Southern Mutual 2013 Benefit Guide
User Manual:
Open the PDF directly: View PDF ![]() .
.
Page Count: 16
June2013
EmployeeBenefitsGuide
Welcome to Your Benefit Guide
for
Who, How, When 3
Medical & Life Carrier Overview & Cost Sheet 4
Medical Insurance Plans- Summary of Benefits 5
Myuhc.com Information 7
Dental & Vision Carrier Overview 9
Dental Plan—Summary of Benefits & Cost 10
Vision Plan– Summary of Benefits & Cost 11
LTD & STD—Summary of Benefits 12
Basic & Supplemental Life—Summary of Benefits 13
Contact Info 16
Premium Saver Plan Info 6
FSA Plan Info 8
Notes Pages 14-15
Table of Contents
Southern Mutual offers you and your eligible family members a comprehensive and valuable benefits program.
We encourage you to take the time to educate yourself about your options and choose the best coverage for you
and your family.
The insurance benefits become effective on your full time date of hire, with the exception of vision, which
becomes effective on the first day of the month following your full time date of hire.
InsuranceManagementGroup 2
Who is Eligible?
If you are a Southern Mutual full-time W2 employee,
working 30 or more hours per week, you are eligible to
enroll in the benefits described in this guide. Your
spouse and eligible dependents may enroll for medical,
dental, vision and supplemental life insurance.
Premiums for all plans are paid thru pre-tax payroll de-
ductions, resulting in approximately 30% savings.
When may I make changes?
Unless you have a qualified change in status, you
cannot make changes to the benefits you elect during the
plan year. Qualified changes in status include: marriage,
divorce, legal separation, birth, adoption of a child, change
in child’s dependent status, death of spouse or child. Invol-
untary loss of other coverage due to a change in spouse
employment or loss of Medicaid eligibility would also apply.
Employee’s have an open enrollment period during the
month of May to make changes to the dental and supple-
mental life benefits.
How do I enroll?
Medical:
You must complete an enrollment form, electing or waiving
coverage. Please be sure to provide a beneficiary for the small
life benefit required by UHC.
Dental:
You must complete an enrollment form, electing or waiving
coverage.
Vision:
You must complete an enrollment form, electing or waiving
coverage.
Long Term & Short Term Disability
You are automatically enrolled in this employer paid benefit.
Group Term Life Insurance:
You are automatically enrolled in this employer paid benefit.
You must complete an enrollment form to select a beneficiary.
Supplemental Life / Dependent Life Insurance:
You must elect or waive coverage on the Group Term Life In-
surance enrollment form.
InsuranceManagementGroup 3

Your Medical Benefits at a Glance for 2013
InsuranceManagementGroup
Medical & Life Insurance
United Healthcare
Policy #0489680
Southern Mutual offers a Traditional Copay Plan with Office Visit and Rx Copays Included.
Southern Mutual pays 100% of the employee only medical plan premium and 45% of any dependent costs.
Employees are responsible for any remaining dependent cost which will be payroll deducted on a pre-tax ba-
sis resulting in approximately 30% savings.
Southern Mutual offers $15,000 of Life and Accidental Death & Dismemberment Insurance to each employee.
Premiums are paid by Southern Mutual.
Care 24 Services offers you access to a wide range of health and well-being information—seven days a
week, 24 hours a day. Call 1-888-887-4114 to speak with a registered nurse and/or master’s-level counselor
who can help with almost any problem ranging from medical and family matters to personal, legal, financial
and emotional needs.
Health Discount Program—even if you already have medical, dental and vision coveage, as an enrollment
health plan member, you can save even more by using the health discount program for things such as teeth
whitening, laser eye surgery, alternative medical care (i.e. chiropractics, acupuncture, etc.), infertility, etc. In
addition, you can save on many wellness resources like weight management programs (i.e. Jenny Craig, Nu-
triSystem, etc.), fitness clubs, smoking cessation programs and more. To find out more visit www.myuhc.com
and select “Extra Programs and Discounts”.
Children are covered to age 26 regardless of student or marital status.
Customer Service: 1-800-357-0978
Website: www.myuhc.com
COVERAGE LEVEL
(rates valid 6/1/13 to 5/31/14)
Medical Plan
SMCI Pays
100% of EE Cost AND
45% of Dependent Cost
Semi-Monthly
Contributions SMIC
Pays on Your Behalf:
EMPLOYEE $266.60
EMPLOYEE & SPOUSE $408.23
EMPLOYEE & CHILD(REN) $372.92
EMPLOYEE & FAMILY $515.27
Medical Plan
Employee Pays
ONLY 55% of their
Dependent Cost!
