CareCentrix Provider Manual (EDRC 746 01242018) VT 9241
User Manual: VT 9241
Open the PDF directly: View PDF ![]() .
.
Page Count: 77

Provider Manual

Provider Manual
2 | P a g e
EDRC 746 - 01242018
Contents
1-1
KEY CONTACTS ................................................................................................................................... 6
GENERAL .................................................................................................................................................. 6
KEY PHONE NUMBERS: AUTHORIZATION, RE-AUTHORIZATION, AUTHORIZATION CORRECTIONS ................................ 7
NETWORK MANAGEMENT KEY CONTACTS ............................................................................................... 7
1-2
WELCOME.......................................................................................................................................... 8
ABOUT THIS PROVIDER MANUAL ..................................................................................................................... 8
1-3
ABOUT CARECENTRIX ......................................................................................................................... 9
ABOUT CARECENTRIX .................................................................................................................................... 9
1-4
CORPORATE COMPLIANCE PROGRAM ............................................................................................... 10
COMPANY OBJECTIVES AND PURPOSE OF THE COMPLIANCE PROGRAM ................................................................... 10
REPORTING SYSTEM .................................................................................................................................... 12
RESPONSE AND CORRECTIVE ACTION TO PROMOTE PROGRAM EFFECTIVENESS .......................................................... 13
COMPLIANCE WITH CENTERS FOR MEDICARE & MEDICAID SERVICES NOTICE OF MEDICARE NON-COVERAGE REQUIREMENT
............................................................................................................................................................... 14
2-1
PERFORMANCE STANDARDS ............................................................................................................. 15
2-2
USE OF OFFSHORE VENDORS .......................................................................................................... 157
3-1
PROVIDER COMMUNICATIONS ......................................................................................................... 17
PROVIDER MANUAL .................................................................................................................................... 18
OUR CUSTOMERS ..................................................................................................................................... 188
PROVIDER ORIENTATION CONFERENCE CALL ..................................................................................................... 19
THE CARECENTRIX PROVIDER PORTAL ............................................................................................................. 19
CARECENTRIX NEWSFLASHES ......................................................................................................................... 20
3-2
NATIONAL CREDENTIALING COMMITTEE ........................................................................................... 21
PURPOSE .................................................................................................................................................. 21
COMMITTEE ATTENDANCE ............................................................................................................................ 21
COMMITTEE MEETING SCHEDULE ................................................................................................................... 21
Provider Manual
3 | P a g e
EDRC 746 - 01242018
3-3 PROVIDER QUALIFICATION AND QUALITY MANAGEMENT ...................................................................... 22
CREDENTIALING .......................................................................................................................................... 22
RE-CREDENTIALING ..................................................................................................................................... 23
PROVIDER PROFILING .................................................................................................................................. 24
CREDENTIALING REQUIREMENTS FOR A NEW LOCATION ....................................................................................... 24
CREDENTIALING REQUIREMENTS FOR ADDING A SERVICE CATEGORY ...................................................................... 24
QUALITY MEASUREMENT.............................................................................................................................. 25
SATISFACTION MEASUREMENT..................................................................................................................... 256
SATISFACTION MEASUREMENT REPORT TO PROVIDERS ....................................................................................... 25
4-1
CHANGES IN YOUR ORGANIZATION .................................................................................................. 26
5-1
HEALTHCARE DELIVERY PROCESS INTRODUCTION ............................................................................. 27
5-2
COORDINATION OF SERVICES AND AUTHORIZATIONS ....................................................................... 27
PROVIDER RECEIVES REFERRAL FROM PRIMARY REFERRAL SOURCE ...................................................................... 279
CARECENTRIX RECEIVES REFERRAL FROM PRIMARY REFERRAL SOURCE ................................................................... 29
REQUESTS FOR ADDITIONAL SERVICES ............................................................................................................. 32
RETROACTIVE SERVICE REQUESTS ................................................................................................................. 333
SERVICE REQUEST INQUIRIES ....................................................................................................................... 333
5-3
UTILIZATION MANAGEMENT ............................................................................................................ 35
THE CARECENTRIX UTILIZATION MANAGEMENT PROCESS .................................................................................... 35
UTILIZATION MANAGEMENT RESPONSIBILITIES ................................................................................................ 377
RETROSPECTIVE CLAIMS REVIEW .................................................................................................................. 398
APPEALING A DENIED REQUEST ...................................................................................................................... 39
6-1
SERVICE DELIVERY ............................................................................................................................ 39
THE PROVIDER’S RESPONSIBILITY ................................................................................................................... 40
THE PROVIDER’S DISCHARGE RESPONSIBILITIES ................................................................................................ 411
6-2 GUIDELINES SPECIFIC TO PROVIDER SPECIALTY ................................................................................ 422

Provider Manual
4 | P a g e
EDRC 746 - 01242018
TRADITIONAL HOME HEALTH (THH) ............................................................................................................. 422
INFUSION NURSING SERVICES ........................................................................................................................ 45
HOME INFUSION THERAPY (HIT) .................................................................................................................. 457
HOME MEDICAL EQUIPMENT AND PROSTHETICS AND ORTHOTICS (DMEPOS) ....................................................... 499
SPECIALTY PROGRAMS ............................................................................................................................... 533
DOCUMENTATION ..................................................................................................................................... 533
6-3
GENERAL CLAIMS AND REIMBURSEMENT INFORMATION ................................................................ 533
CLAIMS PROCESS ...................................................................................................................................... 544
CHECKING REIMBURSEMENT STATUS ............................................................................................................. 555
EXPLANATION OF PAYMENT ........................................................................................................................ 566
6-4
GENERAL BILLING REQUIREMENTS .................................................................................................. 577
CLAIMS SUPPORT CENTER ........................................................................................................................... 577
CLAIM FORM AND CLEAN CLAIM REQUIREMENTS ............................................................................................. 578
TIMELY FILING .......................................................................................................................................... 611
HEALTH EXCHANGE MEMBERS THAT RECEIVE ADVANCE PREMIUM TAX CREDITS .................................................... 612
BILLING WHEN ANOTHER PAYOR IS PRIMARY .................................................................................................. 633
MEDICARE PRIMARY CLAIMS ......................................................................................................................... 63
RECOUPMENT AND ADJUSTMENTS .................................................................................................................. 64
6-5
COMPLAINTS, CLAIMS PAYMENT RECONSIDERATIONS, AND APPEALS ................................................ 65
INTRODUCTION TO COMPLAINT, CLAIMS PAYMENT RECONSIDERATION, AND APPEALS PROCESS ................................... 65
COMPLAINTS ........................................................................................................................................... 655
CREDENTIALING .......................................................................................................................................... 65
UTILIZATION MANAGEMENT ISSUES .............................................................................................................. 666
6-6
CLAIMS PAYMENT ISSUES ................................................................................................................. 66
CORRECTED CLAIMS .................................................................................................................................... 66
CLAIMS INQUIRIES ....................................................................................................................................... 67

Provider Manual
5 | P a g e
EDRC 746 - 01242018
RECONSIDERATION ...................................................................................................................................... 67
APPEALS ................................................................................................................................................... 70
DISPUTE RESOLUTION ................................................................................................................................ 711
BINDING ARBITRATION ................................................................................................................................ 71
6-7
CONTRACT TERMINATION ................................................................................................................ 72
7-1
CUSTOMER ACKNOWLEDGEMENT AND RESOLUTION MANAGEMENT .............................................. 733
Provider Manual
6 | P a g e
EDRC 746 - 01242018
1-1 KEY CONTACTS
GENERAL
Reason for Contact Resource Contact Information
Authorizations
Initial Authorization
CareCentrix Provider
Portal www.CareCentrixPortal.com
Add-On Requests
Re-Authorization
Authorization Edits
Authorization Status
Other Care & Service Center
Aetna: 888-999-9641
Amgen: 888-571-6027
Beech Street and Cofinity:
877-466-0164
Cigna: 844-457-9969
Coventry: 877-415-7864
Fallon: 866-827-2469
Florida Blue: 877-561-9910
Horizon Healthcare Services, Inc.: 855-243-3321
Neighborhood Health Plan (NHP): 866-827-5861
Public Employee Insurance Agency (PEIA): 888-
497-5337
CareCentrix Direct CareCentrix Provider
Portal www.CareCentrixPortal.com
Claims and Payment
Claims Questions Claims Support Team For
Cigna 844-457-9969
Appeal & Reconsideration
Status Claims Support Team for
all other plans 877-725-6525
Rejection Questions EDI Support Team EDISupport@CareCentrix.com
Claims Inquiries
CareCentrix Provider
Portal www.CareCentrixPortal.com
Claims Status
Reconsideration & Appeals
Forms
Register for EDI
EFT & ERA Enrollment
CareCentrix Provider Portal
Admin Accounts: Create or
Unlock Network Management www.CareCentrixPortal.com
User Accounts: Create , Reset,
or Unlock
Provider Portal Admin at
your agency Provider Portal Admin at your agency
Provider Portal Questions Portal Info Box Portalinfo@CareCentrix.com
Provider Manual
7 | P a g e
EDRC 746 - 01242018
Other
Patient Transitions Transition Team 1-866-776-4617
Provider Information Updates Credentialing Department Contract.Department@CareCentrix.com
Compliance Concerns Compliance Hotline 877-848-8229
Policies and Processes Provider Manual www.CareCentrixPortal.com
Click “Provider Manual”
Contractual Questions Network Management www.CareCentrixPortal.com
Reference “Network Management Contact Sheet”
Patient Financial Responsibility Patient Services Team 800-808-1902
Infusion Nursing Services Infusion Nursing Team 844-457-9973
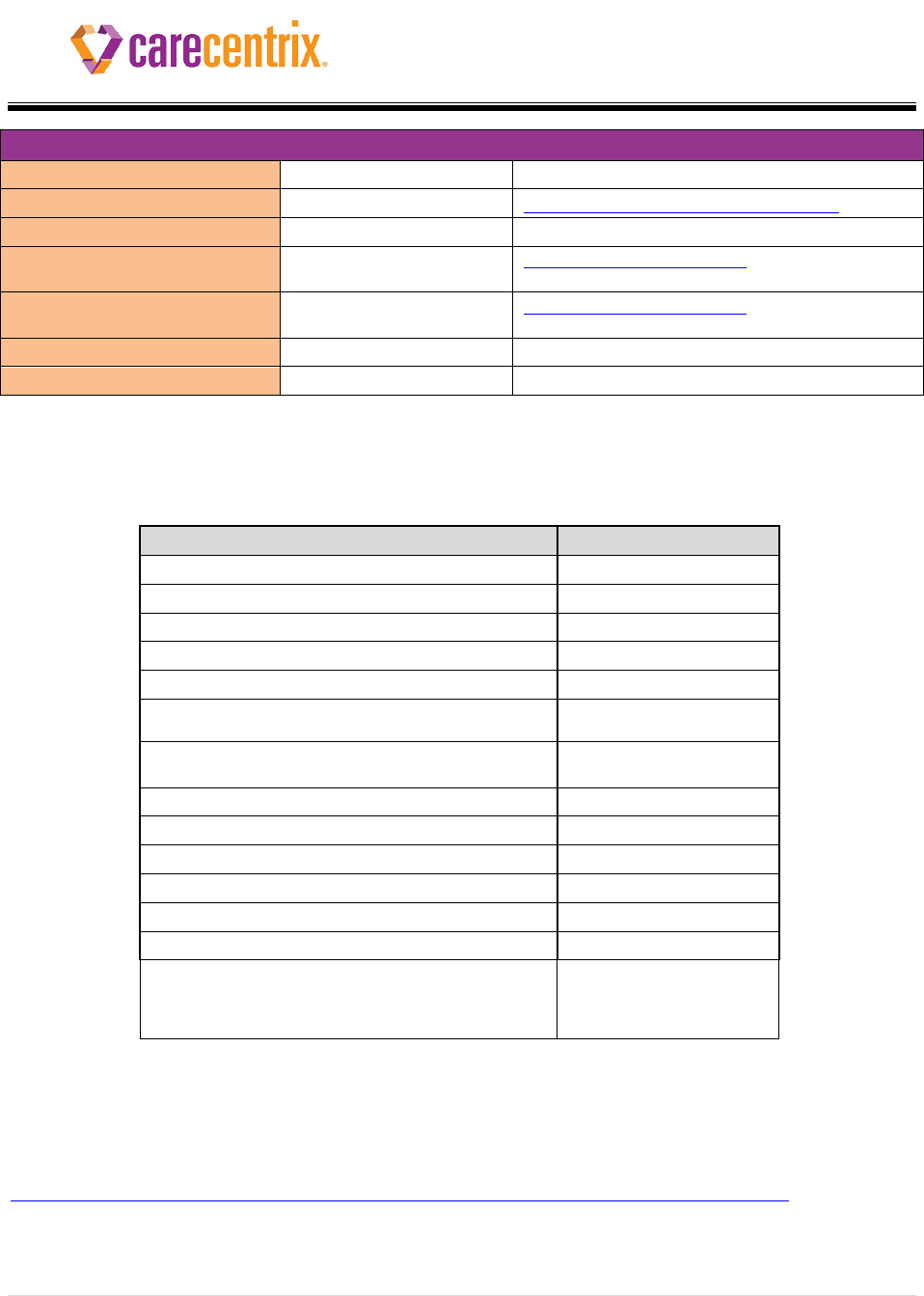
KEY PHONE NUMBERS: Authorization, Re-authorization, Authorization Corrections
Plan
Phone Number
Aetna FL 888-999-9641
Aetna GA 888-999-9641
Amgen 888-571-6027
Beech Street 877-466-0164
CIGNA 844-457-9969
Cofinity 877-466-0164
Coventry 877-415-7864
Fallon 866-827-2469
Florida Blue 877-561-9910
Horizon Healthcare Services, Inc. 855-243-3321
Humana 888-428-4282
Neighborhood Health Plan (NHP) 866-827-5861
Public Employees Insurance Agency (PEIA) 888-497-5337
Walmart
Specialty Pharmacy
Reauthorization
Authorization Edits
877-453-4566
NETWORK MANAGEMENT KEY CONTACTS
http://www.carecentrix.com/ProviderResources/Network_Management_Contact_List.pdf

