UD01eCase Manual Updated May 102013 E Case
User Manual:
Open the PDF directly: View PDF ![]() .
.
Page Count: 129 [warning: Documents this large are best viewed by clicking the View PDF Link!]
υ
Ver 3.2013
.
Introduction to eCase
OVERVIEW
eCase 4.0, formally ACFI manager, was introduced into the aged care industry
ready for the inception of ACFI March, 2008. Since then the product has not
only undergone a name change, but has also significantly grown in its
functionality. Healthmetrics prides itself on producing user friendly interfaces
specifically designed for the Aged and Health care sector.
This philosophy of design ensures that all users, regardless of literacy levels are
able to use the product in its entirety.
eCase is a fully cloud delivered software product which allows users (depending
on security levels) full access to the system anywhere at any time. The ensure
management and executive staff can monitor usage and compliance regardless
of their location.
φ
Ver 3.2013
.
Table of Contents
OVERVIEW .......................................................................................................................................... 1
FUNCTIONALITY ................................................................................................................................ 6
ADMINISTRATION ............................................................................................................................ 7
Screen resolution ......................................................................................................................... 7
‘Back’ function on browser ....................................................................................................... 8
Tokens .............................................................................................................................................. 8
Breadcrumbs .................................................................................................................................. 8
Sliding menu .................................................................................................................................. 9
GETTING STARTED ........................................................................................................................ 10
Logging on to eCase .................................................................................................................. 10
Search resident ........................................................................................................................... 10
Troubleshooting search ............................................................................................................ 11
Main screen overview ............................................................................................................... 12
Message Board. ............................................................................................................................... 13
ADMITTING A RESIDENT ............................................................................................................. 14
Add resident ................................................................................................................................. 14
Admission ...................................................................................................................................... 15
RESIDENT MOVEMENTS............................................................................................................... 16
B2B ...................................................................................................................................................... 16
B2B Overview .............................................................................................................................. 16
B2B instructions for use........................................................................................................... 17
CARE FUNCTIONALITY ................................................................................................................. 20
Care Overview ............................................................................................................................. 20
Workflow .................................................................................................................................... 20
Progress Notes ............................................................................................................................ 24
Care Work Log ............................................................................................................................. 28
Auto-close ..................................................................................................................................... 30
Chart deactivation ...................................................................................................................... 30
Add Activity .................................................................................................................................. 33
Change Activity settings-Work log editor ......................................................................... 37
Charting ......................................................................................................................................... 41
Wound management ................................................................................................................. 52
χ
Ver 3.2013
.
Taking photos of wounds using Toughbook ................................................................. 56
Upload photo to Wound Chart ........................................................................................... 56
Wound Gallery ......................................................................................................................... 57
Schedule ongoing wound management ......................................................................... 59
Change wound management regime via Work Log Editor ..................................... 61
Delete resolved wound from Work Log via Work Log Editor ................................. 64
Assessments ................................................................................................................................. 65
Careplans- interim, full careplan & Summary ................................................................. 70
Incident Management ............................................................................................................... 77
Care Reporting Tools ................................................................................................................ 78
Activity Viewer .................................................................................................................................. 78
Notifications and warnings ............................................................................................................... 83
TOUGHBOOKS ................................................................................................................................. 84
Toughbook Overview ................................................................................................................ 84
Toughbook Operational Guidelines ...................................................................................... 84
ACFI FUNCTIONALITY ................................................................................................................... 90
ACFI Overview ............................................................................................................................. 90
ACFI instructions for use ......................................................................................................... 90
REGISTERS ....................................................................................................................................... 95
Registers Overview .................................................................................................................... 95
Registers instructions for use ................................................................................................ 96
REPORTING ....................................................................................................................................... 99
Reporting Overview ................................................................................................................... 99
DECISION MANAGER .................................................................................................................. 101
ROSTERING .................................................................................................................................... 107
Rostering Overview ................................................................................................................. 107
Rostering instructions for use ............................................................................................. 107
SURVEYS .......................................................................................................................................... 109
Satisfaction survey Overview .............................................................................................. 109
Satisfaction surveys instructions for use ........................................................................ 109
COMPETENCIES ............................................................................................................................. 115
Competency Overview............................................................................................................ 115
Competencies instructions for use .................................................................................... 116
eCONTRACTS ................................................................................................................................. 121
ψ
Ver 3.2013
.
eContracts Overview ............................................................................................................... 121
eContracts instructions for use ........................................................................................... 122
eCase FOR DOCTORS ................................................................................................................. 130
Logging on to eCase ................................................................................................................ 130
Search resident ......................................................................................................................... 131
Troubleshooting search .......................................................................................................... 132
Main screen overview ............................................................................................................. 133
Progress Notes for Doctors ................................................................................................... 133
Work log for Doctors ............................................................................................................... 137
Integration with existing practice software.................................................................... 138
eCase FOR ALLIED HEALTH PROFESSIONALS .................................................................. 139
Logging on to eCase ................................................................................................................ 139
Search resident ......................................................................................................................... 140
Troubleshooting search .......................................................................................................... 141
Main screen overview ............................................................................................................. 142
Progress Notes for AHP’s ....................................................................................................... 142
Work log for AHP’s ................................................................................................................... 146
Integration with existing practice software.................................................................... 147
OVERVIEW ...................................................................................................................................... 149
FUNCTIONALITY ........................................................................................................................ 150
CARE FUNCTIONALITY ............................................................................................................... 151
Care Overview ........................................................................................................................... 151
Workflow......................................................................................................................................... 151
ADMINISTRATION ........................................................................................................................ 153
Screen resolution ..................................................................................................................... 153
‘Back’ function on browser ................................................................................................... 154
Tokens .......................................................................................................................................... 154
Breadcrumbs .............................................................................................................................. 154
Sliding menu .............................................................................................................................. 155
GETTING STARTED ...................................................................................................................... 156
Logging on to eCase ................................................................................................................ 156
Search resident ......................................................................................................................... 156
Troubleshooting search .......................................................................................................... 157
Main screen overview ............................................................................................................. 158
ω
Ver 3.2013
.
Progress Notes .......................................................................................................................... 159
Care Work Log ........................................................................................................................... 164
Daily eCase access and activities ................................................................................................ 164
Management monitoring tools ....................................................................................................... 166
Activity Viewer ............................................................................................................................ 166
Progress note overview .............................................................................................................. 167
Care worklog ............................................................................................................................... 168
Notifications and warnings ............................................................................................................. 169

ϊ
Ver 3.2013
.
FUNCTIONALITY
eCase provides a range of functionality for all levels within the organization.
From basic care charting to CEO reporting, eCase provides a solution.
Functionality available in Ecase 4.0:-
• Full B2B integration with Medicare Australia
• Extensive ACFI functionality
• A fully integrated care system
• Quality registers and forms
• Full suite of BI reporting modules
• Rostering featuring funding optimization
• Satisfaction surveys
• eContracts
• Competencies
2013 release
• Quality Auditing system
• Medication Management
• Community Care
• Apple and Android apps.
• Fully integrated medication compliance system
ϋ
Ver 3.2013
.
ADMINISTRATION
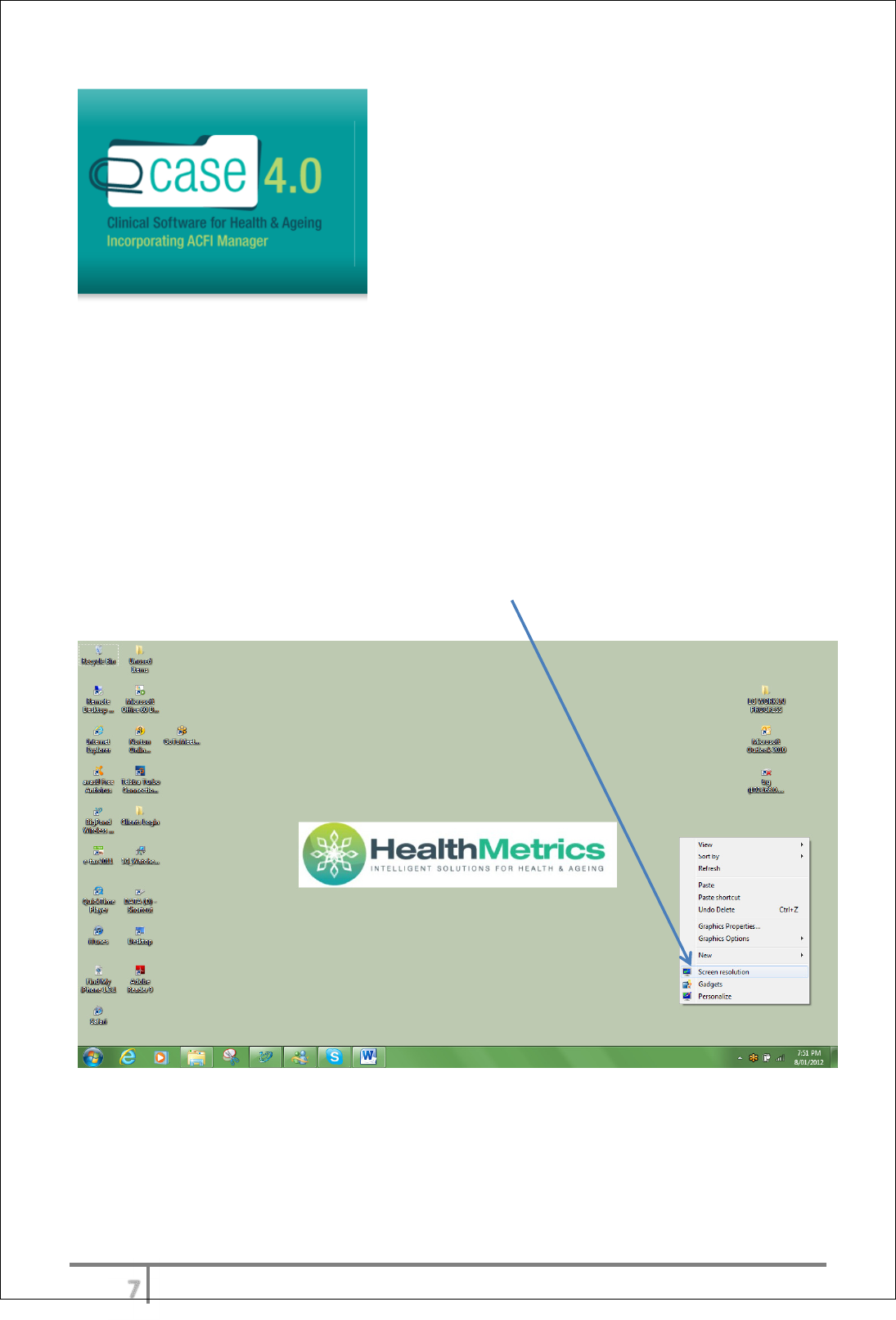
Screen resolution
eCase will run on any type of hardware including touch screens, Samsung
Galaxy, Apple iPad and many more. The optimal resolution to run eCase is using
the resolution 1280 x 1024. This will prevent scrolling and maintain a crisp focus
in all items in the product.
Setting screen resolution
Right click anywhere on the desktop screen. The option for ‘Screen resolution’
will be located at the bottom of the option list.
ό
Ver 3.2013
.
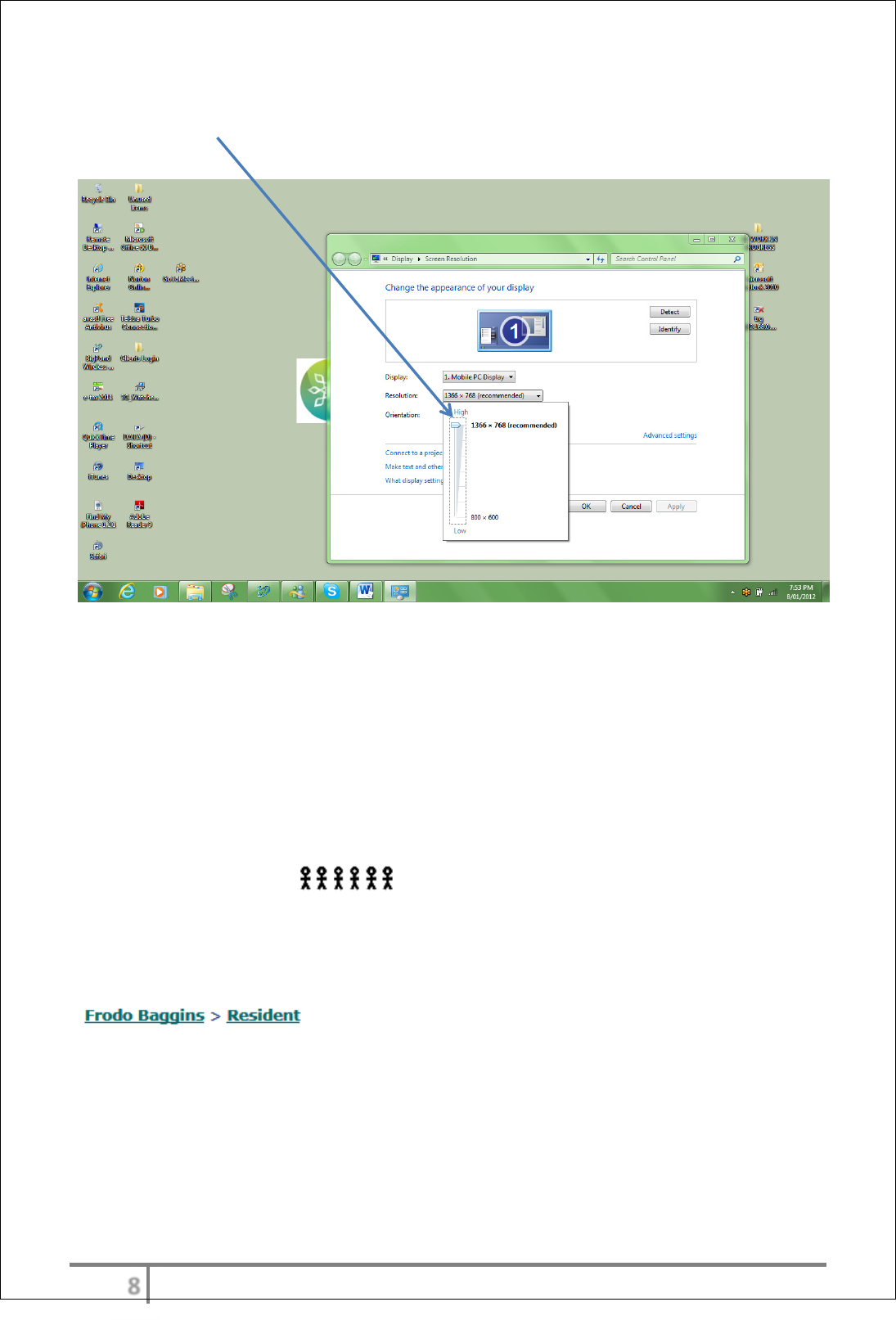
Select the resolution button and slide the scale to the recommended level of
1280 x 1024.
‘Back’ function on browser
The ‘back option’ on the internet browser should not be used to move around
within eCase. The product will provide the user with various alternatives to
change or move from one screen to another. Prompts such as ‘save’, ‘enter’ and
‘back’ will provide the user with the ability to navigate around the entire product.
As an alternative the user can also select the escape key which will take the user
back to the main screen.
Tokens
Recent resident tokens the last 6 resident can be seen at any time
under the main menu ‘Recent Resident’. This information will remain there for
the user after logging off.
Breadcrumbs
Breadcrumbs or breadcrumb trail is a navigation aid available in eCase.
Breadcrumbs appear horizontally across the top the page, below the title bar.
They provide links back to each previous page the user navigated through to get
to the current page. Breadcrumbs provide a trail for the user to follow back to
the starting or entry point.
ύ
Ver 3.2013
.
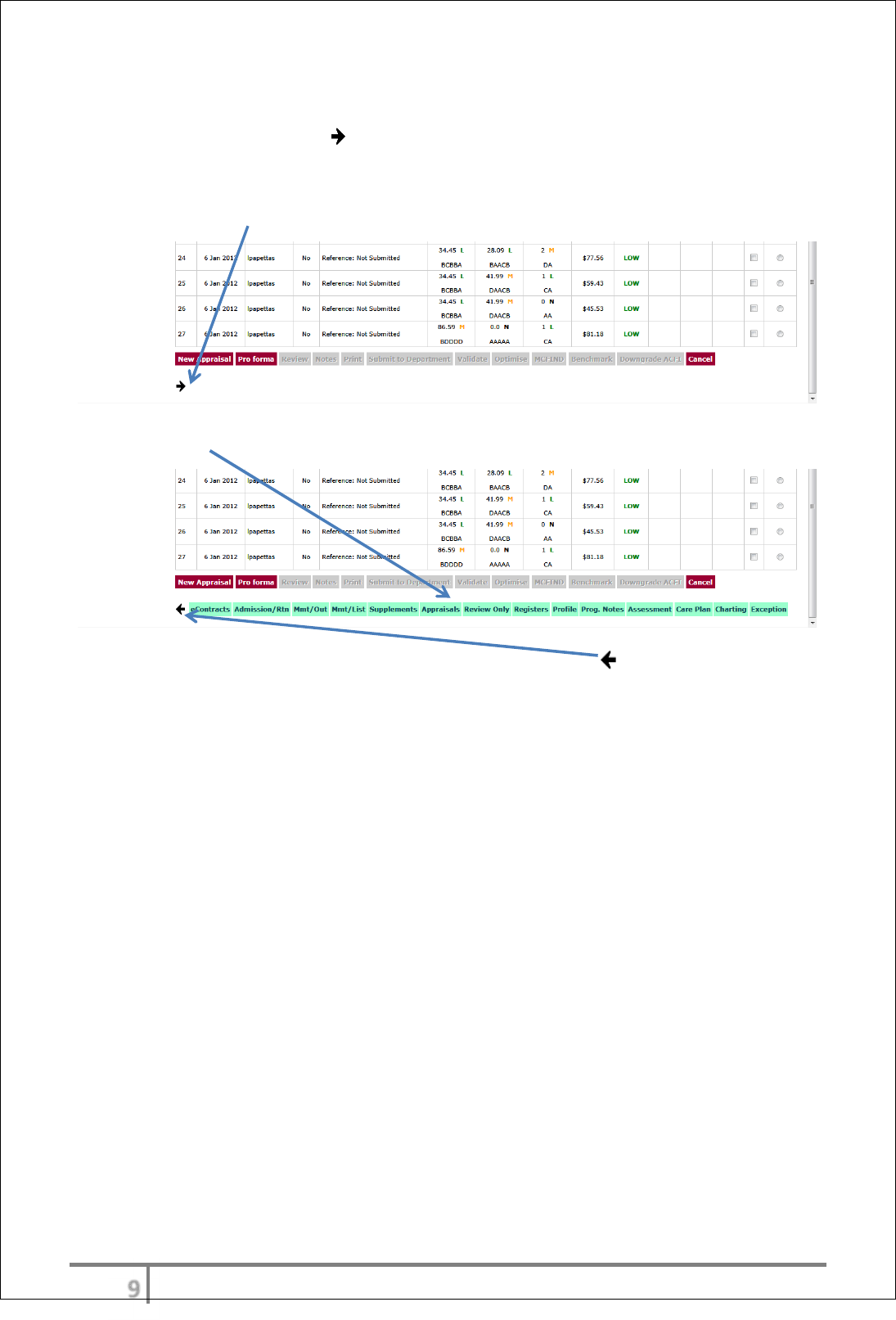
Sliding menu
The menu bar automatically slides open from the left edge of the screen when
the user selects the arrow
To ease navigation, the sliding menu bar displaying ‘Resident Functions’ can be
activated by selecting the arrow.
The ‘Resident Functions’ menu appears.
Re-selecting the arrow will cause the bar to slide back in
υτ
Ver 3.2013
.
GETTING STARTED
• Logging on
• Search function (search for resident)
• Troubleshooting search function
• Main screen overview
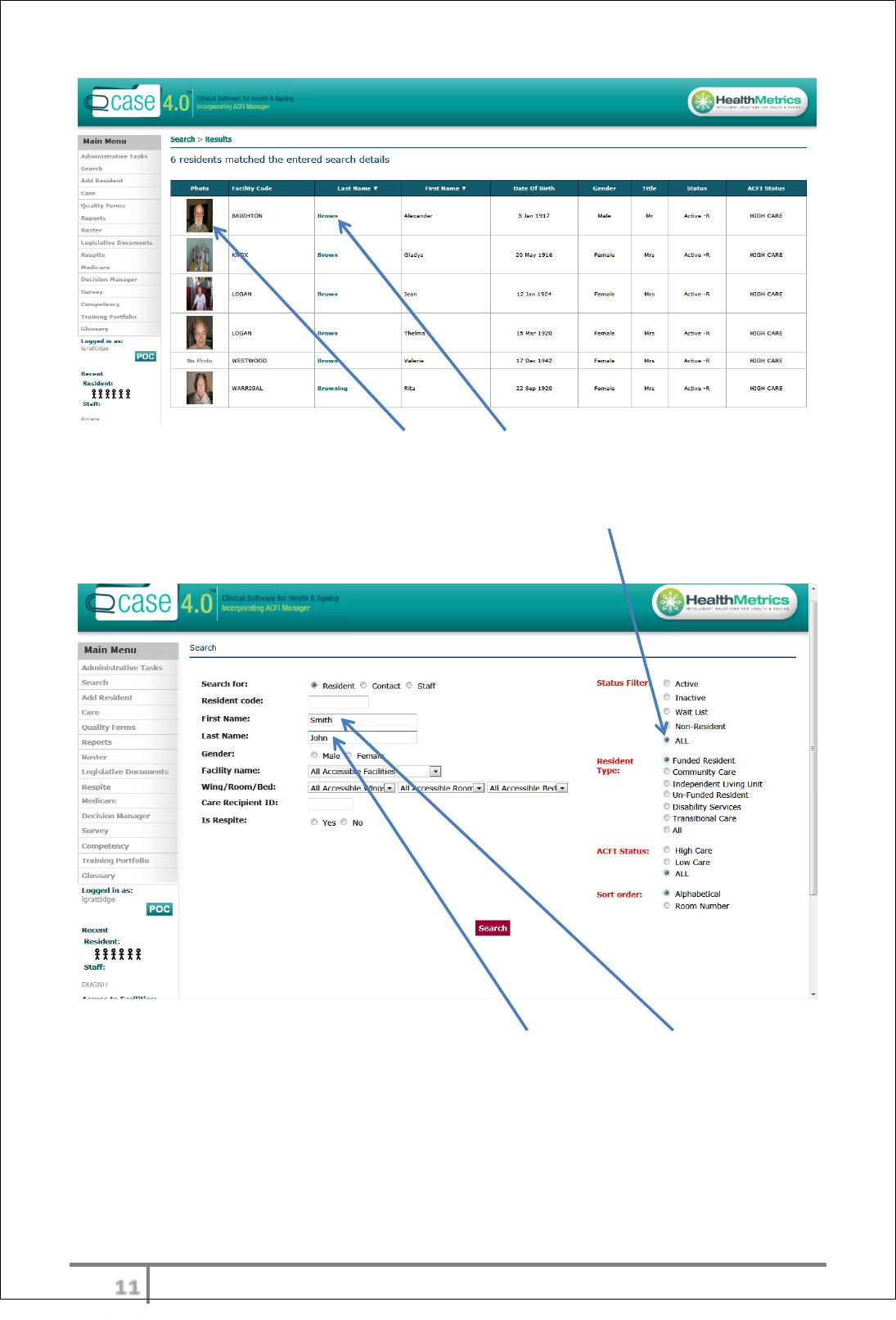
Logging on to eCase
Insert Username and Password and select ‘Login’.
Search resident
Users can search by any of the fields on the search screen. Usually search by
resident’s Last Name. Enter the Last Name and select ‘Search’.
If more than one resident shares the same Last Name, a list of residents will
appear in a list, and can be differentiated by photo, gender, date of birth etc.
υυ
Ver 3.2013
.
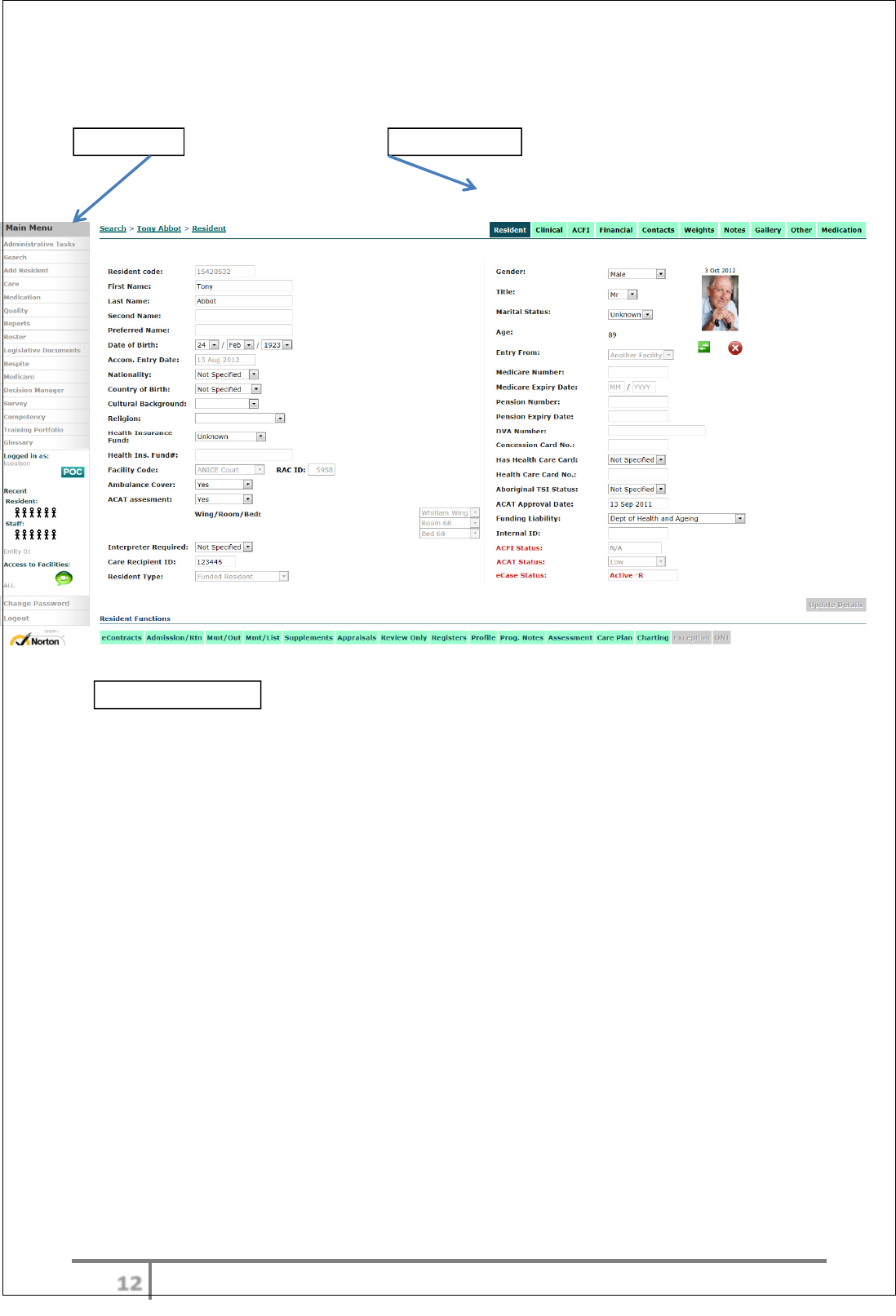
To load the resident page, select Photo or Last Name.
Troubleshooting search
If resident cannot be found, change the Status Filter to ‘ALL’. The resident may
have been added incorrectly or may have been discharged.
The resident may also have been added with Last Name and First Name around
the wrong way. Try searching by switching these around.
υφ
Ver 3.2013
.
Main screen overview
eCase is a very resident centred product. Once on the resident page, the entire
screen will be about that resident.
Main Menu
Resident Menu
Resident Functions
υχ
Ver 3.2013
.
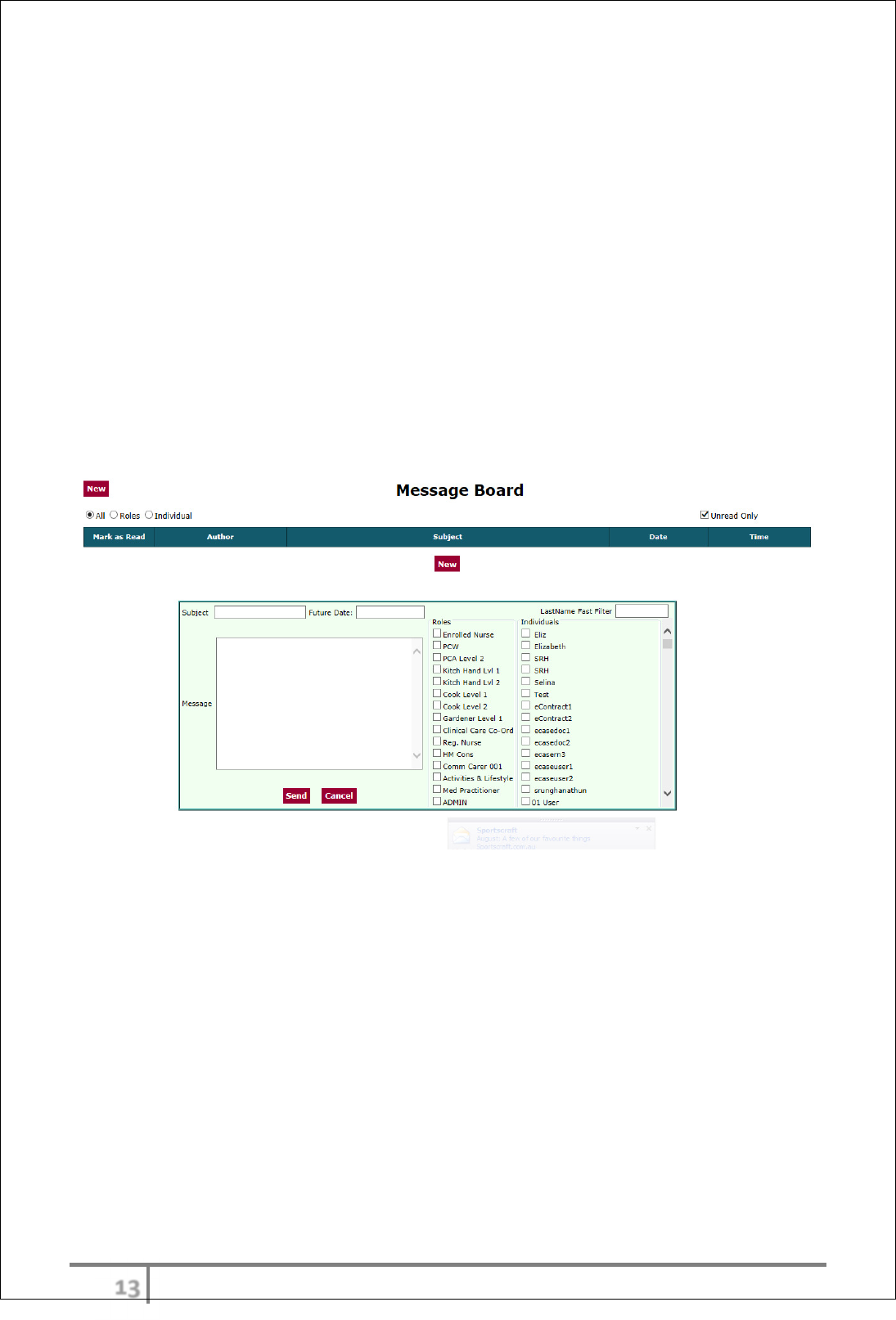
Message Board.
The message board is the facility/organization communication tool. The MB
essentially replaces a facility diary where resident and staff appointments and
notifications would previously have existed.
To send a message > select new > Message Subject > date (can also enter
future date > recipients (can be sent to roles or individuals) and message
content. Then select send.
To receive a message> if a message has been sent to you it will open a first
page when a user logs on. The user can also review messages during the shift
by selected the MB icon under the main menu. To review message simply click
on the message subject and read. Once message is read it will filter out to read
messages off the current list.
υψ
Ver 3.2013
.
ADMITTING A RESIDENT
New residents can be added to the data base prior to admission as a person of
interest. If the resident is interested in being admitted to the facility the status
of the resident can be made to waitlist. (Admit to waitlist) The resident can then
be admitted to the facility from the waitlist.
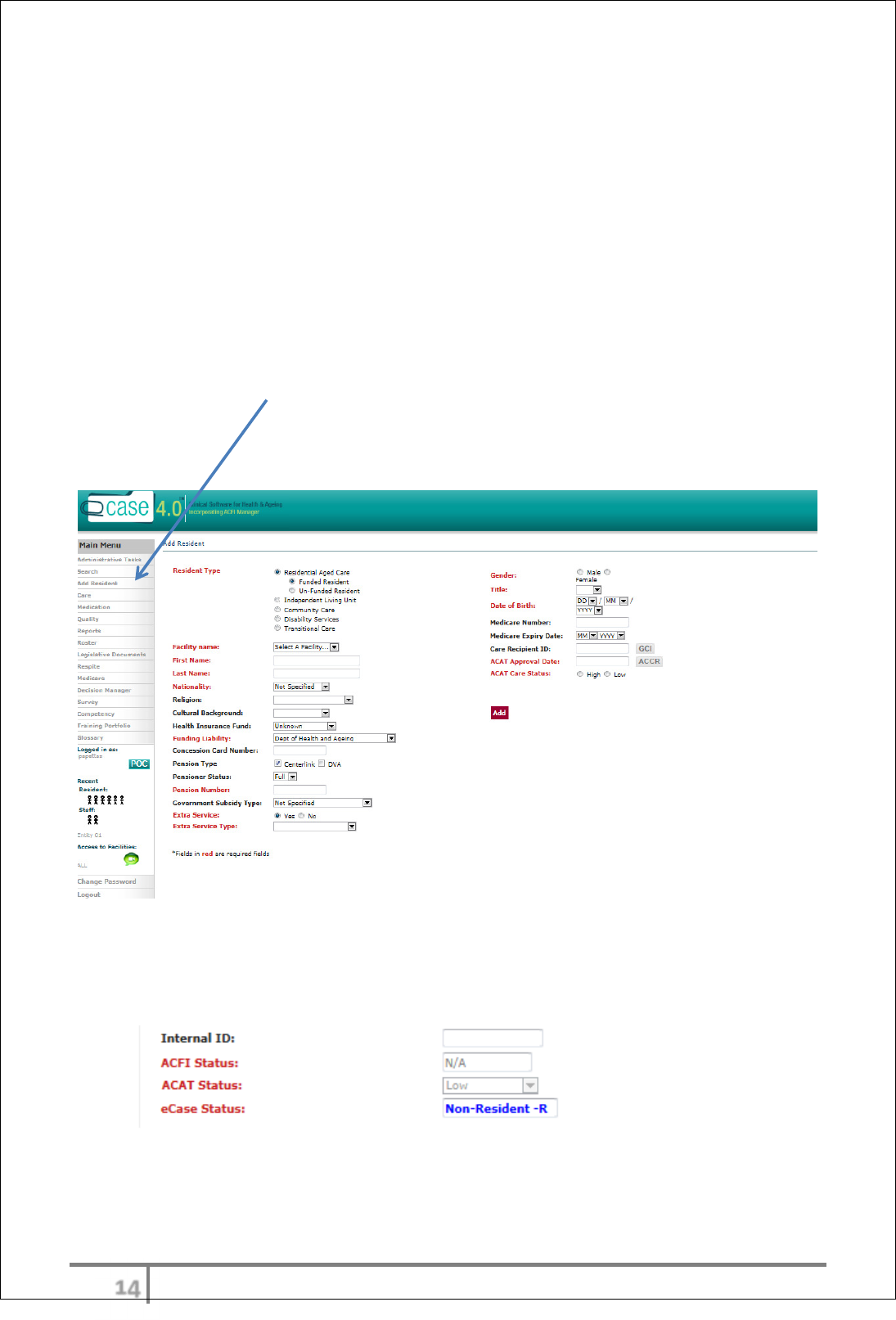
Add resident
Select add from main menu. Complete all relevant fields for pre admission. N.B
red highlighted fields are mandatory fields.
Once the resident has been added to the data base their status becomes a non-
resident
The resident can be admitted from this status or further added to the waitlist.
N.B an interim careplan can be initiated from the status.
υω
Ver 3.2013
.
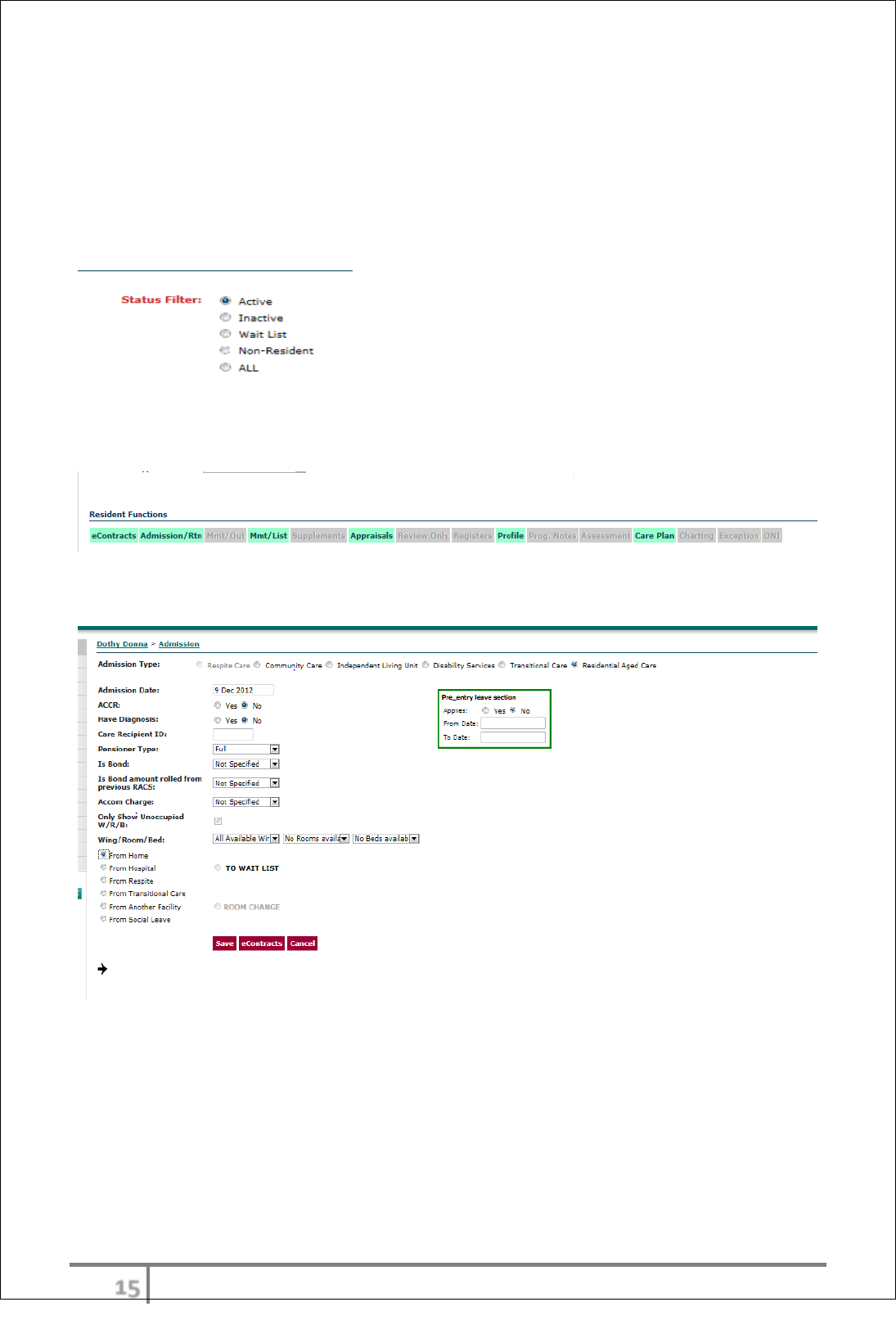
Admission
Select waitlisted resident from search function. Ensure search options are
selected accordingly by changing the status field on the search screen
.
Admitting the resident is completed by selecting the admissions/returns function
button from the function menu
All fields from the admission screen must be completed, then save
The admission transaction will generate numerous activities including:-
1. B2B transaction to Medicare Aust.
2. Creation of ACFI expiry dates
3. Creation of care tasks in care worklog
υϊ
Ver 3.2013
.
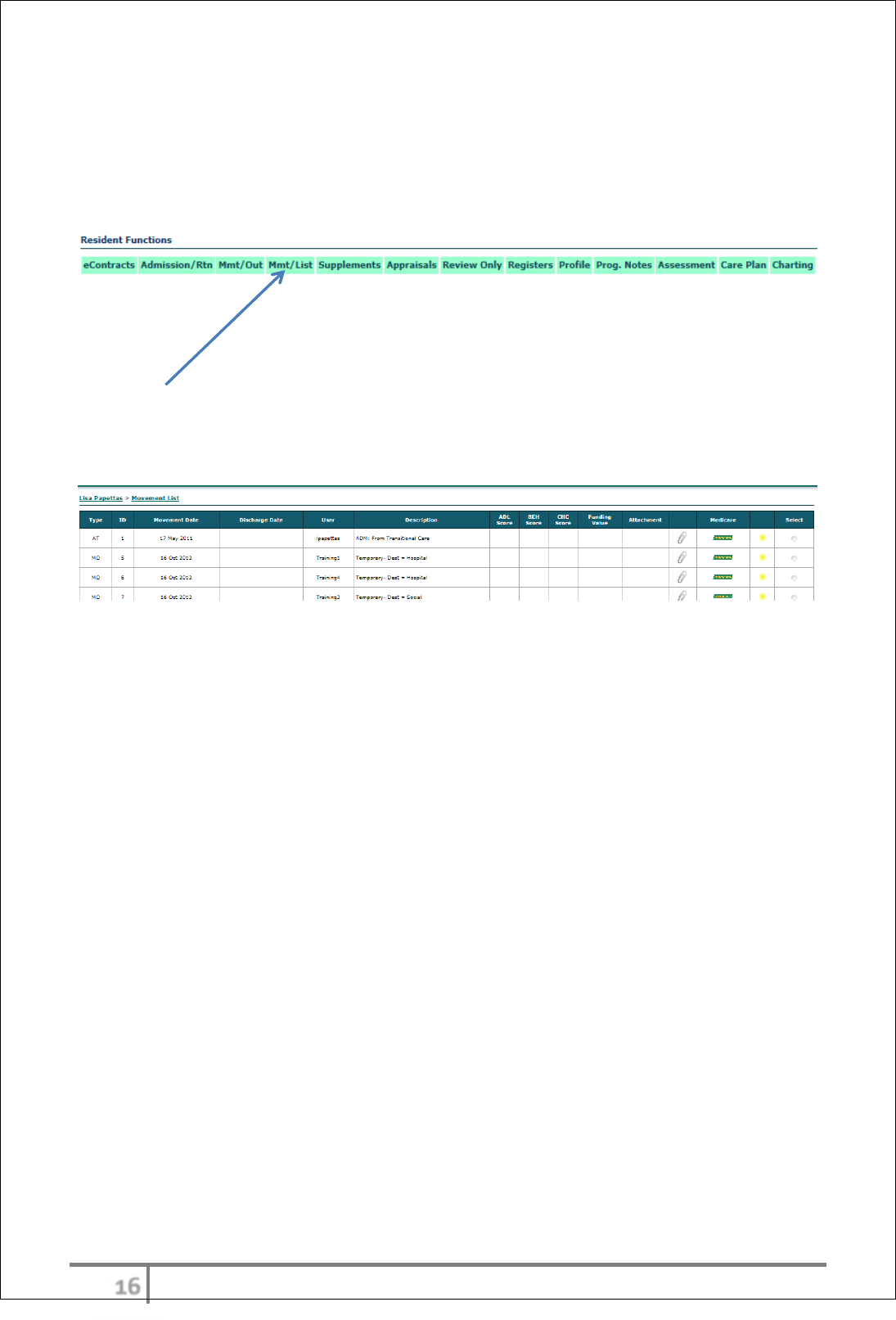
RESIDENT MOVEMENTS
All resident movements are completed using the admission/transfer function
button or the Movement out function button.
All movements are recorded and transmitted via B2B to Medicare Australia.
The resident record of all movements is found under the Movement list function
button.
The movement list provides a full overview of all movements for that resident
with Medicare status of each transaction if relevant
The colored icon will alert the Medicare status of each transaction (ie yellow on
hold, Red rejected, Green accepted)
B2B
Full B2B functionality with Medicare Australia allows users to perform all funding
related tasks using eCase:-
• ACFI submissions
• Register movements
• Resident entry records
• Funding reconciliation and finalization
B2B Overview
eCase B2B is fully integrated into all funding aspects required for Medicare.
Healthmetrics received approval from Medicare in a Notice of integration in
December 2009. Resident admissions, movements, ACFI submissions and
discharges are all seamlessly integrated into the Medicate Australia data base.
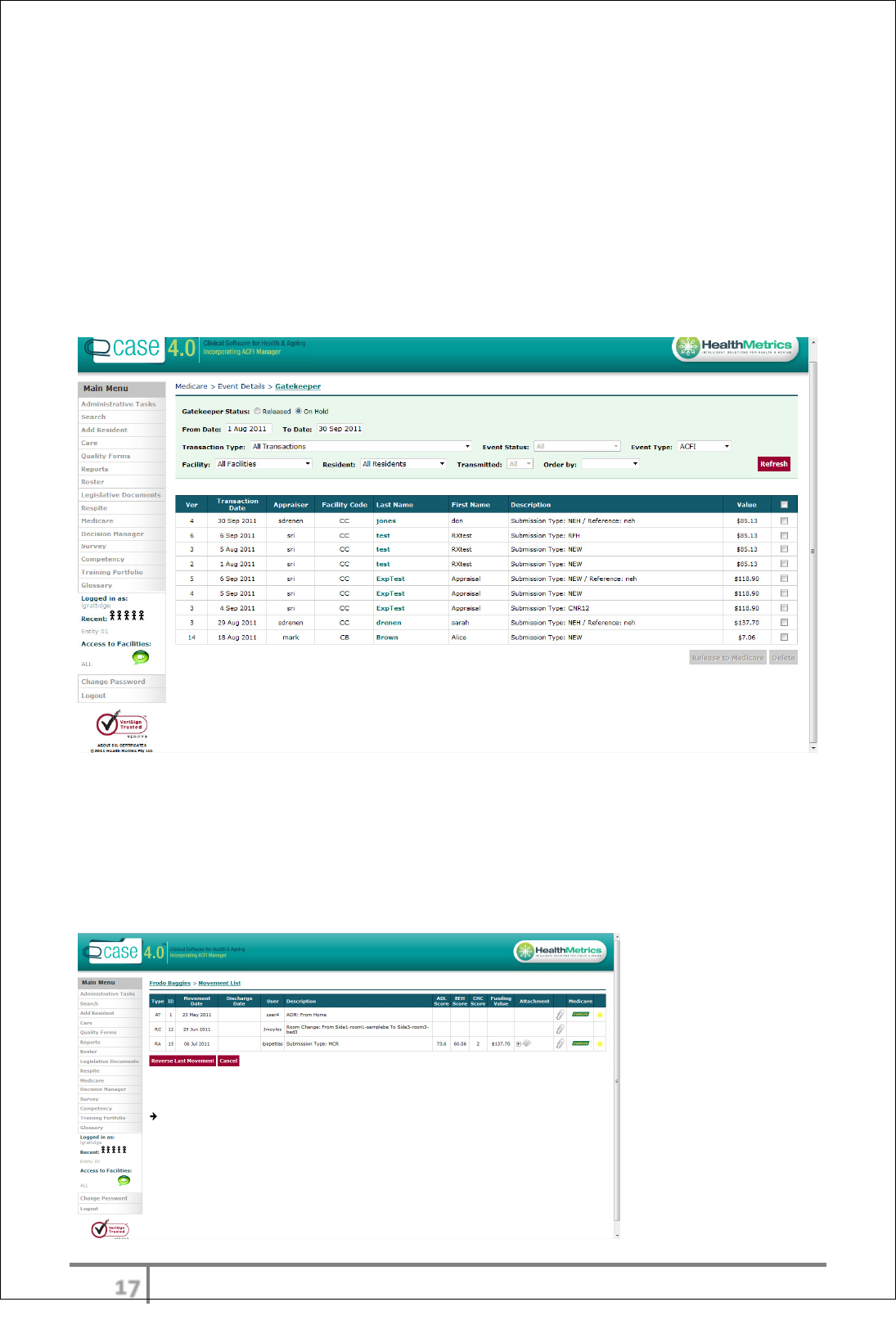
eCase also offers the ‘Gatekeeper’ function which allows all ACFI transactions to
be reviewed and submitted by selected personnel. Appraisals can be submitted
in batches following review and approval.
N.B The Gatekeeper functionality is an optional enhancement and will only be deployed if
requested by the organization.
υϋ
Ver 3.2013
.
B2B instructions for use
ACFI submission
After the user has modelled, reviewed and optimized their appraisal they will
select submit function on the ACFI submission screen.
The submitted appraisal will now ‘park’ in the gatekeeper bay. This appraisal
will not transmit to Medicare until the ‘gatekeeper’ logs in and submits the
appraisal or batch. Approved Gatekeepers are registered and provided with
appropriate level of security for submissions.
Movements (admissions, leave & discharge)
All movement transactions can be transmitted directly to Medicare. This area of
functionality does not have the gatekeeper option. Each user depending on their
level of security will have the ability to directly transmit movements. A record of
each movement is recorded in the resident movement list. Each transmitted
transaction will display the Medicare logo next to it on the movement list.
υό
Ver 3.2013
.
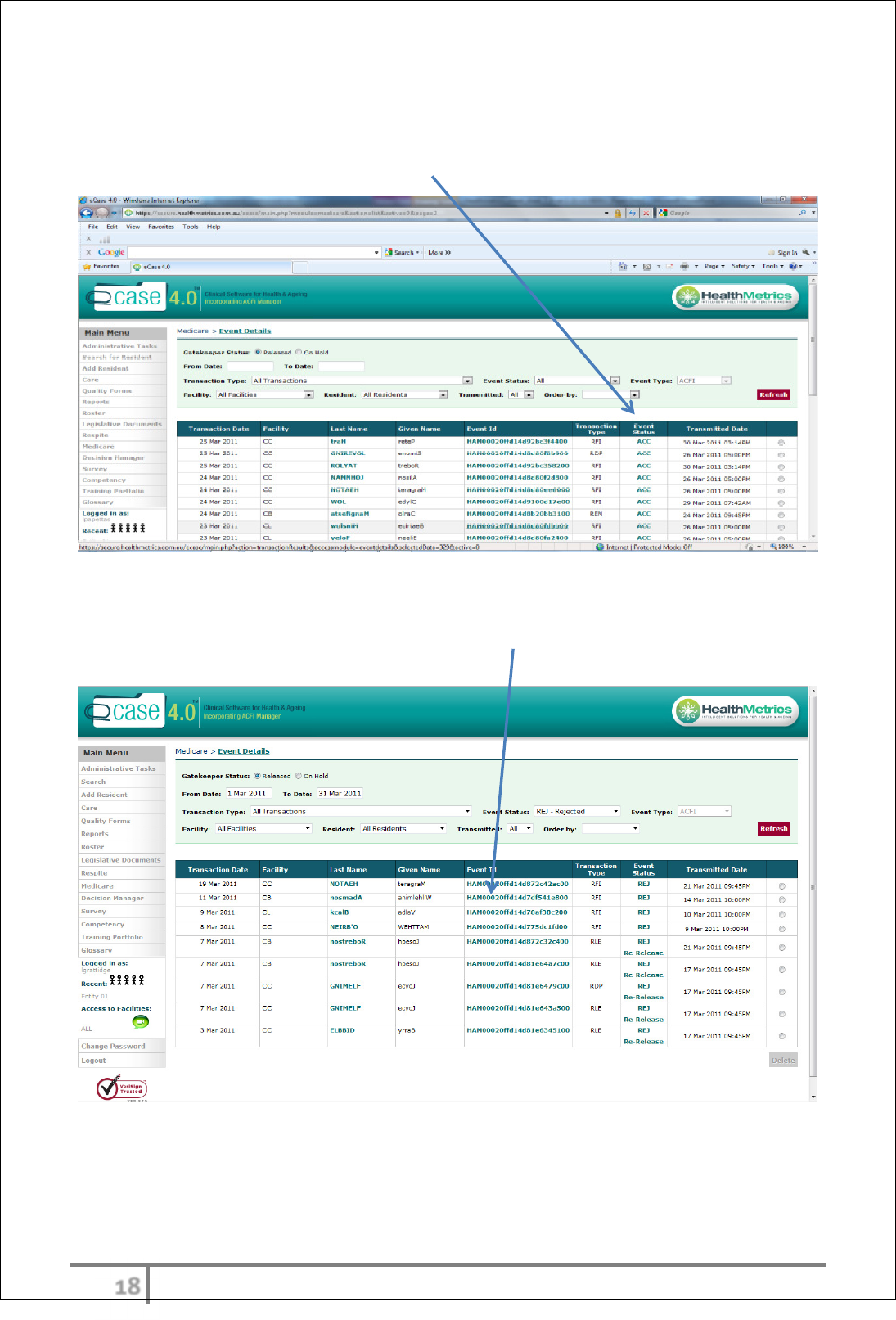
The transmission or ‘event status’ can be monitored in the Medicare item listed
under the main menu. The status will be one of the following:-
Rejected – accepted- being processed – processed – error.
Notice of unsuccessful transactions will be recorded in the Medicare table. Each
transaction receives a status code from Medicare. The code begins with the
letter HAM_______. If user clicks on this code an explanation regarding the
status of this transaction will be provided.
υύ
Ver 3.2013
.
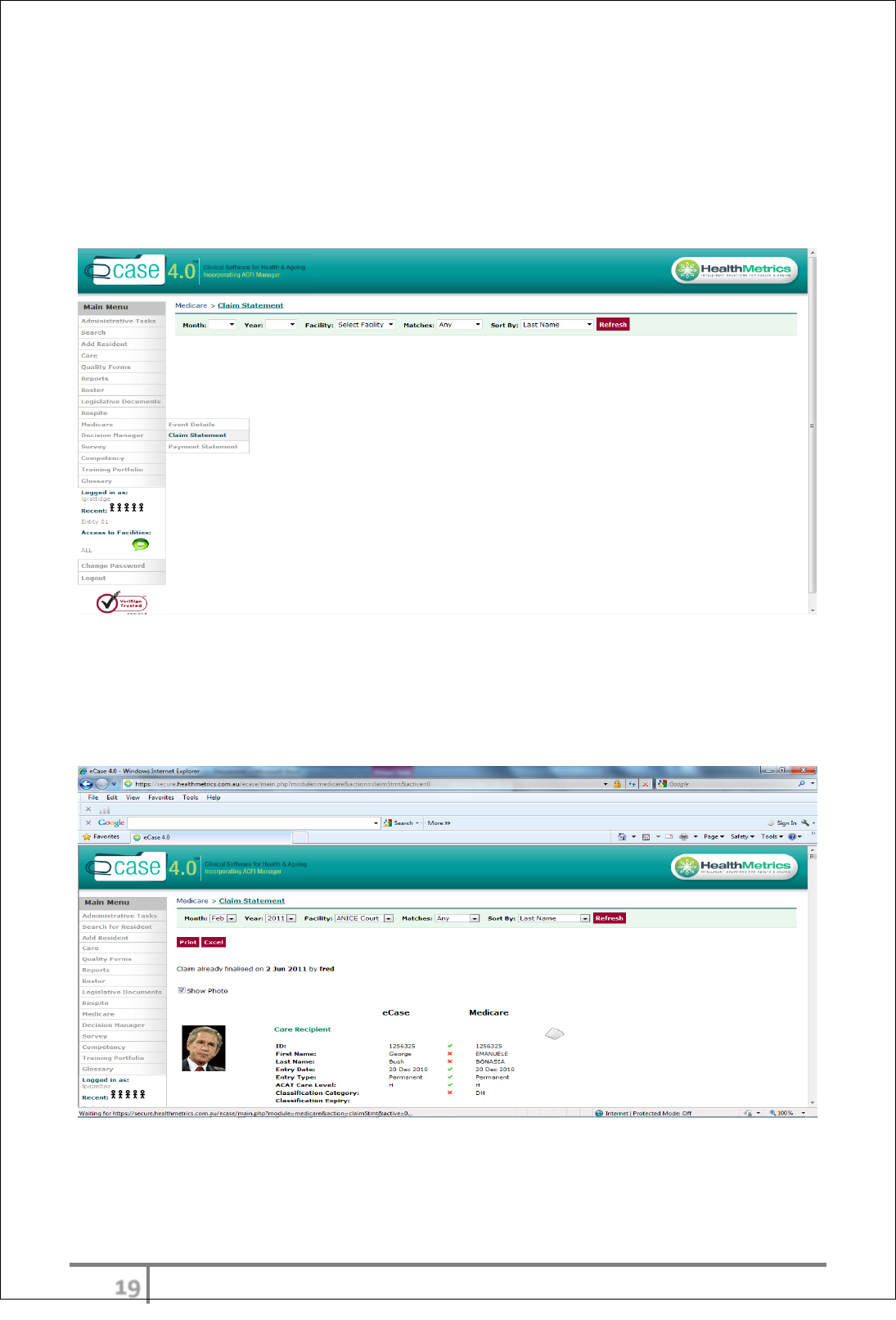
Claim finalization
To access the claim statement the user must ‘call for’ the statement 24 hours
prior to point of use. The populated claim statement will be available for review
after 24 hours. The claim statement provides reconciliation between Medicare
and current eCase data.
Ticks
identify matches and crosses x identify mismatches between Medicare
and eCase. The notes icon provides an option for the user to enter a
summary/explanation regarding the mismatch or transaction.
N.B Mismatches do NOT prevent a user from finalising the claim.
When the user is satisfied with the status of all transactions, click on the ‘Finalise
Claim’ button.
φτ
Ver 3.2013
.
CARE FUNCTIONALITY
eCase care functionality is based and driven by the principle of resident centred
care. This can be seen throughout the product with not only the framework but
words used to refer to the resident
Care Overview
Activities within the care worklog are at the heart of the care system. Everything
comes from and revolves around activities generated into the worklog. Activities
are split into parent and child activities.
The care framework enables Users of the care system to access triggered care
events (activities, parents/children) on the basis of specific events (movements)
in the life of a resident, by progress note trigger or by adding adhoc activities as
required. At a facility level or a resident level, exceptions to the ‘framework’ of
care can be set up. Setting up the original frameworks of care will be configured
by Health Metrics consultants in accordance with the requirements of the
Provider’s operations.
eCase care promotes the person centred care model. After searching for a
resident the entire screen will become related to that particular resident. Each
assessment, chart and careplan will draw the User to the attention of the related
diagnosis including physical and mental. Careplan refers to the resident as ‘I’ or
‘MY’. These basic design features promotes the focus on that particular resident
and on their individual needs for care at all times.
eCase care is also structured to enable the Facility manager or Clinical manager
can have full transparency to all aspects of care delivery and status at all times
from anywhere. This is includes access and review all care documentation that
occurs in the facility at any given time, review care worklogs, progress notes
overview and activity viewer.
