COGNITIVE BEHAVIORAL THERAPY FOR ANXIETY AND SOCIAL PROBLEMS Wood2015 Biaca Manual Update Feb 2014 W Updated Handouts
User Manual:
Open the PDF directly: View PDF ![]() .
.
Page Count: 151 [warning: Documents this large are best viewed by clicking the View PDF Link!]

COGNITIVE BEHAVIORAL THERAPY FOR ANXIETY AND SOCIAL PROBLEMS
IN CHILDREN WITH AUTISM
INTERVENTION MANUAL
JEFFREY J. WOOD, PH.D. KAREN SZE WOOD, PH.D.
AMY DRAHOTA, PH.D.
UNIVERSITY OF CALIFORNIA, LOS ANGELES
REV. 2-2014
Child
Modules
Module Contents
1
Introduction, Information about ASD
2
―K‖ and ―I‖ Steps
3
―C‖ Step
H
Hierarchy of Exposures
4
―K‖—Keep Practicing
KICK
Using the KICK Plan
IV
In Vivo Exposure
FRND
Making Friends
SOC-C
Social Coaching Exposure
ERP
E/RP In Vivo Exposure
MENTOR
Mentoring Skills In Vivo Exposures
X
Support / Emergency session
T
Termination
Parent
Modules
Module Contents
1
Introduction, Information, and the Treatment Plan
IEP
Parent Advocacy and IEP Goals
IND
Encouraging Independence
H
Hierarchy of Exposures
EXP
Negotiating Exposures
REW
Rewards
SOC-C
Social Coaching
PLAY
Play Dates / Friendships
APPROP
Socially Appropriate Activities
MENTOR
Mentoring
X
Support / Emergency session
T
Termination
School
Modules
Module Contents
SOCIAL
Social Interventions at School: Rewards, Peer Buddies,
Gameleading, Social Coaching

Introduction
This program is a modular cognitive behavioral intervention for children with
autism who show signs of acute anxiety and social dysfunction. This program is flexible
in nature, providing therapy techniques that can be individually tailored to the needs of
specific children and their families. Children are taught anxiety management skills
based on the cognitive behavioral therapy (CBT) approach (cf. Barrett, Dadds, &
Rapee, 1996; Kendall, 1994), they participate in social training experiences in a variety
of settings, and parents are taught skills to support children’s social and emotional
development and enhance CBT efficacy.
The Central Role of Exposure and Hierarchical Learning
Exposure therapy involves systematic and repeated confrontation with fearful
stimuli. Exposure is the central therapeutic intervention employed in this program. A
wealth of clinical data supports the efficacy of exposure therapy in treating anxiety
disorders. However, for exposure therapy to work, several ingredients are needed. First,
the child has to experience mastery in feared situations. Hence, the need for repetition
until fear is reduced. Second, the child must experience mastery in as many new
situations as possible. Hence, the need for a systematic program of exposure that
includes all or almost all feared stimuli. Third, in order to promote long-term change,
parents should learn appropriate communication skills to facilitate their children’s
independence, which should become a family routine that continues indefinitely after the
treatment program. Additionally, school personnel may play a crucial role in facilitating
exposures during the school day.
A key learning strategy used in exposure therapy is hierarchical learning.
Approaching emotional and social skills that children do not have in a bottom-up, one-
step-at-a-time manner is consistent in many ways with task analysis. In this therapy
program, hierarchical learning is broadened beyond the bounds of anxiety management
into areas of social skills training and friendship development. In working on these areas
of training, small incremental steps are the underlying teaching approach. A second
characteristic of exposure therapy is also applied to social skills training in this program:
training and practice in the actual settings where social interactions occur, rather than
remaining in the therapy room and practicing ―hypothetical situations‖ as most previous
social skills training programs have done.
Modular Therapy Algorithm
Chorpita (2004) and others advocate a modular therapy approach to CBT. In
modular therapy, there is not a set schedule of sessions, but rather, a range of possible
therapy ―modules‖ (specific therapeutic procedures that can normally be covered in one
session) that may be selected. In this program, there are 14 child modules, 12 parent
modules, and 1 school module (which is generally repeated several times). Modules for

each session are selected on the basis of a simple algorithm that is adapted from
Chorpita (2004). This algorithm essentially highlights the need for a few basic coping
skills to be learned, followed by a primary focus on exposures unless there is a barrier
to the efficacy of such exposures. If barriers occur, then supplementary modules are
used, based on clear decision rules, until exposure becomes successful.
Important information about the modules
Most modules include examples of ways to present key concepts to parents or
children. Such examples are presented in italics. In every case, these examples are
tailored to the personality and cognitive features of the specific child they were used
with. These examples should rarely if ever be repeated verbatim to new clients—they
are general guides for helpful ways to word ideas for some families.
On a related note, each module has a list of Goals at the start of the session. All
of these goals should be accomplished in some manner during the session. However,
the manner of presentation and depth of coverage is flexible—for instance, for a very
verbal child, cartoons might be less helpful, and the use of make-believe stories and
acting-out situations might be a more effective means of psychoeducation. There are
many different means of training that can lead to the same acquisition of knowledge,
and the therapist must use his/her clinical expertise (and/or that of the supervisor) to
determine how best to present information to a particular family. In short, it is important
to cover the main Goals of each session; but it is not necessary to go ―point-by-point‖
through the detailed instructions in each Module—these details are provided primarily
for therapist education and background, and as a guide to a possible ―model session.‖
Note that occasionally parent and child modules have overlapping goals (e.g.,
reviewing or assigning exposure homework). Often goals from both modules may be
accomplished simultaneously in a single parent-child meeting (e.g., by discussing the
previous week’s exposures with both members of the dyad, and then planning together
the next week’s exposures). In such a case, there is no need to have a ―separate‖
conversation with either member of the dyad about such overlapping topics unless the
additional conversation is clinically indicated (i.e., to allow the child to give input without
fear of the parent ―taking over‖ the conversation).
Algorithm for child modules:
1. The first session should involve an introduction to the program and chit-chat or game-
play (Module 1)
2. The child must identify at least one effective coping skill (relaxation, positive self-talk,
or self-reward) prior to initiating exposures. (Child Modules 2-4 & R)
3. When steps 1 & 2 are completed, a fear hierarchy must be developed prior to
beginning exposures, and this should be conducted with a parent present when
possible. (Parent / Child Module H)

4. After step 3 is complete, in vivo exposures (Child Module: IV) and ―homework‖ (out-
of-session) exposures (Child Module: KICK and Parent Module: EXP) should be
conducted continuously until all anxiety symptoms have remitted.
a. If the child co-sleeps, this should be an initial target of exposure.
b. If clinical progress is not being made at step 4 after three successive
―exposure‖ sessions, step 2 must be repeated to build up new coping skills and
motivation before attempting more exposures.
5. If the child has obsessions or compulsions, Child Module: Exposure/Response
Prevention (ER/P) should be conducted concurrently with exposures (Child Module: IV
and Parent Module: EXP).
6. Depending on the child’s social skills training needs, any of the social intervention
modules may be initiated after step 3 (FRND, MENTOR, SOC-C). Exposure homework
is discussed in each of these modules, allowing exposures to be done concurrently with
social skills training efforts.
7. If the child’s special interests or preoccupations interfere with social adjustment, the
Special Interest Suppression module (Child Module: SUPPRESS) should be presented.
8. Treatment may stop when all targeted behaviors have improved, or after 16 sessions.
The final session should be Child Module: T and Parent Module: T.
Algorithm for parent modules:
Parent modules may last 15-60 minutes, to leave sufficient time for the concurrent child
module. At minimum, the ―key points‖ of each parent session must be covered. If one
parent is attending sessions, the same parent should be encouraged to attend all of the
sessions to prevent inconsistency in follow-through. A second parent is welcome to
come when s/he is available.
1. The parent should be given psychoeducation and a treatment plan (Module 1) first.
2. If there are advocacy or IEP issues that would further the goals of therapy (i.e.,
getting a 1:1 aide) Module: IEP should be done next.
3. The parent should be given the Encouraging Independence module (Module IND)
next. Self-help skills are an important on-going emphasis throughout treatment.
4. The parent should participate in the Hierarchy module (Module H) whenever the child
is ready to develop the hierarchy.
5. If there are any questions or concerns about the child’s motivation to do exposure
and self-help tasks, the Reward Module (Module REW) should be presented.
6. The parent should normally complete the Negotiating Exposure module (Module
EXP) each time the child is assigned a ―homework‖ exposure.
7. If the child has few or no friends, the parents should be given the Playdates module
(Module PLAY) as soon as feasible, taking into account the need to monitor and
troubleshoot the other exposures the child is engaging in. Note, Module PLAY is a
specific type of exposure that requires specialized implementation. Most importantly the
child must be prepared (Child Module: FRND).
8. To increase perspective taking and prosocial behavior in older children, implement
Module: MENTOR.
9. If the parent has access to social situations in which the child frequently finds
him/herself, the social coaching module should be conducted (Module: SOC-C).
10. Treatment may stop when all targeted behaviors have improved, or after 16
sessions. The final parent session should be Module T.
Algorithm for school/teacher modules:
1. A school observation should be conducted by the therapist, if clinically feasible.
2. By session 2-3, the school should be contacted (with parent written consent).
Implement School Module: SOCIAL with any teacher/staff member who is able to be
present.
Session structure when parents attend
If the child is waiting in a waiting room, it is important for the child to have a
volunteer college student supervise to them, and to have an enjoyable activity OR
homework to do while they wait for the therapist and parent to meet.
General stance of the therapist
It is important to establish and maintain rapport with the family. The first few
sessions are used to develop and foster the relationship with the family. As part of this
approach, skills training is presented as a collaborative effort, wherein everyone is
working together towards an important goal. The therapist provides a friendly,
accepting, and supportive environment. Parent-blaming is always to be avoided.
Parents should feel that they have not contributed to their child’s anxiety, but may be
able to engage in ―specialized parenting techniques‖ that might not otherwise be
needed with typically developing youth, to assist in the anxiety reduction process.
When talking with children with limited verbal ability, limited attention span,
excessive preoccupations, or tangential speech, adopting an interactive style that
reflects several components may be helpful in maintaining rapport and ensuring the
child’s comprehension of core CBT concepts. These include: (1) explicitly setting the
expectation for on-topic responding, (2) setting a rapid pace for the session, and (3)
consistently checking for child’s comprehension of CBT concepts, repeating illustration
as needed. The following is an example therapist-child dialogue:
T: Hey Andy, we’re going to be talking for about 15 minutes. After that can watch the
Jimmy Neutron video, okay (Sets the expectation for on-topic responding)? C: (Engages
in preoccupations) Did you know that the Santa Ana winds.... T: Andy, listen, remember
what we could do when we’re done talking?
C: Jimmy Neutron video. T: That’s right (quickly proceeds to discussing session topic)!
Great, one thing I want to talk to you about is autism. Have you heard of that term
before? What does it mean? C: Serious something... (tangential response)
T: (Ignores irrelevant response and sets a rapid pace for the session) Well, autism
means that there is something special and different about a kid’s brain....
C: (Reverts to preoccupations).... the weather channel.
T: (Ignores comment and repeats illustration) So autism means that.... (Checks for
child’s comprehension) Andy, what is special and different about a kid with autism?
C: Brain, up here (points to own head).
T: You’re right on! Nice job... (Proceeds to discuss subsequent concept)
Glossary of terms to use
When talking with families, attempt to use non-stigmatizing / non-clinical language
when possible. In particular, it is preferable to refer to parent training and child CBT as a
―program‖ rather than as a ―treatment‖ or ―intervention‖. The following are terms that can
be useful to incorporate into the dialogue with families.
―Building your muscle‖—helping parents become less distressed by their child’s
behavior
―Where the child gets stuck‖—the point when the child cannot make progress in
anxiety-provoking situations
―Learning there is nothing to be afraid of‖—the point of child CBT / exposure
therapy
―Building the child’s confidence‖—the overall goal of the program
Autism Spectrum Disorders Appropriate for this Program
This program has been developed for use with children with high-functioning
autism (children with a full scale IQ equivalent score above 70), pervasive
developmental disorder—not otherwise specified (PDD-NOS), or Asperger syndrome.
The authors advise that children participating in this program have a full-scale IQ score
within the normal range of the child’s chronological age, which ensures that children
have the verbal ability to comprehend and contribute to their treatment.
Child Module 1
Introduction, Information, and Homework
Background
In the first session, the main goal is to establish rapport with the child; in addition, the
therapist introduces the concepts of autism and anxiety and briefly evaluates how well the child
can interpret his/her emotional and behavioral cues for emotional recognition. Psychoeducation
is an important aspect of treatment. Parents and children benefit from naming and being able to
identify behaviors resulting from autism.
Children with ASD have deficits in their ability to read and correctly interpret social and
emotional cues, including emotion recognition and attention to socially relevant details (c.f.
Bauminger, 2002). Consequently, children with ASD have difficulty being able to identify
CUES of their own emotions (the K step of the KICK plan; the necessary element to initiating a
positive coping response) including BODY FEELINGS. Therefore, therapists may initially focus
on the child‘s own BEHAVIORAL CUES of anxiety rather than on the on internal states that
children with ASD have trouble identifying.
Goals
1. Establish rapport with the child by playing, chatting, permitting child to help set the tempo of
the session.
2. Present psychoeducation regarding ASD and anxiety.
3. Assign homework.
Preparations
Review the child‘s intake reports to become familiar with the child‘s primary symptoms.
Review whether the child knows about his/her diagnosis of autism, and what the family
refers to it as (e.g., autism, Asperger syndrome, PDD-NOS).
Be sure parent knows to bring in toys/games/books the child likes to show the therapist.
Prepare handouts: Homework Assignment handout.
Bring a ―business card‖ with the therapist‘s name and pager/voice mail number.
Materials
Homework Assignment handout
CARTOON w/ happy child
Session
WITH PARENTS AND CHILD TOGETHER (10 MINUTES)
Meet briefly and explain the session format (about 30 minutes with child alone and about 30
minutes with parents alone, plus 5 minutes with both, each session). Point out that you‘ll be
working together for approximately 4 months. Remind the family that a volunteer college student
will stay with the child (and his/her siblings, if applicable) during therapist-parent meetings.
WITH CHILD ALONE (30 MINUTES)
1. Build rapport with the child:
Allow the child to explore the room/area; if s/he is interested, tour around the building or select
a toy or game to play later.
- Engage in an activity or conversation that is of particular interest to the child, based on your
knowledge about him/her. This can include looking at the toy/game the child brought with
him/her. Ask questions; let the child indicate what is important, etc. Let the child know that
you will stop engaging in the activity to do some other things, but will be able to engage in the
topic/behavior at the end of the session.
2. Orient the child to the program:
Orient child to goals of program: (a) learning about thoughts and feelings, (b) learning about
making friends and having fun, (c) maybe earning privileges and rewards.
3. Determine what the child already knows about autism/anxiety & provide
psychoeducation:
Make sure to use the exact language used at home (i.e., autism vs. Asperger‘s vs. non-
diagnostic label such as ―learning problems‖).
―Your mom and dad might have talked with you about autism. What does that term mean to
you?‖
If the child does not know that he/she has a diagnosis of autism, casually introduce the topic
without mentioning that the child has the diagnosis: ―One thing I want to talk with you about
today is autism. Have you heard of that word before? What does it mean?‖
o Children who are not yet aware of their diagnosis should not be told by the therapist on
day 1. Check in with the parents over time before disclosing this information to the
child. The present conversation can be kept informational, not personal.
If the child provides a wrong answer, ignore the comment (e.g., do not state that the answer
was incorrect) but do provide corrective and accurate information.
Key points to cover about autism include:
o It means that there is something special and different about a kid‘s brain.
o Some kids have ―different kinds of brains‖ that make it hard for them to see, so they
need to wear glasses.
o Some kids have ―different kinds of brains‖ that make it hard for them to stay calm and
get along with other people, and those kids have autism.
Kids with autism need a little extra coaching to learn to stay calm and get along
with people.
o Other things that can happen to kids with autism (individualize to child if possible):
Hard time making friends
Hard time guessing what people are thinking or feeling (FOR INSTANCE…)
Hard time saying what they want to say (LIKE…)
Hard time getting people to do what they want them to (LIKE…)
Not understanding what people mean by words like fear, sadness
Just wanting to do 1 type of game (like videogames) even though everyone else
wants you to do other stuff (like sports, schoolwork, reading, playing w/
people…)
Link anxiety with autism—personalize to child‘s fears.
o For example: Kids with autism often become nervous or upset easily about some things.
A lot of kids with autism feel really shy about talking on the phone to other kids. And
they often get scared about staying at home with a babysitter. And they worry that
something terrible might happen to their mom when she‘s driving…
4. Externalize autism:
Make autism a discrete ―enemy.‖
―Autism is something that makes us special; but it can also make us do stuff we don‘t want to. Like
sometimes kids really want to behave, but their autism makes them misbehave! And some kids
really want to make friends, but their autism makes it hard for them. Sometimes we get really sick
and tired of autism cause it messes us up. But we can fight back against autism. What could kids
say to their autism? Take a hike, go jump in the lake…?‖
5. Homework Task:
Explain a reward system that will be set up to encourage the child to do their homework tasks.
o Each week the child will be asked to complete a few things at home. It is great if they
write it down. Or if they‘d rather, they can get mom/dad to help and tell them what
they‘d like to say.
o Child will receive two points / stickers (depending on age, gender, maturity) for each
homework. Points will add up to small fun rewards or privileges the child will enjoy.
―We can talk about kinds of rewards next time.‖
Assign homework task of writing about a time when s/he felt good in the past week and, if
possible, thoughts and body feelings. (See homework sheet).
Practice imaging thoughts and body feelings using the ―happy child‖ cartoon.
Reinforce child participation by chatting about his/her special interest or playing favorite
game/activity. This should last approximately 5-10 minutes.
Write about a time this week that you are feeling happy.
What was going on?
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
How did my body feel?
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
What was I thinking about?
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________

Child Module: 2
Emotion Recognition; KICK Plan – ―K‖ and ―I‖ Steps
Background
Children with anxiety disorders have high negative affect as well as catastrophic cognitions.
They need to learn to identify both feelings and thoughts as a first step of coping with anxiety.
Goals
1. Review homework
2. Teach child how to bodily identify cues of anxiety (―K‖ step)
3. Exemplify connection between anxious thoughts and anxious feelings for child (―I‖ step)
4. Maintain rapport with the child by playing, chatting, permitting child to help set the tempo of
the session
5. Assign HOMEWORK task
Preparations
1. Prepare a simple reward chart out of colorful paper with a title such as ―Jimmy‘s Smart
Chart.‖ Make a column of 4 sessions (Meeting 1, Meeting 2…) and leave space to either
write in points or stick stickers
Materials
Reward chart (see above)
Cartoons
2 pages blank paper
Pencil (crayons optional)
WITH CHILD ALONE (30 MINUTES)
1. Build Rapport:
For only a minute or two, build rapport with child by asking about activities or topics of
interest to him/her. Remind child that s/he will be able to engage in activity/topic at the end of
the session.
2. Review HOMEWORK Task:
Review the child‘s HOMEWORK task. If s/he did not write the homework, allow him/her do
complete it verbally by reporting to you. Give gentle corrective feedback to clarify any
misinterpretations of thoughts vs. feelings. Introduce reward chart with appropriate affective
tone (matching child‘s style). Record appropriate points/stickers on his/her reward chart.
3. Identifying Emotions:
Use cartoons of children depicted in various mood states and work with the child to identify
feelings based on expressions and posture.
―Andy, let‘s look at these cartoons. We‘re going to play detective and figure out what people
are feeling. See this guy here? I think that he is… (pause) …happy! Know how I can tell? He
has a big smile on his face! Do you want to take a turn, what do you think this person is feeling
in this picture? Is there anything about her face that gives up clues about what this person is
feeling?‖
Provide scaffolding, as necessary, to help the child identify the emotion and pick out facial and
body cues that inform us about the emotion the character is feeling. The following chart
identifies the key facial and bodily features for the basic emotions that children should learn to
differentiate among:
Emotion
Cues
Fear (―scared‖, ―nervous,‖ ―afraid,‖ ―anxious‖)
Wide eyes; sometimes a frown; sometimes an
open mouth; raised eyebrows; shivering;
sweating
Anger
Squinting; angled eyebrows; furrowed brow
(―wrinkley forehead‖); pursed lips; red face
Sadness
Crying; frown; drooping shoulders; slumped
over (head in hands); looking away from others
Happiness
Smile/grin; laughing; wrinkles on the sides of
eyes
―What about the face, in particular, tells us that he is feeling happy? Is there something about
his mouth that gives us clues? What about his eyes—do they have big wrinkles next to them?
Okay, so let‘s review—what are the main ways we can tell that someone is happy from looking
at their face and body?
Do this for the 4 basic emotions. Some children will want/need to distinguish between surprise
and fear (the former usually has a ―gape-mouthed‖ feature). Others will want to add more
complex emotions such as jealousy—allow them to do so to encourage rapport, but ensure they
understand the key features of the 4 basic emotions.
Help the child understand that when it comes to fear, there are different words for the same
feeling: feeling afraid, scared, nervous, worried or anxious. They all mean the same thing. Ask
which word the child uses and likes best. Be sure to use this word in the future in discussing
fear/anxiety.
4. Identifying Anxiety – the ―K‖ Step:
Disclose a situation that causes the therapist modest anxiety that is socially acceptable such as
going on rollercoasters or giving speeches (avoid examples such as driving on the freeway
which might model novel anxious thoughts for the child that could be deleterious to daily
functioning). Use appropriate affect to engage and maintain the child‘s interest and attention.
Describe the physical cues that the situation elicited (e.g., racing heart, trembling, sweating,
fast breathing, stomach ache, light-headedness, headache, aches and pains—this is often best if
these physical cues match some of the child‘s known somatic expressions of anxiety).
If the child volunteers a feared situation during or after this disclosure, help him/her brainstorm
on the kinds of somatic reactions s/he had. Otherwise, return to the cartoons and select
examples that show clear somatic reactions to fear that can be portrayed in a picture
(trembling, sweating, stomach ache). Ask what kinds of ―things‖ the cartoon-child‘s body is
doing. Ask rhetorically ―if that is one way we could tell the child is afraid.‖ Follow-up noting
that ―yes, the way our body feels is one way we can tell if we‘re afraid/nervous/anxious/etc.‖
Introduce concept of using physical cues as a signal that one is becoming anxious (―before we
know what to do about anxiety, we have to know when we‘re becoming anxious‖). ―We refer to
this as the ―K‖ step: KNOWING I‘M NERVOUS (―K stands for Knowing‖)!‖
o Write down KICK vertically on a blank piece of paper. Fill in the ―K‖ step, Knowing
I‘m Nervous. Explain to the child that ―we‘re going to be learning the ‗KICK plan‘ as a
way to feel better when we become afraid. That‘s what this program is about. And we
just learned the first step, ‗K‘!‖
Say (as drawing an ―inverted U‖ mountain and a stick figure ―kid‖ on a blank piece of paper):
―Let‘s practice: Let‘s say a kid didn‘t like going up to high places. And then he had to go to the
top of a mountain and look down. Then he started shivering and sweating. His eyes got really
wide-open. (Quickly draw squiggles and circles to represent shivers, sweat, and wide eyes).
How do you think he is feeling? How can you tell? Why not happy? Why not sad?‖
If the child is still engaged, ask if s/he can think of something that would make ―most kids‖
afraid. Ask her/him to make up a story (offer to draw a stick-figure of the story, or if the child
would like to do so, offer her/him the pencil/crayons) about a child who was in this situation.
Ask how people could tell the child was afraid by looking at him/her. Use Socratic questioning
to help child distinguish among the different emotions.
Tip: these exercises may need to be repeated in later sessions to ensure they ‗stick‘ and are
completely mastered.
5. Explain the ―I‖ Step:
Return to the cartoons used earlier in the session. Discuss the kinds of thoughts that each
person experiencing fear may be having. Begin with an example: ―Okay let‘s have a look at
this cartoon again. We‘re going to play detective again—figuring out this time what some of
these kids are thinking about. Okay, I‘ll go first… let‘s see, he‘s standing beside a swimming
pool, and we already know he feels afraid because we saw he was shivering and sweating. So,
I think he might be thinking: ‗If I go into the pool, I might sink to the bottom because I‘m not a
good swimmer!‘ Do you think that‘s what he‘s saying to himself?‖
o Negotiate with the child to come up with a reasonable ‗thought‘ that reflects anxiety in
the situation. Once this has been agreed upon, draw a ―thought bubble‖ over the
cartoon-child‘s head and quickly write in the ‗thought‘, while saying it again out loud
with affect (to keep child‘s attention). The child may do the writing, too.
Try a second, third, and even fourth cartoon depending on the child‘s willingness and interest.
Use a scaffolding approach to increasingly transfer the work of developing appropriate
―anxious thoughts‖ for each cartoon situation to the child. However, do so slowly to evaluate
the child‘s grasp of the concept. If s/he is developing thoughts that do not reflect anxiety or
have little to do with the setting of the picture, ignore the incorrect response and ask a

structured question to lead the child to the right response: ―Oh, well, do you think that she is
also afraid about messing up in her speech? What might happen if she said something wrong
when she was giving her speech? What might the other kids do??‖
o If the child provides a response in third person language, transform the thought into
first person language for the child and check-in to see if this is what the child had in
mind (e.g., for ―they‘d laugh at her‖… ―so, she might say to herself, ‘I‘m afraid they‘ll
laugh at me?‘‖) Again, write in the correctly-worded thought into the thought-bubble
while saying it out loud to help model and reinforce the use of ‗thought language‘ in the
first person for this exercise. Continue with cartoon examples to build up the child‘s
level of mastery.
Disclose anxious thoughts that were experienced in the therapist‘s example provided above for
the ―K‖ step (e.g., fear of rollercoasters… ―so remember how I was saying I get nervous about
rollercoasters? Well, do you know what kind of thoughts I had when I once went on a roller
coaster at Magic Mountain? I thought, ‗Oh boy, I‘m afraid the cart is going to fly off the track
and I‘ll get really hurt!‘)‖
If the child volunteers a feared situation during or after this disclosure, help him/her brainstorm
on the kinds of thoughts s/he had.
Explain ―I‖ step—it is important to identify ―icky‖ or ―irritating‖ (depending on the child‘s
maturity level and personality) thoughts, so we know what is bothering us when we are afraid.
o Write the ―I‖ step on the KICK plan: Icky Thoughts
o Review the first two steps of the KICK plan: ―Okay in a minute we‘re going to tell your
mom about the KICK plan. First, lets try to remember what each step is. Okay, the K
step was… (pause)… that‘s right, Knowing I‘m Nervous, and we use that step to figure
out when we‘re feeling nervous. What kinds of things do our bodies do to tell us we‘re
afraid? Okay, now the ―I‖ step was… …right, Icky Thoughts. Can you give me an
example of the kinds of thoughts kids get when they go someplace scary, like a new
roller coaster? …great, okay, we‘re almost ready to tell your mom all about it!‖
Assign child HOMEWORK task of writing about a time when s/he felt anxious, and describe
his/her body feelings and thoughts.
Reinforce child participation by discussing or playing a special topic or game. This should
last approximately 5-10 minutes.
WITH PARENTS AND CHILD TOGETHER (5 MINUTES)
1. Review the content of the child’s session:
Either ask the child to explain, or summarize the child session briefly. Inform parents that the
child is to complete a HOMEWORK task at home, but may not need help with it (unless they
are unable to write independently).

Discuss small rewards the child might earn for doing 4 weeks of homework (e.g., 8
points/stickers). The therapist may provide the first reward, or the parent can. Make
suggestions of privileges or small treats/trinkets (e.g., staying up 15 min late, getting to chose
a favorite dinner or other food, getting a pack of trading cards). Whatever is chosen, the
parent has to be okay with it and the child has to care about it. Note that rewards will be
discussed more fully in later sessions—this is just a start. NOTE: rewards are not optional in
CBT. Parents should be aware that rewards are short term but are necessary for this kind of
program to teach the child skills that they need—to keep them motivated.
Write about a time this week that you are feeling nervous.
What was going on?
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
How did my body feel?
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
What kinds of bad things did I think might happen?
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________

Child Module 3
―C‖ Step
Background
Cognitive restructuring is a basic CBT technique that involves changing fearful thoughts at a
superficial (conscious) level. Although unlikely to lead to long term anxiety reduction by itself,
use of positive thoughts can give children confidence to face feared situations, which then can
lead to habituation and longer-term changes in underlying schemata.
Goals
1. Review homework
2. Reviewing the ―K‖ and ―I‖ steps
3. Learning the ―C‖ step of the KICK plan
4. Maintain rapport with the child by playing, chatting, permitting child to help set the tempo of
the session
5. Assigning HOMEWORK task
Materials
Cartoons from previous sessions
―KICK‖ plan acronym sheet from last session
Blank paper and colored pencils / crayons
Child‘s reward chart
Session
Therapist Note: Prepare the child for the format of the session: after the meeting with the
child, then the therapist will meet with the parents for 30 minutes. Finally, the therapist will ask
the child to come back in the room to make some plans at the end of the session.
WITH CHILD ALONE (30 MINUTES)
1. HOMEWORK Task:
Review the child‘s HOMEWORK task. If s/he did not write the homework, allow him/her to
complete it verbally by reporting to you. Give gentle corrective feedback to clarify any
misinterpretations of thoughts vs. feelings. Record appropriate points/stickers on his/her
reward chart with appropriate affective tone (matching child‘s style).
2. Review ―K‖ and ―I‖ Steps:
See Child Module 2, review as needed.
Review the KICK plan sheet briefly. Ask the child if s/he can recall the first two steps:
Remember what K and I stand for in the KICK plan? …guess what, later today we‘re going to
learn what C stands for!!
3. Introduce the ―C‖ Step:
Return to the cartoons used in session 2. Choose the most favored or salient cartoon from the
child‘s perspective to begin with. Review the kinds of feelings and thoughts that the cartoon-
child may have been having. ―Okay let‘s have a look at this cartoon again. Let‘s try to
remember, what was this boy feeling? How could we tell? Yes, his eyes are wide open, so he‘s
probably afraid. Also, he is shaking, remember? When people shake that is one way we know
they are afraid. And remember what kinds of icky thoughts he had? Yes, we wrote them down—
he‘s afraid he‘s going to sink to the bottom of the pool!‖
o Sticking with the same cartoon, explain that the goal today is to help the boy think
of calm thoughts that will help him feel better. Begin with an example before asking
the child to generate positive thoughts. ―For instance, could he say to himself, ‗I‘ve
taken a lot of swimming lessons and my mom says I am a good swimmer. So I don‘t
think that I‘ll sink if I go in the pool?‘‖
o Assess child‘s initial reactions: ―Do you think that saying this would help him feel
better?‖ If child shows signs of understanding, consider asking the child if there is
something else the cartoon-child could say to himself that could also make him feel
better. If child provides incorrect information, gently provide corrective information
without stating that the child is ―wrong.‖ Write in the positive thought in a thought-
bubble, next to the original ―fearful thought‖ bubble. Often this is best
accomplished using a different-colored pencil or pen for positive thoughts (vs.
fearful ones).
Proceed to additional cartoons. ―We‘re going to play detective again—figuring out this time
what some of these kids can say to themselves to feel calmer. You know, calm thoughts they can
have.‖ Prompt child to re-identify the cartoon-child‘s feelings and fearful thoughts. Then
negotiate with the child to come up with a reasonable ‗calm thought‘ that could reduce anxiety
in the situation. Once this has been agreed upon, draw a ‗thought bubble‘ over the cartoon-
child‘s head and quickly write in the ‗thought‘, while saying it again out loud with affect (to
keep child‘s attention). The child may do the writing, too.
Use a scaffolding approach to increasingly transfer the work of developing appropriate ―calm
thoughts‖ for each cartoon situation to the child. However, do so slowly to evaluate the child‘s
grasp of the concept. If s/he is developing thoughts that have little to do with the problem,
ignore the incorrect response and ask a structured question to lead the child to the right
response: ―Okay, how likely is it that the roller-coaster cart would fly off the track? Have you
ever seen that happen? Me neither! How could she remind herself that she‘s never actually
heard of a roller coaster cart flying off? What could she say to herself? What would her ‗calm
thought‘ be? Something like…‘I‘ve never heard…‘ [allow child to finish the sentence if
possible].‖
o If the child provides a response in third person language, transform the thought into
first person language for the child and check-in to see if this is what the child had in
mind (e.g., for ―she has never messed up a speech before‖… ―so, she might say to
herself, ―I have never messed up a speech before?‖) Again, write in the correctly-
worded thought into the thought-bubble while saying it out loud to help model and
reinforce the use of ‗thought language‘ in the first person for this exercise. Continue
with cartoon examples to build up the child‘s level of mastery.

