TravelExpenseSample Travel Expense Sample
User Manual: TravelExpenseSample
Open the PDF directly: View PDF ![]() .
.
Page Count: 2
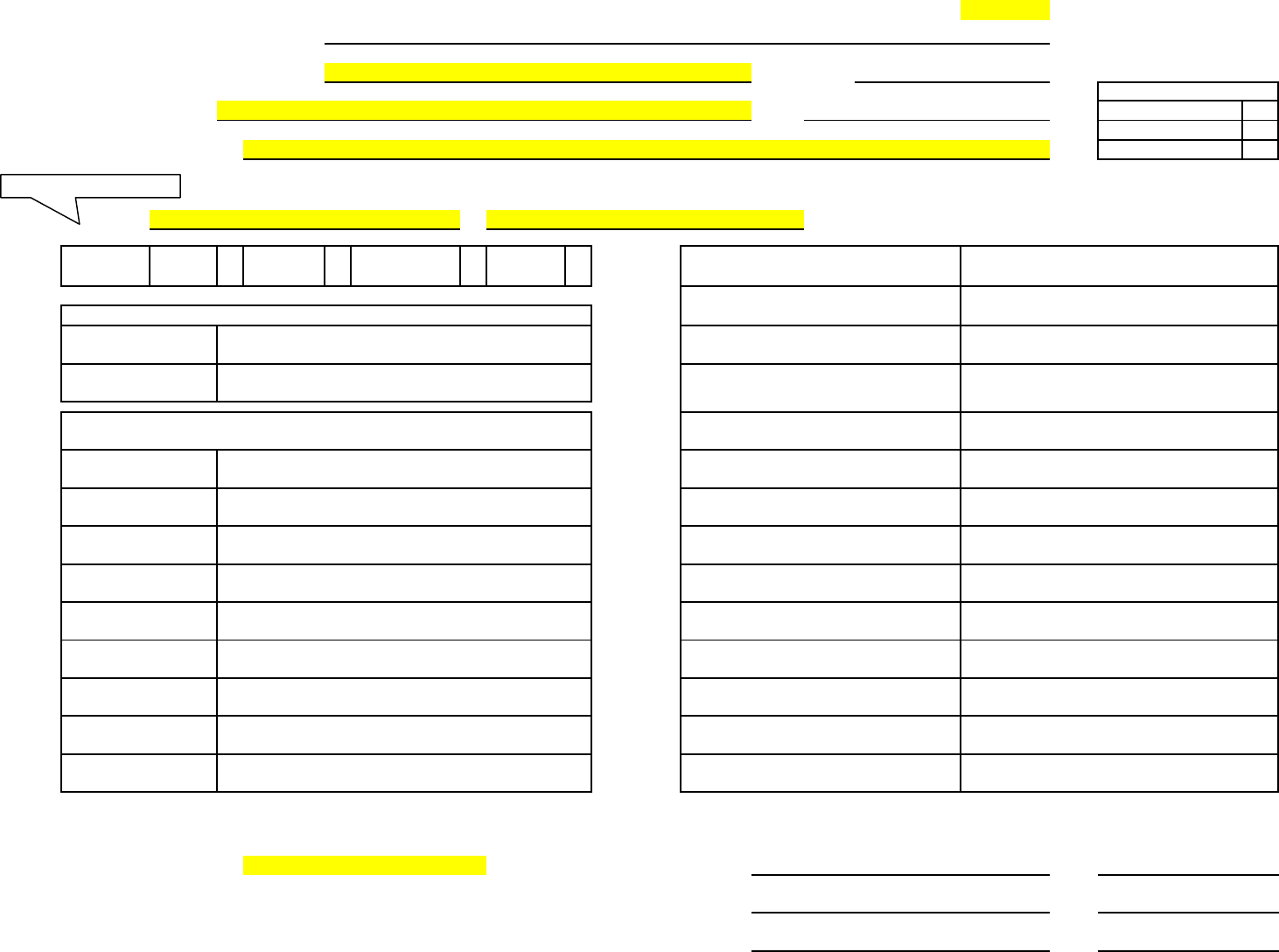
Form 13.20.10 TRAVEL VOUCHER
Revised 05/2005
SAMPLE
State of Mississippi:
Social Security #:
PIN/WIN #:
Name:
PID#:
Employee
Contract Worker
Address:
Board Member
I request reimbursement for subsistence and other authorized expenses paid by me incident to official travel for the State from
to
. The itemized statement follows.
