. It is used for individuals with
previously non-reactive, doubtful, or unrecorded skin tests.
(2) Chest Radiograph. This method is if active TB is suspected in persons with a
previously reactive tuberculin skin test (TST). Routine periodic chest
radiographs will generally not be performed.
b. Summary of Testing Procedures. At a minimum, TB screening is required when a
person enters military service and during periodic physical examinations. A medical
officer or this manual describe when to test more frequently.
c. When to Test Personnel.
(1) Initial Tuberculosis Screening. A PPD is mandatory in the physical
examination of any person entering initial active duty for 30 days or more and
any other active duty member whose records contain no report of a completed
tuberculin test.
(2) Screening Personnel at Low Risk of Exposure.
(a) Tuberculin Non-reactive Personnel. All active duty personnel whose last
recorded reaction was recorded as non-reactive at a minimum must have
a PPD during their quinquennial physical examination.
(b) Tuberculin Reactive Personnel. All personnel whose last recorded TST
reaction was considered reactive receive chest radiographs only when
previous medical follow-up has not been done and properly documented
in the individual's health record, or when a medical officer deems it
clinically indicated. All TST reactors or their medical records must be
medically reviewed annually to screen for indicators of active disease.
(3) Screening Personnel at Increased Risk of Exposure.
(a) Tuberculosis Non-reactive Personnel. Personnel whose last recorded
TST reaction was considered to be nonreactive and who are at increased
risk of TB, such as health care workers, will be skin tested annually,
usually during routine immunizations. EMT or law enforcement and
other personnel, in addition to testing at their quinquennial physical

7-25 CH 17
examination, will be tested after clinically significant contact with high
risk groups (e.g., following interdiction of and prolonged, confined
contact with migrants who have signs of active tuberculosis).
(COMDTINST M6220.9 (series) provides more information regarding
tuberculosis and AMIO, but this instruction is the definitive guidance on
frequency of testing.)
(b) Tuberculin Reactive Personnel. Personnel whose last recorded TST was
considered reactive will receive chest radiographs or sputum smear
examinations only when a medical officer deems necessary.
(4) Separation from Service. Those individuals whose last test was nonreactive
shall have a PPD as part of their separation process. A chest radiograph will be
done for a separation physical only if the individual has a confirmed positive
PPD. Results of the PPD or chest radiograph must be evaluated and recorded
in the health record prior to separation.
d. Testing Procedures.
(1) Tuberculin Skin Test Materials.
(a) Tuberculin, Purified Protein Derivative (PPD). The only approved
tuberculin skin test material for a routine Mantoux test is premixed
Tween-80-stabilized intermediate strength PPD (5 Tuberculin Units (TU)
equivalent). Multiple puncture tuberculin tests (e.g., Tine tests) are not
authorized. A medical officer can direct using first-strength PPD (1 TU)
when a person has a verbal or questionable history of a reactive TST but
no documentation of such.
(b) Syringes and Needles. The disposable 1 ml tuberculin syringe graduated
in 0.1 ml intervals and fitted with a 25-gauge 5/8-inch needle is a
convenient combination for administering the PPD.
(2) Tuberculin Skin Test Methods.
(a) Personnel Authorized to Perform the Tuberculin Test. Only trained
health services personnel are authorized to perform PPDs. The local
medical authority shall verify they are competent to administer and read
the PPD.
(b) Techniques. Following aseptic preparation of the skin, an intradermal
injection of 0.1 ml of the tuberculin solution shall be made upon the
volar aspect of the left forearm. The point of the needle should be visible
just within the dermis, beneath the outer layers of the epidermis. The
results should be a definite wheal, pale and sharply demarcated. Be
careful to avoid subcutaneous or epidermis injection. If it is recognized
that the first test was improperly planted, another test dose can be given
at once, selecting a site several centimeters away from the original
CH 17 7-26
injection. A note in the record should indicate the site chosen for both
the first and second tests.
(c) Documentation. Document the PPD test in the SF-601 under Sensitivity
Tests with the date tested. Do not record results until the actual time of
reading.
(d) Two-Step TST. Because of delayed hypersensitivity, an adult who has
never been skin tested and will receive periodic skin testing should
receive two-step skin testing to distinguish boosted reactions from
reactions due to new infection. Persons in this category include new
accessions to the Coast Guard (officer and enlisted). In such cases
consult a medical officer for procedure.
(e) Measuring and Recording Results.
1 After an interval of between 48 and 72 hours examine the PPD site.
Classify injection response according to the extent of the induration
(not erythema or edema) measured in millimeters (mm) at the widest
diameter transverse to the long axis of the forearm.
2 When reading the PPD, the forearm should be in good light and
flexed a little at the elbow. Lightly pass a forefinger over the test
area. The induration can be felt even when it does not produce a
visible elevation. For those skilled in its use, the pen-tracking
method is both authorized and more accurate. To measure, mark
induration borders with a ball-point pen.
3 To record the result, enter by hand this information under Sensitivity
Tests on SF-601 and PHS 731: date, type of tuberculin, its strength
or dilution (e.g., PPD 5 TU), and the resulting diameter of induration
expressed in millimeters. Report absence of induration as "zero
mm." If induration is present, use Arabic numerals to record the
widest diameter. A sample entry is: "17 SEP 86 PPD (5TU) 6mm
induration." Also measure and record any vesiculation. In red ink
record the result indicating a PPD converter on the Sensitivity
Sticker (section 4-B-2) and the Problem Summary List (section 4-B-
3). Using rubber stamps or automatic imprinting devices to record
results or recording results as “negative” are both prohibited.
4 A medical officer must evaluate grossly vesiculated reactions. Warn
the person about possible secondary bacterial infection from
scratching the reaction.
(f) Failure to Return for Skin Test Reading. Personnel who do not return at
the proper time to have the skin test interpreted must be retested. Do not
7-27 CH 17
under any circumstances record the PPD as "zero mm" if the person does
not return within the prescribed time frame. Each time a person fails to
return for timely reading, document the SF-601 with "no reading done"
and the date.
(g) Interpreting Skin Test Readings. Consider a skin test reactive according
to Figure 7-D-2.
Figure 7-D-2
Size of Induration Considered Reactive for
Reactions < 5mm are considered non-reactive
5 mm · Persons with HIV infection or risk factors for HIV
infection but unknown HIV status;
· Persons who have had recent close contact with
persons who have active TB;
· Persons who have fibrotic chest radiograph consistent
with healed tuberculosis;
· Patients with organ transplants and other
immunosuppressed patient.
10mm · Injecting drug users known to be HIV seronegative;
· Persons with other medical conditions with reported
increased risk for progressing from latent TB infection
to active TB. These medical conditions include
diabetes mellitus, chronic renal failure, some
hematologic disorders and other malignancies, weight
loss of >10% below ideal body weight, silicosis,
gastrectomy, and jejunoileal bypass;)
· Residents and employees of high-risk congregate
settings: prisons, long-term care facilitiess, health-care
facilities, and homeless shelters;
· Some medically underserved, low income populations,
including migrant workers and homeless persons;
· Foreign-born persons recently arrived (i.e., within the
last five years) from countries with a high TB
prevalence;
· Children < 4 years of age, any child or adolescent
exposed to adults in high-risks categories.
15mm · Persons who meet none of the above criteria.
(3) Chest Radiographs. Those individuals who have been determined to need a
chest radiograph will have a standard, erect posteroanterior view. A medical
officer may determine other appropriate views.

CH 17 7-28
e. Responsibility for Local Program Management.
(1) The command holding affected persons’ health records is responsible for
monitoring health records and managing local skin testing and chest radiograph
programs.
(2) The activity maintaining the health record assures the tuberculin skin test status
is clearly and properly documented on SF-601 and PHS-731 Immunization
Records of each active duty member’s health record; the activity also must
clearly, properly record tuberculin reactors’ chest radiograph status on SF-600,
Chronological Record of Medical Care, and NAVMED 6150/20, Problem
Summary List. Further, the activity is responsible for initiating tests for
persons whose health records do not contain appropriate, timely entries.
3. Tuberculosis Contact Investigation Program.
a. Contact Investigation Procedures. On discovering a case of active TB in a command,
take these actions:
(1) Submit a Disease Alert Report. (See Figure 7-B-2, and 7-B-3).
(2) Determine the patient's close contacts.
(3) Screen or give these contacts a TST test for TB and repeat the screening 3, 6, 9,
and 12 months later.
(4) Report summary results of the investigation to Commandant (G-WKH)
through the appropriate chain of command.
(5) Evaluate possible secondary cases.
b. Initiating a Contact Investigation. Initiate a contact investigation when notified a
member of the command has diagnosed active PMTB or when a medical officer so
requests.
c. Performing a Contact Investigation.
(1) Conducting an investigation
Initial Investigation of Contacts. Each person who is a close contact of an
known case of active, infectious tuberculosis shall undergo a screening
examination for TB. Those personnel who are previous tuberculin reactors,
and do not have a document of appropriate medical follow-up, or have signs of
PMTB, shall receive a chest radiograph [unless otherwise contraindicated, see
7-D-4.b.(5)(c)]. All other contacts shall receive a PPD. Individuals identified
to be close contacts who are not eligible for health care through the Coast
Guard should be referred to the local public health department or private
medical facility of choice.
(a) Establishing Limits for Contact Investigations. The infectiousness of a
source case is determined by first evaluating close contacts for evidence
of new infection or disease. If there is no evidence of infection in this
7-29 CH 17
group no further investigation is necessary. Remember that TB is a slow
progressing disease and initial screening results should only be
interpreted as baseline information if it is determined that the source case
may have a recent infection or disease. If there is evidence of infection
in close contacts (as determined after an appropriate time-lapse), extend
the investigation to progressively lower-risk contacts, e.g., casual or
other contacts. This should proceed until the levels of infection detected
approximate the levels of infection in the local community. NOTE: If a
newborn or an immunocompromised person (e.g., HIV infected person)
is identified as a close contact, they should be evaluated for prophylaxis
per current Centers for Disease Control and Prevention Guidelines.
Figure 7.D.3 shows a decision tree for establishing contact limits.
(2) Determining Close Contacts.
(a) Active Tuberculosis at a Shore Facility. The local medical officer must
classify a TB patient’s "close contacts” at a shore facility, generally
including all those sharing the same berthing facilities, in close contact
during duty hours, regular liberty mates, and the patient’s cohabitants.
Consult the appropriate MLC (k) for advice in specific instances.
(b) Active Tuberculosis Aboard a Cutter. When a case of active TB is
discovered aboard the cutter the entire ship’s company shall be
considered close contacts included in the contact investigation.
(c) Other Situations. Commands or activities in which exceptionally close
conditions occur, such as isolated duty stations, shall follow the
procedures listed for cutters.
(3) Follow-up Investigation of Contacts.
(a) Follow-up Period. Follow up tuberculosis contacts for 12 months (see
paragraph 5.a.(3)). Record follow-up results on an SF-600 in each
contact’s medical record. Take particular care to record all items before
an involved member from the command transfers.
4. Protective measures
a. General. Depending on the level, nature, and intensity of exposure, a person’s risk of
TB infection can be reduced. Tuberculosis spreads almost exclusively by airborne
transmission from persons who have active pulmonary TB. The risk of infection is
negligible for those who have casual or brief contact with high-risk persons,
particularly if exposure occurs in a open space. Special personal protective
equipment, e.g., masks, gloves, or gowns, is not required for routine limited contact
in such a setting.
b. Respiratory protective devices (RPD).
CH 17 7-30
(1) RPDs may be warranted if TB exposure is longer or more intense. Coast Guard
personnel will comply with guidelines established by the Centers for Disease
Control and Prevention (CDC), the National Institute of Occupational Safety
and Health (NIOSH), and pertinent Coast Guard directives, e.g., COMDINST
M6260.2 (series), governing using RPDs or other personal protective
equipment.
(2) Surgical masks do not filter small enough particles to protect a wearer from TB
infection, and must not be used for this purpose. However, surgical masks can
help contain infectious droplets from the infected person, and when worn by
this person, may reduce the risk of passing the infection.
(3) The minimum RPD for wearer safety is a NIOSH-approved, high-efficiency
particulate air (HEPA) respirator. Respiratory protective devices must fit and
be worn correctly to be effective. Technical Guide: Practices for Respiratory
Protection, COMDTINST M6260.2 (series), describes how to evaluate, fit, and
train persons to wear RPDs to protect against TB transmission.
c. Air Circulation. At least 6 air exchanges per hour (ACH) are required to reduce
concentrations of droplet nuclei in the air in an enclosed space requires; higher ACH
rates eliminate more bacteria. If possible 12 ACH or more is recommended.
Recirculated air should filter through fixed HEPA filters. Fresh or filtered air should
be provided in optimum airflow patterns that prevent stagnation.
d. Handling High-Risk Populations. When transporting or otherwise in a confined
space with a person known or suspected to have active TB, take these precautions:
(1) If he or she can tolerate one, have the patient wear a mask.
(2) Take measures to increase airflow within the enclosed space. Vent air to the
outside whenever possible.
(3) Avoid unnecessary close contact with the patient.
(4) Separate suspected TB cases from others if conditions permit.
(5) Emergency Medical Technicians (EMTs) should wear HEPA respirators when
working with persons demonstrating clinical signs of TB.
(6) Consult competent medical authority to determine if specific circumstances
warrant HEPA mask use.
5. Managing Personnel with Reactive Tuberculin Tests or Suspected TB.
a. Evaluation for Tuberculosis.
(1) Personnel Requiring Evaluation. As soon as possible evaluate persons who
meet any of these criteria for the presence of active tuberculosis:
(a) Tuberculin reactor on initial testing.
(b) Tuberculin skin test converter.
7-31 CH 17
(c) Close contact of an active case of TB who develops a TST reaction
>5mm..
(d) Previous tuberculin reactor but never evaluated for active TB.
(e) Previous tuberculin reactor, now with suspicious chest radiograph
findings.
(f) Anyone with history, signs, symptoms, or laboratory tests suggesting TB.
(2) Initial Examination. Persons listed in Paragraph 4.a.(1) will have a medical
history, physical examination and chest radiograph.
(3) Further Examination. A medical officer or a civilian physician most evaluate
more thoroughly those individuals whose findings suggest active TB.
b. Managing Tuberculin Reactors Without Evidence of Active TB.
(1) Personnel evaluated and found not to have active TB will be considered for
preventive therapy according to Figure 7-D-3. Prophylaxis is intended to
prevent latent infections from progressing to clinically active disease.
Figure 7-D-3
Age Induration
Size
Risk Factor
Any Age > 5mm Known or suspected HIV infection
Close contact with newly diagnosed active TB
Previously untreated or inadequately treated persons
with chest radiographs showing fibrotic lesions
compatible with old healed tuberculosis. If diagnosis
is doubtful after consulting with a medical officer,
administer a booster TST
> 10mm Injecting drug users
Persons with medical conditions reported to increase
tuberculosis risk including silicosis; gastrectomy;
jejunoileal bypass; weight 10% or more below ideal
body weight; chronic renal failure; conditions
requiring prolonged high-dose corticosteroid therapy
or other immunosuppressive drugs; some hematologic
disorders (leukemia and lymphomas); and other
malignancies
Under 35 > 10mm Foreign-born persons from high-prevalence countries
including those in Asia, Africa, Central and South
America, and eastern Europe
Residents of correctional facilities
> 15mm No risk factors, but not previously treated
CH 17 7-32
Recent TST converters
Under 35 > 10mm increase within a 2 year period
Over 35 > 15mm increase within a 2 year period
Previously known (old) tuberculin reactor not properly evaluated in the past or who
did not complete appropriate preventive therapy
Under 35 If risk factors and induration sizes listed above are
present
Over 35 Generally not a candidate for INH unless specific risk
factors for active disease are present
Note: A previously known tuberculin reactor may be treated without repeat
testing if a properly documented tuberculin TST result is in the medical record. If
a person gives an undocumented history of a tuberculin reaction and INH
prophylaxis may be indicated, a first strength PPD (1 TU) may be administered
under the direction of a medical officer, to confirm the reported reaction.
(2) Initial Evaluation for Prophylaxis. Before initiating a course of prophylaxis a
medical officer must evaluate the person as follows:
(a) An appropriate history and physical examination.
(b) Chest radiograph for newly identified tuberculin reactors, unless
otherwise contraindicated. Give one to previously known reactors only if
no documents exist of proper medical evaluation with radiograph at time
of reactive TST or if clinically indicated.
(c) Baseline liver function tests (LFT), including AST, ALT, LDH, total bili,
and GGT, and a CBC.
(d) Perform HIV antibody testing on all newly identified active duty
tuberculin reactors. Query civilian employees and dependents with
newly-identified reactive TSTs about HIV risk behaviors. Counsel
persons with HIV risk factors and offer them an HIV serological
screening test.
(e) Review conditions that may contraindicate prophylaxis as follows:
pregnancy, breast feeding, ETOH abuse, known sensitivity to the agent,
peripheral neuropathy, IV drug abuse, acute or chronic liver disease,
therapy with medication with a potential for significant interaction
(Tegretol, phenytoin, etc.). If any of these conditions exist, the provider
must decide whether to initiate prophylaxis, weighing therapeutic risks
and benefits.
(3) Prophylaxis. Recommended regimens are listed in Figure 7-D-4. There are
other considerations not listed in the Figure for HIV infected persons.
7-33 CH 17
Figure 7-D-4
Drug Interval and Duration Comments
Daily X 9 Mo1,2 In HIV-infected patients, INH may be administered
concurrently with NRTIs or NNRTIs.
Isoniazid (INH)
2X Weekly X 9 Mo1,2 Directly observed therapy (DOT) must be used.
Daily X 6 Mo2 Not indicated for HIV-infected persons or those with
fibrotic lesions on chest X-ray.
INH
2X Weekly X 6 Mo2 DOT must be used.
Daily X 2 Mo May also be offered to persons who are contacts of
patients with IHN-resistant, rifampin-susceptible TB;
In HIV-infected patients protease inhibitors or NNRTIs
should generally not be administered concurrently with
rifampin.
Rifampin plus
pyrazinamide
2X Weekly X 2-3 Mo DPT must be used
Rifampin Daily X 4 Mo For persons who cannot tolerate pyrazinamide.
Notes: 1Recommended regimen for children younger than 18 years of age.
2Recommended regimen for pregnant women.
(a) Supervision. Persons whose risk of developing active TB is high and
whose compliance is questionable may require directly observed therapy
(DOT).
(b) (b) Monitoring. Appropriately trained personnel must monitor persons
taking INH monthly for the first two months and at least every two
months thereafter. Follow persons 35 and older monthly for the first
three months. Initially dispense a maximum of one month's supply of
medication and up to two months’ supply thereafter to coincide with
follow-up visits. If signs or symptoms of toxicity appear, discontinue
INH immediately; a medical officer should reevaluate. Prophylaxis
should not be prescribed if periodic monitoring cannot be done.
Monitoring consists of:
1 Reviewing significant symptoms of INH side effects: fever, rash,
jaundice, fatigue, anorexia, dark urine, joint pain, paresthesia of
hands, feet, or eyelids.
2 Obtaining follow-up LFTs as follows:
One month after instituting INH; then at least at three month
intervals for all individuals.
At 1, 2, 3, and 5-6 months (8-10 month interval for those with a
one-year course) for all persons 35 and older.
CH 17 7-34
If evidence of possible reaction to therapy occurs.
3 Upon termination of INH prophylaxis, LFTs and a CBC will be
done.
4 The periodic evaluations will be documented in the patient medical
record.
c. Patient Education. The health services representative must ensure the patient
understands the meaning of the skin test result or TB exposure, INH
chemoprophylaxis hazards (hepatitis, drug fever, severe rash, etc.) and benefits, the
warning signs of the drug’s potential side effects; and the danger of alcohol
consumption while taking INH. The necessity for faithful adherence to the course of
treatment, in the absence of side effects, cannot be too strongly stressed. A notation
of the counseling offered shall be made on an SF-600 in the medical record.
d. Persons Leaving the Service While on Chemoprophylaxis.
(1) Members who retire prior to completing chemoprophylaxis shall be advised
that continued treatment is necessary and may be obtained at most Uniformed
Services Medical Treatment Facilities.
(2) Members who are discharged or released to inactive duty prior to completing
Isoniazid chemoprophylaxis shall be advised of the importance of continuing
the program. Care may be provided by the Veterans Administration, county
health department, private physicians, etc. To facilitate follow-up, personnel
shall be provided with a statement signed by a medical officer containing the
date treatment began, the type and dosage of prescribed medications, course of
therapy, and the present status. At a minimum, the local Health Department
where the individual plans to reside should be notified.
(3) A medical board or limiting duties is not indicated for those with no evidence
of active disease except as noted in paragraph 4.b.(6) regardless of the status of
preventive therapy.
(4) Special Situations and Procedures.
(a) Exposure to Drug-resistant TB. Consult with CDC or a state health
department before starting prophylaxis for persons known to be exposed
to patients with drug-resistant strains of TB.
(b) Children. A pediatrician or medical officer with training in pediatrics
must follow children receiving TB prophylaxis.
(c) Pregnant Women. Complete the same initial procedures for adults
except DO NOT PERFORM A RADIOGRAPH unless an actual clinical
indication of pulmonary disease exists. Consult the patient's obstetrician.
Generally, defer treatment until after delivery or breast feeding. Place
7-35 CH 17
the patient's name in a "tickler" so that she can be contacted upon
termination of pregnancy.
(d) Child Care Workers. Child care workers must receive annual PPDs or
medical evaluations, as appropriate.
(5) Aviators.
(a) Personnel on flying status shall be grounded for the first seven days of
chemoprophylaxis because of the slight risk (less than 1%) of
convulsions among persons taking INH. At the end of seven days of
treatment, flight surgeon must be consulted to return the member to
flying status.
(b) A flight surgeon shall evaluate aviators receiving INH monthly to
carefully brief the individual about possible adverse reactions.
(c) Aviation personnel should be considered for grounding if, at any time
during treatment, liver function test are significantly abnormal or
symptoms of liver dysfunction appear.
e. Managing Suspected Cases of Active TB. When a patient is evaluated and suspected
of having TB:
(1) Submit a Disease Alert Report (see Figure 7-B-2).
(2) Expeditiously refer the patient to the nearest USMTF, including those initially
admitted to civilian medical facilities. If at all possible, refer before beginning
definitive treatment.
(3) Initiate contact tracing.
(4) Decontaminate spaces (see Paragraph 7-D-7).
f. Reporting Requirements. The health services division chief of the medical treatment
facility where the diagnosis of active TB is suspected or established, shall notify the
patient’s commanding officer within 48 hours. The notification shall include the date
that the diagnosis was established or suspected and the probability that the patient is
infectious. If, in the case of suspected active TB, the diagnosis of TB is subsequently
ruled out, a message to that effect must be sent to both the patient’s commanding
officer and to the address of the Disease Alert Report, immediately.
(1) Follow-up Procedures. The command investigating TB contacts shall maintain
a "tickler" file or similar effective system to assure prompt evaluation of
persons requiring periodic examination and testing. Medical evaluations and
other indicated procedures are an appropriate part of the periodic examination.
(2) Completing Follow-up. When the 12 months expire, those individuals whose
tuberculin response or chest radiograph were unchanged shall revert to routine
program screening.
CH 17 7-36
(3) Separated Members. Contacts separated from the Coast Guard shall be
counseled regarding the need for medical evaluation and the appropriate
referrals made.
(4) Managing Tuberculin Converters or Possible Cases. Those individuals found
to have “converted” or who developed changes on a chest radiograph shall be
evaluated as outlined in Section 7-D-4 of this manual. Close contacts who
increase the size of induration on a TST, even though the reaction is still
considered nonreactive, should also be considered for evaluation.
(5) Secondary Cases. If a subsequent active TB case is discovered among the
contacts, it is not necessary to begin an entirely new investigation. However,
start contact studies on any personnel exposed to the secondary case not tested
in the original investigation.
g. Responsibility for Managing the Contact Investigation Program.
(1) The commanding officer of the permanent duty station of a person diagnosed
with active TB shall initiate the contact investigation. If the individual has a
permanent change of station during the preceding year, the commanding officer
of the former duty station shall be notified to initiate a contact investigation if
determined appropriate by the medical officer or civilian physician making the
diagnosis. If assistance is required contact the appropriate MLC (k).
(2) The commanding officer of any activity is responsible for successfully
continuing or completing contact studies under way among members assigned
to or transferred to the unit. Additionally, the commanding officer shall
ensure:
(a) The records of members transferred from the unit while undergoing
contact studies are complete (including radiographs) so the member’s
gaining unit can continue the studies.
(b) Prompt submission of the summary letter report on the tuberculosis
contact investigation to Commandant (G-WKH) through the chain of
command.
h. Reporting Requirements. The command initiating the contact investigation shall
prepare and submit study summaries to Commandant (G-WKH) with a copy to the
appropriate MLC (k). Submit progress summary reports and the final
RCS-G-K-13012, Disease Alert Report, with this information:
(1) Unit identification.
(2) Source case(s)’s name, grade, rate, and Social Security Number .
(3) Status of investigation, e.g., initial, 3-, 6-, 9-, or 12-month summary reports.
(4) For each reporting period provide:
(a) Number of tuberculin non-reactive individuals skin-tested.

7-37 CH 17
(b) Number of skin-tested tuberculin non-reactive persons found to be
converters.
(c) Number of tuberculin-reactive individuals receiving chest radiographs.
(d) Number of tuberculin-reactive persons found to have suspicious changes
on the chest radiograph.
(e) Number of contacts placed on or receiving isoniazid chemoprophylaxis.
(f) Name, grade, rate, Social Security Number, and exact diagnosis of each
secondary tuberculosis case.
(g) Comments on investigation including any problems.
6. Tuberculosis Control Among Dependents and Other Civilians.
a. Dependents.
(1) As part of health education efforts, commands shall impress upon dependents
the importance of routine TB preventive measures. Within their capabilities,
commands in known high-risk areas should extend the active duty program to
those dependents residing in the area. Dependent contacts of active cases of
TB shall be given periodic screening with either tuberculin test or chest
radiographs, as appropriate. Chemoprophylaxis will be administered, when
indicated.
(2) If active TB is diagnosed in a military dependent, the medical treatment facility
(MTF) establishing the diagnosis shall notify the appropriate public health
authorities. Dependents may obtain care through the local public health
department, military MTF, or through civilian sources, as appropriate. The
MTF making the diagnosis should provide advice on available treatment
alternatives.
b. Positive Skin Tests in Children Under 6 Years of Age. Preventive treatment is
definitely recommended for all positive tuberculin reactors under six years old. The
Mantoux method shall be used to confirm “positive” responses elicited by other
tuberculin testing methods.
c. Alien Dependents. See "Tuberculosis Among Foreign-Born Persons Entering the
United States," Centers for Disease Control and Prevention, MMWR, Dec 28, 1990
(Vol. 39), and the U.S. Immigration and Naturalization Act for the waiver procedure
an alien with PMTB to enter CONUS.
d. Civilian Personnel. If a civilian employee under Coast Guard cognizance is
discovered to have active TB, the medical administrative officer or the medical
officer of the activity shall make arrangements for contact investigation of close
work associates. Local public health authorities shall be notified. Coast Guard
CH 17 7-38
personnel who are close contacts of the employee shall have detailed entries made in
their medical records and receive appropriate follow-up.
7. Decontaminating Spaces Occupied by Persons with Active PMTB.
a. Pulmonary tuberculosis is transmitted by small airborne droplets or droplet nuclei
from persons in close contact or possibly through ventilation systems, such as on
ships. Other dried secretions and fomites in themselves do not pose significant
hazards unless aerosolized. Therefore, only normal laundry and cleaning procedures
with sodium hypochlorite (household bleach) are necessary for linen and bedding of
a person with active PMTB. Take care not to shake dirty linen to launch particles on
it into the air.
b. When a case of PMTB is discovered aboard a ship, the filters in the ventilation
system exhausting the berthing, messing areas, work spaces, and medical spaces
must be replaced and cleaned. In this situation contact the Commandant (G-WKH)
or appropriate MLC (k), for specific instructions. Increase circulation of fresh air
and, if possible, exposure of spaces to natural light (sunlight) will rapidly clear any
infectious, airborne droplet nuclei from the spaces.
c. No other sanitation measures are necessary. Consult a medical officer for advice in
specific instances.
7-39 CH 17
FIGURE 7-D-1
SUMMARY OF TESTING PROCEDURES
TUBERCULIN (PPD) SKIN TEST RECOMMENDED ACTION
Unknown Perform a PPD, using intermediate strength PPD (5 TU).
History of strongly reactive or
vesiculated reaction Perform a PPD using the regular dose of first strength
PPD (1TU). If this test’s results are negative, follow up
with a subsequent test using a full dose of intermediate
strength PPD (5TU).
Last test reactive Determine if an appropriate medical follow-up and/or
chemoprophylaxis has been pursued. If not, perform a
standard posterior-anterior chest radiograph. If the chest
radiograph and a review of signs and symptoms reveal no
findings, consider prophylaxis. If proper medical follow-
up previously has been pursued, counsel the patient on
the need to monitor him- or herself for signs of active
pulmonary tuberculosis. Further follow-up is not
indicated.
Evaluate these classes of personnel as Section 7-D-4 outlines.
1. Those with unknown or previously nonreactive tuberculin status who are found upon testing
to be PPD reactors.
2. Those with reactive skin tests who have not been medically examined for tuberculoses
before.
3. Those with suspicious chest radiograph findings.
NOTE: A reactive single/multiple puncture TB skin test, i.e., Monovac or Tine Test, to test
children; must always be verified by PPD.
8-i
CHAPTER 8
FISCAL AND SUPPLY MANAGEMENT
A. RESOURCE MANAGEMENT ............................................................................................................................ 1
UNIT ........................................................................................................................................................................ 1
MAINTENANCE AND LOGISTICS COMMAND (MLC) ................................................................................................. 2
HEADQUARTERS ...................................................................................................................................................... 2
B. GENERAL PROPERTY MANAGEMENT AND ACCOUNTABILITY. ........................................................ 3
BASIC POLICIES ....................................................................................................................................................... 3
PHYSICAL PROPERTY CLASSIFICATIONS . ................................................................................................................. 3
PROPERTY RESPONSIBILITY AND ACCOUNTABILITY ................................................................................................ 3
EXPENDING PROPERTY UNNECESSARILY ................................................................................................................. 3
STOCK LEVELS, REORDER POINTS, AND STOCK LIMITS. .......................................................................................... 3
TRANSFERRING AND LOANING PROPERTY ............................................................................................................... 4
C. CUSTODY, ISSUES, AND DISPOSITION ........................................................................................................ 5
TRANSFERRING CUSTODY ....................................................................................................................................... 5
STOREROOMS .......................................................................................................................................................... 5
ISSUING MATERIAL .................................................................................................................................................. 5
INSPECTING STOREROOMS ....................................................................................................................................... 5
DISPOSING OF PROPERTY ......................................................................................................................................... 6
D. HEALTH SERVICES SEGMENT OF THE COAST GUARD SUPPLY SYSTEM ...................................... 8
HEALTH SERVICES CONTROL POINT ........................................................................................................................ 8
RESPONSIBILITY FOR GENERAL STORES ITEMS ........................................................................................................ 8
SUPPLY SUPPORT ASSISTANCE . ...............................................................................................................................8
AUTHORIZED ALLOWANCES .................................................................................................................................... 9
SUPPLY SOURCES .................................................................................................................................................... 9
EQUIPMENT ........................................................................................................................................................... 10
UNIFORM ............................................................................................................................................................... 11
E. EYEGLASSES AND OPHTHALMIC SERVICES...........................................................................................12
GENERAL ............................................................................................................................................................... 12
PERSONNEL AUTHORIZED REFRACTIONS ............................................................................................................... 12
PROCURING AND ISSUING STANDARD PRESCRIPTION EYEWEAR ............................................................................ 12
AVIATION PRESCRIPTION LENSES .......................................................................................................................... 14
CONTACT LENSES .................................................................................................................................................. 14
SUNGLASSES FOR POLAR OPERATIONS .................................................................................................................. 15
SAFETY GLASSES ................................................................................................................................................... 15
DEPENDENT CARE IN ISOLATED AREAS ................................................................................................................. 15
CONTEMPORARY PRESCRIPTION EYEWEAR PROCUREMENT .................................................................................. 15

8-1 CH 15
CHAPTER 8. RESOURCE MANAGEMENT
A. RESOURCE MANAGEMENT. The Health Services Program has three resource
management levels.
1. Unit.
a. A unit’s commanding officer (CO) is charged with ensuring all unit aspects operate
effectively and efficiently. For units with health care facilities, this means using
personnel, funds, equipment, expendable supplies and materials, health care spaces,
and external health care providers economically and efficiently. The CO oversees all
health care equipment maintenance. Commanding officers will ensure management
of command resources provides the best amount of care to all eligible beneficiaries at
the least cost to the Government.
(1) In general, care provided in Coast Guard clinics is more cost-effective than any
other source’s. The fixed cost of physical plant, staff, and equipment is divided
by the number of beneficiaries served; thus, the more care provided, the lower the
cost per visit. Therefore, units should set goals to provide the maximum amount
of care possible. Achieve these goals by operating properly staffed clinics at
times most convenient to beneficiaries, scheduling to decrease the time patients
wait, efficiently managing health care providers’ valuable time, and publicizing
the availability of services to beneficiaries in the surrounding communities.
(2) If the current level or mix of resources is inefficient, the commanding officer will
report this fact through the chain of command and recommend corrections.
Timeliness is extremely important in dealing with changes in resource
requirements. Good resource planning should address these needs long before it
becomes necessary for a unit commanding officer to deny care to any authorized
beneficiary due to lack of resources.
b. The unit commanding officer directly controls the unit's financial plan or budget,
including unit health care resources. Monthly the CO reports medical and dental
workloads, operating targets, adjustments to the targets, and actual expenditures to
Commandant (G-WKH) on the unit's Health Services Statistical Report. From an
oversight or management review perspective, repeated or recurring amounts of unit
Fund Code-57 (AFC-57) moneys dedicated to health care are the "base" funds. COs
must justify additional unit operating funds above this base solely on the criterion of
increased workloads.
c. The unit commanding officer will review all uses of unit funds and reallocate funds
during the current fiscal year. The unit commanding officer must first inform the
chain of command before he or she can reduce the amount of care the unit's clinic
provides to eligible beneficiaries. The CO will report the circumstances supporting

CH 15 8-2
the decision and identify what resources are required to ensure normal health care
facility operations through the end of the fiscal year. The District or Maintenance and
Logistics Commander's Budget Review Board (for district or MLC units respectively)
will address these current fiscal year AFC-57 unit requests.
2. Maintenance and Logistics Command (MLC). Maintenance and Logistics Commands
administer the health services program in their respective area of responsibility.
Administrative functions include:
a. Approving and funding care non-Federal and Department of Veteran's Affairs sources
provide;
b. Approving or disapproving requests to procure health care equipment costing more
than $750.00 for units with CG Clinics/AFC-57 funding and over $300.00 for units
without CG clinics/AFC-57 funding;
c. Approving clinic budgets. Each clinic’s parent command shall submit a zero-based
AFC-57 direct care funding request to the appropriate MLC (k) through the chain of
command. This request should include predicted equipment procurement requests to
Commandant (G-CBU) using the automated ATU budget process according to current
directives. The MLC request should include a line item for each clinic, proposed
equipment funding, and an estimate of non-Federal care cost.
d. Targeting AFC 57 and AFC 73 funds to pay for Department of Defense for all health
care the Army, Navy, Air Force, TRICARE and USTF programs provided to Coast
Guard beneficiaries.
3. Headquarters.
a. Commandant (G-WK) obtains health services program resources from the budget
process for these purposes:
(1) Targeting AFC-57 funds to the MLC (k)s to pay for all non-Federal and VA
medical care provided in each region;
(2) Targeting AFC-57 funds to the MLC (k)s to acquire health care equipment; and
(3) Targeting AFC-57 funds to allotment target units in response to budget requests
the MLC (k)s submit.
b. Commandant (G-WK) is also the program manager for replacing, expanding, or
creating health care facilities with Acquisition, Construction, and Improvement
Appropriation funds and works with Commandant (G-A) and the MLC's Facilities
Design and Construction Center staffs on plans and layouts.
8-3 CH 15
B. GENERAL PROPERTY MANAGEMENT AND ACCOUNTABILITY
1. Basic Policies. The Director of Health and Safety:
a. Establishes procedures to manage and account for health care material pursuant to the
personal property management policies contained in the Property Management
Manual COMDTINST M4500.5A;
b. Directs and coordinates the health care supply system;
c. Determines requirements for health care material; and
d. Establishes allowance lists, advises, and assists field units.
2. Physical Property Classifications. Property is divided into two categories: real property
and personal property. Health care material is personal property and is accounted for in
accordance with Property Management Manual COMDTINST M4500.5A
3. Property Responsibility and Accountability.
a. Clinic administrators are responsible and accountable for the property their facilities
use. Additionally, they serve as the health services finance and supply officer.
b. In the absence of a clinic administrator, the senior commissioned health services
department representative acts as the property custodian.
c. If health services technicians only are assigned to a facility, the senior health services
technician acts as the property custodian.
4. Expending Property Unnecessarily. All persons having custody of health care property
shall avoid any unnecessary expenditures of such property within their authority’s limits
and shall prevent such expenditures by others.
5. Stock Levels, Reorder Points, and Stock Limits.
a. General. Stock levels, reorder points, and stock limits discussed below apply to all
health care facilities, especially those at major shore units such as the Academy, ISC
Alameda, and Training Center Cape May. These large facilities with multiple
components (e.g., pharmacy, laboratory, dental clinic, etc.) need to maintain a greater
stock depth to serve their clientele. COMDTINST M4500.5A (series) contains
overall supply policy and procedures.

CH 15 8-4
b. Terms.
(1) Operating Stock. That quantity of material on hand needed to meet daily
operating needs during the interval between delivery of replenishments.
(2) Safety Stock. That amount of inventory in addition to operating stock needed to
sustain operations if deliveries are delayed or demands unexpectedly heavy.
(3) Reorder Point. Low Limit. Both terms mean the predetermined inventory level
for a specific item at which it is reordered.
c. Stock Inventory and Transactions. All health care facilities shall maintain sufficient
amounts of stock to prevent out-of-stock conditions. To do so, maintain stock
inventory and transaction records, either electronically (on computer) or by using
stock cards, inventory records, etc.
(1) Generally, health services supply activities at facilities with multiple components
are authorized one month's safety stock. Experience may prove this level is not
adequate for certain items or in certain circumstances. These units are authorized
to maintain more a larger supply if and wherever exceptional circumstances
dictate. Establish procedures to ensure reviews of stock records periodically to
identify items reaching a low limit (reorder point) or the authorized allowance and
quantity and to revise low limits if current usage so indicates.
(2) Ships and small shore units may use the minimum quantities indicated in the
Health Services Allowance List to establish reorder points. If the list does not
indicate a minimum allowance, e.g., for "optional" items, establish reorder points
for commonly used items based on current usage rates. Do not order excessive
quantities of material.
(3) When a ship receives orders to deploy or a station notice of a change in operating
conditions that may require additional material, promptly review authorized
allowance quantities to replenish critical items in time for the deployment or
operational change.
(4) Pharmacies procuring drugs through prime vendor systems (either directly or
through pharmacy officer staffed clinics) should try to stock one-month quantities
of regularly used items. Ongoing inventories of these limited quantities are not
required except where applicable for controlled substances. Pharmacies shall
"sight inventory" monthly before ordering.
6. Transferring and Loaning Property. Written approval is required from Commandant (G-
WKH) to loan health care property to any state, community, organization, or private
individual. Property or transferred to other military units is at the commanding officer's
discretion. Obtain custody receipts in such instances. Use NAVSUP 460, Equipment

8-5 CH 15
Stock Card and Custody Record, or a local form for local transactions and DD-1149 to
transfer property from one activity to another.
C. CUSTODY, ISSUES, AND DISPOSITION
1. Transferring Custody. When transferring custody of health services property and supplies
a joint inventory is required, conducted by both the departing and relieving custodians
and an independent person who has no direct interest in the inventory outcome. If a joint
inventory is impossible, the departing custodian shall conduct an inventory and submit a
written report to the commanding officer before departing. As soon as possible after
reporting, the relieving custodian also shall conduct an inventory, report the same to the
commanding officer, and indicate any discrepancies noted between the two. In both
cases, the inventories should include the participation of an independent person.
Additionally, in all cases, an acknowledgment of inventory correctness must be entered in
the unit Health Services Log. See “Pharmacy Operations and Drug Control,” Chapter 10,
for detailed information on controlled substances.
2. Storerooms.
a. At large facilities, bulk stock of health care supplies and materials used by the various
facility components (e.g., pharmacy, laboratory, dental clinic, etc.) shall be kept in a
specifically designated storeroom. If facility layout permits, it may be advantageous
to permit designated individuals responsible for a particular component (pharmacy,
dental clinic, etc.) to manage their area’s expendable supplies. The individual
responsible for medical supply shall process their procurement requests. Otherwise,
manage clinic supplies from a designated storeroom.
b. An individual familiar with supply procedures shall be in charge of the storeroom; he
or she shall report directly to a medical administration officer.
c. In the interest of proper management, centralize clinic procurement request
processing. Medical administrator(s) shall verify all procurement requests, including
prime vendor "ZOA" documents, to ensure funds are available in that component’s
budget allocation.
3. Issuing Material.
a. Supplies issued by or removed from the storeroom should be immediately recorded
on the appropriate stock record. In large facilities where the health services storeroom
is a distinct organizational entity, stores issued shall be made only upon receiving a
properly prepared and authenticated local requisition document.
b. Use DD 1149 to issue, return, or transfer equipment between activity components.
4. Inspecting Storerooms.

CH 15 8-6
a. Health services store items require periodic inspection (every three months for
consumable supplies and equipment) to detect signs of deterioration or expiration.
Accomplish such inspections by physically examining representative samples of
various age groups of stock on hand.
b. It is extremely important to issue oldest stock first (“First in, First out”). This is true
of all items but is mandatory for potency-dated items and those subject to spoilage.
5. Disposing of Property.
a. In disposing of health services personal property, follow COMDTINST M4500.5A
(series) procedures regardless of the circumstances or conditions requiring disposal
(e.g., over-ordering, decline in demand, fair wear and tear requiring survey, or damage
requiring replacement).
b. Certain conditions may require Board of Survey action. COMDTINST M4500.5A
(series) contains procedures for this action.
(1) Take precautions to assure compliance with local health and sanitation
requirements when surveying and destroying poisonous chemicals (e.g., arsenic,
strychnine, cyanide, etc. preparations).
(a) Ordinarily, dispose of small amounts of liquid preparations and soluble
substances through the sewage system. Large quantities of soluble poisonous
material may constitute pollution dangerous to public health or fish and
wildlife.
(b) If destroying large amounts of drugs (including controlled substances),
coordinate this action with local air and water pollution control authorities.
Then destroy by complete incineration with appropriate safeguards against
toxic fumes or by such other methods as local health and sanitation officials
recommend if disposal through sewage system or incineration are
inappropriate.
(c) Never deposit poisonous drugs and chemicals in dump piles or dumpsters.
(2) Either burn or dissipate through the sewage system drugs requiring destruction
other than poisonous chemicals.
c. Dispose of used, contaminated, defective, or expired health care material in a manner
that ensures it is both impossible to reuse and harmless to the environment.
Completely destroy all drugs to preclude reusing them or any portion of them. Follow
these specific procedures:
8-7 CH 15
(1) Sharps. Place all items likely to puncture or lacerate trash handlers in rigid plastic
autoclavable disposable sharp containers. Do not attempt to sterilize or cover
used blades or needles (this is hazardous to personnel); simply place them in the
container. At appropriate intervals, seal, autoclave, and dispose of containers as
regular non-hazardous trash. These containers are NOT reusable.
(2) Tablets, Capsules, Powders. Remove from original container, crush or dissolve
tablets and capsules, and flush into sewage system. Dispose of original container
as trash. Follow biohazardous material disposal regulations when discarding
chemotherapeutic and other hazardous agents (including biologicals).
(3) Syrettes. Cut along syrette’s crimped end and discard contents into sewage
system. Place in a sharps disposable container.
(4) Injectables/Parenterals. Pour bottle contents into the sewage system. Place empty
vials in the trash. Follow biohazardous material disposal regulations when
discarding chemotherapeutic and other hazardous agents (including biologicals).
(5) Auto Injectors. Activate the injector against a hard surface and discard contents
into a suitable container. Dump container contents into the sewage system and
then place the auto injector in a sharps disposable container.
(6) Incinerate biohazardous materials, including used bandaging materials, or if
sterilized, dispose of them as trash.:
(7) Chapter 10 contains detailed instructions on surveying and destroying controlled
substances.
(8) Destroy the above materials in an appropriate area using appropriate personnel
protection: rubber gloves, protective goggles, and proper ventilation.
d. Do NOT dispose of medical materials at sea. Prepare materials for disposal and
retain them on board in a secure area until disposed in accordance with Federal, state,
and local laws.
e. Commandant Notices and other directives requiring disposal of defective material
constitute authorization to effect immediate disposal of any of the suspect items on
hand.
CH 15 8-8
D. HEALTH SERVICES SEGMENT OF THE COAST GUARD SUPPLY SYSTEM
1. Health Services Control Point. Commandant (G-WKH-2) is the Health Services Control
Point for Coast Guard health care material; in that capacity he or she takes these actions.
a. Prepares and distributes the Health Services Allowance List, COMDTINSTs
M6700.5, M6700.6, and M6700.7(series).
b. Informs and assists field units; and
c. Reviews and responds to requests to change units' base operating funds allotment
targets. Annually provides funds for routine health care supplies to the field as part of
the recurring base of funds distributed through the Administrative Target Unit (ATU)
budget process.
2. Responsibility for General Stores Items.
a. Supply Officer.
(1) Procures, receives, stores, issues, ships, transfers, and accounts for command
stores and equipment;
(2) Maintains specified records; and
(3) Submits required reports for stores and equipment.
b. Health Services Department Representative. Except where specific responsibility has
been assigned, the Health Services Department Representative does not determine
general supply requirements but acts in an advisory capacity for those items the
department uses. The Health Services Department Representative will maintain close
contact with the Supply Officer on special department needs and advise the latter
when the requirement for any item will exceed the quantity normally carried in stock.
The individual designated in writing as responsible for Health Services supply
operations shall maintain a supply policy and procedures manual.
3. Supply Support Assistance.
a. Direct problems with supply support of health care supplies (except controlled drugs)
that cannot be resolved through the supply source, to Commander, Maintenance and
Logistics Command (k). Direct problems with supply support of controlled drugs to
Commandant (G-WKH).
b. Commandant (G-WKH) will coordinate initial outfitting of new classes of units and
vessels. Commander, Maintenance and Logistics Command (k) will help in the initial

8-9 CH 15
outfitting process, limited to submitting requisitions and staging, when Commandant
(G-WKH) so requests through Commandant (G-CPM).
4. Authorized Allowances. Coast Guard units are assigned specific minimum required
allowances of health care supplies and equipment as described in COMDTINST M6700.5
(Shore Units), M6700.6 (Vessels), and M6700.7 (Shore Units and Vessels)(series).
5. Supply Sources.
a. Standard Items. Items listed in the DOD Medical Catalog (microfiche) are
"standard". Obtain items with an Advice Acquisition Code (AAC) of "D" from the
Defense Personnel Support Center (DPSC) through the Automated Requisition
Management System (ARMS).
b. Non-standard Items.
(1) Obtain "non-standard" items, i.e., those not described as above, from commercial
sources.
(2) All commercial procurements shall be made under the applicable acquisition
regulations and Coast Guard Acquisition Procedures, COMDTINST M4200.19
(series). Commercial procurement of health care supplies, equipment, and repair
and maintenance service is authorized in these conditions:
(a) Time does not permit obtaining standard items from Government sources; or
(b) A legitimate need exists for nonstandard items;
(c) Equipment requires repair or maintenance.
(3) These items are authorized:
(a) Newly listed standard items not available from government sources;
(b) Necessary non-standard health care supplies and equipment;
(c) Medical Catalog (microfiche) items bearing the Acquisition Advice Code "L";
(d) Equipment repair and maintenance (excluding installation); and
(e) Health care technical books, publications, and professional journals.
(4) Local or commercial procurement is not authorized for these items:
(a) Non-standard items differing only slightly from standard items of identical
capability; and
(b) Preferred trade names and proprietary products in lieu of standard items.
CH 15 8-10
c. Prime Vendor Items.
(1) A prime vendor is one pre-arranged on behalf of the government procurement
system. The Defense Personnel Support Center (DPSC) negotiates prime
vendors, equivalent to Federal "depot" sources, for medical commodities.
(2) Where available, DPSC prime vendors shall serve as the primary source of supply
for pharmaceuticals. Use other sources if it is determined their price or service
better meet the unit's needs.
6. Equipment.
a. New Installations. The appropriate construction project (AC&I) funds normally will
pay for equipment for newly constructed facilities. To ensure standardization,
authorization and approval MUST be obtained from Commandant (G-WKH) before
requisitioning or procuring health care equipment for new installations.
b. Replacement Equipment. See Section 6-A for detailed information on health services
equipment replacement procedures and reporting requirements.
c. Receipts.
(1) The unit shall retain one copy of signed receipts for health services material for
record purposes.
(2) Send one copy of signed receipts for all health care equipment to MLC (k).
(3) Maintain copies of receipts for controlled substances and security materials
separately for record purposes.
d. Maintenance.
(1) Each unit is responsible for maintaining health care equipment in optimum, safe
operating condition. Maintenance shall include:
(a) Measures necessary to ensure the equipment’s operating safety and efficiency
(preventive maintenance);
(b) Manufacturer's representatives’ required checks to meet warranty
requirements;
(c) Removing from service if deficiencies are detected; and
(d) Replacing defective parts.
(2) Preventive maintenance is systematic inspection of and service to equipment to
maintain it in optimum operating condition. A properly executed program will

8-11 CH 15
detect and correct minor problems before they render the equipment inoperable.
Manufacturers usually require preventive maintenance to maintain the warranty.
Maintenance records are also valuable tools for evaluating equipment needs and
justifying future equipment procurement requests.
(3) Each clinic shall designate a Preventive Maintenance Coordinator who ensures the
program is established and functions effectively. If a Biomedical Equipment
Repair Technician (BMET) is assigned to the unit, he or she fills this role. If not,
designate an individual with mechanical aptitude or a desire to work with
equipment to fill this role. Clinics may contract for preventive maintenance
services if funding permits and are encouraged to enter into cooperative
agreements with DOD MTFs whenever possible. Each unit shall:
(a) Establish a preventive maintenance schedule for all health care equipment.
Each unit shall determine maintenance intervals based on manufacturers'
recommendations and frequency of use.
(b) Maintain a written record of all preventive maintenance and repairs performed
on health care equipment using NAVMED 6700/3CG, Medical/Dental
Equipment Maintenance Record; see Figure 8-D-1. Use side A to record
preventive maintenance and safety checks and side B to record repairs.
(c) Charge clinic health care equipment maintenance costs to unit AFC-57 funds
and sickbay health care equipment maintenance costs to unit AFC-30 funds.
(d) MLC and HQ units shall establish and maintain a program to replace their
health care equipment.
7. Uniform. USPHS officers assigned to Coast Guard detail shall wear the Coast Guard
uniform as prescribed in USCG Uniform Regulations, COMDTINST M1020.6 (series).
They shall wear USPHS devices on Coast Guard blue background in place of the Coast
Guard shield on the combination cap, garrison cap, shoulder boards, and sleeve insignias.
For officers transferring from another USPHS assignment to the Coast Guard detail, the
unit shall issue Coast Guard uniforms consisting of one service dress blue uniform with
two pairs of trousers, three light blue long-sleeve shirts, three light blue short-sleeve
shirts, a raincoat and a wind-breaker according to the Comptroller Manual. Vol. III,
COMDTINST M4400.19A (series). Women will receive a hat frame; they may substitute
a skirt for one pair of trousers in their uniform issue. USPHS officers may wear lab coats
and smocks as prescribed in USCG Uniform Regulations, Section 11-B.
CH 15 8-12
E. EYEGLASSES AND OPHTHALMIC SERVICES
1. General. This section describes ophthalmic services (refractions and spectacle issue)
provided.
2. Personnel Authorized Refractions.
a. Coast Guard medical treatment facilities and USMTFs to the extent of available
facilities, including ophthalmologists’ and optometrists’ services, may furnish
refractions to active duty and retired uniformed services members.
b. Where USMTF's are not available, MLC (k) may authorize refractions at other
facilities for active duty members only.
c. USMTFs may furnish non-active duty eligible beneficiaries refractions if facilities are
available. USMTFs may not furnish eyeglasses to dependents at government expense
except as Section 8-E-8 authorizes.
d. Reserve members on active duty for training for more than 30 days are authorized
repair or replacement of standard eyeglasses during the active duty if the member did
not damage or lose the eyeglasses through his or her own negligence.
3. Procuring and Issuing Standard Prescription Eyewear.
a. Coast Guard units shall order standard eyewear from optical laboratories as outlined
in this section.
(1) Civilian sources are acceptable for procuring eyewear providing the prescription is
for standard frames and lenses are available from fabrication labs. Transcribe this
request on DD-771, Eyewear Prescription.
(2) If fabrication would entail a prolonged delay (more than eight weeks) and the
member's vision is so poor he or she cannot safely perform assigned duties,
procure non-standard eyewear from local civilian sources using non-Federal
health care funds.
(3) Members requiring corrective lenses shall have two pair at all times, including
eyeglasses issued from government sources or purchased at their own expense.
(4) Requests for tinted eyewear for non-aviation members must be justified solely on
the duties they perform, e.g., majority of duty time in bright sunlight, etc.
(5) Replacement eyewear may be obtained without repeating a visual acuity check,
provided the replacement prescription is less than two years old. If a corrected
8-13 CH-17
visual acuity check is required and indicates the current prescription is
inadequate, and obtain a refraction.
a. Available Eyewear and Standard Eyewear Sources of Supply.
(1) These types of eyewear are available:
Cellulose acetate frame
Type of Correction Glass Lens Plastic Lens
Single Vision, white 1 X X
Single Vision, tinted 1, 2 X X
Bifocal, 25mm segment, white 1 X X
Bifocal, 25mm segment, tinted 1, 2 X X
Trifocal, white X
Cataract Aspheric X
Trifocal, white and tinted 1, 2 X
(1) Eyewear provided in FG-58 (Flight Goggle) mounting for
authorized personnel
(2) Only N-15 and N-32 tints authorized
(2) Process all requests for standard prescription eyewear through the
below military optical laboratory; this is the only optical laboratory
from which Coast Guard units are authorized to order standard
prescription eyewear.
Naval Ophthalmic Support and Training Activity
Yorktown, VA 23691-5071
(a) The Coast Guard pays only for glasses ordered and processed for
Coast Guard active duty or retired personnel; therefore, it is
extremely important to properly complete the DD-771 service
identification block to indicate the patient's service affiliation.
(3) Procurement Procedures. Order all prescription eyewear using DD-
771, Eyewear Prescription. It is extremely important to accurately
complete the prescription form. If the prescription is wrong, the patient
is inconvenienced; the Coast Guard is required to pay for eyewear even
if it cannot be used; and the supply activity will reject an improperly
prepared prescription, resulting in delay. Use these guidelines to
prepare DD-771. See Section 4-B for more detailed instructions.
(a) Use a separate DD-771 for each type of eyewear.
CH-17 8-14
(b) If no health services personnel are available at the unit, send the
prescription obtained from the health record or local civilian
source to the health record custodian to prepare and submit the
DD-771.
(c) Submit all three DD-771 copies to the approving authority or
supply activity; disregard the distribution instructions. Remove
all carbon sheets before submission. File a photocopy of the DD-
771 in the member's health record.
(d) TRACEN Cape May shall send recruits’ eyewear prescriptions
separately and mark the envelope, "RECRUIT—PLEASE
EXPEDITE".
(e) Report delays longer than eight weeks in receiving eyeglasses to
the appropriate MLC (k).
(4) Health Record Entries. Record on a separate DD-771 the current
prescription, including frame measurements and all other data
necessary to reorder eyewear, for each individual requiring eyeglasses.
4. Aviation Prescription Lenses. These personnel are authorized two pair of clear
aviation spectacles (FG-58) and one pair of tinted spectacles (N-15) in matte
chrome only:
a. Aviators Engaged in Actual Flight Operations. Aviation spectacles may be
ordered for distant vision correction , or for distant vision and near vision
correction (bifocal lenses). Those aviation personnel engaged in flight
operation who desire near vision only correction in aviation frames must
order bifocal lenses containing plano top portion and the near vision
correction on the bottom. Spectacles containing only near vision correction
are not authorized in aviation frames. This type correction will only be order
in cellulose acetate frames.
b. Landing Signal Officers (LSO).
c. Coast Guard Ceremonial Honor Guard personnel.
d. Small Boat Crew required to wear a helmet while performing their assigned
duties.
5. Contact Lenses. Contact lenses are issued only to active duty personnel for
postocular surgical difficulties or to enable a member to overcome a
handicapping disease or impairment. MLC (k) will not approve contact lenses
solely for cosmetic reasons.
8-15 CH 15
a. Submit letter requests for contact lenses to MLC (k) under Section 2-A-6.d.; include
the type of lenses and cost.
b. If MLC (k) approves, he or she will provide an authorization number by return
correspondence. Units will write this number on all correspondence and billings
before submitting to MLC (k).
6. Sunglasses for Polar Operations. Military fabrication laboratories no longer issue polar
operation sunglasses. Activities requiring such glasses may use the process below to
obtain them:
a. Non-prescription Lenses. If issuing, the command must purchase and issue non-
prescription lenses as part of the cold weather clothing allowance and pay the lenses’
costs from operating expenses. The command should issue the lenses on a custodial
basis; departing members should return them to the command for reissue.
b. Prescription Lenses. Procure prescription lenses in the specifications below under the
guidelines in Comptroller Manual, COMDTINST M4400.19A (series), Vol. III.
(1) Aviation-type frames; and
(2) Lenses must contain Type 1 or 1-A metallic coat.
7. Safety Glasses.
a. Non-prescription or prescription safety glasses meeting American National Standards
Institute Standard Z87.1 shall be for industrial wear to military and civilian personnel
working in any environment hazardous to eyes, e.g., welders, machinists, mechanics,
riggers, and grinders.
b. Non-prescription safety glasses shall be furnished on a custody receipt when a
prescription lenses are not required..
c. Prescription safety glasses are no longer available from military optical laboratories.
Procure them under the guidelines in the Financial Resources Management Manual
(COMDTINST M7100.3A).
8. Dependent Care in Isolated Areas. Spectacles may be furnished to command-sponsored
dependents of uniformed services members assigned outside CONUS.
9. Contemporary Prescription Eyewear Procurement. This optional program enables active
duty members to obtain contemporary prescription eyewear on a cost-shared basis.
COMDTINST 6490.1A (series), contains current policies and procedures to obtain
contemporary prescription eyewear.
9-i CH-16
CHAPTER 9
HEALTH SERVICES TECHNICIANS ASSIGNED TO INDEPENDENT DUTY
SECTION A- INDEPENDENT DUTY AFLOAT............................................................................................. PAGE
INTRODUCTION ............................................................................................................................................... 1
MISSION AND RESPONSIBILITIES.................................................................................................................. 1
CHAIN OF COMMAND....................................................................................................................................... 2
OPERATION OF THE HEALTH SERVICES DEPARTMENT.......................................................................... 2
PROVIDING HEALTH CARE AFLOAT............................................................................................................. 5
TRAINING.......................................................................................................................................................... 12
SUPPLY AND LOGISTICS................................................................................................................................ 16
HEALTH SERVICES DEPARTMENT ADMINISTRATION........................................................................... 23
COMBAT OPERATIONS .................................................................................................................................. 27
ENVIRONMENTAL HEALTH .......................................................................................................................... 28
9-1 CH-16
CHAPTER 9. HEALTH SERVICES TECHNICIANS ASSIGNED TO INDEPENDENT
DUTY
Section A - Independent Duty Afloat.
1. Introduction. An independent duty health services technician (IDT) is a Health Services
Technician (HS) assigned to an afloat unit that has no attached medical officer.
Assignment to independent duty is challenging. The role is one of tremendous
responsibility and at times can tax even the most experienced HS’s skill, knowledge and
ability. Along with the increased responsibility and sometimes arduous duty comes the
potential for personal satisfaction unsurpassed by any other job assignment.
2. Mission And Responsibilities.
a. Mission. The Health Services Technician serving independently is charged with the
responsibility for the prevention and control of disease and injury, and the treatment
of the sick and injured.
b. Responsibilities. The Commanding Officer (CO) is responsible for the health and
physical readiness of the crew of the unit. In the absence of a permanently attached
Medical Officer (MO) the vessel's Executive Officer (XO) is designated by Coast
Guard Regulations as the unit's medical officer. The role of the IDT is to assist the
command in maintaining the good health and physical readiness of the crew. To
accomplish this responsibility, the IDT must be informed of planned operations and
anticipate any operational demands resulting from such operations. To this end, the
IDT will consult and advise the Command in all matters with potential to effect crew
readiness or the health of personnel. Some of the duties of the IDT include:
(1) Assessment and treatment of illness and injury;
(2) Prevention of illness and injury through an aggressive environmental health
program. Such a program includes inspection of living and working spaces;
food service and storage areas and food storage and handling practices;
integrated pest management practices; potable water quality surveillance; and
recognition and management of communicable diseases;
(3) Provision of Health Services training aligned with the needs and mission of the
unit;
(4) Security and proper use of Health Services supplies, material and property;
(5) Supply and logistics to ensure supplies, materials and equipment necessary to
carry out the mission of the Health Services Department are obtained and
maintained in sufficient quantity and condition to support the unit mission and
operation;
(6) Health Services Department administration, maintenance and security of health
records;
(7) Strict adherence to Chapter 2 of this Manual which contains information about
general and specific duties of the HS serving independently.
9-2
CH-16
3. Chain Of Command. The IDT will normally be assigned to the Administrative
Department and will report directly to the Executive Officer (XO).
4. Operation Of The Health Services Department. The IDT is tasked with a wide variety
and high volume of duties and responsibilities. This section sets forth policy and
guidelines designed to assist the IDT in carrying out assigned duties and responsibilities.
a. Health Services Department Standard Operating Procedure. In order to successfully
manage the Health Services Department the IDT must use time management and
organizational skills and tools. One such tool is a written Standard Operating
Procedure (SOP) for the Health Services Department. The SOP will govern the
activity of the IDT and has as its guiding precept the goals and missions of the unit.
The SOP will be developed and submitted in written form to the CO for approval via
the chain of command. In addition, the SOP will be reviewed at least annually by the
IDT, XO and CO. The approved SOP will be kept in the Health Services
Department for easy referral. Copies of pertinent sections will be posted as
appropriate. The SOP will include:
(1) A copy of the IDT’s letter of assumption of duties as Health Services
Department Representative;
(2) A written daily schedule of events for both underway and inport periods;
(3) Copies of all letters of designation, assignment, and authority that directly
impact upon the IDT or Health Services Department. Examples include those
granting ”By direction” authority, designation as working Narcotics and
Controlled Substances custodian, and assignment of a Designated Medical
Officer Advisor (DMOA);
(4) A copy of the unit's organizational structure. This document will show
graphically the IDT’s chain of command;
(5) A listing of duties and responsibilities assigned to the IDT and the frequency
that they are to be carried out. The listing will include both primary and
collateral assigned duties;
(6) A listing of all required reports, the format required for submission, the
frequency or date required, required routing and required “copy addressees”.
Incorporation of this information in tabular format provides a quick and easy
guide for reference purposes;
(7) A water bill, for the safe handling of potable water;
(8) A unit instruction or SOP for the management of rape or sexual assault cases.
The document must provide policy for Health Services Department action in
such cases, names of organizations, points of contact and telephone numbers
for local resources as well as contact information for agencies and facilities
which must be notified. It must contain a prearranged mechanism for timely
completion of a physical examination for the purpose of evidence gathering
that meets requirements of all applicable law enforcement agencies.
Additionally, it must define limitations that will exist if the unit is underway at
the time the incident occurs;

