Instruction Manual
User Manual:
Open the PDF directly: View PDF ![]() .
.
Page Count: 9
PHQ and GAD-7 Instructions P. 1/9
INSTRUCTION MANUAL
Instructions for Patient Health Questionnaire (PHQ) and GAD-7 Measures
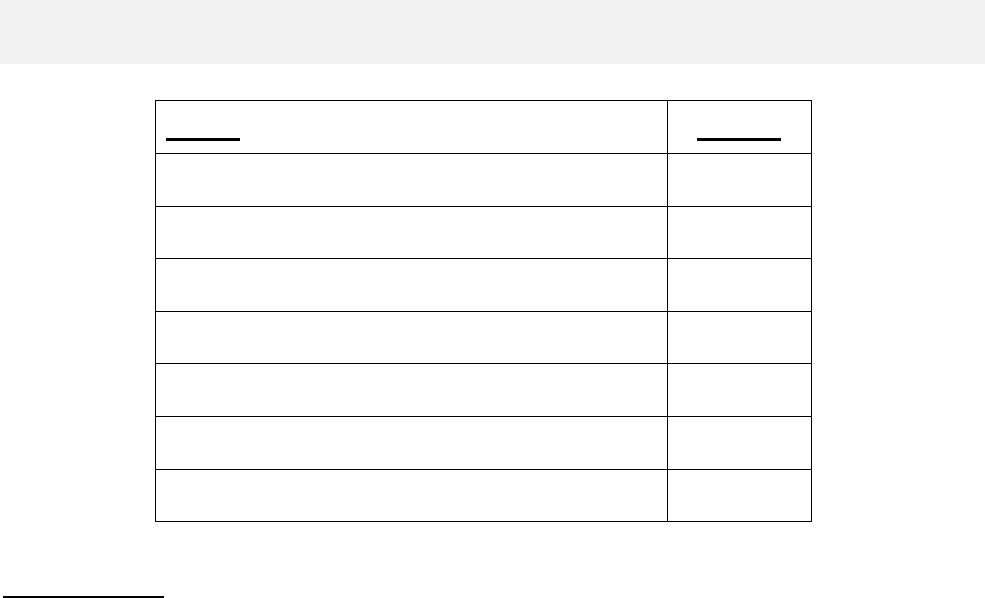
TOPIC
PAGES
Background
1
Coding and Scoring
2, 4, 5
Versions
3
Use as Severity and Outcome Measures
6-7
Translations
7
Website and Other Issues
8
Selected References
9
BACKGROUND
The Primary Care Evaluation of Mental Disorders (PRIME-MD) was an instrument developed and
validated in the early 1990s to efficiently diagnose five of the most common types of mental
disorders presenting in medical populations: depressive, anxiety, somatoform, alcohol, and eating
disorders.[1] Patients first completed a one-page 27-item screener and, for those disorders for
which they screened positive, were asked additional questions by the clinician using a structured
interview guide. However, this 2-stage process took an average of 5-6 minutes of clinician time in
patients without a mental disorder diagnosis and 11-12 minutes in patients with a diagnosis. This
proved to be a barrier to use given the competing demands in busy clinical practice settings.
Therefore, in two large studies enrolling 6000 patients (3000 from general internal medicine and
family practice clinics and 3000 from obstetrics-gynecology clinics), a self-administered version of
the PRIME-MD called the Patient Health Questionnaire (PHQ) was developed and validated.[2,3] In
the past decade, the PHQ in general and the PHQ-9 depression scale in particular [4-6] have gained
increasing use in both research and practice. The original PRIME-MD is now largely of historical
interest and seldom used except in a few types of research studies.