As the scaffolding with the cartoons goes along, weave in two points:
o The ―C‖ step in the KICK plan is Calm Thoughts. Write this down on the sheet.
Explain that all the positive thoughts we‘ve been thinking of today for the cartoon
characters are calm thoughts—thoughts that can make us feel CALM and NOT
ANXIOUS. If the child‘s maturity level is sufficient, directly draw this link: Our
thoughts can change our feelings.
o There are two types of calm thoughts that are often especially helpful: 1) How likely
is the bad thing to happen; 2) if it did happen, so what? Sometimes one of these
types of calm thoughts is more useful than the other. The first question can make us
feel better when we know that something almost never happens (e.g., mom getting
in a horrible car accident on the way to work—it‘s never happened before, right??).
The second question is good if we are pretty sure something ―a little bad‖ could
happen, but it might not be the end of the world (e.g., messing up on a speech—
sometimes I ask myself when I worry about this: ‗but will I remember messing up on
this speech when I‘m an old man? Is it so important that I‘d still care then?‘
Probably not, right?!).
Return to the therapist‘s example provided in session 2 for the ―K‖ and ―I‖ steps (e.g., fear of
rollercoasters… ―so remember how I was saying I get nervous about rollercoasters? And I
worried that I might fall out of the cart? Well, do you know what kind of calm thoughts I had
when I went that roller coaster at Magic Mountain? I thought, ‗I‘ve never actually heard of
someone flying out of their cart… and the roller coasters have good seatbelts just like a car.‘
In fact, I heard that it is as safe going on a roller coaster as it is driving in your car!‖)
o Ask the child if they think the therapist‘s calm thought helped the therapist feel
calmer and less afraid in the situation. Provide feedback and discuss.
If the child volunteers a feared situation during or after this disclosure, help him/her brainstorm
on calm thoughts s/he could have used. Consider writing these down.
Review the first three steps of the KICK plan: Okay in a minute we‘re going to tell your mom
about the first three steps of the KICK plan. First, lets try to remember what each step is.
Okay, the K step was… (pause)… that‘s right, Knowing I‘m Nervous, and we use that step to
figure out when we‘re feeling nervous. What kinds of things do our bodies do to tell us we‘re
afraid?... …great, okay, we‘re almost ready to tell your mom all about it!‖
Assign child HOMEWORK task of writing about a time when s/he felt anxious, and describe
his/her body feelings and thoughts.
Reinforce child participation by discussing or playing a special topic or game. This should
last approximately 5-10 minutes.
WITH PARENTS AND CHILD TOGETHER (5 MINUTES)
1. Review the content of the child’s session:

Either ask the child to explain, or summarize the child session briefly. Inform parents that the
child is to complete a HOMEWORK task at home, but may not need help with it (unless they
are unable to write independently).
Discuss rewards again. Reference child‘s reward chart. Make sure a specific reward for the
first 4 weeks of homework has been agreed on and the child is aware of it. Note that rewards
will be discussed more fully in later sessions—this is just a start. NOTE: rewards are not
optional in CBT. Parents should be aware that rewards are short term but are necessary for
this kind of program to teach the child skills that they need—to keep them motivated.
Write about a time this week when you felt anxious.
What was going on?
____________________________________________________________
____________________________________________________________
____________________________________________________________
How did my body feel?
____________________________________________________________
____________________________________________________________
____________________________________________________________
What were my icky thoughts (what kinds of bad things did I think might
happen)?
____________________________________________________________
____________________________________________________________
____________________________________________________________
MY CALM THOUGHTS!
What can I say to myself to feel calmer and less anxious about this situation?
(Hint: How likely was something bad really going to happen? How bad would it
be if did happen?)
____________________________________________________________
____________________________________________________________
____________________________________________________________
Child Module 4
Keep Practicing / KICK Plan Review
Background
This session completes the basic presentation of CBT skills and the KICK plan. Generally this
session is completed before exposures are initiated.
Goals
1. Review homework
2. Learn the final step of the KICK plan
3. Review the KICK plan
4. Assign homework
5. Maintain rapport with the child by playing, chatting, permitting child to help set the
tempo of the session
Materials
Cartoons from previous sessions
―KICK‖ plan acronym sheet from last session
Blank paper and colored pencils / crayons
Any needed props/toys for Session Topic 3 (below)
Child‘s reward chart
Homework page
Session
WITH CHILD ALONE (15-20 MINUTES)
1. HOMEWORK Task:
Review the child‘s HOMEWORK task. If s/he did not write the homework, allow him/her do
complete it verbally by reporting to you. Give gentle corrective feedback to clarify any
misinterpretations of thoughts vs. feelings. Record appropriate points/stickers on his/her
reward chart with appropriate affective tone (matching child‘s style).
2. Review the KICK plan sheet briefly. Ask the child if s/he can recall the first three steps:
Remember what K, I, and C stand for in the KICK plan? … later today we‘re going to learn
what the other K stands for!!
3. Develop imaginary plotline to practice K-I-C steps. Using any props or toys that may be
useful to engage the child‘s attention, present an imaginary ―fearful situation‖ that matches
previous topics of discussion and interest to the child (e.g., a child who is preoccupied with
arts-and-crafts projects such as making paper snowflakes during sessions may find it
interesting to talk about an imaginary scenario in which a child wants to make a paper
snowflake for the first time, but she cannot because she is too scared of using the scissors…)
Use blank paper and state you‘ll sketch out a quick stick figure for the story. The child can help
if s/he likes.
o Ask what kinds of body feelings the character has (e.g., when the girl ―wants to use
scissors‖) and sketch out squiggles on the stick figure‘s body to represent the body
feelings. Link with the first K step.
o Then brainstorm with the child about reasonable ―icky‖ thoughts and ―calm‖ thoughts
(I and C steps) and write in appropriate thought bubbles.
4. Elaborate on the second ―K‖ step:
Continuing to build upon the imaginary plotline developed above, ask how the character
should behave in the feared situation now that s/he has developed calm thoughts.
o E.G., ―so she now knows that kids almost never get hurt by scissors if they‘re careful
and use safety scissors. But she still has a little bit of a stomach ache—some leftover
nervous feelings. Okay! Now what should she do?? Should she still stay away from the
scissors just cause she still feels a little nervous? Or should she practice with them a
little bit and help herself learn that they are safe?‖
o Make this point: if the imaginary character knows that a situation is safe, s/he should go
ahead and practice the feared behavior. Practice can involve taking a small step (e.g.,
maybe just a few small cuts of a piece of paper), to try it out first and get comfortable,
even if s/he is still feeling a little bit nervous.
Introduce the fourth step, Keep Practicing. Write this step on the child‘s KICK plan sheet.
Point out that the most important step to take after developing Calm Thoughts is to practice
what you‘ll do in the scary situation. ―What do we mean by practice?‖
o ―If we don‘t know how to use scissors very well, we get someone to help us and we start
out with very simple cuts. This is an example of practicing.‖
o ―If we haven‘t been in a swimming pool before, we start out practicing in the shallow
end where our head can always be above water until we‘re sure we are good
swimmers.‖
o ―If we are going to give a speech in front of the whole class, we practice our speech a
couple of times with our mom so we don‘t forget and get embarrassed when we‘re in
front of the class.‖
o Etc. Give relevant examples that may be somewhat close to home for the child.
Initiate conversation about the value of practicing by asking why it helps to practice when
we‘re scared. Include the following points, trying to elicit each from the child through Socratic
questioning:
o When we practice something hard we feel more confident.
o Practice is like taking little (―baby‖) steps. Doing things a little at a time is always
easier than doing a big thing all at once.
E.G.: learning math, it‘s easier to learn adding single numbers together first,
before adding two-digit numbers. Imagine if teachers taught multiplication
before they taught addition—could anyone learn it that way?
o Practicing helps us know what to expect if we‘re going to be doing something new.
―It is a good idea to practice with training wheels before riding a regular bike,
for instance.‖
―It is a good idea to practice an overnight sleepover with a friend before trying
to go to an overnight summercamp for a week.‖
These are little steps that make the ―real thing‖ easier.
Return to cartoons used in earlier sessions. Briefly review the scenario of each cartoon with the
child. Pose the question in each case, how could s/he practice or use baby steps to get used to
the situation that s/he is afraid of—to learn that s/he can handle it and that it is safe?
Return to the therapist‘s self-disclosed ―fear‖ (e.g., roller-coasters) from previous sessions.
Brainstorm with the child how someone with that fear could practice taking small steps to
overcome it (e.g., go on a merry-go-round; then a really little roller coaster like at ToonTown
in Disneyland, perhaps several times; then see if you feel more ready to go on a faster roller-
coaster at Disneyland…)
If the child‘s brings up his/her fears, promote a productive discussion of methods of ‗practice‘.
But do not engage in a disagreement over whether there are any opportunities to ‗practice‘ in
the case of the child‘s fears—move on with the session rather than try to ‗prove‘ that it is
possible for the child to practice facing his/her fears.
Review the four steps of the KICK plan. Explain that the KICK plan can help you deal with
things that make you nervous, and suggest that it is important to think of a KICK plan each
time you feel anxious—before you start practicing with ―baby steps.‖
If time—develop a hypothetical scenario relevant to the child‘s fears that has not been
discussed in detail thus far. Brainstorm with the child on creating a specific KICK plan—each
of the 4 steps—to help the child with the situation. A new cartoon may be useful as a visual
scaffold.
o ―Lets pretend this boy here is afraid of closing his bedroom door at night. When his
mom closes his door, he cries and begs her to keep it open. But he wishes he was brave
enough to sleep with the door closed, like his big brother does. Let‘s make a KICK plan
to help him! Let‘s see, the first K step is… what? …yes, Knowing I‘m Nervous. How do
you think he might tell he‘s getting nervous? Maybe he gets a racing heart and breathes
real fast when his mom closes his bedroom door? Okay, next step, I…‖
5. Telling parents about the KICK plan:
Plan on having the child to explain the KICK plan to the parents during the family meeting.

If needed, role-play the conversation with the child. Then ask if s/he feels prepared to actually
try with the parents. Otherwise, inform him/her that you will explain the steps to the parents
this time and the child can try a different time.
6. Assign homework
o See homework page, and explain briefly.
Reinforce child participation by discussing or playing a special topic or game. This should
last approximately 5-10 minutes.
WITH PARENTS AND CHILD TOGETHER (5 MINUTES)
1. Review the content of the child’s session:
Either ask the child to explain, or summarize the child session briefly.
Inform parents that the child is to complete a HOMEWORK task at home, but may not need
help with it (unless they are unable to write independently).
Discuss rewards. Reference child‘s reward chart. Make sure a specific reward for the first 4
weeks of homework has been agreed on and the child is aware of it. Note that rewards will be
discussed more fully in later sessions—this is just a start. NOTE: rewards are not optional in
CBT. Parents should be aware that rewards are short term but are necessary for this kind of
program to teach the child skills that they need—to keep them motivated.

Let’s Remember the KICK Plan!
Your homework this week is to remember each step of the KICK Plan! Try to
do it from memory—don’t look at your notes! It is okay to ask your mom or dad
to help you write it down if you want.
Knowing… ______________________ (2 words)
Icky… __________________________ (1 word)
Calm… _________________________ (1 word)
Keep… _________________________ (1 word)
Child Module: KICK
KICK Plan Review
Background
This session will be repeated 2-8 times in a typical course of CBT. Children with ASD
often have impaired episodic memory. In addition, they have difficulty generalizing learned
information across situations; therefore, the therapist must provide multiple opportunities for
children to learn the KICK plan. This will not only allow children to remember the order of the
steps, but they will better understand the meaning of each step. It is helpful for children to put the
meaning of each step in their own words. Finally, the therapist should explain in simple, concrete
terms why the KICK plan is important to use—to let the child do the things that s/he‘s afraid of
(or, alternatively, things s/he wants to do).
Goals
1. Review homework
2. Review the KICK Plan
3. Practice using the KICK plan via role-play
4. Plan new exposures and assign as HOMEWORK
5. Maintain rapport with the child by playing, chatting, permitting child to help set the
tempo of the session
Preparations
Review the fear hierarchy for appropriate feared situations to assign for homework (and to
prepare for in-session). It is important to determine what ―lines‖ of exposures still need to be
covered. If problems have been encountered be sure to consider ways to reduce the level of
difficulty of a line of exposures without allowing the child to completely avoid it. See Parent
Module: EXP for complete discussion of the selection of appropriate homework exposures.
Determine whether you will continue with the therapist-directed rewards system or transfer
future rewards/privileges entirely to the parent.
Have the child‘s reward ready for him/her if she is likely to have earned it this session.
Materials
Feelings Thermometer handout
KICK plan written by hand
Cartoons and pictures previously used
Blank paper and colored pencils/crayons
Reward chart
Session
WITH CHILD ALONE (20-30 MINUTES)
1. Review the child’s homework task and record appropriate points on his/her reward
chart. If s/he did not write the homework, allow him/her do complete it verbally by reporting
to you. Give gentle corrective feedback to clarify any misinterpretations of the assignment.
Record appropriate points/stickers on his/her reward chart with appropriate affective tone
(matching child‘s style).
Present the child with his/her reward, if it has been earned. If indicated, explain in very simple
terms any changes that will happen to the reward system (e.g., ―Remember how last time we
talked about how your mom is going to give you a chance to earn even more rewards now that
we‘re starting a new phase of this program? Yes, that‘s right, we‘ll think of some cool stuff for
you to earn!‖)
Therapist Note: Working out the next phase of the rewards program (i.e., therapist- vs.
parent-mediated rewards) is a complex decision process. Review Parent Module:REW
(Rewards & Privileges) for complete discussion of the considerations involved.
2. Review the KICK plan with the child. Encourage the child to recall each step.
Use the KICK plan sheets (including the child‘s homework sheet, if completed) to scaffold this
review as needed. Use the review procedures described in Child Module 4 (Keep Practicing
Step), as needed, focusing on applying the KICK plan to situations that the therapist discloses
or presents, or that the child discloses (potentially related to child‘s recent exposure
experiences or upcoming exposures).
3. Further explanation of the KICK plan:
Explain that the KICK plan can help you deal with things that make you nervous, and suggest
that it is important to think of a KICK plan each time you notice that you are feeling nervous.
o The KICK plan gives us the chance to plan for what we‘re going to do in case we feel
nervous. We should practice using the KICK plan so we can have confidence when we
really need it.
OPTIONAL
If helpful in transitioning to working on the child‘s fears, make a personal disclosure about
when it applied to the therapist. As usual, this should involve only ―normative‖ fears that
anyone could have, which do not model new anxieties (e.g., being lost as a child).
―The KICK plan lets us do the things we want to do even though we may feel nervous about
doing it. Once, when I was in 7th grade, I was at an amusement park with a whole group from my
school. We were on our own and we knew that we had to meet at the front of the park at 8 o‘clock
for the bus. We knew it was getting late but we didn‘t have a watch. We knew we could ask people
what time it was, but we all felt too nervous about asking a stranger for the time. We were afraid
that the strangers would yell at us. But by the time that we decided to go to the front it was 8:30
and we had missed the bus!‖
Brainstorm about a KICK plan for the therapist‘s ―fearful situation.‖
Take turns role-playing an exposure situation using the KICK plan (in the therapy room). This
exposure ideally is one that the child can do for homework in the upcoming week, based.
o Generally, this is a good time to begin the discussions about the child‘s upcoming
exposure tasks for the week, but sometimes it is better to simply practice a possible
exposure that the therapist considers reasonable before discussing the child‘s exposure
homework, in order to raise his/her level of confidence about the exposure and prevent
unnecessary conflict in the session before s/he feels confident with a good KICK plan.
The therapist can go first do one version of an imaginal exposure that is on the child‘s list
(again, this should be relevant to the current level of exposures—low, medium, or high). The
child can ―tag along‖ (Kendall et al., 1990) afterwards and role-play the same or a slight
permutation of the exposure.
Work out a KICK plan for the imaginal exposures.
Step 1. ―K‖ Step – Focus on having the child identify the kinds of body feelings s/he
might get in a specific situation that is likely to make her/him nervous.
Step 2. ―I‖ Step – Review bad things the child thinks could happen if s/he entered the
feared situation. Using scaffolding, as necessary, to help the child explain what
things s/he is afraid will happen
Step 3. ―C‖ Step – Come up with coping thoughts to counter each of the anxious
thoughts. Make sure that the child puts the coping thoughts in his/her own words.
Step 4. ―K‖ Step—Focus on ways of practicing the child‘s responses in the situation in
advance to improve confidence and feelings of preparation.
Step 5. Get ratings on the feelings thermometer.
Reinforce child participation by discussing or playing a special topic or game. This should
last approximately 5-10 minutes.
WITH PARENTS AND CHILD TOGETHER (OR JUST CHILD) (10 MINUTES)
1. Review past week’s homework exposures:
Check on how exposure tasks went the previous week. Give the child praise for trying
exposure tasks during the week.
2. Plan this week’s home-based exposures:
Encourage the family to discuss and agree upon a new set of exposure tasks. It is best for the
child to work on 3 separate exposure tasks at home each week (it is reasonable to spend 20-
30 minutes per day ―practicing‖ these tasks). Plan on a specific (set of) reward(s), privileges,
and/or points (see Parent Module: REW) for the child‘s home-based exposures this week.
Write the exposure assignments down for the child on a blank piece of paper.
Emphasize that the rate of progress on treatment goals is directly related to the frequency and
consistency with which the child and parents do the assigned exposure tasks each week.
3. Rewards program
Check in on the rewards program (see Parent Module: REW). Having rewards that the child
wants is key for motivating them to continue with the exposure tasks.
As necessary, modify the rewards list to exclude reinforcers that are not motivating to the
child. Also, for reinforcers that the child has access to all the time, the parent can either
control the child‘s access to them or exclude them from the reinforcement list. Finally, the
best rewards are things that are renewable, wanted, and already used frequently by the child
(e.g., TV, computer, specific games, etc.). These should be added to the reinforcement list if
not already on it.
Child Module: I.V.
In Vivo Exposure
Background
This session will be repeated 4-10 times in a typical course of CBT. In vivo exposure is
conducted during the therapy session, but is not just imaginal (see Child Module: KICK for
imaginal exposure and home-based exposure preparation). The advantage of in vivo exposure is
that the therapist ensures that some exposures are actually completed; s/he has a chance to see
exactly how the child reacts to feared stimuli, which helps with treatment planning; and s/he may
get the opportunity to scaffold a particularly hard exposure that the parent is unlikely to
supervise successfully. Progressing with exposures is the key for therapeutic success.
Goals
1. Review homework
2. Prepare a KICK plan for an in vivo exposure
3. Conduct an in vivo exposure
4. Obtain fear ratings before and after the exposure
5. Plan new exposures and assign as HOMEWORK
6. Maintain rapport with the child by playing, chatting, permitting child to help set the
tempo of the session
Preparations
Review fear hierarchy for feared situations that are appropriate for the child‘s current spot in
the hierarchy and can be performed in session (see Parent Module: EXP for complete
discussion on the selection of appropriate exposures.)
Make all preparations necessary for the in vivo exposure, e.g., arranging for confederates,
materials, room space, etc.
Have the child‘s reward ready for him/her if she is likely to have earned it this session.
Materials
Feelings Thermometer handout
KICK plan written by hand
Cartoons and pictures previously used
Blank paper and colored pencils/crayons
Reward chart
Session
WITH CHILD ALONE (20-30 MINUTES)
1. Review the child’s homework task and record appropriate points on his/her reward
chart. If s/he did not write the homework, allow him/her do complete it verbally by reporting
to you. Give gentle corrective feedback to clarify any misinterpretations of the assignment.
Record appropriate points/stickers on his/her reward chart with appropriate affective tone
(matching child‘s style).
Present the child with his/her reward, if it has been earned. If indicated, explain in very simple
terms any changes that will happen to the reward system (e.g., ―remember how last time we
talked about how your mom is going to give you a chance to earn even more rewards now that
we‘re starting a new phase of this program? Yes, that‘s right, we‘ll think of some cool stuff for
you to earn!‖)
Therapist Note: Working out the next phase of the rewards program (i.e., therapist- vs.
parent-mediated rewards) is a complex decision process. Review Parent Module: REW
(Rewards & Privileges) for discussion of the considerations involved.
2. Review exposure rationale (if not previously done):
Point out that many of the situations we‘re afraid of are actually safe (review salient examples).
The way we ―teach our brain‖ to not be afraid anymore is to practice being in the situation until
we stop feeling fearful feelings. Cite relevant examples previously discussed, e.g., learning to
swim. If helpful:
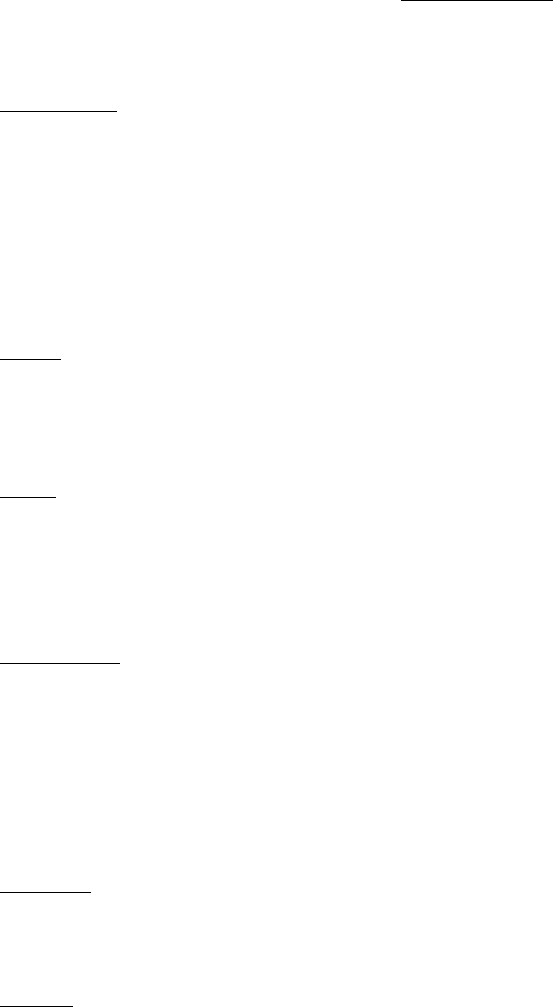
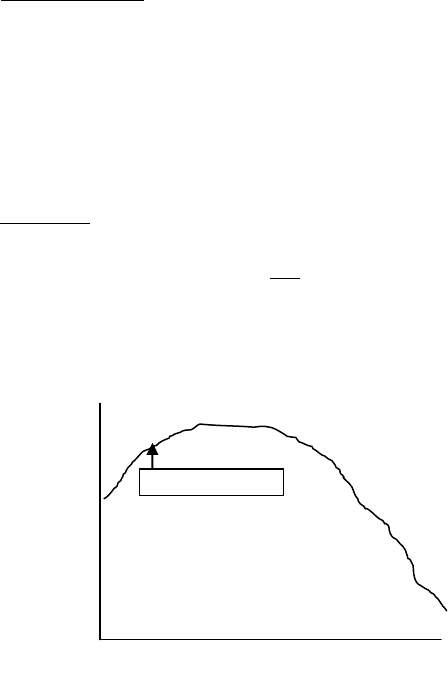
o Demonstrate in graph form that when we enter a situation that makes us fearful, our
feelings of fear initially go up, making us want to leave; but if we stay and ―teach our
brain‖ that nothing bad will happen, the feelings of fear start to go down—somewhat
steadily—until we feel pretty okay and not too fearful.
3. Decide on a specific in vivo exposure with the child.
As noted above, it is important to have several ideas prepared in advance for possible
exposures. These exposures need to be doable during session; must be within several fear-
rating points on the hierarchy of what the child has accomplished to date; must make positive
progress towards advancing a ―line‖ of exposures (see Parent Module: EXP; e.g., reducing
handwashing in small steps); and should perhaps broaden out the child‘s experiences with
exposures into areas the parent has not tried and may be less likely to successfully supervise.
The child may give some input on choosing between several reasonable exposures most of the
time. However, refusing all proffered exposures is not acceptable. For many children, a
Before 1 min. 5 min. 20 min 30 min.
Entering the situation
10 Fear 0
collegial conversation clarifying the importance of exposures and how helpful it will be to the
child when s/he feels ―happy‖ (confident, not afraid, etc.) in the specific situation will be
enough to elicit a more agreeable attitude. For others, also note that the child is earning points
for doing this exposure (if this fits with the reward/privilege system in place), or arrange a
short-term reinforcer on the spot (e.g., time on the office computer, a game with the therapist
later, a treat, etc.). In the end brainstorm with the child on ways of reducing the intensity of one
of the suggested exposures in order to make it more acceptable—but this is to be avoided
whenever possible.
4. Prepare for the in vivo exposure.
Develop a KICK plan for the exposure. Use the KICK plan sheets (including the child‘s
Session 4 homework sheet, if completed) to scaffold this preparation as needed. Use the review
procedures described in Child Module 4, as needed.
Step 1. ―K‖ Step – Focus on having the child identify the kinds of body feeling s/he
might get in the situation.
Step 2. ―I‖ Step – Review bad things the child thinks could happen if s/he entered the
feared situation. Using scaffolding, as necessary, to help the child explain what
things s/he is afraid will happen
Step 3. ―C‖ Step – Come up with coping thoughts to counter each of the anxious
thoughts. Make sure that the child puts the coping thoughts in his/her own words.
Step 4. ―K‖ Step—Focus on ways of practicing the child‘s responses in the situation in
advance to improve confidence and preparation (in the case of in vivo exposures,
this usually involves practicing the child‘s ―lines‖ or ―going through the motions‖
[e.g., dropping papers] in the therapy room before going into a public place to
really try it).
Get ratings on the feelings thermometer before the exposure.
- If needed (based on child‘s need to practice & gain confidence or ―get his lines down‖ in
the case of any exposure involving a social interaction), take turns role-playing the exposure
situation using the KICK plan (in the therapy room). The therapist can go first and do one
version of an imaginal exposure. The child can ―tag along‖ (Kendall et al., 1990) afterwards
and role-play the same or a slight permutation of the exposure.
5. Conduct the exposure and get a rating from the child.
Go to the site of the exposure and allow the child to give it a try. If the opportunity arises to
ensure the situation is a success (but the child will not be aware of any intervention on the
therapist‘s part) it is generally a good idea to do so. For instance, it is permissible to wink or
smile at a stranger or confederate to elicit the desired response. An exception would be times
when the child is to be exposed to a situation that might turn out more or less favorably—in
other words, a truly ‗realistic‘ exposure. Remove the child from the situation only if it is
potentially dangerous or if the child has experienced such significant failure or embarrassment
that there is little chance of ―turning it around‖ in the short-term.
When done, have child rate on feelings thermometer (a) how fearful the situation actually was
and (b) how fearful it would be to do the exposure again. Be sure to draw the child‘s attention
to a drop in ratings of 2 or more points.
A drop in ratings should be the basis of a brief discussion reviewing whether the
child‘s ―Icky Thoughts‖ (fearful cognitions from the ―I‖ step) had been justified, or
whether the ―Calm Thoughts‖ (―C‖ step) had been more realistic. This is a very
important step in helping the child change his/her underlying anxious cognitions
supporting the conditioned fearful response.
A minimal or negligible drop in fear ratings (unless the exposure was initially rated
quite low) requires a careful review of the ―facts‖ of the situation with the child:
Did anything bad actually happen, if so how ―bad‖ was it, and if not, how likely
was it to possibly have happened. Brainstorm together on what steps need to be
taken to make a future exposure easier, perhaps by reducing the level of difficulty
(e.g., number of steps involved, length of time, specific location). Try to change the
child‘s attitude from defeatist to optimistic by focusing on his/her ability to handle a
modified version of the exposure.
6. If time, conduct another exposure.
Note, often an in vivo exposure should be repeated multiple times in the same session without
any additional preparation. An example is, if the child had success in asking for the time from
one individual, it is advisable to get fear ratings, and then repeat the same basic exposure
several times. If the fear rating is going down, the exposure can be changed to something
slightly harder in the same ―line‖ of exposures (e.g., asking for directions) with very minimal
additional preparation in the same session. This often gets maximum benefit from the in-
session preparation efforts and sometimes is superior to trying to prepare for and conduct a
second exposure from a different ‗line‘ of exposures, which of course can require a lot of
―talk‖ and ―imaginal exposure‖ in the therapy room.
Reinforce child participation by discussing or playing a special topic or game. This should last
approximately 5-10 minutes.
WITH PARENTS AND CHILD TOGETHER (10 MINUTES)
1. Review past week’s homework exposures:
Check on how exposure tasks went the previous week. Give the child praise for trying
exposure tasks during the week. Give points/rewards as appropriate.
2. Plan this week’s home-based exposures:
Encourage the family to discuss and agree upon a new set of exposure tasks. It is best for the
child to work on 3 separate exposure tasks at home each week (it is reasonable to spend 20-
30 minutes per day ―practicing‖ these tasks). Plan on a specific (set of) reward(s), privileges,
and/or points (see Parent Module: REW) for the child‘s home-based exposures this week.
Write the exposure assignments down for the child on a blank piece of paper.
Emphasize that the rate of progress on treatment goals is directly related to the frequency and
consistency with which the child and parents do the assigned exposure tasks each week.
3. Rewards program
Check in on the rewards program (see Parent Module: REW). Having rewards that the child
wants is key for motivating them to continue with the exposure tasks.
As necessary, modify the rewards list to exclude reinforcers that are not motivating to the
child. Also, for reinforcers that the child has access to all the time, the parent can either
control the child‘s access to them or exclude them from the reinforcement list. Finally, the
best rewards are things that are renewable, wanted, and already used frequently by the child
(e.g., TV, computer, specific games, etc.). These should be added to the reinforcement list if
not already on it.
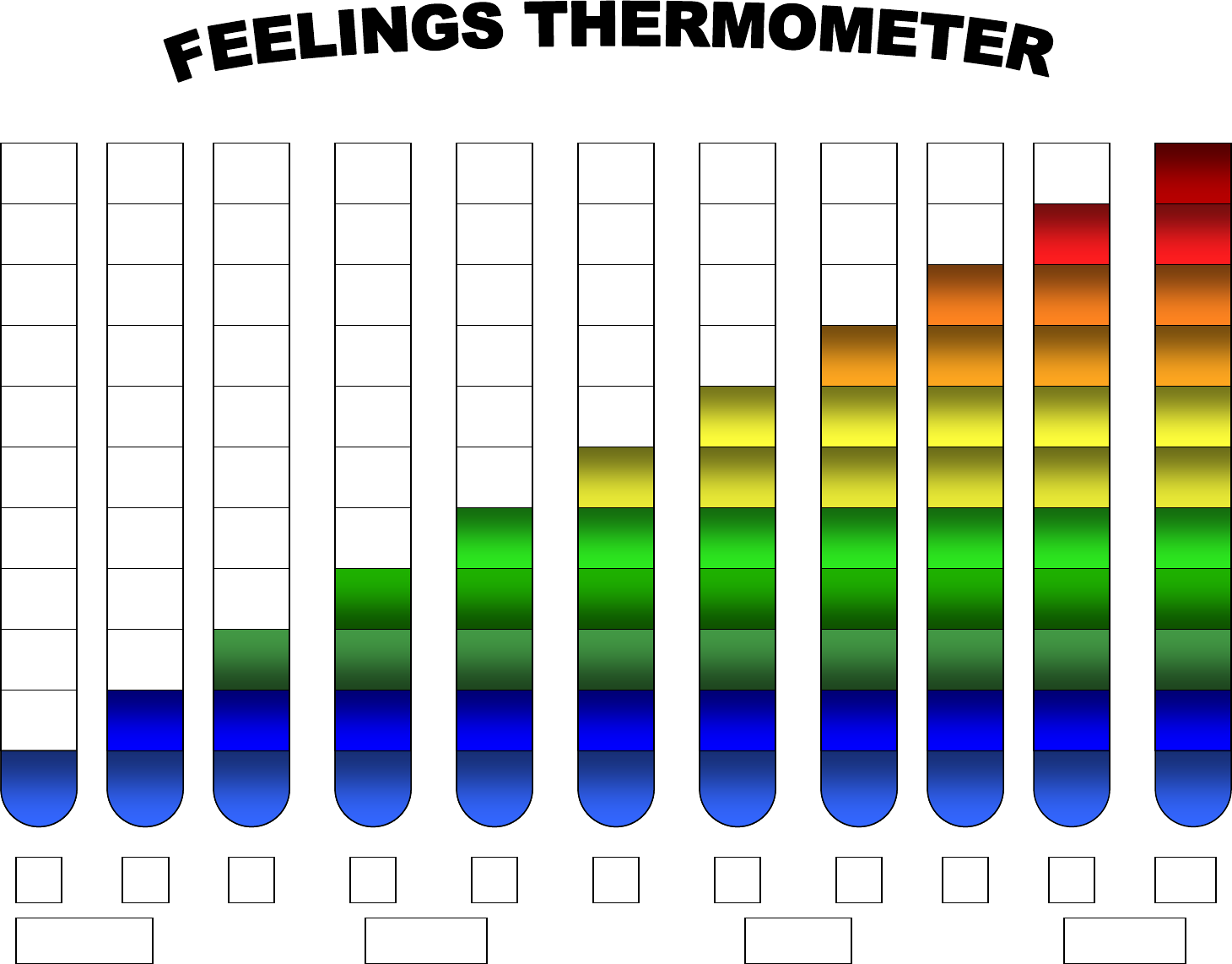
0
1
2
3
4
5
6
7
8
9
10
A little
Not at all
Some
Totally