Semi-Monthly
Payroll Deductions
(Pre-taxed resulting in
approx. 30% savings)
$0.00
$173.10
$129.95
$303.93
Medical Plan
UHC & Premium Saver
TOTAL
MONTHLY
COST:
$533.19
$1,162.65
$1,005.74
$1,638.39
4
InsuranceManagementGroup
Medical Benefits Copay Plan
Individual Deductible: In-Network:
UHC $10,000
EE Pays - $5,000 per Individual
Use Both Cards
Family Deductible (Limit is 2x the Individual): In-Network:
UHC $20,000
EE Pays - $10,000 per Family
Use Both Cards
Calendar or Benefit Year Deductible? Calendar Year
Coinsurance %: In-Network: EE 20% and PS 80%, then UHC 100%
Co-insurance Out of Pocket: In-Network:
EE Pays $1000
Use Both Cards
Co-insurance Limit Per Family: In-Network:
EE Pays $2000 per Family
Use Both Cards
Maximum Annual Exposure *** UHC $10,000
EE Pays $6,000 and PS Pays $4,000
(Deductible + Coinsurance Out of Pocket) Single (In-Network): **
(Deductible + Coinsurance Out of Pocket) Family (In-Network): **
UHC $20,000
EE Pays $12,000 and PS Pays $8,000
PCP / Specialist: $25 / $50
Office Visit Copay Covers: Consultation
Diagnostic Labs & X-Rays?* Yes
High Tech Radiology? Deductible + Coinsurance
In Office Surgery? Deductible + Coinsurance
Outpatient Preferred Labs (covered @ 100%): Any In-Network Lab
PCP Referral Required? No
Urgent Care (Doctors Care): $75
Emergency Room: $150
Network: UHC
Drug Card (generic/preferred/nonpreferred): $100 Rx Ded $10 / $35 / $60
Specialty Medication: n/a
Mail Order (up to 90 day supply): $100 Rx Ded then $25 / $88 / $150
Preventive Care: In Network Benefits
Plan Pa
y
s 100%
No Limit & No Copay
Annual Physicals:
Gyn Exams & Prostate Screenings:
Preventive Mammograms:
Vision Benefit w/ PEP
Maximum Annual Benefit (in/out of network): $5,000,000
Maximum Lifetime Benefit (in/out of network): Unlimited
*Labs & X-Rays must be performed at an in-network physicians office on the same date, billed by the same physician and filed as an office visit.
**Plus Copays.
Customer Service: 1-800-357-0978 Website: www.myuhc.com
5
***YOU MUST USE YOUR UHC & PREMIUM SAVER FOR ALL SERVICES UNTIL THE MEMBER’S MAX ANNUAL EXPOSURE IS MET!!
This is intended as a brief overview of the benefits. Refer to the full Certificates of Coverage for all binding contractual provisions.

Insurance Management Group ♦ www.imgsc.com 6
Premium Saver Plan For Southern Mutual
Group Supplemental Coverage
Health Insurance designed exclusively for those covered under a comprehensive major
medical plan.
This plan picks up where your major medical plan leaves off - on Hospital and Medical
Expenses that you incur when you are in the Hospital.
This plan is designed to help fill the gap between what your current plan pays and what you owe on the
covered expenses from:
The hospital and doctor as the result of an in-patient hospital confinement.
Additional benefits for outpatient expenses.
Supplemental Deductible and Co-Insurance
Annual Deductible - $5,000 Single and $10,000 Family
Co-Insurance - 20% to $1,000 Single and $2,000 Family Out of Pocket
Maximum Annual Exposure - $6,000 Single and $12,000 Family (Deductible + Co-insurance)
This plan will then pay the benefits described below for each insured, after the deductible for this plan has
been satisfied, as provided in the policy until the Premium Saver Plan payments under all benefits reach the
Maximum Total Benefit Amount.
A. Supplemental Benefits for Covered Hospital Confinement
For medically necessary expenses incurred while you are confined in the hospital this plan pays:
Deductible and Co-insurance
Pays the amount applied to your Deductible and Co-insurance by your major medical health plan
for covered charges incurred during the covered hospital confinement not paid by your major
medical plan.