Given the popularity of the PHQ-9 for assessing and monitoring depression severity, a new 7-item
anxiety scale using a response set similar to the PHQ-9 was initially developed to diagnose
generalized anxiety disorder (hence its name, the GAD-7) and validated in 2740 primary care
patients.[7] Though originally developed to diagnose generalized anxiety disorder, the GAD-7 also
proved to have good sensitivity and specificity as a screener for panic, social anxiety, and post-
traumatic stress disorder.[8] Finally, the PHQ-15 was derived from the original PHQ studies and is
increasingly used to assess somatic symptom severity and the potential presence of somatization
and somatoform disorders.[9]

PHQ and GAD-7 Instructions P. 2/9
Each PHQ module can be used alone (e.g. the PHQ-9 if depression is the condition of interest),
together with other modules, or as part of the full PHQ. Also, alternative or abbreviated versions of
the PHQ-9 and GAD-7 are sometimes used in certain screening or research settings [10-14]
Although the PHQ was originally developed to detect five disorders, the depression, anxiety, and
somatoform modules (in that order) have turned out to be the most popular.[10] Also, most primary
care patients with depressive or anxiety disorders present with somatic complaints and co-
occurrence of somatic, anxiety, and depressive symptoms (the SAD triad) is exceptionally common.
This is the rationale behind the PHQ-SADS screener.[15] The most commonly used versions of the
PHQ scales are summarized in Table 1, page 3.
CODING AND SCORING
The full PHQ, Brief PHQ, and PHQ for Adolescents (PHQ-A) can be used to establish provisional
diagnoses for selected DSM-IV disorders. The diagnostic algorithm for the PHQ modules are
included in footers at the bottom of each page of the PHQ, and also reiterated in Table 2, page 4.
The other measures are principally used to derive severity scores (PHQ-9 and PHQ-8 for depressive
symptom severity; GAD-7 for anxiety symptom severity; PHQ-15 for somatic symptom severity) or
as ultra-brief screeners (PHQ-2, GAD-2, PHQ-4). An example in which the PHQ depression module
can be used as both a diagnostic module as well as a depression severity score (PHQ-9 score) is
shown in Table 3, page 5.
Over time, the severity scores have been a particularly popular use of the measures, and are now
used much more commonly than the provisional diagnoses. For example, cutpoints of 5, 10, and 15
represent mild, moderate, and severe levels of depressive, anxiety, and somatic symptoms, on the
PHQ-9, GAD-7, and PHQ-15 respectively. Also, a cutpoint of 10 or greater is considered a ―yellow
flag‖ on all 3 measures (i.e., drawing attention to a possible clinically significant condition), while a
cutpoint of 15 is a ―red flag‖ on all 3 measures (i.e., targeting individuals in whom active treatment is
probably warranted). For the ultra-brief measures (PHQ-2 and GAD-2), a score of 3 or greater
should prompt administration of the full PHQ-9 and/or GAD-7, as well as a clinical interview to
determine whether a mental disorder is present.
The final question on the PHQ (and some of its abbreviated versions) asks the patients to report
―how difficult have these problems made it for you to do your work, take care of things at home, or
get along with other people?‖ This single patient-rated difficulty item is not used in calculating any
PHQ score or diagnosis but rather represents the patient‘s global impression of symptom-related
impairment. It may be useful in decisions regarding initiation of or adjustments to treatment since it is
strongly associated with both psychiatric symptom severity as well as multiple measures of
impairment and health-related quality of life.
A particularly important question is how to assess suicide risk in individuals who answer positively to
the 9th question of the PHQ-9. A four-item screener has been developed that may assist in positive
responses to this 9th question [16], although a final decision about the actual risk of self-harm
requires a clinical interview.