Provider Manual
8 | P a g e
EDRC 746 - 01242018
1-2 WELCOME
Congratulations and welcome to the CareCentrix Provider Network. We are proud to work with you as
we strive to meet high quality of care standards and provide and manage cost-effective health care
solutions for the customers and patients served by our integrated healthcare network.
As a Provider within our network, we value your services and are committed to making your experience
with us as easy as possible. To demonstrate this commitment, we have dedicated resources to support
your participation in our network, and those resources are discussed further in this manual.
About This Provider Manual
This manual, as updated from time to time, serves as the basis for providing services within our network.
It contains both general and Health Plan specific information.
Please read this manual carefully. It explains your rights and responsibilities as a CareCentrix Network
Provider. As indicated in your Provider Agreement, you are obligated to comply with the terms of this
manual. Since this manual is updated regularly, we encourage you to visit our Provider portal frequently
at www.carecentrixportal.com to find the most recent information.
CareCentrix does not own the various third party websites referenced in this manual and makes no
representation relating to the content or accuracy of the information contained therein. You are solely
responsible for your interaction with such third parties, and we encourage you to read the terms of use
and privacy policies before accessing any third-party websites.
Provider Manual
9 | P a g e
EDRC 746 - 01242018
1-3 ABOUT CARECENTRIX
About CareCentrix
CareCentrix is the leader in managing the transition of care to the home. For nearly 20 years, we have
worked with health plans to support patients and providers make healing at home attainable and
sustainable while lowering costs and improving outcomes.
CareCentrix works with health plans to manage care in the home for their 23 million members. We
connect providers with patients, help leverage best practices, and help patients navigate the complex
home health care system.
Our Core Services include:
• Durable Medical Equipment – consisting of four subcategories – home medical equipment,
disposables, respiratory supplies and orthotics/prosthetics.
• Home Infusion – This includes coordination for both specialty pharmacy products and acute
services required for post discharge such as enteral nutrition, anti-infective and hydration.
• Home Health – including nursing services for recuperative care typically following a period of
hospitalization.
• Wound Care Management – Our Wound Care program tracks post-acute healing for wounds
and offers intervention when patients are not healing as expected.
Our Specialty products and services include:
• Sleep Management –Our wholly owned subsidiary, Sleep Management Solutions (SMS),
collaborates with health plans to help manage their patients’ sleep disorders in the most cost
effective way, offering diagnostic sleep testing in the home, as well as remote patient
monitoring.

Provider Manual
10 | P a g e
EDRC 746 - 01242018
• HomeSTAR® (Successful Transitions and Recovery at Home) – HomeSTAR® is designed to
identify patients at risk for hospital readmission. The program provides telephonic coaching and
coordination with home health care with the goal of avoiding costly hospital readmissions.
Employees and Office Locations
CareCentrix operates nationally with employees primarily located in Tampa, Florida; Hartford,
Connecticut; Overland Park, Kansas; and Phoenix, Arizona. For more information, visit the CareCentrix
web site, http://www.carecentrix.com.
1-4
CORPORATE COMPLIANCE PROGRAM
Company Objectives and Purpose of the Compliance Program
CareCentrix is committed to complying with all applicable legal requirements in the course of conducting
its operations and expects each of its associates and network Providers to do the same. CareCentrix’s
Corporate Compliance Program was developed with that commitment in mind.
One purpose of the CareCentrix Corporate Compliance Program (the “Program”) is to help prevent and
detect fraudulent, noncompliant or unethical conduct and to take appropriate corrective actions upon
detection of any such conduct. One activity that the Program is intended to help prevent and detect is
the submission of improper, false or fraudulent claims for payment to the United States government or
other health care payors as prohibited by such payors and/or as prohibited under applicable state and
federal law, including applicable fraud, waste and abuse laws such as False Claims Act(s), Anti-Kickback
Act(s), and the Civil Monetary Penalties law. Violation of such laws can expose a Provider to significant
civil and/or criminal penalties. Whistleblower protections under some of these laws provide protections
for individuals reporting fraud and abuse in good faith and, in some cases; the reporter is entitled to a

Provider Manual
11 | P a g e
EDRC 746 - 01242018
percentage of the proceeds of the case. Refer to the section below entitled Reporting System for
information on how to report suspected fraud and abuse.
Examples of improper conduct include but are not limited to:
• Billing for excessive services (not medically necessary or appropriate);
• Billing for services not rendered, not rendered as billed, and/or not used by the patient/family (e.g.
supplies);
• Failing to comply with government and other payor requirements (including billing for home health
agency visits to patients who are not homebound (when required) or do not require a qualifying
service, submission of cost reports claiming expenses unrelated to patient care or failing to identify
related parties with whom business is conducted, failure to obtain required prior authorizations or
to comply with claim submissions requirements, or using staff who do not meet the payor
requirements (e.g. using physical therapist assistants when the payor does not permit physical
therapist assistants);
• "Upcoding" diagnoses or otherwise entering false or misleading information on assessments, orders,
clinical notes, authorization requests, claims or other documents for the intent and purpose of
obtaining excessive or improper payments;
• Using unlicensed or untrained staff;
• Billing for the services of a higher level practitioner than the practitioner that rendered the service;
• Falsifying physician orders or plans of care;
• Forging signatures;
• Falsifying licensure/certification or falsifying clinical records, cost reports, OASIS assessment
information, or other documents for the purpose of obtaining payment, including but not limited

Provider Manual
12 | P a g e
EDRC 746 - 01242018
to, documenting services not provided, backdating or falsifying dates of services, and falsifying the
condition and status of a patient;
• "Split billing" among payors to circumvent payor coverage restrictions;
• Billing two or more payors for the same services resulting in a duplicate payment ("double dipping");
• Kickbacks and improper relationships with referral sources.
• Billing CareCentrix for any services provided by the Provider’s employees or permitted
subcontractors to themselves or to their immediate family members. An “immediate family
member” is defined to include, but not be limited to, a spouse, domestic partner, parent, step-
parent, child, grandchild, grandparent, and sibling (including natural, step, half or other legally
placed children).
Reporting System
CareCentrix is committed to contracting with a network of Providers that adheres to high ethical
standards. To achieve this goal, it is essential that every employee and contractor associated with your
organization is also committed to this goal and assists your company in assuring compliance.
Accordingly, it is our policy that participating Providers must report potentially criminal, fraudulent or
other illegal activity immediately. Please report any such activity to the CareCentrix toll-free
Compliance Hotline: 877.848.8229
Individuals who make a good faith report to the CareCentrix Compliance Hotline are protected from
retaliation. CareCentrix will take reasonable steps to protect the anonymity of any such reporter and to
ensure no adverse actions are taken against such reporters. This policy is not intended to protect any
individual giving a report which CareCentrix reasonably believes is fabricated, distorted, or exaggerated
to either injure someone else or to protect the reporting individual or others.

Provider Manual
13 | P a g e
EDRC 746 - 01242018
The CareCentrix Compliance Department is responsible for investigating the report. Information
obtained in the course of any such investigation will be considered confidential but may be disclosed to
third parties at the sole discretion of CareCentrix. Any Provider knowingly failing to report unlawful
conduct will be subject to disciplinary action which could include network termination.
Response and Corrective Action to Promote Program Effectiveness
After any offense is detected, CareCentrix takes reasonable steps to respond appropriately to the
offense and to prevent any further similar offenses, including any necessary modifications to its Program
to prevent and detect violations of law. Depending on the individual circumstances, appropriate
responses may include, but shall not be limited to, recoupment of inappropriately billed amounts,
placement on a corrective action plan, network termination, additional training and/or reinforcement
communications, and disclosure to our customers, governmental agencies, and/or law enforcement.
False Claims
Providers are required to comply with all applicable federal and state False Claims Act statutes and
regulations. Any person who violates a federal or state False Claims statute or regulation is subject to all
applicable fines and penalties. Under False Claims Acts, any person who knowingly with intent to injure,
defraud or deceive any insurer or a Medicare or Medicaid entity files a statement of claim or an
application containing any false, incomplete or misleading information is in violation of those laws and
subject to criminal penalties and/or fines.

Provider Manual
14 | P a g e
EDRC 746 - 01242018
Compliance with Centers for Medicare & Medicaid Services (CMS) Notice of Medicare
Non-Coverage Requirement
Providers are required to comply with applicable state and federal laws. With respect to Medicare
patients who are discharged from home health care, CMS requires Providers to timely issue a Notice of
Medicare Non-Coverage (NOMNC) to the patient unless an exception to the NOMNC requirement
applies. The following are some steps Providers should take to ensure compliance with this NOMNC
requirement:
• Prior to discharging a patient from home health services, determine whether the patient is a
Medicare Advantage member.
• If the patient is a Medicare Advantage member, provide the patient with a NOMNC letter at
least 2 calendar days prior to discharge or the second to the last day of service if home health
care is not provided daily unless the patient meets an exception to the NOMNC requirement.
Please note that the patient or the patient’s authorized representative must sign and date the
notice.
• Patients who meet one of the following CMS exceptions should not receive a NOMNC:
o When a patient never received Medicare covered care in one of the covered settings
o When a service is being reduced (i.e. home health agency providing both physical
therapy and occupational therapy and discontinues the occupational therapy)
o When a patient is moving to a higher level of care (i.e. home health care ends because a
beneficiary is admitted to a Skilled Nursing Facility (SNF))
o When a patient has exhausted his/her benefit
o When a patient ends care on his/her own initiative (i.e. patient decides to revoke the
home health benefit and return to standard Medicare coverage)
o When a patient transfers to another provider at the same level of care
o When a provider discontinues care for business reasons
Provider Manual
15 | P a g e
EDRC 746 - 01242018
• Utilize the approved CMS NOMNC letter template and complete the template letter as directed
by CMS.
Please be aware that CareCentrix may audit your records for NOMNC letter compliance. Appropriate
action will be taken if you fail to comply with the CMS NOMNC requirement, which may include a
corrective action plan and/or termination from the network. For more information about NOMNC
letters, including the appropriate form and signature requirements, please refer to the Question and
Answer document posted on our Provider Portal and the CMS website.
2-1 PERFORMANCE STANDARDS
As a participant in the CareCentrix network of Providers, you are required to:
• Provide high quality, compassionate care to patients.
• Effectively and respectfully respond to patients’ linguistic, cultural and other unique needs.
• Accept and treat all patients regardless of race, color, national origin, age, religion, English
proficiency, sexual orientation, gender identity, health status or disability.
• Provide timely oral and written language assistance services at no cost to the patient for patients
with limited English proficiency.
• Conduct ongoing training of staff at all levels regarding culturally and linguistically appropriate
service delivery. For helpful resources and training information, please reference
www.thinkculturalhealth.hhs.gov.
• Submit timely written notice to CareCentrix of changes in your organization as required in your
Provider contract and this Provider Manual.
• Maintain 24 hour on-call coverage 7 days per week and respond to patient and/or CareCentrix
contacts within 30 minutes of call, including weekends, evenings and holidays, unless otherwise
specified by contract.

Provider Manual
16 | P a g e
EDRC 746 - 01242018
• Submit billing for authorized services and/or products to CareCentrix at least monthly and within
timely filing requirements at the designated address for claims and submit no billing to the primary
Health Plan for services/products unless directed to do so by CareCentrix in writing.
• Not bill the patient/member for covered services or for services where payment is denied because
you did not comply with your Provider Agreement or this Provider Manual.
• Not bill the patient/member for any covered services.
• Not, under any circumstance, tell the patient/member that they are not responsible for any co-pays,
coinsurance or deductibles. Providers are paid for authorized covered services in accordance with
their contract rates. Those payments are not reduced by the applicable copay, coinsurance or
deductible, and CareCentrix assumes the Provider’s burden of collecting these amounts. Although
the patient is not responsible to pay copays, coinsurance or deductibles to the Provider since the
Provider has been paid in full, the patient is responsible for remitting those amounts to CareCentrix.
• Promptly return to CareCentrix any overpayments for services provided under your Provider
Agreement.
• For services where payment is denied because the services are not medically necessary or are not
otherwise covered under the member’s plan, not charge the member for such services unless, in
advance of the provision of the services, the member agrees in writing to accept the financial
responsibility for the services.
• Submit medical records, quality assessment, quality improvement, clinical outcomes, program
evaluation, and other reports upon request of CareCentrix personnel and cooperate fully with any
audits conducted by CareCentrix. Requested records must be provided to CareCentrix at no charge
to CareCentrix and within the timeframes requested by CareCentrix. If Provider fails to timely
provide records requested by CareCentrix in order to substantiate services billed, payments on the
claims that are the subject of the record request may be reversed and recovered through a refund
request or offset. CareCentrix further reserves the right to impose a penalty of $50 per day for each
day that the Provider fails to provide records within the requested timeframes.

