CMS 1500 ICD 10 WYOMING Manual CMS1500 4 1 17
User Manual:
Open the PDF directly: View PDF ![]() .
.
Page Count: 366 [warning: Documents this large are best viewed by clicking the View PDF Link!]

DIVISION OF HEALTHCARE FINANCING
CMS 1500 ICD-10
April 1, 2017

General Information____________________________________________________________
CMS 1500 ii Revision 4/1/17
Overview
Thank you for your willingness to serve clients of the Medicaid Program and other
medical assistance programs administered by the Division of Healthcare Financing.
This manual supersedes all prior versions.
Rule References
Providers must be familiar with all current rules and regulations governing the
Medicaid Program. Provider manuals are to assist providers with billing Medicaid;
they do not contain all Medicaid rules and regulations. Rule citations in the text are
only a reference tool. They are not a summary of the entire rule. In the event that the
manual conflicts with a rule, the rule prevails. Wyoming State Rules may be located
at, http://soswy.state.wy.us/Rules/default.aspx.

General Information____________________________________________________________
CMS 1500 iii Revision 4/1/17
Importance of Fee Schedules and Provider’s Responsibility
Procedure codes listed in the following Sections are subject to change at any time
without prior notice. The most accurate way to verify coverage for a specific service
is to review the Medicaid fee schedules on the website (2.1, Quick Reference). Fee
schedules list Medicaid covered codes, provide clarification of indicators, such as
whether a code requires prior authorization and the number of days in which follow-
up procedures are included. Not all codes are covered by Medicaid or are allowed for
all taxonomy codes (provider types). It is the provider’s responsibility to verify this
information. Use the current fee schedule in conjunction with the more detailed
coding descriptions listed in the current CPT-4 and HCPCS Level II coding books.
Remember to use the fee schedule and coding books that pertain to the appropriate
dates of service. Wyoming Medicaid is required to comply with the coding
restrictions under the National Correct Coding Initiative (NCCI) and providers should
be familiar with the NCCI billing guidelines. NCCI information may be reviewed at
http://www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/index.html.
Getting Questions Answered
The provider manuals are designed to answer most questions; however, questions
may arise that require a call to a specific department such as Provider Relations or
Medical Policy (2.1, Quick Reference).
Medicaid manuals, bulletins, fee schedules, forms, and other resources are available
on the Medicaid website or by contacting Provider Relations.

General Information____________________________________________________________
CMS 1500 iv Revision 4/1/17
AUTHORITY
The Wyoming Department of Health is the single state agency appointed as required in the Code
of Federal Regulations (CFR) to comply with the Social Security Act to administer the Medicaid
Program in Wyoming. The Division of Healthcare Financing (DHCF) directly administers the
Medicaid Program in accordance with the Social Security Act, the Wyoming Medical Assistance
and Services Act, (W.S. 42-4-101 et seq.), and the Wyoming Administrative Procedure Act
(W.S. 16-3-101 et seq.). Medicaid is the name chosen by the Wyoming Department of Health for
its Medicaid Program.
This manual is intended to be a guide for providers when filing medical claims with Medicaid.
The manual is to be read and interpreted in conjunction with Federal regulations, State statutes,
administrative procedures, and Federally approved State Plan and approved amendments. This
manual does not take precedence over Federal regulation, State statutes or administrative
procedures.

General Provider Information____________________________________________________
CMS 1500 v Revision 4/1/17
Contents:
Contents: v
Chapter One – General Information .......................................................................... 1
Chapter Two – Getting Help When You Need It ...................................................... 6
Chapter Three – Provider Responsibilities ..............................................................15
Chapter Four – Utilization Review ..........................................................................32
Chapter Five – Client Eligibility ..............................................................................39
Chapter Six – Common Billing Information ...........................................................46
Chapter Seven – Third Party Liability ...................................................................112
Chapter Eight – Electronic Data Interchange (EDI) ..............................................124
Chapter Nine – Wyoming HIPAA 5010 Electronic Specifications ......................132
Chapter Ten – Important Information ....................................................................154
Chapter Eleven – Covered Services – Ambulance ................................................158
Chapter Twelve – Covered Services – Audiology.................................................166
Chapter Thirteen – Covered Services – Behavioral Health ...................................170
Chapter Fourteen – Covered Services – Children’s Mental Health Waiver .........207
Chapter Fifteen – Covered Services – Chiropractic Services ................................210
Chapter Sixteen – Covered Services – Developmental Centers ............................214
Chapter Seventeen – Covered Services – Dietician ..............................................221
Chapter Eighteen – Covered Services – DME Billing ..........................................224
Chapter Nineteen – Covered Services – Family Planning .....................................228
Chapter Twenty – Covered Services – Health Check ...........................................230
Chapter Twenty One – Covered Services – Interpreter Services ..........................245
Chapter Twenty Two – Covered Services – Laboratory Services .........................248
Chapter Twenty Three – Covered Services – Non-Emergency Medical
Transportation ........................................................................................................253

General Provider Information____________________________________________________
CMS 1500 vi Revision 4/1/17
Chapter Twenty Four – Covered Services – Practitioner Services .......................257
Chapter Twenty Five – Covered Services – Pregnant by Choice ..........................334
Chapter Twenty Six – Covered Services – Therapy Services ...............................339
Appendix 346

General Provider Information____________________________________________________
Ch. 1 Index 1 Revision 4/1/17
Chapter One – General Information
1.1 How the CMS-1500 Manual is Organized ............................................................ 1
1.2 Updating the Manual ............................................................................................. 2
1.2.1 RA Banner Notices/Samples ................................................................................. 3
1.2.2 Medicaid Bulletin Notification/Sample ................................................................. 4
1.2.3 Wyoming Department of Health (WDH) State Letter/Sample ............................. 4
1.3 State Agency Responsibilities ............................................................................... 5
1.4 Fiscal Agent Responsibilities ................................................................................ 5
General Provider Information____________________________________________________
Ch. 1 Index 1 Revision 4/1/17
1.1 How the CMS-1500 Manual is Organized
The table below provides a quick reference describing how the CMS-1500 Manual is
organized.
Chapter
Description
Two
Getting Help When You Need It – Quick Reference guide, telephone
numbers and addresses and web sites for help and training.
Three
Provider Responsibilities – Obligations and rights as a Medicaid
provider. The topics covered include enrollment changes, civil rights,
group practices, provider-patient relationship, and record keeping
requirements.
Four
Utilization Review – Fraud and abuse definitions, the review process,
and rights and responsibilities.
Five
Client Eligibility – How to verify eligibility when a client presents their
Medicaid card.
Six
Common Billing Information – Basic claim information, completing
the claim form, cap limits, co-pays, prior authorizations, timely filing,
consent forms, NDC, working the Medicaid remittance advice (RA) and
completing adjustments.
Seven
Third Party Liability (TPL)/Medicare – Explains what TPL/Medicare
is, how to bill it and exceptions to it.
Eight
Electronic Data Interchange (EDI) – Explains the advantages of
exchanging documents electronically. Secured Provider Web Portal
registration process.
Nine
Wyoming Specific HIPAA 5010 Electronic Specifications – This
chapter covers the Wyoming Specific requirements pertaining to
electronic billing. Wyoming payor number and electronic
adjustments/voids.
Ten
CMS-1500 Covered Services – This chapter is alphabetical by
professional service and provides information such as: definitions,
procedure code ranges, documentation requirements, covered and non-
covered services and billing examples.
Appendices
Appendices – Provide key information in an at-a-glance format. This
includes the Provider Manual Version Control Table, and last quarters
Provider Notifications.
General Provider Information____________________________________________________
Ch. 1 Index 2 Revision 4/1/17
1.2 Updating the Manual
When there is a change in the Medicaid Program, Medicaid will update the manuals
on a quarterly (January, April, July, and October) basis and publish them to the
Medicaid website. Most of the changes come in the form of provider bulletins (via
email) and Remittance Advice (RA) banners, although others may be newsletters or
Wyoming Department of Health letters (via email) from state officials. The updated
provider manuals will be posted to the website and will include all updates from the
previous quarter. It is in the provider’s best interest to download an updated provider
manual and keep their email addresses up-to-date. Bulletin, RA banner, newsletter
and state letter information will be posted to the website as it is sent to providers, and
will be incorporated into the provider manuals as appropriate to ensure the provider
has access to the most up to date information regarding Medicaid policies and
procedures.
RA banner notices appear on the first page of the proprietary Wyoming Medicaid
Remittance Advice (RA), which is available for download through the Secured
Provider Web Portal after each payment cycle in which the provider has claims
processed or “in process”. This same notice also appears on the RA payment
summary email that is sent out each week after payment, and is published to the
“What’s New” section of the website.
It is critical for providers to keep their contact email address(es) up-to-date to ensure
they receive all notices published by Wyoming Medicaid. It is recommended that
providers add the “wycustomersvcs@acs-inc.com” email address from which notices
are sent to their address books to avoid these emails being inadvertently sent to junk
or spam folders.
All bulletins and updates are published to the Medicaid website (2.1, Quick
Reference).
NOTE: Provider bulletins and state letter email notifications are sent to the email
addresses on-file with Medicaid and are sent in two (2) formats, plain text
and HTML. If the HTML format is received or accepted then the plain text
format is not sent.

General Provider Information____________________________________________________
Ch. 1 Index 3 Revision 4/1/17
1.2.1 RA Banner Notices/Samples
RA banners are limited in space and formatting options and are used to notify
providers quickly and often refer providers elsewhere for additional information.
Sample RA Banner:
************************************************************************
ICD-10 IMPLEMENTATION OCTOBER 1, 2015
EXPECT:
1) LONGER WAIT TIMES WHEN CALLING PROVIDER RELATIONS OR EDI SERVICES
2) INCREASED POSSIBILITY OF RECEIVING A BUSY DISCONNECT WHEN
EXITING THE IVR
3) DO NOT EXPECT THE AGENTS TO PROVIDE ICD-10 CODES
TROUBLESHOOTING TIPS PRIOR TO CALLING THE CALL CENTERS:
1) IF YOUR SOFTWARE OR VENDOR/CLEARINGHOUSE IS NOT ICD-10 READY--FREE
SOFTWARE AVAILABLE ON THE WY MEDICAID WEBSITE (CANNOT DROP TO PAPER)
2) ICD-10 DX/SURGICAL DENIALS, VERIFY FIRST: CODES ARE BOTH ALPHA & NUMERIC,
DX QUALIFIER, O VS 0, 1 VS I
3) VERIFY DOS, PRIOR TO 10/1/15 BILL WITH ICD-9 AND ON OR AFTER 10/1/15 BILL WITH
ICD-10 CODES
4) INPATIENT SERVICES THAT SPAN 9/2015-10/2015 BILL WITH ICD-10
HTTP://WYMEDICAID. ACS-INC.COM/PROVIDER_HOME.HTML
**************************************************************************
Sample RA Payment Summary (weekly email notification):
-----Original Message-----
From: Wyoming Medicaid [mailto:wycustomersvc@xerox.com]
Sent: Thursday, May 28, 2015 5:17 AM
To: Provider Email Name
Subject: Remittance Advice Payment Summary
On 05/27/2015, at 05:16, Wyoming Medicaid wrote:
Dear Provider Name,
The following is a summary of your Wyoming Medicaid remittance advice 123456 for 05/27/2015, an RA
Banner with important information may follow.
*****************************************************
RA PAYMENT SUMMARY
*****************************************************
To: Provider Name
NPI Number: 1234567890
Provider ID: 111111111
Remittance Advice Number: 123456
Amount of Check: 16,070.85
The RA banner notification will appear here when activated for the provider’s taxonomy (provider type)

General Provider Information____________________________________________________
Ch. 1 Index 4 Revision 4/1/17
1.2.2 Medicaid Bulletin Notification/Sample
Medicaid bulletin email notifications typically announce billing changes, new codes
requiring prior authorization, reminders, up and coming initiatives, etc.
Sample bulletin email notification (HTML format):
1.2.3 Wyoming Department of Health (WDH) State Letter/Sample
WDH email notifications typically announce significant Medicaid policy changes,
RAC and other audits, etc.
Sample WDH email notification (HTML format):
General Provider Information____________________________________________________
Ch. 1 Index 5 Revision 4/1/17
1.3 State Agency Responsibilities
The Division of Healthcare Financing administers the Medicaid Program for the
Department of Health. They are responsible for financial management, developing
policy, establishing benefit limitations, payment methodologies and fees, and
performing utilization review.
1.4 Fiscal Agent Responsibilities
Conduent is the fiscal agent for Medicaid. They process all claims and adjustments,
with the exception of pharmacy. They also answer provider inquiries regarding claim
status, payments, client eligibility, known third party insurance information and
provider training visits to train and assist the provider office staff on Medicaid billing
procedures or to resolve claims payment issues.
NOTE: Wyoming Medicaid is not responsible for the training of the provider’s
billing staff or to provide procedure or diagnosis codes or coding training.

Getting Help When You Need It__________________________________________________
Ch.2 Index 6 Revision 4/1/17
Chapter Two – Getting Help When You Need It
2.1 Quick Reference .................................................................................................... 7
2.2 How to Call for Help ........................................................................................... 11
2.3 How to Write for Help ......................................................................................... 11
2.3.1 Provider Inquiry Form ......................................................................................... 12
2.4 How to Get a Provider Training Visit ................................................................. 12
2.5 How to Get Help Online ...................................................................................... 13
2.6 Training Seminars/Presentations ......................................................................... 13

Getting Help When You Need It__________________________________________________
Ch.2 Index 7 Revision 4/1/17
2.1 Quick Reference
Agency Name &
Address
Telephone/Fax
Numbers
Web Address
Contact For:
Dental Services –
Interactive Voice
Response (IVR)
System
Tel (800)251-1270
24 / 7
N/A
Payment inquiries
Client eligibility
Medicaid client number and
information
Lock-in status
Cap limits
Medicare Buy-In data
Service limitations
Client third party coverage
information
NOTE: The client’s Medicaid ID
number or social security
number is required to verify
client eligibility.
Claims
PO Box 547
Cheyenne, WY
82003-0547
N/A
N/A
Claim adjustment submissions
Hardcopy claims submissions
Returning Medicaid checks
Dental Service
PO Box 667
Cheyenne, WY
82003-0667
Tel (888)863-5806
9-5pm MST M-F
Fax (307)772-8405
http://wymedicaid.acs-
inc.com/
Bulletin/manual inquiries
Claim inquiries
Claim submission problems
Client eligibility
How to complete forms
Payment inquiries
Request Field Representative visit
Training seminar questions
Timely filing inquiries
Verifying validity of procedure
codes
Claim void/adjustment inquiries
WINASAP training
Web Portal training
EDI Services
PO Box 667
Cheyenne, WY
82003-0667
Tel (800)672-4959
OPTION 3
9-5pm MST M-F
Fax (307)772-8405
http://wymedicaid.acs-
inc.com/
EDI Enrollment Forms
Trading Partner Agreement
WINASAP software
Technical support for WINASAP
Technical support for vendors,
billing agents and clearing houses
Web Portal registration/password
resets
Technical support for Web Portal
ACS EDI
Gateway
N/A
http://www.acs-gcro.com
Download WINASAP software

Getting Help When You Need It__________________________________________________
Ch.2 Index 8 Revision 4/1/17
Agency Name &
Address
Telephone/Fax
Numbers
Web Address
Contact For:
Medical Policy
PO Box 667
Cheyenne, WY
82003-0667
Tel (800)251-1268
OPTIONS 1,1,4,3
9-5pm MST M-F
(24/7 Voicemail
Available)
Fax (307)772-8405
http://wymedicaid.acs-
inc.com/manuals.html
Cap limit waiver requests
Prior authorization requests for:
Out-of-State Home Health
Surgeries requiring prior
authorization
Hospice Services: Limited to clients
residing in a nursing home
Provider
Relations
PO Box 667
Cheyenne, WY
82003-0667
(IVR Navigation
Tips available on
the website)
Tel (800)251-1268
9-5pm MST M-F
(call center hours)
Fax (307)772-8405
24 / 7
(IVR availability)
http://wymedicaid.acs-
inc.com/
http://wymedicaid.acs-
inc.com/contact.html
Provider enrollment questions
Bulletin/Manuals inquiries
Cap limits
Claim inquiries
Claim submission problems
Client eligibility
Claim void/adjustment inquiries
Form completion
Payment inquiries
Request Field Representative visit
Training seminar questions
Timely filing inquiries
Troubleshooting prior authorization
problems
Verifying validity of procedure codes
Third Party
Liability (TPL)
PO Box 667
Cheyenne, WY
82003-0667
Tel (800)251-1268
OPTION 2
9-5pm MST M-F
Fax (307)772-8405
Select Option 2 if you
need Medicare or
estate and trust
recovery assistance
THEN
Select Option 2 if you
are with an insurance
company, attorney’s
office or child support
enforcement
OR
Select Option 3 for
Medicare and
Medicare Premium
payments
OR
Select Option 4 for
estate and trust
recovery inquires
N/A
Client accident covered by liability
or casualty insurance or legal
liability is being pursued
Estate and Trust Recovery
Medicare Buy-In status
Reporting client TPL
New insurance coverage
Policy no longer active
Problems getting insurance
information needed to bill
Questions or problems regarding
third party coverage or payers
WHIPP program
Getting Help When You Need It__________________________________________________
Ch.2 Index 9 Revision 4/1/17
Agency Name &
Address
Telephone/Fax
Numbers
Web Address
Contact For:
Transportation
Services
PO Box 667
Cheyenne, WY
82003-0667
Tel (800)595-0011
9-5pm MST M-F
(24/7 Voicemail
Available)
Fax (307)772-8405
http://wymedicaid.acs-
inc.com/client/
Client inquiries:
Prior authorize transportation
arrangements
Request travel assistance
Verify transportation is reimbursable
Qualis Health
DMEPOS
PO Box 33400
Seattle, WA
98133
Tel (800)783-8606
8a-6pm MST M-F
Fax (877)810-9265
http://www.qualishealth.org/
DMEPOS Covered Services manual
Prior authorization request for
Durable Medical Equipment (DME)
or Prosthetic/Orthotic Services
(POS)
Questions related to documentation
or clinical criteria for DMEPOS
WYhealth
(Utilization and
Care
Management)
PO Box 49
Cheyenne, WY
82003-0049
Tel (888)545-1710
Nurse Line:
(OPTION 2)
Fax PASRRs Only
(888)245-1928
(Attn: PASRR
Processing Specialist)
http://www.WYhealth.net/
Medicaid Incentive Programs
Diabetes Incentive Program
ER Utilization Program
P4P
SBIRT
Educational Information about
WYhealth Programs
Prior authorization for:
Acute Psych
Extended Psych
Extraordinary heavy care
Gastric Bypass
Inpatient rehabilitation
Psychiatric Residential Treatment
Facility (PRTF)
Transplants
Vagus Nerve Stimulator
Aids Drug
Assistance
Program (ADAP)
Tel (307)777-5800
Fax (307)777-7382
N/A
1) Prescription medications
2) Program information
Maternal & Child
Health (MCH)
/Children Special
Health (CSH)
6101 N.
Yellowstone Rd.
Ste. 420
Cheyenne, WY
82002
Tel (307)777-7941
Tel (800)438-5795
Fax (307)777-7215
N/A
High Risk Maternal
Newborn intensive care
Program information
Severe
Malocclusion
Tel (307)777-8088
Fax (307)777-6964
N/A
Severe Malocclusion Applications
and Criteria
Social Security
Administration
(SSA)
Tel (800)772-1213
N/A
Social Security benefits
Medicare
Tel (800)633-4227
N/A
Medicare information
Getting Help When You Need It__________________________________________________
Ch.2 Index 10 Revision 4/1/17
Agency Name &
Address
Telephone/Fax
Numbers
Web Address
Contact For:
Division of
Healthcare
Financing
(DHCF)
6101
Yellowstone Rd.
Ste. 210
Cheyenne, WY
82002
Tel (307)777-7531
Tel (866)571-0944
Fax (307)777-6964
http://www.health.wyo.gov
/healthcarefin/index.html
Medicaid State Rules
State Policy and Procedures
Concerns/Issues with state
Contractors/Vendors
DHCF Program
Integrity
6101
Yellowstone Rd.
Ste. 210
Cheyenne, WY
82002
Tel (855)846-2563
N/A
Client or Provider Fraud, Waste and
Abuse
NOTE: Callers may remain
anonymous when reporting
Stop Medicaid
Fraud
Tel (855)846-2563
http://stopmedicaidfraud.w
yo.gov
Information and education
regarding fraud, waste, and abuse in
the Wyoming Medicaid program
To report fraud, waste and abuse
DHCF Pharmacy
Program
6101
Yellowstone Rd.
Ste. 210
Cheyenne, WY
82002
Tel (307)777-7531
Fax (307)777-6964
N/A
General questions
Goold Health
Systems, Inc.
(GHS)
PBM Vendor
Tel (877)209-1264
(Pharmacy Help
Desk)
Tel (877)207-1126
(PA Help Desk)
http://www.wymedicaid.org/
Pharmacy prior authorization
Enrollment
Pharmacy manuals
FAQs
Customer Service
Center (CSC) ,
Wyoming
Department of
Health
2232 Dell Range
Blvd, Suite 300
Cheyenne, WY
82009
Tel (855)294-2127
TTY/TDD
(855)29-5205
(Clients Only, CSC
cannot speak to
providers)
7-6pm MST M-F
Fax (855)329-5205
www.wesystem.wyo.gov
Client Medicaid applications
Eligibility questions regarding:
1) Family and Children’s programs
2) Tuberculosis Assistance Program
3) Medicare Savings Programs
4) Employed Individuals with
Disabilities
Wyoming
Department of
Health Long
Term Care Unit
(LTC)
Tel (855)203-2936
8-5pm MST M-F
Fax (307)777-8399
N/A
Nursing home program eligibility
questions
Patient Contribution
Waiver Programs
Inpatient Hospital
Hospice
Home Health

Getting Help When You Need It__________________________________________________
Ch.2 Index 11 Revision 4/1/17
Agency Name &
Address
Telephone/Fax
Numbers
Web Address
Contact For:
Wyoming
Medicaid
N/A
http://wymedicaid.acs-
inc.com
Provider manuals
HIPAA electronic transaction data
exchange
Fee schedules
On-line Provider Enrollment
Frequently asked questions (FAQs)
Forms (e.g., Claim
Adjustment/Void Request Form)
Contacts
What’s new
Remittance Advice Retrieval
EDI enrollment form
Trading Partner Agreement
Secured Provider Web Portal
Training Tutorials
HealthHelp
Tel (888) 545-1710
Option 2
https://wyhealth.net
PA’s for Radiology, Cardiology
and Radiation Oncology
2.2 How to Call for Help
The fiscal agent maintains a well-trained call center that is dedicated to assisting
providers. These individuals are prepared to answer inquiries regarding client
eligibility, service limitations, third party coverage, electronic transaction questions
and provider payment issues.
2.3 How to Write for Help
In many cases, writing for help provides the provider with more detailed information
about the provider claims or clients. In addition, written responses may be kept as
permanent records.
Reasons to write vs. calling:
Appeals – Include claim, all documentation previously submitted with the
claim, explanation for request, documentation supporting the request.
Written documentation of answers – Include all documentation to support
the provider request.
Rate change requests – Include request and any documentation supporting
the provider request.
Requesting a service to be covered by Wyoming Medicaid – Include
request and any documentation supporting the provider request.
To expedite the handling of written inquiries, we recommend providers use a
Provider Inquiry Form (2.3.1, Provider Inquiry Form). Providers may copy the form
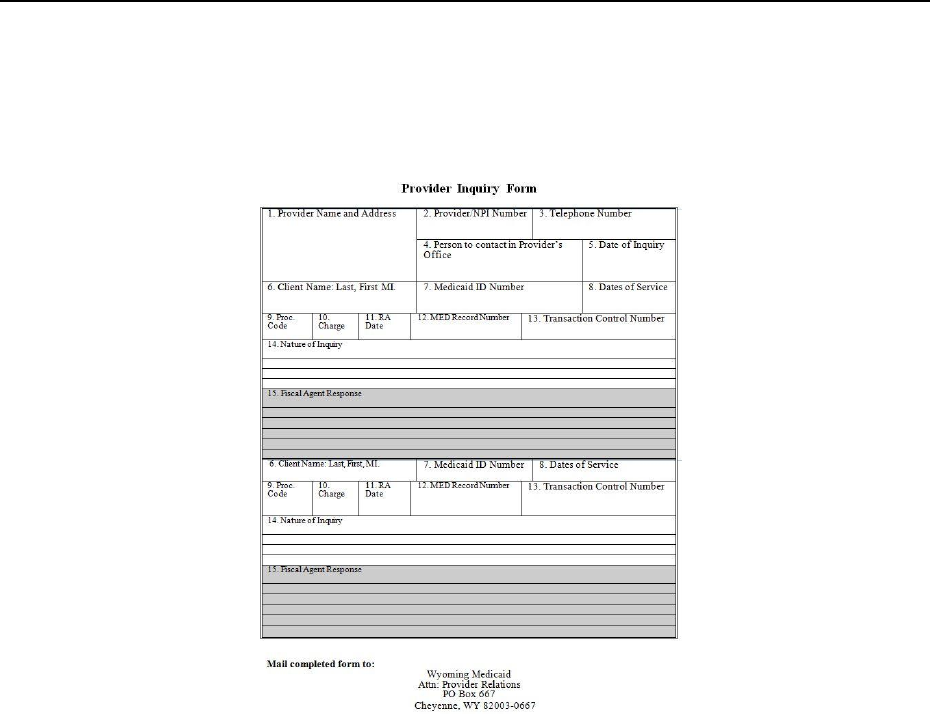
Getting Help When You Need It__________________________________________________
Ch.2 Index 12 Revision 4/1/17
in this manual. Provider Relations will respond to the provider inquiry within ten
business days of receipt.
2.3.1 Provider Inquiry Form
NOTE: Click image above to be taken to a printable version of this form.
2.4 How to Get a Provider Training Visit
Provider Relations Field Representatives are available to train or address questions
the provider’s office staff may have on Medicaid billing procedures or to resolve
claims payment issues.
Provider Relations Field Representatives are available to assist providers with help in
their location, by phone, or webinar with Wyoming Medicaid billing questions and
issues. Generally, to assist a provider with claims specific questions, it is best for the
Field Representative to communicate via phone or webinar as they will then have
access to the systems and tools needed to review claims and policy information.
Provider Training visits may be conducted when larger groups are interested in
training related to Wyoming Medicaid billing. When conducted with an individual
provider’s office, a Provider Training visit generally consists of a review of a
provider’s claims statistics, including top reasons for denials and denial rates, and a
review of important Medicaid training and resource information. Provider Training
Workshops may be held during the summer months to review this information in a
larger group format.
Getting Help When You Need It__________________________________________________
Ch.2 Index 13 Revision 4/1/17
Due to the rural and frontier nature, and weather in Wyoming, visits are generally
conducted during the warmer months only. For immediate assistance, a provider
should always contact Provider Relations (2.1, Quick Reference).
2.5 How to Get Help Online
The address for Medicaid’s public website is http://wymedicaid.acs-inc.com. This site
connects Wyoming’s provider community to a variety of information including:
Answers to the providers frequently asked Medicaid questions.
Claim, prior authorization, and other forms for download.
Free download of latest WINASAP software and latest WINASAP updates.
Free download of WINASAP Training Manuals and Tutorials.
Medicaid publications, such as provider handbooks and bulletins.
Payment Schedule.
Primary resource for all information related to Medicaid.
Wyoming Medicaid Secured Provider Web Portal.
Wyoming Medicaid Secured Provider Web Portal tutorials.
The Medicaid public website also links providers to Medicaid’s Secured Provider
Web Portal, which delivers the following services:
278 Electronic Prior Authorization Requests – Ability to submit and
retrieve prior authorization requests and responses electronically via the web.
Data Exchange – Upload and download of electronic HIPAA transaction
files.
Remittance Advice Reports – Retrieve recent Remittance Advices
o Wyoming Medicaid proprietary RA
835
User Administration – Add, edit, and delete users within the provider’s
organization who can access the Secured Provider Web Portal.
837 Electronic Claim Entry – Interactively enter dental, institutional and
medical claims without buying expensive software.
PASRR entry
LT101 Look-Up
2.6 Training Seminars/Presentations
The fiscal agent and the Division of Healthcare Financing may sponsor periodic
training seminars at selected in-state and out-of-state locations. Providers will receive
advance notice of seminars by Medicaid bulletin email notifications, provider


Provider Responsibilities________________________________________________________
Ch. 3 Index 15 Revision 4/1/17
Chapter Three – Provider Responsibilities
3.1 Enrollment/Re-Enrollment .................................................................................. 16
3.1.1 Notifying Medicaid of Updated Provider Information ........................................ 18
3.1.2 Re-Certification ................................................................................................... 19
3.1.3 Discontinuing Participation in the Medicaid Program ........................................ 19
3.2 Accepting Medicaid Clients ................................................................................ 19
3.2.1 Compliance Requirements .................................................................................. 19
3.2.2 Provider-Patient Relationship .............................................................................. 19
3.2.2.1 Medicare/Medicaid Dual Eligible Clients ....................................................... 21
3.2.2.2 Accepting a Client as Medicaid After Billing the Client ................................. 22
3.2.2.3 Mutual Agreements Between the Provider & Client ....................................... 22
3.2.3 Missed Appointments .......................................................................................... 22
3.3 Medicare Covered Services ................................................................................. 23
3.4 Medical Necessity ............................................................................................... 23
3.5 Medicaid Payment is Payment in Full ................................................................. 24
3.6 Medicaid ID Card ................................................................................................ 25
3.7 Verification of Client Age ................................................................................... 25
3.8 Verification Options ............................................................................................ 25
3.8.1 Free Services ....................................................................................................... 25
3.8.2 Fee for Service ..................................................................................................... 26
3.9 Freedom of Choice .............................................................................................. 26
3.10 Out-of-State Service Limitations ......................................................................... 26
3.11 Record Keeping, Retention and Access .............................................................. 27
3.11.1 Requirements ....................................................................................................... 27
3.11.2 Retention of Records ........................................................................................... 28
3.11.3 Access to Records ............................................................................................... 28
3.11.4 Audits .................................................................................................................. 28
3.12 Tamper Resistant RX Pads .................................................................................. 30
Provider Responsibilities________________________________________________________
Ch. 3 Index 16 Revision 4/1/17
3.1 Enrollment/Re-Enrollment
Medicaid payment is made only to providers who are actively enrolled in the
Medicaid Program. Providers are required to complete an enrollment application,
undergo a screening process and sign a Provider Agreement at least every five (5)
years. In addition, certain provider types are required to pay an application fee,
submit proof of licensure and/or certification. These requirements apply to both in-
state and out-of-state providers.
All providers have been assigned one (1) of three (3) categorical risk levels under the
Affordable Care Act (ACA) and are required to be screened as follows:
Categorical Risk Level
Screening Requirements
LIMITED
Includes:
Physician and nonphysican practitioners,
(includes nurse practitioners, CRNAs,
occupational therapists, speech/language
pathologist audiologists) and medical groups
or clinics
Ambulatory surgical centers
Competitive Acquisition Program/Part B
Vendors:
End-stage renal disease facilities
Federally qualified health centers (FQHC)
Histocompatibility laboratories
Hospitals, including critical access hospitals,
VA hospitals, and other federally-owned
hospital facilities
Health programs operated by an Indian
Health program
Mammography screening centers
Mass immunization roster billers
Organ procurement organizations
Pharmacy newly enrolling or revalidating
via the CMS-855B application
Radiation therapy centers
Religious non-medical health care
institutions
Rural health clinics
Skilled nursing facilities
Verifies provider or supplier meets all applicable Federal regulations and
State requirements for the provider or supplier type prior to making an
enrollment determination
Conducts license verifications, including licensure verification across
State lines for physicians or non-physician practitioners and providers
and suppliers that obtain or maintain Medicare billing privileges as a
result of State licensure, including State licensure in States other than
where the provider or supplier is enrolling
Conducts database checks on a pre- and post-enrollment basis to ensure
that providers and suppliers continue to meet the enrollment criteria for
their provider/supplier type.
MODERATE
Includes:
Ambulance service suppliers
Community mental health centers (CMHC)
Comprehensive outpatient rehabilitation
facilities (CORF)
Hospice organizations
Independent diagnostic testing facilities
Physical therapists enrolling as individuals
or as group practices
Portable x-ray suppliers
Revalidating home health agencies
Revalidating DMEPOS suppliers
Performs the “limited” screening requirements listed above
Conducts an on-site visit
Provider Responsibilities________________________________________________________
Ch. 3 Index 17 Revision 4/1/17
Categorical Risk Level
Screening Requirements
HIGH
Includes:
Prospective (newly enrolling) home
health agencies
Prospective (newly enrolling)
DMEPOS suppliers
Prosthetic/orthotic (newly enrolling)
suppliers
Individual practitioners suspected of
identity theft, placed on previous
payment suspension, previously
excluded by the OIG, and/or
previously had billing privileges
denied or revoked within the last ten
(10) years
Performs the “limited” and “moderate” screening requirements listed
above.
Requires the submission of a set of fingerprints for a national
background check from all individuals who maintain a five (5) percent
or greater direct or indirect ownership interest in the provider or supplier.
Conducts a fingerprint-based criminal history record check of
the FBI’s Integrated Automated Fingerprint Identification
System on all individuals who maintain a five (5 percent or
greater direct or indirect ownership interest in the provider or
supplier
Categorical Risk Adjustment:
CMS adjusts the screening level from limited or moderate to high if any
of the following occur:
Exclusion from Medicare by the OIG
Had billing privileges revoked by a Medicare contractor within
the previous ten (10) years and is attempting to establish
additional Medicare billing privilege by—
o Enrolling as a new provider or supplier
o Billing privileges for a new practice location
Has been terminated or is otherwise precluded from billing
Medicaid
Has been excluded from any Federal health care program
Has been subject to a final adverse action as defined in §424.502 within
the previous ten (10) years
The ACA has imposed an application fee on the following institutional providers:
In-state only
o Institutional Providers
o PRTFs
o Substance abuse centers (SAC)
o Wyoming Medicaid-only nursing facilities
o Community Mental Health Centers (CMHC)
o Wyoming Medicaid-only home health agencies (both newly enrolling
and re-enrolling)
Providers that are enrolled in Medicare, Medicaid in other states, and CHIP are only
required to pay one (1) enrollment fee. Verification of this payment must be included
with the enrollment application.
The application fee is required for:
New enrollments
Enrollments for new locations
Re-enrollments
Medicaid requested re-enrollments (as a result of inactive enrollment statuses)
Provider Responsibilities________________________________________________________
Ch. 3 Index 18 Revision 4/1/17
The application fee is non-refundable and is adjusted annually based on the Consumer
Price Index (CPI) for all urban consumers.
After a providers enrollment application has been approved, a welcome letter will be
sent.
If an application is not approved, a notice including the reasons for the decision will
be sent to the provider. No medical provider is declared ineligible to participate in the
Medicaid Program without prior notice.
To enroll as a Medicaid provider, all providers must complete the on-line enrollment
application available on the Medicaid website (2.1, Quick Reference).
3.1.1 Notifying Medicaid of Updated Provider Information
If any information listed on the original enrollment application subsequently changes,
providers must notify Medicaid in writing 30-days prior to the effective date of
the change. Changes that would require notifying Medicaid include, but are not
limited to, the following:
Current licensing information
Facility or name changes
New ownership information
New telephone or fax numbers
Physical, correspondence or payment address change
New email addresses
Tax Identification Number
It is critical that providers maintain accurate contact information, including email
addresses, for the distribution of notifications to providers. Wyoming Medicaid policy
updates and changes are distributed by email, and occasionally by postal mail.
Providers are obligated to read, know and follow all policy changes. Individuals who
receive notifications on behalf of an enrolled provider are responsible for ensuring
they are distributed to the appropriate personnel in the organization, office, billing
office, etc.
Effective September 1, 2016, if any of the above contact information is found to be
inaccurate (mail is returned, emails bounce, phone calls are unable to be placed or
physical site verification fails, etc.) the provider will be placed on a claims hold.
Claims will be held for 30 days pending an update of the information. A letter will be
sent to the provider, unless both the physical and correspondence addresses have had
mail returned, notifying them of the hold and describing options to update contact
information. If the information is updated within the 30 days, the claim will be
released to complete normal processing; if a claim is held for this reason for more
than 30 days, it will then be denied and the provider will have to resubmit once the
incorrect information is updated. The letter will document the information currently
on file with Wyoming Medicaid and allow you to make updates/changes as needed.
Provider Responsibilities________________________________________________________
Ch. 3 Index 19 Revision 4/1/17
3.1.2 Re-Certification
Sixty (60) days prior to licensure/certification expiration Medicaid sends all providers
a letter requesting a copy of their license or other certifications. If these documents
are not submitted within 60-days of their expiration date, the provider will be
terminated as a Medicaid provider.
3.1.3 Discontinuing Participation in the Medicaid Program
The provider may discontinue participation in the Medicaid Program at any time.
Thirty (30) days written notice of voluntary termination is requested.
Notices should be addressed to Provider Relations, attention Enrollment Services
(2.1, Quick Reference).
3.2 Accepting Medicaid Clients
3.2.1 Compliance Requirements
All providers of care and suppliers of services participating in the Medicaid Program
must comply with the requirements of Title VI of the Civil Rights Act of 1964, which
requires that services be furnished to clients without regard to race, color, or national
origin.
Section 504 of the Rehabilitation Act provides that no individual with a disability
shall, solely by reason of the handicap:
Be excluded from participation;
Be denied the benefits; or
Be subjected to discrimination under any program or activity receiving federal
assistance.
Each Medicaid provider, as a condition of participation, is responsible for making
provision for such individuals with a disability in their program activities.
As an agent of the Federal government in the distribution of funds, the Division of
Healthcare Financing is responsible for monitoring the compliance of individual
providers and, in the event a discrimination complaint is lodged, is required to
provide the Office of Civil Rights (OCR) with any evidence regarding compliance
with these requirements.
3.2.2 Provider-Patient Relationship
The relationship established between the client and the provider is both a medical and
a financial one. If a client presents himself/herself as a Medicaid client, the provider
must determine whether the provider is willing to accept the client as a Medicaid
patient before treatment is rendered.

Provider Responsibilities________________________________________________________
Ch. 3 Index 20 Revision 4/1/17
Providers must verify eligibility each month as programs and plans are re-
determined on a varying basis, and a client eligible one (1) month may not
necessarily be eligible the next month.
NOTE: Presumptive Eligibility may begin or end mid-month.
It is the provider’s responsibility to determine all sources of coverage for any client.
If the client is insured, by an entity other than Medicaid and Medicaid is unaware of
the insurance, the provider must submit a Third Party Resources Information Sheet
(7.7.1, Third Party Resources Information Sheet) to Medicaid. The provider may not
discriminate based on whether or not a client is insured.
Providers may not discriminate against Wyoming Medicaid clients. Providers must
treat Wyoming Medicaid clients the same as any other patient in their practice.
Policies must be posted or supplied in writing and enforced with all patients
regardless of payment source.
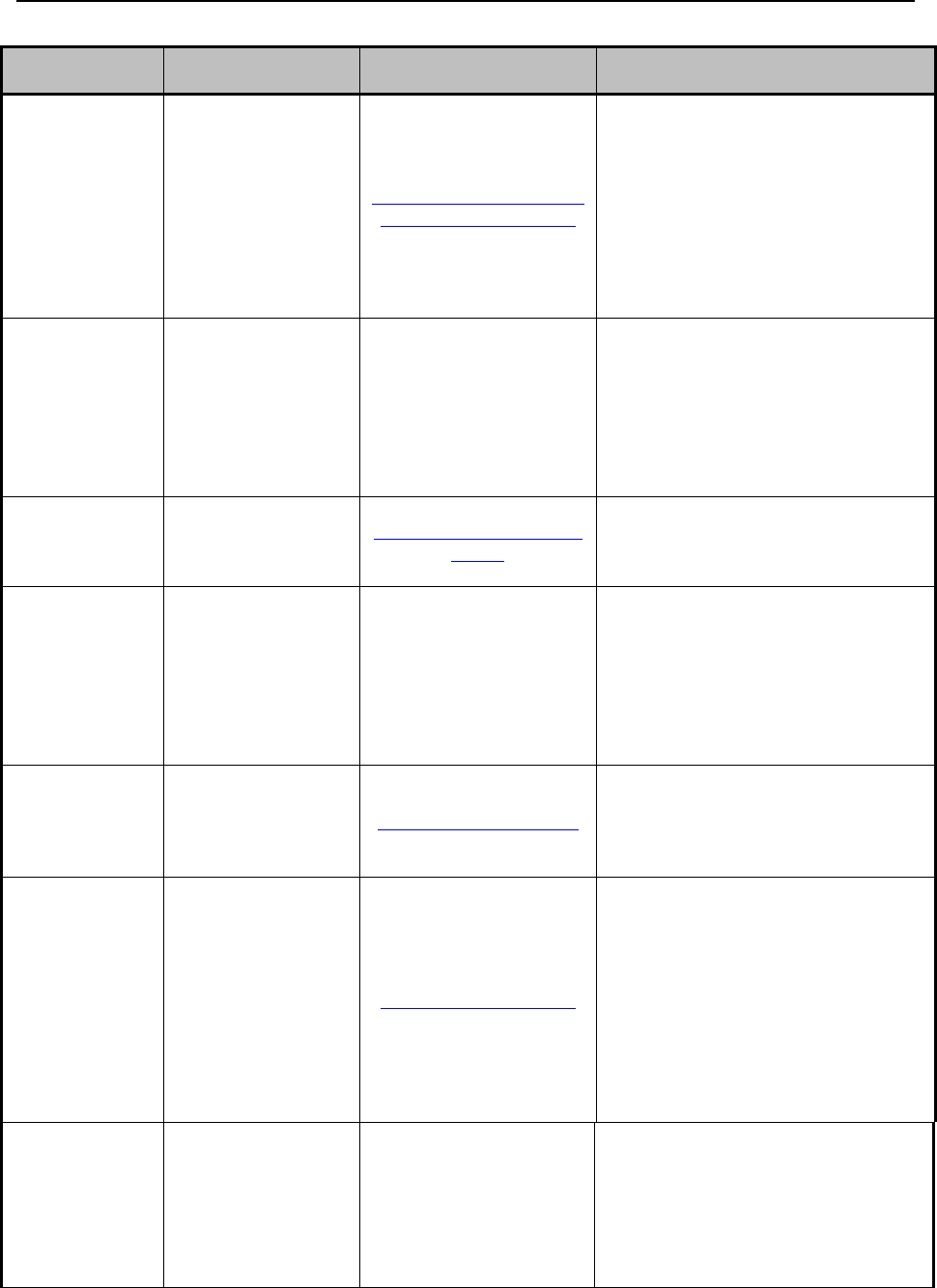
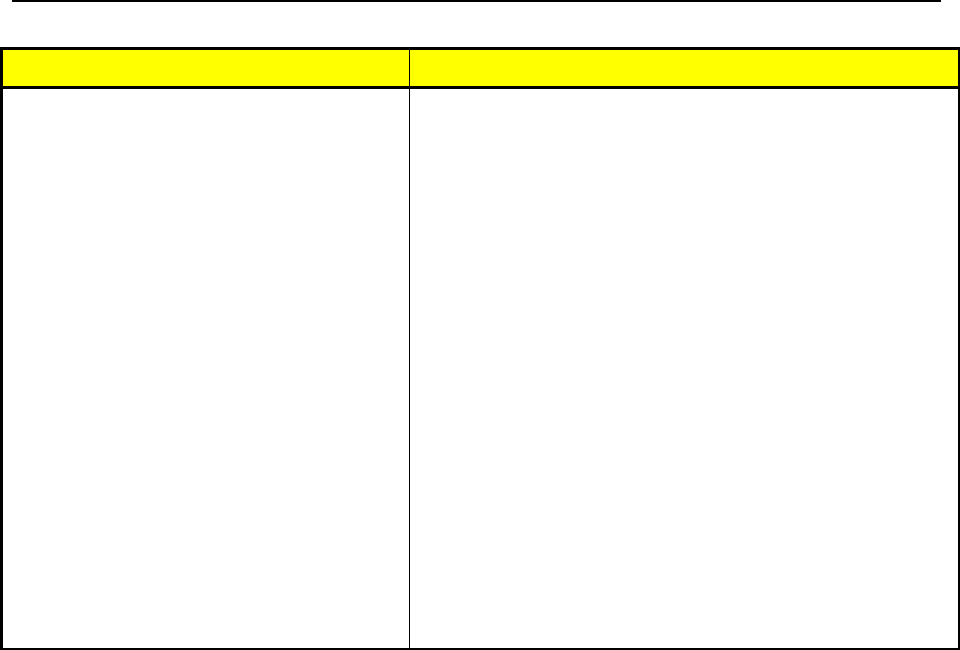
When and what may be billed to a Medicaid client.
Once this agreement has been reached, all Wyoming Medicaid covered services the
provider renders to an eligible client are billed to Medicaid.
Client is Covered
by a FULL
COVERAGE
Medicaid Program
and the provider
accepts the client as
a Medicaid client
Client is Covered by
a LIMITED
COVERAGE
Medicaid Program
and the provider
accepts the client as
a Medicaid client
FULL
COVERAGE or
LIMITED
COVERAGE
Medicaid Program
and the provider
does not accept the
client as a Medicaid
client
Client is not
covered by
Medicaid (not
a Medicaid
client)
Service is
covered by
Medicaid
Provider can bill the
client only for any
applicable copay
Provider can bill the
client if the category
of service is not
covered by the
client’s limited plan
Provider can bill the
client if written
notification has been
Provider may
bill client
Service is
covered by
Medicaid, but
client has
exceeded his/her
service
limitations (cap
limits)
Provider can bill the
client OR provider
Can request cap
limit waiver and bill
Medicaid
Provider can bill the
client OR provider
can request cap limit
waiver and bill
Medicaid
Provider can bill the
client if written
notification has been
given to the client
that they are not
being accepted as a
Medicaid client
Provider can
bill client
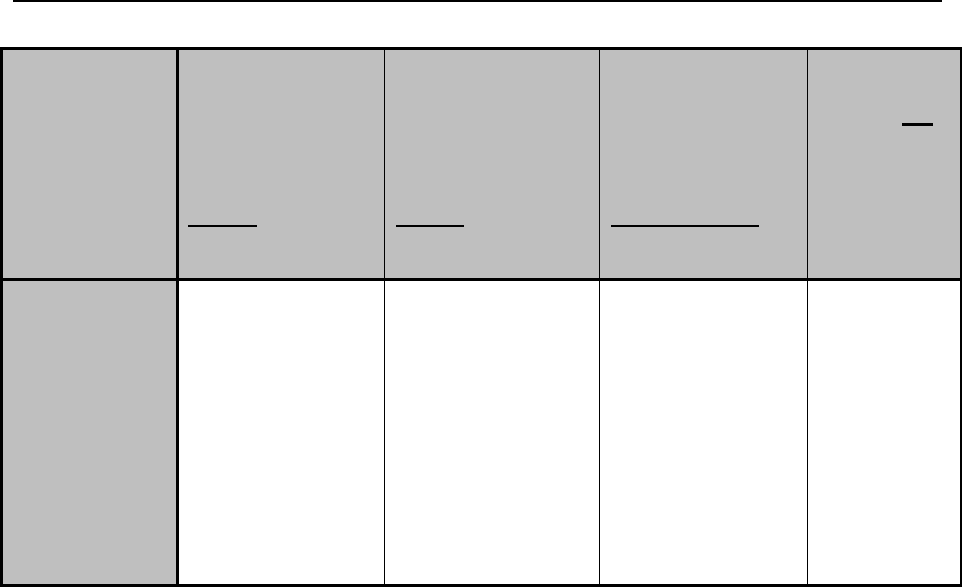
Provider Responsibilities________________________________________________________
Ch. 3 Index 21 Revision 4/1/17
Client is Covered
by a FULL
COVERAGE
Medicaid Program
and the provider
accepts the client as
a Medicaid client
Client is Covered by
a LIMITED
COVERAGE
Medicaid Program
and the provider
accepts the client as
a Medicaid client
FULL
COVERAGE or
LIMITED
COVERAGE
Medicaid Program
and the provider
does not accept the
client as a Medicaid
client
Client is not
covered by
Medicaid (not
a Medicaid
client)
Service is not
covered by
Medicaid
Provider can bill the
client only if a
specific financial
agreement has been
made in writing
Provider can bill the
client if the Category
of service is not
covered by the
client’s limited plan.
If the Category of
service is covered,
the provider can only
bill the client if a
specific financial
agreement has been
made in writing
Provider can bill the
client if written
notification has been
given to the client
that they are not
being accepted as a
Medicaid client
Provider can
bill client
Full Coverage Plan – Plan covers the full range of medical, dental, hospital, and
pharmacy services and may cover additional nursing home or waiver services.
Limited Coverage Plan – Plan with services limited to a specific category or type of
coverage.
Specific Financial Agreement – specific written agreement between a provider and a
client, outlining the specific services and financial charges for a specific date of
service, with the client agreeing to the financial responsibility for the charges.
3.2.2.1 Medicare/Medicaid Dual Eligible Clients
Dual eligible clients are those clients who have both Medicare and Medicaid. For
clients on the QMB plan, CMS guidelines indicate that coinsurance and deductible
amounts remaining after Medicare pays cannot be billed to the client under any
circumstances, regardless of whether you bill Medicaid or not.
For clients on other plans who are dual eligible, coinsurance and deductible amounts
remaining after Medicare payment cannot be billed to the client if the claim was
billed to Wyoming Medicaid, regardless of payment amount (including claims that
Medicaid pays at $0).
If the claim is not billed to Wyoming Medicaid, and the provider agrees in writing
prior to providing the service not to accept the client as a Medicaid client and advises
the client of his or her financial responsibility, and the client is not on a QMB plan,
then the client can be billed for the coinsurance and deductible under Medicare
guidelines.
Provider Responsibilities________________________________________________________
Ch. 3 Index 22 Revision 4/1/17
3.2.2.2 Accepting a Client as Medicaid After Billing the Client
If the provider collected money from the client for services rendered during the
eligibility period and decides later to accept the client as a Medicaid client, and
receive payment from Medicaid:
Prior to submitting the claim to Medicaid, the provider must refund the entire
amount previously collected from the client to him or her for the services
rendered; and
The 12-month timely filing deadline will not be waived (6.20, Timely Filing).
In cases of retroactive eligibility when a provider agrees to bill Medicaid for services
provided during the retroactive eligibility period:
Prior to billing Medicaid, the provider must refund the entire amount
previously collected from the client to him or her for the services rendered;
and
The twelve month timely filing deadline will be waived (6.20, Timely Filing).
NOTE: Medicaid will not pay for services rendered to the clients until eligibility
has been determined for the month services were rendered.
The provider may, at a subsequent date, decide not to further treat the client as a
Medicaid patient. If this occurs, the provider must advise the client of this fact in
writing before rendering treatment.
3.2.2.3 Mutual Agreements Between the Provider & Client
Medicaid covers only those services that are medically necessary and cost-efficient. It
is the providers’ responsibility to be knowledgeable regarding covered services,
limitations and exclusions of the Medicaid Program. Therefore, if the provider,
without mutual written agreement of the client, deliver services and are subsequently
denied Medicaid payment because the services were not covered or the services were
covered but not medically necessary and/or cost-efficient, the provider may not obtain
payment from the client.
If the provider and the client mutually agree in writing to services which are not
covered (or are covered but are not medically necessary and/or cost-efficient), and the
provider informs the client of his/her financial responsibility prior to rendering
service, then the provider may bill the client for the services rendered.
3.2.3 Missed Appointments

Provider Responsibilities________________________________________________________
Ch. 3 Index 23 Revision 4/1/17
Appointments missed by Medicaid clients cannot be billed to Medicaid. However, if
a provider’s policy is to bill all patients for missed appointments, then the provider
may bill Medicaid clients directly.
Any policy must be equally applied to all clients and a provider may not impose
separate charges on Medicaid clients, regardless of payment source. Policy must be
publically posted or provided in writing to all patients.
Medicaid only pays providers for services they render (i.e., services as identified in
1905 (a) of the Social Security Act). They must accept that payment as full
reimbursement for their services in accordance with 42 CFR 447.15. Missed
appointments are not a distinct, reimbursable Medicaid service. Rather, they are
considered part of a provider’s overall cost of doing business. The Medicaid
reimbursement rates set by the State are designed to cover the cost of doing business.
3.3 Medicare Covered Services
Claims for services rendered to clients eligible for both Medicare and Medicaid which
are furnished by an out-of-state provider must be filed with the Medicare
intermediary or carrier in the state in which the provider is located.
Questions concerning a client’s Medicare eligibility should be directed to the Social
Security Administration (2.1, Quick Reference).
3.4 Medical Necessity
The Medicaid Program is designed to assist eligible clients in obtaining medical care
within the guidelines specified by policy. Medicaid will pay only for medical services
that are medically necessary and are sponsored under program directives. Medically
necessary means the service is required to:
Diagnose
Treat
Cure
Prevent an illness which has been diagnosed or is reasonably suspected to:
o Relieve pain
o Improve and preserve health
o Be essential for life
Additionally, the service must be:
Consistent with the diagnosis and treatment of the patient’s condition.
In accordance with standards of good medical practice.
Required to meet the medical needs of the patient and undertaken for reasons
other than the convenience of the patient or his/her physician.

Provider Responsibilities________________________________________________________
Ch. 3 Index 24 Revision 4/1/17
Performed in the least costly setting required by the patient’s condition.
Documentation which substantiates that the client’s condition meets the coverage
criteria must be on file with the provider.
All claims are subject to both pre-payment and post-payment review for medical
necessity by Medicaid. Should a review determine that services do not meet all the
criteria listed above, payment will be denied or, if the claim has already been paid,
action will be taken to recoup the payment for those services.
3.5 Medicaid Payment is Payment in Full
As a condition of becoming a Medicaid provider (see provider agreement), the
provider must accept payment from Medicaid as payment in full for a covered
service.
The provider may never bill a Medicaid client:
When the provider bills Medicaid for a covered service, and Medicaid denies
the providers claim due to billing errors such as wrong procedure and
diagnosis codes, lack of prior authorization, invalid consent forms, missing
attachments or an incorrectly filled out claim form.
When Medicare or another third party payer has paid up to or exceeded what
Medicaid would have paid.
For the difference in the providers charges and the amount Medicaid has paid
(balance billing).
The Provider may bill a Medicaid client:
If the provider has not billed Medicaid, the service provided is not covered by
Medicaid, and prior to providing service, the provider informed the client in
writing that the service is non-covered and he/she is responsible for the
charges.
If a provider does not accept a patient as a Medicaid client (because they
cannot produce a Medicaid ID card or because they did not inform the
provider they are eligible.
If the client is not Medicaid eligible at the time the provider provides the
services or on a plan that does not cover those particular services. Refer to the
table above for guidance.
If the client has exceeded the Medicaid limits on physical therapy,
occupational therapy, speech therapy, behavioral health services, chiropractic
services, prescriptions, and/or office/outpatient hospital visits. (6.9, Cap
Limits)
Provider Responsibilities________________________________________________________
Ch. 3 Index 25 Revision 4/1/17
NOTE: The provider may contact Provider Relations or the IVR to receive cap
limits for a client (2.1, Quick Reference).
If the provider is an out-of-state provider and are not enrolled and have no
intention of enrolling.
3.6 Medicaid ID Card
It is each provider’s responsibility to verify the person receiving services is the same
person listed on the card. If necessary, providers should request additional materials
to confirm identification. It is illegal for anyone other than the person named on the
Medicaid ID Card to obtain or attempt to obtain services by using the card. Providers
who suspect misuse of a card should report the occurrence to the Program Integrity
Unit or complete the Report of Suspected Abuse of the Medicaid Healthcare System
Form (4.9, Referral of Suspected Fraud and Abuse).
3.7 Verification of Client Age
Because certain services have age restrictions, such as services covered only for
clients under the age of 21, and informed consent for sterilizations, providers should
verify a client’s age before a service is rendered.
Routine services may be covered through the month of the client’s 21st birthday.
3.8 Verification Options
One (1) Medicaid ID Card is issued to each client. Their eligibility information is
updated every month. The presentation of a card is not verification of eligibility. It is
each provider’s responsibility to ensure that their patient is eligible for the services
rendered. A client may state that he/she is covered by Medicaid, but not have any
proof of eligibility. This can occur if the client is newly eligible or if his/her card was
lost. Providers have several options when checking patient eligibility.
3.8.1 Free Services
The following is a list of free services offered by Medicaid for verifying client
eligibility:
Contact Provider Relations. There is a limit of three (3) verifications per call
but no limit on the number of calls.
Fax a list of identifying information to Provider Relations for verification.
Send a list of beneficiaries for verification and receive a response within ten
(10) business days.
Provider Responsibilities________________________________________________________
Ch. 3 Index 26 Revision 4/1/17
Call the Interactive Voice Response (IVR) System. IVR is available 24-hours
a day, seven (7) days a week. The IVR System allows 30 minutes per phone
call. (2.1, Quick Reference).
Use the Ask Wyoming Medicaid feature on the Secured Provider Web Portal
(2.1, Quick Reference).
3.8.2 Fee for Service
Several independent vendors offer web-based applications and/or swipe card readers
that electronically check the eligibility of Medicaid clients. These vendors typically
charge a monthly subscription and/or transaction fee. A complete list of approved
vendors is available on the Medicaid website.
3.9 Freedom of Choice
Any eligible non-restricted client may select any provider of health services in
Wyoming who participates in the Medicaid Program, unless Medicaid specifically
restricts his/her choice through provider lock-in or an approved Freedom of Choice
waiver. However, payments can be made only to health service providers who are
enrolled in the Medicaid Program.
3.10 Out-of-State Service Limitations
Medicaid covers services rendered to Medicaid clients when providers participating
in the Medicaid Program administer the services. If services are available in
Wyoming within a reasonable distance from the client’s home, the client must not
utilize an out-of-state provider.
Medicaid has designated the Wyoming Medical Service Area (WMSA) to be
Wyoming and selected border cities in adjacent states. WMSA cities include:
Colorado
Montana
South Dakota
Craig
Billings
Deadwood
Bozeman
Custer
Idaho
Rapid City
Montpelier
Nebraska
Spearfish
Pocatello
Kimball
Belle Fourche
Idaho Falls
Scottsbluff
Utah
Salt Lake City
Ogden

Provider Responsibilities________________________________________________________
Ch. 3 Index 27 Revision 4/1/17
NOTE: The cities of Greeley, Fort Collins, and Denver, Colorado are excluded
from the WMSA and are not considered border cities.
Medicaid compensates out-of-state providers within the WMSA when:
The service is not available locally and the border city is closer for the
Wyoming resident than a major city in Wyoming; and
The out-of-state provider in the selected border city is enrolled in Medicaid.
Medicaid compensates providers outside the WMSA only under the following
conditions:
Emergency Care – When a client is traveling and an emergency arises due to
accident or illness.
Other Care – When a client is referred by a Wyoming physician to a provider
outside the WMSA for services not available within the WMSA. The referral
must be documented in the provider’s records. Prior authorization is not
required unless the specific service is identified as requiring prior
authorization (6.14, Prior Authorization).
Children in out-of-state placement.
If the provider is an out-of-state, non-enrolled provider and renders services to a
Medicaid client, the provider may choose to enroll in the Medicaid Program and
submit the claim according to Medicaid billing instructions, or bill the client.
Out-of-state providers furnishing services within the state on a routine or extended
basis must meet all of the certification requirements of the State of Wyoming. The
provider must enroll in Medicaid prior to furnishing services.
3.11 Record Keeping, Retention and Access
3.11.1 Requirements
The Provider Agreement requires that the medical and financial records fully disclose
the extent of services provided to Medicaid clients. The following elements include
but are not limited to:
The record must be typed or legibly written.
The record must identify the client on each page.
The record must contain a preliminary working diagnosis and the elements of
a history and physical examination upon which the diagnosis is based.
All services, as well as the treatment plan, must be entered in the record. Any
drugs prescribed as part of a treatment, including the quantities and the

Provider Responsibilities________________________________________________________
Ch. 3 Index 28 Revision 4/1/17
dosage, must be entered in the record. For any drugs administered, the NDC
on the product must be recorded, as well as the lot number and expiration
date.
The record must indicate the observed medical condition of the client, the
progress at each visit, any change in diagnosis or treatment, and the client’s
response to treatment. Progress notes must be written for every service,
including, but not limited to: office, clinic, nursing home, or hospital visits
billed to Medicaid.
Total treatment minutes of the client, including those minutes of active
treatment reported under the timed codes and those minutes represented by the
untimed codes, must be documented separately, to include beginning time and
ending time for services billed.
NOTE: Specific or additional documentation requirements may be listed in the
covered services sections or designated policy manuals.
3.11.2 Retention of Records
The provider must retain medical and financial records, including information
regarding dates of service, diagnoses, and services provided, and bills for services for
at least six (6) years from the end of the State fiscal year (July through June) in which
the services were rendered. If an audit is in progress, the records must be maintained
until the audit is resolved.
3.11.3 Access to Records
Under the Provider Agreement, the provider must allow access to all records
concerning services and payment to authorized personnel of-Medicaid, CMS
Comptroller General of the United States, State Auditor’s Office (SAO), the Office of
the Inspector General (OIG), the Wyoming Attorney General’s Office, the United
States Department of Health and Human Services, and/or their designees. Records
must be accessible to authorized personnel during normal business hours for the
purpose of reviewing, copying and reproducing documents. Access to the provider
records must be granted regardless of the providers continued participation in the
program.
In addition, the provider is required to furnish copies of claims and any other
documentation upon request from Medicaid and/or their designee.
3.11.4 Audits
Medicaid has the authority to conduct routine audits to monitor compliance with
program requirements.
Audits may include, but are not limited to:

Provider Responsibilities________________________________________________________
Ch. 3 Index 29 Revision 4/1/17
Examination of records;
Interviews of providers, their associates, and employees;
Interviews of clients;
Verification of the professional credentials of providers, their associates, and
their employees;
Examination of any equipment, stock, materials, or other items used in or for
the treatment of clients;
Examination of prescriptions written for clients;
Determination of whether the healthcare provided was medically necessary;
Random sampling of claims submitted by and payments made to providers;
and/or
Audit of facility financial records for reimbursement.
Actual records reviewed may be extrapolated and applied to all services billed
by the provider.
The provider must grant the State and its representative’s access during regular
business hours to examine medical and financial records related to healthcare billed to
the program. Medicaid notifies the provider before examining such records.
Medicaid reserves the right to make unscheduled visits i.e., when the client’s health
may be endangered, when criminal/fraud activities are suspected, etc.
Medicaid is authorized to examine all provider records in that:
All eligible clients have granted Medicaid access to all personal medical
records developed while receiving Medicaid benefits.
All providers who have at any time participated in the Medicaid Program, by
signing the Provider Agreement, have authorized the State and their
designated agents to access the provider’s financial and medical records.
Provider’s refusal to grant the State and its representative’s access to examine
records or to provide copies of records when requested may result in:
Immediate suspension of all Medicaid payments.
All Medicaid payments made to the provider during the six (6)-year record
retention period for which records supporting such payments are not produced
shall be repaid to the Division of Healthcare Financing after written request
for such repayment is made.
Suspension of all Medicaid payments furnished after the requested date of
service.
Reimbursement will not be reinstated until adequate records are produced or
are being maintained.
Prosecution under the Wyoming Statute.

Provider Responsibilities________________________________________________________
Ch. 3 Index 30 Revision 4/1/17
3.12 Tamper Resistant RX Pads
On May 25, 2007, Section 7002(b) of the U.S. Troop Readiness, Veterans’ Care,
Katrina Recovery, and Iraq Accountability Appropriations Act of 2007 was signed
into law.
The above law requires that ALL written, non-electronic prescriptions for Medicaid
outpatient drugs must be executed on tamper-resistant pads in order for them to be
reimbursable by the federal government. All prescriptions paid for by Medicaid must
meet the following requirements to help insure against tampering:
Written Prescriptions: As of October 1, 2008 prescriptions, must contain all
three (3) of the following characteristics:
1. One (1) or more industry-recognized features designed to prevent
unauthorized copying of a completed or blank prescription form. In
order to meet this requirement all written prescriptions must contain:
Some type of “void” or illegal pantograph that appears if the
prescription is copied.
May also contain any of the features listed within category one,
recommendations provided by the National Council for
Prescription Drug Programs (NCPDP) or that meets the
standards set forth in this category.
2. One (1) or more industry-recognized features designed to prevent the
erasure or modification of information written on the prescription by
the prescriber. This requirement applies only to prescriptions written
for controlled substances. In order to meet this requirement all written
prescriptions must contain:
Quantity check-off boxes PLUS numeric form of quantity
values OR alpha and numeric forms of quantity value.
Refill Indicator (circle or check number of refills or “NR”)
PLUS numeric form of refill values OR alpha AND numeric
forms of refill values.
May also contain any of the features listed within category two,
recommendations provided by the NCPDP, or that meets the
standards set forth in this category.
3. One (1) or more industry-recognized features designed to prevent the
use of counterfeit prescription forms. In order to meet this requirement
all written prescriptions must contain:
Security features and descriptions listed on the FRONT of the
prescription blank.
May also contain any of the features listed within category
three (3), recommendations provided by the NCPDP, or that
meets that standards set forth in this category.

Provider Responsibilities________________________________________________________
Ch. 3 Index 31 Revision 4/1/17
Computer Printed Prescriptions: As of October 1, 2008 prescriptions, must
contain all three (3) of the following characteristics:
1. One (1) or more industry-recognized features designed to prevent
unauthorized copying of a completed or blank prescription form. In
order to meet this requirement all prescriber’s computer generated
prescriptions must contain:
Same as Written Prescription for this category.
2. One (1) or more industry-recognized features designed to prevent the
erasure or modification of information printed on the prescription by
the prescriber. In order to meet this requirement all computer
generated prescriptions must contain:
Same as Written Prescription for this category.
3. One (1) or more industry-recognized features designed to prevent the
use of counterfeit prescription forms. In order to meet this requirement
all prescriber’s computer generated prescriptions must contain:
Security features and descriptions listed on the FRONT or
BACK of the prescription blank.
May also contain any of the features listed within category
three (3), recommendations provided by the NCPDP, or that
meets the standards set forth in this category.
In addition to the guidance outlined above, the tamper-resistant requirement does not
apply when a prescription is communicated by the prescriber to the pharmacy
electronically, verbally, or by fax; when a managed care entity pays for the
prescription; or in most situations when drugs are provided in designated institutional
and clinical settings. The guidance also allows emergency fills with a non-compliant
written prescription as long as the prescriber provides a verbal, faxed, electronic, or
compliant written prescription within 72-hours.
Audits of pharmacies will be performed by the Wyoming Department of Health, to
ensure that the above requirement is being followed. If the provider has any questions
about these audits or this regulation, please contact the Pharmacy Program Manager
at (307)777-7531.

Utilization Review______________________________________________________________
Ch. 4 Index 32 Revision 4/1/17
Chapter Four – Utilization Review
4.1 Utilization Review ............................................................................................... 33
4.2 Complaint Referral .............................................................................................. 33
4.3 Release of Medical Records ................................................................................ 33
4.4 Client Lock-In ..................................................................................................... 34
4.5 Pharmacy Lock-In ............................................................................................... 34
4.6 Hospice Lock-In .................................................................................................. 35
4.7 Fraud and Abuse .................................................................................................. 35
4.8 Provider Responsibilities ..................................................................................... 36
4.9 Referral of Suspected Fraud and Abuse .............................................................. 36
4.9.1 Report of Suspected Abuse of the Medicaid Healthcare System ........................ 37
4.10 Sanctions ............................................................................................................. 37
4.11 Adverse Actions .................................................................................................. 38

Utilization Review______________________________________________________________
Ch. 4 Index 33 Revision 4/1/17
4.1 Utilization Review
The Division of Healthcare Financing (DHCF) has established a Program Integrity
Unit whose duties include, but are not limited to:
Review of claims submitted for payment (pre and post payment reviews)
Review of medical records and documents related to covered services
Audit of medical records and client interviews
Review of client Explanation of Medical Benefits (EOMB) responses
Operation of the Surveillance/Utilization Review (SUR) process
Provider screening and monitoring
Program compliance and enforcement
4.2 Complaint Referral
The Program Integrity Unit reviews complaints regarding inappropriate use of
services from providers and clients. No action is taken without a complete
investigation. To file a complaint, please submit the details in writing and attach
supporting documentation to:
Program Integrity Unit
Division of Healthcare Financing
6101 Yellowstone Rd., Suite 210
Cheyenne, WY 82002
Or contact: (855) 846-2563
Or email: programintegrity@wyo.gov
4.3 Release of Medical Records
Every effort is made to ensure the confidentiality of records in accordance with
Federal Regulations and Wyoming Medicaid Rules. Medical records must be released
to the agency or its designee. The signed Provider Agreement allows the Division of
Healthcare Financing or its designated agent’s access to all medical and financial
records. In addition, each client agrees to the release of medical records to the
Division of Healthcare Financing when they accept Medicaid benefits.
The Division of Healthcare Financing will not reimburse for the copying of medical
records when the Division or its designated agents requests records.

Utilization Review______________________________________________________________
Ch. 4 Index 34 Revision 4/1/17
4.4 Client Lock-In
In designated circumstances, it may be necessary to restrict certain services or “lock-
in” a client to a certain physician, hospice, pharmacy or other provider. If a lock-in
restriction applies to a client, the lock-in information is provided on the Interactive
Voice Response System (2.1, Quick Reference).
A participating Medicaid provider who is not designated as the client’s primary
practitioner may provide and be reimbursed for services rendered to lock-in clients
only under the following circumstances:
In a medical emergency where a delay in treatment may cause death or result
in lasting injury or harm to the client.
As a physician covering for the designated primary physician or on referral
from the designated primary physician.
In cases where lock-in restrictions are indicated, it is the responsibility of each
provider to determine whether he/she may bill for services provided to a lock-in
client. Contact Provider Relations in circumstances where coverage of a lock-in client
is unclear. Refer to the Medicaid Pharmacy Provider Manual (2.1, Quick Reference).
4.5 Pharmacy Lock-In
The Medicaid Pharmacy Lock-In Program limits certain Medicaid clients to receiving
prescription services from multiple prescribers and utilizes multiple pharmacies
within a designated time period is a candidate for the Lock-In Program.
When a pharmacy is chosen to be a client’s designated Lock-In provider, notification
is sent to that pharmacy with all important client identifying information. If a Lock-In
client attempts to fill a prescription at a pharmacy other than their Lock-In pharmacy,
the claim will be denied with an electronic response of “NON-MATCHED
PHARMACY NUMBER-Pharmacy Lock-In”.
Pharmacies have the right to refuse Lock-In provider status for any client. The client
may be counseled to contact the Medicaid Pharmacy Case Manager at (307)777-8773
in order to obtain a new provider designation form to complete.
Expectations of a Medicaid designated Lock-In pharmacy:
Medicaid pharmacy providers should be aware of the Pharmacy Lock-In
Program and the criteria for client lock-in status as stated above. The entire
pharmacy staff should be notified of current Lock-In clients.
Review and monitor all drug interactions, allergies duplicate therapy, and
seeking of medications from multiple prescribers. Be aware that the client is
locked-in when “refill too soon” or “therapeutic duplication” edits occur. Cash
payment for controlled substances should serve as an alert and require further
review. Gather additional information which may include, but is not limited
to, asking the client for more information and/or contacting the prescriber.
Document findings and outcomes. The Wyoming Board of Pharmacy will be

Utilization Review______________________________________________________________
Ch. 4 Index 35 Revision 4/1/17
contacted when early refills and cash payment are allowed without appropriate
clinical care and documentation.
When doctor shopping for controlled substances is suspected, please contact the
Medicaid Pharmacy Case Manager at (307)777-8773. The Wyoming Online
Prescription Database (WORx) is online with 24/7 access for practitioners and
pharmacists. The WORx program is managed by the Wyoming Board of Pharmacy at
http://worxpdmp.com/ to view client profiles with all scheduled II through IV
prescriptions the client has received. The Wyoming Board of Pharmacy may be
reached at (307)634-9636 to answer questions about WORx.
EMERGENCY LOCK-IN PRESCRIPTIONS
If the dispensing pharmacist feels that in his/her professional judgment a prescription
should be filled and they are not the Lock-In provider, they may submit a hand-billed
claim to Goold Health Systems (GHS), an Emdeon company for review (2.1, Quick
Reference). Overrides may be approved for true emergencies (auto accidents, sudden
illness, etc.).
Any Wyoming Medicaid client suspected of controlled substance abuse, diversion, or
doctor shopping should be referred to the Medicaid Pharmacy Case Manager.
Pharmacy Case Manager (307)777-8773 or
Fax referrals to (307)777-6964.
Referral forms may be found on the Pharmacy website (2.1, Quick
Reference).
4.6 Hospice Lock-In
Clients requesting coverage of hospice services under Wyoming Medicaid are locked-
in to the hospice for all care related to their terminal illness. All services and supplies
must be billed to the hospice provider, and the hospice provider will bill Wyoming
Medicaid for covered services. For more information regarding the hospice program,
refer to the Institutional Provider Manual on the Medicaid website (2.1, Quick
Reference).
4.7 Fraud and Abuse
The Medicaid Program operates under the anti-fraud provisions of Section 1909 of
the Social Security Act, as amended, and employs utilization management,
surveillance, and utilization review. The Program Integrity Unit’s function is to
perform pre- and post-payment review of services funded by Medicaid. Surveillance
is defined as the process of monitoring for service and controlling improper or illegal
utilization of the program. While the surveillance function addresses administrative
concerns, utilization review addresses medical concerns and may be defined as
monitoring and controlling the quality and appropriateness of medical services

Utilization Review______________________________________________________________
Ch. 4 Index 36 Revision 4/1/17
delivered to Medicaid clients. Medicaid may utilize the services of a Professional
Review Organization (PRO) to assist in these functions.
Since payment of claims is made from both State and Federal funds, submission of
false or fraudulent claims, statements, documents or concealment of material facts
may be prosecuted as a felony in either Federal or State court. The program has
processes in place for referral to the Medicaid Fraud Control Unit (MFCU) when
suspicion of fraud and abuse arise.
Medicaid has the responsibility, under Federal Regulations and Medicaid Rules, to
refer all cases of credible allegations of fraud and abuse to the MFCU. In accordance
with 42 CFR Part 455, and Medicaid Rules, the following definitions of fraud and
abuse are used:
4.8 Provider Responsibilities
The provider is responsible for reading and adhering to applicable State and Federal
regulations and the requirements set forth in this manual. The provider is also
responsible for ensuring that all employees are likewise informed of these regulations
and requirements. The provider certifies by his/her signature or the signature of
his/her authorized agent on each claim or invoice for payment that all information
provided to Medicaid is true, accurate, and complete. Although claims may be
prepared and submitted by an employee, billing agent or other authorized person,
providers are responsible for ensuring the completeness and accuracy of all claims
submitted to Medicaid.
4.9 Referral of Suspected Fraud and Abuse
If a provider becomes aware of possible fraudulent or program abusive
conduct/activity by another provider, or eligible client, the provider should notify the
Program Integrity Unit in writing. Return a completed Report of Suspected Abuse of
the Medicaid Healthcare System to or call or reference the below website:
Fraud
“An intentional deception or misrepresentation made by a person with the
knowledge that the deception could result in some unauthorized benefit to
himself or some other person. It includes any act that constitutes fraud
under applicable Federal or State law.”
Abuse
“Provider practices that are inconsistent with sound fiscal, business, or
medical practices, and result in an unnecessary cost to the Medicaid
program or in reimbursement for services that are not medically necessary
or that fail to meet professionally recognized standards for healthcare. It
also includes recipient practices that result in unnecessary cost to the
Medicaid Program.”
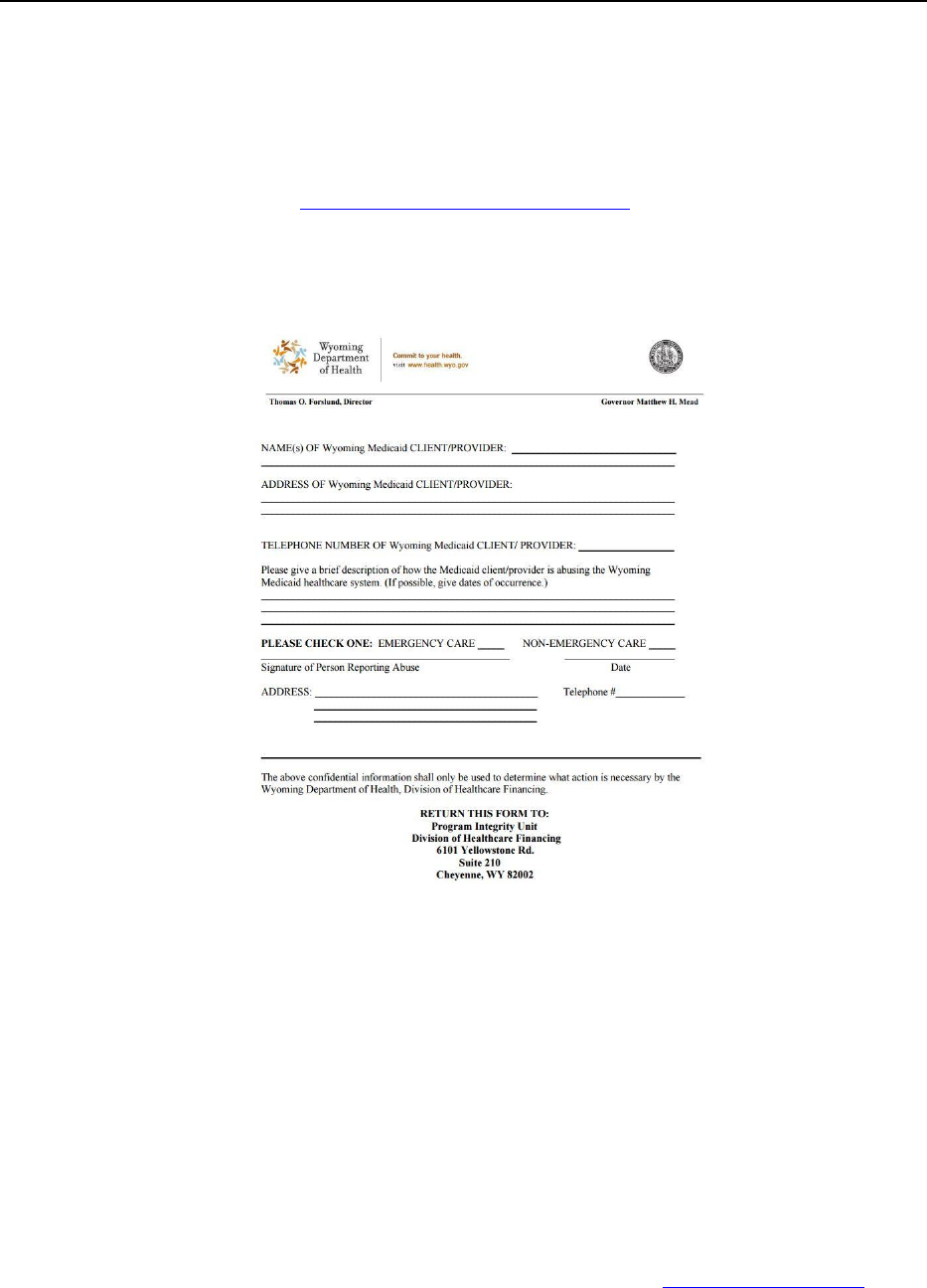
Utilization Review______________________________________________________________
Ch. 4 Index 37 Revision 4/1/17
Program Integrity Unit
Division of Healthcare Financing
6101 Yellowstone Rd., Suite 210
Cheyenne, WY 82002
Or contact: (855)846-2563
http://stopmedicaidfraud.wyo.gov/
4.9.1 Report of Suspected Abuse of the Medicaid Healthcare System
NOTE: Click image above to be taken to a printable version of this form.
4.10 Sanctions
The Division of Healthcare Financing (DHCF) may invoke administrative sanctions
against a Medicaid provider when a credible allegation of fraud abuse, waste, non-
compliance (i.e., Provider Agreement and/or Medicaid Rules) exists or who is under
sanction by another regulatory entity (i.e. Medicare, licensing boards, OIG, or other
Medicaid designated agents).
Providers who have had sanctions levied against them may be subject to prohibitions
or additional requirements as defined by Medicaid Rules (2.1, Quick Reference).

Utilization Review______________________________________________________________
Ch. 4 Index 38 Revision 4/1/17
4.11 Adverse Actions
Providers and clients have the right to request an administrative hearing regarding an
adverse action, after reconsideration, taken by the Division of Healthcare Financing.
This process is defined in Wyoming Medicaid Rule, Chapter 4, entitled “Medicaid
Administrative Hearings”.

Client Eligibility_______________________________________________________________
Ch. 5 Index 39 Revision 4/1/17
Chapter Five – Client Eligibility
5.1 What is Medicaid? ............................................................................................... 40
5.2 Who is Eligible? .................................................................................................. 40
5.2.1 Children ............................................................................................................... 40
5.2.2 Pregnant Women ................................................................................................. 41
5.2.3 Family MAGI Adult ............................................................................................ 41
5.2.4 Aged, Blind and Disabled ................................................................................... 41
5.2.4.1 Supplemental Security Income (SSI) and SSI Related .................................... 41
5.2.4.2 Institution ......................................................................................................... 41
5.2.4.3 Home and Community Based Waiver ............................................................. 42
5.2.5 Other .................................................................................................................... 42
5.2.5.1 Special Groups ................................................................................................. 42
5.2.5.2 Employed Individuals with Disabilities (EID) ................................................ 42
5.2.5.3 Medicare Savings Programs ............................................................................ 42
5.2.5.4 Non-Citizens with Medical Emergencies (ALEN) .......................................... 43
5.3 Maternal and Child Health (MCH) ..................................................................... 43
5.4 Eligibility Determination ..................................................................................... 43
5.4.1 Applying for Medicaid ........................................................................................ 43
5.4.2 Determination ...................................................................................................... 44
5.5 Client Identification Cards .................................................................................. 44
5.6 Other Types of Eligibility Identification ............................................................. 45
5.6.1 Medicaid Approval Notice .................................................................................. 45

Client Eligibility_______________________________________________________________
Ch. 5 Index 40 Revision 4/1/17
5.1 What is Medicaid?
Medicaid is a health coverage program jointly funded by the Federal government and
the State of Wyoming. The program is designed to help pay for medically necessary
healthcare services for children, pregnant women, family Modified Adjusted Gross
Income (MAGI) adults and the aged, blind and disabled.
5.2 Who is Eligible?
Eligibility is generally based on family income and sometimes resources and/or
healthcare needs. Federal statutes define more than 50 groups of individuals that may
qualify for Medicaid coverage. There are four (4) broad categories of Medicaid
eligibility in Wyoming:
Children;
Pregnant women;
Family MAGI Adults; and
Aged, Blind, and Disabled.
5.2.1 Children
Newborns are automatically eligible if the mother is Medicaid eligible at the
time of the birth.
Low Income Children are eligible if family income is at or below 133%
federal poverty level (FPL) or 154% FPL, dependent on age of the child.
Presumptive Eligibility (PE) for Children allows temporary coverage for a
child who meets eligibility criteria for the full Children's Medicaid program
while the full Medicaid application is being processed.
o PE Coverage will end the date a determination is made on the full
Medicaid application or the last day of the next month after PE is
approved if a full Medicaid application is not submitted.
Foster Care Children in Department of Family Services (DFS) custody are
eligible in different income levels including some who enter subsidized
adoption or who age out of foster care until they are age 26.
Presumptive Eligibility (PE) for Former Foster Youth allows temporary
coverage for a person who meets eligibility criteria for the full Former Foster
Youth Medicaid program while the full Medicaid application is being
processed.
o PE Coverage will end the date a determination is made on the full
Medicaid application or the last day of the next month after PE is
approved if a full Medicaid application is not submitted.

Client Eligibility_______________________________________________________________
Ch. 5 Index 41 Revision 4/1/17
5.2.2 Pregnant Women
Pregnant Women are eligible if family income is at or below 154% FPL.
Women with income less than or equal to the MAGI conversion of the 1996
Family Care Standard must cooperate with child support to be eligible.
Presumptive Eligibility (PE) for Pregnant Women allows temporary outpatient
coverage for a pregnant woman who meets eligibility criteria for the full
Pregnant Woman Medicaid program while the full Medicaid application is
being processed.
o PE Coverage will end the date a determination is made on the full
Medicaid application or the last day of the next month after PE is
approved if a full Medicaid application is not submitted.
5.2.3 Family MAGI Adult
Family MAGI Adults (caretaker relatives with a dependent child) are eligible
if family income is at or below the MAGI conversion of the 1996 Family Care
Standard.
Presumptive Eligibility (PE) for Caretaker Relatives allows temporary
coverage for the parent or caretaker relative of a Medicaid eligible child who
meets eligibility criteria for the full Family MAGI Medicaid program while
the full Medicaid application is being processed.
o PE Coverage will end the date a determination is made on the full
Medicaid application or the last day of the next month after PE is
approved if a full Medicaid application is not submitted.
5.2.4 Aged, Blind and Disabled
5.2.4.1 Supplemental Security Income (SSI) and SSI Related
SSI – A person receiving SSI automatically qualifies for Medicaid
SSI Related – A person no longer receiving SSI payment may be eligible
using SSI criteria.
5.2.4.2 Institution
All categories are income eligible up to 300% SSI Standard.
Nursing Home
Hospital
Hospice
ICF ID – Wyoming Life Resource Center
INPAT-PSYCH – WY State Hospital – clients are 65 years and older.

Client Eligibility_______________________________________________________________
Ch. 5 Index 42 Revision 4/1/17
5.2.4.3 Home and Community Based Waiver
All waiver groups are income eligible when income is less than or equal to 300% SSI
Standard.
Acquired Brain Injury
Assisted Living Facilities
Children’s Mental Health
Comprehensive
Long Term Care
Supports
5.2.5 Other
5.2.5.1 Special Groups
Breast and Cervical Cancer (BCC) Treatment Program – Uninsured
women diagnosed with breast or cervical cancer are income eligible at or
below 250% FPL
Presumptive Eligibility (PE) for BCC allows temporary coverage for a woman
who meets eligibility criteria for the full BCC Medicaid program while the
full Medicaid application is being processed.
o PE Coverage will end the date a determination is made on the full
Medicaid application or the last day of the next month after PE is
approved if a full Medicaid application is not submitted.
Tuberculosis (TB) Program – Individuals diagnosed with tuberculosis are
eligible based on the TB Standard.
Program for All Inclusive Care for the Elderly (PACE) – Individuals over
the age of 55 assessed to be in need of nursing home level of care receive all
services coordinated through the PACE provider. This program is currently
available in Laramie County only.
5.2.5.2 Employed Individuals with Disabilities (EID)
Employed Individuals with Disabilities are income eligible when income is less than
or equal to 300% SSI using unearned income and must pay a premium calculated
using total gross income.
5.2.5.3 Medicare Savings Programs
Qualified Medicare Beneficiaries (QMB) are income eligible at or below
100% FPL. Benefits include payment of Medicare premiums, deductibles, and
cost sharing.
Specified Low Income Beneficiaries (SLMB) are income eligible at or below
135% FPL. Benefits include payment of Medicare premiums only.

Client Eligibility_______________________________________________________________
Ch. 5 Index 43 Revision 4/1/17
5.2.5.4 Non-Citizens with Medical Emergencies (ALEN)
A non-citizen who meets all eligibility factors under a Medicaid group except for
citizenship and social security number is eligible for emergency services. This does
not include dental services.
5.3 Maternal and Child Health (MCH)
Maternal and Child Health (MCH) provides services for high-risk pregnant women,
high-risk newborns and children with special healthcare needs through the Children’s
Special Health (CSH) program. The purpose is to identify eligible clients, assure
diagnostic and treatment services are available, provide payment for authorized
specialty care for those eligible, and provide care coordination services. CSH does not
cover acute or emergency care.
A client may be eligible only for a MCH program or may be dually eligible
for a MCH program or other Medicaid programs. Care coordination for both
MCH only and dually eligible clients is provided through the Public Health
Nurse (PHN).
MCH has a dollar cap and limits on some services for those clients who are
eligible for MCH only.
Contact MCH for the following information:
o The nearest Public Health Nurse (PHN)
o Questions related to eligibility determination
o Questions related to the type of services authorized by MCH.
Maternal & Child Health
6101 N. Yellowstone Rd., Ste. 420
Cheyenne, WY 82002
(800)438-5795 or Fax: (307)777-7215
Providers must be enrolled with Medicaid and MCH to receive payment for MCH
services. Claims for both programs are submitted to and processed by the fiscal agent
for Wyoming Medicaid (2.1, Quick Reference). Providers are asked to submit the
medical record to CSH in a timely manner assure coordination of referrals and
services.
5.4 Eligibility Determination
5.4.1 Applying for Medicaid
Persons applying for Children, Pregnant Women and/or Family MAGI Adult
programs may complete the Application for Wyoming’s Healthcare Coverage,
which is also used for the Kid Care CHIP program. The application may be

Client Eligibility_______________________________________________________________
Ch. 5 Index 44 Revision 4/1/17
mailed to the Wyoming Department of Health (WDH). Applicants may also
apply online at https://www.wesystem.wyo.gov/.
Presumptive Eligibility (PE) applicants may also apply through a qualified
provider or qualified hospital for the PE programs.
5.4.2 Determination
Eligibility determination is conducted by the Wyoming Department of Health
Customer Service Center (CSC) or the Long Term Care (LTC) Unit centrally located
in Cheyenne, WY (2.1, Quick Reference).
Persons who want to apply for other programs offered through the Department of
Family Services (DFS), such as Supplemental Nutrition Assistance Program (SNAP)
or Child Care need to apply in person at their local DFS office. Persons applying for
Supplemental Security Income (SSI) need to contact the Social Security
Administration (SSA) (2.1, Quick Reference).
Medicaid assumes no financial responsibility for services rendered prior to the
effective date of client eligibility as determined by the WDH or the SSA. However,
the effective date of eligibility as determined by the WDH may be retroactive up to
90-days prior to the month in which the application is filed, as long as the client
meets eligibility criteria during each month of the retroactive period. If the SSA
deems the client eligible, the period of original entitlement could precede the
application date beyond the 90-day retroactive eligibility period and/or the 12-month
timely filing deadline for Medicaid claims (6.20, Timely Filing). This situation could
arise for the following reasons:
Administrative Law Judge decisions or reversals.
Delays encountered in processing applications or receiving necessary client
information concerning income or resources.
5.5 Client Identification Cards
A Medicaid ID Card is mailed to clients upon enrollment in the Medicaid Program or
other health programs such as the AIDS Drug Assistance Program (ADAP),
Children’s Special Health (CSH), and Prescription Drug Assistance Program (PDAP).
Not all programs receive a Medicaid ID Card, to confirm if a plan generates a card or
not refer to the “card” indicator on the Medicaid and State Benefit Plan Guide.
Sample Medicaid ID card:
Client Eligibility_______________________________________________________________
Ch. 5 Index 45 Revision 4/1/17
5.6 Other Types of Eligibility Identification
5.6.1 Medicaid Approval Notice
In some cases, a provider may be presented with a copy of a Medicaid Approval
Notice in lieu of the client’s Medicaid ID Card. Providers should always verify
eligibility before rendering services to a client who presents a Medicaid Approval
Notice.
NOTE: Refer to “Verification Options” (3.8, Verification Options) on ways to
verify a client’s eligibility.

Common Billing Information ____________________________________________________
Ch. 6 Index 46 Revision 4/1/17
Chapter Six – Common Billing Information
6.1 Electronic Billing ................................................................................................ 49
6.2 Basic Paper Claim Information ........................................................................... 49
6.3 Authorized Signatures ......................................................................................... 50
6.4 Completing the CMS-1500 Claim Form ............................................................. 51
6.4.1 Instructions for Completing the CMS-1500 Claim Form ................................... 51
6.4.2 Place of Service ................................................................................................... 56
6.5 Medicare Crossovers ........................................................................................... 61
6.5.1 General Information ............................................................................................ 61
6.5.2 Billing Information .............................................................................................. 62
6.6 Examples of Billing ............................................................................................. 63
6.6.1 Client has Medicaid Coverage Only or Medicaid and Medicare Coverage ........ 63
6.6.2 Client has Medicaid and Third Party Liability (TPL) or Client has Medicaid,
Medicare and TPL ............................................................................................... 64
6.7 National Drug Code (NDC) Billing Requirement ............................................... 65
6.7.1 Converting 10-Digit NDC’s to 11-Digits ............................................................ 65
6.7.2 Documenting and Billing the Appropriate NDC ................................................. 66
6.7.3 Procedure Code/NDC Combinations .................................................................. 67
6.7.4 Billing Requirements ........................................................................................... 67
6.7.5 Submitting One NDC per Procedure Code ......................................................... 67
6.7.6 Submitting Multiple NDCs per Procedure Code ................................................. 68
6.7.7 Medicare Crossover Claims ................................................................................ 68
6.7.8 CMS-1500 02-12 Billing Instructions ................................................................. 68
6.8 Cap Limits ........................................................................................................... 69
6.8.1 Cap Limit Waiver ................................................................................................ 70
6.8.2 Cap Limit Waiver Request Form ........................................................................ 71
6.8.3 Cap Limit Waiver Request Form Instructions .................................................... 72
6.8.4 Cap Limit Additional Information for Clients Under the Age of 21 ................... 73
6.8.5 Cap Limit Additional Information Instructions ................................................... 74
6.9 Reimbursement Methodologies ........................................................................... 75

Common Billing Information ____________________________________________________
Ch. 6 Index 47 Revision 4/1/17
6.10 Usual and Customary Charges ............................................................................ 75
6.10.1 Invoice Charges ................................................................................................... 75
6.11 Co-Payment Schedule ......................................................................................... 76
6.12 How to Bill for Newborns ................................................................................... 76
6.13 Prior Authorization .............................................................................................. 76
6.13.1 Requesting Prior Authorization from Medical Policy ......................................... 77
6.13.1.1 Medicaid Prior Authorization Form ................................................................ 79
6.13.1.2 Instructions for Completing the Medicaid Prior Authorization Form ............. 79
6.13.2 Requesting an Emergency Prior Authorization ................................................... 81
6.13.2.1 Prior Authorization Approval .......................................................................... 81
6.13.2.2 Sample PA Approval Letter ............................................................................ 82
6.13.2.3 Prior Authorization Denial .............................................................................. 83
6.13.2.4 Sample Prior Authorization Denial Letter ....................................................... 83
6.13.2.5 Prior Authorization Pending ............................................................................ 84
6.13.2.6 Sample Prior Authorization Pending ............................................................... 84
6.14 Order vs Delivery Date ........................................................................................ 85
6.14.1 Order vs Delivery Date Exception Form ............................................................. 86
6.15 Submitting Attachments for Electronic Claims ................................................... 86
6.15.1 Attachment Cover Sheet ...................................................................................... 88
6.16 Sterilization, Hysterectomy and Abortion Consent Forms ................................. 88
6.16.1 Sterilization Consent Form and Guidelines ......................................................... 88
6.16.1.1 Sterilization Consent Form .............................................................................. 90
6.16.1.2 Instructions for Completing the Sterilization Consent Form........................... 90
6.16.2 Hysterectomy Acknowledgment of Consent ....................................................... 90
6.16.2.1 Instructions for Completing the Hysterectomy Acknowledgment of Consent
Form ................................................................................................................ 92
6.16.2.2 Hysterectomy Acknowledgment Consent Form.............................................. 93
6.16.3 Abortion Certification Guidelines ....................................................................... 93
6.16.3.1 Instructions for Completing the Abortion Certification Form ......................... 93
6.16.3.2 Abortion Certification Form ............................................................................ 94
6.17 Remittance Advice .............................................................................................. 94
6.17.1 Sample Professional Remittance Advice ............................................................ 96

Common Billing Information ____________________________________________________
Ch. 6 Index 48 Revision 4/1/17
6.17.2 How to Read the Remittance Advice .................................................................. 97
6.17.3 Remittance Advice Replacement Request Policy ............................................... 98
6.17.3.1 Remittance Advice (RA) Replacement Request Form .................................... 99
6.17.4 Obtain an RA from the Web ................................................................................ 99
6.17.5 When a Client Has Other Insurance .................................................................... 99
6.18 Resubmitting Versus Adjusting Claims ............................................................ 100
6.18.1 How Long do Providers Have to Resubmit or Adjust a Claim? ....................... 100
6.18.2 Resubmitting a Claim ........................................................................................ 101
6.18.2.1 When to Resubmit to Medicaid ..................................................................... 101
6.18.3 Adjustment/Void Request Form Electronically Adjusting Paid Claims via
Hardcopy/Paper ................................................................................................. 101
6.18.3.1 Adjustment/Void Request Form .................................................................... 102
6.18.3.2 How to Request an Adjustment/Void ............................................................ 102
6.18.3.3 How to Complete the Adjustment/Void Request Form ................................. 103
6.18.3.4 When to Request an Adjustment ................................................................... 103
6.18.3.5 When to Request a Void ................................................................................ 104
6.19 Credit Balances .................................................................................................. 104
6.20 Timely Filing ..................................................................................................... 105
6.20.1 Exceptions to the Twelve-Month Limit ............................................................ 105
6.20.2 Appeal of Timely Filing .................................................................................... 106
6.20.2.1 How to Appeal ............................................................................................... 106
6.21 Important Information Regarding Retroactive Eligibility Decisions ................ 106
6.22 Client Fails to Notify a Provider of Eligibility .................................................. 107
6.23 Billing Tips to Avoid Timely Filing Denials .................................................... 107
6.24 Telehealth .......................................................................................................... 108
6.24.1 Covered Services ............................................................................................... 108
6.24.2 Non-Covered Services ....................................................................................... 110
6.24.3 Billing Requirements ......................................................................................... 110
Common Billing Information ____________________________________________________
Ch. 6 Index 49 Revision 4/1/17
6.1 Electronic Billing
As of July 1, 2015 Wyoming Medicaid requires all providers to submit electronically.
There are two (2) exceptions to this requirement:
Providers who do not submit at least 25 claims in a calendar year.
Providers who do not bill diagnosis codes on their claims.
If a provider is unable to submit electronically, the provider must submit a request for
an exemption in writing and must include:
Provider name, NPI, contact name and phone number.
The calendar year for which the exemption is being requested.
Detailed explanation of the reason for the exemption request.
Mail to:
Wyoming Medicaid
Attn: Provider Relations
PO Box 667
Cheyenne, WY 82003-0667
A new exemption request must be submitted for each calendar year. Wyoming
Medicaid has free software or applications available for providers to bill
electronically (Chapter 8, Electronic Data Interchange (EDI)).
6.2 Basic Paper Claim Information
The fiscal agent processes paper CMS-1500 and UB04 claims using Optical
Character Recognition (OCR). OCR is the process of using a scanner to read the
information on a claim and convert it into electronic format instead of being manually
entered. This process improves accuracy and increases the speed at which claims are
entered into the claims processing system. The quality of the claim will affect the
accuracy in which the claim is processed through OCR. The following is a list of tips
to aid providers in avoiding paper claims processing problems with OCR:
Use an original, standard, red-dropout form (CMS-1500 (02-12) and UB04).
Use typewritten print; for best results use a laser printer.
Use a clean, non-proportional font.
Use black ink.
Print claim data within the defined boxes on the claim form.
Print only the information asked for on the claim form.
Use all capital letters.