PHQ and GAD-7 Instructions P. 3/9
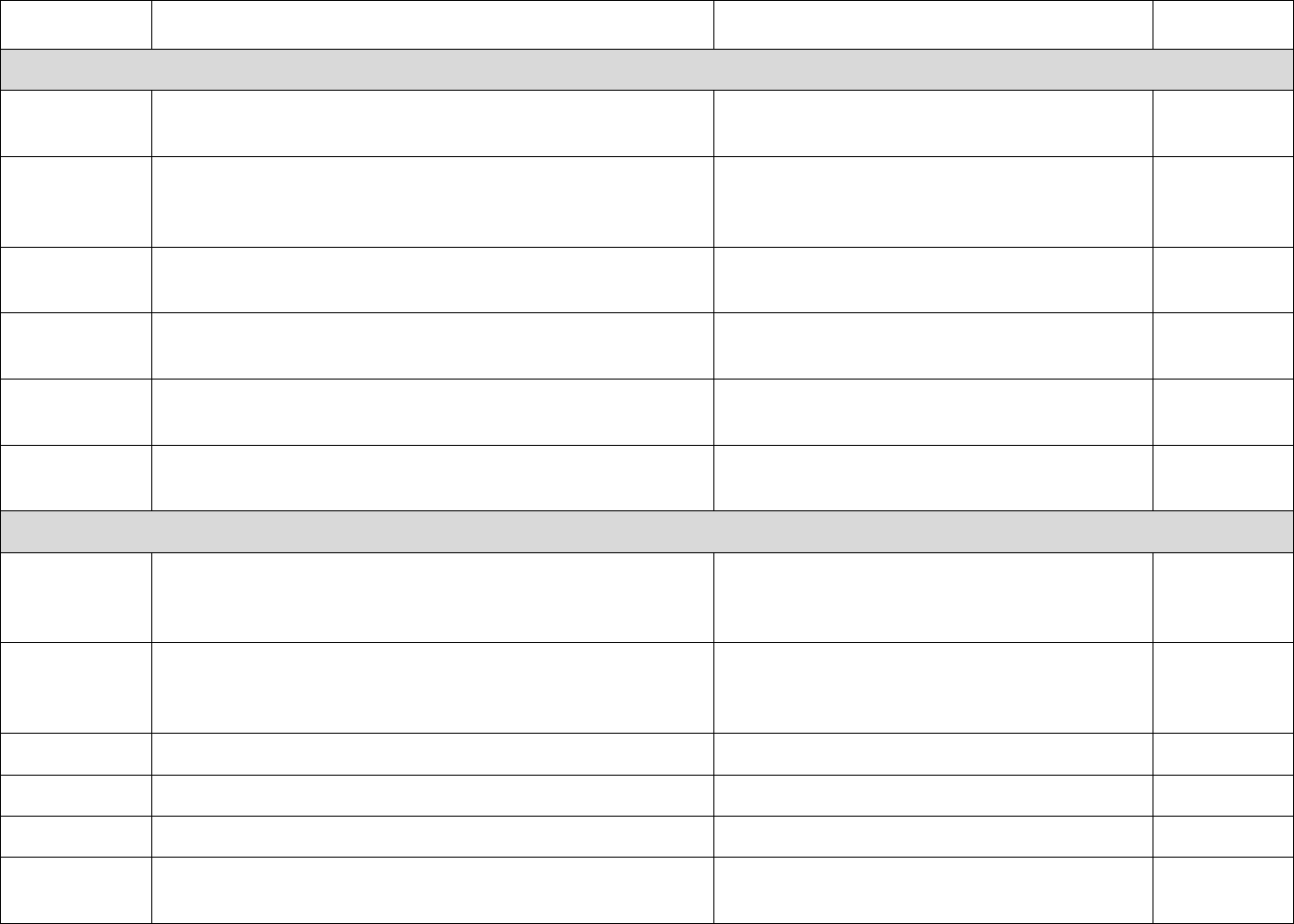
Table 1. Versions: Patient Health Questionnaire (PHQ) Family of Measures
Measure
Description
Scoring
References
Core
PRIME-MD
Predecessor of PHQ, now mainly of historical interest.
Combined self-administered patient
screener with clinician follow-up questions.
1
PHQ
Five modules covering 5 common types of mental
disorders: depression, anxiety, somatoform, alcohol,
and eating.
Selected (but provisional) DSM-IV
diagnoses for all types of disorders except
somatoform.
2, 3
PHQ-9
Depression scale from PHQ.
Nine items, each of which is scored 0 to 3,
providing a 0 to 27 severity score.
1, 4, 5, 6, 10
GAD-7
Anxiety measure developed after PHQ but incorporated
into PHQ-SADS.
Seven items, each of which is scored 0 to
3, providing a 0 to 21 severity score.
7, 8, 10
PHQ-15
Somatic symptom scale from PHQ.
Fifteen items, each of which is scored 0 to
2, providing a 0 to 30 severity score.
9, 10
PHQ-SADS
PHQ-9, GAD-7, and PHQ-15 measures, plus panic
measure from original PHQ.
