REV Medicare
User Manual: REV
Open the PDF directly: View PDF ![]() .
.
Page Count: 13

MKT-080910-03 Rev A © Copyright 2008, AVAZZIA, Inc. All rights reserved.
Innovation in Health and Wellness Technology
Pro-SportTM, BEST PRO 1TM and BEST
RSITM Device
Physician and Patient
Information
Package
Regarding Medicare Reimbursement
This package is presented to physicians and Whole Wellness Club
members for their support in prescribing AVAZZIA Biofeedback
Microcurrent Electro-Stimulation Devices and then patient self-filing
a claim for reimbursement with Medicare without purchasing and
processing through a Medicare DME provider.
Whole Wellness Club is not a Medicare DME provider.

MKT-080910-03 Rev A © Copyright 2008, AVAZZIA, Inc. All rights reserved.
AVAZZIA BEST™
Microcurrent Biofeedback Electro-Stimulation Technology
BEST-Pro1™
BEST-RSITM
The Pro-Sport, BEST-Pro1 and BEST-RSI devices are FDA
cleared Microcurrent Biofeedback Devices
“for symptomatic relief and management of chronic, intractable
pain, and adjunctive treatment in the management of post-
surgical and post-traumatic pain.”
Medicare reimbursement is available, if the correct
procedure is carefully followed
• In-clinic treatments and training
• Device reimbursement
MKT-080910-03 Rev A © Copyright 2008, AVAZZIA, Inc. All rights reserved.
AVAZZIA BESTTM vs. Conventional TENS
AVAZZIA BESTTM devices are FDA cleared as microcurrent biofeedback TENS devices for the
symptomatic relief and management of chronic, intractable pain, and adjunctive treatment in the
management of post surgical and post-traumatic pain.
Technical Comparison
AVAZZIA BEST TM Conventional TENS
21st Century Technology
High intensity, very low current, burst
pulses
Voltage Range: 0-450 volts
Amperage Range: Microamps (10-6
Amps)
Signals in the frequency range of 1Hz
to 1000 Hz
Damped asymmetrical biphasic
sinusoidal waveform
Signaling always varies based upon
changes in impedance of the tissue
The AVAZZIA BEST device
forms a somatic biofeedback
between the device and the
tissue
1970’s Technology
Low intensity, higher current, long
duration pulses
Voltage Range: 0-40 volts
Amperage Range: Milliamps (10-3
Amps)
Signals in the frequency range of 1Hz to
100 Hz
Square waveform, mono-phasic or
biphasic
Symmetrical or asymmetrical
Signaling is typically the same
continuous pattern.
No biofeedback
Performance Comparison
AVAZZIA BESTTM Conventional TENS
Somatic biofeedback prevents
neurological habituation and
accommodation, for more effective
pain management
Effectiveness lasts several hours after
treatment
Develops neurological habituation and
accommodation, which severely limits
effectiveness of pain management
Effectiveness often stops when treatment
ends
MKT-080910-03 Rev A © Copyright 2008, AVAZZIA, Inc. All rights reserved.
AVAZZIA BEST™
Microcurrent Biofeedback Electro-Stimulation Technology
Biofeedback is the body’s response to the stimulus, and
the technology’s ability to detect, measure, analyze and
respond to the body.
As the BEST™ product is applied, a “high voltage,
micro-current” signal is passed through the skin. With
each signal, the electrical properties of the tissue
changes. The device detects the change and responds,
resulting in the very next signal being modified.
BEST™ Technology
• New concept in electro-stimulation
• Micro-current Electro-Neuro Stimulation
• Automatic Interactive Biofeedback
• Electro-therapy
• Handheld
• Battery-operated
• Measures and sends electric pulses as the
unit is moved along the skin
BEST-RSITM, Body-StimTM, and BEST-Pro 1TM micro-current biofeedback devices are FDA
cleared for symptomatic relief and management of chronic, intractable pain, and adjunctive
treatment in the management of post-surgical and post-traumatic pain.