Workflow
Care workflow is generated into the care worklog by several sources. This
includes progress notes, resident movements (admission, leave, and discharge),
generation of particular charts and ádhoc adding clinical tasks to the worklog
itself. (see full description pp23)
Resident movements
Resident movements can be configured to trigger care task events in the care
worklog. As an example the resident admission transaction will set out day by
day the 21 days of assessments required in the work log. As staff log on each
day the corresponding tasks will be allocated to staff depending on the
φυ
Ver 3.2013
.
staff/resident allocation. Other movements also generate tasks in the same
manner.
Progress notes
Progress notes are tagged according to the type that best describes the event
that has occurred. Depending on the tag/s selected, workflow will be generated
for the user accordingly (see progress note overview). This ensure that all
required tasks according to the issue are outlined and completed on all
occasions. Progress of all such tasks can be monitored by senior staff using the
‘activity viewer’.
Chart generated activities and adhoc creation.
Certain charts have the provision to allow automatic generation of an activity in
the care worklog. One example is the blood glucose monitoring chart. The user
can schedule the ongoing task of BGL monitoring in the care worklog. Adhoc
activities can also be added from the care worklog itself as an ‘add activity’. This
may include items such as BP monitoring for week etc.
All tasks generated regardless of the source can be monitored via the ‘activity
viewer’ which displays the status of the activity, who has completed it including
time and date.
All entries must be sighted and signed off by the person completing the task.
The overriding principle ensures compliance with outcomes and the opportunity
to ensure the continuous improvement cycle is closed.
φφ
Ver 3.2013
.
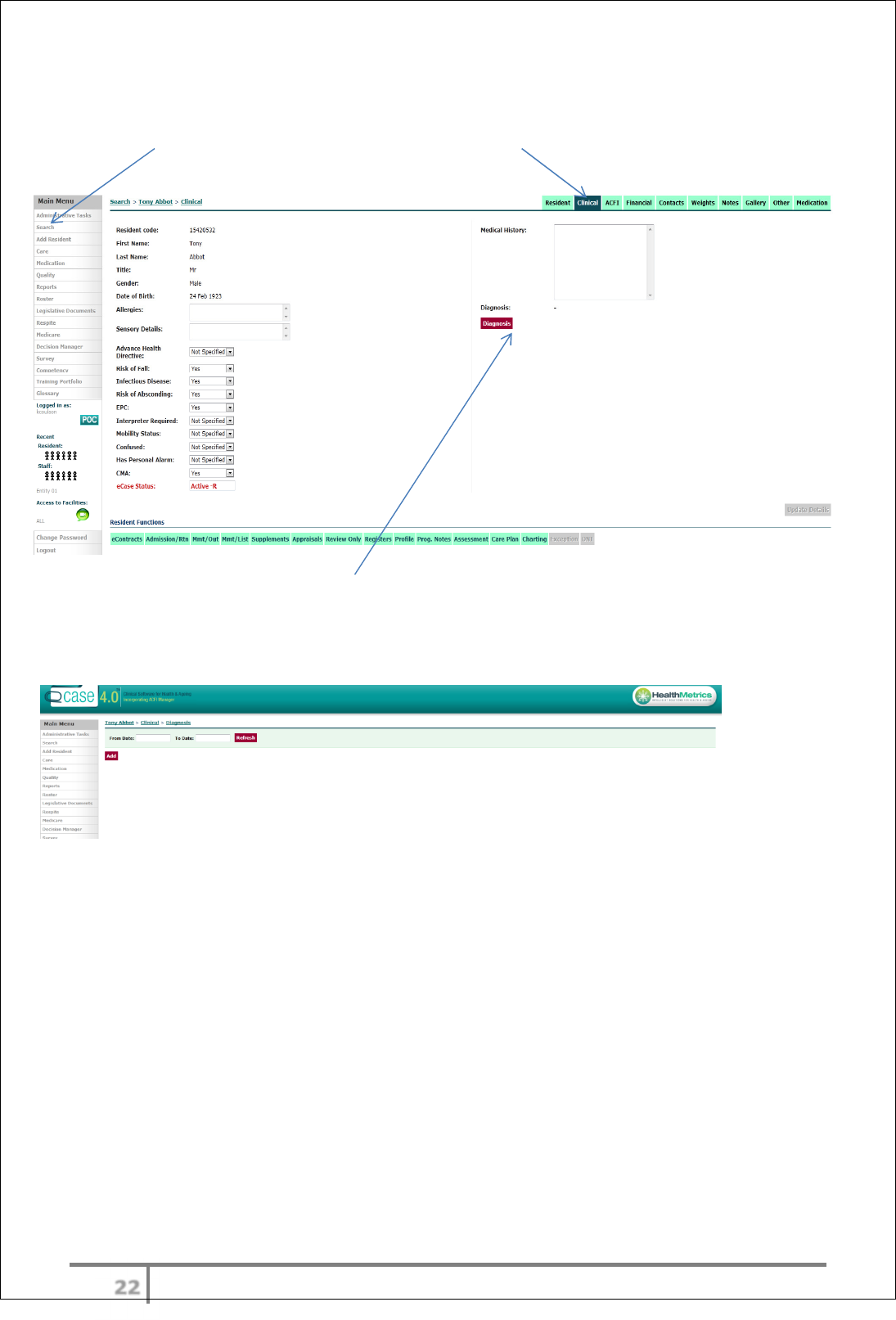
Creating new Diagnosis
‘Search’ for resident’s name, then click on the clinical tab
To create new or add existing diagnosis
To search for a particular diagnosis page that may have been created enter date
range and refresh
φχ
Ver 3.2013
.
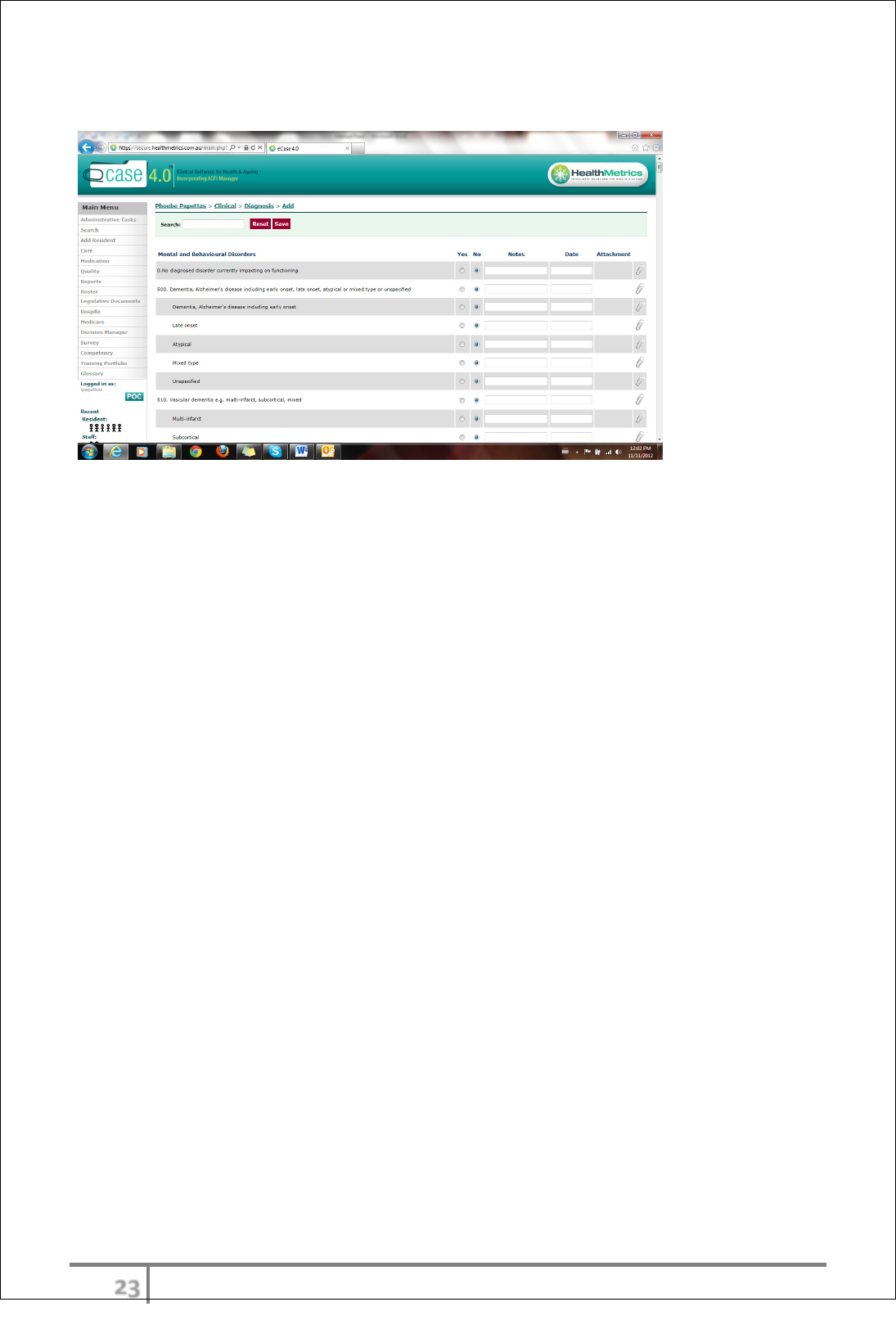
Add new diagnosis page or update existing diagnosis
• Select ‘ADD’ on the diagnosis page. If there is an existing diagnosis you
will need to select on that line and add the new diagnosis to the list. If
there is a totally new diagnosis you will add a new line.
• The user can add notes, attachments and date relevance to any of the
entries. Access to the add function can be security limited by role.
• Diagnoses can then be viewed throughout the care system where relevant
and will also update the ACFI diagnosis list.
φψ
Ver 3.2013
.
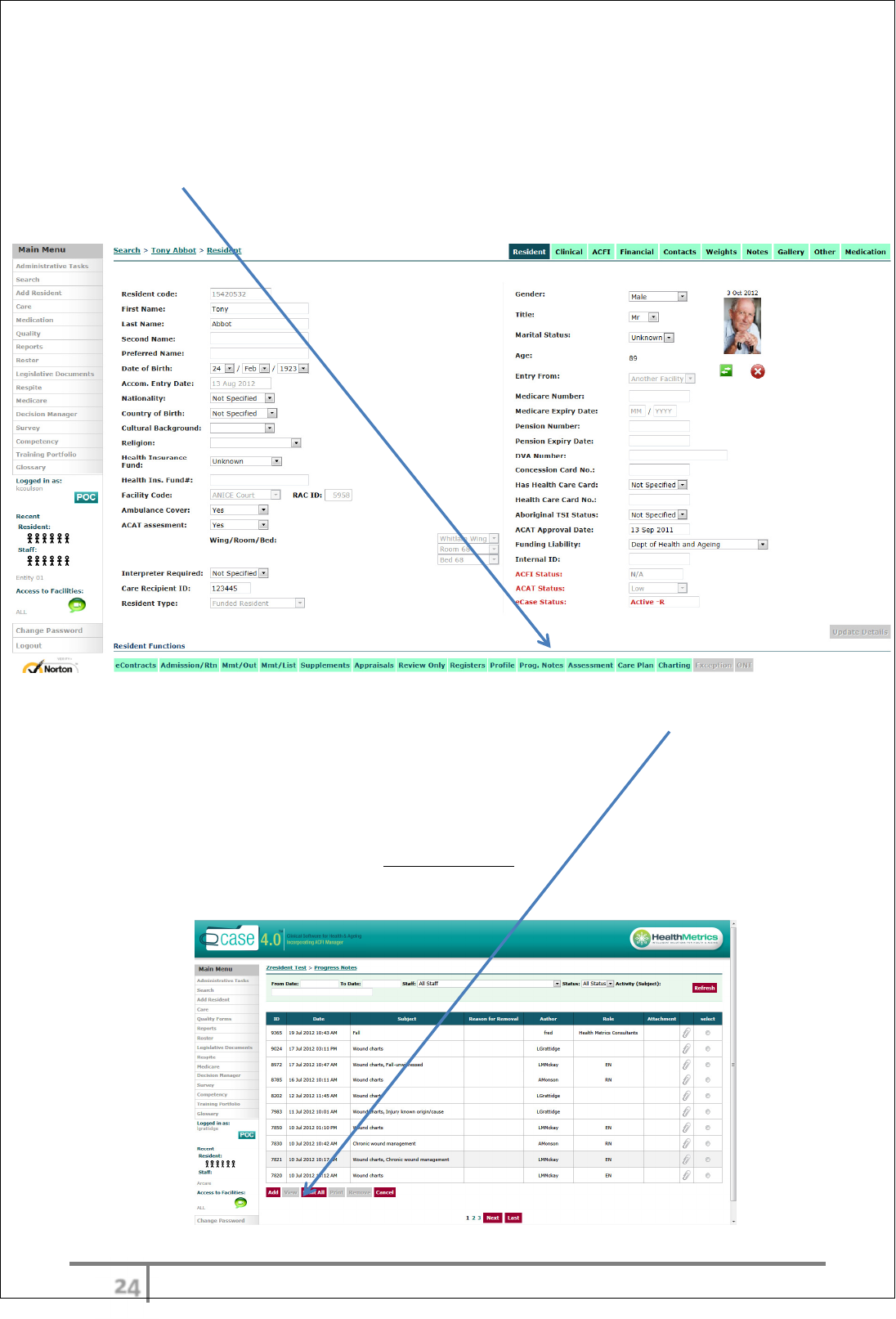
Progress Notes
Adding Progress Notes
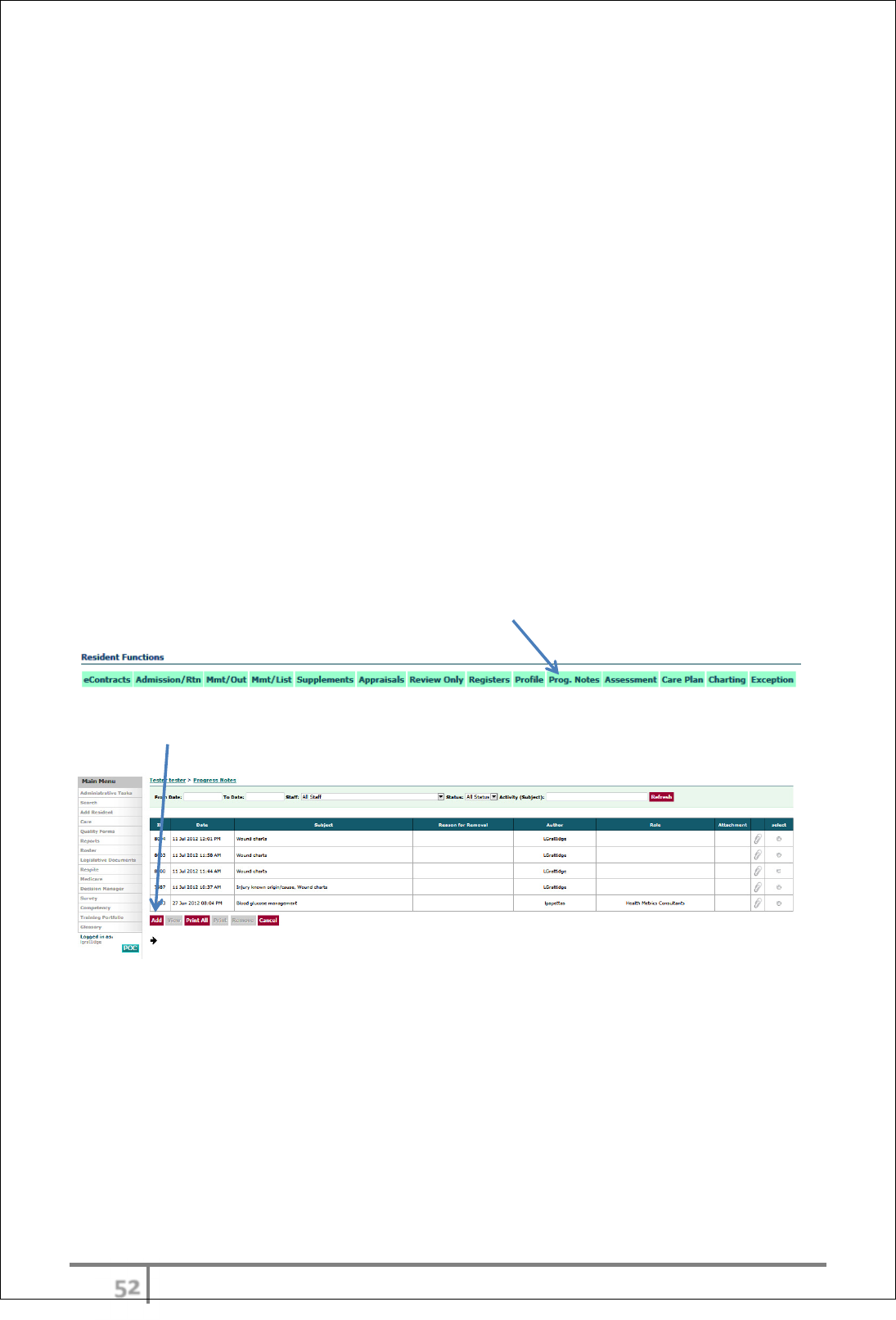
Select ‘Progress. Notes’ from Resident Functions menu
The previous progress notes will show on this screen. Select ‘Add’ to start a new
progress note.
The User can also View, Print All, Print a selected entry and Remove progress
notes from this screen.
Note: Deleted notes will have a strike through and a reason must be provided
for deleting.
φω
Ver 3.2013
.
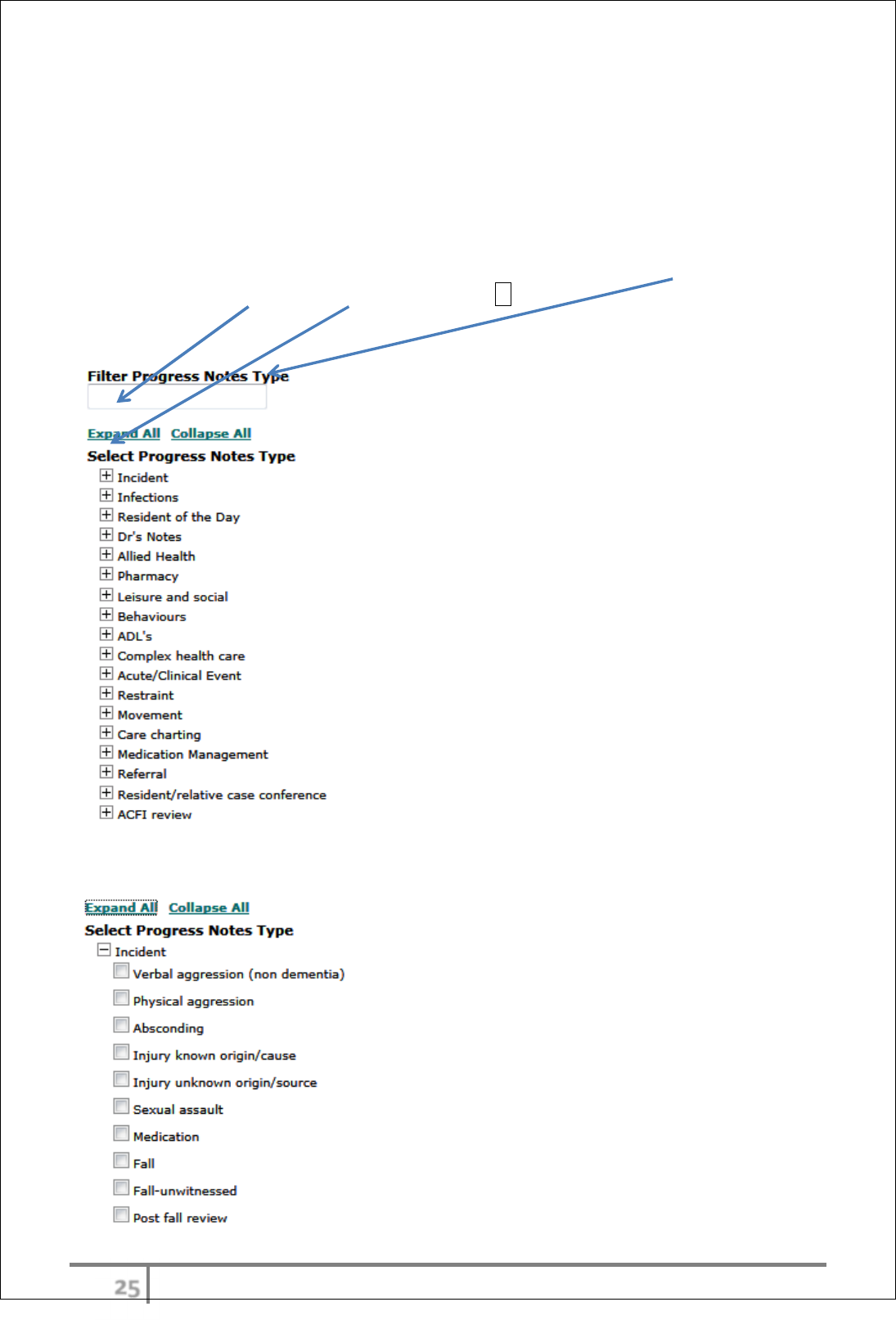
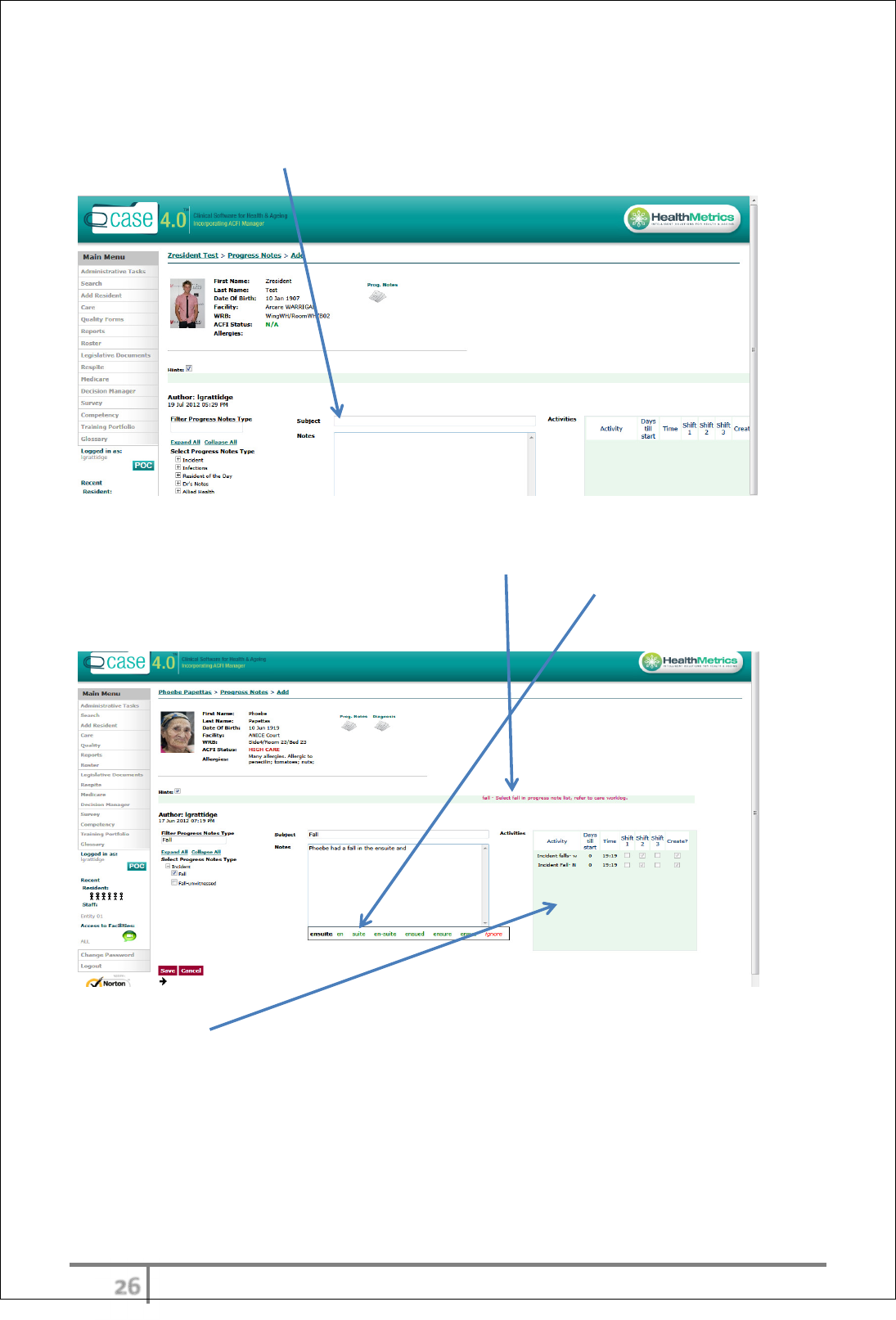
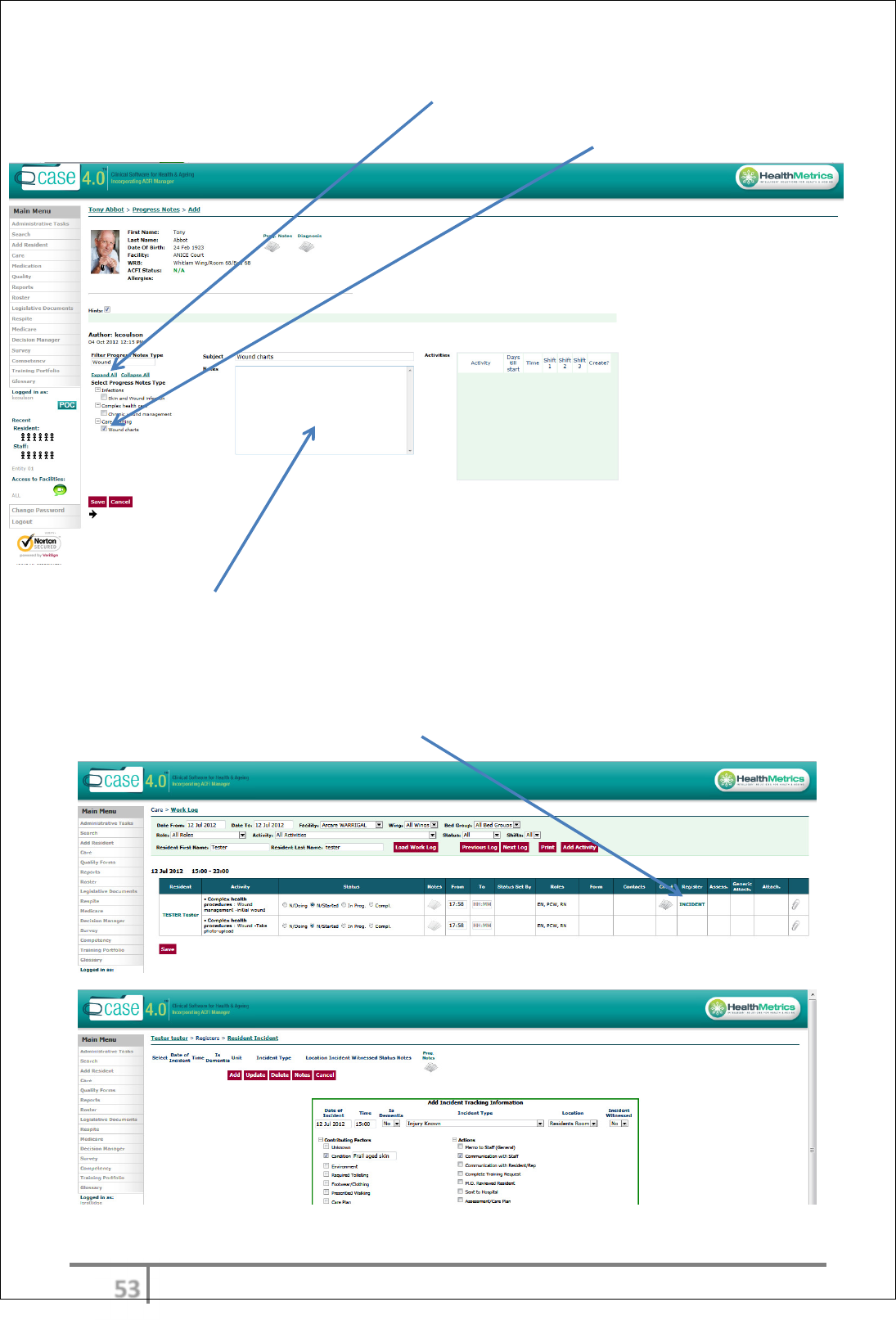
Choosing the ‘type’ of Progress Note
Progress notes are entered by selecting the type of progress note using the
‘Filter Progress Notes Type’. This is very important as it is the type of progress
note that will outline actions/workflow required. The tasks allocated to the ‘type’
(if any) will be found in the Care ‘Work log’. The user will be forced to the
worklog page after saving if an activity exists.
This can be done by either entering a key word (or part thereof) into the ‘Filter
Progress Notes Type’ or using ‘Expand All’ or + which will display progress notes
sub-types.
Example of sub-types of Incidents expanded.
φϊ
Ver 3.2013
.
Multiple types can be chosen by selecting check box/es and will auto populate in
Progress Note > Subject field.
Writing Progress Notes
As the User types the progress note entry ‘Hints’ (remind the User to do certain
tasks) will stream across the screen. Below a spell check will be activated
offering corrections and alternatives for misspelt words.
The Activities screen will show any tasks that may need to be completed if
previously configured. These tasks will be accessed from the worklog.
φϋ
Ver 3.2013
.
Tasks/activities after the progress note
The User will then be automatically taken to the Work Log screen. The Work Log
screen will show the tasks associated with the progress note entered. The User
can access the Work Log screen at any time to see outstanding tasks.
Work Log – The User may have a form/chart/assessment/careplan sitting in the
Work Log related to the entry they have just made. In this example there is an
Incident register , Neurological chart, Dr contact details all generated from an
Incident progress note .
φό
Ver 3.2013
.
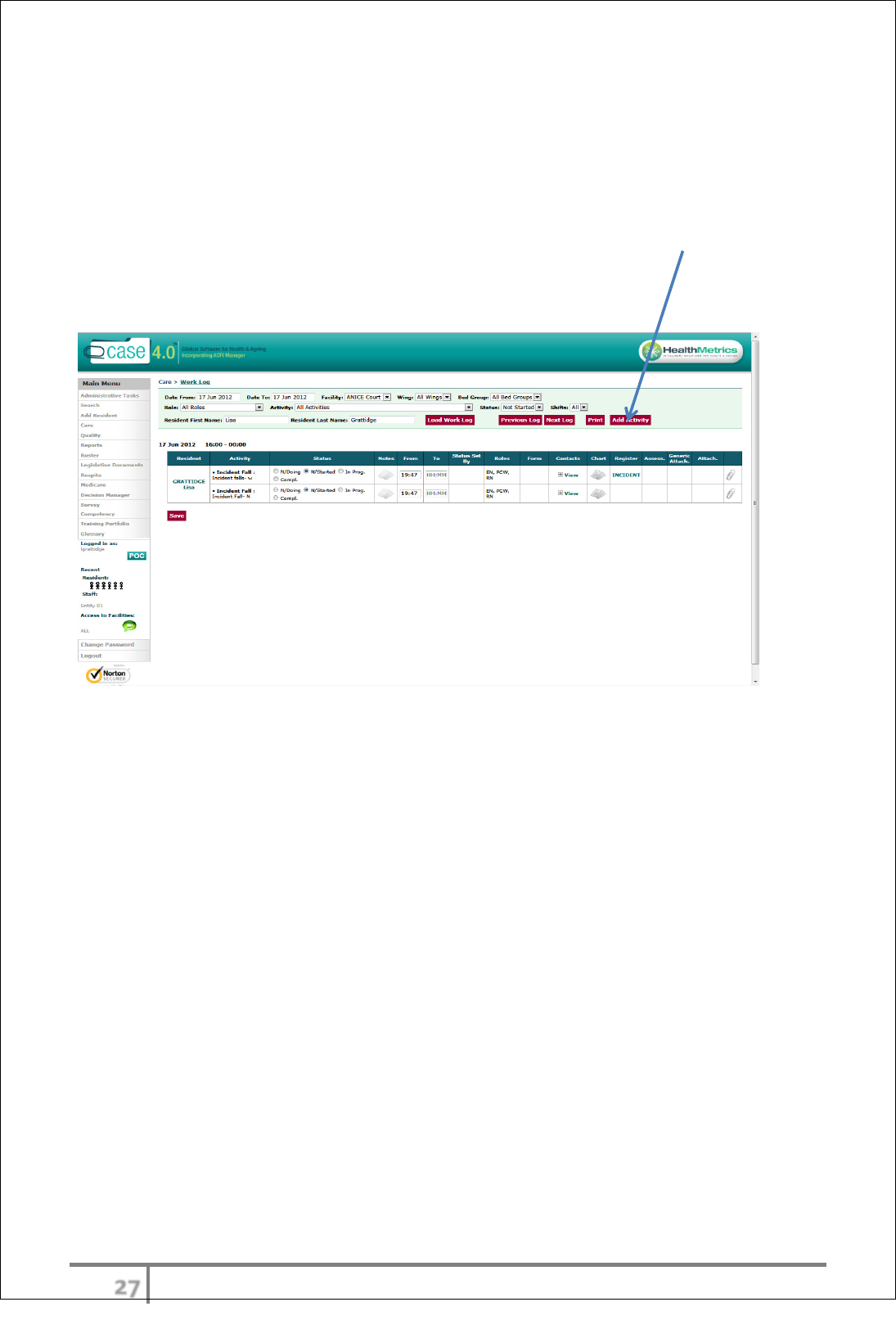
Care Work Log
The Work Log lists tasks that require completion on a designated shift (subject
to filter applied) by designated staff (according to role). The tasks may have
been generated from a progress note, movement, adhoc add activity or by chart
generation.
Each staff member must check their Work Log every shift, to identify any tasks
allocated to them, section/bed group, or individual resident. Senior staff
members will also periodically access the care worklog or activity viewer to
monitor and identify tasks that may not have been completed.
Daily eCase access and activities
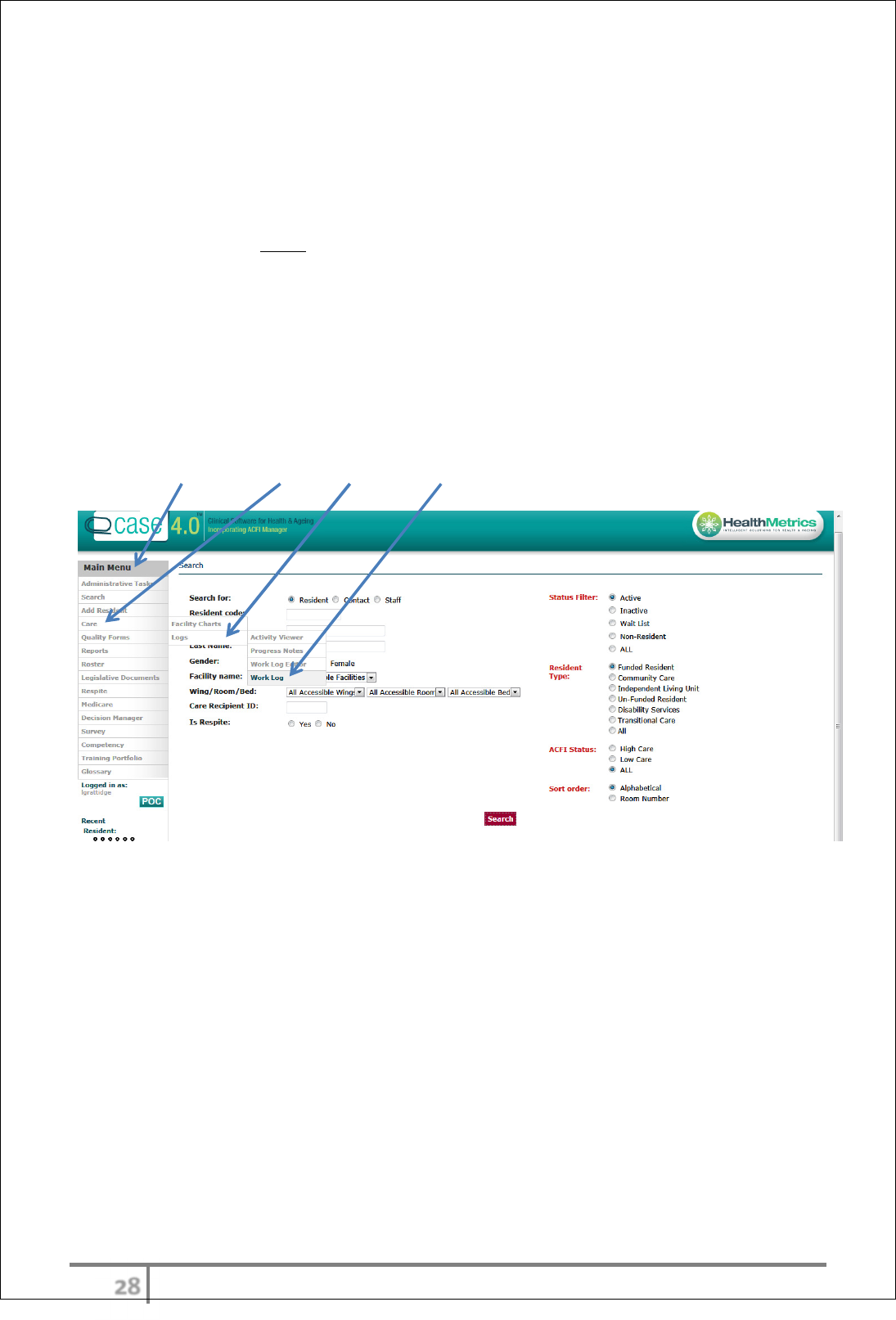
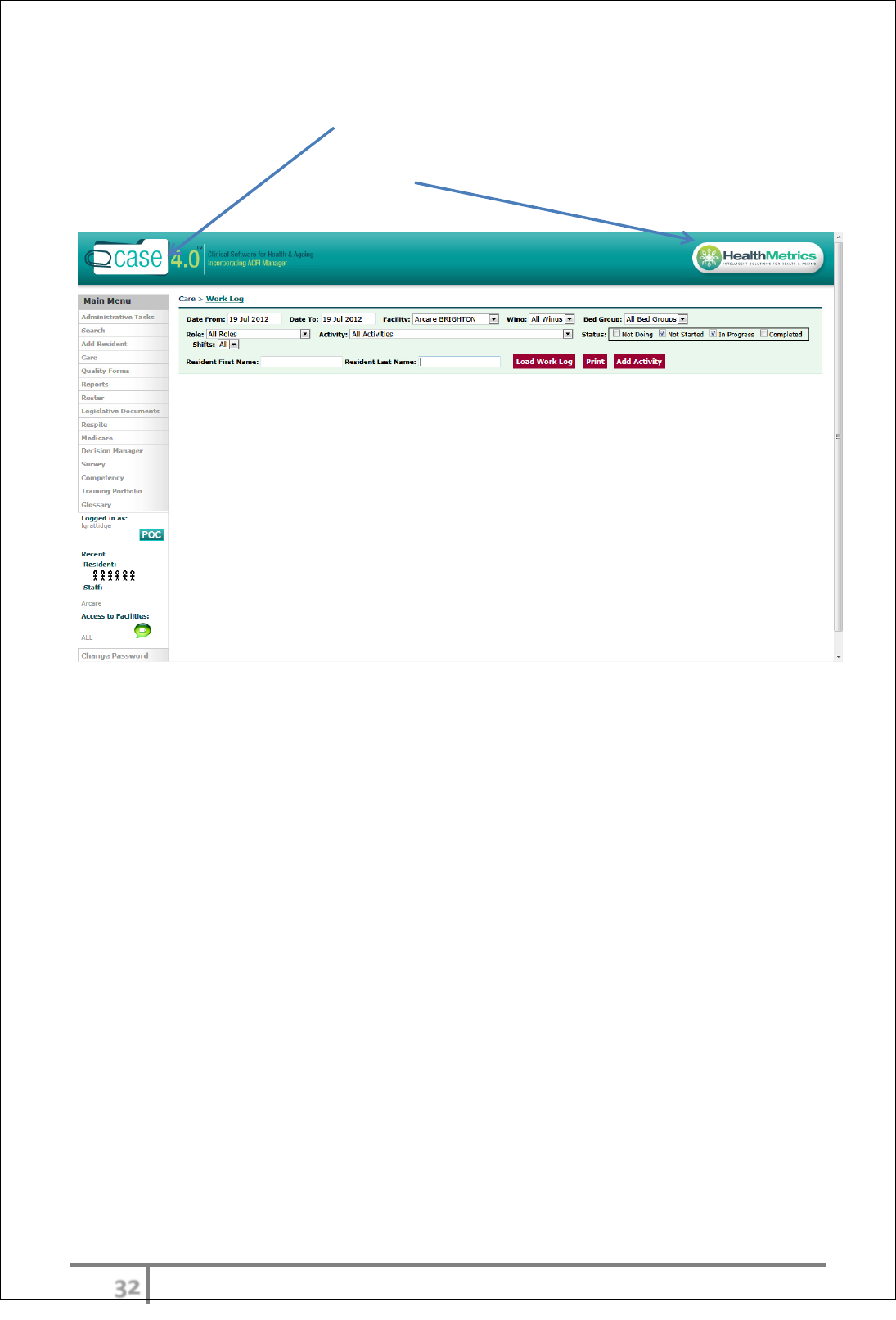
There are two ways to access the Work Log.
Access Work Log – Option 1
Main Menu > Care > Logs > Work Log
Load Work Log
At the top of the page, a range of filters are available – Date Range > Wing >
Bed Group etc. The User will need to apply the relevant filters to query the data
base (the Facility and current date will default) This is based on the residents the
user is responsible for an any given shift.
Staff can also print the worklog for their allocated residents to refer to
throughout the shift
φύ
Ver 3.2013
.
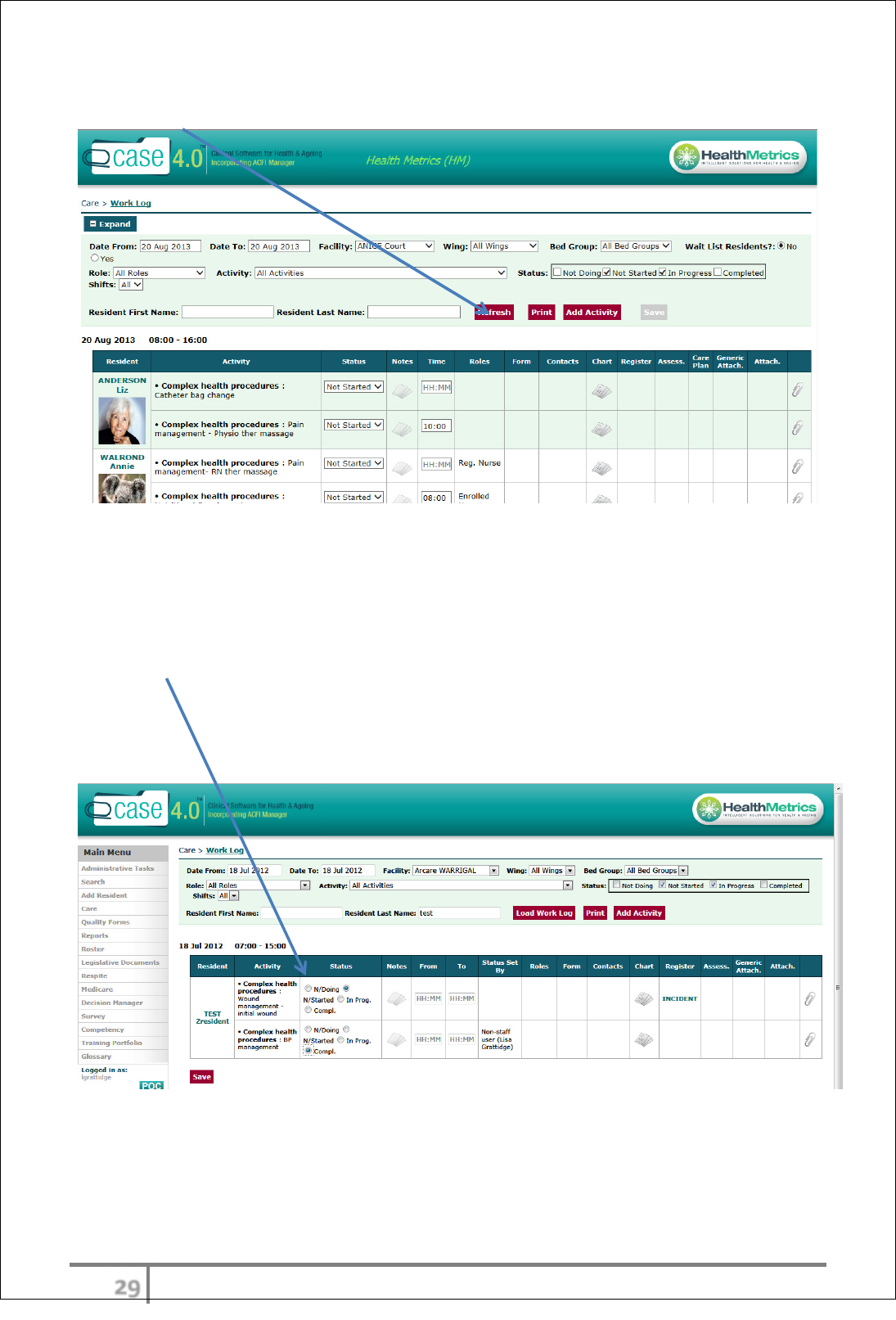
The User can select the ‘Wing’ and ‘Bed Group’ they are working in then select
‘Refresh’.
Work Log activities – tasks allocated for the day
The User will now see all allocated residents and the tasks/work that is required
to complete for the day.
Each task has the corresponding chart/assessment/form to complete. Click
on the chart/assessment/form to complete the tasks. Each task will open in
a separate window; therefore staff don’t have to go in and out of the care
worklog. If auto close does not show after you have completed a task then the
User must then select the status according to the progress of the task. ie select
Compl. (Complete).
χτ
Ver 3.2013
.
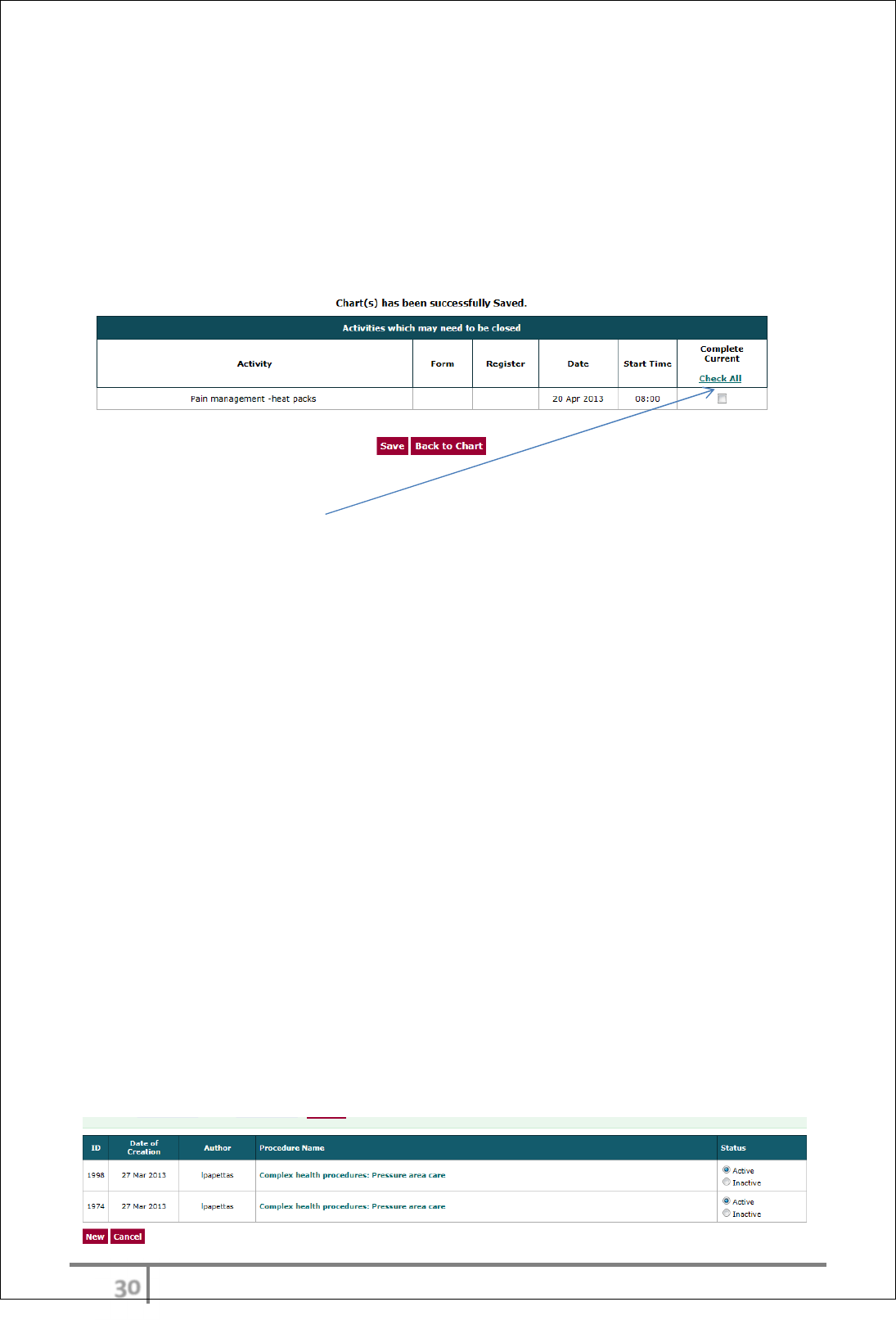
Auto-close
The auto close function currently only applies to the most commonly used
charts. Healthmetrics plans to have this applied to all activities in the worklog
by July 2013.
The auto-close provides the user a second screen after clicking on a chart from a
worklog scheduled activity. Once the chart has had an entry made the following
screen will be displayed
The user then selects ‘Complete current’ task and then saves. This will
automatically sign off the activity in the Worklog.
Currently the auto close applies to the following charts:-
• Bowel charting
• Pain management (Complex health care chart)
• Blood Glucose chart
• Blood Pressure chart
Chart deactivation
The chart deactivation function allows the user to deactivate a chart which is no
longer current or required. This function is however role restricted and is by
default only available to the RN. As per Healthmetrics security model this can be
changed at any time on request from project managers.
All charts have the deactivation function.
Select the inactive button and save. The chart will then be read only.
Chart deactivation

χυ
Ver 3.2013
.
Access Work Log – Option 2
The User can also access the Work Log using the POC (Point Of Care) button.
The User won’t be able to see the entire Work Log for a Bed Group however will
be able to access one resident at a time.
POC (Point Of Care)
Point of Care (POC) is designed to allow a Carer access to all of the relevant
information they would normally require in the course of their duties. Although
accessible from a desk top computer, the POC is primarily designed for
Toughbook’s or other point of care devices (ie ipad, galaxy etc. etc.)
To access POC:
1. Selecting from Main Menu
Or
2. Selecting the Healthmetrics logo
Select Wing > Bed Group and select Refresh
The resident photos will appear as per filter applied. Click on the resident’s
photo and then Work Log. Any items for this resident will now display on the
Work Log.
χφ
Ver 3.2013
.
Accessing POC (Point Of Care) - tips and tricks
If a User selects the eCase logo it will take them back to the search page.
For POC Users, select the Healthmetrics logo and this will return to the POC
page.

χχ
Ver 3.2013
.
Add Activity
Adding an activity can be executed in 2 ways.
1. Via the Work Log (adhoc by RN). Limited activities available
2. Using individual resident charts (most charts).
3. Generated by progress notes automatically.
4. Generated by movements automatically.
The Work Log ‘Add Activity’ is to be used where the chart required does not have
the capacity to generate activities. (See List of charts in Charts heading)
The ‘Add Activity’ by individual chart enables the User to schedule ongoing
activities related to a specific chart. This may include items such as BGL and BP
management.
Scheduling an Activity via the Work Log
Access the Work Log via Main Menu > Care > Logs > Work Log
Filter facility bed group required and resident Load work log.
Select ‘Add Activity’
χψ
Ver 3.2013
.
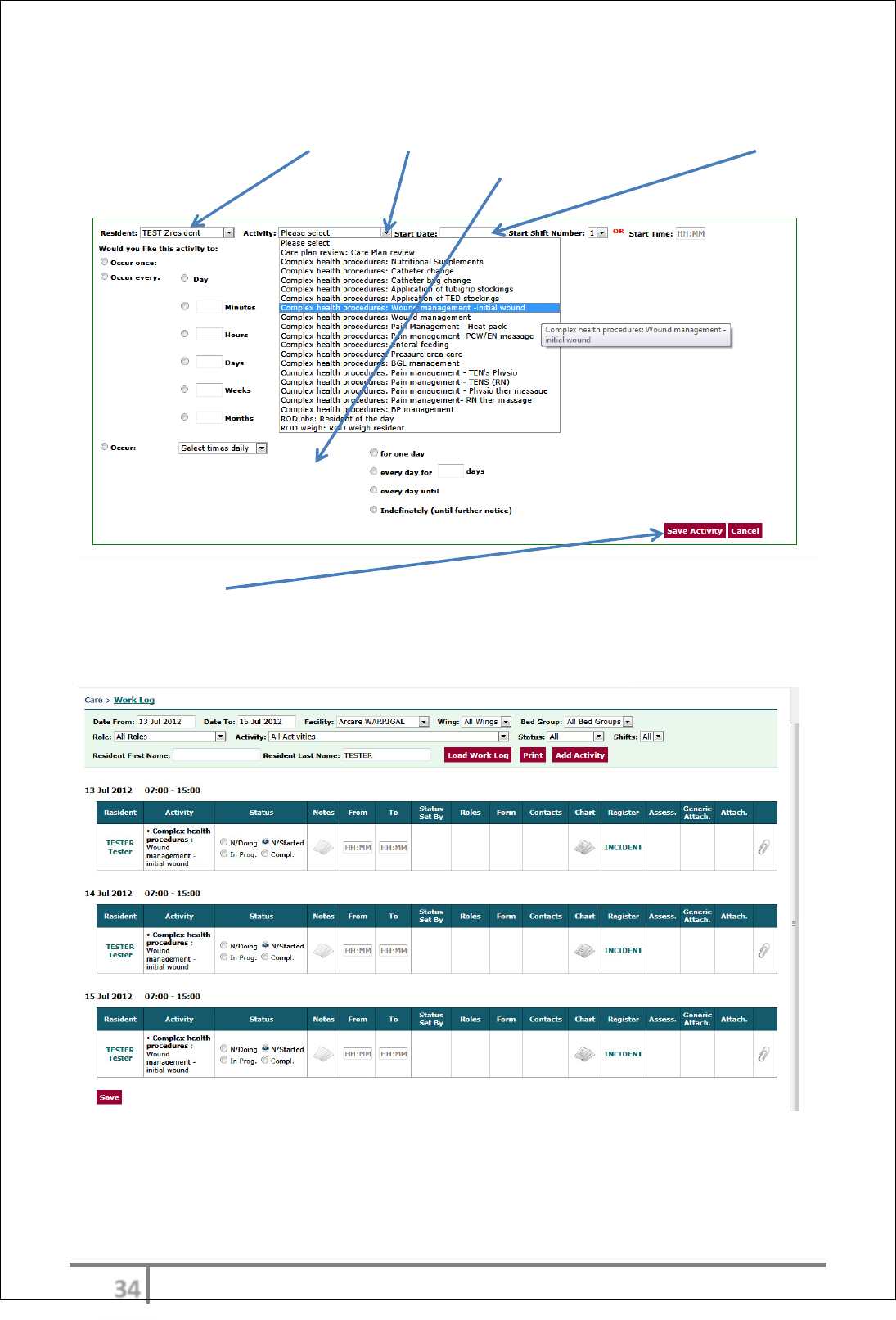
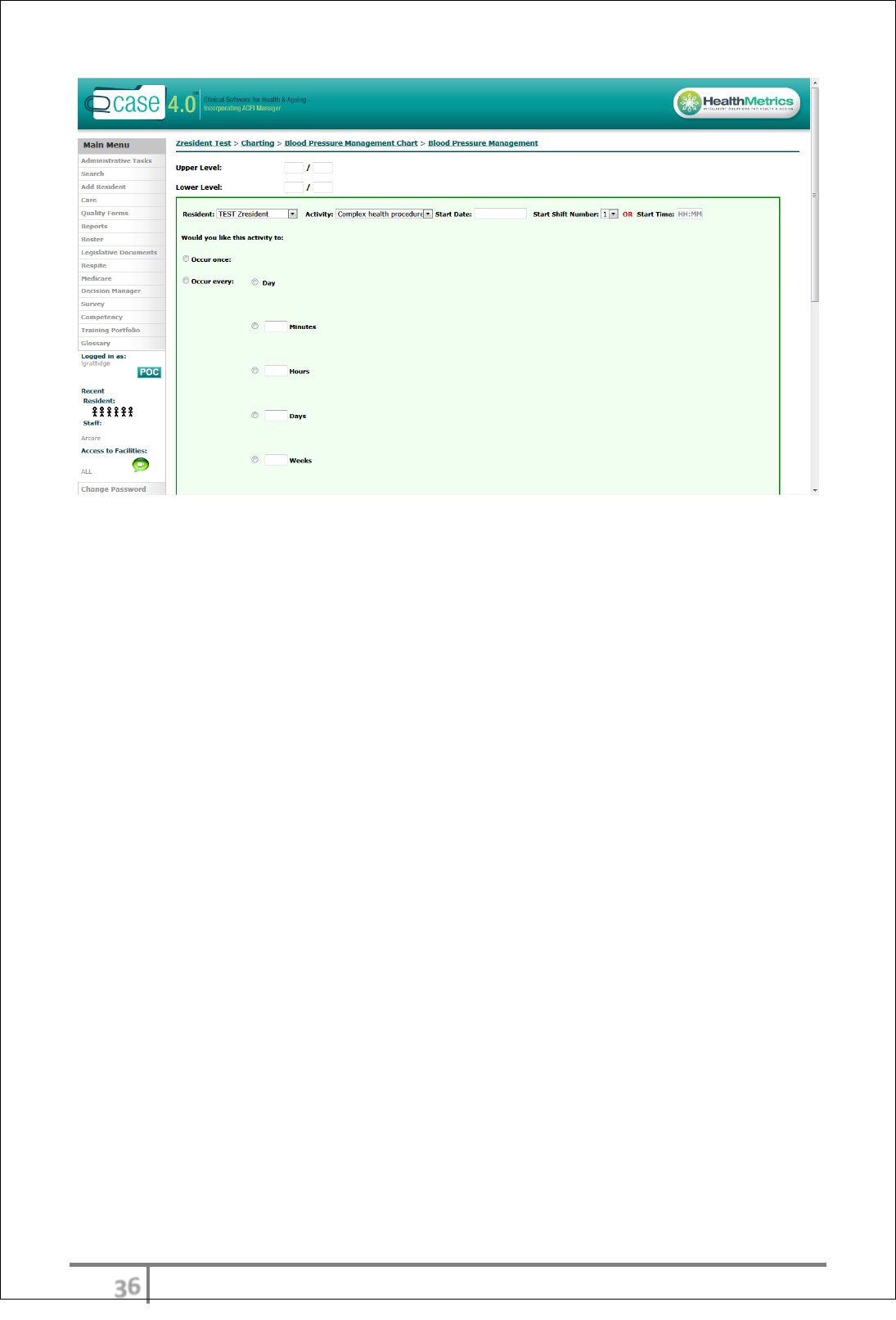
This add activity screen enables the User to schedule a particular activity.
