07 15 Syndesmotic Injuries Syllabus
2015-07-07
: Pdf 07 07 15 Syndesmotic Injuries Syllabus 07_07_15_Syndesmotic_Injuries_Syllabus 7 2015 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 36
7/3/2015
1
Daniël Haverkamp
Syndesmotic Instability
Physical Exam & Imaging
Disclosure
Research Support from:
Implantcast
Mathys Medical
Imove Medical
Cotera
Carbylan
Consultancy agreement
IMove Medical
Cotera
7/3/2015
2
Consensus Meeting Rome 2013
Consensusmeeting Budapest 2015
7/3/2015
3
Acute
High index of suspicion
Rome, consensus meeting 2013
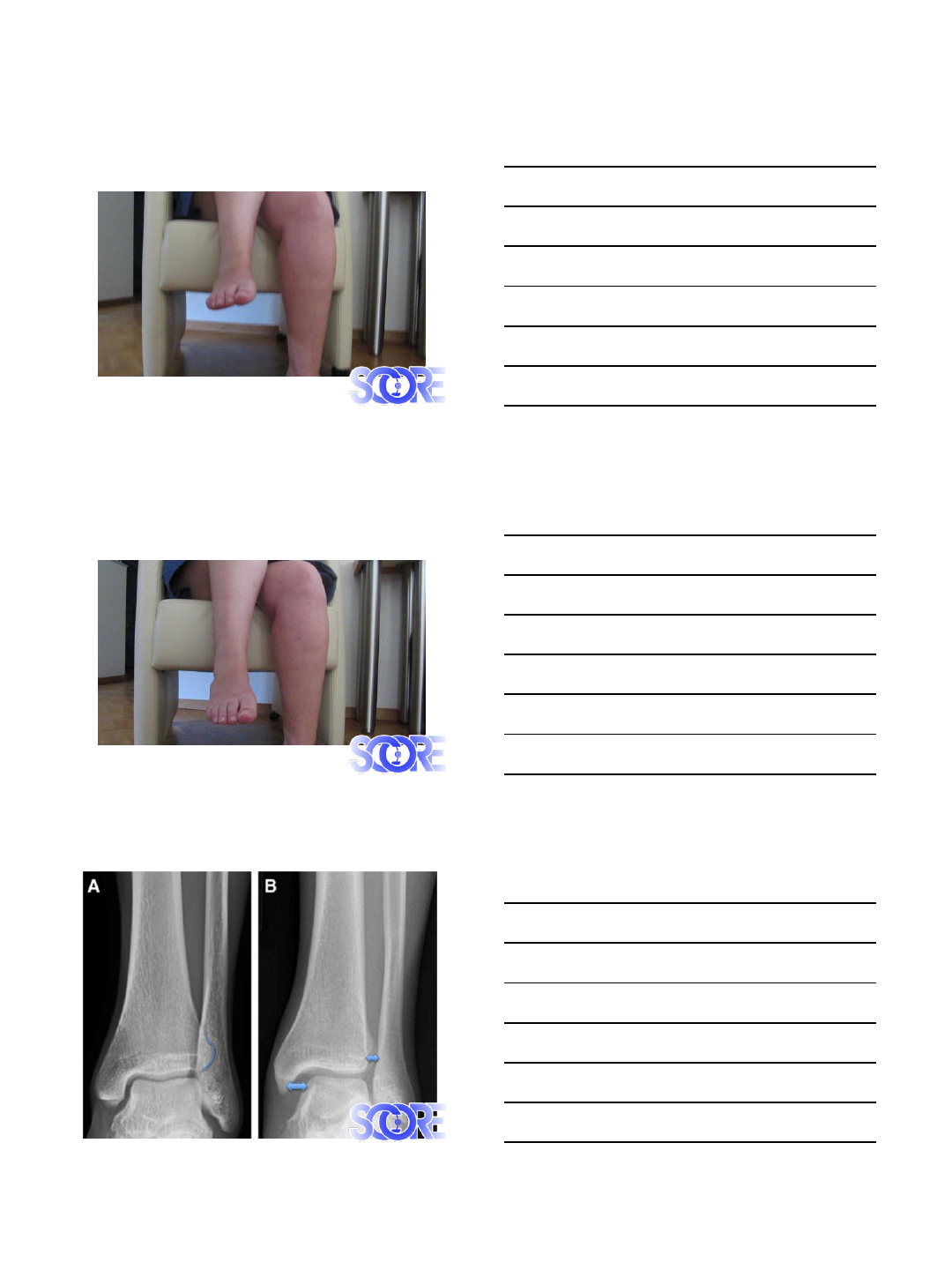
Acute
High index of suspicion
The tenderness length measurement
Rome, consensus meeting 2013
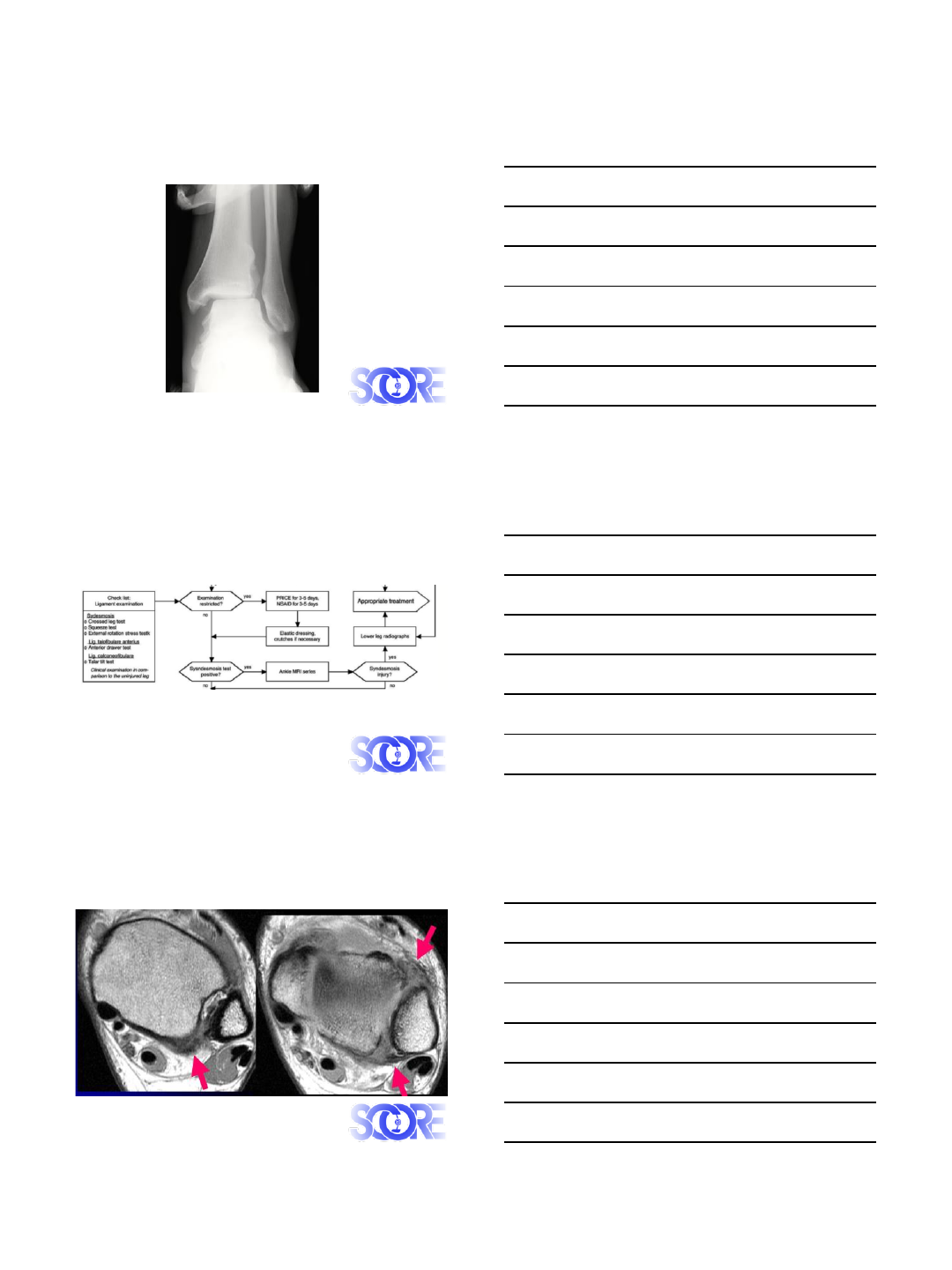
Acute
High index of suspicion
The tenderness length measurement
Deltoid ligament
Rome, consensus meeting 2013
7/3/2015
4
Acute
Rome, consensus meeting 2013
High index of suspicion
The tenderness length measurement
Deltoid ligament
Stable/Unstable
Cotton Test
Squeeze test
7/3/2015
5
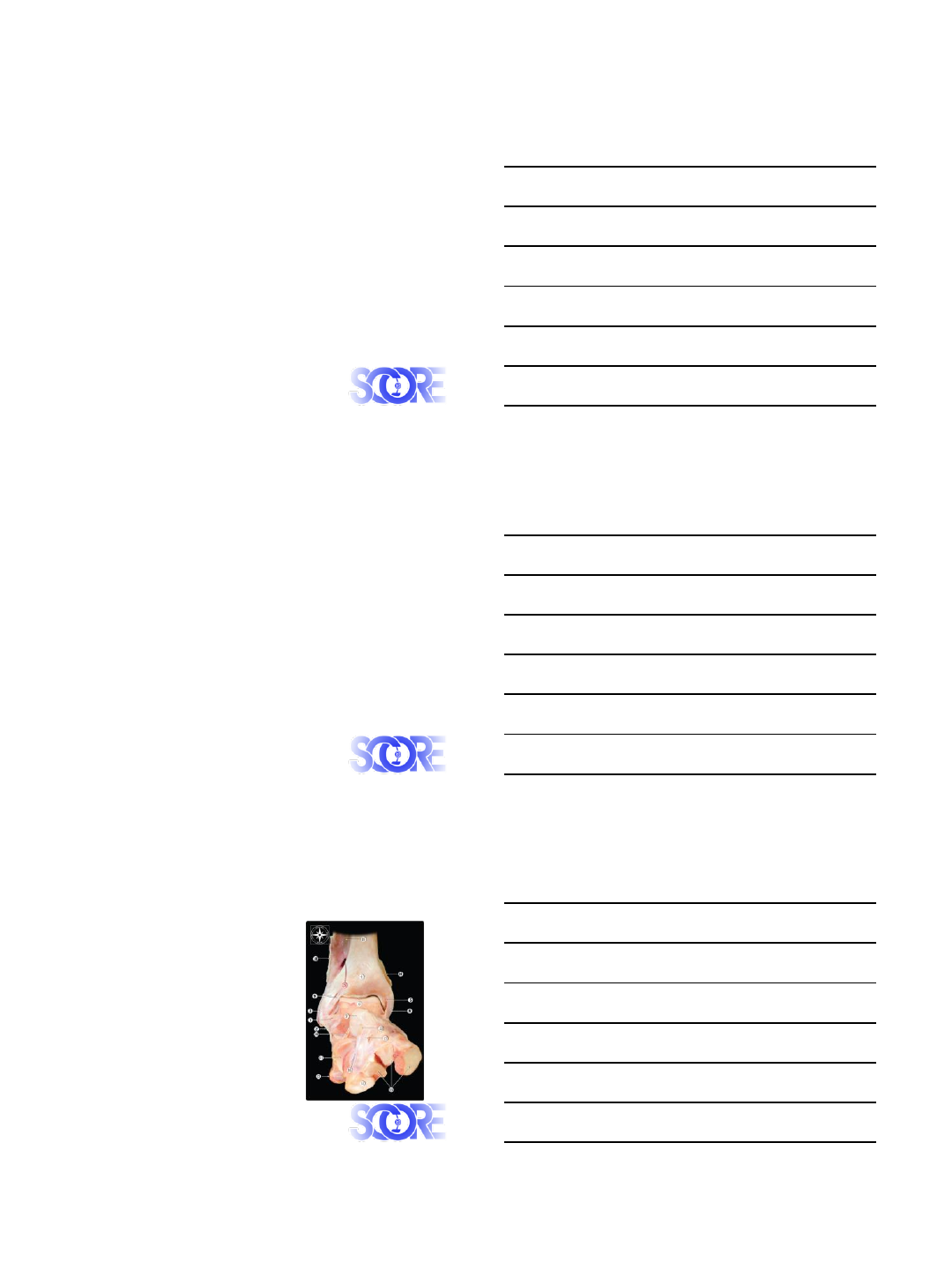
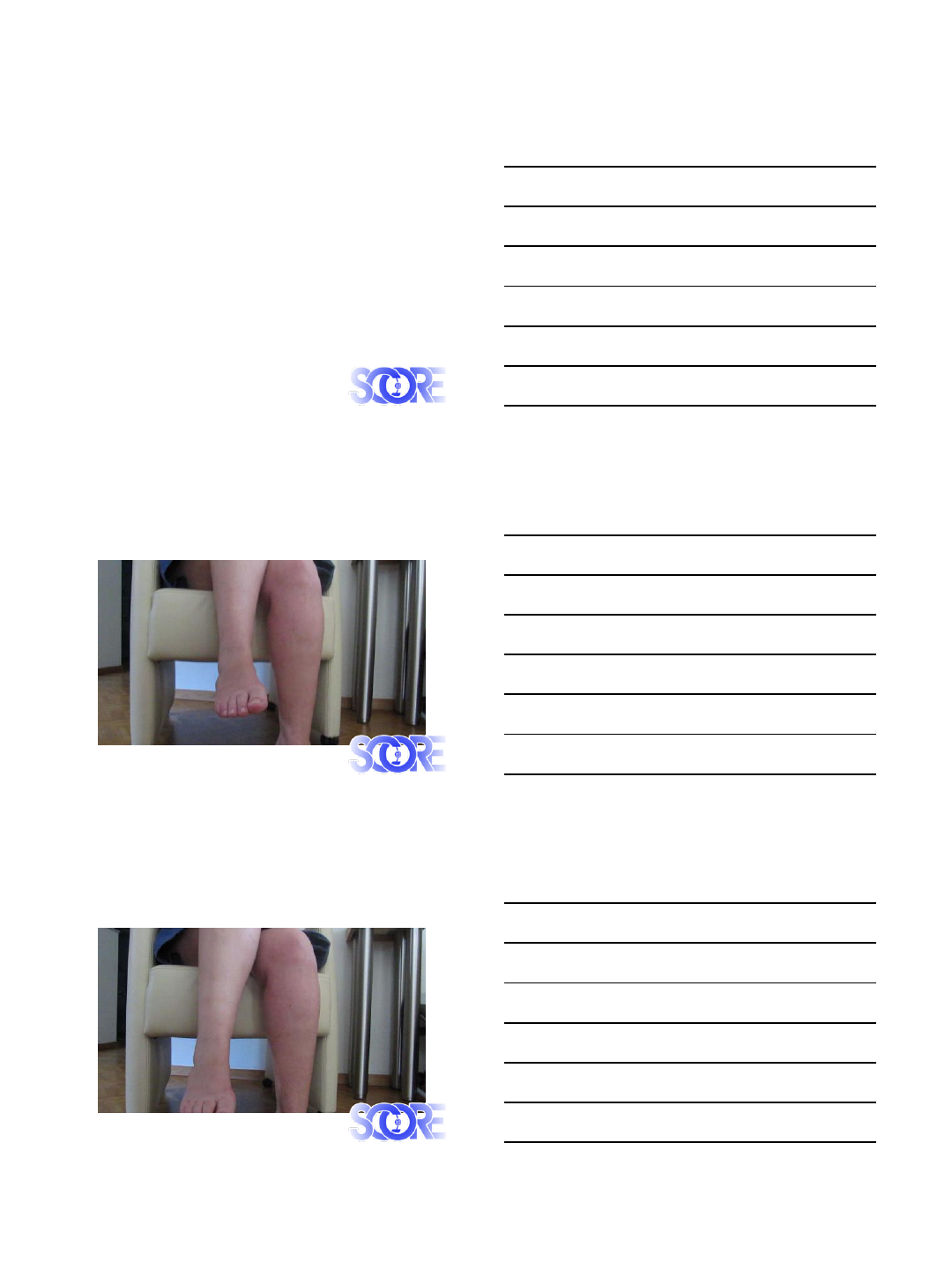
Fibula Translation test
External Rotation test
7/3/2015
6
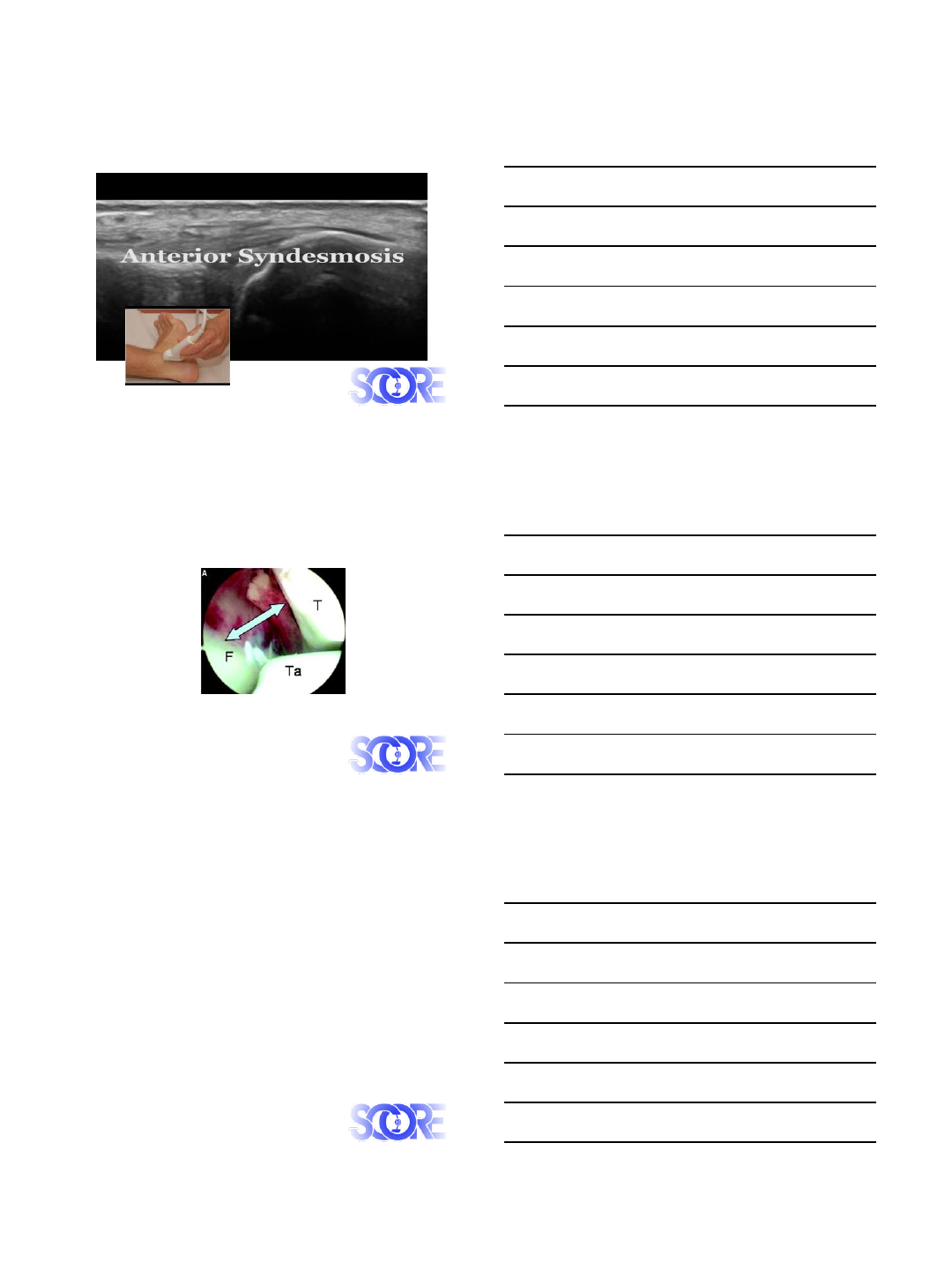
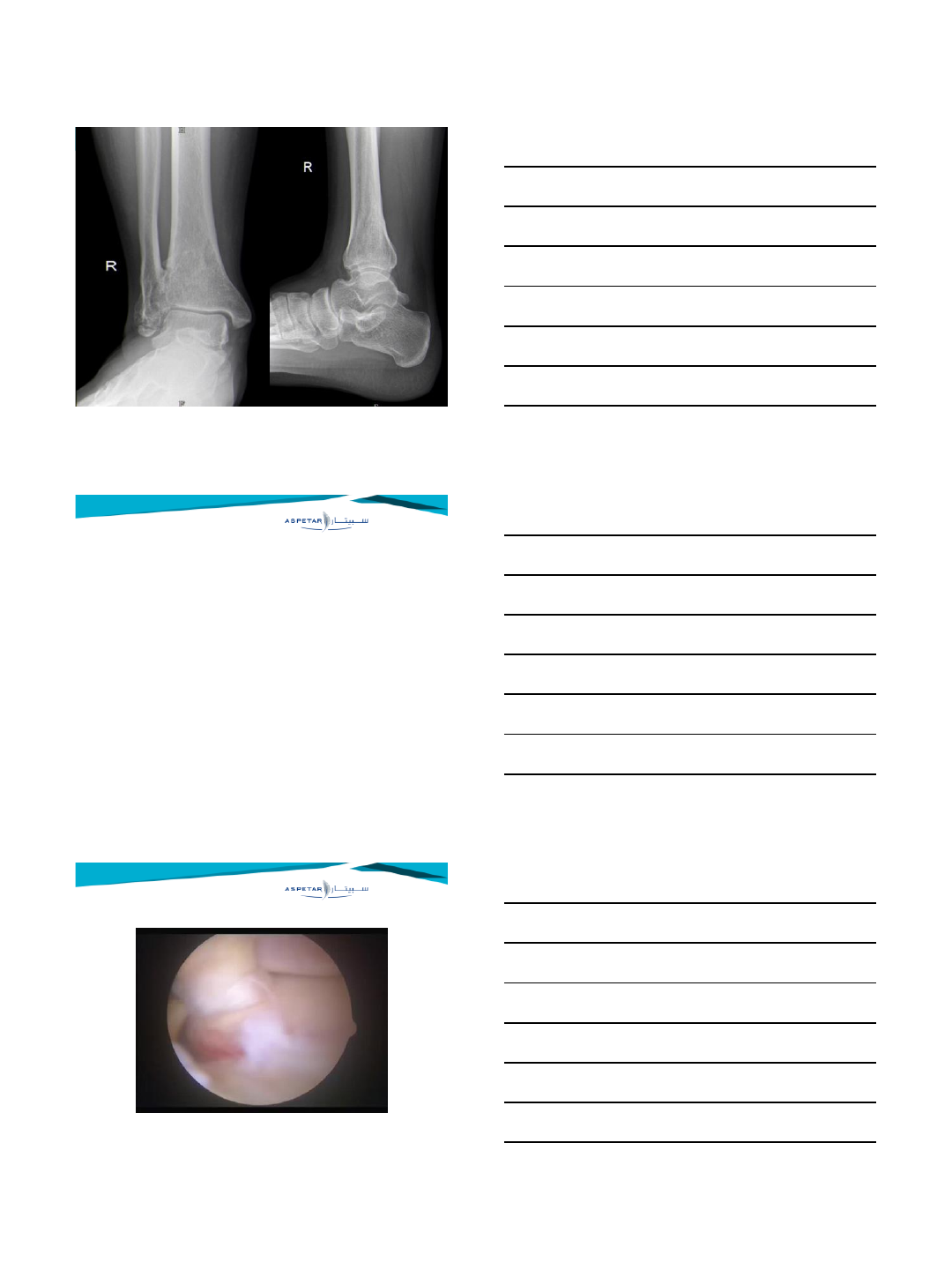
Stress X-ray
Polzer 2012, Orthopedic Reviews
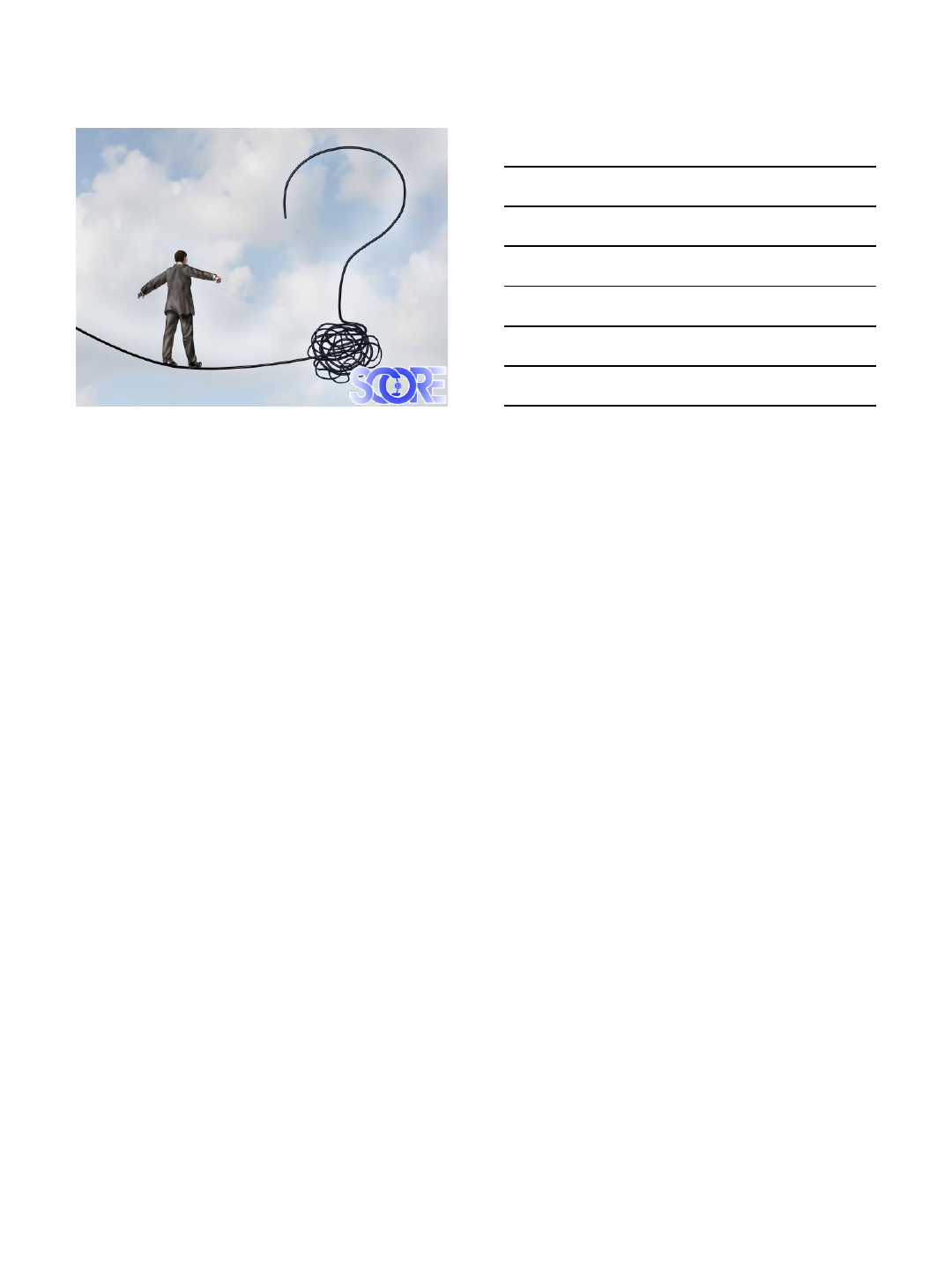
MRI
Howard, Sports Health 2012
7/3/2015
7
Ultrasound
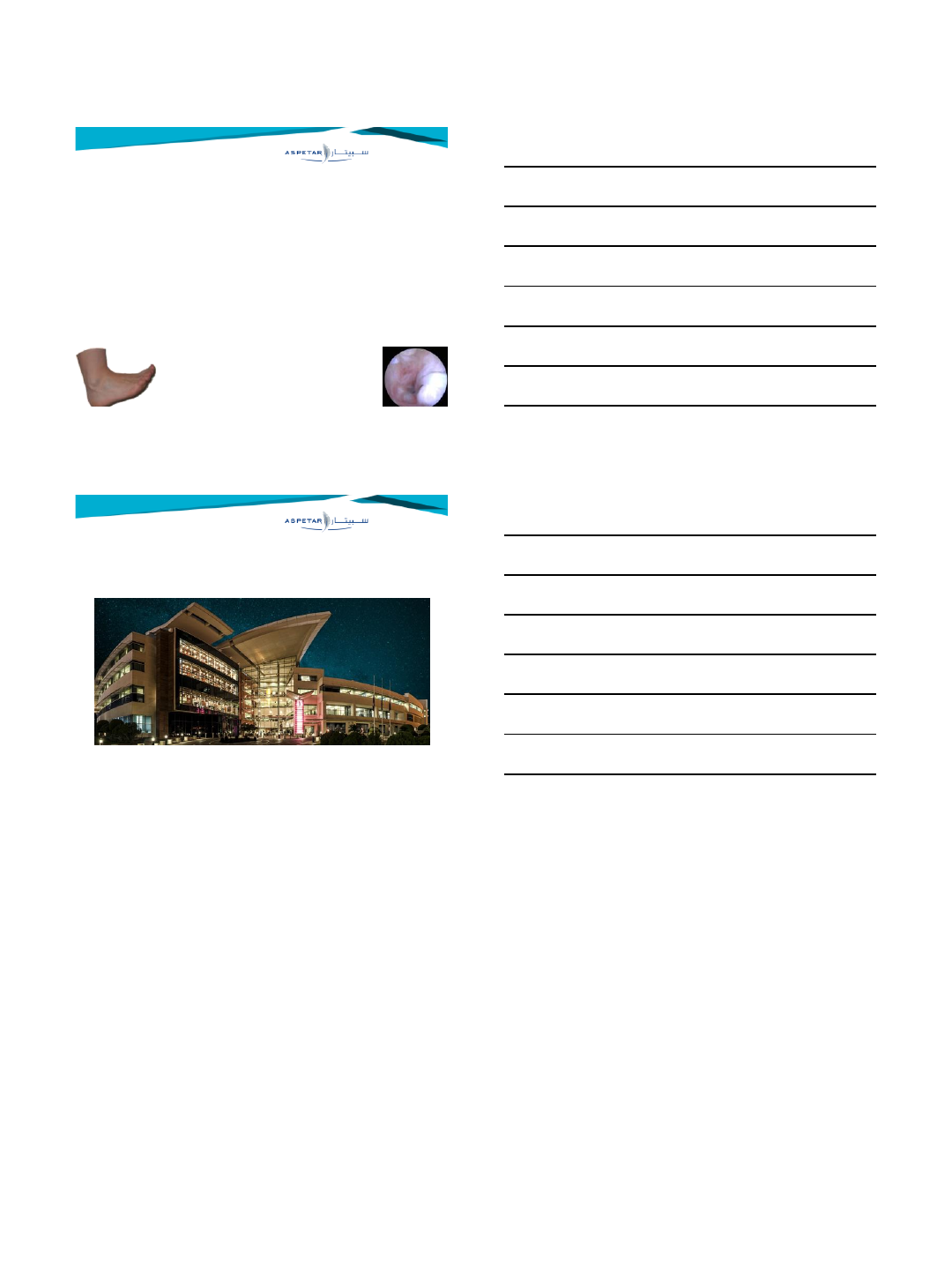
Arthroscopy
Imaging
Consensusmeeting Budapest 2015
Comparative Weightbearing X-rays should be
made
Stress views might be an option
MRI is the most appropriate addiotonial tool
Dynamic Sonography might play a role in
selected centers
Diagnostic arthroscopy can be performed in
cases with a high clinical suspicion with a non-
conclusive MRI (Chronic instability).
7/3/2015
8
7/2/2015
1
Principles of conservative
management of syndesmosis injuries
