MAC5772_0914_Sharing Good Practice_AW AW 7091 Sharinggoodpractice Electronic Holistic Needs Assessmentandcareplanning
User Manual: AW 7091
Open the PDF directly: View PDF ![]() .
.
Page Count: 19
Winter 2014
Sharing good practice
Andrew Brittle
Technical Project Manager – eHNA
Jackie Rowe
Recovery Package
Programme Manager
Leighton Mitchell
Evaluation and Impact Offi cer
Amanda Watson
eHNA Implementation
Project Manager
Noëline Young
Change Project Manager,
Recovery Package
plANnig (HN)
Electroni
h NEeds
ASseSmt
nd Cae
MAC5772_0914_Sharing good practice_AW.indd 1 14/11/2014 10:34

i Winter 2014
eHNA and Care Planning
Introduction
Jackie Rowe describes the background behind developing an
electronic tool for Holistic Needs Assessment (eHNA).
Background to developing the eHNA
There are currently two million people1 in
the UK living with and beyond cancer. This
number is likely to double to four million by
20302, refl ecting an increasing incidence of
cancer and better survival rates. The story
about cancer is changing, and we need to
recognise its long-term impact on people’s
lives, plan better services and develop more
personalised care closer to home. The current
system of follow up is not meeting people’s
needs, and will not cope if the number of
people living with cancer increases at this rate.
The 2014 National Cancer Patient
Experience Survey for England identifi ed that
only 22% of people with cancer received an
assessment of their needs and a written care
plan.3 Feelings of isolation and loneliness are
experienced by many people4 and having an
effective assessment and care plan helps to
ensure that individual needs are identifi ed and
met. Macmillan and its partner organisations
have a vision that everyone living with cancer
should have a tailored care plan5
which addresses their emotional,
physical, spiritual, social and
practical needs.
To do this, we must make sure
we are assessing people’s needs
throughout their cancer journey.
Among clinical nurse specialists
(CNSs), 90% believe a structured
Holistic Needs Assessment
(HNA) and care plan contributes
to person-centred care, with
almost identical proportions
(89%) saying these measures
address people’s needs
that would otherwise
remain unknown.6
HNA and care planning can greatly improve
the coordination of care and outcomes for
people living with and beyond cancer. The
assessment is not an end in itself; it is a means
of ensuring that in the fi rst place, a person’s
needs are identifi ed so that care planning
can provide a structured process to address
those needs.7
The key components of HNA and care
planning are:
• Self assessment using a structured HNA
tool, delivered at key transition points of
the care pathway.
• A conversation between the person with
cancer and the clinician, to discuss the
needs identifi ed in the assessment and
develop a plan of care.
• A simple care plan/action plan that is
co-created by, and owned by, the
person living with cancer.
• Referral or signposting to appropriate
information or support services.
Introducing these components will support:
• A more systematic and proactive approach
to aiding recovery, improving outcomes for
people living with or beyond cancer and
enabling them to live as near a normal life
as possible.
• More emphasis on empowering people
to manage their own care, by giving them
the appropriate information and support.
• A shift in focus from a pathway that is
essentially ‘one size fi ts all’ to a service
that identifi es people’s individual needs,
and which does this using an assessment
process that proactively addresses those
needs. This avoids unnecessary follow up
appointments and unplanned admissions.
Jackie Rowe
Recovery Package
Programme Manager
Macmillan Cancer Support
020 7091 2410
ehna@macmillan.org.uk
MAC5772_0914_Sharing good practice_AW.indd 2 14/11/2014 10:34

Sharing good practice
Winter 2014 ii
• A more integrated model of care through
a better coordinated approach to
shared documentation.
• Improved information-giving between
secondary, primary and community care,
and the person living with cancer.
Working with clinicians and people living with
cancer, we are now testing a prototype of a
new electronic Holistic Needs Assessment tool
(eHNA) across the UK. During 2014, we have
expanded the number of sites and hope to
engage up to 65 sites by the end of the year.
Macmillan’s approach to eHNA
Macmillan’s electronic approach to assessment
is simple but effective. It starts with people
fi lling in a questionnaire about their concerns
on a touch screen computer (a tablet).
The information is then sent to a secure
care-planning website, where the issues
affecting the person are ranked in order
of priority. Using these results, health
professionals develop the care plan with the
person, and also review data to identify trends
and local service development needs.
This innovative approach to care planning
is user-friendly and makes it easier to give
people personalised support. For health
professionals, it immediately shows them
what’s concerning the person in front of them,
as they will have an electronic record of their
questionnaire and care plan. For people with
cancer, it joins up their care, meaning they
are not repeating themselves to different
professionals at different times.
Macmillan is testing and evaluating the
eHNA to record the quality of individual
outcomes and the person-reported experience,
and to calculate the cost of delivery.
This work links to three of Macmillan’s Nine
Outcomes, which are the things that people
affected by cancer have told Macmillan matter
most to them. The overall aim of the eHNA
tool, as outlined above, supports the outcomes
relating to:
• I understand, so I make good decisions.
• I get the treatment and care which are
best for my cancer, and my life.
• I know what I can do to help myself
and who else can help me.
References
1 Macmillan Cancer Support. Two Million Reasons.
2008. London.
2 Maddams J et al. Projections of cancer prevalence in the
UK 2010 to 2040. British Journal of Cancer. 2012. 107:
1195 –120 2.
3 NHS England. National Cancer Patient Experience
Survey 2014 National Report. September 2014.
4 Macmillan Cancer Support. Facing the fi ght alone.
2013. London.
5 Department of Health. Living with and beyond cancer:
Taking action to improve outcomes. 2013. London.
6 Ipsos Mori. Evaluation of eHNA baseline report. 2013.
7 National Cancer Action Team. Holistic Needs
Assessment for people with cancer: a practical guide for
health care professionals. 2011. London.
MAC5772_0914_Sharing good practice_AW.indd 1 14/11/2014 10:34

iii Winter 2014
eHNA and Care Planning
Amanda Watson
eHNA Implementation
Project Manager
Macmillan Cancer Support
020 7840 4771
ehna@macmillan.org.uk
Transforming care
Amanda Watson explains the
development and testing of eHNA.
