Executive_summary__30 11 Pharmax IPR 3000 Wg Pharma2902
User Manual: IPR 3000
Open the PDF directly: View PDF ![]() .
.
Page Count: 178 [warning: Documents this large are best viewed by clicking the View PDF Link!]
i
EXECUTIVESUMMARY
TheIndianpharmaceuticalIndustryhaswitnessedarobustgrowthofaround14%since
thebeginningofthe11thPlanin2007fromaboutRs71000crorestooverRs1laccrores
in2009‐10comprisingsomeRs62,055croresofdomesticmarketandexportsofoverRs
42,154crores.Thisalsoamountstoaround20%oftotalvolumeofglobalgenerics.
However,theIndustryisquitefragmentedandcomprisesofnearly10,500unitswith
majorityoftheminunorganizedsector.Ofthese,about300‐400unitsarecategorizedas
belongingtomediumtolargeorganizedsectorwiththetop10manufacturersaccounting
for36.5%ofthemarketshare.AsregardstheBulkdrugscomponentoftheindustry,the
marketisaroundRs42,000croresgivingitashareofaround50%ofthetotaldomestic
market.ThisgivestheIndianBulkDrugindustryashareofabout9%oftheglobalbulk
drugmarket.
Indiaisamongthetop20pharmaceuticalexportingcountriesandtheexportshave
grownverysignificantlyataCAGRofaround19%inthe11thplanperiod.Indiandrugs
areexportedtoaround200countriesintheworldwithhighlyregulatedmarketsofUSA,
UKetc.Themajortherapeuticcategoriesofexportareantiinfective,antiasthmaticand
antihypertensive.
TheDepartmentofPharmaceuticalshasaVisionforthedevelopmentoftheIndian
PharmaceuticalIndustry.ThisVisionis–
“TomakeIndiatheLargestGlobalProviderofQualityMedicinesatReasonablePrices.”
TheVisionistobeachievedasperthefollowingMission:
• DevelopHumanResourcesforPharmaceuticalIndustryandDrugResearchand
Development
• PromotePublic‐PrivatePartnershipfordevelopmentofpharmaceuticalsIndustry
• PromotePharmaBrandIndiathroughInternationalCooperation
• PromoteenvironmentallysustainabledevelopmentofPharmaceuticalIndustry
• Enableavailability,accessibilityandaffordabilityofdrugs
ii
InordertorealisetheMission,theDepartmenthassetthefollowingGoalsfor12thplan:
• ProductionsizeofUS$60bnandexportsizeofoverUS$25bn.
• UpgradationofSMEstoWHO‐GMPandtrainingofprofessionalstherein.
• EstablishmentofPharmaGrowthClusters.
• FacilitategrowthofCentralpharmaPSUs.
• DevelopPharmaInfrastructureandCatalyzeDrugDiscoveryandInnovation
• DevelopPharmaHumanResourcesthroughincreasedM.PharmaandPh.D
programsinNIPERS
• ProvideInfrastructureandstafffornewNIPERsandstrengthenNIPERMohali
• Open10newNIPERs
• JanAushadiCampaignandimplementationofBusinessPlanforsettingupof3000
JanAushadhiStores(uptoSubdivisionlevelinthecountry)
• IncentivizingPrivateSectorfordevelopmentofnewDrugsfordiseasesendemic
toIndia
FortheachievementoftheseGoals,itisnecessaryfortheIndianPharmaceuticalIndustry
tobecomegloballycompetitivethroughworldclassmanufacturingcapabilitieswith
qualityandcostefficiencyofproductioncapacityandradicalupgradationofresearchand
developmentcapabilitiesfornewdrugsandassociatedactivitieslikeclinicaltrialsand
contractmanufacturing.Thereisneedtodevelopworldclasssupportinfrastructure
bothforproductionandresearch.
Withthisapproach,thepreparationofthe12thPlaninvolvedadetailedSWOTanalysisof
theIndianPharmaceuticalsIndustry.Thisanalysishasrevealedthefollowingstrengths:
(a)StrongLowcostmanufacturingsector(b)Significantbreadthanddepthofproduct
expertise(c)LowcostofgrowingHumanresourcesinthePharmasector.Themajor
weaknessesare–(a)Highemphasisongenericsbothfordomesticandinternational
marketswherefilingandapprovalofANDAsandDMFshaveleftlittleroomforR&Don
drugsdevelopment(b)InadequateR&DInfrastructure(c)PoorIndustry‐Academia
linkage(d)Lackofrequiredhigh‐endproductdevelopmentcapablehumanresources(e)
Lackoftimedrivenregulatoryinfrastructure(f)PoorSMEbaseforhigh‐endmanufacture.
Themajoropportunitiesavailableare‐(a)GlobalopportunityforincreasingGenericsand
iii
bio‐genericsmarketbothindevelopedandemergingcountriesduetopressureon
budgetarylimitationsofthesecountriesaswellasemergentpatentcliffduetooff‐
patentingofmajorhigh‐valuedrugs(c)Lowcostgoodskilldestinationforcontract
researchandmanufacturingandresultantopportunitiesindrugdiscoveryaswellas
clinicaltrials(d)Highgrowthofdomesticmarketattractingmulti‐nationalsbothfor
brownfieldandgreenfieldinvestmentsinproductionandcapacitybuilding.Thethreats
totheindustryarefrom‐(a)Ever‐greeningstrategyofMNCsfordenyingandlimitingthe
patentcliffopportunitieswithdebatablerecoursetoTRIPsandFTAs(b)Increasingly
stringentregulatoryandnon‐tariffbarrierstogenericsmarketsindevelopedcountries(c)
Increasedcompetitionforgenericsandbio‐genericsproductionintermsofhighcapacity
andproductioncosts(d)High‐entrybarrierstoenablemarketshareindevelopmentof
newdrugs.
BasedontheaboveSWOTanalysis,recommendationshavebeenmadeinthe12thPlan
Documentfor–
1) DevelopmentandgrowthoftheIndustry
2) StrengtheningofR&DCapabilities
3) StrengtheningofhumanresourcebaseforIndustry
4) AffordabilityandAccesstoQualityDrugs
ThemajorrecommendationsconcerningsupportforIndustrygrowthare‐(a)Schemes
forUpgradationofSMEstoWHO‐GMP,USFDA/EDQM/TGAandotherInternational
Standards(b)Supportfornewgenericsandbio‐genericsthroughsettingupof
FormulationDevelopmentCentersandManufacturingStandardsTrainingCenters(c)
Regionalcluster‐basedIndustrydevelopmentthroughestablishmentandupgradationof
10PharmaGrowthAreaClusters(d)IndustrysupporttoInternationalmarketaccess
throughcapacitybuildingandinter‐governmentalcooperation.TheMedicalDevice
IndustryisalsoproposedtobesupportedthroughthedevelopmentofaMedicalDevices
ParkinAhmedabad,Gujarat.
iv
IntheareaofR&Dandhumanresourcedevelopmentthemajorrecommendations
concern(a)settingupofNationalExcellenceCentrescomprisingthreeforResearchand
DevelopmentinPhyto‐pharmaceuticals,Nano‐PharmaceuticalsandBio‐Similars,onefor
settingupofNationalfacilitiesforNewDrugsDevelopmentalongwithanotherforEnd
ToEndLarge‐ScaleAnimalHouseandsettingupofaNationalCentreforR&DinAPIs(b)
SchemesforsupportingR&DinIndustrythroughassistanceforsettingupof
GLP/GCP/AnimalHouseLabSchemes(c)SettingupofPharmaVentureCapitalFundto
fundinnovationsindrugdiscoveryincludingincubatordriventranslationalresearch(d)
PharmaInnovationandInfrastructureDevelopmentInitiativeforR&Dinfrastructure
developmentincludingfundingofprivatesectorinitiativesinPPPmode.Emphasison
supportingextramuralresearchindevelopmentofnewdrugsanddosageformsformass
afflictiondiseaseslikeJE,Chikungunya,TB(resistantstrains),leishmeinasis,malaria,and
therecentlifestylediseaseslikediabetesandCVD,etc.
AsregardsstrengtheningofHumanResourcebase,itisestimatedthatdirect
employmentinPharmaceuticalsIndustryhasincreasedfromabout6.9lacspeoplein
2006to8lacspeoplein2008with20%ofthismanpowerbeingengagedinresearchand
testing.Theprojectedhumanresourcerequirementisaroundanestimated21.5lacsby
2020.BasedonthisitisproposedtofilltheHRrequirementsthroughSchemessuchas
(a)ExpandingthestudentoutputatNIPERMohali(b)Developmentof6NewNIPERS
alreadysanctionedinthe11thPlanand(c)Settingupof10NewNIPERsetc.
The12thPlanDocumenthighlightsthevitalroleDrugpriceplayinaccesstoessential
medicinesacrosstheworld.WhileitisafactthatthedrugsmanufacturedinIndiaare
consideredtobeamongstthelowestpricedinternationally,still,avastsectionofIndian
populationisnotinapositiontoaccesstheneededhealthcareaswellasthemedicines
duetovariousreasonsofaccessandaffordability.Accordingly,therecommendations
madebytheTaskForceunderDr.PronabSenmadehavebeenconsideredandadraft
NationalPharmaceuticalsPricingPolicyhasbeenformulatedwhichseekstocontrolthe
pricesofessentialdrugsaspertheNationalListofEssentialMedicines2011(NLEM‐
2011).Furthertothis,theDepartmentwouldtakeupissuespertainingtoprescription
v
andpromotionofunbrandedgenericdrugswiththeDepartmentofHealth.Issues
relatedtopricingofpatentedmedicineswouldalsobesuitablyconsideredinthelightof
needforpromotingindustrygrowthandresearchaswellasdevelopmentofnewdrugs
alongwithaffordabilityofnewpatentedmedicinesforbettertherapeutictreatmentof
themasses,especiallyindiseasespertainingtocancerandHIV.Accordingly,itis
proposedtocontinueschemesforstrengtheningoftheNPPA,forsuchfunctionsas‐(a)
StrengthenMonitoringandEnforcementWork,(b)BuildingConsumerAwareness
aboutpricingandavailabilityand(c)CreationofNPPACellsinStates,etc.
ThepresentmarketsizeofMedicalDevicesandEquipmentsisaroundRs15,000crores.
ThemedicaldeviceIndustryinIndiaisverynascentandislargelyimportdependent.More
than65%ofIndia’srequirementofmedicaldevicesandequipmentsaremetthrough
importswithdomesticproductionbeinglargelyrestrictedtolowtechnologydisposable
equipments.TheSWOTanalysisofMedicalDeviceIndustryshowsthatitsmajorstrengths
are–(a)WelldevelopedMicroelectronic,Telecommunication,SoftwareandPrecision
EngineeringIndustry,(b)Abilitytoattractforeigninvestmentsand(c)Abilitytohandlelow
valuelargevolumeproductionasperglobalqualitystandards.Themajorweaknessesare–
(a)Lowpercapitaexpenditureonhealthcare&lowhealthinsurance,(b)Lackofadequate
andtrainedmanpower,(c)Lackofincubationandsuitableecosystem,(d)Lackof
regulation/standardsetc.Themajoropportunitiesare‐ (a)Hugemarketpotential,(b)
Growingopportunitiesinexportmarket,(c)Growingdemandonaccountofchanging
demographicprofile,increasingincidencesoflifestylediseaseslikecancer,CNSand
diabetics,etc.Themajorthreatsare–(a)Growingcompetitioninexportmarkets,(b)
Increasingdependencyonimports,(c)Unorganizedmarketformedicaldisposables,(d)
Lackofregulationsinmedicaldisposablesandsurgicalitems.Togiveaboosttothe
MedicaldevicesSector,anumberofschemeshavebeenproposedsuchasfor‐(a)
Settingupgreen‐fieldMedicalDevicesParkand(b)SettingupNationalCenterforR&Din
MedicalDevicesatNIPERAhmedabad
The11thPlanaimedatmakingthesickCPSUsfinanciallyviablethroughsupportfor
modernisationandrehabilitationaswellaswaiverofduesandpaymentofVRSpackages.
vi
Accordingly,HindustanAntibioticsLtd(HAL)andBengalChemicalsandPharmaceuticals
Ltd(BCPL)weregivensupportofoverRs.1000croresinthe11thPlanperiodinvolving
waiver,settlementandcashassistanceformodernisation.KarnatakaAntibioticsand
PharmaceuticalsLtd(KAPL)andRajasthanDrugsandPharmaceuticalsLtd(RDPL)were
alsogivenfinancialsupportfollowingtheirdelinkingfromHALandIDPLrespectivelyso
astomakethemindividuallymoreviableandindependentinpursuinggrowthplans.As
aresult,thePharmaPSUshavebeenabletoachieveacombinedbusinessofmorethan
Rs.600crores.Itisexpectedthattheywouldgrowinthe12thPlanforwhich
Governmentsupportformarketingwillberequired.Accordingly,nomajorschemehas
beenproposed.TherehabilitationofIndianDrugsandPharmaceuticalsLtd(IDPL)could
beconsideredduringthe12thPlanasperapprovaloftheCabinet.
Asregardsaccesstoqualitydrugsataffordableprices,apartfromthepricecontroland
monitoringinitiative,theGovernmentproposestofurtherexpandtheJanAushadhi
Schemestartedinthe11thPlanwiththeobjectiveofmakingavailableunbranded
genericmedicinesataffordablepricesthroughtheproposed3000dedicatedoutlets
acrossthecountry.The12thPlandocumenthassupportedtherevisedbusinessplanof
theJanAushadhiSchemewhichhasbeenpreparedafteradetailedanalysisofshortfalls
andpossiblesolutionsincludingspecialfocusonsupplychainmanagement.
Finally,theDepartmentofPharmaceuticalshasnotbeenabletotakeuporlaunchany
majornewactivityinlinewithitsmandateevenafterthreeyearsofitsexistence.The
mainreasonforthisliesinlackoftechnicalcapabilitysinceitsinception.Thereforethere
isanurgentneedofstrengthentheDepartmentintermsofrequiredhumanresources.
Forthis,supportofatechnicalcadrehasbeenproposed.
Itisexpectedthatgoingforwardinthe12thPlan,theDepartmentwouldbeabletoplaya
vitalcatalyticroleinspurringthegrowthofthepharmaceuticalindustryinthecountry
andstrengthenittobecomeagloballeaderinthecomityofnationsintheglobal
economy.
vii
SUMMARYOFSCHEMES
SlNoSchemeBriefdescriptionBudget(Rs
Crores)
1INDUSTRYPROMOTION&DEVELOPMENT
1.1ExistingSchemes–Continued
from11thPlan
(i)PharmaPromotionand
DevelopmentScheme(PPDS)
GrantassistanceforIndustryStudies,Workshops,
Seminars,etc
10
(ii)IntellectualPropertyRights
FacilitationCenters
CapacitybuildingGrantassistance(capitaland
revenue)forsettingupofIPRcentresby
Pharmaexcil,Industrybodies,etctoassistindustryin
IPRmatters
26.5
1.2NewSchemes
(i)InternationalPharma
CooperationInitiative(IPCI)
SettingupofJointtestingandlabfacilitiesfor
certificationofIndianpharmaproducts,
developmentoflocallysustainableformulationsand
drugdeliverysystemsandothermutuallybeneficial
schemes
50
(ii)UpgradationofSMEsto
WHO‐GMPstandards
Interestbasedsubsidyschemeattherateofabout
Rs1crsperunitofassistancetobeimplementedin
partnershipwithIDBI/SIDBIforupgradingSMEsto
WHO‐GMPmanufacturingstandardstocapitalizeon
theGenericsOpportunity–about1200unitsoutof
about10,563SMEsinthecountry
1200
(iii)Capacitybuildingthrough
trainingof5000Working
ProfessionalsinWHO‐GMP
Toprovidemanufacturingcapabilityupgradation
assistanceforcapitalexpenditure,skilldevelopment
ofpersonnelrequiredforsuchupgradationand
sustenanceofsupplyofskilledpersonnel.
250
(iv)UpgradationofSMEsto
USFDA/EDQM/TGAandother
InternationalStandards
SpecificassistanceforstandardshigherthanWHO‐
GMPtoselectedSMEs–250innostobuild
Competitivenessofveryhighstandardsandsecond
lineofinternationallycapableindustryforhighvalue
pharmaproductsforstrongregulatedbuthighvalue
markets
500
(v)SettingupofoneNational
andfiveRegionalFormulation
Developmentand
Manufacturingstandards
trainingcentres
SchemetosetupFormulationdevelopmentcentres
totapthepatentcliffopportunityandbecome
globalleaderinGenericsandBio‐similars
160
viii
(vi)Establishmentand
upgradationof10Pharma
GrowthClusters
Infrastructurebuildingforpharmaindustry
particularlyforSMEs–buildingonstrengthof
existingClusterssoastoprovideinfrastructuregaps
forhigherproductionincludingtakingcareof
environment,powerandlabstesting,etcneeds.
500
(vii)Infrastructuresupportfor
ColdChainforhighenddrugs
forexports
Inordertoenhanceexportscapabilityforhighend
drugsrequiringexactcoldchainstandardstillthe
timetheyareexportedfromthecountryinlightof
stringentdevelopedmarketrequirements
50
(viii)Schemeforenvironment
standardscomplianceand
requiredinfrastructure
supportincludingcapacity
building
providingfinancialandtechnicalassistanceto
improvefinancialsustainabilityofSMEsonone
handandalsosafeguardtheenvironmentfrom
thehazardsassociatedwiththeunplanned
growthoftheindustry.
100
2R&D,CAPACITYBUILDINGANDEMPLOYMENT
2.1ContinuingSchemes
2.1.1ForNIPERMohali
(i)ThecontinuationofthePG
andthePhDeducation
ThecontinuationofthePGandthePhDeducation
atpresentstrengthlevelswouldrequirebudgetary
support
100
(ii)CapacityEnhancementfor
supportingrequiredindustry
humanresourcesandcapacity
buildingrequirementbythe
Institute
a. Additional1000PGsandPhDs
b. TrainingIndustryandRegulatorypersonnel
c. PublicHealthandPharmacovigilanceTrg.
d. InfrastructureUpgradation
200
25
25
250
2.1.2ForNewNIPERs
(i)Permanentestablishmentand
operationof6NewNIPERs
2000
2.1.3OtherSchemes
(i)SettingupofNationalCenter
forPhyto‐pharma
development
MajorcapitalexpenditureofaboutRs100crsbeing
metfromDONER.Presentallocationsoughtfor
initialyearsoperationasperadvicefromDONER
20
(ii)GLP/GCP/AnimalHouseLab
Schemes
ForsettingupofGLPcompliantLabs,GCPcompliant
LabandaAnimalHouseLabonPPPbasisisunder
implementation
50
ix
(iii)ContinuingR&DSchemesFor
NiperMohali
NiperMohaliispresentlyimplementinganumberof
projectsinR&Dforvariouspharmaareaslike
neglecteddiseases,infectiousdiseases,vectorborne
diseases,etc.Inadditionanumberofprojectsare
beingimplementedforPublichealth,
PHarmacovigilance,Regulatorycapacitybuildingfor
academiaandindustry,etc.
50
(iv)ContinuingschemeatNew
Nipers
JointdevelopmentofTuberculosisrelateddrugsat
NiperAhmedabadandAIIMS,Delhi
1
2.2NewSchemes
(i)EstablishmentofNewNew
NIPERs
Inordertomeetthegapofaverylowgraduateto
postgraduatepharmaeducationseatscapacityof
1:10(51000graduateseatsvs5100PGseatsinthe
entirecountry)thereisneedtosetupfurthernew
Nipersapartfromthe6approvedinthe11thplan.It
isproposedtosetup10NewnewNIPERs
3000
(ii)NewSchemesatNiperMohali R&DCentreforBiologicalsandNCEsR&DCentrefor
NDDS,Settingup20NewIncubators,Incentive
SchemeforCROsDevptforNew,DrugDiscovery
PartnershipwithInternationalCentresofExcellence
825
(iii)PharmaVentureCapitalFundToconsiderinvestmentofidentifiedfundsintoa
newlycreatedspecialisedprivateequity/venture
capitalfundthatundertakesR&Dinvestmentsinto
companiesinthepharmaceuticalindustry
500
(iv)PharmaInnovationand
InfrastructureDevelopment
Initiative(PIIDI)
Developtechnicalandinnovationcapacityof
Indianpharmaformanufacturingquality
affordablemedicines,developInternational
competitivenessoftheIndianPharmasoasto
bethelargestproducerofgenericmedicinesin
theworld,TomakeIndiaapreferred
destinationforglobalinitiativesincuringthe
world’sailmentsspeciallythedevelopingworld
inavaluebasedmanner
2000
(v)AtNIPERHyderabad:Setting
upNationalCenterforR&Din
BulkDrugsatNIPER
Hyderabad
BuildcompetitivenessthroughInnovationand
ProductivityefficienciesintheAPIindustry.Alsotap
Genericsopportunityandmeetcompetitionof
China,etc.
56
x
(vi)AtNIPERKolkattaNational
Pharmaceutical
NanotechnologyCenter
TobesetupatNIPERKolkattafordevelopmentof
Nano‐materialsfrominorganicsubstratesfor
innovativedrugsanddrugdeliverysystems
50
(vii)SettingupNationaland
RegionalBiosimilarExpertise
Centers
Toprovideexpertadviceandassistancetoindustry
onregulatoryissuespertainingtoClinicalTrials,
TestingandApprovalprocessforBiosimilars–One
nationalcentreatBangaloreand3regionalcentres
atChandigarh,HyderabadandAhmedabad
60
(viii)SettingupofaIndustry
focusedAnimalHouse
EndtoendservicesfromPrimatestosmallanimals
forpre‐clinicaldrugdevelopment
100
(ix)SupporttoAcademia,
ResearchInstitutionsand
privatesectorforExtraMural
Research
Forfundingbothacademiaindividually,asan
institutionandprivatecompaniesfortargeted
drugdevelopmentincludingassistancefor
clinicaltrials.
100
(x)SupporttoAcademia,
ResearchInstitutionsand
privatesectorforExtra
Labsupgradation
Forfundingupgradationoflabsintheprivateand
governmentsectorwithsharingbasison50‐50
patternforthelabupgradationforequipments
deployedfordrugdevelopmentunderspecifically
identifiableprojects
10
(xi)AllNIPERs:International
cooperationinR&D
TopromoteR&DinCISanddevelopingcountriesfor
mutualadvantages
25
3Pricing
3.1Continuingschemes
(i)MonitoringandEnforcement
Work
StrengtheningtheExistingMonitoringand
EnforcementWork
2
(ii)AwarenessandPublicitytConsumerAwarenessandPublicitythroughPrint,
ElectronicandotherMedium
20
3.2NewSchemes
(i)CreationofNPPA‐State
GovernmentCoordination
CellsinStates
Schemeoriginallyproposedin11thPlanbutnot
approvedbyPlanningCommission.Henceproposed
for12thPlan.Willhelpinstrengtheningthe
MonitoringObjectiveofdrugsprices.
25
(ii)SchemeforInteractionwith
States
Schemeoriginallyproposedin11thPlanbutnot
approvedbyPlanningCommission.Henceproposed
for12thPlan.Willhelpinstrengtheningthe
MonitoringObjectiveofdrugsprices.
2
xi
4MedicalDevicesindustrydevelopment
(i)Settingupgreen‐fieldmedical
devicesandequipmentparks.
TappingtheopportunityUS$200Bnglobalindustry300
(ii)SettingupNationalCenterfor
MedicalDevicesatNIPER
Ahmedabad.
PromotingindigenousR&DinMedicaldevicessector50
5CPSUsandJanAushadhi
(i)IDPL
Tokenallocationforminimalregulatory
compliances.Actualwoulddependontheapproval
byCabinetforrevivalofIDPLpackage
10
(ii)HAL MinimalUpgradationoffacilities 10
(iii)BCPLMeetinggapsintherevivalpackage 10
(iv)JanAushadhiContinuingschemetobestrengthenedinthe12th
planforensuringaccesstoaffordablequality
unbrandedgenericmedicinesforthepoormasses
200
TOTAL12922.5
xii
METHODOLOGY
(A) ConstitutionofWorkingGroup
PlanningCommissionconstitutedaworkinggrouponDrugsandPharmaceuticals,videtheir
letternoI&M‐3(25)/2011,dated10.5.2011.
(a)TermsofReference(TOR)oftheWorkingGroup
TheworkinggroupwasgivenfollowingTermsofReference:
i. Toarticulatethelongtermgoalstobeachievedintermsofgrowth,
competitivenessandshareinglobaltradeforthedomesticDrugs&
PharmaceuticalIndustries.
ii. ToreviewthecurrentstatusofdomesticPharmaceuticalsSectorhighlightingthe
achievementsduringthe11thPlanandreasonsformajordeviation/shortfall,if
any,inrespectoffulfilmentoftargetsandidentifyingareasofstrengthand
weaknessoftheIndianindustryvis‐à‐visinternationalDrugsand
PharmaceuticalsIndustry.
iii. Tobenchmarkindigenousdrugs&pharmaceuticalsindustryagainstinternational
drugs&pharmaceuticalsindustryandsuggestappropriatemeasuresforbridging
thegapswherenecessary,includingtheneedsforfurtherR&Dactivitiesand/or
technologycollaborationforupgradingtechnology.
iv. Toexaminethestructureandcapabilityofthedomesticdrugs&pharmaceutical
industry,itsexporttrend&performanceandidentifyemergingareashaving
specificpotentialforgrowthandcompetitivenessaswellastosuggestmeasures
forputtingtheindigenousindustryonsoundfootingandgrowthpathkeepingin
viewthegoalstobearticulatedunderitem1above.
v. ToreviewthepresentstatusofWHO‐GMP(WorldHealthOrganization–Good
ManufacturingPractice)certificationandschedule‐Mcomplianceandsuggest
measuresforraisingthelevelofcompliancebymanufacturersofdrugsand
pharmaceuticalproductsinthecountry.
xiii
vi. Toexaminetheimpactofnewpatentregimeondomesticpharmaceutical
industryincludingitsimplicationondrugprices.
vii. Tostudytheefficacyandappropriatenessofcurrentdrugpricingsystemaswell
asitscontrolandenforcementmechanismandsuggestmeasuresforfurther
improvement,ifapplicable.
viii. Toassessthepresentcapabilityforinnovationvis‐à‐visR&Dstatusofthe
domesticDrugs&Pharmaceuticalsindustryandtosuggestwaysandmeansto
improvethedomesticefforts,enhanceindustryparticipationandintensify
Industry‐Institutional/academialinkagetopromotedomesticR&Dfor
establishmentofitsinternationalcompetitivenessandmeetingtheemerging
challengesarisingoutoftheWTOregime.
ix. Tostudychangeinstructureofdomesticpharmaceuticalsindustryinthelightof
currenttrendofmerger&acquisitions/takeovers/collaborationsandits
correlationwithrelatedFDInormsandsuggestmeasurestosafeguardnational
interests.
x. ToexaminethetrendofemploymentgrowthintheDrugsandPharmaceuticals
industryandprojectlikelyrequirementofskilledmanpowerduringtheTwelfth
Planperiodaswellastomeetthelongtermgoals.Tosuggestmeasuresfor
puttinginplaceadequateacademicandtraininginfrastructureandfacilitiesto
meettherequirements.
xi. Toassesstheadequacyandrelevanceofpresentregulatorymechanismofdrug
andpharmaceuticalssectorandexamineneedforfurtherstrengtheningtotackle
themenaceofspuriousdrugsetc.andexamineneedforanapexauthorityto
controlprice,qualityandsupplyofdrugs.
xii. Tosuggestmeasurestowardsimprovementofaccessibilityofessential
medicinesforcommonmanparticularlythepoorersectionsofthepopulation
andtoidentifystepsrequiredforfacilitatingimplementationoftheNational
HealthPolicy.
xiii. Toassessthecurrentstatusofdomesticmedical/surgicalequipmentindustry,its
exportpotentialandcompetitivenessandsuggestmeasuresforimprovement
andaugmentationofcapabilities,wherenecessary.
xiv
xiv. Toindicatethemilestonestobeachievedinthe12thPlaninthecontextoflong
termgoalsasperitem‐IoftheToRandrecommend
pogrammes/schemes/measuresthataretobeinitiated,continuedor
discontinuedinthe12thPlanperiodandestimatedfundrequirement.
xv. Tomakeanyotherrecommendationsasmaybeappropriateforsustained
growthandcompetitivenessofthesector.
(b)MembersoftheWorkingGroup
Theworkinggroupconsistedoffollowingmembers:
1.Secretary,DepartmentofPharmaceuticals(DOP) Chairman
2.Secretary,DepartmentofScientific&Industrial
Research/DG,CouncilofScientific&Industrial
ResearchorhisRepresentative
Member
3.PrincipalAdviser/Adviser(Health),Planning
Commission
Member
4.Secretary,MinistryofHealth&FamilyWelfareor
Nominee
Member
5.Secretary,DepartmentofScience&Technologyor
Nominee
Member
6.Secretary,DepartmentofBio‐TechnologyorNominee Member
7.Secretary,DepartmentofConsumerAffairsorNominee Member
8.Chairman,NationalPharmaceuticalPricingAuthority Member
9.AdditionalSecretary&FinancialAdviser,Department
ofPharmaceuticals(DOP)
Member
10.Adviser(I&VSE),PlanningCommission Member
xv
11.JointSecretary(PI),DepartmentofPharmaceuticals
(DOP)
Member
12.JointSecretary(Pharma),Departmentof
Pharmaceuticals(DOP)
Member
13.Director,CentralDrugsResearchInstitute,Lucknow Member
14.Director,NationalInstituteofPharmaceutical
Education&Research,Mohali,Punjab
Member
15.Chairman,PharmaceuticalsExportPromotionCouncil,
Hyderabad
Member
16.President,IndianDrugsManufacturesAssociation Member
17.Chairman,ConfederationofIndianPharmaceuticals
Industry
Member
18.SecretaryGeneral,IndianPharmaceuticalsAlliance Member
19.President,OrganisationofPharmaceuticalsProducers
ofIndia(OPPI)
Member
20.President,BulkDrugManufacturersAssociation Member
21.Chairman,Dr.Reddy’sLaboratoriesLtd.,Hyderabad Member
22.Chairman,CIPLALimited,Mumbai Member
23.Chairman,LupinLimited,Mumbai Member
24.EconomicAdviser,DepartmentofPharmaceuticals
(DOP)
Member
xvi
(B) ConstitutionofSubWorkingGroups
BasedonthethrustoftheToRs,DepartmentofPharmaceuticalsconstitutedfoursub
workinggroups.ThemembersandToRsofthesubworkinggroupsareasbelow:
(a) Sub‐GrouponStatusandStructureofthePharmaceuticalIndustry
CompositionoftheSub‐Group
1.JointSecretary(AJ),DepartmentofPharmaceuticals Chairman
2.NomineeofSecretary,DepartmentofScientific&Industrial
Research
Member
3.NomineeofSecretary,MinistryofHealth&FamilyWelfareMember
4.NomineeofSecretary,DepartmentofScience&Technology Member
5.Adviser(I&VSE),PlanningCommission Member
6.Chairman,PharmaceuticalExportPromotionCouncil,
Hyderabad
Member
7.President,IndianDrugsManufacturersAssociation Member
8.Chairman,ConfederationofIndianPharmaceuticalsIndustry Member
9.SecretaryGeneral,IndianPharmaceuticalsAlliance Member
10.President,OrganisationofPharmaceuticalsProductsof
India(OPPI)
Member
11.President,BulkDrugManufacturersAssociation Member
12.DeputyDirectorGeneral,DepartmentofPharmaceuticals Member
13.Director(BKS)MemberSecretary
TermsofReference(TOR)
(i) Toarticulatethelongtermgoalstobeachievedintermsofgrowth,
competitivenessandshareinglobaltradeforthedomesticDrugs&
PharmaceuticalIndustries.
xvii
(ii) ToreviewthecurrentstatusofdomesticPharmaceuticalsSectorhighlightingthe
achievementsduringthe11thPlanandreasonsformajordeviation/shortfall,if
any,inrespectoffulfilmentoftargetsandidentifyingareasofstrengthand
weaknessoftheIndianindustryvis‐à‐visinternationalDrugsand
PharmaceuticalsIndustry.
(iii) Tobenchmarkindigenousdrugs&pharmaceuticalsindustryagainstinternational
drugs&pharmaceuticalsindustryandsuggestappropriatemeasuresforbridging
thegapswherenecessary,includingtheneedsforfurtherR&Dactivitiesand/or
technologycollaborationforupgradingtechnology.
(iv) Toexaminethestructureandcapabilityofthedomesticdrugs&pharmaceutical
industry,itsexporttrend&performanceandidentifyemergingareashaving
specificpotentialforgrowthandcompetitivenessaswellastosuggestmeasures
forputtingtheindigenousindustryonsoundfootingandgrowthpathkeepingin
viewthegoalstobearticulatedunderitem1above.
(v) Tostudychangeinstructureofdomesticpharmaceuticalsindustryinthelightof
currenttrendofmerger&acquisitions/takeovers/collaborationsandits
correlationwithrelatedFDInormsandsuggestmeasurestosafeguardnational
interests.
(vi) Toassessthecurrentstatusofdomesticmedical/surgicalequipmentindustry,its
exportpotentialandcompetitivenessandsuggestmeasuresforimprovement
andaugmentationofcapabilities,wherenecessary.
(vii) Toindicatethemilestonestobeachievedinthe12thPlaninthecontextoflong
termgoalsasperitemIoftheToR(ByPlanningCommission)andrecommend
pogrammes/schemes/measuresthataretobeinitiated,continuedor
discontinuedinthe12thPlanperiodandestimatedfundrequirement.
(viii) Tomakeanyotherrecommendationsasmaybeappropriateforsustained
growthandcompetitivenessofthesector.
xviii
(b) Sub‐GrouponRegulatoryIssuesinthePharmaceuticalIndustry
CompositionoftheSub‐Group
1.JointSecretary(DC),DepartmentofPharmaceuticals Chairman
2.NomineeofSecretary,MinistryofHealth&FamilyWelfareMember
3.NomineeofSecretary,DepartmentofScience&TechnologyMember
4.NomineeofSecretary,DepartmentofBio‐TechnologyMember
5.PrincipalAdvisor/Advisor(Health)orNominee,Planning
Commission
Member
6.DrugControllergeneralofIndia/NomineeMember
7.President,IndianDrugManufacturersAssociation Member
8.Chairman,ConfederationofIndianPharmaceuticalsIndustry Member
9.SecretaryGeneral,IndianPharmaceuticalsAlliance Member
10.President,OrganisationofPharmaceuticalsProductsof
India(OPPI)
Member
11.President,BulkDrugManufacturersAssociation Member
12.Director(MV),DepartmentofPharmaceuticals MemberSecretary
TermsofReference(TOR)
i. ToreviewthepresentstatusofWHO‐GMP(WorldHealthOrganization–Good
ManufacturingPractice)certificationandschedule‐Mcomplianceandsuggest
measuresforraisingthelevelofcompliancebymanufacturersofdrugsand
pharmaceuticalproductsinthecountry.
xix
ii. Toassesstheadequacyandrelevanceofpresentregulatorymechanismofdrug
andpharmaceuticalssectorandexamineneedforfurtherstrengtheningtotackle
themenaceofspuriousdrugsetc.andexamineneedforanapexauthorityto
controlprice,qualityandsupplyofdrugs.
iii. Toindicatethemilestonestobeachievedinthe12thPlaninthecontextoflong
termgoalsasperitemIoftheToR(ByPlanningCommission)andrecommend
pogrammes/schemes/measuresthataretobeinitiated,continuedor
discontinuedinthe12thPlanperiodandestimatedfundrequirement.
iv. Tomakeanyotherrecommendationsasmaybeappropriateforsustained
growthandcompetitivenessofthesector.
(c)Sub‐GrouponPricingandAvailabilityofDrugs
CompositionoftheSub‐Group
1.Chairman,NationalPharmaceuticalPricingAuthority Chairman
2.NomineeofSecretary,MinistryofHealth&FamilyWelfareMember
3.NomineeofSecretary,DepartmentofConsumerAffairsMember
4.Adviser(I&VSE),PlanningCommission Member
5.MemberSecretary,NPPAMember
6.SecretaryGeneral,IndianPharmaceuticalsAlliance Member
7.President,OrganisationofPharmaceuticalsProductsofIndia
(OPPI)
Member
8.President,IndianDrugsManufacturersAssociation Member
9.Chairman,ConfederationofIndianPharmaceuticalsIndustry Member
10.President,BulkDrugManufacturersAssociation Member
11.Director(Monitoring),NPPAMemberSecretary
xx
TermsofReference(TOR)
i. Toexaminetheimpactofnewpatentregimeondomesticpharmaceutical
industryincludingitsimplicationondrugprices.
ii. Tostudytheefficacyandappropriatenessofcurrentdrugpricingsystemaswell
asitscontrolandenforcementmechanismandsuggestmeasuresforfurther
improvement,ifapplicable.
iii. Tosuggestmeasurestowardsimprovementofaccessibilityofessential
medicinesforcommonmanparticularlythepoorersectionsofthepopulation
andtoidentifystepsrequiredforfacilitatingimplementationoftheNational
HealthPolicy.
iv. Toindicatethemilestonestobeachievedinthe12thPlaninthecontextoflong
termgoalsasperitemIoftheToR(ByPlanningCommission)andrecommend
pogrammes/schemes/measuresthataretobeinitiated,continuedor
discontinuedinthe12thPlanperiodandestimatedfundrequirement.
v. Tomakeanyotherrecommendationsasmaybeappropriateforsustained
growthandcompetitivenessofthesector.
(d)Sub‐GrouponR&D,TrainingandEmploymentGenerationinthePharmaceutical
Industry
CompositionoftheSub‐Group
1.Director,NIPER,Mohali,Punjab Chairman
2.NomineeofDG,CouncilofScientific&IndustrialResearchMember
3.NomineeofSecretary,DepartmentofScience&TechnologyMember
4.NomineeofSecretary,DepartmentofBio‐TechnologyMember
xxi
5.ProjectDirector,NIPER,Hyderabad Member
6.Director,CentralDrugsResearchInstitute,Lucknow Member
7.SecretaryGeneral,IndianPharmaceuticalsAlliance Member
8.President,OrganisationofPharmaceuticalsProductsofIndia
(OPPI)
Member
9.Chairman,Dr.Reddy’sLaboratoriesLtd.,Hyderabad Member
10.Chairman,CIPLALimited,Mumbai Member
11.Chairman,LupinLimited,Mumbai Member
12.DeputyDirectorGeneral,DepartmentofPharmaceuticals. Member
13.Director(SCS),DepartmentofPharmaceuticals MemberSecretary
TermsofReference(TOR)
i. Toassessthepresentcapabilityforinnovationvis‐à‐visR&Dstatusofthe
domesticDrugs&Pharmaceuticalsindustryandtosuggestwaysandmeansto
improvethedomesticefforts,enhanceindustryparticipationandintensify
Industry‐Institutional/academialinkagetopromotedomesticR&Dfor
establishmentofitsinternationalcompetitivenessandmeetingtheemerging
challengesarisingoutoftheWTOregime.
ii. ToexaminethetrendofemploymentgrowthintheDrugsandPharmaceuticals
industryandprojectlikelyrequirementofskilledmanpowerduringtheTwelfth
Planperiodaswellastomeetthelongtermgoals.Tosuggestmeasuresfor
puttinginplaceadequateacademicandtraininginfrastructureandfacilitiesto
meettherequirements.
iii. Toindicatethemilestonestobeachievedinthe12thPlaninthecontextoflong
termgoalsasperitem‐IoftheToR(ByPlanningCommission)andrecommend
xxii
pogrammes/schemes/measuresthataretobeinitiated,continuedor
discontinuedinthe12thPlanperiodandestimatedfundrequirement.
iv. Tomakeanyotherrecommendationsasmaybeappropriateforsustained
growthandcompetitivenessofthesector.
AstheToRswerehavingnomentionofCentralPublicSectorUndertakings(CPSUs)inthe
DepartmentofPharmaceuticals,itwasdecidedtohaveasubgrouponCPSUsalso.
Thesubgroupconsistedoffollowingmembers
1.JointSecretary(DC),DepartmentofPharmaceuticals Chairman
2.CMD,IDPLMember
3.MD,HALMember
4.MD,KAPLMember
5.MD,BCPLMember
6.UnderSecretary(ShriA.K.Sah) MemberSecretary
TheToRsofthesubgroupareasbelow:
i.Toarticulatethelongtermgoalstobeachievedintermsofgrowthand
competitivenessofPharmaPSUs.
ii.Toindicatethemilestonestobeachievedinthe12thPlaninthecontextoflongterm
goalsasperitem(i)aboveandrecommendprogrammes/schemes/measuresthat
aretobeinitiated,continuedordiscontinuedinthe12thPlanperiodandestimated
fundrequirement.
iii.Tomakeanyotherrecommendationsasmaybeappropriateforsustainedgrowth
andcompetitivenessofthesector.
xxiii
TheworkinggrouponDrugsandPharmaceuticalsfirstmeton29.06.2011.Thereafter
differentsubworkinggroupsheldtheirmeetingsseparatelyandfinallysubmittedtheir
reportswhichwasseenandanalysedbytheworkinggroupmeetingheldon12.08.2011.
(C) RearrangementofToRs
TheToRshavebeenarrangedinvariousChaptersbasedonthefocusareaasbelow:
Chapter1‐IndustryStructure&SWOTAnalysisconsistsoffollowingToRs:
(i) Toarticulatethelongtermgoalstobeachievedintermsofgrowth,
competitivenessandshareinglobaltradeforthedomesticDrugs&
PharmaceuticalIndustries.
(ii) ToreviewthecurrentstatusofdomesticPharmaceuticalsSectorhighlightingthe
achievementsduringthe11thPlanandreasonsformajordeviation/shortfall,if
any,inrespectoffulfilmentoftargetsandidentifyingareasofstrengthand
weaknessoftheIndianindustryvis‐à‐visinternationalDrugsand
PharmaceuticalsIndustry.
(iii) Tobenchmarkindigenousdrugs&pharmaceuticalsindustryagainstinternational
drugs&pharmaceuticalsindustryandsuggestappropriatemeasuresforbridging
thegapswherenecessary,includingtheneedsforfurtherR&Dactivitiesand/or
technologycollaborationforupgradingtechnology.
(iv) Toexaminethestructureandcapabilityofthedomesticdrugs&pharmaceutical
industry,itsexporttrend&performanceandidentifyemergingareashaving
specificpotentialforgrowthandcompetitivenessaswellastosuggestmeasures
forputtingtheindigenousindustryonsoundfootingandgrowthpathkeepingin
viewthegoalstobearticulatedunderitem1above.
(v) ToreviewthepresentstatusofWHO‐GMP(WorldHealthOrganization–Good
ManufacturingPractice)certificationandschedule‐Mcomplianceandsuggest
measuresforraisingthelevelofcompliancebymanufacturersofdrugsand
pharmaceuticalproductsinthecountry.
xxiv
(ix) Tostudychangeinstructureofdomesticpharmaceuticalsindustryinthelightof
currenttrendofmerger&acquisitions/takeovers/collaborationsandits
correlationwithrelatedFDInormsandsuggestmeasurestosafeguardnational
interests.
(xi) Toassesstheadequacyandrelevanceofpresentregulatorymechanismofdrug
andpharmaceuticalssectorandexamineneedforfurtherstrengtheningtotackle
themenaceofspuriousdrugsetc.andexamineneedforanapexauthorityto
controlprice,qualityandsupplyofdrugs.
Chapter2:Research&DevelopmentconsistsoftheToR(viii)whichisasbelow:
(viii) Toassessthepresentcapabilityforinnovationvis‐à‐visR&Dstatusofthe
domesticDrugs&Pharmaceuticalsindustryandtosuggestwaysandmeansto
improvethedomesticefforts,enhanceindustryparticipationandintensify
Industry‐Institutional/academialinkagetopromotedomesticR&Dfor
establishmentofitsinternationalcompetitivenessandmeetingtheemerging
challengesarisingoutoftheWTOregime.
Chapter3:CapacityBuildingandEmploymentconsistsofToR(x),whichisasbelow:
(x) ToexaminethetrendofemploymentgrowthintheDrugsandPharmaceuticals
industryandprojectlikelyrequirementofskilledmanpowerduringtheTwelfth
Planperiodaswellastomeetthelongtermgoals.Tosuggestmeasuresfor
puttinginplaceadequateacademicandtraininginfrastructureandfacilitiesto
meettherequirements.
Chapter4:PricingandAvailabilityconsistsofToRs(vi),(vii)and (xii)whichareasbelow:
(vi) Toexaminetheimpactofnewpatentregimeondomesticpharmaceutical
industryincludingitsimplicationondrugprices.
xxv
(vii) Tostudytheefficacyandappropriatenessofcurrentdrugpricingsystemaswell
asitscontrolandenforcementmechanismandsuggestmeasuresforfurther
improvement,ifapplicable.
Chapter5MedicalDevicesconsistsofToR(xiii)whichisasbelow:
(xiii)Toassessthecurrentstatusofdomesticmedical/surgicalequipmentindustry,its
exportpotentialandcompetitivenessandsuggestmeasuresforimprovement
andaugmentationofcapabilities,wherenecessary.
Chapter6isrelatedtoCentralPublicSectorUndertakings.
Chapter7isResourceRequirementintheDepartmentofPharmaceuticals
Chapter8SchemesandProposalsconsistsofToRs(xiv)and(xv)whichreadasbelow:
(xiv) Toindicatethemilestonestobeachievedinthe12thPlaninthecontextoflong
termgoalsasperitem‐IoftheToRandrecommend
pogrammes/schemes/measuresthataretobeinitiated,continuedor
discontinuedinthe12thPlanperiodandestimatedfundrequirement.
(xv) Tomakeanyotherrecommendationsasmaybeappropriateforsustained
growthandcompetitivenessofthesector.
Page 1 of 153
Chapter1
PHARMACEUTICALSINDUSTRY:STRUCTURE&SWOTANALYSIS
1.1 INTRODUCTION
TheIndianpharmaceuticalIndustryisdrivenbyknowledge,skills,lowproduction
costs,quality.Duetothisthereisdemandfrombothdomesticaswellas
internationalmarkets.Thishasresultedinarobustgrowthofaround14%sincethe
beginningofthe11thPlanin2007fromaboutRs71000crorestooverRs1laccrores
in2009‐10comprisingsomeRs62,055croresofdomesticmarketandexportsof
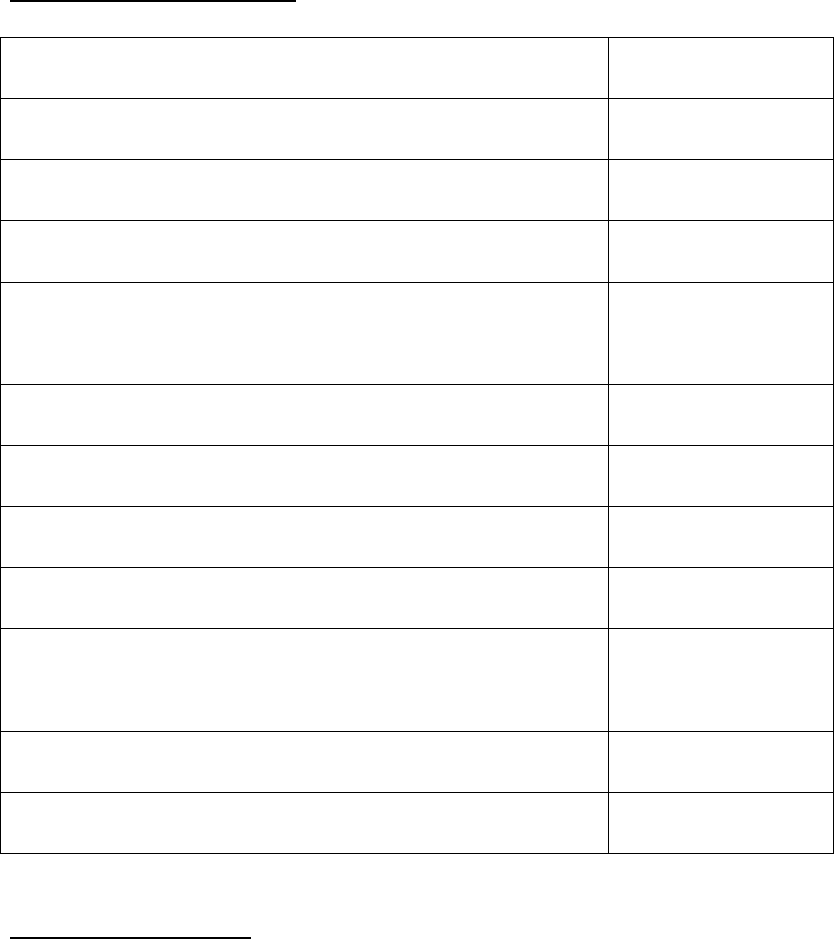
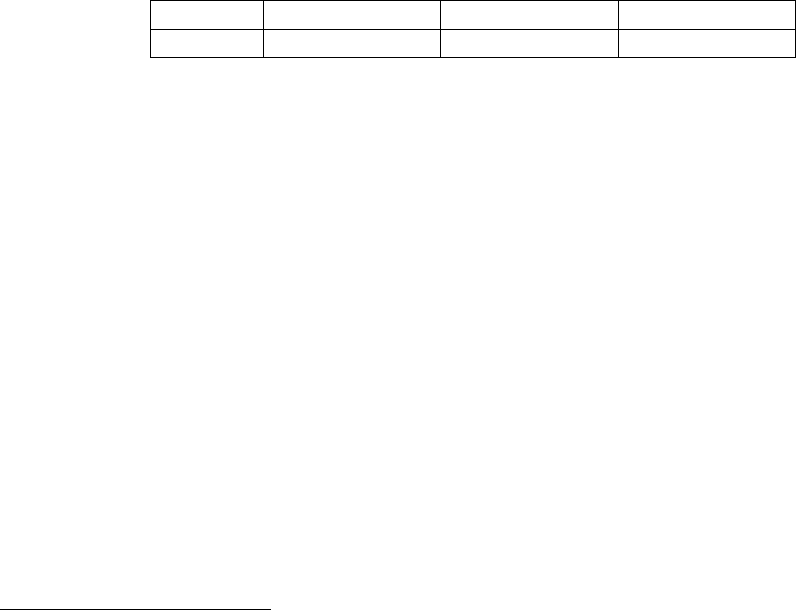
overRs42,154crores(Table‐1).
Table‐1:ExportandDomesticGrowth
*Provisional
TheIndustryisranked3rdgloballyinvolumeand14thinvalue,supplyingaround10%oftotal
globalproduction1.Thisalsoamountstoaround20%oftotalvolumeofglobalgenerics.Thus
every5thTablet,CapsuleandInjectableingenericsdrugsconsumedanywhereintheworld
ismanufacturedinIndia.Infact,Indiamanufactures30%oftheworldrequirementofAnti‐
HIVdrugs.Allofthisgrowthhasbeenwithaffordablepricetothecommonman–oneofthe
lowestintheworld.Goingforward,itisexpectedthatthegrowthwillbesustained
notwithstandingtherecentinitialdecreaseduetoglobaleconomicslowdownas
broughtoutinthedecreasedgrowthratefrom18.65%in2009‐10over2008‐09to
9.38%intheperiod2009‐102.
1.CygnusReport‐CygnusBusinessConsultingandResearchisaservicesorganizationfocusingonanalysisand
researchofEconomies,IndustriesandCompanies
2.FICCI‐IMSReport
YearExportsGrowth DomesticGrowth%TotalGrowth%
Mar20062123023.233998917.176121919.21
Mar20072566620.894536713.457103316.03
Mar20082935414.37 50946 12.30 8030013.04
Mar20093982135.66554548.859527518.65
Mar201042154*5.866205511.901042099.38

