03 14 16 MIS Spine Syllabus
2016-03-14
: Pdf 03 14 16 Mis Spine Syllabus 03_14_16_MIS_Spine_Syllabus 3 2016 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 57
3/14/2016
1
MIS vs Open Surgery for Spinal Deformity:
Treatment Algorithm
Praveen V. Mummaneni, M.D.
Professor
Vice-Chairman
Dept. of Neurosurgery
Co-director: UCSF Spine Center
University of California,
San Francisco
Chair: AANS/CNS Joint Section on
Disorders of the Spine and Peripheral Nerves
Todd D. Vogel, MD.
UCSF spine fellow
Junichi Ohya, MD.
International visiting fellow
Disclosure
•Consultant:
–DePuy Spine
•Other Financial Support (royalty):
–DePuy Spine
–Thieme Publishing
–Quality Medical Publishers/Taylor and Francis
–Springer Publishing
•Stock
–Spinicity/ISD
Burgeoning Adult Deformity Patient
Population
•Need to Treat More Patients with Adult
Spinal Deformity
•Need to Avoid Morbidity
3/14/2016
2
Why Would We Want To Do “Less”
Surgery for Adult Spinal Deformity?
•Complication rates
high
•Pseudarthrosis rates
problematic
Mummaneni et al: Neurosurgery 2008
Degen Vs Deformity
•In Degenerative 1-2 level spinal disease, MIS
approaches decrease hospital stay and EBL
–The operations are interchangeable for Most cases
•Does this hold true for deformity?
–Are the indications for the MIS vs open deformity
surgery similar?
3/14/2016
3
J. Cheng and P. Mummaneni:
NS Focus 2013
•Compared 50 MIS TLIF with 25 open TLIF
•MIS TLIF with fewer complications and
lower EBL
•MIS TLIF had shorter LOS and saved $4k
compared to open TLIF
•Long term outcomes similar
MIS Deformity
•Can decompression be achieved? Yes
•Can hardware be placed safely? Yes (even iliac
screws)
•Can sag balance be restored? Maybe
•Will you match LL-PI within 10 degrees? Maybe
•Will it take a long time to do? Initially - yes
•Can a succesful fusion be established?
– This is the Challenge…
Anand, et al. NS Focus 2010
Complications
3/14/2016
4
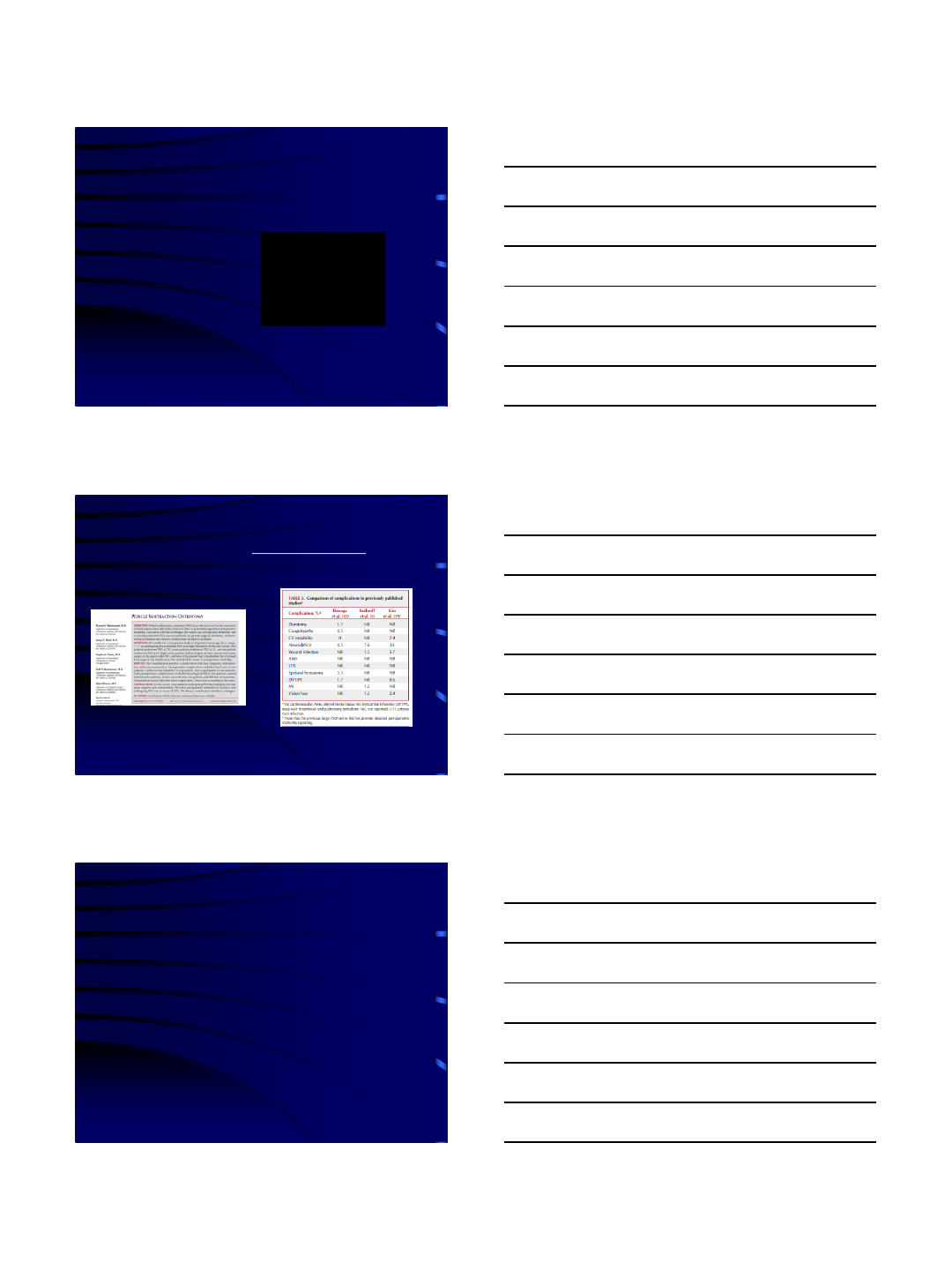
Tormenti, et al.
NS Focus 2010
Complications
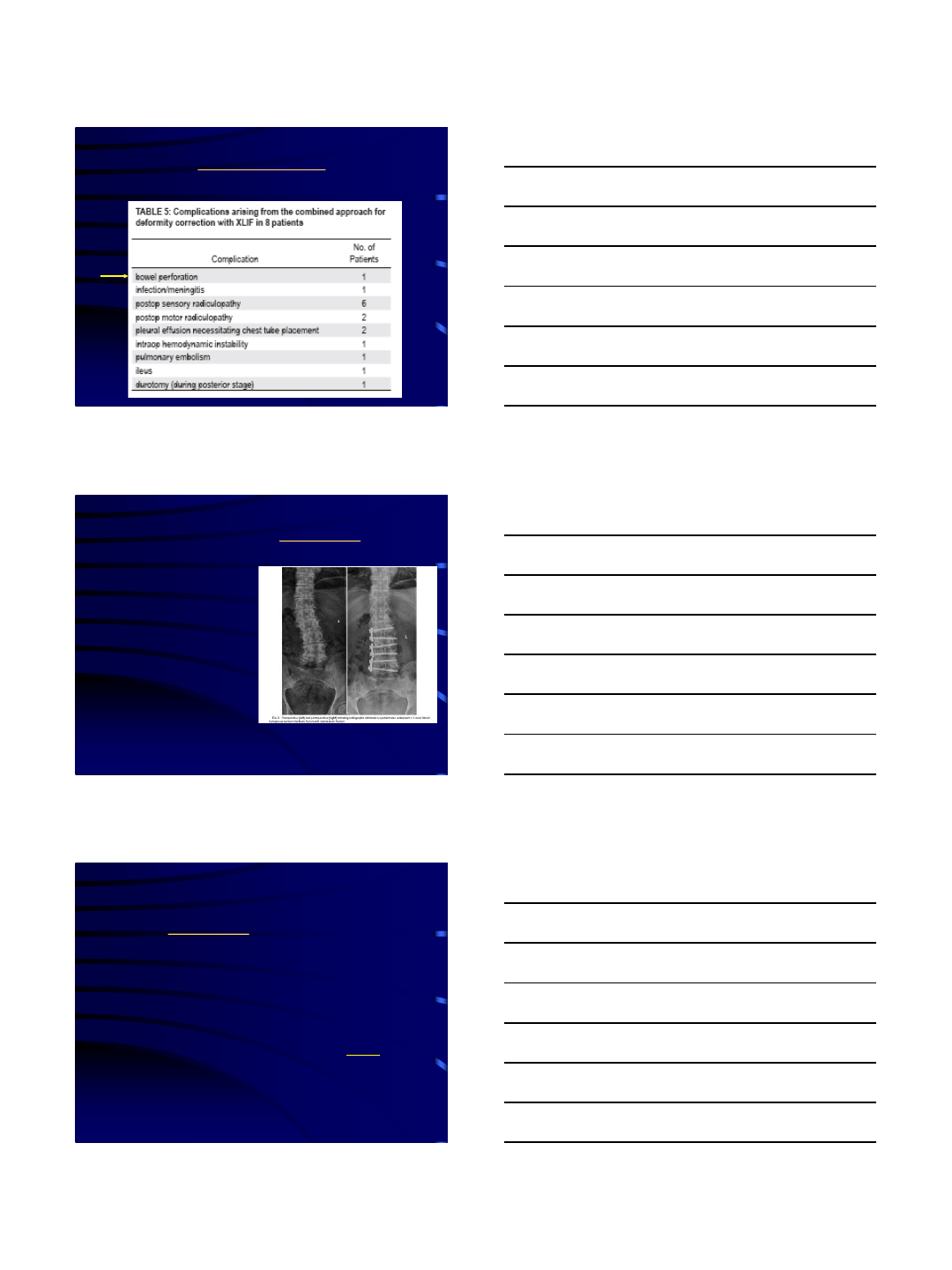
Dakwar and Uribe. NS Focus 2010
•Pitfall:
–The authors
concentrated on
coronal curve and not
on sagittal balance
Dakwar and Uribe:
NS Focus March 2010
•1/3 of the patients did NOT have sagittal
balance restored
•Remember: Coronal correction is NOT as
important as sagittal correction
3/14/2016
5
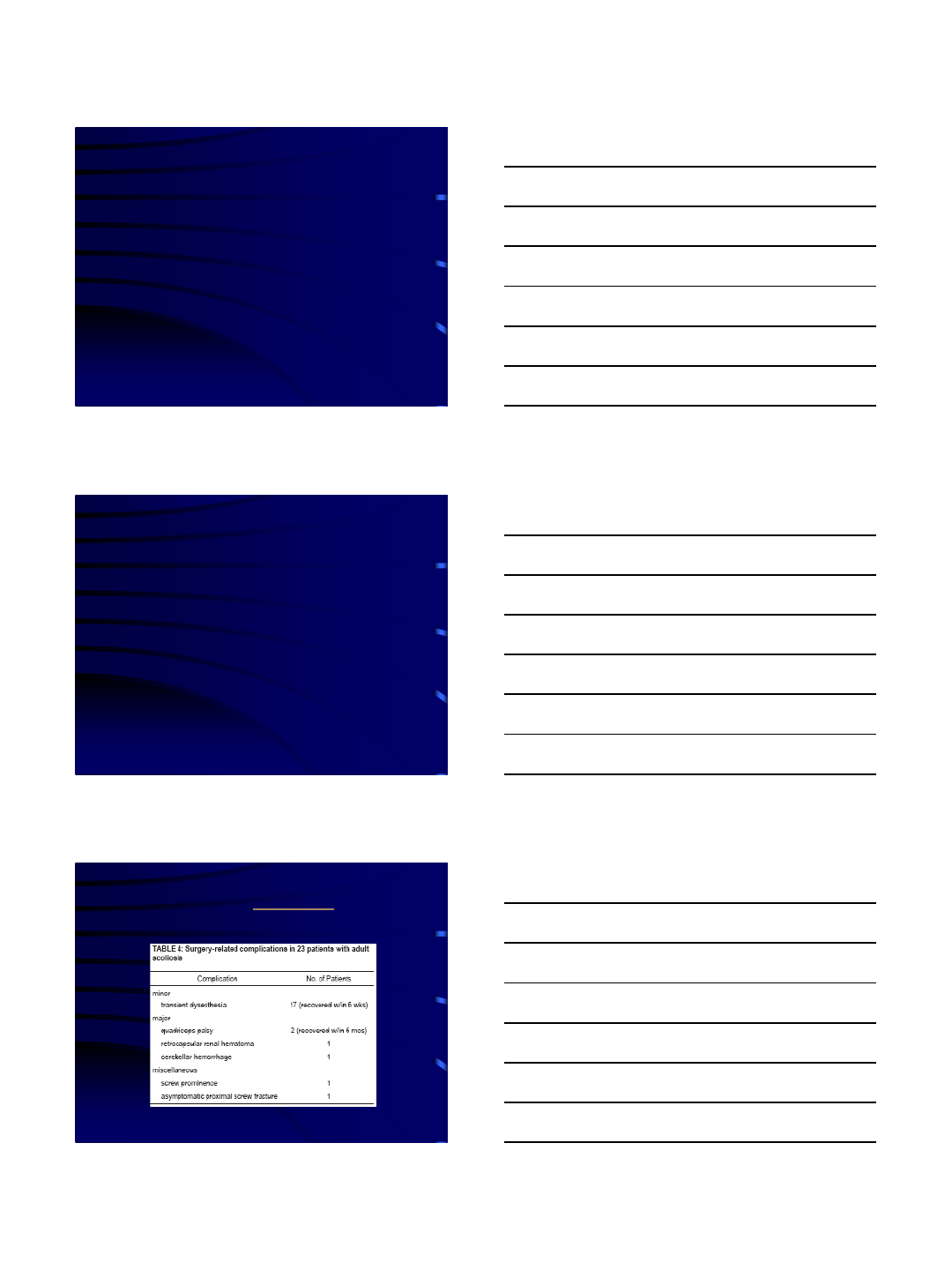
Wang & Mummaneni
NS Focus March 2010
•23 patients,
retrospective review
•High pseudo rate if no
interbody fusion is
done, can not rely on
MIS posterolateral
fusion
When To Do MIS for Deformity?
• Need an algorithm…
NS FOCUS May 2014:
•Praveen Mummaneni
•Chris Shaffrey
•Lawrence Lenke
•Paul Park
•Michael Wang
•Frank LaMarca
•Justin Smith
•Greg Mundis
•David Okonkwo
•Bertrand Moal
•Richard Fessler
•Neel Anand
•Juan Uribe
•Adam Kanter
•Behrooz Akbarnia
•Kai Ming Fu
•MIS ISSG
3/14/2016
6
When To Do MIS for Deformity?
• Need an algorithm…
NS FOCUS May 2014:
•Praveen Mummaneni
•Chris Shaffrey
•Lawrence Lenke
•Paul Park
•Michael Wang
•Frank LaMarca
•Justin Smith
•Greg Mundis
•David Okonkwo
•Bertrand Moal
•Richard Fessler
•Neel Anand
•Juan Uribe
•Adam Kanter
•Behrooz Akbarnia
•Kai Ming Fu
•MIS ISSG
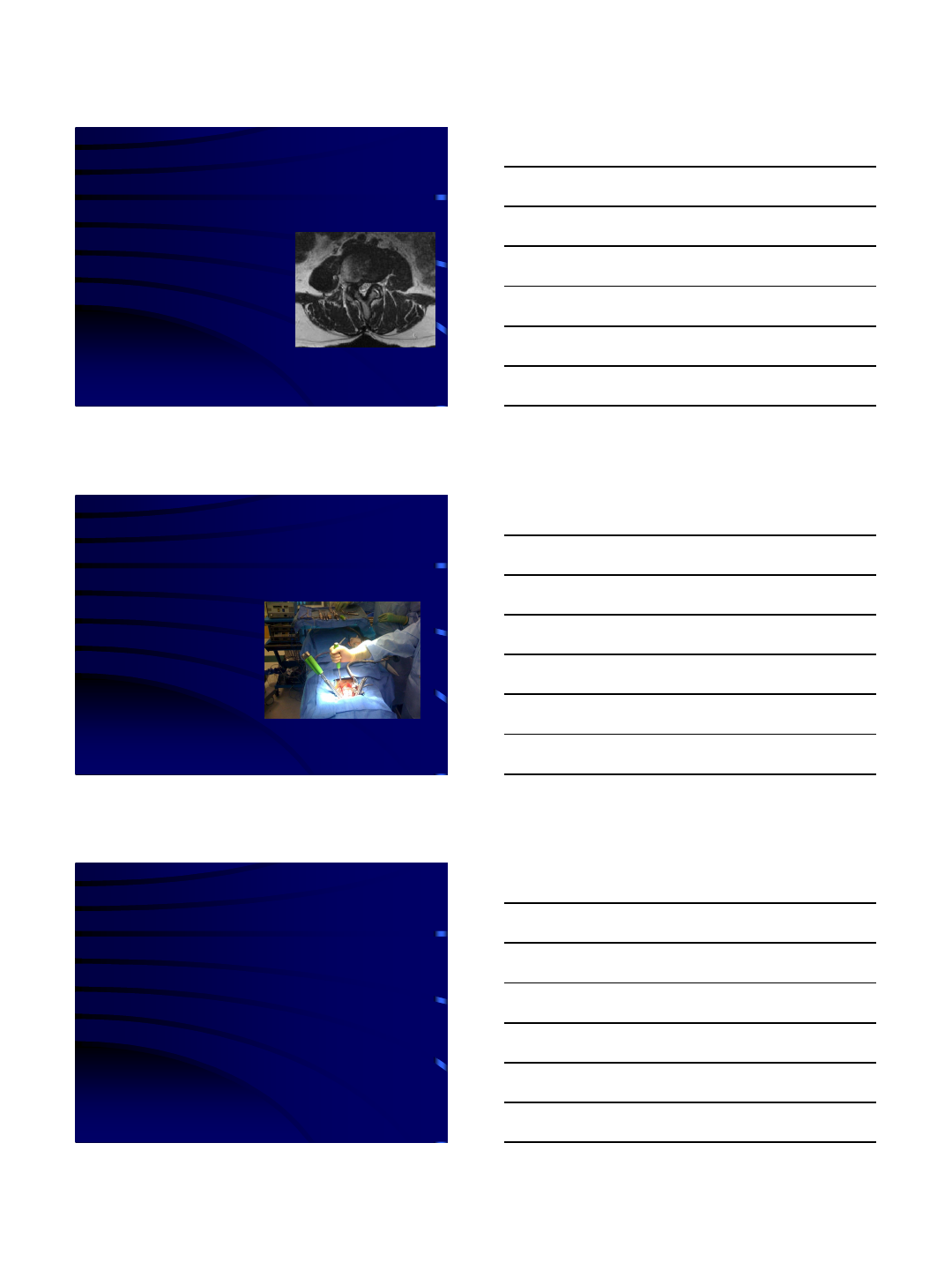
Class I Treatment
•MIS Decompression without fusion or with limited
one level fusion
A D
C
B
52 year old woman with radicular right leg pain. Minimal back pain. MRI with
Right L3-4 lateral recess stenosis from disc bulge (axial shown below).