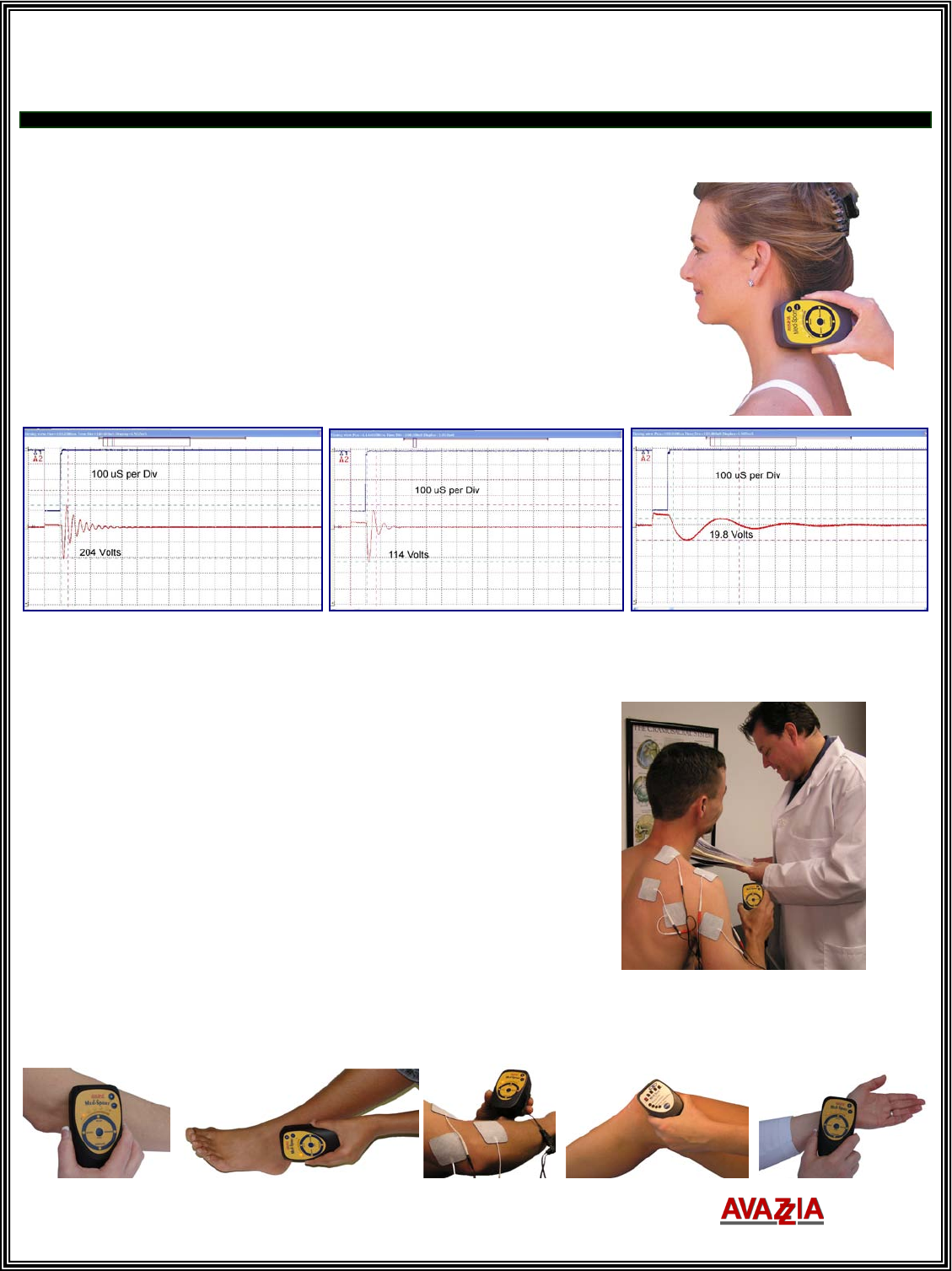
In air, there is no conductivity
between the electrodes. The
output signal waveform appears
as shown.