Page 2 of 153
Indianpharmaceuticalindustryistrulyinternationalwithleadinginternational
manufacturerscompetinginIndiandomesticmarketandseveralIndianpharma
companieshavingasignificantpresenceininternationalmarket,especiallyinthe
genericsegment.However,theIndustryisquitefragmentedandcomprisesofnearly
10,500unitswithmajorityoftheminsmallsector.Ofthese,about300‐400unitsare
categorizedasbelongingtomediumtolargeorganizedsectorwiththetop10
manufacturersaccountingfor36.5%ofthemarketshare3.
Medium&LargeDomesticCompanies:Themediumandlargedomesticcompanies
havebeenthedriversofgrowth,contributing75%ofdomesticsalesandover90%of
exports.Theexportoftop50companiesfortheyear2009‐10revealthat
pharmaceuticalindustry’sforayintheglobalmarketisdrivenmainlybythedomestic
companiesasmaybeseenbelow.Thustop50exportersaccountedfor76%oftotal
exportsofRs36,683crin2009‐10.Itisnoteworthythatonlytwoforeigncompanies
featureinthislistcontributinglessthan2%ofthetotalpharmaceuticalexports.
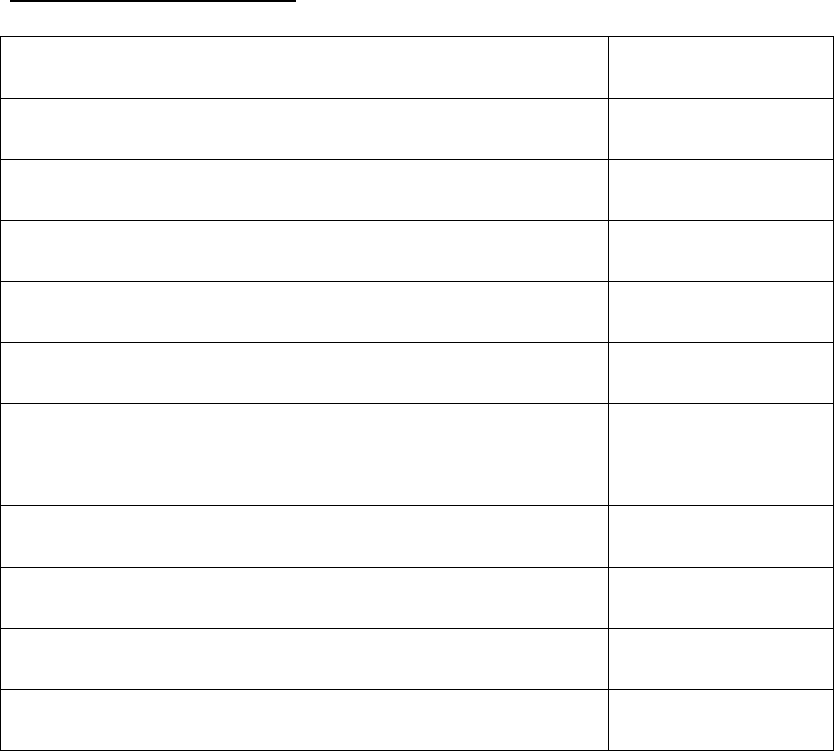
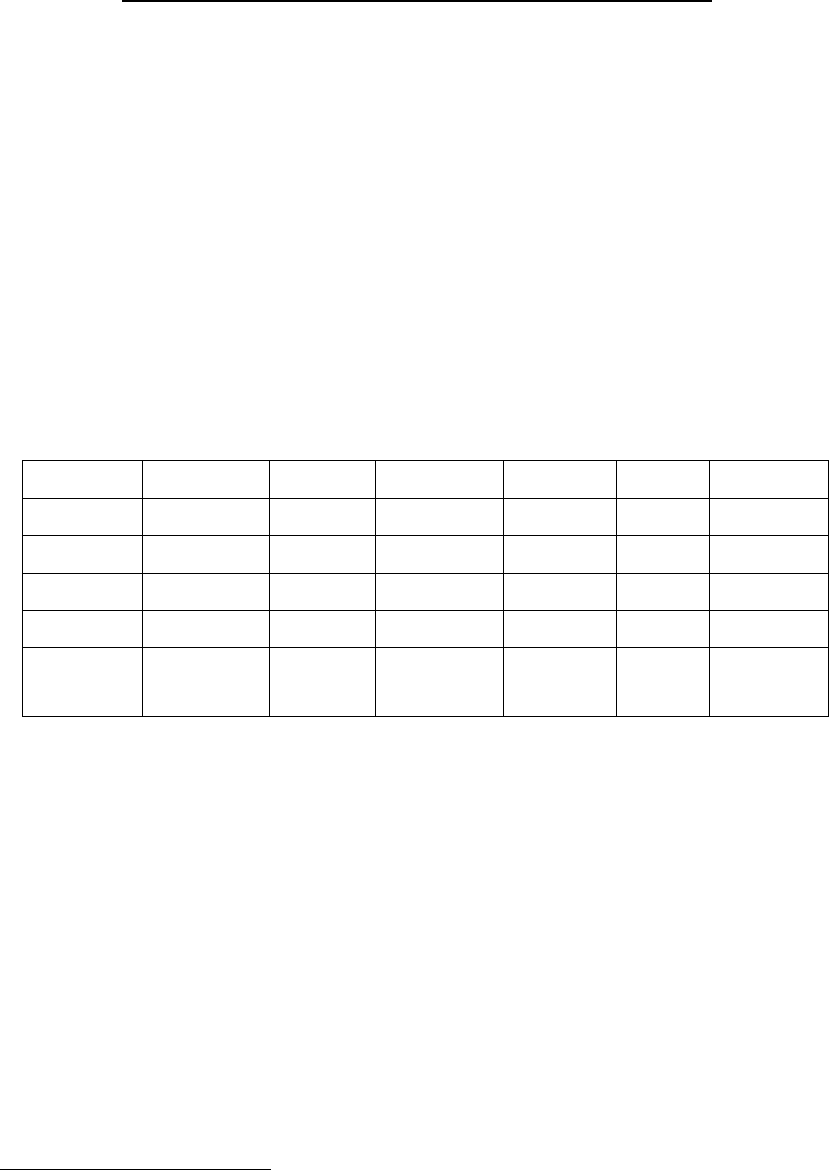
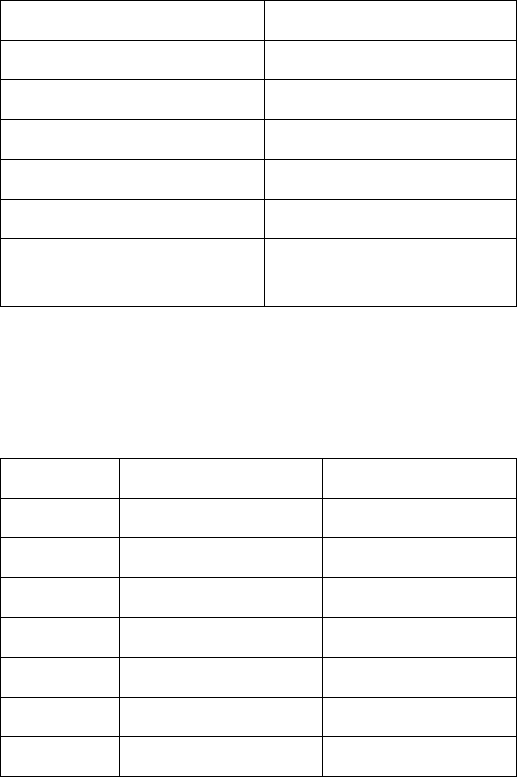
Table–2:Internationalsalesonconsolidatedbasis(Rscrore)2010‐114
3 Indian Institute of Management, Bangalore – Report on “Viable Strategies to make Pharmaceutical CPSEs
Self-Reliant” prepared for DoP in 2009-10
4 Pharmabiz analysis
Consolidated International Exports as % of net sales
net sales sales 2010-11
Ranbaxy Labs 8960.77 6771.74 75.6
Dr Reddy's Labs 7236.80 5940.70 82.1
Lupin 5706.82 3983.08 69.8
Cipla 6130.31 3361.49 54.8
Sun Pharma 5721.43 2898.20 50.7
Wockhardt 3751.24 2709.91 72.2
Jubilant Lifescience 3433.40 2369.11 69.0
Cadila Healthcare 4464.70 2288.70 51.3
Biocon 2300.52 1956.79 85.1
Glenmark Pharma 3089.59 1955.83 63.3
Stride Arcolab 1695.84 1637.67 96.6
Plethico Pharma 1535.20 1367.22 89.1
Piramal Healthcare 2509.86 1280.58 51.0
Divi's Labs 1307.11 1204.95 92.2
Aurobindo Pharma 4381.48 1112.06 25.4
Page 3 of 153
1.2DOMESTICMARKET
1.2.1Structure&GeographicalDistribution
TheDomesticPharmaceuticalMarkethasreachedtooverRs60,000croresin2009‐
10.Understandably,themarketisskewedtowardscitieswiththetop23cities
accountingforalmost25%ofpharmasalesofwhichtheTier‐Itownsaccountforone
thirdofsalesandTier‐IIcities(populationlessthanonelac)includingtherural
marketaccountingforabout40%ofmarketshare.Thisisfortheobviousreasonsof
betterhealthcareaccessibilityandpurchasingpoweroftheresidentmiddleclass
incomegroup.However,duetoshiftingruralandsemi‐urbaneconomicstatusas
wellaslivinglifestyles,theruralareasarewitnessingamarketincreasegrowthof
morethan30%annually.Thisincreaseinthegrowthiscatchingattentionofthe
majorcompanieswhoarenowfocusingonthemforfuturegrowth.
Statewisedistributionis:
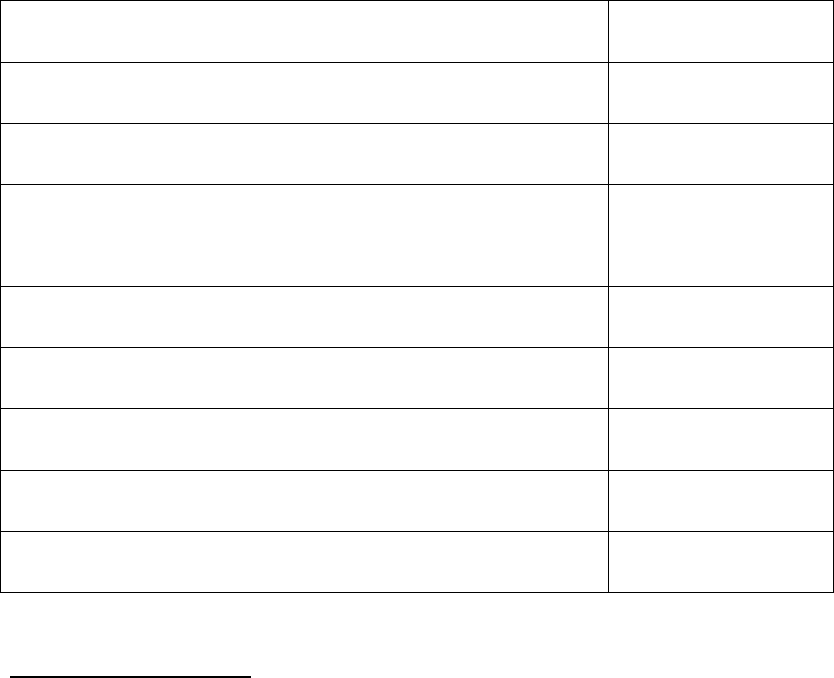
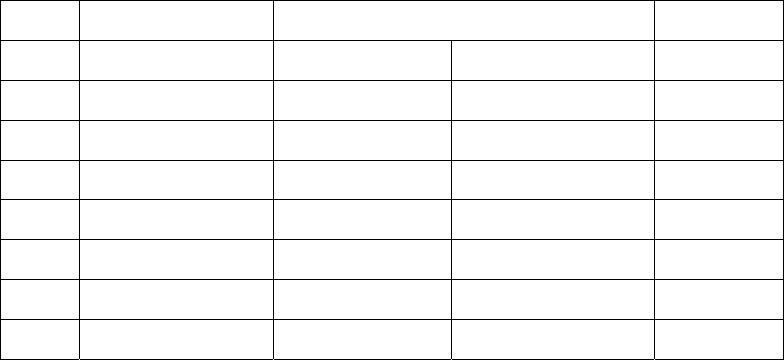
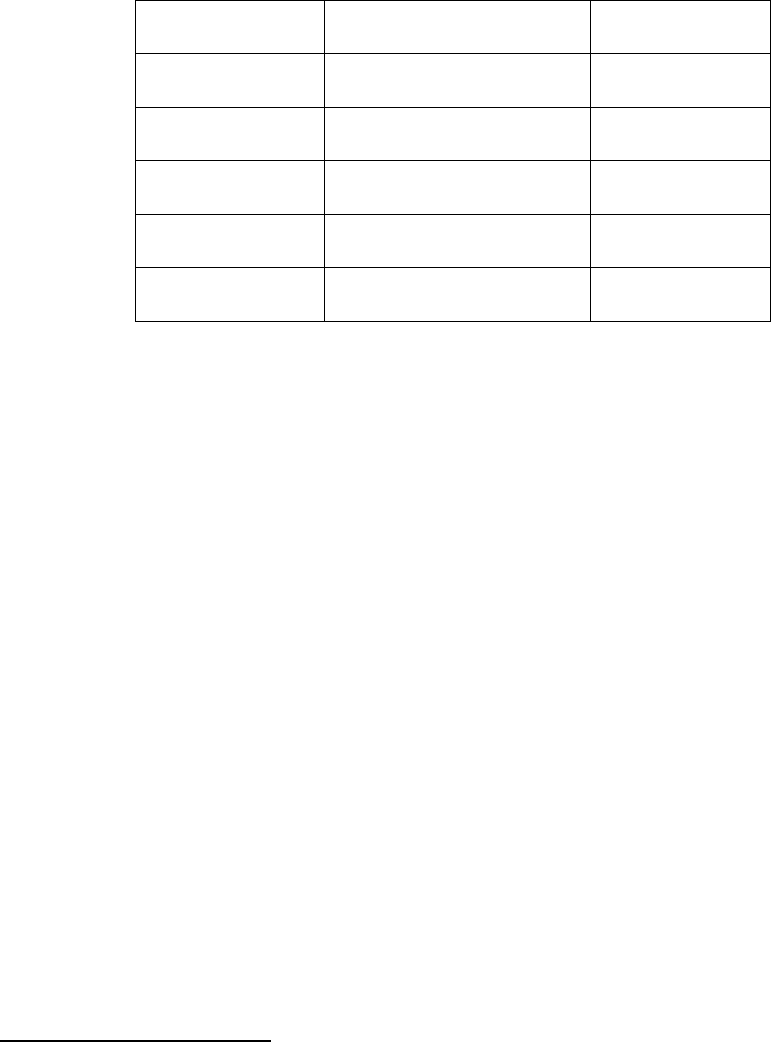
Table‐3:GeographicalDistributionofPharmaCompanies
S.No.StateNumberofManufacturingUnits Total
FormulationBulkDrugs
1.Maharashtra192812113139
2.Gujarat1129 397 1526
3.WestBengal69462756
4.AndhraPradesh528199727
5.TamilNadu47298570
6.Others34234223845
Total8174238910563
Torrent Pharma 2121.97 1101.57 51.9
Ipca Laboratories 1882.54 1025.18 54.5
Dishman Pharma 990.84 911.56 92.0
Orchid Chemicals 1781.79 725.85 40.7
Shasun Chemicals 799.42 676.78 84.7
Panacea Biotec 1143.78 610.44 53.4
Page 4 of 153
1.2.2FormulationsandTherapeuticsegmentsinthedomesticmarket:
WithintheDomesticformulationsmarketthemajortherapeuticcategoriesare‐
anti‐infective,gastrointestinal,cardiac,gynecologyanddermatology5.Theleading
drugclasseswereCephalosporin,Anti‐pepticulcerants,oralanti‐diabeticand
Ampicillin/Amoxycillin,etc.Thetoptendugclassescontributed35%oftotal
domesticmarket.AsperIMS‐Health6themajortherapeuticsegmentsasperMAT
valueare:
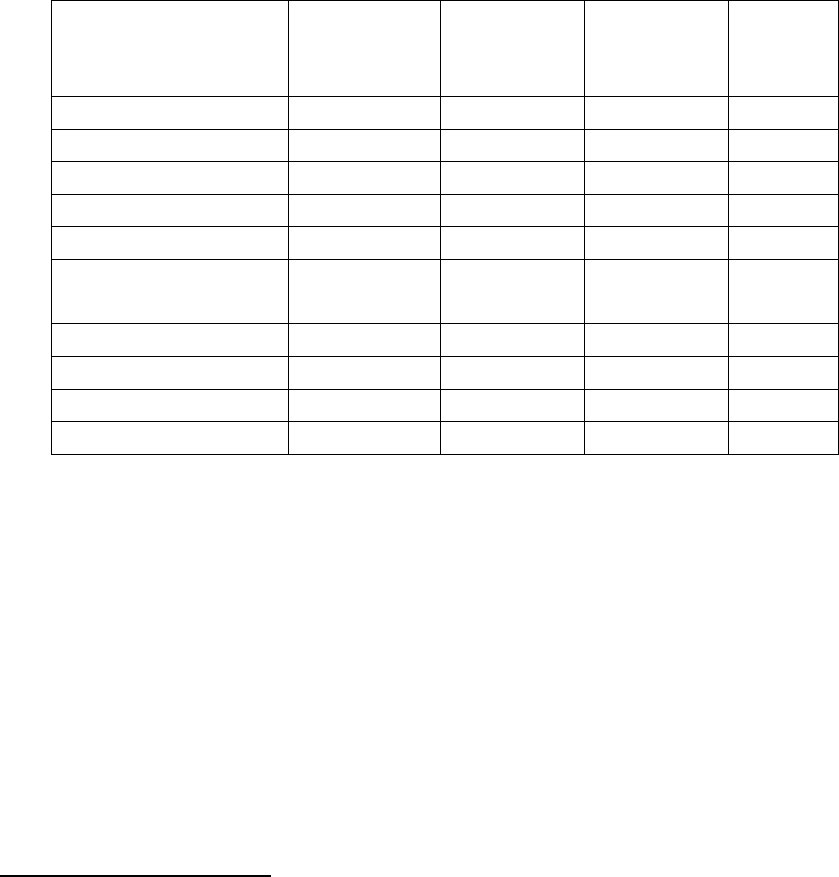
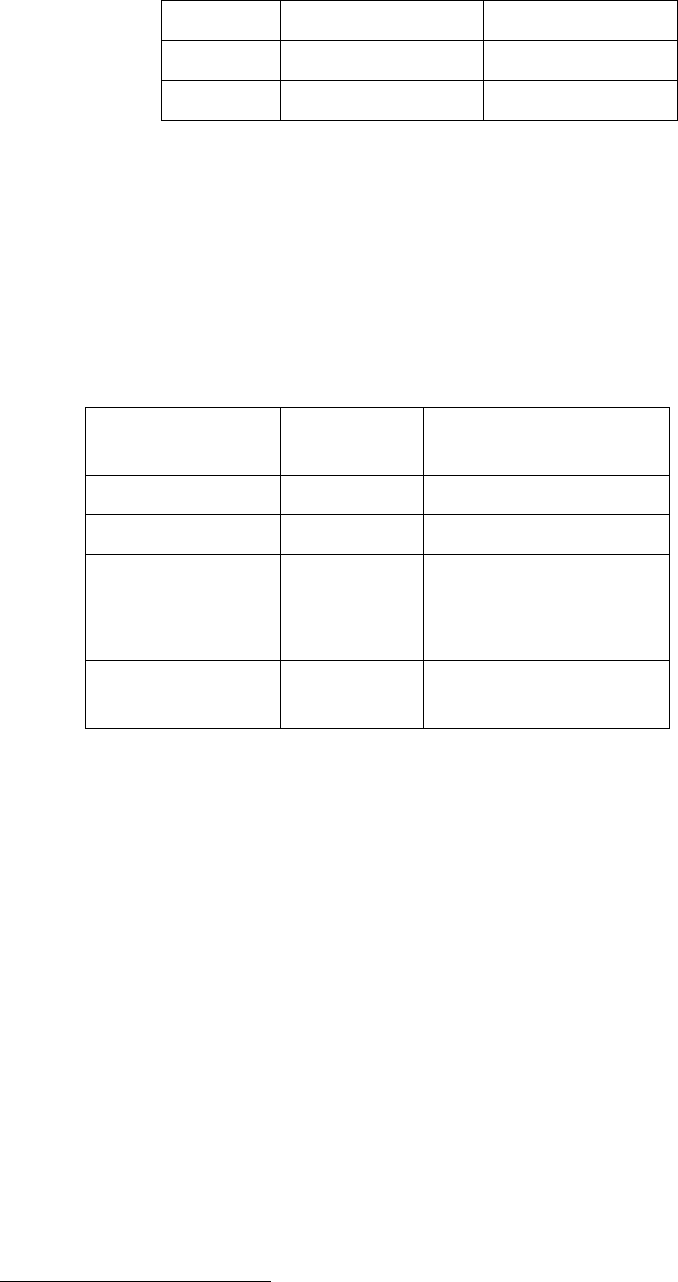
Table‐4:MarketTurnoverofMajorTherapeuticSegments
MajorTherapiesMATDEC'05
(ValinCrs)
%
Contribution
MATDEC'10
(ValinCrs)
%
Contribut
ion
Anti‐infectives4,056 17.6 8,060 17.2
Cardiac2,378 10.3 5,318 11.4
GastroIntestinal2,537 11.0 5,099 10.9
Respiratory2,170 9.4 4,080 8.7
Pain/Analgesics2,059 8.9 4,038 8.6
Vitamins/Minerals/
Nutrients2,1059.13,6257.7
AntiDiabetic 998 4.3 2,743 5.9
Gynaecology1,261 5.5 2,658 5.7
Neuro/CNS1,231 5.3 2,633 5.6
Derma1,255 5.4 2,554 5.5
Source:IMSHealth
Indiaislargelyself‐sufficientincaseofformulations,thoughsomelifesaving,new‐
generation‐technology‐barrierformulationscontinuetobeimported.Thisisevident
fromthefactthatoutofthelistof348medicinesenlistedas“EssentialMedicines”
intheNLEM2011,allaremanufacturedbydomesticpharmaindustry.
1.2.3BulkDrugIndustry
5 IMS-Health
6 IMS-Health
Page 5 of 153
The Bulk drugs component of the domestic industry is around Rs 42,000 crores giving
it a share of around 50% of the total domestic market7. This gives the Indian Bulk
Drug industry a share of about 9% of the global bulk drugs market of about US$ 102
Bn in 20098.
The bulk drugs produced in Indian market fall under 21 major therapeutic classes with
Antibiotics constituting more than 50% of the total production. This is because of
anti-infectives being the therapeutic segment of highest demand in accordance with
the prevailing disease class in India. Analgesics and Anti-pyretics account for 18%
and Anti-Dysentery and Vitamin constitute about 8%.
AsregardstheexportsofBulkdrugsithasshownaCAGRof16.98%inthelast3
years–seeTable‐5below:
Table‐5:BulkIndustryGrowth
(InRsCrores)
2007‐082008‐09 2009‐10 CAGR
12,647.5116,360.71 17,307.02 16.98%
WhiletheIndianbulkdrugindustryiscateringtoaround70%requirementofIndian
PharmaceuticalIndustrythereisgrowingdependenceonChinawithlowimport
costs.ThisdependenceisparticularlymoreinfermentationbaseAPIssuchas
Pencillin,Erythromycin,etcwhereitisalmost100%dependentonChina.Thisissue
hasbeenvoicedatvariousforaincludingbyMoH&FWasbeingofstrategicconcern.
1.2.4BiopharmaIndustry
1.2.4.1OverviewoftheGlobalBiologicsSector
7 BDMA
8 Cygnus- Cygnus Business Consulting and Research is a services organisation focusing on analysis and
research of Economies, Industries and Companies
Page 6 of 153
Withglobalsalesofbiologicsreachingnearly$137billionin2009andthepatentson
atleast48biologicsduetoexpireoverthenextdecade,industryexpertspredictthat
theglobalbiosimilarsmarketcouldbeworthmorethan$43billionby2020.But
biologicsdifferfromconventionalpharmaceuticalsinsomefundamentalways.
1.2.4.2SizeandCompositionoftheGlobalBiologicsMarket
In2009,globalsalesofbiologicstotalled$136.6billion(Table‐6).Avastin
(bevacizumab)headedthelistofbestsellers,withsalesof$5.74billion,while
Rituxan(rituzimab)andHumira(adalimumab)camesecondandthird,respectivelyas
pertablebelow.
Table‐6:TheGlobalMarketforBiologicsin2009
Country 2009Sales($bn)
US69.02
Europe41.68
Japan10.29
Asia/Africa/Australasia14.4.0
LatinAmerica1.20
TotalBiologicDrugs
Market
136.59
Source:Visiongain&PricewaterhouseCoopersanalysis
Table‐7:The10TopSellingBiologicsin2009
BrandDrugName 2009Sales($bn)
Avastinbevacizumab 5.74
Rituxanrituximab5.62
Humiraadalimumab5.48
Herceptintrastuzumab4.86
Lantusinsulinglarine4.29
Enbreletanercept3.87
Remicadeinfliximab 3.51
Page 7 of 153
Neulastapegfilgrastim 3.35
Epogenepoetinalfa 2.56
Avonexinterferonbeta‐1a2.32
Source:EvaluatePharma
1.2.4.3SizeandCompositionoftheGlobalBiosimilarsMarket
Biosimilarsaccountedforsalesofjust$1.23billion–lessthan1%ofthetotal
biologicsmarket–in2009(Table8).However,thereisconsiderablepotentialfor
growth.
Table‐8:TheGlobalMarketforBiosimilarsin2009
Country2009Sales($
bn)
MarketShareof
Biosimilars(%)
US0.06 4.9
Europe0.14 11.4
OtherCountries
(incl.Chinaand
India)
1.03 83.7
TotalBiosimilars
Market
1.23 100
Source:IMSHealth&visiongain
1.2.5GROWTH
1.2.5.1DomesticIndustry:
Asstatedearlierabove,thedomesticpharmaceuticalIndustryhasgrownataround
12%CAGRsincethestartofthe11thPlanin2007,fromRs45,367croresin2007to
aboutRs62,055croresin2009‐10.Thisissustainedbythefollowingfactors‐
a) marketsizeincreaseduetoincreaseinthesizeofmiddlelevelincomeearning
populationsegmentasitgrowsinsizefromthecurrent270Mntosome583
Millionby20259;
b) Increaseinpurchasingpowerofthisgroup;
9 www.Mckinsey.com/mgi/mginews/bigspenders.asp

Page 8 of 153
c) AgingoftheIndianpopulationaslifeexpectancyhasincreasedfromabout42
yearsin1960sto66.95yearsatthebeginningofthe11thplantonow68.45years
in2010‐1110coupledwiththepurchasingpowerofthissegment.Itistobenoted
thatpeopleofoldagespendaround3to4timesmoreondrugsthanpeoplein
youngeragegroupsforobviousreasons;
d) greatermarketpenetrationduetoincreasingspreadofprivatesectormedical
insurancecoverdrivenbyliberalizationoftheinsurancesectorofthisburgeoning
middleclass;and
e) sustainedexpectedgrowthoftheIndianeconomyingeneralataGDPgrowth
rateofsome9%to9.5%inthe12thPlanperiod11
Goingforward,theabovefactorsforsustainedgrowthwillbematchedbythe
inherentabilityoftheIndianmanufacturerstoscaleupproductionwithlesscosts
andtime,aswitnessedintheoverRs29,000croresofinvestmentinsettingupof
newmanufacturingplantsinthecountryinthe11thplanperiod12.
Theproductpatentnowpermittedfollowingthe2005amendmentinthePatentAct
1970hasfurtherencouragedthenowreasonablypreparedIndianpharmaceutical
companiestomovefromitsexpertiseinprocesschemistrywhichhasserveditwell
forgenericsproductstomorecomplexskillsindrugmoleculeResearchand
Development.ThusR&Dinvestmentsofthetop15Indianmanufacturingcompanies
haveincreasedfrom3%ofsalesin2000tosome8.68%ofsalesin201013.Basedon
abovefacts,theprojectedgrowthofthepharmaceuticalsectorasperpresent
outlookis–
Table‐9:ProjectedGrowth
ValueinRscrs/Growthin%
YearDomesticExports Total
10 Census Commission
11 Planning Commission
12 IPA
13 IPA

Page 9 of 153
ValueGrowth Value Growth ValueGrowth
2016‐17130,00021% 158,000 16% 288,00018%
2019‐20233,00022% 248,000 17% 481,00019%
1.2.5.2BulkDrugIndustryGrowthcomponent:
InIndiathebulkdrugsindustryisamajordriverfortheoverallindustrygrowthbeing
drivenbythesame6reasonsasforthepharmaceuticalsformulationssector
mentionedearlier.AspertheestimatesofBulkDrugsManufacturersAssociation
(BDMA),thishighgrowthwillcontinueandthesectorwillbeofUSD20billionsizeby
2015growingataCAGRof20%from2008‐0914.Withtheseprojections,itis
expectedtotouchUS$28billionbyendof12thplanin2017.
1.3EXPORT:
1.3.1Structure
Indiaisamongthetop20pharmaceuticalexportingcountriesgloballyandhas
showncommendableexportperformancewithcontinuouspositivetradeofbalance.
ExportsconstituteamajorpartofIndianpharmaceuticalIndustryandatpresentitis
around45%oftotalturnoveroftheIndustry.AsperDGCIS,theexportduring2010‐
11hasreachedmorethanRs45,000crores.
Indiandrugsareexportedtoaround200countriesintheworldwithhighlyregulated
marketsofUSA,UKetc.ThetopfiveexportingdestinationcountriesareUSA,Russia,
Germany,AustriaandUKwithUSAaloneaccountingforalmost20%oftotalexport.
Themajortherapeuticcategoriesofexportareantiinfective,antiasthmaticandanti
hypertensive.Country‐wise,thepositionisasflows:
1.3.2Growth
14 BDMA
Page 10 of 153
ExportshavegrownverysignificantlyataCAGRofaround19%inthe11thPlan
period,fromRs25,666crsin2007tooverRs45,000croresduring2010‐1115.The
table‐10belowgivesapictureofgrowthofexportforlast5years.
Table‐10:ExportGrowth
YearExports(Rs.crores) Growth%
Mar20072566620.89
Mar20082935414.37
Mar20093982135.66
Mar2010421546.6
Mar2011457457.7
Thesustenanceinexportgrowthrateswillbedrivenbythreefactors–
i. Increaseddependenceongenericsproductionduetopatentexpiriesby
2015,estimatedatsomeUS$300Bnofconventionaland
biopharmaceuticals16;
ii. Slowdownindiscovery/inventionofnewmoleculesindevelopedcountries;
and
iii. pressureonthedevelopedcountrygovernmentslikeUS,Germany,Japan,etc
tocontaintheirhealthcareexpenditure;
Consequently,theglobalMNCsarenowincreasinglydependingontheIndian
genericsproducers,aswitnessedintheacquisitions/mergersofsixmajorIndian
PharmacompaniesataworthofoverUS$10billionsinthe2007‐2010periodwith
anaveragepurchasepriceofabout7to9timesthegrossrevenuesforagiven
company.
1.3.3GlobalShare
15DGCIS
16 McKinsey &Company,”Capturing the India Advantage-page 18
Page 11 of 153
India,atpresentisrecognizedasaleadingglobalplayerandholds3rdpositionin
termsofvolumeand14ththeintermsofvalueoftheproduction.Theglobalmarket
forgenericdrugsin2009wasworthUS$108billion(FICCI‐IMSreportonGlobal
GenericMarket)andIndianpharmamarket,whichaspointedoutearlierconsistsof
almostgenericdrugsonly,contributedaround20%intermsofvalue.Globally,inthe
overallpharmaceuticalsspace,withaturnoverofUS$21billionin2010,Indian
PharmaceuticalIndustryhasashareof2.4%intermsofvalueinglobal
pharmaceuticalindustrywhichishavingaturnoverofUS$878billionin201017.
1.3.4Regulatory
IndiaissignatorytotheWHOcertificationprotocolonthequalityofpharmaceuticals
productsandhasthereforeacceptedtheWHO‐GMPstandardsasanintegralpartof
thestandardsforexportofpharmaceuticalsproducts.Asperarrangement,WHO‐
GMPcertificationisgrantedbytheofficeoftheDCGI(CDSCO)andStateFDAs.The
certificationisfortwoyearsatatime.
Sinceexportofgenericstothehighgrowthemergingmarketsistobeakeystrategy
forgrowthofpharmaindustryinthecountry,henceupgradationofSMEstoWHO‐
GMPstandardswouldenablethemtoexporttheirproductsandtherebyincrease
profitability.Itisestimatedthatatpresentabout800unitsarecertifiedbyCDSCO
forWHO‐GMPproduction.Asthereareabout10,000plusPharmaSMEUnitsinthe
country,therefore,thenumberofWHO‐GMPstandardunitsneedstoberaisedtoat
least2000bytheendofthe12thplanin2017toenabletheSMEsectortoincrease
andsustainitsparticipationinthePharmaIndustrygrowthprocess.Accordingly
giventheambitioustargetofachievingUSD100Bnproductionby2020,itis
estimatedthatabout1000‐1200unitswillhavetobeassistedforraisingtheir
manufacturingstandardstoWHO‐GMPlevels.Atanaverageproductioncontribution
ofUSD10Mnperunit,thiswouldmeanadditionalcontributionofaboutRs.10Bn
fromtheabovetargetachievement.
17 April-10,2010. IMS – forecasts for global pharmaceutical market – Market Prognosis :
www.imshealth.com

Page 12 of 153
Further,thereisneedtoupgradeatleast250unitstoUSFDA/EDQM/TGAandother
InternationalStandardsby2017andtrainingof5000WorkingProfessionalsinWHO‐
GMPandotherInternationalStandardsGMPrequirements.
1.3.5CompetitivenessandBenchmarking
1.3.5.1Competitiveness
GlobalPharmaMarket
Theglobalmarketischaracterizedby‐
• Peakyearsofpatentexpiriesdrivinggrowthtowardgenerics
• Publiclyfundedmarketsfacingslowergrowthandaddeduncertainty
• Chinaonpathtobecomingworld’sthird‐largestmarketin2011
AsperestimatesofIMSHealth–aglobalpharmaconsultingorganization‐thesize
oftheglobalmarketforpharmaceuticalsisexpectedtogrownearly$300billionover
thenextfiveyears,reaching$1.1trillionin2014.The5‐8percentcompoundannual
growthrateduringthisperiodwouldreflecttheimpactofleadingproductslosing
patentprotectionindevelopedmarkets,aswellasstrongoverallgrowthinthe
world’semergingcountries.Itistobestatedthatglobalpharmaceuticalsalesgrew
at7.0percentto$837billionin2009,comparedwitha4.8percentgrowthratein
2008.
Themarketwillcontinuetodrivenbypatientdemanddespitetheongoingeffectsof
theeconomicdownturn.Indevelopedmarketswithpubliclyfundedhealthcare
plans,pressurebypayerstocurbdrugspendinggrowthwillonlyintensify,butthat
willbemorethanoffsetbytheongoing,rapidexpansionofdemandinthe
pharmergingmarkets.Netgrowthoverthenextfiveyearsisexpectedtobestrong
—evenastheindustryfacesthepeakyearsofpatentexpiriesforinnovativedrugs
introduced10‐15yearsagoandsubsequententryoflower‐costgeneric
alternatives.
Page 13 of 153
Goingforward,IMShasidentifiedthefollowingkeymarketdynamics:
i. Geographicbalanceofthepharmaceuticalmarketwillcontinuetoshift
towardpharmergingcountries.Pharmergingmarkets(BRIC,SouthKorea,
Turkey,ASEAN,etc.)areexpectedtogrowata14‐17percentpacethrough
2014,whilemajordevelopedmarkets(US.WestEurope)willgrow3‐6
percent.Asaresult,theaggregategrowththrough2014frompharmerging
marketswillbesimilartothegrowthexperiencedindevelopedmarkets—
about$120‐$140billion.Thiscomparestoaggregategrowthoverthepast
fiveyearsof$69billioninpharmergingmarketsand$126billionindeveloped
markets.TheU.S.willremainthesinglelargestmarket,with3‐6percent
growthexpectedannuallyinthenextfiveyearsandreaching$360‐$390
billionin2014,upfrom$300billionin2009.
ii. TheTherapyareagrowthdynamicswillbedrivenbyinnovationcycleand
areasofunmetneed.Asthepharmaceuticalindustry’sresearchand
developmentprogramsadjusttothebroadavailabilityoflow‐costgeneric
optionsinmanychronictherapyareas,highergrowthwilloccurinthose
therapyareaswherethereissignificantunmetclinicalneed,high‐costburden
ofdisease,andinnovativesciencethatcanbringnewtreatmentoptionsto
patients.Intheareasofoncology,diabetes,multiplesclerosisandHIV,
annualgrowthisexpectedtoexceed10percentthrough2014asnewdrugs
arebroughttomarket,patientaccessisexpandedandfundingisredirected
fromotherareaswherelower‐costgenericswillbeavailable.
iii. Broadcutsinspendingwillbeappliedbypublicpayerstoreducegrowthin
drugbudgets.Publiclyfundedhealthsystemsareunderincreasedpressure
toreducegrowthindrugbudgetsfollowingtheglobaleconomicdownturn.
Page 14 of 153
CountriesincludingTurkey,Spain,GermanyandFrancealreadyhave
announcedplanstoapplyacross‐the‐boardrestrictionsonaccessor
reductionsinreimbursementstoreducedrugspendinggrowth.Governments
inothercountriesseekingtorestorefiscalbalancemaytakesimilaractions,
orshiftmorecoststopatients.
iv. Peakyearsofpatentexpirieswillshiftmajortherapiestogeneric
dominance.Overthenextfiveyears,productswithsalesofmorethan$142
billionareexpectedtofacegenericcompetitioninmajordevelopedmarkets.
Collectively,theimpactofpatientsshiftingtolower‐costgenericsinmajor
therapyareassuchascholesterolregulators,antipsychoticsandanti‐
ulcerantswillreducetotaldrugspendingbyabout$80‐$100billion
worldwidethrough2014.ThisimpactparticularlywillbefeltintheU.S.,
wherenearlytwo‐thirdsofthetotalvalueofpatentexpirieswilloccur.
PatentexpiriesintheU.S.willpeakin2011and2012whensixoftoday’sten
largestproductsareexpectedtofacegenericcompetition.
v. Closerscrutinyofnewproductswillresultinrestrictedcontributestolower
initialspendingbypayers.Thenumberofnewmolecularentitieslaunched
annuallyoverthenextfiveyearsisexpectedtoremainintherangeof30to
35products.However,thesewillbesubjecttomorerigorousandcomplex
assessmentsbypayersbeforebeingacceptedintoclinicalpracticeand
reimbursed.Inmanycountries—includingChina,Spain,ItalyandCanada—
fundingandimplementationofhealthcareatregionalorlocallevelsis
becomingmoresignificant.Thisisexpectedtoextendthetimeittakesfor
newmedicinestobecomeavailabletopatients,andcontributetolower
initialspendingbypayers.
Page 15 of 153
Furtherthattheexpectedglobaleconomicrecoveryremovesanelementof
uncertaintyfortheindustryoverthenextfiveyears,althoughthewaypayers
addresslingeringbudgetdeficitswillremainanissueinmanymarkets.Health
systemreforms,suchasthosetobeimplementedintheU.S.,canspurfundamental
changeinthemarket—butthefullimpactmaynotbefeltuntilthelatterhalfofthis
decade.Leadingupto2020,IMSexpectstoseeacontinuingshifttoward
biopharmaceuticals,specialty‐drivenproducts,andchangesinthemixofdisease
areasofinterest.
1.3.5.2Benchmarking
i. Research,developmentandInnovation
ii. HumanResources
iii. TechnicalCapability
iv. Infrastructure
v. ColdChaininfrastructure
(i) Research,developmentandInnovation
ResearchandDevelopment(R&D)isthebackboneofthegloballeadersinthe
pharmaceuticalindustryallovertheworld.Thepharmacompaniesinthe
developingcountrieswithsomesizeableturnoverarenowincreasinglytherefore
lookingatinnovationandR&Daskeystrategiesforfuturegrowth.TheIndian
pharmaceuticalcompaniescannotaffordtobedifferent.SomeleadingIndian
companieslikeSun,ZydusCadilla,DRL,Lupin,etcareincreasinglyfocusedonR&D
totaptheupcomingopportunitiesfromexpirationofpatentsofseveral
blockbusterproducts.
TheglobalaverageR&Dexpenditurein2010was$68billionwhichwasaround8%
ofglobalPharmaceuticalsalesin2010i.e.$856billion1.Hence,althoughinterms
ofpercentagetheR&DexpenditureofbigPharmacompaniesinIndiaisalso
comparabletoglobalaverage,howeverthetotalexpenditureonR&DbyIndian