9-3 CH-16
(9) A unit instruction or SOP for the management of suicide threat or attempt. The
document must provide policy for Health Services Department action in such
cases, names of organizations, points of contact and telephone numbers for
local resources, contact information for agencies and facilities which must be
notified as well as a listing of required information, reports or actions.
(10) A unit instruction or SOP action required in the event of family violence. The
document must provide policy for Health Services Department action in such
cases, names of organizations, points of contact and telephone numbers for
local resources, contact information for agencies and facilities which must be
notified as well as a listing of required information, reports or actions.
b. Other Necessary Documents. The IDT is an integral part of many unit activities and
various unit bills and doctrines require specific action by the IDT. Since these are
changed frequently, incorporation of Health Services Department responsibilities
contained in these various documents into the Health Services Department SOP is
not recommended. Applicable portions should be kept in the Health Services
Department for quick reference, however. These include:
(1) A battle doctrine for the unit.
(2) Portions of the unit mass casualty bill pertaining to Health Services
Department responsibility;
(3) Portions of the unit general emergency bill pertaining to Health Services
Department responsibility;
(4) Portions of the unit man overboard bill pertaining to Health Services
Department responsibility;
(5) Portions of the unit replenishment at sea, special sea detail, flight quarters and
bomb threat bills pertaining to Health Services Department responsibility.
c. Departure From the Daily Schedule of Events. The day-to-day operation of the
Health Services Department is complex and impacted upon by the operational needs
of the unit. It will of necessity change when events of higher priority or concern
occur. If deviation from the daily schedule of events is required, notification of the
XO (IDT’s Division Officer) will be made at the earliest opportunity. When
deviation from daily schedule of events occurs frequently, the daily schedule of
events will be reviewed and if necessary, changed. Any changes will be incorporated
into the Health Services Department SOP and approved by the Commanding Officer.
d. Relief and Assumption of Duties as the IDT. Proper documentation of the status of
the Health Services Department, the condition of its equipment, stores, and records is
required at the time of relief and assumption of the duties and responsibilities as the
IDT. The process is complex and requires both the incoming and outgoing IDT to
jointly perform the following:
(1) A complete inventory of all medical stores, spaces, and equipment, including
durable medical equipment. The Health Services Allowance List Afloat

9-4
CH-16
(COMDTINST M6700.6D series) provides a listing of supplies and the
equipment required by each class of vessel.
(a) A controlled substances inventory must be done. Use direction provided
in Chapter 10 of this Manual.
(b) A complete inventory of all unit property in custody of the Health
Services Department;
(2) A review of ongoing actions affecting the status of Health Services, e.g.,
outstanding requisitions, survey or repairs, and proper documentation of all
such transactions;
(3) A review of the Health Services Department SOP;
(4) A review of the most recent Maintenance and Logistics Command (MLC)
Quality Assurance Assistance Survey for the unit. A copy of the survey
annotated with any finding of incomplete or uncorrected discrepancies will be
included as an enclosure to the letter of relief;
(5) A review of crew training files required for Tailored Ships Training
Availability (TSTA) evaluation. Paragraph A.6. of this chapter provides a
listing of requirements;
(6) A review of all health records for completeness and accuracy;
(7) A complete health, safety and sanitation inspection of the vessel, to include
status of potable water systems (records of bacteriological, halogen content and
pH testing), food stores inspections, and berthing and habitability of living and
berthing spaces.
e. Letter of Relief and Assumption of Duties. Upon completion of the Health Services
Department review a basic Coast Guard letter will be prepared and submitted by the
oncoming IDT via the chain of command and will advise the Commanding Officer of
the status of the Health Services Department. A copy of the letter will be forwarded
to the cognizant MLC. The letter of Relief and Assumption of Duties will provide
the following:
(1) Date of assumption of duties; a statement that the duties and responsibilities of
the IDT have been assumed; and a statement that a thorough review of the
Health Services Department has been conducted. Any discrepancies of
material or record keeping will be annotated on a copy of the unit's most recent
MLC Quality Assurance site survey and this survey submitted as an enclosure
to the letter of Relief and Assumption of Duties as IDT for the vessel;
(2) Any discrepancies noted upon relief will be handled as a matter of individual
command prerogative. Responsibility for correction, adjustment of account or
inventory records, action required to replace missing items, as well as any
necessary disciplinary action will be determined by the command;
9-5 CH-16
(3) In cases in which no “on site” relief occurs, all of the preceding action will be
completed. The supply officer of the unit will participate in the review process
in place of the outgoing IDT.
f. Actions Upon Proper Relief. Upon assumption of duties as the unit's IDT, one of the
first tasks to complete is a thorough review of all SOPs and department instructions.
Check the references, make contact with any listed Points of Contact. If possible,
make visits and introductions in person. Find out how each system works and how it
is accessed.
5. Providing Health Care Afloat. Provision of health care is undoubtedly the most
challenging and rewarding part of the job of an IDT. An IDT bears a tremendous
responsibility. This responsibility can never be taken lightly. This section is intended to
provide a brief summary of the various facets of providing medical care afloat.
a. Designated Medical Officer Advisor (DMOA). Each independent HS will be
assigned a DMOA in accordance with Chapter 1 of this Manual. Good
communication between the IDT and the unit DMOA can eliminate many problems
affecting health care delivery to the crew. The IDT will schedule a visit to the
DMOA as soon as is practical after reporting aboard. The purpose of the visit is to
allow first-hand communication of expectations, support facility requirements, and
any unique needs or concerns. Open communication can be maintained through
regular visits when practical, or at minimum, regular telephone calls. With regard to
provision of direct care, the IDT will seek DMOA or another MO’s advice whenever
there are questions about a patient’s condition or when the following conditions
exist:
(1) Return to sick call before assigned follow-up because of failure to improve or
condition has deteriorated;
(2) Member cannot return to full duty status after 72 hours duration because of
unresolved illness;
(3) Undetermined fever of 102 degrees Fahrenheit or higher (when taken orally)
persisting for 48 hours;
(4) Fever of 103 degrees Fahrenheit or higher (when taken orally);
(5) Unexplained pulse rate above 120 beats per minute;
(6) Unexplained respiratory rate above 28 breaths per minute or less than 12
breaths per minute.
(7) Depression with suicidal thoughts;
(8) Change in mental status;
(9) Chest pain or arrhythmia;
(10) Unexplained shortness or breath;
(11) Rape or sexual assault.
9-6
CH-16
b. Gender Considerations. Chapter 1.A. of this Manual provides specific direction for
health services technicians about patient privacy, same gender attendant
requirements, and examination restrictions.
c. Avoiding Common Problems. Scheduling and obtaining the routine medical care
needed by crewmembers during short inport periods can tax the organizational skills
of even the most experienced IDT. There are, however, actions that the IDT can take
which will enhance the chances of getting the routine appointments needed for all
members. Some of these are:
(1) Identify the routine medical and dental needs of the crew well in advance of
return to port. The vessel's supporting clinic has an established appointment
scheduling procedure within which the IDT must work whenever operational
schedules allow. Provide requests via message (or other written form as
appropriate) for appointment scheduling ahead of "appointment schedule
opening" for the inport period whenever possible. Request reply by message
prior to the vessel's scheduled return to port. Provide the list of scheduled
appointments to division officers and shop chiefs for the purpose of identifying
in advance operationally related conflicts or leave. Provide request for any
appointment rescheduling or changes by message as soon as possible;
(a) When routine medical or dental care is to be made directly to a DOD
MTF, the IDT must determine the facility requirements for referral of
patients and follow any local procedures.
(2) Communicate with the vessel's supporting clinic. Visit the supporting clinic, if
practical, as soon as possible after return to port. Discuss the crew's medical
and dental needs with the clinic supervisor and DMOA (if located at the
facility);
(3) Post a listing of appointment dates and times as soon as it becomes available.
Provide each division officer and shop chief a listing of the appointments
applicable to the division or shop;
(4) Hold members accountable to be at their appointed place and time. Provide
feedback to division officers and shop chiefs on any appointment failure.
Notify XO of more than one failure.
9-7 CH-16
d. Consultations. During the management of complex or protracted cases, consultations
or specialty referral may be necessary. When such services are needed, the IDT will
normally make referral to a Coast Guard clinic or in some cases, a Department of
Defense medical treatment facility (DoD MTF). When referring a patient to see a
medical officer at a CG health services clinic, the IDT shall ensure that a SF-600
entry is completed using the SOAP format and that an appointment is scheduled.
The clinic will normally provide treatment or arrange care if treatment is beyond its
scope. When consultations or referral for specialty care are made directly to a DOD
MTF, the IDT must determine the facility requirements for referral of patients and
follow any local procedures. Referrals to a DOD MTF will normally be documented
using a Consultation Sheet (SF 513) or a Referral for Civilian Medical Care DD
(2161). The consultation will provide a concise history of the condition to be
evaluated as well as any pertinent findings. A provisional diagnosis is normally
expected by the consultant. Chapter 4 of this Manual provides direction on
completion of a SF 513. The patient and the patient’s supervisor must be informed
of all consultation or referral appointment dates and times. Courtesy is an important
part of maintaining good working relationships with the facilities that the
independent duty HS accesses for consultation and referral. Timely notification of
the referral facility when appointment changes or cancellations occur (along with
brief explanation of why the change is required) help maintain those relationships.
Whenever possible, provide at least 24 hours notice of changes or cancellations.
e. Medical Evacuation (MEDEVAC) of Injured or Ill Crewmembers. Medical
evacuation must be considered when care needed by a patient to preserve life or limb,
provide pain relief beyond capability onboard, or to provide other medical or dental
treatment for which delay until the unit's next scheduled port call would provide
undue hardship or pain for the patient. The unit's ability to MEDEVAC a patient will
be affected by the vessel's current mission, availability of air transport assets, and
location. When considering or executing a MEDEVAC:
(1) Keep the XO informed. At first indication that a MEDEVAC may become
necessary, notify the XO;
(2) Request, via the XO, communication with the IDT's DMOA, a medical officer
familiar with the vessel's current area of operation or a flight surgeon if
MEDEVAC is to be by aircraft. In addition to a thorough patient presentation,
information about the unit's location in relation to medical resources ashore
and realistic estimations of time requirements to reach a point that MEDEVAC
is possible, must be available. Keep the XO and the DMOA/medical
officer/flight surgeon advised of any change in the patient's condition;
(3) Thoroughly document the MEDEVAC process. Ensure that a complete patient
record is maintained in the patient's health record. Maintain a complete record
of events in the Health Services log. Make entries as events occur. It is very
difficult to reconstruct an accurate log entry "after the fact".
(4) Keep the patient informed. Explain in as much detail as possible the actions
being taken and expected outcome of the actions. As time of departure
approaches, describe for the patient what to expect during transport and upon
9-8
CH-16
arrival at destination. If a Coast Guard Beneficiary Representative is attached
to the medical facility to which the patient is being MEDEVACed, provide this
information to the patient.
(5) Ensure that all documentation about the patient's condition is contained in the
health record and that it and any medication needed by the patient during
transport are securely packaged and ready for transport with the patient.
Ensure that information necessary for unit contact and contact of the unit's
supporting clinic are provided and easily located by the receiving medical
facility. Anticipate the patient's need for personal items, including a valid
Armed Forces Identification Card, and ensure these are packaged for transport
with the patient. Limit such items to those that are necessary. Encourage the
patient to limit cash.
(6) Notify the unit's supporting clinic of the MEDEVAC and any needed
assistance for the patient.
(7) Provide an inpatient hospitalization notification message in accordance with
current directives. See Chapter 6.A. of this Manual.
f. Surgical Procedures. Most routine minor surgical procedures will be delayed until
the vessel is in port. Surgical procedures while underway will be limited to only
those procedures that are needed in order to return a patient to a fit for full duty
status. These procedures include:
(1) Placing and removing sutures in a wound;
(2) Incision and drainage;
(3) Unguinectomy;
(4) Paring down painful plantar warts.
g. Refusal of Treatment. Medical, dental, and surgical treatment will not be performed
on a mentally competent member who does not consent to the recommended
procedure except:
(1) Emergency care is required to preserve the life or health of the member;
(2) Isolation and quarantine of suspected or proven communicable diseases as
medically indicated or required by law to ensure proper treatment and
protection of the member or others.
h. Motion Sickness. Members that manifest chronic motion sickness, that do not
respond to conventional therapy, and are unable to perform their duties as a result,
will be considered for administrative separation from active duty as per the Personnel
Manual, COMDTINST M1000.6 (series).
9-9 CH-16
i. Antibiotic Therapy. The IDT may prescribe and administer antibiotics included on
the Health Services Allowance List Afloat. Whenever possible, the IDT should
consult with his/her DMOA or a medical officer for a recommendation or
concurrence prior to administering antibiotic therapy. If consultation is not possible
prior to administration a message must be sent to the DMOA providing case history,
ICD9CM code and treatment provided.
j. Health Services Treatment Space. The Health Services treatment space will be
manned at all times when patients are inside. All items are to be stowed in their
proper place and secured. All medical records shall be locked in a cabinet. At no
time should the Health Services space be left unlocked when the IDT is not onboard.
k. Patient Berthing. Some units have facilities for short term berthing of patients in the
Health Services Department. These facilities are provided to facilitate close patient
observation or treatment. No person other than the sick or injured will be berthed in
the Health Services Department. The IDT may sleep in the Health Services
Department when attending an injured or sick patient, but will have a regularly
assigned berthing space. Personal gear and clothing are not to be stored in the Health
Services Department. The Health Services Department will not be used as berthing
spaces for augmented personnel.
l. Not Fit For Sea Duty. Members who are medically, surgically, or orthopedically
unfit for sea duty (including wearing a cast or needing to use crutches), and unable to
perform their duties will not be placed onboard the vessel. Personnel will either be
placed on Limited Duty ashore or on Convalescent Leave.
m. Convalescent Leave. Convalescent leave is a period of leave not charged against a
member’s leave account. It can be a recommendation to the command when a
patient is Not Fit For Duty (usually for a duration expected to be greater than 72
hours) and whose recovery time can reasonably be expected to improve by freedom
from the confines of quarters. It should be considered only when required as an
adjunct to patient treatment. The command must evaluate each recommendation.
Commands are authorized to grant convalescent leave as outlined in Chapter 4 of the
Personnel Manual.
n. Controlled Substances. Regulations for the handling, storage, and issue of narcotics
and controlled substances are found in Chapter 10 of this Manual. The contents of
this section are not intended to contradict the guidance provided there. This section
serves to amplify policy provided with respect to medicinal narcotics and controlled
substances onboard afloat units.
(1) Narcotics and controlled substances require special handling. All controlled
substances shall be obtained through the unit’s collateral duty pharmacy
officer.
(2) The CO will designate a commissioned officer as the controlled substances
custodian (CSC). The CSC will follow the accounting procedure provided in
Chapter 10 of this Manual. The IDT will normally be assigned as custodian for

9-10
CH-16
narcotics and controlled substances working stock. Such assignment must be
made in writing.
(3) All issues from working stock will be documented with a properly completed,
written prescription. All non-emergent care requires contact with a medical
officer before dispensing any controlled medication. The medical officer’s
orders will be documented on a prescription and in the patient’s health record.
The words “By verbal order of” will precede the ordering medical officer’s
initials, last name, time of order and date of order both on the prescription and
in the patient's health record. In the event of a true emergency, a medical
officer’s order is not needed to dispense a controlled substance. Once the
emergency situation is over or alleviated, the IDT will contact a medical
officer, detail the circumstances and the controlled substances that were
administered. Upon concurrence by the medical officer, the prescription
prepared for the patient will be annotated with the words “By concurrence of”
the ordering physician’s initials, last name, time of concurrence and date of
concurrence.
(4) The XO will countersign all prescriptions prepared by the IDT prior to issue of
any controlled substance or narcotic.
(5) Controlled substances stored aboard cutters shall be limited to amounts in the
Health Services Allowance List (HSAL). If the need exists for the unit to carry
additional quantities of controlled substances based on use or potential for
operational need, a written request signed by the Commanding Officer will be
forwarded to the unit’s cognizant MLC (k). The request must include,
nomenclature, quantity, and brief justification.
o. Dental. It is the duty of the IDT to arrange for the necessary dental examinations of
the crew. All personnel should be Class I or Class II prior to deployment.
(1) All personnel must receive an annual dental exam.
(2) The IDT will arrange, usually via message, for the large group of dental
appointments needed for crewmembers returning from deployment. A signup
sheet and announcement to the crewmembers is advised, and early
communication with the staff of the dental clinic is recommended in order to
allow sufficient time for the scheduling of a large amount of dental visits.
Urgent cases obviously are to be scheduled first, regardless of rank or position
of the member. Once back in port, active communication with a designated
POC in the dental clinic is advised in order to handle cancellations,
substitutions and last minute appointment changes. Although it may be time
consuming, it is easier to deliver patient reminders the morning of the
scheduled appointment than to try and explain a group of no-show
crewmembers to a dental officer or XO.

9-11 CH-16
p. Rape or Sexual Assault. All victims of rape or sexual assault must be treated in a
professional, compassionate and non-judgmental manner. Examination of rape and
sexual assault victims will be limited to only visual examination of any wound or
injury and treated according to present standards of care. In all cases, a medical
officer will be contacted for advice. In the event that no medical officer is available
(underway), an IDT may conduct the visual examination. A chaperone of the same
gender as the patient will be present if such examination is conducted. All aspects of
the patient encounter must be carefully documented. Physical examination to gather
evidence of rape or sexual assault is strictly prohibited. Also, see paragraph A.4.a. of
this chapter.
q. Suicide Prevention. An encounter with a suicidal person is always a deeply
emotional event. It is important for the IDT to act in a caring and professional
manner. Early intervention and good communication skills are essential. If suicidal
ideation is suspected it is important to remember:
(1) Take all threats and symptoms seriously. Immediately seek professional help
from the nearest MTF for any member considering suicide. At no time should
the person be left unattended;
(2) Actively listen to the patient. Do not argue, judge, attempt to diagnose, or
analyze the person’s true intentions. It is important to provide a calm, caring,
professional demeanor throughout the entire situation. Thoroughly document
the patient encounter using the SOAP format;
(3) Arrange for an escort and a driver to transport the patient to the nearest Coast
Guard clinic, MTF or civilian emergency room with facilities appropriate to the
situation. The unit's SOP for suicide threat or attempt should contain this
information for ready use if needed. If underway, then a MEDEVAC must be
considered. An IMARSAT phoncon with a flight surgeon, if MEDEVAC by
aircraft is required, the IDT’s DMOA or a medical officer familiar with the
area of operation is required.
r. Decedent Affairs. Chapter 5 of this Manual contains guidance about action that the
Health Services Department must take when there is a death aboard a Coast Guard
unit. Chapter 11 of the Personnel Manual, COMDTINST M1000.6A (series)
contains further guidance concerning casualties and decedent affairs, as does the
Decedent Affairs Guide, COMDTINST 1770.1C (series). It is unlikely that the IDT
will be assigned as the Casualty Assistance Calls Officer (CACO) for the command,
but the IDT will undoubtedly be heavily involved with the process of proper
disposition of remains, so familiarity with the information required is helpful. The
IDT should also perform the following:
(1) An entry in the Health Services Log will be made detailing all available
information concerning the death;
(2) The health record of the deceased member will be terminated in accordance
with Chapter 4 of this Manual.
s. Disposition of Remains.
9-12
CH-16
(1) As soon as possible, remains will be transferred to the nearest Military
Treatment Facility (MTF) for further disposition. When transfer cannot be
accomplished immediately, the remains will be placed into a body pouch and
refrigerated at a temperature of 36 to 40 degrees Fahrenheit to prevent
decomposition. The space must contain no other items and must be cleaned
and disinfected before reuse. Remains will be identified with a waterproof tag,
marked with waterproof ink, and affixed with wire ties to the right great toe of
the decedent and also to each end of the body pouch. The minimum
information needed on each tag includes the full name, SSN and rate of the
decedent. Whenever possible, do not remove items attached to the deceased at
time of death. Such items may include (for example) IV lines, needles, lengths
of cord or line, etc. These may be important during an autopsy.
(a) Additionally, do not discard or launder clothing of the deceased. These
items are sometimes important to surviving family members and in some
cultures are part of the mourning process for the deceased. This is a
cultural consideration but should be a part of the decision process.
t. Physical Disability Evaluation System. The medical board process is detailed in
Chapter 17.A. of the Personnel Manual, COMDTINST M1000. 6A (series) and the
Physical Disability Evaluation System, COMDTINST M1850.2 (series).
(1) Death Imminent. Chapter 17 A of the Personnel Manual and the Physical
Disability Evaluation System Manual describe the actions a unit must take to
initiate an expedited review process. The purpose of the expedited review
process is to provide a member whose death is imminent, with the counsel to
represent the member's best interests, and an opportunity to make timely
decisions that will maximize applicable benefits for the member's dependents.
The IDT must become familiar with the actions required. As with decedent
affairs, the IDT may not have primary responsibility for completing all actions
in a death imminent case, but will be required to provide necessary information
in a timely manner.
6. Training. The purpose of training provided to the crew of an afloat unit include:
assurance that crewmembers are able to provide aid for themselves and their shipmates in
an emergency or a combat situation; and to promote the general health and well being of
the crew. To this end, a written Health Services Department Training Plan will be
prepared and submitted to the unit training officer for incorporation into the unit training
plan.

9-13 CH-16
a. Health Services Department Training Plan. A plan for training of the crew will be
established. The plan will be established in written form and kept on file. It will be
based on a minimum 12 month cycle and be included in the cutter training schedule.
At a minimum, the following training will be given annually:
(1) Basic first aid;
(2) Shock, hemorrhage control, bandaging;
(3) Airway management and assisted ventilation;
(4) Route to battle dressing stations (BDS), use of items in first aid kits, gunbags
and boxes;
(5) Personal and dental hygiene;
(6) STD/HIV prevention;
(7) Heat and cold stress programs, including hypothermia;
(8) Respiratory protection program;
(9) Hearing conservation;
(10) Poisoning;
(11) Sight conservation;
(12) Blood borne pathogens;
b. Documentation of Training. Documentation of the training is a TSTA requirement
as well as a requirement of several Coast Guard programs. The rule of thumb to
remember is “If it isn’t written down, it didn’t happen.” An outline must be prepared
and kept on file for all training topics presented and a training log maintained for all
training provided. The training log will contain a record of all HS training given to
the crew, stretcher-bearers, and HSs. It will contain the following information:
(1) Date;
(2) Topic;
(3) Duration;
(4) Group or department receiving the training;
(5) Instructor’s name;
(6) Names (signatures of those present) of members trained.
c. Training Format. Training will normally be presented in either lecture format or
demonstration and practical application. Lecture format presentations should be
limited to 15 to 20 minutes and demonstrations and practical application should not
exceed 1 hour.
(1) Practical application must be of high priority in training the crew and stretcher-
bearers in first aid, casualty evaluation, treatment, reports to damage control
central, and transporting casualties to battle dressing stations. There is no

9-14
CH-16
substitute for "hands on" practice in developing effective first aid and patient
transport skills.
d. Departmental Training. Specific training not applicable to the entire crew, but
appropriate to individual departments, should be incorporated into the Health
Services Training Plan. Such departmental training is normally needed because of
workplace exposure to potential health hazards. Training subjects appropriate to
various departments are listed in the following subparagraphs. The list is not all
inclusive. It is provided as a guideline.
(1) Weapons department:
(a) Hearing conservation,
(b) Heat stress (ship's laundry personnel),
(c) Respiratory protection,
(d) Basic life support (fire control personnel),
(e) Review of prevention and treatment of electric shock casualties,
(f) Eyesight protection.
(2) Engineering department:
(a) Hearing conservation,
(b) Potable water,
(c) Heat stress,
(d) Respiratory protection,
(e) Eyesight protection,
(f) Hazards associated with human waste.
(3) Supply department:
(a) Food service sanitation (food service personnel);
(b) Heat stress (scullery personnel).
(4) Operations department:
(a) Basic life support (electronics shop personnel),
(b) Review of prevention and treatment of burns, electric shock and
hemorrhage.
(5) Deck department:

9-15 CH-16
(a) Eyesight protection,
(b) Hearing conservation,
(c) Heat stress,
(d) Respiratory protection.
e. Drills. Drills are a necessary part of unit training. Drills help to reinforce
performance of skills and actions that must be completed during stressful or
potentially dangerous situations. Drills that have close relation to health and safety
of the crew will be incorporated into the Health Services Department Training Plan.
The cutter training board should integrate Health Services Department Training Plan
drills into the unit's training schedule.
(1) The following drills will be conducted semi-annually:
(a) Battle dressing station;
(b) Personnel casualty transportation;
(c) Mass casualty.
(2) The following drills, at minimum, will be conducted quarterly:
(a) Compound fracture;
(b) Sucking chest wound;
(c) Abdominal wounds;
(d) Amputation;
(e) Facial wounds;
(f) Electrical shock;
(g) Smoke inhalation;
(h) Casualty transport.
f. Training and Assignment of Stretcher-Bearers. No less than four stretcher-bearers
will be assigned from each repair locker. The training for stretcher-bearers will
include all subjects given to the crew with emphasis on basic first aid, casualty
evacuation, triage, use of all stretcher types maintained onboard the unit, casualty
carrying methods, Battle Dressing Station (BDS) setup and organization and basic
life support. Stretcher-bearers must also complete the advanced first aid portion of
the Damage Control Personnel Qualification Standards (DC PQS).

9-16
CH-16
g. Training for the IDT. Careful study, practice, and concentration on all facets of the
Health Services Technician rate are necessary to prepare an HS to be successful as an
IDT. In addition to the requirements of the rate, attendance of certain "C" schools is
required. These are:
(1) Air Force Medical Services Craftsman - Independent Duty Medical Technician
or Navy Surface Forces Independent Duty Technician;
(a) Health Services Technicians that have successfully completed an afloat
tour as an HS within five years are exempt from this requirement.
Additionally, members that have successfully completed multiple TAD
periods afloat as an HS may be considered for waiver of this requirement
if in the opinion of his/her Designated Medical Officer (DMO) the
member has the skills and experience needed for independent duty.
Request for waiver are to be submitted in letter format, through the
requesting member’s chain of command to Commandant (G-WKH-1).
Chapter 3 of the Cutter Training and Qualification Manual,
COMDTINST M3502.4 (series) contains information about waiver of
requirements.
(2) Coast Guard Introduction to Environmental Health or Navy Basic Shipboard
Series. (Note: This is not required for graduates of Navy Surface Forces
Independent Duty Technician.);
(3) Emergency Medical Technician - Basic Level. IDTs assigned to floating units
are required to maintain currency with the National Registry of Emergency
Medical Technicians (NREMT) at the Basic level. Short Term Training
Requests are to be completed in accordance with the Training and Education
Manual, COMDTINST M1500.10(series) and forwarded to Commandant (G-
WKH-1). Funding will be provided by Commandant (G-WK). See the
Emergency Medical Services Manual, COMDTINST M16135.4 (series) for
additional information.
7. Supply And Logistics.
a. Custody of Health Services Equipment and Material. As directed by the
Commanding Officer, the IDT is responsible and accountable for the health services
material onboard the cutter. As such, the IDT is the custodian of all health service
equipment and material. The custodian will not permit waste or abuse of supplies or
equipment and will use techniques such as stock rotation, planned replacement and
preventive maintenance to minimize waste of resources.
b. Inventory. An accurate record of medical stores and equipment must be maintained.
The inventory of medical stores, spaces and equipment will be prepared using the
Stock Record Card Afloat (NAVSUP Form 1114) or in line item form (computerized
database is an approved and preferred alternative if all necessary information is
captured) and include:
(1) Quantity and shelf-life of each item currently on board;

9-17 CH-16
(2) Balance on hand, high-level, low-level (reorder point for each item);
(3) Manufacturer, lot number and expiration date (pharmaceuticals);
(4) Quantity placed on order, date received.
c. Unit Property. Unit property in Health Services Department custody must also be
safeguarded and accounted for. The unit property custodian should be contacted
before transfer or destruction of such property.
d. Funding and Account Record Keeping. Funds used to purchase supplies and
equipment, and to pay for the various expenses of operating the unit are broken down
into Account Funding Code (AFC) expenditure categories. This method allows for
efficient budgeting and accounting. Fund categories generally used by IDTs fall
within the AFC subhead 30 or 57 expenditure categories.
(1) AFC 30 is a general ship fund used by the supply department to purchase
generally needed operating supplies and services. Examples include pens,
paper, books, training aids, etc. AFC 30 funding can be used to pay for Health
Services Department supplies and equipment not obtainable through Defense
Supply Center Philadelphia Prime Vendor Program (via the unit's supporting
clinic) or the major medical equipment request process (see Chapters 6 and 8
of this Manual). Restrictions exist on what may be purchased with AFC 30
funds. Specific questions can be answered by unit supply personnel.
(2) AFC 57 is a funding category used to purchase health care related supplies and
equipment, and to pay for health care. AFC 57 funds are distributed to the
MLCs and further allocated by them to the units within their areas of
responsibility.
(3) With the full implementation of the Prime Vendor programs for
Pharmaceuticals and for Medical and Surgical Supplies, AFC 57 fund
allocations will be made to the Prime Vendor ordering point assigned for the
unit.
e. Budgets and Budgeting. In general, IDTs do not need to plan and submit an AFC 57
budget request because medical supplies and equipment funding are controlled by the
MLCs and Prime Vendor ordering points. If additional AFC 57 resource needs are
anticipated, the IDT’s supporting clinic should be contacted for direction on how the
resources are to be requested. The budget build process does have value for the IDT
value, however. AFC 30 funds will need to be planned for and requested and
medical equipment in need of planned replacement must be identified and CG 5211s
submitted. The budget build process is a good way to handle these needs. AFC 30
fund budget planning is relatively straight forward, although it can be time
consuming. AFC 30 expenditures for Health Services should be broken into general
use categories. Examples of categories are books and publications, non consumable
goods and services such as hydro testing and replacement of oxygen cylinders, and
travel for continuing education. Budgeting categories can be as simple or
complicated as the IDT desires to make it. Once categories have been established, a
ledger for the Health Services Department should be "opened" and the expenditure
9-18
CH-16
categories entered into it. The use of a "spreadsheet” program is an efficient way to
keep an accounting record but a ledger book works just as well. Attention to detail is
the key. In general, a system using four to five categories works well.
(1) In preparing a budget for the upcoming year, it is important to look back over
what was purchased in the previous year. To do this, collect all records of
AFC 30 orders and expenditures. Review each line item and record the
amount spent into the appropriate budget category. The steps for preparing a
budget and carrying it out along with general timelines are contained in this
paragraph. They are:
9-19 CH-16
March Look back process. Review amount of funds spent
over the first two quarters of the fiscal year as well
as spending patterns for the previous fiscal year.
Note general categories on which funds were spent
and in which quarter items were ordered. This will
allow projection of quarterly funding needs into the
upcoming year.
April/May Review status of the Health Services Department
medical library and determine which texts and
references must be updated.
Review status of HS certifications and continuing
medical education. Funding for training,
conferences or seminars not normally funded by
AFC 56 funds must be budgeted for as AFC 30
budget line items.
Review preventive maintenance records and
include cost projections in AFC 30 budget. Prepare
and submit CG 5211s for medical equipment to be
replaced.
Seek guidance from XO on known or planned
activities outside normal operations. An example is
a yard period (which will require higher than
normal supplies of various personal protective
equipment (PPE)) or extended deployments in
which normal supply is difficult.
June Submit finalized budget proposal through chain of
command. AFC 30 budget information will be
added to the unit budget. Be prepared to “defend”
the budget request submitted. Documentation of
the data gathering process and retrieval of the raw
data used to justify the funding requested will likely
be required. AFC 56 funds requests will be
consolidated by the command and forwarded to the
unit’s district, MLC or Area commander, as
appropriate.
(2) Careful stewardship, good record keeping and accounting make existing
funding and justification for increased funding levels easier.

9-20
CH-16
f. Obtaining Pharmaceuticals, Medical and Surgical Supplies. Chapter 8-B of this
Manual provides policy applicable to the management of Health Services supplies.
Prime Vendor programs for both Pharmaceuticals and Medical/Surgical Supplies
have been established and it is through these programs that essentially all
pharmaceuticals and supplies will be obtained. Medical Prime Vendor Program
Implementation within the Coast Guard, COMDTINST M6740.2 (series) provides
detailed instruction about this program. From an "afloat" perspective important
aspects of the program include:
(1) Each afloat unit has been assigned a Prime Vendor ordering point for
Pharmaceuticals and for Medical/Surgical Supplies. The cognizant MLC (k)
assigns the POCs and periodically updates the information. The Prime Vendor
ordering point may be different for each of the programs.
(2) Funding for both Prime Vendor for Pharmaceuticals and Prime Vendor for
Medical/Surgical Supplies is provided to the assigned Prime Vendor ordering
point by the cognizant MLC (k).
(a) Internal accounting procedures vary among Prime Vendor ordering
points. Some have established individual "accounts" for the units they
are responsible for while others manage funds from a central account.
Regardless of the accounting method used by the Prime Vendor ordering
point, the IDT must establish and maintain a system to track
expenditures.
(3) Prime Vendor ordering points establish pharmaceutical and medical/surgical
supply ordering procedures for their assigned units. Pharmaceutical and
medical supply items ordered will be those required by the Health Services
Allowance List (HSAL) in quantities required for the unit type. Deviation
from the HSAL requirements will normally occur only after justification of the
need is made by the IDT to the DMOA for the unit. It will be made in writing
and kept on file for review during MLC site surveys.
g. Health Services Supporting Clinic. The supporting clinic for a vessel is the IDT's
partner in providing health care for the vessel's crew. Local agreements and
resources may be available to allow the supporting clinic to provide a broader range
of services to the IDT and the vessel's crew but at a minimum, the following will be
provided.
(1) All supplies and equipment (under $300.00) listed in the HSAL for the class of
vessel and on the HS Core Formulary. The unit no longer receives AFC 57
funding for the operation of the Health Services Department. These funds are
provided instead to the vessel's supporting clinic with the intent that the
supporting clinic will provide all required items for the IDT to operate the
Health Services Department.
(2) Assign the IDT a DMOA in writing. The DMOA shall be available for
questions about patient care, as well as completing record reviews quarterly.
(3) Perform medical boards for the IDT unit as necessary.
9-21 CH-16
(4) Provide a resource for advice and support in all administrative areas of health
care provision to include medical administration; physical examination review
(within the approving authority of the Clinic Administrator), health benefits,
medical billing and bill payment processing assistance, dental care pharmacy
administration, supply and logistics, bio-medical waste management, IDT
continuing education, and quality assurance support. Any services provided at
the clinic shall be extended to the IDT to the maximum extent possible
h. Preventive Maintenance of Health Services Equipment. Chapter 8 of this Manual
details the preventive maintenance program for Health Services equipment. Chapters
1 and 2 of the Health Services Allowance List Afloat, COMDTINST
M6700.6(series) provide guidance on the maintenance of specific items carried
onboard ship (i.e. gunbags, portable medical lockers, stokes litter, etc.). An
important part of medical readiness is a program of preventive maintenance and
planned equipment replacement. Repair and routine replacement part costs should
be recorded on side B of NAVMED 6700/3CG (Medical/Dental Equipment
Maintenance Record). Capture of this data will allow more accurate forecasting of
AFC 30 funding needs for preventive maintenance.
i. Replacement of Health Care Equipment. Chapters 6 and 8 of this Manual provide
direction on how to obtain replacement of healthcare equipment. An effectively
managed planned equipment replacement program minimizes repair costs, and
avoids loss of critical equipment at unscheduled times. Additionally, used but still
serviceable equipment can be used by other facilities by "turn-in and reissue" through
the Defense Reutilization Management Office (DRMO). At least annually, normally
during the budgeting process, review the preventive maintenance costs for each piece
of Health Care equipment. When repair and maintenance costs for the year exceed
50 percent of the current replacement cost of the equipment, then a CG 5211 (U. S.
Coast Guard Health Care Equipment Request) should be submitted to the unit's
cognizant MLC(k) requesting replacement.
j. Disposal of Unserviceable or Outdated Medical Material.
(1) Equipment and Supplies. The Property Management Manual, COMDTINST
M4500.5 (series) provides guidance on when a formal survey is required. In
general, a formal survey is not required except when equipment has been lost
or stolen. If uncertain about whether or not a formal survey should be done,
the unit's supply officer should be consulted.
(2) Pharmaceuticals and Medicinals. Destruction of pharmaceuticals and
medicinals will rarely be required. Chapter 8.C. of this Manual directs that
materials will not be disposed of at sea, rather prepared for destruction and
held in a secure area until the vessel's return to port where they can be disposed
of in accordance with federal, state and local laws.
(a) Prime Vendors provide a partial credit for some materials returned to
them. IDTs and supporting clinics will establish local policy for transfer
of expired or short shelf-life pharmaceuticals. A transfer and

9-22
CH-16
replacement of pharmaceuticals within 6 months of expiration should be
made with the supporting clinic to minimize waste.
(b) If destruction is required, it will be accomplished in a well-ventilated
area. Liquid substances present potential exposure through splash back.
At a minimum, splash proof goggles and neoprene rubber gloves will be
worn when working with liquid substances that may be absorbed through
the skin. The wearing of protective equipment such as a splash apron is
also encouraged. Thorough hand washing after the destruction process
must be accomplished. Medical material must be disposed of in a
manner so as to ensure that the material is rendered non-recoverable for
use and harmless to the environment. Destruction is to be complete, to
preclude the use of any portion of a pharmaceutical. Chapter 8. C. of this
Manual provides detailed information about destruction and disposal of
unsuitable medications.
k. Disposal of Medical Waste. Federal regulation defines how medical waste must be
stored and disposed of, and the records that must be kept to document the storage and
disposal. The information in the following paragraphs is provided as a general
explanation of program requirements rather than an in-depth instruction on handling
of medical waste. Medical waste must be classed in one of two categories:
potentially infectious or non-infectious waste. In depth guidance about storage,
disposal and required record keeping for medical waste can be found in Chapter 13
of this Manual, in Quality Assurance Implementation Guide (QAIG) 16, and in
Chapter 6 of the Safety and Environmental Health Manual, COMDTINST M5100.47
(series). An additional source of information is the unit’s hazardous material control
officer. In general, the disposal and record keeping requirements for the waste
depend on the waste category and are:
(1) Potentially infectious waste is defined as an agent that may contain pathogens
that may cause disease in a susceptible host. Used needles, scalpel blades,
(“sharps”), syringes, soiled dressings, sponges, drapes and surgical gloves will
generate the majority of potentially infectious waste. Potentially infectious
waste (other than sharps) will be double bagged in biohazard bags, autoclaved
if possible and stored in a secure area until disposed of ashore;
(2) Used sharps will be collected in an autoclavable “sharps” container and
retained on board for disposal ashore. “Sharps” will not be clipped. Needles
will not be recapped;
(3) An adequate supply of storage and disposal material (containers, bags, etc.,)
must be maintained on board to ensure availability even on a long or
unexpected deployment;
(4) A medical bio-hazardous waste log must be establish and maintained, and must
be kept on file for a period of 5 years. A medical bio-hazardous waste log
must include the following information:
(a) Date of entry;
9-23 CH-16
(b) Type of waste;
(c) Amount (in weight or volume);
(d) Storage location;
(e) Method of disposal;
(f) Identification number (if required by the state regulating authority). If
such a number is required, the authority will provide it;
(5) Non-infectious waste includes disposable medical supplies that do not fall into
hazardous waste. Non-infectious waste will be treated as general waste and
does not require autoclaving or special handling. It should be placed into an
appropriate receptacle and discarded with other general waste.
8. Health Services Department Administration.
a. Required Reports, Logs, and Records. Clear, accurate record keeping is of
paramount importance for the IDT. The quality of care provided to the unit's crew is
reflected in the thoroughness of record and log entries completed by the IDT. During
compliance inspections, TSTA and customer assistance visits, the IDT and the unit
will be evaluated at least in part on the accuracy and completeness of the reports and
records created and maintained by the IDT.
b. The following records will be maintained in the Health Services Department. They
will be in book/log form and in sufficient detail, to serve as a complete and
permanent historical record for actions, incidents and data.
(1) Health Services Log. A Health Services Department log will be maintained by
the IDT. This log is a legal document. Entries will be clearly written in a
concise, professional manner. The log may be either hand written or prepared
using a typewriter or word processor but must be kept on file in “hard copy”
form. It is used to document the daily operation of the Health Services
Department. Chapter 6.B.8. of this Manual provides the requirement for this
log. At a minimum, it will contain the names of all individuals reporting to
sickcall for treatment, inspections, inventories conducted, and the results of
potable water testing. The log will be signed daily by the IDT and submitted
for review, approval and signature on a schedule to be determined by the
Commanding Officer. It is worth noting that the Health Services Log will
provide the information used in the Binnacle List (see required reports in this
Chapter and Chapter 6 of this Manual), so a complete record containing
information required in the binnacle list as well as other information of interest
will streamline preparation of the report.
(a) Training Log. See “Training” in this chapter.
(b) Potable Water Quality Log. This log will document the date, location
and results of free available Chlorine residual or Bromine testing and
9-24
CH-16
bacteriological testing. Such logs will be maintained in chronological
order, record the date and time of test, type of test, collection site, and
results of testing. Potable water quality logs must be kept onboard for 2
years. A sample Potable Water Quality Log is available for local
reproduction in Chapter 1, Appendix 1.A of the Water Supply and Waste
Water Disposal Manual, COMDTINST M6240.5 (series).
(c) Biohazard waste log. This log will contain information as provided in
Chapter 13 of this Manual. Chapter 6 of the Safety and Environmental
Health Manual, COMDTINST M5100.47 (series) also provides
information and guidance on record retention.
(d) Health Records. Health records will be maintained as outlined in
Chapter 4 of this Manual. They will be checked for accuracy as outlined
in Chapter 4 of this Manual. Navmed 6150/7 Health Record Receipt
Form will be used whenever a Health Record leaves the custody of the
IDT. A quarterly check using the unit's alpha roster will ensure that any
oversight is identified in a reasonably timely manner. All records
checked out and not returned shall be reported to the command. In the
event of Abandon Ship, make necessary arrangements to salvage health
records, if possible. Salvaging health records will be secondary to
treating and evacuating casualties.
(2) Required reports. Numerous reports are required at various intervals. A brief
explanation along with a reference is provided for those not mentioned
elsewhere in this chapter. Additionally, the information is provided in tabular
format at the end of this section.
(a) Binnacle List. The binnacle list is normally a part of the Health Services
Department Log. It is a listing of the names of the members provided
treatment, and the duty status determination resulting from the treatment.
The list must be kept daily and submitted to the command for review as
directed by the CO. It is normally reviewed each week by the XO and
signed by the CO.
9-25 CH-16
(b) Injury Reports. See paragraph 10.a.(16) of this chapter.
(c) Disease Alert Reports. See Chapter 7 of this Manual for requirements.
(d) Inpatient Hospitalization Report. See paragraph 5.e. of this Chapter and
Chapter 6.A. of this Manual
(e) Food Service Sanitation Inspection Report. See the Food Service
Sanitation Manual and paragraph 10.a.(2) of this chapter.
(f) Potable Water Quality Discrepancy Report. Required by chapter 1-K.6
of the Water Supply and Waste Water Disposal Manual, COMDTINST
M6240.5 (series) when potable water quality fails to meet requirements
or is suspect.
Reports Required Weekly
Report Name Format or Form
Required Reference Frequency or
Date
Binnacle List locally designed
form COMDTINST
M6000.1(series)
Chap 6.B.8
Compiled
daily,
submitted
weekly (or as
directed by
command).
Food Service
Establishment
Inspection Report
CG 5145 COMDTINST
M6240.4(series)
Chap 11.
9-26
CH-16
Reports Required Quarterly
Report Name Format or Form
Required Reference Frequency or
Date
Controlled
Substances
Inventory Board
Perpetual
Inventory of
Narcotics, Alcohol
and Controlled
Drugs, NAVMED
6710/5
Chapter 10.B.
of this Manual 5th working
day of the
month
Reports Required "As Needed"
Report Name Format or Form
Required Reference Frequency or
Date
Injury Report for
Not Misconduct
and In-Line-of-
Duty
Determination
CG-3822 See paragraph
10.a.( 16) of
this chapter
As needed.
See paragaph
10.a.( 16) of
this chapter
Disease Alert
Reports RCN 6000-4 See chapter 7.B.
of this Manual As needed
Inpatient
Hospitalization
Report
Message format See chapter 6.A.
of this Manual As needed
Report of
Potential Third
Party Liability
CG 4889 COMDTINST
6010.16 (series)
and chapter 6 of
this Manual
As needed
Potable Water
Quality
Discrepancy
Report
COMDTINST
M6240.5
(series)
when potable
water quality
fails to meet
require-
ments or is
suspect
Emergency
Medical
Treatment Report
CG 5214 COMDTINST
M16135.4
(series)
As needed
9-27 CH-16
9. Combat Operations .
a. Battle Dressing Station (BDS). The Health Services Allowance List contains a list of
all items required in the BDS, provides information about required frequency of
inventory and documentation.
b. Route and Access Marking to the BDS. On cutters that have a BDS, the routes to the
BDS shall be marked in accordance with the Coatings and Color Manual,
COMDTINST M10360.3(series). In general:
(1) Self adhering Red Cross decals in both photo-luminescene (internal) and
nonphoto-luminescene (exterior marking) are authorized;
(2) When establishing and marking the routes to the various stations throughout
the cutter, the markers shall be located frequently enough to enable the person
following the route to have a clear view of the next marker of the route to be
followed;
(a) On the interior surfaces of the cutter, the signs shall be placed not less
than 12 inches above the deck and no higher than 36 inches above the
deck. On exterior surfaces, signs shall be placed approximately 60
inches above the deck.
(3) Label plates with red letters will be installed at each direct access to BDS;
(4) An adhesive reflective marking system will be used and maintained. The
purpose of this system is to provide emergency information during a situation
involving the loss of lighting.
c. Use of BDS. On cutters with separate BDSs, the BDS is not to be used for any
purpose other than the treatment of injured personnel in an emergency situation. No
items are to be placed in a manner which will block access or restrict use of the BDS.
d. First Aid Kits, Gun Bags and Portable Medical Lockers.
(1) Supplies stored in emergency medical kits (first aid kits, gun bags, and portable
medical lockers) must be protected from weather and pilferage, and will be
maintained as directed in the Health Services Allowance List. An inventory
list for each kit will be maintained and a monthly inspection of all first aid kits,
gun bags and portable medical lockers will be performed by the IDT. Each kit
will be secured with a wire seal or other anti-pilferage device that will indicate
when it has been accessed. Each kit will be inspected for tampering (seal
intact). The inspection will be noted in the Health Services Log. Once per
quarter, the contents of all first aid kits, gun bags and portable medical lockers
will be inventoried. The inspection will be noted in the Health Services Log.
(2) Antidote locker. A separate poison control locker, marked with a red cross and
the words “ANTIDOTE LOCKER” will be prominently located immediately
outside the sickbay for ready access by the crew.

9-28
CH-16
(a) The antidote locker will be secured with a wire seal or other anti-
pilferage device that will indicate when the locker has been accessed.
(b) An alphabetical inventory, listing the contents and shelf location, will be
posted on the inside of the locker. The telephone number of the local
poison control center will also be displayed.
(c) The antidote locker will be inspected monthly by the IDT and the results
will be recorded on the inventory list and in the Health Services Log.
e. Oxygen Cylinders. Ensure that oxygen handling and storage precautions are posted
next to all oxygen cylinders onboard the vessel. Oxygen is considered a drug and
under no circumstances will oxygen be used for any purpose other than patient care.
Oxygen cylinders (for ready use) must have the content level read every morning by
the HS in order to ensure readiness in case of an emergency. Empty cylinders will be
clearly tagged as empty and stored separately from full cylinders. Oxygen cylinders
must be hydrostatically tested every 5 years. Damage Control Department personnel
will be a good source of information on where to have Oxygen cylinders refilled or
hydrostatically tested. Oxygen for medical use must be grade D.
10. Environmental Health. Environmental health program related activities make up a large
percentage of the daily responsibility of the IDT. The link between environmental health
and mission accomplishment cannot be over-emphasized. From a military perspective,
environmental health and environmental health related problems accounted for almost
eighty percent of personnel losses during past conflicts in which the United States was
involved. For the purposes of this chapter, environmental health encompasses the
disciplines of preventive medicine, sanitation and occupational health.
a. Environmental Health Program Components. An effective environmental health
program requires the IDT to have a working knowledge of a large number of unit
systems and work processes. An aggressive program of inspection and observation is
required. These include:
(1) Environmental Health Inspection.
(a) The IDT will make routine daily messing and berthing space "walk
through" and make note of any conditions that require immediate action.
These "walk through" should be done in an informal manner but items
requiring correction will be brought to the attention of the department
head responsible for the berthing area.
(2) Food Service Sanitation. The Food Service Sanitation Manual, COMDTINST
M6240.4 (series) provides in-depth information regarding food service
sanitation. This section is intended to provide information specific to the
duties of an IDT on an afloat unit. In general, the IDT will monitor the food
service operation to ensure the protection of the crew from food borne
illnesses. The duties of the IDT will include:
9-29 CH-16
(a) Maintain sanitary oversight of the galley and all food service,
preparation, storage and scullery spaces. Such oversight includes stores
on-load, storage, preparation, and serving of food; disposal of garbage;
proper cleaning and sanitizing of equipment and utensils; personal
hygiene of food handlers; proper storage temperature of food products,
and the condition and cleanliness of the spaces;
(b) Food service areas will be inspected weekly and the findings will be
reported on a Food Services Establishment Inspection Report (CG-5145);
(c) Conduct an inspection of the subsistence items and food for fitness for
human consumption. Ensure that subsistence items were received from
sources approved by the U.S. Department of Agriculture (USDA) or an
approved source from a foreign port that complies with all laws relating
to food and food labeling;
(d) Conduct an initial physical screening of food services personnel for
detection of any condition or communicable disease that could result in
transmission of disease or food borne illness.
(3) Storage of Food Items. Proper storage procedures play a major part in
preventing food borne illnesses. The IDT will make routine inspections of
food storage areas to ensure that spaces are properly maintained to prevent
supplies from being:
(a) Infested by insects and rodents;
(b) Contaminated by sewage, chemicals, or dirt;
(4) Subsistence items will be inspected by the HS upon receipt to determine food
quality and ensure the stores are free from insect or rodent infestation. The
results of this inspection will be recorded in the Health Services Log.
(5) Coffee Mess. Food consumption, with the exception of coffee and condiments,
will be limited to messing areas and lounges. Coffee messes provide a
potential food source for insects and rodents if they are not properly located
and kept scrupulously clean. For these reasons, permission to establish a
coffee mess must be obtained from the Commanding Officer by the department
desiring to establish a mess prior to its establishment. Messes will be
physically located in a place that can be easily cleaned. Food contact areas
(surrounding counter or table tops) must be non porous and kept free of
spillage and food debris. Strict sanitary measures are to be used. Coffee mess
regulations specifying sanitary operation of the mess will be posted. Use of
community cups and spoons are prohibited. Inspection of coffee messes may
be documented using a Food Service Sanitation Inspection Report (CG 5145)
or through a locally generated inspection report forms.
(6) Water Supply. Water is used by all members of ship's company and so a
tremendous potential exists for ship wide illness should potable water not be
9-30
CH-16
properly loaded from sources free from contamination, protected from
contamination onboard, and a halogen residual maintained in the potable water
tanks and throughout the distribution system. The IDT will be notified
whenever the potable water distribution system is opened for maintenance or
repair. Establishment of a working relationship with the ship’s engineering
company, and the "water king" will aid the IDT in maintaining a proactive
stance in regard to prevention of contamination of the vessel's potable water.
The IDT will make a monthly inspection of the potable water system and report
conditions with potential to affect the health of the crew to the Commanding
Officer.
(7) Halogen Residual Testing. Chlorine/Bromine residual testing will be
performed before receiving any water onboard, and also about 30 minutes after
an initial halogenation has been accomplished. A water log shall be kept and
the results of the daily halogen testing recorded in it. The Color Comparator
Test set is used for determining Halogen and pH levels. Nomenclature and
ordering information is available in the HSAL. Four test sites should be
selected: forward, aft, amidships and as far above the 0-1 deck as possible.
This will give the widest range of sample points. Lack of a residual or a
residual reading that is significantly lower than results at the other locations
indicate possible contamination. Systematic testing from areas with low
residuals "backward" to areas with "average" residuals will help locate the
source or general area of contamination.
(8) Bacteriological Test of Water. At least weekly, potable water samples for
bacteriological analysis will be collected from two of the four test sites selected
for halogen residual testing, as well as a sample collected directly from the
potable water tanks. At least weekly, samples of ice must also be collected
from any machines making ice used for human consumption and tested for
bacteriological growth. The results of bacteriological testing will be entered
into the Potable Water Quality Log.
(9) Habitability. The need for sanitary and hygienic living and working spaces is
essential for good health and morale of the crew. General guidance on
habitability standards can be found in Chapter 2 of NAVMED P-5010 (series).
Habitability inspection can most easily be accomplished if it is made a part of
the material inspection of all ship’s spaces normally scheduled by each
command
(10) Barber Shops. Any space used for cutting hair may be designated a Barber
Shop by the command. It will not be located in food service areas or berthing
areas. Sanitation inspection of the ship’s barber shop will be performed on a
schedule determined by the command. General guidance on standards can be
found in Chapter 2 of NAVMED P-5010 (series).
(11) Ship’s Laundry. Laundry spaces will be maintained in a clean and sanitary
condition. Because of the potential for elevated temperature and high humidity
within the space when laundry equipment is in operation, the ship’s laundry
will be identified as a heat stress monitoring space and monitored accordingly.
9-31 CH-16
Sanitation inspection of the ship’s laundry will be performed on a schedule
determined by the command. General guidance on standards can be found in
Chapter 2 of NAVMED P-5010 (series).
(12) Fitness and Exercise Facilities. The fitness and exercise facility will be
inspected for cleanliness and compliance with general sanitation standards on a
schedule determined by the command. General guidance on standards can be
found in Chapter 2 of NAVMED P-5010 (series).
(13) Insect Control. Roaches, stored product pests, and to a lesser degree flies, can
have significant impact on the health and general morale of a ship's company.
Insect control starts in the warehouse from which stores are received. When
practical, a visit by the IDT to assess storage conditions can help decrease
numbers of pests brought on board. Dockside inspection of all food stores
brought on board is a must if insects are to be excluded. Produce with "loose"
husks or skin such as onions provide common harborage for roaches as does
the corrugation of cardboard boxes. Careful inspection with a good light and
adjuncts such as an aerosolized flushing agent can identify harborages from
which cans and stores can be removed prior to their being brought aboard.
(a) Roach Control. A ship provides myriad harborages for roaches.
Frequent and regular surveillance by the IDT using a good light and a
flushing agent can pinpoint areas of infestation. Roach traps containing
pheromones work well in areas with small or isolated infestations.
Larger or more widespread areas must be controlled initially with
insecticide. Insecticide application will be made only by HSs that hold
current certification to apply pesticides. Such personnel have been
properly trained in pesticide selection, application, safety and handling
precautions. This training is available through Navy Environmental
Preventive Medicine Units (NEPMU)s. Pesticide application may be
available through Coast Guard Integrated Support Commands with
attached Preventive Medicine Technicians. Any insect surveillance
activity, general report of findings, or pesticide application, will be
reported in the Health Services Log. Pest control services may also be
contracted for from civilian pest control firms. Such services are paid for
from ships AFC 30 funds and are contracted in the same manner as any
other contract for services. While proper selection and application of the
materials used is the legal responsibility of the licensed pest control
operator, the IDT must be informed of all applications made. The
contractor must provide a report of pest control operations which
includes, trade and chemical name of product used, strength and
formulation applied, type of application (crack and crevice, etc.,) location
of application. Requirement for such a report will be included in the
contract for services. Report of pest control operations will be held on
file for 3 years.
(b) Stored Products Pests. A relatively small infestation of flour, grains,
beans and cereals with stored products pests can spread quickly and lead
9-32
CH-16
to the loss of most or all of such products in a storage area if an
infestation is not identified quickly and action taken to control it. In
general, such action consists of identifying infested or suspect lots,
removing them from storage with other food stuffs with the potential to
become infested, and application of pesticide to control flying insects.
Underway, control is limited to identification of infested or suspect lots
and their removal.
(14) Rodent Control.
(a) Exclusion is by far the most effective means of rodent control available
to the IDT. Proper installation of rat guards is required on all mooring
and service lines when the vessel is in port. Information about proper
installation of rat guards can be found in Chapter 8 of the Manual of
Naval Preventive Medicine (NAVMED P-5010) and in the Safety and
Environmental Health Manual, COMDTINST M5100.47(series). The
IDT will inspect all mooring and service lines upon arrival in any port,
including home port, to verify the proper placement of rat guards on all
of the lines.
(b) In the event that rodents do gain access to the vessel, an aggressive
campaign using traps and/or poisoned bait (if the IDT has been properly
trained to apply and use such substances) must be undertaken. Trapping
is the preferred method. Assistance may be available from Coast Guard
Integrated Support Commands with attached Preventive Medicine
Technicians or through the cognizant MLC (k).
(c) A current deraterization exemption certificate (CDC 75.5(F.4.452)) must
be kept onboard at all times. The certificate may be obtained from Coast
Guard Integrated Support Commands with attached Preventive Medicine
Technicians; Navy units or bases with attached Preventive Medicine
Technicians or NEPMUs. The deraterization certificate must be renewed
every 6 months, and must be included as a pre-deployment checklist
item.
(15) Immunizations and Prophylaxis. The IDT will ensure that all personnel receive
required immunizations in accordance with the Immunizations and
Chemoprophylaxis,COMDTINST 6230.4 (series). MLCs (k) and NEPMUs
can provide up to date information on immunization requirements, disease
intelligence and preventive medicine precautions required for vessels
deploying to OUTCONUS ports.
(16) Safety. A ship is a very dangerous place and dangers inherent to the shipboard
environment are heightened by worker's lack of attention, short-cuts,
"horseplay," inadequate training or understanding of a job or process, fatigue or
over-familiarity. The IDT must remain vigilant in regard to the safety and safe
work practices of the crew. A safe work environment can't be maintained from
the Health Services Department space. The IDT must become familiar with
9-33 CH-16
the work processes that are on-going and be able to recognize when they are
not being done in the proper manner or with the proper materials.
(a) Mishap Reporting. When accidents or mishaps do occur, certain reports
or action may be required. The Safety and Environmental Health
Manual, COMDTINST M5100.47 (series) contains requirements and
guidance about mishap reporting. Such reports are not normally
completed by the IDT, but input may be required regarding severity of
injury and required treatment.
(b) Accident Reports. The Administrative Investigations Manual, (AIM)
COMDTINST 5830.1 (series) contains a requirement that an Injury
Report for Not Misconduct and In-Line-of-Duty Determination (CG-
3822) be completed whenever an injury results in temporary or
permanent disability. This report is referred to in the Physical Disability
Evaluation System, COMDTINST M1850.2(series) as an "Line of Duty
(LOD) Report" and requirement is made that it be completed for all
initial medical boards involving or resulting from trauma. Since it is
difficult to determine the outcome of a serious injury in the early stages
of treatment, a CG-3822 (also commonly known as an "Accident
Report") is usually completed in such cases. It is not necessary to
complete an "Accident Report" for any and all injuries unless command
policy dictates otherwise.
(c) Vessel's Safety Board. The IDT is a required member of the vessel’s
Safety Board. The IDT should strive to be an active participant in the
board, to identify potential problems or accident trends, and suggest
solutions to current or potential safety problems. Be proactive. Educate
supervisors whenever possible.
(17) Hazard Communication. The Hazard Communication Program is a unit wide
program. Each unit will have appointed a Hazardous Materials Control Officer
with overall responsibility for carrying out the program. The Safety and
Environmental Health Manual, COMDTINST M5100.47(series)and Hazard
Communication for Workplace Materials, COMDTINST 6260.21(series)
contain in-depth information about this program. The IDT must be aware of
the program requirements and its impact upon the operation of the Health
Services Department. Additionally, the IDT must know the location of the
unit's central MSDS file and have immediate access to product information
which may be needed to render proper treatment to exposed crewmembers.
Computerized databases available on CD-ROM are acceptable for this purpose
if the Health Services Department contains appropriate access to the
information.
(18) Heat Stress Program. Coast Guard Cutter Heat Stress Program, COMDTINST
M6260.17(series) provides details about this program. All areas of the vessel
that expose crewmembers to extreme heat will have a dry bulb thermometer
9-34
CH-16
installed. Such areas normally include (but are not limited to) ship's laundry,
scullery and engine room spaces.
(a) Wet Bulb Globe Thermometer (WGBT). A WGBT apparatus must be
used to determine stay times of personnel working within heat hazardous
spaces or areas and so familiarity with this equipment is required. The
apparatus is normally operated by the IDT or member of the engineering
department. Recommendations for safe work rest cycles will be
provided by the IDT to the Engineering Watch Officer (EWO). Coast
Guard Cutter Heat Stress Program, COMDT M 6260.17(series) provides
information about the program. The WGBT is listed on the Health
Services Allowance List (HSAL) and is procured as health care
equipment. A CG 5211 (U. S. Coast Guard Health Care Equipment
Request) should be submitted to the unit's cognizant MLC (k). Current
calibration of the ship's WGBT apparatus is a TSTA "critical" item.
Delinquent calibration can result in cancellation of some or all TSTA
drills by the training evaluation team. Contact the cognizant MLC (k) for
locations to send WGBTs for calibration.
(19) Sight Conservation Program. Eye protection and safety should be stressed in
the workplace. Safety glasses or goggles will be provided for all crewmembers
involved in eye-hazardous tasks. Tools with strong potential for eye hazard
will be identified with an adhesive warning label. Fixed machinery with eye
hazard potential will have posted nearby an easily visible warning placard, and
eye protection will be easily accessible and clearly visible.
(20) Eyewash Stations. Eyewash stations will be located in any space or work area
with strong potential for splashes to, or foreign body injury of the eye.
Eyewash stations will be maintained in accordance with the station's
manufacturer requirements. Eyewash stations shall be flushed weekly for 15
seconds and flushed and drained according to the recommendations of the
biostat ingredient manufacturer used in the station. This interval is usually
every six months. Eyewash stations will be "tagged" with a maintenance
record tag and inspection or maintenance activities will be recorded when
performed. Inspections of eyewash stations will be recorded in the Health
Services Log.
10-i
CHAPTER 10
PHARMACY OPERATIONS AND DRUG CONTROL
SECTION A - PHARMACY ADMINISTRATION. ...............................................................................1
RESPONSIBILITIES..................................................................................................................................................... 1
PRESCRIBERS. .......................................................................................................................................................... 3
PRESCRIPTIONS. ....................................................................................................................................................... 4
PRESCRIBING IN THE MEDICAL RECORD................................................................................................................... 5
SIGNATURES............................................................................................................................................................. 6
DISPENSING.............................................................................................................................................................. 6
LABELING................................................................................................................................................................. 9
DRUG STOCK.......................................................................................................................................................... 10
PHARMACY AND THERAPEUTICS COMMITTEE........................................................................................................ 11
SECTION B - CONTROLLED SUBSTANCES. ...................................................................................17
GENERAL. .............................................................................................................................................................. 17
CUSTODY AND CONTROLLED SUBSTANCE AUDITS................................................................................................. 17
PROCURING, STORING, TRANSFERRING, AND DISPOSING OF CONTROLLED SUBSTANCES....................................... 19
PRESCRIBING PRACTICES. ...................................................................................................................................... 21
SECTION C - FORMS AND RECORDS...............................................................................................23
GENERAL ............................................................................................................................................................... 23
PRESCRIPTION FORMS............................................................................................................................................ 23
QUALITY CONTROL FORMS.................................................................................................................................... 24
CONTROLLED DRUG FORMS................................................................................................................................... 24
FORMS AVAILABILITY. ........................................................................................................................................... 26
SECTION D - DRUG DISPENSING WITHOUT A MEDICAL OFFICER. .....................................27
CHILD-RESISTANT CONTAINERS............................................................................................................................. 27
CONTROLLED SUBSTANCES.................................................................................................................................... 27
FORMULARY. ......................................................................................................................................................... 27
NONPRESCRIPTION MEDICATION PROGRAMS. ........................................................................................................ 27
CH 1510-1
CHAPTER 10. PHARMACY OPERATIONS AND DRUG CONTROL
Section A - Pharmacy Administration
1. Responsibilities.
a. The person designated in writing as responsible for the pharmacy is accountable to
the Chief, Health Services Division, or the executive officer for properly storing and
dispensing drugs, record keeping, and maintaining a pharmacy policy and procedures
manual.
b. The person in charge of the pharmacy shall acquire, store, compound, and dispense
medications according to applicable Federal laws (principally Title 42, United States
Code [42 USC] and Title 21, Code of Federal Regulations [21 CFR] ) and observe
the highest standards of professional practice and established pharmaceutical
procedures.
c. Through medical administration persons responsible for daily pharmacy operations
shall request adequate funding to provide the level of pharmaceutical care required in
Section 10.A.2.c.
d. Health Services Division Chiefs shall ensure that all short-term, interim, or
temporarily assigned pharmacy personnel have successfully completed Quality
Assurance Guide (QAIG) #41 (Pharmacy Watchstander Qualification
Guide(PWQG)) and that all regular assigned pharmacy personnel have completed
pharmacy technician “C” school training. These minimum standards of
qualifications must be documented in the training file of all pharmacy watchstanders.
The PWQG does not replace the requirement for “C” school trained pharmacy
technicians, but will assist clinic personnel in becoming more productive members of
the Coast Guard health services team and in doing so further enhance the mission of
the Coast Guard clinics.
e. Pharmacy officer collateral duty oversight shall be provided for all clinics and
sickbays that do not have pharmacy officers assigned. A Pharmacy Officer Collateral
Duty Program shall be administered by the cognizant Maintenance and Logistic
Command (k), who shall:
(1) Determine cost requirements for the pharmacy officer collateral duty program
and submit funding requests to Commandant (G-WKH) in the annual operating
summary of budget estimates (CG-4144) process.
(2) Provide direction and funding to pharmacy officers for matters relating to
assignments in pharmacy officer collateral duty program.
(3) Develop work plans which specifies units for which the pharmacy officer is
responsible.
(4) Ensure that visit schedule will be:
(a) the most cost effective;
CH 15 10-2
(b) feasible to maintain responsibilities at the unit where the pharmacy billet
is assigned; and
(c) coordinated with the unit commanding officer possessing the billet.
(5) Establish the content and frequency of a reporting system for pharmacy officers
on assignment and provide a copy of this report to the unit commanding officer
where the billet is assigned.
(6) Ensure that rating officers of pharmacy officers on assignment in the pharmacy
collateral duty program obtain input for completing the USPHS Commissioned
Officers’ Effectiveness Report from the other units where the pharmacy officer
provides oversight.
(7) Oversees the following pharmacy officer responsibilities.
(a) Report to the Chief, Health Services Division of the unit to which they
are assigned.
(b) Follow the established chain of command.
(c) Serve as a member of the Pharmacy and Therapeutics Committee, and
assist those units to which they are assigned with developing and
maintaining a drug formulary. This formulary shall be standardized to
provide a list of medications stocked in the “therapeutic category”
format.
(d) Provide direct assistance for all aspects of the Pharmaceutical Prime
Vendor Program.
(e) Assist each unit in eliminating or minimizing the purchase of medication
through nonfederal sources by using formulary process and redistributing
medication as needed.
(f) Develop an inventory of limited use pharmaceuticals/pharmaceutical
supplies for distributing to each unit.
(g) Serve as the point of contact for redistribution of medication that are due
to expire or are in excessive supply.
(h) Identify special order medication, label them for each patient and assure
that they are not considered formulary items. These should be marked
for a specific patient only and removed when the patient no longer
requires them.
(i) Analyze and develop the most cost effective methods for providing non-
formulary medication for chronic conditions.
(j) Provide oversight to the health services technician(s) who normally
operate the unit pharmacy and assist in dispensing operation as required.
CH 1510-3
(k) Provide and document in-service training to the clinic staff.
(l) Review all pharmacy operations and policies including controlled
substance activities.
(m) Assist the unit in preparation for MLC Quality Assurance Surveys.
(n) Submit a report of the content and frequency established by MLC (k).
2. Prescribers.
a. Authorized prescribers include:
(1) Medical officers and dental officers as defined in this Manual’s Sections 1.B.1.
and 1.B.4.;
(2) Civilian physicians employed by the Coast Guard;
(3) HSs may prescribe drugs listed in the Coast Guard Health Services Technician
Formulary, COMDTINST 6570.1 (series). While performing isolated duty at
LORAN stations or underway, HSs may prescribe additional drugs listed in
Health Services Allowance List, Part 2 (Vessels), COMDTINST
6700.6(series). HSs in these situations should seek medical advice if available;
and
(4) Civilian physicians, dentists, and allied health care providers (nurse
practitioners, physician assistants, optometrists, etc.) as authorized by State law
in their licensing jurisdiction to write prescriptions in practicing their
profession.
b. Prescriptions by uniformed service physicians and dentists, other than Coast Guard,
shall be honored when ever possible. For example, Department of Defense
prescription policies (TRICARE/TRI SERVICE) shall be considered/observed to the
fullest extent possible within the scope of the primary care nature of Coast Guard
Health Care facilities. Prescriptions by these providers shall be written on the
prescription forms authorized by their service.
c. Prescriptions for eligible beneficiaries from licensed civilian physicians, dentists, or
podiatrists shall be honored for products on the clinic’s formulary. Clinic
formularies shall be established based on the Coast Guard Core Formulary and the
prescribing habits of the providers assigned to that clinic. Items will not be
maintained on the formulary primarily to meet civilian prescription demand.
Military practitioners or contract providers shall not countersign civilian
prescriptions nor shall civilian prescriptions be rewritten during cursory outpatient
visits with the intent of authorizing the prescription for dispensing at the facility. If
additional funding is required for specific, high cost drugs, it shall be requested via
the AFC-57 budget.
d. Authorized prescribers shall not prescribe controlled medications for themselves
and/or their family members. If such medication is required and no other prescriber
CH 15 10-4
is assigned to the facility, the commanding officer or executive officer shall approve
and countersign each prescription before the prescriber fills it.
3. Prescriptions.
a. Prescriptions written by Coast Guard physician's assistants and nurse practitioners
may be filled at the facility where written or at a neighboring MTF as permitted by
local prescribing policy. Prescriptions written by health services technicians shall be
filled only at the facility were written. Coast Guard clinics may agree among
themselves to honor another Coast Guard clinic’s physician assistants’ or nurse
practitioners’ prescriptions if stock shortages so necessitate. Other Coast Guard
facilities may honor Coast Guard physician assistants’ and nurse practitioners’ refills
(for other than controlled substances) if the patient presents his or her health care
record containing the original entry.
b. Accept telephoned and oral prescriptions only in emergencies. The prescriber must
write and sign the prescription as soon afterwards as possible. A clinic may choose
to accept FAXed prescriptions provided it receives the original prescription before
dispensing the medication.
c. Health Services Technicians shall not contact civilian prescribers to resolve
prescription problems but return the problem prescription to the patient and explain
why he or she cannot dispense it. The HS may provide the names of suggested
available products to the patient. Professional supervisors (pharmacy officers or
senior medical officers) may authorize, via the Pharmacy Policy and Procedures
Manual, pharmacy technicians to make telephone contact with civilian prescribers to
resolve problems. All authorized telephone transactions will be clearly defined;
those transactions not listed shall be unauthorized.
d. Prescriptions shall be personalized. If more than one member of a family is
prescribed the same drug, a separate prescription blank must be used for each
member
e. Items prescribed must treat conditions within the normal scope of professional
practice and the ethics of the prescriber.
f. Prescriptions for medications to treat cosmetic conditions (baldness, wrinkles, etc.)
and for weight loss will not be honored nor shall medications for these conditions be
stocked at Coast Guard facilities.
g. Do not fill prescriptions for animals other than those the Government owns.
h. If a physician assistant has clinical privileges at a local DOD facility, he or she may
use its prescription form to write prescriptions to be filled at that facility, provided
the form contains the statement "To be filled only at [insert designated DOD
facility]."
i. The prescriber's facility has the responsibility to procure and dispense all medications
its staff members (including in-house contract prescribers) prescribe. In the rare
CH 1510-5
event a patient must carry a prescription elsewhere for dispensing, the prescriber
shall write the facility’s name in addition to the other required information on the
form.
j. Providers are tasked with the cost-effective use of medications. Commandant (G-
WKH) maintains a list of and prescribing guidelines for selective medications, listed
in Figure 10-A-2. Clinics shall ensure in-house prescriptions meet the requirements
to use these items cost-effectively.
4. Prescribing in the Medical Record.
a. At all clinics and sickbays, prescribe medications on an SF-600 in the medical
record, or when appropriate, SF-558, Emergency Care and Treatment. The medical
record thus becomes a more comprehensive repository for all patient health
information and also ensures the pharmacy staff has access to the necessary clinical
information (age, weight, allergies, lab values, vital signs, etc.) to provide complete
pharmaceutical care. In clinics that maintain dental records separately, the dental
staff may use prescription forms.
b. Procedures.
(1) Document (S.O.A.P. format) the patient visit on an SF-600 or SF-558 in the
chart. Under the "Plan" section list the drug name, strength, directions,
quantity, and refills. Start each new drug entry on a new line (examples:
"HCTZ 50 mg, #1 tab po QD #90 RF X 1"; "Clonidine 0.1 mg, #1 tab po BID
#180 RF X 1"). If prescribing for a dental condition, label the SF-600 section
"Dental Rxs" and list the same information required here and in 10-A-4.b.(2).
(2) In the "Plan" section, state a disposition to assist pharmacy staff in coordinating
quantities of all chronic medications until the next appointment. Complete the
entry with the authorized prescriber’s signature (examples: RTC PRN; F/U
appt. 10 days; RTC 3 months).
(3) The terms chronic and maintenance medications are synonymous. A
maintenance medication is defined as any medication used to treat a chronic
condition. The term “maintenance” implies that a prescriber and patient have
gone through a dosage titration process and have determined that the patient
should be “maintained” on an effective dose of a medication that is well
tolerated. Ultimately, the individuals in a position to make such a
determination are the patient and the prescriber. The standard quantity issued
for chronic conditions is a 90-day supply. If it is necessary to deviate from this
amount, prescribe quantities in 30-day increments (30, 60, 90, etc.) if possible.
If pharmacy staff in consultation with the prescriber deem it advantageous to
the patient due to travel, deployment, operational commitments, packaging,
etc., they may dispense larger quantities.
(4) Pharmacy staff shall completely draw a single horizontal line through errors or
changes and conspicuously write “Error” next to the item. The person
changing the entry shall initial the change or error. Return incorrect or
incomplete entries to the prescriber for revision.