Common Billing Information ____________________________________________________
Ch. 6 Index 50 Revision 4/1/17
Use correction tape for corrections.
To avoid delays in the processing of claims it is recommended that providers avoid
the following:
Using copies of claim forms.
Faxing claims.
Using fonts smaller than 8 point.
Resizing the form.
Handwritten information on the claim form.
Entering “none”, “NA”, or “Same” if there is no information (leave the box
blank).
Mixing fonts on the same claim form.
Using italics or script fonts.
Printing slashed zeros.
Using highlighters to highlight field information.
Using stamps, labels, or stickers.
Marking out information on the form with a black marker.
Claims that do not follow Medicaid provider billing policies and procedures may be
returned unprocessed with a letter or may be processed incorrectly. When a claim is
returned the provider may correct the claim and return it to Medicaid for processing.
NOTE: The fiscal agent and the Division of Healthcare Financing (DHCF) are
prohibited by federal law from altering a claim.
Billing errors detected after a claim is submitted cannot be corrected until after
Medicaid has made payment or notified the provider of the denial. Providers should
not resubmit or attempt to adjust a claim until it is reported on their Remittance
Advice (6.18, Resubmitting Versus Adjusting Claims).
NOTE: Claims are to be submitted only after service(s) have been rendered, not
before. For deliverable items (i.e. dentures, DME, glasses, hearing aids,
etc.) the date of service must be the date of delivery, not the order date.
6.3 Authorized Signatures
All paper claims must be signed by the provider or the provider’s authorized
representative. Acceptable signatures may be either handwritten, a stamped facsimile,
typed, computer generated, or initialed. The signature certifies all information on the

Common Billing Information ____________________________________________________
Ch. 6 Index 51 Revision 4/1/17
claim is true, accurate, complete, and contains no false or erroneous information.
Remarks such as signature on file or facility names will not be accepted.
6.4 Completing the CMS-1500 Claim Form
6.4.1 Instructions for Completing the CMS-1500 Claim Form
Claim
Item
Title
Required
Conditionally
Required
Action/Description
1
Insurance Type
X
Place an "X" in the "Medicaid" box.
1a
Insured’s ID
Number
X
Enter the client’s ten (10) digit Medicaid ID
number that appears on the Medicaid
Identification card.
2
Patient’s Name
X
Enter the client’s last name, first name, and
middle initial.
3
Patient’s Date of
Birth/Sex
Information that will identify the patient and
distinguishes persons with similar names.

Common Billing Information ____________________________________________________
Ch. 6 Index 52 Revision 4/1/17
Claim
Item
Title
Required
Conditionally
Required
Action/Description
4
Insured’s Name
X
Enter the insured’s full last name, first
name, and middle initial. Insured’s name
identifies who holds the policy if different
than Patient information.
5
Patient’s Address
Refers to patient’s permanent residence.
6
Patient’s
Relationship to
Insured
X
If the client is covered by other insurance,
mark the appropriate box to show
relationship.
7
Insured’s Address
X
Enter the address of the insured.
8
Patient Status
Indicates patient’s marital and employment
status.
Instruct
ions for
9a-d
Other Insurance
Information
X
If item number 11d is marked complete
fields 9 and 9a-d.
9
Other Insured’s
Name
X
When additional group health coverage
exists, enter other insured’s full last name,
first name and middle initial of the enrollee
if different from item number 2.
9a
Other Insured’s
Policy or Group
Name
X
Enter the policy or group number of the
other insured.
9b
Reserved for
NUCC Use
9c
Reserved for
NUCC Use
9d
Insurance Plan or
Program Name
X
Enter the other insured’s insurance plan or
program name.
10a-c
Is Patient’s
Condition Related
to?
X
When appropriate, enter an X in the correct
box to indicate whether one or more the
services described in Item Number 24 are
for a condition or injury the occurred on the
job or as a result of an auto accident.
10d
Reserved for Local
Use
11
Insured’s Policy,
group or FECA
Number
X
Enter the insured’s policy or group number
as it appears on the ID card. Only complete
if Item Number 4 is completed.
11a
Insured’s Date of
Birth, Sex
X
Enter the 8- digit date of birth
(MM/DD/CCYY) and an X to indicate the
sex of the insured.
11b
Insured’s
Employer’s Name
or School Name
X
Enter the Name of the insured’s employer or
school.
Common Billing Information ____________________________________________________
Ch. 6 Index 53 Revision 4/1/17
Claim
Item
Title
Required
Conditionally
Required
Action/Description
11c
Insurance Plan
Name or Program
Name
X
Enter the insurance plan or program name
of the insured.
11d
Is there another
Health Benefit
Plan?
X
When appropriate, enter an X in the correct
box. If marked “YES”, complete 9 and 9a-d.
12
Patient’s or
Authorized
Person’s Signature
Indicates there is an authorization on file for
the release of any medical or other
information necessary to process the claim.
13
Payment
Authorization
Signature
Indicates that there is a signature on file
authorizing payment of medical benefits.
14
Date of current
illness, injury or
pregnancy
X
Enter the date of illness, injury or
pregnancy.
15
If Patient has had
Same or Similar
Illness
A patient having had same or similar illness
would indicate that the patient had a
previously related condition.
16
Date Patient
Unable to Work in
Current
Occupation
Time span the patient is or was unable to
work.
17
Name of Referring
Physician
Enter the name and credentials of the
professional who referred, ordered or
supervised the service on the claim.
17a
17a Other ID #
X
Other ID number of the referring, ordering,
or supervising provider is reported in 17a in
the shaded area. The qualifier indicating
what the number represents is reported in
the qualifier field to the immediate right.
17b
NPI #
X
Enter the NPI number of the referring,
ordering, or supervising provider in Item
Number 17b.
18
Hospitalization
Dates Related to
Current Service
The hospitalization dates related to current
services would refer to an inpatient stay and
indicates admission and discharge dates.
19
Reserved for Local
Use
20
Outside lab? $
Charges
Indicates that services have been rendered
by an independent provider as indicated in
Item Number 32 and related Costs.
Common Billing Information ____________________________________________________
Ch. 6 Index 54 Revision 4/1/17
Claim
Item
Title
Required
Conditionally
Required
Action/Description
21
ICD Indicator
Diagnosis or
Nature of Illness or
Injury
X
Enter the ICD-9 or ICD-10 indicator Enter
the patient’s diagnosis/condition. List up to
twelve ICD-PCM codes. Use the highest
level of specificity. Do not provide a
description in this field.
22
Medicaid
Resubmission
Code
The code and original reference number
assigned by the destination payer or receiver
to indicate a previously submitted claim.
23
Prior Authorization
X
Enter the ten (10) digit Prior Authorization
number from the approval letter, if
applicable. Claims for these services are
subject to service limits and the 12 month
filing limit.
24
Claim Line Detail
Supplemental information is to be placed in
the shaded sections of 24A through 24G as
required by individual payers. Medicaid
requires information such as NDC and
taxonomy in the shaded areas as defined in
each Item Number
24A
Dates of Service
X
Enter date(s) of service, from and to. If one
(1) date of service only enter that date under
“from”. Leave “to” blank or reenter “from”
date. Enter as MM/DD/YY. NDC qualifier
and NDC code will be placed in the shaded
area. For detailed information on billing
with the corresponding NDC codes, refer to
the NDC entry information following this
instruction table.
24B
Place of Service
X
Enter the two (2) digit Place of Service
(POS) code for each procedure performed.
24C
EMG
X
This field is used to identify if the service
was an emergency. Provider must maintain
documentation supporting an emergency
indicator. Enter Y for “YES” or leave blank
or enter N for “NO” in the bottom, un-
shaded area of the field. This field is
situational, but required when the service is
deemed an emergency
24D
Procedures,
Services, or
Supplies
X
Enter the CPT or HCPCS codes and
modifiers from the appropriate code set in
effect on the date of service.
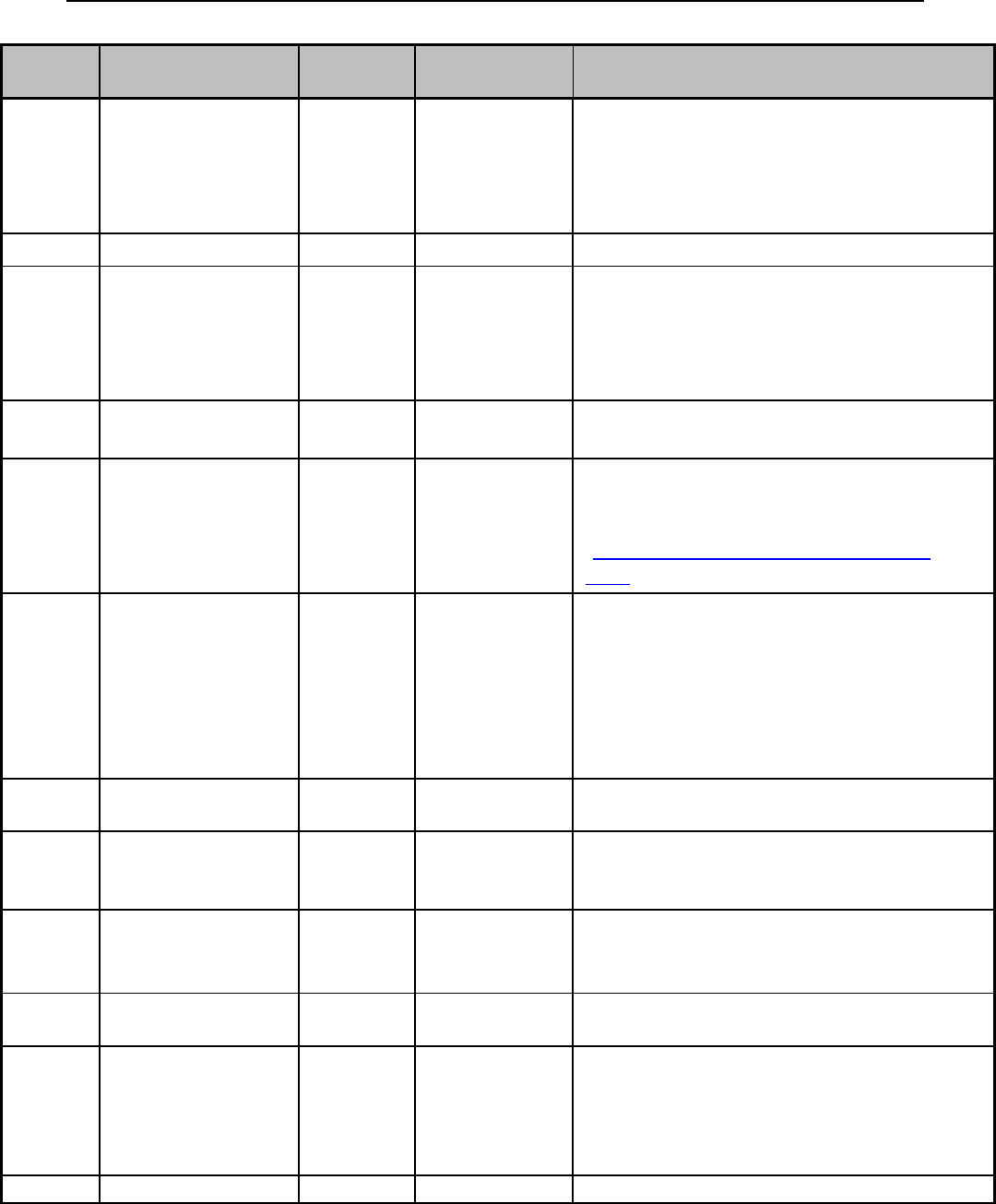
Common Billing Information ____________________________________________________
Ch. 6 Index 55 Revision 4/1/17
Claim
Item
Title
Required
Conditionally
Required
Action/Description
24E
Diagnosis Pointer
X
Enter the diagnosis code reference letter
(pointer) as shown in Item Number 21 to
relate the date of service and the procedures
performed to the primary diagnosis. Do Not
enter any diagnosis codes in this box.
24F
$ Charges
X
Enter the charge for each listed service.
24G
Days or Units
X
Enter the units of services rendered for each
detail line. A unit of service is the number
of times a procedure is performed. If only
one (1) service is performed, the numeral 1
must be entered.
24H
EPSDT/Family
Plan
X
Identifies certain services that may be
covered under some state plans.
24I
ID Qualifier
X
If the provider does not have an NPI
number, enter the appropriate qualifier and
identifying number in the shaded area
(Chapter 9, Wyoming Specific HIPAA
5010).
24J
Rendering
Provider ID #
X
The individual rendering the service is
reported in 24J. Enter the taxonomy code in
the shaded area of the field. Enter the NPI
number in the un-shaded area of the field.
Report the Identification Number in Items
24I and 24J only when different from the
data in Items 33a and 33b.
25
Federal Tax ID
Number
Refers to the unique identifier assigned by a
federal or state agency.
26
Patient’s Account
Number
The patient’s account number refers to the
identifier assigned by the provider
(optional).
27
Accept
Assignment?
X
Enter X in the correct box. Indicated that the
provider agrees to accept assignment under
the terms of the Medicare program.
28
Total Charge
X
Add all charges in Column 24F and enter
the total amount in this field.
29
Amount Paid
X
Enter total amount the patient or other
payers paid on the covered services only.
This field is reserved for third party
coverage only, do not enter Medicare paid
amounts
30
Balance Due
Enter the total amount due.
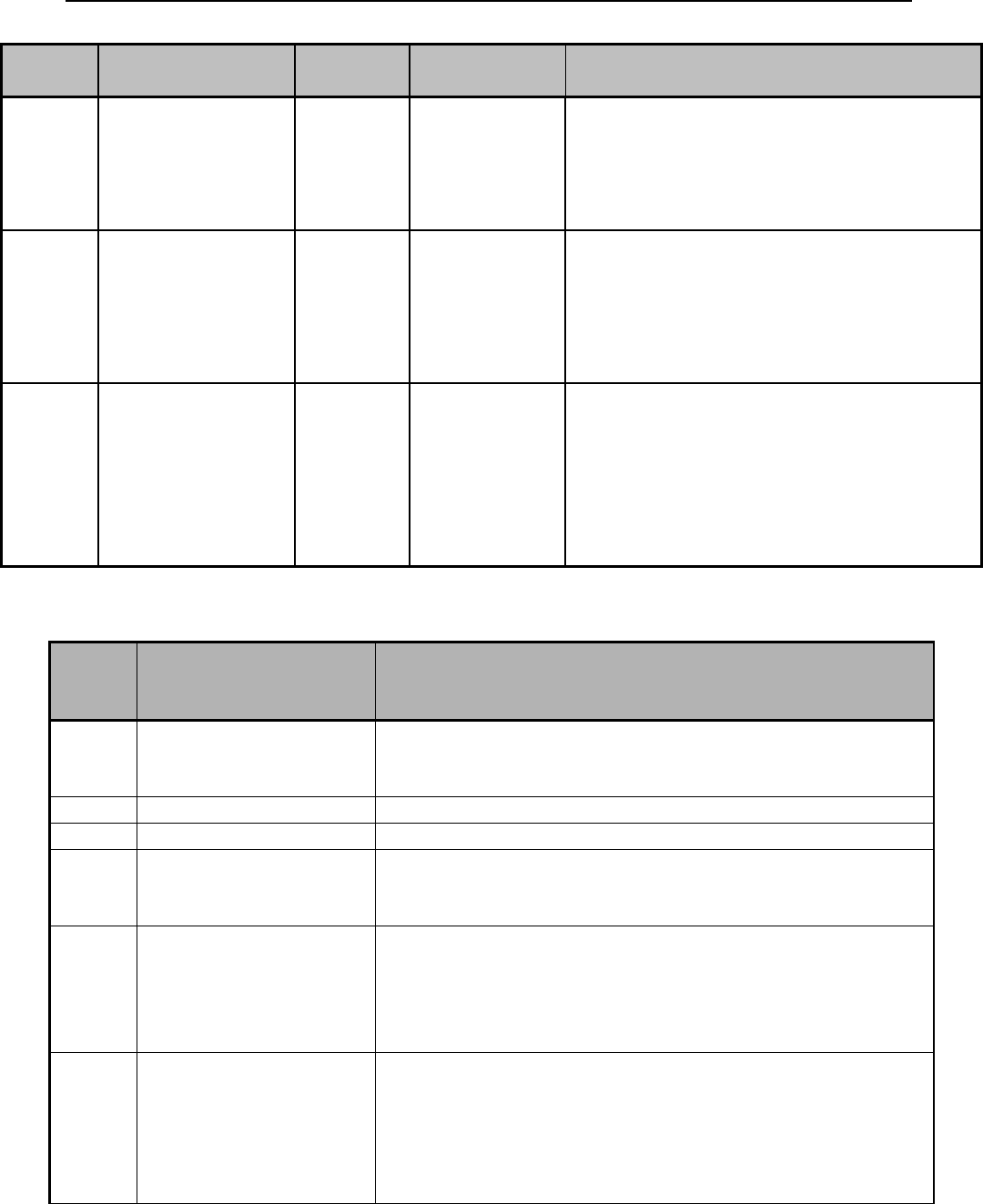
Common Billing Information ____________________________________________________
Ch. 6 Index 56 Revision 4/1/17
Claim
Item
Title
Required
Conditionally
Required
Action/Description
31
Signature of
Physician or
Supplier Including
Degrees or
Credentials
X
Enter the legal signature of the practitioner
or supplier, signature of the practitioner or
supplier representative. Enter date the form
was signed.
32, 32a
and 32b
Split
Field
32 -Service
Facility Location
Information
32a NPI Number
32b Other ID#
X
Enter the name, address, city, state and zip
code of the location where the services were
rendered. Enter the NPI number of the
service facility location in 32a; enter the two
(2) digit qualifier identifying the non-NPI
number followed by the ID number.
33, 33a
and 33b
Split
Field
33 -Billing
Provider Info &
Ph#
33a NPI number
33b taxonomy
X
Enter the provider’s or supplier’s billing
name, address, zip code and phone number.
Enter the NPI number of the billing provider
in 33a. Enter the two (2) digit qualifier
identifying the non-NPI number followed
by the ID number. Enter the provider’s
taxonomy number in 33b.
6.4.2 Place of Service
Place
of
Service
Place of Service Name
Place of Service Description
01
Pharmacy
A facility or location where drugs and other medically
related items and services are sold, dispensed, or
otherwise provided directly to patients.
02
Unassigned
N/A
03
School
A facility whose primary purpose is education.
04
Homeless Shelter
A facility or location whose primary purpose is to
provide temporary housing to homeless individuals (e.g.,
emergency shelters, individual or family shelters).
05
Indian Health
Service Free-
standing Facility
A facility or location, owned and operated by the Indian
Health Service, which provides diagnostic, therapeutic
(surgical and non-surgical), and rehabilitation services to
American Indians and Alaska Natives who do not require
hospitalization.
06
Indian Health
Service Provider-
based Facility
A facility or location, owned and operated by the Indian
Health Service, which provides diagnostic, therapeutic
(surgical and non-surgical), and rehabilitation services
rendered by, or under the supervision of, physicians to
American Indians and Alaska Natives admitted as
inpatients or outpatients.

Common Billing Information ____________________________________________________
Ch. 6 Index 57 Revision 4/1/17
Place
of
Service
Place of Service Name
Place of Service Description
07
Tribal 638 Free-
standing Facility
A facility or location owned and operated a federally
recognized American Indian or Alaska Native tribe or
tribal organization under a 638 agreement, which
provides diagnostic, therapeutic (surgical and non-
surgical), and rehabilitation services to tribal members
who do not require hospitalization.
08
Tribal 638 Provider-
based Facility
A facility or location owned and operated a federally
recognized American Indian or Alaska Native tribe or
tribal organization under a 638 agreement, which
provides diagnostic, therapeutic (surgical and non-
surgical), and rehabilitation services to tribal members
admitted as inpatients or outpatients.
09
Prison/Correctional
Facility
A prison, jail, reformatory, work farm, detention center,
or any other similar facility maintained by either Federal,
State, or local authorities for the purpose of confinement
or rehabilitation of adult or juvenile criminal offenders.
10
Unassigned
N/A
11
Office
Location, Other than a Hospital, Skilled Nursing Facility,
Military treatment Facility, Community Health Center,
State or Local Public Health Clinic, or Intermediate Care
Facility, where the health professional routinely provides
health examinations, diagnosis, and treatment of illness
or injury on an ambulatory basis.
12
Home
Location, other than a Hospital or other Facility, where
the patient receives care in a private session.
13
Assisted Living
Facility
Congregate residential facility with self-contained living
units providing assessment of each resident’s needs and
on-site support 24-hours a day, seven (7) days a week,
with the capacity to deliver or arrange for services
including some healthcare and other services.
14
Group Home
A residence, with shared living areas, where clients
receive supervision and other services such as social and
/ or behavioral services, custodial service, and minimal
services (e.g., medication administration.
15
Mobile Unit
A facility / unit that moves from place-to-place equipped
to provide preventive, screening, diagnostic, and / or
treatment services.
16
Temporary Lodging
A short term accommodation such as a hotel, camp
ground, hostel, cruise ship or resort where the patient
receives care, and which is not identified by any other
POS code.
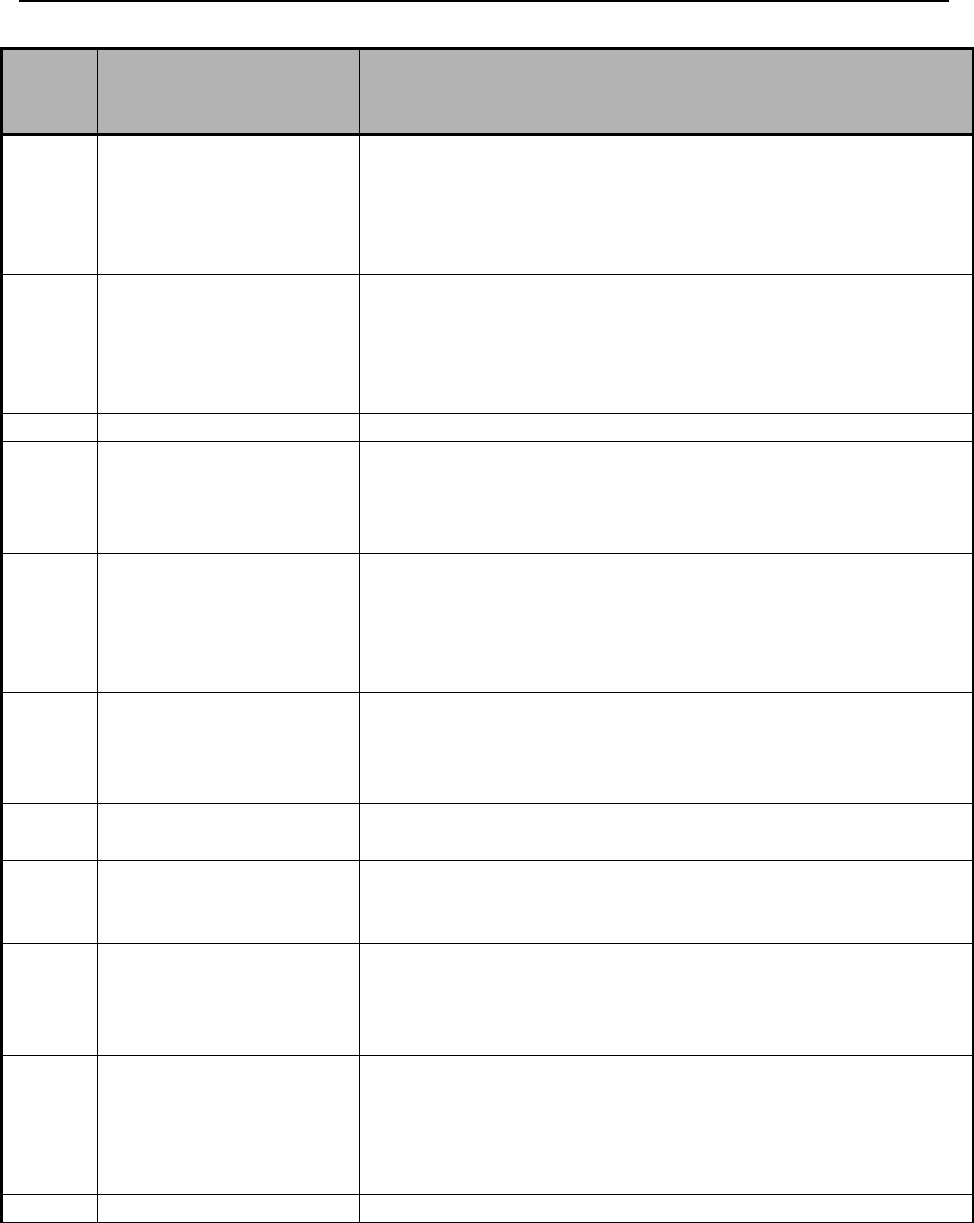
Common Billing Information ____________________________________________________
Ch. 6 Index 58 Revision 4/1/17
Place
of
Service
Place of Service Name
Place of Service Description
17
Walk-in Retail
Health Clinic
A walk-in-health clinic, other than an office, urgent care
facility, pharmacy or independent clinic and not
described by any other Place of Service code, that is
located within a retail operation and provides, on an
ambulatory basis, preventive and primary care services.
18
Place of
Employment-
Worksite
A location, not described by any other POS code, owned
or operated by a public or private entity where the patient
is employed, and where a health professional provides
on-going or episodic occupational medical, therapeutic or
rehabilitative services to the individual.
19
Unassigned
N/A
20
Urgent Care Facility
Location, distinct from a hospital emergency room, an
office, or a clinic, whose purpose is to diagnose and treat
illness or injury for unscheduled, ambulatory patients
seeking immediate medical attention.
21
Inpatient Hospital
A facility, other than psychiatric, which primarily
provides diagnostic, therapeutic (both surgical and non-
surgical), and rehabilitation services by, or under, the
supervision of physicians to patients admitted for a
variety of medical conditions.
22
Outpatient Hospital
A portion of a Hospital, which provides diagnostic,
therapeutic (both surgical and non-surgical), and
rehabilitation services to sick or injured persons who do
not require Hospitalization or Institutionalization.
23
Emergency Room –
Hospital
A portion of a Hospital where emergency diagnosis and
treatment of illness or injury is provided.
24
Ambulatory Surgical
Center
A free standing facility, other than a physician’s office,
where surgical and diagnostic services are provided on an
ambulatory basis.
25
Birthing Center
A facility, other than a hospital’s maternity facilities or a
physician’s office, which provides a setting for labor,
delivery, and immediate post-partum care as well as
immediate care of new born infants.
26
Military Treatment
Facility
A medical facility operated by one (1) or more of the
Uniformed Services. Military Treatment Facility (MTF)
also refers to certain former U.S. Public Health Services
(USPHS) facilities now designated as Uniformed Service
Treatment Facilities (USTF).
27-30
Unassigned
N/A
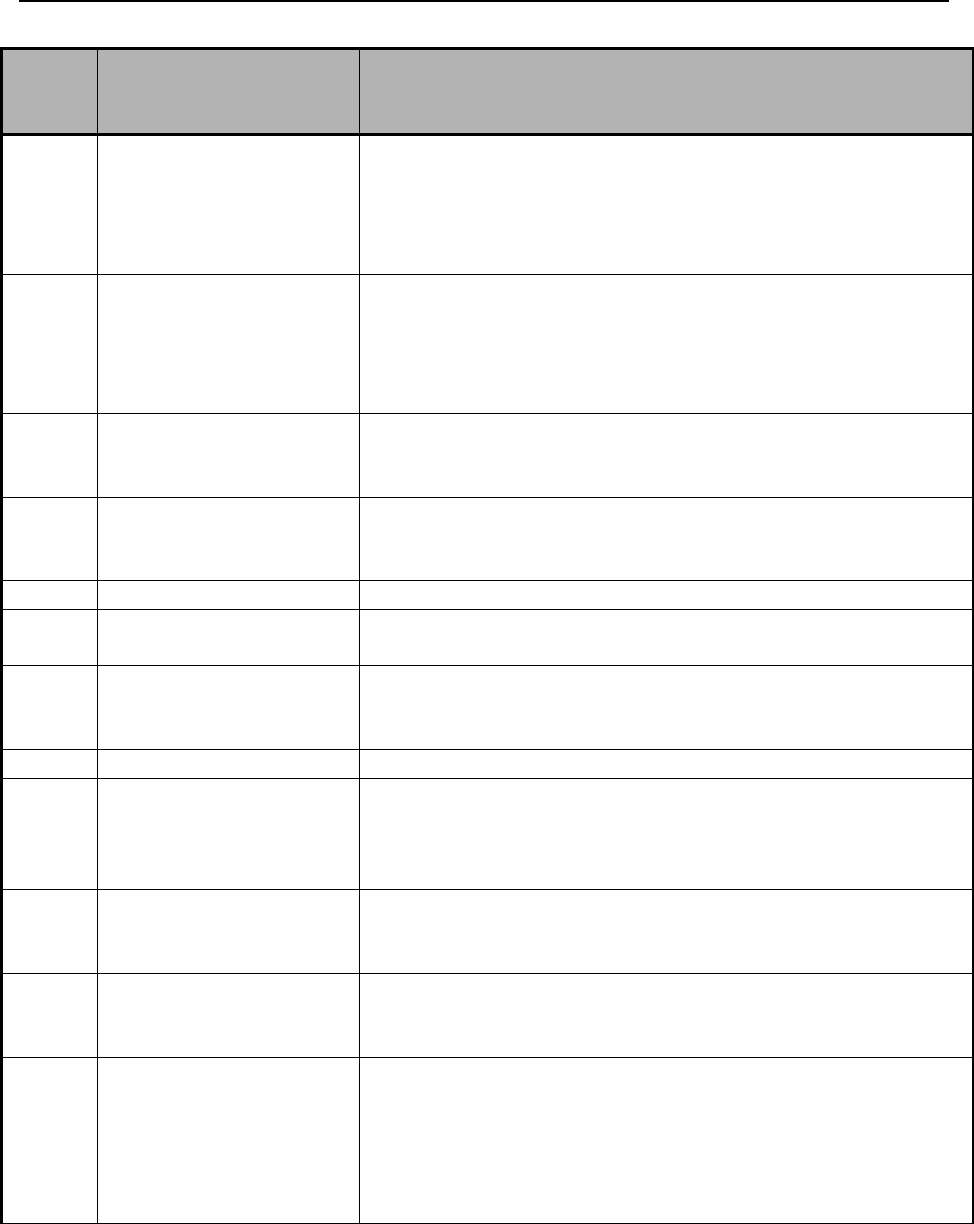
Common Billing Information ____________________________________________________
Ch. 6 Index 59 Revision 4/1/17
Place
of
Service
Place of Service Name
Place of Service Description
31
Skilled Nursing
Facility
A facility, which primarily provides inpatient skilled,
nursing care and related services to patients who require
medical, nursing, or rehabilitation services but does not
provide the level of care of treatment available on a
hospital.
32
Nursing Facility
A facility which primarily provides to residents skilled
nursing care and related services for the rehabilitation of
injured, disabled, or sick persons, or, on a regular basis,
health-related care services above the level of custodial
care to other than mentally retarded individuals.
33
Custodial Care
Facility
A facility which provides room, board and other personal
assistance services, generally on a long-term basis, which
does not include a medical component.
34
Hospice
A facility, other than a patient’s home, in which palliative
and supportive care for terminally ill patients and their
families are provided.
35-40
Unassigned
N/A
41
Ambulance – Land
A land vehicle specifically designed, equipped and
staffed for lifesaving and transporting the sick or injured.
42
Ambulance – Air or
Water
An air or water vehicle specifically designed, equipped
and staffed for lifesaving and transporting the sick or
injured.
43-48
Unassigned
N/A
49
Independent Clinic
A location, not part of a hospital and not described by
any other Place of Service code, that is organized and
operated to provide preventive, diagnostic, therapeutic,
rehabilitative, or palliative services to outpatients only.
50
Federally Qualified
Health Center
A facility located in a medically underserved area that
provides Medicare beneficiaries preventive primary
medical care under the general direction of a physician.
51
Inpatient Psychiatric
Facility
A facility that provides inpatient psychiatric services for
the diagnosis and treatment of mental illness on a 24-
hour basis, by or under the supervision of a physician.
52
Psychiatric Facility-
Partial
Hospitalization
A facility for the diagnosis and treatment of mental
illness that provides a planned therapeutic program for
patients who do not require full time hospitalization, but
who need broader programs than are possible from
outpatient visits to a hospital-bases or hospital-affiliated
facility.
Common Billing Information ____________________________________________________
Ch. 6 Index 60 Revision 4/1/17
Place
of
Service
Place of Service Name
Place of Service Description
53
Community Mental
Health Center
A facility that provides the following services: Outpatient
services, including specialized outpatient services for
children, the elderly, individuals who are chronically ill,
and residents of the CMHC’s mental health services are
who have been discharged from inpatient treatment at a
mental health facility; 24-hour a day emergency care
services; day treatment, other partial hospitalization
services, or psychosocial rehabilitation services.
54
Intermediate Care
Facility / Mentally
Retarded
A facility which primarily provides health-related care
and services above the level of custodial care to mentally
retarded individuals but does not provide the level of care
or treatment available in a hospital or SNF.
55
Residential
Substance Abuse
Treatment Facility
A facility which provides treatment for substance
(alcohol and drug) abuse to live-in residents who do not
require acute medical care. Services include individual
and group therapy and counseling, family counseling,
laboratory test, drugs and supplies, psychological testing,
and room and board.
56
Psychiatric
Residential
Treatment Center
A facility or distinct part of a facility for psychiatric care
which provides a total 24-hour therapeutically planned
and professionally staffed group living and learning
environment.
57
Non-residential
Substance Abuse
Treatment Facility
A location which provides treatment for substance
(alcohol and drug) abuse on an ambulatory basis.
Services include individual and group therapy and
counseling, family counseling, laboratory tests, drugs and
supplies, and psychological testing.
58-59
Unassigned
N/A
60
Mass Immunization
Center
A location where providers administer pneumococcal
pneumonia and influenza virus vaccinations and submit
these services as electronic media claims, paper claims,
or using the roster billing method. This generally takes
place in a mass immunization setting, such as, a public
health center, pharmacy, or mall but may include a
physician office setting.
61
Comprehensive
Inpatient
Rehabilitation
Facility
A facility that provides comprehensive rehabilitation
services under the supervision of a physician to inpatients
with physical disabilities. Services include physical
therapy, occupational therapy, speech therapy, speech
pathology, social or psychological services, and orthotics
and prosthetics services.
Common Billing Information ____________________________________________________
Ch. 6 Index 61 Revision 4/1/17
Place
of
Service
Place of Service Name
Place of Service Description
62
Comprehensive
Outpatient
Rehabilitation
Facility
A facility that provides comprehensive rehabilitation
services to outpatients with physical disabilities. Services
include physical therapy, occupational therapy, and
speech pathology services.
63-64
Unassigned
N/A
65
End-Stage Renal
Disease Treatment
Facility
A facility other that a hospital, which provides dialysis
treatment, maintenance, and /or training to patients or
caregivers on an ambulatory or home-care basis.
66-70
Unassigned
N/A
71
Public Health Clinic
A facility maintained by either State or local health
departments that provide ambulatory primary medical
care under the general direction of a physician.
72
Rural Health Clinic
A certified facility, which is located in a rural medically,
underserved area that provides ambulatory primary
medical care under the general direction of a physician.
73-80
Unassigned
N/A
81
Independent
Laboratory
A laboratory certified to perform diagnostic and/or
clinical tests independent of an institution or a
physician’s office.
82-98
Unassigned
N/A
99
Other Place of
Service
Other place of service not listed above.
6.5 Medicare Crossovers
Medicaid processes claims for Medicare/Medicaid services when provided to a
Medicaid eligible client.
6.5.1 General Information
Dually eligible clients are clients that are eligible for Medicare and Medicaid.
Providers may verify Medicare and Medicaid eligibility through the IVR (2.1,
Quick Reference).
Providers must accept assignment of claims for dually eligible clients.
Be sure Wyoming Medicaid has record of all applicable NPIs under which the
provider is submitting to Medicare to facilitate the electronic crossover
process.
Medicaid reimburses the lesser of the assigned coinsurance and deductible
amounts or the difference between the Medicaid allowable and the Medicare
paid amount for dually eligible clients as indicated on the Medicare
(Explanation of Medicare Benefits) EOMB.

Common Billing Information ____________________________________________________
Ch. 6 Index 62 Revision 4/1/17
o Wyoming Medicaid’s payment is payment in full. The client is not
responsible for any amount left over, even if assigned to coinsurance
or deductible by Medicare.
6.5.2 Billing Information
Medicare is primary to Medicaid and must be billed first. Direct Medicare
claims processing questions to the Medicare carrier.
When posting the Medicare payment, the EOMB (Explanation of Medicare
Benefits) may state that the claim has been forwarded to Medicaid. No further
action is required, it has automatically been submitted.
Medicare transmits electronic claims to Medicaid daily. Medicare transmits all
lines on a claim with any Medicare paid claim – If one (1) line pays, and three
(3) others are denied by Medicare, all four (4) lines will be transmitted to
Wyoming Medicaid.
The time limit for filing Medicare crossover claims to Medicaid is 12-months
from the date of service or six (6) months from the date of the Medicare
payment, whichever is later.
If payment is not received from Medicaid after 45-days of the Medicare
payment, submit a claim to Medicaid and include the COB (Coordination of
Benefits) information in the electronic claim. The line items on the claim
being submitted to Medicaid must be exactly the same as the claim submitted
to Medicare, except when Medicare denies then the claim must conform to
Medicaid policy.
If a paper claim is being submitted, the EOMB must be attached. If the
Medicare policy is a replacement/advantage or supplement, this information
must be noted (it can be hand written) on the EOMB.
NOTE: Do not resubmit a claim for coinsurance or deductible amounts unless the
provider has waited 45-days from Medicare’s payment date. A provider’s
claims may be returned if submitted without waiting the 45-days after the
Medicare payment date.
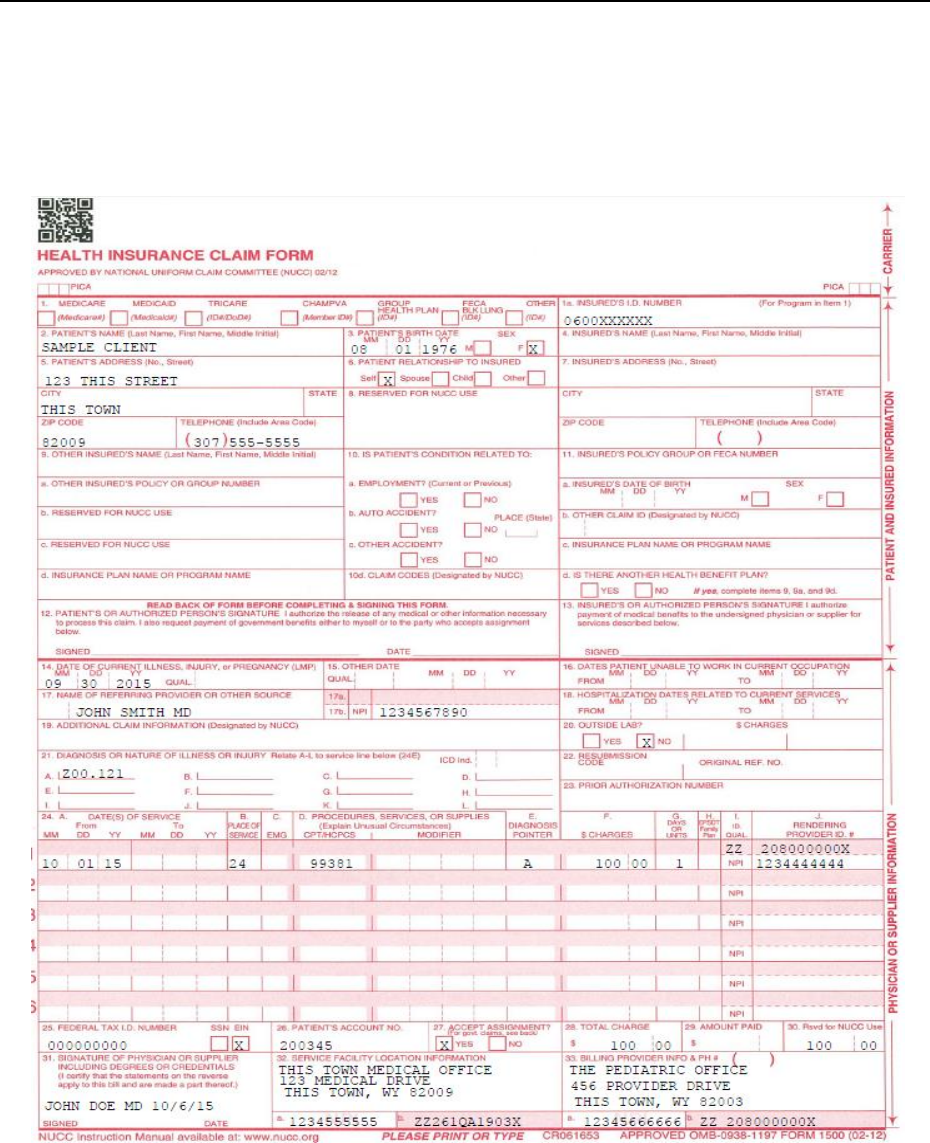
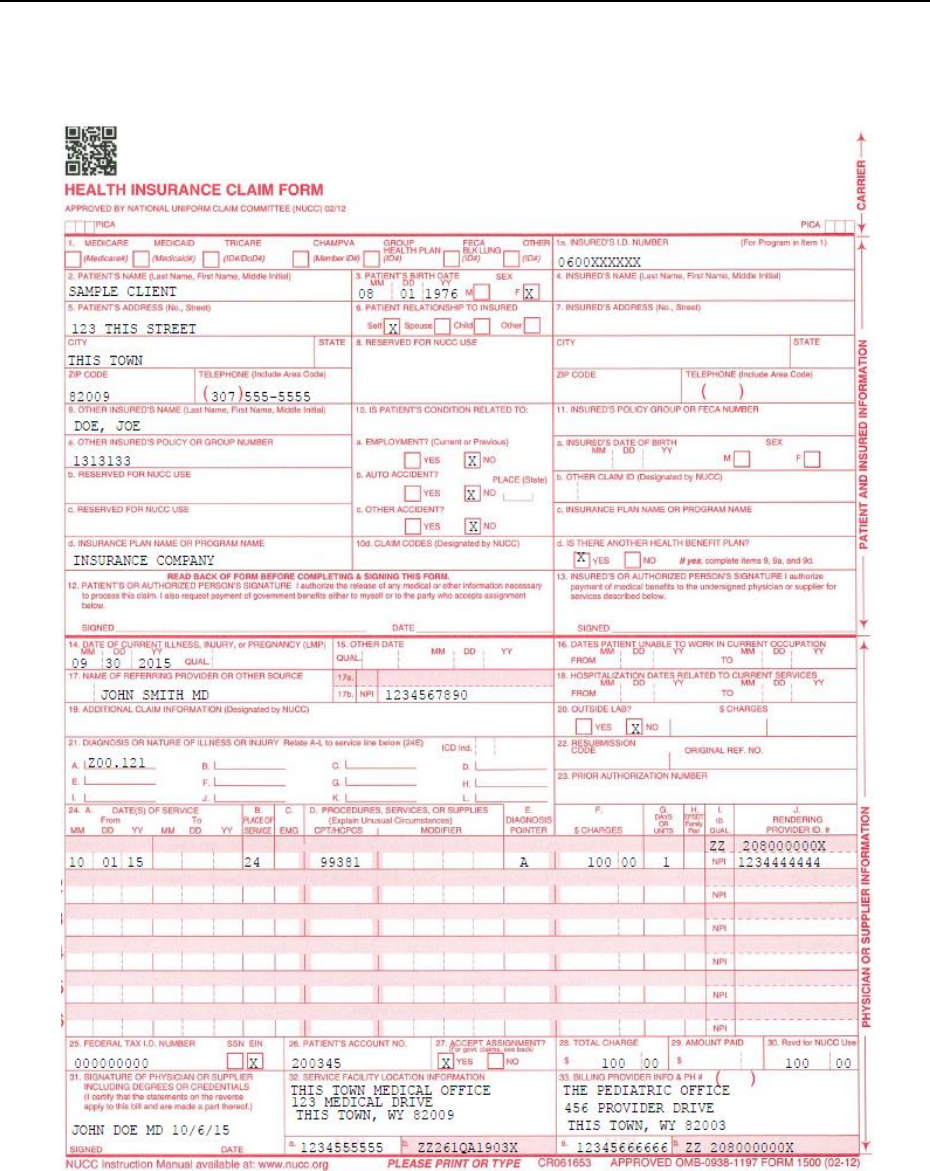
Common Billing Information ____________________________________________________
Ch. 6 Index 64 Revision 4/1/17
6.6.2 Client has Medicaid and Third Party Liability (TPL) or Client
has Medicaid, Medicare and TPL
NOTE: If the client has both Medicare and TPL in addition to Medicaid, attach the
TPL EOB and the Medicare EOMB to the claim. If the client has TPL and
Medicaid but no Medicare, attach the TPL EOB to the claim.
Common Billing Information ____________________________________________________
Ch. 6 Index 65 Revision 4/1/17
6.7 National Drug Code (NDC) Billing Requirement
Effective for dates of service on and after March 1, 2008 Medicaid will require
providers to include National Drug Codes (NDCs) on professional and institutional
claims when certain drug-related procedure codes are billed. This policy is mandated
by the Federal Deficit Reduction Act (DRA) of 2005, which requires state Medicaid
programs to collect rebates from drug manufacturers when their products are
administered in an office, clinic, hospital or other outpatient setting.
The NDC is a unique 11-digit identifier assigned to a drug product by the
labeler/manufacturer under Federal Drug Administration (FDA) regulations. It is
comprised of three (3) segments configured in a 5-4-2 format.
6
5
2
9
3
-
0
0
0
1
-
0
1
Labeler Code Product Code Package Code
(5 Digits) (4 Digits) (2 Digits)
Labeler Code – Five (5) digit number assigned by the Food and Drug
Administration (FDA) to uniquely identify each firm that manufactures,
repacks, or distributes drug products.
Product Code – Four (4) digit number that identifies the specific drug,
strength and dosage form.
Package Code – Two (2) digit number that identifies the package size.
6.7.1 Converting 10-Digit NDC’s to 11-Digits
Many NDCs are displayed on drug products using a ten (10) digit format. However,
to meet the requirements of the new policy, NDCs must be billed to Medicaid using
the 11-digits FDA standard. Converting an NDC from ten (10) to 11-digits requires
the strategic placement of a zero (0). The following table shows three (3) common ten
(10) digit NDC formats converted to 11-digits.
Converting 10-Digit NDCs to 11-Digits
10-Digit Format
Sample 10-Digit
NDC
Required 11-Digit Format
Sample 10-Digit NDC
Converted to 11-Digits
9999-9999-99 (4-4-2)
0002-7597-01 Zyprexa
10mg vial
09999-9999-99 (5-4-2)
00002-7597-01
99999-999-99 (5-3-2)
50242-040-62 Xolair
150mg vial
99999-0999-99 (5-4-2)
50242-0040-62
99999-9999-9 (5-4-1)
60575-4112-1 Synagis
50mg vial
99999-9999-09 (5-4-2)
60575-4112-01

Common Billing Information ____________________________________________________
Ch. 6 Index 66 Revision 4/1/17
NOTE: Hyphens are used solely to illustrate the various ten (10) and 11 digit
formats. Do not use hyphens when billing NDCs.
6.7.2 Documenting and Billing the Appropriate NDC
A drug may have multiple manufacturers so it is vital to use the NDC of the
administered drug and not another manufacturer’s product, even if the chemical name
is the same. It is important that providers develop a process to capture the NDC when
the drug is administered, before the packaging is thrown away. It is not permissible to
bill Medicaid with any NDC other than the one (1) administered. Providers should not
pre-program their billing systems to automatically utilize a certain NDC for a
procedure code that does not accurately reflect the product that was administered to
the client.
Clinical documentation must record the NDC from the actual product, not just from
the packaging, as these may not match. Documentation must also record the lot
number and expiration date for future reference in the event of a health or safety
product recall.

Common Billing Information ____________________________________________________
Ch. 6 Index 67 Revision 4/1/17
6.7.3 Procedure Code/NDC Combinations
The list of rebateable NDCs Medicaid posts to its website will also present providers
a way to validate procedure code/NDC combinations. The table below illustrates a
few sample entries from the list.
NDC
Procedure
Code
Procedure
Description
NDC Label
Rebateable
Rebate
Start
Date
Rebate
End
Date
58468-
0040-01
J0180
Injection,
Agalsidase
Beta, 1 MG
Fabrazyme (PF)
35 MG
Y
01/01/1991
99/99/9999
58468-
0041-01
J0180
Injection,
Agalsidase
Beta, 1 MG
Fabrazyme (PF)
5 MG
Y
01/01/1991
99/99/9999
58468-
1060-01
J0205
Injection,
Alglucerase,
Per 10
Ceredase 80
U/ML
Y
01/01/1991
99/99/9999
00517-
8905-01
J0210
Injection,
Methyldopa
te HCL
Methyldopate
HCL (S.D.V.) 50
Y
10/01/1991
99/99/9999
The first two (2) entries show NDCs 58468-0040-01 and 58468-0041-01 can only be
paired with one (1) procedure code, J0180. These are the only valid procedure code /
NDC combinations when billing Agalsidase. Pairing either NDC with a different
procedure code OR pairing the procedure code with a different NDC would create an
invalid combination. Procedure code / NDC combinations deemed invalid according
to the list will be denied.
6.7.4 Billing Requirements
The requirement to report NDCs on professional and institutional claims is meant to
supplement procedure code billing, not replace it. Providers are still required to
include applicable procedure code information such as dates of service, CPT/HCPCS
code, modifier(s), charges and units.
6.7.5 Submitting One NDC per Procedure Code
If one (1) NDC is to be submitted for a procedure code, the procedure code,
procedure quantity and NDC must be reported. No modifier is required.
Procedure Code
Modifier
Procedure Quantity
NDC
90378
2
60574-4111-01

Common Billing Information ____________________________________________________
Ch. 6 Index 68 Revision 4/1/17
6.7.6 Submitting Multiple NDCs per Procedure Code
If two (2) or more NDCs are to be submitted for a procedure code, the procedure code
must be repeated on separate lines for each unique NDC. For example, if a provider
administers 150 mg of Synagis, a 50 mg vial and a 100 mg vial would be used.
Although the vials have separate NDCs, the drug has one (1) procedure code, 90378.
So, the procedure code would be reported twice on the claim, but paired with
different NDCs.
Procedure Code
Modifier
Procedure Quantity
NDC
90378
KP
2
60574-4111-01
90378
KQ
1
60574-4112-01
On the first (1st) line, the procedure code, procedure quantity, and NDC are reported
with a KP modifier (first drug of a multi-drug). On the second line, the procedure
code, procedure quantity and NDC are reported with a KQ modifier
(second/subsequent drug of a multi-drug).
NOTE: When reporting more than two (2) NDCs per procedure code, the KQ
modifier is also used on the subsequent lines.
6.7.7 Medicare Crossover Claims
Because Medicaid pays Medicare coinsurance and deductible for dual-eligible clients,
the NDC will also be required on Medicare crossover claims for all applicable
procedure codes. Medicaid has verified that NDC information reported on claims
submitted to Medicare will be included in the automated crossover claim feed to
Medicaid. Crossover claim lines that are missing a required NDC will be denied.
6.7.8 CMS-1500 02-12 Billing Instructions
To report a procedure code with a NDC on the CMS-1500 02-12 claim form, enter
the following NDC information into the shaded portion of field 24A:
NDC qualifier of N4 [Required]
NDC 11-digit numeric code [Required]
Do not enter a space between the N4 qualifier and the NDC. Do not enter hyphens or
spaces within the NDC.
CMS-1500 02-12 – One (1) NDC per Procedure Code:
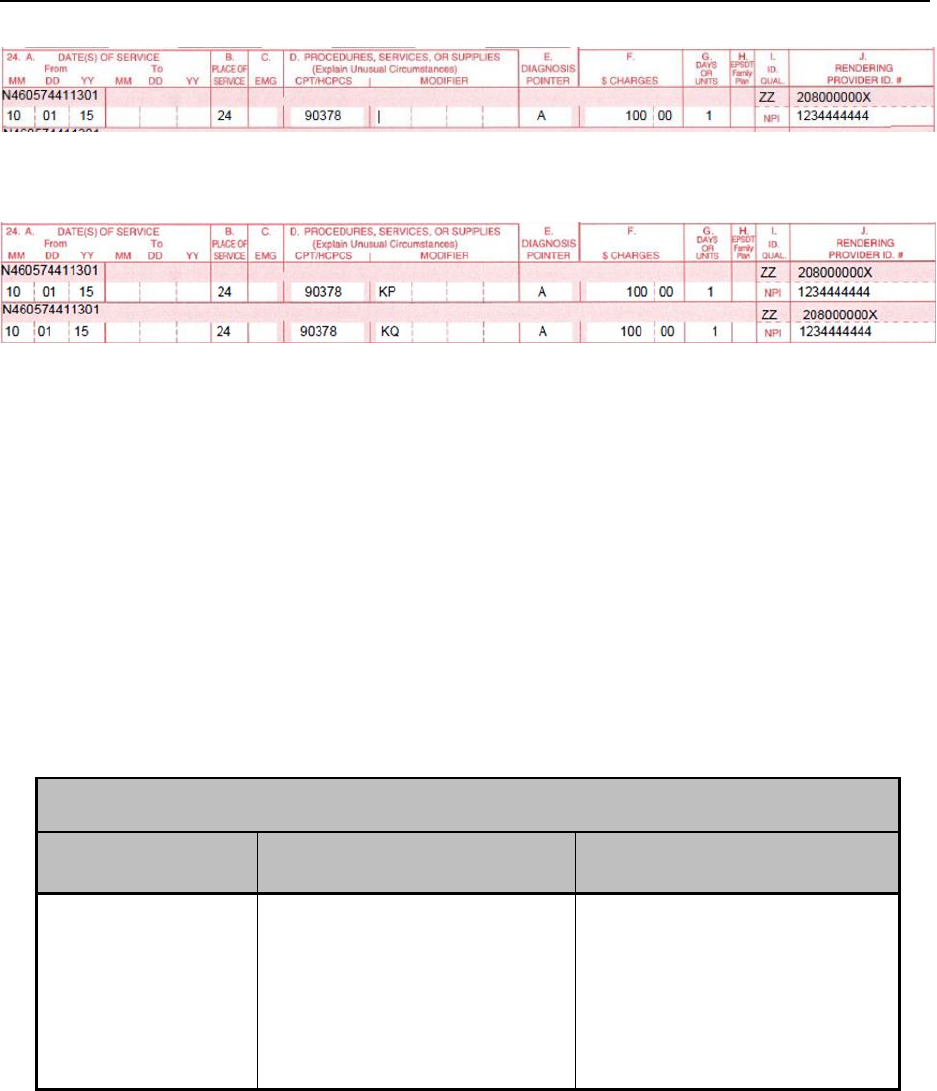
Common Billing Information ____________________________________________________
Ch. 6 Index 69 Revision 4/1/17
CMS-1500 02-12 – Two (2) NDCs per Procedure Code:
NOTE: Medicaid’s instructions follow the National Uniform Claim Committee’s
(NUCC) recommended guidelines for reporting the NDC on the CMS-
1500 02-12 claim form. Provider claims that do not adhere to these
guidelines will be returned unprocessed.
6.8 Cap Limits
Medicaid clients 21 years of age and older are subject to service cap limits on the
number of office/outpatient hospital visits and behavioral health visits. Medicaid
clients of any age are subject to service cap limits on the number of
physical/occupational/speech therapy visits, chiropractic visits, dietician visits and
emergency dental visits they receive.
NOTE: Ancillary services (e.g., lab, x-ray, etc.) provided during an
office/outpatient hospital visit that exceeded the cap limit will still be
reimbursed.
OFFICE AND OUTPATIENT HOSPITAL VISITS
Codes
Limits
Does not apply to:
Procedure Codes:
99281-99285
99201-99215
Revenue Codes:
0450-0459
0510-0519
12 combined visits per
calendar year
Clients Under Age 21
Emergency Visits
Family Planning Services
Medicare Crossovers
Common Billing Information ____________________________________________________
Ch. 6 Index 70 Revision 4/1/17
PHYSICAL THERAPY, OCCUPATIONAL THERAPY, SPEECH THERAPY,
BEHAVIORAL HEALTH VISITS, CHIROPRACTIC VISITS AND DIETICIAN
Codes
Limits
Does not apply to:
Procedure codes:
90785; 90792; 90832-
90834; 90836-90839;
90845-90849; 90853;
90857;92507-92508;
92526; 96101-96125;
97010-97039; 97110-
97546, 97802-97804,
98940-98942; (all
modalities on same date of
service count as 1 visit)
HCPCS Level II codes:
G9012; H0005-H0006;
H0031; H0034; H0047;
H2010; H2014; H2015;
H2017; H2019; H2021;
T1007; T1012; T1017 (all
modalities on same date of
service count as 1 visit)
Revenue codes:
0420,0421, 0422,0 424,
0430, 0431, 0432, 0434,
0439, 0440, 0441, 0442,
0444, and 0449 (each unit
counts as 1 visit)
20 physical therapy
visits per calendar year
20 occupational therapy
visits per calendar year
20 speech therapy visits
per calendar year
20 behavioral health
visits per calendar year
(21 and over only)
20 chiropractic visits per
calendar year
20 dietician visits per
calendar year
Medicare Crossovers
If a client has exceeded the Medicaid limits on office/outpatient hospital visits,
physical/occupational/speech therapy visits, behavioral health visits, chiropractic
visits, or dietitian visits the provider may bill him/her or request the cap limit be
waived.
6.8.1 Cap Limit Waiver
Physicians, nurse practitioners, physical, occupational and speech therapists,
psychiatrist, psychologists, licensed mental health professionals such as licensed
professional counselors, licensed marriage and family therapist, licensed certified
social workers and licensed addiction therapists, community mental health or
substance abuse treatment centers, chiropractors and dieticians may request a waiver
of a cap limit once a limit has been reached.

Common Billing Information ____________________________________________________
Ch. 6 Index 71 Revision 4/1/17
Cap limit waiver requests must be submitted on the Cap Limit Waiver Request form
and cite specific medical necessity. Below is the Cap Limit Waiver Request form for
office visits, therapies (PT, OT, ST and Chiropractic services), dietician visits and
Behavioral Health visits (6.9.2 Cap Limit Waiver Request Form).
The form must be mailed to:
Wyoming Medicaid
Attn: Medical Policy
PO Box 667
Cheyenne, WY 82003-0667
If granted, a cap limit waiver is valid for one (1) calendar year. For additional
information, contact Medical Policy (2.1, Quick Reference).
If a cap limit waiver request is denied, the provider may request reconsideration by
mail by providing additional supporting documentation to include but not limited to a
detailed letter of explanation as to why you feel the denial is incorrect, additional
medical records and/or testing results. This request must be in accordance with
Medicaid rules.
6.8.2 Cap Limit Waiver Request Form
NOTE: Click image above to be taken to a printable version of this form

Common Billing Information ____________________________________________________
Ch. 6 Index 72 Revision 4/1/17
6.8.3 Cap Limit Waiver Request Form Instructions
Field
Action
Pay to (Group) NPI
Complete with the ten digit NPI number for the Pay to/Group Provider
Pay to (Group) Name
Complete with the name of the Pay to/Group Provider
Treating/Rendering NPI
Complete with the ten digit NPI number for the treating provider
Treating/Rendering Name
Complete with the name of the treating provider
Client ID
Complete with the client’s Wyoming Medicaid ID number
Client Name
Complete with the client’s full name
Client Age
Complete with the client’s age at the time of the request
Cap Limit Year
Complete with the requested calendar year for the cap limit waiver
Cap Limit Begin/End Date
Complete with the dates the cap limit waiver will need to begin and when
it will end
Cap Limit Type
Check the appropriate box for which type cap limit waiver you are
requesting
Date of Onset Condition
Complete with the date the onset condition began
Diagnosis Code
Complete with the diagnosis codes – up to four are allowed
Ordering Provider Name & NPI
Complete with the Name and NPI number for the ordering provider – this
section is required for Speech, Occupational or Physical Therapy
Describe injury, illness, surgery or
triggering event that initiated the
need for services
Complete with what caused the acute condition (i.e. post-surgery,
personal injury, auto accident, etc.)
Describe acute condition requiring
rehabilitative services
A detailed explanation as to the diagnosis and rehabilitative need for
services for acute conditions only. Indicate why the client has exceeded
their CAP limit. For Behavioral Health Cap Limit Waiver Request,
ensure to include last 5 progress reports and treatment plan.
Describe anticipated rehabilitative
progress and length of additional
treatment
Describe the rehabilitative progress anticipated and the length needed for
additional treatment. For physical, occupational, or speech therapy Cap
Limit Waiver Requests, ensure you attach a copy of the practitioner’s
order.
Treating provider signature and date
The provider providing the services will need to sign and date the Cap
Limit Waiver Request Form

Common Billing Information ____________________________________________________
Ch. 6 Index 73 Revision 4/1/17
6.8.4 Cap Limit Additional Information for Clients Under the Age of 21
In addition to the completion of the Cap Limit Waiver Request Form, the Additional
Information sheet must be completed for clients under the age of 21.
Common Billing Information ____________________________________________________
Ch. 6 Index 74 Revision 4/1/17
6.8.5 Cap Limit Additional Information Instructions
Cap Limit Additional Information
For Children who are school age:
Field
Action
Is this child on IEP?
Indicate whether or not the child is on an Individualized Education Program (IEP)
What services is the
child receiving
through school
system?
Describe the services the child is receiving through the school system under the IEP
How are the
services you are
provider distinct
from the services
being provided
through the school
system and how are
you avoiding
conflict with the
services being
provided?
Describe how the services you are providing to the client are different from the
services that are being provided through the school system and how you are avoiding
conflict with those services
For kids who are younger than school age
Has this child been
evaluated at a Child
Development
Center?
Indicate whether or not this child has been evaluated at a Child Development Center
(CDC)
What services is the
child receiving
through the CDC?
Describe the services the child is receiving through the Child Development Center
How are the
services you are
providing distinct
from the services
being provided
through the CDC
and how are you
avoiding conflict
with the services
being provided?
Describe the services you are providing and how they are distinct from the services
that are being provided through the Child Development Center and how you are
avoiding conflict with those services being provided through the CDC

Common Billing Information ____________________________________________________
Ch. 6 Index 75 Revision 4/1/17
6.9 Reimbursement Methodologies
Medicaid reimbursement for covered services is based on a variety of payment
methodologies depending on the service provided.
Medicaid fee schedule
By report pricing
Billed charges
Invoice charges
Negotiated rates
Per diem
RBRVS (Resource Based Relative Value Scale)
6.10 Usual and Customary Charges
Charges for services submitted to Medicaid must be made in accordance with an
individual provider’s usual and customary charges to the general public unless:
The provider has entered into an agreement with the Medicaid Program to
provide services at a negotiated rate; or
The provider has been directed by the Medicaid Program to submit charges at
a Medicaid-specified rate.
6.10.1 Invoice Charges
Invoice must be dated within 12-months prior to the date of service being
billed – if the invoice is older, a letter must be included explaining the age of
the invoice (i.e. product purchased in large quantity previously, and is still in
stock)
All discounts will be taken on the invoice.
The discounted pricing or codes cannot be marked out.
A packing slip, price quote, purchase order, delivery ticket, etc. may be used
only if the provider no longer has access to the invoice, and is unable to obtain
a replacement from the supplier/manufacturer, and a letter with explanation is
included.
Items must be clearly marked. (i.e. how many calories are in a can of formula,
items in a case, milligrams, ounces, etc.)
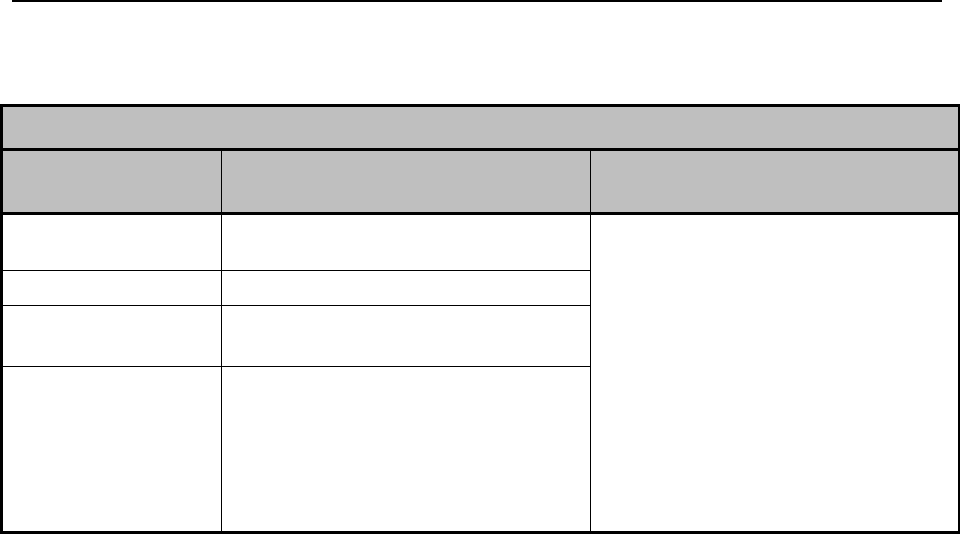
Common Billing Information ____________________________________________________
Ch. 6 Index 76 Revision 4/1/17
6.11 Co-Payment Schedule
$2.45 Co-Payment Schedule
Procedure and
Revenue Code(s)
Description
Exceptions
99201 – 99215
Office Visits only when the place
of service code is 11
Co-payment requirements do not
apply to:
Clients under age 21
Nursing Facility Residents
Pregnant Women
Family planning services
Emergency services
Hospice services
Medicare Crossovers
Members of a Federally recognized
tribe
99341 -99350
Home Visits
92002, 92004,
92014
Eye Examinations
90804 – 90815
Medical psychotherapy – co-
payment only applies when the
place of service code is 11
6.12 How to Bill for Newborns
When a mother is eligible for Medicaid, at the time the baby is born, the newborn is
automatically eligible for Medicaid for one (1) year. However, the WDH Customer
Service Center must be notified of the newborn’s name, gender, and date of birth,
mom’s name and Medicaid number for a Medicaid ID Card to be issued. This
information can be faxed, emailed, or mailed to the WDH Customer Service Center
on letterhead from the hospital where the baby was born or reported by the parent of
the baby. A provider will need to have the newborn client ID in order to bill newborn
claims.
6.13 Prior Authorization
Medicaid requires prior authorization (PA) on selected services and equipment.
Approval of a PA is never a guarantee of payment. A provider should not render
services until a client’s eligibility has been verified and a PA has been approved (if a
PA is required). Services rendered without obtaining a PA (when a PA is required)
may not be reimbursed.
Selected services and equipment requiring prior authorization include, but are not
limited to, the following – use in conjunction with the Medicaid Fee Schedule to
verify what needs PA:
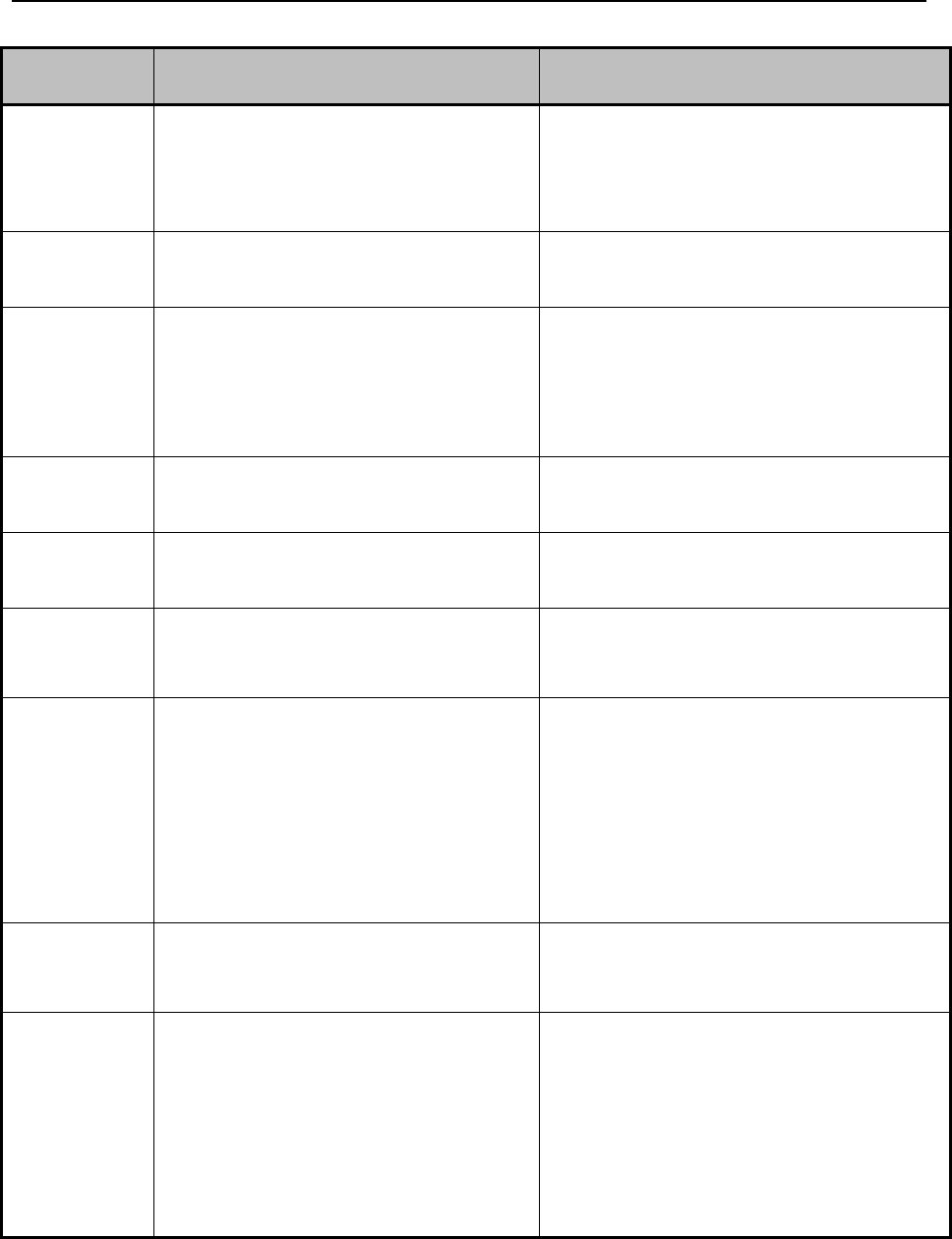
Common Billing Information ____________________________________________________
Ch. 6 Index 77 Revision 4/1/17
Agency
Name
Phone
Services Requiring PA
Division of
Healthcare
Financing
(DHCF)
Contact case manager
Case manager will contact the DHCF
Assisted Living Facility (ALF) Waiver
Long Term Care (LTC) Waiver
Out-of-State Home Health
Out-of-State Placement for LTC
Facilities
Dental
Services
(888)863-5806
Reference Dental Manual for details
Malocclusion (PA)
Implants & fixed bridges (PA)
Maxillofacial Surgeries (PA)
Behavioral
Health
Division
Contact case manager
Case manager will contact the Behavioral
Health Division
Acquired Brain Injury (ABI) Waiver
Services
Developmentally Disabled Adult
Waiver Services
Developmentally Disabled Children
Waiver Services
Goold Health
Systems Inc.
(GHS)
(877)207-1126
Pharmacy
HealthHelp
(888)545-1710
Option 2
Advanced Radiology, Cardiology and
Radiation Therapy
Magellan
(855)883-8740
Children’s Mental Health Waiver
Services
Medical
Policy
(800)251-1268
Option 1, 1, 4, 3
Hospice Services: Limited to clients
residing in a nursing home
Out-of-State Home Health
Surgeries Requiring PA (not listed in
this table)
Tysabri IV Infusion Treatment
Contact Lenses
Certain Eyeglass Lenses
Scleral Cover Shell
Qualis Health
(DMEPOS)
(800)783-8606
Durable Medical Equipment (DME)
Prosthetic and Orthotic Supplies (POS)
Home Health
WYhealth
(Utilization
and Care
Management)
(888)545-1710
Acute Psych
Extended Psych
Extraordinary Care
Gastric Bypass
Inpatient Rehabilitation
PRTF – Psychiatric Residential
Treatment Facility
Transplants
Vagus Nerve Stimulator
6.13.1 Requesting Prior Authorization from Medical Policy
Common Billing Information ____________________________________________________
Ch. 6 Index 78 Revision 4/1/17
This section only applies to providers requesting PA for out-of-state Home Health,
certain surgeries and hospice services (limited to clients residing in a nursing home).
For all other types of PA requests, contact the appropriate authorizing agencies listed
above for their written PA procedures.
Providers have three (3) ways to request and receive a PA:
Medicaid Prior Authorization Form (6.14.1.1, Medicaid Prior Authorization
Form). A hardcopy form for requesting a PA by mail or fax. For a copy of the
form and instructions on how to complete it, refer to the following section.
X12N 278 Prior Authorization Request and Response. A standard electronic
file format used to transmit PA requests and receive responses. For additional
information, refer to Chapter 8, Electronic Data Interchange (EDI) and
Chapter 9, Wyoming Specific HIPAA 5010 Electronic Specifications; or
Web-Based Entry (Limited to Medical Policy PA requests). A web-based
option for entering PA requests and receiving responses via Medicaid Secured
Provider Web Portal. For direction on entering a PA request through the
Secured Provider Web Portal, view the Web Portal Tutorial found on the
website. (2.1, Quick Reference). For additional information, refer to Chapter
8, Electronic Data Interchange (EDI) and Chapter 9, Wyoming Specific
HIPAA 5010 Electronic Specifications.
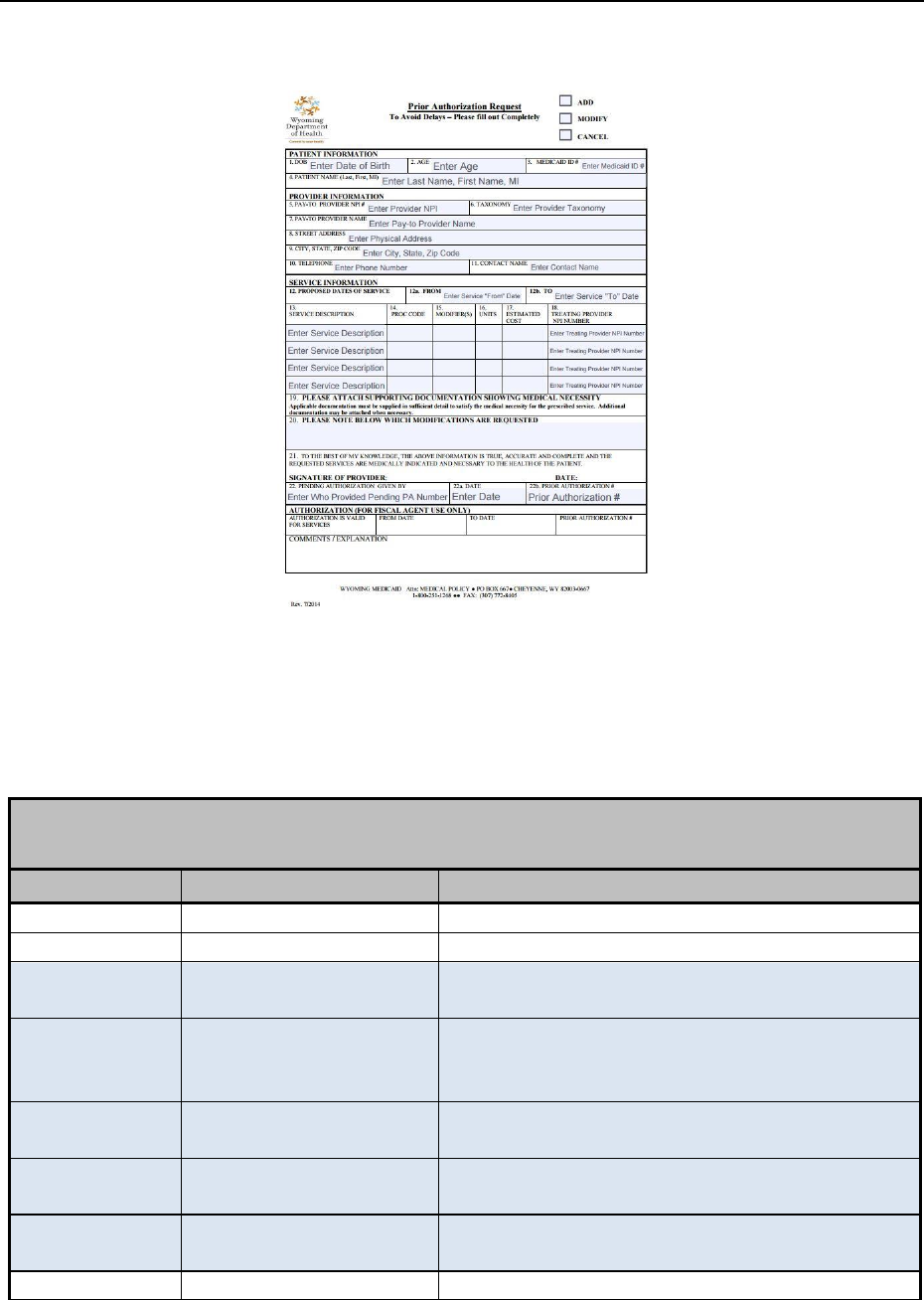
Common Billing Information ____________________________________________________
Ch. 6 Index 79 Revision 4/1/17
6.13.1.1 Medicaid Prior Authorization Form
NOTE: Click image above to be taken to a printable version of this form.
6.13.1.2 Instructions for Completing the Medicaid Prior
Authorization Form
Completing the Medicaid Prior Authorization Form for medical services
*Denotes Required Field
NOTE: Is this an Add, Modify, or Cancel request?
Field Number
Title
Action
1
Date of Birth
Enter MMDDYY of client’s date of birth.
2
Age
Enter client’s age.
3*
Medicaid ID Number
Enter the client’s ten (10) digit Medicaid ID
number.
4*
Patient Name
Enter Last Name, First Name and Middle
Initial exactly as it appears on the Medicaid
ID card.
5*
Pay-To Provider NPI
#
Enter the Pay to Provider NPI Numbers.
6*
Pay To Provider
Taxonomy
Enter the Pay To Provider Taxonomy.
7*
Pay To Provider
Name
Enter the Pay To Provider Name.
8
Street Address
Enter the Pay To Provider Street Address.
Common Billing Information ____________________________________________________
Ch. 6 Index 80 Revision 4/1/17
Completing the Medicaid Prior Authorization Form for medical services
*Denotes Required Field
NOTE: Is this an Add, Modify, or Cancel request?
Field Number
Title
Action
9
City, State, Zip Code
Enter the Pay To Provider City, State and Zip
Code.
10*
Telephone – Contact
Person
Enter phone number of the contact person
for this prior authorization.
11*
Contact Name
Enter the name of the person that can be
contacted regarding this Prior
Authorization.
12*
Proposed Dates of
service
Enter to the best of the providers ability,
what dates of service the provider is looking
for. It can be one (1) day or a date range.
13*
Service Description
Enter the service that the provider is
requesting.
14*
Procedure Code
Procedure Code for the service(s) being
requested.
15*
Modifier(s)
Modifier needed to bill the procedure on the
claim – If no modifiers needed – put N/A.
16*
Unit(s)
Enter number of each service requested.
17*
Estimated Cost
Enter dollar amount times the unit(s) for
each service requested.
18*
Treating Provider
NPI Number
Enter the Treating Provider NPI Number –
Needs to be a Wyoming Medicaid Provider.
19*
Supporting
Documentation
Please attach all documentation to support
medical necessity. Applicable
documentation must be supplied in
sufficient detail to satisfy the medical
necessity for the prescribed service.
Additional documentation may be attached
when necessary.
20
Modifications
This is the entry of changes that are needed by
the provider from the original request.
21*
Signature
The form needs to be signed and dated by
the entity requesting the prior authorization
of services.
22
Pending Authorization
If called in for a verbal authorization, put the
name of the person giving the PA number and
date.
NOTE: The Prior Authorization Request Form must match the lines on the claim
that are being billed.
Common Billing Information ____________________________________________________
Ch. 6 Index 81 Revision 4/1/17
6.13.2 Requesting an Emergency Prior Authorization
In the case of a medical emergency, providers should contact Medical Policy by
telephone, after business hours and on weekends, leave a message. Medical Policy
will provide a pending PA number until a formal request is submitted. The formal
request must be submitted within 30-days of receiving the pending PA number and
must include all documentation required.
NOTE: Contact the other appropriate authorizing agencies for their
pending/emergency PA procedures (6.14, Prior Authorization).
6.13.2.1 Prior Authorization Approval
Once a PA is approved, an approval letter (sample approval letter below) is mailed
that includes the PA number. The PA number must be entered in box 23 of the CMS-
1500 02-12 claim form. For placement in an electronic X12N 837 Professional Claim,
consult the Electronic Data Interchange Technical Report Type 3 (TR3). The TR3 can
be accessed at http://www.wpc-edi.com.
Common Billing Information ____________________________________________________
Ch. 6 Index 82 Revision 4/1/17
6.13.2.2 Sample PA Approval Letter
02/26/15 MEDICAID PRIOR
SAMPLE PROVIDER OF WYOMING AUTHORIZATION NOTICE
LTC WAIVER SERVICES
1234 SAMPLE STREET Client : SAMPLE CLIENT
SAMPLE WY 82001 Client ID: 0000062141
PA-NUMBER 0012900194
Waiver Case Manager :
***PRIOR AUTHORIZATION APPROVAL DOES NOT GUARANTEE ELIGIBILITY***
The prior authorization request submitted on behalf of Sample Client has been determined as follows:
01/01/15-01/31/15 T2041 – SUPPORTS BROKERAGE, SELF DIRECTED, 12 MIN APPROVED
APPR UNITS: 300 UNIT PRICE $ 3.32 USED UNITS: 202
02/01/15-02/28/15 T2041 – SUPPORTS BROKERAGE, SELF DRIECTED, 15 MIN APPROVED
APPR UNITS: 300 UNIT PRICE $ 3.32 USED UNITS: 0
CODE EXPLANATIONS:
NO DENIAL REASON PROVIDED
COMMENT:
A8200RB1
NOTE: PRIOR AUTHORIZATION APPROVAL DOES NOT GUARANTEE ELIGIBILITY. PAYMENT IS
SUBJECT TO THE CLIENT’S ELIGIBILITY AND MEDICAID BENEFIT LIMITATIONS. VERIFY ELIGIBILITY
BEFORE RENDERING SERVICES
PA-NUMBER 0012900194
A8200RB1
NOTE: For lines that are approved, the corresponding item may be purchased or
delivered, or service may be rendered.
Common Billing Information ____________________________________________________
Ch. 6 Index 83 Revision 4/1/17
6.13.2.3 Prior Authorization Denial
If a PA request is denied, the provider may request reconsideration to the appropriate
agency. This request must be in accordance with Medicaid rules.
6.13.2.4 Sample Prior Authorization Denial Letter
01/19/15 MEDICAID PRIOR AUTHORIZATION NOTICE
SAMPLE PROVIDER OF WYOMING
1234 SAMPLE STREET
SAMPLE WY 82001 Client: SAMPLE CLIENT
Client ID: 0000062141
PA-Number: 00198000001
***PRIOR AUTHORIZATION APPROVAL DOES NOT GUARANTEE ELIGIBILITY***
The prior authorization request submitted on behalf of Sample Client has been determined as follows:
01/18/10-01/18/11 V2715 – PRISM, PER LENS DENIED
APPR UNITS: 0 USED UNITS: 0
CODE EXPLANATIONS:
800 SERVICE NOT COVERED BY WYOMING MEDICAID
COMMENT:
DOES NOT FALL WITHIN AGE GUIDELINES FOR PROC CODE
NOTE: PRIOR AUTHORIZATION APPROVAL DOES NOT GUARANTEE ELIGIBILITY. PAYMENT IS SUBJECT TO THE
CLIENT’S ELIGIBILITY AND MEDICAID BENEFIT LIMITATIONS. VERIFY ELIGIBILITY BEFORE RENDERING SERVICES.
PA-Number: 00198000001
A1500RB2
NOTE: For lines that are denied, additional information may be needed before the
item or service can be reconsidered for approval. It is imperative this
information be supplied to the appropriate agency.
Common Billing Information ____________________________________________________
Ch. 6 Index 84 Revision 4/1/17
6.13.2.5 Prior Authorization Pending
If a PA request is in a pending status, it was likely the result of an emergency request
made over the phone to Medical Policy. A claim cannot be billed using a PA number
from a pending request (2.1, Quick Reference).
6.13.2.6 Sample Prior Authorization Pending
10/01/15 MEDICAID PRIOR AUTHORIZATION NOTICE
SAMPLE PROVIDER OF WYOMING
1234 SAMPLE STREET
SAMPLE WY 82001 Client: SAMPLE CLIENT
Client ID: 0000062141
*** PRIOR AUTHORIZATION APPROVAL DOES NOT GUARANTEE ELIGIBILITY***
The prior authorization request submitted on behalf of SAMPLE CLIENT has been determined as follows:
01/18/15-01/18/16 V2715 – PRISM, PER LENS PENDING
APPR UNITS: 2 UNIT PRICE:$ 9.32 USED UNITS: 0
CODE EXPLANATIONS:
NO DENIAL REASON PROVIDED
COMMENT:
RECEIVED GLASSES LESS THAN A YEAR AGO
NEED DOCUMENTATION SAYING WILL REUSE OLD FRAMES
NOTE: PRIOR AUTHORIZATION APPROVAL DOES NOT GUARANTEE ELIGIBILITY. PAYMENT IS SUBJECT TO
THE RECIPIENT’S ELIGIBILITY AND MEDICAID BENEFIT LIMITATIONS. VERIFY ELIGIBILITY BEFORE
RENDERING SERVICES.
PA-Number: 00198000002
A1500RB2

Common Billing Information ____________________________________________________
Ch. 6 Index 85 Revision 4/1/17
6.14 Order vs Delivery Date
All procedures that involve delivering an item to the client can only be billed to
Medicaid on the date the item is delivered to the client. This includes glasses, DME
products/supplies, dental appliances, etc. The provider is responsible for billing these
procedures only on the delivery date.
Wyoming Medicaid will allow a provider to bill using the order date only if one of
the following conditions are present:
Client is not eligible on the delivery date but was eligible on the order date
Client does not return to the office for the delivery of the product
A provider may use the order date as the date of service only if they have obtained a
signed exception form from the State. To obtain this authorization, follow the steps
below.
Print the “Order vs Delivery Date Exception Form” (link to form below)
Complete the form and fax or mail the form to the address at the bottom of the
form
Once the form is signed by the State, it will be returned to the provider and
must be a part of the client’s permanent clinical record
The provider may then bill the claim using the order date as the date of service
NOTE: If an audit of clinical records is performed, and it is found that the provider
billed on the order date but does not have a signed “Order vs Delivery Date Exception
Form” for the client and the DOS, the money paid will be recovered.
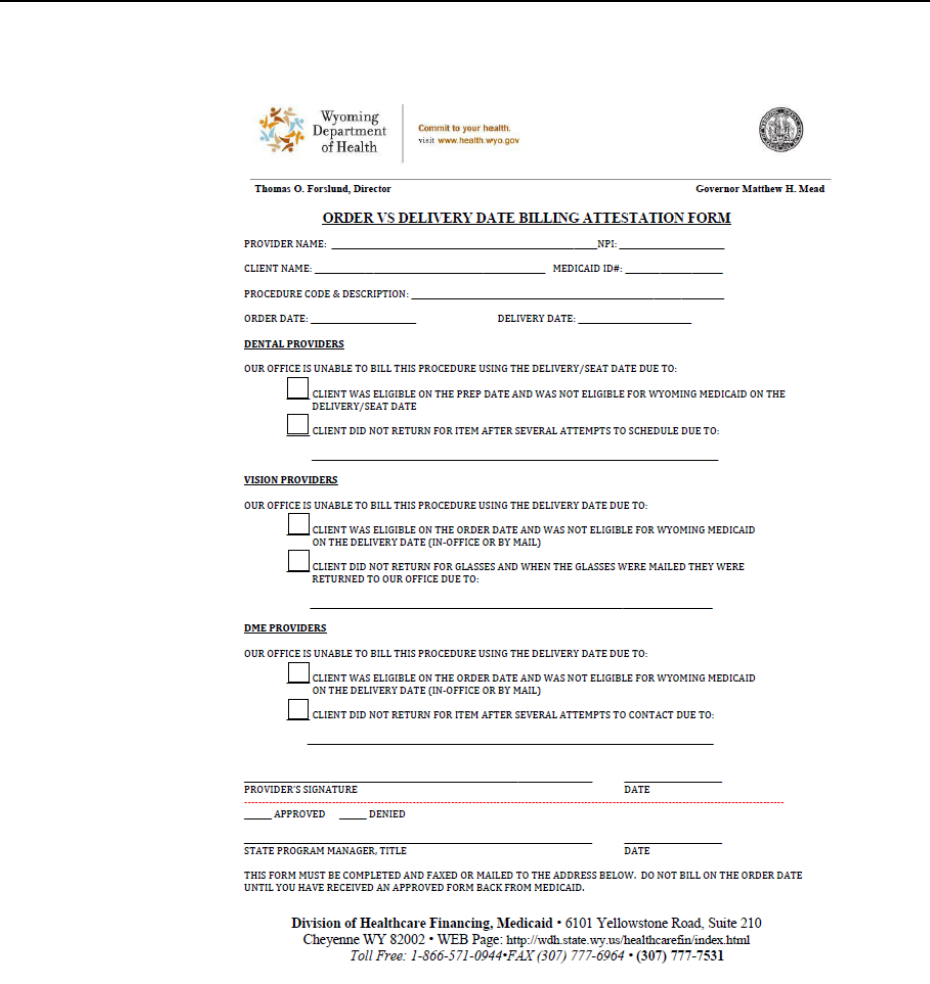
Common Billing Information ____________________________________________________
Ch. 6 Index 86 Revision 4/1/17
6.14.1 Order vs Delivery Date Exception Form
NOTE: Click image above to be taken to a printable version of this form
6.15 Submitting Attachments for Electronic Claims
Providers may either upload their documents electronically or complete the
Attachment Cover Sheet and mail their documents.
Steps for submitting electronic attachments:
1. The fiscal agent has created a process that allows providers to submit
electronic attachments for electronic claims. Providers need only
follow these steps:
Common Billing Information ____________________________________________________
Ch. 6 Index 87 Revision 4/1/17
Mark the attachment indicator on the electronic claim. For
more information on the attachment indicator, consult the
provider software vendor or clearinghouse, or the X12N 837
Professional Electronic Data Interchange Technical Report
Type 3 (TR3). The TR3 can be accessed at http://www.wpc-
edi.com.
Log onto Secured Provider Web Portal.
Under the submissions menu select Electronic Attachments.
Complete required information – Information must match the
claim as submitted i.e., DOS, client information, provider
information, and the name of the attachment must be identical
to what was submitted in the electronic file (with no spaces).
Select Browse
Navigate to the location of the electronic attachment on the
provider’s computer.
Click Upload.
For support and additional information refer to Chapter 8 and
Chapter 9 or contact EDI Services (2.1, Quick Reference).
NOTE: One (1) attachment per claim, providers may not attach one (1) document
to many claims. Also, if the attachment is not received within 30-days of
the electronic claim submission, the claim will deny and it will be
necessary to resubmit it with the proper attachment.
Steps for submitting paper attachments
1. The fiscal agent has created a process that allows providers to submit
paper attachments for electronic claims. Providers need only follow
these two (2) simple steps:
Mark the attachment indicator on the electronic claim and
indicate by mail as the submission method. For more
information on the attachment indicator, consult the provider
software vendor or clearinghouse, or the X12N 837
Professional Electronic Data Interchange Technical Report
Type 3 (TR3). The TR3 can be accessed at http://www.wpc-
edi.com.The data entered on the form must match the claim
exactly in DOS, client information, provider information, etc.
Complete Attachment Cover Sheet (6.15.1, Attachment Cover
Sheet) and mail it with the attachment to Claims (2.1, Quick
Reference).
NOTE: Both steps must be followed; otherwise, the fiscal agent will not be able to
join the electronic claim and paper attachment, and the claim will deny.
Also, if the paper attachment is not received within 30-days of the
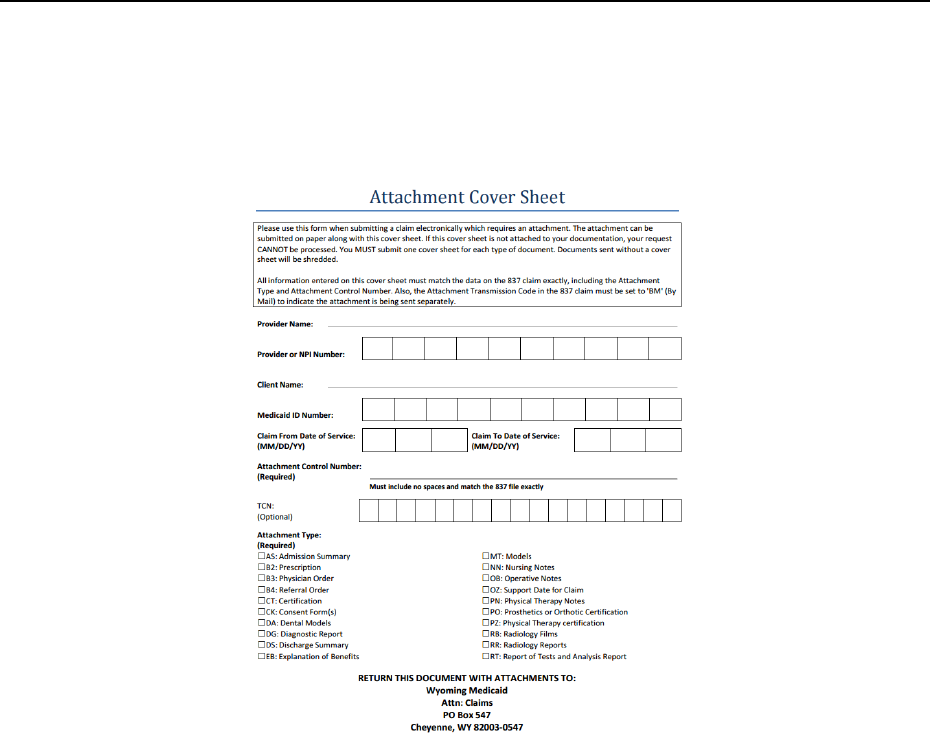
Common Billing Information ____________________________________________________
Ch. 6 Index 88 Revision 4/1/17
electronic claim submission, the claim will deny and it will be necessary
to resubmit it with the proper attachment.
6.15.1 Attachment Cover Sheet
NOTE: Click image above to be taken to a printable version of this form.
6.16 Sterilization, Hysterectomy and Abortion Consent Forms
When providing services to a Medicaid client, certain procedures or conditions
require a consent form be completed and attached to the claim. This section describes
the following forms and explains how to prepare them:
Sterilization Consent Form
Hysterectomy Consent Form
Abortion Certification Form
6.16.1 Sterilization Consent Form and Guidelines
Federal regulations require that clients give written consent prior to sterilization;
otherwise, Medicaid cannot reimburse for the procedure.

