12 14 16 Robotic Spine Syllabus
2016-12-15
: Pdf 12 14 16 Robotic Spine Syllabus 12_14_16_Robotic_Spine_Syllabus 12 2016 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 65
12/14/2016
1
Robotic Spine Surgery
Introduction and Literature Review
Christopher R. Good, MD, FACS
Director of Research
Director of Scoliosis and Spinal Deformity Surgery
Advancements in Robotic Spine Surgery
Agenda
•History of Robotic Surgery and Literature Review
•Christopher R, Good MD, FACS
•Minimally Invasive Robotic Spine Surgery
•Michael Wang, MD, FACS
•Robotic Spinal Deformity Surgery
•Ronald Lehman, Jr, MD
•Robotic Assisted Spinal Tumor Resection
•Samuel Bederman, MD
•Robotic Sacroiliac Joint Fusion
•Bernard Guiot, MD
•The Future of Robotic Spine Surgery
•Christopher R, Good MD, FACS
Disclosures
Consultant Mazor Robotics
Consultant /Travel Reimbursement
MOI: $1000-$10,000
I use “guidance” in ~ 30% of my cases
First Robot Experience - 2005
First Navigation Experience - 2007
Regular use Navigation -2010
Regular use Robot- 2012
12/14/2016
3
7
Spinal fixation
─Pedicle screws
─Transfacet, translaminar-facet screws
─Sacroiliac screws
Spinal deformities
─Scoliosis posterior spinal instrumentation
Cement augmentations
─Kyphoplasty and vertebroplasty
Oncological applications
─Biopsies, tumor resections
Revision Surgery
Robotic-Guided Spine Surgery
Posterior approaches (Open, MIS, Percutaneous)
Robotic-Guided Spine Surgery
Planning Software
Workstation
Guidance Unit
Robotic-Guided Spine Surgery
Pre-op 3D planning
12/14/2016
4
Robot Registration Process
10
Pre-op CT vs intra-op CT “scan and plan”
Robot mounted to patient via bone
Robot Positioning Near Patient
Reference Arc
12/14/2016
5
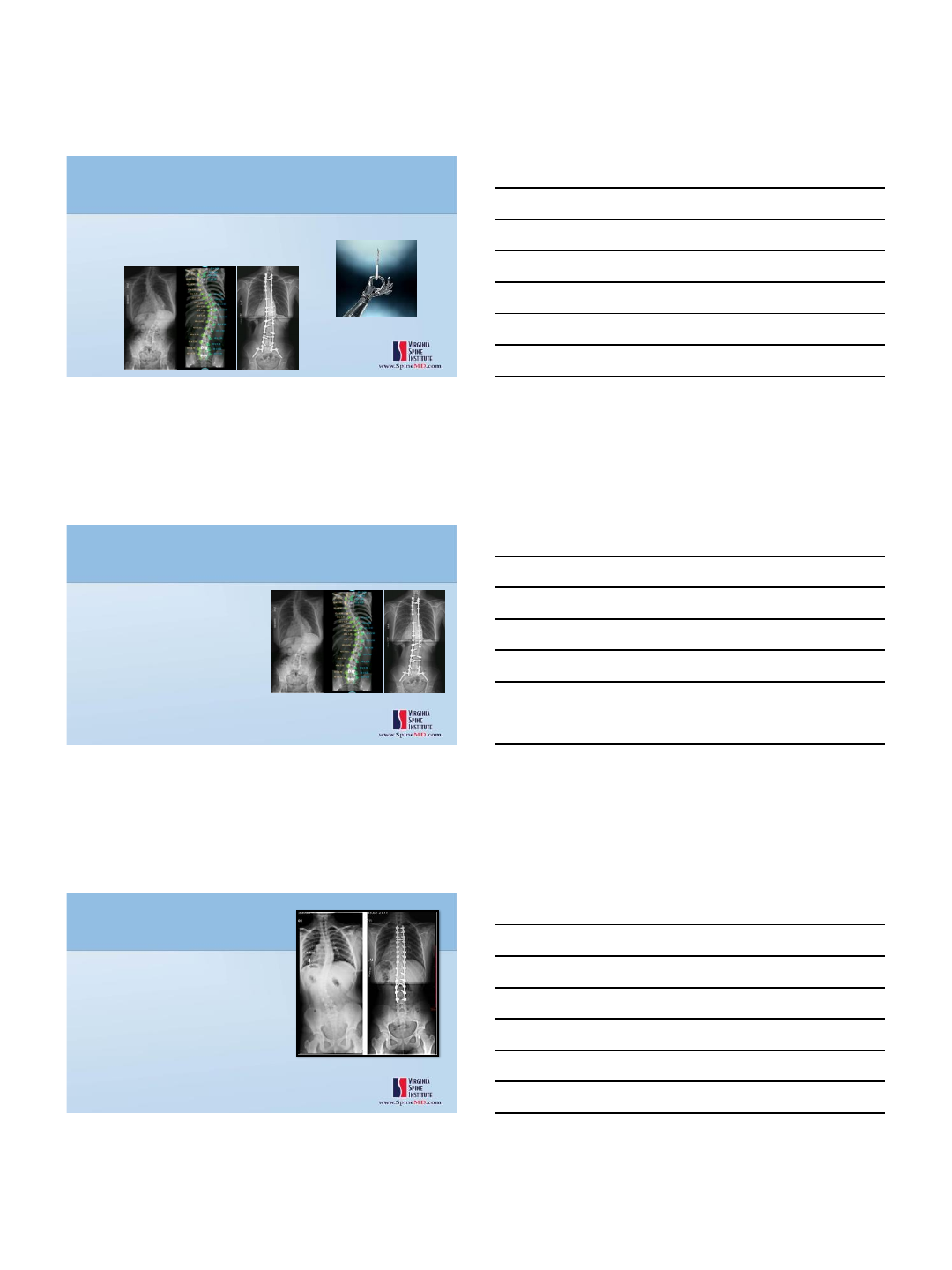
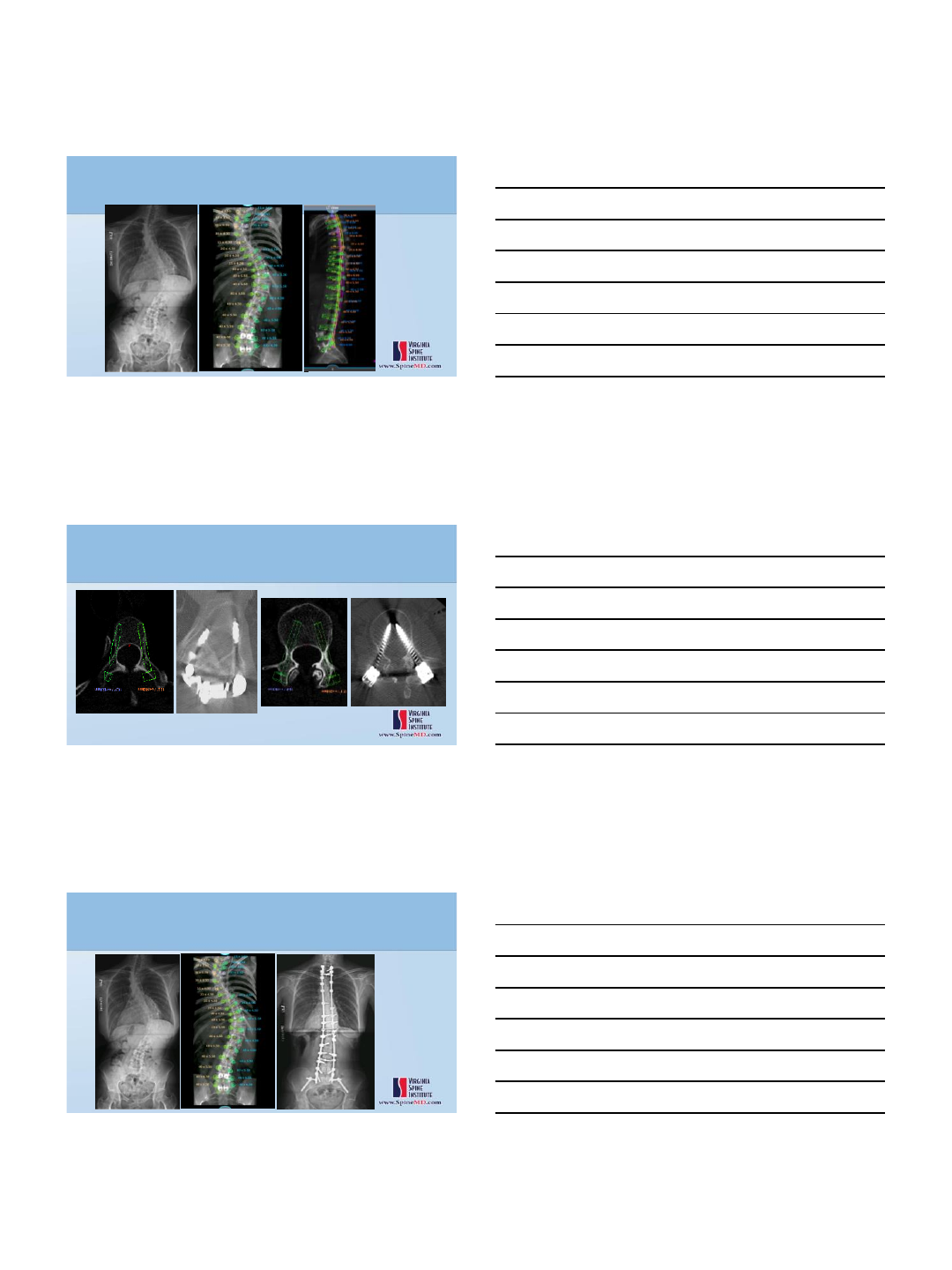
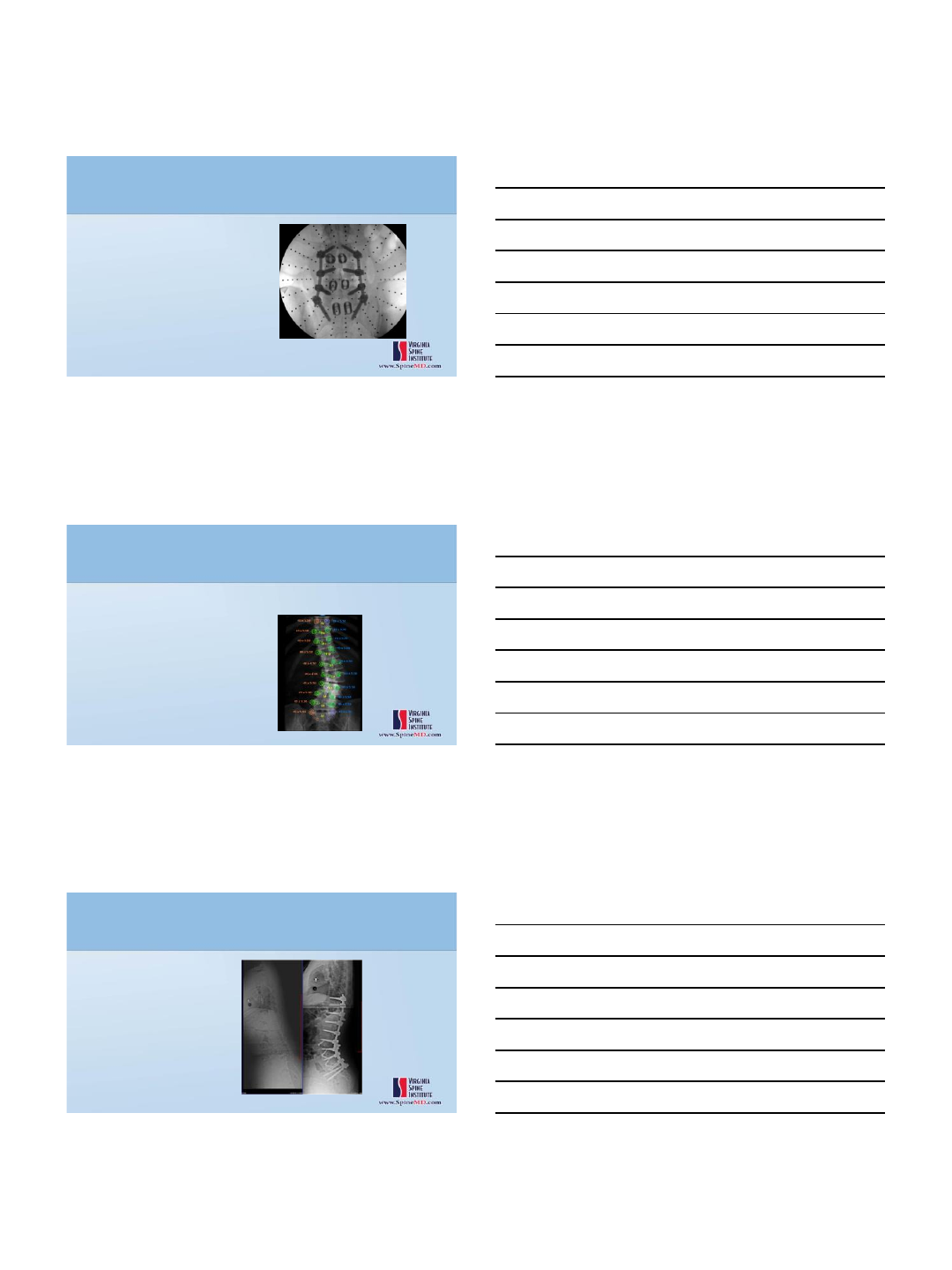
Robotic-Guided Scoliosis Correction
Cortical Pedicles, Severe Osteoporosis
Progressive Deformity, PFTs 47% predicted
L3
T3
Robotic-Guided Scoliosis Correction
Cortical Pedicles, Severe Osteoporosis
Progressive Deformity, PFTs 47% predicted
12/14/2016
6
MIS Deformity
Template skin incisions
12/14/2016
7
n=3,059 n=12,299
•130 studies –37,337 pedicle screws (cadaver and in vivo)
•91% accuracy overall
•Navigation –95.2%
•No Navigation –90.3%
•30 studies
•1973 patients - 9310 pedicle screws
•Results consistent throughout all spinal levels
Type
Data
sets
Total
screws
Accurate
screws
% accurate
Conventional
fluoroscopy
12
3719
2532
68.1
2D fluoroscopic
navigation
8
1223
1031
84.3
3D fluoroscopic
navigation
20
4368
4170
95.5
12/14/2016
8
22
•Retrospective review
•Radiographs (all) and CTs (646 screws)
•635 cases in 14 medical centers
•49% of implants placed percutaneously
•98.3% Accuracy of 3,271 implants
•CT data
•98% safe (<2mm)
•89% contained
23
Retrospective: 112 cases Robot vs freehand
•Improved implant accuracy
•94% vs 91%
•Reduced fluoroscopy by 56%
•34 sec vs 77 sec
•Reduced complication rates by 48%
•Reduced re-operations 46%
•1% vs 12%
•Reduced average length of stay 27%
•10.6 days vs 14.6 days
•Cadaveric Study
–New robotic device
–Coupled with flat panel CT guidance
–38 cadaver screws
•37 (97.4%) fully contained
•1 screw ,1mm lateral breach

12/14/2016
9
•20 patients , 1 surgeon
•10 robot (40 screws)
•10 freehand (50 screws)
•Operating time
•Robot 187 min
•Freehand 119 min
•Accuracy
•Robot
•36/40 successfully placed (4 manually placed)
•97% accurate
•Freehand
•50/50 successfully placed
•92% accurate
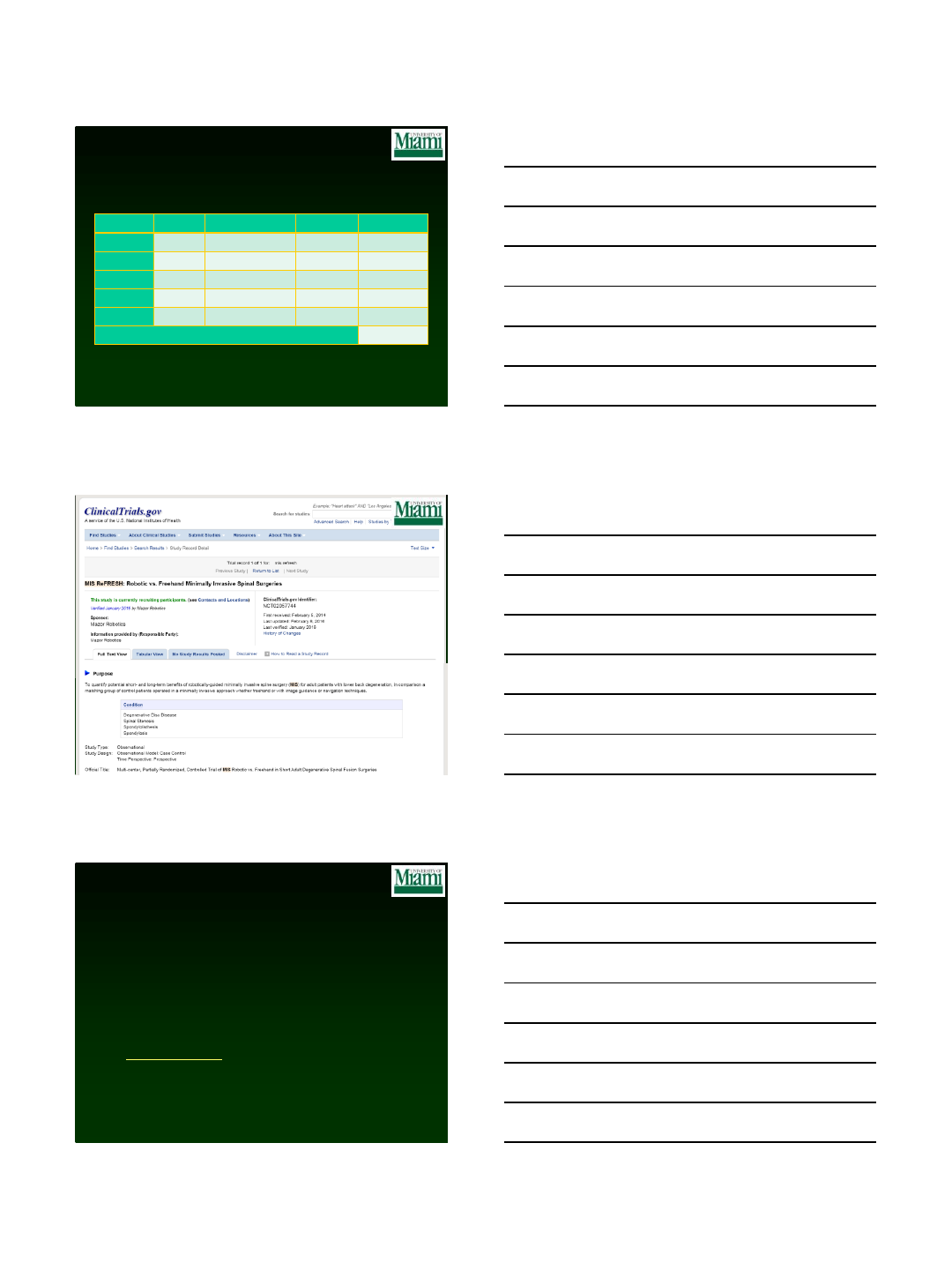
First Report from MIS ReFRESH ‐ a Prospective, Comparative Study of
Robotic‐ Guidance vs. Freehand Pedicle Screw Placement in Minimally
Invasive Lumbar Surgery
IMAST 2016
Zahrawi F1, Schroerlucke SR2, Good CR3, Wang MY4
•Prospective, comparative multi-center study –Robot vs Freehand
•Lumbar instrumented fusions: 1-3 levels
•Complications
•Accuracy
•Rate of revision surgery
•143 cases
•118 robot, 25 freehand
•Fluoro time
•3.2 sec/screw robot
•12.5 sec/screw freehand (p<0.001)
•Complications
•Robot –no complications
•Freehand –1 neuro deficit, 1 infection (p=0.03)
Robotic-Guided Spine Surgery
Potential Advantages
•Improved Accuracy
•Less Intra-op Radiation
•Complex procedure / anatomy
•DOES change my usual technique
•MIS
•Screw cadence facilitates rod placement
•Plan skin incision
140260
12/14/2016
10
Robotic Weaknesses
Maximum ~ 5 levels per scan
Lack of live intra-op
feedback
Cost / availability
Learning curve
Registration issues
Robotic Spine Surgery Conclusions
•Many robots in development, FDA approval/studies ongoing and growing
•First FDA approved robot
–120 systems worldwide, 80 USA
–>18,000 cases
–>120,000 Implants
Time when Robot is most beneficial:
Complicated anatomy
Severe deformity
Congenital anomaly
Previous surgery
Osteoporosis
Morbid Obesity
Minimal visualization

12/14/2016
11
Thank You!
12/14/2016
1
Advances in Robotics and Navigation
for MIS Spinal Surgery
Michael Y. Wang, MD
Professor & Spine Director
Departments of Neurological Surgery & Rehab Medicine
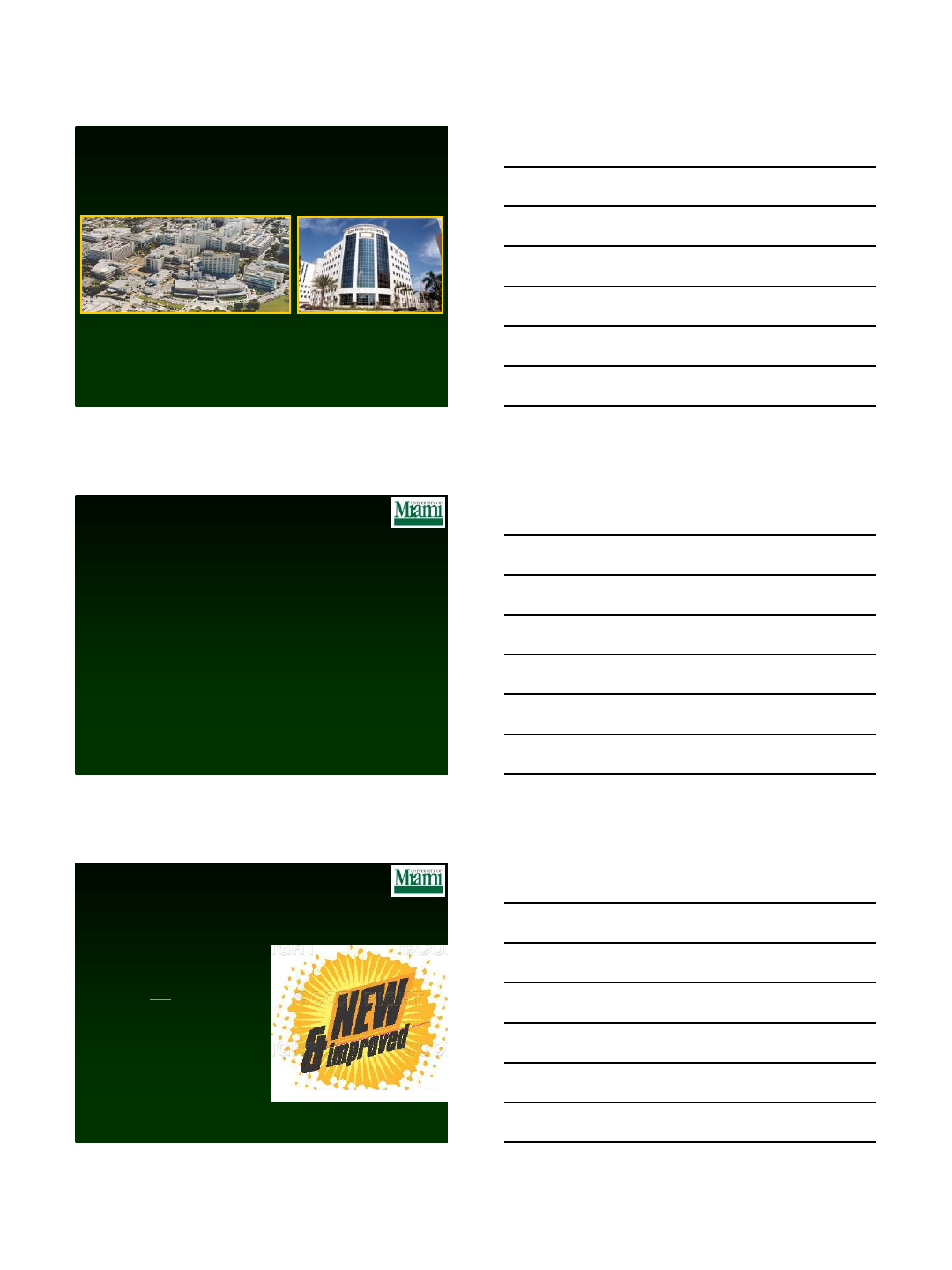
The Miller School of Medicine at the
University of Miami
Disclosures
Consultant: Depuy Spine
Aesculap Spine
JoiMax
K2M
Royalties: Children’s Hospital of Los Angeles
Depuy Spine
Springer Publishing
Quality Medical Publishing
Stock: Innovative Surgical Devices
Spinicity
Grants: Department of Defense
Disclaimer
New does not mean better !
12/14/2016
2
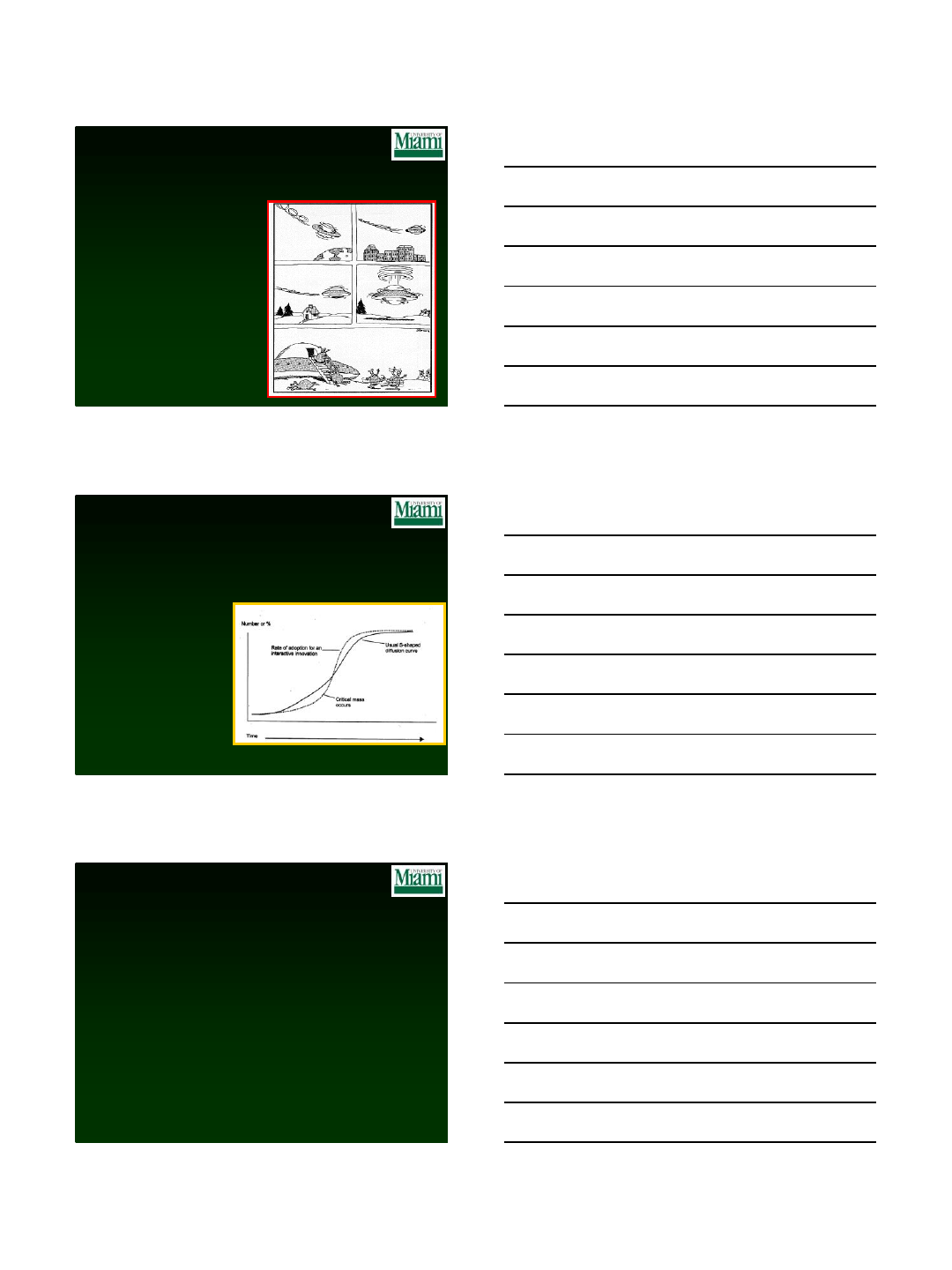
Surgical Obsolescence
The Morbidity of Open Surgery
Pain
Disability
Surgical
Intervention
Inciting
Event Bony Fusion Muscle
Healing
The “Cost” of Surgery
Pain
Surgical
Intervention
Inciting
Event Bony Fusion
“Healthy”
Preop
POD #1
Muscle
Healing
12/14/2016
3
Disadvantages of Minimally
Invasive Spine Surgery
› Technically challenging
› Inadequate visualization
› Disorienting
› Difficult to manipulate
instruments & structures
› ? Iatrogenic neural injury ?