James Calder TD, MD, FRCS(Tr & Orth) FFSEM(UK)
Chelsea & Westminster Hospital, London
The Fortius Clinic, London
www.fortiusclinic.com
Key to success
Accurate assessment
of degree of
instability / grading
Early stabilisation /
immobilisation
Assessment during
rehabilitation Longer recovery than ATFL/CFL injuries
Nussbaum, AJSM 2001
Wright, AJSM 2004
Jones, CORR 2007
What are the aims / pitfalls?
Subtle instability -
antero-lateral
synovitis /
impingement
Chronic instability
Medial deltoid
instability / pain
7/2/2015
2
Which injuries are suitable for
conservative management?
Isolated syndesmosis
injury:
AITFL +/- IOL
?PITFL
ATFL/CFL injury protective?
Which injuries are suitable for
conservative management?
Isolated syndesmosis
injury:
AITFL +/- IOL
?PITFL
ATFL/CFL injury protective?
Concomitant ATFL/CFL
injury indicates:
SER with syndesmosis
extension
Milder injury
Calder & Roche, FA meeting St George’s 2014
Which injuries are suitable for
conservative management?
Isolated syndesmosis
injury:
AITFL +/- IOL
?PITFL
ATFL/CFL injury protective?
Concomitant ATFL/CFL
injury indicates:
SER with syndesmosis
extension
Milder injury
Calder & Roche, FA meeting St George’s 2014
Consider fixation /
intervention:
Medial deltoid injury
Fibula fracture
Posterior malleolar fracture
7/2/2015
3
What does this translate into clinically?
West Point Classification -
syndesmosis no fracture
Gerber Foot Ankle 1998
Grade I –mild AITFL sprain
Conservative Mx
Grade III –definite
instability with complete
disruption of all ligaments
Operative Mx
What does this translate into clinically?
West Point Classification -
syndesmosis no fracture
Gerber Foot Ankle 1998
Grade I –mild AITFL sprain
Conservative Mx
Grade III –definite
instability with complete
disruption of all ligaments
Operative Mx
Grade II – vague “slight
instability” with tear of
AITFL and partial tear IOL