CH 15 10-6
(5) Pharmacy staff shall write the prescription number or put the multi-part strip
label on the SF-600 and initial to identify the person who prepared the
prescription.
(6) Pharmacy staff shall write the manufacturer's name, lot number, and expiration
date to the right of the drug prescription (not required with CLAMS OR
CHCS). Sickbays not on CLAMS OR CHCS also shall maintain a drug
dispensing log containing prescription number, patient's name, patient's SSN,
drug name, drug manufacturer, and lot number. Retain this log for record
purposes for 3 years.
(7) For refills, pharmacy staff shall note the date, pharmacy identity and "Rx
Refill" on the SF-600, followed by medication name, quantity, original
prescription date, manufacturer's name, lot number, expiration date, and
remaining refills. If processing through CLAMS OR CHCS, the only required
information is the pharmacy identity, current date and medication name. The
pharmacy staff member charting the refill shall initial the entry. The use of
personal stamps to further identify pharmacy personnel is encouraged. Any
other services (counseling, vital signs, etc.) provided to the patient shall also be
noted in the medical record. See Figure 10-A-2 for examples.
(8) In addition to the SF-600 or SF-558 entry, written prescriptions are required for
all controlled substances or cases where a prescription must be taken to another
pharmacy.
(9) All prescriptions generated from sources outside the clinic shall be filled or
refilled using CLAMS OR CHCS or the procedures specified in this Chapter
and maintained on file in the pharmacy. The pharmacy need not maintain a
health care record if the patient receives only basic pharmaceutical care from
the facility.
5. Signatures. No prescription or order shall be filled unless it bears the signature of an
individual authorized to write prescriptions. All prescriptions shall be
imprinted/stamped with the prescriber’s name, rank, and professional discipline (MD,
DDS, HS2, etc.). Prescriptions for controlled substances shall also provide the social
security number of the prescriber or DEA number. Pharmacy personnel shall maintain
signature examples for in-house and contract prescribers. Professional judgment shall be
used to verify authenticity of prescriptions from other sources.
6. Dispensing.
a. The pharmacy shall serve as the source of supply from which clinics or satellite
activities normally obtain required pharmaceuticals and related supplies. In addition,
the pharmacy dispenses required, authorized preparations directly to patients.
b. Except for OTC program items, the pharmacy shall dispense all stocked items only
on receiving a properly written, verified prescription. If pharmacy staff receive an
illegible prescription or question its authenticity, dosage, compatibility, or directions
to the patient, staff shall obtain clarification from the prescriber before dispensing the
medication(s).
CH 1510-7
c. Clinics shall have a system (computerized, written, etc.) in place to ensure they can
obtain prescriptions in case of a product recall.
d. Clinics shall submit all pertinent patient adverse reactions or product quality
problems on the FDA MEDWATCH system on FDA Form 3500. Obtain
MEDWATCH forms and information from the FDA at 1-800-FDA-1088.
e. When dispensing medication, the dispenser shall identify the patient and ensure his
or her eligibility.
f. Use child-resistant containers to dispense all prescription legend medications except
nitroglycerin, which is dispensed in the original container. The practitioner or patient
may specifically request a conventional closure; a practitioner must so indicate on the
prescription order. If the patient requests such a closure, enter a statement so saying
on the back of the prescription; have the patient sign it. When refilling prescriptions,
the pharmacy must ensure the safety closure still functions and the label is legible
before dispensing in the original container.
g. Prescriptions (except for controlled substances-see 10-B-4.c.) may be refilled when
authorized by the prescriber. The maximum quantity shall be a year’s supply of
medication. No prescription shall be refilled after more than one year from the date
it was written. PRESCRIPTIONS SHALL NOT BE REFILLED FROM THE
LABEL ON THE CONTAINER ONLY.
h. Coast Guard clinics are encouraged to establish non-prescription medication
programs under the following guidelines:
(1) Commanding Officer of Coast Guard units assigned health care personnel may
elect to operate a nonprescription drug program. Units not staffed with an HS,
may operate a nonprescription medication program if quarterly oversight
(direct visit) is provided by a Coast Guard clinic or supporting Independent
Duty HS. Units electing to offer a nonprescription drug program shall inform
their respective MLC, and verify that they will operate within these guideline.
(2) All Coast Guard health care facilities shall make condoms available to
beneficiaries even if they elect not to offer a nonprescription drug program.
Condoms shall be made available to beneficiaries under 18 years of age unless
specifically forbidden by law.
(3) Items available shall be limited to those specifically identified in the
Nonprescription Medication Program section of the “Core” Formulary
(COMDTINST 6570.2A) Units may elect not to offer every product from this
list but shall not select products other than those listed.
(4) A beneficiary family shall be limited to a maximum of two items per week
from the program. Occasionally, it may be necessary to extend this limit due to
family size. Pharmacy and Therapeutics Committees ( if available) and
collateral duty pharmacy officers shall provide guidance and monitor any such
extensions.
CH 15 10-8
(5) Items shall only be available during normal operating hours of the facility.
(6) Pharmacy or sick bay personnel shall monitor the program for perceived
overuse. Individuals suspected of this shall be referred to a medical officer and
may have their access to this privilege denied.
(7) All products must be dispensed in the Manufacturer’s FDA approved packages
with required instructions and warnings. Other locally packaged items are not
authorized. Local Pharmacy and Therapeutics Committees may develop
supplemental information on sheets to provide additional dosage or drug
information to the patient.
(8) Nonprescription drug program items shall not be dispensed to pregnant patients
or non active duty beneficiaries under 18 years of age. Local flight surgeons,
via the Pharmacy and Therapeutics Committee, shall determine which products
may be acquired by personnel on flight status.
(9) Facilities offering this service shall keep quarterly statistics as to the
quantity of items dispensed and the dollar value expended. This figure shall be
separated from regular pharmacy workload statistics and not be counted as a
prescription number. Only those items which have been dispensed by a written
prescription shall be counted in the facility prescription number totals.
(9) The Patients are responsible for providing an authorized identification card to
verify their eligibility.
(10) To receive a nonprescription item, patients must sign a log request form which
certifies the following:
(a) “I do not wish to see a physician or other health care provider for advise
before receiving these medications. I understand that the medication is
for minor illness or conditions and that if symptoms worsen or persist
longer than 48 hours, the person for whom this medication is intended
should be seen by a health care provider.
(b) “I am not pregnant or under 18 years of age (unless active duty). If on
flight status, I understand that I am only authorized to receive over-the-
counter items approved by the flight surgeon.
(11) Individuals suspected of returning for medication for a non-resolving problem
shall be referred to a medical officer for evaluation.
(12) The log sheet or request form shall also contain the date, patient’s name, and
the name and quantity of the item(s) received.
(13) Beneficiaries requesting medical advice that, in the opinion of the pharmacy or
sick bay personnel, is beyond their expertise, shall be referred to the medical
officer.
(14) Funding for independent duty HS assigned units (vessel, groups, etc.) deciding
to offer this service shall be from their unit’s AFC-30 account.
CH 1510-9
i. When the pharmacy is closed, a medical or dental officer, or a person so authorized,
may dispense medication from a locked cabinet or locker containing pre-packaged or
limited supplies of after-hours medications. These drugs are dispensed under the
same procedures required when the pharmacy is open, including appropriate labeling
and complete as an entry in the health record.
Do not fill prescriptions from civilian prescribers from the after-hours locker except
for emergency pain medications and/or antibiotics to treat acute infection.
j. Bulk items for use in the clinic may be issued on authorized prescription forms or
locally approved requisition forms.
k. A sign shall be posted outside of the pharmacy in a highly visible location stating
“Please inform our pharmacy staff if you are breast feeding or may be pregnant.”
Clinic pharmacies shall maintain a written drug information system (USP, CHCS,
etc.) to provide information to patients when appropriate.
l. Coast Guard pharmacies staffed with one pharmacy technician or HS generally
dispense an average of 75 prescriptions per day. Clinics with a pharmacy officer and
HS can be expected to average 150 prescriptions per day. These workload
expectations account for "background" clinic and pharmacy activities (collateral
duties, OTC program, bulk issues, etc.).
m. Pharmacies shall adhere to applicable state laws governing generic dispensing of
civilian prescriptions. Civilian prescribers may provide the facility with a written
statement giving "blanket approval" to dispense generics for their prescriptions.
n. Dispense drug samples only through the pharmacy; they must have proper labeling
and child-resistant containers. A system shall be maintained to recall sample
products should such action become necessary.
7. Labeling.
a. A label will be prepared for each prescription dispensed to individuals and will be
securely affixed to the container prior to dispensing. The label or appropriate
auxiliary labeling will show as a minimum:
(1) facility identity, including pharmacy address and telephone number;
(2) consecutive identifying number;
(3) prescriber’s name;
(4) definite, concise directions to the patient;
(5) drug name and strength, unless prescriber directs otherwise;
(6) amount dispensed;
(7) patient's first and last name;
(8) initials of person typing the prescription label;
CH 15 10-10
(9) the legend "KEEP OUT OF THE REACH OF CHILDREN" on all
prescription labels;
(10) date prescription filled;
(11) indication of refills;
(12) expiration date (for liquid antibiotics);
(13) the legend "CAUTION: FEDERAL LAW PROHIBITS THE TRANSFER
OF THIS DRUG TO ANY PERSON OTHER THAN THE PATIENT
FOR WHOM IT WAS PRESCRIBED" (for controlled substances only);
(14) any necessary supplemental or auxiliary labels.
b. If prescription contents are for external use only or require further preparation(s) for
use (shaking, dilution, temperature adjustment, or other manipulation or process)
include appropriate directions on the label or affix an additional label to the
container. If liquid preparations for external use are poisonous, affix a "poison" label
to the container. If medicines prescribed for internal use are poisonous, use sound
judgment whether to label them "poison" based on the finished preparation’s potency
in each case.
c. Medicinal preparations compounded or packaged in the pharmacy for subsequent
issue will be identified and labeled with the full generic name, except that trade or
brand names may be used provided trade or brand name product actually is in the
container. The manufacturer’s name, lot number, and expiration date, if any, will be
shown on the label.
d. Drug issued to clinics for subsequent reissue to outpatients shall be adequately
labeled in the pharmacy.
e. All multiple dose injectable vials shall be dated upon opening. Expiration will
normally be thirty days unless:
(1) the product is expensive and manufacturer's information guarantees the product
is usable beyond 30 days, or
(2) product information indicates a shorter expiration date.
8. Drug Stock.
a. The person responsible for the pharmacy’s daily operations must authorize all orders
procuring medications. The clinic finance officer shall verify funds are available for
all procurements. For prime vendor requisitions, verify funds availability before
entering the "ZOA" document entry in the Automated Requisition Management
System (ARMS), not prior to the order being submitted to the prime vendor.
b. The Defense Personnel Support Center is the primary source of medications for
either the "Depot" system or prime vendor contracts. Use other Federal sources
(Perry Point IHS Depot, Federal Supply Schedules, MLC-negotiated purchase
agreements, etc.) may be used when, due to price or service advantages, it is
CH 1510-11
determined to be the most cost-effective procurement method to meet the needs of
the unit. Drug procurement from retail sources shall be done only when absolutely
required for urgent patient needs and when other, less costly, sources cannot meet
this need.
c. Only those items that have been licensed and approved by the Food and Drug
Administration (with the exception of vitamins with an established RDA) are
authorized for use in Coast Guard health care facilities. Coast Guard health care
facilities shall not purchase or dispense "herbal supplements" or "dietary
supplements".
d. In storage, separate external use medications from internal use medications and
ophthalmic and otic preparations. Caustic acids such as glacial acetic, sulfuric,
nitric, concentrated hydrochloric, or oxalic acid shall not be issued to clinics, but
shall be stored in separate lockers, clearly marked as to contents. Methyl alcohol
shall not be stored, used, or dispensed by the pharmacy.
e. Store flammable drugs according to accepted fire safety regulations.
f. Use solid-core doors with 1-inch (minimum), throw key-operated, dead-bolt locks
shall be used for all pharmacy and medical supply areas. On “Dutch” doors, both
sections shall have this type lock.
g. Remove from stock drugs under testing in the FDA/DOD Shelf Life Extension
Program; label them with the project number until results are received. While
pending, use these items only in emergencies. Upon return of results, items should
be destroyed or marked with new expiration dates and returned to stock. Oral
contraceptives, opthalmics, otics, and inhaler medications should not be extended.
These items may be used, while pending, results, to offset medical allowance list
requirements.
h. The pharmacy shall maintain, in the pertinent clinic areas, an adequate supply of
emergency medications, poison antidotes, and the poison control center telephone
number. Containers for these items shall be closed with break-away seals to prevent
the unreported removal of items. The outside of the container shall contain an
inventory list containing the expiration dates of dated items.
i. Where feasible, pharmacies shall establish borrowing policies with local Government
or civilian pharmacies to cover temporary supply shortfalls. The person responsible
for the pharmacy shall maintain a log of items loaned or borrowed, and review and
initial the log weekly to ensure prompt replacement of all items.
9. Pharmacy and Therapeutics Committee.
a. This is a mandatory advisory committee in all Coast Guard health service treatment
facilities having assigned medical officers. It should meet regularly, but at least four
times a year. The committee is composed of, but not limited to the following: at
least one physician, one dental officer, a pharmacy officer (when available), and a

CH 15 10-12
representative from medical administration. The chairman shall be a physician
member. When a pharmacist is assigned, he or she is the secretary of this committee.
b. The committee is an advisory group on all matters relating to the acquisition and use
of medications. Its recommendations are subject to the approval of the Chief, Health
Services Division. The basic responsibilities of this committee are to:
(1) Use the Coast Guard Core Formulary as guidance to develop and maintain a
clinic drug formulary; the group reviews new and deletes unnecessary items.
(2) Maintain a health service technician formulary selected from products
authorized by the Coast Guard Standardized Health Services Technician
Formulary;
(3) Ensure the unit formulary does not include items based primarily on civilian
prescriber demand;
(4) Prevent unnecessary therapeutic duplications of formulary products;
(5) Conduct an ongoing review of all non-formulary items the pharmacy procures
and dispenses. To accomplish this, the clinic and/or P&T committee lists:
(a) A list of all clinic formulary items not currently in the CG Core
Formulary;
(b) A list of all special order items and the number of patients for whom
procured (add special order items procured for seven or more patients to
the unit formulary);
(6) Conduct an ongoing drug usage evaluation (DUE) program for selected
medications;
(7) Monitor the facility’s controlled drug prescribing and usage;
(8) Review pharmacy policies and procedures as necessary;
(9) Monitor the quality and accuracy of prescriptions and patient information the
pharmacy provides and enacts any quality assurance measures it deems
necessary (double checks, etc.) to ensure pharmacy quality and availability of
services; and
(10) Reviews any adverse reaction or product quality reports (VAERS or
MEDWATCH) before any drugs or vaccines are released.
c. Minutes shall be prepared for each meeting and approved by the Chief, Health
Service Division.
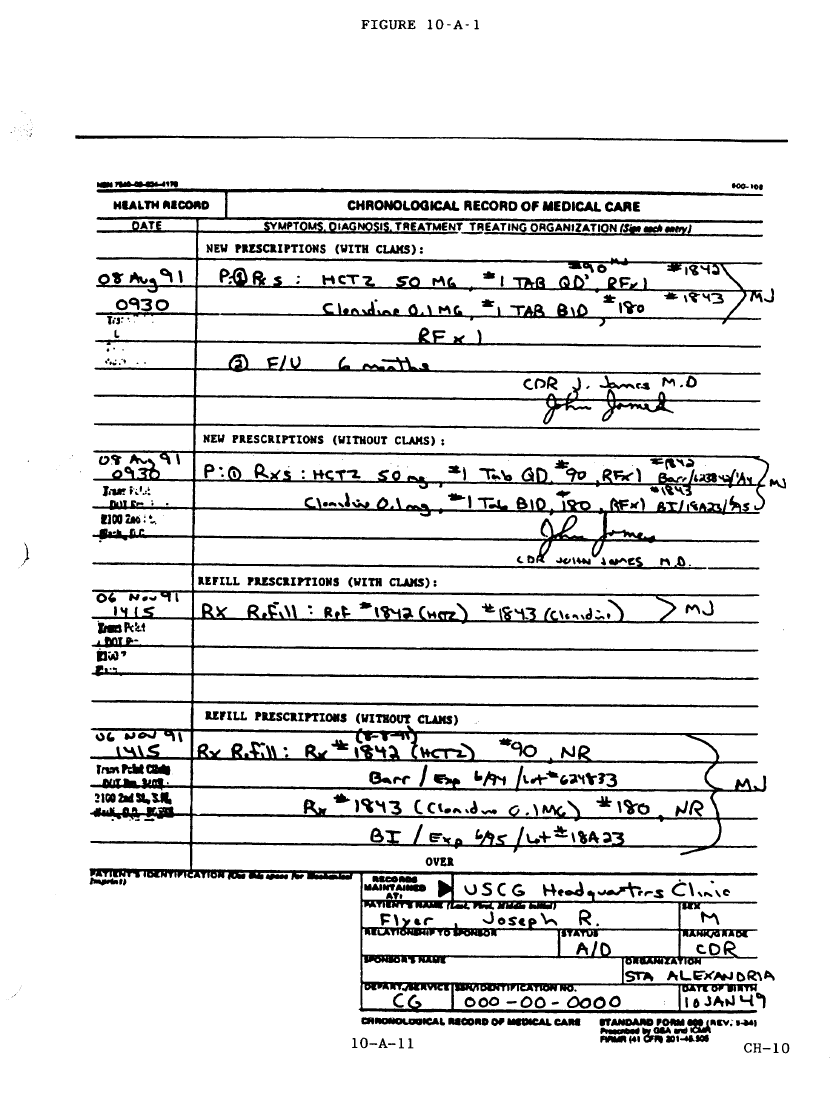
CH 1510-13
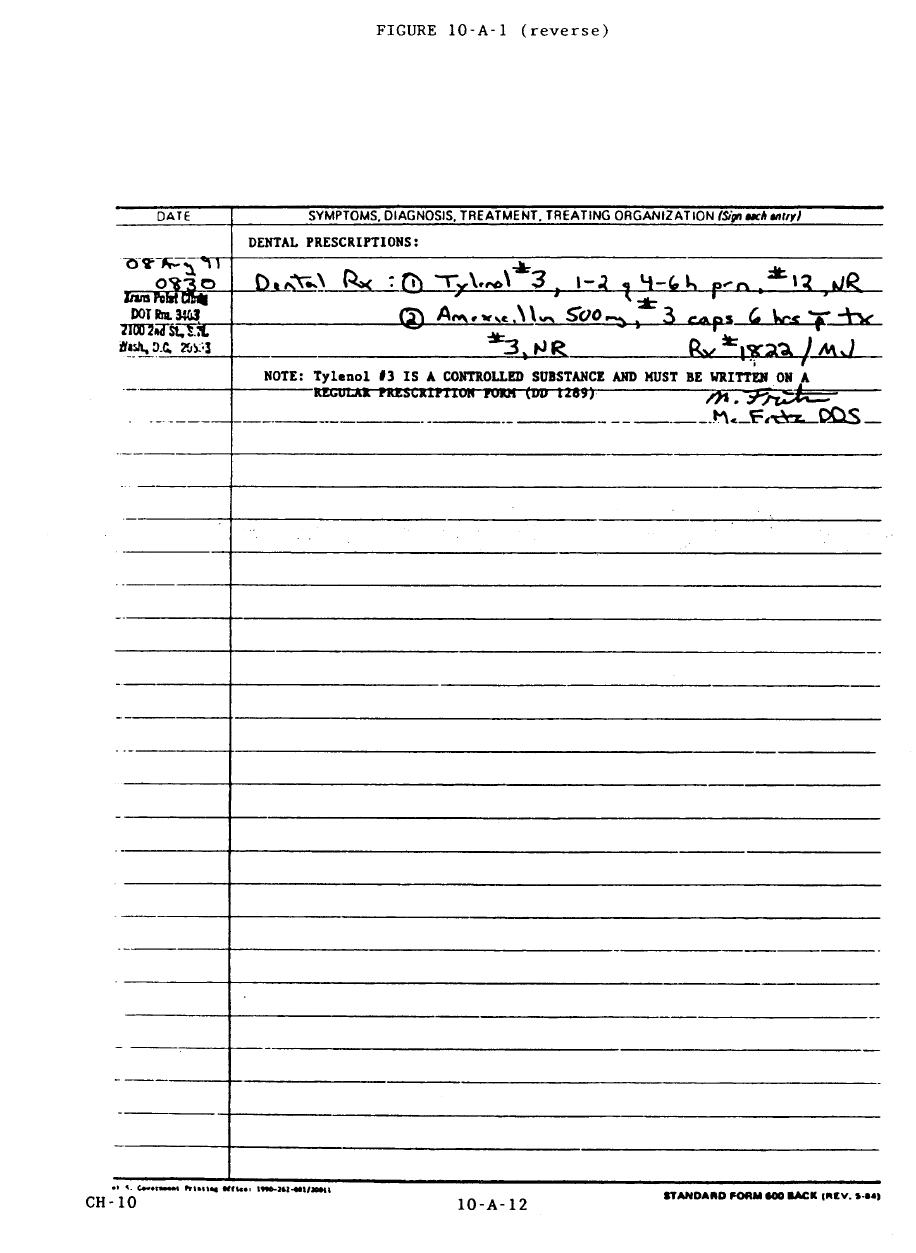
CH 15 10-14
CH 1510-15
FIGURE 10-A-2: PRESCRIBING GUIDELINES FOR EXPENSIVE MEDICATIONS
DRUGS INCLUDED GUIDELINES
1. Cholesterol and Lipid Lowering Agents
Lovastatin and other similar agents
to reduce cholesterol and lipid
levels
Patients prescribed these products shall have:
A. Documented hyperlipidemia confirmed by at least one of these
baseline laboratory values:
1. Fasting Total Serum Cholesterol > 240 mg/dl
2. Fasting serum LDL > 160 mg/dl or > 130 mg/dl if risk factors
present
3. Fasting HDL < 35 mg/dl
4. Fasting Serum Triglyceride Levels > 250 mg/dl
2. Antibiotics
Amoxicillin and Potassium
Clavulanate (Augmentin),
Azithromycin (Zithromax), Cefaclor
(Ceclor), Cefixime (Suprax),
Cefuroxime (Ceftin), Ciprofloxacin
(Cipro), Clarithromycin (Biaxin),
Erythromycin/Sulfasoxazole
(Pediazole)
Limit use of these and other more costly antibiotics to patients who
have unsuccessfully taken more traditional, less expensive antibiotics or
where culture and sensitivity testing confirms organism sensitivity. Use
these drugs for initial therapy only if Sanford's Guide to Antimicrobial
Therapy indicates they are the primary agent of choice.
3. Smoking Cessation Aids
Nicotine gum and patches (any
manufacturer), and other products
used for smoking cessation
Behavioral modification is the primary method of smoking cessation;
do not prescribe smoking cessation aids to patients without proof of
ongoing participation in a "recognized" program that consists of
regularly scheduled patient interaction with a smoking cessation
facilitator. Do not prescribe smoking cessation products for anyone
who continues to smoke after the initial two weeks of therapy.
4. Antihistamines
Fexofenadine (Allegra), Loratadine
(Claritin) All patients prescribed these products shall have:
1. Previously documented failure to obtain relief of symptoms with
at least one antihistamine or one antihistamine-and-decongestant
combination or documented history of intolerance to
antihistamines’ sedative effects.
2. A consulting physician’s prescription for unresolved allergy
problems.
3. Current aircrew qualification with documented allergies.
CH 15 10-16
This Page Intentionally Left Blank
CH 15 10-17
Section B- Controlled Substances
1. General.
a. Controlled substances, as used here, are defined as:
(1) drugs or chemicals in DEA Schedules I-V: (for example, the manufacturers
label for Acetaminophen with Codeine #3(30 mg.) carries the DEA symbol for
Schedule III (C-III) and will be treated as a Schedule III by Coast Guard units.)
(2) precious metals;
(3) ethyl alcohol (excluding denatured);
(4) other drugs or materials the local commanding officer or Pharmacy and
Therapeutics Committee determine to have significant abuse potential.
b. Coast Guard authorized uses for controlled substances are:
(1) medicinal purposes;
(2) retention as evidence in legal or disciplinary actions; or
(3) other uses CG Regulations specifically authorize.
c. Quantity Definitions. Due to the potential for abuse and associated audits required,
Coast Guard units should strive to minimize the quantities of controlled substances
used. Two types of quantities are recognized for controlled substances:
(1) Working Stock. Working stock is defined as a 30 day supply (under routine
conditions) of a controlled substance or limited amounts of emergency drug as
might be required. For smaller facilities, with limited quantities of controlled
substances, working stock may surpass the 30 day limit when quantities are
less than 1000 dosage units (tablets, capsules, etc.). It is also acceptable for
partial containers to temporarily surpass this 1000 dosage unit limit.
(2) Bulk Stock. Bulk stock is defined as a larger quantity beyond the normal
working stock quantity. Bulk stock should primarily be sealed in sealed
manufacturer’s containers.
2. Custody and Controlled Substance Audits.
a. Controlled Substance Custodian (CSC).
(1) Pharmacy officers, when assigned, shall be appointed in writing as the CSC by
the commanding officer.
(2) In the absence of a pharmacy officer, COs shall designate the clinic
administrator as CSC.
(3) Medical and dental officers may serve as alternate CSCs.
(4) Temporarily assigned personnel shall not serve as CSCs or alternates.
(5) Under Coast Guard Regulations, COMDTINST M5000.3A, Chapter 6-2-3-
A.(6), the Executive Officer is directly responsible for medical matters if a

CH 15 10-18
medical officer is not assigned. For sickbays, the CO shall designate a
commissioned officer as the CSC.
(6) CSCs may permit Health Services Technicians to assume custody of a
"working stock" quantity of controlled substances.
(7) An audit of all controlled substances (working and bulk stock) is required
when the CSC is changed. The results of this inventory shall be filled in the
command’s permanent file and in the Health Services Log. All keys should be
transferred and/or combination locks changed at the time of this inventory.
b. Unit Controlled Substance Audits.
(1) Controlled Substance Audit Boards (CSAB). Each unit procuring, storing, or
dispensing controlled substances shall have a CSAB.
(a) Membership: The CSAB shall consist of two or more disinterested
officers or if unavailable, two or more disinterested senior petty officers
(E-6 or above). Designated in writing by the Commanding Officer.
CSAB letters of designation will remain in effect until the members are
relieved in writing or detached from the command. In no case may the
controlled substance custodian be a member of the CSAB.
(b) The CSAB shall conduct monthly audits of controlled substances at
clinics (quarterly at ashore or afloat sickbays) and submit its report to the
commanding officer within 5 working days after its audit. Commands
shall maintain these reports for three years after which they may be
destroyed.
(c) Monthly CSABs shall audit all working and bulk stock of C-II through
C-V controlled substances, precious metals, ethyl alcohol, and drugs or
other items locally designated as controlled substances due to abuse
potential and report all quantities on CG-5353, Monthly Report for
Narcotics and Other Controlled Drugs.
(d) During monthly audits, CSABs shall inspect controlled substances for
expiration, deterioration, and inadequate or improper labeling. Expired
products or those with other discrepancies shall be removed for disposal.
(e) The CSAB shall count required controlled substances; review a
representative random sample of prescriptions, receipts, and issue
documents; and report the results on Monthly Report for Narcotics and
Other Controlled Drugs, CG-5353. For sealed containers, a bottle count
is sufficient; for open containers an exact count is required. For open
liquid containers, an estimate other than an exact volume measurement is
adequate. CSABs may use tamper-proof seals on open containers to
avoid future counting of partial quantities.
CH-17
CH 1510-19
reviewed to ensure that only authorized products are procured in appropriate
quantities. Discrepancies are forwarded to the pertinent MLC (kqa) for follow-
up.
(3) DEA Biennial Inventories. To comply with DEA requirements, all controlled
substances shall be inventoried by the custodian during May of even-numbered
years. This copy of the CG-5353 shall be maintained on file locally and
labeled “FOR DEA BIENNIAL INVENTORY” at the top of the form.
c. Drug Enforcement Administration (DEA) Registration. DEA registration is required
for those CG clinics with Prime Vender Ordering Officers. Purchase of controlled
substances from commercial sources is prohibited unless approved and procured by
pharmacy officers. Sickbays shall not register with the DEA unless in-house
physician services are provided. The unit’s Drug Enforcement Agency Registration
Form (DEA-244A) shall be signed by the Commanding Officer. By direction
signature is not authorized. Forward the signed form to the cognizant MLC (k) for
signature as approver/exemptor. The MLC (k) shall forward the form (DEA-244A)
to the DEA and provide a photostatic copy to the originating unit. The DEA will
issue the registration to the unit.
d. Reporting Theft or Loss. Upon receipt of the CSAB or pharmacy officer monthly
audit noting theft or loss of controlled substances, the command shall::
(1) Designate a command member to contact the cognizant MLC (k), discuss the
circumstances of the discrepancy, and request guidance for further action.
MLC will advise the command in writing or by E-mail of the guidance
provided. Should MLC determine an investigation is warranted, the command
shall: appoint one or more members of the command to investigate the
discrepancy. The command shall not appoint CSAB members to investigate an
incident they have reported.
(2) Review and send to the pertinent MLC (k) the findings of the investigation.
(3) The pertinent MLC (k) shall determine if the theft or loss warrants further
action or DEA notification.
3. Procuring, Storing, Transferring, and Disposing of Controlled Substances.
a. Procurement.
(1) Clinics shall procure controlled substances from the DSCP prime vendor, or
directly through DSCP, if items are available. Coast Guard vessels shall obtain
authorized controlled substances through their collateral duty pharmacy officer.
(2) Documents relating to commercial procurement of controlled substances shall
be endorsed by the CSC prior to processing.
(3) Schedule I controlled substances and alcoholic beverages shall not be procured
or stocked in Coast Guard health care facilities.
(4) Upon receipt, controlled substances shall immediately be placed in the custody
of the designated custodian. The invoice shall be checked against the

CH 15 10-20
requisition to verify receipt of all quantities listed on the invoice. The
custodian shall acknowledge receipt by signing the invoice. Controlled
substance procurement documents shall be maintained in the pharmacy for
three years.
b. Storage.
(1) Bulk stocks of controlled substances shall be stored in an all-purpose Class V
safe or cabinet.
(2) Working stocks shall be stored in a locked cabinet in a secured area (pharmacy,
etc.).
(3) The controlled substance custodian shall record and sign on the NAVMED
6710/5 all transfers of controlled substances from bulk.
(4) Afloat units may use existing "built in" containers to store bulk or working
stocks of controlled substances.
c. Transfer.
(1) Controlled substances may be transferred between CG and other government
facilities using the Requisition and Invoice/Shipping Document (DD-1149).
When completed the document shall include:
(a) names of issuing and receiving facility or unit;
(b) name, strength, and quantity of each drug;
(c) date; and
(d) signatures of the issuing and receiving custodians.
(2) Both units shall adjust inventories as required and file copies of the DD-1149
for three years.
(3) When the transaction cannot be done in person, it may be done by registered
mail. The Registered Mail Return Receipt (PS Form 3806) shall be maintained
by the issuing unit until a signed copy of the DD-1149 is returned.
(4) A copy of the DD-1149 shall be sent to the pharmacy officer with collateral
duty responsibility for the facility.
d. Disposal.
(1) Expired, contaminated, excessive, or inadequately labeled controlled
substances shall be destroyed by the inventory board. CSAB reports shall
include the drug name, quantity, reason for destruction, and mechanism of
destruction. These shall be maintained on file for three years.
(2) Controlled substances identified for destruction must be disposed of in
accordance with state law. The DEA may also be used to dispose of controlled
substances. Contact your pharmacy officer for information on this procedure.
CH 1510-21
4. Prescribing Practices.
a. Authorized prescribers (see 10-A-2.a). are exempt from registration under provision
of 21 CFR 1301.25. The officer’s social security number shall be used in lieu of a
DEA registration number. The exemption does not apply when the officer prescribes
controlled substances outside of their official duties. In that case, the prescriber is
required to register with the DEA, at their own expense, and comply with applicable
state and federal laws.
b. Signatures.
(1) All prescriptions for controlled substances shall be signed by a medical or
dental officer. If none is assigned, the prescription shall be signed by the
senior health services department representative and countersigned by the
executive officer.
(2) All schedule II controlled substance prescriptions by physician assistants or
nurse practitioners shall be countersigned quarterly by their supervising
medical officer.
(3) All controlled substance quantities used in the preparation of other products
(compounding, etc.) shall be accounted for on a prescription form and be
signed by the pharmacy officer or custodian.
(4) The back of all controlled substance prescriptions shall include the wording
"received by," followed by the patient's signature, address, and the date
dispensed.
c. Quantities and Refills.
(1) Controlled substances shall be prescribed in minimal quantities consistent with
proper treatment of the patient's condition.
(2) Out-of-state controlled substance prescriptions may be dispensed if, in the
professional judgment of the pharmacy staff, the prescription is legitimate.
These prescriptions should invoke special scrutiny by pharmacy personnel.
(3) Schedule II prescriptions shall not be accepted more than seven days after the
date the prescription was written. For other controlled substances, 30-days
shall be the limit.
(4) Schedule II prescriptions shall be limited to a 30-day quantity and may not be
refilled. The only exception shall be medication for Attention Deficit Disorder
(ADD) where quantities may be dispensed in up to a 90 day supply with no
refills.
(5) Schedule III, IV, and V prescriptions shall be limited to 30-day quantities with
up to five refills authorized by prescriber. The only exception shall be for
chronic seizure medications, which may be dispensed in up to 90-day
quantities with one refill (six months’ total supply). Civilian prescriptions for
these medications shall only be honored for these quantities. Patients shall be

CH 15 10-22
informed of this quantity/refill limit and be offered the opportunity to have the
prescriptions filled elsewhere.
d. Filing Prescriptions.
(1) Controlled substance prescriptions shall be serially numbered and maintained
in two files:
(a) File #1: All C-II, precious metals, and alcohol prescriptions.
(b) File #2: All C-III, C-IV, and C-V prescriptions.
(2) All prescriptions shall be maintained on file for three years after which they
may be destroyed them by shredding or tearing each prescription in half.
(3) All prescriptions for C-II medications, precious metals, and alcohol shall be
posted on NAVMED 6710/5 by the end of the workday. When this is done, a
line shall be initialed by the pharmacy staff member completing the
transaction.
CH 1510-23
Section C - Forms and Records
1. General. Records shall be maintained for certain procedures conducted within all Coast
Guard Clinics. Among mandatory requirements for record keeping are the prescribing of
drugs, handling of controlled substances, and quality control procedures. Standardized
forms are available for all procedures except quality control.
2. Prescription Forms.
a. The DOD prescription form (DD 1289) or polyprescription (NAVMED 6710/6) shall
be used by Coast Guard prescribers when chart prescribing is not available.
b. All prescriptions shall be filed in one of three files:
(1) All non-controlled drug prescriptions;
(2) Schedule II prescriptions; and
(3) Schedule III, IV, and V prescriptions.
c. Prescriptions in black or blue ink, indelible pencil, or typewritten must show the
information:
(1) Patient's full name;
(2) Date the prescription was written;
(3) Full generic name (or trade name with substitution instructions), dosage form
desired, and dosage size or strength written in the metric system. The quantity
dispensed shall be clearly specified numerically or spelled out in words (“one
bottle” or “one package” are not acceptable). Standard pharmacy abbreviations
may be used in writing dispensing and dosage instructions but not in specifying
the drug to be dispensed.
(4) Complete, explicit directions to the patient (expressions such as "take as
directed," "label," etc. are not adequate directions and not allowed);
(5) Prescriber's legible, legal signature (initials not permitted) with stamped name
and professional discipline (MD, DO, DMD, DDS, PA, HS2, etc.);
(6) All additional requirements when prescribing controlled substances:
(a) Patient's complete address; and
(b) Prescriber's SSN or DEA number.
(c) NOTE: Alterations on prescriptions for controlled substances are
prohibited unless initialed by the prescriber.
d. Multiple prescription forms, such as NAVMED 6710/6 or 6710/10, which are
intended for use when prescribing a number of non-controlled drugs for one patient,
are authorized.
CH 15 10-24
e. Maintain all prescriptions on file, including all "prescription logs" related to chart
prescribing, for three (3) years, after which they may be destroyed by shredding or
tearing each prescription in half.
f. The pharmacy shall have ready access to the patient's medical information including
age, allergies, weight, etc., when preparing and dispensing prescriptions.
3. Quality Control Forms. Quality control is important for proper conformity and safety of
drug products to be dispensed. The two main areas that benefit from quality control are
compounding and prepackaging. A locally prepared form shall be used which will
provide clearly definable material sources (manufacturer’s name, lot numbers, and
expiration dates), procedures used, intermediary and final checks by supervisory
personnel, and sample labeling.
4. Controlled Drug Forms.
a. NAVMED 6710/4—24-Hour Narcotic and Controlled Drug Inventory. This record
shall be maintained at Coast Guard facilities providing inpatient care.
(1) The NAVMED 6710/4 shall be signed by the senior health services technician
on each watch after the drugs have been checked prior to relief. Where feasible
and practical the drugs should checked concurrently by the HS reporting for
duty as well as by the HS being relieved. Any discrepancies noted shall be
reported immediately. The record is used for two (2) weeks, with a one (1)
week period on each side. The night HS shall initiate the record.
(2) The serial numbers of new NAVMED 6710/1’s received from the pharmacy
during each watch shall be entered. The serial numbers of completed
NAVMED 6710/1’s returned to the pharmacy shall be entered and the
pharmacist or authorized representative shall acknowledge receipt by initialing
in the appropriate column.
(3) At the time specified in local instructions, the senior health services technician
shall audit the clinic controlled substances supplies. After the audit the senior
health services technician shall date and sign the NAVMED 6710/4.
b. NAVMED 6710/1—Narcotic and Controlled Drug Account Record.
(1) Upon receipt of a properly completed prescription requisition a separate
Narcotic and Controlled Drug Account Record (NAVMED 6710/1) shall be
prepared by the pharmacy for each schedule II through schedule V drug, and
any other drug which, in the opinion of the commanding officer, requires
control procedures.
(2) All NAVMED 6710/1’s shall be kept in a controlled drug book.
(3) All entries shall be made in blue or black ink. Errors shall be corrected by
drawing a line through the erroneous entry and having the person making the
correction sign the entry. The correct entry shall be recorded on the following
line, if necessary.

CH 1510-25
(4) If a new issue is received before the old issue is completely expended, the new
NAVMED 6710/1 shall be inserted in back of the current record. The serial
number of the new NAVMED 6710/1 shall be entered on the NAVMED
6710/4.
(5) The heading for each NAVMED 6710/1 shall be completed at the time of
issue. The body shall be used for recording expenditures and balances only.
(6) Each time a drug is used, complete information shall be recorded: date, time,
patient, doctor's name, by whom given, amount used, and balance remaining on
hand (NAVMED 6710/1).
(a) Record all amounts in Arabic numerals. Where the unit of measure is a
milliliter (ml) and the amount used is less than one ml, it shall be
recorded as a decimal (e.g., 0.5 ml) rather than a fraction.
(b) When a fraction of the amount is expended to the patient , it shall be
placed in parentheses before the amount recorded in the expended
column; [e.g., an entry of (0.0005)1 on the morphine sulfate 16 mg/ml
record indicates that one-half ml was expended and that 0.008 gm was
administered].
(c) If a single dose of a controlled substance is accidentally damaged or
contaminated during preparation for administration or the patient refuses
after preparation, the dose shall be destroyed and a brief statement of the
circumstances shall be entered on the NAVMED 6710/1. Such
statements shall be signed as witnessed by a second health care provider.
(d) If multiple doses of a controlled substance are damaged, another senior
HS shall record the disposition of the drug, including date, amount of
drug, brief statement of disposition, and new balance. Both the senior
and witnessing HS shall sign the NAVMED 6710/1.
(e) Deteriorated drugs shall be returned to the pharmacy for disposal.
(f) The completed NAVMED 6710/1, along with the counter-type dispenser,
shall be returned to the pharmacy.
(g) Monthly, the pharmacy shall report all NAVMED 6710/1s still
outstanding 30 days from date of issue. The report shall be verified and
returned to the pharmacy for reconciliation. Discrepancies shall be
reported to the commanding officer via the Controlled Substances
Inventory Report.
c. Narcotic and Controlled Drug Book.
(1) Each activity drawing controlled substances from the pharmacy shall maintain
a loose leaf notebook containing NAVMED 6710/4—24-Hour Narcotics and
CH 15 10-26
Controlled Drug Inventory in the first section and individual NAVMED
6710/1—Narcotic and Controlled Account Records in the latter sections.
(2) The senior HS shall remove all filled NAVMED 6710/4’s over three (3)
months old from the Narcotic and Controlled Drug Book and return them to
the pharmacy.
d. NAVMED 6710/5—Perpetual Inventory of Narcotics, Alcohol, and Controlled
Drugs. Separate NAVMED 6710/5 forms are not required for each controlled
substance (C-II through C-V) in bulk and working stock when electronic records or
documentation are available via the Composite Health Care System (CHCS) or
equivalent software programs. The requirement for hard copy report monthly
substance audit board report (CG-5353) is still required, however the CHCS software
prepares and automates controlled substance inventory reports which are acceptable
and can be used as an equivalent to the CG-5353. If software is not available prepare
a separate NAVMED 6710/5 for each controlled substance (C-II through C-V) in
bulk and working stock; All boxes and columns below are self-explanatory except as
noted:
(1) Drug Name. Enter generic or proprietary drug name as appropriate, e.g.,
"Codeine Sulfate."
(2) Strength. Express as gm, mg, etc.
(3) Unit. Enter dosage form as appropriate.
(4) Prescription or Requisition Number. Enter appropriate prescription or
requisition (voucher) number. For issues returned to the pharmacy, enter the
source.
(5) Recipient. Enter "pharmacy" for receipts. Enter clinic or patient name, as
appropriate, for expenditures.
(6) NAVMED 6710/1 Returned. The date the NAVMED 6710/1 is returned to the
pharmacy shall be entered on the appropriate line bearing the same serial
number or prescription number.
5. Forms Availability.
a. Forms CG-5353, DD-1289, NAVMED 6710/1, NAVMED 6710/4, NAVMED
6710/5, and NAVMED 6710/6 are available from the Coast Guard Supply Center.
b. Obtain DEA forms from the nearest DEA office. Consult with a pharmacy officer
for more information.
CH 1510-27
Section D - Drug Dispensing Without a Medical Officer.
HSs dispensing prescriptions without a medical officer’s direct supervision, e.g., at
independent duty shore stations or vessels, shall be conducted in accordance with
provisions of this manual, except that these services shall be provided for active duty
personnel only. HSs in these situations are encouraged to seek consultation with their
assigned collateral duty pharmacy officer when necessary.
1. Child-Resistant Containers. Prepackaged OTC products should be issued in their
original container. For vessels, limited quantities of prescription drugs may be issued in
labeled plastic zip-lock bags while underway. These bags must be inserted in a child
resistant container if they are removed from the vessel.
2. Controlled Substances.
a. All drugs shall be dispensed under the supervision of a health services technician at
activities where there are no officers of the health services department.
b. An officer, designated by the commanding officer, shall keep in a separate locked
compartment, all bulk un-issued controlled substances, alcohol, or items otherwise
controlled. The keys or combination shall always be in the custody of an officer.
The executive officer, or other designated officer, shall arrange for the care and safe
custody of all keys and require strict compliance with instructions concerning the
receipt, custody, and issue of controlled substances and alcohol as contained in the
law, Coast Guar Regulations, and this manual.
c. Custodians or their designated assistants shall retain the keys or combination to the
working stock storage area while on duty. When relieved, they shall deliver the keys
to their relief or to a responsible person designated by local instructions. A copy of
the combination of a safe, if used, shall be sealed in an envelope and deposited with
the commanding officer.
d. Commanding officers may authorize temporary deviations from the controls
established in this Chapter due to operational and/or emergency situations.
3. Formulary. Health Services Technicians on independent duty shall maintain drug
formularies consisting of:
a. Standardized Health Services Drug Formulary items;
b. Health Services Allowance List requirements;
c. Chronic medications prescribed by a physician for active duty members; and
d. Other drugs the HS has agreed to stock for their active duty members for a local
contract prescriber.
4. Non-prescription Medication Programs. Sickbays are encouraged to operate
nonprescription medication programs as described in paragraph 10-A-6.h. of this
manual.
11-i
CHAPTER 11
HEALTH CARE PROCUREMENT
SECTION A - CONTRACTING FOR HEALTH CARE SERVICES.................................................. 1
GENERAL..................................................................................................................................................................1
TYPE OF SERVICES....................................................................................................................................................1
ELIGIBILITY FOR CONTRACT HEALTH CARE SERVICES.............................................................................................2
APPROVAL TO CONTRACT FOR SERVICES..................................................................................................................2
FUNDING...................................................................................................................................................................3
PRE-CONTRACT AWARD ACTIONS. ...........................................................................................................................3
AWARD EVALUATION FACTORS................................................................................................................................5
POST-CONTRACT AWARD ACTIONS. .........................................................................................................................6
SECTION B - HEALTH CARE SERVICES INVOICE REVIEW AND AUDITING...................... 11
GENERAL................................................................................................................................................................11
INVOICES SUBJECT TO REVIEW AND AUDIT. ...........................................................................................................11
REVIEW AND AUDIT PROCEDURES..........................................................................................................................11
SECTION C - CLAIMS PROCESSING ....................................................................................................
GENERAL................................................................................................................................................................13
CERTIFICATION. ......................................................................................................................................................13
ADMINISTRATIVE SCREEN. .....................................................................................................................................13
TECHNICAL SCREEN. ..............................................................................................................................................14
APPROPRIATENESS REVIEW. ...................................................................................................................................14
PEER REVIEW. ........................................................................................................................................................16
GUIDELINES FOR INITIAL APPROPRIATENESS AND PEER REVIEWS. .........................................................................17
11-1 CH 17
CHAPTER 11. HEALTH CARE PROCUREMENT
Section A - Contracting For Health Care Services
1. General. Commandant (G-WK) has fiscal responsibility for health care for all Coast
Guard beneficiaries. The necessary care can be obtained through contracts with private
concerns and individuals and interagency and other agreements with military facilities.
Commanding officers are responsible for obtaining the necessary services for each fiscal
year, subject to MLC (k) review and approval. MLC (k) first authorizes all non-
emergency, non-Federal health care. The MLC is responsible for all health services
contracting in its area and shall comply with Federal Acquisition Regulations Part 37.
The MLC (k) oversees all non-Federal care acquired and minimizes expenses by
ensuring competitive contracting procedures take place.
2. Type of Services. The following services may be procured by contract as determined by
MLC (k).
a. Allergist;
b. Dental Prosthetic Laboratory;
c. Dentist, Dental Hygienist, or chairside Dental Assistant;
d. General medicine (Physician or Midlevel Providers);
e. Group Practice Hospital;
f. Gynecologist;
g. Medical Laboratory;
h. Neurologist;
i. Nurse (Registered or Licensed Practical);
j. Obstetrician;
k. Occupational Health Services (for OCCMED Physicals);
l. Optometrist;
m. Orthopedist;
n. Pharmacist;
o. Physical Therapist or Certified Athletic Trainer;
p. Psychiatrist or Psychologist; and
CH 17 11-2
q. Radiologist.
3. Eligibility For Contract Health Care Services. Eligibility for contract health care
services is the same as described in Chapter 2.
a. The following persons are NOT eligible for health care services rendered by contract
providers:
(1) Family members of Coast Guard personnel and retired and retired members of
the Coast Guard (however, they may receive health care services when the
contractor performs the service at a Coast Guard Clinic or sickbay and/or if the
Coast Guard has contracted with a health care provider as a demonstration
project).
(2) Active duty beneficiaries separated from the Service while undergoing
treatment (eligibility for treatment terminates and becomes the member's
responsibility).
(3) Coast Guard civilian employees except for required Occupational Medical
Surveillance and Evaluation Program (OMSEP) physical examinations and
required pre-appointment examinations, all funded using either MLC (k) or
unit AFC-57 funds.
b. Dental laboratory fees for non-active duty beneficiaries:
(1) Retirees. Retirees are authorized to use private sector dental laboratories. Pay
retirees’ dental laboratory fees in the same manner as for active duty members.
(2) Dependents. The dependent receiving the treatment shall pay all private sector
laboratory fees resulting from space-available treatment . A suggested way to
handle such payments is to require dependents to submit a check or money
order payable to the private sector laboratory before delivery of appliances.
The attending dental officer then photocopies the check or money order, pays
the laboratory, and retains the photocopy in the dental record.
4. Approval to Contract for Services.
a. Units shall submit letter requests for contract health care services through the
appropriate chain of command to MLC (k). All requests must contain this
information:
(1) Description of services required (e.g., general health care, pharmacy, lab, or
specialty care such as OB/GYN, optometry, or psychiatry), including desired
days and hours of availability;
(2) A justification of the need for the service;
(3) Estimated annual cost of the required services;
(4) A list of USMTFs within 40 miles of the unit and whether they could perform
the desired service;
(5) A list of Coast Guard units benefiting from the services;
11-3 CH 17
(6) The number of active duty members assigned to each unit;
(7) Either the names and mailing addresses of all interested, recommended
providers or a justification of other than full, open competition (see paragraph
11-A-7, Pre-contract Award Actions, below);
(8) Preferred solicitation area and the rationale for it (e.g. "provider must be
located within 20 miles of the unit", etc.);
(9) Estimated number of annual Coast Guard visits to the provider; and
(10) A list (by type) of any other approved or requested health care contracts.
b. Each request must be able to stand on its own merits and fulfill cost-to-benefit
criteria. MLC (k) will analyze each request and provide written approval or
disapproval (with alternative proposals) to the requesting unit through the chain of
command. If approved, the MLC contracting officer will undertake procurement.
c. MLC will not renew existing contracts simply as a matter of convenience. Each
contract must continue to prove its value annually on a cost-to-benefit basis before its
renewal. MLC (k) will review each contract’s current fiscal year activity. If the
contract passes review, it may be renewed; if it does not, MLC (k) will so advise the
unit receiving the contract services.
5. Funding.
a. The MLC shall budget, review, and pay for all MLC (k)-authorized non-Federal
health care obtained in its area. These documents contain detailed instructions:
(1) Maintenance and Logistics Command, Atlantic Standing Operating Procedures
(MLCLANT SOP), Annex D; and
(2) Maintenance and Logistics Command, Pacific Instruction M6000.1 (series).
b. Charge all MLC (k)-authorized non-Federal health care expenditures to the MLC
AFC-57 account. MLCs can find detailed object class and cost center information in
the Accounting Manual, COMDTINST M7300.4 (series).
6. Pre-contract Award Actions.
a. The contracting officer issues solicitations to obtain supplies and services from
industry on a competitive (more than 1 source) or non-competitive (1 source) basis.
The Competition in Contracting Act of 1984 (PL-98-369) requires the Government
to contract for supplies and services by means of full, open competition to the
maximum extent possible. This means all responsible firms or individuals who can
provide the supplies or services must be allowed to compete for a government
contract. Contracting officers locate potential contractors by publishing the proposed
procurement in the Commerce Business Daily as required by Federal Acquisition
Regulation (FAR), Part 5.
CH 17 11-4
(1) Non-competitive Procurements. Pre-awarding a firm a Government contract
violates the Competition in Contracting Act of 1984. If it is claimed only one
firm can provide the supplies or service, the purchasing office must justify in
writing other than full, open competition, setting forth the facts and rationale
(see FAR, Part 6) to support this claim. The justification must be certified that
it is accurate and complete and send it with the purchase request when sending
it to the contracting officer for procurement action.
(2) Competitive Procurements. The contracting officer also may require certain
information before contracting on a competitive basis. The contracting officer
may request the types of information below to determinate responsibility
within the meaning of Federal Acquisition Regulation, Part 9.
(a) Organizational structure and plan to accomplish the service;
(b) Summary of experience in performing the same or similar work;
(c) Evidence of pertinent state and local licenses;
(d) Evidence of professional liability insurance, or that the offeror can obtain
such insurance;
(e) Membership in professional organizations;
(f) Resume of key personnel with particular emphasis on academic
achievements pertinent to the proposed services; and
(g) Information about the firm or its key individuals that reflects their status
or professional recognition in their field, e.g., awards, published articles,
and the like.
b. Subject to the contracting officer’s approval, a visit may be made to the offeror's
facility before the award (pre-award survey) to review some of the above data to
reduce submitted data. The following paragraphs are examples of the information
that may be required from an offeror.
(1) Brief description of the facility, how long established, where located relative to
the required mile radius, daily operating hours, weekly operating hours
(include holidays, Saturdays, and Sundays).
(2) Brief description of similar work performed under Government contracts
including the government agency’s name, contract number, contract price, and
name and telephone number of the agency’s contracting officer.
(3) A resume, X pages maximum, including education, past and present experience
over the last X years, certificates, association membership, etc., of the key
persons who will perform the work under the contract and their letter of intent
indicating they intend to work for the offeror if it is awarded the medical
services contract.
11-5 CH 17
c. Minimum qualifications required to perform the contract may be stated; however,
these qualification requirements must be justified. For example:
(1) Personnel.
(a) Physician. At a minimum, a X year degree in medicine from an
accredited college, license to practice medicine in the location where the
services will be performed, member of the AMA; X years’ experience in
practicing general medicine.
(b) Nurse. RN or LPN. B.S. degree (or equivalent) in nursing from an
accredited college; ANA-certified or equivalent; X years’ experience in
handling patients, administering patient records, etc.
(c) Laboratory Technician. HHS certified, ASCP or eligible, X years’
experience in all phases of laboratory work; e.g., x-rays, blood samples,
etc.
(2) Facility.
(a) Within a X mile radius of the Coast Guard facility requiring the services.
(b) Capable of accommodating or rendering services for at least X patients
simultaneously.
7. Award Evaluation Factors.
a. State the steps or procedures to be used to evaluate the proposals.
b. List the evaluation criteria in the descending order of relative importance and state
whether one factor will have predominant consideration over another. For example:
(1) Personnel,
(2) Experience,
(3) Facility, and
(4) Price.
c. Establish the criteria to be used in evaluating the proposal. They must be the same as
the evaluation factors for award the solicitation cited. The weights assigned to the
factors may be in any form, e.g., adjective (acceptable, outstanding), numerical (50).
Give this information to the contracting officer, preferably before he or she issues the
solicitation, but in any event before receiving the proposals for evaluation.
CH 17 11-6
8. Post-Contract Award Actions.
a. Referring for Contract Services. Before referring any person to a medical services
contractor, the cognizant authority shall determine whether:
(1) The person is eligible;
(2) Services are available in-house;
(3) Services are available from a USMTF; and
(4) Services are available from another Federal facility, e.g., Department of
Veterans Affairs, under an interagency support agreement.
b. Contracting Officer's Technical Representative. The contracting office that awarded
the contract administers it. If the requiring office requests, a Contracting Officer's
Technical Representative (COTR) may be assigned to the contract. The COTR is
preferably a health services program manager or medical administration officer
having jurisdiction in the contract services area. The contracting officer designates
the contracting officer's technical representative in a written, signed letter of
appointment describing the COTR’s responsibilities and limitations. These
responsibilities and limitations must strictly be adhered to avoid any conflicts with
the contractor about changes to contract terms and conditions.
c. Health Care Invoices.
(1) Contractor Invoices.
(a) All invoices for health care services contractors by contractors shall be
processed for payment under the applicable contract’s terms and
conditions. This Manual’s Chapter 6-B-8 describes certifying and
processing non-Federal health care invoices. The contracting officer is
responsible for including the applicable invoice and payment clauses
(e.g., Federal Acquisition Regulations 52.204-3, Taxpayer Identification,
52.232-25, Prompt Payment, etc.) in the contract. Ensure the contracting
officer also includes these invoice requirements in the contract so the
invoice is proper for payment:
1 An itemized, priced list of the services by contract or order line item
number; and
2 Any additional information deemed necessary to process the invoice
for payment.
(b) In addition to the invoice requirements above :Any invoice without the
following supporting documentation will not be paid.