To complete select: Resident > Activity type from drop down menu > Start Date
> Start Shift Number OR Start Time > Occurrences.
Select ‘Save Activity’
The ongoing Activities will now be scheduled in the Work Log.
χω
Ver 3.2013
.
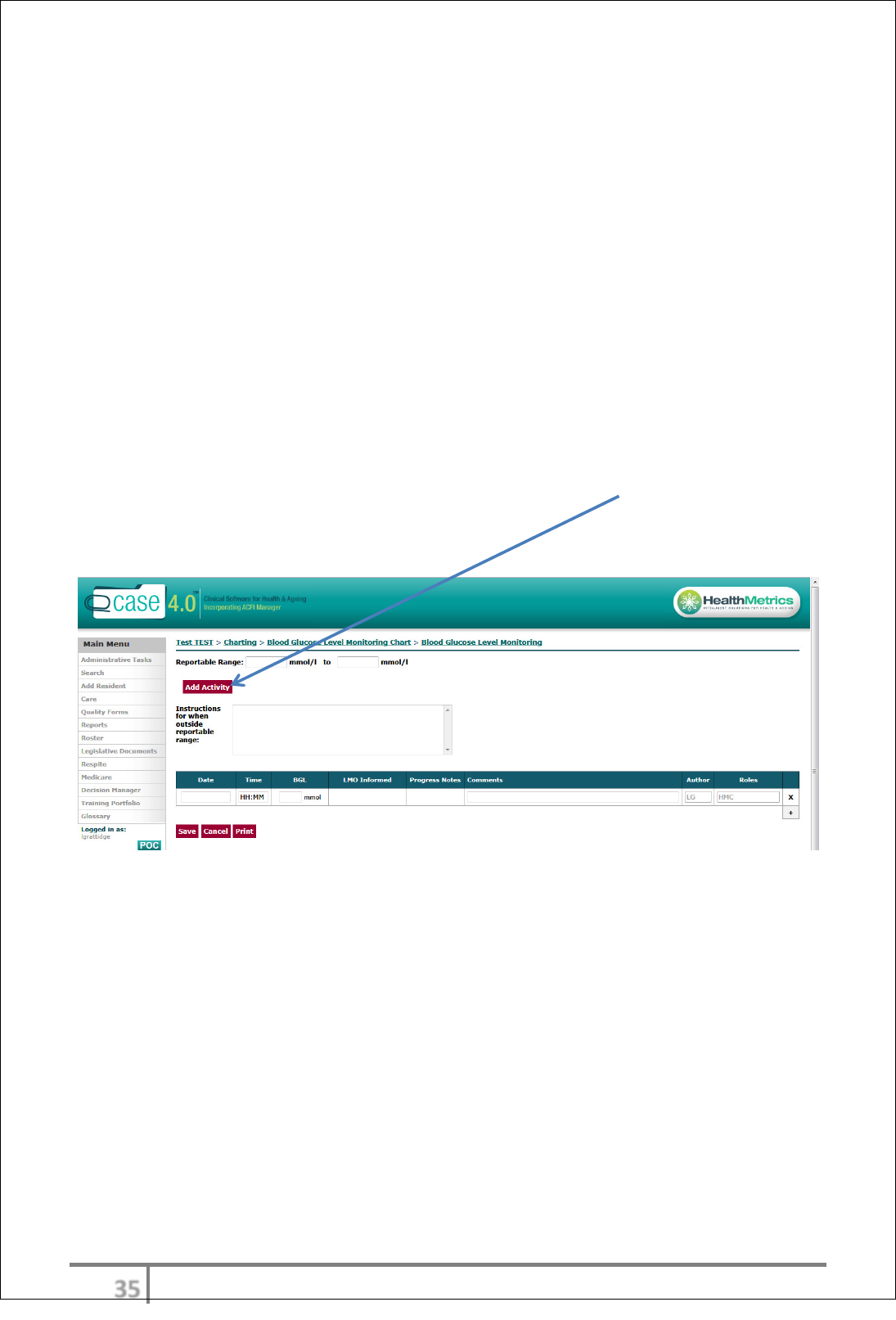
Scheduling an Activity via a Chart
The ‘Add Activity’ function or scheduler is only available when ‘New’ charts are
created and for select Charts only:
• Wound chart
• Catheter colostomy
• CPAP respiration and obs
• Fluid Balance chart
• Food and Fluid record
• Neuro obs
• Nutritional supplements
• Pain Flow chart
• Physiotherapy
• Pressure care
• Wound
An Activity can be added to the Work Log by selecting ‘Add Activity’ within the
chart or the scheduler will appear directly on the page when a new chart is
created.
χϊ
Ver 3.2013
.
χϋ
Ver 3.2013
.
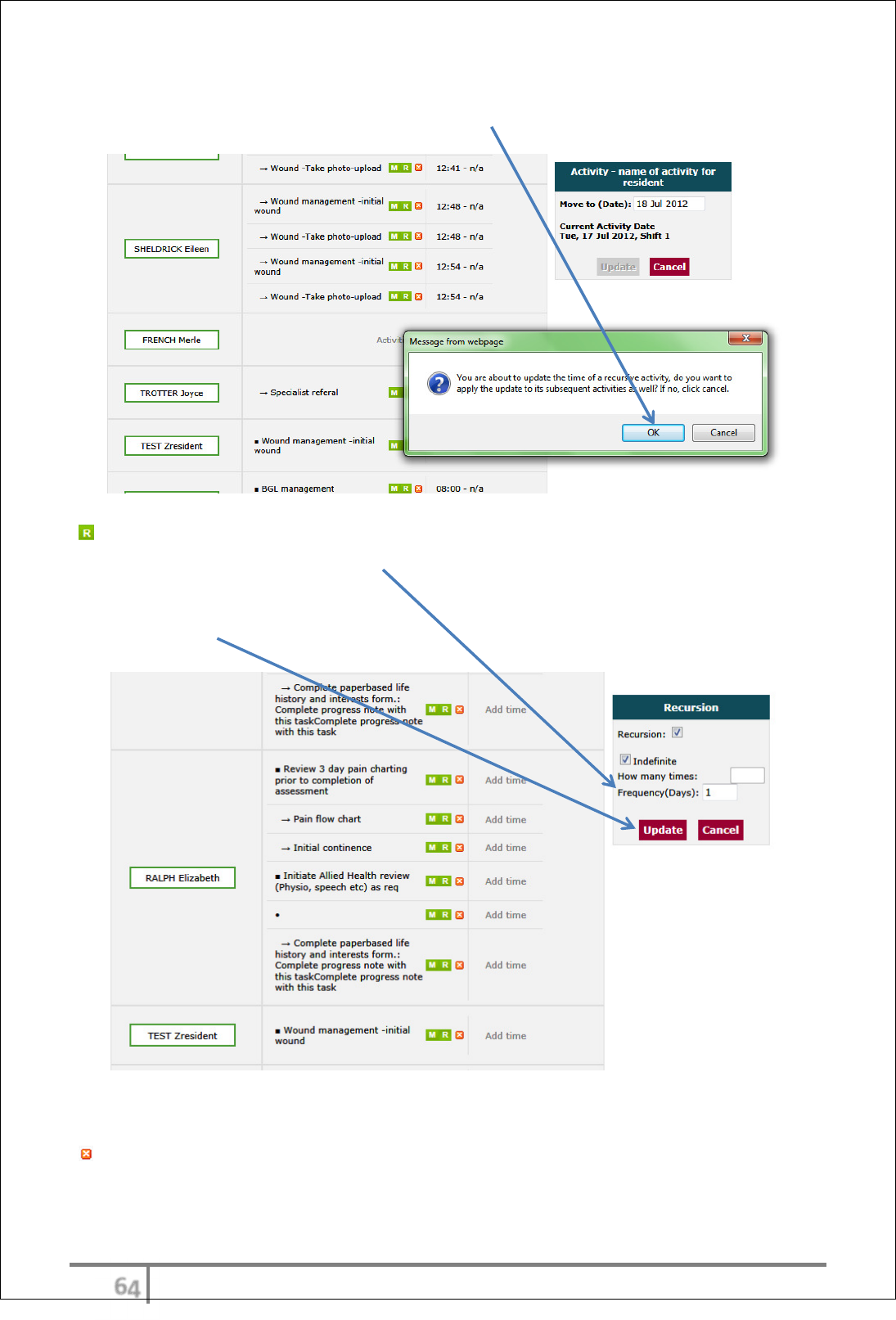
Change Activity settings-Work log editor
Move Activity, change Recursion settings or Delete Activity via the Work
Log Editor
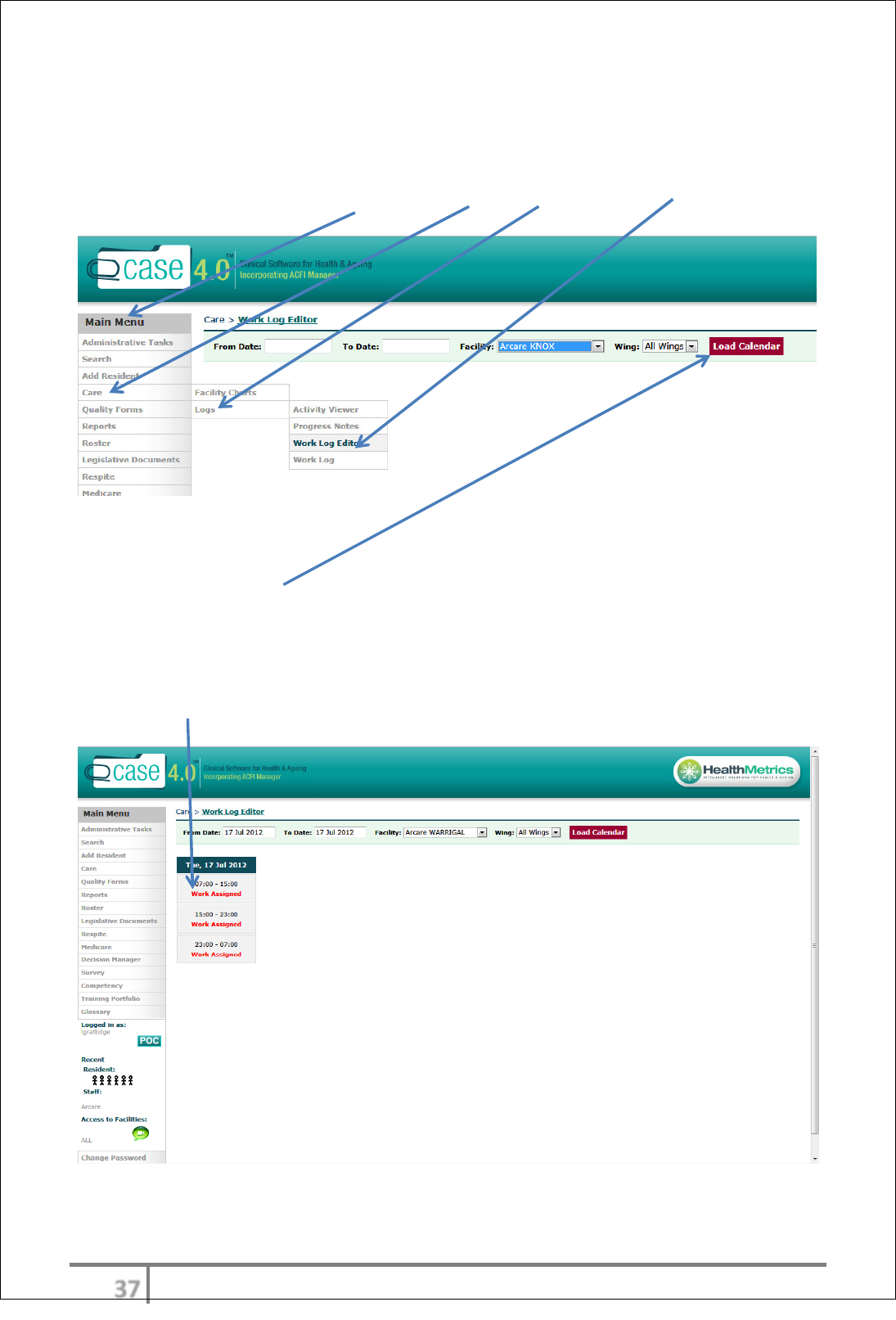
Access Work Log Editor via Main Menu > Care > Logs > Work Log Editor
Enter the date or date range and Wing to isolate Work Log item to be reviewed.
Select ‘Load Calendar’
A calendar of work assigned (Activities) will appear.
Select the date and time frame of the Activity for review by clicking on the red
‘Work Assigned’
χό
Ver 3.2013
.
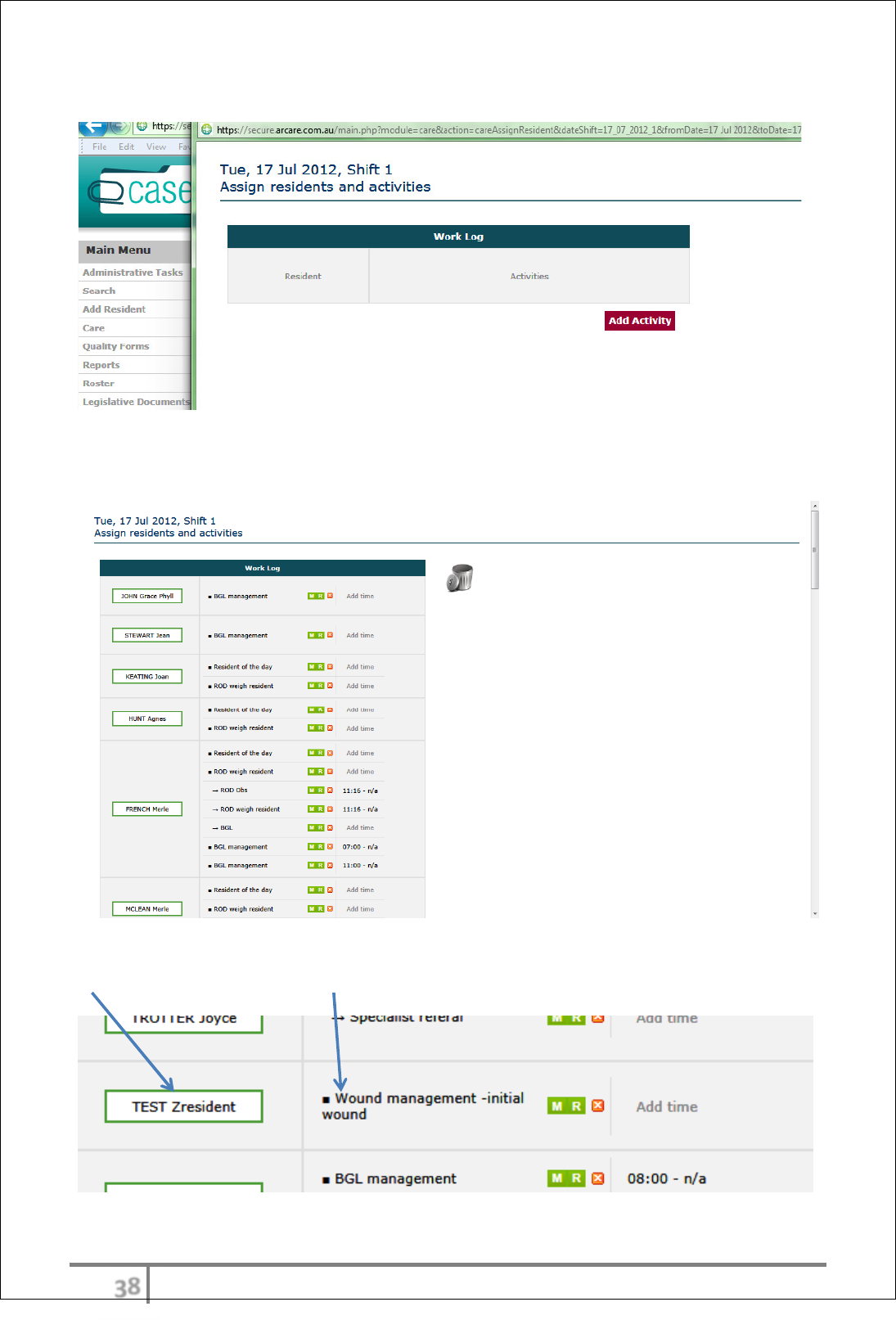
Interim screen will appear
Wait until the next screen is generated (this takes a few seconds). The next
screen will show the Resident’s scheduled Activities for the date chosen.
Scroll down to find resident’s name and relevant entry (example – TEST
Zresident, Wound management –initial wound)
χύ
Ver 3.2013
.
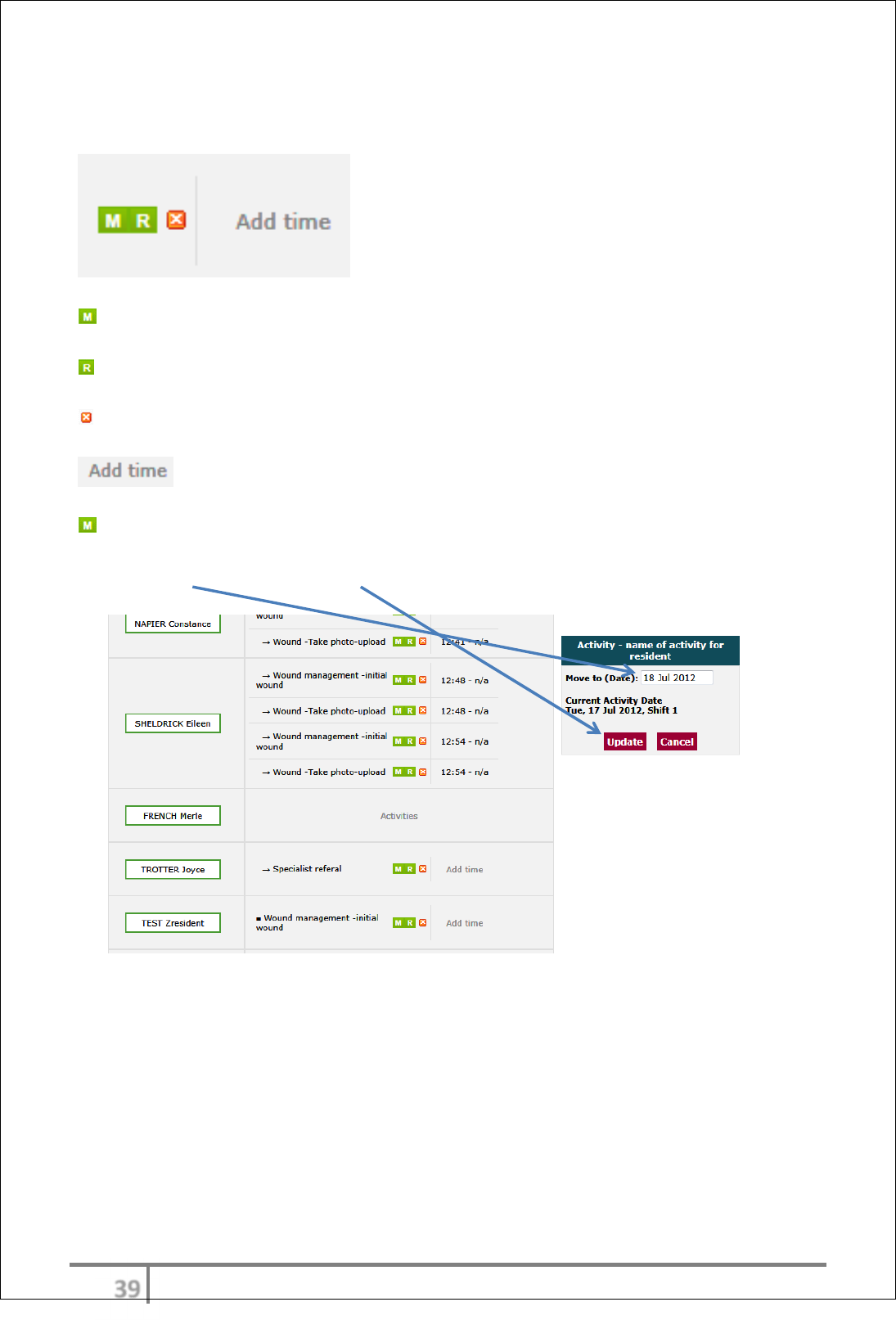
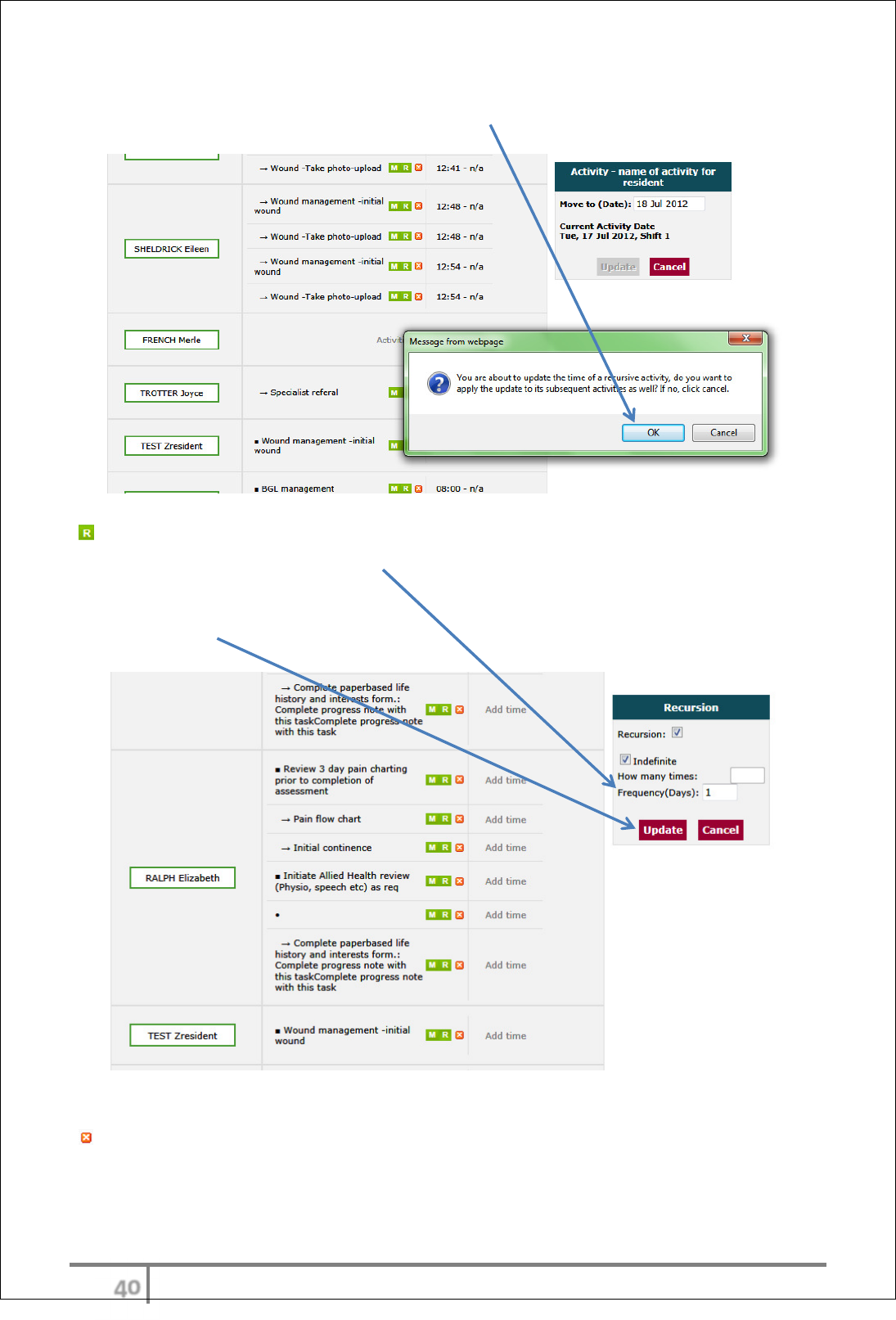
Several options are available to change settings in the Work Log via the
Work Log Editor
Move Activity Settings
Recursion Settings
Delete this activity
Move Activity Settings - enables a change of date
Enter new date and select ‘Update’
ψτ
Ver 3.2013
.
A message prompt will appear to confirm ‘do you want to apply the update to its
subsequent activities as well?’ If yes, click ‘OK’.
Recursion Settings - enables a change to recursion and/or frequency. For
example – changing the frequency of wound dressing regime from daily to 3
rd
daily (replace the 1 with 3).
Select ‘Update’
Delete Activity from Work Log via Work Log Editor
Delete this activity – enables the Activity to be deleted from the Work Log if a
residents care need/directive is no longer required. For Example - a resolved
wound.
ψυ
Ver 3.2013
.
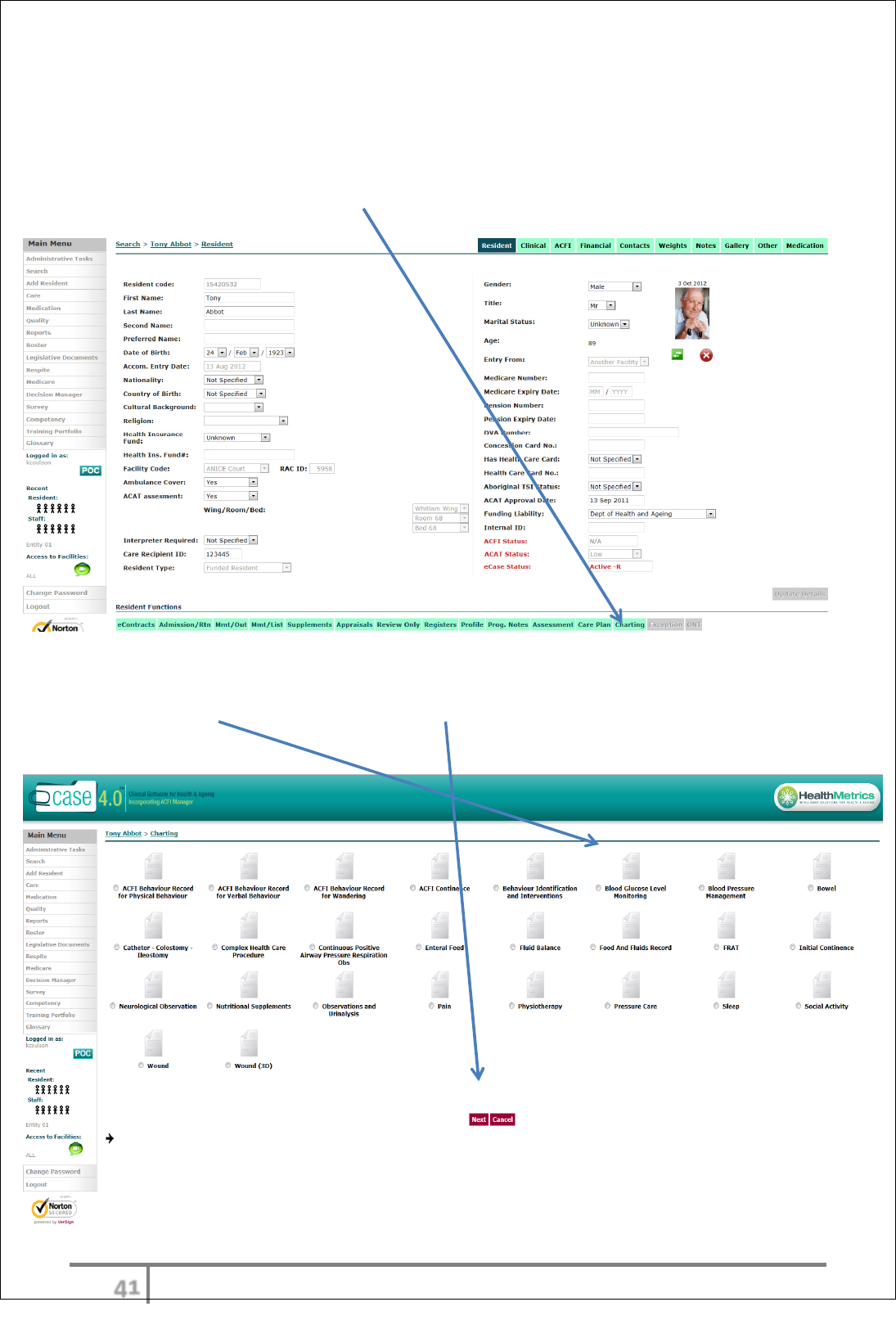
Charting
Charting access
Generally resident charts will be accessed through the care worklog. Only RN’s
will be able to access charts using the resident function menu. eCase Charting is
located under the individual Resident Functions menu.
Select the Chart required and select ‘Next’. Charts that are colored indicate a
chart with data.
ψφ
Ver 3.2013
.
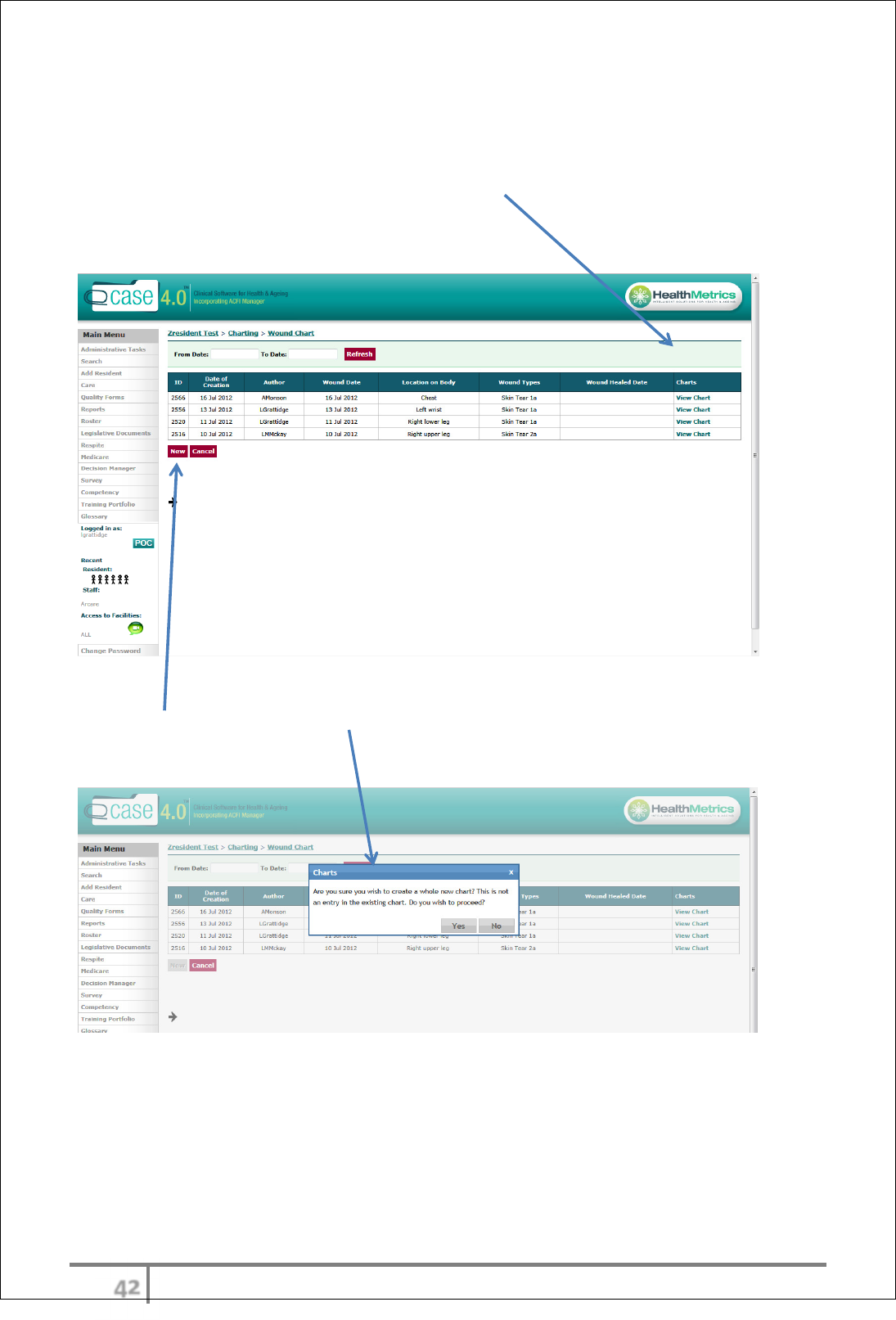
Using an Existing Chart
The most recent chart will automatically be sitting there for the User to complete
if it is still an uncompleted chart. Select ‘View Chart’ and the chart will open.
Once again however the user would normally be accessing this chart using the
worklog as he tasks has been previously scheduled.
Creating a new Chart
Select ‘New’ and a prompt message will appear to confirm whether the User
wishes to create a whole new chart that is not an entry in the existing chart.
ψχ
Ver 3.2013
.
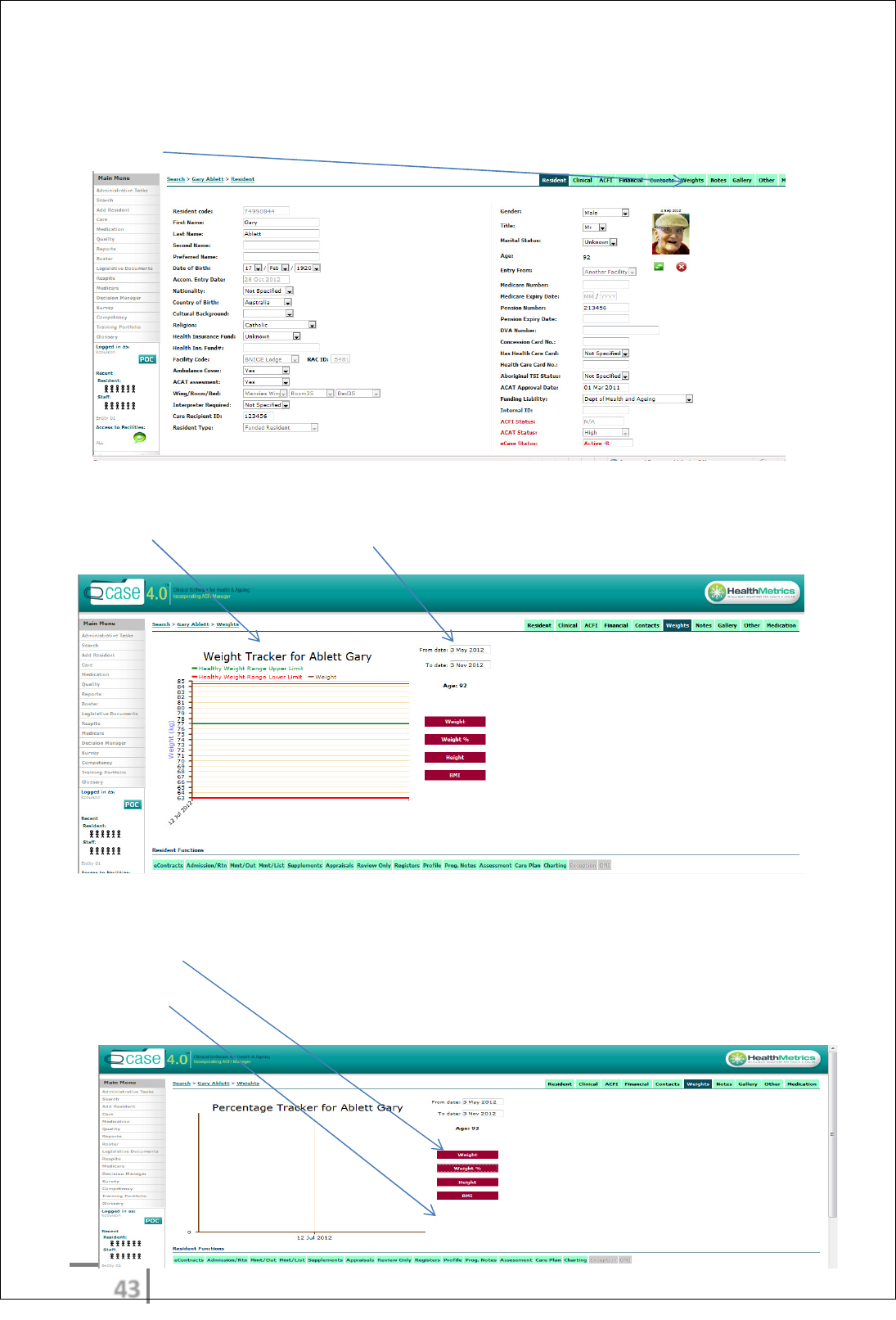
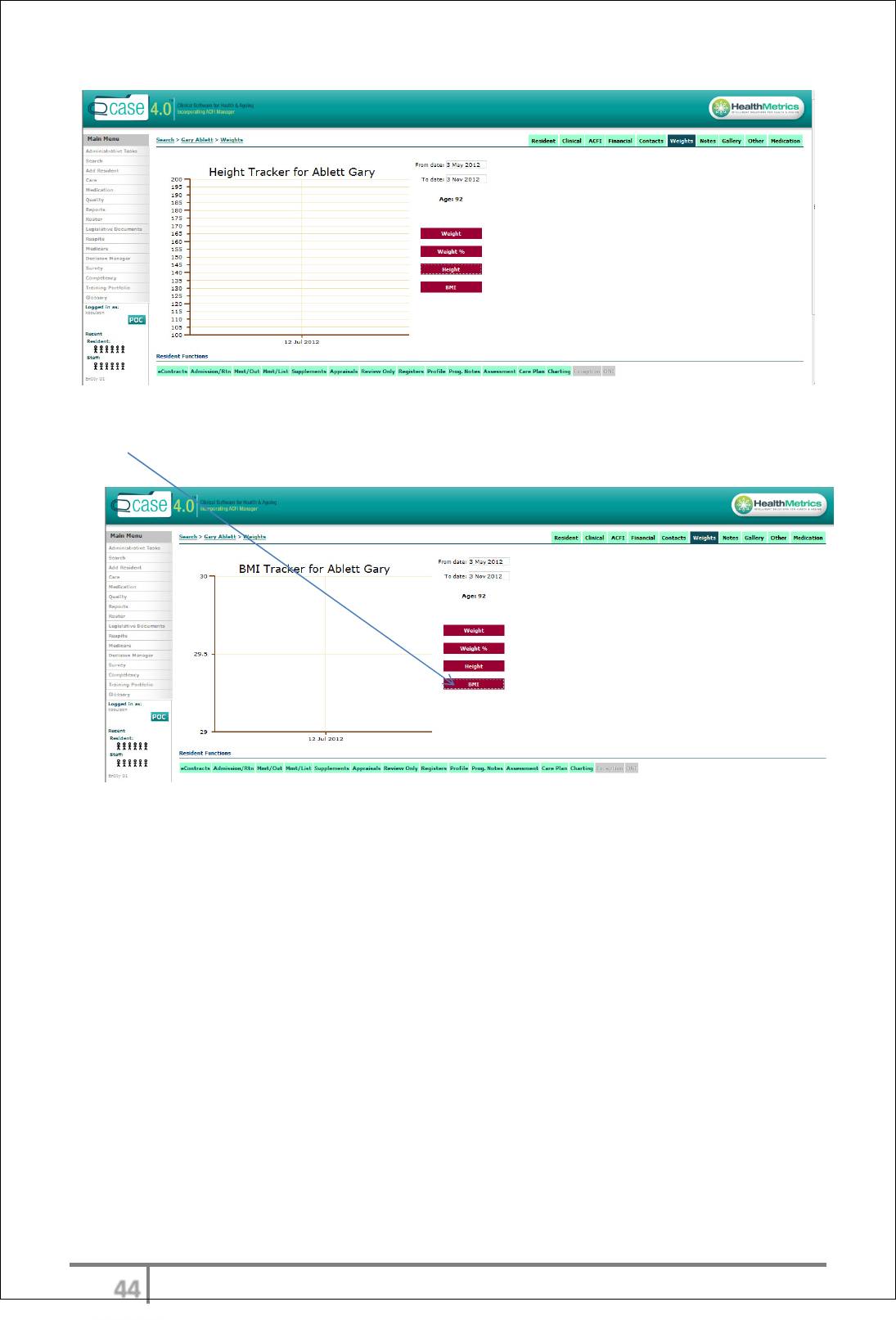
Weight chatting
Click “weights”
Weight Tracker, you must also refine date
Percentage tracker
Height Tracker
ψψ
Ver 3.2013
.
BMI Tracker
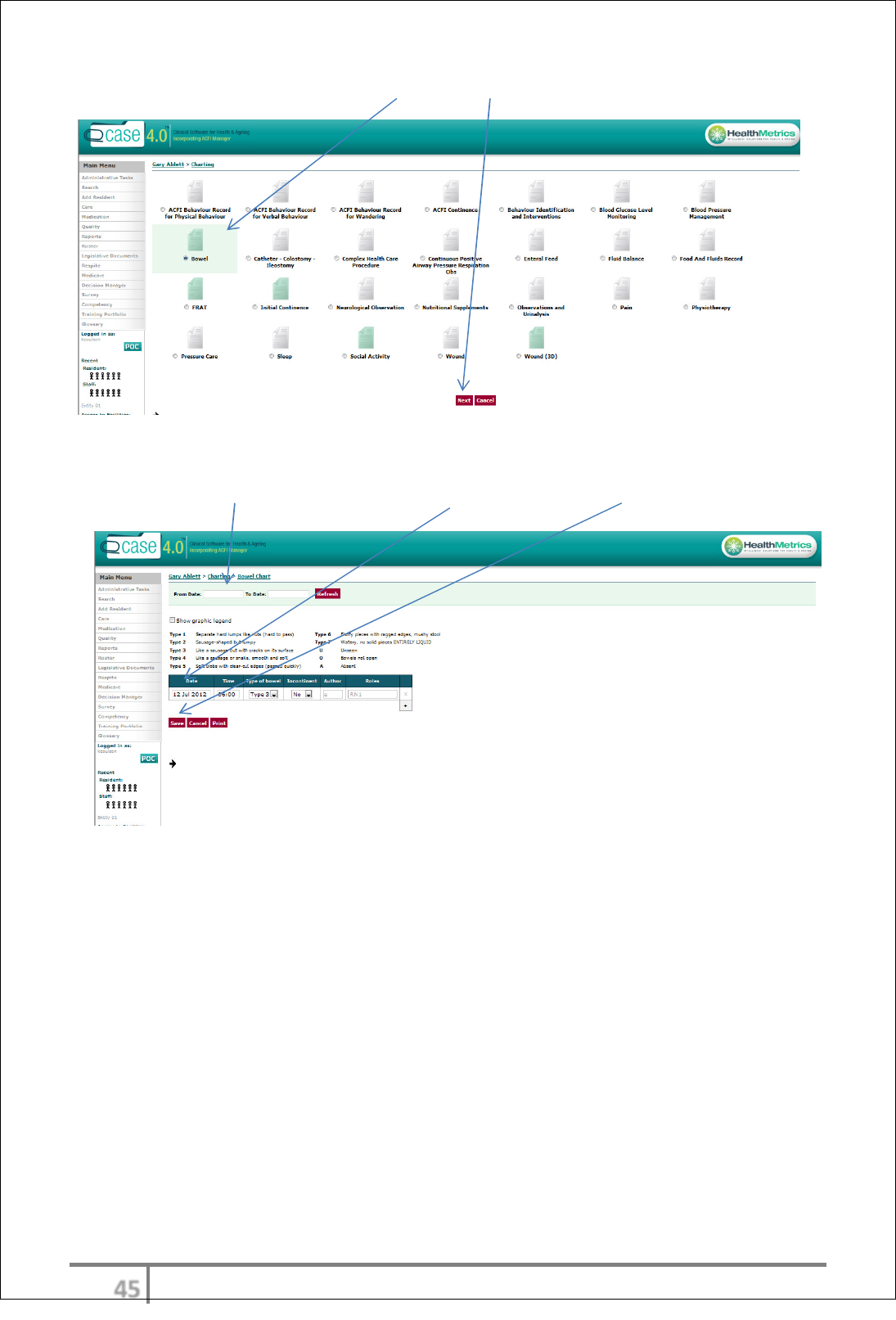
Bowel charting
ψω
Ver 3.2013
.
To create a bowel chart you must click “bowel” then “next”
Must type in date range, Fill out the areas provided, Then click “save” to save all changers
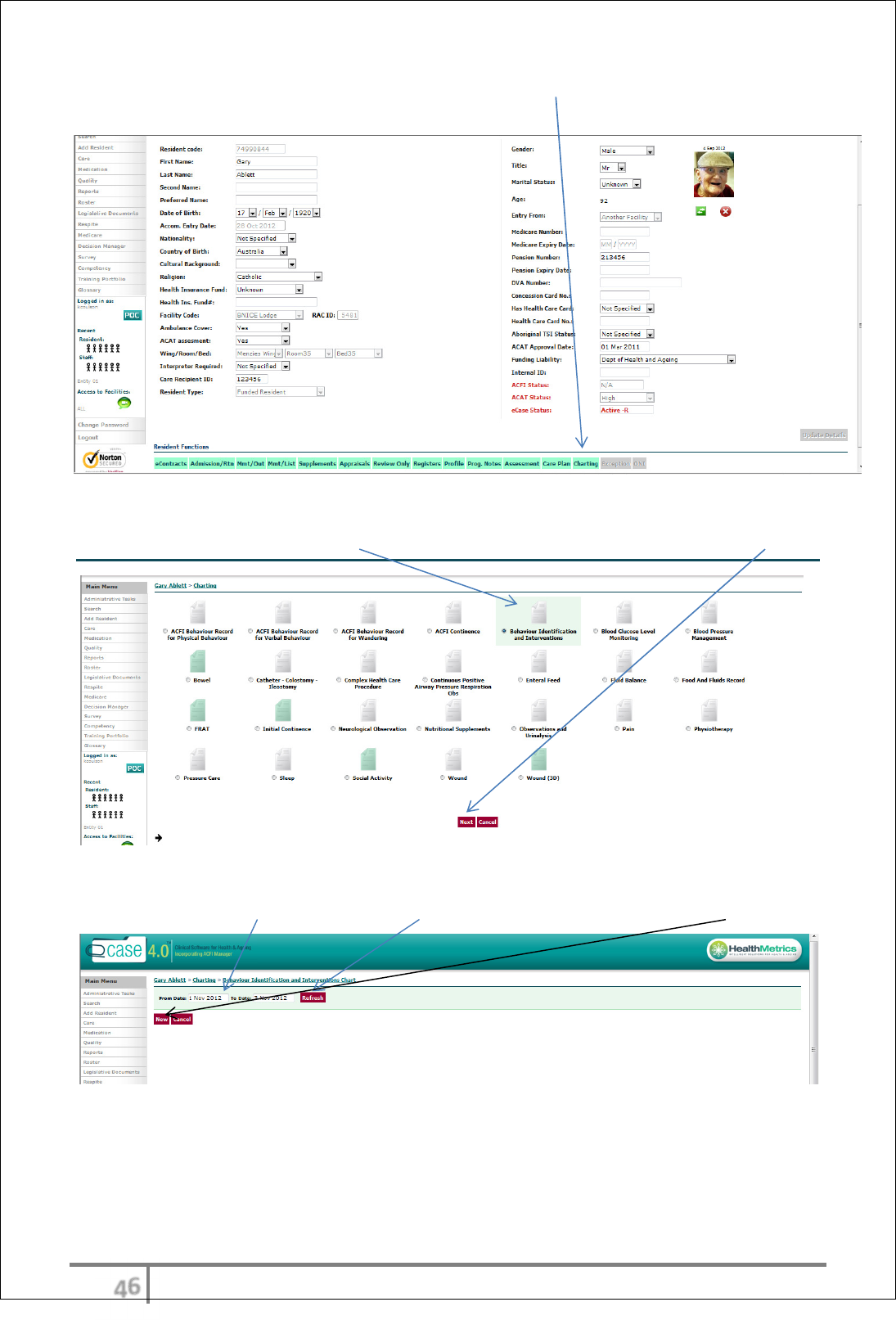
Behaviour identifications chart
ψϊ
Ver 3.2013
.
Creating a new behaviour identification chart you must click on the “charting “in the resident function table
Then you must click on “Behaviour Identification and Interventions Chart” and click “next”
To refine sure fill out “date range” then click “refresh” or to create new behaviour chart click “new”
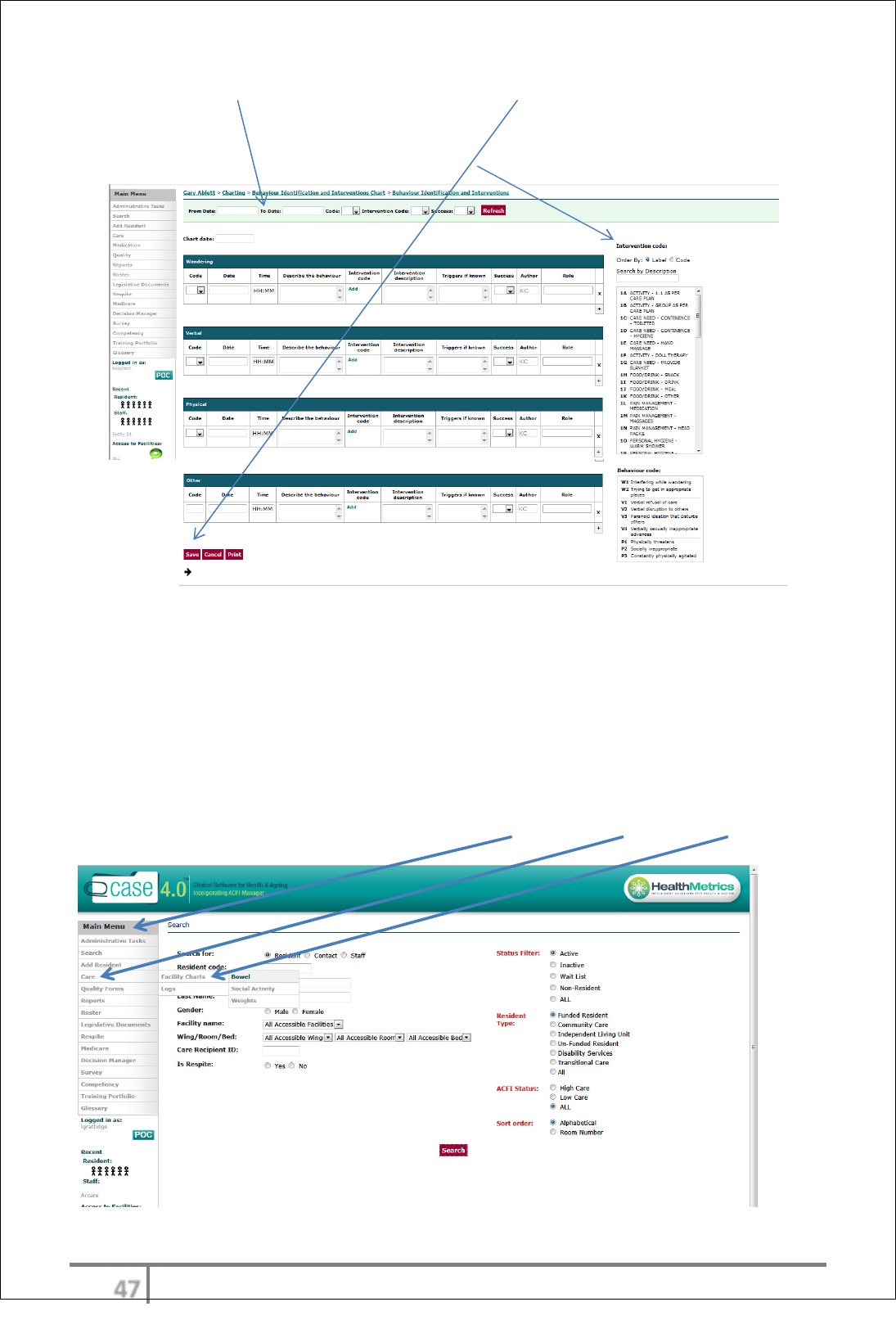
To create new Behaviour chart you must fill out each filed etc wandering, verbal, physical and other
ψϋ
Ver 3.2013
.
You must also add a “date range” when finished you must click “save” if you have complete this chart
successfully it will populate into the work log and active viewer
You must also complete a PAS, The code are also on the side you must put a code in
General resident charts - Bowels, Social Activities & Weights-
Group entry
The User can also add data to a group of residents rather than one resident at a
time. This only applies to the frequently accessed charts – Bowel, Social Activity
and Weights.
Access general (bulk entry) Charts via the Main Menu > Care > Facility Charts
ψό
Ver 3.2013
.
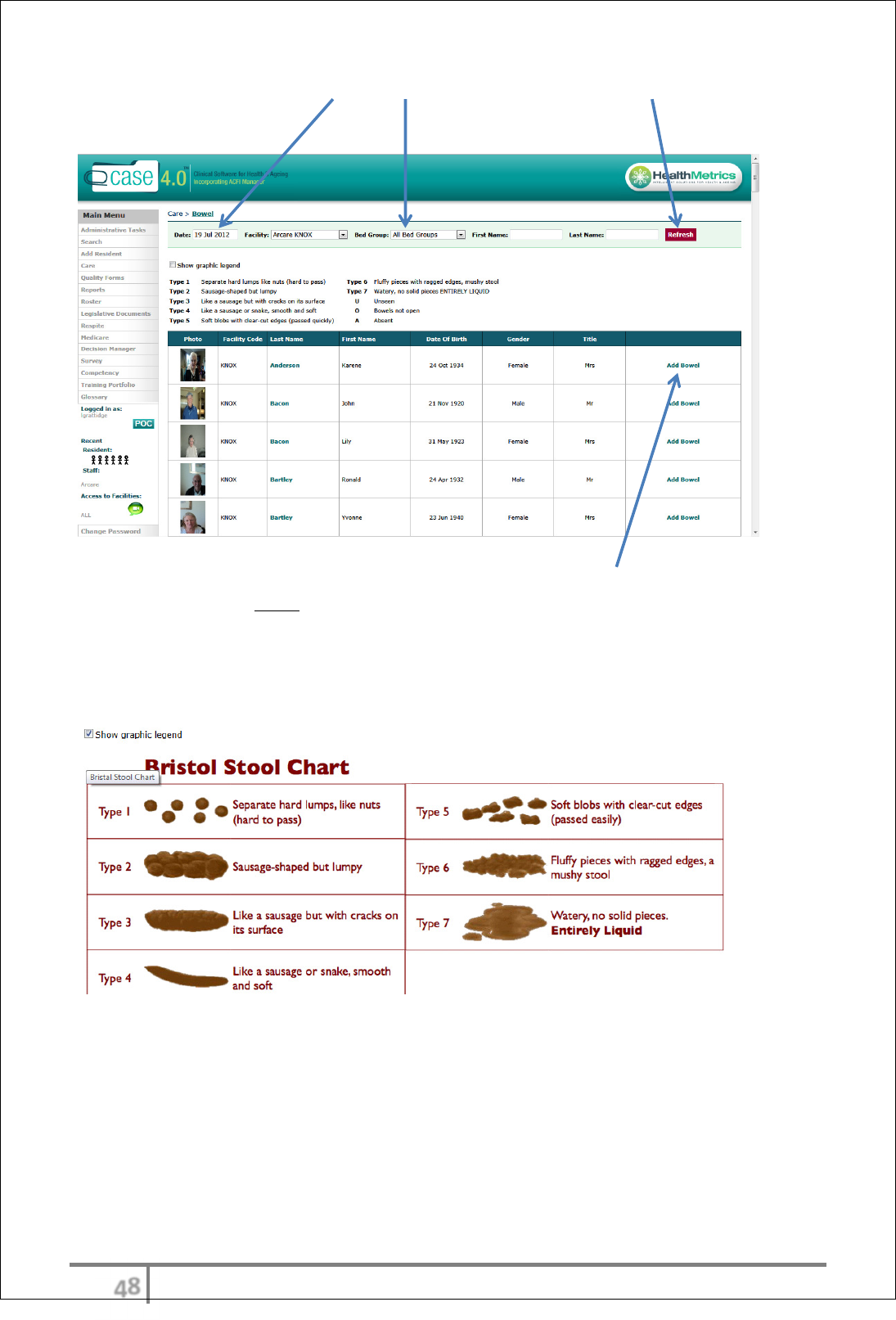
Apply the desired filters: Date, Bed Group etc. and select ‘Refresh’ and the most
recent data template will be generated.
Find the resident you wish to add info to and select ‘Add Bowel’.
Enter the data and Save.
The bowel chart also displays a graphic representing the Bristol stool scale for
user reference and clarification
ψύ
Ver 3.2013
.