What does this translate into clinically?
West Point Classification -
syndesmosis no fracture
Gerber Foot Ankle 1998
Grade I –mild AITFL sprain
Conservative Mx
Grade III –definite
instability with complete
disruption of all ligaments
Operative Mx
Grade II – vague “slight
instability” with tear of
AITFL and partial tear IOL
Arthroscopy Grade II?
Wolf & Amendola, Cur Op Orthop 2002
Grade II a –stable
Conservative Mx
Grade IIb – “latent”
instability
Operative Mx
Mcollum, KSSTA 2013
7/2/2015
4
Conservative Management
- Grade I and IIa injuries
Nussbaum, AJSM 2001
60 pts “aggressive”
rehabilitation
Level 4
Phase I - 1-4 days
immobilisation NWB
Phase II –PWB with ankle
brace (proprioception, ROM,
resistance/functional training)
Phase III –when 10 single leg
toe-hops
RTS –with tape & brace after
functional testing
Conservative Management
- Grade I and IIa injuries
Results
Mean RTS 13.4 days (5-24)
Length of tenderness = longer RTS
At 6/12:
6/53 –pain/stiffness
3/53 –recurrent sprains
1/53 –heterotropic ossification
35/53 –excellent; 18/53 –good
No MRI
?ATFL sprain not syndesmosis
Nussbaum, AJSM 2001
60 pts “aggressive”
rehabilitation
Level 4
Conservative Management
- Grade I and IIa injuries
Hopkinson, FAI 1990
1334 military pts
Partial syndesmosis longer recovery vs ankle sprain
(55 vs. 28 days)
Significant +ve squeeze test @ 20 months
9/10 heterotopic ossification
Problems:
Retrospective; No MRI ?diagnosis; few late f/u
Level 4
7/2/2015
5
Conservative Management Principles
- Grade I and IIa injuries
Few level 4 studies on conservative Mx
No level 2 or 3 studies
Specific conservative management:
Grade I recommendation
Conservative Management Principles
- Grade I and IIa injuries
Few level 4 studies on conservative Mx
No level 2 or 3 studies
Specific conservative management:
Grade I recommendation
What follows is a summary but
Level 5!!