11-7 CH 17
1 Services Rendered Under Non-Emergent Conditions. A referral slip
or written confirmation of patient's eligibility from cognizant health
services department representative.
2 Services Rendered Under Emergent Conditions. A written statement
from the patient describing the emergent condition(s). The
cognizant health services department representative must certify the
patient's eligibility and emergent condition.
(c) If the eligible patient pays the contractor for services rendered under a contract
and requests reimbursement, the reimbursement claim must be submitted to
the appropriate accounting office on SF-1034, Public Voucher for Purchases
or Services Other Than Personal. A patient's invoice cannot be reimbursed
from funds obligated under a contract even though the contractor rendered the
services. These documents must accompany the claim:
1 The contractor’s itemized invoice,
2 A copy of the invoice and receipt showing payment to the contractor,
3 The patient’s written statement of the circumstances justifying the
claim, and
4 The cognizant health services department representative’s approval
of the claim.
(2) Invoices Outside the CONUS.
(a) The nearest Coast Guard facility having an authorized certifying officer
shall process invoices for emergency health care civilian facilities furnish
to Coast Guard members. The invoices and justification explaining the
reasons for the emergency health care must be in duplicate and attached
to SF-1166, Voucher and Schedule of Payments.
(b) Every attempt to pay for emergency health care should be made before
departing from a foreign port to reduce paperwork and pay at the
exchange rate. If payment before departure is not feasible, advise the
facility rendering the service to send all invoices to the United States
Embassy or appropriate consular office for the area.
CH 17 11-8
Figure 11.A.1
STATEMENT OF WORK
1. Scope. Provide all labor, materials, and facilities necessary to perform the tasks herein.
2. Definitions.
a. Patient. An eligible U.S. Coast Guard military member.
b. Emergency. Treatment required to curtail the patient’s undue suffering or loss of life
or limb.
c. Non-Elective Condition. A condition that, if untreated, would render the patient
unfit for duty.
d. Elective Procedure. Treatment the patient desires, e.g., vasectomy, tubal ligation,
sterility test, contact lenses, orthodontics, etc.
e. Duty Status. A determination of the patient's ability to perform the assigned tasks at
the assigned work station. These statuses apply:
(1) Fit for Full Duty (FFFD). Patient is not physically restricted or limited.
(2) Fit for Limited Duty (FFLD). Patient is physically restricted or limited, e.g.,
office work only; no lifting, stooping, prolonged standing, walking, running,
jumping, sea duty, etc.
(3) Not Fit for Duty (NFFD). Patient cannot perform any assigned tasks at
assigned work station.
3. The contractor shall perform these tasks:
a. Task I. Eligibility Determination. Provide service to the Coast Guard military
personnel listed below. Each patient must show the required authorizations before
the Contractor renders service.
b. Task II. Physical Examinations. Examine the patient according to Attachment (1)
requirements. [Attach copy of appropriate section of Medical Manual,
COMDTINST M6000.lA (series).]
c. Task III. Immunization. Immunize the patient and document appropriately on
Standard Form 601 (Immunization Record) or Public Health Form 731 (International
Certificate of Vaccination) in the Coast Guard Health Record the patient presents the
contractor. Record also any sensitivity reactions to the immunization. The
contractor shall use only those immunizing agents approved by the Department of
Health and Human Services. Immunize the patient at the time intervals Attachment
2 specifies. [Attach a copy of Immunization and Chemoprophylaxis, COMDTINST
M6230.4D (series).]

11-9 CH 17
d. Task IV. Emergency Hospitalization. Provide all necessary services to patient while
he or she is hospitalized, to a maximum of seven days. If the patient requires
hospitalization for eight or more days, the contractor shall notify the Coast Guard
Point of Contact by telephone. If the Coast Guard elects to transfer the patient to a
military hospital, the contractor shall complete all necessary documents the civilian
hospital may require to effect the transfer.
e. Task V. Prosthetic and Orthopedic Appliances. The contractor shall provide
prosthetic or orthopedic appliances to the patient only under emergency conditions
(required immediately due to his or her condition). The contractor shall document
the emergency condition on the Coast Guard Health Record. Under non-emergency
conditions, the contractor shall refer the patient to a military hospital to obtain these
appliances.
f. Task VI. Communicable Disease. The contractor shall report all communicable
diseases and recommended control measures to the Coast Guard Point of Contact
immediately after detecting the disease. The contractor also shall report to local
authorities as required by local regulations.
g. Task VII. Notification. The contractor shall notify the Coast Guard Point of Contact
if a patient is seriously ill, injured, or dies.
h. Task VIII. Records and Reports. For all patients the contractor shall maintain a
record with this information:
(1) Outpatient Record. Record the name, rank or rating, Social Security Number,
address, date of treatment, history of present illness, physical findings,
diagnostic procedures including x-rays and laboratory, therapy provided,
fitness for duty determination, duration and limitations if unfit or fit for limited
duty, and the contractor’s printed name and signature.
(2) Inpatient Report. On discharge from the hospital, furnish the patient’s medical
report written using diagnostic nomenclature (standard disease and operation
nomenclature) to summarize the course of the case, laboratory and x-ray
findings, surgeries and treatments, complications, current condition, final
diagnosis, and a fitness for duty determination with duration and limitations if
unfit or fit for limited duty.
i. Task IX. Certificate of Services. After rendering services to the patient, complete
Attachment (3) and obtain the patient’s signature before he or she departs from the
contractor's facility or location where the services were rendered. [Attach copy of
certification form.]
4. The contractor shall not execute any oral or written agreements with the patient to render
a more expensive type of service than that described in the contract in which the patient
pays the difference in price between the contract unit price and the price the contractor
charges (for eyeglasses, see Section 8-E-3
CH 17 11-10
5. The contractor must obtain written authority from the patient's Coast Guard unit before
filling any prescriptions.
6. The contractor must obtain written authority from the patient's Coast Guard unit before
performing any elective procedure.
Personnel Required Authorization
Active Duty 1. Valid Green I.D. Card (DD Form 2CG
(ACTIVE))
2. a referral slip signed by an authorized Coast
Guard official
Reservists (Active Duty) 3. Valid Green I.D. Card (DD Form 2CG
(RESERVE))
4. copy of active duty orders
5. a referral slip signed by an authorized Coast
Guard official
Reservists 6. Valid Green I.D. Card (DD Form 2CG
(RESERVE))
7. a copy of Inactive Duty letter signed by the
Coast Guard Reserve unit’s commanding officer
8. or CG-4671 and a letter signed by the Coast
Guard unit’s commanding officer
PHS Commissioned Officers on
Coast Guard Active Duty Valid Green I.D. Card (DD Form 2CG (ACTIVE))
Prospective Coast Guard Recruit A letter signed by an authorized official at the Coast
Guard recruiting unit
The contractor shall not provide services under this contract to personnel who do not
have the required authorizations listed above.
11-11 CH 17
Section B - Health Care Services Invoice Review and Auditing
1. General.
a. All health care invoices are subject to review and audit to ensure the Coast Guard
pays only for necessary, appropriate health care for its beneficiaries.
(1) The auditing process ensures the contractor’s invoice charges for services
provided at either reasonable fees or those in agreement with the contract.
(2) The review process determines the appropriateness of care for the diagnosis.
b. Personnel performing the review and audit functions must remember if they find
discrepancies, they must give the care provider the opportunity to comment on the
findings.
c. The process of health care invoice auditing and review is complex and lends itself to
errors; thus, most reviews and audit inquiries are not dismissed. Finding must be
presented in a non-threatening manner, demonstrating the Coast Guard's willingness
to cooperate with our health care providers in determining fair, equitable charges.
2. Invoices Subject to Review and Audit. These contract and non-contract health services
invoices are subject to review and audit. The unit processing the invoice should review
bills in these categories before paying them:
a. All outpatient invoices contractors submit;
b. All inpatient and outpatient supplemental care.
3. Review and Audit Procedures. The personnel processing health care invoices should
perform these procedures:
a. Review.
(1) Is the diagnosis compatible with the prescribed care?
(2) Are ancillary services (e.g., lab, x-ray, pharmacy, electrodiagnostic tests, etc.)
prescribed appropriately in amount and frequency?
(3) Is the length of care appropriate for the diagnosis?
b. Audit. Does the contractor's invoice meet the contract definition of a proper invoice?
If not, notify the contracting officer immediately.
(1) Is the bill mathematically correct?
(2) Does it bill only for authorized care and services?
(3) Were services and billed care actually furnished?
(4) Do the charges agree with the provider's regular fee schedule or the prices
listed in the contract?
CH 17 11-12
(5) Does the bill give credit for incomplete, canceled, or partial treatments?
(6) Do dates of care match the time period the patient received the care or
services?
(7) Have previous audits of this provider demonstrated billing errors?
11-13 CH 17
Section C - Claims Processing
1. General. The Maintenance and Logistics Command, Health and Safety Division (MLC
(k)) is responsible for processing Federal and nonfederal health care claims in
compliance with the Federal Law and CG Regulations.
2. Certification. Certification ensures that only authorized payment services to eligible
beneficiaries receiving health care within their entitlements and the care and related
charges are appropriate. Commanders, MLC (k) shall
a. Administratively screen each claim and supporting documents according to
paragraph 3 below. Claims submission procedures from field units is provided by
the MLC (k) Standard Operating Procedures.
b. Technically screen claims and supporting document according to paragraph 4.
below.. In screening, perform these actions:
(1) Refer claims that do not satisfy the Technical Screen criteria to a medical audit
staff for Appropriateness Review and/or audit.
(2) Enter information from these claims into the Non-Federal Invoice Processing
System (NIPS) data base and approve them for payment in this manner:
(a) Claims that satisfy Administrative and Technical Screen criteria
(including Active Duty Claims Program (ADCP) claims coded through a
TRICARE Fiscal Intermediary).
(b) Claims referred for Appropriateness Review and/or audit recommended
for payment.
c. Transmit payment data electronically to the Coast Guard Finance Center.
d. Certify batch transmissions.
e. Correct batch errors.
f. Update vendor files.
3. Administrative Screen.
a. Administrative screening of a claim package determines the patient's authorization
and eligibility to receive billed services and also ensures the package contains all
appropriate, necessary documents. At a minimum, administrative screening includes:
(1) Patient information is present and complete.
(2) Public Voucher for Purchases and Services other than Personal (SF-1164) is
completed for reimbursement requests.
(3) The claim is a complete, itemized original.

CH 17 11-14
(4) A copy of CG-4899, Report of Potential Third Party Liability, is attached if a
third party potentially is liable.
(5) Verification of pre-authorization number.
(6) Support documentation is complete for Reservists’ bills.
(7) Claims for formal contracts have the contracting officer's signature and amount
to be paid.
(8) Claims for clinic support contracts have a Coast Guard beneficiary breakdown.
b. Ensure that all claims that fail to satisfy the administrative screening are corrected by
the unit through the most expeditious means possible.
4. Technical Screen.
a. Health care claims must be reviewed to ensure they comply with Federal regulations.
Part of that process compares claim packages to standard criteria to withstand the
scrutiny of Departmental Accounting and Financial Information System (DAFIS) for
payment. Technical screening of claim packages includes:
(1) Comparing charges against contract fee schedules, pre-authorizations, blanket
purchase agreements, or the geographic area’s usual and customary fees;
claims falling within ADCP guidelines are exempt from fee review;
(2) Entering relevant claim information into NIPS;
(3) Determining whether services were appropriate for the diagnosis; and
(4) Identifying claims requiring further review under these circumstances:
(a) Unrelated charges to the initial diagnosis or injury.
(b) Duplicate charges for services received on a given day.
(c) Care was unauthorized or unnecessary.
(d) Claims submitted by different providers for the same service (e.g.,
anesthesiology charges from more than one provider).
(e) NIPS "flagged" the claim.
(f) The reviewer "feels" a need for further review.
b. Claims a Technical Screen identifies for further review and/or audit require:
(1) Documentation of the problem, and
(2) A recommended course of action.
5. Appropriateness Review.
a. An appropriateness Review is performed under these circumstances:
11-15 CH 17
(1) MLC (k) selects or NIPS flags a claim for further review and/or audit for a
Technical Screen; and/or
(2) Periodically for quality assurance.
b. An Appropriateness Review requires:
(1) An itemized claim;
(2) A patient’s signed "Request for Medical Records" DD-877 or it’s equivalent,
to request medical records and other information about an individual’s care.
Various records, which may include:
(a) Hospital records,
(b) Physician's orders,
(c) Physician and nursing progress notes,
(d) Lab and x-ray reports,
(e) Operative or endoscopic reports,
(f) Admission records (history and physical examinations), and
(g) Discharge summaries.
c. An Appropriateness Review process often involves these activities:
(1) Reviewing records to verify:
(a) The treatment or therapy was:
1 Appropriate for the diagnosis,
2 Consistent with currently accepted medical practice, and
3 Not duplicated unnecessarily.
(b) The length of inpatient hospitalization was appropriate for the diagnosis
and course of care.
(c) The charges were reasonable; claims falling within ADCP guidelines are
exempt from fee review.
(2) Obtaining additional documentation and/or correspondence from health care
providers.
(3) Initially notifying health care providers of this information:
(a) Their claims are being reviewed and audited.
CH 17 11-16
(b) The audit is a normal part of the Coast Guard’s health care review
process and does not indicate or allege the health care provider
committed a offense; and
(c) If reviewing cases for longer than 30 days, periodically communicate
with health care providers to inform them of claim status.
d. An Appropriateness Review may recommend:
(1) Full payment for services. Enter data into and process through NIPS.
(2) Partial payment for services. Attach decision documents; recommend the
amount of payment; and enter data into NIPS. Initiate a reimbursement request
if the claim initially was overpaid.
(3) Consulting a specialist for peer review.
(4) Referral to a contractor for further review or an on-site hospital audit.
(5) Closing the case with no further action.
e. An Appropriateness Review includes:
(1) Fully documenting the decision process,
(2) Initiating payment or the provider’s reimbursement, and
(3) Drafting appropriate correspondence.
6. Peer Review.
a. A Peer Review will be performed under these circumstances:
(1) A health care provider objects to other reviews’ findings, or
(2) An Appropriateness Review reveals the need for a more sophisticated
evaluation of the diagnosis, prognosis, or specific medical procedures
employed.
b. Send the case and health care provider's additional documentation (if any) to a
qualified medical, pharmaceutical, or dental specialist for review. These services
should be contracted if in-house specialists are not available
c. Peer Review may include these detailed examinations:
(1) Diagnosis;
(2) Prognosis;
(3) Appropriateness of the care provided;
(4) Claims submitted to a Fiscal Intermediary for pricing are exempt from fee
review.
(5) Selection of the most cost-effective therapy.

11-17 CH 17
d. Among other things a pharmacist's review of pharmaceutical bills and supporting
documents may:
(1) Determine the efficacy of prescribed medication;
(2) Identify cost-effective choices; or
(3) Recommend stocking pharmaceuticals for future issuance.
7. Guidelines for Initial Appropriateness and Peer Reviews. These common health care
services guidelines are not all-inclusive. Appropriateness and Peer Reviews should be
used to assist reviewers in deciding whether in-hospital audits or contracted review
services are required.
a. Trauma. Answer these questions:
(1) Does the level of care correspond to the diagnosis?
(2) Were appropriate facilities used?
(3) Were laboratory and x-ray procedures appropriate? Include justification for:
(a) Repeating procedures on a given day;
(b) Repeating normal procedures;
(c) Failing to follow up abnormal tests.
(4) Were iatrogenic complications were identified appropriately? Include:
(a) Sepsis,
(b) Wound dehiscence,
(c) Hemorrhage,
(d) Pulmonary complications,
(e) Cardiovascular complications (thrombophlebitis, etc.),
(f) Urinary tract infection,
(g) Anesthetic or other drug reactions (appropriate drug and dosage, known
allergies), and
(h) Other associated injuries.
(5) The length of stay was appropriate for the diagnosis and indicated
complications.
(6) The discharge diagnosis was compatible with admission diagnosis and the
patient's history.

CH 17 11-18
(7) The patient's physical status on discharge:
(a) Alive,
(b) Complications were controlled,
(c) Wound(s) condition was satisfactory,
(d) Required follow-up arrangements are listed, and/or
(e) Medications were prescribed.
(8) Follow-up care was appropriate, including:
(a) Therapy,
(b) Office visits, and
(c) Additional hospitalization was for a good reason, e.g., iatrogenic
complications, continued therapy, or additional surgeries.
(9) Fees are usual and customary for the geographic area (claims falling within
ADCP guidelines are exempt from fee review).
(10) The use of multiply providers is explained.
(11) Providers’ and reviewers’ differences in medical opinion (particularly
involving altered treatment and length of hospital stay) are significant enough
to warrant negotiation.
b. Laboratory Services. Answer these questions:
(1) Are tests related to or necessary for the diagnosis?
(2) Were ICU standing orders in effect?
(3) Were tests repeated excessively?
(4) Were charges duplicated for the same procedure on the same day?
(5) Were tests repeated due to equipment or operator error?
(6) Were tests repeated despite normal previous test(s) (justification is required)?
(7) Were there multiple charges for the same or similar tests?
(8) Were multiple tests performed in a logical sequence (i.e., the most invasive or
sophisticated performed last)?
(9) Were fees usual and customary (claims falling within ADCP guidelines are
exempt from fee review);
(10) For a laboratory under Coast Guard contract, were:
(a) Tests covered by the contract?

11-19 CH 17
(b) Charges within fee schedule?
c. Radiology Services. Considerations:
(1) Was the examination required given the diagnosis?
(2) Were charges for portable radiology of an ambulatory patient?
(3) Were examinations repeated?
(4) Were bilateral x-rays appropriate (patients over 12 years of age)?
(5) Were charges or exams of the same anatomical part duplicated?
(6) Do examinations and in-patient dates coincide?
(7) Were examinations repeated despite normal findings in previous
examinations?
d. Physical Therapy. Considerations:
(1) Was the injury or diagnosis properly documented? Did it include:
(a) Objective findings?
(b) Functional findings?
(c) Multiple provider discrepancies?
(d) Documentation of improvement?
(2) Did a physician prescribe treatment?
(3) Were injury management and treatments reasonable and necessary? Did they
cover these:
(a) Was the treatment plan documented?
(b) Did objective findings permit the therapist and/or physician to monitor
treatment results?
(c) Were changes in the treatment program due to unsuccessful results?
(d) Was treatment only for subjective complaints?
(e) Was the treatment related to diagnosis?
(f) Did the treatment follow standard procedures and protocols?
(g) Did the treatment plan include goals and objectives?
(4) Was the length or number of treatments excessive?
(5) Was treatment consistent or continuous or did patient attend sporadically?

CH 17 11-20
(6) Did therapy continue after "Fit-For-Duty" status?
(7) Did therapy charges continue during stays in cardiac or intensive care units.
(8) Were charges duplicated for same-day, apparently inappropriate treatments?
(9) Was therapy frequency within accepted standards?
(10) Were same-day charges for three or more modalities during a single therapy
session.?
(11) Were charges usual and customary (claims falling within ADCP guidelines are
exempt from fee review).
e. Dentistry.
(1) For provider contract care, were:
(a) Services within the contract scope?
(b) Charges within fee schedules?
(2) For emergency care, were:
(a) Services within the scope of entitlements?
(b) Charges reasonable and customary?
(3) For care pre-authorized in Chapter 2-A-6, did any of these occur?
(a) Did the MLC assign a pre-authorization number?
(b) Were services within the authorized, standard treatment plan?
(c) Were treatments split to circumvent pre-authorization requirements?
(4) For all dental services, do any of these apply?
(a) Were services duplicated?
(b) Were billings for the same service duplicated?
(c) Were diagnosis charges consistent with services received?
(d) Were crowns constructed of precious metals?
(e) Are laboratory charges consistent with the service provided (bridges,
crowns, partial or full dentures)?
f. Pharmacy.
(1) For contract providers, were services within the scope of the contract?
(2) For inpatient care, do any of these apply?
11-21 CH 17
(a) Were billings duplicated?
(b) Was credit received for returned or unused medications?
(c) Did medication and in-patient dates coincide?
(d) Did medications’ cost exceed 250 percent of Annual Pharmacists'
Reference (“Red Book”) average wholesale price (Note: This equals a
150 percent markup.)? Claims falling within ADCP guidelines are
exempt from fee review.
12-i
CHAPTER 12
OCCUPATIONAL MEDICAL SURVEILLANCE AND EVALUATION PROGRAM
(OMSEP)
SECTION A - GENERAL REQUIREMENTS. .................................................................................. 1
1. DESCRIPTIONS. ............................................................................................................................ 1
2. ENROLLMENT .............................................................................................................................. 1
3. REPORTING REQUIREMENTS ........................................................................................................ 2
4. MEDICAL REMOVAL PROTECTION ................................................................................................ 4
5. ROLES AND RESPONSIBILITIES..................................................................................................... 4
SECTION B - ADMINISTRATIVE PROCEDURES........................................................................ 9
1. GENERAL..................................................................................................................................... 9
2. EXAMINATIONS TYPES. ............................................................................................................... 9
3. USE OF OMSEP FORMS. ........................................................................................................... 11
4. MEDICAL REMOVAL STANDARDS.............................................................................................. 13
5. REPORTING OF EXAMINATION RESULTS.................................................................................... 13
SECTION C - MEDICAL EXAMINATION PROTOCOLS........................................................... 26
1. GENERAL................................................................................................................................... 26
2. ASBESTOS.................................................................................................................................. 26
3. BENZENE. .................................................................................................................................. 28
4. CHROMIUM COMPOUNDS........................................................................................................... 31
5. HAZARDOUS WASTE. ................................................................................................................. 32
6. LEAD. ........................................................................................................................................ 34
7. NOISE. ....................................................................................................................................... 36
8. PESTICIDES. ............................................................................................................................... 39
9. RESPIRATOR WEAR.................................................................................................................... 41
10. RESPIRATORY SENSITIZERS....................................................................................................... 43
11. SOLVENTS. ................................................................................................................................ 45
12. TUBERCULOSIS. ......................................................................................................................... 47
13. UNSPECIFIED. ............................................................................................................................ 48

12-ii
CH-17
This page left blank

12-1 CH-17
CHAPTER 12. OCCUPATIONAL MEDICAL SURVEILLANCE AND EVALUATION
PROGRAM (OMSEP)
Section A - General Requirements.
1. Description.
a. The work environment and occupational activities inherent to Coast Guard missions can
expose personnel to health hazards with the potential for disease or injury. The
Occupational Medical Surveillance and Evaluation Program (OMSEP) is designed to
identify work related diseases or conditions, through baseline and periodic examinations,
at a stage when modifying the exposure or providing medical intervention could
potentially arrest disease progression or prevent recurrences. The fundamental purpose
of this program is to identify pre-existing health conditions, provide risk specific
periodic screenings, and monitor clinical laboratory tests and biologic functions
suggestive of work related environmental exposures. All OMSEP enrollees receive
periodic physical examinations, in accordance with Occupational Safety and Health
Administration (OSHA) requirements, for the duration of their health hazard exposure or
end of their employment. Individuals are released from active surveillance at the end of
their exposure. In accordance with OSHA regulations, the OMSEP personnel tracking
database containing the name, social security number, billet or occupation code,
applicable examination protocols, and next physical examination due date remains active
for an additional 30 years.
b. The OMSEP is the physical examination process for the Coast Guard’s Occupational
Health Program. The guidance for this program is outlined in the Safety and
Environmental Health Manual, COMDTINST M5100.47 (series). OMSEP replaces the
present version of the physical exam process described in the SEH Manual as the
Occupational Medical Monitoring Program (OMMP).
2. Enrollment.
a. Coast Guard Medical Surveillance Action Level: The medical surveillance action level
(MSAL) is the level of worker exposure, determined by workplace sampling, at or above
which occupational medical surveillance examinations will be performed. The Coast
Guard MSAL will be 50% of the most stringent of the current OSHA permissible
exposure limit (PEL),or, the most current American Conference of Governmental
Hygienists (ACGIH) Threshold Limit Value (TLV).
b. Determination of Occupational Exposure.
(1) An employee is considered occupationally exposed for OMSEP purposes if a noise
exposure or hazardous condition is likely to occur 30 or more days per year.
Documentation of the exposure must meet the following criteria: quantitative
work-site sampling measurements indicate hazard levels at or above the MSAL or
that the exposure can reasonably be determined, in the absence of quantitative
sampling, to exceed the MSAL.
(2) Quantitative sampling is the primary and definitive means to characterize
workplace health hazards, although personal sampling measurement is preferred to
workplace sampling. Coast Guard Safety and Environmental Health Officers

12-2
CH-17
(SEHOs) using guidance contained in the Safety and Environmental Health
Manual, COMDTINST M5100.47 (series) will generally perform this function.
SEHOs will normally characterize workplaces by frequency of exposure, type of
exposure, and risk groups.
(3) Certain occupations or exposures may require surveillance by federal statutes,
DOT regulations, or Safety and Environmental Health Manual, COMDTINST
M5100.47 (series) without regard to the 30-day exposure threshold.
(4) Competent environmental health authority is considered to be the cognizant SEHO
but the authority may be delegated to other recognized and approved personnel
with the necessary technical training and abilities. Qualitative assessments must
be based on expected type, frequency, mode, and duration of hazard exposure, and
are considered temporary until validated by quantitative means.
c. Enrollment Criteria: Recommendations for enrollment are based on specific job
assignments and the level of worker exposure. This process is initiated at the unit level
and must be finalized by the IH or cognizant SEHO, with recommendations from the
supervising medical officer (if necessary), before forwarding to Maintenance and
Logistics Command (MLC (k)) for inclusion into the OMSEP database (see section 12-
A-3-(a)-3). This centralized database will be maintained by MLC (k) and will be
accessible to the commands in accordance with privacy act requirements. Personnel will
be enrolled in the OMSEP if either of the following criteria are met:
(1) Personnel identified as occupationally at risk/exposed to hazardous chemicals or
physical agents at levels documented or reasonably determined to be above the CG
Medical Surveillance Action Level (MSAL) for that hazard,
(2) Personnel actively engaged for 30 or more days per calendar year in the following
occupations will be enrolled in OMSEP, unless an IH investigation determines
individuals are not exposed to toxic chemicals or physical hazards: resident
inspectors, pollution investigators, marine safety (general), port safety (general),
vessel inspectors or marine investigators; and fire fighters.
(3) Note: New OMSEP enrollees maybe considered for enrollment under the
guidelines of the Hazardous Waste protocol, which provides the most through
surveillance for those with unknown hazardous risks and no prior history of
exposures. However, the unit IH or cognizant SEHO may recommend enrollment
using the medical surveillance protocol considered most appropriate.
3. Reporting Requirements.
a. Examination Reports:
(1) Required forms: OMSEP physical examinations require completion of the most
current version of CG Form 5447 (6-01) in addition to forms DD-2808 and DD-
2807-1. Other OMSEP specific forms and their uses are presented in Section 12-B
(also see Table 12-B-1.) Uses of routine medical record forms are presented in
Chapter 4 of this Manual.
(2) Record keeping: OMSEP personnel records will be handled in the same manner
as other medical records (see Chapter 4 of this Manual) with the following
exceptions: all x-ray, laboratory test, and related reports of examinations or
12-3 CH-17
procedures done for OMSEP purposes, as well as the medical record cover, shall
be clearly labeled "OMSEP." All OMSEP examination reports, including all
laboratory data, must be entered into the individual’s health record and maintained
in accordance with OSHA regulations. The member’s medical record custodian
will maintain all OMSEP medical records on file for the duration of employment.
Upon separation or retirement, all records concurrently labeled “OMSEP” will be
maintained, for an additional 30 years, as required by OSHA regulations [29 CFR
1915.1120].
(3) OMSEP database: MLC (k)’s will maintain an electronic database of all OMSEP
enrollees based on enrollment information provided by the local units. The
OMSEP personnel tracking database should include, at a minimum, the member's
name, social security number (SSN), billet or occupation code, applicable
examination protocols, and next physical examination due date. The handling of
all data in the OMSEP database will comply with Privacy Act requirements.
(4) Substitutions: OMSEP examination forms may not be substituted for other
examination forms. If another examination is anticipated/required, (i.e. FLIGHT,
RELAD) at the same time as the OMSEP examination the appropriate forms for
each particular examination should be provided to the examiner so they may be
completed at the same time. Duplicate laboratory tests are not required, so long as
all specific tests and procedures required for each exam are completed and
reported.
(5) Exposure data records: Any available exposure data, from workplace surveys,
industrial hygiene personal or area monitoring, material safety data sheets, or
assigned IH/SEHO other appropriate sources, will be provided by OMSEP
coordinator to the examining medical officer as part of the examination packet.
These data should be supplied by the local unit, in coordination with the
supporting industrial hygienist, prior to the examination. The protocols in Section
12-C, in addition to OSHA regulations, specify what exposure surveillance data
must be maintained and made available to the examining medical officer.
b. Tracking Report: Individual units, in coordination with the cognizant SEHO, are
responsible for creating and managing a roster of all OMSEP enrollees and providing the
designated medical officer advisor (DMOA)/clinic and MLC(k)'s with an updated report.
Once fully implemented medical officers will be able to access this information through
the OMSEP database. Updates to the tracking report will be possible by placing the
information directly into the database. This will preclude the need for any additional
written reports. The report should include all information cited in Section 12-A-3(a)(3)
and will form the basis for the OMSEP database.
c. Sentinel Occupational Health Event Reporting: The occurrence of a new illness or
disease, which is likely associated with an occupational exposure or condition, may be
considered a "sentinel event." Such an event may serve as a warning signal that the
quality of preventive measures may need to be improved. In order to facilitate timely
intervention, the initial diagnosis of any such diseases must be reported IAW Section 7-
B of this Manual. A complete list of reportable occupational diseases is found in Figure
7-B-2.
12-4
CH-17
4. Medical Removal Protection. It is the responsibility of the commanding officer to assure a
safe and healthy working environment. The finding of a work-related illness or injury,
which could be further exacerbated by continued exposure to a workplace hazard or
condition, requires immediate evaluation to determine whether the worker must be at least
temporarily removed from further exposure. A recommendation to remove the member
should be made by the examining medical officer and cognizant SEHO, in coordination with
the unit’s Commanding Officer. (See section 12-B-4-b).
5. Roles and Responsibilities. The OMSEP is part of a larger and more comprehensive
surveillance process requiring the coordinated effort of various district units and local
commands working to secure the safety and health of Coast Guard workers. Key personnel
have been identified as essential in maintaining a sound occupational health prevention
program. Following is a description of their expected roles and responsibilities in this
process: NOTE: For the purposes of this Chapter all references to employees, workers,
personnel will be assumed to be part of the ONE DOT/CG TEAM concept. Rules,
regulations, and directives apply equally to ALL unless otherwise specified.
a. Units/Commands: Each unit must appoint an OMSEP coordinator, usually the Safety
Coordinator (SC) or the Safety and Occupational Health Coordinator (SOHC), or
Independent Duty Corpsman. Even if units are under one servicing clinic, the unit is
still required to appoint an OMSEP coordinator and manage their respective database.
The OMSEP coordinator is responsible for updating the roster of OMSEP enrollees and
maintaining the unit's OMSEP personnel tracking report, ensuring OMSEP examinations
are completed in a timely fashion, and ensuring all available exposure data is available
to the medical officer at the time of the OMSEP examination.
b. MLC (k): MLC (k)’s will ensure that SEHO/IH work-site monitoring and reporting is
completed and entered into the appropriate database. Additionally they will provide
oversight to the local units ensuring the accuracy and completeness of the OMSEP
personnel tracking report. The MLC (k)’s medical officers will provide oversight over
the physical examination consultation and referral process. MLC (k)’s will also provide
indicated guidance and or training to HS personnel on examination practices and
procedures.
c. SEHOs: SEHOs will be required to review all requested OMSEP enrollments from the
unit OMSEP Coordinators. SEHOs will approve or disapprove requested enrollments
through the on-line database. Disapprovals need to be explained to the requesting unit.
To substantiate enrollments, SEHOs will be required to conduct and update quantitative
and/or qualitative IH assessments of their units’ workplace environment. SEHOs will be
required to have these written assessments available to the medical officer for review, if
requested, to determine the appropriate medical surveillance protocol to use. SEHOs
will also be required to provide training and day-to-day consultation with their unit
OMSEP Coordinators on database management.
d. Commandant (G-WKS): Commandant (G-WKS) will provide planning, development,
and expertise on occupational health issues. G-WKS is responsible for policy making,
procedural decisions, and ensuring currency of Chapter 12 of the Medical Manual with
OSHA standards. The G-WKS occupational medicine medical officer will provide
support on physical examination problems and review all diagnosed occupational health
related abnormalities encountered by the on-site provider. A yearly report, updating the

12-5 CH-17
status of the member's abnormalities, will be provided to onsite providers. G-WKS is the
final authority on decisions of any OMSEP related problems.
e. Medical Officer’s Responsibilities:
(1) Medical Diagnosis coding. The examining medical officer is responsible for
explaining and/or following any abnormalities through to a resolution. All
diagnoses made must be appropriately coded using ICD-9CM diagnostic coding,
or most current version. ICD codes should be noted in parentheses next to the
diagnosis on the examination report and be reported to the fifth digit.
(2) Written assessment or opinion. Whenever a physical exam is performed, the
examining medical officer must include the following information in writing as
part of the record of each examination. This information should be included in the
appropriate blocks.
(a) The occupationally pertinent results of the medical examination.
(b) An opinion about adequacy of the information available to support any
diagnosed occupational disease(s), if appropriate.
(c) Any recommended limitations to the employee’s assigned work.
(d) A statement that the employee has been informed about the results of the
examination.
(e) Any additional written information required by the protocols listed in
Section 12-C.
f. Medical Administrators:
(1) Support. Medical Administrators are responsible for providing administrative
assistance on all OMSEP related matters. This support should extend to :
(a) All units within the designated AOR.
(b) Contracted medical providers and their respective facilities.
(c) IDT’s.
(2) OMSEP report/worksite data. Medical Administrators should interact with
OMSEP coordinators within their AOR to ensure currency of the roster of
enrollees and ensure that work-site information is received in a timely matter.
Worksite exposure information, reported history of past exposures and safety data
sheets should precede the physical examination to give the medical officer ample
time to reach an educated decision.
(3) Physical Examinations/Medical Records. The Medical Administrator is
responsible for the following clinic functions in support of OMSEP:
(a) Timely scheduling of physicals.

12-6
CH-17
(b) Providing qualified technicians to perform the indicated laboratory and
radiological procedures.
(c) Ensuring proper calibration of equipment, and
(d) Compliance with quality assurance standards.
g. Civilian Employees: Civilian OMSEP enrollees may be entitled to services provided by
Coast Guard medical facilities should a determination be made by a medical provider,
that an adverse health condition resulted from a work place exposure. Employees are
expected to report and explain any illnesses or injuries resulting from exposure sources
outside their primary duty station or from other non-occupational settings. Should a
determination of an injury or illness, resulting from an exposure at the workplace, be
made by a medical provider, civilian appropriated fund employees should contact their
servicing civilian Command Staff Advisor (CSA) for assistance in making a claim with
the Department of Labor. Non-appropriated fund employees (NAF) should contact their
immediate supervisor and/or personnel liaison office. The services provided by the Coast
Guard facilities will be only to establish an occupationally-related illness/injury. Further
medical care should be provided by the civilian employee’s health care provider.
h. Others: In the event of an emergency situation with heavy exposure (e.g., fire, spill),
24-hour assistance is available from the Agency for Toxic Substances Disease
Registry (ATSDR) at the Centers for Disease Control and Prevention. Call 404-498-
0210.

12-7 CH-17
Disease Registry (ATSDR) at the Centers for Disease Control and Prevention. Call 404-
639-0615-6360.
LIST OF ABBREVIATIONS
ACGIH
ALT
AST
BUN
American Conference of Governmental Industrial Hygienists
Alanine aminotransferase
Aspartate amino transferase
Blood u
r
ea nitrogen
CBC Complete blood count
CNS Central nervous system
CXR Chest x-ray
DOT Department of Transportation
EL
FVC
FEV-1
Excursion limit (OSHA mandated maximal “safe” airborne concentration of
a substance)
Forced vital capacity
Forced expiratory volume at one second
ICD-9 International Classification of Diseases, 9th Revision (coding system for
medical diagnoses.)
IH
LDH
MCV
MCH
MCHC
Industrial hygiene or industrial hygienist
Lactic dehydrogenase
Mean corpuscular volume
Mean corpuscular hemoglobin
Mean corpuscular hemoglobin concentration
MLC (k)/(kse) Maintenance and Logistics Command: (k)-medical; ((kse)-safety &
environmental health.
MO Medical officer (physician, physician’s assistant or nurse practitioner )
MSAL Medical surveillance action level (Defined in 12-A-3)
OMSEP Occupational Medical Surveillance and Evaluation Program
OSHA Occupational Safety and Health Administration
PEL Permissible exposure limit (The OSHA mandated TWA airborne exposure
limit)
PFTs Pulmonary function tests

12-8
CH-17
LIST OF ABBREVIATIONS (continued)
RBC red blood cell
SC Safety Coordinator
SEHO Safety and Environmental Health Officer
SOHC Safety and Occupational Health Coordinator
STEL Short-term exposure limit (The maximal “safe” airborne concentration of a
substance)
STEL/C Short-term exposure limit/ceiling (maximal “safe” airborne concentration of
a substance)
STS Significant threshold shift
TB Tuberculosis
TLV Threshold limit value (ACGIH) (The TWA airborne concentration of a
substance)
TST tuberculin skin test (Mantoux)
TWA time-weighted average
U/A Urinalysis
12-9 CH-17
Section B - Administrative Procedures.
1. General: All medical examinations and procedures required under the OMSEP shall be
performed by or under the supervision of a licensed medical officer and an accredited
laboratory shall perform all laboratory tests. Timely completion and monitoring of
scheduled examinations is essential in identifying work related health hazards and any
specific health effects. All tests required as part of an OMSEP examination should be
completed prior to and the results made available to the health care provider at the time of
the physical examination. This requirement may be waived if travel or time costs make
separate visits impractical. The provider is required to review, approve (sign), and
explain any abnormalities. Any unexplained, examination finding, laboratory
abnormality, or test result must be referred to a certified Occupational Health
Clinic/provider for further evaluation.
2. Examination Types.
a. Initial/baseline. Baseline examinations are required before placement in a specific job in
order to assess whether the worker will be able to do the job safely, to meet any
established physical standards, and to obtain baseline measurements for future
comparison. Each baseline examination shall consist of all of the elements specified
under the appropriate surveillance protocol(s) in Section 12-C. Table 12-B-1 also
summarizes the required forms and tests for a baseline examination under each of the
surveillance protocols. In the event that the employee is being monitored under more
than one protocol, each unique form or test need only be completed once for a particular
examination.
(1) An initial examination is required for all employees prior to employment. The
employee may not be exposed to a potential health hazard until the physical
examination is completed. In the event of scheduling delays, this requirement may
be waived, if the employee completes ALL the necessary laboratory tests specified
under the appropriate surveillance protocol(s). The physical examination must
still be completed at the earliest possible date, but not beyond 30 days after the
initial date of employment. Longer delays will require temporary removal.
Workers who transfer from operational to administrative positions on a frequent
basis during the same duty assignment may, with medical officer approval, receive
a periodic physical vice a complete baseline examination upon re-entering the
hazardous work site.
(2) All employees must have a physical examination prior to reassignment to any
position with an occupational health hazard exposure as defined in Section 12-A-
2-b. This requirement is subject to the stipulation described above in Section 12-
B-2-a-1.
(3) Any employee actively monitored in the OMSEP, identified, as at risk of exposure
to a new health hazard requiring additional protocols, should have an initial
examination performed for the new potential exposure(s). The employee may not
be placed at risk of exposure until the examination is completed. During such an
examination, both the initial examination requirements for the additional protocol
and the periodic examination requirements for the original protocol(s) should be
met. This requirement is subject to the stipulation described above in Section 12-
B-2-a-1.
12-10
CH-17
b. Periodic.
(1) Once enrolled in the OMSEP, periodic examinations will be performed at the
required interval for the duration of the health hazard exposure. Periodic
examinations are generally provided at twelve-month intervals, though under some
exposure protocols, the period between exams may vary. Each periodic
examination shall consist of all of the elements specified under the appropriate
surveillance protocol(s). See Section 12-C. and Table 12-B-1. If an employee is
being monitored under more than one protocol, each form or test need only be
completed once during a particular examination.
(2) Periodic laboratory monitoring may be required under certain protocols (e.g., lead,
pesticides) or special situations. These examinations consist of the specified
laboratory tests only, and are usually performed in accordance with the specific
protocol or as often as deemed necessary by the medical provider.
c. Acute Exposure.
(1) An acute health hazard exposure examination is required, under some protocols,
(e.g., benzene, hazardous waste, noise, solvents), when the applicable short-term
exposure limit (STEL) ceiling limit of the substance(s) in question is exceeded.
The requirement applies whether or not the employee exhibits any overt symptoms
of acute exposure. Specific requirements, if any, for an acute exposure
examination are found under the protocols in Section 12-C.
(2) An acute health hazard exposure examination is recommended if the employee
exhibits any adverse effects following an acute exposure to a suspected hazardous
substance. If the substance(s) is identified, an examination should be performed
following the specific protocol(s) for that substance(s). In the event no specific
substance is identified, an examination should be directed according to the
“Unspecified” examination protocol and presenting symptoms. The Acute
Chemical Exposure Information form (Figure 12-B-1) should be used to collect
and organize information when an acute exposure occurs. The information on this
form must accompany the employee to his/her examination.
(3) All HAZMAT response personnel with a documented exposure event, including
Coast Guard Strike Team members and firefighters, must complete an Acute
Chemical Exposure Information form (Figure 12-B-1) at the end of each
HAZMAT response. Special attention must be provided to the type, duration and
degree of toxicity of the agent(s) encountered as well as the type of contact
(inhalation, skin absorption, ingestion). The type of PPE utilized, type of respirator
(if any), and protective clothing worn should also be noted. This information is to
be entered in the member’s medical record.
d. Exit/Separation (Employment/Exposure). Exit exams are designed to assess pertinent
aspects of the worker’s health when the worker leaves employment or when exposure to a
specific hazard has ceased. Results may be beneficial in assessing the relationship of any
future medical problem to an exposure in the workplace. Exit physical examinations
must be completed within 30 days of the last day of exposure or employment. The
worker may not be re-assigned to a hazardous area once the examination is completed. In
the event the worker is exposed to a hazardous substance, after completing the
examination, ALL laboratory tests required by the specific protocol for that particular
12-11 CH-17
substance must be repeated (see Table 12-B-1 and Section 12-C). The following
conditions also apply:
(1) End of Exposure:
(a) OMSEP enrollees assigned to a non-hazardous work environment but likely
to be assigned to a designated area later in their career.
(b) Workers who transfer from operational to administrative positions on a
frequent basis may, with medical officer approval, receive an update to their
periodic physical vice a complete exit (end of exposure) examination. This
does not preclude a complete exit/separation examination upon the end of
employment.
(c) Individuals enrolled in the OMSEP, with exposures to known carcinogens or
agents with prolonged latency periods for disease development (e.g.,
asbestos, benzene), will receive an end of exposure exam upon reassignment
to non-hazardous area and continue to receive updates to their periodic
physicals according to the designated protocol(s). These individuals will be
monitored for the duration of their Coast Guard career unless the responsible
supervising medical officer or other cognizant medical authority determines
such monitoring is not required.
(2) End of Employment:
(a) OMSEP enrollees permanently separating from Coast Guard employment
should receive an end of employment examination.
(b) The member’s permanent home of record and phone number must be
secured for notification of any abnormalities.
(c) A copy of the member’s occupational health history, including all potential
exposure agents, severity and duration of exposure, and any
recommendations on future protocol testing or examinations, must be placed
in the member’s medical record. A personal copy should also be provided to
the member. (see Section 12-B-3-j).
e. Timing of next examination. The default interval between examinations is one year for
all protocols except respirator wear and prior (not current) exposure to asbestos, in
which case the default interval is five years. However, exams may be recommended as
infrequently as biennially for employees monitored solely under the protocols for
chromium compounds, hazardous waste, solvents, and unspecified exposures. A
medical officer may recommend for any individual patient a shorter interval
between examinations than the default period, if such is medically indicated. Any
recommendation on the timing of the next examination should be included as part of the
physician’s written assessment.
3. Use of OMSEP Forms.
a. CG Form 5447 (6-01) (History and Report of OMSEP Examination).
12-12
CH-17
(1) This form must be completed whenever an OMSEP physical examination is
required, except when only annual hearing conservation program is needed.
Ensure that the examinee and medical officer identifying information are
accurately recorded, including phone numbers.
(2) For an initial examination, all history sections on the CG-5447 must be completed.
For subsequent examinations, as an alternative to completing all the blocks in
history Sections I through IV, the examinee may choose to initial the statement
above each section noting that there have been no changes during the interval from
the last examination.
b. OSHA Respirator Medical Evaluation Questionnaire-(mandatory). This questionnaire is
to be completed by any worker who is to be issued a respirator or assigned to a task that
may require a respirator.
c. CG-5140 (Audiometric Biological Calibration Check). This form is to be used to record
calibration of the audiometric equipment.
d. CG-5552 (Audiology History Questionnaire). This form provides a chronological
record of audiologic symptoms and recreational noise exposure. It should be initiated at
the time of enrollment in the hearing conservation program and OMSEP surveillance for
occupational noise exposure. This form must be updated at each subsequent annual
audiogram and reviewed by the responsible medical officer.
e. DD Form 2215 (Reference Audiogram). This form is used to record initial audiometric
test results.
f. DD Form 2216 (Hearing Conservation Data). This form is used to record the results of
periodic and follow-up audiometry for individuals routinely exposed to hazardous noise.
This form should be preceded by a reference audiogram (DD Form 2215 or other record)
already on file in the individual’s health record.
g. Notification of Summary Results. A sample of this form is provided in Figure12-B-2. A
photocopy or a locally generated form may be used to provide the required notification
to the enrollee of the results of his/her OMSEP examination.
h. Acute Chemical Exposure Information Form. This form is used to record the results of
any unexpected exposures and for verification of notification of the appropriate
agencies. A sample of this form is provided in Figure 12-B-1.
i. Separation Letter. This letter serves as notification of the member’s documented
exposure(s) while serving in the US Coast Guard. It provides the nature and levels of
exposure(s), if known, and the medical provider’s comments and recommendations A
copy is to be placed in the member’s record and another provided directly to the
member. A sample of the separation letter is provided as Figure 12-B-4.
j. Patient Notification. The medical officer is responsible for notifying the patient of any
and all abnormalities found or diagnoses made, whether or not they are occupationally
related or simply an incidental finding. Notification must be made within 30 days of
12-13 CH-17
completion of the examination and should be documented as a medical record entry (see
Figure 12-B-2).
4. Medical Removal Standards
a. The following abnormal laboratory findings during an OMSEP examination mandate
immediate removal of the employee from further workplace exposure to the hazard
listed, pending resolution of the abnormality or a determination that the abnormality is
not due to a workplace exposure. The medical officer should coordinate all medical
removal recommendations with the cognizant SEHO before forwarding to the
commanding officer (CO).
(1) Benzene (any of the following):
(a) The hemoglobin/hematocrit falls below the laboratory’s normal limit and/or
these indices show a persistent downward trend from the individual’s pre-
exposure norms; provided these findings cannot be explained by other
means.
(b) The thrombocyte (platelet) count varies more than 20% below the
employee’s most recent prior values or falls below the laboratory’s normal
limit.
(c) The leukocyte count is below 4,000 per mm3 or there is an abnormal
differential count.
(2) Lead: A blood lead level at or above 40µg/100 ml of whole blood.
(3) Noise: A loss of hearing of > 35 dB in either ear at one or more of the speech
frequencies (500, 1,000, 2000, or 3000 Hz), compared with the current reference
audiogram.
(4) Organophosphate pesticides: cholinesterase level at or below 50% of the pre-
exposure baseline.
b. Pregnancy is not a reason for automatic medical removal from the workplace. A
decision to remove or restrict a pregnant woman must be based on sound clinical
judgment after careful consideration of the workplace environment and the woman’s
physical capabilities. The woman’s pre-natal health care provider (obstetrician) should
be apprised early of any/all potential hazards and safety precautions available.
5. Reporting of Examination Results.
a. Coast Guard medical officers will have 30 days from completion of the examination to
meet all medical officer responsibilities in Section 12-B-4.
b. Contractual providers, IDTs, and other detached HSs/units must forward all OMSEP
examination questions, problems, and any unresolved matters, with accompanying
supporting information, to the assigned CG medical officer for review within 15 days of
receipt (includes the examination and any additional testing or consultations).
c. All records must be forwarded to the record custodian upon compliance with Sections
12-B-6- (a) and 12-B-6 (b) above.
12-14
CH-17
TABLE 12-B-1
REQUIRED FORMS AND TESTS FOR VARIOUS OMSEP EXAMINATIONS AND PROTOCOLS
Exam Type
Exposure
Protocol
Initial/
Baseline Periodic Exit/Separation Acute
Exposure Biological
Monitoring
Asbestos CG 5447
*OSHA
Resp. Quest.
DD-2808/
DD-2807-1
Stool guaiac
(a)*
PFTs
“B” reader
CXR
CBC
Multichem
panel
U/A w/
micro
CG 5447
(update)
Stool guaiac
(a)*
PFTs
“B” reader
CXR(b)*
CBC
Multichem
panel
U/A w/ micro
CG 5447 (update)
Stool guaiac (a)*
PFTs
“B” reader CXR
CBC
Multichem panel
U/A w/ micro
N/A N/A
Benzene CG 5447
DD-2808/
DD-2807-1
CBC w/ diff
Multichem
panel
U/A w/
micro
CG 5447
(update)
CBC w/ diff
Multichem
panel
U/A w/ micro
CG 5447 (update)
CBC w/diff
Multichem panel
U/A w/ micro
CG 5447
(update)
Urinary
phenol
CBC w/ diff
Acute
Exposure
Form
Only under
special
circumstances
. Contact G-
WKS-3.
Chromates CG 5447
DD-2808/
DD-2807-1
CXR
PFTs
CBC
Multichem
panel
U/A w/
micro
CG 5447
(update)
PFTs
CBC
Multichem
panel
U/A w/ micro
CG 5447 (update)
CXR
PFTs
CBC
Multichem panel
U/A w/ micro
N/A N/A
* OSHA Medical Evaluation Respiratory Questionnaire. Note: DD Forms 2493-1/2493-2 Asbestos
Report may be required at medical DOD facilities.
12-15 CH-17
TABLE 12-B-1 (Continued)
Exam Type
Exposure
Protocol
Initial/
Baseline Periodic Exit/Separation Acute
Exposure Biological
Monitoring
Hazardous
Waste CG 5447
DD-2808/
DD2807-1
vision
screening
CXR
PFTs
CBC w/
diff
Multichem
panel
U/A w/
micro
CG 5447
(update)
vision
screening
PFTs
CBC w/ diff
Multichem
panel
U/A w/ micro
CG 5447 (update)
vision screening
CXR
PFTs
CBC w/ diff
Multichem panel
U/A w/ micro
CG 5447
(update)
Acute
Exposure
Form
PFTs
CBC w/
diff
Multichem
panel
U/A w/
micro
Heavy
metal
screen (c)*
Only under
special
circumstan
ces.
Contact G-
WKS-3.
NOTES: *(a) only if patient is age 35+ or otherwise clinically indicated.
*(b) B-reader chest x-rays will be done at periodic examinations according to the following
schedule:
Years since Age of examinee
first exposure 15 to 35 36 to 45 over 45
0 to 10 Every 5 yrs. Every 5 yrs. Every 5 yrs.
Over 10 Every 5 yrs. Every 2 yrs. Annually
*(c) Heavy metal screen includes blood lead, cadmium, mercury, and arsenic levels.
12-16
CH-17
TABLE 12-B-1 (Continued)
Exam Type
Exposure
Protocol
Initial/
Baseline Periodic Exit/Separation Acute
Exposure Biological
Monitoring
Lead CG 5447
DD-2808
DD-2807-1
Blood lead
& ZPP
CBC w/
diff
Multichem
panel
U/A w/
micro
CG 5447
(update)
Blood lead &
ZPP
CBC w/ diff
Multichem
panel
U/A w/ micro
CG 5447 (update)
Blood lead & ZPP
CBC w/ diff
Multichem panel
U/A w/ micro
CG 5447
(update)
Acute
Exposure
Form
Blood lead
& ZPP
CBC w/
diff
Multichem
panel
U/A w/
micro
Blood lead,
ZPP
Noise CG-5552
DD Form
2215 *
CG-5552
(update)
DD Form
2216 *
CG-5552 (update)
DD Form 2216 *
CG-5447
(update)
DD Form
2216 *
N/A
Pesticides CG 5447
DD-2808
Dd-2807-1
Blood
cholin-
esterase,
twice
PFTs
CBC w/
diff
Multichem
panel
U/A w/
micro
CG 5447
(update)
Blood cholin-
esterase (d)*
PFTs
CBC w/ diff
Multichem
panel
U/A w/ micro
CG 5447 (update)
Blood cholin-
esterase (d)*
PFTs
CBC w/ diff
Multichem panel
U/A w/ micro
CG 5447
(update)
Acute
Exposure
Form
Blood
cholin-
esterase
(d)*
PFTs
Blood
cholinester
ase (c)*
Note: DD Forms 2215/2216 remain active and are to be properly recorded and maintained in the member’s
medical record. DOD facilities continue to use these forms or an electronic equivalent.
CG facilities may continue to use these forms; an equivalent locally reproduced form or electronic version
as long as they comply with regulations set forth in Chapter 4 of this Manual.
NOTES: *(d) Blood cholinesterase only required if exposure includes organophosphate and/or carbamate
pesticides.
12-17 CH-17
TABLE 12-B-1 (Continued)
Exam Type
Exposure
Protocol
Initial/
Baseline Periodic Exit/Separation Acute
Exposure Biological
Monitoring
Respiratory
Sensitizers CG 5447
DD-2808
DD-2807-1
PFTs
CBC w/
diff
Multichem
panel
U/A w/
micro
CG 5447
(update)
PFTs
CBC w/ diff
Multichem
panel
U/A w/ micro
CG 5447 (update)
PFTs
CBC w/ diff
Multichem panel
U/A w/ micro
CG 5447
(update)
Acute
Exposure
Form
PFTs
N/A
Solvents CG 5447
DD-2808
DD-2807-1
CBC w/
diff
Multichem
panel
U/A w/
micro
CG 5447
(update)
CBC w/ diff
Multichem
panel
U/A w/ micro
Biological
moni-toring
(if possible)
CG 5447 (update)
CBC w/ diff
Multichem panel
U/A w/ micro
CG 5447
(update)
Acute
Exposure
Form
Specific
blood or
urine tests
for specific
solvents.
Specific
blood or
urine tests
for specific
solvents.
(See
Section 12-
C-11.d.)
Respirator
wear only CG 5447
** OSHA
Resp Quest
**ORQ
(update) N/A N/A N/A
* Respiratory: OSHA Respiratory Questionnaire, this form is provided at the unit level (worksite),
(Reference Section 12-c-9.
12-18
CH-17
TABLE 12-B-1 (Continued)
Exam Type
Exposure
Protocol
Initial/
Baseline Periodic Exit/Separation Acute
Exposure Biological
Monitorin
g
Tuberculosis CG 5447
DD-2808
DD-2807-1
Mantoux
skin test
(e)*
Mantoux skin
test (e)* Mantoux skin test
(e)* Mantoux
skin test
(e)*
N/A
Unspecified CG 5447
DD-2808
DD-2807-1
CBC
Multichem
panel
U/A w/
micro
CG 5447
(update)
CBC
Multichem
panel
U/A w/ micro
CG 5447 (update)
CBC
Multichem panel
U/A w/ micro
CG 5447
(update)
CBC
Multichem
panel
U/A w/
micro
Only
under
special
circumsta
nces.
Contact
G-WKS-
3.
NOTES: *(e) Personnel with a history of reactive tuberculin skin tests should be monitored for
development of symptoms of active TB. A CXR should be done only if the skin test is newly reactive.
12-19 CH-17
FIGURE 12-B-1
ACUTE CHEMICAL EXPOSURE INFORMATION
Last Name, First Name, M.I. Rank/Rate SSN
1. Name(s) of chemical(s): _________________ _________________ _________________
2. CAS number(s), if known: _________________ _________________ _________________
3. Physical form: 0 Solid 0 Liquid
0 Gas/Vapor
0 Aerosol
0 Solid 0 Liquid
0 Gas/Vapor
0 Aerosol
0 Solid 0 Liquid
0 Gas/Vapor
0 Aerosol
4. Chemical form: 0 Acid 0 Alkali
0 Organic solvent
0 Acid 0 Alkali
0 Organic solvent
0 Acid 0 Alkali
0 Organic solvent
5. Modes or routes of
exposure:
0 Inhalation
0 Ingestion 0 Skin
0 Inhalation
0 Ingestion 0 Skin
0 Inhalation
0 Ingestion 0 Skin
6. Exposure date, time &
duration:
Date/time _________________
Duration ___________ minutes
Date/time _________________
Duration ___________ minutes
Date/time _________________
Duration ___________ minutes
7. Brief description of the incident:
8. Observed symptoms:
9. Associated injuries:
10. Personal Protective
Equipment Used:
Notify District/ISC Safety & Environmental Health Officer, cognizant MLC (kse), and G-WKH-3.
11 Further guidance
received:
Contact ATSDR emergency response line at 404-498-0210 to obtain further guidance.
12. ATSDR
guidance: Prescribed tests: Time limits for
specimens Other
Attach Material Safety Data Sheet (MSDS) and shipping manifest to this form, if available.
(Use reverse for continuation or reporting of additional information.)
12-20
CH-17
FIGURE 12-B-2
OMSEP
NOTIFICATION OF SUMMARY RESULTS
Date of Examination: __________________
Patient: _____________________________________________ SS#:__________________
Address: Phone #
Reference. (a) Medical Manual, COMDTINST M6000.1(series).
1) An environmental health evaluation has determined that you may have been exposed to the
following health hazards at your workplace:
_____________________________________________________________________________
___________________________________________________________________________
2) Your physical examination was conducted in accordance to reference (a).
There ARE / ARE NOT abnormalities in your physical examination and laboratory testing.
NOTED ABNORMAL PHYSICAL FINDINGS OR
LABORATORY TESTS RESULT/INTERPRETATION
3) Additional comments on your Occupational Medical Surveillance and Evaluation physical
Name and Title of Health Care Provider: ________________________________________
________________________________________
Signature of Health Care Provider: _________________________________________
Date:__________________
12-21 CH-17
FIGURE 12-B-3
HISTORY AND REPORT OF OMSEP EXAMINATION
1. Last Name, First Name, M.I. 2. Grade/Rate/Rank SSN Date of Examination
6. Work/duty phone
( )
8. Unit Name and Location (city & state)
5. Home Address (apt#, street#, street name, city, state, zip)
7. Home phone
( )
9. Unit OPFAC# 10. Unit Zip Code
11. Date of birth & age 12. Sex (M or F) 13. Race or Ethnicity 14. Occupation or usual duties (describe)
16. Examining facility name & location (○city,
state) 17. Purpose of Examination
O Initial/Baseline O Periodic
O Acute exposure O Exit/Separation 15. How many years have you worked in
this occupation?
I. Occupational History (patient must complete)
_____ Initial here if there have been NO changes to your occupational
history since your last exam and go to section II.
II. Family History (patient must complete)
______Initial here if there have been NO changes in the answers to the
following questions since your last exam and go to section III.
18. Are you exposed to any of the following in your present job,
yes or no? 26. Have any of your blood relatives (mother, father, brother,
sister, grandparents, aunts, uncles, children) had any of the
following illnesses or problems, yes or no?
Y N
Y N Y N
Asbestos (fibers, dust)
Hazardous waste(oil spill) Anemia, blood disease, or bleeding tendency
Benzene (liquid or vapor)
Radiation x-ray, microwave Asthma, hayfever, or allergies
Lead (dust or fumes) Loud noise Birth defects or multiple miscarriages
Liquid chemicals (various) Vibration (jackhammer) Cancer, leukemia, or other malignancy
Chemical vapors or gases Extreme heat Diabetes (high blood sugar)
Dust (sawdust, blasting) Extreme cold Eye trouble or blindness
Metals or metal fumes Mental or emotional stress Epilepsy, fits, or convulsions
Hearing trouble or deafness
Entry into closed spaces
(tanks, voids) Human bodily fluids, or
infectious agents Heart trouble, high blood pressure, or stroke
Kidney trouble (stones or kidney failure)
19. Do you wear any of the following on your present job, yes or
no? Lung trouble (cystic fibrosis, bronchitis, emphysema)
Y N Y N
Some other disease or condition which runs in your family, if so
list:
Earplugs or muffs Safety glasses
Dust mask Welding face-mask
Half-face respirator Rubber gloves
Full-face respirator Protective body suit
Air-line respirator Other, list below:
Y N 20. Have you had any difficulty wearing your protective clothing
or equipment? (If you don’t need to wear any, answer “no.”)
21. Have you had any work-related illness or injury?
22. Have you been limited in your work for health reasons?
23. Have you left or changed jobs due to health reasons?
III. Social History(patient must complete)
_______Initial here is there have been NO changes in the
answers to the following questions since your last exam and go
on to section IV.
24. Have you had a work-related experience, which you believe
may have affected your health or the health of fellow workers? 27. Cigarette smoking history.
Y N
Do you smoke cigarettes now?
If NO: Did you ever smoke cigarettes?
If you smoked before, what year did you stop?
How many years had you smoked?
25. Do you have any hobbies or outside activities, which would
expose you to any of the hazards listed in 18, above? If Yes,
explain:
How many packs per day?
If YES: How many years have you smoked?
How many packs per day?
DEPT. OF TRANSP., USCG, CG-5447 (Rev 6/01) Previous editions are obsolete Page 1
12-22
CH-17
FIGURE 12-B-3 (cont’d)
Section III. Social History (continued)
28. Other smoking history: 29. Alcohol use history:
Y N Y N
Do you smoke cigars or a pipe now? Do you drink any alcoholic beverages (beer, wine, liquor)?
If NO: Did you ever smoke cigars or a pipe? If YES: How many bottles/cans of beer per week?
If you smoked before, what year did you stop? How many glasses of wine per week?
How many years had you smoked? How many ounces of liquor per week?
How many cigars or pouches per week? 30. Do you use any other recreational drugs? If so, list below.
If YES: How many years have you smoked?
How many cigars or pouches per week?
IV. Personal Health History (patient must complete)
_______ Initial here if the answers to the following questions are all “NO” and there have been no changes since your last exam, then go to
item 32.
31. Have you recently had or do you now have any of the following symptoms or complaints, yes or no?
Y N Unexplained weight loss Y N Difficulty sleeping Y N Chest pain or angina Y N Birth defects in your
children
Fever or chills Red or irritated eyes Palpitations or irregular
heart Pain or blood with
urination
Skin rashes or ulcers Visual disturbances or
changes Other heart trouble Muscle pain or weakness
Lumps you can feel Sinus trouble (pain,
discharge) Abdominal pain Joint pain or swelling
Severe or recurrent
headaches Nosebleeds Gastritis or peptic ulcers Limitations of motion
Dizziness or vertigo Sore throat, trouble
swallowing Jaundice or yellowing skin Back pain
Fainting or passing out Pain or swelling in neck Nausea or vomiting Numbness, tingling in
extremities
Seizures or epilepsy Frequent coughing Constipation Anemia (“low blood”)
Trouble concentrating Coughing phlegm or
blood Diarrhea or runny stools Easy bruising or bleeding
Mood changes, irritability Wheezing or asthma Bloody or tarry stools HIV/AIDS
Tiredness or fatigue Shortness of breath Infertility or miscarriages Cancer or leukemia
32. In general, would you say your health is (check one): Excellent 9 Very Good 9 Good 9 Fair 9 Poor 9
33. List any medications you are currently using, or state “none”.
34. List any allergies you know you have, or state ‘none”.
35. Additional space for comments and explanations of your “yes” answers:
All information provided will be handled in accordance with Privacy Act requirements, and will not be otherwise disclosed.
I hereby certify that I have reviewed the foregoing information
supplied by me and that it is true and complete to the best of
my knowledge.
Signature of patient Date
DEPT. OF TRANSP., USCG, CG-5447 (Rev 6/01) Previous editions are obsolete Page 2
12-23 CH-17
FIGURE 12-B-3 (cont’d)
Occupational Exposure History
_____Patient initial here if there have been NO changes in the answers to
the following questions since last exam and proceed to Part 2.
_____Medical Officer/SEHO initial here for verification of
hazardous exposure and monitoring.
INSTRUCTIONS: Please complete the following history beginning with present job or military assignment.
Additional copies of this sheet may be added if necessary
36. List all known hazardous exposures:
Agents(s) (noise-metals-solvents) Date (from - to) Location (work site) Protective equipment used
All information provided will be handled in accordance with Privacy Act requirements, and will not be otherwise disclosed.
I hereby certify that I have reviewed the foregoing information supplied by
me and that it is true and complete to the best of my knowledge. Signature of patient Date
DEPT. OF TRANSP., USCG, CG-5447 (Rev 6/01) Previous editions are obsolete Page 3
12-24
CH-17
FIGURE 12-B-3 (cont’d)
MEDICAL OFFICER’S SECTION
Part 2
1. Last Name, First Name, M.I. (of patient) 2. Grade/Rate/Rank (of patient) 3. SSN (of patient) 4. Date of Examination
5. Examining facility or examiner name and address: 6. Facility phone number
( )
7. Surveillance protocols followed (check all that apply)
9 Asbestos 9 Chromium compounds 9 Lead 9 Pesticides 9 Respiratory sensitizers 9 Unspecified
9 Benzene 9 Hazardous waste 9 Noise 9 Respirator wear 9 Solvents £ Other:____
8. Medical Officer Initial Here: _________ Verify completion of DD-2808 & DD-2807-1. Initial Baseline ________________
9. General prevention counseling provided to patient 9check any that were addressed with patient)
£ Tobacco cessation £ Physical activity £ Weight reduction £ HIV/STD’s avoidance £ Injury prevention
£ Alcohol or drug abuse £ Nutrition (low-fat/salt) £ Stress reduction £ Breast/testicular self exam £ Other:_____
10. List current diagnoses by ICD-9 code number and name: (If no exactly corresponding ICD-9 code is available, use the closest code
to the named diagnosis.)
ICD-9 Diagnosis ICD-9 Diagnosis
11. In your opinion, was the information to you adequate to support any listed diagnoses of occupational disease? 9 YES 9 NO
12. Respirator wear This examinee
9
9
Is medically approved for respirator wear. (Comment on any restrictions or limitations)
Is not
13. CONCLUSIONS: This examinee
9
9
Has medical conditions which limit his/her performance of duties. (Specify any limitations)
Does not have
14. Next OMSEP examination should be in 9 12 mos. 9 Other____________
15. Examinee was informed about the results of this examination____________(date).
Printed or typed name (rank) and degree of examining medical officer Signature of examining medical officer Date
DEPt. OF TRANSP., USCG, CG-5447 (REV 6/01) Previous editions are obsolete Page 4
12-25 CH-17
FIGURE 12-B-4
OMSEP
SEPARATION LETTER
NAME: ____________________________ SSN:___________________
DATE:_______________
You have been enrolled in the Coast Guard’s OCCUPATIONAL MEDICAL SURVEILLANCE
AND EVALUATION PROGRAM (OMSEP). During the past __________years you received
periodic physical examinations based on Occupational Health Safety Organization (OSHA)
protocols for the following known potentially hazardous exposures:
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________
Your occupational (work-related) history also indicates suspected exposure to the following agents:
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
____________________________________________________________
At the time of your EXIT/SEPARATION medical examination you were found to be in good health
with no evidence occupational induced disease. However, it is recommended that you continue to
receive medical examinations on a periodic basis based on age indicated guidelines. In addition, the
periodicity of the examination should be modified to allow for adequate detection and prompt
intervention on disease processes resulting from the latent effects of occupational hazardous
substances. Your medical provider should follow OSHA mandated recommendations, for the
aforementioned hazardous substances, in determining the frequency and level of care you require.
NOTE: if a member is found to have an occupational related disease process at the time of
separation, indicated medical referral measures will be instituted.
Any questions relating to this member’s occupational health history can be obtained by contacting
the US Coast Guard’s Office of Safety and Environmental Health at # 202-267-1883.
Medical officer signature
· This letter should printed on official Coast Guard Letterhead for inclusion in members official
health record.