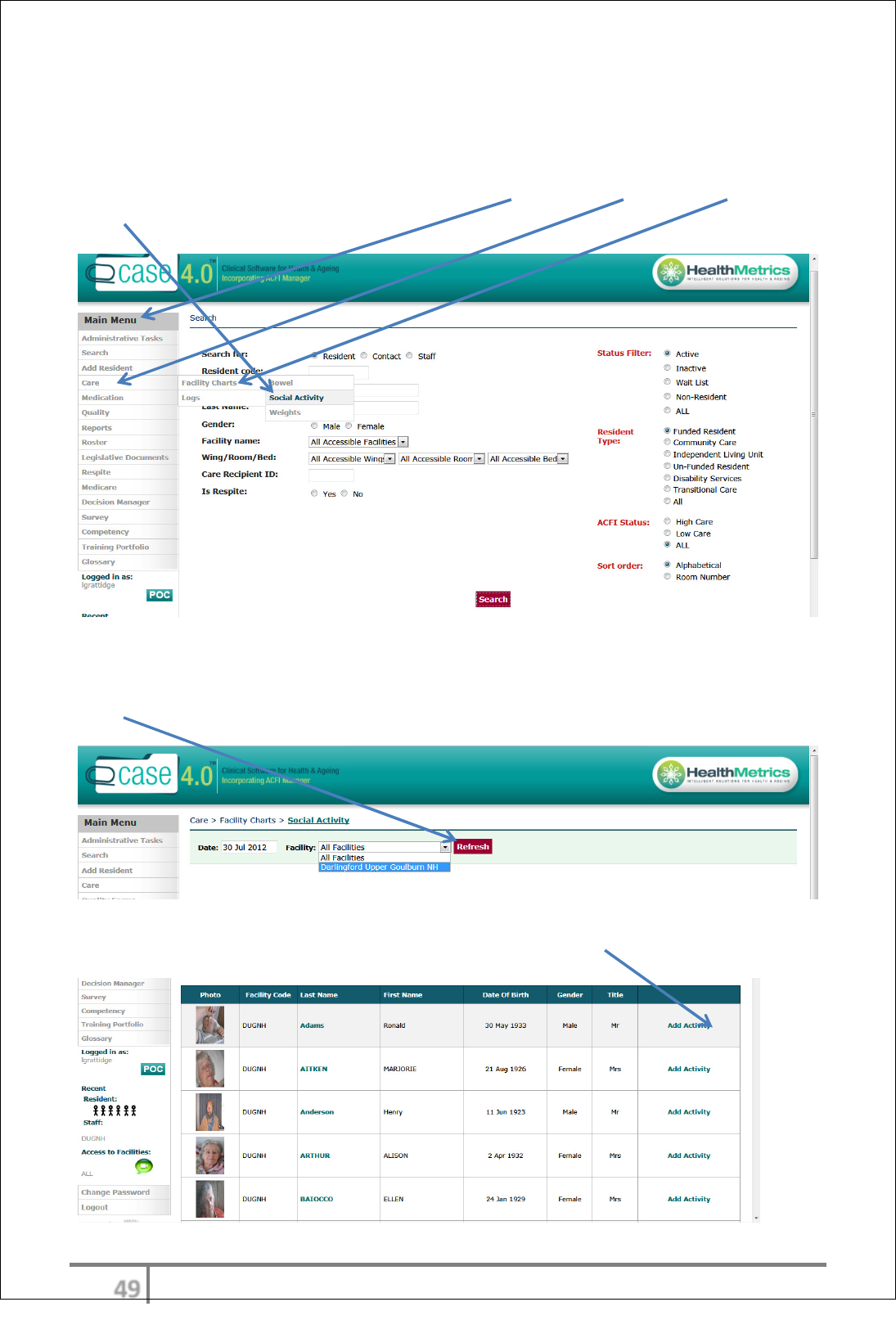
General resident charts - Social Activities
The User can add data to a group of residents rather than one resident at a
time.
Access general (bulk entry) Charts via the Main Menu > Care > Facility Charts >
Social Activity
Apply the desired filters: Date, Facility from drop down menu and select
‘Refresh’ and the most recent data template will be generated.
Find the resident you wish to add info to and select ‘Add Activity’.
ωτ
Ver 3.2013
.
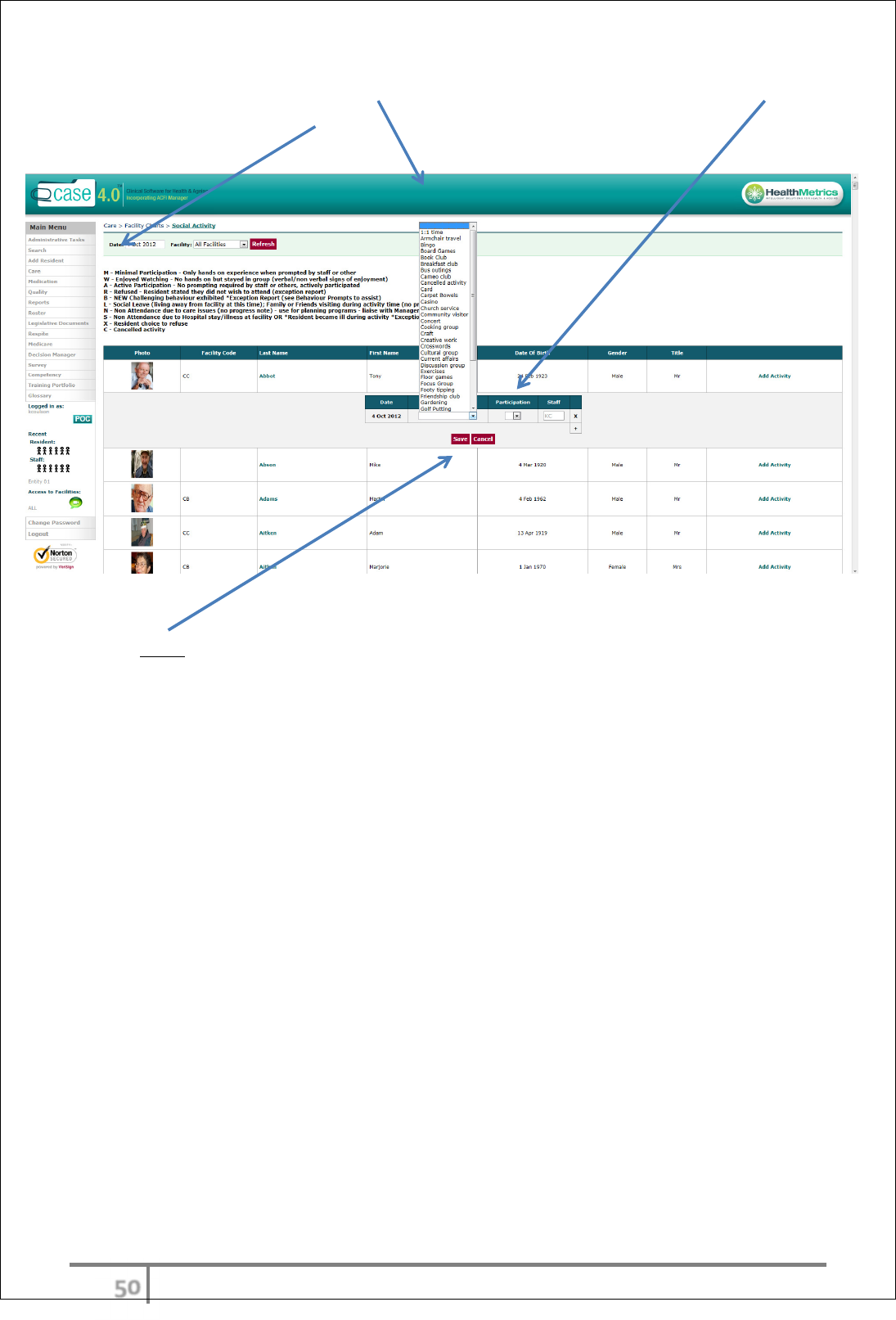
Enter relevant data: Select Activity from drop down menu and level of
participation using coded table.
Select Save
ωυ
Ver 3.2013
.
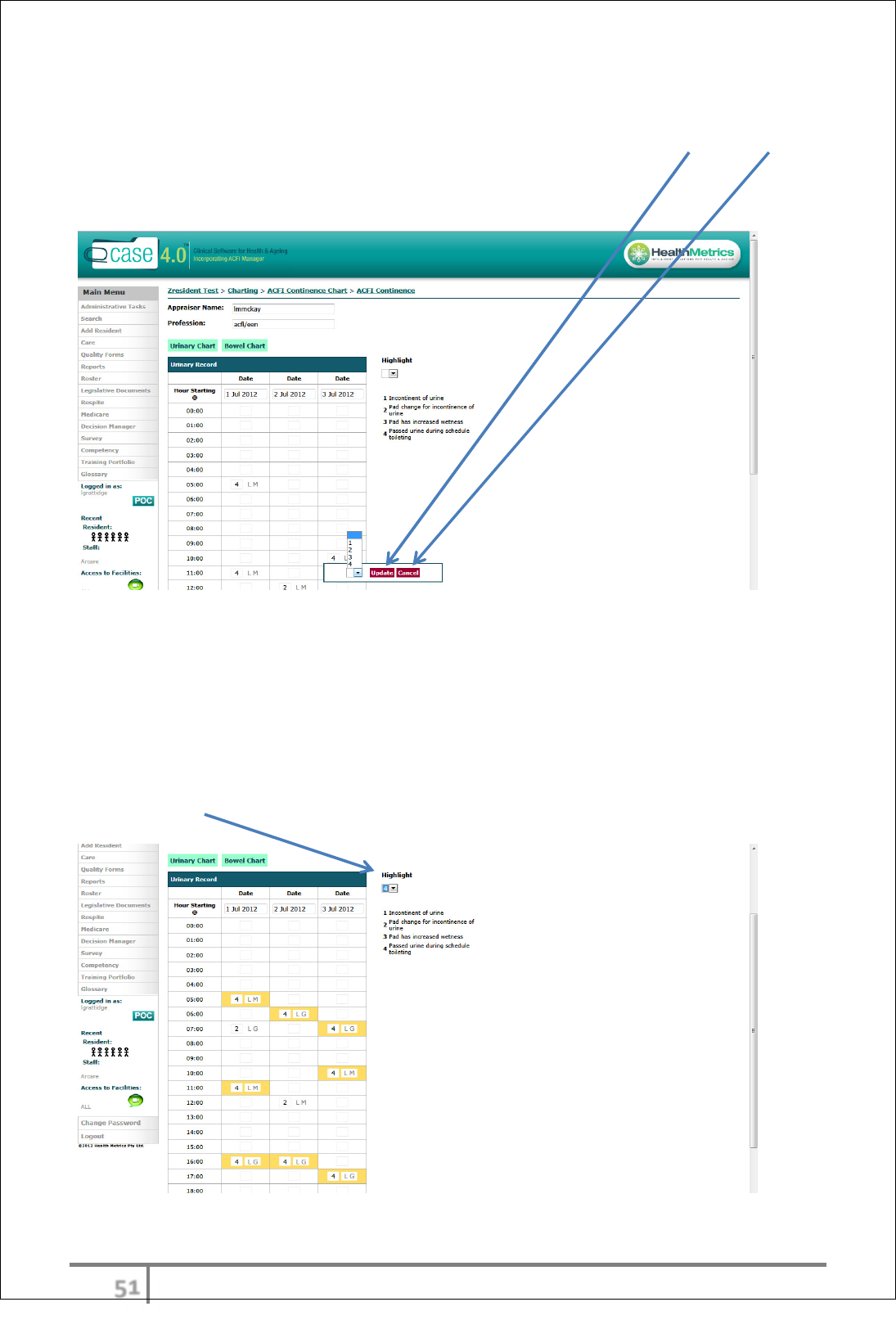
Making entries to charts
The User can add to charts depending on how they have been scheduled in the
worklog. If a chart entry is being completed, options for each box will be
provided with an Update or Cancel option. The Update option will save the
change/addition and the Cancel option will delete it.
Depending on the chart, there may be a set of options to choose from or open
fields for changeable data such as BGL readings.
eCase charting allows the User to record charted evidence that may be used to
establish care outcomes or patterns of care indicators. This includes all relevant
ACFI charting. ACFI charting has the option to be included in an ACFI appraisal if
the User is satisfied with the outcomes established. To ascertain a pattern, select
the ‘Highlight’ option.
ωφ
Ver 3.2013
.
Wound management
• Add Progress Note
• Complete Resident Incident
• Complete Wounds Tracking linked to Wound Chart
• Take wound photo using tablet
• Upload photo to Wound Chart
• Wound Gallery
• Update Work Log
• Schedule ongoing wound management
Also,
• Change wound management regime
• Delete resolved wound from Work Log
Wound management – New Wound
Add Progress Note
In the ‘Resident Functions’ menu, select ‘Prog. Notes’
Select ‘Add’
ωχ
Ver 3.2013
.
In ‘Filter Progress Notes Type’ enter ‘wound’
In expanded menu, Select Progress Note Type ‘Wound charts’
Enter (type in open field) progress ‘Notes’ and ‘Save’
Work Log screen will appear
Complete Resident Incident
Complete incident report via
‘INCIDENT’
link in Work Log
‘Save’ Resident Incident
ωψ
Ver 3.2013
.
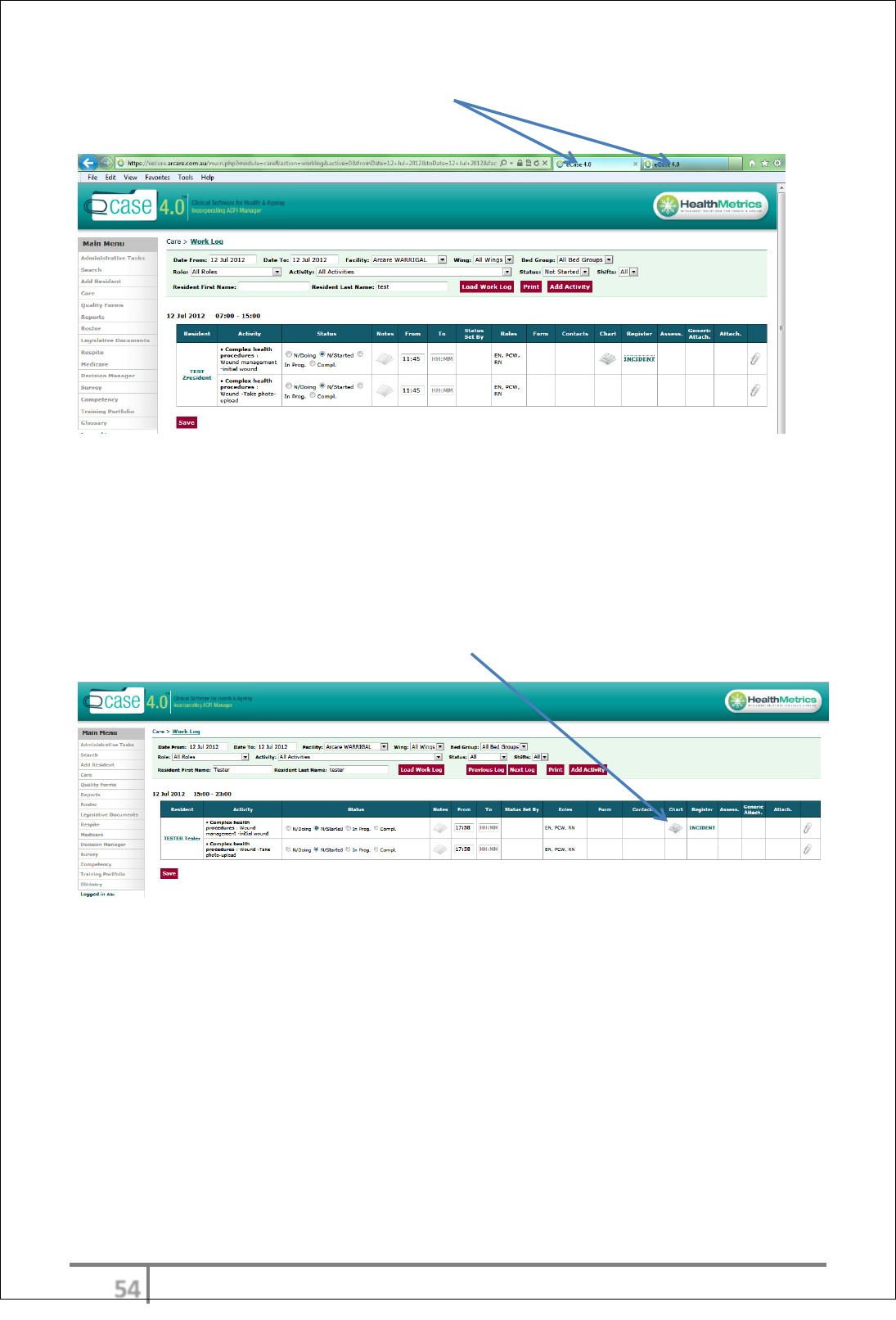
Navigate back to Work Log screen via tab in top menu bar (able to alternate
between open screens)
Note: Users do not need to go in and out of the Work Log to complete tasks.
Each item will open in a new window. Depending on the computer you are using
this will display in various ways. As above, each window will present as a tab
alternatively on a large screen, each window may just ‘pop up’ on top of the
Work Log.
Wound Tracking > Wound Chart
Complete wound tracking and chart via Chart link in Work Log
ωω
Ver 3.2013
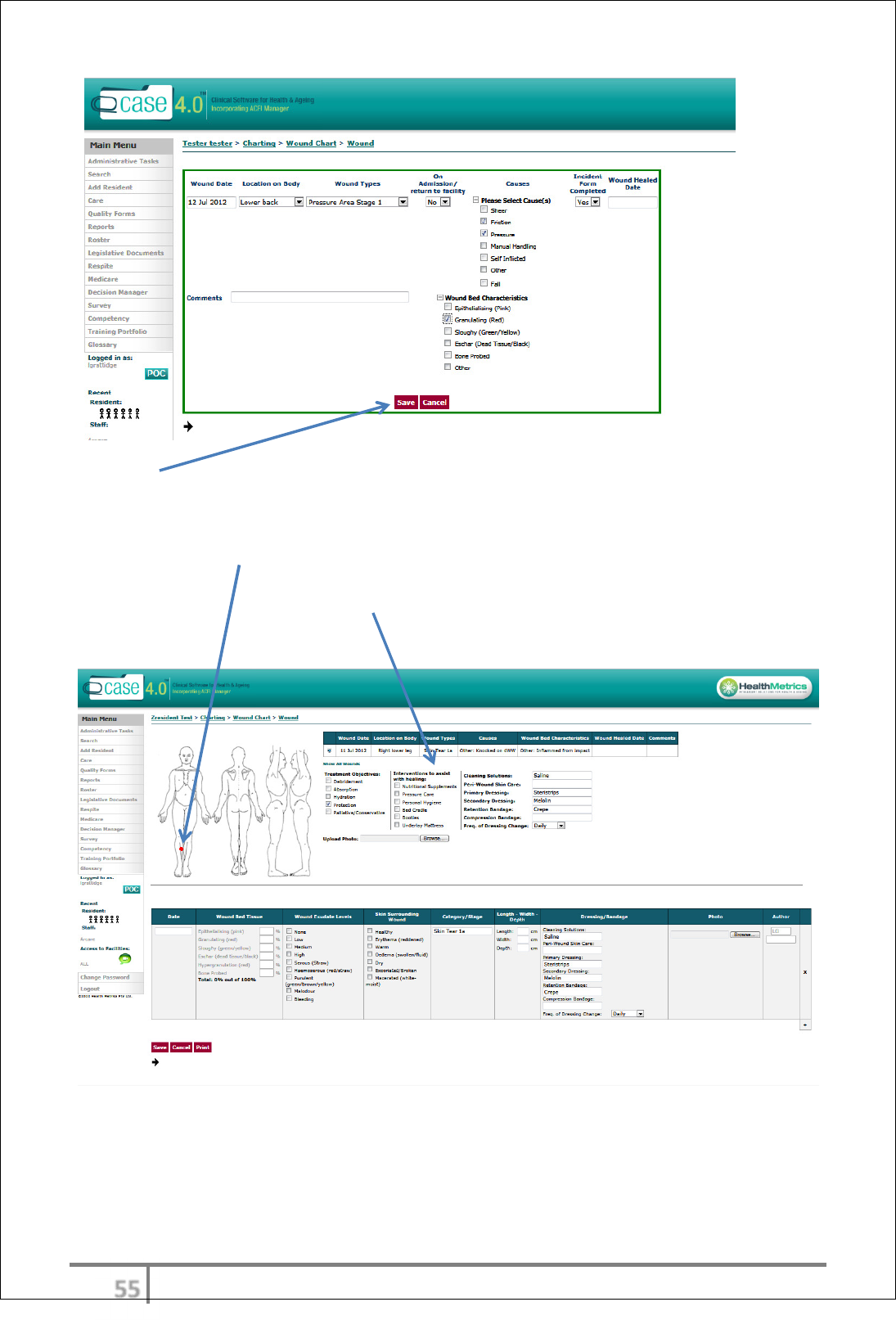
.
After ‘Save’ the comprehensive Wound Chart will appear
Hover over body image using mouse and click left mouse button, a red dot will
indicate wound location.
Fill out other wound information: Treatment Objectives; Interventions to assist
with healing; and dressing details.
ωϊ
Ver 3.2013
.
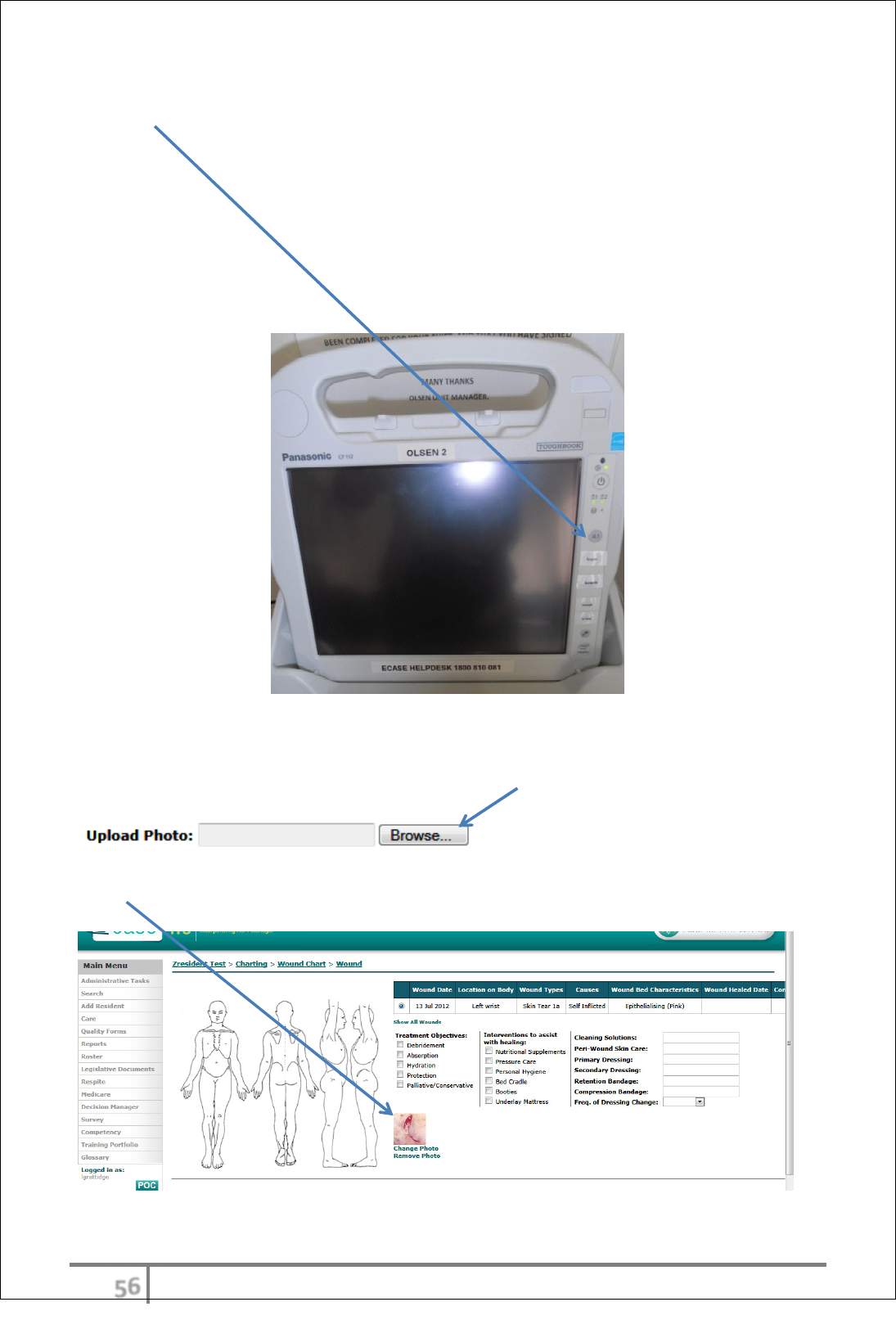
Taking photos of wounds using Toughbook
Press A1 button is camera.
The photo must be labelled in order to be easily retrievable when uploading to
Wound Chart.
Labelling protocol: ‘Resident’s Last Name’, ‘Resident’s Initial’ and ‘Location of
wound’ (e.g. Smith C Lower Leg)
The photo will be automatically saved into a designated directory on the Server.
Upload photo to Wound Chart
In the Wound Chart, via the Upload Photo: Browse button, search for applicable,
labelled photo in Toughbook Pictures file (browser will default to this file)
Choose file to upload and double click left mouse button or select ‘Open’. The
photo will now appear in Wound Chart
ωϋ
Ver 3.2013
.
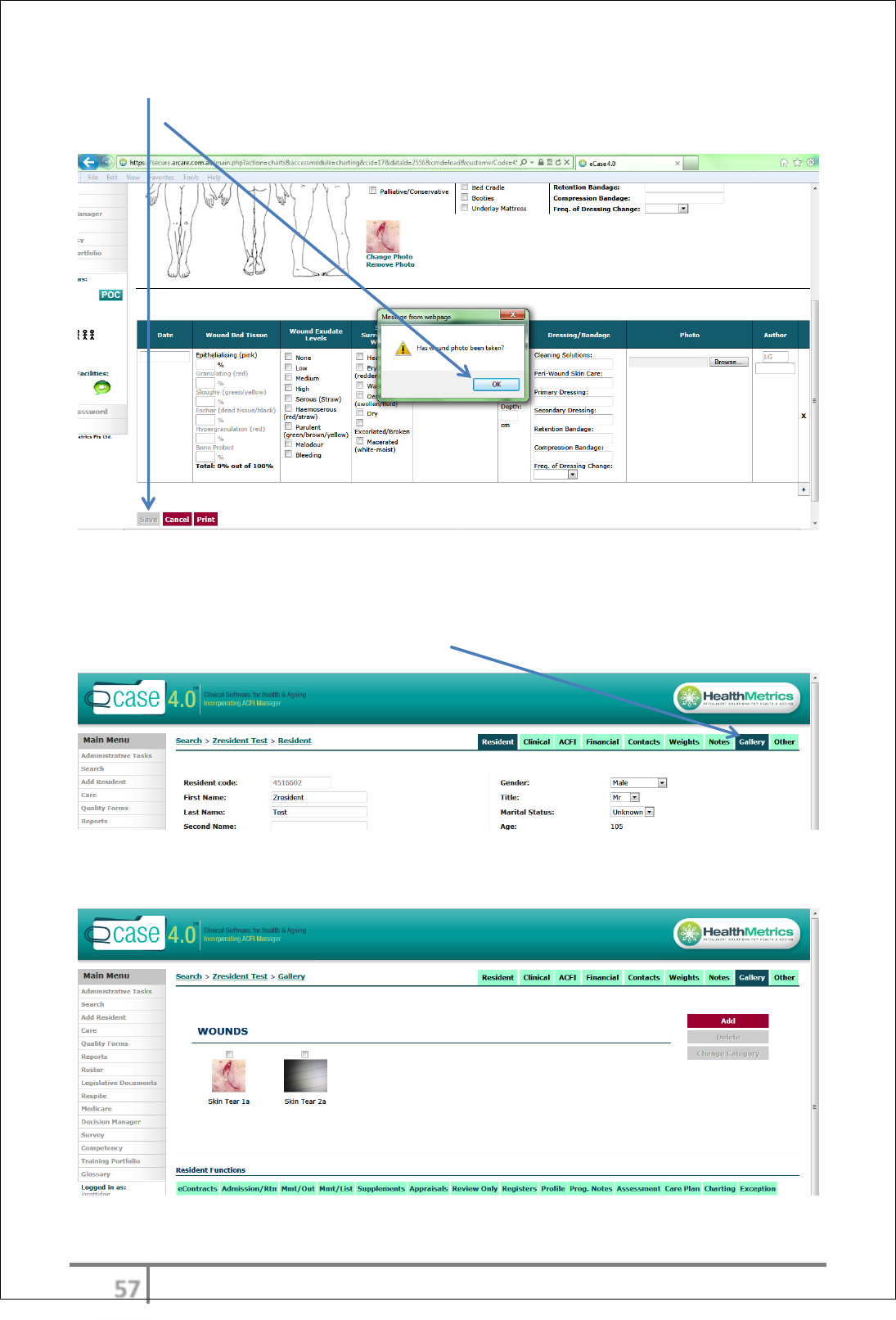
Select ‘Save’, a prompt message will appear to ensure a photo has been taken,
select ‘OK’
Wound Gallery
All wound images from the wound chart will be stored in the Gallery > WOUNDS.
To access the wound gallery, select ‘Gallery’ from Resident Menu.
An historical ‘WOUNDS’ gallery will now appear.
ωό
Ver 3.2013
.
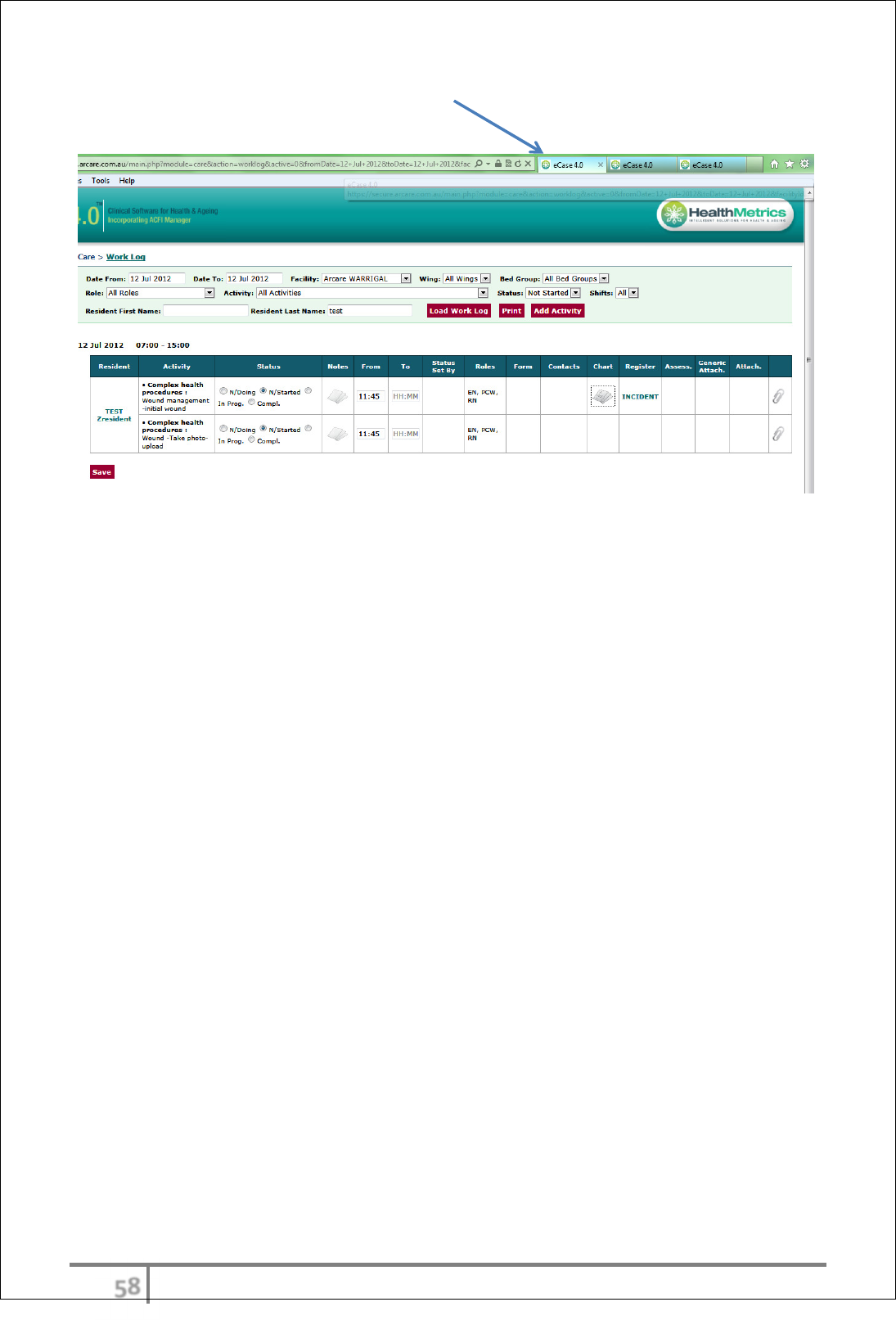
Navigate back to Work Log screen via tab in top menu bar (able to alternate
between open screens)
ωύ
Ver 3.2013
.
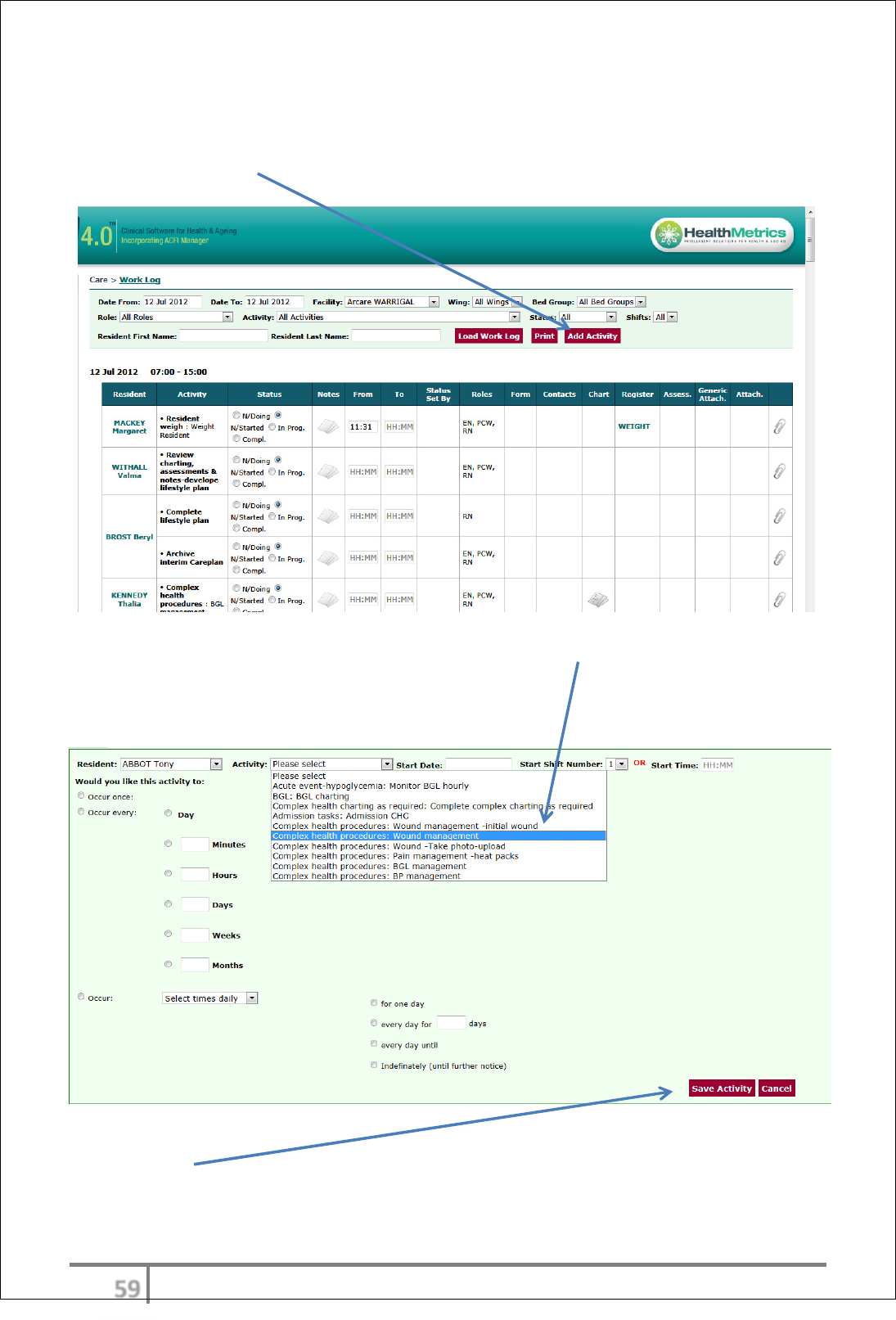
Schedule ongoing wound management
Schedule ongoing wound management regime via Work Log, Add Activity
Select ‘Add Activity’
Fill out information: Resident, Activity (select ‘Wound management –initial
wound’) from drop down menu and schedule accordingly (Start Date, Start Shift
Number OR Start Time and occurrences.
Select ‘Save Activity’
ϊτ
Ver 3.2013
.
The ongoing wound management regime will now be scheduled and appear in
the Work Log
ϊυ
Ver 3.2013
.
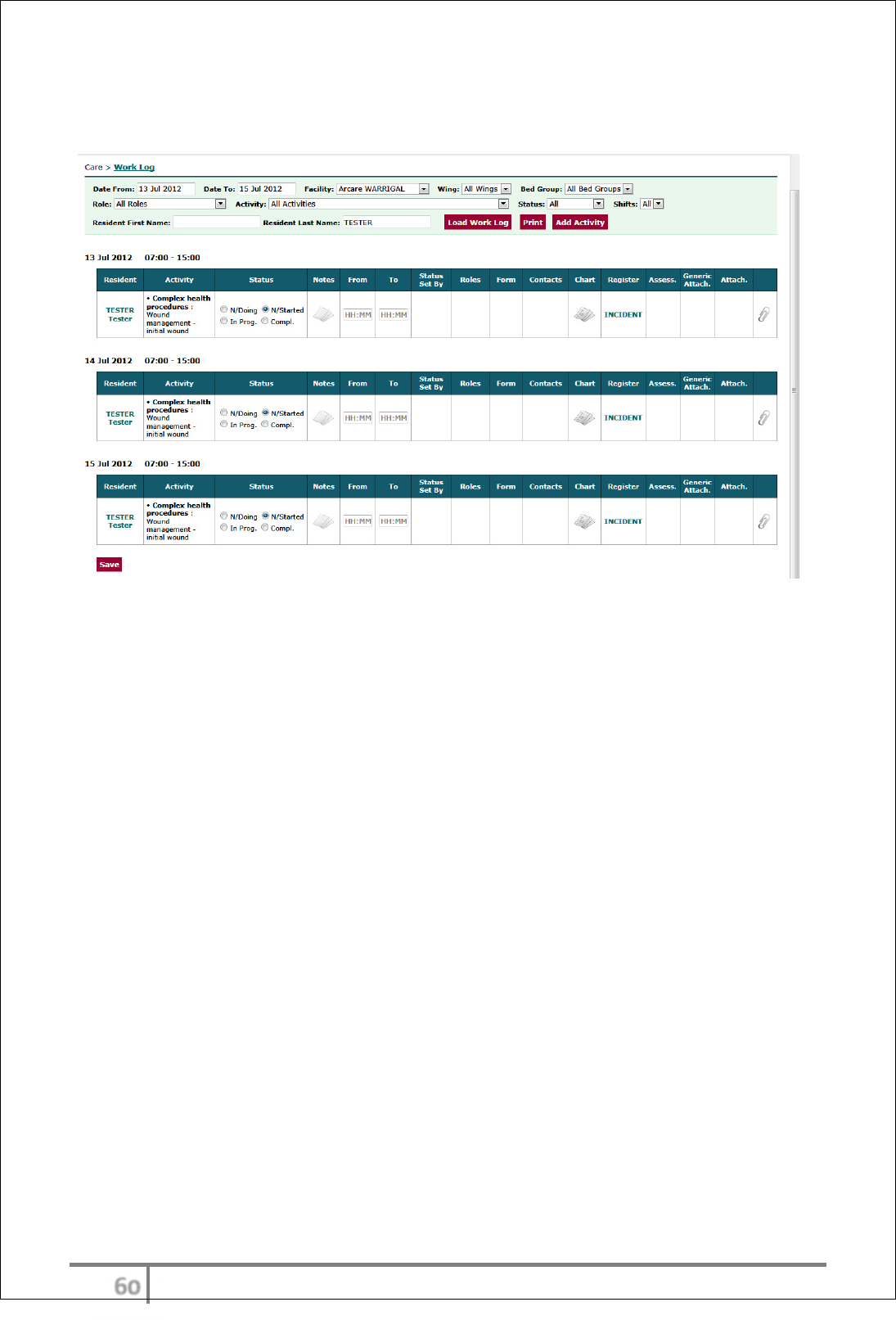
Change wound management regime via Work Log Editor
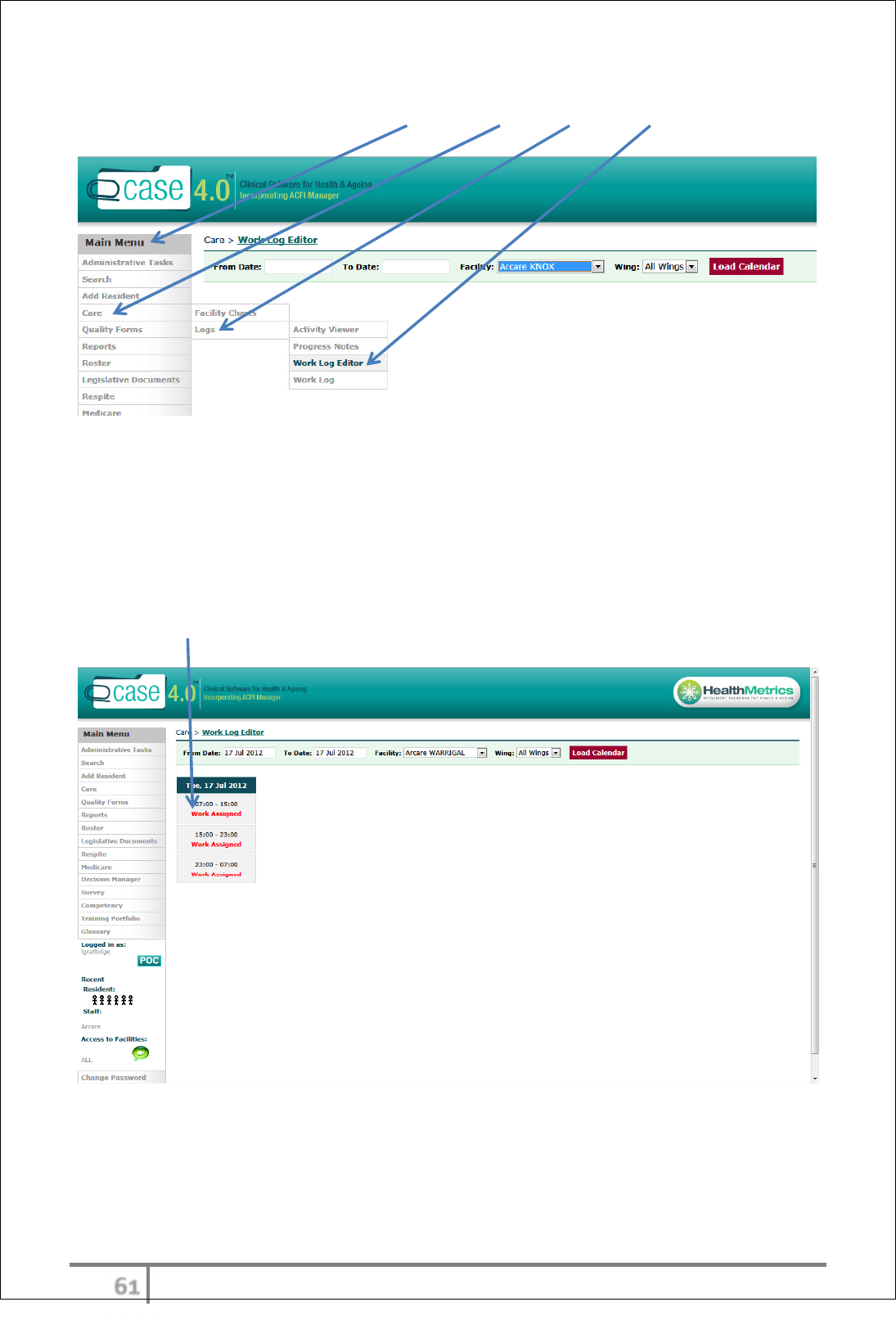
Access the Work Log Editor via Main Menu > Care > Logs > Work Log Editor
Enter the date or date range and Wing to isolate Work Log item to be reviewed.
Select ‘Load Calendar’
A calendar of work assigned (Activities) will appear.
Select the date and time frame of the Activity for review by clicking on the red
‘Work Assigned’
ϊφ
Ver 3.2013
.
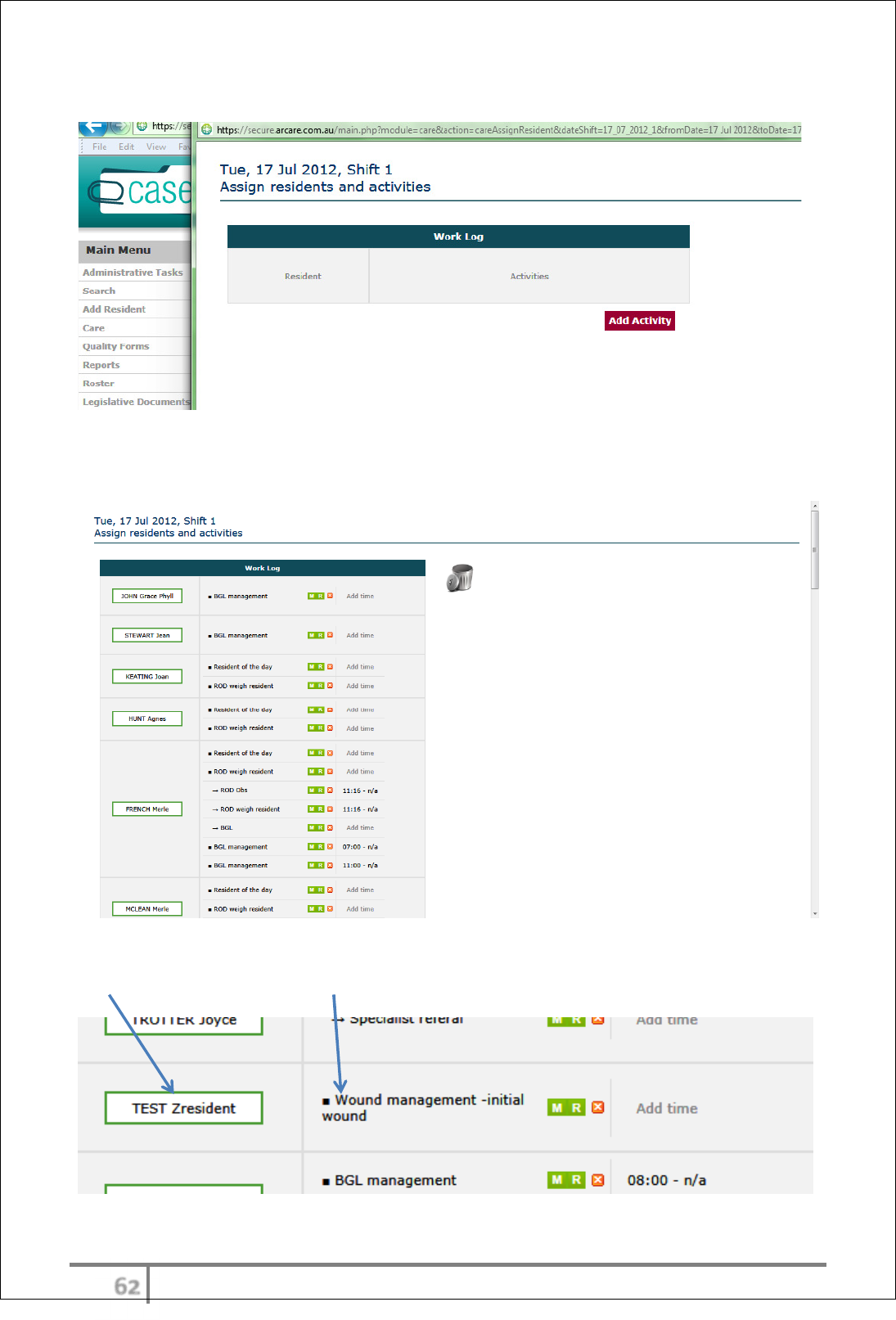
Interim screen will appear
Wait until the next screen is generated (this takes a few seconds). The next
screen will show the Resident’s scheduled Activities for the date chosen.
Scroll down to find resident’s name and relevant entry (example – TEST
Zresident, Wound management –initial wound)
ϊχ
Ver 3.2013
.
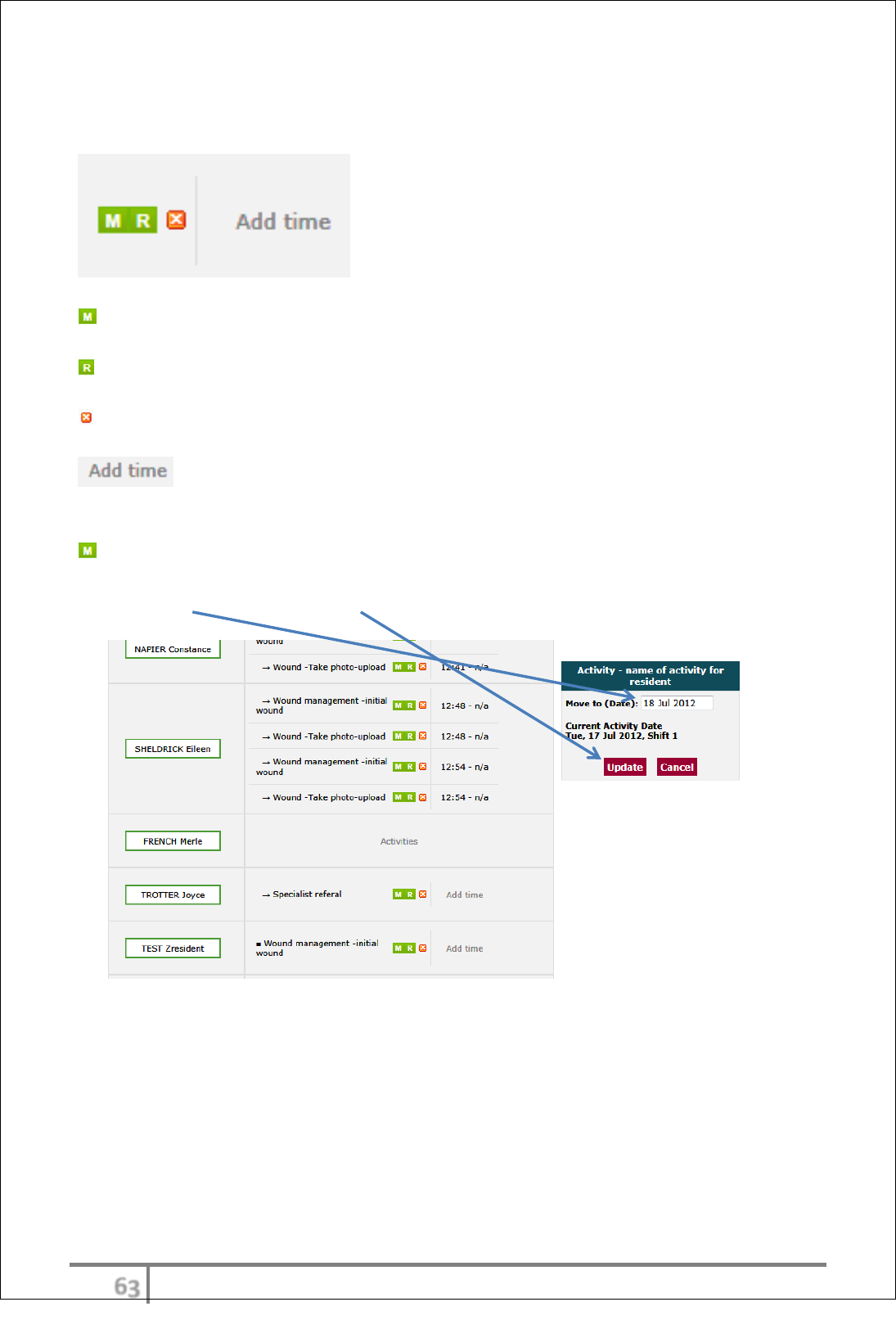
Several options are available to change settings in the Work Log via the
Work Log Editor
Move Activity Settings
Recursion Settings
Delete this activity
Move Activity Settings - enables a change of date
Enter new date and select ‘Update’
ϊψ
Ver 3.2013
.
A message prompt will appear to confirm ‘do you want to apply the update to its
subsequent activities as well?’ If yes, click ‘OK’.
Recursion Settings - enables a change to recursion and/or frequency. For
example – changing the frequency of wound dressing regime from daily to 3
rd
daily (replace the 1 with 3).
Select ‘Update’
Delete resolved wound from Work Log via Work Log Editor
Delete this activity – enables the Activity to be deleted from the Work Log.
For example – delete activity from Work Log when wound has resolved.
ϊω
Ver 3.2013
.
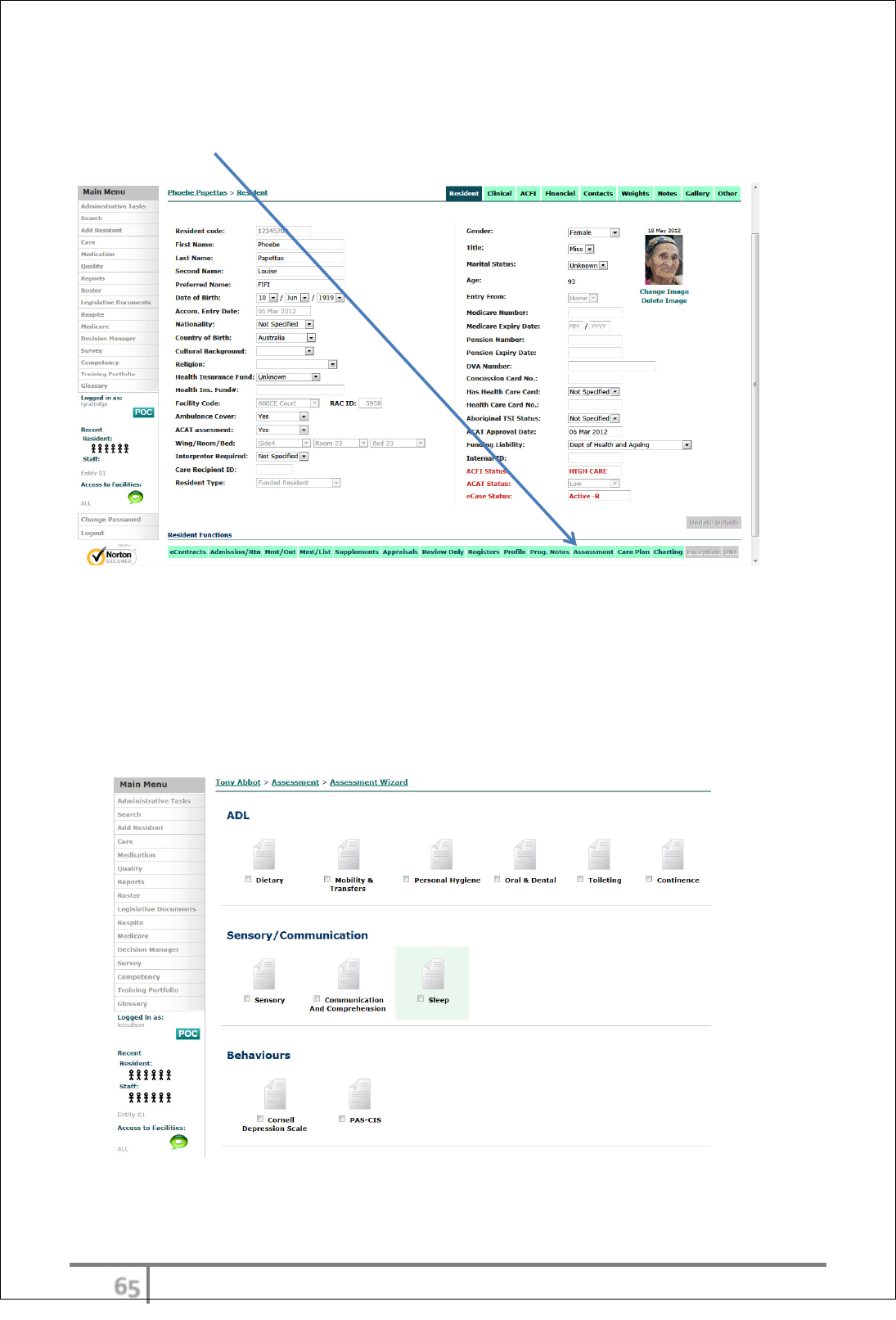
Assessments
Assessment access
eCase Assessments are located under the individual Resident Functions menu.
The User can choose to do one or multiple assessments at any given time
depending how they have been set out in the care worklog . Assessments are
not completed at that time, will remain in the assessment list for completion or
care plan development and then when careplan is completed the can be
published. . Assessment tasks will be set out in the care worklog and generally
not accessed through the main screen
ϊϊ
Ver 3.2013
.
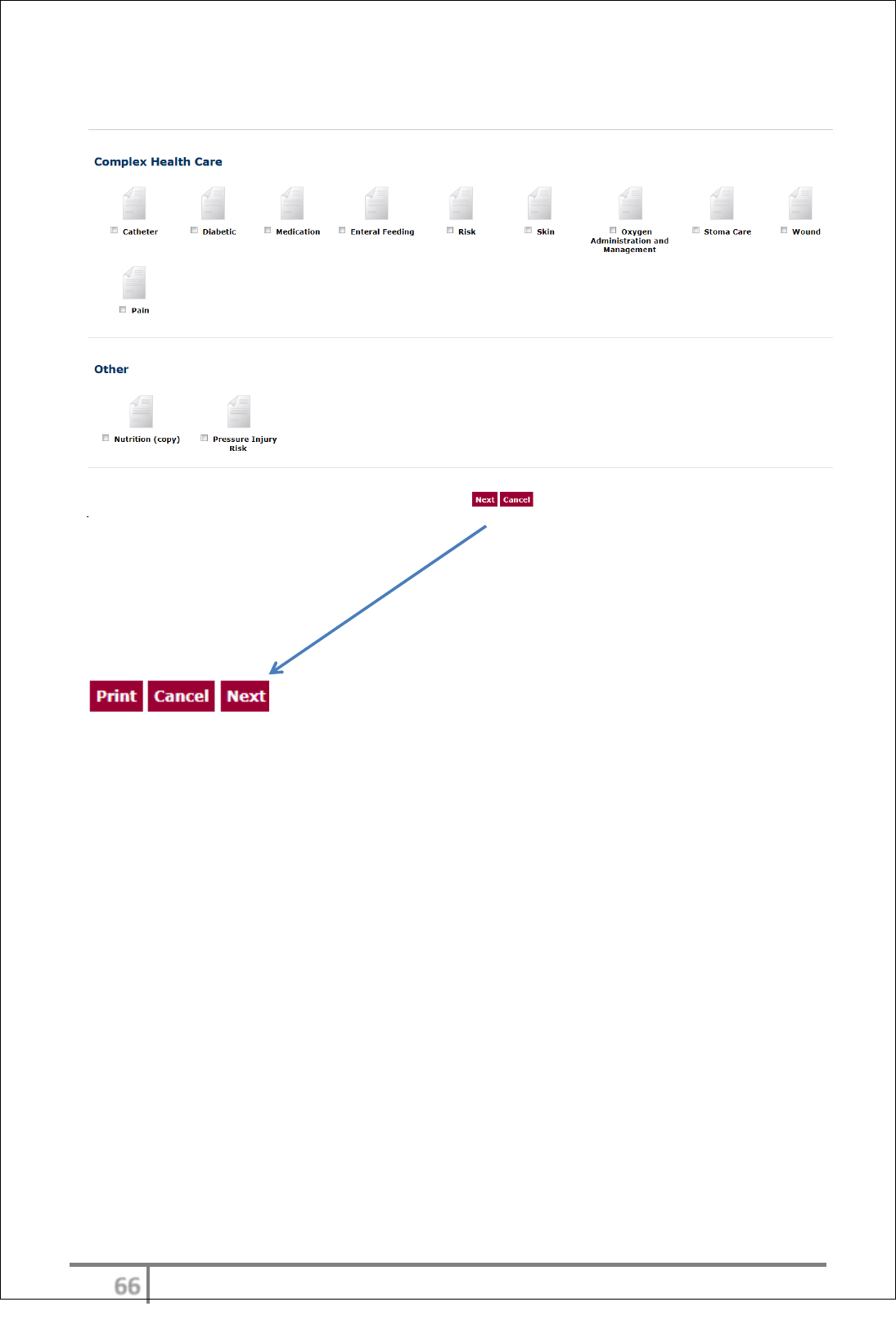
If multiple assessments have been selected, the Wizard will prompt the User to
continue to the ‘Next’ after each one is completed.