Common Billing Information ____________________________________________________
Ch. 6 Index 89 Revision 4/1/17
The Sterilization Consent Form may be obtained from the fiscal agent or copied from
this manual. As mandated by Federal regulations, the consent form must be attached
to all claims for sterilization-related procedures.
All sterilization claims must be processed according to the following Federal
guidelines:
FEDERAL GUIDELINES
The waiting period between consent and sterilization must not exceed 180 days and must be at least 30
days, except in cases of premature delivery and emergency abdominal surgery. The day the client signs
the consent form and the surgical dates are not included in the 30-day requirement. For example, a
client signs the consent form on July 1. To determine when the waiting period is completed, count 30-
days beginning on July 2. The last day of the waiting period would be July 31; therefore, surgery may
be performed on August 1.
In the event of premature delivery, the consent form must be completed and signed by the client at
least 72-hours prior to the sterilization, and at least 30-days prior to the expected date of delivery.
In the event of emergency abdominal surgery, the client must complete and sign the consent form at
least 72-hours prior to sterilization.
The consent form supplied by the surgeon must be attached to every claim for sterilization related
procedures; i.e., ambulatory surgical center clinic, physician, anesthesiologist, inpatient or outpatient
hospital. Any claim for a sterilization related procedure which does not have a signed and dated, valid
consent form will be denied.
All blanks on the consent form must be completed with the requested information. The consent form
must be signed and dated by the client, the interpreter (if one is necessary), the person who obtained
the consent, and the physician who will perform the sterilization.
The physician statement on the consent form must be signed and dated by the physician who will
perform the sterilization on the date of the sterilization or after the sterilization procedure was
performed. The date on the sterilization claim form must be identical to the date and type of operation
given in the physician’s statement.
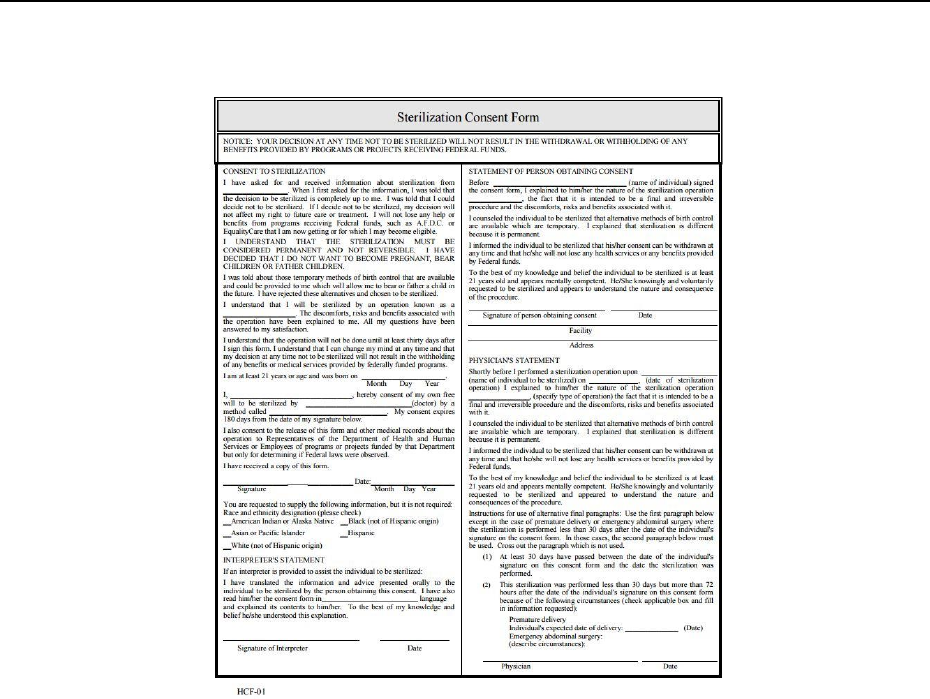
Common Billing Information ____________________________________________________
Ch. 6 Index 90 Revision 4/1/17
6.16.1.1 Sterilization Consent Form
NOTE: Click image above to be taken to a printable version of this form.
6.16.1.2 Instructions for Completing the Sterilization Consent Form
Important tips for completing the Sterilization Consent Form
Print legibly to avoid denials – The entire form must be legible.
The originating practitioner has ownership of this form and must supply
correct, accurate copies to all involved billing parties.
Fields 7, 8 and 15, 16 must be completed prior to the procedure.
All fields may be corrected however corrections must be made with one (1)
line through the error and must be initialed.
The person that signed the line is the only person that can make the alteration.
“Whiteout” will not be accepted when making corrections.
Every effort should be taken to complete the form correctly without
any changes.
6.16.2 Hysterectomy Acknowledgment of Consent
The Hysterectomy Acknowledgment of Consent Form must accompany all claims for
hysterectomy-related services; otherwise, Medicaid will not cover the services. The
Common Billing Information ____________________________________________________
Ch. 6 Index 91 Revision 4/1/17
originating physician is required to supply other billing providers (e.g., hospital,
surgeon, anesthesiologist, etc.) with a copy of the completed consent form.
NOTE: Instructions for attaching documents to claims refer to Section 6.15.
Section
Field
#
Action
Consent to
Sterilization
1
Enter the name of the physician or the name of the clinic from
which the client received sterilization information.
2
Enter the type of operation (no abbreviations)
3
Enter the client’s date of birth (MM/DD/YY). Client must be at
least 21 years
4
Enter the client’s name
5
Enter the name of the physician performing the surgery
6
Enter the name of the type of operation (no abbreviations)
7
The client to be sterilized signs here
8
The client dates signature here
9
Check one (1) box appropriate for client. This item is requested
but NOT required.
Interpreter’s
Statement
10
Enter the name of the language the information was translated to
11
Interpreter signs here
12
Interpreter dates signature here
Statement of
person obtaining
consent
13
Enter clients name
Statement of
person obtaining
consent
Physician’s
Statement
14
Enter the name of the operation (no abbreviations)
15
The person obtaining consent from the client signs here
16
The person obtaining consent from the client dates signature here
17
The person obtaining consent from the client enters the name of
the facility where the person obtaining consent is employed. The
facility name must be completely spelled out (no abbreviations)
18
The person obtaining consent from the client enters the complete
address of the facility in #17 above. Address must be complete,
including state and zip code
19
Enter the client’s name
Physician’s
Statement
20
Enter the date of sterilization operation
21
Enter type of operation (no abbreviations)
22
Check applicable box:
If premature delivery is checked, the provider must write in
the expected date of delivery here.
If emergency abdominal surgery is checked, describe
circumstances here.
23
Physician performing the sterilization signs here
24
Physician performing the sterilization dates signature here
Common Billing Information ____________________________________________________
Ch. 6 Index 92 Revision 4/1/17
6.16.2.1 Instructions for Completing the Hysterectomy
Acknowledgment of Consent Form
Section
Field #
Action
Part A
1
Enter the name of the physician performing the surgery.
2
Enter the narrative diagnosis for the client’s condition.
3
The client receiving the surgery signs here and dates.
4
The person explaining the surgery signs here and dates.
Part B
5
Enter the date and the physician’s name that performed the hysterectomy.
6
Enter the narrative diagnosis for the client’s condition.
7
The client receiving the surgery signs here and dates.
8
The person explaining the surgery signs here and dates.
Part C
9
Enter the narrative diagnosis for the client’s condition.
10
Check applicable box:
If other reason for sterility is checked, the provider must write what was
done.
If previous tubal is checked, the provider must enter the date of the tubal.
If emergency situation is checked, the provider must enter the
description.
11
The physician who performed the hysterectomy signs here and dates.
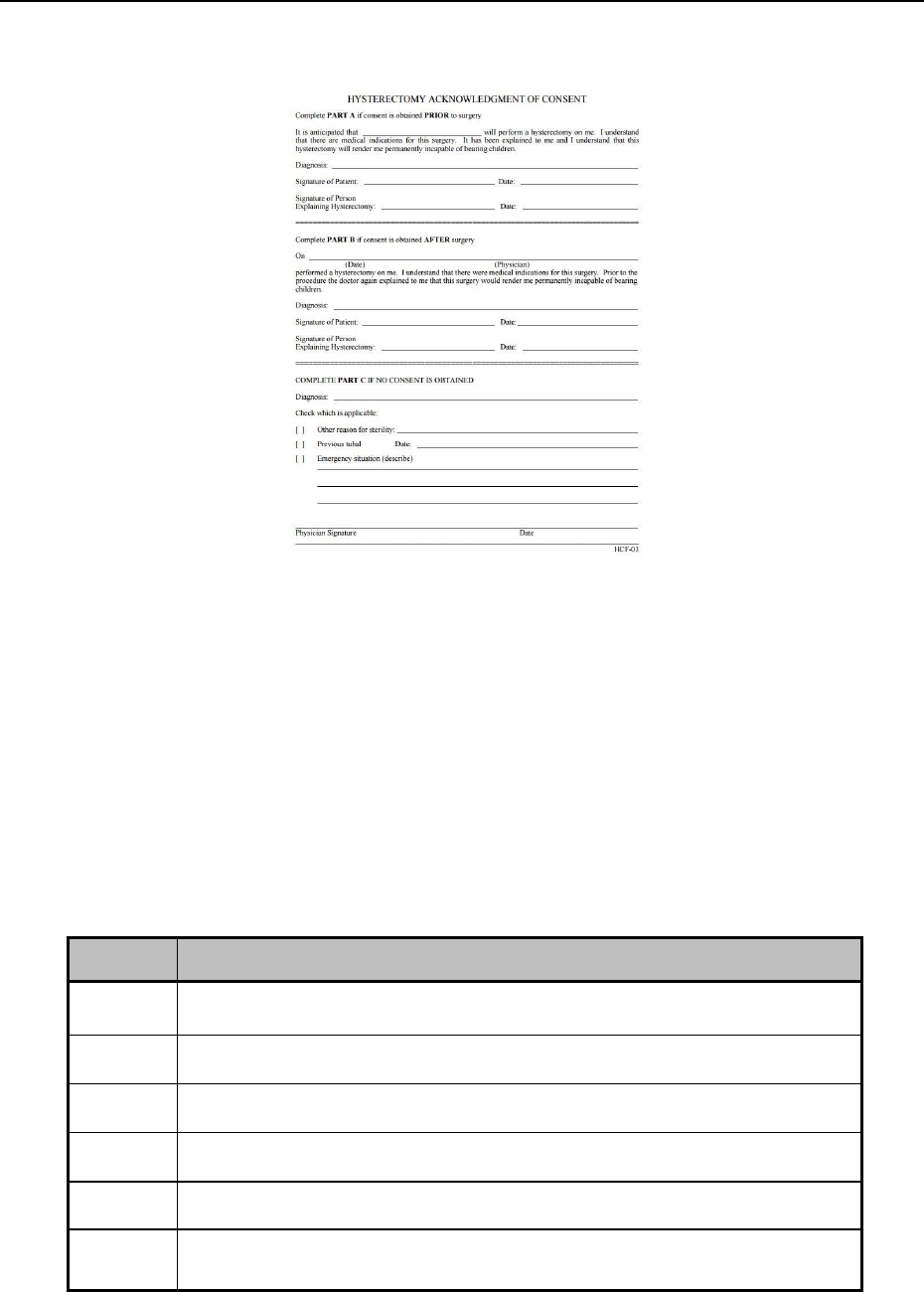
Common Billing Information ____________________________________________________
Ch. 6 Index 93 Revision 4/1/17
6.16.2.2 Hysterectomy Acknowledgment Consent Form
NOTE: Click image above to be taken to a printable version of this form.
6.16.3 Abortion Certification Guidelines
The Abortion Certification Form must accompany claims for abortion-related
services; otherwise, Medicaid will not cover the services. This requirement includes,
but is not limited to, claims from the attending physician, assistant surgeon,
anesthesiologist, pathologist, and hospital.
6.16.3.1 Instructions for Completing the Abortion Certification
Form
Field #
Action
1
Enter the name of the attending physician or surgeon.
2
Check the option (1, 2 or 3) that is appropriate
3
Enter the name of the client receiving the surgery
4
Enter the client’s address
5
The physician or surgeon performing the abortion will sign and date
here.
6
Enter the performing physician’s address.
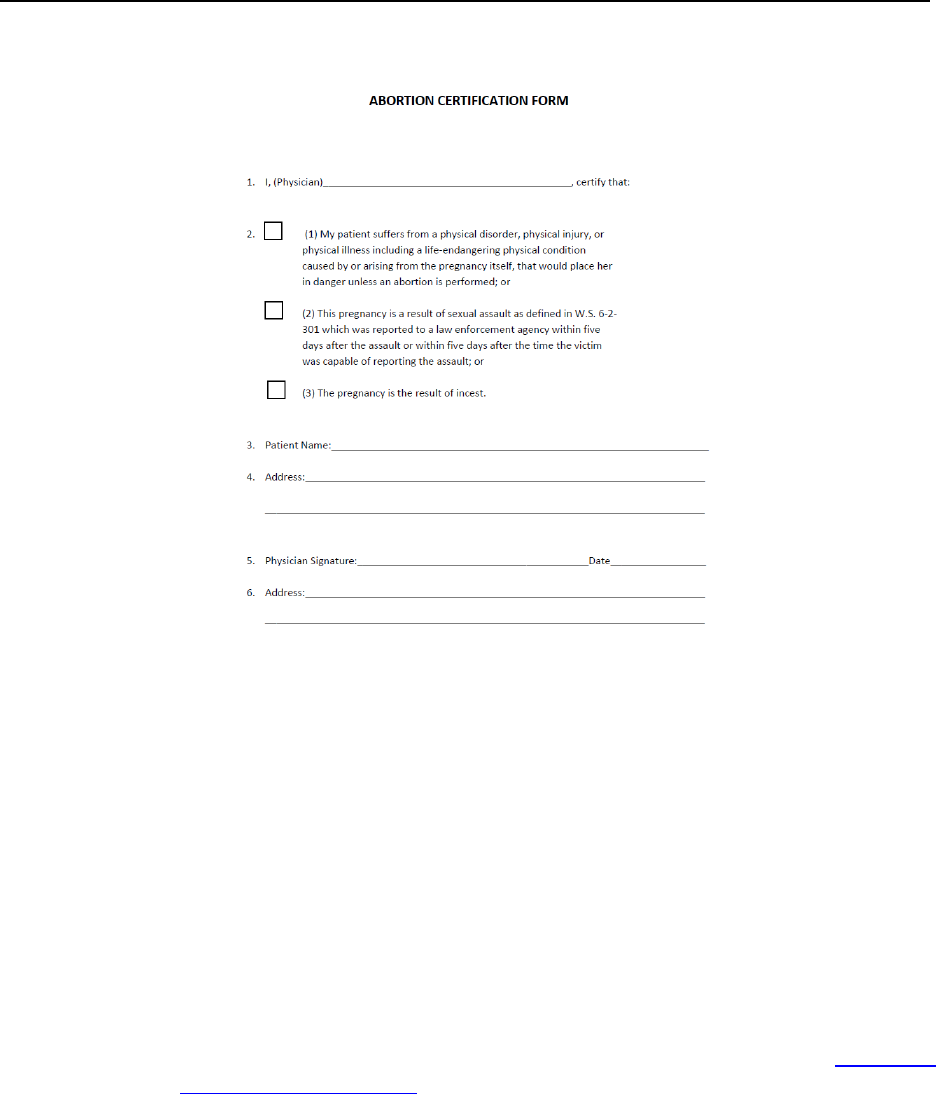
Common Billing Information ____________________________________________________
Ch. 6 Index 94 Revision 4/1/17
6.16.3.2 Abortion Certification Form
NOTE: Click image above to be taken to a printable version of this form.
6.17 Remittance Advice
After claims have been processed weekly, Medicaid distributes a Medicaid
proprietary Remittance Advice (RA) to providers. The Remittance Advice (RA) plays
an important communication role between providers and Medicaid. It explains the
outcome of claims submitted for payment. Aside from providing a record of
transactions the RA assists providers in resolving potential errors. Providers receiving
manual checks will receive their check and RA in the same mailing.
The RA is organized in the following manner:
The first page or cover page is important and should not be over looked it may
include an RA Banner notification from Wyoming Medicaid (1.2.1, RA
Banner Notices/Samples).
Claims are grouped by disposition category.
o Claim Status PAID group contains all the paid claims.
o Claim Status DENIED group reports denied claims.
o Claim Status PENDED group reports claims pended for review. Do
not resubmit these claims. All claims in pended status are reported
each payment cycle until paid or denied. Claims can be in a pended
status for up to 30-days.
o Claim Status ADJUSTED group reports adjusted claims.
Common Billing Information ____________________________________________________
Ch. 6 Index 95 Revision 4/1/17
All paid, denied, and pended claims and claim adjustments are itemized
within each group in alphabetic order by client last name.
A unique Transaction Control Number (TCN) is assigned to each claim. TCNs
allow each claim to be tracked throughout the Medicaid claims processing
system. The digits and groups of digits in the TCN have specific meanings, as
explained below:
0 05180 22 001 0 001 00
Claim Number
Type of Document (0=new claim, 1=credit, 2=adjustment)
Batch Number
Imager Number
Year/Julian Date
Claim Input Medium Indicator___________ 0=Paper Claim
1=Point of Sale (Pharmacy)
2=Electronic Crossovers sent by Medicare
3=Electronic claims submission
4=Medicaid initiated adjustment
5=Special Processing required
The RA Summary Section reports the number of claim transactions, and total
payment or check amount.

Common Billing Information ____________________________________________________
Ch. 6 Index 96 Revision 4/1/17
6.17.1 Sample Professional Remittance Advice
WYOMING DEPARTMENT OF HEALTH
MEDICAID MANAGEMENT INFORMATION SYSTEM RUN DATE 00/00/00
R E M I T A N C E A D V I C E
TO: SAMPLE PROVIDER R.A. NO.: 0101010 DATE PAID: 00/00/00 PROVIDER NUMBER: 123456789/1234567890 PAGE: 1
TRANS-CONTROL-NUMBER BILLED MCARE COPAY OTHER DEDUCT- COINS MCAID WRITE TREATING
LI SVC-DATE PROC/MODS UNITS AMT. PAID AMT. INS. IBLE AMT. PAID OFF PROVIDER S PLAN
* * * CLAIM TYPE: HCFA 1500 * * * CLAIM STATUS: DENIED
ORIGINAL CLAIMS:
* BRADY TOM RECIP ID: 0000012345 PATIENT ACCT #: 00000
0-03000-22-000-0006-10 80.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
HEADER EOB(S): 300 147
01 04/28/15 42830 1 80.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 1234567890 K LTCS
* MANNING PEYTON RECIP ID: 0800000001 PATIENT ACCT #: 00001
0-03000-22-000-0006-12 80.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
HEADER EOB(S): 300 147
01 05/02/15 69436 1 80.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 1234567890 K NH
REMITTANCE ADVICE
TO: SAMPLE PROVIDER R.A. NO.: 0101010 DATE PAID: 00/00/00 PROVIDER NUMBER: 1234567890 PAGE: 2
REMITTANCE T O T A L S
PAID ORIGINAL CLAIMS: NUMBER OF CLAIMS 0 --------- 0.00 0.00
PAID ADJUSTMENT CLAIMS: NUMBER OF CLAIMS 0 --------- 0.00 0.00
DENIED ORIGINAL CLAIMS: NUMBER OF CLAIMS 4 --------- 320.00 0.00
DENIED ADJUSTMENT CLAIMS: NUMBER OF CLAIMS 0 --------- 0.00 0.00
PENDED CLAIMS (IN PROCESS): NUMBER OF CLAIMS 0 --------- 0.00 0.00
AMOUNT OF CHECK: ------------------------------------------------------------ 0.00
---- THE FOLLOWING IS A DESCRIPTION OF THE EXPLANATION OF BENEFIT (EOB) CODES THAT APPEAR ABOVE: COUNT:
147 THE TREATING PROVIDER TYPE IS NOT VALID WITH THE PROCEDURE CODE. 4
300 THE PROVIDER NUMBER CANNOT BE BILLED ON THIS CLAIM TYPE. VERIFY THE PROVIDER IS 4
USING THE CORRECT PROVIDER NUMBER FOR THIS CLAIM TYPE AND RESUBMIT.
Common Billing Information ____________________________________________________
Ch. 6 Index 97 Revision 4/1/17
6.17.2 How to Read the Remittance Advice
Each claim processed during the weekly cycle is listed on the Remittance Advice
with the following information:
FIELD NAME
HEADER DESCRIPTION
To
Provider Name
R.A. Number
Remittance Advice Number assigned.
Date Paid
Payment date.
Provider Number
Medicaid provider number/NPI number
Page
Page Number
Last, MI, and First
The client’s name as found on the Medicaid ID Card.
Recip ID
The client’s Medicaid ID Number.
Patient Acct #
The patient account number reported by the provider on the claim.
Trans Control Number
Transaction Control Number: The unique identifying number assigned to each claim submitted.
Billed Amt.
Total amount billed on the claim
Mcare Paid
Amount paid by Medicare
Copay Amt.
The amount due from the client for their co-payment.
Other Ins.
Amount paid by other insurance.
Deductible
Medicare deductible amount.
Coins Amt.
Medicare coinsurance amount.
Mcaid Paid
The amount paid by Medicaid
Write off
Difference between Medicaid paid amount and the provider’s billed amount.
Header EOB(s)
Explanation of Benefits: A denial code. A description of each code is provided at the end of the RA
Li
The line item number of the claim.
Svc date
The date of service.
Proc / Mods
The procedure code and applicable modifier.
Units
The number of units submitted.
Billed Amt.
Total amount billed on the line.
Mcare Paid
Amount paid by Medicare
Copay Amt.
The amount due from the client for their co-payment.
Other Ins.
Amount paid by other insurance.
Deductible
Medicare deductible amount.
Coins Amt.
Medicare coinsurance amount.
Mcaid Paid
The amount paid by Medicaid
Write off
Difference between Medicaid paid amount and the provider’s billed amount.
Treating Provider
The treating provider’s NPI number.
S
How the system priced each claim. For example, claims priced manually have a distinct code. Claims paid according
to the Medicaid fee schedule have another code. Below is a table which describes these pricing source codes:
A= Anesthesia
B= Billed Charge
C= Percent-of-Charges
D= Inpatient Per Diem Rate
E= EAC Priced Plus Dispensing Fee
F= Fee Schedule
G= FMAC Priced Plus Dispensing Fee
H= Encounter Rate
I= Institutional Care Rate
K= Denied
L= Maximum Suspend Ceiling
M= Manually Priced
N= Provider Charge
O= Relative Value Units TC
P= Prior Authorization Rate
R= Relative Value Unit Rate
S= Relative Value Unit PC
T= Fee Schedule TC
X= Medicare Coinsurance and Deductible
Y= Fee Schedule PC
Z = Fee Plus Injection
Plan
The Medicaid and State Healthcare Benefit Plan the client is eligible for (Section A.3).
Line EOB(s)
Explanation of Benefits: A denial code. A description of each code is provided at the end of the RA
Common Billing Information ____________________________________________________
Ch. 6 Index 98 Revision 4/1/17
6.17.3 Remittance Advice Replacement Request Policy
If you are unable to obtain a copy from the web portal, a paper copy may be requested
as follows:
To request a printed replacement copy of a Remittance Advice, complete the
following steps:
Print the Remittance Advice (RA) replacement request form
For replacement of a complete RA contact Provider Relations (2.1, Quick
Reference) to obtain the RA number, date and number of pages
Replacements of a specific page of an RA (containing a requested specific
claim/TCN) will be three (3) pages (the cover page, the page containing the
claim, and the summary page for the RA)
Review the below chart to determine the cost of the replacement RA (based
on total number of pages requested – For multiple RAs requested at the same
time, add total pages together)
Send the completed form and payment as indicated on the form
o Make checks to Division of Healthcare Financing
o Mail to Provider Relations (2.1, Quick Reference)
The replacement RA will be emailed, faxed or mailed as requested on the form. Email
is the preferred method of delivery, and RAs of more than ten (10) pages will not be
faxed.
RAs less than 24 weeks old can be obtained from the Secured Provider Web Portal,
once a provider has registered for access (8.5.2.1, Secured Provider Web Portal
Registration Process).
Total Number of RA Pages
Cost for Replacement RA
1-10
$2.50
11-20
$5.00
21-30
$7.50
31-40
$10.00
41-50
$12.50
51+
Contact Provider Relations for rates

Common Billing Information ____________________________________________________
Ch. 6 Index 99 Revision 4/1/17
6.17.3.1 Remittance Advice (RA) Replacement Request Form
NOTE: Click image above to be taken to a printable version of this form.
6.17.4 Obtain an RA from the Web
Providers have the ability to view and download their last 24 weeks of RAs from the
Medicaid website, refer to Chapter 8, Electronic Data Interchange (EDI).
6.17.5 When a Client Has Other Insurance
If the client has other insurance coverage reflected in Medicaid records, payment may
be denied unless providers report the coverage on the claim. Medicaid is always the
payor of last resort. For exceptions and additional information regarding Third Party
Liability, refer to Chapter 7 of this manual. To assist providers in filing with the other
carrier, the following information is provided on the RA directly below the denied
claim:
Insurance carrier name;
Name of insured;
Policy number;
Insurance carrier address;
Group number, if applicable; and
Group employer name and address, if applicable.
Common Billing Information ____________________________________________________
Ch. 6 Index 100 Revision 4/1/17
The information is specific to the individual client. The Third Party Resources
Information Sheet (7.7.1, Third Party Resources Information Sheet) should be used
for reporting new insurance coverage or changes in insurance coverage on a client’s
policy.
6.18 Resubmitting Versus Adjusting Claims
Resubmitting and adjusting claims are important steps in correcting any billing
problems. Knowing when to resubmit a claim versus adjusting it is important.
Action
Description
Timely Filing Limitation
VOID
Claim has paid; however, the provider
would like to completely cancel the claim as
if it was never billed.
May be completed any time
after the claim has been
paid.
ADJUST
Claim has paid, even if paid $0.00;
however, the provider would like to make a
correction or change to this paid claim
Must be completed within
six (6) months after the
claim has paid UNLESS the
result will be a lower
payment being made to the
provider, then no time limit.
RESUBMIT
Claim has denied entirely or a single line
has denied, the provider may resubmit on a
separate claim.
One (1) year from the date
of service.
6.18.1 How Long do Providers Have to Resubmit or Adjust a Claim?
The deadlines for resubmitting and adjusting claims are different:
Providers may resubmit any denied claim or line within 12-months of the date
of service.
Providers may adjust any paid claim within six (6) months of the date of
payment.
Adjustment requests for over-payments are accepted indefinitely. However, the
Provider Agreement requires providers to notify Medicaid within 30-days of learning
of an over-payment. When Medicaid discovers an over-payment during a claims
review, the provider maybe notified in writing, in most cases, the over-payment will
be deducted from future payments. Refund checks are not encouraged. Refund checks
are not reflected on the Remittance Advice. However, deductions from future
payments are reflected on the Remittance Advice, providing a hardcopy record of the
repayment.

Common Billing Information ____________________________________________________
Ch. 6 Index 101 Revision 4/1/17
6.18.2 Resubmitting a Claim
Resubmitting is when a provider submits a claim to Medicaid that was previously
submitted for payment but was either returned unprocessed or denied. Electronically
submitted claims may reject for X12 submission errors. Claims may be returned to
providers before processing because key information such as an authorized signature
or required attachment is missing or unreadable.
How to Resubmit:
Review and verify EOB codes on the RA/835 transaction and make all
corrections and resubmit the claim.
o Contact Provider Relations for assistance (2.1, Quick Reference).
Claims must be submitted with all required attachments with each new
submission.
If the claim was denied because Medicaid has record of other insurance
coverage, enter the missing insurance payment on the claim or submit
insurance denial information, when resubmitting the claim to Medicaid.
6.18.2.1 When to Resubmit to Medicaid
Claim Denied. Providers may resubmit to Medicaid when the entire claim has
been denied, as long as the claim was denied for reasons that can be corrected.
When the entire claim is denied, check the explanation of benefits (EOB) code
on the RA/835 transaction, make the appropriate corrections, and resubmit the
claim.
Paid Claim With One (1) or More Line(s) Denied. – Providers may submit
individually denied lines.
Claim Returned Unprocessed. – When Medicaid is unable to process a claim
it will be rejected or returned to the provider for corrections and to resubmit.
6.18.3 Adjustment/Void Request Form Electronically Adjusting Paid
Claims via Hardcopy/Paper
When a provider identifies an error on a paid claim, the provider must submit an
Adjustment/Void Request Form. If the incorrect payment was the result of a keying
error (paper claim submission), by the fiscal agent contact Provider Relations to have
the claim corrected (2.1, Quick Reference).
NOTE: All items on a paid claim can be corrected with an adjustment EXCEPT
the pay-to provider number. In this case, the original claim will need to be
voided and the corrected claim submitted.
Denied claims cannot be adjusted.
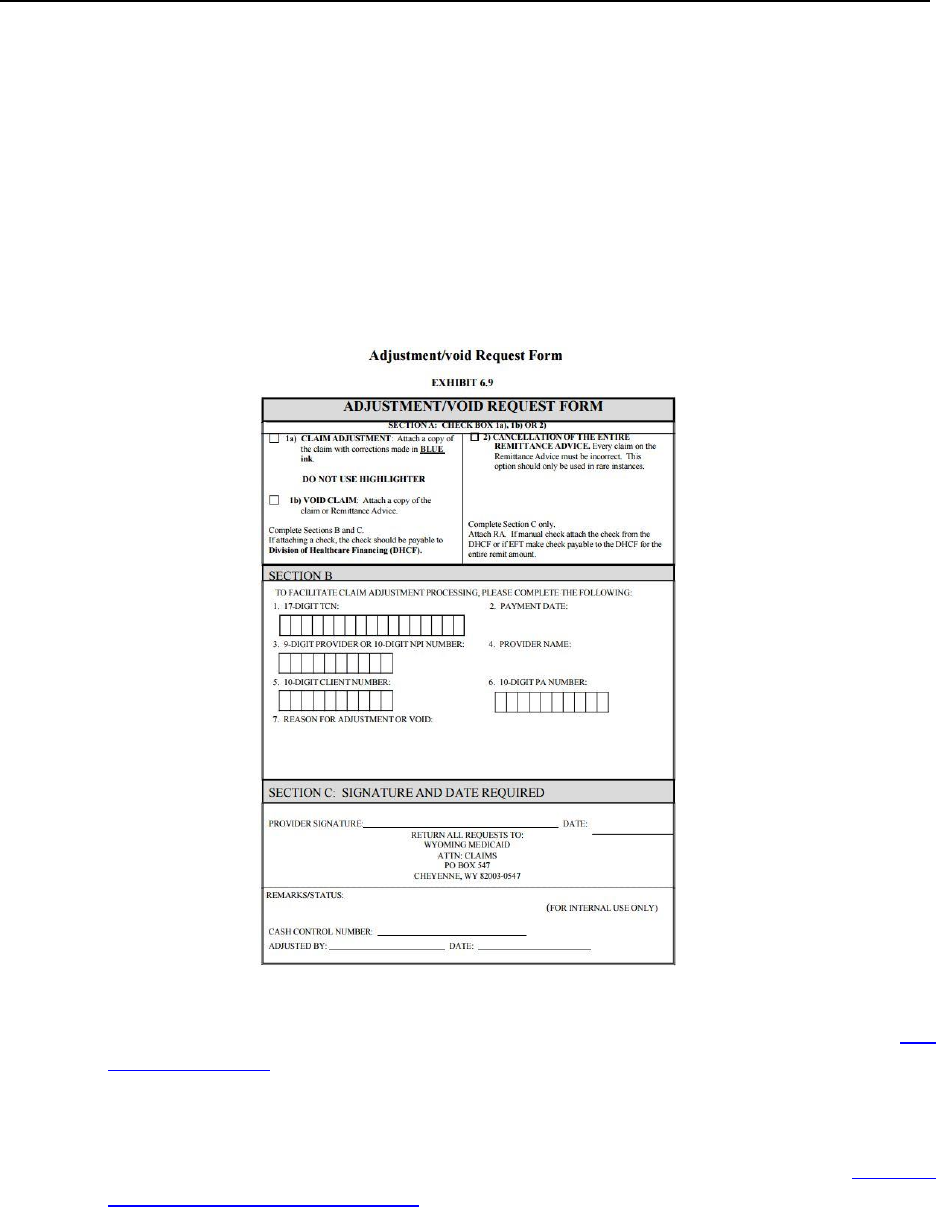
Common Billing Information ____________________________________________________
Ch. 6 Index 102 Revision 4/1/17
When adjustments are made to previously paid claims, Medicaid reverses the original
payment and processes a replacement claim. The result of the adjustment appears on
the RA/835 transaction as two (2) transactions. The reversal of the original payment
will appear as a credit (negative) transaction. The replacement claim will appear as a
debit (positive) transaction and may or may not appear on the same RA/835
transaction as the credit transaction. The replacement claim will have almost the same
TCN as the credit transaction, except the 12th digit will be a two (2), indicating an
adjustment, whereas the credit will have a one (1) in the 12th digit indicating a debit.
6.18.3.1 Adjustment/Void Request Form
NOTE: If a provider wants to void an entire RA, contact Provider Relations (2.1,
Quick Reference). Click image above to be taken to a printable version of this form.
6.18.3.2 How to Request an Adjustment/Void
To request an adjustment, use the Adjustment/Void Request Form (6.18.3.1,
Adjustment/Void Request Form). The requirements for adjusting/voiding a claim are
as follows:
An adjustment/void can only be processed if the claim has been paid by
Medicaid.
Common Billing Information ____________________________________________________
Ch. 6 Index 103 Revision 4/1/17
Medicaid must receive individual claim adjustment requests within six (6)
months of the claim payment date.
A separate Adjustment/Void Request Form must be used for each claim.
If the provider is correcting more than one (1) error per claim, use only one
(1) Adjustment/Void Request Form, and include all corrections on one form.
o If more than one (1) line of the claim needs to be adjusted, indicate
which lines and items need to be adjusted in the “Reason for
Adjustment or Void” section on the form or simply state, refer to the
attached corrected claim.
6.18.3.3 How to Complete the Adjustment/Void Request Form
Section
Field #
Field Name
Action
A
1a, 1b
Claim Adjustment
Void Claim
Mark this box if any adjustments need to be made to
a claim. Attach a copy of the claim with corrections
made in BLUE ink (do not use red ink or highlighter)
or the RA. Attach all supporting documentation
required to process the claim, i.e. EOB, EOMB,
consent forms, invoice, etc.
Mark this box if an entire claim needs to be voided.
Attach a copy of the claim or the Remittance Advice.
Sections B and C must be completed.
B
1
17-digit TCN
Enter the 17-digit transaction control number
assigned to each claim from the Remittance Advice.
2
Payment Date
Enter the Payment Date
3
Nine (9) digit Provider
or ten (10) digit NPI
Number
Enter provider’s nine (9) digit Medicaid provider
number or ten (10) digit NPI number, if applicable.
4
Provider Name
Enter the provider name.
5
Ten (10) digit Client
Number
Enter the client’s ten (10) digit Medicaid ID number.
6
Ten (10) digit PA
Number
Enter the ten (10) digit Prior Authorization number,
if applicable.
7
Reason for
Adjustment or Void
Enter the specific reason and any pertinent
information that may assist the fiscal agent.
C
Provider Signature
and Date
Signature of the provider or the provider’s authorized
representative and the date.
Adjusting a claim electronically via an 837 transaction.
Wyoming Medicaid accepts claim adjustments electronically, refer to Chapter 9, Wyoming
Specific HIPAA 5010 Electronic Specifications, for complete details.
6.18.3.4 When to Request an Adjustment
When a claim was overpaid or underpaid.
Common Billing Information ____________________________________________________
Ch. 6 Index 104 Revision 4/1/17
When a claim was paid, but the information on the claim was incorrect (such
as client ID, date of service, procedure code, diagnoses, units, etc.)
When Medicaid pays a claim and the provider subsequently receives payment
from a third party payor, the provider must adjust the paid claim to reflect the
TPL amount paid.
Attach a corrected claim showing the insurance payment and attach a copy of
the insurance EOB if the payment is less than 40% of the total claim charge.
For the complete policy regarding Third Party Liability refer to Chapter 7.
NOTE: Cannot complete an adjustment when the mistake is the pay-to provider
number or NPI.
6.18.3.5 When to Request a Void
Request a void when a claim was billed in error (such as incorrect provider number,
services not rendered, etc.).
6.19 Credit Balances
A credit balance occurs when a provider’s credits (take backs) exceed their debits
(pay outs), which results in the provider owing Medicaid money.
Credit balances may be resolved in two (2) ways:
1. Working off the credit balance: By taking no action, remaining credit balances
will be deducted from future claim payments. The deductions appear as
credits on the provider’s RA(s)/835 transaction(s) until the balance owed to
Medicaid has been paid.
2. Sending a check payable to the “Division of Healthcare Financing” for the
amount owed. This method is typically required for providers who no longer
submit claims to Medicaid or if the balance is not paid within 30-days. A
notice is typically sent from Medicaid to the provider requesting the credit
balance to be paid. The provider is asked to attach the notice, a check and a
letter explaining the money is to pay off a credit balance. Include the provider
number to ensure the money is applied correctly.
NOTE: When a provider number with Wyoming Medicaid changes, but the
provider’s tax-id remains the same, the credit balance will be moved
automatically from the old Medicaid provider number to the new one, and
will be reflected on RAs/835 transactions.
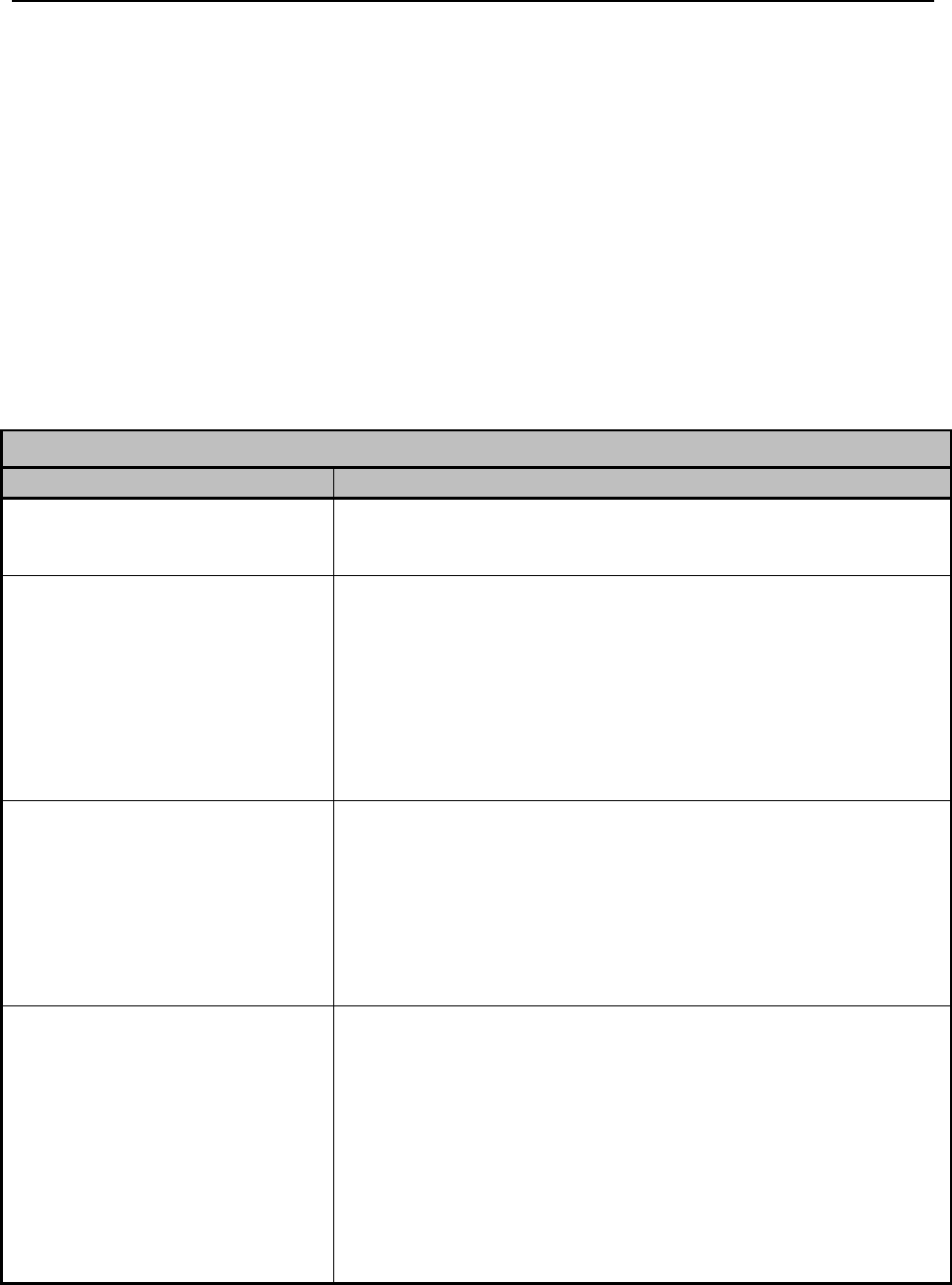
Common Billing Information ____________________________________________________
Ch. 6 Index 105 Revision 4/1/17
6.20 Timely Filing
The Division of Healthcare Financing adheres strictly to its timely filing policy. The
provider must submit a clean claim to Medicaid within 12-months of the date of
service. A clean claim is an error free, correctly completed claim, with all required
attachments, that will process and approve to pay within the twelve-month time
period. Submit claims immediately after providing services so when a claim is
denied, there is time to correct any errors and resubmit. Claims are to be submitted
only after the service(s) have been rendered, and not before. For deliverable items
(i.e. dentures, DME, glasses, hearing aids, etc.) the date of service must be the date of
delivery, not the order date.
6.20.1 Exceptions to the Twelve-Month Limit
Exceptions Beyond the Control of the Provider
When the Situation is:
The Time Limit is:
Medicare Crossover
A Claim must be submitted within 12-months of the date of service
or within six (6) months from the payment date on the Explanation
of Medicare Benefits (EOMB), whichever is later.
Client is determined to be eligible
on appeal, reconsideration, or court
decision (retroactive eligibility)
Claims must be submitted with in six (6) months of the date of the
determination of retroactive eligibility. The client must provide a
copy of the dated letter to the provider to document retroactive
eligibility. If a claim exceeds timely filing and the provider elects to
accept the client as a Medicaid client and bill Wyoming Medicaid, a
copy of the notice must me attached to the claim with a cover letter
requesting an exception to timely filing. The notice of retroactive
eligibility may be a SSI award notice or a notice from WDH.
Client is determined to be eligible
due to agency corrective actions
(retroactive eligibility)
Claims must be submitted within six (6) months of the date of the
determination of retroactive eligibility. The client must provide a
copy of the dated letter to the provider to document retroactive
eligibility. If a claim exceeds timely filing and the provider elects to
accept the client as a Medicaid client and bill Wyoming Medicaid, a
copy of the notice must be attached to the claim with a cover letter
requesting an exception to timely filing.
Provider finds their records to be
inconsistent with filed claims,
regarding rendered services. This
includes dates of service,
procedure/revenue codes, tooth
codes, modifiers, admission or
discharge dates/times, treating or
referring providers or any other
item which makes the
records/claims non-supportive of
each other.
Although there is no specific time limit for correcting errors, the
corrected claim must be submitted in a timely manner from when
the error was discovered. If the claim exceeds timely filing, the
claim must be sent with a cover letter requesting an exception to
timely filing citing this policy.
Common Billing Information ____________________________________________________
Ch. 6 Index 106 Revision 4/1/17
6.20.2 Appeal of Timely Filing
A provider may appeal a denial for timely filing ONLY under the following
circumstances:
The claim was originally filed within 12-months of the date of service and is
on file with Wyoming Medicaid; and
The provider made at least one (1) attempt to resubmit the corrected claim
within 12-months of the date of service; and
The provider must document in their appeal letter all claims information and
what corrections they made to the claim (all claims history, including TCNs)
as well as all contact with or assistance received from Provider Relations
(dates, times, call reference number, who was spoken with, etc.) or
A Medicaid computer or policy problem beyond the provider’s control
prevented the provider from finalizing the claim within 12-months of the date
of service
Any appeal that does not meet the above criteria will be denied. Timely filing will not
be waived when a claim is denied due to provider billing errors or involving third
party liability.
6.20.2.1 How to Appeal
The provider must submit the appeal in writing to Provider Relations (2.1, Quick
Reference) and should include the following:
Documentation of previous claim submission (TCNs, documentation of the
corrections made to the subsequent claims);
Documentation of contact with Provider Relations
An explanation of the problem; and
A clean copy of the claim, along with any required attachments and required
information on the attachments. A clean claim is an error free, correctly
completed claim, with all required attachments, that will process and pay.
6.21 Important Information Regarding Retroactive Eligibility
Decisions
The client is responsible for notifying the provider of the retroactive eligibility
determination and supplying a copy of the notice.
A provider is responsible for billing Medicaid only if:
They agreed to accept the patient as a Medicaid client pending Medicaid
eligibility; or
Common Billing Information ____________________________________________________
Ch. 6 Index 107 Revision 4/1/17
After being informed of retroactive eligibility, they elect to bill Medicaid for
services previously provided under a private agreement. In this case, any
money paid by the client for the services being billed to Medicaid would need
to be refunded prior to a claim being submitted to Medicaid.
NOTE: The provider determines at the time they are notified of the client’s
eligibility if they are choosing to accept the client as a Medicaid client. If
the provider does not accept the client, they remain private pay.
In the event of retroactive eligibility, claims must be submitted within six (6) months
of the date of determination of retroactive eligibility.
NOTE: Inpatient Hospital Certification: A hospital may seek admission
certification for a client found retroactively eligible for Medicaid benefits
after the date of admission for services that require admission certification.
The hospital must request admission certification within 30-days after the
hospital receives notice of eligibility. To obtain certification, contact
WYhealth (2.1, Quick Reference).
6.22 Client Fails to Notify a Provider of Eligibility
If a client fails to notify a provider of Medicaid eligibility and is billed as a private-
pay patient, the client is responsible for the bill unless the provider agrees to submit a
claim to Medicaid. In this case:
Any money paid by the client for the service being billed to Wyoming
Medicaid must be refunded prior to billing Medicaid;
The client can no longer be billed for the service; and
Timely filing criterion is in effect.
NOTE: The provider determines at the time they are notified of the client’s
eligibility if they are choosing to accept the client as a Medicaid client. If
the provider does not accept the client, they remain private pay.
6.23 Billing Tips to Avoid Timely Filing Denials
File claims soon after services are rendered.
Carefully review EOB codes on the Remittance Advice/835 transaction (work
RAs/835s weekly).

Common Billing Information ____________________________________________________
Ch. 6 Index 108 Revision 4/1/17
Resubmit the entire claim or denied line only after all corrections have been
made.
Contact Provider Relations (2.1, Quick Reference):
o With any questions regarding billing or denials.
o When payment has not been received within 30-days of submission,
verify the status of the claim.
o When there are multiple denials on a claim, request a review of the
denials prior to resubmission.
NOTE: Once a provider has agreed to accept a patient as a Medicaid client, any
loss of Medicaid reimbursement due to provider failure to meet timely
filing deadlines is the responsibility of the provider.
6.24 Telehealth
Telehealth is the use of an electronic media to link beneficiaries with health
professionals in different locations. The examination of the client is performed via a
real time interactive audio and video telecommunications system. This means that the
client must be able to see and interact with the off-site practitioner at the time services
are provided via telehealth technology.
It is the intent that telehealth services will provide better access to care by delivering
services as they are needed when the client is residing in an area that does not have
specialty services available. It is expected that this modality will be used when travel
is prohibitive or resources won’t allow the clinician to travel to the client’s location.
Each site will be able to bill for their own services as long as they are an enrolled
Medicaid provider (this includes out-of-state Medicaid providers).
6.24.1 Covered Services
Originating Sites (Spoke Site)
The Originating site or Spoke site is the location of an eligible Medicaid client at the
time the service is being furnished via telecommunications system occurs.
Authorized originating sites are:
Hospitals
Office of a physician or other practitioner (this includes medical clinics)
Office of a psychologist or neuropsychologist
Community mental health or substance abuse treatment center
(CMHC/SATC)
Office of an advanced practice nurse (APN) with specialty of psych/mental
health
Office of a Licensed Mental Health Professional (LCSW, LPC, LMFT, LAT)

Common Billing Information ____________________________________________________
Ch. 6 Index 109 Revision 4/1/17
Federally Qualified Health Center (FQHC)
Rural Health Clinic (RHC)
Skilled nursing facility (SNF)
Indian Health Services Clinic (IHS)
Hospital-based or Critical Access Hospital-based renal dialysis centers
(including satellites). Independent Renal Dialysis Facilities are not eligible
originating sites.
Developmental Center
Distant Site Providers (Hub Site)
The location of the physician or practitioner providing the professional services via a
telecommunications system is called the distant site or Hub site. A medical
professional is not required to be present with the client at the originating site unless
medically indicated. However, in order to be reimbursed, services provided must be
appropriate and medically necessary. Physicians/practitioners eligible to bill for
professional services are:
Physician
Advanced Practice Nurse with specialty of Psychiatry/Mental Health
Physician’s Assistant
Psychologist or Neuropsychologist
Licensed Mental Health Professional (LCSW, LPC, LMFT, LAT)
Speech Therapist
Provisionally licensed mental health professionals cannot bill Medicaid
directly. Services must be provided through an appropriate supervising
provider. Services provided by non-physician practitioners must be within
their scope(s) of practice and according to Medicaid policy.
For Medicaid payment to occur, interactive audio and video
telecommunications must be permitting real-time communication between the
distant site physician or practitioner and the patient with sufficient quality to
assure the accuracy of the assessment, diagnosis, and visible evaluation of
symptoms and potential medication side effects. All interactive video
telecommunication must comply with HIPAA patient privacy regulations at
the site where the patient is located, the site where the consultant is located,
and in the transmission process. If distortions in the transmission make
adequate diagnosis and assessment improbable and a presenter at the site
where the patient is located is unavailable to assist, the visit must be halted
and rescheduled. It is not appropriate to bill for portions of the evaluation
unless the exam was actually performed by the billing provider. The billing
provider must comply with all licensing and regulatory laws applicable to the
provider’s practice or business in Wyoming and must not currently be
excluded from participating in Medicaid by state or federal sanctions.

Common Billing Information ____________________________________________________
Ch. 6 Index 110 Revision 4/1/17
6.24.2 Non-Covered Services
Telehealth does not include a telephone conversation, electronic mail message
(email), or facsimile transmission (fax) between a healthcare practitioner and a
patient.
6.24.3 Billing Requirements
In order to obtain Medicaid reimbursement for services delivered through telehealth
technology, the following standards must be observed:
The services must be medically necessary and follow generally accepted
standards of care.
The service must be a service covered by Medicaid.
Claims must be made according to Medicaid billing instructions.
The same procedure codes and rates apply as for services delivered in person.
Quality assurance/improvement activities relative to telehealth delivered
services need to be identified, documented and monitored.
Providers need to develop and document evaluation processes and patient
outcomes related to the telehealth program, visits, provider access, and patient
satisfaction.
All service providers are required to develop and maintain written
documentation in the form of progress notes the same as is originated during
an in-person visit or consultation with the exception that the mode of
communication (i.e. teleconference) should be noted.
Medicaid will not reimburse for the use or upgrade of technology, for
transmission charges, for charges of an attendant who instructs a patient on
the use of the equipment or supervises/monitors a patient during the telehealth
encounter, or for consultations between professionals.
o The modifier to indicate a telehealth service is “GT” which must be
used in conjunction with the appropriate procedure code to identify the
professional telehealth services provided by the distant site provider
(e.g., procedure code 90832 billed with modifier GT). Using the GT
modifier does not change the reimbursement fee.
o When billing for the originating site facility fee, use procedure code
Q3014. A separate or distinct progress note isn’t required to bill
Q3014. Validation of service delivery would be confirmed by the
accompanying practitioner’s claim with the GT modifier indicating the
practitioner’s service was delivered via telehealth. Medicaid will
reimburse the originating site provider the lesser of charge or the
current Medicaid fee.
o Additional services provided at the originating site on the same date as
the telehealth service may be billed and reimbursed separately
according to published policies and the national correct coding
initiative guidelines.
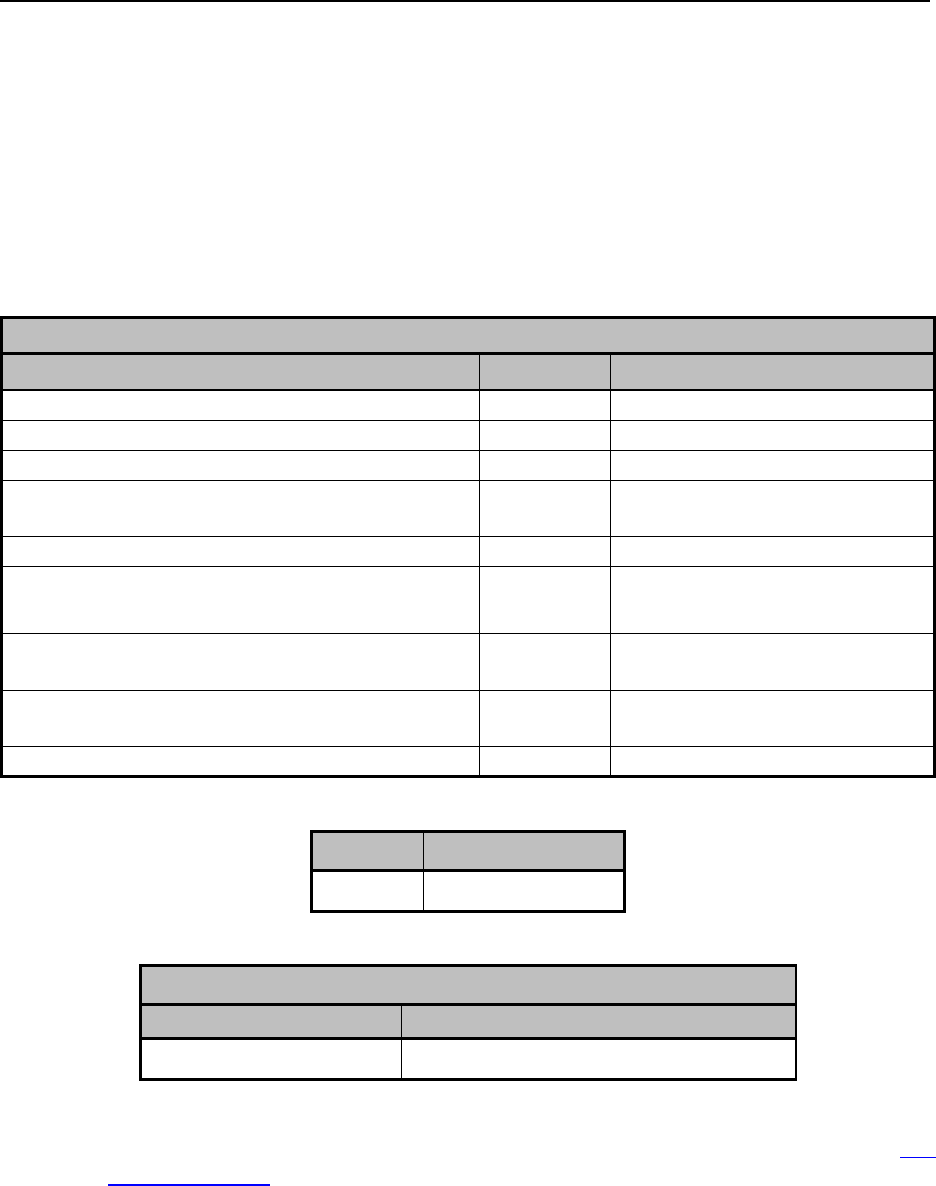
Common Billing Information ____________________________________________________
Ch. 6 Index 111 Revision 4/1/17
o For ESRD-related services, at least one (1) face-to-face, “hands on”
visit (not telehealth) must be furnished each month to examine the
vascular access site by a qualified provider.
NOTE: If the patient and/or legal guardian indicate at any point that he/she wants
to stop using the technology, the service should cease immediately and an
alternative appointment set up.
Hub Sites Billing Code(s) (site with provider)
CPT-4 and HCPCS Level II Codes
Modifier
Description
99241-99255
GT
Consultations
99201-99215
GT
Office or other outpatient visits
90832-90838
GT
Psychotherapy
90791-90792
GT
Psychiatric diagnostic
interview examination
96116
GT
Neurobehavioral status exam
90951,90952,90954,90955,90957,90958,90960
and 90961
GT
End stage renal disease related
services
G0270
GT
Individual medical nutrition
therapy
H0031, H2019, T1007, T1017, H0006, G9012
GT
Mental Health and Substance
Abuse Treatment Services
92586, 92602, 92604, 92626
GT
Remote Cochlear Implant
Modifier
Description
GT
Telehealth Service
Spoke Site Billing Code (site with patient)
HCPCS Level II Code
Description
Q3014
Telehealth originating site facility fee
For accurate listing of codes, refer to the fee schedule on the Medicaid website (2.1,
Quick Reference).

Third Party Liability_______ ____________________________________________________
Ch. 7 Index 112 Revision 4/1/17
Chapter Seven – Third Party Liability
7.1 Definition of a Third Party Liability ................................................................. 113
7.1.1 Third Party Liability (TPL) ............................................................................... 113
7.1.2 Third Party Payer ............................................................................................... 113
7.1.3 Medicare ............................................................................................................ 114
7.1.4 Medicare Replacement Plans ............................................................................ 114
7.1.5 Disability Insurance Payments .......................................................................... 114
7.1.6 Long-Term Care Insurance ............................................................................... 114
7.1.7 Exceptions ......................................................................................................... 114
7.2 Provider’s Responsibilities ................................................................................ 115
7.2.1 Third Party Resources Information Sheet ......................................................... 116
7.2.2 Provider is not enrolled with TPL Carrier ......................................................... 116
7.2.3 Medicare Opt-Out .............................................................................................. 117
7.3 Billing Requirements ......................................................................................... 117
7.3.1 How TPL is applied ........................................................................................... 119
7.3.1.1 Previous Attempts to Bill Services Letter ..................................................... 120
7.3.2 Acceptable proof of Payment or Denial ............................................................ 120
7.3.3 Coordination of Benefits ................................................................................... 121
7.3.4 Blanket Denials and Non-Covered Services ..................................................... 121
7.3.5 TPL and Copays ................................................................................................ 121
7.4 Medicare Pricing ............................................................................................... 122
7.4.1 Medicaid Covered Services ............................................................................... 122
7.4.2 Medicaid Non-Covered Services ....................................................................... 122
7.4.3 Coinsurance and Deductible .............................................................................. 123

Third Party Liability_______ ____________________________________________________
Ch. 7 Index 113 Revision 4/1/17
7.1 Definition of a Third Party Liability
7.1.1 Third Party Liability (TPL)
TPL is defined as the right of the department to recover, on behalf of a client, from a
third party payer the costs of Medicaid services furnished to the client (Wyoming
Department of Health, Medicaid Rules, Chapter 1, Section 3 Part (b) subpart
(ccxlviii)).
In simple terms, third party liability (TPL) is often referred to as other insurance,
other health insurance, medical coverage, or other insurance coverage. Other
insurance is considered a third-party resource for the client. Third-party resources
may include but are not limited to:
Health insurance (including Medicare)
Vision coverage
Dental coverage
Casualty coverage resulting from an accidental injury or personal injury
Payments received directly from an individual who has either voluntarily
accepted or been assigned legal responsibility for the health care of one or
more clients.
7.1.2 Third Party Payer
Third Party Payer is defined as a person, entity, agency, insurer, or government
program that may be liable to pay, or that pays pursuant to a client’s right of recovery
arising from an illness, injury, or disability for which Medicaid funds were paid or are
obligated to be paid on behalf of the client. Third party payers include, but are not
limited to:
Medicare
Medicare Replacement (Advantage or Risk Plans)
Medicare Supplemental Insurance
Insurance Companies
Other
o Disability Insurance
o Workers’ Compensation
o Spouse or parent who is obligated by law or by court order to pay all
or part of such costs (absent parent)
o Client’s estate
o Title 25
Medicaid is the payor of last resort. It is a secondary payer to all other payment sources
and programs and should be billed only after payment or denial has been received from
such carriers.

Third Party Liability_______ ____________________________________________________
Ch. 7 Index 114 Revision 4/1/17
7.1.3 Medicare
Medicare is administered by the Centers for Medicare and Medicaid Services (CMS) and
is the federal health insurance program for individuals age 65 and older, certain disabled
individuals, individuals with End Stage Renal Disease (ESRD) and amyotrophic lateral
sclerosis (ALS). Medicare entitlement is determined by the Social Security
Administration. Medicare is primary to Medicaid. Services covered by Medicare must
be provided by a Medicare-enrolled provider and billed to Medicare first.
7.1.4 Medicare Replacement Plans
Medicare Replacement Plans are also known as Medicare Advantage Plans or Medicare
Part C and are treated the same as any other Medicare claim. Many companies have
Medicare replacement policies. Providers must verify whether or not a policy is a
Medicare replacement policy. If the policy is a Medicare replacement policy, the claim
should be entered as any other Medicare claim.
7.1.5 Disability Insurance Payments
If the disability insurance carrier pays for health care items and services, the payments
must be assigned to Wyoming Medicaid. The client may choose to receive a cash
benefit. If the payments from the disability insurance carrier are related to a medical
event that required submission of claims for payment, the reimbursement from the
disability carrier is considered a third party payment. If the disability policy does not
meet any of these, payments made to the Wyoming Medicaid client may be treated as
income for Medicaid eligibility purposes.
7.1.6 Long-Term Care Insurance
When a long-term care (LTC) insurance policy exists, it must be treated as TPL and be
cost-avoided. The provider must either collect the LTC policy money from the client or
have the policy assigned to the provider. However, if the provider is a nursing facility
and the LTC payment is sent to the client, the monies are considered income. The funds
will be included in the calculation of the client’s patient contribution to the nursing
facility.
7.1.7 Exceptions
The only exceptions to this policy are referenced below:
Children’s Special Health (CSH) – Medical claims are sent to Wyoming
Medicaid’s MMIS fiscal agent
Indian Health Services (IHS) – 100% federally funded program
Ryan White Foundation – 100% federally funded program
Wyoming Division of Victim Services/Wyoming Crime Victim
Compensation Program

Third Party Liability_______ ____________________________________________________
Ch. 7 Index 115 Revision 4/1/17
Policyholder is an absent parent
Upon billing Medicaid, providers are required to certify if a third party has
been billed prior to submission. The provider must also certify that they have
waited 30 days from the date of service before billing Medicaid and has not
received payment from the third party
Services are for preventative pediatric care (Early and Periodic Screening,
Diagnosis, and Treatment/EPSDT), prenatal care.
NOTE: Inpatient labor and delivery services and post-partum care must be cost
avoided or billed to the primary health insurance. See State Medicaid Manual Section
3904.3B – Prenatal and Preventative Pediatric Care. An internet search may be
performed to locate this citation by performing an internet query of the State Medicaid
Manual, select Chapter 3 and go to Section sm_3_3900_to_3910.15.
The probable existence of third-party liability cannot be established at the
time the claim is filed.
Home and community based (HCBS) waiver services as most insurance
companies do not cover these types of services.
NOTE: It may be in the provider’s best interest to bill the primary insurance themselves,
as they may receive higher reimbursement from the primary carrier.
7.2 Provider’s Responsibilities
Providers have an obligation to investigate and report the existence of other third-
party liability information. Providers play an integral and vital role as they have direct
contact with the client. The contribution providers make to Medicaid in the TPL arena
is significant. Their cooperation is essential to the functioning of the Medicaid
Program and to ensuring prompt payment.
At the time of client intake, the provider must obtain Medicaid billing information
from the client. At the same time, the provider should also ascertain if additional
insurance resources exist. When a TPL/Medicare has been reported to the provider,
these resources must be identified on the claim in order for claims to be processed
properly. Other insurance information may be reported to Medicaid using the Third
Party Resources Information Sheet. Claims should not be submitted prior to billing
TPL/Medicare.
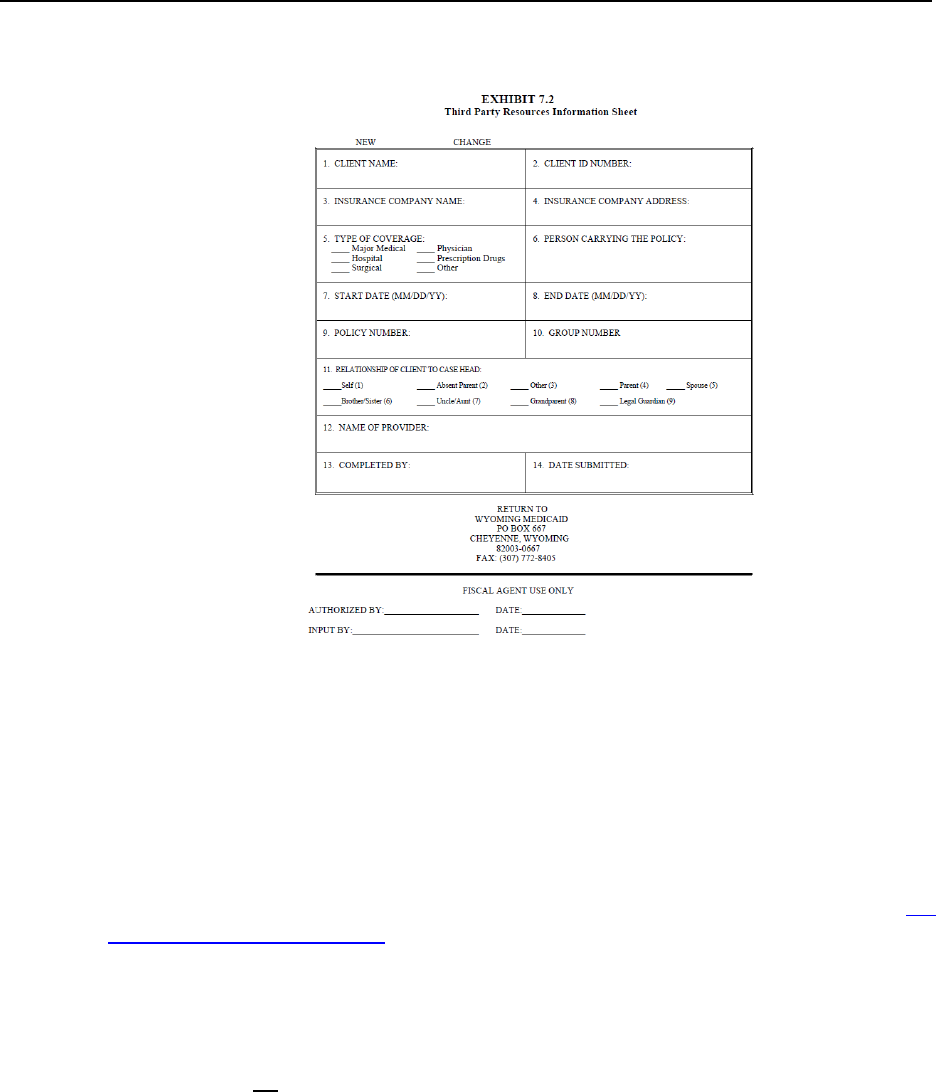
Third Party Liability_______ ____________________________________________________
Ch. 7 Index 116 Revision 4/1/17
7.2.1 Third Party Resources Information Sheet
NOTE: Click image above to be taken to a printable version of this form.
Medicaid maintains a reference file of known commercial health insurance as well as
a file for Medicare Part A and Part B entitlement information. Both files are used to
deny claims that do not show proof of payment or denial by the commercial health
insurer or by Medicare. Providers must use the same procedures for locating third
party payers for Medicaid clients as for their non-Medicaid clients.
Providers may not refuse to furnish services to a Medicaid client because of a third
party’s potential liability for payment for the service (S.S.A. §1902(a)(25)(D)) (3.2
Accepting Medicaid Clients)
7.2.2 Provider is not enrolled with TPL Carrier
Medicaid will no longer accept a letter with a claim indicating that a provider does
not participate with a specific health insurance company. The provider must work
with the insurance company and/or client to have the claim submitted to the carrier.
Providers cannot refuse to accept Medicaid clients who have other insurance if their
office does not bill other insurance. However, a provider may limit the number of
Medicaid clients s/he is willing to admit into his/her practice. The provider may not
discriminate in establishing a limit. If a provider chooses to opt-out of participation
with a health insurance or governmental insurance, Medicaid will not pay for services
covered by, but not billed to, the health insurance or governmental insurance.

Third Party Liability_______ ____________________________________________________
Ch. 7 Index 117 Revision 4/1/17
7.2.3 Medicare Opt-Out
Providers may choose to opt-out of Medicare. However, Medicaid will not pay for
services covered by, but not billed to, Medicare because the provider has chosen not
to enroll in Medicare. The provider must enroll with Medicare if Medicare will cover
the services in order to receive payment from Medicaid.
NOTE: In situations where the provider is reimbursed for services and Medicaid later
discovers a source of TPL, Medicaid will seek reimbursement from the TPL source.
If a provider discovers a TPL source after receiving Medicaid payment, they must
complete an adjustment to their claim within 30 days of receipt of payment from the
TPL source.
7.3 Billing Requirements
Providers should bill TPL/Medicare and receive payment to the fullest extent possible
before billing Medicaid. The provider must follow the rules of the primary insurance plan
(such as obtaining prior authorization, obtaining medical necessity, obtaining a referral or
staying in-network) or the related Medicaid claim will be denied. Follow specific plan
coverage rules and policies. CMS does not allow federal dollars to be spent if a client
with access to other insurance does not cooperate or follow the applicable rules of his or
her other insurance plan.
Medicaid will not pay for and will recover for payments made for services that could
have been covered by the TPL/Medicare if the applicable rules of that plan had been
followed. It is important that providers maintain adequate records of the third-party
recovery efforts for a period of time not less than six (6) years after the end of the state
fiscal year. These records, like all other Medicaid records, are subject to audit/post-
payment review by Health and Human Services, the Centers for Medicare and Medicare
Services (CMS), the state Medicaid agency, or any designee.
NOTE: If a procedure code requires a prior authorization (PA) for Medicaid payment,
but not required by TPL/Medicare, it is still highly recommended to obtain a PA through
Medicaid in case TPL/Medicare denies services.
Once payment/denial is received by TPL/Medicare, the claim may then be billed to
Medicaid as a secondary claim. If payment is received from the other payer, the provider
should compare the amount received with Medicaid’s maximum allowable fee for the
same claim.
If payment is less than Medicaid’s allowed amount for the same claim, indicate
the payment in the appropriate field on the claim form.
o CMS 1500 – TPL paid amount will be indicated in box 29 Amount Paid
Third Party Liability_______ ____________________________________________________
Ch. 7 Index 118 Revision 4/1/17
o CMS 1500 – Medicare paid amount will not be indicated on the claim, a
COB must be attached for claim processing
o UB-04 –TPL/Medicare amount will be indicated in box 54 Prior Payments
o Dental – TPL/Medicare amount will be indicated in box 33A Other Fees
If the TPL payer paid less than 40% of the total billed charges, include the
appropriate claim reason and remark codes or attach an explanation of benefits
(EOB) with the electronic claim (Electronic Attachments).
If payment is received from the other payer after Medicaid already paid the claim,
Medicaid’s payment must be refunded for either the amount of the Medicaid
payment or the amount of the insurance payment, whichever is less. A copy of the
EOB from the other payer must be included with the refund showing the
reimbursement amount.
NOTE: Medicaid will accept refunds from a provider at any time. Timely filing
will not apply to adjustments where money is owed to Medicaid (6.20 Timely
Filing).
If denial is obtained from the third party payer/Medicare that a service is not
covered, attach the denial to the claim (6.15 Submitting Attachments for
Electronic Claims). The denial will be accepted for one (1) calendar year, but will
still need to be attached with each claim.
If verbal denial is obtained from a third party payer, type a letter of explanation on
official office letterhead. The letter must include:
o Date of verbal denial
o Payer’s name and contact person’s name and phone number
o Date of Service
o Client’s name and Medicaid ID number
o Reason for denial
If the third party payer/Medicare sends a request to the provider for additional
information, the provider must respond. If the provider complies with the request
for additional information and after ninety (90) days from the date of the original
Third Party Liability_______ ____________________________________________________
Ch. 7 Index 119 Revision 4/1/17
claim and the provider has not received payment or denial, the provider may
submit the claim to Medicaid with the Previous Attempts to Bill Services Letter.
NOTE: Waivers of timely filing will not be granted due to unresponsive third
party payers.
In situations involving litigation or other extended delays in obtaining benefits
from other sources, Medicaid should be billed as soon as possible to avoid timely
filing. If the provider believes there may be casualty insurance, contact TPL Unit
(2.1 Quick Address and Telephone Reference) TPL will investigate the
responsibility of the other party. Medicaid does not require providers to bill a
third party when liability has not been established. However, the provider cannot
bill the casualty carrier and Medicaid at the same time. The provider must choose
to bill Medicaid or the casualty carrier (estate). Medicaid will seek recovery of
payments from liable third parties. If providers bill the casualty carrier (estate)
and Medicaid, this may result in duplicate payments.
If the client receives reimbursement from the primary insurance, the provider
must pursue payment form the patient. If there are any further Medicaid benefits
allowed after the other insurance payment, the provider may still submit a claim
for those benefits. The provider, on submission, must supply all necessary
documentation of the other insurance payment. Medicaid will not pay the provider
the amount paid by the other insurance.
Providers may not charge Medicaid clients, or any other financially responsible
relative or representative of that individual any amount in excess of the Medicaid
paid amount. Medicaid payment is payment in full. There is no balance billing.
7.3.1 How TPL is applied
The amount paid to providers by primary insurance payers is often less than the
original amount billed, for the following reasons:
Reductions resulting from a contractual agreement between the payer and the
provider (contractual write-off); and,
Reductions reflecting patient responsibility (copayment, coinsurance, deductible,
etc.). Wyoming Medicaid will pay no more than the remaining patient responsibility
(PR) after payment by the primary insurance.
Wyoming Medicaid will reimburse the provider for the patient liability up to the
Medicaid Allowable Amount. A provider must include the contract write-off amount
and the amount paid by the other insurance as the third party liability payment. (See
the State Medicaid Manual Chapter 3, Section 3904.7 for more information.)
TPL is applied to claims at the header level. Medicaid does not apply TPL amounts
line by line.
Example:
Total claim billed to Medicaid is for $100.00, with a Medicaid allowable for
the total claim of $50.00. TPL has paid $25.00 for only the second line of the
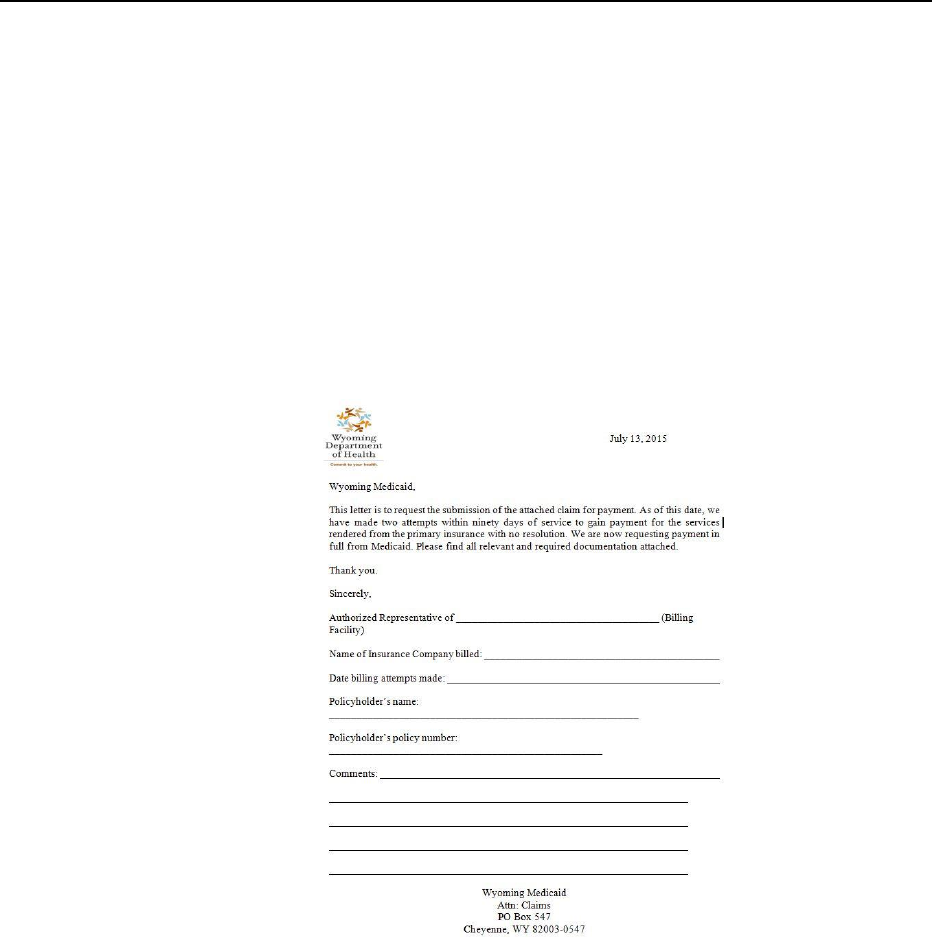
Third Party Liability_______ ____________________________________________________
Ch. 7 Index 120 Revision 4/1/17
claim. Claim will be processed as follows: Medicaid allowable ($50.00) minus
the TPL paid amount ($25) = $25.00 Medicaid Payment.
If the payer does not respond to the first attempt to bill with a written or electronic
response to the claim within sixty (60) days, resubmit the claims to the TPL. Wait an
additional thirty (30) days for the third party payer to respond to the second billing. If
after ninety (90) days from the initial claim submission the insurance still has not
responded, bill Medicaid with the Previous Attempts to Bill Services Letter.
NOTE: Waivers of timely filing will not be granted due to unresponsive third party
payers.
7.3.1.1 Previous Attempts to Bill Services Letter
NOTE: Do not submit this form for Medicare or automobile/casualty insurance.
Click image above to be taken to a printable version of this form.
7.3.2 Acceptable proof of Payment or Denial
Documentation of proper payment or denial of TPL/Medicare must correspond with
the client’s/beneficiary’s name, date of service, charges, and TPL/Medicare payment
referenced on the Medicaid claim. If there is a reason why the charges do not match
(i.e. other insurance requires another code to be billed, institutional and professional
charges are on the same EOB, third party payer is Medicare Advantage plan,
replacement plan or supplement plan) this information must be written on the
attachment.

Third Party Liability_______ ____________________________________________________
Ch. 7 Index 121 Revision 4/1/17
7.3.3 Coordination of Benefits
Coordination of Benefits (COB) is the process of determining which source of
coverage is the primary payer in a particular situation. COB information must be
complete, indicate the payer, payment date and the payment amount.
If a client has other applicable insurance, providers who bill electronic and web
claims will need to submit the claim COB information provided by the other
insurance company for all affected services. For claims submitted through the
Medicaid website, see the Web Portal Tutorials on billing secondary claims.
For clients with three insurances, tertiary claims cannot be submitted through the
Medicaid Web Portal and will need to be sent in on paper, with both EOBs and a
cover sheet indicating that the claim is a tertiary claim.
7.3.4 Blanket Denials and Non-Covered Services
When a service is not covered by a client’s primary insurance plan, a blanket denial
letter should be requested from the TPL/Medicare. The insurance carrier should then
issue, on company letterhead, a document stating the service is not covered by the
insurance plan. The provider can also provide proof from a benefits booklet from the
other insurance, as it shows that the service is not covered or the provider may use
benefits information from the carrier’s website. Providers should retain this statement
in the client’s file to be used as proof of denial for one calendar year. The non-
covered status must be reviewed and a new letter obtained as the end of one calendar
year.
If a client specific denial letter or EOB is received, the provider may use that denial
or EOB as valid documentation for the denied services for that member for one
calendar year. The EOB must clearly state the services are not covered. The provider
must still follow the rules of the primary insurance prior to filing the claim to
Medicaid.
7.3.5 TPL and Copays
A client with private health insurance primary to Wyoming Medicaid is required to
pay the Wyoming Medicaid copay. Submit the claim to Wyoming Medicaid in the
usual manner, reporting the insurance payment on the claim with the balance due. If
the Wyoming Medicaid allowable covers all or part of the balance billed, Wyoming
Medicaid will pay up to the maximum Wyoming Medicaid allowable amount, minus
any applicable Wyoming Medicaid copay. Wyoming Medicaid will deduct the copay
from its payment amount to the provider and report it as the copay amount on the
provider’s RA. Remember, Wyoming Medicaid is only responsible for the
client’s liability amount or patient responsibility amount up to its maximum
allowable amount.
Submit claims to Wyoming Medicaid only if the TPL payer indicates a patient
responsibility. If the TPL does not attribute charges to patient responsibility or non-
covered services, Wyoming Medicaid will not pay.

Third Party Liability_______ ____________________________________________________
Ch. 7 Index 122 Revision 4/1/17
7.4 Medicare Pricing
Effective dates of service beginning January 1, 2017, Wyoming Medicaid changed
how reimbursement is calculated for Medicare crossover claims. This change applies
to all service providers.
Part B crossovers are processed and paid at the line level (line by line)
Part A inpatient crossovers, claims are processed at the header level
Part A outpatient crossovers, claims are priced at the line level (line by line)
totaled, and then priced at the header level
7.4.1 Medicaid Covered Services
For services covered under the Wyoming Medicaid State Plan, the new payment
methodology will consider what Medicaid would have paid, had it been the sole
payer. Medicaid’s payment responsibility for a claim will be the lesser of the
Medicare coinsurance and deductible, or the difference between the Medicare
payment and Medicaid allowed charge(s).
Example:
Procedure Code 99239
o Medicaid Allowable - $97.67
o Medicare Paid - $83.13
o Medicare assigned Coinsurance and Deductible - $21.21
First payment method option: (Medicaid Allowable) $97.67 –
(Medicare Payment) $83.13 = $14.54
Second payment method option: Coinsurance and deductible =
$21.21
o Medicaid will pay the lesser of the Medicaid payment methodology or
the coinsurance and deductible
This procedure code would pay $14.54 since it is less than
$21.21
NOTE: If the method for Medicaid covered services results in a Medicaid
payment of $0 and the claim contains lines billed for physician-administered
pharmaceuticals, the line will pay out at $0.01.
7.4.2 Medicaid Non-Covered Services
For specific Medicare services which are not otherwise covered by Wyoming
Medicaid State plan, Medicaid will use a special rate or method to calculate the
amount Medicaid would have paid for the service. This method is Medicare allowed
amount, divided by 2, minus the Medicare paid amount.

Third Party Liability_______ ____________________________________________________
Ch. 7 Index 123 Revision 4/1/17
Example:
Procedure Code: E0784 – (Not covered as a rental – no allowed amount has
been established for Medicaid)
o Medicaid Allowable – Not assigned
o Medicare Allowable - $311.58
o Medicare Paid – $102.45
o Assigned Coinsurance and Deductible - $209.13
First payment method option: [(Medicare Allowable 311.58 ÷
2)] – 102.45 Medicare paid amount = $155.79 (Calculated
Medicaid allowable) – (Medicare Paid Amount) 102.45 =
$53.34
Second payment method option: Coinsurance and deductible =
209.13
o Medicaid will pay the lesser of the Medicaid payment methodology or
the coinsurance and deductible
This procedure code would pay $53.34 since it is less than
$209.13
NOTE: If the method for Medicaid non-covered services results in a
Medicaid payment of $0 and the claim contains lines billed for physician-
administered pharmaceuticals, the line will pay out at $0.01.
7.4.3 Coinsurance and Deductible
For clients on the QMB plan, CMS guidelines indicate that coinsurance and
deductible amounts remaining after Medicare pays cannot be billed to the client under
any circumstances, regardless of whether you bill Medicaid or not.
For clients on other plans who are dual eligible, coinsurance and deductible amounts
remaining after Medicare payment cannot be billed to the client if the claim was
billed to Wyoming Medicaid, regardless of payment amount (including claims that
Medicaid pays at $0).
If the claim is not billed to Wyoming Medicaid, and the provider agrees in writing
prior to providing the service not to accept the client as a Medicaid client and advises
the client of his or her financial responsibility, and the client is not on a QMB plan,
then the client can be billed for the coinsurance and deductible under Medicare
guidelines.

Electronic Data Interchange (EDI)________________________________________________
Ch. 8 Index 124 Revision 4/1/17
Chapter Eight – Electronic Data Interchange (EDI)
8.1 What is Electronic Data Interchange (EDI)? ..................................................... 125
8.2 Benefits .............................................................................................................. 125
8.3 Standard Transaction Formats ........................................................................... 125
8.4 Sending and Receiving Transactions ................................................................ 126
8.5 EDI Services ...................................................................................................... 127
8.5.1 Getting Started ................................................................................................... 127
8.5.2 Web Portal ......................................................................................................... 128
8.5.2.1 Secured Provider Web Portal Registration Process ....................................... 128
8.5.2.2 Creating an Office Administrator .................................................................. 128
8.5.2.3 Creating Additional Users ............................................................................. 129
8.5.3 WINASAP ......................................................................................................... 129
8.5.3.1 WINASAP Start-up ....................................................................................... 129
8.6 Additional Information Sources ........................................................................ 131
8.7 Scheduled Web Portal Downtime ..................................................................... 131

Electronic Data Interchange (EDI)________________________________________________
Ch. 8 Index 125 Revision 4/1/17
8.1 What is Electronic Data Interchange (EDI)?
In its simplest form, EDI is the electronic exchange of information between two (2)
business concerns (trading partners), in a specific, predetermined format. The
exchange occurs in basic units called transactions, which typically relate to standard
business documents, such as healthcare claims or remittance advices.
8.2 Benefits
Several immediate advantages can be realized by exchanging documents
electronically:
Speed – Information moving between computers moves more rapidly, and
with little or no human intervention. Sending an electronic message across the
country takes minutes or less. Mailing the same document will usually take a
minimum of one (1) day.
Accuracy – Information that passes directly between computers without
having to be re-entered eliminates the chance of data entry errors.
Reduction in Labor Costs – In a paper-based system, labor costs are higher
due to data entry, document storage and retrieval, document matching, etc. As
stated above, EDI only requires the data to be keyed once, thus lowering labor
costs.
8.3 Standard Transaction Formats
In October 2000, under the authority of the Health Insurance Portability and
Accountability Act (HIPAA), the Department of Health and Human Services (DHHS)
adopted a series of standard EDI transaction formats developed by the Accredited
Standards Committee (ASC) X12N. These HIPAA-compliant formats cover a wide
range of business needs in the healthcare industry from eligibility verification to
claims submission. The specific transaction formats adopted by DHHS are listed
below.
X12N 270/271 Eligibility Benefit Inquiry and Response
X12N 276/277 Claims Status Request and Response
X12N 278 Request for Prior Authorization and Response
X12N 277CA Implementation Guide Error Reporting
X12N 835 Claim Payment/Remittance Advice
X12N 837 Dental, Professional and Institutional Claims
X12N 999 Functional Acknowledgement
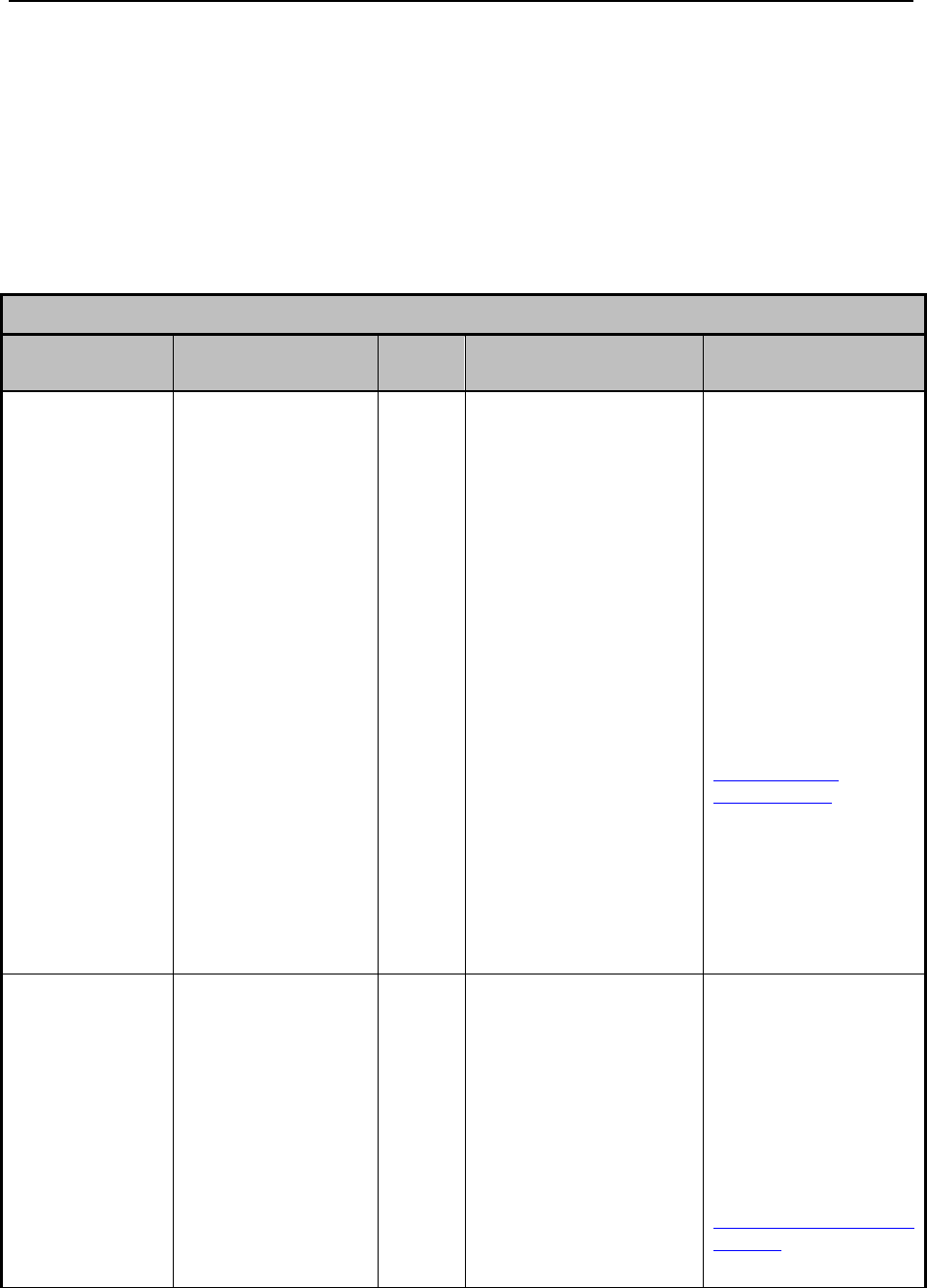
Electronic Data Interchange (EDI)________________________________________________
Ch. 8 Index 126 Revision 4/1/17
NOTE: As there is no business need, Medicaid does not currently accept nor
generate X12N 820 and X12N 834 transactions.
8.4 Sending and Receiving Transactions
Medicaid has established a variety of methods for providers to send and receive EDI
transactions. The following table is a guide to understanding and selecting the best
method.
EDI Options
Method
Requirements
Access
Cost
Transactions
Supported
Contact
Information
Bulletin Board
System (BBS)
The BBS is an
interactive, menu-
driven bulletin
board system for
uploading and
downloading
transactions.
Computer
Hayes-compatible
9600-baud or greater
asynchronous modem
Dial-up connection
utility (e.g., ProComm,
Hyperterminal, etc.)
File decompression
utility
Software capable of
formatting and reading
EDI transactions
Telephone connectivity
Free
X12N 270/271 Eligibility
Benefit Inquiry and
Response
X12N 276/277 Claims
Status Request and
Response
X12N 278 Request for
Prior Authorization and
Response
X12N 277CA
Implementation Guide
Error Reporting
X12N 835 Claim
Payment/Remittance
Advice
X12N 837 Dental,
Professional and
Institutional Claims
X12N 999 Functional
Acknowledgement
EDI Services
Telephone:
(800)672-4959
9-5pm MST M-F
OPTION 3
Website:
http://www.acs-
gcro.com/gcro/
Web Portal
The Medicaid
Secure Web Portal
provides an
interactive, web-
based interface for
entering individual
transactions and a
separate data
exchange facility
for uploading and
downloading batch
transactions.
Computer
Internet Explorer 5.5
(or higher) or Netscape
Navigator 7.0 (or
higher). Whichever
browser version is
used, it must support
128-bit encryption
Internet access
Additional
requirements for
Free
X12N 270/271 Eligibility
Benefit Inquiry and
Response
X12N 276/277 Claims
Status Request and
Response
X12N 278 Request for
Prior Authorization and
Response
X12N 277CA
Implementation Guide
EDI Services
Telephone:
(800)672-4959
9-5pm MST M-F
OPTION 3
Website:
http://wyequalitycare.acs-
inc.com/
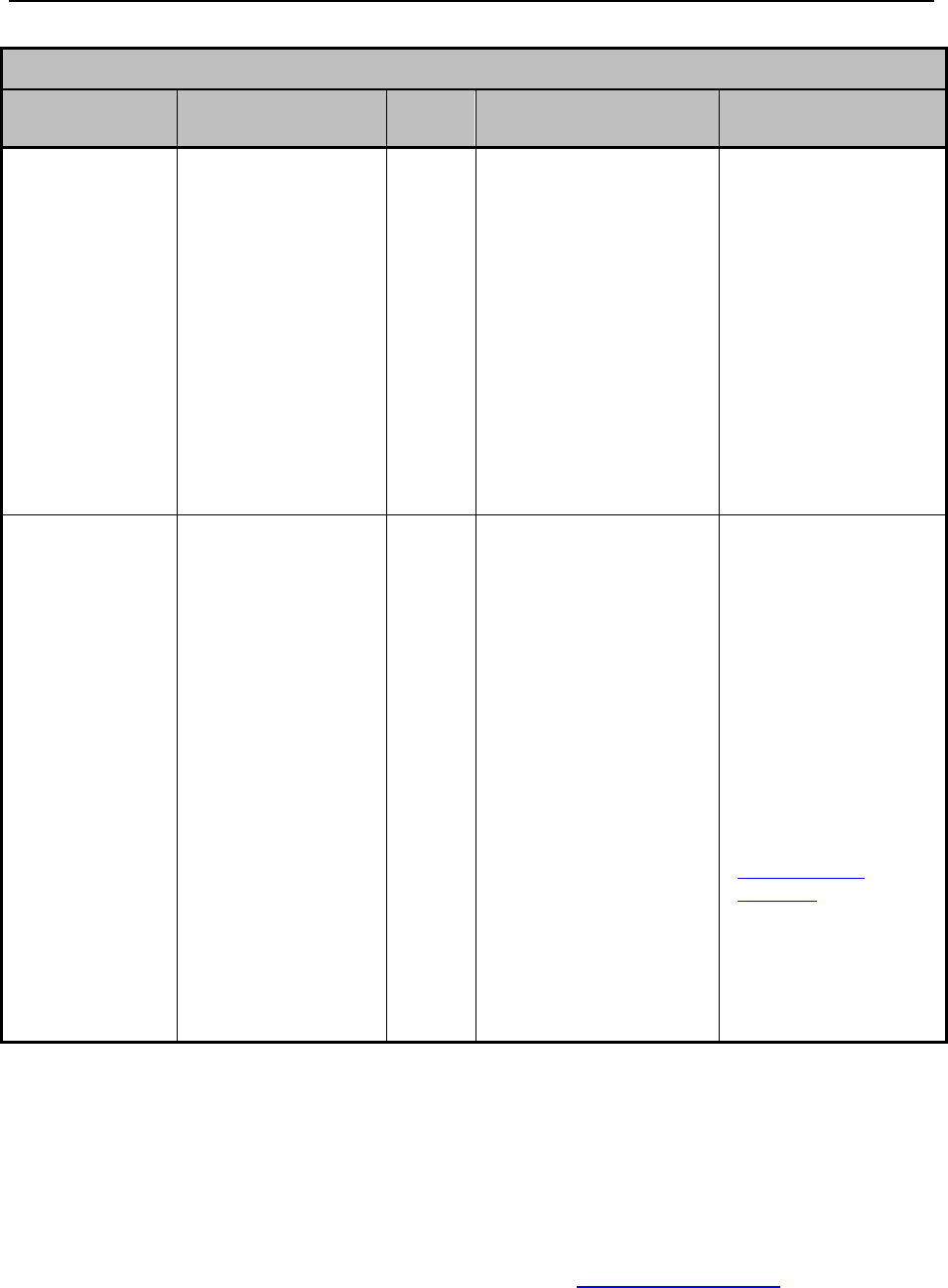
Electronic Data Interchange (EDI)________________________________________________
Ch. 8 Index 127 Revision 4/1/17
EDI Options
Method
Requirements
Access
Cost
Transactions
Supported
Contact
Information
uploading and
downloading batch
transactions:
File decompression
utility. Software
capable of formatting
and reading EDI
transactions
Error Reporting
X12N 835 Claim
Payment/Remittance
Advice
X12N 837 Dental,
Professional and
Institutional Claims*
X12N 999 – Functional
Acknowledgement
NOTE: Only the 278 and
837 transactions can be
entered interactively.
WINASAP 2003
Windows
Accelerated
Submission and
Processing
(WINASAP) is a
Windows-based
software
application that
allows users to
enter and submit
dental,
professional and
institutional claims
electronically
using a personal
computer.
Computer
Hayes-compatible
9600-baud
asynchronous modem
Windows 98 (or
higher) operating
system
Pentium processor
25 megabytes of free
disk space
128 megabytes of
RAM
Monitor resolution of
800 x 600 pixels
Telephone
connectivity
Free
X12N 837 Dental,
Professional and
Institutional Claims
X12N
277CAImplementation
Guide Error Reporting
X12N 999 – Functional
Acknowledgement
EDI Services
Telephone:
(800)672-4959
9-5pm MST M-F
OPTION 3
Website:
http://www.acs-
gcro.com/
8.5 EDI Services
8.5.1 Getting Started
The first step the provider needs to complete before the provider is able to start
sending electronic information is to complete the EDI Enrollment Application. The
application is located on the Medicaid website (2.1, Quick Reference) under “Forms”
and “Enrollment/Agreement Forms”.
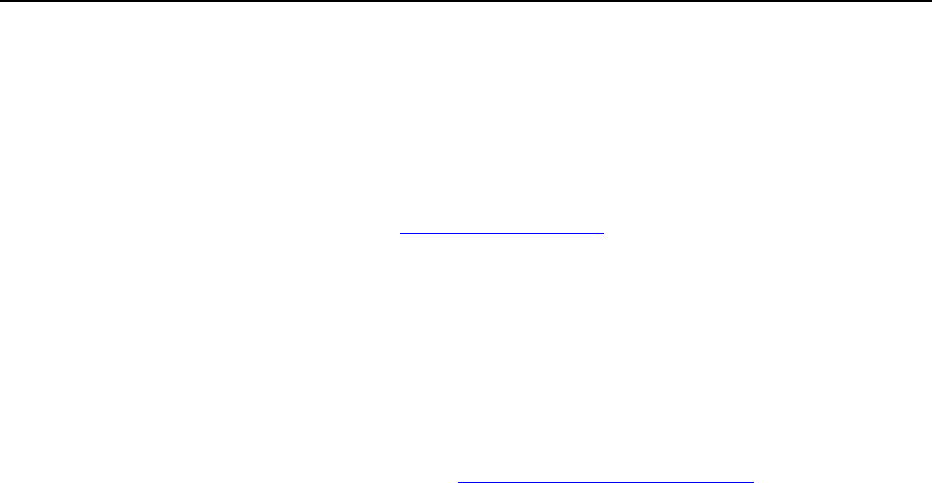
Electronic Data Interchange (EDI)________________________________________________
Ch. 8 Index 128 Revision 4/1/17
Once the form is completed and sent to Medicaid the provider will be sent an EDI
Welcome Letter which will include a User Name and Password. Below are the
benefits of using Web Portal and WINASAP and instructions for registering.
NOTE: Web Portal Tutorials and WINASAP Tutorials are published to the
Medicaid website (2.1, Quick Reference).
8.5.2 Web Portal
The Web Portal allows all trading partners to retrieve and submit data via the internet
24-hours a day, seven (7) days a week from anywhere.
8.5.2.1 Secured Provider Web Portal Registration Process
Go to the Medicaid website: http://wymedicaid.acs-inc.com.
Select Provider.
Select Provider Portal from the left hand menu.
Under “New Providers” select Web Portal to register.
Enter the following information from the EDI Welcome Letter:
o Provider ID: Trading Partner/Submitter ID.
o Trading Partner ID: Trading Partner/Submitter ID.
o EIN/SSN: The Providers tax-id as entered on the EDI application.
o Trading Partner Password: Password/User ID – Must be entered
exactly as shown on the welcome letter.
Select Continue
o Confirm that the information that the provider has entered is correct. If
it is, choose Continue, if not re-enter information.
Additional Trading Partner IDs:
o If the provider needs to enter additional Trading Partner IDs enter the
ID and the Trading Partner password on this page.
o If the provider does not have any additional Trading Partner IDs select
continue.
8.5.2.2 Creating an Office Administrator
The providers Office Administrator will be the person responsible for adding and
deleting new users as necessary for the provider’s organization along with any other
privileges selected.
1. Select Create a new user.
a. Enter a unique user ID, last name, first name, email address and phone
number for the person that the provider wants to be the office
administrator.
b. Confirm the information entered is correct.
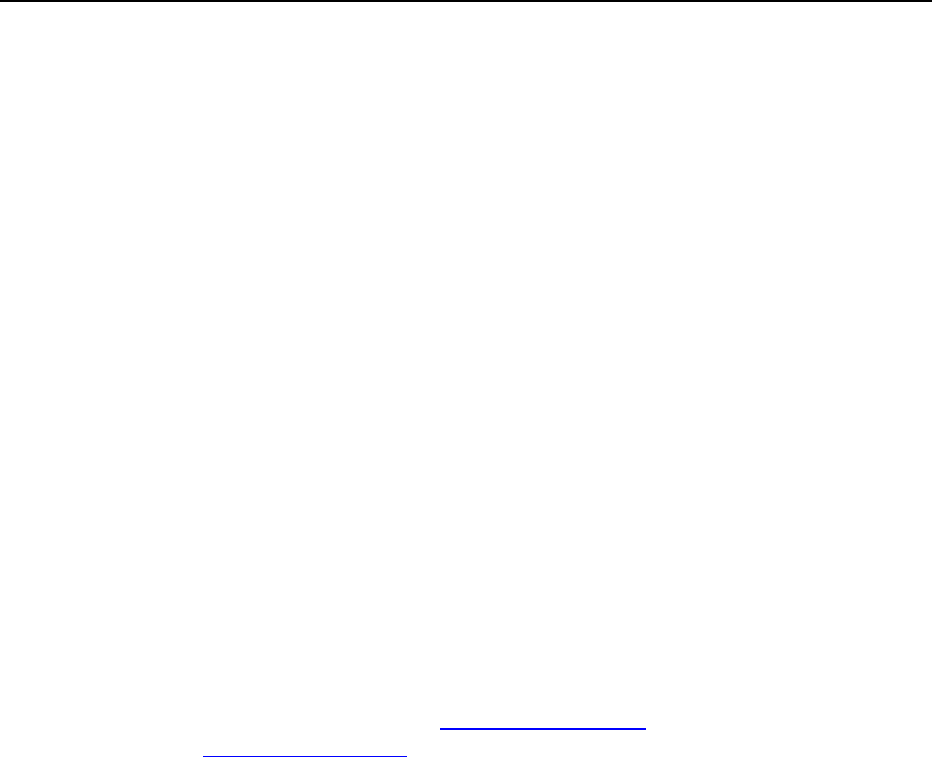
Electronic Data Interchange (EDI)________________________________________________
Ch. 8 Index 129 Revision 4/1/17
c. This completes the web registration for the office administrator, an
email will be sent to the email address entered with a one (1) time use
password.
d. Once the provider receives the single use password, (it is easiest to
copy and paste this directly from the email to avoid typographical
errors) and must be changed upon logging in for the first (1st) time.
Return to the home page and log in.
2. All permissions will be set once the provider has logged in. To do this, select
update or remove users. Enter the provider user ID and select search. When
the user information is brought up, click on the user ID link.
a. Select which privileges the provider wishes to have. Once the provider
has chosen these privileges click Submit.
8.5.2.3 Creating Additional Users
1. Return to the home page and choose Manage Users.
a. Follow the steps as listed above.
8.5.3 WINASAP
WINASAP allows all Trading Partners to submit claims 24-hours a day, seven (7)
days a week from any computer with a dial up modem over an analog phone line that
the provider has installed the software on. WINASAP can be downloaded from the
ACS EDI Gateway, Inc. website (2.1, Quick Reference) or the provider can call EDI
Services (2.1, Quick Reference) and request a CD to be mailed to the provider.
Requirements:
Windows 98 Second Edition, Windows NT, Windows 2000 (Service Pack 3),
Windows XP or Windows 7 operating system
Pentium processor
CD-ROM drive
25 Megabytes of free disk space
128 Megabytes of RAM
Monitor resolution of 800 x 600 pixels
Hayes compatible 9600 baud asynchronous modem
Telephone connectivity
8.5.3.1 WINASAP Start-up
1. Download program from the ACS EDI Gateway, Inc. website or install the
program from the CD the provider requested.
a. When the welcome screen appears click next
b. Read and accept the terms of the Software License Agreement

Electronic Data Interchange (EDI)________________________________________________
Ch. 8 Index 130 Revision 4/1/17
c. Enter User Information
d. Choose Destination Location
e. Confirm provider current settings and choose Next
f. Check Yes, launch the program file and Finish.
2. Creating a WINASAP login
a. The user ID auto fills as ADMIN
b. Tab to password and type ASAP
i. The user ID and password are the same for everyone using
WINASAP, we suggest that the provider does not change them
c. After successfully logging in choose ok
3. Steps that must be completed
a. The screen will automatically open the first (1st) time the provider
runs the program that says Open Payer
i. Select Wyoming Medicaid and choose OK
ii. Choose File and Trading Partner – Enter the following
iii. Primary Identification: Enter the provider Trading Partner ID
from the EDI Welcome Letter
iv. Secondary Identification – Re-enter the provider Trading
Partner ID (primary and secondary identification will be the
same)
b. Trading Partner Name:
i. Entity Type: select person or non-person.
1. Choose person if the provider is an individual such as; a
waiver provider, physician, therapist, or nurse
practitioner
2. Choose non-person if the provider is a facility such as;
a hospital, pharmacy or nursing home.
c. Enter the providers last name, first name and middle initial (optional)
OR the organization name
i. Contact Information:
1. Contact Name: provider Name
2. Telephone Number: Enter provider phone number
3. Fax Number: Enter provider fax number (optional)
4. Email: Enter provider email address
4. The following criteria must be completed:
a. WINASAP2003 Communications:
i. Host Telephone Number: This phone number is listed as the
Submission Telephone Number on the EDI Welcome Letter.
Enter it with no spaces, dashes, commas, or other punctuation
marks.
ii. User ID Number: Enter providers Password/User ID exactly as
it appears.
iii. User Name: Enter providers User Name exactly as it appears.
iv. Choose Save
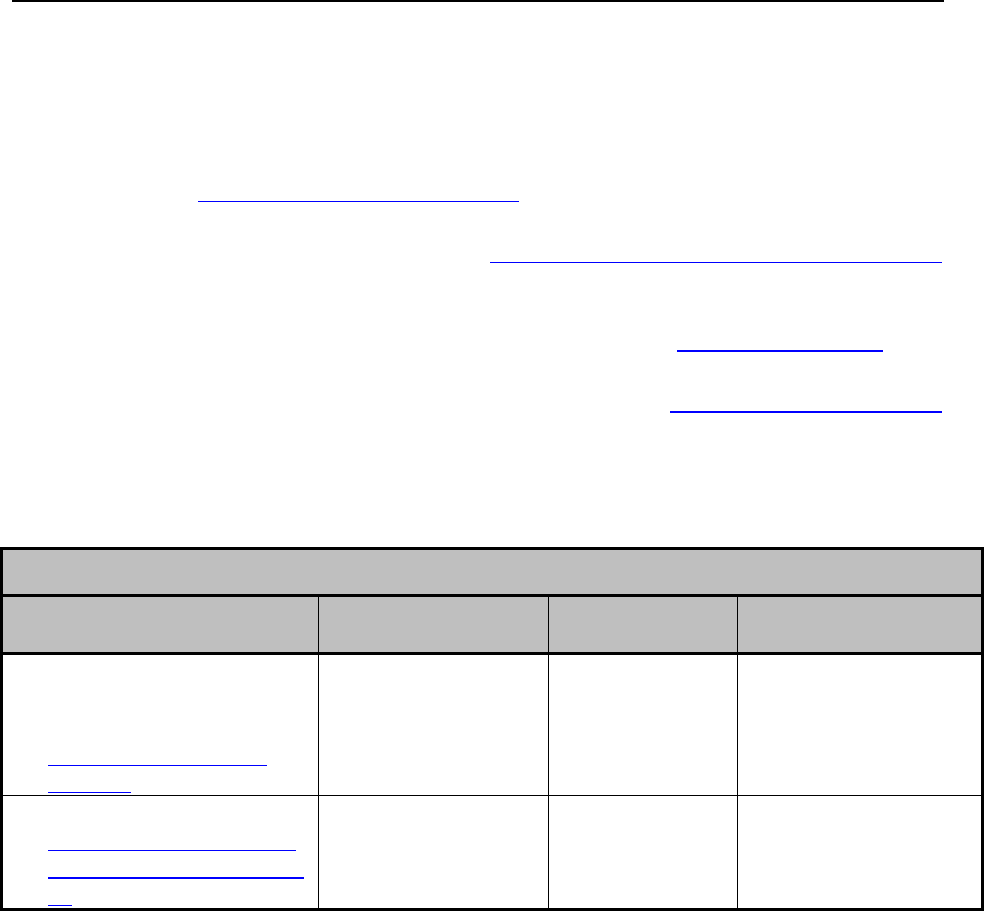
Electronic Data Interchange (EDI)________________________________________________
Ch. 8 Index 131 Revision 4/1/17
8.6 Additional Information Sources
For more information regarding EDI, please refer to the following websites:
Centers for Medicare and Medicaid Services:
www.cms.gov/hipaa2/default.asp. This is the official HIPAA website of the
Centers for Medicare & Medicaid service.
Washington Publishing Co.: http://www.wpc-edi.com/hipaa/HIPAA_40.asp.
This website is the official source of the implementation guides for each of the
ASC X12 N transactions.
Workgroup for Electronic Data Interchange: http://www.wedi.org/. This
industry group promotes electronic transactions in the healthcare industry.
Designated standard maintenance organizations: http://www.hipaa-dsmo.org/.
This website explains how changes are made to the transaction standards.
8.7 Scheduled Web Portal Downtime
Scheduled Web Portal Downtime
What is Impacted
Functionality
Impact
Why
Downtimes
Entire website
(Provider/Client) Static web
pages
http://wymedicaid.acs-
inc.com/
Website not available
Regular
scheduled
maintenance
4 a.m. – 4:30 a.m.
MST Saturdays
3 p.m. – 6 p.m.
MST Sundays
Secured Provider Web Portal
http://wyequalitycare.acs-
inc.com/wy/general/home.
do
Verification of
claims submission
will not be available
Regular
scheduled
maintenance
10 p.m. – 12 a.m.
(midnight)
Sundays

Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 132 Revision 4/1/17
Chapter Nine – Wyoming HIPAA 5010 Electronic Specifications
9.1 Wyoming Specific HIPAA 5010 Electronic Specifications .............................. 134
9.2 Transaction Definitions ..................................................................................... 134
9.3 Transmission Methods and Procedures ............................................................. 134
9.3.1 Asynchronous Dial-up ....................................................................................... 134
9.3.1.1 Communication Protocols ............................................................................. 135
9.3.1.2 Teleprocessing Requirements ........................................................................ 135
9.3.1.3 Teleprocessing Settings ................................................................................. 135
9.3.1.4 Transmission Procedures ............................................................................... 136
9.3.2 Web Portal ......................................................................................................... 137
9.3.3 Managed File Transfer (MOVEit) ..................................................................... 137
9.4 Acknowledgement and Error Reports ............................................................... 138
9.4.1 Confirmation Report .......................................................................................... 138
9.4.2 Interchange Level Errors and TA1 Rejection Report ........................................ 138
9.4.3 999 Implementation Acknowledgements .......................................................... 139
9.4.3.1 Batch and Real-Time Usage .......................................................................... 139
9.4.4 Data Retrieval Method ...................................................................................... 140
9.5 Testing ............................................................................................................... 140
9.5.1 Testing Requirements ........................................................................................ 140
9.6 270/271 Eligibility Request and Response ........................................................ 141
9.6.1 ISA Interchange Control Header ....................................................................... 141
9.6.2 GS Functional Group Header ............................................................................ 142
9.6.3 The Following are Access Methods Supported by Wyoming Medicaid ........... 142
9.6.4 270 Eligibility Request ...................................................................................... 143
9.6.5 271 Eligibility Response ................................................................................... 143
9.7 276/277 Claim Request and Response .............................................................. 143
9.7.1 ISA Interchange Control Header ....................................................................... 143
9.7.2 GS Functional Group Header ............................................................................ 143
9.7.3 276 Claim Status Request .................................................................................. 144

Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 133 Revision 4/1/17
9.7.4 277 Claim Status Response ............................................................................... 144
9.8 278 Request for Review and Response ............................................................. 144
9.8.1 ISA Interchange Control header ........................................................................ 144
9.8.2 GS Functional Group Header ............................................................................ 145
9.8.3 278 Prior Authorization Request – Data Clarifications Inbound ...................... 145
9.8.4 X12N 278 Health Care Services Review – Response to Request for Review –
Outbound for Wyoming Medicaid .................................................................... 145
9.9 835 Claim Payment/Advice ............................................................................... 145
9.9.1 Payment/Advice ................................................................................................ 145
9.10 837 Professional Claims Transactions Wyoming Medical Professional Claims
........................................................................................................................... 146
9.10.1 ISA Interchange Control Header ....................................................................... 146
9.10.2 GS Functional Group Header ............................................................................ 146
9.10.3 837 Professional ................................................................................................ 147
9.11 837 Institutional Claims Transactions Wyoming Medicaid Institutional Claims
........................................................................................................................... 150
9.11.1 ISA Interchange Control header ........................................................................ 150
9.11.2 GS Functional Group Header ............................................................................ 151
9.11.3 837 Institutional ................................................................................................. 151
9.12 837 Dental Claims Transactions Wyoming Medicaid Dental Claims .............. 151
9.12.1 ISA Interchange Control Header ....................................................................... 152
9.12.2 GS Functional Group Header ............................................................................ 152
9.12.3 Dental ................................................................................................................ 152

Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 134 Revision 4/1/17
9.1 Wyoming Specific HIPAA 5010 Electronic Specifications
This chapter is intended for trading partner use in conjunction with the ASC X12N
Standards for Electronic Data Interchange Technical Report Type 3 (TR3). The TR3
can be accessed at http://www.wpc-edi.com. This section outlines the procedures
necessary for engaging in Electronic Data Interchange (EDI) with the Xerox
Government Healthcare Solutions EDI Clearinghouse (EDI Clearinghouse) and
specifies data clarification where applicable.
9.2 Transaction Definitions
270/271 – Health Care Eligibility Benefit Inquiry and Response.
276/277 – Health Care Claim Status Request and Response.
278/278 – Health Care Services – Request for Review and Response; Health
Care Services Notification and Acknowledgement.
835 – Health Care Claim Payment/Advice.
837 – Health Care Claim (Professional, Institutional, and Dental), including
Coordination of Benefits (COB) and Subrogation Claims.
Acknowledgement Transaction Definitions.
TA1 – Interchange Acknowledgement.
999 – Implementation acknowledgement for Health Care Insurance .
277CA – Health Care Claim Acknowledgement.
9.3 Transmission Methods and Procedures
9.3.1 Asynchronous Dial-up
The Host System is comprised of communication (COMM) servers with modems.
Trading partners access the Host System via asynchronous dial-up. The COMM
machines process the login and password, then log the transmission.
The Host System will forward a confirmation report to the trading partner providing
verification of file receipt. It will show a unique file number for each submission.
The COMM machines will also pull the TA1s and 999s from an outbound
transmission table, and deliver to the HIPAA BBS Mailbox system. The trading
partner accesses the mailbox system via asynchronous dial-up to view and/or retrieve
their responses.

Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 135 Revision 4/1/17
9.3.1.1 Communication Protocols
The EDI Clearinghouse currently supports the following communication options:
XMODEM
YMODEM
ZMODEM
KERMIT
9.3.1.2 Teleprocessing Requirements
The general specifications for communication with EDI Clearinghouse are:
Telecommunications: Hayes-compatible 2400-56K BPS asynchronous
modem
File Format: ASCII text data
Compression Techniques – EDI Clearinghouse accepts transmission with any
of these compression techniques, as well as non-compression:
o PKZIP will compress one (1) or more files into a single ZIP archive.
o WINZIP will compress one (1) or more files into a single ZIP archive.
Data Format:
o 8 data bit
o 1stop bit
o no parity
o full duplex
9.3.1.3 Teleprocessing Settings
ASCII Sending
o Send line ends with line feeds (should not be set)
o Echo typed characters locally (should not be set)
o Line delay 0 millisecond
o Character delay 0 milliseconds
ASCII Receiving
o Append line feeds to incoming line ends should not be checked
o Wrap lines that exceed terminal width
o Terminal Emulation VT100 or Auto
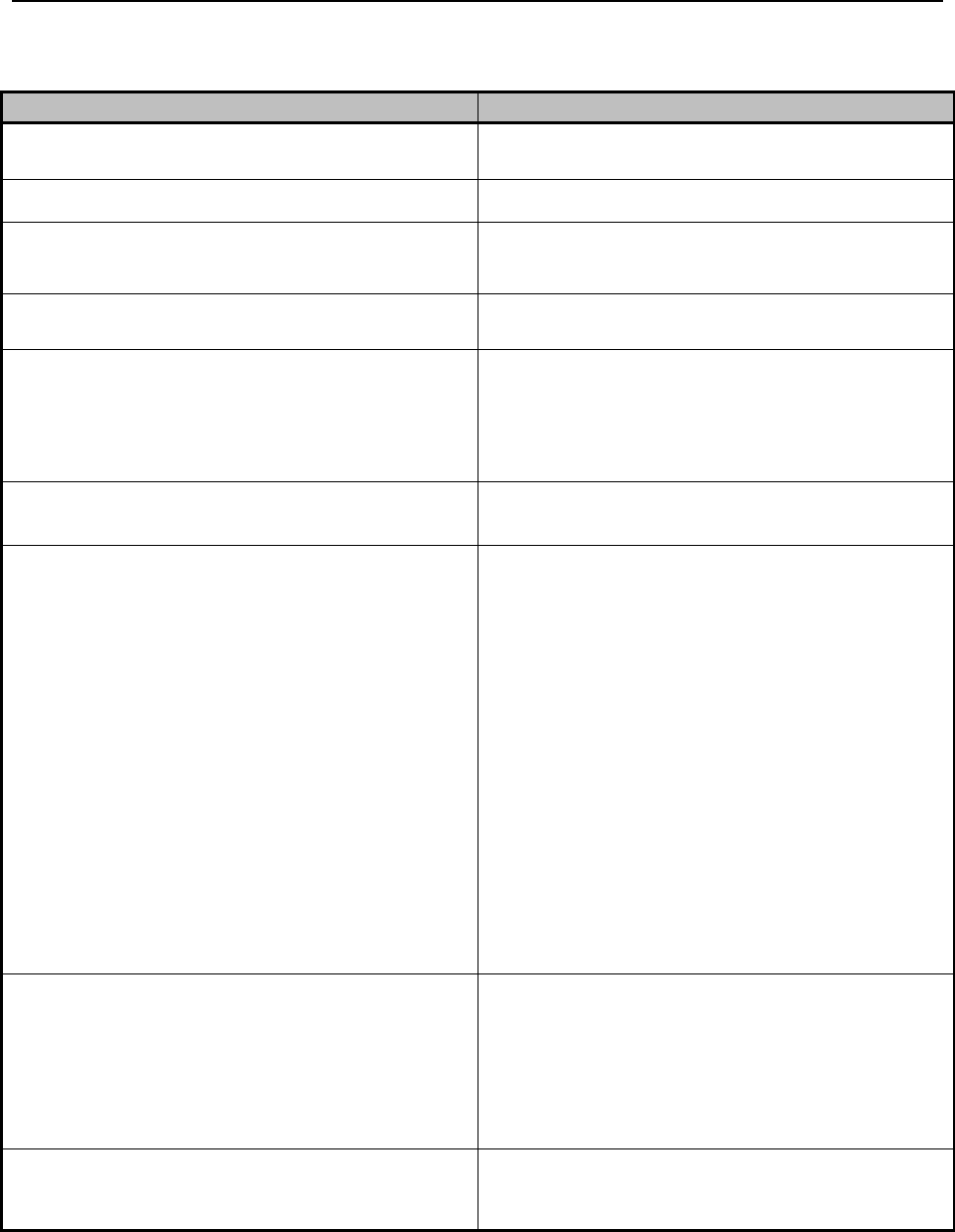
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 136 Revision 4/1/17
9.3.1.4 Transmission Procedures
SUBMITTER
HOST
Dials Host 1(800) 334-2832 or (800) 334-4650
Answers call, negotiates a common baud rate,
and sends to the Trading Partner:
Prompt: “Please enter provider Logon=>”
Enters User Name (From the EDI Welcome
Letter) <CR>
Receives User Name and sends prompt to the
Trading Partner:
Prompt: “Please enter provider
password=>”
Enters Password/User ID (From the EDI
Welcome Letter) <CR>
Receives Password/User ID and verifies if
Trading Partner is an authorized user. Sends
HOST selection menu followed by a user
prompt:
Prompt: “Please Select from the Menu
Options Below=>”
Enters Desired Selection <CR>
#1. Electronic File Submission: Assigns and
sends the transmission file name then waits for
ZMODEM (by default) file transfer to be
initiated by the Trading Partner.
#2. View Submitter Profile
#3. Select File Transfer Protocol: Allows the
provider to change the protocol for the current
submission only. The protocol may be changed
to (k) ermit, (x) Modem, (y) Modem, or (z)
Modem. Enter selection [k, x, y, z]:
#4. Download Confirmation
#9. Exit & Disconnect: Terminates
connection.
Enters “1” to send file <CR>
Receives ZMODEM (or other designated
protocol) file transfer. Upon completion,
initiates file confirmation. Sends file
confirmation report. Sends HOST selection
menu followed by a user prompt=>
Prompt: “Please Select from the Menu
Options Below=>”
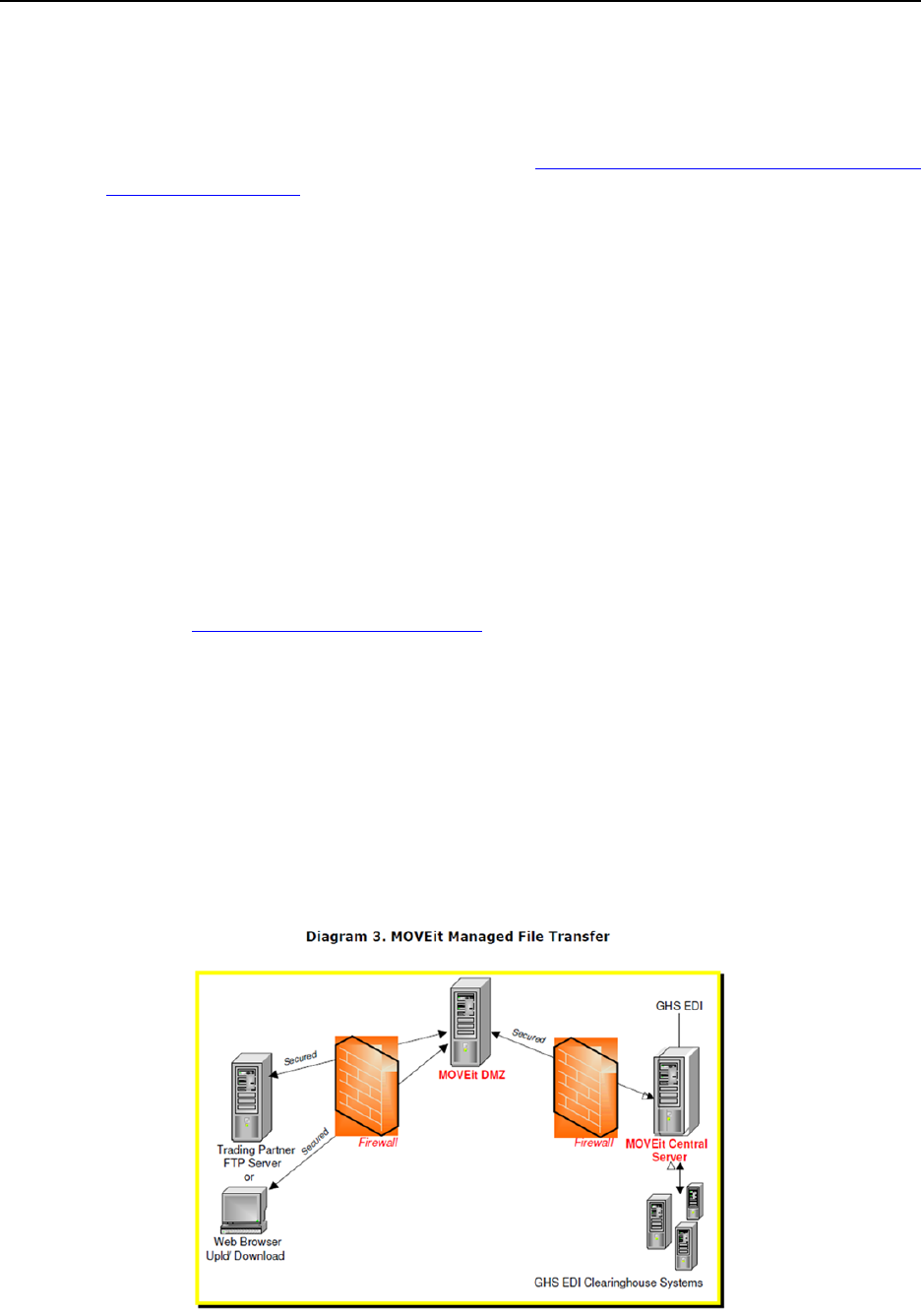
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 137 Revision 4/1/17
9.3.2 Web Portal
The trading partner must be an authenticated portal user who is a provider. Only
active providers are authorized to access files via the web. Provider must have
completed the web registration process. (8.5.2.1, Secured Provider Web Portal
Registration Process)
Trading partners can submit files via the web portal in two (2) ways:
Upload an X12N transaction file – The trading partner accesses the web portal
via a web browser and is prompted for login and password. The provider may
select files from their PC or work environment and upload files.
Enter X12N data information through a web interface – The trading partner
accesses the web portal via a web browser and is prompted for login and
password. Data entry screens will display for entering transaction information.
NOTE: Providers can retrieve their response files via the web portal by logging in
and accessing their transaction folders.
Transaction files can be uploaded and downloaded through the Secured Provider Web
Portal at http://wymedicaid.acs-inc.com.
Transaction transmission is available 24-hours a day, seven (7) days a week. This
availability is subject to scheduled and unscheduled host downtime.
9.3.3 Managed File Transfer (MOVEit)
EDI Clearinghouse supports Managed File Transfer using a product suite called
MOVEit. In the diagram below, trading partners can deliver files to or retrieve files
from the MOVEit DMZ site. EDI Clearinghouse does corresponding pickups from
and deliveries to the DMZ via an agreed upon schedule with Medicaid and trading
partner.

Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 138 Revision 4/1/17
9.4 Acknowledgement and Error Reports
The following acknowledgement reports are generated and delivered to trading
partners:
TA1 – Will be used to report invalid Trading Partner Relationship Validation
to Provider/Trading Partner.
999 – Will be used to acknowledge Syntax Validation (Positive, Negative or
Partial) – to Provider/Trading Partner.
277CA – Claims Acknowledgement will be used to provide accept/reject
information regarding submitted claims/request – to Provider/Trading Partner.
9.4.1 Confirmation Report
When a trading partner submits an X12N transaction, a receipt is immediately sent to
the trading partner to confirm that EDI Clearinghouse received a file, and shows a
unique file number for each submission. The Host System will forward a
Confirmation Report to the trading partner indicating:
Verification of file receipt.
If the file is accepted or rejected.
Identified as an X12N at a high level.
If a file fails this preliminary check, it will not continue processing.
The Confirmation Report includes the following information:
Date and time file was received
File number
Payer code (Wyoming Medicaid 77046)
Submission format
Type of transaction
Number of claims and batches
Status of Production or Test
Additional messages that can be added as a communication to trading partners
or may indicate the reason the file is invalid.
9.4.2 Interchange Level Errors and TA1 Rejection Report
A TA1 is an ANSI ASC X12N Interchange Acknowledgement segment used to report
receipt of individual interchange envelopes. An interchange envelope contains the
sender, receiver, and data type information within the header. The term "interchange"
connotes the ISA/IEA envelope that is transmitted between trading/business partners.
Interchange control is achieved through several "control" components. Refer to the
TR3 documents for a description of Envelopes and Control Structures.

Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 139 Revision 4/1/17
The TA1 reports the syntactical analysis of the interchange header and trailer. The
TA1 allows EDI Clearinghouse to notify the trading partner that a valid X12N
transaction envelope was received; or if problems were encountered with the
interchange control structure or the trading partner relationship.
The TA1 is unique in that it is a single segment transmitted without the GS/GE
envelope structure.
If the data can be identified, it is then checked for trading partner relationship
validation.
If the trading partner information is invalid, the data is corrupt or the trading
partner relationship does not exist, a negative confirmation report is returned
to the submitter. Any major X12N syntax error that occurs at this level will
result in the entire transaction being rejected, and the trading partner will need
to resubmit their X12N transaction.
If the trading partner information is valid, the data continues processing for
complete X12N syntax validation.
9.4.3 999 Implementation Acknowledgements
The 999 informs the submitter that the functional group arrived at the destination. It
may include information about the syntactical quality of the functional group and the
implementation guide compliance.
For more information on the relationship between the 999 transaction set and other
response transaction sets, refer to the ASC X12N Standards for Electronic Data
Interchange Technical Report Type 3 (TR3).
The 999 contains information indicating if the entire file is HIPAA 5010 compliant or
not.
9.4.3.1 Batch and Real-Time Usage
There are multiple methods available for sending and receiving business transactions
electronically. Two (2) common modes for EDI transactions are batch and real-time.
Batch – In a batch mode the sender does not remain connected while the
receiver processes the transactions. Processing is usually completed according
to a set schedule. If there is an associated business response transaction (such
as a 271 Response to a 270 Request for Eligibility), the receiver creates the
response transaction and stores it for future delivery. The sender of the
original transmission reconnects at a later time and picks up the response
transaction.
Real-Time – In real-time mode the sender remains connected while the
receiver processes the transactions and returns a response transaction to the
sender.
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 140 Revision 4/1/17
The 999 contains information indicating if the entire file is HIPAA 5010 compliant or
not.
9.4.4 Data Retrieval Method
Secured Web Portal
The web portal allows all trading partners to retrieve data via the internet 24-hours a
day, seven (7) days a week. Each provider has the option of retrieving the transaction
responses and reports themselves or allowing billing agents and clearinghouses to
retrieve on their behalf. The trading partner will access the Secured Provider Web
Portal system using the user ID and password provided upon completion of the
enrollment process (8.5.2.1, Secured Provider Web Portal Registration Process).
Contact the EDI Services for more information (2.1, Quick Reference).
9.5 Testing
Submitters (software vendors, billing agents, clearinghouses, and providers) who
have created their own electronic X12 transaction software are required to test their
software. Contact EDI Services for more information (2.1, Quick Reference). By
testing the submitter is validating their software prior to submitting production
transactions.
While in test mode for HIPAA 5010 the provider will not be able to submit
production files until testing is complete and the providers software is approved.
If a production HIPAA 5010 file is submitted while in test mode the file will fail with
a TA1 error (9.4.2, Interchange Level Errors and TA1 Rejection Report).
9.5.1 Testing Requirements
Contact EDI Services and explain that the provider is ready to test the provider
software.
Testing via EDIFECS
o Submitters cannot obtain direct Internet access to EDIFECS, the EDI
Services call center staff will set this up at the provider’s request.
o A user ID and password will be generated for the providers use.
o The provider is required to submit test files through EDIFECS.
o The provider is required to address any errors discovered during
testing prior to moving on to testing with the EDI Clearinghouse.
o After the provider’s software has received approval provide EDI
Services with the EDIFECS certification.
Testing with EDI Clearinghouse
o The call center will have the provider submit a test file.
o After 24-hours contact the call center for test file results.

Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 141 Revision 4/1/17
o Make corrections based on the TR3s and Wyoming Specific HIPAA
5010 Specifications.
o Resubmit test files as necessary.
o Successful completion of the testing process is required before a
submitter will be approved for production.
A separate testing process must be completed for each type of transaction i.e.
270/271, 276/277, 837 etc.
Each test transmission is validated to ensure no format errors are present. Testing is
conducted to verify the integrity of the format not the integrity of the data. However,
in order to simulate a true production environment, we request that test files contain
realistic healthcare transaction data. The number of test transmissions required
depends on the number of format errors in a transmission and the relative severity of
these errors. Additional testing may be required in the future to verify any changes
made to Wyoming Specific HIPAA 5010 Specifications or HIPAA mandated
changes.
9.6 270/271 Eligibility Request and Response
Health Care Eligibility Benefit Inquiry Request and Response for Wyoming
Medicaid.
This section is for use along with the ANSI ASC X12 Health Care Eligibility Request
& Response 270/271. It should not be considered a replacement for the TR3’s, but
rather used as an additional source of information. This section contains data
clarifications derived from specific business rules that apply exclusively to Wyoming
Medicaid.
NOTE: The page numbers listed below in each of the tables represent the
corresponding page number in the Technical Report Type3 (TR3) ANSI
ASC X12N Consolidated Guide; Health Care Eligibility Benefit Inquiry
and Response for the 270/271 005010X279 & 005010X279A1, June 2010.
9.6.1 ISA Interchange Control Header
TR3 Page
Loop
Segment
Reference
Description
Wyoming Requirements
Appendix C Page C.5
Header
ISA
08
100000 Followed by spaces
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 142 Revision 4/1/17
9.6.2 GS Functional Group Header
TR3 Page
Loop
Segment
Reference
Description
Wyoming Requirements
Appendix C page C.7
Header
GS
03
Enter 77046
9.6.3 The Following are Access Methods Supported by Wyoming
Medicaid
Access by Member ID number for subscriber.
Access by Member Card ID number.
Access by Social Security Number, and Date of Birth (Format CCYYMMDD)
for the subscriber.
Access by Social Security Number, and Name for the subscriber (Any non-
alphanumeric character including spaces that are included in the last name or
the first name may cause the inquiry to not be successfully processed).
Access by Name (Any non-alphanumeric character including spaces that are
included in the last name or the first name may cause the inquiry to not be
successfully processed), Sex, and Date of Birth for the subscriber.
NOTE: References to “Subscriber” are taken from the ANSI ASC X12N
Consolidated Guide; Health Care Eligibility Benefit Inquiry and Response
for the 270/271 005010X279 & 005010X279A1 and are synonymous with
Member.
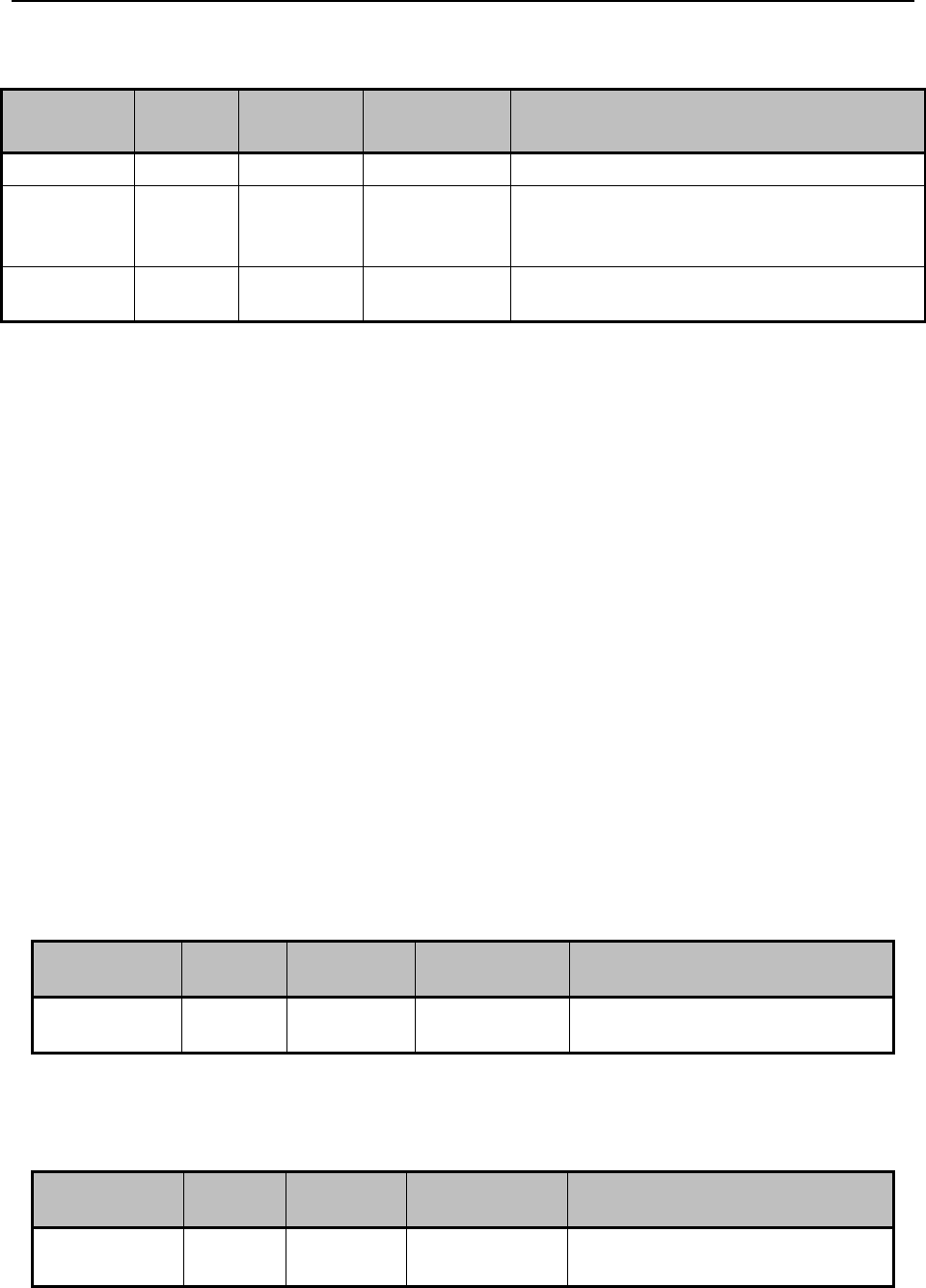
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 143 Revision 4/1/17
9.6.4 270 Eligibility Request
TR3 Page
Loop
Segment
Reference
Description
Wyoming Requirements
Page 72
2100A
NM1
03
Wyoming Medicaid
Page 79
2100B
NM1
08
NOTE: SV should be used only when a
Wyoming Provider is an Atypical
Provider/non-medical.
Page 80
2100B
NM1
09
NOTE: Enter Wyoming Medicaid
Provider ID when NM108 is SV.
9.6.5 271 Eligibility Response
No Wyoming Specific Requirements.
9.7 276/277 Claim Request and Response
Health Care Claim Status Request and Response for Wyoming Medicaid.
This section is for use along with the ANSI ASC X12 Health Care Claim Status
Request and Response 276/277. It should not be considered a replacement for the
TR3’s, but rather used as an additional source of information. This section contains
data clarifications derived from specific business rules that apply exclusively to
Wyoming Medicaid.
NOTE: The page numbers listed below in each of the tables represent the
corresponding page number in the Technical Report Type3 (TR3) ANSI
ASC X12N Health Care Claim Status Request and Response for the
276/277 005010X212, August 2006.
9.7.1 ISA Interchange Control Header
9.7.2 GS Functional Group Header
TR3 Page
Loop
Segment
Reference
Description
Wyoming Requirements
Appendix C
Page C.7
Header
GS
03
Enter 77046
TR3 Page
Loop
Segment
Reference
Description
Wyoming Requirements
Appendix C
Page C.5
Header
ISA
08
Enter 100000 followed by
spaces
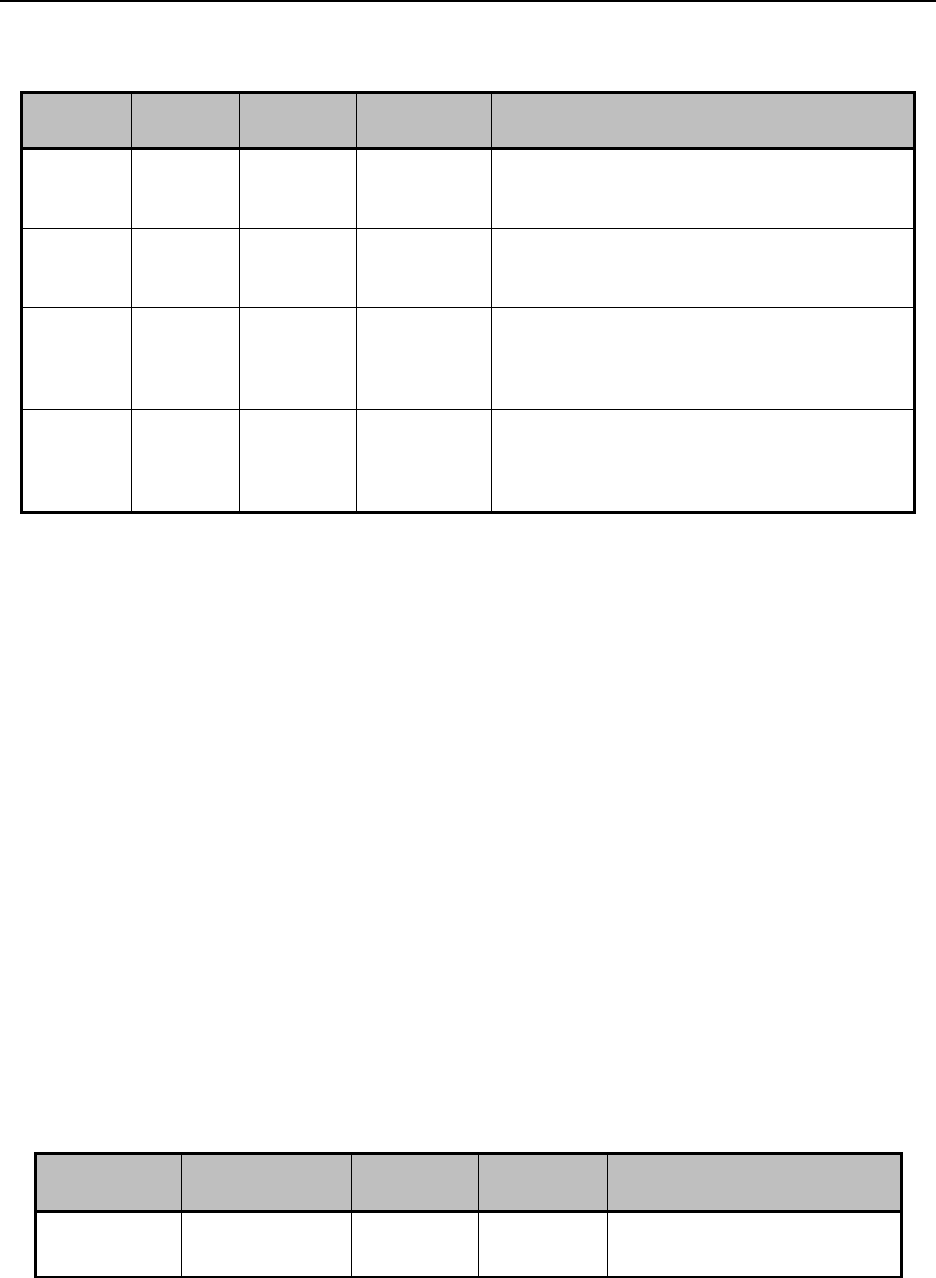
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 144 Revision 4/1/17
9.7.3 276 Claim Status Request
TR3
Page
Loop
Segment
Reference
Description
Wyoming Requirements
Page 46
2100B
NM1
09
NOTE: Enter the nine (9) digit Wyoming
Medicaid Provider ID when a Wyoming
Provider is an Atypical Provider/non-medical
Page 51
2100C
NM1
08
NOTE: SV should be used only when a
Wyoming Provider is an Atypical
Provider/non-medical.
Page 73
2210D
REF
01
The Line Item Control Number inquiry is not
supported by Wyoming Medicaid. The Claim
Status Response will return all claim line
items.
Page 73
2210D
REF
02
The Line Item Control Number inquiry is not
supported by Wyoming Medicaid. The Claim
Status Response will return all claim line
items.
9.7.4 277 Claim Status Response
No Wyoming Specific Requirements.
9.8 278 Request for Review and Response
Health Care Services Request for Review/Response for Wyoming Medicaid
This section is for use along with the ANSI ASC X12 Health Care Prior
Authorization Request and Response 278. It should not be considered a replacement
for the TR3’s, but rather used as an additional source of information. This section
contains data clarifications derived from specific business rules that apply exclusively
to Wyoming Medicaid.
NOTE: The page numbers listed below in each of the tables represent the
corresponding page number in the Technical Report Type3 (TR3) ANSI
ASC X12N Health Care Services Review – Request for Review and
Response for the (278) 005010X217, May 2006.
9.8.1 ISA Interchange Control header
TR3 Page
Loop
Segment
Data
Element
Wyoming Requirements
Appendix C
Page C.5
Interchange
Control Header
ISA
08
Enter 100000 followed by
spaces
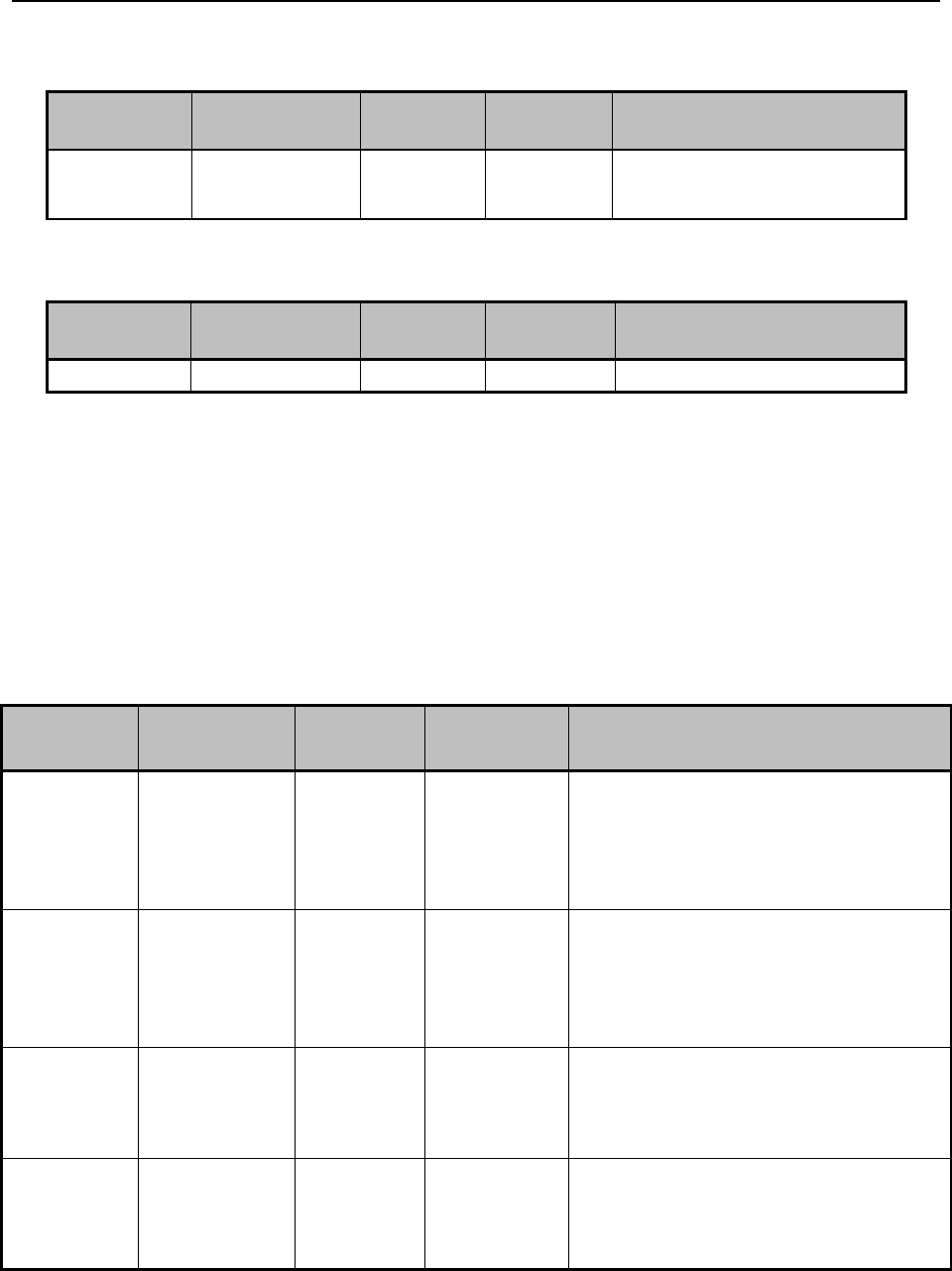
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 145 Revision 4/1/17
9.8.2 GS Functional Group Header
TR3 Page
Loop
Segment
Data
Element
Wyoming Requirements
Appendix C
Page C.7
Functional
Group Header
GS
03
Enter 77046
9.8.3 278 Prior Authorization Request – Data Clarifications Inbound
TR3 Page
Loop
Segment
Data
Element
Wyoming Requirements
Page 73
2010A
NM1
09
Enter 77046
9.8.4 X12N 278 Health Care Services Review – Response to Request for
Review – Outbound for Wyoming Medicaid
9.9 835 Claim Payment/Advice
Health Care Claim Payment Advice for Wyoming Medicaid.
9.9.1 Payment/Advice
TR3 Page
Loop
Segment
Data
Element
Wyoming Requirements
Page 107
1000B
REF
01
If the provider does not have an NPI
then REF01 will contain “PQ”
(Payee Identification) and REF02
will contain the Wyoming Medicaid
Provider ID.
108
1000B
REF
02
If the provider does not have an NPI
then REF01 will contain “PQ”
(Payee Identification) and REF02
will contain the Wyoming Medicaid
Provider ID.
Page 207-
208
2110
REF
01
Either HPI or G2 will be displayed.
NOTE: G2 will be displayed only
for WY Medicaid Atypical Providers.
Page 208
2110
REF
02
NOTE: Enter the nine (9) digit
Wyoming Medicaid Provider ID
when a Wyoming Provider is an
Atypical/non-medical.
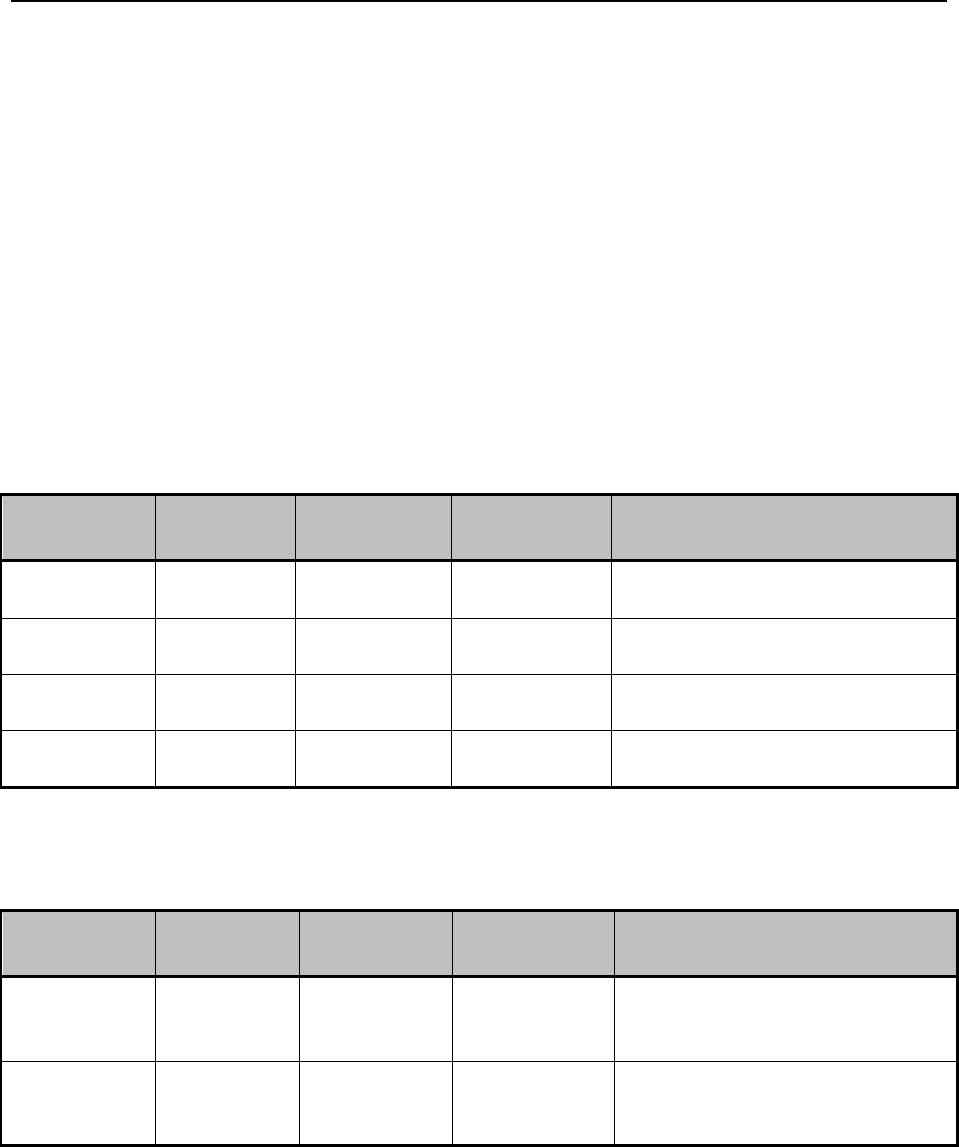
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 146 Revision 4/1/17
9.10 837 Professional Claims Transactions Wyoming Medical
Professional Claims
This section is for use along with the ANSI ASC X12 Health Care 837 Claims
Transactions. It should not be considered a replacement for the TR3s, but rather used
as an additional source of information. This section contains data clarifications
derived from specific business rules that apply exclusively to Wyoming Medicaid.
NOTE: The page numbers listed below in each of the tables represent the
corresponding page number in the Technical Report Type3 (TR3) ANSI
ASC X12N Consolidated Guide Health Care Claim: Professional (837),
005010X222/005010X222A1, June 2010
9.10.1 ISA Interchange Control Header
TR3 Page
Loop
Segment
Reference
Description
Wyoming Requirements
Appendix C
Page C.3
Header
ISA
01
Enter 00
Appendix C
Page C.4
Header
ISA
03
Enter 00
Appendix C
Page C.4
Header
ISA
06
Enter Trading Partner ID
Appendix C
Page C.5
Header
ISA
08
Enter 100000 followed by spaces
9.10.2 GS Functional Group Header
TR3 Page
Loop
Segment
Data
Element
Wyoming Requirements
Appendix C
Page C.7
Functional
Group
Header
GS
02
Enter Trading Partner ID
Appendix C
Page C.7
Functional
Group
Header
GS
03
Enter 77046
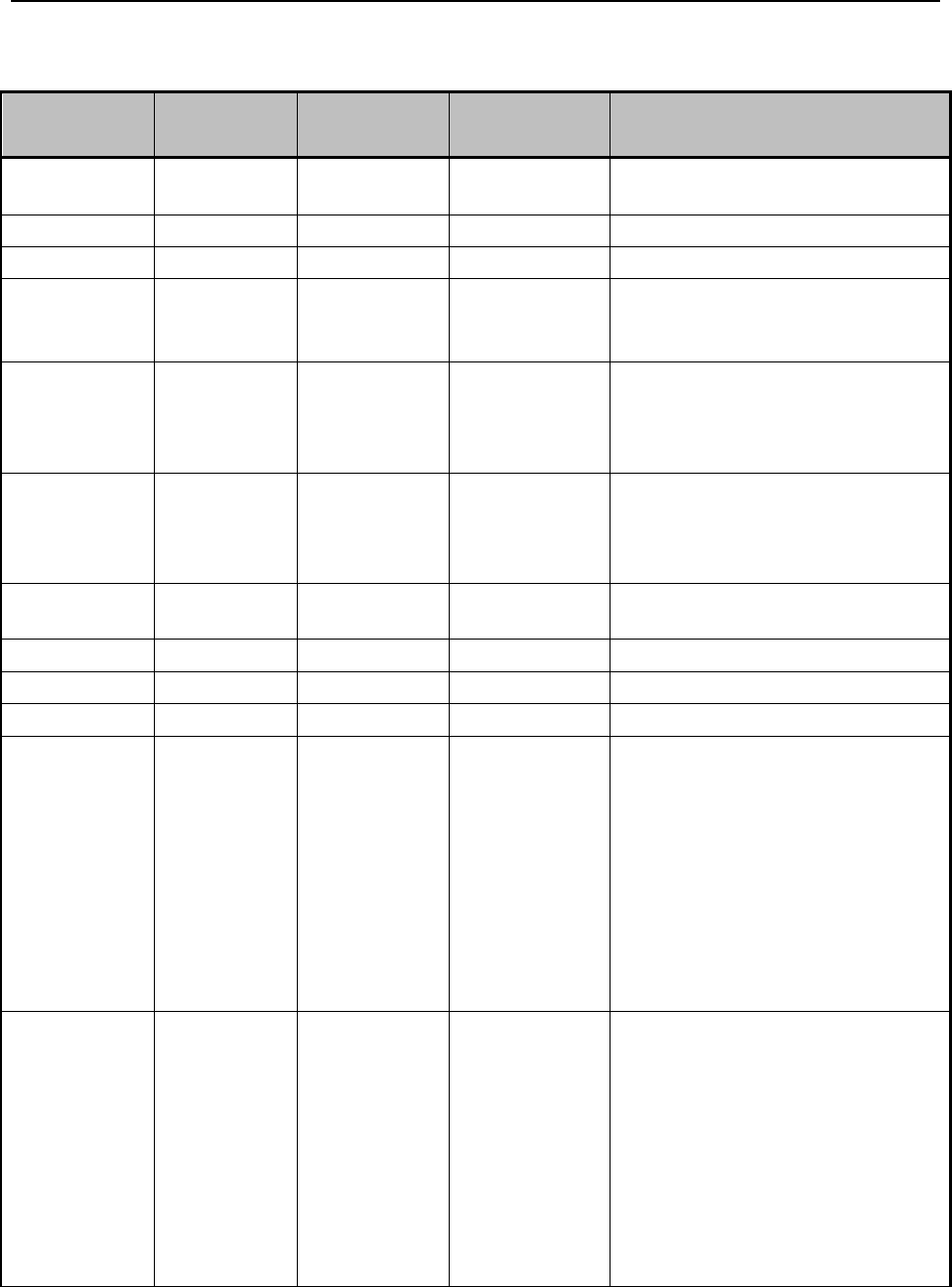
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 147 Revision 4/1/17
9.10.3 837 Professional
TR3 Page
Loop
Segment
Reference
Description
Wyoming Requirements
Page 72
Header
BHT
06
Wyoming Medicaid only accepts
the CH code.
Page 80
1000B
NM1
03
Enter Wyoming Medicaid.
Page 80
1000B
NM1
09
Enter 77046.
Page 83
2000A
PRV
03
If the NPI is registered with
Wyoming Medicaid, the
Taxonomy Code is required.
Page 115
2000B
HL
04
Enter 0. The subscriber is always
the patient; therefore, the
dependent level will not be
utilized.
Page 116-117
2000B
SBR
01
Enter P (Primary-Payer
Responsibility Sequence
Number code) Client has only
Medicaid Coverage.
Page 123
2010BA
NM1
09
Enter the ten (10) digit Wyoming
Medicaid Client ID.
Page 134
2010BB
NM1
03
Enter Wyoming Medicaid.
Page 134
2010BB
NM1
08
Enter PI (Payer Identification).
Page 134
2010BB
NM1
09
Enter 77046.
Page 140
2010BB
REF
01
If ‘XX’ is used to pass the NPI
number in 2010AA, NM109,
then Medicaid Provider Number
is no longer allowed, do not
submit this segment. If no NPI
was submitted then submit ‘G2’
(Provider Commercial Number)
in 2010BB REF01, and submit
the Wyoming Medicaid Provider
Number in the 2010BB REF02.
Page 140-141
2010BB
REF
02
If ‘XX’ is used to pass the NPI
number in 2010AA, NM109,
then Medicaid Provider Number
is no longer allowed, do not
submit this segment. If no NPI
was submitted then submit ‘G2’
(Provider Commercial Number)
in 2010BB REF01 and submit
the Wyoming Medicaid Provider
number in 2010BB REF02.
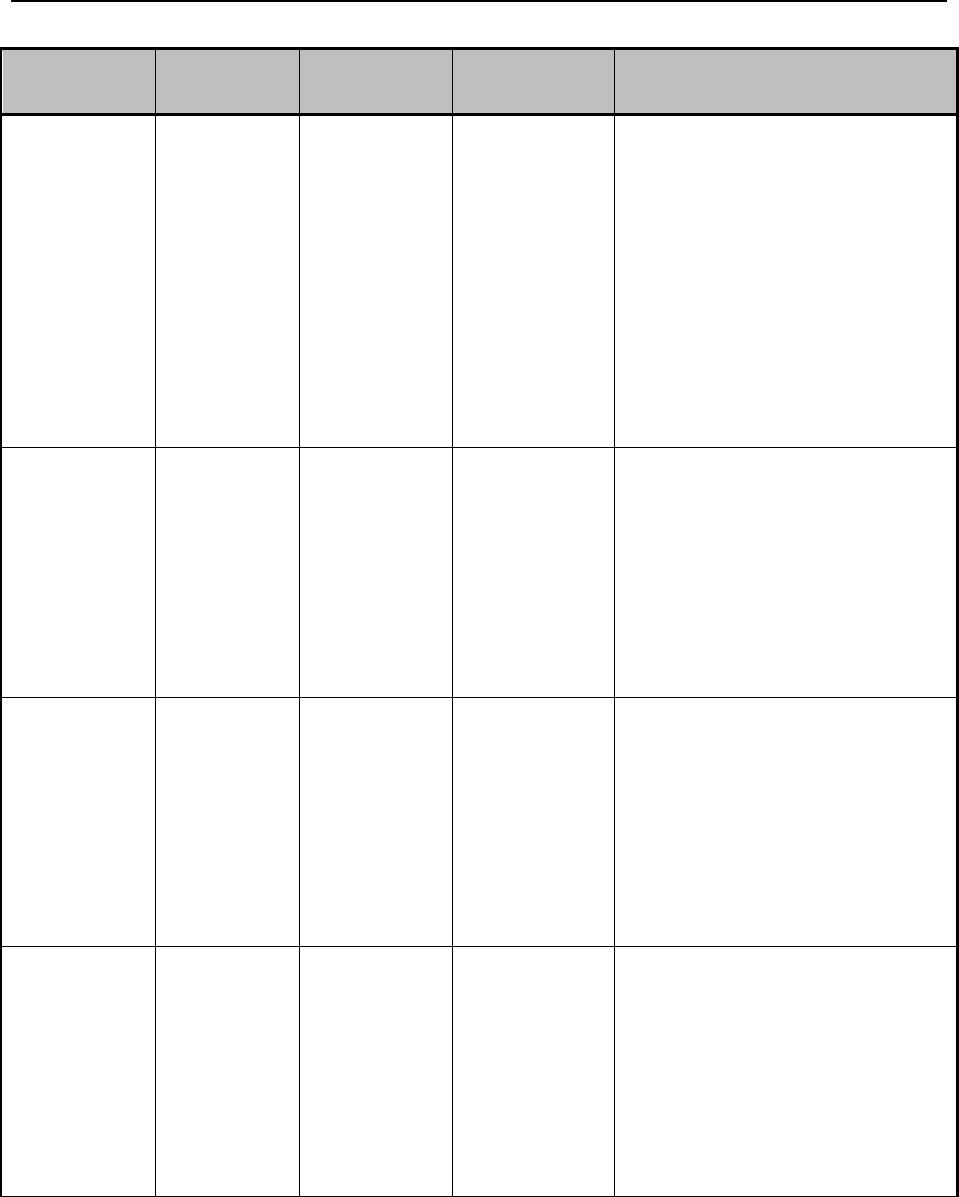
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 148 Revision 4/1/17
TR3 Page
Loop
Segment
Reference
Description
Wyoming Requirements
Page 161
2300
CLM
05:3
Void/Adjustment (Frequency
Type Code) should be six (6)
(Adjustment) only if paid date
was within the last six (6)
months (12-month timely filing
will be waived), or seven (7)
(Void/Replace) which is subject
to timely filing. Adjustments can
only be submitted on a
previously paid claim. Do not
adjust a denied claim. For non-
adjustment options see the TR3.
Page 262-263
2310A
REF
01
If ‘XX’ is used to pass the NPI
Number in NM109, Medicaid
Provider Number is no longer
allowed, do not submit this
segment. If no NPI was
submitted then enter ‘G2’
(Provider Commercial Number)
in REF01 and the Wyoming
Medicaid Provider ID in REF02.
Page 262-263
2310A
REF
02
If ‘XX’ is used to pass the NPI
number in NM109, Medicaid
Provider Number is no longer
allowed, do not submit this
segment. If no NPI was
submitted then enter ‘G2’
(Provider Commercial Number)
in the REF01 and the Wyoming
Medicaid Provider ID in REF02.
Page 269-270
2310B
REF
01
If ‘XX’ is used to pass the NPI
number in NM10, then Medicaid
Provider Number is no longer
allowed, do not submit this
segment. If no NPI was
submitted then enter ‘G2’
(Provider Commercial Number)
in REF01 and the Wyoming
Medicaid Provider ID in REF02.
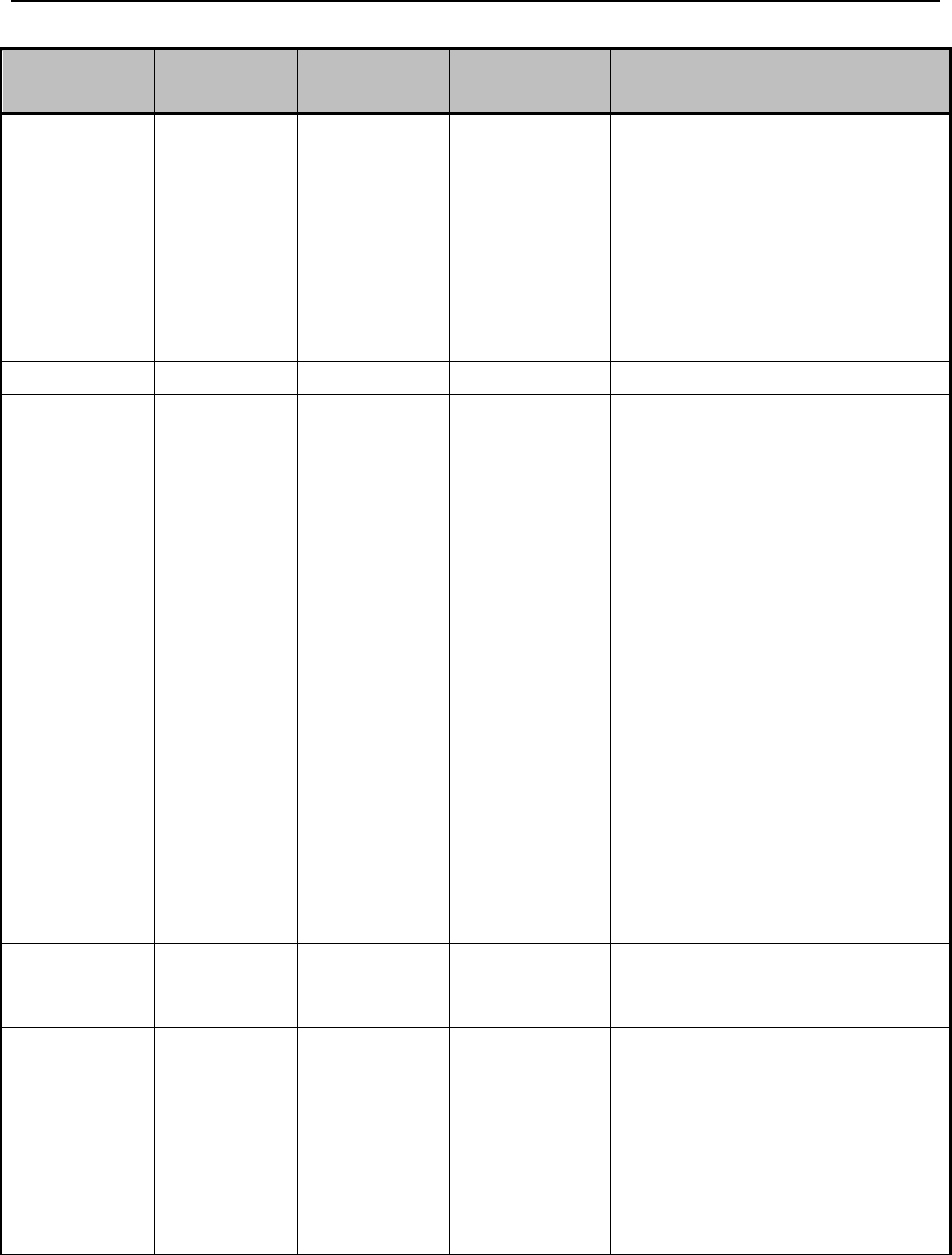
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 149 Revision 4/1/17
TR3 Page
Loop
Segment
Reference
Description
Wyoming Requirements
Page 269-270
2310B
REF
02
If ‘XX’ is used to pass the NPI
number in NM109, Medicaid
Provider Number is no longer
allowed, do not submit this
segment. If no NPI was
submitted the enter ‘G2’
(Provider Commercial Number)
in REF01 and the Wyoming
Medicaid Provider ID in REF02.
Page 300
2320
SBR
09
Do not use code MC.
Page 427
2410
LIN
03
Enter the 11 digit National Drug
Code (NDC). NDC’s less than
11-digits will cause the service
line to be denied by Wyoming
Medicaid. Do not enter hyphens
or spaces within the NDC.
NOTE: Only the first iteration
of Loop 2410 will be used for
claims processing. If two (2) or
more NDCs need to be reported
for the same procedure code on
the same claim, the procedure
code must be repeated on a
separate service line with the
first iteration of Loop 2410 used
to report each unique NDC. For
more information consult the
Wyoming Medicaid website
(http://wymedicaid.acs-inc.com).
Page 436
2420A
PRV
03
If the NPI is registered with
Wyoming Medicaid, the
Taxonomy Code is required.
Page 437
2420A
REF
01
If ‘XX’ is used to pass the NPI
number in NM109, Medicaid
Provider Number is no longer
allowed, do not submit this
segment. If no NPI was submitted
then enter ‘G2’ (Provider
Commercial Number) in REF01
and the Wyoming Medicaid
Provider ID in REF02.
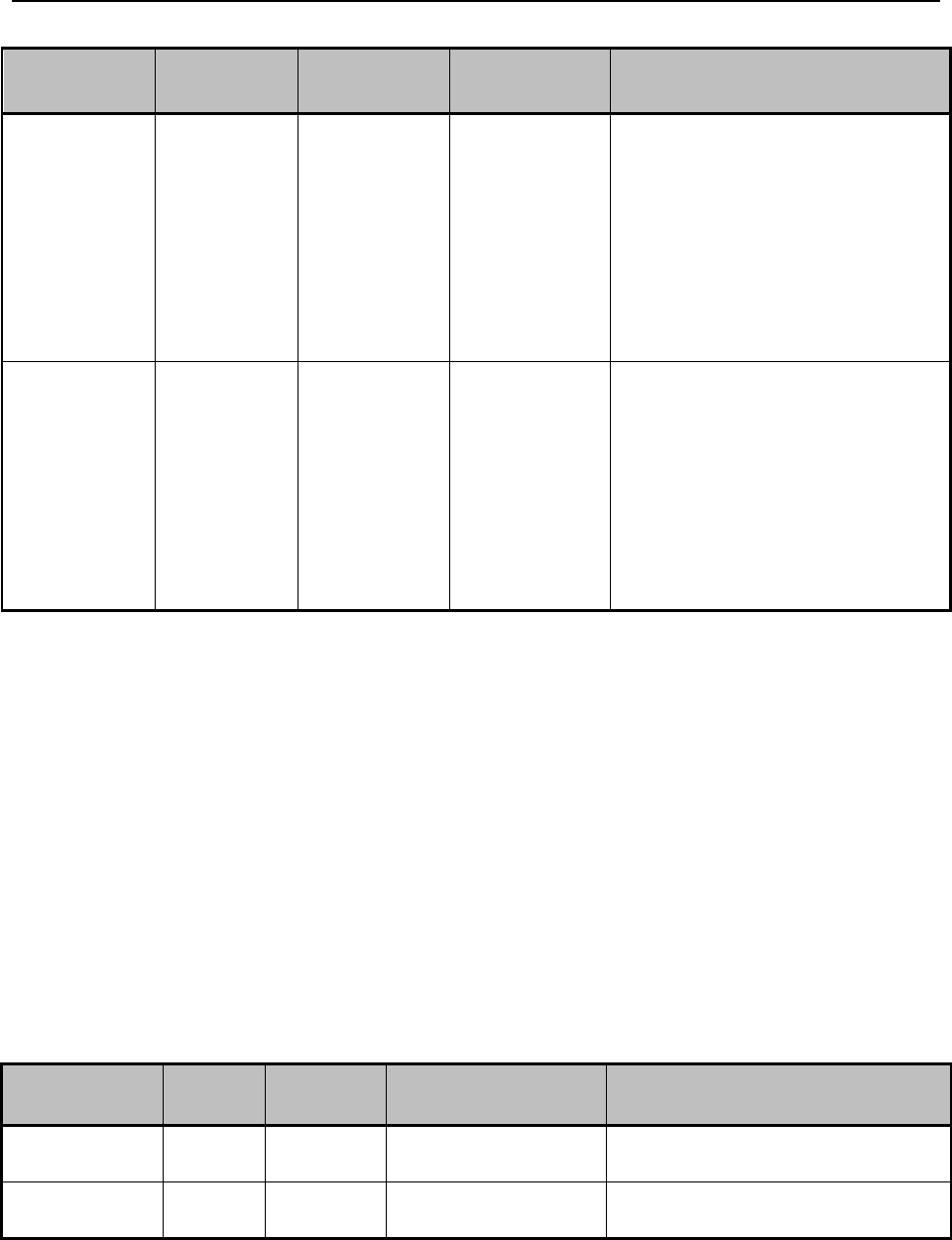
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 150 Revision 4/1/17
TR3 Page
Loop
Segment
Reference
Description
Wyoming Requirements
Page 471
2420 F
REF
01
If ‘XX’ is used to pass the NPI
number in NM109, Medicaid
Provider Number is no longer
allowed, do not submit this
segment. If no NPI was
submitted then enter ‘G2’
(Provider Commercial Number)
in REF01 and the Wyoming
Medicaid Provider ID in REF02.
Page 472
2420F
REF
02
If ‘XX’ is used to pass the NPI
number is NM109, Medicaid
Provider Number is no longer
allowed, do not submit this
segment. If no NPI was
submitted then enter ‘G2’
(Provider Commercial Number)
in REF01 and Wyoming
Medicaid Provider ID in REF02.
9.11 837 Institutional Claims Transactions Wyoming Medicaid
Institutional Claims
This section is for use along with the ANSI ASC X12 Health Care 837 Claims
Transactions. It should not be considered a replacement for the TR3s, but rather used
as an additional source of information. This section contains data clarifications
derived from specific business rules that apply exclusively to Wyoming Medicaid.
NOTE: The page numbers listed below in each of the tables represent the
corresponding page number in the Technical Report Type3 (TR3) ANSI
ASC X12N Consolidated Guide Health Care Claim: Institutional (837),
005010X223/005010X223A/1005010X223A2, June 2010.
9.11.1 ISA Interchange Control header
TR3 Page
Loop
Segment
Reference
Description
Wyoming Requirements
Appendix C
Page C.4
Header
ISA
06
Enter Trading Partner ID
Appendix C
Page C.5
Header
ISA
08
Enter 100000 followed by spaces
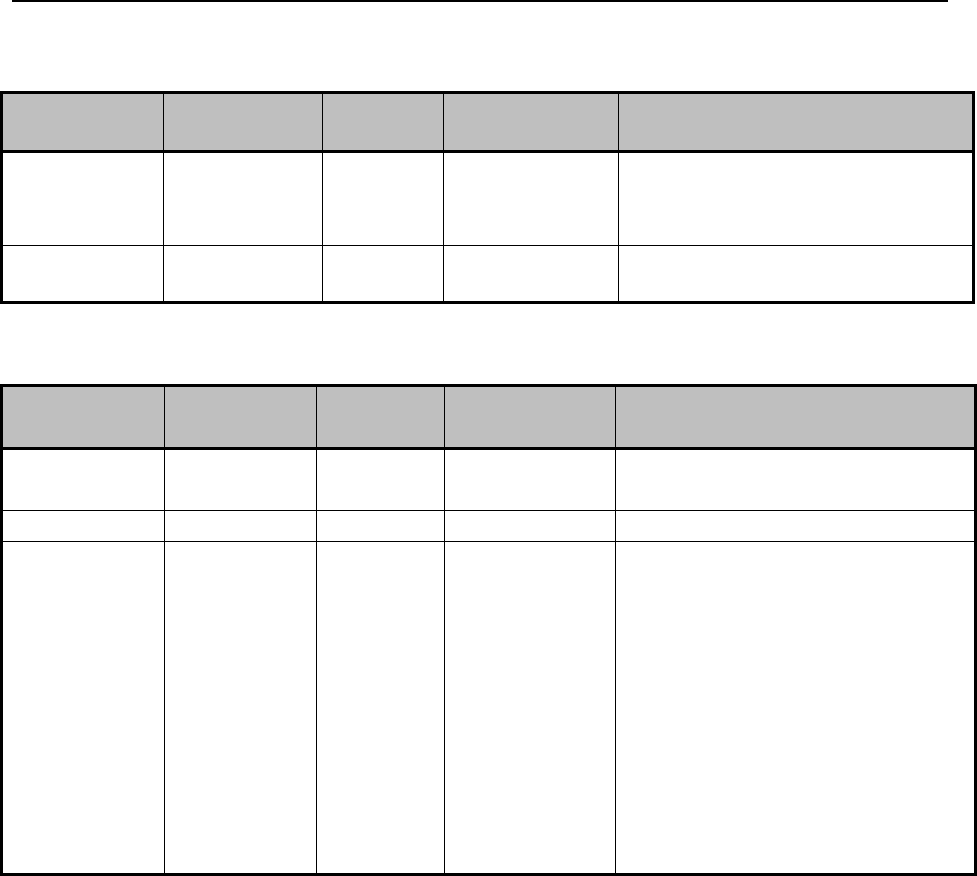
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 151 Revision 4/1/17
9.11.2 GS Functional Group Header
TR3 Page
Loop
Segment
Data Element
Wyoming Requirements
Appendix C
Page C.7
Functional
Group Header
GS
02
Enter Trading Partner ID
Appendix C
Page C.7
Functional
Group Header
GS
03
Enter 77046
9.11.3 837 Institutional
TR3 Page
Loop
Segment
Reference
Description
Wyoming Requirements
Page 77
1000B
NM1
03
Enter Wyoming Medicaid
Page 77
1000B
NM1
09
Enter 77046
Page 147
2300
CLM
05:3
Void/Adjustment (Frequency Type
Code) should be 6 (Adjustment)
only if paid date was within the
last six (6) months (12 month
timely filing will be waived), or
seven (7) (Void/Replace) which is
subject to timely filing.
Adjustments can only be
submitted on a previously paid
claim. Do not adjust a denied
claim. For non-adjustment options
see the TR3.
9.12 837 Dental Claims Transactions Wyoming Medicaid Dental
Claims
NOTE: The page numbers listed below in each of the tables represent the
corresponding page number in the Technical Report Type3 (TR3) ANSI
ASC X12N Consolidated Guide Health Care Claim: Dental (837),
005010X224/005010X224A1/005010X224A2, June 2010.
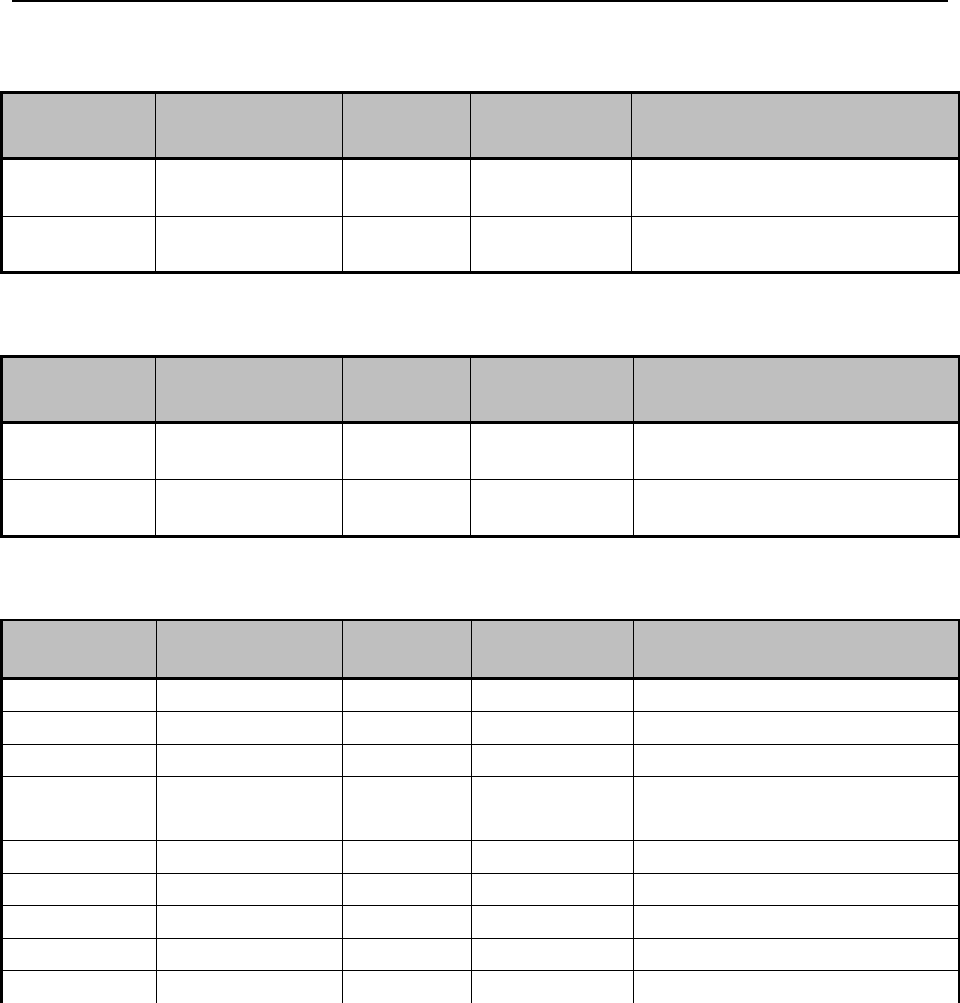
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 152 Revision 4/1/17
9.12.1 ISA Interchange Control Header
TR3 Page
Loop
Segment
Reference
Description
Wyoming Requirements
Appendix C
Page C.4
Header
ISA
06
Enter Trading Partner ID
Appendix C
Page C.5
Header
ISA
08
Enter 100000 followed by
spaces
9.12.2 GS Functional Group Header
TR3 Page
Loop
Segment
Data Element
Wyoming Requirements
Appendix C
Page C.7
Functional
Group Header
GS
02
Enter Trading Partner ID
Appendix C
Page C.7
Functional
Group Header
GS
03
Enter 77046
9.12.3 Dental
TR3Page
Loop
Segment
Reference
Description
Wyoming Requirements
Page 75
1000B
NM1
03
Enter Wyoming Medicaid
Page 75
1000B
NM1
09
Enter 77046
Page 125
2010BB
NM1
03
Enter Wyoming Medicaid
Page 125
2010BB
NM1
08
Enter PI (Payor Identification)
Page 125
2010BB
NM1
09
Enter 77046
Page 126
2010BB
N3
01
Enter PO Box 547
Page 127
2010BB
N4
01
Enter Cheyenne
Page 128
2010BB
N4
02
Enter WY
Page 128
2010BB
N4
03
Enter 82003
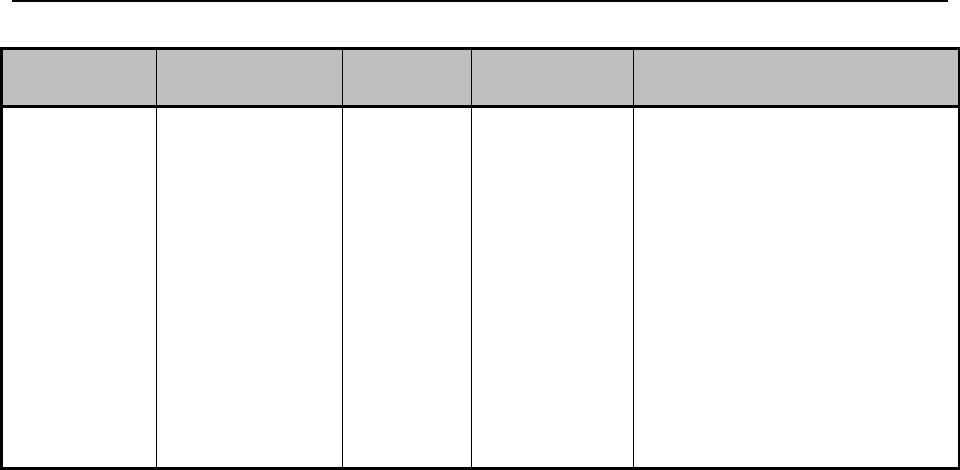
Wyoming Specific HIPAA_5010 Electronic Specifications_____________________________
Ch. 9 Index 153 Revision 4/1/17
TR3Page
Loop
Segment
Reference
Description
Wyoming Requirements
Page 149
2300
CLM
05:3
Void/Adjustment (Frequency
Type Code) should be six (6)
(Adjustment) only if paid date
was within the last six (6)
months (12 month timely filing
will be waived), or seven (7)
(Void/Replace) which is
subject to timely filing.
Adjustments can only be
submitted on a previously paid
claim. Do not adjust a denied
claim. For non-adjustment
options see the TR3.

Important Information__________________________________________________________
Ch. 10 Index 154 Revision 4/1/17
Chapter Ten – Important Information
10.1 Claims Review .................................................................................................. 155
10.2 Physician Supervision Definition ...................................................................... 155
10.3 Coding ............................................................................................................... 155
10.4 Importance of Fee Schedules and Provider’s Responsibility ............................ 156
10.5 Face-to-Face Visit Requirement ........................................................................ 156

Important Information__________________________________________________________
Ch. 10 Index 155 Revision 4/1/17
10.1 Claims Review
Medicaid is committed to paying claims as quickly as possible. Claims are
electronically processed using an automated claims adjudication system and are not
usually reviewed prior to payment to determine whether the services provided were
appropriately billed. Although the computerized system can detect and deny some
erroneous claims, there are many erroneous claims that it cannot detect. For this
reason, payment of a claim does not mean the service was correctly billed or the
payment made to the provider was correct. Periodic retrospective reviews are
performed which may lead to the discovery of incorrect billing or incorrect payment.
If a claim is paid and Medicaid later discovers the service was incorrectly billed or
paid, or the claim was erroneous in some other way, Medicaid is required by federal
regulations to recover any overpayment, regardless of whether the incorrect payment
was the result of Medicaid, fiscal agent, provider error or other cause.
10.2 Physician Supervision Definition
Supervision is defined as the ready availability of the supervisor for consultation and
direction of the individual providing services. Contact with the supervisor by
telecommunication is sufficient to show ready availability, if such contact is sufficient
to provide quality care. The supervising practitioner maintains final responsibility for
the care of the client and the performance of the mental health professional in their
office.
Supervisor is defined as an individual licensed to provide services who takes
professional responsibility for such services, even when provided by another
individual or individuals.
The physical presence of the supervisor is not required if the supervisor and the
practitioner are, or can easily be, in contact with each other by telephone, radio, or
other telecommunications.
The supervised individual may work in the office of the supervisor where the primary
practice is maintained and at sites outside that office as directed by the supervisor.
Fiscal responsibility and documentation integrity for claims remains with the
supervisor.
Those provider types able to enroll with Wyoming Medicaid, even if working under
the supervision of another practitioner, must enroll and be noted on the claim as the
rendering provider.
10.3 Coding
Standard use of medical coding conventions is required when billing Medicaid.
Provider Relations or the Division of Healthcare Financing cannot suggest specific
Important Information__________________________________________________________
Ch. 10 Index 156 Revision 4/1/17
codes to be used in billing services. The following suggestions may help reduce
coding errors and unnecessary claim denials:
Use current CPT-4, HCPCS Level II, and ICD-9-CM/ICD-10 coding books.
NOTE: The DSM-V, while useful for diagnostic purposes, is not considered a
coding manual, and should be used only in conjunction with the above.
Always read the complete description and guidelines in the coding books.
Relying on short descriptions can result in inappropriate billing.
Attend coding classes offered by certified coding specialists.
Use the correct unit of measurement. In general, Medicaid follows the
definitions in the CPT-4 and HCPCS Level II coding books. One (1) unit may
equal “one (1) visit” or “15 minutes.” Always check the long version of the
code description.
Effective April 1, 2011, the National Correct Coding Initiative (NCCI)
methodologies were incorporated into Medicaid’s claim processing system in
order to comply with Federal legislation. The methodologies apply to both
CPT Level I and HCPCS Level II codes.
Coding denials cannot be billed to the patient but can be reconsidered per
Wyoming Medicaid Rules, Chapter 16. Send a written letter of
reconsideration to Wyoming Medicaid, Medical Policy (2.1, Quick
Reference).
10.4 Importance of Fee Schedules and Provider’s Responsibility
Procedure codes listed in the following sections are subject to change at any time
without prior notice. The most accurate way to verify coverage for a specific service
is to review the Medicaid fee schedules on the website (2.1, Quick Reference). Fee
schedules list Medicaid covered codes, provide clarification of indicators such as
whether a code requires prior authorization and the number of days in which follow-
up procedures are included. Not all codes are covered by Medicaid or are allowed for
all taxonomy codes (provider types). It is the provider’s responsibility to verify this
information. Use the current fee schedule in conjunction with the more detailed
coding descriptions listed in the current CPT-4 and HCPCS Level II coding books.
Remember to use the fee schedule and coding books that pertain to the appropriate
dates of service.
10.5 Face-to-Face Visit Requirement
For practitioners ordering new Durable Medical Equipment (DME) or
Prosthetic/Orthotic Supplies (POS) for a client, the client must have a face-to-face
visit related to the condition for which the item(s) are being ordered within the
previous six (6) months with the ordering or prescribing practitioner. The supplying

Important Information__________________________________________________________
Ch. 10 Index 157 Revision 4/1/17
provider will need the date and the name of the practitioner with whom the face-to-
face visit occurred for their records in order to bill Wyoming Medicaid for the DME
or POS supplied.
Note: This requirement is waived for renewals of existing DME or POS orders.

Covered Services - Ambulance___________________________________________________
Ch. 11 Index 158 Revision 4/1/17
Chapter Eleven – Covered Services – Ambulance
11.1 Ambulance Services .......................................................................................... 159
11.2 Covered Services ............................................................................................... 159
11.2.1 Emergency Transportation ................................................................................ 159
11.2.2 Non-Emergency Transportation ........................................................................ 160
11.2.3 Definitions of Service Levels ............................................................................ 160
11.3 Disposable Supplies .......................................................................................... 161
11.4 Oxygen and Oxygen Supplies ........................................................................... 161
11.5 Mileage .............................................................................................................. 162
11.6 Non-covered Services ........................................................................................ 162
11.7 Multiple Client Transportation .......................................................................... 163
11.8 Usual and Customary Charge ............................................................................ 163
11.9 Billing Requirements ......................................................................................... 164

Covered Services - Ambulance___________________________________________________
Ch. 11 Index 159 Revision 4/1/17
11.1 Ambulance Services
Ambulance providers are independent ambulances or hospital-based ambulances.
Medicaid covers ambulance transports, with medical intervention, by ground or air to
the nearest appropriate facility.
An appropriate facility is considered an institution generally equipped to provide the
required treatment for the illness or injury involved.
Each ambulance service provided to a client (transport, life support, oxygen, etc.)
must be medically necessary to be covered by Medicaid.
Procedure Code Range: A0380-A0436
11.2 Covered Services
11.2.1 Emergency Transportation
Medicaid covers emergency transportation by either Basic Life Support or Advanced
Life Support ambulance under the following conditions:
A medical emergency exists in that the use of any other method of
transportation could endanger the health of the patient; and
The patient is transported to the nearest facility capable of meeting the
patient’s medical needs; and
The destination is an acute care hospital where the patient is admitted as an
inpatient or outpatient.
For purposes of this section, a medical emergency is considered to exist under any of
the following circumstances:
An emergency situation, due to an accident, injury, or acute illness; or
Restraints are required to transport the patient (often when a psychiatric
diagnosis is made); or
The patient is unconscious or in shock; or
Immobilization is required due to a fracture of the possibility of a fracture; or
The patient is experiencing symptoms of myocardial infarction or acute
stroke; or
The patient is experiencing severe hemorrhaging.

Covered Services - Ambulance___________________________________________________
Ch. 11 Index 160 Revision 4/1/17
11.2.2 Non-Emergency Transportation
Non-emergency transportation is covered when any other mode of transportation
would endanger the health or life of a client and at least one (1) of the following
criteria is met:
Continuous dependence on oxygen.
Continuous confinement to bed.
Cardiac disease resulting in the inability to perform any physical activity
without discomfort.
Receiving intravenous treatment.
Heavily sedated.
Comatose.
Post pneumo/encephalogram, myelogram, spinal tap, or cardiac
catheterization.
Hip spicas and other casts that prevent flexion at the hip.
Requirement for isolette in perinatal period.
State of unconsciousness or semi-consciousness.
11.2.3 Definitions of Service Levels
Basic Life Support Services – A Basic Life Support (BLS) ambulance is one which
provides transportation in addition to the equipment, supplies, and staff required for
basic services such as the control of bleeding, splinting of fractures, treatment for
shock, and basic cardiopulmonary resuscitation (CPR).
Basic Life Support – Emergency – Basic Life Support emergency services must
meet one (1) of the criteria listed under Emergency Transportation and the definition
of Basic Life Support Services.
Basic Life Support Services – Non-Emergency – Basic Life Support non-
emergency services must meet one (1) of the criteria listed under Non-Emergency
Transportation and the definition of Basic Life Support Services.
Advanced Life Support Services – Advanced Life Support (ALS), means treatment
rendered by highly skilled personnel, including procedures such as cardiac
monitoring and defibrillation, advanced airway management, intravenous therapy
and/or the administration of certain medications.
Advanced Life Support Level 1 – Emergency (ALS1-emergency) – This level of
service is transportation by ground ambulance with provision for medically necessary
supplies, oxygen, and at least one (1) ALS intervention. The ambulance and its crew
must meet certification standards for ALS care. An ALS intervention refers to the
provision of care outside the scope of an EMT-basic and must be medically necessary
(e.g. medically necessary EKG monitoring, drug administration, etc.) An ALS
assessment does not necessarily result in a determination that the client requires an
ALS level of service.

Covered Services - Ambulance___________________________________________________
Ch. 11 Index 161 Revision 4/1/17
Advanced Life Support Level 1 – Non-Emergent (ALS1 non-emergent) – This
level of service is the same as ALS1-emergency but in non-emergent circumstances.
Advanced Life Support Level 2 (ALS2) – Covered for the provision of medically
necessary supplies and services including:
1. At least three (3) separate administrations of one (1) or more medications by
intravenous push/bolus or by continuous infusion (excluding crystalloid
fluids); or
2. Ground ambulance transport, medically necessary supplies and services, and
the provision of at least one (1) of the ALS2 procedures listed below:
Manual defibrillation/cardio version.
Endotracheal intubation.
Central venous line.
Cardiac pacing.
Chest decompression.
Surgical airway.
Intraosseous line.
Air Ambulance Services – Medicaid covers both conventional air and helicopter
ambulance services. These services are only covered under the following conditions:
The client has a life threatening condition which does not permit the use of
another form of transportation; or
The client’s location is inaccessible by ground transportation; or
Air transport is more cost effective than any other alternative.
Medicaid covers air ambulance transfers of a client who is discharged from one (1)
inpatient facility and transferred and admitted to another inpatient facility when
distance or urgency precludes the use of ground ambulance.
11.3 Disposable Supplies
Medicaid covers disposable and non-reusable supplies such as gauze and dressings,
defibrillation supplies, and IV drug therapy disposable supplies. When medically
necessary, each service is allowed to be billed up to five (5) units.
11.4 Oxygen and Oxygen Supplies
Medicaid covers oxygen and related disposable supplies only when the client’s
condition at the time of transport requires oxygen. Medicaid does not cover oxygen
when it is provided only on the basis of protocol.

Covered Services - Ambulance___________________________________________________
Ch. 11 Index 162 Revision 4/1/17
11.5 Mileage
Although mileage may be billed in addition to the base rate for ground transport, it is
only paid for loaded miles (client on board) from pickup to destination.
Loaded mileage is covered in addition to the base rate for all air transports.
Mileage must be medically necessary, which means that mileage should equal the
shortest route to the nearest appropriate facility. Exceptions may occur such as road
construction or weather.
When billing for mileage, one (1) unit is equal to one (1) statute (map) mile for both
air and ground transport. Mileage must be rounded to the nearest mile.
11.6 Non-covered Services
Medicaid does not reimburse for the following ambulance services:
Transportation to receive services that are not covered services.
No-load trips and unloaded mileage (when no patient is aboard the
ambulance), including transportation of life-support equipment in response to
an emergency call.
Transportation of a client who is pronounced dead before an ambulance is
called.
When a client is pronounced dead after an ambulance is called but before
transport.
Transportation of a family member or friend to visit a client or consult with
the client’s physician or other provider of medical services.
Transportation to pick up pharmaceuticals.
A client’s return home when ambulance transportation is not medically
necessary or a client’s return back to a nursing facility.
Transportation of a resident of a nursing facility to receive services that are
available at the nursing facility.
Transportation to a mental health facility if no other appropriate ambulance
criteria is met.
Air ambulance services to transport a client from a hospital capable of treating
the client to another hospital because the client or family prefers a specific
hospital or practitioner.
Transportation of a client in response to detention ordered by a court or law
enforcement agency.
Transportation based on a physician’s standing orders.
Stand-by time.
Special attendants.
Specialty Care Transport (SCT).
Paramedic Intercept (PI).