CA 15
PT 3
PI-LL -7
SVA<5
3/14/2016
7
Class I Treatment
•Decompression alone
–Neurogenic claudication secondary to central stenosis
•Requires limited decompression
•Minimal or no back pain
–Radiographic findings
•Decompression w/ limited instrumented PL Fusion
–Stenosis with minimal back pain
–Anterior supporting osteophytes
–No global imbalance, cobb <20,
–No LL-PI Mismatch
–Caution: Deformity progression and worsening of
symptoms
Class 2 “Medium”MIS Treatment
•Apex of lumbar curve is
included in instrumented fusion,
plus necessary decompression
–back pain associated with
deformity
•Radiographic
–LL-PI mismatch 10-30
degrees
–May have grade 1,2
spondylolisthesis or lateral
listhesis
–PT<25
–Coronal cobb over 20
degrees
Silva FE, Lenke LG: Adult degenerative scoliosis: evaluation and management. Neurosurg Focus 28
(3): E1, 2010
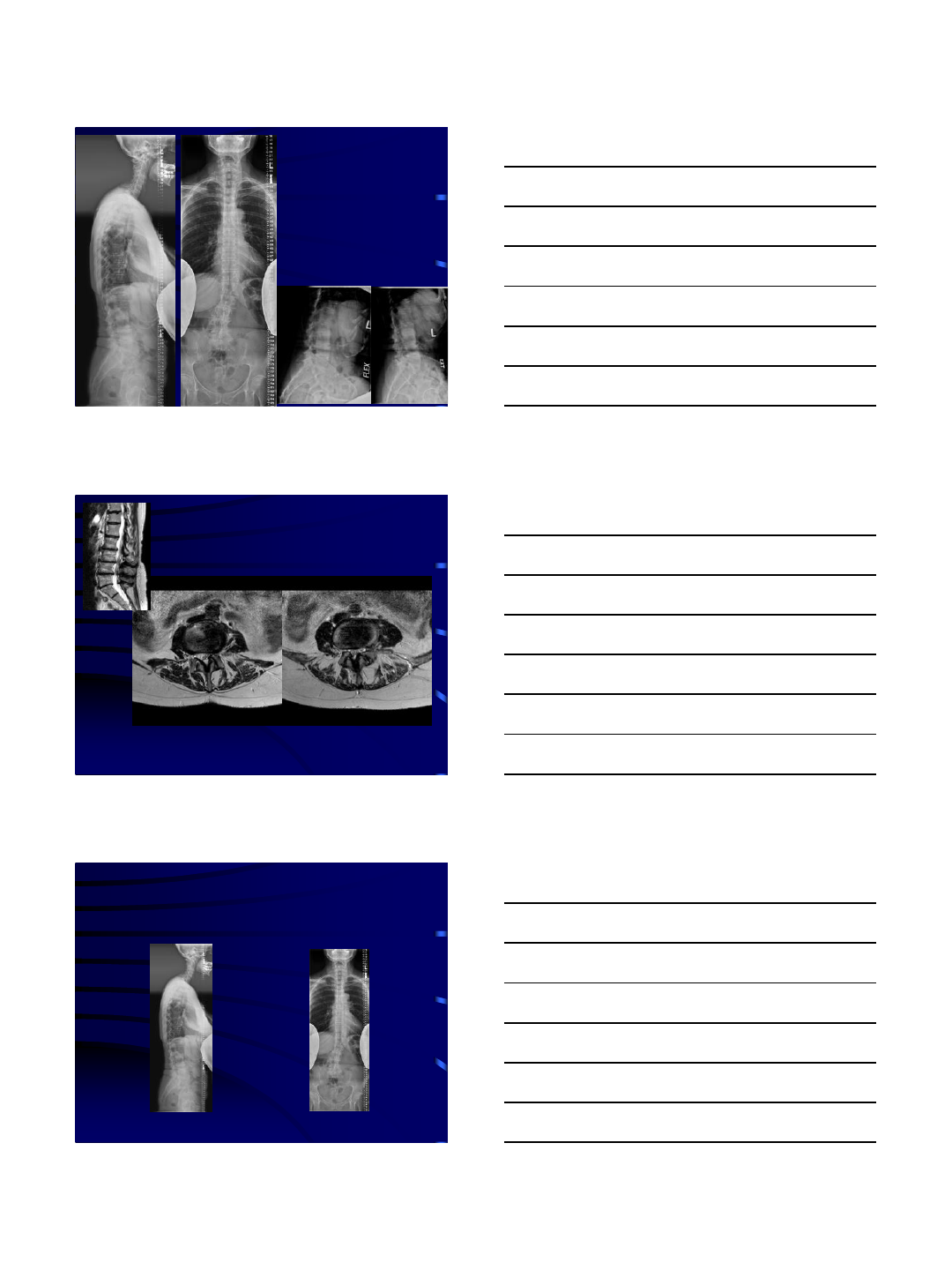
Case Example
•67 year old woman with low back pain and
bilateral sciatica and anterior thigh pain
–Failed multiple steroid injections
–On oral narcotics
3/14/2016
8
36-Inch X-rays revealed
L2-3 lateral listhesis
SVA: 4.3cm
Lumbar lordosis: 27°
Dynamic X-rays
MRI
L3/4 L4/5
What Levels to Treat?
3/14/2016
9
•1st stage surgery:
–Lateral interbody fusion at L2-3, L3-4, L4-5
•2nd stage surgery:
–Posterior MIS L2-S1 pedicle screw fixation and
right iliac screw fixation
–TLIF at L5-S1

3/14/2016
10
AB
D
C
3/14/2016
11
Iliac Screws May Be Placed MIS
Initial Results
•24 patients underwent percutaneous iliac screw fixation
-indications: infection, neoplasm, trauma, deformity
•47 screws placed with fluoroscopic guidance
•All screws confirmed with CT
–correct placement of all screws.
•No hardware complications
•One patient died of unrelated medical comorbidities
-Wang MY, Williams S, Mummaneni PV, Sherman JD. Minimally
invasive percutaneous iliac screws: Initial 24 case experience with CT
confirmation
MIS techniques in selected cases
may diminish complications
3/14/2016
12
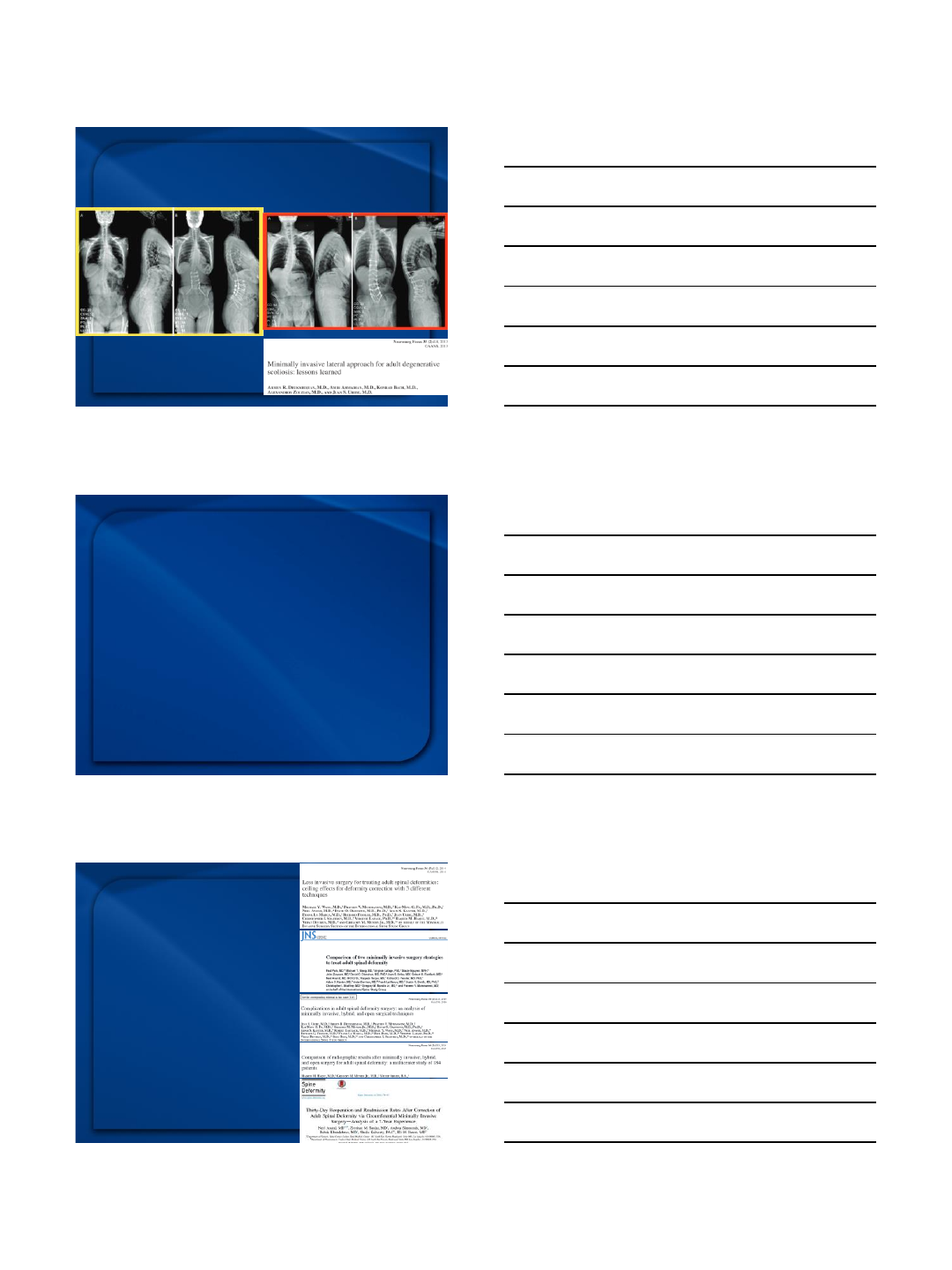
There is a limit (ceiling effect) to deformity
correction using current MIS techniques
Conclusion:
MIS is NOT Ideal for Class 3
•Avoid
–Curves with Cobb >300
–Apical rotation > Grade II
–Lateral olisthesis >6mm
–Sag imbalance requiring PSO
–Thoracic kyphosis
•These characteristics predict
failure with limited MIS
decompression/fusion surgery
•Need to do OPEN surgery
Conclusions
•PI is a fixed parameter
•PT may increase to
compensate for loss of
sagittal balance
•Goal LL = PI +/- 10
degrees
–Match PI within 10
degrees of the lumbar
lordosis
3/14/2016
13
Conclusions
•Minimally invasive techniques:
–Useful for MISDEF Class 1, 2 deformities
–Don’t forget to restore sagittal balance
–Currently, MIS techniques are not ideal for cases
requiring 3 column osteotomies for correction of spinal
imbalance
3/7/2016
1
MIS Deformity Management
using the Lateral Approach
Luiz Pimenta, MD PhD
1Instituto de Patologia de Coluna - São Paulo –Brazil
2UCSD, San Diego, CA –USA
2016
•Decompress neural structures
•Promote fusion
•Preserve/ correct alignment
–CORONAL/ SAGITTAL
ADULT DEFORMITY
Surgical Principles
•Previous surgery?
•Free levels
•Focal deformity?
•More correction in lower levels
•Risks
–Bleedind
–Surgery duration
–ICU
–Neurological risks
–PJK
Method and approach selection
REDUCE
REDUCE
REDUCE
3/7/2016
2
ASD
LLIF ACR
Posterior
Osteotomies
PSO, SPO,
VCR
ALIF
ALIF
ACR
TLIF/PLIF
LLIF
LLIF + SPO
Method and approach selection
MIS
OPEN
HYBRID
ALIGNED COMPENSATED DECOMPENSATED
The majority of the cases are
“ALIGNED to COMPENSATED”…
3/7/2016
3
Not only SVA
but also PI-LL
Disability is underappreciated in compensated cases
Decompensated
x SVA
xPI-LL
Compensated
SVA
xPI-LL
Both groups
experienced similar
improvements with
sagittal correction
Examples
3/7/2016
4
Examples
MIS X HYBRID X OPEN
ALIF
LLIF
MIS post
ALIF
LLIF
Limited open posterior
Open posterior osteot/fixation
•Complications
MIS < HYB < OPEN
•Surgery duration
OPEN = MIS < HYB
•EBL
MIS < HYB < OPEN
•Power of correction
OPEN > HYB > MIS
Summary
MIS; HYB; OPEN
3/7/2016
5
PLF/ TLIF/ PLIF and Alignment
PLF alone average
reported pre- to post-
op lordosis change
per level treated
was -10.7°to 0°in
lordosis (1)
PLIF/TLIF alone
average reported pre-
to post-op lordosis
change per level
treated was -5.6°to
0°in lordosis (2)
PLIF/TLIF plus SPO
average reported pre- to
post-op lordosis change
per level treated was
15°to 20°lordosis per
level (3)
1. Hsieh, P. C., Koski, T. R., O'Shaughnessy, B. A., Sugrue, P., Salehi, S., Ondra, S., & Liu, J. C. (2007). Anterio r lumbar interbody fusion in comparison with transforaminal lumbar interbody fusion: implications for the restoration of
foraminal height, local disc angle, lumbar lordosis , and sagittal balance.
2. Kepler, C. K., Rihn, J. A., Radcliff, K. E., Patel, A. A., Anderson, D. G., Vaccaro, A. R., ... & Albert, T. J. (2012). Restoration of lordosis and disk height after single‐level transforaminal lumbar inter body fusion. Orthopaedic
surgery,4(1), 15-20.
3. Jagannathan, J., Sansur, C. A., Oskouian Jr, R. J., Fu, K. M., & Shaffrey, C. I. (2009). Radiographic restoration of lumbar alignment after trans foraminal lumbar interbody fusion. Neurosurgery,64(5), 955-964.
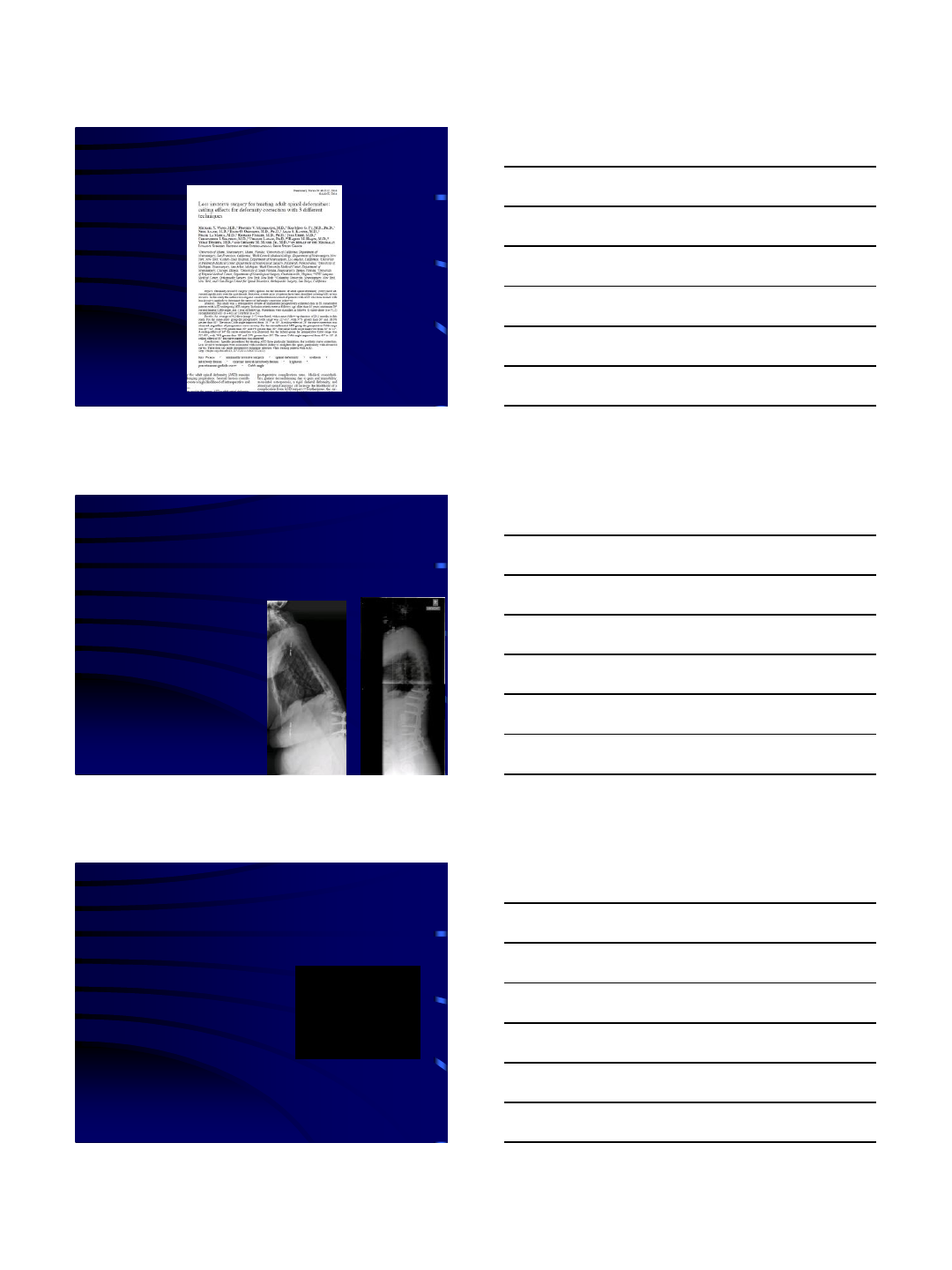
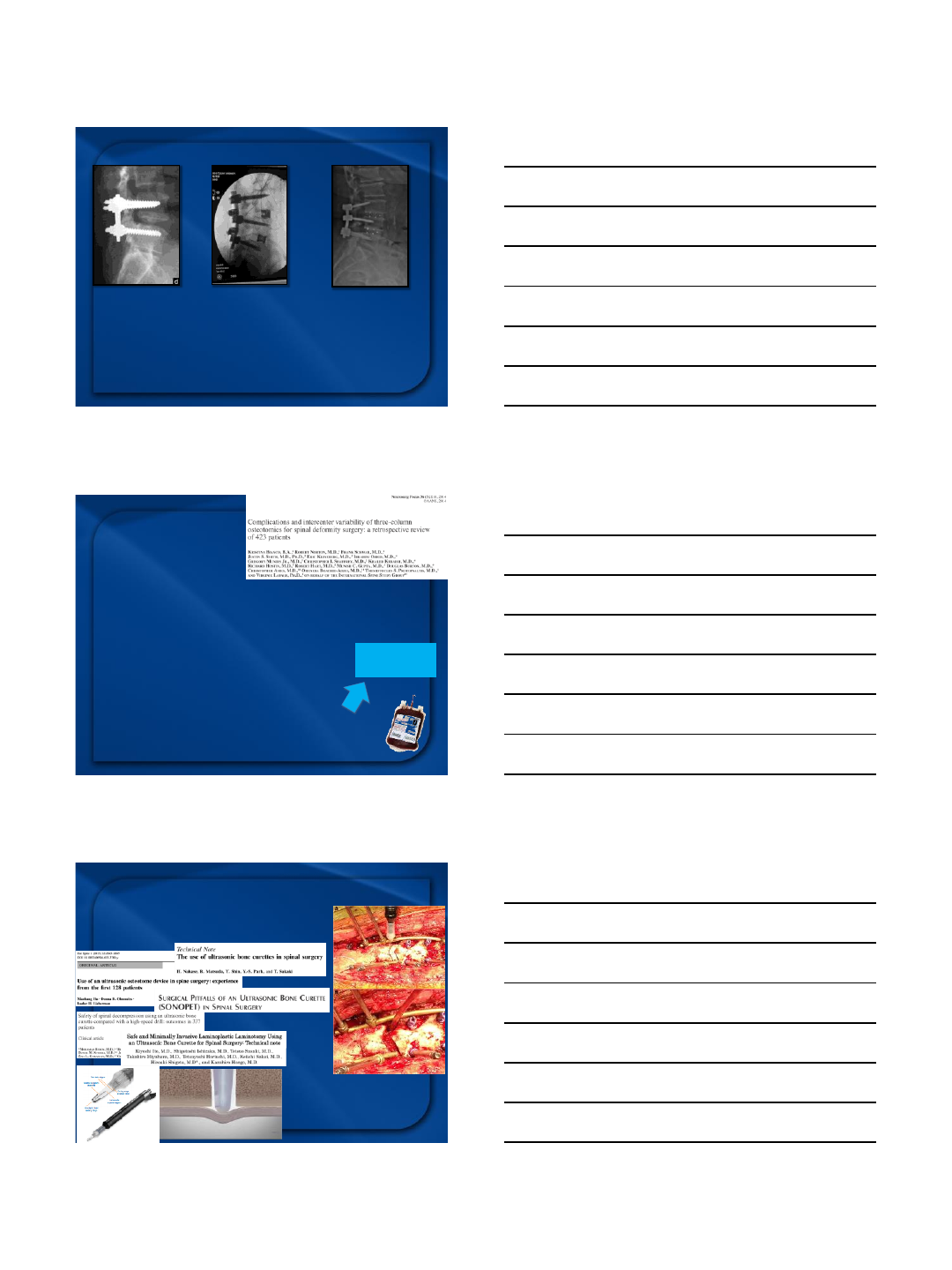
3-column
osteotomy
423 consecutive patients (8 Surgical centers)
•Major Intraop complications –7%
–spinal cord deficit (2.6%)
•Major Periop complications –39%
–Unplanned reop (19.4%)
•Major overall complications –42%
average % of total blood volume lost - 55% !!!