In 2010 Macmillan, in partnership with the
National Cancer Survivorship Initiative, began
testing HNAs with 11 NHS test communities.
This led to a small pilot project to trial the
concept of an eHNA with four test sites.
The aim of this project was to understand the
impact an electronic assessment tool would
have on the HNA process and its impact on
assessment and care planning for the future.
The initial testing was conducted over one
year, and began with scoping and developing
the eHNA tool. Macmillan sought expressions
of interest from sites that had been involved in
the testing of the paper HNA tools, as they had
the experience and knowledge of the HNA
process. The sites chosen to test were Guy's
and St Thomas’ NHS Foundation Trust, North
Bristol NHS Trust, East Kent Hospitals NHS
Foundation Trust, and St Helens and Knowsley
Hospitals NHS Trust.
Working together with these sites, Macmillan
identifi ed how and where the assessments would
be carried out and the type of technology that
would be needed to support this.
A six months live test period
followed. All sites were keen to
continue using the system and
the test period was therefore
extended to twelve months.
Overall the testing had a positive
impact. Both staff and people
living with cancer told us it was
generally easy to use and had
the potential to save time.
There were some initial
concerns around security of
equipment and that the elderly
would struggle to use the tablets.
However, the fi nal project report
for the pilot project highlighted that these
were not issues. Although not originally part
of the project scope, it was recognised that
the aggregated data from the assessment and
care plans could be used to support service
development and commissioning.
As this was only a small pilot to test the
concept across four test sites, Macmillan
needed to identify how the eHNA could be
scaled up.
Moving forward
Testing the eHNA helped to defi ne a standard
process for delivering assessments, and
a format for care planning that could be
measured through the use of live aggregated
data. The data could identify the needs and
concerns of the person affected by cancer at
key points of their cancer journey.
Realising the future potential of the eHNA
to transform cancer services was a defi ning
moment, and helped to change the small
pilot to one of Macmillan’s bigger projects
for investment.
In 2012 the decision was made to move
to a larger ‘prototype’ project phase, which
would include more cancer service providers
from across the whole of the UK. Our early
evaluation showed that sites found it much
easier to move to an electronic approach
if they were already providing paper
assessments and care planning routinely.
Macmillan therefore made it a requirement
of the prototype sites that they needed to have
used a paper assessment tool for a minimum
of six months before adopting the eHNA.
The project has recently been extended and
will now end in June 2016.
For further information, please email
ehna@macmillan.org.uk
MAC5772_0914_Sharing good practice_AW.indd 2 14/11/2014 10:34
Winter 2014 iv
Sharing good practice
Andrew Brittle
Technical Project Manager
– eHNA
Macmillan Cancer Support
020 7091 2130
eHNA@macmillan.org.uk
Developing the eHNA
earlier diffi culties have now been overcome.
Being a pilot project, both the eHNA
assessment tool and the care planning website
have been developing and growing, as new
requirements have arisen and new suggestions
have been made. Macmillan has worked closely
with a third party supplier to develop these tools,
and we are continually assessing and updating
them, taking into account some of the ideas and
good practice we fi nd within the trusts.
Alongside the technical issues faced by
prototype sites, information governance (IG)
requirements around storing identifi able
NHS data within the NHS network prompted
further development to ensure the eHNA met
with trust and national policies. We continue
to work with trusts to make sure that these
standards continue to be met.
IG has been one of the biggest challenges
in the development of eHNA. Each trust has
a responsibility to protect the confi dentiality
of individuals’ data, while at the same time
sharing it appropriately in the interest of each
person’s care. As the national requirements
change, we’re working with the trusts, and the
Health and Social Care Information Centre,
to make sure eHNA takes these changes into
account and continues to give the assurance
that the trusts and the public need.
Macmillan sits outside of the NHS network,
and consequently has no access to individual
identifi able data – this is restricted to the trust
that carried out the assessment. However, it is
recognised that there is tremendous value in
having access to aggregated data to identify
areas of concern, and more importantly to
highlight potentially unmet needs. This data is
an exciting new area that could in time lead
to the delivery of a more timely and effective
range of services to the people who need them
the most.
Andrew Brittle looks at the
technical development of eHNA
and how information governance
(IG) has informed it so far.
One of the main drivers for developing the
eHNA was to help deliver the components
of assessment and care planning identifi ed
on page i of this document. Making the
assessment and care planning process
easier for the person affected by cancer
and their healthcare professional allows
more assessments to be carried out, more
care plans to be written, and potentially
more needs to be met.
A key decision at the start of the pilot
project was to use tablets for the assessment
process. This allows the person to complete
the assessment on their own with express
consent, and to highlight concerns that
would be diffi cult to bring up in a normal
conversation. Keeping the focus tightly on
the needs of the individual in this way is one
of the main benefi ts of the eHNA.
Although Macmillan took this innovative
approach in using tablets, many of the pilot
sites had no policies in place to
manage and control their use,
meaning that the teams trying
to pilot eHNA were pioneering
this technology in their trusts.
The reliance of the tablets on
the availability of a WiFi signal
was another unexpected area
of diffi culty. In many areas of
trusts, clinical areas were not
covered by WiFi at all, or the
coverage was patchy at best.
Trusts worked hard to overcome
this, and tablets and WiFi are
now more widely accepted and
established, so many of these
MAC5772_0914_Sharing good practice_AW.indd 3 14/11/2014 10:34

v Winter 2 014
eHNA and Care Planning
Evaluating the eHNA
Leighton Mitchell looks at the evaluation of the eHNA
programme so far. What does it tell us?
Evaluating the eHNA
The initial eHNA pilot phase to test the
concept in 2012 was evaluated by Ipsos Mori.1
The evaluation highlighted a number of key
fi ndings, including staff and user satisfaction
with the ease of use of
the eHNA, and time
savings for staff. People
living with cancer felt their
holistic needs were being
met, experienced better
and more personalised
support, and perceived
assessment and care
planning to be useful.
Healthcare professionals placed greater
recognition on the importance of assessments
and care planning, and they had greater
confi dence to deliver them. Any reluctance
among staff to administer eHNAs tended to
stem from logistical diffi culties of embedding
the process in their daily routines, rather
than a lack of appreciation of its value. The
potential barriers to success were reported as
IG, time and logistics (limited availability of
clinic space and reliable WiFi).
