EQ 5D 5L User Guide 2015
User Manual:
Open the PDF directly: View PDF ![]() .
.
Page Count: 28

EQ-5D-5L User Guide
Basic information on how to use the EQ-5D-5L instrument
Prepared by
Mandy van Reenen / Bas Janssen
Version 2.1
April 2015
Table of contents
1. INTRODUCTION .................................................................................................................. . 4
1.1. THE EUROQOL GROUP .................................................................................................... 4
1.2. EQ-5D ........................................................................................................................... 4
1.2.1. EQ-5D-3L ................................................................................................................. 4
1.2.2. EQ-5D-5L ................................................................................................................. 5
1.3. WHAT IS A HEALTH STATE? .............................................................................................. 9
2. SCORING THE EQ-5D-5L DESCRIPTIVE SYSTEM .......................................................... 10
3. SCORING THE EQ VAS ..................................................................................................... 11
4. CONVERTING EQ-5D-5L STATES TO AN INDEX VALUE ............................................... 12
4.1. THE EQ-5D-5L CROSSWALK PROJECT ........................................................................... 12
4.2. CROSSWALK VALUE SETS FOR THE EQ-5D-5L ................................................................ 12
5. ORGANISING EQ-5D-5L DATA ......................................................................................... 14
6. PRESENTING EQ-5D-5L RESULTS .................................................................................. 15
6.1. HEALTH PROFILES ......................................................................................................... 15
6.2. EQ VAS ...................................................................................................................... 17
6.3. EQ-5D-5L INDEX VALUE ................................................................................................ 17
7. EQ-5D PRODUCTS ............................................................................................................ 19
7.1. EQ-5D-5L TRANSLATIONS AND OTHER FORMATS ............................................................ 19
7.2. OTHER EQ-5D PRODUCTS ............................................................................................ 19
7.2.1. EQ-5D-3L Translations and formats ....................................................................... 19
7.2.2. EQ-5D-Y Translations ............................................................................................ 19
7.3. TRANSLATION PROCESS ................................................................................................ 20
7.4. HOW TO OBTAIN EQ-5D-5L? ......................................................................................... 20
8. FAQS .................................................................................................................................. 21
8.1. GENERAL ..................................................................................................................... 21
8.2. REGISTRATION ............................................................................................................. 23
8.3. COPYRIGHT .................................................................................................................. 23
9. REFERENCES AND PUBLICATIONS ............................................................................... 24
9.1. KEY EUROQOL GROUP REFERENCES ............................................................................. 24
9.2. REFERRING TO THE EQ-5D-5L INSTRUMENT IN PUBLICATIONS .......................................... 24
9.3. EQ-5D BOOKS ............................................................................................................. 25

Page | 4
1. Introduction
This guide has been developed in order to give users basic information on how to use the EQ-5D-5L version.
Topics include administering the instrument, setting up a database for data collected using EQ-5D-5L as well
as information about how to present the results. Also included are several frequently asked questions
dealing with common issues regarding the use of EQ-5D-5L and a list of currently available EuroQol
products.
1.1. The EuroQol Group
The EuroQol Group is a network of international multidisciplinary researchers devoted to the
measurement of health status. Established in 1987, the EuroQol Group originally consisted of
researchers from Europe, but nowadays includes members from North America, Asia, Africa, Australia,
and New Zealand. The Group is responsible for the development of EQ-5D, a preference based
measure of health status that is now widely used in clinical trials, observational studies and other health
surveys.
The EuroQol Group has been holding annual scientific meetings since its inception in 1987.
The EuroQol Group can be justifiably proud of its collective scientific achievements over the last 20
years. Research areas include: valuation, EQ-5D use in clinical studies and in population surveys,
experimentation with the EQ-5D descriptive system, computerized applications, interpretation of EQ-5D
ratings and the role of EQ-5D in measuring social inequalities in self-reported health.
The EuroQol website (www.euroqol.org) contains detailed information about EQ-5D, guidance for users,
a list of available language versions, EQ-5D references and contact details.
1.2. EQ-5D
EQ-5D is a standardised measure of health status developed by the EuroQol Group in order to
provide a simple, generic measure of health for clinical and economic appraisal1.
Applicable to a wide range of health conditions and treatments, it provides a simple descriptive profile and a
single index value for health status that can be used in the clinical and economic evaluation of health care as
well as in population health surveys. EQ-5D is designed for self-completion by respondents and is ideally
suited for use in postal surveys, in clinics, and in face-to-face interviews. It is cognitively undemanding,
taking only a few minutes to complete. Instructions to respondents are included in the questionnaire.
1.2.1. EQ-5D-3L
The EQ-5D 3 level version (EQ-5D-3L) was introduced in 1990. The EQ-5D-3L essentially consists of 2
pages - the EQ-5D descriptive system (page 2) and the EQ visual analogue scale (EQ VAS) (page 3). The
EQ-5D-3L descriptive system comprises the following 5 dimensions: mobility, self-care, usual activities,
1 EuroQol Group. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy 1990;16:199-208