Child Module: FRND
Making Friends
Background
This session is usually done together with Parent Module: PLAY. Many children with ASD
lack friends. Deficits in social communication and reciprocity contribute directly to this problem.
Barriers such as social anxiety add to this difficulty by preventing children with ASD from
repeating attempts at making friends. While some families may have attempted to facilitate
playdates for their children, parents often lose motivation when little success is evident. Other
families simply have not facilitated regular playdates for their children. Playing with friends
provides an unmatched opportunity to develop and practice social skills, and to overcome social
anxiety. Developing closer peer relationships also gives children a new role that can replace less
positive roles and self-perceptions such as ―the weird kid‖ or ―the shy kid‖. Making friends
enhances self-esteem and helps children feel normal and accepted. The key to making and keeping
close friends is repeatedly arranging successful playdates with peers who the child likes (or might
like) (cf. Frankel, 1996). But the child with ASD must develop skills as an ―ideal‖ host of
playdates in order to accommodate for inherent deficits in social communication that might
otherwise make them unattractive choices as friends for most typical peers.
Therapist Note: Although the term "playdate" is not always appropriate for children over the
age of 11, the principles of this session still apply to early adolescents (up to age 13). Try replacing
"playdate" terminology with "get-togethers" or "having friends over," when talking with the
family, if needed. If parents continue to use the term ―playdate,‖ it may be beneficial to actively
replace the term with more age-appropriate terms listed above, depending on the maturity level of
the child‘s peer group.
Goals
1. Review homework
2. Teach child social rules to follow during play dates
3. Plan and/or practice making phone calls and/or hosting playdates
4. Optional smiling practicum
5. Plan new exposures and assign as HOMEWORK
6. Maintain rapport with the child by playing, chatting, permitting child to help set the tempo of
the session
Preparations
Be sure to read the three chapters that are assigned to the parents prior to the session.
Review the fear hierarchy for appropriate feared situations to assign for homework (and to
prepare for in-session). It is important to determine what ―lines‖ of exposures still need to be
covered. If problems have been encountered be sure to consider ways to reduce the level of
difficulty of a line of exposures without allowing the child to completely avoid it. See Parent
Module: EXP for complete discussion of the selection of appropriate homework exposures.
Determine whether you will continue with the therapist-directed rewards system or transfer
future rewards/privileges entirely to the parent.
Have the child‘s reward ready for him/her if she is likely to have earned it this session.
Materials
Child-appropriate magazine
Feelings Thermometer handout
KICK plan written by hand
Cartoons and pictures previously used
Blank paper and colored pencils/crayons
Reward chart
Session
WITH CHILD ALONE (30 MINUTES)
Review the child’s homework task and record appropriate points on his/her reward chart. If
s/he did not write the homework, allow him/her do complete it verbally by reporting to you.
Give gentle corrective feedback to clarify any misinterpretations of the assignment. Record
appropriate points/stickers on his/her reward chart with appropriate affective tone (matching
child‘s style).
Present the child with his/her reward, if it has been earned. If indicated, explain in very simple
terms any changes that will happen to the reward system (e.g., ―remember how last time we
talked about how your mom is going to give you a chance to earn even more rewards now that
we‘re starting a new phase of this program? Yes, that‘s right, we‘ll think of some cool stuff for
you to earn!‖)
1. Introduce the concept of a having a friend over to play at the child’s house.
If appropriate, provide rationale for having playdates with peers: You can have fun, you can
make friends, it is nice to get along with the other kids.
Pose the question (w/ scaffolding as needed) about whether kids (1) want to come to a playdate
where the host is bossy and chooses all the games (and plays them); or (2) whether they want
to come to a playdate where the host is friendly, lets them choose what games to play, and
makes it fun for them.
Therapist Note: This point COULD be exemplified by two cartoon-based stories
(―which would be a more fun play date‖ would be the eventual question). These could be
sketched quickly out with stick figures, as in Child Module 2.
Suggest that the point of a playdate is to make closer friends with someone we like. We need to
help kids who come to our house to have a good time so that they want to be our friend too,
and so they want to come back again.
Conclude that a playdate should be with someone who the child may like to get to know better.
Ask the child for information about people who they might want to invite to play. (―Who
would be on a list like that?‖ ―Who would be on the top of a list like that?‖)
Therapist Note: Although much of this session will seem very self-evident to the typically
developing child, these insights and skills on friendships are very novel to most children with
ASD. Assume nothing, and do not be afraid to correct distorted and erroneous conceptions about
the nature of friendship and related social skills that may come up in this session. Generally,
children with ASD have significant deficits in this area no matter how ―high-functioning‖ they
appear.
2. Teach child rules of hosting a playdate.
The guest should choose all the games.
o We want to make sure our friend has fun. So, do you think that it is a good idea for us
to choose the games when s/he comes over, or is it a better idea to let our friend choose
the game?
Always stay with the guest. It is never acceptable to go off and play by oneself when a guest is
over, even if the guest wants to play a less-desired game. Play only with the guest and don‘t
leave the guest alone.
o Okay, so the two main rules we know about having a play date are… (1) the guest gets
to choose all the games we play, and (2) always stay with the guest, and make sure I am
playing with him/her!
Give compliments. The host should praise the guest by giving compliments, saying ―nice try,‖
etc. The child should not criticize the guest or the types of things that the guest wants to do.
4. Optional: Introduce the concept of smiling as a way to make others like us more.
Using cartoons, the therapist describes the situation in a cartoon that hasn‘t been used before.
- The therapist helps the child to determine what the cartoon characters might be thinking
based on their smiling or not smiling. The therapist helps the child to identify how smiling makes
others like us more and want to be our friend more.
―If we were in this cartoon, walking up to these kids, which child would I want to talk to
more? Why?‖ ―The reason that the kids in this cartoon are talking with him/her is
because he is smiling, right?‖ ―If the kid who isn‘t smiling tried smiling more, then
maybe more of the characters would want to talk with him/her.‖
Practice smiling in session. Help the child experience the effect of his/her smile on the
therapist (―it makes me feel like you like me, and I want to be your friend when you smile!‖)

For homework, the child is to smile at peers and family members during the next week.
Therapist and child specify specific times for the child to smile (or smile more). Note: The
therapist must put this assignment in concrete terms (e.g., ―when you are in a conversation, like
right now, smile each time someone smiles at you, and even smile sometimes when you just
feel like it; let‘s practice right now—try to remind yourself that you want to smile when we
talk to your mom in a minute!‖).
Therapist asks child how much this assignment makes the child nervous. Therapist may follow
up with questions regarding child‘s beliefs about smiling (e.g., ―Do you think that there is
anything bad about smiling? Do bad things happen when you smile?‖). Determine the child‘s
anxiety level regarding smiling.
5. Introduce the concept of making a phone call to the child.
If appropriate to the child‘s ability level and status in the social group, role-play making a
phone call to invite a peer to a playdate. See parent readings from Parent Module: PLAY for
specifics. In brief, the child must make an appropriate greeting, ask how the child is doing, ask
if s/he‘d like to come over for a playdate sometime soon, and if so, find out what the peer
would like to do at the playdate.
Suggest that the child ―play detective‖ by asking the friend what sorts of things he/she would
want to play when coming over so that the child can have those things ready.
―This is important to do because it will make the playdate more fun so that your friend
will want to come back.‖
Parents generally should be closely consulted at this point in the phone call with regard to
making specific plans for a time and day.
Prepare what the child will say (and think) if the friend can‘t make it over for a playdate
sometime soon. The child should be prepared with lines such as, ―That‘s okay, maybe some
other time,‖ and should remind him/herself that often other children are just busy and might
want to come over in the future.
Determine child‘s anxiety regarding calling a friend. Develop a KICK plan as needed.
Reinforce child participation by discussing or playing a special topic or game. This should
last approximately 5-10 minutes.
WITH PARENTS AND CHILD TOGETHER (OR JUST CHILD) (10 MINUTES)
1. Review past week’s homework exposures:
Check on how exposure tasks went the previous week. Give the child praise for trying
exposure tasks during the week.

2. Plan this week’s home-based exposures, including building towards a playdate:
Encourage the family to discuss and agree upon a new set of exposure tasks. One of these
exposures may be a playdate, or activities that could lead to a playdate, if appropriate and
feasible for the family. It is best for the child to work on 3 separate exposure tasks at home
each week (it is reasonable to spend 20-30 minutes per day ―practicing‖ these tasks). Plan on
a specific (set of) reward(s), privileges, and/or points (see Parent Module: REW) for the
child‘s home-based exposures this week.
Write the exposure assignments down for the child on a blank piece of paper.
Emphasize that the rate of progress on treatment goals is directly related to the frequency and
consistency with which the child and parents do the assigned exposure tasks each week.
3. Rewards program
Check in on the rewards program (see Parent Module: REW). Having rewards that the child
wants is key for motivating them to continue with the exposure tasks.
As necessary, modify the rewards list to exclude reinforcers that are not motivating to the
child. Also, for reinforcers that the child has access to all the time, the parent can either
control the child‘s access to them or exclude them from the reinforcement list. Finally, the
best rewards are things that are renewable, wanted, and already used frequently by the child
(e.g., TV, computer, specific games, etc.). These should be added to the reinforcement list if
not already on it.
Child Module: SOC-C
Social Coaching Exposure
Background
Children with ASD have impaired social interactions. But social skills training programs
have been ineffective; children seem to be unable to generalize training in ―hypothetical
situations‖ in the therapy room to ―real life‖ situations and social partners. ―Social coaching‖
addresses these weaknesses in traditional social skills training by providing children with
planning and preparation for social interactions in real life situations. Social coaching is most
effective when in vivo, taking place just a few minutes before, and certainly no more than 30
minutes before the social interaction is to take place. Social coaching is intended to be enacted in
support of peer interactions—for this reason, child-settings such as school recess-time or parks
and community centers are best for this kind of exposure.
Goals
1. Review homework
2. Prepare child for an exposure using social coaching
3. Conduct a social exposure experience immediately after the social coaching
4. Plan new exposures and assign as HOMEWORK
5. Maintain rapport with the child by playing, chatting, permitting child to help set the tempo of
the session
Preparations
Review intake materials and fear hierarchy to identify social situations that may be good
targets for social coaching. Note, the child need not feel ―anxious‖ about the social situation—
s/he simply must be functioning below age-expectation in that situation. Examples of target
situations include eating with peers during lunch at school; playing with peers during recess at
school; joining free play games in parks or other community child-settings. Often the child
simply has a deficit in social abilities in these situations, and may not be fearful of the
situations per se. The overarching goal of social coaching is to augment the child‘s social skills
in the exact situations where s/he finds him/herself and exhibits a significant social deficit. Of
course this will differ from child to child and just as with other exposures, social coaching
exposures must be tailored to each child individually.
Make all preparations necessary for the social coaching exposure. This may involve arranging
to meet the child or family at school or an appropriate community setting. This may also
involve arranging for peer confederates with the teacher or parent, if necessary.
Have the child‘s reward ready for him/her if she is likely to have earned it this session.

Materials
Feelings Thermometer handout
KICK plan written by hand
My Own Cartoon handout and colored pencils/crayons
Blank paper
Reward chart
Session
WITH CHILD ALONE (30 MINUTES)
1. Review HOMEWORK Task:
Review the child‘s HOMEWORK task and record appropriate points on his/her reward chart.
2. Introduce purpose of module:
―Sometimes we have a hard time talking to other kids our own age because we don‘t quite
know when to join the conversation or what to say. To make sure things go well, we have to
plan and prepare what we are going to say or do. A lot of times it can be really helpful to plan
and prepare with someone else.‖
Let the child know that you and he/she will be trying this out. Before heading out to the
exposure, it can be useful to prepare the child with a summary of what you will be doing, as
described below. However, keep in mind that simply role-playing with the therapist in the
therapy room is not social coaching per se—it is limited to a ―hypothetical situation‖ when
done in the therapy room and will not generalize. Only spend enough time on the preparation
so the child knows what is expected of him/her and s/he indicates readiness to try out the
exposure.
3. Social Coaching Exposure:
1) Go to the location of the social coaching exposure. Somewhere a bit removed from the exact
situation (e.g., the periphery of a playground; on a bench near the school lunch arbor) help the
child prepare appropriate social behavior for the situation.
Identify the goal of the interaction (e.g., greeting, giving compliments, gathering
information, etc.) with a specific person or class of people (e.g., a specific friend; or a
group of children like classmates at the lunch table).
o ―Okay, so what we want to do today is join Pat, Jo, and Mike at the lunch table.
You know, we want to eat lunch with them. So we want to ask if we can join them in
a polite way.‖
Initiate a discussion of appropriate conversation topics for the given situation. Some
children may need suggestions before they are likely to provide relevant responses. With
some children, it may be possible to ask directly what s/he thinks s/he could talk about
during the interaction. However, avoid the latter approach initially if it is likely to only lead
to a failure experience; rather, provide some examples first. Be sure to include basic but
critical non-verbal behaviors in the plan.
o ―So we‘re going to get ready to join those guys for lunch. A good thing to do first is
look right at the kids who are seated, and say ―Hi,‖ or ―Hey guys,‖ or, ―Mind if I
sit with you?‖ Which one of those sounds good to you? Which one is how the other
kids talk?‖
o ―Okay now we want to think about something we can say to the kids after we start
eating lunch together. You said that Pat likes to play with matchbox cars. It is nice
to ask people about things they like to do. Can you think of something to ask him
about his cars? What about if he‘s got any new ones recently? How could you ask
that? Let‘s practice.‖
o Andy, what do you think you would like to say first to the person who you‘ll be
going up and talking to?
Role-play the interaction verbally, being mindful of confidentiality and the need to keep the
nature of this conversation private. Of course, this may be best done sitting down with the
child using a quiet voice if others are nearby, rather than standing and using noticeable
gestures.
o Take the role of the child first. Provide direct modeling of the words to use. Ask the
child to tag-along next, while you role-play as the interlocutor. Provide scaffolding
to the child about how to approach and what to say if s/he does not exhibit
appropriate social behavior during the role-playing. Repeat role-playing as needed
until mastery is achieved and the child is ―ready.‖
o Make sure that the child uses his/her own words for the upcoming social
interaction. This will allow the child to remember and use the words practiced, as
well as to sound authentic in his/her interaction.
o If the child seems nervous, prepare a KICK plan or review relevant aspects of the
plan (i.e., icky thoughts and calm thoughts) as needed. If helpful, remind the child
of the reinforcer that is being used with this exposure. Have the child give a fear
rating.
Therapist Note: One way to plan a social interaction with the child is to use Cartoon
Script handout. Write down the goal of the interaction, and together identify the steps for
what to do to meet the goal.
When the child is ready, prompt him/her to approach the target person/group and engage in
the planned social behavior.
o As necessary, pull the child aside during the conversation to participate in more
social coaching. Ideally, social coaching should occur during natural breaks in the
conversation so the target children are not aware that social skills training is
occurring.
When the child returns from the exposure, get a fear rating. Review how the child
experienced the interaction, focusing on dispelling any fearful s/he may have had. Provide
feedback to the child.
o ―Andy, you did a fantastic job saying ‗hello‘ to the receptionist and asking her how
she was doing! How did you do that!?! You showed a lot of confidence when you
looked at her in the eyes to tell her that you were having a good day, too. Way to
power up!‖
If time, conduct more social coaching exposures (often, only time for 1-2 in vivo exposures
per session).
Only if the social coaching is going well, invite parents to observe the social coaching.
Reinforce child participation by discussing or playing a special topic or game. This should last
approximately 5-10 minutes.
WITH PARENTS AND CHILD TOGETHER (10 MINUTES)
1. Review past week’s homework exposures:
Check on how exposure tasks went the previous week. Give the child praise for trying
exposure tasks during the week. Give points/rewards as appropriate.
2. Plan this week’s home-based exposures:
Encourage the family to discuss and agree upon a new set of exposure tasks. It is best for the
child to work on 3 separate exposure tasks at home each week (it is reasonable to spend 20-
30 minutes per day ―practicing‖ these tasks). Plan on a specific (set of) reward(s), privileges,
and/or points (see Parent Module: REW) for the child‘s home-based exposures this week.
Write the exposure assignments down for the child on a blank piece of paper.
Emphasize that the rate of progress on treatment goals is directly related to the frequency and
consistency with which the child and parents do the assigned exposure tasks each week.
3. Rewards program
Check in on the rewards program (see Parent Module: REW). Having rewards that the child
wants is key for motivating them to continue with the exposure tasks.
As necessary, modify the rewards list to exclude reinforcers that are not motivating to the
child. Also, for reinforcers that the child has access to all the time, the parent can either
control the child‘s access to them or exclude them from the reinforcement list. Finally, the
best rewards are things that are renewable, wanted, and already used frequently by the child
(e.g., TV, computer, specific games, etc.). These should be added to the reinforcement list if
not already on it.
M
MY
Y
O
OW
WN
N
C
CA
AR
RT
TO
OO
ON
N
Directions: For each situation, develop a plan!
1) What is my GOAL? ____________________________________________________________
2) Plan the steps to take, coming up with what I’ll do.
3) Power up and do it!
1
2
3
4
G
GR
RE
EA
AT
T
J
JO
OB
B!
!!
!

Child Module: ERP
E/RP In Vivo
Background
This session is optional; however, literature suggests that it is common for individuals with
HFA to experience some obsessions and compulsions (McDougle et al., 1995). Obsessions are
―intrusive thoughts, urges, images, or ideas characteristic of OCD, usually accompanied by a dysphoric
affect (e.g., doubt, feeling of incompleteness, anxiety, disgust, or aggression); compulsions are ―an
intentional behavior, often performed in a stereotyped or ritualized fashion, designed to reduce an
obsession and accompanying dysphoric affects‖ (see March and Mulle, 1998 for review of obsessions
and compulsions). For example, an individual may have obsessional fears of being contaminated;
therefore, engages in washing or checking rituals to reduce his/her feelings of dysphoric affect. Thus,
the plan for this session is to introduce Exposure plus Response Prevention techniques (E/RP; March
& Mulle, 1998) as another exposure strategy to be used in this program. E/RP is defined by March and
Mulle as a ―contrived or uncontrived exposure plus refraining from performing the accompanying
compulsions‖; that is, ―not doing the ritual—for example, washing—after either contrived or
uncontrived exposure—for example, touching a toilet seat.‖
Therapist Note: Many children with OCD have obsessive thoughts about harming themselves or
other people, or behaving in socially inappropriate ways. It is important for parents and children to be
told that it is okay to think anything. There is no such thing as a wrong thought.
Goals
1. Review homework
2. Prepare a KICK plan for an in vivo exposure
3. Create and conduct in vivo exposure using E/RP
4. Obtain fear ratings before and after the exposure
5. Plan new exposures and assign as HOMEWORK
6. Maintain rapport with the child by playing, chatting, permitting child to help set the tempo of the
session
Preparations
Review the child‘s hierarchy, Diagnostic Evaluation materials, and the CY-BOCS in particular, for
an appropriate E/RP for this session (see Parent Module: EXP for complete discussion on the
selection of appropriate exposures.)
Make all preparations necessary for the in vivo exposure, e.g., arranging for confederates, materials,
room space, etc.
Have the child‘s reward ready for him/her if s/he is likely to have earned it this session
Materials
Feelings Thermometer handout
KICK plan written by hand
Cartoons and pictures previously used
Blank paper and colored pencils/crayons
Reward chart
Session
WITH CHILD ALONE (20-30 MINUTES)
1. Review the child’s homework task and record appropriate points on his/her reward chart. If
s/he did not write the homework, allow him/her do complete it verbally by reporting to you. Give
gentle corrective feedback to clarify any misinterpretations in the assignment. Record appropriate
points/stickers on his/her reward chart with appropriate affective tone (matching child‘s style).
Present the child with his/her reward, if it has been earned. If indicated, explain in very simple
terms any changes that will happen to the reward system (e.g., ―remember how last time we
talked about how your mom is going to give you a chance to earn even more rewards now that
we‘re starting a new phase of this program? Yes, that‘s right, we‘ll think of some cool stuff for
you to earn!‖)
Therapist Note: Working out the next phase of the rewards program (i.e., therapist- vs. parent-
mediated rewards) is a complex decision process. Review Parent Module:REW (Rewards &
Privileges) for discussion of the considerations involved.
2. Review ERP rationale (if not previously done):
Externalize the obsessions and compulsions from the child—―blame‖ the anxiety.
o ―Sometimes we get thoughts in our heads, like feeling like we might jump out of the car when
it‘s moving. These thoughts are okay to have, but we need to remember that it‘s only our
anxiety trying to mess us up! Today we‘re going to do something about it, and fight back
against anxiety!‖
Explain that the way to ―fight back‖ against anxiety is to do things that will make us braver, more
courageous. Thinking about scary thoughts on purpose; maybe doing things that make us a little
nervous. When we do things like this, we feel more nervous at first, but eventually the anxiety goes
away and we feel brave and confident.
3. Identify, using the exposure hierarchy, an appropriate E/RP (e.g., fear of contamination would
suggest having the child put a sticky substance on his/her hands without engaging in washing, fear of
getting shoes dirty would get shoes dirty and not take them off or wash them).
As noted above, it is important to have several ideas prepared in advance for possible exposures.
These exposures need to be doable during session; must be within several fear-rating points on the
hierarchy of what the child has accomplished to date; must make positive progress towards
advancing a ―line‖ of exposures (see Parent Module: EXP; e.g., reducing handwashing in small
steps).
The child may give some input on choosing between several reasonable ERP exposures most of the
time. However, refusing all proffered exposures is not acceptable. For many children, a collegial
conversation clarifying the importance of exposures and how helpful it will be to the child when s/he

feels ―happy‖ (confident, not afraid, etc.) in the specific situation will be enough to elicit a more
agreeable attitude. For others, also note that the child is earning points for doing this exposure (if this
fits with the reward/privilege system in place), or arrange a short-term reinforcer on the spot (e.g.,
time on the office computer, a game with the therapist later, a treat, etc.). In the end brainstorm with
the child on ways of reducing the intensity of one of the suggested ERP exposures in order to make it
more acceptable—but this is to be avoided whenever possible.
4. Use the in vivo exposure procedure described in Child Module: IV to prepare for and conduct the
ERP exposure. The following points should be considered for the ERP components of the exposure,
specifically.
Focus on cognitions such as, ―It‘s only my anxiety. I know that feeling anxious about _____
(obsession) will go away in a little bit; I don‘t need to _____ (compulsion).‖
Focus on ―hanging in there‖ for exposures to unpleasant substances, thoughts, or tasks. The longer
you do it, the more you‘ll get used to it and not care! After awhile your anxiety will go away!!
Use rewards/privileges to ‗back up‘ prohibitions against compulsions and safety behaviors.
Remember, the way to earn the candy bar is to not wash our hands for at least 20 minutes while we
have this gooey stuff on our fingers!!
Even if the child eventually engages in a permitted safety behavior (e.g., washing hands after getting
them really dirty for part of the session), encourage him/her in advance to go about the safety
behavior CALMLY and not act like it is ―such a relief‖ to get to end the exposure. Encourage
her/him to think in this way too, and to reject cognitions that focus on how ―disgusting, terrible, or
fearful‖ the exposure is—that is, engage in some cognitive restructuring (I and C steps) during the
ERP exposure, as needed.
Often, get ratings of the child‘s fear level throughout the ERP exposure, to chart out any changes
over the course of the ERP.
Provide the child positive feedback for successful ERP exposures such as, ―How did you do it?! That
was awesome.‖
5. If time, conduct another ERP exposure.
Note, often an ERP exposure should be repeated multiple times in the same session without any
additional preparation. An example is, if the child had success in touching one bothersome substance,
it is advisable to get fear ratings, and then repeat the permutations of the same basic exposure several
times. If the fear rating is going down, the exposure can be changed to something slightly harder in
the same ―line‖ of exposures (e.g., ―contamination‖) with very minimal additional preparation in the
same session. This often gets maximum benefit from the in-session preparation efforts and
sometimes is superior to trying to prepare for and conduct a second exposure from a different ‗line‘
of exposures, which of course can require a lot of ―talk‖ and ―imaginal exposure‖ in the therapy
room.
Reinforce child participation by discussing or playing a special topic or game. This should last
approximately 5-10 minutes.
WITH PARENTS AND CHILD TOGETHER (10 MINUTES)
1. Review past week’s homework exposures:
Check on how exposure tasks went the previous week. Give the child praise for trying exposure
tasks during the week. Give points/rewards as appropriate.
2. Plan this week’s home-based exposures:
Encourage the family to discuss and agree upon a new set of exposure tasks. Of course, in keeping
with the theme of the ERP session, it is advisable to include an ERP exposure or two on the child‘s
homework list. It is best for the child to work on 3 separate exposure tasks at home each week (it is
reasonable to spend 20-30 minutes per day ―practicing‖ these tasks). Plan on a specific (set of)
reward(s), privileges, and/or points (see Parent Module:REW) for the child‘s home-based
exposures this week.
Write the exposure assignments down for the child on a blank piece of paper.
Emphasize that the rate of progress on treatment goals is directly related to the frequency and
consistency with which the child and parents do the assigned exposure tasks each week.
3. Rewards program
Check in on the rewards program (see Parent Module: REW). Having rewards that the child wants
is key for motivating them to continue with the exposure tasks.
As necessary, modify the rewards list to exclude reinforcers that are not motivating to the child.
Also, for reinforcers that the child has access to all the time, the parent can either control the
child‘s access to them or exclude them from the reinforcement list. Finally, the best rewards are
things that are renewable, wanted, and already used frequently by the child (e.g., TV, computer,
specific games, etc.). These should be added to the reinforcement list if not already on it.
Child Module: MENTOR
Mentoring
Background
Children with ASD have significant impairments in taking other individual‘s perspectives,
termed ―theory of mind‖. Previous experiments attempting to teach theory of mind abilities to children
with ASD have yielded mixed results. However, these have typically involved hypothetical situations,
which may not generalize to dynamic naturalistic situations. Providing mentoring opportunities to
children with ASD, which necessitates taking another‘s perspective, may lead to the development of
theory of mind, and may facilitate generalization across settings and people.
Goals
1. Review homework
2. Introduce the concept of mentoring to child.
3. Discuss rules of being a mentor.
4. Plan new exposures and assign as HOMEWORK
5. Maintain rapport with the child by playing, chatting, permitting child to help set the tempo of the
session
Preparations
Review Parent Module: MENTOR. Also suggested for review are Parent Module: PLAY and Child
Module: FRND for additional background on social interventions in ASD.
Review the fear hierarchy for appropriate feared situations to assign for homework (and to prepare
for in-session). It is important to determine what ―lines‖ of exposures still need to be covered. If
problems have been encountered be sure to consider ways to reduce the level of difficulty of a line of
exposures without allowing the child to completely avoid it. See Parent Module: EXP for complete
discussion of the selection of appropriate homework exposures.
Determine whether you will continue with the therapist-directed rewards system or transfer future
rewards/privileges entirely to the parent.
Have the child‘s reward ready for him/her if she is likely to have earned it this session.
Materials
Feelings Thermometer handout
KICK plan written by hand
Blank paper and colored pencils/crayons
Reward chart
Session
WITH CHILD ALONE (30 MINUTES)
1. Review the child’s homework task and record appropriate points on his/her reward chart. If
s/he did not write the homework, allow him/her do complete it verbally by reporting to you. Give
gentle corrective feedback to clarify any misinterpretations of the assignment. Record appropriate
points/stickers on his/her reward chart with appropriate affective tone (matching child‘s style).

