ImThera Medical IPG MedRadio User Manual
ImThera Medical, Inc. MedRadio
User Manual

THN Sleep Therapy® System
Implant Manual
0344
2012
C

Explanation of symbols on product or package labeling
h Model number
f Serial number
N Manufacturing date
M Manufacturer
H Use by
Y Caution: Consult instructions for use
i Consult instructions for use
D Do not reuse
L Do not use if package damaged
l Storage temperature
IQ Sterilization: ethylene-oxide gas
Implantable pulse generator
Lead length
Non-pyrogenic
C Conformite Europeene (European Conformity). This symbol means that
the device fully complies with AIMD Directive 90/385/EEC (NB 0344)
and R&TTE Directive 1995/5/EC
Operating Instructions
©2014 ImThera Medical, Inc. All Rights Reserved. aura6000, ImThera and THN Sleep Therapy
Manufacturer M
ImThera Medical, Inc.
12555 High Bluff Drive, #310
San Diego, CA 92130 USA
Authorized Representative P
in the European Community
Cormedics Medizintechnik GmbH
Bahnhofstrasse 32
82041 Deisenhofen Germany
2014-10 EN LBL-00086-01-AR
are registered trademarks, and THN and is a trademark of ImThera Medical, Inc. The ImThera
system is covered by one or more claims of U.S. Patents No. 7,725,195; 7,937,159; 8,428,725 and
8,751,005. Additional U.S. and foreign patent applications are pending.

aura6000 Implant Manual | 19
LIMITED WARRANTY
ImThera Medical, Inc., (referred to as ImThera) warrants to the patient who receives an aura6000
System (referred to as “aura6000”) that the aura6000 will be free from defects in workmanship and
materials for a period of one year from the date of surgical implant. This warranty applies only to
the patient who has the implanted device and no other person or entity. If the aura6000 fails to
function within normal ranges within one year after the date it is implanted, ImThera will repair or
replace the aura6000 component with a functionally equivalent device made by ImThera. No other
relief whatsoever is available under this limited warranty. The limited warranty for a repaired or
replacement aura6000 will last only for one year from the date of surgical implant of the original
aura6000. Claims under this limited warranty are subject to the following additional conditions and
limitations:
1. The product registration form must be completed and returned to ImThera within 30 days of
surgery.
2. The device must be implanted before the “use before” date.
3. Failure of the device must be confirmed by ImThera.
4. The device must be returned to ImThera (or ImThera’s authorized agent) within 30 days after it
fails to function within normal ranges. That device becomes ImThera’s property.
5. This limited warranty does not include failures to function within normal ranges caused by:
a) fire, floods, lightning, natural disasters, water damage and other calamities commonly
defined as “Acts of God”;
b) accident, misuse, abuse, negligence, or the customer’s failure to operate the aura6000 in
accordance with manufacturer’s instructions;
c) unauthorized attempts to repair, maintain, or modify the aura6000 by the patient or any
unauthorized third party; or
d) attaching equipment to the aura6000 that is not supplied or expressly authorized by
ImThera.
This limited warranty is the only warranty that applies to the aura6000, and ImThera expressly
disclaims any other warranty, express or implied, including any warranty of merchantability or
fitness for a particular purpose. Under this limited warranty, ImThera will be responsible only for
repair or replacement of the aura6000 with a functionally equivalent device made by ImThera and
will not be liable for any damages (whether direct, indirect, consequential, or incidental) caused by
the aura6000, whether the claim is based on warranty, contract, tort or any other theory.
Any translation of this Limited Warrant is done for local requirements and/or convenience only. In
the event of a dispute between the English and any non-English versions, the English version of this
Limited Warranty shall govern.
18 | aura6000 Implant Manual
Interference Type / Description How to Minimize Effects
EMI
Conductive current—current
introduced by something touching the
body, e.g. electrocautery, defibrillation.
Turn the device off. Keep the IPG/lead out of the
conductive path. In surgery, use only bipolar
electrocautery. Do not place external defibrillator
paddles over the IPG.
Induced/coupled current—current
introduced by an electric or magnetic
field where the energy travels through
the air (no physical contact).
Lead wires will act as an antenna to electric fields, and
lead loops will act to “pickup” magnetic fields. The
electric/magnetic field strength decreases with distance,
so move away from EMI sources to reduce EMI effects.
Radiated energy—energy traveling
through the air, e.g. x-rays, radioactive
materials.
High dose radiation can temporarily or permanently
damage an IPG or lead. If possible, avoid placing the
IPG/lead directly in the radiation beam. This type of
damage to the device may not be immediately
detectable.
Mechanical
Mechanical interference—pressure
waves generated by vibrating or
ultrasonic transducers.
Avoid placing the IPG/lead directly in the path of the
pressure beam. The beam may damage the device, or
the device may inadvertently concentrate therapeutic
ultrasound and cause harm.