See scoring for these scales above.
10
Variants
Brief PHQ
PHQ-9 and panic measures from original PHQ plus
items on stressors and women‘s health.
See scoring for PHQ above. Stressor and
women‘s health items are not diagnostic or
scored.
3
PHQ-A
Substantially modified version of PHQ developed for use
in adolescents. Moderate data exists for validity but
much less than for original PHQ.
Diagnostic scoring described in manual,
available upon request.
11
PHQ-2
First 2 items of PHQ-9. Ultra-brief depression screener.
Two items scored 0 to 3 (total score of 0-6)
10, 12
GAD-2
First 2 items of GAD-7. Ultra-brief anxiety screener.
Two items scored 0 to 3 (total score of 0-6)
8, 10, 12
PHQ-4
PHQ-2 and GAD-2.
See PHQ-2 and GAD-2 above.
10, 12, 13
PHQ-8
All items of PHQ-9 except the 9th item on self-harm.
Mainly used in non-depression research studies.
Eight items, each of which is scored 0 to 3,
providing a 0 to 24 severity score.
5, 10, 14
PHQ and GAD-7 Instructions P. 4/9
Table 2. Diagnostic Algorithms for the PHQ
Page 1
Somatoform Disorder if at least 3 of #1a-m bother the patient ―a lot‖ and lack an adequate biological
explanation.
Major Depressive Syndrome if #2a or b and five or more of #2a-i are at least ―More than half the days‖
(count #2i if present at all) .
Other Depressive Syndrome if #2a or b and two, three, or four of #2a-i are at least ―More than half the days‖
(count #2i if present at all).
Note: the diagnoses of Major Depressive Disorder and Other Depressive Disorder requires ruling out normal
bereavement (mild symptoms, duration less than 2 months), a history of a manic episode (Bipolar Disorder)
and a physical disorder, medication or other drug as the biological cause of the depressive symptoms.
Page 2
Panic Syndrome if #3a-d are all ‗YES‘ and 4 or more of #4a-k are ‗YES‘.
Other Anxiety Syndrome if #5a and answers to three or more of #5b-g are ―More than half the days‖.
Note: The diagnoses of Panic Disorder and Other Anxiety Disorder require ruling out a physical disorder,
medication or other drug as the biological cause of the anxiety symptoms.
Page 3
Bulimia Nervosa if #6a,b, and c and #8 are ‗YES‘;
Binge Eating Disorder the same but #8 is either ‗NO‘ or left blank.
Alcohol abuse if any of #10a-e are ―YES‖.
Additional Clinical Considerations. After making a provisional diagnosis with the PHQ, there are
additional clinical considerations that may affect decisions about management and treatment.
Have current symptoms been triggered by psychosocial stressor(s)?
What is the duration of the current disturbance and has the patient received any treatment for it?
To what extent are the patient’s symptoms impairing his or her usual work and activities?
Is there a history of similar episodes, and were they treated?
Is there a family history of similar conditions?