Provider Manual
17 | P a g e
EDRC 746 - 01242018
• Participate in CareCentrix quality initiatives as requested.
• Notify patients of FDA recalls impacting them and facilitate the repair, replacement and/or
resolution of the recall according to the guidelines issued by the manufacturer in the FDA
notification
• Adhere to all other principles, practices and procedures found in the Provider Agreement,
CareCentrix Provider Manual, and contractual relationships between CareCentrix and its Health
Plan customers.
• Bill CareCentrix only for services that have been provided in accordance with the applicable
health plan and member benefits, medical coverage guidelines, claims requirements and
applicable laws, rules and regulations.
• Not bill CareCentrix for any services provided by the Provider’s employees or permitted
subcontractors to themselves or to their immediate family members. An “immediate family
member” is defined to include, but not be limited to, a spouse, domestic partner, parent, step-
parent, child, grandchild, grandparent, and sibling (including natural, step, half or other legally
placed children). Any such services billed to CareCentrix are not payable and, to the extent such
services are billed to and paid by CareCentrix, will be subject to recovery and/or recoupment by
CareCentrix.
2-2 USE OF OFFSHORE VENDORS
Except as otherwise permitted by CareCentrix in writing, Provider and any of its sub-vendors,
subcontractors, or agents may not (1) perform or engage with business agents to perform any functions,
activities or services under its agreement with CareCentrix from a location outside the United States; or
(2) send or transmit to, or access, Members’ PHI or other personal information from outside the United
States.
Provider Manual
18 | P a g e
EDRC 746 - 01242018
3-1 PROVIDER COMMUNICATIONS
In keeping with our commitment to support our Network Providers, we have a variety of Provider
orientation and training communications and opportunities.
Provider Manual
Our Provider Manual is intended to inform our providers of their responsibilities as a CareCentrix
Network Provider. This Manual also serves as an ongoing reference that is updated periodically.
Providers have a responsibility to ensure they are following the most up to date policies and procedures
implemented by CareCentrix. Providers must check the CareCentrix Provider Portal
(www.carecentrixportal.com) frequently for any information updates, including updates to this manual.
Changes may include:
• A change in policy, process and/or procedure that impacts the Provider and/or Provider
Management.
• A change in the expectations or conditions of contract(s) with CareCentrix customers.
• New carrier contracts which the Provider may service.
Our Customers
Our customers include Aetna (Florida and Georgia), Florida Blue, Horizon Healthcare Services, Inc.,
Beech Street, Cigna (including Great West), ConnectiCare, Coventry, Public Employees Insurance Agency
(PEIA), Neighborhood Health Plan (NHP), Amgen, Fallon, Humana, Cofinity and Walmart Specialty
Pharmacy. You may request a complete and current list of our customers at any time by contacting your
Network Management Representative. Please note that, when a patient presents an insurance
identification card that includes the name or logo of one of our customers and the Covered Service
required by that patient is included within the scope of your Provider Agreement and our customer
contract, your CareCentrix Provider Agreement will apply to that service, and you must direct claims for

Provider Manual
19 | P a g e
EDRC 746 - 01242018
that service to CareCentrix for processing as specified in this Provider Manual. Note that some
CareCentrix customers have only contracted with CareCentrix to arrange for select home care services.
Please contact your Network Management Representative with any questions regarding the applicability
of your Provider Agreement to a particular service.
Provider Orientation Conference Call
Our Provider orientation conference call provides important information on Provider responsibilities and
CareCentrix operational procedures as outlined in this manual. If you are a new provider, our Provider
Services Department will contact you to set a date and time for an orientation conference call. Network
Providers may also request an orientation call at any time to give a refresher of this manual’s contents.
Providers should review this manual prior to the call to obtain the most benefit from their participation.
The CareCentrix Provider Portal
The CareCentrix Provider Portal (www.carecentrixportal.com) is the best place to find the most up to
date information about how to work with CareCentrix. In addition to providing educational resources,
our Provider Portal gives you access to several self-service tools. When you access our Provider Portal,
you can:
• Request an authorization or re-authorization
• Add a service to an existing authorization request
• Edit an authorization request
• Upload clinical documentation
• Look up claim and authorization status
• Submit a claims inquiry*
• Submit a request for reconsideration and/or appeal*

Provider Manual
20 | P a g e
EDRC 746 - 01242018
• Enroll in EDI (Electronic Claims Submission)
• Sign Up For ERA/EFT Submissions
• Enroll In CareCentrix Direct
• Review the CareCentrix claims billing crosswalk
• Access our Provider Manual
• Access self-guided Provider education tools on several topics
Not using the portal?
Contact your assigned Network Management Representative to register an
administrator account on the Portal.
*Applicable only to those Payors that have migrated to our enhanced claims platform. For more
information, go to Section 6 of this Provider Manual.
CareCentrix Newsflashes
CareCentrix uses the newsflash tool to provide updates and other important information to our network
Providers, including action items that Providers are expected to comply with. Newsflashes are
distributed to Providers via fax or email communication. If you have any questions regarding
newsflashes, please contact your Network Management Representative.
Provider Manual
21 | P a g e
EDRC 746 - 01242018
3-2 NATIONAL CREDENTIALING COMMITTEE
Purpose
The purpose of the Credentialing Committee is to establish a credentialing plan and process for
verification and review of qualifications when a Provider seeks to participate in the CareCentrix Provider
network.
Committee Attendance
The Credentialing Committee represents varied specialties from the home health care industry and is
comprised of 5 voting and 4 non-voting members. The CareCentrix Medical Director reviews and
approves clean credentialing files for acceptance and admission into the CareCentrix Network. The
Credentialing Committee does not review such files. “Clean” credentialing files are those files that meet
all of the criteria for inclusion into the Provider Network and do not require additional review by the
Committee. All other complete files are submitted to the Committee.
Committee Meeting Schedule
The Credentialing Committee generally meets monthly. Ad hoc meetings may also be scheduled to
address quality issues.

Provider Manual
22 | P a g e
EDRC 746 - 01242018
3-3 PROVIDER QUALIFICATION AND QUALITY MANAGEMENT
Credentialing
Our credentialing process requires, but is not limited to, the following:
• Completed CareCentrix Credentialing Application. The application must contain a current signature
of the CEO, Administrator or other appropriate designated representative, attesting that all
information provided in conjunction with the application is true, correct, and complete.
• Copies of current licensure as required by applicable law.
• Proof of professional and general liability insurance. Required limits are generally one million dollars
($1,000,000) per occurrence and three million dollars ($3,000,000) in aggregate and a copy of a
current fidelity bond for fifty thousand dollars ($50,000) or other crime and theft coverage in an
amount satisfactory to CareCentrix.
• Five year malpractice history.
• Copies of current accreditation or certification. For non-accredited, non-certified Providers,
CareCentrix may perform a site visit. QA/QI program description - The quality program must
address patient care in general detail, including the overall steps that are taken to maintain quality
control over internal processes as they relate to patient care. Quality Improvement Plans should
contain the following:
1. The implementation of the plan, analysis and progress on QI initiatives.
2. The purpose, goals, objectives, and scope of the quality improvement program.
3. The organizational authority, organization of responsibility, general methodology and quality
improvement methodology.

Provider Manual
23 | P a g e
EDRC 746 - 01242018
Re-Credentialing
CareCentrix Network Providers are re-credentialed every two to three years (as determined by
applicable law or plan requirements). However, a Provider’s credentialing status may be evaluated by
the Credentialing Committee at any time during the two to three year credentialed period, including
when a Provider adds a new service category, or malpractice or quality of care/service issues are
brought to the Committee’s attention. In addition, if a Provider adds or acquires a new location,
subsidiary or affiliate, that location or entity must be credentialed.
When a potential quality of care or service issue is brought to the Committee’s attention, the
Committee reviews the issue and, based on the findings, takes appropriate action, which may include
the implementation of a corrective action plan or termination of the Provider’s participation.
The standard re-credentialing process begins approximately six months before the credentialing
anniversary. Our re-credentialing process requires, but is not limited to, the following:
• Completion of re-credentialing application
• Copies of current licensure.
• Proof of professional and general liability insurance. Required limits are generally one million dollars
($1,000,000) per occurrence and three million dollars ($3,000,000) in aggregate; a copy of current
fidelity bond for fifty thousand dollars ($50,000) or other crime and theft coverage in an amount
satisfactory to CareCentrix.
• Three year malpractice history.
• Copies of current accreditation or certification. For non-accredited, non-certified Providers,
CareCentrix may perform a site visit.
• QA/QI program description and program evaluation.

Provider Manual
24 | P a g e
EDRC 746 - 01242018
Provider Profiling
In addition to the information listed in the previous section, the re-credentialing process includes a
review of the Provider’s performance during their participation with CareCentrix.
This may include but is not limited to:
• Satisfaction surveys.
• All incidents and follow-up correspondence.
• All complaints and follow-up correspondence.
• Any correspondence received complimenting the Provider’s service.
• Compliance with CareCentrix credentialing and other policies.
Credentialing Requirements for a New Location
Providers that wish to add a new location must contact their Network Management Representative in
writing to request the addition of the new location. New locations must be credentialed following the
initial credentialing process outlined above. CareCentrix reserves the right to refuse to add new
Provider locations. Decisions are based on a variety of factors, including satisfaction of our credentialing
criteria and the network’s needs at the time of the request, subject to applicable law.
Credentialing Requirements for Adding a Service Category
Providers that wish to add a new service category (i.e. staffing, DME, infusion) must notify the Network
Management Department in writing. New service categories must be credentialed following the initial
credentialing process outlined above. Providers must maintain the licensure necessary to provide the
new service category. CareCentrix reserves the right to refuse to add new service categories. Decisions
are based on a variety of factors, including satisfaction of our credentialing criteria and the network’s
needs at the time of the request, subject to applicable law.

Provider Manual
25 | P a g e
EDRC 746 - 01242018
Quality Measurement
We assess the quality of our Providers in a variety of ways including assessing quality against industry,
regulatory, and accreditation body standards.
Satisfaction Measurement
In compliance with our own policies and procedures, and in keeping with NCQA and URAC standards and
the contractual requirements of our customers, we or our Health Plan customers may sample and
report findings regarding:
• Patient satisfaction
• Physician satisfaction
• Customer (Health Plan) satisfaction
In addition, we are concerned with your satisfaction as a participant in the CareCentrix Provider
Network. Therefore, we may assess your satisfaction or request your input through various means,
including but not limited to:
• Provider satisfaction surveys via email, web, letter and telephone.
• Provider focus groups
• Joint Operating Committee meetings
Satisfaction Measurement Report To Providers
We may periodically report satisfaction data results, analyses and related quality improvement
initiatives to our Providers for purposes of providing feedback on CareCentrix performance and
improvement efforts and to foster improved relations between and among your patients, physicians,
CareCentrix Providers, Health Plans and CareCentrix associates.
Provider Manual
26 | P a g e
EDRC 746 - 01242018
4-1 CHANGES IN YOUR ORGANIZATION
You must notify CareCentrix of changes in your demographic information or changes to the information
submitted with your credentialing application in writing on company letterhead within 7 days of the
change. The written notice should be directed to the credentialing department at the following address:
Contract.Department@carecentrix.com
Changes may affect receipt of referrals and reimbursements. Please be diligent in timely reporting
changes to such information including changes to the following:
• Address(es), including the remit to address
• Telephone number(s) and/or fax number(s)
• Name of key organizational contact(s)
• Names(s) of key local operations contact(s)
• Tax Identification Number
• Days/hours of operations
• Service/product capabilities
• Populations served (adults, children, geriatric)
• Service area
• Accreditation status, including revocations
• New malpractice actions
• Licensing status, including sanctions
• Liability insurance coverage
• Change in business structure or ownership
• Closure of operations/business site

Provider Manual
27 | P a g e
EDRC 746 - 01242018
5-1 HEALTHCARE DELIVERY PROCESS INTRODUCTION
CareCentrix has contracts with many payors. The processes that CareCentrix applies to a given patient’s
referral are based upon the specifics of the contract between CareCentrix and the applicable payor.
5-2 COORDINATION OF SERVICES AND AUTHORIZATIONS
CareCentrix Providers may receive referrals for new patients in one of two ways:
1. A Primary Referral Source, typically a physician, hospital discharge planner, other Provider, etc.,
contacts the Provider with the referral. In all cases, subject to patient choice, CareCentrix
reserves the right to select an alternative Provider to service the referral.
2. CareCentrix receives a request from the Primary Referral Source and directs the referral to the
Provider.
Provider Receives Referral From Primary Referral Source
Unless otherwise directed, Providers should submit requests to provide a service/item via the
CareCentrix on-line Provider Portal (www.CareCentrixportal.com). The Provider Portal identifies the
information necessary to complete a request. The required information generally includes, but is not
limited to, the following:
A. Patient first and last name
B. Patient date of birth
C. Patient insurance company and insurance subscriber ID number
D. Patient physical address (not PO Box) including zip code
E. Patient phone number
F. Patient gender

Provider Manual
28 | P a g e
EDRC 746 - 01242018
G. Diagnosis
H. If recently discharged from hospital or other inpatient setting, facility name and full address
I. Ordering physician first and last name, full address and telephone number
J. Service description or HCPCS code and modifier
K. Miscellaneous codes without a known description will require the Provider to manually enter a
description with request
L. Number of requested units, start and stop date of requested authorization
M. Medical necessity justification for the service or item requested
N. Confirmation that physician orders exist for services for which authorization is being requested
If the Provider does not submit all of the required information, the request will not be accepted by
CareCentrix.
The type of review applied to a request depends on the patient’s Health Plan. For example, an item or
service may be reviewed for medical necessity under one Health Plan but not another. In addition, the
type of review may change from time to time. Receipt of a Service Authorization Form (SAF) from
CareCentrix does not guarantee that the service was reviewed for medical necessity. If medical
necessity is later determined not to exist, the Provider’s claim for service may be denied or payments
may be recouped.
In many cases, requests submitted via the Portal can be processed immediately and the Provider
receives an electronic notification of authorization.
Some requests require verification of administrative information or clinical review. These requests are
routed to a CareCentrix associate for processing. Reasons for routing include, but are not limited to:
1. Other insurance
2. Medical necessity review
3. Obtaining authorization from the Health Plan