Major blood loss (over 4 L) –25%
Higher risk of
complications
3-column osteotomy –
Minimize colateral damage Hu et al
Safe and effective
Decrease the risk of soft tissue injury
Decrease blood loss
•ultrasonic bone ressectors

3/7/2016
6
“Standard” Lateral LIF
Good for coronal realignment
Poor for sagittal correction
Posterior Osteotomies (SPO)
Pedicle subtraction osteotomy (PSO)
Vertebral column resection (VCR)
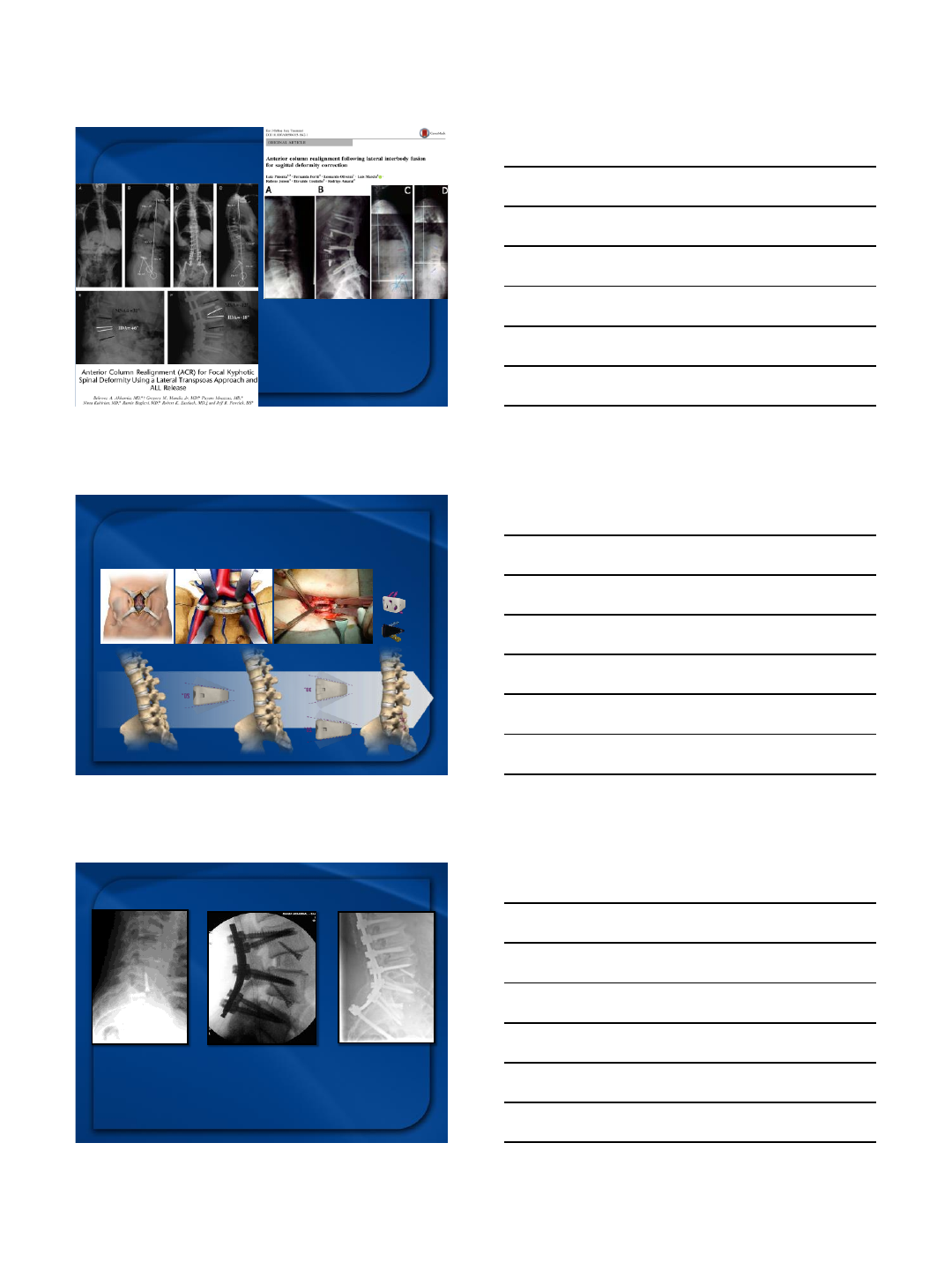
Anterior Column Realignment (ACR)
NEW OPTIONS FOR
MIS powerful
correction
Posterior shortening
x
Anterior elongation
LLIF and Alignment
LLIF average
reported pre- to post-
op lordosis change per
level treated was
1.2°to 3.6°in
lordosis
LLIF with SPO
average reported pre-
to post-op lordosis
change per level
treated 27.6°in
lordosis
LLIF ACR average
reported pre- to post-op
lordosis change per level
treated was 10°to
30°in lordosis
Rodgers, W. B., Gerber, E. J., & Patterson , J. R. (2010). Fusion after minimally disruptive anterior lumbar interbody fusion: analysis of extreme lateral interbody fusion by computed tomography. SAS Journal ,4(2), 63-66

3/7/2016
7
Anterior Column Realignment (ACR)
by the lateral approach
•Segmentar Sagittal Correction →
–Lateral/ Anterior access
–ALL ressection
–Hyperlordotic cages
Regional/
Global
changes
20/30°
Anatomical Considerations - ALL
•RADIOGRAPHIC ANALYSIS
–36”XRAYS, CT, and MRI
–Sagittal parameters
–Pelvic parameters
–Mobile interbody disc
–Hyper-extension view to
evaluate disk space motion
•CLINICAL ANALYSIS
–Hip flexion contractures
–Neuromuscular conditions
–Dynamic flexibilty supine vs.
Prone vs. standing
–Neurologic impairment (UMN)
Planning for a lateral ACR

3/7/2016
8
37°
Dynamic X-Rays
Dorsal Decubitus + Bolster
Courtesy: Dr Akbarnia
CT/ MRI
Free levels
Can give a
clue about
flexibility
orthostatic supine
LLIF= 25
ACR= 9
ACR correction (per level):
Lordosis 12°
SVA 3.1cm
ACR equivalent to SPO
Selection bias...
3/7/2016
9
Lessons learned:
limited posterior osteotomies
(Pontè) can give superior
correction
Hyperlordotic ALIF
ALIF and Alignment
ALIF Alone
average reported
pre- to post-op
lordosis change per
level treated was
5.6°in lordosis
ALIF + SPO average
reported pre- to post-op
lordosis change per level
treated was 15°to
20°in lordosis
ALIF ACR average
reported pre- to post-op
lordosis change per
level treated was 10°
to 30°in lordosis
Lu, Y., Falcone, M. M. , Wang, M. Y., & Wu, S. (2014). Multilevel TLIF for Spinal Deformity. In Minimally Invasive Spinal Deformity Surgery (pp. 173-183). Springer Vienna.
Dorward, I. G., Lenke, L. G. , Bridwell, K. H., O'Leary, P. T., Stoker, G. E., Pahys, J. M. , ... & Koester, L. A. (2013). Tran sforaminal versus anterior lumbar interbody fusion in long deformity constructs: a matched cohort
analysis.Spine,38(12), E755-E762.
3/7/2016
10
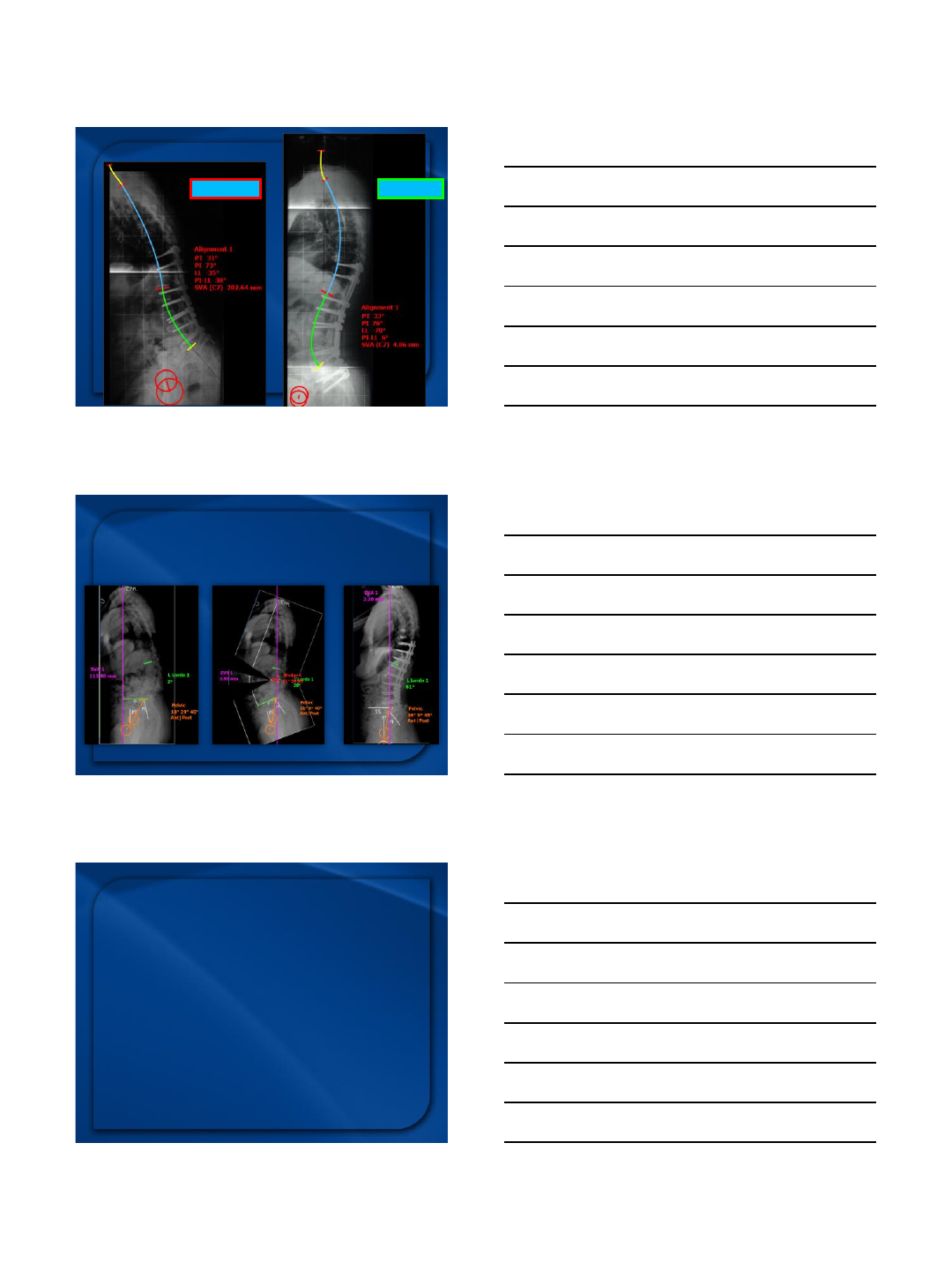
PI-LL = 30°PI-LL = 6°
Case example –
1-level HL ALIF
Pre-Op Surgical Plan Post-Op Result
Importance of PLANNING
Summary
Anterior colunm reconstruction
•Proper indication and planning
•Adequate exposure
•Safety (protection of neurovascular &
monitoring)
•Complete release (ALL & annulus; any posterior?)
•Proper cage position & size
•Cage fixation & screw
•Good stabilization & fusion technique
•Achievement of Goal
3/7/2016
11
www.patologiadacoluna.com.br
3/8/2016
1
MIS Applications for
Pediatric Deformity
Firoz Miyanji MD, FRCSC
VuMedi Seminar
2016
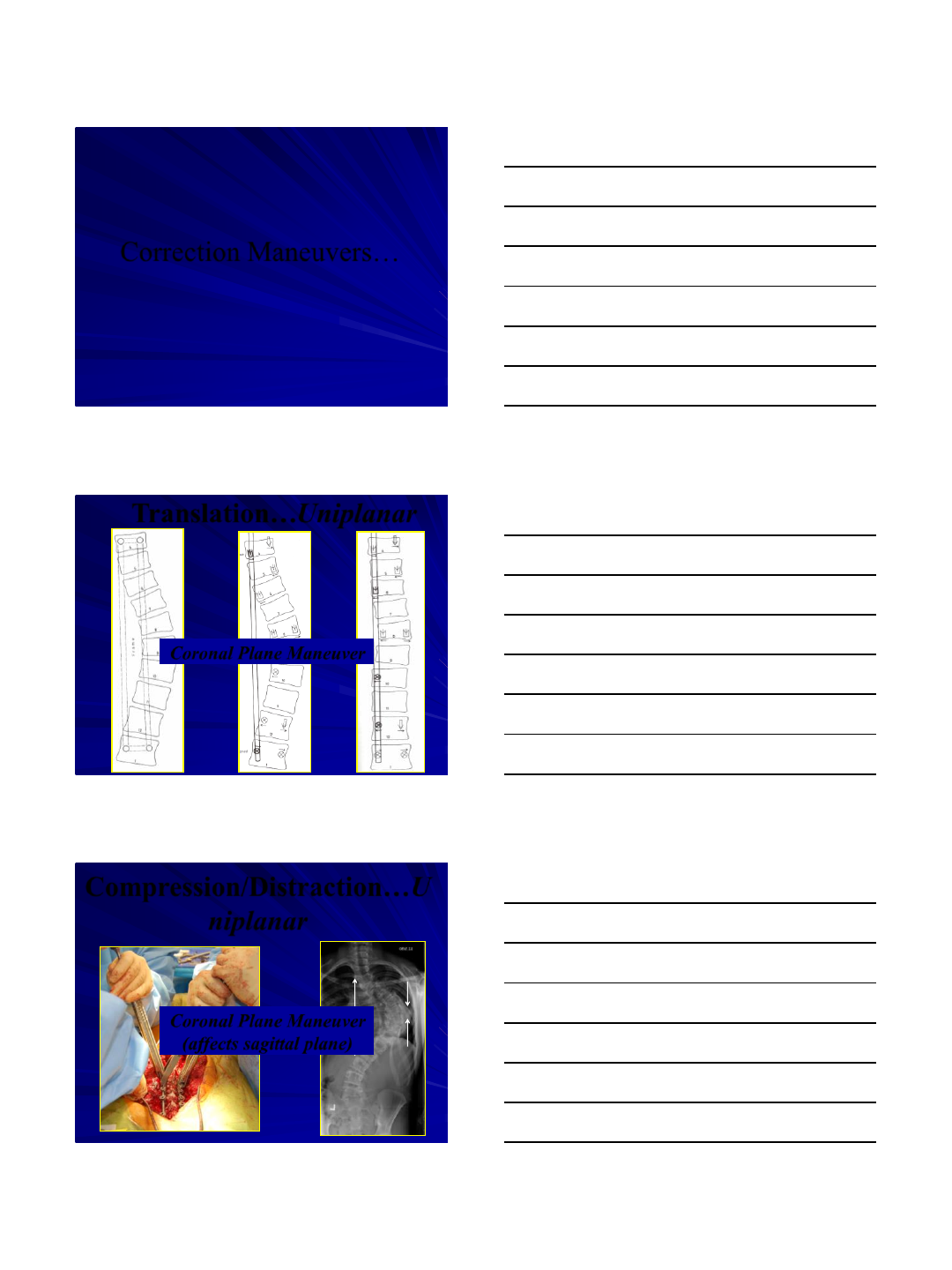
12 yo
Lenke 1B
How can we
achieve the
correction
through MIS?