ϊϋ
Ver 3.2013
.
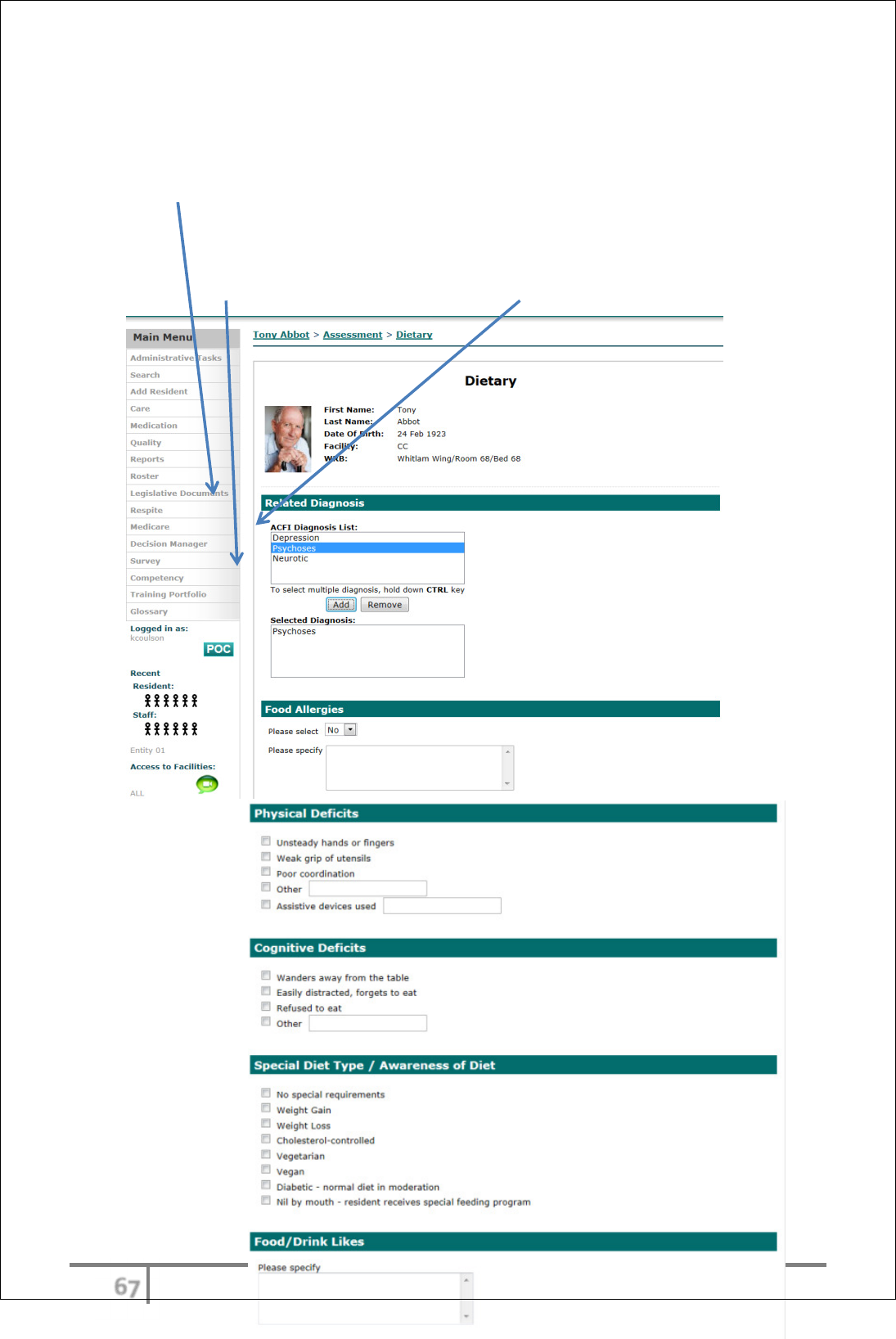
Care assessments are primarily used to establish the assessed Need/choices for
care for the resident. Each assessment is also initiated by the selection of
relevant diagnoses.
All diagnoses from the admission process/ACFI Appraisals will be available for
the User to select from. The diagnoses selected will be those that are related to
the assessment being completed and can be selected one at a time or by holding
down the CTRL key to select multiple diagnoses. All relevant diagnoses can be
added to the Selected Diagnosis: field via the ‘Add’ button.
ϊό
Ver 3.2013
.
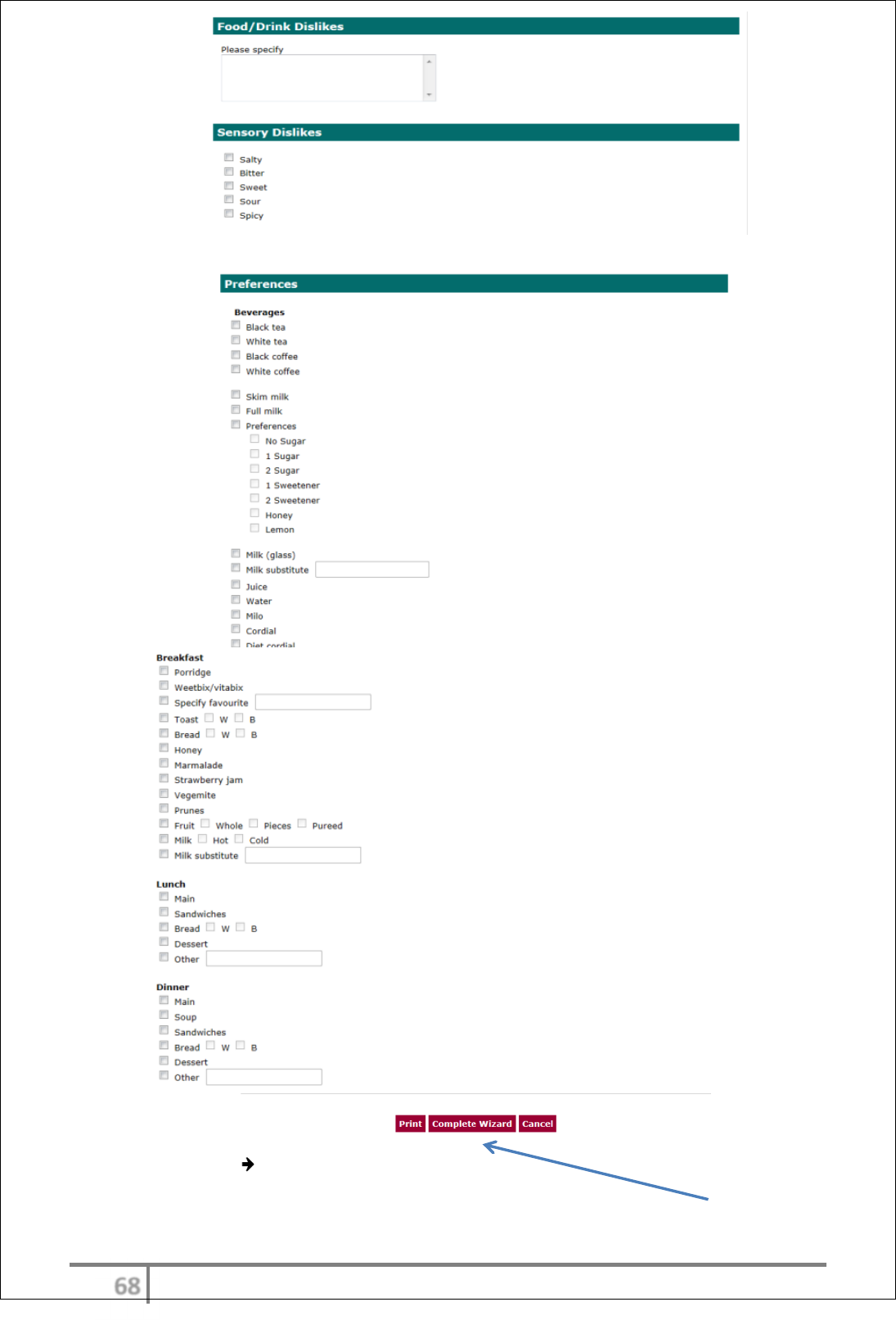
When all assessments are complete, the Wizard will display ‘Complete Wizard’
ϊύ
Ver 3.2013
.
Each assessment can also be printed as they are completed.
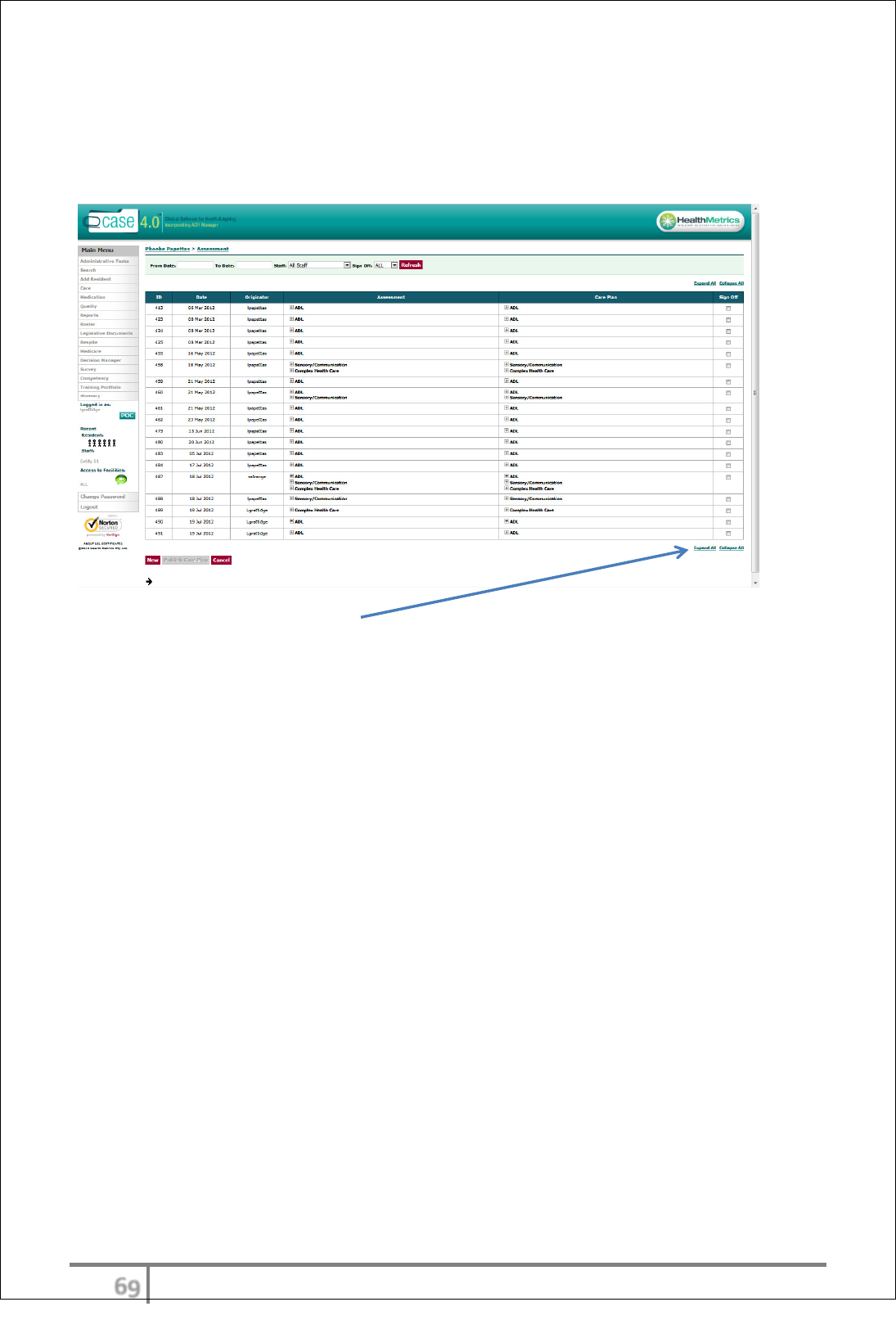
The Complete Wizard option will take the User to the Wizard completion page.
All assessments and careplans are stored within this area.
The page has an ‘Expand All’ or ‘Collapse All’ viewing option.
eCase care is designed to ensure that all assessments have a relevant careplan
following.
ϋτ
Ver 3.2013
.
Careplans- interim, full careplan & Summary
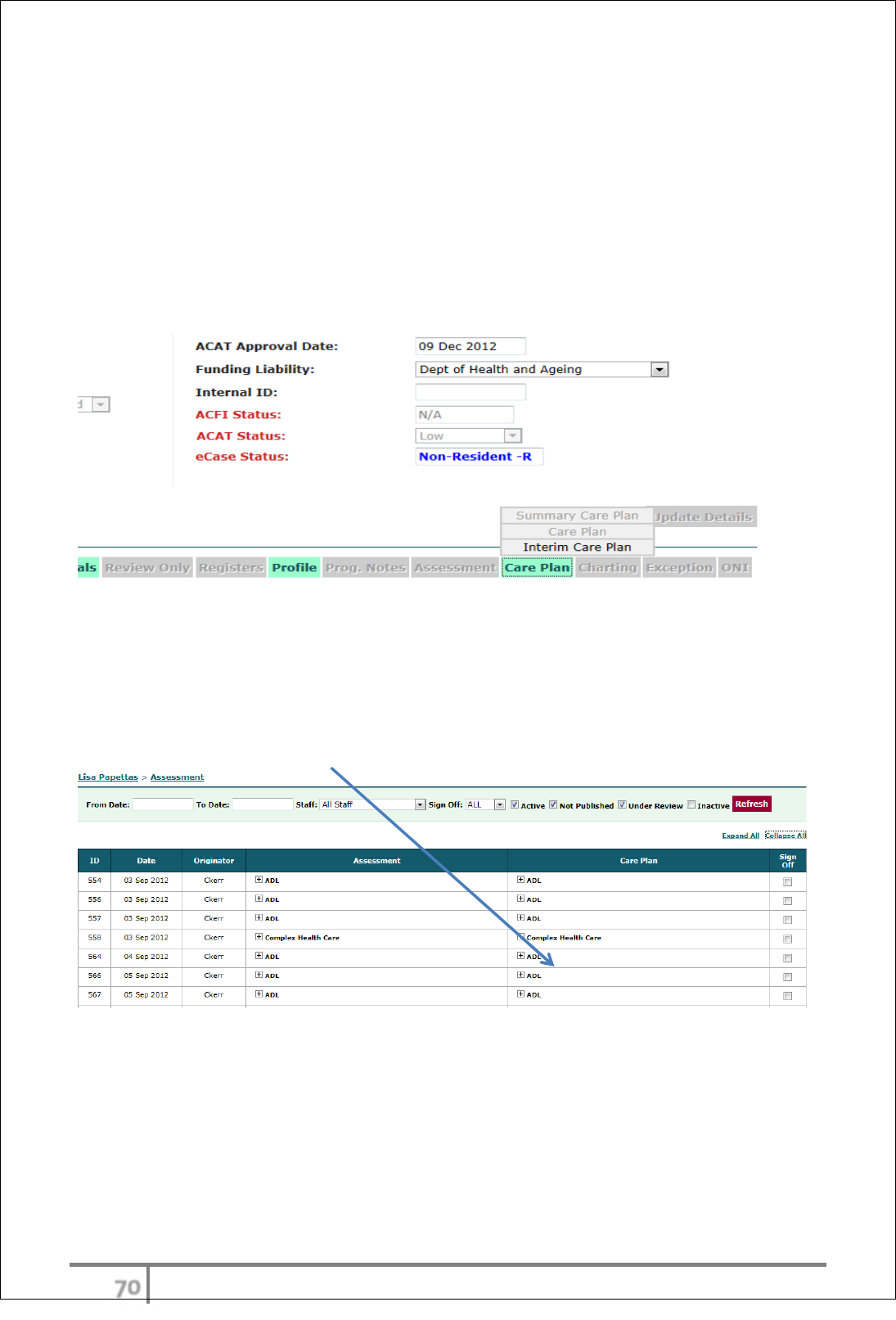
Interim Careplan
The interim careplan is available to residents from the period of admission until
the full resident careplan suite is developed. Once this is complete the Interim
careplan will be inactivated (greyed out). The interim careplan is also available
to complete during the pre-admission phase.
Completing a Careplan
The initial creation of a careplan begins on the assessment page. eCase workflow
ensures that an assessment must be created first to provide relevant needs for
care details for the corresponding careplan. Choose the assessment/careplan
required for completion.
ϋυ
Ver 3.2013
.
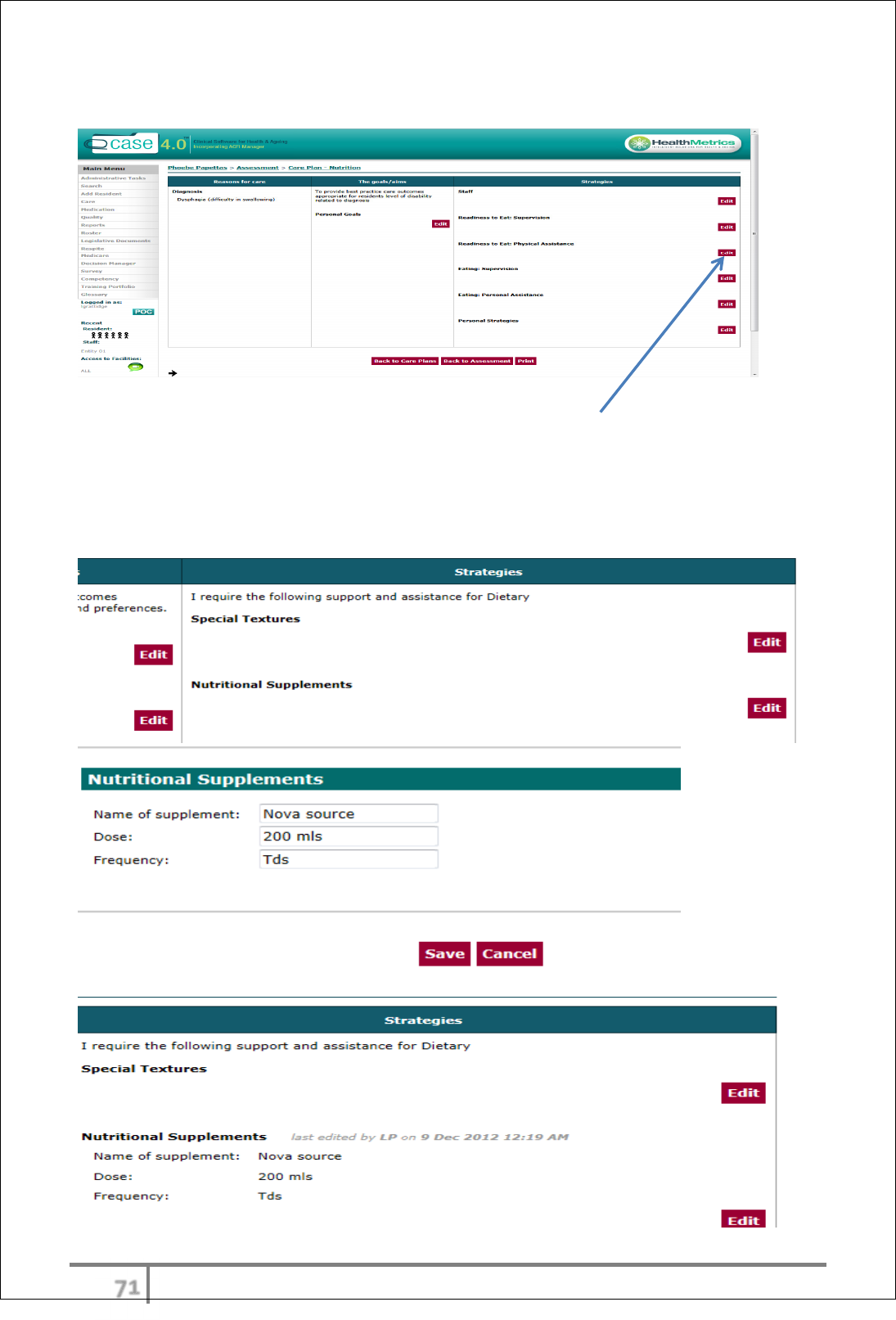
The careplan options will then be available for completion
Entries can be made to the care plan by selecting the EDIT button next to the
goals/aims and strategies. The reason for care has been automatically
transferred from the assessment previously completed.
Any mapped data from other fields including charts will be located within the edit
button and will need to be initiated. (see example below nutritional supplements
chart data)
ϋφ
Ver 3.2013
.
eCase careplans include the resident’s need and choices (which come from
assessment), Goals and relevant interventions. Associated charting outcomes
will also be included in the relevant care interventions. Careplans provide
suggested clinical interventions as well as the option for the User to include
personalised strategies.
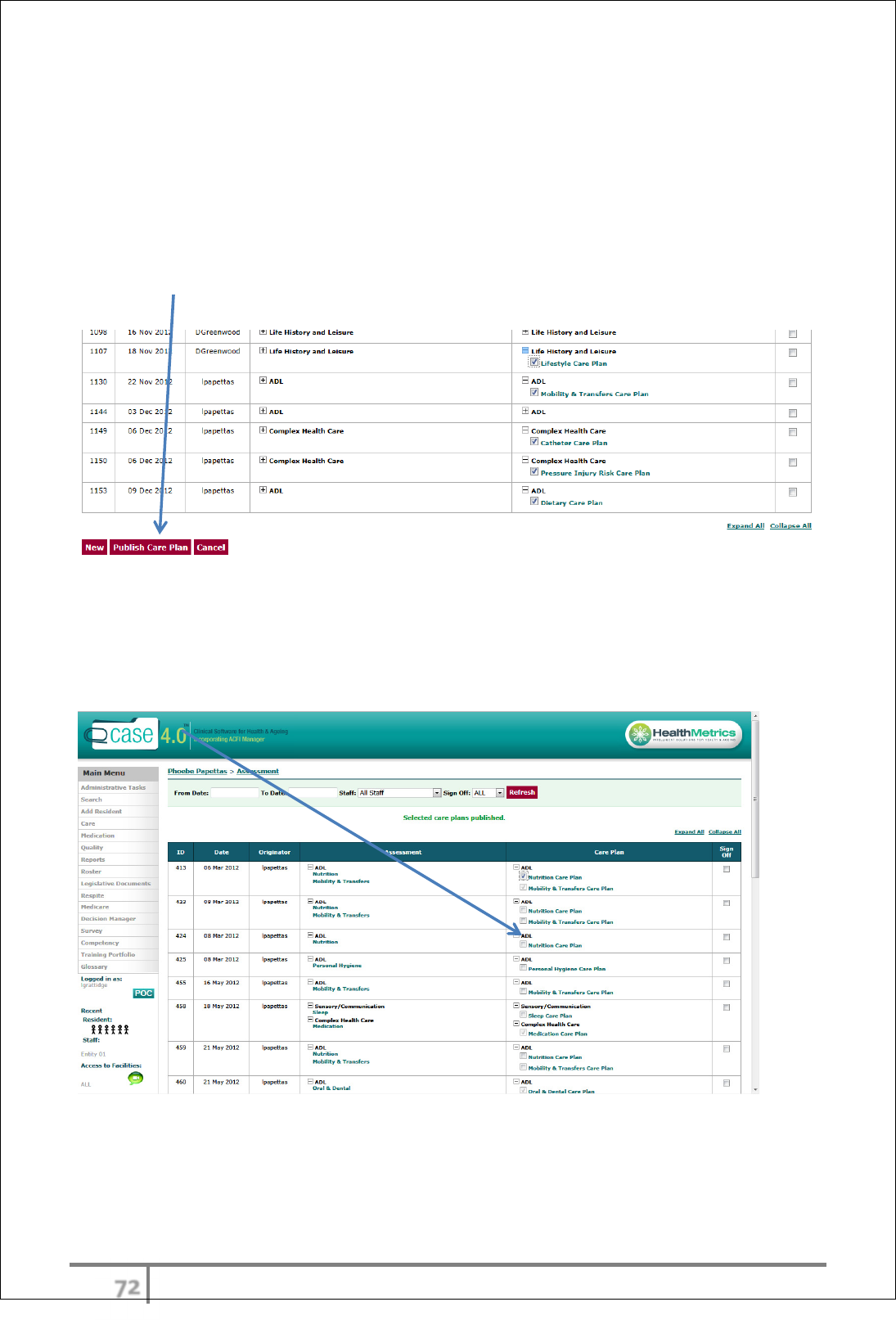
Once the careplan is finished it is now ready for publishing. The publishing
function is role restricted (usually to RN’s) Publishing the careplan is initiated in
the assessment page. The user selects the careplan/s for publishing and then
selects publish. These published careplans will now be visible from the careplan
menu icon.
Changes to Careplan
Once the careplan has been published, changes are made using the ‘quick edit’
or careplan evaluation function. When the careplan has been published the
published careplan will be denoted in the careplan list with a permanent tick.
ϋχ
Ver 3.2013
.
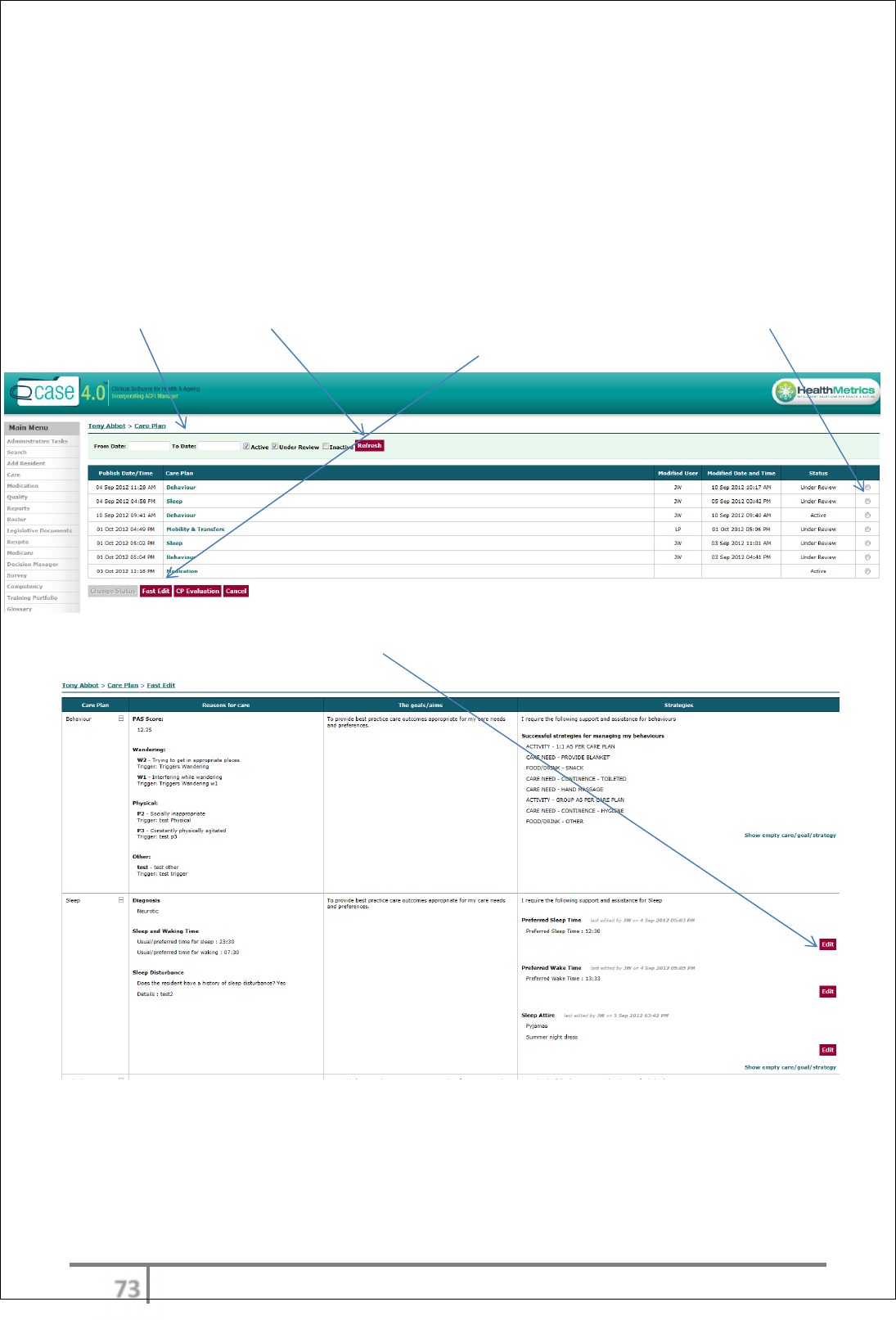
Care plan fast edit
The fast edit allows for small changes to the care plan strategies in-between full
care plan evaluation
The Fast edit screen will initially display only the fields that have been selected
on the initial published careplan. There is an icon at the bottom of the page
which will allow the user to open up and display all existing fields from that
careplan. The user can make changes to the strategies using the option.
Add date then Click ‘Refresh’ then click on the area you would like to fast edit by
clicking the box then click ‘fast edit’
To edit the different areas click ‘Edit’, you will not have to press save as for every time
anything is enter into the edit box it will auto save
All changes to the care plan will have auto initial time and date stamps
Changes to reasons of care and goals will need a full assessment and care plan
for that particular care plan
ϋψ
Ver 3.2013
.
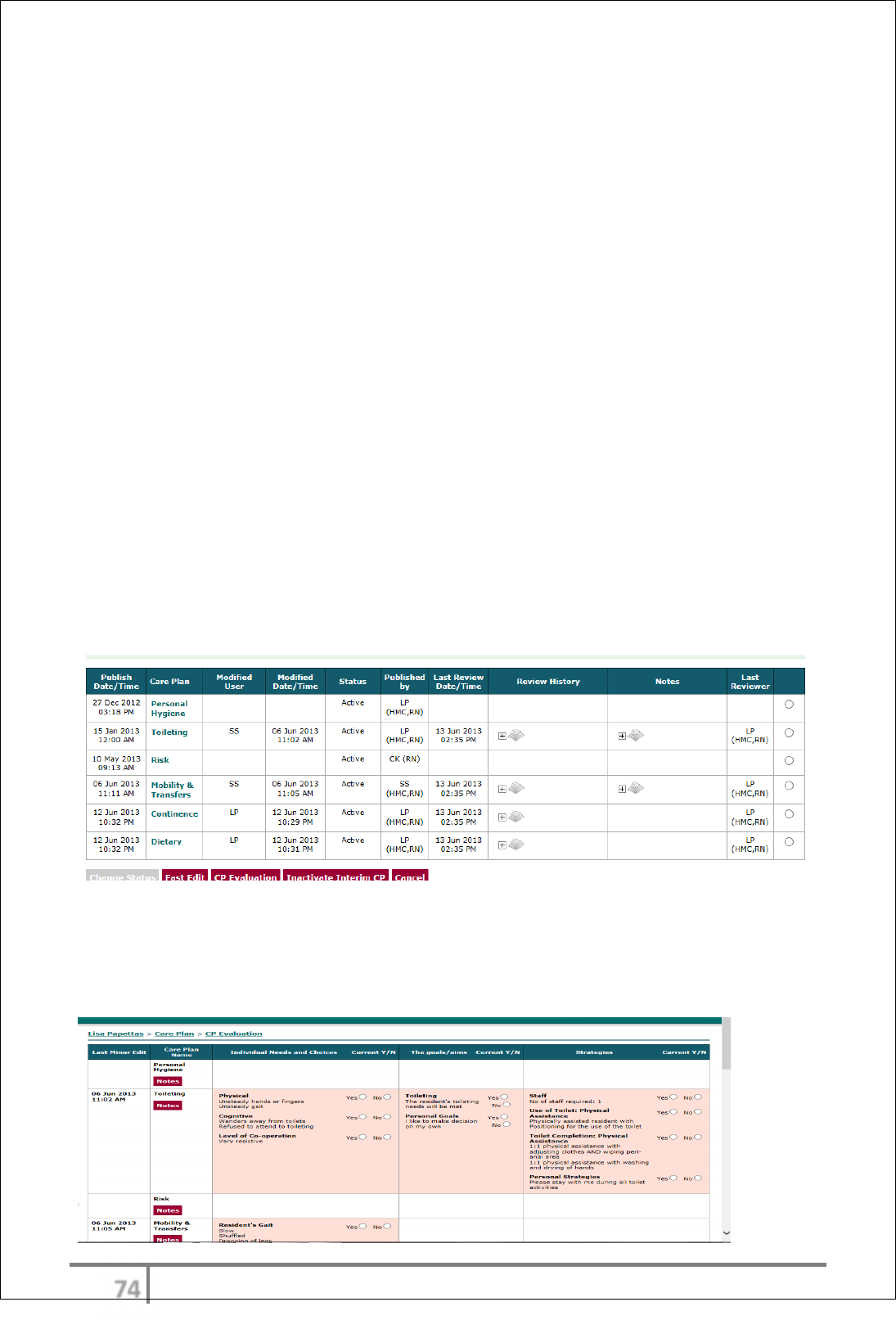
Care plan evaluation
The careplan evaluation ensures that every option in the existing careplan
including Reason for care, Goals and Strategies is fully reviewed on a 3 month
basis (or as per organizational policy). The user must acknowledge every field on
each careplan with a Yes/No identifying if the item is current/ affective or not. If
any item on any given careplan is selected as No, the care plan becomes ‘under
review’. When the care plan evaluation is complete a task with be created in the
work log to commence a full review of the care plan that has been selected with
‘no’ . Users are forced to select Yes or No on each aspect of every careplan.
When an option is selected for each item the save button will come alive and the
entire review can be saved.
There is also a notes option on each individual careplan where the appraiser can
make further comments regarding the review/evaluation. The notes will also
display on the careplan table.
The layout of the careplan table is as follows:-
• Date and time careplan published
• Modified user and date modified
• Careplan status
• Published by
• Review history (display changes made by date/time /user
• Notes from careplan evaluation page
• Credentials of last reviewer
Careplan evaluation – each item must be addressed as Yes/No regarding status
of information. The user can also include additional notes regarding the
evaluation. The save button will not come alive until each item on all careplans
have been addressed.
ϋω
Ver 3.2013
.
Careplan evaluation cont’d
If the user selects the yes option to all items in any given careplan, that
careplan will remain active. If any item is selected as NO (not current ) that
careplan will become under review.
If the No was selected from the assessment side of the careplan a complete new
assessment and careplan will need to be commenced.
If the NO was selected on the interventions or goals the user can make relevant
changes on the fast edit.
When the changes are made the user can then change that careplan back to
active status.
Care plan workflow
CAREPLAN FAST EDIT/CAREPLAN EVALUATION
Care plan fast edit is designed to make small changes in between full 3 monthly
careplan reviews. This may be a result of a fall, hospital admission etc etc. It is
not a full careplan review/evaluation and will not be scheduled in the worklog.
The careplan evaluation ensures that every option in the existing careplan
including Reason for care, Goals and Strategies is fully reviewed on a 3 month
basis.
The Fast edit screen will initially display only the fields that have been selected
on the initial published careplan. There is an icon at the bottom of the page
which will allow the user to open up and display all existing fields from that
careplan. The user can make changes to the strategies using the option.
ϋϊ
Ver 3.2013
.
ECase CAREPLAN WORK FLOW
ASSESSMENT/CAREPLAN WIZARD
ACCESS CARE ASSESSMENT FROM CARE WORKLOG
COMPLETE ASSESSMENT ALLOCATED ON THE DAY YOU ARE VIEWING
MOBILITY ASSESSMENT
COMPLETE CORRESPONDING CAREPLAN READY FOR RN TO AUTHORIZE
/PUBLISH
CAREPLAN EDIT
CAREPLAN BECOMES
ACTIVE
PUBLISH CAREPLAN
-
ONLY THE RN HAS THE AUTHORITY TO PUBLISH
CAREPLANS. This allows for EN’s and Senior PCW to complete a careplan
however RN only needs to authorize/approve.
PUBLISH CAREPLAN
CAREPLAN FAST EDIT
FAST EDIT
FAST EDIT CHANGES
CAREPLAN EVALUATION
REVIEW CAREPLAN -EVALUATION
ϋϋ
Ver 3.2013
.
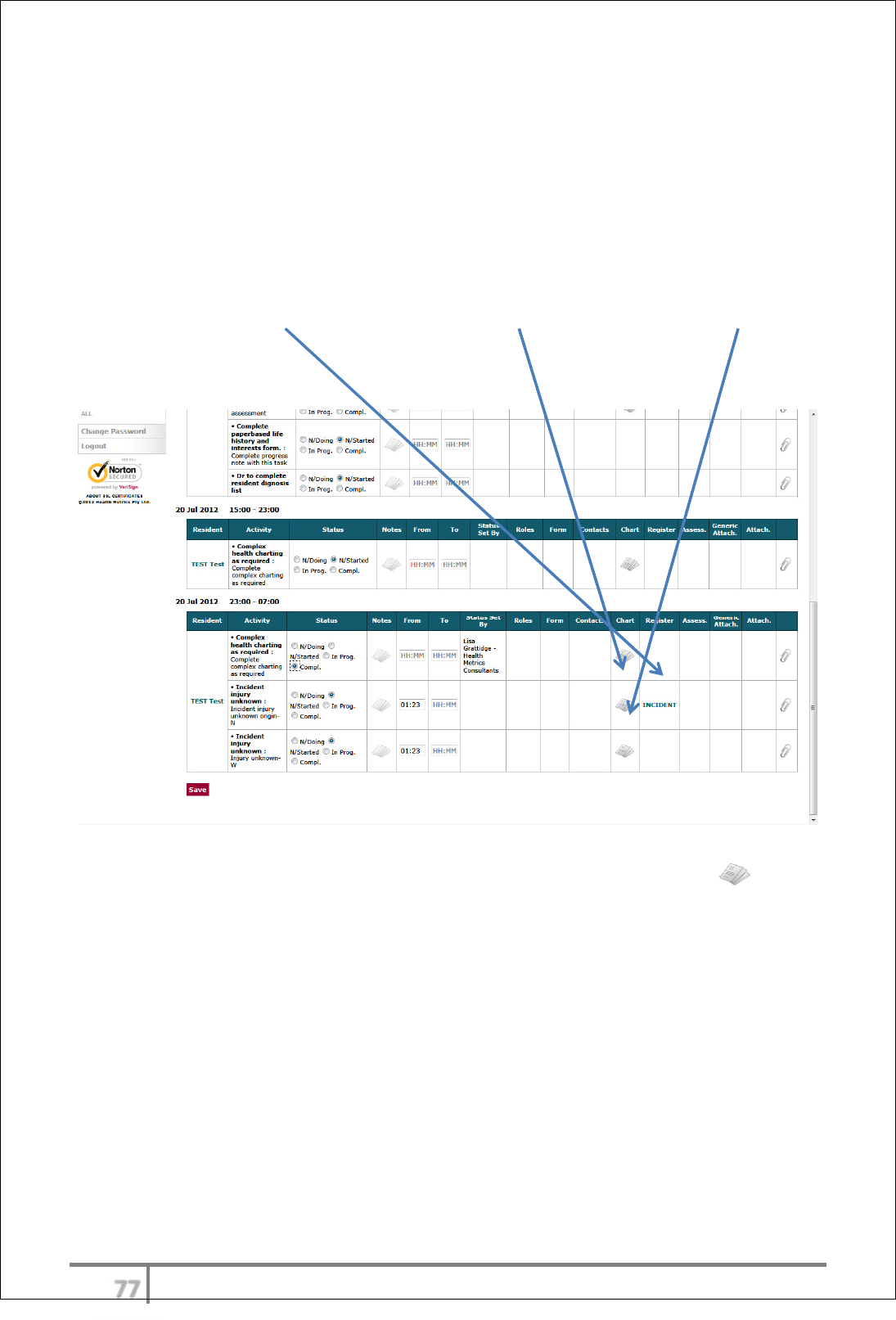
Incident Management
Integration with clinical registers
A progress note entry with the correctly selected ‘Progress Note Type’ will trigger
an
‘INCIDENT’
form in the Work Log for completion.
For example – A progress note entry tagged ‘Injury unknown origin/source’ will
generate a Resident Incident form, Neurological Observation chart and Wound
chart in the Work Log to complete if applicable.
Complete incident report via
‘INCIDENT’
link in Work Log and charts via icon.
Resident infections are also logged using the same workflow however will be
tagged as a particular infection type in the progress note.
ϋό
Ver 3.2013
.
Care Reporting Tools
In Charge of Shift/Clinical Managers/Facility Manager
eCase has a variety of standard care reports/views. In addition to this the super
User can also call the Health Metrics helpdesk at any time and request an adhoc
report. If adhoc reports are requested more than once they will be made a
regular report for the organization.
In addition power users can product unlimited dashboard reports using the BI
reporting tool.
A Business Intelligence module of eCase is also available (acquired separately)
which will enable all senior users to generate infinite reports, using a dashboard
presentation.
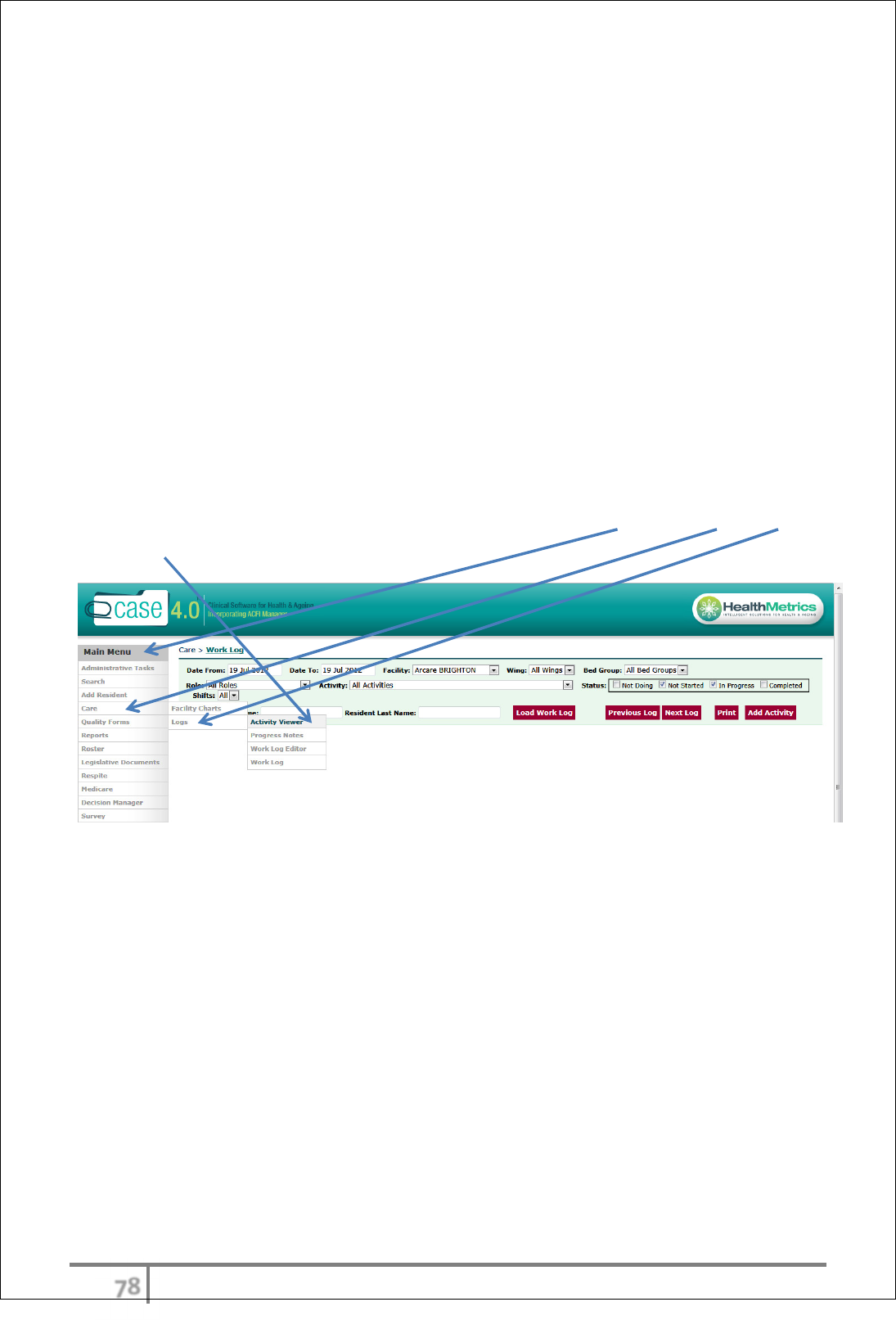
Report/View One: Activity Viewer for In Charge of Shift/Clinical Managers/Facility
Managers
Activity Viewer
The Activity Viewer can be accessed by selecting form Main Menu > Care > Logs
> Activity Viewer.
This allows the super User to view and monitor the status of tasks that have
been generated from the care Work Log.
There are 4 possible statuses for any particular task: Not Started, Work in
Progress, Complete and Not Doing (default filter - All Statuses)
ϋύ
Ver 3.2013
.
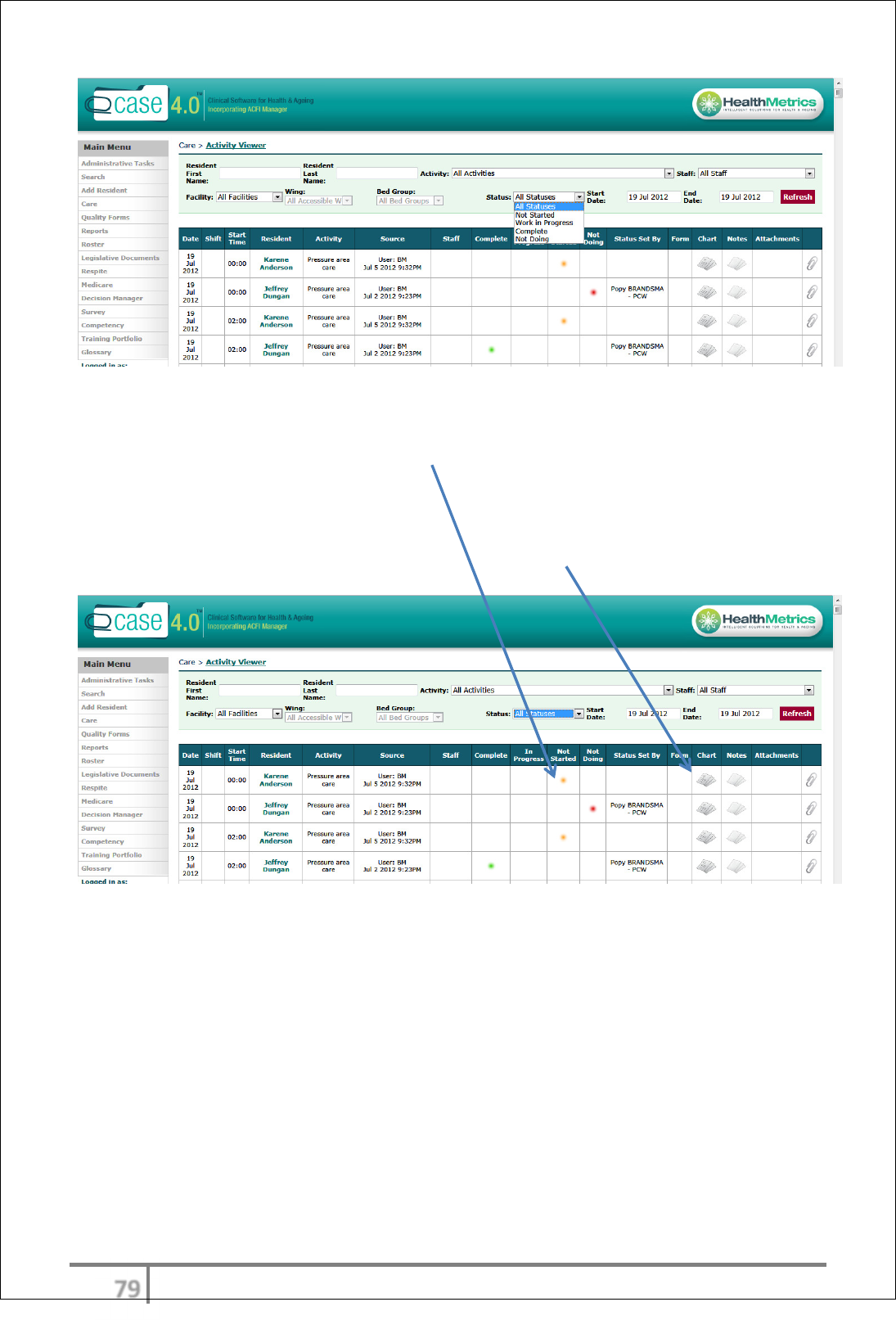
The super User can use the filter at the top of the screen to filter and identify all
statuses at any time. As an example all ‘Not started’ tasks by a particular date
range can be listed and if staff have not started or not doing an item and have
not attached a note explaining why, the super User can then contact the staff
member who has generated that task and follow up on a 1:1 basis.
The super User can also review any completed forms/charts from this view.
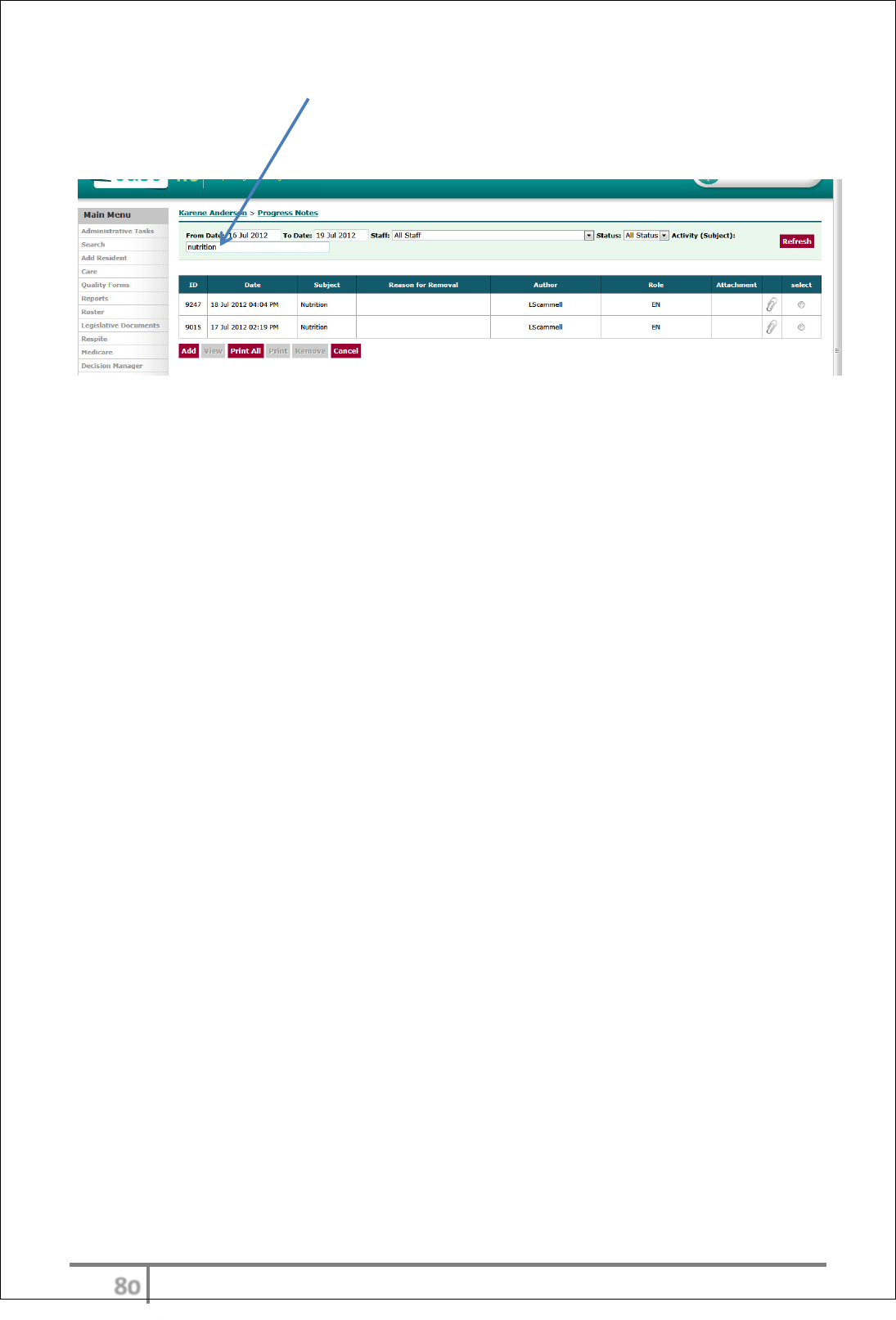
Report/View Two: Progress Notes
The full progress notes list is an invaluable tool for senior staff to view and
monitor all progress notes for any given period. There are also filters for each
variable for this list.
Senior staff can monitor particular progress note types, by staff or by resident
depending on the requirement. As an example the RN coming on duty may wish
to review all acute events that may have occurred in the proceeding shift.
ότ
Ver 3.2013
.
In the filter on the Activity (Subject) heading the User can put in any key word
or part there-of and any progress note similar to the key word will display.
See example below – Activity (Subject): entered was nutrition.
όυ
Ver 3.2013
.
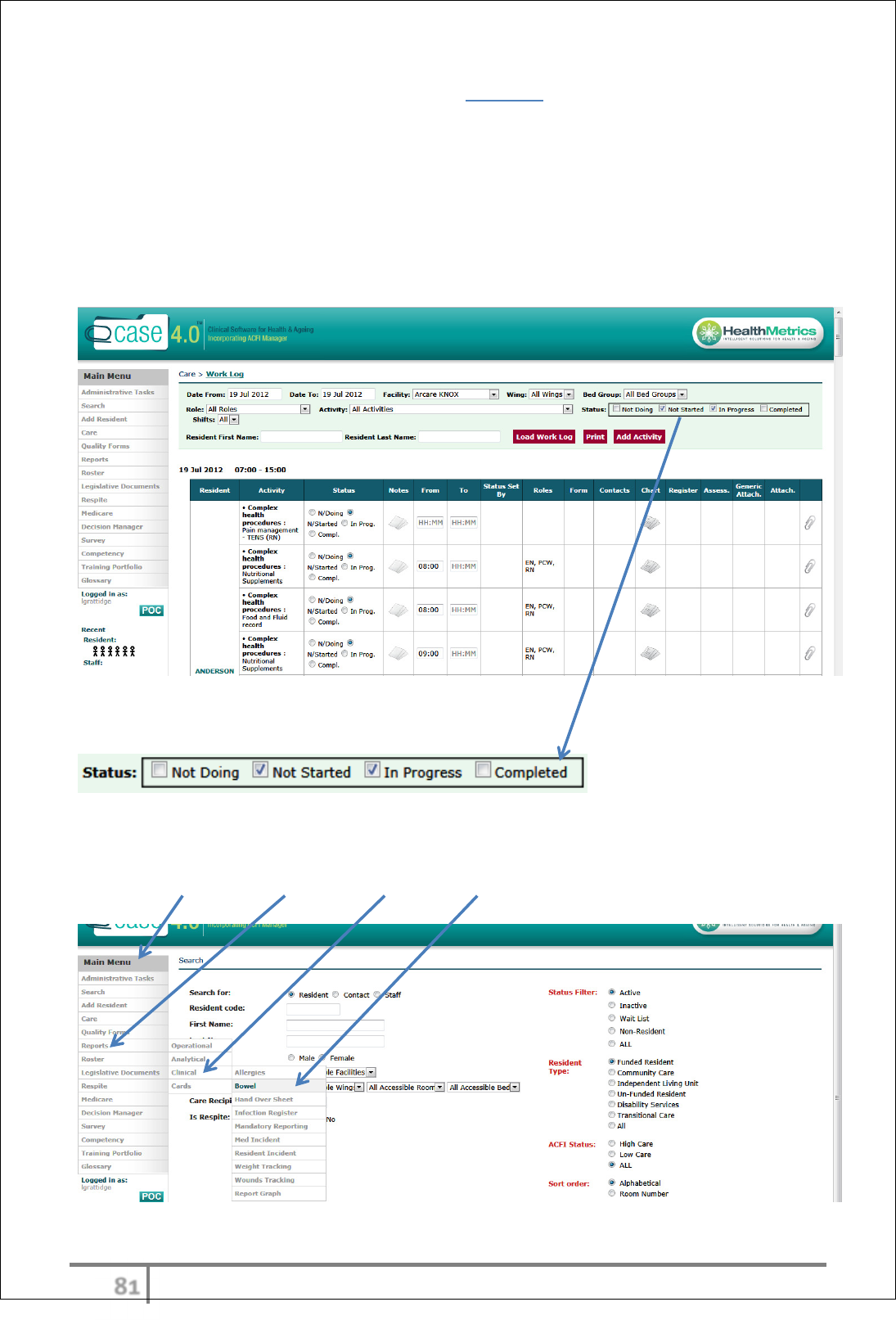
Report/View Three: Care Work Log for All Staff
All Users should be accessing this report each day to view the tasks allocated
depending on their designation and/or work area they are allocated.
Managers and senior staff can also use this view to identify incomplete or tasks
needed to be done for any given time frame. The filters at the top of the screen
allow the super User to identify particular roles, work areas, and any particular
activity.
There are 4 possible statuses for any particular task:
(Default filter - Not Started and In Progress).