Conservative Management Principles
- Grade I and IIa injuries
Phase I
Week 1:
RICE
NWB boot
Avoid NSAIDs
Week 2:
PWB as tolerate boot
Physio supervised ROM &
proprioception

7/2/2015
6
Conservative Management Principles
- Grade I and IIa injuries
Phase 2
Week 3
FWB boot / if no pain - tape
Strength & proprioception
Plyometric exercises (leg press, aero-
mat, toe standing, single leg hop)
Clinical marker:
Improved pain with forward lunge
Conservative Management Principles
- Grade I and IIa injuries
Phase 2
Week 4+
Support brace / tape
Light running:
30 sec single leg toe hop
Improved knee-to-wall
?Progress to multi-
directional training
Conservative Management Principles
- Grade I and IIa injuries
Phase 2
Week 4+
Support brace / tape
Light running:
30 sec single leg toe hop
Improved knee-to-wall
?Progress to multi-
directional training
7/2/2015
7
Conservative Management Principles
- Grade I and IIa injuries
Phase 2
Week 4+
Support brace / tape
Light running:
30 sec single leg toe hop
Improved knee-to-wall
?Progress to multi-
directional training
Conservative Management Principles
- Grade I and IIa injuries
Phase 2
Week 4+
Support brace / tape
Light running:
30 sec single leg toe hop
Improved knee-to-wall
?Progress to multi-
directional training
Conservative Management Principles
- Grade I and IIa injuries
Phase 2
Week 4+
Support brace / tape
Light running:
30 sec single leg toe hop
Improved knee-to-wall
?Progress to multi-
directional training
Clinical markers:
Forward lunge test
Pain-free single leg toe hop 30 secs
Pain-free ext rotation on exam couch
7/2/2015
8
Conservative Management Principles
- Grade I and IIa injuries
Phase 3
Continue taping 12
weeks
Return to training
Running –Alter-G
treadmill
Multi-directional
training
Conservative Management Principles
- Grade I and IIa injuries
Phase 3
Continue taping 12
weeks
Return to training
Running –Alter-G
treadmill
Multi-directional
training
Summary
Accurate assessment of
grade
ATFL injury “good sign”
Beware higher grade injury:
Medial deltoid & PITFL injury
+ve squeeze test
“high ankle pain”
Consider arthroscopy to
differentiate Grade IIa/b
7/2/2015
9
Summary
Accurate assessment of
grade
ATFL injury “good sign”
Beware higher grade injury:
Medial deltoid & PITFL injury
+ve squeeze test
“high ankle pain”
Consider arthroscopy to
differentiate Grade IIa/b
Early “aggressive”
immobilisation (not
rehabilitation)
Progress depends on
clinical assessment
Maintain taping
Warn of RTS 6-10
weeks
7/6/2015
1
Acute Syndesmotic Injury in the Athlete:
Indications & Approach for Operative Treatment
Presenter: Umile Giuseppe Longo MD, MSc, PhD
University Campus Bio-Medico of Rome
Department of Trauma and Orthopaedic Surgery
Head Prof Vincenzo Denaro
No conflicts to declare
Conflicts of interest
“Acute” injury: Definition
M.Vd Bekerom, CN van Dijk - 2009
•Acute
•Subacute > 6 w
•Chronic > 6 m
Espinoza 2012
•Acute < 3 weeks
•Subacute > 3 weeks
•Chronic> 3 months
Valkering 2012 - Scraton - 2000
•Acute < 6 weeks
•Subacute > 6 weeks
•Chronic > 3 months
Porter - 2009
•Acute < 4 weeks
•Subacute > 4 weeks
•Chronic > 3 months
Magan A, Golano P, Maffulli N, Khanduja V. Br Med Bull. 2014;111(1):101-15.
7/6/2015
2
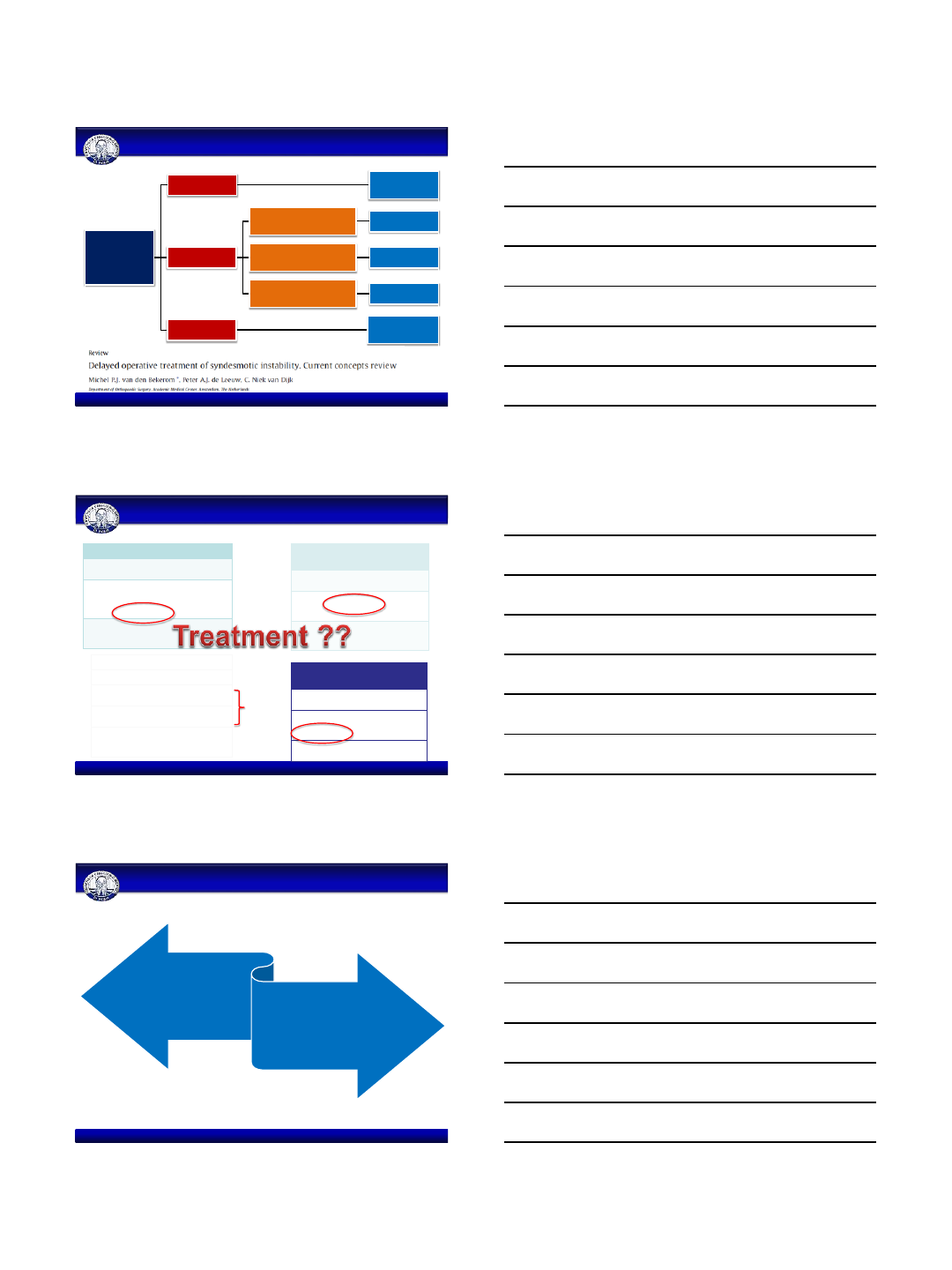
“Acute” injury: Definition
Syndesmotic
Ligament Repair
Acute < 6w Syndesmotic screw fixation
Subacute > 6w
Inadeguate remnants of ligaments Ligamentoplay + screw
placement
Adequate remnants of ligaments Suturing + screw
placement
Slack but continuos ligament Traslation + screw
placement
Chronic > 6m Synostosis/fusion + screw
placemnt
Treatment of syndesmotic instability - Flow Chart
Porter Classification
I. injury is characterized by lesion of the AITFL,
IOL and anterior deltoid ligament
II.
injury is characterized by lesion of a
significant portion of the
syndesmosis, and
disruption of the anterior and deep deltoid
ligaments.
Occult instability.
III. injury consists of extensive disruption of the
syndesmosis
and complete disruption of the
deltoid ligament
West Point Ankle Grading
System
I.
injury consists of a mild sprain or tear of
the AITFL with no instability of the ankle
.
II.
lesion of the AITFL and partial tear of
the IOL with slight instability of the joint
.
Latent instability.
III.
complete disruption of all the ligaments
with frank instability of the ankle
Edwards and
DeLee
classification
I.
lesion of the AITFL without involvement
of the deltoid ligament
.
II. rupture of the AITF and deltoid ligaments
leading to occult instability
III.
fibular bowing (plastic deformation of
fibula) and widening of
tibiofibular space
visible on standard plain radiographs
.
Sikka Classification
I.
lesion is an isolated injury of the AITFL
II.
injury of the AITFL, IOL and
interossesous
membrane.
III
. injury of the AITFL, IOL, interossesous
membrane and PITFL
.
IV.
disruption of all the previous ligaments
associated
with the rupture of the deltoid
ligament
.
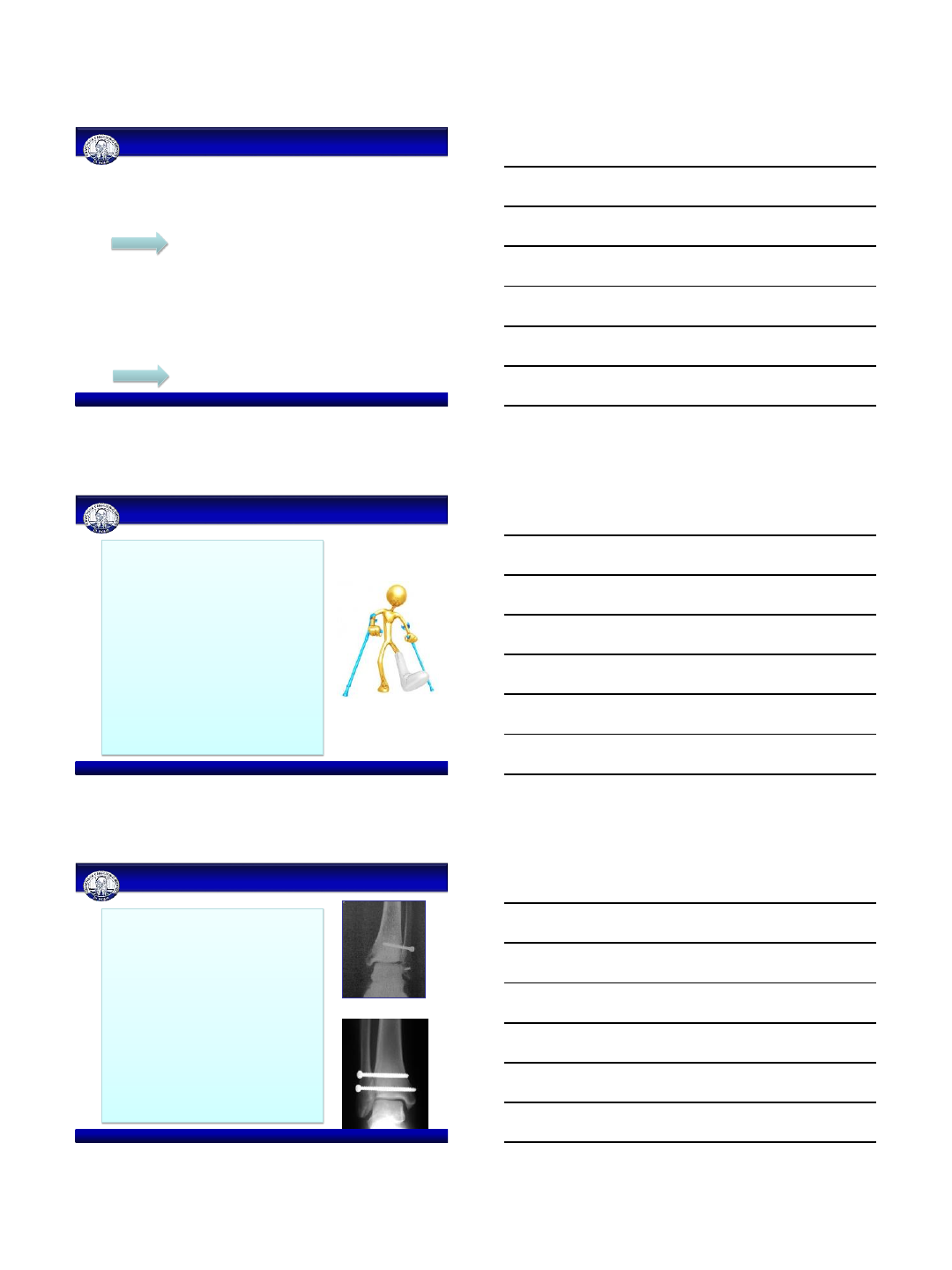
Classifications
Magan A, Golano P, Maffulli N, Khanduja V. Br Med Bull. 2014;111(1):101-15.