Deformity Correction
•Remains a delicate balance between construct
and application of forces and surgical technique
of mobilizing the spine
•With changes in available instrumentation,
techniques for deformity correction have also
evolved
•A number of traditional techniques exist for
open procedures not all of which are available
for MIS
3/8/2016
2
Correction Maneuvers…
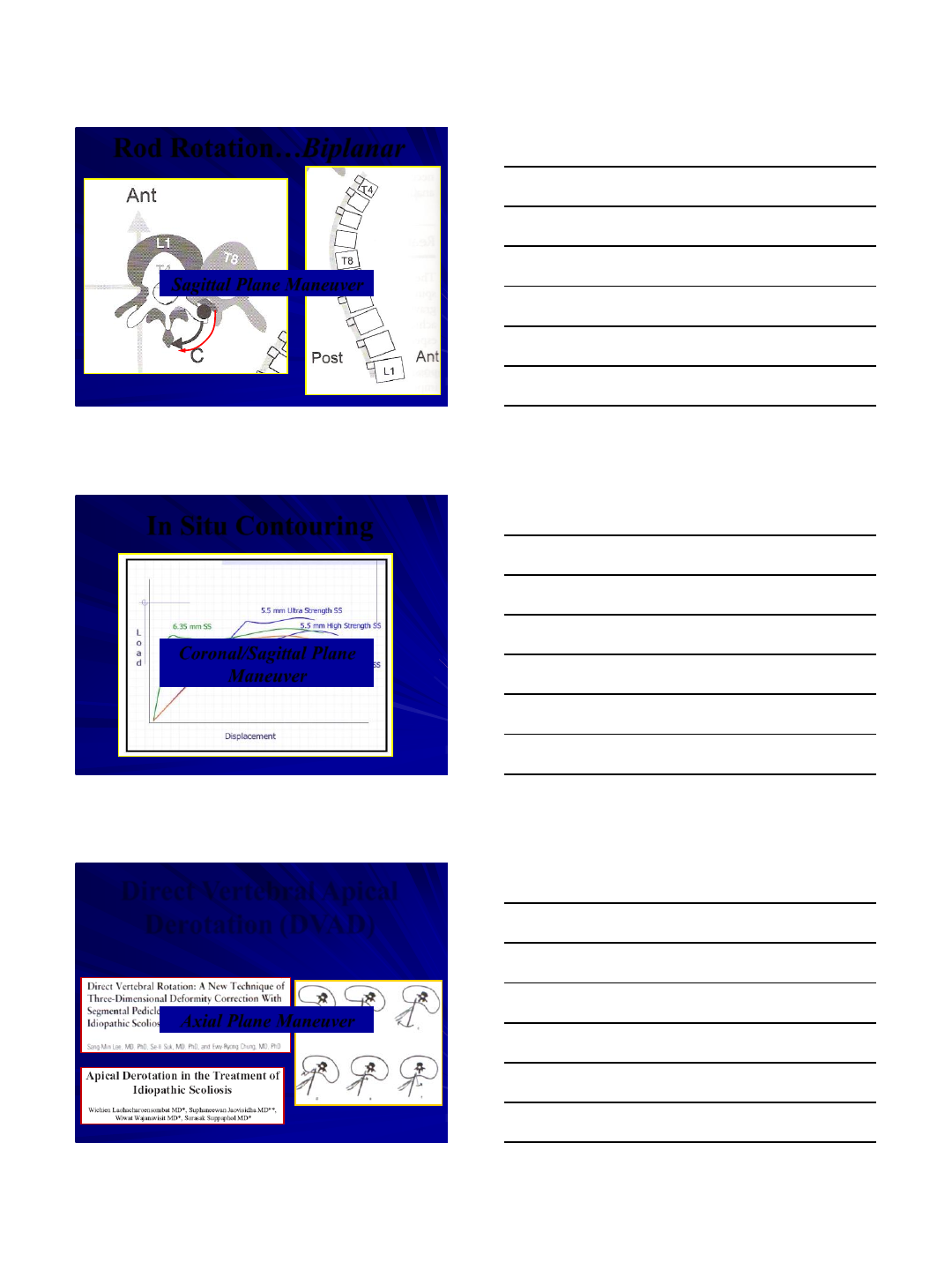
Translation…Uniplanar
Coronal Plane Maneuver
Compression/Distraction…U
niplanar
Coronal Plane Maneuver
(affects sagittal plane)

3/8/2016
3
Rod Rotation…Biplanar
Rod Rotation…Biplanar
Coronal Plane Maneuver
Rod Rotation…Biplanar
3/8/2016
4
Rod Rotation…Biplanar
Sagittal Plane Maneuver
In Situ Contouring
Coronal/Sagittal Plane
Maneuver
Direct Vertebral Apical
Derotation (DVAD)
Axial Plane Maneuver

3/8/2016
5
Direct Vertebral Apical
Derotation (DVAD)
Differential Rod Contouring :
“Newtonian Principle”
Axial Plane Maneuver
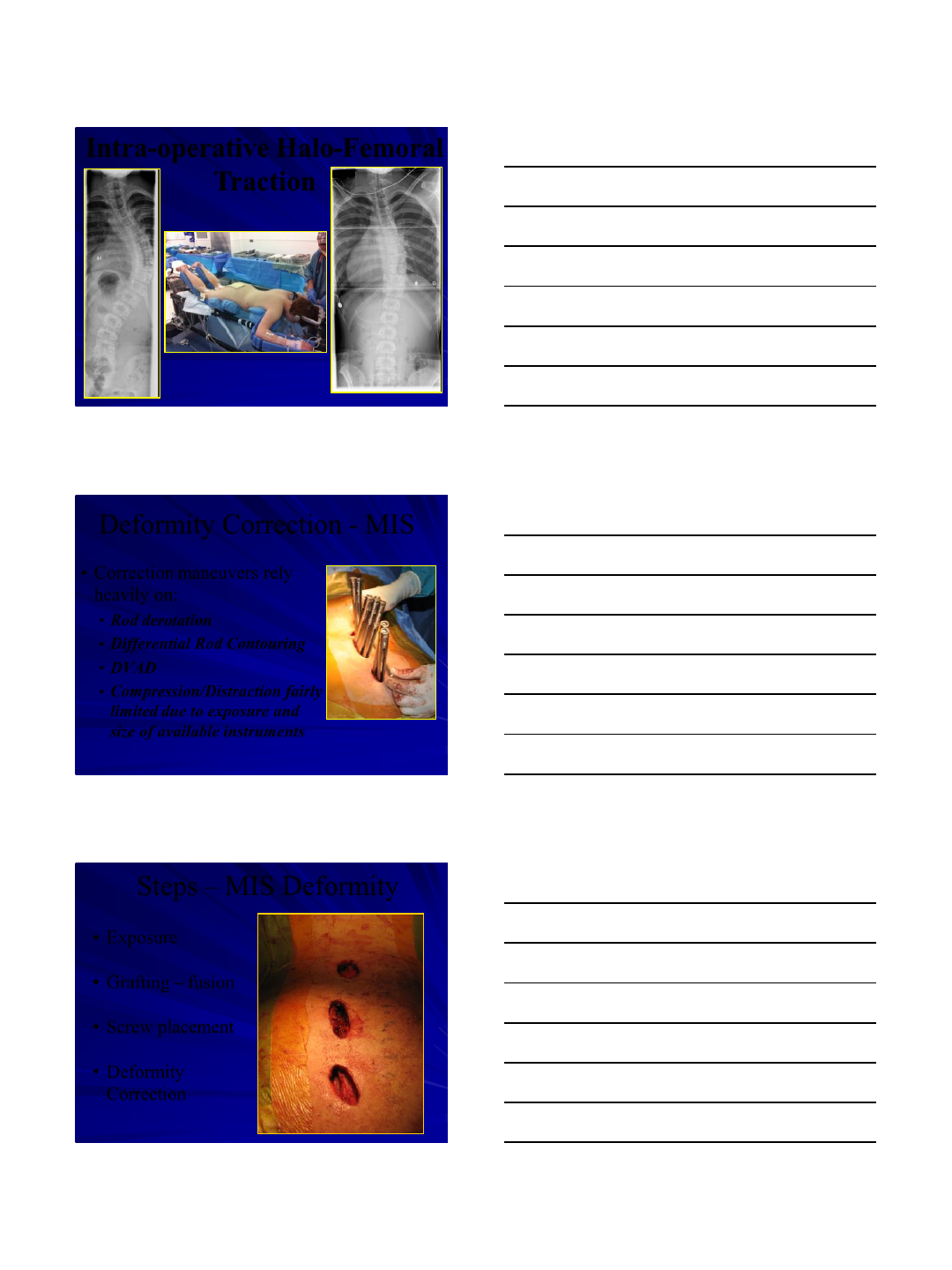
Intra-operative Halo-Femoral
Traction
•Increasingly popular in
open deformity procedures
for large, stiff curves
•Advantage in MIS –
powerful indirect deformity
correction away from
operative field
3/8/2016
6
Intra-operative Halo-Femoral
Traction
•Correction maneuvers rely
heavily on:
•Rod derotation
•Differential Rod Contouring
•DVAD
•Compression/Distraction fairly
limited due to exposure and