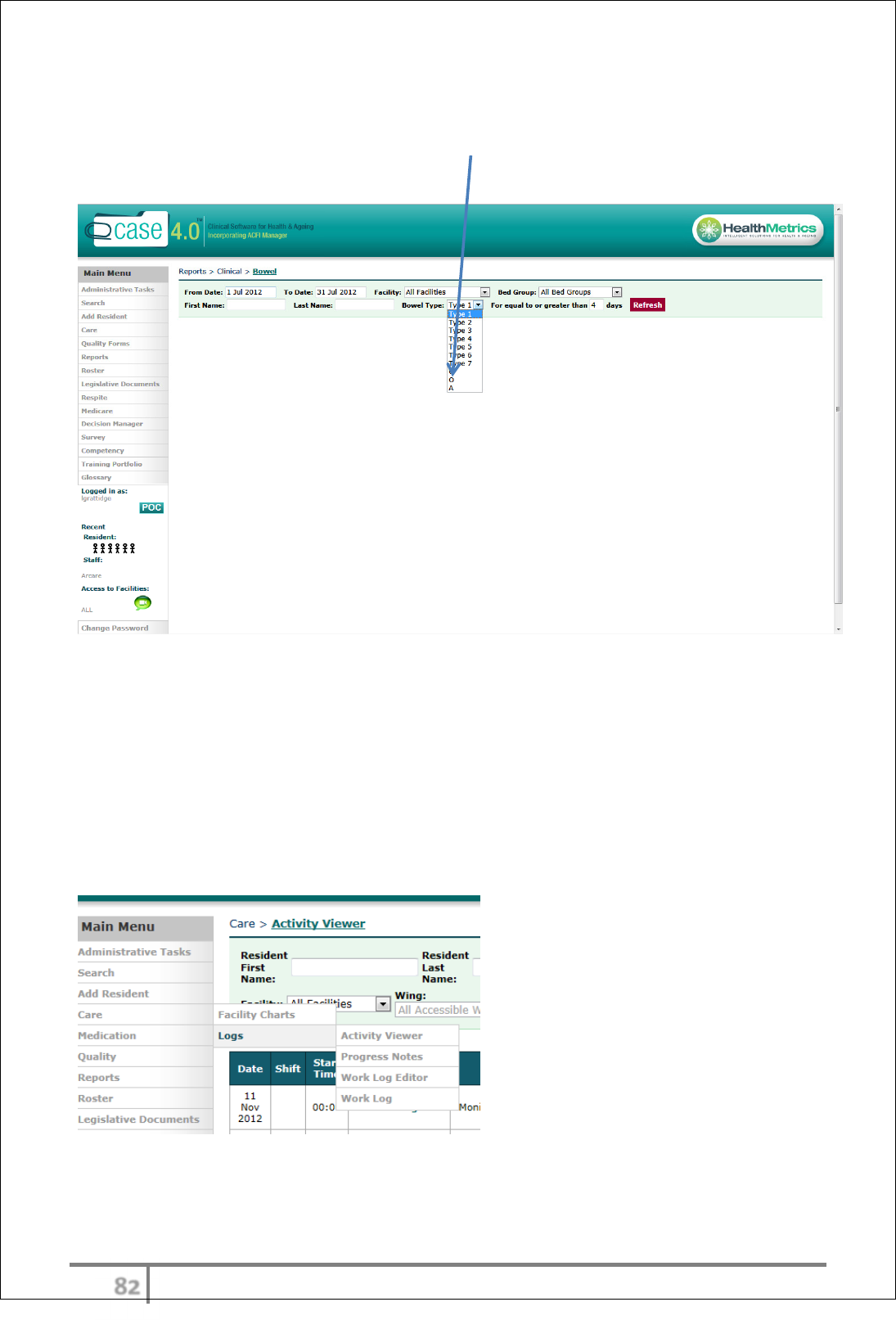
Report/View Four: Bowels
Go to Main Menu > Reports > Clinical > Bowel.
όφ
Ver 3.2013
.
This report also has filters for bowel action type. For example, the User can
identify bowels not open for any given date range by selecting a date, a length
of time for bowels not open and selecting ‘O’. All bowel motion types can be
audited by this manner.
Health Metrics highly recommends that all senior staff/Users identify any regular
reporting they would like to have in the suite of reports/views.
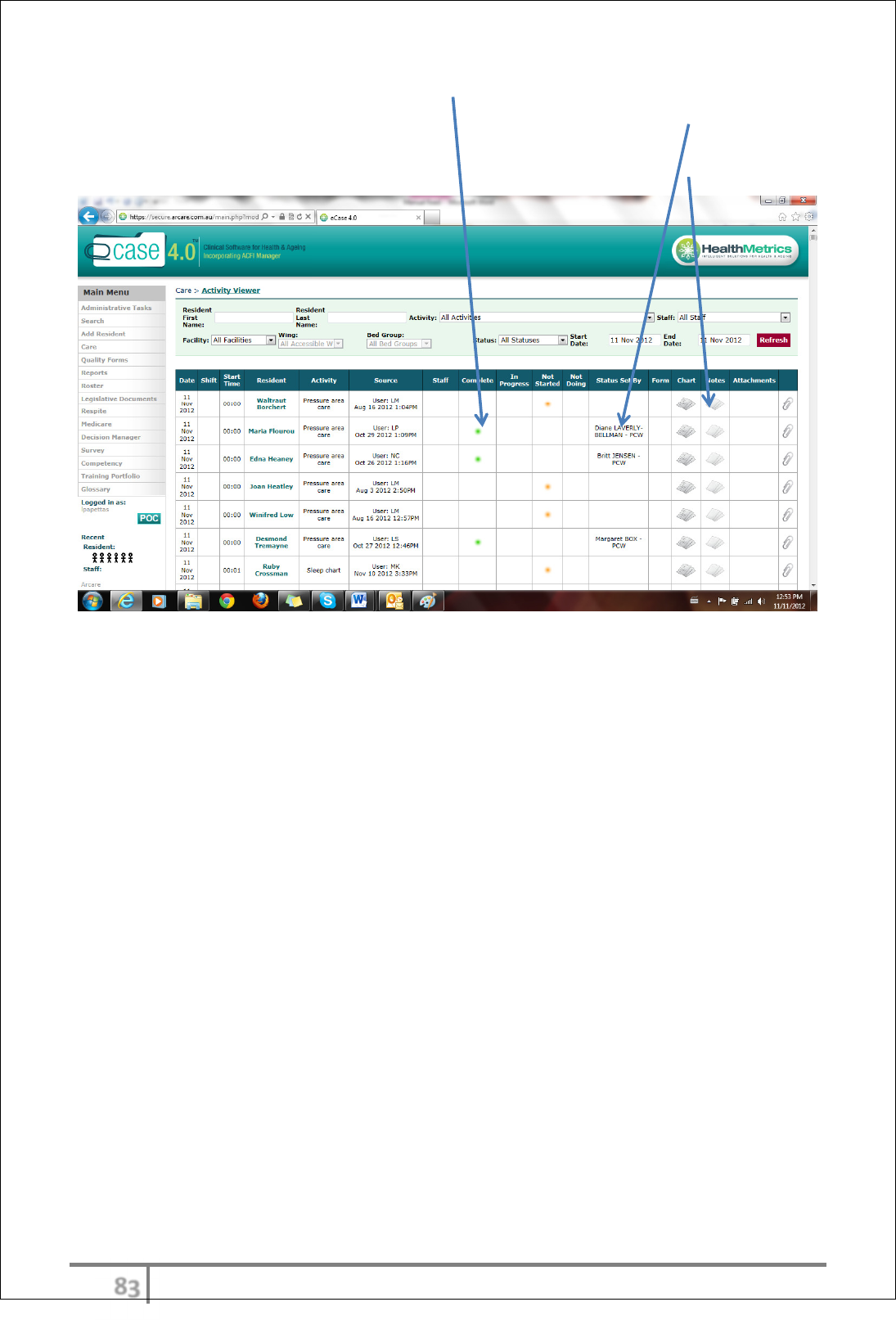
Activity viewer
The activity viewer provides an instant snap shot for senior management,
auditors or managers to address the status of all tasks in a facility at any given
time or day. The Activity viewer is accessed through main
menu>care>logs>Activity viewer
όχ
Ver 3.2013
.
The status of the tasks is highlighted by color (Green complete, yellow not
started red not doing, blue in progress for easy reference and the user details
will be outlined next to tasks that have been addressed. The senior staff member
can also view the actual assessment/chart that requires completion.
Notifications and warnings
eCase has the capacity to generate warnings and notifications via email or SMS to Dr’s, RN, senior
clinicians, pharmacy, in fact to any person who has a valid email address or phone number .
The trigger point for notifications can be generated from progress note generation, charts with
reportable ranges and movement transactions.
This functionality allows auditors to track and monitor notification workflow and compliance. Some
examples are outlined below.
1. Progress note notifications: - incidents, movements to hosp, mandatory reporting, acute
clinical events.
2. Reportable range settings: - BGL management, BP management, weight loss/gain.
3. Movement transactions:- notify pharmacy of hospital transfer, notify funeral director
όψ
Ver 3.2013
.
TOUGHBOOKS
Toughbook Overview
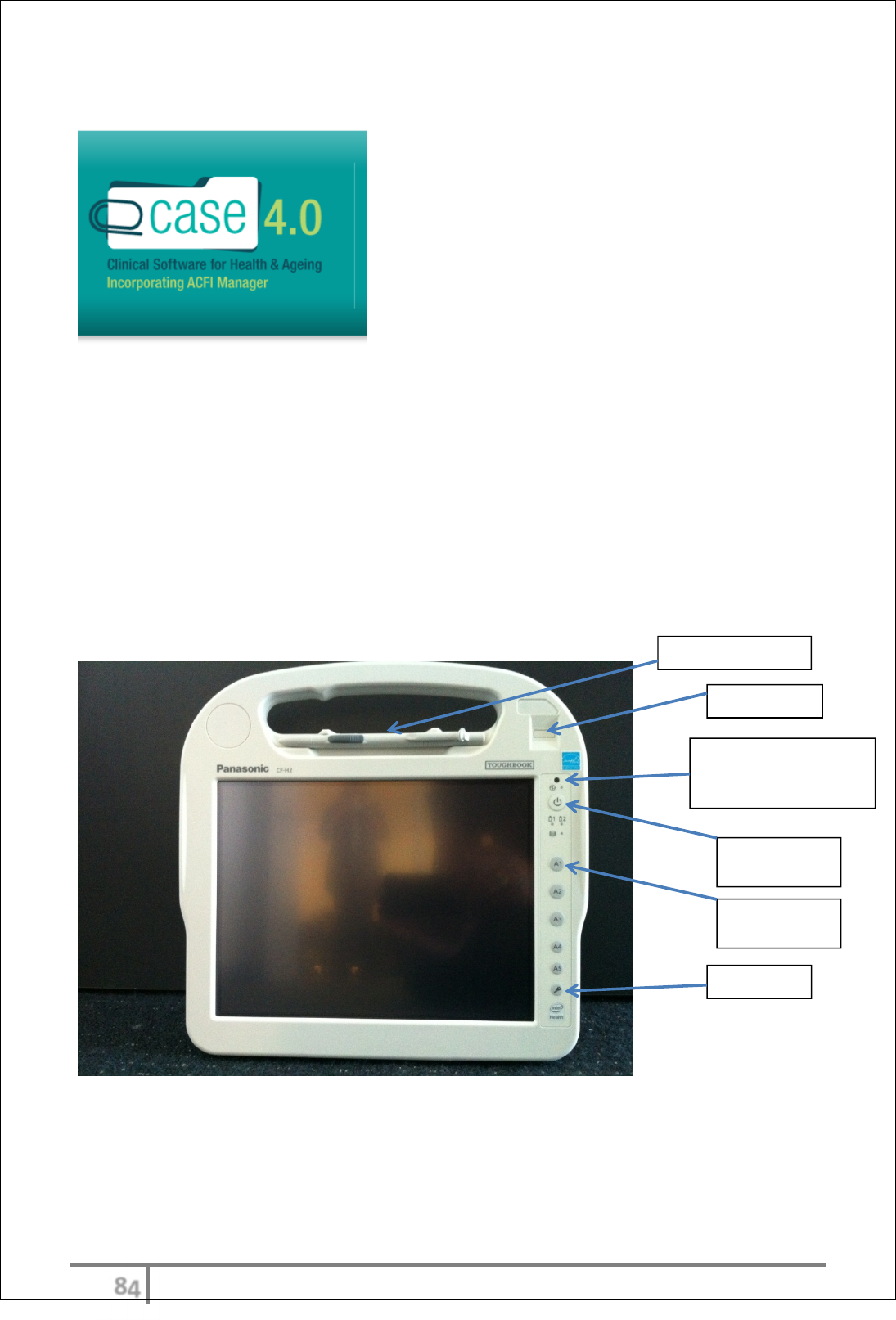
Panasonic’s Toughbook H2 Tablet
The lightweight Toughbook is the ultimate tool for mobile care staff, helping
them to stay productive by delivering constant access to eCase information and
data input capabilities at the point of care (right through to the resident’s
bedside).
Toughbook Operational Guidelines
Pen and pen holder
Finger reader
Power (light) indicator:
Green - Power ON
Blinking Green – SLEEP
Pre-set button
A1 - Camera
Lock screen
Turn-On and
Turn-Off
όω
Ver 3.2013
.
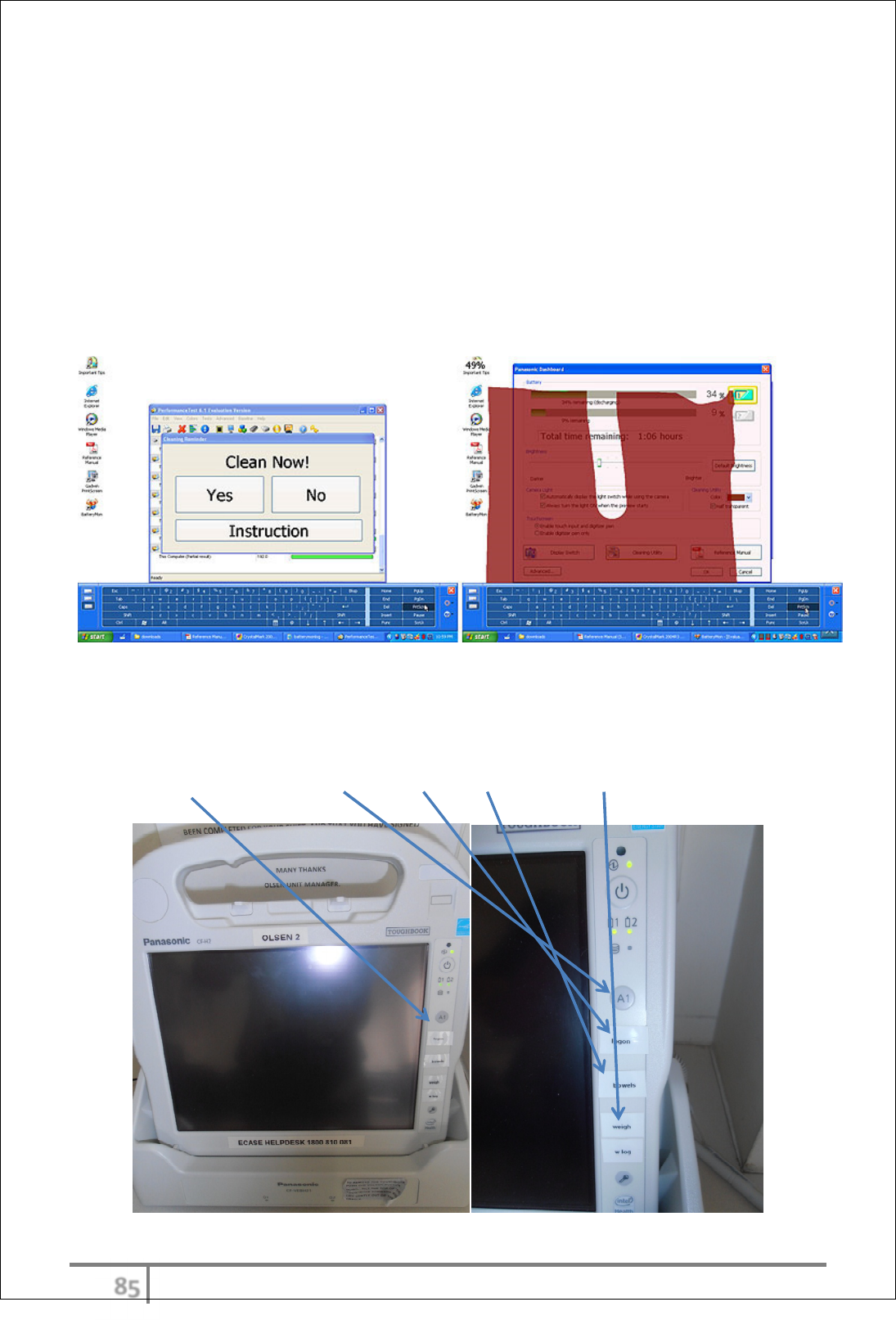
Cleaning Your Tablet
The H2 has a "Cleaning Reminder" tool. In a clinical environment, germs are
potentially anywhere and cleanliness is everything. This means that equipment is
frequently cleaned and scrubbed down with disinfectants. Panasonic made the
H2 easy to clean with a minimum of places where germs can hide and
accumulate. The utility will pop up at certain intervals or upon certain activities
and ask, the User to clean the display. To make sure every part is cleaned, the
Toughbook colours the display and then the User has to carefully wipe off all
colour. This ascertains that the entire screen is cleaned. Cleaning to be done
using standard alcohol screen wipes.
Pre-set buttons
The H2 device has 4 to 5 pre-set buttons. This allows for quick access to any
particular function in eCase without having to search or go through the product.
Pre-set buttons include: Camera, Log-on, Bowels and Weights.
όϊ
Ver 3.2013
.
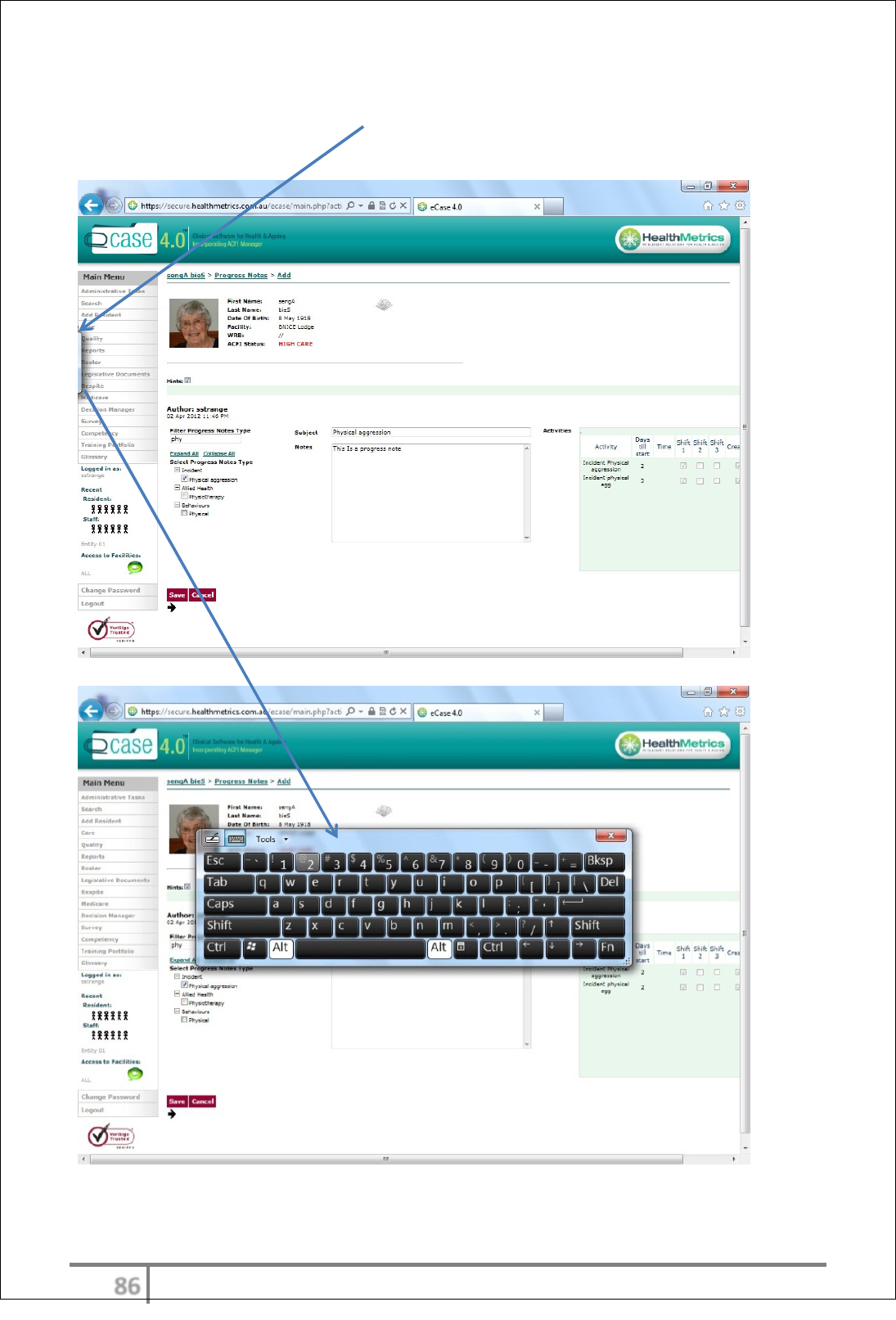
Handwriting recognition
Pull out key board- touch this icon and the key board/handwriting recognition
panel be displayed.
όϋ
Ver 3.2013
.
Typing or text recognition
The User can choose between typing OR writing for text recognition. This can be
done by clicking on the screen icon.
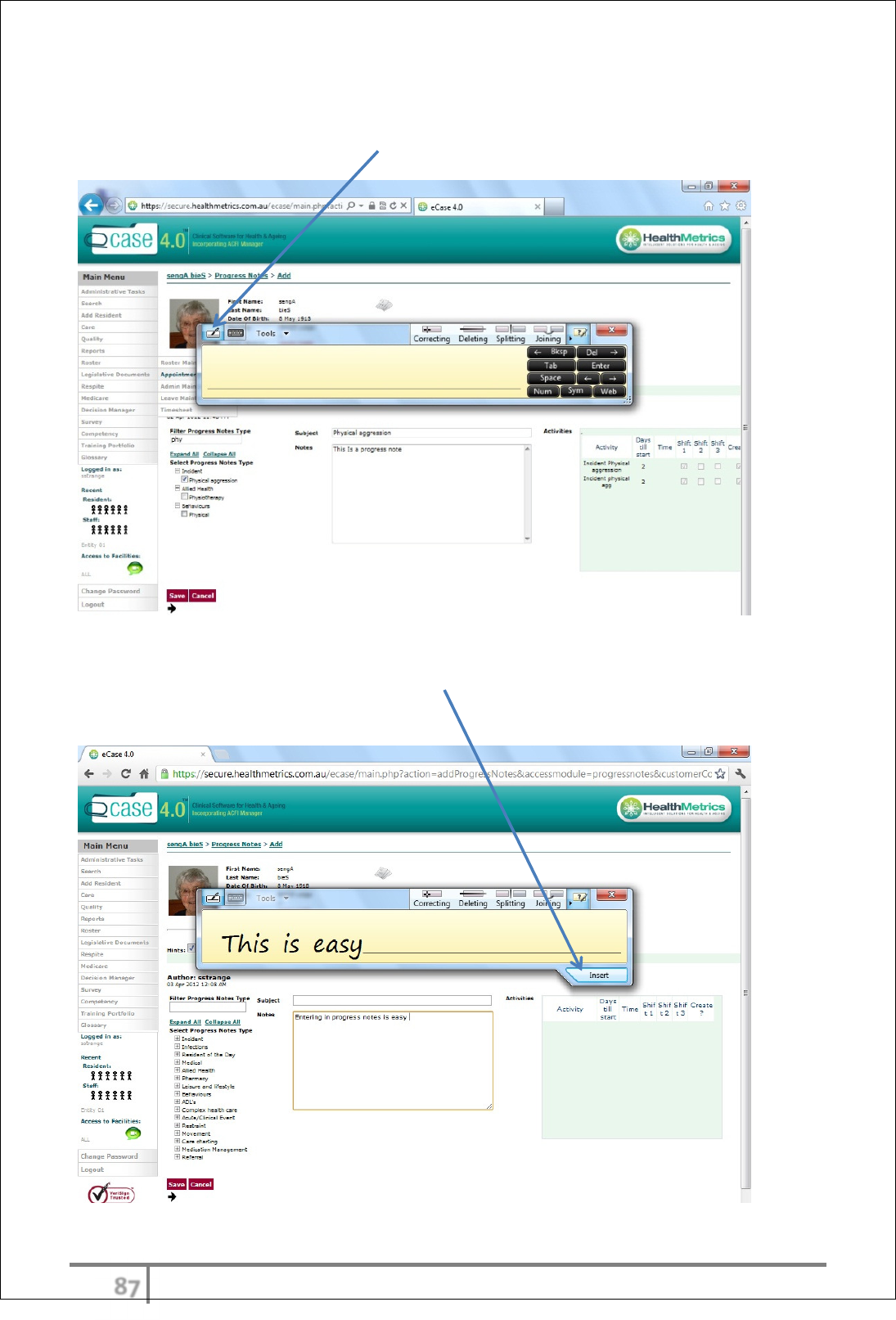
Text recognition
After writing an entry, simply select ‘Insert’ and the data will be entered into the
chosen field.

όό
Ver 3.2013
.
Crossing out text
If the User wishes to delete or remove the writing, simply place the pin on the
word that needs to be removed and ‘flick’ across it. Alternatively select
backspace or delete.
Holding the device

όύ
Ver 3.2013
.
Docking and charging
Ensure the unit is placed in the charger or docking station when not in use. This
will ensure the H2 device ready for action at all times.
ύτ
Ver 3.2013
.
ACFI FUNCTIONALITY
ACFI functionality is managed ensuring all aspects of ACFI are captured and
maintained. This includes:-
• Creation of ACFI
• Modelling ACFI’s
• Optimize ACFI
• Validate ACFI
• Management of dates includes documentation commencement, all
expiry’s, and diagnosis due by
• Full suite of reporting
• Revenue mining
ACFI Overview
eCase provides extensive ACFI functionality ensuring ACFI submissions are
optimized and meet all validation criteria whilst ensuring the best possible care
outcomes.
eCase ACFI related reporting provided allows all levels of users to have up-to-
date ACFI related details on a host of topics and indicators. eCase provides
numerous reports, graphs and pie charts as standard. Users may also request
additional reports and indicators as required.
ACFI instructions for use
Create, model, optimize and validate an appraisal
The first step to achieve a fully optimized appraisal, from a financial and care
perspective the user must first create a modelled appraisal.
Select ‘Appraisals’ from ‘Resident Functions’ menu.
ύυ
Ver 3.2013
.
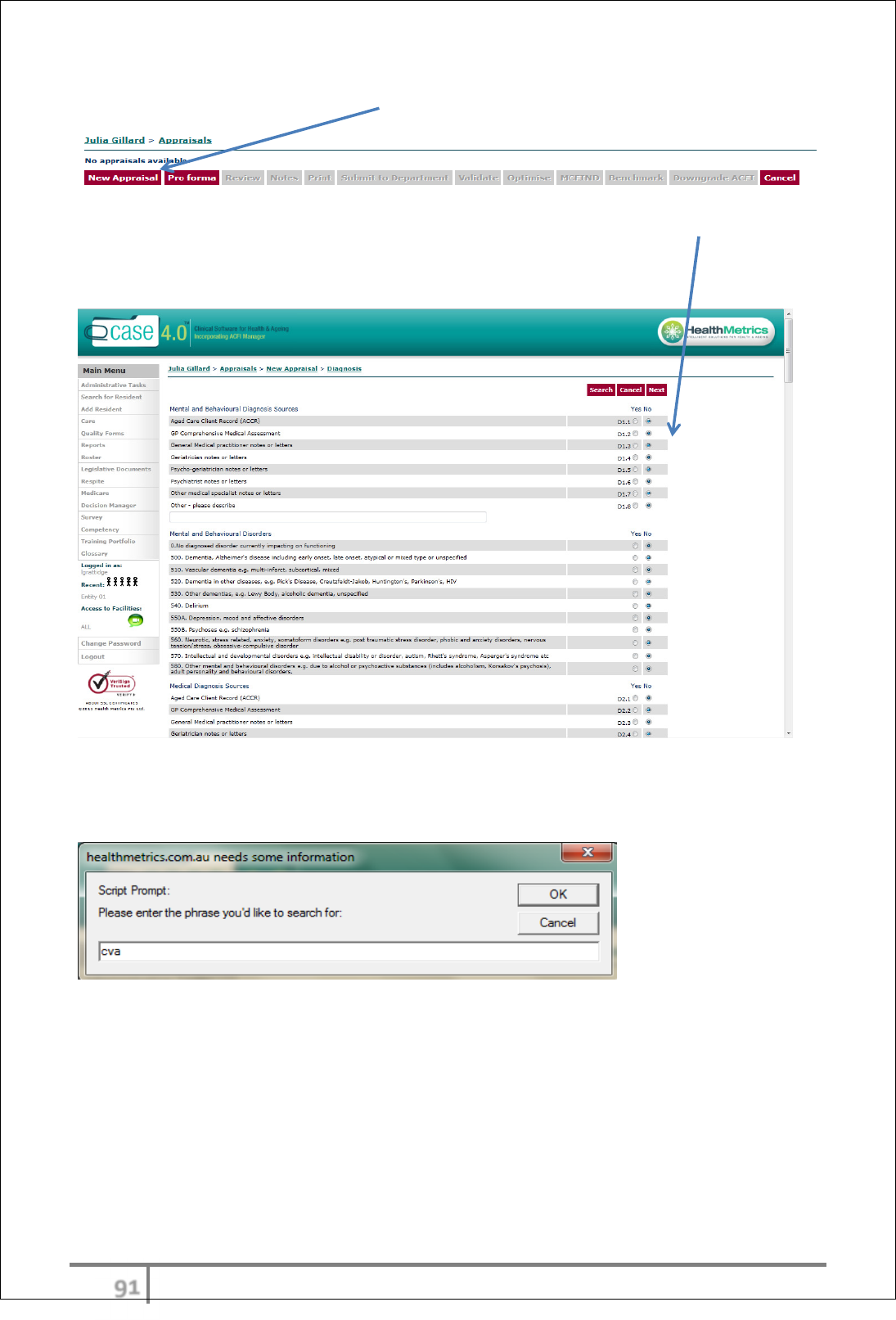
Creating an appraisal. Select ‘New Appraisal’ and begin the ACFI apppraisal.
Select diagnosis by scrolling down the page and manually selecting the radio
button ‘Yes’.
N.B The default is ‘No’.
Search for diagnosis using the search button entering name of diagnosis, part of
diagnosis, or by code number.
ύφ
Ver 3.2013
.
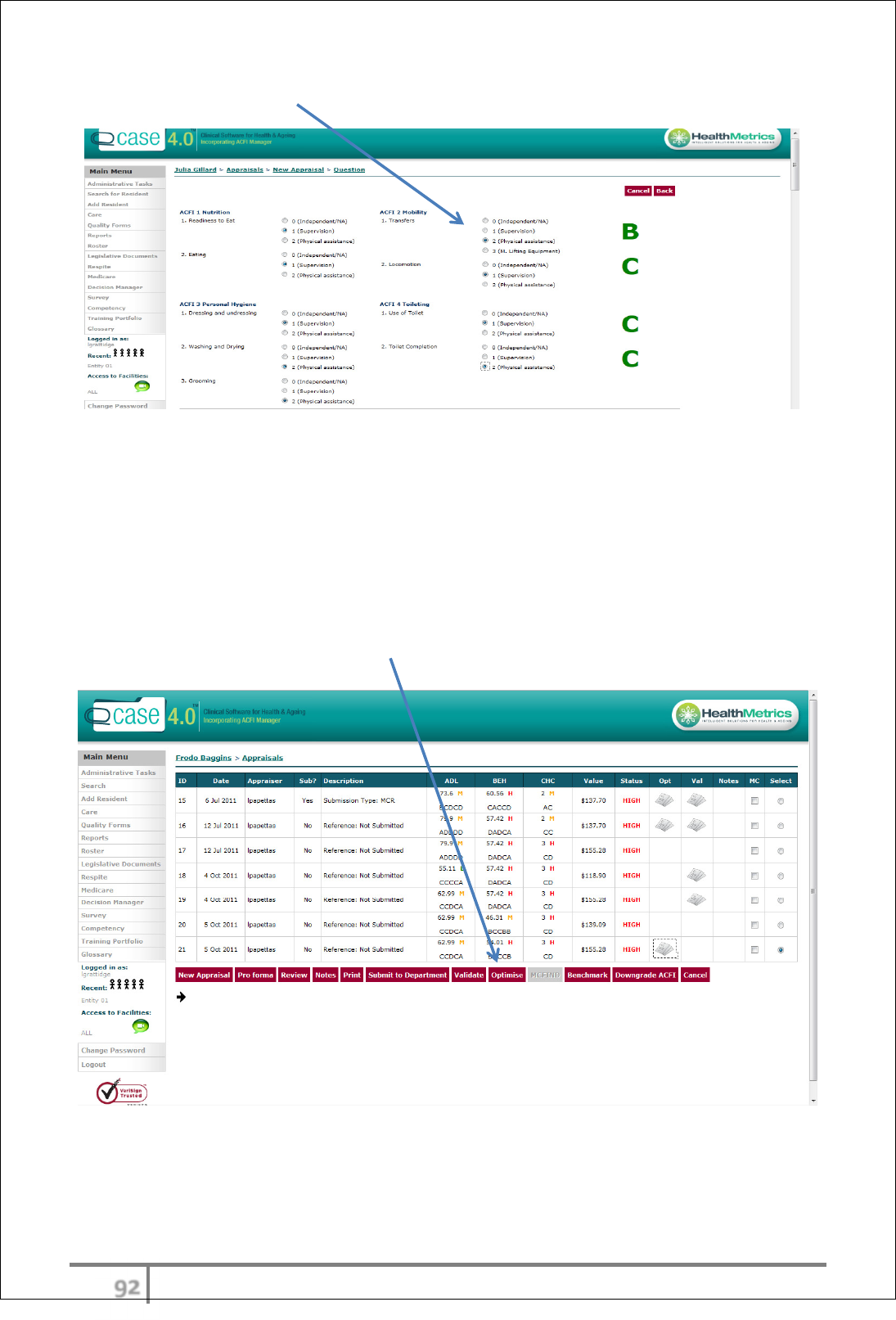
Complete ACFI questions 1-12
Optimising the appraisal
Will provide a comprehensive list of suggested care outcomes based on
diagnosis driven care outcomes. The recommended suggestions can be
implemented by user discretion. The Optimisation report will be emailed to the
logged on user and will also be presented in an envelope icon next to the
appraisal.
The user can review and change the appraisal as many times as required to
achieve the outcome objective.
ύχ
Ver 3.2013
.
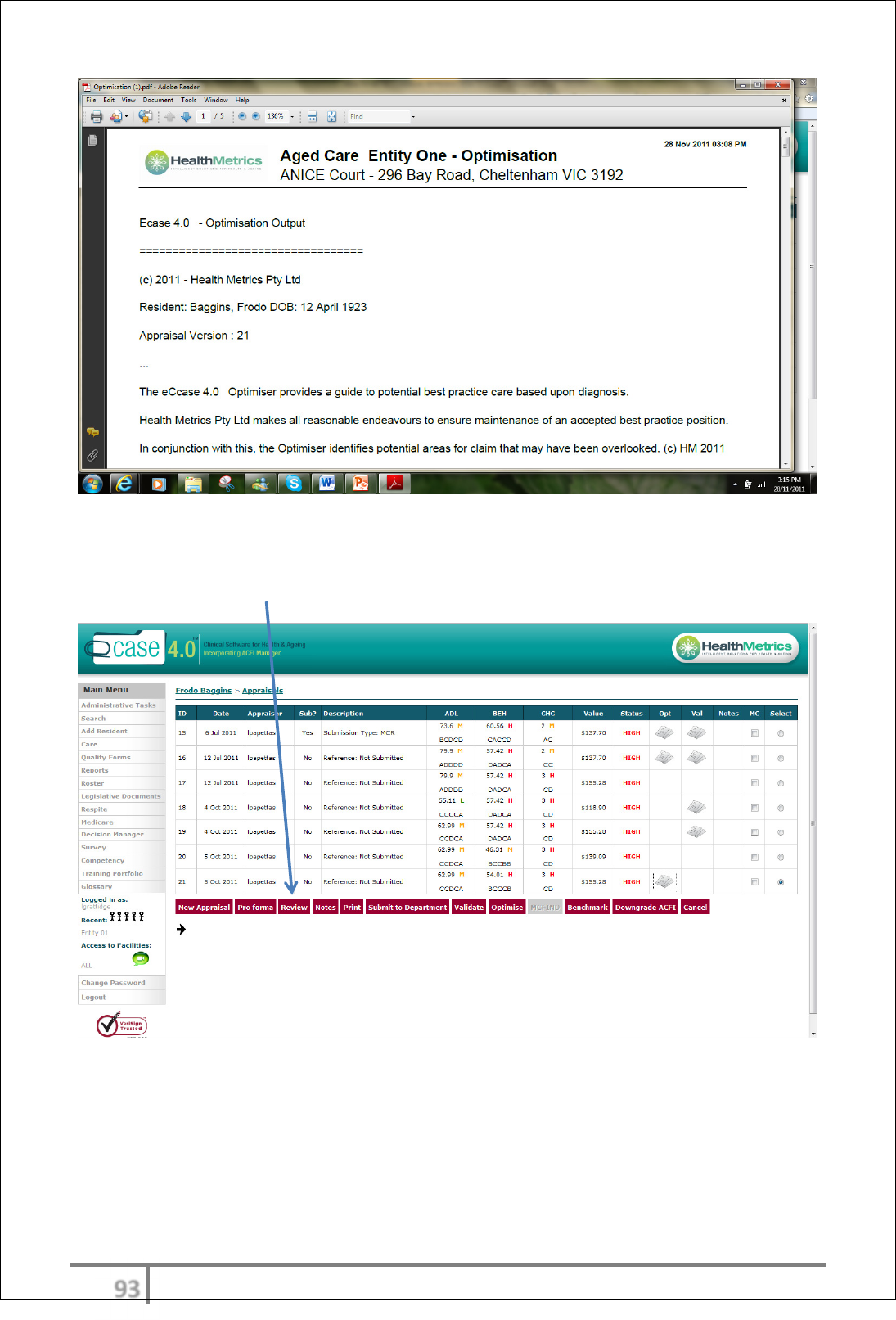
To change the modelled appraisal after reviewing the Optimisation Output
report, select the appraisal last created and then click ‘Review’. Changes can
then be made and changes thus recorded and calculated.
ύψ
Ver 3.2013
.
Reviewing appraisal list
Any appraisal can be reviewed and changed. The result of a review will be a
new appraisal created with the relevant changes made by the user. Any dollar,
score, or domain change will also be shown for user reference.
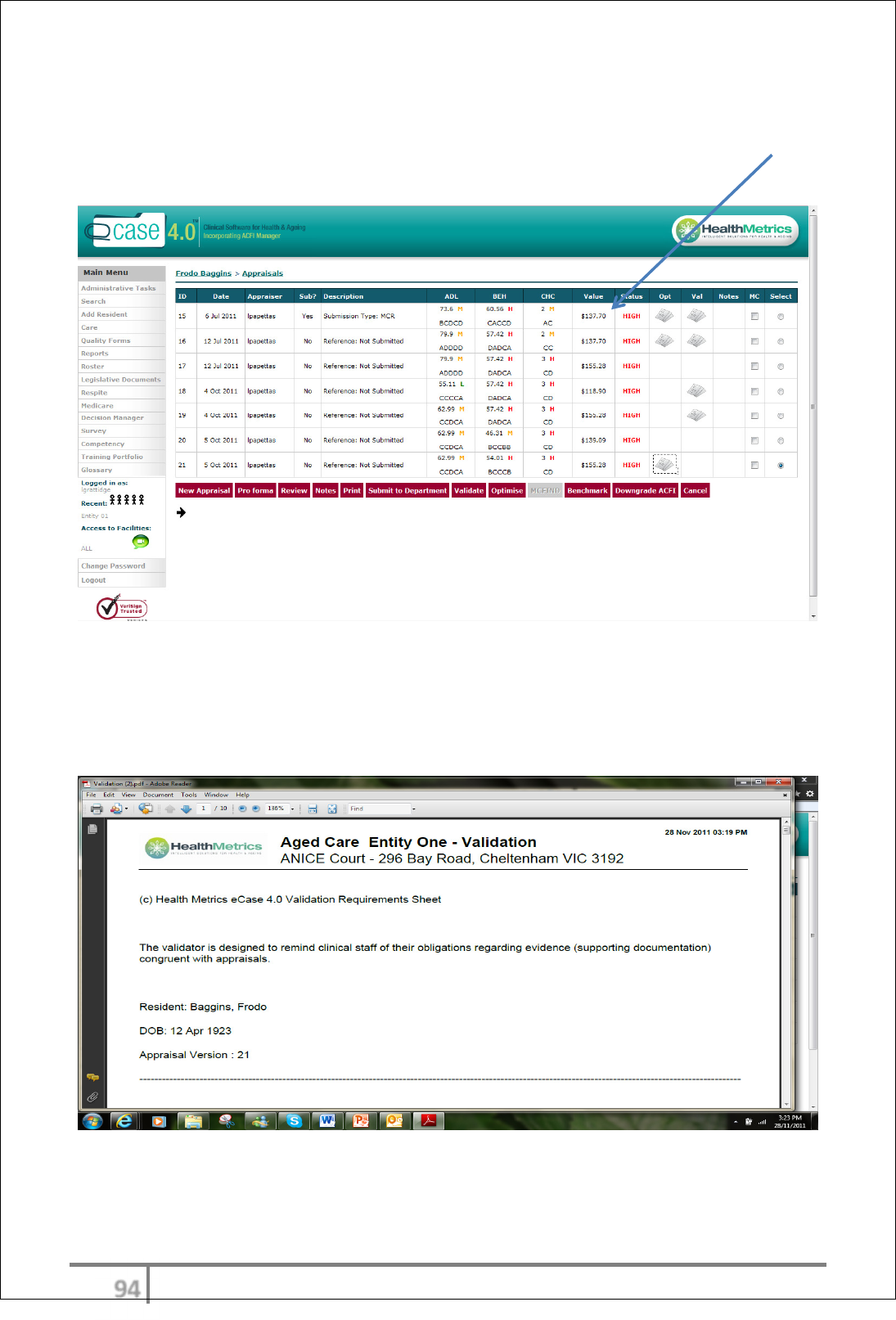
Validating the appraisal
Validating the appraisal will provide the user with a list of required
documentation for that specific appraisal. Users should ensure all
recommendations to ensure Validation outcomes are met in all circumstances.
Submitting the appraisal- see B2B
ύω
Ver 3.2013
.
REGISTERS
Clinical registers can function with or without the care module. If using the care
module registers will auto-populate. From this the following reporting outcomes
will be produced:-
• Summary reports
• Graphical representation
• Month end analysis
• Warning indicators
If not using the clinical module registers can be maintained by manual entry of
data collected with the same reporting outcomes available.
Registers Overview
eCase registers can be used as part of the integrated care systems or manually
entered if users are not using eCase. The monthly data entered will be reported
on in groups of key indicators. The user can also choose to export to excel thus
allowing further clinical indicators to be identified and listed.
Graphical representation of each clinical outcome and associated indicators are
also available for month end report.
The user will enter their own month end analysis based on analysis of reports
and graphs. This will be displayed on the end of month report.
If using eCase care graphs and reports will be automatically generated from
progress note entries and associated form completion.
ύϊ
Ver 3.2013
.
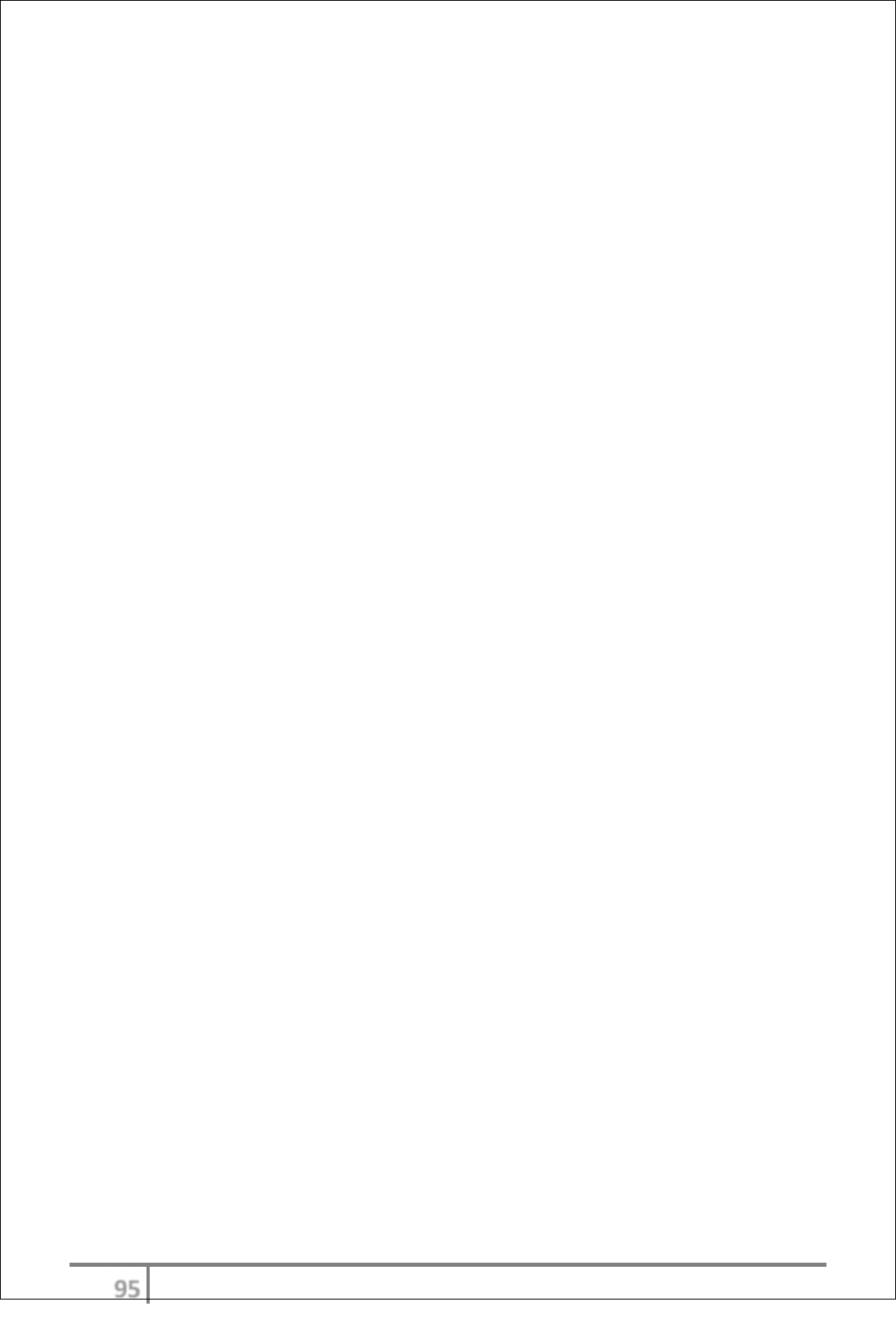
Registers instructions for use
Entering data manually
Select type of register for data entry from resident function.
Data is entered by selecting ‘Add’ from the option list. All available fields must
be completed, and then select ‘Save’.
All existing entries will be listed for either review or ‘Update’ changes or ‘Delete’.
‘Notes’ can also be added and will appear as an envelope icon within the table
next to the relevant entry.
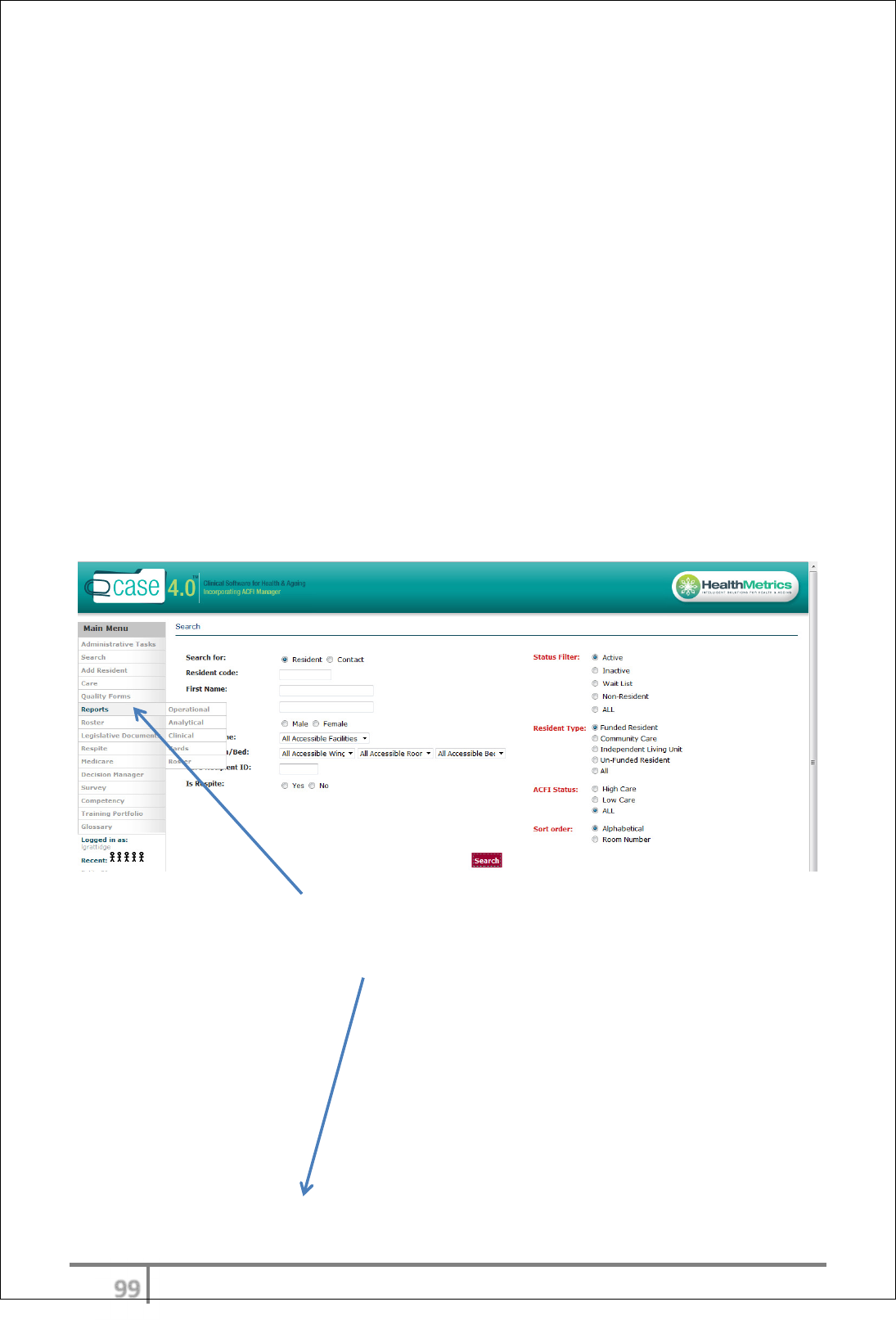
Review data and month end analysis
From the main menu select ‘Reports’, ‘Clinical’, and the chosen area for
reporting.
ύϋ
Ver 3.2013
.
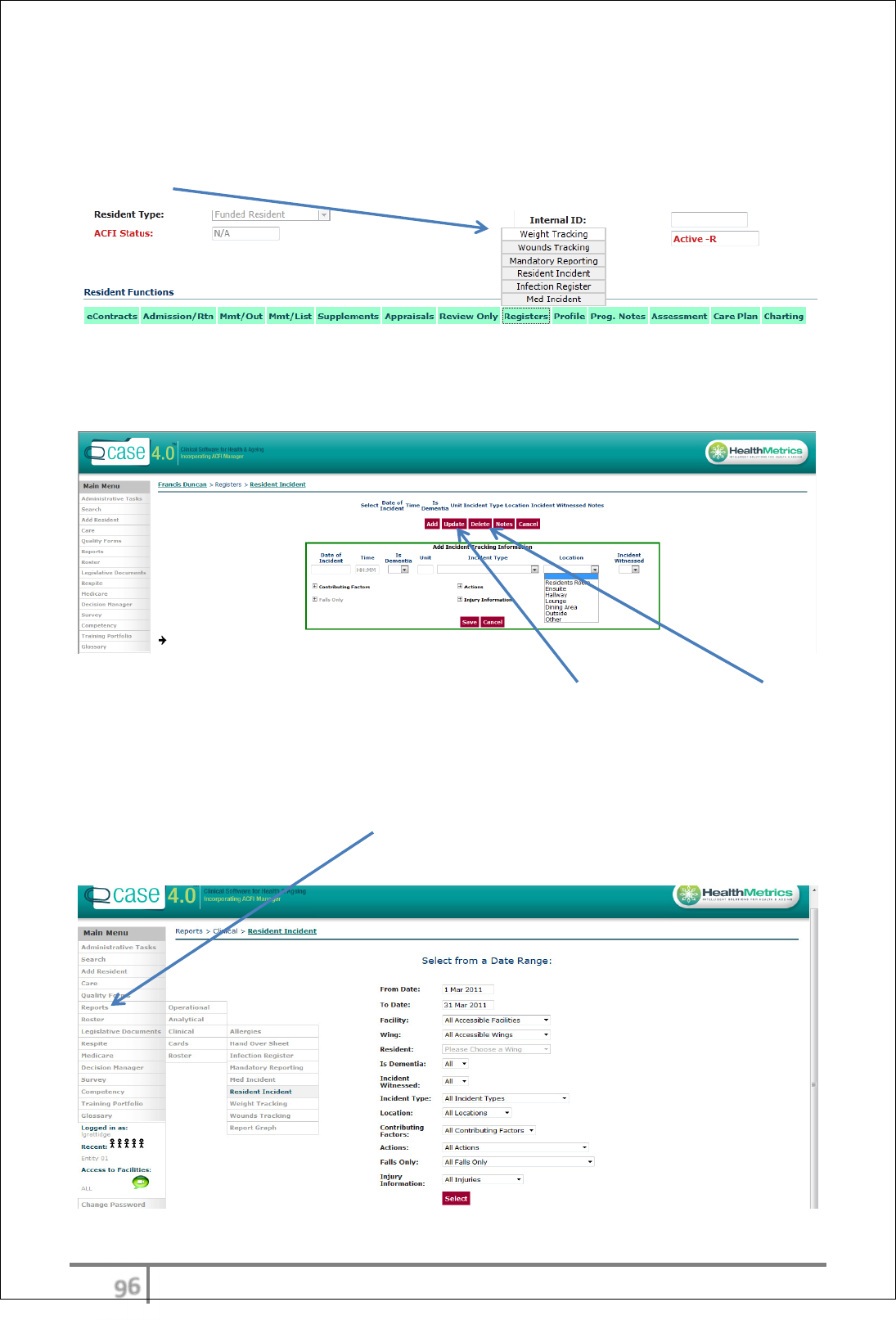
Reports
Reports are ordered according to type of incident. The user may also choose to
export to Excel to isolate further data trends.