Page 16 of 153
firmsismuchlessascomparedtotheglobalexpenditure.Moredetailsofthisis
discussedinChapter3onR&D.
(ii) HumanResources
ThesubjectofHumanresourcesrequiredindetailintheChapter3onCapacity
BuildingandEmployment.Forsakeofacompletediscussionbrieflyitmaybe
mentionedherethattheGovernmentandtheprivatesectordoofferauseful
institutionalstructureforprovidingdiplomatoPhDlevelknowledgedevelopment
inthepharmaceuticalssector.TheGovernmentofIndia‐throughthehighend
NationalInstituteofPharmaceuticalEducationandResearchestablishedat
Mohali,Chandigarhin1997followedbysettingupofsixNationalInstitutesof
PharmaceuticalsEducationandResearch(NIPER)atRaeBareilly,Hajipur(Patna),
Hyderabad,Ahmedabad,GuwahatiandKolkata.Theseprovidepostgraduateand
PhDleveleducationandcontributetosome1800MastersandPhDsperyear.
Othercentralgovernmentinstitutesinclude–TheIndianInstituteofChemical
Technology(IICT),CentreforCellularandMolecularBiology(CCMB),National
InstituteofNutrition(NIN),CentreforDNAFingerprintingandDiagnostics(CDFD),
IndianImmunologicalLtd(IIL),etc.
AnumberofStateGovernmentUniversitiesandCollegesalsoofferbothgraduate
andpostgraduateeducationinpharmaceuticalsciences.Theaboveresourcesare
alsosupplementedbytheinstitutesandcollegesintheprivatesector.Together
boththegovernmentandprivatesectorrolloutsome51000graduatesand5200
PGsinpharmaceuticalsscienceseveryyear18.
(iii) TechnicalCapability
Thechemistryskillsproducedinthecountrythroughitscollegesanduniversities
supportedbytheirdemandinthegenericsdominatedproductionpatternin
IndianpharmahasplayedakeyroleinbuildingIndiandominanceintheglobal
genericssector.Thatthisskillhascomeatlowcostshasresultedamongstvarious
18 Report by Deloitte 2010 for DoP on setting up of new NIPERs
Page 17 of 153
otherfactorsinenablingIndianpharmatoproduceoneofthecheapestgood
qualitydrugsintheworld.AcomparisonofthedrugpricesinIndiaandPakistan
illustratesthispoint.Withhardlyanymanufacturingbasefordrugs,thepricesof
drugsinPakistanaremuchhigherthaninIndia(3to14times)eventhoughper
capitaincomesinboththecountriesaremoreorlesssame.HoweverwithChina
thereisatoughcompetitiononthisfront.Nevertheless,Indiaisamongstthefew
developingcountriestosucceedinbuildingstronglocalcapabilityinthe
technology‐intensivepharmaceuticalsector.
However,onceagainthetechnologydevelopmentbeinglimitedtogenericsAPIs
orformulationhasbeenmostlylimitedtocost‐effectiveprocessdevelopment.
Thishasresultedinpoordevelopmentofnewproducts.Howeveritcanbeargued
thatsincetheIndianpharmastarteddevelopmentonlyasfrom1960salbeitina
MNCdominatedenvironment,itisacredittoittobeabletodevelopeventothe
currentskillsascomparedtorestoftheworld.Surelyhighriskandhighskill
demandfornewdrugdevelopmentcanpossiblynotbedoneinbarely25yearsof
ahightechnologyindustryandtheIndianpharmarightlyfirstmettheneedsof
country’sdrugneedsinthemuchrequiredanti‐infectivessector(themoleculesin
thissegmentwereinearly1940‐50s)andisnowperhapswellplacedtotakeon
thenewdrugdevelopmentchallenges.Wereitnotso,Indiawouldnothavebeen
abletotaptheglobalizationandliberalizationopportunitynowwideopeninthe
genericssectorwithitslowcostgoodqualitybase.Thisisdiscussedmoreinthe
Section1.7onSWOTAnalysis.Goingforward,Indianpharmaindustrywould
needtofocusondevelopingcompetenceinadvancedareasofdrugmanufacture
e.g.biopharmaceuticals,DNAbaseddrugsetc.
(iv)Infrastructure
AlthoughIndianpharmahasgloballyrecognizedcapabilitiesingenerics
production,ChinaisforgingaheadwithhugeinvestmentsinAPIproductionwhich
requiresinter‐aliacheappowerandotherinfrastructurefacilities.Israel,Germany,
BrazilandTurkeyarealsobuildinglargestrengths.Inthefieldofmedicaldevices,
Page 18 of 153
theIndianindustryisinnascentstage.So,thereisaneedofdevelopingcommon
infrastructureindrugdiscoveryanddevelopment,manufacturing,distribution,
exports,medicaldevices,etc.
Thekeyareasare:
(a) GLPCompliantAnimalFacilities:Pre‐Clinicaltestingrequiresprimatebased
largeanimaltesting.Howevertherearelimitedprimatefacilitiesinthe
country.WhileICMRhasproposalsfortransgenicanimalfacilitiesanda
Nationalcenterfornon‐humanprimatebreedingcenterthereisneedtobuild
capacityinthisareaandtodoitfast.Thiswouldrequirelicensedbreeders
meetingandmaintainGLPstandards.
(b) BiologicalSampleStorageFacilities:Accesstostoragefacilitiesadheringto
appropriatebio‐safetylevelsisrequired,asIndiaaddresseschallengesof
infectiousdiseases.Currently,samplesusedinmanyoftheclinicaltrialsare
beingstored/archivedoutsideIndia.ManyIndianpharmaceuticalcompanies
outsourcesafety,pharmacologyandregulatorytoxicitystudiestoother
countries,duetolackofcomprehensivefacilityexistinginthecountry,which
couldcarryoutthesestudiesinanintegratedmanner.
(c)SharedInfrastructureforOptimalCapacityUtilization:Everyscientistore
R&Dinstitution/Industryfacilitydoesnotrequirecompleteself‐sufficiencyin
termsofin‐houseinfrastructure.Poolingofresourcesbetweengovernment
andindustryasalsoacademiaevenwhilesecrecyconditionswouldgoalong
wayinbuildingmutuallybeneficialpartnerships.
(v)ColdChainInfrastructure
ThePharmaceuticalSupplyChainisverycomplexandhighlyresponsibletoensure
thattheconcerneddrugreachesthetargetpeoplewithoutlosingitsefficacy
whereverthedrugsaretemperaturesensitivewheretheColdChainInfrastructure
Page 19 of 153
isparamount.ThisisparticularlyimportantforVaccinesandrelatedtreatments
likePolio,etc.
ThisfactisincreasinglyofimportancenowintheIndianmarketgiventhegrowing
accessalongwiththelargeandoftenpoorlyconnecteddistantplaceswhere
treatmentmedicinesaretobecarriedto.Hence,pharmaceuticalcompaniesin
IndiahaverealizedtheimportanceofSCMrelatedColdChainInfrastructureand
areaggressivelylookingforwaystoimprovethecostsassociatedwithSCM.
DistributioninIndiaisproportionallymuchmorecostlythanitisintheUSorEU
duetoinherentlypoortransportstructureavailablefordrugs.Uptoone‐thirdof
therevenuesareoftenspentonSCM.BecauseoflackofdevelopedSCM
infrastructurefordrugs,thecostishigherinIndiaascomparedtoUSandEU(2%
ofsalesinUS/EUascomparedto4‐%inIndia).(BioPharmInternational
www.biopharminternational.comSeptember200).
OneotherreasonfortheabsenceofamodernSCMinfrastructureisthatthe
medicinessupplychaininIndiaishighlyfragmentedwithmorethan550,000retail
pharmaciesspreadacrossvastdistancesoftenpoorlyconnectedinthecountry.
Thisalsoleadstosuchproblemsasconcerningrecallofdrugs.Newertechnologies
wouldhelpinkeepingtrackofproductsalongtheentirechainandwouldlimit
counterfeitdrugstoenterintothesystem.Theproblemsareobviously
compoundedwhenmandatedcoldchainrequirementsaretobemet.Thisisone
ofthemajorchallengesfacedbytheindustryiftheyaretoretainproductquality
duringshipmentspeciallythebiotechproducts.Thereforetheorganizeddrugretail
facesdauntingchallengeswhichwouldthereforebeakeyfactortoimprove
affordableandqualityhealthcareaccesstoall.
1.4IPRandInternationalCooperationIssues
1.4.1ThesubjectofIPR,TRIPS,PatentLinkage,FTAs,DataExclusivity,etc.aremuch
debatedinthenationalandinternationalfora.BothlargeandSMEunitsarefinding
itdifficulttocopeupwiththeincreasinglynewdemandsbeingplacedonthese
Page 20 of 153
issuesbythedevelopedmarkets.Itisalsowidelybelievedthatthisistobuildnon‐
tariffbarriersagainstthecapabilitiesoftheIndianpharmatogarneralargermarket
shareinthedevelopedmarketsnowhavingincreasingneedforgenericsforcost
containmentinthecontextoflimitedgovernmentbudgetsandthecontinuingslow
downoftheeconomies.
IndianPharmaIndustryconsistsof60%domesticand40%ofexportmarketon
accountofwhichtheexportswouldbeaffectedduetosuchanapproachofthe
developedmarketregulators.TheStandardOperatingProcedures(SOPs)ofdifferent
governmentsisdifferentinternationally.Thereforethereisarequirementto
educateSMEunitsaboutcountryspecificSOPsfortestingtheirproducts.
Inthisregard,thesituationisalreadypitiableevenfortestingofproductsforIndian
marketsduetolackofavailabilityofreferencestandardproductsasperIndian
Pharmacopeia(IP).Thuswhilemorethan1000moleculesarebeingmanufacturedor
marketedinthecountry,IPChasreferencestandardsforabout200productsonly.
Thusthesebatchspecificandtimelimitedreferenceproductshavetobeeither
importedorgotmanufacturedin‐houseorthroughotherunitswhichisavery
tediousandexpensiveprocess.Thereisaneedtolaunchpartnershipprogrammes
byDoPinpartnershipwithMoHFW/IPCtomakereferencestandardproducts
availablenotonlyforIPbutalsoforothercountrieswheremajorexportsare
focused.ThereisalsoneedforincreasedtrainingforSMEsregardingtheSOPsand
ensuringavailabilityofreferencestandardproductsfortestingandfulfilmentof
exportsrequirements.
1.4.2Non‐TariffBarriers(NTBs): Theexportingunitsbothbulkdrugsand
formulationsfacethreetypesofnon‐tariffbarriersrelatedtoregulatory
requirementsfromhighexportmarketsliketheEU.
Page 21 of 153
i. ThereisarequirementtoensurecompliancetoEDQMstandardswhichis
availableforonly3yearsatatimewithsuchhighcostsasEuro15,000
perdrugpertime.
ii. TheninadditiontoEDQMthereisfurtherneedtoobtaincertification
fromeachimportingcountry.
iii. Furtherinthecaseofbulkdrugs,athirdadditionalrequirementisofa
thirdpartyaudit.Thisauditcompelscompaniestodivulgetheir
intellectualpropertyinfringingontheirrighttoprotectdataguaranteed
underTRIPs.
iv. Then,EUisinsistingonverificationofpedigreeofActivePharmaceutical
Ingredientsincaseofexportofformulations.
Clearly,ifsuchNTBsaretobeaddressedthereisaneedtocreategreatersynergy
amongvariousgovernmentdepartments/ministriesviz.DepartmentofCommerce
(DoC),Pharmexcil,M/oHealth&FW,DoPforformulatinganintegratedstrategyto
tacklesuchbarriersandmayincludetakingcountermeasures.
Additionallythereseemstobelackofclarityinthemultipletradeagreementsviz.
TradeRelatedIntellectualPropertyRights(TRIPs)ofWTO,AntiCounterfeitTrade
Agreement(ACTA),etcduetoexportersarefacingproblemsinensuringtheir
compliancewhichisaffectingtheirexports.Theseissuesneedtobetackledina
comprehensivemannerbyjointeffortsofDoPandDoC.
Anotherissueconcernsarecentsteptakenbysomedevelopedcountiesintheform
ofTransPacificPartnershipAgreement(TPPA),anewregionalfreetradeagreement
whichincludetheUnitedStates,Australia,Peru,VietnamandMalaysia,Japan,etc.
TPPAhasdiscriminatoryarrangementsbetweensignatoryandnon‐signatory
countrieswhichisaviolationofTRIPs.
Page 22 of 153
AdditionalbarriersarealsobeingraisedinemergingmarketslikeArgentinawherein
thereisadiscriminationinimportregulationsbetweenbulkdrugs(whichare
allowed)againstformulationswhicharebanned.Hereinthereisalsoatrustdeficit
betweentheindustryandthegovernmentespeciallyinthecontextofgovernment
signingFreeTradeAgreement(s)withvariouscountrieswhereinfacilityofzeroduty
isbeingextendedthereiseverylikelihoodofcreationoffurtherproblemswithout
properinvolvementoftheIndustry.
InthespecialcontextoftheseregulationsimpingingonIndianPharma’sleadership
intheAPIsector,thereisaneedtostudythedetailsofAPIsproductionespeciallyin
Spain,Italy,PortugalandEasternEuropeandprepareareportonexportofIndian
APIs/formulationdrugstoEUanddetailsofAPIsbeingmanufacturedinthese
countries.Thereisaneedtotackletheseissuesinorganizedmannerwherein
representativesoftheindustryneedtobeco‐optedintheefforts.Itisproposedto
establishacellinIPA,tobefundedbyDoP,onallissuesrelatedtoIPR,regulatory
issues,etc.actingasbarriers.
Inthisconnectionthereisneedtotapanewdevelopment–Theadoptionof
recommendationsofPharmaceuticalInspectionConventionandPharmaceutical
InspectionCo‐operationScheme(jointlyreferredtoasPIC/S).Thisagreement
providesforinteraliacooperationbetweencountriesandpharmaceuticalinspection
authoritiesforenablinginternationaldevelopment,implementationand
maintenanceofharmonisedGoodManufacturingPractice(GMP)standardsand
qualitysystemsofinspectoratesinpharmaproducts.Thisistobeachievedby
developingandpromotingharmonisedGMPstandardsandguidancedocuments,
trainingcompetentauthoritiesandregulatorsinthepharmasector.
1.52DBarcoding
2DBarcodinghasbeenmadearegulatoryrequirementforexportofmedicinesby
DGFTtopreventfakemedicinesandmis‐representationofIndianexportsinthe

Page 23 of 153
nameofothercountrieslikeChinaetc.TheSSIunitsdoingcontractmanufacturefor
tradinghousesandotherpharmaneedtobesupportedbygovernmentschemesfor
buildingthiscompetenciesbothbywayofinfrastructureandfinancialsupport.
Furthertheimplementationof2DBarcodingattertiaryleveli.e.atstriplevelalso
envisagedbyDoCcouldbecomeveryexpensiveandoffsetIndianprice
competitivenessinemergingmarkets.TheMNCswhoexporthighpricedpatented
drugshavenosuchproblem.Inthe11thplanrecommendationhadbeenmadefora
Rs.100croresassistanceforassistingSMEstobuildexportcompetitive
infrastructureandtechnologysupport.Howeverthesamecouldnotbe
implemented.Thereisneedtodoitnowforthe12thPlan.
1.5.1ApexAuthoritytoControlPrices,Quality&SupplyofDrugs
NPPAismandatedforpricingofdrugsandDCGIistheauthorityforensuring
standardsformanufacturingandqualityofdrugsinadditiontothebasicelementof
introducingthedrugitselfinthecountryforanytherapeutictreatment.Aneedfora
commonauthorityhasbeenfeltinthepastseveralyears(PronabSenReportof
200519)forensuringsupplyofsufficientgoodqualitydrugs.TheviewoftheDoPis
thatsuchanauthorityliketheNationalAuthorityonDrugsandTherapeutics(NADT)
addressingalltheseissuesinasinglewindowmodeifconstitutedshouldbepartof
theDepartmentofPharmaceuticalswiththeDoPitselfbeingpartofMinistryof
ChemicalsandFertilisersorotherwise.
1.6Environmentalissues:
1.6.1 PresentStatus
TheIndianpharmaindustryhasevolvedaroundindustrialdevelopmentclustersset
upbyvariousstategovernments.Inearlieryears,mostofthemanufacturingand
R&Dunitscouldtakebenefitofthethenprevalentlaxorotherwiseenvironmental
laws.Butnowinternationalcustomersfromdevelopednationsarebecomingmore
19 Dr. Pronab Sen Report Sept.2005
Page 24 of 153
stringentonensuringlocalenvironmentstandardcompliancestandardsandwant
companiestoadheretothesestandards.Thishasledtoabigchallengeforthe
Indianpharmaindustry,particularlysmallscaleunits,whicheitherhaveinvestment
concernsorlimitationsofgrowthbeyondtheirallottedunitareasintheindustrial
clusterssetupearlierwithantiquatedenvironmentstandardscompliancepotential.
DoPisexpectedtoplayavitalrolebyprovidingfinancialandtechnicalassistanceto
improvefinancialsustainabilityofSMEsononehandandalsosafeguardthe
environmentfromthehazardsassociatedwiththeunplannedgrowthofthe
industry.Thisisparticularlychallengingforthebulkdrugindustryalreadyasource
ofadversereactioninthepublicinareasaroundHyderabadandalsofornew
possiblegrowthcentersforthepharmasector.ThemissionshouldbeClean
business=morebusiness=BetterHealthCaremedicinesforall.
1.7SWOTANALYSIS
TheIndianPharmaceuticalindustryhasemergedasaleadinglowcosthighquality
genericmedicinessuppliertotheworld.Itsfuturegrowthispebbledwithseveral
aspectsofitsstrengths,weaknesses,opportunitiesandweaknesses.
1.7.1Strengths
(1)StrongLowcostmanufacturingsector
LiketherestoftheIndianmanufacturingandserviceseconomy,ascomparedtothe
EuropeanandUSlevels,thepharmasectorhasthestrengthof‐
i. lowwagecosts;
ii. lowmaterialcostslikethebulkdrugsandthechemicalsintermediates
requiredtomanufacturethebulkdrugsaswellastheexcepientswhichgo
intoformulationsmanufacture;and
iii. lowcostofliving.
ThusoveralldrugsmanufacturinginIndiaisupto50%cheaperthaninwestern
industrialcountries.

Page 25 of 153
Intermsofbreadthoftheindustry,theIndianPharmaceuticalsectorishaving
around10563manufacturersinthecountry20comprisingsome300largeand
mediumunitsandbalanceinthesmallscaleandunorganizedsector.Theemphasis
ongenericsandtheexistenceofprocesspatentonlyregimebetween1970and2005
helpedtheSMEsectortogrow.ItenabledIndiatosourcemorethan85%ofits
domesticdemandforbulkdrugs,drugintermediatesandisalmostselfreliantin
pharmaceuticalformulations,chemicals,tablets,capsules,oralsandinjectiblesup
fromdomesticproductionwith20%in1950s.
Thisgrowthwasinalargemeasuretriggeredbythegovernmentinitiativesinthe
publicsectorwiththesettingupoflargeplantsformanufacturingantibiotics–HAL
in1951,IDPLin1961KAPLin1981etc.Thisgrowthsharedasynergywiththegrowth
ofthechemicalssectorandthewholegamutofchemicalbasedindustriesprovided
thebasictechnologyandscienceskillfordrugsmanufacture.
Followingliberalizationthecontributionofthepublicsectorhasexpectedly
decreasedinanincreasinglycommoditizedmarket.Atpresent,theleading250
pharmaceuticalcompaniescontrol70%ofthemarketwithmarketleaderholding
nearly7%ofthemarketshare.
(2)CompetitivenessofIndianGenerics
AnimportantcharacteristicoftheIndianpharmaindustryisitsexportsaspointed
outearlier.Thisissustainedbytheincreasingcompetitivenessoftheindustryvis‐a‐
visthedevelopedandregulatedmarketswhichisreflectedinthelargenumberof
AbbreviatedNewDrugApplications(ANDA)andFirsttoFile(FTF)fillingsforthe
formulationssectorandDrugMasterFiles(DMF)filingsforthebulkdrugsbyIndian
companiesintheUSFDAforexportstoUSmarketwhichbyitselfisvaluedatUS$
20 DoP survery 2007 done in collaboration with MSME –First Pharmaceutical Census – DoP Annual Report
2010.

Page 26 of 153
300Bnin200921.Thus,in2010,over30%ofDMFapprovalsbyUSFDAwerefrom
India.ThisshowsthecompetitivenessoftheIndianpharmaascomparedtothe
otherleadinggenericsproducerslikeChina,IsraelandGermany.Itisnoteworthy
thatthisproportionoffilingsbyIndiancompanieshasincreasedfrom14%in200022.
ThiscompetitivenessisfurtherextendedintheEUmarketsaswitnessedbythefact
thatIndiahasaround461CertificateofSuitabilityi.e.19.78%ofthetotalgrantedby
EuropeanDirectorateofQualityMedicine(EDQM).Also,theproductsregisteredby
Indiavaryincomplexityandrangeoftherapeuticareas.Thisensuresthat
competitionfortheproductsofferedbyIndiancompaniesisrestrictedensuring
steadydemand.
(3)HumanSkill
ThehumanresourcesavailabilityinIndiaischaracterizedby:
• Significantbreadthanddepthinengineeringandscience
• Lowercostofinnovationandhighlymotivatedscientists.
• LargepoolofEnglishspeakingemployees,acomfortforinternational
customersandregulatoryagencies.
• Lowcostscientificpoolonshopfloorleadingtohighquality
documentationandprocessunderstanding
• Outsourcingservicesculture
Thereisabundanceoflowtomiddlelevelskillsinscienceandtechnologyingeneral
andasalsointhepharmaceuticalsciencessector.Thetable‐11belowmakesthis
clear.
Table‐11:HumanresourcepositioninIndia
SlItemTotalnumbers
1NoofUniversities 409
21IMS Health , Spring 2010
22 Cygnus Report
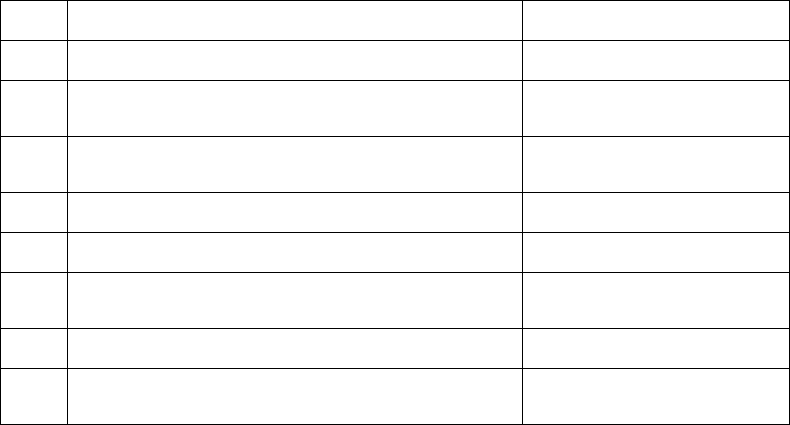
Page 27 of 153
2Noofcolleges25990
3Noofsciencecolleges 4696
4Annualstudentoutputatdegreelevelin
science
2000374
5Annualstudentoutputatdegreelevelin
engineering
1663619
6Totalnoofpharmacycolleges1162
7NumberofBPharmcolleges848
8NumberofMastersinpharmaceuticalsarea
andPhDofferingcolleges
191
9NoofBPharmstudentsinpharma51716
10NoofMastersandPhdstudentsoutputin
pharma
5648
Sufficeittosaythatthelevelofavailabilityofmanpowerinnumbersinageneral
skillcapacityisquiteabundant.Fordomesticpharmaindustrythisisadequatein
termsofbasicneeds.Tothatextentthesituationofdemand–supplyissimilarfor
theMNCsoperatinginIndia.Theskillbasehassofarservedwellformeetingthe
needsforchemistryskills,R&Dandmanufacturinginfrastructurewithproventrack
recordinadvancedchemistrycapabilities,designofhightechmanufacturing
facilitiesandregulatorycompliance.Thisisevidencedbythefactthatthelargest
numberofUSFDAapprovedplantsoutsideUSareinIndia.Still,thereisshortageof
skillinhigh‐techarea.
Lately,inthelast3to5years,therehasbeenanincreasingdemandforthecontract
researchandclinicaltrialsindustryfromtheMNCendaswellasfromdomestic
entities.Thisisfurthercatalysedbytheavailabilityofabundantdrugnaïve
populationandvarietyofgenepool.
1.7.2WEAKNESSES:
(1)LowR&DBudget:
AlthoughtheIndianpharmaceuticalindustryislargebyIndianstandards,onthe
worldmarketitsshareismerely2.4%.TheestimatedinvestmentinR&Dbymajor
IndianPharmacompaniesisaround8.68%oftheirsalesturnover.Asapercentageof

Page 28 of 153
totalproductionthisworksouttoonly4.4.%ofthetotalproduction.Comparedto
theR&Dinvestmentinthedevelopedmarketsofsome8%23theIndianinvestmentis
quitelow.Onereasonforthisistheemphasissofarongrowthbasedgenerics
productionandtheprevalentdiseasepatternofhighneedofgenericanti‐infectives,
antihistamines,painmanagementandotherthirdworldvectorbornediseaseslike
Malaria,Filariasis,Anti‐heleminthic,etc.Allthedrugsforthesetreatmentshave
beenalreadyinthegenericspacegloballyformorethan40yearsandhencethe
growthofgenericsisnotoutofcontext.Thepictureiscompletegiventhelow
purchasingpowerofthemiddleclassandtheruralareasupto1980s.
ThushighendR&Dwasnotarequirementanddiseasecontrolwasmoreanissueof
accesstopublichealthinfrastructureandlowcostmedicines.Tothatextentthe
Indianmanufacturingmodelhasservedwellfromthemanufacturingpointofview.
HowevernowthatIndiaispoisedforagreaterroleintheglobaleconomyingeneral
andalsointhepharmasectorforreasonsdiscussedearlierintermsofthegrowth
drivers,theweaknessinthesystemofpoorR&Disquiteevident.Theindustry’stotal
R&Dbudgetiscomparativelyverysmallascomparedtotheglobalcompetitors.Thus
individualR&DbudgetsofmanyUScompaniesprobablyamounttomuchmorethan
thecumulativeR&DbudgetsofallthecompaniesinIndia(in2009,Pfizerspent
around18%ofitssalesturnoverofUS$9.9Billion)24.Thisisfurthermanifestinsome
newareaslikepharmaco‐genomicsleadingtopersonalizedmedicineasthebasisof
therapeutictreatmentwithdrugtherapytailoredtoindividuals.Theemergingareas
ofbio‐pharmaceuticalswithhighlycapitalintensivehighfailurefeaturesfurther
raisestheentrybarriertomoderndaypharmaR&D.
TheproblemofR&DinvestmentisenhancedbyLackofsupportivefundingfrom
governmentashasbeenpossibleinothercompetingcountrieslikeIsrael,Singapore
andMalaysia.TheR&Disnowherenearthepossiblefundingindevelopedcountries
23 Pharma Times, June 11, 2011
24www.evaluatepharma.com/Universal/View.aspx?type=Story&id=217946§ionID=&isEPVantage=yes
Page 29 of 153
likeUSundertheNationalInstitutesofHealthfundingprograms.Thishasalso
resultedinpoortappingofopportunitypresentedbytheintroductionofproduct
patentregimein2005.
MoredetailsonR&DmaypleasebereadinChapter‐2onR&D.
(2)InadequateInfrastructure
Whilethereisanestablishedbasicweaknessinbasicinfrastructurelikepower,roads
andcoldchainstheLackofadvancedlabandrelatedinfrastructurefordrugstesting
anddevelopedisacutelyperceivedintheneedofgreateremphasisonresearchand
developmentaswellaslargecapacitiesrequiredforAPIsandformulationsonthe
scaleatwhichcompetitorslikeChinaandIsraeloperate.Thisisparticularlytruefor
suchsectorslikeantibioticswherethecountryhasmigratedfromastateof
completeindependencetototaldependenceonimportsfromChinafor
fermentationbulkproductsduetounmatchedcostsofpowerandhighcapacity
buildupleadingtolowcostsofproduction.Thisinasenseisalsoastrategicissue
andhasassumedsignificancefollowingtheHINISwineFluepidemic.
Thedevelopmentofinfrastructureisakeytosuccess,andtheIndianPharmaceutical
Industryandsothereisneedtotakemoredefinitivestepstoovercomethis
weakness.
(3)DiffusedIndustrystructure
DiffusednatureoftheIndianpharmaceuticalindustrywhereby,onlyabout20to30
companiesarelargeenoughtobearthetransactionscostsassociatedwithsustained
productionincludingexportsparticularlyinthelightofincreasinglystringent
complianceentryregulationsofthedevelopedandemergingmarkets.Thusthereis
Lackofdepthandbreadthnowinthecontextoftheinternationalscenario.
(4)PoorIndustry‐Academialinkage
Page 30 of 153
ThereisaconspicuousLackofstronglinkagesbetweenindustryandacademiawhich
areessentialforgrowthoftheindustry.
(5)Limitationstodomesticmarketsize
Limitationsingrowthofthedomesticmarketsizeduetoconstraintsoflowmedical
andhealthcareexpenditureintheruralareasofthecountryinspiteofspecific
projectslikeNRHM,DOTS,NSAIDSandPulsePolio.
(6)Decreasinglabourarbitrage
Nowrapidlyincreasingcostsofskilledmanpowersuchasscientists/regulatory
compliancepersonnel/pharmaceuticallawyers/internationalbusiness
developmentpersonnelispushingupthecostofinnovationleadingtolossof
arbitrageoflabourascomparedtodevelopedandotheremergingmarketcountries.
(7)Poorworldclassprojectskills
Projectmanagementcapabilitiestoevaluatecontracts/alliancesetc.,isavailable
onlyintopcompanies.
(8)Non‐availabilityofmajorintermediatesforbulkdrugs
(9)Inadequateoverseasmarketinginfrastructure
TheIndiancompaniesareseverelyLackinginaglobalmarketingworkforcenodoubt
constrainedbysurpluscapitalandrecurringexpenditurecostsmuchrequiredfor
globaldominance.Thishasresultedinanumberofmarketingtie‐upsofIndian
companieswithMNCs.Thesetie‐upswhilebeingpresentedassuccessful
partnershipsmissthefactthatthelucrativeemergingmarketsarelostduetoLackof
abilitytotapthembyindigenousefforts.Whiletheexacttermsofdealarenot
publicprivy,thewin‐winsituationrequiresadeeperstudytoanlaysethelossof
opportunityduetotheweaknessofthemarketingforce.
(10)Lackofregulatoryinfrastructure
DuetomajorunderstaffingandLackofresourceswiththeCentralDrugsStandards
andControlOrganisation(CDSCO)undertheMinistryofHealththereisamajor

Page 31 of 153
bottleneckfortimelyclearancesfornewdrugtrials,pharmacovigilanceand
assistancetothewillingindustrymemberstoshoreuptheirtechnicalcapacitiesfor
betterregulatorycompliances.TheLackofdruginspectors,bothatthecentreand
thestatelevelintheFDAsisamajorhindranceinthesmoothgrowthoftheindustry.
Nowhereisthismoreevidentthaninthepoorpaceofclinicaltrialclearancesand
theFDCssegment.
(11) LackofproperRegulatoryFrameworkforbiosimilardrugs
Presently,biosimilarsareregulatedundertheprovisionsofEnvironmentProtection
Actof1970andtheDrugs&CosmeticsActof1940.Therearenosetofspecific
rulestoenablespeedierandunambiguousclearanceforproductionofbiosimilars.
Thisisimportantinthecontextofthefactthatbiosimilarsisaverystrongemerging
marketopportunityforthecountry.
(12)Regulationoffixeddrugcombinations.
Anotherimportantissueconcernsregulationforapprovalforfixeddrug
combinations.Thisneedstobeevolvedinconsultationwiththeindustry.TheDTAB
undertheDCGIshouldhavearepresentativeofDoPsoastoensurethatthePharma
Industryconcernsareaddressedinaspeedyandunambiguousmanner.
1.7.3OPPORTUNITES:
(1)Generics
AsperMcKenseystudyconductedbyDoP25,US$300Bnareexpectedtogooff
patentby2015forconventionalmoleculesandbiopharma.Factoringforthe
reductioninpriceandtheconsequentmarketvaluefrompatenttogenericsthisis
estimatedtobeatleast30‐35%whichtranslatestosomeUS$100Bn.
CompulsorylicensingprovisionsnegotiatedintheDohaRound,allowsforcountries
toimportcheapergenericversionsofpatenteddrugsintheinterestsofpublic
25 McKinsey &Company,”Capturing the India Advantage-page 18
Page 32 of 153
health.ThailandandSouthAfricahavealreadystartedsuchinitiativesfromwhich
Indianfirmshavebenefited.Thisisanopeningopportunityalbeitnotverylargefor
Indianpharma.
(2)Bio‐generics&BioPharma
Bio‐genericsarenothingbutgenericversionsofbiologicalproducts.India's
biotechnologysectorisgrowingfastandisintheearlystagesofdevelopmentwith
initialemphasisonvaccinesandbio‐services.Theindustrycurrentlyhasaround340
companieswhichemploymorethan25,000technologists.TheIndianBio‐Pharma
industryhasalreadyastrongglobalpresence,producingthefourthlargestvolumeof
productsintheworld.India’svastpoolofskilledmanpower,hugepatientbaseand
relativelylowcostsdrivesmanyglobalbiotechgiantstopartner,acquireor
outsourcetoIndiancompanies.Likewise,someofthelargerIndiancompanieshave
evenbegunacquiringforeignentitiesintheUnitesStatesandEurope,toretailtheir
productsandexpandproductofferings.
Internationallyspeaking,in a study conducted on behalf of Datamonitor by Bornadata
Bain, vice-president and global director of research and analysis, healthcare, and John
Shortmoor head of company analysis, both at Datamonitor Group, it has been stated
that the product mix of pharmaceutical companies' pipelines and commercial drugs is
of crucial importance to contract development and manufacturing organizations as
they evaluate their service capabilities and tailor them to demand. Market
fundamentals are changing. The erosion of the blockbuster-drug model, traditionally
supported by small-molecule drugs (i.e., drugs with a molecular weight of < 500 Da),
in favour of an increased emphasis on biologic-based development is an important
consideration not only for pharmaceutical companies' product strategies, but for
contract service providers that offer drug-substance and finished-product
manufacturing.
Page 33 of 153
Although small-molecule drugs will continue to dominate the overall pharmaceutical
market, market growth in small-molecule drugs will contract in the near term. In
biologics, mAbs will drive growth and so enticing a growing number of companies to
expand in this field with the hope of ensuring long-term growth. In fact, 36 of the top
50 pharmaceutical companies (excluding generics companies) will have a presence in
the mAb, therapeutic protein, or vaccines sector by 2014. Currently, 32 of the top 50
companies are now in those sectors. Vaccines will grow at a 5.5% compound annual
growth rate (CAGR) between 2009 and 2014, partly because of the emergence of new
technologies and the recent commercial success of several novel products such as
Pfizer's pneumococcal vaccine Prevnar and Merck & Co.'s human papillomavirus
vaccine Gardasil.
Biotechnologycompanieshavefocusedprimarilyonbiologics,butfrom2008to
2014,thedominanceoftherapeuticproteinswithinthemolecularclassmixwill
declinesteadilyasmAbsgainmarketshare.Nevertheless,therapeuticproteinswill
remainthedominantmoleculetypethroughout,accountingfor68.0%of2014sales.
ThisshiftinfocustowardmAbswillbespurredbythismolecularclass'srelatively
stronggrowthof$4.4billionin2008–2014,whichresultedprimarilyfromthelaunch
ofAmgen'sProliaandcontinuedsalesgrowthofMerckKGaA'sErbitux.Interestingly,
therapeuticproteinswilldelivergreatersalesgrowthuntil2014(i.e.,$5.2billion)
becauseofNovoNordisk'sinsulin‐analogportfolio,whichincludesNovoRapid,
NovoMix,andLevemir.Small‐moleculegrowthwilltotallessthanhalfofthat
deliveredbybiologics,at$3.1billion.
BiogenIdechasthebiggestmAbfocusandalsothebiggestbiologicsfocus;mAbs
andtherapeuticproteinsaccountedfor98.9%ofits2008sales.NovoNordiskwill
accountforthemajorityofthepeerset'stherapeutic‐proteinsalesgrowth,withan
increaseof$4.7billionforecastbetween2008and2014,tobesupportedprimarily
byGenzyme(Cambridge,MA,$1.3billion).Bycontrast,declinesof$741millionand
$221millionareforecastforBiogenIdecandAmgen'stherapeutic‐proteinportfolios,
respectively
Page 34 of 153
Reflecting the pharmaceutical industry's burgeoning interest in high-growth biologic
markets, 27% (seven out of 26) of US Food and Drug Administration new drug
approvals in 2009 were for biologic license applications (BLAs). This number
represents the highest proportion of biologic approvals since 2003 (2). In fact, the
growth in approved BLAs offset the decline in approved new molecular entities
(NMEs). Furthermore, the number of US orphan-drug designations has more than
doubled in the past decade, from 208 (2000–2002) to 425 (2006–2008) (3). The
number of orphan drug approvals grew from 32 to 47, an increase of 47%. In 2009,
the European Medicines Agency (EMA) granted orphan status to 103 medicines, the
highest number since European orphan-medicines legislation was introduced in 2000.
Injectable drugs will drive market growth
Despite the current dominance of oral drugs, which typically are associated with
small-molecule drug delivery, injectable drugs enjoyed strong growth between 2002
and 2008 at 20.8% CAGR. Injectables will continue to enjoy the fastest growth rate of
all delivery mechanisms (i.e., 4.9% CAGR) until 2014, aided by the development of
vaccines and mAb therapies which are typically delivered by this mechanism. The
loss of patent protection for blockbuster brands such as Pfizer's Lipitor (atorvastatin)
and Effexor (venlafaxine), and AstraZeneca's Seroquel (quetiapine) will trigger strong
generic-drug competition and sales erosion for oral drugs.
Secondary-care therapy areas would become a priority
Historically, small-molecule drugs dominated therapeutic areas such as cardiovascular
and central nervous system (CNS) conditions and contributed to significant sales
growth. However, these markets are not only saturated with me-too drugs, but also
suffer from rapid market erosion because of the influx of generic drugs after the
patent expirations of key brands. For example, in 2009, sales of cardiovascular drugs
totalled $99 billion; they are forecast to decline at 2.8% CAGR (2009–2014). The
forecast contraction in this market is likely the reason for Pfizer's announcement in
September 2008 that the company was ending its research and development (R&D)
investment in this therapy area—a landmark move, given the dominance of
cardiovascular drugs in Pfizer's portfolio.
Page 35 of 153
Now pharmaceutical companies are shifting their R&D focus toward developing
novel—often biologic—therapies for the treatment of niche indications, which should
ensure longer-term growth given biosimilars' minimal impact to date. Examples of
target therapy areas are oncology, immunology and inflammation, and endocrine
diseases, which are forecast to grow at rates of 5.9%, 4.0%, and 6.3% CAGR,
respectively, between 2009 and 2014.
In 2009, several noteworthy therapies were launched, representing truly novel drugs
that target unmet needs. Johnson & Johnson's (New Brunswick, NJ) Stelara
(ustekinumab) for plaque psoriasis stands out as a first-in-class agent with efficacy
superior to that of traditional therapies. Also, Takeda's Uloric (febuxostat) is the first
new treatment for gout in 40 years, and Forest's Savella (milnacipran) is the first drug
indicated solely for fibromyalgia .
In addition, these target markets—oncology, endocrinology, and immunology and
inflammation—will experience the highest sales growth and become the principal
growth drivers for the top 50 pharmaceutical companies (excluding generic-drug
companies), collectively generating an additional $45 billion by 2014. It is therefore
expected that an increasing number of companies will focus on these more profitable
markets.
Factors driving the shift away from the primary-care model
The cash-strapped payers now scrutinizing drugs' costs and clinical benefits and so it
is not surprising that the pharmaceutical industry is now focused on biologic therapies
in secondary care and niche markets. Additional factors that attract pharmaceutical
companies toward niche indications include the faster and cheaper R&D process that
results from the smaller patient populations and clinical-trial sizes. In addition, several
regulatory agencies provide incentives and subsidize R&D in the development of
orphan drugs. The agencies offer tax credits, regulatory assistance, and accelerated
approval. Also, one of the largest cost-saving factors for companies with a niche
product is that large-scale patient and physician marketing through various channels is
largely irrelevant. In fact, annual average marketing costs for an orphan drug are
seven times lower than those for nonorphan products. Figure 1 summarizes the factors
Page 36 of 153
inspiring the shift away from the primary-care blockbuster model toward niche
indications.
Big Pharma will remain dependent on small molecules, but biologics will spur
growth
The Big Pharma business model essentially was built on small-molecule products,
which are relatively inexpensive to develop and manufacture, thus allowing
companies to concentrate on fuelling growth with an assertive sales and marketing
strategy. However, once patent protection is lost, small molecules are easy for
generic-drug companies to manufacture. Manufacturers of generic drugs do not have
to support large R&D teams and they are able to compete aggressively on price. The
resulting commoditization of the small-molecule market has forced the Big Pharma
players to seek diversification into areas of high unmet need (e.g., oncology) or, in
terms of molecule type, into biologics. The Big Pharma shift to biologics will be led
by mAbs, which are forecast to grow by $22.1 billion during 2008–2014 at a 9.5%
CAGR, thus making them the biggest growth factor for this sector. Therapeutic
proteins also will experience strong growth during 2008–2014, contributing an
increase in sales of $9.2 billion at a CAGR of 3.6%. By contrast, small molecules—
which accounted for 80.4% of Big Pharma's 2007 sales—will decline by $25.6 billion
during 2008–2014. Despite these shifts, Big Pharma will remain dependent on small-
molecules, which will account for 71.4% of its sales in 2014. Biologics (i.e., mAbs
and therapeutic proteins combined) will account for 21.8% of sales, up 6.7% from
2008.
At a company level, a clear correlation can be drawn between small molecules and
declining sales versus biologics and sales growth. Of the top 16 Big Pharma
companies, only Novartis, Bayer, Merck & Co, and Boehringer Ingelheim will see net
positive growth from their small-molecule portfolios. By contrast, the remaining 12
companies are forecast to see a net growth in their biologics portfolios.
Roche - primarily through its acquisition of Genentech contributes about 51.4% of the
mAb growth for Big Pharma. Aside from Roche, Abbott Laboratories also will exhibit
strong growth in the mAb sector. Its growth is attributable to its acquisition of Knoll
and its licensing of international rights to Synagis and Numax from MedImmune.
Page 37 of 153
Johnson & Johnson also will exhibit strong growth, spurred by the growth of Simponi
(golimumab), Stelara (ustekinumab), and its share of bapineuzumab sales.
Growth from therapeutic proteins will be spread more evenly across Big Pharma.
Sanofi-Aventis, primarily through insulin analog Lantus; Pfizer, through Enbrel; and
Bristol-Myers Squibb, through Orencia and belatacept, will make significant
contributions. Novartis also will report growth in therapeutic proteins, primarily
attributable to its launch of biosimilar drugs through its generic-drug division Sandoz.
However, none of these companies will experience biologics growth remotely close to
the level of mAb growth forecast for Roche.
Looking forward
For the foreseeable future, blockbuster drugs will provide the bulk of sales for the top
50 pharmaceutical companies (excluding generic-drug companies). These drugs
generated $344 billion collectively in 2008, representing 66% of prescription sales.
However, the outlook for these drugs is less than stellar; 66 drugs with blockbuster
status in 2010 will see a sales decline of more than $200 million by 2014, in response
to me-too and direct or indirect generic competition. As a result, total forecast sales
for blockbusters will decline by 2.1% CAGR from 2009 to 2014. Pfizer will be the
hardest hit, with 2014 blockbuster drugs sales forecast to decline by $8.3 billion
versus its 2009 level. The Wyeth merger will soften the blow slightly for Pfizer, but
the company will remain the most strongly affected in terms of blockbuster
expirations and total sales losses over the 2009–2014 periods. Bristol-Myers Squibb
and Sanofi-aventis are also forecast to experience losses of $5.0 billion in
blockbuster-drug sales by 2014 versus 2009 because of the generic erosion of
blockbuster brands.
As the industry moves away from the old primary-care blockbuster model toward
targeting specialty secondary-care indications, several novel drugs launched in 2009
still have the potential for blockbuster status, including sanofi-aventis's antiarrhythmia
agent Multaq (dronedarone), Johnson & Johnson's Simponi (golimumab) indicated for
rheumatoid arthritis, and Bristol-Myers Squibb and AstraZeneca's Onglyza
(saxagliptin) for the treatment of type 2 diabetes. Nevertheless, entering a
Page 38 of 153
multibillion-dollar therapy area cannot guarantee blockbuster status, particularly in
today's price-conscious environment.
Key factors that will be important for determining blockbuster success within the
biologic markets include the ability to gain first-mover advantage within a given
indication, the subsequent horizontal expansion across disease stages and indications,
and the creation of high barriers to competition through the accumulation of clinical
safety and efficacy data. In addition, with the increasing cost pressures facing payers,
manufacturers will need to demonstrate comprehensive pharmacoeconomic data and
drug benefits for these therapies in relation to the disease frequency and severity.
They may also need to demonstrate an advantage in comparative effectiveness over
existing products. This competitive advantage may be achieved best through coupling
drugs with companion diagnostics or creating disease-management solutions.
Pharmaceutical companies frequently employ risk-sharing agreements as a means of
securing a place on reimbursement lists, thus sharing the risk between the payer and
the manufacturer. These schemes also encourage responsible prescribing by
healthcare professionals and ensure that resources are not wasted on ineffective
treatments. By addressing payer concerns regarding both economic and clinical
outcomes, risk-sharing schemes have the potential to change the pricing landscape of
high-cost drugs.
These very factors have led to the dominance of mAb products such as Roche's
Avastin (bevacizumab), Herceptin (trastuzumab), and MabThera (rituximab); Abbott's
Humira (adalimumab); and Johnson & Johnson and Merck & Co's Remicade
(infliximab), which together accrued a 72% share of mAb sales in 2008. However, the
market share of these top five brands will fall to 57% in 2014 because of increasing
competition from newly launched mAbs. In fact, from 2008 to 2014, the number of
mAbs achieving blockbuster status will increase from five to 15. Nine other mAbs
will generate sales of more than $500 million in 2014. Overall, the mAbs market will
remain healthy.
Clearly, a paradigm shift is taking place in the pharmaceutical industry, as the small-
molecule business model that historically inspired sales growth is replaced by a high-
value specialty-biologics model to fend off further sales erosion. As the patent cliff
approaches, it will be increasingly important for all pharmaceutical companies to

Page 39 of 153
consider putting a biologics strategy in place, either through organic means or through
partnerships, to avoid being left behind in this dynamic, competitive environment.
(3)AttractivedestinationforContractManufacturing&Research:
Theglobalpharmaceuticalindustryisatthecrossroads.Withmanyofthe
blockbusterdrugsgettingoff‐patentedandwithincreasingR&Dcosts,itshardbythe
companiestomaintaintheirbottom‐lineandremainunaffected.Theyhavefound
recoursetooutsourcingsomeoftheirresearchandmanufacturingactivitiesand
savingcostintheprocess.Thishasledtothegrowthofcontractresearchand
manufacturingservicesorCRAMSmakingthecompaniesinIndiatorejoice.Business
ofCRAMShascomeasaboontothemid‐cappharmacompaniesinIndia,these
companiesaremerrilyembracingCRAMStakingfulladvantageofthefeatures
enjoyedbyIndiaasacountryofdiverseoriginandstrongmanufacturingbasein
pharmaforyears.Indiacouldpotentiallycapture10%oftheglobalCRAMSmarketof
almostUS$200billionby201126.Overall,theCRAMSsegmentisexpectedtogrow
30‐35%perannumontopofagrowthof40‐50percentinthelastfewyears.In
termsofcontractresearch,someoftheknownfactsinrecentdrugdiscoveryare:
(4)DrugDiscovery
Inthedrugdiscoveryvaluechain,therearekeyblockslikebiology,chemistry,drug
evaluation,preclinicaltrialsandclinicaltrials.Buildingtheskillsetandinvestingin
theinfrastructuretoachievecriticalmasswillhelpdrawtheresearchworkintothe
countryperhapsinapiece‐mealinitially.Asthecomponentsgetbuilt,
entrepreneurialinitiativeswillkickoffonabroaderscale,establishingtheindustry.
VarioussurveysindicatethatIndiahasquiteanumberofresourcefulfirmsinthe
fieldofChemistryprovidinghighqualityoutputintimelyschedules,allowingmore
leadstopursue.Indiaissignificantlyaheadinchemistryservicessuchasanalog
preparation,analyticalchemistry,focuslibrary,combinatorialchemistry,structural
chemistry,structuraldrugdesign,computeraideddrugdesign,highthroughput
screeningandassaydevelopment.
26 Cygnus research

Page 40 of 153
IndiaatthispointisaheadofChinainchemistrybuttheimpressioninmany
countriesisthatIndiaisweakonbiologyfront.ItisfoundthatIndia’sstrengthin
biologysectorisverylimitedespeciallyingeneticallymodifiedanimals,biochipsand
basicmolecularbiology.Thebiologycapabilitiesaremainlyingovernmentinstitutes
withahandfulofcompanieshavingskillsinmolecularbiologyandprotein
expression.However,onlyahandfulofGLPlabsexistandtheavailabilityofclinical
investigatorsandclinicalpharmacologistsarenegligibleincomparisontoother
countriesinthefield.
Throughstrategicbuildingofinfrastructure,suchasorganizationsconducting
chemistryresearch,preclinicaltrialsandclinicaltrialsandlaterbiologyresearch,
Indiacancreateastrongvendorbaseallowingvariouscompaniesintheworldto
undertakenewdrugresearch.Biologyresearchservicesmarketandinfrastructure
shouldbedevelopedwithconsciouseffort.Suchservicesinallkeysegmentsbuilt
eveninpiecemealwillcreategoodvendorbaseandaugurswellinconvertingthe
countryintoanNCEhub.Obviously,sucheffortwillbeasuccessfuldrivertoearn
fromexportofpharmaceuticalservices.
(5)ClinicaltrialsIndustry
ThepressuresofdecliningR&Doutputandincreasingcostshasresultedinthe
globalizationofclinicalresearchandemergingmarketshavebegunplayinga
significantroleinthedrugdevelopmentvaluechain.Indiatoohasseenasurgein
clinicalresearchactivitywithanevolutionoverthelastdecade,frombeingan
industryfocusedonBA/BEservicestoincreasinglybeingviewedasserviceprovider
ofchoicebytheglobalpharmaceuticalandbiotechnologycommunityinthearenaof
PhaseI‐IVtrialsandalliedservices.
EmergingmarketslikeIndiaarenomoreanoptionbutastrategicimperativefor
globalclinicalresearch27.
27 “The Global Metamorphosis- Compelling reasons for doing clinical research in India – Report by E&Y and
FICCI, 2009
Page 41 of 153
TheUSD64Bnglobalclinicalresearchindustryiswitnessingatransitionaslife
sciencecompaniesareturningtowardemergingmarketsinAsia,LatinAmericaand
EasternEurope,topursueclinicalresearch.Increasingcosts,decliningproductivity
andrisingdrugdevelopmenttimelines,combinedwiththestrategicadvantages
offeredbytheseemergingmarkets,isdrivingresearch‐drivenpharmaceuticaland
biotechnologycompaniestoconductclinicalresearchbeyondestablishedmarkets.
Emergingmarketsnowcontributeto~36%ofglobalpatientenrolmentascompared
to~20%in2001.
Indiaisoneofthefastestgrowingclinicalresearchdestinationswithagrowthrate
thatistwoandahalftimestheoverallmarketgrowth.
Indiaparticipatedin7%ofglobalPhaseIIIand3.2%ofPhaseIItrialswithindustry‐
sponsoredtrialshavinggrownataspectacular39%CAGRbetween2004and2008.
ThenumberofinvestigatorsinIndiahasalsogrownthefastestamongAsian,Latin
AmericanandEasternEuropeancountrieswitha42%CAGRbetween2002and
2008.Indiahasoneofthelatestsubjectrecruitmentratesglobally(nearlythreeto
fivetimestheglobalaverage),withscreenfailureanddropoutrateslowerbynearly
40‐50%,ascomparedtoglobalaverages.Asaresult,Indiacontributes15‐30%of
globalenrolmentinmulti‐centricstudieswhereitisaparticipant.Indiaisranked
thirdacrossallcountriesaftertheUSAandChinaintermsofitsoverall
attractivenessasaclinicaltrialdestinationaccordingtoarecentATKearneyglobal
survey.
Further,India’sclinicalresearchlandscapeisundergoingaglorious
metamorphosis,aidedbymanyuniquelydifferentiatingcapabilities,arapidly
transforminghealthcaremarketandanenablingenvironmentthatisrapidly
adaptingitselftoglobalstandards.Theseare–
(i)Scientificfeasibility:
Indiaconstitutes16%oftheglobalpopulationwith20%oftheglobaldisease
burden.With~32millionpatientsinurbanareasand~72millionpatientsin
Page 42 of 153
ruralareasatanygivenpointoftime,Indiahasadiversemixofsubjectswho
arerelativelytreatmentnaïveaswellassubjectswithahighstandardofcare
tomeetdiversestudyprotocols.
Thecountry’sdiseaseburdenisalsowellalignedwiththenewdrug
developmenttherapyfocusofglobalpharmaandbiotech,withashifttoward
non‐communicablediseases.Indiahas65millionpatientswithCNSdisorders,
31milliondiabetics,29millioncardiacpatients,41millionCOPDandasthma
patients,0.8millioncancerpatients,withmostoftheseailmentsexpectedto
increasebyover50%inthenumberofcasesby2015.
Allthefivemajorracialtypes–AustraloidMongoloid,Europoid,Caucasian
andNegroid–findrepresentationamongthepeopleofIndia,withCaucasian
beingthemostprevalent.
(ii)MedicalInfrastructure:
Theurbanhealthcareinfrastructure,intermsofthenumberofbeds/
physicians/nursesper1000,iscomparablewiththeglobalaverage,Indiahas>
8,40,000urbanbeds.Thereareover6,00,000English‐speakingphysiciansand
nearly1,00,000specialists,withmanyofthemhavingbeentrainedinthebest
globalinstitutes.Thereare41hospitalsaccreditedunderInternationalSociety
forQualityinHealthcarebyNationalAccreditationBoardforHospitaland
HealthcareProviders(NABH)andJointCommissionInternational(JCI),while
84hospitalsarecurrentlyintheprocessofapplyingforNABH.
(iii)Regulatoryreforms:TheClinicalestablishment(Registrationand
Regulation)Act,whichisbeingpromulgatedbythegovernmenttoregulate
privatehospitalsandlaboratoriesacrossthecountry,willplayasignificant
roleindevisingandimplementinguniformstandardsoffacilities/servicesand
furtherenhancethequalityofcareprovidedbytheIndianhealthcaredelivery
system.