High Complication Rates
Resulted in a previous
generation of spine
surgeons being
disabused of MIS
The “Disconnect”
MIS Adoption remains at less than 20% of lumbar
fusion surgeries
Reasons:
• Safety concerns
• Lack of familiarity
• Limited applications
• Increased work effort
• Financial disincentive
So what is the role of
Robotics & Navigation?
12/14/2016
4
Different Surgical Robots
Da Vinci®
Cyberknife®
Who Needs Robotics?
•Too expensive
•It will slow me down
• I’m doing just fine
• Don’t fix what isn’t broken
•Just helps place K-wires
•Marketing ploy
“Maybe it’s good for other surgeons, but I don’t
need it”
12/14/2016
5
13
Doesn’t technology add to cost?
Complication Avoidance
12/14/2016
6
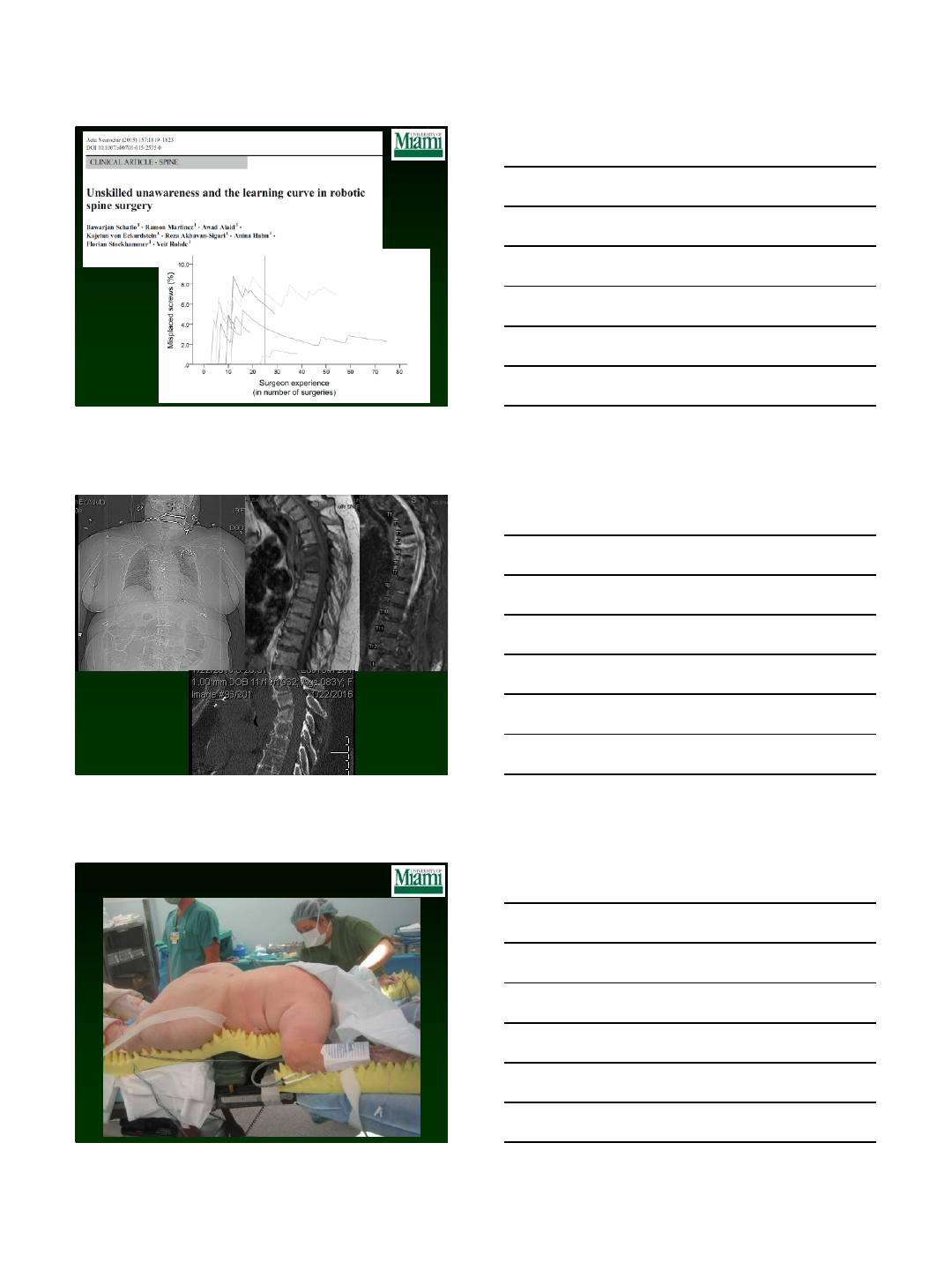
Pedicle Screw Misplacement
Problem:
The radiographic breach rate is > 5% in open surgeries
Solutions:
1. Experience
2. Intra-operative visualization/palpation
3. Proper X-ray guidance
4. Neuronavigation
5. Neuromonitoring
Good judgment comes from experience, and
experience comes from bad judgment
Can MIS Techniques Get You There?
12/14/2016
8
Bed Mount
24
12/14/2016
9
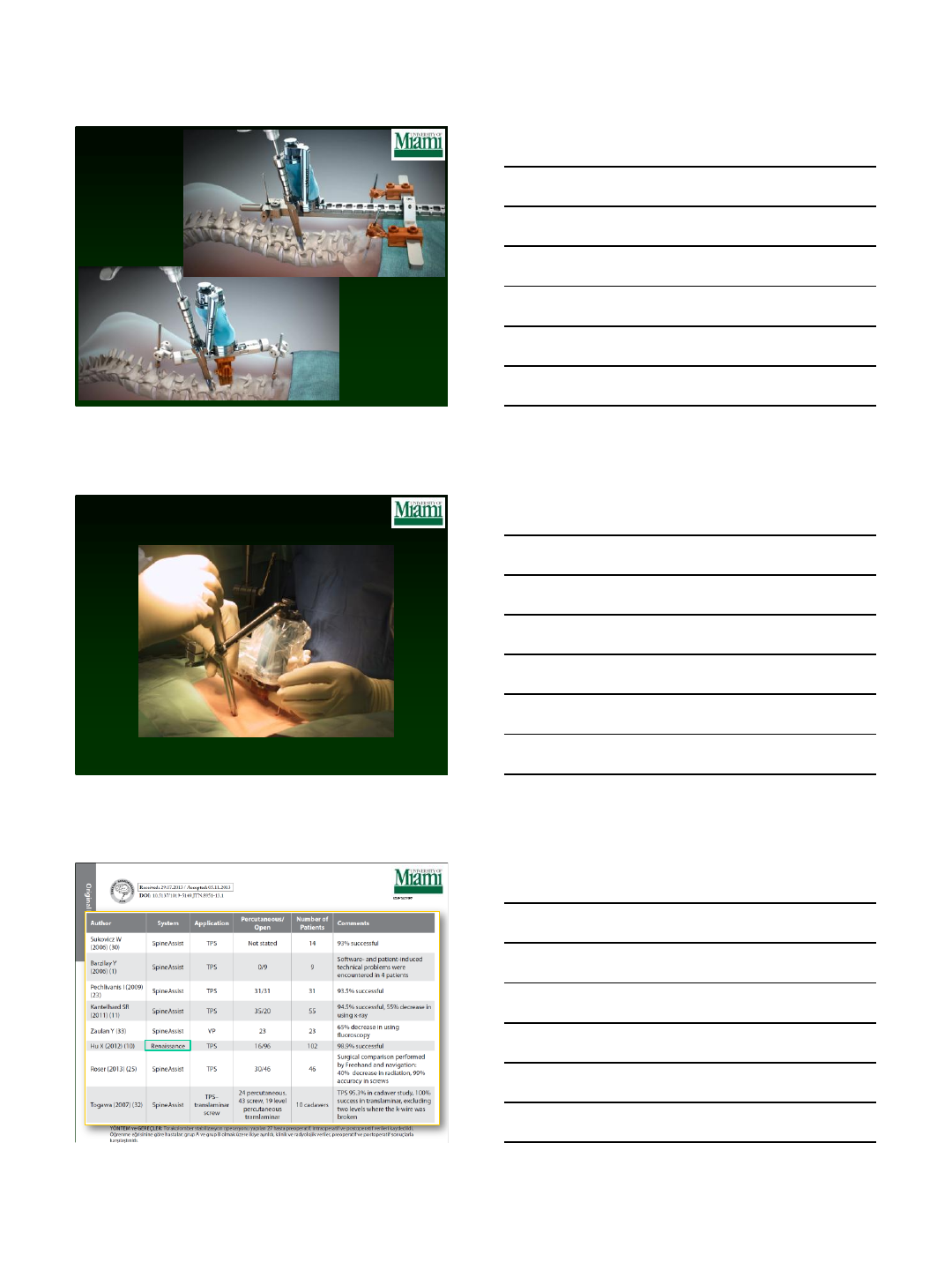
Review of evidence on
Renaissance accuracy
Author
Year
Study type
# screws
Safe Screws
Hu
2013
Retrospective
960
98.9%
Onen
2014
Prospective
136
98.5%
Kim
2015
RCT**
80
100%
Fujishiro
2015
Cadaveric study
216
100%
Kuo
2016
Retrospective
317
98.7%
Weighted average
99.0%
* Fully within the pedicle or breaching <2mm
** RCT = Randomized Control Trial
MIS ReFRESH
26
MIS ReFRESH
•Prospective
•Multi-center (currently 6 sites)
•Controlled, partially randomized study
•Adult degenerative lumbar disease
•Fusion surgery of 1 to 3 levels
Outcome Measures
•Surgical complications
•Revision surgeries
•Intra-operative fluoroscopy
12/14/2016
10
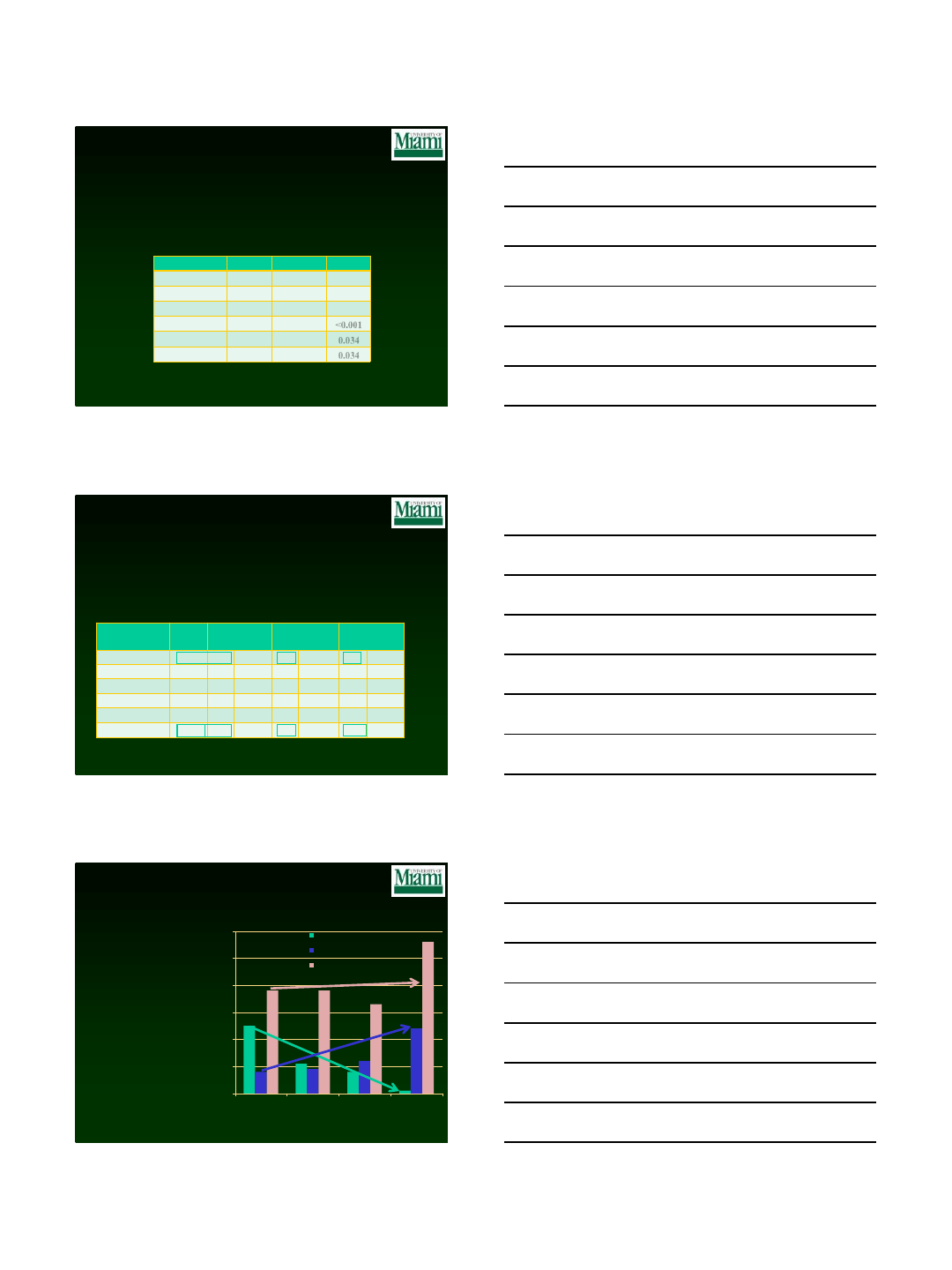
MIS ReFRESH - Surgical Outcomes
•No significant differences in:
–Charleson comorbidity Index (0.5)
–Gender (60% female)
–Age (58)
–BMI (30.8)
Robotic
Freehand
P-value
Sites*
3
2
Patients
118
25
# levels
1.4 (1-3)
1.1 (1-2)
0.006
Fluoro/screw
3.2±2.8
12.5±7.9
<0.001
Complications
0
2
0.034
Revisions
0
2
0.034
*1 surgeon randomized patients to both arms
Retrospective Comparative Analysis
Sweeney et al.
Parameter
Robot
MIS
Total Freehand
Freehand MIS
Freehand Open
# of patients
167
99
p vs. robot
46
p vs. robot
53
p vs. robot
% female
48.5
42.4
>0.05
50.0
>0.05
35.8
>0.05
Age
68.3
62.6
<0.001
60.5
0.001
64.6
0.093
BMI
31.4
31.2
>0.05
30.3
>0.05
31.7
>0.05
Screws per case
8.2
7.2
<0.001
5.6
<0.001
8.7
>0.05
% complications
4.8
10.1
>0.05
6.5
>0.05
13.2
0.034
Robotics MIS vs. Freehand MIS & Open
Doctor’s Hospital, Sarasota, FL
268 patients
Adults, thoracolumbar degenerative spine disease
Parameter
Robot
MIS
Total Freehand
Freehand MIS
Freehand Open
# of patients
167
99
p vs. robot
46
p vs. robot
53
p vs. robot
% female
48.5
42.4
>0.05
50.0
>0.05
35.8
>0.05
Age
68.3
62.6
<0.001
60.5
0.001
64.6
0.093
BMI
31.4
31.2
>0.05
30.3
>0.05
31.7
>0.05
Screws per case
8.2
7.2
<0.001
5.6
<0.001
8.7
>0.05
Parameter
Robot
MIS
Total Freehand
Freehand MIS
Freehand Open
# of patients
167
99
p vs. robot
46
p vs. robot
53
p vs. robot
% female
48.5
42.4
>0.05
50.0
>0.05
35.8
>0.05
Age
68.3
62.6
<0.001
60.5
0.001
64.6
0.093
BMI
31.4
31.2
>0.05
30.3
>0.05
31.7
>0.05
Parameter
Robot
MIS
Total Freehand
Freehand MIS
Freehand Open
# of patients
167
99
p vs. robot
46
p vs. robot
53
p vs. robot
% female
48.5
42.4
>0.05
50.0
>0.05
35.8
>0.05
Age
68.3
62.6
<0.001
60.5
0.001
64.6
0.093
Parameter
Robot
MIS
Total Freehand
Freehand MIS
Freehand Open
# of patients
167
99
p vs. robot
46
p vs. robot
53
p vs. robot
% female
48.5
42.4
>0.05
50.0
>0.05
35.8
>0.05
Parameter
Robot
MIS
Total Freehand
Freehand MIS
Freehand Open
# of patients
167
99
p vs. robot
46
p vs. robot
53
p vs. robot
Case Mix by Surgical Approach
Sweeney et al.
•Clear preference for
Freehand MIS in short
fusions
–Freehand MIS performed
mainly in 1 level cases
–Single case of 4 levels
Freehand MIS
•Robotics enables MIS in
all types of cases
0
10
20
30
40
50
60
1-4
5-6
7-8
9+
FH MIS
FH Open
RO MIS
Screws Executed
Number of cases
12/14/2016
11
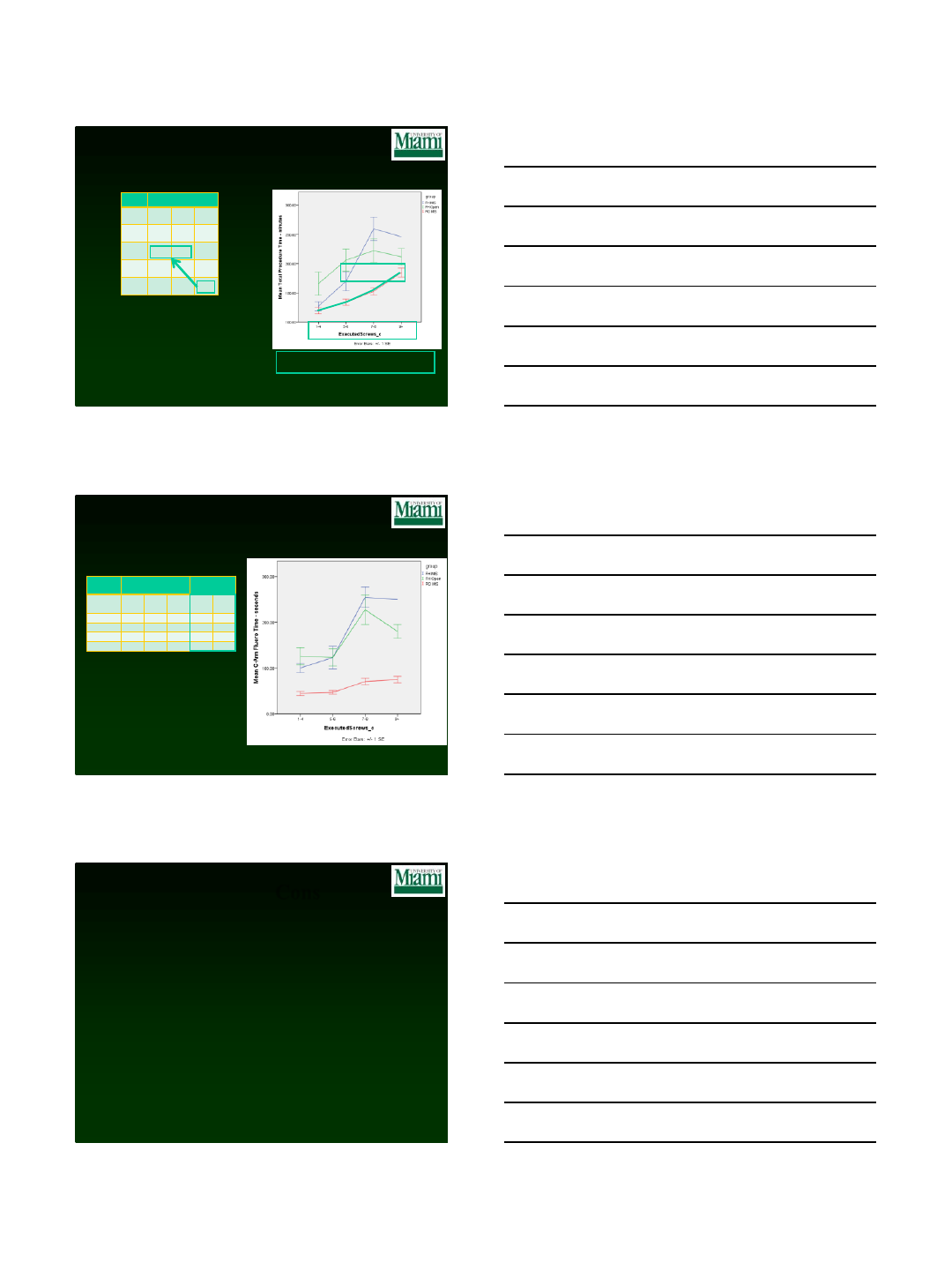
Procedure Time by Technique –
Sweeney et al.
•Robotics MIS is significantly
faster than freehand MIS or open
Robotic
MIS
Freehand
Open
Freehand
MIS
Skin-to-skin (min)
Levels
FH
Open
FH
MIS
RO
MIS
1
166
127
120
2
206
170
134
3
222
260
153
4+
212
246
185
Multi-level Robotic MIS case takes about as long
as a 2-level freehand case
Fluoro Exposure by Technique –
Sweeney et al.
•Robotics reduces fluoro by:
Robotics MIS requires significantly
less fluoro than freehand MIS or open Robotics MIS
Freehand Open
Freehand MIS
Fluoro time - seconds
Reductions in
%
Levels
FH
Open
FH
MIS
RO
MIS
vs.
open
vs.