Ipsos Mori have carried out further
evaluation of the prototype sites using a mixed
method approach to collecting data on the
eHNA process, impact and cost effectiveness.
It is both formative, informing the ongoing
development of the eHNA, and summative,
providing a thorough understanding of its
impact. The evaluation included:
• Collection of data from Macmillan and
the software developer.
• Online surveys with staff.
• In-depth exploration of eHNA
implementation in a number of
case study sites.
• A detailed examination of the benefi ts and
costs of the eHNA from the perspective of
people living with cancer.
• In-depth interviews with key stakeholders.
Progress so far
An Ipsos Mori survey
compared the experiences
of people who had
completed an eHNA,
people who had
completed a paper HNA,
and those who had neither
assessment. A very brief
overview of some of the
main fi ndings is provided below.
• Most people living with cancer, particularly
those who completed an eHNA, felt that
they had received support at the right time:
’I’m not sure there’s ever a good time, but
for me at that particular point I knew I
was going to be having surgery and it
was a good time to think about what I
was going through.’
• The holistic needs of people living with
cancer appear to be better met for
those who have completed an electronic
assessment, compared with those that
recall completing a paper assessment
or can’t recall an assessment at all.
‘I remember it being quite interesting
because it covered a lot of things I didn’t
think we would talk about – emotional as
well as physical needs really.’
’I’m not sure there’s ever a
good time, but for me at
that particular point I knew
I was going to be having
surgery and it was a good
time to think about what I
was going through.’
MAC5772_0914_Sharing good practice_AW.indd 4 14/11/2014 10:34
Winter 2014 vi
Sharing good practice
‘[There] was something on the
questionnaire that I might not have thought
was in [the nurse’s] sphere without the
questionnaire.’
• The data shows that there is an 80%
conversion rate of electronic assessments
into care plans.
Using the eHNA for research, service
planning and commissioning
The eHNA not only helps clinicians to better
tailor the care and support provided to
address people’s needs, but also gives a
valuable source of information for research
purposes and local service planning and
commissioning. The aggregated data gives
Macmillan an opportunity to investigate the
needs of people living with cancer and how
these are addressed.
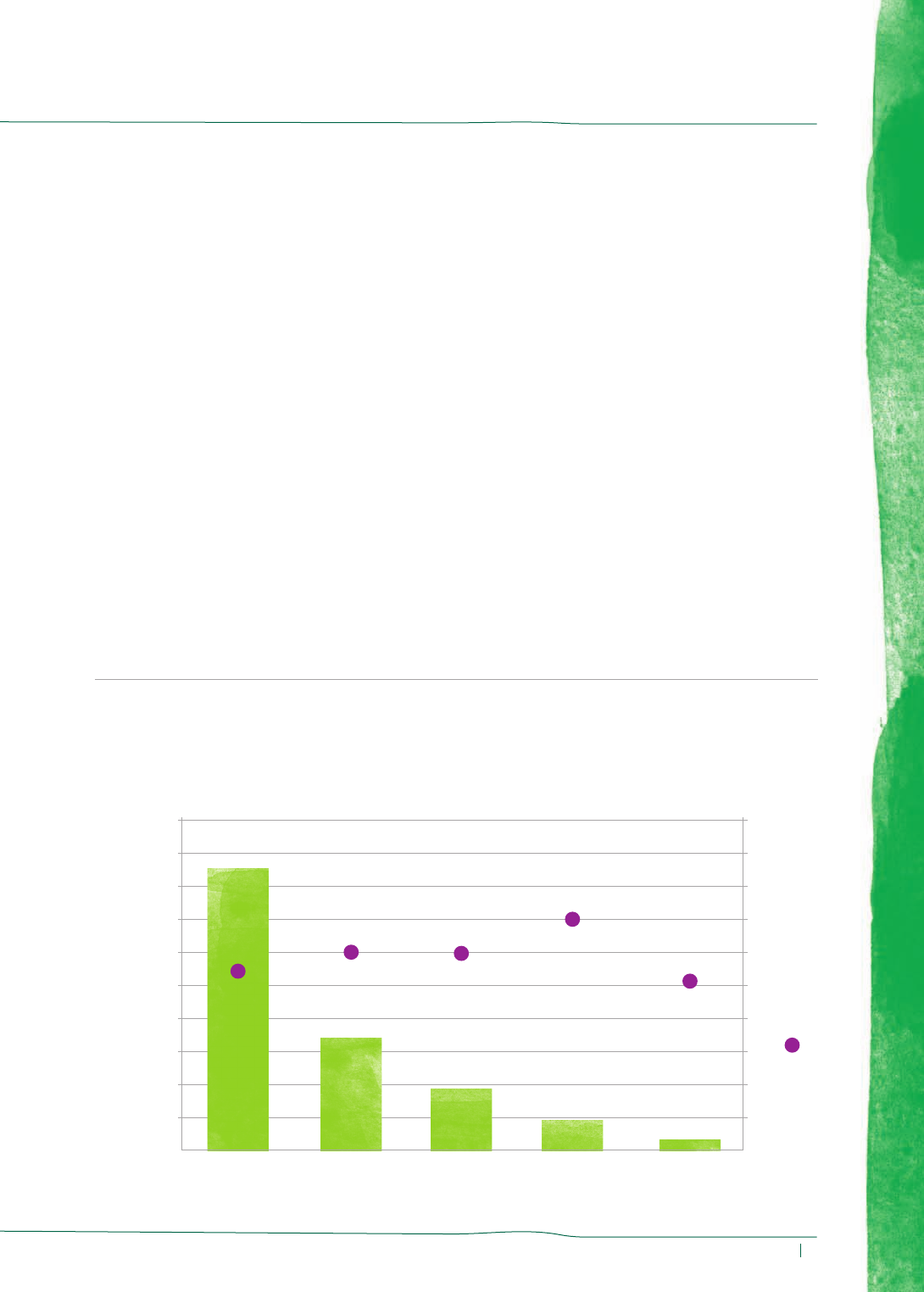
Wide range of concerns expressed
Our early analysis2 showed that half of the
concerns raised by people living with cancer
using the eHNA relate to physical aspects
of cancer survivorship (fi gure 1). A further
quarter related to emotional concerns, with
anxiety being the most frequently reported.