The device immediately detects
when the electrodes are placed
on reactive tissue as shown.
In Relax/Assess mode, the
device will ‘RING’ when it detects
the optimum characteristics.

MKT-080910-03 Rev A © Copyright 2008, AVAZZIA, Inc. All rights reserved.
MKT-080910-03 Rev A © Copyright 2008, AVAZZIA, Inc. All rights reserved.
Office Visit and Reimbursement Process
Step 1: Physician – patient conference for chronic, intractable pain
o Patient appointment and evaluation with physician
o Physician prescribes BESTTM technology to start a trial period
BESTTM device must be used by patient on trial basis for a minimum of 1 month
(30 days) but not more than 2 months (60 days) to qualify for Medicare
reimbursement
Physician must document location of pain, duration patient has had the pain, and
the presumed etiology of pain
Physician must document that pain has been present for at least 3 months and what
other treatments have been tried and that these treatments failed
o Physician’s office or patient faxes, mails, or personally delivers prescription to Medicare
Step 2: Whole Wellness Club delivers the BESTTM device to patient
Step 3: Trial period
o Physician must monitor patient during trial period to determine effectiveness of BESTTM
device in modulating pain
o For purchase of BESTTM device, physician must determine that patient is likely to receive
significant therapeutic benefit from continuous use of the device over a long period of time
o Physician records must document re-evaluation of patient at end of trial period
Step 4: Patient returns to physician’s office after 30-day trial
o Physician documents the trial evaluation confirming effectiveness
o Physician completes and signs Medicare form CMS-848 (included here)
o Physician’s office or patient faxes, mails, or personally delivers the CMS-848 and 1490S
forms to Medicare. Click on the hyperlink to retrieve form 1490S from Medicare's
website.
In this way, the patient is filing their own claim for reimbursement. The 1490S form is for
the purpose of filing your own Medicare claim.
Whole Wellness Club is not a Medicare DME provider.
Your local Medicare center may tell you that you must purchase the device from and file a
claim through a Medicare DME provider. This is not true.
Step 5: Medicare reimburses patient
Note: Conductive garment is not covered for use with BESTTM device during the trial period

MKT-080910-03 Rev A © Copyright 2008, AVAZZIA, Inc. All rights reserved.
Conductive Garment
Conductive garments are covered by Medicare if ordered by physician for use in delivering a covered
BESTTM (TENS) device and one of the following conditions is met:
1. Patient cannot manage without conductive garment because there is such a large area or multiple
sites to be stimulated and stimulation must be delivered so frequently that electrodes are not
feasible
2. Patient cannot manage without conductive garment for treatment because areas or sites to be
stimulated are inaccessible with use of conventional electrodes
3. Patient has documented medical condition, such as skin problem, that preclude the application of
conventional electrodes, adhesive tapes
4. Patient requires electrical stimulation beneath a cast to treat chronic, intractable pain
MKT-080910-03 Rev A © Copyright 2008, AVAZZIA, Inc. All rights reserved.
For Therapist’s Records
Patient Letter of Medical Necessity BESTTM Therapy
Patient name (insert patient info or sticker here)
Symptoms: ____ Pain ____ Stiffness ____ weakness ____ instability ____ other
ICD9 codes: __________________________________________________________
Diagnosis ____________________________________________________________
Therapy is ordered for this patient for AVAZZIA biofeedback micro-current electro-stimulation.
Therapy goals (check goals that apply)
____ Pain relief
____ Pain management at home
Restorative Potential: ____ 25% ____ 50% ____ 75% ____ 90% ____ 100%
Clinical procedures and modalities:
____ Biofeedback ____ Micro-current stimulation – BEST-PRO 1™ or BEST RSI™ Device
____ Self care training
Individual therapy sessions are 30 to 45 minutes in length. Number of therapy sessions required is
expected to be ______________
At follow up office visit, it will be determined if additional therapy sessions are needed.
Reevaluation in _____ days _____ weeks
Patient should begin treatment AS SOON AS POSSIBLE.