Page | 5
pain/discomfort and anxiety/depression. Each dimension has 3 levels: no problems, some problems, extreme
problems. The respondent is asked to indicate his/her health state by ticking (or placing a cross) in the box
against the most appropriate statement in each of the 5 dimensions. The EQ VAS records the respondent’s
self-rated health on a vertical, visual analogue scale where the endpoints are labelled ‘Best imaginable
health state’ and ‘Worst imaginable health state’. This information can be used as a quantitative measure of
health outcome as judged by the individual respondents.
The EQ-5D-3L has now been translated into more than 170 languages and is used worldwide. However
ceiling effects have been reported, particularly when used in general population surveys but also in some
patient population settings. In order to address these criticisms, and encouraged by demand from clinicians
and other users, the EuroQol Group decided to explore ways of improving the EQ-5D’s measurement
properties.
1.2.2. EQ-5D-5L
In 2005, a Task Force was established within the EuroQol Group to investigate methods to improve the
instrument’s sensitivity and to reduce ceiling effects. After much discussion, the Task Force decided that
there should be no change in the number of dimensions for a new version of EQ-5D. However, previously
published studies by EuroQol Group members showed that experimental 5-level versions of EQ-5D could
significantly increase reliability and sensitivity (discriminatory power) while maintaining feasibility and
potentially reducing ceiling effects. The Group therefore decided that the new version of the EQ-5D should
include five levels of severity in each of the existing five EQ-5D dimensions and that it would be called the
EQ-5D-5L (Figure 1)2. The existing EQ-5D was renamed the EQ-5D-3L.
The EQ-5D-5L still consists of 2 pages – the EQ-5D-5L descriptive system (page 2) and the EQ Visual
Analogue scale (EQ VAS) (page 3). The descriptive system comprises the same 5 dimensions as the EQ-
5D-3L (mobility, self care, usual activities, pain/discomfort, anxiety/depression). However, each dimension
now has 5 levels: no problems, slight problems, moderate problems, severe problems, and extreme
problems. The respondent is asked to indicate his/her health state by ticking (or placing a cross) in the box
against the most appropriate statement in each of the 5 dimensions. This decision results in a 1-digit number
expressing the level selected for that dimension. The digits for 5 dimensions can be combined in a 5-digit
number describing the respondent’s health state. It should be noted that the numerals 1-5 have no
arithmetic properties and should not be used as a cardinal score. During the development of the EQ-
5D-5L, the opportunity was also taken to improve some of the wording in the dimensions to enhance
consistency and facilitate understanding. For example, the old wording of ‘confined to bed’ to indicate the
upper extreme in the EQ-5D-3L has been replaced with ‘I am unable to walk about’ which is more consistent
with the wording within the Mobility dimension and with the extreme levels on other dimensions.
The EQ VAS records the respondent’s self-rated health on a 20 cm vertical, visual analogue scale with
endpoints labelled ‘the best health you can imagine’ and ‘the worst health you can imagine’. This information
can be used as a quantitative measure of health as judged by the individual respondents. The instructions
2 Herdman M, Gudex C, Lloyd A, Janssen MF, Kind P, Parkin D, Bonsel G, Badia X. Development and preliminary testing of the new
five-level version of EQ-5D (EQ-5D-5L). Quality of Life Research.
Page | 6
for the EQ VAS task have been changed and simplified in the EQ-5D-5L. The EuroQol Group had received
feedback over the years that respondents sometimes found it difficult to draw a line from the box to the scale.
It was also cumbersome for administrators to record their scores. The EQ-5D-5L now asks respondents to
simply ‘mark an X on the scale to indicate how your health is TODAY’ and then to ‘write the number you
marked on the scale in the box below’. This should make the task easier for both respondents and users.

Page | 7
Figure 1: EQ-5D-5L (UK English sample version)
Under each heading, please tick the ONE box that best describes your health TODAY
MOBILITY
I have no problems in walking about
I have slight problems in walking about
I have moderate problems in walking about
I have severe problems in walking about
I am unable to walk about
SELF-CARE
I have no problems washing or dressing myself
I have slight problems washing or dressing myself
I have moderate problems washing or dressing myself
I have severe problems washing or dressing myself
I am unable to wash or dress myself
USUAL ACTIVITIES (e.g. work, study, housework, family or leisure activities)
I have no problems doing my usual activities
I have slight problems doing my usual activities
I have moderate problems doing my usual activities
I have severe problems doing my usual activities
I am unable to do my usual activities
PAIN / DISCOMFORT
I have no pain or discomfort
I have slight pain or discomfort
I have moderate pain or discomfort
I have severe pain or discomfort
I have extreme pain or discomfort
ANXIETY / DEPRESSION
I am not anxious or depressed
I am slightly anxious or depressed
I am moderately anxious or depressed
I am severely anxious or depressed
I am extremely anxious or depressed

Page | 8
• We would like to know how good or bad your health is TODAY.
• This scale is numbered from 0 to 100.
• 100 means the best health you can imagine.
0 means the worst health you can imagine.
• Mark an X on the scale to indicate how your health is TODAY.
• Now, please write the number you marked on the scale in the box below.
YOUR HEALTH TODAY =
Page | 8
• We would like to know how good or bad your health is TODAY.
• This scale is numbered from 0 to 100.
• 100 means the best health you can imagine.
0 means the worst health you can imagine.
• Mark an X on the scale to indicate how your health is TODAY.
• Now, please write the number you marked on the scale in the box below.
YOUR HEALTH TODAY =

Page | 9
1.3. What is a health state?
Each of the 5 dimensions comprising the EQ-5D descriptive system is divided into 5 levels of perceived
problems:
Level 1: indicating no problem
Level 2: indicating slight problems
Level 3: indicating moderate problems
Level 4: indicating severe problems
Level 5:indicating extreme problems
A unique health state is defined by combining 1 level from each of the 5 dimensions.
A total of 3125 possible health states is defined in this way. Each state is referred to in terms of a 5 digit
code. For example, state 11111 indicates no problems on any of the 5 dimensions, while state 12345
indicates no problems with mobility, slight problems with washing or dressing, moderate problems with doing
usual activities, severe pain or discomfort and extreme anxiety or depression.