CONTENTS
ABOUT THIS MANUAL .................................................................................. 1
DEVICE DESCRIPTION ................................................................................. 1
PACKAGE CONTENTS ................................................................................... 1
INDICATIONS .................................................................................................. 2
CONTRAINDICATIONS ................................................................................. 2
WARNINGS ....................................................................................................... 3
PRECAUTIONS ................................................................................................ 4
Clinician Training ............................................................................................. 4
Storage, Sterilization, Implantation and Disposal .......................................... 4
Patient Information ........................................................................................... 6
Adverse Effects .................................................................................................. 7
SURGICAL GUIDELINES .............................................................................. 8
Pre-Operative .................................................................................................... 8
Lead Placement ................................................................................................. 8
IPG Placement ................................................................................................. 10
IPG Replacement ............................................................................................ 14
CUSTOMER SERVICE INFORMATION ................................................... 15
Technical Service ............................................................................................ 15
Product Registration Information ................................................................. 15
Radiopaque Identification .............................................................................. 15
Rechargeable System Information................................................................. 15
SPECIFICATIONS AND TECHNICAL DATA ........................................... 16
APPENDIX A: ELECTROMAGNETIC INTERFERENCE AND
MECHANICAL ENERGY ............................................................................. 17
LIMITED WARRANTY ................................................................................. 19

aura6000 Implant Manual | 17
APPENDIX A: ELECTROMAGNETIC INTERFERENCE AND
MECHANICAL ENERGY
Electromagnetic interference (EMI) is a field (electrical, magnetic or both) that can be
produced by various types of electrical devices found in the home, work or medical
environment. There are three types of EMI—conductive current, induced/coupled
current and radiated energy—which can occur alone or in combination and potentially
produce enough interference to:
turn the IPG on or off;
change the stimulation parameters;
temporarily change the IPG output;
cause a shocking/jolting sensation to the patient;
induce/conduct excessive current in the lead causing tissue damage; or
damage the IPG or lead.
In addition, certain mechanical devices, e.g. ultrasound, may produce mechanical energy
that is strong enough to be a source of interference.
Whenever possible, the device should first be deactivated, or care should be taken to
monitor the functioning of the device during the initial stages of, and after exposure to,
any procedure that produces EMI or mechanical energy.
16 | aura6000 Implant Manual
SPECIFICATIONS AND TECHNICAL DATA
IPG Characteristics
Case Titanium
Header Epoxy
Dimensions 45 x 32 x 8 mm
Weight 16 g
Lead connector Ring type, 6 contact
Retention strength > 10 N
Radiopaque marking AURA 6000
Telemetry type MICS 400 MHz
Storage temperature -10 to 55 °C
Battery Lithium-ion secondary cell
Capacity 50 mA·h
Charging Inductive coupling
Estimated Lifetime (to EOL) 15 years
Stimulation Parameters
Waveform Biphasic, charge-balanced with cathodic phase pulse 4x amplitude and
¼ duration of the anodic phase.
Output current amplitude 0 to 3000 µA
Pulse frequency 1 to 100 Hz
Pulse width 50 to 1000 µsec
Lead Characteristics
Electrode type Self-sizing cuff
Electrode pattern 6 contacts, 50º radial spacing
Electrode cuff inner diameter 2.5 mm
Connector 1.5 mm diameter, 2.3 mm contact spacing
Overall length 25 cm
Material Stainless steel, silicone, platinum-iridium, polyurethane
Storage temperature -10 to 55 °C
Declaration of Conformity
ImThera Medical declares that this product is in conformity with the essential
requirements of Directive 1995/5/EC on Radio and Telecommunications Terminal
Equipment and Directive 90/385/EEC on Active Implantable Medical Devices. For
additional information, contact ImThera Technical Services.
aura6000 Implant Manual | 1
ABOUT THIS MANUAL
This manual provides information about the implantable pulse generator (IPG) and lead
components of the aura6000® targeted hypoglossal neurostimulation (THN™) Sleep
Therapy System.
Refer to the information packaged with the other system components for
contraindications, warnings, precautions, adverse events and other additional information
associated with the use of those devices.
DEVICE DESCRIPTION
The aura6000 IPG and lead are part of the THN Sleep Therapy® System for the
treatment of obstructive sleep apnea (OSA). Other components include the handheld
remote control and charger (RCC or remote; model 500.0100), charging antenna
(antenna; model 500.0300), and aura6000 clinical manager (aCM; model 700.0100)
software.
PACKAGE CONTENTS
Model 100.0100 300.0100
IPG 1 -
Torque Wrench 1 1
Suture Sleeve 1 1
Lead - 1
Instructions for use 1 1
Product registration form 1 1
Temporary Patient ID card 1 -

2 | aura6000 Implant Manual
INDICATIONS
The aura6000 System is indicated for use in patients who cannot or will not tolerate
positive airway pressure (PAP) therapy for the treatment of obstructive sleep apnea. The
aura6000 System is for use by or on the order of a physician.