Physician’s Name (print):______________________________ NPI number:______________
Clinic Name: ______________________________________ Phone#: ___________________
Physician’s Signature:____________________________________ Date:________________
Physician’s Address:__________________________________________________________
Confidential Information
MKT-080910-03 Rev A © Copyright 2008, AVAZZIA, Inc. All rights reserved.
“Add clinic name, address
phone number and logo”
Physician’s Statement of Medical Necessity (Prescription)
Please Complete, Sign, Date and Fax to Medicare
Patient’s Name: ___________________________________ Date of Birth: ___________ SS#: ___________
Patient’s Address: _________________________________________________________________________
Patient’s Phone #: _________________________________________________________________________
Date of Injury/Onset: _____________________________
Diagnosis / ICD9:
_____
Chronic Pain
338.4
_____
Pain: Joint: Ankle
719.47
_____
Pain: Joint: shoulder (region)
719.41
_____
Pain: Postoperative
338.18
_____
Pain: Joint: Elbow
719.42
_____
Pain: Joint: wrist
719.43
_____
Pain: Postoperative: Acute
338.18
_____
Pain: Joint: Foot
719.47
_____
Pain: face, facial
784.0
_____
Pain: Postoperative: Chronic
338.28
_____
Pain: Joint: Hand
719.44
_____
Pain: face, facial: Atypical
350.2
_____
Pain: Extremity (lower) (upper)
729.5
_____
Pain: Joint: Hip
719.45
_____
Pain: face, facial: Nerve
351.8
_____
Pain: Back (postural)
724.5
_____
Pain: Joint: Knee
719.46
_____
Pain: Finger
729.5
_____
Pain: Back: Low
724.2
_____
Pain: Joint: Multiple Sites
719.49
_____
Pain: Foot
729.5
_____
Pain: Joint
719.40
_____
Pain: Joint: Pelvic Region
719.45
_____
Pain: Hand
729.5
Other ICD-9 Codes: __________________________
Other Diagnosis : _______________________________________________________________________________________
Previous Treatment(s)/Medications: ________________________________________________________________________
Product Description:
Micro-current Biofeedback TENS ____BEST-PRO 1™ or ___ BEST RSI™ or ___ Pro-Sport™ Device with
one lead wire, 1 set conductive pads
Conductive Garment ____ is ____ is not medical necessity. Check any that apply:
___ large area to be treated
___ multiple sites to be treated
___ areas are inaccessible with the use of conventional electrodes, adhesive tapes, and lead wires.
___ medical conditions, such as skin problems, that preclude the application of conventional electrodes
___ therapy required beneath a cast
Left
Right
Both
Carpal wrap
ankle wrap
low back wrap (6 inches tall)
high back wrap (8 inches tall)
elbow wrap
shoulder wrap
arm or leg wrap
cervical wrap
conductive glove
conductive sleeve
conductive sock
conductive leg sleeve
Length of Need:
_______# of Months (short term) _______6-9 months (long term) _______Purchase
I certify that the above prescribed treatment is medically necessary for the patient’s well being. In my
opinion, the treatment is effective and is reasonable in the treatment of this patient’s condition. I also
certify that the information noted above is accurate to the best of my knowledge.
Physician’s Signature:____________________________________ Date:____________________
Physician’s Name (print):_________________________________ NPI number:______________
Clinic Name: ___________________________________________ Phone#: _________________
Physician’s Address:______________________________________________________________
DO NOT SUBSTITUTE CONFIDENTIAL INFORMATION
MKT-080910-03 Rev A © Copyright 2008, AVAZZIA, Inc. All rights reserved.
MKT-080910-03 Rev A © Copyright 2008, AVAZZIA, Inc. All rights reserved.
For Doctor’s Files
Patient Record of In-Office Therapy
Date of Therapy _________
Patient name (insert patient info or sticker here)
Diagnosis (ICD9) ____________________________________________________________
Therapy is ordered for this patient for AVAZZIA biofeedback micro-current electro-stimulation.