Page | 10
2. Scoring the EQ-5D-5L descriptive system
The EQ-5D-5L descriptive system should be scored, for example, as follows:
.
This example identifies the health state ‘12345’.
NB: There should be only ONE response for each dimension
NB: Missing values can be coded as ‘9’.
NB: Ambiguous values (e.g. 2 boxes are ticked for a single dimension) should be treated as missing
values.
Mobility
Self
-
-
Usual Activities
I have some problems with performing my usual activities
(e.g. work, study, housework, family or leisure activities)
Pain/Discomfort
By placing a tick in one box in each group, please indicate whic
h
statements best describe your health today.
Under each heading, please tick the ONE box that best describes your
health TODAY
MOBILITY
I have no problems in walking about
I have slight problems in walking about
I have moderate
problems in walking about
I have severe problems in walking about
I am unable to walk about
SELF
-CARE
I have no problems washing or dressing myself
I have slight problems washing or dressing myself
I have moderate problems washi
ng or dressing myself
I have severe problems washing or dressing myself
I am unable to wash or dress myself
USUAL ACTIVITIES
(e.g. work, study, housework,
family or leisure activities)
I have no problems doing my usual activities
I hav
e slight problems doing my usual activities
I have moderate problems doing my usual activities
I have severe problems doing my usual activities
I am unable to do my usual activities
PAIN / DISCOMFORT
I have no pain or discomfort
I have slight pain or discomfort
I have moderate pain or discomfort
I have severe pain or discomfort
I have extreme pain or discomfort
ANXIETY / DEPRESSION
I am not anxious or depressed
I am slightly anxious or depressed
I am moderately anxious or depressed
I am severely anxious or depressed
I am extremely anxious or depressed
Levels of perceived
problems are coded as
follows:
Level 1 is
coded as
a ‘1’
Level 2 is
coded as
a ‘2’
Level 3 is
coded as
a ‘3’
Level 4 is
coded as
a ‘4’
Level 5 is
coded as
a ‘5’

Page | 11
3. Scoring the EQ VAS
The EQ VAS should be scored, for example, as follows:
NB: Missing values should be coded as ‘999’.
NB: If there is a discrepancy between where the respondent has placed the X and the number he/she has
written in the box, administrators should use the number in the box.
For example this
response should be
coded as 77

Page | 12
4. Converting EQ-5D-5L states to an index value
EQ-5D-5L health states, defined by the EQ-5D-5L descriptive system, may be converted into a
single index value3. The index values, presented in country specific value sets, are a major
feature of the EQ-5D instrument, facilitating the calculation of quality-adjusted life years (QALYs)
that are used to inform economic evaluations of health care interventions. Studies that directly
elicit preferences from general population samples to derive value sets for the EQ-5D-5L are
under development in a number of countries; however, these studies will take time to complete
and for results to be disseminated.
4.1. The EQ-5D-5L Crosswalk Project
In the interim, the EuroQol Group coordinated a study4 that administered both the 3-level and 5-
level versions of the EQ-5D, in order to develop a “crosswalk” between the EQ-5D-3L value sets
and the new EQ-5D-5L descriptive system, resulting in crosswalk value sets for the EQ-5D-5L. A
total of 3691 respondents completed both the 3L and 5L across 6 countries: Denmark, England,
Italy, the Netherlands, Poland and Scotland. Different subgroups were targeted, and in most
countries, a screening protocol was implemented to ensure that a broad spectrum of levels of
health would be captured across the dimensions of EQ-5D for both the 5L and 3L descriptive
systems.
Several methods were consequently tested to optimize the link function between the two
descriptive systems. The crosswalk link function resulting from this exercise can be used to
calculate index values for EQ-5D-5L, based on the existing value sets for the EQ-5D-3L. Value
sets have been derived for EQ-5D-3L in several countries using visual analogue scale (VAS)
technique or time trade-off (TTO) valuation techniques. The list of currently available value sets
with the number of respondents and valuation technique applied is presented in table 1. Most of
the EQ-5D-3L value sets have been obtained using a representative sample of the general
population, thereby ensuring that they represent the societal perspective. For anyone working
with EQ-5D-3L data, an essential guide to the Group’s available value sets can be found in:
EuroQol Group Monograph series: Volume 2: EQ-5D value sets: inventory, comparative review
and user guide, published by Springer (see section 9.3 for more information).
4.2. Crosswalk value sets for the EQ-5D-5L
EQ-5D-5L value sets are available for each country that performed a valuation study for the EQ-
5D-3L (table 1). By using the crosswalk link function and the individual responses to the EQ-5D-
5L descriptive system, index values for the EQ-5D-5L can be calculated. Documents containing
information on the crosswalk project, tables of values for all 3125 health states and the ‘EQ-5D-5L
Crosswalk Index Value Calculator’ can be downloaded from the EuroQol website. The SAS and
SPSS syntax files can be ordered from the EuroQol Office.
3 Many different terms are in use for these index values, such as preference weights, preference-based values, utilities,
QALY weights, etc. Here, we use the term 'index value'.
4Van Hout B, Janssen MF, Feng YS, Kohlmann T, Busschbach J, Golicki D, Lloyd A, Scalone L, Kind P, Pickard AS.
Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value in Health.

Page | 13
Table 1: List of available value sets for the EQ-5D-3L (references available on the website)
Country
N
Valuation method
Belgium
722
EQ-5D VAS
Denmark
1686
EQ-5D VAS
Denmark 1332 TTO
Europe
8709
EQ-5D VAS
Finland
1634
EQ-5D VAS
France
443
VAS/TTO
Germany 339 EQ-5D VAS
Germany
339
TTO
Japan
621
TTO
Netherlands
309
TTO
New Zealand 1360 EQ-5D VAS
Slovenia
733
EQ-5D VAS
Spain
300
EQ-5D VAS
Spain
1000
TTO
Thailand 1324 TTO
UK
3395
EQ-5D VAS
UK
3395
TTO
US
4048
TTO
Zimbabwe 2440 TTO