Stable ankle
Conservative
Unstable ankle
Surgery
7/6/2015
3
Stable ankle:
•Syndesmotic ruptures without injury of the deltoid ligament
Indications
Unstable ankle
•Frank diastasis or
•Latent instability with proved deltoid ligament rupture
Conservative Management
Surgical Management
Indications
Sprains without instability:
nonoperative
•Short leg cast or brace
•Rehab program as pain allows
•Double the time to recover
compared to a typical lateral
ankle sprain
Indications
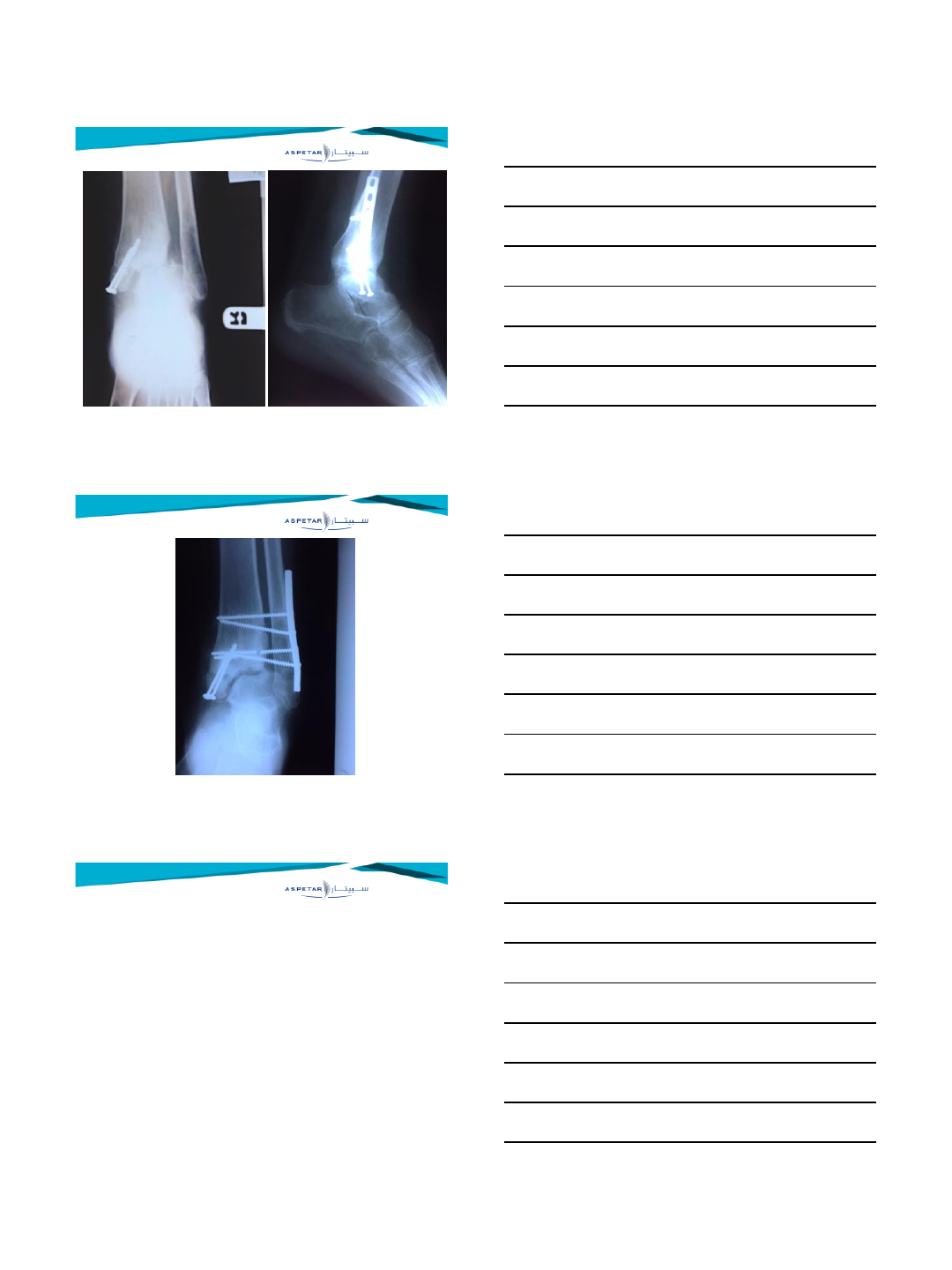
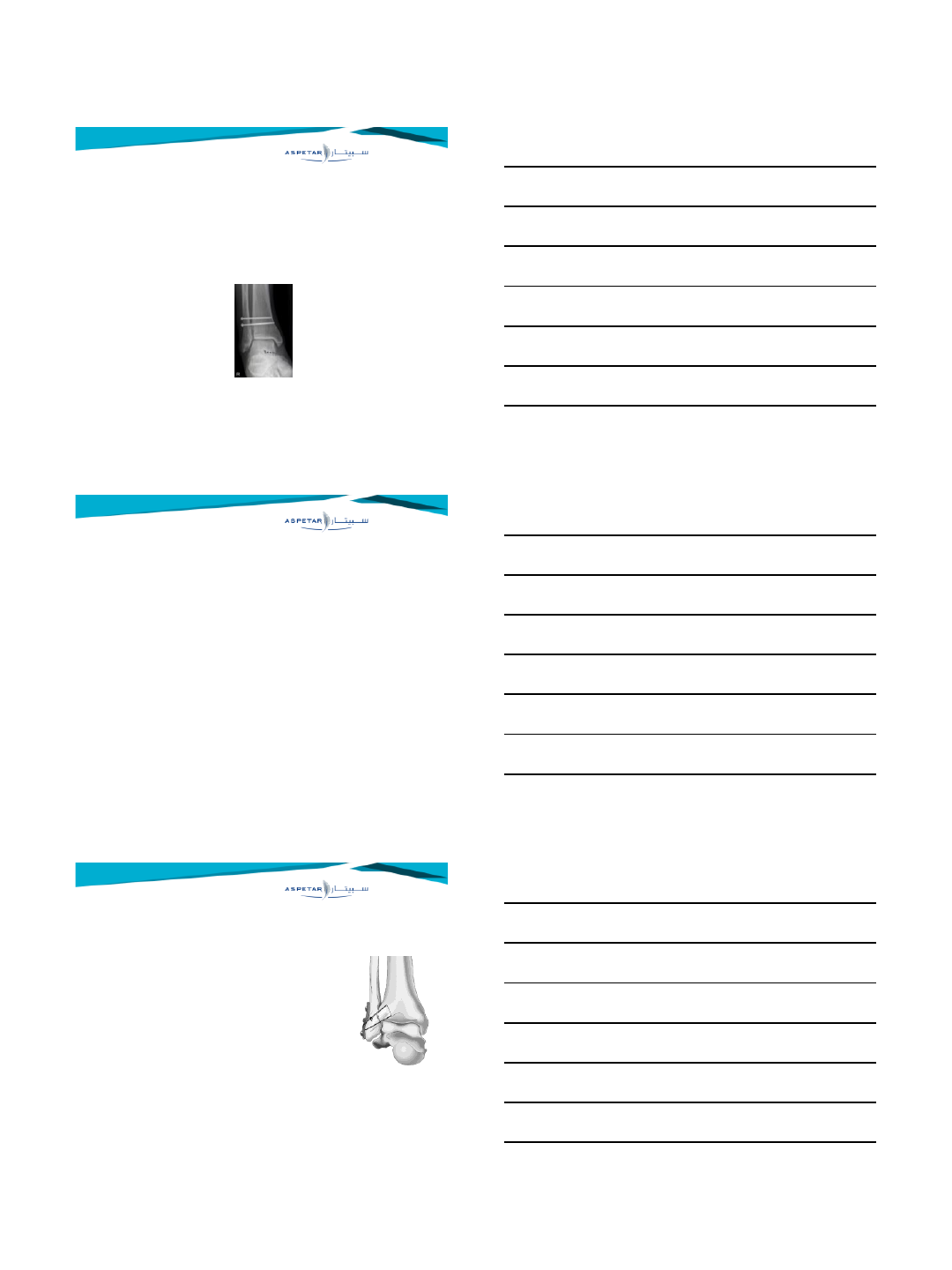
Frank diastasis: operative
•Repair of the ligament?