Family concerns, on the other hand, had the
highest average rating. Such a wide spread of
concerns further highlights the need for more
holistic support for people living with cancer.
Before and during treatment, people are
more likely to be concerned and ask about
nutrition, and tend to ask more questions about
physical activity and lifestyle (fi gure 2). This
suggests the potential for promotion of physical
activity and lifestyle changes in cancer survivors
at an earlier stage in the cancer care pathway –
a potential ‘teachable moment’. The emotional
concerns reported suggest a higher need for
emotional support during the cancer pathway.
Figure 1 – Showing the range of concerns expressed
Number of concerns
Physical
concerns
Emotional
concerns
Practical
concerns
Family
concerns
Spiritual or
religious
concerns
Average score (0-10)
Number of concerns reported by people with cancer
using e-HNA and their average score by category
2,000 10
9
8
7
6
5
4
3
2
1
0
1,800
1,600
1,400
1,200
1,000
800
600
400
200
01,696
5
682
6
375
6
184 63
5
7
MAC5772_0914_Sharing good practice_AW.indd 5 14/11/2014 10:34
vii Winter 2014
eHNA and Care Planning
The early data indicates that following eHNA
and care planning, women are more likely to
be referred to general support services (CNS
and counselling) while men tend to receive
more clinical help (medicine review, psychiatric
referral). This was a small sample size and
therefore is worth investigating further.
As the number of eHNA sites increases,
we will continue evaluating the tool and
drawing population-level conclusions on the
relationship between age, gender, cancer
type, cancer pathway and treatment intent,
in relation to the needs of people living
with cancer.
This is early data and a more detailed
report will follow in the fi nal evaluation,
which is due in 2015.
References
1 Ipsos Mori. Evaluation of Holistic Needs Assessment:
Final Report for NCSI Macmillan Cancer Support.
October 2012. London. (accessible at http://www.
ncsi.org.uk/wp-content/uploads/e-HNA-Final-
re p or t - 011112-.p df )
2 Internal analysis of data for the 3-month period of
01/09/13–30/11/13 from 17 participating sites that
have fully launched the eHNA
Leighton Mitchell
Evaluation and Impact Offi cer
Evidence Department
Macmillan Cancer Support
020 7091 2411
lemitchell@macmillan.org.uk
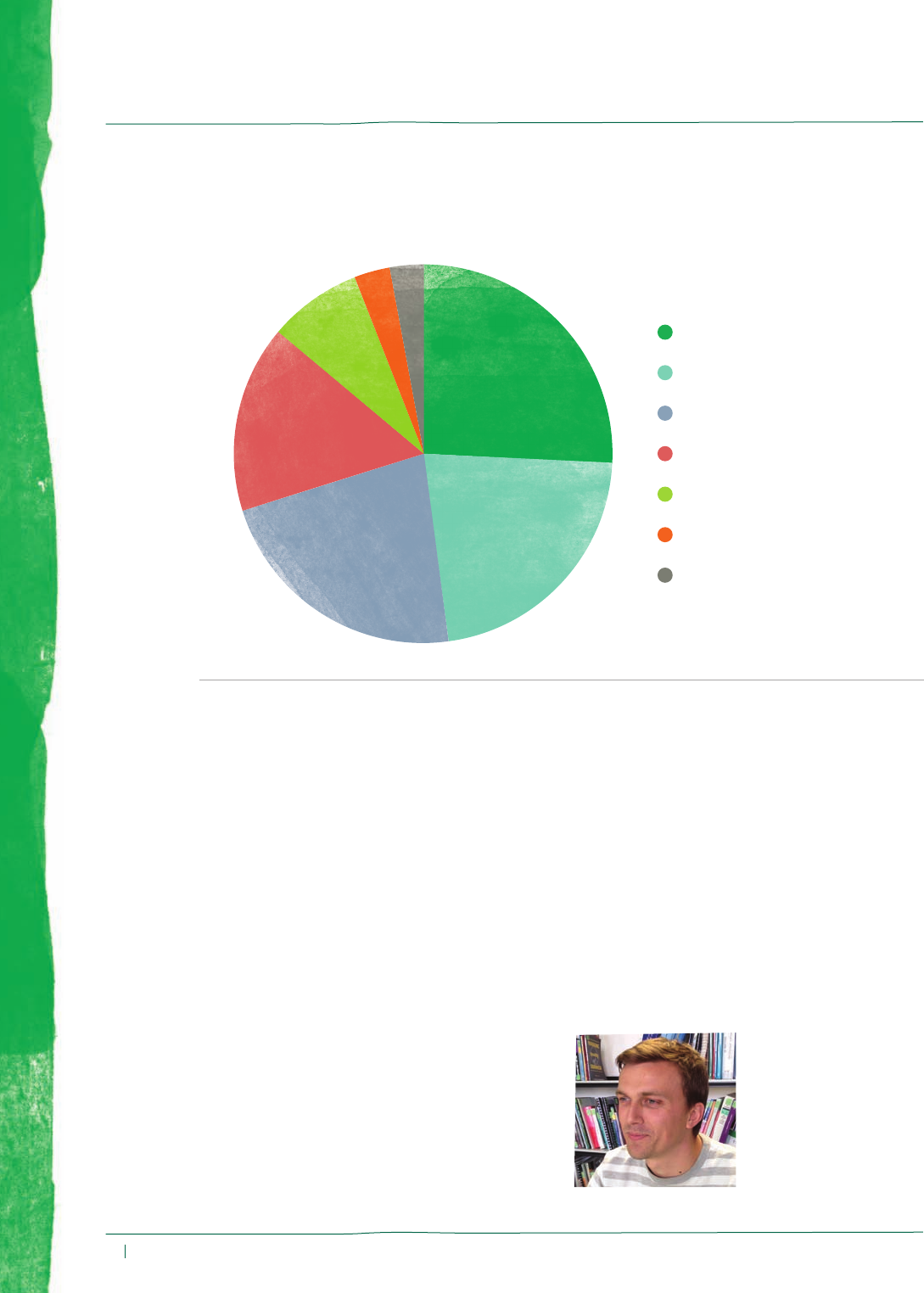
Figure 2 – Showing the opportunity for physical activity and lifestyle information
Breakdown of the information needs reported
by people living with cancer using eHNA
26% Diet and nutrition
22% Physical activity
22% Complementary therapies
16% Support groups
8% Hobbies
3% Sun protection
3% Smoking, alcohol and drugs
MAC5772_0914_Sharing good practice_AW.indd 6 14/11/2014 10:34

Winter 2014 viii
Sharing good practice
Evidence base
Noëline Young describes the evidence that supports the change
towards using eHNA rather than a paper format.