Covered Services - Ambulance___________________________________________________
Ch. 11 Index 163 Revision 4/1/17
When a client can be transported by a mode other than ambulance without
endangering the client’s health, regardless of whether other transportation is
available.
If a client is an inpatient at a hospital, Medicaid does not pay separately for
round trip ambulance transport for an outpatient service (e.g., e-ray or other
procedure) at a different hospital. This type of transport is included in the
Medicaid payment to the hospital for the inpatient stay.
Transportation of a client having suicidal ideations, if no other appropriate
ambulance criteria is met.
Transports related to Emergency/Involuntary Detainment/Title 25.
11.7 Multiple Client Transportation
When more than one (1) client is transported during the same trip, Medicaid will
cover one (1) base rate and one (1) mileage charge per transport, not per client.
Medicaid will reimburse for each client’s supplies and oxygen.
11.8 Usual and Customary Charge
Providers should bill Medicaid their usual and customary charge for each service; that
is, the same charge that would be billed to other payers for that service.
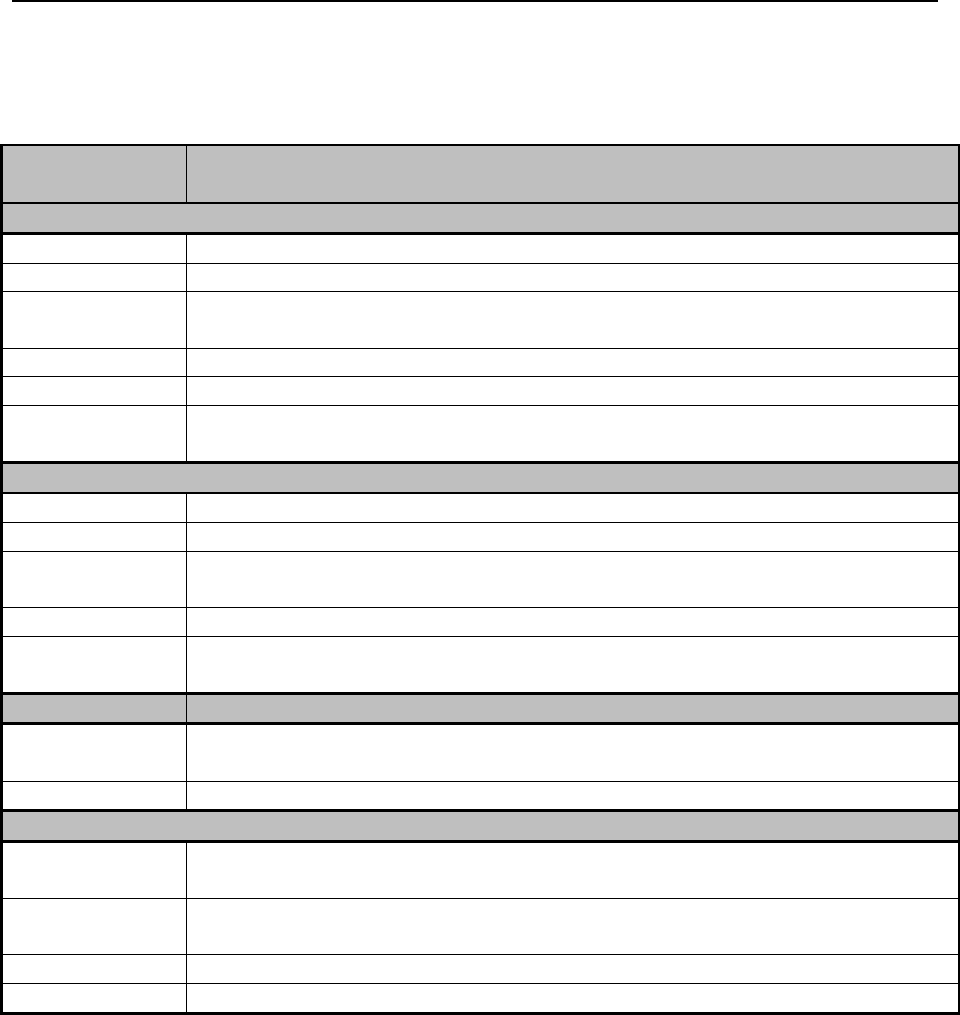
Covered Services - Ambulance___________________________________________________
Ch. 11 Index 164 Revision 4/1/17
11.9 Billing Requirements
The following are the procedure codes accepted for ambulance services:
Procedure
Code
Description
GROUND/Basic Life Support (BLS)
A0380
BLS mileage (per mile)
A0382
BLS routine disposable supplies
A0422
Ambulance (ALS or BLS) oxygen and oxygen supplies, life sustaining
situation
A0425
Ground mileage, per statute mile
A0428
Ambulance service, basic life support, non-emergency transport, (BLS)
A0429
Ambulance service, basic life support, emergency transport (BLS,
emergency)
GROUND/Advanced Life Support (ALS)
A0390
ALS mileage (per mile)
A0398
ALS routine disposable supplies
A0422
Ambulance (ALS or BLS) oxygen and oxygen supplies, life sustaining
situation
A0425
Ground mileage, per statute mile
A0426
Ambulance service, advanced life support, non-emergency transport, level 1
(ALS1)
Procedure Code
Description
A0427
Ambulance service, advanced life support, emergency transport, level 1
(ALS1-emergency)
A0433
Advanced life support, level 2 (ALS 2)
Air Ambulance
A0430
Ambulance service, conventional air services, transport, one (1) way (fixed
wing)
A0431
Ambulance services, conventional air services, transport, one (1) way (rotary
wing)
A0435
Fixed wing air mileage, per statute mile
A0436
Rotary wing air mileage, per statute mile
Wyoming Medicaid does not require a separate trip report provided the request for
service has been entered appropriately into the Wyoming Ambulance Trip Reporting
System (WATRS https://health.wyo.gov/publichealth/ems/watrs/), and marked
appropriately for Wyoming Medicaid to review.
In order for Wyoming Medicaid to be able to view the report, EMS providers or
billing agents must select either the "Primary Method of Payment" or "Insurance
Company Name" as Wyoming Medicaid. Both of these data elements are in the
Billing section of WATRS. Failure to select the proper data element will prohibit

Covered Services - Ambulance___________________________________________________
Ch. 11 Index 165 Revision 4/1/17
Wyoming Medicaid staff from being able to review your entered information, and
your claim will be denied for not having a Trip Report.
Effective June 1, 2017 Wyoming Medicaid will no longer accept paper trip reports for
any billed claim, and will only review the data entered into WATRS. Please see the
Rules and Regulations for Wyoming Emergency Medical Services W.S. 33-36-101
through -115 Chapter 4, Section 4 for reporting requirements.
The WATRS reporting requirements apply if:
The call originates in Wyoming and ends in Wyoming. (e.g. Wyoming -
Wyoming)
If the ambulance itself starts in Wyoming, goes somewhere out of state and
comes back to Wyoming. (e.g. Wyoming - Denver - Wyoming.)
If the ambulance itself starts in Wyoming, goes somewhere out of state and
ends out of state. (e.g. Wyoming - Denver - Salt Lake.)
Transports that do not touch ground in Wyoming at any point will still be permitted to
submit paper trip reports.
If submitting a paper trip report, the claim should be submitted through the usual
electronic billing method, and the claim should indicate that an attachment will be
coming and by what method, electronic or mail (6.15, Submitting Attachments for
Electronic Claims).
The paper trip report must include the following:
Documentation in the narrative to support the level of service billed
(ALS/BLS, Emergent/Non-Emergent, and if air transport rotary/fixed wing).
Documentation in the narrative to support the medical necessity of the
transport.
Documentation in the narrative of the use and medical necessity of any
supplies.
Documentation in the narrative of the use and medical necessity of any
oxygen.
Documentation of the patient loaded miles (must match the number of units
billed on the claim).

Covered Services – Audiology____________________________________________________
Ch. 12 Index 166 Revision 4/1/17
Chapter Twelve – Covered Services – Audiology
12.1 Audiology Services ........................................................................................... 167
12.2 Requirements ..................................................................................................... 167
12.3 Reporting Standards .......................................................................................... 167
12.4 Billing Procedures ............................................................................................. 168
12.5 Reimbursement .................................................................................................. 169
12.6 Hearing Aid Repair ........................................................................................... 169
12.7 Hearing Aid Insurance ....................................................................................... 169

Covered Services – Audiology____________________________________________________
Ch. 12 Index 167 Revision 4/1/17
12.1 Audiology Services
Audiology Services – A hearing aid evaluation (HAE) and basic audio assessment
(BAA) provided by a licensed audiologist, upon a licensed practitioner referral, to
individuals with hearing disorders.
Hearing Aid – An instrument or device designed for or represented as aiding or
improving defective human hearing and includes the parts, attachments or accessories
of the instrument or device.
Hearing Aid Dispenser – A person holding an active license to engage in selling,
dispensing, or fitting hearing aids.
Procedure Code Range: V5000-V5275 and 92550-92700
12.2 Requirements
Clients must be referred by a licensed practitioner. The practitioner must indicate on
the referral there is no medical reason for which a hearing aid would not be
appropriate in correcting the client’s hearing loss.
Written orders from the licensed practitioner, diagnostic reports and evaluation
reports must be current and available upon request.
Basic Audio Assessment (BAA) under earphones in a sound attenuated room must
include, at a minimum, speech discrimination tests, speech reception thresholds, pure
tone air thresholds, and either pure tone bone thresholds or tympanometry, with
acoustic reflexes.
Hearing Aid Evaluation (HAE) includes those procedures necessary to determine the
acoustical specifications most appropriate for the individual’s hearing loss.
12.3 Reporting Standards
The audiologist’s report for Medicaid clients must contain the following information:
The client’s name, date of birth, and Medicaid ID number;
Results of the audiometric tests at 500, 1,000, 2,000, and 3,000 hertz for the
right and left ears, and the word recognition or speech discrimination scores
obtained at levels which insure pb max;
The report shall include the audiologist’s name, address, license number, and
signature of the audiologist completing the audiological evaluation, including
the date performed; and
A written summary from the licensed audiologist regarding the results of the
evaluation indicating whether a hearing instrument is required, the type of
hearing instrument (e.g., in-the-ear, behind-the-ear, body amplifier, etc.), and
whether monaural or binaural aids are requested.

Covered Services – Audiology____________________________________________________
Ch. 12 Index 168 Revision 4/1/17
A copy must be sent to the referring practitioner for the client’s permanent record.
If binaural aids are requested, all of the following criteria must be met:
Two-frequency average at 1 KHZ and 2 KHZ must be greater than 40 decibels
in both ears;
Two-frequency average at 1 KHZ and 2 KHZ must be less than 90 decibels in
both ears;
Two-frequency average at 1 KHZ and 2 KHZ must have an interaural
difference of less than 15 decibels;
Interaural word recognition or speech discrimination score must have a
difference of not greater than 20%;
Demonstrated successful use of a monaural hearing aid for at least six (6)
months; and
Documented need to understand speech with a high level of comprehension
based on an educational or vocational need.
A hearing aid purchased by Medicaid will be replaced no more than once in a five (5)
year period unless:
The original hearing aid has been irreparably broken or lost after the one (1)-
year warranty period;
The provider’s records document the loss or broken condition of the original
hearing aid; and
The hearing loss criteria specified in this rule continues to be met; or
The original hearing aid no longer meets the needs of the client and a new
hearing aid is determined to be medically necessary by a licensed audiologist.
The audiologist should provide a copy of the report to the Medicaid client to take to
the hearing aid dispenser (if the audiologist is not the provider for the hearing aid).
The audiologist retains the original report in the client’s medical file.
12.4 Billing Procedures
Providers must bill for services using the procedure codes set forth and according to
the definitions contained in the HCPCS Level II and CPT coding book. Providers are
responsible for billing services provided within the scope of their practice and
licensure. It is essential for providers to have the most current HCPCS and CPT
editions for proper billing.
The date of service is the date the hearing aid is delivered or the date that the repairs
are completed. A copy of the invoice must be attached to the claim. No other
attachments are required (6.15, Submitting Attachments for Electronic Claims).
Covered Services – Audiology____________________________________________________
Ch. 12 Index 169 Revision 4/1/17
The provider bills Medicaid for hearing aids using two (2) separate procedure codes;
one (1) for the hearing aid and one (1) for the dispensing fee. The hearing aid must be
billed under the appropriate procedure code(s).
12.5 Reimbursement
Medicaid payment for audiology services will be based on the Medicaid fee schedule.
Medicaid reimburses for hearing aids either by fee schedule or invoice plus shipping
plus 15%. The dispensing fee is payable on the day the hearing aid was delivered.
NOTE: These fees are subject to change. The most accurate way to verify
coverage for a specific service is to review the Medicaid fee schedule on
the website (2.1, Quick Reference).
12.6 Hearing Aid Repair
The following guidelines apply to the repair of hearing aids:
Repairs covered under warranty are not billable to Medicaid.
V5014 is used to bill for repairs that are not covered under warranty.
Re-dispensing fees may be applicable. When re-dispensing the hearing aid
after the repair, use the RP modifier with the appropriate dispensing code.
Claims must have an invoice attached.
Claims are reimbursed at invoice plus shipping only
12.7 Hearing Aid Insurance
Hearing aid insurance is covered for services not covered under warranty or when the
warranty expires. Use the following codes:
X5612 Standard hearing aid insurance, per aid, annual fee.
X5613 Advanced hearing aid insurance, per aid, annual fee.

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 170 Revision 4/1/17
Chapter Thirteen – Covered Services – Behavioral Health
13.1 Behavioral Health Services ............................................................................... 172
13.2 Requirements for Community Mental Health Centers (CMHC) and Substance
Abuse Centers .................................................................................................... 172
13.2.1 Provider’s Role .................................................................................................. 173
13.2.2 Responsibilities of Mental Health/Substance Abuse Providers ........................ 173
13.2.3 Qualification for Participating Provider and Staff ............................................ 174
13.3 Covered Services for Community Mental Health and Substance Abuse
Treatment Centers ............................................................................................. 175
13.3.1 Rehabilitative Option Services .......................................................................... 175
13.3.2 Targeted Case Management .............................................................................. 177
13.3.3 EPSDT Mental Health Services or Ongoing Case Management ...................... 177
13.3.4 Limitations to Mental Health/Substance Abuse Services ................................. 178
13.3.5 Quality Assurance ............................................................................................. 178
13.4 Community Mental Health & Substance Abuse Treatment Centers Billing
Procedures ......................................................................................................... 179
13.4.1 Psychiatric Services ........................................................................................... 179
13.5 Eligible Providers .............................................................................................. 189
13.5.1 Psychiatric Services ........................................................................................... 191
13.5.1.1 Psychologists ................................................................................................. 192
13.5.1.2 Licensed Mental Health Professionals .......................................................... 192
13.5.1.3 Provisional Licensed Mental Health Professionals ....................................... 192
13.5.1.4 Supervision .................................................................................................... 193
13.5.2 Behavioral Health Providers Eligible for Medicare Enrollment ....................... 193
13.5.3 Covered Services ............................................................................................... 193
13.5.4 Non-Covered Services ....................................................................................... 194
13.5.5 Provisions of Mental Health and Substance Abuse Treatment Services to
Residents of Nursing Facilities .......................................................................... 195
13.5.6 Billing Codes ..................................................................................................... 195
13.6 Applied Behavioral Analysis Treatment ........................................................... 197
13.6.1 Covered Services ............................................................................................... 197

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 171 Revision 4/1/17
13.6.2 Applied Behavior Analysis Providers ............................................................... 199
13.7 Limitations for Behavioral Health Services ...................................................... 200
13.8 Cap Limits ......................................................................................................... 200
13.9 Documentation Requirements for All Behavioral Health Providers ................. 200
13.9.1 Provider Agreement .......................................................................................... 201
13.9.2 Documentation of Services ............................................................................... 201
13.9.3 Client Records ................................................................................................... 202
13.9.3.1 Requirements ................................................................................................. 202
13.9.3.2 Clinical Records Content Requirement ......................................................... 204
13.9.4 Treatment Plans ................................................................................................. 205
13.9.5 Billing Requirements ......................................................................................... 205
13.9.6 Time and Frequency .......................................................................................... 206
13.9.7 Pre-Admission Screening and Resident Review (PASRR) Assessments ......... 206
13.9.7.1 Billing Requirements ..................................................................................... 206

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 172 Revision 4/1/17
13.1 Behavioral Health Services
Outpatient Behavioral Health Services are a group of services designed to provide
medically necessary mental health or substance abuse treatment services to Medicaid
clients in order to restore these individuals to their highest possible functioning level.
Services may be provided by any willing, qualified provider. Services are provided on
an outpatient basis and not during an inpatient hospital stay.
Wyoming Medicaid covers medically necessary therapy services, including mental
health and substance abuse (behavioral health) treatment services via the federal
authority guidelines granted by the Centers for Medicare and Medicaid Services
(CMS) and specified in the Code of Federal Regulation's (CFR) rehabilitative
services option section. All Medicaid clients who meet the service eligibility
requirements and have a need for particular rehabilitative option services are entitled
to receive them.
"Medical necessity" or "Medically necessary" means a determination that a
health service is required to diagnose, treat, cure or prevent an illness, injury
or disease which has been diagnosed or is reasonably suspected to relieve pain
or to improve and preserve health and be essential to life. The service must be:
o Consistent with the diagnosis and treatment of the client's condition;
o In accordance with the standards of good medical practice among the
provider's peer group;
o Required to meet the medical needs of the client and undertaken for
reasons other than the convenience of the client and the provider; and,
o Performed in the most cost effective and appropriate setting required
by the client's condition.
Restorative (Rehabilitative) Services – Services that help patients keep, get
back, or improve skills and functioning for daily living that have been lost or
impaired because the client was sick, hurt or suddenly disabled.
Maintenance (Habilitative) Services – Services that help patients keep, learn,
or improve skills and functioning for daily living. Examples would include
therapy for a child who isn’t walking or talking at the expected age.
13.2 Requirements for Community Mental Health Centers
(CMHC) and Substance Abuse Centers
Community Mental Health Centers (CMHC) and Substance Abuse Treatment Centers
(SATC) shall meet the following criteria to be enrolled as a Medicaid provider. Prior
to enrollment as a Medicaid provider, a mental health center shall have received
certification from the Behavioral Health Division as evidence of compliance. The
center shall also have resolved any compliance deficiencies within time lines
specified by the certifying Division.
To become a provider of Medicaid mental health services, an agency shall apply for
certification as a mental health and/or substance use Medicaid provider by submitting

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 173 Revision 4/1/17
the Medicaid provider certification application form and its required attachments to
the Behavioral Health Division. To become a provider of Medicaid mental health
services, an agency shall be under contract with the Behavioral Health Division; and
be certified by the Behavioral Health Division for the services for which the agency
provides under the contract.
13.2.1 Provider’s Role
Each Medicaid provider shall be certified under state law to perform the
specific services.
Certify that each covered service provided is medically necessary,
rehabilitative and is in accordance with accepted norms of mental health and
substance use practice.
Providers are required to maintain records of the nature and scope of the care
furnished to Wyoming Medicaid clients.
13.2.2 Responsibilities of Mental Health/Substance Abuse Providers
Each client shall be referred by a licensed practitioner who attests to medical
necessity as indicated by the practitioner’s signature, date on the clinical
assessment and on the initial and subsequent treatment plans which prescribe
rehabilitative, targeted case management or ESPDT mental health services.
Licensed practitioners who are eligible to refer and to sign for medical
necessity are persons who have current license from the State of Wyoming to
practice as a:
o Licensed Professional Counselor
o Licensed Addictions Therapist
o Licensed Psychologist
o Licensed Clinical Social Worker
o Licensed Marriage and Family Therapist
o Licensed Physician
o Licensed Psychiatric Nurse (Masters)
o Licensed Advanced Practitioner of Nursing (Specialty area of
psychiatric/mental health nursing)
For a licensed practitioner to be authorized to refer and to sign for medical
necessity, the agreement between the licensed practitioner and the provider by
which the practitioner’s responsibilities under the Medicaid Mental Health
Rehabilitative Option, Targeted Case Management Option and EPSDT mental
health services are specified.
Any licensed practitioner under contract with, or employed by, a provider
shall be required to submit Medicaid claims through the provider and to
indicate the provider as payee. All individuals providing services must have
their own provider number.
Prior to the provider’s billing Medicaid for Mental Health Rehabilitative
Option, Targeted Case Management Option and EPSDT mental health

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 174 Revision 4/1/17
services a licensed practitioner shall sign, date and add their credentials to the
client’s clinical assessment, written treatment plan and clinical notes.
Licensed practitioners who sign for services that are not medically necessary
and rehabilitative in nature are subject to formal sanctions through Wyoming
Medicaid and/or referral to the relevant licensing board.
13.2.3 Qualification for Participating Provider and Staff
TO BE ELIGIBLE TO PROVIDE MEDICAID MENTAL HEALTH
CLINICAL SERVICES STAFF SHALL:
Be employed or under contract with the Behavioral Health Division as a
certified mental health center and enrolled Medicaid provider, and
Be licensed, provisionally licensed, or certified by the State of Wyoming, or
Be a registered nurse (R.N.), licensed in the State of Wyoming, who has at
least two years of supervised experience and training to provide mental health
services after the awarding of the R.N.
Be a clinical professional, clinical staff, or qualified as a case manager per the
requirements of the service provided as pursuant to Wyoming Medicaid
Rules, Chapter 13- Mental Health Services.
TO BE ELIGIBLE TO PROVIDE MEDICAID SUBSTANCE USE
TREATMENT SERVICES, STAFF SHALL:
Be employed or under contract with the Behavioral Health Division as a
certified substance use treatment center and enrolled Medicaid provider, and
Be a licensed, provisionally licensed or certified by the State of Wyoming, or
Be a registered nurse (R.N.), licensed in the State of Wyoming, who has at
least two years of supervised experience and training to provide mental health
services after the awarding of the R.N.
Be a clinical professional, clinical staff, or qualified as a case manager per the
requirements of the service provided as pursuant to Wyoming Medicaid
Rules, Chapter 13- Mental Health Services.
TO BE ELIGIBLE TO PROVIDE MEDICAID INDIVIDUAL
REHABILITATIVE SERVICES, STAFF SHALL:
Be employed or under contract with the Behavioral Health Division certified
Medicaid provider.
Be eighteen years of age or older.
Complete a basic training program, including non-violent behavioral
management, and
Be supervised and meet the qualifications of a certified mental health worker
as pursuant to Wyoming Mental Health Professions Board, Chapter 1-
General Provisions.
Under the direct supervision of the primary therapist for that client.

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 175 Revision 4/1/17
TO BE ELIGIBLE TO PROVIDE PEER SPECIALIST SERVICES, STAFF
SHALL:
Be employed or under contract with the Behavioral Health Division certified
Medicaid provider. Self-identify as a person in recovery from mental illness
and/or substance use disorder.
Be eighteen years of age or older.
Be credentialed by the Behavioral Health Division as a peer specialist, and
Be supervised for the position by a person licensed by the Wyoming Mental
Health Professions Licensing Board or by a person with at least five (5)
contiguous years of experience as a Credentialed Peer Specialist. Supervisors
of Peer Specialists must complete at least 16 hours of direct contact training
on the supervision of Peer Specialists.
Be under the direct supervision of the primary therapist for that client.
TO BE ELIGIBLE TO PROVIDE CASE MANAGEMENT SERVICES, STAFF
SHALL:
Be employed or under contract with the Behavioral Health Division certified
mental health or substance use treatment center and enrolled as a Medicaid
provider, and
Be a mental health or substance use treatment professional, a mental health or
substance use treatment counselor, a mental health or substance use treatment
assistant as pursuant to Wyoming Medicaid Rules, Chapter 13- Mental Health
Services, or
Be a registered nurse (R.N.), licensed in the State of Wyoming, who has at
least two years of clinical experience after the awarding of the R.N.
Knowledgeable of the community and have the ability to work with other
agencies
All documentation, including required signatures, must be completed at the time
the service is completed.
13.3 Covered Services for Community Mental Health and
Substance Abuse Treatment Centers
The following rehabilitative services are allowable for outpatient community mental
health and substance abuse treatment services:
13.3.1 Rehabilitative Option Services
Adult Psychosocial Rehabilitation: Skills addressed may include:
o Emotional skills, such as coping with stress, managing anxiety, dealing
constructively with anger and other strong emotions, coping with
depression, managing symptoms, dealing with frustration and
disappointment and similar skills.

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 176 Revision 4/1/17
o Behavioral skills, such as managing overt expression of symptoms like
delusions and hallucinations, appropriate social and interpersonal
interactions, proper use of medications, extinguishing
aggressive/assaultive behavior.
o Daily living and self-care, such as personal care and hygiene, money
management, home care, daily structure, use of free time, shopping,
food selection and preparation and similar skills.
o Cognitive skills, such as problem solving, concentration and attention,
planning and setting, understanding illness and symptoms, decision
making, reframing, and similar skills.
o Community integration skills, which focus on the maintenance or
development of socially valued, age appropriate activities.
o And similar treatment to implement each enrolled client’s treatment
plan.
o Excludes the following services, academic education, recreational
activities, meals and snacks and vocational services and training.
Agency/Based Individual/Family Therapy
Peer Specialist Services
Children’s Psychosocial Rehabilitation: This service is designed to address the
emotional and behavioral symptoms of youth diagnosed with childhood
disorder, including ADHD, Oppositional Defiant Disorder, Depression,
Disruptive Behavior Disorder and other related children’s disorder. Within
this service there are group and individual modalities and a primary focus on
behaviors that enhance a youth’s functioning in the home, school, and
community. Youth will acquire skills such as conflict resolution, anger
management, positive peer interaction and positive self-esteem. Treatment
interventions include group therapy, activity based therapy, psycho-
educational instruction, behavior modification, skill development, and similar
treatment to implement each enrolled client’s treatment plan. The day
treatment program may include a parent group designed to teach parents the
intervention strategies used in the program.
Clinical Assessment
Community-Based Individual/Family Therapy
Comprehensive Medication Services
Group Therapy
Individual Rehabilitative Services
Intensive Individual Rehabilitative Services
Substance Use Intensive Outpatient Treatment Services: Direct contact with
two or more enrolled clients (and collaterals as necessary) for the purpose of
providing a preplanned and structured program of group treatment which may
include education about role functioning, illness and medications; group
therapy and problem solving, and similar treatment to implement each
enrolled client’s treatment plan.
Psychiatrist Services: These mental health and substance abuse treatment
services are covered by Medicaid when it is determined to be medically
necessary and rehabilitative in nature.

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 177 Revision 4/1/17
13.3.2 Targeted Case Management
Targeted Case Management for adults with serious mental illness age twenty-one (21)
and over is an individual, non-clinical service which will be used to assist individuals
under the plan in gaining access to needed medical, social, educational, and other
services.
The purpose of targeted case management is to foster a client’s rehabilitation from a
diagnosed mental disorder or substance use disorder by organizing needed services
and supports into an integrated system of care until the client is able to assume this
responsibility.
Targeted case management activities include the following:
Linkage: Working with clients and/or service providers to secure access to
needed services. Activities include communication with agencies to arrange
for appointments or services following the initial referral process, and
preparing clients for these appointments. Contact with hospitalized clients,
hospital/institution staff, and/or collaterals in order to facilitate the client’s
reintegration in to the community.
Monitoring/Follow-Up: Contacting the client or others to ensure that a client
is following a prescribed service plan and monitoring the progress and impact
of that plan.
Referral: Arranging initial appointments for clients with service providers or
informing clients of services available, addresses and telephone numbers of
agencies providing services.
Advocacy: Advocacy on behalf of a specific client for the purpose of
accessing needed services. Activities may include making and receiving
telephone calls, and the completion of forms, applications and reports which
assist the client in accessing needed services.
Crisis Intervention: Crisis intervention and stabilization are provided in
situation requiring immediate attention/resolution for a specific client. The
case manager may provide the initial intervention in a crisis situation and
would assist the client in gaining access to other needed crisis services.
The client’s primary therapist (employed or contracted by the community mental
health or substance use treatment center) will perform an assessment and determine
the case management services required.
13.3.3 EPSDT Mental Health Services or Ongoing Case Management
Ongoing Case Management: Ongoing Case Management for persons under age
twenty one (21) is an individual, non-clinical service which will be used to assist
individuals under the plan in gaining access to needed medical, social, educational,
and other services.
The purpose of Ongoing case management is to foster a client’s rehabilitation from a
diagnosed mental disorder or substance use disorder by organizing needed services
and supports into an integrated system of care until the client or family is able to
assume this responsibility.

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 178 Revision 4/1/17
Ongoing case management activities include the following:
Linkage: Working with clients and/or service providers to secure access to
needed services. Activities include communication with agencies to arrange
for appointments or services following the initial referral process, and
preparing clients for these appointments. Contact with hospitalized clients,
hospital/institution staff, and/or collaterals in order to facilitate the client’s
reintegration into the community.
Monitoring/Follow-up: Contacting the client or others to ensure that a client is
following a prescribed service plan and monitoring the progress and impact of
that plan.
Referral: Arranging appointments for clients with service providers or
informing clients of services available, addresses and telephone numbers of
agencies’ providing services.
Advocacy: Advocacy on behalf of a specific client for the purpose of
accessing needed services. Activities may include making and receiving
telephone calls, and the completion of forms, applications and reports which
assist the client in accessing needed services.
Crisis Intervention: Crisis Intervention and stabilization are provided in
situations requiring immediate attention/resolution for a specific client. The
case manager may provide the initial intervention in a crisis situation and
would assist the client in gaining access to other needed crisis services.
The client’s primary therapist will perform an assessment and authorize the case
management services required.
13.3.4 Limitations to Mental Health/Substance Abuse Services
Medicaid Mental Health Rehabilitative Targeted Case Management Option
and EPSDT mental health services are limited to those eligible persons who
have a primary diagnosis of a mental/substance use disorder in the most
current edition of the Diagnostic and Statistical Manual Disorders (DSM) or
ICD equivalent.
Specifically excluded from eligibility for Rehabilitative Option, Targeted
Case Management Option and EPSDT mental health services are the
following diagnosis resulting from clinical assessment:
o Sole DSM diagnosis of mental retardation
o Sole DSM diagnosis of any Z code and services provided for a Z code
diagnosis (exception for young children)
o Sole DSM diagnosis of other unknown and unspecified cause of
morbidity and mortality
o Sole DSM diagnosis of specific learning disorders
Habilitative services are not covered for clients twenty-one (21) years of age
or older.
13.3.5 Quality Assurance
The quality assurance program of a provider shall, at minimum, meet these criteria:
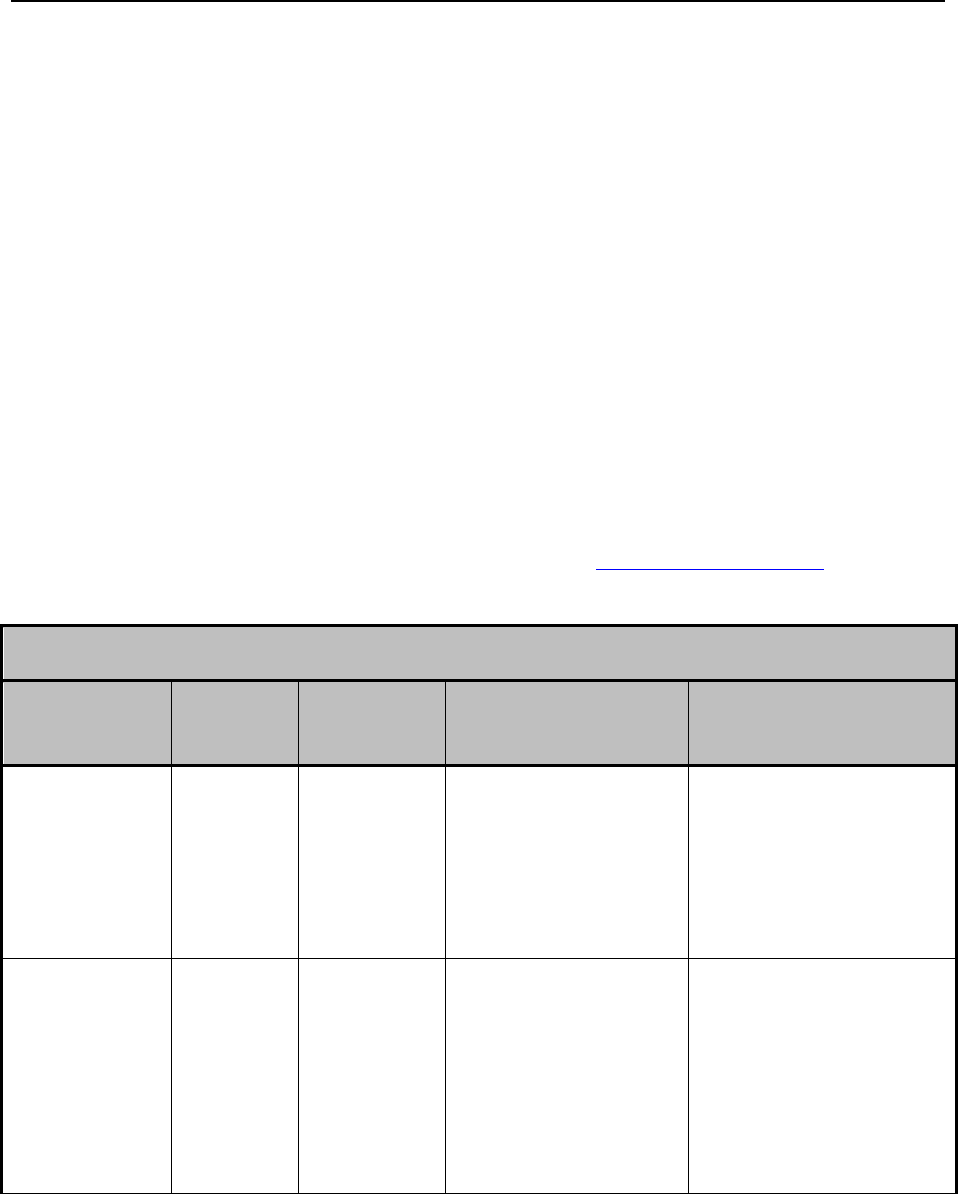
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 179 Revision 4/1/17
Utilization and quality review criteria
Agency standards for completeness review and criteria for clinical records
Definition of critical incidents which require professional review and review
procedures
13.4 Community Mental Health & Substance Abuse Treatment
Centers Billing Procedures
The following matrix indicates the HCPCS Level II code, the Medicaid defined unit
(for codes without a specific time span in the HCPCS Level II coding book) and
acceptable modifiers (when applicable).
13.4.1 Psychiatric Services
Community Mental Health Centers will be reimbursed for psychiatric services at the
same fee currently established for psychiatrists in private practices. Community
Mental Health Centers must use current CPT codes when billing for these services.
Refer to Psychiatric and Mental Health Services (13.6, Eligible Providers).
Community Mental Health & Substance Abuse Centers
HCPCS Level
II Code
Modifier(s)
1 Unit
Equals
Description
Taxonomies Allowed
G9012
Per 15 minutes
Ongoing Case
Management(<21)
101YA0400X, 101YP2500X,
101Y00000X, 103G00000X,
103TC0700X, 106H00000X,
163W00000X, 171M00000X,
2084P0800X, 364SP0808X,
1041C0700X, Taxonomies
beginning with 20 (Physicians)
T1017
Per 15 minutes
Adult Case Management –
Targeted Case
Management (>21)
101Y00000X, 101YP2500X,
101YA0400X, 103TC0700X,
103G00000X, 1041C0700X,
106H00000X, 163W00000X,
171M00000X, 2084P0800X,
251B00000X, 364SP0808X,
Taxonomies beginning with
20 (Physicians),
261QM0801X, 261QR0405X
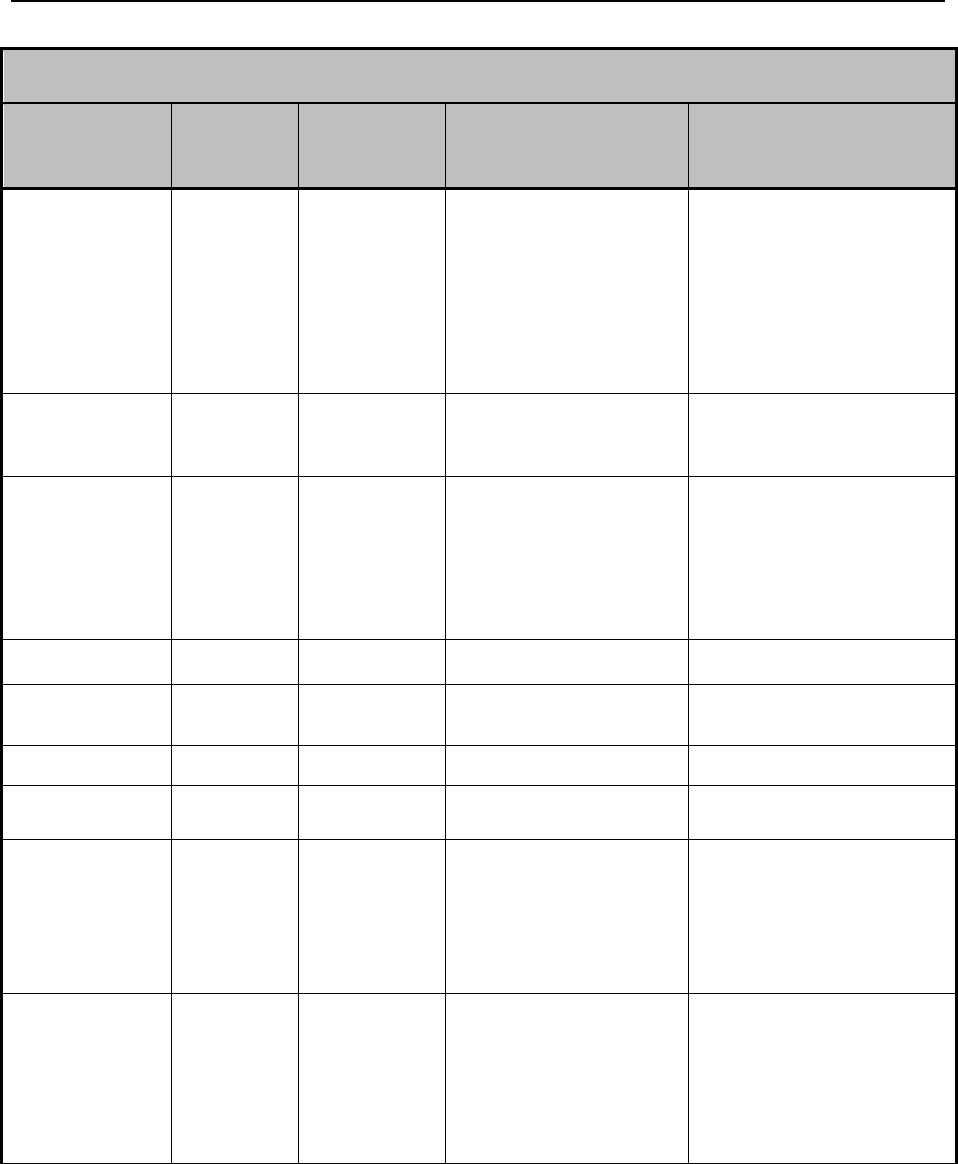
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 180 Revision 4/1/17
Community Mental Health & Substance Abuse Centers
HCPCS Level
II Code
Modifier(s)
1 Unit
Equals
Description
Taxonomies Allowed
H0031
Per 15 minutes
Clinical Assessment –
Mental Health Assessment
by non-physician
101Y00000X, 101YP2500X,
101YA0400X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 163W00000X,
2084P0800X, 364SP0808X,
Taxonomies beginning with
20 (Physicians),
261QM0801X, 261QR0405X
H0034
Per 15 minutes
Comprehensive Medication
Service – Medication
Training and Support
101YP2500X, 163W00000X,
164W00000X, 364SP0808X,
261QM0801X
H2014
Per 15 minutes
Individual Rehabilitative
Service – Skills Training
and Development
101Y00000X, 101YP2500X,
101YA0400X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 163W00000X,
164W00000X, 171M00000X,
172V00000X, 261QM0801X
H2014
HH
Per 15 minutes
Certified Peer Specialists
172V00000X, 261QM0801X
H2014
HH + HQ
Per 15 minutes
Certified Peer Specialists
172V00000X, 261QM0801X
H2015
HH
Per 15 minutes
Certified Peer Specialists
172V00000X, 261QR0405X
H2015
HH, HQ
Per 15 minutes
Certified Peer Specialist –
Group
172V00000X, 261QR0405X
H2017
Per 15 minutes
Psychosocial Rehabilitation
Services
101Y00000X, 101YP2500X,
101YA0400X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 163W00000X,
171M00000X, 2084P0800X,
364SP0808X, 261QM0801X
H2017
EP
Per 15 minutes
Children’s Psychosocial
Rehabilitation Services
101Y00000X, 101YP2500X,
101YA0400X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 163W00000X,
171M00000X, 2084P0800X,
364SP0808X, 261QM0801X

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 181 Revision 4/1/17
Community Mental Health & Substance Abuse Centers
HCPCS Level
II Code
Modifier(s)
1 Unit
Equals
Description
Taxonomies Allowed
H2019
Per 15 minutes
Agency Based
Individual/Family Therapy
101Y00000X, 101YP2500X,
101YA0400X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 163W00000X,
2084P0800X, Taxonomies
beginning with 20
(Physicians), 261QM0801X
H2019
HQ
Per 15 minutes
Group Therapy – Group
Counseling by Clinician
101Y00000X, 101YP2500X,
101YA0400X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 163W00000X,
2084P0800X, Taxonomies
beginning with 20
(Physicians), 261QM0801X
H2021
Per 15 minutes
Community-Based
Individual/Family Therapy
101Y00000X, 101YP2500X,
101YA0400X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 163W00000X,
2084P0800X, Taxonomies
beginning with 20
(Physicians), 261QM0801X
H2010
Per 15 minutes
Comprehensive Medication
Therapy
101YP2500X, 163W00000X,
164W00000X, 171M00000X,
172V00000X, 261QR0405X
H0047
Per 15 minutes
Alcohol/Drug Services –
NOS, Community Based
Individual/Family Therapy
101Y00000X, 101YA0400X,
101YP2500X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 163W00000X,
2084P0800X, 261QR0405X
T1012
Per 15 minutes
Alcohol/Drug Services –
Skill Development
(Psychosocial Rehab
Service)
101Y00000X, 101YA0400X,
101YP2500X, 1041C0700X,
106H00000X, 163W0000X,
171M00000X, 261QR0405X
H0005
Per 15 minutes
Alcohol/Drug Services –
Group Counseling by
Clinician
101Y00000X, 101YA0400X,
101YP2500X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 163W00000X,
261QR0405X
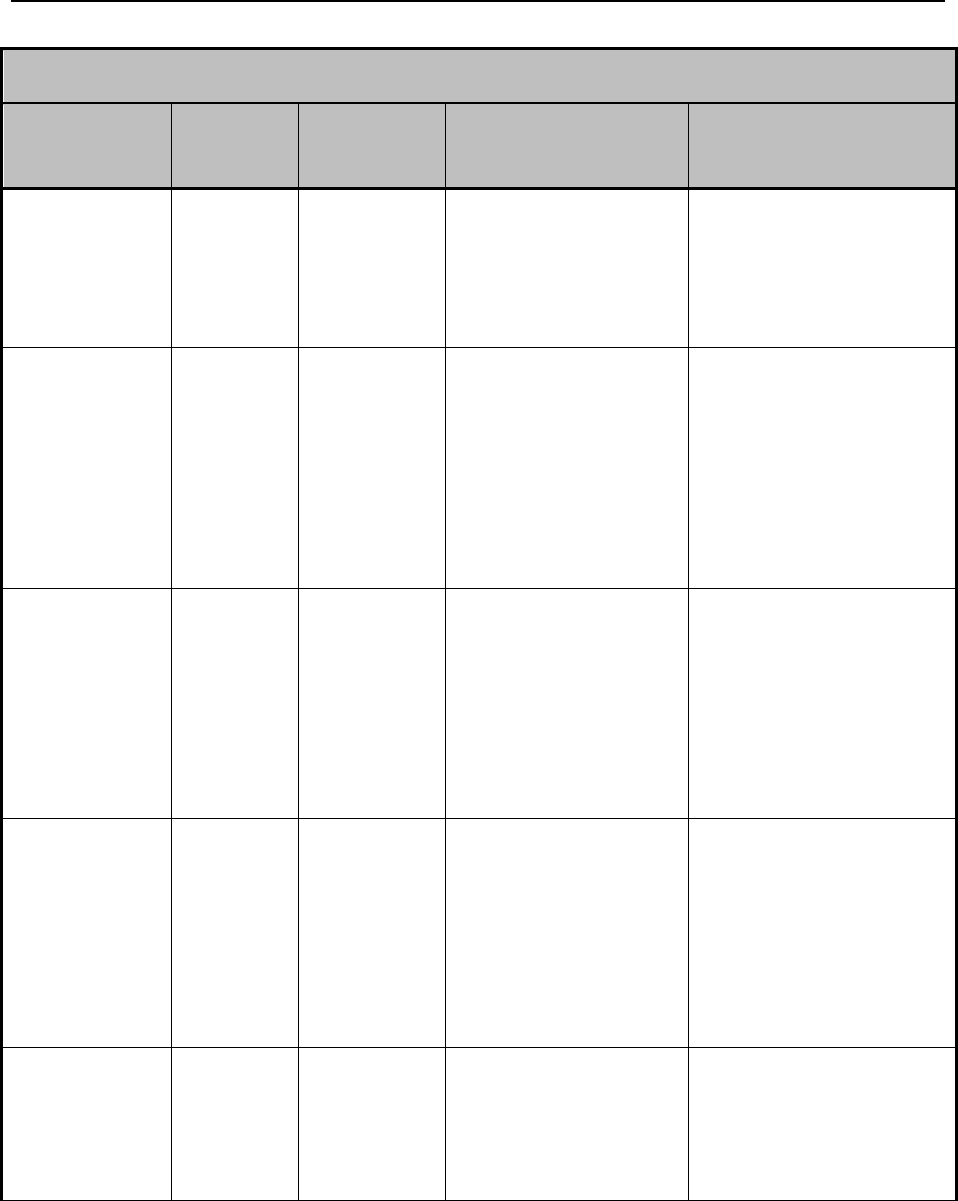
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 182 Revision 4/1/17
Community Mental Health & Substance Abuse Centers
HCPCS Level
II Code
Modifier(s)
1 Unit
Equals
Description
Taxonomies Allowed
H2015
Per 15 minutes
Comprehensive
Community Support
Services – Individual Rehab
Services
101Y00000X, 101YA0400X,
101YP2500X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 163W00000X,
164W00000X, 171M00000X,
172V00000X, 261QR0405X
H0006
Per 15 minutes
Alcohol/Drug Services –
Case Management
101Y00000X, 101YA0400X,
101YP2500X, 103TC0700X,
103G00000X, 1041C0700X,
106H00000X, 163W00000X,
171M00000X, 2084P0800X,
364SP0808X, Taxonomies
beginning with 20
(Physicians), 261QM0801X,
261QR0405X
H0006
EP
Per 15 minutes
Substance Abuse Case
Management (Youth)
101Y00000X, 101YA0400X,
101YP2500X, 103TC0700X,
103G00000X, 1041C0700X,
106H00000X, 163W00000X,
171M00000X, 2084P0800X,
364SP0808X, Taxonomies
beginning with 20
(Physicians), 261QM0801X,
261QR0405X
H0006
HQ
Per 15 minutes
Alcohol/Drug Services –
Case Management – Group
101Y00000X, 101YA0400X,
101YP2500X, 103TC0700X,
103G00000X, 1041C0700X,
106H00000X, 163W00000X,
171M00000X, 2084P0800X,
364SP0808X, Taxonomies
beginning with 20
(Physicians), 261QM0801X,
261QR0405X
T2011
PASRR Level II
Psychiatric
Evaluation/Determination
of Appropriate Placement
101Y00000X, 101YP2500X,
103G00000X, 103TC0700X,
1041C0700X, 106H00000X,
2084P0800X, 364SP0808X,
Taxonomies beginning with
20 (Physicians),261QM0801X
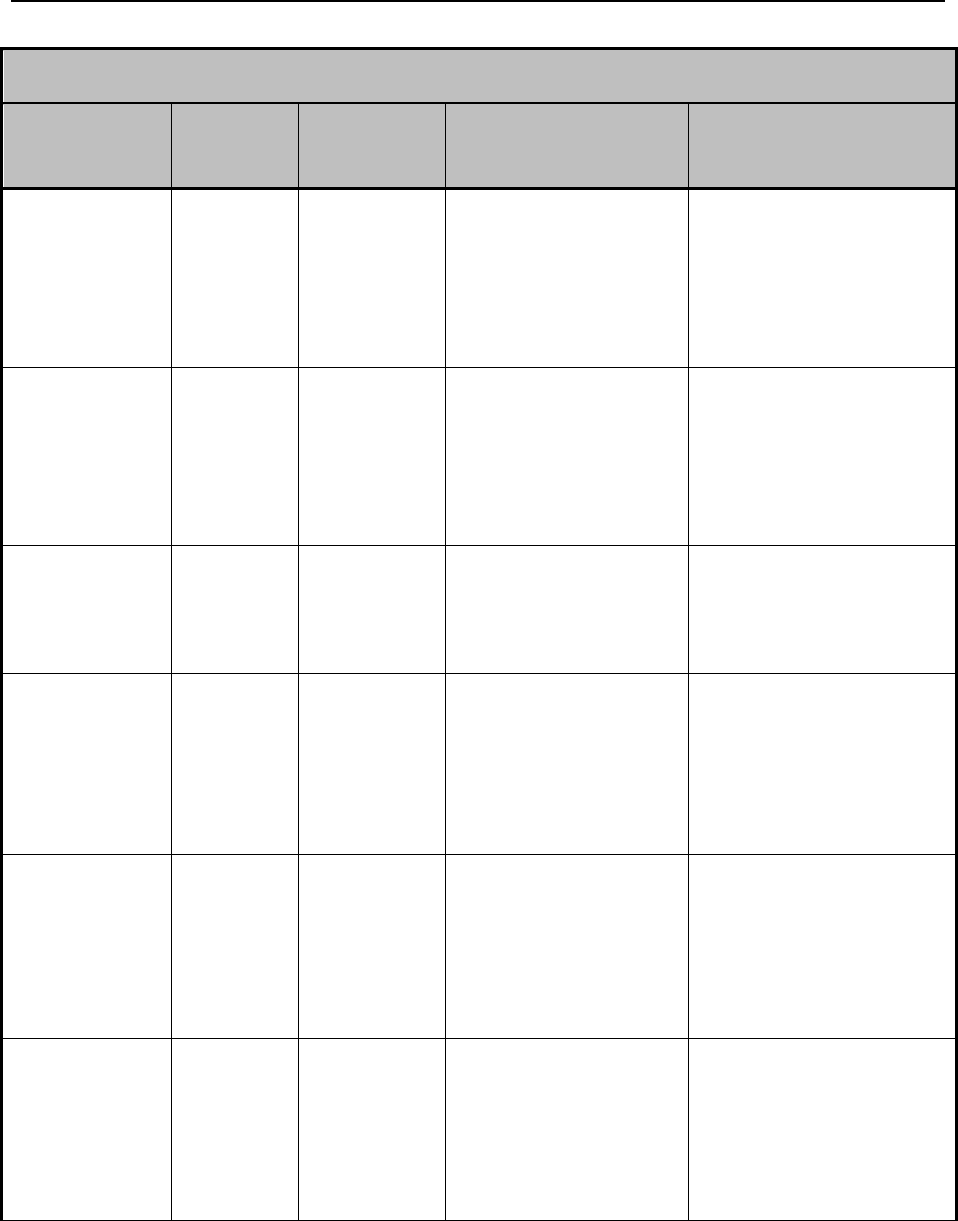
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 183 Revision 4/1/17
Community Mental Health & Substance Abuse Centers
HCPCS Level
II Code
Modifier(s)
1 Unit
Equals
Description
Taxonomies Allowed
90785
CPT Defined
Interactive complexity (list
separately in addition to the
code for primary procedure)
101Y00000X, 101YP2500X,
101YA0400X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 364SP0808X,
Taxonomies beginning with
20 (Physicians),
261QM0801X, 261QR0405X
90791
CPT Defined
Psychiatric Diagnostic
Evaluation
101Y00000X, 101YP2500X,
101YA0400X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 364SP0808X,
Taxonomies beginning with
20 (Physicians),
261QM0801X, 261QR0405X
90792
CPT Defined
Psychiatric diagnostic
evaluation with medical
services
103G00000X, 103TC0700X,
364SP0808X, Taxonomies
beginning with 20
(Physicians), 261QM0801X,
261QR0405X
90832
CPT Defined
Psychotherapy, 30 minutes
with patient and/or family
member
101Y00000X, 101YA0400X,
101YP2500X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 364SP0808X,
Taxonomies beginning with
20 (Physicians),
261QM0801X, 261QR0405X
90833
CPT Defined
Psychotherapy, 30 minutes
with patient and/or family
member when performed
with an evaluation and
management service (list
separately in addition to the
code for primary procedure)
103TC0700X, 103G00000X,
364SP0808X, Taxonomies
beginning with 20
(Physicians). 261QM0801X,
261QR0405X
90834
CPT Defined
Psychotherapy, 45 minutes
with patient and/or family
member
101Y00000X, 101YA0400X,
101YP2500X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 364SP0808X,
Taxonomies beginning with
20 (Physicians),
261QM0801X, 261QR0405X

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 184 Revision 4/1/17
Community Mental Health & Substance Abuse Centers
HCPCS Level
II Code
Modifier(s)
1 Unit
Equals
Description
Taxonomies Allowed
90836
CPT Defined
Psychotherapy, 45-minutes
with patient and/or family
member when performed
with an evaluation and
management service (list
separately in addition to the
code for primary procedure)
103TC0700X, 103G00000X,
364SP0808X, Taxonomies
beginning with 20
(Physicians), 261QM0801X,
261QR0405X
90837
CPT Defined
Psychotherapy, 60 minutes
with patient and/or family
member
101Y00000X, 101YA0400X,
101YP2500X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 364SP0808X,
Taxonomies beginning with
20 (Physicians),
261QM0801X, 261QR0405X
90838
CPT Defines
Psychotherapy, 60 minutes
with patient and/or family
member when performed
with an evaluation and
management services (list
separately in addition to the
code for primary procedure)
103G00000X, 103TC0700X,
364SP0808X, Taxonomies
beginning with 20
(Physicians), 261QM0801X,
261QR0405X
90845
CPT Defined
Psychoanalysis
101Y00000X, 101YA0400X
103G00000X, 103TC0700X,
1041C0700X, 106H00000X,
2084P0800X, 364SP0808X,
Taxonomies beginning with
20 (Physicians),
261QM0801X, 261QR0405X
90846
CPT Defined
Family Medical
Psychotherapy (without the
patient present)
101YP2500X, 103G00000X,
103TC0700X, 2084P0800X,
364SP0808X, Taxonomies
beginning with 20
(Physicians), 261QM0801X,
261QR0405X
90847
CPT Defined
Family Psychotherapy
101Y00000X, 101YA0400X,
101YP2500X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 2084P0800X,
364SP0808X, Taxonomies
beginning with 20
(Physicians), 261QM0801X,
261QR0405X
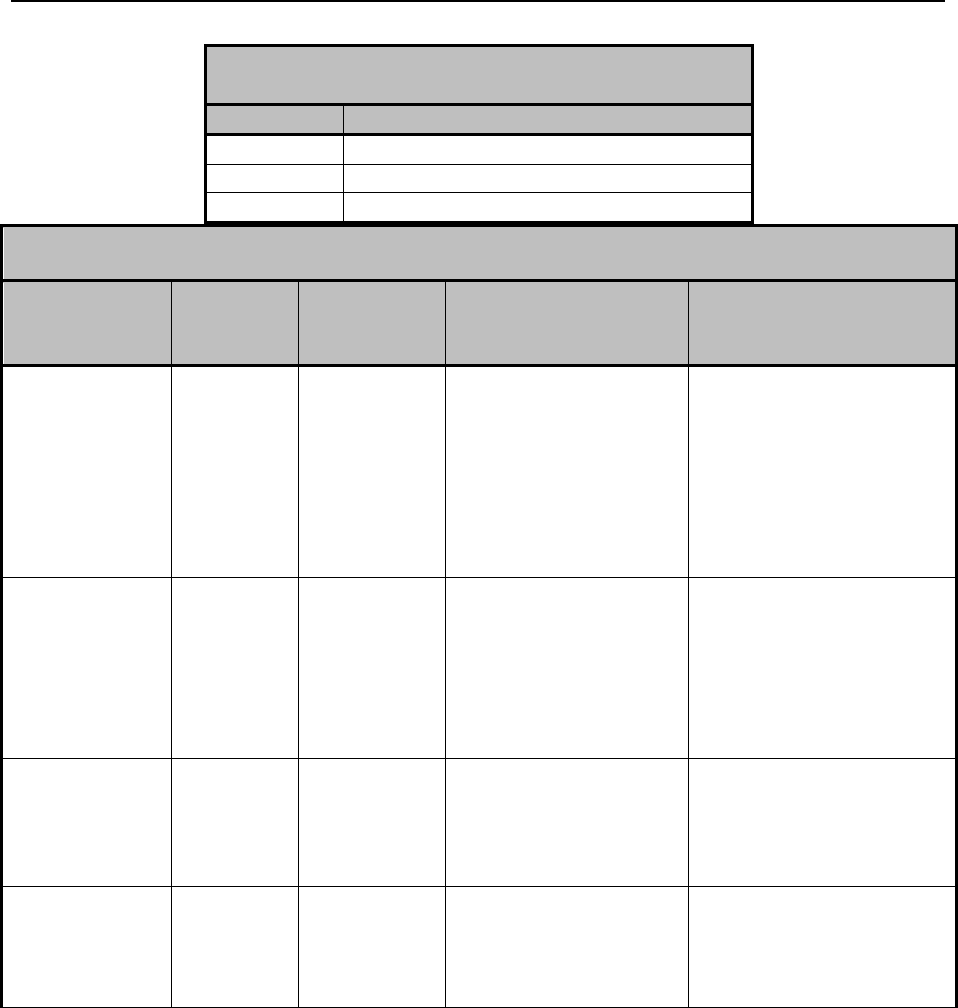
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 185 Revision 4/1/17
Community Mental Health & Substance Abuse Centers
HCPCS Level
II Code
Modifier(s)
1 Unit
Equals
Description
Taxonomies Allowed
90849
CPT Defined
Multiple-Family Group
Psychotherapy
101Y00000X, 101YA0400X,
101YP2500X, 103G00000X,
103TC0700X, 1041C0700X,
106H00000X, 2084P0800X,
364SP0808X, Taxonomies
beginning with 20
(Physicians), 261QM0801X,
261QR0405X
90853
CPT Defined
Group Medical
Psychotherapy
101Y00000X, 101YA0400X
103G00000X, 103TC0700X,
1041C0700X, 106H00000X,
2084P0800X, 364SP0808X,
Taxonomies beginning with
20 (Physicians),
261QM0801X, 261QR0405X
96101-96103,
96120
CPT Defined
Central Nervous System
Assessments/Psychological
Testing
103G00000X, 103TC0700X,
2084P0800X, 364SP0808X,
Taxonomies beginning with
20 (Physicians),
261QM0801X
96105, 96110-
96111, 96116,
96118-96119,
96125
CPT Defined
Central Nervous System
Assessments/Psychological
Testing
103G00000X, 103TC0700X,
2084P0800X, 364SP0808X,
Taxonomies beginning with
20 (Physicians)
Community Mental Health & Substance Abuse
Treatment Centers
Modifier(s)
Description
EP
Services provided as part of EPSDT
HH
Peer Specialist
HQ
Group setting
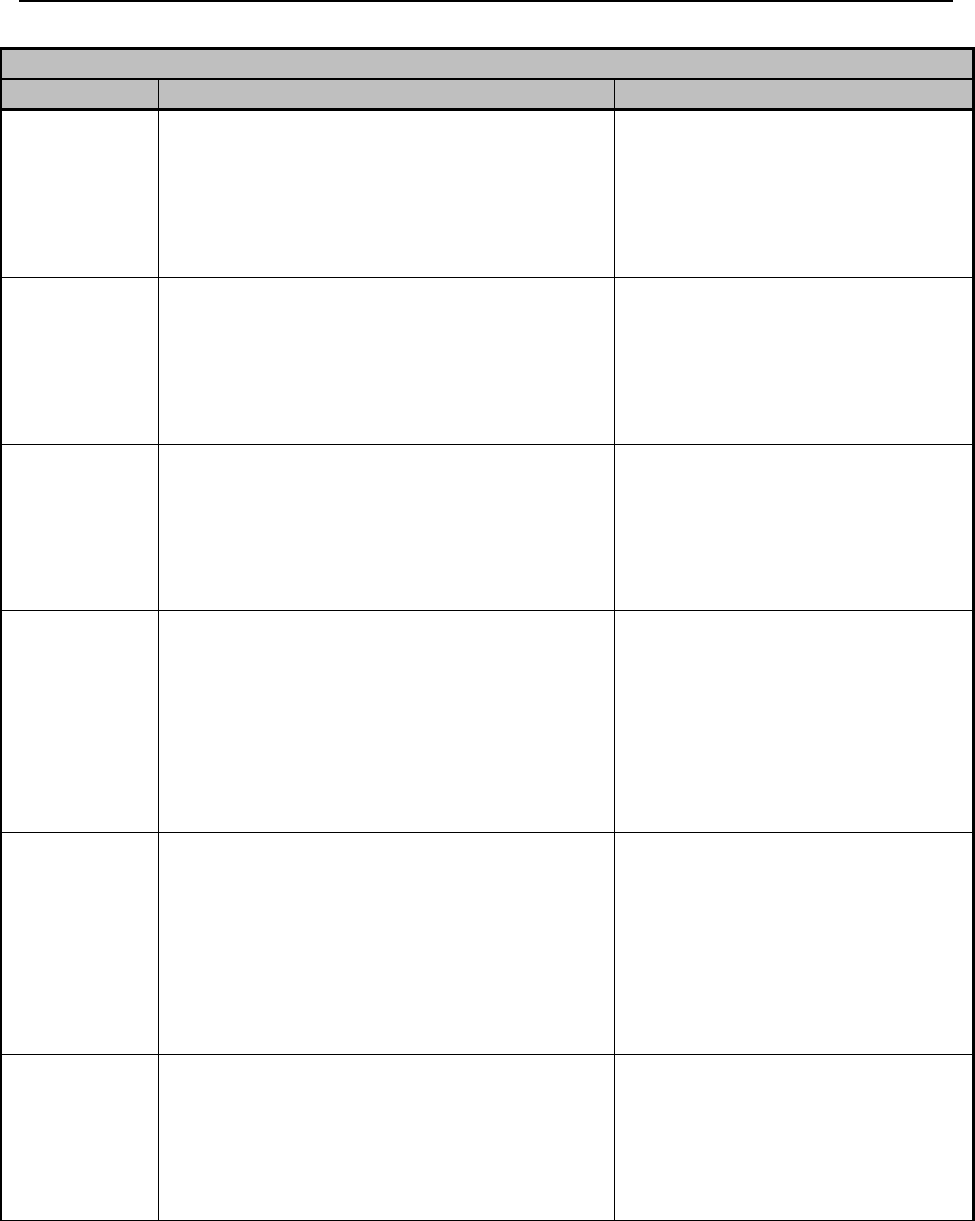
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 186 Revision 4/1/17
Community Mental Health Centers
Taxonomy
Provider Types
Allowed Codes
101Y00000X
Provisional Professional Counselor (PPC),
Certified Mental Health Worker
G9012, H0031, H2014, H2014 +
HK, H2017, H2017 + EP, H2019,
H2019 + HQ, H2021, T1017,
T1017 + EP, T2011, 90785,
90791, 90832, 90834, 90837,
90845, 90847, 90849, 90853
101YA0400X
Licensed Addictions Therapist (LAT),
Provisionally Licensed Addictions Therapist
(PLAT), Certified Addictions Practitioner
(CAP)
G9012, H0031, H2014, H2014 +
HK, H2017, H2017 + EP, H2019,
H2019 + HQ, H2021, T1017,
T1017 + EP, T2011, 90785,
90791, 90832, 90834, 90837,
90845, 90847, 90849, 90853
101YP2500X
Licensed Professional Counselor (LPC)
G9012, H0034, H2014, H2014 +
HK, H2017, H2017 + EP, H2019,
H2019 + HQ, H2021, T1017,
T1017 + EP, 90791, 90785,
90832, 90834, 90837, 90846,
90847, 90849, 90853, H0031,
103G00000X
Neuropsychologist
G9012, H0031, H2014, H2014 +
HK, H2017, H2019, H2021,
T1017, T1017 + EP, T2011,
90785, 90791, 90792, 90832-
90834, 90836-90839, 90845-
90847, 90849, 90853, 96101-
96103, 96105, 96110-96111,
96116, 96118-96120, 96125
103TC0700X
Clinical Psychologist
G9012, H0031, H2014, H2014 +
HK, H2017, H2019, H2021,
T1017, T1017 + EP, T2011,
90785, 90791, 90792, 90832-
90834, 90836-90839, 90845-
90847, 90849, 90853, 96101-
96103, 96105, 96110-96111,
96116, 96118-96120, 96125
1041C0700X
Licensed Clinical Social Worker (LCSW),
Certified Social Worker (CSW)
G9012, H0031, H2014, H2014
+HK, H2017, H2017 + EP,
H2019, H2019 + HQ, H2021,
T1017, T1017 + EP, T2011,
90785, 90791, 90832, 90834,
90837, 90845
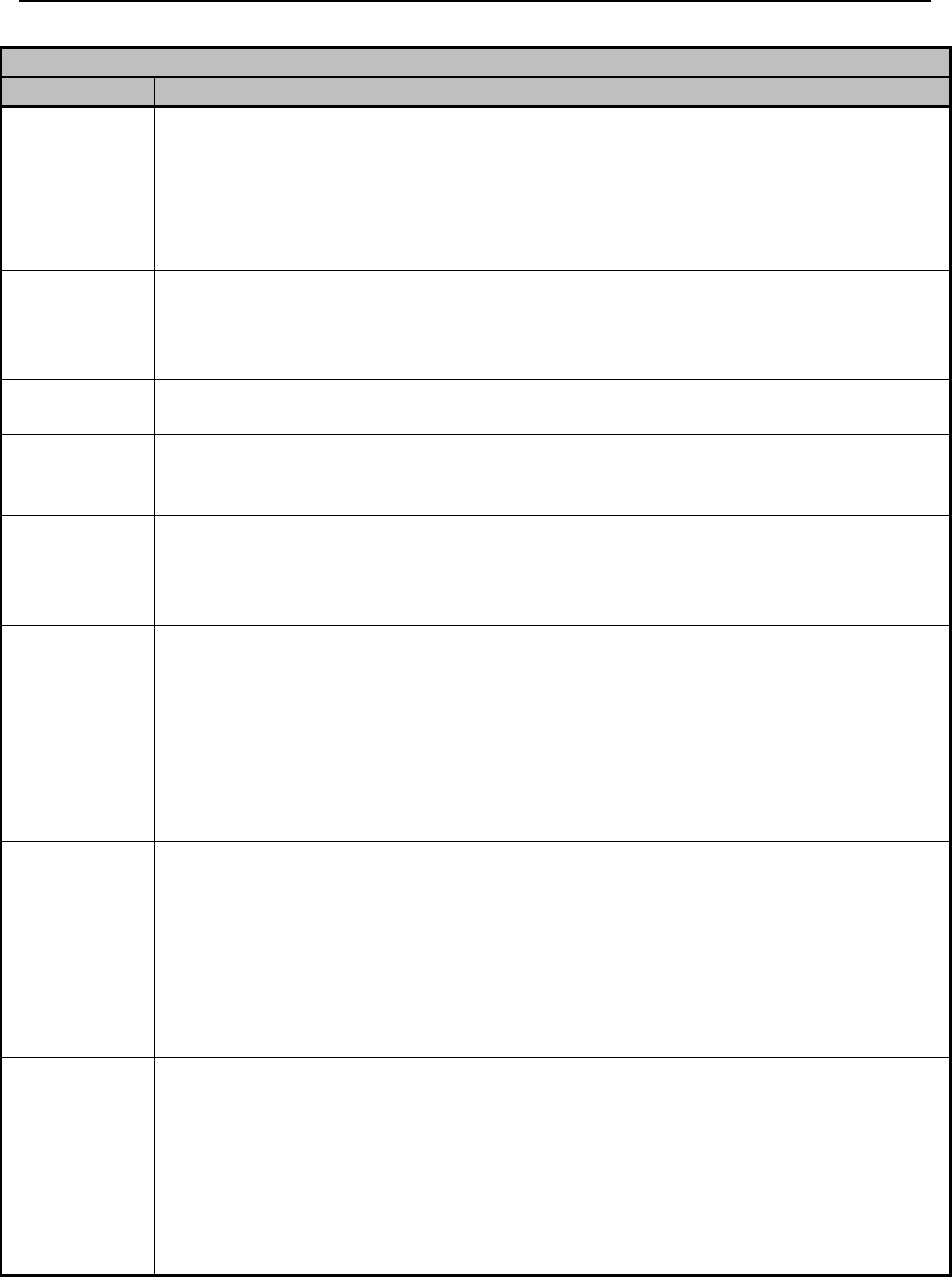
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 187 Revision 4/1/17
Community Mental Health Centers
Taxonomy
Provider Types
Allowed Codes
106H00000X
Marriage and Family Therapist (MFT),
Provisionally Licensed Marriage and Family
Therapist (PMFT)
G9012, H0031, H2014, H2014 +
HK, H2017, H2017 + EP, H2019,
H2019 + HQ, H2021, T1017,
T1017 + EP, T2011, 90785,
90791, 90832, 90834, 90837,
90845, 90849, 90853
163W00000X
RN
G9012, H0031, H0034, H2014,
H2014 + HK, H2017, H2017+EP,
H2019, H2021, T1017, T1017 +
EP
164W00000X
LPN
G9012, H0034,
H2014,H2014+HK
171M00000X
Case Manager
G9012, H2014, H2014 + HK,
H2017, H2017 + EP, T1017,
T1017 + EP
172V00000X
Community Health Worker – Individual
Rehabilitative Services Worker (IRS),
Certified Peer Specialist, Certified
Addictions Practitioner Assistant (CAPA)
H2014, H2014 + HK, H2014 +
HH, H2014 + HH+ HQ
Taxonomies
beginning
with 20
Physicians
G9012, H0031, H2019, H2019 +
HQ, H2021, T1017, T1017 + EP,
90785, 90791, 90792, 90832-
90834, 90836-90839, 90845
90846, 90847, 90849, 90853,
96101-96103, 96105, 96110-
96111, 96116, 96118-96120,
96125
2084P0800X
Psychiatry and Neurology, Psychiatry
G9012, H0031, H2017, H2017 +
EP, H2019, H2019 + HQ, H2021,
T1017, T1017 + EP, T2011,
90785, 90791, 90792, 90832-
90834, 90836-90839, 90845-
90847, 90849, 90853, 96101-
96103, 96105, 96110-96111,
96116, 96118-96120, 96125
364SP0808X
Nurse Practitioner, Advanced Practice,
Psychiatric/Mental Health
G9012, H0031, H0034, H2017,
H2017 + EP, H2021, T1017,
T1017 + EP, T2011, 90785,
90791, 90792, 90832-90834,
90836-90839, 90845-90847,
90849, 90853, 96101-96103,
96105, 96110-96111, 96116,
96118-96120, 96125
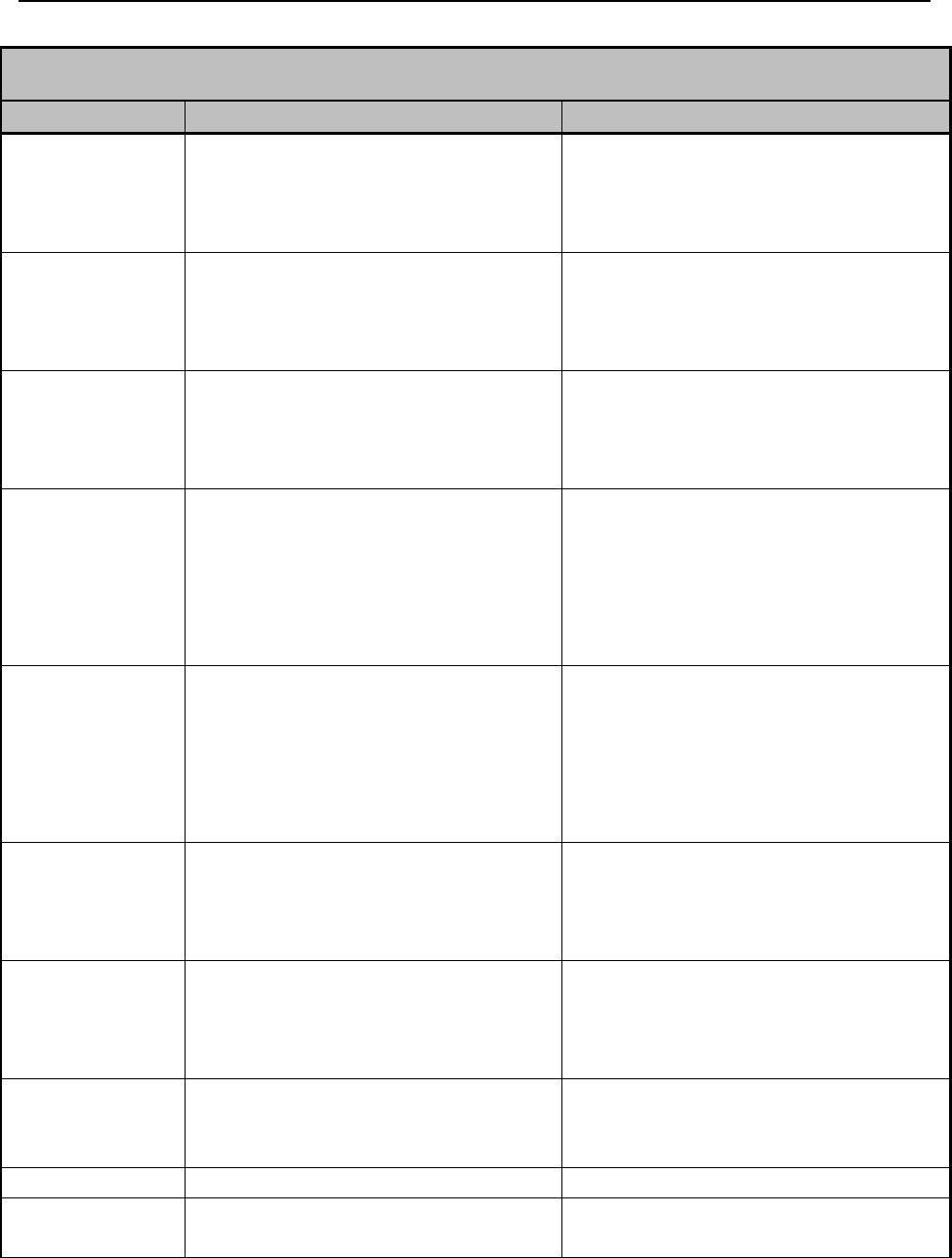
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 188 Revision 4/1/17
Substance Abuse Treatment Centers
Taxonomy
Provider Types
Allowed Codes
101Y00000X
Provisional Professional Counselor (PPC),
Certified Mental Health Worker
G9012, H0031, H0005, H0006, H0006 + EP,
H0006 + HQ, H0047, H2015, H2015 + HK,
T1017, T1012, 90785, 90791, 90832, 90834,
90837, 90847, 90849, 90853
101YA0400X
Licensed Addictions Therapist (LAT),
Provisionally Licensed Addictions Therapist
(PLAT), Certified Addictions Practitioner
(CAP)
G9012, H0031, H0005, H0006, H0006 + EP,
H0006 + HQ, H0047, H2015, H2015 + HK,
T1017, T1012, 90785, 90791, 90832, 90834,
90837, 90847, 90849, 90853
101YP2500X
Licensed Professional Counselor (LPC)
G9012, H0031, H0005, H0006, H0006 + EP,
H0006 + HQ, H0047, H2015, H2015 + HK,
T1017, T1012, 90785, 90791, 90832, 90834,
90837, 90846, 90847, 90849, 90853
103G00000X
Neuropsychologist
G9012, H0005, H0006, H0006 + EP, H0006 +
HQ, H2015, H2015 + HK, T1017, 90785,
90791, 90792, 90832-90834, 90836-90838,
90845- 90847, 90849, 90853, 96101-96103,
96105, 96110-96111, 96116, 96118-96120,
96125
103TC0700X
Clinical Psychologist
G9012, H0005, H0006, H0006 + EP, H0006 +
HQ, H2015, H2015 + HK, T1017, 90785,
90791, 90792, 90832-90834, 90836-90838,
90845- 90847, 90849, 90853, 96101-96103,
96105, 96110-96111, 96116, 96118-96120,
96125
1041C0700X
Licensed Clinical Social Worker (LCSW),
Certified Social Worker (CSW)
G9012, H0031, H0005, H0006, H0006 + EP,
H0006 + HQ, H0047, H2015, H2015 + HK,
T1017, T1012, 90785, 90791, 90832, 90834,
90837, 90847, 90849, 90853
106H00000X
Marriage and Family Therapist (MFT),
Provisionally Licensed Marriage and Family
Therapist (PMFT)
G9012, H0031, H0005, H0006, H0006 + EP,
H0006 + HQ, H0047, H2015, H2015 + HK,
T1017, T1012, 90784, 90791, 90832, 90834,
90837, 90847, 90849, 90853
163W00000X
RN
G9012, H0005, H0006, H0006 + EP, H0006 +
HQ, H2010, H2015, H2015 + HK, H0047,
T1017, T1012
164W00000X
LPN
H2010, H2015, H2015 + HK
171M00000X
Case Manager
G9012, H0006, H0006 + EP, H0006 + HQ,
H2015, H2015 + HK + T1012
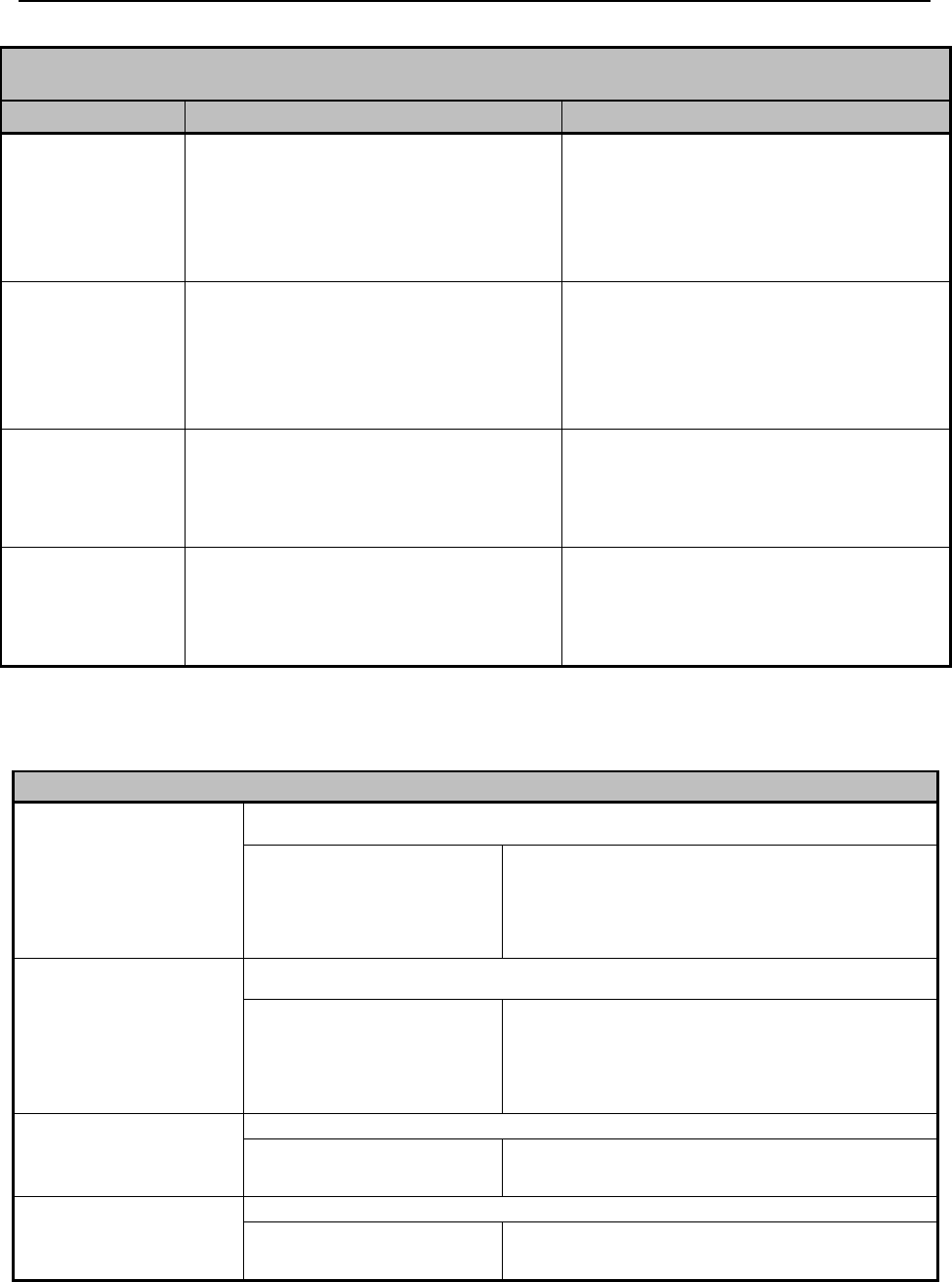
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 189 Revision 4/1/17
Substance Abuse Treatment Centers
Taxonomy
Provider Types
Allowed Codes
172V00000X
Community Health Worker – Individual
Rehabilitative Services Worker (IRS),
Certified Peer Specialist, Certified Addictions
Practitioner Assistant (CAPA)
H2010, H2015, H2015 + HK, H2015 + HH,
H2015 + HH + HQ
2084P0800X
Psychiatry and Neurology, Psychiatry
G9012, H0006, H0006 + EP, H0006 + HQ,
T1017, 90785, 90791, 90792, 90832-90834,
90836-90838, 90846, 90849, 90853, 96101-
96103, 96105, 96110-96111, 96116, 96118-
96120, 96125
Taxonomies
beginning with 20
Physicians
G9012, H0006, 90785, 90791, 90792, 90832-
90834, 90836-90838, 90845-90847, 90849,
90853, 96101-96103, 96105, 96110-96111,
96116-96120, 96125
364SP0808X
Nurse Practitioner, Advanced Practice,
Psychiatric/Mental Health
G9012, H0006, H0006 + EP, H0006 + HQ,
90785, 90791, 90792, 90832-90834, 90836-
90838, 90845-90847, 90849, 90853, 96101-
96125
13.5 Eligible Providers
Individual and/or Group Providers
Licensed Professional
Counselor (LPC)
101YP2500X
Shall be enrolled as an individual or in one (1) of the following groups:
Psychiatry
CMHC
SATC
Developmental Center
Psychologist
Neuropsychologist
Physician
Licensed Addictions
Therapist (LAT)
101YA0400X
Shall be enrolled as an individual or in one (1) of the following groups:
Psychiatry
CMHC
SATC
Developmental Center
Psychologist
Neuropsychologist
Physician
Neuropsychologist
103G00000X
Shall be enrolled as an individual or in one (1) of the following groups:
CMHC
Physician
SATC
Clinical Psychologist
103TC0700X
Shall be enrolled as an individual or in one (1) of the following groups:
CMHC
Physician
SATC
LAT
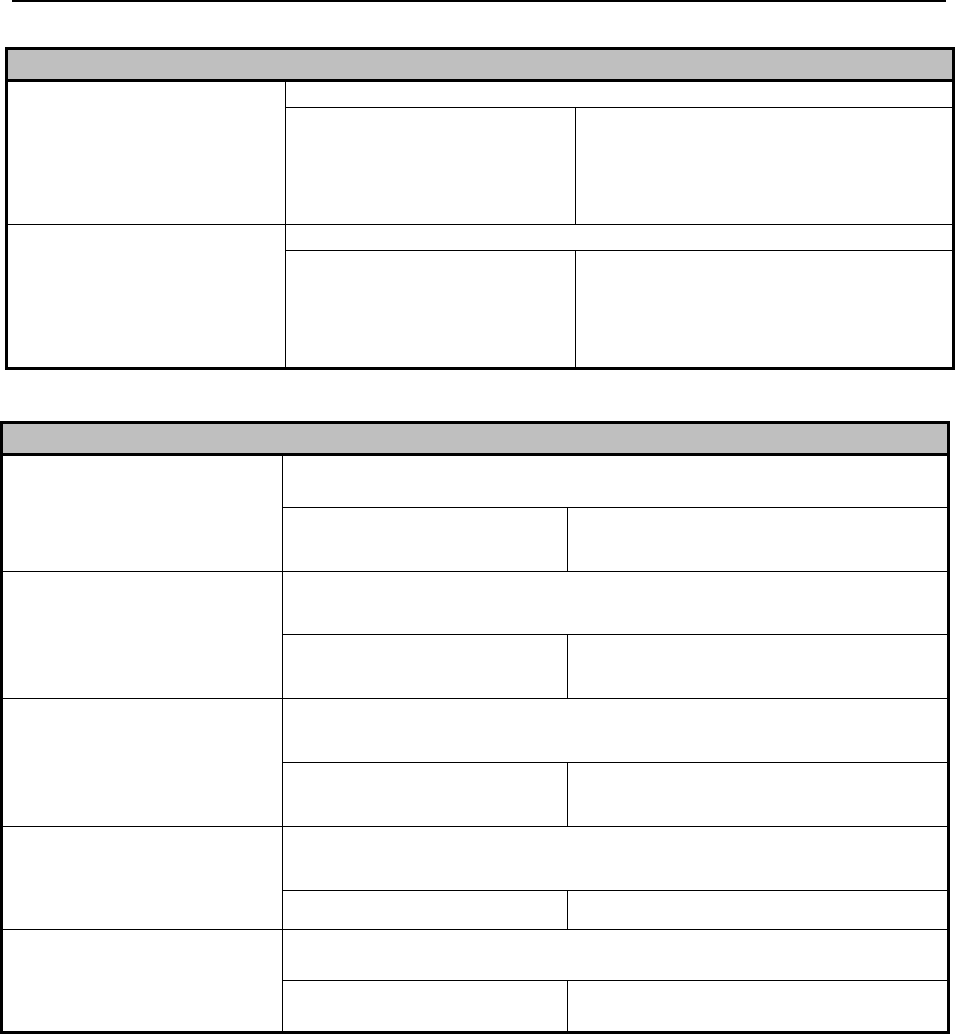
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 190 Revision 4/1/17
Individual and/or Group Providers
Licensed Clinical Social
Worker (LCSW)
1041C0700X
Shall be enrolled as an individual or in one (1) of the following groups:
Psychiatry
CMHC
SATC
Developmental Center
Psychologist
Neuropsychologist
Physician
Licensed Marriage and
Family Therapist (LMFT)
106H00000X
Shall be enrolled as an individual or in one (1) of the following groups:
Psychiatry
CMHC
SATC
Developmental Center
Psychologist
Neuropsychologist
Physician
Only Enrolled Under Supervision
Certified Mental Health
Worker (CMHW)
101Y00000X
Shall be under the supervision of a Qualified Clinical Supervisor and
employer; AND Shall be enrolled in one (1) of the following groups:
Psychologist
CMHC
Neuropsychologist
SATC
Certified Addictions
Practitioner (CAP)
101YA0400X
Shall be under the supervision of a Licensed Professional and Employer;
AND Shall be enrolled in one (1) of the following groups:
Psychologist
CMHC
Neuropsychologist
SATC
Certified Social Worker
(CSW)
1041C0700X
Shall be under the supervision of a Qualified Clinical Supervisor and
employer; AND Shall be enrolled in one (1) of the following groups:
Psychologist
CMHC
Neuropsychologist
SATC
Community Health Worker –
Individual Rehabilitative
Services Worker (IRS)
172V00000X
Shall be under the supervision of a Licensed Professional and Employer;
AND Shall be enrolled in one (1) of the following groups:
CMHC
SATC
Certified Addictions
Practitioner Assistant
(CAPA)
172V00000X
Shall be under the supervision of a Licensed Professional and Employer;
AND Shall be enrolled in one (1) of the following groups:
CMHC
SATC
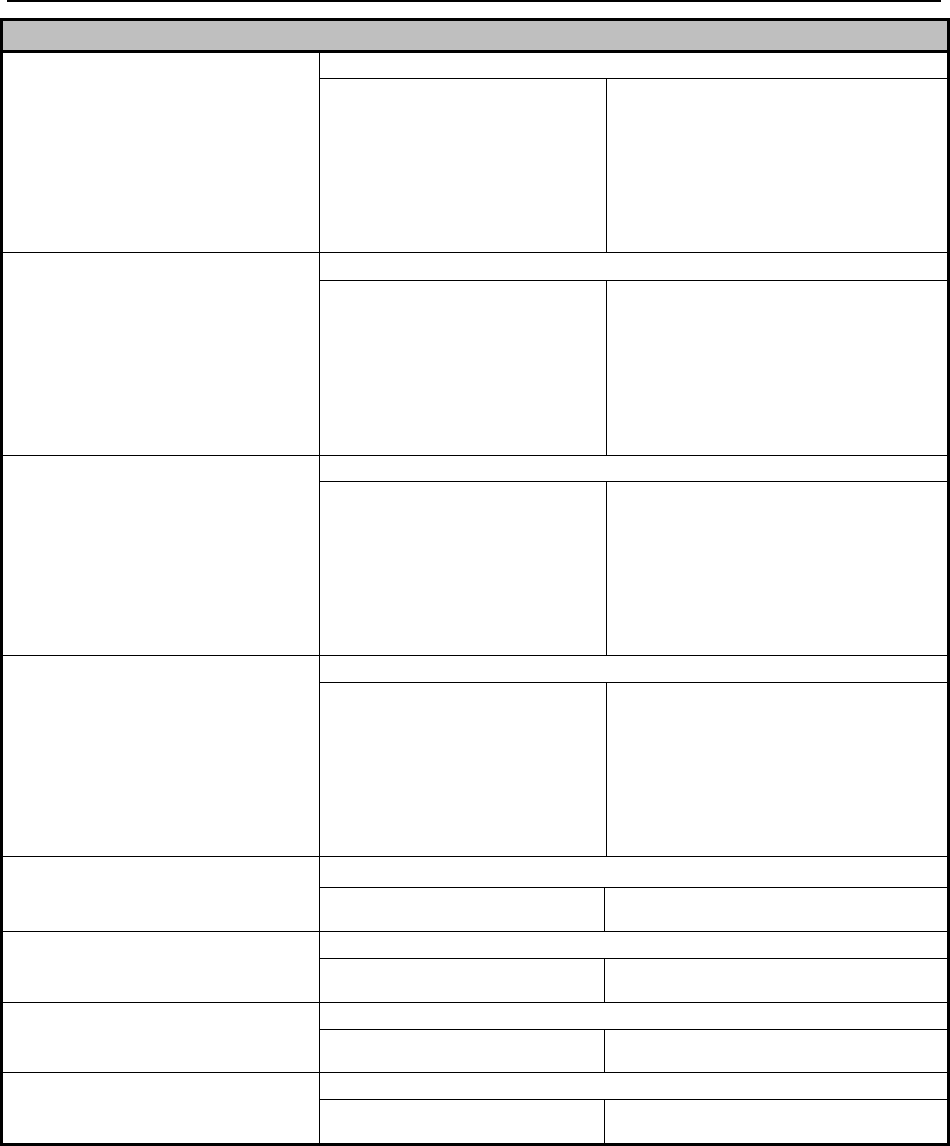
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 191 Revision 4/1/17
13.5.1 Psychiatric Services
Psychiatric Services – Medicaid covers medically necessary psychiatric and
mental health services when provided by the following practitioners:
o Psychiatrists or Physicians; or
Providers MUST be enrolled in a group
Provisional Professional
Counselor (PPC)
101Y00000X
Shall be enrolled in one (1) of the following groups:
CMHC
Psychiatry
Neuropsychologist
LPC
LAT
Developmental Center
SATC
Psychologist
Physician
LCSW
LMFT
Provisional Licensed Addictions
Therapist (PLAT)
101YA0400X
Shall be enrolled in one (1) of the following groups:
CMHC
Psychiatry
Neuropsychologist
LPC
LAT
Developmental Center
SATC
Psychologist
Physician
LCSW
LMFT
Master of Social Worker (MSW)
with Provisional License
(PCSW)
1041C0700X
Shall be enrolled in one (1) of the following groups:
CMHC
Psychiatry
Neuropsychologist
LPC
LAT
Developmental Center
SATC
Psychologist
Physician
LCSW
LMFT
Provisional Marriage and Family
Therapist (PMFT)
106H00000X
Shall be enrolled in one (1) of the following groups:
CMHC
Psychiatry
Neuropsychologist
LPC
LAT
Developmental Center
SATC
Psychologist
Physician
LCSW
LMFT
Registered Nurse (RN)
163W00000X
Shall only be enrolled in one (1) of the following groups:
CMHC
SATC
Licensed Practical Nurse (LPN)
164W00000X
Shall only be enrolled in one (1) of the following groups:
CMHC
SATC
Case Manager
172V00000X
Shall only be enrolled in one (1) of the following groups:
CMHC
SATC
Certified Peer Specialist
172V00000X
Shall only be enrolled in one (1) of the following groups:
CMHC
SATC

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 192 Revision 4/1/17
o APN/PMHNP (Advance Practice Nurse/Psychiatric Mental Health
Nurse Practitioner.
APN/PMHNP Services – Medicaid covers medically necessary psychiatric
services when provided by an APN/PMHNP.
o The APN/PMHNP must have completed a nursing education program
and national certification that prepares the nurse as a specialist in
Psychiatric/Mental Health and is recognized by the State Board of
Nursing in that specialty area of advance practice.
13.5.1.1 Psychologists
Medicaid covers medically necessary mental health and substance abuse disorder
treatment and recovery services provided by psychologists and/or the following
mental health professionals, when they are directly supervised by a licensed
psychologist:
Persons who are provisionally licensed by the Mental Health Professions
Licensing Board pursuant to the Mental Health Professions Practice Act.
Psychological residents or interns as defined by the Wyoming State Board of
Psychology Rules and Regulations.
Certified social worker or certified mental health worker, certified by the
Mental Health Professions Licensing Board pursuant to the Mental Health
Professions Practice Act.
13.5.1.2 Licensed Mental Health Professionals
Medicaid covers medically necessary mental health and substance abuse disorder
treatment and recovery services provided by Licensed Mental Health Professionals
(LMHPs). The LMHPs include Licensed Professional Counselors, Licensed Certified
Social Workers, Licensed Addictions Therapists and Licensed Marriage and Family
Therapists. LMHPs may enroll independently and must bill using their own National
Provider Identifier (NPI) or may enroll as members of a Mental Health group and are
required to bill with the group’s National Provider Identifier (NPI) as the pay to
provider, and the individual treating providers NPI as the rendering provider at the
line level.
13.5.1.3 Provisional Licensed Mental Health Professionals
Medicaid covers medically necessary mental health and substance abuse disorder
treatment and recovery services provided by Provisional Licensed Mental Health
Professionals which includes Provisional Professional Counselors, Provisional
Licensed Addictions Therapists, Master of Social Work with Provisional License, and
Provisional Marriage and Family Therapists. The Provisional Licensed Mental Health
Professionals may enroll with a CMHC or SATC, physician, psychologist, or under
the supervision of a LMHP. They must bill using their own National Provider
Identifier (NPI) or may enroll as members of a Mental Health group and are required
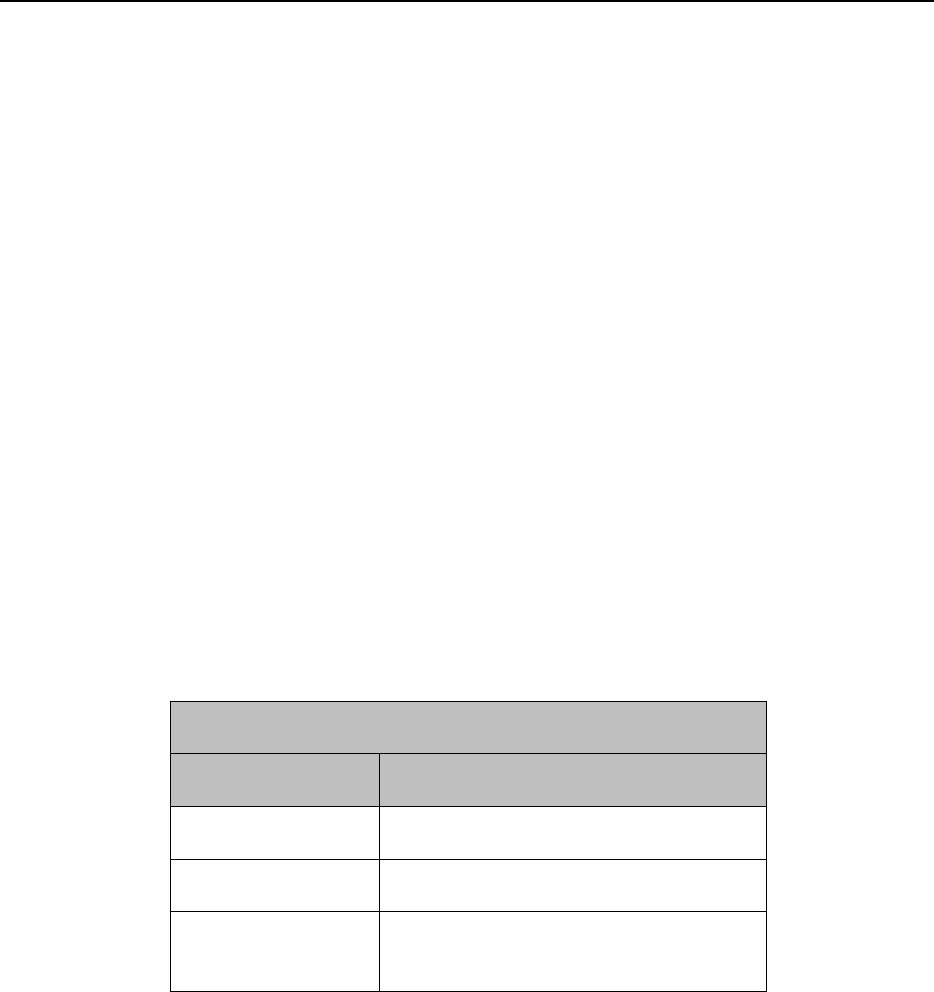
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 193 Revision 4/1/17
to bill with the group’s National Provider Identifier (NPI) as the pay to provider, and
their individual treating provider NPI as the rendering provider at the line level.
13.5.1.4 Supervision
Supervision is defined as the ready availability of the psychiatrist/physician,
psychologist or LMHPs for consultation and direction of the activities of the mental
health professionals in the office. Contact with the supervising practitioner (physician
/psychiatrist, psychologist, or LMHPs) by telecommunication is sufficient to show
ready availability, if such contact provides quality care. The supervising practitioner
maintains final responsibility for the care of the client and the performance of the
mental health professional in their office.
13.5.2 Behavioral Health Providers Eligible for Medicare Enrollment
Taxonomy codes listed in the table below can enroll in Medicare and are required to
bill Medicare prior to billing Medicaid for services rendered to clients that have
Medicare as primary insurance. If a group is enrolled with one of the taxonomy codes
listed in the table, the group MUST bill Medicare prior to billing Medicaid. For these
groups, the rendering provider treating a client with Medicare as primary MUST also
be enrolled in Medicare. If the rendering provider cannot enroll in Medicare due to
taxonomy code, they will not be able to treat clients that have Medicare as primary.
Taxonomy Codes Eligible for Medicare Enrollment
Taxonomy
Description
2084P0800X
Psychiatrist
103TC0700X
Licensed Psychologist
1041C0700X
Licensed Clinical Social Worker
(LCSW)
For behavioral health providers that cannot enroll in Medicare due to taxonomy code,
and do not belong to a group with the taxonomy codes listed in the table, these
providers can bill Medicaid directly for services rendered to clients with Medicare as
primary.
13.5.3 Covered Services
Clinical Assessment - Contact with the recipient (and collaterals as
necessary) for the purposes of completing an evaluation of the recipient’s
mental health and/or substance abuse disorder(s) to determine treatment needs

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 194 Revision 4/1/17
and establish a treatment plan. This service may include psychological testing
if indicated.
Agency or Office-based individual/family therapy services - Direct contact,
within the provider’s office or agency, with the recipient and/or collaterals for
the purpose of developing and implementing the treatment plan for an
individual or family. This service is targeted at reducing or eliminating
specific symptoms or behaviors which are related to a recipient’s mental
health or substance abuse disorder as specified in the treatment plan.
Community-based individual/family therapy services - Direct contact,
outside of the provider’s office or agency, with the recipient and/or collaterals
for the purpose of developing and implementing the treatment plan for an
individual or family. This service is targeted at reducing or eliminating
specific symptoms or behaviors which are related to a recipient’s mental
health or substance abuse disorder as specified in the treatment plan.
Group Therapy – Direct contact with two or more unrelated recipients and/or
collaterals as necessary for the purpose of implementing each recipient’s
treatment plan. This service is targeted at reducing or eliminating specific
symptoms or behaviors related to a recipient’s mental health and/or substance
abuse disorder(s) as identified in the treatment plan.
Ongoing Case management – Direct contact with a client under age 21 to
provide individual, non-clinical service which will be used to assist
individuals under the plan in gaining access to needed medical, social,
educational, and other services. Ongoing case management activities include
linkage, monitoring of follow-up, referrals, advocacy and crisis intervention
13.5.4 Non-Covered Services
Hospital liaison services that include institutional discharge functions that are
Medicaid reimbursable to the institution.
Consultation to other persons and agencies about non-clients, public
education, public relations activities, speaking engagements and education.
Clinical services not provided through face-to-face contact with the client,
other than collateral contacts necessary to develop/implement the prescribed
plan of treatment.
Residential room, board, and care.
Substance use and mental health prevention services.
Recreation and socialization services.
Vocational services and training.
Appointments not kept.
Day care.
Psychological testing done for the sole purpose of educational diagnosis or
school placement.
Remedial or other formal education.
Travel time.
Record keeping time.