B. Supplemental Benefits for Covered Outpatient Expenses
For medically necessary expenses incurred on an outpatient basis this plan pays:
Deductible and Co-insurance Pays the amount applied to your Deductible and Co-insurance by
your major medical plan.
Charges for the professional fees of a physician in a doctor’s office or medical clinic and
outpatient prescription drugs are not covered.
Maximum Total Benefit Amount Premium Saver Pays: $4,000 Single and $8,000 Family
Premium Saver pays the same benefit regardless of whether Members go in-network or out-of-network.
It is in the best interest of the Member to ALWAYS seek out in-network providers to receive discounted services,
maximize their benefits and minimize their cost!
Customer Service: 1-888-859-3795 Claims Assistance: 1-888-888-2519
InsuranceManagementGroup7
How to register on myuhc.com
By registering on myuhc.com, you can find the answers to your health and benefits questions and the infor-
mation you need in one easy-to-use, convenient location online.
Registration is quick and simple:
1.) Go to myuhc.com
2.) Click the
Register Now
button
3.) Enter ID card information or your Social Security number and date of birth
4.) Enter or confirm your e-mail address or sign up for a free e-mail account
5.) Check to receive informational e-mails and confirm enrollment for electronic documents
6.) Create a username and password—then start using myuhc.com
On myuhc.com you can:
~ Check past and current statements and claims status
~ Review eligibility and look up benefits
~ Find a hospital or doctor
~ Print a temporary ID card or request a replacement card
~ Estimate health care costs - compare hospitals in quality and cost at the procedure level
~ “Chat” with a nurse online in real-time
~ Take a health assessment and participate in online health coaching programs
~ Learn about health conditions, symptoms and the latest treatment options
~ Use the Personal Health Record to organize health data and receive condition-specific information
to organize your overall health
~ Track your medical expenses, manage prescriptions and organize your claims
Online Health Assessment on myuhc.com
Take your first step towards a healthier lifestyle by taking a free, personalized health assessment at
myuhc.com. You can identify your personal health needs, learn healthy habits and compare your “lifestyle
score” to others of the same age and gender. Based upon your score, an interactive Health Coach may recom-
mend up to three health improvement goals to help you achieve your personal health goals such as:
~ Weight Management ~ Excercise
~ Nutrition ~ Tobacco Cessation
~ Stress Management ~ Heart Health Lifestyle
~ Diabetes Lifestyle
To access the Health Assessment, log onto myuhc.com and click on the “Health Assessment” tab on the right
side of the home page.
Personal Health Record on myuhc.com
It’s your health history, a medical library and a customizable organizer rolled into one secure and easy-to-use
tool. With the Personal Health Record you can
~ Review medical and pharmacy claims information, as well as lab results
~ Record allergies, immunizations, your family health history and personal contacts
~ Utilize Health Trackers to track progress such as blood pressure, cholesterol and weight
~ Print or download Personal Health History using historical claims data
Insurance Management Group 8
1. WHAT IS A MEDICAL EXPENSES FLEXIBLE
SPENDING ACCOUNT?
A Health Care Flexible Spending Account (FSA) is an
account to which you contribute part of your pay before
Social Security, Medicare and Federal Income (withholding)
Tax, to pay for qualified medical, dental and certain vision
expenses for yourself, your spouse, and/or your dependents.
2. WHAT ARE QUALIFIED EXPENSES?
Visit www.shdr.com and log-in for a complete list.
3. WHY SHOULD I PARTICIPATE IN A MEDICAL EXPENSES
FLEXIBLE SPENDING ACCOUNT?
Normally, you would receive an income tax deduction for
qualifying medical, dental and vision expenses that exceed
10% of your adjusted gross family income. (Few taxpayers
ever meet that qualification or receive a tax deduction.)
With the medical expenses Flexible Spending Account, every
dollar contributed to your account escapes both FICA and
Federal Withholding taxes. For example, if you and your
family incur $1,000 in qualified medical, dental and vision
out-of-pocket expenses, you will save about $256 in taxes by
using the medical expenses Flexible Spending Account (Federal In-
come Tax 20% + Medicare and Social Security 5.65%).
4. HOW DO I PARTICIPATE?
A) Determine regular medical, dental and vision expenses
you and your dependent(s) will incur during this plan year
(1/1 to 12/31). The worksheet on this page can help you calculate
your expenses. B) Enter the amount you want to set aside before
taxes on the Election Form. Each pay period, Chicora Affiliated Com-
panies will deduct this amount from your paycheck and deposit the
funds directly into your Flexible Spending Account.