Background
In the management of cancer, good
communication between people living with
cancer and their healthcare teams, and the
assessment of people’s needs, treatment
outcomes, psychosocial factors and quality of
life, are crucial in decision making.1
The busy nature of outpatient clinics
and short consultations may limit a detailed
assessment of people’s needs. This could
constitute a barrier to delivering high-quality
care and improving quality of life. Taenzer et
al1 identifi ed that information technology (IT)
was an easy and acceptable way to overcome
this barrier and enables more precise
assessment and data collection. The data from
this study suggests a marked improvement in
quality of life.
The advent of IT has offered an opportunity
to have a more comprehensive assessment
of how a person thinks and feels. Velikova et
al2 identifi ed that using IT-based assessment
tools enables the transfer of critically important
information that helps to initiate and stimulate
discussion. People felt that if the clinician had
the results of the assessment, they were more
likely to enquire about the issues raised and
their quality of life, and satisfaction with the
care they received increased.
Early work by Velikova et al3 identifi ed
that IT was well-received as a method for
assessment and preferred over paper, as
it was quicker. Responses were legible and
good software design meant it was less easy
to skip questions and therefore data was
more complete. Viewing fewer questions at
a time on the screen was also considered
an advantage over the paper where all the
questions are visible on one page.
Feasibility
Many studies have piloted the use of
computers for assessment and have found that
it is a reliable method to assess quality of life
and people’s needs. Touch screen technology
is mouse and keyboard-free, allowing input
to the screen using fi nger or pen.4 Cull et al5
identifi ed that IT was a practical and effective
method of easing the administration burden,
and that there was scope for using touch
screens to enable more precise assessment
and data collection. Wright et al6 recognised
manual methods were laborious and time-
consuming, and that the use of self-reporting
methods showed better detection rates. See
also Ibottson.7
The validity of data gathered through touch
screens was found to be stable when compared
to paper formats. Gwaltney et al8 identifi ed that
paper and IT formats gave directly comparable
scores. This meta-analysis identifi es the validity
of using an IT solution. Gwaltney et al and
Ashley et al9 also identifi ed that the answers
to electronic questionnaires were equivalent to
those on paper. Frennered et al10 recognised
the psychometric characteristics and score
equivalents when using a touch screen for
assessments were highly correlated, with no
signifi cant difference when compared to the
paper format.
Effectiveness
The major aim of introducing technology is to
improve the HNA and care planning process,
in order to improve treatment outcomes and
satisfaction with services.
The completion of a touch screen
questionnaire signifi cantly increases the
discussion of chronic symptoms by clinicians.
MAC5772_0914_Sharing good practice_AW.indd 7 14/11/2014 10:34

ix Winter 2014
eHNA and Care Planning
Noëline Young
Change Project Manager
Recovery Package
Macmillan Cancer
Support
0142 547 8965
recoverypackage@
macmillan.org.uk
It also has a positive clinical improvement on
a person’s health and well-being.1, 2
Compared to paper, computerised
assessments require less comparable time
to complete, provide better data and result in
a reliable format.11 Bickmore et al12 identifi ed
that people were generally receptive to
technology and Velikova et al2 recognised that
the assessment enhanced communications and
triggered appropriate referrals. Only half the
people living with cancer in this study wanted
a printed copy of the results; however, they
felt that the process resulted in a signifi cant
improvement in the content of the consultation
and improved doctor-patient relationships.
There was a strong preference for the use
of graphics.
Acceptance and user satisfaction
Despite concerns related to computer literacy
and skills, touch screen instruments have been
widely accepted by people living with cancer.13,
14 Touch screens do not require typing or
computer skills and with the minimum of
training, there have been few problems
reported related to use.6 A high degree of
user satisfaction with touch screen solutions
has been found across all genders and age
groups, irrespective of computer skills, literacy
or ethnic background.15 Wright et al6 identifi ed
that 94% of people in their
study had no problem using a
touch screen device, however
Velikova et al2 identifi ed that
those who had severe disease
were less inclined to complete
an assessment using a touch
screen. This paper also identifi ed
that staff had a crucial role in
infl uencing compliance and there
was a need for commitment,
training and skills for health
care professionals.
Evidence of use
The use of computers has
been widely adopted in the
NHS as an alternative means to paper, and
offers many benefi ts to improving effi ciency
and effectiveness in outcome assessments,
including holistic needs.
The evidence to date suggests that
computerisation of the HNA minimises missing
data and duplication, while improving analysis,
storage, retrieval and backup of information
and data. It could aid in the scheduling and
selection of appropriate assessment tools,
ensuring that assessments are completed
consistently across the population of people
living with cancer.
References
1 Taenzer P, Bultz et al. Impact of computerised quality
of life screening on physician behaviour and patient
satisfaction in lung cancer outpatients. Psycho-oncology.
2000. 9:203–213.
2 Velikova G, Wright E P et al. Self reported quality of life
of individual cancer patients: concordance of results
with disease course and medical records. Journal of
Clinical Oncology. 2001. 19(7): 2064–2073.
3 Velikova G, Wright E P et al. Automated collection
of quality of life data: a comparison of paper and
computer touch screen questionnaires. Journal of
Clinical Oncology. 1999. 17(3): 998–1007.
4
Clark K, Bardwell W et al. Implementing touch screen
technology to enhance recognition of distress. Psycho
Oncology. 2009. 18:822–830.
5 Cull A, Gould A et al. Validating automated screening
for psychological distress by means of computer
touchscreens for use in routine oncology practice. British
Journal of Cancer. 2001. 85(12):1842–1849.