MIS
1
126
100
45
64%
55%
2
123
123
47
62%
62%
3
227
255
71
69%
72%
4+
180
250
75
58%
70%
All results are statistically significant
Pros
•Improved planning
•Implant management
•Enables surgeons to do
complex surgery
•Axial rotation &
deformity are no
longer a challenge
•Stepping-stone
technology
Cons
•Requires one mm CT
scan
•Capital equipment costs
•Learning curve
•Attachment to the
patient or bed
•Dependence on
technology
•Unrecognized screw
misplacement
12/14/2016
12
34
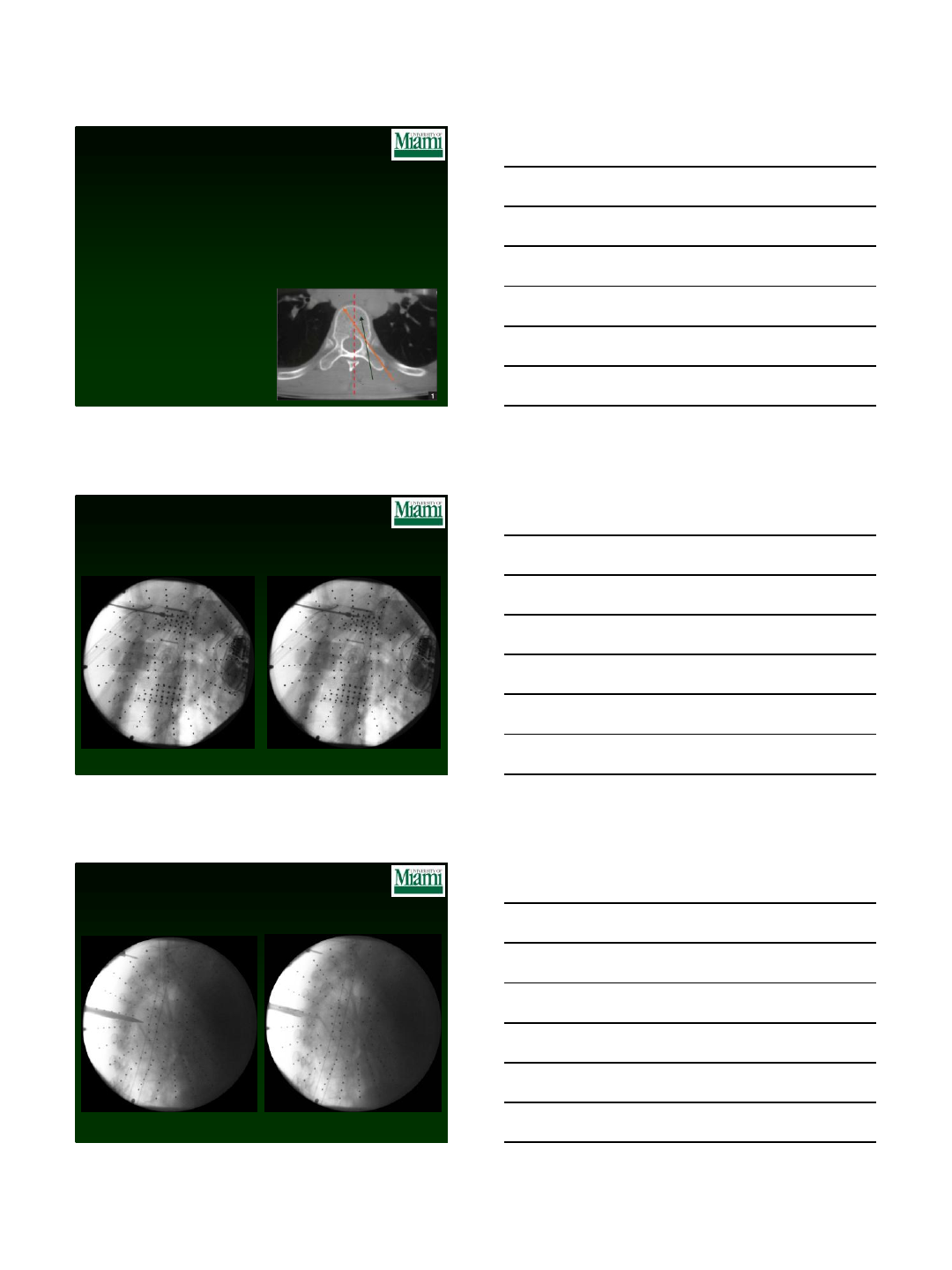
12/14/2016
13
Challenges in this case
•Obesity
•Level localization (T4)
•Surrounding structures (blood vessels, lung,
spinal cord, ribs, intercostal nerves)
•Access trajectory
•Medical co-mobidities
Robot Registraiton
Access at T4
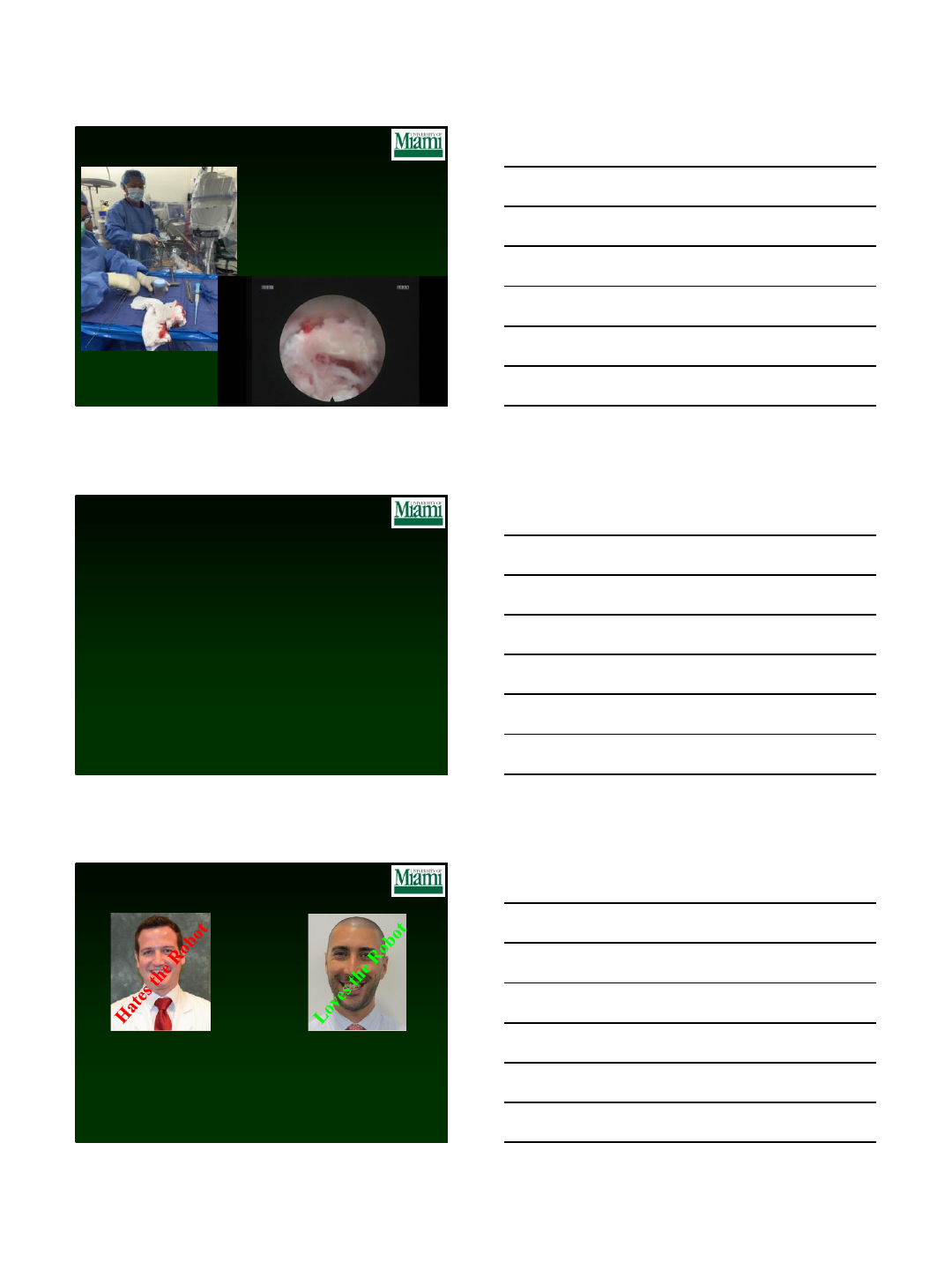
12/14/2016
14
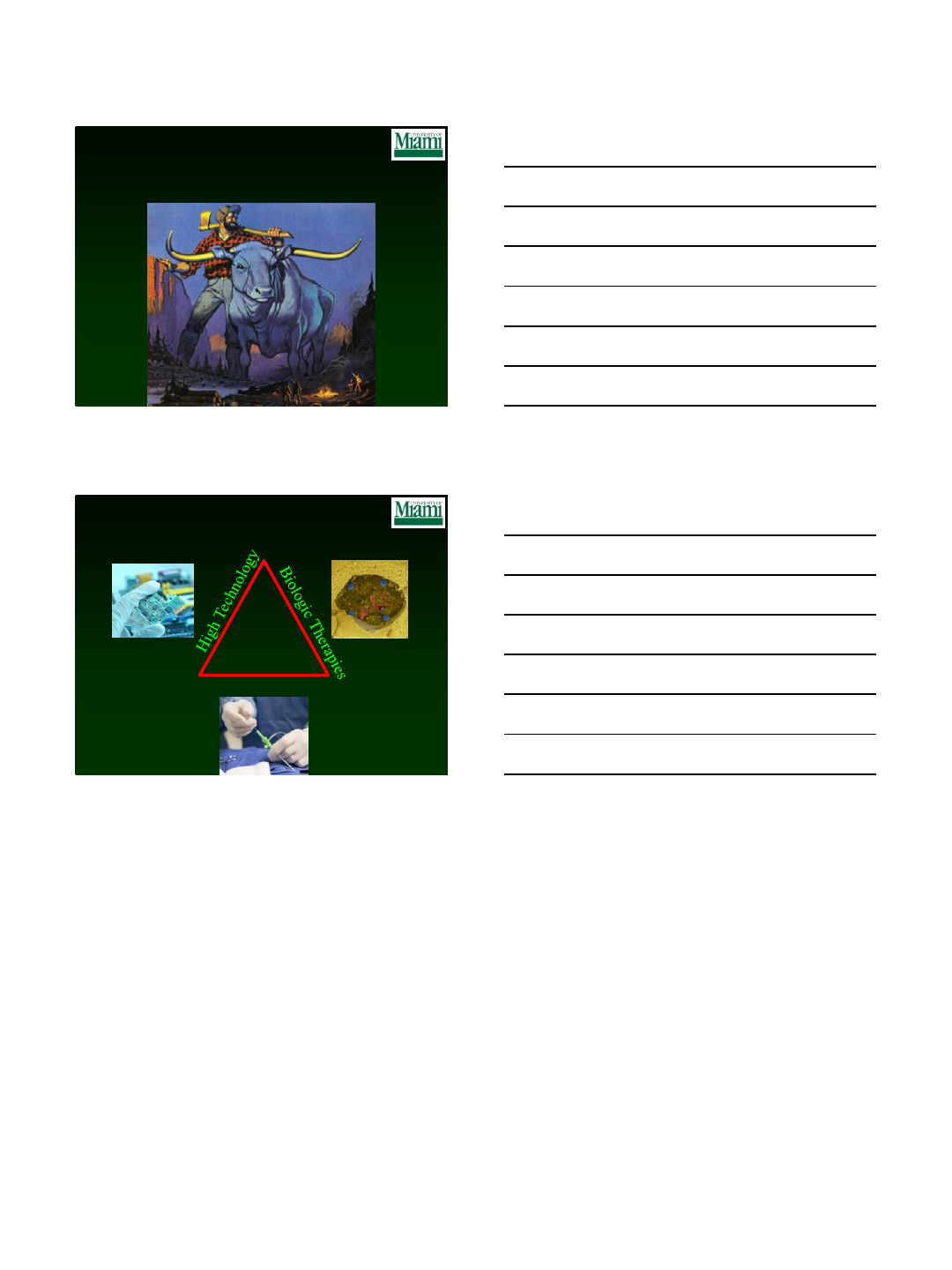
Endoscopic Debridement
A Marriage of Technologies
Robotic localization, trajectory, & access
+
Endoscopic debridement
7th year resident
Performed > 500 spine surgeries
From Missouri
Married w/ two dogs
IQ ~ 145
Who likes the robot?
1st year resident (intern)
Performed < 10 spine surgeries
Worked at Blackrock in NYC
Single (but monogamous)
IQ ~ 154
12/14/2016
15
Paul Bunyan & Babe vs. New
Technology
The Future of Medicine
Minimally Invasive
12/14/2016
1
Ronald A. Lehman, Jr., MD
Professor of Orthopedic Surgery, Tenure
Chief, Degenerative, Minimally Invasive and Robotic Spine Surgery
Director, Robotic Spine Surgery
Complex Pediatric and Adult Scoliosis Service
Co-Director, Spine Fellowship
Director, Clinical Spine Research
Co-Director, Orthopaedic Clinical Research
THE SPINE HOSPITAL
New York – Presbyterian
The Allen Hospital
Robotic Assisted Spine
Surgery (RASS)
Use in Deformity
Why Surgical Guidance
•Surgical Planning
•Create total 3D custom plan for patient
•Consider challenging anatomy
•Optimize implant size and placement
•Accommodate MIS (proximal facet joint, tulip head
alignment, rod passage)
•Intra-op Guidance
•Allows OR staff to be in sync with surgical plan
•Streamline implant sizing and sequence to OR staff
•Execute surgical plan
•Lock trajectory any point, regardless of patient position
Robotic Assisted Spine Surgery
12/14/2016
2
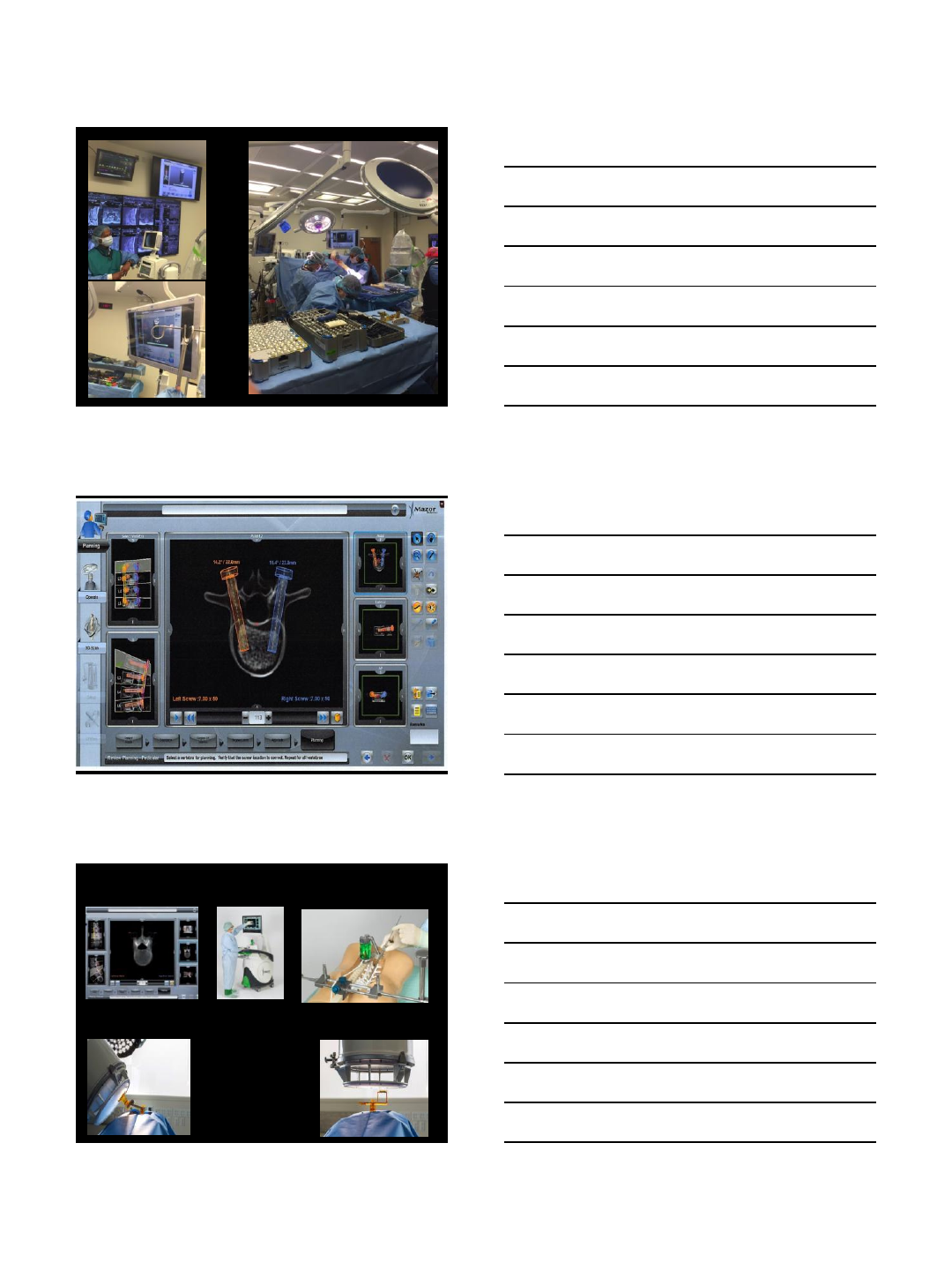
How it Works
•Upload pre-op CT
•Position implants with
Planning software
•Assess in all 3 planes
•Consider global
alignment
1. Create Surgical Plan
Can also create plan Intra-op with O-arm scan (“Scan and Plan”)
CT-based
3D Planning Robot Unit
Workstation
Robotic Assisted Spine Surgery
Registration
AP/Oblique
12/14/2016
3
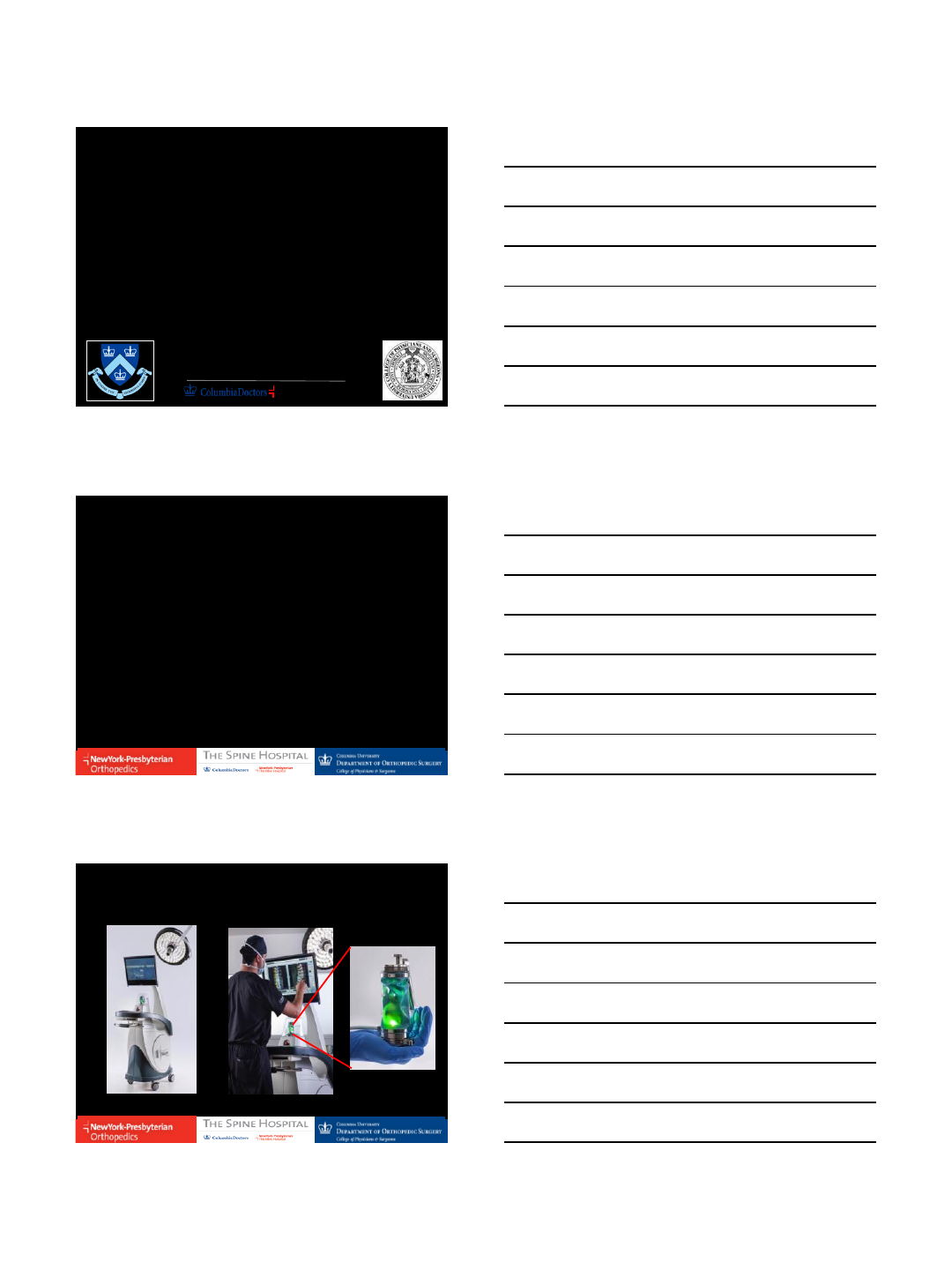
How Does it Work?
Registration
Step 4:
Operate
Step 2:
Mount
Step 3:
3D Sync
Preoperative blueprint of the ideal surgery
is created using CT-based 3D planning
Step 1: Pre Operative Planning
12/14/2016
4
Step 4:
Operate
Step 2:
Mount
Step 3:
3D Sync
Preoperative blueprint of the ideal surgery
is created using CT-based 3D planning
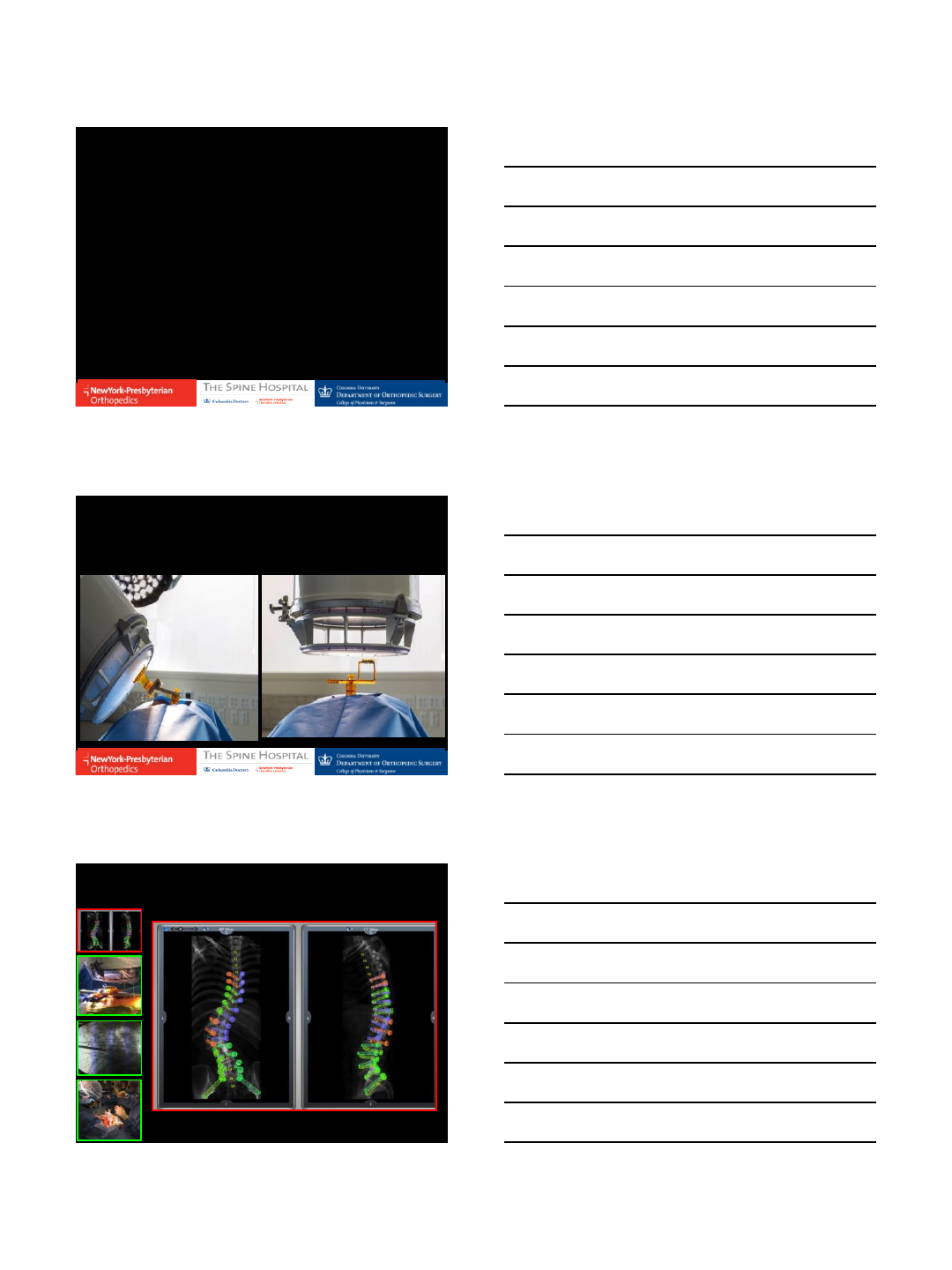
Step 2: Mount Robot Unit
Step 4:
Operate
Step 2:
Mount
Step 3:
3D Sync
Preoperative blueprint of the ideal surgery
is created using CT-based 3D planning
Step 3: Acquire and Sync
Step 4:
Operate
Step 2:
Mount
Step 3:
3D Sync
Preoperative blueprint of the ideal surgery
is created using CT-based 3D planning
Step 4: Operate
S2AI
12/14/2016
5
•Less radiation
– Surgical Team vs. MISS with Flouroscopic Assist
–? Patient (requires preop or intraop CT scan (similar to
navigation)
•Less exposure
–If employed in MISS or MAST Setting
•Accuracy = Big Question
–Freehand?
–Navigation?
–Flouro Assist?