12-26
CH-17
Section C - Medical Examination Protocols.
1. General.
a. The following protocols follow the same format. Each contains a brief description of the
hazard and its possible effects; the conditions required for an individual to be surveyed
under that protocol; information which must be provided to the examining medical
officer; specific requirements of the history and physical, including laboratory tests and
special procedures; and any additional written requirements on the part of the examining
medical officer. The protocols are summarized in Figures 12-C-1 through 12-C-12.
Copies of these figures may be locally reproduced. The unit OMSEP coordinator should
complete the information in the first eight blocks at the very top, and the appropriate
protocol summary figure(s) should be provided to the examining medical officer with
the examination packet.
b. Multiple protocols for a single individual. In the event that an individual is being
monitored on more than one protocol (e.g., asbestos and noise), the final examination
packet must include each of the required items for each of the protocols. However, each
required form or test need only be completed once.
c. Past exposure. Personnel who have a documented history of workplace exposure to
known carcinogens, but who are not currently exposed, shall be offered an annual
medical examination, according to this protocol until end of employment. Undergoing
this examination is strictly voluntary.
2. Asbestos (Figure 12-C-1).
a. Exposure effects. Asbestos exposure can cause asbestosis, bronchogenic carcinomas,
mesothelioma, and gastric carcinoma. It may also be associated with multiple myeloma
and renal carcinoma. Disease risk is dose dependent. There is a synergistic effect
between asbestos exposure and cigarette smoking, so that the risk of lung cancer is
roughly ten times greater in asbestos-exposed workers who smoke as opposed to
nonsmoking asbestos-exposed workers. The primary route of exposure is inhalation,
though ingestion of fibers may also occur.
b. Required surveillance.
(1) All personnel with current employment exposure to airborne asbestos, who meet
the MSAL criteria in Section 12-C-2- (4) below, shall undergo medical
surveillance. These personnel shall be included in the OMSEP and be examined
according to the protocol in Section 12-C-2.d below. Medical examinations shall
be provided upon enrollment and at least annually thereafter, throughout the
duration of exposure or until end of employment, whichever comes first. Under
current Coast Guard policies for management of asbestos, very few non-shipyard
workers should be currently exposed at or above the PEL or EL.
(2) Construction worker standard. The OSHA standard for asbestos applies to, but is
not limited to, workers who demolish, remove, alter, repair, maintain, install, clean
up, transport, dispose of, or store asbestos containing materials.
(3) The current MSALs are based on the OSHA exposure standard for shipyards [29
CFR 1915.1001].
12-27 CH-17
(a) For other than shipyard and construction workers, medical surveillance is
required for those employees who are or will be exposed at or above the
PEL as an 8 hour time-weighted average, or above the EL averaged over 30
minutes, regardless of the number of days of exposure.
(b) For shipyard and construction workers, medical surveillance is required for
those workers:
1 Who remove any asbestos-containing materials, or who perform repair
and maintenance operations in which asbestos-containing materials are
likely to be disturbed, is such work is performed for a combined total of
30 or more days per year, regardless of fiber levels;
2 Who are exposed at or above the PEL or EL for a combined total of 30
or more days per year; or
3 Who are required to wear positive pressure respirators while performing
asbestos-related work, regardless of the number of days respirators are
worn.
c. Information to medical officer. The following information must be provided to the
examining medical officer, by the OMSEP coordinator, prior to the examination taking
place:
(1) A copy of the OSHA asbestos standards [29 CFR 1915.1001], with appendices D
and E.
(2) A description of the affected employee’s duties as they relate to the employee’s
exposure.
(3) The employee’s representative exposure level or anticipated exposure level.
(4) A description of any personal protective or respiratory equipment used or to be
used.
d. Examination protocol.
(1) Each initial, periodic, and exit examination shall include, as a minimum:
(a) A medical and work history. Emphasis should be placed on the member’s
history of tobacco use (smoking), and associated symptoms of dyspnea on
exertion, recurrent epigastric discomfort, pleuritic chest pains or unexplained
cough.
(b) Completion of the OSHA Respiratory Medical Evaluation Questionnaire
Appendix C to RP Standard 29CFR 1910.134. Note: additional information
on asbestos reporting guidelines may be found at www.osha.gov.
(c) A complete physical examination of all systems, with emphasis on the
respiratory system, the cardiovascular system, and digestive tract.
(d) A stool guaiac test, if the patient is age 35 or over.
12-28
CH-17
(e) PFTs, including FVC and FEV1.
(f) Routine screening labs, including a CBC, multichemistry panel (including
glucose, BUN, creatinine, total protein, total bilirubin, AST, ALT, LDH, and
alkaline phosphatase), and U/A with microscopic.
(g) A postero-anterior (PA) CXR, in accordance with the schedule and
interpretation requirements in Section 12-C-2-d(2) below;
(h) Any other tests or procedures deemed appropriate by the examining
physician, including specialty consultations.
(2) Chest x-ray requirements:
(a) A PA CXR shall be performed at the initial examination and then according
to the following schedule:
Years since Age of examinee
First exposure 15 to 35 36 to 45 over 45
0 to 10 Every 5 yrs. Every 5 yrs. Every 5 yrs.
Over 10 Every 5 yrs. Every 2 yrs. Annually
(b) A PA chest-x-ray shall be performed at the exit examination.
(c) All CXRs shall be interpreted and classified in accordance with a
professionally accepted classification system and recorded following the
format of the CDC/NIOSH (M) 2.8 form. A B-reader or a board
eligible/certified radiologist using the ILO-U/C International Classification
of Radiographs for Pneumoconiosis references shall only do the
interpretation.
(d) Assistance in obtaining the location of the nearest B-reader is available from
MLC (k).
e. Specific written requirements. In addition to the general requirements specified in
Section 12-B-4-b, the examining physician must address the following in writing:
(1) Any detected medical conditions placing the employee at increased risk of health
impairment from further asbestos exposure.
(2) The employee’s ability to use respiratory and other personal protective equipment
(see Section 12-C-9), and any limitations thereof.
(3) Employee notification of the results of the examination and any medical
conditions resulting from asbestos exposure that might require follow-up.
(4) Employee notification of the increased risk of lung cancer attributable to the
synergistic effects of asbestos and smoking.
3. Benzene (Figure 12-C-2).
a. Exposure effects. Benzene exposure can cause central nervous system depression,
leukemia, aplastic anemia, and dermatitis. The primary route of exposure is inhalation
12-29 CH-17
of vapors, though skin absorption may also occur. Within the Coast Guard, most
benzene exposure occurs among marine inspectors and oil spill responders.
b. Required surveillance.
(1) The Coast Guard MSALs are based on the OSHA action level and PEL standards.
Enrollment in the OMSEP is required for all personnel:
(a) who are or may be exposed to benzene at or above the current average
exposure action level 30 or more days per year,
(b) who are or may be exposed to benzene at or above the current short-term
exposure action level 10 or more days per year, or
(c) who served as resident inspectors, pollution investigators, marine safety
officers, port safety officers, vessel inspectors, or marine investigators prior
to 1990. These personnel are considered to have been exposed at/or above
the MSAL unless otherwise documented.
(2) In addition to routine surveillance requirements above, if an employee is exposed
to benzene in an emergency (fire, spill) situation, a urine specimen will be
collected as soon as possible thereafter, but not later than 24 hrs. after the
exposure, and an acute exposure examination will be performed within 72 hrs. of
the exposure. Such an examination must contain a urinary phenol test on the
collected urine specimen.
c. Information to medical officer. The following information must be provided to the
examining physician, by the OMSEP coordinator, prior to the examination taking place:
(1) A description of the affected employee’s duties as they relate to the employee’s
exposure.
(2) The employee’s representative exposure level or anticipated exposure level.
(3) A description of any personal protective or respiratory equipment used or to be
used.
d. Examination protocols.
(1) Each routine (non-acute exposure) initial, periodic, and exit examination shall
include, as a minimum:
(a) A detailed history which includes:
1 past occupational exposure to benzene or any other hematological
toxins, at work or at home;
2 a family history of blood dyscrasias, including hematological
neoplasms;
3 a personal history of blood dyscrasias, including genetic hemoglobin
abnormalities, bleeding abnormalities, abnormal function of formed
blood elements; and of renal or liver dysfunction;

12-30
CH-17
4 history of exposure to ionizing radiation;
5 smoking history, alcohol usage history, and all medicinal drugs
routinely taken;
6 any current history of headache, difficulty concentrating, decreased
attention span, short-term memory loss, mood lability, fatigue, dry skin,
abnormal bleeding, anemia, or weight loss.
(b) a complete physical examination, (Ensure the patient is examined for mental
status changes, dermatitis, and pallor.);
(c) a CBC and differential, with platelet count and RBC indices (MCV, MCH,
MCHC);
(d) a multichemistry panel (includes glucose, BUN, creatinine, total protein,
total bilirubin, AST, ALT, LDH, and alkaline phosphatase) and U/A with
microscopic;
(e) any other tests or procedures deemed appropriate by the examining
physician.
(2) Each acute exposure examination shall include, as a minimum:
(a) a brief summary of the nature of the exposure and investigation of any
symptoms or complaints;
(b) a total urinary phenol level (mg/L) or a urinary phenol adjusted for urinary
creatinine (mg/g creatinine), plus a CBC and differential, with platelet count,
and RBC indices (MCV, MCH, MCHC). Plasma folate and B12 levels to
rule out megaloblastic anemia if the MCV is elevated.
(c) any other test or procedure deemed appropriate by the examining physician
may be performed, if available. Coast Guard medical providers are
encouraged to contact G-WKS for advise and consultation in selecting the
most applicable test or procedure. Alternatively, medical providers may
contact any certified Occupational Health clinic provider, available in the
local community.
(d) If either the total urinary phenol level is below 50 mg phenol/L of urine, or
the urinary phenol adjusted for urinary creatinine is less than 250 mg/g
creatinine, and the CBC is normal, no further testing is required. Otherwise,
contact Commandant (G-WKS-3) for further requirements.
e. Specific written requirements. In addition to the general requirements specified in
Section 12-B-4-b, the following must be addressed in writing by the examining medical
officer:
(1) Any detected medical conditions, which would place the employee’s health at
greater than normal risk of material impairment from exposure to benzene.
12-31 CH-17
(2) The medical officer’s recommended limitations upon the employee’s exposure to
benzene or upon the employee’s use of protective clothing or equipment and
respirators.
(3) A statement that the employee has been informed by the medical officer of the
results of the examination and any medical conditions resulting from benzene
exposure which require further explanation or treatment.
4. Chromium Compounds (Figure 12-C-3).
a. Exposure effects. Hexavalent chromium compounds are known human carcinogens.
They may also cause dermatitis, skin ulceration, occupational asthma, and nasal septum
perforation. The primary routes of exposure are percutaneous absorption and inhalation.
Chromates may be found in certain metal alloys, paints, and masonry cements. Within
the Coast Guard, most chromate exposure is from the use of chromium containing
paints.
b. Required surveillance. The Coast Guard MSALs are based on the ACGIH threshold
limit values (TLVs). Medical surveillance is required for all personnel who are or may
be exposed to chromium IV compounds at or above the current exposure action level 30
or more days per year.
c. Information to medical officer. The following information must be provided by the
OMSEP coordinator to the examining physician prior to the examination taking place:
(1) A description of the affected employee’s duties as they relate to the employee’s
exposure.
(2) The employee’s representative exposure level or anticipated exposure level.
(3) A description of any personal protective or respiratory equipment used or to be
used.
d. Examination protocols. Each routine initial, annual (periodic), and exit examination
must include:
(1) A detailed history, which includes:
(a) Past and current occupational exposures to chromate, asbestos, or any other
pulmonary carcinogens at work or at home;
(b) Smoking history and alcohol usage history;
(c) Any past or current history of dry skin, skin ulcers—usually painless,
nosebleeds, asthma, shortness of breath, wheezing, or cough;
(2) A directed physical examination, with attention to the skin, mucous membranes,
and respiratory tract, both upper and lower (ensure the patient is examined for
erosion of the nasal mucosa and septum, respiratory rhonchi, dermatitis, and
cutaneous ulcers);
(3) A CBC, multichemistry panel (includes glucose, BUN, creatinine, total protein,
total bilirubin, AST, ALT, LDH, and alkaline phosphatase), and a U/A with
microscopic;
12-32
CH-17
(4) PFTs (including FVC & FEV1);
(5) A PA CXR only for an initial/baseline or exit examination, unless there is a
current clinical indication (cough, shortness of breath, wheezing, etc.);
(6) Any other tests or procedures deemed appropriate by the examining physician.
e. Specific written requirements. Other than the general requirements specified in Section
12-B-4-b, the physician should address:
(1) The periodicity of the next routine medical surveillance examination.
Examinations will be provided annually unless the physician recommends a longer
interval.
(2) The employee’s ability to use respiratory and other personal protective equipment
(see Section 12-C-9), and any limitations thereof.
5. Hazardous Waste (Figure 12-C-4).
a. Exposure effects. The OSHA medical surveillance protocol for hazardous waste
operations and emergency response (HAZWOPER)[29 CFR 1910.120] involves medical
surveillance for potential exposure to numerous metals and chemicals, usually in
uncontrolled—spill, fire, disposal—situations. Therefore, there are no specific exposure
effects to describe.
b. Required surveillance.
(1) Routine medical surveillance is required for employees involved in hazardous
waste operations when any of the following conditions are met:
(a) Exposure or potential exposure to hazardous substances or health hazards at
or above the MSAL for that substance (as defined in Section 12-A-4),
without regard to the use of respirators or personal protective equipment, for
30 or more days per year.
(b) All hazardous waste operation employees who wear a respirator for 30 or
more days per year or as required under Section 12-C-9.
(c) All employees who are injured, become ill, or develop signs or symptoms
due to possible overexposure involving hazardous substances or health
hazards from an emergency response or hazardous waste operation.
(d) Members of HAZMAT response teams, including all Coast Guard Strike
Team members and firefighters.
(2) In addition to routine surveillance requirements above, if an employee is exposed
to a hazardous substance above the Coast Guard MSAL in an emergency (fire,
spill) situation, a urine specimen will be collected as soon as possible thereafter,
but not later than 24 hrs after the exposure, and an acute exposure examination
will be performed within 72 hrs of the exposure.
c. Information to medical officer. The examining medical officer shall be provided, by the
OMSEP coordinator, one copy of the OSHA HAZWOPER standard [29 CFR 1910.120]
and its appendices, plus the following specific information:
12-33 CH-17
(1) A description of the employee’s duties as they relate to the employee’s exposures.
(2) The employee’s exposure levels or anticipated exposure levels.
(3) A description of any personal protective equipment used or to be used, including
any respirators.
(4) Information from previous medical examinations of the employee which is not
readily available to the examining physician.
d. Examination protocols.
(1) Each routine (non-acute exposure) initial, periodic, and exit examination shall
include, as a minimum:
(a) A medical and occupational history which includes:
1 past and current occupational exposure to hazardous chemicals, metals,
dusts, fumes, and heat stress;
2 any history of heat illness, allergies, sensitivities, or physical
abnormalities;
3 current medications, and immunization history;
4 smoking history, and alcohol usage history;
5 a complete review of organ systems.
(b) A complete physical examination with attention to the skin, eyes, nose,
throat, and respiratory, cardiovascular, genitourinary, and neurologic
systems;
(c) A CBC and differential, with platelet count, and RBC indices (MCV, MCH,
MCHC);
(d) A multichemistry panel (includes glucose, BUN, creatinine, total protein,
total bilirubin, AST, ALT, LDH, and alkaline phosphatase) and U/A with
microscopic;
(e) PFTs (including FVC & FEV1);
(f) Vision screening;
(g) A PA CXR only for an initial/baseline or exit examination, unless there is a
current clinical indication (cough, shortness of breath, wheezing, etc.);
(h) Any other tests or procedures deemed appropriate by the examining
physician. (Consider a stool guaiac and/or electrocardiogram, if indicated by
age or physical findings).
(2) Each acute exposure examination shall include, as a minimum:
12-34
CH-17
(a) A brief summary of the nature of the exposure and investigation of any
symptoms or complaints;
(b) A CBC and differential, with platelet count, and RBC indices (MCV, MCH,
MCHC), a multichemistry panel (includes glucose, BUN, creatinine, total
protein, total bilirubin, AST, ALT, LDH, and alkaline phosphatase) and a
U/A with microscopic;
(c) PFTs (including FVC & FEV1);
(d) Appropriate biological monitoring tests (e.g., blood metal screen) depending
on the exposure in question. Contact Commandant (G-WKS-3) for further
information and requirements.
e. Specific written requirements. Other than the general requirements specified in Section
12-B-4-b, the physician should address:
(1) Whether the employee has any detected medical conditions which would place the
employee at increased risk of material impairment of the employee’s health from
work in hazardous waste operations or emergency response, or from respirator use.
(2) The employee’s ability to use respiratory and other personal protective equipment
(see Section 12-C-9), and any limitations thereof.
(3) The periodicity of the next routine medical surveillance examination.
Examinations will be provided annually unless the physician recommends a longer
interval.
6. Lead (Figure 12-C-5).
a. Exposure effects. In adults, excessive lead exposure can cause hypertension, anemia,
peripheral neuropathy, encephalopathy, spontaneous abortions in women, and decreased
fertility in men. The primary route of exposure in adults is inhalation of lead containing
dust or fumes. Most exposure in the Coast Guard occurs during removal of previously
applied lead-based paint coatings, or during environmental recovery of previously
discarded lead-acid batteries. Some welders may be exposed to lead fumes.
b. Required surveillance. The Coast Guard MSAL is based on the OSHA PEL standard for
shipyards [29 CFR 1915.1025]. Enrollment in the OMSEP is required for all personnel
who are or may be exposed to lead at or above the current exposure action level for 30 or
more days per year.
c. Information to medical officer. The OMSEP coordinator shall provide the medical
officer with one copy of the OSHA lead standard [29 CFR 1915.1025] and its
appendices, plus the following specific information:
(1) A description of the employee’s duties as they relate to the employee’s exposure.
(2) The employee’s exposure level or anticipated exposure levels to lead and to any
other toxic substance (if applicable).
(3) A description of any personal protective equipment used or to be used, including
any respirators (if known).

12-35 CH-17
(4) Prior blood lead determinations.
(5) Information from previous medical examinations of the employee which is not
readily available to the examining physician. This includes all available prior
written medical opinions concerning the employee.
d. Examination protocols.
(1) Biological monitoring or “blood lead only” examinations must be provided to each
employee exposed at or above the OSHA action level (currently TWA of 30 mg/
m3 air) every six months. Otherwise, only annual examinations must be
performed, unless an employee’s blood lead level is found to be elevated at or
above 40 mg/100 ml of whole blood.
(2) Each routine initial, periodic, exit, and acute exposure examination shall include,
as a minimum:
(a) A detailed work history and a medical history, with particular attention to:
1 past lead exposure (occupational and non-occupational);
2 personal habits (smoking, handwashing after work and before eating);
3 past and current gastrointestinal, hematological, renal, cardiovascular,
reproductive, and neurological problems.
(b) A complete physical examination with particular attention to:
1 occular fundi, teeth, gums, hematological, gastrointestinal, renal,
cardiovascular, and neurological systems;
2 blood pressure (must be recorded);
3 pulmonary status should be evaluated if respiratory protection is to be
used. (See Section 12-C-9).
(c) The following routine laboratory tests:
1 a CBC and differential, with platelet count, and RBC indices (MCV,
MCH, MCHC), plus examination of peripheral smear morphology;
2 blood lead level and zinc protoporphyrin (must be performed by a
laboratory licensed by the CDC for proficiency in blood lead testing);
3 a multi-chemistry panel (includes glucose, BUN, creatinine, total
protein, total bilirubin, AST, ALT, LDH, and alkaline phosphatase);
4 a U/A with microscopic examination; and,
5 PFTs (including FVC & FEV 1).
12-36
CH-17
(d) Any other tests or procedures deemed appropriate by the examining
physician (pregnancy testing, laboratory examination of male fertility).
e. Specific written requirements. In addition to the general requirements specified in
Section 12-B-4-b, the physician should address:
(1) Any detected medical conditions which would place the employee at increased
risk of material impairment of the employee’s health from exposure from lead, or
from respirator use.
(2) The employee’s ability to use respiratory and other personal protective equipment
(see Section 12-C-9), and any limitations thereof.
(3) The results of the blood lead determinations.
7. Noise (Figure 12-C-6).
a. Exposure effects. The primary effect of excessive noise is to cause loss of hearing. This
hearing loss may be described by three “p-words:” painless, progressive, and permanent.
Cumulative overexposures to hazardous noise levels cause millions of people to lose
hearing during their working lives.
b. Required surveillance. The Coast Guard MSAL is based on DOD Instruction 6055.12,
DOD Hearing Conservation Program, as well as OSHA guidance [29 CFR 1910.95].
Enrollment in the OMSEP is required for all personnel who are or may be exposed to
hazardous noise at or above the current exposure action level for 30 or more days per
year. However, personnel who infrequently or incidentally enter designated “hazardous
noise areas” need not participate in the audiometric testing program.
(1) Enrollment is required in accordance with the following criteria:
(a) When the member is exposed to continuous and intermittent noise that has
an 8-hour time-weighted average (TWA) noise level of >85 decibels A-
weighted (dBA), or is exposed to impulse noise sound pressure levels
(SPLs) of 140 decibels (dB) peak, or greater, or
(b) When a threshold shift of > 35 dB is noted in the speech frequencies.
(2) Reference (baseline) audiograms:
(a) All personnel shall receive a reference audiogram prior to any Coast Guard
occupational noise exposure or before they are assigned to duties in
“hazardous noise areas”.
(b) Every effort should be made to schedule the reference audiogram on civilian
workers in order to avoid conflicts with assigned duties; military personnel
shall receive their reference audiogram at initial entry training.
(c) Testing to establish a reference audiogram shall be preceded by at least 14
hours without exposure to workplace noise. Hearing protectors that
attenuate workplace noise below a TWA of 85 dBA, may be used to meet
this requirement, in place of exclusion from the noisy workplace.
12-37 CH-17
(3) Exit audiograms: shall be conducted on all employees, previously enrolled in the
“hearing conservation program”, if it is determined the employee no longer works
in a designated “hazardous noise area,” unless that employee is moving to another
Coast Guard position that also involves work in such areas. However, if the
employee’s audiogram shows hearing losses (compared to the reference
audiogram) of greater than 35 dB in the speech frequencies (500 - 3000 Hz) the
employee must continue to receive annual audiograms until end of employment.
c. Information to medical officer. The OMSEP coordinator must provide the examining
medical officer with a description of the employee’s duties as they relate to the
employee’s exposure, the dB level of the hazardous work area and a description of any
personal protective equipment used or to be used (e.g., earplugs or earmuffs).
d. Examination protocols.
(1) Each routine (non-acute exposure) initial, periodic, and exit examination shall
include completion or updating of an Audiology History Questionnaire (CG 5552)
and audiometric testing (audiogram). All audiometric testing shall:
(a) Be performed by a licensed or certified audiologist, otolaryngologist, or
other physician; or by a technician who is certified by the Council for
Accreditation in Occupational Hearing Conservation or who has completed
CG HS “A” school. A technician who performs audiometric tests shall be
responsible to an audiologist, otolaryngologist, or other physician. Standard
instructions shall be given to individuals before testing.
(b) Be conducted in a testing environment with background octave band SPLs
not greater than 27 dB at 500 Hz, 29 dB at 1000 Hz, 34 dB at 200 Hz, 39 dB
at 4000 Hz, and 41 dB at 8000 Hz. The test environment shall be surveyed
annually to ensure these levels are not exceeded.
(c) Include pure tone, air conduction, and hearing threshold examinations of
each ear at the test frequencies of 500, 1000, 2000, 3000, 4000, and 6000
Hz.
(d) Be performed on audiometers conforming to the most current calibration
specifications of the American National Standards Institute (ANSI).
Audiometers currently in operation must receive annual electroacoustic
calibration to maintain certification.
(e) Occur on audiometers that have received a functional operations check
before each day’s use for specifications in the OSHA Occupational Noise
Exposure standard [29 CFR 1910.95]
(f) Be recorded on DD Form 2215 (Reference Audiogram), or DD Form 2216
(Hearing Conservation Data), or equivalent locally reproduced versions as
appropriate.
(2) Significant Threshold Shift (STS). Transcribe the reference audiogram test results
into the “Reference Audiogram” spaces on the DD Form 2216, Hearing
12-38
CH-17
Conservation Data (or equivalent). The reference levels are subtracted from the
current levels at 2000, 3000, and 4000 Hz. The differences in hearing levels
calculated at 2000, 3000, and 4000 Hz are added together and divided by three, for
each ear. STS exists if the resulting average hearing loss in either ear is greater
than or equal to +10 dB [29 CFR 1910.95]. Additionally, any change of +15 dB at
2000, 3000, or 4000 Hz in either ear shall constitute an STS. Results shall be
recorded on DD Form 2216. Aging (presbycusis) can contribute to the change in
hearing level. When determining whether an STS has occurred, note the
following: The TRACOR microprocessor audiometer automatically corrects for
aging. The National Institute for Occupational Safety and Health (NIOSH) age
corrections shall not be applied when determining STS if a microprocessor
audiometer is used for the test.
(3) A follow-up audiogram shall be conducted when an individual’s audiogram shows
an STS, in either ear, relative to the current reference audiogram. Medical
evaluation is required to validate the existence of a permanent noise-induced
threshold shift and/or to determine if further medical referral is required. An
audiologist, otolaryngologist, or other knowledgeable physician shall perform the
evaluation and determine if the noise-induced STS is/is not work-related or
has/has not been aggravated by occupational noise exposure.
(4) When a negative STS (improvement in hearing threshold from the reference
audiogram) is noted on the periodic audiogram, one 14-hour noise-free follow-up
test is required. That may be administered on the same day as the periodic test.
The results of the follow-up test may be used to create a re-established reference
audiogram.
(5) When a positive STS (decrease in hearing threshold form the reference audiogram)
is noted on the periodic audiogram, two consecutive 14-hour noise-free follow-up
tests must be administered to confirm if the decrease in hearing is permanent. The
follow-up exams may not be performed on the same day as the periodic audiogram
The results of the second follow-up test may be used to reestablish a reference
audiogram, if the required medical evaluation validates the existence of a
permanent noise induced threshold shift (see Section 12-3-d.(3) above). If the
results of the first follow-up test do not indicate an STS, a second follow-up test is
not required.
(6) A new reference audiogram shall replace the original reference audiogram when
the medical evaluation confirms that the STS noted during the annual and follow-
up audiograms is permanent. The original reference audiogram shall be retained
in the patient’s medical record.
(7) Acute exposure examinations (formerly called the Detailed Surveillance Program).
These examinations are designed to observe any dynamic hearing loss, to identify
those who demonstrate unusual noise sensitivity, or to monitor personnel acutely
exposed to unprotected high levels of noise (impulse >140dba).
(a) The initial acute exposure examination shall consist of all elements
described in Sections 12-C-7.d. (1)-(6), above. Additional follow-up
audiograms will be performed at 30 and 90 days, or at more frequent
intervals at the discretion of the medical officer.
12-39 CH-17
(b) If any of the follow-up audiograms demonstrate an average loss of no more
than 10 dB in 2000, 3000, and 4000 Hz in either ear, when compared to the
revised reference audiogram, hearing may be considered stable. The
reference audiogram (per Section 12-C-7-d (5) and (6)) remains the
audiogram against which further testing is compared. The individual is
returned to annual monitoring.
(c) If these reevaluation audiograms exhibit a loss greater than an average
threshold of 10 dB in 2000, 3000, and 4000 Hz in either ear when compared
to the revised reference audiogram, the individual must be referred to an
otolaryngologist for a consultation. Final disposition will depend on the
consultant’s diagnosis and recommendations.
e. Specific written requirements. In addition to the general requirements specified in
Section 12-B-4-b, the medical officer must do the following:
(1) The employee shall be notified in writing within 21 days, when an audiologist or a
physician confirms a threshold shift is permanent. Such determination must be
entered in the employee’s medical record.
(2) Supervisors shall be notified, in writing, that the worker has experienced a
decrease in hearing. Release of medical information must conform to privacy act
requirements.
(3) Document that the patient was counseled concerning the potential seriousness of
repeated unprotected exposures to excessive noise and provided additional
information on hearing protection and avoidance of hazardous noise exposures.
8. Pesticides (Figure 12-C-7).
a. Exposure effects. There are over 1,200 chemical compounds currently classified as
pesticides. However, this surveillance protocol is primarily concerned with only two
classes of pesticides: organophosphate and carbamate insecticides, and
chlorophenoxyacetic acid herbicides. Organophosphates and carbamates are inhibitors
of the enzyme acetylcholinesterase and they cause parasympathetic nervous system
hyperactivity (miosis, urination, diarrhea, defecation, lacrimation, salivation),
neuromuscular paralysis, CNS dysfunction (irritability, anxiety, impaired cognition,
seizures, coma), peripheral neuropathy, and depression of RBC cholinesterase activity.
Chlorophenoxyacetic acid herbicides cause skin, eye, and respiratory tract irritation,
cough, nausea, vomiting, diarrhea, abdominal pain, and peripheral neuropathy. In the
past, some chlorophenoxyacetic herbicides were contaminated with dioxins during
manufacture.
b. Required surveillance. The Coast Guard MSALs for carbaryl, chlorpyrifos, malathion,
parathion, 2,4, -D, and 2,4,5,-T are based on the ACGIH threshold limit values.
Enrollment in the OMSEP is required for all personnel who are or may be exposed to
any identified pesticide at or above the MSAL (as defined in Sect. 12-A-2) for 30 or
more days per year.
c. Information to medical officer. The OMSEP coordinator must provide the examining
medical officer with:
12-40
CH-17
(1) A description of the employee’s duties as they relate to the employee’s exposure.
(2) The employee’s exposure level or potential exposure level to any pesticides.
(3) A description of any personal protective equipment used or to be used, including
any respirators.
d. Examination protocols.
(1) Biological monitoring or “RBC cholinesterase only” examinations must be
provided at least every six months to each employee exposed to organophosphate
or carbamate pesticides at or above the MSAL. If an employee’s RBC
cholinesterase activity is found on any testing to be less than 80% of the pre-
exposure baseline, the frequency of biological monitoring will be increased to at
least every three months during the application season. Non-seasonal, acute
exposures will be monitored at a frequency determined by the supervising medical
officer based on exposure information data.
(2) Each routine (non-acute exposure) initial, periodic, and exit examination shall
include, as a minimum:
(a) A detailed work history and a medical history, with particular attention to:
1 past and current exposure to pesticides or other chemicals (occupational
and non-occupational);
2 smoking and alcohol use history;
3 any symptoms of eye, nose, or throat irritation; cough; nausea,
vomiting, diarrhea, or abdominal pain; irritability, anxiety, difficulty
concentrating, impaired short-term memory, fatigue, or seizures;
numbness, tingling, or weakness in the extremities; and
4 allergic skin conditions or dermatitis.
(b) A complete physical examination, with attention to the skin, respiratory, and
nervous systems, including a mental status examination, should be
performed. Pulmonary status must be evaluated if respiratory protection is
used. (See Section 12-C-9).
(c) The following routine laboratory tests:
1 A CBC, a multichemistry panel (includes glucose, BUN, creatinine,
total protein, total bilirubin, AST, ALT, LDH, and alkaline
phosphatase), and a dipstick U/A;
2 An erythrocyte (RBC) cholinesterase level.
3 Initial examination only—two RBC cholinesterase tests must be
drawn at least 24 hrs. apart. The results of these two tests will be
averaged to provide the pre-exposure baseline for future reference,
unless they differ by more than 15% from each other, in which case,
12-41 CH-17
additional testing must be performed until successive tests do not differ
by more than 15%. The pre-exposure baseline blood tests must be
drawn after a period of at least 60 days without known exposure to
organophosphates.
(d) Any other tests or procedures deemed appropriate by the examining
physician (e.g., cognitive function testing). Pulmonary function testing
should be performed at least once every 4 years if the employee wears a
respirator.
(3) Each acute exposure examination shall include, as a minimum:
(a) A medical and work history with emphasis on any evidence of eye, nose, or
throat irritation; cough; nausea, vomiting, diarrhea, or abdominal pain;
irritability, anxiety, difficulty concentrating, impaired short-term memory,
fatigue, or seizures; numbness, tingling, or weakness in the extremities.
(b) A complete physical examination with attention to any reported symptoms
as well as the skin, respiratory, and nervous systems. A mental status
examination must be performed.
(c) An erythrocyte (RBC) cholinesterase level.
(d) Any other tests or procedures deemed appropriate by the examining
physician (e.g., CBC, CXR, cognitive function testing, urinary
metabolites—if less than 24 hrs. post acute exposure). Pulmonary function
testing should be performed at least every 4 years if the employee wears a
respirator.
e. Specific written requirements. In addition to the general requirements specified in
Section 12-B-4, the physician should address:
(1) Any detected medical conditions, which would place the employee’s health at
increased risk from exposure to identified pesticides or from respiratory wear.
(2) Counseling on the possible increased risk of health impairment from working with
certain pesticides, in the event that the employee was found to have skin disease,
chronic lung disease, or abnormalities of the central or peripheral nervous system
that could directly or indirectly be aggravated by such exposure.
9. Respirator Wear (Figure 12-C-8).
a. Exposure effects. The OSHA medical surveillance protocol for respirator wear is a
means to assess the effectiveness of respiratory protection among exposed workers.
Periodic examinations are required to assess continued fitness for duties and to assess
whether the present respiratory protection program provides adequate protection against
illness. Respirators are often extremely uncomfortable to wear for long periods.
Workers with asthma, claustrophobia, angina, and other conditions may not be able to
wear respirators effectively. The worker should be questioned for a history or symptoms
of past and current exposures to hazardous chemicals; fumes and dusts; smoking and
alcohol use histories; wheezing or abnormal breath sounds; clubbing; and cardiac
arrhythmia.
12-42
CH-17
b. Required surveillance.
(1) Initial Medical Determination. An initial/baseline examination will be performed
at the time of assignment to a job requiring respirator wear. Before an employee
may be issued a respirator or assigned to a task that may require a respirator, that
worker must complete a mandatory OSHA Respirator Medical Evaluation
Questionnaire. This questionnaire will be provided, at the local unit by the
cognizant SEHO, to all workers expected to require the use of a respirator. This
questionnaire serves as the initial medical examination. A health care professional
(nurse, nurse practitioner, physician assistant, and physician) must review this
questionnaire to determine if a follow- up medical examination is required.
Independent duty technicians (IDT’S) are authorized to review the questionnaire
but must refer any positive responses on questionnaire (or any other concerns) to
the supervising medical officer for further review. Any employee who gives a
positive response to any questions among questions 1-8 in section two of the
questionnaire shall be subject to a follow-up medical examination. This
examination will determine whether the worker is physically and mentally capable
of performing the work and using a respirator [29 CFR 1910.134].
(2) Additional Medical Evaluation and Medical Examination.
(a) Additional medical examinations maybe required to assess continued fitness
for duties involving respirator wear. The following conditions will dictate
the need for a follow-up evaluation:
1 The member reports signs and symptoms related to the ability to use a
respirator;
2 The health care provider, supervisor, or respirator program coordinator
informs the command of the need for evaluation;
3 Observations are made during fit testing, respirator use, or program
evaluation that indicate the need for evaluation;
4 When changes in workplace conditions such as physical work effort,
protective clothing or climate conditions result in substantial increase in
physiological burden;
5 A member’s scheduled quintennial physical examination.
(b) Periodic physical examinations will be provided at least once every five
years. The periodic physical examination requires a review and update of
the respirator questionnaire. A health care provider must review the
questionnaire to determine the need for a follow-up examination. A follow-
up medical examination is required for anyone with positive responses to
questions 1-8 in section two of the questionnaire.
c. Information to medical officer. The OMSEP coordinator must provide the examining
medical officer with:
12-43 CH-17
(1) A description of the employee’s duties as they relate to the employee’s respirator
wear.
(2) The employee’s exposures or potential exposures to any hazardous chemicals or
physical agents.
(3) A description of the respirator(s) used or to be used.
d. Examination protocol. Each routine (non-acute exposure) initial and periodic
examination shall include, as a minimum the completion of the mandatory OSHA
Respirator Medical Evaluation Questionnaire.
e. Specific written requirements. In addition to the general requirements specified in
Section 12-B-4, the physician should address:
(1) Any detected medical conditions that would place the employee at increased risk
of material impairment of the employee’s health from respirator use.
(2) Asthmatics with normal or mildly impaired lung function should be evaluated
based on the job requirements, but disapproval should be strongly considered for
asthmatics that require regular medications to maintain airflow, or who have a
history of airway reactivity or sensitization to extrinsic materials (dusts, fumes,
vapors, or cold).
(3) Note: There currently exists no consensus standard by which physicians may
assess a worker’s ability to wear a respirator. As a general rule, however, anyone
with documented respiratory impairment of moderate to severe degree (FEV1 or
FVC <70% of predicted) should not be routinely approved to wear a respirator.
10. Respiratory Sensitizers (Figure 12-C-9).
a. Exposure effects. Respiratory sensitizers include numerous compounds which cause
both occupational asthma and/or hypersensitivity pneumonitis (extrinsic allergic
alveolitis). Respiratory sensitizers include vegetable dusts and woods, molds and spores,
animal danders, metals (platinum, chromium, nickel, cobalt, vanadium), and chemicals
(isocyanates, formaldehyde, trimellitic anhydride).
b. Required surveillance. The Coast Guard MSALs for formaldehyde, toluene
diisocyanate, and vanadium, are based on the ACGIH threshold limit values. Enrollment
in the OMSEP is required for all personnel who are or may be exposed to any identified
respiratory sensitizer at or above the MSAL (as defined in Sect. 12-A-2) for 30 or more
days per year. In the Coast Guard, exposure to respiratory sensitizers is primarily
associated with industrial operations, though some marine inspection activities may also
lead to exposures.
c. Information to medical officer. The OMSEP coordinator must provide the examining
medical officer with:
(1) A description of the employee’s duties as they relate to the employee’s exposure.
(2) The employee’s exposure level or anticipated exposure level to any respiratory
sensitizers.
12-44
CH-17
(3) A description of any personal protective equipment used or to be used, including
any respirators.
d. Examination protocols.
(1) Each routine (non-acute exposure) initial, periodic, and exit examination shall
include, as a minimum:
(a) A detailed work history and a medical history, with particular attention to:
1 past and current exposure to respiratory sensitizers (occupational and
non-occupational);
2 smoking history;
3 any symptoms of eye, nose, or throat irritation;
4 chronic airway problems or hyperactive airway disease; and
5 allergic skin conditions or dermatitis.
(b) In the event that the employee is not required to wear a respirator and the
history and routine laboratory tests are unremarkable, the medical officer
may determine that a complete physical examination is not required.
Otherwise, at a minimum, a system specific physical examination with
attention to the respiratory system must be completed. Pulmonary status
must be evaluated if respiratory protection is used. (See Section 12-C-9).
(c) The following routine laboratory tests:
1 a CBC, a multichemistry panel (includes glucose, BUN, creatinine, total
protein, total bilirubin, AST, ALT, LDH, and alkaline phosphatase), and
a dipstick U/A;
2 PFTs (including FVC & FEV1).
(d) Any other tests or procedures deemed appropriate by the examining
physician (e.g., CXR, bronchial provocation tests).
(2) Each acute exposure examination shall include, as a minimum:
(a) A medical and work history with emphasis on any evidence of upper or
lower respiratory problems, allergic conditions, skin reaction or
hypersensitivity, and any evidence of eye, nose, or throat irritation.
(b) A directed physical examination with attention to the respiratory system.
(c) PFTs (including FVC & FEV1).
(d) Any other tests or procedures deemed appropriate by the examining
physician (e.g., CBC, CXR, bronchial provocation tests).

12-45 CH-17
e. Specific written requirements. In addition to the general requirements specified in
Section 12-B-4-b, the physician should address:
(1) Any detected medical conditions which would place the employee at increased
risk of material impairment of the employee’s health from exposure to identified
respiratory sensitizers, or from respirator use.
(2) The employee’s ability to use respiratory and other personal protective equipment
(see Section 12-C-9), and any limitations thereof.
11. Solvents (Figure 12-C-10).
a. Exposure effects. There are over 30,000 industrial solvents. This protocol is designed
to survey for the most frequent health effects of solvents when considered as an
admittedly broad group. These effects are skin disorders (acute irritant dermatitis,
chronic eczema), acute CNS effects (headache, nausea and vomiting, dizziness, light-
headedness, vertigo, disequilibrium, fatigue, weakness, nervousness, irritability,
depression, confusion, coma), and chronic CNS effects (chronic solvent intoxication,
neurobehavioral abnormalities, cognitive dysfunction). Some other less frequent effects
of solvents involve the hematopoietic, hepatic, peripheral nervous system, renal,
reproductive, and respiratory systems. Most solvents are not carcinogenic to humans;
benzene being a notable exception (see Section 12-C-3, above). In the Coast Guard,
exposure to solvents is primarily associated with industrial and maintenance operations
(e.g., painting).
b. Required surveillance. The Coast Guard MSALs for ethylene glycol, methyl ethyl
ketone, VM & P naphtha, and xylene are based on the ACGIH threshold limit values.
Enrollment in the OMSEP is required for all personnel who are or may be exposed to
any identified hazardous solvent at or above the MSAL (as defined in Section 12-A-2)
for 30 or more days per year. An acute exposure examination is required in the event of
any documented overexposure (above the TLV or STEL) to a solvent or any presumed
overexposure where symptoms are present. In the case of an acute overexposure, an
appropriate urine or blood specimen should be collected as soon as possible after the
overexposure incident.
c. Information to medical officer. The OMSEP coordinator must provide the examining
medical officer with:
(1) A description of the employee’s duties as they relate to the employee’s exposure.
(2) The employee’s exposure level or potential exposure level to any solvents.
(3) A description of any personal protective equipment used or to be used, including
any respirators.
d. Examination protocols.
(1) Each routine (non-acute exposure) initial, periodic, and exit examination shall
include, as a minimum:
(a) A detailed work history and a medical history, with particular attention to:

12-46
CH-17
1 past and current exposure to solvents (occupational and non-
occupational);
2 smoking history and alcohol use history;
3 any symptoms of dry skin, skin irritation, or dermatitis;
4 any CNS symptoms, including headache, nausea and vomiting,
dizziness, light-headedness, vertigo, disequilibrium, fatigue, weakness,
nervousness, irritability, depression, difficulty concentrating, mood
changes, or confusion;
5 a review of symptoms with attention to the hematopoietic, hepatic,
peripheral nervous system, renal, reproductive, and respiratory systems.
(b) A system specific physical examination, with attention to the skin and
nervous systems, including a mental status examination, should be
performed. Pulmonary status must be evaluated if respiratory protection is
used. (See Section 12-C-9).
(c) The following routine laboratory tests:
1 a CBC and differential, with platelet count, and RBC indices (MCV,
MCH, MCHC); and
2 a multichemistry panel (includes glucose, BUN, creatinine, total protein,
total bilirubin, AST, ALT, LDH, and alkaline phosphatase) and a U/A
with microscopic.
(d) Consideration should be given to biological monitoring tests for ongoing
overexposure to certain solvents, if specimens can be obtained in a timely
manner during the exposure period. For non-acute exposures, a timely
manner generally implies that the specimen be obtained at the end of a work
shift or the end of a workweek.
1 For toluene, measure urinary hippuric acid, at the end of a full work
shift.
2 For xylene, measure urinary methyl-hippuric acid, at the end of a full
work shift.
3 For methylethylketone (MEK), measure urinary MEK, at the end of a
full work shift.
4 For trichloroethylene, measure urinary trichloroacetic acid, at the end of
a full workweek.
(e) Any other tests or procedures deemed appropriate by the examining
physician (e.g., cognitive function tests. Note that skin (patch) testing is
generally of little value in solvent-induced dermatitis, since the
12-47 CH-17
pathophysiology is generally not allergic. Pulmonary function testing
should be performed at least once every 4 years if the employee wears a
respirator.
(2) Each acute exposure examination shall include, as a minimum:
(a) A medical and work history with emphasis on any evidence of skin disorders
or acute CNS effects (headache, nausea and vomiting, dizziness, light-
headedness, vertigo, disequilibrium, fatigue, weakness, nervousness,
irritability, depression, confusion, coma).
(b) A system specific physical examination with attention to the skin and
nervous systems.
(c) If at all possible, a biological monitoring test for overexposure to the solvent
in question should be performed, if such a test is available and a specimen
can be obtained in a timely manner. For acute exposures, a timely manner
implies within the first half-life of the chemical within the human body,
generally a matter of a few hours after the overexposure.
(d) Any other tests or procedures deemed appropriate by the examining
physician (e.g., CBC, CXR, and bronchial provocation tests).
e. Specific written requirements. In addition to the general requirements specified in
Section 12-B-4-b, the physician should address:
(1) Any detected medical conditions, which would place the employee at increased
risk of material impairment of the employee’s health from any identified
exposures to solvents, or from respirator use.
(2) The periodicity of the next routine medical surveillance examination.
Examinations will be provided annually unless the physician recommends a longer
interval.
12. Tuberculosis (Figure 12-C-11).
a. Exposure effects. Tuberculous droplet nuclei are coughed, spoken, or sneezed into the
air by an individual with active pulmonary tuberculosis. Exposure to these airborne
droplet nuclei may cause infection with the bacterium that causes tuberculosis.
b. Required surveillance. Employees who are occupationally exposed to active TB cases
will be enrolled in the OMSEP and undergo annual screening for tuberculosis. See
section 7-D-3 of this Manual, Tuberculosis Screening Program, for complete details. In
the Coast Guard, medical personnel and personnel involved in alien migrant interdiction
operations (AMIO) are at potential risk for exposure to active TB cases.
c. Information to medical personnel. In order to assess whether the employee should
remain under active surveillance for TB exposure, the OMSEP coordinator must provide
the examining medical officer with the following information:
(1) A description of the employee’s duties as they relate to the employee’s exposure.
(2) The employee’s exposure level or potential exposure level active TB cases.
12-48
CH-17
(3) A description of any personal protective equipment used or to be used.
d. Examination protocols.
(1) Routine screening for exposed individuals is covered in section 7-D-3.
(a) Personnel with a history of non-reactive tuberculin skin tests will receive
annual skin testing. Routine skin testing does not require an examination by
a medical officer.
(b) Personnel with a history of reactive skin test(s) will be monitored for
development of symptoms of active TB (cough, hemoptysis, fatigue, weight
loss, night sweats) annually. A health services technician or a medical
officer may complete such monitoring. Routine annual CXRs will not be
done.
(2) Evaluation of personnel with newly reactive tuberculin skin tests or suspected
active TB is covered in section 7-D-4. A medical officer shall perform a physical
examination and obtain a complete medical history in such personnel. A CXR
should be done.
e. Specific written requirements. Requirements for recording routine skin test results are
covered in Section 7-D-3-c. In addition, medical personnel should make a written
recommendation as to whether continued annual TB surveillance is required.
13. Unspecified (Figure 12-C-12).
a. Exposure effects. Individuals undergoing surveillance in this category have exposures to
hazards, which are not included in any of the other protocols. Exposure effects will vary
with the nature of the exposure, so there are no specific effects to describe.
b. Required surveillance. Enrollment in the OMSEP is required whenever an employee is
exposed to an identified hazard, at or above the MSAL, for 30 or more days per year.
c. Information to medical officer. The OMSEP coordinator must provide the examining
medical officer with:
(1) A description of the employee’s duties as they relate to the employee’s exposure.
(2) The employee’s exposure level or anticipated exposure level to any hazardous
chemicals or physical agents.
(3) A description of any personal protective equipment used or to be used.
d. Examination protocols. Each routine initial, periodic, and exit examination shall
include, as a minimum:
(1) A medical and work history. Ensure the patient is questioned about past exposure
to chemical and physical hazards, smoking history and alcohol use, a complete
review of systems.
(2) A complete physical examination of all systems, with attention to any organ
systems with a significant history or current symptoms. Pulmonary status must be
evaluated if respiratory protection is used. (See Section 12-C-9).