CONTRAINDICATIONS
Implantation of the aura6000 System is contraindicated in individuals with any of the
following:
Central sleep apnea
Performing any of the following procedures is contraindicated in patients implanted with
an aura6000 System:
Diathermy—Shortwave, microwave, and/or therapeutic ultrasound (all now referred to
as diathermy) energy can be transferred through the stimulation system, causing damage
to the implant and tissue damage resulting in severe injury or death. Diathermy can also
damage the neurostimulation system components resulting in loss of therapy and
requiring additional surgery for explantation and replacement. Advise your patient to
inform all their healthcare professionals that they must not be exposed to diathermy
treatment. Injury to the patient or damage to the system components can occur during
diathermy treatment: i) whether the system is on or off; ii) wherever diathermy is used
on the body (not just over the system component); and iii) whether diathermy delivers
heat or not.
aura6000 Implant Manual | 15
CUSTOMER SERVICE INFORMATION
Technical Service
Contact your local ImThera representative for technical support. For additional support,
ImThera Medical Technical Service may be reached at +1-858-259-2980 between
9:00am and 5:00pm Pacific Time or via email at support@ImTheraMedical.com.
Product Registration Information
A product registration form is packaged with each ImThera Medical IPG and lead. The
purpose of this form is to maintain traceability of all products and to secure warranty
rights. It also allows the institution involved in the evaluation or replacement of a
specific implanted lead, accessory, or IPG to gain quick access to pertinent data from
ImThera. Complete the registration form and: i) return one copy to ImThera Medical; ii)
keep one copy for your records; and iii) provide one copy to the patient.
Customer Service Department
ImThera Medical, Inc.
12555 High Bluff Drive, Suite 310
San Diego, CA 92130 USA
Radiopaque Identification
A radiopaque identifier is visible on standard x-ray,
and identifies the IPG as the ImThera model
100.0100.
Rechargeable System Information
The aura6000 IPG has a rechargeable battery. At typical stimulation settings and usage,
IPGs will require charging at least twice a week, and possibly daily. More frequent
charging may be required at higher stimulation settings or when the system is used for
more hours of therapy per day. Charging sessions may range from 30 minutes to 2.5
hours. Patients should be instructed to charge the IPG until the RCC beeps, signaling the
full replenishment of the IPG battery.
Over time the IPG battery will lose its ability to recover to full capacity. This may result
in more frequent charging sessions. The IPG will need replacement when stimulation can
no longer be maintained with acceptable charging intervals.

14 | aura6000 Implant Manual
Never suture directly to the lead.
Figure 6
15. Close and dress all incisions.
Caution: Do not use surgical staples to close the IPG pocket. The staples may
heat when the IPG is charged.
16. Complete the product registration form and return it to ImThera Medical.
IPG Replacement
1. Surgically open the IPG pocket and withdraw the IPG.
2. Use the torque wrench provided with the replacement IPG to unscrew the setscrew
in the old IPG, and then gently pull the lead out of the old IPG header.
3. Follow steps 5 through 15 of “IPG Placement” to complete the surgical procedure.
4. If possible, use the aCM to place the old IPG into shelf mode and return it to
ImThera Medical for analysis and disposal. See the aCM Operator's Manual for
instructions on placing an IPG into shelf mode.
a
b
aura6000 Implant Manual | 3
WARNINGS
Magnetic Resonance Imaging (MRI)—Implanted patients should not be subjected to
MRI. MRI exposure may result in dislodgement of implanted components, heating of the
IPG, lead and/or electrode(s) which may in turn cause tissue damage, damage to the
device electronics, and/or voltage induction through the lead and IPG.
Implant Damage—Severe burns may result if the IPG case is pierced and tissue is
exposed to battery chemicals. Never implant a damaged IPG.
Interaction with Cardiac Devices—When a patient’s medical condition requires both
this device and an implanted cardiac device (e.g. pacemaker, defibrillator), clinicians
involved with both devices should discuss the possible interactions between the devices
before surgery. Interactions could include:
Defibrillation therapy from an implanted defibrillator may damage the
neurostimulator.
The cardiac device may sense the neurostimulator pulses and respond
inappropriately.
Electromagnetic Interference (EMI)—The IPG contains features that provide
protection from EMI. Most electrical devices and magnets encountered in a normal day
are unlikely to affect the IPG, however strong EMI sources can cause:
Serious patient injury or death—The lead can act as an antenna that “picks up” EMI
and delivers excess current causing nerve or tissue damage.
IPG operational changes or system damage—EMI can cause a loss of, or change in,
stimulation requiring reprogramming or surgical replacement.