6 Wright E P, Selby P J et al. Feasibility and compliance of
automated measurement of quality of life in oncology
practice. Journal of Clinical Oncology. 2003. 21(2):374–
382.
7 Ibbotson T, Maguire P et al. Screening for anxiety and
depression in cancer patients: the effects of disease and
treatment. European Journal of Cancer. 1994. 30A:37–
40.
MAC5772_0914_Sharing good practice_AW.indd 8 14/11/2014 10:34

Sharing good practice
Winter 2014 x
8 Gwaltney C J, Shields A L and Shiffman S. Equivalence
of electronic and paper and pencil administration of
patient reported outcome measures; A meta-analytic
review. International Society for pharmoeconomics
and Outcomes Research. 2007. 1098(3015/08/322):
332–333.
9 Ashley L, Keding A et al. Score equivalence of electronic
and paper versions of the social diffi culties inventory
(SDI): a randomised crossover trial in cancer patients.
Quality of Life Research. 2013. 22(6):1435–1440.
10 Frennered K, Hägg O et al. Validity of a computer
touch screen questionnaire system in back patients.
Spine. 2010. 15(35):697–703.
11 Carpenter J S, Rawi S et al. Oncology outpatient
and provider responses to a computerised symptom
assessment system. Oncology Nurse Forum. 2008.
35(4):661–669.
12 Bickmore T, Gruber A et al. Establishing the computer
– patient working alliance in automated health
behaviour change interventions. Patient Education and
Counselling. 2005. 59:21–30.
13 Crawley J A, Kleinman L et al. User Preference for
computer administration of quality of life instruments.
Therapeutic and Innovation & Regulatory Science. 2000.
34(1):137–14 4.
14 Bischoff-Ferrari H A, Vondechend M et al. Validation
and patient acceptance of computer touch screen
versions of the WOMAC 3.1 osteoarthritis index.
Annuals of Rheumatic Disease. 2005. 64:80.
15 Nicholas D, Huntington P et al. Three years of digital
consumer health information: a longitudinal study of
the touch screen health kiosk. Information Processing
and Management. 2003. 39:479–502.
MAC5772_0914_Sharing good practice_AW.indd 9 14/11/2014 10:34

xi Winter 2014
eHNA and Care Planning
Case studies
Nicola Easton and Paul Worrall describe their experience
of being among the fi rst sites to test the concept of eHNA.
Guy’s and St Thomas’ NHS Foundation
Trust (GSTT)
Setting the scene
Guy’s and St Thomas’ is one of England’s
leading cancer centres, treating more people
with cancer than any other provider in London.
Leading cancer experts are based onsite
and work as part of the cancer team. That
means joined-up care, all in one place, for
an all-round better experience of healthcare.
Cancer care is about much more than medical
treatment. That’s why we do a HNA for
everyone who joins our services, to fi nd out
what cancer means to them, and what support
they need. From psychological support to
fi nancial advice, we will work with the person
to understand how cancer is affecting them
and their family. It was important to us to fi nd
a more effective and effi cient way of assessing
people's holistic needs.
Challenges and solutions
GSTT were accepted as one of the fi rst test
sites for eHNA. WiFi was one of the fi rst
challenges. We couldn’t get the tablets to
connect and stay connected without them
timing out and requiring a personal password.
Using a mobile WiFi device worked; we could
connect and stay connected. However, this
didn’t work in the lower fl oors or where there
was high lead shielding.
Nicola Easton
Quality and Improvement
Lead
Cancer Programme
King's Health Partners
Integrated Cancer Centre
Guy’s and St Thomas’ NHS
Foundation Trust
020 7188 9569
nicola.easton@gstt.nhs.uk
MAC5772_0914_Sharing good practice_AW.indd 10 14/11/2014 10:34

Sharing good practice
Winter 2014 xii
Top tips
Involve the IT department really early. Ask for
an IT representative to be the contact for the
project and work with your team to solve IT
issues and processes. This works best when
there is a member of the IT team willing to be
‘hands on’. The IT contact can be the main
contact with the IG department and can
respond to any IG issues.
Further challenges came at the start of the
pilot, as tablets were not yet approved for use
in the trust. It took some time for the use of
iPads for this work to be approved. In addition,
the iPads were not a standard procurement
item at the time. Testing included making
sure that, if an assessment was not completed,
the tablet would automatically return to
the welcome screen after a certain time.
Once iPads were procured through IT, the
uptake of eHNA advanced rapidly. Now all
clinical teams in all areas have access to an
iPad to use for eHNA.
eHNA is offered to people living with cancer
in a variety of ways: in clinics by the clinic
staff, by a volunteer who assists the person
to complete the eHNA, and in some clinics,
the doctors identify who needs an eHNA.
They are completed in some specifi c clinics,
such as end of treatment clinics, HNA clinics
or at radiotherapy review meetings. The care
planning discussions may happen at the clinic
appointments, at the next appointment, or over
the phone after the hospital appointment.
Benefi ts to people living with cancer
The benefi ts to people living with cancer
have been identifi ed by Sarah Thompson,
CNS at GSTT, as:
’Holistic Needs Assessment is an important
part of the person’s treatment because it allows
us as nurses to be able to focus on individual
needs and their primary concerns.’
One person I was caring for commented that:
’Having a CNS supporting my treatment
made a huge difference. Even now treatment
has fi nished, I still require physical and
psychological support, which has been
highlighted and demonstrated by the Holistic
Needs Assessment.’
Team benefi ts
The IT project team saw the extra benefi t of
the tablet and that it could be used for other
surveys, for example the Staff, Friends and
Family Test. IT ensured that mobile device
management software was used to enable
more than one survey to be loaded on the iPad.
This also means that the care planning
website is on the iPad, so the assessment
can be viewed by the clinician without them
needing to go to a computer. This is useful in
areas with limited access to computers, such as
on the wards and certain clinics. You will need
IG agreement to view or do care planning on
the iPad.