•If reduction blocked by deltoid
ligament:
exploration and repair
Removal of interposed soft tissue
•Syndesmosis screw
•NWB short leg cast
7/6/2015
4
Available surgical techniques:
–Traditional metal screw fixation
–Bioabsorbable screws
–Suture-Button
–Fixation with a staple
–Cerclage wires
–Kirschner wires
Approach for Operative Treatment
Syndesmotic screw
–Aims to temporarily stabilize the reconstructed
mortise
–Potential complications
•Synostosis or ossification of the distal tibiofibular joint
•Impairment of full ankle dorsiflexion, limit tibiotalar range of
movement in terms of rotation (Data from Experimental cadaveric
studies)
Approach for Operative Treatment
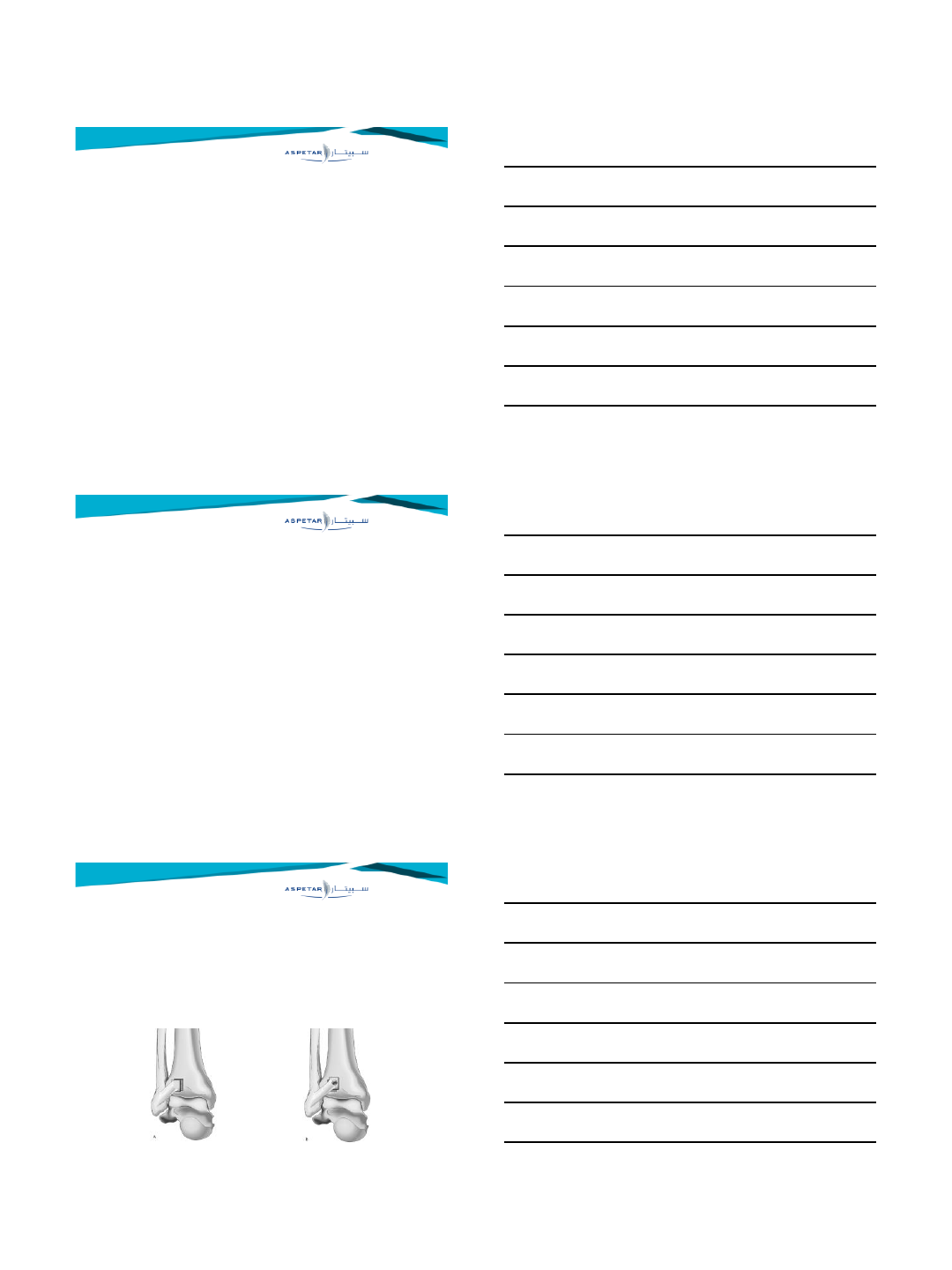
Suture-button (TightRope®)
–Similar outcome compared with the
syndesmotic screw or bolt fixation
–Might lead to a quicker return to work
–Rate of implant removal is lower compared
to the syndesmotic screw
–Insufficient evidence on the long-term
effects of the TightRope®
Approach for Operative Treatment
7/6/2015
5
Diameter of the screw
•No consensus on the optimal screw size for
syndesmotic fixation (3.5 mm or 4.5 mm cortical
screw)
•Experimental data: screw of larger diameter provide
greater resistance to an applied load
Approach for Operative Treatment
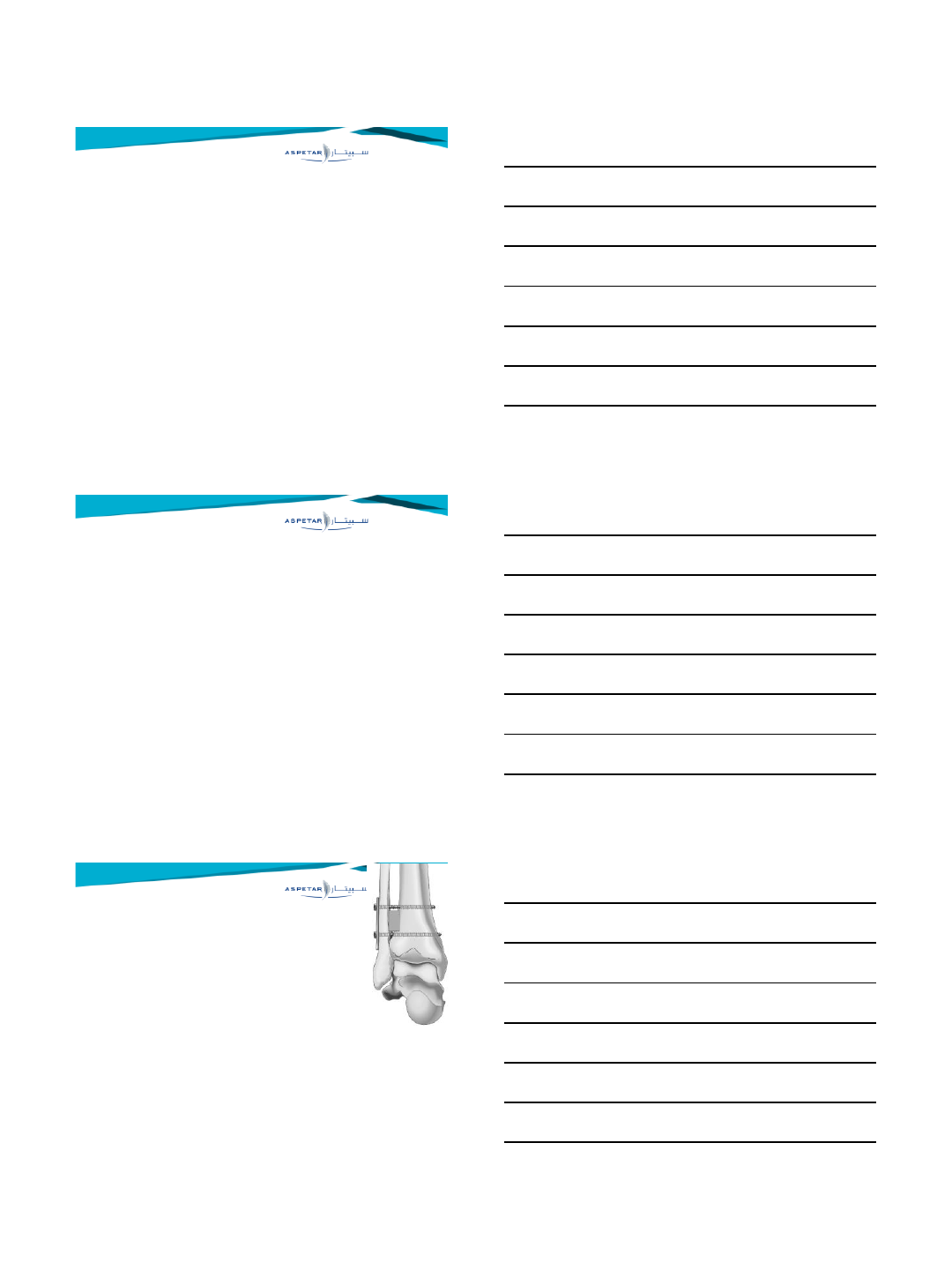
Number of cortices
–No consensus (three or four cortices)
–Four-cortical fixation: more rigidity and
stability of the ankle, but higher risk of
screw breakage
–Three-cortical fixation: better syndesmosis
biomechanics (possibility of hardware
failure is diminished while the risk of
loosen the screw is increased than four-
cortical fixation)
Approach for Operative Treatment
Absorbable screw
–To prevent the removal of the screw and
the risks associated with this procedure
–Inferior biomechanical properties
compared with those of conventional
metallic implants.
–Good clinical outcomes
–No differences compared to metallic
screws
Approach for Operative Treatment
7/6/2015
6
Position of the ankle during fixation
–Debated issue.
–Recommended to fix an injured
syndesmosis with the foot in dorsiflexion
to prevent a limited dorsiflexion of the
ankle.
–Recent studies show that the position of
the ankle during syndesmotic fixation is
probably irrelevant
Approach for Operative Treatment
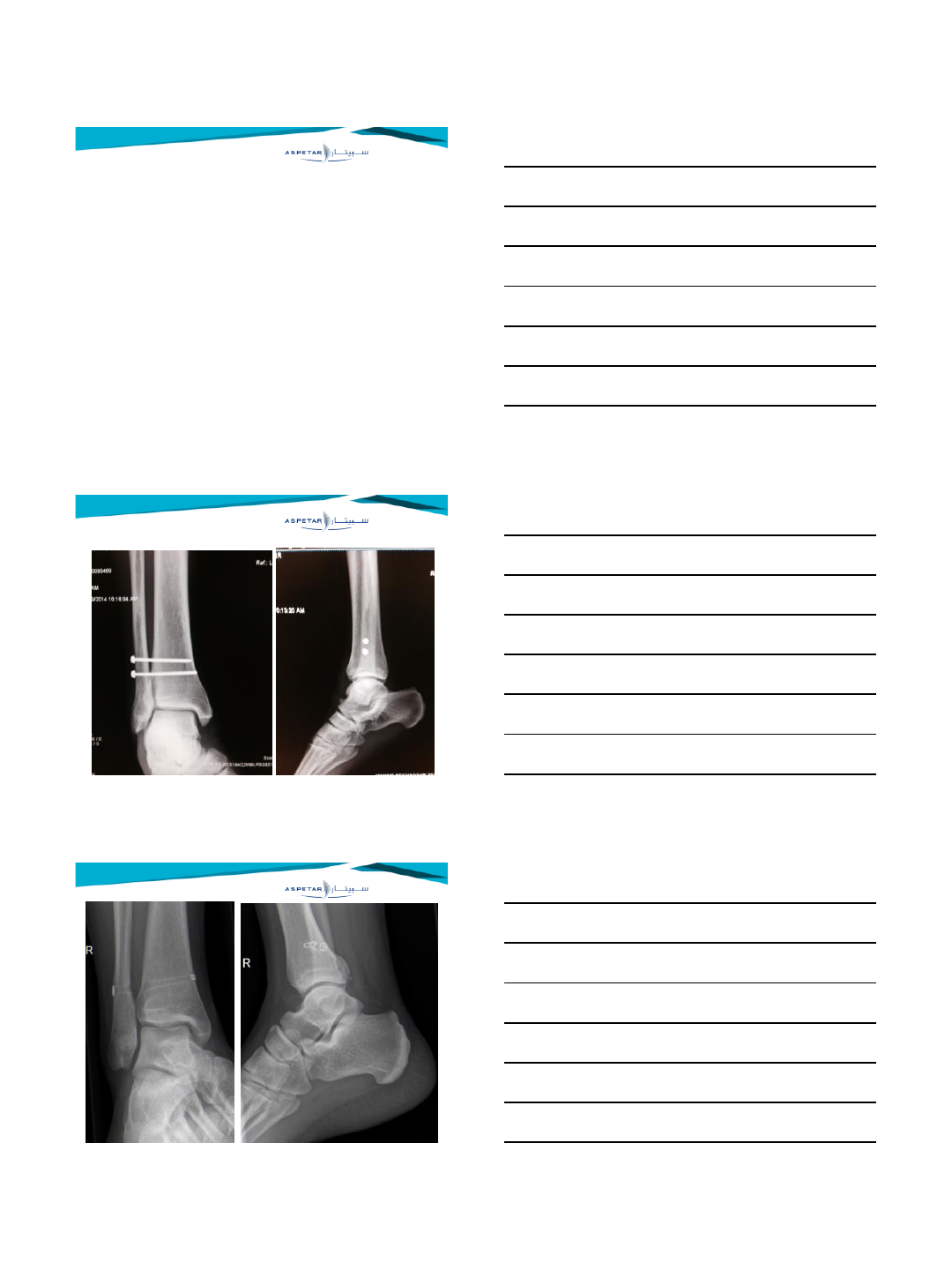
Positioning of the screw
•Screw should be positioned parallel to the joint line and
angled about 30° anteriorly (anatomically the fibula is
posterior and lateral to the tibia)
•Optimal position of the screw with respect to the tibial
plafond is still debated
–Sproule et al.: the screw 4 cm proximal to the ankle joint
–McBryde et al. less syndesmotic widening when using the
screw at 2 cm than at 3.5 cm.
•Screw positioned too far proximally, it can deform the
fibula and the mortise is more likely to widen.
Approach for Operative Treatment
Retain or remove a syndesmotic screw prior to
weight-bearing
–Still debated
–At 6–8 weeks to prevent the possibility of
breakage of the screw?
–Leaving the screw in place may save patients
from one extra surgical procedure
–Outcome appears to be similar or better
when the screw is retained
–Van den Bekerom et al.: removal of four-
cortical screws after 6–8 weeks, and removal
on indication in three-cortical screws.