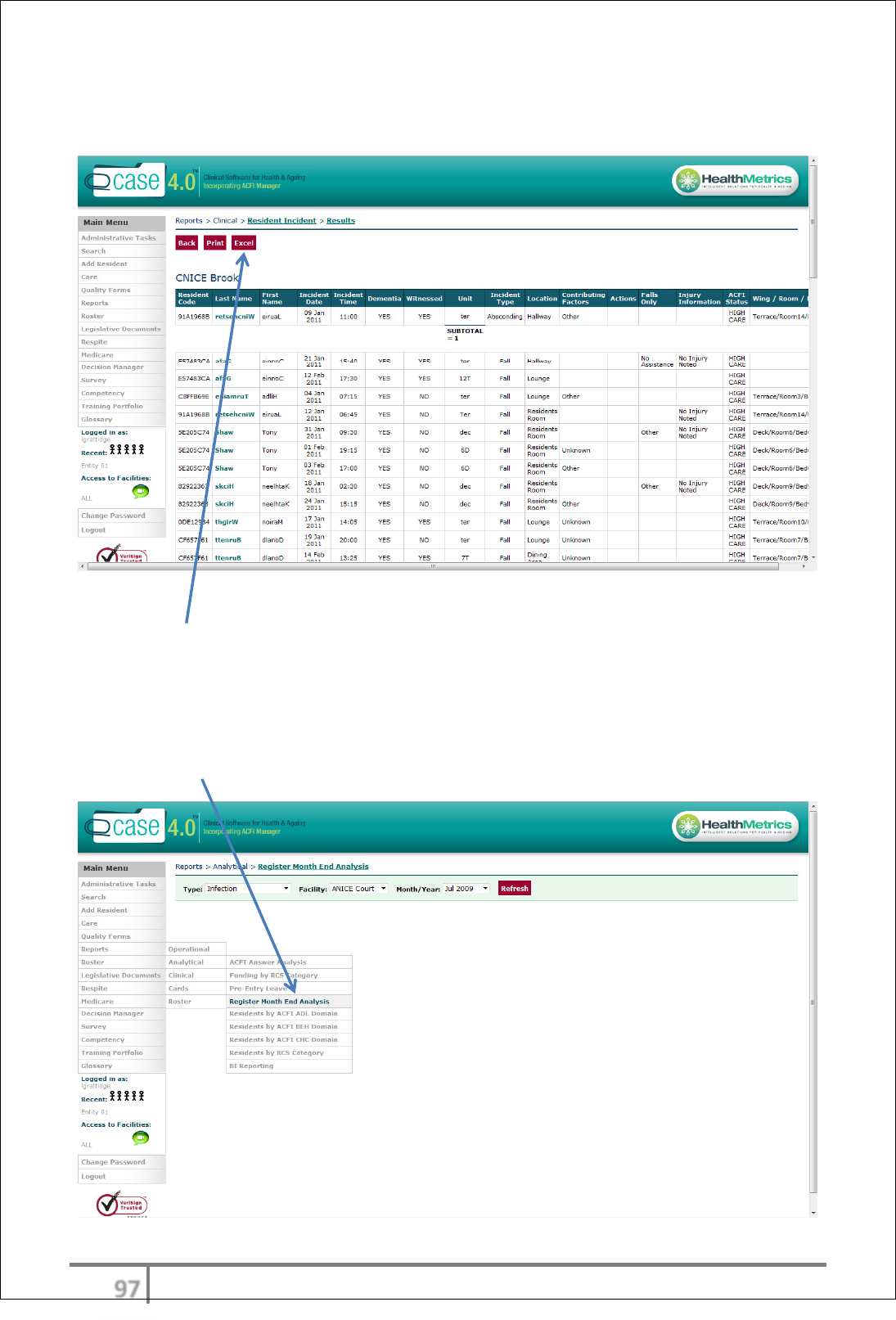
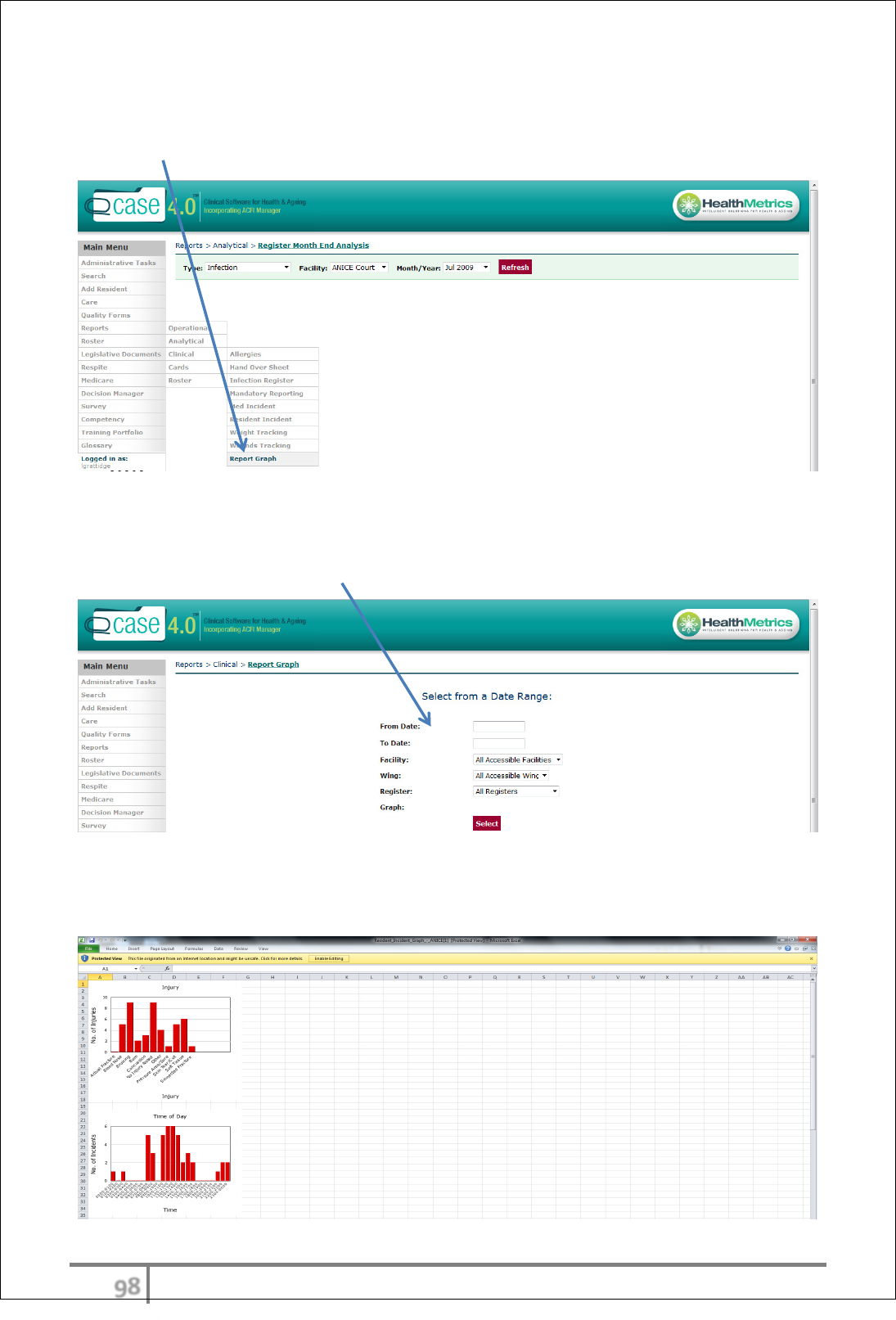
Month end analysis
After the data has been reviewed the user can now write their month end
analysis. This is completed within the ‘Reports’, ‘Analytical’ tab, under ‘Register
Month End Analysis’.
ύό
Ver 3.2013
.
Creating graphs
Graphs are also located within the ‘Reports’ menu (Main Menu) under ‘Clinical’,
‘Report Graph’.
Complete required sections to meet graph requirements including, date range,
facility, wing and type of register. Under each type of register there are
additional indicators that can also be selected.
The user can now print report with month end analysis and corresponding
graphs for relevant record keeping.
ύύ
Ver 3.2013
.
REPORTING
eCase provides reports for all modules. A full suite of standard reports are
available for users. Additional reporting modules can be requested by users as a
one-off or integrated into your program.
Reporting Overview
eCase has a broad range of reporting requirements located not only under report
options but also within the Decision Manager.
Report menu
The reports menu option includes Operational, Analytical and Clinical reports.
Users can select which report they require ensuring all required option fields are
completed on each report. Additional reporting options are configurable and are
available on request.
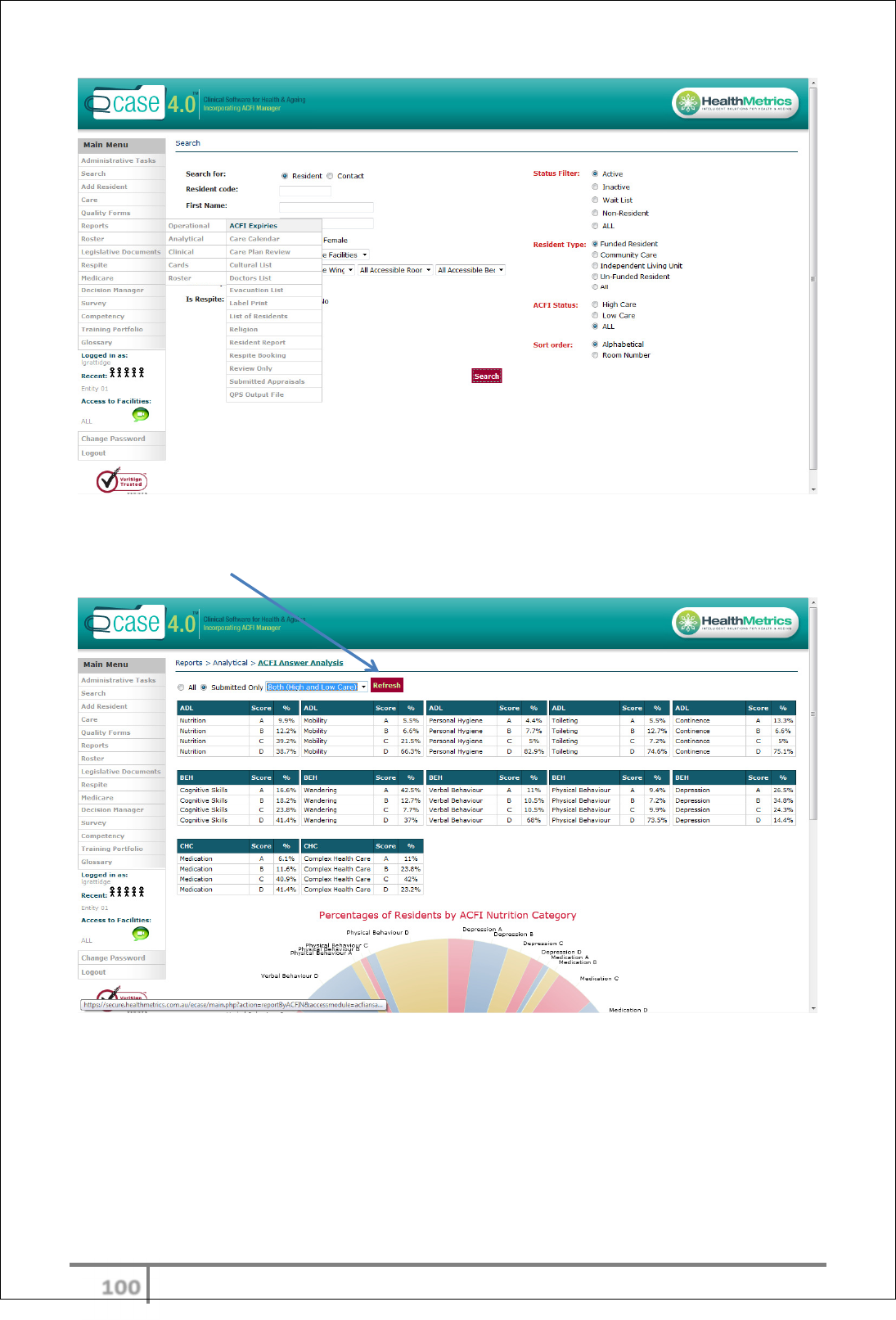
Reporting instructions for use
From the main menu select Report, then Operational, Analytical or Clinical.
Each Report heading has a variety of standard reports.
υττ
Ver 3.2013
.
Each report is required to have different types of indicators entered and must
always be refreshed with new reports.
υτυ
Ver 3.2013
.
DECISION MANAGER
Decision manager and reports
The decision manager has a comprehensive range of reports and graphs to
assist the users in quality reporting and decision making.
Decision manager headings include:-
• ACFI
• Occupancy
• Supported information
• Clinical indicators
• Profiler
• Modeller
• Procurements
• Mining
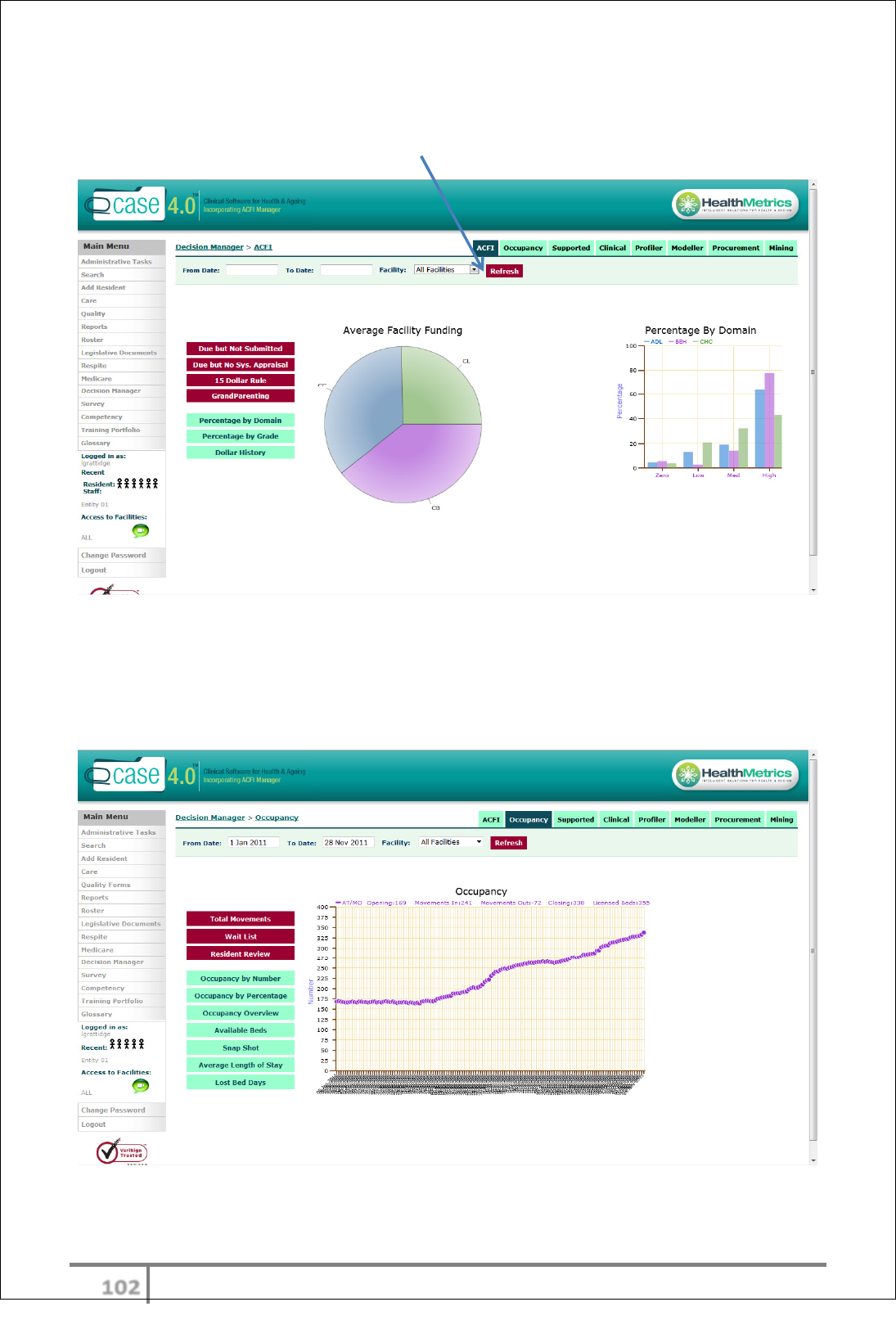
Decision Manager ACFI
The ACFI tab contains data reflected in PIE charts and graphs. Types of
indicators include:-
• Appraisal due but not submitted
• Average funding per facility
• Submissions due but no data
• 15 dollar rule
• GrandParenting
• Percentage by Domain
• Percentage by Grade
• Dollar history
υτφ
Ver 3.2013
.
Data can be reviewed by facility comparison or within one site. All reports are
printable and exportable to Excel. Various date ranges can be viewed by
selecting relevant date range and refreshing.
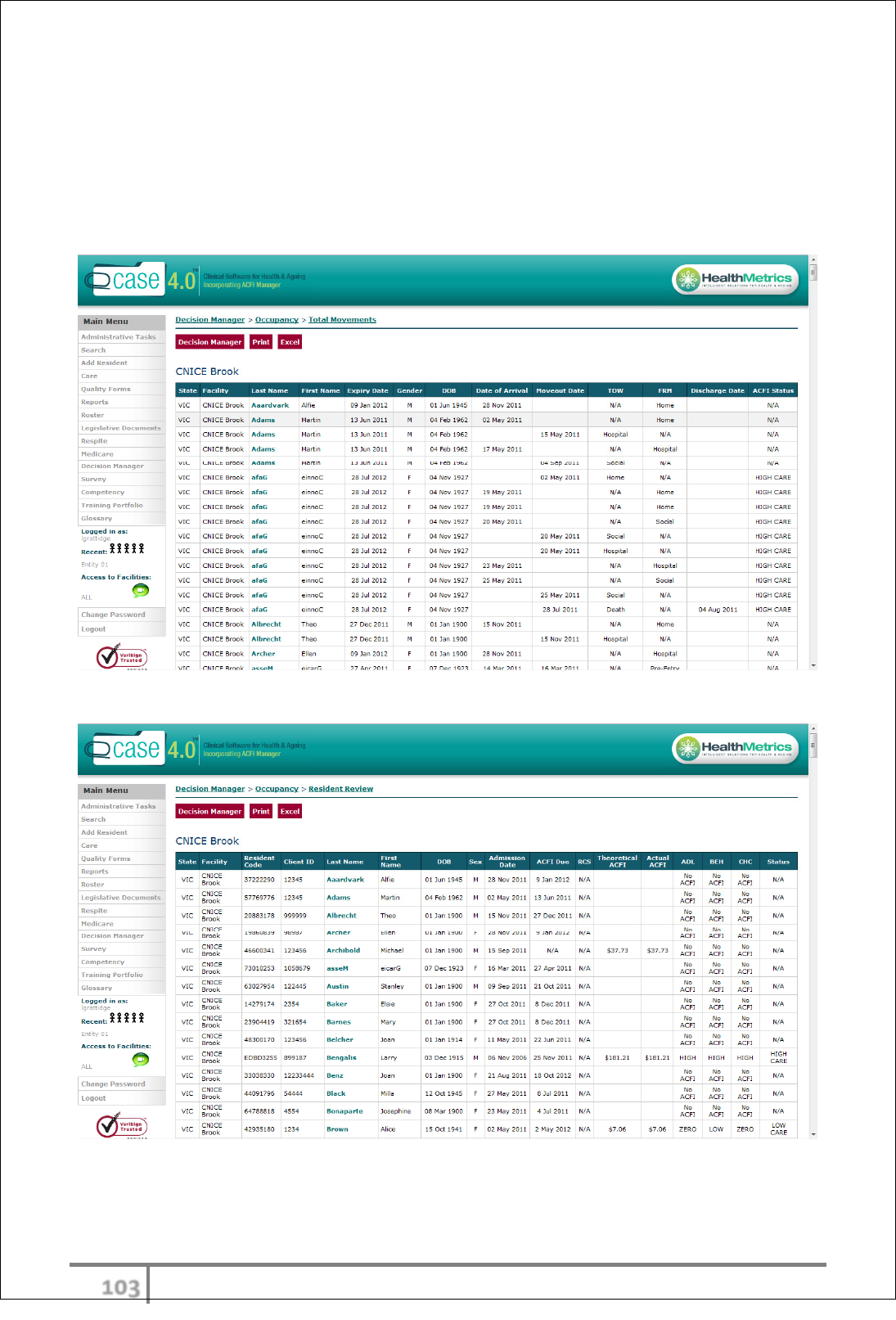
Decision manager - Occupancy Tab
The Occupancy tab provides a host of reports, graphs and charts which will
empower the most senior stakeholder to ascertain KPI’s on all Occupancy
indicators.
υτχ
Ver 3.2013
.
As with all Decision Manager reports the user must select a date range and
refresh the data for review. The ‘Total Movements’ and ‘Resident Review’
provides a full overview of each resident including all movments and ACFI
funding.
‘Total Movements’
‘Resident Review’
υτψ
Ver 3.2013
.
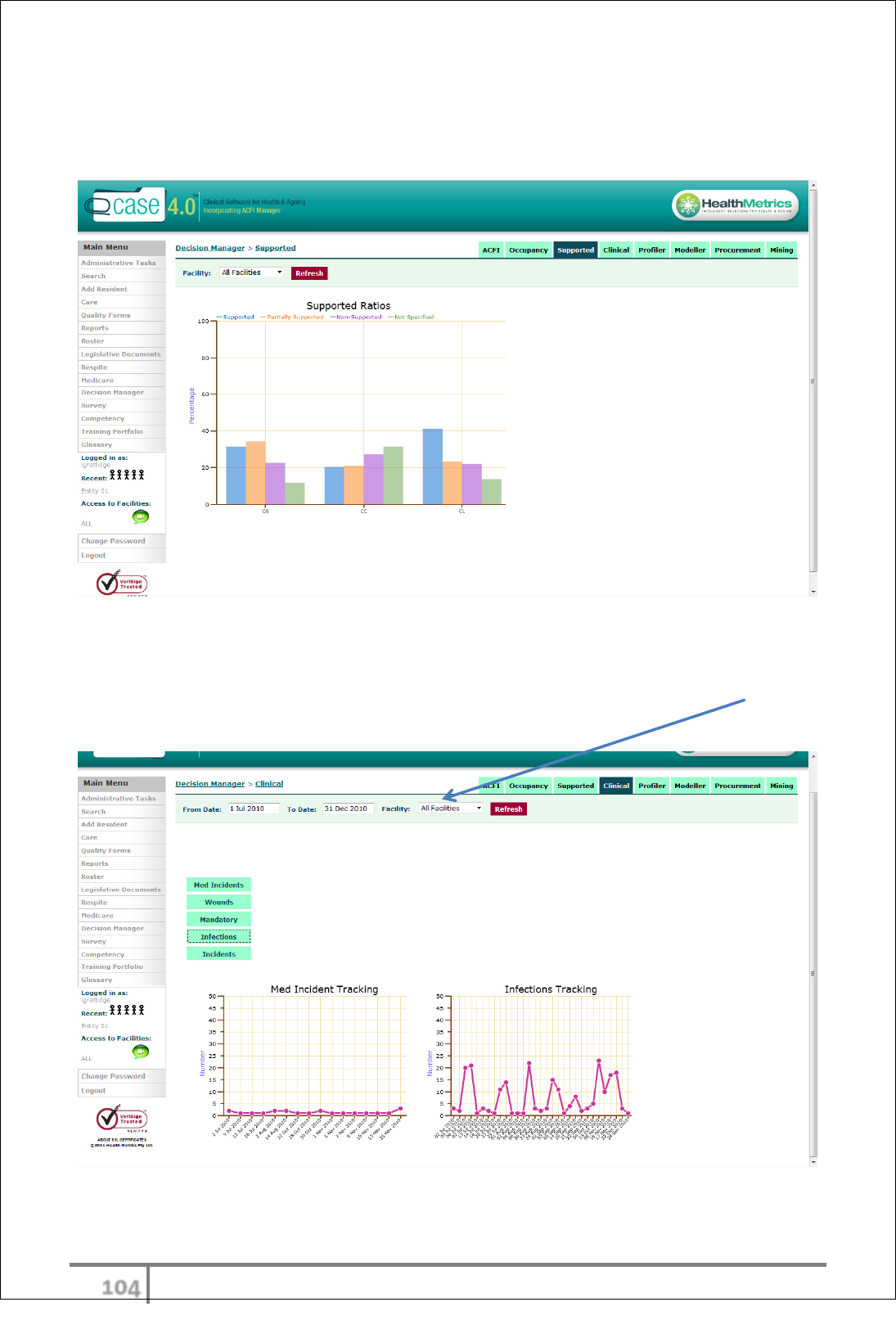
Decision Manager – Supported
The ‘Supported’ tab displays supported resident ratios by facility.
Decision Manager – Clinical
The ‘Clinical’ tab provides a snapshot of basic clinical indicators by facility or
comparing several facilities. This can be achieved by changing the facility filter
and date filter at the top of the screen.
υτω
Ver 3.2013
.
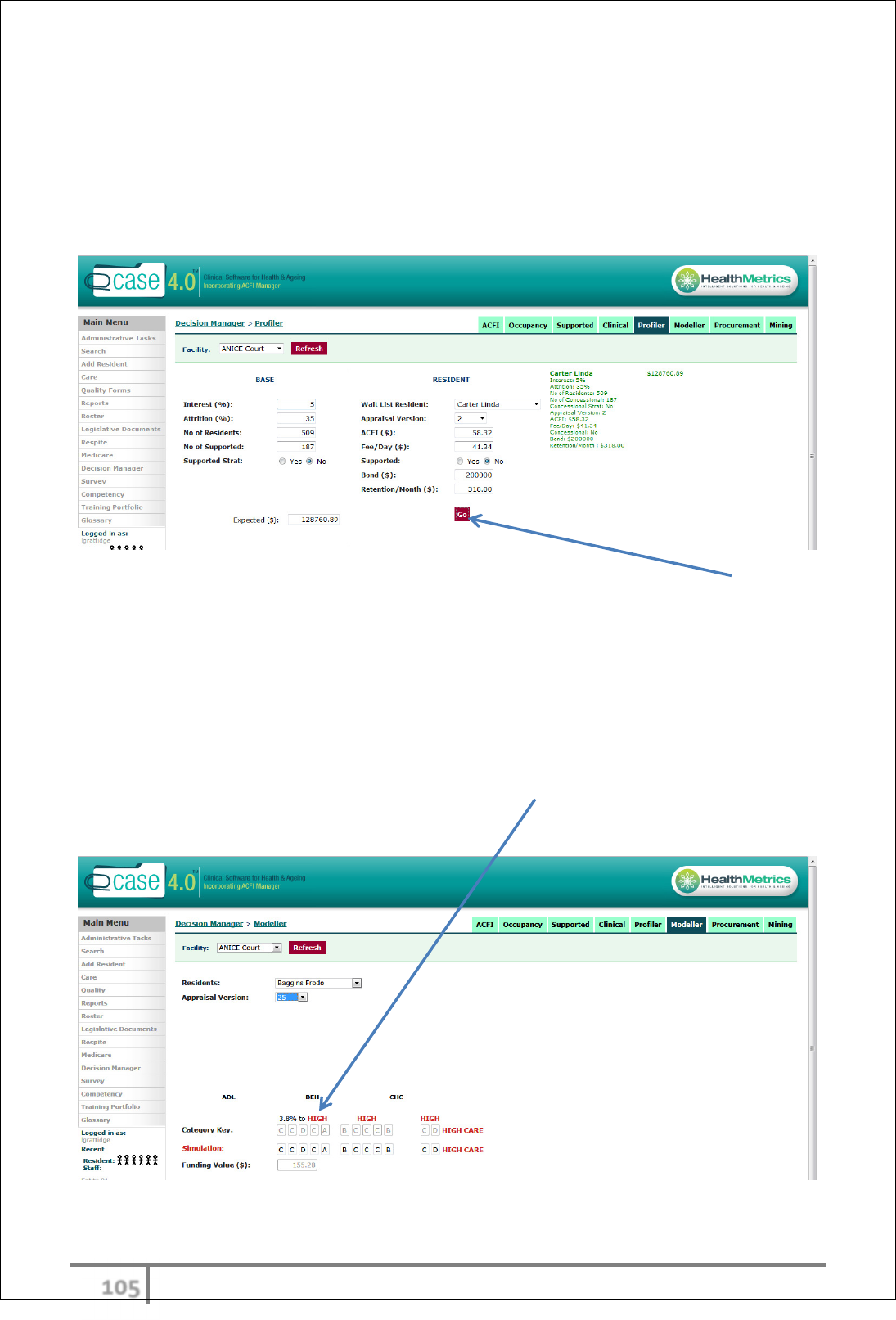
Decision Manager – Profiler
The Profiler is a powerful tool that can be used to ascertain the life value of
waitlisted residents. This enables the user to apply a variety of selction criteria
to the resident admission process. Resident can be pre-appraised on the Waitlist
which allows a comprehensive mathematical calculation to be made.
Enter all fields with relevant and appropriate information and select ‘Go’. The
profiler will prioritize residents and display as RED< AMBER and GREEN with the
overall value indicated for each resident.
Decision Manager – Modeller
The Modeller is an insightful tool that can be used to simulate potential ACFI
funding by comparing existing appraisal scores with proposed scores across the
12 ACFI questions. The Modeller provides sensitivity analysis and identifies % to
reach next domain category jump – for example 3.8% to HIGH in ADL domain.
It also combines scores to confirm HIGH or LOW care status and Funding Value.
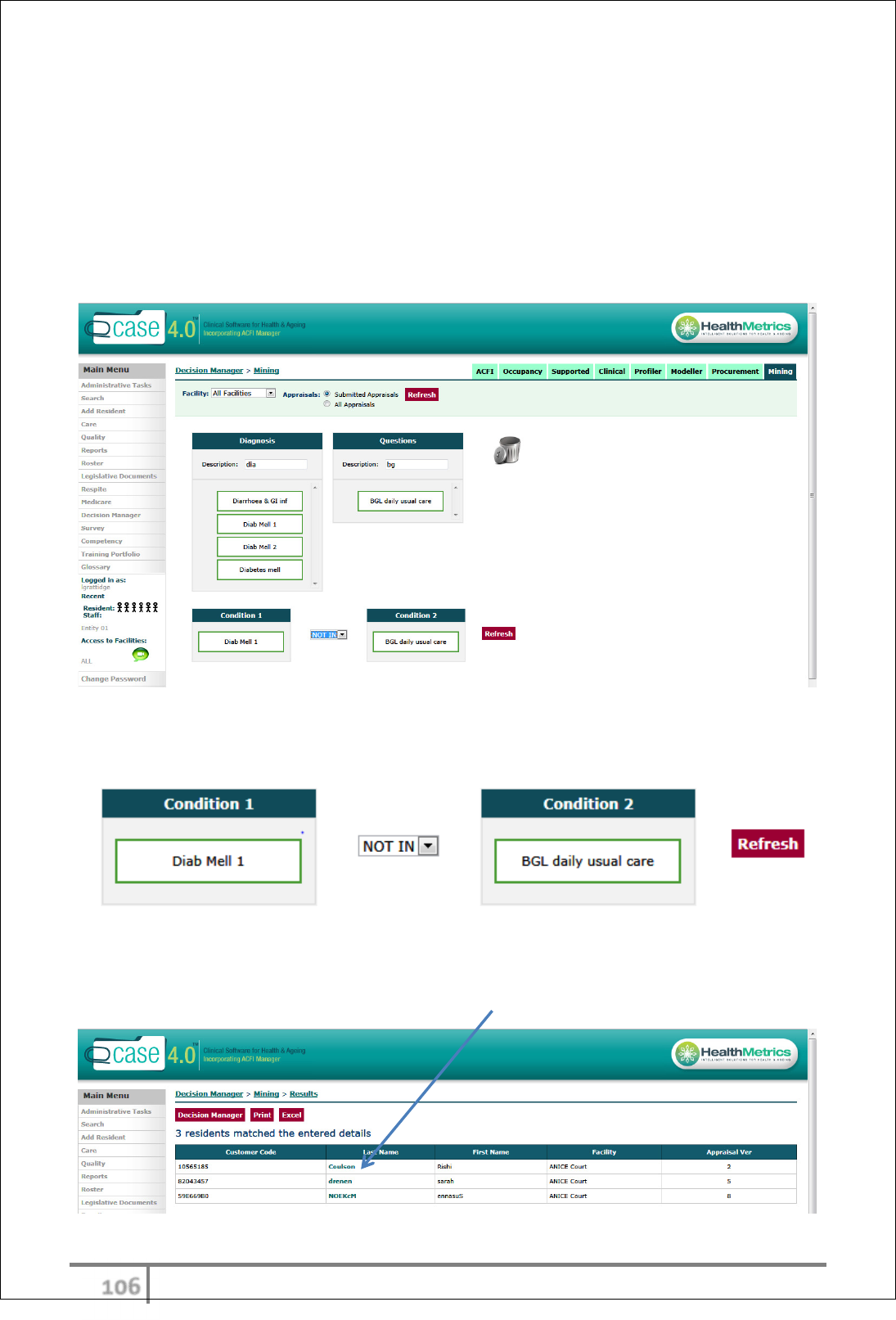
υτϊ
Ver 3.2013
.
Decision Manager – Mining
The data ‘Mining’ tool searches/drills data variables in relation to ACFI appraisals
revealing opportunities for potential ACFI funding uplift.
Data variables (Diagnosis & or Question) can be dragged and dropped into
Condition fields with the option to filter AND, OR, NOT IN or IN. Selecting the
‘Refresh’ button brings up all appraisals that meet the selected criteria.
For example:
Condition 1 (Type 1 Diabetes Mellitis) NOT IN Condition 2 (BGL daily usual care)
Three residents meet this criteria. This provides a trigger to review their
appraisals which can be directly accessed by a single click on the resident’s Last
Name.

υτϋ
Ver 3.2013
.
ROSTERING
eCase rostering module provides the following:-
• Roster development
• Roster modelling
• Roster optimization based on care funding
• Roster costing
• Roster reporting
• Roster gap reporting
• Roster overtime reporting
Rostering Overview
eCase rostering is not a payroll system; however it is a comprehensive easy to
use rostering module that allows the user to optimize rosters against ACFI
funding. eCase rostering also provides as extensive suite of reports including
daily, weekly and overall costing’s, average costing’s and gap analyses.
Rostering instructions for use
Select Roster from main menu.
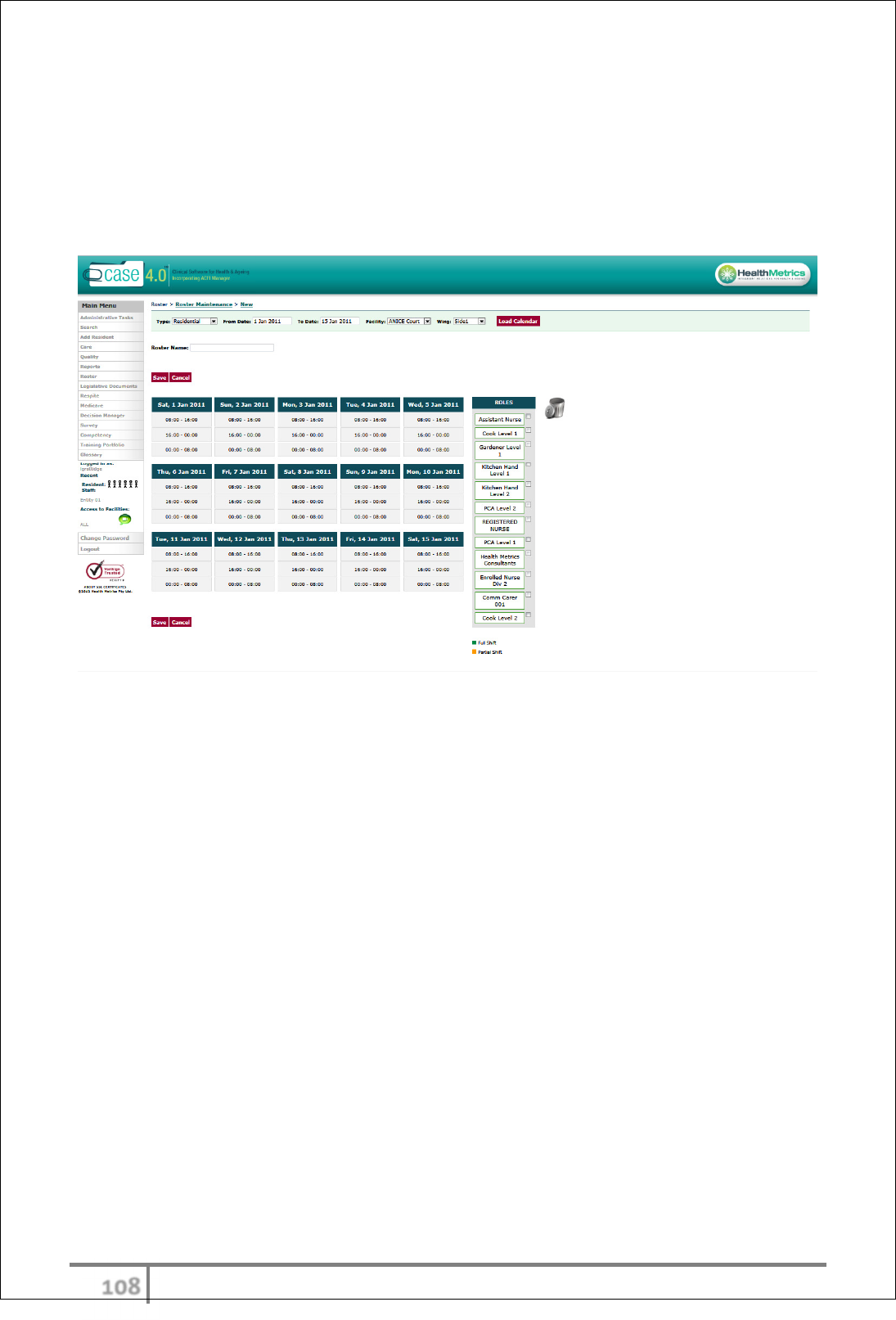
υτό
Ver 3.2013
.
Creating a roster
Select ‘Roster Maintenance’ from roster tab in main menu. Select ‘New’. Enter
date range for new roster and facility. The roster Wizard allows the user to drag
and drop positions thus creating the base roster. Once the base roster is built,
personnel can be added to positions.
Roster reporting
eCase roster module allows the user to process numerous reports. Reports
available as standard include:-
• Summary daily with total time and total cost
• Summary weekly with total time and total cost
• Summary of roles
• Total summary of entire roster
• Optimize roster
Additional reports are available and configurable based on customer needs and
requests.
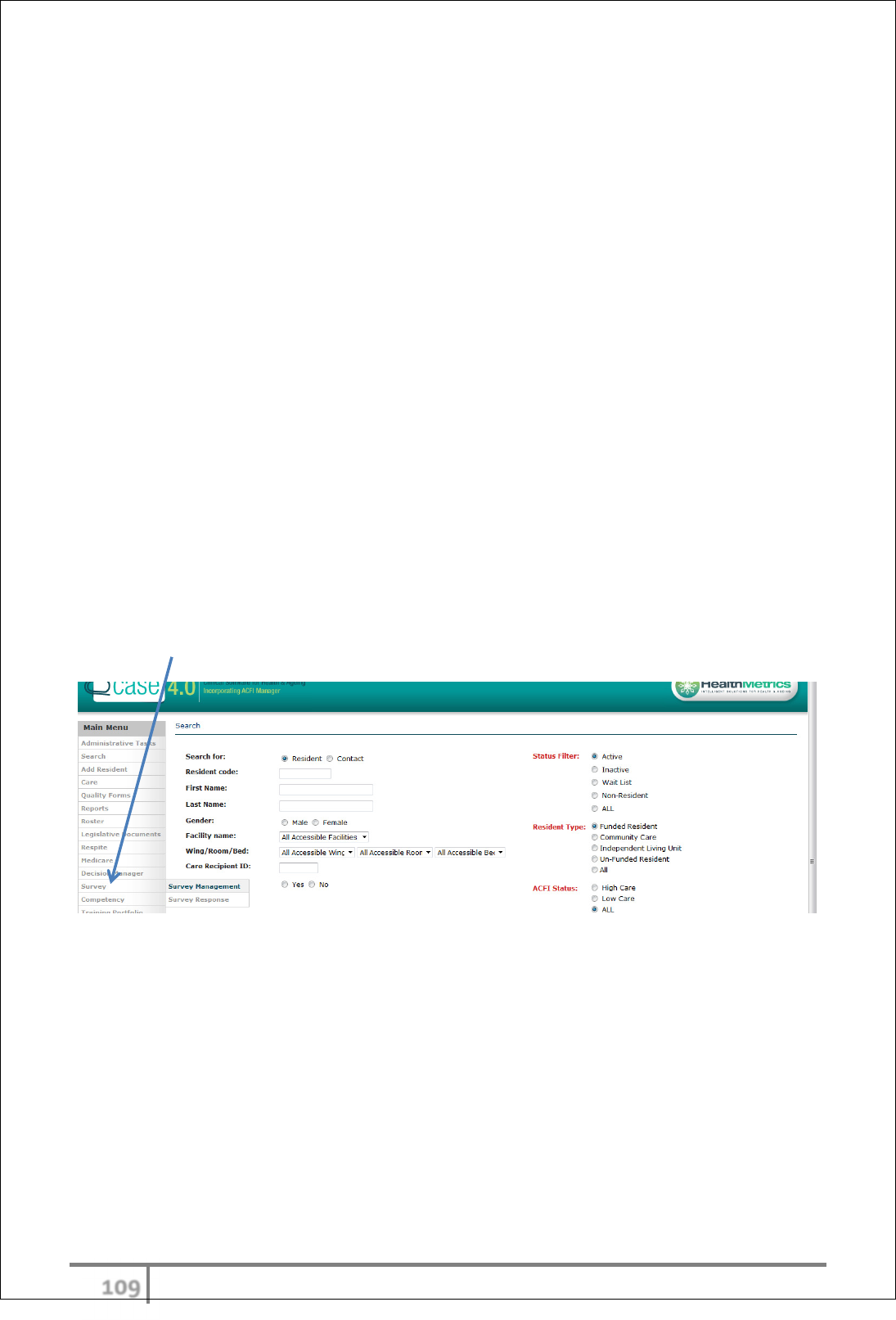
υτύ
Ver 3.2013
.
SURVEYS
eCase Survey module provides the following:-
• Survey development
• Survey on-line deployment
• Survey permissions
• Survey response reporting
Satisfaction survey Overview
The Survey builder allows users to create their own online surveys, quickly and
easily and process responses.
This enables the user to receive feedback and collect vital information needed to
improve performance and develop new strategies along with satisfying
compliance requirements. eCase surveys can be used on a variety of
respondents, including residents, staff, and relatives.
Surveys can be completed either on line or manually for all participants.
Satisfaction surveys instructions for use
Select Survey from main menu.
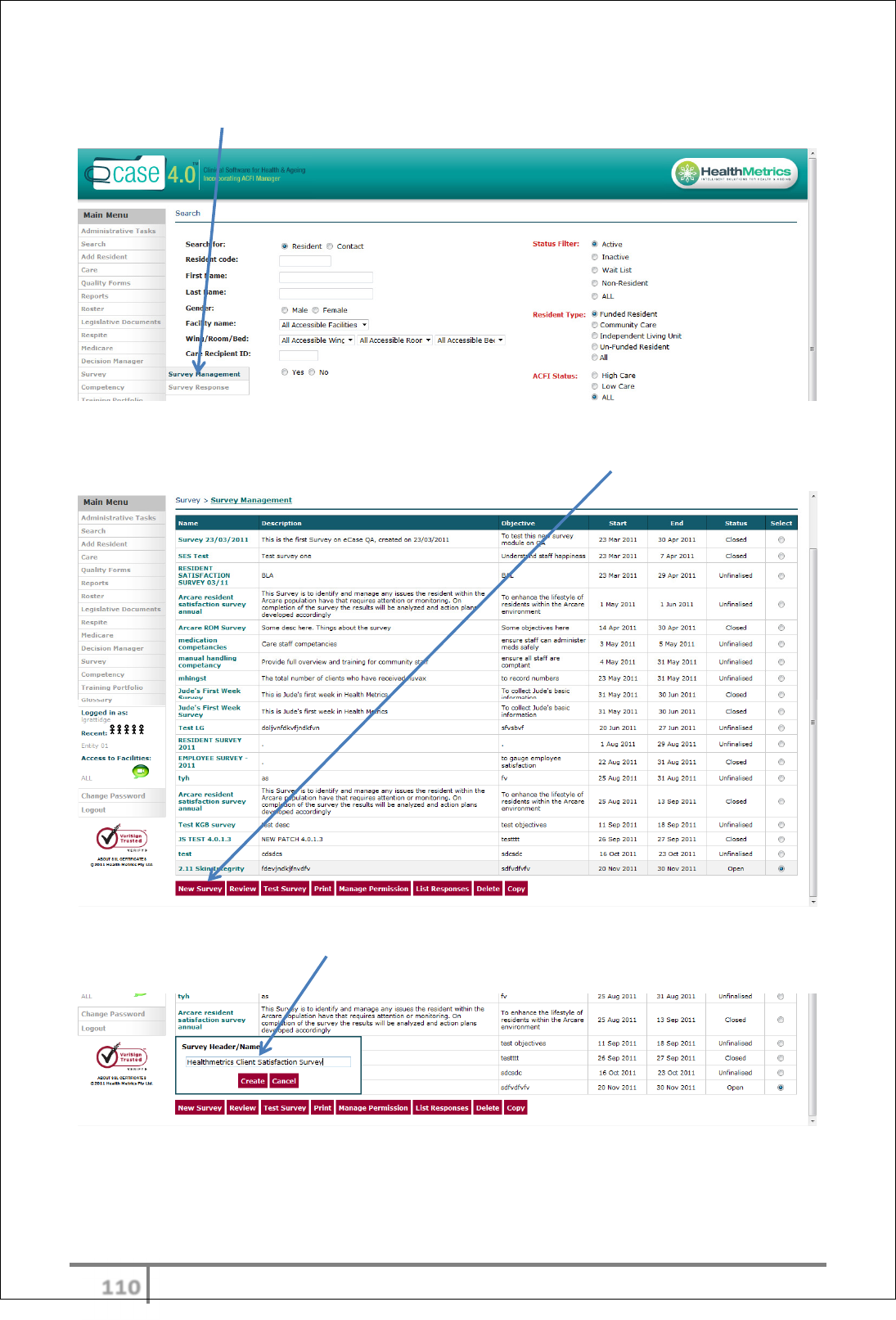
υυτ
Ver 3.2013
.
Creating a survey
Select ‘Survey Management’ from survey tab in main menu.
A list of existing surveys will appear on the page defining Name, Description,
Objective, Start Date, End Date and Status. Select ‘New Survey’.
A ‘Survey Header/Name:’ box will appear. Enter preferred name and select
‘Create’.
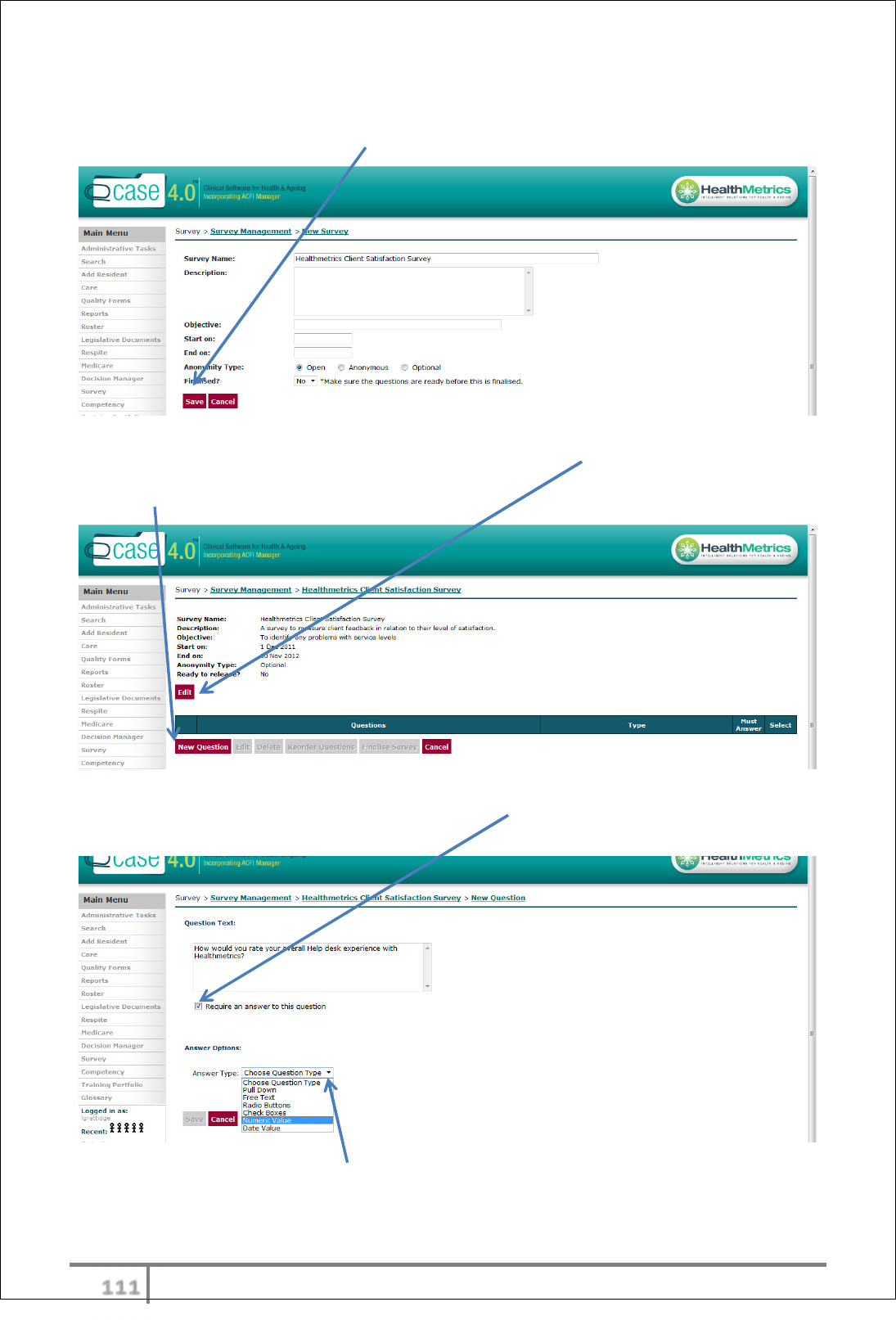
υυυ
Ver 3.2013
.
Enter a description of the survey, objective, start date, end date, anonymity
type (default open) and click ‘Save’ button.
The information previously entered can be edited via ‘Edit’ button.
Select ‘New Question’ to commence formulation of survey questions.
Enter ‘Question Text’ in open field box and check box as to whether an answer is
required to this question.
Select the preferred ‘Answer Type’ from the drop down menu: Pull Down, Free
Text, Radio Buttons, Check Boxes, Numeric Value or Date Value.
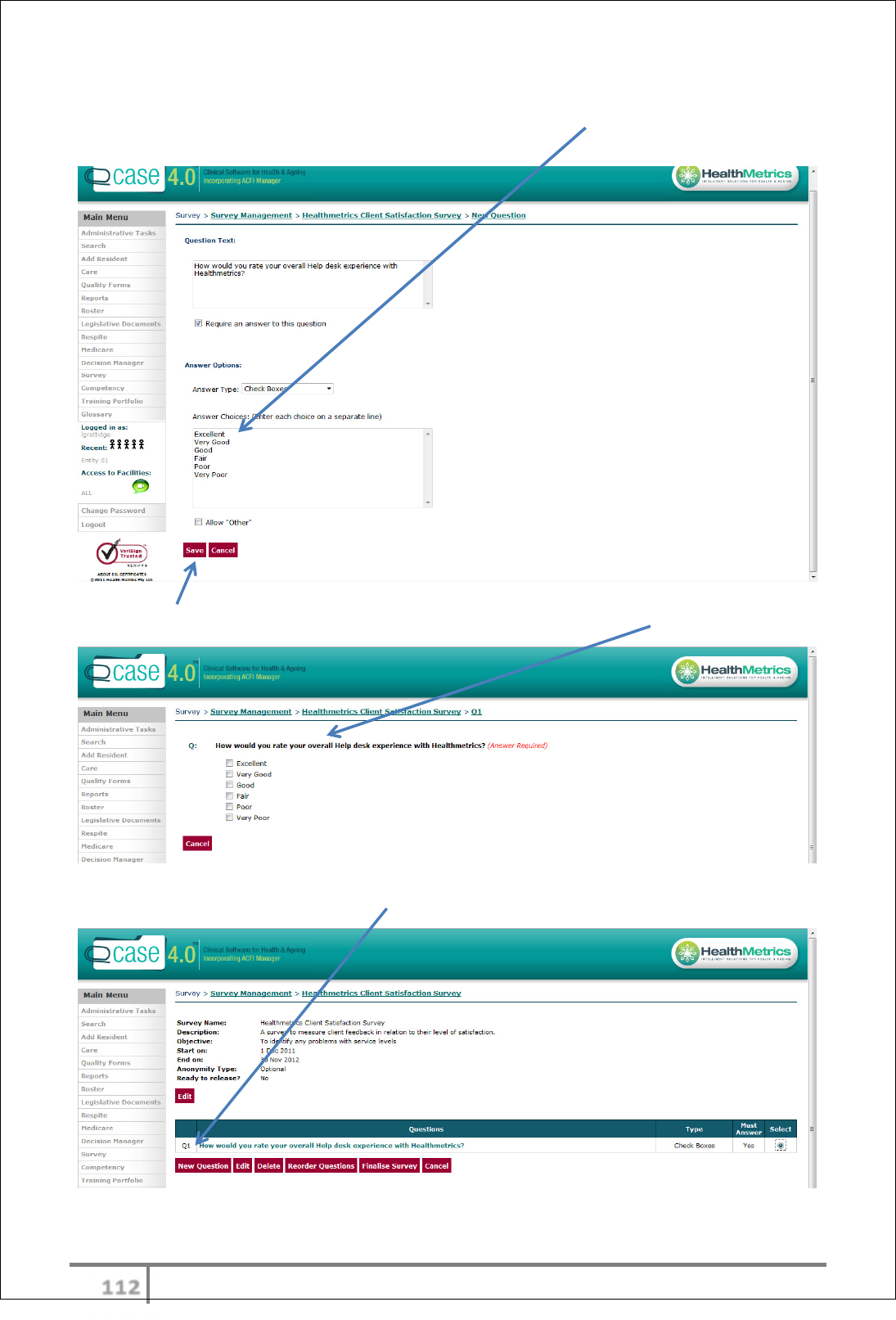
υυφ
Ver 3.2013
.
For example – Answer Type ‘Check Boxes’. Type in Answer Choices (ensuring
each choice starts on a separate line).
Select ‘Save’ button and a screen will appear displaying question format.
Each question created will be listed.
Continue to add ‘New Questions’ until complete.
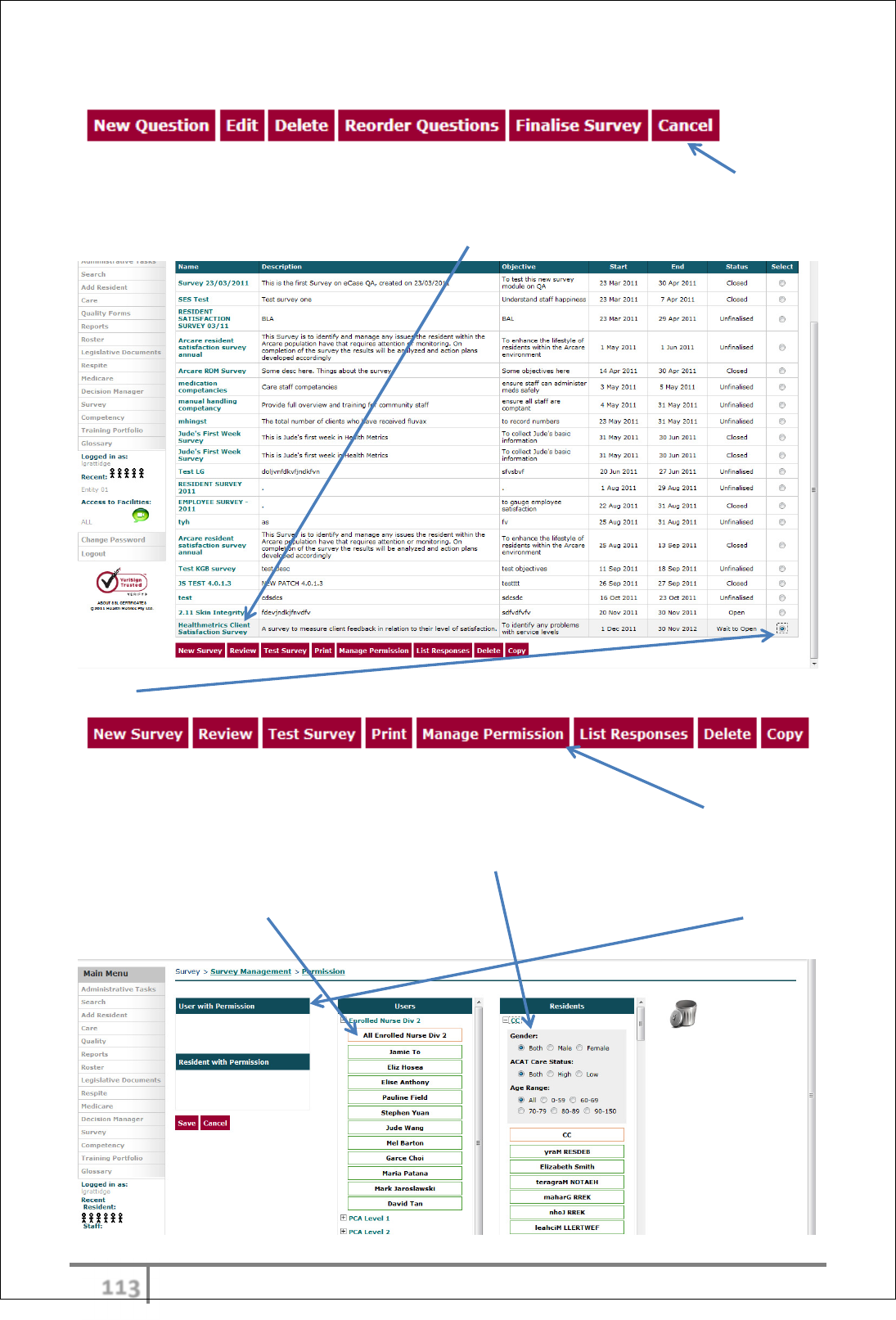
υυχ
Ver 3.2013
.
Options are available to Edit, Delete and Reorder Questions.
It is recommended to test survey and manage survey permissions prior to
finalising. Select ‘Cancel’. The newly created Survey will appear in the list along
with other existing surveys.
‘Select’ survey to highlight the following options:
Survey Access – Manage Permissions
User access to a particular Survey can be managed via the ‘Manage Permission’
function. Simply drag and drop users and/or residents into the ‘User/Resident
with Permission’ fields. There are also smart filters to group particular residents
by Gender, HIGH/LOW status and Age Range. Individual users or groupings such
as ‘All Enrolled Nurse Div 2’ can be dragged and dropped into ‘User with
Permission’ field.
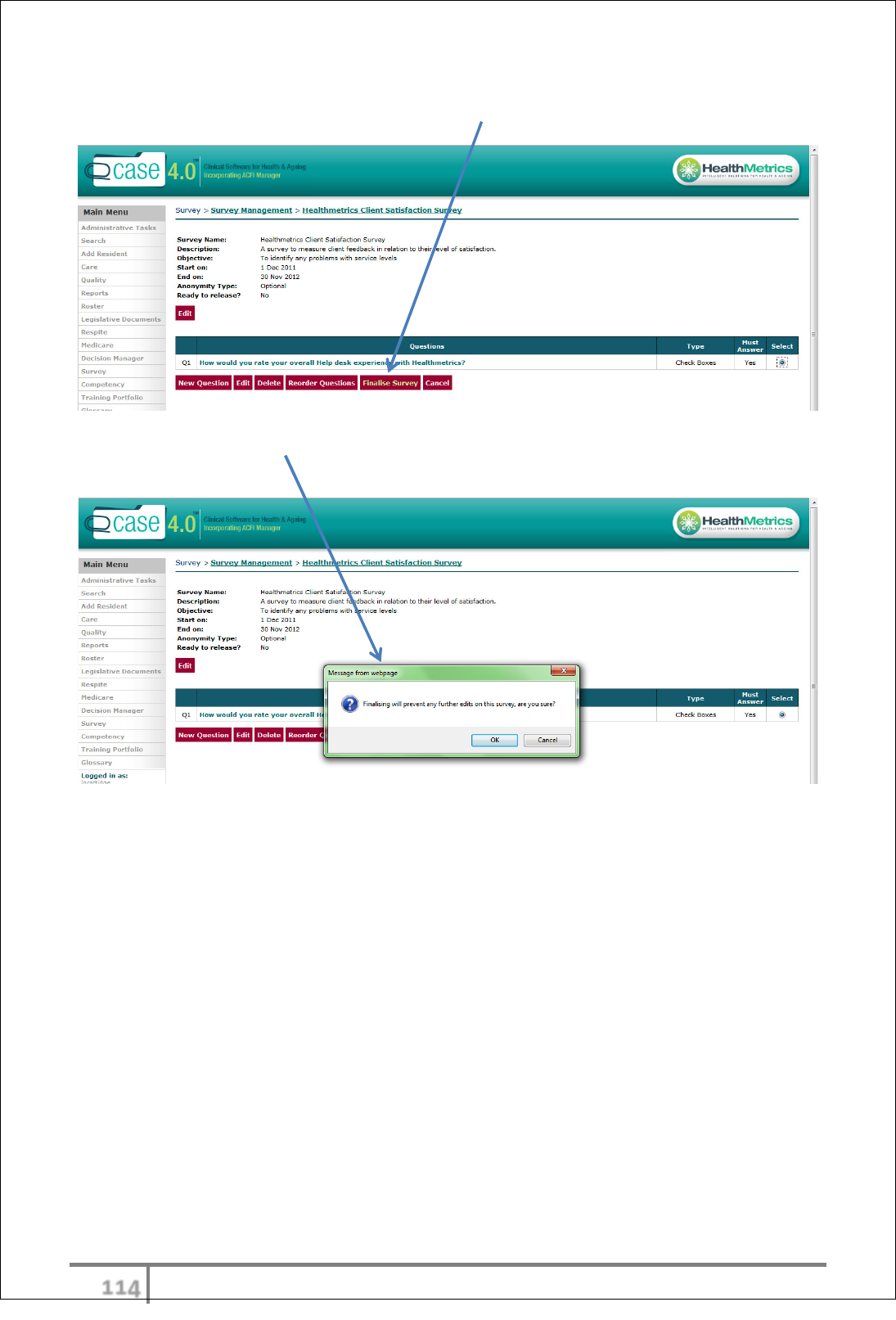
υυψ
Ver 3.2013
.