5. CAN I REVOKE MY ANNUAL ELECTION AMOUNT?
Generally, no. However, if you have a qualified change in
status (marriage, divorce, birth, adoption, unpaid leave of
absence, change in employment status of you or your spouse
from full-time to part-time or vice-versa) you can revoke
your annual elected amount and make a new election for the re-
mainder of the plan year.
6. WHAT IS THE “USE IT OR LOSE IT” PROVISION?
You may submit a request for reimbursement for expenses
incurred
through December 31, 2013. You will have a 90-day grace
period to submit the Reimbursement Request Form for expenses
incurred during that time. IRS regulations stipulate that any unused
or unclaimed balances remaining in your account, are forfeited.
7. WHEN DO I ELECT TO PARTICIPATE AND HOW MUCH
MAY I CONTRIBUTE:
Each year, during the Open Enrollment period and prior to
the Plan renewal date, you must complete a new Election
Form for the upcoming Plan Year. The annual contribution limit for
Healthcare Reimbursement is $2,500.
8. ARE THERE ANY NEGATIVES?
You must use all the funds for eligible expenses between 1/1/13 and
12/31/13. Unused funds are forfeited.
9. WHAT EXPENSES ARE NOT ELIGIBLE?
• Expenses reimbursed by other sources or insurance
• Expenses
not incurred
during the Plan Year
• Non-qualifying expenses per IRS Code Section 213D
10. WHAT HAPPENS IF MY REQUEST FOR HEALTH CARE
REIMBURSEMENT IS GREATER THAN THE AMOUNT OF MONEY
IN MY ACCOUNT?
The annual amount is available to you from the beginning of the
1/1/13 plan year.
HEALTH CARE
FLEXIBLE SPENDING ACCOUNT WORKSHEET
Estimate expenses for yourself, spouse and dependents
between (1/1/13 to 12/31/13).
MEDICAL Estimated Amount
Deductibles ________________
Copayments ________________
Prescriptions ________________
Other (misc.) ________________
DENTAL
Copayments ________________
Crowns, bridges ________________
Other (misc.) ________________
VISION
Exams ________________
Lenses, frames ________________
Contact lenses ________________
Total Health Care Expenses ________________
Your Tax Bracket (15% to 35%) x_______________
(Income tax plus 5.65% FICA) ________________
Your Estimated Savings ________________
1/1/2013 1/1/2013 1/1/2013 —
—
— 12/31/201312/31/201312/31/2013
Flexible Benefits Program
Flexible Benefits Program
Flexible Benefits Program
Health Care Reimbursement
Health Care Reimbursement
Health Care Reimbursement
Questions and answers about how a Flexible Spending Account works
Your Ancillary Benefits at a Glance for 2013
InsuranceManagementGroup
MetLife Dental Plan Info
Policy #TBA
Southern Mutual pays 100% of the employee only dental premium. Employees are responsible for any
dependent costs, which will be payroll deducted on a pre-tax basis, resulting in approximately 30%
savings.
Members are free to choose any dentist, but can avoid balance billing and receive better discounts if a
MetLife participation provider is used. Search for providers at www.metlife.com/dental. On the side of
the web page under “Find a Dentist”, click “Advanced Search”. Under Network Type, click “PDP Plus”,
enter your search criteria and click “Search” at the bottom.
Children are covered to age 26 regardless of student status.
Customer Service: 1-800-275-4638 Website: www.metlife.com/dental
PEP Vision Plan Info
Policy #TBA
The Vision Plan is voluntary. Employees pay 100% of the premium, which will be pre-taxed thru payroll
deductions, resulting in approximately 30% savings.
Members must use an In-Network Provider to take full advantage of their benefits. Search for Vision
providers by visiting www.physicianseyecareplan.com.
Children are covered to age 26 regardless of student status.
9

InsuranceManagementGroup
DENTAL INSURANCE COSTS:
This is intended as a brief overview of the benefits. Refer to the full Certificate of Coverage for all binding contractual provisions.