Approach for Operative Treatment
7/6/2015
7
–Syndesmotic injuries require an early recognition
–Late repairs are less favourable
–3.5 or 4.5 screw? Proposal: 3.5 mm
–3 cortices or 4 cortices? Proposal: 4 cortices in heavy
patient, 3 in patients with low BMI
–Screw or suture-button? Proposal: both
–Absorbable non absorbable? Proposal: non absorbable
–Position for fixation Proposal: neutral to slightly dorsiflexion
position
–Lag or positioning screw? Proposal: Both possible (prob
positioning more safe)
–Removal of soft tissue Proposal: between 3-6 weeks
–Removal of screw Proposal: at 8 weeks
–Partial weightbearing: Proposal: 6-8 weeks
Approach for Operative Treatment
Umile Giuseppe Longo - Email: ug.longo@gmail.com
University Campus Bio-Medico of Rome
Department of Trauma and Orthopaedic Surgery
7/5/2015
1
Operative Techniques for chronic syndesmotic
injury
Pieter D'Hooghe
Aspetar Orthopaedic Surgery Dept, Doha, Qatar
•Orthopaedic Sportssurgeon
•ISAKOS Chair "Leg, Ankle & Foot Committee
•ESSKA AFAS Member
•No disclosures
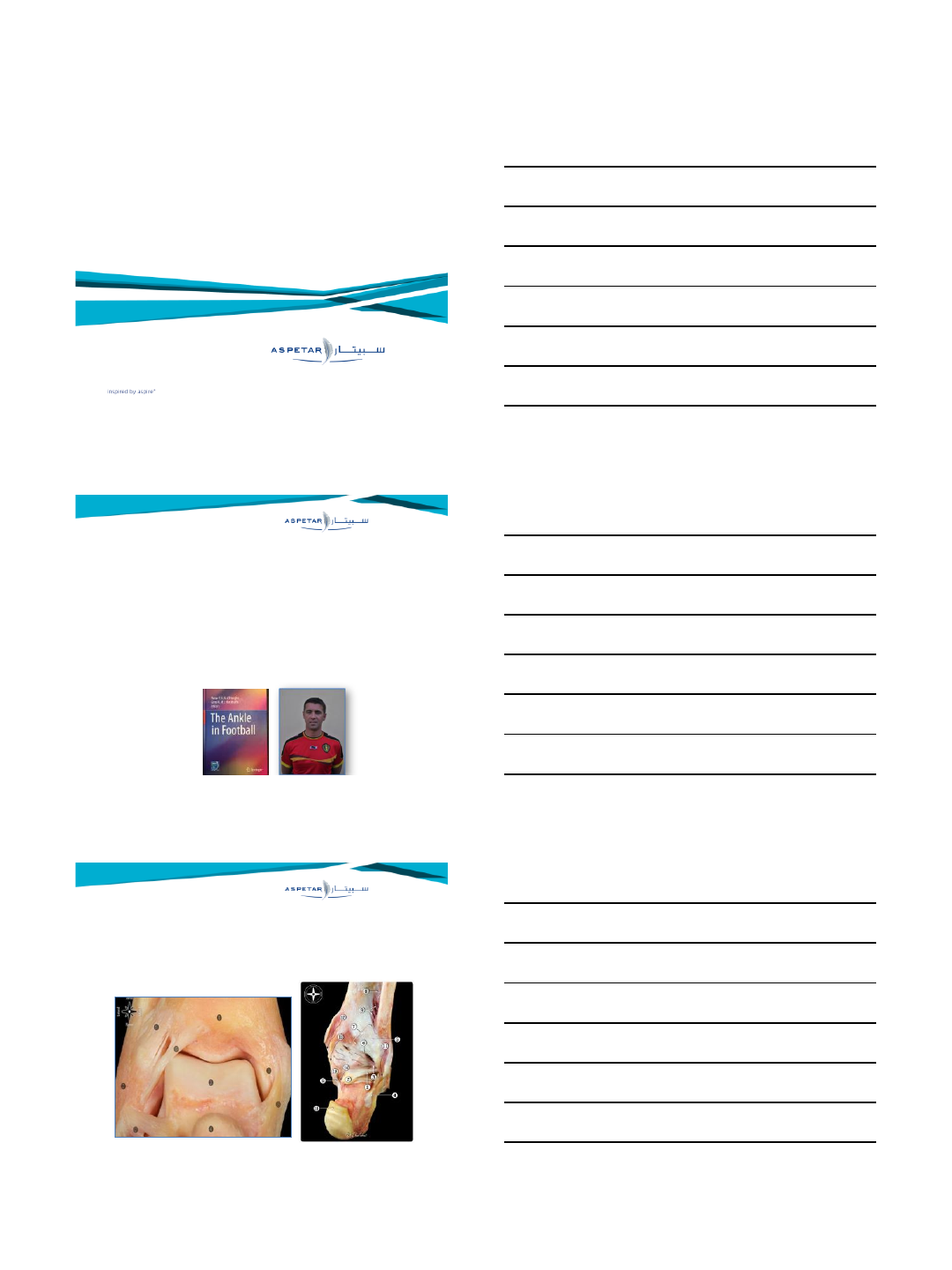
Courtesy Pau Golano - Niek van Dijk
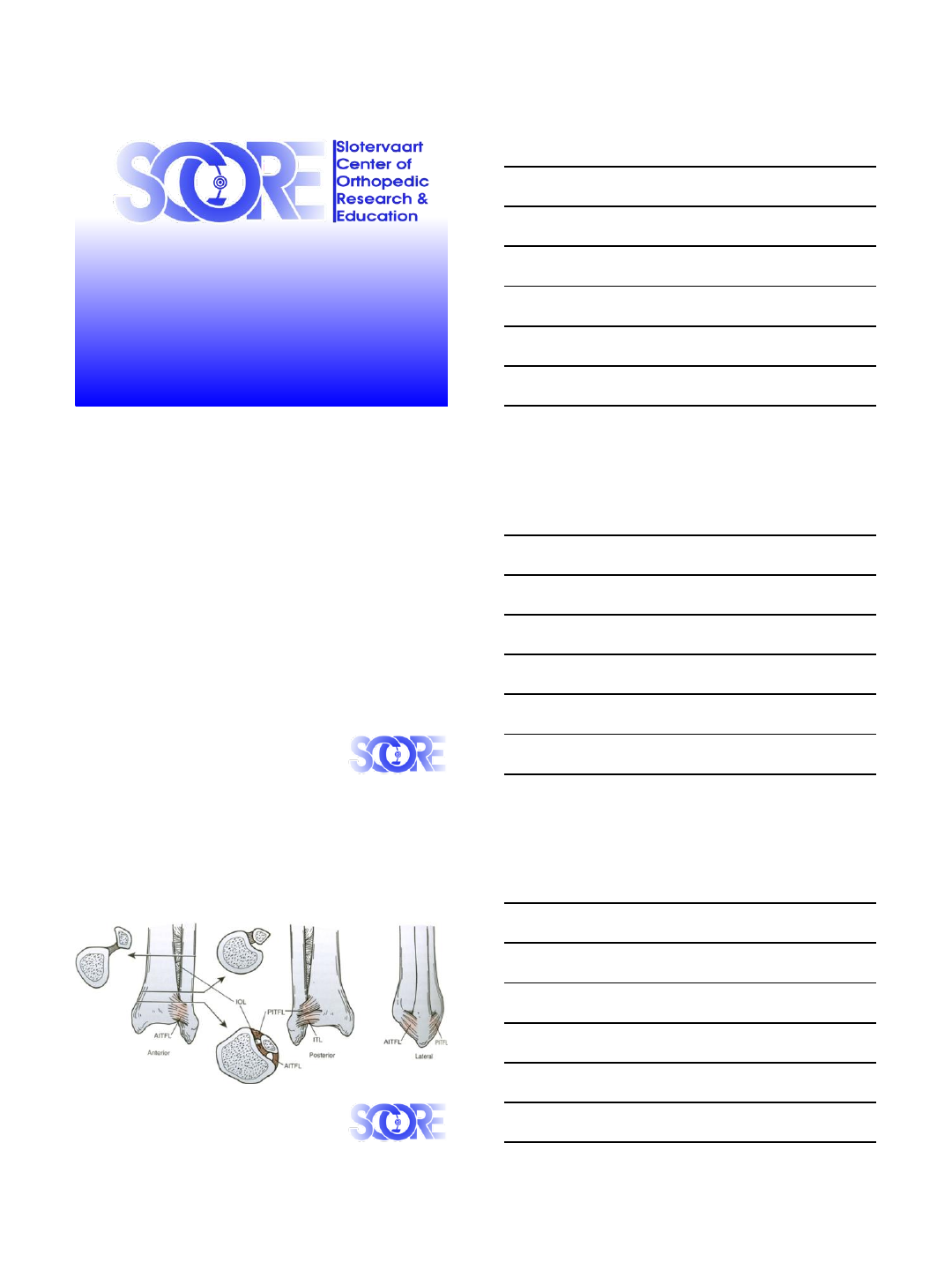
anterior and posterior inferior tibiofibular ligaments (AITFL
and PITFL) as well as the interosseous tibiofibular ligament
(IOL). The transverse tibiofibular ligament (TTFL) is
considered a continuation or deep portion of the posterior
PITFL
7/5/2015
2
Mechanism of injury
Courtesy James Calder

7/5/2015
3
7/5/2015
4
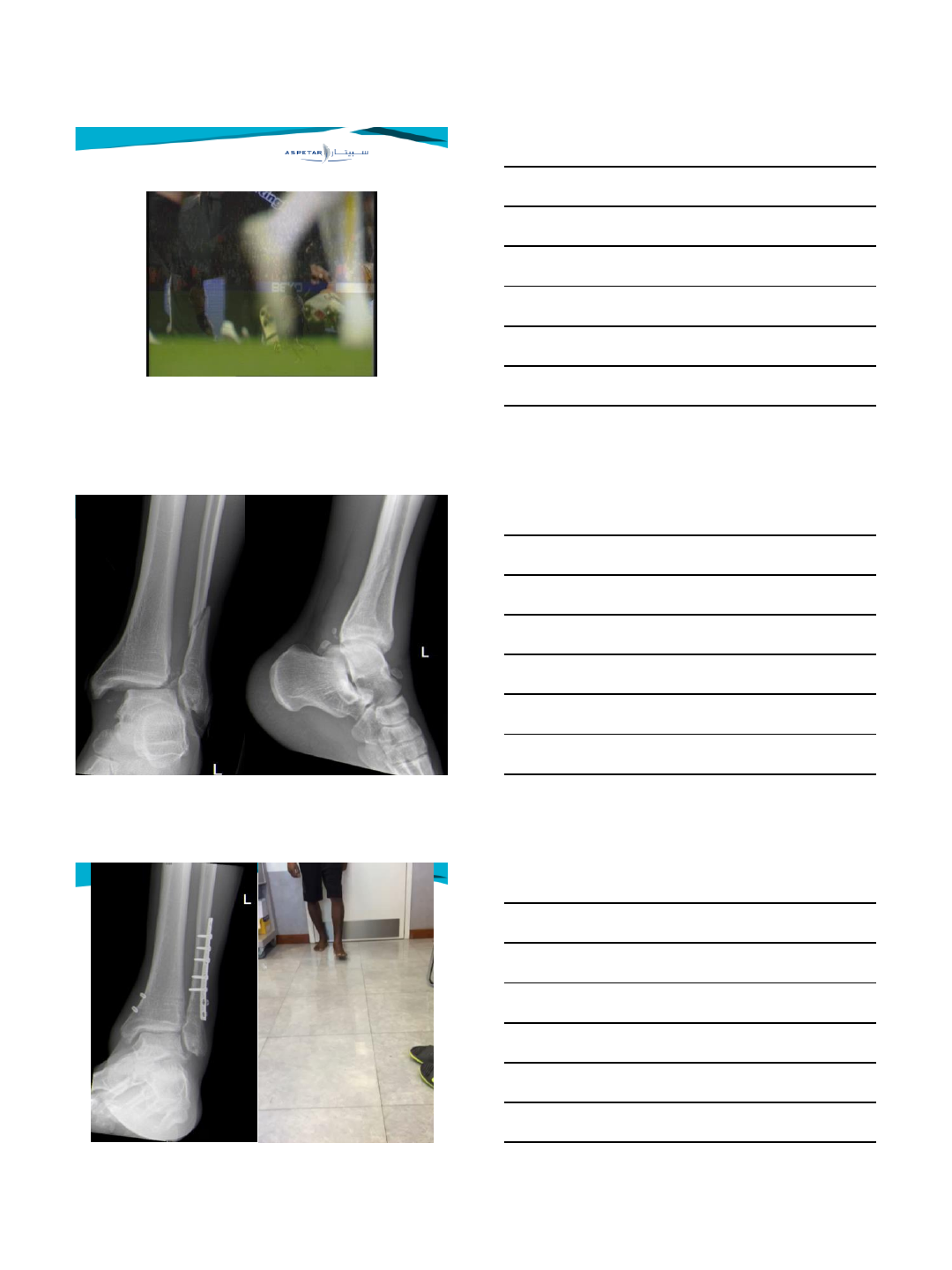
Late syndesmotic widening
History:
•Persistent pain after fracture/sprain
•Giving way
•Difficulty with walking on uneven ground
Delayed operative treatment of syndesmotic instability. Current concepts review.