size of available instruments
Deformity Correction - MIS
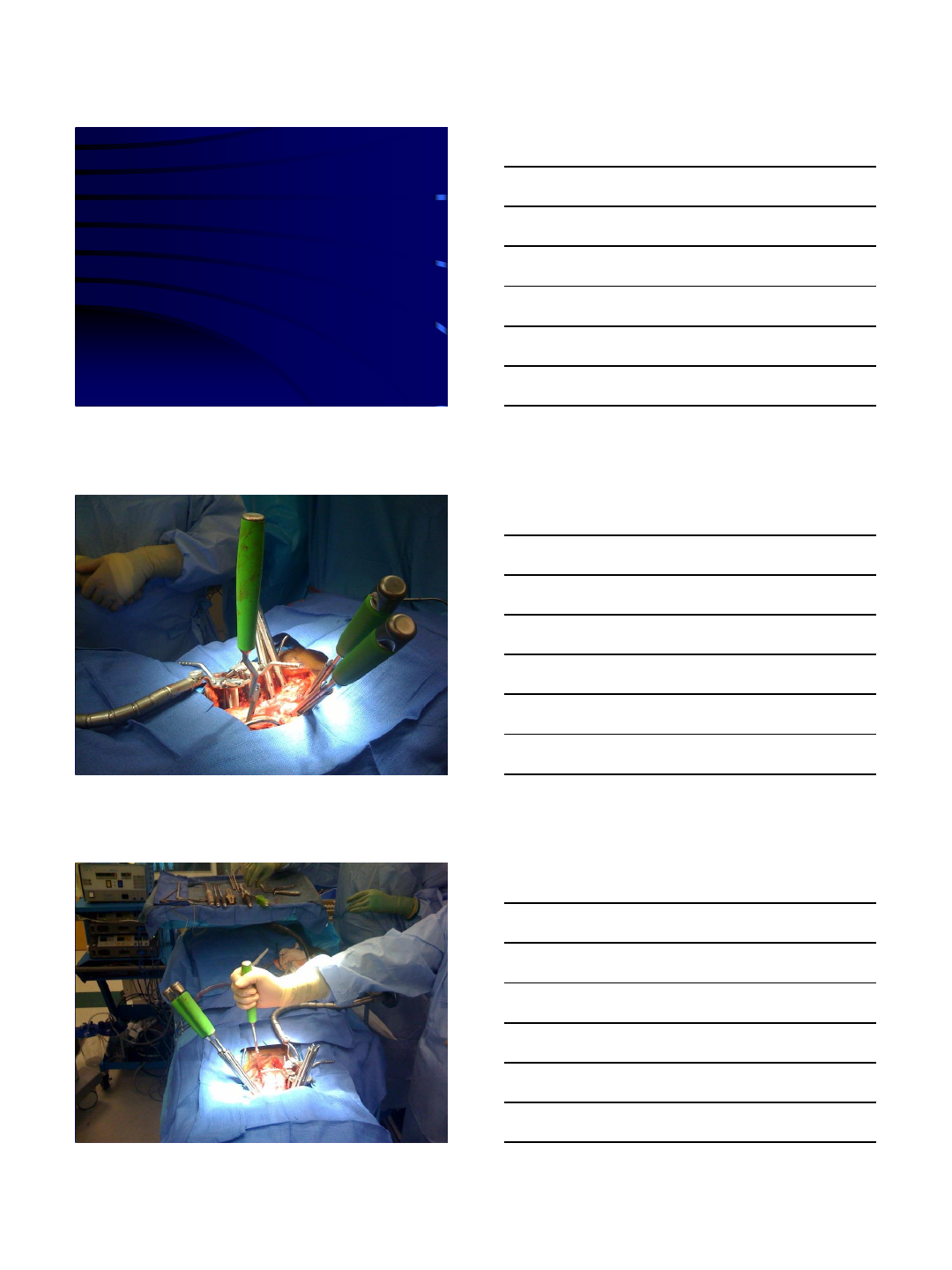
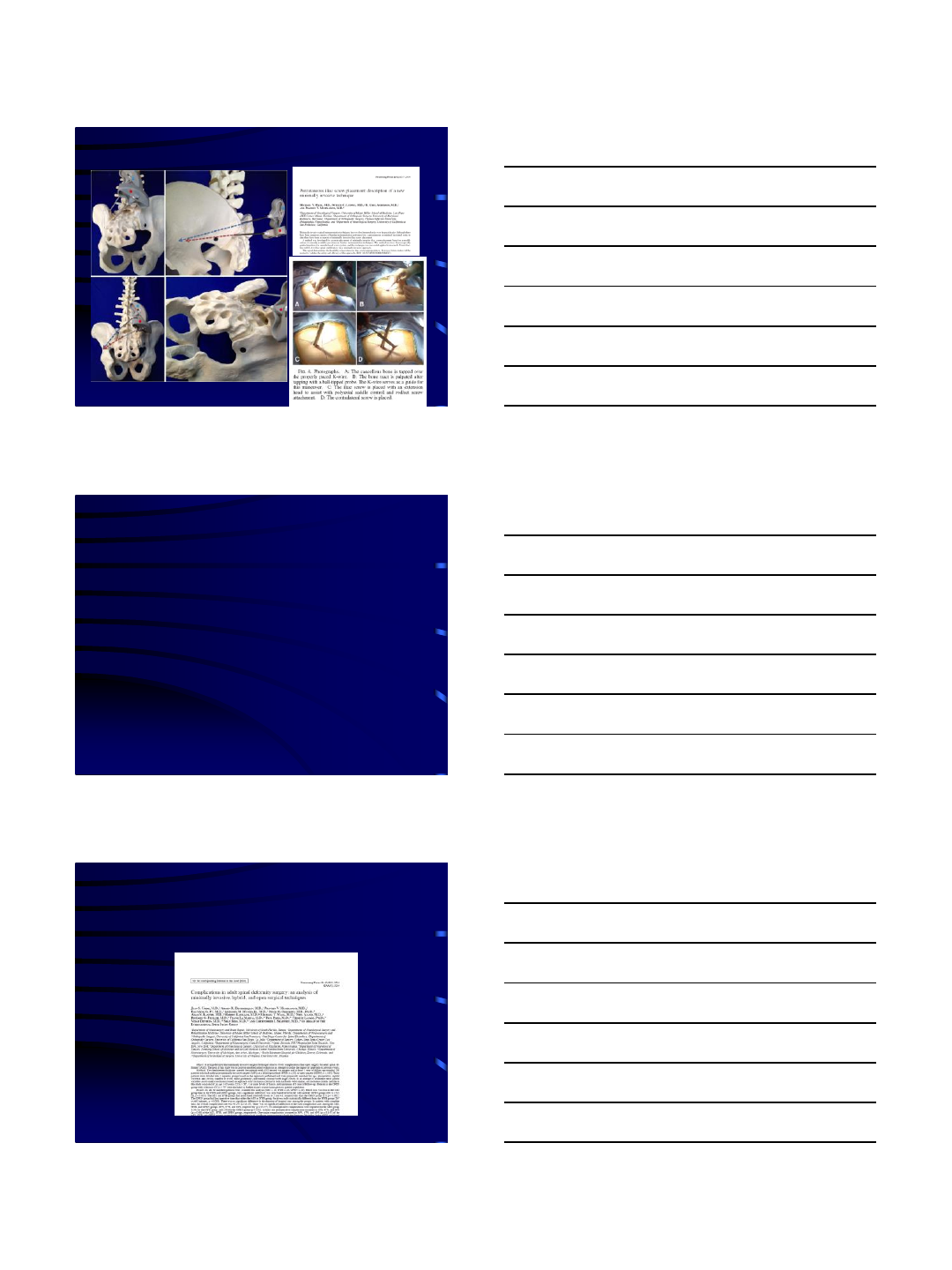
Steps –MIS Deformity
•Exposure
•Grafting –fusion
•Screw placement
•Deformity
Correction
3/8/2016
7
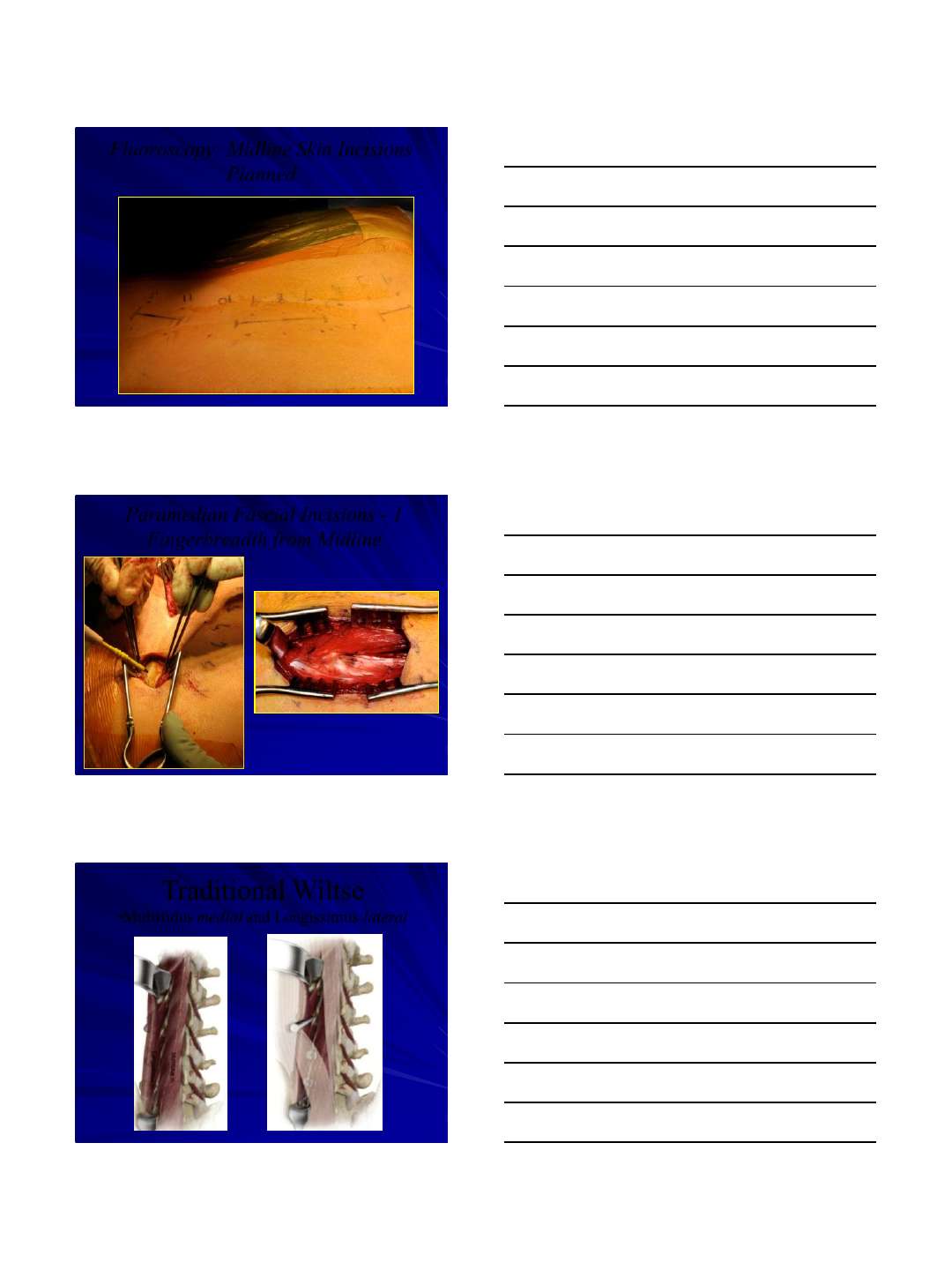
Fluoroscopy: Midline Skin Incisions
Planned
Paramedian Fascial Incisions - 1
Fingerbreadth from Midline
Blunt muscle splitting approach in
line with fibres
Traditional Wiltse
•Multifidus medial and Longissimus lateral
3/8/2016
8
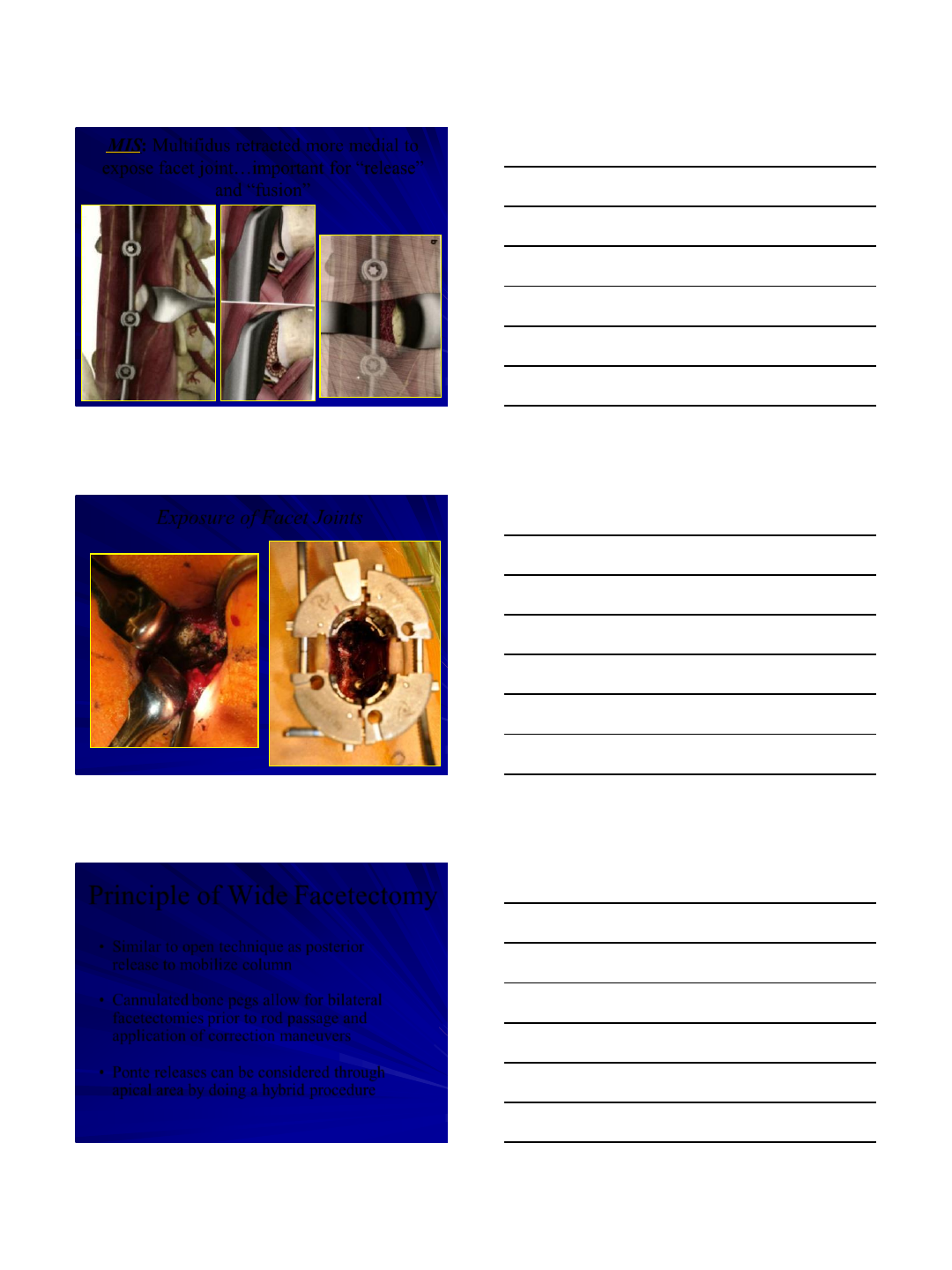
MIS:Multifidus retracted more medial to
expose facet joint…important for “release”
and “fusion”
Exposure of Facet Joints
Principle of Wide Facetectomy
•Similar to open technique as posterior
release to mobilize column
•Cannulated bone pegs allow for bilateral
facetectomies prior to rod passage and
application of correction maneuvers
•Ponte releases can be considered through
apical area by doing a hybrid procedure
3/8/2016
9
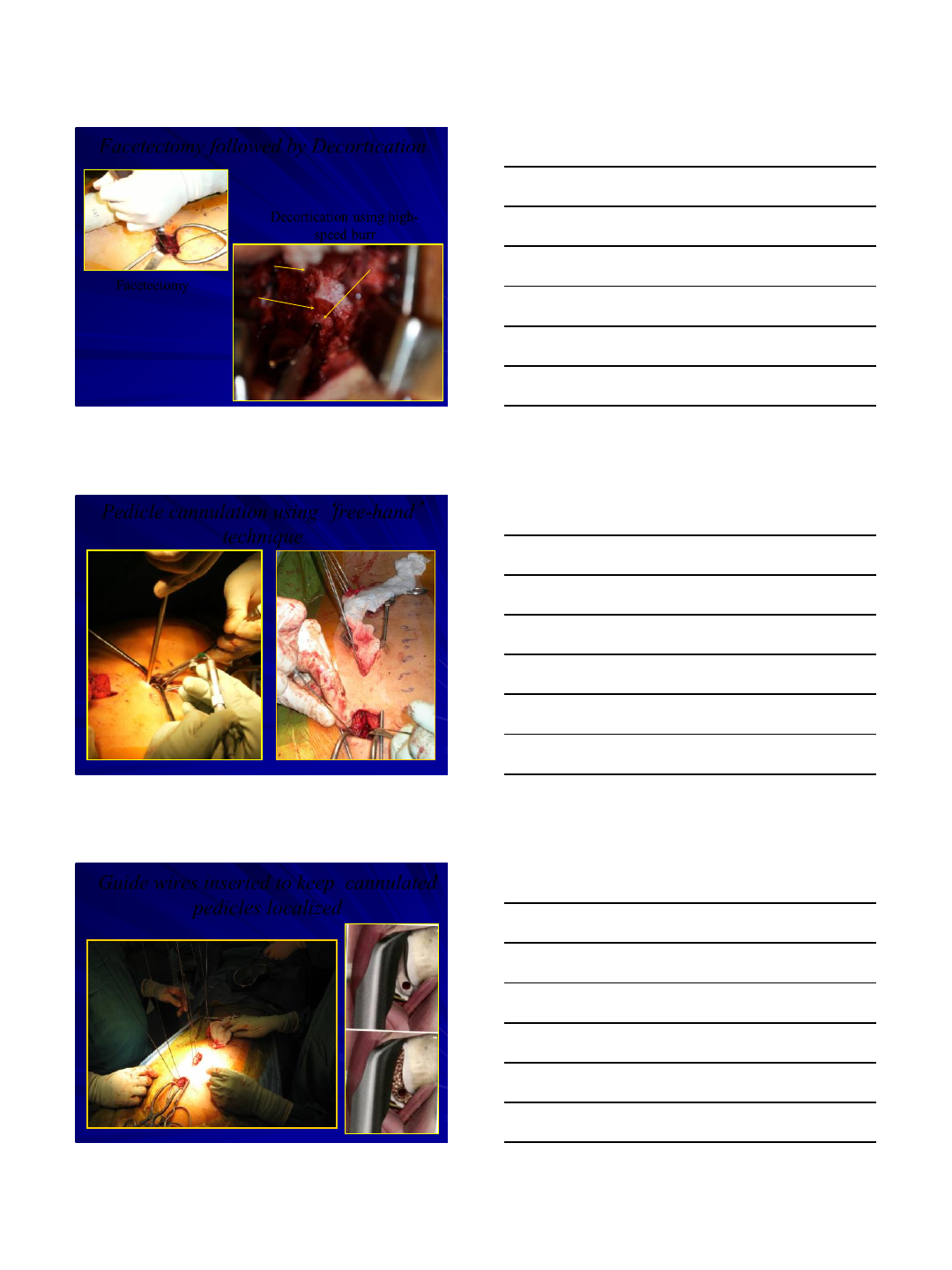
Facetectomy followed by Decortication
Facetectomy
Superior facet
TP
Facetectomy
Decortication using high-
speed burr
Pedicle cannulation using
‘
free-hand
’
technique
Guide wires inserted to keep cannulated
pedicles localized
3/8/2016
10
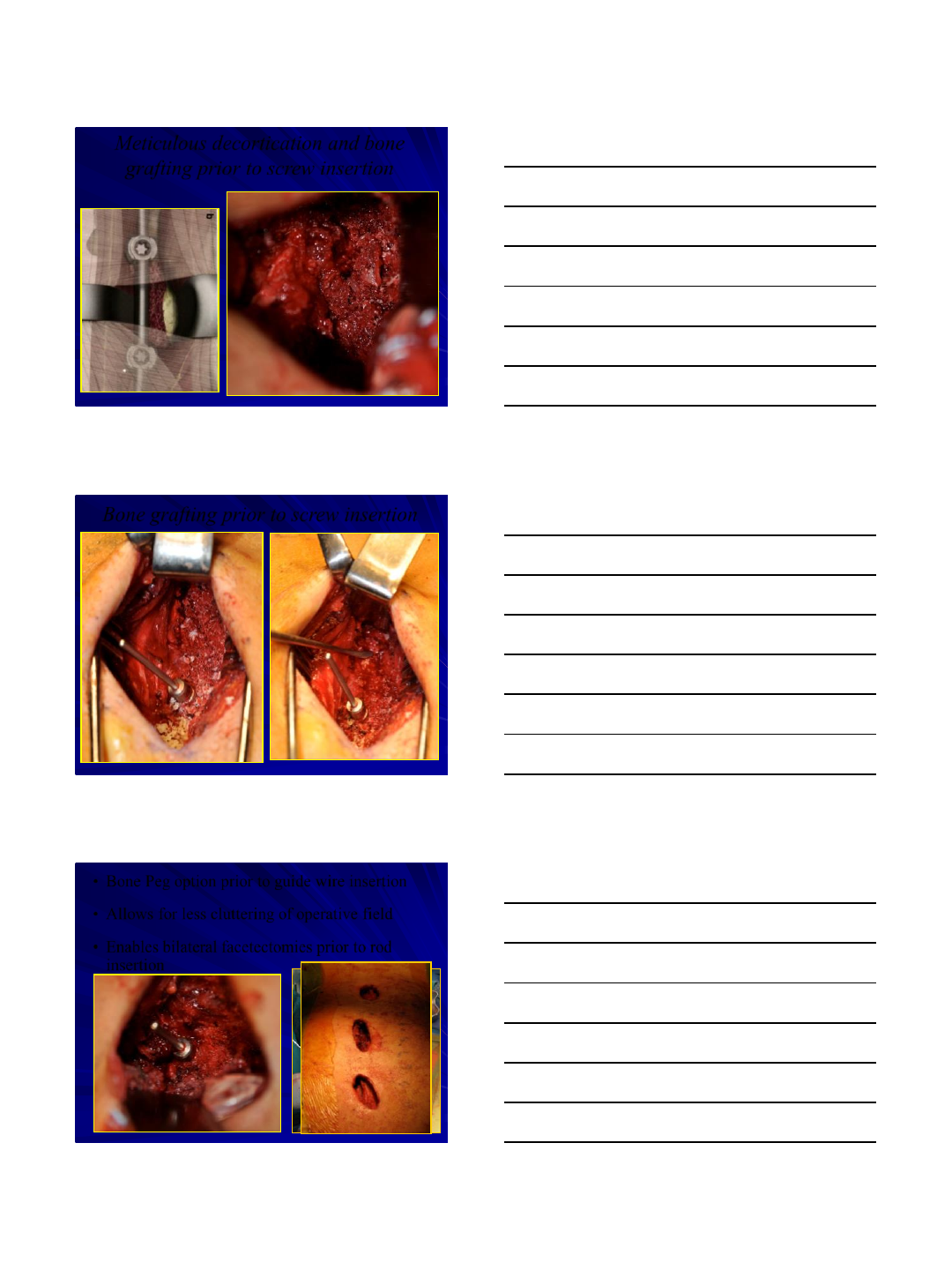
Meticulous decortication and bone
grafting prior to screw insertion
Bone grafting prior to screw insertion