10
PREVENTIVE SERVICES
No Waiting Period
BASIC SERVICES
Waiting Period
6 Month - Fillings
12 Month - All Other Services
MAJOR SERVICES
24 Month Waiting Period
Zero Deductible
100% Coverage
$50 Calendar Year Deductible
80% Coverage
$50 Calendar Year Deductible
50% Coverage
Oral Exams / Cleanings
(1 per 6 months)
Fillings
Full Mouth X-rays
(1 per 60 months)
Inlays, Onlays, Crowns
Oral Surgery & General Anesthesia
Oral Exams / Problem Focused
(Combined w/ Exam Limit)
Endodontics & Periodontics
(root canals)
Bridges and Dentures
Bitewing x-rays
(<14: 1 per 12 months)
(19+: 1 per 12 months)
Labs Repair & Maintenance of Crowns,
Bridges & Dentures
Oral Cancer Screening
Fluoride Treatment
(<14: 1 per 12 months)
Sealants & Space Maintainers
(age & frequency limits apply)
Implants
Welcome to MetLife! We are pleased to offer Dental benefits for you and your family. GRP# TBA
GRP# TBA
Calendar Year Annual
Maximum:
$1,500 per member
ORTHODONTICS—$1,000 Lifetime Maximum per member
(dependents to age 19 only)
Customer Service: 1-800-275-4638
Website: www.metlife.com/dental
COVERAGE LEVEL
(rates valid 6/1/13 to 5/31/14)
Dental Plan
SMCI Pays
100% of the EE Cost
Semi-Monthly
Contributions on Your
Behalf
EMPLOYEE $14.54
EMPLOYEE & SPOUSE $14.54
EMPLOYEE & CHILD(REN) $14.54
EMPLOYEE & FAMILY $14.54
Dental Plan
Employee Pays
Dependent Cost Only!
Semi-Monthly
Payroll Deductions
(Pre-taxed resulting in
approx. 30% savings)
$0.00
$15.38
$16.50
$34.93
Dental Plan
TOTAL
MONTHLY
COST
$29.08
$59.84
$62.07
$98.94
InsuranceManagementGroup
COVERAGE LEVEL
(rates valid 6/1/2013 to 5/31/2014)
Employee Pays Total Cost
Semi-Monthly Payroll Deductions
(Pre-taxed resulting in approx. 30% savings)
EMPLOYEE $3.90
EMPLOYEE & SPOUSE $7.40
EMPLOYEE & CHILD(REN) $7.65
EMPLOYEE & FAMILY $11.70
VISION INSURANCE COSTS:
This is intended as a brief overview of the benefits. Refer to the full Certificates of Coverage for all binding contractual provisions.
11
Welcome to Physicians Eyecare Plan! We are pleased to offer Vision benefits for you and your family. GRP# TBA
GRP# TBA
IN NETWORK
BENEFITS
C
o
mp
r
e
h
en
sive eye exam eve
r
y 12 months with a $15 co
pa
y.
$150
material
allowance eve
r
y 12 months towards gl
as
ses and/or contact lens* with a one-time $25 co
pa
y.
After your
material
allowance has been used, receive a 20
%
discount on glasses and a 15% discount on con-
tact lens at
mos
t
providers
**.
Discounts of
10%-15%
on
refractive
surgery including
L
A
SIK
at
participating
prov
iders.
$49
standard
contact lens fitting fee or 15% discount off
t
h
e usual and
customary
fitting for
non-standard
contact lens***
at
most
pr
ovi
der
s*.
No claims or
paperwork
to file.
*Material allowance does not cover non-prescription lenses, non-prescription or cosmetic contact lenses, or non-prescription sun-
glasses.
**Certain providers such as JC Penney Optical, Pearle Vision, Sears Optical, and Target Optical do not offer discounts on disposa-
ble contact lens. Participating Walmart Vision Centers do not offer discounts on glasses, contacts, or contact lens fitting fees. Not
all Walmart Vision Centers provide eye exam services
*** Spherical daily wear, extended wear and disposable contact lens are considered standard contact lens; any other contact lens
types are considered non-standard.
OUT OF NETWORK
BENEFITS
If you choose to use an out-of-network provider, you will be reimbursed the following amounts:
Exam including contact lens fitting: $55 less exam copay
Materials: 65% of the material allowance that was used, less material copay
Please submit a claim form (available at www.physicianseyecareplan.com) along with your itemized receipts to: Physicians Eyecare
Plan, Attn: Claims Department, 48 Courtenay Dr., Charleston, SC 29403.
IMPORTANT INFORMATION:
- You will be mailed a membership card.