Organisational benefi ts
The Deputy Chief Nurse for Cancer is using
the data from eHNA within performance
review meetings and is reporting results to
the cancer locality meeting with the Clinical
Commissioning Group. Now that more
assessments have been carried out, we can
look at the top concerns of people with cancer
overall, or by individual tumour groups by using
the ‘Data Store’ function on the care planning
website. This helps us to see where there are
capacity issues or gaps in services across the
different tumour groups, and it will therefore
assist in future planning to ensure we have the
right type of services to address these concerns.
MAC5772_0914_Sharing good practice_AW.indd 11 14/11/2014 10:34
xiii Winter 2 014
eHNA and Care Planning
University Hospitals Coventry and
Warwickshire NHS Trust (UHCW)
Setting the scene
Cancer site specifi c CNSs are often assigned
the role of ‘key worker’ for people living with
cancer and their relatives from the point of
diagnosis. As a result, CNSs play a central
role in the initial coordination of the care
planning process.
University Hospitals Coventry and
Warwickshire is a regional cancer centre
covering a wide geographical area, including
Coventry and Warwickshire. Depending
on the type of cancer a person has been
diagnosed with, the subsequent treatment plan
will determine where they are cared for. As a
result, people are often referred to the centre
for all or part of their treatment.
At UHCW, fi ve cancer sites (skin, breast,
colorectal, neurology, and head and neck)
were already using the paper-based concerns
checklist and distress thermometer assessment
tools for HNA. As these sites were already
experienced with undertaking HNAs, they
were approached by the Lead Cancer Nurse
for UHCW to determine interest in applying to
participate in the pilot study. The CNSs already
using paper versions saw this as an ideal
opportunity to further develop their existing
HNA practice.
Following a successful
application to be involved in the
pilot, a steering group was set
up to ascertain how the eHNA
would be implemented. The
steering group also involved
representatives from the IT
and governance department,
to ensure correct IT and
governance procedures were
adhered to.
Following initial training for
the touch screen tablets and the
care planning website, provided
by the Macmillan Cancer
Support eHNA project team,
the cancer sites began using the eHNA in
June 2013.
Challenges and solutions
Once the pilot was in progress, regular
steering group meetings were held to identify
any challenges the sites encountered. The
meetings also provided an ideal forum to
formulate potential solutions.
Initially it was felt that completion of
the eHNA and care plans was more time
consuming. To overcome this, specifi c
clinics were developed to ensure there were
protected times for individuals to complete
the assessment and for the CNSs to produce
the care plans. Some CNSs asked people
living with cancer to arrive 10 minutes
earlier for their clinic appointment to enable
completion of the eHNA, and this reduced
the time spent in their consultation.
The limitation of language barriers
was raised as a concern, but it was felt
this was addressed by using the in-house
interpretation service.
The colorectal team discussed the option
of using the eHNA during community
assessments. The option of purchasing a
3G-enabled tablet and the ongoing cost has
also been discussed with the IT department.
Other technical issues such as the tablets
freezing when submitting the assessment
were easily resolved via the support team.
Benefi ts for people living with cancer
The steering group has also discussed the
benefi ts of the eHNA for people living with
cancer. Primarily it was felt that the process
was person-centred and that consultations
were more person-focused rather than being
health professional-led. This encourages more
in-depth exploration of people’s concerns,
supporting individualised care. The eHNA
has also provided CNSs with the ability to
demonstrate a ‘before and after’ treatment
picture for people, enabling them to see an
improvement in areas such as treatment-
related symptoms.
Paul Worrall
Macmillan Head and Neck
Clinical Nurse Specialist
University Hospitals
Coventry and Warwickshire
NHS Trust
0247 6966 452
paul.worrall@uhcw.nhs.uk
MAC5772_0914_Sharing good practice_AW.indd 12 14/11/2014 10:34
Sharing good practice
Winter 2014 xiv
Team benefi ts
The eHNA has allowed cancer teams to share
the HNA outcomes with other members of the
multidisciplinary team, GPs and community
teams, creating more focused discussions
about the management of care for people
living with cancer.
Organisational benefi ts
Producing the eHNA not only provides people
with individualised care plans, but also benefi ts
the organisation, by ensuring compliance with
peer review measures and national projects. It
also aids data collection of specifi c concerns,
which in turn supports service development.
Following a successful implementation of
the eHNA in the pilot sites, the intention is now
to roll out the eHNA to the remaining cancer
CNSs across the trust.
MAC5772_0914_Sharing good practice_AW.indd 13 14/11/2014 10:34

xv Winter 2 014
eHNA and Care Planning
Policy
As part of the UK government’s information
revolution, it wishes to see greater collection
and sharing of data and information.
It has challenged the NHS to be paperless
by 2018.1 It wants to empower people so that
they can make more informed choices about
their health, treatment and care. The eHNA
process supports this aspiration and aims to
give people the personalised care and the
information they need to enable supported
self management.2
Information Governance (IG)
The IG Toolkit is an online system that
allows NHS organisations and partners to
assess themselves against Department of
Health IG policies and standards. One such
standard calls for the handling and storage of
identifi able patient data to be within the NHS
N3 network. Access to this network is restricted
to organisations that are compliant with the IG
Toolkit, and have reached at least level two.
Visit www.igt.hscic.gov.uk
The Health and Social Care
Information Centre is the national provider
of information, data and IT systems for health
and social care. It documents information
standards about personal data protection and
safety. Specifi cally, ISB0129 sets clinical risk
management requirements for manufacturers
of health IT systems and this covers the
requirements for eHNA. Visit
systems.hscic.gov.uk/clinsafety
England
Living With and Beyond Cancer: Taking
Action to Improve Outcomes details advice
for commissioners and providers about the
types of services that need to be available
for cancer survivors. It starts to develop
an evidence base, as a basis for action for
commissioners and providers, about what
support people living with cancer need, and
how that support can be provided in the most
cost effective way. Visit tinyurl.com/livingwbc
The NHS Outcomes Framework
(NHSOF) is used to monitor the progress
of the NHS Commissioning Board and to
measure the quality of cancer services at
a national level. HNA will be essential for
achieving the outcomes under Domain 2
(Enhancing quality of life for people with
long-term conditions) and Domain 4 (Ensuring
that people have a positive experience of
care). Visit tinyurl.com/nhsof2014
The Clinical Commissioning Group
Outcomes Indicator Set (CCG OIS) is
a key part of the NHS Commissioning
Board's approach to quality improvement. Its
main aim is to support and enable Clinical
Commissioning Groups (CCGs) and health
and well-being partners to plan for health
improvement by providing information for
measuring and benchmarking outcomes
of services commissioned by CCGs. It is
also intended to provide clear, comparative
information for healthcare users and the
MAC5772_0914_Sharing good practice_AW.indd 14 14/11/2014 10:34

Sharing good practice
Winter 2014 xvi
public about the quality of health services
commissioned by CCGs and the associated
health outcomes. Visit
www.england.nhs.uk/ccg-ois
Improving Outcomes: A Strategy
for Cancer, 2011 puts people with cancer
at the heart of cancer services, notably by
aiming to reduce the proportion of people
who report unmet physical or psychological
support needs following cancer treatment.