Provider Manual
29 | P a g e
EDRC 746 - 01242018
Once any necessary verification or routing is completed or when a request is automatically processed
and approved, a SAF is faxed to the Provider and/or is posted to the Provider Portal for Providers to
retrieve.
Providers must in every instance, whether receiving a referral from CareCentrix or a primary referral
source, verify eligibility and benefits with the patient’s Health Plan prior to providing any service,
equipment or supply item. Providers should maintain documentation to evidence this verification of
eligibility and benefits. CareCentrix does not conduct electronic eligibility and benefit verification
transactions, but our health plan customers do. Please remember that eligibility and benefit verification
and receipt of a Service Authorization Form are not a guarantee of payment for services such as, but not
limited to, items provided when the member is not eligible or there is no available benefit. Providers
are responsible for ensuring that they maintain, and have available upon request, all documentation
necessary to support the services rendered, including but not limited to, the medical necessity of such
services.
Requests for service, whether for the initial start of care or reauthorization for continued care, must be
requested prior to the service being provided. If a Provider fails to submit a request for service prior to
providing services, those services performed may not be reimbursable and are not billable to the
patient. Exceptions to this requirement may exist for certain Plans.
CareCentrix Receives Referral from Primary Referral Source
Provider staffing is the process of identifying a Provider to meet the needs of a specific patient. Many
referrals will initially be sent to the Provider via CareCentrix Direct. CareCentrix Direct is CareCentrix’s
electronic application that allows Providers to receive referrals quickly and entirely on-line. Providers
who enroll in CareCentrix Direct are offered referrals preferentially to those not enrolled. For
information about how to enroll in CareCentrix Direct, please contact your Network Management
Representative. For cases not staffed through CareCentrix Direct, a CareCentrix Provider Staffing
Associate will facilitate the referral. Referrals are made based on a variety of factors, including but not

Provider Manual
30 | P a g e
EDRC 746 - 01242018
limited to:
• The location where the patient will receive service and corresponding location of the Provider
• The services/products for which a Provider is credentialed to perform or supply
• The lines of business for which a Provider is credentialed (e.g. Medicaid, Medicare)
• The Provider’s ability to provide the service or item for the required start of care date
CareCentrix makes no representations or guarantees about the number of patients that will be referred
to a CareCentrix Network Provider as a result of the Provider’s participation in the CareCentrix Network
and reserves the right to direct and/or redirect patients to selected CareCentrix Network Providers. In
addition, CareCentrix customers reserve the right to exclude certain CareCentrix Network Providers
from the network accessed by their members.
The process for Provider Staffing is as follows:
A. CareCentrix receives a request for a service or item from the primary referral source.
B. Except with respect to services falling under BlueCard, the referral is either sent out
electronically to Providers via CareCentrix Direct or telephonic outreach is made to Providers.
i. The Provider accepts the referral.
ii. SAF is faxed to the Provider. Providers may opt out of receiving faxed SAFs and manage
all of their authorizations online via the CareCentrix Provider Portal. For information
about how to go paperless, please contact your Network Management Representative.
Regardless of the staffing route, Providers must verify eligibility and benefit availability with the Health
Plan prior to providing any service, equipment or supply item. Receipt of a Service Authorization Form is
never a guarantee of payment for services/items provided and is subject to factors that include, without
limitation eligibility, benefit coverage, timely and proper claims submission and compliance with the
terms of the Provider Agreement and this Provider Manual. In addition, Providers must carefully
consider their ability to accept every case and only do so when the Provider is confident that the
patient’s needs can be met. Referral turn-backs can delay the start of care and can cause quality of care
and service issues.

Provider Manual
31 | P a g e
EDRC 746 - 01242018
After accepting a referral and receiving a Service Authorization Form, it is the Provider’s responsibility to
abide by all of the terms of the Provider Agreement and this Provider Manual including, without
limitation, the following:
• Notify the CareCentrix Care and Service Centers immediately and in no event more than 2 hours
after Provider learns that the start of care/delivery must be delayed or if unable to continue the
case. In all instances, the Provider should contact the Care and Service Centers prior to the start of
care/delivery date to allow CareCentrix adequate time to secure an alternate Provider if needed. It is
also the Provider’s responsibility to obtain approval from the patient’s physician if the start of
care/delivery date is delayed.
• Render no service unless ordered by the appropriate physician.
• Provide after hours (on call) home visits as appropriate and necessary in situations that cannot be
resolved by telephone consultation.
• Notify the CareCentrix utilization management staff of changes in patient/family status within 24
hours upon occurrence and/or identification, including:
o Illness
o Hospitalization
o Death
o Any other adverse incident or change affecting continued service delivery.
• Immediately notify CareCentrix of complaints made by the patient, family, physician or Health Plan
upon occurrence.
• Except as otherwise provided in this Provider Manual, submit requests for service/product re-
authorization at least 72 hours prior to expiration date of the previous authorization.

Provider Manual
32 | P a g e
EDRC 746 - 01242018
• Obtain authorization for any previously unauthorized emergency or urgent services 24 hours a day,
seven days a week, 365 days per year. CareCentrix provides 24/7 on-call access for emergency and
urgent situations.
• Provide assessment reports, progress reports, organizational forms or other organizational
documents within 48 hours of request by CareCentrix.
• Respond to grievances/complaints filed against the CareCentrix Provider within 24 hours and pursue
timely resolution as acceptable by CareCentrix staff.
• Notify CareCentrix if other insurance or additional sources of reimbursement are identified.
• Provide all other documentation and records which may be requested by CareCentrix from time to
time, within the time frames set forth in the request.
Requests for Additional Services
If additional dates of service and/or units or services are needed beyond the date span or units/services
listed on the previously issued Service Authorization Form, Providers must submit an additional request
for services.
Except as otherwise set forth in this Provider Manual, Providers must submit requests for additional
services at least 72 hours prior to the expiration of the date span specified in the Service Authorization
Form and provide clinical status and objective reasons for the additional services. Such requests should
not be submitted more than 7 days prior to the expiration of the date span specified in the Service
Authorization Form. Requests received prior to that timeframe may be rejected, and the Provider will
be required to resubmit the request. By submitting a request for services, the Provider is certifying that
it has confirmed eligibility, benefits and medical necessity and that it has on hand all supporting
documentation.

Provider Manual
33 | P a g e
EDRC 746 - 01242018
Additional services should be requested via the Provider Portal at www.carecentrixportal.com. The
Provider Portal identifies the information required in order to complete your request. That information
includes, but is not limited to, the following:
i. Intake ID
ii. Patient’s Last Name
iii. Service description or HCPCS Code and modifier for services requested
iv. Number of requested units, start and stop date of requested services
v. Medical necessity for the service requested
vi. Physician orders for all services requested
If the Provider does not submit all of the required information, the request will not be accepted by
CareCentrix.
Retroactive Service Requests
Providers must submit requests for service/items prior to the service/item being provided or delivered.
If a Provider fails to submit a request prior to providing services, those services performed may not be
reimbursed and are not billable to the patient.
Service Request Inquiries
After submitting a service request, Providers may check the status of their request by accessing the
CareCentrix Provider Portal at www.carecentrixportal.com
Providers can view completed service requests made within the last 60 days. The following information
is available on our Provider Portal:

Provider Manual
34 | P a g e
EDRC 746 - 01242018
• Request type – referral or reauthorization
• Intake ID
• HCPCS and modifier combination requested/approved
• Service code
• Description of HCPCS code
• Date request received
• Status of request
o Approved
o Cancelled
o Denied
o Denied by the Health Plan
o In process – elevated to the Health Plan
o In process – pending additional information
o In process – under review
• Authorization ID if applicable
• Name of Rendering Provider (if approved)
• Number of units for HCPCS code approved
• Unit of Measure for HCPCS code approved
• Service start and stop date

Provider Manual
35 | P a g e
EDRC 746 - 01242018
5-3 UTILIZATION MANAGEMENT
The CareCentrix and Sleep Management Solutions (SMS) Utilization Management
Process
Utilization Management is the evaluation of the appropriateness, medical necessity and efficiency of
healthcare services according to established criteria or guidelines under the provisions of the patient’s
benefit plan. When CareCentrix or Sleep Management Solutions (SMS) is responsible for conducting a
review of the medical necessity of a proposed service, the following is our standard medical necessity
definition:
•
Appropriate and consistent with the diagnosis of the treating Provider and the omission of which
could adversely affect the eligible Member’s medical condition;
•
Compatible with the standards of acceptable medical practice in the community;
•
Provided in a safe, appropriate, and cost-effective setting given the nature of the diagnosis and the
severity of the symptoms;
•
Not provided solely for the convenience of the Member or the convenience of the Health Care
Provider or hospital; and
•
Not primarily custodial care unless custodial care is a covered service or benefit under the Member’s
evidence of coverage.
The above definition is subject to the requirements of the applicable and plan and applicable law (for
example, the mandated definition for medical necessity for Medicare and Medicaid plans will apply to
patients covered under such plans; a state mandated definition for medical necessity for insured
commercial plans will apply to patients covered under such plans). Medical necessity reviews can be
conducted for both initial and reauthorization requests and can be required for all types of service.
Providers may request a copy of the utilization review criteria applied by CareCentrix or Sleep
Management Solutions (SMS) when completing a medical necessity review. Providers may also provide

Provider Manual
36 | P a g e
EDRC 746 - 01242018
input regarding the utilization review criteria by contacting CareCentrix direct by email at
CCXMedPolicy@CareCentrix.com.
The utilization review criteria that CareCentrix and/or Sleep Management Solutions (SMS) uses when
completing medical necessity reviews is accessible through the links to health plan medical coverage
policies below. Links to these medical coverage policies are also available on the CareCentrix Portal at
www.CareCentrixPortal.com and the Sleep Management Solutions (SMS) Portal at www.SleepSMS.com.
CareCentrix
• Aetna and Coventry Clinical Policy Bulletins
• Amgen Medical Criteria
• Cigna Coverage Policies
• Florida Blue Medical Policies
• Horizon Medical Policies
• ConnectiCare Medical Policies
Sleep Management Solutions (SMS), a subsidiary of CareCentrix
• Fallon Medical Criteria
• Neighborhood Health Plan (NHP) Medical Criteria
• Public Employees Insurance Agency (PEIA) Medical Criteria
Health plans update medical coverage policies regularly. Please reference these medical coverage
policies frequently to become aware of any updates. The above listed websites may also be referenced
to identify clinical documentation that may be required to be submitted with a claim by the above-
referenced plans.

Provider Manual
37 | P a g e
EDRC 746 - 01242018
Under the CareCentrix Utilization Management Program:
• Utilization Management decisions are made independently and impartially and based solely on the
appropriateness of care and service and the existence of coverage.
• CareCentrix decisions regarding hiring, compensation, termination, or promotions of Utilization
Management personnel are not based on the likelihood that the individual will support the denial of
benefits.
• Performance of associates who make Utilization Management decisions is measured based on the
consistent and appropriate application of the approved coverage criteria to the clinical situation
presented. Performance is not measured based on redirection rates or denial rates.
• CareCentrix does not specifically reward practitioners or others for issuing denials of coverage, and
financial incentives for Utilization Management decision makers do not encourage decisions.
Utilization Management Responsibilities
Providers have the following Utilization Management responsibilities:
• Provide and maintain appropriate documentation to establish the existence of medical necessity.
• Obtain authorization prior to beginning services/products. Services/products performed without
authorization may be denied for payment, and any such denial of payment is not billable to the
patient by the Provider.
• Verify the information on the SAF (service codes, HCPCS, modifier, number of units, start and stop
date, Provider name and location) upon receipt. While the CareCentrix utilization management staff
work to assure the accuracy of the information on the SAF/SRF, mistakes can occur. Should you
identify an error, call CareCentrix within 24 hours to correct the error.

Provider Manual
38 | P a g e
EDRC 746 - 01242018
• Timely notify the patient and the patient’s referring physician that services were authorized
consistent with applicable legal and accrediting body requirements.
• Notify CareCentrix immediately if, when the services or equipment are delivered, the diagnosis is
determined to be different than the diagnosis information obtained from CareCentrix.
• Notify CareCentrix if the services ordered will not meet the needs of the patient. You may be asked
to assist in identifying alternatives and discussing with CareCentrix and the ordering physician.
• Participate in case conferences
• Respond to all requests for contact from CareCentrix within 24 hours
• Respond to all requests for contact from the Health Plan case manager within 1 business day. In
most cases, CareCentrix will act as a liaison when a Health Plan case manager requests information.
Providers should not initiate contact with a Health Plan case manager unless directed to do so by
CareCentrix.
• If requested by CareCentrix, provide assessment reports, progress reports, organization forms or
other organization documents within 48 hours of request.
• Verify all initial physician orders with the physician and obtain physician orders for additional
services/products as necessary.
• Provide all other documentation and records which may be requested by CareCentrix from time to
time, within the time frames set forth in the request.

Provider Manual
39 | P a g e
EDRC 746 - 01242018
Retrospective Claims Review
Paid claims can be subject to retrospective audits, and Providers have the obligation to maintain and
make available documentation to support the medical necessity of services rendered and billed. Such
documentation must be made available to CareCentrix and/or the applicable Health Plan at no cost to
CareCentrix or the Health Plan and within the timeframes requested. CareCentrix may recover any
payment for services determined not to meet medical necessity or benefit requirements, including
recovery through recoupment.
Appealing a Denied Request
If services/products have been denied in their entirety and new and/or additional information is
obtained, the Provider should contact the CareCentrix utilization management staff to relay the new
information and have the authorization request reviewed.
If services/products have been denied in their entirety and there is no new information available, the
patient or physician may submit an appeal to the patient’s Health Plan in accordance with the Health
Plan’s appeals process.
6-1 SERVICE DELIVERY
To help ensure seamless patient care and timely and accurate payment, it is important that a Provider
clearly understand the responsibilities for service/product delivery and the discharge of patients from
service.