PHQ and GAD-7 Instructions P. 5/9
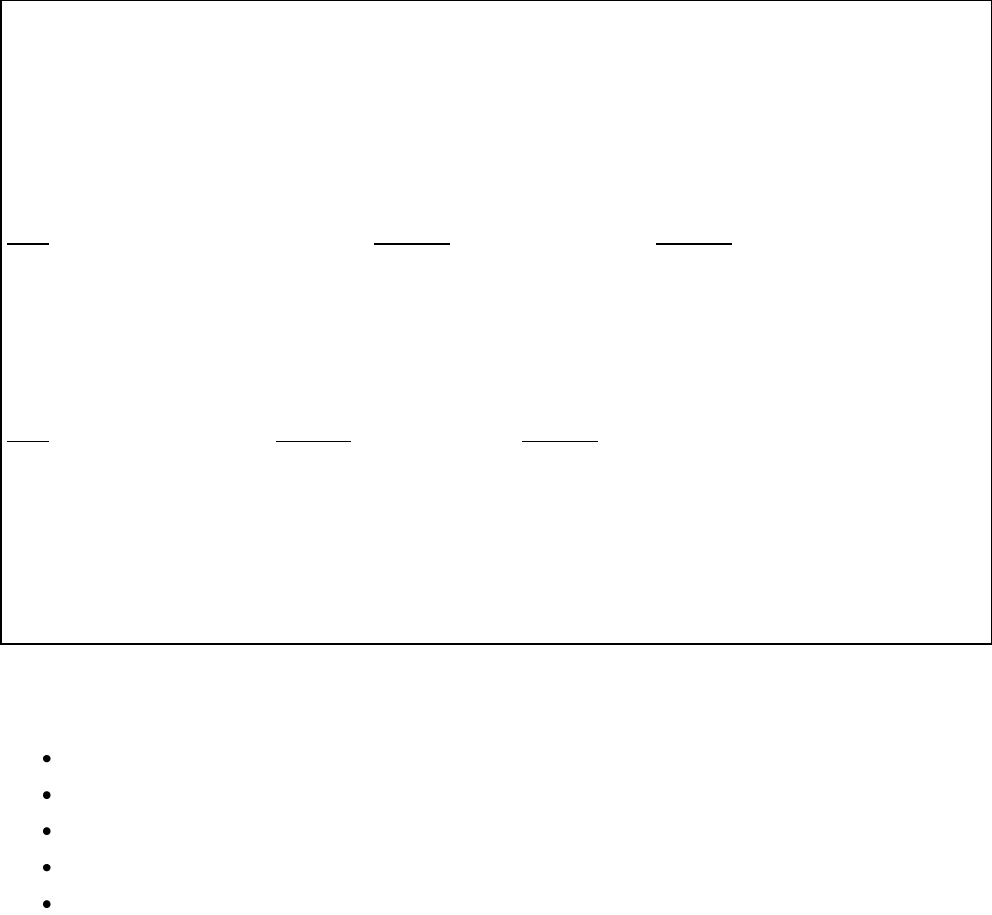
Table 3. Example of PHQ Depression Module for both Diagnostic and Severity
Purposes
Patient: A 43-year-old woman who looks sad and complains of fatigue for the past month.
2. Over the last 2 weeks, how often have you been bothered by
any of the following:
Not at all
Several
days
More than
half the
days
Nearly
every
day
(0)
(1)
(2)
(3)
a. Little interest or pleasure in doing things?………………..
b. Feeling down, depressed, or hopeless?………………..…
c. Trouble falling or staying asleep, or sleeping too much?
d. Feeling tired or having little energy?.........……….....…..
e. Poor appetite or overeating?......................………….….
f. Feeling bad about yourself—or that you are a failure or
have let yourself or your family down?…………………..
g. Trouble concentrating on things, such as reading the
newspaper or watching television? ……………………..
h. Moving or speaking so slowly that other people could
have noticed? Or the opposite—being so fidgety or
restless that you have been moving around a lot more
than usual?.............………………………………………..
i. Thoughts that you would be better off dead or of hurting
yourself in some way? …………………………………….
________________________________________________________________________________________________
FOR OFFICE CODING: Maj Dep Syn if #2a or b and five or more of #2a-i are at least ―More than half the
days‖ (count #2i if present at all) . Other Dep Syn if #2a or b and two, three, or four of #2a-i are at least ―More
than half the days‖ (count #2i if present at all).
Major Depressive Disorder Diagnosis. The criteria for Major Depressive Syndrome are met since
she checked #2a ―nearly every day‖ and five of items #2a to i were checked ―more than half the
days‖ or ―nearly every day‖. Note that #2i, suicidal ideation, is counted whenever it is present.
In this case, the diagnosis of Major Depressive Disorder (not Syndrome) was made since
questioning by the physician indicated no history of a manic episode; no evidence that a physical
disorder, medication, or other drug caused the depression; and no indication that the depressive
symptoms were normal bereavement. Questioning about the suicidal ideation indicated no
significant suicidal potential.
PHQ-9 Depression Severity. This is calculated by assigning scores of 0, 1, 2, and 3, to the
response categories of ―not at all,‖ ―several days,‖ ―more than half the days,‖ and ―nearly every day,‖
respectively. PHQ-9 total score for the nine items ranges from 0 to 27. In the above case, the PHQ-
9 depression severity score is 16 (3 items scored 1, 2 items scored 2, and 3 items scored 3).