Page | 14
5. Organising EQ-5D-5L data
Data collected using EQ-5D-5L can be entered in a database according to the following schema:
Variable
name
ID
SEX
AGE
EDU
COUNTRY
YEAR
MOBILITY
Variable
description
patient
ID
number
1=Male
2=Female
9=Missing
value
999=Missing
value
1=Low
2=Medium
3=High
9=Missing
value
Country
where data
was
collected
Year in
which data
was
collected
1=No problems,
2=Slight problems
3=Moderate
problems
4=Severe problems
5=Unable to
9=Missing value
Data row 1
1001
1
43
1
UK
2011
4
Data row 2
1002
2
24
2
UK
2011
2
Variable
name
SELFCARE
ACTIVITY
PAIN
ANXIETY
STATE
EQ_VAS
Variable
description
1=No problems
2=Slight
problems
3=Moderate
problems
4=Severe
problems
5=Unable to
9=Missing value
1=No problems
2=Slight
problems
3=Moderate
problems
4=Severe
problems
5=Unable to
9=Missing value
1=No pain
2=Slight pain
3=Moderate
pain
4=Severe pain
5=Extreme pain
9=Missing
value
1=Not anxious
2=Slightly anxious
3=Moderately
anxious
4=Severely
anxious
5=Extremely
anxious 9=Missing
value
5 digit code
for EQ-5D-5L
999=Missing
value
Data row 1
1
3
2
5
41325
60
Data row 2
1
1
1
1
21111
90

Page | 15
6. Presenting EQ-5D-5L results
Data collected using EQ-5D-5L can be presented in various ways. A basic subdivision can be
made according to the structure of the EQ-5D-5L:
1. Presenting results from the EQ-5D-5L descriptive system as a health profile
2. Presenting results of the EQ VAS as a measure of overall self-rated health status
3. Presenting results from the EQ-5D-5L index value
The way results can be presented is determined both by the data and by what message you, as a
researcher, wish to convey to your audience.
6.1. Health profiles
One way of presenting data as a health profile is by making a table with the frequency or the
proportion of reported problems for each level for each dimension. These tables can be broken
down to include the proportions per subgroup, such as age, before vs. after treatment, treatment
vs. comparator, etc.
Sometimes it is more convenient to dichotomise the EQ-5D-5L levels into 'no problems' (i.e. level
1) and 'problems' (i.e. levels 2 to 5), therefore changing the profile into frequencies of reported
problems. This can be the case, for example, in a general population survey where the numbers
of reported problems are low. Tables 2 and 3 are examples of how to present EQ-5D-5L data in
tabulated form.
Table 2: Percentage of a general population sample reporting levels 1 to 5 by dimension and by age group
AGE GROUPS
EQ-5D DIMENSION 18-29 30-39 40-49 50-59 60-69 70+
TOTAL
MOBILITY
Level 1 95,2% 90,7% 87,2% 67,8% 78,9% 47,1% 86,0%
Level 2 4,4% 8,1% 10,1% 18,6% 14,1% 41,2% 10,2%
Level 3 0,4% 0,6% 2,1% 10,2% 4,2% 5,9% 2,7%
Level 4 0,0% 0,6% 0,5% 3,4% 2,8% 5,9% 1,1%
Level 5 0,0% 0,0% 0,0% 0,0% 0,0% 0,0% 0,0%
SELF-CARE
Level 1 98,0% 96,9% 97,3% 91,5% 91,5% 88,2% 95,9%
Level 2 0,4% 1,9% 2,7% 6,8% 8,5% 5,9% 3,0%
Level 3 0,8% 1,2% 0,0% 0,8% 0,0% 5,9% 0,7%
Level 4 0,4% 0,0% 0,0% 0,0% 0,0% 0,0% 0,1%
Level 5 0,4% 0,0% 0,0% 0,8% 0,0% 0,0% 0,2%
USUAL
ACTIVITY
Level 1 66,5% 64,6% 54,3% 37,3% 50,7% 41,2% 57,1%
Level 2 30,7% 29,8% 36,7% 41,5% 39,4% 41,2% 34,5%
Level 3 1,6% 5,0% 8,5% 14,4% 7,0% 17,6% 6,6%
Level 4 0,8% 0,6% 0,5% 6,8% 2,8% 0,0% 1,7%
Level 5 0,4% 0,0% 0,0% 0,0% 0,0% 0,0% 0,1%