•Bone Peg option prior to guide wire insertion
•Allows for less cluttering of operative field
•Enables bilateral facetectomies prior to rod
insertion
3/8/2016
11
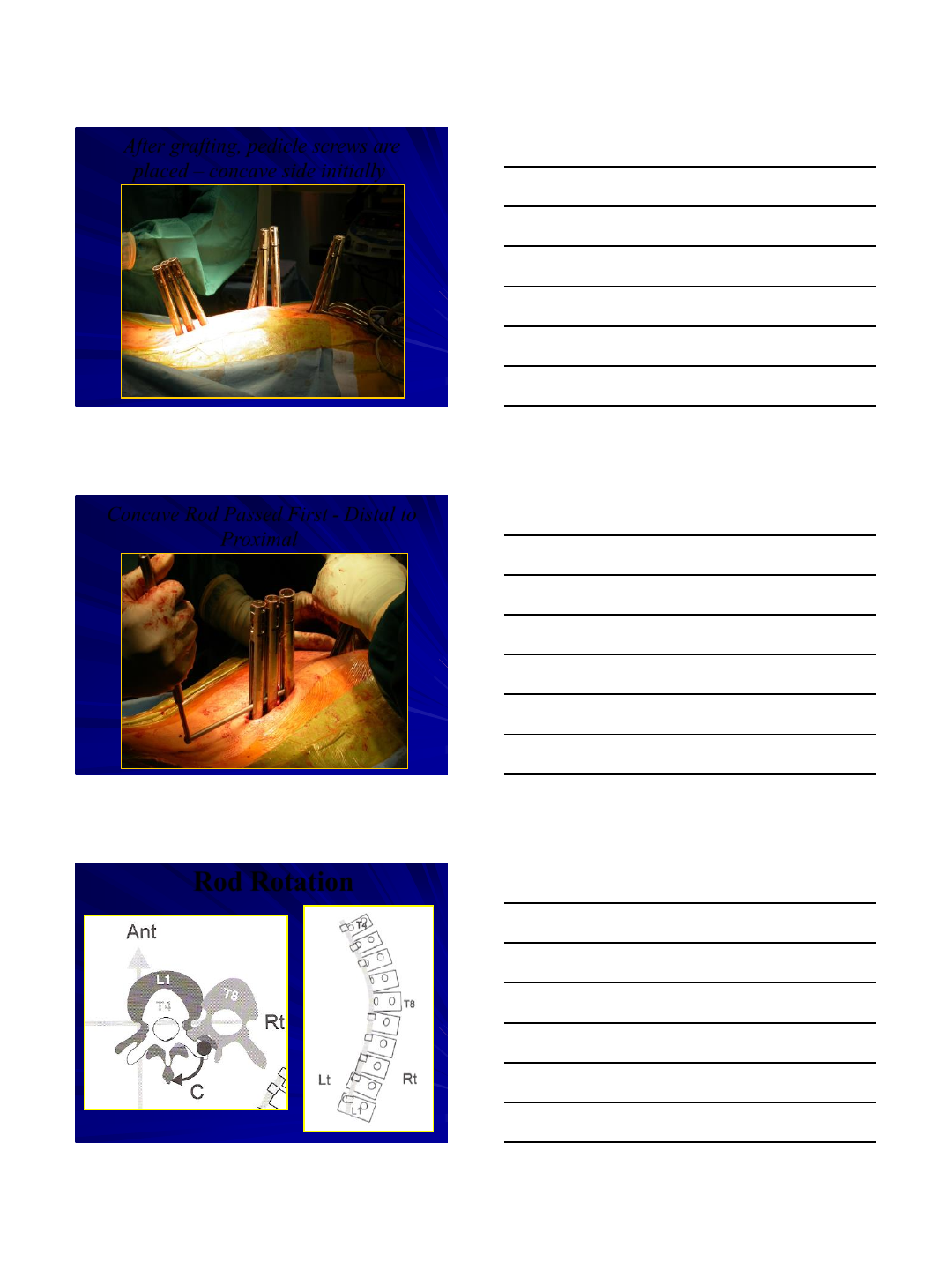
After grafting, pedicle screws are
placed –concave side initially
Concave Rod Passed First - Distal to
Proximal
Rod Rotation
3/8/2016
12
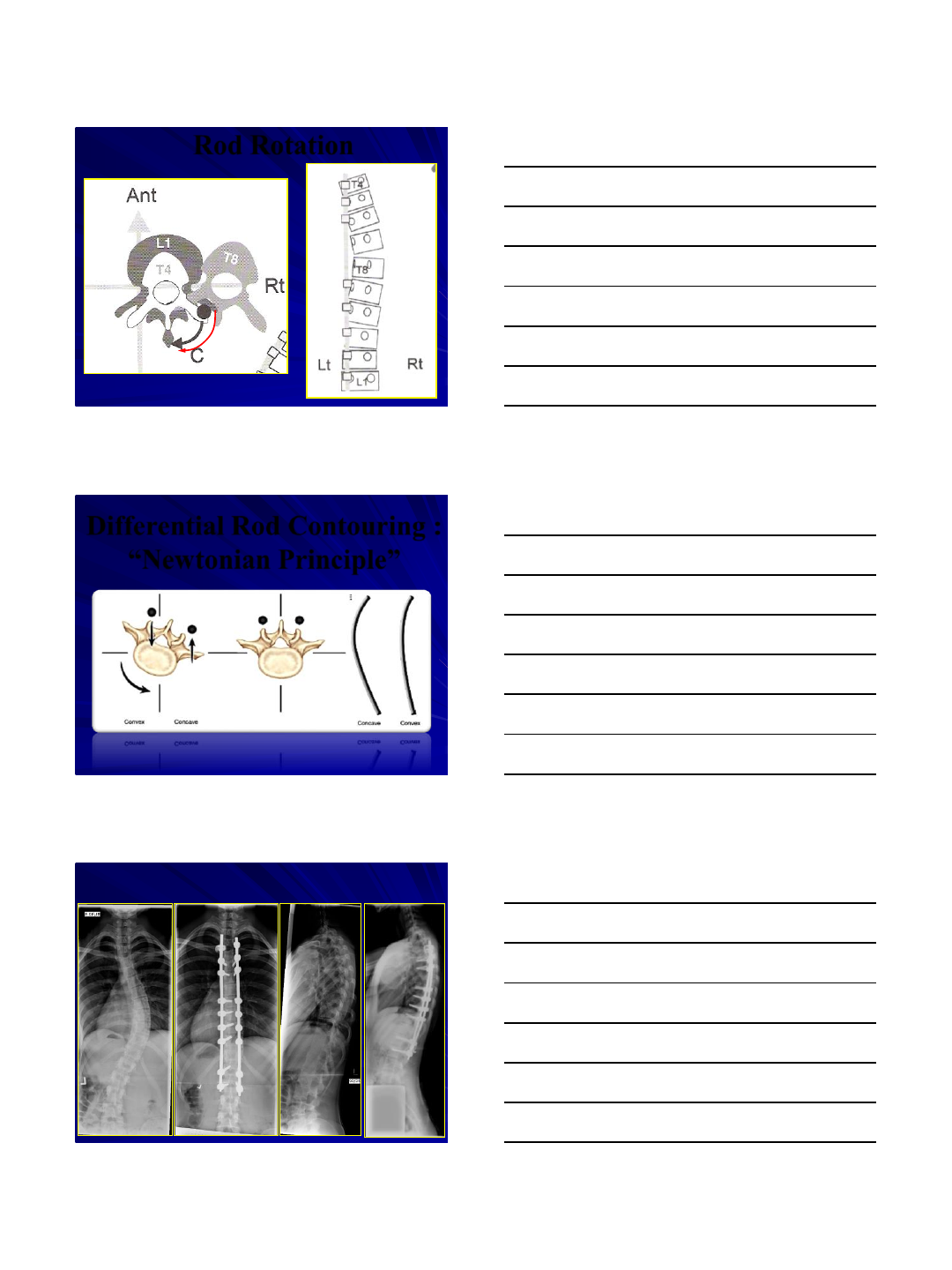
Rod Rotation
Differential Rod Contouring :
“Newtonian Principle”
3/8/2016
13
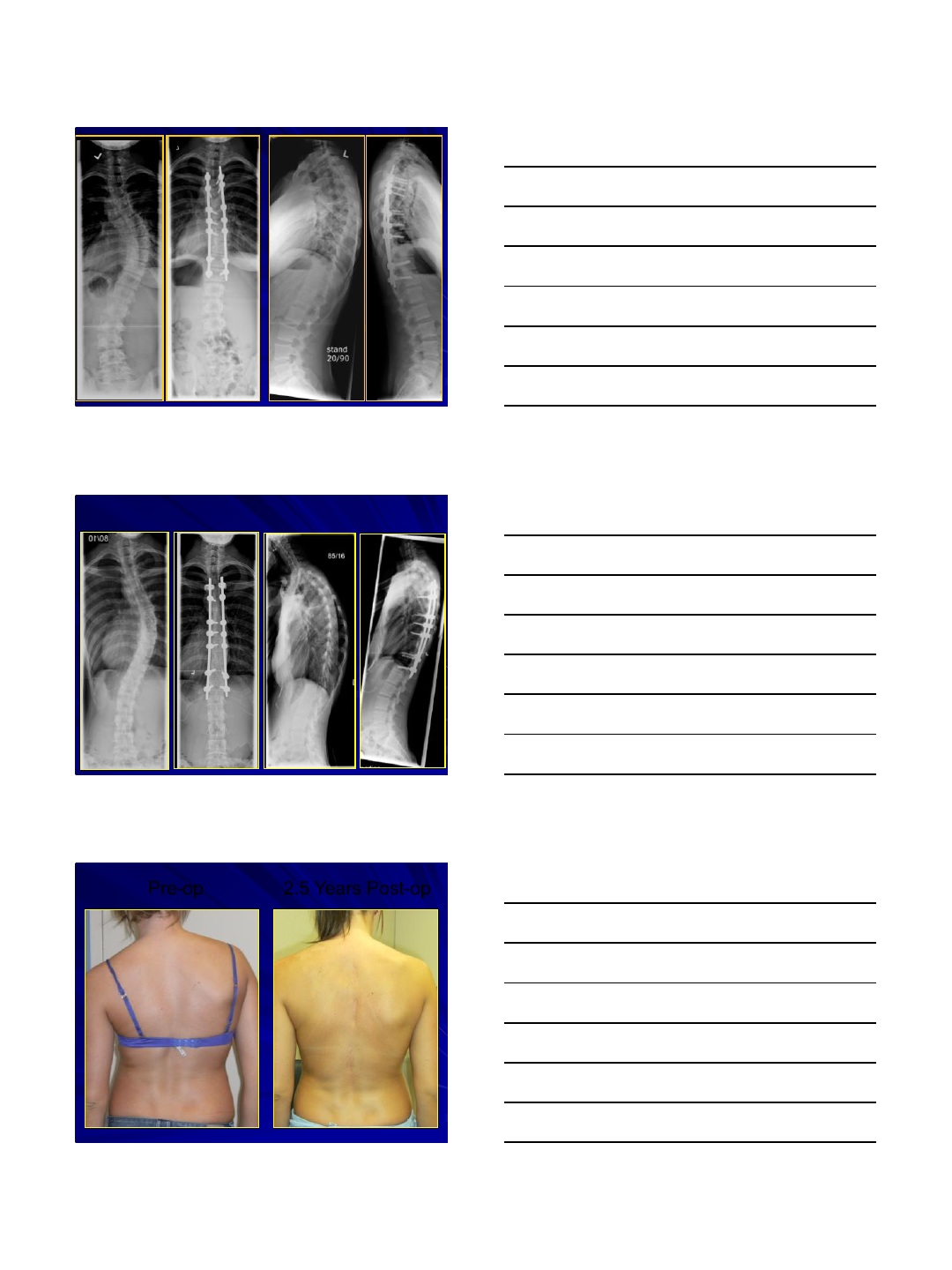
Pre-op 2.5 Years Post-op
3/8/2016
14
2.5 Years Post-op
Pre-op
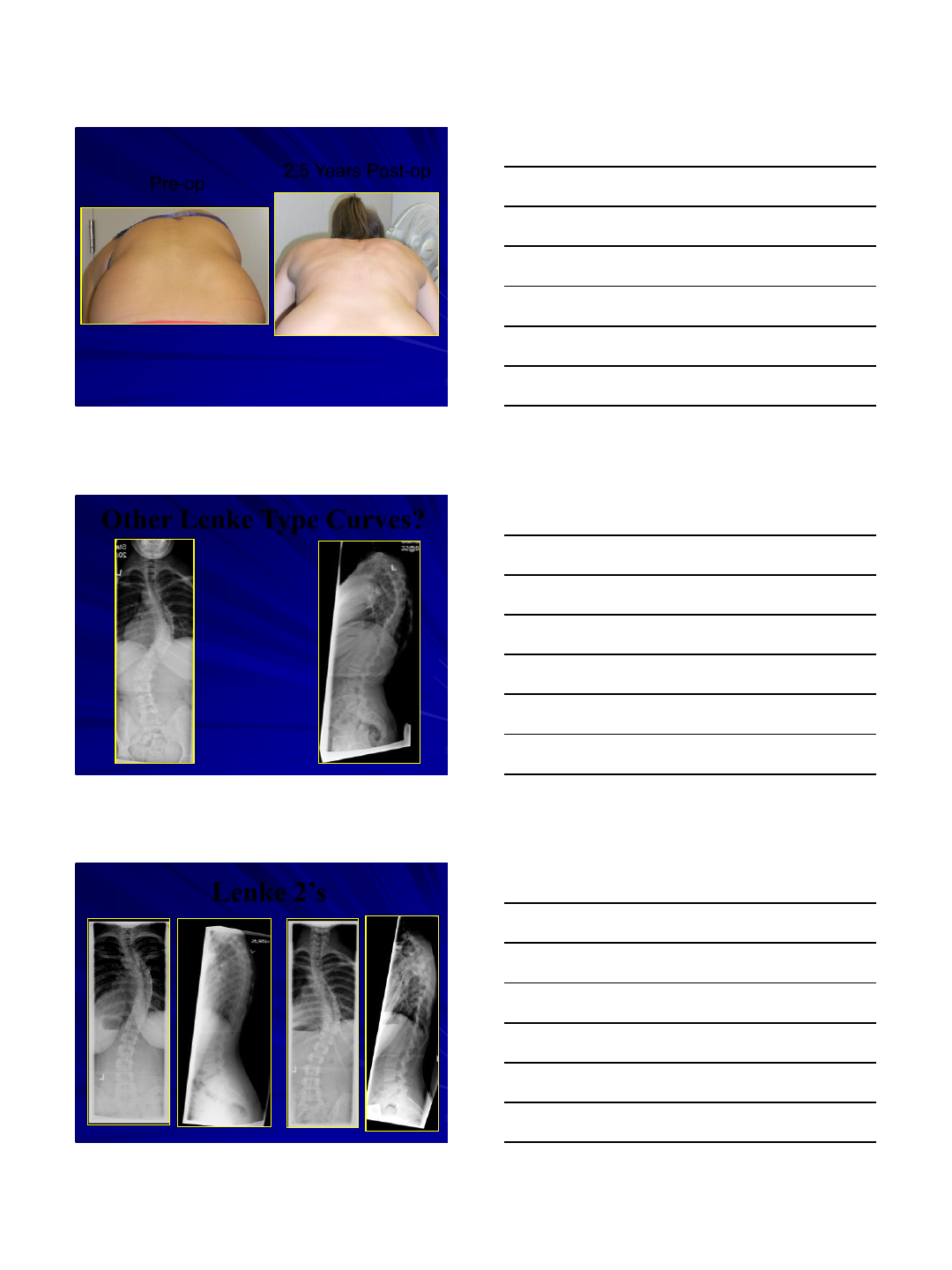
Other Lenke Type Curves?
Lenke 2’s
3/8/2016
15
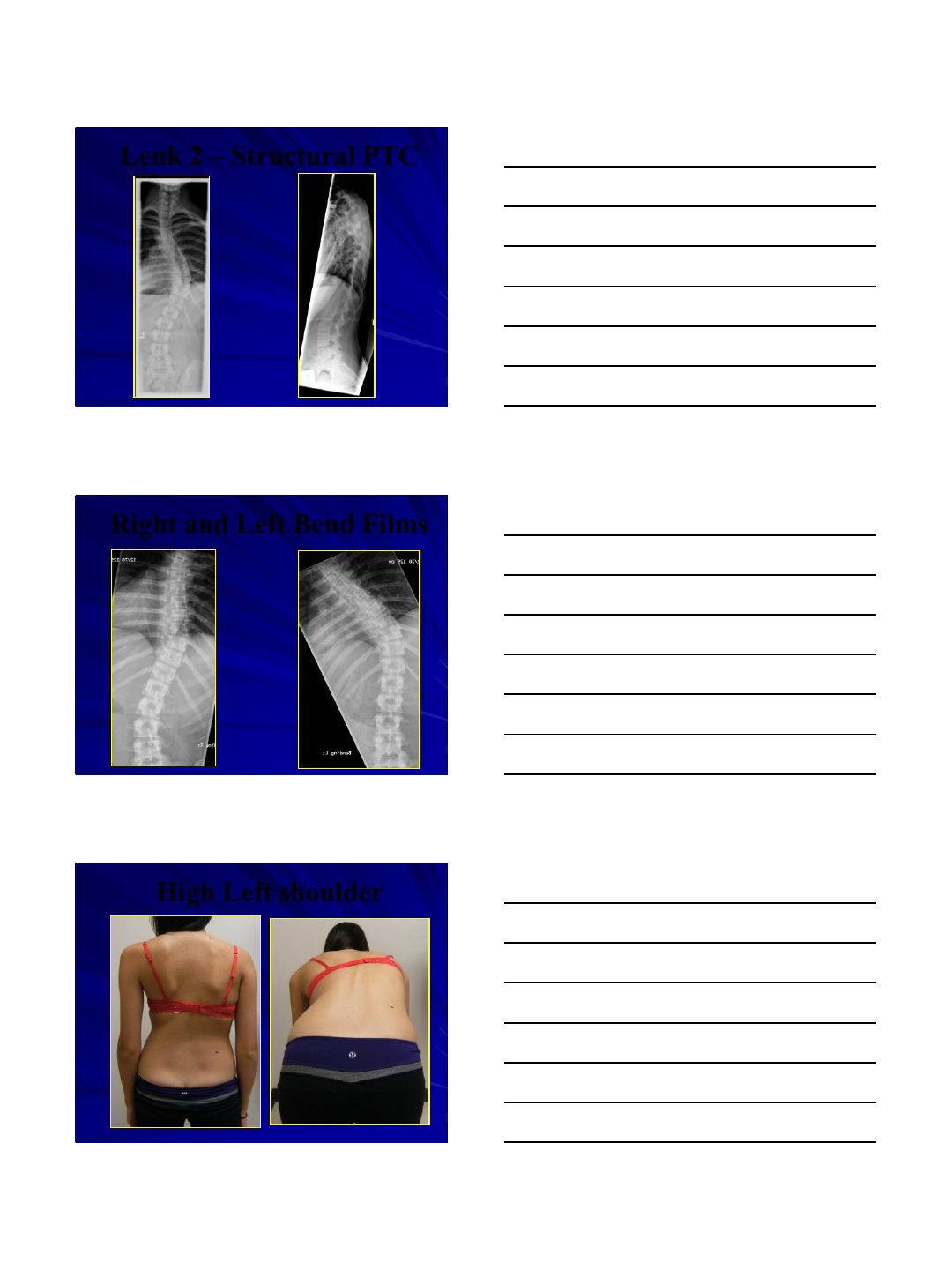
Lenk 2 –Structural PTC
Right and Left Bend Films
High Left shoulder
3/8/2016
16
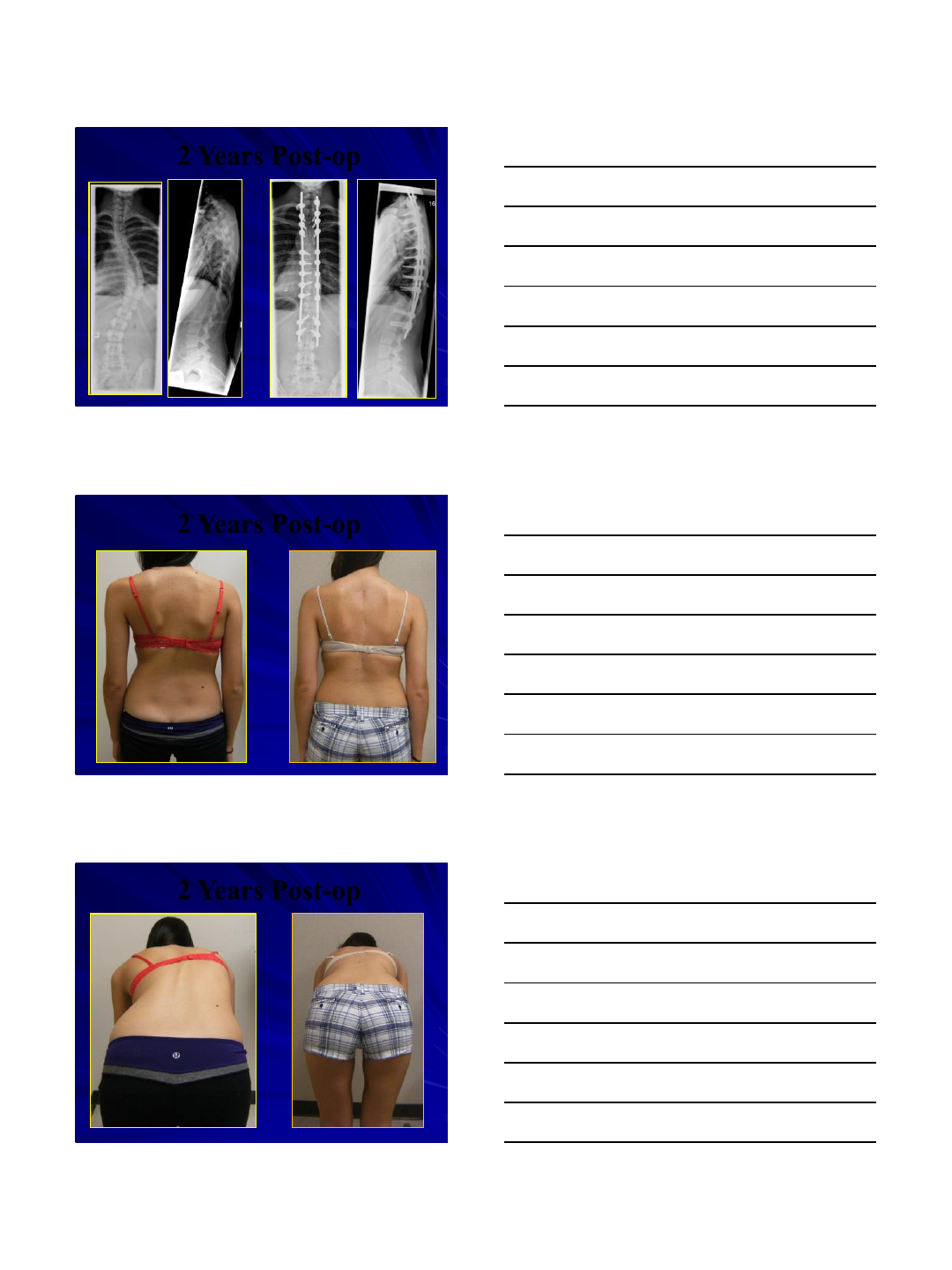
2 Years Post-op
2 Years Post-op
2 Years Post-op
3/8/2016
17
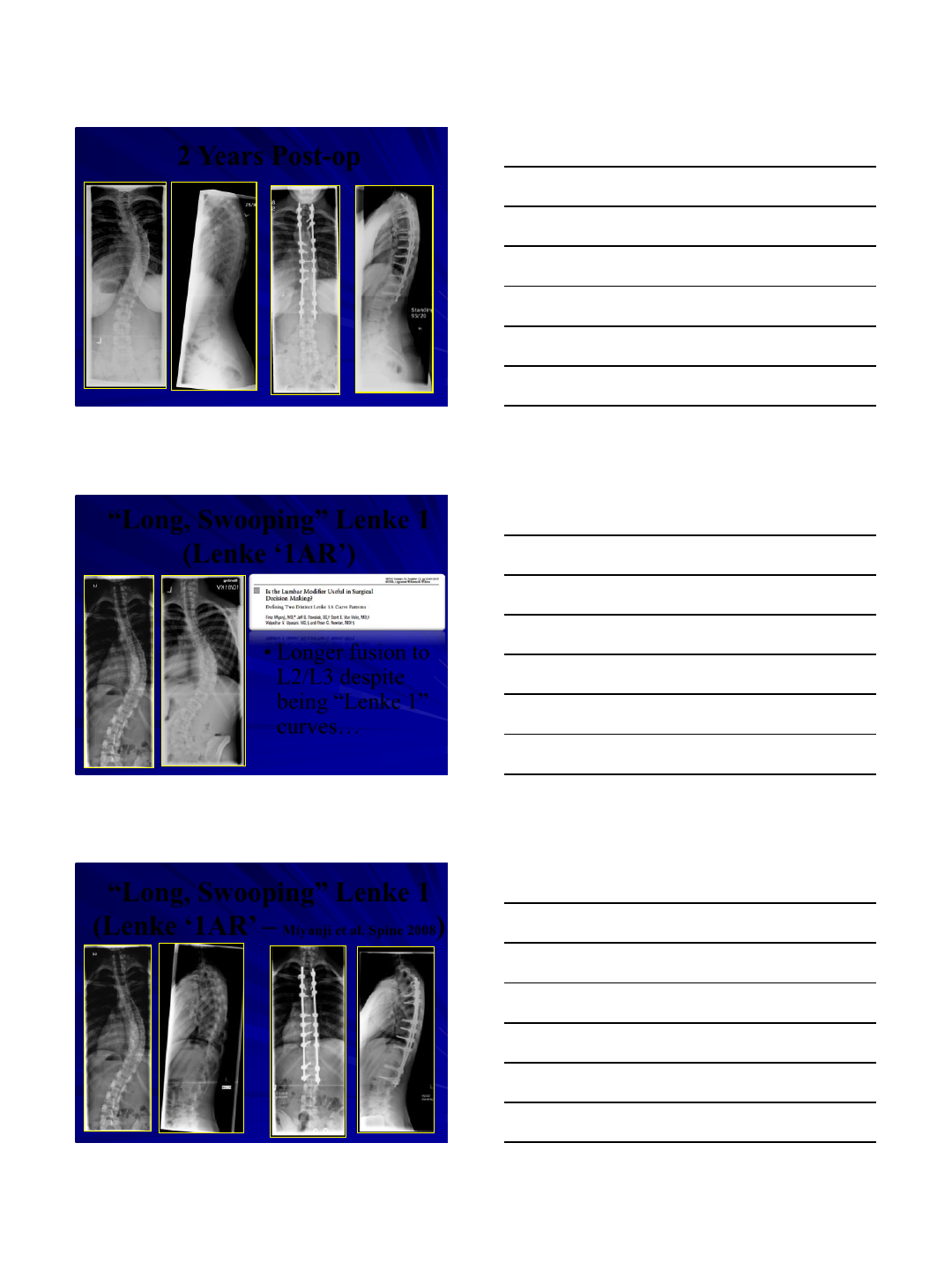
2 Years Post-op
“Long, Swooping” Lenke 1
(Lenke ‘1AR’)
•Longer fusion to
L2/L3 despite
being “Lenke 1”
curves…
“Long, Swooping” Lenke 1
(Lenke ‘1AR’ – Miyanji et al. Spine 2008)
3/8/2016
18
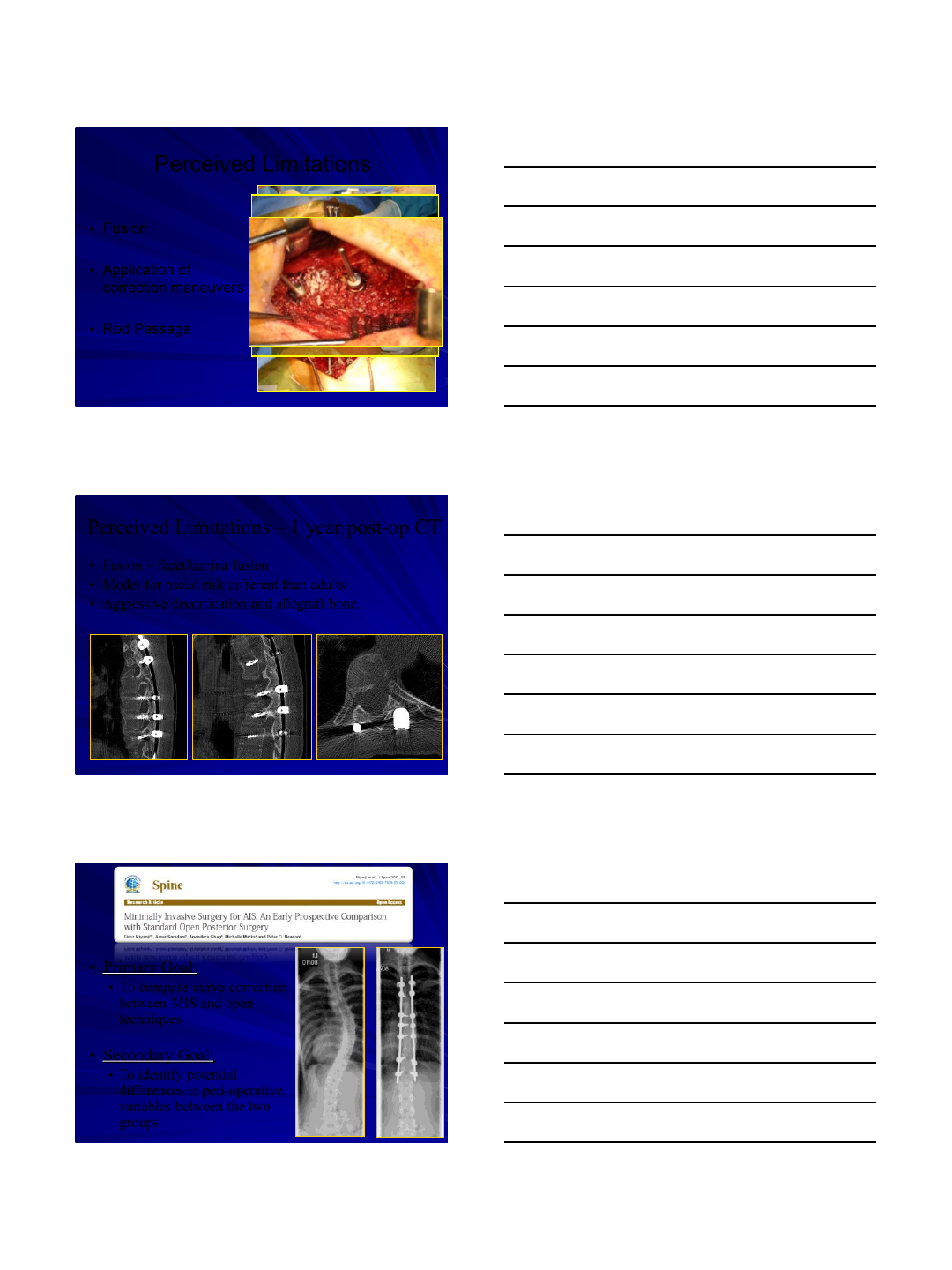
Perceived Limitations
•Fusion
•Application of
correction maneuvers
•Rod Passage
Perceived Limitations –1 year post-op CT
•Fusion –facet/lamina fusion
•Model for pseud risk different than adults
•Aggressive decortication and allograft bone.