Unexpected stimulation—EMI can cause a transient increase in, or interruption of,
stimulation which could be perceived as a tingling or shocking.
4 | aura6000 Implant Manual
PRECAUTIONS
Clinician Training
Prescribing Clinicians—Prescribing clinicians should be experienced in the diagnosis
and treatment of the condition for which the system is being prescribed and should be
familiar with the use of neurostimulation systems.
Patient Selection—The safety and effectiveness of this neurostimulation system has not
been established for pediatric use.
Implanting Physicians—Implanting physicians should be experienced in cranial nerve
anatomy and surgical techniques, and should review this manual before surgery.
Storage, Sterilization, Implantation and Disposal
Storage—All system components must be stored within the storage conditions listed on
their package.
Sterilization—The products have been sterilized according to the process indicated on
the package label. This device is for single use only and is not intended to be resterilized.
Component Handling—Handle the implantable components of this system with
extreme care. In particular:
Never sharply bend or kink the lead body or cuff electrode.
Do not tie suture(s) directly on the lead.
Always provide a strain relief loop to minimize tension on the electrode cuff.
Avoid handling the lead with sharp instruments.
Use caution when using sharps near the lead and IPG.
Component Packaging—Do not implant a system component if any of the following
have occurred:
the sterile package has been pierced or altered;
the component shows signs of damage; or
the use-by date has passed.
aura6000 Implant Manual | 13
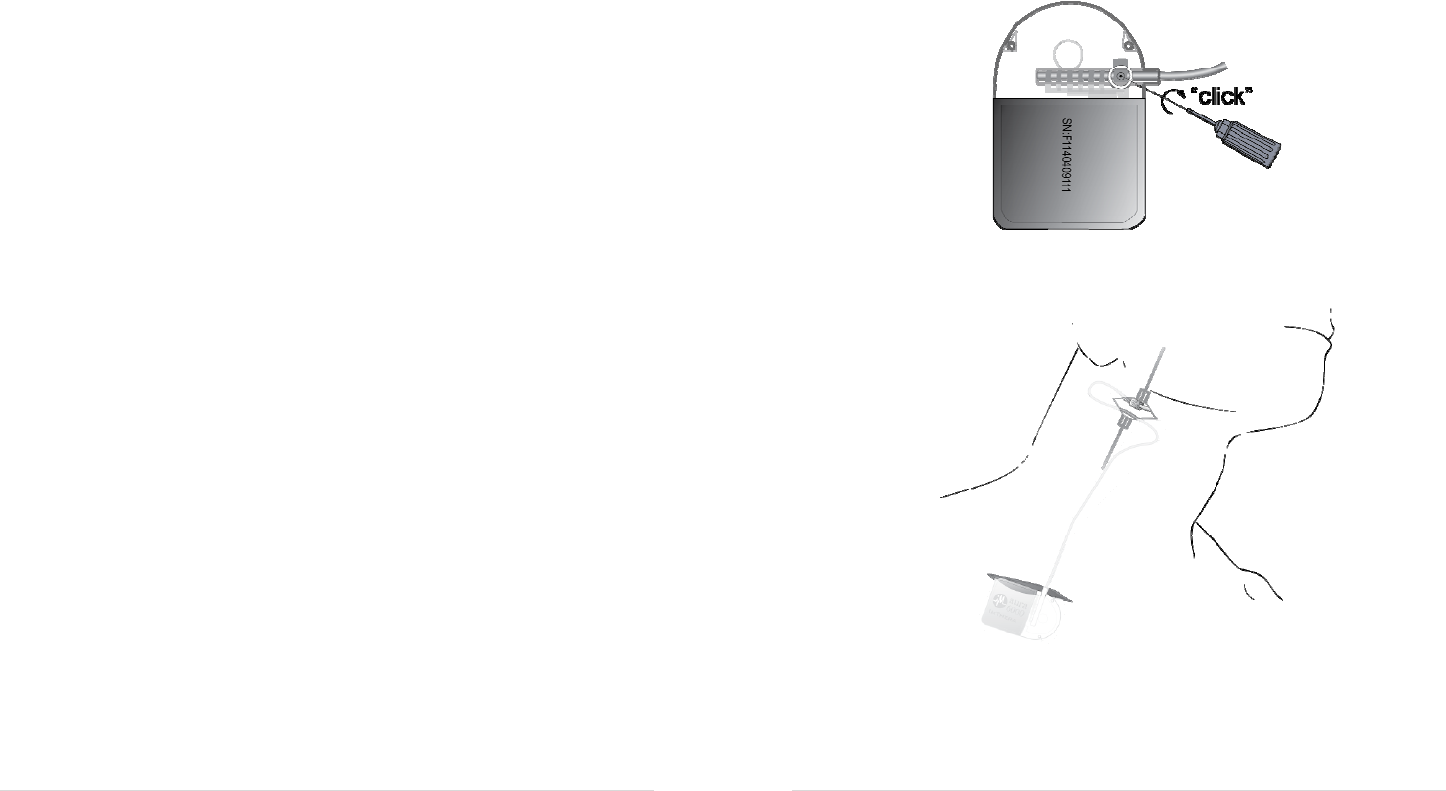
13. Gently pull the lead back toward the electrode cuff and create an S-shaped section of
lead near the neck incision as shown in Figure 5.