•Based on “segmentation” vs Navigation (alignment)
Potential Advantages
Work Flow
Freehand
1. Exposure
2. Facetectomies
3. Decompression(s)
4. PCOs
5. Screws (benefit open canal)
6. TLIFs
7. Correction
Robotic Assistance
1. Exposure
2. Wires/Tap +/- Screws
3. Facetectomies
4. Decompressions
5. PCOs
6. TLIFs
7. Correction
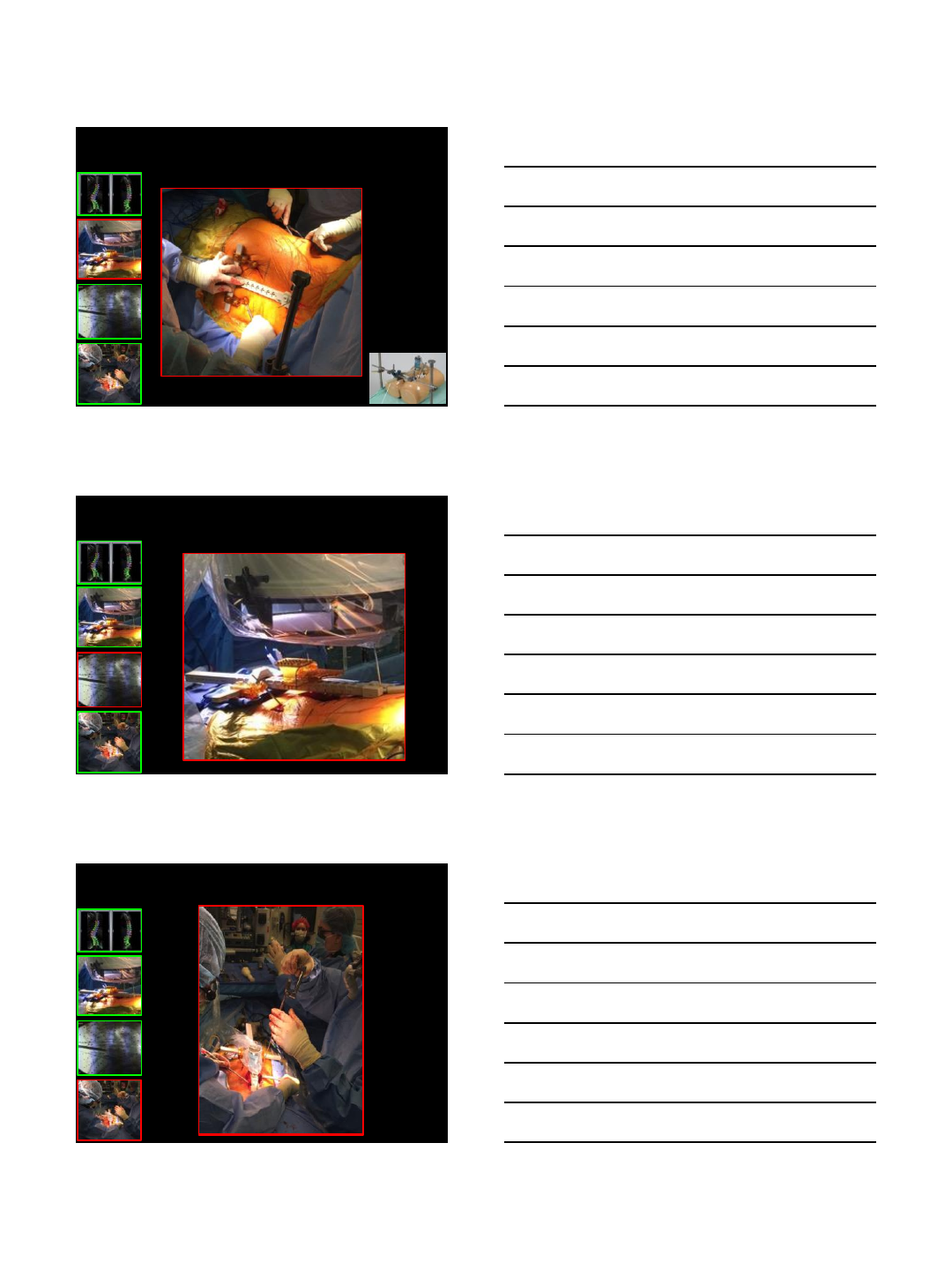
Screw Placement
12/14/2016
6
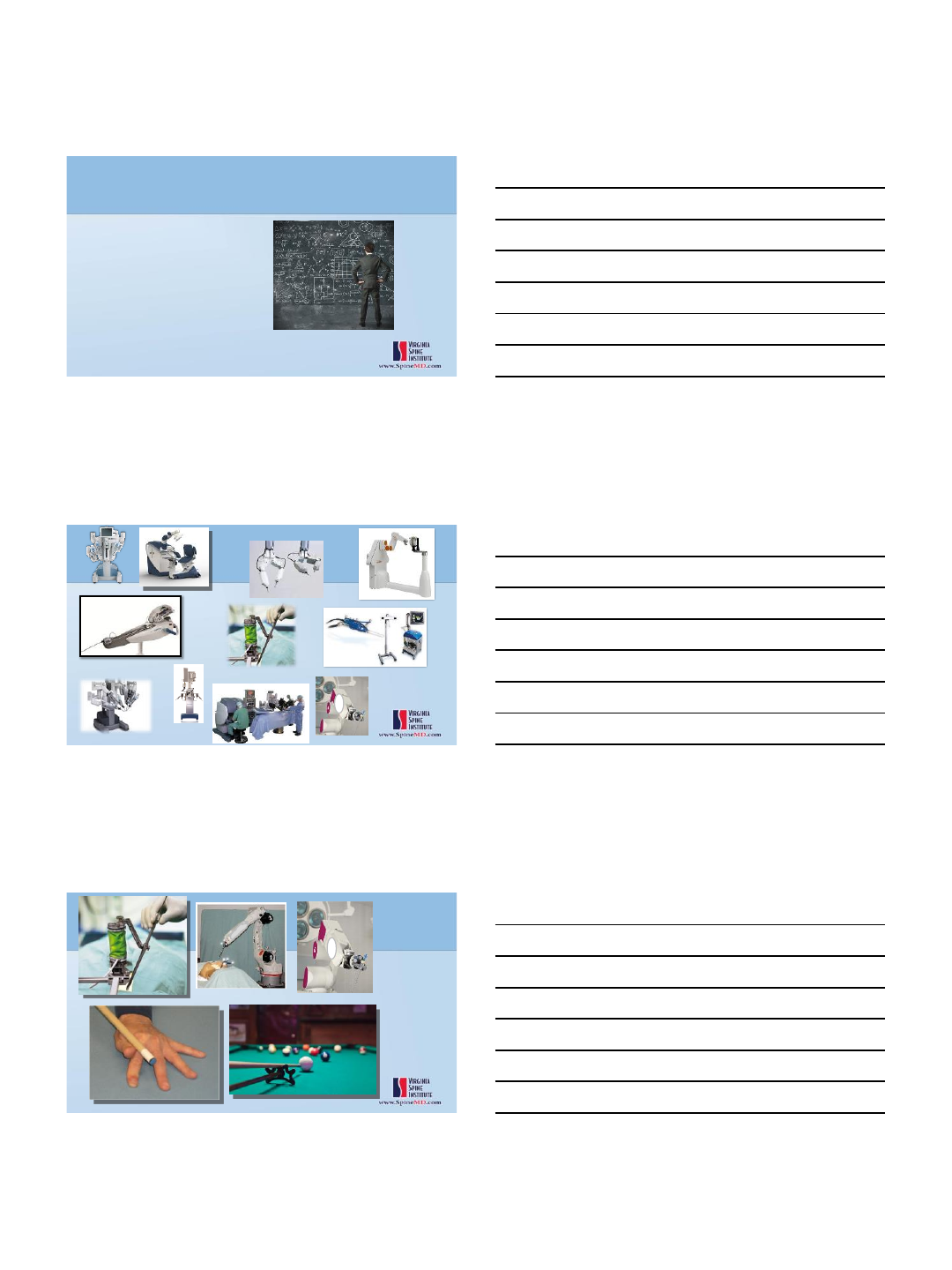
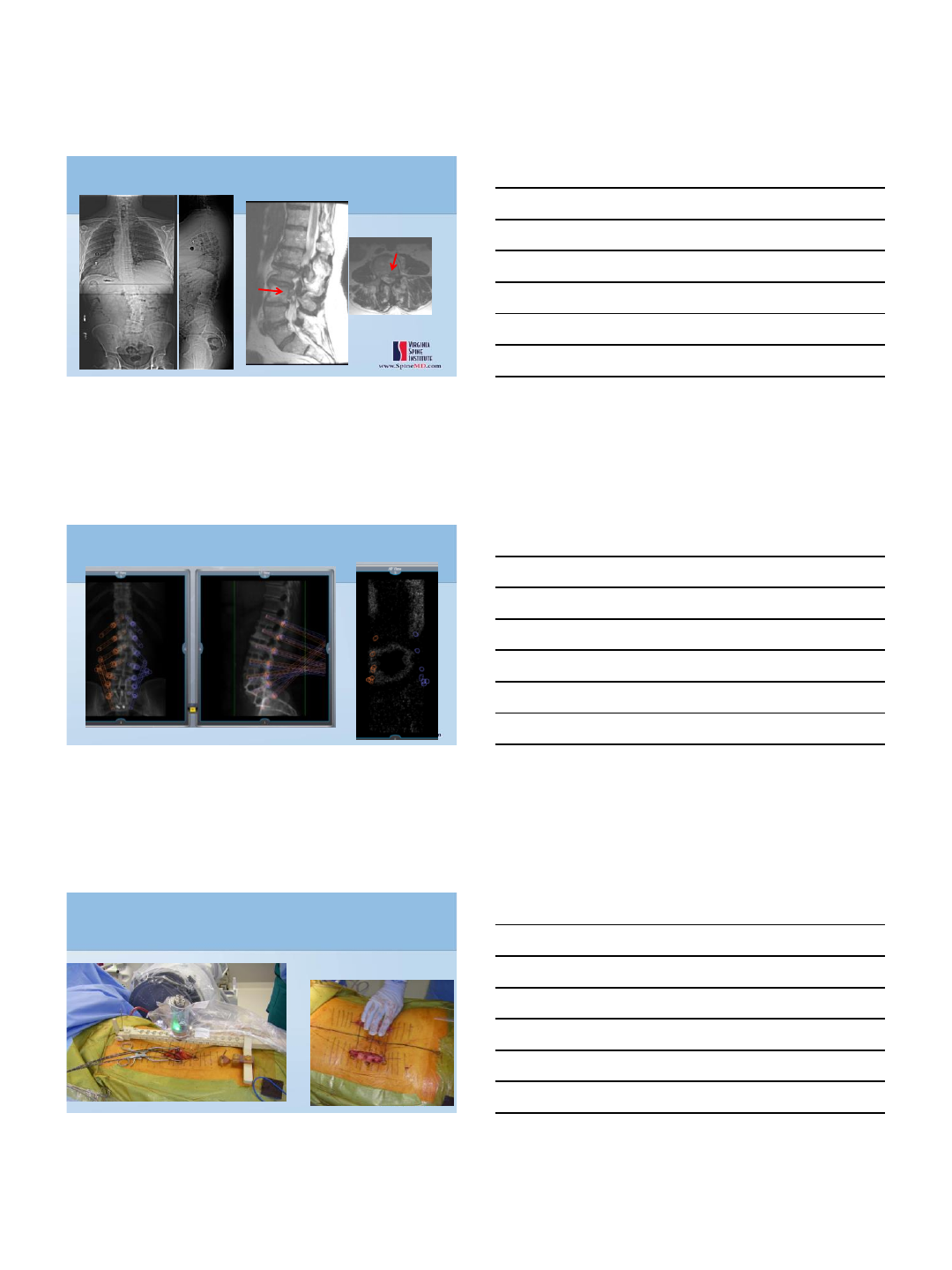
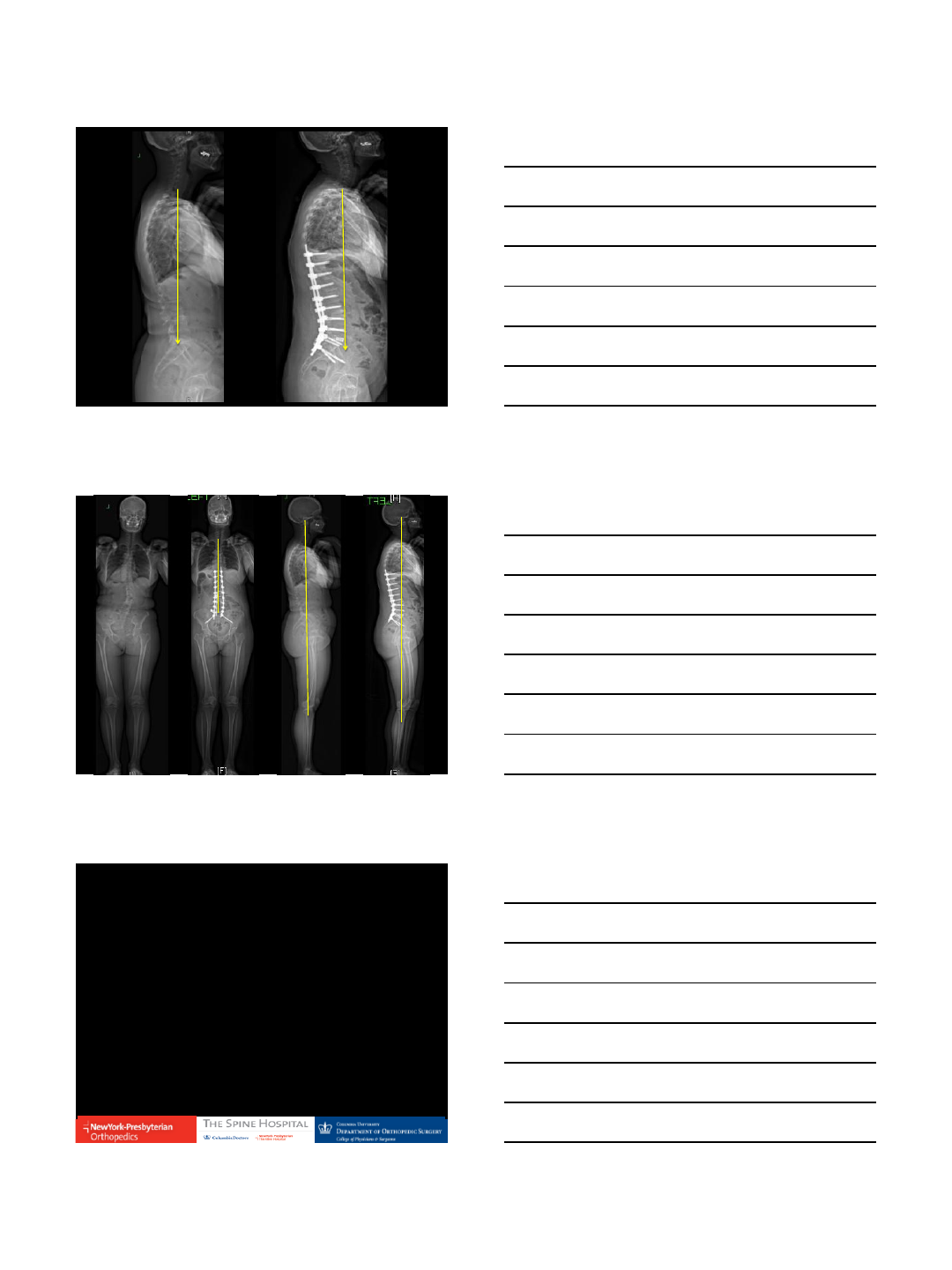
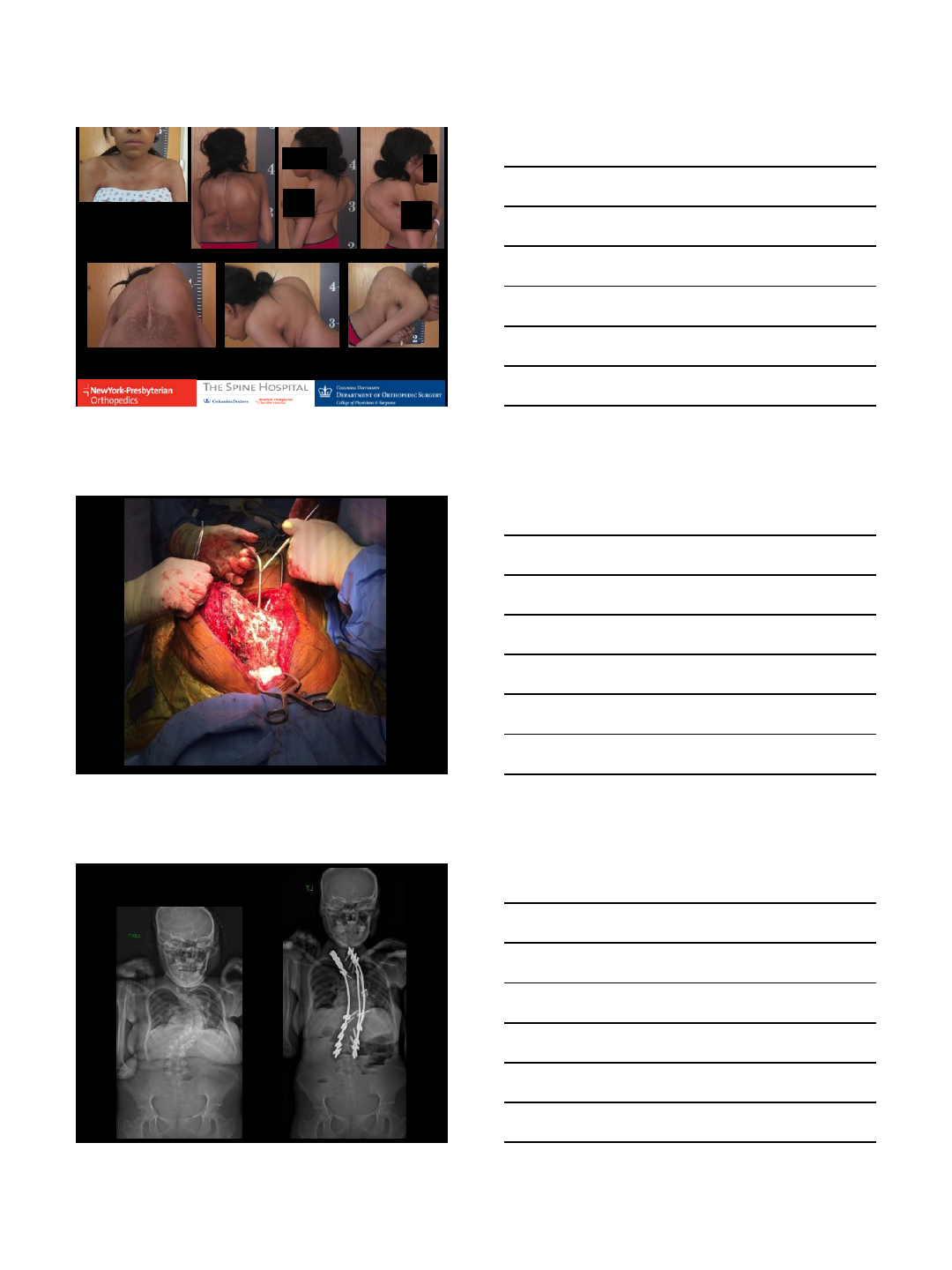
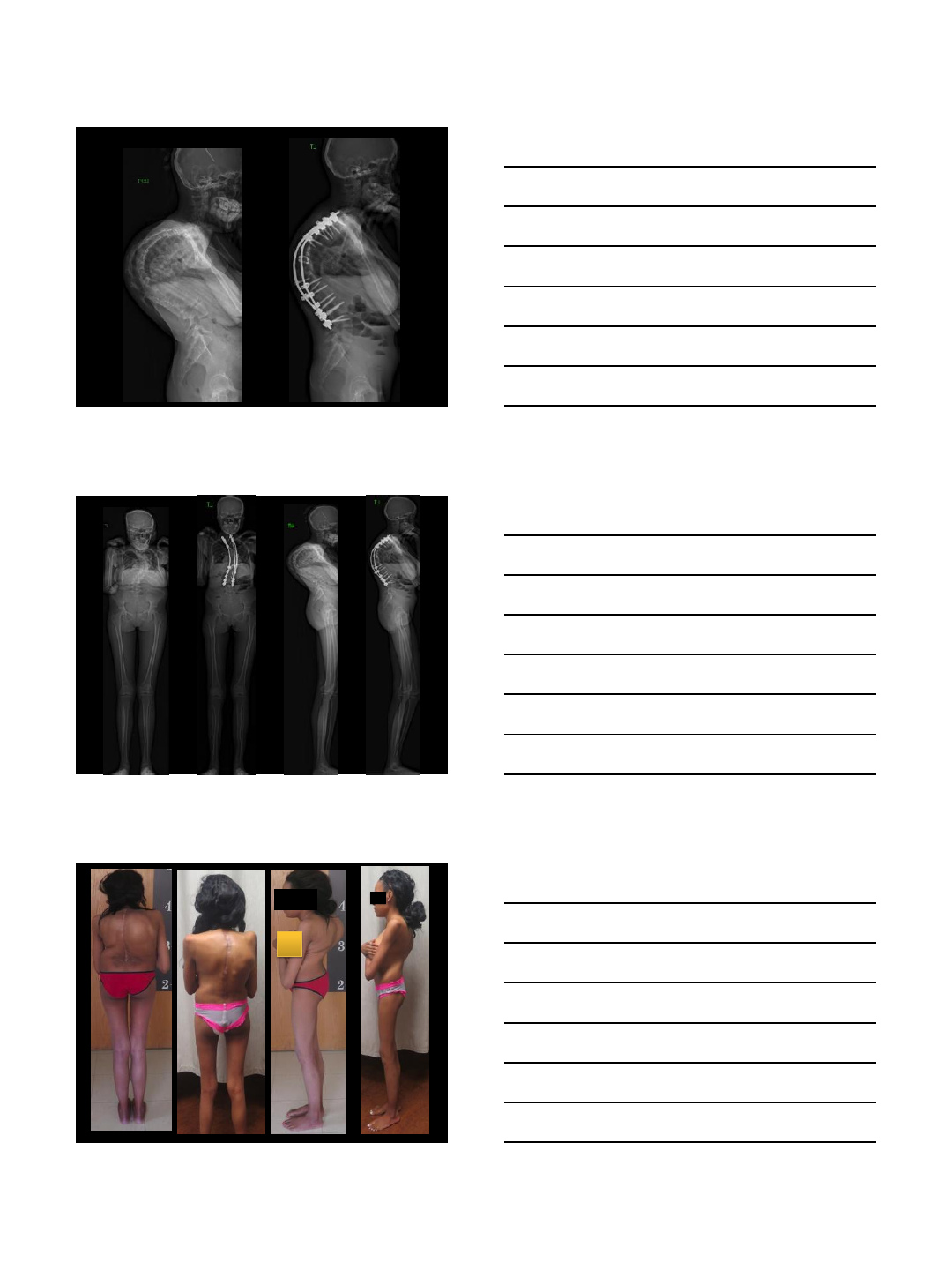
Adult Deformity
HISTORY OF PRESENT ILLNESS:
57 yo F with several years of back and leg pain with scoliosis
- Low back pain 70%
- Leg pain 30%. right hip and right calf pain
- Has right calf weakness and numbness
- Had an injection 3 months ago, which helped her for a little it.
PHYSICAL EXAMINATION:
- Right EHL 4/5, gastroc 4/5
- Decreased sensation on the lateral aspect of right leg and right foot
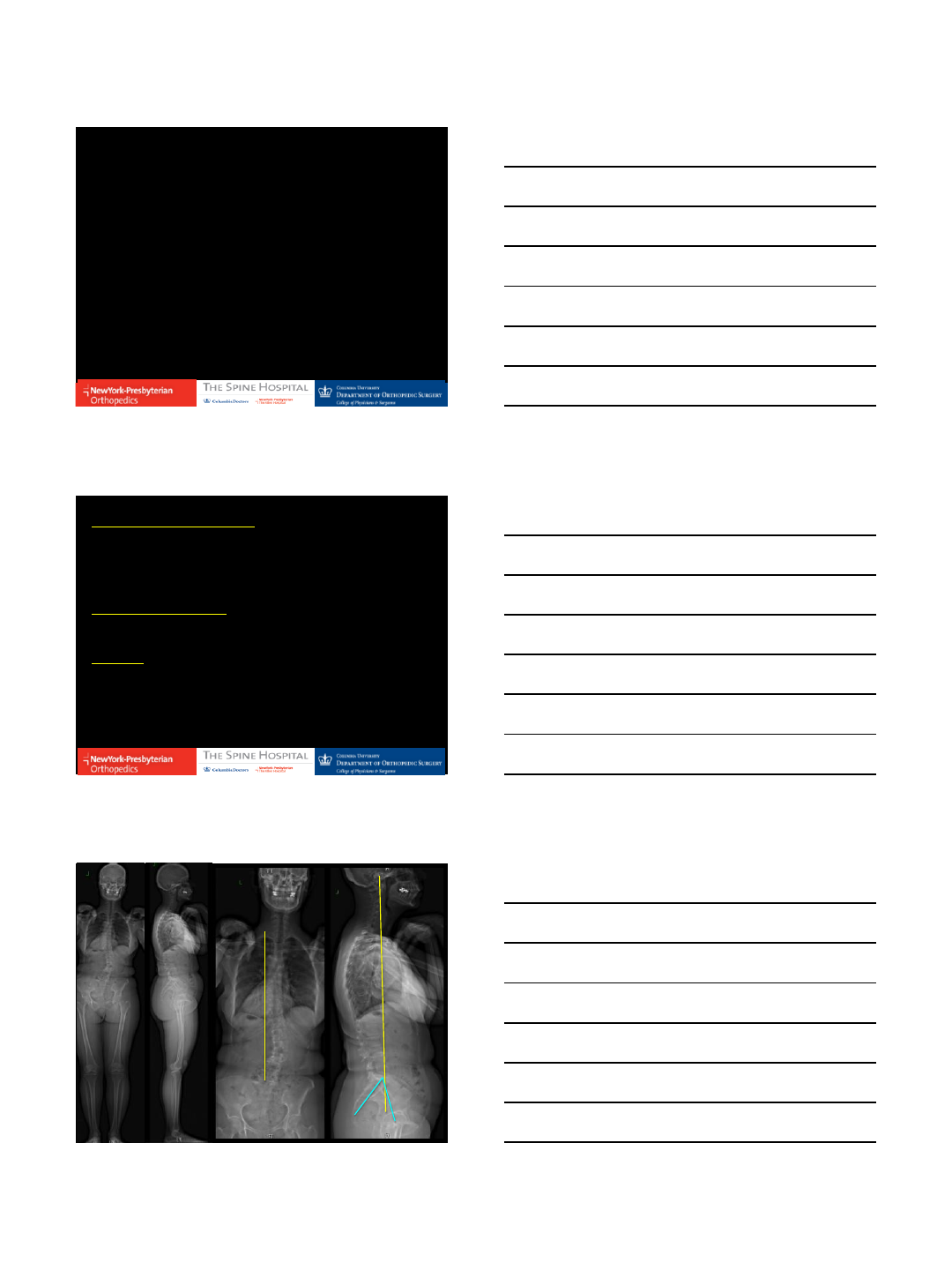
IMAGING:
-Xray: scoliosis of approximately 50 degrees, fractional concavity on the right
hand side. She has overall good sagittal balance.
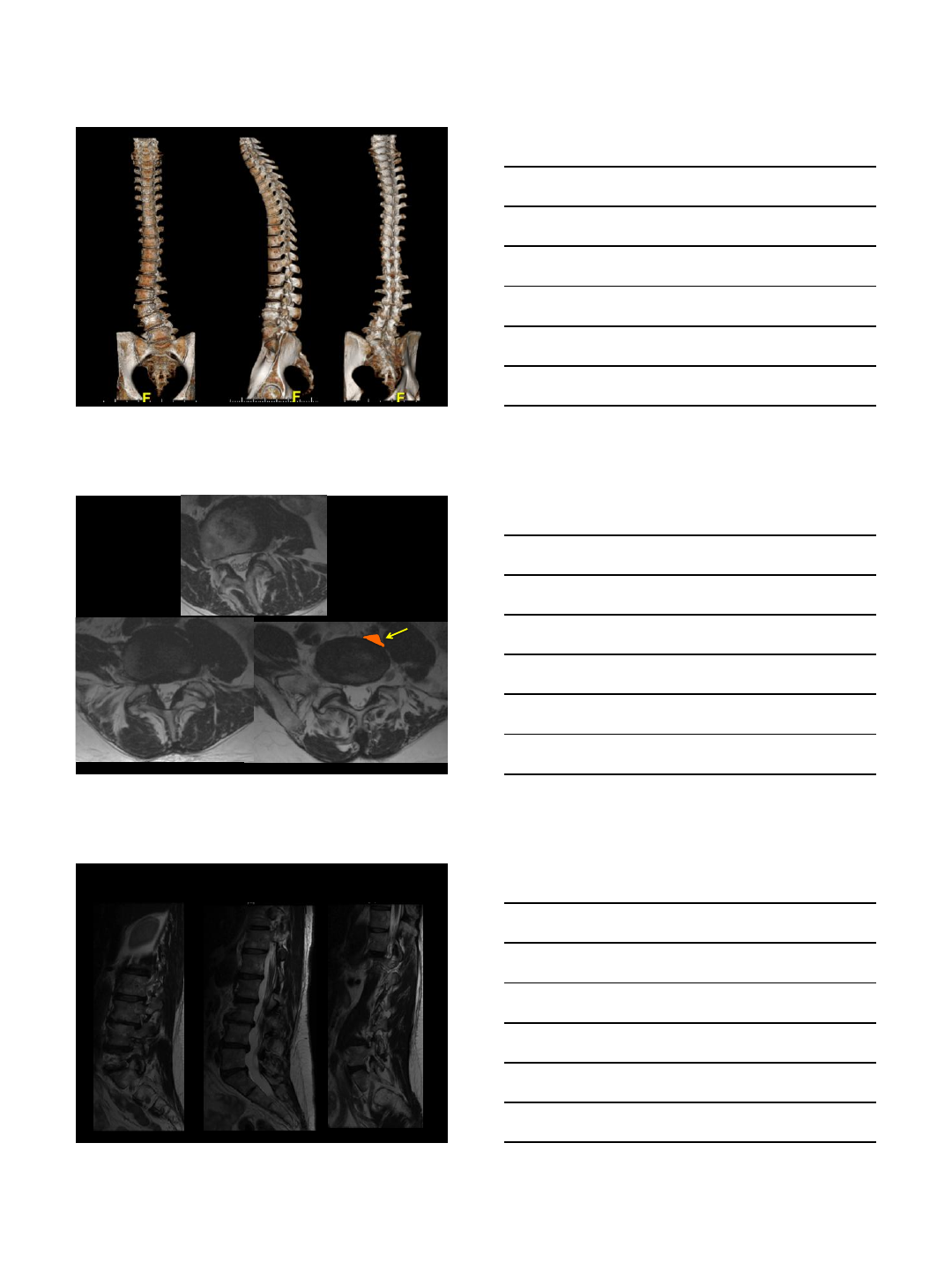
-MRI: disc desiccation most prevalent at L4-L5 and L5-S1. She also has
spondylosis and degenerative disc disease as well as facet hypertrophy.