Page 43 of 153
ThusitmaybeseenthatIndiahassignificantvalidpopulationtoparticipatein
clinicaltrialsandthecountryalsohasprovencapabilitiesinmedicalskills,hospital
bedsandITcapability.Thisoffersanopportunitytocapturethemarketsharein
globalclinicalR&Dmarketsuchasclinicaltrials,datamanagement,testing,etc.By
buildingtheabovekeyblocksinthedrugdiscoveryvaluechain,Indiacanreachthe
statusofintegratedproviderinchemistryandbiologyservices.Thecountrycanlearn
skillswhileearning,atleastincertainpartsofdrugdiscoveryprocess.Thiscould
enablethecountrytoattractdrugdiscoveryfirmstoconductresearchinIndiawith
spin‐offbenefitsinmakingIndiaasanR&Dhubinthelongterm.
CostsofclinicaltrialsinIndiaarearoundone‐tenthoftheirlevelsintheU.S.
Currently,IndiaisexperiencingagrowingnumberofcollaborationsbetweenIndian
andforeignfirmsinthedomesticmarket,especiallyinvolvingthebiotechnology
sector,inawidevarietyofareassuchascollaborativeR&Dincludingdrugdiscovery
andclinicaltrials.However,scarcityofspecialistclinicalpharmacologists,clinical
investigatorsismostcriticalissuefacingIndianclinicaltrialindustry.
Anotherimportantareaisthelackofproperregulatoryframework.Someofthe
importantpointsinthisconnectionare28:
(i)SingleWindowClearance
Therearemultiplegovernmentdepartmentsthatmayhavetobeaddressedduring
theexecutionoftheclinicaltrialsforpermissionsandapprovals.TheyareDCGI‐
MinistryofHealthandFamilyWelfare,DirectorateGeneralofForeigntrade–
MinistryofCommerceandIndustry,DepartmentofBiotechnology–Ministryof
ScienceandTechnology,MinistryofEnvironmentandForestforbiotechproducts.
Theindustryfeelstheneedtohaveasinglewindowforapprovals.Whereasthe
specificdepartmentscancontinuetobethedecisionmaker,fortheindustryall
applicationstobemadeforpermissionshouldbeasinglewindow.
28 FICCI Report on Clinical Trials Industry, 2009 prepared for DoP
Page 44 of 153
(ii)HarmonizationOfTechnicalRequirementsWithICHRequirements
TohelpIndiagloballycompeteandgetnewtherapiestopatientsfasterandalso
buildearlydevelopmentalcapabilitiesandexperience.
(iii)Pre‐ClinicalRequirements
Today,regulatoryrequirementsforearlydrugdevelopmentinIndiaareseenas
beingmorerestrictivethanfacilitatingwhencomparedtootherglobalregulatory
bodies.ForexamplethedraftICHguidelinesforNonClinicalEvaluationforAnti‐
CancerPharmaceuticalsrequirea1monthtoxicologypackageintwospecies(rodent
andnon‐rodent)fortheevaluationofnewinvestigationaldrugsforthetreatmentof
advancedcancerinPhase1clinicaltrials.A3‐monthtoxicologypackageisonly
neededtosupportPhase3registrationstudies.AsperScheduleYthecurrent
toxicologyrequirementforIndiaisa6‐monthtoxicologypackagetoinitiatethefirst‐
in‐mantrialforallagentsincludinganticancercompounds.Duringtheprocessof
drugdevelopmenttheabovementionedpre‐clinicalstudiesareconductedlate,
beforePhase‐III.
IncertainareassuchascancertheIndianregulatorscaneasilyadopttheuniversal
regulatoryguidance(i.e.ICH–InternationalConferenceonHarmonizationof
TechnicalrequirementforPharmaceuticalsforhumanuse)toallowevaluationof
treatmentoptionsforthisdebilitatingdisease.Itshouldberecognizedthatsincethe
longevityofpatientswithadvancedcancerislimited,thePhase1evaluationmay
providesomenewertreatmentmodalitiesforsuchpatients.Patientsmayactually
benefitfromthenewerexperimentaloption.
(iv) DefinitionofPhase‐IClinicalTrials
ThePhase‐1studiesfallwithintherealmofexperimentalscienceandrequirearange
ofskillsandexpertiseofthehighestorder.Becauseofthehigh‐risknatureofthese
studies,theregulatorybodyiscalledupontoplayapivotalrole.PhaseItrialsare
Page 45 of 153
allowedonlyformolecules‘discovered’inIndia.Thesafety/tolerabilityissuesata
PhaseIstagearerelevantandapplicableformoleculeswhetherdiscoveredinIndia
oroutsideofIndia.USFDAandmanywesterncountriesallowtheevaluationofIndia
discoveredmoleculesintherespectivegeographiesaslongastheycleartheIND
(investigationalNewDrugs)and/orCTA(ClinicalTrialApplication)hurdles.Itshould
benotedthatthesameyardstickandrigorshouldbefollowedfortheevaluationof
Indiadiscoveredcompoundsversuscompoundsdiscoveredelsewhere.
Withmoreandmorepartnershipsandco‐developmentthereisneedtohavea
uniformunderstandingandinterpretationofIndianversusForeignmolecules.Itis
unclearwhatconstitutesanIndianmolecule.Therearemanyvariantsincluding
DiscoveredandDevelopedinIndia,DiscoveredoutsideIndiabutDevelopedinIndia,
DiscoveredinIndiaandDevelopedoutsideIndia,DiscoveredoutsideIndiabutare
partiallyorcompletelyownedbyIndiancompanies,DiscoveredoutsideIndiabut
handedovertoanIndiancompanywhichischargeofdevelopment.
Thedecisionsondevelopmentstrategiesfornewmedicineandtheexperimental
approachesusedtoassembleinformationrelevanttothesafetyoffirst‐in‐manand
Phase‐Iclinicaltrialsmustbescience‐based.
(v)CapacityBuilding
(a)Ethics:RegistrationandTrainingofEthicsCommittees
IndiahasalargenumberofResearchInstitutesandMedicalCollegesandHospitals
involvedinclinicalresearch.Duringthelastfewyearstheseinstitutionshavesetup
ethicscommittees.Variousindependentethicscommitteeshavealsocomeinto
existence.Thepurposeofethicscommitteeistoensurethattheresearchis
conductedinanethicalmanner,forwhichenablingethicalguidelines,lawsand
effectivereviewmechanismshouldbeinplace.TodaythereareICMRandthe
CDSCOGuidelinesforthispurpose.
Page 46 of 153
However,thefunctioningandoperationsofthesecommitteesisvariabledespite
havingtheguidelinesinplace.CurrentlyEthicsCommitteesacrossthecountrydo
nothaveacentralbodythatwouldeitherregisteroraccreditthesecommitteesto
ensureeffectivefunctioning.TheIndianCouncilofMedicalResearchhadinitiated
somestepstowardsregistrationofInstitutionalEthicsCommitteessometimeback
butnothingconcretehascomeoutsofar.Theimmediateneedsare:
• RegistrationofEthicsCommitteesbyacentralbodyandthedetailsofthese
committeesthatoverseetheclinicalstudiesofallphasesshouldbe
availableinpublicdomain.
• AccreditationofEthicsCommittees–Theprocessfollowedcouldbethatof
FERCAP(ForumforEthicsReviewCommitteesinAsiaandWesternPacific
Region).TwoEthicsCommitteesinMumbai‐KEMHospitalandTata
MemorialCentreareundergoingthisprocesscurrently
ABioethicscurriculumhasbeendevelopedundertheICMR‐NIHProgramme
Inthesecondphaseadistancelearningprogrammeisbeingdevelopedbythis
projectincollaborationwithIndiraGandhiOpenUniversity.
(b)InvestigatorTraining
InvestigatorsneedtobetrainedtobeabletoparticipateinClinicalResearch.The
trainingneedsarenotjustconfinedtoGCP.Aspracticingdoctors,theapproachto
traininghastobenovel.Theyhavetobetrainedinevaluatingprotocolfeasibility
anditsethicaladministration.
(c)NursesTraining
Nursesarekeyelementintheoverallhealthcaredeliverymechanism.Specificallyin
clinicalresearch,mostofstudycoordinatorsareNurses.UnfortunatelyinIndia,due
tolackoftrainednurses,theresponsibilitiesofastudycoordinatorisprimarily
shoulderedbyanInvestigator.Afocusedtrainingprogramfornursesinclinical
Page 47 of 153
researchcangoalongwayinreducingthecurrentburdenoninvestigators,andalso
offerenhancedopportunitiestothenursingprofession.
(d)RegulatoryCapacityBuildingforSiteInspections
ForthelastfewyearsregulatoryauthoritiesliketheUSFDAandEMEAhave
conductedvariousinvestigatorsiteinspectionsinIndia.Itisincommonknowledge
thattheDCGIofficeincollaborationwiththeUSFDAistrainingafleetofinspectors
forconductingregulatoryinspections.Thoughthisisawelcomestepanditneedsto
beviewedmorebroadly.Thereneedstobeanestablishedprocessforthese
inspectionsthattheseinvestigatorsaregoingtoundertake.Sincethesecapabilities
ofinspectionsarebeingdevelopeditisimportanttopredefinethecapabilities,the
qualifications,themethods/SOPsinatransparentwayreflectingandassuringgood
governance.
ItisalsoimportanttonotethatGCPcomplianceistakenasaresponsibilitysolelyof
themonitoringorganizationandsponsorbuttheinvestigatorsitesalsoshouldbe
equallyheldaccountableandresponsibleasrequiredbyvariousregulatoryagency
guidelinesincludingtheIndianGCPguidelines.Therehastobeamechanismfor
reportingscientificmisconduct/fraud.
Itmaybeimportanttohaveabasicmandatorytrainingforthe
investigators/coordinators/nursesthatiscertifiedbyabodyrecognizedbythe
competentauthorityandalistofsuchGCPtrainedandcertifiedinvestigatorscanbe
availableontheCDSCOwebsite.
Theregulatoryauthoritiesshouldmakeavailabletothepublic,inunderstandable
language,negativeandpositiveassessmentreportsoftheinspectiononlyafter
completingtheinspectionprocess
(e)InfrastructureforClinicalResearch
Page 48 of 153
ThereisaneedforClinicalResearchCentresforhighrisktrialslikePhaseI.The
availabilityofsuitablytrainedmanpower,andfacilityforcriticalcareisimportant.
Whereas,facilityforcriticalcarewillbelinkedtothehospital,theavailabilityof
trainedinvestigators,specialistfromnumerousdisciplinestrainednursesandtrained
studycoordinatorsarekeyelementsofanyworldclassclinicalresearchcentre.
(6)ITinPharmaR&D
ThereisagrowingimportanceofITinthepharmaindustry.Thus,eventhoughthepharma
industryisalifesavingproductsandhealthcareindustry,ithasbeenaslowandlate
implementerofITtools.UseofITcanhelpin–
i. Dataanalysisformolecularscreening
ii. Clinicalresearchdatamanagement(CDM)
iii. Animalmodeling
iv. Biomarkersforsafetyandeffectiveness
v. Bio‐statistics
vi. Bio‐informatics
vii. Genomeresearch
viii. ProcessimplementationintermsofERPs,Regulatorysubmissions
Developmentoftoolsfortheseandotheractivitiesisacontinuousandexpensiveprocess
particularlyfortheSMEsector.AtpresentDIT,DBT,DST,etcdonothaveanyschemeto
assistSMEsforcapacitybuildingandITtoolsdeploymentforbetter,newerandcheaper
drugs.Thisisespeciallyimportantinthebio‐pharmaindustrywhereIndianpharma
industryneedstodevelopskillsasgoodasinmedicinalchemistrytotakethenext
generationdrugrevolutionleadershipglobally.
Inthiscontextitmaybeusefultoconsideraschemetoforfillingthisgapandensure
capacitybuildingandtechnologyenhancementofthepharmaindustrytomakeitglobally
morecompetitive.
1.7.4THREATS
(1)FormulationsSector

Page 49 of 153
Thegenericsmarketindevelopedcountriesisbeingcurrentlyaffectedbyanumber
offactors:
a) Ever‐greeningstrategyofMNCstoprotectmarketlossduetoexpiryofpatents
b) IncreasedcompetitiontocountrieslikeIndiafromemergingmanufacturersin
ChinaandEastEuropenotonlyfromthemanufacturingpointofviewbutalso
barriersbeingraisedbythemtoprotectanddeveloplocalindustry.Thisisbeing
donebysuchprocessesaslongapprovaltimeandcostsforregistrationof
drugs.Insistenceoncompletinglongprocessforregistrationfordrugs
registeredearlierbywayofspecificrequirementsoffreshclinicaltrials
(marketslikeRussianFederation).
c) KeymarketsliketheUnitedStatesareenteringintoanumberofFTA’swith
differentcountrieswithintenttocontainIndianexports
d) PreventionfrombiddingforgovernmentcontractsasUSpermitsbidders
onlyfromcountriesthataresignatoriestoWTOAgreementon
GovernmentProcurement.
e) Submissionofseparatestatelevelapplicationsformarketingdrugsinthe
UnitedStatesasthereisnonation‐widesystemofapplicationeven
whereFDAapprovalhasbeenreceived.
(2)BulkDrugIndustry
StiffcompetitionfromChinaoncostfronthasledtotheIndianBulkDrugIndustry
particularlytheFermentationindustry,toastageofclosureduetovariousfactors
includingsubsidizedpowerandfinancecostsinthecomputingcountry.Asaresult,
nocompanyinIndiaismanufacturingantibioticslikePenicillinandErythromycinetc.
1.8GOALSANDRECOMMENDATIONS
(1)GrowthRate
Theglobalgrowthrateprojectedis6%withtheexpectedmarketsizebeingUSD$
1200Bnby2017.TheTable‐12belowmakesitclear29.
29IMS-2009
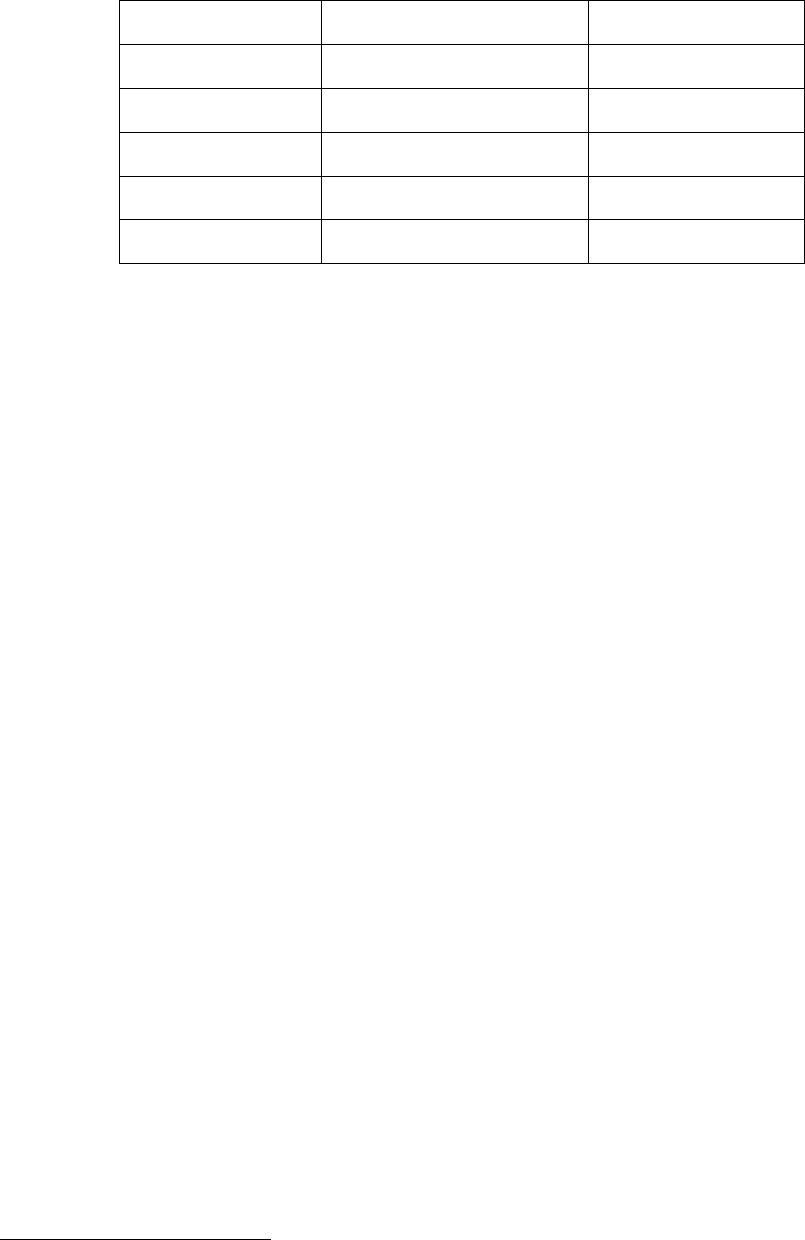
Page 50 of 153
Table‐12:GlobalPhamamarketgrowthrate
YearMarketinBillionUS$ %growthrate
2004620 7.9
2005664 7.2
2006710 6.9
2007756 6.4
2008801 4.9
ToplayaroleofgloballeaderinPharmaceuticalsIndustry,inlongrun,the
departmentofpharmaceuticalsissettingagoalofachievingaproductionsizeofUS$
60billionbyendof12thplanin2017withaCAGRof18%fortheplanperiodand
finallytouchingUS$100Bnby2020.
Asregardsbulkdrugindustry,itwillalsocontinuetogrowandthesectorwill
contributeanestimatedUSD20billionsizeby2015growingataCAGRof20%from
2008‐0930.Withtheseprojections,itisexpectedtotouchUS$28billionbyendof
12thplanin2017.
(2)GlobalShare
Theemergingmarketsaretargetedtogrowat14%.Inthiscontext,theIndian
marketisprojectedtogrowat18%.Accordinglygiventhecurrentdemandandthe
abilityoftheIndianpharmamanufacturingsectortocontinuetomeetthedemand
push,itisexpectedthattheIndianpharmasectorwouldbeofaboutUS$60billion
sizein2017.HenceitisexpectedthatIndianPharmaceuticalsindustrywillhavea
shareof5%inglobalpharmaceuticalindustrybytheendof12thFiveYearPlan.
(3)Exports
TheexportswhichhavegrownverysignificantlytooverRs45,000croresin2010‐11,
isprojectedtotoucharound130,000croresbytheendof12thfiveyearplan.
30 BDMA estimates
Page 51 of 153
1.9 INDUSTRYDEVELOPMENTSCHEMES
Onthebasisofanalysisofweaknesses,threatsandgaponotherinternational
parametersasexplainedabove,followingIndustryDevelopmentSchemesare
proposed:
(1)IndustryPromotion
i. PharmaPromotionandDevelopmentScheme(PPDS):Thisisanongoing
schemeforpromotionanddevelopmentofPharmasectorinthe
country.
ii. TheongoingschemeofIntellectualPropertyRightcentersinHyderabad
andChandigarhshouldbecontinued.NewIPRFCsatMumbai,Chennai
andAhmedabadcanbeopenedforeasyaccessofthecentersbythe
industry.
(2)IndustryUpgradationandCapacityBuilding
iii. ACapitalSubsidyofRs.1200croresfor1200unitsattherateofRs.1
croresperunitforupgradingtheunitstoWHO‐GMP.
iv. Toupgradeatleast250unitstoUSFDA/EDQM/TGAandother
InternationalStandardsby2017
v. Totrain5000WorkingProfessionalsinWHO‐GMPandother
InternationalStandardsGMPrequirements.
vi. Openinganational“InternationalManufacturingStandardsTraining
Centre”atNIPERMohaliandfiveregionalcentersatHyderabad,
Chennai,Ahmadabad,MumbaiandKolkata,especiallyfortheindustry
regulatoryskillbuilding.
vii. OpeningaNationalFormulationDevelopmentCentre(NFDC)toassist
theSMEsforthedevelopmentofnewformulationswhicharethe
sourceofincreasingproductioninthedomesticandexportmarket.
viii. Developasoftware,underthetechnicalguidanceofDCGI,forhelping
theSMEsinachievingvariousregulatorycomplianceswhichwouldbe
distributedbytheDepartmenttotheindustryfreeofcost.
ix. Establishmentandupgradationof10PharmaGrowthClustersby2017.

Page 52 of 153
OtherRecommendations:
i. MoHFW/IPCtoexplorethepossibilityofputtingPharmacopeiaontheinternetas
isthepracticeforseveralinternationalpharmacopeiasuchasUSPandBP.
ii. IncreasingthelimitofSSIcategorizationofpharmaunitsfromRs.5crorestoat
leastRs.8croresbothforDPCOincentivisationandMSMEassessment.Similarly
intheDPCO,theexemptionfrompricecontrolshouldbeprovidedtoPharma
UnitshavingappropriatelycertifiedinvestmentofuptoRs.8croresinplantand
machineriesandhavingWHO‐GMPcertification.
iii. Levelplayingfield:IndianBulkDrugIndustryismainlycomparedwiththat
odChina.InChina,theindustryisfullysupportedbyGovernment,right
fromprovidinginfrastructuretovariousbenefitsintermsofTaxesincase
ofexport.TopromoteourBulkDrugIndustry,governmenthastocomeup
withvarioussupportiveschemes.
iv. AntiDumping:Immediateactionneedstobeinitiatedforimpositionof
AntiDumpingDutyonPen‐Gand6APA.
v. SubsidizedElectricitySupply:Electricityneedstobesuppliedatsubsidized
ratesof@Rs.3.00‐3.50perunitatparoftheprevailingratesinChinain
ordertoenableIndianfermentationIndustrycompeteatalevelplaying
field.Thiswillleadtoreductionof~10%productioncostofPen‐G.
vi. SubsidizedSugar:Sugar,beinganimportantinputconstitutingaround30%
ofthetotalcost,needstobesuppliedtoPen‐Gmanufacturing
fermentationunitsatasubsidizedpriceofRs.20perKg.Thissubsidymay
resultinareductionof~7%intheproductioncostofPen‐G.
Thedetailsoftheschemeandbudgetaryrequirementsarementionedin
Chapter‐8.
‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐

Page 53 of 153
Chapter2:
RESEARCH&DEVELOPMENT
2.1Introduction
IndianPharmaceuticalIndustryhasalreadybeenplacedamongthetopfour
emergingmarketsinpharmaindustrybythemarketresearchreportpublishedby
IMSHealthInc.Theglobalpharmaceuticalindustry,inthelastfewyears,hasshown
highinterestinIndiapharmaindustrybecauseofitssustainedeconomicgrowth,
healthcarereformsandpatent‐relatedlegislation.Indiandomesticpharmaceutical
markethasseengrowthataCAGRofabout12%sincethestartof11thFiveYear
Plan.Thepositiveapproachtowardsproductpatentproducthasencouragedthe
IndianpharmaceuticalcompaniestoinvestmoreinResearchandDevelopment.
India’straditionalstrengthliesinsmallmoleculeAPIsandgenerics.Indiaranksthird
inworldwidevolumeofproductionandis14thlargestbyvalue.Themainreasonfor
thisdiscrepancyhasbeendeterminedtobethelowercostofsuchdrugsinIndia,
comparednotonlytothetraditionalmarketsbuttosmallermarketslikeZimbabwe
andSiLanka.However,intoptenglobalgenericsplayers,onlyoneIndiancompanyis
present.
Table‐13:TopGlobalGenericPlayers
(Source:CapitalIQ,EvaluatePharmaandDeutscheBankReport)
RankCompany
1Teva
2Sandoz
3Mylan/MerckGX
4WatsonAndrx
5Barr
6Actavis
7Ratiopharm
8Stada
9Ranbaxy
10Perrigo
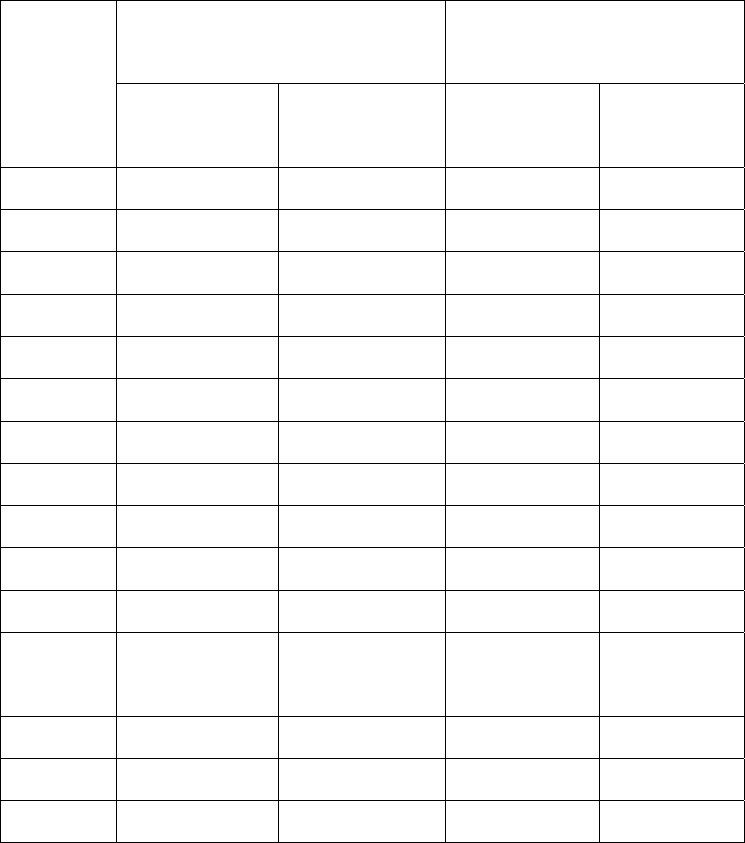
Page 54 of 153
2.2ResearchandDevelopmentexpenditure
TheprivateinvestmentonR&DinPharmaceuticalSectorbydomesticcompanieshas
increased40‐foldoverthelast15yearsfromRs80.61crin1994‐95toRs3,342.32crin2009‐
10representing4.5%ofdomesticsalesin2009‐10.
Table14:ResearchandDevelopmentExpenditure
Year
GrowthinR&DExpenditure
–
Rs
Cr
R&DExpenditureAs%of
Sales
Domestic
Companies
Foreign
Companies
Domestic
Companies
Foreign
Companies
Mar199580.6164.131.340.77
Mar1996142.5083.37 1.71 0.91
Mar1997148.1289.41 1.55 0.95
Mar1998154.1590.651.430.88
Mar1999218.6679.781.560.70
Mar2000256.8090.171.560.66
Mar2001435.07109.812.300.72
Mar2002597.91110.04 2.64 0.65
Mar2003686.74232.73 2.93 0.71
Mar20041084.26346.693.811.10
Mar20051527.24510.504.981.63
Mar20061850.97816.025.352.39
Mar20072371.79695.625.012.67
Mar20082772.63700.184.782.86
Mar20093316.14846.054.893.84
Mar20103342.32934.404.504.01
Source: CMIE
Page 55 of 153
AscomparedtothisasregardsglobalR&Dinvestment,accordingtoThomsonReuters’2011
PharmaceuticalR&DFactbook,GlobalexpenditureonR&Dhasdroppedtoanestimated
$68billionfromthe$70billionspentineachof2008and2009.Thethree‐yearlow
demonstratestherecedingtrendsofdrugsuccess,theamountofdrugsenteringPhaseIand
IItrialsandthenumberofnewmolecularentities(NMEs)launchedintheglobalmarket.On
thecontrarydomesticcompanieshavebeenincreasingtheirresearchexpenditure,andnow
investaround4.5%oftheirsalesinpursuingR&D.Asagainstthis,globalspendisaround
8.68%ofthesalesininnovation.Worldwide,bigpharmacompanieswhoinvestin
"research''inpursuitofnewchemicalentities(NCE),havestartedcuttingbackasclinical
trialsareexpensive,andjackupdevelopmentcoststobillionsofdollars,whichsometimes
givedisappointingreturns.Incontrast,domesticcompanieshavebeeninvestingin
"development''ofcopiesofexistingmoleculeshavingmorethanabillionUS$annualsales
androllingoutgenericdrugsversionatafractionofdevelopmentcostofnewmedicines.
ThishasledtheglobalMNCstosetuptheirresearchfacilitiesincountrieslikeChinawhere
besideslowcostworkforceahugemarketisalsoleveraged.Theseare:31:
31 Mckinsey Draft Report for DoP, 2009
7
Sources: Interviews; literature search; company Web sites; analyst reports
Location
Shanghai
Business model
Captive
Time
2004
Size
•
Initial investment $12mn
•
~40 scientists
Research focus
•
Medicinal chemistry for drug discovery
programs in antiviral and anticancer areas
Shanghai,
Beijing Partner with National
Genome Centers 2001
•
More than $1mn
•
Epidemiology projects, focusing on genetic
predispositions to diabetes and Alzheimer's
disease
Shanghai Partner with Chem-
Explorer, Synchem 2003
•
100-200 local scientists
•
Custom synthesis and other chemistry
services
Shanghai Captive 2004
•
Investing $175mn
•
New regional headquarter and first clinical
trial center in Shanghai, including biometrics
capability to support regional and global trials
Partner with Shanghai
Huashan Hospital
Shanghai 2004
•
N.A.
•
Jointly setting up infectious disease
diagnosis and treatment center
CaptiveShanghai 2002
•
More than 40 staff
members
•
Established clinical research unit – East
Asia to support regional and global trials
Partner with WuXi
PharmaTech
Shanghai 2003
•
Multiyear, multimillion $
agreement
•
Dedicated full-time equivalents (FTEs) to
provide discovery chemistry services (e.g.,
library synthesis)
Partner with Shanghai
Institute of Meteria
Medica (SIMM)
Shanghai 2004
•
Multiyear agreement
•
Joint program to develop natural compounds
in traditional Chinese medicine (TCM)
CaptiveBeijing 2002
•
20, growing to 60
scientists in the next few
years
•
Center of excellence for molecular biology,
protein chemistry, and cell biology
This has resulted in a number of R&D centers being set up by
multinational pharmacos
ILLUSTRATIVE
DRAFT
Page 56 of 153
Thishasalsobeencatalysedbymassiveexpendituresupportofthegovernment.
Thus,ifonecompareswithChinathesituationisquitechallengingasseenbelowand
asbroughtoutbyMckinseyinaReportfortheDoPin200932.
Ascomparedwiththis,theR&Dspendscenarioisnotveryencouraging.Thus,the
R&DexpensesforIndiandomesticcompaniesarefirstofallinthedevelopmentand
filingdrugmasterfilings(DMF),andabbreviatednewdrugapplications(ANDA),
throughconductofbio‐equivalenceandbioavailabilitystudies.Eveninthisspace
thereareselectedfewbigspenderslike‐Lupin,DrReddy's,RanbaxyandSun
Pharmawithroughly8.5%,8%,5.6%&5.3%oftheirannualturnoversrespectively,
forthefinancialyearendedMarch2011.IfthisiscomparedwiththeR&Dspendof
bigpharmathesituationisquitechallengingasmaybeseeninthetablebelow:
32 Mckinsey in a Report for the DoP in 2009
6
China has made large investments to provide a congenial environment to
encourage R&D activities
Infrastructure
Policy
Description
•
Development of more than 20 high-tech parks (e.g.,
Shanghai Zhangjiang, Beijing Zhongguancun)
•
Six drug screening centers established to focus on
lead compound selection
•
QC procedures implemented in three good
laboratory practice (GLP) evaluation centers and
several GLP standard laboratories
•
10 good clinical practice (GCP) testing centers
established
•
Favorable policies toward life sciences investment
•
Strong government support for partnerships
between MNCs and domestic companies
•
Increased government funding for university
programs in science and engineering
•
Chinese government is actively encouraging
educated Chinese to return (e.g., free visits with
paid plane tickets and hotel rooms, development of
centers such as Shanghai Pudong Center for
Returned overseas Students to assist returnees)
100
2010E
8,800
2005
1,200
2001
Government investment in
biotechnology research
USD million
Tax
•
2 year tax exemptions on profitability for companies
involved in life science research
•
50% rebate on enterprise tax for the next 3 years,
usually extended for another 3 years
DRAFT
Page 57 of 153
Table‐15:R&DspendingofleadingIndianandGlobalpharmaceuticalMNEs,FY200933
IndianPharmaceuticalCompaniesGlobalPharmaceuticalCompanies
Rank
in
R&D
spendi
ng
Company
R&Dexp.
FY
2008/09,
millionUS$
RankinR&D
spendingCompany
R&Dexp.
2009,
millionUS$
1Ranbaxy*991Roche,CH8,570
2Dr.Reddy’s895GlaxoSmithKlin,UK6,286
3SunPharma6710ElliLilly,USA4,300
4Cipla5125Lundbeck,DNK615
5LupinLabs5050Watson,USA197
*RanbaxywasacquiredbyDaiichiSankyofromJapaninMarch2009.
2.3Bio‐pharmaConvergence
Biotechnologyhasemergedasoneofthekeytechnologiesofthiscentury.
Biopharmaceuticalshavebeenprojectedaspotentialdrugscuringmanydiseases.
Manyresearchpapershaveopinedthatchemistrybasedmedicalinnovationsofthe
previouscenturyarebecomingtorecedeinimportance,tobereplacedbyadvances
inbiopharmaceuticalresearchthatwillboostthegrowthofrevenuesandprofitsin
theyearstocome.Givenitspotential,mostoftheglobalpharmaceuticalcompanies
areshowinginterestinthebiopharmaceuticalssector.Thistrendislikelyto
32.Gert Bruche,- ‘Emerging challengers in knowledge-based industries? The Case of Indian pharma
Multinationals,’ Columbia FDI Perspectives, No. 41, July 1, 2011.