Page | 16
AGE GROUPS
EQ-5D DIMENSION 18-29 30-39 40-49 50-59 60-69 70+
TOTAL
PAIN /
DISCOMFORT
Level 1 79,3% 75,2% 75,0% 78,0% 78,9% 94,1% 77,5%
Level 2 16,3% 19,3% 19,7% 17,8% 15,5% 0,0% 17,5%
Level 3 2,8% 4,3% 4,3% 2,5% 5,6% 5,9% 3,7%
Level 4 1,2% 1,2% 1,1% 1,7% 0,0% 0,0% 1,1%
Level 5 0,4% 0,0% 0,0% 0,0% 0,0% 0,0% 0,1%
ANXIETY /
DEPRESSION
Level 1 92,4% 85,1% 83,5% 65,3% 84,5% 82,4% 84,0%
Level 2 6,8% 9,3% 11,7% 19,5% 9,9% 11,8% 10,7%
Level 3 0,0% 4,3% 3,2% 11,9% 4,2% 5,9% 3,8%
Level 4 0,4% 1,2% 1,6% 3,4% 1,4% 0,0% 1,4%
Level 5 0,4% 0,0% 0,0% 0,0% 0,0% 0,0% 0,1%
Table 3: Frequency of reported problems for a general population sample by dimension and age group
AGE GROUPS
EQ-5D DIMENSION 18-29 30-39 40-49 50-59 60-69 70-79 TOTAL
MOBILITY No problems 239 146 164 80 56 8 693
Problems 12 15 24 38 15 9 113
SELF-CARE No problems 246 156 183 108 65 15 773
Problems 5 5 5 10 6 2 33
USUAL ACTIVITY No problems 167 104 102 44 36 7 460
Problems 84 57 86 74 35 10 346
PAIN / DISCOMFORT No problems 199 121 141 92 56 16 625
Problems 52 40 47 26 15 1 181
ANXIETY /
DEPRESSION
No problems 232 137 157 77 60 14 677
Problems 19 24 31 41 11 3 129
In addition to presenting the results in tabulated form, you can also use graphical presentations.
Two (or three) dimensional bar charts can be used to summarise the results in a single graph
(see Figure 2). Figure 2 shows the sum of the proportion of reported levels 2 to 5 for each of the 5
EQ-5D-5L dimensions for 3 different age groups. Older people reported more problems on all
dimensions but the effect of age was strongest for mobility and weakest for anxiety/depression.
Figure 2: Profile of the population (% reporting problem
Page | 17
6.2. EQ VAS
In order to present all aspects of the EQ VAS data, you should present both a measure of the
central tendency and a measure of dispersion. This could be the mean values and the standard
deviations or, if the data are skewed, the median values and the 25th and 75th percentiles. An
example is presented in table 4.
Table 4: EQ VAS values by age – mean + standard deviation and median + percentiles
AGE GROUPS
EQ VAS
18-29 30-39 40-49 50-59 60-69 70+ TOTAL
Mean 85,7 84,3 83,7 79,7 86,1 79,0 84,0
- Std Dev 10,1 12,6 13,3 14,0 11,1 22,6 12,6
Median 88,0 89,0 88,0 80,5 90,0 80,0 86,0
- 25th 80,0 80,0 75,0 73,3 79,0 73,5 80,0
- 75th 93,0 91,0 93,8 90,0 95,0 92,0 92,0
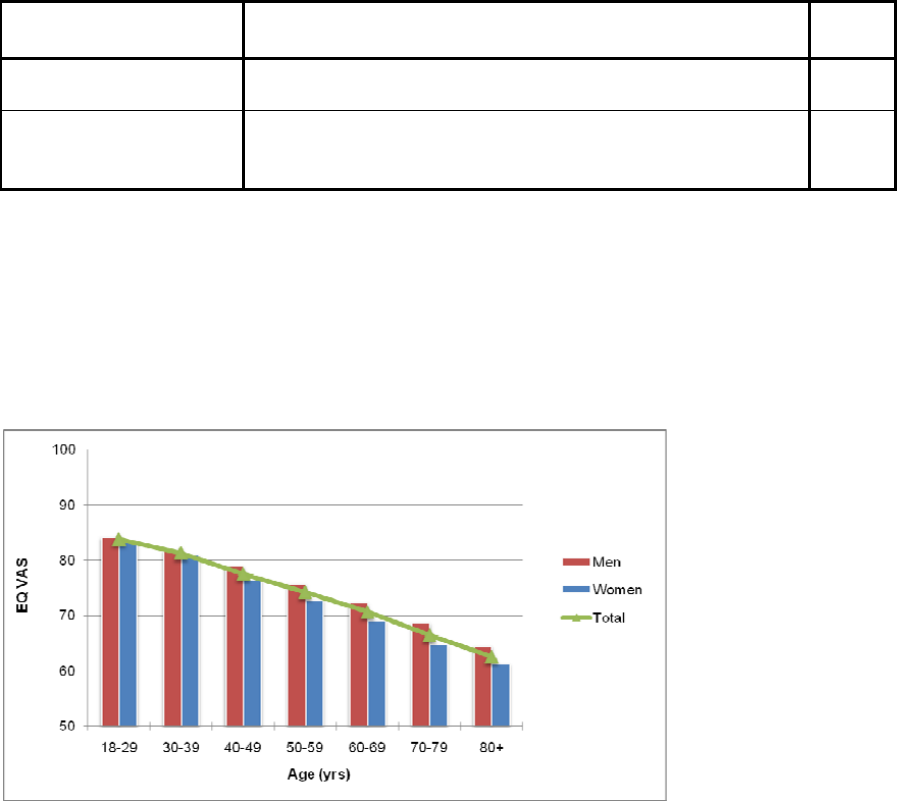
You can present a graphical representation of the data by using bar charts, line charts, or both
(see figure 3). Figure 3 shows the mean EQ VAS scores reported by men, women and both for 7
different age groups. Mean EQ VAS scores are seen to decrease with increasing age. Also, men
in all age groups reported higher EQ VAS scores than women.
Figure 3: Mean population EQ VAS scores by age group and sex
6.3. EQ-5D-5L index value
EQ-5D-5L index values can be presented in much the same way as EQ VAS data, i.e. using both
a measure of central tendency and a measure of dispersion. These can be mean values and
standard deviations (or standard errors, or 95% confidence intervals) or again, if the data are
skewed, median values and the 25th and 75th percentiles. Tables 5 and 6 and figures 4 and 5
show 2 examples of how to present EQ-5D-5L index value results. Table 5 and figure 4 present
the results from a study in which the effect of a treatment on health status is investigated. Table 6
and figure 5 show results for a patient population and 3 subgroups.