Present the child with his/her reward, if it has been earned. If indicated, explain in very simple
terms any changes that will happen to the reward system (e.g., ―remember how last time we
talked about how your mom is going to give you a chance to earn even more rewards now that
we‘re starting a new phase of this program? Yes, that‘s right, we‘ll think of some cool stuff for
you to earn!‖)
2. Introduce the concept of being a positive role model to another child.
Draw a set of stick figures to explain why mentoring is a benefit to the child. Draw a large stick
figure and state that s/he is a ―superhero.‖ This may be individualized to the child‘s interests. Draw
a smaller stick figure and note that this is a ―regular kid.‖
o Initiate a conversation about what the ―kid‖ has to learn from the superhero. Predictably,
some initial suggestions from the child may include flying, fighting, saving the world, etc.
Accept these suggestions good naturedly and suggest that even if the kid never learns to fly,
the superhero could teach him/her a lot about (a) how to get along with other kids in school,
(b) how to do well on schoolwork, (c) how to be ―good‖ at sports and games, (d) how to
follow the rules, etc. This can be individualized to the individual child‘s developmental
level and community. The point is that older people know a lot of things that they can teach
younger people.
o Point out that when older people help younger people it is fun for both parties. The younger
person gets to learn a lot and has someone to look up to—even if they‘re not really a
superhero. The older person has fun seeing how much s/he can help the younger person
become good at something or deal with his/her problems.
Point out that superheroes are like older mentors / buddies / friends / role models. Use whatever
term is most appropriate for the family and community. Help the child understand the term with
examples and discussion. Ideally, drawing in the child‘s preoccupations / obsessional interests to
present the topic of mentoring is useful to pique the child‘s interest. This may require learning
more about the plotline of the child‘s favorite stories/shows.
o Remember that one ―Dragon Rider‖ episode when Brom teaches little Jasper how to
become strong? He shows him how to magnify gravity until just walking takes a lot of
effort, and that makes you strong, remember? Brom was an older buddy to Jasper in that
episode—someone who helped him learn something new, someone who was nice to him.
But remember who looked the happiest at the end of the episode? Brom—he had a big smile
on his face! Do you know why? Because he was proud of how strong Jasper became!
Because Brom knew he was the one who had helped Jasper become a Dragon Rider!
It is useful for therapists to tell anecdotes about specific children they have known who have been a
mentor, and had positive results from the role. I know a kid who was older buddy to a first grader
who was new at school. She showed her how to go to the cafeteria, get lunch, and how to play hand
ball. She played hand ball with her each day to keep her company. The older girl felt like she had a
new little sister; the younger girl felt so lucky to have an older buddy, so she loved going to school
every day! Both of them had a lot of fun.

Then note that the child with HFA would be great at doing that: ―I was thinking that you would be
really good at being an older buddy for a younger kid, too! Being a buddy is like being a super
hero to one kid. The type of person who can be a really good older buddy is a kid who is well
mannered and polite and is nice to younger people. It‘s a big responsibility and a grown-up thing
to do.‖‖
Depending on what specific mentoring ideas have been worked out with the parents in Parent
Module: MENTOR, describe the pragmatics of the possible mentoring situation to the child (e.g.,
spending an hour a week). Evaluate his/her level of interest and willingness. Some additional effort
may need to be spend in selling the idea if the child is not enthusiastic.
3. Discuss rules of being a mentor:
If appropriate, review principles from Child Module: FRND regarding being a good host with the
child.
Discuss patience. ―You might have to be a little bit patient and you want to try to make it fun for
the younger friend because you‘re trying to help them learn how to be a good player. It requires
some effort but it is an important responsibility and everyone thinks you are mature enough to do
it!‖
If the child states that he doesn‘t like the child to be mentored, the therapist may inform the child
that he/she doesn‘t have to ―like‖ the mentored child to begin with. ―We are trying to help them
and we are trying to show them how to be more grown up. So, those are some things that you can
actually help your buddy with and maybe you‘ll find over time you‘ll like him more because you
help him.‖
4. What to do when the mentored child is disobedient:
Explain that disobedience is normal.
Plan and role-play how to handle disobedience (e.g., have a list of activities that the mentored child
likes and be prepared to suggest another preferred activity if disobedience occurs; give the
mentored child choices in the activity to play).
Reinforce child participation by discussing or playing a special topic or game. This should last
approximately 5-10 minutes.
WITH PARENTS AND CHILD TOGETHER (Or JUST CHILD) (10 MINUTES)
1. Review past week’s homework exposures:
Check on how exposure tasks went the previous week. Give the child praise for trying exposure
tasks during the week.
2. Plan this week’s home-based exposures, including building towards a get-together with the
―younger buddy‖:

Encourage the family to discuss and agree upon a new set of exposure tasks. One of these
exposures may be a get-together with a younger buddy, if appropriate and feasible for the family. It
is best for the child to work on 3 separate exposure tasks at home each week (it is reasonable to
spend 20-30 minutes per day ―practicing‖ these tasks). Plan on a specific (set of) reward(s),
privileges, and/or points (see Parent Module: REW) for the child‘s home-based exposures this
week.
Write the exposure assignments down for the child on a blank piece of paper.
Emphasize that the rate of progress on treatment goals is directly related to the frequency and
consistency with which the child and parents do the assigned exposure tasks each week.
3. Rewards program
Check in on the rewards program (see Parent Module: REW). Having rewards that the child wants is
key for motivating them to continue with the exposure tasks.
As necessary, modify the rewards list to exclude reinforcers that are not motivating to the child.
Also, for reinforcers that the child has access to all the time, the parent can either control the
child‘s access to them or exclude them from the reinforcement list. Finally, the best rewards are
things that are renewable, wanted, and already used frequently by the child (e.g., TV, computer,
specific games, etc.). These should be added to the reinforcement list if not already on it.
Parent or Child Session X
Support / Emergency Session
Background
In any therapy, occasional unexpected events arise that must be addressed which do not fit into
the guidelines of a particular module. In these cases, previous clinical training (and, if needed,
supervision or consultation) must serve as the guide of the session content, as there is inherently no
way to provide a treatment plan for all possible eventualities. It should be noted, however, that the
more that non-manualized sessions are used, the less treatment effect on the target symptoms (e.g.,
anxiety) one can expect. Therefore, it is a priority to limit off-protocol clinical interventions to a very
infrequent basis if possible.
Goals
1. Identify problems that have arise for the client
2. Help client problem-solve to develop solutions
3. Provide support and empathy
4. Redirect clinical interventions back to manualized procedures as soon as clinically appropriate
Materials
Variable.
Session
Content is variable. See Background, above.
Child Module T
Termination Session
Background
The goal of the Termination Session is to help children feel good about their accomplishments
and to plan for the future.
Goals
1. Help child develop a positive attitude about his/her progress in the program
2. Review skills learned in this program and plan for the future
3. Discuss termination issues
Preparations
Prepare any ―party‖ materials (e.g., snacks), and certificate, card, and/or small gift for child. For most
children, a certificate of completion from the web (color-printed), a small assortment of treats that the
child likes (e.g., some cookies, chips, soda), and perhaps a small gift (if there is an obvious gift for this
particular child that is easily obtainable), are sufficient.
Materials
Party materials
Session
WITH CHILD ALONE (15 MINUTES)
1. Review the child‘s homework task and record appropriate points on his/her reward chart.
2. Explain the format of the session: a brief meeting to talk about how the child has done in the
program, including a small ―celebration‖ party.
3. Present snacks, certificates, etc., to the child and compliment him/her for effort in the program.
4. Review the child‘s progress in the program with him/her, including focus on positive
accomplishments and solicitation of the child‘s self-perceptions of his/her progress.
5. Discuss termination issues: how it has been a pleasure to work with the child; it is normal to miss
people you like when you can‘t see them much anymore; and how you‘re sure you‘ll miss the child
and think about him/her a lot after today.
Ask the child how s/he feels about ending the program, and ask her/him to name 1 good thing
and 1 bad thing about the program being over. Empathize as appropriate, and reflect positively on
the child‘s pleasure at finishing the program (e.g., ―I know what you mean about being glad you
have your Tuesdays free again! You‘ve worked really hard coming here every Tuesday for 16
weeks—I bet you‘ve got a ton of other things you could be doing on Tuesday like playing with

your new friend in the neighborhood!‖) The child is free to disclose his/her feelings or not during
this conversation—there is no benefit to pressuring the child on this.
6. Review importance of continuing to use the KICK plan with situations that make the child feel
nervous—everyone become nervous about some things, and only some people are lucky enough to
know how to deal with these feelings!
WITH PARENTS AND CHILD TOGETHER (15 MINUTES)
Therapist Note: Only conduct the joint parent-child meeting in this session with families that have
made significant progress on anxiety symptoms.
1. Briefly review past week’s home-based exposures:
Focus on any positives from the exposure tasks and give the child praise for his/her effort.
2. Review progress with the parents and child:
Explain that it can be helpful to evaluate if there are still areas to work on by briefly rating fears of
the original hierarchy items. Read several of the key fears listed on the original hierarchy and ask
the parents and child to re-rate these situations with the Feeling Thermometer. Do not disclose the
child’s original ratings prior to obtaining the new ratings.
If the child has several items that are currently rated lower than they were at the start of the
program, provide this information to the family and emphasize the child‘s progress in reducing
his/her anxiety.
o Wow, before the program, you rated ‗Keeping your room messy‘ as a 9! Now you rated
it as a 1! Wow, that‘s a big change—you really got over that fear!
If the child has made minimal improvement on the core anxiety symptoms, according to the new
ratings, but the family views the child as having made improvements, reiterate the family‘s sense
of improvement, but do not draw attention to the lack of improvement on the numerical ratings,
which may not accurately reflect the child‘s progress.
3. Focus on the child’s progress, provide compliments, congratulate family on hard work.
Certificate of
Accomplishment
presented to
for completing the
Building Confidence Program
THERAPIST NAME, PROGRAM NAME Date

Parent Module 1
Setting Up Session 1
Either in-person at the pre-treatment assessment or on the phone, an initial appointment should be
made for the parent and child to come in for the first session. If possible, encourage both parents to
attend the first session.
1. In general, the parent and child will meet with the therapist together for about 10 minutes, the child
will work alone with the therapist for about 30 minutes, and then the parent will spend the next 30
minutes with the therapist while the child plays games, reads, or does another enjoyable activity
(sessions will last 80-90 minutes, total). Encourage the parent to bring two types of activities for
the child: the first should be an activity that is of special interest (e.g., games or objects of
particular interest) for the child to do for the half-hour that the parent will spend with the therapist,
and the second should be an interactive activity (e.g., quick board game, things that can be looked
at together) that the therapist and child will play with during their sessions. This must also be an
activity of particular interest to the child. Baker, Koegel, & Koegel (1998) found that creating
games using the obsessions of children with ASD increased the child‘s time of engagement and
interaction with peers and adults. Increased interaction time was maintained when switching from
the original game to others. Additionally, significant increases in positive affect were found for the
child with ASD and others. Therefore, allowing the child and therapist to engage in activities that
the child enjoys will build rapport and positively reinforce the child‘s participation during the
sessions. However, the activity to be played during the session should not be games or toys that can
be played alone (e.g., gameboys or electronic toys, videos, television programs, etc.).
2. Explain that usually a volunteer college student will keep an eye on the child in the waiting room
or a separate office during this time. Otherwise the child will be asked to work quietly in the room
while the parent and therapist talk.
3. Explain that the first session focuses on collecting background information, providing
psychoeducation regarding anxiety and autism spectrum disorders, and developing the child‘s
treatment plan.
Some parents may be reluctant to have their child‘s autism diagnosis disclosed to them.
Reasons for this may include concern that their children will will feel more isolated and
less confident, use the diagnosis as an excuse to not achieve, or may disclose this
information to individuals without understanding potential consequences. However,
informing children of their psychological diagnosis—―externalizing‖ the problem—has
been found to ameliorate therapeutic alliance between the therapist, child, and parent(s)
(White & Epston, 1990).
For parents who are reluctant to disclose their child‘s ASD diagnosis to the child:
Explain that children with high-functioning autism typically are aware that they are ―different‖
or have more difficulty than their peers in social situations, communicating, or interacting with others.
Providing a label for these feelings allows children to know that it is ―not because of them‖ but due to
their diagnosis. This can assist children begin to feel more confident.
Inform parents that the goal of the session is for children to understand that the program will
teach them how to work to overcome the difficulties resulting from their diagnoses (both anxiety and
autism). ―We will talk about how anxiety and autism get in the way of doing things that we want to do
like making friends and playing with kids.‖
Finally, explain that it will be emphasized that children talk more with their parents about their
diagnosis, and when it is appropriate to tell others including peers and teachers.
4. Discuss the importance of getting both parents to participate in treatment. Evaluate feasibility.
Some parents feel very certain their spouse/the other parent will detract from or undermine the
program and this should be respected (e.g., a non-psychologically minded person, someone who
denies the child‘s disability, etc.). Ideally, the secondary parent (usually the father) should come for
at least two sessions, especially the third (Encouraging Independence) and forth (Negotiating
Exposures) sessions.
Parent Module 1
Introduction, Information, and Treatment Planning
Background
In the first session, the main goals are to (1) conduct a functional analysis of behavior by
inquiring about the antecedents, behaviors, and consequences (ABCs) associated with the child‘s
anxiety symptoms, with particular emphasis on parental responses to anxious behavior (i.e.,
consequences, which may reinforce the child‘s anxiety), (2) provide psychoeducation about ASD and
anxiety, and (3) briefly present the child‘s treatment plan.
Psychoeducation is found to be an important aspect of treatment. Parents and children benefit
from naming and being able to identify behaviors resulting from their disorder. A connection between
child ―misbehavior‖ and his/her comorbid disorders is emphasized. It is important for the parents to see
this connection to help reduce blame, hostility, and other kinds of tension between the parents and
child that may have arisen because of the child‘s autistic symptoms and deficient coping responses to
anxiety (i.e., tantrums, avoidance).
Goals
1. Establish rapport with parents
2. Conduct a functional analysis of the child‘s most severe symptoms of anxiety
3. Provide psychoeducation regarding ASD and anxiety
Preparations
Review questionnaire measures to acquire background information on the parent-child relationship
Review the child‘s intake reports to become familiar with the child‘s primary symptoms
Prepare parent handouts: Building Confidence Program handout, Homework Assignment handout,
Behavior Record Form
Bring a business card with the therapist‘s name and pager/voice mail number
Materials
Behavior Record Form handout
Common Patterns of Child Anxiety handout
Cognitive Behavioral Therapy handout

WITH PARENTS ALONE (30 MINUTES):
1. Review the content of the child’s session:
Mention that the child has a short homework task to complete and bring to the next session.
Encourage parent to provide support but the least amount of help that is actually needed.
2. Introduce purpose of session:
To get to know each other better, provide general information about the program to the parents, and
collect information about the child so we can develop an effective treatment plan.
3. Introduce self:
The therapist should briefly describe his/her background in psychology (e.g., doctoral student in
ed-psych at UCLA), general experience working with children and families (e.g., several years as
special ed teacher), and express enthusiasm about having the opportunity to work with the present
family. No need to say ―first time as a therapist‖ per se or ―I‘m learning to do CBT.‖
4. Orient parents to the parenting sessions:
Cover the following points with the parents:
Child was referred to the program because s/he has both ASD and a diagnosable anxiety disorder.
This program addresses the anxiety disorder with ‗cognitive-behavioral therapy‘.
However some of the aspects of the program also target problems caused by ASD such as
friendship skills deficits and as a result both reduced anxiety and improved social adjustment are
primary goals for the program.
But it is not intended as a ‗cure for ASD‘ per se—too short, not comprehensive in coverage of all
ASD symptoms.
Because they spend many more hours with their child, parents have a great opportunity to help the
child use the new skills they are learning in therapy.
Parents benefit from learning how to help their child employ his/her new coping skills. Dealing
with anxiety and ASD is difficult, and this program provides parents with the skills and the
confidence needed to help their children handle tough situations. This point may benefit from a
humorous presentation (i.e., ―We want to build up your muscle to deal with your child‘s
behavior when they become anxious‖).
The program is fairly structured: Each session, we will have an agenda and try to systematically set
up a plan to help the child with corresponding homework assignments. Some sessions focus on
developing techniques aimed at helping the child; some sessions are used for trouble-shooting.
How quickly the family attains their treatment goals is directly related to how often and completely
the parents and child complete the weekly assigned homework tasks.
5. Conduct a functional analysis of behavior (ABCs):
For at least one of the target anxious behaviors (ideally the most salient or distressing for the
parents), discuss in depth about the process of the problem. It is not necessary to adhere to the
following order of questions:
a) Step 1 – Assess specific Antecedents of the current anxious behavior (e.g. what leads up to the
child refusing to go into school). What is the main ―cue‖ that triggers anxiety in the child? (e.g.,
when the child gets in the car on the way to school, is this when it becomes clear he is
anxious?)
After the child‘s anxiety has become noticeable, what makes it ―get worse‖—how does the anxious behavior escalate,
what factors seem to make the anxiety increase (e.g. driving into the parking lot of the school, the child begins
trembling)?
Ask what the parent is thinking and feeling at each stage of the child‘s anxiety buildup (e.g.
when the child is asking many questions, what is the parent thinking/feeling; when the child
becomes angry, what is the parent thinking/feeling, etc.)
b) Step 2 – Assess the child‘s Behavior when the anxiety reaches its peak (e.g. the child refuses to
go into school and starts to cry).
How does the parent respond to the child‘s behavior as they build up to the peak phase? Has
anything been effective/ineffective at getting the child through feared situations? Does the child
act the same with both parents?
c) Step 3- Assess the Consequences of the child‘s anxious behavior (e.g. when the child refuses to
go into school, what happens?) Does the child face the perceived threat or avoid it? If they
avoid, how do they do so?
What is the parent‘s emotional reaction once the child has reduced their anxiety? Is the parent
relieved, guilty, angry with the child, frustrated, etc.?
6. Present information on the nature of autism spectrum disorder:
Pass out The Nature of ASD sheet and discuss with the parents. Highlight relevant information that
pertains to their child (i.e., ―you told me about your child‘s preoccupation with certain cartoon
characters. Preoccupations are a symptom of ASD…‖). Emphasize: (a) the main features of ASD,
(b) variability of symptoms, and (c) looking to the future and independence of the child.
7. Discuss the nature and causes of anxiety, and the child’s pattern of anxiety:
Describe the behavioral (avoidance), cognitive (worry), and affective (moodiness,
physiological arousal) components of anxiety.
o Link with threat—occurs when a danger is perceived (accurately or otherwise).
o Brain-based: studies show that the limbic system and especially the amygdala are sensitive to cues
of danger in the world.
Once they get triggered by the perception or worry about a danger (even just
being laughed at in gym class the next day) these brain structures set off the
―fight/flight reflex‖ which involves adrenalin release, racing heart, etc., and poor
concentration and attention to anything other than the feared situation.

o Emphasize: (a) anxiety is experienced by everyone, but becomes a problem when it interferes with
important areas of life (e.g., friends or family), and (b) because it is normal, the aim is not to
eliminate anxiety, but simply to reduce its intensity and help the child cope better with it.
o Present the Common Patterns of Child Anxiety handout to the parents. With input from the parents,
fill in the blanks for the ways that the child manifests his/her anxiety during one of the child‘s most
salient ―anxious situations‖, and what s/he does to reduce anxiety and regulate emotions (seeking
help or avoiding).
8. Describe the treatment plan, personalized to the family:
Present the Cognitive Behavioral Therapy handout to the parents. Use relevant information
about the child and parents to help personalize the presentation.
―ASD is a disorder that adds barriers to your child‘s getting along in the world. And anxiety
makes many children feel helpless and frightened in certain situations. They lose confidence in
themselves and their abilities.‖
―In this program, we teach children coping skills, like positive thinking skills and identification
of their own negative feelings, that help them manage their anxiety.
―We will spend several sessions teaching you communication skills that will help when your
child is feeling anxious. For example, children often do not know what they are feeling and
helping children identify their feelings can help them learn when the time has come to use their
coping skills.‖ ―Also we can provide incentive and reinforcement to children when they face
their fears by providing them with some type of reward system.‖
Children also need to learn basic ―friendship skills‖ in order to make progress in developing
friendships. We use a very specific research-supported CBT technique to help this occur.
―A very important part of the program is helping children to gradually face their fears. This
helps them feel more confident and in control of their anxiety.‖
Additionally, we work to increase the quality and flexibility of playdates and social interactions
at school by working with parents and the school using structured protocol we call ―social
coaching,‖ ―mentoring,‖ and ―peer buddies.‖
Finally, there is a significant problem in ASD with children‘s independent self-help skills such
as washing hair, keeping one‘s room tidy, and so forth. Children must have these basic skills
when planning for eventual independent living. We have a successful structured protocol that
helps children implement these skills and gain confidence and self-esteem.
9. Give the parents a business card with the therapist’s voice mail or pager number.
10. Describe the homework assignment briefly.
Autism is a disorder that falls on a wide spectrum. Some children have more
difficulties than others. ASD refers to a pattern of behaviors. The main
symptoms of ASD are listed below.
1. Impairment in social interactions.
Typically developing children in grades K–8 develop close friendships
with children of the same gender and age. These relationships involve
feelings of closeness, reciprocity, and shared interests. In contrast,
children with ASD usually have few friendships, and may display:
Impaired nonverbal behaviors (eye contact, facial expression, body postures).
For example, children with ASD may not smile while talking with others even when
having a great time.
Failure to spontaneously share enjoyment or interests with other people.
Children with ASD often don’t initiate conversations. They fail to bring up things that
make them interesting and unique without being prompted to do so.
Lack of social or emotional reciprocity.
Children with ASD may not be aware when others are feeling sad/annoyed/etc. They
do not know to be sympathetic with others—or know when they’ve done something
annoying & need to stop their current behavior. Also sharing, turn-taking, and “being
there for others” are not “natural” social behaviors for the child with ASD.
Impairment in the ability to sustain a conversation.
Children with ASD have a very hard time knowing what to say. They are hard pressed
to think of appropriate responses to others’ conversational topics and often seem
awkward (without a response) or insensitive (change topics abruptly).
2. Restricted repetitive and stereotyped patterns of behavior, interests,
and activities:
Preoccupation with restricted patterns of interest.
Children may have one or two obsessive interests: Videogames, cartoon characters,
trains, fire hydrants, special books or musicians, etc. The child talks about the interest
excessively or when it would be more appropriate to discuss other topics. The interest
usually interferes with social relationships.
Excessive routines or rituals and lacking ―flexibility‖.
Children may insist on the exact same schedule every day; going places via the same
route; organizing their belongings just so; or having things done over again and again.
List some situations your child
finds difficult:
How do you know when your child
has become anxious or fearful? (What
behaviors tip you off?)
How does your child behave when s/he
is feeling highly anxious?
What does your child do to reduce
his/her anxiety?
Child enters a difficult
situation (the ―cue‖)
Child becomes
anxious or fearful
Child avoids the situation
or asks others to help
(Short Term Anxiety
Relief)
Child continues to
think the situation is
dangerous and remains
fearful of it in the future.
Anxious behaviors
escalate (child gets stuck)
Problem:
ASD interferes with key
coping skills. Anxiety
undermines child‘s
confidence
Friendship /
playdate
skills
Step 1:
Develop
cognitive and
behavioral
skills.
Solution:
Build skills and
confidence.
Coping skills:
positive thoughts,
emotion
recognition
Specialized
parenting
techniques
Gradually
face feared
situations
Engage in
self-help skills
independently
Develop peer
relationships
at home &
school
Step 2: Apply
the skills in
―the real
world.‖
Building Confidence Program—Session 1
1. Track your child’s behavior! Use the Behavior Record Form and fill in 2 or
3 of your child’s typical anxious behaviors. This week, record if your child
engages in these behaviors each day and how you respond. This form is not
for research—it is to help you and the therapist identify what is leading to and
helping with your child’s anxiety problems.
Remember to bring the Behavior Record Form to the next session!
Directions: Each day, record your child’s anxious behavior and your response.
I am tracking these 2-3 behaviors:
Example:
Behavior: My child refused to get out of the car and go into school by himself.
My response: I said I could tell he was nervous about leaving this morning and I waited.
Child’s reaction: After several minutes of waiting, he grumbled and walked into school.
Date
Anxious Behavior
My Response To My Child
My Child’s Reaction
Parent Module: IEP
Parent Advocacy and IEP Goals
Background
Parent advocacy is one of the most important aspects of the intervention. Effective special
education services are expensive and may be portrayed as a limited resource. The Individual Education
Plan (IEP) offered by public schools is a mandate to provide tailored education to address the child‘s
academic social and emotional needs in the school setting if the regular education curriculum is not
leading to appropriate progress. Often children with ASD require more services than they currently
have been offered by the schools. Parents often become their child‘s primary advocate in the IEP
process.
Various issues surround parent advocacy and the IEP process for children with ASD. Children
with high-functioning autism have IQ scores above the cut-off for mental retardation and often are
fully included in regular education classrooms. Since major deficits of autism include communication
and social functioning, parents must be aware of educational services that can address these deficits.
Parents must always advocate in the IEP for services that will allow their child to get a ―free and
appropriate public education.‖
In helping parents with advocacy issues, it is important to note that the therapist not portray
him/herself to be an expert in litigation, or in occupational therapy, speech and language, medication,
or classroom education. Because this program is focused on child psychopathology, behavioral
features of autism, and anxiety in particular, advocacy consultation should be limited to these areas.
Goals
1. Review homework
2. Discuss principles of parent advocacy with family
3. Help family set up specific advocacy plan for child
Preparations
Review Parent Module: SOC-C, Child Module: SOC-C, and School Module: SOCIAL in preparation
for discussion of possible school accommodations that could be introduced for the child.
Carefully review the Parent Advocacy Tips handout and IEP chapter to become familiar with basic
laws and terminology
Read ahead to become familiar with the 3 school intervention sessions in this manual to have the key
aspects (as well as details) of these interventions on the top of your mind
Materials
Parent Advocacy Tips handout
Possible School Accommodations handout
Involving Parents in the IEP Process chapter
Session
WITH PARENTS ALONE (35 MINUTES)
1. Inquire about parents’ completion of homework.

2. Introduce purpose of module:
Explain the important role that parents play in generating IEP goals. Since most educational
systems don‘t effectively focus on social development for children with ASD, parents must
advocate for this service. Only through effective parent advocacy can IEP goals targeting social
skills and anxiety be added to their child‘s educational plan.
3. Introduce parent advocacy lesson:
Ask parents about their current experience with their child‘s IEP team, and satisfaction with their
child‘s IEP goals. ―What has been your role in your child‘s IEP team? What are your child‘s goals
and services? How satisfied are you?‖
Review the Advocating for Your Child handout. Ask parents what they think about the handout.
Ask parents ―Have you felt like you‘ve played a role in determining _____‘s (child) services? Are
there any services that you would like for _____ (child)?‖ Attempt to ascertain why particular
services are wanted, and why they have not been obtained yet.
4. Introduce IEP Goals:
Parents must always be looking towards the future development of their child, especially when
assessing the priority of goals on their child‘s IEP. Educators without extensive knowledge of
autism may not be clear about symptoms of autism, and the interaction between autism and
anxiety. Since major deficits of autism include communication and social reciprocity, educational
services often need to include opportunities for social interactions, and social skills building.
Provide parents the ―Involving Parents in the IEP Process‖ chapter. Point out that it is a very
important chapter to read for understanding their role in the IEP process and for reducing barriers
to the process.
Present possible accommodations that may be attained through the child‘s IEP. Present these fairly
briefly with an eye towards the individual child‘s needs as well as fit with her/his strengths.
1. One-on-one aide.
Parents may consider their child‘s need for a one-on-one aide to provide assistance for
behavior management as well as the autism-related interventions suggested below in points
2-4. An aide can assure that the child is receiving the support needed for his/her social
interactions.
When is an aide indicated? If the child is exhibiting severe social adaptation deficits
including aggression, severe noncompliance, emotionality unresponsive to lesser
interventions such as counseling and behavior management, school refusal, or being the
chronic victim of bullying. An aide is viewed by the school as a step below sending the
child to a special class or school (a very expensive intervention) but will not provide it ―just
because‖ the child has ASD—it must be required based on the child‘s specific behaviors at
school.
2. Live social coaching.
See Child Module: SOC-C and Parent Module: SOC-C. Describe the ―gist‖ of social
coaching to parents—the purpose, goals, and methods.