•Primary Goal:
•To compare curve correction
between MIS and open
techniques
•Secondary Goal:
•To identify potential
differences in peri-operative
variables between the two
groups
3/8/2016
19
Results
MIS
OPEN
Demographics
Gender M:F
2:14
1:15
Lenke Class (n)
1(8); 2(5);
3(2); 4(1)
1(9); 2(2);
3(3); 4(1);
6(1)
Mean
SD
Mean
SD
Age (yrs)
16.8
1.2
16.4
1.2
BMI
21
3
22
4
Risser
4.5
0.5
4.5
0.5
Pre Op Major Cobb
56
5
56
8
Primary Outcome
Mean
SD
Mean
SD
95% CI
Lower
95% CI
Upper
Post-Op Major Cobb
20
8
18
4
-2.4
7.2
Post-Op Thoracic
Kyphosis (T5-T12)
21
9
17
5
-1.7
9.4
Percent Curve
Correction
63%
13
68%
8
-0.12
0.04
Secondary Variables
Mean
SD
Mean
SD
95% CI
Lower
95% CI
Upper
OR Time (min)
444
89
350
76
34.8
154.0
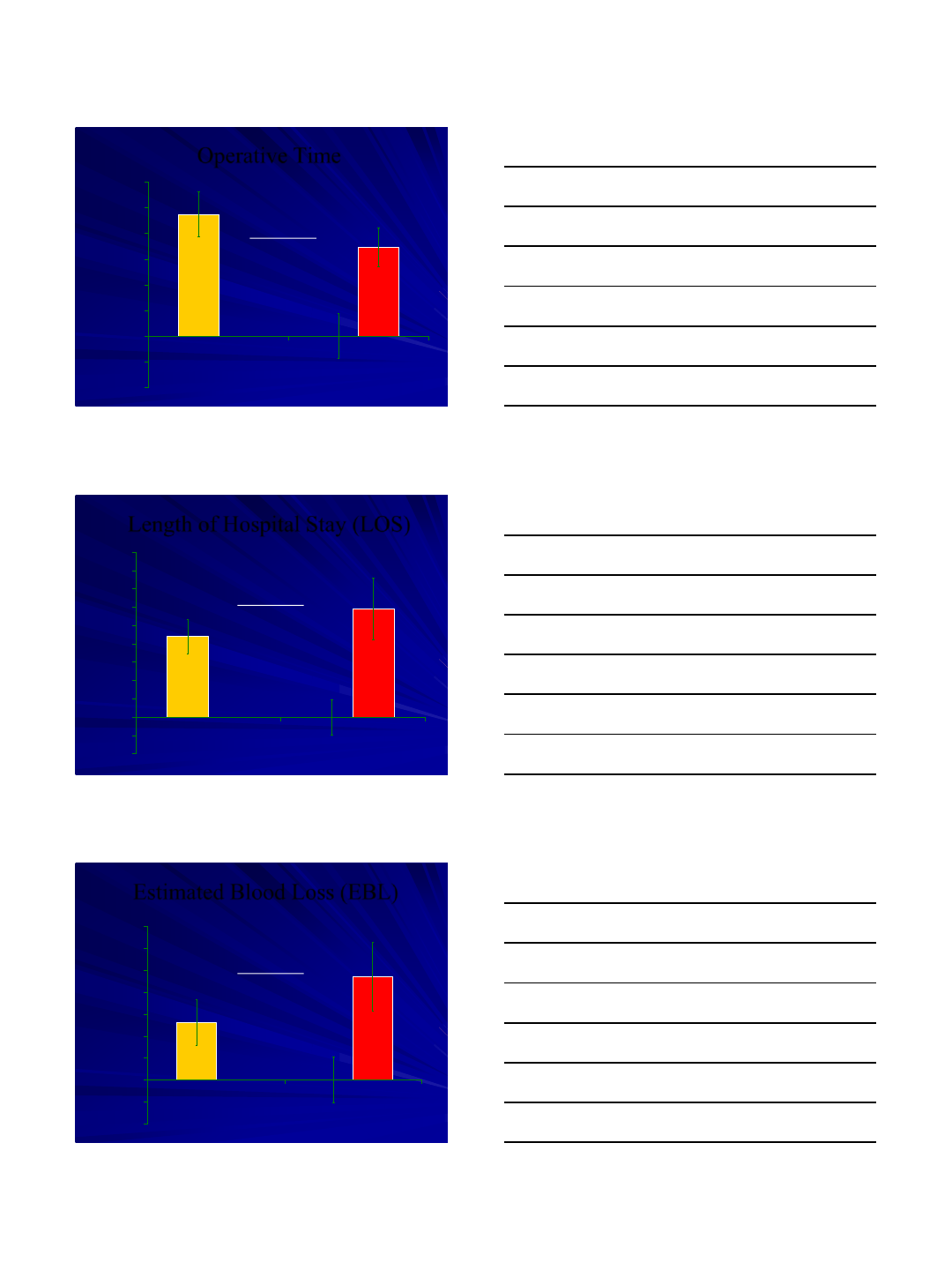
EBL (ml)
277
105
388
158
-207.8
-14.1
LOS (days)
4.63
.96
6.19
1.68
-2.6
-0.6
Conclusions
Perceived Limitations
•Prospective and long-term studies are critical to
evaluate possible limitations and to demonstrate
the true clinical benefits of minimally invasive
surgery in the setting of deformity
3/8/2016
20
Results
Patient Demographics MIS (n=23) PSIF (n=23)
Gender M:F 3:20 4:19
Lenke Class (n) 1: 20
2: 2
4: 1
1: 12
2: 8
3:3
Mean Age (yrs) 16.8±0.40
(14-20) 16.4±0.28
(13-19)
Mean Weight (kg) 59.1±1.74
(43-72) 56.4±1.57
(44.6-76.2)
Mean Preop Major Cobb
(°)56.7±1.62
(45-77) 58.1±1.57
(46-71)
Mean Preop Lat (T5-T12) 20.5±2.08
(-2-39) 22.6±3.38
(-4-54)
No. of Fusion Levels 10.2 12.2
Peri-op Outcomes
3/8/2016
21
Operative Time
-200
-100
0
100
200
300
400
500
600
MIS OPEN
OR Time (min)
P= 0.000
Length of Hospital Stay (LOS)
-2
-1
0
1
2
3
4
5
6
7
8
9
MIS OPEN
Number of Days
P= 0.000
Estimated Blood Loss (EBL)
-200
-100
0
100
200
300
400
500
600
700
MIS OPEN
ml
P= 0.000
3/8/2016
22
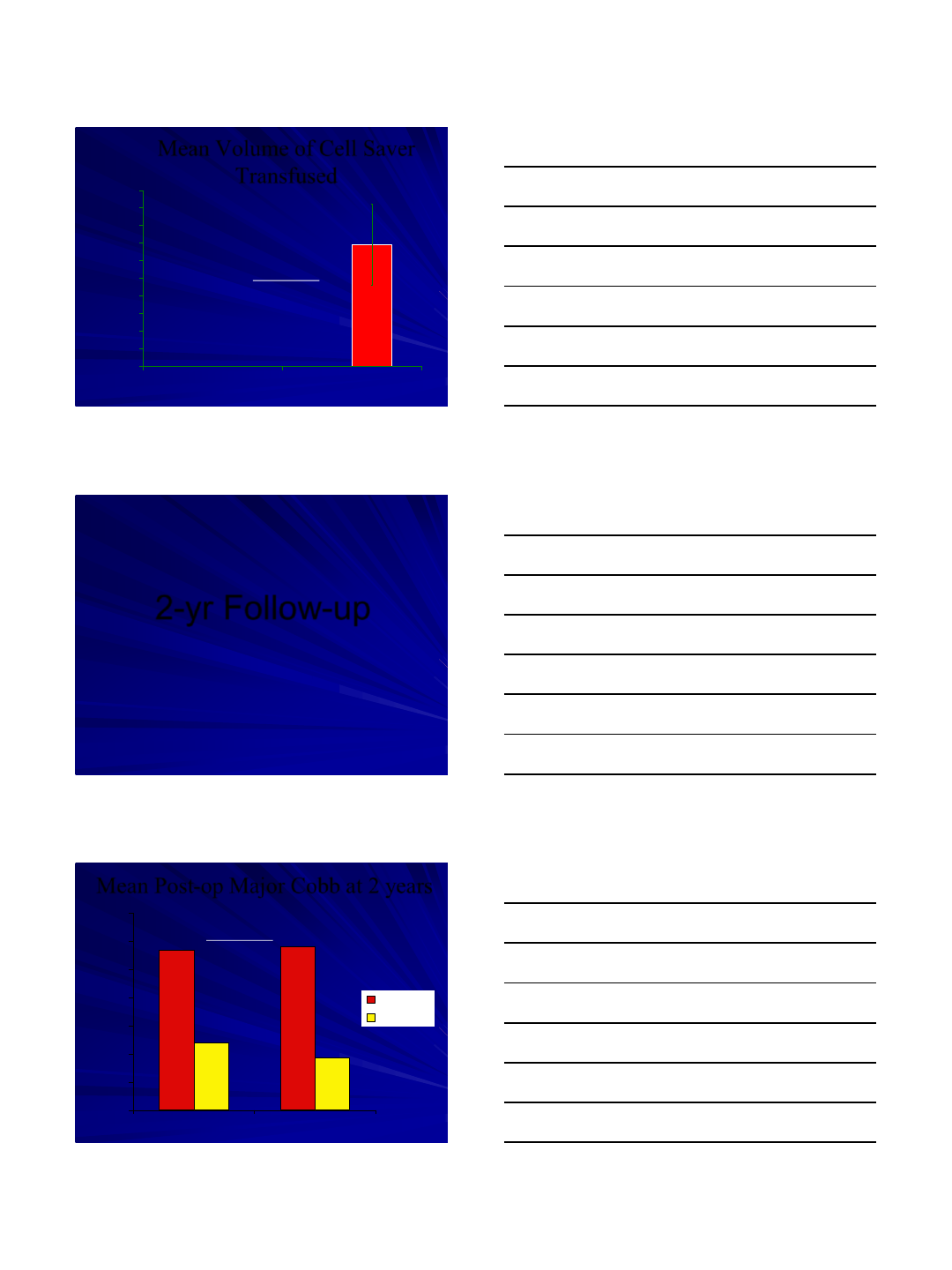
Mean Volume of Cell Saver
Transfused
0
10
20
30
40
50
60
70
80
90
100
MIS OPEN
ml
P= 0.005
69.0
0
2-yr Follow-up
Mean Post-op Major Cobb at 2 years
0
10
20
30
40
50
60
70
MIS OPEN
Major Cobb (degrees)
Pre-op
Post-op
58.1% 68%
P= 0.017
3/8/2016
23
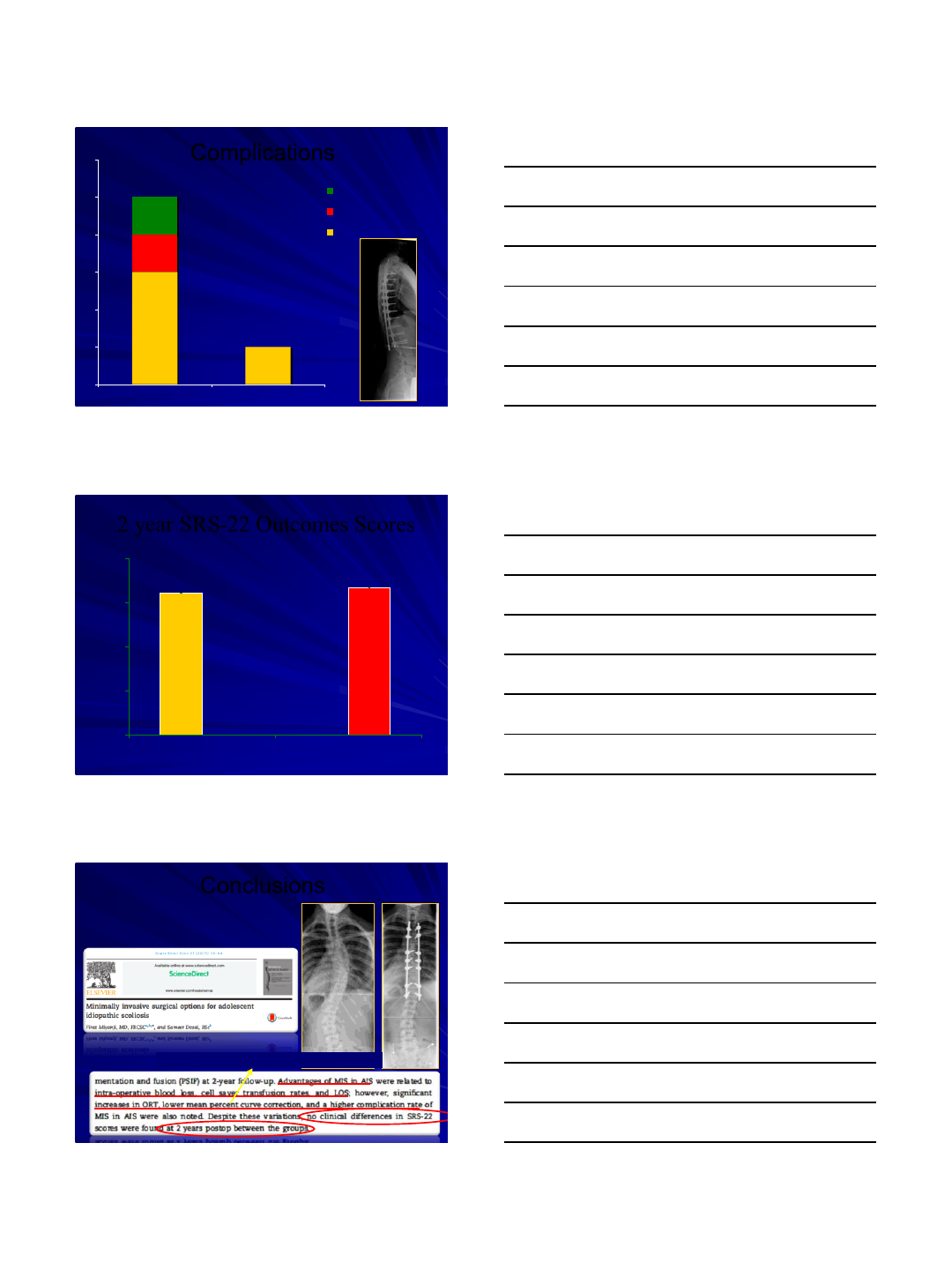
Complications
0
1
2
3
4
5
6
MIS OPEN
Pseudarthrosis
Hardware Failure
Infection
P= 0.08
21.7%
4.3%
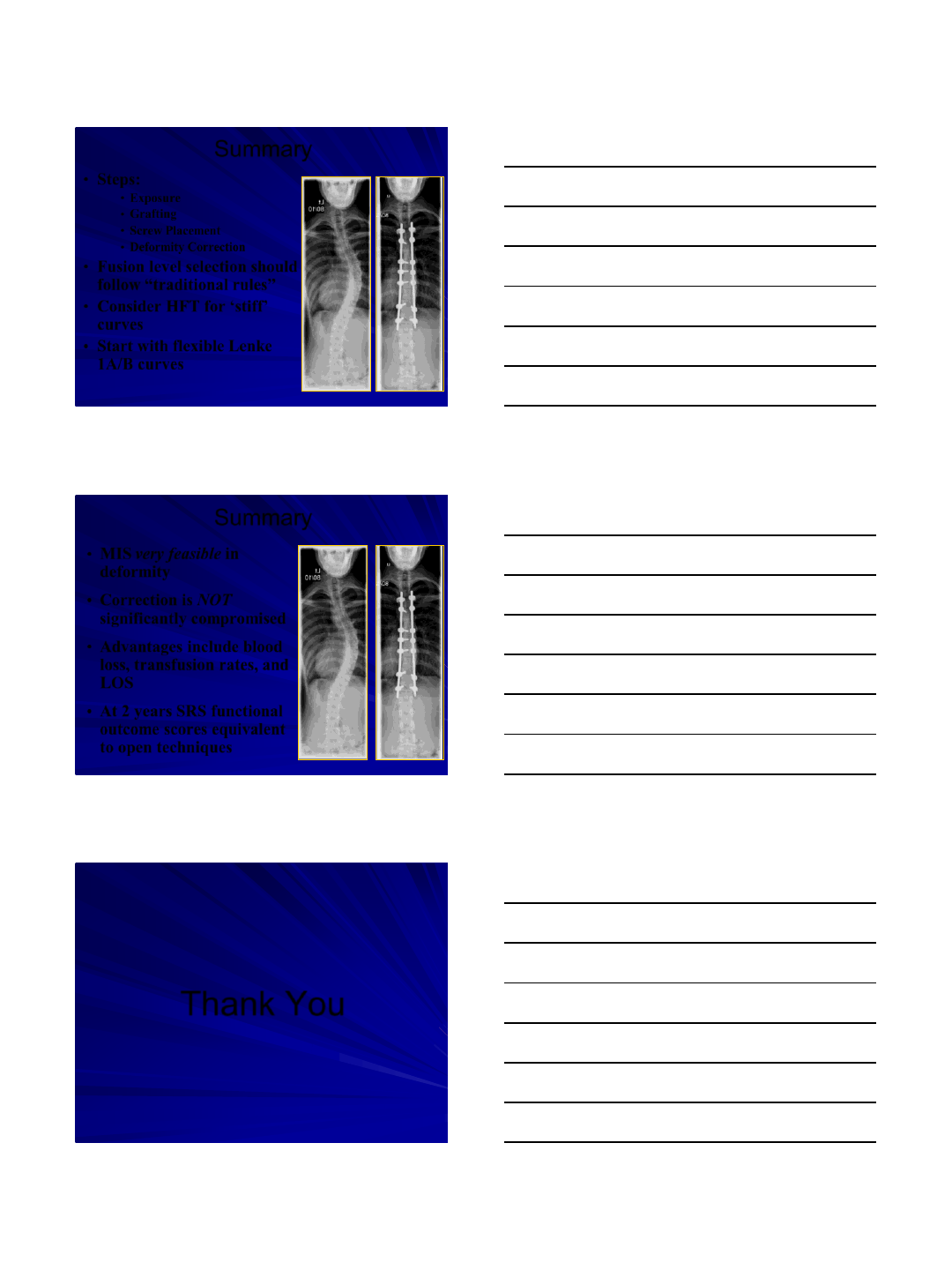
2 year SRS-22 Outcomes Scores
1
2
3
4
5
MIS OPEN
ml
P= 0.715
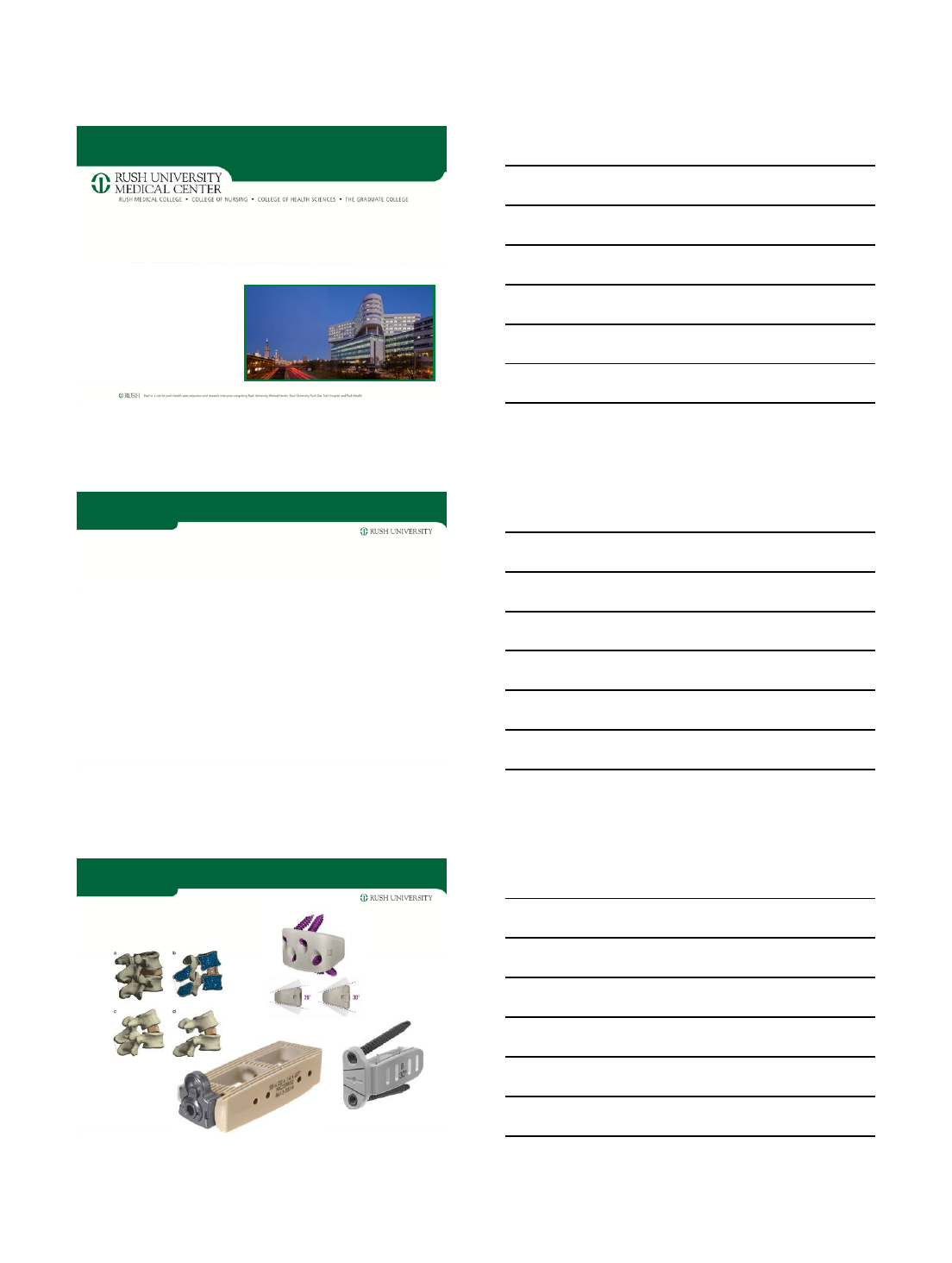
Conclusions
Mean 5.2°difference –Clinical significance?