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 195 Revision 4/1/17
Time spent writing test reports with the exception of three hours allowed for
report writing by a licensed psychologist for the purpose of compiling a
formal report of test findings and time spent completing reports, forms and
correspondence covered under case management services.
Time spent in consultation with other persons or organizations on behalf of a
client unless:
o The consultation is a face-to-face contact with collateral in order to
implement the treatment plan of a client receiving Rehabilitative Option
services. OR
o The consultation is a face-to-face or telephone contact in order to
implement the treatment plan of a client receiving EPSDT Mental Health
Services. OR
o The consultation is a face-to-face or telephone contact in order to
implement the treatment plan of a client receiving Targeted Case
Management Services.
Groups such as Alcoholics Anonymous, Narcotics Anonymous, and other
self-help groups, and
Driving while under the influence (DUI) classes.
Services provided by a school psychologist
13.5.5 Provisions of Mental Health and Substance Abuse Treatment
Services to Residents of Nursing Facilities
Eligibility for Medicaid mental health and substance use services provided to enrolled
clients in the nursing facility is limited to the following services under the
Rehabilitative Services Option:
Clinical Assessment
Community-Based Individual/Family Therapy
Group Therapy
Psychiatric Services
13.5.6 Billing Codes
The following matrix indicates the Psychiatrist and APN/PMHNP CPT-4 codes.
Please refer to the most current version of the CPT book.
Interpretations or explanation of results of psychiatric services to family members or
other responsible persons is included in the fee for psychotherapy.
This list of codes is not all-inclusive; it does not contain all codes that
Psychiatrists/Physicians & APN/PMHNP may bill.
Psychiatrists/Physicians & APN/PMHNP Billing Codes
CPT-4 Code
Unit
99201-99205
CPT Defined
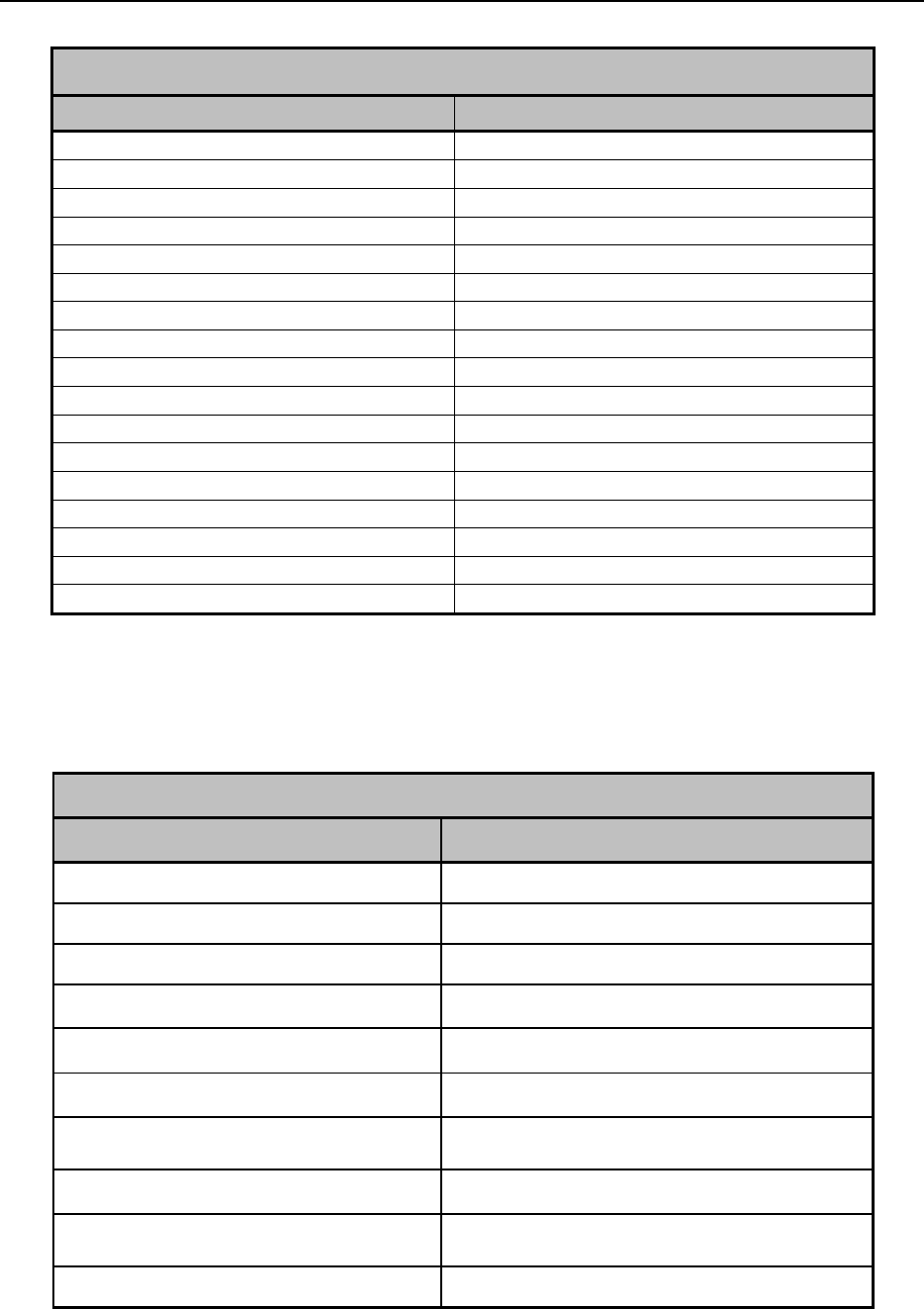
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 196 Revision 4/1/17
Psychiatrists/Physicians & APN/PMHNP Billing Codes
CPT-4 Code
Unit
99211-99215
CPT Defined
99217-99226
CPT Defined
99231-99236
CPT Defined
99238-99239
CPT Defined
99241-99245
CPT Defined
99251-99255
CPT Defined
99304-99318
CPT Defined
99324-99337
CPT Defined
99341-99359
CPT Defined
90785
CPT Defined
90791-90792
CPT Defined
90832-90834
CPT Defined
90836-90838
CPT Defined
90845-90847
CPT Defined
90849
CPT Defined
90853
CPT Defined
G9012
15 minutes
The following matrix indicates the CPT-4 codes specific to psychological services.
Please refer to the most current version of the CPT book.
Psychologist Billing Codes
CPT-4 Code
Unit
90785
CPT Defined
90791
CPT Defined
90832-90834
CPT Defined
90836-90838
CPT Defined
90845-90847
CPT Defined
90849
CPT Defined
90853
CPT Defined
96101-96125
CPT Defined
99366
CPT Defined
G9012
15 minutes
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 197 Revision 4/1/17
Licensed Mental Health Professionals have the following HCPCS Level II codes
available to them for service provision:
Billing Codes for Licensed Mental Health Professionals LMHP (LAT, LCSW,
LMFT, LPC) and supervised Mental Health Professionals working under a
physician/psychiatrist, LMHP or psychologist (CMHW, CSW and provisionally
licensed mental health professionals-PAT, PCSW, PMFT, PPC)
H0031
Clinical Assessment
H2019
Office-Based Individual/Family
Therapy
H2019+HQ modifier
Group Therapy
H2021
Community-Based
Individual/Family Therapy
G9012
Ongoing Case Management for
Clients <21
13.6 Applied Behavioral Analysis Treatment
Applied Behavior Analysis (ABA) treatments are allowable to children between the
ages of 0-20 years of age with a diagnosis of Autism Spectrum Disorder. Applied
Behavior Analysis are individualized treatments based in behavioral sciences that
focus on increasing positive behaviors and decreasing negative or interfering
behaviors to improve a variety of well-defined skills. ABA is a highly structured
program that includes incidental teaching, intentional environmental modifications,
and reinforcement techniques to produce socially significant improvement in human
behavior. ABA strategies include reinforcement, shaping, chaining of behaviors and
other behavioral strategies to build specific targeted functional skills that are
important for everyday life.
13.6.1 Covered Services
Behavior identification assessment – Direct contact with the recipient (and
collaterals as necessary) for the purposes of identification of deficient adaptive
or maladaptive behaviors, completing an evaluation of the recipient’s mental
health and/or substance abuse disorder(s) to determine treatment needs and
establish a treatment plan. This service may include psychological testing if
indicated.
Observational behavioral follow-up assessment – Direct contact with the
recipient (and collaterals as necessary) for the purposes of identification and
evaluation factors that may impede the expression of adaptive behavior. This
assessment utilizes structured observation and/or standardized and non-
standardized test to determine adaptive behavior. This service may include
psychological testing if indicated.
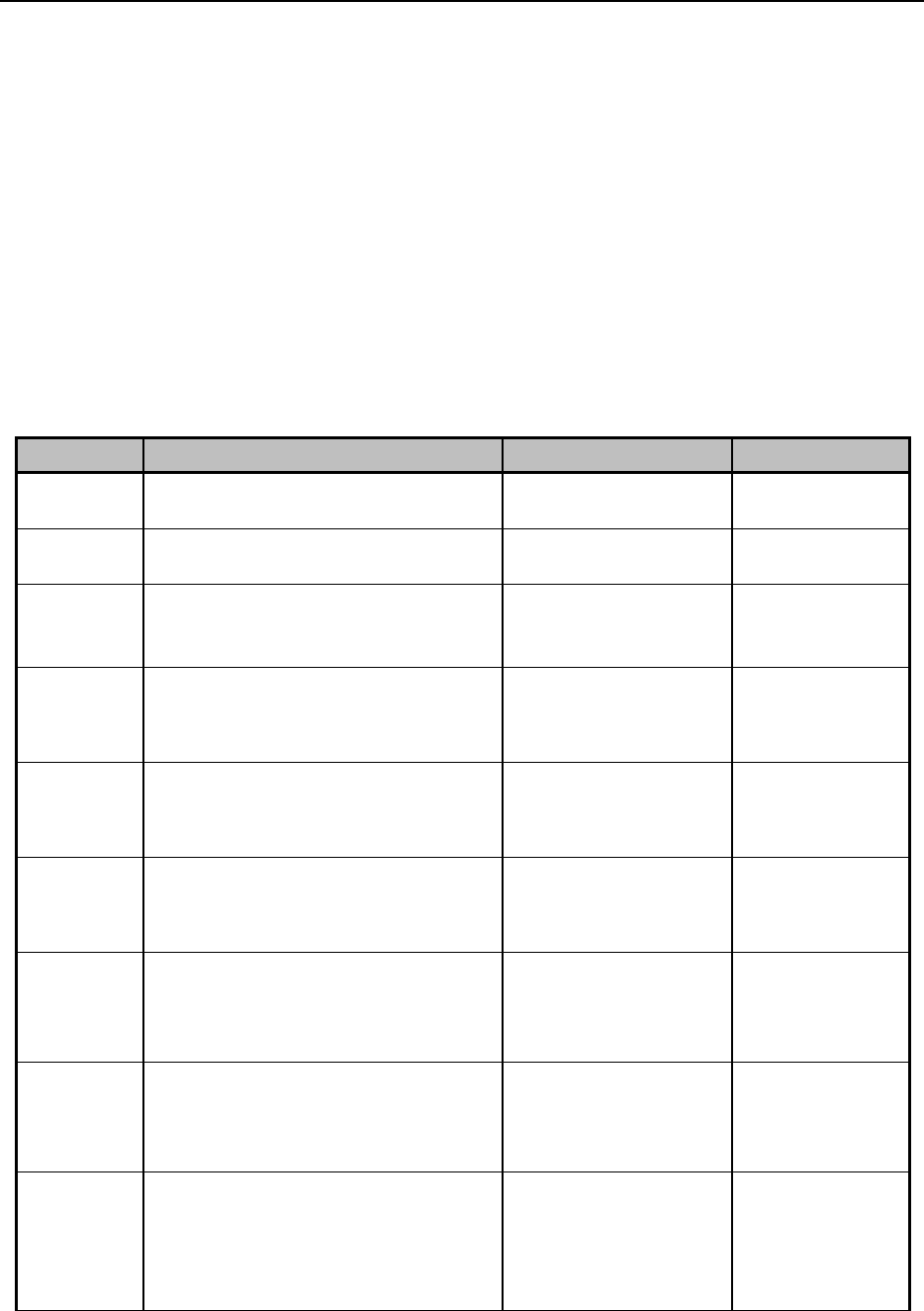
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 198 Revision 4/1/17
Adaptive behavior treatment – Direct contact with the recipient (and
collaterals as necessary) for the purpose of addressing the patient’s specific
target problems and treatment goals as defined by the assessments. Adaptive
behavior treatment is based on principles including analysis and alteration of
contextual events and motivating factors, stimulus-consequence strategies and
replacement behavior, and monitoring of outcome metrics.
Family adaptive behavior treatment guidance – Direct contact with the
family/caregiver to provide specialized training and education to assist with
the child’s needs and development. The provider will observe, instruct and
train the family/caregivers on the child’s development status, and techniques
and strategies to promote the child’s development that is established in the
treatment plan.
Code
Description
Taxonomy Allowed
Limits
0359T
Behavior identification assessment
+ plan of care.
103K00000X
Twice A Year
0360T
Observational Follow Up
Assessment - 1st 30 minutes.
103K00000X
30 Minutes
0361T
Observational Follow Up
Assessment - Additional 30
minutes.
103K00000X
30 Minutes
0364T
Behavior treatment by protocol
administered by technician first 30
minutes.
106E00000X,
106S00000X,
103K00000X
30 Minutes
0365T
Behavior treatment by protocol
administered by technician each
additional 30 minutes.
106E00000X,
106S00000X,
103K00000X
30 Minutes
0366T
Group behavior treatment by
protocol administered by
technician first 30 minutes.
106E00000X,
106S00000X,
103K00000X
30 Minutes
0367T
Group behavior treatment by
protocol administered by
technician additional 30 minutes /
Group.
106E00000X,
106S00000X,
103K00000X
30 Minutes
0368T
Behavior treatment with protocol
modification administered by
physician or other qualified health
care professional first 30 minutes.
103K00000X
Quarterly
0369T
Behavior treatment with protocol
modification administered by
physician or other qualified health
care professional each additional
30 minutes.
103K00000X
30 Minutes
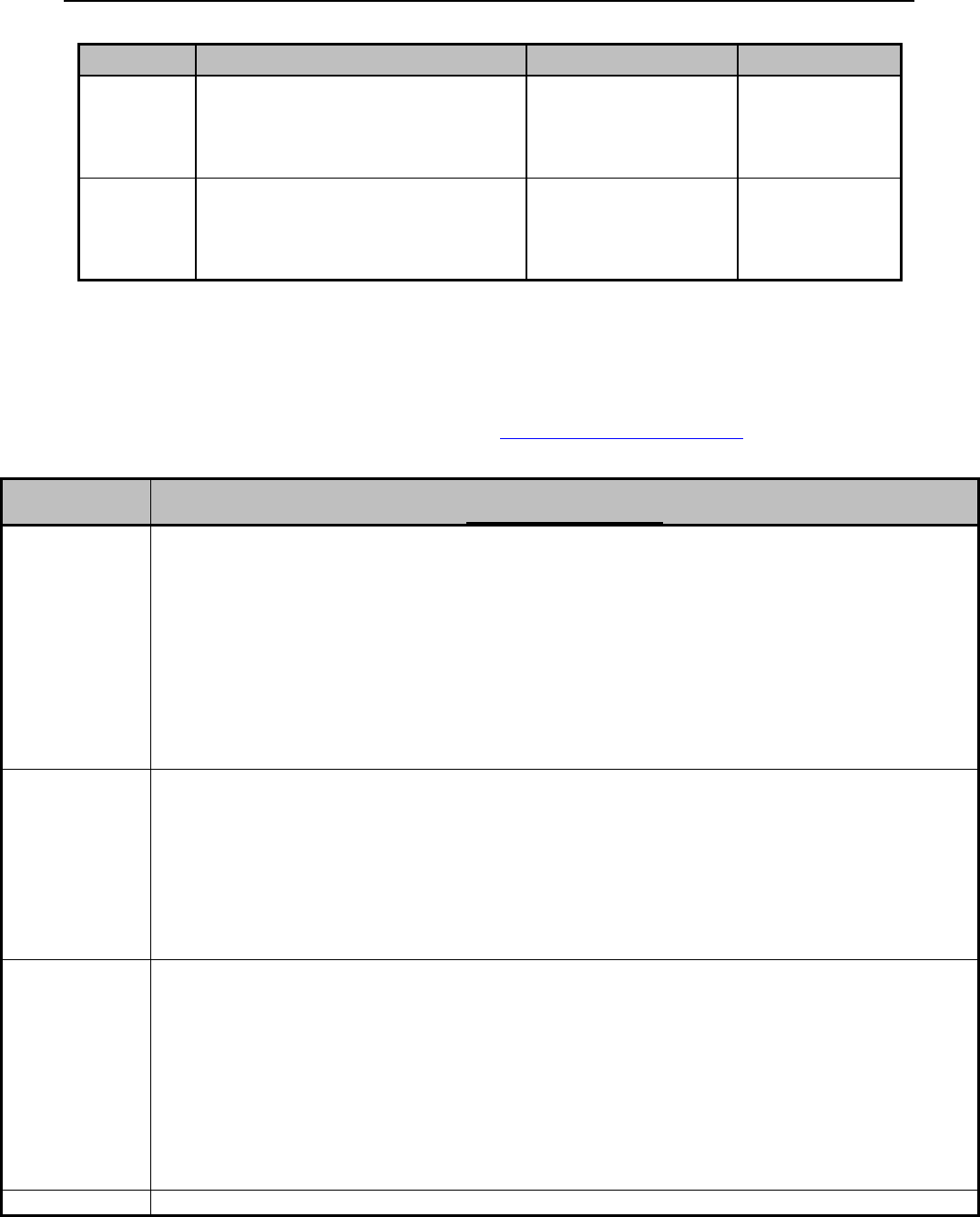
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 199 Revision 4/1/17
Code
Description
Taxonomy Allowed
Limits
0370T
Family behavior treatment
guidance administered by qualified
health care professional 60 - 75
min.
103K00000X
60-75 Minutes
0371T
Family behavior treatment
guidance administered by qualified
health care professional 60 - 75
min. / Group.
103K00000X
60-75 Minutes
13.6.2 Applied Behavior Analysis Providers
Applied Behavior Analysis Providers must follow the requirements set by the Board
of Certified Behavior Analysts as per http://bacb.com/credentials/ in order to provide
applied behavior analysis treatment services to Wyoming Medicaid clients.
Name
Abbreviation and Requirements
http://bacb.com/credentials/
Board Certified
Behavior
Analysts –
Doctoral
103K00000X
BCBA-D
Be actively certified as a BCBA in Good Standing
Have earned a degree from a doctoral program accredited by the Association for Behavior Analysis
International or;
A certificant whose doctoral training was primarily behavior-analytic in nature, but was not obtained from an
ABAI-accredited doctoral program, may qualify for the designation by demonstrating that his or her doctoral
degree met the following criteria:
(a.)The degree was conferred by an acceptable accredited institution; AND
(b.) The applicant conducted a behavior-analytic dissertation, including at least 1 experiment; AND
(c.) The applicant passed at least 2 behavior analytic courses as part of the doctoral program of study; AND
(d.) The applicant met all BCBA coursework requirements prior to receiving the doctoral degree.
Board Certified
Behavior
Analysts
103K00000X
BCBA
Option 1 requires an acceptable graduate degree from an accredited university, completion of acceptable
graduate coursework in behavior analysis, and a defined period of supervised practical experience to apply for
the BCBA examination.
Option 2 requires an acceptable graduate degree from an accredited university, completion of acceptable
graduate coursework in behavior analysis that includes research and teaching, and supervised practical
experience to apply for BCBA examination.
Option 3 requires an acceptable doctoral degree that was conferred at least 10 years ago and at least 10 years
post-doctoral practical experience to apply for the BCBA examination.
Board Certified
Assistant
Behavior
Analyst
106E00000X
BCaBA
1. Degree
Applicant must possess a minimum of a bachelor’s degree from an acceptable accredited institution. The
bachelor’s degree may be in any discipline.
2. Coursework
Course work must come from an acceptable institution and cover the required content outlined in the BACB’s
Fourth Edition Task List and Course Content Allocation documents.
3. Experience
Applicants must complete experience that fully complies with all of the current Experience Standards.
4. Examination
Applicants must take and pass the BCaBA examination.
Registered
RBT
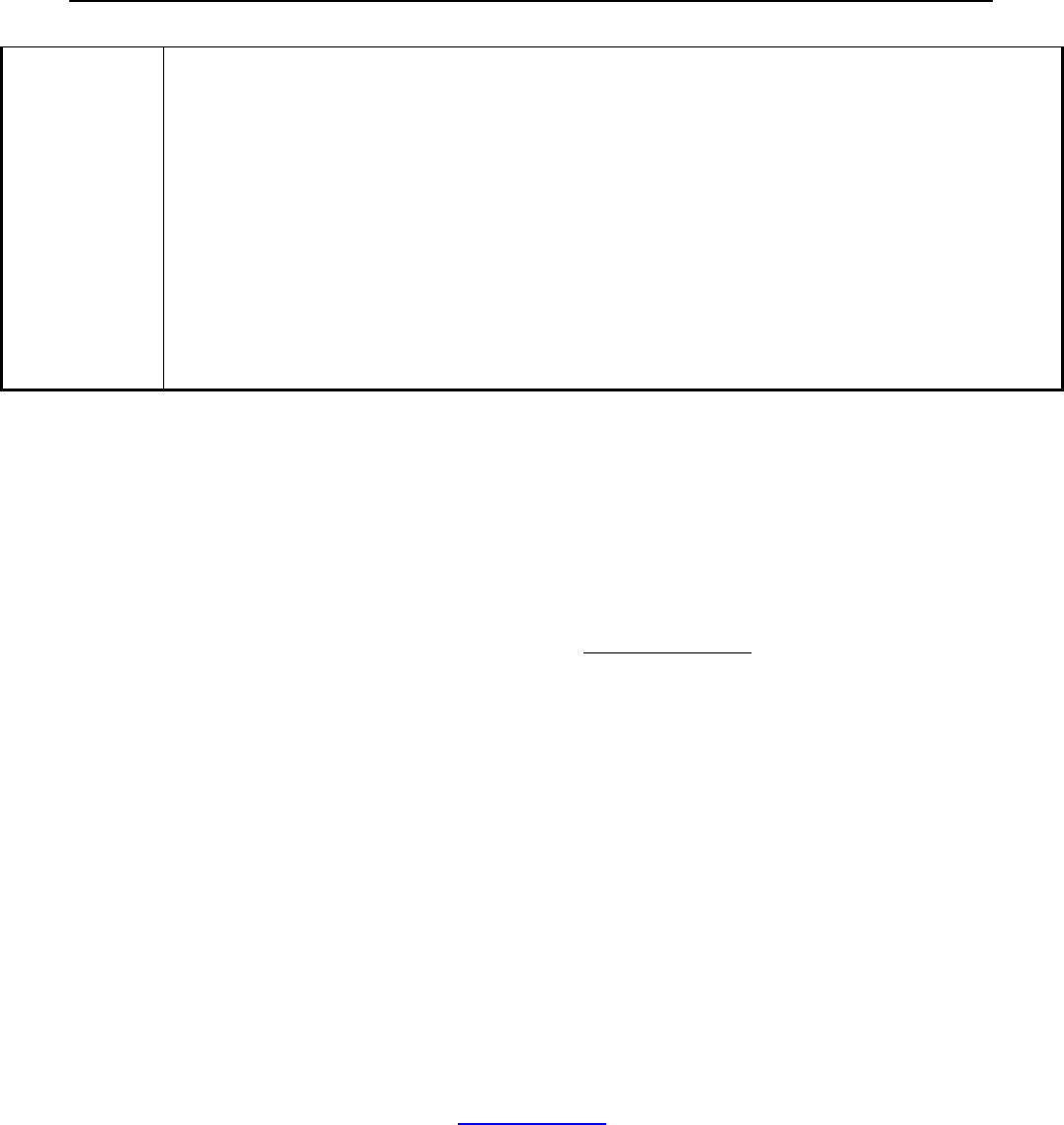
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 200 Revision 4/1/17
Behavior
Technician
106S00000X
1. Age and Education
RBT applicants must be at least 18 years of age and have demonstrated completion of high school or
equivalent/higher.
2. Training Requirement
The 40-hour RBT training is not provided by the BACB but, rather, is developed and conducted by BACB
certificants.
3. The RBT Competency Assessment
The RBT Competency Assessment is the basis for the initial and annual assessment requirements for the RBT
credential.
4. Criminal Background Registry Check
To the extent permitted by law, a criminal background check and abuse registry check shall be conducted on
each RBT applicant no more than 45 days prior to submitting an application.
5. RBT Examination
All candidates who complete an RBT application on or after December 14, 2015 will need to take and pass an
examination before credential is awarded.
13.7 Limitations for Behavioral Health Services
The report writing segment, for the purpose of compiling a formal report of
psychological test findings, is limited to a maximum of three (3) hours.
Span billing is not allowed for fee for service behavioral health services. Each date of
service must be billed on its own separate line.
The following conditions do not meet the medical necessity guidelines, and therefore
will not be covered:
Clients age 21 and over are limited to restorative/rehabilitative services only.
Restorative/rehabilitative services are services that assist an individual in
regaining or improving skills or strength.
Maintenance therapy can be provided for clients age 20 and under.
Services are not medically necessary.
Treatment whose purpose is vocationally or recreationally based.
Diagnosis or treatment in a school-based setting.
13.8 Cap Limits
Medicaid clients age 21 and over will be limited to 20 behavioral health service visits
per year. If the client has exceeded the Medicaid limits on behavioral health visits, the
provider may bill him/her, or request the cap limit be waived, as long as the services
are still medically necessary (6.9, Cap Limits).
13.9 Documentation Requirements for All Behavioral Health
Providers

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 201 Revision 4/1/17
13.9.1 Provider Agreement
The Provider Agreement requires that the clinical records fully disclose the extent of
treatment services provided to Medicaid clients. The following elements are a
clarification of Medicaid policy regarding documentation for medical records:
The record shall be typed or legibly written.
The record shall identify the client on each page.
Entries shall be signed and dated by the qualified staff member providing
service.
A mental health/substance use therapeutic record note must show length of
service including time in and time out (Standard or Military time).
The record shall contain a preliminary working diagnosis and the elements of
a history and mental status examination upon which the diagnosis is based.
All services, as well as the treatment plan, shall be entered in the record. Any
drugs prescribed by medical personnel affiliated with the provider, as part of
the treatment, including the quantities and the dosage, shall be entered in the
record.
The record shall indicate the observed mental health/substance abuse
therapeutic condition of the client, any change in diagnosis or treatment, and
client’s response to treatment. Progress notes shall be written for every contact
billed to Medicaid.
The record must include a valid consent for treatment signed by the client or
guardian.
Pursuant to Wyoming Medicaid Rules, Chapter 3-Provider Participation,
“Documentation requirements,” a provider must have completed all required
documentation, including required signatures, before or at the time the provider
submits a claim to the Division (Division of Healthcare Financing, Medicaid).
Documentation prepared or completed after the submission of a claim will be deemed
to be insufficient to substantiate the claim and Medicaid funds shall be withheld or
recovered.
13.9.2 Documentation of Services
Documentation of the services must contain the following:
Name of the client
Identify the covered services provided and the procedure code billed to
Medicaid
Identify the date, length of time (start and end times in standard or military
format), and location of the service
Identify all persons involved
Be legible and contain documentation that accurately describes the services
rendered to the client and progress towards identified goals
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 202 Revision 4/1/17
Full signature, including licensure or certification of the treating provider
involved
Providers shall not sign for a service prior to the service being completed
No overlapping behavioral health services
NOTE: When providing behavioral health services to a Medicaid client, the
documentation kept must be accurate with the date and times the services were
rendered (3.11 Record Keeping, Retention and Access, 13.9 Documentation
Requirements for All Behavioral Health Providers). Behavioral health services cannot
overlap date and time for a client. For example, a client being seen for group therapy
on February 28th from 11:00 to 12:00 cannot also be seen for targeted case
management on February 28th from 11:00 to 12:00. These are overlapping services
and cannot be billed to Medicaid. The importance of proper documentation of
services is important to differentiate the times of services being rendered, as you
cannot bill times on a CMS 1500.
13.9.3 Client Records
Providers of mental health/substance use services under the Medicaid shall maintain
clinical and financial records in a manner that allows verification of service provision
and accuracy in billing for services. Billed services not substantiated by clinical
documentation shall be retroactively denied payment. The provider shall be
responsible for reimbursing any Medicaid payments that are denied retroactively.
Late entries made to the client’s record are allowable to supplement the clinical
record. Late entries are not allowable for the purpose of satisfying record keeping
requirements after billing Wyoming Medicaid.
13.9.3.1 Requirements
In addition to the general documentation requirements listed above, the following
requirements shall be met:
There shall be a separate clinical note made in each client’s clinical record for
every treatment contact that is to be billed to Medicaid. More frequent
documentation is acceptable and encouraged
o A separate progress note in the clinical record for each face-to-face
contact with the client and with others who are collaterals to
implement the client’s treatment plan. Progress notes shall include:
The name of the Medical reimbursable service rendered and
procedure code billed to Medicaid
The date, length of time (time in and time out in standard or
military time format) and location of the contact
Persons involved (in lieu or in addition to the client)
Summary of client condition, issues addressed, and client
progress in meeting treatment goals
Signature, date and credentials of treating staff member
o The note for Psychosocial Rehabilitation shall document:

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 203 Revision 4/1/17
The date and length of time (time in and time out in standard or
military time format) of each day’s contact
A separate progress note describing therapeutic activities
provided, the procedure code billed to Medicaid, and client’s
progress in achieving the treatment goal(s) to be accomplished
through psychosocial rehabilitation
Signature, date and credentials of treating staff member
Co-signature of the primary therapist on progress notes for
services provided by non-licensed, certified staff or qualified
case managers
o Individual Rehabilitative Services (IRS), a separate chart note shall
document each contact to be billed, including:
The date and length of time (time in and time out in standard or
military time format) of each day’s contact
Activities of the skill trainer and activities of the client
Any significant client behavior observed
The date and signature of the skill trainer
The location of service and the procedure code billed to
Medicaid
The signature, date and credentials of the primary therapist
o Peer Specialist Services, a separate chart note shall document for each
contact to be billed, including:
The date and length of time (time in and time out in standard or
military time format) of each day’s contact
Activities of the skill trainer and activities of the client
Any significant client behavior observed
The date and signature of the skill trainer
The location of service and the procedure code billed to
Medicaid
The signature, date and credentials of the primary therapist
o Ongoing Case Management Services and Targeted Case Management
Services, a separate chart note shall document each contract to be
billed, including:
The date and length of time (time in and time out in standard or
military time format) of each day’s contact
The date and signature of the case manager
Type and description of each service and the procedure code
billed to Medicaid
Each note shall show length of service, time in and time out in standard or
military format.
The provider shall adhere to clinical records standards defined in Section 3.5.
The provider shall maintain an individual ledger account for each Medicaid
client who receives services. The ledger account shall indicate, at a minimum:
o The length of contact rounded to the nearest 15- minute unit, per
billing instructions. If seven (7) minutes or less of the next fifteen (15)

Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 204 Revision 4/1/17
minute unit is utilized, the unit must be rounded down. However, if
eight (8) or more minutes of the next fifteen (15) minute unit are
utilized, the units can be rounded up. Date ranges are not acceptable. O
The date and type of each treatment contact.
o The appropriate Medicaid charge.
o Date that other third-party payers were billed and the result of the
billing. Services noted on the individual ledger account and billed to
Medicaid shall be substantiated by the clinical record documentation.
13.9.3.2 Clinical Records Content Requirement
Each Medicaid provider shall establish requirements for the content, organization,
and maintenance of client records. The content of clinical records shall include, at a
minimum:
Documentation of client consent to treatment at the agency. If an adult client
is under guardianship, consent shall be obtained from the guardian. In the case
of minors, consent shall be obtained from a parent or the guardian. Wyoming
Medicaid shall not reimburse for services delivered before a valid consent is
signed.
A client fee agreement, signed by the client or guardian. For Medicaid, this
agreement shall include authorization to bill Medicaid, and other insurance if
applicable, using the following statement, “I authorize the release of any
treatment information necessary to process Medicaid/insurance claims.”
A specific fee agreement for any Medicaid non-covered service, and the fee
that an enrolled client agrees to pay.
Documentation that each client has been informed of his or her client rights.
A clinical assessment completed prior to the provision of treatment services
which shall include at a minimum:
o The specific symptoms/behaviors of a mental/substance use disorder
which constitute the presenting problem.
o History of the mental/substance use disorder and previous treatment.
o Family and social data relevant to the mental/substance use disorder.
o Medical data, including a list of all medications being used, major
physical illnesses, and substance use (if not the presenting problem).
o Mental status findings.
o A diagnostic interpretation.
o A DSM (current edition) diagnosis
A diagnostic interpretation or a treatment plan shall be completed prior to or
within five (5) working days of the third face-to-face contact with a licensed
mental health professional.
Properly executed release of information, as applicable, and chart
documentation of information received or released as a result of the written
client consent.
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 205 Revision 4/1/17
Testing, correspondence, and like documents or copies.
For any client receiving ten or more therapeutic contacts, a discharge
summary which includes each type of Medicaid service received client
progress in achieving treatment goals, and plans for follow-up, necessary. The
discharge summary shall be completed within 90 days of the last contact. Any
clinical record shall document the reason for case closure.
13.9.4 Treatment Plans
Treatment plans for services must be based on a comprehensive assessment of an
individual’s rehabilitation needs, including diagnoses and presence of a functional
impairment in daily living, and be reviewed every 90-days.
Treatment plans must also:
Be developed by qualified provider(s) working within the State scope of
practice acts with significant input from the client, client’s family, the client’s
authorized healthcare decision maker and/or persons of the client’s choosing;
Ensure the active participation of the client, client’s family, the client’s
authorized healthcare decision maker and/or persons of the client’s choosing
in the development, review and modification of these goals and services;
Specify the client’s rehabilitation goals to be achieved, including recovery
goals for persons with mental health and/or substance related disorders;
Specify the mental health and/or substance related disorder that is being
treated;
Specify the anticipated outcomes within the goals of the treatment plan;
Indicate the type, frequency, amount and duration of the services;
Be signed by the individual responsible for developing the rehabilitation plan;
Specify a timeline for reevaluation of the plan, based on the individual’s
assessed needs and anticipated progress, but not longer than 90-days;
Document that the individual or representative participated in the
development of the plan, signed the plan, and received a copy of the
rehabilitation plan; and
Include the name of the individual; and
The date span of services the treatment plan covers; and
The progress made toward functional improvement and attainment of the
individual’s goals.
13.9.5 Billing Requirements
In order to obtain Medicaid reimbursement for services, the following standards must
be observed.
The services must be medically necessary and follow generally accepted
standards of care.
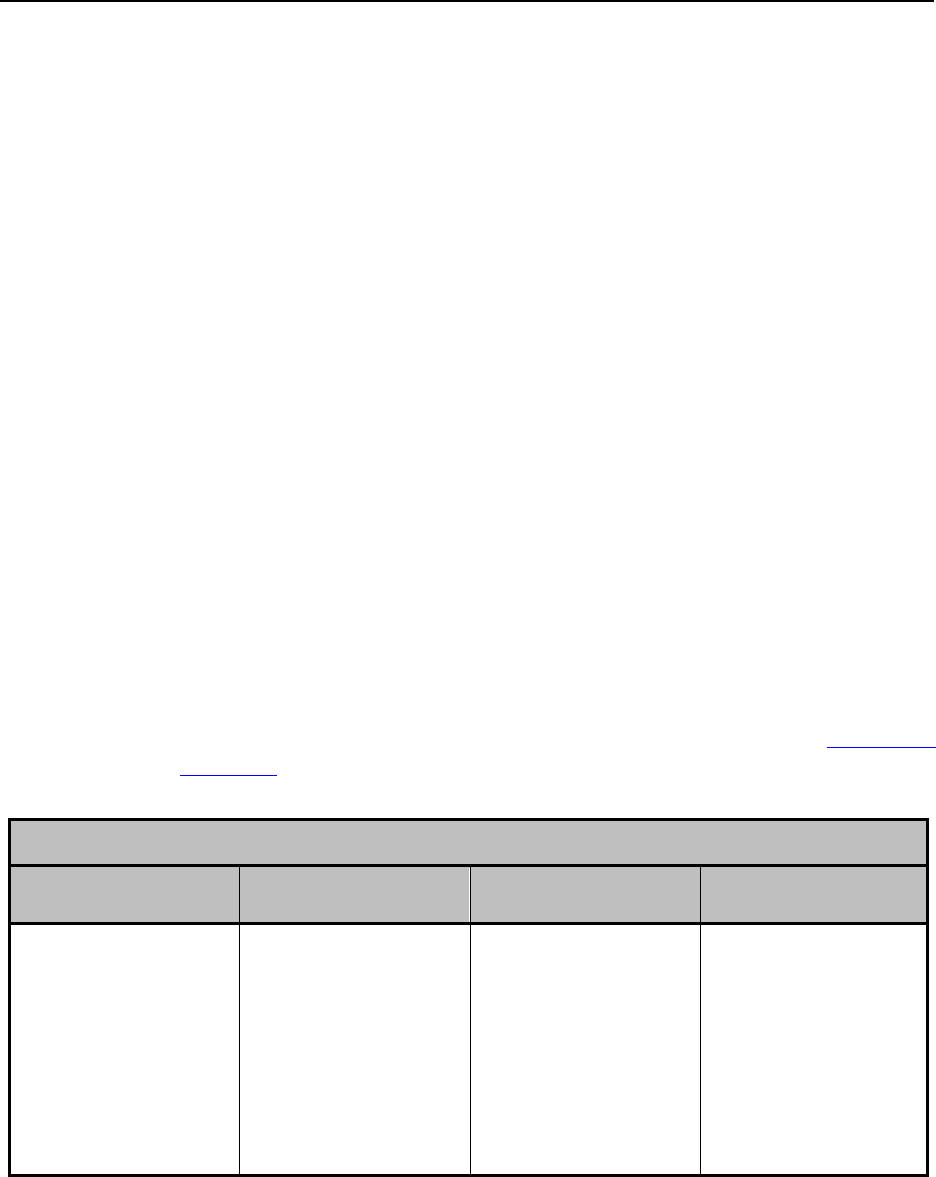
Covered Services –_Behavioral Health_____________________________________________
Ch. 13 Index 206 Revision 4/1/17
Bill using the appropriate code set.
The service must be a service covered by Medicaid.
Claims must be made according to Medicaid billing instructions.
13.9.6 Time and Frequency
Time and frequency are required on all documentation and must be specific so time in
and time out must be reflected on the document in standard or military format. Time
can be a unit of 15 minutes depending on the Current Procedural Terminology (CPT)
code or Healthcare Common Procedure Coding System (HCPCS) Level II code used
to bill the service. For example, if the code is a fifteen (15) minute unit, then follow
the guidelines for rounding to the nearest unit. If seven (7) minutes or less of the next
15 minute unit is utilized, the unit must be rounded down. However, if eight (8) or
more minutes of the next 15 minute unit are utilized, the units can be rounded up.
Date ranges are not acceptable. Please refer to the CPT and HCPCS coding books for
more information on how to round a unit per code.
13.9.7 Pre-Admission Screening and Resident Review (PASRR)
Assessments
13.9.7.1 Billing Requirements
Submit PASRR Level II claims to the Medicaid Program.
PASRR Level II assessments should be sent to WYhealth (2.1, Quick
Reference).
PASRR Level II Billing Code(s)
HCPCS Level II
Code
1 Unit Equals
Description
Taxonomies
Allowed
T2011
Per Visit
PASRR Level II
Psychiatrist
101Y00000X,
101YP2500X,
103G00000X,
103TC0700X,
1041C0700X,
106H00000X, 20
(Physicians),
2084P0800X,
364SP0808X

Covered Services – Children’s Mental Health Waiver________________________________
Ch. 13 Index 207 Revision 4/1/17
Chapter Fourteen – Covered Services – Children’s Mental Health
Waiver
14.1 Children’s Mental Health Waiver (CMHW) Services as Administered by
Magellan healthcare, Inc., Through the Care Management Entity ................... 208
14.2 Child and Adolescent Service Intensity Instrument (CASII) Evaluations ........ 208
14.2.1 Requirements ..................................................................................................... 208
14.2.2 Billing Requirements ......................................................................................... 209
Covered Services – Children’s Mental Health Waiver________________________________
Ch. 13 Index 208 Revision 4/1/17
14.1 Children’s Mental Health Waiver (CMHW) Services as
Administered by Magellan Healthcare, Inc., Through the
Care Management Entity
The Care Management Entity (CME) is a short-term home and community based
program that utilizes an intensive care coordination model (high fidelity wraparound)
designed to provide a community-based alternative for youth with serious emotional
disturbance who might otherwise be hospitalized and whose parents may be required
to relinquish custody of their child in order for them to receive needed mental health
treatment and services. The Children’s Mental Health Waiver via the CME seeks to
(1) prevent custody relinquishment in order for youth to receive mental health
treatment; (2) prevent or reduce the length of costly psychiatric hospital stays; and (3)
provide a mechanism to offer mental health support services to youth with serious
emotional disturbance and their families in identified service areas. The Children’s
Mental Health Waiver is not a long-term care waiver. Children who are not
financially eligible for Medicaid and who meet the clinical eligibility criteria for Care
Management Entity (CME) services may apply for CME participation through the
CMHW.
For additional information on the CME contact Magellan at:
1-855-883-8740
TDD/TTY: 1-800-424-6259
http://www.magellanofwyoming.com
To apply for participation in the CME through the Children’s Mental Health Waiver
please refer to the Children’s Mental Health Waiver website at:
https://health.wyo.gov/healthcarefin/medicaid/childrens-mental-health-waiver/
14.2 Child and Adolescent Service Intensity Instrument (CASII)
Evaluations
CASII evaluations are performed for waiver applicants initially as a step in the
eligibility process in order to receive waiver services, then again every 12-months for
re-certification.
14.2.1 Requirements
Reimbursement for CASII evaluations will be made to providers approved by the
Children’s Mental Health Waiver program, and only after all billing requirements are
met.
Covered Services – Children’s Mental Health Waiver________________________________
Ch. 13 Index 209 Revision 4/1/17
14.2.2 Billing Requirements
Upon completion of the CASII the provider must submit the following
documentation to the Children’s Mental Health Waiver staff:
o CASII scoring sheet– completed and signed.
o CASII instrument identifying selected letter items for each numbered
anchor point.
o Waiver services application.
Claims cannot be submitted for at least 72-hours after all required
documentation is sent to Children’s Mental Health.
Clients who are not eligible for any other Medicaid plan will be made eligible
for the date of the CASII evaluation for the processing of these claims. The
CASII score sheet needs to contain the following information to add the client
to the system for claims payment:
o Client Name.
o Address.
o Social Security Number.
o Date of Birth.
All services billed in relation to the CASII evaluation will be billed on a single
date of service. This date should be the date listed with the evaluators’
signature on the submitted forms.
o Example – The CASII evaluation process was conducted on August 1,
August 8, and August 9. The CASII evaluation was signed and
submitted on August 9 therefore one (1) unit will be billed with a date
of service of August 9.
CASII Evaluation Procedure Codes
Code
Modifier(s)
1 Unit Equals
Procedure Quantity
Description
H0002
1 evaluation
1 Max Unit
CASII Evaluation
CASII evaluators, who assist the client and/or their family to complete the full
Care Management Entity (CME) enrollment packet, including completion of
the application and assistance with arranging completion of the level of care
form, may add the modifier “CG” to the procedure code H0002 for a
reimbursement increase of 25%.
Supporting documentation for the use of modifier CG with procedure code H0002
includes an accurately completed ECSII or CASII evaluation, a completed CME
application, and a completed level of care form submitted to and accepted by the
CME.

Covered Services –_Chiropractic Services__________________________________________
Ch. 15 Index 210 Revision 4/1/17
Chapter Fifteen – Covered Services – Chiropractic Services
15.1 Coverage Indications ......................................................................................... 211
15.2 Definitions ......................................................................................................... 211
15.3 Medical Necessity ............................................................................................. 211
15.4 Limitations ......................................................................................................... 212
15.5 Covered CPT Codes .......................................................................................... 212
15.6 Documentation Requirements ........................................................................... 213
Covered Services –_Chiropractic Services__________________________________________
Ch. 15 Index 211 Revision 4/1/17
15.1 Coverage Indications
Coverage of chiropractic service is specifically limited to treatment by means of
manual manipulation, i.e., by use of the hands. Manual devices (i.e., those that are
hand-held with the thrust of the force of the device being controlled manually) may
be used by chiropractors in performing manual manipulation of the spine, however,
no additional payment is available for use of the device, nor does Medicaid recognize
an extra charge for the device itself.
The word "correction" may be used in lieu of "treatment." The following terms, or
combination of may be used to describe manual manipulation as defined above:
Spine or spinal adjustment by manual means;
Spine or spinal manipulation;
Manual adjustment; and
Vertebral manipulation or adjustment.
15.2 Definitions
Acute: A patient's condition is considered acute when the patient is being
treated for a new injury, identified by x-ray or physical exam as specified
above. The result of chiropractic manipulation is expected to be an
improvement in or arrest of the progression of the patient's condition.
Maintenance therapy: Maintenance therapy includes services that seek to
prevent disease, promote health and prolong and enhance the quality of life, or
maintain or prevent deterioration of a chronic condition. When further clinical
improvement cannot reasonably be expected from continuous ongoing care,
and the chiropractic treatment becomes supportive rather than corrective in
nature, the treatment is then considered maintenance therapy. Maintenance
therapy is not a Wyoming Medicaid covered service.
15.3 Medical Necessity
ALL of the following criteria must be met to substantiate medical necessity:
1. The client has a neuromusculoskeletal disorder.
2. The medical necessity for treatment is clearly documented.
3. Improvement is documented within the initial two (2) weeks of chiropractic
care.
The service will NOT be considered medically necessary if:
1. No improvement is documented within the initial two (2) weeks unless the
treatment is modified.

Covered Services –_Chiropractic Services__________________________________________
Ch. 15 Index 212 Revision 4/1/17
2. No improvement is documented within 30-days despite modification of
chiropractic treatment.
3. The maximum therapeutic benefit has been achieved.
4. The chiropractic manipulation is being performed in asymptomatic person or
persons without an identifiable clinical condition.
5. The chiropractic care is occurring in persons whose condition is neither
regressing nor improving.
15.4 Limitations
Evaluation & Management (E & M) Cap Limits:
Medicaid clients 21 years of age and older are subject to a service cap limit of
12 office/outpatient hospital visits per calendar year. This includes all E & M
procedure codes.
Chiropractic Services Cap Limits:
Medicaid clients are subject to a service cap limit of 20 chiropractic visits per
calendar year.
15.5 Covered CPT Codes
99201-99205, 99211-99215
These office visit codes are subject to a $2.45 co-pay for adults >21 years of
age.
A full schedule of co-pays and exceptions is located in Chapter 6 of the CMS
1500 Manual.
98940, 98941, 98942
70100 -77086 Diagnostic Radiology codes
Refer to the Wyoming Medicaid CMS 1500 Manual for additional
information regarding radiology services.
Some diagnostic radiology services require prior authorization. A complete
list of codes and requirements may be viewed at WYhealth or by contacting
(888)545-1710 prompt 4.

Covered Services –_Chiropractic Services__________________________________________
Ch. 15 Index 213 Revision 4/1/17
15.6 Documentation Requirements
1. History as stated above.
2. Description of the present illness including:
Mechanism of trauma.
Quality and character of symptoms/problem.
Onset, duration, intensity, frequency, location, and radiation of
symptoms.
Aggravating or relieving factors.
Prior interventions, treatments, medications, secondary complaints.
Symptoms causing client to seek treatment.
These symptoms must bear a direct relationship to the level of subluxation. The
symptoms should refer to the spine (spondyle or vertebral), muscle (myo), bone
(osseo or osteo), rib (costo or costal) and joint (arthro), and be reported as pain
(algia), inflammation (itis), or as signs such as swelling, spasticity, etc. Vertebral
pinching of spinal nerves may cause headaches, arm, shoulder, and hand problems as
well as leg and foot pains and numbness. Rib and rib/chest pains are also recognized
symptoms, but in general other symptoms must relate to the spine as such. The
subluxation must be causal, i.e., the symptoms must be related to the level of the
subluxation that has been cited. A statement in the client's file/chart that there is
"pain" is insufficient. The location of pain must be described and whether the
particular vertebra listed is capable of producing pain in the area determined.
3. Evaluation of musculoskeletal/nervous system through physical examination.
4. Diagnosis (ICD-10 diagnosis codes will be required for dates of service
10/1/2015 and after): The primary diagnosis must be subluxation, including
the level of subluxation, either so stated or identified by a term descriptive of
subluxation. Such terms may refer either to the condition of the spinal joint
involved or to the direction of position assumed by the particular bone named.
5. Treatment Plan: The treatment plan should include the following:
Recommended level of care (duration and frequency of visits).
Specific treatment goals.
Objective measures to evaluate treatment effectiveness.
6. Date of the initial treatment.

Covered Services –_Developmental Centers________________________________________
Ch. 16 Index 214 Revision 4/1/17
Chapter Sixteen – Covered Services – Developmental Centers
16.1 Development Centers ........................................................................................ 215
16.2 General Documentation Requirements ............................................................. 215
16.3 Location ............................................................................................................. 215
16.4 Time and Frequency .......................................................................................... 215
16.5 Missed Appointments/Make-up Session ........................................................... 216
16.6 Diagnosis ........................................................................................................... 216
16.7 Covered Services ............................................................................................... 216
16.8 Billing Requirements ......................................................................................... 218
Covered Services –_Developmental Centers________________________________________
Ch. 16 Index 215 Revision 4/1/17
16.1 Development Centers
A developmental center is a public or privately funded facility, which provides
services to clients (infants/toddlers or preschool age children, ages 0-5) with
developmental disabilities who have been determined to require early intervention
programs, care, treatment and supervision in an appropriate setting.
A licensed practitioner is a person that is licensed within the state of Wyoming to
perform specialized services (e.g., physician or nurse practitioner).
16.2 General Documentation Requirements
The Provider Agreement requires that medical records fully disclose the extent of
services provided to Medicaid clients. The following elements are a clarification of
Medicaid policy regarding documentation for medical records (3.11.1,
Requirements):
The record must be typed or legibly written.
The record must identify the client on each page.
The record must contain a preliminary working diagnosis and the elements of
a clinical assessment upon which the diagnosis is based.
All services, as well as the treatment plan, must be entered in the record.
The record must indicate the observed condition of the client, the progress at
each visit, any change in diagnosis of treatment, and the client’s response to
treatment. Progress notes must be written for every service billed to Medicaid.
The type, frequency and duration of service must be specified in the treatment plan.
All services provided must track back to the client’s treatment plan.
16.3 Location
If the location on the physician’s order is different from the location where the child
is seen, the therapist must document the deviation from the Plan of Care in the child’s
record. If this occurs on a regular basis, there must be a modification of the Plan of
Care.
16.4 Time and Frequency
Time and frequency are required on the physician’s order and must be specific so
time in and time out must be reflected on the document in standard or military format.
Time is a unit of 15 minutes. If seven (7) minutes or less of the next 15 minute unit is
utilized, the unit must be rounded down. However, if eight (8) or more minutes of the

Covered Services –_Developmental Centers________________________________________
Ch. 16 Index 216 Revision 4/1/17
next 15 minute unit are utilized, the units can be rounded up. Date ranges are not
acceptable. For example, six (6) months duration three (3) times per day is an
acceptable time and frequency.
16.5 Missed Appointments/Make-up Session
Medicaid clients have the right to refuse services. If numerous therapy sessions are
missed, the therapist may offer make-up sessions; however, if the child is continually
non-compliant with attendance for whatever reason, the practitioner must be informed
of the missed sessions and non-compliance of the child. All communication with the
child, child’s family and practitioner must be documented in the child’s records.
Clients should be seen for the amount of time and frequency noted on the physician’s
order. An extra session may be billed only if the need for a make-up session is
documented within the record. Billing cannot exceed the Plan of Care.
16.6 Diagnosis
When billing Medicaid for services provided at Developmental Centers, the diagnosis
codes used must be:
Consistent with the diagnosis identified by the ordering practitioner;
Related directly to the need for the services billed; and
Coded to the greatest degree of specificity.
Developmental Centers may not assign diagnosis codes. Diagnosis codes must be
provided by the practitioner or healthcare provider.
16.7 Covered Services
Diagnostic Evaluations/Assessments – A comprehensive multi-disciplinary
evaluation performed by an appropriate Wyoming certified or licensed
practitioner is required for all children referred and all areas will be evaluated
to gain a complete developmental overview of the child.
o Areas to be assessed will include physical development including fine
and gross motor skills, cognitive development, speech development,
and social and emotional development.
o Service is limited to children five (5) years of age and under.
o A licensed practitioner shall provide diagnostic evaluation services.
o Must have a written referral and the referral must list areas of concern.
o Use standardized assessment tools or criterion based assessment.
o Written report includes:
Assessment tools used

Covered Services –_Developmental Centers________________________________________
Ch. 16 Index 217 Revision 4/1/17
Procedures followed
Findings of the evaluation/assessment shall be developed
Provide a copy to the referring practitioner
NOTE: Based on the individual needs of the child, the evaluation may take place
in a Regional Developmental Center, the child’s primary placement (if
other than a Developmental Center) or the child’s home.
Mental Health Services – Medicaid will pay for mental health services
provided by licensed mental health professionals at a Developmental Center to
include licensed professional counselors (LPC), licensed marriage and family
therapists (LMFT), licensed clinical social workers (LCSW), licensed
addiction therapists (LAT), and provisional licensed mental health
professionals under the supervision of a licensed mental health professional.
Physical, Occupational, and Speech Therapy – Medicaid covers restorative
therapy services when provided by or under the direct supervision of a
licensed physical, occupational or speech therapist upon written orders from a
practitioner.
o Restorative services are services that assist an individual in regaining
or improving skills or strength.
o Speech therapy includes any therapy to correct a speech disorder
resulting from injury, trauma, or a medically based illness or disease.
o Service is limited to children five (5) years of age and under
o Therapy shall be provided only after a written order is received from a
licensed practitioner
o Group therapy or field trips cannot exceed five (5) children
o If “individual” is indicated on the Physician’s Order and the child is
seen in a group session, the therapist may not bill for a group session
for that child.
Specific Documentation Requirements – Prior to providing any therapy
services, the following must occur and be documented in the client’s
permanent clinical record:
o A comprehensive medical diagnostic examination by a licensed
practitioner as well as a multi-disciplinary comprehensive evaluation
must be completed as part of the Individual Education Plan/Individual
Family Services Plan (IEP/IFSP). The IFSP must be completed for
children ages 0-36 months.
o Services must:
Be determined, in writing, to be medically necessary by a
licensed practitioner;
Appear on the practitioner’s plan of treatment/care; and
Have original and subsequent renewal written orders, not to
exceed six (6) months duration.
o The practitioner’s plan of treatment/care shall contain:
Covered Services –_Developmental Centers________________________________________
Ch. 16 Index 218 Revision 4/1/17
Diagnosis and onset date of client’s condition;
Client’s rehabilitation potential;
Restorative and/or maintenance program goals;
Therapy modalities determined to be medically necessary to
attain the program goals;
Therapy duration (not to exceed six (6) months); and
Practitioner’s signature and date signed.
o Each therapy ordered, either independently or in combination, must:
State treatment goals in terms of specific outcomes associated
with referral diagnosis;
Outline each therapy regime relative to stated goals, including
modalities, frequency of each treatment session and duration of
each treatment session;
Be updated with every change or renewal of physician orders
(not to exceed six (6) months);
Be signed, including professional title, and dated by each
appropriate therapist; and
Be attached to the client’s IEP/IFSP.
o Ongoing documentation of services provided (progress notes) is
required by each type/discipline of therapy billing Medicaid for
services provided and shall include each of the following:
Identification of the client on each page of the treatment
record;
Identification of the type/discipline of therapy being
documented on each entry (i.e., speech vs. occupational
therapy);
Date and time(s) spent in each therapy session;
Description of therapy activities, client reaction to treatment
and progress being made to stated goals/outcomes; and
Full signature or counter signature of the licensed therapist,
professional title and date that entry was made and the
signature of the therapy assistant and date the entry was made.
Licensed therapist must sign progress notes of assistants within
30-days.
16.8 Billing Requirements
The following procedure codes can be billed by enrolled Developmental Centers:
Developmental Centers
HCPCS
Level II
Code
Modifier
1 Unit
Equals
Description
92507
Per Instance
Individual treatment of speech language voice
communication and/or auditory processing disorder
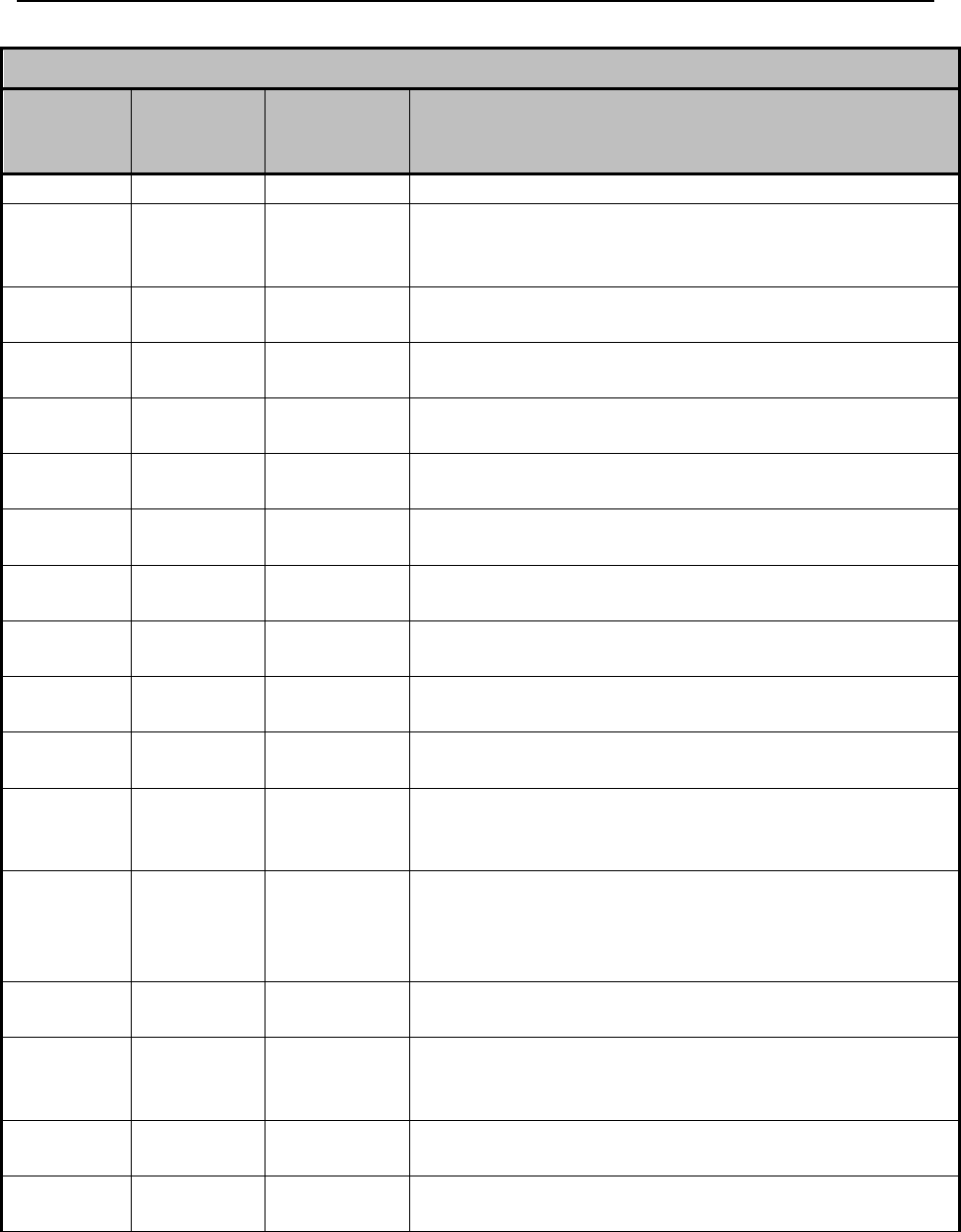
Covered Services –_Developmental Centers________________________________________
Ch. 16 Index 219 Revision 4/1/17
Developmental Centers
HCPCS
Level II
Code
Modifier
1 Unit
Equals
Description
(including aural rehab).
92508
Per Instance
Treatment of speech, language, voice communication,
and/or auditory processing disorder (including aural
rehab); group, two (2) or more individuals.
92521
Per
Evaluation
Evaluation of speech fluency.
92522
Per
Evaluation
Evaluation of speech fluency.
92523
Per
Evaluation
Evaluation of speech sound production with evaluation
of language comprehension and expression.
92524
Per
Evaluation
Behavioral and qualitative analysis of voice and
resonance.
92526
Per Instance
Treatment of swallowing dysfunction and or oral
function for feeding.
97001
Per 15
minutes
Physical therapy evaluation.
97002
Per 15
minutes
Physical therapy re-evaluation.
97003
Per 15
minutes
Occupational therapy evaluation.
97004
Per 15
minutes
Occupational therapy re-evaluation.
97110
Per 15
minutes
Therapeutic procedure, one (1) or more areas;
therapeutic exercises to develop strength and
endurance, range of motion and flexibility.
97112
Per 15
minutes
Therapeutic procedure, one (1) or more areas;
neuromuscular reeducation of movement, balance,
coordination, kinesthetic sense, posture, and/or
proprioception for sitting and/or standing activities.
97113
Per 15
minutes
Therapeutic procedure, one (1) or more areas; aquatic
therapy with therapeutic exercises.
97124
Per 15
minutes
Therapeutic procedure, one (1) or more areas;
massage, including effleurage, petrissage and/or
tapotement (stroking, compression, percussion).
97150
Per 15
minutes
Therapeutic procedure(s); group, two (2) or more
individuals.
97530
Per 15
minutes
Therapeutic activities, direct (one to one) client contact
by the provider.
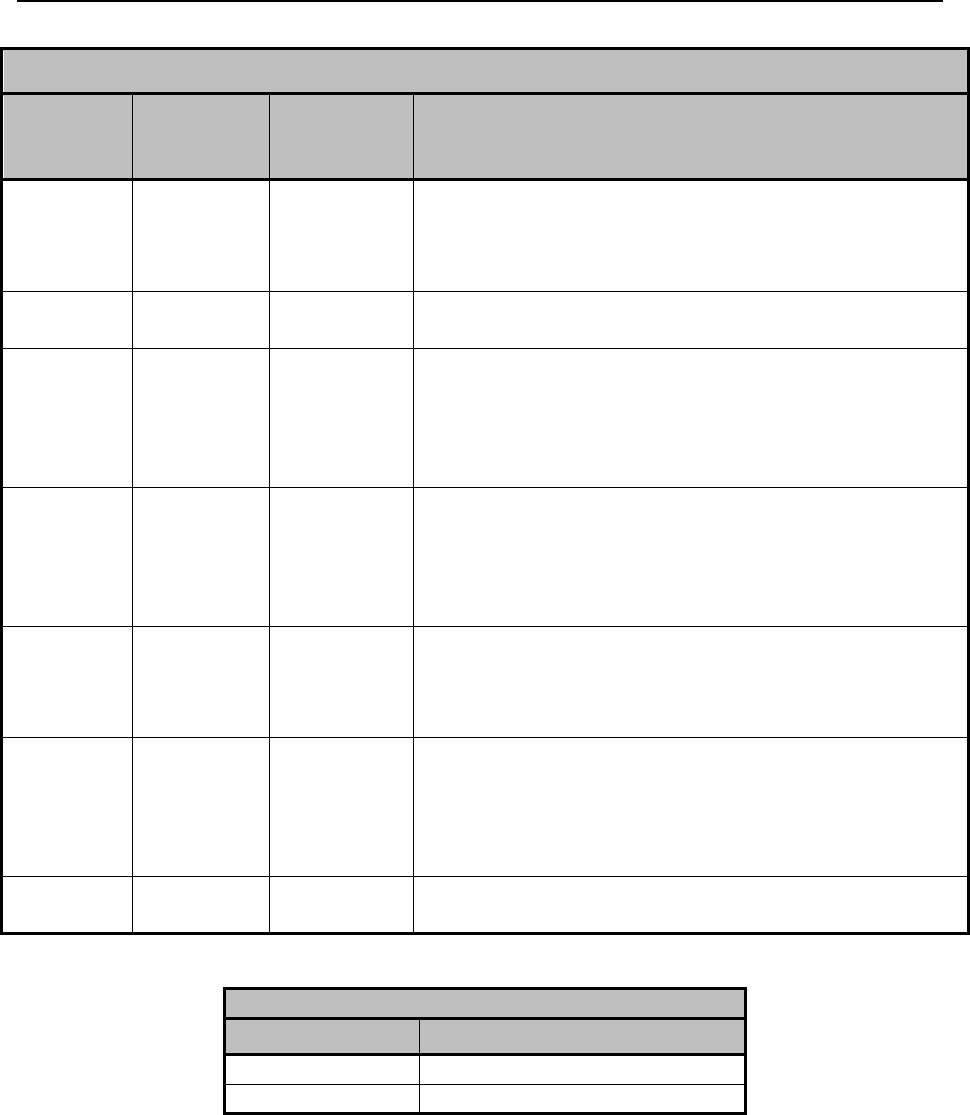
Covered Services –_Developmental Centers________________________________________
Ch. 16 Index 220 Revision 4/1/17
Developmental Centers
HCPCS
Level II
Code
Modifier
1 Unit
Equals
Description
97533
Per 15
minutes
Sensory integrative techniques to enhance sensory
processing and promote adaptive responses of
environmental demands, direct (one-on-one) client
contact by the provider.
G9012
Per 15
minutes
Other specified case management service not
elsewhere classified.
H0031
Per 15
minutes
Clinical assessment – Therapist contact with the client
and/or collaterals as necessary, for the purpose of
completing an evaluation of the client’s mental health
and substance abuse disorder(s) and treatment needs,
including psychological testing if indicated.
H2019
Per 15
minutes
Agency Based Individual/Family Therapy – Therapist
contact at the developmental center with the enrolled
client and/or collaterals as necessary, for the purpose
of developing and implementing the treatment plan for
the enrolled client.
H2019
HQ
Per 15
minutes
Group Therapy – Therapist contact with two (2) or
more unrelated clients and/or collaterals as necessary,
for the purpose of implementing each client’s
treatment plan.
H2021
Per 15
minutes
Community-Based Individual/Family Therapy –
Therapist contact outside the developmental center
with the enrolled client and/or collaterals as necessary,
for the purpose of developing and implementing the
treatment plan for the enrolled client.
T2011
N/A
PASRR Level II Developmental Disabilities
Evaluation.
Developmental Centers
Modifier
Description
HI
Multi-Disciplinary Team
HQ
Group Setting

Covered Services –_Dietician_____________________________________________________
Ch. 17 Index 221 Revision 4/1/17
Chapter Seventeen – Covered Services – Dietician
17.1 Limitations ......................................................................................................... 222
17.2 Covered CPT Codes and Documentation .......................................................... 222
17.3 Medical Nutrition Therapy Documentation Requirements ............................... 222

Covered Services –_Dietician_____________________________________________________
Ch. 17 Index 222 Revision 10/1/16
17.1 Limitations
Dietician services must be ordered by a physician or nurse practitioner.
Medicaid clients are subject to a service cap limit of 20 visits per calendar
year.
17.2 Covered CPT Codes and Documentation
97802 – Medical nutrition therapy; initial assessment and intervention, individual,
face-to-face with the patient, each 15 minutes – Maximum allow 4 units per day.
97803 – Medical nutrition therapy; re-assessment and intervention, individual, face -
to-face with the patient, each 15 minutes – Maximum allow 4 units per day.
97804 – Medical nutrition therapy; group (2 or more individual(s)), each 30 minutes –
Maximum 2 units per day.
17.3 Medical Nutrition Therapy Documentation Requirements
For Medical Nutrition Therapy, the following elements must be in the documentation:
1. Date of MNT visit along with Beginning and Ending Time of visit;
2. ICD-10 code – defines type of visit/counseling;
3. Subjective Data:
a. Client’s reason for visit
b. Primary care physician
c. History
i. Past and present medical
ii. Nutrition including food patterns and intake
iii. Weight
iv. Medication
v. Exercise
4. Objective Data:
a. Laboratory results (if available)
b. Height, Weight
c. BMI
d. Calorie Needs
e. Drug/Nutrient Interactions
5. Individual Assessment of Diet/Intake:
a. Laboratory results (if available)
b. Height, Weight
c. BMI
d. Calorie Needs
e. Drug/Nutrient Interactions
6. Plan:

Covered Services –_Dietician_____________________________________________________
Ch. 17 Index 223 Revision 10/1/16
a. Individualized dietary instruction that incorporates diet therapy
counseling and education handouts for nutrition related problem.
b. Plan for follow-up.
c. Documentation of referral for identified needs.
d. Send a letter to the client’s physician describing dietary instruction
provided and progress. A copy of the letter should be placed in the
client’s medical record.
7. Date and legible identity of provider:
a. All entries must be signed and dated by the provider.

Covered Services –_DME Billing_________________________________________________
Ch. 18 Index 224 Revision 4/1/17
Chapter Eighteen – Covered Services – DME Billing
18.1 Order vs Delivery Date ...................................................................................... 225
18.2 DME Billing Requirement Exception ............................................................... 225
18.2.1 K0108/E1399 Crossover Claim Form ............................................................... 227
Covered Services –_DME Billing_________________________________________________
Ch. 18 Index 225 Revision 4/1/17
18.1 Order vs Delivery Date
If the client is not eligible on the delivery date or does not return for the delivery, the
provider may submit an “Order vs Delivery Date Exception Form” for authorization
to bill on the order date. (6.14 Order Vs Delivery Date)
18.2 DME Billing Requirement Exception
For clients who are dual eligible Medicare and Medicaid, in situations where the
provider is billing for multiple units of either K0108 or E1399, and Medicare
approves some units but not all units, the provider may complete the billing
requirements and exception process/steps below for additional Medicaid
reimbursement, if applicable. The Medicaid claim will be processed according to
Wyoming Medicaid’s policy for the units Medicare denied.
NOTE: K0108 and E1399 only and the client is dual eligible, Medicare and
Medicaid.
Refer to the DME Covered Services manual and Chapters 1-10 of this manual for the
complete Medicaid policy.
Provider must obtain a prior authorization (PA) through the Medicaid DME vendor
1. Submit the claim first to Medicare according to Medicare instructions.
2. Medicare should crossover the claim electronically to Medicaid, and any units
approved by Medicare will be processed to pay co-insurance and deductible as
per usual. Lines that Medicare denied will deny on the crossover claim as
exact duplicates conflicting with the paid lines of the same code, but the
crossover claim will be in a paid status.
a. If crossover claim is not received electronically from Medicare the
providers will need to submit this crossover claim electronically to
Medicaid (Refer to the Web Portal Tutorials)
3. Providers need to wait for the paid crossover to appear on the Medicaid
remittance advice (RA)/835 before continuing the DME billing requirement
exception process (Step 5).
4. Once the paid crossover claim appears on the Medicaid RA, the provider will
need to complete a CMS-1500 paper claim form. Complete the paper claim
form according to Medicaid’s billing requirements, not the way it was
previously submitted to Medicare.
a. Bill according to Medicaid’s PA, enter the PA number in box 23
b. All units denied by Medicare must be combined onto one line with
multiple units or they will deny as exact duplicates.
i. Billed charge/units must add up and match the Medicare
EOMB.

Covered Services –_DME Billing_________________________________________________
Ch. 18 Index 226 Revision 4/1/17
5. Review the invoice(s) for each item and clearly mark for each line item
a. Medicaid must be able to match descriptions from the PA to the
invoice(s), to assist with this process complete the K0108/E1399
Crossover Claim Form (18.1.1 K0108/E1399 Crossover Claim Form)
6. Completing the K0108/E1399 Crossover Claim Form – the purpose of this
form is to assist in matching up the descriptions of the items/components of
the PA to the appropriate items on the invoice(s).
a. When entering the first item description on line 1 of the form place (1)
on the invoice next to the item on the invoice that matches it, continue
the same process until all items are documented on the form.
i. Complete as many forms as necessary.
7. Finalization and mailing process: Providers must include all of the following
in the mailing
a. K0108/E1399 Crossover Claim Form (place on top to ensure
appropriate routing)
b. Completed CMS-1500 paper claim form
c. Medicare’s EOMB
d. Invoice(s)
e. Mail the documents to:
Wyoming Medicaid
ATTN: Medical Policy
PO Box 667
Cheyenne, WY 82003-0667
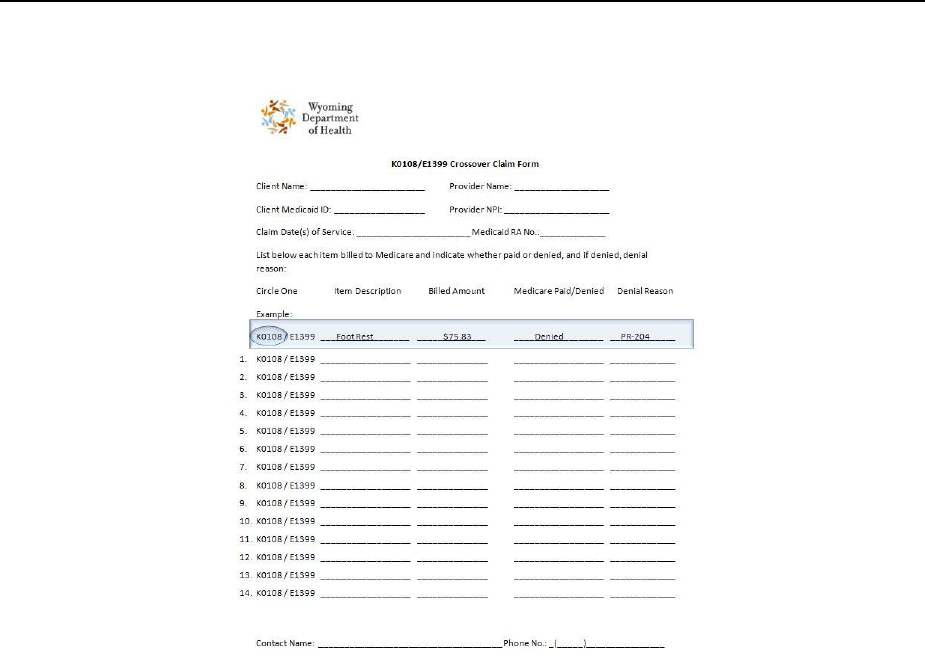

Covered Services –_Family Planning______________________________________________
Ch. 19 Index 228 Revision 4/1/17
Chapter Nineteen – Covered Services – Family Planning
19.1 Family Planning Clinics .................................................................................... 229
19.2 Covered Services ............................................................................................... 229
19.3 Non-Covered Services ....................................................................................... 229

Covered Services –_Family Planning______________________________________________
Ch. 19 Index 229 Revision 4/1/17
19.1 Family Planning Clinics
Family planning clinics provide services that are prescribed to clients of childbearing
age for the purpose of enabling them to freely determine the number and spacing of
their children.
19.2 Covered Services
The following services are covered by Medicaid:
Appropriate office visits according to CPT guidelines.
Contraceptive supplies and devices as prescribed by a healthcare provider
(limited to a three (3) month supply).
Insertion or removal of implantable capsules are allowed with appropriate
E&M procedure code.
Insertion or removal of intrauterine devices (IUD’s) are allowed with an
appropriate E&M procedure code.
Pap smears.
Pregnancy tests.
19.3 Non-Covered Services
The following services are not covered by Medicaid:
Reversal of Sterilizations.
Artificial insemination.
Fertility testing.
Infertility counseling.
NOTE: Pregnant by Choice/Family Planning Waiver has specific covered and
non-covered services (25.1, Pregnant By Choice/Family Planning
Waiver).

Covered Services –_Health Check_________________________________________________
Ch. 20 Index 230 Revision 4/1/17
Chapter Twenty – Covered Services – Health Check
20.1 Health Check – EPSDT ..................................................................................... 231
20.2 Periodicity Schedule .......................................................................................... 232
20.3 Reimbursement .................................................................................................. 232
20.4 Detailed Information for Well Child Screens .................................................... 236
20.5 Initial/Interval History ....................................................................................... 237
20.6 Assessments ....................................................................................................... 237
20.7 Comprehensive Unclothed Physical Examination ............................................ 238
20.8 Head Circumference .......................................................................................... 238
20.9 Blood Pressure ................................................................................................... 239
20.10 Vision Screen .................................................................................................... 239
20.11 Topical Fluoride Varnish ................................................................................... 239
20.12 Hearing Screen .................................................................................................. 240
20.13 Laboratory Tests ................................................................................................ 241
20.13.1 Hematocrit and Hemoglobin ............................................................................. 241
20.13.2 Blood Lead Level .............................................................................................. 241
20.13.3 Tuberculin Screening ........................................................................................ 242
20.13.4 Urinalysis ........................................................................................................... 243
20.13.5 Other .................................................................................................................. 243
20.14 Immunizations ................................................................................................... 243
20.15 Dental Screen .................................................................................................... 244
20.16 Speech and Language Screens .......................................................................... 244
20.17 Discussion and Counseling ............................................................................... 244

Covered Services –_Health Check_________________________________________________
Ch. 20 Index 231 Revision 4/1/17
20.1 Health Check – EPSDT
The Early and Periodic, Screening, Diagnosis and Treatment Program (EPSDT):
Brings comprehensive healthcare to children from birth up to and including
20-years of age who are eligible for Medicaid.
Has a preventive health philosophy of discovering and treating health
problems before they become disabling and far more costly to treat in terms of
both human and financial resources.
Examines all aspects of a child’s well-being and corrects any problems that
are discovered.
Is administered by the Division of Healthcare Financing (DHCF), Medicaid.
EPSDT is a statewide program that provides children with comprehensive health
screenings, diagnostic services, and treatment of any health problem detected.
Defining each word of the program title will help explain the concept of EPSDT.
Procedure Code Range: 99381-99394
Early – Well Child Screens will be performed as soon as possible in the child’s life
(in case of a family already receiving assistance) or as soon as a child’s eligibility for
Medicaid is established.
Periodic – Means Well Child Screens will be performed at intervals established by
medical, dental, and other healthcare experts. Periodic screens assure diseases or
disabilities are detected in the early stages. Types of procedures performed will
depend on age and health history of the child.
Screening – The use of examination procedures for early detection and treatment of
diseases of abnormalities. Referrals are made for those in need of specialized care.
Diagnosis – The determination of the nature or cause of physical or mental disease
(abnormality). A diagnosis is made through the combined use of a health history,
physical, developmental and psychological evaluations, laboratory tests, and x-rays.
Practitioners who complete EPSDT examinations may diagnosis and treat health
problems uncovered by the screen or may refer the child to other appropriate sources
for care.
Treatment – Care provided by practitioners enrolled with Medicaid to prevent,
correct, or ameliorate disease or abnormalities detected by screening and diagnostic
procedures. Practitioners may screen, diagnosis, and treat during one (1) office visit.

Covered Services –_Health Check_________________________________________________
Ch. 20 Index 232 Revision 4/1/17
20.2 Periodicity Schedule
The periodicity schedule contains an easy reference table for Well Child Screens
defined by the age of the child. Refer to the Well Child Screen Requirements table for
all ages.
Key: = to be performed = to be performed for clients at risk s =
subjective, by history o = objective, by a standard testing method s/o =
objective at 12, 15, and 18 years old, subjective, by history for all other
years.
20.3 Reimbursement
If an abnormality(ies) is encountered or a pre-existing problem is addressed in the
process of performing preventative medicine E&M service, and if the
problem/abnormality is significant enough to require additional work to perform the
key components of a problem oriented E&M service, then the appropriate
office/outpatient code 99201-99215 should also be reported. Modifier 25 must be
added to the office/outpatient code to indicate that a significant, separate identifiable
E&M service was provided by the same physician on the same day as the
preventative service. The appropriate preventative medicine service is additionally
reported.

Covered Services –_Health Check_________________________________________________
Ch. 20 Index 233 Revision 4/1/17
Well Child Screen Requirements
For Ages Birth through 21 Years Old
Newborn – 12
months
15 months to
4 years
5-10 years
11-21 years
History
Initial/Interval
Measurements
Height & Weight
Head circumference
(up to 24
mo.)
Blood Pressure
(start at 3
yrs)
Sensory Screening
Vision
s
s
o
o
Hearing
s
s
o
s/o
Developmental / Behavioral Assessment
Immunizations
Health Check Immunizations
Procedures
Lead Screening
(9-12 mo)
(24 mo)
Tuberculin Test
(12 mo)
Topical Fluoride Varnish
(6–12mo)
(15 m-3
yrs)
Cholesterol Screening
(24 mo-4
yrs)
STD Screening
Pelvic Exam
Anticipatory Guidance
Injury Prevention
Violence Prevention
Sleep Positioning Counseling
(up to 6 mo)
Nutrition Counseling
Dental
(12 mo)
All abnormalities detected during the Health Check exam should be referred to the
appropriate specialist, including but not limited to a vision, dental and /or hearing
specialist as necessary. The appropriate way to indicate that the provider has referred
the child is to add Modifier 32 to the preventative service code.
Covered Services –_Health Check_________________________________________________
Ch. 20 Index 234 Revision 4/1/17
If any insignificant or trivial problem/abnormality is encountered while performing
the preventative medicine E&M services, and does not require additional work, the
office/outpatient code should not be reported.
It is of utmost importance that the appropriate CPT, modifier and diagnosis codes are
reported. For the provider’s convenience, the codes, modifiers, and diagnosis codes
for EPSDT-Health Check and the most current fee schedule for the above mentioned
codes are attached. Fees are subject to change without notice.
At a minimum, these screenings must include, but are not limited to:
Comprehensive health and developmental history.
Comprehensive unclothed physical examination.
Dental screening.
Appropriate vision testing.
Appropriate hearing testing.
Appropriate laboratory test (Blood Lead Level testing is required at 12 and 24
months for all children).
The most current copy of the immunization schedule may be found at
http://www.cdc.gov/vaccines/schedules/index.html.
Diagnosis Codes to be used when Billing for EPTSD – Well Child Checks
Diagnosis Code
Description
Z76.1
Health Supervision of Foundling.
Z76.2
Other Healthy Infant or Child Receiving Care.
Z00.121, Z00.129
Routine Infant or Child Health Check.
Topical Fluoride
Procedure Code
Modifier
Description
D1206
32
Topical Fluoride Varnish.
Preventative Medicine Services
Procedure Code
Modifier
Description
99381
32
Initial Comprehensive Preventative Medicine Age 0 through
11 Months.
99382
32
Early Childhood Age 1-4 Years.
99383
32
Late Childhood Age 5-11 Years.
99384
32
Adolescent Age 12-17 Years.
99385
32
Age 18-20 Years.
Modifier
32
Mandated Services – Referral.
Covered Services –_Health Check_________________________________________________
Ch. 20 Index 235 Revision 4/1/17
Evaluation and Management Services – New Patient
Procedure
Code
Modifier
Description
99201
25
Office or other outpatient visit for the E&M of a new patient
requires three (3) key components:
A problem focused history.
A problem focused exam.
Straight forward medical decision making.
99202
25
Office or other outpatient visit for the E&M of a new patient
requires three (3) key components:
An expanded focused history.
An expanded focused exam.
Straight forward medical decision making.
99203
25
Office or other outpatient visit for the E&M of a new patient
requires three (3) key components:
A detailed history.
A detailed exam
Medical decision making of low complexity.
99204
25
Office or other outpatient visit for the E&M of a new patient
requires three (3) key components:
A comprehensive history.
A comprehensive exam.
Medical decision making of moderate complexity.
99211
25
Office or other outpatient visit for the E&M of an established
patient that may not require the presence of a physician.
Usually the presenting problems are minimal. Typically five
(5) minutes are spent performing or supervising these
services.
99212
25
Office or other outpatient visit for the E&M of an established
patient which requires at least of these three (3) components:
A problem focused history.
A problem focused exam.
Straight forward medical decision making.
99213
25
Office or other outpatient visit for the E&M of an established
patient which requires at least of these three (3) components:
An expanded problem focused history.
An expanded problem focused exam.
Straightforward medical decision making.
Covered Services –_Health Check_________________________________________________
Ch. 20 Index 236 Revision 4/1/17
Evaluation and Management Services – New Patient
Procedure
Code
Modifier
Description
99214
25
Office or other outpatient visit for the E&M of an established
patient which requires at least of these three (3) components:
A detailed history.
A detailed exam.
Medical decision making of low complexity.
99215
25
Office or other outpatient visit for the E&M of an established
patient which requires at least of these three (3) components:
A comprehensive history.
A comprehensive exam.
Medical decision making of high complexity.
NOTE: Please refer to the current CPT for additional information regarding
preventative services.
20.4 Detailed Information for Well Child Screens
In some instances, Well Child Screens may not be completed at the suggested
age (example: immunizations); the healthcare professional must follow
recommended practices to ensure the child becomes current.
Results may indicate further testing or referrals are needed. Healthcare
professionals should complete tests or make referrals according to standard
procedures and practices.
Well Child Screens must be completed when there is no acute diagnosis
applicable (i.e. otitis media).
May show that a high risk factor is present based on the child’s environment,
history, or test results. Healthcare professionals should proceed with
required/recommended tests. Evaluation methods used may be different from
what is indicated on the Well Child Screen Requirements table (example: a
tuberculin test performed on a child who is nine (9) months of age because the
child’s sibling had an active case of diagnosed tuberculosis).
The following information contains additional guidelines to be used when performing
Well Child Screens.

Covered Services –_Health Check_________________________________________________
Ch. 20 Index 237 Revision 4/1/17
20.5 Initial/Interval History
The initial/interval history should be obtained from a parent or other responsible adult
who is familiar with the child’s health history. This must include, but is not limited
to:
Family history
Details of birth, prenatal, neonatal periods
Nutritional status
Growth and development
Childhood illness
Hospitalizations
Immunization history
NOTE: If a health history has been obtained previously, then update it each visit.
20.6 Assessments
Appropriate Developmental Screening – Providers should administer a
developmental screen appropriate to the age of the child during each Well Child
Screen. The following screening tools are recommended for children age birth to six
(6) years:
1. Prescreening Developmental Questionnaire
2. Denver Developmental Screening Test
3. Battelle Screening Test
Children five (5) years of age and older should have a general developmental
assessment including gross-motor and fine-motor skills, social-emotional
skills, and cognitive and self-help skills development.
Results of development screens need to be considered in combination with
other information gained through the history, physical examination,
observations of behavior and reports of observations by the parents/caregivers.
Any abnormalities detected during a Well Child Screen outside of the
attending physician’s scope of practice should be referred to the appropriate
specialist, including vision, dental and hearing specialists as necessary. All
services provided must be medically necessary and provided in the most cost-
effective manner.
Nutritional Screen – Providers should assess the nutritional status at each Well
Child Screen through the following activities:

Covered Services –_Health Check_________________________________________________
Ch. 20 Index 238 Revision 4/1/17
o Inquire about dietary practices to identify unusual eating habits.
Unusual eating habits include pica behavior, extended use of bottle
feedings, or diets deficient or excessive in one (1) or more nutrients;
A complete physical examination including an oral inspection;
Accurate measurements of height and weight (all measurements should be
plotted on the National Center for Health Statistics Growth Charts); and
Screening for iron deficiency at the appropriate ages and/or intervals.
NOTE: Children with nutritional problems may be referred to a licensed
nutritionist or dietician for further assessment, counseling, or education
as needed.
20.7 Comprehensive Unclothed Physical Examination
Each comprehensive unclothed physical examination should include the following:
Height measurement
Weight measurement
Standard body systems evaluation
Observation for any signs of abuse
Observation of any physical abnormality
During each Well Child Screen, providers need to assess the child’s growth. All
measurements should be plotted on the National Center for Health Statistics (NCHS)
Growth Chart.
Growth assessments should be documented in the medical record and any
abnormality should be addressed as abnormal if:
If a child’s height and/or weight is below the 5th percentile or above the 95th
percentile; or
If weight for height is below the 10th percentile or above the 90th percentile
(using the weight for height graph).
20.8 Head Circumference
An Occipital Frontal Head Circumference (OFHC) should be measured on each child
four (4) years and younger at each Well Child Screen. This measurement should be
plotted on the NCHS Growth Chart. OFHC should be reported abnormal if:
It is below the 5th percentile or above the 95th percentile;
Size of the head is not following a normal growth curve; or
Head is grossly disproportionate to the child’s length.

Covered Services –_Health Check_________________________________________________
Ch. 20 Index 239 Revision 4/1/17
Deviations in the shape of the head may warrant further evaluation and follow-up.
20.9 Blood Pressure
All children three (3) years and older must have a blood pressure reading at
each Well Child Screen.
Measurements should be taken in a quiet environment, with the correct size
cuff, and with the fourth (4th) and fifth (5th) phase Korotkoff sound noted for
the diastolic pressure.
Blood pressure is considered abnormal if the systolic and/or diastolic or both
are above the 95th percentile. Any child with a blood pressure reading above
the 95th percentile should have it repeated in 7-14 days. If the blood pressure
is still elevated, the child should be rechecked again in 7-14 days. If blood
pressure is elevated on the third visit, the child should receive appropriate
medical evaluation and follow-up, as recommended by the American
Academy of Pediatrics.
20.10 Vision Screen
A vision screen appropriate to the age of the child should be conducted at each Well
Child Screen. Further evaluations and proper follow up should be recommended if the
following conditions are present:
Infants and children who show evidence of infection, squinting, enlarged or
lazy cornea, crossed eyes, amblyopia, cataract, excessive blinking, or other
eye abnormality;
An infant or child who scored abnormal on the fixation test, papillary light
reflex test, alternate cover test, or the corneal light reflect test in either eye;
Three (3) to nine (9) year old children who demonstrate a visual acuity of less
than 20/40 in either eye or who demonstrate a one (1) line difference in visual
acuity between the two (2) eyes within the passing range; or
Children ten (10) years and older whose vision is 20/30 or worsen in either
eye or who demonstrate a one (1) line difference in visual acuity between the
two (2) eyes within the passing range.
20.11 Topical Fluoride Varnish
Physicians can apply a topical fluoride varnish for patients who are at a moderate to
high risk for dental caries:
This application should be done in conjunction with EPSDT well child visits.
Physician offices may bill the CPT code 99188 on the CMS-1500 form.

Covered Services –_Health Check_________________________________________________
Ch. 20 Index 240 Revision 4/1/17
Fluoride varnish application can be done up to three (3) times a year on
children ages six (6) months (or when the first teeth erupt) through age three
(3) years.
The American Academy of Pediatric Dentistry recommends the establishment
of dental home no later than 12-months of age.
20.12 Hearing Screen
A hearing screen appropriate to the age of the child should be conducted at each Well
Child Screen. Further evaluations and proper follow up should be recommended if
one (1) of the following conditions is present:
Infants and children who are positive on one (1) or more of the Eight (8) Hi-
Risk register items:
o Visible congenital or traumatic deformity of the ear.
Congenital, such as atresia (no ear canal) or abnormally small ear canals.
Traumatic deformity, collapsed canals or a deformed ear that might
contraindicate presence of mold or aid.
History of active drainage from the ear within previous 90-days.
History of sudden or rapidly progressive hearing loss within the previous 90-
days possibly due to viral attack, trauma, etc. should be seen by a medical
doctor immediately.
Acute or chronic dizziness indicates possible problems with semi-circular
canals (balance).
Unilateral hearing loss of sudden or recent onset within the previous 90-days.
Could be caused by mumps, virus, head trauma, Meniere's disease, and
various vascular disorders.
Audiometric air-bone gap equal to or greater than 15 decibels (dB) at 500Hz,
1000Hz, 2000Hz and 3,000Hz. Conductive or middle ear pathology can cause
a difference of greater that 15dB between the air conduction test results and
results by bone conduction.
Visible evidence of significant cerumen accumulation or a foreign body in the
ear canal.
Pain or discomfort simply indicates there is something wrong and should be
seen by a medical doctor.
Infants and children whose medical, physical, or developmental history
indicates possible hearing loss:
Positive family history of hearing loss.
Viral or other non-bacterial transplacental infection.
o Defects of ear, nose or throat system; malformed, low-set to absent
pinnae; cleft lip or palate.
o Birth weight under 1500 grams.

Covered Services –_Health Check_________________________________________________
Ch. 20 Index 241 Revision 4/1/17
o Unconjugated bilirubin over 24 mg/100 ml or over infant’s weight
in decagrams.
o Bacterial meningitis.
o Sever asphyxia with arterial flow less than 7.25, coma, seizures or
need for continuous assisted ventilation.
o Children found positive when tested with pure tone screening.
20.13 Laboratory Tests
Providers who conduct Well Child Screens must use their medical judgment when
determining the applicability of performing specific laboratory tests and/or analyses.
The following are basic laboratory tests that should be performed when a child
reaches the required age.
20.13.1 Hematocrit and Hemoglobin
Hematocrit or Hemoglobin is completed at the following ages:
Newborns (for high risk infants),
Two (2) months (for high risk infants),
8-12 months,
18-24 months,
Three to four (3-4) years, and
11-12 years.
20.13.2 Blood Lead Level
A venous blood lead level determination must be performed on children at 12
and 24 months of age.
Children who have a history of pica behavior, an environment suspect of lead
exposure, or whose history/physical examination findings are suspicious
should have a blood lead level follow-up.
Lead poisoning is an elevated venous blood lead level (that is greater than or
equal to 10 micrograms per deciliter (ug/dl).
If an elevated blood level is discovered, a child should be re-screened every
three (3) to four (4) months until lead levels are within normal limits. In
addition, a venipuncture blood lead level should be performed annually
through at least age six (6).
Beginning at six (6) months of age and at each visit thereafter until six (6) years of
age providers must discuss with parent(s)/caregiver(s) about childhood lead poisoning
interventions and assess the child’s risk for exposure. A verbal interview or written
questionnaire, such as the following may identify those children at high risk of lead

Covered Services –_Health Check_________________________________________________
Ch. 20 Index 242 Revision 4/1/17
exposure. Blood lead testing should be carried out on those children identified as high
risk by this or a similar questionnaire:
Does your child live in or regularly visit an old house built before 1950? Is
your child’s day care center / preschool / babysitter’s home built before 1978?
Does the house have peeling or chipping paint?
Does your child live in a house built before 1978 with recent, ongoing, or
planned renovation or remodeling (within the last six (6) months)?
Do any of your children or their playmates have or had lead poisoning?
Does your child frequently come in contact with an adult who works with
lead? Examples are construction, welding, pottery, or other trades practiced in
your community.
Does your child live near a lead smelter, battery recycling plant, or other
industry likely to release lead?
Do you give your child any home or folk remedies that may contain lead?
Does your child live near a heavily traveled major highway where the soil and
dust may be contaminated with lead?
Does your home’s plumbing have lead pipes or copper with lead solder joints?
Ask any additional questions specific to situations existing in the provider’s
community. Risk is determined from responses to a verbal or written questionnaire
risk assessment. A subsequent verbal risk assessment can change a child’s risk
category. Any information suggesting increased lead exposure for previously low risk
children must be followed up with a blood lead test. Medicaid will pay for samples to
be taken from the home and sent to state laboratory for testing.
If answers to all questions are negative, a child is considered low risk for high doses
of lead exposure. Practitioners will need to determine whether to perform additional
blood lead level test beyond those required at 12 and 24-months of age.
If the answers to any questions are positive, a child is considered high risk for high
doses of lead exposure. Practitioners are required to perform a venous blood lead
level on children determined to be high risk. Tests need to be repeated every three (3)
to four (4) months until lead levels are within normal limits. Tests should continue to
be completed if the child is still considered high risk.
20.13.3 Tuberculin Screening
Tuberculin testing should be completed as indicated on the Well Child Screen
Requirements table or more often on clients in high-risk populations (Asian refugees,
Indian children, migrant children, etc.), or if historical findings, physical
examinations or other risk factors so indicate.

Covered Services –_Health Check_________________________________________________
Ch. 20 Index 243 Revision 4/1/17
20.13.4 Urinalysis
Urinalysis using a multiple dipstick method should be completed on all children at
two (2) years and 13-15 years.
Because of heightened incidence of bacteriuria in girls, they should have
additional tests around three (3) years, five (5) years and eight (8) years.
Children who have had previous urinary tract infections should be re-screened
more frequently.
If test results are positive but the history and physical examination are
negative, the child should be tested again in seven (7) days.
If the results are positive a second (2nd) time or if there are supportive findings
in the history and physical examination from the first (1st) positive test, further
follow-up is required.
If a male child has a urinary tract infection, a referral for further testing should
be completed immediately.
20.13.5 Other
Other laboratory tests (i.e., chest x-ray, Pap smear, sickle cell testing, etc.) should be
completed if medically necessary.
20.14 Immunizations
The immunization status of each child should be reviewed at each Well
Child Screen.
Reviewing the immunization status of a child includes interviewing
parents/caretakers, reviewing immunization history/records, and reviewing
known high risk factors to which the child may be exposed.
Immunizations needed by children at their Well Child Screen should be given
on-site, provided there are not existing contradictions.
Immunizations are to be given according to the Advisory Committee on
Immunization Practices (ACIP).
Arrangements should be made with the parents/responsible adult for the
completion of immunizations.
If immunizations have not been completed at the recommended age, the
healthcare professional should set up a schedule to ensure the child
becomes current.
NOTE: The Recommended Immunization Schedule can be found at
http://www.cdc.gov/vaccines/schedules/index.html.
Covered Services –_Health Check_________________________________________________
Ch. 20 Index 244 Revision 4/1/17
20.15 Dental Screen
Oral inspections are included in Well Child Screens. Results should be included in the
child’s Initial/Interval History. Although an oral inspection is part of Well Child
Screens, it does not substitute for an examination through a direct referral to a dentist.
A child should be referred to the dentist as follows:
When the first tooth erupts and at least yearly thereafter.
If an oral inspection reveals cavities, infection, or the child has or is
developing a handicapping malocclusion or significant abnormality.
NOTE: Refer back to Topical Fluoride (20.11, Topical Fluoride Varnish).
20.16 Speech and Language Screens
Speech and language screens identify delays in development of children.
Referrals for further speech and hearing evaluations may be appropriate if one (1) or
more of the following exists:
Child is not talking at all by the age of 18 months.
Suspected hearing impairment.
Child is embarrassed or disturbed by his/her own speech.
Voice is monotone, extremely loud, largely inaudible, or of poor quality.
There is noticeable hypernasality or lack of nasal resonance.
There is undue parental concern.
Where speech is not understandable at three (3) years of age, a referral may be
appropriate, as the condition may be caused by an unsuspected hearing
impairment or a variety of undiagnosed conditions.
20.17 Discussion and Counseling
Parents should have the opportunity to ask questions, to have them answered and to
have sufficient time allotted for unhurried discussions. Practitioners should discuss
and interpret examination results in accordance with the parents’ level
of understanding.
NOTE: Interpretation services are available upon request (21.1, Interpreter
Services).