Scores of 5, 10, 15, and 20 represent cutpoints for mild, moderate, moderately severe and severe
depression, respectively. Sensitivity to change has also been confirmed.

PHQ and GAD-7 Instructions P.6/9
USE OF SOME SCREENERS AS SEVERITY AND OUTCOME MEASURES
PHQ-9 Depression Severity. This is calculated by assigning scores of 0, 1, 2, and 3, to the
response categories of ―not at all,‖ ―several days,‖ ―more than half the days,‖ and ―nearly every
day,‖ respectively. PHQ-9 total score for the nine items ranges from 0 to 27. In the above case
(see table 3, page 5), the PHQ-9 depression severity score is 16 (3 items scored 1, 2 items
scored 2, and 3 items scored 3). Scores of 5, 10, 15, and 20 represent cutpoints for mild,
moderate, moderately severe and severe depression, respectively. Sensitivity to change has
also been confirmed. The PHQ-8 is scored just like the PHQ-9 and its total score ranges from
0 to 24. Cutpoints on the PHQ-8 are identical to the PHQ-9.
GAD-7 Anxiety Severity. This is calculated by assigning scores of 0, 1, 2, and 3, to the
response categories of ―not at all,‖ ―several days,‖ ―more than half the days,‖ and ―nearly every
day,‖ respectively. GAD-7 total score for the seven items ranges from 0 to 21. Scores of 5, 10,
and 15 represent cutpoints for mild, moderate, and severe anxiety, respectively. Though
designed primarily as a screening and severity measure for generalized anxiety disorder, the
GAD-7 also has moderately good operating characteristics for three other common anxiety
disorders – panic disorder, social anxiety disorder, and post-traumatic stress disorder. When
screening for anxiety disorders, a recommended cutpoint for further evaluation is a score of 10
or greater.
PHQ-2 and GAD-2 Severity. These consist of the first two items of the PHQ-9 and GAD-7
respectively, and constitute the two core DSM-IV items for major depressive disorder and
generalized anxiety disorder, respectively. Each ranges from a score of 0 to 6. The operating
characteristics of these ultra-brief measures are quite good; the recommended cutpoints for
each when used as screeners is a score of 3 or greater. When used together, they are referred
to as the PHQ-4 a 4-item screening measure which ranges from a score of 0 to 12, and serves
as a good measure of ―caseness‖ (i.e., the higher the score, the more likely there is an
underlying depressive or anxiety disorder). In particular, the PHQ-2 and GAD-2 subscores of
the PHQ-4 provide separate depressive and anxiety scores, and can be used as screeners for
depression and anxiety.
PHQ-15 Somatic Symptom Severity. This is calculated by assigning scores of 0, 1, and 2 to
the response categories of ―not at all‖, ―bothered a little‖, and ―bothered a lot‖, for the 13
somatic symptoms of the PHQ (items 1a-1m). Also, 2 items from the depression module (sleep
and tired) are scored 0 (―not at all‖), 1 (―several days‖) or 2 (―more than half the days‖ or ―nearly
every day‖). Thus, a PHQ-15 score can be derived from page 1 of the PHQ, or from separate
administration of the PHQ-15 scale or the PHQ-SADS. PHQ-15 scores of 5, 10, and 15
represent cutpoints for low, medium, and high somatic symptom severity, respectively.
Sensitivity to Change for Monitoring Treatment Outcomes. A particularly important use of
a measure is its responsiveness to changes of condition severity over time. This is well-
established for the PHQ-9 which is increasingly used as a measure to assess the level of
depression severity (for initial treatment decisions) as well as an outcome tool (to determine
treatment response).[6,10] An example of how different PHQ-9 severity levels might guide
treatment is shown in Table 4, page 7. There is preliminary evidence that the PHQ-15 may be
responsive to changes as individuals with somatoform disorders or high somatization are
treated.[10] The GAD-7 has demonstrated change as a secondary anxiety outcome in several
depression trials, but has not yet been studied as a primary outcome in anxiety trials. Also,
since there is more diagnostic splitting for anxiety than for depressive disorders, it remains to
be determined whether a single anxiety measure can suffice as an outcome measure. It is
likely the GAD-7 will be useful but not yet certain it will be sufficient.