3. Peer buddy.
See School Module: SOCIAL. Present a summary of school-based peer intervention.
4. Gamesleader.
See School Module: SOCIAL. Describe the rationale and procedures for this intervention.
Ask parents for feedback on these possible school-based interventions.
1. Assess the parent‘s level of enthusiasm for the different school-based interventions that
have been described. Note problems that they foresee with these interventions, either for
their child per se, or within the school setting (i.e., there is no one who would be willing
to do social coaching).
2. Determine whether these programs would be better suited to informal working into the
school system by meeting with school personnel and teachers, versus helping the
parents prepare for formal advocacy in the IEP setting.
3. Inform parents that of the school programs that seem to make the most sense for their
child, there will be more specific focus in later sessions on setting the programs up—
including one or more direct school visits.
If appropriate, discuss the need to request an IEP immediately. Schools can delay the IEP for a
number of weeks after it is requested, so beginning the process soon is the only way it may end up
coinciding with this brief CBT program.
Therapist Note: Parents will most likely need the presence of the therapist at the IEP if the
proposed school interventions are to have a chance of being implemented.
As a parent, you are a natural advocate for your child. You know what skills your child needs
assistance with, and what types of accommodations may best prepare your child for an
independent future and high quality of life. Because of this, you must play an active role in
planning for your child’s educational services. The law gives you the power to make
educational decisions for your child.
As the parent of a child with autism, you should have two goals in mind:
Ensuring that the school provides your child with a ―free appropriate public education‖ that
includes ―specially designed instruction… to meet [your child’s] unique needs‖ (20 U.S.C.
§ 1401).
Building an advantageous relationship with personnel at your child’s school.
7 Tips for Parent Advocates
Gather information. Gather information and organize documents; learn about your child’s
symptoms of autism. Knowing as much as you can about autism will prepare you to identify services
that the school can provide for your child and allow you to identify when a service does not target your
child’s needs. Using facts and documentation about autism will assist you in resolving disagreements
with the school.
Learn the rules of the game. Educate yourself about the local school district. Know how decisions
are made and by whom. Educate yourself about your child’s legal rights, such as knowing that
children with autism are entitled to an ―appropriate‖ education.
Identify problems. Define and describe your child’s challenges clearly and concisely. If possible,
provide concrete examples.
Plan and prepare. Adequate planning prevents problems. Research special education laws and
regulations to answer your questions. Prepare for meetings by entering with an agenda, write
objectives for your child, and focus discussions on interventions and services for your child’s needs.
This can help prevent meetings from focusing solely on your child’s challenges.
Keep written records / notes. Because documents are needed for appropriate implementation,
parents must keep written records. We recommend tape-recording IEPs, too. If a statement is not
written down, it can be ―lost‖. Make requests in writing and write polite follow-up letters to documents
events, discussions, and meetings.
Ask questions and listen to the answers. Do not be afraid to ask questions, but make sure to
listen carefully to the answers. Remember to use ―Who, What, Why, When, Where, and How‖
questions to clarify responses and services that your child will receive.
Plan for the future. Always keep in mind your child’s future as an independent, and self-sufficient
adult. Plan what your child needs to be prepared for before leaving the school system. What services
and supports will your child need to meet this goal?
(Adapted from ―Advocating for Your Child – Getting Started‖ at www.wrightslaw.com)
Every child has individualized needs. Your child is no different. One goal in this
program is to assist with brainstorming what will provide the most benefit to your child.
Some accommodations benefit many children with ASD by providing
opportunities to successfully interact with peers in social situations. Possible school
accommodations for your child include:
One-on-One Aide
Aides provide assistance for behavior management and can assist with
autism-related interventions implemented at school.
Live Social Coaching
At school, an aide or other school personnel can help your child learn
fundamental of appropriate social interactions by helping him/her prepare for
peer interactions right before an unstructured social event requiring
spontaneous social communication (such as lunchtime or recess).
Peer Buddy
Two to four friendly peers of the same gender may be trained to invite
your child to engage in an enjoyable activity during lunch or recess a few times
a week. This can serve as the basis for learning to interact with peers ―the right
way‖—and can sometimes be the basis of a true friendship, too.
Games Leader
Children with ASD can learn to take the perspective of others by acting as
a playground assistant, games leader, tutor or buddy for younger children. Of
course they require ongoing ―training‖ and feedback to become increasingly
independent and competent in this role. Perspective taking is a key skill children
with ASD lack which contributes to their difficulties in relationships with others.
What are some of your child’s other needs at school?
What services may accommodate these needs?
Parent Module: IND
Encouraging Children’s Independence
Background
Most children with ASD have significant adaptive deficits (Liss, Harel, Fein, Allen, Dunn,
Feinstein, Morris, Waterhouse, & Rapin, 2001; Volkmar, Sparrow, Goudreau, & Cicchetti, 1987).
These deficits may be related to the fact that about 90% of children with ASD are unable to live
independently as young adults.
Children develop self-confidence when they are able to do activities that other children their age can
do. This enhances self-esteem and increases feelings of control. In contrast, children feel incompetent
and anxious when they have not mastered age-appropriate adaptive skills. Thinking towards the future,
basic self-help skills as well as self-confidence and feelings of control are needed for successful
development into young adulthood and independent living. It is important for parents to assist in the
development of adaptive skills that facilitate independent functioning in children with ASD.
Goals
1. Explain the importance of developing independence
2. Plan on 3 self-help skills for the child to begin doing independently
3. Teach parents 2 communication skills: respecting a child‘s struggle and giving choices
Preparations
Be sure to read the ―Autonomy‖ chapter prior to the session
Review the Vineland Adaptive Behavior Scales (Self-Care) and Skills of Daily Living Checklist for
self-help areas that should be emphasized
Materials
Self-Help Skills handout
Five Tips for Parents handout
Building Self-Confidence handout
Homework Assignment handout
Self-Help Skills Diary handout
―Encouraging Autonomy‖ chapter
Session
WITH PARENTS ALONE (40 MINUTES)
1. Inquire about parents’ completion of homework:
Briefly inspect the Behavior Record Form and screen for unusual or extreme child symptoms. (Note,
for future reference, how the parent responded to the child‘s anxious behaviors.)
2. Introduce purpose of module:
Explain that an important role that parents can play in helping to improve their child‘s anxiety
problems involves helping the child to become more independent. Refer to the Cognitive Behavioral
Therapy sheet from Session 1, and remind the parents that children can build their self-confidence by
engaging in self-help skills independently. This can help children feel mature and confident.
3. Emphasize the importance of helping children develop self-help skills:
Initiate a conversation about the value of developing independence in self-help skills. Make the
following points:
Children with ASD have about a 90% chance of not living fully independently as young adults
according to a variety of research studies, such as Sir Michael Rutter‘s study in England.
One feature of ASD that makes it hard for youth to function independently is the lack of ―self-
help skills.‖ These are the skills of daily living such as dressing, bathing, preparing food,
managing personal belongings, getting around in the community, and engaging in day-to-day
activities safely so that there is not a need for constant monitoring of the individual. Youth with
ASD have substantial deficits in self-help skills—these deficits are partly due to ASD itself (poor
motor coordination; poor organization).
But oftentimes youth with ASD have many self-help skills that they ARE already capable of
doing for themselves—or would be capable of with just a little teaching (not full-blown
occupational therapy). But they have fallen into a rut of having things done for them.
Paradoxically, however, doing so few things for themselves also makes children feel helpless and
dependent, which generally increases anxiety and clinginess.
In planning for an independent adulthood, it is never too early to begin mastering and USING
self-help skills for children with ASD.
Moreover, the double-benefit of developing such skills is that they increase children‘s confidence
and self-esteem, and tend to reduce anxiety and feelings of helplessness/dependency.
Personalize for the family: Refer to specific self-help behaviors that you know that the child does not
typically perform, based on parents‘ report or your own observations:
―Self-help skills include things like choosing clothes, grooming independently, etc. (choose relevant
examples). We have found that it can be very helpful for parents to encourage their children to
engage in these tasks without help. Over the course of our program, we‘ve seen this lead to increases
in self-confidence, and more courageous behavior in many children.‖
4. Identify 3 self-help skills to target:
Present the Self-Help Skills worksheet to the parents. Propose that this week, the child should be
encouraged to engage in 3 age-appropriate self-help skills that s/he does not normally perform
independently (i.e., needs a parent‘s help with). Encourage the parents to review the list of
examples on the Self-Help Skills worksheet.
Therapist Note: It is important to distinguish between what the child is capable of doing and
what s/he actually does. Many parents state that their child is capable of certain behaviors (e.g.,
independent bathing), but when questioned further, parents acknowledge that in practice they still
assist with part of the task (e.g., helping the child out of the bath / wash hair). Priority should be
given to the more private self-help skills, if relevant (i.e., dressing or bathing).
Review the 5 ―tips‖ on the worksheet with the parents.

5. Prepare parents for the possibility that children may resist new self-help skills:
Children may resist changes in the daily routine, especially if they perceive doing self-help skills as
a ―chore‖. The goal is to have the child do the tasks without providing help, even if the child
struggles. Suggest that there are two useful ways of responding to problems that arise as the child
tries to perform these tasks: respecting the child‘s struggle and giving choices.
6. Showing respect for a child's struggle and giving choices:
Pass out the Building Self-Confidence handout. Note that ―respecting a child‘s struggle‖ helps
children master new skills; it involves waiting patiently and giving children time to figure out their
own solutions.
With respect to ―giving choices‖, the choices do not always have to be significantly different from
each other—it is the feeling of having a choice that helps (e.g., ―Do you want to wait 1 minute
before starting your bath, or would you prefer 2 minutes?‖). Discuss how even small choices give
children a sense of control that can be very helpful.
7. Trouble-shoot the self-help skills task with the parents:
Ask the parents how they think their child will react to being asked to do this task. Will any of the
3 self-help tasks be especially hard for the child to perform independently?
Have the parents describe what they imagine their child would do and say if s/he was resistant or
having difficulty with the tasks. Take the role of the parent in responding to the child in these
situations. Then, switch roles.
Explore the parents‘ affect and difficulty with using the techniques after the role-playing. Inquire if
the parent‘s emotional reactions to struggle or resistance in the child would make it difficult to
―respect the child‘s struggle‖ and wait patiently? Empathize with the parents‘ reactions.
8. Plan for the conversation with the child:
Mention to the parents that an important part of starting the child on his/her new self-help skills is
initially presenting the idea to him/her. Plan on how to introduce the idea to the child when s/he
joins the therapist and family at the end of the session. It is important for the parent to be the one to
explain the new expectations to the child, in order for them to ―own‖ the exercise and for the child
to take it seriously. The therapist‘s role in the conversation is to scaffold and fill in extra details
that will help the child and parent understand and develop a specific plan of what to do in the
coming week.
WITH PARENTS AND CHILD TOGETHER (15 MINUTES)
1. Briefly explain the purpose of the exercise to the child:
―Your parents and I were just talking about things to work on at home this week. Remember how
we were talking about learning to do some things by yourself in this program? You know, like
learning how to calm yourself down without anyone‘s help when you‘re nervous? I also wanted to
see if we could all talk about making a plan to do some other things by yourself this week. Your
parents had some ideas about some things that they thought you would do a good job on without
any help.‖
Encourage the parents to explain the 3 targeted self-help skills to the child.
Therapist Note: It is important for the parents to ―own‖ some of the responsibility for suggesting
that the child work on the 3 specific self-help skills by having them describe these to the child
during the family meeting.
2. Encourage the family to plan on how the child will engage in the 3 self-help skills:
Ask the child if s/he feels that s/he would be able to do the 3 self-help skills without any help this
week. Help the family trouble-shoot if the child does not feel comfortable doing these tasks
independently. If the child cannot perform a skill without help, encourage the family to provide a
reduced level of help this week on this skill, with the goal of making the child independent
eventually. If the child is highly resistant to a task, switch to an easier task for now. Write the
agreed-upon 3 tasks on the Self-Help Skills handout.
3. Explain the Homework assignment to the parents.

Self-Help Skills
Think of three daily self-help tasks that your child could do independently. Here are
some tasks that other parents have successfully worked on with their children:
Age Norm Skill
4+ Toilet-trained during the night
5+ Brushing teeth
6+ Turning faucets on and adjusting temperature by adding hot or cold water
6+ Wearing appropriate clothing during wet or cold weather
6+ Tying shoes
7+ Bathing or showering and drying self independently
7+ Washing and drying hair (with towel or hair dryer)
7+ Using microwave oven for heating, baking or cooking (sets time, etc.)
8+ Putting own dirty clothes in hamper
9+ Making breakfast or a bag lunch
9+ Putting own homework in backpack
10+ Getting up in the morning without a reminder (using an alarm)
11+ Being responsible for own bedroom (neatness, decorations…)
12+ Arranging own transportation to certain places (i.e. bike, bus…)
The tasks should have to do with care of self and one‘s own space, not ―family
chores‖ like washing dishes or doing yard work.
The skills we will work on this week are:
1. _________________________________________
2. _________________________________________
3. _________________________________________
See ―Tips for Parents‖ on the next page!
Children who usually get help with these skills will need to learn how to perform
these tasks successfully. Talk with them about it this week. Here are some tips:
1. Point out that it's really important for kids to learn to do some things for
themselves—it can make them feel more grown up. It can also help to say
that you've been helping her/him do some things that s/he could probably do
by her/himself.
2. Consider finding a small reward that the child might want to work for. For
instance, if a child is able to start a bath and wash her hair by herself, she
may watch 15 minutes of TV after the bath before going to bed.
3. MOST IMPORTANT, once the child agrees to do the self-help tasks, do not
help him/her do it. Respect the child's struggle and allow him/her to try and
fail and try again. It is ok to provide occasional reminders at first. But try not
to do the task for the child.
4. If your child is having a hard time with a task, help him/her become
independent by reducing the amount of help you are giving him/her slowly.
5. Give your child a compliment each time s/he does a self-help task by
him/herself! This is a big accomplishment, and should be fun for everyone!
Anxious children often have low self-confidence and rely on others for help with
tasks that they could actually do by themselves. It helps children to become
more independent and learn that they can do a fine job on their own. There are
two principles for encouraging independence in children:
1. Show respect for the child's struggle. Children learn by trying, failing, and
trying again. Rather than doing their tasks for them, it helps to stay calm
and show children that it’s ok not to be perfect: "That can be very hard!" or
"You’re trying your best!"
You can give information that children may not have. "When you button
your shirt, it helps to start with the bottom button." When you hang back, it
gives children room to try again (and again, if necessary).
2. Give choices. Giving children several choices about how they might do a
task can make them more willing to try. For instance, with a child trying to
make a bag lunch by himself, you might ask, ―Well, do you think you want
peanut butter or tuna today?”
Choices can help when children are anxious, too. For instance, if a child is
feeling shy at a birthday party and asks to be taken home early, you might
say, ―We’re going to stay, but you could always watch the girls play on
that computer over there, or we could ask if you could join in the treasure
hunt. It’s up to you.‖
Be positive and firm about the choices. If your child thinks of a good alternative
choice, that is ok, too! If your child will not make a decision, it is best to wait and
use "planned ignoring". If you are patient, most children will eventually make a
choice!
Encouraging Independence Lesson
1. Read the ―Encouraging Autonomy‖ chapter. This is a very important
chapter for this program!!
2. Have your child practice 3 self-help skills. Each day, record on the "Self-
Help Skills Diary" any new self-help tasks which you encouraged your child to
do and how your child reacted.
3. Spread the word! If other important people in your child‘s life were not able to attend
the session, please mention the 3 self-help skills that your child is working on to
them—and explain that the child is doing these skills without any help this week.
Also, encourage them to read the chapter.
Remember to bring the Self-Help Skills Diary to the next session!
Directions: Each day, encourage your child to do the 3 self-help routines. Record how it goes on this form.
Example:
Behavior: I encouraged my child to tie shoes by herself.
My child's reaction: She tied them, but she forgot to tie a double loop. She showed me proudly.
My response: I praised her. I did not say anything about the double loop.
Date
I Encouraged My Child To Do
This Self-Help Skill
My Child’s Reaction
My Response To My Child
Parent / Child Module H
Developing the Exposure Hierarchy
Background
Children with excessive anxiety avoid facing feared situations and never learn that they can
handle the situations without excessive difficulty. The principle of exposure therapy is to gradually
expose a child to increasingly worrisome situations. Working through a ―hierarchy‖ of feared
situations helps reduce anxiety and allows children to try out new coping skills. Exposures are thus
instrumental for treating most child anxiety problems. Normally parents are involved in exposures
from the beginning. There is little time in this session to discuss new problems. Setting up a good
hierarchy with the family takes most of the session. Leave some time to discuss potential pitfalls
and help the parent think of useful response strategies. If parents are completely uninvolved with
the treatment, this session may be done with the child alone—although this is clinically
contraindicated.
Goals
1. Review homework
2. Teach principles of exposure to the family
3. Build hierarchy of child fears
4. Assign 1-2 low-level exposure tasks for HOMEWORK, and prepare rudimentary coping
plan
Preparations
Review intake report and progress notes for clues about possible feared situations for the
hierarchy. Make a preliminary list of 10-20 feared situations that range in intensity—these
should reflect all of the major anxiety symptoms (including social phobias, SAD, GAD, OCD,
panic, and simple phobia symptoms) experienced by the child. It is generally good to prepare
2-4 ―steps‖ for anxious situations that are moderately to highly fearful (e.g., for fear of the
phone: calling a trusted person like the child‘s grandmother; calling an unknown person like a
store clerk; calling an old friend; and, at the highest difficulty level, calling a new friend to
come over to play). These will be rated by the family in the session and serve as the ―roadmap‖
for the homework and the rest of therapy.
In preparing the preliminary list, keep the following key considerations in mind:
o Perfectionism (needing to be on time, needing to get all A‘s, never be tardy, etc.) is
targeted by the paradoxical intervention of having the child intentionally fall short of
perfection; for instance, being late, not turning in assignments, not getting help or
editing on homework, doing a poor job on homework or test items, etc. When
developing the hierarchy with the family, the question to ask is: ―How nervous would it
make you to… [e.g., be 5 minutes late to 1st period at school?]‖ There is no need to
justify the rationale for including such items on the list at this time, although parents
will need careful explanation of the need for such exposures when they are addressed
and practiced later in treatment.
o Worries (e.g., wondering if assignments will receive good grades; ruminating over
events of the day; worrying about keeping things tidy/clean/in order; concerns about
homelessness, etc.) are cognitive in nature but may or may not have a behavioral
expression too, which is easier to target in exposure. Behavioral exposures that can
target worries include tasks such as turning in poorly done assignments; intentionally
making a bedroom messy; or intentionally breaking a minor rule (e.g., not talking in the
library). Worries that cannot be addressed with such an approach (e.g., worries about
homelessness) can be addressed by focusing on positive thoughts (e.g., a variant of the
―C‖ step), as well as by engaging in behaviors other than exposure (such as
volunteering in a soup kitchen with a family member) that allows the child to ―take
action‖ in dealing with the worry. Sometimes imaginal exposures are appropriate for
worries, too (e.g., thinking of an abuser‘s face; drawing a bully‘s face; telling a story
about traumatic experiences that still induce worry; etc.) and can be included on a fear
hierarchy.
o Fears/avoided activities (e.g., dogs; playdates; talking to new people; going to school)
generally are treated by going into the feared/avoided situation, and exposure tasks are
directly worded in this way, e.g., ―Spending 10-15 minutes playing with other kids
from class at recess,‖ ―Going to school for 2 hours each day, with mom waiting in the
office.‖
o Obsessions and compulsions should be included but may need a special presentation.
Often the task is for the child to not engage in a compulsion; and to intentionally think
about an upsetting obsession. E.G., children may be asked to only ask a repetitive
question (a compulsion) about the same topic 5X per day; then 3X; then 1X; or to
spend less and less time per day organizing and cleaning an already tidy bedroom.
However, if there are frightening obsessions, children may need to think about them
intently without engaging in compulsions or other safety behaviors (e.g., think for 4
min about a disturbing image without praying; then, draw a picture of the image; then,
tell a story about it), or they may need to have a behavioral task to confront the
obsession (e.g., for obsessions about germs, children may need to use the bathroom
without washing hands; touch various dirty surfaces such as tabletops and doorknobs
without cleaning their hands; etc.)
o Some ASD symptoms may belong on the list. Failure to initiate social interactions may
not reflect anxiety/fear, but rather a lack of interest. Nonetheless, social interaction with
peers is a primary goal of this program. If this is an area of deficit, include it on the
hierarchy (e.g., eating lunch with kids from class; playing four-square with kids at
recess; inviting a kid from class over for a playdate). Some restricted interests and
rituals are not OCD but, rather, ASD symptoms. Nonetheless they should go on the
hierarchy (e.g., ―not playing with Thomas trains for 1 day,‖ ―not discussing the Beatles
for a 2-hour period once per day,‖ etc.).
Carefully review the Exposure Therapy Handout (parent handout in this module) in addition to
the therapist instructions below. This form includes the key ―tips‖ and ―parameters‖ and
includes important points to address with parents as well as ways of describing conditioning
and reinforcement to the parents without using jargon.
Materials
Parent Homework Handout
Exposure Therapy Handout
Feeling Thermometer sheet
My Fear List handout
Session
Therapist Note: Prepare the child for the format of the session: after the meeting with the parent
for 10 minutes, the entire family will meet with the therapist for the rest of the session to make
some plans together. The child and therapist will also meet 1:1 for about 15-20 minutes.
WITH PARENT ALONE (10-20 MINUTES)
1. Introduce the purpose of the module:
When people face their fears, they often learn that they can deal with situations better than they
expected, and they begin to get more confident—they stop avoiding these situations. This is the
single best way of reducing anxiety.
Pass out and review the Exposure Therapy sheet. Cover each point carefully. People
reinforce their anxiety when they avoid situations that they fear (personalize: i.e., school,
play-dates, speaking with unknown people, staying with a babysitter, etc.).
Use examples of gradual learning processes, e.g., learning to swim, to illustrate exposure
concept.
The child has learned a plan for how to cope with anxiety in situations—the KICK plan.
Using a hierarchy of feared situations, ordered from easiest to hardest, the child will practice
these coping skills during the treatment sessions and at home. Explain to the parent that the
child will begin with very mild situations and that this builds up confidence for facing harder
situations.
2. Introduce rationale for fear hierarchy:
Explain that the session will largely consist of setting up the fear hierarchy, which will act as
the guide for future sessions. Therefore, it is important for most of the child‘s fears to be
identified on the fear hierarchy.
However, IT IS ESSENTIAL THAT THE CHILD NOT KNOW THAT HE/SHE WILL BE
FACING THE SITUATIONS ON THE HIERARCHY! If the child knows he/she will face the
fears, the ratings of how difficult the situation is will be inaccurate. Inform the parent that
she/he must keep the purpose of the hierarchy ambiguous while they are forming the list.
WITH PARENTS AND CHILD TOGETHER (OR JUST WITH CHILD) (40 MINUTES)
1. Briefly review the content of the child’s session with parent.

2. Inquire about the family’s completion of homework (this must be done—briefly—to
teach the family the critical importance of homework). Offer brief consultation regarding
any modifications to the previous week‘s assignment, if indicated. This is a good time to
encourage the family to continue working on self-help skills, either increasing the child‘s
independence in the skills already identified, or adding additional skills for the child to work
on.
3. Set up hierarchy (this will take 20-40 minutes):
Explain that this is when the parents, child, and therapist will need to work together to make
an important list. Both parent and child will have a say in rating each situation.
Present and explain the Feelings Thermometer—it will be used to rate each situation in terms
of how anxious/nervous it makes the child.
Explain you‘ll be coming up with a list of different situations, some of which will only cause
a little anxiety, and some which will cause a lot of anxiety. Using the list of feared situations
you compiled before the session, explain that you have thought of some situations to rate
already; the family may have additional suggestions or permutations. Key pointers:
1. Situations should be very specific (e.g. "Getting into bed without help and staying in own
bed during night") rather than general ("going to bed").
2. Most situations should be things that the child is able to do on a frequent basis (e.g.
"Walking to school by self") not on an occasional basis (e.g. "Going to a friends birthday
party by self").
3. See the Preparations section, above, for additional suggestions on what to target and how
to word exposures of different kinds.
4. Use My Fear List and have the parents and child make ratings on the 0-10 point Feeling
Thermometer for each situation. Write each situation and each ranking on the My Fear
List form.
Therapist Note: It is important to note that children with ASD may not accurately report
their level of anxiety associated with an exposure. Be sure to obtain ratings from the parent
too, and give their input credence! This can be done by soliciting the child‘s rating first, then
turning to the parent and inquiring, ―Mom, what would you say about this situation? Do you
think a rating of 5 is pretty right-on?‖ However, in the end, it is the child‘s rating that must
be taken most of the time to maintain the alliance; ratings can be adjusted later after the
family leaves, if the therapist is fairly sure a rating should be higher or lower. The most
important thing is to have the hierarchy be fairly accurate in terms of what to target first.
4. Set up first home-based exposure:
Explain that in this program, children try the situations at the bottom of the list (the easier
ones), test them out, and if things go well, they move up to try situations that are slightly
more difficult.
Use examples of other gradual learning processes, e.g., learning to swim, riding roller-
coasters, etc. Try to personalize it by referring to normative developmental situations that the
child has mastered. Also, use self-disclosure, if appropriate.
―For instance, Andy, you‘ve told me that you used to be pretty nervous about going on all of the roller-coasters
at Disneyland. Well, that‘s pretty understandable to be nervous about those when you were in third grade! But, I
know that this year, you decided you were going to try it—and do you feel nervous about riding the rides at
Disneyland now? Is it hard to go on even bigger rides like Space Mountain now? See, after trying things that
make you nervous, you often become more confident and can do the things that you want to do! Well, that is the
purpose of this program: to take little steps on trying new things that still make you nervous, use your new skills
like the KICK plan, and test out if they‘re really so bad.‖
Use the metaphor of a scientist—―This program involves experimenting with how to do
things (feared situations) so that they can become easy. Each week, we will test out a few of
these—sometimes during the session, and sometimes at home for a HOMEWORK task.‖
Engage the family in a brief discussion to choose the first 1 or 2 home-based exposure(s).
Encourage the family to choose exposures rated 0-2 on the 0-10 scale.
The exposures should be ―easy‖ for the child; have a high probability of success; and
have some relevance to eventual goals the family wishes to reach.
Tasks that involve aspects of daily routines (e.g., answering the phone, going to school by
oneself) should be practiced at least once per day; tasks that are more out-of-the-ordinary
(e.g., watching a scary movie) may be done only once or twice during the week.
Emphasize the importance of the KICK plan for preparing for these exposure(s). Encourage
the child to develop a specific KICK plan for these exposure(s), and coach him/her through
each step of the plan.
Discuss in some detail what the child and the parents will do in the home-based exposure(s).
Plan specific dates and times. The child should feel fairly comfortable with the exposure or
else it may be too hard.
Remind the child that this is part of his/her HOMEWORK for the week and that s/he will
earn 2 points/stickers from the therapist next week for doing these tasks.
UCLA Anxiety Intervention Program—Rationale
Children’s fears are unrealistic: Children in this program tend to fear situations that are
actually ―no big deal.‖ For instance…
o Many children fear being away from their parents even when they are in safe places
such as school or at a friend’s house
o Others fear saying the wrong thing, so they avoid speaking in public or talking to new
people
o Some children have a lot of worries about day-to-day matters such as their
homework or quizzes at school (even if they are doing well in school), about always
being perfect and on-time, their appearance, etc.
Children need to experience feared situations head-on. It is never enough just to talk about
the safety of a feared situation. Children can use logic to understand something is safe, but
they will still experience anxiety until they see for themselves that they can ―handle‖ the
situation.
o As one example, children who avoid talking in public benefit from learning through
direct experience that they are not humiliated by others when they give speeches.
This experience allows children’s deep-seated beliefs about the ―danger‖ of the
situation to change: It is direct evidence—more than ―just an adult saying it’s okay.‖
―Don’t jump in the deep end of the pool first!‖ Although facing fears is the most effective
strategy for fighting fears, it has to be done carefully. You would never try jumping in the
deep end of the pool before learning if you can handle the shallow end, after all! Here are
several key principles about exposure therapy (facing fears):
o Take baby steps!!! Ideally, every feared situation is broken down into a series of
steps that the child can take to build up to the final target behavior. For example, for
a child who is very fearful of making phone calls, s/he might start by (1) calling a
trusted person like his/her grandmother… then (2) calling an unknown person like a
store clerk… then (3) calling an old friend… and, (4) at the highest difficulty level,
calling a new friend to ask him/her to come over to play.
o Once is not enough! In most cases, a single experience of any ―exposure‖ to a
feared situation is not enough to completely change a person’s fearful beliefs. People
might say to themselves, ―Oh I got lucky, but better not try my luck again!‖ That is
why multiple exposures to the same fear over the course of days and weeks is
critical.
o Use the KICK plan—this is what it is for! In order to feel more confident about facing
feared situations one baby step at a time, children should prepare and use a KICK
plan each time before trying a feared activity.
o Avoidance is not an option! Avoiding feared situations strengthens the child’s belief
that the situation is dangerous and increases the difficulty they will face in ―jumping
back in the pool.‖ When children attempt to face fears, they should not change their
minds and back out at the last minute—this can make matters even worse!!
FEAR LEVEL
FEAR RATING
(0-10)
SITUATION
HIGH
MEDIUM
LOW

Exposure Therapy Lesson
Have your child do his/her first ―exposure‖ tasks, as arranged with
the therapist. Remember, the more children practice exposure tasks, the
faster they will overcome their fears.
Spread the word! If other important people in your child’s life were not
able to attend the session, please discuss with them the reasons for
doing ―exposures.‖ Encourage them to participate in your child’s
―exposure‖ tasks this week.
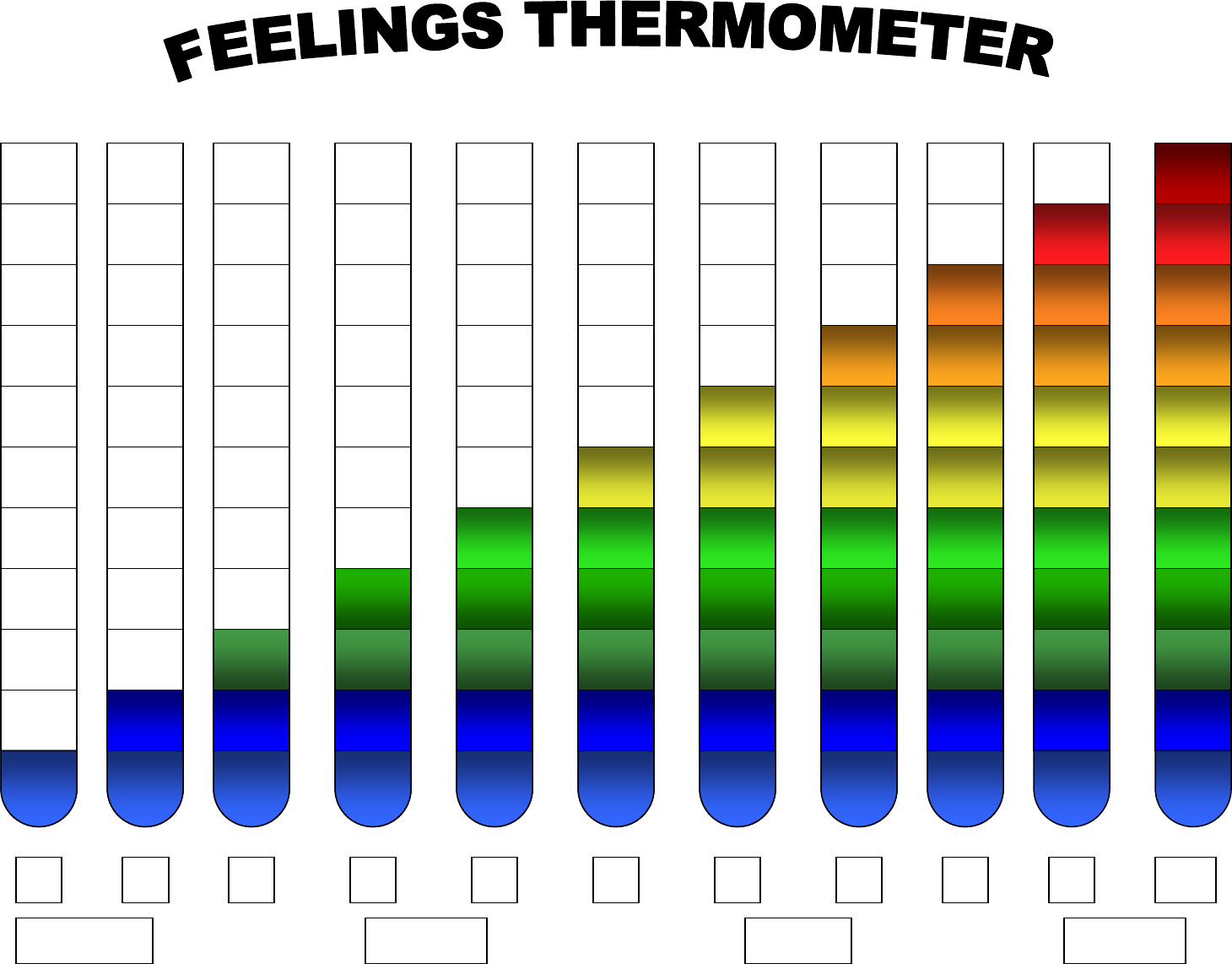
0
1
2
3
4
5
6
7
8
9
10
A little
Not at all
Some
Totally
Parent Module: EXP
Negotiating and Planning Exposures
Background
This session will be repeated 2-10 times in a typical course of CBT. Working up the exposure
hierarchy is an art form. The therapist and family must brainstorm on which exposures to introduce at
any given time. Children may begin to resist engaging in exposures as the exposures increase in level
of difficulty. Likewise, parents may begin to feel like the exposures are burdensome, or may feel
unmotivated to continue with the behavioral rewards plan. However, maintaining the exposures and
rewards is the key for therapeutic success.
Goals
1. Review Homework
2. Brainstorm on which exposures to introduce next, and how to conduct the exposures
3. Meet with (a) parent and (b) parent/child dyad separately to discuss exposures &
rewards/privileges
4. If necessary, introduce CALM & planned ignoring strategies for assisting with exposures.
5. Assign exposure tasks for HOMEWORK; link with rewards/privileges
Preparations
Review fear hierarchy in advance to develop ideas for what ―lines‖ of exposures still need to be
covered. If problems have been encountered be sure to consider ways to reduce the level of difficulty
of a line of exposures without allowing the child to completely avoid it.
Materials
Child‘s Fear List
―ABC‖ Handout, if needed
CALM handout, if needed
Planned Ignoring handout, if needed
Blank paper and pen to write down NEW exposure assignments and any changes to
rewards/privileges system
Session
Prepare the child for the format of the session: after the meeting with the parents, the entire family will
meet with the therapist for awhile to make some plans together, then the child will meet with the
therapist.
Therapist Note: It is sometimes better to begin with the child session depending on child‘s
energy level, attention, and ability to transition. Whatever the order of meetings, inform the
child so s/he is aware of the expected schedule.
WITH PARENTS ALONE (10-40 MINUTES)
1. Inquire about child’s functioning during the past week:
Keep brief, but screen for unusual or extreme child symptoms.