Covered Services –_Interpreter Services___________________________________________
Ch. 21 Index 245 Revision 4/1/17
Chapter Twenty One – Covered Services – Interpreter Services
21.1 Interpreter Services ............................................................................................ 246
21.2 How it Works .................................................................................................... 246
21.3 Covered Services ............................................................................................... 247
21.4 Non-Covered Services ....................................................................................... 247
21.5 Billing Procedures ............................................................................................. 247
21.6 Required Documentation ................................................................................... 247
Covered Services –_Interpreter Services___________________________________________
Ch. 21 Index 246 Revision 4/1/17
21.1 Interpreter Services
Enrolled providers assisting Medicaid clients with oral interpretation or sign language
interpretation must adhere to national standards developed by the National Council on
Interpreting in Healthcare (NCIHC). These include:
Accuracy – To enable other parties to know precisely what each speaker
has spoken.
Confidentiality – To honor the private and personal nature of the healthcare
interaction and maintain trust among all parties.
Impartiality – To eliminate the effect of interpreter bias or preference.
Role Boundaries – To clarify the scope and limits of the interpreting role, in
order to avoid conflicts of interest.
Professionalism – To uphold the public’s trust in the interpreting profession.
Professional Development – To attain the highest possible level of
competence and service.
Advocacy – To prevent harm to parties whom the interpreter serves.
Procedure Code: T1013
21.2 How it Works
A need for interpreter services is determined by a medical appointment.
The healthcare provider accesses the Medicaid website or contact Provider
Relations for a current list of enrolled interpretation providers (2.1, Quick
Reference).
The healthcare provider will contact and provide the interpretation service the
following information:
o Name of client
o Client’s Medicaid ID number
o Name of referring provider
o Time and date service will be required
o Location where services will take place (telephonically or in person)
o Estimated length of time service will be required
The appointment takes place and interpretation services are provided.
If any follow-up appointments are needed after the initial appointment, the
interpretation services may be arranged at that time.

Covered Services –_Interpreter Services___________________________________________
Ch. 21 Index 247 Revision 4/1/17
21.3 Covered Services
The interpretation provider may only bill Medicaid for time spent with the client in
conjunction with Medicaid healthcare services delivered by different providers.
21.4 Non-Covered Services
Medicaid will not pay for interpreter services in conjunction with the
following services:
o Inpatient or outpatient hospital services.
o Intermediate Care Facilities for persons with Intellectual Disability
(ICF-ID).
o Nursing facilities.
o Ambulance services by public providers.
o Psychiatric Residential Treatment Facilities.
o Comprehensive inpatient or outpatient rehabilitation facilities.
o Other agencies/organizations receiving direct federal funding.
Interpreter services provided by family members or by a volunteer, associate
or friend.
Reimbursement for travel to and from the appointment.
Services provided to a client on an ALEN program that are not emergency
services.
21.5 Billing Procedures
Following are the interpretation services billing procedures or requirements:
Interpreters may bill for the same client on the same day more than once if
provided in conjunction with Medicaid healthcare services delivered by
different providers.
The diagnosis code for interpretation services is Z71.0.
The procedure code for interpretation services is T1013 and should be billed
with the appropriate number of units provided.
o One (1) unit = 15 minutes of service.
When not providing services in-person the GT modifier must be used.
21.6 Required Documentation
Interpretation providers must maintain documentation to support that the service
occurred. This should include (at minimum) the client’s name, date of service, times
in and out, service provided, and signature of provider.

Covered Services –_Laboratory Services___________________________________________
Ch. 22 Index 248 Revision 4/1/17
Chapter Twenty Two – Covered Services – Laboratory Services
22.1 Laboratory Services ........................................................................................... 249
22.2 CLIA Requirements .......................................................................................... 249
22.3 Genetic Testing .................................................................................................. 251
22.3.1 BRCA Testing and Counseling ......................................................................... 251
22.3.2 Counseling ......................................................................................................... 252
22.3.3 Billing Requirements ......................................................................................... 252

Covered Services –_Laboratory Services___________________________________________
Ch. 22 Index 249 Revision 4/1/17
22.1 Laboratory Services
Medicaid covers tests provided by independent (non-hospital) clinical laboratories
when the following requirements are met:
Services are ordered by physicians, dentists, or other providers licensed within
the scope of their practice as defined by law.
Services are provided in an office or other similar facility, but not in a hospital
outpatient department or clinic.
Providers of lab services must be Medicaid certified.
Providers of lab services must have a current Clinical Laboratory
Improvement Amendments (CLIA) certification number.
Providers may bill Medicaid only for those lab services they have performed
themselves. Medicaid does not cover reference lab services.
Procedure Code Range: 80047-89356
NOTE: Non-covered services include routine handling charges, stat fees, post-
mortem examination and specimen collection fees for throat culture or Pap
Smears.
22.2 CLIA Requirements
The type of CLIA certificate required to cover specific codes is listed in the table
below. These codes are identified by Center for Medicare and Medicaid Services
(CMS) as requiring CLIA certification; however, Medicaid may not cover all of the
codes listed. Refer to the fee schedule (2.1, Quick Reference) located on Medicaid
website for actual coverage and fees. Content is subject to change at any time,
without notice.
NOTE: Codes within the below table are NOT Wyoming Medicaid specific. It is
the provider’s responsibility to ensure the codes being billed are covered
by Wyoming Medicaid.
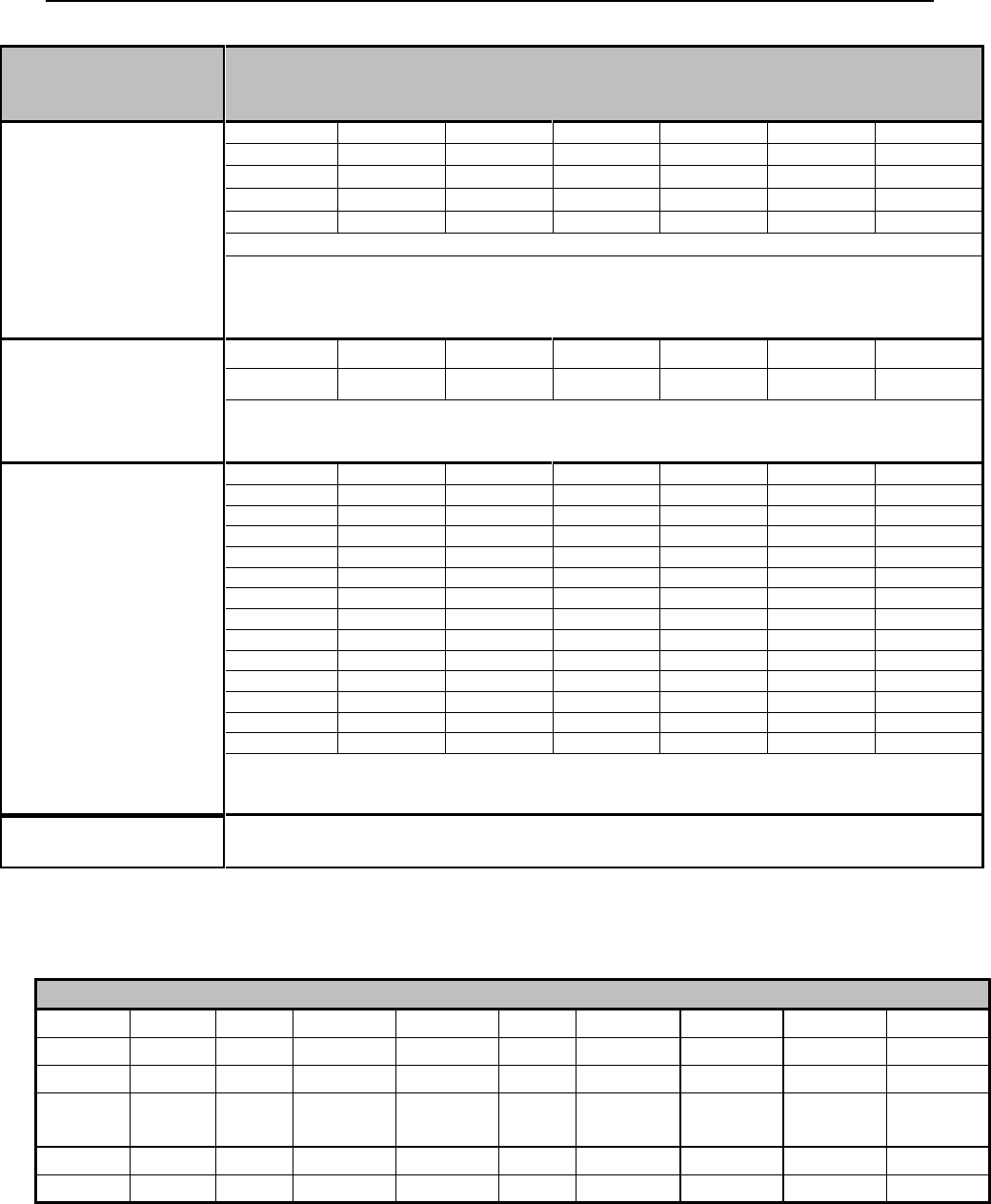
Covered Services –_Laboratory Services___________________________________________
Ch. 22 Index 250 Revision 4/1/17
CLIA
CERTIFICATE
TYPE
ALLOWED TO BILL
REGRISTRATION,
COMPLIANCE, OR
ACCREDITATION
(LABORATORY) (1)
G0103
G0123
G0124
G0141
G0143
G0144
G0145
G0147
G0148
G0306
G0307
G0328
G0416
G0432
G0433
G0434
G0477
G9143
P3000
17311
17312
17313
17314
17315
78110
78111
78120
78121
78122
78130
78191
78270
78271
78272
80000-89999 (UNLESS OTHERWISE SPECIFIED ELSEWHERE IN THIS TABLE)
PROVIDERS WITH THIS CLIA TYPE MAY BILL THE CODES WITHIN THE LABORATORY
(CLIA TYPE 1) SECTION AND ALL CODES FOR PPMP (CLIA TYPE 4) SECTION AND WAIVER
(CLIA TYPE 2) SECTION AND THE CODES EXCLUDED FROM CLIA REQUIREMENTS (REFER
TO TABLE BELOW)
PROVIDER-
PERFORMED
MICROSCOPY
PROCEDURES
(PPMP) (4)
81000
81001
81015
81020
89055
89190
G0027
Q0111
Q0112
Q0113
Q0114
Q0115
PROVIDERS WITH THIS CLIA TYPE MAY BILL THE CODES WITHIN THE PPMP (CLIA TYPE 4)
SECTION AND ALL CODES FOR WAIVER (CLIA TYPE 2) SECTION AND THE CODES
EXCLUDED FROM CLIA REQUIREMENTS (REFER TO TABLE BELOW)
WAIVER (2)
80047 QW
80048 QW
80051 QW
80053 QW
80061 QW
80069 QW
80178 QW
81003 QW
81007 QW
82010 QW
82040 QW
82043 QW
82044 QW
82120 QW
82150 QW
82247 QW
82271 QW
82274 QW
82310 QW
82330 QW
82374 QW
82435 QW
82465 QW
82523 QW
82550 QW
82565 QW
82570 QW
82679 QW
82947 QW
82950 QW
82951 QW
82952 QW
82977 QW
82985 QW
83001 QW
83002 QW
83036 QW
83037 QW
83516 QW
83605 QW
83655 QW
83718 QW
83721 QW
83861 QW
83880 QW
83986 QW
84075 QW
84132 QW
84155 QW
84295 QW
84443 QW
84450 QW
84460 QW
84478 QW
84520 QW
84550 QW
84703 QW
85014 QW
85018 QW
85576 QW
85610 QW
86294 QW
86308 QW
86318 QW
86386 QW
86618 QW
86701 QW
86803 QW
87077 QW
87210 QW
87449 QW
87804 QW
87807 QW
87808 QW
87809 QW
87880 QW
87899 QW
89300 QW
89321 QW
G0328 QW
G0433 QW
G0434 QW
G0477 QW
81002
81025
82270
82272
82962
83026
84830
85013
85651
PROVIDERS WITH THIS CLIA TYPE MAY BILL THE CODES WITHIN THE WAIVER (CLIA
TYPE 2) SECTION AND ALL CODES EXCLUDED FROM CLIA REQUIREMENTS (REFER TO
TABLE BELOW)
NO
CERTIFICATION
PROVIDERS WITHOUT A CLIA MAY BILL ALL CODES EXCLUDED FROM CLIA
REQUIREMENTS (SEE BELOW)
NOTE: QW next to a laboratory code signifies that a QW modifier must be used.
CODES EXCLUDED FROM CLIA REQUIREMENTS
80500
80502
81050
82075
83013
83014
83987
84061
86077
86078
86079
86485
86486
86490
86510
86580
86891
86910
86923
86927
86930
86931
86932
86945
86950
86960
86965
86985
86999
87900
88125
88240
88241
88304
TC
88305
TC
88311
88312
TC
88313
TC
88314
TC
88329
88720
88738
88741
88749
89049
89220
89240
89251
89255
89261
89272
89281
89290
89354
89398

Covered Services –_Laboratory Services___________________________________________
Ch. 22 Index 251 Revision 4/1/17
For updated Medicare CLIA information visit:
http://www.cms.gov/Regulations-and-Guidance/Legislation/CLIA/Categorization_of_Tests.html
22.3 Genetic Testing
Procedure Codes: 81201-81507; 96040
Prior Authorization is required for all genetic testing codes. Prior authorization
documentation must document the following:
There is reasonable expectation based on family history, risk factors, or
symptomatology that a genetically inherited condition exists; and
Test results will influence decisions concerning disease treatment or
prevention; and
Genetic testing of children might confirm current symptomatology or predict
adult onset diseases and findings might result in medical benefit to the child or
as the child reaches adulthood; and
Referral is made by a genetic specialist (codes 81223 and 81224) or a
specialist in the field of the condition to be tested; and
All other methods of testing and diagnosis have met without success to
determine the client’s condition such that medically appropriate treatment can
be determined and rendered without the genetic testing. (6.14, Prior
Authorization).
Codes 81420, 81507 - Mother must be documented as high-risk to include:
advanced maternal age >35 (at EDC), previous "birth" of embryo/fetus/child
with aneuploidy, parent with known balanced translocation, screen positive on
standard genetic screening test (FTCS, multiple marker screen of one type or
another, etc), ultrasound finding on embryo/fetus consistent with increased
risk of aneuploidy
22.3.1 BRCA Testing and Counseling
The U.S. Preventive Services Task Force (USPSTF) recommends that women whose
family history is associated with an increased risk for deleterious mutations in
BRCA1 or BRCA2 genes be referred for evaluation for BRCA testing (81211-
81217). Medicaid covers BRCA testing when the following criteria are met:
Personal and/or family history of breast cancer, especially if associated with
young age of onset; or
Multiple tumors; or
Triple-negative (i.e., estrogen receptor, progesterone receptor, and human
epidermal growth factor receptor 2-negative) or medullary histology; or
History of ovarian cancer; and
18 years or older; and
Pre-test genetic counseling has been prior authorized.

Covered Services –_Laboratory Services___________________________________________
Ch. 22 Index 252 Revision 4/1/17
22.3.2 Counseling
Medicaid covers appropriate genetic counseling (96040) when it is provided in
conjunction with performance or consideration of medically necessary BRCA testing
that meets the criteria listed above. This includes follow-up genetic counseling to
discuss the results of these tests. Three (3) 30 minute units (for a total of 90 minutes)
are allowed per day.
Genetic counseling services may be billed by a physician when the genetic counselor
is under physician supervision and is an employee of the physician. Services provided
by independent genetic counselors are not a benefit of Wyoming Medicaid.
Physician specialties that may bill for BRCA genetic counseling are:
Clinical genetics
Family practice
OB/GYN
Internal medicine
Internal medicine, medical oncology
General surgery
22.3.3 Billing Requirements
Prior authorization is required for BRCA pre-test counseling and must be
submitted by a physician with a specialty listed above.
BRCA testing CPT codes will only be paid with an approved prior
authorization for pre-test counseling.
Prior authorization requests will need to be submitted to Medical Policy (2.1,
Quick Reference)
Prior authorization documents should include:
o The reason for the test(s); and
o Previous lab results; and
o How the test results will be utilized; and
o How the test results will contribute to improved health outcomes; and
o How the test results will alter the client’s treatment management.
Providers may contact Medical Policy (2.1, Quick Reference) by telephone for verbal
prior authorization. Medical Policy will provide a pending PA number until a formal
request is submitted. The formal request must be submitted within 30-days of
receiving the pending PA number and must include all documentation required.

Covered Services –_Non-Emergency Medical Transportation_________________________
Ch. 23 Index 253 Revision 4/1/17
Chapter Twenty Three – Covered Services – Non-Emergency
Medical Transportation
23.1 Non-Emergency Medical Transportation (NEMT) ........................................... 254
23.1.1 Covered services ................................................................................................ 254
23.1.1.1 Taxi and non-taxi rides .................................................................................. 254
23.1.1.2 Lodging .......................................................................................................... 254
23.2 Billing Information ............................................................................................ 254
23.2.1 Taxi Rides .......................................................................................................... 254
23.2.2 Non-Taxi Rides ................................................................................................. 255
23.2.3 Lodging ............................................................................................................. 256

Covered Services –_Non-Emergency Medical Transportation_________________________
Ch. 23 Index 254 Revision 4/1/17
23.1 Non-Emergency Medical Transportation (NEMT)
Wyoming Medicaid provides non-emergency medical transportation (NEMT)
services to clients who are in need of assistance traveling to and from medical
appointments to enrolled providers to obtain covered services.
Wyoming Medicaid enrolls taxi providers (344600000X), non-taxi ride providers
(347C00000X), and lodging providers (177F00000X) to provide covered services.
23.1.1 Covered services
23.1.1.1 Taxi and non-taxi rides
Covered for adults and children
Client must call in the ride to the Transportation Call Center (800-595-0011)
o Transportation Call Center will verify client is covered for the ride and
meets criteria
Transportation Call Center will contact Ride Provider once the ride is
approved
Transportation Call Center will supply client ID for billing purposes to Ride
provider
23.1.1.2 Lodging
Covered for clients 20 years of age and younger
Client must be inpatient or outpatient at a medical facility that is enrolled with
Wyoming Medicaid
Client must call in the transportation request to the Transportation Call Center
and indicate that they are staying with an enrolled lodging provider
Client must live more than 400 miles round trip from medical facility
o Exceptions may be granted for special circumstances (several
appointments over several days; very early appointments; need for
direct medical supervision during outpatient recovery; etc. The client
must contact Transportation Call Center (800-595-0011) to request
exceptions)
23.2 Billing Information
23.2.1 Taxi Rides
Procedure codes A0100, S0215

Covered Services –_Non-Emergency Medical Transportation_________________________
Ch. 23 Index 255 Revision 4/1/17
Taxi provider must receive authorization for the taxi ride from the
Transportation Call Center
Transportation Call Center will provide client ID and TAC number for billing
purposes
o The TAC number will be entered as the client’s account number on the
claim when billing
Bill procedure code A0100 – Base Rate – 1 unit for each one way trip
Bill procedure code S0215 – mileage for each mile or part of a mile
o Mileage is always rounded up. Example: 5.2 miles would be billed as
6 miles.
Mileage without the client on board is not eligible for billing
Wait time is not a covered service
No show or late clients are not a covered service, however, they should be
reported to the Transportation Call Center (800-595-0011)
All rides billed are subject to post payment review and as such records should
be kept with detail including:
o Authorization from Transportation Call Center
o Client information
o Date and time of pick-up
o Pick up address
o Destination address
o Total mileage
o Total charge
23.2.2 Non-Taxi Rides
Procedure Codes: A0110, A0080
Ride provider must receive authorization for the ride from the Transportation
Call Center
Transportation Call Center will provide client ID and TAC number for billing
purposes
o The TAC number will be entered as the client’s account number on the
claim when billing
Bill procedure code A0110 – Base Rate – 1 unit for each one way trip
Bill procedure code A0080 – mileage for each mile or part of a mile above 15
miles
NOTE: The first 15 miles are INCLUDED with the base rate and are not billed
o Mileage is always rounded up

Covered Services –_Non-Emergency Medical Transportation_________________________
Ch. 23 Index 256 Revision 4/1/17
o Example – A trip of 23.2 miles would be billed with code A0110 as
the base rate (1 unit) and A0080 for the mileage (9 units: 23.2 miles -
15 base miles = 8.2 miles, round up to 9 miles = 9 units)
Mileage without the client on board is not eligible for billing
Wait time is not a covered service
No show or late clients are not a covered service, however, they should be
reported to the Transportation Call Center (800-595-0011)
All rides billed are subject to post payment review and as such records should
be kept with detail including:
o Authorization from Transportation Call Center
o Client information
o Date and time of pick up
o Pick up address
o Destination address
o Total mileage
o Total charge
23.2.3 Lodging
Procedure Code: A0180
Client must call in transportation to the Transportation Call Center (800-595-
0011) and indicate they are staying with an enrolled lodging provider and
provide the TAC number to the lodging provider for billing purposes
o The TAC number will be entered as the client’s account number on the
claim when billing
Client must provide client ID of child to the lodging provider for billing
purposes
Bill procedure code A0180 for each night of lodging – child client must be
inpatient in medical facility or outpatient and staying at lodging provider
All lodging claims are subject to post payment review and as such records
should be kept with detail including:
o Client information
o Medical facility client was patient of
o Inpatient/outpatient status
o Dates of stay
o Total nights
o Total charge
The client’s family will need a copy of receipt/documentation to receive their
per diem for the stay

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 257 Revision 4/1/17
Chapter Twenty Four – Covered Services – Practitioner Services
24.1 Practitioner Services .......................................................................................... 263
24.2 Covered Services ............................................................................................... 263
24.2.1 Abortion ............................................................................................................. 263
24.2.1.1 Covered Services ........................................................................................... 263
24.2.1.2 Reimbursement Requirements ....................................................................... 264
24.3 Anesthesia Services ........................................................................................... 264
24.3.1 Covered Services ............................................................................................... 264
24.3.2 Billing Guidelines .............................................................................................. 265
24.3.3 Obstetrical Exceptions ....................................................................................... 266
24.3.4 Modifiers ........................................................................................................... 268
24.3.5 Documentation Requirements ........................................................................... 268
24.4 Dermatology ...................................................................................................... 268
24.4.1 Covered Services ............................................................................................... 269
24.4.2 Benign Lesion Removal and Destruction of Benign or Premalignant Lesions . 269
24.4.3 Covered Services ............................................................................................... 269
24.4.4 Billing Requirements ......................................................................................... 269
24.4.5 Documentation Requirements ........................................................................... 270
24.5 Diabetic Training ............................................................................................... 270
24.5.1 Covered Services ............................................................................................... 271
24.5.2 Billing Requirements ......................................................................................... 271
24.5.3 Documentation .................................................................................................. 271
24.6 Family Planning Services .................................................................................. 271
24.6.1 Covered Services ............................................................................................... 272
24.6.2 Hysterectomies .................................................................................................. 272
24.7 Immunizations ................................................................................................... 272
24.7.1 Billing Procedures: WyVIP Supplied or Private Stock ..................................... 273
24.7.2 Billing Examples ............................................................................................... 277
24.7.3 Other Immunizations ......................................................................................... 279
24.8 Injections ........................................................................................................... 281

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 258 Revision 4/1/17
24.8.1 Belimuab (Benlysta®) Criteria ........................................................................... 281
24.8.1.1 Covered Services ........................................................................................... 281
24.8.1.2 Billing Requirements ..................................................................................... 281
24.8.2 Botox®, Dysport® and Myobloc® ...................................................................... 282
24.8.2.1 Covered Services ........................................................................................... 282
24.8.2.2 Billing Requirements ..................................................................................... 282
24.8.3 Synvisc® Injections............................................................................................ 284
24.8.3.1 Covered Services ........................................................................................... 284
24.8.3.2 Limitations ..................................................................................................... 284
24.8.3.3 Billing Requirements ..................................................................................... 285
24.8.4 Tysabri® ............................................................................................................. 285
24.8.4.1 Covered Services ........................................................................................... 285
24.8.4.2 Billing Requirements ..................................................................................... 286
24.8.4.3 Documentation Requirements ....................................................................... 286
24.9 Interpretation Services ....................................................................................... 286
24.10 Laboratory Services ........................................................................................... 287
24.10.1 CLIA Requirements .......................................................................................... 288
24.10.2 Genetic Testing .................................................................................................. 290
24.10.2.1 Covered Services ........................................................................................... 290
24.10.2.2 BRCA Testing and Counseling ..................................................................... 290
24.10.2.3 Billing Requirements ..................................................................................... 291
24.11 Maternity Care ................................................................................................... 291
24.11.1 Billing Requirements ......................................................................................... 291
24.12 Medical Supplies (Disposable) .......................................................................... 295
24.13 Phototherapy for High Bilirubin Levels ............................................................ 295
24.13.1 Billing Requirements ......................................................................................... 296
24.13.2 Phototherapy Maximum Allowable Appeal Process ......................................... 296
24.14 Practitioner Visits .............................................................................................. 296
24.14.1 New Client ......................................................................................................... 297
24.14.2 Established Client .............................................................................................. 297
24.14.3 After Hours Services ......................................................................................... 297
24.14.4 Consultation Services ........................................................................................ 298

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 259 Revision 4/1/17
24.14.4.1 Billing Requirements ..................................................................................... 298
24.14.4.2 Documentation............................................................................................... 298
24.14.5 Emergency Department Services ...................................................................... 298
24.14.5.1 Covered Services ........................................................................................... 298
24.14.6 Home Visits ....................................................................................................... 299
24.14.6.1 Documentation............................................................................................... 299
24.14.6.2 Limitations ..................................................................................................... 299
24.14.6.3 Billing Requirements ..................................................................................... 300
24.14.7 Critical Care Services ........................................................................................ 301
24.14.8 Prolonged Service .............................................................................................. 301
24.14.9 Practitioner Standby Service ............................................................................. 302
24.14.10 Inpatient Pediatric/Neonatal Critical Care ........................................................ 302
24.14.10.1 Covered Services ........................................................................................... 302
24.14.10.2 Billing Requirements ..................................................................................... 303
24.14.11 Nursing Facilities .............................................................................................. 304
24.14.11.1 Covered Services ........................................................................................... 304
24.14.11.2 Billing Requirements ..................................................................................... 304
24.14.11.3 Nursing Facility Discharge Services ............................................................. 304
24.14.12 Office Visits ...................................................................................................... 305
24.14.12.1 Billing Requirements ..................................................................................... 305
24.14.12.2 Telephone Services ........................................................................................ 305
24.14.12.3 Billing Requirements ..................................................................................... 305
24.15 Preventive Medicine .......................................................................................... 305
24.15.1 Covered Services ............................................................................................... 305
24.16 Public Health Services ....................................................................................... 306
24.17 Radiology Services ............................................................................................ 306
24.17.1 Covered Services ............................................................................................... 306
24.17.2 Billing Requirements ......................................................................................... 306
24.17.3 Limitations ......................................................................................................... 307
24.18 Screening, Brief Intervention, Referral and Treatment (SBIRT) ...................... 307
24.18.1 Covered Services and Billing Codes ................................................................. 308
24.18.2 Limitations ......................................................................................................... 309

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 260 Revision 4/1/17
24.19 Sterilizations and Hysterectomies ..................................................................... 309
24.19.1 Elective Sterilization ......................................................................................... 309
24.19.2 Hysterectomies .................................................................................................. 310
24.20 Surgical Services ............................................................................................... 311
24.20.1 Surgical Packages, Separate Surgical Procedures and Incidental Surgical
Procedures ......................................................................................................... 311
24.20.2 Covered Services ............................................................................................... 312
24.20.3 Limitations ......................................................................................................... 312
24.20.4 Billing Requirements ......................................................................................... 312
24.20.5 Assistant Surgeon .............................................................................................. 313
24.20.5.1 Surgical Assistant Service ............................................................................. 313
24.20.5.2 Two (2) Surgeons .......................................................................................... 314
24.20.5.3 Modifiers ....................................................................................................... 314
24.20.6 Cosmetic Services ............................................................................................. 314
24.20.7 Oral and Maxillofacial Surgeons ....................................................................... 315
24.20.7.1 Covered Services ........................................................................................... 315
24.20.7.2 Covered Services ........................................................................................... 315
24.20.7.3 Billing Requirements ..................................................................................... 315
24.20.8 Breast Reconstruction ........................................................................................ 316
24.20.8.1 Covered Services ........................................................................................... 316
24.20.8.2 Billing Requirements ..................................................................................... 316
24.20.9 Breast Reduction ............................................................................................... 316
24.20.9.1 Covered Services ........................................................................................... 316
24.20.9.2 Billing Requirements ..................................................................................... 316
24.20.9.3 Documentation Requirements ....................................................................... 317
24.20.10 Cochlear Device, Implantation and Replacement ............................................. 317
24.20.10.1 Covered Services ........................................................................................... 317
24.20.10.2 Billing Requirements ..................................................................................... 317
24.20.10.3 Documentation............................................................................................... 318
24.20.11 Gastric Bypass Surgery ..................................................................................... 319
24.20.12 Lumbar Spinal Surgery ..................................................................................... 319
24.20.12.1 Covered Services ........................................................................................... 319

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 261 Revision 4/1/17
24.20.12.2 Reimbursement .............................................................................................. 319
24.20.12.3 Scoliosis ......................................................................................................... 320
24.20.13 Panniculectomy/Abdominoplasty ..................................................................... 320
24.20.13.1 Covered Services ........................................................................................... 320
24.20.13.2 Reimbursement .............................................................................................. 320
24.20.14 Pectus Excavatum and Poland’s Syndrome ...................................................... 321
24.20.14.1 Covered Services ........................................................................................... 321
24.20.14.2 Reimbursement .............................................................................................. 321
24.20.15 Ptosis and Blepharoplasty Repair ...................................................................... 322
24.20.15.1 Covered Services ........................................................................................... 322
24.20.15.2 Ptosis (Belpharoptosis) .................................................................................. 322
24.20.15.3 Reimbursement .............................................................................................. 323
24.20.16 Septoplasty and Rhinoplasty ............................................................................. 324
24.20.16.1 Covered Services ........................................................................................... 324
24.20.16.2 Documentation Requirements ....................................................................... 325
24.20.16.3 Reimbursement .............................................................................................. 325
24.20.17 Vagus Nerve Simulation (VNS) for Epilepsy ................................................... 325
24.20.18 Varicose Vein Treatment ................................................................................... 326
24.20.18.1 Covered Services ........................................................................................... 326
24.20.18.2 Billing Requirements ..................................................................................... 326
24.21 Transplant Policy ............................................................................................... 327
24.21.1 Outpatient Stem Cell/Bone Marrow .................................................................. 327
24.21.1.1 Non-Covered Services ................................................................................... 327
24.22 Vision Services .................................................................................................. 327
24.22.1 Eye and Office Examinations ............................................................................ 327
24.22.1.1 Covered Services ........................................................................................... 328
24.22.1.2 Non Covered Services ................................................................................... 329
24.22.2 Eyeglasses/Materials ......................................................................................... 329
24.22.2.1 Covered Services ........................................................................................... 329
24.22.2.2 Non Covered Charges .................................................................................... 330
24.22.2.3 Reimbursement .............................................................................................. 330

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 262 Revision 4/1/17
24.22.3 Contact Lenses .................................................................................................. 331
24.22.3.1 Covered Services ........................................................................................... 331
24.22.3.2 Non-Covered Services ................................................................................... 331
24.22.4 Vision Therapy .................................................................................................. 331
24.22.4.1 Covered Services ........................................................................................... 332

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 263 Revision 4/1/17
24.1 Practitioner Services
Practitioners Include:
Physicians (MD/DO).
Locum Tenens.
Nurse Practitioners.
Physician’s Assistants, prior to 7/1/16 can only bill for Medicare
crossover claims.
Mental Health Providers.
Ordering, Rendering and Prescribing Providers.
24.2 Covered Services
Abortion
Anesthesia Services
Dermatology
Diabetic Training
Family Planning
Hysterectomies
Imaging Services
Immunizations
Injections
Interpretation Services
Laboratory Services
Locum Tenens
Maternity Care
Medical Supplies
Practitioner Visits
Pregnant By
Choice/Family Planning
Waiver
Preventive Medicine
Psychiatric Services
Public Health Services
Screening, Brief
Intervention, Referral and
Treatment (SBIRT)
Sterilization
Surgical Services
Transplant Policy
Vision Service
24.2.1 Abortion
24.2.1.1 Covered Services
Legal (therapeutic) abortions and abortion services will only be reimbursed by
Medicaid when a physician certifies in writing that one (1) of the following
conditions has been met:
The client suffers from a physical injury, or physical illness, including
endangering the physical condition caused by or arising from the pregnancy
itself, that would place her in danger of death unless an abortion was
performed; or

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 264 Revision 4/1/17
The pregnancy is the result of sexual assault as defined in Wyoming Statute
W.S. 6-2-301, which was reported to a law enforcement agency within five
(5) days after the assault or with five days after the time the victim was
capable of reporting the assault; or
The pregnancy is the result of incest.
24.2.1.2 Reimbursement Requirements
The Abortion Certification Form (6.16.3.2, Abortion Certification Form) must
accompany all claims from the attending physician, assistant surgeon,
anesthesiologist, pathologist and hospital. The attending physician is required to
supply all other billing providers with a copy of the consent form.
In cases of sexual assault, submission of medical records is not required prior
to payment; however, documentation of the circumstances of the case must be
maintained in the client’s medical records.
Other abortion-related procedures, including spontaneous, missed, incomplete,
septic, and hydatiform mole, do not require the certification form; however,
all abortion related procedure codes are subject to audit, and all pertinent
records must substantiate the medical necessity and be available for review.
Pregnancies that terminate in spontaneous abortion/miscarriage in any
trimester must bill with the appropriate CPT-4 code and documentation is
required in the client’s record. Prenatal visits and additional services may be
billed in addition to the abortion code.
RU-486 under the same guidelines as the legally induced abortion is covered
when administered by a practitioner in the practitioner’s office.
NOTE: Reimbursement is available for those induced abortions performed during
periods of retroactive eligibility only if the Abortion Certification Form
(6.16.3.2, Abortion Certification Form) is completed prior to performing
the induced abortion.
24.3 Anesthesia Services
Anesthesia is the process of blocking the perception of pain and other sensations. This
allows clients to undergo surgery and other procedures without the distress and pain
they would otherwise experience.
Procedure Code Range: 00100-01999
24.3.1 Covered Services
Medicaid covers anesthesia only when administered by a licensed anesthesiologist or
a certified registered nurse anesthetist (CRNA) who remains in attendance for the sole
Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 265 Revision 4/1/17
purpose of rendering general anesthesia in order to afford the client anesthesia care
deemed optimal during any procedure.
The American Society of Anesthesiologists (ASA) relative value guide is accepted as
the basis for coding and definition of anesthesia provided to Medicaid clients.
NOTE: The lower conversion factor of 21 is used in the reimbursement rate for
CRNAs. This conversion factor is lower than the conversion factor for
anesthesiologists. The most accurate way to verify coverage for a specific
service is the review the Medicaid fee schedule on the website or contact
Provider Relations (2.1, Quick Reference).
24.3.2 Billing Guidelines
When billing ASA procedure codes, enter actual minutes for procedures
where time is necessary. Fractions of time are always rounded up to the next
full number.
o For example, enter 65 minutes, rather than one (1) hour five (5)
minutes.
o For example, nine (9) minutes would be rounded up to 15 minutes.
Anesthesia units must be billed in minutes. Do not convert or change time by
dividing by 15, the Medicaid’s claims processing system does this
automatically.
Anesthesia CPT Codes are reimbursed based on the units of the anesthesia
procedure and the time units allowed. The total units are multiplied by a
conversion factor to determine the allowed amount. Medical supervision is not
reimbursed.
o For example, claim is billed with 105 units: 105(units billed)/15 = 7
(Anesthesia Units). Add the anesthesia units to the base value (RVU)
assigned to the procedure code: 7 + 7= 14. Times that total by the
conversion factor for that procedure code: 14 x 27.04 = $378.56 = total
paid.
Note: The conversion factor and RVU for each anesthesia procedure
code can be found on the fee schedule on the Wyoming Medicaid
website.
Anesthesia time begins when the anesthesiologist starts to prepare for the
induction of the anesthesia and ends when the anesthesiologist is no longer in
personal attendance. Anesthesia time is the total number of minutes the
surgery(ies) is performed.

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 266 Revision 4/1/17
o For example, preparation of the induction began at 11:00 am and the
anesthesiologist was no longer in attendance by 2:15 pm, total minutes
would be 195 and is also the number of units to be billed.
Providers should bill the appropriate CPT-4 procedure codes for
induction/injection of anesthetic agent.
When multiple procedures are performed during a single anesthetic
administration, Medicaid will pay the anesthesia code representing the most
complex procedure reported. The time reported is the combined total for all
procedures.
Anesthesia is a global service just as the surgical procedure for which it is
given. No pre or postoperative services will be recognized for separate
payment, including those for:
o Pain Management on the same day as surgery.
o Routine monitoring is included in the primary anesthesia and not
reimbursed separately. For specific information regarding routine
monitoring, refer to the current version of the ASA relative value
guide.
o Laryngoscopy codes 31505, 31515, and 31527 are incidental or
included within the anesthesia time.
o Any anesthesia substance administered at the time of the procedure for
circumcision, cannot be billed separately as this is considered part of
the global package.
If two (2) anesthesia codes are billed on the same day, (i.e. tubal ligation
following vaginal delivery), documentation must be submitted with the claim
to support the necessity of these services.
NOTE: Anesthesiologists and CRNA’s are not required to request prior
authorization (PA) directly from Medicaid for any anesthesia procedure.
24.3.3 Obstetrical Exceptions
Procedure code 01967 is a global fee per the fee schedule and should be billed
as one (1) unit, not the number of minutes. The Global fee includes:
o Establishing and maintaining the anesthesia for the time the client
requires it.
o If the anesthesia should continue into the next day, use procedure code
01996.
Anesthesia for multiple obstetrical procedures may be paid for both
procedures in the following circumstances.
o Neuraxial analgesia/anesthesia for planned vaginal delivery which
becomes a Cesarean delivery.
Use procedure code 01967 to begin the procedure and
discontinue its use when a C-section is imminent, then begin

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 267 Revision 4/1/17
using procedure code 01968 and continue on with straight time
(minutes) as for a general surgery.
o Neuraxial analgesia/anesthesia for planned vaginal delivery followed
by tubal ligation on same or the next day following delivery.
Use procedure code 01967 for delivery.
Use procedure code 00851 for intraperitoneal lower abdomen,
tubal ligation/ transection.
NOTE: Medicaid does not allow CPT 01996 on the same day as placement of an
epidural catheter.
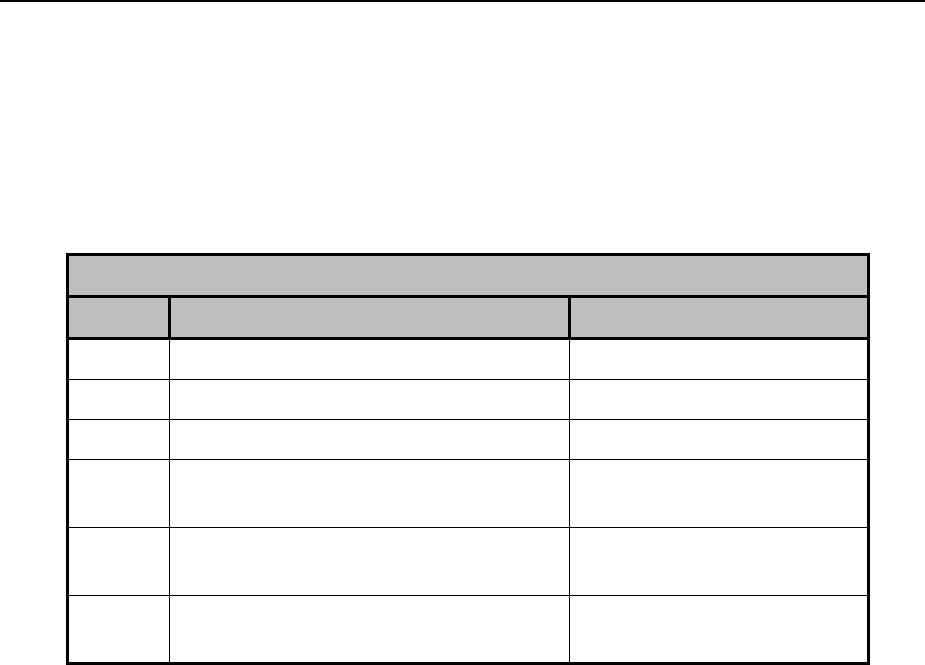
Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 268 Revision 4/1/17
24.3.4 Modifiers
When billing for anesthesia, indicate the appropriate physical status modifier. These
modifiers indicate various levels of complexity of the anesthesia service provided. If
a physical status modifier is billed, additional payment will be added, if appropriate to
the claim payment.
Physical Status Modifiers
Modifier
Description
Reimbursement
P1
A normal healthy client.
No change
P2
A client with mild systemic disease.
No change
P3
A client with severe systemic disease.
Additional 5%
P4
A client with severe systemic disease
that is a constant threat to life.
Additional 10%
P5
A moribund client who is not expected
to survive without the operation.
Additional 15%
P6
A declared brain-dead client whose
organs are removed for donor purposes
Not covered
NOTE: The use of other optional modifiers may be appropriate.
24.3.5 Documentation Requirements
Begin and end times must be documented in the anesthesia record and must
be legible.
Anesthesia time begins when the anesthesiologist begins to prepare the client
for anesthesia care in the operating room or an equivalent area and ends when
the anesthesiologist is no longer in personal attendance and the client is
safely placed under post-anesthesia supervision.
If two (2) anesthesia codes are billed on the same day, (i.e. tubal ligation
following vaginal deliver), documentation must be submitted with the claim
to support the necessity of these services.
24.4 Dermatology
Medicaid covers medically necessary services rendered in the treatment of
dermatological illnesses.

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 269 Revision 4/1/17
24.4.1 Covered Services
Acne surgery due to disfigurement requires prior authorization. (6.14, Prior
Authorization)
Removal of lesions suspected to be precancerous.
Removal of a benign lesion, ganglion cyst, skin tag, keloid, or wart, may be
covered when medically necessary.
24.4.2 Benign Lesion Removal and Destruction of Benign or
Premalignant Lesions
Procedure Code: 11200 (Removal of Skin Tags
Procedure Code: 11310 (Removal / Shave Lesion)
Procedure Code Range: 11400-11446 (Removal)
Procedure Code Range: 17106-17111 (Destruction)
24.4.3 Covered Services
Benign skin lesions include seborrheic keratosis, sebaceous (epidermoid) cysts, skin
tags, milia (keratin-filled cysts), nevi (moles) acquired hyperkeratosis (keratoderma),
papillomas, hemangiomas and viral warts.
24.4.4 Billing Requirements
Wyoming Medicaid considers removal of benign skin lesions as medically
necessary, and not cosmetic, when any of the following is met and is clearly
documented in the medical record, operative report or pathology report:
The lesion is symptomatic as documented by any of the following:
o Intense itching
o Burning
o Irritation
o Pain
o Tenderness
o Chronic, recurrent or persistent bleeding.
o Physical evidence of inflammation (e.g., purulence, oozing, edema,
erythema, etc.)
The lesion demonstrates a significant change in size or color.
The lesion obstructs an orifice or clinically restricts vision.
There is clinical uncertainty as to the likely diagnosis, particularly where
malignancy is a realistic consideration based on lesional appearance, change
in appearance and/or non-response to conventional treatment.
The lesion is likely to turn malignant as documented by medical peer-
reviewed literature or medical textbooks.
A prior biopsy suggests the possibility of lesional malignancy.

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 270 Revision 4/1/17
The lesion is an anatomical region subjected to recurrent physical trauma that
has in fact occurred and objective evidence of such injury or the potential for
such injury is documented.
Wyoming Medicaid considers destruction of benign or malignant skin lesions as
medically necessary, and not cosmetic, when any of the following is met and is
clearly documented in the medical record, operative report or pathology report.
An over-the-counter (OTC) product has been tried and was ineffective (when
applicable)
Lesion causes symptoms of such a severity that the patient’s normal bodily
functions/activities of daily living are impeded (e.g., palmar or plantar warts)
Periocular warts associated with chronic recurrent conjunctivitis thought
secondary to lesion virus shedding;
Warts showing evidence of spread from one (1) body area to another,
particularly in immunosuppressed patients.
Lesions are condyloma acuminata or molluscum contagiosum.
Cervical dysplasia or pregnancy associated with genital warts.
Port wine stains and other hemangiomas when lesions are located on the face
and neck.
o Only three (3) sessions per PA.
o Must include progress notes and photos documenting improvement.
NOTE: Wyoming Medicaid does not consider removal of skin lesions to improve
appearance as medically necessary. Removal of certain benign skin lesions
that do not pose a threat to health or function are considered cosmetic, and
as such, are not medically necessary. In the absence of any of the above
indications, removal of seborrheic keratoses, sebaceous cysts, nevi (moles)
or skin tags is considered cosmetic. Wart removal can be requested for 3
units at a time.
24.4.5 Documentation Requirements
One (1) or more of the above conditions, clearly documented in the medical record,
operative report or pathology report.
24.5 Diabetic Training
Procedure Code Range: G0108-G0109
Physicians, public health nurses, and nurse practitioners managing a client’s diabetic
condition are responsible for ordering diabetic training sessions. Certified Diabetic

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 271 Revision 4/1/17
Educators (CDE) or dieticians employed by a physician, nurse practitioner, or facility
may furnish outpatient diabetes self-management training.
24.5.1 Covered Services
Individual and group diabetes self-management training sessions are covered.
Curriculum will be developed by individual providers and may include, but is not
limited to:
Medication education.
Dietetic/nutrition counseling.
Weight management.
Glucometer education.
Exercise education.
Foot/skin care.
Individual plan of care services received by the client.
24.5.2 Billing Requirements
HCPCS Level II codes, G0108 (individual session) and G0109 (group
session) should be used.
Do not bill a separate office visit on the same date of service.
For individual services, one (1) unit equals 30 minutes. A maximum of two
(2) units applies.
For group services, one (1) unit equals 30 minutes. A maximum of five (5)
units per individual per training session applies.
Billing is to be done under the physician, nurse practitioner or hospital’s
provider number.
24.5.3 Documentation
Documentation should reflect an overview of relative curriculum and any
services received by the client.
The Diabetic Education Certificate is not required to be submitted with each
claim.
24.6 Family Planning Services
Family planning services are to assist clients of childbearing age with learning the
choices available to them to freely determine the number and spacing of their
children.
Family planning services include the following:
Initial visit
Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 272 Revision 4/1/17
Initial physical examination
Comprehensive history
Laboratory services
Medical counseling
Annual visits
Routine visits
24.6.1 Covered Services
Sterilization procedures are covered only when all Medicaid guidelines have
been met (6.16.1.1, Sterilization Consent Form).
Contraceptives
Cervical caps
Male/female condom
Contraceptive injections
Creams
Diaphragms
Foams
Insertion/removal of implantable contraceptives (Norplant and Implanon).
Insertion/removal of IUDs.
Oral contraceptives when prescribed by a physician or nurse practitioner and
dispensed a participating pharmacy.
Spermicides
Sponges
NOTE: Pregnant by Choice/Family Planning Waiver has specific covered and
non-covered services. The plan information can be found in Section 25.1.
24.6.2 Hysterectomies
Procedure Code Range: 58150-58294
Refer to the following sections for information:
6.16.2, Hysterectomy Acknowledgement of Consent.
Section 6.16.2.1, Instructions for Completing the Hysterectomy
Acknowledgement Consent Form.
Section 6.16.2.2, Hysterectomy Consent Form.
24.7 Immunizations
Wyoming Vaccinates Important People (WyVIP) Program (formerly VFC).

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 273 Revision 4/1/17
Providers must enroll with the WyVIP program to receive and distribute WyVIP
vaccines. The WyVIP program makes available, at no cost to providers, selected
vaccines for eligible children 18 years old and under. Medicaid will therefore pay
only for the administration of these vaccines (oral or injection). WyVIP covered
vaccines may change from year to year. For more information on the WyVIP program
current WyVIP covered vaccines or how to enroll as a WyVIP provider contact the
Wyoming Immunization Program at (307)777-7952.
24.7.1 Billing Procedures: WyVIP Supplied or Private Stock
Use the following guidelines when submitting claims to Medicaid:
Providers must use a WyVIP provided vaccine when available and client
appropriate. If the vaccine is supplied by WyVIP, bill the appropriate
procedure code and use the SL modifier. Codes 90477-90748 identify the
vaccine product only. To report the administration of vaccine/toxoid, the
appropriate administration code (see table below) must be reported in addition
to the vaccine/toxoid code. Reimbursement will be made for the
administration only.
When Medicaid is the secondary payer, the provider must submit the claim
according to Medicaid guidelines. Bill other potential payers before billing
Medicaid.
Providers are reminded that use of any vaccine or immunization solely for the
purpose of travel is not covered by Medicaid.
According to WyVIP policy, providers may not impose a charge for the
administration of the vaccine that is higher than the maximum fee established
by the Centers for Medicaid and Medicare Services (CMS) regional cap of
$21.72 per dose.
A previous policy from our office indicated that additional units could be
billed for each antigen in the combination vaccination. Separate codes are
available for combination vaccines. It is inappropriate to code each
component of a combination vaccine separately.
Codes 90477-90748 identify the vaccine product only. To receive
reimbursement for administration they must be reported in addition to an
immunization administration code from the tables below.
When a vaccine is privately obtained due to lack of availability through the
WyVIP program, it will be reimbursed at 100% of purchase invoice. DO
NOT USE the SL modifier in this instance. This policy applies exclusively to
situation where the WyVIP Program has issued a notice of vaccine shortage
and has specified which vaccines are affected.
For vaccines administered to adults over 18 years of age, or for
vaccines/toxoids not supplied by WyVIP, report the appropriate CPT code and
administration fee. DO NOT USE the SL modifier. Medicaid will reimburse
for the vaccine/toxoid and the administration.

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 274 Revision 4/1/17
When the vaccine/toxoid product code does not contain the SL modifier, a
manufacturers’ invoice must be attached to the claim. The vaccine/toxoid will
be reimbursed at 100% of the invoice cost. Exception:
o For procedure codes 90656, 90660, 90703, 90707, and 90714, an
invoice is only required for those clients age 18 years and younger.
Those claims for clients 19 years and older will be reimbursed at a flat
rate of $15.00 for these codes.
o For procedure code 90658, an invoice is only required for those clients
age 18 years and younger. Those claims for clients 19 years and older
will be reimbursed at a flat rate of $20.00 for this code.
o For procedure code 90715 an invoice is only required for those clients
age 18 years and younger. Those claims for clients 19 years and older
will be reimbursed at a flat rate of $30.00 for this code.
Human Papilloma Virus (HPV) Vaccine
o For Codes & 90650 90649
Use CPT-4 code, 90649, for HPV Types 6, 11, 16, and 18
(quadrivalent)
Administer intramuscularly as three (3) separate doses. Use
CPT code 90650, for HPV Types 16, 18 (bivalent)
Administer intramuscularly as three (3) separate doses.
If the client turns 19 years of age between the 1st and 2nd
doses administration, a VFC supplied vaccine cannot be used
to complete the series. Any HPV vaccine administered at age
19 or older must be administered from a provider’s private
stock vaccine.
If the vaccine is supplied by VFC, bill code 90649 or 90650
with the SL modifier. Also bill the appropriate administration
code (see table below). Only the administration code will be
reimbursed.
If the vaccine is supplied from private stock, bill code 90649
without the SL modifier and attach the manufacturers’ invoice.
Also bill the appropriate administration code (see table below).
The vaccine will be reimbursed at 100% of invoice cost along
with the administration code.
For Code 90651
o Use CPT-4 code, 90651, for HPV Types 6, 11, 16, 18, 31, 33, 45, 52,
and 58 nonvalent (HPV) for females only
Administer intramuscularly as three (3) separate doses. If the
client turns 19 years of age between the first (1st) and second
(2nd) doses administration, a VFC supplied vaccine cannot be
used to complete the series. Any HPV vaccine administered at
age 19 or older must be administered from a provider’s private
stock vaccine.

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 275 Revision 4/1/17
The vaccine must be supplied by VFC, bill code 90651 with
the SL modifier. Also bill the appropriate administration code
(see table below). Only the administration code will be
reimbursed.
Influenza Vaccine
o Medicaid covers influenza vaccines for clients age 6 months and older.
If the vaccine is supplied by WyVIP, bill the appropriate
procedure code and use the SL modifier. Also bill the
appropriate administration code (see table below). Only the
administration code will be reimbursed.
o For codes 90656 and 90660:
If the vaccine is supplied from private stock and the client is 18
years of age or younger, DO NOT USE the SL modifier, and
attach a manufacturers’ invoice. Also bill the appropriate
administration code (see table below). The vaccine will be
reimbursed at 100% of invoice cost, along with the
administration code.
If the vaccine is supplied from private stock, and the client is
19 years of age or older, DO NOT USE the SL modifier. No
manufacturers’ invoice is necessary. Also bill the appropriate
administration code (see table below). The vaccine will be
reimbursed at a flat $15.00 rate along with the administration
code.
For code 90658:
o If the vaccine is supplied from private stock and the client is 18 years
of age or younger, DO NOT USE the SL modifier, and attach a
manufacturers’ invoice. Also bill the appropriate administration code
(see table below). The vaccine will be reimbursed at 100% of invoice
cost, along with the administration code.
o If the vaccine is supplied from private stock, and the client is 19 years
of age or older, DO NOT USE the SL modifier. No manufacturers’
invoice is necessary. Also bill the appropriate administration code (see
table below). The vaccine will be reimbursed at a flat $20.00 rate
along with the administration code.
All other influenza vaccine codes:
o If the vaccine is supplied from private stock and the client is of any
age, DO NOT USE the SL modifier, and attach a manufactures’
invoice. Also bill the appropriate administration code (see table
below). The vaccine will be reimbursed at 100% of invoice cost, along
with the administration code.
Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 276 Revision 4/1/17
o When a Medicaid client is a resident of a long-term care facility, the
vaccine and administration are included in the nursing home per diem
rate, and not paid separately.
Pneumococcal Vaccine
o Medicaid covers pneumococcal vaccines for where it is medically
indicated.
o If the vaccine is supplied by WyVIP, bill the appropriate procedure
code and use the SL modifier. Also bill the appropriate administration
code (see table below). Only the administration code will be
reimbursed.
o If the vaccine is supplied from private stock and the client is of any
age, DO NOT USE the SL modifier, and attach a manufacturers’
invoice. Also bill the appropriate administration at 100% of invoice
cost, along with the administration code.
o When a Medicaid client is a resident of a long-term care facility, the
vaccine and administration are included in the nursing home per diem
rate, and not paid separately.
NOTE: If a significant separately identifiable Evaluation and Management service
(e.g. Office or other outpatient services, preventive medicine services) is
performed, the appropriate E&M service code should be reported in
addition to the vaccine and toxoid administration codes.
Administration Codes – Physician Provides Face-to-Face Vaccine Counseling
CPT Code
Description
90460
Immunization administration 0-18 years of age via any route of
administration, with counseling by physician or other qualified health
care professional; first vaccine/toxoid component
90461
Each additional vaccine/toxoid component (list separately in addition to
code for 1st component) for age 0-18
Administration notes: For vaccines where physician or other qualified health care
professional provides counseling, code 90460 will be reported once for each vaccine
administered. For any vaccine with multiple components (i.e. DtaP or Tdap), 90461
will be reported for each additional component. If multiple vaccines are administered,
“like codes” must be combined onto the same line, using multiple units to avoid
denials for duplicates. Medicaid will pay up to the allowable on each unit of 90460,
and $0.00 for each unit of 90461. Providers should bill their usual and customary fee
for 90460 and $0.00 for 90461.
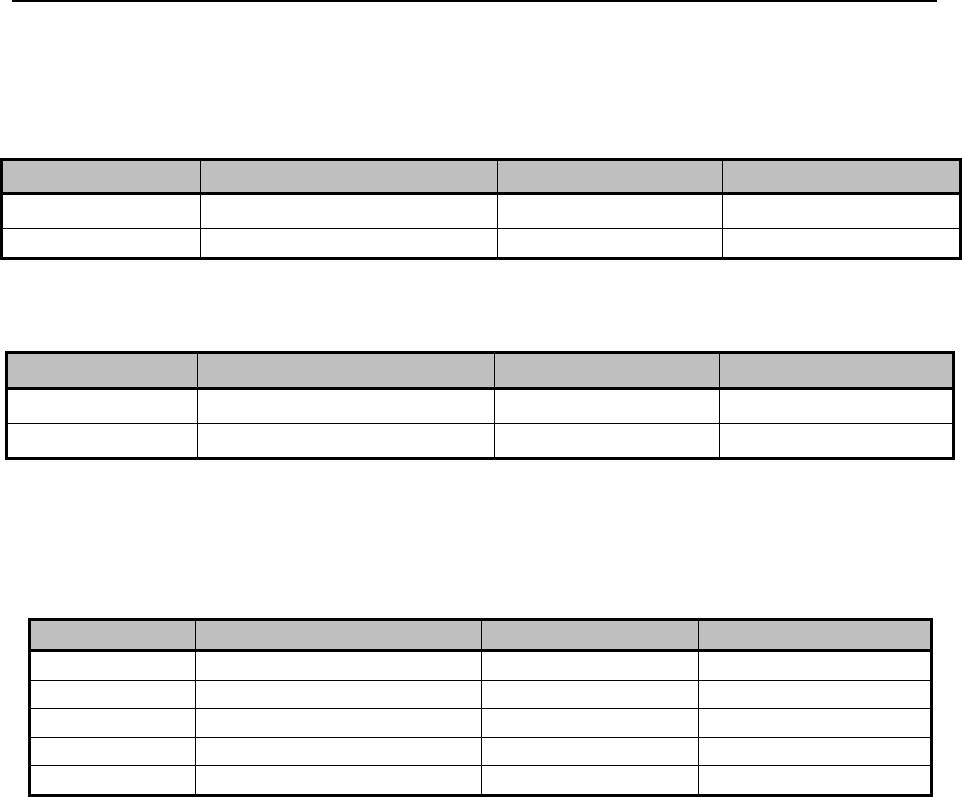
Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 277 Revision 4/1/17
24.7.2 Billing Examples
Example 1: Provider administers the HPV vaccine, state supplied with physician
counseling:
DOS (24A)
Procedure Code (24C)
Charges (24F)
Units (24G)
01/01/15
90649 SL
$0.00
1
01/01/15
90460
$21.72
1
Example 2: Provider administers Tdap, MMR and Influenza. All are state supplied
with physician counseling:
DOS (24A)
Procedure Code (24C)
Charges (24F)
Units (24G)
01/01/15
90707 SL
$0.00
1
01/01/15
90715 SL
$0.00
1
01/01/15
9065 SL
$0.00
1
01/01/15
90460
$65.16
3
01/10/15
90461
$0.00
4
Explanation of Example 2: Three (3) units of 90460 (one (1) for each vaccine
administered to indicate each 1st component) and four (4) units of 90461 (one (1) for
each additional component in the Tdap and the MMR vaccine beyond the 1st.
DOS (24A)
Procedure Code (24C)
Charges (24F)
Units (24G)
01/01/15
90651 SL
$0.00
1
01/01/15
90460
$21.72
1
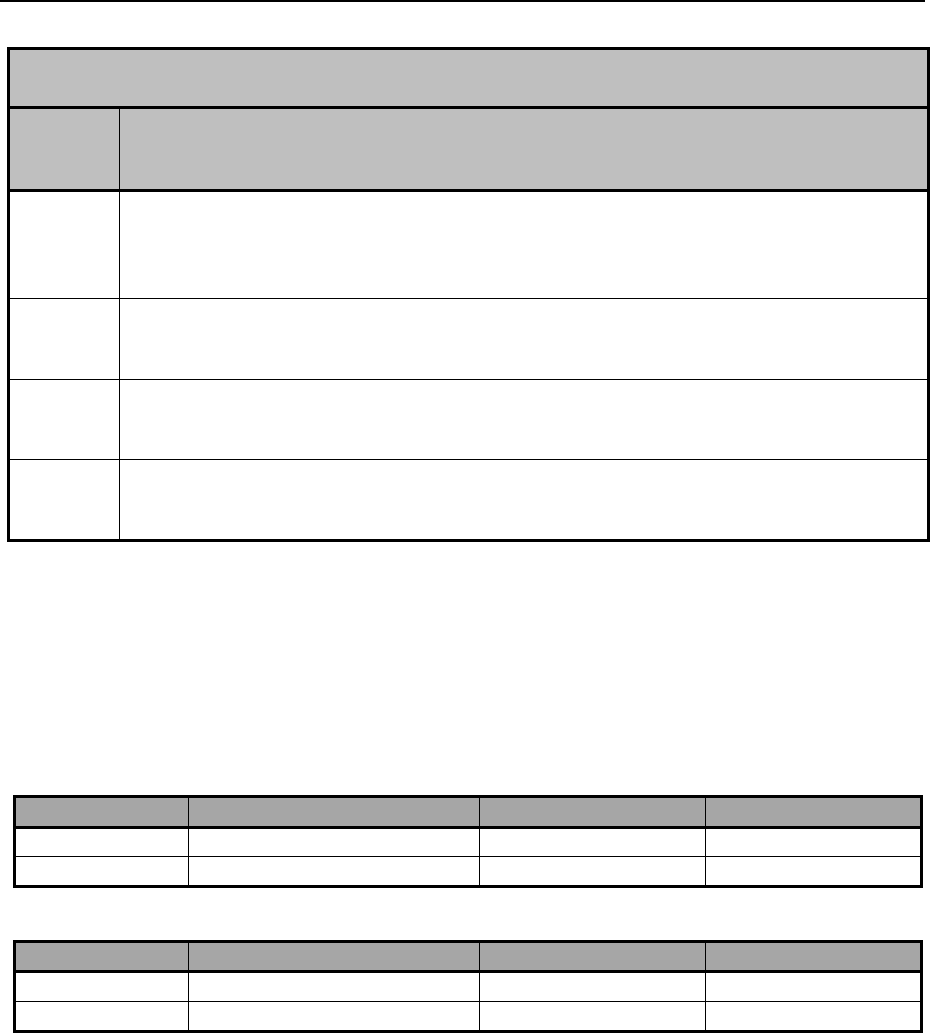
Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 278 Revision 4/1/17
Administration Codes – Face-to-Face Vaccine Counseling Not Provided by Physician
CPT
Code
Description
90471
Immunization administration (includes percutaneous, intradermal, subcutaneous,
or intramuscular injections); one (1) vaccine (single or combination
vaccine/toxoid). Do not report in conjunction with 90473.
90472
Each additional vaccine (single or combination vaccine/toxoid). List separately in
addition to code for primary procedure (90471 or 90473).
90473
Immunization administration by intranasal or oral route; one (1) vaccine (single
or combination vaccine/toxoid). Do not report with 90471.
90474
Each additional vaccine (single or combination vaccine/toxoid). List separately in
addition to code for primary procedure (90471 or 90473).
For vaccinations where face to face counseling is not provided, 90471 or 90473 is
reported for the first vaccine, and 90472 or 90474 (units combined for multiples) for
each additional vaccine.
Example 4: Provider administers the HPV vaccine, state supplied, without physician
counseling:
DOS (24A)
Procedure Code (24C)
Charges (24F)
Units (24G)
01/01/15
90649 SL
$0.00
1
01/01/15
90471
$14.00
1
DOS (24A)
Procedure Code (24C)
Charges (24F)
Units (24G)
01/01/15
90651 SL
$0.00
1
01/01/15
90471
$14.00
1
Example 5: Provider administers Tdap, MMR and Influenza, all state supplied,
without physician counseling:
Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 279 Revision 4/1/17
Explanation of Example 5: One (1) unit of 90471 for the first (1st) vaccine, and two
(2) units of 90472 for the other two (2) vaccines.
NOTE: WyVIP is not intended for private pay patients.
24.7.3 Other Immunizations
Other immunizations include, but are not limited to:
Synagis
o Synagis is used for the prevention of serious lower respiratory tract
disease caused by respiratory syncytial virus (RSV) in infants and
children under two (2) years of age with chronic lung disease who
have required medical therapy for their chronic lung disease within six
(6) months before the anticipated RSV season (American Academy of
Pediatrics Committee on Infectious Diseases and Committee on Fetus
and Newborns).
o Wyoming Medicaid will pay for Synagis when ordered by a physician
to prevent RSV when the following conditions are met:
Chronic Lung Disease: Client is < 24-months of age at start of
therapy and has chronic lung disease of prematurity (i.e.
bronchopulmonary dysplasia), continues to require medical
intervention (chronic corticosteroid or diuretic therapy) or
required supplemental oxygen for at least 28 days after birth.
Congenital Heart Disease: Client is < 12 months of age at start
of therapy and has hemodynamically significant congenital
heart disease and one (1) or more of the following:
Is receiving medication to control congestive heart
failure.
Has a diagnosis of moderate to severe pulmonary
hypertension.
Has a diagnosis of cyanotic heart disease.
Prematurity:
Client is < 12 months of age at start of RSV season and
born at < 28 weeks, six (6) days gestational age.
Client is < 12 months of age at start of RSV season and
born at 34-weeks, six (6) days or less gestational age
DOS (24A)
Procedure Code (24C)
Charges (24F)
Units (24G)
01/01/15
90707 SL
$0.00
1
01/01/15
90715 SL
$0.00
1
01/01/15
90656 SL
$0.00
1
01/01/15
90471
$14.00
1
01/01/15
90472
$28.00
2

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 280 Revision 4/1/17
and has either severe neuromuscular disease or
congenital abnormalities, either of which compromise
handling of respiratory secretions.
Client is < six (6) months of age at start of RSV season
and born between 29 weeks, zero (0) days and 35
weeks, six (6) days gestational age.
o If Synagis is prescribed outside the normal prescribing guidelines, the
physician will need to supply documentation of medical necessity to
support prescribing.
o Synagis may be provided in a physician’s office or in an outpatient
hospital or clinic setting. Because of the short stability once mixed (six
(6) hours) and the expense of this medication, every effort should be
made to ensure the least amount of waste. Scheduling multiple clients
that are in need of this medication within the six (6) hour allotment is
suggested.
o Synagis may be billed one (1) of two (2) ways:
Supplied by a pharmacy and injected at the physician’s office.
The physician’s office may bill the appropriate
Evaluation and Management code, procedure code
90772 for the injection fee.
The physician’s office supplies the medication and gives the
injection.
The physician submits a claim for the appropriate
Evaluation and Management code, procedure code
90378 and appropriated NDC for the Synagis and the
90772 for the injection fee.
NOTE: Because of the cost associated with Synagis, only one (1) month’s dose
should be billed at a time.
Additional Vaccines, Toxoids
o CPT-4 codes for vaccines are to be used to bill for the vaccine product
itself and are reported in addition to the immunization administration
codes (90471, 90472) unless the WyVIP program supplied the
vaccine.
o Separate codes are available for combination vaccines. It is
inappropriate to code each component of a combination vaccine
separately.
NOTE: The most accurate way to verify coverage for a specific service is to
review the Medicaid fee schedule on the website (2.1, Quick Reference).
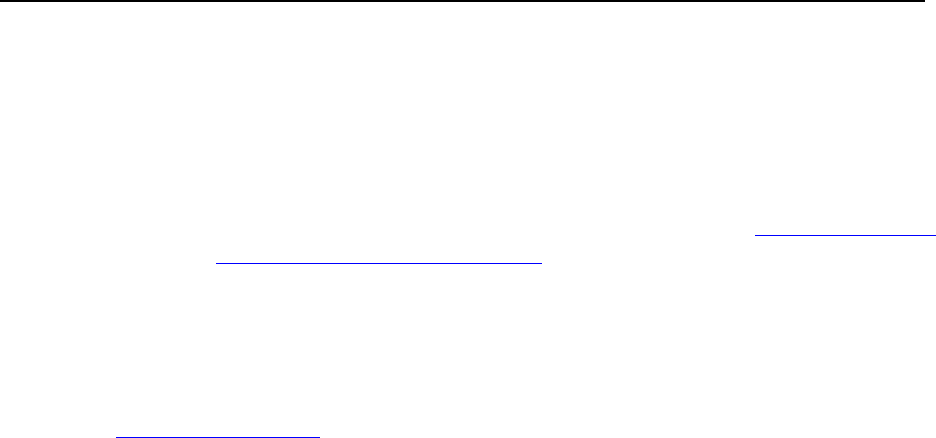
Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 281 Revision 4/1/17
24.8 Injections
Reimbursement for J-codes and therapeutic injections include the cost of the
administration fee. This cost is already calculated into the fee for each code.
NOTE: Therapeutic injections may not be billed with a J-code (6.8, National Drug
Code (NDC) Billing Requirement).
If multiple drugs are included in a single injection, separate codes may be billed for
the drugs, however, the administration fee should be included with only one (1) code.
For an accurate listing of codes, refer to the fee schedule on the Medicaid website
(2.1, Quick Reference).
24.8.1 Belimuab (Benlysta®) Criteria
Procedure Code: J0490
24.8.1.1 Covered Services
Belimumab is covered and considered medically necessary if the below requirements
are met.
24.8.1.2 Billing Requirements
Prior authorization requirements:
Wyoming Medicaid considers Belimumab medically necessary, when all of the
following is met and is clearly documented in the medical record, operative report or
pathology report:
The patient is 18 years of age or older.
The patient has a diagnosis of active systemic lupus erythematosus (SLE)
disease.
The patient has positive autoantibody test results [positive antinuclear
antibody (ANA >1:80) and/or anti-dsDNA (>30 IU/mL)].
ONE (1) of the following:
o The patient is currently on a standard of care SLE treatment regimen
comprised of at least one (1) of the following: corticosteroids,
hydroxychloroquine, chloroquine, nonsteroidal anti-inflammatory
drugs (NSAIDS), aspirin, and/or immunosuppressives (azathioprine,
methotrexate, cyclosporine, oral cyclophosphamide, or
mycophenolate).
o The patient has a documented intolerance, FDA labeled
contraindication, or hypersensitivity to the standard of care drug
classes listed above.

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 282 Revision 4/1/17
Benlysta® (belimumab) PA Criteria Page two (2) of four (4) Current
Procedural Terminology copyright American Medical Association. All Rights
Reserved. Contains Public Information.
The patient does NOT have severe active lupus nephritis [proteinuria >6 g/24-
hour or equivalent or serum creatinine >2.5 mg/dL OR required hemodialysis
or high-dose prednisone >100 mg/day] within the past 90-days.
The patient does NOT have severe active central nervous system lupus [e.g.
seizures, psychosis, organic brain syndrome, cerebrovascular accident,
cerebritis, CNS vasculitis requiring therapeutic intervention] within the past
60-days.
The patient has NOT been treated with intravenous cyclophosphamide in the
previous six (6) months.
The patient is NOT currently using another biologic agent.
The patient is NOT currently being treated for a chronic infection.
The dose is within the FDA labeled dosage of 10 mg/kg intravenously at two
(2) week intervals for the first three (3) doses and at four (4) week intervals
thereafter.
NOTE: Length of Approval: 12 months.
24.8.2 Botox®, Dysport® and Myobloc®
Procedure Code Range: J0585-J0587
24.8.2.1 Covered Services
Botulinum toxin type A (e.g., onabotulinumtoxinA [Botox®], or abobotulinumtoxinA
[Dysport®]) or B (fimabotulintoxinB [Myobloc®] for the treatment of the following
conditions and are considered medically necessary when specific criteria is met.
24.8.2.2 Billing Requirements
Prior authorization requirements:
Wyoming Medicaid considers Botulinum toxin A (onabotulinumtoxinA [Botox®] and
abobotulinumtoxinA [Dysport®]) appropriate for the treatment of the following
conditions and meet medical necessity criteria where it is stated:
Strabismus with ALL of the following:
1. Associated with dystonia (impaired or disordered tonicity)
2. ABSENCE of ALL of the following:
a. Duane’s syndrome with lateral rectus weakness.
b. Restrictive strabismus.
c. Strabismus secondary to prior surgical over-recession of the
antagonist.

Covered Services –_Practitioner Services__________________________________________
Ch. 24 Index 283 Revision 4/1/17
d. Strabismus deviations more than 50 prism diopters.
e. Chronic paralytic strabismus except when used with surgical
repair to reduce antagonist contracture.
Severe primary hyperhidrosis with ALL of the following:
1. Location is ANY ONE (1) of the following:
a. Axillary
b. Palmar
2. Treatment is not adequately managed with topical agents
3. The condition causes ANY ONE (1) of the following:
a. Functional impairment
b. Medical complications
Urinary incontinence with ALL of the following:
1. Individual has undergone urodynamic studies with diagnosis of
idiopathic detrusor over-activity (IDO).
2. Anticholinergic therapy has failed to provide adequate control.
NOTE: Not allowed when an individual has a urinary tract infection, in patients
with urinary retention and in patients with post-void residual (PVR) urine
volume > 200 mL who are not routinely performing clean intermittent
self-catheterization (CIC).
Blepharospasm
Cranial nerve VII disorders (eg. Hemifacial spasms)
Wyoming Medicaid considers Botulinum toxin type A (e.g., onabotulinumtoxinA
[Botox®], or abobotulinumtoxinA [Dysport®]) or B (fimabotulintoxinB [Myobloc®]
for the treatment of the following conditions are considered medically necessary:
Achalasia
Cervical Dystonia
Chronic anal fissure
Hereditary spastic
paraplegia
Idiopathic torsion
dystonia
Infantile cerebral palsy,
spastic
Organic writer’s cramp
Orofacial dyskinesia
Oromandibular dystonia
Spasmodic dysphonia
Spasmodic torticollis
Spastic hemiplegia
Symptomatic torsion
dystonia

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 284 Revision 4/1/17
Botulinum toxin type A (e.g., onabotulinumtoxinA [Botox®]) for the prevention of
migraine headaches is considered medically appropriate if the headaches are
chronic with ANY ONE (1) the following criteria met:
Initial six (6) month trial for migraine headaches with ALL the following:
o Occur 15-days or more per month.
o Last four (4) hours a day or longer.
o Experienced for three (3) months or more.
o Symptoms persist despite adequate trials of a minimum of two (2)
agents from different classes used in the treatment of chronic
migraines (e.g. Angiotensin-converting enzyme inhibitors/antiotensin
II receptor blockers, anti-depressants, anti-epileptics, beta blockers and
calcium channel blockers), unless the individual has contraindications
to such medications.
Continuation of therapy after six (6) month trial for the prevention of
migraines with ANY ONE (1) of the following:
o Frequency reduced by at least seven (7) days per month.
o Duration of headache reduced by at least 100 hours per month.
NOTE: Botox® can only be requested one (1) session at a time, with medical
necessity provided for each session and only 360 units (three (3) month
supply) per limb.
24.8.3 Synvisc® Injections
(Hyaluronan, Hyaluronic acid, Sodium Hyaluronate, Hylan polymers)
Procedure Code: J7323-J7326
24.8.3.1 Covered Services
Hyaluronic Acid Derivatives are injected directly into the knee joint to improve
lubrication and reduce the pain associated with osteoarthritis of the knee. Hyaluronic
Acid Derivatives are subject to prior authorization as well as step therapy. When prior
authorization criteria is met and approval given, step therapy must still be followed.
The FDA has not approved intra-articular hyaluronan for joints other than the knee.
24.8.3.2 Limitations
Euflexxa® – Is injected into the affected knee, 20 mg once (1) weekly for
three (3) weeks, a total of three (3) injections.
Synvisc One® – Is injected into the affected knee, 48 mg for one (1) dose
only.
Synvisc – Is injected into the affected knee, 16 mg once weekly for three (3)
weeks, a total of three (3) injections.

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 285 Revision 4/1/17
Hyalgan® – Is injected into the affected knee, 20 mg once (1) weekly for a
total of five (5) injections.
Orthovisc – Is injected into the affected knee, 30 mg once (1) weekly for
three (3) or four (4) injections.
Supartz® – Is injected into the affected knee, 25 mg once (1) weekly for a
total of five (5) injections.
Gel-One® – Is injected into the affected knee, 30 mg, for one (1) dose only.
24.8.3.3 Billing Requirements
Prior authorization requirements:
Wyoming Medicaid considers Synvisc injections as medically necessary when any of
the following is met and is clearly documented in the medical record, operative report
or pathology report. The following criteria must be met for approval of coverage:
Documented diagnosis of symptomatic osteoarthritis of the knee.
Trial of conservative nonpharmacologic treatment, (education, physical
therapy, weight loss if appropriate) has not resulted in functional
improvement. Medical records documenting these therapies must be
submitted.
Trial of pharmacotherapy (NSAIDs, COX II Inhibitors, acetaminophen) has
not resulted in functional improvement.
Pain interferes with functional activities such as ambulation and prolonged
standing.
Prior therapy with at least one (1) intra-articular corticosteroid injection.
Repeat doses of any viscosupplement will be approved only when the following
criteria are met:
At least six (6) months has elapsed since the previous injection or completion
of the prior series of injections.
Medical records must document significant improvement in pain and
functional capacity of the knee joint.
24.8.4 Tysabri®
Procedure Code: J2323
24.8.4.1 Covered Services
Tysabri® is a treatment for MS to delay the accumulation of physical disability and
reduce the frequency of clinical exacerbations. It is used as a monotherapy. Tysabri®
is recommended for patients who have had an inadequate response to, or are unable to
tolerate alternate MS therapies.

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 286 Revision 4/1/17
NOTE: Tysabri® increases the risk of Progressive Multifocal
Leukoencephalopathy (PML), an opportunistic viral infection of the brain
that usually leads to death or severe disability.
24.8.4.2 Billing Requirements
Prior authorization (PA) requirements:
Tysabri® must be prescribed by a neurologist enrolled in the Touch Program.
Both the provider administering the Tysabri® and the patient receiving the
Tysabri® must be enrolled in the Touch Program.
Medicaid will only authorize Tysabri® for clients that have a diagnosis of MS.
Length of PA: 12 months
For continued PA the neurologist must submit documentation to show
improvement or stabilization.
Dosage: 300 mg IV infusion every four (4) weeks.
Must be billed using the NDC number and the appropriate J-code.
NOTE: Medicaid will not cover Tysabri® when used in conjunction with other
medications for the treatment of progressive MS.
24.8.4.3 Documentation Requirements
Physician’s prescription
Complete Prior Authorization Form (6.14, Prior Authorization)
Must document an inadequate response to, or inability to tolerate an
appropriate trial with at least one (1) of the following interferon agents:
o Betaseron
o Avonex
o Rebif
o Copaxone
This documentation must include information that states when the drug(s) was started
and discontinued, and the reason the drug(s) was discontinued.
Documentation must state the date the treating provider and patient were
enrolled in the Touch Program, and both must meet all eligibility requirements
of that program. As of 11/18/2015, the first infusion can be documented with
Initial Notice of Patient Authorization.
24.9 Interpretation Services
The Office for Civil Rights (OCR) of the U.S. Department of Health and Human
Services (DHHS) enforces Federal laws that prohibit discrimination by healthcare and

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 287 Revision 4/1/17
human service providers that receive funds from the DHHS. Such laws include Title
VI of the Civil Rights Act of 1964, Section 504 of the Rehabilitation Act of 1973, and
Title II of the Americans with Disabilities Act of 1990.
In efforts to maintain compliance with this law and ensure that Medicaid clients
receive quality medical services, interpretation services should be provided for clients
who have Limited English Proficiency (LEP) or are deaf/hard of hearing. The
purpose of providing services must be to assist the client in communicating
effectively about health and medical issues.
Interpretation between English and a foreign language is a covered service for
Medicaid clients who have LEP. LEP is defined as “the inability to speak,
read, write, or understand the English language at a level that permits an
individual to interact effectively with healthcare providers.”
Interpretation between sign language or lip reading and spoken language is a
covered service for Medicaid clients who are deaf or hard of hearing. Hard of
hearing is defined as “limited hearing which prevents an individual from
hearing well enough to interact effectively with healthcare providers.”
Medicaid providers should arrange this service for their clients by contacting an
enrolled interpretation provider prior to the medical appointment. A current list of
enrolled interpretation providers and is available on the Medicaid website or upon
request from Provider Relations (2.1, Quick Reference). Interpretation services may
be provided telephonically (via a language line service) or in person. When
coordinating interpreter services for a client it will be necessary to provide the
enrolled interpretation provider with the following information:
Name of client.
Client’s Medicaid ID number.
Name of referring provider.
Time and date service will be rendered.
Location of where service will take place (telephonically or in person).
Estimated length of time service will be rendered.
24.10 Laboratory Services
Medicaid covers tests provided by independent (non-hospital) clinical laboratories
when the following requirements are met:
Services are ordered and provided by physicians, dentists, or other providers
licensed within the scope of their practice as defined by law.
Services are provided in an office or other similar facility, but not in a hospital
outpatient department or clinic.
Providers of lab services must be Medicaid certified.

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 288 Revision 4/1/17
Providers of lab services must have a current Clinical Laboratory
Improvement Amendments (CLIA) certification number.
Providers may bill Medicaid only for those lab services they have performed
themselves. Medicaid does not cover reference lab services.
Procedure Code Range: 80048-89331
NOTE: Non-covered services include routine handling charges, stat fees, post-
mortem examination and specimen collection fees for throat culture or Pap
smears.
24.10.1 CLIA Requirements
The type of CLIA certificate required to cover specific codes is listed in the table
below. These codes are identified by Center for Medicare and Medicaid Services
(CMS) as requiring CLIA certification; however, Medicaid may not cover all of the
codes listed. Refer to the fee schedule located on Medicaid website for actual
coverage and fees. Content is subject to change at any time, without notice (2.1,
Quick Reference).
NOTE: Codes within the below table are Wyoming Medicaid specific. It is the
provider’s responsibility to ensure the codes being billed are covered by
Wyoming Medicaid.
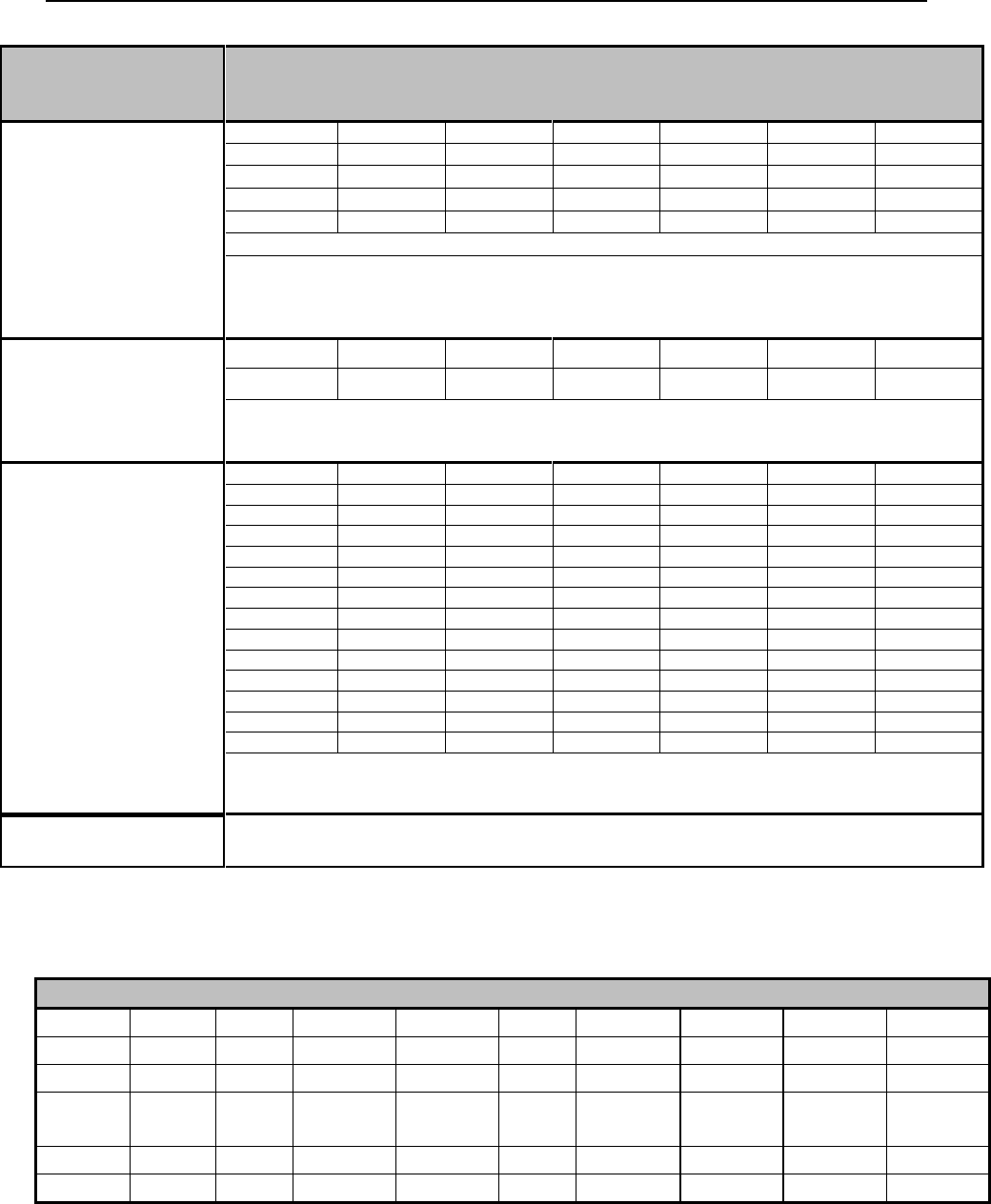
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 289 Revision 4/1/17
CLIA
CERTIFICATE
TYPE
ALLOWED TO BILL
REGRISTRATION,
COMPLIANCE, OR
ACCREDITATION
(LABORATORY) (1)
G0103
G0123
G0124
G0141
G0143
G0144
G0145
G0147
G0148
G0306
G0307
G0328
G0416
G0432
G0433
G0434
G9143
P3000
17311
17312
17313
17314
17315
78110
78111
78120
78121
78122
78130
78191
78270
78271
78272
80000-89999 (UNLESS OTHERWISE SPECIFIED ELSEWHERE IN THIS TABLE)
PROVIDERS WITH THIS CLIA TYPE MAY BILL THE CODES WITHIN THE LABORATORY
(CLIA TYPE 1) SECTION AND ALL CODES FOR PPMP (CLIA TYPE 4) SECTION AND WAIVER
(CLIA TYPE 2) SECTION AND THE CODES EXCLUDED FROM CLIA REQUIREMENTS (REFER
TO TABLE BELOW)
PROVIDER-
PERFORMED
MICROSCOPY
PROCEDURES
(PPMP) (4)
81000
81001
81015
81020
89055
89190
G0027
Q0111
Q0112
Q0113
Q0114
Q0115
PROVIDERS WITH THIS CLIA TYPE MAY BILL THE CODES WITHIN THE PPMP (CLIA TYPE 4)
SECTION AND ALL CODES FOR WAIVER (CLIA TYPE 2) SECTION AND THE CODES
EXCLUDED FROM CLIA REQUIREMENTS (REFER TO TABLE BELOW)
WAIVER (2)
80047 QW
80048 QW
80051 QW
80053 QW
80061 QW
80069 QW
80178 QW
81003 QW
81007 QW
82010 QW
82040 QW
82043 QW
82044 QW
82120 QW
82150 QW
82247 QW
82271 QW
82274 QW
82310 QW
82330 QW
82374 QW
82435 QW
82465 QW
82523 QW
82550 QW
82565 QW
82570 QW
82679 QW
82947 QW
82950 QW
82951 QW
82952 QW
82977 QW
82985 QW
83001 QW
83002 QW
83036 QW
83037 QW
83516 QW
83605 QW
83655 QW
83718 QW
83721 QW
83861 QW
83880 QW
83986 QW
84075 QW
84132 QW
84155 QW
84295 QW
84443 QW
84450 QW
84460 QW
84478 QW
84520 QW
84550 QW
84703 QW
85014 QW
85018 QW
85576 QW
85610 QW
86294 QW
86308 QW
86318 QW
86386 QW
86618 QW
86701 QW
86803 QW
87077 QW
87210 QW
87449 QW
87804 QW
87807 QW
87808 QW
87809 QW
87880 QW
87899 QW
89300 QW
89321 QW
G0328 QW
G0433 QW
G0434 QW
G0477 QW
81002
81025
82270
82272
82962
83026
84830
85013
85651
PROVIDERS WITH THIS CLIA TYPE MAY BILL THE CODES WITHIN THE WAIVER (CLIA
TYPE 2) SECTION AND ALL CODES EXCLUDED FROM CLIA REQUIREMENTS (REFER TO
TABLE BELOW)
NO
CERTIFICATION
PROVIDERS WITHOUT A CLIA MAY BILL ALL CODES EXCLUDED FROM CLIA
REQUIREMENTS (SEE BELOW)
NOTE: QW next to a laboratory code signifies that a QW modifier must be used.
CODES EXCLUDED FROM CLIA REQUIREMENTS
80500
80502
81050
82075
83013
83014
83987
84061
86077
86078
86079
86485
86486
86490
86510
86580
86891
86910
86923
86927
86930
86931
86932
86945
86950
86960
86965
86985
86999
87900
88125
88240
88241
88304
TC
88305
TC
88311
88312
TC
88313
TC
88314
TC
88329
88720
88738
88741
88749
89049
89220
89240
89251
89255
89261
89272
89281
89290
89354
89398

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 290 Revision 4/1/17
24.10.2 Genetic Testing
Procedure Codes: 81201-81479; 96040
Prior Authorization is required for all genetic testing codes. Prior authorization
documentation must document the following:
24.10.2.1 Covered Services
Medicaid covers genetic testing under the following conditions:
There is reasonable expectation based on family history, risk factors, or
symptomatology that a genetically inherited condition exists; and
Test results will influence decisions concerning disease treatment or
prevention (in ways that not knowing the test results would not); and
Genetic testing of children might confirm current symptomatology or predict
adult onset diseases and findings might result in medical benefit to the child or
as the child reaches adulthood; and
Referral is made by a genetic specialist (codes 81223 and 81224) or a
specialist in the field of the condition to be tested; and
All other methods of testing and diagnosis have met without success to
determine the client’s condition such that medically appropriate treatment can
be determined and rendered without the genetic testing. (6.14, Prior
Authorization).
Codes 81420, 81507 - Mother must be documented as high-risk to include:
advanced maternal age >35 (at EDC), previous "birth" of embryo/fetus/child
with aneuploidy, parent with known balanced translocation, screen positive on
standard genetic screening test (FTCS, multiple marker screen of one type or
another, etc), ultrasound finding on embryo/fetus consistent with increased
risk of aneuploidy
24.10.2.2 BRCA Testing and Counseling
The U.S. Preventive Services Task Force (USPSTF) recommends that women whose
family history is associated with an increased risk for deleterious mutations in
BRCA1 or BRCA2 genes be referred for evaluation for BRCA testing (81211-
81217). Medicaid covers BRCA testing when the following criteria are met:
Personal and/or family history of breast cancer, especially if associated with
young age of onset; or
Multiple tumors; or
Triple-negative (i.e., estrogen receptor, progesterone receptor, and human
epidermal growth factor receptor 2-negative) or medullary histology; or
History of ovarian cancer; and
18 years or older; and
Pre-test genetic counseling has been prior authorized.
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 291 Revision 4/1/17
24.10.2.3 Billing Requirements
Enrolled laboratories should bill Medicaid directly for genetic testing, refer to Section
20.3.
The following billing procedures must be followed when the physician agrees to act
as a third party agent for a non-enrolled laboratory:
The following documents must be attached to the claim (6.15, Submitting
Attachments for Electronic Claims):
The physician’s letter justifying the genetic testing must be attached to the
claim. The letter must document the necessity for the genetic testing by
meeting the covered service conditions mentioned above.
Manufacturer’s invoice (Reimbursement will be invoice plus 15%).
No prior authorization is required.
NOTE: Post payment claim review will be conducted.
24.11 Maternity Care
Maternity services include antepartum, delivery & postpartum care of a pregnant
woman, according to guidelines set forth in the current edition of the CPT-4 book.
Procedure Code Range: 59000-59898
24.11.1 Billing Requirements
Global Care for Routine Obstetric Care
According to the AMA, if the global care is provided by the same physician or same
physician group, then the appropriate global code must be reported. Global services
are to be billed in all cases of a single physician or group providing uncomplicated
maternity care.
59400 – Routine OB care including antepartum care, vaginal delivery (with or
without episiotomy, and/or forceps) and postpartum care.
59510 – Routine OB care including antepartum care, cesarean delivery and
postpartum.
59610 – Routine OB care including antepartum care, vaginal delivery (with or
without episiotomy, and/or forceps) and postpartum care, after previous C-
section.
59618 – Routine OB care including antepartum care, C-section and
postpartum care, following attempted vaginal delivery after previous C-
section.

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 292 Revision 4/1/17
NOTE: The E&M services (visits) provided within the Global package are
included in the antepartum care and are not to be coded separately. The
date of service is the date of delivery.
The services normally provided in uncomplicated maternity cases include antepartum
care, delivery and postpartum care. Antepartum care includes:
The initial and subsequent.
Physical examination.
Recording of the weight, blood pressures and fetal heart tones.
Routine chemical urinalysis.
Monthly visits up to 28-week’s gestation, biweekly visits to 36 week’s
gestation and then weekly visits until delivery.
Non-Global Services for Routine Obstetric Care
Use the following billing procedures when a patient is seen by a different physician or
a different physician group for their antepartum care:
If the total antepartum visits with the patient is 1-3, bill the appropriate E&M
(Evaluation and Management) code for each visit.
Bill only one (1) of the following two (2) antepartum procedure codes
(depending on the total number of antepartum visits):
o 59425 – Antepartum care only; four (4) to six (6) visits. This code
would be used in the case where the patient was only seen for four (4)
to six (6) visits and then quit seeing that provider. The provider would
not be providing services of delivery or postpartum care. If the
provider saw the patient at least four (4) times and no more than six (6)
times, this is the correct code the provider would submit.
o 59426 – Antepartum care only; seven (7) or more visits. This code
would be used for the patient who was seen for seven (7) or more
antepartum visits, but the provider did not provide services for
delivery or postpartum care.
Bill procedure code 59430 for postpartum care only (separate procedure). This
code is to be used when the provider did not provide the service of the
delivery, but they may have provided the antepartum care.
NOTE: It is not appropriate to separately report the antepartum, delivery and
postpartum care when provided by the same physician or same physician
group. However, any other visits or services provided within the
antepartum period, other than those listed above, should be coded and
reported separately. The date of service is the date of delivery.
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 293 Revision 4/1/17
Patient has Other Medical Conditions, or a Complicated Pregnancy
Use the following billing procedures when the patient has other medical conditions,
or a complicated pregnancy:
If the provider needs to treat the patient for additional services due to
complication of pregnancy, use the proper CPT and ICD codes to reflect the
complication.
If the provider attempts to bill a separate E&M visit and only code the
encounter as a normal pregnancy code, the claim will be denied and
considered unbundling of the Global Maternity package.
These codes cover attendance at delivery when requested by the provider delivering
and initial stabilization of newborn. These codes may be reported in addition to the
CPT-4 code for history and examination, but not in addition to the newborn
resuscitation code.
When billing for a twin delivery, modifier 22 should be added to the delivery
code and documentation must accompany the claim. Providers cannot bill two (2)
separate delivery codes for the delivery of twins except, when one (1) twin is
delivered vaginally and the other by cesarean.
Pregnancies that terminate in abortion/miscarriage in any trimester must bill with the
appropriate CPT-4 code and documentation is required. Prenatal visits and additional
services may be billed in addition to the abortion code.
NOTE: When billing for an assistant surgeon at a delivery, use the procedure code
for delivery only with an 80 or AS modifier as appropriate. Refer to
Section 6.16.1, Sterilization Consent Guidelines for more information if
the client is considering sterilization.
Elective Inductions and Medical Necessity
Induction of labor for medical reasons is appropriate when there may be health risks
to the woman or baby if the pregnancy were to continue. Some indications for
inducing labor include:
High blood pressure caused by the pregnancy.
Maternal health problems affecting the pregnancy.
Infection in the uterus.
Water has broken too early.
Fetal growth problems.
Documentation, which substantiates that the patient’s condition meets the coverage
criteria, must be on file with the provider.