Page | 18
Table 5: EQ-5D-5L index values before and after treatment
EQ-Index Before treatment After treatment
Mean 0,59 0,76
- Std error 0,012 0,015
Median 0,60 0,70
- 25th 0,50 0,65
- 75th 0,70 0,80
N 120 110
Table 6: EQ-5D-5L index values for the total patient population and the 3 subgroups
EQ-Index All patients Subgroup 1 Subgroup 2 Subgroup 3
Mean 0,66 0,45 0,55 0,90
- Std error 0,010 0,013 0,015 0,010
Median 0,55 0,40 0,55 0,95
- 25th 0,50 0,30 0,50 0,80
- 75th 0,70 0,50 0,60 1,00
N 300 100 75 125
Figure 4: EQ-5D-5L index values before and after treatment: mean values and 95% confidence intervals
Figure 5: Mean EQ-5D-5L index values and 95% confidence intervals for the total patient population and 3
subgroups.
Page | 19
7. EQ-5D Products
7.1. EQ-5D-5L Translations and other formats
The EQ-5D-5L self-complete paper version is currently available in more
than 120 different language versions. Likewise, although the EQ-5D-5L was
primarily designed as a pen-and-paper, self-complete instrument, it is now
available in alternative formats and modes of administration, and in multiple
translations:
PDA
Telephone
Proxy paper
Web
Tablet
If you want to know whether an EQ-5D-5L version exists for your country, please
consult the EuroQol website.
7.2. Other EQ-5D Products
7.2.1. EQ-5D-3L Translations and formats
The EQ-5D-3L (EQ-5D 3 level) self-complete paper version is currently
translated in more than 170 language versions. Likewise, although the EQ-5D-
3L was also primarily designed as a pen-and-paper self-complete instrument, it is
now available in alternative formats and modes of administration, and in multiple
translations e.g.:
Face-to-face and proxy
paper
Tablet
IVR
Telephone
PDA
Web
If you want to know whether an EQ-5D-3L language version exists for your
country, please consult the EuroQol website.
7.2.2. EQ-5D-Y Translations
The EQ-5D-Y is an EQ-5D-3L self complete youth version has been
developed specifically for children and adolescents aged 8-15 years (or
respectively 8-18 years; see Youth User Guide). At present, this version is
available in more than 30 different languages. Likewise, although the EQ-5D-Y
was primarily designed as a pen-and-paper, self-complete instrument, it is now
available in the following alternative formats:
PDA
Tablet
Proxy paper
Page | 20
7.3. Translation process
All translation/adaptations of the EQ-5D-5L are produced using a standardized translation
protocol that conforms to internationally recognized guidelines. These guidelines aim to ensure
equivalence to the English ‘source’ version and involve a forward/backward translation process
and cognitive debriefing. Only the EuroQol Office can give permission for a translation to be
performed and translations can only be stamped as official if they are performed in cooperation
with EuroQol reviewers.
7.4. How to obtain EQ-5D-5L?
If you require a version that is not available, please first check with the EuroQol Office to ascertain
whether the version is in progress. If the version is not in progress and you are interested in
getting the version (or versions) translated, the policy of the EuroQol Research Foundation is that
you use a specialist agency to carry out the work. The EuroQol Office will refer you to their
preferred agencies who cooperate with the Foundation regularly and are aware of our
requirements. Please note that copyright of all translations remains with the Foundation.