Provider Manual
40 | P a g e
EDRC 746 - 01242018
The Provider’s Responsibility
For service/product delivery, a Provider must:
• Verify physician’s orders and obtain physician signature within the time specified by state
regulations and licensure.
• Meet the start of care date set forth by CareCentrix and/or the Primary Referral source. Any
inability to meet start of care or delay in start of care requires notification to CareCentrix by
calling the Care and Service Centers and the referring physician as soon as the Provider becomes
aware of the delay. In all instances, approval must be obtained from the patient’s physician if
the start of care will be delayed. Obtain patient signature to validate the patient’s receipt of
services/products delivered.
• Notify CareCentrix by calling the Care and Service Centers immediately if unable to continue
service delivery to the patient.
• Notify CareCentrix within 24 hours if the information obtained during the CareCentrix
authorization process has changed or was incorrect. The utilization management staff will
review to determine if a change to an authorization is required. (For example: An authorization
is given for Ampicillin. When the primary care physician is contacted, the Provider is notified of
a drug, dosage or frequency change. An initial referral and authorization is given for diabetic
teaching. The Provider, upon completing the initial assessment, identifies a need for wound
care visits and supplies. DME Provider identifies the equipment is not the correct size/type to
meet the patient need.)
• Bill CareCentrix only for services/products that have been ordered by an appropriate physician,
meet medical necessity and benefit requirements and are approved by CareCentrix. Provide
after hours (on-call) home visits as appropriate and necessary in situations that cannot be
resolved by telephone consultation.
• Report adverse incidents to CareCentrix within 24 hours of occurrence. Do not contact the
Health Plan unless instructed to do so by CareCentrix.

Provider Manual
41 | P a g e
EDRC 746 - 01242018
• Report complaints and problems with services/products to CareCentrix within 24 hours of
occurrence. Do not contact the Health Plan unless instructed to do so by CareCentrix.
• Comply with state and federal licensing requirements and other applicable laws.
• Conduct and document discharge planning on an on-going basis during the care and document
that discharge needs were met upon discharge.
• Not auto ship supplies. Medical necessity must be confirmed and documented with each supply
shipment.
• Not provide equipment without first confirming medical need.
• Not deliver or ship supplies unless, in advance of delivery or shipment, you have verified with
the patient or their treating physician that the patient needs additional supplies.
• Discharge the patient to a Provider who is in-network with the applicable Health Plan if the
patient requires ongoing services not covered by Provider.
The Provider’s Discharge Responsibilities
Providers are required to notify CareCentrix prior to discharging a patient in the following
circumstances:
• The Provider cannot provide the services/products ordered because of lack of staffing or expertise.
• The patient relocates outside of the geographic service area.
• The patient completes the Plan of Care.
• The patient and/or family are capable of assuming care. The patient’s physician should be notified
of the patient/family’s request before stopping services/picking up equipment.

Provider Manual
42 | P a g e
EDRC 746 - 01242018
• The patient no longer wishes to receive services/products. The patient’s physician should be
notified of the patient/family’s request before stopping services/picking up equipment.
• The patient/family refuses to comply or is incapable of compliance.
• The physician does not provide the needed orders.
• The patient is institutionalized.
• The patient expires.
• Home care is no longer appropriate due to risk factors.
As applicable, Providers are required to cooperate and assist in transitioning a discharged patient’s care
to another Provider in order to ensure continuity of care.
6-2 GUIDELINES SPECIFIC TO PROVIDER SPECIALTY
This section outlines the guidelines specific to the specialty area of a Provider. Guidelines are prescribed
for traditional home health (THH), infusion nursing services , home infusion therapy (HIT) and durable
medical equipment (DME).
Traditional Home Health (THH)
Traditional home health consists of skilled nursing (intermittent and hourly), physical therapy,
occupational therapy, speech therapy, social workers and home health aides.
• A visit (2 hours) is defined as an episode of service (treatment or procedure) performed in a
predetermined period of time with a predictable outcome. Providers must submit a request for
services to CareCentrix for any service that will be billed in excess of one visit in advance.

Provider Manual
43 | P a g e
EDRC 746 - 01242018
• Services performed on the same day with the same HCPCS and modifier combination must be billed
on the same claim. For example, if two nursing visits were completed in 1 day, both nursing visits
need to be submitted on one claim and billed as 2 units on one claims line.
• Provider subcontracting is not allowed.
• Any laboratory tests collected by a Provider must be taken to the laboratory participating in the
patient’s insurance plan. Lab studies are not included in the CareCentrix Provider Agreement.
• The reimbursement for a skilled nursing visit includes the following routine supplies:
o Dressing supplies-gauze pads, sterile/unsterile gloves, ABDs, Kerlix, tape
o Betadine wipes
o Peroxide
o Syringes for nurse administered injections (excludes specialty syringes, special order items)
o Lab tubes and needles for drawing lab work
o KY jelly
o Cotton balls and alcohol sponges
o Gloves
o Band-aids
o Thermometers
o Vacutainers
• Excluding the list above, certain supplies may be billed to CareCentrix but must be requested prior
to delivery. The list of supplies, itemized cost, and the amount used daily must be submitted to
CareCentrix via portal or phone. If you do not submit a request to CareCentrix l for these supplies,
you cannot be reimbursed for them.
• Supplies for care rendered by the patient or family are to be obtained from the insurance carrier’s
supply Provider unless the nursing Provider has supplies in its contract with CareCentrix.
• In the event that the Provider wishes to substitute an LVN/LPN for an RN, it is the Provider’s
responsibility to ensure that:
Provider Manual
44 | P a g e
EDRC 746 - 01242018
1. The substitution is allowed by the patient’s plan and applicable law;
2. The care to be rendered is within the scope of practice for the LVN/LPN as defined by applicable
law;
3. The treating physician is in Agreement with the substitution; and
4. The Provider’s contract includes a rate for LVNs/LPNs and the Provider bills at that contract rate.
• Rehab para-professionals (COTA, PTA) used to support a physical or occupational therapy plan of
treatment must be authorized as a paraprofessional. Paraprofessionals are only authorized when
permitted by applicable law and the patient’s Health Plan and included in the Provider’s contract,
and must be billed at the Provider Agreement rate applicable to the rehab para-professional.
Does the Payor allow substitution of PTA and OTA?
Aetna Yes
Coventry Yes
Florida Blue Yes
Horizon Healthcare Services, Inc. No
Beech Street No
CIGNA/Great West Yes
Cofinity No
• The coordinating Provider is responsible for:
o Coordinating services/products such that vital services/products are received in compliance with
physician orders and meeting patient needs.
o Ensuring assessment/services/products by other Providers are started after they have assessed
the patient but within 48 hours.
o Obtaining and providing to CareCentrix the clinical information needed for re-authorization.
Notifying other involved Providers of authorization decisions, eligibility issues, etc.

Provider Manual
45 | P a g e
EDRC 746 - 01242018
Infusion Nursing Services
The home health Infusion Nursing Services product provides nursing services associated with drug
therapy when CareCentrix is not the source for the drug. Services included in the home health Infusion
Nursing Services product are specialty and standard drug infusion administration and the administration
or training for other injectable drugs appropriate for administration in the home by a certified Home
Health Agency (HHA).
• Upon accepting a referral, the Provider will contact the patient to welcome them on service and to
provide appropriate contact information.
• Within 24 hours of each scheduled visit, the Provider must confirm with the patient that all
necessary medication and supplies, including pump if needed, have arrived. In the event that the
patient has not received all necessary medication and supplies, the Provider must contact the
appropriate Specialty Pharmacy to confirm when medications and supplies will be delivered to the
member and will reschedule visit as appropriate.
• In the event of any adverse reactions to the drugs being infused, Provider will:
o Notify the prescribing physician immediately.
o Notify CareCentrix by the next business day or earlier if necessary.
o Include any details regarding the adverse reaction(s) in the clinical documentation.
• In the event there is any clinically significant deterioration in the patient’s condition, Provider will:
o Notify the prescribing physician immediately.
o Notify CareCentrix by the next business day or earlier if necessary.
o Include any details regarding the clinically significant deterioration in the clinical documentation.

Provider Manual
46 | P a g e
EDRC 746 - 01242018
• Walmart Specialty Pharmacy Requirements
o Both the drug and supplies will be coordinated by Walmart Specialty Pharmacy.
o If a first dose is being requested in the home, Provider will have a policy in place regarding
administration for first dose in home.
o Require nurses performing Infusion Nursing Services to maintain CPR certification.
o Do not use the Provider Portal: HomeBridge
SM
for reauthorization or edits to
authorizations. Requests for reauthorization can be faxed directly to Walmart Specialty
Pharmacy at 866-537-0877. Include the following information when requesting reauthorization:
Patient Intake Number
Patient First / Last Name
Walmart Subscriber ID (WALMART + 9 numeric digits)
Services Requested (either 99601 or 99602)
Start Date Requested
o Should you need additional hours per visit due to flow rate or other patient specific criteria,
please contact Walmart Specialty Pharmacy directly at 877-453-4566.
o There is no need to check eligibility or benefits as the Specialty Pharmacy will check eligibility
and benefits prior to issuing authorization to CareCentrix.
o Never, under any circumstance, tell the patient/member that they are not responsible for any
co-pays, coinsurance or deductibles. Providers are paid for authorized services in accordance
with their contract rates. Those payments are not reduced by the applicable copay, coinsurance
or deductible, and Walmart Specialty Pharmacy assumes the Provider’s burden of collecting
these amounts. Although the patient is not responsible to pay copays, coinsurance or
deductibles to the Provider since the Provider has been paid in full, the patient is responsible for
remitting those amounts to Walmart Specialty Pharmacy.

Provider Manual
47 | P a g e
EDRC 746 - 01242018
o Provider is required to fax clinical notes and documentation to CareCentrix within 3 business
days of the provision of service to 877-254-6121.
o Provider is required to use the patient Subscriber ID list on the Service Authorization Form when
submitting a claim using the following format WALMART + 9 numeric (e.g.,
WALMART123456789).
Home Infusion Therapy (HIT)
Consistent with industry standards, reimbursement for medications is based on HCPCS units of measure
and is Average Wholesale Price (AWP) based. Most infusion service authorizations consist of three
components: the drug, a per diem/dispensing fee and nursing. Exceptions to this authorization
methodology are Total Parenteral Nutrition (TPN) and hydration therapy, which are reimbursed on a
bundled per diem basis. Utilization management staff provides via the SAF the infusion therapy-specific
codes for authorization and billing. TPN and hydration therapy have only a per diem code plus nursing.
The standard per diem includes:
• All administrative overhead including: on-call pay, overtime, travel and facility expenses.
• All pharmacy, warehouse and delivery expenses.
• All emergency kits including: anaphylactic kits, extravasation kits, narcotic antidote kits, etc.
• All clinical monitoring: vital signs, lab draws, etc. Labs should be transported to the patient’s (Health
Plan’s) participating laboratory.
• All infusion-related supplies including stationary, ambulatory, disposable, syringe or other infusion
devices.
• Nursing is authorized separately to the per diem and includes but is not limited to; patient
assessment, first dose administration, teaching, IV catheter insertion (including mid-lines and PICC
lines,) and maintenance, troubleshooting of products and services, lab draws, resolving patient
complaints, etc. Services performed on the same day with the same HCPCS and modifier

Provider Manual
48 | P a g e
EDRC 746 - 01242018
combination must be billed on the same claim. For example, if two infusion nursing visits were
completed in 1 day, both nursing visits need to be submitted on one claim. For Florida Blue and
Horizon Healthcare Services, Inc. patients, the first visit should be billed with CPT code 99601 and
the second visit on the same day should be billed using CPT code 99602
• Ambulatory Infusion Suite (AIS) visits should be billed with place of service (POS) 12. For Florida Blue
members, AIS visits should be billed with POS 11 and the ‘SS’ (Home infusion services provided in
the infusion suite of the IV therapy Provider) modifier
• Providers are responsible for managing the inventory of patient supplies. Overstocked drugs or
supplies may not be reimbursed.
• If a patient or caregiver wastes medication or supplies, the Provider must notify CareCentrix and
provide documentation to the events.
• Reimbursement for drugs will be based on the HCPCS unit of measure and maximum allowable costs
(MAC) as calculated by CareCentrix. Generic drugs are encouraged when clinically appropriate. The
CareCentrix MAC can be viewed on the Provider Portal.
• Drugs and per diems will be reimbursed on the lesser of the date span specified on the Service
Authorization Form or actual dates of patient care.
• Provider may utilize a home health agency contracted with CareCentrix to perform the nursing
component of an infusion case. Utilization management staff will make the determination of which
per diem to attach to an ordered medication. The per diem is determined by the type of
medication, if there is more than one medication prescribed, and what services/products will
actually be provided. Example: Ampicillin q6 and Vancomycin q8. Provider would receive the
following per diems:
o anti-infective (Ampicillin) q6 primary per diem and;
o anti-infective (Vancomycin) q8 multiple second (more than one (1) medication ordered)
• It is important to maintain an accurate record of patient authorizations so that claim payment is not
delayed or denied. Payment may be denied or reduced if the service billed does not match the
services on the Service Authorization Form.

Provider Manual
49 | P a g e
EDRC 746 - 01242018
• Requests for additional services should not be made more than 7 days prior to the expiration of the
date span specified on the Service Authorization Form. Exceptions to this rule are specialty
medications, such as Immune Globulin, where additional clinical documentation and review is
required by the Health Plan prior to approval.
Durable Medical Equipment and Prosthetics and Orthotics (DMEPOS)
Durable medical equipment is durable medical equipment that is appropriate for home use. It does not
include unrelated consumable supplies, orthotics or prosthetics. However, for some Health Plans, it
may or may not include consumable supplies, orthotics and prosthetics.
• Initial authorization for rental DME will generally be 1 billing month, unless the physician order or
actual use period will be for less time or unless more than one billing cycle is approved. When
Provider requests a rental of durable medical equipment for a member that was renting or
purchased that durable medical equipment either prior to Provider’s start of care date with the
member or prior to the date the member became eligible under a CareCentrix customer benefit
plan, Provider must notify CareCentrix of that prior rental or purchase, the amount previously paid
for that equipment, and the prior rental period. Provider shall not request or bill and shall not be
entitled to receive reimbursement for any durable medical equipment if the amount already paid
for such equipment prior to Provider’s start of care date with the member or prior to the date the
member became eligible with the CareCentrix customer exceeds either the purchase price cap or
rental period cap for that equipment under either the member’s prior benefit plan or the member’s
current CareCentrix customer benefit plan. If such dollar amount or rental period did not exceed
such cap, then Provider may request a continued rental of the durable medical equipment provided
that the accumulator for the purchase price cap and rental period cap will include the prior amounts
paid and prior rental period. CareCentrix will review requests for vendor or brand-specific
equipment on a case-by-case basis.

