12 9 15 Endovascular Syllabus
2015-12-09
: Pdf 12 9 15 Endovascular Syllabus 12_9_15_Endovascular_Syllabus 12 2015 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 33
12/8/2015
1
Endovascular Treatment of Acute Ischemic
Stroke: Review of Recent Trials
Venu Vadlamudi, MD
NeuroInterventional Radiology
Vascular & Interventional Radiology
Association of Alexandria Radiologists, PC
INOVA Alexandria Hospital
No relevant disclosures
Objectives
•Review 2015 endovascular stroke trials and
impact on clinical practice
•Review updated AHA/ASA guidelines for
endovascular treatment of acute ischemic stroke
12/8/2015
2
2015 Endovascular Stroke
Trials
•MR CLEAN –Multicenter Randomized Clinical Trial of
Endovascular Treatment for Acute Ischemic Stroke in the
Netherlands
•ESCAPE –Endovascular Treatment for Small Core and Proximal
Occlusion Ischemic Stroke
•EXTEND-IA –Extending the Time for Thrombolysis in
Emergency Neurological Deficits - Intra-Arterial
•SWIFT PRIME –Solitaire With the Intention For Thrombectomy
as Primary Endovascular Treatment
•REVASCAT –Endovascular Revascularization With Solitaire
Device Versus Best Medical Therapy in Anterior Circulation
Stroke Within 8 Hours
•THRACE –Trial and Cost Effectiveness Evaluation of Intra-
arterial Thrombectomy in Acute Ischemic Stroke
•THERAPY –Assess the Penumbra System in the Treatment of
Acute Stroke
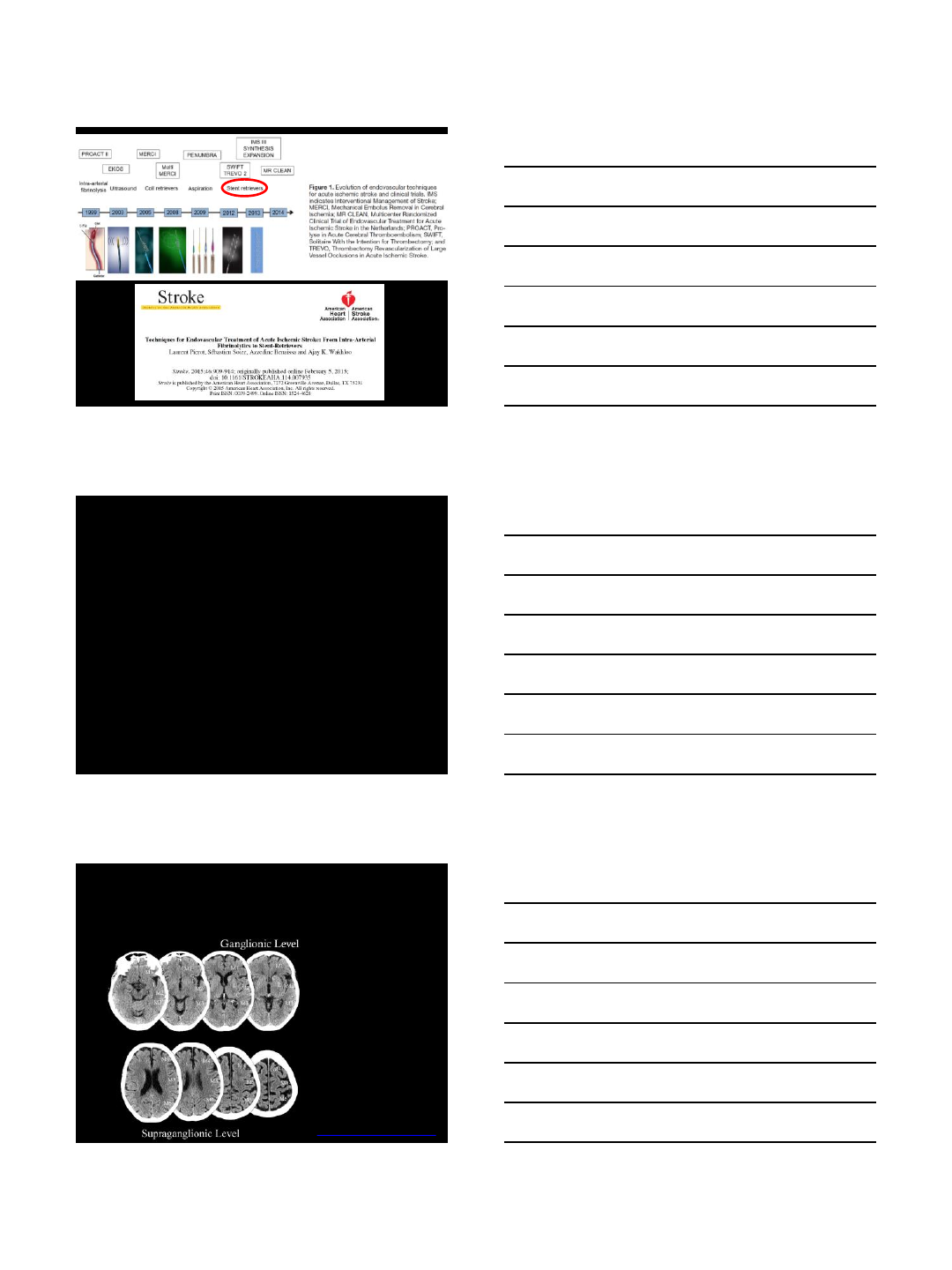
ASPECTS
•Alberta Stroke Program Early CT Score
Caudate
Putamen
Internal capsule