2. Present purpose of module:
The overarching goal is to move forward in the exposure hierarchy while ensuring the child is
getting maximal benefit by participating willingly and not engaging in excessive cognitive
avoidance (self-distraction, or dissociative types of responses) or behavior problems that s/he is not
habituating properly.
3. Review exposure homework.
Get parent report on past week‘s exposures.
Any problems with completing the exposures should be carefully analyzed: were they too difficult or
was there insufficient motivation? If the former, brainstorm an easier version of the exposures for the
coming week. In both cases, the use of more effective rewards/privileges should be discussed.
Consider whether any exposures can be ―taken off the list‖ of weekly assignments. Sometimes a
child has become habituated to facing a previously feared situation, or has simply stopped engaging
in a nonproductive ―habit.‖ The family should ―free up space‖ on the exposure list and rewards
program by removing such targets from future homework assignments. E.G., a child may now eat
lunch with a group of peers every day and enjoy it; s/he no longer needs external rewards or
encouragement to do this.
4. Brainstorm with parent about upcoming exposures.
It is crucial not to get stuck in any one ―line‖ of exposures (e.g., reducing handwashing; increasing
class participation) while neglecting important other treatment targets. Here are some
considerations in determining additional ‗exposures‘ to add:
a. By session 4-5, it is important to directly or indirectly ascertain the parent‘s highest
immediate priorities—anxiety related or otherwise. Some parents have social or behavioral
goals that are not related to anxiety per se, but still may be amenable to a hierarchical and
behavioral program (i.e., step-by-step plan augmented by rewards/privileges). For example,
a child with little interest in peer interaction still needs to engage in such interaction to learn
social skills, and many parents rightly view this as a high priority. Whatever the priorities
are, it is very desirable from the perspective of consumer satisfaction to include any such
parent goals—if there is a reasonable chance of success in the CBT timeframe—in the
hierarchy.
b. Review the Fear List. Think of the relative adaptive significance of the child‘s various
anxieties. Fear of participating in class is probably more important to focus on than fear of
heights, for example. Broaden the lines of exposures into key areas fairly early on so any
problems that may arise can be addressed before time runs out in therapy.
c. Keep in mind certain ASD-related behaviors (which may resemble anxiety) are unlikely to
be amenable to short term CBT. Language deficits are one example. Sensitivity to touch,
sound, and taste are another. Exposures can be tried for the latter type of symptoms (e.g., a
child who refuses to eat anything off a restricted menu of 10 items) but with limited early
success, must be moved to the side for longer-term parental follow-up after active CBT is
complete.
d. The goal is to get to the top of the hierarchy for each line of exposures. Do not stop with a
―middling‖ exposure that would ideally culminate in a more challenging one (e.g., sleeping
only part of the night in parent‘s bed rather than not at all; calling a friend but not asking
them over; asking 10 repeated questions a day rather than 2…).
Discuss any relevant details regarding the set-up for the upcoming exposures that should not be
discussed in front of the child (e.g., the parent may phone a peer‘s mother to double-check the peer
would like to have a playdate with the child before suggesting that a phone call be made.)
Address the rewards/privileges system to ensure the parent is following-through exactly as
planned, as close to 100% of the time as possible. Review Parent Session 5 for additional tips.
5. IF CHILD HAS ENGAGED IN NONCOMPLIANT/AVOIDANT BEHAVIOR (especially
around exposures): Present parents with strategies for dealing with child’s anxious behavior /
behavioral challenges:
Use the ABC handout to delineate the specific problems going on in an illustrative exposure via
functional analysis.
a. Suggest that fear/anxiety can often lead to anger, disobedience, aloofness, etc.
Explain how fear and anxiety can lead to a variety of ―negative‖ emotions and behaviors.
Personalize for the family: (a) If the parents have provided relevant examples in previous
sessions, refer to these specifically, and/or (b) If you have observed the child‘s coping responses
in-session refer to these specific behaviors. When personalizing for the family, BE SURE to both
describe the specific behavior AND relate that behavior to its function (i.e., how it represents a
―coping response‖ because it reduces anxiety).
―For instance, a child who is very scared of going to school may have angry outbursts in the
morning because that behavior ultimately lets the child stay home from school. It is helpful to
remind yourself that even though the child might be acting angry, this simply represents a coping
response that the child has adopted to deal with anxiety. The child is not being naughty—he is
just very nervous and dealing with the situation the best way he knows how. We are teaching him
new coping responses and the communication techniques that I am going to teach you today will
help him develop these skills.‖
b. Teach the CALM approach to dealing with children’s negative feelings:
[BRIEFLY] Explain that when children are feeling anxious or upset, they have very little
attention for dealing with conversation, logic, and suggestions. This is a result of how the brain
deals with fear—everything else gets ignored when the ―fear center‖ of the brain gets triggered.
Because of the way the brain handles emotions, fear, anxiety, and anger go away slowly but
surely. That is, fear shows a consistent decrease the longer a person stays in a feared situation.
Point out that in order to help children learn to manage their fear and anxiety, it is important to
be very calm and patient and not rush to react. Waiting patiently can provide the child with an
opportunity to use their new skills, such as relaxation. In other words, by giving the child time,
one can help the child develop new coping responses—the child needs to be able to practice
using his/her new coping skills when s/he is anxious without having problems ‗solved‘ for
him/her.

Pass out the CALM handout. Review the steps on the handout and discuss them. Special emphasis
should be placed on labeling feelings.
Acknowledge that many parents question the appropriateness of ―accepting‖ negative feelings
and behaviors. Address this in the following manner:
―Remaining calm and labeling feelings when children are upset has two benefits. It allows the
child to experience their bad feelings without ―adding‖ to the bad feelings—trying to talk kids
out of bad feels often make the feelings worse. It also provides the child with a model of calm
behavior. The parent shows s/he can cope with the child‘s bad feelings, and the child may
slowly learn from the parent‘s example.‖
Personalize this technique by describing how it would be used in a situation relevant to the
family:
―When Andy gets mad in the morning when you are trying to get him in the car, he is
experiencing anxiety—he is afraid of being separated from you. During these times it is
important to accept his bad mood (when he is yelling at you), label his feelings (e.g., ―you are
really scared right now‖), and show him that you are going to be patient with him—model for
him how to be ―calm‖. That will help him develop new coping responses because he is able to
learn about his emotions, your behavior will help calm him down, and eventually you both will
be able to more easily negotiate the morning routine.‖
c. Describe the Planned Ignoring technique:
Explain that a logical extension of the CALM approach involves not responding to certain
anxious behaviors. It is important to avoid giving too much attention when children are feeling
scared. This could cause the fear to become even worse by ―reinforcing‖ it with attention.
Pass out and discuss the Planned Ignoring handout with the parents. Emphasize that ―planned
ignoring‖ is a good technique to use in situations that the child has agreed to attempt but is now
avoiding. It is used after labeling children‘s feelings and demonstrating a CALM, accepting
attitude towards the child. Explain that if the child remains anxious after CALM responses,
planned ignoring can be used to quickly reduce (a) tantrums, complaining, and negative
comments, and (b) repeated questions and other ―irrational‖ dialogue. This will help the child
return to a lower state of anxiety.
Try to personalize this technique to situations relevant to the family. Several kinds of situations
well-suited to planned ignoring are:
a) A child sits in the car outside of school and cries, begging not to have to go to class. The
parent sits quietly and ignores the child‘s tantrum, waiting until the child has calmed down
and then reiterates the child‘s reward for going to school that day.
b) A child won‘t get in line at McDonalds to order himself a hamburger due to social anxiety,
and asks to go home repeatedly. The parent uses the labels the child‘s feelings, explains that
s/he expect the child to calm down before making any decisions, and then uses planned
ignoring.
c) A child repeatedly states that his homework is too hard and he can‘t do it and he hates it and he
needs help on every problem. The parent feels frustrated, acknowledges the child‘s anxiety,
and then excuses herself, explaining that she would like the child to try the next 20 problems
and she needs to take a ―time out‖ herself and will check on him in a while.
d. Warn the parents that these communication techniques may not feel natural at first:
Most parents feel awkward and unnatural the first times they try labeling feelings, waiting
patiently or ignoring, and not responding with advice, suggestions, etc. This is to be expected,
and most find that they have to try this approach with their children several times before it begins
to feel smoother and more ―genuine‖.
e. Assess the parents’ reactions:
Ask the parents how the child might respond to these techniques. If they express doubt or
disagreement, try to identify and respond to their objections. Refer to the ―Common Parental
Reactions‖ section below for guidance.
Ask the parents how they typically feel and how they respond to their child when the child
becomes anxious or worried. What emotions do they experience at these times? What do these
feelings make them feel like doing at these times?
Problem-solve with the parents about where they think they might run into difficulties with the
use of these techniques. What kinds of situations would make it hard to use these techniques?
How has the child responded in the past? Do the parents‘ own feelings in some situations with
their child make it difficult to act ―CALM‖?
6. If the parent is expressing reluctance or a motivational barrier:
Explain that the exposures and rewards system can take a lot of work to implement effectively.
Encourage parents to continue with the exposures and rewards program. Assure parents that the
child will begin to experience easier exposures and will come to not fear the stimulus in the
exposures.
“I understand that it is hard work to set up the opportunity for exposures. It sounds like you
have made great efforts in doing this. As you remember, we have started with easier exposures;
that is, exposures that ____ (child) has rated as not difficult. We will be moving up the list of
exposures and your child will start facing more difficult exposures. While it may not be difficult
for your child to move up the hierarchy, some children have shown some resistance. Some parents
have wanted to give up when their child started showing some resistance to the program, but I
want to caution you about this. These parents don‘t get a chance to experience the benefit from the
downhill slope that occurs when the child displays more self-confidence and less anxiety, and is
able to do more things on their own. The moral is to keep up with the exposures, even if ____
(child) begins showing resistance to them.”
Reassure parents that the child will habituate eventually to the exposure stimuli. Especially with
the low to moderately feared stimuli, rewarding the child will no longer be required. The child will
just naturally act more independently / less scared in situations with such stimuli.
Therapist should explain to parents, however, that there might be a time when the child is not as
eager or willing to face an exposure. This may occur when the child is asked to face a moderate to
highly fear stimulus. Explain to parents that this is when the behavioral rewards program is most
important. Sticking with the program is key. Parents can consult with the therapist to determine
what are reasonable levels of rewards for each exposure, based on what the child has put on his/her
rewards menu.
WITH PARENTS AND CHILD TOGETHER (10-20 MINUTES)
1. Briefly Review the content of the child’s session.
2. Inquire about the family’s completion of homework (this must be done—briefly—to teach the
family the critical importance of homework). Offer brief consultation regarding any modifications
to the previous week‘s assignment, if indicated. This is a good time to encourage the family to
continue working on self-help skills, either increasing the child‘s independence in the skills already
identified, or adding additional skills for the child to work on.
3. As a group, discuss upcoming exposures and rewards/privileges. Even though these have already
been arranged to some extent in the earlier parent session, the child must be aware and at some level
agree to the plans. Such agreement is often obtained by reviewing the rewards/privileges associated
with compliance.
Therapist Note: In some cases, most or all of the exposure planning should be done with just
the child, or with parent and child together. Variables affecting this choice are the child‘s
maturity, motivation, and sense of (and desire for) independence and respect; and the parent‘s
attitude about children‘s input (very laissez faire parents may have children who expect to be
consulted carefully.)
4. Homework. Using blank paper and pen, write down all exposure assignments and any changes to
rewards/privileges system.
Parents may track their child‘s behavior during exposures on the ABC form, if they have shown
interest in recording observations previously.
It is important to know what happened to make an exposure more difficult
to complete, to identify barriers, and troubleshoot how to make the next
exposure go more smoothly. However, while the exposure is taking place, it can
be hard to figure out what happened.
Let’s take some time to figure out the ABCs.
Antecedents – What happened right before the exposure took place?
How did you present the exposure to your child? How did your child
respond?
___________________________________________________________________________
___________________________________________________________________________
___________________________________________________________________________
___________________________________________________________________________
Behaviors during Exposure – What happened during the exposure?
How were you reacting to your child’s exposure? How was your child
handling the exposure?
___________________________________________________________________________
___________________________________________________________________________
___________________________________________________________________________
___________________________________________________________________________
Consequences – What happened right after the exposure took place?
What did you do? What did your child do? Did you provide the reward?
If so, when? If not, was there a reason?
___________________________________________________________________________
___________________________________________________________________________
___________________________________________________________________________
___________________________________________________________________________
Helping children cope with their feelings
Catch Your Breath (Pause to think or withdraw briefly to become calm
and plan a response)
Accept Negative Feelings (wait patiently and respond to angry or worried
comments with "hmm..oh...I see")
Label Emotions ("You seem really nervous")
Model Coping Skills (Show your child, through your behavior, how to
remain calm and collected)
Example:
C: "I need a minute to think about this, myself. Hold on a second, and then we can talk about this."
A: Wait patiently as the child complains about having to go to a social event. Express acceptance by
nodding and using active listening: ―Oh... I see...‖
L: "Gee, you seem upset right now. Your face is red and you look really unhappy."
M: Don‘t say anything! Just use your own coping skills to remain calm and keep in mind how
helpful it can be to your child to have a chance to cool down and work through the anxiety
on his/her own.
Attention. A basic but powerful principle is that PAYING ATTENTION to a
behavior INCREASES IT, and REMOVING ATTENTION from a behavior
REDUCES IT. When children engage in anxious behavior that gets a lot of
attention, the anxious behavior is more likely to happen again in the future.
Therefore, it is important to minimize giving attention to anxious behavior.
Planned ignoring. It is very important to provide acceptance and
understanding. But, it is also important to avoid giving too much attention
when children are feeling scared. This could cause the fear to increase. To
prevent this, label the child’s feelings in an accepting tone of voice (―You seem
scared…‖). Then, use planned ignoring:
1. If the child expresses fear or anger, do not respond frequently. Wait
patiently. Occasionally label the child’s feelings in a calm voice without
giving advice or suggestions (Child: ―You’re mean!‖ Parent: ―You sound
angry.‖)
2. If the child asks repeated questions (such as, ―You’re coming home at
nine o’clock, right?‖), answer the question once and then remind the
child that he/she already knows the answer—or, do not respond at all.
3. If the child demands to leave a feared situation, give a choice. Remind
the child that he/she needs to stay in or near the situation, but he/she
has several options (such as, ―You can either go into school, or wait here
in the car with me.‖)
Avoid reassurance, advice, suggestions, or lectures. When anxious,
children cannot be convinced that things will be ok. Also, children usually
ignore advice and suggestions when they are worried. Save logic and advice
for a time when the child is calm.
Consistency. Consistently applying this approach, like other parenting
techniques, is important. Try to use this approach at least 70% of the time.
(Adapted from Coping Kids Group Parent Workbook; Rapee, 1998)
Gather the ABCs
1) Have your child do his/her exposure tasks, as arranged with the therapist.
Remember, the more children practice exposure tasks, the faster they will
overcome their fears.
2) Track your child’s exposure tasks on the record form.
3) Spread the word! If other important people in your child’s life were not
able to attend the session, please discuss the new exposure tasks with
them and ask them to participate, if possible.
Directions: Record the ABCs for your child’s exposure tasks this week.
I am tracking these 2-3 exposures:
Example:
Antecedents (What happened before): I reminded Andy that he would be able to get to watch 10 minutes
of extra TV tonight if he asked his coach a question during basketball practice.
Behaviors During Exposure: He raised his hand and asked the coach a question.
Consequences (What happened after): At home, I let him watch 10 extra minutes of TV.
Date
Antecedents
Behaviors During Exposure
Consequences
Parent Module: REW
Rewards
Background
In order to promote the child‘s compliance with exposure therapy, a reward system is set
up. Setting up a good rewards system with the family often takes most of the session. Leave some
time to discuss potential pitfalls and help the parent think of useful response strategies.
Goals
1. Check in about initial exposures
2. Teach principles of reward to the family
3. Establish a list of highly motivating rewards
Preparations
Carefully review the Just Rewards Handout in addition to the therapist instructions below. This
form include the key ―tips‖ and ―parameters‖ for both aspects of this session, and includes
important points to address with parents as well as ways of describing reinforcement to the
parents without using any jargon.
Materials
Parent Homework Handout
Just Rewards Handout
Rewards Menu handout
Session
Therapist Note: Prepare the child for the format of the session: after the meeting with the
parent for 10 minutes, the entire family will meet with the therapist for the rest of the session to
make some plans together. The child and therapist will also meet 1:1 for about 15-20 minutes.
WITH PARENT ALONE (20 MINUTES)
1. Introduce the concept of rewards:
Pass out and review the Just Rewards sheet. Explain that doing exposure tasks (or
―HOMEWORK‖ / ―practice‖ tasks) is ―hard work.‖ They take a lot of concentration and
energy. Just as with other kinds of work, it helps if people have something that they can work
for. Use relevant examples: parents go to work to earn money; children do their schoolwork
to get good grades so that they can get into college. Doing work in this program is just the
same. We try to find things that children can work for that will give them extra motivation.
Review pros and cons of using rewards vs. privileges (or both) with the parent. It is often
easiest if rewards include the simple point system described on the handout. But for lower-
functioning or very young children, consider a specific daily reward (i.e., an extra treat, etc.)
for each time the child does an exposure.

Privileges may or may not need to have points assigned. If the child is earning the daily
privilege of computers/TV/etc. by doing his/her exposure tasks, then points are not needed.
But if the child is working up to earn a special privilege such as a favorite meal, a trip to the
park or other outing, etc. (something that would not be supplied on the same day), then points
are needed and the ―privilege‖ should be included on the child‘s reward menu.
Points should be arranged so that the child gets 1 per exposure. The points-per-reward
formula should be calibrated so s/he can earn 1 or more small/medium items on the rewards
menu each week if s/he does all of her assigned exposure tasks for the week. [Occasionally
older children can delay gratification and work up to a larger reward over the course of
weeks or months, but this is rare in ASD.]
Use Possible Reinforcers handout to help brainstorm rewards and/or privileges. Do not forget
that earning highly valued privileges that are currently taken for granted is an extremely
effective (and cheap and easy) means of encouraging compliance. Examples: Daily TV time,
videogame time, gameboy time, computer time, use of art supplies at home, time outside
skateboarding, playing with favored card games, engaging in games related to special
interests, etc.
MOST IMPORTANTLY, CHOOSE REWARDS THAT ARE HIGHLY REINFORCING
TO THE CHILD!
The child CAN and SHOULD help put together the rewards menu with the parent; however,
s/he may only earn rewards for which s/he has sufficient points—pleading/begging for a
highly desired reward cannot serve as a substitute for points!!
The parents should not negotiate with the child about rewards after the exposures. A specific
number of points (generally 1), or a specific reward/privilege, should be set in advance for
each exposure. This is the only reward/privilege that should be provided for successful
completion of the exposure.
Emphasize that when a child has done an exposure task, it is important to provide the reward
on the spot, if that was the agreement. Rewards are not given on the basis of whether the
child did the exposure task perfectly, but whether s/he tried hard. THE USE OF
IMMEDIATE REWARDS FOLLOWING EACH EXPOSURE IS ESPECIALLY USEFUL
FOR CHILDREN WITH ASD! Remember that children with ASD seem to have impaired
episodic memory. Therefore, providing a reward for an exposure after time has passed may
not allow the child to associate the positive salience of the reward with facing the feared
stimulus.
Inform the parent that we‘ll be talking about rewards/privileges with the child and will begin
compiling a list of items to work towards.
WITH PARENTS AND CHILD TOGETHER (40 MINUTES)
1. Briefly review the content of the child’s session.

2. Inquire about the family’s completion of homework (this must be done—briefly—to teach
the family the critical importance of homework). Offer brief consultation regarding any
modifications to the previous week‘s assignment, if indicated. This is a good time to encourage
the family to continue working on self-help skills, either increasing the child‘s independence in
the skills already identified, or adding additional skills for the child to work on.
Any problems with completing the exposure should be carefully analyzed: was it too
difficult or was there insufficient motivation. If the former, focus on an easier version of
the exposures for the coming week. In both cases, the use of more effective
rewards/privileges will be discussed in this session, which should increase motivation.
3. Introduce Concept of Rein forcers:
If rewards are being used, explain that the child will have the opportunity to earn ―stuff
you like‖ for doing some tasks in this program.
If only daily privileges (such as earning TV time) are being used, parents should be
involved in explaining this new expectation to children, so parental ownership and
authority over the policy is established, and to protect the therapeutic alliance.
Use Possible Reinforcers handout to help brainstorm rewards and/or longer-term
privileges, if indicated (that is, if the reinforcement system will involve more than just
earning daily privileges such as TV time).
Have the family develop some initial ideas about rewards/privileges on the
Rewards/Privileges Menu. Suggest the family think more about this at home and report
back to the therapist next session.
Help the family assign point values or arrange a reasonable ratio of rewards: exposures
based on the type of rewards/privileges that emerge on the menu (i.e., ―trivial‖ such as a
cookie vs. ―big‖ such as going to a restaurant or ballgame). Keep the general points-
formula noted above in mind.
4. Discuss with the family the rewards/privileges that could result from the current week’s
exposure tasks.
Set up 2-3 new exposure tasks, at an appropriate small increment above the previous week‘s
tasks (if there was success).
Help the child and parent understand how points/rewards/privileges will work for this current
week‘s assignment. Walk them through the logic so they understand what to expect. If you
are discontinuing the rewards chart you started with the child and transferring it to a parent-
based rewards system, explain this to the family, too. [This decision is made on a case-by-
case basis depending partly on whether just privileges are being used by the family (then
consider keeping the therapist-based reward chart)].
UCLA Anxiety Intervention Program—Rationale
Compensation for Hard Work: Facing fears takes a lot of concentration and energy. Children
are unlikely to think facing their fears is valuable or enjoyable (until they experience the
results first-hand!) Just as with other kinds of work, it helps if people have something that
they can work for. Therefore, to keep children’s motivation, enthusiasm, and participation at
a high level, they need some kind of compensation. Compensation for hard work is not a
―bribe.‖
Rewards and privileges are an essential part of CBT—they are ―compensation‖ from a child’s
point of view. Here are a few tips for making them work as a therapeutic tool.
a. They are used in the short-term for the duration of therapy to get children to face their
fears. The great thing about fears is that once children find out that a situation is safe,
the fear generally goes away permanently! Therefore, rewards are only needed to
encourage the child to face the situation until s/he feels comfortable doing so. They do
not need to be continued when a child’s fears subside.
b. Rewards and privileges are an extremely effective child behavior management tool—
more fun for everyone than yelling, arguing, etc. The same approach that we use in this
program can be used to encourage children to engage in any important educational or
social task that they are reluctant to try.
c. Choose rewards and privileges that are highly reinforcing to the child! It goes without
saying that a new pair of socks is unlikely to motivate most children to face their fears!
d. Follow-through every time!! Whatever the reward or privilege that was agreed-upon,
parents must try hard to come through on their end of the bargain, on time. If a cookie
was promised right after the child makes a phone call, for instance, it will not help
matters to wait until a trip to the store the following day to get the cookie!
e. Never give the reward if it was not earned. For example, if the reward is TV time after
school, children should not be allowed to watch TV until they do their ―UCLA work!‖
f. Rewards/privileges encourage children’s independence. Generally, if the reward system
is working (with the ―right‖ rewards/privileges on the list), child can make up their own
minds about whether to do their UCLA work or not. They will usually feel very motivated
to do it, but this provides them with the sense of having had a ―choice!‖
3. Distinction between rewards and privileges.
a. Rewards: Small items the child can earn for engaging in a specific behavior or set of
behaviors. Generally, give 1 point or sticker for each exposure task that is completed.
The ―rewards menu‖ will have a specific ―price‖ (in points) for each item, so the child can
earn a reward 1 or more times per week for doing what is asked of him/her.
b. Privileges: Can be even more effective than rewards! With this approach, children must
do their ―UCLA work‖ in order to earn the privilege of doing favored activities such as
watching TV or playing on the computer. It can also involve going special places, staying
up 20 minutes later than usual, having a favorite meal, engaging in a special activity
(e.g., baking a cake)—as long as the child only gets the privilege if s/he does his/her
―UCLA work.‖ Activities like this can be incorporated into the point/sticker system
mentioned above. Only include privileges you’re comfortable with!
Daily rewards & privileges
1.
2.
3.
4.
Medium rewards & privileges
1.
2.
3.
4.
Long term rewards & privileges
1.
2.
3.
4.
REINFORCEMENT IDEAS
1. Favorite dessert
2. Favorite meal
3. Special snack
4. Small toy
5. Sports equipment
6. CD’s/ITUNES Gift cards
7. Rent special DVDs
8. Attention
9. Praise
10. Special privileges
11. Private time in room
12. Special TV privileges
13. Stay up late
14. Have a friend over for dinner or for sleepover
15. Special time with one parent
16. Go to a movie
17. Go to a concert
18. Go on a special trip
19. Attend a sporting event
20. Camping
21. Traveling
22. Have a party
23. Use of TV for 2 hours during 1 day
24. Use of computer/video game/ipad/Wii for 2 hours during 1 day
25. Take a 30-minute walk with Mom
26. Play one-on-one basketball with Dad for 30 minutes
27. Special snack at bedtime
28. Bike riding with both parents for 30 minutes
29. Dad cooks a favorite meal
30. Get to have a friend over for dinner
31. Go to a favorite restaurant
32. Outing to Game Stop
33. Earn one point per day until earns five points to exchange for a movie
34. Earn one point per day until earns 7 points to exchange for a 1-day outing to the
beach/museum/amusement park
35. Mystery reinforcer
Note. Make sure the reward is motivating for the child and is realistic for the parent to give to
the child.
Rewards & Privileges Lesson
Have your child do his/her exposure tasks, as arranged with the
therapist. Remember, the more children practice exposure tasks, the
faster they will overcome their fears.
Think about rewards and privileges. What additional items should
be added to the Rewards & Privileges Menu? Please brainstorm with
your child about this; the therapist will help you set point-values for
each item next session.
Spread the word! If other important people in your child’s life were
not able to attend the session, please discuss with them the concept
of rewards & privileges.
Parent Module: SOC-C
Social Coaching
Background
This module is generally done concurrently with Child Module: SOC-C. Parents should
know that social skills training as traditionally done, is quite ineffective. ―Social coaching‖
overcomes the hypothetical nature of social skills training by prompting the child to engage in
specific positive social behaviors in actual social situations. This ―bottom-up‖ approach—similar
to learning phonics rather than whole words at a time—can help the child amass social skills
over time. S/he will be reinforced and naturally shaped by receiving positive feedback from
others based on the appropriate social behavior s/he is prompted to use.
Goals
1. Review Homework
2. Introduce the concept of mentoring to parent.
3. Teach parents how to conduct social coaching
4. Assign HOMEWORK
Preparations
Review fear hierarchy in advance to develop ideas for what ―lines‖ of exposures still need to
be covered. If problems have been encountered be sure to consider ways to reduce the level of
difficulty of a line of exposures without allowing the child to completely avoid it.
Materials
My Own Cartoon handout
Homework Assignment handout
Social Coaching handout
Child‘s Fear List
Blank paper and pen to write down NEW exposure assignments and any changes to
rewards/privileges system
Session
WITH PARENTS ALONE (30 MINUTES)
1. Inquire about the family’s completion of homework.
Briefly screen for problems experienced by the family. Briefly inquire if the child is continuing
to practice the new self-help skills.
2. Introduce purpose of module:
Many children with ASD have difficulty interacting with others in social situations. Planning
and preparing are keys to successful interactions with others. ―Social coaching‖ is a method

of ensuring that children have prepared for a social interaction, and planned for events that
might happen during the social exchange.
Social skills training as traditionally done is ineffective. Social coaching is a ―bottom-up‖
approach—similar to learning phonics rather than whole words at a time. This method can
help children amass social skills over time which will be relevant to the actual situations they
find themselves in. S/he will be reinforced by receiving positive feedback from others, which
will train him/her to use the same type of skill in future similar situations.
Give parents a copy of the Social Coaching handout.
3. Examples of social coaching that might be provided by parents when entering school
with the child in the morning (use as iconic examples to give parents the ―gist‖ of the idea of
social coaching; it may be best to include examples of situations parents have brought up, too):
1. In the morning, parents could help the child prepare to make a verbal greeting to a target
peer, plan for the specific wording s/he will use, the use of eye contact and a smile.
a. Later this can be expanded to include a compliment about the target peer (e.g.,
―That is a cool shirt,‖) following the greeting.
b. After establishing success doing this for awhile (one or more weeks), the child
can add ONE question for the child to prepare to ask the target peer after greeting
him/her in the morning.
c. Through the process of chaining, additional verbal behaviors can be slowly added
for this interaction situation via social coaching until fluency is attained.
Disclosures about personal interests or observations that are relevant to peers
would be added eventually, for example.
4. Teach parents how to conduct social coaching with their child:
The social coaching session should occur no more than 30 minutes before the real
conversation—but for some children, even a few minutes delay will be too long! Generally, the
more proximal, the better.
Step 1. Parents inform the child of the goal of the interaction (e.g., greetings, giving
compliments, making disclosures of personal interests, gathering information, etc.).
o It is important to do the coaching in a location that feels private enough to the
child so that s/he does not feel too self-conscious.
o It is important to remind him/her that s/he will earn rewards/privileges for trying
out the greetings / conversational items.
Step 2. Parents and child are to think in advance about what the child is going to talk about
during the interaction. If needed to assist the child, introduce the My Own Cartoon
handout to the parents. The child can draw a social situation and write in what they
would say next in the interaction.