Finalise Survey
Once satisfied Survey is ready, select ‘Finalise Survey’.
A message box will appear as a reminder that finalising will prevent any further
edits on the survey.
The status of the Survey will now appear as ‘Open’.
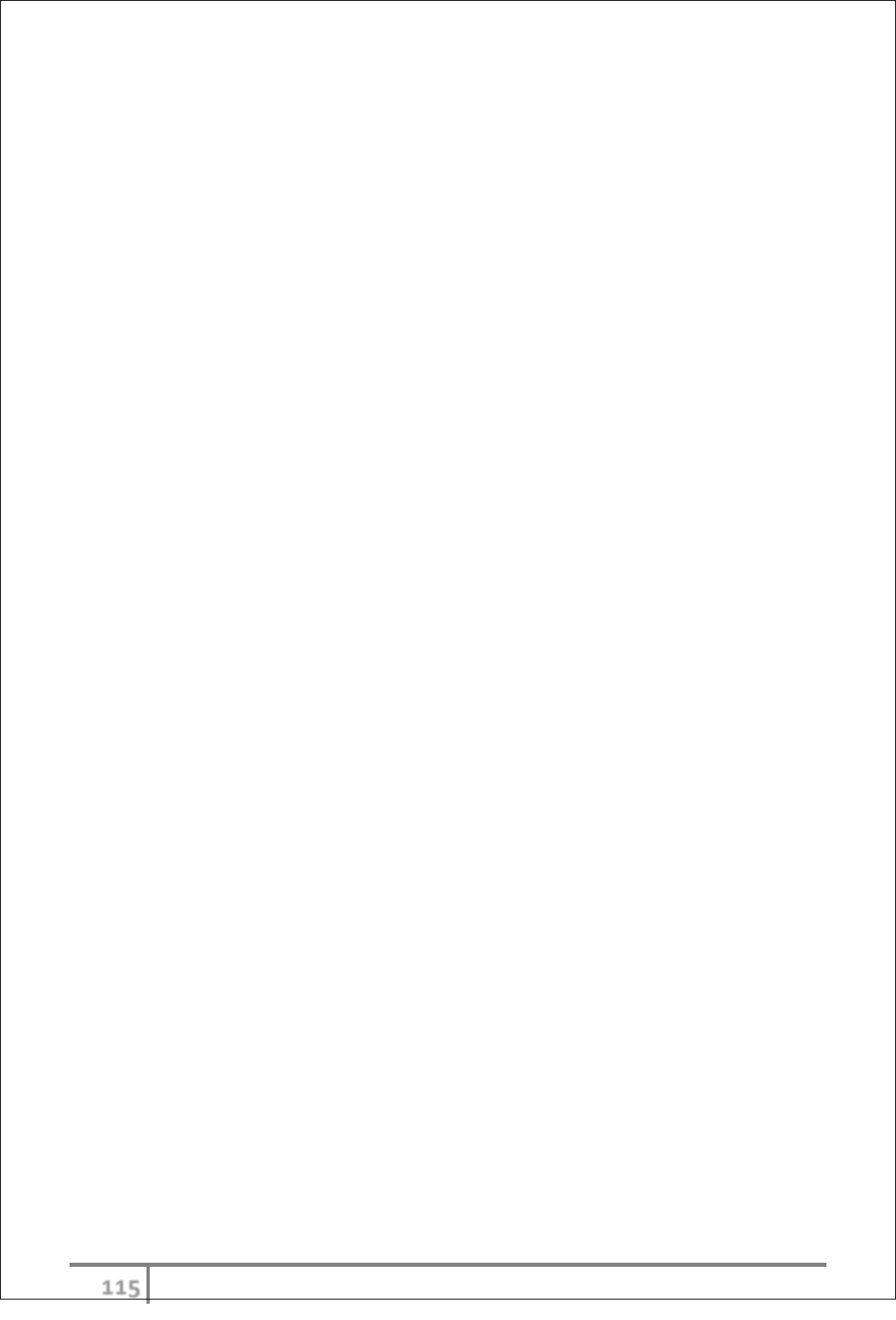
υυω
Ver 3.2013
.
COMPETENCIES
eCase Competencies module provides the following:-
• Competency development
• Competency on-line deployment
• Competency permissions
• Scoring to determine whether a prescribed level of competency has been
met
Competency Overview
The Competency builder allows users to create their own online competencies,
quickly and easily and process responses measuring levels of competency.
eCase provides a secure, on-line resource centre to align contemporary
education with an organisations unique processes, policies and procedures to
meet accreditation and compliance obligations and the continuing professional
development needs of staff. eCase Competency module provides a systematic
approach to ensure that staff have the appropriate knowledge and skills for
effective performance of their job role.
Competencies can be completed either on line or manually for all participants.
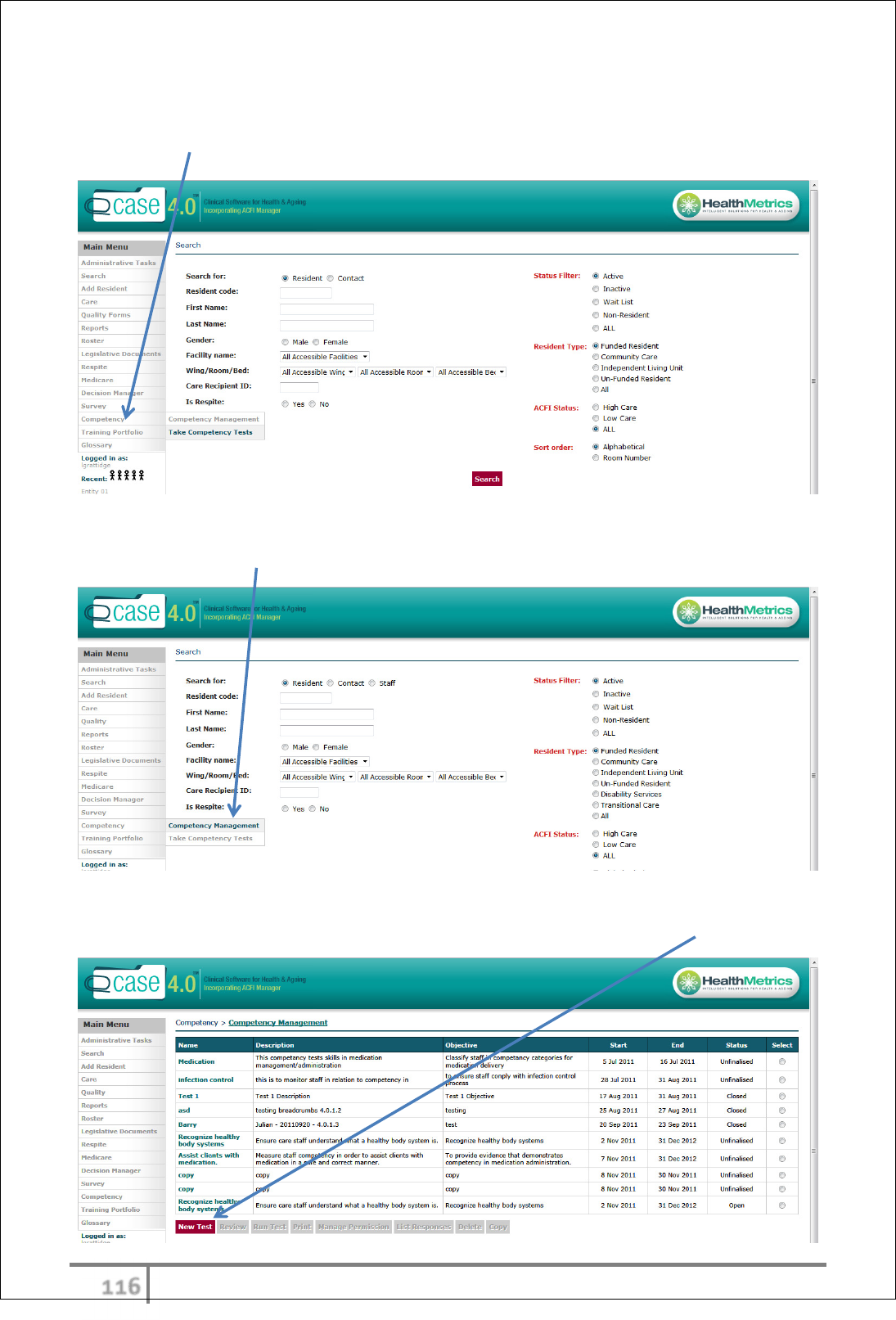
υυϊ
Ver 3.2013
.
Competencies instructions for use
Select Competency from main menu.
Creating a competency test
Select ‘Competency Management’ from competency tab in main menu.
A list of existing competencies will appear on the page defining Name,
Description, Objective, Start Date, End Date and Status. Select ‘New Test’.
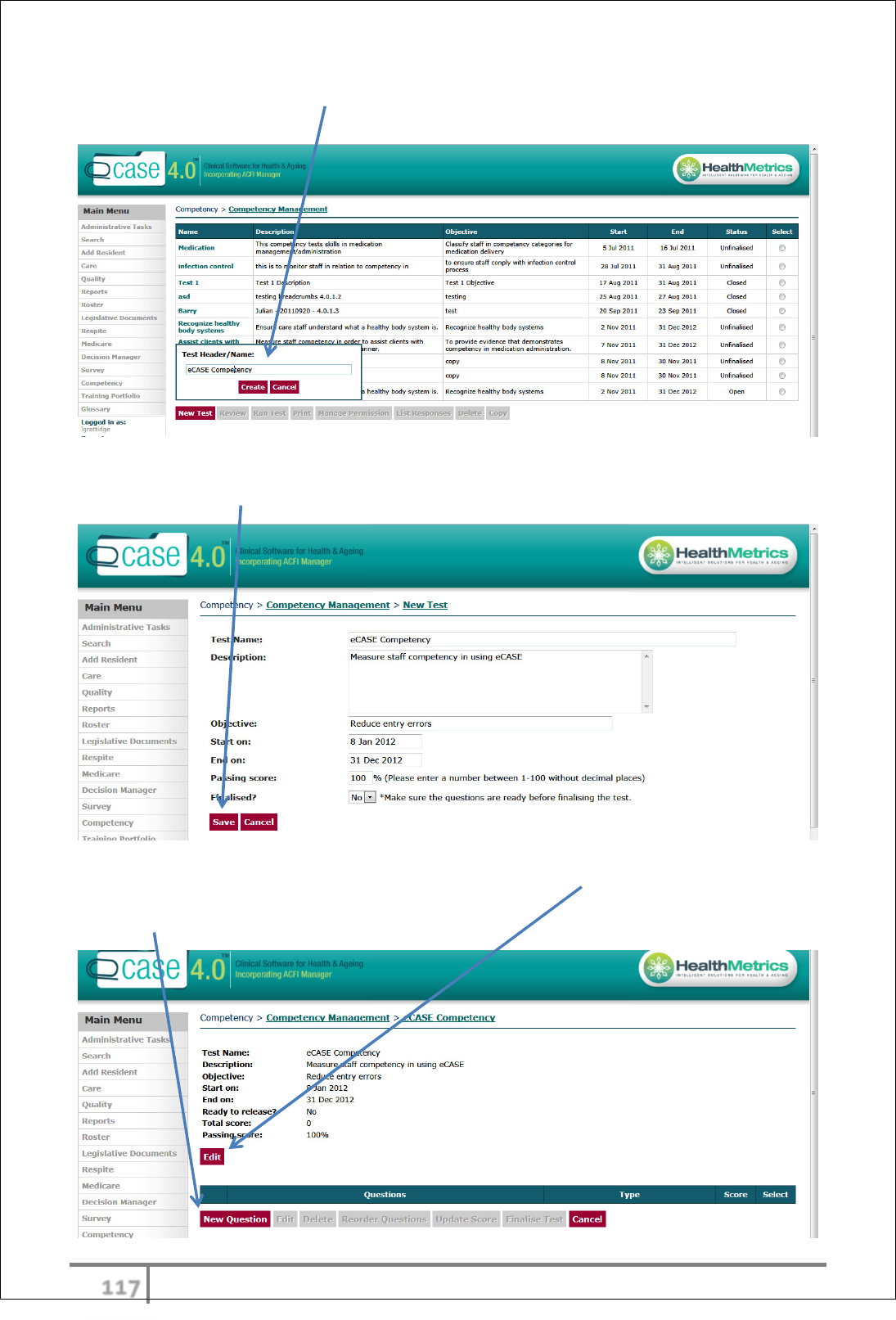
υυϋ
Ver 3.2013
.
A ‘Test Header/Name:’ box will appear. Enter preferred name and select
‘Create’.
Enter a description of the competency, objective, start date, end date, passing
score and click ‘Save’ button.
The information previously entered can be edited via ‘Edit’ button.
Select ‘New Question’ to commence formulation of competency questions.
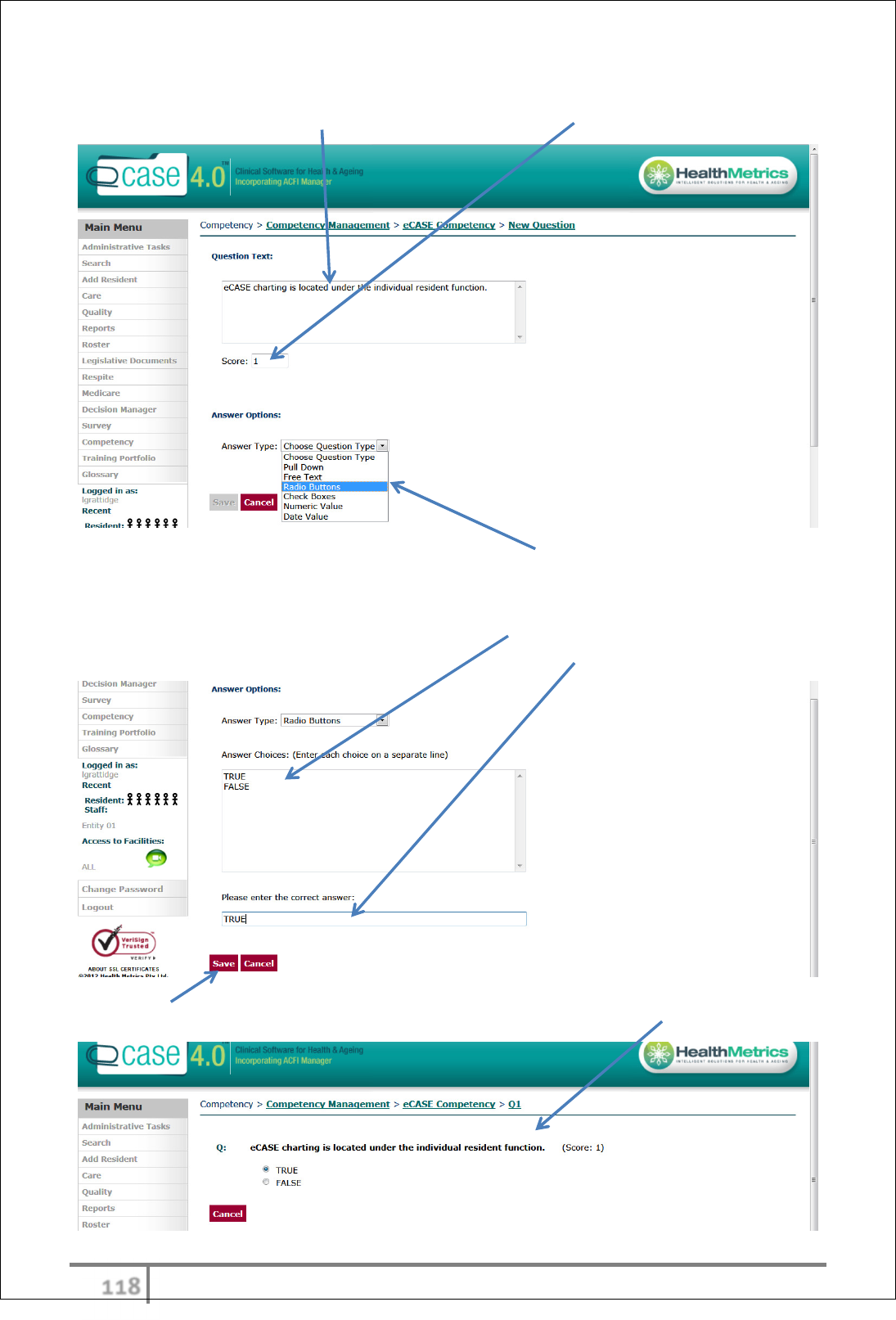
υυό
Ver 3.2013
.
Enter ‘Question Text’ in open field box and proposed score for question.
Select the preferred ‘Answer Type’ from the drop down menu: Pull Down, Free
Text, Radio Buttons, Check Boxes, Numeric Value or Date Value.
For example – Answer Type ‘Radio Buttons. Type in Answer Choices (ensuring
each choice starts on a separate line). Enter the correct answer in next field.
Select ‘Save’ button and a screen will appear displaying question format.
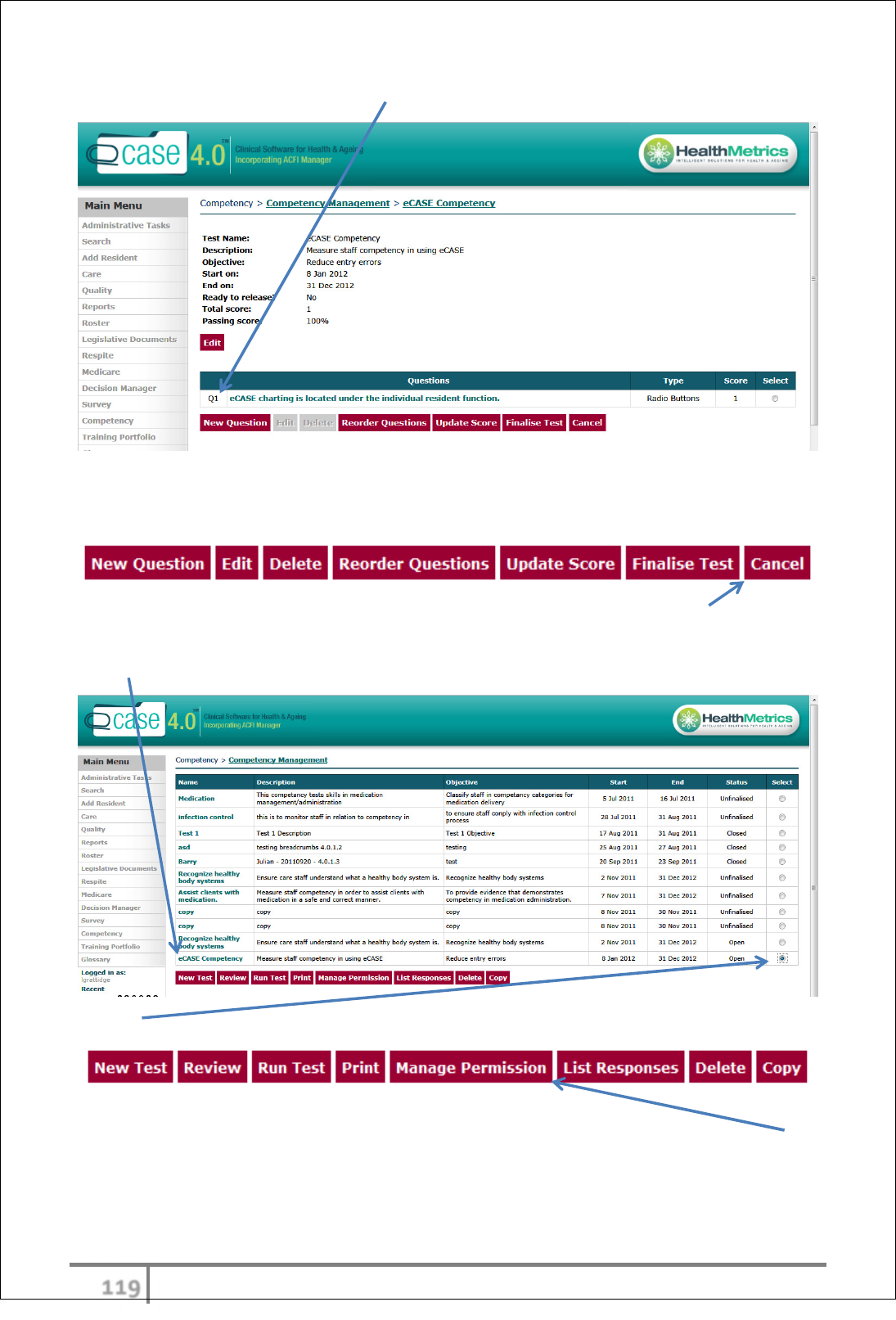
υυύ
Ver 3.2013
.
Each question created will be listed.
Continue to add ‘New Questions’ until complete.
Options are available to Edit, Delete, Reorder Questions and Update Score.
It is recommended to run test and manage competency permissions prior to
finalising. Select ‘Cancel’. The newly created Competency will appear in the list
along with other existing competencies.
‘Select’ competency to highlight the following options:
Competency Access – Manage Permissions
User access to a particular Competency can be managed via the ‘Manage
Permission’ function.
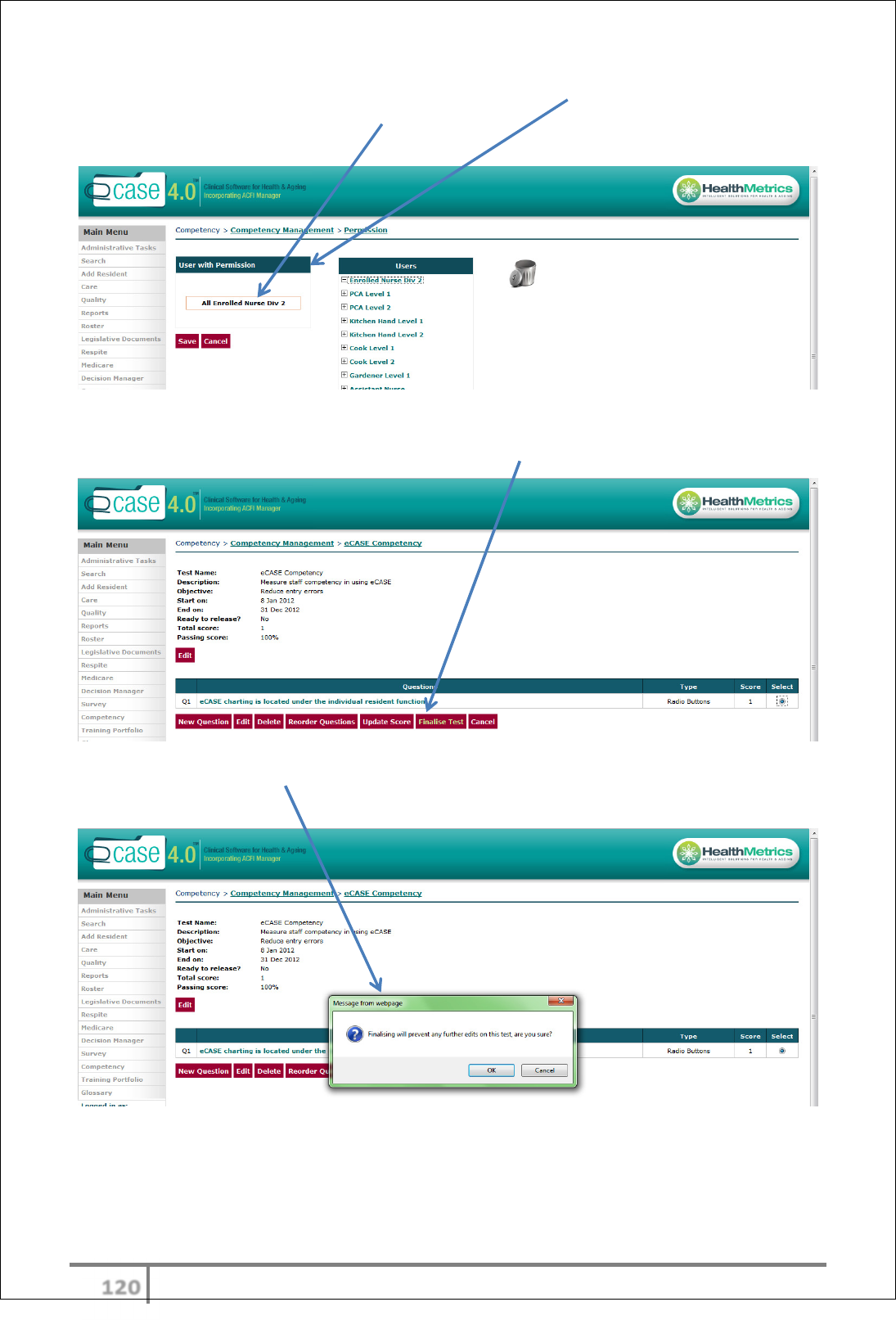
υφτ
Ver 3.2013
.
Simply drag and drop users into the ‘User with Permission’ field. Individual users
or groupings such as ‘All Enrolled Nurse Div 2’ can be dragged and dropped into
‘User with Permission’ field.
Finalise Test
Once satisfied Competency is ready, select ‘Finalise Test’.
A message box will appear as a reminder that finalising will prevent any further
edits on the test.
The status of the Competency will now appear as ‘Open’.
υφυ
Ver 3.2013
.
eCONTRACTS
eCase eContracts module includes the following:-
• Preparation of Residential Agreements (Low Care, High Care, Respite,
Extra Service etc.)
• Auto populated fields with Department of Health and Ageing scheduled
fees as default values that can be overwritten for individually negotiated
agreements
• Auto upload of .pdf (portable document format) eContract to the
resident’s movement list
• Attach scanned documents (signed contract pages etc.) to eContract
transaction
• Print function
• Secure environment with user permissions
eContracts Overview
eContracts module generates Residential Agreements as required by the Aged
Care Act 1997. Healthmetrics maintains the currency of agreements by pre-
loading default data supplied periodically by the Department of Health and
Ageing (Funding Tables) including - interest rates, retention amounts and daily
care fees etc. eContracts feature tailor-able fields which are unique to specific
facilities and individuals – Logo’s, clauses, schedules, Extra Service fees etc.
A full suite of contract templates can be uploaded and reside on eCase. eCase
serves as a central repository for eContracts facilitating easy, on-line access for
key stakeholders (Facility Management, Admissions Officers, Legal and Finance
personnel etc.).
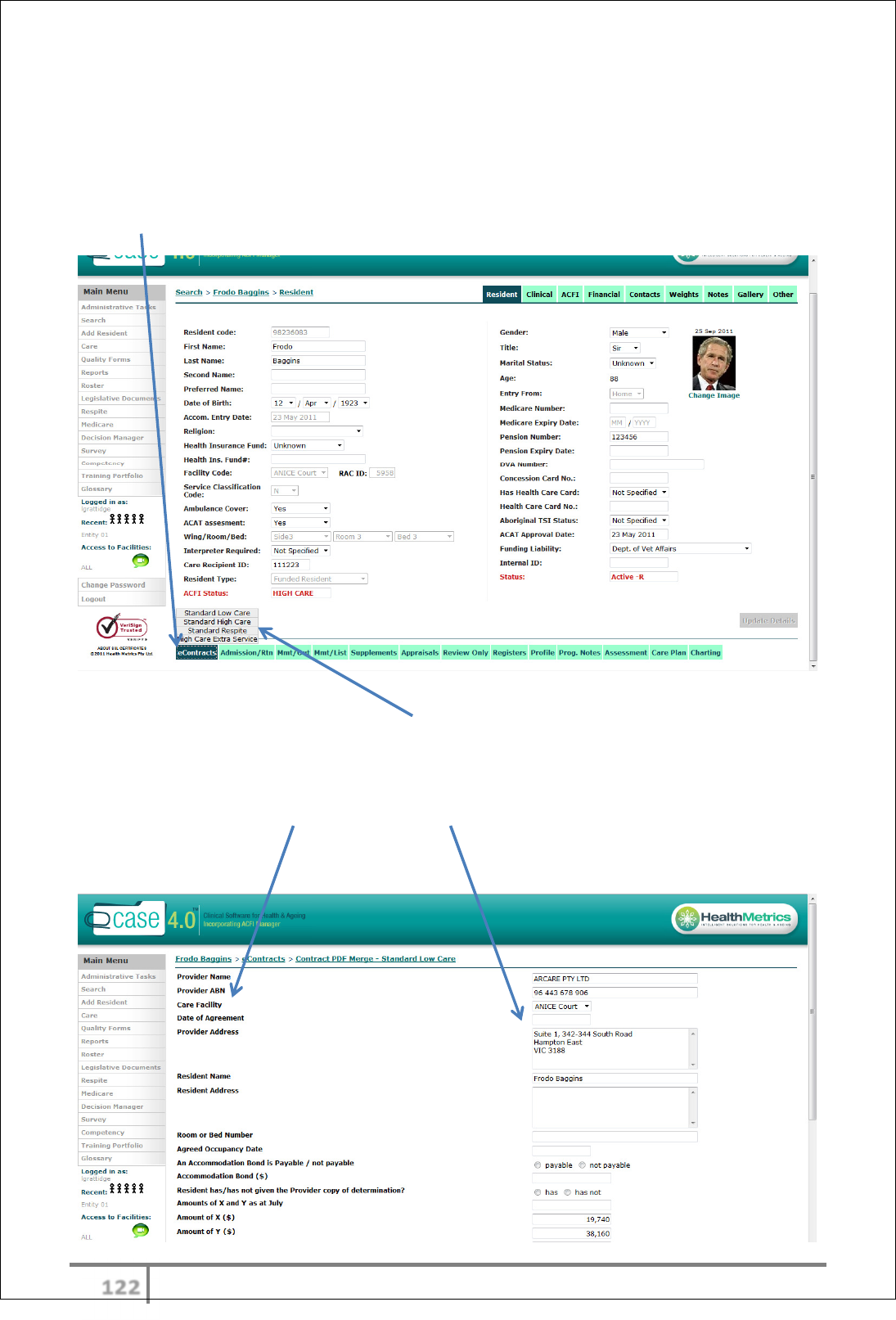
υφφ
Ver 3.2013
.
eContracts instructions for use
N.B Resident must be added to the database prior to creating an eContract. Once
resident is added to eCase, a contract can be created pre-admission or anytime
thereafter.
Select eContracts from ‘Resident Functions’ menu.
Creating an eContract
Pop up menu displays all available contracts. Select required contract subject to
type of service being offered to prospective resident or current resident requiring
a new contract type due to change of status.
The contract field titles and field contents appear on a page which can be
scrolled down. These match all fields that are configurable in the contract
template.
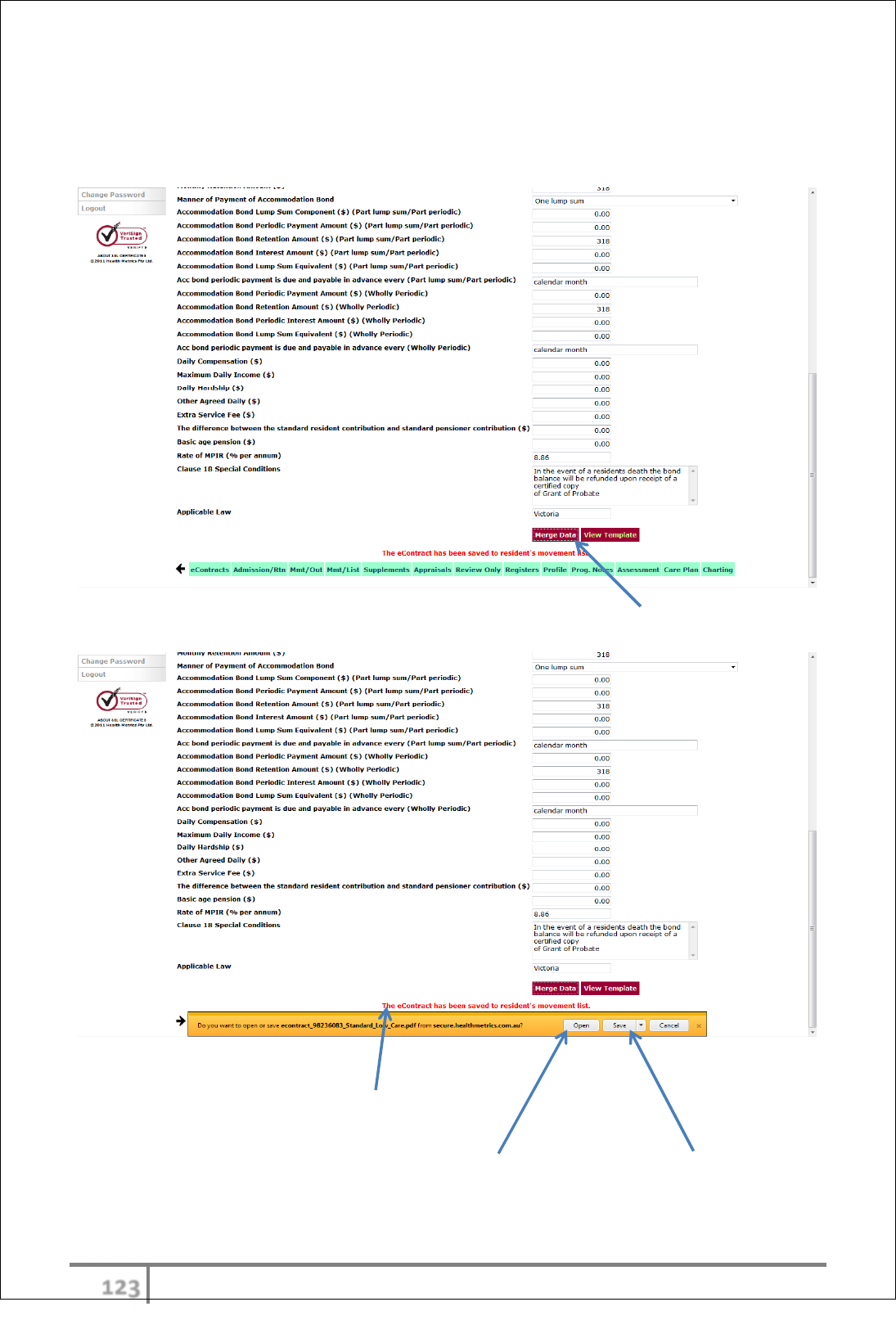
υφχ
Ver 3.2013
.
Many of the fields are auto filled with default data which can be overwritten as
necessary. There are a combination of date pickers, drop down menus, default
dollar values, percentages and open entry fields. The fields are displayed in a
logical order, consistent with the sequence of the contract template.
Once satisfied that all fields have been entered, select ‘Merge Data’ button.
Opening, Viewing and Saving
An on-screen alert in red notifies the user that the eContract has been (auto)
saved to the resident’s movement list.
The completed .pdf eContract can also be opened to view and/or saved onto the
users own filing system (independent of eCase). This is useful if the user intends
to email the eContract to the recipient (Power of Attorney etc.).
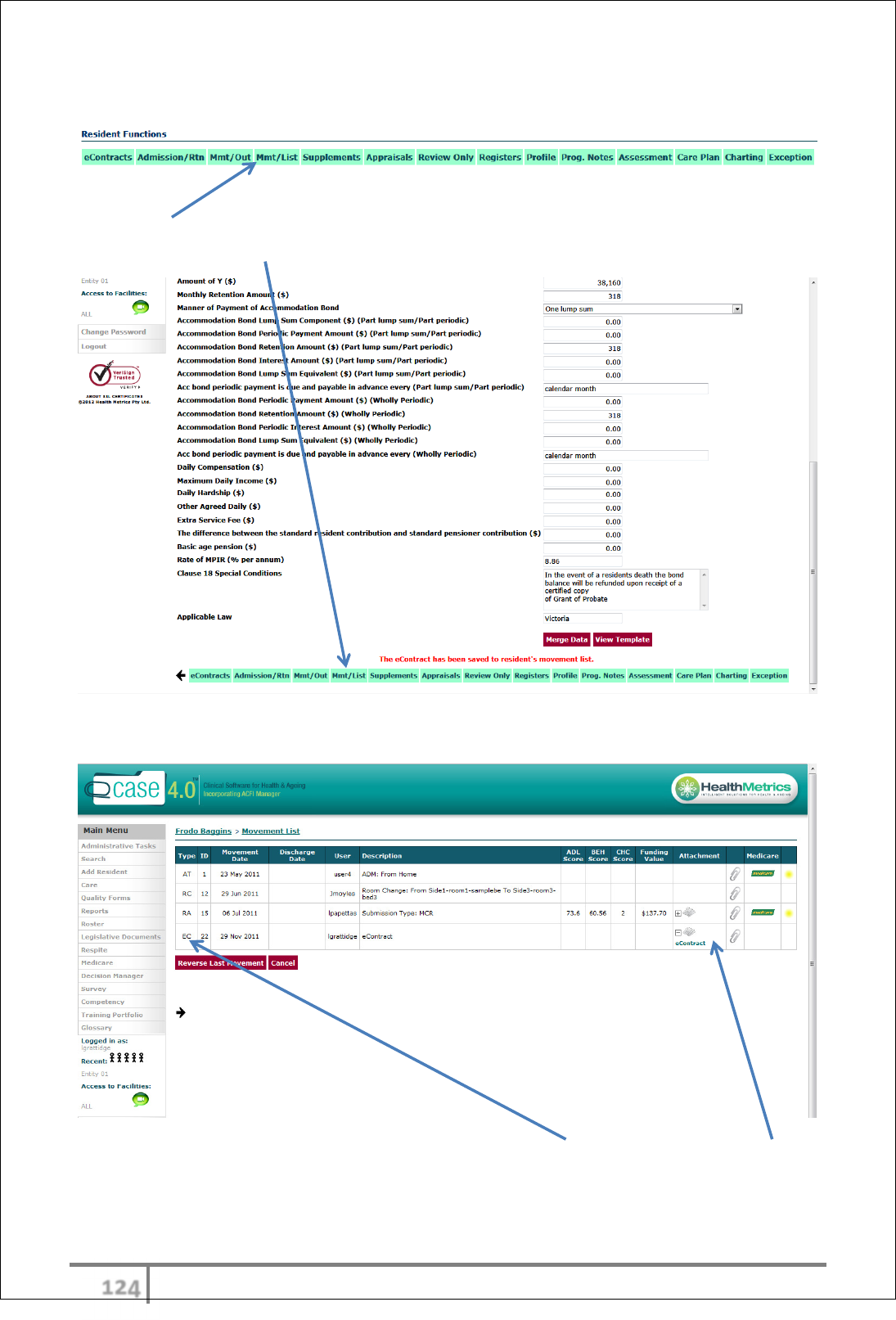
υφψ
Ver 3.2013
.
Movement List Access
The newly created eContract will appear in the resident’s movement list
(‘Mmt/List’). The movement list is accessed in the Resident Functions Menu also
available via Sliding menu.
Movement List – EC (eContract) Transaction
The movement list will display transaction type ‘EC’ and an envelope icon,
eContract hyperlink (click-on text to jump to) and paperclip will appear in the
table.
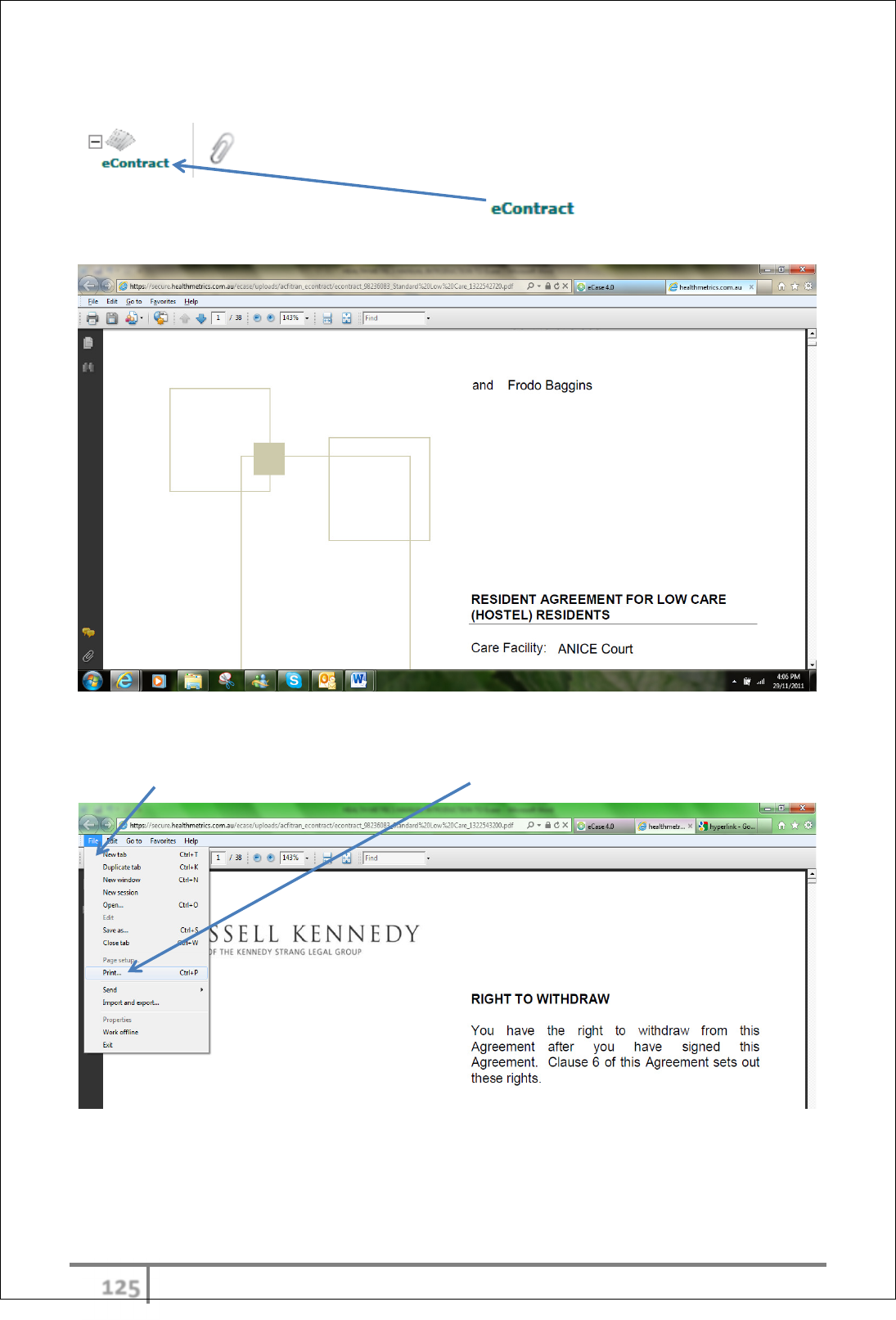
υφω
Ver 3.2013
.
Opening and Viewing eContract
To open the eContract click directly on and the contract will be
displayed in .pdf format.
Printing eContract
Select ‘File’ in the menu bar and select ‘Print’ from the drop down menu.
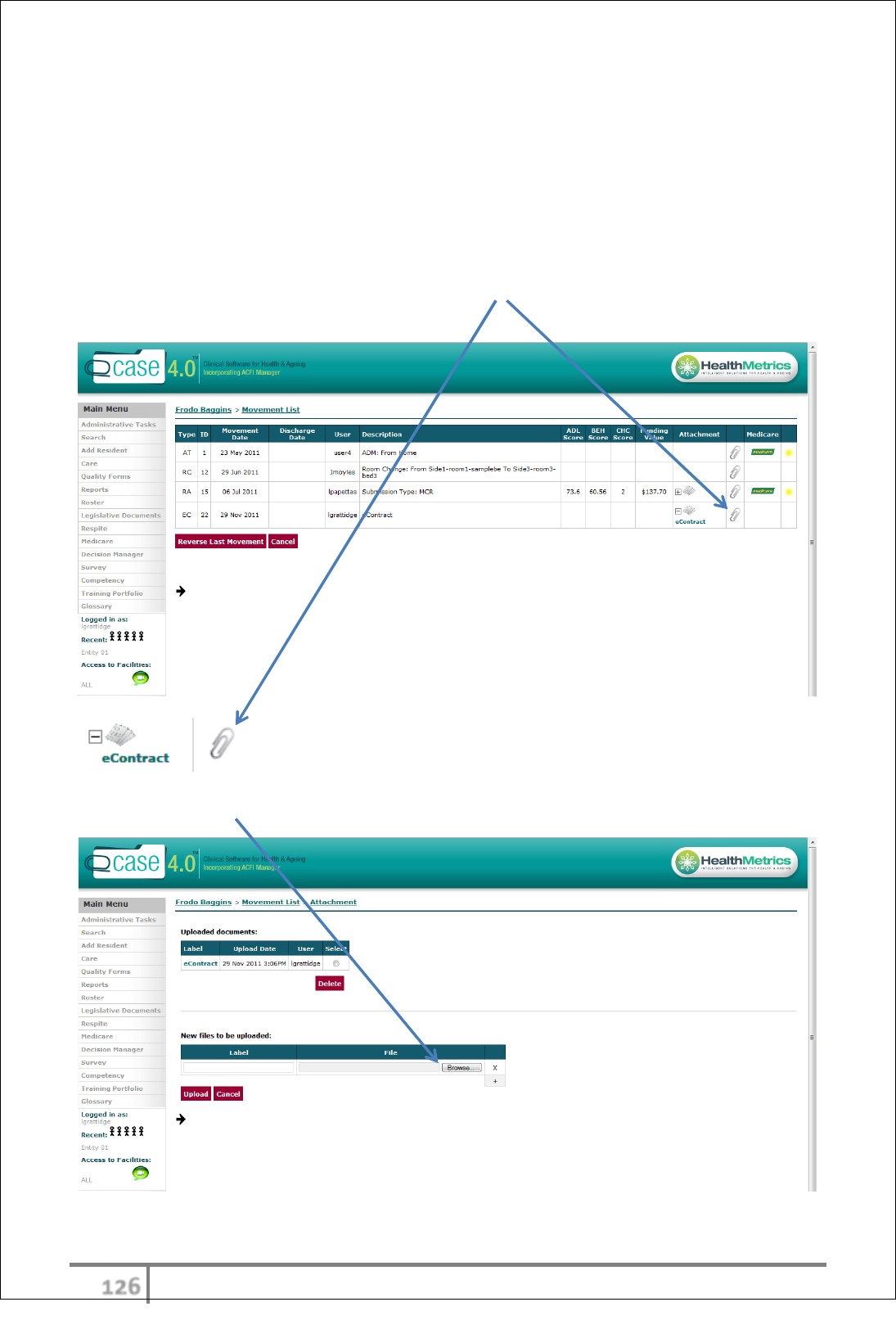
υφϊ
Ver 3.2013
.
Attaching documents to eContract transaction
When a contract has been executed (signed-off) or amended manually in any
way, a scanned copy of the relevant (signed/amended) pages can be uploaded
onto eCase residing next to the applicable movement list transaction. This is a
central, tidy and secure means to access the most up-to-date records quickly.
Multiple attachments can be uploaded and may include other documentation
relevant to contract negotiation.
To attach a document, click directly on the paperclip icon next to the relevant EC
transaction in the movement list.
Click the ‘Browse’ button in the ‘New files to be uploaded:’ section.
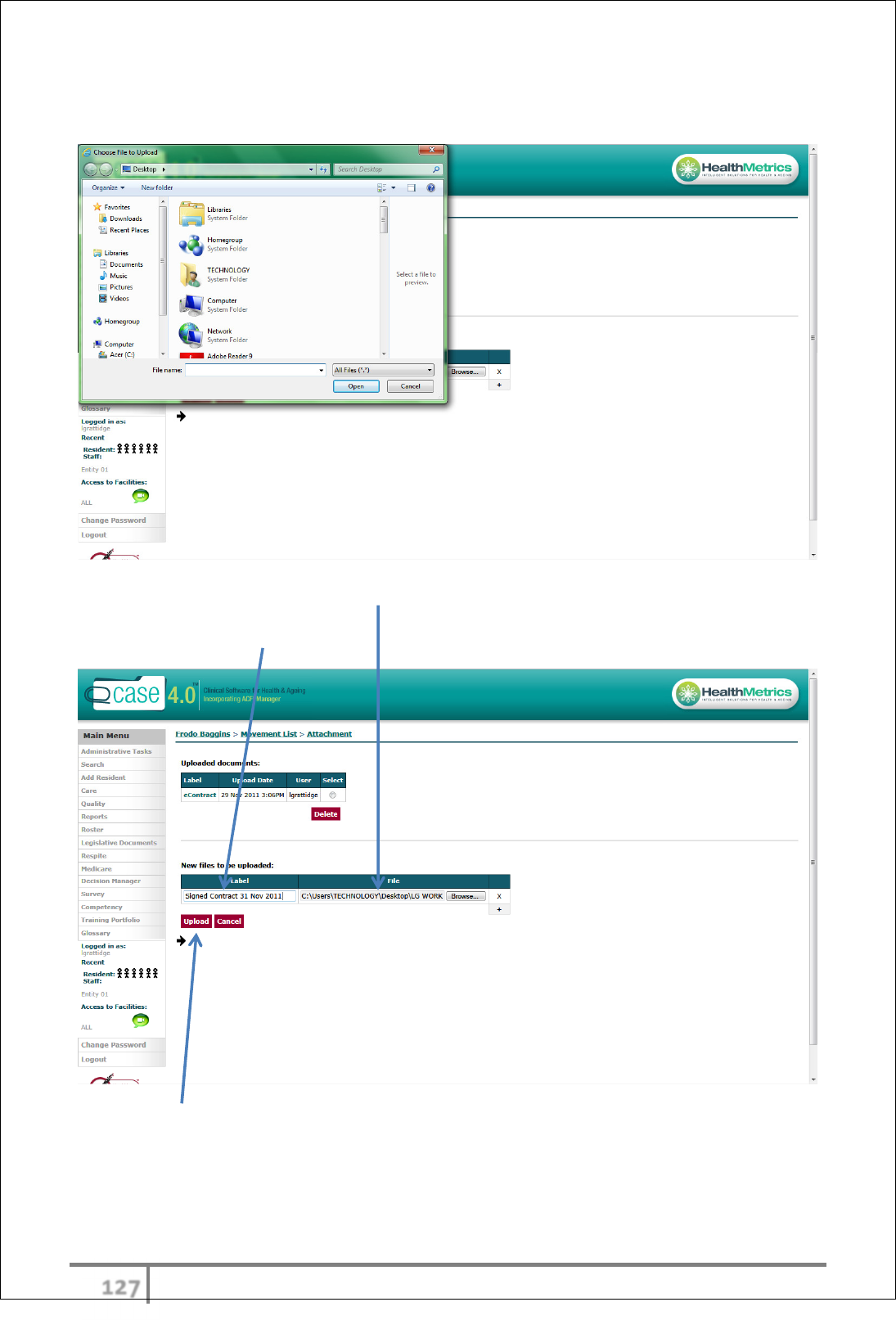
υφϋ
Ver 3.2013
.
The Browser function will prompt a search in user files to choose relevant file to
upload.
The selected file will appear in table as below.
A brief descriptive label should also be applied to the attachment.
Click ‘Upload’ button.
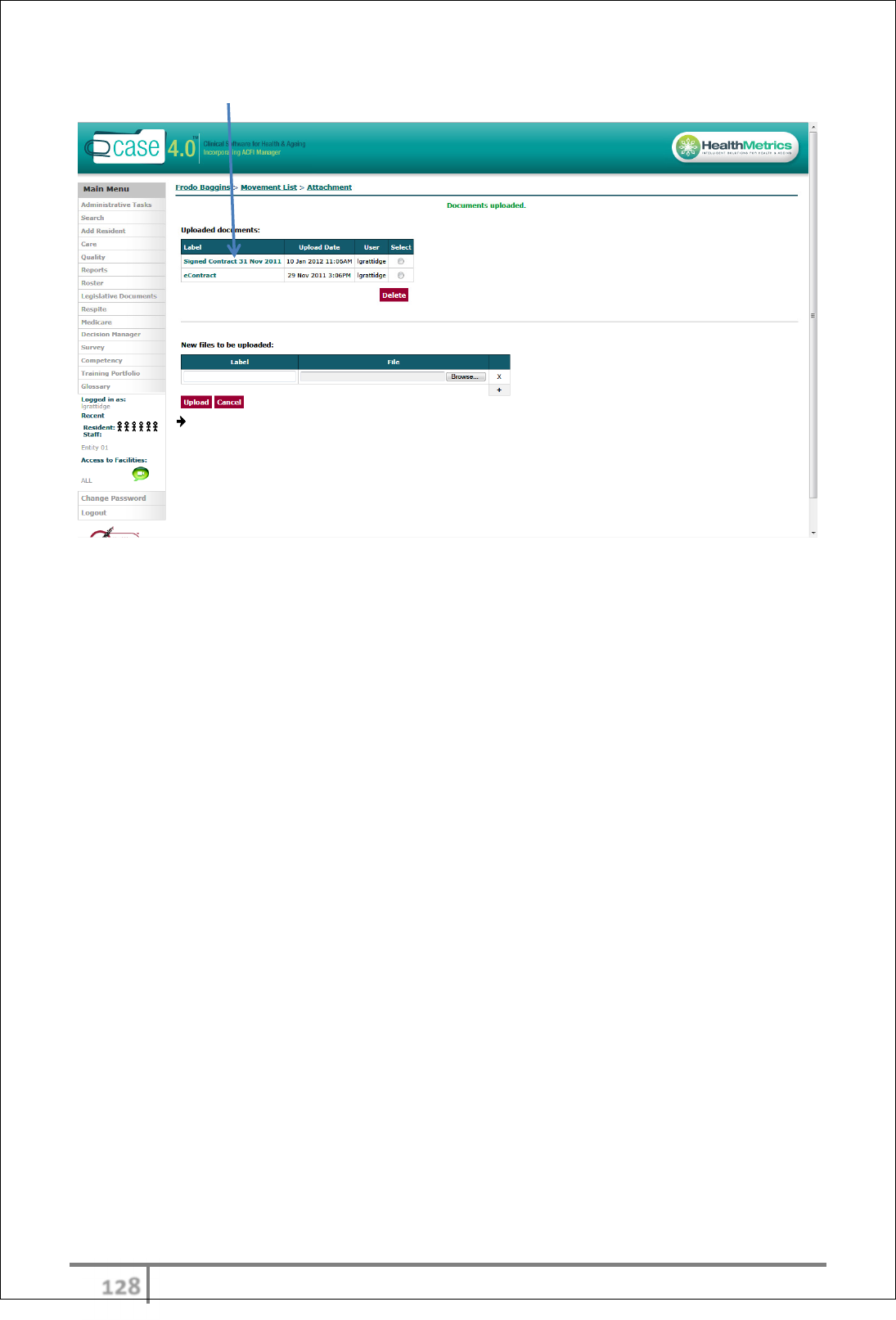
υφό
Ver 3.2013
.
The uploaded document will appear as below.
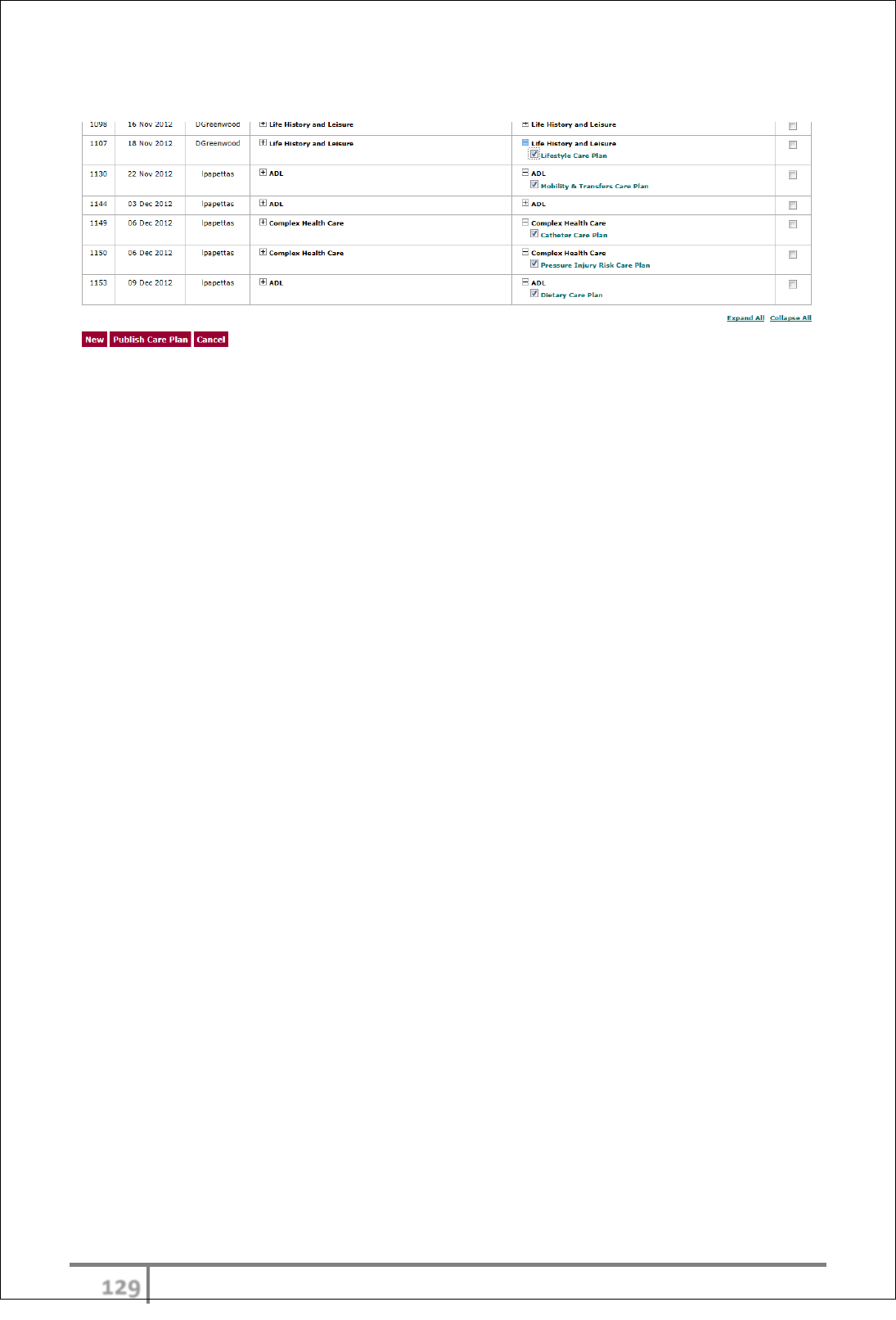
υφύ
Ver 3.2013
.