PI
12/14/2016
7
L3/4
L4/5 L5/S1
Right Foramen Mid-Sagittal
Left Foramen
12/14/2016
8
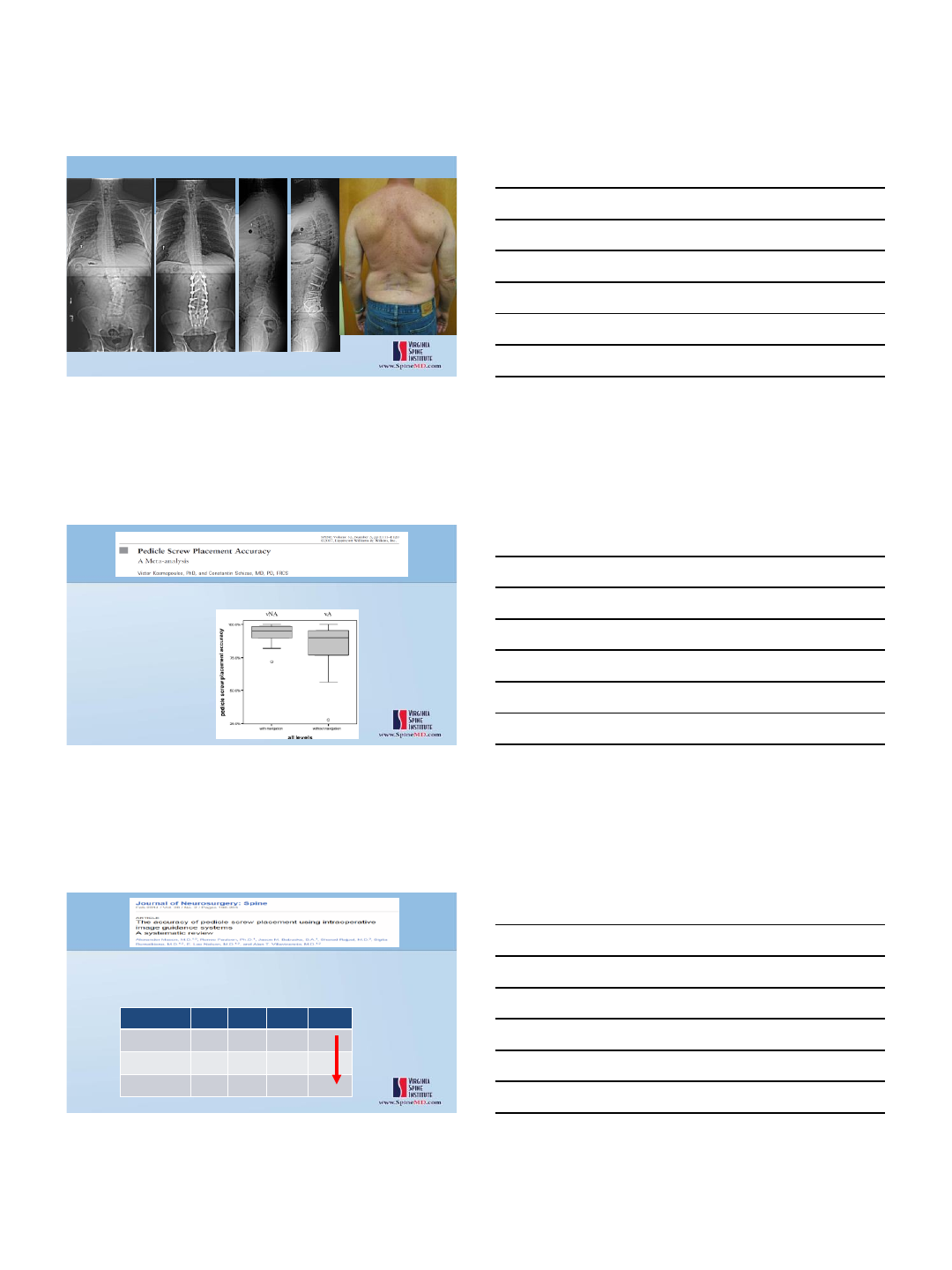
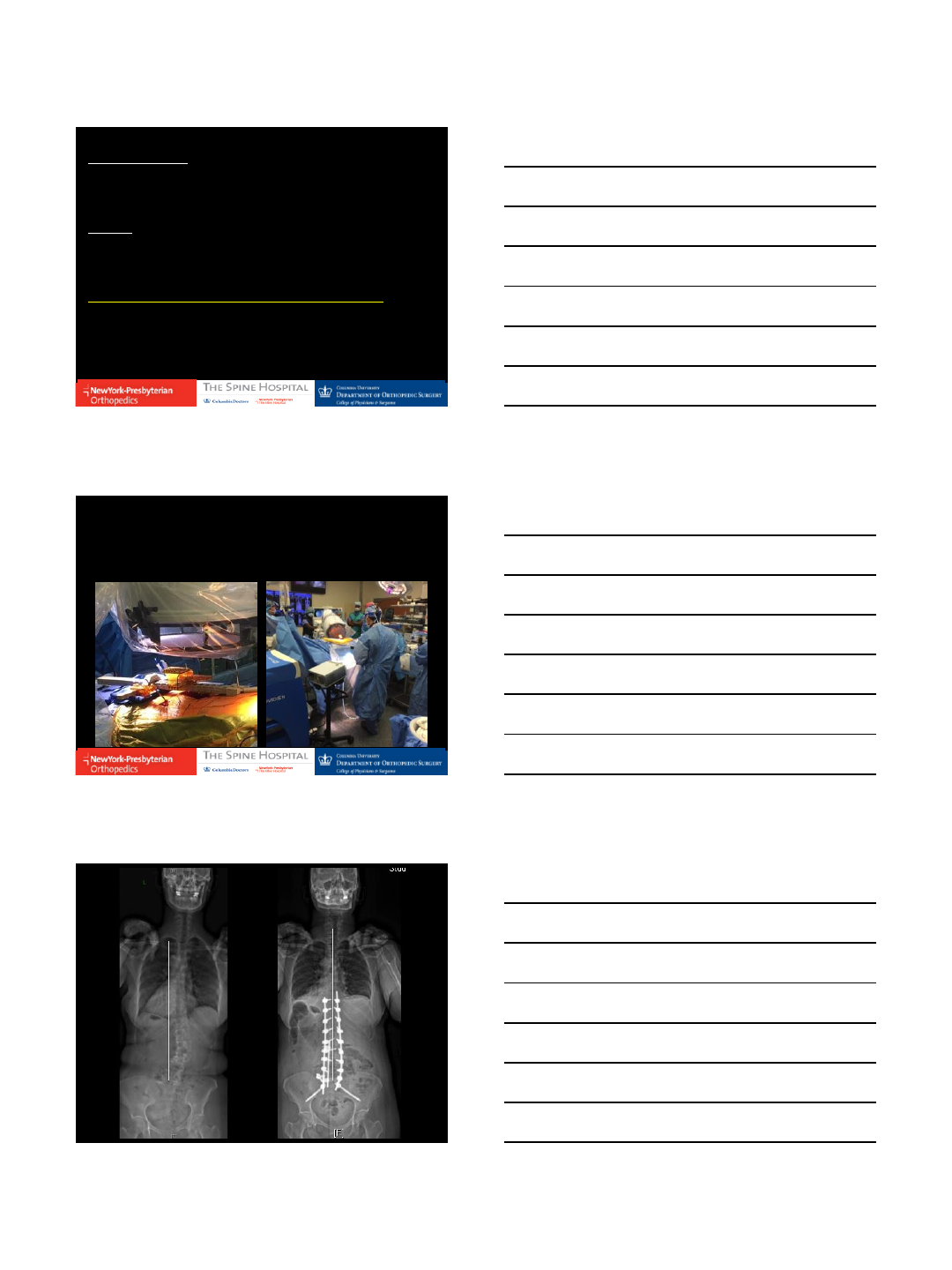
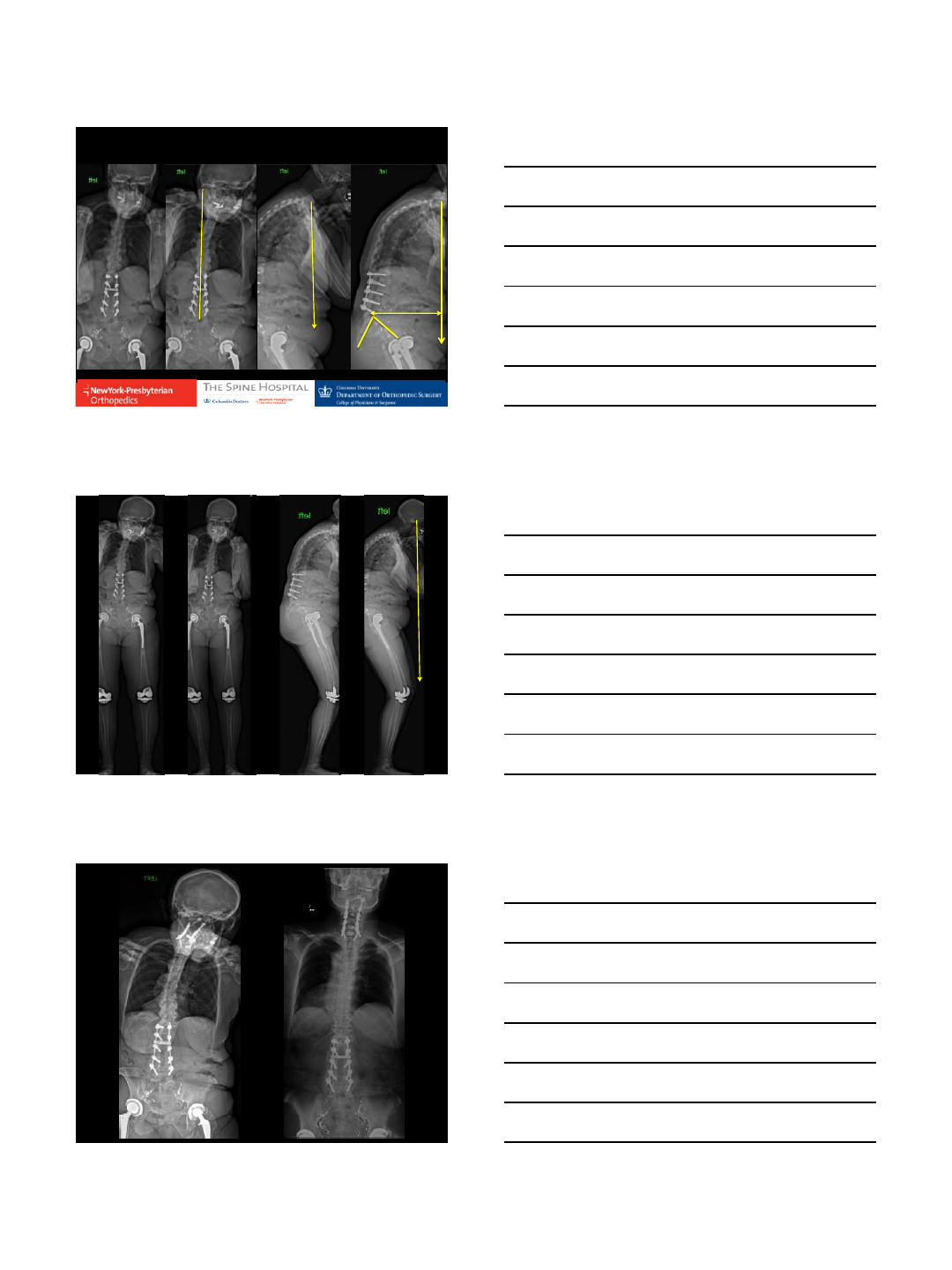
ASSESSMENT:
57 yo F with degenerative scoliosis and olisthesis,
radiculopathy
PLAN:
OLIF vs TLIF at L5/S1
PSF T10 to ilium
Decompression R L4/5 and L5/S1
Robotic Assistance – Left; Freehand on the Right
12/14/2016
9
Three Column
Osteotomies (3CO)
12/14/2016
10
12/14/2016
11
Pedicle Subtraction Osteotomy (PSO)
12/14/2016
12
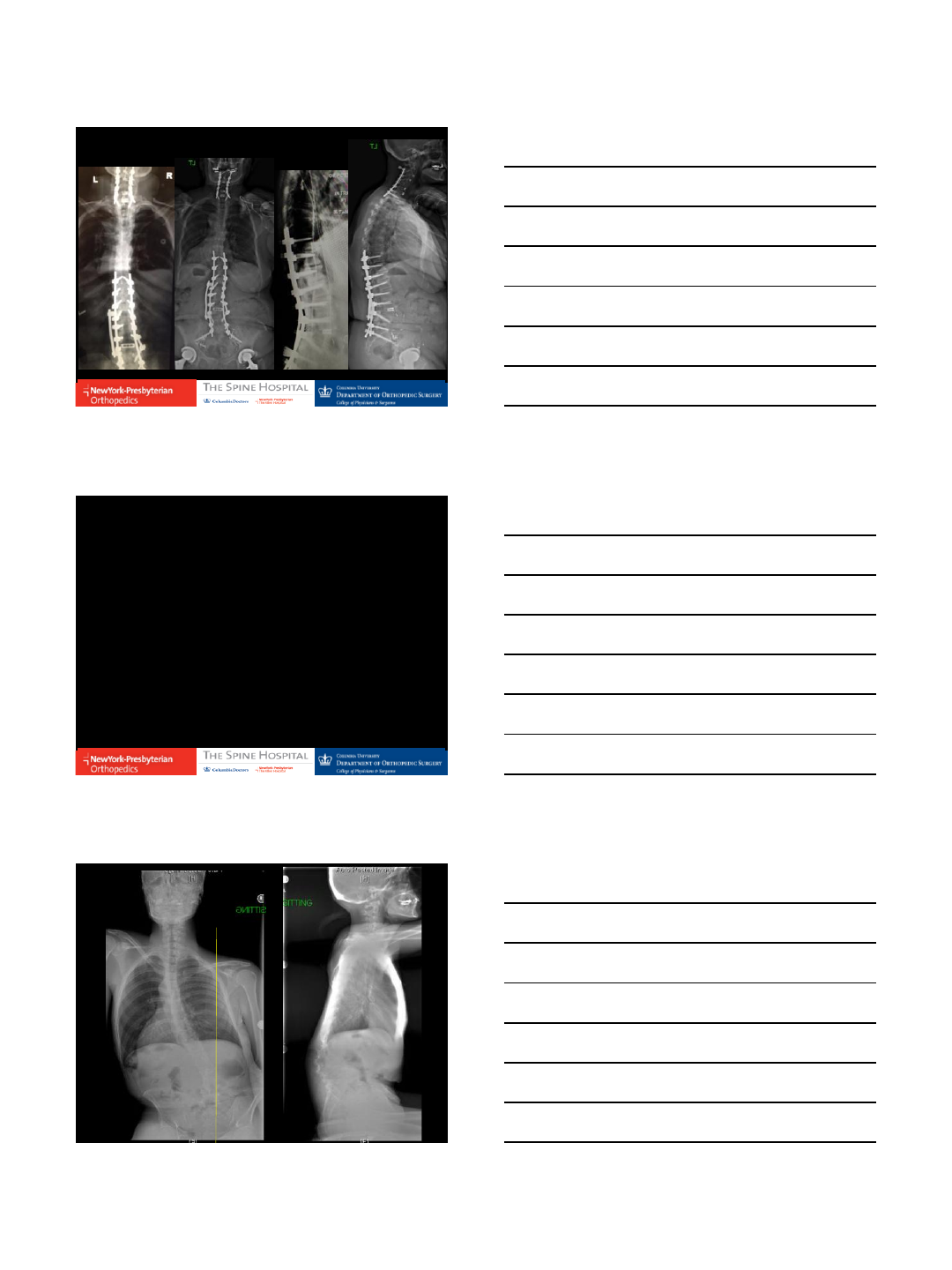
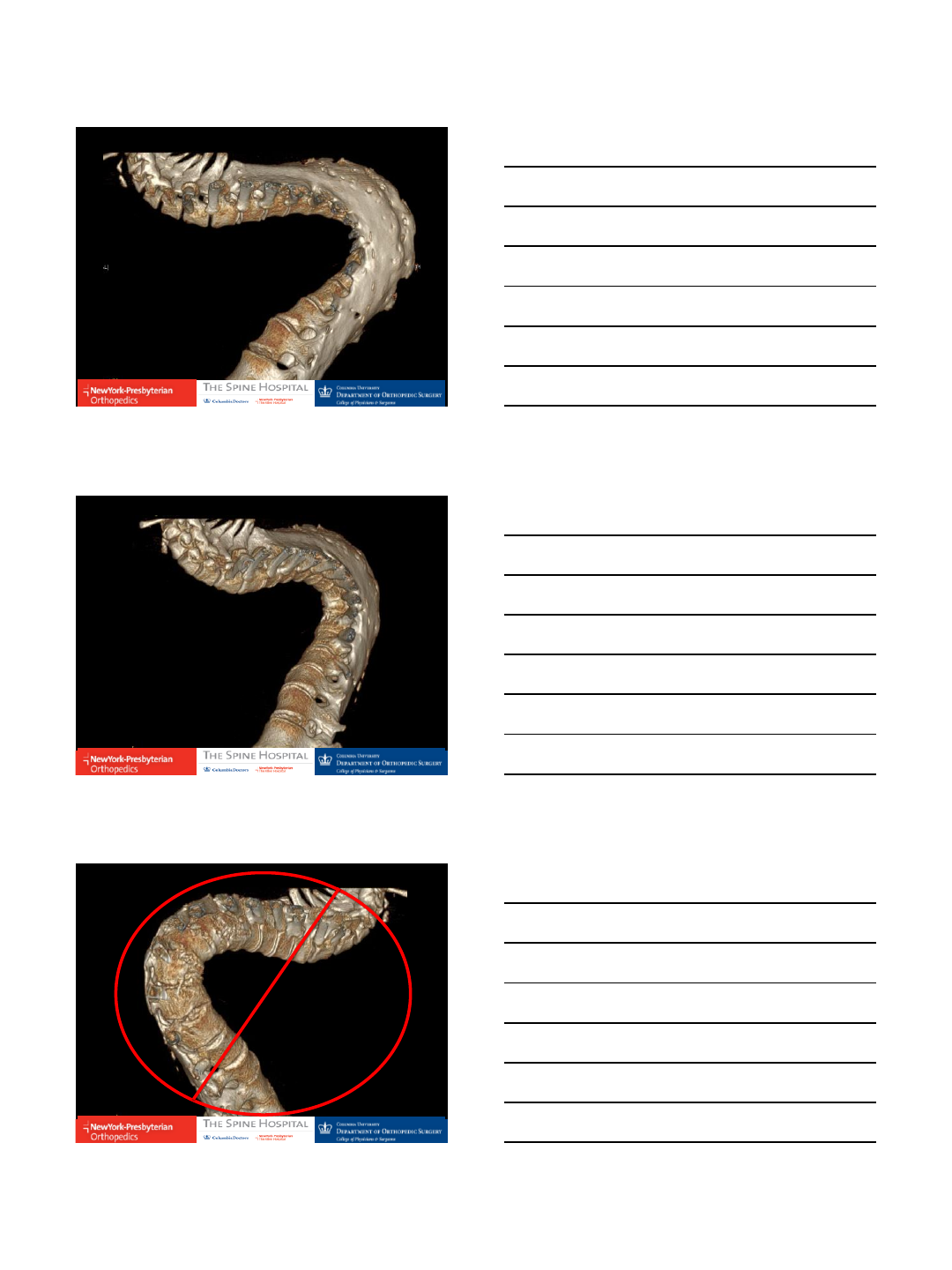
COMPLEX CASES
12/14/2016
13
L3 L4
L5 S1
12/14/2016
14
T12-L1 L1-L2
L2
L3
L4 L5 L5-S1
12/14/2016
15
12/14/2016
16
Current Limitations
1. Work Flow Changes
1. Requires screw preparation first
2. Cannot remove bone
2. Mandates CT scan (pre or intraop)
1. Less radiation for OR Team (vs. flouro)
2. More radiation for patient (vs Freehand or flouro)
3. Time
1. More than Freehand Technique
2. </= Flouro and Navigation
4. Accuracy
5. Unable to negotiate difficult deformities
All Adult Deformity is NOT the same
adult deformity ADULT DEFORMITY
12/14/2016
17
ROBOT
12/14/2016
18
12/14/2016
19

12/14/2016
20
Future and Now
Intraoperative
Alignment Correction Improved DOF / Less Constraint
Thank You!