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 294 Revision 4/1/17
All clams are subject to both pre-payment and post-payment review for medical
necessity by Medicaid. Should a review determine that services do not meet all the
criteria listed above, payment will be denied or, if the claim has already been paid,
action will be taken to recoup the payment for those services.
Induction is not a covered service unless it meets the guidelines listed above.
Inductions without medical necessity will be subject to post pay reviews and possible
recoupment of payments to both the physician and hospital.
Obstetrical Ultrasound
Procedure Code Range: 76801-76828
Acceptable Modifiers: TC, 22, 26 and 52
Medicaid covers obstetrical ultrasounds during pregnancy when medical necessity is
established for one (1) or more of the following conditions:
Establish date of conception
Discrepancy in size versus fetal age
Early diagnosis of ectopic or molar pregnancy
Fetal Postmaturity Syndrome
Guide for amniocentesis
Placental localization associated with abnormal vaginal bleeding (placenta
previa)
Polyhydramnios or Oligohydramnios
Suspected congenital anomaly
Suspected multiple births
Other conditions related directly to the medical diagnosis or treatment of the
mother and/or fetus.
NOTE: Maintain all records and/or other documentation that substantiates medical
necessity for OB ultrasound services performed for Medicaid clients as
documentation may be requested for post-payment review purposes.
Medicaid will only pay for two (2) routine ultrasounds per pregnancy.
Medicaid will not reimburse obstetrical ultrasounds during pregnancy for any of the
following reasons:
Determining gender
Baby pictures
Elective
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 295 Revision 4/1/17
Post-payment review will be conducted on obstetrical ultrasound claims after
payment is made to the provider in order to ensure claims meet the Medicaid policies
contained in this manual.
24.12 Medical Supplies (Disposable)
Procedure Code: 99070
Disposable medical supplies are intended for one (1) time use, not re-use, and
specifically related to the active treatment or therapy of the client for a medical illness
or physical condition. These supplies have a medical purpose, are consumable and/or
expendable and non-durable. This does not include personal care items. They are not
to be confused with durable medical supplies/equipment. The following is a partial
list:
Ace bandage
Sling
Rib belt
Straight Catheter Kit
Surgical tray
Reimbursement may be allowed for a surgical tray if minor surgery necessitates local
anesthesia and other supplies (i.e., gauze, sterile equipment, suturing material) and the
surgery is performed in the provider’s office. Examples of procedures requiring a
major surgical tray include:
Diagnosis biopsies.
Wound closures.
Removal of cysts or other lesions.
Expendable medical supplies such as gauze, dressing, syringes and culture plates, are
included in the reimbursement rate for the office visit or test performed. The most
accurate way to verify coverage for a specific service/supply is to review the fee
schedule on the Medicaid website (2.1, Quick Reference).
Supplies and materials, which do not have procedure codes, may be billed with CPT
code 99070, which will reimburse billed charge up to $10.00. Claims for more than
$10.00 require an attached invoice. These claims will be reimbursed at invoice plus
shipping and handling plus 15%. Claims billed with this code will be subject to pre-
and post-payment review (6.15, Submitting Attachments for Electronic Claims).
24.13 Phototherapy for High Bilirubin Levels
Procedure Code: E0202 RR
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 296 Revision 4/1/17
Effective with dates of service April 1, 2015 and forward, in order to provide better
access to home therapy for newborns with high bilirubin levels, and reduce the
number of hospital readmissions for Wyoming Medicaid infants, Wyoming Medicaid
will be allowing the below taxonomies to bill the E0202 RR (phototherapy – rental)
HCPCS code.
All physicians (20s)
Nurse Practitioners (363Ls, 367A00000X)
Durable Medical Equipment Suppliers (332B00000X)
Public Health Nurse’s Offices (251K00000X)
24.13.1 Billing Requirements
Procedure code E0202 with the RR (rental only) modifier may be billed using daily
units with a maximum of five (5) per lifetime.
Practitioner services, such as home or office based visits, home health visits, lab tests,
etc., should be billed as appropriate in addition to the rental of the Biliblanket or other
phototherapy device.
For clinical requirements, refer to the DME Covered Services Manual on the website
(2.1, Quick Reference).
24.13.2 Phototherapy Maximum Allowable Appeal Process
Wyoming Medicaid encourages providers to submit the initial claim to receive
reimbursement for the initial five (5) days. Then, when appealing, submit an
Adjustment/Void Request Form (6.18.3.1, Adjustment/Void Request Form) with a
corrected claim that has the additional units included along with medical necessity
and an appeal letter to the below address.
Providers may choose to submit only one (1) claim which includes the additional
units along with the medical necessity and the appeal letter to:
DME Provider Services Manager
6101 Yellowstone Road, Suite 210
Cheyenne, WY 82002
24.14 Practitioner Visits
Procedure Code Range: 99201-99443
Practitioner services are provided in inpatient and outpatient settings and include:
Consultation services
Emergency department services
Home visits
Hospital services
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 297 Revision 4/1/17
Nursing facilities
Office visits
Telephone services
NOTE: Practitioner services provided to a client between ages 22 and 64 at an
Institution for Mental Disease (IMD) are a non-covered service pursuant to federal
Medicaid regulation. This includes Medicare crossover claims for dual eligible
clients. An IMD is defined as a hospital, nursing facility, or other institution of 17
beds or more that is primarily engaged in providing diagnosis, treatment, or care of
people with mental diseases.
24.14.1 New Client
Procedure Code Range: 99201-99205
Medicaid considers a new client to be a client who is new to the practitioner and
whose medical and administrative records need to be established. A new client visit
should be submitted once per client lifetime per provider. An exception may be
allowed when a client has been absent for a period of three (3) years, or more.
24.14.2 Established Client
Procedure Code Range: 99211-99215
Medicaid considers an established client to be a client that has been seen by the
practitioner and whose medical and administrative records have been established.
24.14.3 After Hours Services
Medicaid reimburses physicians and practitioners who see clients in their offices
rather than the emergency room, when appropriate. The following codes are only to
be used when the client is seen in the physician/practitioner’s office. The following
codes may be billed in addition to Evaluation and Management codes.
Physician/Practitioner’s After Hours Billing Codes
CPT-4 Code
Description
99050
Services provided in the office times other than regularly scheduled office
hours, or days when the office is normally closed (e.g. holidays, Saturday, or
Sunday) in addition to basic service
99051
Service(s) provided in the office during regularly scheduled evening, weekend,
or holiday office hours, in addition to basic service
99058
Service(s) provided on an emergency basis in the office, which disrupts other
scheduled office services, in addition to basic service
NOTE: Do not use these codes for seeing clients in the emergency room.
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 298 Revision 4/1/17
24.14.4 Consultation Services
Procedure Code Range: 99241-99245
Consultation services are when a practitioner’s opinion or advice is sought by another
practitioner for further evaluation and/or management of a client for a specific
problem.
24.14.4.1 Billing Requirements
The request and need for a consultation from the attending practitioner, along
with the consultant’s opinion and any service that was ordered or performed,
must be documented in the client’s record and communicated to the
requesting practitioner.
If subsequent to the completion of a consultation, the consultant assumes
responsibility for management of all or a portion of the client’s condition(s),
the follow-up consultation codes should not be used.
If an additional request for an opinion or advice regarding the same or new
problem is received from the attending practitioner and documented in the
medical record, the office consultation codes may be used again.
When billing for a consultation, the NPI of the referring practitioner must be
provided on the claim.
NOTE: For an accurate listing of codes, refer to the fee schedule on the Medicaid
website (2.1, Quick Reference).
24.14.4.2 Documentation
Medicaid requires Documentation of Medical Necessity (3.4, Medical Necessity) to
be attached to a claim submitted by the consulting practitioner when a client is seen
for an additional consultation within one (1) year of the initial consultation.
24.14.5 Emergency Department Services
Procedure Code Range: 99281-99288
Emergency department services provide evaluation, management, treatment and
prevention of unexpected illnesses or injuries. Emergency Department is defined as
an organized hospital-based facility for the provision of unscheduled, episodic
services to clients who present themselves for immediate attention. The facility must
be available 24-hours a day.
24.14.5.1 Covered Services
Medicaid covers practitioner services performed by:
A hospital-based emergency room practitioner;
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 299 Revision 4/1/17
A private practitioner who furnished emergency room services through
arrangement with the hospital; or
A private practitioner who is called to the hospital to treat an emergency.
The practitioner must document in the client’s medical record if the client’s
visit to the emergency room was actually an emergency situation.
NOTE: Practitioners are requested to report any potential abuse of emergency
room visits to Provider Relations (2.1, Quick Reference).
24.14.6 Home Visits
Procedure Code Range: 99341-99350
Home visits are evaluation and management services provided by a practitioner in a
private residence.
This benefit is not intended to replace those services available in the community
through other agency programs, (Best Beginnings, Public Health Nurse, Home
Health, etc.) but to offer the attending practitioner another alternative to care for
clients.
24.14.6.1 Documentation
The following documentation must be included in the client’s medical record:
Documentation of practitioner order and treatment plan of care.
Documentation of observed medical condition, progress at each visit, any
change in treatment, and the client’s response to treatment.
Documentation of coordination of care between office and home visit.
24.14.6.2 Limitations
Medicaid will reimburse the admitting practitioner for only one (1) initial visit
per client for each hospital stay.
A comprehensive inpatient hospital visit is not allowed within 30-days of a
previous hospital admission with the same diagnosis.
Medicaid will not reimburse a comprehensive hospital inpatient exam on the
same day as an office visit, nursing home visit or ER visit by the same
provider.
NOTE: For initial inpatient encounters by practitioners other than the admitting
practitioner use initial inpatient consultation codes or subsequent hospital
care codes.

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 300 Revision 4/1/17
24.14.6.3 Billing Requirements
Initial Hospital Care (99221-99223) – All E&M services (e.g., office visits)
related to and provided on the same date as an inpatient hospital admission are
considered part of that hospital admission.
Subsequent Hospital Care (99231-99233) – Subsequent visits are limited to
one (1) visit per day unless a Documentation of Medical Necessity is attached
and approved by Medicaid. All subsequent hospital care visits are to include
the medical record and the results of diagnostic studies and changes in the
status since the last assessment by the practitioner (3.4, Medical Necessity).
Observation or Inpatient Care Services (99234-99236) – These codes are
used when the client is admitted and discharged on the same day. These codes
are used to report observation or inpatient hospital care services provided to
clients admitted and discharged on the same date of service. It is not required
that the client be located in an observation area designated by the hospital as a
separate unit. These codes are to be used based on the level of care the client
received rather than location.
Hospital Discharge Services (99238-99239) – Practitioners may bill for the
final day of an inpatient hospital stay when they provide a final examination,
discussion of the stay, instructions for continuing care and preparation of
discharge records. These codes are only allowed when an initial or subsequent
hospital visit is billed on the day of discharge.
o To report services provided to a client admitted to the hospital after
receiving hospital observation care services on the same date, refer to
the hospital inpatient billing instructions. For a client admitted to the
hospital on a date subsequent to the date of observation status, the
hospital admission is reported using the appropriate initial hospital
care codes. Do not report the observation discharge in conjunction
with the hospital admission.
o All evaluation and management services related to and provided on the
same day as an admission to observation status are considered part of
that admission. Do not report them separately. This applies regardless
of the setting in which the services are provided (e.g., a hospital
emergency department, a physician’s office or a nursing facility, etc.).
o These codes apply to all practitioner services provided on the same
date of client admission to observation status. Do not use these codes
for postoperative recovery if the procedure is considered a global
procedure.
Concurrent Care – Inpatient hospital care provided by two (2) or more
practitioners to the same client on the same day. Practitioners who are
providing concurrent care should use the subsequent hospital care billing
codes. Medicaid will reimburse for these services when all of the following
criteria are met:
o The practitioners have different specialties or subspecialties;
o The condition or injury involves more than one (1) body system;

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 301 Revision 4/1/17
o The condition or injury is so severe or complex that one (1)
practitioner alone cannot handle the client’s care; and
o The practitioners are actively co-managing the client’s treatment.
24.14.7 Critical Care Services
Procedure Code Range: 99291
Critical care is the treatment of critically ill clients experiencing medical emergencies
requiring constant attendance of the practitioner. Critical care is typically provided in
a critical care unit. Critical care involves high complexity decision making to assess,
manipulate, and support vital system function(s) to treat single or multiple vital organ
system failure and/or to prevent further life threatening deterioration of the client’s
condition Critical Care services include:
The interpretation of cardiac output measurements (93561, 93562)
Chest x-rays (71010, 71015, 71020)
Blood gases
Data stored in computers
Gastric intubation (43752, 91105)
Temporary transcutaneous pacing (92953)
Ventilator management (94002-94003, 94660, 94662)
Vascular access procedures (36000, 36410, 36415, 36600)
Pulse oximetry (94760, 94762)
The critical care codes are used to report the total duration of time spent by a
practitioner providing constant attention to a critically ill client. The procedure code
99291 is to report the first 30-74 minutes of critical care should be used only once per
day even if the time spent by the physician is not continuous that day. Another
procedure code 99292 is used to report each additional 30 minutes (30 minutes = 1
unit) beyond the first 74 minutes.
24.14.8 Prolonged Service
Procedure Code Range: face-to-face 99354-99357 and non-face-to-face 99358-
99359
Prolonged physician services either direct face-to-face or non-face-to-face contact
may be billed to Medicaid in addition to other physician’s services. This service is
reported when the service is beyond the usual service in either the inpatient or
outpatient setting. In addition to other physician service, including E&M services at
any level.
NOTE: Prolonged services that exceed three (3) hours on the same date of service
must be documented as medically necessary in the patient’s medical

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 302 Revision 4/1/17
record, including the purpose and actual time the physician was detained
(3.4, Medical Necessity).
24.14.9 Practitioner Standby Service
This procedure code is used to report physician standby service that is requested by
another physician and that involves prolonged physician attendance without direct
(face-to-face) client contact. The physician may not be providing care or services to
other clients during this period. This code is not used if the period of standby ends
with the performance of a procedure subject to a “surgical” package by the physician
who was on standby.
Standby service of less than 30-minutes duration on a given day is not reported
separately.
Second and subsequent periods of standby beyond the first 30-minutes may be
reported only if a full 30-minutes of standby was provided for each unit of service
reported.
NOTE: This code may not be reported in addition to CPT-4 code 99464 for
attendance at delivery.
Procedure Code Range: 99360
24.14.10 Inpatient Pediatric/Neonatal Critical Care
Procedure Code Range: 99291
24.14.10.1 Covered Services
Critical care codes include the following:
Management
Monitoring treatment of the client
Parent counseling
Direct supervision of the healthcare team in the performance of cognitive and
procedural activities
Cardiac and respiratory monitoring
Continuous and/or frequent vital sign monitoring
Heat maintenance
Enteral and/or parenteral nutritional adjustments
Laboratory service
Oxygen

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 303 Revision 4/1/17
24.14.10.2 Billing Requirements
Services start with the date of admission to the NICU and may be reported only once
per day, per client. Once the neonate is no longer considered to be critically ill, the
appropriate codes for subsequent hospital care should be utilized.
The following procedures are also included as part of the global descriptors:
Interpretation of chest x-rays.
Cardiac output measurements.
Pulse oximetry.
Blood gases and other information stored in computers.
Gastric intubation.
Ventilation management.
Temporary transcutaneous pacing.
Vascular procedures.
Chest X-rays.
Umbilical venous and arterial catheters.
Arterial, central venous or peripheral vessel catheterization.
Vascular access procedures.
Vascular punctures.
Oral or nasogastric tube placement.
Endotracheal intubation.
Lumbar puncture.
Suprapubic bladder aspiration.
Bladder catheterization.
CPAP management.
Surfactant administration.
Intravascular fluid administration.
Blood transfusion.
Monitoring of electronic vital signs.
Bedside pulmonary function testing and/or monitoring or interpretation of
blood gases or O2 saturation.
In addition, specific services are included in the parenthetic note following each
NICU code.
NOTE: The most accurate way to verify coverage for a specific service is to
review the CPT-4 book for the appropriate date of service.

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 304 Revision 4/1/17
24.14.11 Nursing Facilities
Procedure Code Range: 99304-99318
A nursing facility is an entity that provides skilled nursing care and rehabilitation
services to people with illnesses, injuries or functional disabilities. Most facilities
serve the elderly. However, some facilities provide services to younger individuals
with special needs such as the developmentally disabled, mentally ill and those
requiring drug and alcohol rehabilitation.
24.14.11.1 Covered Services
Practitioner services are covered when they are medically necessary and are
performed to meet the requirements of continued long-term care.
24.14.11.2 Billing Requirements
When a client is admitted to the nursing facility in the course of an encounter in
another site of service, such as office or emergency room, all evaluation and
management service in conjunction with the admission is considered part of the initial
nursing facility care if performed on the same date, and will not be reimbursed
separately.
Initial client care may be billed only once per long-term care stay unless the client has
moved to a different facility and/or changes providers.
Evaluation and management codes billed in addition to procedure code 99304 are not
reimbursed when performed on the same date as the admission.
Hospital discharge or observation discharge services performed on the same date of
nursing facility admission or readmission may not be reported separately.
Discharge planning codes may not be billed on date of the client’s death.
Two (2) subcategories of nursing facility services are recognized. Both subcategories
apply to new or established clients; and must be billed by the provider.
24.14.11.3 Nursing Facility Discharge Services
Nursing facility discharge day management codes are to be used to report the total
duration of time spent by a physician for the final nursing facility discharge of a
client.
99315 Nursing Facility discharge day management; 30-minutes or less.
99316 Nursing Facility discharge day management, more than 30-minutes.
NOTE: For an accurate listing of codes, refer to the fee schedule on the Medicaid
website (2.1, Quick Reference).
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 305 Revision 4/1/17
24.14.12 Office Visits
An office visit is considered evaluation and management services provided in a
practitioner’s office or in an outpatient or other ambulatory facility.
24.14.12.1 Billing Requirements
Office visits for new clients must be billed using CPT-4 codes 99201-99205.
Established clients must be billed using CPT-4 codes 99211-99215.
Several codes may be used in addition to the above codes when services are
provided in a physician or practitioner’s office for emergency care after
scheduled routine office hours.
Documentation must support the CPT-4 code(s) billed by the practitioner.
NOTE: For an accurate listing of codes, refer to the fee schedule on the Medicaid
website (2.1, Quick Reference).
24.14.12.2 Telephone Services
Procedure Code Range: 99441-99443, limited to physician use only
24.14.12.3 Billing Requirements
Telephone evaluation and management service provided by a physician to an
established patient, parent, or guardian not originating from a related evaluation and
management service provided within the previous seven (7) days nor leading to an
evaluation and management service or procedure within the next 24-hours or soonest
available appointment.
Procedure code 99441: 5 to 10 minutes of medical discussion.
Procedure code 99442: 11 to 20 minutes of medical discussion.
Procedure code 99443: 21 to 30 minutes of medical discussion.
24.15 Preventive Medicine
Procedure Code Range: 99381-99379
24.15.1 Covered Services
For specific information on preventive health services for clients under age 21, refer
to Section 18.1, Health Check – EPSDT.
Preventive health services for clients over 21 are:
Cancer screening services.

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 306 Revision 4/1/17
Screening mammographies are limited to a baseline mammography between
ages 35 and 39; one (1) screening mammography per year after age 45. All
mammograms require a referral.
Annual gynecological exam including a Pap smear. One (1) per year
following the onset of menses. This should be billed using an extended office
visit procedure code. The actual Lab Cytology code is billed by the lab where
the test is read and not by the provider who obtains the specimen.
24.16 Public Health Services
Public health clinic services are physician and mid-level practitioner services
provided in a clinic designated by the Department of Health as a public health
clinic.
Services must be provided directly by a physician or by a public health nurse
under a physician’s immediate supervision (i.e., the physician has seen the
client and ordered the service).
24.17 Radiology Services
Procedure Code Range: 70010-79999
Radiology services are ordered and provided by practitioners, dentists, or other
providers licensed within the scope of their practice as defined by law. Radiology
providers must be supervised by a practitioner licensed to practice medicine within
the state the services are provided. Imaging providers must meet state facility
licensing requirements. Facilities must also meet any additional federal or state
requirements that apply to specific tests (e.g., mammography). All facilities providing
screening and diagnostic mammography services are required to have a certificate
issued by the Federal Food and Drug Administration (FDA).
24.17.1 Covered Services
Medicaid provides coverage of medically necessary radiology services, which are
directly related to the client’s symptom or diagnosis when provided by independent
radiologists, hospitals and practitioners.
24.17.2 Billing Requirements
For most radiology services and some other tests, the fee schedules indicate different
fees, whether the practitioner provided only the technical component (performed the
test), only the professional component (interpreted the test), or both components (also
known as the global service). Practitioners must bill only for the services they provide
(2.1, Quick Reference).
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 307 Revision 4/1/17
Technical components of imaging services must be performed by
appropriately licensed staff (e.g., x-ray technician) operating within the scope
of their practice as defined by state law and under the supervision of a
practitioner.
Multiple procedures performed on the same day must be billed with two (2)
units to avoid duplicate denial of service.
24.17.3 Limitations
Screening mammographies are limited to a baseline mammography between
ages 35 and 39; one (1) screening mammography per year after age 45. All
mammograms require a referral by a practitioner.
X-rays performed as a screening mechanism or based on standing orders.
Separate consultations or procedures unless ordered by the attending
practitioner.
24.18 Screening, Brief Intervention, Referral and Treatment
(SBIRT)
SBIRT is a comprehensive, integrated, public health approach to the delivery of early
intervention and treatment services for persons with substance abuse use disorders, as
well as those who are at risk of developing these disorders. Primary care centers,
hospital emergency rooms, trauma centers and other community settings provide
opportunities for early intervention with at-risk substance users before more severe
consequences occur. The goal of SBIRT is to make screening for substance abuse a
routine part of medical care.
Screening is a quick, simple way to identify patients who need further
assessment of treatment for substance use disorders. It does not establish
definitive information about diagnosis and possible treatment needs.
Brief intervention is a single session or multiple sessions of motivational
discussion focused on increasing insight and awareness regarding substance
use and motivation toward behavior change. Brief intervention can be tailored
for variance in population or setting and can be used as a stand-alone
treatment for those at-risk as well as a vehicle for engaging those in need of
more extensive levels of care.
Brief treatment is a distinct level of care and is inherently different from both
brief intervention and specialist treatment. Brief treatment is provided to those
seeking or already engaged in treatment, who acknowledges problems related
to substance use. Brief treatment in relation to traditional or specialist
Modifier
Description
Reimbursement
26
Professional Component
30% of allowed fee
TC
Technical Component
70% of allowed fee

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 308 Revision 4/1/17
treatment has increased intensity and is of shorter duration. It consists of a
limited number of highly focused and structured clinical sessions with the
purpose of eliminating hazardous and/or harmful substance use.
Referral to specialized treatment is provided to those identified as needing
more extensive treatment than offered by the SBIRT program. The
effectiveness of the referral process to specialty treatment is a strong measure
of SBIRT success and involves a proactive and collaborative effort between
SBIRT providers and those providing specialty treatments to ensure access to
the appropriate level of care.
A key aspect of SBIRT is the integration and coordination of screening and treatment
components into a system of services. This system links a community’s specialized
treatment program with a network of early intervention and referral activities that are
conducted in medical and social service settings.
24.18.1 Covered Services and Billing Codes
Acceptable billing providers for SBIRT include:
Physician – All 20X taxonomy types
Public Health Clinic – 251K00000X
FQHC – 261QF0400X
RHC – 261QR1300X
Nurse Practitioners – 363L
Advanced Practitioner of Psych/Mental Health Nursing – 364SP0808X
Certified Nurse Midwives – 367A00000X
Nurse Anesthetists – 357500000X
Medicaid covers SBIRT services for clients 18 years of age and older.
H0049 – Alcohol and/or drug screening, per screening. WY SBIRT Screening
Tool – ASSIST – The Mental Health and Substance Abuse Services Division
has chosen the Alcohol, Smoking and Substance Involvement Screening Test
(ASSIST) developed by the World health organization (WHO) The ASSIST
screening tool can be accessed through their web site at:
http://www.who.int/substance_abuse/activities/assist/en/
H0050 – Alcohol and/or drug services, brief intervention, per 15 minute units
– Maximum of four (4) units.
NOTE: Providers are to bill these codes in addition to the code they will bill for
the primary focus of the visit. Screening and brief intervention are not
stand alone services, rather they may be part of a medical visit with
another problem focus. For example, a patient presents for migraine

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 309 Revision 4/1/17
headaches and is given the ASSIST (H0049 – screening). The ASSIST
tool indicates the need for brief intervention (H0050 – brief intervention).
The physician would bill the most appropriate code for their services
related to the initial complaint of migraine headache, in addition to the
appropriate SBIRT codes.
24.18.2 Limitations
SBIRT will not be covered for clients with services limited to emergency services
only.
24.19 Sterilizations and Hysterectomies
Procedure Code Range: 58150-58294, 58541-58554, 58600-58720
24.19.1 Elective Sterilization
Elective sterilizations are sterilizations completed for the purpose of becoming sterile.
Medicaid covers elective sterilizations for men and women when all of the following
requirements are met:
Clients must complete and sign the Sterilization Consent Form at least 30-
days, but not more than 180-days, prior to the sterilization procedure. There
are no exceptions to the 180-day limitation of the effective time period of the
informed consent agreement (e.g., retroactive eligibility). This form is the
only form Medicaid accepts for elective sterilizations. If this form is not
properly completed, payment will be denied. A complete Sterilization Consent
Form must be obtained from the primary physician for all related services
(6.16.1, Sterilization Consent Guidelines).
The 30-day waiting period may be waived for either of the following reasons:
Premature Delivery – The Sterilization Consent Form must be completed
and signed by the client at least 30-days prior to the estimated delivery date
and at least 72-hours prior to the sterilization.
Emergency Abdominal Surgery – The Sterilization Consent Form must be
completed and signed by the client at least 72-hours prior to the sterilization
procedure.
o Clients must be at least 21 years of age when signing the form.
o Clients must not have been declared mentally incompetent by a
federal, state or local court, unless the client has been declared
competent to specifically consent to sterilization.
o Clients must not be confined under civil or criminal status in a
correctional or rehabilitative facility, including a psychiatric hospital
or other correctional facility for the treatment of the mentally ill.

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 310 Revision 4/1/17
Before performing sterilizations, the following requirements must be met:
The client must have the opportunity to have questions regarding the
sterilization procedure answered to his/her satisfaction.
The client must be informed of his/her right to withdraw or withhold consent
any time before the sterilization without being subject to retribution or loss of
benefits.
The client must understand the sterilization procedure being considered is
irreversible.
The client must be made aware of the discomforts and risks, which may
accompany the sterilization procedure being considered.
The client must be informed of the benefits associated with the sterilization
procedure.
The client must know that he/she must have at least 30-days to reconsider
his/her decision to be sterilized.
An interpreter must be present and sign for those clients who are blind, deaf,
or do not understand the language to assure the client has been informed
(19.1, Interpreter Services).
Informed consent for sterilization may not be obtained under the following
circumstances:
If the client is in labor or childbirth.
If the client is seeking or obtaining an abortion.
If the client is under the influence of alcohol or other substances which may
affect his/her awareness.
24.19.2 Hysterectomies
When sterilization results from a procedure performed to address another medical
problem, it is considered a medically necessary sterilization. These procedures
include hysterectomies, oophorectomies, salpingectomies and orchiectomies. Every
claim submitted to Medicaid for a medically necessary sterilization must be
accompanied by one (1) of the following:
A complete Hysterectomy Acknowledgement of Consent Form must be
obtained from the primary practitioner for all related services. Complete only
one (1) section (A, B or C) of this form. When no prior sterility (section B) or
life-threatening emergency (section C) exists, the client must sign and date
section A of this form (see 42 CFR 441.250 for the federal policy on
hysterectomies and sterilizations). The client does not need to sign this form
when sections B or C apply. If this form is not properly completed, payment
will be denied (6.16.2, Hysterectomy Acknowledgement of Consent).
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 311 Revision 4/1/17
For clients that become retroactively eligible for Medicaid, the practitioner
must verify in writing that the surgery was performed for medical reasons and
must document one (1) of the following:
o The client was informed prior to the hysterectomy that the operation
would render the client permanently incapable of reproducing.
o The client was already sterile at the time of the hysterectomy and the
reason for prior sterility.
NOTE: Pregnant by Choice/Family Planning Waiver has specific covered and
non-covered services (25.1, Pregnant by Choice/Family Planning Waiver).
24.20 Surgical Services
Procedure Code Range: 10021-69990
Medicaid only covers surgical procedures that are medically necessary. In general,
surgical procedures are covered if the condition directly threatens the life of a client,
results from trauma demanding immediate treatment, or had the potential for causing
irreparable physical damage, the loss or serious impairment of a bodily function, or
impairment of normal physical growth and development.
These policies follow Medicare guidelines but in cases of discrepancy, the Medicaid
policy prevails.
24.20.1 Surgical Packages, Separate Surgical Procedures and Incidental
Surgical Procedures
Surgical Packages – Procedures that are commonly performed as an integral
part of a total service and may not be billed separately. The following services
are included in the surgical package in addition to the operation:
o Local infiltration, metacarpal/metatarsal/digital block or topical
anesthesia
o Subsequent to the decision for surgery, one (1) related Evaluation and
Management (E&M) encounter on the date immediately prior to or on
the date of procedure (including history and physical)
o Immediate postoperative care, including dictating operative notes,
talking with the family and other physicians
o Writing orders
o Evaluating the patient in the postanesthesia recovery area
o Typical post-operative follow-up care.
Separate Surgical Procedures – When a procedure is performed
independently of, and is not immediately related to, other services, it may be
reported separately under its unique procedure code (e.g., a tonsillectomy and
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 312 Revision 4/1/17
an adenoidectomy may be billed separately), only if performed on a different
day.
Incidental Surgical Procedures – Incidental procedures are those procedures
performed subsequent to surgery which do not add significantly to the major
surgery or are rendered incidental and performed at the same time as the
major surgery (e.g., incidental appendectomies, incidental scar excisions).
24.20.2 Covered Services
Normal preoperative and postoperative care includes:
Pre-Op lab and radiology.
Office examinations.
Emergency room visits, and hospital visits, including discharge management
Routine post-operative care (The number of post-operative days for each
procedure is listed within the fee schedules.).
24.20.3 Limitations
Consultations and hospital admission are not considered part of the surgical package.
NOTE: Services provided to diagnose or treat conditions unrelated to the surgery
may be billed with a separate examination code if the primary diagnosis
code reflects a different complaint or service.
For an accurate listing of codes and the number of postoperative days for each
procedure, refer to the fee schedule on the Medicaid website (2.1, Quick Reference).
24.20.4 Billing Requirements
All surgical claims for reimbursement for multiple surgical procedures must have an
operative report attached (6.15, Submitting Attachments for Electronic Claims). The
following methodology applies to reimbursement for surgical procedures (refer to the
CPT-4 book for correct use of modifiers):
Unusual Procedural Services – When the service(s) provided is greater than
that usually required for the listed procedure, it may be identified adding
modifier 22 to the usual procedure number. An operative report must
accompany the claim for payment.
Multiple Procedures – When multiple procedures are performed during the
same session, the primary procedure will be paid at 100% of the fee assigned
on the fee schedule. The primary procedure must be billed on the first line; the
subsequent procedure(s) must be billed on the following line(s) using the 51
modifier, if applicable. Operative reports are required for multiple procedures.
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 313 Revision 4/1/17
Refer to the Medicaid website for the most accurate fee schedule (2.1, Quick
Reference).
NOTE: The 51 modifier pays at 50% of the customary rate.
Bilateral Procedures – When bilateral procedures are performed during the
same session, the second procedure will be paid at 75% of the customary rate.
If the procedure performed is bilateral, providers should report the procedure
with 1 unit of service on line 1 and 1 unit of service on line two (2) using the
same procedure code with the 50 modifier. Care should be taken not to
designate a procedure as bilateral when the procedure is already identified as a
bilateral service in the CPT-4 definition. An example of a bilateral procedure
would be a client having a tympanostomy (tubes inserted in the ears)
performed on both the left and right ears; it should be billed as follows:
Line
Unit
CPT Code
Modifier
01
1
69433
02
1
69433
50
NOTE: Operative reports are required for bilateral procedures.
24.20.5 Assistant Surgeon
Assistant surgeon fees are billed with an 80 modifier using the same procedure code
billed by the primary surgeon.
24.20.5.1 Surgical Assistant Service
Physician assistant, nurse practitioner or clinical nurse specialist service fees
are billed with an AS modifier using the same procedure code billed by the
primary surgeon.
Non-physician providers (NPP) should bill with the AS modifier using the
same procedure code billed by the primary surgeon.
The provider should report the services using his/her own provider
identification number with the appropriate site of service.
The modifier AS is appended to the CPT-4 code(s) for the procedure(s) the
NPP/APP assisted with.
Do not use modifier AS if the APP/APP acts as an “extra” pair of hands and
not a surgical assistant in place of another surgeon.
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 314 Revision 4/1/17
24.20.5.2 Two (2) Surgeons
When two (2) surgeons work together as primary surgeons performing distinct part(s)
of a procedure, each surgeon should report his/her distinct operative work by adding
modifier 62 to the procedure code and any associated add-on code(s) for that
procedure as long as both surgeons continue to work together as primary surgeons.
Each surgeon should report the co-surgery once using the same procedure code. If
additional procedure(s) (including add-on procedure(s) are performed during the
same surgical session, separate code(s) may also be reported with modifier 62.
NOTE: If the co-surgeon acts as an assistant in the performance of additional
procedure(s) during the same surgical session, those services may be
reported using separate procedure code(s) with modifier 80 or modifier AS
added, as appropriate. If the procedure code(s) require Prior Authorization,
it is the responsibility of the individual practitioner to obtain that
authorization. Example; two surgeons perform a surgery and utilize the 62
modifier; both surgeons MUST receive Prior Authorization.
24.20.5.3 Modifiers
Medicaid recognizes the following list of modifiers when used in conjunction with
CPT-4 surgical procedure codes:
Modifier
Description
Reimbursement
22
Unusual Procedural Services – An
operative report is required.
Allowed fee plus 20%
50
Bilateral Procedures
75% of allowed fee
51
Multiple Procedures
50% of allowed fee
62
Two (2) Surgeons – An operative
report is required.
100% of allowed fee
80
Assistant Surgeons
20% of allowed fee
AS
Physician Assistant, Nurse
Practitioner, or Clinical Nurse
Specialist services for assistant at
surgery
15% of allowed fee
24.20.6 Cosmetic Services
Medicaid covers cosmetic services only when it is medically necessary (e.g., restore
bodily function or correct a deformity). Before cosmetic services are performed, they
must be prior authorized.
NOTE: Refer to Section 6.14 for Prior Authorization procedures and the fee
schedule on the Medicaid website indicates which codes require prior
authorization (2.1, Quick Reference).

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 315 Revision 4/1/17
24.20.7 Oral and Maxillofacial Surgeons
Procedure Code Range: 21010-21499
Oral and maxillofacial surgery is surgery to correct a wide spectrum of diseases,
injuries and defects in the head, neck, face, jaws and the hard and soft tissues of the
oral and maxillofacial region.
24.20.7.1 Covered Services
Removal of tumor
Maxillofacial Prosthetics – Introduction and Removal
Repair, Revision and/or Reconstruction
Temporomandibular Joint (TMJ) Treatment
Procedure Code Range: 40490-42999
24.20.7.2 Covered Services
Lips (excision and repair)
Vestibule of mouth (incision, excision and repair)
Tongue and Floor of mouth (incision, excision and repair)
Dentoalveolar Structures (incision, excision and other)
Palate and Uvula (incision, repair and other)
Salivary Gland and Ducts (incision, excision, repair and other)
Pharynx, Adenoids, and Tonsils (incision, excision, repair and other)
24.20.7.3 Billing Requirements
In order to obtain Medicaid reimbursement for services, the following standards must
be observed.
The services must be medically necessary and follow generally accepted
standards of care
The service must be a service covered by Medicaid
Claims must be made according to Medicaid billing instructions
Review the entire surgical section to verify appropriate use of modifiers
When billing dental codes refer to the dental manual
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 316 Revision 4/1/17
NOTE: The most accurate way to verify coverage for a specific service is to
review the CPT-4 book, the CDT book and the Medicaid fee schedule on
the website (2.1, Quick Reference).
24.20.8 Breast Reconstruction
Procedure Code Range: 19316-19499
24.20.8.1 Covered Services
Breast reconstruction following breast cancer treatment
24.20.8.2 Billing Requirements
Prior authorization requirements (6.14, Prior Authorization):
Wyoming Medicaid covers surgical reconstruction following breast cancer treatment.
Additional revisions may only be approved for a repeated constructive surgery based
on medical necessity such as the procedures listed below:
Secondary surgery includes implant rupture.
Wound dehiscence (bursting open).
Wound infection.
Tattooing of the nipple (included in 19350, 19357-19369 unless the procedure
is done after the global setting – then 11920-11921 is appropriate).
24.20.9 Breast Reduction
Procedure Code Range: 19318
24.20.9.1 Covered Services
Breast reductions are covered and considered medically necessary if the below
requirements are met.
24.20.9.2 Billing Requirements
Prior authorization requirements (6.14, Prior Authorization):
Wyoming Medicaid considers breast reduction surgery as medically necessary, when
all of the following is met and is clearly documented in the medical records.
Client must be 18 years or older.
Amount to be removed from each breast is greater than or equal to 500 grams,
or the total to be removed from both breasts exceeds 1000 grams.
Preoperative indications for breast surgery must include one (1) or more of the
following symptoms:
o Breast pain

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 317 Revision 4/1/17
o Shoulder, neck, or back pain
o Other persistent neurological symptoms attributable to breast size or
weight.
o Refractory intertrigo
o Significant activities
This procedure may be done as a hospital inpatient, hospital outpatient, or in
an ASC.
24.20.9.3 Documentation Requirements
Documentation must show medical necessity. The patient’s clinical records must be
specific and contain the following information:
Current clinical notes including history, physical, and preoperative indications
for breast surgery.
Height and weight.
Current bra size.
Proposed amount of tissue to be removed from each breast.
Duration of time that symptoms have persisted.
Conservative methods of treatment tried, such as weight loss or support bras.
Photographs of the shoulder to waist, front and lateral.
24.20.10 Cochlear Device, Implantation and Replacement
Procedure Code: 69930
24.20.10.1 Covered Services
Wyoming Medicaid has instituted the following policy for Cochlear Device
Implantation and Replacement. Medicaid reimburses for the implant, external
processor and headset.
24.20.10.2 Billing Requirements
Prior authorization is required for the procedure, device and replacement device only.
(6.14, Prior Authorization) Medicaid clients must meet all the following criteria:
There must be a diagnosis of bilateral profound (90db hearing loss)
sensorineural hearing impairment that cannot be mitigated by the use of a
hearing aid in clients whose auditory cranial nerves can be stimulated.
The client must have demonstrated that they cannot benefit from hearing
amplification through a trial period of a minimum of six (6) months.
There must be freedom from middle ear infection, an accessible cochlear
lumen that is structurally suited to implantation, and be free of lesions in the
auditory nerve and acoustic areas of the central nervous system.

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 318 Revision 4/1/17
There must not be a contraindication to having the surgery.
The client must have the cognitive ability to use auditory clues.
The procedure may only be performed using FDA-approved devices.
Evaluation and continued treatment for cochlear transplants must be
completed by a Board Certified Specialist.
Only one (1) cochlear implant per five (5) year period. An exception may be
possible if the implant is proven to no longer be working sufficiently and the
manufacture warranty has expired.
Initial first year calibration visits are part of the global fee for implementation.
Follow up calibration visits will be covered one (1) per year if the implant is
authorized or if the client had an existing cochlear device that needs
calibration.
Additional equipment will be allowed only to replace defective equipment and
will not be allowed solely to update equipment. Upgrade equipment can be
evaluated once every five (5) years.
In addition, the following criteria must be met for adults 21 and older:
Must be highly motivated and have appropriate expectations to complete
prescribed pre- and post-surgical treatment.
In addition the following criteria must be met for children 20 and under:
o Implantation will not be considered before the age of 12-months.
o Children may be pre-linguistically deafened.
o Family members or caregivers must have appropriate expectations,
motivation, and resources to assist in completion of treatment and
educational services.
o Family members must agree to accompany a young child to training
sessions and be able to reinforce learning.
NOTE: Only the procedure for implantation needs prior authorization; the device
does not require a separate prior authorization and must be supplied by the
hospital.
24.20.10.3 Documentation
The client’s clinical records must be specific and contain the following information:
A complete history and physical indicating how the diagnosis of sensorineural
hearing impairment was determined.
Demonstration of lack of benefit from hearing amplification through a trial
period of six (6) months, using appropriate fitted amplification.
Documentation of other health conditions.
Notation that there has been active family involvement during the diagnosis
and treatment sessions for a child who is to have a cochlear transplant.

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 319 Revision 4/1/17
24.20.11 Gastric Bypass Surgery
Procedure Code Range: 43644, 43770, 43842-43843, 43846-43848
For prior authorization for the above listed procedure codes, please contact WYhealth
at (888)545-1710.
24.20.12 Lumbar Spinal Surgery
Procedure Code Range: 22207, 22214, 22224, 22533, 22534, 22558, 22612, 22630,
22633, 22800-22808, 22812, 22818, 22840, 22857 and 22862
24.20.12.1 Covered Services
Authorization for lumbar spinal surgery has been separated into three (3) general
categories:
Surgery related to the treatment of sciatica or other nerve root impingements
where primary intervention is related to removal of an offending herniated
disk.
Surgery related to mechanical and anatomical abnormalities for which spinal
fusion may be appropriate treatment.
Spinal fracture or dislocation, spinal infection (These can be approved with
documentation of said fracture/dislocation or infection.).
24.20.12.2 Reimbursement
Prior Authorization requirements:
In the absence of red flag symptoms or progressive neurological symptoms or signs,
members presenting with:
Low back pain should undergo conservative therapy, which may include the
use of anti-inflammatory medications, aggressive physical therapy with home
exercise program, activity modification, physical.
Reconditioning or facet or epidural injections. A patient should undergo at
least 12-weeks of conservative management for symptomatic spinal stenosis
or spondylolisthesis.
Patients with only axial low back pain (absence of leg or neurological
symptoms) and without demonstrable instability, spondylolisthesis or spinal
stenosis should go through conservative therapy for at least six (6) months.
Documentation Requirements:
Office notes, including history and physical.
Detailed documentation of extent and response to conservative therapy (PT,
Steroids, Anti-inflammatory Medications, etc.).
Radiology reports for MRI’s, CT’s, etc.

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 320 Revision 4/1/17
Complete the prior authorization form with specific procedures with CPT
codes.
NOTE: The requesting surgeon must personally evaluate the patient on at least
two (2) occasions prior within the preceding six (6) months to requesting
surgery.
24.20.12.3 Scoliosis
The treatment of idiopathic scoliosis medically necessary for any of the following
conditions:
An increasing curve (greater than 40 degrees) in a growing child; or
Scoliosis related pain that is refractory to conservative treatments; or
Severe deformity (curve greater than 50 degrees) with trunk asymmetry in
children and adolescents; or
Thoracic lordosis that cannot be treated conservatively.
In the absence of the above-mentioned criteria, idiopathic scoliosis surgery is
considered experimental and investigational.
Documentation Requirements:
Office notes, including history and physical.
Detailed documentation of extent and response to conservative therapy (PT,
Steroids, Anti-inflammatory Medications, etc.).
Radiology reports for MRI’s, CT’s, etc.
Complete the prior authorization form with specific procedures with CPT
codes.
NOTE: The requesting surgeon must personally evaluate the patient on at least
two (2) occasions prior within the preceding six (6) months to requesting
surgery.
24.20.13 Panniculectomy/Abdominoplasty
Procedure Code Range: 15830 and 15847
24.20.13.1 Covered Services
Panniculectomies/Abdominoplasties are covered and considered medically necessary
if the below requirements are met.
24.20.13.2 Reimbursement

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 321 Revision 4/1/17
Prior Authorization requirements (6.14, Prior Authorization):
Wyoming Medicaid considers a Panniculectomy/Abdominoplasty as medically
necessary, when all of the following is met and clearly documented in the medical
records.
Pannus hangs at or below the level of the symphysis pubis.
Pannus causes a chronic and persistent skin condition that is refractory to at
least six (6) months of medical treatment. In addition to good hygiene
practices, treatment should include topical antifungals, topical and/or systemic
corticosteroids, and/or local or systemic antibiotics.
NOTE: If the procedure is being performed following significant weight loss, in
addition to meeting the criteria noted above, there should be evidence that
the individual has maintained a stable weight for at least six (6) months. If
the weight loss is the result of bariatric surgery,
abdominoplasty/panniculectomy should not be performed until at least 18
months after bariatric surgery and only when weight has been stable for at
least the most recent six (6) months.
Medicaid does not cover abdominoplasty or panniculectomy when performed
primarily for ANY of the following indications because it is considered not medically
necessary (this list may not be all-inclusive).
Treatment of neck or back pain.
Improving appearance (i.e. cosmesis).
Repairing abdominal wall laxity or diastasis recti.
Treating psychological symptomatology or psychosocial complaints.
When performed in conjuncture with abdominal or gynecological procedures
(e.g., abdominal hernia repair, hysterectomy, obesity surgery) unless criteria
for panniculectomy or abdominoplasty are met separately.
24.20.14 Pectus Excavatum and Poland’s Syndrome
Procedure Code Range: 21743
24.20.14.1 Covered Services
Surgical repair of severe pectus excavatum deformities that cause functional deficit
are covered and considered medically necessary when done for medical reasons in
clients who meet the criteria listed below.
24.20.14.2 Reimbursement
Prior Authorization requirements (6.14, Prior Authorization):

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 322 Revision 4/1/17
Wyoming Medicaid considers a Pectus Excavatum medically necessary, when all of
the following is met and clearly documented in the medical records.
Medical documentation outlining evidence of complications from the sternal
deformity. Complications may include but are not limited to:
o Asthma
o Atypical chest pain.
o Cardiopulmonary impairment documented by respiratory and/or
cardiac function tests.
o Exercise limitation.
Frequent lower respiratory tract infections.
An electrocardiogram or echocardiogram is documented in the instance(s) of
known heart disease in order to define the relationship between the sternal
deformity and cardiac issues; and
A CT scan of the test is completed and demonstrates a pectus index of greater
than 3.25. The pectus index is calculated by dividing the transverse diameter
of the chest by the anterior-posterior diameter.
In the absence of the above-mentioned criteria, surgery for pectus excavatum is
considered cosmetic.
The following interventions are considered experimental and investigational
secondary to their effectiveness in the treatment of pectus excavatum:
The magnetic min-mover procedure.
The vacuum bell.
Dynamic Compression Syndrome.
Surgery for reconstruction of musculo-skeletal chest wall deformities
associated with Poland’s Syndrome are considered medical necessary if
syndrome causes functional deficits.
24.20.15 Ptosis and Blepharoplasty Repair
Procedure Code Range: 67900-67909
24.20.15.1 Covered Services
Surgical repair of ptosis and blepharoplasty that cause functional deficit are covered
and considered medically necessary when done for medical reasons in clients who
meet the criteria listed below.
24.20.15.2 Ptosis (Belpharoptosis)
Repair for laxity of the muscles of the upper eyelid causing functional visual
impairment when photographs in straight gaze show the margin reflex difference
(distance from the upper lid margin to the reflected corneal light reflex at normal
gaze) of 2mm or less.

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 323 Revision 4/1/17
Brow ptosis repair for laxity of the forehead muscles causing functional visual
impairment when photographs show the eyebrow below the supra-orbital rim.
Eyelid ectropion or entropion repair is considered medically necessary for corneal or
conjunctival injury due to ectropion, entropion or trichiasis.
Upper eyelid tightening procedures (block resection or tarsal strip with lateral canthal
tightening) for member who has refractory corneal or conjunctival inflammation
related to exposure from floppy eyelid syndrome.
Canthoplasty – Is considered medically necessary as part of a blepharoplasty
procedure to correct eyelids that sag so much that they pull down the upper eyelid so
that vision is obstructed.
NOTE: Visual field testing is not routinely necessary to determine the presence of
excess upper eyelid skin, upper eyelid ptosis, or brow ptosis. Each of these
three (3) components can be present alone or in any combination, and each
may require correction. If both a blepharoplasty and ptosis repair are
requested, two (2) photographs may be necessary to demonstrate the need
for both procedures: one (1) photograph should show the excess skin
above the eye resting on the eyelashes, and a second (2nd) photograph
should show persistence of lid lag, with the upper eyelid crossing or
slightly above the pupil margin, despite lifting the excess skin above the
eye off of the eyelids with tape. If all three (3) procedures (i.e.,
blepharoplasty, blepharoptosis repair, and brow ptosis repair) are
requested, three (3) photographs may be necessary.
Congenital Ptosis – Surgical correction of congenital ptosis is medically necessary to
allow proper visual development and prevent amblyopia in infants and children with
moderate to severe ptosis interfering with vision. Surgery is considered cosmetic if
performed for mild ptosis that is only of cosmetic concern. Photographs must be
available for review to document that the skin or upper eyelid margin obstructs a
portion of the pupil.
24.20.15.3 Reimbursement
Prior Authorization requirements (6.14, Prior Authorization):
Wyoming Medicaid considers surgical repair for Ptosis and Blepharoplasty when the
criteria below are met.
Blepharoplasty is considered medically necessary for any of the following
indications:
To correct prosthesis difficulties in an anophthalmia socket; or
To remove excess tissue of the upper eyelid causing functional visual
impairment when photographs in straight gaze show eyelid tissue resting on or

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 324 Revision 4/1/17
pushing down on the eye lashes (Excess tissue beneath the eye rarely obstructs
vision, so the lower lid blepharoplasty is rarely covered for this indication); or
To repair defects predisposing to corneal or conjunctival irritation:
o Corneal exposure
o Ectropion (eyelid turned outward)
o Entropion (eyelid turned inward)
o Pseudotrichiasis (inward misdirection of eyelashes caused by
entropion); or
To relieve painful symptoms of blepharospasm; or
To treat peri-orbital sequelae of thyroid disease and nerve palsy, and peri-
orbital sequelae of other nerve palsy (e.g., the oculomotor nerve).
24.20.16 Septoplasty and Rhinoplasty
Procedure Code Range: 30520, 30400-30420, 30430-30450 and 30460-30462
24.20.16.1 Covered Services
Septoplasty and Rhinoplasty are covered and considered medically necessary if the
below requirements are met.
Septoplasty is medically necessary when any of the following clinical criteria
is met.
o Asymptomatic septal deformity that prevents access to other intranasal
areas when such access is required to perform medical necessary
surgical procedures (e.g., ethmoidectomy); or
o Documented recurrent sinusitis felt to be due to a deviated septum not
relieved by appropriate medical and antibiotic therapy; or
o Recurrent epistaxis (nosebleeds) related to a septal deformity; or
o Septal deviation causing continuous nasal airway obstruction resulting
in nasal breathing difficulty not responding to appropriate medical
therapy; or
o When done in association with cleft palate repair.
NOTE: Septoplasty is considered experimental and investigational for all other
indications (e.g., allergic rhinitis) because its effectiveness other than the
ones listed above has not been established.
Rhinoplasty may be considered medically necessary only in the following
limited circumstances:
o When it is being performed to correct a nasal deformity secondary to
congenital cleft lip and/or palate;
o Upon individual case review, to correct chronic non-septal nasal
airway obstruction from vestibular stenosis (collapsed internal valves)

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 325 Revision 4/1/17
due to trauma, disease, or congenital defect, when all of the following
criteria are met:
Prolonged, persistent obstructed nasal breathing; and
Physical examination confirming moderate to severe vestibular
obstruction; and
Airway obstruction will not respond to septoplasty and
turbinectomy alone; and
Nasal airway obstruction is causing significant symptoms (e.g.,
chronic rhinosinusitis, difficulty breathing); and
Obstructive symptoms persist despite conservative
management for three (3) months or greater, which includes,
where appropriate, nasal steroids or immunotherapy; and
Photographs demonstrate an external nasal deformity; and
There is an average 50 % or greater obstruction of nares (e.g.,
50 % obstruction of both nares, or 75 % obstruction of one nare
and 25 % obstruction of other nare, or 100 % obstruction of
one nare), documented by nasal endoscopy, computed
tomography (CT) scan or other appropriate imaging modality.
24.20.16.2 Documentation Requirements
Documentation of duration and degree of symptoms related to nasal
obstruction, such as chronic rhinosinusitis, mouth breathing, etc.; and
Documentation of results of conservative management of symptoms; and
If there is an external nasal deformity, pre-operative photographs showing the
standard 4-way view: anterior-posterior, right and left lateral views, and base
of nose (also known as worm's eye view confirming vestibular stenosis; this
view is from the bottom of nasal septum pointing upwards); and
Relevant history of accidental or surgical trauma, congenital defect, or disease
(e.g., Wegener’s granulomatosis, choanal atresia, nasal malignancy, abscess,
septal infection with saddle deformity, or congenital deformity); and
Results of nasal endoscopy, CT or other appropriate imaging modality
documenting degree of nasal obstruction.
When rhinoplasty for nasal airway obstruction is performed as an integral part
of a medically necessary septoplasty and there is documentation of gross nasal
obstruction on the same side as the septal deviation
24.20.16.3 Reimbursement
Prior Authorization requirements (6.14, Prior Authorization)
24.20.17 Vagus Nerve Simulation (VNS) for Epilepsy
Procedure Code Range: 61850-61888, 64570, 64573
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 326 Revision 4/1/17
For prior authorization for the above listed procedure codes, please contact WYhealth
at (888)545-1710.
24.20.18 Varicose Vein Treatment
Procedure Code Range: 36471- 36479, 37770-37785
24.20.18.1 Covered Services
Wyoming Medicaid considers the following procedures medically necessary for
treatment of varicose veins:
Great saphenous vein or small saphenous vein ligation/division/ stripping,
Radiofrequency endovenous occlusion (VNUS procedure)
Endovenous laser ablation of the saphenous vein (ELAS) – also known as
endovenous laser treatment (EVLT)
24.20.18.2 Billing Requirements
Prior authorization requirements (6.14, Prior Authorization):
Incompetence at the saphenofemoral junction or saphenopopliteal junction is
documented by Doppler or duplex ultrasound scanning, and all of the following
criteria are met.
Documented reflux duration of 500 milliseconds (ms) or greater in the vein to
be treated; and
Vein size is 4/5mm or greater in diameter (not valve diameter at junction); and
Saphenous varicosities result in any of the following:
o Intractable ulceration secondary to venous stasis; or
o More than 1 episode of minor hemorrhage from a ruptured superficial
varicosity; or a single significant hemorrhage from a ruptured
superficial varicosity , especially if transfusion of blood is required; or
o Saphenous varicosities result in either of the following and symptoms
persist despite a three (3) month trial of conservative management
(e.g., analgesics and prescription gradient support compression
stockings).
NOTE: A trial conservative management is not required for persons with
persistent or recurrent varicosities who have undergone prior endovenous
catheter ablation procedures or stripping/division/ligation in the same leg
because conservative management is unlikely to be successful.
o Recurrent superficial thrombophlebitis; or

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 327 Revision 4/1/17
o Severe and persistent pain and swelling interfering with activities of
daily living and requiring chronic analgesic medication.
Endovenous ablation procedures are considered medically necessary for the treatment
of incompetent perforating veins with vein diameter of 3.5mm or great with outward
flow duration of 500 milliseconds duration or more, located underneath an active or
healed venous.
24.21 Transplant Policy
For prior authorization for transplant services, please contact WYhealth at (888)545-
1710.
24.21.1 Outpatient Stem Cell/Bone Marrow
The hospital performing a bone marrow/stem cell transplant on an outpatient basis
must bill using procedure code 38240 or 38241 and will be reimbursed at 55% of
billed charges.
24.21.1.1 Non-Covered Services
Transportation of organs from one (1) facility to another is not covered.
24.22 Vision Services
Vision and dispensing services are benefits for client’s ages 0-20. Limited office
visits for the treatment of an eye injury or eye disease is available for clients 21 &
older. A licensed ophthalmologist, optometrist, or optician, within the Scope of the
Practice Act within their respective profession, may provide vision services and
dispensing services.
Vision services for clients 21 and older are only reimbursable for the treatment of eye
disease or eye injury based on the appropriate ICD diagnosis code and client records
must support billing of any vision services. Routine eye exams and/or glasses are not
a covered benefit for clients 21 and older.
NOTE: Wyoming Medicaid will pay the deductible and/or coinsurance due on
Medicare crossover claims for post-surgical contact lenses and/or eyeglasses, up
to the Medicaid allowable.
24.22.1 Eye and Office Examinations
Procedure Code Range: 92002-92014, 99201-99215, 92018-92060, 92081-92226,
92230-92287

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 328 Revision 4/1/17
24.22.1.1 Covered Services
For clients under the age of 21 years:
Eye exams determine visual acuity and refraction, binocular vision, and eye
health.
o 92002-92004 - New patient eye exams are a covered benefit for clients
who are new to the provider’s practice.
o 92012-92014 - Established patient eye exams are a covered benefit
once in a 365 day period unless there is medical necessity to support
an additional exam.
Office visits for the treatment of eye disease or eye injury.
o 99201-99215 – May be billed by ophthalmologists for office exams.
Documentation: Eye care provider records must reflect
medical necessity and include interpretation and report, as
appropriate, of the procedure.
92018-92060, 92081-92226, 92230-92287 - Special Ophthalmological
Services should be performed only when medically necessary. 99283 requires
a prior authorization.
For clients 21 years and older:
Eye exams to diagnose an eye disease or eye injury.
o 92002-92004 - New patient eye exams are a covered benefit for clients
who are new to the provider’s practice.
o 92012-92014 - Established, patient eye exams are a covered benefit
once in a 365 day period unless there is medical necessity to support
an additional exam.
NOTE: Routine eye exam are not covered for adult clients. Do not
bill for routine eye exams for clients 21 years and older. Exam codes
may pay, and then upon audit, be taken back as Medicaid abuse
recovery. These codes are not limited by diagnosis at this time and
should only be billed when medical necessity can be documented to
show an eye disease or injury.
Office visits as for the treatment of eye disease or eye injury.
o 99201-99215 - Ophthalmologists may bill these codes for office exams
Documentation: Eye care provider records must reflect
medical necessity and include interpretation and report, as
appropriate, of the procedure.
92018-92060, 92081-92226, 92230-92287 - Special ophthalmological services
should be performed only when medically necessary and will be subject to

Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 329 Revision 4/1/17
post-payment review of the client’s records. 92283 will require a prior
authorization.
24.22.1.2 Non Covered Services
Exam codes should not be billed for routine eye exams for clients over 21
years old.
24.22.2 Eyeglasses/Materials
Procedure Code Range: V2020, V2100-V2499, V2627, V2784
24.22.2.1 Covered Services
For Clients under the age of 21 years:
One (1) pair of eyeglasses is covered per 365 days
V2020 – Standard frames are covered up to $73.49. The provider may not
“balance bill” the client for frames that cost more than the allowable amount.
o NOTE: Balancing billing example – When the client selects $120
frames and Medicaid allows up to $73.49 then the optometrist should
either, mutually agree in writing with the client that the client is
responsible for the payment of the frames ($120), or, the provider may
bill Medicaid for $73.49 and accept this payment as payment in full
for the frames.
Covered eye glass lenses:
o V2100-V2121 (V2199 requires prior authorization) - Single lenses
o V2200-V2221 (V2299 requires prior authorization) – Bifocal lenses
o V2300-V2321 (V2399 requires prior authorization) – Trifocal lenses
o V2410-V2430 (V2499 requires prior authorization) - High Index
Aspheric lens-
Aspheric lenses will only be covered when medically necessary
and when they meet the following guidelines listed below:
When the power in the highest meridian is - (minus) 6
diopters or more. For example:
o A spectacle prescription of -2.00 -4.00 x 180 -
4.00 + -2.00 = -6.00. This Rx would qualify
o A spectacle prescription of -2.00 +5.00 x 180 -
2.00 + +5.00 = +3.00. This Rx would not
qualify for high index aspheric material
When the power in the highest meridian is + (plus) 4.00
diopters or more. For example:
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 330 Revision 4/1/17
o A spectacle prescription of -2.00 -4.00 x 180 -
4.00 + -2.00 = -6.00. This Rx would qualify
o A spectacle prescription of -2.00 + +5.00 =
+3.00. This Rx would not qualify for a high
index aspheric material
o V2784 – Polycarbonate lens (billed as an add on to a standard C-39
lens)
o Lenses must be ordered as pairs. If the lens on one (1) side is aspheric
or high index, then the matching lens should also be aspheric or high
index, even if it does not meet the threshold.
Medicaid will allow one (1) replacement of lenses and frames within the 12
month period if:
o There is a change in the prescription for the lenses, use the existing
frames if possible.
o Eyeglasses are lost or broken beyond repair – This will require
documentation stating it was not due to blatant abuse or neglect
NOTE: The provider will need to submit an electronic claim and attach
necessary documentation of the medical necessity to substantiate why the
replacement glasses are needed. The claim will then be review and
processed if criteria is met. (6.15 Submitting Attachments)
Repair of eyeglasses may be billed upon expiration of the warranty
V2623, V2629 (Prosthetic eyes) V2627 (Scleral cover shell) –requires a
prior authorization. (6.14 Prior Authorizations)
24.22.2.2 Non Covered Charges
Reimbursement for dispensing of frames, frame parts, and/or lenses is not
allowed in addition to reimbursement for dispensing of total eyeglasses
Clients 21 years of age and older are not covered for eyeglasses
24.22.2.3 Reimbursement
Obtain eligibility information from Medicaid prior to placing order for
eyewear
Verify with client and Provider Relations (1-800-251-1268) if the benefit has
been used in the past year
Deliver glasses in a reasonable amount of time (typically within one to two
weeks)
Verify client eligibility for the date of delivery
Bill Medicaid on the delivery date of the glasses. The date of delivery must
be used as the date of service on a claim.
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 331 Revision 4/1/17
If the client does not return to receive their glasses, the glasses should be
mailed to the client and the mail date used as the date of service.
NOTE: If the client is not eligible on the delivery date or does not return for the
delivery, the provider may submit an “Order vs Delivery Date Exception
Form” for authorization to bill on the order date. (6.14 Order Vs Delivery
Date)
24.22.3 Contact Lenses
Procedure Code Range: V2500-V2599, 92072
Contact lenses are covered for correction of pathological conditions when useful
vision cannot be obtained with regular lenses.
24.22.3.1 Covered Services
For Clients under the age of 21 years:
V2500-V2599 – Contact lenses require prior authorization (PA) and
documentation provided must show medical necessity and state why the
client’s vision cannot be corrected with eyeglasses. (6.14 Prior
Authorizations)
Contact lenses will be reimbursed at the cost of invoice, plus shipping and
handling, plus 15% (6.15, Submitting Attachments for Electronic Claims).
92072 – Fitting of contact lens does not require PA, however, should only be
billed when PA has been obtained for the lens.
24.22.3.2 Non-Covered Services
Contact lenses are not covered for clients 21 and older.
24.22.4 Vision Therapy
Procedure Code: 92065, 99070
Vision therapy is a sequence of activities individually prescribed and monitored by
the doctor to develop efficient visual skills and processing. It is prescribed after a
comprehensive eye examination has been performed and has indicated that vision
therapy is an appropriate treatment option. The vision therapy program is based on
the results of standardized tests, the needs of the patient, and the patient’s signs and
symptoms.
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 332 Revision 4/1/17
Research has demonstrated vision therapy can be an effective treatment option for
individuals under the age of 21 or individuals with Acquired Brain Injury:
Ocular motility dysfunctions (eye movement disorders)
Non-strabismic binocular disorders (inefficient eye teaming)
Strabismus (misalignment of the eyes)
Amblyopia (poorly developed vision)
Accommodative disorders (focusing problems)
Visual information processing disorders, including visual-motor integration
and integration with other sensory modalities.
24.22.4.1 Covered Services
92065 – Vision Therapy can be billed for clients under the age of 21 and
clients eligible for the Acquired Brain Injury Waiver benefit plan with a
qualifying medical diagnosis (See tables below)
When administered in the office under the guidance of a practitioner.
It requires a number of office visits and depending on the severity of the
diagnosed conditions
The length of the program typically ranges from several weeks to several
months
Activities paralleling in-office techniques are typically taught to the patient to
be practiced at home to reinforce the developing visual skills
Vision therapy visits are capped at 32 per 365-days for treatment of ICD
diagnosis
o Additional visits or exceptions to these diagnosis codes will be
considered on a case by case basis only
99070 - Vision Therapy training aids will be reimbursed at cost of invoice.
Invoices must be submitted with documentation of medical necessity to
Medial Policy (2.1, Quick Reference) for consideration (6.15, Submitting
Attachments for Electronic Claims)
Diagnosis Codes for Clients under 21 years old
Diagnosis Codes
Description
Amblyopia
H53.031, H53.032, H53.033
Strabismic amblyopia
H53.011, H53.012, H53.013
Deprivation amblyopia
H53.021, H53.022, H53.023
Refractive amblyopia
Strabismus (Concomitant)
Covered Services –_Practitioner Services__________________________________________
Ch. 25 Inedx 333 Revision 4/1/17
H50.11, H50.012
Monocular esotropia
H50.05
Alternating esotropia
H50.11, H50.112
Monocular exotropia
H50.15
Alternating exotropia
H50.311, H50.312
Intermittent esotropia, monocular
H50.32
Intermittent esotropia, alternating
H50.331, H50.332
Intermittent exotropia, monocular
H50.34
Intermittent exotropia, alternating
H50.43
Accommodative component in esotropia
Non-strabismic disorder of binocular eye movements
H51.11
Convergence insufficiency
H51.12
Convergence excess
H51.8
Anomalies of divergence
Ocular Motor Dysfunction
H55.81
Deficiencies of saccadic eye movements
H55.89
Deficiencies of smooth pursuit movements
Heterophoria
H50.51
Esophoria
H50.52
Exophoria
General Binocular Vision Disorder
H53.30
General Binocular Vision Disorder
Nystagmus
H55.01
Nystagmus
Diagnosis Codes for Clients on Acquired Brain Injury Waiver Benefit Plan
Diagnosis Codes
Description
I69.998
Disturbances of vision
S06 Family of Codes
Late effect injury intracranial injury without mention of skull fracture.

Covered Services –_Pregnant by Choice__________________________________________
Ch. 25 Inedx 334 Revision 4/1/17
Chapter Twenty Five – Covered Services – Pregnant by Choice
25.1 Pregnant by Choice/Family Planning Waiver ................................................... 335
25.1.1 Covered Services ............................................................................................... 335
25.1.2 Non-Covered Services ....................................................................................... 335
25.1.3 Eligibility Criteria .............................................................................................. 335
25.1.4 Enrollment Process ............................................................................................ 336
25.2 Pregnant by Choice Covered Codes .................................................................. 336

Covered Services –_Pregnant by Choice___________________________________________
Ch. 25 Inedx 335 Revision 4/1/17
25.1 Pregnant by Choice/Family Planning Waiver
Pregnant by Choice provides family planning service to women who have received
Medicaid benefits through the Pregnant Women Program. This program extends
family planning options to women who would typically lose their Medicaid benefits
up to two (2) months postpartum.
25.1.1 Covered Services
Initial physical exam and health history, including client education and
counseling related to reproductive health and family planning options,
including a pap smear and testing for sexually transmitted diseases.
Annual follow up exam for reproductive health/family planning purposes,
including a pap smear and testing for sexually transmitted diseases where
indicated.
Brief and intermediate follow up office visits related to family planning.
Necessary family planning/reproductive health-related laboratory procedures
and diagnostic tests.
Contraceptive management including drugs, devices and supplies.
Insertion, implantation or injection of contraceptive drugs or devices.
Removal of contraceptive devices.
Sterilization services and related laboratory services (when properly
completed sterilization consent form has been submitted).
Medications required as part of a procedure done for family planning
purposes.
Services must be provided by an enrolled Medicaid provider.
25.1.2 Non-Covered Services
Services are limited to approved family planning methods and products
approved by the Food and Drug Administration (FDA).
Sterilization reversals, infertility services, treatments or abortions.
25.1.3 Eligibility Criteria
The client must be transitioning from the Pregnant Women Program.
She is not eligible for another Medicaid program.
Does not have health insurance including Medicare.
Is a Wyoming resident.
Is a US Citizen.
Her age is 19 through 44 years.
Covered Services –_Pregnant by Choice___________________________________________
Ch. 25 Inedx 336 Revision 4/1/17
She is not pregnant.
25.1.4 Enrollment Process
The Customer Service Center, Wyoming Department of Health (WDH) must
be notified of the pregnancy and birth of the baby.
The Customer Service Center, WDH will send a review form and a Pregnant
by Choice Questionnaire to women eligible for the Pregnant Women Program
while in the two (2) month postpartum period to determine if they are
interested in the program.
If a mother allows her Medicaid benefits to lapse after the two (2) month
postpartum period she will not be eligible for the Pregnant by Choice
Program.
Eligibility is determined yearly.
25.2 Pregnant by Choice Covered Codes
Pregnant By Choice Covered Codes
Covered Diagnosis
Codes
Diagnosis Code Description
Z30.011
General counseling on prescription of oral contraceptives
Z30.013, Z30.014,
Z30.018, Z30.019
General counseling on initiation of other contraceptive
Z30.012
Encounter for emergency contraceptive counseling and prescription
Z30.02
Natrl Family pln – avoid preg
Z30.09
Other general counseling and advice on contraception
Z30.430
Encounter for insertion of intrauterine contraceptive device
Z30.432
Encounter for removal of intrauterine contraceptive device
Z30.433
Encounter for removal & insertion of IUD
Z30.2
Sterilization
Z30.40
Contraceptive surveillance, unspecified
Z30.41
Surveillance of contraceptive pill
Z30.431
Surveillance of intrauterine contraceptive device
Z30.49
Surveillance of implantable sub dermal contraceptive
Z30.42, Z30.49
Surveillance of other contraceptive method
Z30.019, Z30.49
Surveillance of previously prescribed contraceptive methods
Z30.8
Other specified contraceptive management
Z32.02
Pregnancy examination or test, negative result
Z32.01
Pregnancy examination or test, positive result
Z11.3
Screening examination for venereal disease
Pregnant By Choice Covered Codes
Covered Procedures
Procedure Code Description
99201-99203
Office/Outpatient New
Covered Services –_Pregnant by Choice___________________________________________
Ch. 25 Inedx 337 Revision 4/1/17
Pregnant By Choice Covered Codes
Covered Diagnosis
Codes
Diagnosis Code Description
99211-99213
Office/Outpatient Established
11976
Removal, implantable contraceptive capsules
11980
Implant hormone pellet(s)
11981
Implant hormone pellet(s)
11982
Remove drug implant device
11983
Remove/insert drug implant
57170
Diaphragm or cervical cap fitting with instructions
58300
Insertion of Intrauterine device (IUD)
58301
Removal of intrauterine device (IUD)
58600
Division of fallopian tube
58615
Occlude fallopian tube(s)
58670
Laparoscopy tubal cautery
58671
Laparoscopy tubal block
90772
Therapeutic, prophylactic or diagnostic injection (specify substance or
drug); subcutaneous or intramuscular
96372
Therapeutic, prophylactic or diagnostic injection (specify substance or
drug); subcutaneous or intramuscular
80048
Basic metabolic panel (calcium, total)
80076
Hepatic function panel
81000-81015
Urinalysis
81025
Urine pregnancy test
82465
Cholesterol
82947-82948
Glucose
84703
Gonadotropin, Chorionic (HCG)
85013
Blood count
85014-85018
Blood smear exam
86592
Syphilis Test
86593
Syphilis test non-trep quant
86689
HTLV or HIV antibody, confirmatory test (EG, Western Blot)
86701
HIV – 1 – Antibody
86702
HIV – 2 – Antibody
86703
HIV – 1 and HIV – 2, single assay – antibody
87070-87081
Culture, bacterial
87110
Culture, Chlamydia
87205-87207
Smear, primary source
87209
Smear complex stain
87210
Smear wet mount saline/ink
87270
Infectious agent antigen detection Chlamydia
87274
Infectious agent antigen detection Herpes Simplex virus type 1
87320
Infectious agent antigen detection multiple step method; Chlamydia
Trachomatis
87340
Infectious agent antigen detection Hepatitis B surface antigen (HBSAG)
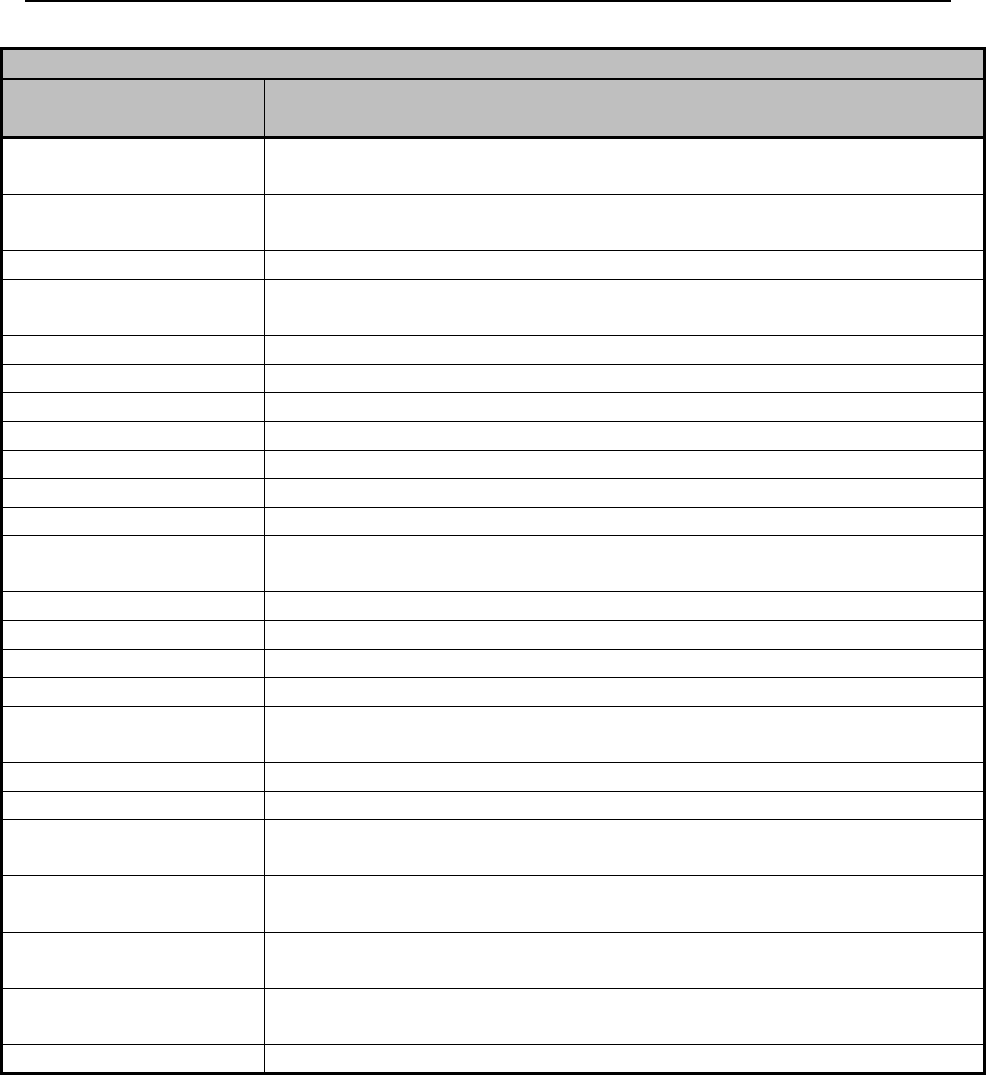
Covered Services –_Pregnant by Choice___________________________________________
Ch. 25 Inedx 338 Revision 4/1/17
Pregnant By Choice Covered Codes
Covered Diagnosis
Codes
Diagnosis Code Description
87490
Infectious agent detection by Nucleic Acid (DNA or RNA); Chlamydia
Trachomatis, direct probe technique
87491
Infectious agent detection by Nucleic Acid (DNA or RNA); Chlamydia
Trachomatis, amplified probe technique
87590
N.Gonorrhoeae DNA dir prob
87591
Infectious agent detection by Nucleic Acid (DNA or RNA); Neisseria
Gonorrhoeae, amplified probe technique
88141-88143
Cytopathology
88164-88167
Cytopathology
88175
Cytopath C/V auto fluid redo
A4266
Diaphragm for contraceptive use
A4267
Contraceptive supply, condom, male, each
A4268
Contraceptive supply, condom, female, each
J0696
Injection, Ceftriaxone sodium, Per 250MG
J1050
Injection, medroxyprogesterone acetate, contraceptive 150 MG (Depo-
Provera)
J7300
Intauterine copper contraceptive
J7301
Skyla 13.5MG
J7303
Contraceptive supply, hormone containing vaginal ring, each
J7304
Contraceptive patch
J7307
Etonogestrel (Contraceptive) implant system, including implant and
supplies
S4993
Contraceptive pills for birth control
T1015
Clinic encounter, per visit
58600
Ligation or transaction of fallopian tube(s) abdominal or biginal
approach, unilateral or bilateral
58615
Occlusion of fallopian tube(s) by devices (EG, Bank, Clip, Falope Ring)
Vaginal or suprapubic approach
58670
Laparoscopy, surgical; with fulguration of oviducts (with or without
tran-section)
58671
Laparoscopy, surgical; with occlusion of oviducts by device (EG, Bank,
Clip or Falope ring)
00851
Laparoscopy; tubal ligation/transaction

Covered Services – Therapy Service_______________________________________________
Ch. 26 Index 339 Revision 4/1/17
Chapter Twenty Six – Covered Services – Therapy Services
26.1 Therapy Services ............................................................................................... 340
26.2 Physical and Occupational Therapy .................................................................. 340
26.2.1 Covered Services ............................................................................................... 340
26.2.2 Limitations ......................................................................................................... 341
26.2.3 Documentation .................................................................................................. 341
26.3 Speech Therapy ................................................................................................. 342
26.3.1 Covered Services ............................................................................................... 342
26.3.2 Limitations ......................................................................................................... 343
26.3.3 Documentation .................................................................................................. 344
26.3.4 Cap Limits ......................................................................................................... 345

Covered Services – Therapy Service_______________________________________________
Ch. 26 Index 340 Revision 4/1/17
26.1 Therapy Services
Physical Therapy – The treatment of physical dysfunction or injury by the use of
therapeutic exercise and the application of modalities intended to restore of facilitate
normal function or development; also called physiotherapy.
Occupational Therapy – Occupational therapy addresses the physical, cognitive,
psychosocial, sensory, and other aspects of performance in a variety of contexts to
support engagement in everyday life activities that affect health, well-being, and
quality of life.
Speech Therapy – Services that are necessary for the diagnosis and treatment of
speech and language disorders, which result in communication disabilities and for the
diagnosis and treatment of swallowing disorders (dysphagia), regardless of the
presences of a communication disability.
Restorative (Rehabilitative) Services – Services that help patients keep, get back, or
improve skills and functioning for daily living that have been lost or impaired
because the client was sick, hurt or suddenly disabled.
Maintenance (Habilitative) Services – Services that help patients keep, learn, or
improve skills and functioning for daily living. Examples would include therapy for a
child who isn’t walking or talking at the expected age.
26.2 Physical and Occupational Therapy
26.2.1 Covered Services
Services must be directly and specifically related to an active treatment plan.
Independent physical therapy services are only covered in an office or home setting.
Physical Therapy & Occupational Therapy – Services may only be
provided following physical debilitation due to acute physical trauma or
physical illness. All therapy must be physically rehabilitative and provided
under the following conditions:
o Prescribed during an inpatient stay continuing on an outpatient basis;
or as a direct result of outpatient surgery or injury.
Manual Therapy Techniques – When a practitioner or physical therapist
applies physical therapy and/or rehabilitation techniques to improve the
client’s functioning.
Occupational Therapy interventions may include:
o Evaluations/re-evaluations required to assess individual functional
status.
o Interventions that develop, improve or restore underlying impairments.
Covered Services – Therapy Service_______________________________________________
Ch. 26 Index 341 Revision 4/1/17
26.2.2 Limitations
Reimbursement includes all expendable medical supplies normally used at the time
therapy services are provided. Additional medical supplies/equipment provided to a
client as part of the therapy services for home use will be reimbursed separately
through the Medical Supplies Program.
Physical and occupational therapy visits are limited to 20 per calendar year
o 20 visits per physical therapy; 20 visits per occupational therapy. (6.9,
Cap Limits, 6.9.4 Cap Limit for Therapies Request Form)
Visits made more than once daily are generally not considered reasonable.
There should be a decreasing frequency of visits as the client improves.
Clients age 21 and over are limited to restorative services only. Restorative
services are services that assist an individual in regaining or improving skills
or strength.
Maintenance therapy can be provided for clients 20 and under.
26.2.3 Documentation
The practitioners and licensed physical therapist’s treatment plan must contain the
following:
Diagnosis and date of onset of the client’s condition.
Client’s rehabilitation potential.
Modalities.
Frequency.
Duration (interpreted as estimated length of time until the client is discharged
from physical therapy).
Practitioner signature and date of review.
Physical therapist’s notes and documented measurable progress and
anticipated goals.
Initial orders certifying the medical necessity for therapy.
Practitioner’s renewal orders (at least every 180-days) certifying the medical
necessity of continued therapy and any changes. The ordering practitioner
must certify that:
o The services are medically necessary.
o A well-documented treatment plan is established and reviewed by the
practitioner at least every 180-days.
o Outpatient physical therapy services are furnished while the client is
under their care.
Total treatment minutes of the client, including those minutes of active
treatment reported under the timed codes and those minutes represented by the
untimed codes, must be documented, to include beginning time and ending
time for services billed.

Covered Services – Therapy Service_______________________________________________
Ch. 26 Index 342 Revision 4/1/17
Practitioners and licensed physical therapist’s progress notes must be completed for
each date of service and contain the following:
Identification of the client on each page of the treatment record;
Identification of the type of therapy being documented on each entry (i.e.,
97530 vs. 97110);
Date and time(s) spent in each therapy session; total treatment minutes of the
client, including those minutes of active treatment reported under timed codes
and those minutes represented by the untimed codes, must be documented, to
include beginning time and ending time for each service billed;
Description of therapy activities, client reaction to treatment and progress
being made to stated goals/outcomes;
Full signature or counter signature of the licensed therapist, professional title
and date that entry was made and the signature of the therapy assistant and
date the entry was made. Licensed therapist must sign progress notes of
assistants within 30-days.
26.3 Speech Therapy
Speech (pathology) therapy services are those services necessary for the diagnosis
and treatment of speech and language disorders, which result in communication
disabilities and for the diagnosis and treatment of swallowing disorders (dysphagia),
regardless of the presences of a communication disability.
26.3.1 Covered Services
Speech therapy services provided to Medicaid clients must be restorative for clients
21 and over. Maintenance therapy can be provided for clients 20 and under. The
client must have a diagnosis of a speech disorder resulting from injury, trauma or a
medically based illness. There must be an expectation that the client’s condition will
improve significantly.
To be considered medically necessary, the services must meet all the following
conditions:
Be considered under standards of medical practice to be a specific and
effective treatment for the client’s condition.
Be of such a level of complexity and sophistication, or the condition of the
client must be such that the services required can be performed safely and
effectively only by a qualified therapist or under a therapist’s supervision.
Be provided with the expectation that the client’s condition will improve
significantly.
The amount, frequency and duration of services must be reasonable.

Covered Services – Therapy Service_______________________________________________
Ch. 26 Index 343 Revision 4/1/17
In order for speech therapy services to be covered, the services must be related
directly to an active written treatment plan established by a practitioner and must be
medically necessary to the treatment of the client’s illness or injury.
In addition to the above criteria, restorative therapy criteria will also include the
following:
If an individual’s expected restoration potential would be insignificant in
relation to the extent and duration of services required to achieve such
potential, the speech therapy services would not be considered medically
necessary
If at any point during the treatment it is determined that services provided are
not significantly improving the client’s condition, they may be considered not
medically necessary and discontinued.
26.3.2 Limitations
The following conditions do not meet the medical necessity guidelines, and therefore
will not be covered:
Clients age 21 and over are limited to restorative services only. Restorative
services are services that assist an individual in regaining or improving skills
or strength.
Maintenance therapy can be provided for clients age 20 and under.
Self-correcting disorders (e.g., natural dysfluency or articulation errors that
are self-correcting).
Services that are primarily educational in nature and encountered in school
settings (e.g., psychosocial speech delay, behavioral problems, attention
disorders, conceptual handicap, mental retardation, developmental delays,
stammering and stuttering).
Services that are not medically necessary.
Treatment of dialect and accent reduction.
Treatment whose purpose is vocationally or recreationally based.
Diagnosis or treatment in a school-bases setting.
Maintenance therapy consists of drills, techniques, and exercises that preserve the
present level of function so as to prevent regression of the function and begins when
therapeutic goals of treatment have been achieved and no further functional progress
is apparent or expected.
NOTE: In cases where the client receives both occupational and speech therapy,
treatments should not be duplicated and separate treatment plans and goals
should be provided.

Covered Services – Therapy Service_______________________________________________
Ch. 26 Index 344 Revision 4/1/17
26.3.3 Documentation
The practitioners and licensed speech therapist’s treatment plan must contain the
following:
Diagnosis and date of onset of the client’s condition.
Client’s rehabilitation potential.
Modalities.
Frequency.
Duration (interpreted as estimated length of time until the client is discharged
from speech therapy).
Practitioner signature and date of review.
Speech therapist’s notes and documented measurable progress and anticipated
goals.
Initial orders certifying the medical necessity for therapy.
Practitioner’s renewal orders (at least every 180-days) certifying the medical
necessity of continued therapy and any changes. The ordering practitioner
must certify that:
o The services are medically necessary.
o A well-documented treatment plan is established and reviewed by the
practitioner at least every 180-days.
o Outpatient speech therapy services are furnished while the client is
under their care.
Total treatment minutes of the client, including those minutes of active
treatment reported under the timed codes and those minutes represented by the
untimed codes, must be documented, to include beginning time and ending
time for services billed.
Practitioners and licensed speech therapist’s progress notes must be completed for
each date of service and contain the following:
Identification of the client on each page of the treatment record;
Identification of the type of therapy being documented on each entry (i.e.,
97530 vs. 97110);
Date and time(s) spent in each therapy session; total treatment minutes of the
client, including those minutes of active treatment reported under timed codes
and those minutes represented by the untimed codes, must be documented, to
include beginning time and ending time for each service billed;
Description of therapy activities, client reaction to treatment and progress
being made to stated goals/outcomes;
Full signature or counter signature of the licensed therapist, professional title
and date that entry was made and the signature of the therapy assistant and
date the entry was made. Licensed therapist must sign progress notes of
assistants within 30-days.

Covered Services – Therapy Service_______________________________________________
Ch. 26 Index 345 Revision 4/1/17
26.3.4 Cap Limits
Medicaid clients will be limited to 20 speech therapy visits per year. If the client has
exceeded the Medicaid limits on speech therapy visits, the provider may bill him/her,
or request the cap limit be waived, as long as the services are still medically necessary
(6.9, Cap Limits).

APPENDIX A – CMS1500 Manual Version Control Table
Revision
Date
Change(s)
4/1/17
2.1 Quick Reference – Added HealthHelp to the table of contacts
3.2.3 Missed Appointments – Section re-written
6.8.1 Cap Limit Waiver – Form and instruction updated
6.14 Prior Authorization – Added HealthHelp to the table
Chapter Seven – TPL/Medicare - Completely re-written
Chapter Thirteen – Behavioral Health – Several changes throughout chapter
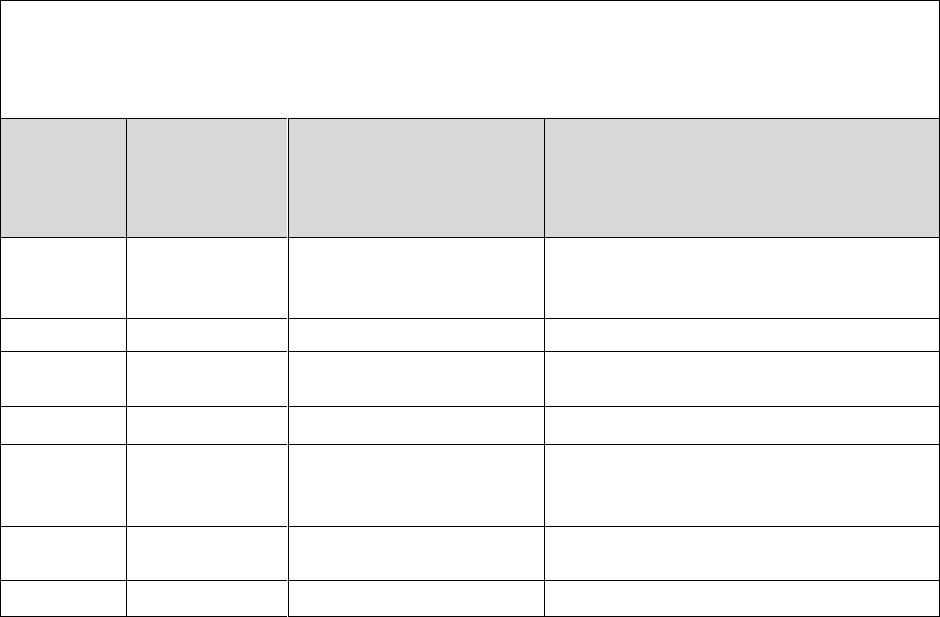
APPENDIX B – Provider Notifications Log
Email /
Mail /
Active
Date(s)
Notification
Type
Title
Audience
1/26/17
Email Notice
Child Development
Center Enrollment
Requirements
All Providers
1/30/17
RA Banner
Humidifier RA Banner
DME
2/1/17
Email Notice
Physician Administered
Drugs
Physicians, Nurses
2/27/17
Email Notice
FCBC
DME, Home Health
3/1/17
Email Notice
Behavioral Health &
Substance abuse Option
Manual
Behavioral Health
3/6/17
RA Banner
Colorectal Cancer
Screening Program
Physicians, Hospitals
3/23/17
RA Banner
Medicare Pricing
All Providers
Wyoming Medicaid Provider Enrollment Requirement – ACTION REQUIRED
Wyoming Medicaid is mandated by federal policy to enroll all providers rendering services to clients
for reimbursement through the Medicaid program. Currently, the CDCs are enrolled as individual pay-
to entities. This means that on any given claim from a CDC, there is no listing of which therapist
provided services to the client for which Wyoming Medicaid is reimbursing. In order to comply with
federal regulations, this process must be updated to have the CDCs enrolled as groups (the pay-to
provider) with treating (rendering) providers.
Wyoming Medicaid will require that the CDCs begin billing as groups with dates of service 6/1/17 and
newer. Before this date, each CDC will need to enroll as a group and enroll the providers who are
providing services to the clients in their facility. This includes Physical, Occupational, and Speech
Therapists and Behavioral Health providers (licensed professional counselors (LPC), licensed marriage
and family therapists (LMFT), licensed clinical social workers (LCSW), licensed addiction therapists
(LAT), and provisional licensed mental health professionals) The enrollment process is conducted
online. After submitting the online portion of the enrollment, you will mail in the documents that
require signature and copies of supporting documentation as required (license, NPI confirmation,
etc.). Once all of the paperwork is received, it generally takes about 4 – 6 weeks for the enrollment to
complete processing, so, please do not wait until the last minute to begin this process. You will not be
able to bill for any dates of service 6/1/17 or after until this process is completed. The first enrollment
you will need to complete will be for the CDC to establish the group, then complete enrollments for
– http://wymedicaid.acs-
lect
–
When enrolling the CDC as a group, the Type of Enrollment will be Group Practice. For all individual
treating providers enrolled, the Type of Enrollment w
selecting the taxonomy for the CDC enrollment, choose the Taxonomy Category DHCF Allowances and
Taxonomy Description of 261Q00000X –
the therapists, choose either Respiratory, Developmental, Rehabilitative & Restorative Service
Providers (PT/OT), Speech, Language and Hearing Service Providers (ST) or Behavioral Health & Social
Service Providers (Behavioral Health Providers) and then select the appropriate taxonomy under
“Are you a member of a group practice, or do you work for a hospital that bills for you?” as yes – this
will allow you to enter the CDCs NPI to link the individual therapist to the CDC for billing purposes.
Enrollment tutorials are available on the web site here: https://wyequalitycare.acs-
inc.com/aca_reenrollment.html. Although these were created for the DD Waiver providers, they are
still very useful for other providers to get an idea of the enrollment process. If you have any questions,
contact Provider Relations at 800-251-1268, options 2, 1, 2 to speak with enrollment. While I am
happy to try to answer questions for you, I do not have access to the tools and resources to review
enrollment information, and the Provider Relations Call Center will be able to assist you much more
timely and effectively. If you wish to contact me, email is the best choice, and I can be reached at
amy.buxton@wyo.gov.
Begin Date: 1/26/17
End Date: 2/23/17
Audience: DME
**********************************************************************
Effective with dates of service 2/1/17 - Wyoming Medicaid will cover
the purchase of the humidifier (E0562) with a CPAP or BiPAP machine
when the item is not an integrated part of the machine.
**********************************************************************
To view this email as a web page, go here.
2/1/17
Medicaid Website
Manuals & Bulletins
Fee Schedules
What's New
Links
IVR Navigation Tips
Web Portal Tutorials
Effective March 1, 2017, Wyoming Medicaid will be
standardizing its methodology for the reimbursement of
physician administered drugs. Rates will be established
by using the drug's Average Sales Price (ASP) rate as
published by Center for Medicare and Medicaid Services
(CMS).
Rates will be reviewed at least annually. For drugs that are not listed on the ASP file
published by
CMS, Wyoming Medicaid will first reimburse the Wholesale Acquisition Cost (WAC), and if no
WAC is available, will default to the Average Wholesale Price (AWP) for the drug based on the
CPT/HCPCS submitted on the claim form. Rates will be made available for viewing on the
Wyoming Medicaid fee schedule no later than February 20 th, 2017 to allow providers to evaluate
specific impacts based on common drugs administered to Wyoming Medicaid clients.
As an important reminder for providers billing physician administered drugs, the units billed
MUST be the CPT/HCPCS units appropriate for the dose administered. The units reported on
the claim should NOT be the NDC-based units. Additionally, the applicable NDC for the drug
administered must also be included on each claim.
Help identify and combat Medicaid Fraud by visiting the website or
contacting the Fraud Hotline:
• http://stopmedicaidfraud.wyo.gov
• 1-855-846-2563
WYhealth is a Medicaid health management and utilization management program
offered by the Wyoming Department of Health through Optum. Medicaid clients and
providers will benefit from a wide array of programs and services offered and
coordinated by Optum. Visit www.wyhealth.net for more information
This bulletin was sent on:
Date:
2/1/17
Time:
3:00pm
MST
Audience: Physicians and Nurses
2/27/17
Medicaid Website
Manuals & Bulletins
Fee Schedules
What's New
Links
IVR Navigation Tips
Web Portal Tutorials
As required under 42 CFR 455.434, starting July 1,
2017 Wyoming Medicaid will require all currently
enrolled, newly enrolling and re-enrolling Home
Health and Durable Medical Equipment/ Prosthetics
and Orthotics Suppliers (DME/POS) to complete a full
criminal background check as a condition of
continued participation (if you haven't already done
so through Medicare or another state's Medicaid
program). This will require submitting fingerprints to the Wyoming
Division of Criminal Investigation (DCI).
Any Home Health or DME/POS owner who reported more than a 5% direct or indirect ownership interest upon
enrollment with Medicaid will also be subject to the same fingerprint and background check requirements.
Wyoming Medicaid is in the process of auditing current enrollment records to identify which enrolled providers will be
required to complete this process. If your office is determined to need additional background checks completed, you
will receive a more detailed letter with instructions on how to complete the fingerprinting process and a timeframe for
completion.
Any provider who has failed to comply with the fingerprinting and background check requirements by July 1, 2017 will
be dis-enrolled from the WY Medicaid program.
Please watch all upcoming communications carefully for more detailed information. For any further questions, please
contact Andrew Chapin, Quality Assurance Manager Andrew.Chapin@wyo.gov.
Help identify and combat Medicaid Fraud by visiting the website or contacting the Fraud
Hotline:
• http://stopmedicaidfraud.wyo.gov
• 1-855-846-2563
WYhealth is a Medicaid health management and utilization management program offered by the Wyoming
Department of Health through Optum. Medicaid clients and providers will benefit from a wide array of programs
and services offered and coordinated by Optum. Visit www.wyhealth.net for more information
Deployed:
Date: 2/27/17
Time: 3pm MST
Audience: DME and Home Health
To view this email as a web page, go here.
3/3/17
Medicaid Website
Manuals & Bulletins
Fee Schedules
What's New
Links
IVR Navigation Tips
Web Portal Tutorials
Attention Behavioral Health Providers
Wyoming Medicaid Program, Community Mental Health & Substance Abuse Treatment
Services Manual
Effective April 1, 2017, the Wyoming Medicaid Program, Community Mental Health & Substance
Abuse Treatment Services Manual, also known as the Medicaid Policies and Procedures
Manual for Mental Health Substance Abuse Option Services will be discontinued. Any of the
pertinent information that was in that manual has been transferred over to the CMS-1500
Provider Manual.
Limitations for Behavioral Health Services
When providing behavioral health services to a Medicaid client, the documentation kept must be
accurate with the date and times the services were rendered (CMS-1500 Provider Manual 3.11
Record Keeping, Retention and Access, 13.9 Documentation Requirements for All Behavioral
Health Providers). Behavioral health services cannot overlap date and time for a client. For
example, a client being seen for group therapy on February 28th from 11:00 to 12:00 cannot
also be seen for targeted case management on February 28th from 11:00 to 12:00. These are
overlapping services and cannot be billed to Medicaid. Proper documentation of services
includes the start and end times of the services being rendered.
Rehabilitative vs. Habilitative Services
Wyoming Medicaid coverage of rehabilitative services such as mental health and/or substance
abuse treatment is limited to restorative treatment only. Maintenance therapy is not a covered
service by Wyoming Medicaid.
Health Resources and Services Administration has historically differentiated between habilitation
and rehabilitation services and does not allow for the inclusion of habilitation services under the
rehabilitation benefit category (State Plan Medicaid). Habilitation services, which are services to
assist an individual in obtaining a skill, are not included in the section 1905(a) list of services and
are only available in an institution for the developmentally disabled or under a home and
community based services waiver. Habilitation services cannot be covered as "rehabilitative"
when they are furnished to individuals, for example, suffering from a mental retardation or to
children experiencing development delays, because services are assisting the child in obtaining
a skill rather than restoring lost capabilities.
To better understand the difference between habilitative and rehabilitative services, the key is
whether or not the person ever had the skill or function. If the person did have it and lost it due to
a disease or accident then it would be a rehabilitative service. If the person never had it then it is
a habilitative service.
Because Wyoming Medicaid is restricted to the reimbursement of services that are exclusively
rehabilitative and restorative in nature, the Medicaid Developmental Disability Waiver Program
(operating as the Comprehensive and Supports Waiver in Wyoming) also includes coverage for
habilitative therapy services (physical, speech, occupational, community integration and
supported living services) beneficial to clients with a developmental disability, recognizing that
most often the services needed by these clients are habilitative in nature, and do not meet the
requirements of the rehabilitative services covered by traditional Medicaid.
Behavioral Health Cap Limits and Waiver Requests
Clients 21 years of age and older have a cap limit of 20 visits for behavioral health services.
After a client has used all 20 of his or her visits, the therapist may complete the Cap Limit Waiver
Request form to request additional visits. Click on the link to be taken to the Cap Limit Waiver
Request Form : https://wymedicaid.acs-
inc.com/forms/Cap_Limit_Waiver_Request_Form_1_1_17.pdf.
Be aware that cap limit waivers will only be granted for those requests that meet Wyoming
Medicaid policy. The Cap Limit Waiver Request form will require both the narrative diagnosis
and the ICD-10 diagnosis code(s) that apply to the client's condition. Please also note the form
requests the pay-to provider information, NOT the treating therapist's information; however, the
treating therapist must sign the form. Forms that do not contain all of the correct information
when they are reviewed may cause claims to deny or may be returned for correction, depending
on the information provided or missing.
Note: For clients over the age of 21 served by the Developmental Disabilities Comprehensive or
Supports waiver, additional services may be available as part of the client's waiver plan. These
services have different rules and requirements. Please contact the client's case manager or the
Behavioral Health Division for questions related to waiver services, plans of care, or IBAs.
Help identify and combat Medicaid Fraud by visiting the website or
contacting the Fraud Hotline:
• http://stopmedicaidfraud.wyo.gov
• 1-855-846-2563
WYhealth is a Medicaid health management and utilization management program
offered by the Wyoming Department of Health through Optum. Medicaid clients and
providers will benefit from a wide array of programs and services offered and
coordinated by Optum. Visit www.wyhealth.net for more information
Unsubscribe
Be sure to add wycustomersvc@conduent.com to your address book to ensure the proper delivery of your Wyoming
Medicaid updates and weekly payment summary information.
Wyoming Medicaid, Provider Relations, PO BOX 667, Cheyenne, WY 82003
Please do not reply to this email with any customer service issues. Specific account inquiries will not be read. For


********************************************************************
The Colorectal Cancer Screening Program has changed the screening
vouchers to an enrollment card. Effective immediately, the program
will be issuing enrollment cards to newly eligible clients. For
questions please call 1-800-264-1296.
********************************************************************
Running:
Date: 3/6/17-5/6/17
Audience: Physicians, Nurses, Hospitals
**********************************************************************
Attention All Providers:
If you have questions regarding paid and/or denied Medicare X-Over
claims, please see the Wyoming Medicaid website - What's New Section
https://wymedicaid.acs-inc.com/new.html.If you are calling Wyoming
Medicaid Provider Relations for questions regarding Medicare X-Over
claims, please note due to increased call volumes, longer wait times
can be expected.
***********************************************************************
Deployed:
Date: 3/22/17
Audience: All Providers