Figure 4
Figure 5
14. Place the suture sleeve around the lead approximately 4-5 cm from the cuff, then
secure the lead to the tissue by first tying a 2-0 non-absorbable braided suture to the
tissue approximately 1-2 cm ventral to the electrode cuff (Figure 6a), and then tying
the tails of the suture around the center groove of the suture sleeve (Figure 6b).
12 | aura6000 Implant Manual
9. Use the aCM programmer to verify that acceptable impedances exist for all
electrode contacts. See the aCM Operator’s Manual for instructions on operating
the aCM.
Impedance (Ω) Interpretation/Action
< 200 Low. Troubleshoot, see below
200 - 3000 OK.
> 3000 High. Troubleshoot, see below.
For low impedance: inspect the fit of the electrode cuff to ensure that it has
sufficient contact with the nerve and reposition the cuff as necessary. If an
acceptable motor response is obtained at an acceptable amplitude, then a low
impedance is OK.
For high impedance: i) ensure that the IPG is in the IPG pocket or otherwise making
tissue contact; ii) ensure that the lead is properly inserted into the IPG (see Figure
2); iii) confirm that there is no visible blood or tissue on the lead terminal bands; iv)
confirm that there is no air gap/bubble between the electrode contact and nerve by
flushing the incision with saline.
If the issue persists, then explant and replace the lead; and failing that explant and
replace the IPG.
10. Use the aCM to verify that noticeable and acceptable muscle movements occur
when stimulated.
Stimulation Level
(μA)
Interpretation/Action
< 500 Optimal.
500-2500 Acceptable. Confirm that the electrode cuff is around the nerve (not
a tendon or other nearby structure).
> 2500 Recheck impedances, and reposition the electrode cuff as necessary
until movements can be seen at lower stimulation levels.
11. Remove the IPG from the pocket and use the torque wrench provided to tighten the
setscrew until it “clicks” (Figure 4). Do not tighten the setscrew any further after the
clicking sound.
12. Tie the IPG sutures to stabilize the IPG within the IPG pocket.
aura6000 Implant Manual | 5
IPG Implant Location—Select an IPG implant location that is:
on the opposite side of the body from another active implanted device to minimize
the potential of interaction between the devices;
away from bony structures and areas of restriction/pressure to minimize the potential
for discomfort and skin erosion;
accessible to the patient for proper operation of the RCC and charging coil; and
close enough for the lead to reach the IPG with a strain relief loop.
Also take into account: i) the patient’s cosmetic needs; and ii) possible future cardiac
needs (e.g. pacemaker, defibrillator). Implanting a neurostimulator on the patient’s right
side allows for possible future placement of cardiac devices on the patient’s left side.
Disposal—If possible, return any explanted devices to ImThera for analysis and disposal.
Do not autoclave the returned devices or expose them to ultrasonic cleaners. Devices that
are not returned should be disposed of according to local environmental regulations. The
IPG contains a battery. Never incinerate or cremate the IPG because it may explode.
Medical Devices/Therapies—The following medical therapies or procedures may
interfere with stimulation or may cause permanent damage to the system, particularly if
used in close proximity to the device. See Appendix A for more information.
electrocautery: Do not use monopolar cautery.
internal or external defibrillation
radiation therapy
lithotripsy
high-output ultrasound
magnetic stimulation, TENS, FES, or any other form of electrical stimulation
6 | aura6000 Implant Manual
Patient Information
Clinicians should convey the following information to patients implanted with the
aura6000 System.
Patient Identification Card—Tell the patient to carry the aura6000 patient
identification card at all times.
Post-operative activities—Following implantation, patients should avoid:
disturbing the implant location, lifting heavy objects, and making extreme head or
neck movements to avoid changing the position of the electrode cuff on the nerve;
and
activities that could damage the IPG or lead by mechanical force or direct impact.
Twiddling—Patients should never attempt to change the orientation, invert or otherwise
manipulate the IPG. Doing this may damage the lead or flip the IPG and make it
impossible to charge or communicate with the IPG, and may require surgery to correct.
Regular IPG Charging—Patients must charge the IPG on a regular basis to keep the
IPG from overdischarging. Overdischarging may permanently damage the IPG. Direct
patients to the aura6000 User’s Manual for information on the IPG charging
requirements and procedure.
Wound Contact—Do not place charging antenna on an unhealed wound. The remote
and antenna are not sterile.