Provider Manual
50 | P a g e
EDRC 746 - 01242018
• For custom equipment, a manufacturer’s specification sheet, including retail and CareCentrix
pricing, must be submitted with a request. Note: For custom equipment, CareCentrix may instruct
the Provider to complete 2 claims, if required for the specific CareCentrix contract. If this
requirement is not met, the all-inclusive claim will be denied.
• Re-authorization can be for 90 to 180 days depending upon the equipment, diagnosis and prognosis.
• CareCentrix should be notified immediately of any rental equipment returned before the end of the
service date span specified on the Service Authorization Form.
• Provider must submit the accurate units billed based on services rendered and service date span.
CareCentrix will validate the To date and From date span against the units billed for the services.
• CareCentrix does not accept and process claims billed by the Provider with future dates of service.
• Multiple monthly rentals submitted on the same claim should be listed on separate claim lines and
billed as individual units in correct chronological order.
• CareCentrix will convert the To Date of service to equal the From Date of service for rentals for the
Health Plan to accurately perform benefit adjudication for these services. Provider will receive the
updated To Date of service on the 835/EOP and in the Provider Portal Remittance Advice tab.
• All equipment and supplies will be delivered and set up in accordance to the Payor’s guidelines and
in compliance with all federal, state and local guidelines.
• Wheelchair pricing includes all patient evaluation, delivery, fitting and set-up.
• Supplies for the following services are included in the monthly rental and must not be billed
separately (for purchased equipment, supplies should be billed directly to the patient):
o Apnea Monitors
o Pulse Oximeter
o Oxygen
o TENS Units

Provider Manual
51 | P a g e
EDRC 746 - 01242018
• Usual and necessary ventilator accessories including circuits, filters, batteries and humidifiers are
included in the monthly rental unless specifically noted by the Payor in their clinical guidelines and
under prescribed conditions
• If a patient is prescribed an Oxygen concentrator only, excluding a prescription for an additional
oxygen device for portability or mobility usage by the patient then Provider shall provide to the
patient a “Back-up” System that is selected by CareCentrix and approved by the patient’s physician,
the costs of such “Back-up” Equipment are included with the rental fee for the oxygen concentrator.
If a patient is prescribed a ventilator that is for use in excess of twelve (12) hours a day or if patient
cannot breathe independently for four (4) consecutive hours, then patient will be provided with a
"back-up" system that is in accordance with the Payor clinical guidelines and selected by CareCentrix
and approved by patient's physician. CareCentrix will approve payment for the "back-up" system per
the Payor guidelines. If such additional payment is permitted, in addition to the monthly rental
charge for the primary ventilator, Provider will be paid an additional charge at fifty percent (50%) of
the charges listed above for the ‘back-up’ system.
• Supplies and accessories that are factory installed and required for proper operation of equipment
are included in the initial purchase or rental price and should not be billed separately. Replacement
supplies and accessories that are required for proper use of equipment in the capped rental
category can be authorized per physician orders and patients need.
• One download per month for pneumograms, sleep studies and apnea monitors are included in the
rental price. CareCentrix does not reimburse for interpretations unless specifically requested and
authorized. CareCentrix does not pay for physician professional fees. These should be billed by the
physician to the Health Plan.
• Provider subcontracting is not allowed under this contract, however, it is allowable for the Provider
to sub-rent equipment if Provider will deliver, set-up and train patient and caregiver.
• Providers may provide an upgraded piece of equipment from that which is authorized if ordered in
writing by the physician and if the patient agrees (in writing, prior to delivery) to pay the difference
between the contract price and the cost of the upgrade. Providers are prohibited from disclosing

Provider Manual
52 | P a g e
EDRC 746 - 01242018
their CareCentrix contracted rate to the patient and shall not market to the patient. This cost
difference is billable only to the patient, not CareCentrix or the Health Plan.
• Equipment maintenance is to be done in compliance with the Safe Medical Device Act and
manufacturers maintenance recommendations and noted on the patient’s records chart if done
while the equipment is in use by the patient.
• CareCentrix must authorize repairs to member-owned equipment in advance of Provider providing
the service.
• For all life support, sustaining or patient monitoring equipment, Providers must verify with the
ordering physician all changes to orders up to and including discontinuation.
• Providers should supply the least costly alternative that meets the physician’s order and patient’s
needs.
• All HCPCS codes and modifiers listed and contracted for a Provider may not be applicable to all
Payor contracts.
• Respiratory Therapist visits or consultations for non-routine equipment support or set up will be
authorized in accordance to the plan guidelines and charged per visit or consultation (up to two
hours). Non-routine visits are visits provided in accordance with a physician's plan of care, or are
required by State regulations and not considered part of a routine set-up. Most plans do not
authorize separate payment to DME Providers for routine RT visits, fittings or consultation.
• Providers are required to have as part of their operations a Disaster / Emergency Preparedness plan
to protect members on service.

Provider Manual
53 | P a g e
EDRC 746 - 01242018
Specialty Programs
Some CareCentrix contracts with Health Plans include the provision of specialty programs such as, but
not limited to, Transitional Care programs (HomeSTAR®), Nurse Practitioner Assessments, sleep
management, disease management, and hospital early release. For these specialty programs, select
contracted Providers are contacted and invited to participate if they satisfy and agree to the terms and
conditions of the program. Program training is mandatory for the Provider to participate in the specialty
program. Provider performance in the specialty program is reviewed for compliance with specialty
program requirements. Such compliance is required for continued participation in the specialty
program.
Documentation
CareCentrix does not maintain medical records. Providers are required to maintain all medical records
and other documentation necessary to support services rendered in accordance with applicable laws,
rules, regulations, this Provider Manual and the Provider Agreement and to provide CareCentrix and
Provider’s patients with access to and/or copies of such records upon request and at no charge.
6-3 GENERAL CLAIMS AND REIMBURSEMENT INFORMATION
This section of our Provider Manual will provide you with information about our claims process.
CareCentrix is currently in the process of implementing an enhanced claims platform. This enhanced
claims platform is referred to in this Provider Manual as Claims 2.0. Most of our claims requirements
and processes will remain the same. In this section, we will highlight the new tools and functionality
available with Claims 2.0 and some of the differences between our existing claims platform and our
enhanced Claims 2.0 platform. We are in the process of migrating our customers to this enhanced

Provider Manual
54 | P a g e
EDRC 746 - 01242018
claims platform. Florida Blue was fully migrated in April of 2015, Horizon Healthcare Services, Inc. in July
2015, and we will notify you as other clients are migrated.
Claims Process
Claims are processed consistent with the services specified in the Service Authorization Form issued to
the Provider.
As with all plans, providers are responsible for confirming eligibility and benefits with the member’s
health plan for ongoing or add-on services. Failure to do so could lead to claim rejections and denials. It
is imperative to check eligibility and benefits to ensure the member’s plan has not changed.
To expedite payment of claims, the Provider should match the billable services against the Service
Authorization Form and your contracted Provider crosswalk. Claims for services, date of service or units
that do not exactly match the Service Authorization Form may be rejected or denied in part or in whole.
Alternatively, if the Provider bills for a higher level of service, equipment or supply than the level
specified in the Service Authorization Form, payment may be made in accordance with the rate
associated with the service, equipment or supply referenced in the Service Authorization Form, and
Provider will accept that rate as payment in full.
Claims will be paid based on the lower of the Provider’s usual billed charge or the contracted/negotiated
rate.
Receipt of a Service Authorization Form is not a guarantee of payment, and payment of services
rendered is subject to the patient’s eligibility and coverage on the date of service, the medical
necessity of the services rendered, coverage requirements, the applicable payor’s payment policies,
including but not limited to, applicable the payor’s claim coding and bundling rules, CareCentrix’s
claim coding and bundling rules and compliance with the Provider’s contract with CareCentrix. Such
payment policies and claim coding and bundling rules require that services must be properly
documented and billed in accordance with industry standard documentation and coding and billing
practices and the Centers for Medicare and Medicaid Services (CMS) guidelines, including but not

Provider Manual
55 | P a g e
EDRC 746 - 01242018
limited to, such guidelines that prohibit inappropriate unbundling of supplies/services, require proof
of delivery (delivery tickets signed and dated by the patient), and requirements regarding medical
record signatures, certificates of need/medical necessity, and eligible provider types. By submitting a
claim for payment to CareCentrix, the Provider is certifying that it has met the above requirements,
that the service has been rendered and that it has a record of all necessary documentation to support
the foregoing. Claims that are not submitted within the timeframes set forth in the Provider
Agreement and in accordance with the requirements of the Provider Agreement, this Provider Manual
and the applicable health plan may be denied.
Checking Reimbursement Status
Providers should utilize the CareCentrix Provider portal to check the status of their claims.
After checking the Provider portal, any further questions regarding the status of claims should be
directed to the CareCentrix Claim Support Team (CST). The CST is available Monday through Friday
between the hours of 9:00 a.m. and 6:00 p.m. Eastern Standard Time. The CST phone number is 1-877-
725-6525. Please follow the prompts for claims and service category.
Under our Claims 2.0 enhanced claims platform, providers have access to more information about the
status of their claims and enhanced search capabilities. Through our Provider Portal, Providers can:
• View current status and history of each claim submitted
• View Health Plan determination information for each claim submitted
• View a replica of their submitted claim within the Provider Portal
• View the 277CA acceptance or rejection information
Provider Manual
56 | P a g e
EDRC 746 - 01242018
Explanation of Payment (EOP)
An Explanation of Payment (EOP) is issued in connection with each payment to a network Provider for
services rendered. The EOP contains detailed explanation on payments and denials for each claim line
per claim/invoice.
EOPs are also used to communicate adjustments to claims that have already been processed when it is
determined that additional payment will be made on the claim. An adjustment may be made as a result
of a Claims Reconsideration Request or an appeal. The amount of the adjustment will be detailed by
claim line item.
CareCentrix uses industry standard ANSI Codes to communicate on 835 transmissions and EOPs. The
835 transmissions and EOPs will have ANSI Claim Adjustment Reason Codes (CARC) and Remittance
Adjustment Reason Codes (RARC) when required. A CARC provides a general explanation for adjustment
or denial, and a RARC provides a more detailed description of the basis for the denial. The CARC and
RARC can also be found on the CareCentrix Provider Portal.
Providers may receive an EOP that includes a credit or amount due to CareCentrix. The credit will be
applied against amounts due the Provider and the net amount will appear on the accompanying check.
CareCentrix offers Electronic Remittance Advice (ERA) and Electronic Funds Transfer (EFT). Providers
that wish to enroll in ERA and EFT can do so by downloading the enrollment form posted on our
Provider portal at www.carecentrixportal.com.
Please note that, for claims covered by Health Plans that have migrated to our Claims 2.0 claims
platform, providers may receive an EOP for more claim lines than originally billed. This can occur when
the Health Plan or CareCentrix was required to split the claim lines in order to process the claim. In
addition, in certain instances, Providers may receive more than one denial for a specific claim since
CareCentrix may receive more than one denial from the Health Plan, and CareCentrix passes each such
denial to the Provider. While CareCentrix acts as a billing representative of the Provider solely for
purposes of submitting a claim to the Health Plan, the Provider is solely and completely responsible for
the timeliness, accuracy and completeness of its claim to CareCentrix, for timely submission of all

Provider Manual
57 | P a g e
EDRC 746 - 01242018
necessary documentation (including clinical documentation), for compliance with the terms of the
Provider Agreement and this Provider Manual and compliance with all Health Plan billing, claim,
coverage and benefit requirements. Failure to comply with any of the above may result in nonpayment
to the provider.
6-4 GENERAL BILLING REQUIREMENTS
In this section, we specify our billing requirements as they relate to the address, format, form, and
timeframe for claim submissions, billing when another Payor is primary, authorization requirements,
adjustments, and recoupments. Compliance with our billing requirements is required and can help
ensure the timely processing and reimbursement of Provider claims.
Claims Support Center
The Revenue Cycle Management Center (RCM) is where Provider claims are processed. We encourage
our network Providers to submit claims to CareCentrix electronically because electronic claims can be
processed more efficiently and quickly. If you choose to submit paper claims, please direct your paper
claims to the address at the bottom of the SAF. Always check the SAF for the claims address, as
occasionally a contract with a Health Plan will dictate a deviation from usual operating procedure.
Contracted Providers are strongly encouraged to enroll in EDI by visiting the CareCentrix Provider Portal
at www.carecentrixportal.com.
Claim Form and Clean Claim Requirements

Provider Manual
58 | P a g e
EDRC 746 - 01242018
Claims must be submitted electronically or on standard paper claims forms (CMS 1500 or UB-04). Home
Health Providers must submit claims on an 837I or UB-04. Private duty nursing providers must submit
claims on a 837P or CMS 1500 form for Horizon Healthcare Services, Inc. only and for all other plans, an
837i or UB-04 is required. Our required clean claim data elements for both electronic and paper claims
include the following:
• Patient name, Subscriber ID number (including any prefix and/or suffix as appropriate), address,
relationship to subscriber, gender, and date of birth
• Insurance name, group name and group number
• Subscriber name, address, and gender
• Place of service code
• Primary diagnosis code(s) V codes will not be accepted as the primary diagnosis code and Provider is
expected to follow all ICD coding rules
• Rendering Provider name, service location, and billing address
• Rendering Provider National Provider Identifier (NPI) number, Federal Tax ID number, Medicaid ID
number (Medicaid network Providers only), and Taxonomy Code
• Referring Provider/physician name and NPI number (837P)
• Attending Provider/physician name and NPI number (837I)
• Individual line level charge for each service
• Number of invoiced units for each claim line
• CareCentrix HCPCS/ CPT code(s) and modifier combination
• NDC codes, NDC description, NDC unit of measure, and NDC units (i.e. prescription drugs)