Page | 21
8. FAQs
8.1. General
Is the EQ-5D-5L instrument validated?
The EQ-5D-5L has been validated in a diverse
patient population in 6 countries, including 8
patient groups with chronic conditions
(cardiovascular disease, respiratory disease,
depression, diabetes, liver disease,
personality disorders, arthritis, stroke) and a
student cohort. Redistribution of responses
from the EQ-5D-3L to EQ-5D-5L was
validated for all dimensions and all levels. The
measurement properties of EQ-5D-5L were
superior to the EQ-5D-3L in terms of
feasibility, ceiling effects, discriminatory power
and convergent validity. Reliability and
responsiveness remain to be assessed for the
EQ-5D-5L.
Can the EQ-5D-5L now be used instead of
the EQ-5D-3L?
Yes, the EQ-5D-5L can be used instead of the
EQ-5D-3L but please bear in mind that
currently there are no value sets available that
are directly elicited from representative
general population samples.
For the purpose of comparing EQ-5D results
with previous research based on the EQ-5D-
3L, or when used in longitudinal research
based on the EQ-5D-3L, it is advised to use
the EQ-5D-3L, or both the EQ-5D-3L and EQ-
5D-5L
For what period of time does EQ-5D-5L
record health status?
Self-reported health status captured by EQ-
5D-5L relates to the respondent’s situation at
the time of completion. No attempt is made to
summarise recalled health status over the
preceding days or weeks, although EQ-5D-3L
has been tested in recall mode. An early
decision taken by the EuroQol Group
determined that health status measurement
ought to apply to the respondent’s immediate
situation - hence the focus on ‘your health
today’.
Can I use only the EQ-5D-5L descriptive
system or only the EQ VAS?
We cannot advise this. EQ-5D-5L is a 2-part
instrument so if you only use one part you
cannot claim to have used EQ-5D-5L in your
publications.
How long should the EQ VAS be?
Officially, for paper versions, the EQ VAS
scale should be 20 cm. All methodological and
developmental work has been carried out
using this length. To ensure that you print the
correct length, make sure your paper size is
set at A4 and the box in your printing
instructions labelled ‘scale to paper size’ is set
at ‘no scaling’.
Can I publish our study using EQ-5D?
Yes, you are free to publish your results. If you
are reproducing the EQ-5D-5L, we request
that you use the sample version of EQ-5D-5L.
Also, please include the copyright statement
stated in the footer of the specific EQ-5D-5L
language version.
What is the difference between the EQ-5D-
5L descriptive system, the EQ VAS and the
EQ-5D index values?
The descriptive system can be represented as
a health state, e.g. health state 21143
represents a patient who indicates slight
problems on the mobility dimension, no
Page | 22
problems on the self-care and usual activities
dimensions, severe pain or discomfort, and
moderate problems on the anxiety/depression
dimension. These health states can be
converted to a single index value using the
crosswalk link function based on the existing
value sets for the EQ-5D-3L described in
Section 4 above. These EQ-5D-3L value sets
are based on VAS or TTO valuation
techniques, and reflect the opinion of the
general population. The EQ VAS self-rating
records the respondent’s own assessment of
their health status and are therefore not
representative of the general population.
Since, the EQ VAS scores are anchored on
100 = the best health you can imagine and 0 =
the worst health you can imagine these scores
are not suitable for QALY calculations,
whereas the value sets are anchored on
11111 = 1 and dead = 0 and can therefore be
used in QALY calculations.
What is the difference between the VAS
and TTO techniques?
The difference between the TTO- and VAS-
based value sets is that the techniques used
to elicit the values on which the models are
based differ. In the TTO task, respondents are
asked to imagine that they will live in a certain
health state (e.g. 33333) for 10 years and
have to specify the amount of time they would
be willing to give up to live in full health
instead (i.e. 11111). For example, someone
might find 8 years in 11111 equivalent to 10
years in 33333. The VAS technique on the
other hand, asks people to indicate where, on
a vertical thermometer-like scale ranging from
best imaginable health to worst imaginable
health, they think a health state should be
positioned.
General population value sets vs. patient
population value sets
If you want to undertake a utility analysis you
will need to use a value set. Generally
speaking, utility analysis requires a general
population-based value set (as opposed to a
patient-based set). The rationale behind this is
that the values should reflect the preferences
of local taxpayers and potential receivers of
healthcare. Additionally, patients tend to rate
their health states higher than the general
population because of coping or other factors,
and may therefore underestimate their need
for healthcare. EQ-5D-5L value sets are
therefore based on general population values.
Multinational clinical trials
Information relating to EQ-5D-5L health states
gathered in the context of multinational trials
may be converted into a single index value
using the crosswalk link function based on the
available EQ-5D-3L value sets as described in
Section 4 above. There are different options
available to do this using appropriate value
sets-however the choice depends on the
context in which the information will be used
by researchers or decision makers. In cases
where data from an international trial are to be
used to inform decision makers in a specific
country, it seems reasonable to expect
decision makers to be interested primarily in
value sets that reflect the values for health
states in that country. So for example, if
applications for reimbursement of a drug are
rolled out from country to country, country-
specific value sets should be applied and
reported in each pharmaco-economic report.
This is no different from the requirement to
use country specific costs. In the absence of a
country-specific value set, the researcher
should select another set of values for a
population that most closely approximates that
Page | 23
country. Sometimes however, information
about index values ('utilities') is required to
inform researchers or decision makers in an
international context. In these instances, one
value set applied over all health states data is
probably more appropriate. The decision
about which value set to use will also depend
on whether the relevant decision making body
in each country specifies any requirements or
preferences in regard to the methodology
used in different contexts (e.g. TTO, standard
gamble (SG), VAS or discrete choice
modelling (DCM)). These guidelines are the
topic of an on-going, international debate but
the EuroQol website is planning to provide a
summary of health care decision-making
bodies internationally together with their stated
requirements regarding the valuation of health
states. Detailed information on valuation
protocols together with guidelines on which
value set to use and tables of all available
value sets has been published by Springer in:
EuroQol Group Monograph series: Volume 2:
EQ-5D value sets: inventory, comparative
review and user guide’ (see section 9.3 for
more information).
8.2. Registration
I am not conducting a study but would like
to use the EQ-5D to measure routine
clinical outcomes or to set-up a registry.
Do I still need to register?
Yes. You can only obtain EQ-5D versions by
completing the EQ-5D Registration Form.
8.3. Copyright
Is the EQ-5D-5L a copyrighted instrument?
Yes. Please note that without the prior written
consent of the EuroQol Office, you are not
permitted to i.e. use, reproduce, alter,
amend, convert, translate, publish or make
available in whatever way (digital, hard-copy
etc.) the EQ-5D-5L and related proprietary
materials. The EuroQol Research Foundation
stresses that any and all copyrights in the EQ-
5D, its (digital) representations, and its
translations exclusively vest in the EuroQol
Research Foundation. EQ-5D™ is a trade
mark of the EuroQol Research Foundation.
Page | 24
9. References and Publications
9.1. Key EuroQol Group references
1. The EuroQol Group (1990). EuroQol-a new facility for the measurement of health-related
quality of life. Health Policy 16(3):199-208.
2. Brooks R (1996). EuroQol: the current state of play. Health Policy 37(1):53-72.
3. Dolan P (1997). Modeling valuations for EuroQol health states. Med Care 35(11):1095-108.
4. Roset M, Badia X, Mayo NE (1999). Sample size calculations in studies using the EuroQol
5D. Qual Life Res 8(6):539-49.
5. Greiner W, Weijnen T, Nieuwenhuizen M, et al. (2003). A single European currency for EQ-
5D health states. Results from a six country study. Eur J Health Econ; 4(3):222-231.
6. Shaw JW, Johnson JA, Coons SJ (2005). US valuation of the EQ-5D health states:
development and testing of the D1 valuation model. Med Care; 43(3): 203-220.
7. Herdman M, Gudex C, Lloyd A, Janssen MF, Kind P, Parkin D, Bonsel G, Badia X.
Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L).
Quality of Life Research.
8. van,Hout B., Janssen,M.F., Feng,Y.S., Kohlmann,T., Busschbach,J., Golicki,D., Lloyd,A.,
Scalone,L., Kind,P., Pickard,A.S. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L
to EQ-5D-3L value sets. Value in Health. 2012 Jul-Aug;15(5):708-15
9. The development of new research methods for the valuation of EQ-5D-5L. European Journal
of Health Economics. Volume 14, Issue 1 Supplement, July 2013.
9.2. Referring to the EQ-5D-5L instrument in publications
When publishing results obtained with the EQ-5D-5L, the following references can be used:
1. The EuroQol Group (1990). EuroQol-a new facility for the measurement of health-related
quality of life. Health Policy 16(3):199-208.
2. Brooks R (1996). EuroQol: the current state of play. Health Policy 37(1):53-72.
3. Herdman M, Gudex C, Lloyd A, Janssen MF, Kind P, Parkin D, Bonsel G, Badia X.
Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L).
Quality of Life Research.
4. Janssen MF, Pickard AS, Golicki D, Gudex C, Niewada M, Scalone L, Swinburn P,
Busschbach J. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across
eight patient groups: a multi-country study
If you used the crosswalk value sets for the EQ-5D-5L in your study you can also include a reference
to the publication regarding that crosswalk value set. The appropriate reference is:
1. van,Hout B., Janssen,M.F., Feng,Y.S., Kohlmann,T., Busschbach,J., Golicki,D., Lloyd,A.,
Scalone,L., Kind,P., Pickard,A.S. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to
EQ-5D-3L value sets. Value in Health. 2012 Jul-Aug;15(5):708-15