- To find an in-network provider near you, go to
www.physicianseyecareplan.com
or call 1-800-368-9609.
- Please visit
www.physicianseyecareplan.com
for participating refractive surgery providers and discounts.
- To make an appointment, call an in-network provider and let them know that you are a PEP member.
- You are responsible for payment to the in-network provider of any amount exceeding the material allowance, any
copays and any contact lens fitting fees.
- This is a routine vision program. Medical and surgical treatments of the eyes are not covered benefits.
- Members will not be able to terminate coverage during their 12 month plan except for a termination resulting from a
change in employment or family status.
- Dependent children are covered to age 26 regardless of student status.

Insurance Management Group 12
Benefit is 60% of your weekly pre-disability earnings, to a maximum of $1,500 per week.
Payable on the 31st day of an accident or the 31st day for an illness.
9 Week benefit duration.
Your benefit will be taxable, as Southern Mutual pays 100% of your monthly premiums.
EMPLOYER PAID SHORT-TERM DISABILITY GROUP#612074GROUP#612074
Benefit is 60% of your monthly pre-disability earnings, to a maximum of $7,500 per month.
Payable after 90 days of a total or partial disability.
Own Occupation Period is 24 months.
Maximum duration of benefits is to Social Security Normal Retirement Age (SSNRA).
Unlimited Return to Work Incentive.
3 months survivor benefit.
Your benefit will be taxable, as Southern Mutual pays 100% of your monthly premiums.
EMPLOYER PAID LONG-TERM DISABILITY GROUP#612074GROUP#612074
This is intended as a brief overview of the benefits. Refer to the full Certificates of Coverage for all binding contractual provisions.
Employee Assistance Program (EAP): One America (AUL) will provide assistance for all
members and their dependents, for a variety of personal and professional matters, in-
cluding: stress, resiliency, depression, addictive behavior, parenting, financial
issues, life changes, mental health, grief, etc. Services are available 24 hours a day,
7 days a week. Call an EAP Professional at 1-800-869-0276. Members can also visit
www.eapconsultants.com and use the password “OneAmerica”.