Step 3. Child and parents practice / role-play the social interaction, so the child can have the
actual words in mind before s/he goes into a situation. Parents should be sure to include
basic non-verbal behaviors in the plan.
Parents are to take the role of the child first. Parents must provide direct modeling
of the words to use and key nonverbal behavior such as smiling.
During the practice, parents are to provide scaffolding to facilitate the interaction
if the child can‘t think of things that he/she should say (e.g., ―Well, do you want to
ask about the kinds of activities that I‘ve been doing? Something like that?‖).
Parents must note that it is important for the child to put the conversation in
his/her own words. This will increase the chance that the child will remember and
use the dialogue that has been practiced.
It is important that the practiced conversation shouldn‘t be hypothetical; it should
be very close to what might really happen in the conversation.
Step 4. When the child is ready, the parent prompts him/her to approach the target person/group
and engage in the planned social behavior on the spot.
As necessary, pull the child aside during the conversation to participate in more
social coaching. Ideally, social coaching should occur during natural breaks in the
conversation so the target children are not aware that social skills training is
occurring.
Step 5. Parents should be prepared to pull the child to the side and do more social coaching in
the middle of the actual conversation, preferably if there is a natural break in the
interaction. This will probably be necessary early on. For example, parents might notice
the peer is initiating social interactions and only getting a yes or no response from the
child. Parents should intervene to make sure that (a) the peer is still having a good time,
and (b) the child has a chance to re-enter the conversation and find a way to participate
even more.
5. Parents and therapist role-play social coaching.
First, the therapist must act as the parent and model how to provide social coaching to the
child. After this role-play, the therapist and parents should switch.
6. Develop a list of social coaching opportunities:
Inform parents that any situation in which children are not engaging in socially appropriate
behavior (e.g., greetings, initiating a conversation, asking questions, etc.) may allow parents
for opportunity for social coaching. However, four situations are particularly likely
opportunities:
o Interacting with siblings at home
o Interacting with family members such as the other parent, grandparents, etc.
o Interacting with peers in the neighborhood
o School situations in the mornings (this should only be done with children whose
parents walk them into school)
WITH PARENTS AND CHILD TOGETHER (15 MINUTES)
1. Inquire about the family’s completion of homework (this must be done—briefly—to
teach the family the critical importance of homework). Offer brief consultation regarding
any modifications to the previous week‘s assignment, if indicated. This is a good time to
encourage the family to continue working on self-help skills, either increasing the child‘s
independence in the skills already identified, or adding additional skills for the child to work
on.
2. Plan the mentoring experience as a family, if it is to occur this week:
Refer to Child Module: MENTOR (Parent-Child meeting section). Be sure to discuss
expectations and details of the meeting with a ―younger buddy,‖ if one is tentatively planned.
3. As a group, discuss and agree upon upcoming exposures and rewards/privileges. Assign
additional exposure tasks that ―move along‖ the current lines of exposure at an appropriate
level. Three exposure lines should be active at any one time. Agreement is often obtained by
reviewing the rewards/privileges associated with compliance.
Therapist Note: In some cases, most or all of the exposure planning should be done
with just the child, or with parent and child together. Variables affecting this choice are
the child‘s maturity, motivation, and sense of (and desire for) independence and respect;
and the parent‘s attitude about children‘s input (very laissez faire parents may have
children who expect to be consulted carefully.)
4. Homework. Using blank paper and pen, write down all exposure assignments and any
changes to rewards/privileges system.
Many children with autism spectrum disorders (ASD) have difficulty interacting with
others in social situations. Planning and preparation are keys to success! Social
coaching is a method of ensuring that children have prepared adequately for
conversations so they can begin to experience social success and ―learn by doing.‖
Use social coaching as frequently as you can!!
Steps for Social Coaching
Social coaching involves taking your child aside right before s/he enters a conversation
(or several minutes beforehand). Cover the following points:
1. Identify the goal of the interaction. Is this a simple ―hello,‖ giving compliments,
asking questions, joining a game? Tell her/him what s/he is trying to accomplish.
2. Brainstorm with your child about the specific topic, if needed. For instance,
what would be some good questions to ask? Be sure to give some suggestions—
s/he may not have a great idea of what is appropriate. It is good to say things like:
―Well, do you want to ask about the kinds of activities that he’s been doing?”
3. Plan and practice the social interaction. This will allow your child to have the
actual words in his/her mind before going into the situation. Be sure to incorporate
eye contact, smiling, and other ―nonverbal communication‖ in the plan.
First, take the role of your child. Act out what he/she is to do.
Have your child take a turn. Make sure that your child puts the interaction in
his/her own words. This will increase the chance that your child will remember
and use the dialogue that has been practiced.
4. Once your child has prepared a reasonable plan, prompt him/her to
approach the target person or group and engage in the planned social interaction.
5. Be prepared to pull your child aside for more social coaching during natural
breaks in the conversation.
Possible situations for social coaching:
Interacting with family members: siblings, grandparents, etc.
Interacting with peers in the neighborhood.
Play dates.
School situations in the mornings (if you walk or drop off your child at school).
Social coaching provided by school staff prior to lunch or recess activities.

Social Coaching
1. Identify opportunities for his/her first social coaching tasks, as
arranged with the therapist. Remember, the more varied opportunities
that children have to engage in positive social interactions, the more likely
they are to learn social skills.
2. Plan and practice the social interactions with your child. If helpful,
use the My Own Cartoon handout to help plan.
3. Reward your child for making a good try at doing the first social
interaction task.
4. Spread the word! If other important people in your child’s life were not
able to attend the session, please explain the reasons for doing ―social
coaching‖. Encourage them to participate in your child’s ―social
coaching‖ this week.
M
MY
Y
O
OW
WN
N
C
CA
AR
RT
TO
OO
ON
N
Directions: For each situation, develop a plan!
1) What is my GOAL? ____________________________________________________________
2) Plan the steps to take, coming up with what I’ll do.
3) Power up and do it!
1
2
3
4
G
GR
RE
EA
AT
T
J
JO
OB
B!
!!
!
Parent Module: PLAY
Facilitating Play-Dates
Background
Most peer social skills come through direct experience with one-on-one interactions with
other children (cf. Frankel, 1996). In modern American culture, a key institution in which such
interactions occur is the ―playdate.‖ Children with ASD paradoxically get less of this form of
social skills training than do typically developing peers, when in fact they really need more
experience with playdates to catch up to typical peers in social skills. They tend to faller further
and further behind in social skills over the course of years, as a result—the earlier this pattern is
reversed, the better the possible outcomes for the child.
Parents have a great deal of influence over the playdates of their school age children, up to
age 13 years or so. A main focus of this CBT program is the expansion of the child‘s current group
of friends. A modest operational goal for every child in this program is to develop one new
friendship with a peer by initiating a series of playdates with him/her. Crucially, these playdates
should be hosted at the child‘s house, so the parent may have maximal control over the tempo and
outcome of early get-togethers. See Background for Child Module: FRND for additional
discussion of the importance of friendships in ASD.
The PLAY module is usually done concurrently with Child Module: FRND. The parent
readings come from Good Friends are Hard to Find (Frankel, 1996). The therapist is advised to
review the entire book, but particularly the three assigned chapters. Parents should be given a copy
of the book or encouraged to purchase it.
Therapist Note: Although the term "playdate" is not always appropriate for children over the
age of 11, the principles of this session still apply to early adolescents (up to age 13). Try replacing
"playdate" terminology with "get-togethers" or "having friends over," when talking with the
family, if needed. If parents continue to use the term ―playdate,‖ it may be beneficial to actively
replace the term with more age-appropriate terms listed above, depending on the maturity level of
the child‘s peer group.
Goals
1. Review homework
2. Teach parents importance of developing regular play dates
3. Teach parents how to identify potential friends for play dates
4. Teach parents how to make play dates run smoothly
5. Assign play-dates and other exposure tasks for HOMEWORK; link with rewards/privileges
Preparations
Be sure to read the three chapters that are assigned to the parents prior to the session.
Carefully review the Play Date Checklist and think of ways it may apply to the child.
Materials
"Using Organized Activities to Find Friends‖ chapter
"Using the Telephone to Make Closer Friends / Having Fun Play Dates‖ chapter
Play Date Checklist
Homework assignment

Making Closer Friends record form
Child‘s Fear List
Blank paper and pen to write down NEW exposure assignments and any changes to
rewards/privileges system
Session
WITH PARENTS ALONE (30-40 MINUTES)
1. Inquire about parents’ completion of homework:
Provide the family feedback on the child‘s progress with exposures.
2. Introduce purpose of module:
This week the topic is finding ways to make the child develop closer relationships with friends.
3. Describe the rationale for helping children with friendships and play-dates:
Explain that friendships teach important social skills that will make relationships in
school, work, family, and personal life more rewarding and successful. Children
with ASD have great difficulty making and keeping friends. The most meaningful
opportunity for developing friendship skills and making friends is during 1:1 play-
dates. They are unique in giving children practice that they need to develop social
skills in a safe and protected environment.
Suggest that when children who like each other spend unsupervised time together in a play-
date, they get to know each other and find enjoyable activities to do together that enhance their
friendship. Repeated enjoyable play-dates help children become close friends and learn to trust
and rely on each other. This can provide the children with a valuable form of support from the
friend and help both children develop new ways of relating to others in a meaningful way.
It is important for children with ASD to learn to make NEW friends and not just rely on the
same old guard. There is always a need to make new friends throughout life. A goal of this
program is to help the family learn principles for the development of new friendship that can
be applied in the future (e.g., in a new school; during a camp; etc.) Furthermore, since
friendship circles tend to be very limited in ASD, most children have an immediate need for
more close friends—so this is more than just an exercise for most children, it can affect their
current social life positively.
4. Help parents brainstorm sources of new friends:
Ask parents how many friends their child has regular play-dates with. What are the play-dates
like and how frequent are they?
Mention that there are typical main sources of friends—school, the neighborhood, and extra-
curricular activities—but that these may have been tried. The sources which have yielded the
best results for new friends from our previous experience are (prioritized):
(1) previous successful play-dates (but children who have not come over for a long
time, perhaps due to inertia or schedule problems)
(2) school/class—either very empathic classmates, or perhaps somewhat younger
children at school. The therapist should conduct a school visit to get an idea of
possible classmates for this job. The teacher should be consulted re: his/her
recommendations, too.
(3) developmentally equivalent (not necessarily same-age) peers with HFA or ASD or
other disabilities. These kids may be accessed through Regional Centers, parent
support groups, etc. It is recommended that an email chain be arranged through
parent groups or the Regional Center, initiated by the parent (but s/he may need
help in identifying the right specific contact person) in which the child is described
(age, sex, developmental level, temperament, and SPECIAL INTERESTS/preferred
activities) and recommendations for a suitable peer friend with disabilities is
requested. It is easiest if the parent provides his/her contact information to pass
along to prospective families.
(4) involvement in specialized extra-curricular activities, summer programs, etc.
(5) family friends
(6) cousins (problem: blurry distinction between ―friend‖ and ―family‖)
Explain the key step to yielding play-dates from these places: ask the child if s/he likes the
proposed target child enough to ask her/him over. Sometimes, this step can be presaged by
asking the child which children s/he likes in settings such as school or community groups, if
such resources are the best place for a particular child with ASD to attain play-dates. Parents
may also observe the child in such settings and see whom s/he interacts with. Once a
potential playmate is identified who is acceptable to the child, arrange for a play date with
the other child using the approach described below.
Give parents ―Using Organized Activities to Find Friends‖ chapter.
5. Review extra-curricular activities as a potential source of friends:
Ask how many and what extra-curricular activities the child participates in. Provide feedback
that the main benefit of extra-curricular activities for children with ASD is the potential for
developing 1:1 friendships. If a given extra-curricular activity is a poor prospect in this regard
(i.e., few peers who live close by; wrong ages; everyone is too mature for the child with ASD
to develop a real friendship with) then it may not be a good use of the child‘s time—that is, it is
more important for the child to develop basic social skills than to learn to square dance (or
paint, play soccer, act, etc.).
It is ideal for the child to be involved in 1-2 extra-curricular activities with children of his/her
own age who live close enough to the child to be able to come over without much
inconvenience.
Not enough extra-curriculars? Suggest sports, art/crafts, or scouting (close by to child‘s house)
as good places to make play date contacts. Help trouble-shoot specific possible extra-curricular
activities for the child.
Too many extra curriculars (more than 2)? Explain that this is more than necessary for the
child to have possible ―contacts‖ with other kids, and the time they are spending on the
additional activities might be better spent in one-on-one play dates where closer friendships
can be developed.
6. Compile a list of possible peers available for play-dates:
Review the child‘s list of possible peers, based on the priorities established in point 4, above.
Encourage parents to come up with possibilities from their social network.
7. For all children, help parents plan for successful play-dates for new (and) existing
friends:
o Present the Play Date Checklist to the parents. Review the suggestions for successful play-
dates with the parents, and discuss skills or techniques with them in greater depth that they
do not currently use. Emphasize need for parent to:
1) host the play-date
2) review ―rules of a good friend‖ with the child prior to the playdate (as discussed with
the child in Child Module: FRND)
3) keep it brief initially (30-90 min?)
4) ban electronics until the end of the play date
5) listen to the progress of the playdate from a nearby room and politely intervene when
necessary—using social coaching, if needed (Parent Module: SOC-C)
Give parents copy of "Using the Telephone / Having Fun Play Dates‖ chapter (it appears to be
for preteens, but a lot of the advice is appropriate for ages 11-13, too).
8. Discuss the feasibility of a regular playdate schedule for the child:
Trouble-shoot with parent on how 2 supervised play-dates of 30-90 min. each could be
arranged starting this week. How might the parents need to alter their schedule to make it
feasible? (Weekend playdates are fine, too!) How might the child need to alter his/her schedule
to make it feasible? (E.G. by dropping excessive extra-curricular activities or reducing their
TV/videogame playing—which could be used as contingent rewards instead).
If parents comment on the amount of work involved in this, remind them that it is
unfortunately a major time commitment early on to help children with ASD develop the skills
and resources they need. Remind parents of the crucial importance of playdates for children
with autism.
WITH PARENTS AND CHILD TOGETHER (15 MINUTES)
1. Inquire about the family’s completion of homework (this must be done—briefly—to
teach the family the critical importance of homework). Offer brief consultation regarding
any modifications to the previous week‘s assignment, if indicated. This is a good time to
encourage the family to continue working on self-help skills, either increasing the child‘s
independence in the skills already identified, or adding additional skills for the child to work
on.
2. Plan the phone call / play date:
Refer to Child Module: FRND (Parent-Child meeting section), which is integrated here.
With compiled list of peers from child and parents, discuss peers who may be available for a
play-date. Once a peer is selected to be called, the therapist and child can review with the
parent what the child will do during his/her call to the play-date peer.
Make the parent aware of the ―rules of a good friend‖ (good host behavior) from
the FRND module, as well as the importance of the child ―playing detective‖ on
the phone to determine what the guest would like to do on the playdate (see
FRND module)
Remind child and parent that child is to practice smiling.
Therapist Note: Characteristics of an ideal initial play date would include, (1) a peer who
will say ―yes‖ to a play-date, (2) a peer who has previously have a play-date with the child,
but quite a while in the past, (3) the child with autism is excited to get together with that peer.
Exclude peers who frequently get together with the child.
3. As a group, discuss and agree upon upcoming exposures and rewards/privileges. Assign
additional exposure tasks that ―move along‖ the current lines of exposure at an appropriate level.
Three exposure lines should be active at any one time. Agreement is often obtained by reviewing
the rewards/privileges associated with compliance.
Therapist Note: In some cases, most or all of the exposure planning should be done
with just the child, or with parent and child together. Variables affecting this choice are
the child‘s maturity, motivation, and sense of (and desire for) independence and respect;
and the parent‘s attitude about children‘s input (very laissez faire parents may have
children who expect to be consulted carefully.)
4. Homework. Using blank paper and pen, write down all exposure assignments and any changes
to rewards/privileges system.

If the playdate is at my house, then I’ll stick to:
The Rules of a Good Host
1. Always let the guest choose all the games
2. Always stay with the guest
3. Give compliments (say nice things to guest)
If I‘m invited by a friend, then I’ll stick to:
The Rules of a Good Guest
1. Always go along with the host, unless given
a choice
2. Always stay with the host
3. Give compliments (say nice things to host)

Interacting with close friends is the most important ―social skills training‖
experience for kids, and children develop friendships by having one-on-one
playdates. Children with close friends feel more confident and accepted.
Parents of school-aged children can help! Review the following questions
about playdates and consider strategies that you have not tried yet.
Do you usually:
____Host the playdates, in order to have more control over how playdates
turn out?
____Review “rules of a good friend” with your child just before the playdate?
____Set up an incentive for appropriate behavior just before the playdate?
____Ensure that the children agree on at least one activity to do BEFORE
the playdate occurs (e.g., while talking on the phone)?
____Keep playdates short (1-2 hour) early in a friendship, so boredom and
bad feelings are prevented?
____Ensure that siblings are busy so they don’t join in the playdate? It is
important that most playdates remain one-on-one.
____Clean up and set up the place where the agreed-upon play activity will
happen (such as a clear spot on the bedroom floor for a board game)?
____Make TV and videogames off-limits (or save the last 30 minutes for TV /
videogames to use as an incentive for appropriate behavior)?
____Make yourselves available to intervene if there is a big problem, but
otherwise let the children play separately from you?
____Check with the child on how playdates go? His/her feedback will help
determine if it is worth it to try another playdate with the same child.
―Making Closer Friends‖ Lesson
1. Read "Using the Telephone" and / or ―Using Organized Activities‖
chapters, as assigned by the therapist. We will discuss the chapter in
the session next week.
2. Arrange 2 play dates this week! Try to host the play dates and have
them last at least an hour. Use the Making Friends Record Sheet form to
track how the play dates went.
3. Practice facing fears! Have your child practice their other exposure
task(s) as arranged with the therapist.
4. Spread the word! If other important people in your child’s life were not
able to attend the session, please encourage them to do the reading, as
well.
When your child has a get-together or playdate, record how it was set up and how
it went. This week take notes on the outcome of one get-together.
Example of the Kinds of Notes to Take
―I helped my child identify a friend by: Noticing my son talking to a boy named Brian in his karate class. I
asked him if he‘d like to invite Brian over and he agreed.
The activity my child arranged in advance to do with his/her guest was: Play ―Monopoly‖.
This is what happened during the playdate: They played Monopoly for an hour and seemed to have fun. I
gave them a snack, and I took Brian home.‖
PlayDate Notes
Date and place of playdate:
I helped my child identify a friend by:
The activity my child arranged in advance to do with his/her guest was:
This is what happened during the playdate:
Parent Module: APPROP
Socially Appropriate Activities and Appearance
Background
Parents may not be cognizant of the developmental changes in games and topics engaged
in by typically developing peers. Moreover, parents of children with ASD may not be aware of
developmental changes in appearance and dress. Therefore, obsessional topics and behaviors
engaged in by their child with ASD and his/her style of dress might seem socially appropriate to
parents. However, this can be far from the truth. In fact, as children with ASD age, they may not
change or modify the types of activities they use to entertain themselves (restrictive and
repetitive interests) nor change their appearance (due to a lack of perspective taking). While this
may not appear significant at younger ages, as the child reaches later childhood and adolescence,
participating in activities not age appropriate can negatively affect social relationships.
The purpose of this session is to expand the child‘s interests, increase his/her ability to
engage other children by playing games that are socially and age-appropriate, and modify the
child‘s appearance (e.g., style of dress, haircut) if necessary to reduce social stigma. Such
changes may potentiate friendships for the child with ASD.
Pay careful attention to the ―parental concerns‖ and suggested therapist responses in point
2 of the session outline, below. This module often elicits predictable reactions from parents that
are well intentioned but fail to take into account the big picture (i.e., the child‘s biggest problem
is poor social adjustment and all concerned wish to change that, over and above other goals.)
Therapist Note: Previous to the session, the therapist should think of 1-3 appropriate activities
for the child, given his/her age-group and community, as well as consider any significant
abnormalities with the child's appearance that could interfere with peer relations. Since activities
should potentiate the child‘s ability to have successful play-dates, the game will generally fall
into one of two categories: (1) indoor games with rules, such as board games, or (2) outside
games with rules, such as sport games (e.g., basketball, croquet, badminton).
Goals
1. Review Homework
2. Present rational for ―socially appropriate activities and appearance‖ to parents
3. Plan strategies for increasing age appropriate activities
4. Present potential modifications in child‘s appearance
5. Assign exposure tasks for HOMEWORK; link with rewards/privileges
Preparations
Review fear hierarchy in advance to develop ideas for what ―lines‖ of exposures still need to
be covered. If problems have been encountered be sure to consider ways to reduce the level of
difficulty of a line of exposures without allowing the child to completely avoid it.
Materials
Child‘s Fear List
Blank paper and pen to write down NEW exposure assignments and any changes to
rewards/privileges system
Reducing Barriers handout
Session
WITH PARENTS ALONE (30 MINUTES)
1. Inquire about the family’s completion of homework.
Briefly screen for problems experienced by the family. Briefly inquire if the child is continuing
to practice the new self-help skills.
2. Present rationale for socially-appropriate appearance and activities:
As much as adults find it superficial and distasteful, part of increasing acceptance and
improving peer relationships in childhood is appearing like a typical kid (based on the
child's age and community norms). This includes the appearance of children and the
types of activities that they participate in.
Due to a lack of perspective taking, children with ASD oftentimes are unaware of the
effect of their appearance on their relationships, and are oblivious to subtle trends in
dress/appearance in their peer group.
Explain to parents that in playdates, children get to know each other and find enjoyable
activities to do together that enhance their friendship. To increase the likelihood of this
happening for the child with ASD, they may need to develop interest and proficiency in
activities that many other children in their community find enjoyable. Children with ASD
who are unaware of trends and standards may be reducing the likelihood of other children
befriending them.
Additionally, restricted and developmentally immature interests held by children with
ASD may bring on unwanted censure, teasing, and rejection from peers. Even if these
interests are maintained, they may need to be kept more private and not disclosed
indiscriminately.
Address parental concerns:
My child is an individual and I don‘t want to make him/her a conformist. The point is
not to take away the child‘s individuality, but rather to add some interests that give
them common ground with important people in their lives, namely, peers. The choice
is not between conformity and individuality. The choice is between affiliation and
isolation.
I believe s/he should be allowed to make his/her own fashion statement. In responding
to this point, try to take this line of reasoning to its logical limit and apply it to the
workplace: no one would last long working in an office if they dressed in a chicken
outfit, for instance. Then help the parent understand that the child is not making a
―fashion statement‖ along the lines of an artist or model—rather, it is his/her autism
that makes him/her incapable of recognizing social expectations with regard to dress
(and interests). Rather than assume s/he is consciously rejecting such expectations

and making a statement, it is much more realistic to assume that s/he is unaware and
needs the expectations brought to his/her attention explicitly.
There is nothing wrong with having unique interests. This is true. However, the
functional outcome of not also having some ―common‖ interests is social isolation
and rejection. It is important to challenge the notion that the child‘s eccentric
interests are an unassailable part of his/her personality. Often their interests are
―cute‖ and charming to adults, but they also reflect the child‘s disability, and must be
seen for what they are: impairing to successful peer relationships. The choice often
comes down to putting modest curbs on a ―cute‖ interest or not doing so and
accepting that the child is unlikely to make any friends.
3. Encourage parents to become aware of age appropriate appearance and behaviors:
Give parents a copy of the Reducing Barriers handout and review it with them.
There are various ways to determine socially appropriate appearance and activities: noticing
other children‘s appearance, listening to activity requests made by children over for a
playdate, talking with neighborhood parents and children, observing children of the same age
and gender at the child‘s school or after-school activities, asking the child‘s teacher, and
watching children‘s programming.
Assuming the therapist has specific suggestions for improvements in the child‘s appearance,
these can be discussed frankly with parents in a problem-solving manner (e.g., eliminating
high-waters from wardrobe, pushing socks down, untucking t-shirts, more modern haircut
[particularly one that would be easy to care for by oneself, e.g., for boys, a "buzz" or a
"step"/"children's cut"; and, for families with some financial resources, one or two new
pieces of clothing influenced by popular culture, such as skating or surfing culture). It is
important to elicit parent's feedback and ask questions using stems such as, "What do you
think about___" and making descriptive comments like, "I've noticed your son wears his
pants_______."
Discuss with parents the child‘s immature or eccentric restricted interests and their ill-effects
on social development.
o In a problem-solving manner, brainstorm modifications in activities (e.g., reducing
play with Pokeman and replace with Yu-Gi-Oh, Battleship, card games). Again, it is
important to elicit parent‘s feedback and ask questions using stems such as, ―What do
you think about _____‖ and making descriptive statements like, ―I noticed that your
son has continued to play with _____ for many years.‖
o Make the point that the child does not have to eliminate an eccentric interest. Rather,
s/he may need to learn to suppress discussing the interest in public, especially with
peers. S/he may also need to increase fluency with and willingness to discuss more
typical children‘s activities and interests with peers. Such relative decreases in
eccentricities and increases in common activities/interests form the basis of the
specific assignments that may be given to children for their homework.
4. Introduce appearance- and activity-related exposures to parents:
Brainstorm specific steps to take to slowly suppress display and discussion of immature/odd
interests and activities in public (e.g., not bringing toy trains to middle school any more;
restricting discussions about ―Beatles tribute bands‖ to the home setting with family
members only).
Brainstorm specific activities that are age- and/or socially appropriate for the child to be
introduced to (the ―replacement‖ activities) that will assist the child in playing with peers
during the child‘s playdates. In so doing, focus on activities that seem likely to be of interest
to the child, which would enhance his/her ―common ground‖ with peers in his/her
community.
Brainstorm specific changes in appearance that could be beneficial to social acceptance.
Therapist Note: The therapist must exercise caution when presenting the replacement
activities to parents; some activities considered standard in playdates between typically
developing children might prove too difficult for a child with autism to master (e.g., due to
impairment in motor skills; e.g., basketball). The therapist must realistically assess the child‘s
ability to learn and engage in the selected activities. The replacement activity must be attainable
for the child and facilitate the development of successful playdates.
WITH PARENTS AND CHILD TOGETHER (15 MINUTES)
1. Inquire about the family’s completion of homework (this must be done—briefly—to teach
the family the critical importance of homework). Offer brief consultation regarding any
modifications to the previous week‘s assignment, if indicated. This is a good time to encourage
the family to continue working on self-help skills, either increasing the child‘s independence in
the skills already identified, or adding additional skills for the child to work on.
2. Present appearance- and activity-related discussion to child.
The parents and therapist should attempt to take the role of a fashion consultant "to the
stars"—i.e., being very respectful and indirect. It is most useful for adults to tell anecdotes
about specific kids they have known who changed their appearance in some positive way,
had positive results come from the change, and then note that the ASD kid looks a lot like the
anecdotal kid; "I was thinking that that kind of haircut would look really cool on you, too!"
Another approach is to say, ―A lot of kids your age are getting this/that, it's cool!!‖ A third
approach is to link the suggested change with the child's cartoon heroes: ―This will help you
power up and be like _____!!‖
A similar approach should be taken when talking about new activities. For example, an adult
can say, ―You know, I know a bunch of kids who are totally into Pokeman and they just told
me about how they tried Yu-Gi-Oh and really thought it was cool and found a bunch of new
friends who liked Yu-Gi-Oh! Now they all play together after school. You know, that game
would be totally fun to play with the kids at your school!‖ Another approach is to say, ―A lot
of kids at your school are playing with Yu-Gi-Oh nowadays, it‘s really cool!!‖ A third
approach is to link the suggested change with the child‘s cartoon heroes.
It is necessary to have come up with a couple of ―appearance‖ and ―activity‖ items that could
be presented to the child, and then give them a choice, if they seem resistant to the change.