Ronald A. Lehman, Jr., MD
Professor of Orthopedic Surgery, Columbia University
Chief, Degenerative, Minimally Invasive & Robotic Spine
Complex Pediatric and Adult Scoliosis Service
Co-Director, Spine Fellowship
Director, Clinical Spine Research
Co-Director, Orthopaedic Clinical Research
www.spinesurgeonlehman.com
THE SPINE HOSPITAL
New York – Presbyterian
The Allen Hospital
12/13/2016
1
S. SAMUEL
BEDERMA N
MD PhD
FRCSC
SC O L I O SIS A ND
SPINE SUR G E ON
RES TO R E
ORT H OPED I C S
AN D S P I N E
CE N T ER
ORA N GE C OU N T Y
CA L I FORNIA
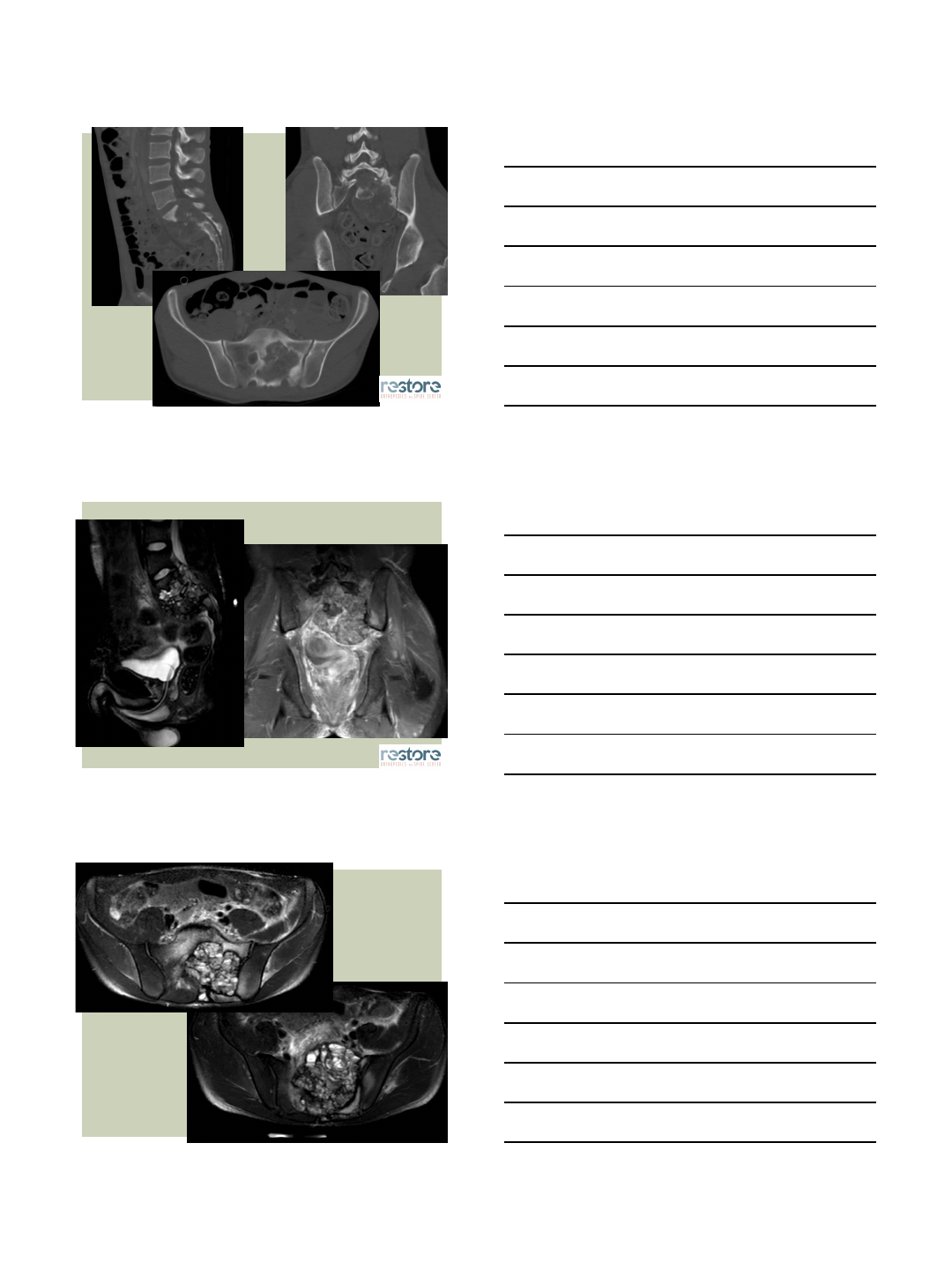
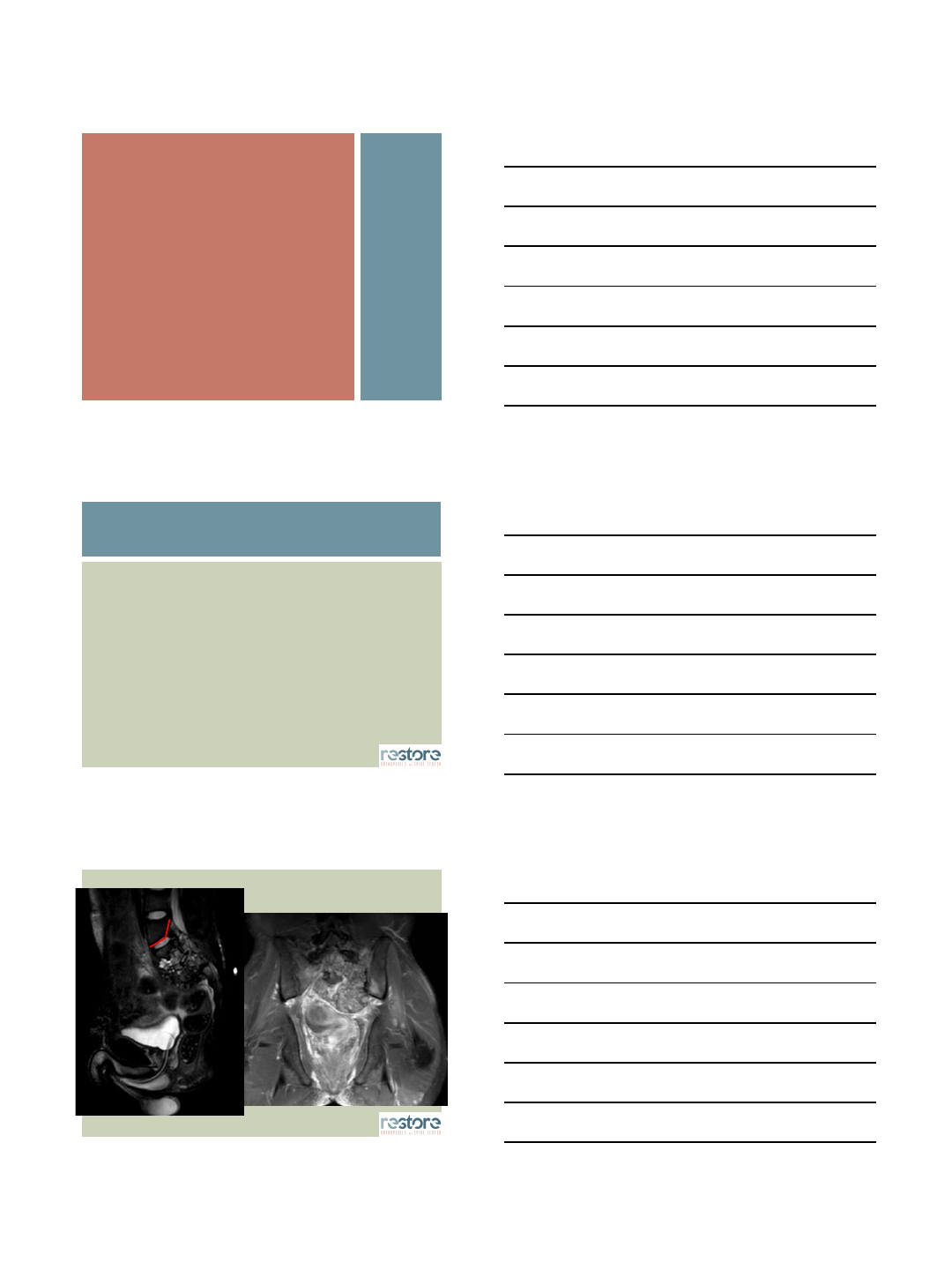
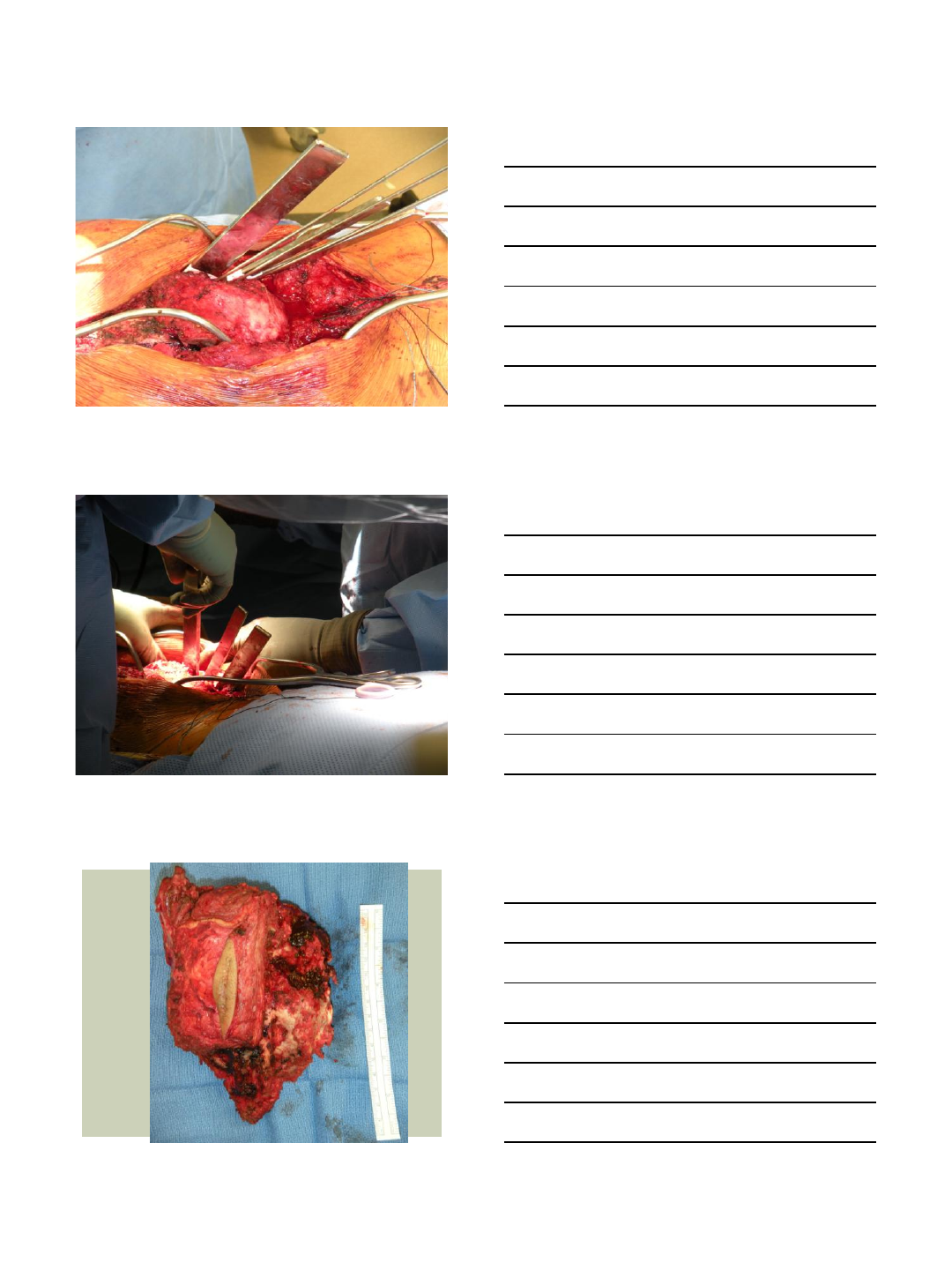
CASE REPORT:
ROBOTIC-ASSISTED
EN BLOC SACRAL
OSTEOSARCOMA
RESECTION
MAZOR ROBOTICS
Consulting/Surgeon Education
SPINEART
Royalties
Consulting
Stock Options
DISCLOSURES
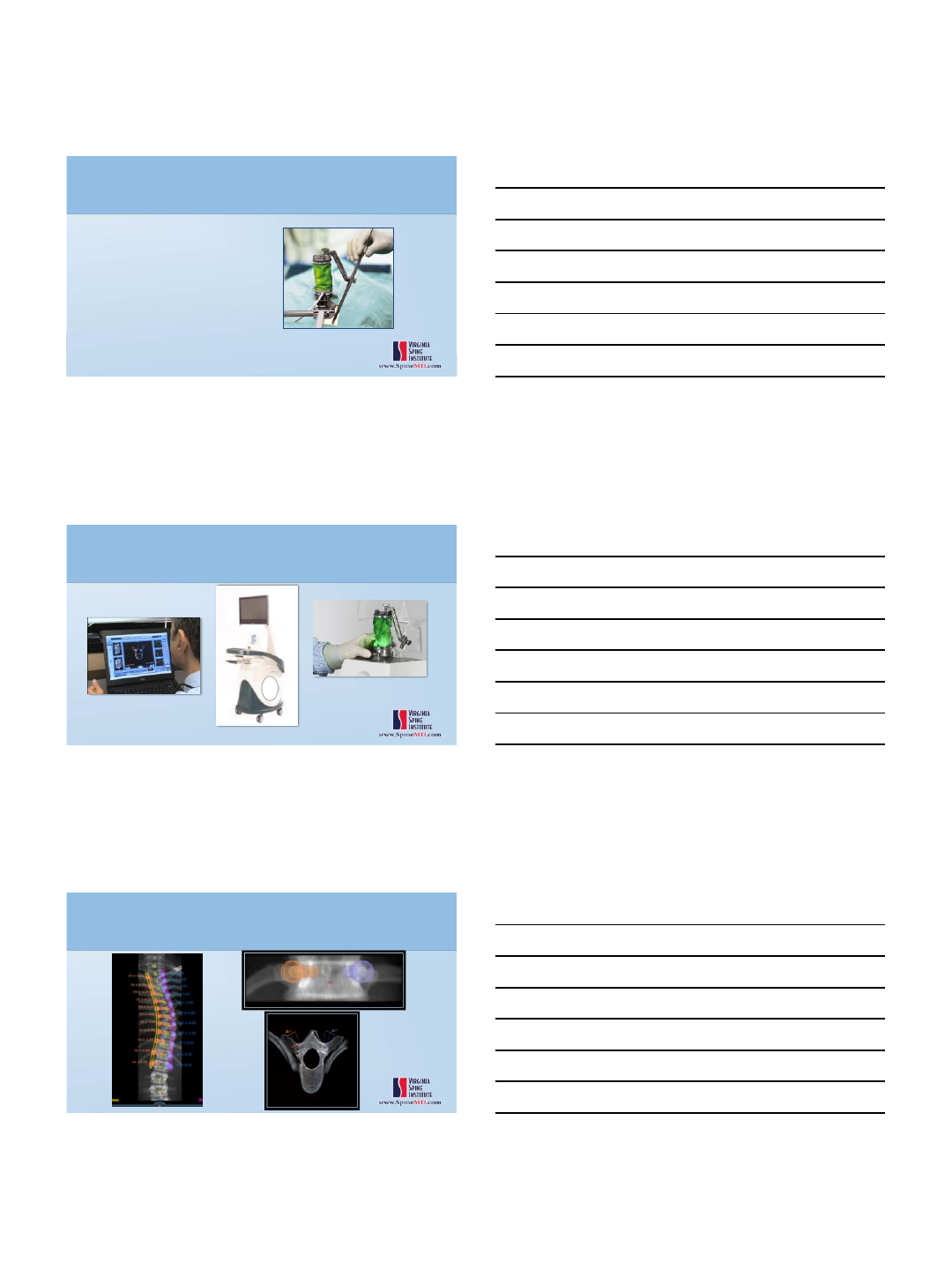
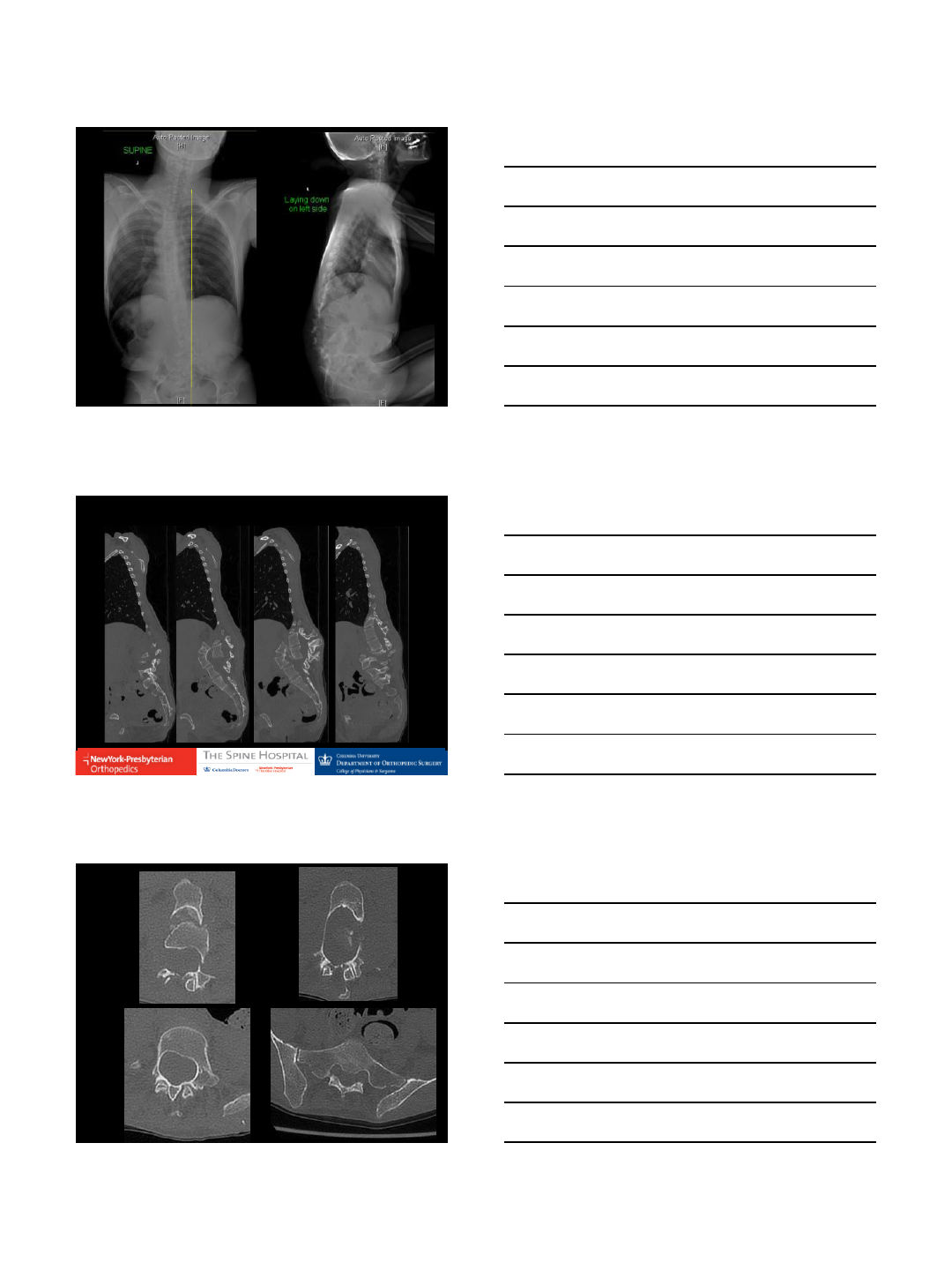
22M with one year history of progressive low back
pain followed by bilateral leg pain.
Developed urinary retention, scrotal numbness, and
progressive difficulty ambulating secondary to pain
Examination:
saddle anesthesia and S1 numbness
Full motor strength in bilateral lower extremities with
normal patellar and Achilles reflexes
HISTORY
12/13/2016
2
12/13/2016
3
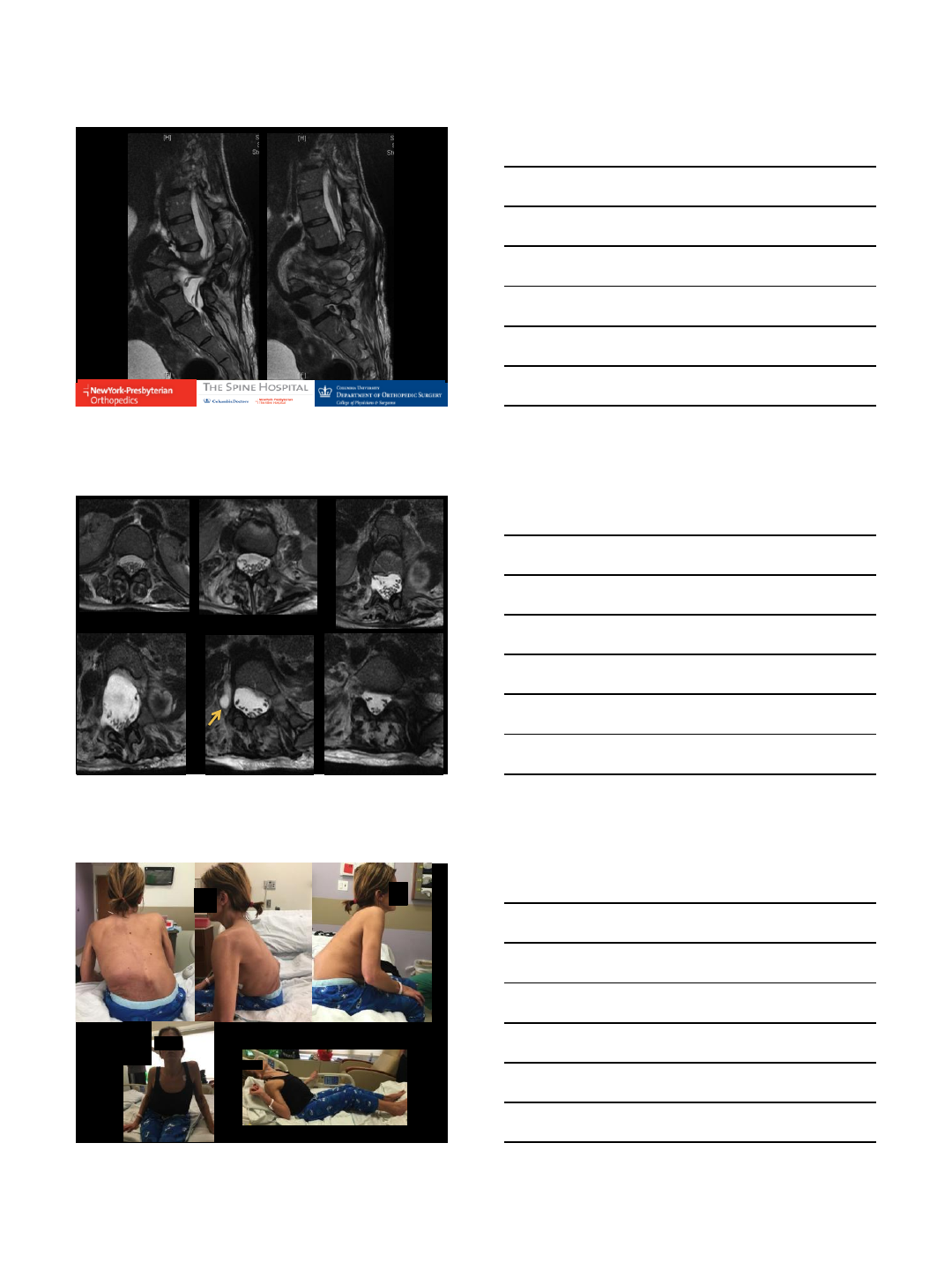
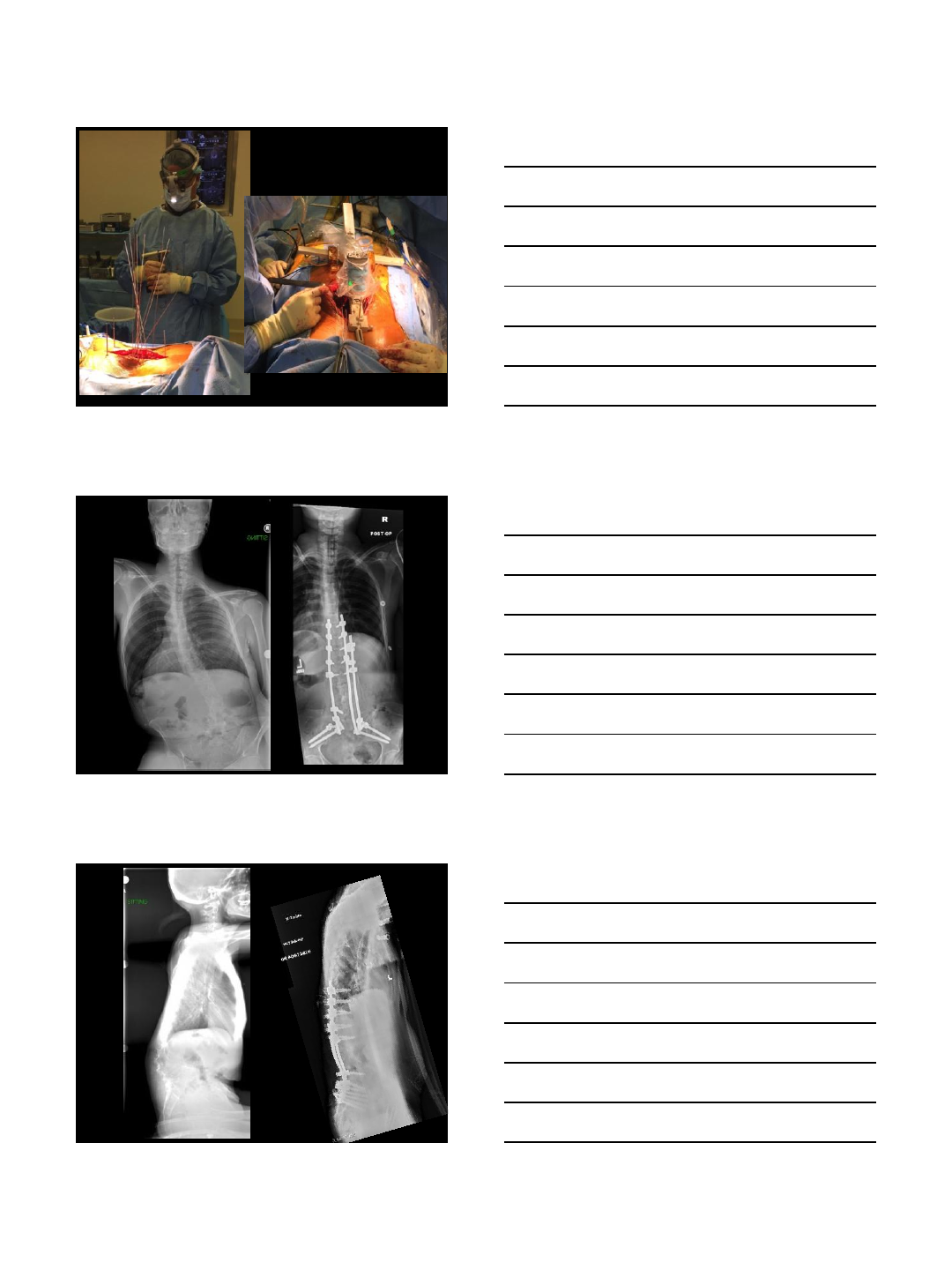
DIAGNOSIS BY OPEN
BIOPSY
SACRAL
TELANGIECTATIC
OSTEOSARCOMA
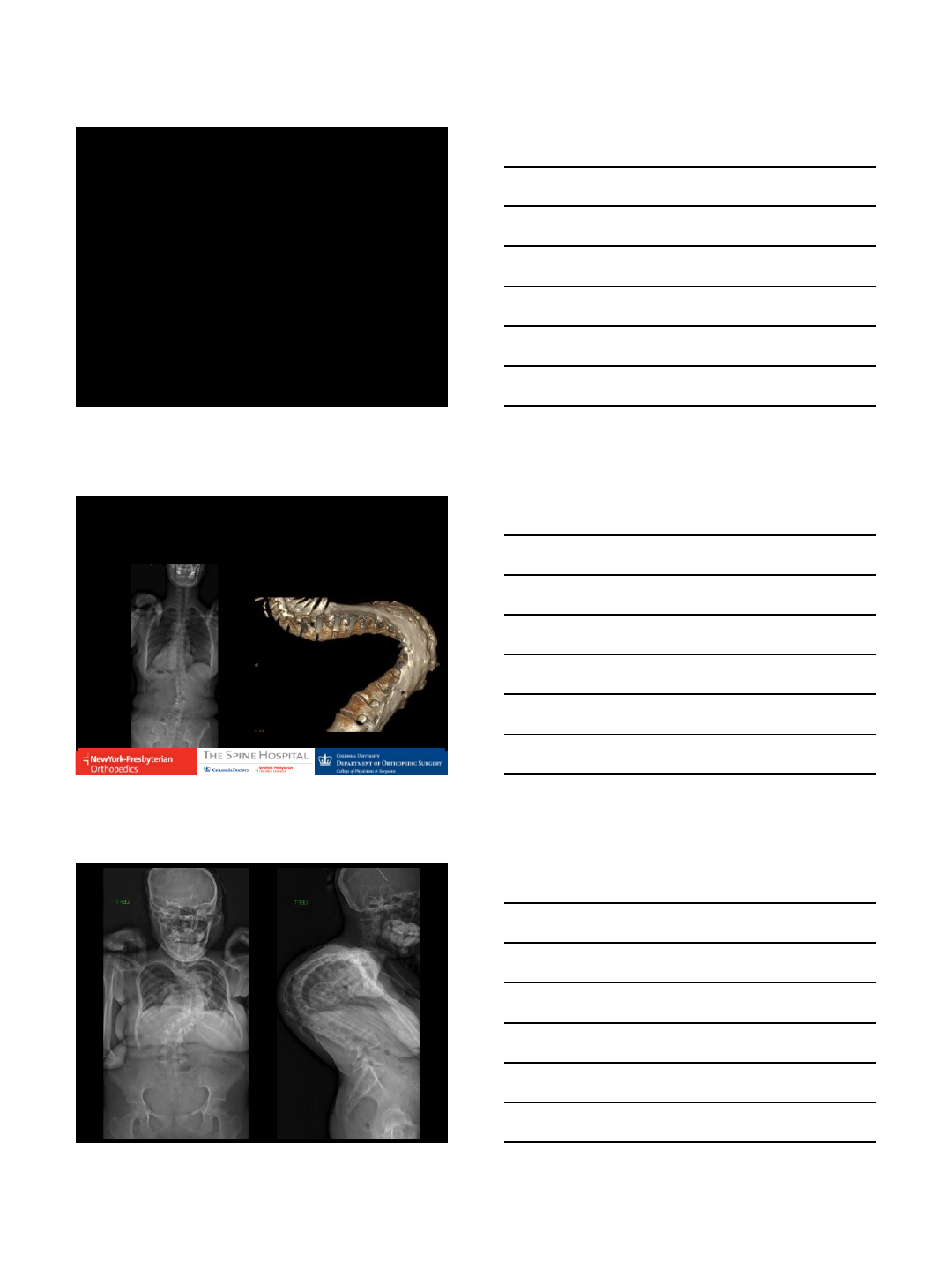
Pre-op chemo
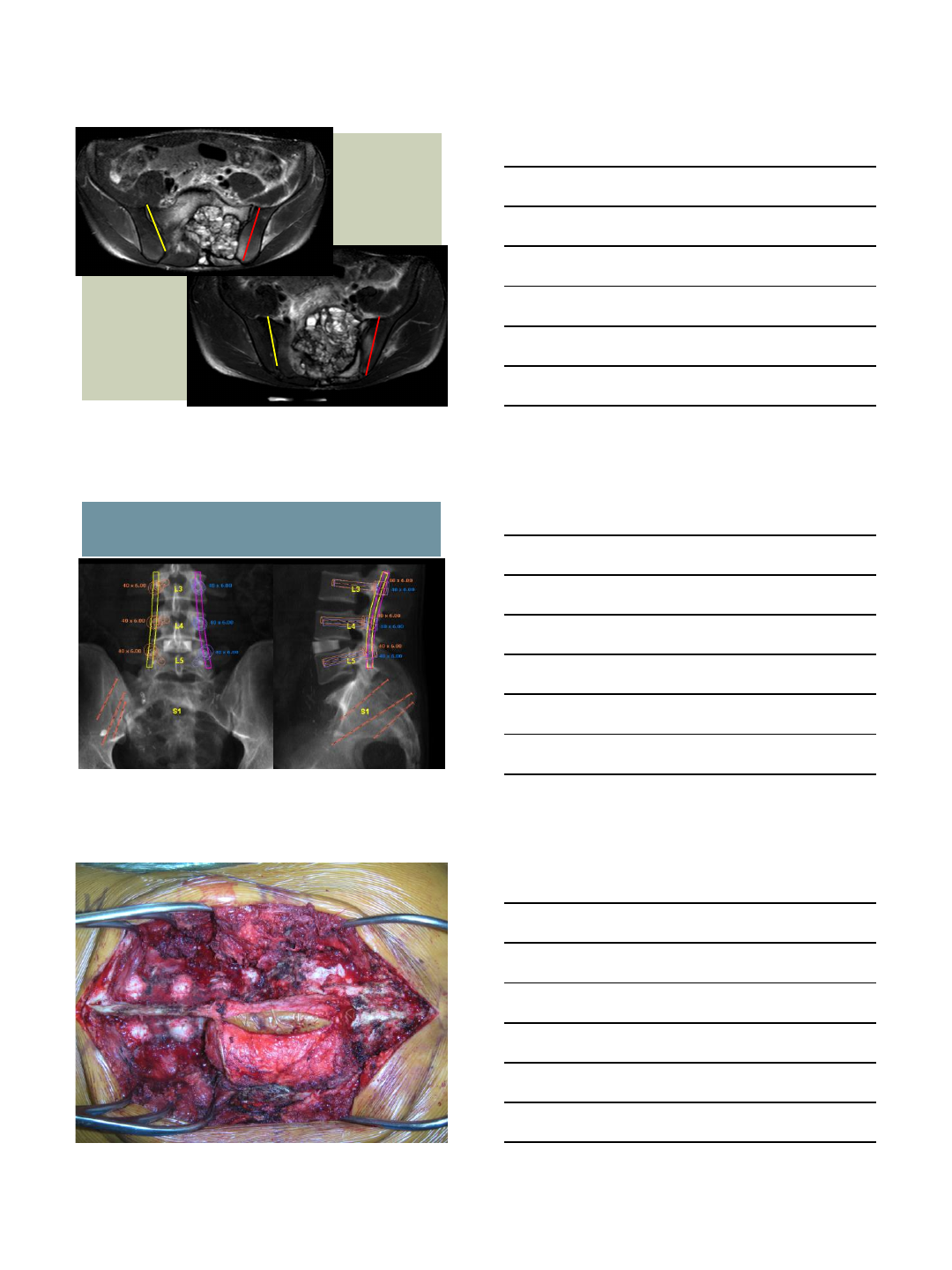
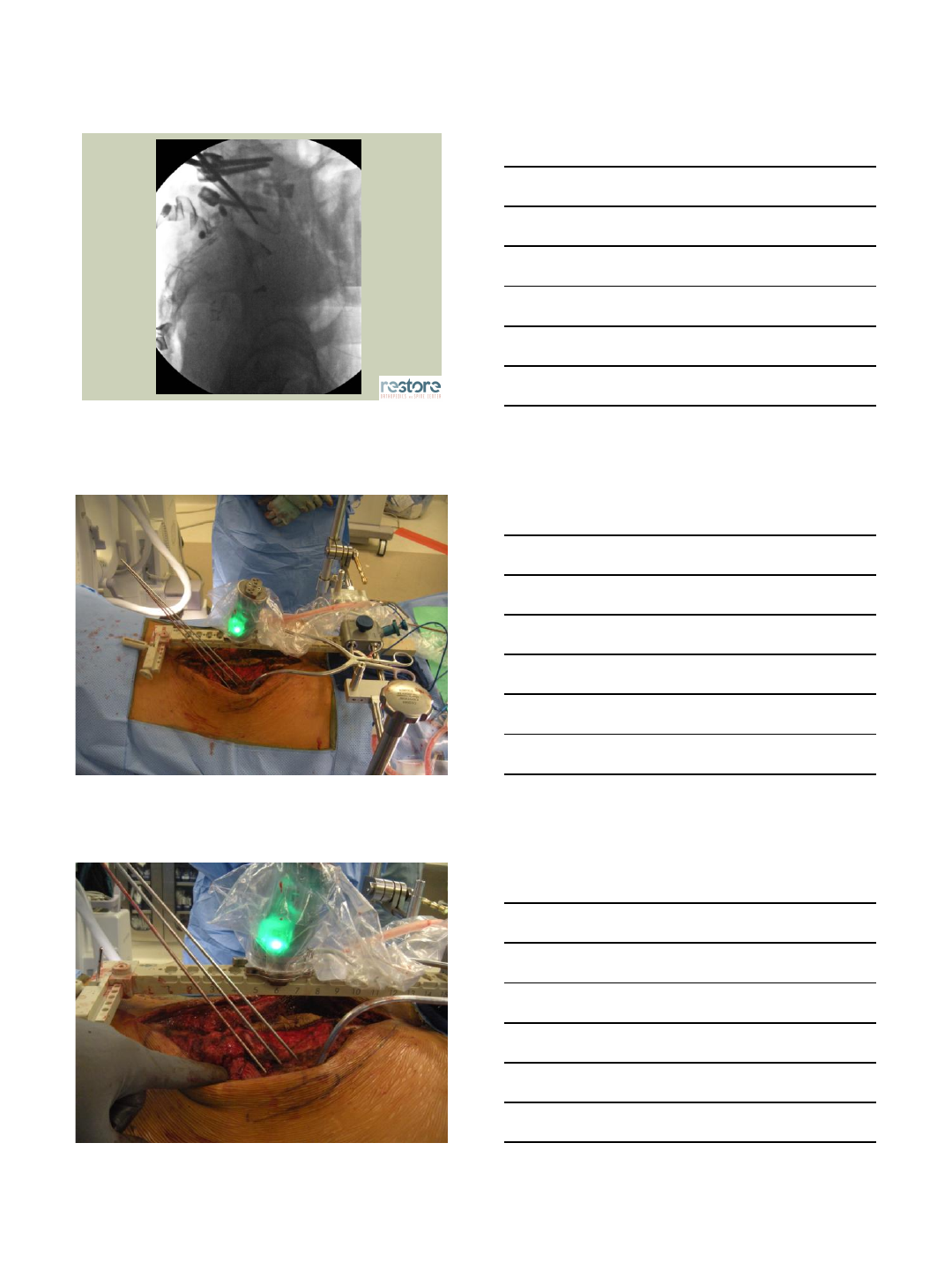
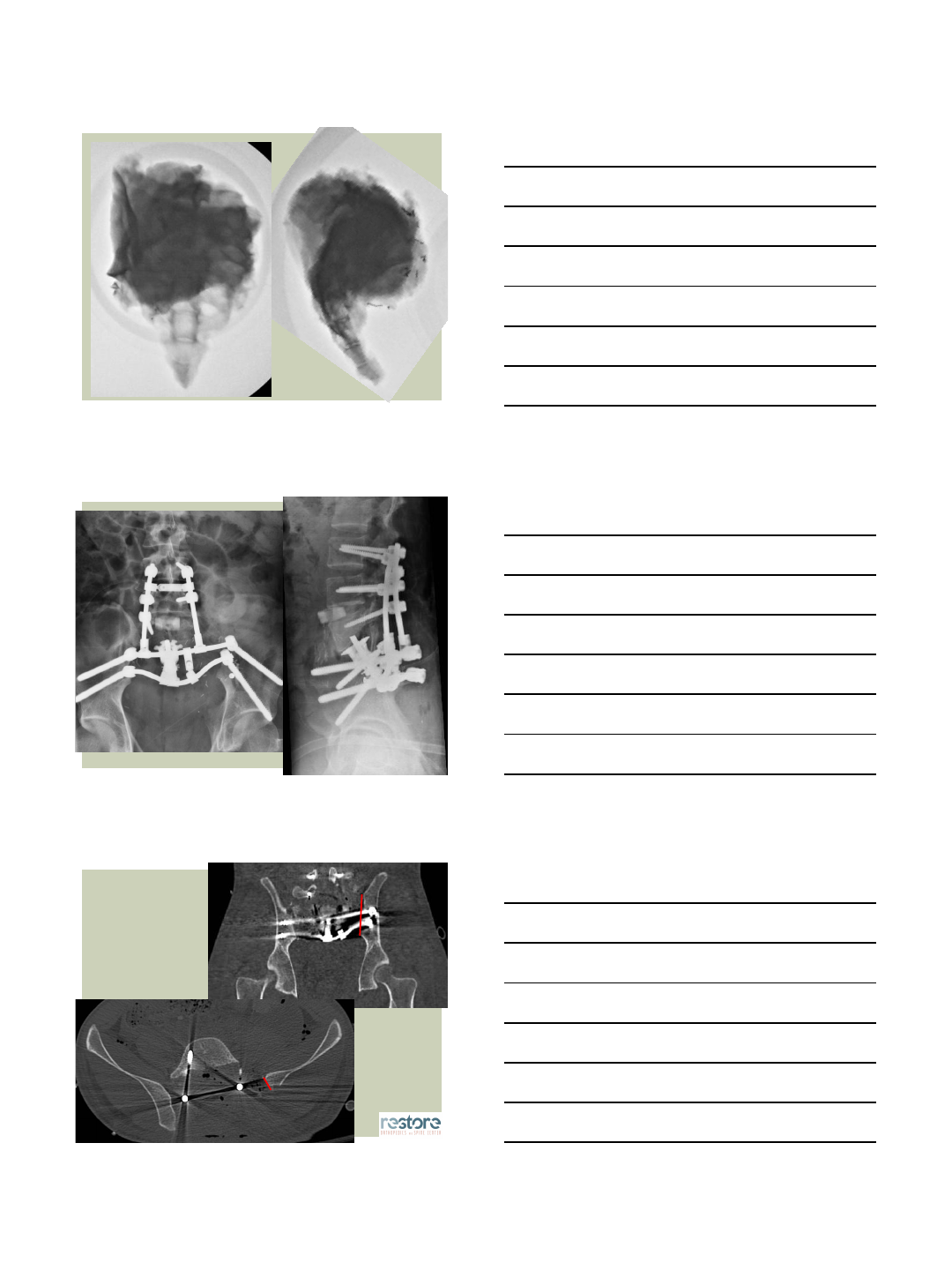
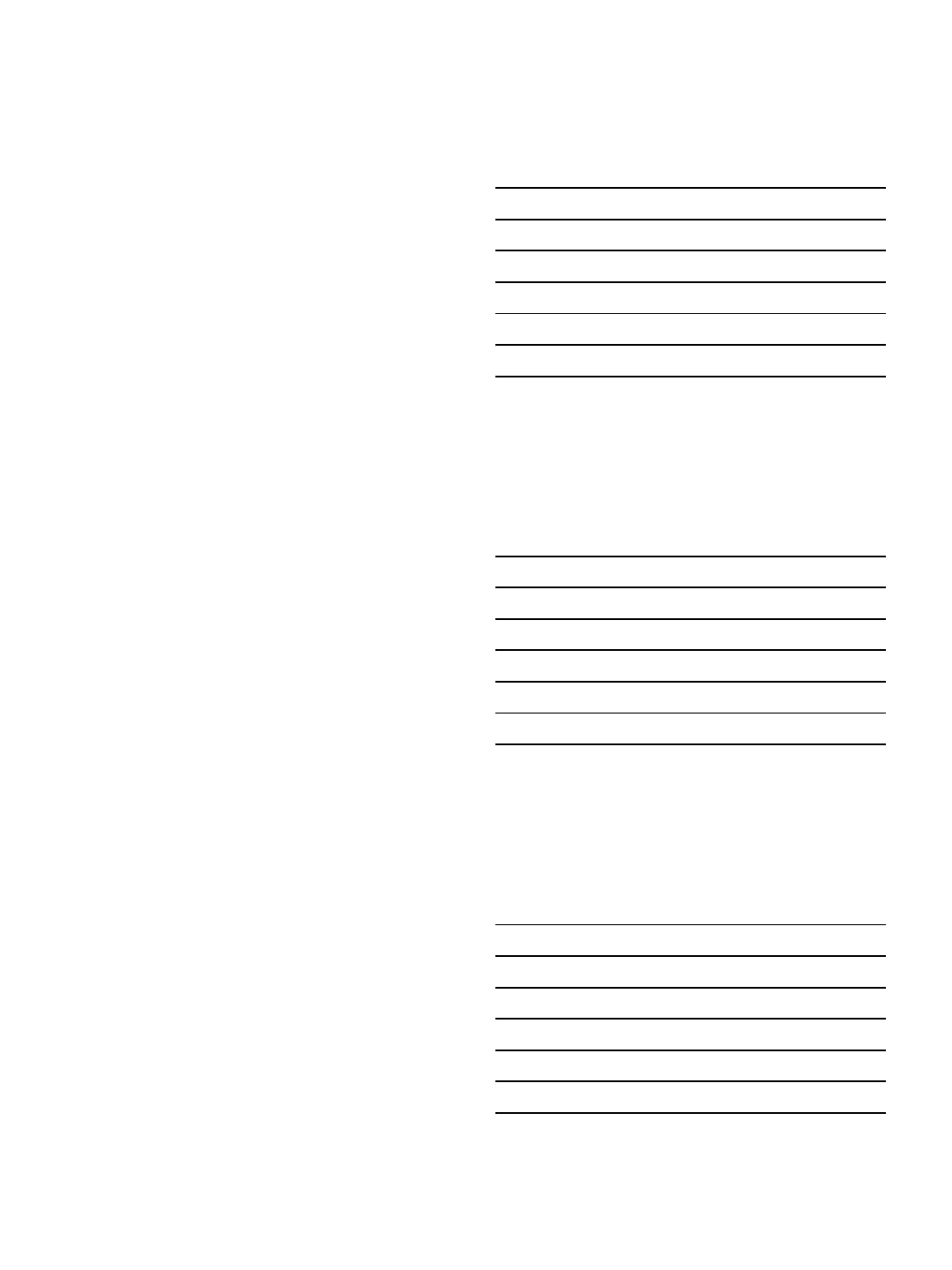
Wide en-bloc sacrectomy with L3-Pelvis PSIF
Stage 1 (anterior)
L5-S1 disc release with anterior dissection
L4-L5 ALIF
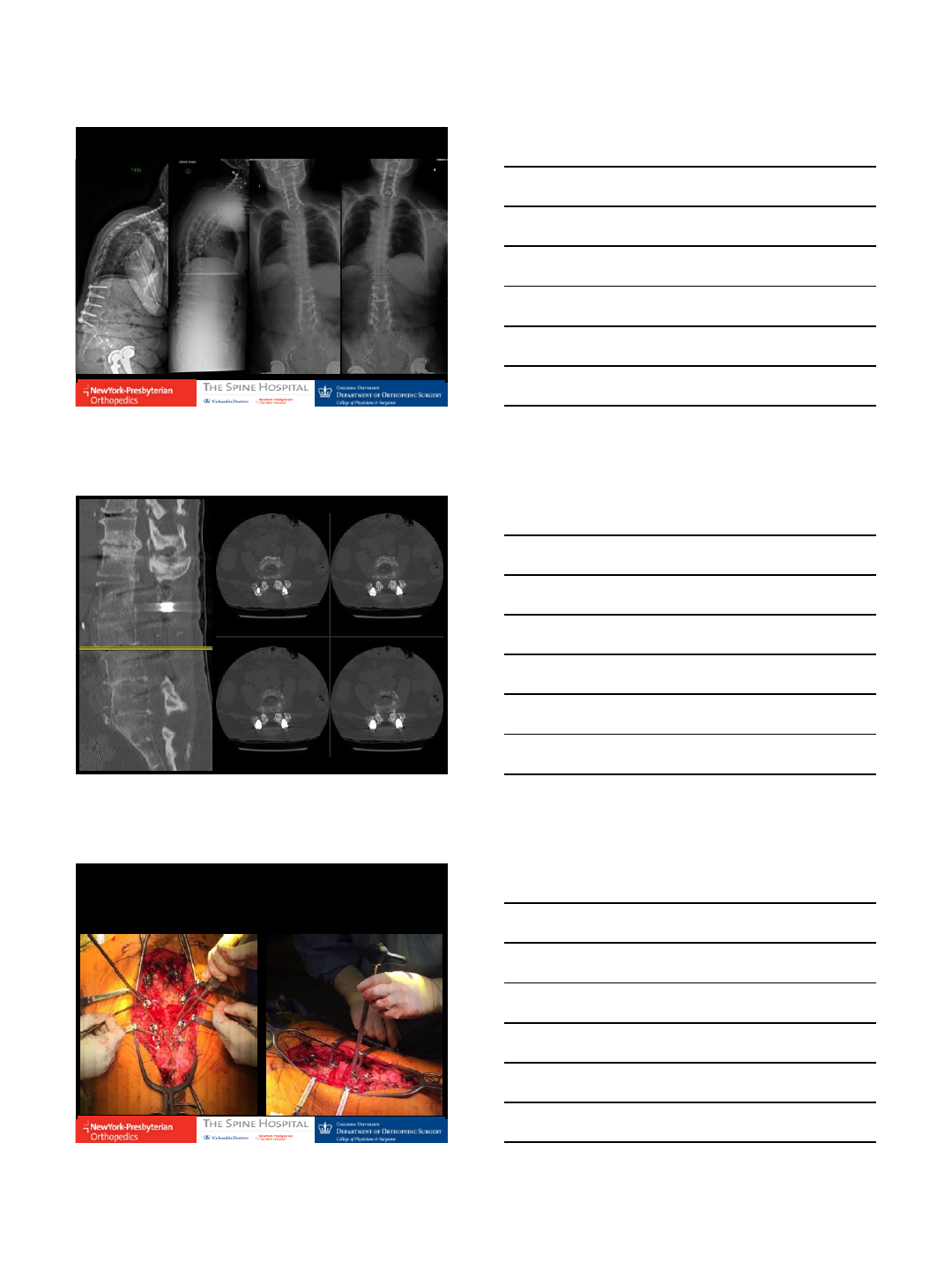
Stage 2 (posterior)