Provider Manual
59 | P a g e
EDRC 746 - 01242018
• Date of service (FROM and TO required; FROM date must be before the claim receipt date and
before or equal to the TO date)
• Whether the patient’s condition is related to employment, auto accident or other accident
• Other insurance information (if other insurance, include other insured’s name, date of birth, other
insurer’s name, group or policy number)
• Coordination of benefits information for secondary claims (explanation of payment from primary
carrier)
• Service authorization number
• Revenue Code (institutional claims)
• HIPPS code on all home health claims submitted for Medicare Advantage members
• Treatment Authorization Code (TAC) on all home health claims submitted for Medicare Advantage
members
• Description of miscellaneous code
HCPCS codes must be billed in whole units of 1 or greater. Units greater than 1 must be rounded up or
down to the nearest whole number. NDC quantities may be submitted in fractional units with up to 2
decimal points.
Claims missing required information, containing incorrect required information, or billed inconsistent
with the requirements of this Provider Manual may not be processed. Paper claims without the correct
required information may be returned, and the Provider will be informed of the information that is
missing or incorrect. Claims submitted electronically without correct required information may be
rejected by the clearinghouse with corresponding reasons for the rejection. Such incomplete claims
must be resubmitted by the Provider to CareCentrix so that a complete or clean claim is received by
CareCentrix within the original timely filing timeframe as specified below subject to applicable law.
Provider Manual
60 | P a g e
EDRC 746 - 01242018
CareCentrix reserves the right to update, modify, and/or clarify HCPCS codes in accordance with federal,
state, or other regulatory bodies. It is the Provider’s responsibility to regularly check the CareCentrix
portal for updates to HCPCS codes, descriptions, and the CareCentrix billing crosswalk. The current
billing crosswalk can be found at: www.carecentrixportal.com.
CareCentrix will only accept original documents for payment consideration that are typed in indelible ink
without erasures, strikeovers, whiteout or stickers. Dot matrix printers should not be used when typing
information onto paper claims forms. Claims with handwritten information will be rejected. Also, it is
important that the name of the Provider organization and service location on the claim match the
Provider name on the related Service Authorization Form(s).
With regard to services delivered, the claim must include a description of the service provided (i.e. “RN
visit” or “CPAP rental”) as well as the relevant HCPCS, CPT or revenue code and applicable modifier(s)
found on the CareCentrix Service Authorization Form or the billing crosswalk (located at
www.carecentrixportal.com). Claims without a description of the service provided will be returned. The
address to which claims should be sent is found in the lower portion of the Service Authorization Form.
Services should be billed at the contracted rates or authorized rates as appropriate. The Provider
Agreement rate is payment in full for covered services and is all inclusive. Provider is not entitled to
receive additional compensation for covered services, including but not limited to, compensation for
copies of records, sales tax, reports, or other services contemplated by the Provider Agreement.
No
billing to the patient or Health Plan of the difference between the negotiated or contracted rate and
the Provider’s list price is permitted. If Provider’s billing system is unable to support billing at the
contracted rate, the difference between the contract rate and Provider’s list price must be adjusted off
Provider’s accounts receivable. Doing so can help Provider avoid repeated claims inquiries. In addition,
when billing for custom equipment, the claim must reflect the full rate, the discount as negotiated, and
the net price. Provider must attach to the claim the manufacturer’s specification sheet for the
equipment. For custom equipment, you may be instructed to complete 2 claims if required for specific
CareCentrix Health Plan contracts.
Claims submitted without all required information may be rejected or denied.

Provider Manual
61 | P a g e
EDRC 746 - 01242018
With respect to applicable sales tax, as indicated above, your network contract rate is inclusive of any
applicable sales tax. It is your obligation to 1) calculate and identify on your claim that portion of your
contract rate that is attributable to applicable sales tax; and 2) remit the applicable sales tax amount to
the appropriate regulatory authority.
For electronic claims processed through our Claims 2.0 platform, CareCentrix will utilize the following
electronic transaction messaging:
• CareCentrix will transmit a 277CA - Accepted without Adjudication (AWA) for each 837 received and
accepted by CareCentrix. Providers will not receive a full acceptance (277CA – Acceptance) until
CareCentrix receives the 277CA acceptance from the Health Plan.
• CareCentrix will transmit a 277CA - Acceptance after the Health Plan sends CareCentrix a 277CA
acceptance response.
• CareCentrix will transmit a 277CA - Rejection, as applicable. The reasons for rejection will be
included in a single notification.
Timely Filing
Clean claims must be filed at the address designated by CareCentrix within the time frame described in
your Provider Agreement or within the period of time required by applicable law if longer. Claims
received by CareCentrix after the filing deadline may be denied, and Providers cannot bill the patient for
such services. Note that CareCentrix may pay some claims that were not submitted timely to
CareCentrix if we believe there may still be time to timely bill and receive payment from the Health Plan.
However, please be aware that, if the Payor does not pay the claim in full, CareCentrix may later deny
the claim for failure to timely file and recoup the prior payment.

Provider Manual
62 | P a g e
EDRC 746 - 01242018
Health Exchange Members That Receive Advance Premium Tax Credits
• Under the Affordable Care Act, health exchange members that receive an Advance Premium Tax
Credit (APTC Members) are afforded a 90-day grace period to pay outstanding premiums. Providers
can obtain grace period status information on APTC Members directly from the APTC Member’s
health plan using the same means by which the health plan provides that information to its network
providers. If a health plan provides this information via an online tool, please obtain access to that
online tool if you do not already have it. A health plan’s toll free phone number can be obtained
from the health plan member identification card.
• CareCentrix will process and pay provider claims for APTC Members and their covered
dependents(s) for authorized covered services throughout the first month of the premium grace
period in accordance with your provider agreement. For services provided during months 2 and 3 of
the grace period, CareCentrix may pend the claims until the health plan provides CareCentrix with
the information necessary to verify eligibility.
• If a claim is pended, it will remain in pended status until CareCentrix can verify eligibility with the
health plan. For those members that paid the required premium timely, the pended claims for
covered services will be processed for payment in accordance with your provider contract. For
those APTC Members that failed to pay the required premium timely, any pended claims for services
provided in months 2 and 3 will be denied on the basis of lack of eligibility and, if CareCentrix paid a
claim for services provided during months 2 and 3, CareCentrix will recoup that payment. If, prior to
receiving such services during months 2 and 3, the APTC Member agreed in writing to accept
financial responsibility for non-covered services, you can bill the patient for the non-covered
services in accordance with your provider contract.

Provider Manual
63 | P a g e
EDRC 746 - 01242018
Billing When another Payor is Primary
When a CareCentrix customer is the secondary payor and, under that CareCentrix customer contract,
CareCentrix is responsible for processing secondary claims, Providers should immediately notify
CareCentrix so that services can be appropriately authorized. Please note, when the CareCentrix
customer is the secondary payor, any claims submitted to CareCentrix must include a copy of the related
denial or explanation of benefits/payment from the primary payor. Such clean claims must be
submitted to CareCentrix with the primary payor’s EOB attached within the timeframe described in your
Provider Agreement or within such longer period of time required by applicable law. Secondary claims
are submitted in paper format or, for those payors that have migrated to our enhanced Claims 2.0
platform, Providers can submit secondary claims electronically by submitting the secondary loops and
segments on the electronic 837.
Medicare Primary Claims
For those members where Florida Blue or Horizon Healthcare Services, Inc. is a secondary payor to
Medicare, all claims for Covered Services are to be submitted directly to Medicare. Through the
Medicare Crossover Process, the claim will then be routed by Medicare to Florida Blue or Horizon
Healthcare Services, Inc.. Florida Blue will process payments in accordance with the Patient’s Health
Plan Benefits Agreements and Medicare requirements, and directly compensate the Provider in
accordance with Florida Blue’s applicable Provider fee schedule equivalent to 100% of Medicare
allowable rate.
Provider Manual
64 | P a g e
EDRC 746 - 01242018
The grid below provides coordination of benefit information for both authorizations and claims when
the CareCentrix payor is not primary.
Payer Name Contact CareCentrix
for authorization
Bill CareCentrix Contact CareCentrix
for authorization
Bill CareCentrix
Aetna FL No No No No
BCBS FL COMM Yes Yes No Yes
BCBS FL Medicare No No No No
Cigna Yes Yes No Yes
Great West Yes Yes Yes Yes
Cofinity Yes Yes Yes Yes
Primary Payor Does Not Cover
(CCX Payor Becomes Primary) Primary Payor Covers
Recoupment and Adjustments
There may be instances in which a refund request or recoupment of an overpayment is required. For
example, we reserve the right to recoup or adjust payment (or request a refund) for amounts paid for
services delivered. This can occur in a number of situations, including but not limited to:
• The patient was not eligible on the date of service or the services were otherwise not covered under
the patient’s Health Plan.
• The CareCentrix customer is discovered to be the secondary payor
• The Provider did not bill CareCentrix timely and CareCentrix was unable to secure reimbursement
from the Health Plan
• Based upon a post service audit or review, the services did not meet medical necessity criteria,
benefit requirements, was not authorized or were otherwise billed incorrectly
• The Provider was paid twice for the same service or received more than the allowable for the
service

Provider Manual
65 | P a g e
EDRC 746 - 01242018
• The services were not reimbursable by the applicable payor or Health Plan, including but not limited
to, were not reimbursable under the applicable payor’s payment policies
• The Provider did not timely provide records requested by CareCentrix to substantiate services billed
by Provider
• The Health Plan otherwise does not pay CareCentrix
Recoupments will appear on the CareCentrix Explanation of Payment (EOP) as a “credit” adjustment.
When applicable, we will provide appropriate information so that the Provider may bill the responsible
party. Also see Service Specific Billing Requirements.
6-5 COMPLAINTS, CLAIMS PAYMENT RECONSIDERATIONS, AND APPEALS
Introduction to Complaint, Claims Payment Reconsideration, and Appeals Process
Our Complaint, Claims Payment Reconsideration, and Appeals process is a continuous process
improvement mechanism that establishes a consistent process for responding to complaints and
credentialing, claims payment, and other issues.
Complaints
• Provider complaints should be communicated to the appropriate Network Management
Representative.
Credentialing
• Credentialing issues should be directed to our Credentialing Department at:
CredentialingDepartment2@CareCentrix.com.

Provider Manual
66 | P a g e
EDRC 746 - 01242018
Utilization Management Issues
Unless otherwise indicated by CareCentrix, CareCentrix does not perform appeals of utilization
management decisions, and the member appeal process is not delegated to CareCentrix. Appeals of
utilization management decisions by or on behalf of the member should be directed to the appropriate
payor.
6-6 CLAIMS PAYMENT ISSUES
Corrected Claims
If you receive a denial from CareCentrix, and you agree with the denial, you can correct the issue
identified in the denial and resubmit the claim as a corrected claim. If submitted on paper, the corrected
claim must include clearly visible markings that indicate the claim has been corrected.
• Providers must send paper corrected claims to:
CareCentrix – Claims
PO BOX 30722-3722
Tampa, FL 33630
• Providers that wish to submit paper corrected claims via Federal Express, UPS or Certified Mail
must send the corrected claims to:
CareCentrix – Claims
5401 W. Kennedy Blvd, Ste 150
Tampa, Florida 33609
Provider Manual
67 | P a g e
EDRC 746 - 01242018
• For claims covered by payors that have migrated to our Claims 2.0 enhanced claims platform,
Providers can submit corrected claims electronically to CareCentrix through a Frequency Code 7
which indicates a void and replace of the original claim submitted. Providers must modify at least
one data element on the claim in order to submit a Frequency Code 7. Providers may not submit a
Frequency Code 7 until they have received the 835/EOP from CareCentrix for the original claim. If
necessary, Providers may submit a Frequency Code 8 which will void the claim in its entirety.
Please note that corrected claims must be received by CareCentrix within the original timely filing
timeframe in order to be payable.
Claims Inquiries
For claims covered by payors that have migrated to our Claims 2.0 claims platform, Providers can submit
claims inquiries through the CareCentrix Provider Portal to interact with the Claims Support Team (CST).
There are three types of claims inquiries to choose from: General, Financial and Denial. To access the
claims inquiry function, visit carecentrixportal.com and click the ‘Submit a Claims Inquiry, Appeal or
Reconsideration’ link.
Reconsideration
If you receive a payment from CareCentrix that is different from what you expected, you should first try
to understand the difference and reconcile the discrepancy. If you cannot reconcile the discrepancy and
wish to request reconsideration, you must submit a request for reconsideration in writing using our
Claim Reconsideration Form which can be found on our Provider portal at www.carecentrixportal.com.
A claim reconsideration form may not be submitted for a FEP member claim as this plan type does not
permit reconsiderations. The Provider should instead submit an appeal for FEP members. In addition,
for New Jersey providers that elect to initiate a New Jersey statutory claims appeal for a claim that is
eligible for such appeal process and for which CareCentrix is delegated to handle such statutory claims

Provider Manual
68 | P a g e
EDRC 746 - 01242018
appeals, submit an appeal using the New Jersey claims appeal form posted on the CareCentrix Provider
Portal.
Prior to submitting a reconsideration request, you should confirm:
1. If the claim was rejected or denied. Rejected claims can be resubmitted without submitting a
reconsideration request.
2. If the member is a FEP member. The provider should not submit a reconsideration request for an
FEP member claim. The Provider should instead submit an appeal for FEP members.
3. If the original claim has been altered in response to the denial. Only original claims that do not
require changes in response to the denial should be submitted as a claims reconsideration request.
Claims requiring correction to address the issue causing the denial should be submitted as corrected
claims.
• Providers must send requests for reconsideration to:
CareCentrix – Reconsiderations
PO BOX 30720-3720
Tampa, FL 33630
• Providers that wish to submit a request for reconsideration via Federal Express, UPS or
Certified Mail must direct the request for reconsideration to:
CareCentrix – Reconsiderations
5401 W. Kennedy Blvd, Ste 150
Tampa, Florida 33609
• For claims covered by payors that have migrated to our Claims 2.0 enhanced claims platform,
Providers can submit a request for reconsideration electronically through our Provider Portal.
• Under Claims 2.0, depending on the applicable Health Plan and claim denial reason, CareCentrix
will either process the reconsideration request itself or will submit the reconsideration request
on behalf of the Provider to the Health Plan for processing.

