D6545 Patient Encounter Form
User Manual: D6545
Open the PDF directly: View PDF ![]() .
.
Page Count: 2
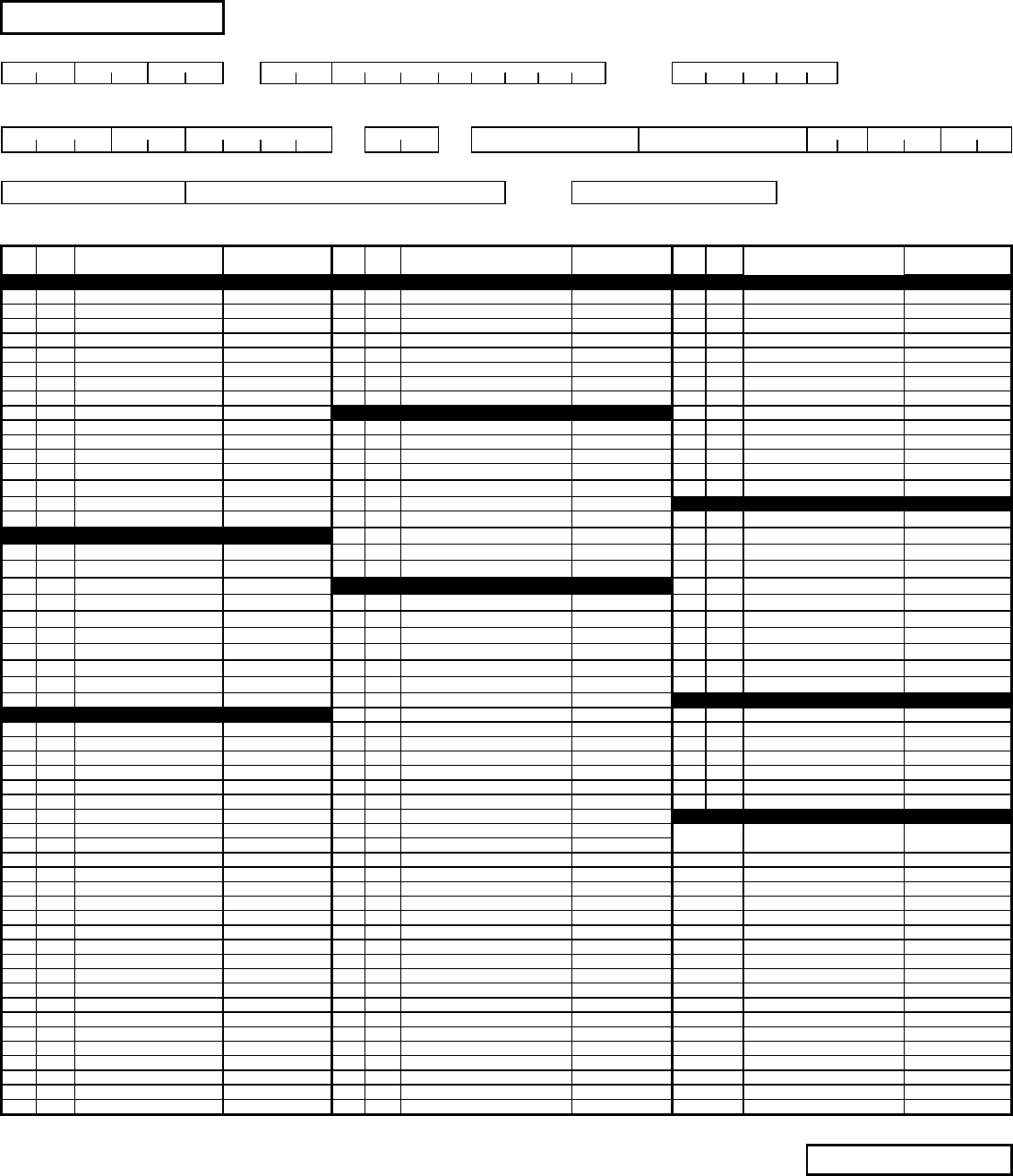
PLEASE PRINT AND FILL IN ALL BLANKS DENTAL NETWORK OF AMERICA
PATIENT ENCOUNTER FORM
DATE OF SERVICE STATE CENTER NUMBE
R
PROVIDER LICENSE
#
MO DAY YR
MEMBER I.D. # (SEE ELIGIBILITY LIST) PN# FIRST LAST NAME PATIENT BIRTH DATE
FIRST NAME OF SUBSCRIBER LAST NAME (IF DIFFERENT FROM PATIENT) GROUP NUMBER
ADA
CODE SERVICE TOOTH # &
SURFACE/QUAD
ADA
CODE SERVICE TOOTH # &
SURFACE/QUAD
ADA
CODE SERVICE TOOTH # &
SURFACE/QUAD
D0100-D0999 DIAGNOSTIC D3000-D3999 ENDODONTICS D6200-D6999 PROSTHODONTICS (FIXED)
D0120 Periodic Oral Eval. D3110 Pulp Cap Direct/Exc Rest D6241 Pontic/Porcelain Base Metal
D0140 Limited Oral Eval. D3120 Pulp Cap Ind/Exc Rest D6545 Ret. For Resin Bonded Br.
D0150 Comprehensive Oral Eval. D3220 Theraputic Pulpotomy D6751 Crown/Porcelain Base Metal
D0160 Detailed/Extensive Oral Eval. D3310 Endodontic Therapy - Anterior D6752 Crown/Porcelain Noble Metal
D0210 Intraoral Comp. Series D3320 Endodontic Therapy - Bicuspid D6791 Crown/Full Cast Base Metal
D0220 Intraoral Periapical 1st D3999 Use for Con't care Appts. D6930 Recement Bridge
D0230 Intraoral Periap. Ea. Add. D3 D6970 Post and Core, Indirect Fab
D0240 Intraoral Occlusal D3 D6972 Prefab Post and Core
D0272 Bitewing - Two Films D4000-D4999 PERIODONTICS D6999 Use for Con't care Appts.