PHQ and GAD-7 Instructions P.7/9
Psychometrics. The psychometrics of the PHQ and its component scales are described in the
validation articles for specific measures (see Selected References on page 9) and are
summarized in a review article on the PHQ-9, GAD-7, and PHQ-15.[10]
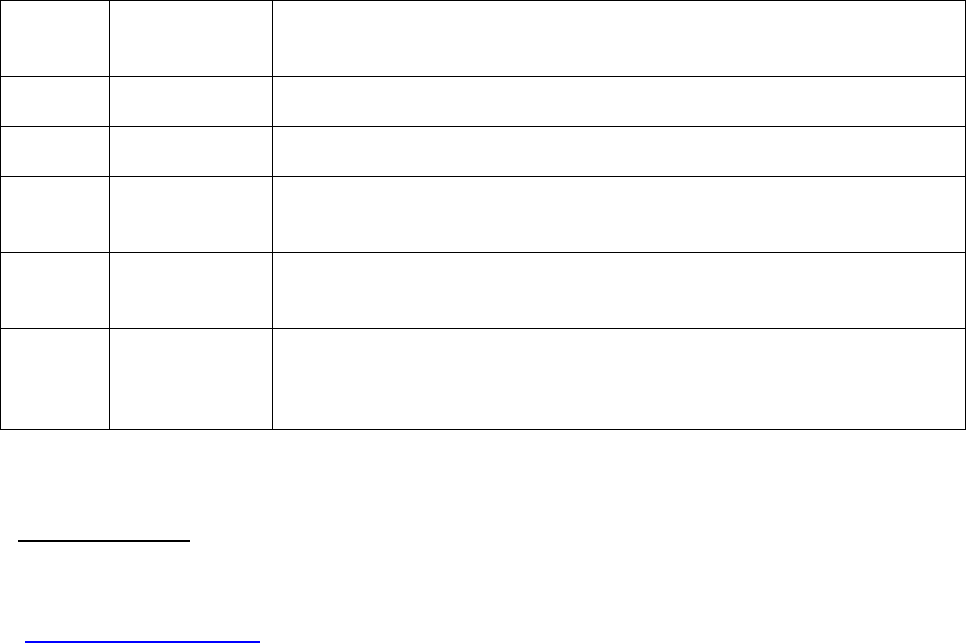
Table 4. PHQ-9 Scores and Proposed Treatment Actions *
PHQ-9
Score
Depression
Severity
Proposed Treatment Actions
0 – 4
None-minimal
None
5 – 9
Mild
Watchful waiting; repeat PHQ-9 at follow-up
10 – 14
Moderate
Treatment plan, considering counseling, follow-up and/or
pharmacotherapy
15 – 19
Moderately
Severe
Active treatment with pharmacotherapy and/or psychotherapy
20 – 27
Severe
Immediate initiation of pharmacotherapy and, if severe impairment or
poor response to therapy, expedited referral to a mental health
specialist for psychotherapy and/or collaborative management
* From Kroenke K, Spitzer RL, Psychiatric Annals 2002;32:509-521
TRANSLATIONS
There are numerous translations of the PHQ as well as the PHQ-9 and GAD-7 available in
many languages, which are freely downloadable on the PHQ website
(www.phqscreeners.com). The abbreviated versions of these measures – PHQ-8, PHQ-2,
GAD-2, and PHQ-4 – can simply be derived from the translations by selecting the relevant
items (see Table 1, page 3). The PHQ-15 can also be simply derived by selecting the 13
somatic items (1a-1m), plus the sleep and tired items (2c and 2c) from the PHQ translations.
Many of the translations have been developed by the MAPI Research Institute using an
internationally accepted translation methodology. Thus, most of the translations are
linguistically valid. However, unlike the English versions of the PHQ and GAD-7, few of the
translations have been psychometrically validated against an independent structured
psychiatric interview.
PHQ and GAD-7 Instructions P.8/9
WEBSITE
Copies of the PHQ family of measures, including the GAD-7, are available at the website:
www.phqscreeners.com
Also, translations, a bibliography, an instruction manual, and other information is provided on
this website.