Heat Due to Charging—While charging, the remote, antenna, and/or IPG may become
warm. If heating occurs, patients should stop charging until the heat dissipates or try
charging more frequently for a shorter duration; and if heating persists, contact their
doctor. Patients should not charge while sleeping.
Device Failure—Tell the patient that, if the device stops working, they should turn off
the IPG and contact their doctor so that the device can be evaluated.
Hospital or Medical Environment—Instruct the patient to always inform any other
health care personnel that they have an implanted medical device before undergoing any
medical procedure or exam. See Appendix A for more information.
Home or Work Environment—ImThera Medical neurostimulators should not be
affected by normal operation of equipment such as household appliances, machine shop
tools, microwave ovens, cell phones, or AM/FM radios. Nonetheless, tell the patient that
if they suspect interference with any electrical device to avoid using the system near that
aura6000 Implant Manual | 11
Note: The setscrew may move during transit and it may be necessary to retract
the setscrew slightly to permit the lead to enter the header.
Caution: Use only ¼ turns to retract the setscrew.
Caution: Do not tighten the setscrew yet.
7. Prepare to secure the IPG in the pocket as follows:
a. Determine where the IPG anchor holes will lay within the IPG pocket.
b. Place and tie a 2-0 non absorbable braided suture in the deep fascia at the
inferior IPG anchor hole location leaving long suture tails (see Figure 3).
Cut the needle from the suture.
c. Repeat step 7b at the superior IPG anchor hole.
d. Thread the inferior and superior sutures through the inferior and superior
IPG anchor holes respectively (see Figure 3).
Note: Do not tie the suture to the IPG until the impedance and motor
thresholds have been tested according to steps 9 and 10.
Figure 3
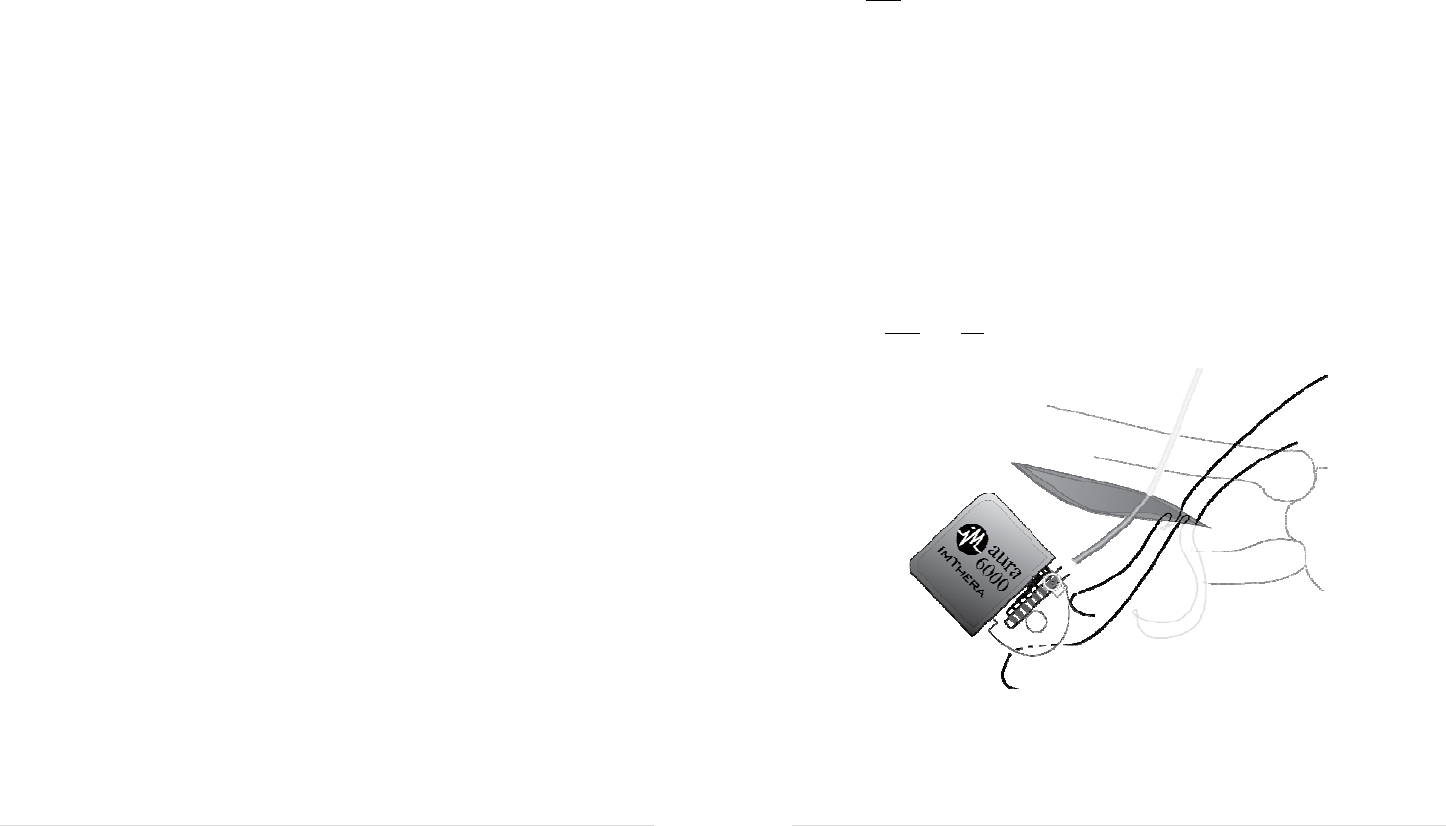
8. Place the IPG into the IPG pocket (metal portion first) with the ImThera logo facing
outward as shown in Figure 5. Ensure that the lead is not sharply bent.