Clinical procedures and modalities:
CPT code
Descriptions
Time
started
Time
ended
Duration
(mins)
Therapist
Initials
97032
Attended electrical stimulation
(15 mins)
G0283
Electrical stimulation unattended
(wkrs comp 97014) (15 mins)
97112
Neuromuscular re-education
(15 mins)
90901
Biofeedback
(15 mins)
97535
Self care / home management training to use device _______yes ______no
Patient Signature _________________________________________ Date ______________
Therapist Signature:________________________________________ Date:________________
Therapists Name (print):_________________________________ NPI number:______________
Clinic Name: _________________________________________ Phone#: __________________
Address:_______________________________________________________________________
CONFIDENTIAL INFORMATION

MKT-080910-03 Rev A © Copyright 2008, AVAZZIA, Inc. All rights reserved.
Therapy Codes for
Micro-Current Biofeedback Electro-Stimulation
Technology
CPT codes
Code Description
G0283
Electrical stimulation unattended (wkrs comp 97014) (15 mins)
97032 Attended electrical stimulation (15 mins)
97112 Neuromuscular re-education (15 mins)
90901 Biofeedback (15 mins)
97535 Self care / home management training
97001 Pt evaluation – Complete Specialist examination
97002
Pt re-evaluation – Complete Orthopedic examination
99243 Office consultation detailed
ICD9 codes for Pain
Acute and Chronic Pain
338.0
Central Pain Syndrome
338.11
Acute Pain due to trauma
338.12
Acute post-thoracotomy pain
338.18
Other acute post-operative pain
338.19
Other acute pain
338.21
Chronic pain due to trauma
338.22
Chronic post-thoracotomy pain
338.28
Other chronic post-operative pain
338.4
Chronic Pain Syndrome
Joint Pain
719.40
Unspecified, joint pain
719.41
Shoulder (region) pain
719.42
Upper arm or elbow pain
719.43
Forearm or wrist pain
719.44
Hand pain
719.45
Hip pain
719.46
Lower leg or knee pain
719.47
Ankle and foot pain
719.48
Other specified site pain
719.49
Multiple sites
729.5
Pain in limb, pain in extremity (lower)
(upper), finger or hand
Neck and Back Pain
723.1
Neck pain
724.1
Thoracic spine pain
724.2
Low back pain
724.5
Backache unspecified - back
(postural)
Facial Pain
784.0
Face, facial pain
350.2
Atypical Facial pain
351.8
Nerve facial pain
NO promises are made and NO liability for any damages due to information related to insurance
coverage are made or accepted.
MKT-080910-03 Rev A © Copyright 2008, AVAZZIA, Inc. All rights reserved.
Instructions for Physician's Statement of Medical Necessity
Prescription Form
Under "Other Diagnoses"
Be certain to indicate "Chronic Intractable Pain"
Under Previous Treatments/Medications
Be certain to indicate at least 3 attempted modalities. E.G. aspirin, Tylenol, massage, etc
Have your physician fill out this prescription form and file it yourself with Medicare to open a claim file.
They may tell you that you must purchase such a device from an authorized Medicare DME provider and
have them file the claim. This is not true. Just tell them your doctor prescribed the device and you could
not find a Medicare DME provider with the device but purchased it from the Whole Wellness Club. Tell
them you want to file the claim yourself using form 1490S or by any other self-filing procedure they
advise you to use.