Provider Manual
69 | P a g e
EDRC 746 - 01242018
Your request for reconsideration must be received by CareCentrix at the designated address within 45
days after the date of our explanation of payment, or within the period of time permitted by applicable
law if longer.
After receipt of your completed request for reconsideration, we will research your concern and respond
to you as soon as possible. For reconsideration requests that are submitted to the Health Plan on
behalf of the Provider, the following review timeframes will apply (subject to applicable law):
Reconsideration Review Time
Payor
Product Type
Review Time
Florida Blue
Loca
l and
State
30
-
60 Days
Horizon Healthcare Services, Inc.
Local and
State
30
-
60 Days
Florida Blue
BlueCard
60
-
90 Days
Horizo
n Healthcare Services, Inc.
BlueCard
60
-
90 Days
CareCentrix will communicate the plan decision to the provider within on average 10 days of receipt of
that decision or the period of time required by applicable law if shorter. If the request for
reconsideration is resolved in your favor, the claim will be adjusted and an explanation of payment
(EOP) issued. If it is not resolved in your favor, you will be advised to submit an appeal in writing using
our Appeal Form which can be found on our Provider portal at www.carecentrixportal.com. Please note
that, if changes are required to the original claim, in lieu of submitting an appeal, Providers should
submit a corrected claim in accordance with our corrected claim process.
• Providers must send completed Appeal Forms to:
CareCentrix – Appeals
PO BOX 30721-3721
Tampa, FL 33630

Provider Manual
70 | P a g e
EDRC 746 - 01242018
• Providers that wish to submit an appeal via Federal Express, UPS or Certified Mail must direct the
completed Appeal Form to:
CareCentrix – Appeals
5401 W. Kennedy Blvd, Ste 150
Tampa, Florida 33609
• For claims covered by payors that have migrated to our Claims 2.0 enhanced claims platform,
Providers can submit the completed Appeal Form through our Provider Portal.
• Under Claims 2.0, depending on the applicable Health Plan and claim denial reason, CareCentrix will
either process the appeal itself or will submit the appeal on behalf of the Provider to the Health Plan
for processing.
Your appeal must be received by CareCentrix within 30 days from the date of our written notice
(EOP, letter, etc.) advising that your request for reconsideration was not resolved in your favor or
within the period of time permitted by law if longer.
Appeals
If CareCentrix processes the appeal itself, the CareCentrix Appeals Unit will endeavor to complete the
review of your appeal within 30 days of receipt of all information necessary to review your appeal or
within the period of time required by applicable law if shorter. If CareCentrix submits the appeal on the
Provider’s behalf to the Health Plan for processing, the timeframes specified in the grid below will apply
(subject to applicable law):
Appeals Review Time
Payor
Product Type
Review Time
Florida Blue
Loca
l,
State
and FEP
30
-
60 Days
Horizon Healthc
are Services, Inc.
*
Including NJ statutory appeals
Local,
State and FEP
30
-
60 Days
Florida Blue
BlueCard
60
-
90 Days
Horizon Healthcare Services, Inc.
*
Including NJ statutory appeals
BlueCard
60
-
90
Days

Provider Manual
71 | P a g e
EDRC 746 - 01242018
CareCentrix will communicate the plan decision to the provider within on average 10 days of receipt of
that decision or the period of time required by law if shorter. We will communicate the results of our
review of your Appeal in writing which may include, when payment is issued, a check along with an
explanation of payment.
CareCentrix Network Providers may not bill a patient or that patient’s insurance company (if the
insurance company is a CareCentrix client) during the reconsideration or appeals process or for a
balance remaining after a decision has been made on a CareCentrix Network Provider appeal.
Dispute Resolution
If the Provider is not satisfied with the resolution of the appeal, the Provider may request in writing that
the parties attempt in good faith to resolve the dispute promptly by negotiation between
representatives of the parties who have authority to settle the dispute within 60 days of the date of the
appeal decision letter. If the matter is not resolved within 60 days of the Provider’s written request for
such negotiation, the Provider may submit the matter for resolution in accordance with the dispute
resolution process outlined in the Provider’s contract with CareCentrix. The right to submit the matter
for dispute resolution will be waived if the matter is not submitted for dispute resolution within 120
days of the date of the appeal decision letter or within the time period required by applicable law if
applicable law requires a time period longer than such 120 day period. If the Provider Agreement does
not provide for a specific dispute resolution mechanism, the following dispute resolution process shall
apply to the extent permitted by applicable law:
Binding Arbitration
If, after exhausting the CareCentrix appeal process, a Provider is not satisfied with the resolution, the
Provider has the option to pursue binding arbitration in accordance with the rules of the American
Arbitration Association as are in effect at the time of the arbitration’s initiation. The sole and exclusive
venue for any such arbitration shall be Hartford, Connecticut. In connection with the foregoing, each
party shall select an arbitrator and the two arbitrators selected by the parties shall select a third,

Provider Manual
72 | P a g e
EDRC 746 - 01242018
mutually agreeable arbitrator. Arbitration shall then proceed before the panel of the three arbitrators.
The timeframe for discovery and hearing shall be mutually agreed upon by the parties, which agreement
shall not be unreasonably withheld. Arbitration shall be the exclusive remedy for the resolution of all
disputes that may arise between the parties, including but not limited to all disputes arising under the
Provider Agreement. The award or decision of the arbitrators shall be final and binding. The initial filing
fee shall be borne by the party initiating the claims or counter claims in arbitration. Thereafter, the cost
of retaining the arbitrators shall be shared equally by the parties. Each party shall be responsible for all
of its own costs associated with the arbitration including without limitation attorneys, expert, and audit
fees. The arbitrators are expressly prohibited from awarding either party attorneys’ fees or any other
fees, costs or expenses incurred by such party in connection with any arbitration proceeding or
judgment. Judgment upon the award rendered by the arbitrators may be entered in any court of
competent jurisdiction. The Agreement will remain in full force and effect during any such period of
arbitration unless otherwise terminated pursuant to the termination provision(s) of the Agreement
which termination provision(s) shall not be affected or overridden by this Binding Arbitration provision.
This Binding Arbitration provision shall survive any termination of the Agreement.
6-7 Contract Termination
Both CareCentrix and the Provider may exercise their option to terminate the Provider Agreement in
accordance with the terms of the Provider Agreement. In the event of a termination, the Provider must
comply with the Provider’s post termination continuity of care obligations as specified in the Provider
Agreement, this Provider Manual and applicable law. The Provider Agreement rates will apply to
authorized covered services provided during the post termination continuity of care period. Provider
shall provide a list of patients currently on service at the time of the notice of termination, with a
description of the services they are receiving. Provider will maintain a professional attitude regarding
CareCentrix to patients and the community, regardless of the reason for the contract termination.
Provider shall assist in transitioning the care of patients whose services will continue beyond the
continuity of care period to new CareCentrix Network Providers (e.g. provide a case summary and status

Provider Manual
73 | P a g e
EDRC 746 - 01242018
upon discharge; provide all necessary documentation (including current prescriptions) to CareCentrix or
the new Provider). In the event that Provider wishes to appeal the termination of the Provider’s
Contract, Provider may submit a request for an appeal, along with supporting documentation, to their
Network Management Representative.
Your appeal must be received by CareCentrix within 30 days from the date of CareCentrix’s termination
notice or the period of time required by law and accrediting body requirements if longer. Your appeal
will be handled in accordance with any appeal processes required by applicable law and accrediting
body requirements. We will endeavor to complete our review of your appeal within 30 calendar days of
the date we receive your appeal or the period of time required by applicable law or accrediting body
requirements if shorter. We will communicate the results of our review of your appeal in writing. If you
are dissatisfied with the results of your appeal, you may request that the termination be reviewed in
accordance with the Dispute Resolution and Binding Arbitration provisions set forth above.
7-1
CUSTOMER ACKNOWLEDGEMENT AND RESOLUTION MANAGEMENT
Complaint, audit and resolution management allows for the prompt resolution of inquiries, complaints
and concerns expressed from an external source, whether that is a member, Provider or other
complainant. As a Provider, you are expected to submit patient records or to provide additional
information and documentation, as requested and at no charge, so that a complaint or audit may be
investigated and resolved. It is important that documents are submitted to CareCentrix within the
requested timeframe. If a request for records is received directly from a Health Plan, please notify your
CareCentrix Network Management Representative.
Provider specific complaint data is tracked, trended, analyzed and used during the re-credentialing
process and to promote on-going process improvement. If an adverse trend is identified, CareCentrix
may initiate appropriate corrective action. This action may be in the form of, but is not limited to, verbal
counseling, written warning, a formal corrective action plan or, in the most severe instances,
termination from the network. Providers are required to comply with corrective action plans required

Provider Manual
74 | P a g e
EDRC 746 - 01242018
by CareCentrix to address quality of care, quality of service or other issues related to the Provider’s
failure to comply with the Provider’s obligations under the Provider Contract, this Provider Manual, or
applicable law.

Provider Manual
75 | P a g e
EDRC 746 - 01242018
Massachusetts Managed Medicaid Addendum
The following provisions are added to the Provider Manual to comply with Massachusetts Managed
Medicaid requirements. These provisions apply only to services rendered by Providers to patients
covered under a Massachusetts Managed Medicaid plan (“MA Medicaid Members”) and only to the
extent required by law. To the extent this Addendum applies and there is a conflict between a provision
of this Addendum and the base Provider Manual, the provision in this Addendum shall control.
1. Specific information regarding Covered Services for MA Medicaid Members can be obtained by
contacting CareCentrix or the applicable Payor listed on the MA Medicaid Member’s insurance
identification card.
2. Under the Massachusetts Managed Medicaid Program, MA Medicaid Members have specified
rights and shall be allowed to exercise such rights without having their treatment adversely
affected. MA Medicaid Members may file a grievance with the applicable Payor if Provider
violates any such rights, and such Payor will resolve such grievance in accordance with the
Payor’s MA Medicaid Member grievance process. Provider shall cooperate with such process and
supply any information required to resolve any such grievance.
3. Provider shall cooperate with the MA Medicaid Member’s Integrated Care Team (ICT) as required
by applicable law.
4. MA Medicaid Member health information will be treated as confidential and protected in
accordance with applicable law.
5. Provider shall provide assistance to MA Medicaid Members who require language assistance,
including providing interpreter services as needed.
6. Provider shall accept and treat all MA Medicaid Members regardless of race/ethnicity, age,
English proficiency, gender identity, sexual orientation, health status, or disability.
7. Provider written communications to MA Medicaid Members regarding the services provided
hereunder, including marketing materials (if any), must be submitted to CareCentrix for approval
prior to distribution.

Provider Manual
76 | P a g e
EDRC 746 - 01242018
8. Provider shall make MA Medicaid Members aware of available clinical options and all available
care options.
9. Provider may not charge MA Medicaid Members, CareCentrix or the Payor for any service that (a)
is not a Medically Necessary Covered Service or non-covered service; (b) for which there may be
other Covered Services or non-covered services that are available to meet the MA Medicaid
Member’s needs; and (c) where the provider did not explain items (a) and (b) and (c), that the
MA Medicaid Member will not be liable to pay Provider for the provision of any such services.
Provider shall document compliance with this provision.
10. Provider shall conform to advance directive requirements as defined in 42 C.F.R. § 489.100, and
pursuant to 42 C.F.R. § 422.108. CareCentrix and Payors have authority to audit the presence of
advance directives in medical records.
11. Prior authorization and/or registration is required for all services provided under the Agreement.
12. New MA Medicaid Members shall have the right to an initial continuity-of-care period as
provided under applicable law.
13. MA Medicaid Members have the right to access and correct medical records information
maintained by Provider.
14. Updates to policies impacting Provider are communicated through Provider Newsflashes,
Provider Manual, and/or the CareCentrix Provider Portal.
15. Utilization management decisions made by CareCentrix are rendered and communicated in
accordance with the process specified in the Provider Manual and timeframes required by
applicable law. The frequency of any reauthorization requirement will depend on the services
provided and will be identified in the authorization notification.
16. Provider may request a reconsideration of a claim determination in accordance with
CareCentrix’s reconsideration and appeals process as specified in the Provider Manual. Appeals
of CareCentrix utilization management decisions should be directed to the applicable Payor and
Provider Manual
77 | P a g e
EDRC 746 - 01242018
will be handled in accordance with such Payor’s appeals process. Other issues will be resolved in
accordance with the terms specified in Provider’s contract with CareCentrix.
17. Provider is prohibited from balance billing MA Medicaid Members as specified in the Provider
Manual and this Addendum.
18. CareCentrix facilitates communication to and from network providers through Provider
Newsflashes, the CareCentrix Provider Portal and/or periodic provider meetings.
19. Except as otherwise required or authorized by CMS, the Executive Office of Health and Human
Services (“EOHHS”) or by operation of law, Providers will receive 30 days advance notice in
writing of policy and procedure changes that impact Provider and maintain a process to provide
education and training for providers regarding any changes that may be implemented, prior to
the policy and procedure changes taking effect; and
20. CareCentrix will work in collaboration with network providers to actively improve the quality of
care provided to MA Medicaid Members consistent with the quality improvement goals and all
other requirements of Payor contracts with CMS and the EOHHS.