12-49 CH-17
(3) A CBC, a multichemistry panel (includes glucose, BUN, creatinine, total protein,
total bilirubin, AST, ALT, LDH, and alkaline phosphatase), and a dipstick U/A.
(4) Any other tests or procedures deemed appropriate by the examining physician.
Pulmonary function testing should be performed at least once every 4 years if the
employee wears a respirator.
e. Specific written requirements. In addition to the general requirements specified in
Section 12-B-4-b, the physician should address:
(1) Any detected medical conditions which would place the employee at increased
risk of material impairment of the employee’s health from any identified
exposures to identified hazards, or from respirator use.
(2) The periodicity of the next routine medical surveillance examination.
Examinations will be provided annually unless the physician recommends a longer
interval.
12-50
CH-17
FIGURE 12-C-1
Date: Unit: OPFAC: Unit POC:
Patient name: SSN: Unit Phone:
Exam type: 0 Initial/Baseline 0 Periodic 0 Exit/Separation 0 Other ___
Acute Exposure
Examination Protocol for Exposure to
ASBESTOS
IF EXAM TYPE IS ü DO or COMPLETE THESE ITEMS
Initial/Baseline ____
____ CG-5447 History and Report of OMSEP Examination /
DD-2808/DD-2807-1
____
DD Form 2493-1 or OSHA Respiratory Disease Questionnaire (Part 1)
(optional)
Periodic/Separation
or Acute Exposure
____
____
DD Form 2493-2 or OSHA Respiratory Disease Questionnaire (Part 2)
(optional)
CG 5447 (update)
All types ____ Complete blood count (CBC); multichemistry panel (includes liver
function tests, BUN, creatinine); urinalysis with microscopic (U/A).
All types ____ Pulmonary function tests (FVC & FEV1).
Acute Exposure ____ Acute Exposure Form
All types ____ Chest x-ray (PA) with “B-reader” or board certified radiologist evaluation
at initial exam then per table:
Years since first exposure
Age 15-35 Age 36-45 Age >45
0-10 Every 5 years Every 5 years Every 5 years
Over 10 Every 5 years Every 2 years Every year
All types _____ Physician’s notification regarding examination results. (Final action.)
To the examining medical officer:
You must follow-up any significant abnormality through to a physical diagnosis. Provide ICD codes.
Ensure that the patient is questioned about the following history or symptoms: smoking history, dyspnea on exertion,
cough, pleuritic pain, heartburn or epigastric pain. (See OSHA Respiratory Disease Questionnaire.)
Ensure that the patient is examined for the following possible signs: clubbing, basilar rales.
You must address the following four items in writing: 1) whether the employee has any detected medical conditions
placing him/her at increased risk of health impairment from further asbestos exposure; 2) any recommended limitations
on use of personal protective equipment; 3) that the employee has been informed by you of the results of the examination
and any medical conditions resulting from asbestos exposure that require follow-up; 4) that the employee has been
informed of the increased risk of lung cancer attributable to the synergistic effects of asbestos and smoking.
Asbestos exposure can cause asbestosis, bronchogenic carcinomas, mesothelioma, and gastric carcinoma. It may also
be associated with multiple myeloma and renal carcinoma. Disease risk is dose dependent.
Asbestos was used in shipbuilding until the 1970s. Exposure among OMSEP participants is mostly associated with
repair and overhaul of vessels built prior to that time
If the patient is on multiple monitoring protocols, ensure each unique item is completed. However, it is not necessary
to duplicate tests and forms.
12-51 CH-17
FIGURE 12-C-2
Date: Unit: OPFAC: Unit POC:
Patient name: SSN: Unit Phone:
Exam type: 0 Initial/Baseline 0 Periodic 0 Exit/Separation 0 Acute exposure 0
Other ______________
Examination Protocol for Exposure to
BENZENE
IF EXAM TYPE IS ü DO or COMPLETE THESE ITEMS
Initial/Baseline ____
____ CG-5447 History and Report of OMSEP Examination.
DD-2808/DD-2807-1
All types ____ CBC and differential, with platelet count and RBC indices (MCV,
MCH, MCHC).
Initial/Baseline, Periodic,
or Separation
____
____
Multichemistry panel (includes glucose, BUN, creatinine, total
protein, total bilirubin, AST, ALT, GGT, LDH, and alkaline
phosphatase)
U/A with microscopic
Periodic /Separation/Acute
Exposure ____ CG 5447 (update)
Acute exposure ____
____
Urinary phenol. (Only immediately after acute exposure) Blood or
breath benzene level (optional-if available)
Acute Exposure Form
All types ____ Physician’s notification regarding examination results. (Final
action.)
To the examining medical officer:
¨ You must follow-up any significant abnormality through to a physical diagnosis. Provide ICD codes.
¨ Ensure that the patient is questioned about the following history or symptoms: smoking history, headache,
difficulty concentrating, decreased attention span, short-term memory loss, mood lability, fatigue, dry skin,
abnormal bleeding, anemia, weight loss.
¨ Ensure that the patient is examined for the following signs: mental status changes, dermatitis, pallor.
¨ Benzene exposure causes CNS depression, leukemia, aplastic anemia, and dermatitis.
¨ The employee should be medically removed from the workplace if any of the following are noted on the exam:
* The hemoglobin/hematocrit is below the laboratory’s normal limit and/or these indices show a
persistent downward trend from the individual’s pre-exposure norms; provided these findings
cannot be explained by other means.
* The thrombocyte (platelet) count has dropped more than 20% below the employee’s most recent
prior values or falls below the laboratory’s normal limit.
* The leukocyte count is below 4,000 per mm3 or there is an abnormal differential count.
¨ Benzene is commonly associated with petrochemical manufacturing. Exposure among OMSEP participants is
generally related to marine vessel inspection or disaster response (oil spill, fire). Commercial gasoline is about
3% benzene.
¨ If the patient is on multiple monitoring protocols, ensure each unique item is completed. However, it is not
necessary to duplicate tests and forms.
12-52
CH-17
FIGURE 12-C-3
Date: Unit: OPFAC: Unit POC:
Patient name: SSN: Unit Phone:
Exam type: 0 Initial/Baseline 0 Periodic 0 Exit/Separation 0 Other ______________
Acute Exposure
Examination Protocol for Exposure to
CHROMATES
IF EXAM TYPE IS ü DO or COMPLETE THESE ITEMS
Initial/Baseline ____
____ CG-5447 History and Report of OMSEP Examination/
DD-2808/DD-2807-1
Initial/Baseline or
Separation ____ Chest x-ray (PA)
Periodic/Separation/
Acute Exposure ____
CG 5447 (update)
All types ____ Pulmonary function tests (FVC & FEV1).
All types ____ Complete blood count (CBC)
All types ____ Multichemistry panel (includes glucose, BUN, creatinine, total protein,
total bilirubin, AST, ALT, LDH, and alkaline phosphatase)
All types ____ U/A with microscopic
All types ____ Physician’s notification regarding examination results. (Final action.)
To the examining medical officer:
¨ You must follow-up any significant abnormality through to a physical diagnosis. Provide ICD codes.
¨ Ensure that the patient is questioned about the following history or symptoms: smoking history, shortness of
breath, wheezing, cough, dry skin, skin ulcers.
¨ Ensure that the patient is examined for the following signs: erosion of nasal mucosa and septum, respiratory
rhonchi, dermatitis, cutaneous ulcers.
¨ Make a recommendation as to when the next OMSEP examination for this employee should take place. The
default interval is 1 year, but you may recommend a longer period of 18 or 24 months, if exposures are limited
and there is no evidence of occupationally significant illness.
¨ Chromium exposure causes lung cancer, dermatitis, skin ulcers, and nasal septum perforation.
¨ Chromic acid may cause acute burns or irritation to skin, eyes, and upper respiratory tract. Inhalation may cause
acute epiglottitis, laryngospasm, pneumonitis, and pulmonary edema.
¨ Some chromium compounds cause occupational asthma.
¨ Chromium compounds are commonly associated with steel and chemical manufacturing. Exposure among
OMSEP participants is generally related to working with chromium containing paints.
¨ If the patient is on multiple monitoring protocols, ensure each unique item is completed. However, it is not
necessary to duplicate tests and forms.
12-53 CH-17
FIGURE 12-C-4
Date: Unit: OPFAC: Unit POC:
Patient name: SSN: Unit Phone:
Exam type: 0 Initial/Baseline 0 Periodic 0 Exit/Separation 0 Acute exposure 0
Other ______________
Examination Protocol for Exposure to
Hazardous Waste
IF EXAM TYPE IS ü DO or COMPLETE THESE ITEMS
Initial/Baseline ____
____ CG-5447 History and Report of OMSEP Examination
DD-2808/DD-2807-1
Initial/Baseline or
Separation ____ Chest x-ray (PA)
Periodic/Separation /Acute
Exposure ____ CG 5447 (update)
All types except acute
exposure ____ Vision screening (distant and near)
All types ____ Pulmonary function tests (FVC & FEV1).
All types ____ CBC and differential, with platelet count and RBC indices (MCV,
MCH, MCHC).
All types ____ Multichemistry panel (includes glucose, BUN, creatinine, total
protein, total bilirubin, AST, ALT, LDH, and alkaline phosphatase)
All types ____ U/A with microscopic
Acute exposure ____ Blood lead and/or heavy metal screen, if indicated.
All types ____ Physician’s notification regarding examination results. (Final
action.)
To the examining medical officer:
¨ You must follow-up any significant abnormality through to a physical diagnosis. Provide ICD codes.
¨ Ensure that the patient is questioned about the following history or symptoms: smoking history, weight loss,
headache, visual disturbances, difficulty concentrating, decreased attention span, short-term memory loss,
confusion, mood lability, fatigue, ataxia, peripheral numbness or paresthesias, weakness, shortness of breath,
anemia.
¨ Ensure that the patient is examined for the following signs: gingivitis, sialorrhea, tremor, mental status changes,
decreased deep tendon reflexes, decreased vibratory sensation, respiratory rhonchi and hyperresonance,
dermatitis, edema.
¨ Make a recommendation as to when the next OMSEP examination for this employee should take place. The
default interval is 1 year, but you may recommend a longer period of 18 or 24 months, if exposures are limited
and there is no evidence of occupationally significant illness.
¨ The hazardous waste protocol involves medical surveillance for effects of exposure to a variety of heavy metals
and chemical compounds. Neurotoxicity, pulmonary disease, dermatitis, and cancer are possible effects of
excessive exposures to hazardous wastes.
¨ OMSEP participants monitored under this protocol are primarily members of HAZMAT and spill response
teams, firefighters, and marine safety inspectors. Individual, specific exposure histories are often ill defined. If
the patient is on multiple monitoring protocols, ensure each unique item is completed. However, it is not
necessary to duplicate tests and forms.
12-54
CH-17
FIGURE 12-C-5
Date: Unit: OPFAC: Unit POC:
Patient name: SSN: Unit Phone:
Exam type: 0 Initial/Baseline 0 Periodic 0 Exit/Separation 0 Acute exposure 0
Other ______________
Examination Protocol for Exposure to
Lead
IF EXAM TYPE IS ü DO or COMPLETE THESE ITEMS
Initial/Baseline ____
____ CG-5447 History and Report of OMSEP Examination
DD-2808/DD-2807-1
All types ____ Blood lead and zinc protoporphyrin (ZPP)
All types ____ CBC and differential, with platelet count and RBC indices
(MCV, MCH, MCHC), plus examination of peripheral
smear morphology.
Periodic/Separation/Acute
Exposure ____ CG 5447 (update)
All types ____ Multichemistry panel (includes glucose, BUN, creatinine,
total protein, total bilirubin, AST, ALT, LDH, alkaline
phosphatase, and uric acid)
Acute Exposure ____ Acute Exposure Form
All types ____ U/A with microscopic
All types ____ Physician’s notification regarding examination results.
(Final action.)
To the examining medical officer:
¨ You must follow-up any significant abnormality through to a physical diagnosis. Provide ICD codes.
¨ Ensure that the patient is questioned about the following history or symptoms: past lead exposure, smoking
history, abdominal pain and cramping, joint and extremity pain, difficulty concentrating, irritability, short-term
memory loss, confusion, mood lability, fatigue, ataxia, peripheral numbness or paresthesias, weakness, anemia,
and infertility.
¨ Ensure that the patient is examined for the following signs: hypertension, papilledema, gum “lead lines”, pallor,
mental status changes, decreased deep tendon reflexes, decreased vibratory sensation, extensor motor weakness.
¨ Lead exposure can cause fatigue, anemia, arthralgias and myalgias, peripheral motor neuropathy,
neurobehavioral disturbances and encephalopathy, acute abdominal pain, gout and gouty nephropathy, acute
and chronic renal failure, spontaneous abortions, and male infertility.
¨ If the blood lead level is greater than 40 µg/100 g of whole blood, the employee must be medically removed
from any workplace exposure.
¨ If the patient is on multiple monitoring protocols, ensure each unique item is completed. However, it is not
necessary to duplicate tests and forms.
12-55 CH-17
FIGURE 12-C-6
Date: Unit: OPFAC: Unit POC:
Patient name: SSN: Unit Phone:
Exam type: 0 Initial/Baseline 0 Periodic 0 Exit/Separation 0 Acute exposure 0
Other ______________
Examination Protocol for Exposure to
Noise
IF EXAM TYPE IS ü DO or COMPLETE THESE ITEMS
Initial/Baseline
____
____
____
____
CG-5447 History and Report of OMSEP Examination
DD-2808/DD-2807-1
CG-5552 Audiology History Questionnaire
DD Form 2215 (optional) or equivalent locally reproduced version.
Periodic, Separation, or
Acute Exposure ____ DD Form 2216 (optional) or equivalent locally reproduced version.
All types ____ Physician’s notification regarding examination results. (Final action.)
To the examining medical officer:
¨ You must follow-up any significant abnormality through to a physical diagnosis. Provide ICD codes.
¨ Review and initial the CG-5552 Audiology History Questionnaire and the audiogram results.
¨ A significant threshold shift (STS) exists if the average change in hearing from the reference audiogram at,
2000, 3000, and 4000 Hz is greater than or equal to +10 dB in either ear.
¨ Additionally, any change of +15 dB at 1000, 2000, 3000, or 4000 Hz in either ear constitutes an STS.
¨ Do not apply the National Institute for Occupational Safety and Health (NIOSH) age corrections when
determining STS.
¨ Follow-up audiograms must be conducted when an individual’s audiogram shows an STS relative to the current
reference audiogram in either ear. When a positive STS (decrease in hearing threshold) is noted, two 14-hour
noise-free follow-up tests must be administered to confirm that the decrease in hearing is permanent. When a
negative STS (improvement in hearing) is noted, one 14-hour noise-free follow-up tests must be administered.
¨ Medical evaluation is required to validate the existence of a permanent noise-induced threshold shift and/or to
determine if further medical referral is required. That evaluation must be performed by an audiologist, and
otolaryngologist, or other knowledgeable physician.
¨ If, compared with the current reference audiogram, a loss of hearing of > 35 dB in either ear at one or more of
the speech frequencies (500, 1,000, 2000, or 3000 Hz) is noted , the employee must be medically removed from
further workplace exposure.
¨ If the patient is on multiple monitoring protocols, ensure each unique item is completed. However, it is not
necessary to duplicate tests and forms.
12-56
CH-17
FIGURE 12-C-7
Date: Unit: OPFAC: Unit POC:
Patient name: SSN: Unit Phone:
Exam type: 0 Initial/Baseline 0 Periodic 0 Exit/Separation 0 Acute exposure 0
Other ______________
Examination Protocol for Exposure to
Pesticides
IF EXAM TYPE IS ü DO or COMPLETE THESE ITEMS
Initial/baseline
____
____
____
CG-5447 History and Report of OMSEP Examination
DD-2808/DD-2807-1
Blood cholinesterase level, two specimens at least 24 hrs. apart
Periodic/ Separation or
Acute Exposure ____
____
Blood cholinesterase level, if current exposure involves organophosphate
or carbamate pesticides
CG 5447 (update)
All types ____ Pulmonary function tests (FVC & FEV1).
All types except acute
exposure ____ CBC and differential, with platelet count and RBC indices (MCV, MCH,
MCHC)
All types except acute
exposure ____ Multichemistry panel (includes glucose, BUN, creatinine, total protein,
total bilirubin, AST, ALT, LDH, alkaline phosphatase)
All types except acute
exposure ____ U/A with microscopic
Acute Exposure ____ Acute Exposure Form
All types ____ Physician’s notification regarding examination results. (Final action.)
To the examining medical officer:
¨ You must follow-up any significant abnormality through to a physical diagnosis. Provide ICD codes.
¨ Ensure that the patient is questioned about the following history or symptoms: past and current exposures to
pesticides, smoking and alcohol use history; eye, nose or throat irritation; cough; nausea, vomiting, diarrhea or
abdominal pain; irritability, anxiety, difficulty concentrating, impaired short-term memory, fatigue, or seizures;
numbness, tingling, or weakness in the extremities; allergic skin conditions or dermatitis.
¨ Ensure the patient is examined for the following possible signs: dermatitis, meiosis, rhinitis, mental status
changes. Pulmonary system must be examined if respiratory protection is used.
¨ If the cholinesterase level is at or below 50% of the pre-exposure baseline, the employee must be medically
removed from any further workplace exposure.
¨ Organophosphates and carbamates are inhibitors of the enzyme acetylcholinesterase. They cause
parasympathetic nervous system hyperactivity, neuromuscular paralysis, CNS dysfunction, peripheral
neuropathy, and depression of RBC cholinesterase activity. Chlorophenoxyacetic acid herbicides cause skin,
eye, and respiratory tract irritation, cough, nausea, vomiting, diarrhea, abdominal pain, and peripheral
neuropathy.
¨ If the patient is on multiple monitoring protocols, ensure each unique item is completed. However, it is not
necessary to duplicate tests and forms.
12-57 CH-17
FIGURE 12-C-8
Date: Unit: OPFAC: Unit POC:
Patient name: SSN: Unit Phone:
Exam type: 0 Initial/Baseline 0 Periodic 0 Exit/Separation 0 Other
______________
Examination Protocol for Exposure to
Respirator Wear
IF EXAM TYPE IS ü DO or COMPLETE THESE ITEMS
Initial/Baseline ____ OSHA Respiratory Medical Evaluation Questionnaire
Periodic/Exit/Separation ____ OSHA Respiratory Medical Evaluation Questionnaire (update).
All types ____ Physician’s notification regarding examination results. (Final
action.)
To the examining medical officer:
¨ You must follow-up any significant abnormality through to a physical diagnosis. Provide ICD codes.
¨ This protocol applies to all employees required to wear a respirator in the course of their work.
¨ Ensure that the patient is questioned about the following history or symptoms: past and current exposures to
hazardous chemicals, fumes, and dusts; smoking and alcohol use history; any history of claustrophobia, asthma,
angina, syncope, and other respiratory or cardiovascular disease.
¨ Ensure the patient is examined for the following possible signs: wheezing or other abnormal breath sounds,
clubbing, and cardiac arrhythmias.
¨ You must address whether the employee as any detected medical conditions which would place him or her at
increased risk of material health impairment from the required respirator use. Consider whether the employee’s
health will allow him or her to tolerate respirator wear.
* Note: There currently exists no consensus standard by which physicians may assess a worker’s
ability to wear a respirator. As a general rule, however, anyone with documented respiratory
impairment of moderate to severe degree (FEV1 or FVC <70% of predicted) should not be
routinely approved to wear a respirator. Asthmatics with normal or mildly impaired lung function
should be evaluated based on the job requirements, but disapproval should be strongly considered
for asthmatics that require regular medications to maintain airflow, or who have a history of
airway reactivity or sensitization to extrinsic materials (dusts, fumes, vapors, or cold).
¨ If the patient is on multiple monitoring protocols, ensure each unique item is completed. However, it is not
necessary to duplicate tests and forms.
12-58
CH-17
FIGURE 12-C-9
Date: Unit: OPFAC: Unit POC:
Patient name: SSN: Unit Phone:
Exam type: 0 Initial/Baseline 0 Periodic 0 Exit/Separation 0 Acute exposure 0
Other ______________
Examination Protocol for Exposure to
Respiratory Sensitizers
IF EXAM TYPE IS ü DO or COMPLETE THESE ITEMS
Initial/Baseline ____
____ CG-5447 History and Report of OMSEP Examination
DD-2808/DD-2807-1
Periodic/Exit/Acute
Exposure ____ CG 5447 (update)
All types ____ Pulmonary function tests (FVC & FEV1).
All types except acute
exposure ____ CBC (complete blood count)
All types except acute
exposure ____ Multichemistry panel (includes glucose, BUN, creatinine, total
protein, total bilirubin, AST, ALT, LDH, alkaline phosphatase)
All types except acute
exposure ____ U/A (dipstick sufficient)
Acute Exposure ____ Acute Exposure Form
All types ____ Physician’s notification regarding examination results. (Final
action.)
To the examining medical officer:
¨ You must follow-up any significant abnormality through to a physical diagnosis. Provide ICD codes.
¨ Ensure that the patient is questioned about the following history or symptoms: past and current exposures to
respiratory sensitizers, smoking history; eye, nose or throat irritation; cough; asthma or other chronic airway
problems; allergic skin conditions or dermatitis.
¨ In the event that the employee is not required to wear a respirator, and the history and routine laboratory tests
are unremarkable, the medical officer may determine that a complete physical examination is not required.
Otherwise, at a minimum, a directed physical examination with attention to the respiratory system must be
completed. Pulmonary status must be evaluated if respiratory protection is used.
¨ Respiratory sensitizers include numerous compounds which cause both occupational asthma and/or
hypersensitivity pneumonitis (extrinsic allergic alveolitis). Respiratory sensitizers include vegetable dusts and
woods, molds and spores, animal danders, metals (platinum, chromium, nickel, cobalt, vanadium), and
chemicals (isocyanates, formaldehyde, trimellitic anhydride).
¨ In the Coast Guard, exposure to respiratory sensitizers is primarily associated with industrial operations, though
some marine inspection activities may also lead to exposures.
¨ If the patient is on multiple monitoring protocols, ensure each unique item is completed. However, it is not
necessary to duplicate tests and forms.
12-59 CH-17
FIGURE 12-C-10
Date: Unit: OPFAC: Unit POC:
Patient name: SSN: Unit Phone:
Exam type: 0 Initial/Baseline 0 Periodic 0 Exit/Separation 0 Acute exposure 0
Other ______________
Examination Protocol for Exposure to
Solvents
IF EXAM TYPE IS ü DO or COMPLETE THESE ITEMS
Initial/Baseline ____
____ CG-5447 History and Report of OMSEP Examination
DD-2808/DD-2807-1
All types ____ Pulmonary function tests (FVC & FEV1).
All types except acute
exposure ____ CBC and differential, with platelet count and RBC indices (MCV,
MCH, MCHC)
Periodic/Exit/Acute
Exposure ____ CG 5447 (update)
All types except acute
exposure ____ Multichemistry panel (includes glucose, BUN, creatinine, total
protein, total bilirubin, AST, ALT, LDH, alkaline phosphatase)
All types except acute
exposure ____ U/A with microscopic
Acute exposure ____ Acute Exposure Form
All types ____ Physician’s notification regarding examination results. (Final
action.)
To the examining medical officer:
¨ You must follow-up any significant abnormality through to a physical diagnosis. Provide ICD codes.
¨ Ensure that the patient is questioned about the following history or symptoms: past and current exposures to
solvents, smoking and alcohol use history; allergic skin conditions, dry skin, or dermatitis ; eye, nose or throat
irritation; headache, nausea, vomiting, dizziness, vertigo; fatigue, weakness, irritability, depression, difficulty
concentrating, or impaired short-term memory; and numbness, tingling, or weakness in the extremities.
¨ Ensure the patient is examined for the following possible signs: dermatitis, peripheral neuropathy, cognitive
dysfunction, and mental status changes.
¨ If the particular solvent exposure is well characterized and specific laboratory tests are available, biological
monitoring should be considered.
¨ Make a recommendation as to when the next OMSEP examination for this employee should take place. The
default interval is 1 year, but you may recommend a longer period of 18 or 24 months, if exposures are limited
and there is no evidence of occupationally significant illness.
¨ There are over 30,000 industrial solvents. This protocol is designed to survey for the most frequent health
effects of solvents when taken as a broad group. These effects are skin disorders, and acute and chronic CNS
effects. Some other less frequent effects of solvents involve the hematopoietic, hepatic, peripheral nervous
system, renal, reproductive, and respiratory systems. Most solvents are not carcinogenic in humans; benzene
being a notable exception.
¨ In the Coast Guard, exposure to solvents is primarily associated with industrial and maintenance operations
(e.g., painting).
¨ If the patient is on multiple monitoring protocols, ensure each unique item is completed. However, it is not
necessary to duplicate tests and forms.
12-60
CH-17
FIGURE 12-C-11
Date: Unit: OPFAC: Unit POC:
Patient name: SSN: Unit Phone:
Exam type: 0 Initial/Baseline 0 Periodic 0 Exit/Separation 0 Acute exposure 0
Other ______________
Examination Protocol for Exposure to
Tuberculosis
IF EXAM TYPE IS ü DO or COMPLETE THESE ITEMS
Initial/Baseline ____
____ CG-5447 History and report of OMSEP Examination
DD-2808/DD-2807-1
All types, no history of
prior reactive skin test ____ Mantoux tuberculin skin test (TST)
Enter results on SF 601 and PHS 731
All types, history of prior
reactive skin test ____ SF 600 entry
Follow-up on newly
reactive TST ____
____
CG-5447 (update)
CXR (only if TST is newly reactive)
All types ____ Physician’s notification regarding examination results. (Final
action.)
To the examining medical officer:
¨ You must follow-up any significant abnormality through to a physical diagnosis. Provide ICD codes.
¨ For personnel with a prior history of a reactive TST, ensure the patient is questioned about the following
symptoms of active TB: fever, night sweats, weight loss, cough, and hemoptysis. This questioning may be
completed by a nurse or health services technician.
¨ See section 7-D of the Medical Manual for full information on the tuberculosis control program.
¨ Forward a copy of all test results to the unit OMSEP coordinator.
¨ If the patient is on multiple monitoring protocols, ensure each unique item is completed. However, it is not
necessary to duplicate tests and forms.
12-61 CH-17
FIGURE 12-C-12
Date: Unit: OPFAC: Unit POC:
Patient name: SSN: Unit Phone:
Exam type: 0 Initial/Baseline 0 Periodic 0 Exit/Separation 0 Acute exposure 0
Other ______________
Examination Protocol for Exposure to
Unspecified
IF EXAM TYPE IS ü DO or COMPLETE THESE ITEMS
Initial/Baseline ____
____ CG-5447 History and Report of OMSEP Examination
DD-2808/DD-2807-1
All types ____ CBC (complete blood count)
All types ____ Multichemistry panel (includes glucose, BUN, creatinine, total
protein, total bilirubin, AST, ALT, LDH, alkaline phosphatase)
Periodic/Exit/Acute
Exposure ____ CG 5447 (update)
All types ____ U/A (dipstick)
Acute exposure ____ Acute Exposure Form
All types ____ Physician’s notification regarding examination results. (Final
action.)
To the examining medical officer:
¨ You must follow-up any significant abnormality through to a physical diagnosis. Provide ICD codes.
¨ Ensure that the patient is questioned about his or her general medical and work history, including: past and
current exposure to chemical and physical hazards, smoking history and alcohol use, and a complete review of
systems.
¨ Ensure the patient is receives a complete physical examination of all systems, with attention to any organ
systems with a significant history or current systems.
¨ Make a recommendation as to when the next OMSEP examination for this employee should take place. The
default interval is 1 year, but you may recommend a longer period of 18 or 24 months, if exposures are limited
and there is no evidence of occupationally significant illness.
¨ Individuals under going surveillance in this protocol have exposures to hazards which are not included in any of
the other protocols.
¨ If the patient is on multiple monitoring protocols, ensure each unique item is completed. However, it is not
necessary to duplicate tests and forms.
13-i CH 13
CHAPTER 13
QUALITY ASSURANCE
SECTION A - QUALITY ASSURANCE PLAN. 1
PURPOSE...................................................................................................................................................................1
BACKGROUND. .........................................................................................................................................................1
APPLICABILITY AND SCOPE.......................................................................................................................................1
QAP OBJECTIVES. ....................................................................................................................................................2
DEFINITIONS. ............................................................................................................................................................2
ORGANIZATIONAL RESPONSIBILITIES ........................................................................................................................3
CONFIDENTIALITY STATEMENT.................................................................................................................................6
QAP REVIEW AND EVALUATION.. ............................................................................................................................6
SECTION B - CREDENTIALS MAINTENANCE AND REVIEW 9
BACKGROUND.. ........................................................................................................................................................8
DEFINITIONS. ............................................................................................................................................................8
PRE-SELECTION CREDENTIALS REVIEW. ...................................................................................................................9
PRACTITIONER CREDENTIALS FILE (PCF).................................................................................................................9
DOCUMENTATION...................................................................................................................................................10
VERIFICATION.........................................................................................................................................................11
CONTRACT PROVIDER CREDENTIALS REVIEW. .......................................................................................................12
REVERIFICATION.....................................................................................................................................................12
NATIONAL PRACTITIONER DATA BANK. .................................................................................................................12
SECTION C - CLINICAL PRIVILEGES 14
PURPOSE.................................................................................................................................................................14
BACKGROUND. .......................................................................................................................................................14
DEFINITIONS. ..........................................................................................................................................................14
APPLICABILITY AND SCOPE.....................................................................................................................................15
CLINICAL PRIVILEGES. ............................................................................................................................................15
SECTION D - QUALITY ASSURANCE CHECKLISTS. Error! Bookmark not defined.
BACKGROUND. .......................................................................................................................................................26
USAGE. ...................................................................................................................................................................26
AMENDMENTS. .......................................................................................................................................................26
SECTION E - QUALITY ASSURANCE IMPLEMENTATION GUIDE (QAIG) 27
BACKGROUND.. ......................................................................................................................................................27
RESPONSIBILITIES. ..................................................................................................................................................27
SECTION F - QUALITY ASSURANCE SITE SURVEY Error! Bookmark not defined.
PROCEDURES.. ........................................................................................................................................................28
SURVEY FORMAT....................................................................................................................................................28
SURVEY REPORT.....................................................................................................................................................28
CUSTOMER ASSISTANCE VISITS..............................................................................................................................29
SECTION G - COAST GUARD CLINIC CERTIFICATION AND ACCREDITATION 30
CH-13 13-ii
CLINIC CERTIFICATION PROGRAM...........................................................................................................................30
CLINIC ACCREDITATION PROGRAM.........................................................................................................................31
LABORATORY CERTIFICATION.. ..............................................................................................................................31
SECTION H - MONITORING AND EVALUATION PROGRAM. 32
BACKGROUND. .......................................................................................................................................................32
RESPONSIBILITIES. ..................................................................................................................................................32
IMPLEMENTATION...................................................................................................................................................32
USING THE MONITORING AND EVALUATION SCHEDULE AND CLINICAL ASPECTS OF CARE LISTING. ......................32
MONITORING AND EVALUATION REPORT FORMS....................................................................................................33
SECTION I - PEER REVIEW PROGRAM. 67
SECTION J - UTILIZATION REVIEW PROGRAM. 68
SECTION K - INFECTION CONTROL PROGRAM (EXPOSURE CONTROL PLAN) 69
BACKGROUND. .......................................................................................................................................................69
POLICY. ..................................................................................................................................................................69
UNIVERSAL PRECAUTIONS......................................................................................................................................70
PRECAUTIONS FOR INVASIVE PROCEDURES.. ..........................................................................................................71
PRECAUTIONS FOR MEDICAL LABORATORIES. ........................................................................................................72
HANDLING BIOPSY SPECIMENS...............................................................................................................................73
USING AND CARING FOR SHARP INSTRUMENTS AND NEEDLES................................................................................73
INFECTION CONTROL PROCEDURES FOR MINOR SURGERY AREAS AND DENTAL OPERATORIES. ............................73
STERILIZING AND DISINFECTING. ............................................................................................................................76
LAUNDRY.. .............................................................................................................................................................81
CLEANING AND DECONTAMINATING BLOOD OR OTHER BODY FLUID SPILLS..........................................................81
INFECTIOUS WASTE. ...............................................................................................................................................81
MANAGING EXPOSURES (NEEDLE STICK PROTOCOL) .............................................................................................82
TRAINING PERSONNEL FOR OCCUPATIONAL EXPOSURE. ........................................................................................85
SECTION L - RISK MANAGEMENT PROGRAM 88
PURPOSE.................................................................................................................................................................88
BACKGROUND. .......................................................................................................................................................88
DEFINITIONS. ..........................................................................................................................................................88
INFORMED CONSENT. .............................................................................................................................................88
OCCURRENCE MONITORING AND REPORTING.........................................................................................................91
MEDICAL INCIDENT MONITORING AND REPORTING................................................................................................91
SECTION M - TRAINING AND EDUCATION 93
DEFINITIONS. ..........................................................................................................................................................93
UNIT HEALTH SERVICES TRAINING PLAN (IN-SERVICE TRAINING).........................................................................93
EMERGENCY MEDICAL TRAINING REQUIREMENTS.................................................................................................94
HEALTH SERVICES TECHNICIAN "A" SCHOOL. .......................................................................................................95
HEALTH SERVICES TECHNICIAN "C" SCHOOLS.......................................................................................................96
CONTINUING EDUCATION PROGRAMS.....................................................................................................................96
LONG-TERM TRAINING PROGRAMS. .......................................................................................................................97
13-iii CH 13
Section N - PATIENT AFFAIRS PROGRAM 99
PATIENT SENSITIVITY..............................................................................................................................................99
PATIENT ADVISORY COMMITTEE (PAC).................................................................................................................99
PATIENT SATISFACTION ASSESSMENT...................................................................................................................100
PATIENT GRIEVANCE PROTOCOL..........................................................................................................................100
CONGRESSIONAL INQUIRIES..................................................................................................................................101
PATIENT BILL OF RIGHTS AND RESPONSIBILITIES..................................................................................................101
13-1 CH 13
CHAPTER 13. QUALITY ASSURANCE
Section A - Quality Assurance Plan
1. Purpose.
The Commandant and Chief, Office of Health and Safety are committed to providing the
highest quality health care to Coast Guard beneficiaries. The Health Services Quality
Assurance Program (QAP) described here establishes policy, prescribes procedures, and
assigns responsibility for Quality Assurance (QA) activities at Coast Guard health
services facilities. It is intended to function as an integral component in a Total Quality
Management (TQM) system aimed at achieving patient satisfaction by using quantitative
methods to continuously improve the health services program. It is essential that the
QAP integrates into the Coast Guard's overall TQM concept to improve the health care
delivery system at all organizational levels. The Office of Health and Safety,
Maintenance and Logistics Commands, unit commanding officers, health care providers,
and patients must cooperate to ensure successful implementation of the TQM concept in
the health care arena.
2. Background.
Health care QA includes monitoring and evaluating performance against generally
accepted medical and dental standards to improve performance. For QA activities to be
successful, health care providers and managers must directly involve themselves in the
on-going process of monitoring, evaluating, and reviewing records, etc., to allow effective
adjustments at the local level. For many years, Coast Guard health care facilities have
conducted QA activities, usually as a normal outgrowth of conforming with this Manual’s
directives and the consequence of Coast Guard practitioners’ good medical and dental
practices. However, until 1988, no attempts were made to standardize QA activities
among all Coast Guard health care facilities to ensure consistently high-quality
performance. Formal QA mechanisms were lacking and documentation was sketchy.
Since Maintenance and Logistics Commands were established in 1987 and the Quality
Assurance Branch was reorganized in 1989 in the Office of Health and Safety, a
concerted effort has been made to develop a Coast Guard-wide QA program designed to
address quality-of-care issues at our facilities. The program has been tailored the
program to Coast Guard medical and dental practices and incrementally phased it in over
an extended time period. This dynamic program continues to evolve in an ever-changing
health care environment. Directives will be amend as necessary.
3. Applicability and Scope.
All Coast Guard health care facilities with medical or dental officers assigned shall have a
QAP to organize efforts to achieve and document quality health care for eligible
CH-13 13-2
beneficiaries. The QAP described here contains the essential elements required at all
Coast Guard facilities and assigns responsibilities for program initiatives. All active duty,
reserve, and civilian health care providers treating patients at Coast Guard clinics must
participate in on-going monitoring and evaluation processes designed to assess the quality
and appropriateness of the services they provide.
4. QAP Objectives.
a. Communicate important QA information to enable sound clinical and management
decision-making at all organizational levels.
b. Review credentials; approve privileges.
c. Establish criteria to certify clinics and ensure facilities attain and sustain compliance
with established standards.
d. Systematically monitor health services to identify opportunities to improve patient
care, implement corrective actions when required.
e. Integrate, track, and analyze QA information to identify significant patterns that may
require additional review or intervention.
f. Identify and justify resources required to maintain acceptable patient care standards.
g. Conduct safety and infection control surveillance.
h. Identify, assess, and decrease risk to patients and staff, thereby reducing liability
exposure.
i. Identify educational and training requirements and assure satisfactory education and
training standards are established and maintained.
j. Establish and maintain adequate systems to monitor and assess patient satisfaction;
respond to patient and command concerns about access and quality of care.
5. Definitions.
a. Quality. The desired level of performance as measured against generally accepted
health care standards.
b. Quality Health Care. According to the Joint Commission on Accreditation of
Healthcare Organizations, quality is the prompt, well-documented, effective,
efficient, and appropriate organization and delivery of care which maximizes the
probability of positive outcomes and minimizes the probability of negative outcomes.
Additionally, Coast Guard health care also must meet these criteria:
(1) Consistent with Coast Guard policies, guidance, and Medical Manual
directives;
(2) Consonant with practices in the applicable professional community; and
(3) Perceived by beneficiaries as caring, competent, and effective.
13-3 CH 13
c. Quality Assurance. Those functions which attempt to ensure the desired level of
performance by systematically documenting, monitoring, evaluating, and, where
necessary, adjusting health care activities. These functions’ goal is to improve
clinical performance and patient care by striving to meet established high standards.
d. Professional Oversight. Monitoring and evaluating services provided by Coast
Guard health care personnel and non-Federal providers, including, among others,
technical guidance and assistance, peer review, resource utilization review and QA
site surveys conducted by Maintenance and Logistics Commands to ensure
compliance with the Coast Guard Health Care QAP.
e. Governing Body. The agency that has ultimate authority and responsibility for
establishing policy, maintaining quality patient care, and providing organizational
management and planning.
6. Organizational Responsibilities. See Figure 13-A-1.
a. Chief, Office of Health and Safety.
(1) Establish at all Coast Guard health care facilities a comprehensive QAP which
meets industry standards such as those published by the Joint Commission on
the Accreditation of Health Care Organizations or similar independent
accrediting organizations (the MLC implements the QAP);
(2) Govern Coast Guard health care facilities, with delegated responsibilities to the
Chief, Health Services Division at each facility.
(3) Establish and promulgate health care policy, including professional
performance standards against which quality can be measured;
(4) Establish and promulgate productivity and staffing standards for the health
services program;
(5) Conduct periodic Quality Assurance Meetings for Headquarters and MLC QA
staffs to coordinate and implement program policy at all organizational levels;
(6) Review credentials and grant privileges for all Coast Guard medical and dental
officers;
(7) Establish criteria for Coast Guard clinic certification and, based on MLC site
surveys, certify those facilities meeting established standards;
(8) Develop and promulgate the Quality Assurance Implementation Guide; and
(9) Identify education and training requirements and assure satisfactory standards
are established and maintained. Coordinate and fund continuing professional
education for all health services personnel.
b. Maintenance and Logistics Commands.

CH-13 13-4
(1) Ensure the Commandant's Health Care QA Program is executed at the field
level;
(2) Periodically conduct QA site surveys of all health services facilities in their
area in accordance with Section 13.F. provisions. Based on survey findings,
recommend clinic certification status to Commandant (G-WK) in accordance
with Section 13.G. provisions; pay customer assistance visits when necessary;
(3) Develop and maintain standard operating procedure manuals and/or health
services support program guides necessary to provide operational guidance for
clinic activities;
(4) Develop and maintain Quality Assurance Checklists for QA site surveys;
(5) Perform utilization review of clinic expenditures, staffing, equipment, supplies,
and facilities; review and process all requests for non-Federal medical care
from units in its jurisdiction; and
(6) Provide technical and professional advice regarding health services to units, as
required.
c. Commanding Officers.
(1) Ensure the unit actively pursues health services QAP standards;
(2) Appoint in writing an individual to serve as Health Services Quality Assurance
Coordinator in accordance with Paragraph 13.A.6.e.;
(3) Appoint health services staff members to serve on a Health Services Quality
Assurance Focus Group in accordance with Paragraph 13.A.6.f.; and
(4) Send copies of QA Focus Group meeting minutes to cognizant MLC (K).
d. Chief, Health Services Division. Represents the Governing Body locally for Quality
Assurance and related activities.
e. Health Services QA Coordinator.
(1) The Health Services QA Coordinator should be a senior health services staff
member with these characteristics:
(a) demonstrates the ability and motivation to provide and ensure quality
health care;
(b) knows the requirements of the Medical Manual, COMDTINST M6000.1
(series);
(c) communicates well both in writing and orally;
(d) well versed in delivering Coast Guard health care and supports the goals
of health care quality assurance; and
(e) is an E-6 or above.
(2) The Health Care QA Coordinator fulfills these responsibilities:

13-5 CH 13
(f) Directs Health Services QA Focus Group activities;
(g) Implements the health care QA program locally by identifying and
coordinating resolution of health care QA problems;
(h) Develops and promulgates an annual QA calendar which sets the agenda
for all QA activities at the unit, including among other activities QA
Focus Group meetings and all monitoring and evaluation functions; and
(a) Other health care QA functions as necessary.
(3) The Chief, Health Services Division or Clinic Administrator may be appointed
as the Health Services QA Coordinator.. However, this is not recommended in
larger clinics since these two individuals are expected to provide necessary
management expertise and clinical guidance in conducting the health care QA
program and effecting any required program adjustments. The Health Services
QA Coordinator's relationship to the Chief, Health Services Division is
advisory.
f. Health Services QA Focus Group.
(1) The Health Services QA Focus Group shall consist of three to 15 members,
depending on unit size, including both enlisted members and officers who
broadly represent the health care services provided at that unit.
(2) Members will include at least a medical or dental officer, a clinic supervisor,
and department representatives, e.g., pharmacy, physical therapy, x-ray,
laboratory, etc. If desired, the Health Care QA Focus Group at small units may
operate as a "Committee of the Whole" of all staff members.
(3) The Health Services QA Focus Group advises the Chief, Health Services
Division about the quality of the facility’s health care and performs these
functions:
(a) Identifies and resolves problems which affect the quality of health care
delivery at the facility (The Chief Health Services Division may delegate
investigating and resolving a particular QA problem to the staff member
responsible for the clinical area where the problem has been identified,
e.g., laboratory, patient reception, etc.).
(b) Ensures all required health services committee meetings are held
according to the provisions of the Coast Guard Medical Manual, MLC
standard operating procedures and operational guides, and local
instructions, including, among others, the Pharmacy and Therapeutics
Committee (see Paragraph 10.A.8.) and Patient Advisory Committee (see
Paragraph 13-N-2)
(c) Uses existing USCG standards, MLC QA checklists, and monitoring and
evaluation exercises to monitor and evaluate the quality of services
delivered both in-house and by contract providers.

CH-13 13-6
(d) Performs systematic, documented reviews of health records for
compliance and adherence to Medical Manual standards and MLC
standard operating procedures, health and safety support program guides,
and QA checklists.
(e) Solicits and monitors patient perceptions and satisfaction by surveys and
questionnaires.
(f) The Health Care QA Focus Group shall meet at least quarterly and more
often as local needs dictate. The MTF will maintain these meetings’
original minutes; forwarding copies of the minutes along with
monitoring and evaluation reports through the chain of command for the
cognizant MLC (K) and Commandant (G-WKH) to review.
7. Confidentiality Statement. All documents created under authority of this instruction are
health services quality assurance records and part of the Coast Guard's QAP. They are
confidential and privileged under 14 USC 645 provisions. Releasing health services QA
documents is expressly prohibited except in limited circumstances listed in 14 USC 645.
8. QAP Review and Evaluation. The Chief, Office of Health and Safety will annually
review and evaluate the QAP. The review will reappraise the QA Plan and incorporate
comments from the Commanders of the Maintenance and Logistics Commands on
implementation activities at field units during the preceding year.
a. By 30 November annually MLC Commanders shall provide to Commandant
(G-WK)a written QA Review and Evaluation Report addressing these topics during
the previous fiscal year:
(1) Summary of clinical certifications and accreditations;
(2) Summary of significant clinical problems identified;
(3) Summary of peer review activities;
(4) Recommended QAP modifications; and
(5) MLC QA Plan for upcoming calendar year.
b. By 31 January annually the Chief, Office of Health and Safety will issue to all units a
written QA report addressing these topics:
(1) Summary of clinical certifications and accreditations during past fiscal year;
(2) Summary of significant clinical problems identified during past year;
(3) QAP modifications for the current fiscal year; and
(4) QA Plan for the current fiscal year.
13-7 CH 13
FIGURE 13-A-1
ORGANIZATIONAL CHART FOR QUALITY ASSURANCE PROGRAM
COMMANDANT
COMMANDER, MLC PACIFIC CHIEF, OFFICE OF HEALTH AND SAFETY COMMANDER, MLC ALTLANTIC
CHIEF, CHIEF, CHIEF,
HEALTH AND SAFETY DIVISION OPERATIONAL MEDICINE DIVISION HEALTH AND SAFETY DIVISION
CHIEF, QA BRANCH CHIEF, QA BRANCH CHIEF, QA BRANCH
MEDICAL DENTAL PHARM MED ADMIN MEDICAL DENTAL PHARM MED ADMIN MEDICAL DENTAL PHARM MED ADMIN
OFF OFF OFF OFF OFF OFF OFF OFF OFF OFF OFF OFF
FIELD UNITS COMMANDING OFFICER
CHIEF, HEALTH SERVICES DIVISION
QA COORDINATOR
QA FOCUS GROUP
CH-13 13-8
Section B – Credentials Maintenance and Review
1. Background. Commandant (G-WK) is responsible for ensuring health care providers in
Coast Guard facilities are competent and capable. Verifying medical or dental officer
qualifications is essential to assure providers are prepared for the scope of practice for
which they are employed. To maintain quality health care the credentials review process
must be effective. Primary sources must certify as valid certain credentials, including
qualifying professional degree(s), license(s), graduate training, and references before a
provider may practice independently in Coast Guard health care facilities. All candidates
for USCG employment, USCG civil service employees, assigned USPHS commissioned
corps officers, and contract providers who provide direct patient care in Coast Guard
health care facilities will comply with this chapter’s provisions as applicable. The
credentials shall be reviewed for each medical or dental officer appointed to a position
providing patient care. Clinical responsibilities will be assigned based on this review.
2. Definitions.
a. Contract Provider. An individual physician, dentist, physician assistant or nurse
practitioner, other than uniformed services personnel, who provides care in a Coast
Guard health services facility under a contractual agreement with the Coast Guard.
b. Credentials. Documents constituting evidence of education, clinical training,
licensure, experience, clinical competence and ethical behavior.
c. Credentials Maintenance. Filing, updating, modifying or completing files or
documents about practitioner credentials.
d. Credentials Review. The process of checking a practitioner's verified credentials and
other supporting documents to evaluate potential assignments, assign or rescind
clinical privileges, or take administrative or personnel actions.
e. Dental Officer. A U.S. Public Health Service (USPHS) commissioned officer
assigned to the Coast Guard, who is a graduate of an accredited school of dentistry
and holds a valid, current state license to practice dentistry.
f. Intake Credentials Verification. The process of verifying a practitioner's license,
education, training, and competence before initial assignment or employment.
g. License (Current, Valid). A certificate issued by one of the 50 states, District of
Columbia or U.S. Territories (Guam, Puerto Rico, Virgin Islands) that permits a
person to practice medicine, dentistry, or other allied health profession.
h. Medical Officer. A commissioned USCG or USPHS officer assigned to the Coast
Guard who has graduated from an accredited educational institution and is currently
licensed as a physician or nurse practitioner; or a physician assistant holding valid
certification from the National Association on Certification of Physician Assistants.
13-9 CH 13
i. Primary Source Verification. Verification of a credential with an individual or
institution possessing direct knowledge of the validity or authenticity of the particular
credential.
j. Provider. A person granted individual clinical privileges to diagnose and treat
diseases and conditions, including physicians, dentists, physician assistants, nurse
practitioners, podiatrists, optometrists, and clinical psychologists.
3. Pre-selection Credentials Review.
a. Commandant (G-WKH) PHS liaison officer in cooperation with the PHS Division of
Commissioned Personnel (DCP) shall perform a pre-employment review and verify
minimum standards before appointing Commissioned personnel. The DCP also
screens individuals and certain credentials as part of the commissioning process.
Coast Guard procedures are designed to complement the DCP’s; the Coast Guard
may alter its policies as DCP modifies them.
b. The cognizant MLC or local command by direction shall perform a pre-employment
review of and verify Civil Service employees, contractors providing care in Coast
Guard health care facilities, and students.
c. To review and verify student credentials, obtain a letter from the school stating the
student is in good academic standing. Document malpractice coverage arrangements
through an appropriate affiliation agreement. (Student Extern Programs,
COMDTINST 6400.1 (series).
4. Practitioner Credentials File (PCF). Commandant (G-WKH-2) shall initiate and maintain
PCFs for all Civil Service and Uniformed Service licensed practitioners for the entire
length of their employment or service. Persons unable or unwilling to provide required
information may be disqualified for employment or accession. These files must contain
this information:
a. A current curriculum vitae accounting for all time since the qualifying degree was
received.
b. Copies of qualifying educational degrees (diploma, certificate) needed to perform
clinical duties with the documents’ primary source verification; see Section 13-B-6.
c. Copies of required postgraduate training certificates for the area of work; for
example, internship, residency, fellowship, nurse practitioner or physician assistant
training, and primary source verification of these documents’ authenticity.
d. Copies of state licenses for all states in which the practitioner is licensed (active or
inactive), current renewal certificates, and Educational Commission for Foreign
Medical Graduates (ECFMG) certification if the practitioner graduated from a
medical school not in the Continental U. S., Hawaii, Alaska, or from a medical
school not accredited by the American Association Liaison Committee on Medical
Education in Puerto Rico. The practitioner must attach a statement of explanation
CH-13 13-10
for lapsed state licenses or those subject to disciplinary action. The primary source
must verify all licenses or renewal certificates.
e. Copies of specialty board and fellowship certificates with primary source verification
of these documents.
f. Proof of current (within one year) competence, i.e., two letters of reference for initial
appointment and a description of recent clinical privileges held (practitioner's
supervisor must note concurrence with and approval of privilege performance).
(1) The official reviewing letters of reference is authorized to contact the author of
the letters to verify authorship and authenticity of letters. The official is also
authorized to request a second letter of reference from an author when the first
letter is deemed unclear. The official reviewing a letter of reference is
authorized to contact the author via telephone in cases in which the author
declines to respond in writing. In such cases, the official will document in a
telephone log the site, date, time, identity of call participants and a detailed
description of the conversation.
g. A statement explaining any involvement in malpractice cases and claims, including a
brief review of the facts about the practitioner's involvement.
h. A statement about any hospitals’, licensing boards’, or other agencies’ disciplinary
action.
i. A copy of current certification in Cardiopulmonary Resuscitation from the American
Heart Association or American Red Cross.
j. Copies of all current and prior Drug Enforcement Agency (DEA) registration, as
appropriate.
k. National Practitioner Data Bank (NPDB) query.
5. Documentation.
a. Documents will be placed into a U. S. Coast Guard Training Record (CG-5285)
folder. Commandant (G-WKH-2) will maintain files in a locked cabinet. PCFs and
their contents are Class III (maximum security) records and protected from disclosure
under the Privacy Act. Do not release documents in the PCF to any other individual
or entity unless the provider has given express written permission.
b. Place documents in the six-section folder are as follows:
(1) Section One: Coast Guard clinical privilege documents.
(2) Section Two: Reference letters.
(3) Section Three: Adverse actions, malpractice documents, proof of malpractice
coverage, statements about adverse information or malpractice claims.
CH-17
13-11 CH 13
(4) Section Four: Copies of CPR certification cards, continuing education
certificates (CME), other military or civilian courses other than initial
qualifying degree.
(a) By 31 December every other year, each provider shall submit a
summary of CME completed during the prior 2 years to Commandant
G-WKH-2.
(b) The CME summary will be in the form of a list in tabular format and will
include the name of the course, date taken, sponsoring organization and
CME earned.
(c) Providers who are members of the professional organizations that
maintain transcripts can submit a transcript in lieu of a summary of
CME.
(5) Section Five: JCAHO-accredited hospital letter on admitting privileges,
privileges granted by other or previous institutions, curriculum vitae.
(6) Section Six: Copies of license(s), diploma(s) or degree certificates, ECFMG
certificate (if applicable), Internship certificate, Residency Certificate,
Fellowship documents, and Board Certification. Primary sources must verify
all documents in Section Six.
c. See Figure 13-B-1 for a list of required documents by provider category.
6. Verification.
a. To verify education, training, licensure or registration, certification, ECFMG and
board certification, obtain either an original letter from the educational institution or
certifying body attesting to successful completion of specialty training, or verify by
telephone call between the Coast Guard representative and educational institution or
specialty board. Record telephone verification on the document itself and on official
letterhead signed and dated by the person making the call. Place all verification
documents with their source documents in PCF Section Six.
b. Commandant (G-WKH) will verify uniformed services persons before appointment.
c. Before selection of Civil Service and contract providers, there will be a verification
of education, training, licensure, experience, certification or registration, and current
competence.
d. To verify experience and current competence requires at least two recommendation
letters from appropriate sources as listed below. Commandant (G-WKH-2) or the
appropriate MLC shall receive direct letters from the person providing the reference.
Verify descriptions of recent clinical privileges as above.
(1) A letter either from the hospital chief of staff, clinic administrator, professional
head, or department head if the individual has professional or clinical
privileges or is associated with a hospital or clinic; or
CH-17
CH-13 13-12
(2) A letter from the director or a faculty member of the individual's training
program if he or she has been in a training program in the previous two years;
or
(3) A letter from a practitioner in the appointee's discipline who is in a position to
evaluate the appointee's peer and a professional association or society
association (mandatory if the appointee is self-employed).
7. Contract Provider Credentials Review.
a. All contract providers who perform any part of their work in a Coast Guard health
care facility will submit credentials documents to the appropriate MLC per Paragraph
13.B.6. above and MLC SOPs.
b. The contracting officer will verify documents.
c. At the contracting officer’s request, MLC (K) will perform a technical review of the
providers’ credentials.
8. Reverification.
a. These credentials are renewable and will be primary source on renewal: License, PA
certification, Board certification, and contract providers’ malpractice coverage.
Reverify contract providers’ credentials at contract renewal.
b. Reverify these credentials by original letter or telephone contact. The person making
the call will record telephone contact on the document and by a separate, signed
memorandum.
9. National Practitioner Data Bank.
a. Commandant (G-WK) possesses sole authority to report to the National Practitioner
Data Bank. Commandant (G-WKH-2) is designated as the appropriate entity for
National Practitioner Data Bank queries. Coordinate all queries for patient care
providers through this branch.
b. A reply from the NPDB is not required before the practitioner begins providing
services. However, any provider whose credential verification is not fully completed
will be considered to have a conditional appointment until all credentials are verified
as required.
CH-17
13-13 CH 13
FIGURE 13-B-1
REQUIRED CREDENTIALS BY PROVIDER CATEGORY
A B C D E F G H I J K
Physicians X X X X X X X X X X X
General Practice Physicians* X X X X X X X X X X
Dentists X X X X X X X X X
Physician Assistants X X X X X X X X
Nurse Practitioners X X X X X X X X
Optometrists X X X X X X X
Physical Therapists X X X X X X X X
Dental Hygienists X X X X X X X
A. Current curriculum vitae
B. Copies of qualifying educational degrees
C. Copies of required postgraduate training certificates for the area of work; for example,
internship, residency, fellowship, nurse practitioner or physician assistant schooling
D. Copies of state license(s)
E. Copies of specialty board certification and fellowship certificates
F. Proof of current competence, recent clinical privileges
G. Proof of malpractice coverage (contractors only)
H. Statement explaining malpractice claims, other adverse actions
I. CPR certification
J. DEA certification
K. NPDB query
___________________
* General Practitioners. Physicians who have completed one year of Graduate Medical
Education (Internship) and have not completed a full residency in a medical specialty.
CH-17

CH-13 13-14
Section C – Clinical Privileges
1. Purpose. Granting individual clinical privileges to independent practitioners providing
services in health care organizations is an essential component of quality assurance.
Clinical privilege granting and rescinding activities define the organization’s scope of
care and services available to patients. The privileging process is directed solely and
specifically at providing quality patient care; it is not a disciplinary or personnel
management system. However, privileging actions may accompany administrative or
judicial actions or engender them. Granting and rescinding clinical privileges is highly
confidential, and must be conducted according to strict rules to prevent improper or
prejudiced actions. This section establishes processes and procedures to grant and
rescind clinical privileges. These provisions fall outside the scope of Administrative
Investigations Manual, COMDTINST M5830.1 (series).
2. Background. Commandant (G-WK) is responsible for planning, developing, and
administering a comprehensive, high-quality health care program which must ensure the
persons providing care have appropriate, verified licenses, education, and training.
Coast Guard health care practitioners must adhere to commonly accepted standards for
treatment and therapeutic modalities. In the Coast Guard, adherence to accepted
standards is achieved by rigorous quality assurance (QA) and providers' peer reviews.
3. Definitions.
a. Abeyance. Temporarily assigning a provider to non-clinical duties while an internal
(focused) or external review or investigation is conducted.
b. Clinical Privileges. Type of practice activities authorized to be performed in the
facility, within defined limits, based on the providers' education, professional license
as appropriate, experience, current competence, ability, judgment, and health status.
c. External Review. Administrative, non-judicial, or criminal investigations initiated
by entities other than the Coast Guard health services program.
d. Focused Review. An internal administrative mechanism to evaluate information
about clinical care or practice. Coast Guard health services officers conduct focused
reviews as part of the quality assurance program.
e. Full Staff Privileges. Unrestricted privileges as defined by "Clinical Privileges"
above, reevaluated and renewed every two years.
f. Peer Review. Review by an individual (or individuals) who possesses relevant
professional knowledge or experience, usually in the same discipline as the
individual under review.
g. Privileging. The process through which providers are given the authority and
responsibility to make independent decisions to diagnose illnesses and/or initiate,
alter, or terminate a regimen of medical or dental care.

13-15 CH 13
h. Professional Review Committee. A committee appointed by Commandant (G-WK),
composed of the Deputy Director of Health and Safety (G-WKd) and the Chiefs of
the Operational Medicine Division (G-WKH), Operational and Clinical Medicine
(G-WKH-1), and Quality Assurance Branch (G-WKH-2) or their designees. At least
two physicians and one dentist shall be members.
i. Provider. For this chapter, an individual granted clinical privileges to independently
diagnose and treat diseases and conditions. Physicians, dentists, physician assistants,
nurse practitioners, podiatrists, optometrists, and clinical psychologists are provider
disciplines within the Coast Guard health services program.
j. Provisional Clinical Privileges. Initial privileges, generally effective 365 days from
issue date, Commandant (G-WK) grants providers when they begin practice in the
Coast Guard health services program or earn a new or changed clinical privilege.
New Coast Guard providers are eligible for full staff privileges after successfully
completing one year of provisional privileges.
k. Expiration of Credentials. It is ultimately the responsibility of the provider to ensure
that all credentials required for clinical privileges are renewed prior to their
expiration dates. If any credential required for clinical privileges is allowed to
expire, the provider may have clinical privileges suspended or terminated. This will
remove the provider from direct patient care and may also render the provider
ineligible to receive any special pay for clinical duties while the provider is in this
status.
4. Applicability and Scope. All military and salaried civilian, and contract civilian Coast
Guard health care providers shall have clinical privileges assigned. Health services
personnel (other than providers) who function under a standard job or position
description or standard protocol, policies, and procedures, or who must consult with
another provider before or during medical or dental treatment will not receive clinical
privileges.
5. Clinical Privileges.
a. General.
(1) Commandant (G-WK) will grant clinical privileges based on education,
specific training, experience, license or certification status, and current
competence. He or she shall consider facility, support staff, equipment
capability, etc. limitations which may prevent a provider from conducting
certain activities. Commandant (G-WK) shall assign or require providers to
perform professional duties only if their education, training, and experience
qualifies them to perform such duties. Commandant (G-WK) also shall
consider the provider's health status and ability to treat coworkers and patients
with dignity and respect (i.e., the presence or absence of good interpersonal
skills and "bedside manner") when granting privileges.

CH-13 13-16
(2) At defined intervals the provider shall use form CG-5575, Request for Clinical
Privileges, to initiate a request for clinical privileges. Chief, Health Services
Division (HSD) shall recommend whether to approve or disapprove clinical
privileges and submit the recommendation to Commandant (G-WK) through
MLC (K). The Professional Review Committee shall review the privileges
requested and recommend a response to Commandant (G-WK). The actions of
the Professional Review Committee actions will not be considered final until
Commandant (G-WK) approves them.
(3) Absence of clinical privileges must not delay treatment in an emergency—a
situation in which failure to provide treatment or hospitalization would result
in undue suffering or endanger life or limb. In such cases the providers are
expected to do everything in their power to save the patient's life or treat the
condition.
(4) On transfer, the gaining Chief, Health Services Division shall evaluate the
provider's clinical privileges to determine whether to continue all previously
granted privileges, or whether the facility, patient population, or other factors
require adjusting privileges. If a change is indicated, the provider shall submit
a revised request for privileges form as delineated below for the Professional
Review Committee’s review and approval.
(5) (5) When providers in the Coast Guard are assigned TAD, Commandant (G-
WKH-2) shall transmit a copy of the provider’s clinical privileges to the host
SMO/SDO who will evaluate the privileges and advise the provider which if
any privileges will be restricted at that site. When assigned TAD to a clinic
that is accredited by JCAHO, AAAHC or other external accrediting agencies,
Commandant (G-WKH-2) will also transmit a credentials transfer brief (CTB)
to the host command.
(6) (6) When providers from DoD are assigned TAD to Coast Guard clinics, their
parent command shall transmit a copy of their clinical privileges as well as a
CTB to the host command prior to their arrival. The SMO/SDO will determine
if any of the privileges will be restricted.
b. Procedures.
(1) Commandant (G-WKH) will inform new Coast Guard providers they must
request provisional clinical privileges in writing before accession to active duty
or formal employment. New Coast Guard providers shall send written requests
for provisional clinical privileges to Commandant (G-WKH) by facsimile or
mail at least 45 days before accession. Privilege requests for persons already
employed by or assigned to the Coast Guard shall be forwarded by mail for
facsimile (FAX) to Commandant (G-WKH) through the cognizant MLC (k)
for Professional Review Committee action.
(2) Providers do not require Professional Review Committee approval before
reporting for duty. Until credentials review is completed and privileges are
granted, new providers may deliver care under supervision, i.e., peers shall
oversee the provider's work by reviewing monthly a random sample of at least

13-17 CH 13
5% of the provider’s charts. Any problems detected during this review will be
documented in writing and copies given to the provider. Providers who fail to
have the deficiencies corrected in 60 days may have their privileges restricted.
(3) Provisional clinical privileges are effective for one year. When granting
provisional privileges, the risks associated with the activities for which a new
provider seeks privileges and the frequency with which he or she performs the
procedures shall be considered.
(4) Privilege request documents, Professional Review Committee actions, and any
other documents relating to the granting, maintaining, reviewing or rescinding
clinical privileges will be maintained in the individual provider's credentials
file.
(5) The Chief, HSD shall evaluate the provider's provisional privileges after one
year. Providers may apply for full staff privileges after one year of successful
performance.
(6) The Professional Review Committee will evaluate full staff privileges every
two years. Providers will submit written privilege requests to Commandant
(G-WKH) through MLC(kqa) 90 days before privileges are due for renewal.
c. Routine Operations of the Professional Review Committee (PRC)
(1) The Quality Assurance (QA) Division, Commandant (G-WKH-2) will have the
responsibility of monitoring and administering the granting of clinical
privileges for all health care workers (HCW’S) in the Health and Safety
Program that require the formal granting of clinical privileges in order to
perform their duties.
(a) Commandant (G-WKH-2) will maintain a Practitioner Credentials File
(PCF) for HCW’s in the CG Health and Safety Program that will be used
for granting clinical privileges.
(b) The local QA Coordinator at each field unit will have the responsibility
of maintaining a list of the expiration dates of all significant documents
required to grant clinical privileges as stipulated in Section 13-B and will
notify the HCW when these documents are within 90 days of expiration.
(c) It is ultimately the responsibility of the HCW to take appropriate actions
to prevent these documents from expiring and to ensure that current
documents are entered in the PCF.
(d) Commandant (G-WKH-2) will also monitor the expiration dates on these
documents and will coordinate through the local QA coordinators.
(e) The Professional Review Committee (PRC) will make recommendations
to Commandant (G-WK) on the granting of clinical privileges.
CH-13 13-18
(f) The PRC will routinely review requests for clinical privileges for HCWs
upon reporting to new CG duty stations and every 2 calendar years.
(g) The PRC can also be convened by Commandant (G-WK) to review
PCF’s for situations other than the routine review of clinical privileges.
This is described further in section 13-C-5-d.
(2) Commandant (G-WKH-2) will conduct a preliminary review of the requests for
clinical privileges as well the entire PCF'S selected to be presented before the
PRC.
(3) Commandant (G-WKH-2) will forward requests for clinical privileges as well
as the PCF'S to the cognizant Program Coordinators who will evaluate the
PCF'S and decide if they should be presented before the PRC or if further
information or action is required before being submitted before the PRC.
(4) After Commandant (G-WK-2) and Program Coordinators have decided which
records will be presented to the PRC, Commandant (G-WKH-2) will prepare
an agenda and will schedule a PRC meeting.
(5) The PRC will included:
(a) Commandant (G-WKd) as President of the PRC
(b) At least 2 physicians
(c) At least 1 dentist
(d) At least 1 PA or NP
(e) 1 member of Commandant(G-WKH-2), non-voting, to act as recorder
(f) Other members of Commandant (G-WKH-2)
(6) The PRC will evaluate each PCF and can recommend any of the following
actions for each case:
(a) Grant all requested privileges.
(b) Revoke all current privileges or certain specific privileges.
(c) Restrict all current privileges or certain specific privileges.
(d) Suspend all current privileges or certain specific privileges.
(e) Hold in abeyance all current privileges or certain specific privileges.
(f) Monitor or supervise of performance of clinical privileges.
(g) Request that any decision regarding privileges be deferred until more
information is submitted to the PRC.
13-19 CH 13
(h) Maintain or modify current privileges while more information is
forthcoming or an investigation is being conducted.
(i) Request a document focused review or other type of internal
investigation.
(j) Request an external review or investigation.
(k) Other actions as dictated by circumstances.
(7) In accordance with the terminology adopted by the National Practitioner Data
Bank (NPDB) and Federal Credentialing Program (FCP), an adverse
privileging action is considered to be any action that revokes, restricts or
suspends current privileges for over 30 days.
(8) The PRC will vote on each case but the decision to approve or reject a
recommendation for a privileging action will be made by WKd..
(9) The PRC will forward its recommendations for privileging actions in the
minutes of the meeting to Commandant (G-WK) via: Commandant (G-WKH-
2), Commandant(G-WKH), and Commandant (G-WKH), and Commandant
(G-WKd)
(a) Commandant (G-WK) will prepare the minutes for each meeting of the
PRC.
(b) The minutes will specific the privileging action recommended.
(c) In the case of a recommendation by the PRC for an adverse privileging
action or any privileging action less than granting full privileges
requested, the minutes will specify the reasons or justification for that
recommendation.
(10) After Commandant (G-WK) receives the minutes, Commandant (G-WK) will
make a decision on how to act on the recommendations of the PRC.
(a) In cases where the PRC has recommended the granting of full privileges
and Commandant (G-WKd) concurs, the request for Clinical Privileges
will be submitted to Commandant (G-WK) for final approval.
(b) In cases where the PRC has recommended an adverse privileging action
or a status less than the granting of all clinical privileges requested and
Command (G-WK) may forward the case to General Legal Counsel,
Commandant (G-LGL) for a legal opinion prior to taking action.
(11) In cases that have been forward to Commandant (G-LGL) for a legal opinion
regarding the intended privileging action, Commandant (G-WK) will have 3
working days to make the final decision on how to act after receiving the
results of the legal opinion.
CH-13 13-20
(a) Commandant (G-WK) will attempt to contact the HCW by telephone and
inform about the action.
(b) Commandant (G-WK) will forward a letter to the HCW by mail.
(c) Commandant (G-WK) will inform the relevant MLC(k) or MLC(m) by
letter.
(d) MLC will notify the local command and the Chief, Health Services
Division,
(12) In cases where Commandant (G-WK) requests a document or focused review
or investigation prior to acting on the recommendations of the PRC, MLC will
have the responsibility of organizing and funding this activity and coordinating
with the local command.
(a) The officer or team conducting the inquiry will be convened within 10
working days after MLC has received written notification from
Commandant (G-WK)
(b) Within 5 working days after MLC has received written notification from
Commandant (G-WK), the local Commanding Officer and the Chief,
Health Services Division will be notified of the identity of the officer or
team conducting the inquiry.
(c) The inquiry will be completed within 3 working days after it has been
initiated.
(d) Before departing, the officer or team will brief the local Commanding
Officer and the Chief, Health Services Division on the findings and
recommendations.
(e) When the review or investigation has been completed, the officer or team
conducting the inquiry will forward a written report of their findings and
recommendations to MLC within 10 working days.
(f) MLC will forward the results to Commandant (G-WK) within 5 working
days After receiving it.
(13) After receiving written notification from Commandant (G-WK) of the
enactment of an adverse privileging action that does not grant full privileges, if
the HCW has 30 calendar days to contact Commandant (G-WK) in writing to
request a hearing
(14) After receiving written notification from Commandant ( G-WK) of the
enactment of an adverse privileging action or a privileging action that does not
grant full privileges, if the HCW does not request a hearing within 30 calendar
days, it will be presumed that the HCW accepts and will comply with the
privileging action.
13-21 CH 13
Commandant (G-WK) will make the decision to notify the NPDB in the case of an
adverse privileging action.
(a) The Coast Guard Health and Safety Program is considered a health care
entity under the Health Care Quality Improvement Act of 1987.
1 Health care entities are requires to report any adverse privileging
action that is enacted for over 30 calendar days for all physicians and
dentists.
2 Health care entities are not required to report adverse privileging
actions for other HCW'S
(b) Commander (G-WK) will make the final decision to report adverse
privileging actions
(c) Commandant (G-WKH-2) will submit the report to the NPBD when
directed by Commandant (G-WK) in accordance with current NPDB
d. Non-Routine Privileging Actions.
(1) The objective of a non -routine privileging action is to affect a change in
clinical privileging that is motivated by an urgent set of circumstances that
precludes waiting for the routinely schedule evaluation for clinical privileges
by the PRC.
(2) In these cases, the local command will normally initiate a request for
modification or termination of clinical privileges based on events at the local
field unit level.
(a) The request will be in the form of a letter from the local command
MLC(k).
(3) The letter must describe in detail the exact circumstances leading up to the
decision to request a modification or termination of clinical privileges.
(4) The letter must identify the individuals who initiated the complaint or action
and every member of the staff and chain of command who had any
involvement in the case.
(a) In extreme cases, the local command may elect to communicate
immediately with MLC(k) by telephone. However this must be followed
by the issuance of a letter
(b) Local commanding officers may have questions or concerns about
providers and under what circumstances requests for restrictive actions
should be made.
(5) The local command should use the cognizant MLC(k) as the POC for these
queries.