10 | aura6000 Implant Manual
IPG Placement
1. Select the site for the IPG pocket. See the Precautions section of this manual for
important information on selecting the IPG pocket site.
2. Make a ~5 cm medio-lateral incision (equal to the width of the IPG).
3. Create a subcutaneous pocket. Make the pocket just large enough to contain the
IPG, and so that the incision will not be over the IPG.
Caution: Ensure that the IPG is placed no deeper than 1 cm (ideally 5-7 mm)
below the skin and is parallel to the skin. Charging may be inefficient or
unsuccessful if the IPG is too deep or not parallel to the skin.
4. Use a shunt passer, or other suitable method, to tunnel the proximal end of the lead
to the IPG pocket.
5. Use sterile gauze to wipe any visible blood or tissue from the metal contact bands on
the proximal end of the lead.
6. Holding the lead 5 mm from its proximal end, insert the lead into the IPG header.
Continue to insert in 5mm increments until the lead is fully seated. You will feel the
lead bottom out in the header and see that the proximal end of the most distal band
on the lead is within the setscrew block (Figure 2).
Fi
g
ure 2
aura6000 Implant Manual | 7
device. Avoid prolonged exposure to RFID sources. RFID sources may not necessarily
be located near the door of a building.
Handling—The remote and charging antenna are sensitive medical devices and should
be handled with care. Dropping the devices on hard surfaces or in water, or other rough
handling, may permanently damage them.
Cleaning—The remote and charging antenna may be cleaned using a damp cloth. Do
not submerge or use abrasive cleansers.
Component Disposal—Never dispose of batteries in fire. Dispose of used batteries in
accordance with local regulations.
Adverse Effects
Potential adverse events from hypoglossal nerve stimulation may include but are not
limited to the following. These events may result in hospitalization, prolongation of
hospitalization, unanticipated surgery, tracheotomy, revision or replacement of system
components, or death.
Medical/Surgical Complications—Infection; bleeding, hematoma, or seroma; scarring;
excessive fibrotic tissue growth around the implanted device; temporary or permanent
hypoglossal or other nerve damage resulting in paresis, paralysis or other dysfunction
including difficulty or inability to swallow or speak; complications from anesthesia or
extended procedure time; heart attack; persistent pain at the implant site; allergic or
immune system response to the implanted materials; and component migration or erosion
through the skin can occur.
Device Complications—Lead migration, dislodgement, disconnection, fracture,
insulation breakage or erosion; failure of IPG component, battery, software or telemetry;
and IPG migration or flipping can occur.
Stimulation Complications—Paresthesia or tingling; loss of therapeutic effect;
extrahypoglossal stimulation; and worsening of OSA condition can occur.
8 | aura6000 Implant Manual
SURGICAL GUIDELINES
Pre-Operative
1. Charge the IPG before opening the shelf box. For charging instructions, see the
aura6000 User’s Manual.
2. Before opening the IPG sterile package, verify that the IPG is operable by using the
aCM to interrogate the IPG and read the IPG battery charge level. See the aCM
Operator’s Manual for instructions on how to operate the aCM.
3. Confirm that the RCC-to-IPG RF range will be sufficient to communicate with the
IPG without placing the RCC into the sterile field. Place the RCC in a sterile bag if
the RCC needs to enter the sterile field to communicate with the IPG.
Lead Placement
1. Determine on which side of the body the IPG (and lead) will be placed, and prep
that side of the neck and infraclavicular region for surgery.
Caution: If possible, place the IPG contralateral to any other active implanted
device to minimize the potential of interaction between the devices.
2. Make a 5-6 cm incision approximately ~2 cm below the mandibular body and
centered over the lesser cornu of the hyoid bone.