D0274 Bitewing - Four Films D4210 Gingivectomy/4+ teeth D6
D0330 Panoramic Film D4240 Ging Flap incl Rt. Plane/4+ teeth D6
D0460 Pulp Vit. Test D4260 Osseous Surg./4+ teeth D6
D0470 Diagnostic casts D4270 Pedicle Soft Tiss Graft D6
D0 D4341 Perio Sc. Rt. Plane/4+ teeth D6
D0 D4355 Full Mouth Debridement D7000-D7999 ORAL SURGERY
D0 D4910 Perio Maintenance D7140 Ext. erupted tooth/exp root
D1000-D1999 PREVENTIVE D4999 Use for Con't care Appts. D7310 Alveo with Ext./4+ teeth
D1110 Prophylaxis, Adult D4 D7320 Alveo not with Ext./4+ teeth
D1120 Prophylaxis, Child D4 D7999 Use for Con't care Appts.
D1203 Fl Excl Pro Child D5000-D5899 PROSTHODONTICS (REMOVABLE) D7
D1351 Sealant - Per Tooth D5110 Complete Upper Denture D7
D15 Space Maintainer D5120 Complete Lower Denture D7
D1999 Use for Con't care Appts. D5130 Immediate Upper Denture D7
D1 D5140 Immediate Lower Denture D7
D1 D5211 Upper Partial - Resin D7
D1 D5212 Lower Partial - Resin D7
D1 D5213 Upper Partial - Metal D9000-D9999 ADJUNCTIVE GENERAL SERVICES
D2000-D2999 RESTORATIVE D5214 Lower Partial - Metal D9110 Palliative Treatment
D2140 Amal 1 Surface D5410 Adj Complete Denture Upper D9951 Occlusal Adj Limited
D2150 Amal 2 Surface D5411 Adj Complete Denture Lower D9952 Occlusal Adj Complete
D2160 Amal 3 Surface D5421 Adj Partial Denture Upper D9999 Use for Con't care Appts.
D2161 Amal 4+ Surface D5422 Adj Partial Denture Lower D9
D2330 Resin 1 Surf Anterior D5510 Repair Comp Denture Base D9
D2331 Resin 2 Surf Anterior D5520 Repl Teeth Comp Denture Ea. D9
D2332 Resin 3 Surf Anterior D5610 Repair Resin Base LIST ALL PROCEDURES OVER MAX OR NOT COVERED
D2335 Resin 4+ Surf Anterior D5620 Repair Framework ADA CODE SERVICE FEE COLLECTED
D2391 Resin 1 Surf Posterior D5630 Repair/Replace Clasp
D2392 Resin 2 Surf Posterior D5640 Replace Broken Tooth Each
D2393 Resin 3 Surf Posterior D5750 Reline Comp Upper Denture
D2740 Crown/Porcelain D5751 Reline Comp Lower Denture
D2750 Crown/Porcelain Hi Noble D5760 Reline Upper Partial Denture
D2751 Crown/Porcelain Base Metal D5761 Reline Lower Partial Denture
D2791 Crown/Full Cast Base Metal D5899 Use for Con't care Appts.
D2950 Core Build Up w/Pins D5
D2951 Pin Ret In add to Rest/Tooth D5
D2952 Post and Core, Indirect Fab D5
D2954 Prefab Post and Core D5
D2999 Use for Con't care Appts. D5
D2 D5
D2 D5
D2 D5
D2 D5
D5
D5
D5
© Dental Network of America 12/08 Current Dental Terminology @ American Dental Association. INSTRUCTIONS FOR COMPLETION ON REVERSE
SIDE
INSTRUCTIONS FOR COMPLETING
THE PATIENT ENCOUNTER FORM
Please complete all necessary information. All procedures are listed by ADA code and blank lines
are available so you may write in any procedures not included on the form. Use only ADA codes.
Forms that are missing information will be returned to the dental office.
1. Refer to your eligibility list while completing the top section of the form.
2. Check each procedure performed and add tooth# and surface when appropriate.
3. Use one line per procedure code.
4. Submit only one procedure code for procedures which require more than one appointment to
complete, example: endodontics, dentures, crown and bridge. For continued care
appointments, use the 999 code in the appropriate category for try-in and delivery of
prosthetics and endodontic completion appointments.
5. Services over the patient’s annual maximum or non-covered services should be reported in
the lower right box. List the ADA code, service description and the fee for service collected.
6. Submit PEFs to DNoA by the 20th of the month. All treatment data received by the 20th of the
month will be reported in that month’s utilization. Treatment data received after the 20th will
be keyed in the following month’s utilization.
LABORATORY AND PROSTHETIC FUND REIMBURSEMENT
Some subscribers are members of groups which offer dental laboratory reimbursement. Follow
the instructions below for submitting laboratory bills:
1. Once the procedure is completed, attach the original laboratory statement(s) to the Patient
Encounter Form.
2. Include the patient’s name and member I.D. number, procedure code and tooth#(s) on the
laboratory statement.
3. Non-covered laboratory charges are the patient’s financial responsibility, for example:
precision attachments or characterizations.
4. Lab bills received after 365 days of the date of service will not be processed
Mail all completed forms directly to:
Dental Network of America
P.O. Box 23089
Belleville, IL 62223-0089
12/08