Van den Bekerom M, de Leeuw P, van Dijk CN
Injury 2009
Late syndesmotic widening
Delayed operative treatment of syndesmotic instability. Current concepts review.
Van den Bekerom M, de Leeuw P, van Dijk CN
Injury 2009
Physical examination
1. Swelling pressure pain over syndesmosis
2. Stiffness/ limited dorsiflexion upper ankle joint
3. Cotton test, fibular translation test
4. External rotation test is not reliable ( false negatives )
Late syndesmotic widening
Delayed operative treatment of syndesmotic instability. Current concepts review.
Van den Bekerom M, de Leeuw PAJ, van Dijk CN
Injury 2009
Radiology:
•Arthrogaphy (Olsen 1981) (Katznelson 1983)
•MRI (Han 2007) (Kim 2007)
•Arthroscopy (Lui 2005) (Sri-Ram 2005)
7/5/2015
5
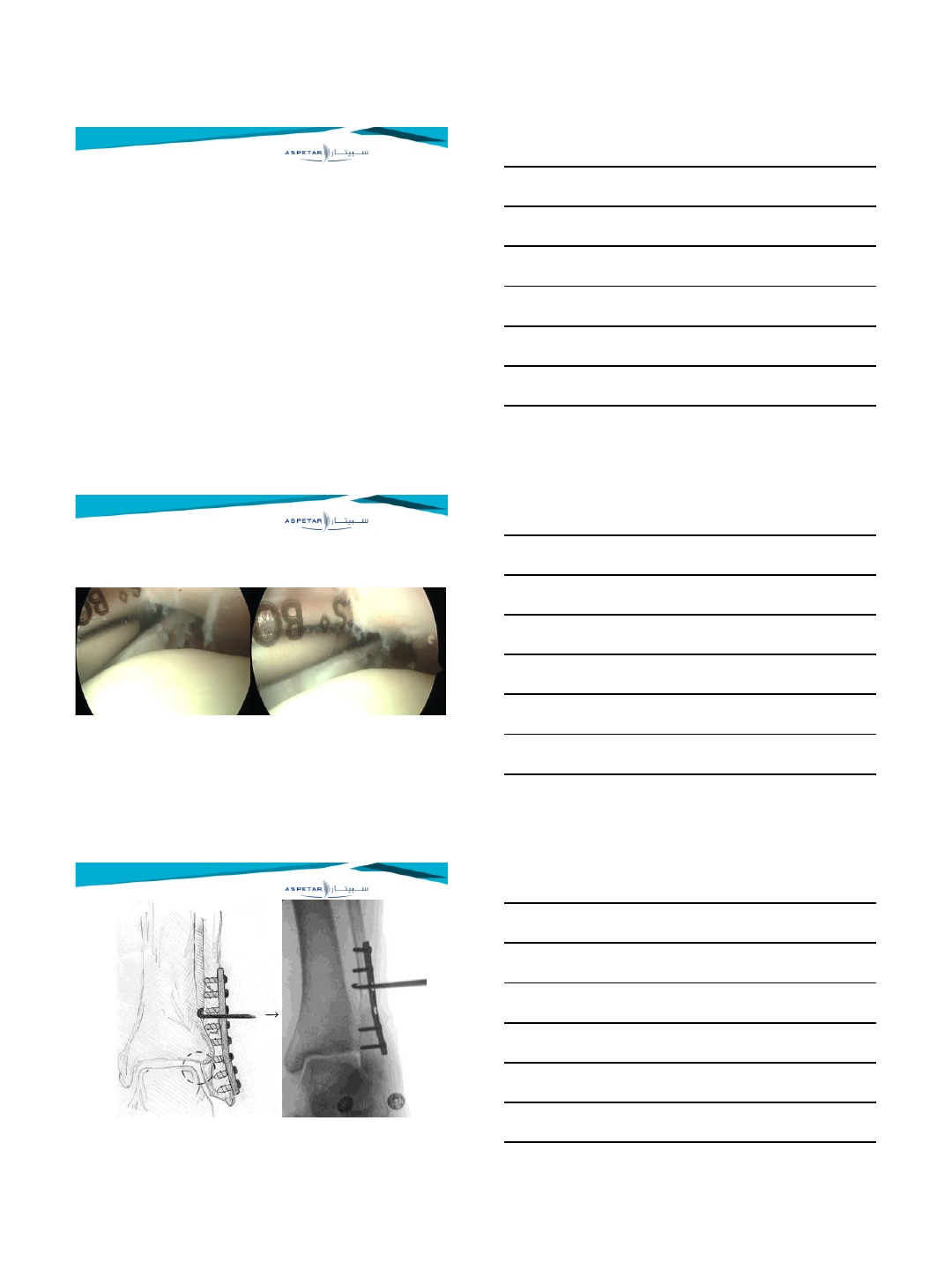
IMAGING
•Comparative weightbearing X-rays should be made
•MRI is the most appropriate additionial tool
•CT (comparitive) might be usefull in assessing
rotational deformities
•Dynamic sonography might play a role in selected
centers
•Diagnostic arthroscopy can be performed in cases
with a high clinical suspicion with a non-conclusive
MRI.
Arthroscopic syndesmotic instability assessment
Hook test
Delayed operative treatment of syndesmotic instability. Current concepts review.
Van den Bekerom M, de Leeuw PAJ, van Dijk CN
Injury 2009
7/5/2015
6
TREATMENT
•Untreated have poor prognosis
•No distinction between subacute and chronic
•Syndesmotic enhancement with lag screw or
positioning screw (3 or 4 cortices) or suture
button technique or combination
•Arthroscopic debridement with lag screw or
positioning screw (3 or 4 cortices) or suture
button technique or combination
7/5/2015
7
Late syndesmotic widening
•Treatment options for late syndesmotic widening
•Syndesmotic screw fixation
•Debridement (with screw fixation)
•Repair (with screw fixation)
•Reconstruction (with screw fixation)
•Bone block transfer (with screw fixation)
•Correction osteotomy
•Arthrodesis
Delayed operative treatment of syndesmotic instability. Current concepts review.
Van den Bekerom M, de Leeuw PAJ, van Dijk CN
Injury 2009
7/5/2015
8
Late syndesmotic widening
Delayed operative treatment of syndesmotic instability. Current concepts review.
Van den Bekerom M, de Leeuw P, van Dijk CN
Injury 2009
Syndesmotic screw stabilisation
•Late syndesmotic screw fixation was advocated by Key (1934)
and Mullins (1958)
•Opinion: only screw fixation for chronic instability is not
sufficient
Late syndesmotic widening
Delayed operative treatment of syndesmotic instability. Current concepts review.
Van den Bekerom M, de Leeuw PAJ, van Dijk CN
Injury 2009
Arthroscopic debridement and screw stabilisation
•Harper MC, FAI, 2001
–6 patients, 4 males, 2 females, mean age 41
–PER stage IV
–15 months post-trauma
–23 months follow-up
–5/6 patients are satisfied
•Opinion: only debridement to aim for a fibrotic union (with
screw fixation) is not sufficient
Late syndesmotic widening
Delayed operative treatment of syndesmotic instability. Current concepts review.
Van den Bekerom M, de Leeuw P, van Dijk CN
Injury 2009
Repair ( + arthroscopic debridement and screw stabilisation)
•Mosier-LaClair, Foot Ankle Clin, 2000
–8 patients
–5 Weber C #, 3 ankle sprains
–48 months post-trauma
–24 months follow-up
–8/9 satisfied. 1/9 dissatisfied
•Opinion: only possible when there are adequate remnants of
the syndesmotic ligament.
7/5/2015
9
Late syndesmotic widening
Reconstruction (+ arthroscopic debridement and screw stabilisation)
•Grass, FAI, 2003
–Reconstruction with peroneus longus
–16 patients, 2 males, 14 females, mean age 40
–14 PER, 2 PA
–14 months post-trauma
–16 months follow-up
–16 are relieved of chronic instability, 15 are relieved of pain
Delayed operative treatment of syndesmotic instability. Current concepts review.
Van den Bekerom M, de Leeuw P, van Dijk CN
Injury 2009
Late syndesmotic widening
Reconstruction (arthroscopic debridement and screw stabilisation)
•Other options
–Extensor Dig V (Kelikian)
–Plantaris tendon (van Dijk, Kelikian)
–Fascia (Kelikian)
–Dura mater (Kelikian)
•Opinion: Reconstruction with plantaris tendon or gracilis tendon
is a good option when there are no adequate remnants and
there is no slack intact ligament
Delayed operative treatment of syndesmotic instability. Current concepts review.
Van den Bekerom M, de Leeuw P, van Dijk CN
Injury 2009
Late syndesmotic widening
Bone block transfer (screw stabilisation)
•Beumer, Acta Orthop Scand, 2000
–Bone block transfer with syndesmotic screw fixation, 9 patients.
–45 months post-trauma
–9/9 are relieved of chronic instability, 2 developed dystrophy, 1 nerve
entrapment
•Van Dijk, Tech Foot Ankle Surg, 2006
–Bone block transfer with syndesmotic screw fixation, 6 patients.
–No patient was symptom free, 2 patients had a later synostosis
7/5/2015
10
Late syndesmotic widening
Bone block transfer ( + screw stabilisation)
•Opinion: a good technique when there is a slack but intact
ligament
•Beumer (2000) stated that even in late cases, the ligament was
slack but always present
•Bahr (1997) stated that anatomic repair with the original
(TibioFibular) ligament should be better
Delayed operative treatment of syndesmotic instability. Current concepts review.
Van den Bekerom M, de Leeuw P, van Dijk CN
Injury 2009
Late syndesmotic widening
Correction osteotomy ( + arthroscopic debridement)
•Opinion: when there is a syndesmotic widening and a malunion,
an osteotomy is regarded the first treatment step.
•All components of the malunion should be corrected
•When there is a severly disturbed ankle function, an arthrodesis
should be considered.
Delayed operative treatment of syndesmotic instability. Current concepts review.
Van den Bekerom M, de Leeuw P, van Dijk CN
Injury 2009
Late syndesmotic widening
Tibiofibular fusion
•Katznelson et al, Injury, 1983
–5 patients, 3 males, 2 females, mean age 20 yr.
–Ankle sprains
–10 months post trauma
–5/5 pain free, 4/5 free ROM
•Opinion: this technique can be used for syndesmotic instability
lasting > 6 months.
Delayed operative treatment of syndesmotic instability. Current concepts review.
Van den Bekerom M, de Leeuw P, van Dijk CN
Injury 2009
7/5/2015
11
Chronic Syndesmotic injury
TAKE HOME MESSAGE
•First consider the fibular malalignment
•Repair of the ligament with/when adequate remnants
•Otherwise a reconstruction ( ligamentoplasty )with gracilis
tendon is advised
•When there is a slack but intact ligament: a bone block
translation osteotomy is advised
•Debridement to aim for a fibrotic union
•Tibiofibular joint fusion ( synostosis with graft )
7/5/2015
12
Syndesmotic impingment
Arthroscopically resection of the distal fascicle of the AITFL should be
considered when there:
(1) is contact between the AITFL and the talus,
(2) is increased contact between the talus and the ligament and this
continued until maximum dorsiflexion with abrasion of the
articular cartilage,
(3) bending of the fascicle on the anterolateral edge of the talus with
dorsiflexion and dorsiflexion-inversion,
(4) is a distally inserting fascicle on the fibula, close to the origin of
the ATFL on the fibula. This finding may be missed if the
distraction is preserved throughout the procedure
The distal fascicle of the anterior inferior tibiofibular ligament as a cause of tibiotalar
impingement syndrome: a current concepts review. van den Bekerom MP, Raven EE. Knee Surg
Sports Traumatol Arthrosc 2007
Thank You