3. Use blunt dissection to expose a 1.5 – 2.0 cm length of hypoglossal nerve distal to
the ansa cervicalis branch and proximal to the first branch innervating the tongue
muscles (usually the styloglossus branch of the hypoglossal nerve) leaving the
perineural tissues intact. Take care not to disrupt the blood vessels or lymphatics
surrounding the hypoglossal nerve.
4. Place the electrode cuff ventrolateral to the exposed nerve such that the lead cable
exits posteriorly.
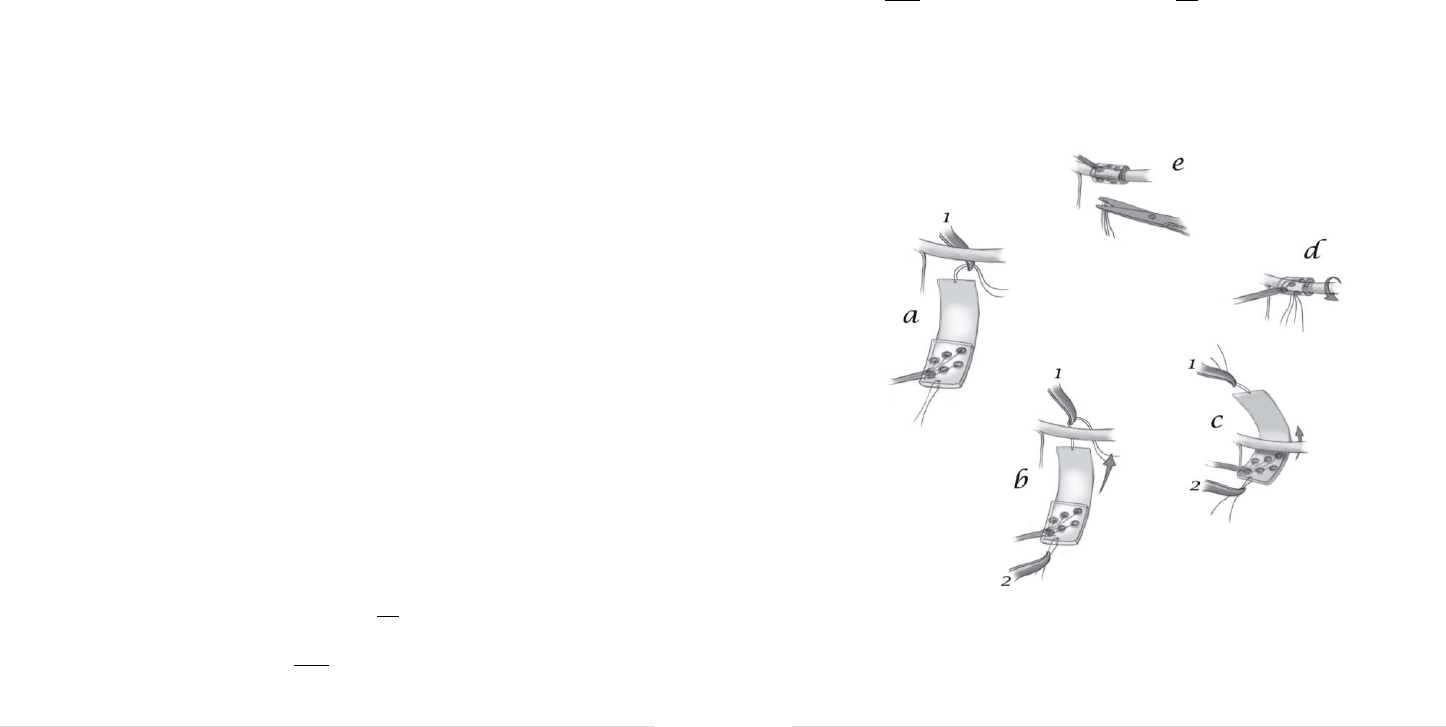
5. Position the electrode cuff around the nerve as follows:
a. [Optional] Instruct an assistant to use a vein retractor to gently lift the
hypoglossal nerve.
b. Position forceps #1 ventromedial to the nerve, then advance its angled tip
laterally beneath the nerve to grasp the red thread on the medial edge of the
electrode cuff (Figure 1a).
c. Use forceps #2 to grasp the blue thread on the lateral edge of the electrode
cuff and spread the electrode cuff open (Figure 1b).
aura6000 Implant Manual | 9
d. Use forceps #1 to pull the cuff under the nerve to the medial side (Figure 1c)
and release forceps #2 (blue thread) when the lateral edge of the cuff reaches
the nerve.
e. Allow the electrode cuff to completely furl around the nerve (Figure 1d).
Note: Ensure that the cuff flap with the red thread is on the outside of the
cuff, and not against the hypoglossal nerve which would preclude the
electrodes from contacting the nerve.
f. Cut and remove both the red and blue threads from the cuff (Figure 1e).
g. Rotate the cuff so that the lead cable is on the superficial side of the nerve.
Figure 1