CH-13 13-22
(6) Requests for information guidance can be made via telephone, electronic or
written correspondence.
(7) MLC(k) will evaluate the request from the local command and will have up to
5 working days to determine what action will be taken including:
(a) No action.
(b) Request more information from the local command.
(c) Immediate action such as placing the HCW in abeyance.
1 Normally Commandant (G-WK) will make the decision to hold the
privileges of the HCW in abeyance.
2 Incases where circumstances are extreme MLC(k) may temporarily
hold the privileges in abeyance and then contact Commandant (G-
WK) as soon as possible.
(d) Convening a document or focused review.
(e) Submitting the case for disposition to Commandant (G-WK).
(8) If MLC (K) determines that a document or focused review is indicated, an
officer or team will be on site within 10 working days if the decision.
(a) The HCW will notified of the decision as soon as possible by telephone
and this will be followed by a letter from MLC (k) to the HCW
describing the circumstances that led to this action.
(b) The local Commanding Officer and Chief, Health Service Division will
be appraised of the identity of the officer or team that will be convened
for the document or focused review within 5 working days after the
decision to convene has been made.
(c) The review will be completed within 3 working days after it has been
initiated.
(d) The officer or team will brief the local a Commanding Officer as well as
the Chief, Health Services Division on the findings and
recommendations.
(e) The officer or team will forward a written report on the findings and
recommendations to MLC(k) within 10 working days after the review
has been concluded.
(9) MLC(k) will review the findings and recommendations of the document or
focused review and will determine what action to take within 5 working days
including:

13-23 CH 13
(a) No action.
(b) Request more information from the local command.
(c) Forward the written report from the document or focused review to
Commandant (G-WK) for disposition with recommendations from
MLC(k)
(10) After receiving the written report if the document or focused review and the
recommendations from MLC(k), Commandant (G-WK) will decide what
action to take within 5 working days including:
(a) No action.
(b) Request for more information.
(c) Forward the report from the document or focused review with
recommendations from the MLC(k) to the PRC and convene an
impromptu meeting with instructions to make recommendations to
Commandant (G-WK) on the issue of privileging for this particular case.
1 The PRC will convene within 5 working days.
2 The PRC will vote on the case but the decision to enact a privileging
action will made by WKd.
3 The PRC will forward its recommendations to Commandant (G-
WK) within 3 working days.
(d) Summary adverse privileging action or grant less than full privileges
(11) In the event that Commandant (G-WK) decides to enact an adverse privileging
action or not grant full privileges either as a summary action or on the basis of
recommendations from the PRC, the following actions will be taken by
Commandant(G-WK):
(a) Commandant (G-WK) will attempt to contact the HCW by telephone to
inform.
(b) Commandant (G-WK) will forward a letter describing the privileging
action and justification to the HCW.
(c) Commandant (G-WK) will forward a letter to MLC informing of the
privileging action.
(d) MLC will forward the letter to the local command and Chief, Health
Services Division.
(12) After receiving written notification from Commandant (G-WK) of the
enactment of an adverse privileging action or a privileging action that does not
CH-13 13-24
grant full privileges, the HCW has 30 calendar days to contact Commandant
(G-WK) in writing to request a hearing.
(13) After receiving written notification from Commandant (G-WK) of the
enactment of an adverse privileging action or a privileging action that does not
grant full privileges, if the HCW does not request a hearing within 30 calendar
days, it will be presumed that the HCW accepts and will comply with the
privileging action.
(14) Commandant (G-WK) will make the decision to notify the NPDB in the case
of an adverse privileging action.
(a) The Coast Guard Health and Safety Program is considered a health care
entity under the Health Care Quality Improvement Act of 1986.
1 Health care entities are required to report any adverse privileging
action that is enacted for over 30 calendar days for all physicians and
dentists.
2 Health care entities are not required to report adverse privileging
actions for other HCW'S.
(b) Commandant (G-WK) will submit make the final decision to report
adverse privileging actions.
(c) Commandant (G-WKH-2) will submit the report to the NPDB when
directed by Commandant (G-WK) in accordance with current NPDB
protocols.
e. Hearing Process
(1) After receiving written notification from Commandant (G-WK) of the
enactment of an adverse privileging action or a privileging action that does not
grant full privileges, the HCW has 30 calendar days to contact Commandant
(G-WK) in writing to request a hearing.
(2) Commandant (G-WK) has 10 working days to convene a hearing committee
after receiving request from the HCW for a hearing.
(a) Commandant (G-WK) will notify MLC that a hearing has been
requested.
(b) Normally hearings will be schedule at Commandant (G-WK) unless
otherwise specified.
(3) A hearing committee will consist of at least three Coast Guard Public Health
Service (CG/PHS) officers with the rank of Lieutenant Commander or above
and a representative Commandant (G-LGL) to act as legal advisor. At least
two of the CGPHS officers on the hearing committee will have board
13-25 CH 13
specialties the same as the provider requesting the hearing. Each (CGPHS)
officer will have one vote.
(a) The HCW will bear all expenses of transporting witnesses or legal
advisors.
(b) The HCW has the right to:
(c) Have an attorney or legal advisor present who can provide legal advice to
the HCW. The legal advisor will not participate directly in the
proceedings.
(d) To record of the proceedings.
(e) To call and cross-examine witnesses.
(f) To present relevant written evidence.
(g) To submit a written statement at the conclusion of the hearing.
(4) The hearing committee will convey its findings in a written report within 3
working days after the conclusion of the hearing to Commandant (G-WK).
(5) Commandant (G-WK) will have 3 working days to act on the findings of the
hearing.
(a) Commandant (G-WK) will attempt to contact the HCW by telephone and
inform about the results of the hearing and the action to be taken
(b) Commandant (G-WK) will forward a letter to the HCW by mail.
(c) Commandant (G-WK) will inform the relevant MLC(k) or MLC(m) by
letter.
(d) MLC will notify the local command and Chief, Health Services Division.
CH-13 13-26
Section D - Quality Assurance Checklists.
1. Background. The MLC Health and Safety Divisions develop and maintain Quality
Assurance Checklists, which detail in question-and-answer format the essential criteria
against which to assess the quality of health services. These criteria are derived from
primarily from the Coast Guard Medical Manual and MLC Standard Operating
Procedures and Health and Safety Support Program Guide. MLC commanders will
make every effort to ensure uniformity among MLC Checklists to the extent permitted
by regional command policies.
2. Usage. QA Checklists will be used primarily to assess compliance with quality assurance
standards, which may focus on structure, process, or outcome measures of quality care.
Their design will allow clinics and sick bays to self-assess performance by answering the
series of questions the checklist poses. Compliance with checklist standards will be
scored on a percentage basis. Resulting scores will determine each clinic's certification
status.
a. Key Elements. Because of their critical nature and importance governing quality of
care, certain clinic checklist items will be designated "key elements." Complying
with key elements is essential for clinic success. A high degree of conformity with
key elements will be required to certify a clinic.
b. Elements. “Elements” are certain other checklist items of a less critical (but still
important) nature than key elements. Required compliance for clinic certification is
lower for elements than for key elements.
c. Information Items. The checklist also contains a number of questions included for
informational purposes only and not scored for certification.
3. Amendments. The MLC is responsible for Checklist amendments and may amend its
Checklist at any time based on policy changes, program requirements, or suggestions and
recommendations from clinic personnel or Commandant (G-WK). QA checklists are
"living documents" and expected to change regularly to reflect changes in clinic
operations and policy. Therefore, clinics will be given updated checklist copies long
before QA site surveys.
13-27 CH 13
Section E – Quality Assurance Implementation Guide (QAIG)
1. Background. The QAIG is a series of exercises designed to assist commands to meet
Health Services QA Program requirements. Serving as a guideline, the QAIG minimizes
the QA program administrative requirements by providing direction and, in many cases,
templates for addressing critical QA issues. The exercises often eliminate the need for
each clinic to develop its own policies and procedures by providing generic frameworks
clinics can adapt to local conditions. In some cases, clinics may be required to submit
evidence of completing an exercise to the MLC Health and Safety Division for data
evaluation purposes.
2. Responsibilities.
a. COMMANDANT (G-WKH) develops as many as 10 exercises per year on critical
QA issues for inclusion in the QAIG. The MLCs distribute the exercises.
b. COMMANDER, MLC (K) ensures exercises are distributed to appropriate
commands for clinic personnel to complete and also reviews each facility's QAIG
during quality assurance site surveys.
c. Unit QA Coordinators ensure staff promptly complete all QAIG exercises and
maintain a complete, up-to-date QAIG.
CH-13 13-28
Section F- Quality Assurance Site Survey.
1. Procedures. All Coast Guard health care facilities are subject to periodic QA site
surveys designed to assess compliance with QA checklist elements, and in the case of
clinics, to attain Commandant (G-WK) certification; see Section 13-G. MLC Health and
Safety Divisions conduct clinic site surveys in accordance with Coast Guard Clinic
Certification Program requirements. MLCs survey independent duty sick bays according
to schedules promulgated by the MLC. Facilities will be given notice at least eight
weeks before the scheduled survey date regarding survey format and schedule and
include with the notice the current QA Checklist against which performance is to be
evaluated. MLCs will make every effort to schedule QA site surveys during time periods
that allow maximum clinic staff participation.
2. Survey Format. The MLC site survey team will conduct all surveys according to this
format:
a. On arrival brief the Commanding Officer.
b. Review on-site clinic or sick-bay procedures and spaces according to QA checklist.
c. Health Records Review.
(1) Review selected records for documentation as required by QA checklist and
verify accuracy of clinic data collection.
(2) Review selected records for pertinent diagnosis and care (see Section 13.I.,
Peer Review).
d. Review clinical monitoring and evaluation program.
e. Clinic All-Hands Meeting to review the QA site survey team’s preliminary findings
and solicit clinic staff’s suggestions and recommendations for improvement.
Feedback from the staff is encouraged on the Quality Assurance Program and the
staff may present problems for troubleshooting with MLC QA Staff. A training
component focusing on Quality Assurance and its incorporation into the Coast
Guard's total quality management philosophy may be included
f. Clinical services review with branch heads (e.g., medical services, dental services,
pharmacy, etc.).
g. Brief Senior Medical Officer, Senior Dental Officer, and Medical Administrative
Officer.
h. Brief Commanding Officer.
3. Survey Report. Commander, MLC (k) will provide a written QA site survey report to
the Commanding Officer within six weeks after the completed survey. Clinics which are
determined to be performing at a level below that required for certification will receive
the survey report or interim action report within two weeks of the site survey and will be
re-survey within 180 days according to Section 13-G provisions. The report will consist

13-29 CH 13
of an executive summary of major survey findings, an itemized account of facility
performance measured against QA checklist elements, corrective actions required, and
for clinics, certification status based on parameters described in the clinic certification
program in Section 13-G. Commanding Officers must provide a written plan for
corrective action to Commander, MLC (k), within 45 days of receiving the written
evaluation. MLC (k) personnel will be available to assist all facilities in meeting
program requirements.
4. Customer Assistance Visits. Customer assistance visits are interim, abbreviated visits by
MLC (kqa) staff members. Units may request or MLC (k) initiate them to review
compliance with applicable clinic regulations and offer assistance in meeting regulatory
requirements.
CH-13 13-30
Section G - Coast Guard Clinic Certification and Accreditation
1. Clinic Certification Program.
a. Background. Commandant (G-WK) must certify all Coast Guard clinics with
assigned medical and dental officers to provide health services. Clinic certification is
based on complying with standards set forth in the Medical Manual, COMDTINST
M6000.1 (series), and MLC Quality Assurance (QA) Checklists. Commandant (G-
WK) certifies facilities based on the results of Quality Assurance site surveys
conducted by Maintenance and Logistics Commands.
b. Responsibility.
(1) Unit. The unit commanding officer is responsible for ensuring the command's
health care facility complies with standards set forth in the Coast Guard
Medical Manual and MLC QA Checklists and for meeting the minimum
requirements set forth for clinic certification.
(2) Maintenance and Logistics Command. Chief, Health and Safety Division is
responsible for developing and coordinating QA Checklists and periodically
conducting Quality Assurance Site Surveys at facilities in their area of
responsibility. These surveys will assess compliance with existing directives
and recommend the facility’s certification status based on survey results.
(3) Headquarters. Chief, Office of Health and Safety coordinates and directs the
certification program, issues certificates to certified clinics, adjudicates
appeals, and promulgates appropriate standards governing Coast Guard
providers’ delivery of health care and policies on managing and operating
Coast Guard health care facilities.
c. Certification Standards.
(1) Certified. Commandant (G-WK) will certify clinics complying with at least
90% of both key elements and all other elements on the QA Checklist. Clinics
must earn re-certification every three years.
(2) Provisionally Certified. Commandant (G-WK) will provisionally certify
clinics complying with at least 80% of key elements and at least 80% of all
other elements on the QA Checklist. MLC Health and Safety Divisions will
annually re-survey provisionally certified facilities until they attain full
certification.
(3) Not Certified. A facility failing to achieve either certification or provisional
certification under this Section’s provisions will be subject to a follow-up
MLC QA site survey within 180 days after notice of non-certification. During
this remedial period, the MLC will assist the facility to promptly address QA
survey discrepancies and may impose restrictions limiting the scope of services
the facility can provide. The facility must request a follow-up survey during
this period. If the facility does not receive at least provisional certification
CH-17
13-31 CH 13
(4) MLC will notify the Commanding Officer the health care facility is not
certified by letter through the chain of command and detail appropriate specific
restrictions on care delivery in that facility.
(a) The Commanding Officer shall submit weekly message reports of
progress attained in eliminating disqualifying discrepancies to the
cognizant MLC (k), with an information copy to Commandant (G-
WKH), through the chain of command.
d. Notice of Certification Status. The Maintenance and Logistics Command will send
each surveyed facility a copy of the survey report and recommendations for
corrective action within 6 weeks of the site survey. If a facility is not certified, the
MLC(k) will send the survey report or an interim action report within two weeks of
the site survey. Certified and provisionally certified facilities will receive certificates
which they are to display prominently within.
e. Appeal of Certification Status. A Unit Commanding Officer (CO) may appeal the
certification status awarded as a result of the MLC Quality Assurance site survey
within 30 days of the site survey report date. The Commanding Officer appeals in
writing to Commandant (G-WK) through the chain of command; the appeal must
specify the particular disputed QA checklist elements and reasons for the appeal.
The CO must not base the appeal on corrective actions taken after the QA site survey
or local misinterpretation of QA checklist elements or Medical Manual guidelines.
Commandant (G-WK) will consider the appeal and render a final verdict on
certification status within 30 days of receiving the appeal.
2. Clinic Accreditation Program.
a. All Coast Guard-certified health care facilities with four or more medical officers
assigned are expected to pursue accreditation from an external accrediting
organization such as the Joint Commission on Accreditation of Health Care
Organizations. The cognizant MLC and G-WKH must approve pursuit of this
accreditation. Once a clinic achieves full or provisional external accreditation, that
facility will automatically receive Coast Guard certification and be required to
maintain external accreditation. A non-scored MLC QA survey will also be
performed to ensure compliance with Coast Guard regulations and compliance with
G-WK quality assurance program standards.
b. The respective Maintenance and Logistics Command will provide any technical and
professional assistance the health care facility requires to prepare for external
accreditation. On the command’s letter request, Commandant G-WK will provide
funding for external accreditation surveys through the respective MLC (K).
3. Laboratory Certification. All ashore medical facilities that test human specimens to
provide information to diagnose, prevent, and/or treat any disease or assess a human
being’s health must comply with the regulations for laboratory testing as stated in the
Clinical Laboratory Improvement Amendments of 1988 (CLIA), administered by the
Department of Health and Human Services.
CH-13 13-32
Section H- Monitoring and Evaluation Program
1. Background. Monitoring and Evaluation (M&E) is an on-going program that examines
important areas of clinical care and assesses how well the facility provides that care. The
Joint Commission of the Accreditation of Health Care Organizations describes M&E as
the "heart" of quality assurance, a process of continuously seeking areas of potential
improvement in the health care delivery system. Participants identify areas of care
needing improvement, implement actions to improve care, and continually monitor these
areas to ensure the improvements are effective and the quality of care satisfactory.
2. Responsibilities.
a. Commandant (G-WKH-2) will monitor and update the M&E program as appropriate.
b. Commander, Maintenance and Logistics Commands (k) shall review each facility's
M&E log during Quality Assurance site surveys.
c. Unit QA Coordinators shall ensure the Quality Assurance Focus Group (QAFG)
performs on-going M&E according to schedule. They shall retain logs or their
equivalent on file for three years for MLC QA site survey teams to review.
3. Implementation. The Monitoring and Evaluation Report Form (Figures 13-H-2 through
13-H-31) is the basic instrument documenting Coast Guard clinics’ M&E. Each clinic
will complete a separate form for each aspect of care monitored. M&E Reports and the
M&E Data Collection Log, CG-5544 (Figure 13-H-32), are the only forms required to
document M&E activity.
4. Using the Monitoring and Evaluation Schedule and Clinical Aspects of Care Listing.
a. Monitoring. M&E exercises for each category—medical (MED), dental (DEN) and
drug utilization review (DUR)—are numbered, e.g., MED-1 to MED-9. Units may
select any appropriate exercise from the designated category each quarter; choose
optional exercises from any category, or develop their own exercises to address unit-
specific issues. Units must record exercises they developed on Figures 13-H-30 and
13-H-31 and obtain cognizant MLC (k) approval. All selected exercises must
address high-risk, high-volume, or problem-prone clinic procedures.
b. Submit M&E Reports to the QAFG prior to the last work day of each quarter.
Therefore, start collecting data for each exercise at the beginning of each quarter.
c. Follow-Up
Reports.
(1) Studies Meeting Thresholds. The facility must follow up each initial M&E
Report in 6 months with a follow-up report (Figure 13-H-31).
(2) Studies Not Meeting Thresholds. The facility must produce a follow-up report
3 months after the initial report, and every 3 months thereafter until it meets
that threshold(s).
13-33 CH 13
d. Use the M&E Data Collection Log, CG-5544 (Figure 13-H-32), to evaluate health
records or other information sources for compliance with the indicator criteria.
Record each record reviewed as meeting or not meeting the indicator. Retain
completed logs on file for three years for MLC QA site survey teams to review.
5. Monitoring and Evaluation Report Forms (Figure 13-H-2 through 31). M&E report
forms contain ten (10) sections: Sections 1 through 7 on the front (Figures 13-H-2
through 30) and Sections 8 through 10 on the back (figure 13-H-31).
a. Aspect of Care (Section 1). If the M&E program is to be meaningful, it must focus
on clinical issues that have the greatest potential to affect our patients: high-volume,
high-risk, or problem-prone aspects of care.
b. Clinical Indicator (Section 2). A component of care which shall be measured to
determine compliance with standards. Commandant (G-WKH-2) establishes clinical
indicators with suggestions from MLCs (k) and the professional staff at all clinics.
c. Thresholds for Evaluation (Section 3). Evaluate compliance with indicator criteria.
If the evaluation does not meet a threshold, then the QAFG or its designee(s) must
investigate the aspects of care and recommend specific action(s) for improvement.
d. Data Collection Methodology (Section 4). M&E exercises’ data collection processes
are designed to be simple. Any staff member can collect the data. One method is to
review clinical records for specific indicator criteria, which are assessed as either
"met" or "not met" and recorded accordingly. The "not met" column on the Data
Collection Log allows the data collector to identify the specific unmet criteria, so
follow-up action can be started.
e. Evaluation Report (Section 5). Calculate the percentage of reviewed cases that meet
and do not meet the indicator criteria and enter results
f. Recommended Action (Section 7). The QAFG must act on completed M&E
Reports. If the M&E does not meet a threshold, its QAFG must recommend
action(s) to improve this aspect of care.
g. Follow-Up Reports (Sections 8-10). Generate either 3 or 6 months after the initial
report by completing Section 8 on the M&E Report Form reverse. If possible, the
same person responsible for the initial report should prepare the follow-up report. In
some cases, a clinic may need to continue a quarterly M&E of a particular aspect of
care indefinitely. Use Form Sections 9 and 10 for this purpose.
h. Figure 13-H-33 depicts an M&E flow chart.

CH-13 13-34
Figure 13-H-1
ANNUAL MONITORING AND EVALUATION SCHEDULE
QUARTER 1st 2
nd 3rd 4th
INITIAL MED DENT DUR OPTIONAL
*FOLLOW-UP DUR OPTIONAL MED DENT
CLINICAL ASPECTS OF CARE FOR MONITORING AND EVALUATION
MED 1. Strep Throat
2. Urinary Tract Infection
3. Gastroenteritis
4. Hypertension
5. Non-specific Vaginitis
6. Otitis Externa
7. Preventive Health Activities (Healthy Lifestyle Assessment)
8. Diagnosis of Acute Minor Illness: Acute Contact Dermatitis
9. Diagnosis of Acute Minor Illness: Herpes Zoster (Shingles)
DENT 1. Exodontia Informed Consent
2. Annual Dental Examinations
3. Dental Emergencies
4. Post-operative Infections
5. Restoration Replacements
6. Biopsies
7. Cast Restorations
8. Dental Radiographs
9. Endodontics
10. Dental Radiology
11. Periodontics
DUR 1. NSAID Therapy
2. Antibiotic Therapy
3. Antihistamine Therapy
4. Antilipemic Therapy
5. Intranasal Steroid Therapy
6. Oral Contraceptive Therapy
7. Smoking Cessation Aids
8. Oral Histamine H2 Antagonists

13-35 CH 13
Figure 13-H-1 (continued)
USING THE MONITORING AND EVALUATION SCHEDULE AND CLINICAL ASPECTS
OF CARE LISTING
Each clinic shall monitor at least one clinical aspect of care each quarter. The schedule above
determines the required category examined in each quarter. Clinics shall select an aspect of care
from the menu below the specified category. For example, each year in the first quarter, M&E
must be performed for a Medical (MED) aspect of care on the category menu (e.g., Strep Throat).
Submit completed M&E reports to the Quality Assurance Focus Group (QAFG) before the last
work day of each quarter. Data collection for each exercise should begin on the first day of each
quarter to allow time to collect and evaluate a representative data sample before the end of the
quarter. It is recommended that the QAFG assign responsibility for each exercise before the start
of each quarter, so that person may collect data promptly. Whenever possible, the same person
responsible for the initial M&E report also should generate follow-up reports.
FOLLOW-UP REPORTS
For studies that meet thresholds:
Each initial M&E report must be followed six months later by a follow-up report.
For studies that do not meet thresholds:
A follow-up report is required three months after the initial report and every three months
after that, until the evaluation meets thresholds.
Record follow-up reports on the M&E Report Form reverse in Sections 8, 9, and 10.
USING THE M&E DATA COLLECTION LOG, CG-5544
Use this form or a locally produced equivalent to evaluate health records or other information
sources for compliance with the indicator criteria. Record each health record reviewed as
meeting or not meeting the indicator. M&E Report Section 2 lists indicator criteria, signify
unmet indicator criteria by marking the log’s appropriate column (e.g., (a), (b), etc.).
Retain completed logs or equivalent on file for three years for MLC QA site survey teams’
review.
CH-13 13-36
Figure 13-H-2
MED-1
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Diagnosis of acute minor illnesses: Strep throat.
2. Indicator All patients diagnosed with strep throat have these documents in their health record
(SF-600) (record must meet all three criteria):
a. A positive either throat culture or “Rapid Strep;” or a documented history of
two of these three findings: Fever, purulent tonsils, or lympadenophathy; and
b. A temperature was taken and recorded; and
c. A description of the condition of the tonsils and/or oropharynx
3. Threshold 90% of the records reviewed shall meet the criteria contained in the indicator.
4. Data
Collection
Methodology
a. Use CLAMS and/or a review of patient records and/or a review of lab records
to retrospectively identify all patients with a diagnosis of “strep throat,” up to a
maximum random sample size of 25 patients.
b. The QAFG or its designee will review all identified patients’ health records to
determine whether they meet the indicator criteria. Record the result on the
M&E Data Log for each case before reporting results in Section 5.
c. If the records do not meet the threshold, the QAFG shall review all cases which
do not meet the criteria before recommending improvement in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse

13-37 CH 13
Figure 13-H-3
MED-2
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Diagnosis of acute minor illnesses: Urinary Tract Infection.
2. Indicator All patients diagnosed with Urinary Tract Infection must have these documents in
their health record (SF-600) (record must meet all three criteria):
a. Temperature recorded,
b. Documented exam (positive or negative) for cva/flank tenderness; and
c. Urinalysis results.
3. Threshold 90% of the records reviewed shall meet the criteria contained in the indicator.
4. Data
Collection
Methodology
a. Use CLAMS and/or a review of patient records and/or a review of lab records
to retrospectively identify all patients with a diagnosis of “urinary tract
infection,” up to a maximum random sample size of 25 patients.
b. The QAFG or its designee will review all identified patients’ health records to
determine whether they meet the indicator criteria. Record the result on the
M&E Data Log for each case before reporting results in Section 5.
c. If the records do not meet the threshold, the QAFG shall review all cases which
do not meet the criteria before recommending improvement in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
CH-13 13-38
Figure 13-H-4
MED-3
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Diagnosis of acute minor illnesses: Acute Gastroenteritis.
2. Indicator All patients diagnosed with Acute Gastroenteritis must have these documents in
their health record (SF-600) (record must meet all five criteria):
a. History (presence or absence) of nausea or vomiting, and/or diarrhea (if
present, number of stools in past 24 hours,
b. Temperature recorded,
c. History (positive or negative) of blood in stools.
d. Abdominal exam, and
e. Current weight of children 11 and younger.
3. Threshold 90% of the records reviewed shall meet the criteria contained in the indicator.
4. Data
Collection
Methodology
a. Use CLAMS and/or a review of patient records and/or a review of lab records
to retrospectively identify all patients with a diagnosis of “acute
gastroenteritis,” up to a maximum random sample size of 25 patients.
b. The QAFG or its designee will review all identified patients’ health records to
determine whether they meet the indicator criteria. Record the result on the
M&E Data Log for each case before reporting results in Section 5.
c. If the records do not meet the threshold, the QAFG shall review all cases which
do not meet the criteria before recommending improvement in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
13-39 CH 13
Figure 13-H-5
MED-4
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Out-patient management of chronic illnesses: Hypertension.
2. Indicator All patients diagnosed as hypertensive must have these documents in their health
record (SF-600) (record must meet all four criteria):
a. A treatment plan as evidenced in a “SOAP” entry on the SF-600,
b. Blood pressure recorded at least once in preceding six months,
c. Documented evaluation of EKG, electrolytes, BUN or creatinine, and
d. A recommended follow-up visit.
3. Threshold 90% of the records reviewed shall meet the criteria contained in the indicator.
4. Data
Collection
Methodology
a. Use CLAMS or a review of the hypertensive prescription files to
retrospectively identify all patients diagnosed as hypertensive during a six-
month period which begins one year before the date the M&E exercise begins..
b. The QAFG or its designee will review all identified patients’ health records to
determine whether they meet the indicator criteria. Record the result on the
M&E Data Log for each case before reporting results in Section 5.
c. If the records do not meet the threshold, the QAFG shall review all cases which
do not meet the criteria before recommending improvement in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
CH-13 13-40
Figure 13-H-6
MED-5
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Diagnosis of acute minor illnesses: Non-specific Vaginitis.
2. Indicator All patients diagnosed with Non-specific Vaginitis must have these documents in
their health record (SF-600) (record must meet five out of six criteria):
a. History of present illness, including sexual behavior;
b. Past medical history;
c. Medication history;
d. Temperature recorded;
e. Documented pelvic examination (positive or negative), including description of
vaginal discharge; and
f. Microscopic examination of discharge, including KOH prep (yeast), wet prep
(clue cells), and testing for chlamydia and GC.
3. Threshold 90% of the records reviewed shall meet five criteria contained in the indicator.
4. Data
Collection
Methodology
a. Use CLAMS and/or a review of patient records and/or a review of lab records
to retrospectively identify all patients with a diagnosis of “non-specific
vaginitis,” up to a maximum random sample size of 25 patients.
b. The QAFG or its designee will review all identified patients’ health records to
determine whether they meet the indicator criteria. Record the result on the
M&E Data Log for each case before reporting results in Section 5.
c. If the records do not meet the threshold, the QAFG shall review all cases which
do not meet the criteria before recommending improvement in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
13-41 CH 13
Figure 13-H-7
MED-6
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Diagnosis of Acute External Otitis (Otitis Externa)
2. Indicator All patients diagnosed with Acute External Otitis must have these documents in
their health record (SF-600) (record must meet three out of four criteria):
a. History of present illness;
b. Past medical history;
c. Temperature recorded;
d. Physical examination of the external ear, including:
1. Movement of the tragus or auricle to elicit pain;.
2. Description of the external ear canal, and
3. Description of any discharge found in the canal or external ear.
3. Threshold 90% of the records reviewed shall meet three criteria contained in the indicator.
4. Data
Collection
Methodology
a. Use CLAMS and/or a review of patient records and/or a review of lab records
to retrospectively identify all patients with a diagnosis of “Acute External
Otitis,” up to a maximum random sample size of 25 patients.
b. The QAFG or its designee will review all identified patients’ health records to
determine whether they meet the indicator criteria. Record the result on the
M&E Data Log for each case before reporting results in Section 5.
c. If the records do not meet the threshold, the QAFG shall review all cases which
do not meet the criteria before recommending improvement in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
CH-13 13-42
Figure 13-H-8
MED-7
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Preventive Health Activities (Healthy Lifestyle Assessment)
2. Indicator Adult patients’ health records should assess annually these factors with health
education and counseling as needed::
a. Diet;
b. Tobacco use (cigarettes, smokeless tobacco, pipes, cigars);
c. Alcohol use;
d. Seat belt use;
e. Exercise type and frequency;
f. Stress identification and reduction;
g. TSE/BSE; and
h. Immunizations.
3. Threshold 60% of the random sample of patients seen in the study time frame should have had
a health assessment performed.
4. Data
Collection
Methodology
a. Use CLAMS or the patient appointment log to identify a random selection of
adult patients who present for non-emergent conditions and/or physical exams
during the study time frame.
b. The QAFG or its designee will review all identified patients’ health records to
determine whether they meet the indicator criteria. Record the result on the
M&E Data Log for each case before reporting results in Section 5.
c. If the records do not meet the threshold, the QAFG shall review all cases which
do not meet the criteria before recommending improvement in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
13-43 CH 13
Figure 13-H-9
MED-8
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Diagnosis of acute minor illness: Acute Contact Dermatitis
2. Indicator All patients diagnosed with Contact Dermatitis must have these documents in their
health record (SF-600) (record must meet all criteria)
a. History of present illness, including any recent changes in habits, detergents,
soaps, lotions, topical medications, and known contact substance cause;
b. Problem-focused medical history;
c. Physical examination, including the description and distribution of lesion(s)
(rash).
3. Threshold 90% of the records reviewed shall meet all criteria contained in the indicator.
4. Data
Collection
Methodology
a. Use CLAMS and/or a review of patient records to retrospectively identify all
patients with a diagnosis of “contact dermatitis,” “industrial dermatitis,” or
“poison ivy.” Select a random sample of 25 patients.
b. The QAFG or its designee will review all identified patients’ health records to
determine whether they meet the indicator criteria. Record the result on the
M&E Data Log for each case before reporting results in Section 5.
c. If the records do not meet the threshold, the QAFG shall review all cases which
do not meet the criteria before recommending improvement in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
CH-13 13-44
Figure 13-H-10
MED-9
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Diagnosis of acute minor illness: Herpes Zoster (Shingles)
2. Indicator All patients diagnosed with herpes zoster or shingles must have these documents in
their health record (SF-600):
a. History of present illness, including:
1. Course of illness and constitutional symptoms, if any, such as low
grade temperature and malaise; and
2. 2 subjective complaints, such as pain;
b. Problem-focused medical history;
c. Temperature recorded;
d. Physical examination, including these symptoms:
1. Description and distribution of primary lesions; and
2. Description and distribution of secondary lesions (if present).
3. Threshold 90% of the records reviewed shall meet all criteria contained in the indicator.
4. Data
Collection
Methodology
a. Use CLAMS and/or a review of patient records to retrospectively identify all
patients with diagnoses including “herpes zoster,” “herpes,” or “shingles.”
Select a random sample of 25 patients.
b. The QAFG or its designee will review all identified patients’ health records to
determine whether they meet the indicator criteria. Record the result on the
M&E Data Log for each case before reporting results in Section 5.
c. If the records do not meet the threshold, the QAFG shall review all cases which
do not meet the criteria before recommending improvement in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
13-45 CH 13
Figure 13-H-11
DENT-1
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Patient Education: Informed Consent for Dental Procedures.
2. Indicator The dental record documents informed consent before all exodontia procedures,
evidenced by the presence of a dated informed consent document (e.g., SF-522)
describing the procedure, associated risks, and alternatives; the dentist, a witness,
and the patient have signed the form.
3. Threshold 100% of the records reviewed shall meet the indicator criteria.
4. Data
Collection
Methodology
a. Use CLAMS and/or a review of patient records to retrospectively identify all
patients who have undergone exodontia procedures, up to a maximum random
sample of 25 patients.
b. The QAFG or its designee will review all identified patients’ health records to
determine whether they meet the indicator criteria. Record the result on the
M&E Data Log for each case before reporting results in Section 5.
c. If the records do not meet the threshold, the QAFG shall review all cases which
do not meet the criteria before recommending improvement in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
CH-13 13-46
Figure 13-H-12
DENT-2
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Preventive Dentistry: Annual Type II Dental Examination for Active Duty
USCG Personnel.
2. Indicator Active duty USCG members’ dental record (SF-603) contains documentation of a
Type II dental examination within the past 12 months.
3. Threshold 90% of the records reviewed shall meet the indicator criteria.
4. Data
Collection
Methodology
a. The QAFG or its designee will randomly select 50 active duty members’ dental
records.
b. The QAFG or its designee will review each record (SF-603) to determine
whether a dental officer performed a documented Type II dental examination
during the past 12 months. Record the result on the M&E Data Log for each
case before reporting results in Section 5.
c. If the records do not meet the threshold, the QAFG shall review all cases which
do not meet the criteria before recommending improvement in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
13-47 CH 13
Figure 13-H-13
DENT-3
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Treatment of Dental Emergencies..
2. Indicator Patients treated for dental emergencies make unscheduled return visits with the
same complaint within 72 hours of the original sick call visit.
3. Threshold 90% of the patients seen for a dental emergency or sick call visit do NOT return for
an unscheduled visit for the same complaint within 72 hours..
4. Data
Collection
Methodology
a. Maintain a daily log of all patients reporting to the clinic for dental
emergencies or sick call during a 60-day period. Be sure each patient is logged
and note the date.
b. After this 60-day period, the QAFG or its designee will review the emergency
or sick call log and screen the records of all emergencies or sick call visits to
identify any patients paying a return visit for the same complaint within 72
hours of the first visit. The QAFG or its designee will review these records to
determine whether they meet the indicator criteria. Record the result on the
M&E Data Log for each case before reporting results in Section 5.
c. If the records do not meet the threshold, the QAFG shall review all cases which
do not meet the criteria before recommending improvement in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
CH-13 13-48
Figure 13-H-14
DENT-4
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Post-Operative Infections
2. Indicator Note surgical sites that develop infections after oral surgery on SF-603/603A and
on CLAMS forms with an audit code. Post-operative inflections display these
characteristics:
a. Elevated oral temperature (>100° F.) in the absence of other disease; and
b. Increase in purulent drainage from the surgical site; and
c. Increased inflammatory signs and symptoms.
3. Threshold Fewer than 10% of the surgical site(s) will develop post-operative infections.
4. Data
Collection
Methodology
a. Use CLAMS or a log to determine the number of surgical procedures
performed in a month to a maximum of 30 cases.
b. Use a record review, a log, or a CLAMS audit code to determine the number of
surgical procedures performed which resulted in post-operative infections.
c. The QAFG or its designee will review these records to determine whether they
exceed the threshold.
d. If the records exceed the threshold, the QAFG shall review all post-operative
infection and recommend action to the SDO.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
13-49 CH 13
Figure 13-H-15
DENT-5
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Replacing Dental Restorations
2. Indicator Note either in a log or with a CLAMS audit code all dental restorations performed
to replace a restoration that has failed within one year of placement. Characteristics
of failed restorations include:
a. Caries;
b. Lost tooth structure, including fractures;
c. Fractured or displaced restoration; and
d. Open contact or margin.
3. Threshold Fewer than 10% of restorations placed will need replacing within one year.
4. Data
Collection
Methodology
a. Use CLAMS to record the number of restorations each dental officer places in
one month.
b. Use a CLAMS audit code or a log to record the number of each dental officer’s
replacement restorations required fewer than 12 months after original
placement.
c. The QAFG or its designee will review these records to determine whether they
exceed the threshold.
d. If the records exceed the threshold, the QAFG shall review all premature that
specific dental officer’s restorative failures and recommend action to the SDO.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
CH-13 13-50
Figure 13-H-16
DENT-6
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Biopsies
2. Indicator Biopsies are submitted properly:
a. Specimens are properly prepared and shipped them according to USN SF-515
guidelines; and
b. Adequate amounts of tissues are submitted.
3. Threshold Fewer than 10% of biopsies submitted have SF-515 forms returned with
notes indicating inadequate tissue sampling or improper preparation and
shipping..
4. Data
Collection
Methodology
a. Use CLAMS or a log to identify the number biopsy procedures performed each
month, to a maximum of 10 cases.
b. Perform a record review of all biopsy cases (up to 10) to determine the number
of cases returned with improper samples, tissue preparation, or shipping.
c. The QAFG or its designee will review these records to determine whether they
exceed the threshold.
d. If the records exceed the threshold, the QAFG shall review all premature that
specific dental officer’s restorative failures and recommend action to the SDO.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
13-51 CH 13
Figure 13-H-17
DENT-7
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Cast Restorations
2. Indicator Treatment is properly planned.
a. Periapical radiographs and periodontal probings are evaluated before preparing
the teeth, and
b. Provisional (temporary) restorations are placed.
3. Threshold More than 90% of castings show a record of recent (<6 months) evaluation
of periapical radiographs and periodontal probings and more than 90% of
prepared teeth show a record of a successful provisional restoration.
4. Data
Collection
Methodology
a. Use CLAMS or a log to identify the number of castings performed each month,
to a maximum of 10 cases.
b. Perform a record review of all casting cases (up to 10) to determine the number
without pre-operative radiographs and probings or successful provisional
restorations.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
CH-13 13-52
Figure 13-H-18
DENT-8
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Dental Radiographs
2. Indicator Radiographs are of diagnostic quality and display these characteristics:
a. Apices of subject teeth visible on PA films;
b. Open interproximals on BW films;
c. Films are appropriately developed and fixed; and
d. Films exhibit appropriate contrast
3. Threshold More than 90% of films will display appropriate technique and development.
4. Data
Collection
Methodology
a. Review all recent (i.e., < 1 year old) dental radiographs in 50 randomly selected
records, recording the number of films with technical and developing errors.
b. The QAFG or its designee will review these records to determine whether they
exceed the threshold.
c. If the records exceed the threshold, the QAFG shall recommend action to the
SDO.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
13-53 CH 13
Figure 13-H-19
DENT-9
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Endodontics
2. Indicator Appropriate radiographs have been obtained.
3. Threshold More than 90% of cases include annotated pre- and post-operative
radiographs.
4. Data
Collection
Methodology
a. Identify endodontic cases with a CLAMS audit code; select 10 cases at random;
review those 10 records’ films; note the number of records with missing pre- or
post-operative films.
b. The QAFG or its designee will review these records to determine whether they
exceed the threshold.
c. If the records exceed the threshold, the QAFG shall recommend action to the
SDO.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
CH-13 13-54
Figure 13-H-20
DENT-10
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Dental Radiology
2. Indicator Radiographs are appropriately ordered and correctly interpreted.
3. Threshold Appropriate radiographs are ordered in 85% of cases and noted pertinent
radiographic finds in 85% of cases.
4. Data
Collection
Methodology
a. Select 25 dental records at random; review films and forms SF-603/603A for
all 25; record the number of inappropriate orders and flawed interpretations.
b. The QAFG or its designee will review these records to determine whether they
exceed the threshold.
c. If the records exceed the threshold, the QAFG shall recommend action to the
SDO.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
13-55 CH 13
Figure 13-H-21
DENT-11
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Periodontics
2. Indicator PSR recorded and treated appropriately.
3. Threshold More than 90% of records indicate PSRs within the last 12 months and
appropriate follow-up in sextants with PSR of 3 or greater.
4. Data
Collection
Methodology
a. Select 50 dental records at random; review forms SF-603/603A for all 50; note
the number of records with absent or elevated and untreated PSRs.
b. The QAFG or its designee will review these records to determine whether they
exceed the threshold.
c. If the records exceed the threshold, the QAFG shall recommend action to the
SDO.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
CH-13 13-56
Figure 13-H-22
DUR-1
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Drug Utilization: Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
2. Indicator If treated with NSAIDs other than Aspirin, Indomethacin, and Ibuprofen, adults
(>18 years old) with soft tissue injuries, musculo-skeletal disorders, and dental
conditions must meet these criteria:
a. The patient’s health record documents a history of hypersensitivity, adverse
reaction, or specific contraindication to using Aspirin and either Indomethacin
and Ibuprofen, OR
b. The patient has a documented failure with Aspirin and Indomethacin and
Ibuprofen when used at appropriate therapeutic dosages (see below) for the
indication for which currently prescribed, OR
c. The record documents a specialist prescribed or recommended the NSAID.
Therapeutic Dosage Ranges Aspirin 325-650 mg every four hours
Indomethacin Up to 150 mg/day
Ibuprofen Up to 3.2 gram/day, divided doses
3. Threshold 90% of cases of records reviewed meet one of the criteria contained in the
indicator.
4. Data
Collection
Methodology
a. Use CLAMS or review prescription files to retrospectively identify all patients
receiving NSAIDs prescriptions except Aspirin, Indomethacin, and Ibuprofen
during a one-month period. Then use CLAMS or review these records to
identify patients who received the NSAIDs for the indicated conditions.
b. The QAFG or its designee will review these records to determine whether they
meet the criteria in the indicator. Record the result on the M&E Data Log for
each case before reporting results in Section 5.
c. If the records exceed the threshold, the QAFG or its designee shall review all
cases which do not meet the criteria and recommend action in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
13-57 CH 13
Figure 13.H.23
DUR-2
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Drug Utilization: Antibiotics
2. Indicator Health records document patients diagnosed with Otitis Media (OM) receive
prescriptions from a clinic practitioner for Amoxicillin, Penicillin, or Septra
UNLESS (record may meet any one of these criteria):
a. Current episode’s symptoms or signs persisted after an initial regimen of listed
antibiotics at therapeutic doses, OR
b. The diagnosis is expanded to recurrent OM (3 or more document OM episodes
in the last 6 months), OR
c. The patient has a documented allergy to Amoxicillin, Penicillin, or Septra, OR
d. Resistant strains are so prevalent in the community using listed antibiotics is
contraindicated.
3. Threshold 90% of records reviewed meet one of the four criteria in the indicator.
4. Data
Collection
Methodology
a. Use CLAMS or keep a log book to identify all patients with a reported OM
diagnosis in a one-month period. Then use CLAMS, review patient records, or
audit the prescription files to retrospectively identify which patients received
prescriptions for antibiotics other than the three listed.
b. The QAFG or its designee (e.g., Pharmacy and Therapeutics Committee) will
review these patients’ records to determine whether they meet the criteria in the
indicator. Record the result on the M&E Data Log for each case before
reporting results in Section 5.
c. If the records exceed the threshold, the QAFG shall review all cases which do
not meet the criteria before recommending corrective action.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse

CH-13 13-58
Figure 13-H-24
DUR-3
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Appropriate use of Antihistamines: Terfenadine (Seldane) and Astemizole
(Hismanal)
2. Indicator Health records document patients prescribed these products have:
a. Previously documented unsuccessful trial with at least one other antihistamine
or documented history of intolerance to the sedative effects of antihistamines;
b. No concurrent therapy with ketoconazole and/or macrolide antibiotics
(Terfenadine only), and
c. No evidence of impaired hepatic function or disease (see Problem Summary
List).
3. Threshold 95% of all records reviewed meet the indicator criteria.
4. Data
Collection
Methodology
a. Use CLAMS or review the prescription files to retrospectively identify all
patients receiving prescriptions for Terfenadine and/or Astemizole.
b. The QAFG will review these patients’ records to determine whether they meet
the criteria in the indicator. Record the result on the M&E Data Log for each
case before reporting results in Section 5.
c. If the records exceed the threshold, QAFG or its designee shall review all cases
which do not meet the criteria, evaluate, and recommend action in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse

13-59 CH 13
Figure 13-H-25
DUR-4
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Antilipemic agent therapy (HMG-CoA Reductase inhibitors, Gemfibrozil)
2. Indicator Patients placed on therapy with the above agents have documented hyperlipidemia
confirmed by at least one of these baseline laboratory values:
a. Fasting total serum cholesterol 8 240 mg/dl
b. Fasting serum LDL 8 160 mg/dl
c. Fasting serum HDL 7 35 mg/dl
d. Fasting serum triglyceride levels 8 250 mg/dl
Note: In borderline cases, additional laboratory values should be sought before
initiating drug therapy.
3. Threshold 80% of all records reviewed meet the indicator criteria.
4. Data
Collection
Methodology
a. Use CLAMS to review the prescription files to retrospectively identify all
patients receiving prescriptions for these medications.
b. The QAFG or its designee will review these patients’ records to determine
whether they meet the criteria in the indicator. Record the result on the M&E
Data Log for each case before reporting results in Section 5.
c. If the records exceed the threshold, QAFG or its designee shall review all cases
which do not meet the criteria, evaluate, and recommend action in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
CH-13 13-60
Figure 13-H-26
DUR-5
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Appropriate use of intranasal steroids (Flunisolide, Beclomethasone,
Dexamthasone, Triamcinone, etc.) in seasonal and vasomotor rhinitis
2. Indicator All patients prescribed these medications will have:
a. Documented histories of seasonal or vasomotor rhinitis (characterized by
moderate to severe symptoms lasting 4 or more weeks per episode) combined
with a history of unsuccessful treatment with conventional therapy including
antihistamines, decongestants, or combination product therapy, and
b. Administration dosage and frequency within the product manufacturer’s and
FDA’s approved guidelines; and
c. Documented evidence instruction is provided in using these medications
properly.
3. Threshold 95% of all records reviewed meet the indicator criteria.
4. Data
Collection
Methodology
a. Use CLAMS to review the prescription files to retrospectively identify all
patients receiving prescriptions for intranasal steroids.
b. The QAFG or its designee will review these patients’ records to determine
whether they meet the criteria in the indicator. Record the result on the M&E
Data Log for each case before reporting results in Section 5.
c. If the records exceed the threshold, QAFG or its designee shall review all cases
which do not meet the criteria, evaluate, and recommend action in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
13-61 CH 13
Figure 13-H-27
DUR-6
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Appropriate use of oral contraceptive medications
2. Indicator All patients prescribed these medications will have:
a. Documented history of physical exams within the past year including personal
and family medical history, pelvic exam (including pap smear), breast exam,
and vital signs, and
b. Documented evidence of instruction in the proper use of these medications,
including an explanation of side effects, missed doses, increased risk factors
(smoking, etc.), and drug interactions (antibiotics, etc.).
3. Threshold 95% of all records reviewed meet the indicator criteria.
4. Data
Collection
Methodology
a. Use CLAMS to review the prescription files to retrospectively identify all
patients receiving prescriptions for oral contraceptives.
b. The QAFG or its designee will review these patients’ records to determine
whether they meet the criteria in the indicator. Record the result on the M&E
Data Log for each case before reporting results in Section 5.
c. If the records exceed the threshold, QAFG or its designee shall review all cases
which do not meet the criteria, evaluate, and recommend action in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
CH-13 13-62
Figure 13-H-28
DUR-7
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Appropriate use of smoking cessation aids (nicotine patches or gum)
2. Indicator All patients prescribed these medications will have:
a. Documented enrollment in a recognized smoking cessation behavioral
modification program advocating using nicotine products as adjunct therapy.
b. Health record documentation of counseling about using this medication
properly, its side effects, and the member shall not smoke while undergoing
this therapy.
c. Documentation therapy has been 12 or fewer weeks in duration.
3. Threshold 95% of all records reviewed meet the indicator criteria.
4. Data
Collection
Methodology
a. Use CLAMS to review the prescription files to retrospectively identify all
patients receiving prescriptions for smoking cessation aids.
b. The QAFG or its designee will review these patients’ records to determine
whether they meet the criteria in the indicator. Record the result on the M&E
Data Log for each case before reporting results in Section 5.
c. If the records exceed the threshold, QAFG or its designee shall review all cases
which do not meet the criteria, evaluate, and recommend action in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse

13-63 CH 13
Figure 13-H-29
DUR-8
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care Appropriate use of oral histamine H2 antagonist medications (Cimetidine,
Ranitidine, etc.)
2. Indicator All patients prescribed these medications will have:
a. Documented diagnosis of duodenal or gastric ulcer, a hypersecretory condition,
gastroesophageal reflux disease, or another appropriate indication before
initiating therapy as listed in the current Facts and Comparisons.
b. Documented case review within 4-6 weeks and shift to maintenance dose
regimen unless active disease still is present (except reflux esophagitis).
c. Documented monitoring of phenytoin serum levels (for cimetidine only) and
prothrombin times (all warfarin patients) for patients taking these drugs.
d. Documented counseling on lifestyle modification (smoking cessation, dietary
habits).
3. Threshold 95% of all records reviewed meet the indicator criteria.
4. Data
Collection
Methodology
a. Use CLAMS to review the prescription files to retrospectively identify all
patients receiving prescriptions for oral histamine H2 antagonist medications.
b. The QAFG or its designee will review these patients’ records to determine
whether they meet the criteria in the indicator. Record the result on the M&E
Data Log for each case before reporting results in Section 5.
c. If the records exceed the threshold, QAFG or its designee shall review all cases
which do not meet the criteria, evaluate, and recommend action in Section 7.
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
CH-13 13-64
Figure 13-H-30
OPTIONAL
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care
2. Indicator
3. Threshold
4. Data
Collection
Methodology
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse
13-65 CH 13
Figure 13-H-30
OPTIONAL
MONITORING AND EVALUATION REPORT
Facility__________________________ QA Coordinator_____________________________
1. Aspect of Care
2. Indicator
3. Threshold
4. Data
Collection
Methodology
5. Evaluation
Report
% Meeting _____ % Not Meeting Indicator Criteria _____
6. Evaluator Name: ___________________________ Date Evaluated _____
7. Recommended
Action
______________________________ / ______
Signature Date
Continued on Reverse

CH-13 13-66
Figure 13-H-31
8. 3 to 6-Month
Follow-up
Report
Evaluation Criteria: _____ % Meeting _____ % Not Meeting
_____Continue M&E _____ Discontinue M&E
Recommended Action:
________________________ / ___________
Signature Date
9. 3 to 6-Month
Follow-up
Report
Evaluation Criteria: _____ % Meeting _____ % Not Meeting
_____Continue M&E _____ Discontinue M&E
Recommended Action:
________________________ / ___________
Signature Date
10. 3 to 6-Month
Follow-up
Report
Evaluation Criteria: _____ % Meeting _____ % Not Meeting
_____Continue M&E _____ Discontinue M&E
Recommended Action:
________________________ / ___________
Signature Date
Facility ____________________________________________
Aspect of Care ______________________________________
Data Collector __________________________ Date _______

13-67 CH 13
M & E DATA COLLECTION LOG
[Ed. Note: Not reviewed.]
DEPT. OF TRANSP., USCG CG 5544 (9-91)
LOCAL REPRO
SECTION I PEER REVIEW PROGRAM.
[Ed. Note: Text to come.]

CH-13 13-68
SECTION J UTILIZATION REVIEW PROGRAM.
[Ed. Note: Text to come.]
13-69 CH 13
Section K - Infection Control Program (exposure control plan).
1. Background.
a. A standard set of infection control strategies is essential to prevent transmitting
infectious diseases. Because history, physical examination, and/or readily available
laboratory tests cannot identify all infected patients, use these procedures when
providing health care to any patient to prevent transmitting infectious agents.
b. Health services personnel (officers, enlisted, and civilian) and emergency medical
technicians (EMTs) may be exposed to infection through direct contact, droplets, or
aerosols from a wide variety of microorganisms in their patients’ blood, secretions,
excretions, and other body fluids. Direct contact may transmit infection by
contaminated instruments (e.g.; needle sticks). Everyone has the potential to transmit
infectious diseases to others. All health services personnel and emergency medical
technicians must know how infectious diseases spread and take appropriate
precautions.
c. While Coast Guard health services personnel and emergency medical technicians
must be seriously concerned with the risk of exposure to human immunodeficiency
virus (HIV), the risk of contracting other infectious diseases, such as hepatitis B virus
(HBV), is much greater. HBV infection can result in serious physical debilitation
and adversely affect a practitioner’s ability to provide health care. Once infected, a
person also poses a potential risk to future patients as an HBV infection “carrier.”
Infection control practices that prevent HVB transmission also prevent HIV
transmission. Since 1982 a safe, effective vaccine to prevent Hepatitis B has been
available; it stimulate active immunity against HBV infection and provides over 90%
protection against the virus for 7 or more years after vaccination.
2. Policy.
a. Health services personnel will adhere to infection-control principles, general hygiene
measures, and the Center for Disease Control and Prevention’s (CDC’s) “universal
precautions” to prevent transmitting infectious disease between themselves and their
patients.
b. Hepatitis B vaccination is mandatory for all Coast Guard health services personnel
and recommended for emergency medical technicians. Civilian administrative staff
and E-8 and E-9 Health Services Technicians filling administrative positions are
exempt; however, these personnel are encouraged to receive Hepatitis B vaccination.
EMTs and clinic administrative personnel declining to receive HBV vaccination
must sign this statement on an SF-600, and it shall be retain in the individual’s health
record:
I understand due to my occupational exposure to blood or other potentially
infectious materials I may be at risk of acquiring Hepatitis B virus (HBV)
infection. I have been given the opportunity to be vaccinated free with
Hepatitis B vaccine. However, I now decline Hepatitis B vaccination. I
understand by declining this vaccine, I continue to risk acquiring Hepatitis B,
CH-13 13-70
a serious disease. If in the future I continue to have occupational exposure
to blood or other potentially infectious materials and I want to be vaccinated
with Hepatitis B vaccine, I can receive the vaccination series free.
c. Emergency medical technicians will adhere to the “universal precautions” described
in Chapter 13-K-3.
d. Under the OSHA Blood-Borne Pathogen (BBP) Standard, all health services
administrative and clinical personnel are occupationally exposed. All clinics shall
provide the health care professional responsible for vaccinating employees with
Hepatitis B vaccine a copy of the OSHA BBP Standard.
3. Universal Precautions.
a. Since medical history and examination cannot reliably identify all patients infected
with HIV or other blood-borne pathogens, care providers must consistently use blood
and body-fluid precautions with all patients, including those in emergency care
settings in which the risk of blood exposure is greater and the patient’s infectious
status usually is unknown. CDC currently recommends the “universal blood and
body-fluid precautions” approach or “universal precautions.”
(1) All health care workers will routinely use appropriate barrier precautions to
prevent skin and mucous-membrane exposure when anticipating contact with
any patient’s blood or other body fluids. Personnel will wear gloves to touch
patients’ blood and body fluids, mucous membranes, or broken skin; to handle
items or surfaces soiled with blood or body fluids; and to perform venipuncture
and other vascular access procedures. Personnel will change gloves after
contact with each patient. Personnel will wear masks and protective eyewear
or face shields during procedures likely to generate blood droplets or other
body fluids to prevent exposure to oral, nasal, or optic mucous membranes.
Personnel will wear gowns or aprons during procedures likely to generate
blood splashes or other body fluids.
(2) If contaminated with blood or other body fluids, personnel immediately will
wash hands and other skin surfaces thoroughly. All persons shall wash their
hands after completing activities likely to expose them to BBPs and remove
protective clothing before leaving the work area.
(3) All health care workers will take precautions to prevent injuries caused by
needles, scalpels, and other sharp instruments or devices during procedures or
when cleaning used instruments, disposing of used needles, and handling sharp
instruments after procedures. To prevent needle stick injuries, personnel will
not by hand directly recap needles, purposely bend or break them, remove them
from disposable syringes, or otherwise manipulate them. After using
disposable syringes and needles, scalpel blades, and other sharp items,
personnel will dispose of them by placing them in puncture-resistant containers
located as close to the use area as practical. The Coast Guard does not
authorize using reusable needles.
13-71 CH 13
(4) Although research has not definitively implicated saliva in HIV transmission, it
is prudent to use mouthpieces, resuscitation bags, or other ventilation devices
instead of mouth-to-mouth resuscitation. These devices must be available for
use in areas where the need for resuscitation is predictable.
(5) Health care workers who have exuding lesions or weeping dermatitis will not
provide any direct patient care or handle patient care equipment until the
condition resolves.
(6) Eating, drinking, smoking, applying cosmetics or lip balm, and handling
contact lenses are prohibited in work areas with a reasonable likelihood of
occupational exposure to BBPs.
(7) Personnel shall not keep food and drink in refrigerators, freezers, shelves, drug
storage areas, or cabinets or on countertops or benchtops where blood or other
potentially infectious materials are present.
(8) Personnel shall perform all procedures involving blood or other potentially
infectious materials in a manner that prevents droplets of these substances from
splashing, spraying, splattering, and generating.
(9) Pregnant health care workers apparently do not face greater risk of contracting
HIV infection than non-pregnant health care workers; however, if a health care
worker develops HIV infection during pregnancy, the infant risks infection due
to prenatal or perinatal transmission. Therefore, pregnant health care workers
will thoroughly learn and strictly adhere to universal precautions to minimize
the risk of HIV transmission.
b. Implementing universal blood and body fluid precautions for all patients eliminates
the need for the “Blood and Body Fluid Precautions” isolation category CDC
previously recommended for patients known or suspected to be infected with blood-
borne pathogens. Personnel will use isolation precautions as necessary if they
diagnose or suspect associated conditions, such as infectious diarrhea or tuberculosis.
4. Precautions for Invasive Procedures. The universal blood and body fluid precautions
listed above and those listed below shall be the minimum precautions for all invasive
procedures, defined as surgical entry into tissues, cavities, or organs; repair of major
traumatic injuries in an operating or delivery room, emergency department, or out-patient
setting, including both physicians’ and dentists’ offices; a vaginal delivery;
manipulating, cutting, or removing any oral or perioral tissues, including tooth structure,
during which bleeding occurs or the potential for bleeding exists.
a. All health care workers who participate in invasive procedures routinely shall take
appropriate barrier precautions to prevent skin and mucous membrane contact with
all patients’ blood and other body fluids. Personnel shall wear gloves and surgical
masks for procedures that commonly generate droplets, splash blood or other body
fluids, or generate bone chips, such as those using rotary dental instrumentation.
Personnel shall wear gowns or aprons made of materials that provide an effective
barrier during invasive procedures likely to splash blood or other body fluids. All
health care workers who perform or assist in vaginal deliveries shall wear gloves and
CH-13 13-72
gowns when handling the placenta or infant until after they remove blood and
amniotic fluid from the infant’s skin and during post-delivery care of the umbilical
cord.
b. If a glove is torn, cut, or punctured, the wearer will remove it, re-scrub, and put on a
new glove as promptly as patient safety permits. The needle or instrument involved
in the incident shall also be remove from the sterile field.
5. Precautions for Medical Laboratories. Blood and other body fluids from all patients will
be considered infectious. To supplement the universal blood and body fluid precautions
listed above, these following precautions are recommended for health care workers in
clinical laboratories.
a. All blood and body fluid specimens shall be placed in a well-constructed, labeled
container with a secure lid to prevent leaking during transport, taking care when
collecting each specimen to avoid contaminating the container’s exterior or the
laboratory form accompanying the specimen.
b. All persons obtaining or processing blood and body fluid specimens (e.g., removing
tops from vacuum tubes) shall wear gloves. Personnel shall wear masks and
protective eyewear if they anticipate contact with mucous membrane with blood or
body fluids, change gloves, and wash hands after completing specimen processing.
c. For routine procedures such as histologic and pathologic studies or microbiologic
culturing, a biological safety cabinet is not necessary. However, personnel shall use
biological safety cabinets (Class I or II) whenever performing procedures with a high
potential for generating droplets, including activities such as blending, sonicating,
and vigorous mixing.
d. Use mechanical pipetting devices to manipulate all liquids in the laboratory. Never
pipette by mouth.
e. Use needles and syringes only in situations in which no alternative exists. Personnel
will follow the recommended universal precautions to prevent needle injuries.
f. Decontaminate laboratory work surfaces with an appropriate chemical germicide
after spilling blood or other body fluids and completing work activities.
g. Decontaminate contaminated materials (including gauze pads) used in laboratory
tests before reprocessing or place such materials in bags and dispose of them
according to institutional policies for disposing of infectious waste.
h. Decontaminate scientific equipment contaminated with blood or other body fluids
with an appropriate chemical germicide and clean such equipment before repairing it
in the laboratory or transporting it to the manufacturer.
i. All persons shall wash their hands after completing laboratory activities and remove
protective clothing before leaving the laboratory.
13-73 CH 13
6. Handling Biopsy Specimens. Generally, personnel must put each specimen in a sturdy
container with a secure lid to prevent leaking during transport and take care when
collecting specimens to avoid contaminating the container’s exterior. If the outside of
the container is visibly contaminated, clean and disinfect it or place it in an impervious
bag before delivery to the appropriate destination for examination
7. Using and Caring for Sharp Instruments and Needles.
a. Personnel will consider sharp items (needles, scalpel blades, dental burs, and other
sharp instruments) potentially infectious and handle them with extreme care to
prevent unintentional injuries.
b. Personnel must place disposable syringes and needles, scalpel blades, anesthetic
carpules and other sharp items in closable, leak-proof, puncture-resistant containers.
Cardboard containers are not appropriate for this purpose. To prevent unintentional
needle stick injuries, personnel will not by hand directly recap disposable needles,
purposefully bend or break them, remove them from disposable syringes, or
otherwise manipulate them after use.
c. If multiple injections of anesthetic or other medications from a single syringe are
required, personnel may use these techniques in lieu of directly recapping by hand:
(1) Use an approved shielding device specifically designed to recap safely (e.g.,
“On-Guard”).
(2) Use the “scoop” recapping technique. Affix the empty needle sheath to a flat
surface and “scoop” it onto the exposed needle. A hand does not touch the
sheath until the needle is securely inside.
(3) Use a hemostat to recap by securing the empty sheath well away from the
health care worker’s hand.
d. All Coast Guard Health Care Units shall establish a needle stick protocol; see
Section 13-K-13. If a needle stick occurs, the affected person shall report the
accident to his or her immediate supervisor, who will document the incident in a
memorandum to the Chief, Health Services Division or health services department
head, with a copy to the affected person. The memorandum will detail the needle
stick’s time, date, and circumstances and any medical treatment received. The Chief,
Health Services Division or health services department head shall ensure the
established needle stick protocol is observed in all cases.
8. Infection Control Procedures for Minor Surgery Areas and Dental Operatories.
a. Medical History. Always obtain a thorough medical history. For dental procedures,
have the patient complete a Dental Health Questionnaire, NAVMED 6600/3, as
Section 4-C requires. Amplify this information by asking the patient specific
questions about medications, current illnesses, hepatitis, recurrent illness,
unintentional weight loss, lymphadenopathy, oral soft tissue lesions, results of last
HIV test, or other infections. Completely review the individual’s health record or
consult with a physician if the history reveals active infection or systemic disease.