Page | 25
9.3. EQ-5D Books
Self-Reported Population Health: An International Perspective based on EQ-
5D. Eds. Szende A, Janssen MF, Cabases J. Springer, 2014.
This book captures up-to-date and expanded information of EQ-5D self-reported
health and index values. EQ-5D population norms and cross-country analyses are
provided from representative national surveys of 20 countries and additional regional
surveys. The book can be obtained from Springer at www.springeronline.com and is
also available as open-access book.
The EuroQol Group after 25 years, Brooks R. Springer, 2013.
This book describes the history of the institutional and administrative framework
within which the EuroQol Group operated. It also presents how the EQ-5D's
descriptive system was determined, how translation and language issues were
handled, and how valuations were provided. The book and e-book can be obtained
from Springer at www.springeronline.com.
EQ-5D value sets: Inventory, comparative review and user guide. Eds. Szende
A, Oppe M, Devlin N. EuroQol Group Monographs Volume 2. Springer, 2006.
This book provides an essential guide to the use of the EuroQol Group’s value sets
for anyone working with EQ-5D data and can be obtained from Springer at
www.springeronline.com.
EQ-5D concepts and methods: a developmental history. Eds Kind P, Brooks R,
Rabin R. Springer, 2005.
This book is a collection of papers representing the collective intellectual enterprise
of the EuroQol Group and can be obtained from Springer at
www.springeronline.com.
The Measurement and valuation of health status using EQ-5D: A European
perspective. Eds Brooks R, Rabin R, de Charro F. Kluwer Acacemic
Publishers, 2005
This book reports on the results of the European Union-funded EQ-net project which
furthered the development of EQ-5D in the key areas of valuation, application and
translation. The book can be obtained from Springer at www.springeronline.com.
Page | 25
9.3. EQ-5D Books
Self-Reported Population Health: An International Perspective based on EQ-
5D. Eds. Szende A, Janssen MF, Cabases J. Springer, 2014.
This book captures up-to-date and expanded information of EQ-5D self-reported
health and index values. EQ-5D population norms and cross-country analyses are
provided from representative national surveys of 20 countries and additional regional
surveys. The book can be obtained from Springer at www.springeronline.com and is
also available as open-access book.
The EuroQol Group after 25 years, Brooks R. Springer, 2013.
This book describes the history of the institutional and administrative framework
within which the EuroQol Group operated. It also presents how the EQ-5D's
descriptive system was determined, how translation and language issues were
handled, and how valuations were provided. The book and e-book can be obtained
from Springer at www.springeronline.com.
EQ-5D value sets: Inventory, comparative review and user guide. Eds. Szende
A, Oppe M, Devlin N. EuroQol Group Monographs Volume 2. Springer, 2006.
This book provides an essential guide to the use of the EuroQol Group’s value sets
for anyone working with EQ-5D data and can be obtained from Springer at
www.springeronline.com.
EQ-5D concepts and methods: a developmental history. Eds Kind P, Brooks R,
Rabin R. Springer, 2005.
This book is a collection of papers representing the collective intellectual enterprise
of the EuroQol Group and can be obtained from Springer at
www.springeronline.com.
The Measurement and valuation of health status using EQ-5D: A European
perspective. Eds Brooks R, Rabin R, de Charro F. Kluwer Acacemic
Publishers, 2005
This book reports on the results of the European Union-funded EQ-net project which
furthered the development of EQ-5D in the key areas of valuation, application and
translation. The book can be obtained from Springer at www.springeronline.com.
Page | 25
9.3. EQ-5D Books
Self-Reported Population Health: An International Perspective based on EQ-
5D. Eds. Szende A, Janssen MF, Cabases J. Springer, 2014.
This book captures up-to-date and expanded information of EQ-5D self-reported
health and index values. EQ-5D population norms and cross-country analyses are
provided from representative national surveys of 20 countries and additional regional
surveys. The book can be obtained from Springer at www.springeronline.com and is
also available as open-access book.
The EuroQol Group after 25 years, Brooks R. Springer, 2013.
This book describes the history of the institutional and administrative framework
within which the EuroQol Group operated. It also presents how the EQ-5D's
descriptive system was determined, how translation and language issues were
handled, and how valuations were provided. The book and e-book can be obtained
from Springer at www.springeronline.com.
EQ-5D value sets: Inventory, comparative review and user guide. Eds. Szende
A, Oppe M, Devlin N. EuroQol Group Monographs Volume 2. Springer, 2006.
This book provides an essential guide to the use of the EuroQol Group’s value sets
for anyone working with EQ-5D data and can be obtained from Springer at
www.springeronline.com.
EQ-5D concepts and methods: a developmental history. Eds Kind P, Brooks R,
Rabin R. Springer, 2005.
This book is a collection of papers representing the collective intellectual enterprise
of the EuroQol Group and can be obtained from Springer at
www.springeronline.com.
The Measurement and valuation of health status using EQ-5D: A European
perspective. Eds Brooks R, Rabin R, de Charro F. Kluwer Acacemic
Publishers, 2005
This book reports on the results of the European Union-funded EQ-net project which
furthered the development of EQ-5D in the key areas of valuation, application and
translation. The book can be obtained from Springer at www.springeronline.com.

© EuroQol Research Foundation 2015
EuroQol Research Foundation
Marten Meesweg 107
3068 AV Rotterdam
The Netherlands
Tel: +31 (0)88 4400190
Email: userinformationservice@euroqol.org
www.euroqol.org