En bloc sacrectomy
Trans-articular margin on right
Trans-iliac margin on left (ROBOTIC-ASSISTED)
Partial L5 corpectomy
L3 to Pelvis instrumentation with anterior cage
Post-op chemo
TREATMENT
12/13/2016
4
OSTEOTOMY PLANNING
12/13/2016
5
12/13/2016
6
12/13/2016
7

12/13/2016
8
THANK YOU
RES TO R E
ORT H OPED I C S
AN D S P I N E
CE N T ER
ORA N GE C OU N T Y
CA L I FORNIA
12/14/2016
1
SI Joint Fusion with Mazor Renaissance
Ben Guiot, MD, FRCSC
December 2016
1
Case Presentation
•58 year old male
•Sharp stabbing pain overlying the L SI joint
•24/7. Worse with activity
•non radiating
•no radicular symptoms or signs
Case Presentation - continued
•Imaging:
•Plain x-rays reveal normal alignment
•CT scan – DDD and facet arthropathy. Vacuum phenomenon in L SI joint.
•MRI – DDD and facet arthropathy. No focal compression
12/14/2016
2
Case Presentation - continued
•Non operative management:
•PT
•SI joint injections – 100% pain relief in the anesthetic phase. No long term
relief
•RFA – no long term relief
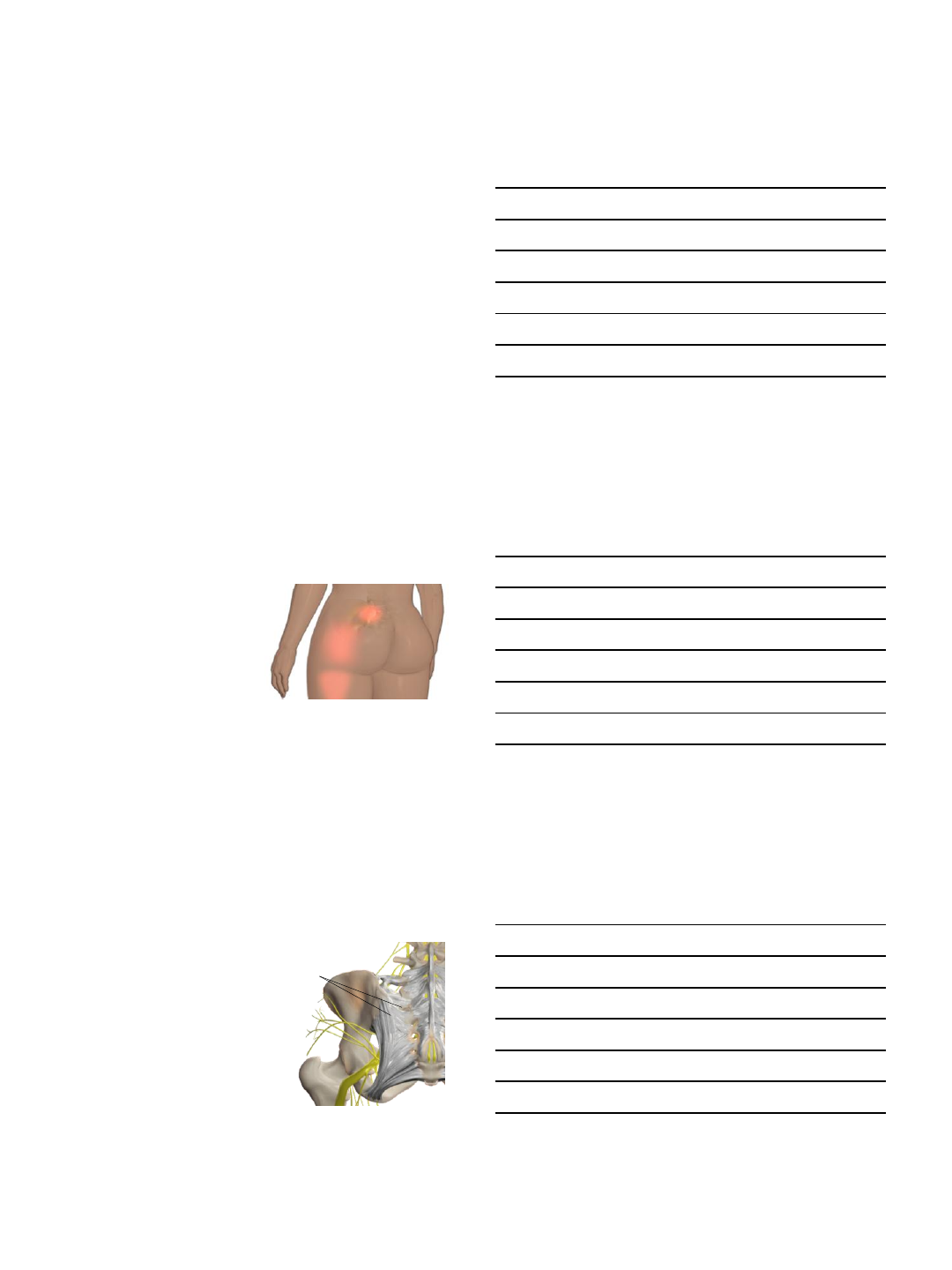
SI Joint: Symptom Presentation
•Low back pain
•Buttock pain
•Thigh pain
•Sciatic-like symptoms
•Difficulty sitting in one place for too long
due to pain
•Poor sleep habits
5
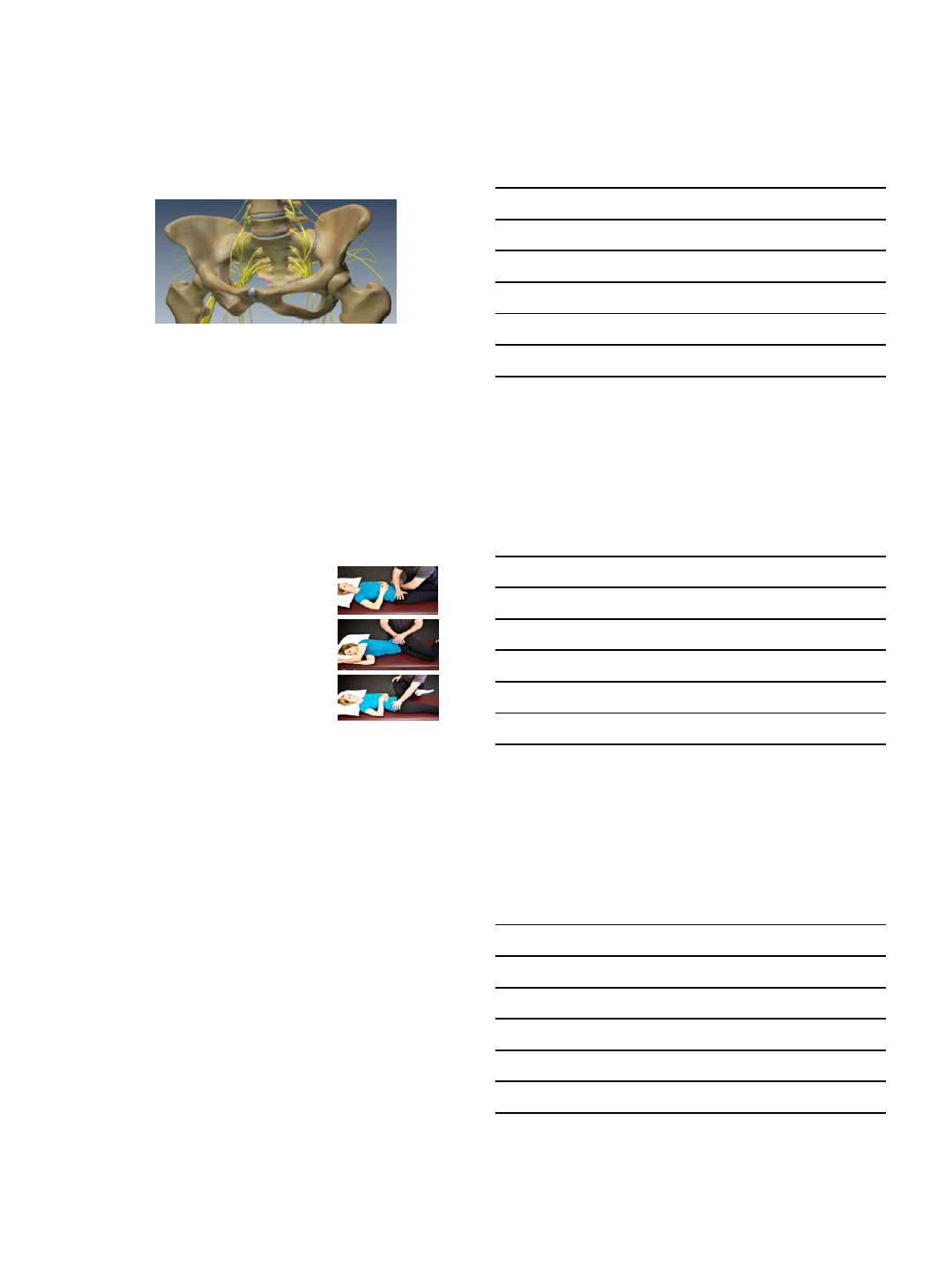
Anatomy – Ligaments
•Strong ligaments encase each joint
•Ligaments affect stability
•If damaged, may have excessive motion
•Excessive motion may inflame and
disrupt the joint and surrounding nerves
6
Sacroiliac
ligaments
12/14/2016
3
Anatomy – Nerve Supply of Pelvis
7
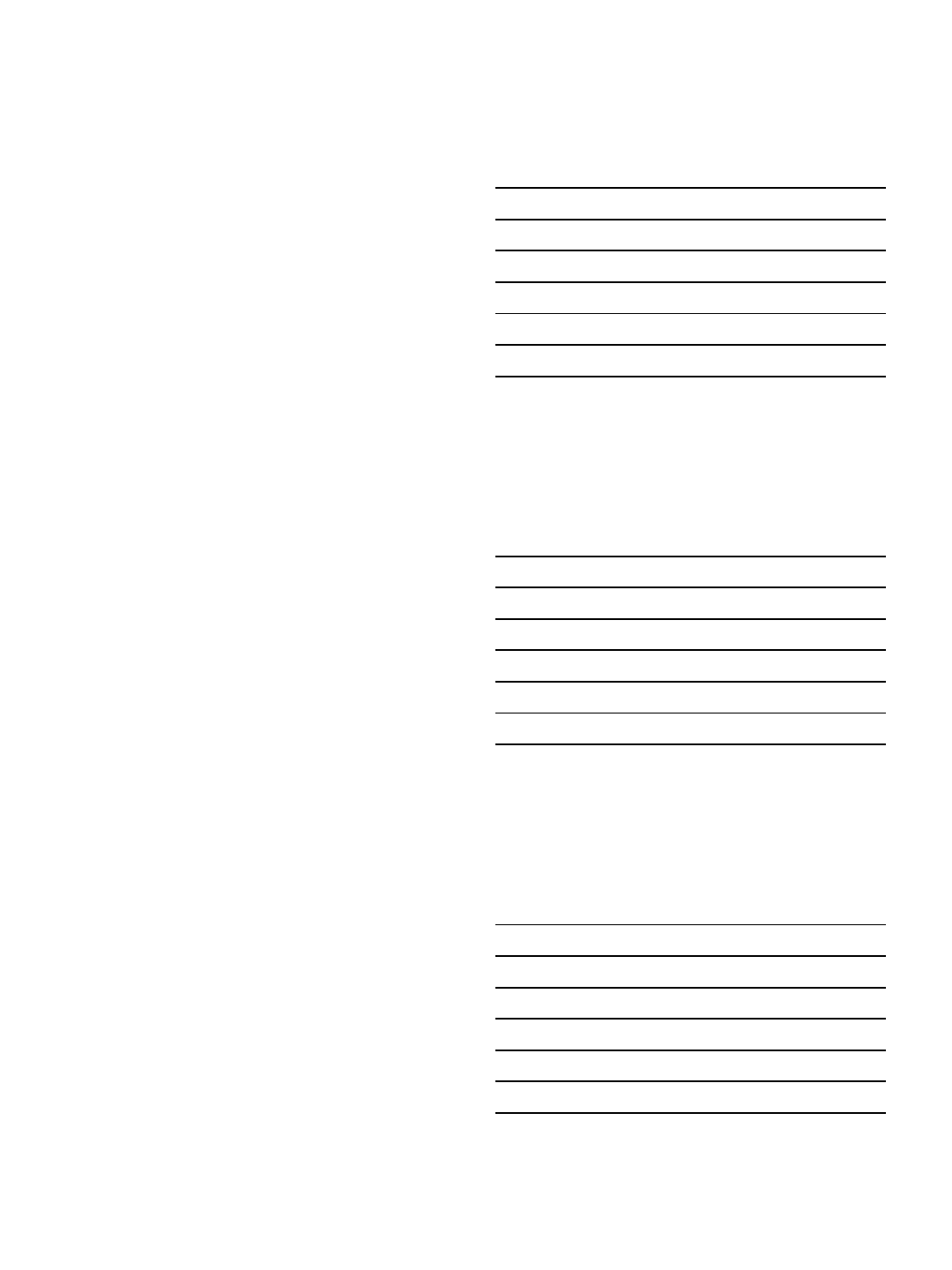
Diagnosing: Provocative Tests
Distraction Test
•The sacroiliac joint is stressed by the examiner,
attempting to pull the joint apart
Compression Test
•The two sides of the joint are forced together. Pain may
indicate that the sacroiliac joint is involved.