Insular cortex
M1: frontal operculum
M2: anterior temporal lobe
M3: posterior temporal lobe
M4: anterior frontal lobe
M5: middle/posterior frontal lobe
M6: parietal lobe
www.aspectsinstroke.com
12/8/2015
3
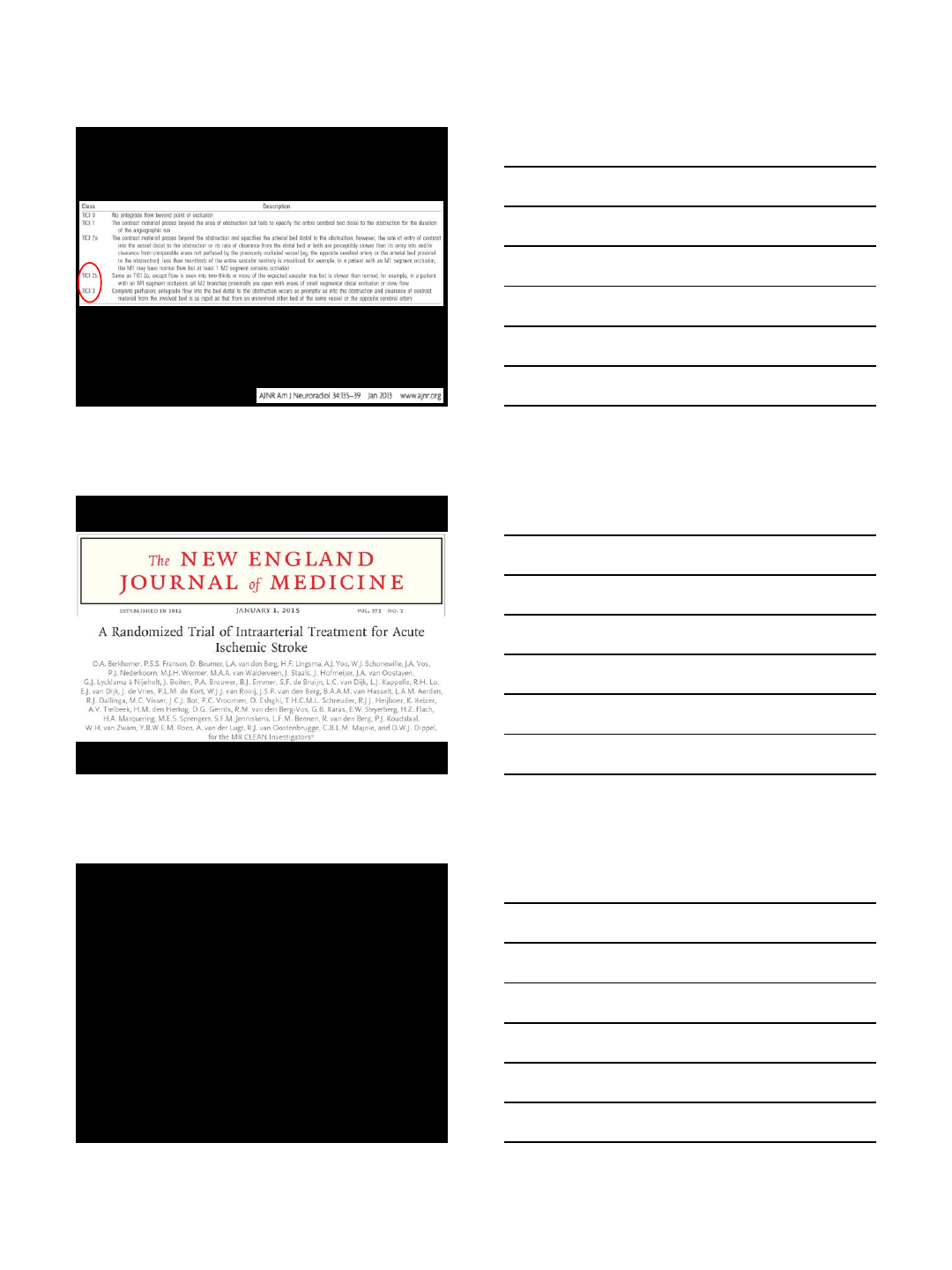
TICI Score
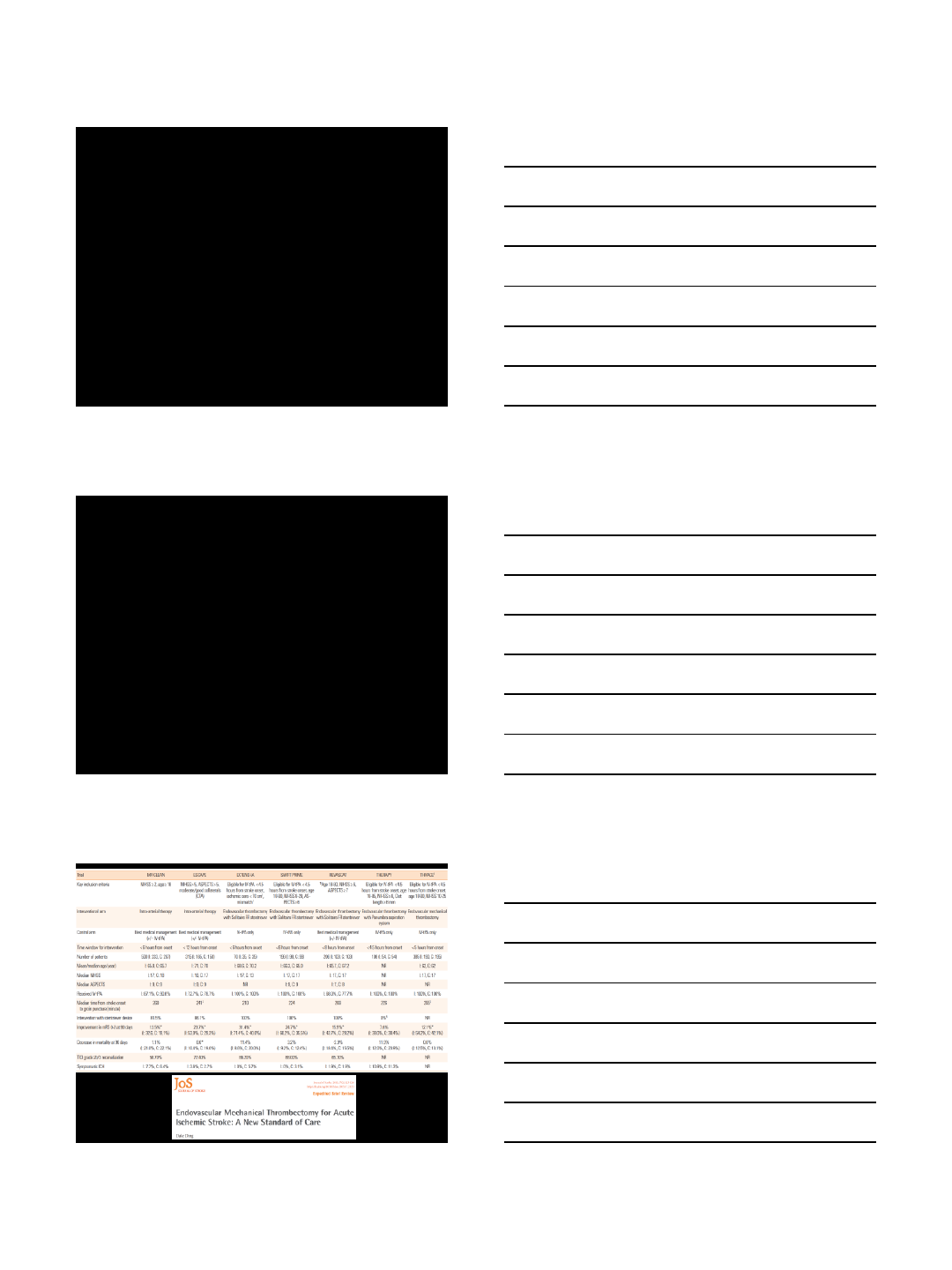
MR CLEAN (2015)
•Netherlands
•N = 500
• Age ≥ 18
•Pre-stroke mRS –no cutoff
•ASPECTS > 5
•Endovascular treatment w/in 6 hours
–Allowed GA
12/8/2015
4
MR CLEAN (2015)
•Primary outcome: mRS at 90 days
•Secondary outcomes:
–NIHSS at 24 hours and 1 week
–Barthel index at 90 days
–EuroQoL at 90 days
MR CLEAN (2015)
•233 endovascular arm vs 267 medical arm
–IV TPA in most (87% in endovascular arm and
91% in medical arm)
–Median ASPECTS 9
–Median NIHSS 17
–Acute carotid stenting in 13% of cases
–Stent retriever in 97% of cases
•TICI 2b/3 in 58.7%
–33% mRS 0-2 (c/w 19% in medical arm)
–No significant difference in hemorrhage (7.7% vs
6.4%) or death
MR CLEAN (2015)
•RCT clearly showed benefit of
endovascular treatment for LVO in AIS
•Domino effect on other
concurrent/subsequent endovascular
trials!
12/8/2015
5
ESCAPE (2015)
•Canada and US
•N = 500 (halted at 316)
• Age ≥ 18
•Pre-stroke mRS ≤ 1
•ASPECTS > 5
•Multiphase CTA (Menon et al. Radiology, 2015)
•Endovascular treatment w/in 12 hours
–CT to groin 60 min; CT to recanalization 90 min
–Discouraged GA or CAS
ESCAPE (2015)
•165 endovascular arm vs 150 medical arm
–IV TPA in most (73% in endovascular arm and
79% in medical arm)