Check
In-
Out-of-
Out-of-
PTE
Box(es):
State
State
Country
Request
Other:
Subject to any difference determined by verification, I certify that the above amount claimed by me for travel expenses for the period indicated is true and accurate in all respects, and that payment for any part has not been
received. In the event of overpayment, I agree that any future salary/travel disbursements may be debited to correct the overpayment.
Signature of Payee: ___________________________________________________________
Associate Signature (no pencil)
Title:
Date:
Verified by: _________________________________________________________________
MSFA Staff Member Signature
Title:
Date:
Approved for Payment: ________________________________________________________
Title:
Date:
PENALTY FOR FRAUDULENT CLAIM - fine of not more than $250; civilly liable for full amount received illegally; removal from office or position held (Section 25-1-81 and 25-1-91, Miss. Code Ann.-1972)
(Agency or Institution)
Associate Instructor
MSFA Staff Member
Project / Sub Proj
Org / Sub Org
Rpt Category
Fund # 3502
Activity / Location 5021
SAAS Ag # 0502
SPAHRS Ag # 502
Payment Information (Traveler complete, if known)
Trip #
Travel Voucher #
Less: PTE Public Carrier
Net Payment (Overpayment) 300.00
Less: Travel Advance
Less: PTE Lodging
Sub Total 300.00
Travel in Public Carrier
0.00
Travel in Private Vehicle 300.00
Travel in Rented Vehicle
Non-Taxable Meals
Lodging
0.00
123 Main St Brandon MS 39042