Page 58 of 153
continue,asthesecompanieswouldtrytoreapthebenefitoftheirsalesand
marketingcapabilitiesalongwithtechnicalexpertiseofbiotechnology.
Lastyear,thepharmaceuticalindustryspentabout$2billiononassortedR&D
activitiesinIndia.However,thisfigurecanreachupto$25billionby2025if
concertedeffortsaremadebyvariousstakeholderslikethegovernment,academia
andindustryondevelopingR&Dandinnovationinthebio‐pharmafield.Thisgrowth
wouldbedrivenbytappingthesynergybetweenexpandingactivitiesofIndian
companies,additionalgovernmentinvestmentandagrowingpoolofqualified
researchers,accordingtoanewreporttitled,'LifeSciencesR&D:“Changingthe
innovationEquation”bytheBostonConsultingGroupinitspositionpaper.
2.4PatentsProgress
Amongotherimpactofthe2005amendments,thenumberofpatentfilingsinIndia
forpharmaceuticalproductsincreasedsteadily.Thetotalnumberofpatentsgranted
inIndiajumpedfrom1911in2004‐05to4320in2005‐06.Thecurrentstatusof
pharmaR&DinIndiaisbestreflectedbythegrowthofdomesticpharmaindustryin
lastdecadeintermsofavailabilityoftrainedmanpower,publicationsandpatents,
valueandvolumeAPIfinishedformulationmarket,NDDSlaunched,INDs/NDAfiled,
Clinicaltrialpermissionsobtained,andannualgrowthinBiopharmaceuticals,Clinical
researchactivity.
Asper2009‐2010annualreportof“INTELLECTUALPROPERTYINDIA”,GOVERNMENT
OFINDIA,(MINISTRYOFCOMMERCE&INDUSTRY)themajorcontributiontopatents
wasfromCSIRandIIT.ThecontributionfromtheIndianuniversitieswasextremely
poor.NIPERMohalicontributedonly4patentsin2009‐10.Thisemphasizestheneed
todevelopNIPERsonIITpatterntoboostgrowthinpharmaR&Dsector,whichalso
performedpoorlyinpatentfilingrace.
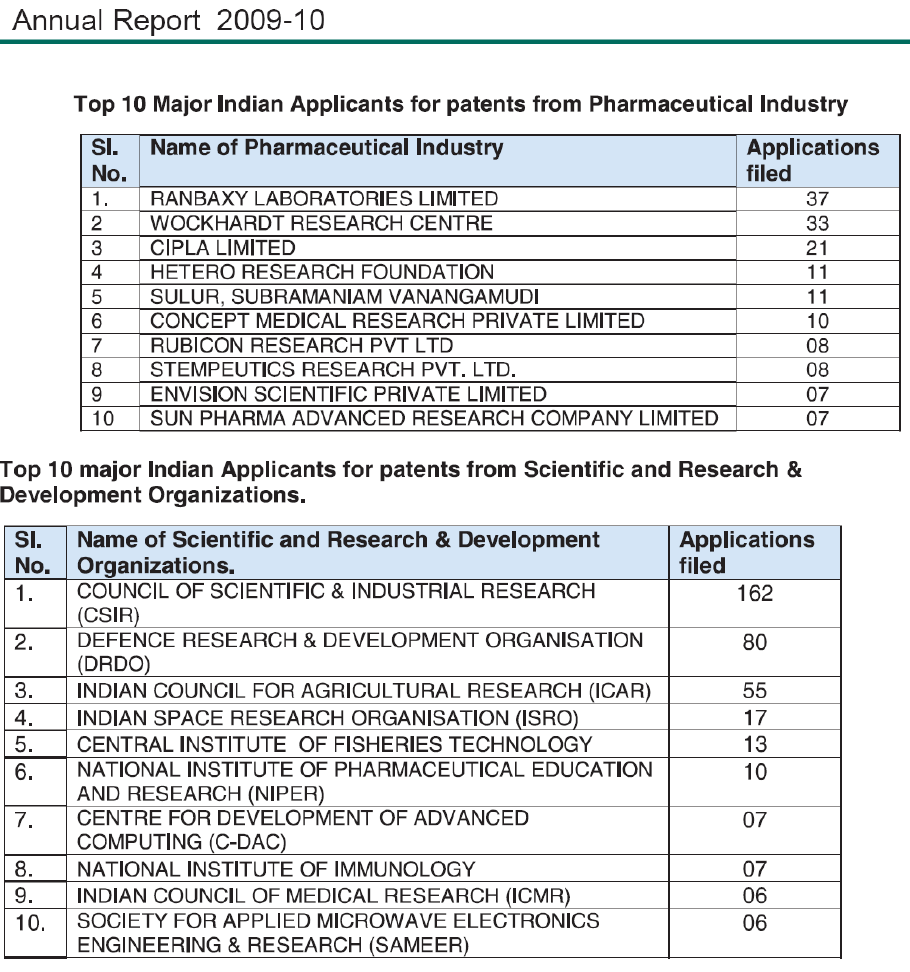
Page 59 of 153
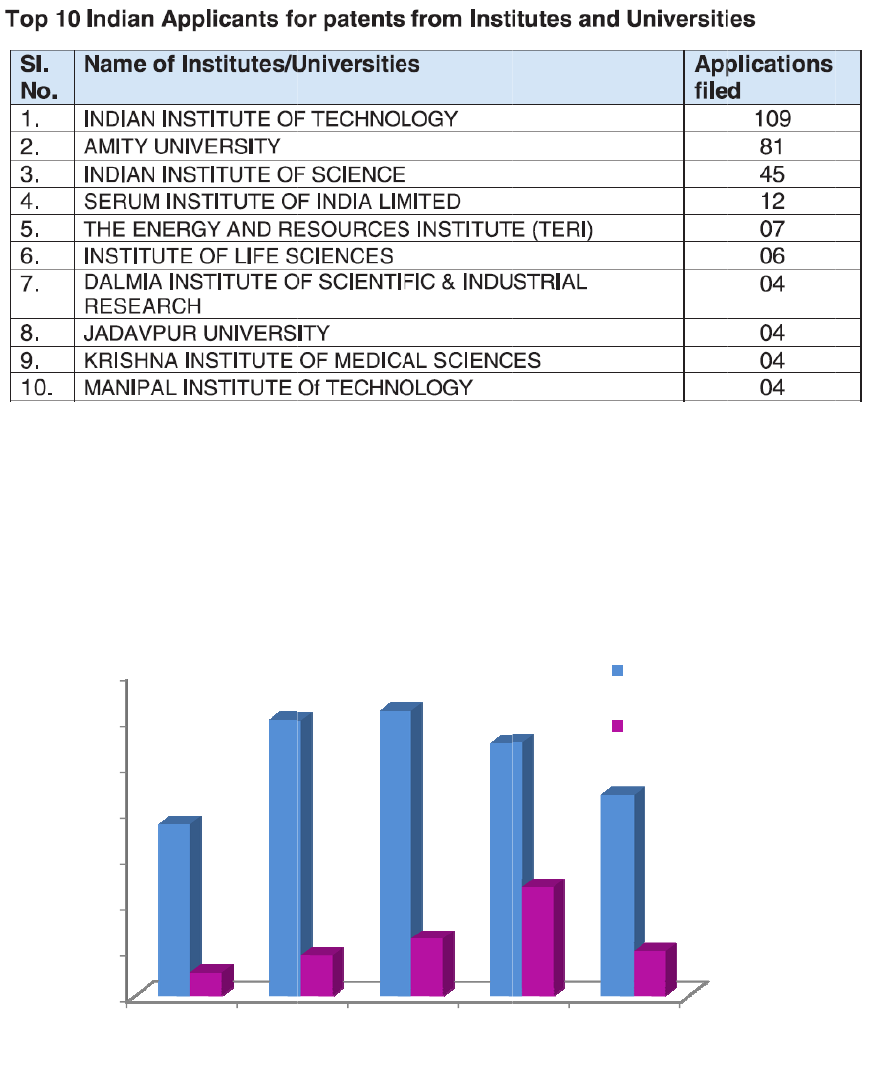
Thereh
a
biotech
s
Total(p
h
*
p
p
c
o
1
0
2
0
3
0
4
0
5
0
6
0
7
0
a
sbeenno
g
s
ectorsinIn
d
h
arma+bio
t
Thetotal
atentsfiled
atentsfiled
o
ntributed
b
0
0
00
0
00
0
00
0
00
0
00
0
00
0
00
2005‐
2
g
rowthsinc
e
d
ia.
t
ech)Paten
t
patentsfil
e
byIndian
a
inIndiadur
i
b
ynonIndia
n
2
006 2006‐
2
e
2005inth
e
t
sFiled/Gr
a
e
d/granted
a
swellfore
i
i
ng2009‐10
n
entities.
2
007 2007
‐
e
numbero
a
ntedbyIn
d
aboveincl
u
i
gncompan
bypharma
+
‐
2008 2008
‐
fpatentsfil
e
d
ianpatent
u
deboth;t
h
ies/intstitu
t
+
biotechse
c
‐
2009 200
9
e
donwards
office*
h
eprocess
tions.Out
c
tor,moret
h
9
‐2010
TotalPaten
t
TotalPaten
t
bypharma
andprodu
c
oftotal43
7
h
an75%we
r
t
sFiled
t
sGranted
+
c
t
7
3
r
e
T
m
b
H
r
e
i
n
0
50
100
150
200
250
300
0
5
1
0
1
5
2
0
heproduct
m
arketinga
u
yDCGI.Bo
t
H
oweverthe
e
venueand
n
ourinnova
2003
Glob
a
0
5
0
5
0
2003 2
0
Ph
a
ivityofph
a
u
thorization
s
t
htheyard
sefiguresa
manpower
d
tioncapabil
2004 20
0
Cli
n
a
lClinicalTrials
0
04 2005
a
sewised
i
a
rmaIndus
t
s
(productl
a
sticksinth
renotvery
d
eployedsi
n
ityinterms
0
5 2006
n
icalTrial
s
permitted
2006 2007
i
stributio
n
D
t
rycanbe
a
unched)an
d
eplotsbel
o
impressive
i
n
ce2003on
ofourR&D
2007
s
from20
0
Market
i
2008 20
0
n
ofClinica
D
CG(I)
bestindic
a
d
/orclinical
o
wshows
t
i
fwecomp
a
wards.The
r
productivit
y
2008 20
0
0
3‐2010
i
ngAuthorizati
o
0
9 2010
lTrialPer
m
a
tedbyth
e
trialpermis
t
eadyyear
a
reitalong
w
r
eseemsto
y
.
0
9 2010
o
nGranted
m
ittedby
Phase
Phase
Phase
Total
e
number
o
sionsgrant
e
wisegrowt
w
iththeR
&
bestagnati
o
I
II
III
o
f
e
d
h.
&
D
o
n
Page 62 of 153
2.5SWOTANALYSIS
2.5.1Strengths
i. Costcompetitiveness;thecostofdevelopinganewmoleculeinIndiaisless
than30%oftheAmericancost.Clinicaltrialscostapproximately$300to
$350millionabroad,whileitcostsonlyabout$20million(Rs100crores)in
India(Mr.VijayMoza,Vice‐ChairmanInstituteofClinicalResearch,India).
ii. EdgeinreverseengineeringforgenericproductsandglobalANDAfiling
iii. WelldevelopedchemistryR&Dandmanufacturinginfrastructure
iv. LowcostEnglishspeakingworkforce
v. Large,diverse,therapy‐naïvepoolofpatientpopulationinallkindofacute/
chronicdiseasesegments:Anidealforclinicalresearch
2.5.2Weakness
i. Lackofdevelopmentskillsincomplexanddifficulttoduplicategeneric
producttechnologies
ii. Lackofcultureforinnovation
iii. Poorindustry‐ academiainteractionandallaroundinfrastructure,
includingeducationalinstitutions
iv. Lowdoctortopatientratioinhospitals,renderingthemnon‐availablefor
clinicalresearch
v. Lackofexperience,capabilityandresourcesinindustryandinstitutions
engagedinnewdrugdiscovery
vi. Lowcapabilityandmotivationforcuttingedgeresearch,especiallyin
areasrelatedtounderstandingofdisease,andplatformtechnologiesfor
drugproducts
vii. Poorinfrastructure,trainingandnonavailabilityoftrainedmanpowerfor
clinicalresearch
viii. LowappetitetoriskandR&Dinvestment
ix. RatioofPhDtoMastersdegreeholdersinR&Dislow(1:10)against
target(1:5)
Page 63 of 153
x. Lowlevelofeducation&traininginthepharmacyinstitutionsand
universities
xi. Small,inefficientandin‐experiencedworkforcelackingcompetencyand
capacityinourconservativeregulatoryenvironmentisunabletosupport
innovation&newdrugdiscovery.
2.5.3Opportunities
i. Developmentofcriticalandhigh‐techmanpower(capacitybuilding)for
pharmaR&Dandalliedsectors
ii. ConvertinglowcostgenerictovalueaddedbrandedgenericbySME
sector
iii. Developplatformtechnologies(Newdrugdeliverysystems)for
improvisingconventionalgenerics
iv. Developmentofnewbio‐molecules,vaccinesandbio‐similar
v. ExploitationofclinicalresearchpotentialofIndia.Accordingto"Booming
ClinicalTrialsMarketinIndia<http://www.rncos.com/>",anewresearch
reportbyRNCOS,anumberoffactorssuchaslowcost,largepatientpool,
easyrecruitment,stronggovernmentsupportandstrengtheningofits
intellectualpropertyenvironmentwillenableIndiatoconductnearly5%
oftheglobalclinicaltrialsby2012.
vi. Indiaassumingleadershiproleamongstdevelopingcountriesforpharma
research,manpowerdevelopmentetc.
2.5.4Threats
ChinaisquiteaheadinAPI,naturalremediesandherbals,Clinicalresearchand
medicaldevices.
Page 64 of 153
2.6RECOMMENDATIONS
Indiaacknowledgedtheuniversalityofintellectualpropertyrightsbyembracingthe
harmonizedTRIPSpatentregimeandenforceditfromJanuary1st,2005.Sincethen,
anewwaveofprogresshassweptthecountry.Post2005,pharmaceuticaland
medicalbiotechnologycompaniesexperiencedsomeverycriticalchanges,andsince
then,theonlyrealdifferentiatorhasbeeninnovation.
2.6.1ENHANCEDINDUSTRY–ACADEMIALINKAGES
2.6.1.1StepsRequiredfromIndustry:
i. Indianacademia,especiallyinchemicalandlifesciences,isequivalenttoany
world‐classfaculty.Theindustrymusttakeadvantageofthisopportunityand
approachthemwithdefinedproblems.
ii. Industryshouldprovideopportunitytoacademicianstointeractwithindustry
scientistsandgetexposuretostyleoffunctioningofindustrialR&D.
iii. VariousschemestopromoteindustrialR&Dshouldbewidelycirculatedto
createawareness.
iv. Industriesshouldinteractwiththeacademiatobecomeawareofthestate‐
of‐the‐artfacilitiesavailableandinuse.
2.6.1.2StepsRequiredfromAcademia:
i. Academicinstitutionsshouldwintheconfidenceofindustrywithrespectto
confidentialityandactivecollaborationwhichisbeneficialtobothparties.
ii. Theacademianeedtointroducecoursesmorerelevanttothedevelopment
ofthepharmasector.Forexample,integratedmasters’coursesin
pharmaceuticaldevelopmentwithfocusonbio‐pharmaceuticalsandNCEs,
intellectualpropertiesissuesrelatedtopharmaceuticals,etc.canbe
developed.ThesecoursesshouldbecreatedafterconsultingOPPI,IDMAand
similarbodies.
Page 65 of 153
iii. TheacademicInstitutionsshouldinviteIndustrypartnerstoteachpartsof
thesecoursessothattheindustryviewpointcanbeconveyedtothenext
generationworkers.
iv. Facultymembersofpremierinstitutescanvisitindustriesandspendashort
periodtoapprisethemselvesofchangingindustryneeds.
2.6.1.3StepsRequiredFromGovernment
i. Thegovernmentneedstocreateastrongplatformforincentivisingthe
innovativeapproachtoproducesafeandaffordablemedicine.
ii. Public‐private‐partnershipswithindustryandleadingacademicpartners/
interestedstakeholdersmaybearrangedtoaddressinnovationissues.
iii. Theimportanceofcommerciallyorientedneedsshouldbeconveyedtothe
publicinstitutions.Otherwisetheserelationshipsmaynotsurviveinthelong
run.
iv. ProgrammeslikePRDSFneedtobeencouragedandtheirscopebroadened.
v. Governmentshouldgivesubsidisedloans/grants/fundingforNewDrug
Development.
vi. Start‐upcompaniesbasedonacademiageneratedIPthroughequitylinked
fundingshouldbeencouraged.Thiswillbeagoodstarttoanindustry
focusedapproach.
vii. Industryneedstobeincentivisedthroughattractivelicensingschemes.
Also,ithasbeenfoundbothstrategicalternativeswhichareusuallyfollowed–
genericmedicinesandinnovativeproducts–ascomplementary.Ifoneconsidersthe
hypothesisthatthegreatexpenseinR&Disproportionaltothecashflowofprevious
periods,thesuccessdomesticfirmsaregettingbysellingtheirgenericswillmake
themabletostrengthentheirfinancialmuscles,addingtotheirR&Dinvestments.
Evidencesexist,evenifincipient,toconfirmpreliminarilythisassertive.Additionally,
asthecompaniesstrengthentheirlinkswiththeinnovationsystems,theyreinforce
theirqualificationsintermsofR&D,openingthepossibilityofpartnerships
arrangementswithuniversities,localandforeigncompanies,andresearchinstitutes
–bothpublicandprivate.
Page 66 of 153
2.6.2MAKINGTHEDOMESTICR&DINTERNATIONALLYCOMPETITIVE
FormakingdomesticR&Dinternationallycompetitiveandalsoviable,onehasto
reviewnotonlythecurrentstateofindustrialR&Dgoingon,butalsoreviewthe
researchactivitiestakingplaceinvariouscentresorinstitutes.Thereviewcouldthen
befurthercategorizedkeepinginviewtherequirementofthevastconsumer
market,andthetimeframesfordevelopment.Suchactionsarehelpfultocurb
excessofimportsandbringingthepricingofhealthcare/biopharmaproductsin
control.Weneedtofocusonfollowingaspects:
2.6.2.1Regulatorysystemandfunding:
i. ThepresentweightedaveragetaxdeductionaccordedtoR&Dshouldcover
internationalpatentingcosts,regulatoryconsultants,outsourcedR&D
servicesandpatentlitigationexpenses.
ii. Regulatoryreformsarerequiredwhichcanreducethecurrentlyprevalent
approvaltimelines.Thecostadvantageisnegatedbytheinordinatedelaysin
approvalwhicherodepatentlife.
iii. A25%subsidyonsalariesofNRIspecialists/expertscouldhelpcompanies
attractandaffordhighendtalent.Industryshouldalsobepreparedtopay
competitivesalariestobench‐levelworkersandmiddlemanagementandnot
onlythehigh‐tiergroup.
iv. Indiancompaniesspend~4‐5%oftheirsalesonR&D,whichisonequarterof
thespendingbyproportionbyglobalpharmacompanies(Source:IDMA).
Governmentfundingandcollaborationwithacademicresearchinstitutesis
theneedofthehour.
v. Reductioninexciseandcustomsdutyofchemicalsandrawmaterialsthatare
importedforbiotechproductsisveryimportanttoreducethemanufacturing
Page 67 of 153
costs;alsotaxexemptionforexportmarketforacertainperiodhasbeen
suggested.
vi. Skilldevelopmentisthenextbigchallenge.Wehavetoencouragepeople
abroadtoreturnandsetstandardsinIndiainsomeoftheseareas.Asthe
academiahasbeenabletoattractthebestoftheIndianbrainsfromabroad
atmuchlowersalaries,industriesneedtolookattheirset‐uptoidentifythe
lacunaeandcorrectthem.
vii. Focusonresearchcapabilitiesshouldshifttoencompassbiopharma
development.Sincethisinvolveshigh‐endandcapital‐intensiveresearch,the
initialsupportfromgovernmentwillbewelcome.
viii. Anothersuggestionhasbeenintroductionofpartnershipbetweenpharma
giantsforeachpharmaceuticalinstitutedealingwithhighereducationinthis
area.Thecoreareasoftheseinstitutesneedtobestrengthenedtoensure
complementarygrowthofeach.Thiswillalsoleadtomorecollaborative
researchandnotcompetingwitheachother.BodieslikeOPPI,IDMA,etc.can
beconsultedforthispurpose.
2.6.2.2In‐houseR&Defforts:
i. AdefinedmechanismtostandardizethedomesticR&Deffortsagainstglobal
standardsneedstobeinplace.Thiscouldincludetheprocess/data/
informationstandardslikeISO/OECD/WHOguidelines.DSIR/NABL
certificationsaregoodmilestonesinthisprocess.
ii. Limitedmargins,duetolowpriceofproductsleadtoLackforinvestingin
R&Dandneedstobeincreasedbyallcompanies.
iii. SettingupanationalBiosimilarCenteratBangaloreandthreeRegional
BiosimilarCentersatChandigarh,HyderabadandAhmedabad.
iv. SettingupofaNationalPharmaceuticalNanotechnologyCenteratNIPER
Kolkota/Mohali.
Page 68 of 153
2.6.2.3Greaterfiscalsupportandincentivesareneededforinnovation.Tax
incentivesforproductsdesignedbydomesticcompaniesandforapplication
withinIndiae.g.grant‐in‐aidfunding,softloans,higherweightedaveragetax
deductionfordruginnovation,5yearNPPAexemptionfornoveldrugs,5year
taxanddutyexemptionfornewdrugs,etc.
2.6.2.4Supportfortheclinicaltrialssector:
i. OrientationprogrammesonClinicalResearchorganizedbyindustry
associations,MedicalSchoolsviaconferences,CMEsetc
ii. Regulartrainingofsitestaffbysponsors/CRO
iii. Orientationprogrammesforadministrativeandlegaldepartmentsofthe
hospitals
iv. CRO/SponsortofacilitatedevelopmentofsiteSOPs
v. RegularRegulatoryinspectionsofsites/IRBs/CROs/Sponsorstoensure
quality
vi. Methodologyforreportingnon‐compliantinvestigators/sites
2.7NIPERMohali
Inordertostrengthenthepharmaandhealth‐caresectors,thereisadireneedto
strengthenNIPERsonthemodelsofnewlyset‐upIISERsandIITs.Thereisaneedto
thereforetheexistingalreadydevelopedNIPER‐SASNagarasaHubtoprovidefull
rangeofservicestodomesticpharmaR&D.
2.7.1RoleofnewNIPERs
ThenewlyestablishedNIPERsneedtobesupportedintermsofbasicinfrastructure
andrecruitmentoffaculty.Theycanworkasspecialisedinnovationhubssuchasfor
‐ thrustonnewchemicalandbiologicalentitiesIndustryneedstoconcentrateon
biologicsasanimportanttherapeutictoolbydevelopingfacilitiesforthesame,with
thehelpofacademia.NIPERscanplayothersignificantroles,intermsof:
(i) EndtoendsolutiontoIndianpharmaR&D,engagedindiscoveryand
developmentofNCEandBiologics.Thishadbeenamajorbottleneckforour
industryintakingupmoleculesallthewaytophaseIII.
Page 69 of 153
(ii) Train&developmanpowerintheseclinicalandnonclinicalstudieswith
labelledcompounds.
(iii) GiveaboosttoGenericsIndustrybyofferingsolutionsfor“difficult”
formulations,suchasthosefordrugswithpoorsolubility,poorbioavailability
orotherpropertiesthatpreventAPIsfromreachingthemarketorachieving
theirfulltherapeuticpotential.
(iv) SupportNovelDrugDeliverySystem(NDDS)groupsinNIPERandIndustry
speciallythoseofferinginhalationdeliverysystems.
2.7.2SynergismbetweenAcademiaandindustry:ANecessity
Inthefirstyearofthe12thfiveyearplan,consolidationofexistingdataisrequired.A
listofthelaboratoriesundergovernmentsector,engageddrugdiscoveryand
developmentrelatedareasisprovidedinAnnexure–A.Thelostleadsgeneratedin
theselaboratoriesneedtoberesuscitated.Thiscanbedonebycreatingadatabase
ofleadswiththesupportofDST,DBT,ICMR,etc.Analysisofthedatabasewillallow
onetoassessthegapsintheexistingknowledgebase.Thiswillbeagoodstarting
pointforinnovativeresearch,sincetheleadsfordrugdiscoveryarealreadypresent.
Tillnow,drugdiscoveryinacademiahasremainedapublicationtool.Themoney
investedbyvariousfundingagencieshasresultedintrainingofhumanresourceand
publicationsinpeer‐reviewedjournals.Onemajorreasoncouldbethatthefunds
investedinextramuralresearchprojectsarewaybelowthoserequiredforserious
drugdiscoveryefforts.Acleardemarcationoftherolesofvariouslaboratoriesis
required.Insteadofinvestinginallfacilitiesinalllaboratories,theinherentexpertise
ofeachinstituteneedstobeutilizedtothefullest.Thatwillresultinoptimum
utilizationoffundsandskillsetavailable.Thus,theaimofthenextfiveyearsofXII
planwillbetoprovidevalue‐addedreturntothepharmasector,bywayofproduct
development.
Basedonaboverecommendations,thedetailsoftheschemesproposedarein
Chapter8(Section8.2).
‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐
Page 70 of 153
CHAPTER:3
CAPACITYBUILDING&EMPLOYMENT
3.1STATUSOFEMPLOYMENTOFTECHNICALMANPOWER
TheemploymentdataforthepharmaceuticalsectorfromtheAnnualSurveyof
Industries(ASI)isgivenbelow:
Table–16:EmploymentDataforPharmaceuticalSector
Source:AnnualSurveyofIndustriesMinistryofStatistics&Programme
Implementation.
AccordingtoCMIEdatabase,thewagebillofthedomesticcompaniesreported
morethantwelve‐foldincreaseover15‐yearperiodfromRs664crin1994‐95toRs
8,172crin2009‐10.
3.2FUNCTIONALDISTRIBUTIONOFHUMANRESOURCESINTHEPHARMASEGEMENT*
YearNoofEmployees
Mar1995 1,81,497
Mar19962,04,609
Mar19972,11,614
Mar19981,89,295
Mar19992,13,999
Mar20002,43,410
Mar2001 2,33,704
Mar2002 2,26,416
Mar20032,23,556
Mar20042,40,791
Mar20052,65,396
Mar20062,90,021
Mar2007 3,36,211
Mar2008 3,53,692
Page 71 of 153
R&Dinthepharmaindustryismulti‐facetedanddrawsupontheexpertiseof
pharmacists,chemists,biologists,chemicalengineers,pharmacologistsandmedical
practitionerstonameafew.Thedifferentactivitiesincludedrugdevelopment
(synthesisandmanufacture),formulation,clinicaltrialsandevaluationandfinally,
launchingofthedrug.
WhilethesubjectofR&DhasbeendiscussedindetailinChapter3ofthisPlan
Document,therelatedsubjectofCapacityBuildingandEmploymentisdiscussed
herein.
Inthisconnection,itistobestatedthatcloselyassociatedwiththeR&Dand
regulatory/qualityassurancefunctionsistheneedtorelatetheimplementationof
thesefunctions/responsibilitieswithmanpowerrequirements,itwillleadto
increaseddemandforpharmacistsbesidesotherprofessionals.Contract
manufacturingisestimatedtogrowUS$30Billion,whereascontractresearchis
estimatedtoreachUS$6‐10Billionandthisispavingwayfornewjobopportunities
beingcreatedintheIndianPharmaceuticalmarket.Thissectorisexpectedtogrow
atarate17.2%in2011.
Itisestimatedthatabout20%ofthe3.53lacmanpoweraboveisengagedin
researchandtestingasshownbelowinthetable.
Table17:PercentagedistributionofMan‐powerinPharmaIndustry
FunctionDistribution
Production&QualityControl50% 50%
Research/Lab/Testing 20%
Sales,Marketing,Medicalassistance5‐10%
Purchase,Logistics,SupplyChain 5‐10%
Supportfunctions(HR,Finance,etc.)10‐12%
*NSDCreport
EducationalqualificationsofpersonnelemployedintheChemicalsand
PharmaceuticalsSegmentinthisrespectareestimatedtobeasfollows:*
Page 72 of 153
Table18:QualificationsofpersonnelemployedintheChemicalsand
PharmaceuticalsSegment
QualificationDistribution
Ph.D/MTech/MScetc.5‐8%
GraduateEngineers15‐25%
DiplomaEngineers10%
ITIandothervocationalcourses 15‐20%
Graduates(BA/BSc/BCom/others)15‐25%
12thstandardorbelow20‐25%
*NSDCreport
Withtheincreaseinnewtherapeuticinterventionsandintroductionof
genomics/proteomictechnologies,anupsurgeindemandforskilledmanpowerto
fuelthisgrowingsectorhasbeenseen.Ithasopeneddifferentjobprofilesfor
aspirantswhoarelookingforacareerinthisfield.AspirantsInterestedinR&Dsector
canworkondrugdiscovery,developmentofnewgenericproduct,analyticalR&D,
APIorbulkdrug,andformulationR&D.Drugdeliveryisalsoanotherareawhere
aspirantscanlookinto.RegulationinpharmaIndustryhasbeenthereforalongtime
nowanditisgettingstringentdaybyday.Professionalswithexpertiseinregulatory
affairsaregrowingindemandallovertheworld.WithIndia’sincreasingexportsand
growingdomesticindustryregulatoryaffairprofessionalwillbeakeytoany
organization’srapidgrowth.Intellectualpropertyandpatentservicesisanother
area,whichareanintegralpartofprotectingtheintellectualpharmaresearch
bringingnewertherapeutics.
Thereisanacuteneedofhumanresourcesintheareasof:
i. PharmaceuticalandBiopharmadevelopment
ii. Clinicaldevelopmentprogramswithcollaborationwithmedical
institutes.
AMckinseyReport34hasbroughtoutthisgapasbelow:
34 A Mckinsey Report for DoP 2009

Page 73 of 153
Pharma R&D talent gaps assessment in India
Aspertheindustry,thedemandofqualityprofessionalsisnotbeenwellsupported
bythesupplyofquantitymanpowerandthisleadstoanemploymentinequilibrium.
Thereisnecessitytoexpandhighereducationinpharmaandcertainareasasper
industryneedandforthisindustryparticipationmaybeneeded.
Inthepharmaceuticalsector,directemploymenthasbeensteadilyincreasing.Inthe
year2006therewere6.9lacspeopleengaged,whichhasrisensteadilyto8lacssin
theyear2008.
3.3GEOGRAPHICALDISTRIBUTION
Goa,Mumbai,PuneandHyderabadhavebeenthepreferreddestinationsfor
formulationplayersinthepast.However,BaddiinHimachalPradeshandPantnagar
includingHaridwarinthestateofUttrakhandaretheupcomingformulationclusters,
attractingformulationmanufacturersfromacrossthecountryduetofiscal
38
However, capability gaps exist around core health-care
innovation skills
* R. Maiti and M. Raghavendra, “Clinical Trials in India,” Pharmacological Research 56 (July 2007): 1-10
** MD Gupte, epidemiologist, Indian Council of Medical Research
Sources: Interviews; FICCI; HRI, 2006; Frost and Sullivan, 2005; literature searches
Degree of
bottleneck Rationale Impact
Principal
investigators
High
•
Only 700 ICH/GCP trained physicians
•
Investigators required for pharma
companies to do trials
•
Causes delay in patient
recruitment (6 to 8 months)
•
Affects quality of data
Clinical Research
Associates (CRA)
•
Three institutions train CRAs*; however
quality very low
•
CRAs trained in theory, not practice
Medium
•
Pharma companies have
to train internally
•
Impacts quality of data
Biostatisticians
•
Small number of institutes
•
Limited career opportunities
•
Migration to higher-value industries
Medium
•
Reduces ability to establish
research or pharmaco-
vigilance facilities
Epidemiologists Medium
•
Deep shortage of epidemiologists:
at least 1,000 required**
•
Reduces pharmacos’
ability to establish PV
facilities
Toxicologists Medium
•
Not enough institutions provide
this training
•
Talent attracted to other areas
•
Reduces pharmacos’
ability to conduct research
NOT EXHAUSTIVE
Biologists High
•
Lack of talent and experience in key R&D
processes (e.g., mammalian expression
systems)
•
Hinders ability to compete
in biologics, a $63bn
business in 2007
Medical device
specialists
High
•
$200bn industry in which India has a very
small presence and is falling further
behind China
•
Reduces willingness of
global device companies to
work in India
DRAFT
Page 74 of 153
incentivesofferedbythegovernment.Traditionalbulkdrugclustersarelocated
primarilyinGujarat,Maharashtra,AndhraPradesh,TamilNadu,Goa,Pondicherry
andKarnataka.VisakhapatnaminAndhraPradeshistheupcomingbulkdrugcluster
thathasgeneratedsignificantinterestintheAPIplayers.TheR&Dclustershave
followedasimilardevelopmentpattern.ApartfromtheNationalcapitalRegion
(NCR),otherR&Dclustershavebeenlimitedtotheestablishedpharmaceutical
regionsinthecountry.
3.4LIKELYREQUIREMENTOFSKILLEDMANPOWER
3.4.1Requirementby2015
Theprojectedhumanresource,keepinginmindthepharmaceuticaldomesticas
wellasglobalmarket,willbearoundapprox.15lacsby2015[Source:Human
ResourceandSkillRequirementsfortheChemicals&PharmaceuticalsSector(2022)
‐AReportbyNSDC].AsthepharmaIndustryislikelytogrowwitharateofaround
18%peryearandthisgrowthwillbefurtherenhancedbytheopportunitypresented
byUS$300bnworthofdrugs(includingBio‐Drugs)settogooff‐patentinnextfive
years,theindustrywillneedbulkofqualityprofessionalsinvariousareas,viz.
regulatoryaffairs,QC/QA,production,environmentandaffluentplanninganddrug
R&D.Industrialgrowthinthissectorisexpectedtocreatejobsforpeoplewith
mastersandPhDs.Singapor’sBiopolisistakingaleadingeneratingnearly7500
PhD’sforthatcountry.InIndia,weneedtohaveplanstobringasynergyamongthe
differentstatesengagedinlifesciences.
Druginnovationwillrequireaplethoraofspecialisedskills:medicinalchemists,
molecularbiologists,geneticists,microbiologists,immunologists,bioinformaticians,
pharmacologists,clinicalresearchers,biostatisticians,chemicalandbiochemical
engineers,clinicians,veterinarians,etc.Indianacademiaandindustrywouldrequire
atleast100,000professionalsby2015topursuemeaningfuldruginnovationof
globalscale.Someindustryexpertshoweveranticipateonlymarginalincrease,not
enoughtoabsorblargenumberofpharmagraduatescomingoutoftheuniversities.
Page 75 of 153
3.4.2Requirementby2020
Itisdifficulttopredicttherequirementatthismoment.Futureappearstobegood
providedweareabletocontainproductcosts(throughcontroloninflationand
prices,increasedproductivity,etc.)andproducevalueaddedproductsthrough
continuousinnovationandintellectualinputs.By2020,therequirementfor
manpowerisexpectedtobearound21.5lacs[Source:HumanResourceandSkill
RequirementsfortheChemicals&PharmaceuticalsSector(2022)‐AReportby
NSDC]keepinginviewthealreadymentionedgrowth.Astheeffortstowardsmaking
personalizedmedicinearealityareincreasing,inadditiontotheabovementioned
skillset,expertsinareaslikepharmacogenetics/pharmacogenomics/toxicogenomics
willbeneeded.Asmoreandmoredrugswillbemanufacturedandmarketed(off‐
patentsdrugs),therewillbeaneedtohaveastrongvigilanceframeworkandhence
hundredsofprofessionalsfrompharmacovigilance,PMS(postmarketing
surveillance),clinicalepidemiplogyandpopulationgeneticsbackgroundwillneedto
bemadeavailable.
3.5RECOMMENDATIONS:
i. Greatertransparencybetweenindustryandacademiaisapre‐requisiteforany
successfuldrugdiscoveryanddevelopmenteffort.AlthoughIndianacademiais
ratedamongthebestintheworld,ithasnottranslatedintoanynoticeable
successintermsofproductdevelopmentinthepharmasector.Essentially,a
‘culture’needstobefosteredwhereintransparencyandefficiencyaretheonly
operationalkeywords.
ii. Anappropriateclimatethatisconducivetoencourageinnovationneedstobe
createdinthecountry.Thiscouldbeachievedbybuildingateamofreturning
Indians,encouragingstudents’finishingschoolsabroad,trainingstudentsto
thinkoutoftheboxandfindcosteffectivesolutionssuitedtothecountry.
Page 76 of 153
iii. Thepresenceofdemographicandgeographicdiversitiesaswellasthe
multiplicityofproductrangeallowsfortheexistenceofanumberofbusiness
modelsandplayersofdifferentlevels.Thus,insteadofassumingan‘either‐or’
attitudebetweenthesmall‐and‐mediumscaleversusmultinationalentities,a
comprehensivestudyofthemarketanditsrequirementneedstobecarried
out.Thiswillhelpidentifythegapsandallowforthebestpossibleutilizationof
theavailableexpertise.
iv. IthasbeenprojectedthatIndiacouldcapture8‐10%oftheglobaloutsourcing
industryby2015(Source:McKinsey&Co.).Indiahasalargepoolofhighly
trainedbiologists,chemists,trainedinvestigatorsforclinicaltrials,
biostatisticiansandhospitalswithstate‐of‐the‐artfacilities.Whatisrequiredis
theidentificationofspecificareasinwhichtheIndianpharmasectorcould
contributeandmakeadifference.InordertoachieveIndia’struepotential,a
visionaryoutlookbackedbystronggovernmentpolicy,willbetheneedofthe
hour.However,mostoftheacademicinstitutes,outsideaselectfew,Lack
‘trainedtrainers’.Itisimperativethatthismiddletierbestrengthened.
Otherwise,thefunctionofthetopresearchinstitutesremainslimitedto
bringingthematparandnotgettinganyhigh‐endresearchdoneinthissector.
v. AsperAllIndiaCouncilforTechnicalEducation(AICTE)websiteinformationof
year2010,morethan75000studentsgraduateinPharmacy.Thisisadequate
tocatertothecurrentrequirementoftheindustry.However,thereisneedto
focusonhigherskillatthelevelofMPharmaandPh.Dinidentifiedareasof
expertiseforaddressingtheneedforResearchandDevelopment,whichisthe
keytolongtermgrowthofPharmaindustry.
Basedonaboverecommendations,thedetailsoftheschemesproposedarein
Chapter8(Section8.2).
------------
Page 77 of 153
Chapter4
PRICING
4.1INTRODUCTION
Drugpriceplaysavitalroleinaccesstoessentialmedicinesacrosstheworld.Itisa
factthatthedrugsmanufacturedinIndiaareconsideredtobeamongstthelowest
pricedinternationally.Still,avastsectionofIndianpopulationisnotinapositionto
accesstheneededhealthcareaswellasthemedicinesduetovariousreasonsof
accessandaffordability.
Undeniably,universalaccessofqualitymedicinesataffordablepricesisofcritical
importance.CentralGovernmenthasbeentakingvariousstepsinthisregardand
fromtimetotime,drugpolicieshavebeenadoptedtostrikeabalancebetweenthe
oftenconflictinginterestsofindustryandconsumersinmovingtowardsthe
objectiveofgreateraccessibilityandaffordabilityofdrugs.Unlikeinmostother
developedcountries,wherepublichealthcareandotherformsofsubsidizedor
prepaidcoverageaccountforasubstantialhealthcareexpenditure,outofpocket
expendituresonhealtharequitehighinIndia.Therefore,anyincreaseinany
componentofhealthcarecoststendstofallacrossaverywidecross‐sectionofour
people,whohavenofall‐backoptions.Thisisoneoftheprincipalreasonswhy
internationalexperiencesandpricecontrolmodelsmaynotbereadilyadaptable
fullytooursituation.Butcertainly,therelevantpartsofthosemodelsneedtobe
consideredonmerit.
Itis,therefore,necessarytoevolveastrategywhichwouldmeetthetwinobjectives
ofensuringthattherelativepriceofdrugsdoesnotdeviatesharplyfromthepattern
andgrowthofpurchasingpowerincountry,andontheother,theIndian
pharmaceuticalindustrycontinuestomaintainitsrobustgrowthpath.
4.2DRUGSUNDERDPCO’95:CURRENTPRICINGSYSTEM
Page 78 of 153
TheDrugsPricesControlOrder,1995(DPCO’95)waspromulgatedbythe
GovernmentofIndiaon6thJanuary;1995inexerciseofthepowersconferredby
Section3oftheEssentialCommoditiesAct.UnderDPCO’95,76bulkdrugs(now74
drugsasAmikacinSulphateandMefenamicAcidwereomittedbyS.O.626(E)dated
2/9/1997),thepricesofwhicharecontrolledunderDPCO1995,havebeenenlisted
intheFirstScheduleofthisOrder.Underpara3ofDPCO’95Governmentis
empoweredtofixtheMaximumSalePricesofBulkDrugsspecifiedintheFirst
Schedulewithaviewtoregulatetheequitabledistributionandincreasingsupplyof
BulkDrugsspecifiedintheFirstScheduleandmakingitavailableatafairpricefrom
differentmanufacturers.TheGovt.mayaftermakingsuchenquiryasitdeemsfit,fix
fromtimetotimebynotificationintheOfficialGazette,MaximumSalePriceat
whichsuchBulkDrugsshallbesold.
4.2.1ScheduleDrugs
Para8ofDPCO,1995empowerstheGovernmenttofixfromtimetotimeretail
priceofscheduledformulationsinaccordancewiththeformulalaiddowninpara7
oftheDPCO.Underpara9ofDPCO,theGovernmentisempoweredtofixceiling
pricesofscheduledformulationsfromtimetotime,inaccordancewiththeformula
laiddowninpara7keepinginviewthecostforefficiencyforboth,ofmajor
manufacturersofsuchformulationsandsuchpriceshalloperateastheceilingsale
priceforallsuchpacksincludingthosesoldundergenericnameandforevery
manufacturerofsuchformulations.Thesepricesarefixed/revisedfromtimetotime
andnotifiedinofficialgazette.Themanufacturersandformulatorsarerequiredto
followthepricesfixed/revisedbytheGovernmentfromtimetotime(bothforbulk
drugsandformulationsincludingceilingprices)within15daysfromtheissuedof
suchorderbytheGovernment.Noonecansellanyscheduleddrug/formulationat
apricehigherthanthepricefixedbyNPPA/Government.
4.2.2NonScheduledDrugs
Inrespectofdrugs,notcoveredundertheDrugs(PricesControl)Order,1995i.e.
non‐scheduleddrugs,manufacturersfixthepricesbythemselveswithoutseeking
approvalofGovernment/NPPA.Suchpricesarenormallyfixeddependingon
Page 79 of 153
variousfactorslikethecostofbulkdrugsusedintheformulation,costofexcipients,
costofR&D,costofutilities/packingmaterial,salespromotioncosts,trademargins,
qualityassurancecost,landedcostofimportsetc.Asapartofpricemonitoring
activity,NPPAregularlyexaminesthemovementinpricesofnon‐scheduled
formulationsonthebasisofmonthlyreportsofORG‐IMS(nowIMS‐Health)andthe
informationfurnishedbyindividualmanufacturersinfollowingconditions–
(i) Increaseinpriceofmorethan10%inoneyear
(ii) IftheannualturnoveroftheformulationpackexceedsRs.1crores.
(iii) Theshareofformulationsinthatsegmentoftheformulationisrequiredto
beatleast20%ofthemarketorthemedicineisoneofthetop3brandsof
thatgroup.
Ifaformulation/packmeetstheabovecriteria,thenthemanufacturerand/or
distributorisaskedtogivejustificationforpriceincreaseofmorethan10%per
annum.Ifnoinformationisreceivedaftertheletterandreminderorthereplyofthe
companyisnotsatisfactory,showcausenoticeisissuedtothemanufacturerstating
astowhyactionshouldnotbeinitiatedforpricefixationunderpara10(b)of
DPCO’95inlargerpublicinterest.Althoughthisprovisionhasnotreallybeenused,
thereisevidencethatitspresencehasmoderatedthepaceofpriceincreasesin
drugs.
4.2.3PricingofImported&DomesticFormulations
Inrespectofformulationsmanufacturedinthecountry,ex‐factorypriceworkedout
byadoptingthenorms/guidelinesformsthebasiswhereasinthecaseofimported
formulations,landedcostofimportformsthebasisofpricefixations.Vastdifference
betweenimportedandindigenouslyproducedmedicinescontainingthesamesaltis
observedinalmostallcaseswhereverequivalentsubstitutesareavailablein
domesticmarkets.ThisisdespitethefactthattheprovisioninDPCOwas
incorporatedtoconsider/allowlowermargini.e.upto50%forimported
formulationsasagainstthe100%forindigenouslyproducedmedicinesunderpara7
ofDPCO1995.Eveninsuchcasesofimportedformulationswhenreducedmarginof
Page 80 of 153
35%isallowedbytheNPPA,thepricesworkedout/approvedarestillmanifold
higherand,hence,thereisnocomparisonwiththosethataremanufactured
indigenouslyduetothefactthatthereisnocontrol/examinationoftheCost,
InsuranceandFreight(CIF)/landedcostoftheimportedformulations.Thereisno
systemforcross‐checkingorexaminationoftheC.I.F./landedpriceoftheimported
formulationsdespitethefactthatNPPAhasbeenaskingforthesame.These
formulationsaremostlyimportedbythecompaniesfromtheirparentcompanies.In
theabsenceofdetailsrelatingtothecostofproductionofimportedformulations,
NPPAisnotallowing/consideringpriceincreasesbasedontheincreasedCIFprice
claimedbytheimportingcompanies.
4.3PRICING&NEWPATENTREGIME
4.3.1.Impact
Theimpactofnewpatentregimeondomesticpharmaindustryismarginalasof
now,asmostofthedrugspatentedbefore1995arefreelyavailable.However,with
thepassingoftheyears,moreandmorepatentprotecteddrugswillbelaunchedin
India,beingaverylargemarket,atwhichtimetheimpactonpricingwillbesevere,
unlessgovernment/regulatorimplementsproperchecksandbalances/price
approvalmechanismforpatentprotectedproducts.
Since2005only11moleculesunderproductpatenthavebeenlaunchedinthe
Indianmarket.Thuspatentedproductscontributelessthaneven0.5%oftotal
pharmaceuticalmarket.Thesearetherapeuticoptionsavailableataffordableprices
forthediseaseconditionsaddressedbythesepatentedmolecules.Thismeansthat
lifesavingdugsareavailableatdifferentpricepointstomeettheneedsofdifferent
socio‐economicgroups.Oneoftheotherpositiveoutcomesofthenewpatent
regimesince2005hasbeentheincreasedcollaborativeagreementsbetween
globalizedIndiancompanies(Sun,ZydusCadila,Aurobindo,Torrentetc)andMNCs
(MSD,Pfizer,GSK,AstraZenecaetc).Thisaugurswellforcollaborativeresearchand
partnershipstoaddressaffordablenewinventionstomeettherequirementsofthe
developingworld.
Page 81 of 153
InthisregardtheTaskForceunderDr.PranabSen,initsreportsubmittedin
September,2005hadmaintainedthatallpatenteddrugsandtheirformulations
shouldbebroughtunderpricenegotiationpriortothegrantofmarketingapproval.
4.3.2IndustryObservations
Researchbasedpharmaceuticalcompanies,whoareintroducingthepatented
products,haveadoptedvaryingmodelstoensureappropriateaccesstosuch
medicinesbythepoor.
• Somecompanieshaveadopteddifferentialpricingstrategiestoextendaccesstolow
andmiddleincomegrouppatients.Somehaveloweredtheirinternationalpricesto
maketheirproductsaffordabletotheIndianmarket.
• AsperOPPIthepatenteddrugsarenewinventionsandresultoftime‐consumingR
&Dinitiativesand,hence,suchmoleculescannotbecomparedwithexistinggeneric
moleculesforpricingpurpose.
IPAstatedthatthereintroductionofproductpatentfrom1995hasbroughtabout
profoundchangesinthepharmaceuticalsector.Thesignificantamongthemaretwo
aslistedbelow:
• Transitionofthedomesticcompaniesfromgenerictoinnovativewiththe
ultimatefocusontheoriginalresearch.Thedomesticcompaniesare
consciousthatitisabigchallengebuthavestartedmovinginthisdirection.
TheincreasedspendonR&Disindicativeofthistransformation.
• Therevivalofforeigncompanies’interestinthedomesticmarket,leadingto
greaterpushforTRIPsplusIntellectualPropertyRights(IPR)regime.Thishas
ledtoshiftinfocusfromthemanufacturingtothemarketingandtheclinical
research(servicessector),resultinginslowdownininvestmentinfixed
assets,rushfordivestmentofmanufacturingplants,outsourcingof
manufacturingandimportingoffinishedformulations.
Boththesedevelopmentswillcontinuetoimpactthepricesofmedicinesinthe
country
Page 82 of 153
BDMAmaintainedthatinthenext3to4years,brandeddrugsintheUSAand
Europeworthabout$100Billionaregoingoffpatent.Indianproducerscanseizethis
opportunitybyexpandingtheircapacitiesinproducinggenerics.Howeverthere
couldbecostlypatentlitigations.Thegovernmentsshouldhelpthesmalland
mediumsectorunitsbymakingprovisionforfreelegalconsultancyservice.
4.3.3CompulsoryLicense
AlthoughcompulsorylicensingisaweaponinthehandsoftheGovernmentto
containpriceriseintheeventofsteepincreaseinthepricesofdrugsaffectedbythe
patentholderbutthatshouldnotsendawrongsignaltothepatentapplicantorto
theprospectiveinventor.Hence,theGovt.shouldspecifyvariousgroundsbasedon
whichtochannelofcompulsorylicensingcouldbeappliedandstipulationstobelaid
downforitsoperation.
Theobjectiveofcompulsorylicensingistoensureaccessibilityofpeopleatlargeto
thepatentedmedicinesatreasonableprice.Thismeasure,inturn,helpsin
protectionofpublichealthandnutrition.TheCompulsoryLicensingallowsthird
parties(otherthanthepatentholder)toproduceandmarketapatentedproduct
withouttheconsentofthepatentholder.ThissystemhasbeenmadeuseofinUSA,
Canada,UnitedKingdom,Italy,Brazil,SouthAfrica,KenyaandEcuador.Therefore,
recognizingthefactthatalmost70%ofthepopulationstillremainsuncoveredby
modernmedicines,itbecomesessentialtoincreasetheavailabilityofmedicinesat
affordablepricesthroughsuchameasure.Thisisexpectedtoimproveavailabilityof
medicinesespeciallyanti‐cancer,anti‐AIDS,severalmedicalimplants,etc.
4.3.4OTHERPRICINGMETHODOLOGIES
4.3.4.1ReferencePricing
Thereferencepricestobeusedfornegotiationsofthepricesofpatenteddrugs
shouldbebasedonthepremiumenjoyedbythedruginthelowestpricedmarket
abroadcomparedtoitsclosesttherapeuticequivalentinthesamecountry.This
premiumcanthenbeappliedtothecorrespondingpriceofthesametherapeutic
Page 83 of 153
equivalentprevailinginthedomesticmarkettodeterminethereasonablepricein
Indianconditions.Inotherwords,thepatenteddrugsshouldbeallowedthe
premiumitcommandselsewhere,butappliedtothepricesprevailinginIndia.
Evenfornonpatenteddrugs,asrecommendedbyPronabSenCommittee,the
pricingcanbebasedonreferencebasisratherthancostbasis.
4.3.4.2PricingofPatentedMedicinesinOtherCountries
(i) Canada:CanadahasapublicfundedHealthscheme,knownas“Medicare”,
whichprovidescomprehensivecoverage.Forthepricingofpatented
medicineunder“Medicare”,thereisPatentedMedicinesPriceReview
Board(PMRB),aquasi‐judicialbody,whichensuresthatpricesofferedby
manufacturersofpatentedmedicinesarenotexcessive.TheBoardcompares
theproposedCanadianpriceunder“Medicare”eithertopricesofexisting
drugsinCanada,ortopricesinsevenmarketsdesignatedintheregulation
(France,Germany,Italy,Sweden,Switzerland,theUnitedKingdomandthe
UnitedStates).Itensuresthatthepricechargedbypatentees,thefactory
gateprice,forpatenteddrugssoldinCanadatowholesalers,hospitals,
pharmaciesorotherforhumanandveterinaryusearenotexcessive.Ifthe
priceexceedsthenitconductsaninvestigationaspertheSchedule5ofthe
CompendiumofGuidelines,PoliciesandProcedures.Thisinvestigationmay
indicatethateitherthepriceiswellwithintheGuidelinesorthepatenteeis
requiredtoreducethepriceandtakemeasurestocomplybyaVoluntary
ComplianceUndertakingorapublichearingiscalledtodetermineifpriceis
excessive.Oncetheintroductorypriceisestablished,subsequentprice
increasesarelimitedtochangesintheConsumerPriceIndex.
(ii) France:InFrance,pharmaceuticalcompaniesselltheirproductsatanyprice.
Ifcompanieswantthenationalhealthcaresystemtoreimbursepatientsfor
thecostofthedrug,theymustagreetoanegotiatedprice.Negotiatedprices
andreimbursementratespaidbythehealthcaresystemarebasedonthe
therapeuticvalueofthedrugandthepriceofthedruginothercountries.
Page 84 of 153
(iv) OtherCountries:FreepricingisapplicableinGermanyandU.Konly.Pricesettingis
negotiatedmainlyonthebasisofnegotiationbetweenauthoritiesandcompaniesin
Belgium,France,Italy,NetherlandsandSpain.Formulationregulationofpremium
pricesbylawisonlythereinItaly.Therapeuticreferencepricingisavailablein
GermanyandNetherlands.Newdrugsareincludedinpositivelistsincaseof
Belgium,France,ItalyandNetherlands.Reimbursementisautomaticallygranted
oncemarketapprovalisobtainedinGermany,SpainandU.K.
4.4 ACCESSTOESSENTIALMEDICINES
4.4.1IncomelevelandAccessibility
Consideringthattheincomelevelsarelow(particularlyinruralareas)andtheoutof
pocketexpensesareasmuchas80%,thepricesofmedicinesplayavitalrolein
ensuringaccessibilityofthecommonpeople.InsurancecoverinIndiaisstillata
nascentstage,althoughprivatesectorhasbeenropedintoplaythisrole.The
contributionoftheStateandCentrealsoisonlyabout14%.
Itisquiteevidentthattheavailabilityofmedicinesandhealthfacilitiesinthehilly,
tribalandinaccessibleareasareeitherabsentorinadequate.Arelativelymuchlower
levelofpercapitaexpenditureonhospitalizationandmedicinesinruralareasandby
thepoorersegmentofpopulationsupportssuchasituation.Therefore,suchareas
needtobegivenspecialtreatmentinamission‐modeapproach,throughwhichthe
healthservicesandmedicinesareprovidedataffordablerates/prices.TheJan
AushadhiSchemeneedstobeexpandedtocovertheseareas.Oneofthemajor
componentsthatcanhelpreducingthisoutofpocketexpensesliesinprovidingbetter
publichealthinfrastructureingeneralbutspecificallyinensuringavailabilityofdrugs
atreasonableprices.TheDepartmentofConsumerAffairsstatedthatanassured
supplyofmedicinesinpublichospitalsandhealthcentreswillreduceunaffordable
sectionsofthepopulationinapproachingtheprivatesectorfortreatment.
Page 85 of 153
ItisquiteencouragingtofindthatseveralStateshavetakentheinitiativetoprovide
medicinesatamuchlowerpricethanthoseinthemarket.TheseStatesinclude
TamilNadu,Bihar,OrissaandRajasthan.Forinstance,Rajasthanhasdemonstrated
thatthroughtenderandnegotiationsifcompetitioncouldbeactivatedamong
differentreputedmanufacturers,thesuppliesofmedicinescouldbemadeavailable
atmuchmoreaffordableratesandinaviableandsustainablemanner.
Inthisregard,ifthetendersystemismeticulouslyfollowedandthepricesof
requiredmedicinesarecentrallydecidedatthestatelevelbyasingleagency,
essentialmedicinesofmassconsumptioncanbemadeavailableataboutonetenth
oftheprintedprice.Themodeldoesnotrequiregovernmentfundingorsubsidy,
unlesstheseareprovidedfreeofcost.Buttheproceduresandsystemsneedtobe
mademoretransparentforensuringsmoothsupplies.Thiswouldalsore‐assurethe
manufacturersofacontinuousandrisingdemandwhichwouldenablethemtoplan
theirproductionprogrammeinadvance.
4.4.2PromotionofUnbrandedGeneric
PromotionofunbrandedgenericsthroughJanAushadhiStores(JAS)needstobe
implementedassoonaspossibleforwhichtheMinistryofHealthneedstobringout
legislationforprescriptionofmedicinesingenericsnomenclaturebythedoctorson
amandatorybasisasdoneeveninadvancedcountrieslikeUS.ThiswouldhelpJAS
tobedevelopedasabrand.IncreasingprovisionofunbrandedgenericsthroughJAS
andpublichealthprogrammescanalsoaugmentavailability.
Affordabilitydoesnotmeanlowcostdrugsonly.Throughpromotionoftheindustry
includingassistancetoqualitystandards,moreunitswouldbesetup(includingSSI
units)resultinginhigherproductionofmedicines.Thiswillenhanceavailability.
Accessisasimportantasaffordability.Industryassociationsfeltalongthefollowing
lines:
Page 86 of 153
• IDMAmaintainedthattheGovernmentshouldincreaseprocurementofmedicines
andshouldmakethemavailableinRuralHealthCareCentres.Sincethis
procurementisdonebytendermechanism,itisalreadyatahighlycompetitive
price.Astheroads,electricity,communicationandotherinfrastructureimprovethe
accessibilitytomedicineswillimprove.ForBPLfamilies,medicinesshouldbegiven
free,whereasforAPLfamilies;costshouldberecoveredfully/partly.
• OPPIobservedthatthechallengeistochangecurrentperceptionsthrough
realizationthatmedicinesarejustapartofmuchbiggeraccessissueofaccessto
healthcarebythecommonman.Thisneedstobeaddressedjointlybywell‐
structuredpublic‐privatepartnershipinitiatives.Thereisaneedtostrengthenthe
linkagebetweenpricingandhealthcareinfrastructure,whichacollectivelyincrease
accesstomedicinesataffordableprices.
AcommongroundwasthattheGovernmentneedstopartnerwiththeprivatesector
toaddressIndia’sacutehealthcarechallengesthroughpublic‐private‐partnerships
(PPPs).RecentexamplesofsuccessfulPPPsinthehealthsectorincludeoutsourcing
ambulanceservices,mobilemedicalunits,diagnosticsandurbanhealthcentersin
severalstatestoprivateNGOs,hospitalsandclinics.PPPsinIndiashouldadequately
coverprimaryandspecialtyhealthcare,includingclinicalanddiagnosticservices,
insurance,telemedicine,hospitalsandmedicalequipment.
Allocatingresourcesfromnationalwelfareschemestowardshealthinsurance
coverageisastepintherightdirection.Forexample,aportionoftheMGNREGS
(MahatmaGandhiNationalRuralEmploymentGuaranteeScheme)fundscouldbe
spentonhealthinsurancepremiumsforlabourersengagedinsuchwork.
Oncethehealthinfrastructureisinplace,differentialpricingpoliciescomplemented
byaccessprogrammesofferedbypharmaceuticalcompaniesconstitutethebestway
forward.AccordingtotheOPPImarketcompetition,monitoringofpricesbyNPPAand
abundantavailabilityofgenericswillstabilizedrugpricesandnopricecontrolbythe
Governmentwouldberequired.
Page 87 of 153
4.4.4 Dr.PronabSenRecommendations
TheTaskForceunderDr.PronabSen(Reportdated20thSept2005)madecertain
importantrecommendations:
i. Inthecaseofproprietarydrugs,particularlyanti‐HIV/AIDSandCancerdrugs,
theGovernmentshouldactivelypursueaccessprogrammesincollaboration
withdrugcompanieswithdifferentialpricingandalternativepackaging,if
necessary.
ii. PublicSectorEnterprises(PSEs)involvedinthemanufactureofdrugsshouldbe
revivedwherepossibleandusedaskeystrategicinterventionsforaddressing
bothpriceandavailabilityissues.Arrangementsmayneedtobemadeto
ensuretheircontinuingviability.
iii. Availabilityofessentialmedicinesthroughpublichealthfacilitiesshouldbe
ensuredboththroughbulkpurchasesbygovernmentagencies,cooperativesor
consumerbodies,throughpublic‐privatepartnershipsifnecessary.
iv. Insurancecompaniesshouldbeencouragedtoextendhealthinsuranceto
covermedicines.
v. Aprocessofactivepromotionofgenericdrugsshouldbeputinplaceandall
publichealthfacilitiesshouldberequiredtoprescribeanddispensegeneric
drugs,exceptwherenogenericalternativeexists.
vi. Allpatenteddrugsandtheirformulationscouldbebroughtunderprice
negotiationspriortothegrantofmarketingapproval.Thereferencepricesto
beusedforsuchnegotiationscouldbebasedonthepremiumenjoyedbythe
druginthelowestpricedmarketabroadcomparedtoitsclosesttherapeutic
equivalentinthatsamecountry.Thispremiumcanthenbeappliedtothe
correspondingpriceofthesametherapeuticequivalentprevailinginthe
domesticmarkettodeterminethereasonablepriceinIndianconditions.
Page 88 of 153
vii. Acentralizedagencycanbecreatedfornegotiationofpricesofpatented
medicinesandtoensureitsavailabilitybycomparingpricesbasedon(i)same
activeingredient;(ii)drugsinapharmacologicalclass;and,(iii)drugswith
similartherapeuticeffect.
viii. IntheIndiancontext,itcouldalsobepossibletodrawfromtheCanadian
modelandsomeofthepracticesinEuropeancountries.
ix. Pricecontrolsshouldbeimposednotonthebasisofturnover,butonthe
‘essentiality’ofthedrugandonstrategicconsiderationsregardingtheimpact
ofpricecontrolonthetherapeuticclass.Thismustbeadynamicprocess.
x. Pricecontrolsshouldbeappliedonlytoformulations,i.e.themedicineactually
usedbytheconsumer,andnottobulkdrugs.Intra‐industrytransactions
shouldnotbecontrolledunlesstherearecompellingreasonsfordoingso.
xi. Theceilingpricesofcontrolleddrugsshouldnormallynotbebasedoncostof
production,butonreadilymonitorablemarket‐basedbenchmarks.
xii. Allotherdrugsshouldbebroughtunderacomprehensivepricemonitoring
systemwithappropriatemarketbasedreferencepricesandwithmandatory
pricenegotiations,ifnecessary.
xiii. TheNationalListofEssentialMedicines(NLEM)shouldformthebasisofdrugs
tobeconsideredforintensivepricemonitoring,ceilingpricesandfor
impositionofpricecontrols,ifnecessary.
Page 89 of 153
xiv. InthecaseofdrugsnotcontainedintheNLEM,intensivemonitoringshouldbe
carriedoutofalldrugsfallingintoapre‐specifiedlistoftherapeuticcategories.
Anysignificantvariationinthepriceswouldbeidentifiedfornegotiation.
xv. Overaperiodoftimemoreeffectivepricemonitoringneedstobeadopted.All
non‐controlleddrugscouldbebroughtunderacomprehensiveprice
monitoringsystemwithappropriatemarketbasedreferencepriceandwith
mandatorypricenegotiations,ifnecessary.Theceilingpricesofcontrolled
drugscouldbebasedonreadilymonitorablemarket‐basedbenchmarks.
GeneralRecommendationsofthePronabSenReport
i. Thereisaneedtobalancetheinterestsofconsumersandpharmaceutical
industry.Pricingofdrugsshouldneitheraffectthepharmaindustry,northe
patients.Hence,StateinterventionthroughschemesliketheNationalRural
HealthMission(NRHM)isimportant.
ii. India,beingaverylargemarket,overtheyearsmoreandmorepatent
protecteddrugswillbelaunchedhereatwhichpointoftimetheimpacton
pricingcouldbelarge;hence,theGovernment/regulatorwouldhaveto
implementproperchecksandbalances/priceapprovalmechanismforpatent
protectedproducts.
iii. Underthenewpatentregime,thetransitionofthedomesticcompaniesfrom
generictoinnovativewiththeultimatefocusontheoriginalresearchis
takingplaces.TheGovernmentneedstosupporttheR&Deffortonoriginal
research.
iv. ThegreaterpushforTRIPsplusIntellectualPropertyRights(IPR)regime
needstobeaddressed.IndiashouldrestricttoexistingprovisionsofTRIPS.
v. Theoptionofusingcompulsorylicensingcouldbeexploredincertaincases,
therebyallowingthirdparties(otherthanthepatentholder)toproduceand
Page 90 of 153
marketapatentedproductwithouttheconsentofthepatentholder.This
wouldensurebetteravailabilityofthemedicine.
vi. Thefocuscouldbeshiftedtoanessentialitycriterionassuggestedbythe
MinistryofHealth&FamilyWelfare.Theysuggestedthatifitisdifficultto
includethe348drugsandtheirformulationsunderDPCOwiththesame
trademargins;therecouldbeagradedsystemoftrade/profitmarginsfor
differentcategories.
vii. NewdrugsdevelopedthroughindigenousR&Dhavingproductpatentunder
theIndianPatentAct1970maybeexemptedfrompriceregulationfora
periodoftenyears.AlsoproductsofNewDrugDeliverySystem(NDDS)
developedthroughindigenousR&Dmaybeexemptedfrompriceregulation
foraperiodoffiveyears.
viii. Lackofproperinfrastructure,particularlyhealthinfrastructure;andpoor
deliverymechanismaremajorhindrancesfordistribution.Hence,thekeyto
healthcareisnotnecessarilypricingcontrolbutcouldbebetterachieved
throughanimproveddeliverymechanism,publicfundingandpromotionof
thepharmaindustry.
ix. Affordabilitydoesnotmeanlowcostdrugsonly.Throughpromotionofthe
industryincludingassistancetoqualitystandards,moreunitswouldbesetup
(includingSSIunits)resultinginhigherproductionofmedicines.Thiswill
enhanceavailability.
x. Thereisaneedtoensureaccessofcommonman(poorersection)to
medicinesthroughpublichospitalsetc.Thesuccessofdistribution/
procurementsystemoftheTamilNaduMedicalServicesCorporationisworth
replicating.
xi. ThesuccessofPPPmodelsinhealthsectorlikeoutsourcingambulance
servicesetc.toprivateNGOsasdoneincertainStatescouldbestudiedin
Page 91 of 153
otherStatesalso.PPPsinIndiamayhelpincoveringprimaryandspecialty
healthcare,includingclinicalanddiagnosticservices,insurance,telemedicine,
hospitalsandmedicalequipments.
xii. Allocatingresourcesfromnationalwelfareschemestowardshealthcoverage
couldalsobeconsidered.Forexample,fromthefundsallocatedforMNREGS,
someportioncouldbemadeavailableforpayingforhealthcoverageofthe
labourersengagedinsuchworks.
xiii. PromotionofunbrandedgenericsthroughJanAushadhiStores(JAS)needsto
beexplored.JAScouldbedevelopedasabrand.Increasingprovisionof
unbrandedgenericsthroughJASandpublichealthprogrammescanalso
augmentavailability.
xiv. Theavailabilityofmedicinesandhealthfacilitiesinthehilly,tribaland
inaccessibleareasareeitherabsentorinadequate.Therefore,suchareas
needtobegivenspecialtreatmentinamission‐modeapproach,through
whichthehealthservicesandmedicinesareprovidedataffordable
rates/prices.TheJanAushadhiSchemeneedstobeexpandedtocoverthese
areas.
xv. Inthecaseofproprietarydrugs,particularlyanti‐HIV/AIDSandCancerdrugs,
theGovernmentshouldactivelypursueaccessprogrammesincollaboration
withdrugcompanieswithdifferentialpricingandalternativepackaging,if
necessary.
xvi. PublicSectorEnterprises(PSEs)involvedinthemanufactureofdrugsshould
berevivedwhereverpossibleandusedaskeystrategicinterventionsfor
addressingbothpriceandavailabilityissues.Arrangementsneedtobemade
toensuretheircontinuingviability.
‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐
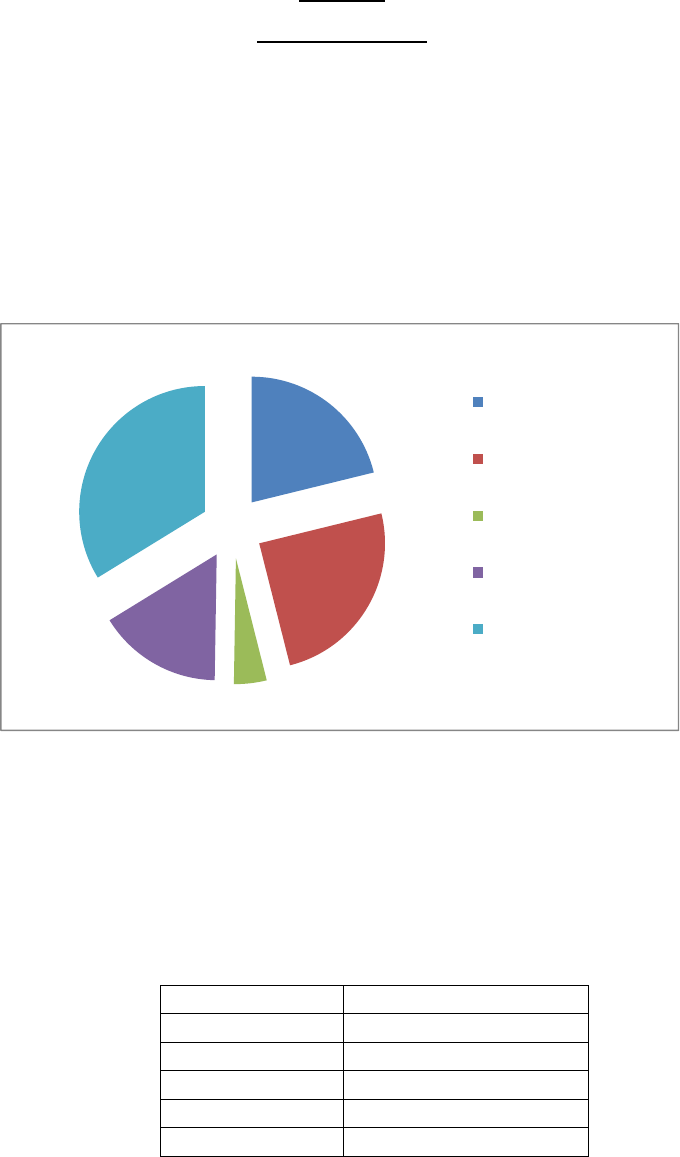
Page 92 of 153
Chapter5
MEDICALDEVICES
5.1StatusofDomesticMedical/surgicalIndustry:
AspertheestimatesofAllIndiaMedicalequipmentsandDevicesAssociation,the
presentmarketsizeofMedicalDevicesandEquipmentsisaroundRs15,000crores
withbreakupsaspertablebelow:
AspertheestimatesofAIMED,therearenearly750manufacturingunitswith
distributionofunitsbasedontheirsizeasbelow:
Table‐19:Turnover‐wisedistribution
Turnover%Distribution
0‐10Cr.70
10‐50Cr.20
50‐100Cr.5
100‐500Cr.3
500+Cr. 2
PresentStatusofIndianmedicaldeviceIndustry:
21.20%
24.90%
4.20%
16%
33.80%
consumables
DiagnosticImaging
Dentalproducts
orthoandImplantable
products
others
Page 93 of 153
(i) ThemedicaldeviceIndustryinIndiaisverynascentandislargelyimport
dependent.Morethan65%ofIndia’srequirementofmedicaldevicesand
equipmentsaremetthroughimportswithdomesticproductionbeinglargely
restrictedtolowtechnologydisposableequipments.
(ii) Asshowninabovetable,thedomesticmedicaldeviceindustryishighly
unorganizedandfragmentedinnature.Thehightechendofmedicaldevices
aredominatedbymultinationalswhichareimportedinthecountry.
(iii) Diagnosticimaging,withthemarketshareof24.9%andMedicalconsumable,
withmarketshareofaround22%dominatestheIndianMarket.
(iv) TheregulatoryregimeisstilldevelopingandDCGIisgoingtobringdetail
guidelinesonMedicalDevicesverysoon.
5.2Export&GlobalMarketPotential:
GlobalmarketformedicaldevicesisvaluedataroundUS$200billion,growingatan
averagegrowthrateofaround4.5%compoundedannuallyduringlast5years.
Growingawarenessabouthealth,newtechnologicalinnovationsintheareaof
diagnosisandtreatment,increasingoldagepopulation,changingdiseasepatterns
towardslongtermtreatmentsetc.,aresomeofthefactorsleadingtogrowthof
industry.
Thehealthcareindustryisshowingrapidgrowthinalleconomiesoftheworld
havingpopulationspreadacrossallagegroups.Inviewofthis,thegrowthof
medicaldeviceindustryisunquestionable.
“ConvergentMedicalTechnologies”arenowbeingdevelopedbymanycompanies.
Thesetechnologiesarebasedontwoormoreexistingtechnologiesplatforms.
Variousmedicaltechnologycompaniesaswellasgrowingenhancedmedical
technologycompaniesinvariouspartsoftheworldhaveemerged,wherecompanies
andresearchersareworkingtogethertoharnessthepotentialofconvergentmedical
technologies.Thekeysupportingtechnologiesintheseeffortsincludemedical
Page 94 of 153
diagnostics,therapeuticandsurgicaldevices,informatics,wirelessmonitoring
devices,nano‐technologies,tissueregenerationandspecializedmaterialsand
quoting.Thishasopenednewareaformedicaldevices.
WiththegrowingincomeinnewworldeconomiessuchasthoseofIndia,Brazil,
SouthAfrica,China,Singaporeetc.,hasopenedavastnewmarketformedical
devicesindustry.However,IndianMedicalDeviceIndustry,atpresentisnotina
positiontoreapthebenefitofthisglobalmarketpositionduetoitsnascentstage.
5.3SWOTAnalysis
5.3.1Strengths
i. WelldevelopedMicroelectronic,Telecommunication,SoftwareandPrecision
EngineeringIndustry,whicharesupportingindustriesformedicaldevices&
equipmentindustry
ii. Abilitytoattractforeigninvestmentsbecauseofstrongfinancialandlegal
system,ruleoflaw,democraticformofGovernment,goodI.P.laws
iii. Industry’sabilitytohandlelowvaluelargevolumeproductionasperglobal
qualitystandards
5.3.2Weaknesses
i. Lowpercapitaexpenditureonhealthcare&lowhealthinsurancewithan
underdevelopedhealthcareawarenessandinfrastructure
ii. Lackofadequateandtrainedmanpower
iii. Lackofincubationandsuitableecosystemencouraginginnovationandnew
products
iv. Absenceoflinkagesbetweenacademiaandindustry
v. Absenceofpropergovernmentalpromotionalpolicytoencourageexports
fromthesector
vi. Tariffstructureworkingagainstlocalmanufacturinginmanycases.
vii. Lackofregulation/standards
Page 95 of 153
5.3.3Opportunities
i. Hugemarketpotentialwithagrowingmiddleclassandrisingexpenditureon
healthcare
ii. GrowingopportunitiesinexportmarketparticularlyinEUmarketwhereEU’s
importsfromdevelopingcountriesareincreasingatover25%
iii. Growingdemandonaccountofchangingdemographicprofile,increasing
incidencesoflifestylediseaseslikecancer,CNSanddiabetics,etc.
iv. Lifecyclesofhighendmedicalequipmentsbecomingshorterduetohigh
levelofinnovation
5.3.4 Threats
i. GrowingcompetitioninexportmarketsfromcountrieslikeThailand,China,
Malaysia,Taiwanetc.
ii. Increasingdependencyonimports,whichisalready65%ofthetotal
demand
iii. Unorganizedmarketformedicaldisposables
iv. Lackofregulationsinmedicaldisposablesandsurgicalitemsleadingto
spuriousproducts
5.4 Recommendations:
i. Thereisaneedofindependentdefinitionformedicaldevicesandaseparate
provisionfortheregulationofthesedevices.TheMinistryofHealthand
FamilyWelfareworkingovertheseissues.
ii. Thereisaneedforinfrastructurecreationforsettingupgreen‐fieldmedical
devicesandequipmentparks.ThisparkmaycontainfacilitieslikeResearch
andDevelopmentCentrefocusedonMedicalDeviceIndustry,Testing
Laboratory,CommonSterilizationfacility,MedicalInstruments/Equipment
calibrationandvalidationfacility,EngineeringServices,atrainingcentreto
trainlabours,managersandentrepreneursetc.Thedetailsofthefacilities
areexplainedintheToRrelatedtobudgetandschemes.
Page 96 of 153
iii. ThereisalsoaneedforNationalCenterforMedicalDevices,whichmayfocus
onnewproductdevelopmentandassessmentformedicaldeviceproducts.
Thiscentercancomplementthegreen‐fieldmedicaldevicesandequipment
parkasstatedabove.
ThedetailsoftheschemesareinChapter8.
‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐

Page 97 of 153
Chaper‐6:
CPSUs
6.1INTRODUCTION
TherearefiveCPSUsnamely,IndianDrugsandPharmaceuticalsLtd(IDPL),Hindustan
AntibioticsLtd(HAL),BengalChemicalsandPharmaceuticalsLtd(BCPL),Karnataka
AntibioticsandPharmaceuticalsLtd(KAPL)andRajasthanDrugsandPharmaceuticals
Ltd(RDPL).ThesefivePharmaPSUshaveacombinesbusinessbetweenINR600and
700crores.Thisworksouttobemere1%ofthedomesticPharmaIndustryturnover.
Thenaturalquestionthenwillbe“whatistherelevanceofPublicSectorunitsinsuch
acrowdedandlargelyself‐sufficientfield?”Theanswertothisliesinthehistorical
developmentofthedrugsectorandalsocurrentscenariowhenitcomestomaking
availablelowvaluelowmarginproductsforpublicgood.
6.2HISTORICALBACKGROUND
Historically,itcanbeseenthatwhennoprivateplayerwasreadytoinvestinthe
capital‐intensivedrugsectorinfiftiesandsixties,GovernmentofIndiainvestedhuge
capitalininfrastructureofthissectorestablishingpublicsectorunitstomakelife‐
savingmedicinesavailableataffordablepricesforgovernmenthealthprograms.This
alsosubstantiallyreduceddependenceonimportssavingthevaluableforeign
exchangewhenthecountryneededitmost.Evenwhenineighties,whenprivate
playersstartedenteringthisfield,publicsectorhelpedthegovernmenttokeepthe
pricesofessentialmedicinesundercontrol.Eventodaythecurrentscenariowith
respecttopovertyandpublichealthinIndiaposesseriousproblemsofaffordability
andavailabilityofkeymedicines.Additionally,incaseslikeepidemics,natural
calamitiesetcwhereemergencyinterventionsarerequired,Publicsectorunitsarea
vitaltoolinthehandsofthegovernmenttomakedesiredproductsavailablein
volumesandatareasonableprice.WhileitisadmittedthattheshareofPublic
SectorisminusculeinPharmasectortheycanhavesomestrategicimportance.It
couldbeusefultomaketheseunitscompetitiveandself‐sustaininginthelongrun
byprovidingthenecessaryfillipatthisjuncture.
Page 98 of 153
6.3CURRENTSTATUSOFCPSUs:
ThePharmaPSUSpresentamixedbagwithrespecttofinancialperformance.While
KAPLandRDPLhavebeendeclaringprofitsovertheyears,theremainingthree
companieshadturnedsickandwerereferredtotheBureauofIndustrialand
FinancialReconstruction(BIFR).BCPLandHALareonapathofrevivalpost
rehabilitationthroughinfusionoffundsandwaiverofinterest,penaltiesand
renegotiationoftermsforfinancialliabilities,IDPL’scaseforrehabilitationispending
beforethegovernment.CollectivelythefivepharmaPSUsgeneraterevenueof
aboutINR600crorestoINR700crores.Exportearningsarecurrentlyasmallfraction
ofKAPLandHALturnoverbutitisgrowing.
6.4 PerformanceofCPSUs:
Table‐20:PerformanceofCPSUs
ParameterKAPLRDPL BCPLHAL IDPLTOTAL
Sales(08‐09) 225.0180.7577.63147.3956.70594.37
TO/Employees
Rslacs
3052 10 11 23 19
TO/Sales
employeesRs
lacs
65304 134 134 236106
PATRscr5.880.01 ‐5.35 ‐22.08 ‐37900.9
Total
Employees
739181 742 1224 2433129
SalesStrength34531 58 105 24 563
Sales(08‐09) 225.0180.75 77.63 147.39 56.70594.37
6.5Personnel:
Thedistributionofpersonnelacrossfunctionsreflectstheorganizationalorientation.
KAPLandtoalesserextentHALhasasalesandmarketingorientationwithlarge
salesforcewhileothershavetraditionallyderivedalmostalloftheirsalesfrom
institutionalmarkets,mainlyfromthegovernmentandmanagethebusinesswith
limitedfieldsalesforceandseveralpersonnelinmanufacturingandoperations.In
Page 99 of 153
termsofeducationalprofile,theLackofR&Disunderlinedbythenearabsenceof
PhDsinthetalentpool.HALhasahighlyqualifiedworkforcewiththelargest
percentage(39%)ofemployeeswithpostgraduatedegreeamongitspeers.
6.6 SourceofRevenue
ThepharmaPSUShavebeengeneratingmostoftheirsalesthroughinstitutional
customers,includingtheCentralandStategovernments.Theshareofinstitutional
salesofpharmaproductsrangesfromabout60%forKAPLtoaround80%forHAL
andcloseto100%forRDPL,IDPLandBCPL.Attheaggregatelevel,thepharmaPSUS
generateabout70%ofsalesofpharmaproductsfromtheinstitutionalsegment.This
biasforinstitutionalsalesgetsreflectedinthecompositionofthesalespersonnel
wherebymostpeopleinthesalesdepartmentsaremanaginginstitutionalorders
andclients.KAPLhasthestrongestandtheyoungestfieldsalesforcefollowedby
HAL,whichhasover100salespersonnel.
KAPLandHALhavebeenexportingtheirproductsprimarilytothesemi‐regulated
marketsinAsia,AfricaandEasternEurope.KAPL’sexportsrepresentslessthan5%of
itsturnoverofRs.225croresin2008‐09whileHAL’sRs.4.73croresworthofexports
representsabout3%ofitsturnoverofRs.147croresin2008‐09.
6.7 SWOTAnalysis:
Overall,thesingularstrengthofmostPharmaPSUsistheirmanufacturingfacilities,
manyofwhicharebeingmodernizedandupgradedforWHOGMPcompliance.
Moreover,beingpartofagovernmentorganization,thereisaperceptionof‘good
quality’associatedwiththeirproducts,whichisanimportantdifferentiatorinan
otherwisecommoditizedmarketforgenericdrugs.SomePharmaPSUshave
developedproductsthatenjoydominanceinnichesegments(e.g.,agrovetproducts
forHAL,OTCandhomecleaningproductsfromBCPL)thathavepotentialforscaling
up.However,theabilitytoderiveadvantagefromtheirgoodqualitymanufacturing
processesandgainmarketshareiscriticallydependentonthecompetenciesthat
PharmaPSUsdevelopintradeandinstitutionalsales.Thisisfoundtobeinadequate
atpresent.MostofthePharmaPSUsaredependentoninstitutionalsalesthat
Page 100 of 153
happenasaresultofgovernment’spreferentialpurchasepolicy(PPP).Eveninthese
cases,PharmaPSUsarefeelingtheneedfordevelopingforecastingtechniquesand
needforhavinginventorybecausemarketpressuresarenolongerallowingthe
supplierstooperateonthebasisofmanufactured‐to‐order.Thebiggestinadequacy
ishoweverfeltintheareaoftradesaleswhere,apartfromKAPLandHAL,thefield
personnelforallPharmaPSUsaretoolow.Mostofthemhavenotbeenableto
attractandretainyoungfieldsalespersonnel,asaresultofwhichtheexistingfield
salespersonnelareagingandabouttoretirewithinthenextfewyears,whichwill
resultinseveretalentcrunch.TrademarketingwouldbecomePharmaPSUskey
sourceofrevenuegeneration,especiallywhenPPPiswithdrawn.Thiswouldinvolve
developingsophisticatedsystemsfordemandestimation,manufacturingresource
planning,inventorymanagement,brandbuildingandsalesforcemanagement–
noneofwhichisvisibleinmostofthePharmaPSUsatpresent.PharmaPSUshave
considerableoverlapinproductsandsometimescompetewithoneanother.
ManyofthePharmaPSUsarehamstrungwithinadequateworkingcapitalfinance.
Thisoftenresultsinthemoutsourcingtheirmanufacturingtothirdparty
manufacturers.Whileoutsourcingasashorttermmeasureisacceptable,thiscan
harmthereputationofPharmaPSUsinthelongrun,giventhefactthat
manufacturingofgoodqualitygenericdrugsisperceivedasthe“corecompetence”
oftheseorganizations.MostofthePharmaPSUshaveplansforexports.However,
theirstrategyordifferentiationinexportsmarketsisunclear.Whilesomeofthem
haveinstitutionalsalesinsemi‐regulatedmarkets,scalingupexportswillneeda
concertedeffortinbrandbuildingaswellasnegotiatingtheregulatoryenvironment
inthosemarkets.
6.8 Goals
ThemainvisionistomakealltheCPSUsself‐sustainingbyyear2020.Towardsthat
end,theroad‐mapforthe12thFiveYearPlanincludestheactionstobetakenin
immediatefuture,thesupportneededforthat,thechangeoforientationtoachieve
propermixofsociallyrelevantbusinessandcommerciallyviablerevenuegenerating
business.Moreovertherewillbesomegeneralgoalscommontoallfivethe
Page 101 of 153
commonpurposebeingthesocialrelevanceof,whiletherewillbePSU‐ specific
goalsdependingonindividualPSU’shistory,strengthandpresentpositiononmarket
ladder.
ItispertinenttomentionherethatalltheresourcesrequiredbytheCPSUsto
becomeselfsustainable,havetobegeneratedbythem,maybebysellingthe
surpluslandavailablewiththem.Thegovernmentassistancewillbelimitedtothe
casesofstrategicimportance.
6.8.1 ShortTermGoals:
Thiswillcoverfirstthreeyearsofthe12thFiveYearPlan.
1) ToupgradetheexistingmanufacturingfacilitiestoWHO‐GMPcompliance.
2) Toidentifyandintroducetheproductinkeytherapeuticsegmentsformass
publicuse
3) TointroducetheproductsfromlatestsociallyrelevantdiseaseslikeAIDS,
Canceretc.
4) Torationalizehumanresourcesforoptimalproductivity.
5) Toengageandexpandintheprescriptionmarket.
Thiswillprovidenecessarybaseandcriticalmasstolaunchintomorecomplexareas
inthelaterhalfoftheFiveYearPlanandbeyond.
6.8.2 LongTermGoals:
Thiswillcovertheperiodoflasttwoyearsof12thFiveYearPlanandbeyond.
1) Bio‐pharmadrugswithemphasisonVaccines
2) IVfluidsbothcurativeandnutritive.
3) Anti‐HIVandOncologymedicines
4) CVDandNon‐Communicablediseasesmedicines.
5) StrategicAPIs
Page 102 of 153
6.8.3 SalesGoalsforFiveCPSUs:
Table‐21:SalesProjectionofCPSUs
RsCrores
YearIDPLHAL BCPL KAPL RDPL
2012‐1351.7 189 153.37 320108
2013‐1470215 176.57 360122
2014‐1580264204.73 425135
2015‐1692290237.6490150
2016‐17125.4319275.83 560165
6.9 Recommendationstoachievethegoals:
ThepharmaceuticalindustryinthecountrygrewataCAGRof14%during11thFive
Yearplan.Logically,PSUsshouldmakeanattempttokeeppacewiththeindustry.
However,thefactthatPSUswillhavetokeeponservicingthelowmarginsocially
relevantproductsandwillhavesignificancepresenceintheinstitutionalmarket,the
CAGRforPSUsneedssometempering.Alsothefactthreeoutoffivearepresently
notintheprescriptionmarketputssomerestrictionontherateatwhichtheycan
growintheimmediatefuture.Theself‐sustaininggrowthassumesthattheprofits
willbeinvestedingrowingthebusiness.AttheprojectedCAGRandROElevels,the
businessgeneratesenoughresourcestofunditsgrowth.Thecross‐linkagesbetween
strategy,operationalefficiencyandfinancialleveragegeneratereturnstothe
shareholders.Achangeinstrategyfrom‘lowcost’to‘differentiation’bychanging
theproductmixinfavorofhighermarginproductsinthechronictherapy,improving
operationalefficiencybygeneratingmoresaleswiththesameassetbaseanda
judiciousmixofdebtandequitycantakethefirmsonanacceleratedgrowth
trajectories.
6.9.1.Therapies:
Page 103 of 153
Thetop7therapiesinIndianpharmaformulationsproductsbelongtoAlimentary
Tract&Metabolism,SystemicAnti‐Infectives,CardiovascularSystem,Respiratory
System,Musculo‐SkeletalSystem,CentralNervousSystemandDermatologicals.
TheyhavegrownataCAGRofbetween12to17%andcontributetoover83%ofthe
industrysales.Ineachtherapy,thereisatremendousamountofconcentrationof
sub‐therapiesaswellasproductswithineachsub‐therapy.Therefore,itisrelatively
easytoidentifyandselectproductsfordrivinggrowthbyusingthecriteriaofannual
salesandgrowth.Atthesametime,theproductswithlargesalesandhighgrowth
arealsothemostcompetitive.Therefore,onemustlookatothercriteriaincluding
profitability,capabilitiesaswellasstrategicintenttoplayincertainproduct–
marketstocreateaportfoliothatwilldrivesustainablegrowth..
6.9.2.Marketstobeconcentrated:
UP,MaharashtraandAndhraPradesharethelargestmarketsfordomestic
formulations.IfoneincludesMumbai,thenMaharashtratakesthetopspotwitha
shareof17.5%ofthetotalsales.Theregionaldistributionofsalesisusefulin
identifyingandfocusingonmarketstoallocatethefieldsalesforceforgrowingsales
throughtrade.Whilethelargemarketsseemattractivefromtheperspectiveofsize,
theyarealsolikelytobethemostcompetitive.Atthesametime,severalofthe
smallerstates,intermsofphysicalsizeaswellassalesofformulations,maybe
underservicedbyleadingindustryplayersthusprovidingthepotentialfor
establishingstrongbrandsovera5‐6yeartimehorizon.Similarly,themetrosand
largecitiesaresaturatedwithcompetitorswhilethesmallertownsandruralareas
remainunderserviced.Anaddedadvantagewouldbetherelativelylowerexpenses
towardssalesforcecompensationandtheabilitytocreateforcemultiplierthrough
partialoutsourcingoffieldsalesstaffthroughBusinessAssociates(BA)/Franchisees.
6.9.3.Newproductsandverticals:
PSUshavetraditionallyremainedwithmainlytheproductsaddressedtothe
institutionalrequirements.Mostoftheseproductsfallunderthecategorieslikeanti‐
infectives,painmanagementmedicines,GItractandgynaecologyrequirements.
Furtherforreasonsofpricetheseareoldproducts.Inrunuptotheself‐sustainable
Page 104 of 153
performance,PSUswillidentifythenewmoleculesintheirareasofcompetence.At
thesametimesnewverticalsbothsociallyrelevantandcommerciallyattractivewill
beenteredinto.Additionaltherapieswillincludedermatologyproducts,
neutraceuticals,cardio‐diabeticmedicinesandAyurvedicproducts.
Twoothertherapiesneedaspecialmention.Theyareantiretroviraldrugsand
VaccinesandSera.
6.9.4 Antiretroviraldrugs:
WithspreadofHIVandsocialstigmaattachedtoit,Governmenthastakenupon
itselftoprovidethenecessarymedicationfortheaffectedindividuals.Thepurposeis
notonlytocurethespecificindividualbutalsotoarrestthespreadandprovide
betterqualityoflife.Thereareprivatecompaniesthatmanufacturethesemedicines
butconcentrateonexportbusinessforprofitabilityatthecostofdomesticpatient.
Therearealsothenewermedicinesthatfallunderpatentregimeandthereforenot
economicallyavailable.PSUscanplayamajorrolebyofferingtheirfacilitiesfor
formulationofthesemedicines.Governmentsupportintheformoflong‐term
contractatanassuredviablepricewillbenecessary.
6.9.5 VaccinesandSera:
ThisisanotherareaidentifiedbyPSUsintheirlong‐termstrategy.Governmentof
Indiaundertakesvaccinationofchildrenforcertainspecificailments.Thenumberof
suchailmentscoveredismuchlessascomparedtotheonesadvisedbyWHO.
Furthercertainepidemicsalsocallforinterventionatshorternotice.PSUswouldlike
toenterthisareastartingwithmarketingtogenerateaclientbase.Thiswillbe
followedbybackwardintegrationintomanufacturing.Thisofcoursewillrequire
establishingadedicatedstateoftheartfacilitythatiscapital‐intensiveactivityand
willneedbudgetarysupport.Thevaccinesthatcouldbelookedintoareinfluenza
vaccine,BCG,Tuberculin,AntiRabies,Hib,TT,Measles,RubellaandJapanese
Encephalitis.SimilarlySeraforrabies,SnakeVenomcanbehandledinthese
facilities.