–Median ASPECTS 9
–Median NIHSS 16
–Stent retriever in 86% of cases
•TICI 2b/3 in 72.4%
–53% mRS 0-2 (c/w 29% in medical arm)
–No significant difference in hemorrhage (3.6%
vs 2.7%) or death
12/8/2015
6
ESCAPE (2015)
•Halted following MR CLEAN results and
showed similar clear benefit for
endovascular treatment for LVO
EXTEND-IA (2015)
•Australia
•N = 100 (halted at 70)
• Age ≥ 18
•Pre-stroke mRS ≤ 1
•No minimum ASPECTS or NIHSS
•RAPID software for CTP or MRI/P
assessment
•Endovascular treatment w/in 6 hours
–Allowed GA
–Discouraged CAS
12/8/2015
7
EXTEND-IA (2015)
•35 endovascular arm vs 35 medical arm
–IV TPA in all
–Median ASPECTS 9
–Median NIHSS 17
–Stent retriever in 100% of cases (Solitaire)
•TICI 2b/3 in 86.2%
–71% mRS 0-2 (c/w 29% in medical arm)
–No significant difference in hemorrhage (0%
vs 5.7%) or death
EXTEND-IA (2015)
•Halted following MR CLEAN results and
showed similar clear benefit for
endovascular treatment for LVO
12/8/2015
8
SWIFT PRIME (2015)
•US and Europe
•N = 477 (halted at 196)
•Age 18-80
•Pre-stroke mRS ≤ 1
• ASPECTS ≥ 6
•NIHSS 8-29
•Endovascular treatment w/in 6 hours
SWIFT PRIME (2015)
•98 endovascular arm vs 98 medical arm
–IV TPA in all
–Pre-stroke mRS 0
–Median ASPECTS 9
–Median NIHSS 17
–Stent retriever in 100% of cases (Solitaire)
•TICI 2b/3 in 88%
–60.2% mRS 0-2 (c/w 35.5% in medical arm)
–No significant difference in hemorrhage (0% vs
3.1%) or death
SWIFT PRIME (2015)
•Halted following MR CLEAN results and