3/8/2016
24
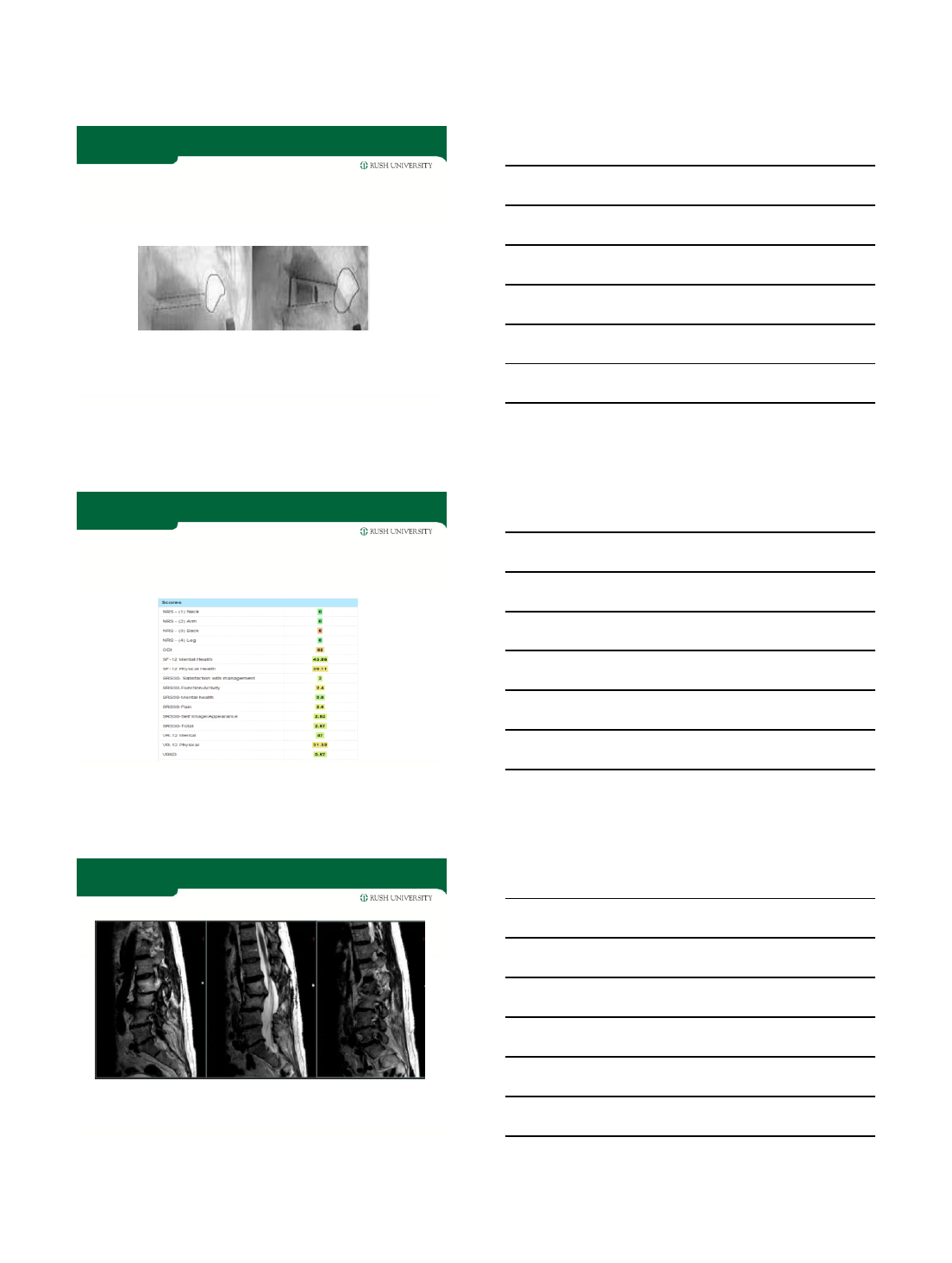
Summary
•Steps:
•Exposure
•Grafting
•Screw Placement
•Deformity Correction
•Fusion level selection should
follow “traditional rules”
•Consider HFT for ‘stiff’
curves
•Start with flexible Lenke
1A/B curves
Summary
•MIS very feasible in
deformity
•Correction is NOT
significantly compromised
•Advantages include blood
loss, transfusion rates, and
LOS
•At 2 years SRS functional
outcome scores equivalent
to open techniques
Thank You
3/14/2016
1
EMERGING TRENDS
IN
MIS DEFORMITY SURGERY
Richard G. Fessler, MD, PhD
Professor
Department of Neurosurgery
Rush University Medical Center
CATEGORIES
•DEVICES
–Hyperlordotic cages
–Patient specific pre-contoured rods
–“Growing” rods for MIS
•BIOLOGICS
–Non-BMP fusion augmentation
•TECHNIQUE
–Expandable disc space distractors
–Sectioning the ALL
–Technique for bending rods into lordosis
•PLANNING
–Computer programs for optimal correction 2
DEVICES
•HYPERLORDOTIC CAGES
3/14/2016
2
Recent modifications
•65 yo male with 20 years of worsening back pain s/p L2-4
laminectomy 6 years ago
•Unable to stand or walk for more than a few minutes; failed
PT, injections, chiro, meds
Courtesy of
John O’Toole
T2 sagittal
3/14/2016
3
•Stage 1:
–L5S1 ALIF with 15 degree cage
–R L2-5 LLIF (10 and 20 degree cages at L23,
45)
•L3-4 ALL release with 30 degree cage
•Stage 2:
–L3-4 MIS posterior osteotomies
–L2-S1 percutaneous screws w/ navigation
3/14/2016
4
Pre to postop PRO scores
•Has severe knee arthritis affecting VAS leg and ODI
DEVICES
•PATIENT SPECIFIC PRE-
CONTOURED RODS
DEVICES
•GROWING RODS FOR MIS
3/14/2016
5
BIOLOGICS
•NON-BMP BONE GROWTH
AUTMENTATION
–Protein
–Calciumphosphosilicate
P-15 PROTEIN
TECHNIQUE: EXPANDABLE DISTRACTORS and CAGES
LORDOTIC
MIS
3/14/2016
6
TECHNIQUE: CUTTING ALL
TECHNIQUE FOR BENDING RODS
Haque, R., Fessler, R.G.: “Push-Through” Rod Passage Technique for
the Improvement of Lumbar Lordosis and Sagittal Balance in Minimally
Invasive Adult Degenerative Scoliosis Surgery.
Journal of Spinal Disorders and Techniques, 2014.
3/14/2016
7
PUSH THROUGH AND BEND INTO LORDOSIS
EMERGING TRENDS: WHERE ARE WE GOING?
3/14/2016
8
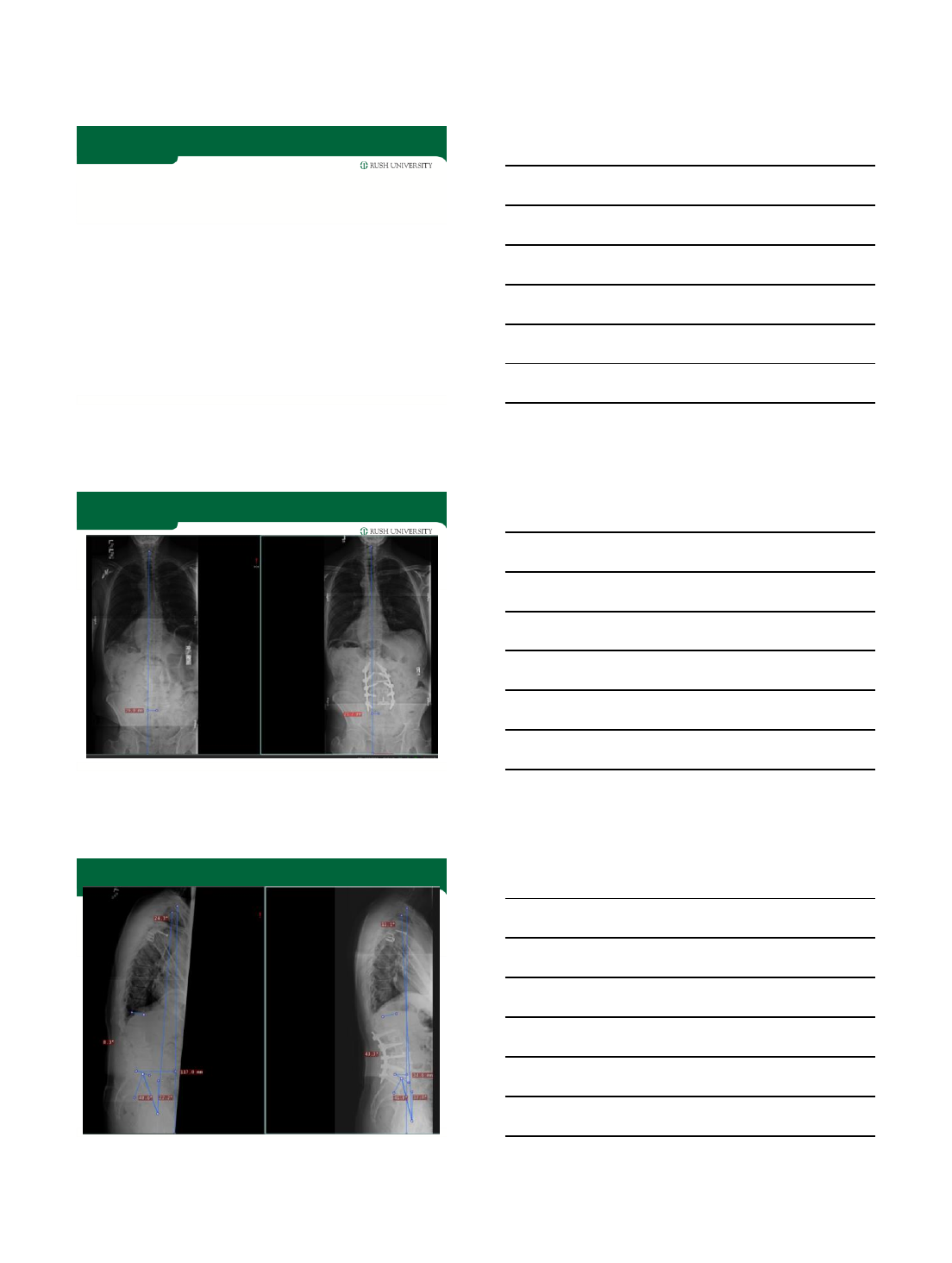
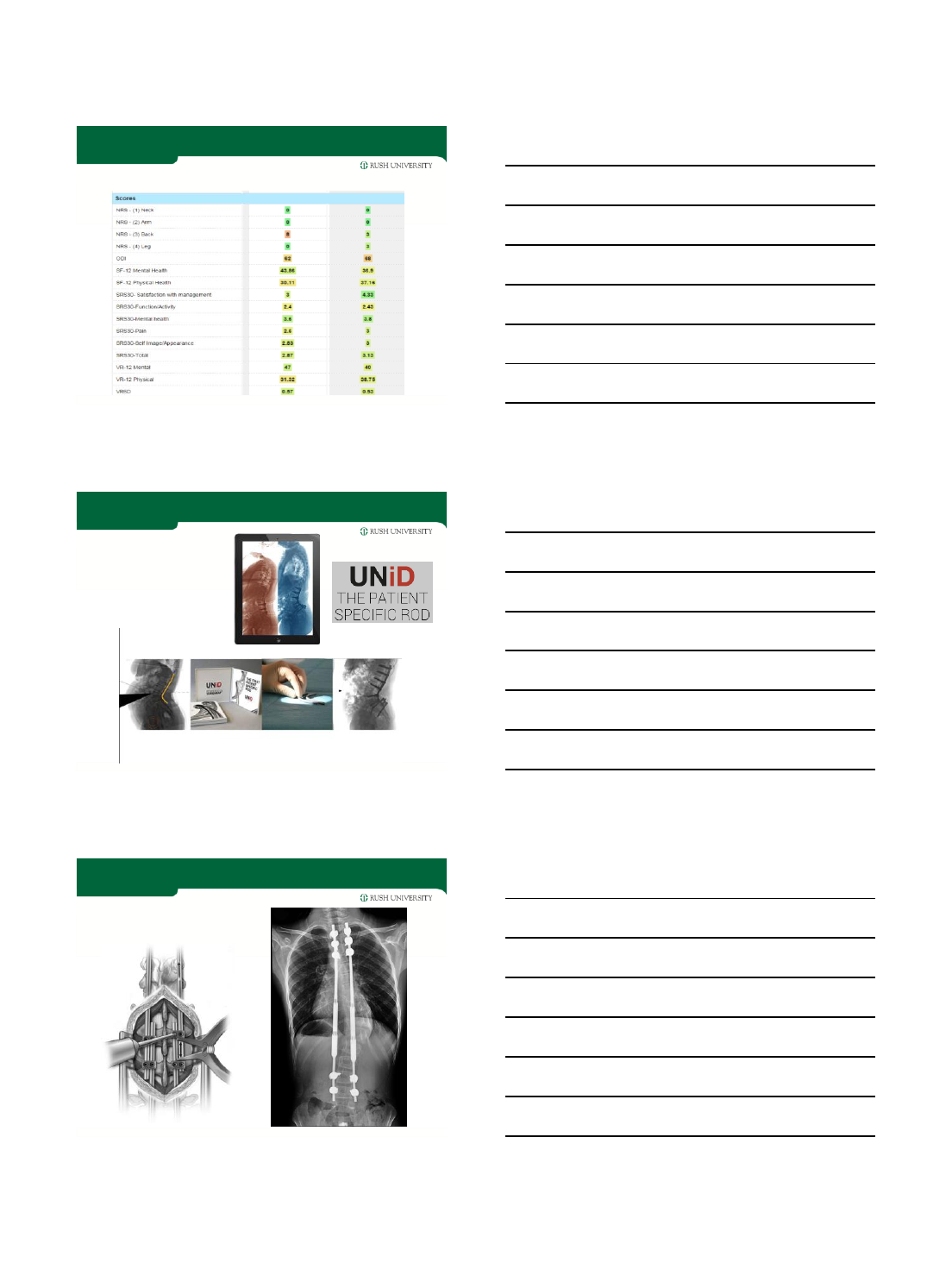
16 Y/O FEMALE
Coronal balance: 28 mm; Sagittal balance: -113 mm;
PI=39.4; PT=0; SS=29; LL=43
58.6º
56º
POST MIS CORRECTION
0º
24.2º
Coronal balance: 26mm; Sagittal balance: 0 mm
PI=52.3; PT=24.4; SS=26.1 LL=30.9
PLANNING
•SURGIMAP
EOS
3/14/2016
9
PLANNING
GOAL: EMERGING TRENDS
•All deformity correction performed through MIS technique!
THANK YOU