Customer Service: 1-800-553-5318 Website: www.oneamerica.com
Insurance Management Group 13
Class I—Officers & Managers / Class II—All Other Employees
Class I—$100,000 Life and Accidental Death & Dismemberment Insurance
Class II—$50,000 Life and Accidental Death & Dismemberment Insurance
Southern Mutual pays 100% of the premium.
EMPLOYER PAID BASIC LIFE INSURANCE GRP#52925GRP#52925
Employee Max Benefit—Lesser of 5x annual earnings or $100,000 in increments of $10,000,
rounded to the next higher $1,000. Guarantee Issue = $100,000.
Spouse Max Benefit—50% of employee amount, up to $20,000. Guarantee Issue = $20,000.
Child Max Benefit—$10,000. Guarantee Issue = $10,000.
VOLUNTARY SUPPLEMENTAL LIFE INSURANCE GRP#52925GRP#52925
This is intended as a brief overview of the benefits. Refer to the full Certificates of Coverage for all binding contractual provisions.
Customer Service: 1-800-778-2255 Website: www.prudential.com
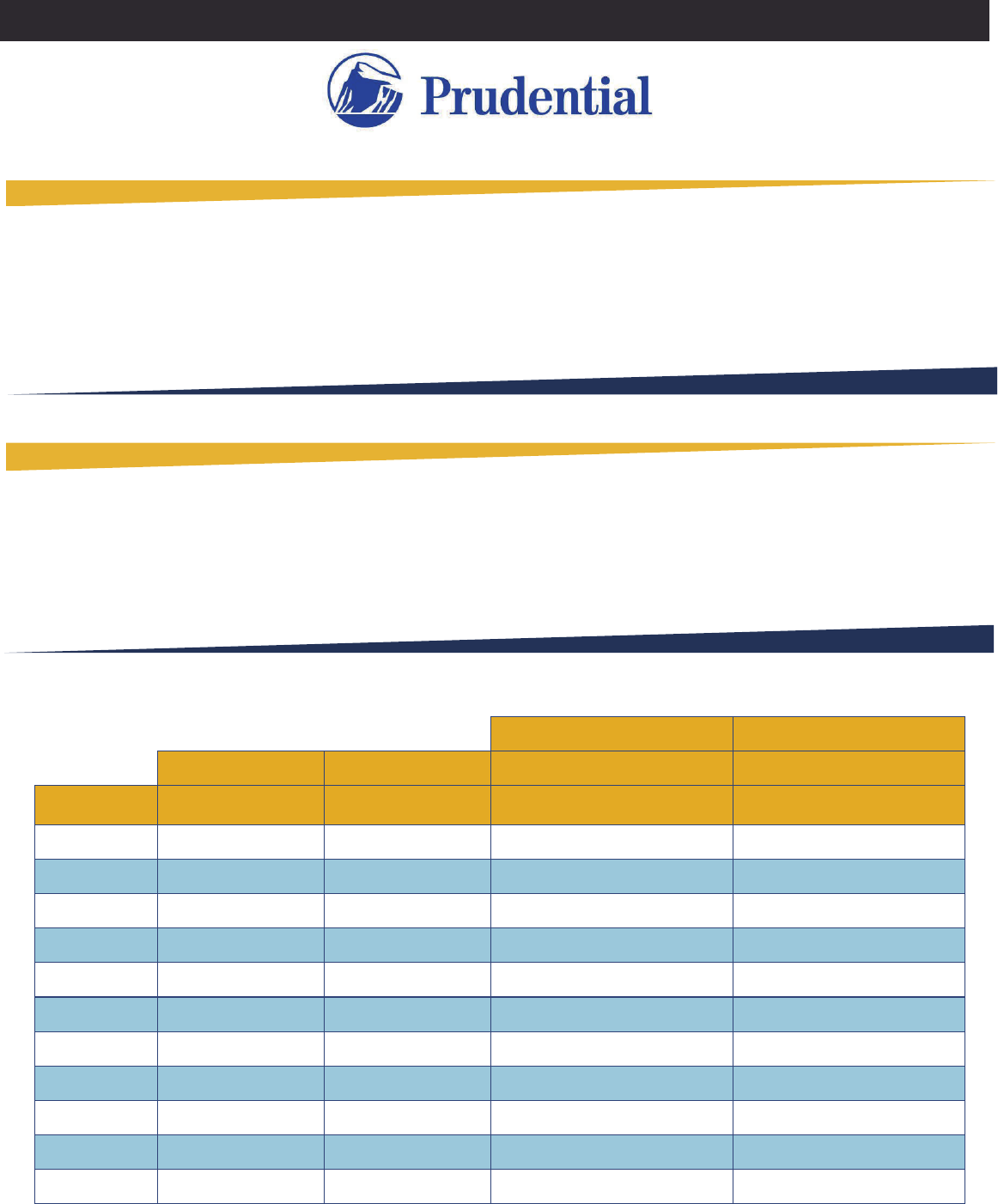
VOLUNTARY SUPPLEMENTAL LIFE INSURANCE RATES
Employee Spouse Per-Pay-Period Per-Pay-Period
Age Bracket Cost Per $1,000 Cost Per $1,000 Cost for $20,000 Cost for $100,000
0-29 $0.09 $0.09 $0.90 $4.50
30-34 $0.10 $0.10 $0.98 $4.90
35-39 $0.12 $0.12 $1.22 $6.10
40-44 $0.16 $0.16 $1.62 $8.10
45-49 $0.24 $0.24 $2.42 $12.10
75-79 $5.04 $5.04 $50.38 $251.90
70-74 $3.01 $3.01 $30.06 $150.30
65-69 $1.72 $1.72 $17.24 $86.20
50-54 $0.39 $0.39 $3.94 $19.70
60-64 $1.05 $1.05 $10.46 $52.30
55-59 $0.66 $0.66 $6.64 $33.20
Sample Employee Sample Employee
NOTES:
Insurance Management Group 14
NOTES:
Insurance Management Group 15

CONTACT INFORMATION
Tammie J. King
T 888-252-1766 x107
P 803.799-1444
tking@imgsc.com
Emily A. Colston
T 888.252.1766 x114
P 803.461.5912
emilyc@imgsc.com
Katy B. Kingsmore
T 888.252.1766 x100
P 803.799.6072
katyk@imgsc.com
Kate Odom
T 888.252.1766 x108
P 803.252.3267
kodom@imgsc.com
This Guide is only intended to offer an outline of bene-
fits. All details and contract obligations of plans are
stated in the group contract/insurance documents. In the
event of conflict between this guide and the group con-
tract/insurance documents, the group contract/insurance
documents will prevail. Please contact your Human
Resources Department for further information.