showed similar clear benefit for
endovascular treatment for LVO
12/8/2015
9
ESO 2015
•European Stroke Organisation 2015
meeting (late April)
•Results of REVASCAT announced
•Preliminary results of THRACE and
THERAPY announced
REVASCAT (2015)
•Spain
•N = 690 (halted at 206)
•Age 18-80 (extended to 85 in mid 2014 if
ASPECTS 9-10)
•Pre-stroke mRS ≤ 1
• ASPECTS ≥ 7
• NIHSS ≥ 6
•Endovascular treatment w/in 8 hours
12/8/2015
10
REVASCAT (2015)
•103 endovascular arm vs 103 medical arm
–IV TPA in most (68% in endovascular arm and
78% in medical arm)
–Pre-stroke mRS 0 in 83-86%
–Median ASPECTS 7-8
–Median NIHSS 17
–Stent retriever in 100% of cases (Solitaire)
•TICI 2b/3 in 65.7%
–43.7% mRS 0-2 (c/w 28.2% in medical arm)
–No significant difference in hemorrhage (1.9% in
both) or death
REVASCAT (2015)
•Halted following MR CLEAN, ESCAPE,
EXTEND-IA and SWIFT-PRIME results
and showed similar clear benefit for
endovascular treatment for LVO
THRACE (2015)
•France
•N = 414
•Age 18-80
•Symptoms < 4 hours
•NIHSS 10-25
•All received IV TPA
–Assigned to endovascular arm if no/minor (< 5
points) NIHSS improvement
–Endovascular treatment to be completed by 6
hours
12/8/2015
11
THRACE (2015)
•190 endovascular arm vs 195 IV TPA arm
•Mean NIHSS 17
•85% had M1 occlusion
•54.2% mRS 0-2 (c/w 42.1% in IV TPA arm)
•No reported significant difference in
hemorrhage or death
THERAPY (2015)
•N = 692 (halted at 108)
•Use of Penumbra aspiration thrombectomy
devices rather than stent retrievers