CH-13 13-74
b. Using Protective Attire and Barrier Techniques.
(1) Health care workers will consider all patients’ blood, saliva, and other body
fluids infectious. To protect themselves and patients, personnel must always
wear gloves when touching:
(a) blood;
(b) saliva;
(c) body fluids or secretions;
(d) items or surfaces contaminated by the above; and
(e) mucous membranes.
(2) Further, personnel must completely treat one patient, if possible, and wash and
re-glove hands before performing procedures on another patient. Repeatedly
using a single pair of gloves is not allowed; such use can produce defects in the
glove material which reduce its effectiveness as a barrier to microorganisms.
Additionally, when gloves are torn, cut, or punctured, the wearer immediately
must remove them, thoroughly wash his or her hands, and put on new gloves
before completing minor surgical or dental procedures.
(3) Personnel shall wear surgical masks and protective eyewear or a chin-length
plastic face shield. Personnel shall change masks after lengthy examinations or
procedures, most especially after any which produce spatter. Patient protective
eyewear shall be provide during all treatment procedures likely to splash or
spatter blood, saliva, gingival fluids, or foreign objects. Personnel will use
rubber dams, pre-procedural mouth rinsing, high-speed evacuation, and proper
patient positioning, when appropriate, to minimize droplet generation and
spatter in the dental operatory.
(4) When examining or treating any patient personnel must wear smocks, gowns,
or laboratory coats. If wearing a reusable gown, personnel shall wash it using a
normal laundry cycle. Personnel shall change gowns at least daily, when
visibly soiled, or after any surgical procedure. All treatment team members
must wear long-sleeved gowns or smocks during all surgical procedures
employing rotary instrumentation.
c. Washing and Caring for Hands.
(1) Personnel must always wash hands after removing gloves between patient
treatment contacts, after touching inanimate objects blood or saliva likely has
contaminated, and before leaving the minor surgery area or dental operatory
because gloves knowingly or unknowingly may become perforated during use.
These perforations allow bacteria to enter and multiply rapidly beneath the
glove material.
(2) Whenever possible wash hands at sinks that provide hot and cold water
through a single mixing valve and preferably readily accessible to the treatment

13-75 CH 13
room or operatory. After scrubbing, rinse hands in cool water to reduce the
likelihood and severity of latex reactions.
(3) For certain routine dental procedures, such as examinations and non-surgical
techniques, hand-washing with plain soap is adequate, since soap and water
will remove transient microorganisms. For surgical procedures, personnel
must use an antimicrobial surgical hand scrub. Clinics may need to stock non-
allergenic soap for allergic individuals.
(4) Health services personnel who have exuding lesions or weeping dermatitis
must refrain from all direct patient care and handling patient-care equipment
until the condition resolves.
d. Sterilizing and Disinfecting Dental Hand Pieces, Ultrasonic Scalers, and Dental
Units.
(1) After each use with each patient, personnel will sterilize dental hand pieces
(including high-speed, low-speed components used intraorally and ultrasonic
scalers) because the device may aspirate a patient’s blood, saliva, or gingival
fluid into the hand piece or waterline. Clinics should purchase sufficient
numbers of autoclavable hand pieces to meet this requirement. Dry heat is the
recommended method of sterilizing dental burs.
(2) Because water retraction valves within dental units may aspirate infectious
materials back into the hand piece and water line, check valves must be
installed to reduce the risk of transferring infectious material. To physically
flush out contaminants run high-speed hand pieces and discharge the water into
a sink or container for 3 minutes at the beginning of each day and 30 seconds
between patients. Additionally, flush high-speed hand pieces with a 1:10
hypochlorite solution for 3 minutes at the end of each week.
(3) Disinfect all dental unit surfaces with a suitable chemical germicide between
patients or cover such surfaces during use. Use impervious backed paper,
aluminum foil, or clear plastic wrap to cover surfaces difficult or impossible to
disinfect (e.g., light handles or x-ray tube heads). Remove the covering while
gloved, discard the covering, remove used and don fresh gloves, and then
recover with clean material after each patient.
(4) Dental laboratory personnel will observe infection control protocols. They will
thoroughly, carefully clean blood and saliva from material used in the mouth
(e.g., impression materials, occlusal registrations), especially before polishing
and grinding intra-oral devices. They will clean and disinfect contaminated
materials, impressions, and intra-oral devices before handling them in the
dental laboratory and before putting them in a patient’s mouth. They will
disinfect laboratory instruments (e.g. spatulas, knives, and wax carvers), plastic
benches, chucks, handles, switches, tubing, air hoses, and lab hand pieces
every day. Rubber mixing bowls require overnight immersion to disinfect.
Workstations, including exposed equipment, drawers, work surfaces, and
sinks, require weekly surface disinfecting. Because of the increasing variety of
CH-13 13-76
dental materials used intra-orally, dental providers should consult with
manufacturers about specific materials’ stability in disinfecting procedures.
(5) Use sterile saline or sterile water as a coolant or irrigator when performing
surgical procedures involving cutting soft tissue or bone.
e. Dental Radiology Sterilization and Disinfecting Procedures.
(1) Film-Holding and –Aiming Devices. When practical, heat-sterilize film-
holding and –aiming devices between patients. For those items unable to
withstand heat sterilization, use a chemical sterilant. Immerse for 6 to 10 hours
depending on the sterilant manufacturer’s instructions. If sterilization is not
practical, immerse these items in chemical disinfectant between patients
according to manufacturer’s instructions.
(2) Panoramic Unit Bite Blocks. Use disposable bite block covers between
patients. If disposable covers are not available, treat bite blocks similarly to
film-holding devices.
(3) Handling Intra-oral Film Packets. Place intra-oral film removed from a
patient’s mouth directly into a disposable container such as a paper cup or
towel for transfer to the darkroom. Discard wrappers directly into a refuse
container or into a disposable towel to prevent contaminating the darkroom
counter.
(4) X-ray Chair. Between patients wipe arm- and headrests with a chemical
surface disinfecting solution. If using paper or plastic headrest covers, replace
them after each patient.
(5) Intra-oral X-ray Tubehead and Exposure Buttons. Wipe these items with a
surface disinfectant or cover them after each patient visit. Do not allow
disinfectant liquid to leak into the tubehead seams or the exposure button
switch.
9. Sterilizing and Disinfecting.
a. Instrument Categories (Spaulding Classification). The Spaulding Classification
defines as critical instruments that normally penetrate soft tissue, teeth, or bone (e.g.,
forceps, scalpels, bone chisels, scalers, surgical burs, etc.). They must be heat-
sterilized after each use. Instruments not intended to penetrate soft or hard tissues
(e.g., amalgam carvers, plastic instruments, etc.) but which may come into contact
with tissues are semi-critical and also should be heat-sterilized after each use. If heat
sterilization is not possible, semi-critical instruments must receive chemical
sterilization. Non-critical instruments never contact tissue. Sterilization is
recommended for non-critical instruments, but high-level disinfection is acceptable.
b. Instrument Preparation.
(6) Initially Storing Contaminated Instruments. Immerse contaminated
instruments in a container of soapy water immediately after use or completing
the patient visit.
13-77 CH 13
(7) Cleansing Instruments. Instruments must be cleansed for sterilization to be
effective. Cleanse them using an ultrasonic cleaner according to the
manufacturer’s instructions. Hand-scrubbing instruments is prohibited.
Persons who cleanse instruments must wear heavy-duty (“Nitrile”) rubber
utility gloves to reduce the risk of injury. Inspect instruments for cleanliness
before preparing them for packaging.
(8) Packaging and Wrapping Instruments. Depending on intended use, wrap or
package most instruments individually or in sets. Packaging in metal or plastic
trays reduces set-up time; instruments and other materials arranged
systematically are more convenient. Package size and sterilization method
generally determine the best wrapping material, most commonly paper, plastic,
nylon, cloth, or combinations of these materials. Seal packages by heat, tape,
and self-sealing methods. Wrap instruments loosely to allow the sterilizing
agent to circulate freely throughout the pack. Pack scissors, hemostats, and
hinged instruments in the open position so the sterilizing agent can reach all
parts. When wrapping in an easily punctured material, cover the tips of sharp
instruments with 2 x 2 gauze or cotton roll. If using plastic or nylon
sterilization tubing, the pack should be approximately 20% larger than the
longest instrument to allow the inside air to expand when heated. Clear tubing
is relatively puncture-resistant and enables rapid identification of contents.
When using cloth to wrap critical items, use a double thickness. Date all
packs.
c. Heat Sterilization.
(1) The best way to minimize cross-contamination is to sterilize all instruments
that can withstand sterilizing conditions. The most practical, dependable
sterilization method, heat, when appropriate, is preferable to chemical means.
These are the most common heat sterilization techniques:
(a) Steam Vapor Under Pressure Sterilizer (Autoclave). Steam vapor under
pressure is an excellent sterilization method. Moist heat kills the bacteria
by causing their proteins to denature and coagulate within the microbial
cell. The steam’s high temperature, not the pressure, kills the
microorganisms. Steam can rust cutting edges made of carbon steel;
however, antirust agents reduce this process.
(b) Chemical Vapor Under Pressure Sterilizer (Chemiclave). This sterilizer
uses chemical vapor under pressure and kills bacteria in much the same
manner as the steam sterilizer. It is an excellent sterilization method.
Because chemical vapors are less corrosive than steam, they do not dull
sharpened instruments. Chemical vapor sterilizers use a specific mixture
of formaldehyde, alcohols, ketone, acetone, and water. If the
manufacturer’s recommended chemical solution is not available, distilled
water may be used for a short time Use chemical solutions only once. A
disadvantage of the chemical vapor sterilizer is the residual chemical
vapor that escapes into the air when the chamber door is opened. While
CH-13 13-78
non-toxic and non-mutagenic, its odor can be objectionable. Allowing
the sterilizer to cool for at least 20 minutes before opening will
significantly reduce the residual vapor level. A commercial purging
system that reduces residual vapor levels is available.
(c) Dry Heat Sterilizer. Dry heat kills bacteria by an oxidation process. Dry
heat sterilization will not corrode instruments, but dry heat sterilizers can
destroy metal instruments’ temper and melt solder joints if not monitored
properly. Some dry heat units are not able to sterilize large trays and
require special wrapping and bagging materials. For these reasons, dry
heat sterilization is not recommended for critical instruments, and should
be monitored carefully and used judiciously with semi-critical and non-
critical instruments. Because sterility is destroyed as soon as items are
touched or left open to the environment, do not place loose instruments
in dry heat sterilizers. Wrap and bag all instruments; they must remain
wrapped or bagged until used.
d. Sterilization Monitoring.
(1) Chemical Indicators. External and internal chemical indictors provide a quick
visual check to verify instruments have been exposed to elevated temperatures.
They do not guarantee the instruments are sterile. External chemical indicators
(autoclave tape or sterilizing bags with heat-sensitive printing) identify at a
glance which instruments have been processed but show only the outside of the
pack was exposed to an elevated temperature. An external chemical indicator
must be on every pack processed. If using see-through packages, a chemical
indicator placed inside the pouch is acceptable. Internal chemical indicators,
available in strips, cards, or labels, react to time/temperature/ sterilizing agent
combinations.
(2) Biological Spore Monitors (BSM). Bacterial spores resist heat destruction
better than do vegetative forms of bacteria and viruses. Therefore, the spores
are used to verify a sterilizer’s effectiveness. Place them in the most
challenging area of the load being tested and wrap the pack in the usual
fashion. Monitor all chemical vapor, water vapor, and dry heat sterilizers with
a spore test either weekly or each cycle, whichever is less frequent.
(a) These systems require a either medical laboratory service or an in-house
incubator to incubate the test spore. Dry heat sterilizers require an
alternate system using a glassine envelope with enclosed spore strips.
Regardless of the system used, document spore monitoring, including
identification test date, test results, and operator, and maintain the
records for two years.
(b) If a spore monitor tests positive (spores are still alive), check the
sterilizer for proper use and function and repeat the spore test. Items
need not be recalled because of a single positive spore test. However, do
not routinely use the unit in question until after obtaining a second test.
13-79 CH 13
If the second test also is positive, the unit requires service or repair.
When the unit is returned to use, perform a spore test to ensure the unit is
in proper operating condition.
(3) Storage and Shelf Life. Store sterile instruments and packs in a cabinet or
drawer to reduce contact with aerosols and dust. Handle them as little as
possible before using them. Instrument pack life varies according to wrapping
material as follows:
Metal or Plastic Container 30 days
Paper Wrap 30 days
Cloth (Double Thickness) 2 months
Nylon, Plastic, or Plastic-Paper Combination (Tape Sealed) 6 months
Nylon, Plastic, or Plastic-Paper Combination (Heat Sealed) 12 months
Rewrap and resterilize outdated packs or packs suspected of being contaminated.
Rotate packs to use the oldest ones first. Keep loose (unwrapped or unpacked)
instruments to an absolute minimum as their sterility cannot be ensured. Recycle
loose reusable instruments through a sterilizer at least once every two weeks.
Disinfect drawers and instrument holders containing loose instruments monthly.
e. Chemical Sterilization and High-Level Disinfection. Although heat is the preferred
sterilization method, certain instruments and plastics will not tolerate heat
sterilization and require chemical sterilization or high-level disinfection. These
disinfectants destroy microorganisms by damaging their proteins and nucleic acids.
Most formulae contain 2% glutaraldehyde and come in two containers. Mixing the
proper amounts from each container activates the solution. Sterilization monitors
cannot verify glutaraldehyde sterilization. The solution is caustic to the skin, so use
forceps or rubber gloves to handle instruments immersed in glutaraldehyde and
always follow manufacturer’s directions carefully. Label each container of fresh
solution with an expiration date. Uninterrupted immersion for 7 to 10 hours in a
fresh glutaraldehyde solution usually will achieve sterilization; uninterrupted
immersion for 10 minutes will kill most pathogenic organisms, but not spores.
Heavily soiled or contaminated instruments render glutaraldehydes ineffective.
Debride instruments thoroughly to disinfect effectively. Glutaraldehydes are not
recommended for surface disinfection.
f. Surface Disinfection.
(1) Extraordinary efforts to disinfect or sterilize environmental surfaces such as
walls, floors, and ceilings generally are not required because these surfaces
generally do not transmit infections to patients or health care workers.
However, routinely clean and remove soil from them.
CH-13 13-80
(2) After contamination, wipe all other treatment room surfaces such as
countertops, dental chairs, light units, exam tables, and non-sterile objects in
the operating field with absorbent toweling to remove any extraneous organic
material, and then disinfect them with a suitable chemical germicide.
Personnel shall wear heavy-duty (“Nitrile”) rubber utility gloves when applying
surface disinfectants. Many different chemical disinfectants possessing
varying degrees of effectiveness are available. The following three surface
disinfectants are recommended.
(a) Iodophor. Iodophor compounds contain 0.05 to 1.6% iodine and surface-
active agents, usually detergents, which carry and release free iodine.
Iodophor’s antimicrobial activity is greater than that of iodine alone: 10
to 30 minutes of contact produces intermediate levels of disinfection.
Iodophors are EPA-approved as effective when diluted 1:213 with water.
Because iodine’s vapor pressure is reduced in iodophor, its odor is not as
offensive. In addition, iodophors do not stain as readily as iodine.
(b) Phenolics. In high concentrations, phenolic compounds are protoplasmic
poisons. In low concentrations, they deactivate essential enzyme
systems. As disinfectants, phenolics are usually combined with a
detergent; 10 to 20 minutes of contact produces disinfection. Phenolics
are less corrosive to treated surfaces.
(c) Sodium Hypochlorite. Sodium hypochlorite is thought to oxidize
microbial enzymes and cell wall components. A 1:10 dilution of 5.25%
sodium hypochlorite in water produces a solution which disinfects at an
intermediate level in 10 minutes. Sodium hypochlorite solution tends to
be unstable, so prepare a fresh solution daily. It possesses a strong odor
and can harm eyes, skin, clothing, upholstery, and metals (especially
aluminum
(3) Chemical Disinfectants Not Recommended For Use.
(a) Alcohol. Alcohol is bacteriocidal against bacterial vegetative forms by
denaturing cellular proteins. Diluted in water, a 70 to 90% solution is
more effective than a more concentrated solution. Alcohol’s
disadvantages are: (1) rapid evaporation, (2) lack of sporicidal or
viricidal activity, and (3) rapid inactivation by organic material. Since
alcohol interferes with proper surface cleansing, it has no place in the
disinfection protocol.
(b) Quaternary Ammonium Compounds. In the past, benzalkonium
chlorides and other “quats” were used as disinfectants because they were
thought to be safe and inexpensive and have low surface tension. Their
biocidal activity breaks down the bacterial cell membrane, producing an
altered cellular permeability. As a group, these compounds have serious
13-81 CH 13
deficiencies. Being positively charged, they are attracted to not only
bacteria but also to glass, cotton, and proteins, which decrease their
biocidal activity. Common cleaners’, soaps’, and other compounds’
negatively charged ions neutralize “quats.” Research has shown some
“quats” support the growth of gram-negative organisms. Quats are
ineffective against most spore formers, the Hepatitis B virus, and the
tubercle bacillus.
10. Laundry. Although research has identified soiled linens as a source of large numbers of
certain pathogenic microorganisms, the risk of linens actually transmitting disease is
negligible. Rather than rigid procedures and specifications, hygienic and common-sense
storage and processing of clean and soiled linen are recommended. Wearing gloves
while handling soiled linen is recommended. Handle it as little as possible and with
minimum agitation to prevent gross microbial contamination of the air and persons
handling the linen. Carefully check linen for sharps objects and remove them before
washing. Bag all soiled linen where used; do not sort or rinse it in patient care areas.
Place and transport linen soiled with blood or body fluids in bags that prevent leakage.
Use normal laundry cycles according to the washer and detergent manufacturers’
recommendations.
11. Cleaning and Decontaminating Blood or Other Body Fluid Spills. Use an EPA-approved
germicide or recommended surface disinfectant agent to promptly clean all blood and
blood-contaminated fluid spills. Health care workers must wear gloves. First remove
visible material with disposable towels or other appropriate means that prevent direct
contact with blood. If anticipating splashing, wear protective eyewear and an impervious
gown or apron that provides an effective barrier to splashes. Next decontaminate the
area with disinfectant solution or an appropriate EPA-approved germicide. Clean and
decontaminate soiled cleaning equipment or put it in an appropriate container and
dispose of it according to clinic policy. Use plastic bags clearly labeled as containing
infectious waste to remove contaminated items from the spill site. Remove gloves; then
wash hands.
12. Infectious Waste.
a. Epidemiological evidence does not suggest most clinic waste is any more infectious
than residential waste. However, public concern about the risk of medical wastes
must not be ignored. Identifying wastes for which special precautions are necessary
include those wastes which potentially cause infection during handling and disposal
and for which special precautions appear prudent, including sharps, microbiology
laboratory waste, pathology waste, and blood specimens or products. While any item
that has touched blood, exudates, or secretions potentially may be infectious, it is
usually not considered practical or necessary to treat all such waste as infectious.
Materials containing small amounts of blood, saliva, or other secretions such as
tainted gauze pads, sanitary napkins, or facial tissues are not considered infectious
waste. Generally, autoclave or incinerate infectious waste before disposing of it in a
sanitary landfill. Infectious waste autoclaving standards are different from normal
sterilization standards. Carefully pour bulk blood, suctioned fluids, excretions, and
CH-13 13-82
secretions down a drain connected to a sanitary sewer. Or for materials capable of it,
grind and flush such items into sanitary sewers (some states prohibit this practice).
b. The Environmental Protection Agency classifies health care facilities as generators of
infectious waste based on the weight of waste generated. Coast Guard classification
is based on facility type. All Coast Guard clinics are considered generators. Each
Coast Guard health care facility must have a written infectious waste management
protocol consistent with state and local regulations in the unit’s area.
c. Biohazard warning labels shall be affixed to regulated waste containers; refrigerators,
and freezers containing blood or other potentially infectious material; and other
containers used to store, transport, or ship blood or other potentially infectious
materials with these exceptions:
(1) Substitute red bags for labels on regulated waste bags or containers. OSHA
believes red bags protect personnel because they must comply with OSHA
BBP Standard Paragraph (g)(2)(iv)(M), which requires training personnel to
understand the meaning of all color coding.
(2) Individual containers of blood or other potentially infectious materials placed
in a labeled container during storage, transport, shipment or disposal.
13. Managing Exposures (Needle Stick Protocol)
a. Exposure.
(1) An exposure occurs if a health care worker comes in contact with blood or
other body fluids in one of these ways:
(a) Parenteral—through a needle stick or cut;
(b) Mucous membrane—from a splash to the eye or mouth;
(c) Cutaneous—contact with large amounts of blood or prolonged contact
with blood when the health care worker’s exposed skin is chapped,
abraded, or afflicted with dermatitis.
(2) All individuals so exposed shall report the exposure to their immediate
supervisor, who will document the incident in a memorandum detailing the
exposure’s time, date, and circumstances and any medical treatment received to
the Chief, Health Services Division or health services department head, with a
copy to the exposed person. The QA coordinator or his or her designee also
will retain a copy and ensure all required follow-up treatment and testing is
documented. The Chief, Health Services Division or health services
department head shall ensure that the following this management protocol is
adhered.
(3) After an exposure, obtain the source person’s consent, making sure to follow
local laws governing consent for testing non-active duty source persons and
incompetent or unconscious persons. At a location where appropriate pre-test
counseling is available for the source person, draw a blood sample and test it

13-83 CH 13
for Hepatitis B Surface Antigen (HbsAg) and Human Immunodeficiency Virus
(HIV) antibody. Provide the source person post-test counseling and treatment
referrals. Inform the exposed person of the source person’s test results and
applicable laws and regulations on disclosing the source person’s identity and
infectious status. It is extremely important all persons who seek consultation
for any HIV-related concerns receive appropriate counseling from a USMTF or
other medical facility capable of providing this service.
(4) All clinics shall ensure the health care professional evaluating an employee
after an exposure incident has this information:
(a) A copy of the OSHA BBP Standard,
(b) A description of the exposed employee’s duties as they relate to the
exposure incident,
(c) Documentation of the route(s) of exposure and circumstances under
which exposure occurred,
(d) Results of the source individual’s blood tests, if available; and all records
on the employee’s appropriate treatment, including vaccination.
(5) The SMO shall obtain and give the exposed person a copy of the evaluating
health care professional’s written opinion within 15 days after the evaluation is
complete.
(6) Figure 13-K-1 presents a sample needle stick injury flow sheet.
b. Hepatitis B Virus Post-exposure Management.
(1) For a worker exposed to a source individual found to be positive for HbsAg:
(a) The exposed worker who has not previously received Hepatitis B vaccine
will receive the vaccine series. A single dose of Hepatitis B immune
globulin (HBIG) if it can be given within 7 days of exposure is also
recommended.
(b) Test the exposed worker who has previously received Hepatitis B
vaccine for antibody to Hepatitis B surface antigen (anti-HBs). If the
antibody level in the worker’s blood sample is inadequate (i.e., less than
10 SRU by RIA, negative by EIA) give the exposed employee one dose
of vaccine and one dose of HBIG.
(2) If the source individual is negative for HbsAg and the worker has not been
vaccinated, the worker shall receive Hepatitis B vaccination.
(3) If the source individual refuses testing or cannot be identified, the unvaccinated
worker should receive the Hepatitis B vaccine series. Consider administering
HBIG on an individual basis if the source individual is known or suspected to
be at high risk of HBV infection. At his or her discretion the responsible

CH-13 13-84
medical officer will manage and treat as needed previously vaccinated workers
who are exposed to a source who refuses testing or is not identifiable.
c. Human Immunodeficiency Virus Post-exposure Management.
(1) If a worker is exposed to a source individual found positive for HIV infection
or who refuses testing, counsel the exposed worker about the risk of infection
and evaluate him or her clinically and serologically for evidence of HIV
infection as soon as possible after the exposure. In view of the evolving nature
of HIV post-exposure management, the health care provider must be well
informed of current Centers for Disease Control (CDC) guidelines on this
subject.
(a) Advise the exposed worker to report and seek medical evaluation for any
acute febrile illness occurring within 12 weeks after exposure. Such an
illness, particularly one characterized by fever, rash, or
lymphadenopathy, may indicate recent HIV infection.
(b) After the initial test at the time of exposure, retest seronegative workers 6
weeks, 12 weeks, and 6 months after exposure to determine whether HIV
transmission has occurred. During this follow-up period (especially the
first 6 to 12 weeks after exposure, when most infected persons
seroconvert), exposed workers must follow CDC recommendations to
prevent transmitting HIV, including refraining from blood donation,
informing health care workers rendering treatment of his or her status,
and using appropriate protection during sexual intercourse. During all
phases of follow-up, it is vital to protect worker confidentiality.
(2) If the source individual’s tests are seronegative, perform a baseline testing of
the exposed worker with optional follow-up testing 12 weeks later if the
worker desires or the health care provider recommends it. After the initial test
at the time of exposure, at the responsible medical officer’s discretion, retest
consenting seronegative source individuals at 12 weeks and 6 months
afterward.
(3) If the source individual cannot be identified, decide appropriate follow-up on
an individual basis. All workers concerned they have been infected with HIV
through an occupational exposure should undergo serologic testing
(4) Follow CDC recommendations for preventing HIV and HBV transmission to
patients during exposure-prone procedures, defined as those invasive
procedures with a recognized risk of percutaneous injury to health care
workers.
(a) All health care workers shall adhere to universal precautions. Health
care workers with exuding lesions or weeping dermatitis shall refrain
from all direct patient care. Health care workers shall comply with
current CDC guidelines for disinfecting and sterilizing equipment and
supplies.
13-85 CH 13
(b) All health care workers performing exposure-prone procedures shall
know their HIV and HBV status.
(c) All health care workers who are HIV or HBV positive shall refrain from
performing exposure-prone procedures.
14. Training Personnel For Occupational Exposure. All Health Services Divisions or
Branches will inform and train personnel in occupational exposure initially on
assignment and annually thereafter. Personnel who have taken appropriate training
within the past year need receive additional training only on subjects not previously
covered. The training program shall contain at least these elements:
a. An accessible copy and explanation of the regulatory text of this standard (Federal
Register 56 (235):64175, December 6, 1991 [29 USC 1910.1030]).
b. A general explanation of the epidemiology and symptoms of bloodborne diseases.
c. An explanation of bloodborne pathogen transmission modes.
d. An explanation of the exposure control plan outlined in Section 13-K.
e. An explanation of the appropriate methods to recognize tasks and other activities that
may involve exposure to blood and other potentially infectious materials.
f. An explanation of methods to reduce or prevent exposure, such as barrier techniques,
and their limitations.
g. Information on the types and properly using, locating, removing, handling,
decontaminating, and disposing of personal protective equipment.
h. An explanation of the basis for selecting personal protective equipment.
i. Information on the Hepatitis B vaccine, including efficacy, safety, administration,
and benefits. This vaccination is mandatory for all Health Services Technicians
except E-8 and E-9 personnel in administrative positions. It is recommended and
available for EMTs and E-8 and E-9 Health Services Technicians in administrative
positions.
j. Information on appropriate actions to take and persons to contact in an emergency
involving blood or other potentially infectious materials.
k. An explanation of the procedure to follow if an exposure incident occurs, including
the method of reporting the incident and available medical follow-up described in
Section 13-K-13.
l. Information on the post-exposure evaluation and follow-up the SMO or designee is
required to provide for the employee after an exposure incident.

CH-13 13-86
m. An explanation of the signs, labels, and/or color coding required for sharps and
biohazardous materials.
n. A question-and-answer period with the person conducting the training session.

13-87 CH 13
Figure 13-K-1
SAMPLE NEEDLESTICK INJURY FLOWSHEET
(CONFIDENTIAL)
Health Care Worker’s Name: _____________________________________________________
Source’s name, status, and contact information (if known): ______________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Date of Incident: _______________________________________________________________
Type of Exposure (check one)
❑ Needle stick, cut, or puncture wound with contaminated instrument
❑ Splash to the eye or mouth
❑ Contact with large amounts of blood when the exposed skin is chapped, abraded, or
afflicted with dermatitis
❑ Other: ______________________________________________________________
No Yes
Have consent to test and pretest information been given? ❑ ❑
Is source test positive for HBV? ❑ (2) ❑ (next)
Is Health Care Worker (HCW) vaccinated for hepatitis? ❑ (2) ❑ (next)
HCW Hepatitis B surface antigen (anti-HBs) adequate (i.e., more
than 10 SRU by RIA, positive by EIA)? ❑ (3) ❑ (next)
Less than 7 days since exposure? ❑ (7) ❑ (4)
Is source test positive for HIV? ❑ (5) ❑ (1, 6)
ACTION TAKEN
1. Post exposure counseling
2. Initiate and complete HBV vaccination series
3. Give one dose of HBV vaccine
4. Give one dose of HBIG
5. HIV testing (baseline, optional 12 weeks )
6. HIV Testing (baseline, 6 weeks, 12 weeks, 6 months)
7. No action required
SENT TO QA COMMITTEE:____________________
CH-13 13-88
Section L - Risk Management Program
1. Purpose. The risk management program supports quality medical care by identifying,
analyzing, and preventing actual and potential risks to patients and staff. The program
provides mechanisms to detect and prevent accidents and injuries and reduces the cost of
claims and loss of other resources.
2. Background. Risk management programs are most effective if they are prospective,
preventive, and comprehensive. All staff members, beneficiaries, contract providers, and
volunteers shall be aware of risks in the clinical environment and act safely and
responsibly to implement program requirements. Risk management activities are not
limited to claims activities but examine all instances of actual and potential risk or loss.
3. Definitions.
a. Medical Incident: An adverse or unexpected medical outcome resulting in death or
significant morbidity.
b. Occurrence: Any event or situation in which there is an actual or potential injury or
patients or staff raise a significant complaint or concern about treatment delivered.
4. Informed Consent.
c. Background. Every person, with a few exceptions, has the right to be examined and
treated only in the manner they authorize. This individual prerogative is based on the
concept a competent patient has the right to make informed decisions about health
care. Consent for health care must be informed, voluntary, competent, and specific,
and is clearly an important issue in quality patient care. The objective of informed
consent is improved patient-provider communication in non-emergent situations,
which should result in patients’ realistic expectations about the nature of treatment
and the expected outcome, and reduced liability for the government. Clear
documentation demonstrating the patient was properly informed is necessary to
protect the patient, the provider, and the government. Although patients must be
informed of treatment options, military members who refuse treatment necessary to
render them fit for duty (including immunization) are subject to separation and/or
disciplinary action (see Chapter 2-A-4-b.).
d. Responsibilities.
(1) Chief, Health Services Division (CHSD): The CHSD must publish facility-
specific implementing instructions that ensure providers carry out the spirit and
intent of this Section. The CHSD and cognizant MLC should monitor
compliance with consent policies and procedures as a regular part of medical
and dental records review.
(2) Health Care Providers: Responsible health care providers must counsel
patients before treatment and document receiving the patient’s informed
consent.
13-89 CH 13
e. Types of Consent. Consent may be expressed or implied.
(1) Expressed Consent: This type of consent is obtained by open discussion
between the provider and patient and must include a statement the patient
consents to the proposed procedure. Expressed consent may be oral or written.
(a) Oral Consent. Except where this regulation specifically requires written
consent, oral consent is sufficient authorization for treatment. However,
oral consent is difficult to prove. If a health care provider receives oral
consent to treatment, he or she must document it by an entry in the
treatment record. Consent received from competent authority by
telephone is a form of oral expressed consent; a person not directly
involved in the patient’s care should witness such consent; and it must be
document it by an entry in the treatment record.
(b) Conditions Requiring Written Consent. Document written consent by
having the patient sign forms authorizing treatment and including an
entry in the treatment record that discusses the requirements outlined in
Paragraph 13-L-4. Except in emergencies, written consent is required for
these situations:
1 All surgical procedures (including, among others, placing sutures,
incision and drainage, removing a foreign body(s), cauterizing,
removing wart(s), injecting medications into a joint(s), etc.)
2 Invasive tests and procedures to diagnose and treat disease or
remove tissue specimens (e.g., biopsies), except routine phlebotomy.
3 Anesthesia, except local dental anesthesia.
4 Dental procedures other than routine restorative dentistry.
5 Genitourinary procedures including vasectomies, IUD insertion or
removal, etc.
(2) Implied Consent. Implied consent is derived from the patient’s conduct even if
he or she does not communicate specific words of consent. Assume implied
consent only if one can reasonably presume the patient knows the risks,
benefits, and alternatives to treatment. For example, a patient's presence at
dental sick call is implied consent for a dental exam. Never accept implied
consent to treatment involving surgical therapy or invasive diagnostic
procedures except in emergencies.
f. Emergencies. Consent before treatment is not necessary when immediate treatment
is required to preserve life or prevent deterioration of the patient's condition. The
provider will document the existence and scope of the emergency and describe the
events precluding obtaining consent.

CH-13 13-90
g. Who May Consent. Generally, competent adult patients who have the capacity to
manage their own affairs who present themselves for treatment have the authority to
consent. If a patient is incompetent due either to statutory incompetence (e.g., a
minor) or mental impairment, then it must determined who the individual with legal
capacity to consent and obtain his or her consent before examining or treating the
patient. Laws defining minors and to what they may legally consent differ by state.
The law of the state where the facility is located governs legal capacity to consent.
Each clinic will develop a policy for treating minors.
h. Information To Provide. The provider must advise the patient of the nature of his or
her condition; describe the proposed treatment in terms the patient can understand;
and explain the material risks and expected benefits of the proposed treatment
course, available alternative health care options, and the option of non-treatment. A
material risk is one a reasonable person likely would consider significant in deciding
whether to undertake therapy and is a function of the likelihood of occurrence, the
severity of the injury it threatens to cause, and existing reasonable alternatives. A
provider is not required to explain risk that are considered extremely remote unless
the patient requests an explanation or the potential adverse consequences are so grave
a reasonable person in the patient’s particular circumstances would consider the risk
important.
i. Informing the Patient. Health care providers will provide information in a manner
that allows a patient of ordinary understanding to intelligently weigh the risks and
benefits when faced with the choice of selecting among the alternatives or refusing
treatment altogether. Health care providers must communicate in language one can
reasonably expect the patient to understand. Although open discussions between the
responsible health care provider and the patient should be the standard, each
department may develop internal methods to acquaint patients with the benefits,
risks, and alternatives to procedures requiring consent. In some departments,
prepared pamphlets or information sheets may be desirable.
j. Documentation. Regardless of the method used to inform the patient or the form of
consent (oral or written), the provider must document the disclosure and the patient's
reactions in the medical or dental record. It is highly recommended progress notes
even if the patient has signed a preprinted "consent" form. Progress notes written to
document disclosing information to the patient will be specific about the information
provided. The notes must specifically enumerate risks, alternative forms of
treatment, and expected benefits the provider discussed with the patient. Use SF
522, "Request for Administration of Anesthesia and for Performance of Operations
and Other Procedures," to document consent in all surgical, anesthetic and
reproductive procedures other than local dental anesthesia and routine restorative
dentistry.
k. Witness to Consent. All consent forms require a witness's signature. The witness
may be a health care facility member who is not participating in the procedure or
treatment. Patients’ relatives are not acceptable as witnesses. The witness confirms
the patient signed the form, not that he or she received all relevant information.

13-91 CH 13
l. Duration of Consent. Consent is valid as long as no material change in
circumstances occurs between the date the patient consented and the procedure or
treatment date. Obtain new consent if a material change in circumstances occurs, for
example the provisional diagnosis changes. If more than seven (7) days elapse
between the date the patient signed the consent and the date treatment begins,
provider and patient must re-sign, re-initial, and re-date the consent form. A new
consent is not required for each stage in a series of treatments for a specific medical
condition, e.g., repeated application of liquid nitrogen to warts.
5. Occurrence Monitoring and Reporting. (To be developed).
6. Medical Incident Monitoring and Reporting.
a. Definition. In the Coast Guard's Health Services Program, a medical incident is an
event involving an unexpected death or permanent disability of a patient to whom
Coast Guard health services personnel have rendered health care. The event is not
reviewed to place blame or discipline those involved, but rather to assess the health
care process(es) involved and identify potential areas for improvement. The Coast
Guard uses the resulting recommendations to determine health care policy,
personnel, equipment, and training needs to prevent future adverse health care
outcomes. A single event may result in initiating a Mishap Board as the Safety and
Environmental Health Manual, COMDTINST M5100.47 (series), requires and a
legal investigation conducted concurrently with a medical incident review of the
same event (e.g., a vessel collision with injuries). In most cases however, a medical
incident review will occur solely within a Coast Guard health care facility or with
medical or dental services rendered its only issue.
b. Reporting Procedure. Within 24 hours after a medical incident occurs, the command
shall submit copy(s) of SF-558, Emergency Care and Treatment Report , and/or SF-
600 for events occurring within the clinic and/or CG-5214, Emergency Medical
Treatment Report, for events occurring outside the clinic to the appropriate MLC (k).
Clearly mark "Incident Report" in large print across the top of these forms. Stamp or
print this statement on the top of each document: "This is a medical quality
assurance document. It is protected by Federal law (14 USC 645)." MLC (k) shall
send copies of the documents to Commandant (G-WKH) within three days of receipt.
c. Review Procedure. On receiving one of the three forms, MLC (k) or Commandant
(G-WKH), if appropriate, shall review the document(s); verify the event meets the
Paragraph 13-L-6-a criteria for an incident; determine whether an on-site medical
review shall be conducted; and designate a single point of contact at MLC (k) or
Commandant (G-WKH).
(1) If MLC (k), or Commandant (G-WKH), determines a medical incident review
is unnecessary, they shall notify the command by letter within 10 working days
of the event and send a copy of the letter to Commandant (G-WKH).
(2) If conducting an on-site medical incident review, MLC (k) or Commandant
(G-WKH), as appropriate, shall notify the involved command as soon as
possible and designate an officer to conduct a review or convene a panel of

CH-13 13-92
qualified professional staff, including a member of the involved facility, to
review all aspects of the incident. To ensure confidentiality, the panel shall
consist of only the designated facility point of contact and the persons MLC (k)
or Commandant (G-WKH) appoint.
d. The incident review officer or panel shall request and review all relevant documents
and reports, interview personnel as required, and when the review is complete,
submit a written letter report with this information on the incident to Commandant
(G-WKH) through the cognizant MLC (k) (see Paragraph 13-L-6-e below):
(1) Synopsis. A brief summary of the incident and injuries and/or fatalities
involved.
(2) Factual Information. Factual information and data about the incident and
personnel involved shall consist of at least these topics:
(a) History. The chronological order of any significant events preceding,
during, and after the incident, including any written logs or transcripts of
radio logs substantiating this chronology, such as the SF-558, CG-5214,
or SF-600.
(b) Injuries. Describe each injury, or in the case of fatalities, the cause of
death. Include autopsy findings when available.
(c) Professional qualifications of all persons who delivered health care,
including all recent applicable training and certificates (e.g., ACLS, BLS,
EMT, HS, etc.).
(d) Equipment Performance. List all pertinent medical equipment used
during the incident and any failures due to mechanical malfunction,
operator error, inadequate training, or other factors. Describe whether
equipment involved was maintained or serviced according to
manufacturers' specifications.
(3) Analysis and Conclusions. The individual's or panel's hypothesis of the
circumstances surrounding the event, emphasizing the health care aspect,
developed using all available information and including a brief conclusion
about the health care rendered and how it contributed to the event’s outcome.
(4) Recommendations. Recommended modifications to policy, personnel staffing,
equipment, training, or any other health care delivery system aspect which
might improve to avoid similar incidents in the future.
e. Routing Incident Review Reports. The cognizant MLC (k) shall send the completed
report to Commandant (G-WKH) for review and appropriate action.
13-93 CH 13
Section M - Training and Education
1. Definitions.
a. ACLS (Advanced Cardiac Life Support): Sponsored by the American Heart
Association (AHA), this 16-hour program (8 hours for recertification) emphasizes
cardiac-related diagnostic and therapeutic techniques and grants a completion
certificate valid for two years on completion. An ACLS certificate of completion
recognizes a person completed the course and does not in any way authorize him or
her to perform skills taught there. ACLS also sometimes refers to the cardiac
component of Advanced Life Support.
b. Advanced Life Support (ALS): A general term applied to pre-hospital skills beyond
the basic life support level including, among others, EKG interpretation, medication
administration, and advanced airway techniques.
c. Basic Life Support (BLS): Rudimentary pre-hospital skills including CPR, bleeding
control, splinting, patient assessment, oxygen administration, etc., associated with the
basic level emergency medical technician.
d. Cardio-Pulmonary Resuscitation(CPR): A program sponsored by the AHA and
American Red Cross which, on completion, grants certificates of completion for 1 to
2 years. The course curriculum includes basic skills (airway maintenance and
cardiac compression) necessary to sustain heart and brain function until advanced
skills can be administered.
e. Emergency Medical Technician (EMT): A general term referring to the certification
of pre-hospital care providers routinely recognizes at three skill levels (EMT-Basic,
EMT-Intermediate, EMT-Paramedic), but functions performed at each level vary
significantly by jurisdiction. When the term EMT is used alone, assumes it refers to
the EMT-Basic level, which performs BLS skills.
f. Paramedic: An individual certified by the National Registry of Emergency Medical
Technicians as an Emergency Medical Technician-Paramedic (NREMTP) or certified
by a local governing body to perform ALS procedures under a physician's license.
2. Unit Health Services Training Plan (In-Service Training).
a. Clinics, sickbays, and independent duty health services technicians must have an on-
going in-service training program aimed at all providers with emphasis on the Health
Services Technicians' professional development. It is expected of clinic staff
members attending outside training to share new information with other staff
members. In-service training sessions allow clinics to ensure issues of clinical
significance are presented to their staff.

CH-13 13-94
b. In-service training must include these topics, among others:
(1) Quality Assurance Implementation Guide Exercises;
(2) Annual review of clinic protocols on suicide, sexual assault, and family
violence;
(3) Patient satisfaction issues;
(4) Patient sensitivity;
(5) Emergency I.V. therapy;
(6) Pneumatic anti-shock garment (MAST) review;
(7) Emergency airway management;
(8) Cardiac monitor and defibrillator familiarization;
(9) Cervical spine immobilization and patient transport equipment;
(10) Emergency vehicle operator's training (where operated);
(11) Section 13-K infection control policy and procedures.
c. The Chief, Health Services Division, must designate in writing a Health Services
Training Coordinator (HSTC) who coordinates clinic in-service training, distributes a
quarterly training schedule, and maintains the unit's health services training record.
The HSTC’s responsibilities include these:
(1) Establishes and maintains a Health Services Training Record to document all
training conducted within the clinic. Records should include presentation
outline, title, program date, name of presenter, and list of attendees. Maintain
training records for 3 years from the date on which training occurred.
(2) Ensures all emergency medical training is documented in the individual's Coast
Guard Training Record (CG-5285) for credit toward the 48-hour National
Registry EMT continuing education requirement.
(3) Maintains a Training Record section that records personnel certifications
including CPR, ACLS, EMT, and flight qualifications, including expiration
dates and copies of the current certificate. The HSTC should ensure assigned
personnel obtain recertification before current certificates expire.
3. Emergency Medical Training Requirements.
a. All active duty, civilian, and contract civilian personnel working in Coast Guard
clinics and sick bays shall maintain current CPR certification at the health care
provider level (AHA "C" Course or equivalent).
b. Every Health Services Technician who participates in SAR or MEDEVAC
operations must be a currently certified EMT. At least one currently certified EMT
will staff Coast Guard emergency vehicles. Unit commanding officers shall ensure
HSs are trained in sufficient numbers under Section 13-M-3.h to meet this
requirement.
CH-17
13-95 CH 13
c. At least one medical officer per clinic will maintain current ACLS certification.
d. Only licensed or certified physicians, nurse practitioners, physician assistants, or
Nationally Registered advanced life support providers (EMT-P and EMT-I) will
perform ALS procedures, except as Section 13-M-3.e stipulates. Paramedics may
perform functions authorized by their certifying jurisdiction’s protocols with written
medical officer authority.
e. Other than those permitted in the Standardized Health Services Technician
Formulary, (COMDTINST 6570.1), an HS in SAR or MEDEVAC situations may
provide ALS procedures and medications only if his or her supervising medical
officer authorizes such provision in writing and assumes responsibility for those
procedures and medications. In emergencies, the supervising medical officer may so
authorize by radio.
f. Other than those described in Sections 13-M-3.d and 13-M-3.e, persons who have
completed an ACLS course should note certification means only they have
completed the course and does not convey a license to perform any skill. Individuals
completing ACLS courses shall serve as a clinic resource on current standards for
pre-hospital care in training and equipment areas.
g. Emergency vehicles shall be equipped to provide basic life support (BLS) only. The
clinic shall maintain equipment (monitor-defibrillator, advanced airway kit etc.) and
medications to provide ALS services at in a reserve status and add them when
necessary if authorized ALS providers are available.
h. To obtain required EMT training (basic course or recertification), commands shall
use local military sources if available. Usually most public service training agencies
or community colleges offering training can accept Coast Guard personnel. If the
required training is not available from a civilian or military source within a 50-mile
radius, commands may use other cost-effective training sources. Submit requests
through the chain of command to Commandant (G-WKH) with these items:
(1) CG-5223, Short-Term Resident Training Request;
(2) SF-182, Request, Authorization, Agreement and Certification of Training;
(3) Requests for training outside a 50-mile radius which incur per diem expense
require the unit commanding officer’s or officer-in-charge’s statement local
training sources are unavailable.
4. Health Services Technician "A" School.
a. The Office of Personnel and Training operates the 20-week introductory course for
Health Services Technicians, including the Emergency Medical Technician (EMT)
course, at TRACEN Petaluma. As program manager, Commandant (G-WKH)
provides professional comments to the TRACEN on curriculum and qualifying
requirements. Commandant (G-PRF) controls HS "A" School personnel quotas. The
Training and Education Manual, COMDTINST M1500.1 (series), outlines selection
requirements and procedures.
CH-13 13-96
5. Health Services Technician "C" Schools.
a. Due to the specialized nature of health care, the Coast Guard requires health services
technicians to complete training in medical specialty fields such as aviation
medicine, preventive medicine, medical and dental equipment repair, physical
therapy, eye specialist, laboratory, radiology, pharmacy, and independent-duty
specialties. The usual sources are Department of Defense training programs.
b. Selection for HS "C" Schools is based on qualification code requirements for HS
billets at clinics and independent duty sites as specified in personnel allowance lists.
Secondary selection criteria include command requests, personnel requests, and
deficiencies noted on MLC Quality Assurance Site Surveys.
c. HS personnel should submit a CG-5223, Short-Term Resident Training Request,
with Command endorsement to Commandant (G-WKH) through the appropriate
chain of command. Commandant (G-WKH) must receive this request at least 45
days before the training convening date.
d. HS personnel wishing to pursue "C" school training in courses of 20 weeks or longer
require a permanent change of duty station coordinated by Military Personnel
Command (CGPC). Submit requests on CG-3698A, Assignment Data Form, to
Military Personnel Command (CGPC-emp).
6. Continuing Education Programs.
a. All U.S. Public Health Service Officers and Coast Guard physician assistants must
maintain active professional licenses and/or certification to practice their professional
specialty while assigned to the Coast Guard. Licensing and/or recertification
requirements often demand continuing professional education, which enhances the
practitioner’s skills and professional credentials.
b. The Office of Health and Safety attempts to fund one continuing education course
annually for all licensed health services professionals. The program coordinator for
an applicant's professional specialty must approve all training requests. Generally
training should provide at least six documentable continuing education credits per
day pertinent to the applicant's Coast Guard billet. Personnel should obtain training
at the nearest possible geographic location.
c. Medical and dental officers’ licensing and certification exams will not be funded as
continuing education. Coast Guard-sponsored Physician Assistant (PA) programs’
graduates may request funding for examination fees (primary care only), travel to the
testing site nearest their current duty station, and per diem associated with obtaining
initial certification from the National Commission on Certification of Physician
Assistants. The Coast Guard funds this one-time exception because it sponsors the
PA training program and requires certification for employment. PAs may take the
recertification examination in conjunction with the annual physician assistant
conference. Travel and per diem will be authorized as annual CME. The member
pays recertification examination fees.
13-97 CH 13
d. Except for Health Service Technician "C" School applicants, Health and Safety
Program personnel requesting continuing education must follow these procedures:
(1) Each person requesting training must complete CG-5223, Short-Term Resident
Training Request, with proper endorsements.
(2) Accompany each training request with course literature (e.g., a descriptive
brochure) or a brief written description.
(3) Submit SF 182, Request, Authorization, Agreement and Certification of
Training (10 parts) with proper endorsements if using a government purchase
order to pay tuition or fees.
(4) Send all completed forms to Commandant (G-WKH) for processing. Send one
information copy of the Short Term Training Request to the appropriate
Maintenance and Logistics Command, Quality Assurance Branch.
(5) Training requests must arrive at Commandant (G-WKH) 8 weeks before the
anticipated training convening date. Coast Guard Training Quota Management
Center (TQC), Portsmouth, VA, processes approved requests and issues orders.
7. Long-Term Training Programs.
a. Long-Term Post-graduate Training for Medical Officers (Physicians, Physician
Assistants, and Nurse Practitioners). This 1- to 2-year program for medical officers
principally emphasizes primary care (family practice, general internal medicine, and
pediatrics). Consideration may be given for non-primary care specialties such as
occupational health, public health, and preventive medicine. Training in orthopedics
is a potential option for mid-level practitioners only. The Health Services Program
Manager will consider non-primary care post-graduate medical training only when
needed. Applicants also must have applied to their chosen training program and
meet its requirements before requesting training. Applicants should have served with
the Coast Guard Health Services Program for at least 2 years for each year of training
received. For physician applicants, highest consideration will be given first to those
who have not completed an initial medical residency. Commandant (G-WKH) has
more information.
b. Advanced Dental Training Programs. This 2-year program provides dental officers
advanced training in general dentistry, enabling them to give more effective,
comprehensive dental care to Coast Guard beneficiaries. The Department of the
Navy, Naval Medical Command, Bethesda, MD, conducts the training, designed to
qualify dental officers to meet the American Dental Association and Federal Services
Board of General Dentistry requirements for specialty board examination. Dental
officers chosen for this program are expected to pursue board certification. For
program prerequisites and applications procedures, see the Coast Guard Training and
Education Manual, COMDTINST M1500.1 (series).
c. Health Services Administration. This program provides instruction in facility and
personnel management, program planning, cost containment, quality assurance,
third-party payment and liability, and medical-legal issues. The program provides

CH-13 13-98
training at the undergraduate (bachelor’s degree) level for Chief Warrant Officers
and senior enlisted HS personnel (Medical Administrators) and post-graduate
(master’s degree) level for officers in grades O-2, O-3, and O-4. See the Coast
Guard Training and Education Manual, COMDTINST M1500.1 (series) for
eligibility requirements, prerequisites, and application procedures.
d. Physician Assistant Program. Conducted at the U.S. Intra-service Physician
Assistant Program, Fort Sam Houston TX, this program trains Coast Guard personnel
interested in becoming Physician Assistants. Program graduates receive a
baccalaureate degree from the University of Nebraska. If they meet eligibility
requirements, graduates are offered a direct commissions as ensigns as described in
the Personnel Manual, COMDTINST M1000.6 (series), Article 1.A.7. Each year
three Coast Guard students are selected for training based on Service needs. Training
at other institutions is not authorized. See the Coast Guard Training and Education
Manual, COMDTINST M1500.1 (series) for eligibility requirements, prerequisites,
and application procedures.
13-99 CH 13
Section N - Patient Affairs Program
1. Patient Sensitivity.
a. The Coast Guard considers patient sensitivity issues of paramount importance in
delivering health care. Important issues in this area include medical record
confidentiality, privacy during medical examination and treatment, respect for patient
concerns, and enhancing the patient's perception of the quality of services delivered.
b. All clinics shall conduct continuing patient sensitivity training. The "Treat Everyone
As Myself" (TEAM) Program, developed by the U.S. Navy and Service Quality
Institute available through each MLC Health and Safety Division, is the
recommended course. It provides the structure for an internal review of patient-
provider interaction and suggestions on ways to improve this relationship.
2. Patient Advisory Committee (PAC).
a. The Coast Guard's health services program provides primary health care to a wide
array of beneficiaries authorized by law and regulation. Medical Treatment Facilities
(MTFs) often are unaware of their population’s health problems until patients voice
complaints or criticisms to the command. To enable beneficiaries to express their
concerns, a PAC must be available to open lines of communication between health
care providers and care recipients.
b. Each Coast Guard MTF shall establish a PAC and specify criteria for committee
functions. PACs shall include one officer and one enlisted member not assigned to
the clinic; an active duty representative from each Coast Guard command in the
clinic's service area; an active duty representative from each of the other uniformed
services using the MTF; a retired representative; and an active duty dependent
representative from both officer and enlisted communities.
c. MTF shall conduct PAC meetings at least quarterly.
d. The Chief, Health Services Division or his or her designee shall chair the meeting.
Meeting minutes shall include recommended actions and an attendance list; and will
be forwarded to the commanding officer with a copy to each PAC member. Specific
PAC objectives include:
(1) Advise the Chief, Health Services Division on the range of services the
beneficiary population requires;
(2) Serve as a communications link between the MTF and the beneficiaries the
members represent;
(3) Serve as a patient advocacy group to assure all patients are accorded their
rights as described in the Commandant's Patient Bill of Rights and
Responsibilities;
CH-13 13-100
(4) Assist the Chief, Health Services Division in advising patients of their
responsibilities as described in the Commandant's Patient Bill of Rights and
Responsibilities;
(5) Assist the Chief, Health Services Division in establishing patient education
programs; and
(6) Advise the Chief, Health Services Division on the acceptability and
convenience of the services provided.
3. Patient Satisfaction Assessment.
a. Assessing patient satisfaction through patient satisfaction surveys has become an
effective, efficient method to investigate and measure the quality of the Coast Guard
health care delivery system from the patient's perspective.
b. A patient satisfaction survey form shall be available to every patient who receives
care at a Coast Guard facility.
c. Satisfaction surveys will be conducted annually for all patient visits during a
randomly selected one-week period.
d. Locally prepared patient satisfaction surveys are authorized for use.
e. Patient satisfaction survey results shall be provided to the quality assurance focus
group for discussion and action and documented in meeting minutes. Survey results
shall report and recommended actions to the unit commanding officer.
f. Persons distant from a Coast Guard clinic can comment about care received from
civilian providers by sending a mail-in Maintenance and Logistics Command survey
form available from unit Health Services Technicians.
4. Patient Grievance Protocol.
a. The Coast Guard expects health services personnel to maintain a professional attitude
at all times. Our goal to provide the highest quality health care within allotted
resources to all beneficiaries with the least personal inconvenience. Despite our best
efforts, occasionally a patient will be dissatisfied with the care received.
b. Whenever possible individuals with grievances should seek out or be referred to the
clinic supervisor, health benefits advisor (HBA), or clinic administrator (CA) for
complaint resolution before leaving the clinic. Refer written or telephone complaints
to the appropriate clinic staff member. At a minimum, the complainant shall be
given the name of his or her unit Patient Advisory Committee representative and
advise the complainant of the time and place of the next PAC meeting.
c. If the clinic supervisor, HBA, or CA cannot resolve the complaint, he or she shall
refer the complainant to the senior medical or dental officer as appropriate.
13-101 CH 13
d. Refer the complainant to the commanding officer or higher authority only if the
patient believes the clinic or PAC has not resolved the complaint.
e. MLC (kqa) shall review concerns reported on forms mailed to the Maintenance and
Logistics Command for quality assurance purposes, action, or referral to an
appropriate level for resolution and follow up.
5. Congressional Inquiries.
a. Occasionally, circumstances arise in which beneficiaries exercise their right to solicit
assistance from their elected Congressional Representative to resolve their complaint
with the Coast Guard health care system.
b. The Coast Guard maintains a Congressional liaison staff to direct inquiries to the
appropriate Headquarters office that can best address the issue and respond
satisfactorily. Normally Commandant (G-WK) replies to health care problems.
c. Congressional inquiries require a complete investigation of the circumstances
surrounding the issues the beneficiary addresses. To this end, the command, health
care facility, and individuals involved must supply supporting documentation and/or
statements to assist in the investigation.
6. Patient Bill of Rights and Responsibilities. Each Coast Guard health care facility shall
conspicuously display the Commandant's "Patient Bill of Rights and Responsibilities."

14-i CH-17
CHAPTER 14
TABLE OF CONTENTS
Section A - Medical Information Systems (MIS) Plan....................................................................1
1. Purpose. ..............................................................................................................................1
2. Background.........................................................................................................................1
3. Coast Guard Policy.............................................................................................................2
4. Applicability and Scope......................................................................................................2
5. Objectives...........................................................................................................................3
6. Definitions. .........................................................................................................................3
7. Organizational Responsibilities..........................................................................................4
Section B - Medical Information System.........................................................................................6
1. Background.........................................................................................................................6
2. Systems...............................................................................................................................6
Section C - Medical Readiness System (MRS). ............................................................................11

14-1 CH-17
CHAPTER 14. MEDICAL INFORMATION SYSTEMS (MIS) PROGRAM
Section A - Medical Information Systems (MIS) Plan.
1. Purpose.
a. The Medical Information System (MIS) program described here follows the
policy established by the Office of Health Services, outlines systems and
assigns responsibility for the administration of the MIS. The MIS is a key
component for the overall management of Coast Guard clinics and sickbays.
MIS is a dynamic tool, which will provide a comprehensive electronic
solution for tracking operational medical readiness, health systems
management, and patient access to care. The Health and Safety Directorate,
Maintenance and Logistics Commands, unit Commanding Officers, and
health care providers are responsible for ensuring successful implementation
of the Coast Guard Medical Information Systems.
2. Background.
a. There is an ongoing need for Commandant, Area Commanders, and field
level Commanding Officers to assess medical operational readiness.
Additionally, the Coast Guard Health Services program needs to accurately
capture workload, performance, and productivity through standardized
methodology. Proper analysis of health care data provides the ability to
realign assets where they are most needed to deliver timely quality health
care. The full implementation of the Composite Health Care System I/II
(CHCS), Shipboard Automated Medical System (SAMS), Dental Common
Access System (DENCAS), and Third Party Collections Program (TPC) will
significantly enhance our ability to provide this information as needed.
b. Federal statutes impose strict requirements for managing government
information. The most pertinent Federal statutes that govern information
include:
(1) Federal Records Act (Public Law 81-754): Sets policy for and
mandates establishment of agency programs for the management of
Federal records.
(2) Freedom of Information Act (Public Law 90-23): Provides policy to
ensure public access to Federal government information.
(3) Paperwork Reduction Act (Public Law 96-511): Recognizes
information as a Federal resource and directs agencies to establish
specific programs for management of the resource and associated
elements.
(4) Paperwork Reduction Reauthorization Act (Public Law 99-500):
Defines information resources management and directs further program
management requirements.
CH-17 14-2
(5) Privacy Act (Public Law 93-579): Provides policy and safeguards to
protect privacy of individuals.
(6) Health Insurance Portability and Accountability Act (HIPAA),
(Public Law 104-191): Requires health plans to assure the security
and privacy of individually identifiable health information, and to use
specified standards and code sets for electronic transactions involving
medical information.
3. Coast Guard policy concerning the privacy rights of individuals and the Coast
Guard’s responsibilities for compliance with operational requirements
established by the The Coast Guard Freedom of Information Acts Manual,
COMDTINST 5260.3, Privacy Act and HIPAA are as follows:
a. Protect, as required by the Privacy Act of 1974, as amended, and HIPAA, the
privacy of individuals from unwarranted intrusion. Individuals covered by
this protection are living citizens of the United States and aliens lawfully
admitted for permanent residence.
b. Collect only the personal information about an individual that is legally
authorized and necessary to support Coast Guard operations. Disclose this
information only as authorized by the Privacy Act and HIPAA, and described
in Chapter 4 of this Manual.
c. Keep only personal information that is timely, accurate, complete, and
relevant to the purpose for which it was collected.
d. Safeguard personal information to prevent unauthorized use, access,
disclosure, alteration, or destruction.
e. Let individuals know what records the Coast Guard keeps on them and let
them review or get copies of these records, subject to exemptions authorized
by law.
f. Permit individuals to amend records about themselves contained in Coast
Guard systems of records, as authorized by HIPAA, which they can prove are
factually in error, not up-to-date, not complete, or not relevant.
g. Allow individuals to ask for an administrative review of decisions that deny
them access to or the right to amend their records.
h. Maintain only information about an individual that is relevant and necessary
for Coast Guard purposes, as required to be accomplished by statute or
Executive Order.
i. Act on all requests promptly, accurately, and fairly.
4. Applicability and Scope.
14-3 CH-17
a. All health care facilities (clinics, super sickbays, and sickbays) shall comply
with the MIS operating guidelines as set forth. The MIS program described
here contains the essential elements required at all Coast Guard facilities with
medical personnel assigned and assigns responsibilities for the program’s
initiatives. The Chief of Health Services shall ensure all healthcare providers
and support staff; which include Medical Officers, Dental Officers, Pharmacy
Officers, Clinic Administrators, HS’s; HSD’s and Medical and Dental
contractors; shall participate. Information technology is not static in nature
but rapidly changing and dynamic, and requires the diligence of all concerned
to create and maintain a sound program.
5. Objectives.
a. The Director of Health and Safety has established a MIS that provides
necessary tools and capabilities to assist in making sound business decisions
for those Commands having healthcare facilities.
b. Identify and justify resources required to maintain a quality MIS.
c. Establish access and connectivity for Coast-Guard wide comprehensive
utilization of CHCS, continuing local DoD host site affiliation for electronic
referrals and consultations.
d. Establish and maintain clinic and sickbay Microcomputer Allowance Lists
(MAL) that provide appropriate access to medical information systems for
managing clinical and administrative operations.
e. Establish a standardized equipment list for peripherals. (i.e. pharmacy
printers, Local Area Network Interface Unit (LIU) devices, etc.)
f. Identify systems training requirements and ensure required education and
training standards are established and maintained.
g. Provide direction as new adjuncts to existing programs are developed and
deployed. (i.e. CHCS II, Theatre Medical Information Program (TMIP), etc.)
h. Participate in DoD sponsored software and product development for use in
the medical arena.
6. Definitions.
a. Intranet: A privately owned network based on the Transmission Control
Protocol/Internet Protocol (TCP/IP) suite.
b. Internet: A voluntary interconnected global network of computers based
upon the TCP/IP protocol suite, originally developed by the U.S. Department
of Defense Advanced Research Projects Agency.
CH-17 14-4
c. NIPERNET: Non-Classified Internet Protocol Routing Network. The
Defense Information Systems network (DISN) Internet line for unclassified
DoD and federal agency Internet traffic.
d. CGDN+: Coast Guard Data Network Plus. Secure closed Coast Guard wide
area network (WAN).
e. Firewall: Security measure which blocks unwanted/unauthorized entry to
computer systems from outside the internal system.
f. Host (site): Medical facility where a CHCS server platform resides.
g. TelNet: Telecommunications Network. A protocol that facilitates remote
logins to host site server and functions via the Internet.
h. IP address: Internet Provider address. An assignable 32 bit numeric
identifier, which designates a device’s location on an intranet network or on
the Internet.
i. LIU: Local Area Network Interface Unit. Device designed to provide
external access and interface with the local area network (LAN).
7. Organizational Responsibilities.
a. Chief, Office of Health Services.
(1) Establish a comprehensive MIS using the DoD Composite Health Care
System (CHCS) and Dental Common Access System (DENCAS) at all
Coast Guard health care facilities ashore and afloat.
(2) Establish and promulgate MIS policy, including performance standards
for use of all systems/applications contained within the program.
(3) Develop and promulgate MIS operation guidance detailing the various
functional/operational requirements and adjuncts of the MIS program.
(4) Identify education and training requirements, and ensure satisfactory
standards are established.
(5) Establish and maintain a Third Party Collection system for the recovery
of reimbursable medical costs through Other Health Insurance (OHI).
b. Maintenance and Logistics Commands.
(1) Ensure the Health and Safety Directorate’s MIS is executed at the field
level.
(2) Provide technical and professional advice regarding medical
information systems, software, and hardware to units as required.
(3) Coordinate professional training for MIS and health services personnel.
c. Commanding Officers.

14-5 CH-17
(1) Ensure the unit actively pursues implementation and compliance with
the health service MIS standards.
d. Chief, Health Services Division.
(1) Designate in writing an individual to serve as Health Services MIS Unit
Site Manager for the Health and Safety Directorate’s MIS.
(2) Implement and adhere locally to the Health and Safety Directorate’s
MIS policy.
(3) Ensure all health care facility personnel as prescribed, are in
compliance of all provisions contained in this chapter.
e. MIS Unit Site Manager.
(1) Provide local level oversight of the Health and Safety Directorate’s
MIS.
(2) Coordinate and provide MIS training to health care facility staff.
(3) Coordinate and provide local systems hardware and software support.
(4) Coordinate with the cognizant Maintenance and Logistics Command
(MLC) regarding hardware/software support issues beyond their ability
to resolve.
(5) Establish liaison with medical appointment referral DoD Medical
Treatment Facility (MTF) for MIS issues.

CH-17 14-6
Section B - Medical Information System.
1. Background.
a. Information technology is not static in nature but dynamic and rapidly
changing. Commandant (G-WKH) is responsible for ensuring that the
Health and Safety Directorate’s MIS continues to evolve. The MIS has
evolved from manual data collection systems of old, such as the old Daily
Dental Workload sheets, to the Clinic Automated Management System
(CLAMS) in the early 1990’s. The late 1980’s brought the DoD deployment
of a hospital-based medical information system, the Composite Health Care
System (CHCS). Concurrently, as the old Convergent Technology
Operating System (CTOS) was phased out of the Coast Guard in the mid
1990’s, CLAMS II was developed internally and deployed to Coast Guard
clinics. The advent of TRICARE in the mid 1990’s has necessitated
integration of Coast Guard health care information with that of DoD’s
medical information infrastructure.
2. Systems. The following outlines current automated information systems,
applications and program components that come under the Coast Guard MIS
program.
a. Composite Health Care System (CHCS) I & II.
(1) CHCS is the primary clinic/hospital based automated medical
information system for DoD and is the legacy system, which will
eventually transition to CHCS II. Major DoD commands generally act
as host sites within their AOR. A “host” site is where the CHCS
servers and database reside. Access to the functionality and modules of
CHCS are accomplished through several options such as a closed
internal network, through web based applications (i.e. Persona) or
TelNet protocols . With the deployment of CHCS II, over 40 legacy
and migration systems will integrate into a seamless clinical
information system which will support readiness of forces, provide
clinical data to enable health care providers to deliver quality managed
care, and capitalize on technological advances to make a computer-
based patient record (CPR) a reality. CHCS II will be the primary
automated information system supporting the clinical business area
within the DoD Health Affairs program.
(2) Definitions.
(a) Modules: Particular functional features of the CHCS system.
(b) Keys: Security access tokens allowing access to modules within
CHCS programs.
(3) Modules.
14-7 CH-17
(a) PHR: Pharmacy. This module is used to input and process
inpatient and outpatient medication orders and prescriptions. It is
also used to maintain and record formulary files, bulk and clinic
issues.
(b) MCP: Managed Care Program. This module is used to perform
patient enrollment, manage appointment referrals, perform
provider searches, and to create and book appointments for
enrolled and non-enrolled patients.
(c) ORE: Order Entry. This module allows providers to enter
orders that are immediately transmitted to other health care
workers for implementation. Providers can create, modify sign,
or counter-sign orders. Additionally, order information for
individual patients can be retrieved for review.
(d) ERT: Electronic Referral Tracking. This module allows
providers to track the status and progress of patient referrals
(e) LAB: Laboratory. This module allows health care professions
to enter lab test orders, access test status, access test results,
receive notification of problems running a test, and track patient
test history.
(f) RAD: Radiology. This module allows users to enter or modify
radiological orders, view order status, and review the radiological
impression.
(g) ADM: Ambulatory Data Module. This module is used to track
provider workload statistics, patient disposition, and patient
diagnosis and procedure history.
b. SNAP Automated Medical System (SAMS).
(1) The U.S. Navy’s primary shipboard and sickbay medical information
system program is SAMS. This application provides a user-friendly
product that allows the Independent Duty Technician (IDT) to
document all facets of health care; including patient encounters,
medical and dental tickler system, and immunization tracking. SAMS
functionality also offers users tools to produce binnacle lists, document
shipboard training, and monitor environmental health issues such as
heat stress and potable water testing. The fully functional tickler
system flags crewmembers in need or past due for items such as
physical examinations and immunizations, greatly enhancing
operational readiness. Currently, SAMS functionality resides at the
Headquarters/MLC level to track members in the anthrax immunization
program and is set for deployment to the entire Coast Guard IDT
community.

CH-17 14-8
(2) Definitions.
(a) Modules: Particular functional features of the SAMS system.
(b) AMMAL: Authorized Minimum Medical Allowance Level.
This is analogous to the medical portion of the Health Services
Allowance List.
(c) AMDAL: Authorized Minimum Dental Allowance Level. This
is analogous to the dental portion of the Health Services
Allowance List.
(3) Modules.
(a) Master Tickler: This module is used to document, update,
report and transfer medical information on a crewmember. This
module tracks demographic, physical examinations (routine,
occupational and special duty), women's health maintenance
examinations, allergies, immunization tracking, vision, hearing,
dental readiness tracking, laboratory results, and sexually
transmitted diseases.
(b) Medical Encounters: This module is used to document and
report health care encounters with the medical department.
Specific encounters include routine sick call using the SOAP
format, vital sign monitoring/tracking, follow-up
examinations/visits, consultations and referrals, patient
disposition accident and injury reporting.
(c) Occupational/Environmental Health: This module documents
environmental conditions that may affect the health of Coast
Guard personnel. This module includes heat stress monitoring,
potable water testing, and pest control.
(d) Supply Management: This module supports the inventory
management of medical material and pharmaceuticals. Support
is provided for AMMAL and AMDAL inventory management.
Users can requisition, store, distribute, and track all medical
materials. The module produces a variety of inventory reports
and maintains the Operating Target (OPTAR) log. The Coast
Guard version of SAMS will utilize the Heath Services
Allowance List.
(e) Training Management: This module tracks both crew and
medical department personnel training. The module can be
customized by the user to suit the needs of the unit.
14-9 CH-17
(f) Periodic Duties: This module provides supervisory personnel
with a method to schedule, assign and track the completion of
assigned tasks.
(g) System Management: This module maintains unit specific
information, user table maintenance, and system utilities.
c. Dental Common Access System (DENCAS).
(1) The Dental Common Access System is an enterprise-wide, world class e-
business system that functions seamlessly between ship and shore to
provide a complete picture of Navy and Coast Guard personnel dental
readiness. DENCAS also provides an accurate, real-time, comprehensive
administrative reporting system. The dental data is centralized in a single
database for query by authorized staff over the NIPRNET. The DENCAS
system is designed with security features that prevent unauthorized access,
data transmission interception, and alteration. Navy Dental Treatment
Facilities (DTF) and Coast Guard dental clinics are able to access dental
data on individual active duty members from either service. However,
summary dental data for each clinic is only available to their respective
commands.
(2) Definitions.
(a) Modules: Particular functional features of the DENCAS system.
(b) DIRS: Dental Information Retrieval System. This system
collects dental procedure codes.
(c) NMIMC: Naval Medical Information Management Center.
Responsible for DENCAS application support.
(3) Modules.
(a) DTF User: This module maintains patient dental records. It
automatically updates Dental Class status, recall appointment
intervals, documents dental treatment needs, allows for the
transfer of patient dental data, tracks dental provider information,
and records DIRS (dental productivity) data. Additionally, this
module can generate a variety of dental reports.
(b) Command User: Command User functions are designed for use
by dental officers to review dental information on active duty
members within their respective geographic areas of
responsibility (AOR). This module displays the current dental
readiness and dental health statistics for each command within
their AOR. Command Users have access to the reports
concerning individual patient dental class, recall appointments,

CH-17 14-10
and treatment needs. In addition, DIRS data for each provider
and the Command User’s dental clinic is available.
(c) Corporate User: This module provides patient and DIRS
reports for all Coast Guard active duty members and Coast Guard
dental clinics to the Coast Guard Maintenance and Logistics
Commands and Office of Health Services.
(d) External User: This module provides access to a number of
useful reports on the real-time status of dental health within the
External User’s own command. When an External User first logs
on to DENCAS, the Home Page displays the current status of
dental readiness and dental health for the External User’s own
customer command. With a click on any of the report links on
the page, the External User can view reports summarizing dental
class, exam recall, members requiring routine dental care, and
members requiring urgent dental care.
(e) System Management: This module provides for system setup,
table maintenance, and maintains system-related information
such as user access, password configuration, and the access log.
Responsibility for this module is shared between NMIMC and
the Coast Guard Office of Health Services.
d. Third Party Collections Program: Other Health Insurance (OHI).
(1) The United States Coast Guard is required by law to collect money
from all third party insurance payers for the cost of medical services
provided to military beneficiaries. This requirement, under Title 10 of
the United States Code, Section 1095 is known as the Third Party
Collection Program (TPC).
(2) This program applies to family members and retirees who have health
insurance coverage other than TRICARE, Medicare or Medicaid.
Commanding Officers and Chiefs of Health Services will ensure that
clinic staffs market the program and educate eligible beneficiaries
based on guidelines provided by the G-WKH program manager.
(3) Each CG clinic will follow guidelines established by the Office of
Health Services for documenting in CHCS any Other Health Insurance
information non-active beneficiaries may have and facilitate the
recovery of health care costs by adhering to guidelines provided by the
G-WKH program manager.

14-11 CH-17
Section C - Medical Readiness System (MRS).
To be developed pending implementation of a functional system.