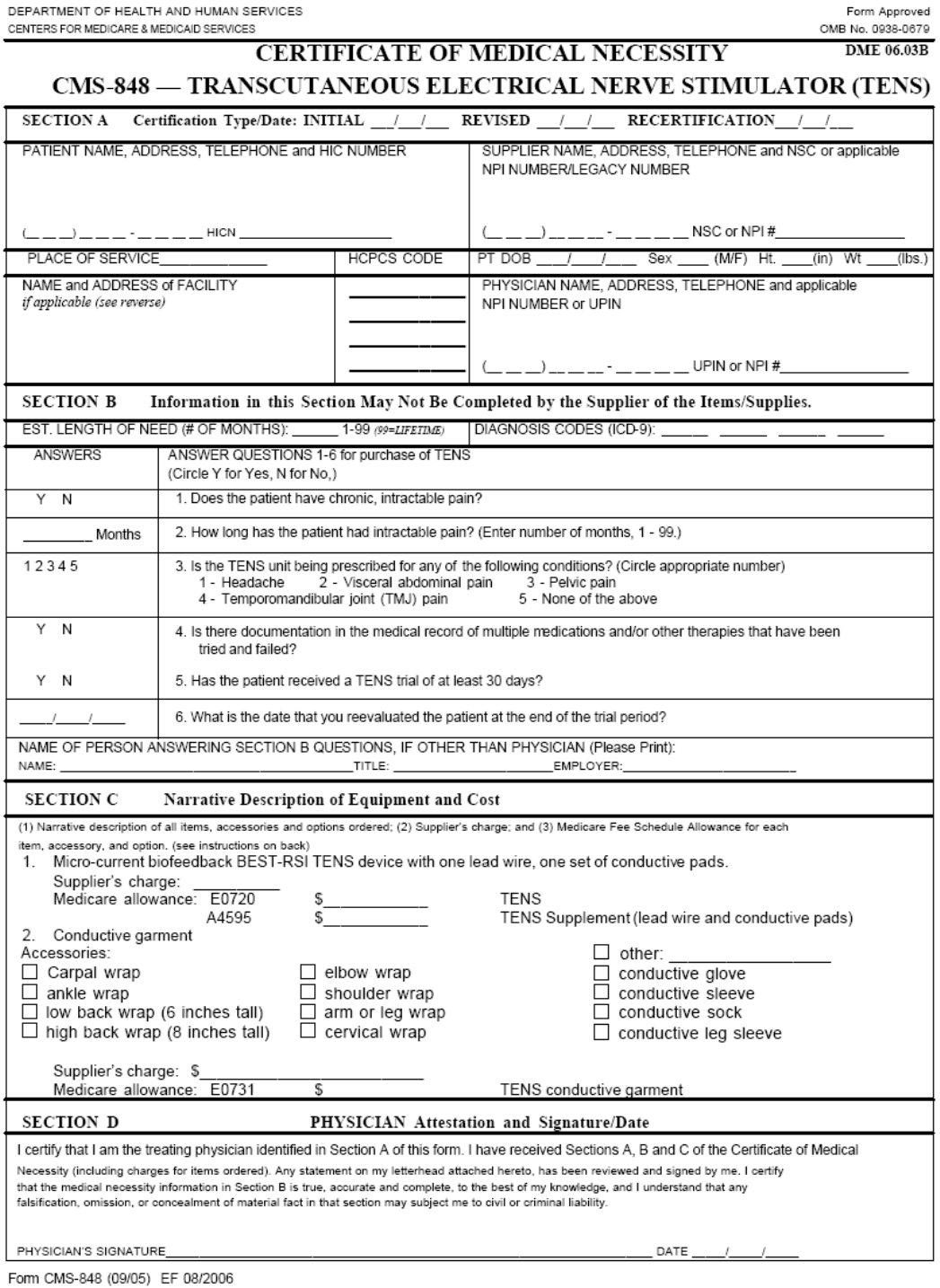
Instructions for CMS 848
Certificate of Medical Necessity
BESTTM device must be used by patient on trial basis for a minimum of 1 month (30 days) but not more
than 2 months (60 days) to qualify for Medicare reimbursement
Under Supplier Name and Address, write:
Whole Wellness Club
503 Lincoln Dr
Sun Prairie, WI 53590
Phone: 866-549-0267
Section B
To be qualified for reimbursement from Medicare the true and honest answer to questions 1, 4, and 5 must
be "Yes" or circle "Y". Question 3 must indicate "5. None of the above"
Fill out and include Form 1490S
with your submission to Medicare
If you need help, call 1-800-MEDICARE (1-800-633-4227)