Chapter 5 (Improving outcomes for cancer
patients: quality of life and patient experience)
acknowledges that people's needs include:
psychological support, fi nancial advice,
support to self-manage, and information
about treatment and care options.
Visit tinyurl.com/improvingo
The NICE quality standards are a set
of statements designed to measure quality
improvements within a certain area of care.
HNA is included in some quality standards but
is absent in some others, showing that HNA is
not yet considered throughout the whole care
pathway and for all conditions. Visit nice.org.
uk/standards-and-indicators
Scotland
The NHS Scotland Quality Strategy underpins
the development of the NHS in Scotland.
It has three ambitions related to quality
(person-centred, safe, effective), all of which
support assessment and care planning
through a focus on self management and
continuity of care. Quality outcomes two
(People are able to live well at home or in the
community) and four (Everyone has a positive
experience of healthcare) are particularly
relevant to HNA and care planning.
Visit tinyurl.com/scotqualitystrat
The Transforming Care After Treatment
programme is being delivered by the Scottish
Government in partnership with Macmillan.
It’s a new work stream of the Scottish Cancer
Taskforce and assessment and care planning
will be a major part of the programme.
Visit tinyurl.com/tcatscot
Wales
Together For Health – Cancer Delivery Plan
sets out the Government expectations of NHS
Wales in tackling cancer up to 2016. Local
health boards are expected to assign a named
key worker, to assess and record the clinical
and non-clinical needs of everyone diagnosed
with cancer in a care plan. This includes regular
assessment of the consequences of treatment,
and other needs, such as access to fi nancial,
emotional and spiritual advice and support, to
ensure a holistic, person-centred approach. Visit
tinyurl.com/togetherfh
Northern Ireland
The Service Framework for Cancer
Prevention, Treatment and Care sets
standards that span the whole care pathway,
from prevention through to survivorship. Several
standards include performance indicators on
HNA and care planning to be achieved over
three years to 2014. It was developed by the
Northern Ireland Cancer Network on behalf of
the Department for Health, Social Services and
Public Safety. Visit tinyurl.com/servicefc
Transforming Your Care – A Review
of Health and Social Care in Northern
Ireland is a 2011 review that set out plans for
the transformation of health and social care in
Northern Ireland over fi ve years. It promotes
joined-up assessment and care planning.
Visit tinyurl.com/tycni
References
1 Department of Health. NHS challenged to go paperless
by 2018. Press release. 16 January 2013 (accessible
online at https://www.gov.uk/government/news/jeremy-
hunt-challenges-nhs-to-go-paperless-by-2018--2)
2 Department of Health. Equality and excellence:
Liberating the NHS. 2010. London.
MAC5772_0914_Sharing good practice_AW.indd 15 14/11/2014 10:34

xvii Winter 2 014
eHNA and Care Planning
Resources
Macmillan resources for health and social care professionals
eHNA Handbook – You’re Transforming
Patients’ Experiences
This booklet provides guidance to prototype
sites when implementing the eHNA. It is
provided as part of the eHNA site set-up.
HNA videos
All of the fi lms that were produced in 2013/14
are now available on YouTube.
• Electronic Holistic Needs Assessment:
http://youtu.be/V9jwh6-9VZU
• Holistic Needs Assessment and Care
Planning: http://youtu.be/q6PCBkfEks4
• Training for Holistic Needs Assessment
and Care Planning:
http://youtu.be/F6iQv4aJePA
Assessment and care planning
for people with cancer
This booklet for patients outlines the process
of assessment and care planning, what to
expect and what they can prepare for.
be.macmillan.org.uk
Order code: MAC12957
Assessment and care planning folder
This pack contains two triplicate pads for the
assessment and the care plan, suffi cient for
100 assessments. This enables the user to
give a copy to the patient, a copy to the GP or
audit, and place a copy in the medical records.
be.macmillan.org.uk
Order code: MAC13689
Replacement pads are also available for the
concerns checklist (MAC13689_concern) and
the care plan (MAC13689_care).
Macmillan Organiser
The Macmillan Organiser is designed to
help people keep track of treatment, make
notes and fi nd information and support. It
enables people to record useful information
to help them self-manage and contains useful
assessment tools such as the concerns checklist
and mood and food diaries.
be.macmillan.org.uk
Order code: MAC13281
MAC5772_0914_Sharing good practice_AW.indd 16 14/11/2014 10:34

Sharing good practice
Winter 2014 xviii
My Organiser
The My Organiser app is now live on the app
stores. My Organiser is a great new mobile app
that can help people affected by cancer plan
and record everything that’s important to them,
from appointment times and contact details
to reminders for when to take medication.
Visit macmillan.org.uk/myorganiser
Assessment and Care planning for cancer
survivors: a concise evidence review (2014)
A concise structured literature review of the
evidence for holistic needs assessment for
cancer survivors, and the implications for
developing services. Download a PDF or
order a copy at be.macmillan.org.uk
Order code: MAC14699_ACP
Innovation to implementation:
A ‘how to guide’
Stratifi ed pathways of care for people living
with or beyond cancer. This document
complements Living With and Beyond Cancer:
Taking Action to Improve Outcomes and
is a practical ‘how to’ guide based on the
experience of test sites who have developed
and implemented a new model of care for
people living with cancer. A PDF is available
from be.macmillan.org.uk
Order code: MAC14481
MAC5772_0914_Sharing good practice_AW.indd 17 14/11/2014 10:34