Page 105 of 153
6.9.6 PurchasePreferencePolicy:
Overlastfiveyears,throughcabinetapprovedscheme,Governmenthasprovided
purchasepreferencefor102medicinesmanufacturedbyPSUs.Thishashelpedalot
inincreasingcapacityutilisation,improvingtop‐line,improvingbottom‐lineforprofit
makingPSUslikeKAPLandRDPLwhilehelpinginreductionoflossforthePSUsin
rehabilitationmode.Withdrawalofthispreferenceatthiscrucialjuncturewillnullify
thebenefitsofalltheeffortsmadeoverlast5yearsandendangerthebenefitsof
thebudgetarysupportenvisagedinthe12thFiveYearPlan.Thereforeitisabsolutely
essentialtocontinuethispreferencefortheperiodof12thFiveTearPlan.Since
MinistryofHealth&FamilyWelfareisalreadyplanningtoestablishacommon
procurementagencyforthemedicinesrequiredforthegovernmentaluse,along
termcontractcanbesignedbyPharmaPSUswithMOH&FWunderthisPurchase
PreferencePolicyinsteadofthebiddingsystemfollowedpresently.Thiscontract
shouldbeoveraperiodoffiveyearswithpricesbeingfixedinconsultationwithNPPA
andthedrugslistidentificationbytheMoH&FWaswellasotherprocuringagencies
likeRailways,ESIC,DGAFMS,etc..ThiswillprovideassuredrevenuetoPSUsinthe
earlyyearswhilethegovernmentwillbeassuredofsupplyofqualitymedicines.
6.9.7 WHO‐GMP:
Thelong‐termsustainabilityalsoincludesafactorofinternationalpresence.Thisis
possiblebyup‐gradingthefacilitiestointernationalstandardsasperWHO‐GMP.
Whilethenewprojectplannedinthe12thPlanwillfactorthisattheprojectstage
itself,theexistingfacilitiesmayneedface‐lifttoachievethosestandards.While
beyond3rdyearoftheplan,internalrevenuegenerationshouldnormallysupport
this,somebudgetarysupportmayberequiredoncase‐to‐casebasis.
6.9.8 R&Dinitiative:
Inadynamicindustrylikepharmaceuticals,thelong‐termsustenancecanonlybe
ensuredwiththeaccesstoknowledgedriventechnologies,eitherintheformofnew
moleculeornewdrugdeliverysystem.ArobustR&Disnecessaryforthis.To
achieveself‐relianceby2020,effortsinthisdirectionhavetostartinthesecondhalf
Page 106 of 153
ofthe12thPlan.Abasicinfrastructureneedstobeputplacseasacommonfacility
forallthefivePSUswithcontributioncomingfromthePSUsaswellasfundingfrom
government.
6.10Janaushadhi:
ThisisaflagshipprogramofDepartmentofPharmaceuticalsunderwhich
commonlyrequiredmedicineswillbemadeavailableundergenericnamesand
affordablepricesthroughdedicatedoutletsacrossthecountry.Apartfrommaking
themedicinesaccessibletopoorsectionsofthesociety,thisalsowillprovidea
platformforPSUstohavefootholdinthetrademarketandinthelongrun
eliminatetheneedofthecrutchesofpurchasepreference.Thepurposeofmaking
availablesociallyrelevantmedicineswillalsobesimultaneouslyserved.
6.10.1 ThekeyfeaturesoftheJanAushadhiSchemeare:
i. Makingavailablequalitymedicinesataffordablepricesforall,typically
thepoorandthedisadvantagedthroughspecializedoutletscalledJan
AushadhiStores(JAS)tobeopenedindistricthospitalsinthefirst
instanceasthisistheplacsewheretypicallythepoorersectionsofthe
massescomefortreatment.
ii. ProvisionofbuiltupspaceforJASindistricthospitalsbytheState
GovernmentswiththeoperationofJASbystateGovernmentnominated
OperatingAgencieslikeNGOs,CharitableOrganistionsandpublic
societieslikeRedCrossSociety,RogiKalyanSamitistypicallyconstituted
forthepurpose
iii. Operationalcoststobemetfromtrademarginsadmissibleforthe
medicines.
iv. SupplyofthegenericmedicinesinthefirstinstancebytheCentral
PharmaPSUssoastoensurebothqualityandtimelysupply.However
Page 107 of 153
wherevertherewouldbeneedandgap,medicinescouldbesourcedfor
qualitySMEunits.ThiswouldalsogivesupporttothePharmaSMEsector
alsoaswellaspromotepublic‐privatepartnershipandavenuesfor
achievementofcorporatesocialresponsibilities,goalsgearedtowards
affordablemedicareforthemasses.
v. StateGovernmentstoensureprescriptionofunbrandedgeneric
medicinesbytheGovernmentdoctors.Hencethelinkofdistricthospital
locatedJAStobeginwith.
6.10.2.StatusofJANAUSHADHIScheme
Thecentralobjectiveoftheschemetobeginwithwastomakemedicinesavailable
tothepooranddisadvantagedsectionsofthesocietythroughtheopeningoftheJan
AushadhiStores–oneineverydistricthospitalofthecountryieatotalof630.This
wastobeexpandedtoSub‐divisionandBlocklevelslater.However,only102stores
couldbesetupin9statesinthelasttwoyearswhichisacauseofconcern.
Severalreasonshavebeenidentifiedforthispoorprogress:
i. FirstlythatmostStatesdidseemtobesensitivetotheissueofavailability
ofqualitymedicinesataffordableprices,especiallyforBPLfamiliesbutstill
advocatedfreemedicinedisbursementfromthehospitaldispensary
withoutadmittingtotheLackofmedicinesavailabilityontimeandin
requiredquantitieswithassuredqualitytopatientsvisitingthese
dispensariesinthehospitalsatdistrict,subdivisionandblocklevels.The
freesupplyinanycaseisaburdenwhichcanbereducedifunbranded
genericmedicinesareprescribedandused,butforvariousreasonsthejan
aushadhiunbrandedgenericmedicineswasperceivedtobeagainstthefree
medicinesconcept.ThefeebleattemptsbysomegovernmentslikeBihar,
TamilNadu,APandsomedistrictsofRajasthanlikeNagaurandChittorgarh
donotlendthemselvestosustainableandtrueunbrandedgenericmedicines
supportasrequiredwhichiswhytheyhavenotbeenabletomakeanydent
intheproblem.ThesupportofthecentralgovernmentintheMinistryof
Page 108 of 153
Healthhasalsonotbeenadequateinasmuchthatthereisneedfor
supportingopeningofjanaushadhistoresincentralgovernmenthospital
premisescoupledwithmonitoredprescriptionofunbrandedgenericdrugsto
theout–patientsandindoorpatients.
ii. Lackofprescriptionofgenericdrugsbygovernmentdoctorswasabighurdle.
Fewstategovernmentscameforwardtoissueguidelinestogovernment
doctorstoprescribegenericmedicines.EventhosethatdidlikeRajasthan,
Punjab,Odhisa,Delhicouldnotenforceitproperly.Eventhenotification
dated19thMay2011bytheMinistryofHealthoftheGovernmentofIndiafor
allcentralgovernmenthospitalsandrelatedinstitutionshasnotbeenof
muchhelp.
iii. Boththeabovereasonsledtoverylessnumberofstores(102in9states)
whichdoesnotlenditselftoviableeconomicoperationbothfromthe
productionofgenericmedicinesinunbrandedgenericformandtheirsupply.
6.10.3Recommendations
i. Toovercometheaboveweaknessrevisedschemehasbeenprepared.Herein
focusedeffortswouldbemadeinthefirstinstanceinschemefriendlystatesandthe
MinistryofHealthwouldbeencouragedtoassistinimplementingtheschemein
centralgovernmenthospitals,MinistrieslikethoseofRailways,ESIC,Labouretc.A
schemeofRs200.00crsisbeingproposed.
ii. Makingtheschemeimplementationmandatoryaspartofthehealthsectorfunds
allocationforsupportingtheschemethroughstategovernmentrunhospitals.This
couldbeensuredthroughamechanismtyingupthereleaseoffundsfromthe
Centralschemetothestatedependantontheprogressofthescheme.Appropriate
deliverableparameterstobeputinplaceforthisinconsultationwithDepartmentof
PharmaceuticalsandthePlanningCommission.
Page 109 of 153
iii. Mandatoryprescriptionofunbrandedgenericmedicinesbystategovernmentand
centralgovernmentinstitutionsdoctorsandmechanismtoensureitscomplianceby
appropriateauditprocesses
iv. InvolvementoftheDepartmentofConsumerAffairsandInformationand
Broadcastingalongwithrelatedstategovernmentdepartmentsformediaassisted
coveragesoastoensurewidespreadruralandtargetgroupoutreachononehand
andtogeneratedemandsidesupplypushsoastomaketheoperations
economicallyviableontheother.
‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐
Page 110 of 153
Chapter7
RESOURCEREQUIREMENTINTHE
DEPARTMENTOFPHARMACEUTICALS
7.1IntheDepartment
TheDoPhasnotbeenabletotakeuporlaunchanynewactivityinlinetoits
BusinessAllocationevenafterthreeyearsofitsexistence.Themainreasonforthis
liesinlackoftechnicalcapabilitysinceitsinception.
7.1.1ExistingTechnicalresponsibilities
i. Examination&processingofapplicationsforImportofitemsrestrictedfor
imports.
ii. Examination&processingofapplicationsforDSIR'srecognitionofin‐house
R&DunitsofPharmaIndustry.
iii. AlltechnicalmatterspertainingtoNLEM®ulatorysystemsunderDrugs&
CosmeticsAct,DPCO,NDPSAct,
iv. AlltechnicalmattersconcerningIPR,WTO,patenteddrugs&medical
devices.
v. Inter‐DepartmentalmattersincludingFreeTradeAgreementsandJoint
Commissionsandotherbilateraltechnicalmatters
vi. TechnicalissuesrelatedtoPharmaPolicy.
vii. ProjectplansforsettingupNationalCentreofR&DinPhytopharmaceuticals
(NCRDP)tobesetupatNIPER,Guwahati.
viii. Examination&processingofapplicationsconcerningfixationofStandard
Input‐OutputNorms(SION)fordrugsandpharmaceuticals
ix. Examination&processingofapplicationsconcerninglicensingmatters,
foreigncollaborationetc.
x. Examination&processingofreferencesaboutdevelopmentofInfrastructure,
manpowerandskillsforthePharmaceuticalssectorandmanagementof
relatedinformation.
Page 111 of 153
xi. Educationandtrainingincludinghighendresearchandgrantoffellowshipin
Indiaandabroad,exchangeofinformationandtechnicalguidanceonall
mattersrelatingtoPharmaceuticalssector.
xii. PromotionofPublic–Private–PartnershipinPharmaceuticalsrelatedareas.
xiii. Inter‐sectoralcoordinationincludingcoordinationbetweenorganizationsand
institutionsandinstitutesundertheCentralandStateGovernmentinareas
relatedtothesubjectentrustedtotheDepartment.
xiv. TechnicalsupportfordealingwithnationalhazardsinPharmaceuticalsector.
7.1.2DifficultiesduetoUnavailabilityofTechnicalOfficers
OwingtounavailabilityofTechnicalOfficers,theDepartmentisfacingalotof
problemsinconsiderationofvariousissuescoveringdevelopmentsofthepharma
industry.Additionally,itisnotabletocontributetointer‐departmentalissueswith
DST/DBT,etc.anddisposalofvariousreferencesreceivedfromdifferentsources
dependinguponthenatureofabovereferredactivities.Insomecases,theschemes
cannotbepursuedatrequiredpace.TheR&DsectionintheDepartmentisvirtually
defunctasitisdifficulttodevelopnewschemesformuchrequiredR&Deffortsin
drug/pharmadepartment.Insomeofthehighlevelcommittees,suchasGLPExpert
CommitteeandDPRPExpertCommittee,properrepresentationfromthe
DepartmentcouldnotbemadeduetolackofseniorlevelTechnicalOfficers.The
requirementoftechnicalofficersisverycrucialinevaluatingmanyproposals
receivedfromDGFTintheDepartmentaboutfixationofSIONforbulkdrugs,drug
intermediatesandformulationsbeingexportedfromIndia
7.1.3Actionneeded
Inviewoftheforegoingitisproposedthatactionforcreatingthepostsmaybetakenas
proposedbelow:
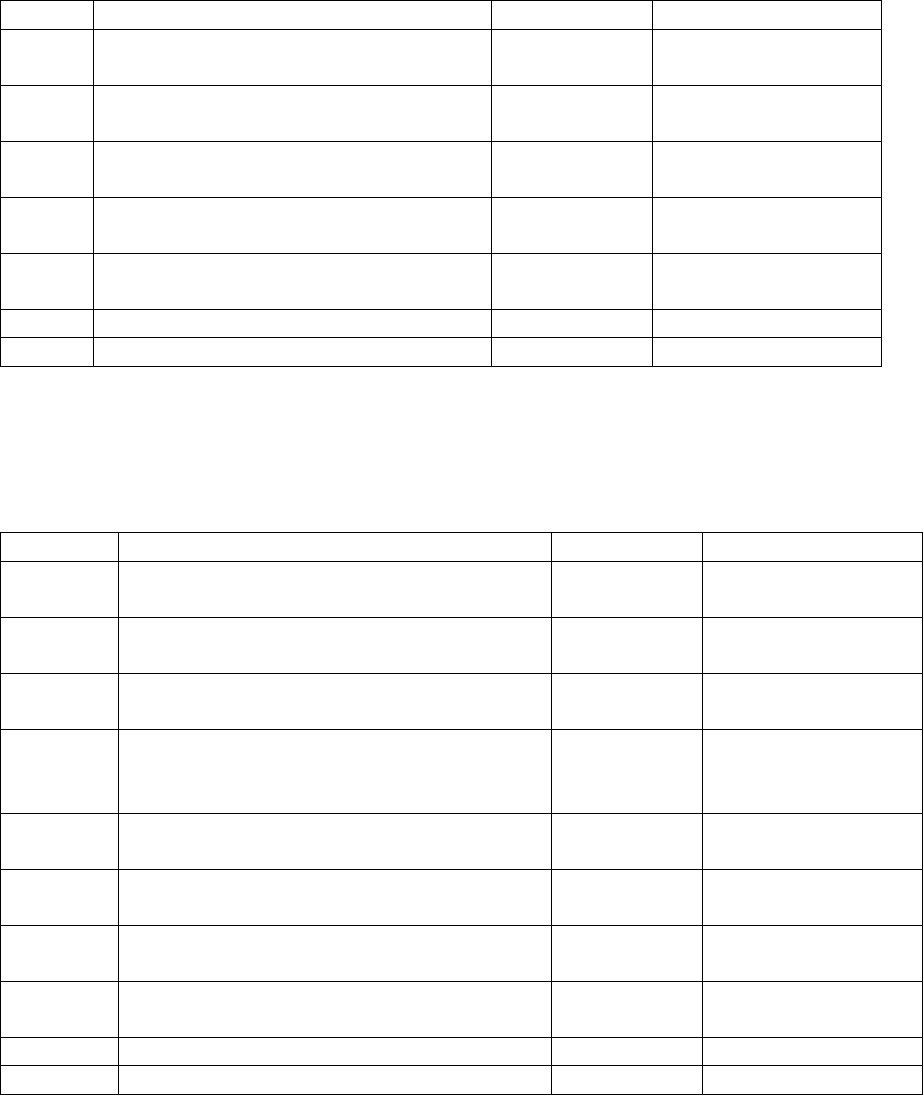
Page 112 of 153
(i)DrugsPriceControlDivision
Table‐22
S.No.Nameofpost/PayscaleNo.ofPostsExpenditure
1JointDirector(Cost)
(Rs.15600‐39100,GP‐7600)
170762
2ScientistGd.C
(Rs.15600‐39100,GP‐6600)
168882
3DeputyDirector(Cost)
(Rs.15600‐39100,GP‐6600)
168882
4AssistantDirector(Cost)
(Rs.15600‐39100,GP‐5400)
266626x2=1,33,252
5JuniorAnalyst
(Rs.9300‐34800,GP‐4600)
252630x2=1,05,260
Total(for1month)4,47,038
Total(for1year)53,64,456
(ii)ProjectsAndTradeRegulatoryDivision
Table‐23
S.No.Nameofpost/PayscaleNo.ofPostsExpenditure(in`)
1DeputyDirectorGeneral(DDG)
(Rs.37400‐67000,GP‐10000)
1121992
2ScientistGd.C
(Rs.15600‐39100,GP‐6600)
168882
3DeputyDirector(Statistical)(Rs.15600‐
39100,GP‐6600)
168882
4ResearchOfficer/AssistantDirector
(EconomicService)(Rs.15600‐39100,GP‐
5400)
166626
5(a)SeniorInvestigator(StatisticalService)
(Rs.9300‐34800,GP‐4800)
253006x2=1,06,012
5(b)JuniorAnalyst(ScienceCadre)
(Rs.9300‐34800,GP‐4600)
252630x2=1,05,260
6(a)JuniorInvestigator(StatisticalService)
(Rs.9300‐34800,GP‐4600)
252630x2=1,05,260
6(b)JuniorTechnicalAssistant(ScienceCadre)
(Rs.9300‐34800,GP‐4200)
251878x2=1,03,756
Total(for1month)7,46,670
Total(for1year)89,60,040
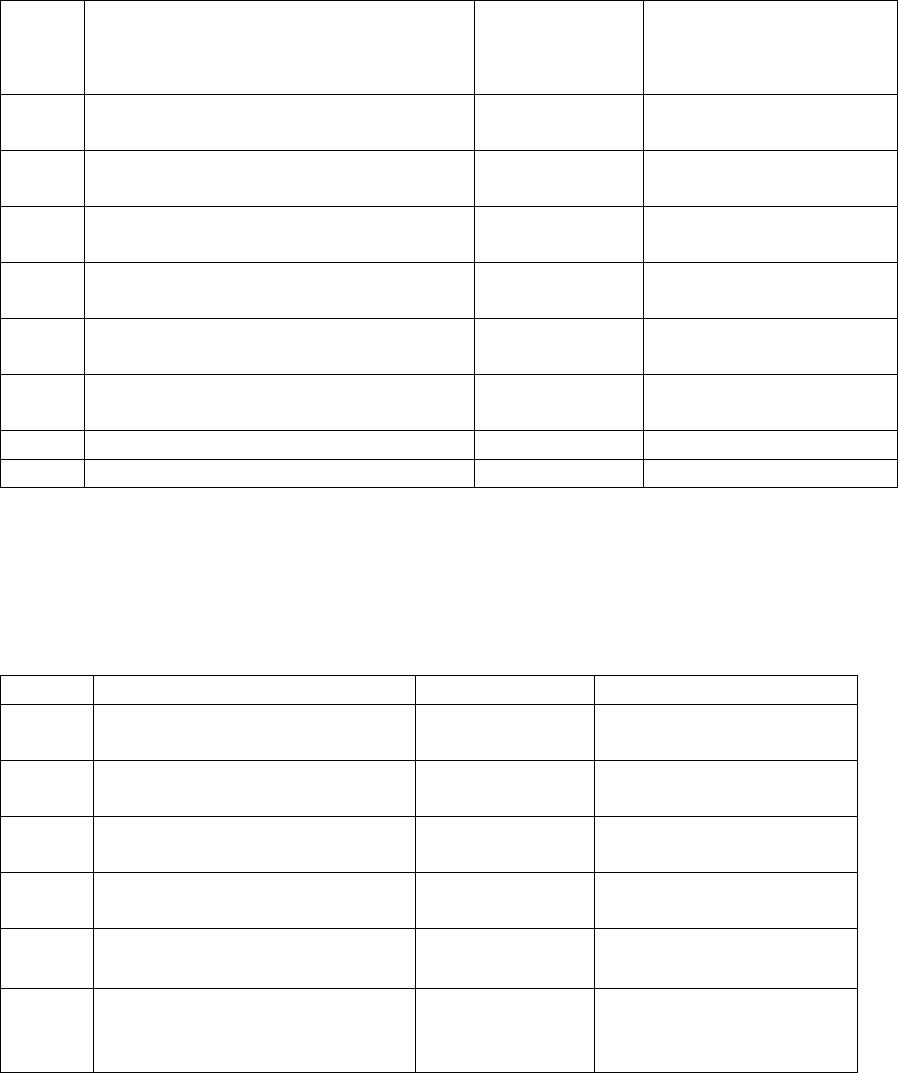
Page 113 of 153
(iii)ResearchAndDevelopmentDivision
Table‐24
S.No.Nameofpost/PayscaleNo.ofPostsExpenditure
1ScientistGd.E
(Rs.37400‐67000,GP‐8700)
1119548
2ScientistGd.D
(Rs.15600‐39100,GP‐7600)
270762x2=1,41,524
3ScientistGd.C
(Rs.15600‐39100,GP‐6600)
268882x2=1,37,764
4ScientistGd.B
(Rs.15600‐39100,GP‐5400)
266626x2=1,33,252
5JuniorAnalyst
(Rs.9300‐34800,GP‐4600)
252630x2=1,05,260
6JuniorTechnicalAssistant
(Rs.9300‐34800,GP‐4200)
251878x2=1,03,756
Total(for1month)7,41,104
Total(for1year)88,93,248
(iv)EducationAndTrainingDivision
Table‐25
Thetotalexpenditureonthesalary,forimplementingaboveproposalwouldbe
approximatelyRs2.9croresperannum.
S.No.Nameofpost/Payscale No.ofPosts Expenditure
1ScientistGd.C
(Rs.15600‐39100,GP‐6600)
268882x2=1,37,764
2ScientistGd.B
(Rs.15600‐39100,GP‐5400)
266626x2=1,33,252
3JuniorAnalyst
(Rs.9300‐34800,GP‐4600)
252630x2=1,05,260
4JuniorTechnicalAssistant
(Rs.9300‐34800,GP‐4200)
251878x2=1,03,756
Total(for1month)4,80,032
Total(for1year)57,60,384
Page 114 of 153
7.2NationalPharmaceuticalPricingAuthority
7.2.1PresentStatus
NPPAsinceitsinceptionishavingtotalsanctionedstrengthof60regularpostsincluding
costing,technicalandadministrativeofficials.SinceNPPAdoesnothaveitsowncadrefor
recruitmentoftheirofficials,therequiredmanpowerisbeingprovidedtoNPPAbydifferent
cadrecontrollingauthoritiessuchasIndianCostsAccountsService,Departmentof
Fertilizers,DepartmentofChemical&Petrochemicals,IndianEconomicServiceetc.
7.2.2StudiesforManpower
StaffInspectionUnit(SIU)hadconductedastudyin2003forassessmentofworkandstaff
requirementforNPPA.However,nofinaldecisioncouldbetakenonthisreport.
Subsequently,aWorkStudywasconductedbyIndianInstituteofPublicAdministrations
(IIPA),whichsubmittedareporton23.11.09.Further,IIPAsubmittedasupplementary
reportinJanuary,2011.
7.2.3ObservationsofIIPAStudy
AsperreportofIIPA,thefunctioningofNPPAisheavilydependentuponthe
outsourced/contractualstaffsi.e.DEOs/YPsasNPPAhashired40DEOs/YPsinorderto
supportits31regularstaffsoutofthetotal71workingstrengthofNPPAasonJanuary
2011.AsperobservationofIIPA,NPPAneedadditionalregularstaffforsmoothrunningof
followingmainfunctionsIIPAhasreassessedthetotalstaffstrengthto132posts.
7.2.4NPPAProposal
NPPAsubmitteddetailsforcreationof44additionalpostsatvariouslevelsand
simultaneouslyabolishmentof15,thusincreasingthestaffstrengthofNPPAfrom60
presentsanctionedstrengthto89.
ThusthetotalsanctionedstrengthofNPPAwouldbeasunder:‐
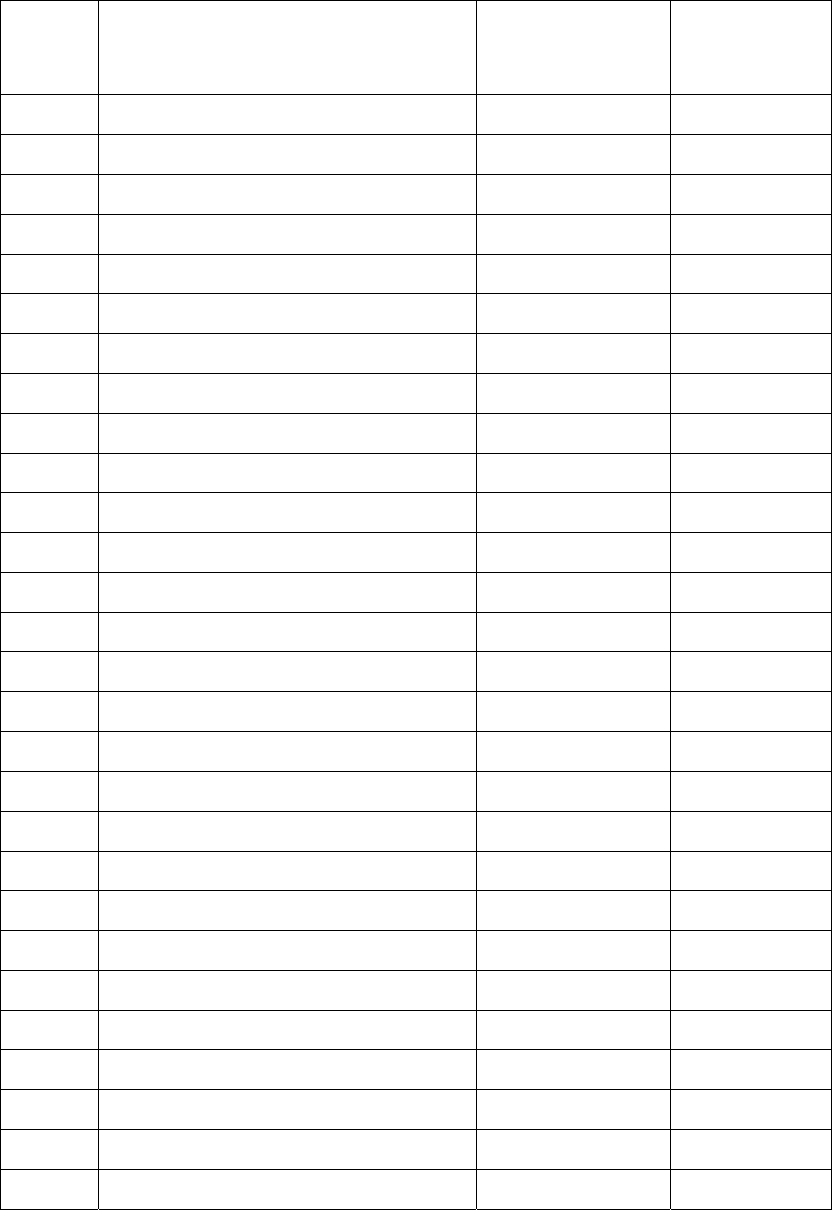
Page 115 of 153
Table‐26
Sl.
No.
DesignationofPostExisting
Sanctioned
Strength
Concurredby
IFD
1234
01Chairman11
02MemberSecretary1 1
03Advisors/Directors54
04 DeputySecretary(Legal)01
05UnderSecretary01
06Dy.Directors(Cost)75
07Dy.Directors(Tech.) 34
08DeputyDirector(Econ)01
09SectionOfficer3 2
10Asstt.Director(Tech.)103
11Asstt.Director(Cost)20
12Asstt.Director(Stat.)001
13PrivateSecretary11
14PersonalAssistant/StenoGrade‘C’25
15PPS11
16SeniorInvestigator1 2
17Assistant16
18LawOfficer/LegalAssistant02
19TechnicalAssistant28
20JuniorInvestigator10
21HindiTranslator11
22StenoGrade‘D’8 1
23UDC1 1
24LDC/Typist816
25StaffCarDriver22
26Daftry21
27Peon/Messenger59
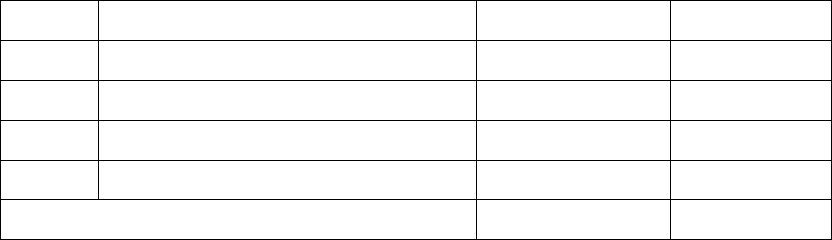
Page 116 of 153
Consequentuponimplementationoftheabovere‐structuringofNPPA,thenetfinancial
implicationwillbeRs.74.89lacsperannum
‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐
28Safaiwala1 2
29Group‘D’0 3
30DatabaseOperator01
31Sr.CounselOperator ‐‐ 1
32DEO02
Total6089
Page 117 of 153
CHAPTER‐8
SCHEMEPROPOSALS
8.1IndustryPromotionandDevelopment
8.1.1ExistingSchemes–Continuedfrom11thPlan
8.1.1.1PharmaPromotionandDevelopmentScheme(PPDS):
ThisisacontinuingschemeforpromotionanddevelopmentofPharmasectorinthe
country.Underthescheme,followingactivitiesareundertaken:
i. OrganizingSeminars,Conferences,exhibitions,mountingdelegationsto
andfromIndiaforpromotionofexportsaswellasinvestments,
conductingstudies/consultanciesforfacilitatinggrowth,exportsand
criticalissuesaffectingPharmaSector.
ii. AnyotheractivityrelatingtothepromotionofPharmaSector,exportand
investment.
Anumberofstudiesareproposedtobeconductedforproperscheme
planningandprojectdevelopment.Thesecouldbe–
• CensusofMSMEincollaborationwithDCGI,MSMEandMinistryofStatistics
&PI
• Studyonpharmaceuticalindustryanalysisofcompetingcountries–study
couldbedoneoravailablereportsprocuredoff‐shelf.
• Studiesrequiredforthedetailedformulationofvariousschemesgiveninthis
PlanDocumentandfurtherasmayberequired
Itisproposedtocontinuetheschemeforthe12thPlanforthesamesetofactivities
whichwouldberequiredmoresonowthatthedepartmentwouldbeableto
implementitmoreeffectivelybasedontheexperiencegainedinthelastthreeyears
followingthesettingupofthedepartmentinJuly2008.
Budgetaryrequirement:Accordingly,thebudgetaryrequirementforthescheme,
attherateofRs.2.0croresperannumwillbeRs10.0crores.
Page 118 of 153
8.1.1.2IntellectualPropertyRightsFacilitationCenters:
Thisisacontinuingschemeandwasstartedin11thFiveYearPlanandtwocenters
oneatPharmexcilHyderabadandotheratNIPERMohalihavebeenopened.The
existingobjectivesoftheseIPRFacilitationCenters(IPRFCs)are:
i. StrengtheningofinteractionbetweenPharmaIndustry,Pharmaindustry
supportinstitutionsandassociations,IPofficesandotherrelevant
governmentorganizationswithaviewtobetteridentifyingtheneedsof
PharmaIndustryfacilitatingtheimplementationofcustomizedtargeted
activitiesaddressingthespecificIPneedsofeachsector,grouporcluster.
ii. SupporttonationalandinternationaleffortsforfurtherintegrationofIP
issuesinprogramsandpolicyinitiativesaimingatfosteringthetechnological
andinnovativecapacityandtheexportpotentialofPharmaIndustry.
iii. IncreaseawarenessandunderstandingofIPissueswithinthePharma
businesscommunitythroughawarenessraisingcampaignsandtargeted
trainingprogramswiththeoptimaluseofmoderninformationand
communicationtechnologiestomaximizetheirbenefitsfromtheuseofIP
systems.
iv. AdvisegovernmenttotakeintoaccountthespecificneedsofPharma
IndustryintheirIPPolicies.
v. DisseminateinformationonbestpracticesontheuseofIPbyPharma
Industryandoftheirexploitationoftechnologicalknowledge.
vi. Makeanaccesstotechnologicalknowledgeeasierandcheaperforthe
industry.
vii. AdetailedstudywouldbegotdoneontheimpactofIPRissuesonthedrug
pricesandavailabilityindevelopingcountries.Forthisfundingwouldbe
donefromthebudgetaryresourcesofPPDSscheme.
Thereisacontinuedneedtofurtherstrengthenthesecentersandbroadenthe
scopeofworkbyhelpinginfilingapplicationsrelatedtoDMF,ANDA,MHRA,etc
giventheincreasingemphasisonpatentissuesbythecompetitivemarketsand

Page 119 of 153
companiesasalsothekeyrolewhichIndianpharmacompaniescanplayinbringing
outnewproductpatentsaswelladvancetheirshareoftheFirst‐to‐fileapplications
intheregulatedmarketslikeUS,JapanandEU.Accordingly,newIPRFCsatMumbai,
ChennaiandAhmedabadcanbeopenedforeasyaccessofthecentersbythe
industry.
Budgetaryrequirement:Thebudgetaryrequirementwouldbe:
• OneTimeCostofsettingupthreeCenters Rs.1.5crores
@Rs0.50crspercentre
• RecurringCostforfivecenters Rs5croresperannum
TotalBudgetfor12thFiveyearPlan: Rs26.5crores
8.1.2NewSchemes
8.1.2.1InternationalPharmaCooperationInitiative(IPCI)
WiththeincreasinginfluenceofIndiainglobalpharmaproduction,mutually
beneficialinternationalpartnershipsisacrucialissuewithrespecttogainingaccess
toemergingmarketsandsustaininggenericscapabilitiesinthedevelopedmarkets.
Forthisatwofoldapproachisproposed‐
i. HereinthefocuswouldbeonBRIC,IBSA,CIS,EE,WA,AfricaandASEAN
marketswhicharegrowingat10%+annuallybutwhereinIndianpharma
productsarebeingtargetedbycompetitiveMNCsonvariousgrounds
includingqualityandmanufacturingstandards.Theschemeaimstomeetthis
challengehead‐on.Itisaccordinglyproposedtohavemutuallybeneficial
capitalinvestmentprojectsonapartnershipbasistotacklesuchneedssuch
as–
• SettingupofJointtestingandlabfacilitiesforcertificationofIndian
pharmaproductsimportedintotheaboveidentifiedimporting
countries–ThiswillenableIndianproductstoenablefaster
registrationandlatercontinuedexportssustainabilityduetobuilding
ofmutualtrustinrespectofqualityofdrugsimportedascertifiedby
thejointfacilities
Page 120 of 153
• Developmentoflocallysustainableformulationsanddrugdelivery
systemsforimportingcountrybyjointpartnershipprograms
• Capacitybuildingofregulatorsofimportingcountrytoenablebetter
appreciationofIndianmanufacturingstandards
• Othermutuallybeneficialdrugdevelopmentandcapacitybuilding
projects
• Capitalsupportforexportcapacitybuildingsuchas2Dbarcodingand
suchotherrequirements
• DossierspreparationsupportforSMEsforregistrationoftheir
productsintargetedcountries
• Studiesandreportsofcompetingcountriesontheirpharmaindustry
developmentandopportunities.
• Jointfinancingofresearchanddrugdevelopmentprojectsofmutual
interest
ii. Hereinthefocuswouldbeongettingagreatershareofthegenericsinthe
developedmarketsliketheUS,EUandJapanwhichwhilegrowingata
comparativelyslowpaceareneverthelessofhighunitvaluefortheproducts
exported.Thispossiblegainishoweverrestrainedbythelackoftechnology
forproductionandfilingofsuchinitiativesas–FirsttoFileincaseofUS
markets,multipletestingrequirementsofTestinginEUcountriesandnow
increasinglyinCISandWestAsianmarkets.Similarlyaccessingmarketshare
innewlyopenedgenericsmarketslikeJapanareofkeyimportance.For
meetingthesechallengesandtakingadvantageofthesenewopportunities,it
isproposedtolaunchJointPartnershipProgramssuchas‐
• Developmentofgenericsfortheconcernedmarkets
• Supportforfilingofgenericsdrugsintheconcernedmarketsintermsof
dossierfiling,clinicaltrialssupportandothersupportasrequiredtogain
accesstothehighvaluemarket
• Jointfundingofschemesforcollaborationinpharmasector
developmentasinnewdrugsorareasofmutualinterest

Page 121 of 153
TheimplementationoftheseprojectswouldbeprecededbyMoUsfor
mutualpartnershipatInter‐governmentallevelandappropriate
implementationthroughSPVsasmayberequired.Theprojectsthemselves
wouldrequirebothcapitalandrevenueexpenditure.
OnthewholetherewillbeanemphasisontheMoUmechanismforbridging
partnershipswithcountriesacrosswhereverIndianpharmahaskeymarket
interests.
ItisproposedtoallocateRs50crsforthisforthe12thPlan.
8.1.2.2UpgradationofSMEstoWHO‐GMPstandards
Inthe11thPlanupgradationofSMEstoSchedule‐MGMPwasenvisaged.This
assistancedidnotincludeupgradationtoWHO‐GMPandhigherInternational
standardsrequirementswhicharenowincreasinglyrequiredformakingtheSME
Pharmasustainableinanincreasinglycompetitiveanddemandglobal
manufacturingenvironment.AccordinglyitisproposedtolaunchaSchemein
the12thPlanforupgradationof1200SMEpharmaunitstoWHO‐GMPand
Internationalstandardsmanufacturingstandards.Forthis,asregards,MSME,it
wouldaccordinglyincludetherequiredupgradationlistinthelistofequipmentsfor
financialassistancetoSSIs.Howeverthiscouldpresentdifficultiesintotalproject
admissibleundertheon‐goingschemeofCLCSSoftheMSMEfortechnical
upgradationofSSIsasitisestimatedthatupgradationtoWHO‐GMPstandards
wouldrequireacostofaboutRs.3crores.
Accordingly,itisproposedthatassistancetoSSIPharmaUnitsundertheCLCSSmay
beprovidedforprojectcostofuptoRs.3croreswithcapitalsubsidyofRs.1crores
fromthecurrentlevelofRs.25lakhscapitalsubsidyonatotalprojectcostofRs.1
crores.Also,theassistanceshouldbedovetailedtoprovidesoftloaninterestrates
of5%bytheBanksforthisupgradation.Similarassistancewouldbeprovidedto

Page 122 of 153
themediumscaleenterpriseswhoarenotWHO‐GMPstandardbutwishtoachieve
thelevelforincreasingtheircompetitiveness.
Onthewholefor1200unitsattherateofRs.1croresperunitwouldrequiretotal
financialassistanceofRs.1200croresassubsidyfortheperiodupto2017.The
subsidyisbettergivenasinterest‐basedsubsidywhichwouldhelpstaggertheplan
allocationsonayearlybasisandtakecareofthewageandmeanslimitationsofthe
budget.
HencetotalBudgetaryrequirementisRs.1200crores
8.1.2.3Trainingof5000WorkingProfessionalsinWHO‐GMP/International
manufacturingstandards:
Whileschemesabovewouldprovidemanufacturingcapabilityupgradation
assistanceforcapitalexpenditure,skilldevelopmentofpersonnelrequiredforsuch
upgradationandsustenanceofsupplyofskilledpersonnelwouldalsoberequired.
Itisestimatedthatforthisthereisaneedfortrainingofatleast5000working
professionalsinWHO‐GMPandotherInternationalStandardsGMPrequirements
by2017.ThiswouldentailexpenditureofaboutRs50,000lacperperson.
AccordinglyasumofRs250crsisproposedforthis.
HencetotalBudgetaryrequirementisRs.250crores
8.1.2.4UpgradationofselectedPharmamanufacturingfacilitiesincludingbio‐
pharmatoHighRegulatedmarketofUSFDA/EDQM/TGAandother
InternationalStandardstoenableGlobalGenericsandBiosimilars
capabilities:
TheexportofPharmaceuticalproductsconstitutesnearly45%oftotalturnoverof
IndianpharmaIndustry.Inviewofthegrowingimportanceofgenericmedicines
andtheadventofBio‐similarsinhighregulatedworldmarketIndianPharma
Page 123 of 153
manufacturersneedtobuildcapacityforcompliancetothestringentstandardsof
highregulatedyethighvaluemarketcountries–US,WestEU,AustraliaandSouth
Africa.Therefore,itisproposedthat250selectunitsbeprovidedassistanceby
2017toupgradetheirfacilitiesaspertherequirementofthesecountriesandother
internationalstandards.Thiswillbedoneattherateof50unitsperyearatthecost
ofRs.2croresperunitandatotalcostofRs.500crores.Theassistanceproposedto
begivenwouldbeone‐timecapitalassistancetoenablequicktimebound
implementationgiventheurgencyofcapacitybuildinginlightofthesteeppatent
cliffofsmallandlargemoleculesvaluedatUS$300Bnby2015.
TheTotalBudgetaryrequirementisRs.500crores
8.1.2.5SettingupofoneNationalandfiveRegionalFormulationDevelopmentand
ManufacturingstandardtrainingCentres(FDC):
Developmentofgenericformulationsfrompatentproductsforsmallandbig
molecules(Biosimilars)isachallengefortheSMEs.Forthis,itisaccordingly,
proposedtosetupFormulationDevelopmentCenterswhichwouldassisttheSME
Pharmafordevelopmentofnewformulationswithaviewtotapingthevast
opportunityopeningupduetooffpatentingofanumberofmoleculesvaluedat
aboutUS$300Bn.(traditionalgenericsandbio‐similars)inthenextfivetoseven
years.ItisproposedtosetupofatleastoneRegionalFormulationDevelopment
Centre(RFDC)ineachoftheidentifiedclustergrowthareasofthepharmasectorin
thecountry.ThismaycostRs.100crores.
Consequenttotheneedofcapacitybuildingofthemanufacturingpersonnel
requiredformanufacturingstandardsupgradation,itisproposedtosetupofone
NationalandfiveRegionalmanufacturingstandardstrainingcentresatthetotal
costofRs.60crores.
HencetotalBudgetaryrequirementisRs.160crores
Page 124 of 153
8.1.2.6EstablishmentandUpgradationof10PharmaGrowthClusters
Thereisaneedofsynergystrategiestoaddressinfrastructuredevelopmentissues
forpromotingintegratedgrowthofthepharmaindustries.Forthis,Clusterbased
approachisanimportantstrategyandisnowincreasinglybeingrecognizedasan
effectiveandsustainablestrategyforcompetitiveenhancementofMSMEs.
Accordingly,itisproposedtoimplementaSchemeforClusterDevelopmentof
PharmaCompaniestoprovideanintegratedsetupforenablingQuality,
Productivity&InnovativemanufacturingbythePharmaSMEsinexistingandnew
clusters.Identifiedclustersare‐Baddi(HP),Hardwar(Uttarakhand)andGurgaon
(Haryana)inthenorth,Pattancheru,PashmalyramandKhazipalli(inA.P),Alandur
andAmbattur(bothinTN)intheSouth,Thane,Nashik,Aurangabad(allin
Maharashtra),VadodaraandAhmedabadinGujaratintheWestandGoa/Sikkimin
otherspecialareas.Theproposedcentralinfrastructurewhichwouldbedeveloped
couldinclude:
• CentralfacilitiesforEnvironmentstandardscompliance
• CentralFacilitiesCentreforQualityTestingandRegulatorycompliances.
• ColdChainfacilities
• FormulationandProductDevelopmentFacilities.
TheassistancewouldbeintheformofaGranttorecognizedbodies–associationof
industriesintheconcernedclusterswithpropersafeguardmechanismsand
procedures.Theassistancewouldberestrictedtoassistanceforbuildingand
machineries.Theoperationalcostofthecentralfacilitiessoestablishedtothe
extentof70%wouldbemetbytheindustryonarecurringbasis.
Itisaccordinglyproposedtoestablishsuchfacilitiesat10PharmaClustersbythe
endofthe12thPlanandsuchclusterswouldbelabeledasPharmaGrowth
Page 125 of 153
Clusters.ItisestimatedthateachclusterwouldrequireassistanceofaboutRs.50
crores.Accordingly,thetotalbudgetaryrequirementwouldbeofRs.500crores.
HencetotalBudgetaryrequirementisRs.500crores
8.1.2.7InfrastructuresupportforColdChainforhighenddrugsforexports
Inordertoenhanceexportscapabilityforhighenddrugsrequiringexactcoldchain
standardstillthetimetheyareexportedfromthecountryinlightofstringent
developedmarketrequirements,thereisaneedtoestablishcoldchainfacilities.
TheDepartmentofPharmaceuticalproposestoprovideassistanceforsettingupof
suchcoldchainfacilitiesandaprovisionofRs.50croresisbeingmadein12thFive
YearPlan.
HencetotalBudgetaryrequirementisRs.50crores
8.1.2.8Schemeforenvironmentstandardscomplianceandrequiredinfrastructure
supportincludingcapacitybuilding.
Theinternationalcustomersfromdevelopednationsarebecomingmorestringent
onensuringlocalenvironmentstandardcompliancestandardsandwantcompanies
toadheretothesestandards.ThishasledtoabigchallengefortheIndianpharma
industry,particularlysmallscaleunits,whicheitherhaveinvestmentconcernsor
limitationsofgrowthbeyondtheirallottedunitareasintheindustrialclusterssetup
earlierwithantiquatedenvironmentstandardscompliancepotential.DoPis
expectedtoplayavitalrolebyprovidingfinancialandtechnicalassistanceto
improvefinancialsustainabilityofSMEsononehandandalsosafeguardthe
environmentfromthehazardsassociatedwiththeunplannedgrowthofthe
industry.
AbudgetaryprovisionforRs100croresisproposedin12thFiveyearplan
Page 126 of 153
8.2.R&D,CapacityBuildingandEmployment
ThefollowingaretheSchemes,aspertherecommendationsmadeearlierinthis
PlanDocument:
8.2.1ContinuingSchemes
8.2.1.1NIPERMohali:
(i)ThecontinuationofthePGandthePhDeducationatpresentstrengthlevels
wouldrequirebudgetarysupport.
ForthisbudgetaryallocationofRs100crswouldberequiredforthe12thPlan
period.
(ii)GiventhehugedemandforHRdevelopmentatMastersandPhDlevelitis
proposedtoexpandthestudentoutputundertheexistingschemeofNIPERMohali
anditisaccordinglyenvisagedtoexpandasperbelow:
Physicaltarget Budget(Rscrs)
a. Additional1000PGsandPhDs 200
b. TrainingIndustryandRegulatorypersonnel25
c. PublicHealthandPharmacovigilanceTrg.25
d. InfrastructureUpgradation 250
Total500
Thiswouldinvolvebothcapitalandrevenueexpenditure.
8.2.1.2ForHRDevelopmentat6NewNIPERS–Raebareilly,Kolkatta,Guwahati,
Hajipur(Patna),AhmedabadandHyderabad
Thesettingupofthe6newNiperswasstartedfollowingtheapprovaloftheScheme
inthe11thPlan.TheCabinetfirstapprovedthesettingupoftheNIPERsin2007.
Followingtheprogressmade,nowtheCabinethasapprovedthepermanent
establishmentoftheNIPERsinOctober,2011.Thiswouldnowenablethefullscale
workforestablishmentoftheNIPERs.Asperestimatespreparedbytheexpert

Page 127 of 153
consultants,Deloitte,TouchandTohamatsu,aboutRs2000crswouldberequired
bothforcapitalandrevenueexpenditure.
ItisaccordinglyproposedtoallocateRs2000crsforthese6newNIPERs.
8.2.1.3OtherSchemes
8.2.1.3.1SettingupofNationalCentreforPhyto‐pharmadevelopment
MajorcapitalexpenditureofaboutRs100croresbeingmetfromDONER.Present
allocationsoughtforinitialyearsoperationasperadvicefromDONER.Aprovisionof
Rs20croresisbeingmadein12thFiveyearPlanfromDoP.
Hence,totalbudgetaryrequirementisRs20Crores.
8.2.1.3.2GLP/GCP/AnimalHouseLabSchemes:
UndertheR&D/ERPSchemealreadyapprovedforthe11thPlantheSchemefor
settingupofGLPcompliantLabsonPPPbasis,GCPcompliantLabonPPPbasisanda
AnimalHouseLabonPPPbasisisunderimplementation.Theselectionof
ConsultantsforimplementationoftheschemeisunderwayattheDepartmentlevel.
Preparationofreportanditssubsequentimplementationwouldcontinueinthe11th
Plan.ItisproposedtoallocateRs25crsforthisschemeforthe12thplanperiod
accordingly.AsregardstheERPcomponentoftheexistingapprovedschemeprojects
forthesamewouldbefinalisedinthe12thPlanforthePrivatesector.Additional
allocationofRs25crsisproposedforthiscomponent.
HencetotalbudgetaryrequirementisRs50Croresin12thFiveyearPlan.
8.2.1.3.3ContinuingR&DSchemesforNiperMohali
NiperMohaliispresentlyimplementinganumberofprojectsinR&Dforvarious
pharmaareaslikeneglecteddiseases,infectiousdiseases,vectorbornediseases,etc.
InadditionanumberofprojectsarebeingimplementedforPublichealth,
Pharmacovigilance,Regulatorycapacitybuildingforacademiaandindustry,etc.
NIPERMohaliwouldacompleteassessmentregardingtheobjectivessetforthese

Page 128 of 153
projectsandtheachievementssofar.Thereafterassestheadditionalbudget
requirementsforsuccessfulcompletionofsuchprojectswouldbeassessed.After
thirdpartyassessmenttherationaleforcontinuanceofsuchprojectsinproper
schemeformatwouldbeconsidered.Thentheconcernedprojectswouldbesought
tobecontinued.
BasedonthismethodologyitisproposedtoallocateRs50crsforsuchprojectsfor
the12thPlan.
8.2.1.3.4ContinuingschemeatNewNipers
AtpresentthereisonlyoneprojectunderimplementationwhichisforJoint
developmentofTuberculosisrelateddrugsatNiperAhmedabadandAIIMS,Delhi.
Thisprojectwouldspilloverforoneyearofthe12thPlan.AccordinglyaBudget
requirementofRs1.00crsisenvisaged.
8.2.2NewSchemes
8.2.2.1SettingupofNewNewNIPERs
AspointedoutinthediscussioninChapter3ofthisPlanDocument,thereisa
shortageof45,000seatsgiventhe1:10ratioofPGseatsvsGraduateSeatsfor
Pharmacystudiesinthecountry.Accordingly,itisproposedtomeetthisgapto
someextentbysettingupof10newNiperswhichwouldprovideabout5000more
PGseatsandalsocatertothePhDrequirements.ThisisnecessaryalsoasIndiais
targetedtobecomeaglobalhubfordrugdiscoveryandinnovationforwhicha
globalstudybyErnst&Younghasalreadybeencommissioned.Thesettingupof
these10NewNewNiperswouldrequireabudgetallocationofaboutRs3000crs.
TheseNiperswouldfollowthesametestedmodelimplementedhithertoandthe
required100acreslandforeachforthemwouldbeprovidedfreeofcostbythe
stategovernments.
RequiredBudgetAllocation: Rs3000crs
8.2.2.2NewSchemesatNiperMohali
ItisproposedtolaunchnewschemesasbelowatNiperMohali‐

Page 129 of 153
SchemeBudget(Rscrs)
a. R&DCentreforBiologicalsandNCEs 250
b. R&DCentreforNDDS 250
c. Settingup20NewIncubators 100
d. IncentiveSchemeforCROsDevptforNew 200
DrugDiscovery
e. PartnershipwithInternationalCentres 25
ofExcellence
Total825
ThustomakeIndiaselfreliantandgloballycompetitiveinnicheareasofdrugsand
pharmaceuticalsinHR,R&DandtoboostEmploymentledgrowththefund
allocationofaroundRs825croresisprojected.
8.2.2.3PharmaVentureCapitalFund
ThegrowthoftheIndianpharmaceuticalindustryoverthepastfewdecadeshas
predominantlyarisenfrommanufacturinggenericdrugsforexportsanddomestic
use.R&Dinthepharmaceuticalindustryhaswitnessednosuccessincreatinganew
drug,despiteitseffortsforthepastsixteenyears.Thisismainlyduetolackof
venturefundindustryinIndiaascomparedtodevelopedcountriesforthepharma
sector.Itneedstobepointedoutthatinvestinginafledglingstart‐upfirm,aiming
forR&Dinthepharmaceuticalindustry,isriskybecauseofthehighrateoffailure
amongnewfirms.Establishedfirmspreferastrategyhingedonsteadyreturnsas
opposedtothehigh‐riskR&Dpathtohighreturns.Thisliabilityofnewness"(botha
newfirmandthenewuncertainidea)formsthebasisfortheneedforchannelling
publicresourcesintodrugdesign,discoveryanddevelopment.
Afterconsultationwiththeindustry,ithasbeenfeltthatitwouldbeappropriateto
harnesstheventurecapitalindustrytechnicalandfinancialacumenforthedelivery
ofpublicresourcesintodrugdesign,discoveryanddevelopment.Venturecapitalists
Page 130 of 153
(VC)havetheexpertiseinhandlingallaspectsofahighriskundertaking;theyraise
fundsforsuchinvestmentandareprofessionalswithspecificindustryexperience.
Theyalsoprovideassistanceofotherkindsthatareimportantforthesuccessofa
newventure:keypersonnel,strategicadvice,financialmanagement,andmost
importantlyestablishkeygovernanceparametersforconstantmonitoringand
evaluation.
TheDoPthereforeproposestoconsiderinvestmentofidentifiedfundsintoanewly
createdspecialisedprivateequity/venturecapitalfund(IPIF)thatundertakesR&D
investmentsintocompaniesinthepharmaceuticalindustry.Thisinvestmentwillbe
subjecttoamarkettestattheleveloftheprivateequity/venturecapitalfunds
wherethefundunderquestionwouldhaveraisedalargesubstantiveportionof
capitalventurefundthemselveswhereininvestmentdecisionsaretakenby
impartial,experienced,andhighlycompetent,motivatedandtrainedfund
managers.
AtpresenttherearenosuchexistingventurecapitalfundsinIndiathatinvestin
innovationinthepharmaceuticalindustry.Accordingly,DoPhasdecidedtowork
closelywiththeNationalInstituteofPublicFinanceandPolicy(NIPFP)underthe
MinistryofFinanceforcreationofsuchafundandthemechanismforits
implementation.ItisproposedtoinvestaboutRs500crsinthefundforthe11th
Plansothatthesamecouldbeleveragedwiththesupportoftheprivatesector.
AbudgetallocationofRs500crsisenvisagedforthisscheme.
8.2.2.4 PharmaInnovationandInfrastructureDevelopmentInitiative(PIIDI)
AsdiscussedinChapter‐8,thereisneedto
Page 131 of 153
• DeveloptechnicalandinnovationcapacityofIndianpharmaformanufacturing
qualityaffordablemedicinesforthecommonmaninIndiaatparwiththe
world
• DevelopInternationalcompetitivenessoftheIndianPharmasoastobethe
largestproducerofgenericmedicinesintheworld
• TomakeIndiaapreferreddestinationforglobalinitiativesincuringthe
world’sailmentsspeciallythedevelopingworldinavaluebasedmanner
ToachievetheseobjectivesitisproposedtoimplementaPharmaInfrastructureand
InnovationDevelopmentInitiativewiththefollowingbasicstrategyelements:
a. Multiplepartnershipsasakeydenominatorbecauseinnovativedrug
developmentisnolongerasingleagencyorentityinitiativepossibility.Thisis
becauseindividualentities(governments,companies,academicbodies,etc)
cannoteasilyperceivethecompleteorsignificantlyholisticcommitments
required,thepossiblegainsandtheircontributiontoindividualandcollective
growthinanInternationallyCompetitiveenvironment.Norcantheindividual
entrepreneurialcompaniesandinitiativescommandadequateresourcesfor
creatingthecriticalmassforsuccessfulclosureandexecutionoflarge
projectsintermsofmanagerialandfinancialcapacitymuchlessthe
innovationcapabilityrequiredtobringuponapossiblesuccessfulproject.
PIIDItherefore,intendstoestablishamechanismforseekingthe
involvementofMultipleStakeholdersinsucheffortsthroughassistance
linkedtoInternationalCompetitivenessperformance.
b. CoordinatedeffortsbytheCentralandstateGovernmentsincludingthe
academiaandtheindustryarenecessaryfordevelopmentofPharmainan
internationallycompetitivescenario.Inthiscontextitisimportantto
understandthatthegrowthinIndianpharmahasbeenpossiblelargely
throughdiffusedandunconnectedeffortswithsomeopportunitiesthrown