Gaenslen's Test
•Lay on a table, one leg drops over the edge and the
supported leg is flexed. In this position, sacroiliac joint
problems will cause pain because of stress to the joint.
FABER Test
•The leg is brought up to the knee, and the knee is
pressed on to test for hip mobility.
8
Diagnosis
•Clinical
•Imaging – limited benefit
•Injections
12/14/2016
4
Treatment Options
•Non operative
•NSAIDs
•Analgesics
•PT
•SI belt
•Injections
•RFA
•Operative
Surgery
•Why use navigation?
•Poor visualization of relevant anatomy on fluoroscopy
•Superior aspect of the sacral ala
•Anterior aspect of sacrum – ala and body
•S1 neural foramina
•Percutaneous
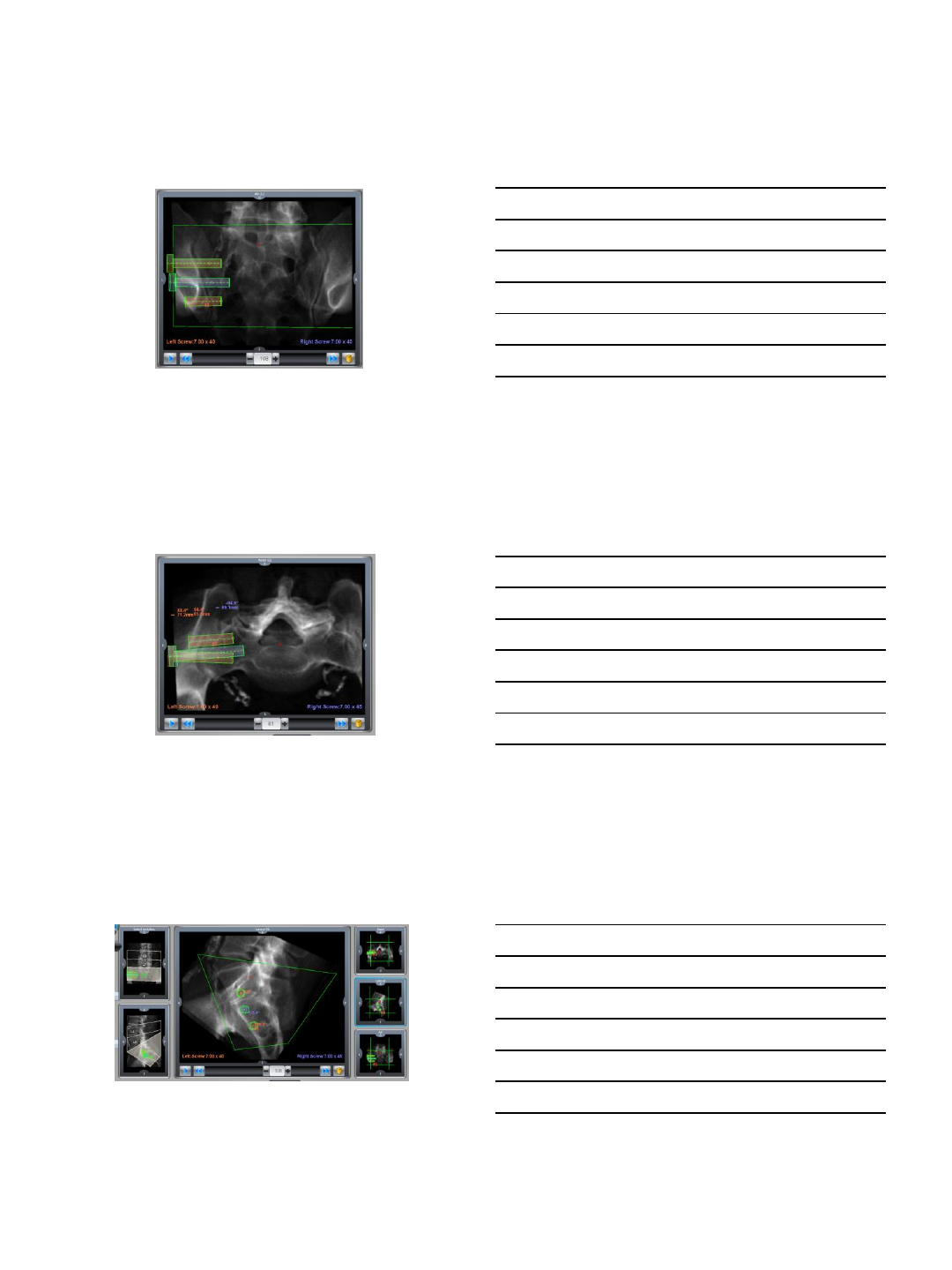
Surgery
•Robotic guided SI joint immobilization:
•Pre operative CT scan of lower lumbar spine, sacrum and pelvis
•Pre operative planning for placement of device across the joint
•GPS speaks to robot
12/14/2016
5
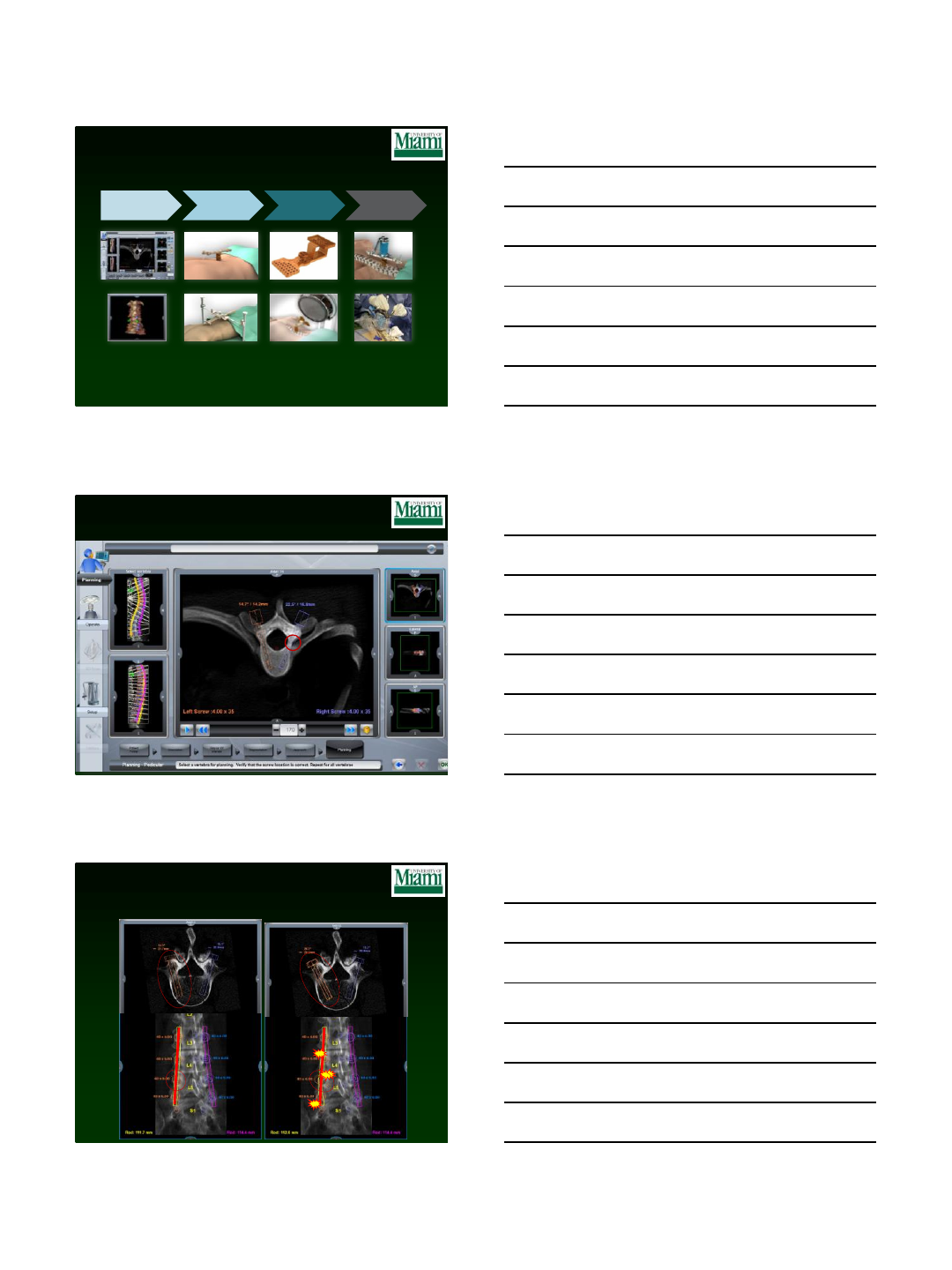
Planning in Coronal View
13
Planning in Axial View
14
Planning in Sagittal View
15
12/14/2016
6
Planning in Axial Video
16
Planning in Coronal Video
17
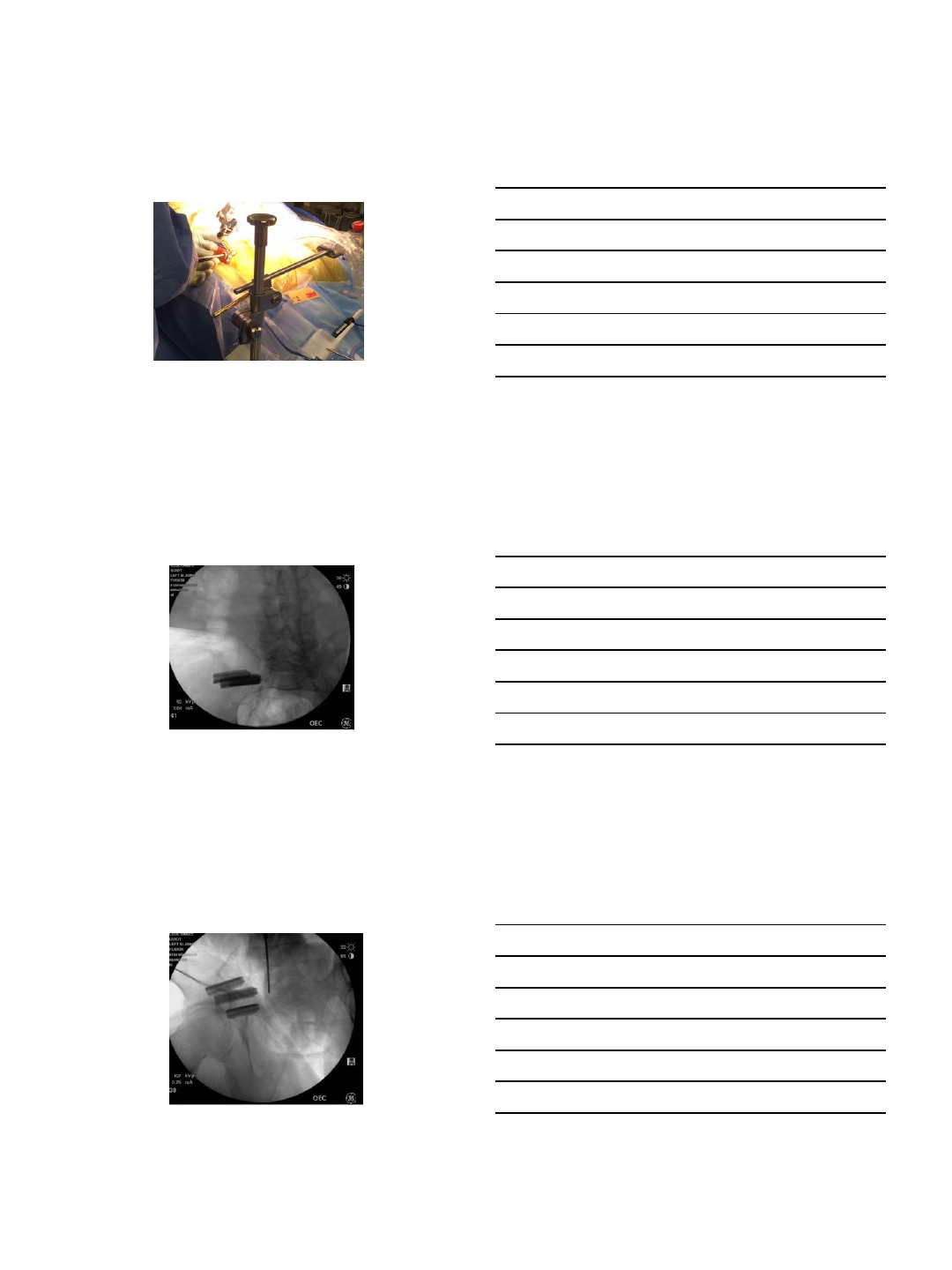
Mounting Multi Directional Bridge
18
12/14/2016
7
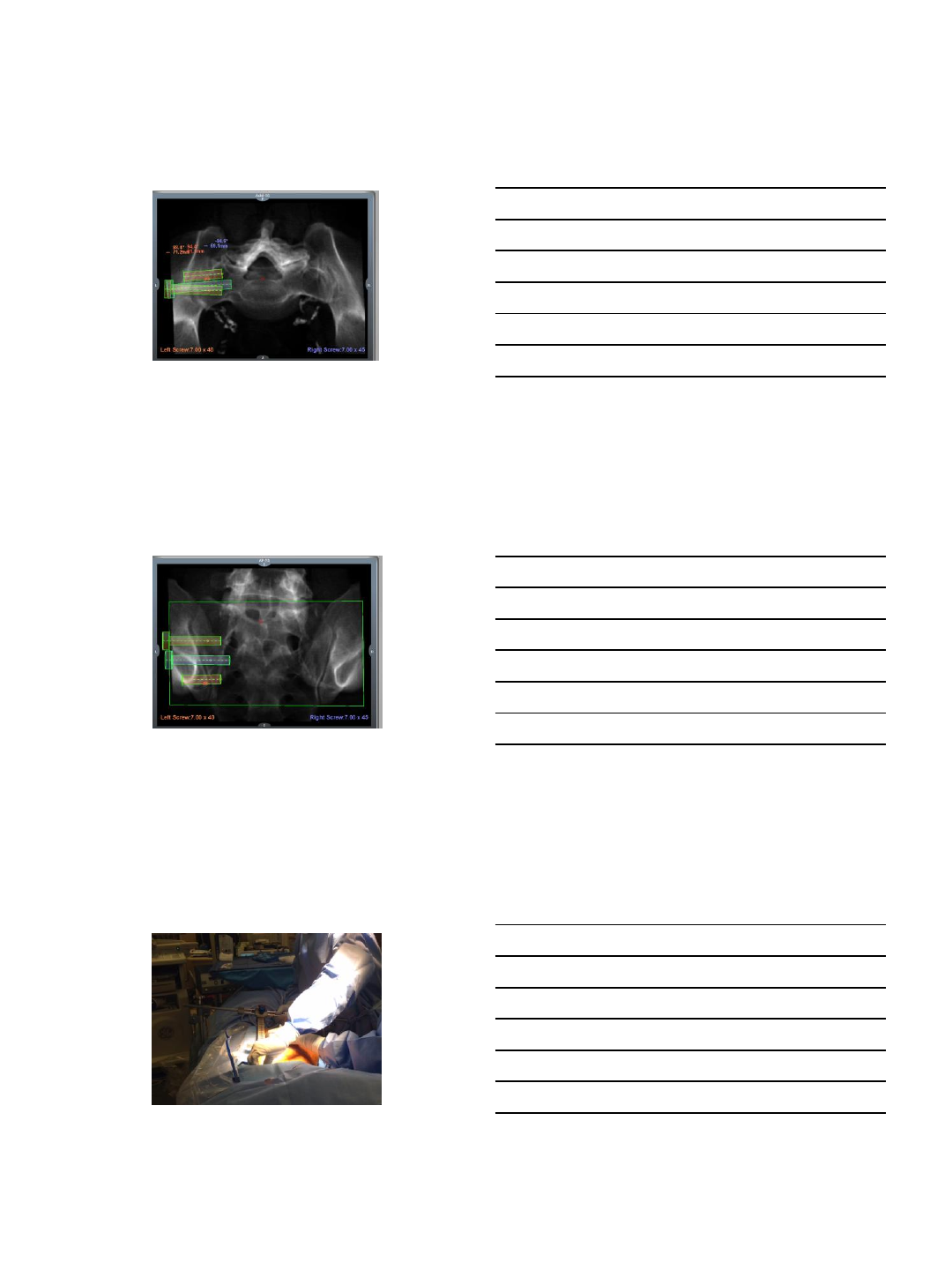
Operating
19
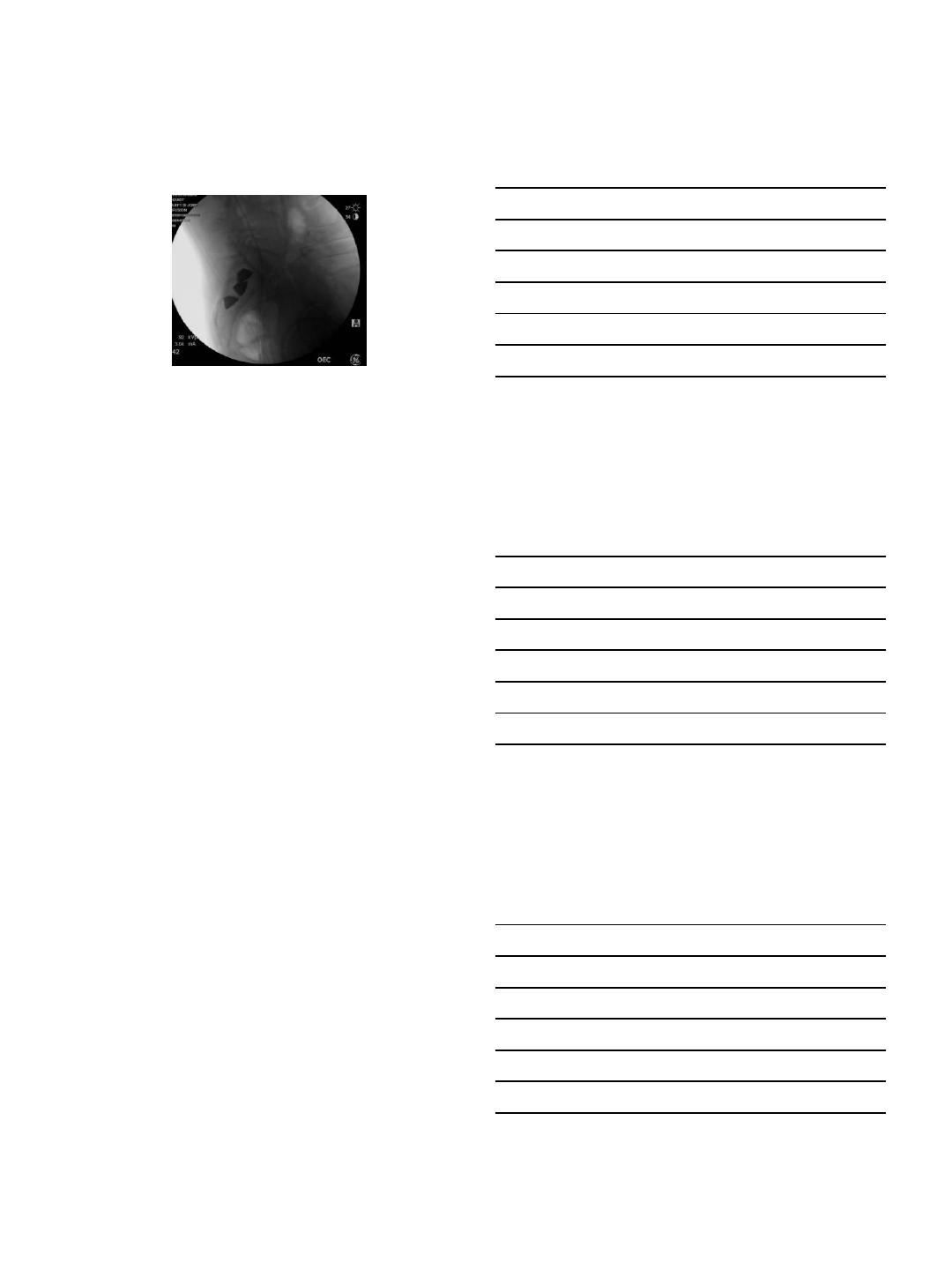
Post Operative View - 1
20
Post Operative View - 2
21
12/14/2016
8
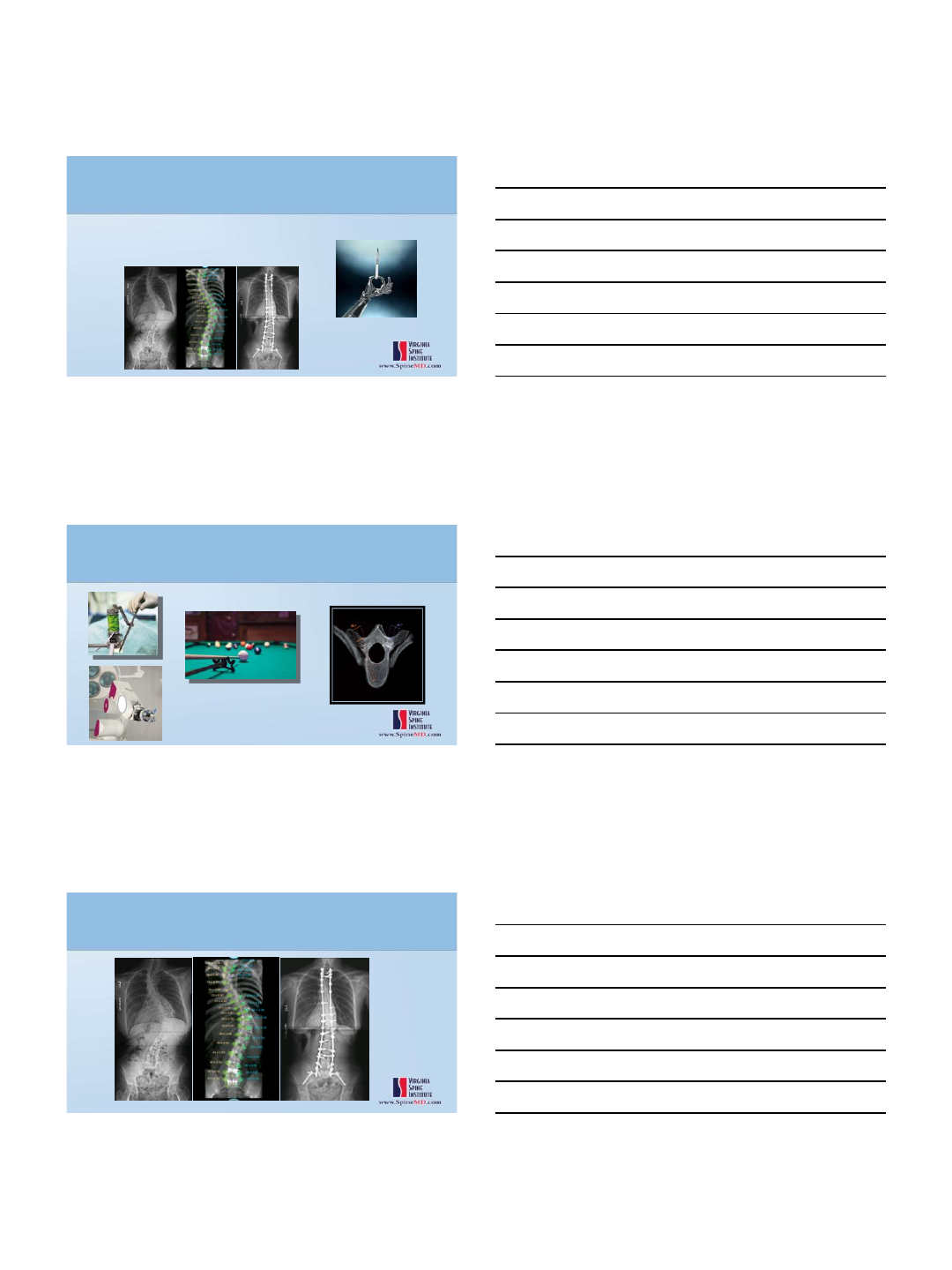
Post Op Lateral View
22
Case Information and Data Points
•Start Time: 1:56pm
•End Time: 2:38pm
•Registration Fluoro Time: Seven Seconds
•Total Fluoro: 41 seconds
23
Questions?
Thank You
12/13/2016
2
Robotic Spine Surgery – The Future
Current or developing technical advancements:
Improved 3D pre-op anatomy
Merging pre-op imaging studies
CT, Scoli X-rays, Flexibility X-rays
Incorporate developing planning software
Stronger Robotic Arms
More accurate trajectories
More tools available
Drills, burrs, bone cutters
Merge with Navigation
Real-time feedback
Merge with implants
Contour/cuts rods
Assist in Correction
Pre-op
Spinal Alignment Assessment
Combine X-ray / CT / MRI
Global parameters
3D rotation assessment
Segmental analysis
Pre-op Planning
Implant Positioning
Deformity Correction
Osteotomy Planning
Decompressions
Robotic Spine Surgery – The Future
Pre-operative Assessment
Intra-op
Trajectory Guidance
Improved Reachability
Implants
Screws
SI fusion
Tumor
Osteotomy
Decompression
Live intra-op Feedback
Rob bend based on robot plan
Deformity Correction
Robotic Spine Surgery – The Future
Intra-op

12/13/2016
3
Robotic Spine Surgery – The Future
Conclusions
•Many robots in development, FDA approval/studies ongoing and growing
•Growing Literature
–>30 Studies
–Increased accuracy
–Decreased radiation
–Decreased complications
•First FDA approved robot
–120 systems worldwide, 80 USA
–>18,000 cases
–>120,000 Implants
•2 systems currently FDA approved
–More to follow