Finally, a back-up plan may be that the parent tells their child that they are going to just ―try
it‖ and then provide the child with a small reward after the attempt.
3. As a group, discuss and agree upon upcoming exposures and rewards/privileges. Assign
additional exposure tasks that ―move along‖ the current lines of exposure at an appropriate level.
Three exposure lines should be active at any one time. Agreement is often obtained by reviewing
the rewards/privileges associated with compliance.
Therapist Note: In some cases, most or all of the exposure planning should be done
with just the child, or with parent and child together. Variables affecting this choice are
the child‘s maturity, motivation, and sense of (and desire for) independence and respect;
and the parent‘s attitude about children‘s input (very laissez faire parents may have
children who expect to be consulted carefully).
4. Homework. Using blank paper and pen, write down all exposure assignments and any
changes to rewards/privileges system.
R
Re
ed
du
uc
ci
in
ng
g
B
Ba
ar
rr
ri
ie
er
rs
s
t
to
o
F
Fr
ri
ie
en
nd
ds
sh
hi
ip
p
Parents play an important role in reducing the ―external‖ barriers to forming friendships among
children with autism spectrum disorders (ASD). External barriers can include the way that
children dress, toys they play with, and interests they discuss.
Dress
At the beginning of a friendship, peers must want to get to know your child better. Several factors
will determine whether peers will be interested in him/her. Unfortunately, one factor includes
dress. Believe it or not, how a child dresses can determine whether peers will have an interest in
getting to know him/her better or not.
Barrier: Children with ASD who are unaware of trends and standards in contemporary dress—
based on age and community norms—may reduce the likelihood of other children befriending
them.
Play and Conversational Interests
At school and during playdates, children naturally seek common interests that will help a
friendship develop. To increase the likelihood of success, it is extremely helpful to develop an
interest and proficiency in activities that other children value.
Barrier: Unusual or immature interests held by children with ASD may bring on teasing and
undermine friendship. Everyone is entitled to their own interests. However, adding some more
typical interests may help children find common ground with their peers.
Reducing Barriers
Become aware of age-appropriate dress and interests. What are the trends in dress, play, and
activities among your child‘s peers? It does not make him/her a ―conformist‖ to learn more about
these trends and see if a few of them catch his/her fancy. This can help your child have more in
common with potential friends. Especially important will be interests and activities beyond TV and
videogames, which tend to be ―dead ends.‖ Focus on dress style, interests, and activities that seem
likely to fit your child‘s style and would enhance his/her ―common ground‖ with peers in the
community.
Do his/her unusual or immature interests need limits? While it is not realistic to eliminate a
―special‖ interest completely, children with ASD benefit from guidelines. When is the right time to
discuss a special interest? With whom should a topic not be discussed (for instance, with peers)?
Children with ASD benefit from direct advice, even if it seems to be a ―touchy‖ or ―personal‖
topic. Help him/her plan to keep his/her unusual/immature interests and activities private
(restricted to conversations at home). Examples:
A middle school boy is advised to keep his ‗Thomas the Tank Engine‘ trains at home,
rather than bringing them to school in his backpack each day
A 5th grade girl is asked to restrict her conversations about ―Beatles tribute bands‖ to the
home setting with family members only
Parent Module: MENTOR
Mentoring
Background
This module is usually conducted in the same session as Child Module: MENTOR. It
should be noted that mentoring actually has two distinct potential benefits for children with
ASD. First, mentoring necessitates taking another‘s perspective, and may lead to the
development of theory of mind. But a second, less self-evident benefit may be the development
of an actual friendship for both parties. Often younger children—even those with disabilities—
are at the same social-developmental level as children with ASD. Although a relationship like
this must start out as ―mentoring‖ to maintain the older child‘s self-esteem, a relationship of this
sort is an implicit set-up for potential movement into the realm of friendship and mutually
enjoyable interactions and activities. Age of the child with ASD is a consideration: for many
children, particularly those who are hyperactive, cognitively impaired, or inappropriate, this
approach is unlikely to be helpful under the age of 9-10.
Goals
1. Review Homework
2. Introduce the concept of mentoring to parent
3. Brainstorm possible sources of a child to be mentored
4. Teach parents how to facilitate mentoring activities
5. Assign exposure tasks for HOMEWORK; link with rewards/privileges
Preparations
Review fear hierarchy in advance to develop ideas for what ―lines‖ of exposures still need to
be covered. If problems have been encountered be sure to consider ways to reduce the level of
difficulty of a line of exposures without allowing the child to completely avoid it.
Materials
Mentoring Handout
Supervision Hierarchy Handout
Child‘s Fear List
Blank paper and pen to write down NEW exposure assignments and any changes to
rewards/privileges system
Session
Prepare the child for the format of the session: After meeting with the parent for 30 minutes, the
therapist will meet with the child. Finally, the therapist will ask the parent to come back in the
room to make some plans at the end of the session.
WITH PARENT ALONE (30 MINUTES)
1. Inquire about the child’s exposures over the past week.
Ask how the child responded to exposures, and the effectiveness of the rewards system.

2. Introduce purpose of the module:
Review psychoeducation on ASD from Parent Module 1 with parents; in particular, review
children‘s inability to take another‘s perspective as a core symptom of ASD. Explain that
theory of mind underlies appropriate social communication. Deficits in theory of mind limit
children‘s ability to understand emotions and experiences of others and respond
appropriately. This can have deleterious effects on social relationships.
Discuss idea of and importance of mentoring:
Providing opportunity for the child to take another person‘s perspective by trying to be a
positive role model for someone else.
A second, less self-evident benefit may be the development of an actual friendship for
both parties. Often times, younger children—even those with disabilities—are at the
same social-developmental level as children with ASD.
We begin by calling the relationship ―mentoring‖ to maintain the older child‘s
self-esteem. Some children with ASD have commented early on that the ―younger
buddy‖ is ―a little kid,‖ with a certain amount of distaste. Defining the
relationship as hierarchical helps the child with ASD accept the younger buddy
and feel proud of the responsibility that has been given to him/her in this role.
Nonetheless, a relationship of this sort is an implicit set-up for potential
movement into the realm of friendship and mutually enjoyable interactions and
activities, over the course of time. Even if it does not, the perspective taking
benefits are significant.
Increasing self-confidence as a younger child looks up to him/her, and knowing that
s/he‘s doing a good thing for another person.
Elicit feedback from parents: ―What do you think about this regarding Andy?‖
3. Brainstorm sources for getting a ―younger buddy‖:
The mentored child should be younger than the child with ASD, may or may not have a
developmental disability, or even be a younger cousin (or even a sibling if all else fails!). For
example, children with mild to moderate Down syndrome may be good candidates for being
mentored. It is important to note that it may or may not be ideal for the mentored child to
have ASD as well. Due to the rigidity of individuals with ASD, this may prove particularly
difficult. If the mentored child has a diagnosis of mental retardation, it is important to ensure
that the child has mild to moderate mental retardation rather than more significant
retardation. Typically, children more severe mental retardation also have chronic health
conditions and extremely limited communication abilities.
Mention that there are sources for finding children who would be willing to be mentored:
children of parents in ASD-related parenting groups, university-based programs that serve
children with developmental disabilities, schools, and the Regional Center. (See Parent
Module: PLAY for extended discussion of some of these sources and methods for ―enlisting‖
them.)

A school-based alternative is the ―games leader‖ intervention described in Parent Module 2.
This will need to be implemented directly with school providers in School Module: SOCIAL.
This should be considered if there are no available ―younger buddies‖ that the parent can
find, or if s/he does not feel capable of overseeing this type of interaction.
4. Teach parents how to supervise a mentoring activity:
Present parents with the Mentoring checklist.
Review with parents the Supervision Hierarchy to emphasize the parents role during
mentoring.
5. Discuss feasibility of a regular mentoring schedule.
Trouble-shoot with parent on how 1 supervised mentoring time of at least 1 hour each could be
arranged starting this week. How might the parents need to alter their schedule to make it
feasible? (Mentoring on the weekends is fine, too!) How might the child need to alter his/her
schedule to make it feasible? (e.g., by dropping excessive extra-curricular activities or reducing
their TV/videogame playing—which could be used as contingent rewards instead).
If parents comment on the amount of work involved in this, remind them that it is
unfortunately a major time commitment early on to help children develop the skills and
resources they need. Remind parents of the importance of mentoring and learning to take
another‘s perspective.
Discuss the reward system for this exposure. Of course, part of the reward will be that the
child knows he/she is doing something good for another person (being a positive role model).
Parents must reinforce this. However, the child must receive some other motivating
reinforcer that should be associated with the type of tasks the child is undergoing. Therefore,
the reward should be some type of social reward. For example, if the child himself has a
mentor, the next time that s/he and the mentor meet after the child acts as a mentor, the child
could choose what to do during the meeting. This type of reward may not work for all
children; flexibility and knowledge of the child will be key for motivating the child to
complete this type of assignment.
WITH PARENTS AND CHILD TOGETHER (15 MINUTES)
Inquire about the family’s completion of homework (this must be done—briefly—to
teach the family the critical importance of homework). Offer brief consultation regarding
any modifications to the previous week‘s assignment, if indicated. This is a good time to
encourage the family to continue working on self-help skills, either increasing the child‘s
independence in the skills already identified, or adding additional skills for the child to work
on.
Plan the mentoring experience as a family, if it is to occur this week:
Refer to Child Module: MENTOR (Parent-Child meeting section). Be sure to
discuss expectations and details of the meeting with a ―younger buddy,‖ if one is
tentatively planned.

As a group, discuss and agree upon upcoming exposures and rewards/privileges. Assign
additional exposure tasks that ―move along‖ the current lines of exposure at an appropriate
level. Three exposure lines should be active at any one time. Agreement is often obtained by
reviewing the rewards/privileges associated with compliance.
Therapist Note: In some cases, most or all of the exposure planning should be done
with just the child, or with parent and child together. Variables affecting this choice are
the child‘s maturity, motivation, and sense of (and desire for) independence and respect;
and the parent‘s attitude about children‘s input (very laissez faire parents may have
children who expect to be consulted carefully.)
4. Homework. Using blank paper and pen, write down all exposure assignments and any changes
to rewards/privileges system.

Being a mentor or ―older buddy‖ makes children feel more confident and
skilled, and teaches them to take another person’s perspective. Parents
can help! Review the following tips to assist in facilitating mentoring
relationships.
____Host the mentoring “get-together” at your house.
____Remind your child that he/she is to ensure that the ―younger buddy‖
child has fun and talk about specific ways your child can do this.
____Brainstorm with your child on what the ―younger buddy‖ might enjoy
doing, why s/he acts in certain ways, and how s/he may perceive your
child (i.e., ―I bet he really looks up to you & wants to be like you!‖).
____Work with your child to prepare 2 or 3 activities that the ―younger
buddy‖ enjoys.
____Keep the mentoring get-together short (1 hour), so boredom and bad
feelings are prevented.
____Ensure that siblings are busy so they don’t join in the mentoring get-
together.
____Clean up and set up the place where the agreed-upon play activity will
happen (such as a clear spot on the bedroom floor for a board game).
____Make TV and videogames off-limits (or save the last 30 minutes for TV /
videogames to use as an incentive for appropriate behavior).
____Verbally praise your child acting as a positive role model, keeping the
‖younger buddy‖ having fun, teaching good skills, etc. immediately after
the mentor get-together.
See the supervision hierarchy on the next page!

Supervising the mentoring activity is quite important. Children with ASD
experience difficulty taking other people‘s perspectives. Mentoring calls for
your child to act as a good host, be patient, and try to teach the mentored child
to play well.
It is important for you to be present for the entire mentoring session until
your child can consistently (at least 2 sessions in a row without needing much
social coaching) do the following:
1. Greet the younger buddy positively.
2. Pay attention to and talk with the younger buddy the whole time.
3. Make sure the younger buddy is having a good time by asking him/her
what to play, playing the suggested game, and playing in a way that
makes it ―fun‖ (i.e., ―going easy‖ on the younger buddy).
4. Demonstrate patience with the younger buddy for 20 minutes.
Once your child meets the above 4 goals, you can reduce your direct
supervision to half time. If the younger buddy comes over for 1 hour, you
should still supervise 30 minutes of the mentoring session.
Continue to supervise half time until your child consistently does the
following without social coaching:
1. Changes games when the mentored child wants to.
2. Asks the mentored child questions to see if he / she is having fun.
3. Asks if the mentored child needs anything.
4. Demonstrates patience with the mentored child for 40 minutes.
Once your child does the above consistently without much social
coaching, you can reduce your direct supervision to quarter time. However,
when you are not present, it is a good idea for you to be within close
proximity (e.g., the next room or hallway), so you can listen to the children’s
activities. Parents should enter and provide supervision and support as
needed.
Parent or Child Session X
Support / Emergency Session
Background
In any therapy, occasional unexpected events arise that must be addressed which do not
fit into the guidelines of a particular module. In these cases, previous clinical training (and, if
needed, supervision or consultation) must serve as the guide of the session content, as there is
inherently no way to provide a treatment plan for all possible eventualities. It should be noted,
however, that the more that non-manualized sessions are used, the less treatment effect on the
target symptoms (e.g., anxiety) one can expect. Therefore, it is a priority to limit off-protocol
clinical interventions to a very infrequent basis if possible.
Goals
1. Identify problems that have arise for the client
2. Help client problem-solve to develop solutions
3. Provide support and empathy
4. Redirect clinical interventions back to manualized procedures as soon as clinically appropriate
Materials
Variable.
Session
Content is variable. See Background, above.
Parent Module: T
Termination
Background
If termination is not planned for Session 12, the treatment material described below for
the ―Termination‖ session should be saved for the final session, whenever it is planned. If the
treatment will last longer than 12 sessions, Session 12 should be used as a ―review‖ session (see
―Review / Processing the Theme‖ module) rather than a termination session. The goal of the
Termination Session is to help parents plan for the future. Specifically, the therapist emphasizes
that treatment gains will be maintained if the parents continue to use appropriate communication
and exposure techniques.
Goals
1. Help family develop a positive attitude about the child‘s progress in the program
2. Review skills learned in this program with the parents and plan for the future
3. Discuss termination issues
Preparations
Prepare any ―party‖ materials (e.g., snacks), and certificate, card, and/or small gift for child
Materials
Planning for the Future handout
Session
WITH PARENTS ALONE (15 MINUTES)
1. Introduce purpose of module:
Point out that this is the final session of the program, that this meeting will be brief, and that
the purpose is to review progress and plan for the future.
2. Review child’s progress and family participation:
Congratulate the parents on their dedication and involvement in the program (as appropriate).
Ask about parents‘ reactions to ending the program.
Provide brief assessment of the child‘s strengths and areas that may need further work.
Present the Planning for the Future handout. Emphasize that the child will probably continue
to have some difficulties with anxiety in the future. Therefore, continued parental vigilance
for cues of child anxious behavior will help parents understand that new negative behaviors
exhibited by the child in some situations may in fact reflect child anxiety.
―For instance, a child who resists attending a new after-school program because it is
―stupid‖ may actually be experiencing anxiety about some aspect of this program.‖
Point out that it is easy for children with anxiety to view themselves (and be viewed by
others) as ―weird‖, ―shy‖, etc. Helping the child see themselves in a new light (e.g. ―brave‖),
and, from the parent‘s perspective, learning to think of the child in more positive terms
(―sometimes sensitive, but often courageous‖) will help the child find alternate roles in the
world to being ―the anxious child‖.
Remind the parents that a check-in call will be made in three months, or they may call to
check in earlier if something comes up.

Congratulations! Your family has completed the UCLA Building Confidence
Program. Be sure to give yourself a pat on the back for the effort you put in
for your child! It is important to make plans to continue helping your child
cope with anxiety. Here are some ideas to keep in mind:
1. Negotiate with your child to keep facing their fears, and provide
rewards for their effort, just like we did in this program.
Identify situations, activities, or thoughts that still frighten your child.
Then, set up a list of increasing ―exposures‖ to these situations, all the
way up to completely facing the fears.
Reward your child for each step he/she takes as he/she faces fears.
2. Find ways to free your child from the role of being ―an anxious
child‖.
Search for and point out to your child times when he/she acts
courageously.
Make an effort to think of your child’s behavior in new ways. For
instance, rather than thinking of a child as ―shy‖, try to find the positives,
such as ―She’s a very considerate child who also values time by herself.‖
3. Use communication skills with your child.
When your child is feeling anxious or angry, avoid giving reassurance,
giving advice, or criticizing. Label your child’s feelings and wait CALMLY
while your child copes with his/her feelings.
4. Make sure that your child continues to develop his / her self-help
skills. This builds confidence and self-esteem.
Ask yourself: is my child as independent as the other children his / her
age?
For instance, are the other children dressing themselves, walking home
by themselves, or being responsible for their own room before my child?
If so, it is time to encourage your child catch up!
5. Encourage your child to develop and maintain his / her friends.
Children with good friends have higher self-esteem and fewer anxiety
problems.
Weekly play-dates are an essential part of developing close friends.
Remember, parents should play an active role in arranging play-dates.
School Module: SOCIAL
Promoting Prosocial Behavior at School
Background
This session requires written consent from the parent to communicate with the child‘s
school about the child‘s diagnosis and treatment plan. This module may repeated on return visits
to the school. Teachers and school staff may have limited knowledge of or experience working
with children with autism. While Individual Education Plans (IEPs) provide some assistance to
teachers and staff regarding the specific impairments experienced by the target child in their
classroom, general knowledge regarding ASD, promotion of friendships, and management of
difficult behaviors may be lacking.
Therapist Note: Many of the interventions being proposed in this module (e.g., peer buddies)
require follow-up on the therapist‘s part. As an example, it is likely the therapist will need to be
directly involved in the initial training of peer buddies. The practicalities of potential follow-up
visits must be considered before going to the school so that the role of the therapist can be clearly
delineated and offers of assistance can be made to the school without ambivalence.
Therapist Note: Setting this session up requires direct phone contact with the child‘s
teacher/staff. Typically, such contact is difficult to attain. Daily phone calls to the school during
the teacher‘s lunch time or immediately after-school are strongly recommended. It is also good
to leave messages that specify times when the therapist is likely to be available at his/her desk
for a callback. This process can drag out for weeks if this approach is not taken. When contact is
made, let the teacher/staff know how important they are to the child‘s intervention, and that you
would welcome an opportunity to collaborate with the teacher/staff on improving the child‘s
behavior and academic success.
Goals
1. Identify and prioritize or review the child‘s needs at school.
2. Establish or review a behavioral program to reduce negative behaviors or increase social
interaction, including rewards systems, social coaching, gameleading, or peer buddies.
Materials
Handouts from any of the relevant parent modules (e.g., REW, SOC-C) that are relevant to the
material being presented to the teachers/staff.
WITH TEACHER / SCHOOL STAFF (30 MINUTES)
1. Review psychoeducation regarding ASD and anxiety.
Review Parent Module 1 information with teacher.
Be sure to disclose enough detail about the child‘s diagnosis and treatment plan to
2. Identify and prioritize (or review) child’s needs at school:
List the child‘s strengths and weaknesses from the teacher‘s point of view.

Ask the teacher what weaknesses seem to provide the most significant barriers. Explain that
there are typically three general categories of difficult behaviors: oppositional behaviors and
behavioral challenges, avoidant behaviors, and peer and social difficulties.
3. If needed, establish (or review) a behavioral rewards program for the teacher.
Ascertain the teacher‘s need, willingness, and ability to implement a behavioral rewards
program.
If the child is having significant behavioral problems in the classroom:
o Review Parent Module: REW and use all strategies described therein, as appropriate
o Therapist must be aware that the teacher has probably tried behavioral strategies
previously. The therapist must determine with the teacher what went wrong with the
behavioral plan (lack of specificity of target behaviors; too many target behaviors;
unrealistic target behaviors out of child‘s range). The therapist should encourage the
teacher to describe what the behavioral plan was, and what happened.
o The therapist must select 2-3 behaviors that the child is displaying at school and
instruct the teacher to implement a behavioral rewards system targeting those
behaviors, and no others at present.
The teacher must provide reinforcement (stickers, points, privileges) on a
multiple time per day basis—consistently.
The therapist may suggest, if helpful, that the child‘s home point system be
incorporated with school behavioral targets. But it is often easier if the
reinforcers are provided at school on an immediate basis.
Encourage teachers to think of ways to reward target behaviors with the
child‘s special interests (e.g., 5-10 minutes playing on the computer)
If the child‘s most significant problems involve avoidant behaviors:
o Classroom avoidant behaviors and playground avoidant behaviors are both important
to target if possible.
4. If needed, develop (or review) a social coaching plan for the child.
If the child is adapting poorly to school activities requiring peer interaction:
o Review Parent Module: SOC-C and use all strategies described therein, as
appropriate.
o Example 1: At recess, school providers could plan for ―Andy‖ to make a verbal
greeting to a target peer, plan for the specific wording he will use, the use of eye
contact and a smile.
d. Later this can be expanded to include a compliment about the target peer (e.g.,
―That is a cool shirt,‖) following the greeting.

e. After establishing success doing this for awhile (one or more weeks), ―Andy‖ can
add a compliment about any peer‘s performance during the game (he would need
help thinking of how to spontaneously devise an appropriate compliment about a
specific event during the games—something he could brainstorm with a provider
and practice right before he joins the group).
o Example 2: Before lunch, school staff could help ―Andy‖ observe the seating
arrangements of his peers:
a. The staff member would, based on knowledge of who would and would not be
receptive to Andy‘s company, help provide Andy with multiple choice options for
whom to sit with.
b. Staff would then help Andy plan to sit close enough to a specific peer to actually
be a ―part‖ of the group.
c. Finally, the staff would help Andy prepare an appropriate greeting to say as soon
as he sits (possibly including a compliment of the peer). [During social skills
training, the timing of such a greeting, including use of smile, tone and volume of
voice, etc., might be practiced].
d. Once successful with this routine, staff could add ONE question for Andy to
prepare to ask a peer during lunch in order to increase his social initiations and
provide an opportunity for conversation.
The most realistic staff member to implement social coaching outside of the classroom is a
1:1 aide. Brainstorm with the teacher/staff who could play the role of social coach at lunch
and on the playground.
o Ideally, the therapist would come back to the school at least once to model live social
coaching for the staff who is assigned to this job.
It is important for teachers/staff to warn the child ahead of time that social coaching will be
implemented, and get his/her feedback on how to do it comfortably.
o Do the coaching at lunch/recess in a location that feels private enough to the child so
that s/he does not feel too self-conscious.
o Remind him/her that s/he will earn points for trying out the greetings / conversational
items.
5. If needed, develop (or review) a gamesleading opportunity for the child.
This intervention is for children who need to improve perspective taking and who may be
able to develop satisfying relationships with younger peers. As noted in Parent Module:
SOC-C, this exercise is ostensibly for development of prosocial skills, but in fact could set
the stage for the develop of actual friendships with younger children who are closer to the
patient‘s developmental level. For instance, a child who begins as a ―helper‖ in the
kindergarten playground may find that s/he enjoys participating in the fantasy games with the
younger children and actually has a positive role that s/he can ―handle‖ in this play.
See Parent Module 2 and Parent Module: SOC-C. A gamesleading intervention is most
likely to succeed with children 8 years or older, of relatively calm temperament, rule-abiding,
and without excessive cognitive delay.
With appropriate supervision, training, and assistance, a child can benefit from being in the
role of playground assistant/gamesleader for younger children.
o Interactions with younger children are often easier to manage for children with
autism, as the demands are less.
o The tendency to be bossy and controlling seen in autistic communication are more
appropriate in an ―authority‖ role such as gameleader than in peer interactions; thus,
the child‘s style might receive greater acceptance in this situation.
o It is possible that the child, with a level of maturity that is more congruent with
younger children in some respects, may find interests in common with younger
children (e.g., Pokemon) that s/he would not foresee, potentially leading to possible
friendships (which would be a good start and developmentally appropriate).
Important to introduce this to the child as a privilege s/he has EARNED due to the
responsibility s/he has displayed, maturity, and trust the staff have in him/her.
Plan for as few as 1-2 recess or lunches per week, but as many as 5 recesses or lunches per
week (but never twice on the same day), depending on his/her initial response/enjoyment of
this role.
S/he will need clear pointers and guidelines on what is expected of him/her in this role prior
to engaging in it. An aide or other staff should be available during his/her gamesleading, but
in a watch-and-wait role to help scaffold the task for him/her if s/he needs assistance.
Even a fairly easy but central role such as pitcher or umpire (e.g., calling outs, fouls, etc.) in a
1st or 2nd grade kickball game would be a good starting point. ―Supervising‖ kindergarteners
or 1st graders in the sandbox (e.g., helping them dig, monitoring for unsafe behavior, giving
suggestions of how to expand sandbox projects) could be successful, too. Too much
responsibility will be hard to manage early on.
This will be a good trial of what could be a useful social integration strategy in other settings
(e.g., camps, after-school programs with younger children).
The therapist will play an important role in preparing the child for this role (adapting Child
Module: SOC-C). S/he would ideally come back to the school at least once to assist in setting
up the gamesleading with the child and the school staff who is assigned to oversee this
intervention.
6. If needed, work with the teacher/staff to arrange ―peer buddies‖ for the child.
This intervention is useful for children who do not have close friends at school.
It is desirable to recruit 2-4 prosocial peers and TRAIN them to invite the patient to engage
in an enjoyable target activity (one that the patient likes) 1-2 recesses/lunches per week (i.e.,
each child could be assigned 1-2 recesses per week, so their own recesses are not too
disrupted).
o The peer buddies would be trained:
To approach and ask him/her to engage in a preferred activity (e.g., handball)
even if the peer would rather play something else.
How to initiate conversation with him on topics that s/he is most likely to
respond to (e.g., interests such as cartoons, Pokemon, gameboy).
That small responses from the child and any interaction at all are actually
signs that s/he is having fun and appreciates being included (since kids might
otherwise think that s/he is bored/uninterested in their company).
o Same-gender peer buddies are recommended. Ages can vary depending on
circumstances.
o Popular and trusted teachers or staff should determine and approach the target peers
to ask them to be the child‘s peer buddies. Students may need to be offered some
small appropriate incentives.
o Staff with social skills training experience should then be assigned to ―train‖ the peers
appropriately prior to beginning this assignment. The Peer Buddy Training Outline
included in this module is recommended for conducting this training.
o A variant of the peer buddy intervention includes the child receiving or providing
peer tutoring. In any case, peers should receive training as above in order to cue
appropriate responses from them. Tutoring is more structured than play and may be
easier for some children to achieve success. S/he could provide tutoring in areas of
strength (e.g., math) to promote his/her self-esteem and social status in the class. S/he
could receive tutoring in order to provide a structured interaction with age-peers in
which to practice conversational skills.
Ideally, the therapist would participate in at least the initial peer buddy training session.

UCLA Behavioral Interventions Program
Dr. Jeffrey Wood, Dr. Karen Sze Wood, and Dr. Amy Drahota
To assist children with certain kinds of disabilities (such as Asperger‘s) in developing their social
skills, it can be very helpful to assign them ―peer buddies.‖ Unfortunately most typically
developing children and youth do not have a good idea of what to do as a ―buddy,‖ even though
they want to be helpful. Therefore, we need to take their natural motivation and good-will, and
train them to engage in specific social behaviors that will permit the development and
maintenance of a relationship with a child with special needs.
Identifying and Recruiting Peer Buddies
o Same-gender peer buddies are recommended. Ages can vary depending on
circumstances—consider the child‘s developmental level and choose peers who are at
or a little above or a little below this level, even if this means that they are younger.
For many elementary school children, it is especially helpful to consider classmates
first, as the class setting promotes friendship development.
Perhaps the biggest single factor to consider in choosing peer buddies is their
level of empathy and patience. The more the better, at all age groups!!
o It is desirable to recruit 2-4 peers as buddies.
o Teachers or staff who are known and trusted by the potential ―peer buddies‖ should
initially approach the students. This presentation is best if presented as an opportunity
and a big responsibility reflecting the child‘s maturity and positive traits (―being a
really nice kid.‖) Students may need to be offered some small appropriate incentives,
but in the end self-motivation should be the driving factor in their participation.
o Staff with relevant experience should ―train‖ the peers prior to beginning this
assignment, and check-in / supervise them regularly to ensure the relationship is
working out.
Training the Peer Buddies (outline of talking points for facilitator (teacher, counselor, etc.)
The following topics are useful to cover in the initial training. This can be done 1:1 or in small
groups of ―peer buddies.‖ It is recommended that the following points be made:
1. You‘ve been selected because you are really good at making friends, you are mature and
responsible, and (teacher / staff) say you‘re ―really nice kids.‖
2. There‘s a special job that I need help with: A boy/girl in your class (or school) who is a
very nice kid also has a few special things about him/her—s/he has a hard time figuring
out what other people are feeling and thinking. S/he also does not understand how to
make friends or what is ―cool.‖ It is not his/her fault—he was just born that way—but
just like any other kid, s/he wants to fit in. When you get to know him/her, he‘s really

nice and has a good sense of humor. There‘s nothing wrong with him/her, s/he‘s a regular
kid—just different socially.
3. So, s/he could really use some friends at this school. And because of all the great things
I‘ve heard about you, you were one of the few kids selected in ___ grade to be a buddy to
__. Do you think you‘d like to give it a try? There‘s no specific reward, just knowing that
you‘ve done a good thing, helped another kid out, and that ____ and the teachers are
proud of you and would really appreciate your help.
4. Here‘s what I‘d like to ask you to do: Once a week, at lunch, I‘d like to see if you can go
and find __ and invite him/her to eat lunch with you and whoever else you normally eat
with. And, if you‘re in class with him/her and s/he seems to be having a hard time, see if
there is anything you can do that would help.
5. Now, this may sound easy, but I didn‘t ask you to meet up with me just to ask you to do
something simple. There‘s a couple things you‘ll need to know, so you can learn how to
be a good buddy to ____:
a. _____ can be very shy. So it‘s important to be enthusiastic when you invite
him/her to lunch so s/he knows s/he‘s really welcome.
b. Sometimes kids like _____ have a hard time making conversation. You‘re
someone who is great at conversation—it will help a lot by trying to include
him/her in conversations during lunch.
c. Who can think of way to include shy people in conversations?
i. Talk / ask questions about ―stuff‖ they‘re interested in.
d. _____ has a few things s/he‘s really into—
i. E.g., cartoons
ii. E.g., videogames
iii. Can you think of any ways you might have something in common with
him/her?
iv. (If true) S/he isn‘t a big sports person, but the one exception is…. (e.g., if
you invited him/her to play handball, s/he‘d probably love it.)
e. It is possible s/he will do things that seem a little weird. What are some weird
things kids do around here at school? Some things you might notice are:
i. S/he might not smile or seem excited
ii. S/he might not always remember to be polite like saying hi, bye, or thanks
iii. S/he might talk in a way that you think is different
f. The key thing to do if s/he does something you think is kind of strange are:
i. Ignore it and keep being friendly. Talk with him/her about stuff s/he likes,
especially early on. Ask him/her questions about things s/he‘s interested
in, it will help him/her get more into the conversation.

1. Remind yourself it‘s not his/her fault. After hanging around other
nice kids s/he‘ll eventually learn from you. And, even if s/he
doesn‘t seem that excited, s/he loves being included.
g. Help him/her know what people are into:
i. It is also good to tell him/her nicely the ―normal‖ way to do things. For
instance, if s/he talks a lot about Pokemon you could say, ―Pokemon is
cool, but what all the kids are watching now is Dragon Ball Z…‖
ii. When s/he does things socially that are ―cool‖ or nice, be sure to tell him
that it was cool…
h. If he doesn‘t join you, leaves early, or is quiet, just ignore it and try again next
time. What could you say to yourself if that happens?
i. E.g., ―Oh well, I know s/he is still learning how to make friends and
doesn‘t know that it was rude or weird… s/he didn‘t mean anything by it!‖
Be sure to cover these three points:
1. Ask if the peer buddies have any questions about their role.
2. Set up a specific day of the week (for each of them) to invite ______ to lunch.
(NOTE: children may volunteer to do this more than once per week. This is
completely permissible. Every day is not recommended initially, however, because
the buddies may not have a good idea of what they are committing to.)
3. Problem solve on how the peers can remember to do this each week, and on where to
find _______ at the beginning of lunch. (NOTE: To ―hook up‖ peer buddies with the
child, some kind of adult facilitation is helpful for the first few weeks until a pattern
is established.)