Page 132 of 153
upfromtimetotimethroughpolicymeasureslikeprocesspatentonone
handfollowedbyproductpatentontheotherlaterintheday.Alongwitha
generalindustry,thepharmasectoralsogrewandnotspeciallysoasa
specificsector.Thestateandthecentralgovernmentshavetakenrather
uncoordinatedstepstoenablethegrowthwhichjusthappenedinagrowing
industrialeconomy.Nowwithincreasingcompetitionandvariouscountries
takingfocusedstepsthereisneedtoputupanintegratedeffortalsofrom
Indiaifitissustainitsleadershipandbuildonitwiththenewopportunities
onoffer.
c. ThePIIDIstrategywouldthereforerestonwaystore‐structureandsynergise
severalhithertounconnectedgovernmentalandprivatesectoreffortssuch
asforfundingofrelevantdrugdiscoveries,upgradationtointernational
standardsofmanufacture,qualityandbrandpromotionforgreateraccess
andprojectstoreduceproductionandprocesscosts,valuebased
technologiesinclinicaltrialsanddrugproduction.
d. Thereneedstobespecialdispensationalsobythegovernmenttoenable
governmentrelatedacademiatoparticipateintheSPVwithappropriate
permissionfromtheemployeeinstitution.AccordinglyprojectsunderPIIDI
couldformpartofthepermissibleprojectactivitieswithintheemployee
institution.Asrequired,theHeadoftheconcernedinstitutionwouldbe
memberoftheappropriatemonitoringcommitteefortheprojectsunder
PIIDIconstitutedforthepurpose.Thisarrangementisnecessarytoharness
thelargelatentpotentialoftheIndianscientificgroupworkingin
governmentprojectsinthecountryandattunethemforidentifiedgainswith
thesupportoftheprivateentrepreneurshiprightfromtheconceptionstage
itself.AppropriatePhDprojectsbeingconductedbyvariousUniversities
wouldalsobeharnessedforthispurpose.ThepromotersoftheSPVselected
Page 133 of 153
forimplementationoftheprojectwouldbepermittedtoappropriatesweat
andotherequitytosuchpersona.
e. Inordertokickstartthis,aninventorywouldbemadeofallthecurrentR&D
projectsunderwaywithvariousleadinstitutionsofnationalimportancealong
withresidentresearchcapabilities.
AbudgetallocationofRs2000crsisenvisagedforthisscheme.
8.2.2.5SettingupNationalCenterforR&DinBulkDrugsatNIPERHyderabad:
IndianBulkDrugIndustryisfacingproblemsofinnovationandcapacitybuildinginan
increasinglycompetitiveenvironmentspeciallyfromcountrieslikeChina,Israel,
Brazil,etc.TheindustrybeingpopulatedbySMEsishighlyfragmented.Hencethe
industrylacksinitsabilitytoinvestinR&D,makeprocessesmorecosteffectiveand
scaleupoperations.ThereforeaneedhasbeenfelttofocusonR&DinBulkDrugs
Sector.ItisaccordinglyproposedtoestablishaR&DcenterforBulkDrugsatNIPER
Hyderabadasaround30%ofbulkdrugproducersareinAndhraPradesh.
Thecenterwillbenefitboth,theinternalstakeholdersi.e.studentsandfacultyof
NIPERaswellastheexternalstakeholderslikeindustry,entrepreneursandindustry
associations.Thestudentsandfacultywillhavefacilitiesofacademicresearch,
processorientedresearch,trainingforindustrypracticesetc.Ontheotherhand
industrywillgetprocessinnovation,productrelatedR&D,Analyticalfacilities,
consultancyservices,developmentofbetterandgreenerprocessetc.
Thekeyobjectivesofthecenterwouldbe:
a. TobecomeaninnovativeR&Dproviderinthefieldofbulkdrugsandoffer
solutionsforcompetitiveandenvironmentallyfriendlytechnologies.
b. Toprovidecentralizedresearchfacilitiesandequipments,analytical
facilitiesfordrugtestingandconsultingservices.
Page 134 of 153
c. Toestablishaplatformfor,maintainingindustry‐academiaandacademia‐
academialinkages.
d. ToenhancethecapacityofstudentsandfacultyatNIPERHyderabadby
providinghigheracademiccourses.
e. Totranslateconceptsdevelopedinbasicbulkdrugresearchto
commerciallyviabletechnologies.
ThebudgetaryrequirementforsettingupthiscenteratNIPERHyderabadisRs
56crores.
8.2.2.6 NationalPharmaceuticalNanotechnologyCenter
‘Pharmaceuticalnanotechnology’involvesuseofnanomaterialsforemerging
industrieslikemedicaldevicesindustryandfornewinnovativedrugdelivery
systems,diagnostic,imagingandbiosensorequipments,etc.Medicaldevices
industryisgrowingat30%perannum.Accordingly,thereisaneedtodevelop
indigenousproductdevelopmentcapacityinthefieldofnano‐technology.Itis
accordinglyproposedtosetupaNationalCenterforPharmaceutical
NanotechnologyatNIPERKolkata,withfollowingobjectives:
(a) DevelopmentofNanomaterials
(b) NewDrugDeliverysystemsbasedonnanotechnology
(c) Medicaldevices
(d) Nano‐toxicologyandRegulatoryaspectsconcerningnanodrugsand
devices
Budgetaryrequirement: Rs.50crores
8.2.2.7SettingupNationalandRegionalBiosimilarCenters
Thefirstgenerationofbiologicaldrugs,whichhaveintroducedmanyrevolutionary
treatmentstolife‐threateningandrareillnesses,iscurrentlyfacingpatent
expiration.Asaresult,research‐basedandgenericspharmaceuticalcompaniesalike
Page 135 of 153
arepursuingtheopportunitytodevelop“generic”substitutestooriginalbiologics,
whicharealsoknownasbiosimilars.
Yetthefieldofbiosimilarspresentsseveralimportantchallenges–safety,
regulatory,legalandeconomic–whicharethetopicofdiscussionacrosstheglobe.
Mostofthesediscussionsstemfromtheideathat,unliketherelatively
straightforwardprocessofintroducingagenericequivalenttoanoriginaldrug
basedonanewchemicalentity(NCE),theprocessofintroducingabiosimilartoan
originalbiologicaldrugisfarmorecomplex.
Thesafetyandregulatoryissues,arealsoequallyimportant,includingtheamount
ofclinicalstudiesthatshouldberequiredaspartofthetestingandapproval
process,aswellaswhetherthebiosimilarsshouldbeconsidered“automatically”
interchangeablewiththeoriginalbiologic.
Theresearchinfrastructure,talentpoolandacademicnetworkinIndiaareatthe
nascentstagesofarasbiosimilarsindustryisconcerned.Theregulatoryhurdlesare
bothatdomesticaswellasgloballevel.Thecostsandtechnologyrelatedchallenges
forbiosimilararealsohigher.
Inviewofabovefacts,tofacilitatethegrowthofbiosimilarindustry,thereisa
proposaltoopenoneNationalBiosimilarCenteratBangaloreandthreeRegional
BiosimilarCentersatChandigarh,HyderabadandAhemedabad,wherefollowing
activitiesmaybeundertaken:
(a) ConsultingActivity:TheissuesrelatedtoIPRandotherregulatoryaspects
like,regulationsofdifferentcountriesonbiosimilars,domesticand
internationalregistrationrequirementsetcwouldbediscussedandexpert
groupswouldbetheretoguidetheindustry.Therewouldbeexpertgroups
forguidancerelatedtoissuesonclinicaltrialsandtestingandapproval
processofbiosimilar.
(b) Providingcommoninfrastructure:Theequipments,whichcouldbeusedby
industryoracademiaforcarryingoutbasicresearchworkrequiringhigh
precisioninstruments.Thiswillhelpinreducingthecostofdevelopmentof
biosimilars.
Page 136 of 153
Foropeningofonenationalandthreeregionalcenters,thebudgetaryrequirements
wouldbe:
(a) OnetimecostRs31crores
(b) Recurringcostfor4centers1styearRS01crores
(c) Recurringcostfor4centers2ndyearRs04crores
(d) Recurringcostfor4centers3rdyearRs06crores
(e) Recurringcostfor4centers4thyearRs08crores
(f) Recurringcostfor4centers5thyearRs10crores
TotalBudgetrequirementisRs60crores.
8.2.2.8SettingupofaIndustryfocusedAnimalHouse
TheAnimalhousewillmeettherequirementofendtoendservicesfromPrimates
tosmallanimalsforpre‐clinicaldrugdevelopment.
AbudgetaryprovisionofRs100croresisbeingproposedforthishouse.
8.2.2.9SupporttoAcademia,ResearchInstitutionsandprivatesectorforExtra
MuralResearch
TheAcademia,variousR&DinstitutionsinthegovernmentasinCSIR,etcandthe
privatesectorcompaniesaredoingresearchindrugrelatedareas.Howeveras
discussedinChapter8onR&D,anevaluationrevealsthat–whilethegovernment
fundedresearchwhetherbyCSIR,CentralLabs(CDRI,etc),DSTandDBTwithatotal
ofsome51researchinstitutionsaredoingresearchinanon‐appliedmannerwith
clearlackoftargeteddrugdevelopmentasinstagesofNCEdevelopment,pre‐
clinicalstudies,etc,theprivatesectorismostlylimitedtoformulationanddrug
deliverysystemsdevelopment.Onlyafewcompaniesareconcentratingnewdrug
developmentandanumberofcompanieslikeGlenmark,Suven,etchadto
outlicensetheirinitialdevelopmentstoothercompaniesforfurtherdevelopment
thusnotbeingabletotakefulladvantageofthefulldrugdevelopmentcycle.Itis
accordinglyproposedtolaunchaschemeforfundingbothacademiaindividually,as
Page 137 of 153
aninstitutionandprivatecompaniesfortargeteddrugdevelopmentincluding
assistanceforclinicaltrials.Thedetailedschemewouldbepreparedafterathorough
studyastotheoutputsfromtheexistingfundinginthissectorbyvarious
governmentbodiesandorganizations/schemesandtofillthegapasmaybe
required.TheindividualprojectscouldbeimplementedbyNipersincollaborative
partnershiporundertheiraegisandguidance.
ItisproposedtoallocateRs100crsforthisscheme.
8.2.2.10SupporttoAcademia,ResearchInstitutionsandprivatesectorforExtra
Labsupgradation
Theschemewillalsohaveprovisionforfundingupgradationoflabsintheprivate
andgovernmentsectorwithsharingbasison50‐50patternforthelabupgradation
forequipmentsdeployedfordrugdevelopmentunderspecificallyidentifiable
projects.Thiscapacitybuildingasaformofinfrastructuresupportwillalsobe
deployedfortraininginadvancedlabtechniquesofpersonnelintheindustryona
mutualsharingbasis.Thetrainingpartwillrequire25%fundingfromtheprivate
sectorside.
ItisproposedtoallocateRs10crsforthisscheme.
8.2.2.11InternationalcooperationinR&D
ThereisaneedtopromoteR&DinCISanddevelopingcountriesformutualadvantages.
ItisproposedtoallocateRs25crsforthisscheme.
8.3Pricing
TheroleofNPPAwouldcontinueunderexistingandpotentiallynewdrugspolicy
followingtheorderoftheSupremeCourtin2003.Inthisconnection,NPPAhadalready
submittedfiveNewPlanschemesforthe11thFiveyearPlan2007‐08to2011‐12tothe
PlanningCommission.Thesecouldnotbefinalisedduetodelayinfinalisationofthe
Page 138 of 153
newpolicy.Itisexpectedthatthenewpolicywouldbefinalisedinthe12thPlanandthe
Planschemesenvisagedforthe11thPlanwouldneedtocontinueforthe12thPlan.
Accordingly,followingbudgetaryrequirementsareenvisaged:
Table‐27
OutoftheaboveschemeatSr.No.1titled“Proposalforbuildingrobust&
responsivestatisticalsystemforNPPA”wasapprovedbythePlanningCommission
andimplementedduringthe11thfiveyearplan.Ithasalsobeenimplementedwith
thehelpofNIC.TowardstheendofSeptember2011,PlanningCommissionhas
accordedin‐principleapprovalfortheSchemeonBuildingAwareness.Detailsof
implementationofthisschemearebeingworkedoutbyNPPAincollaborationwith
DepartmentofConsumerAffairsasrequiredbythePlanningCommission.
AnotherimportantneedofNPPAistheavailabilityofPrimaryDataBaseonpricingof
drugs.Presentlyitsourcesthemfromonlyoneavailablesource–IMSHealth–aprivatesector
organization.Thislackofindependentofficialdatahasbeenadverselyremarkedinseveralcourt
judgmentsunderDPCO’95fromtimetotime.Evenotherwisedependantonaprivatesource
andthattooonlyone,isacauseofconcernforapublic/governmentbodychargedwiththe
responsibilityoffixingofpricesforanentireindustry.TheDPCOprovisionsthemselveshavenot
helpedincollectionofdataascompaniesdonotgivedataasperprescribedformsona
voluntarybasis.Coercionisnotthebestoption.Henceitisproposedtolaunchaschemefor
collectionofpricingandrelateddatabyNPPAthroughpossiblepartnershipswithdatacollection
agenciesandasfaraspossiblewithMinistryofStatisticsandProgramImplementationinthe
GovernmentofIndia.
SrNoSchemeAmount
(Rs.Crs)
ContinuingScheme
1MonitoringandEnforcementWork2.00
2BuildingConsumerAwarenessaboutpricingand
availability
20
NewSchemes
1CreationofNPPACellsinStates25.00
2SchemeforinteractionwithStates2.00
TOTAL49.00

Page 139 of 153
8.4DevelopmentofMedicalDevicesSector
8.4.1 Settingupgreen‐fieldMedicalDevicesPark:
Inordertotapthehighgrowingmedicaldevicesmanufacturingindustry,particularly
inthecontextofIndia,itisproposedtosetupaspecializedParkinthegreenfield
whereintegratedsetoffacilitieswouldbeprovidedforpromotinggrowthofMedical
Devicesindustry.TheenvisagedMedicalDevicesParkwouldfocuson:
• TestingLaboratoryandCommonSterilizationfacilityforMedical
Devices
• MedicalInstruments/Equipmentcalibrationandvalidationfacility
• EngineeringServiceslikesurfacetreatment,coating,electricaland
mechanicalmaintenanceetc.
• Atrainingcentretotrainshop‐floor,managersandentrepreneurs
levelskillsforMedicalDevicesIndustry
• Facilitationofbusinessdevelopmentonregulatorycertifications,and
productdevelopments.
TheGovtofGujarathasalreadyearmarkedlandfortheprojectandthiswouldhelp
theprojecttotakebenefitsfromtherecentlyannouncedNationalManufacturing
Policy2011.
ThebudgetforthesettingupofthePark:Rs300crores.
8.4.2SettingupNationalCenterforR&DinMedicalDevicesatNIPERAhmedabad.
AsacomplimentaryfacilitytotheMedicalDevicesPark,itisproposedtosetupa
dedicatedR&DCentreforMedicalDevicesIndustry.ThisCentrewillprovidehigh
endeducationalfacilitiesforteachingandresearchwithamulti‐disciplinary
approachtowardsinnovationinmedicaldevices.Therewillbeincubatorfacilitiesas
wellasreferencetestfacilitiesforstandardscertificationofmedicaldevices.
FacilitieswouldalsoexistforPreclinicaltestingofmedicaldevices.Itisproposedto
setuptheCentreatNIPERAhmedabad.
Page 140 of 153
TheenvisagedbudgetaryrequirementisRs.50Crores.
8.5CPSUsandJanAushadhi
8.5.1CPSUs
ForHALMinimalUpgradationoffacilities,forIDPLtomeettheregulatory
ComplianceandforBCPLtomeetthegapinrevivalpackage,aprovisionofRs10
croresforeachitemandatotalofRs30croresisbeingmadeinthe12thPlan.
HencetotalbudgetaryrequirementforCPSIUsisRs30crores
8.5.2Janaushadhi
Asdiscussedearlier,theCampaigntomakeavailableaffordabledrugswithensured
qualityatlowpricestothemassesisacontinuingcommitmentfromthe11thPlan.
Accordingly,theJanAushadiSchemelaunchedin11thPlanandfurtherstrengthened
throughtherevisedBusinessPlanwouldbefurtherwidenedanddeepenedinitsreach
bothintermsofgeographyandtherapeuticcoverage.Itisenvisagedthatforcovering
thewholecountryataneffectivelevel,aboutRs.200Croreswouldberequiredinthe
12thPlan.
Budgetaryrequirement: Rs.200Crores

Page 141 of 153
Annexure‐I
GOVERNMENTINSTITUTIONSENGAGEDINPHARMAR&D
A.UnderCSIR:
1. InstituteofIntegrativeandGenomicBiology(IIGB),Delhi
2. InstituteofMicrobialtechnology(IMTech),Chandigarh
3. CentralDrugsResearchInstitute(CDRI),Lucknow
4. CentralInstituteofMedicinalandAromaticPlants(CIMAP),Lucknow
5. IndianInstituteofToxicologicalResearch(IITR),Lucknow
6. IndianInstituteofIntegrativeMedicine(IIIM),Jammu
7. InstituteofHimalayanBioresourceTechnology(IHBT),Palampur
8. IndianInstituteofChemicalTechnology(IICT),Hyderabad
9. CentreforCellularandMolecularBiology(CCMB),Hyderabad
10. CentralSaltandMarineChemicalsResearchInstitute(CSMCRI),Bhavnagar
11. NationalChemicalLaboratory(NCL),Pune
12. IndianInstituteofChemicalBiology(IICB),Kolkata
13. NorthEastInstituteofScienceandtechnology(NEIST),Jorhat
B.UnderDBT
1. NationalInstituteofImmunology(NII),NewDelhi
2. NationalInstituteofPlantGenomeResearch(NIPGR),NewDelhi
3. IndianVaccinesCorporationLimited(IVCOL),Gurgaon
4. NationalAgri‐FoodBiotechnologyInstitute(NABI),SASNagar
5. BharatImmunologicalsandBiologicalsCorporationLimited(BIBCOL),Bulandshahar
6. NationalCentreforCellSciences(NCCS),Pune
7. CentreforDNAFingerprintingandDiagnostics(CDFD),Hyderabad
8. InstituteofLifeSciences(ILS),Bhubaneswar
9. RajivGandhiCentreforBiotechnology,Thiruvananthapuram
10. InstituteofBioresourcesandSustainableDevelopment(IBSD),Imphal
11. BiotechConsortiumIndiaLimited(BCIL),Delhi
C.UnderDepartmentofHealthResearch
1. NationalInstituteofMalariaResearch(NIMR),Delhi
2. NationalInstituteofPathology(NIOP),Delhi
Page 142 of 153
3. NationalInstituteofMedicalStatistics(NIMS),Delhi
4. InstituteofCytologyandPreventiveOncology(ICPO),Noida
5. NationalJALMAInstituteforLeprosy&OtherMycobacterialDiseases(NJILMOD),
Agra
6. NationalInstituteforResearchinEnvironmentalHealth(NIREH),Bhopal
7. DesertMedicineResearchCentre,Jodhpur
8. NationalInstituteforResearchinReproductiveHealth(NIRRH),Mumbai
9. NationalInstituteofImmunohaematology(NIIH),Mumbai
10. EnterovirusResearchCentre(ERC),Mumbai
11. NationalinstituteofVirology(NIV),Pune
12. NationalAIDSResearchInstitute(NARI),Pune
13. RegionalMedicalResearchCentre,Bhuvaneshwar
14. RegionalMedicalResearchCentre,Dibrugarh
15. RegionalMedicalResearchCentre,Jabalpur
16. RajendraMemorialResearchInstituteofMedicalSciences(RMRIMS),Patna
17. RegionalMedicalResearchCentre,Belgaum
18. NationalInstituteofCholeraandEntericDiseases(NICED),Kolkata
19. NationalInstituteofOccupationalHealth(NIOH),Ahmedabad
20. TuberculosisResearchCentre(TRC),Chennai
21. NationalInstituteofEpidemiology(NIE),Chennai
22. NationalInstituteofNutrition(NIN),Hyderabad
23. CentreforResearchinMedicalEntomology(CRME),Madurai
24. VectorControlResearchCentre(VCRC),Puducherry
25. RegionalMedicalResearchCentre,PortBlair
Page 143 of 153
Annexure‐II
ListofAbbreviations
APIsActivePharmaceuticalIngredients
CAGRCompoundAnnualGrowthRate
CDSCO CentralDrugStandardControlOrganisation
CEP CertificateofSuitability
CMIECentreforMonitoringIndianEconomy
CROsContractResearchOrganisations
CSIRCouncilofScientificandIndustrialResearch
DBTDepartmentofBiotechnology
DCG(I) DrugcontrollerGeneral(India)
DMFSDrugMasterFiles
DoPDepartmentofPharmaceuticals
EDQMEuropeanDirectoratefortheQualityofMedicine&HealthCare
EHSEnvironmentHealthandSafety
FICCIFederationofIndianChambersofCommerceandIndustry
GDPGrossDomesticProduct
GLPGoodLaboratoryPractice
GMPGoodManufacturingPractice
GXPGoodXPractice
ICMRIndianCouncilofMedicalResearch
IDMAIndianDrugManufacturingAssociation
IMSInstituteofManagementStudies
IOMAInstituteofManagementandAdministration
IPAIndianPharmaceuticalAssociation
IRBInstitutionalReviewBoard
MOHMinistryofHealth
NCEsNewChemicalEntities
NDDNewDrugdevelopment
NPPANationalPharmaceuticalPricingAuthority
NSDCNationalSkillDevelopmentCorporation
OPPIOrganisationofPharmaceuticalProducersofIndia
Page 144 of 153
PPPPublicPrivatePartnership
PRDSF PharmaceuticalResearch&DevelopmentSupportFund
R&DResearchandDevelopment
SMESmallMediumEntrepreneur
SOPsStandardOperatingProcedures
TORTermofReference
WTOWorldTradeOrganisation
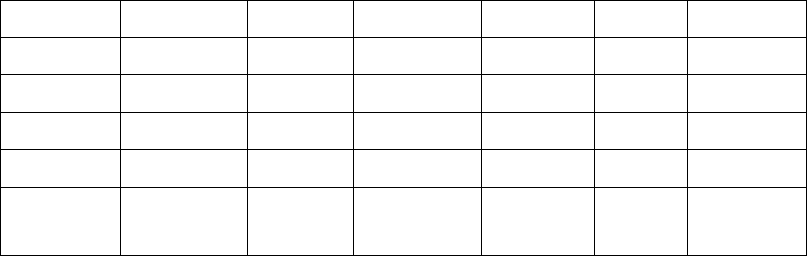
Page 145 of 153
Table‐1:ExportandDomesticGrowth
Table–2:Internationalsalesonconsolidatedbasis
YearExportsGrowth DomesticGrowth%TotalGrowth%
Mar20062123023.23 39989 17.17 6121919.21
Mar20072566620.894536713.457103316.03
Mar20082935414.375094612.308030013.04
Mar20093982135.66554548.859527518.65
Mar201042154*5.866205511.901042099.38
Consolidated International Exports as % of net sales
net sales sales 2010-11
Ranbaxy Labs 8960.77 6771.74 75.6
Dr Reddy's Labs 7236.80 5940.70 82.1
Lupin 5706.82 3983.08 69.8
Cipla 6130.31 3361.49 54.8
Sun Pharma 5721.43 2898.20 50.7
Wockhardt 3751.24 2709.91 72.2
Jubilant Lifescience 3433.40 2369.11 69.0
Cadila Healthcare 4464.70 2288.70 51.3
Biocon 2300.52 1956.79 85.1
Glenmark Pharma 3089.59 1955.83 63.3
Stride Arcolab 1695.84 1637.67 96.6
Plethico Pharma 1535.20 1367.22 89.1
Piramal Healthcare 2509.86 1280.58 51.0
Divi's Labs 1307.11 1204.95 92.2
Aurobindo Pharma 4381.48 1112.06 25.4
Torrent Pharma 2121.97 1101.57 51.9
Ipca Laboratories 1882.54 1025.18 54.5
Dishman Pharma 990.84 911.56 92.0
Orchid Chemicals 1781.79 725.85 40.7
Shasun Chemicals 799.42 676.78 84.7
Panacea Biotec 1143.78 610.44 53.4
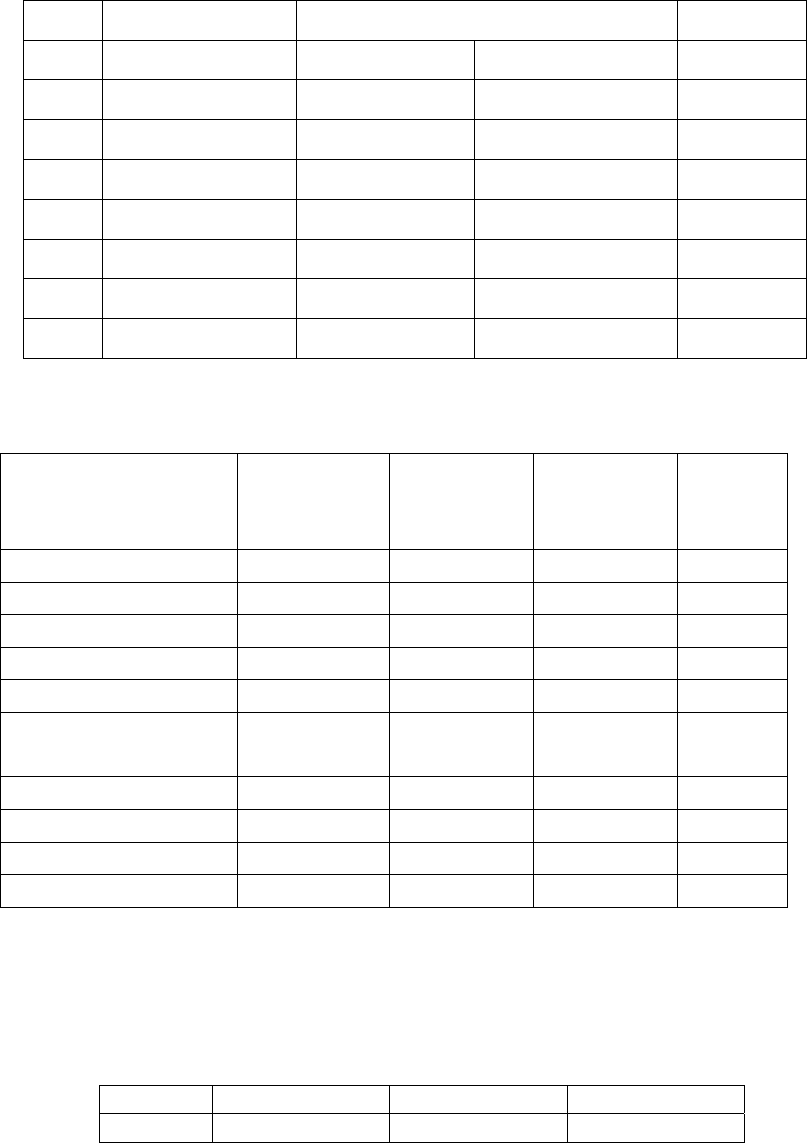
Page 146 of 153
Table‐3:GeographicalDistributionofPharmaCompanies
S.No.StateNumberofManufacturingUnits Total
FormulationBulkDrugs
1.Maharashtra192812113139
2.Gujarat11293971526
3.WestBengal69462756
4.AndhraPradesh 528 199 727
5.TamilNadu47298570
6.Others34234223845
Total8174238910563
Table‐4:MarketTurnoverofMajorTherapeuticSegments
MajorTherapiesMATDEC'05
(ValinCrs)
%
Contribution
MATDEC'10
(ValinCrs)
%
Contribut
ion
Anti‐infectives4,056 17.6 8,060 17.2
Cardiac2,378 10.3 5,318 11.4
GastroIntestinal2,537 11.0 5,099 10.9
Respiratory2,170 9.4 4,080 8.7
Pain/Analgesics2,059 8.9 4,038 8.6
Vitamins/Minerals/
Nutrients2,1059.13,6257.7
AntiDiabetic 998 4.3 2,743 5.9
Gynaecology1,261 5.5 2,658 5.7
Neuro/CNS1,231 5.3 2,633 5.6
Derma1,255 5.4 2,554 5.5
Table‐5:BulkIndustryGrowth
(InRsCrores)
2007‐082008‐092009‐10CAGR
12,647.5116,360.7117,307.0216.98%
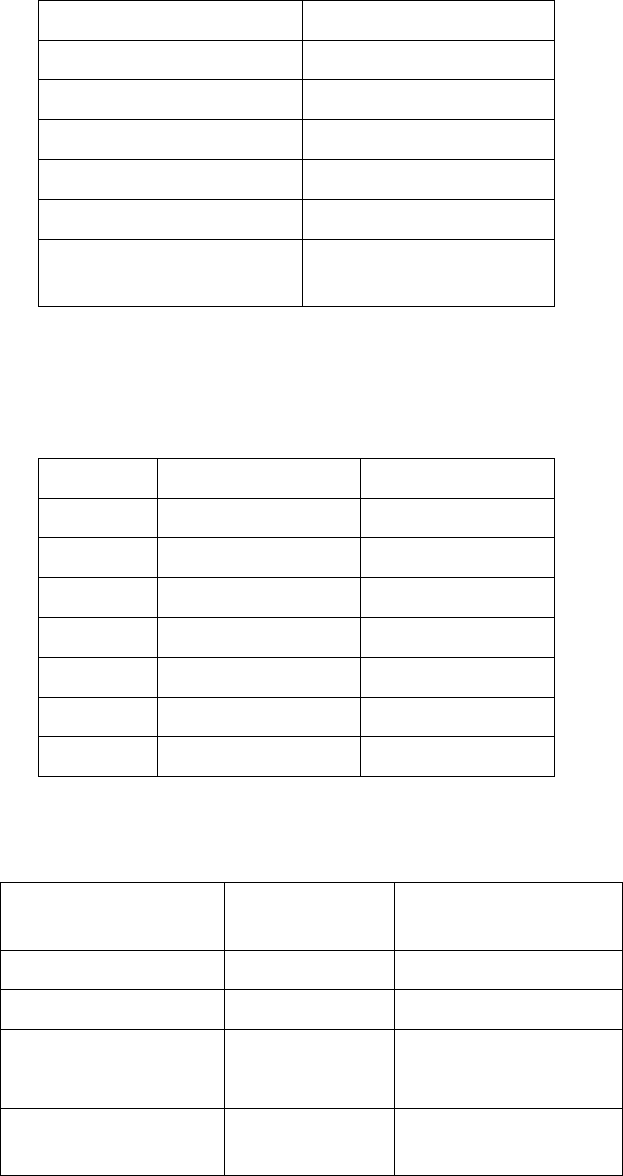
Page 147 of 153
Table‐6:TheGlobalMarketforBiologicsin2009
Country2009Sales($bn)
US69.02
Europe41.68
Japan10.29
Asia/Africa/Australasia14.4.0
LatinAmerica1.20
TotalBiologicDrugs
Market
136.59
Table‐7:The10TopSellingBiologicsin2009
BrandDrugName2009Sales($bn)
Avastinbevacizumab5.74
Rituxanrituximab 5.62
Humiraadalimumab 5.48
Herceptintrastuzumab4.86
Lantusinsulinglarine4.29
Enbreletanercept3.87
Remicadeinfliximab3.51
Table‐8:TheGlobalMarketforBiosimilarsin2009
Country2009Sales($
bn)
MarketShareof
Biosimilars(%)
US0.06 4.9
Europe0.14 11.4
OtherCountries
(incl.ChinaandIndia)
1.03 83.7
TotalBiosimilars
Market
1.23 100
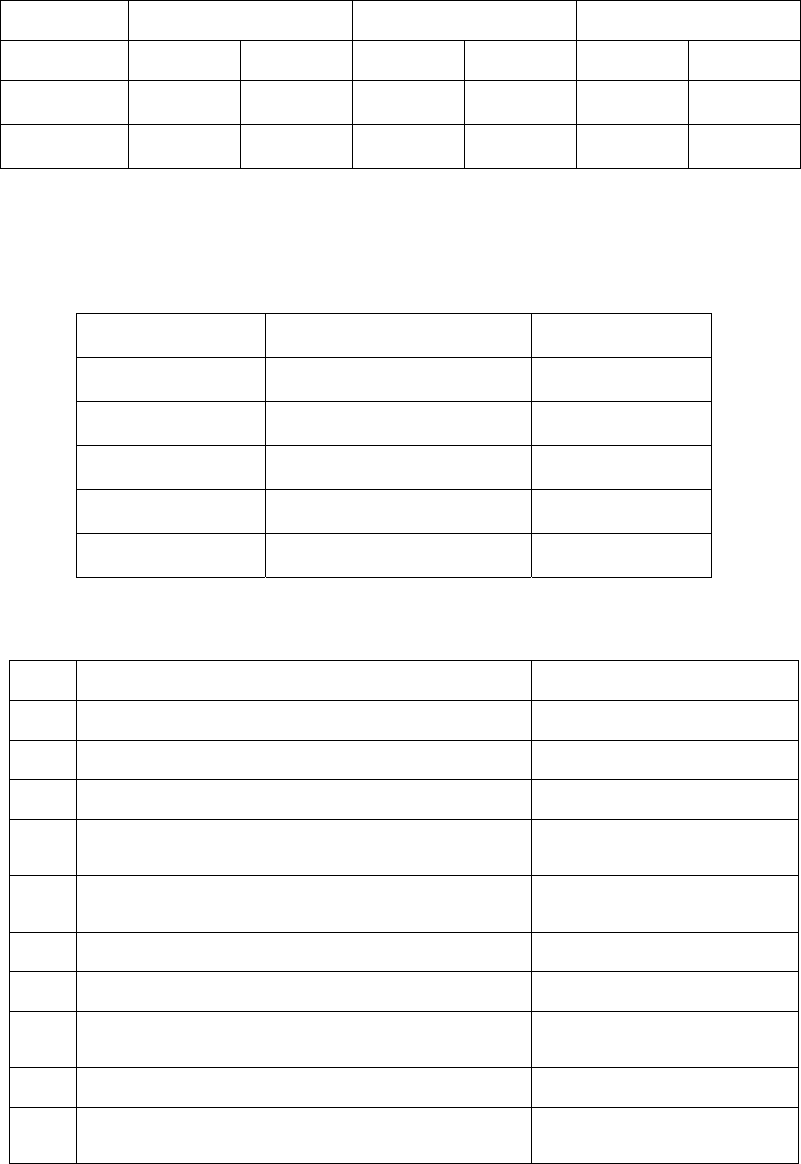
Page 148 of 153
Table‐9:ProjectedGrowth
ValueinRscrs/Growthin%
YearDomesticExportsTotal
ValueGrowthValueGrowthValueGrowth
2016‐17130,00021% 158,000 16% 288,00018%
2019‐20233,00022% 248,000 17% 481,00019%
Table‐10:ExportGrowth
YearExports(Rs.crores)Growth%
Mar200725666 20.89
Mar200829354 14.37
Mar200939821 35.66
Mar201042154 6.6
Mar201145745 7.7
Table‐11:HumanresourcepositioninIndia
SlItemTotalnumbers
1NoofUniversities 409
2Noofcolleges25990
3Noofsciencecolleges4696
4Annualstudentoutputatdegreelevelin
science
2000374
5Annualstudentoutputatdegreelevelin
engineering
1663619
6Totalnoofpharmacycolleges1162
7NumberofBPharmcolleges848
8NumberofMastersinpharmaceuticalsarea
andPhDofferingcolleges
191
9NoofBPharmstudentsinpharma51716
10NoofMastersandPhdstudentsoutputin
pharma
5648
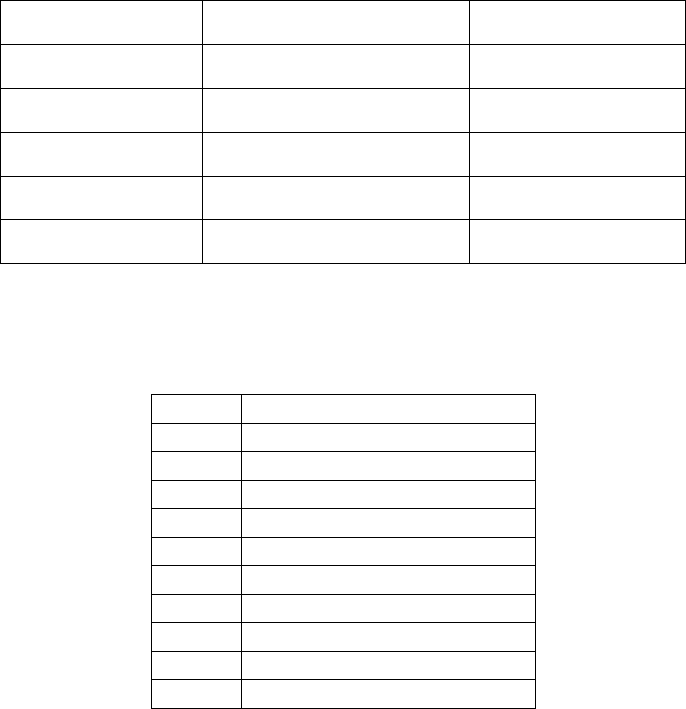
Page 149 of 153
Table‐12:GlobalPhamamarketgrowthrate
YearMarketinBillionUS$ %growthrate
2004620 7.9
2005664 7.2
2006710 6.9
2007756 6.4
2008801 4.9
Table‐13:TopGlobalGenericPlayers
RankCompany
1Teva
2Sandoz
3Mylan/MerckGX
4WatsonAndrx
5Barr
6Actavis
7Ratiopharm
8Stada
9Ranbaxy
10Perrigo
Page 150 of 153
Table14:ResearchandDevelopmentExpenditure
Year
GrowthinR&DExpenditure–Rs
Cr
R&DExpenditureAs%of
Sales
Domestic
Companies
Foreign
Companies
Domestic
Companies
Foreign
Companies
Mar199580.6164.13 1.34 0.77
Mar1996142.5083.371.710.91
Mar1997148.1289.411.550.95
Mar1998154.1590.651.430.88
Mar1999218.6679.781.560.70
Mar2000256.8090.171.560.66
Mar2001435.07109.81 2.30 0.72
Mar2002597.91110.042.640.65
Mar2003686.74232.732.930.71
Mar20041084.26346.693.811.10
Mar20051527.24510.504.981.63
Mar20061850.97816.025.352.39
Mar20072371.79695.625.012.67
Mar20082772.63700.184.782.86
Mar20093316.14846.054.893.84
Mar20103342.32934.40 4.50 4.01
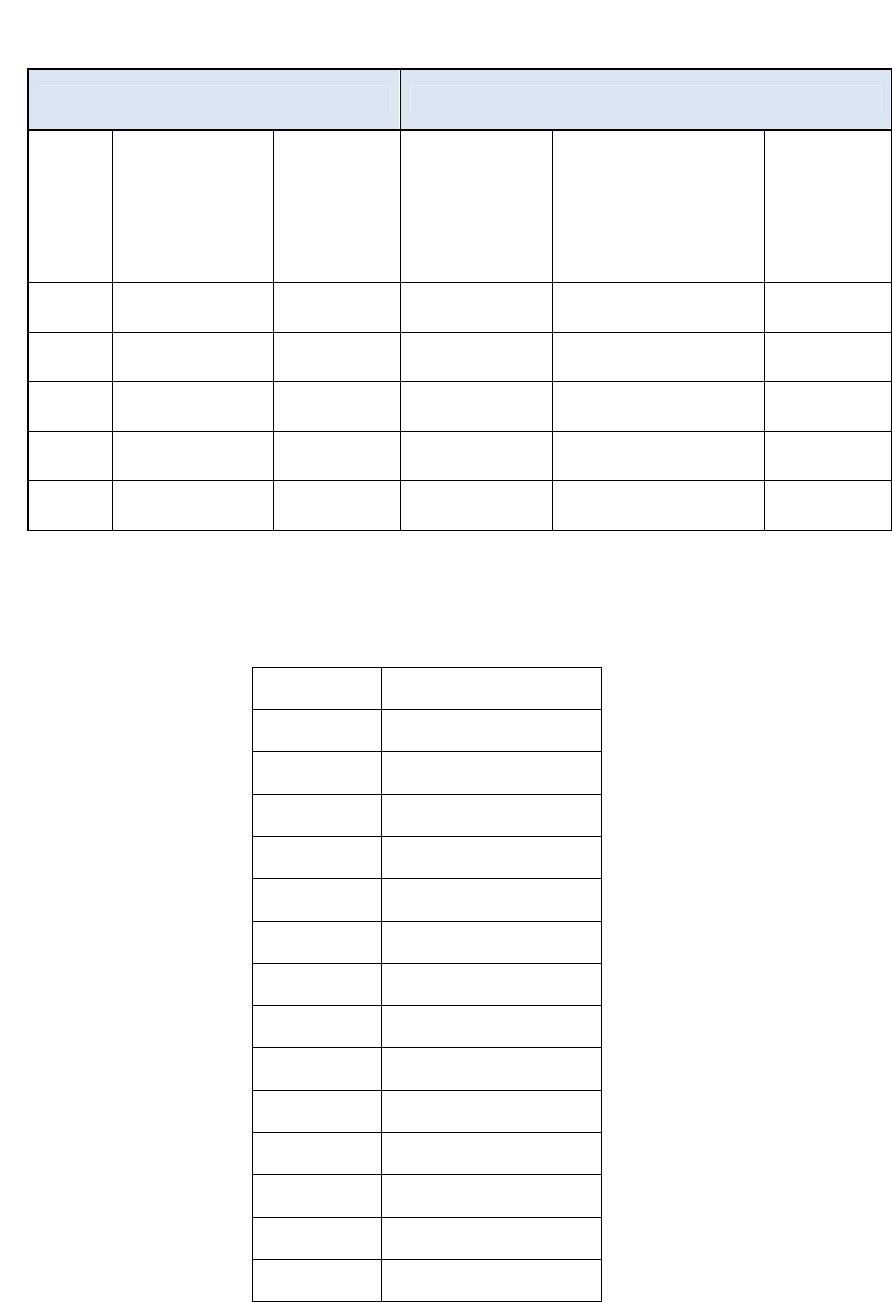
Page 151 of 153
Table‐15:R&DspendingofleadingIndianandGlobalpharmaceuticalMNEs,FY2009
IndianPharmaceuticalCompaniesGlobalPharmaceuticalCompanies
Rank
in
R&D
spendi
ng
Company
R&Dexp.
FY
2008/09,
millionUS$
RankinR&D
spendingCompany
R&Dexp.
2009,
millionUS$
1Ranbaxy*991Roche,CH8,570
2Dr.Reddy’s895GlaxoSmithKlin,UK6,286
3SunPharma6710ElliLilly,USA4,300
4Cipla5125Lundbeck,DNK615
5LupinLabs5050Watson,USA197
Table–16:EmploymentDataforPharmaceuticalSector
YearNoofEmployees
Mar19951,81,497
Mar19962,04,609
Mar19972,11,614
Mar1998 1,89,295
Mar19992,13,999
Mar20002,43,410
Mar20012,33,704
Mar20022,26,416
Mar20032,23,556
Mar2004 2,40,791
Mar2005 2,65,396
Mar20062,90,021
Mar20073,36,211
Mar20083,53,692
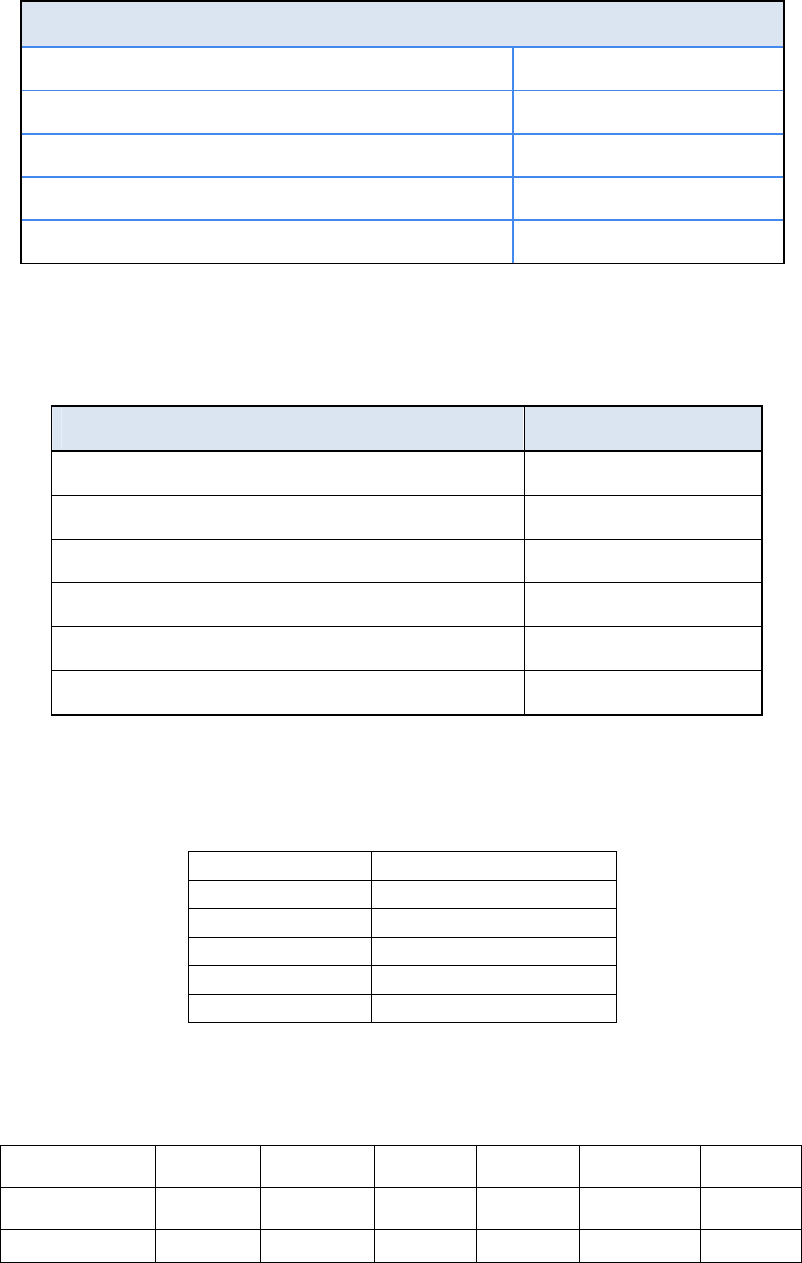
Page 152 of 153
Table17:PercentagedistributionofMan‐powerinPharmaIndustry
FunctionDistribution
Production&QualityControl50% 50%
Research/Lab/Testing 20%
Sales,Marketing,Medicalassistance5‐10%
Purchase,Logistics,SupplyChain 5‐10%
Supportfunctions(HR,Finance,etc.)10‐12%
Table18:QualificationsofpersonnelemployedintheChemicalsand
PharmaceuticalsSegment
QualificationDistribution
Ph.D/MTech/MScetc.5‐8%
GraduateEngineers15‐25%
DiplomaEngineers10%
ITIandothervocationalcourses 15‐20%
Graduates(BA/BSc/BCom/others)15‐25%
12thstandardorbelow20‐25%
Table‐19:Turnover‐wisedistribution
Turnover %Distribution
0‐10Cr. 70
10‐50Cr. 20
50‐100Cr. 5
100‐500Cr.3
500+Cr.2
Table‐20:PerformanceofCPSUs
ParameterKAPLRDPL BCPLHAL IDPLTOTAL
Sales(08‐09) 225.0180.7577.63147.3956.70594.37
TO/Employees3052 10 11 23 19
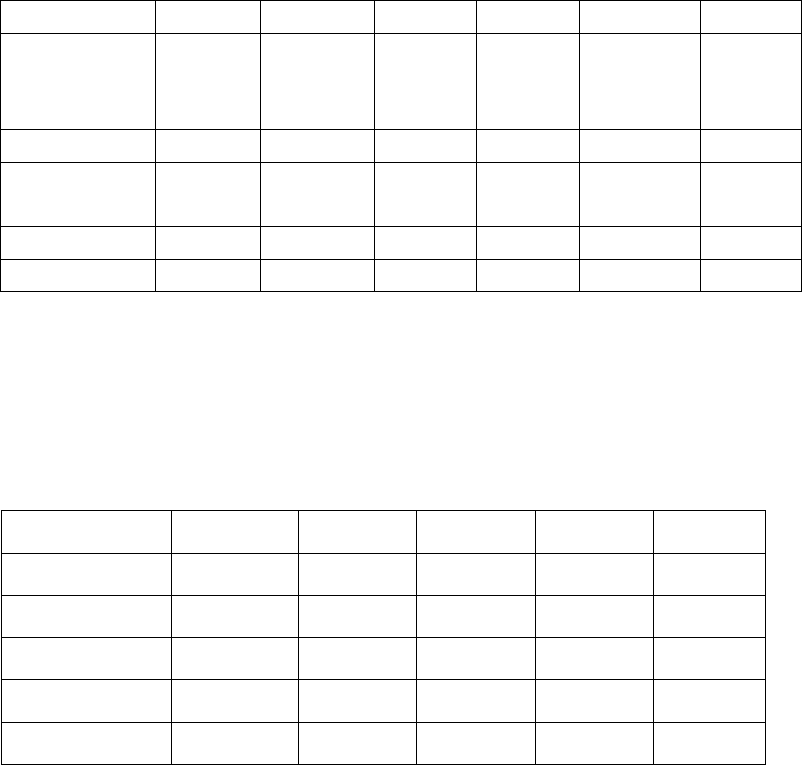
Page 153 of 153
Rslacs
TO/Sales
employeesRs
lacs
65304 134 134 236106
PATRscr5.880.01 ‐5.35 ‐22.08 ‐37900.9
Total
Employees
739181 742 1224 2433129
SalesStrength34531 58 105 24 563
Sales(08‐09) 225.0180.75 77.63 147.39 56.70594.37
Table‐21:SalesProjectionofCPSUs
RsCrores
YearIDPLHAL BCPL KAPL RDPL
2012‐1351.7189153.37 320108
2013‐1470215176.57 360122
2014‐1580264204.73 425135
2015‐1692290 237.6 490150
2016‐17125.4 319 275.83 560165