QUESTIONS REGARDING DEVELOPMENT, ACKNOWLEDGMENTS AND USE
The PHQ family of measures (see Table 1, page 3), including abbreviated and alternative
versions as well as the GAD-7, were developed by Drs. Robert L. Spitzer, Janet B.W. Williams,
Kurt Kroenke and colleagues, with an educational grant from Pfizer Inc.
All of the measures included in Table 1 are in the public domain. No permission is required to
reproduce, translate, display or distribute.

PHQ and GAD-7 Instructions P.9/9
SELECTED REFERENCES
1. Spitzer RL, Williams JBW, Kroenke K, Linzer M, deGruy FV, Hahn SR, Brody D, Johnson
JG. Utility of a new procedure for diagnosing mental disorders in primary care: The
PRIME-MD 1000 study. JAMA 1994;272:1749-1756.
2. Spitzer RL, Kroenke K, Williams JBW, for the Patient Health Questionnaire Primary Care
Study Group. Validation and utility of a self-report version of PRIME-MD: the PHQ Primary
Care Study. JAMA 1999;282:1737-1744.
3. Spitzer RL, Williams JBW, Kroenke K, et al. Validity and utility of the Patient Health
Questionnaire in assessment of 3000 obstetrics-gynecologic patients. Am J Obstet
Gynecol 2000; 183:759-769
4. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: Validity of a brief depression severity
measure. J Gen Intern Med 2001;16:606-613.
5. Kroenke K, Spitzer RL. The PHQ-9: a new depression diagnostic and severity measure.
Psychiatric Annals 2002;32:509-521. [also includes validation data on PHQ-8]
6. Löwe B, Unutzer J, Callahan CM, Perkins AJ, Kroenke K. Monitoring depression treatment
outcomes with the Patient Health Questionnaire-9. Med Care 2004;42:1194-1201
7. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized
anxiety disorder: the GAD-7. Arch Intern Med 2006;166:1092-1097.
8. Kroenke K, Spitzer RL, Williams JBW, Monahan PO, Löwe B. Anxiety disorders in primary
care: prevalence, impairment, comorbidity, and detection. Ann Intern Med 2007;146:317-
325. [validation data on GAD-7 and GAD-2 in detecting 4 common anxiety disorders)]
9. Kroenke K, Spitzer RL, Williams JBW. The PHQ-15: Validity of a new measure for
evaluating somatic symptom severity. Psychosom Med 2002;64:258-266.
10. Kroenke K, Spitzer RL, Williams JBW, Löwe B. The Patient Health Questionnaire somatic,
anxiety, and depressive symptom scales: a systematic review. Gen Hosp Psychiatry 2010
(in press).
11. Johnson JG, Harris ES, Spitzer RL, Williams JBW. The Patient Health Questionnaire for
Adolescents: Validation of an instrument for the assessment of mental disorders among
adolescent primary care patients. J Adolescent Health. 2002;30:196-204.
12. Kroenke K, Spitzer RL, Williams JBW. The Patient Health Questionnaire-2: validity of a
two-item depression screener. Med Care 2003; 41:1284-1292.
13. Kroenke K, Spitzer RL, Williams JBW, Löwe B. An ultra-brief screening scale for anxiety
and depression: the PHQ-4. Psychosomatics 2009;50:613-621
14. Kroenke K, Strine TW, Spitzer RL, Williams JBW, Berry JT, Mokdad AH. The PHQ-8 as a
measure of current depression in the general population. J Affective Disorders
2009;114:163-173.
15. Löwe B, Spitzer RL, Williams JBW, Mussell M, Schellberg D, Kroenke K. Depression,
anxiety, and somatization in primary care: syndrome overlap and functional impairment.
Gen Hosp Psychiatry 2008;30:191-199.
16. Dube P, Kroenke K, Bair MJ, Theobald D, Williams L. The P4 screener: a brief measure
for assessing potential suicidal risk. J Clin Psychiatry Primary Care Companion 2010 (in
press). [Algorithm for following up on positive responses to 9th item of PHQ-9]