January 1, 2009
January 4, 2009
Prior to Trip Expenses (PTE) Request:
Per Diem in Lieu of Subsistence
Taxable Meals
Lodging
Public Carrier
State Fire Academy
000-00-0000
Check One:
John Q. Public
Dates Go Here
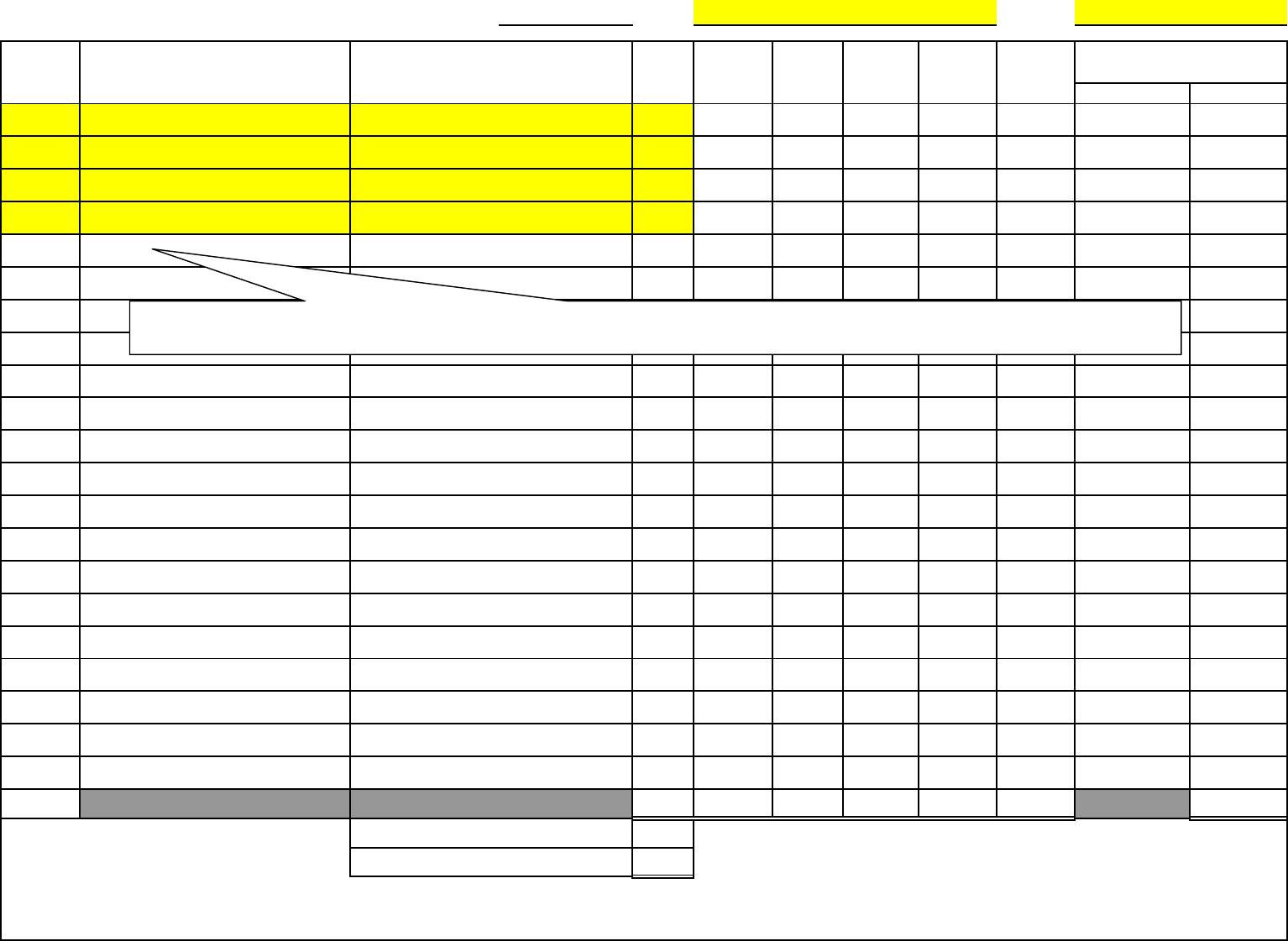
Itemized Statement of Travel Expense SPAHRS Ag #: 502 SS#:
Daily
Actual Actual Actual Meals
Date Purpose Points of Travel Miles Breakfast Lunch Dinner Allowed Hotel Item Amount
1/1/09 Teach Automobile Extrication-Clay County 150
1/2/09 Teach Automobile Extrication-Clay County 150
1/3/09 Teach Automobile Extrication-Clay County 150
1/4/09 Teach Automobile Extrication-Clay County 150
Total 600.00 0.00 0.00 0.00 0.00 0.00 0.00
0.50
300.00
Note: (1) Receipts for amounts paid for lodging and other expenses must accompany this voucher. (2) All activity pertaining to a certain date should be shown on the associated line or
lines completely across the form. (3) Daily Meals Allowed equals the total of Actual Meals, not to exceed the Maximum Daily Meal Reimbursement. (4) If Tips are included in Other,
then the type of tip must be identified. (5) A continuation sheet may be used if necessary.
Other Authorized Expenses
John Q. Public
Brandon-West Point-Brandon
#REF!
Brandon-West Point-Brandon
Brandon-West Point-Brandon
Brandon-West Point-Brandon
Mileage Reimbursement Rate
Total Mileage Dollar Amount
Purpose: LIST CLASS NAME and LOCATION IN COLUMN
Points of Travel: LIST STARTING POINT, DESTINATION, RETURN LOCATION (IF ALL IN SAME DAY)