•Looked at clot length (≥ 8 mm)
• NIHSS ≥ 8
•Inclusion w/in 4.5 hours of onset
•Final results pending but preliminary results
indicate benefit in endovascular treatment vs
IV alone
12/8/2015
12
2015 Endovascular Stroke Trials
2015 AHA Guidelines
2015 AHA Guidelines
•Recommendations:
–Give IV TPA when able (up to 4.5 hrs per ECASS
III)
–Do no wait to look for improvement after IV TPA
–Pre-stroke mRS 0-1
–Baseline CT head – ASPECTS ≥ 6
–NIHSS ≥ 6
–Proceed with CTA or MRA to look for LVO
–Benefits of CTP/MRP not clear
12/8/2015
13
2015 AHA Guidelines
•Recommendations:
–Groin puncture w/in 6 hrs
–Favor conscious sedation rather than GA when
possible
–Use stent retriever or other thrombectomy device
–Use balloon-guide catheter or large-bore distal
access catheter
–Aim for TICI 2b/3 reperfusion
–Salvage IA TPA can be used if needed
Take Home Points
•Endovascular thrombectomy for AIS
has become a standard of care
•Important considerations:
–Pre-stroke mRS ≤ 1
–Baseline CT head – ASPECTS ≥ 6
– NIHSS ≥ 6
–CTA or MRA with LVO and (ideally) good
collaterals
–Take for revascularization ASAP (< 6 hrs to groin
puncture)
Thank You!
12/8/2015
1
0 |
Devices and
Techniques: Review
of stent retrievers,
suction, and
combination therapy
Joseph J Gemmete, MD, FACR, FSIR
Professor of Radiology and Neurosurgery
University of Michigan Hospitals
1 |
Outline
•Access issues
•Balloon guides / Sheaths
•Stent retrievers
•Solitare
•Trevo
•Suction thrombectomy
•ADAPT technique
•Solumbra
•Summary
2 |
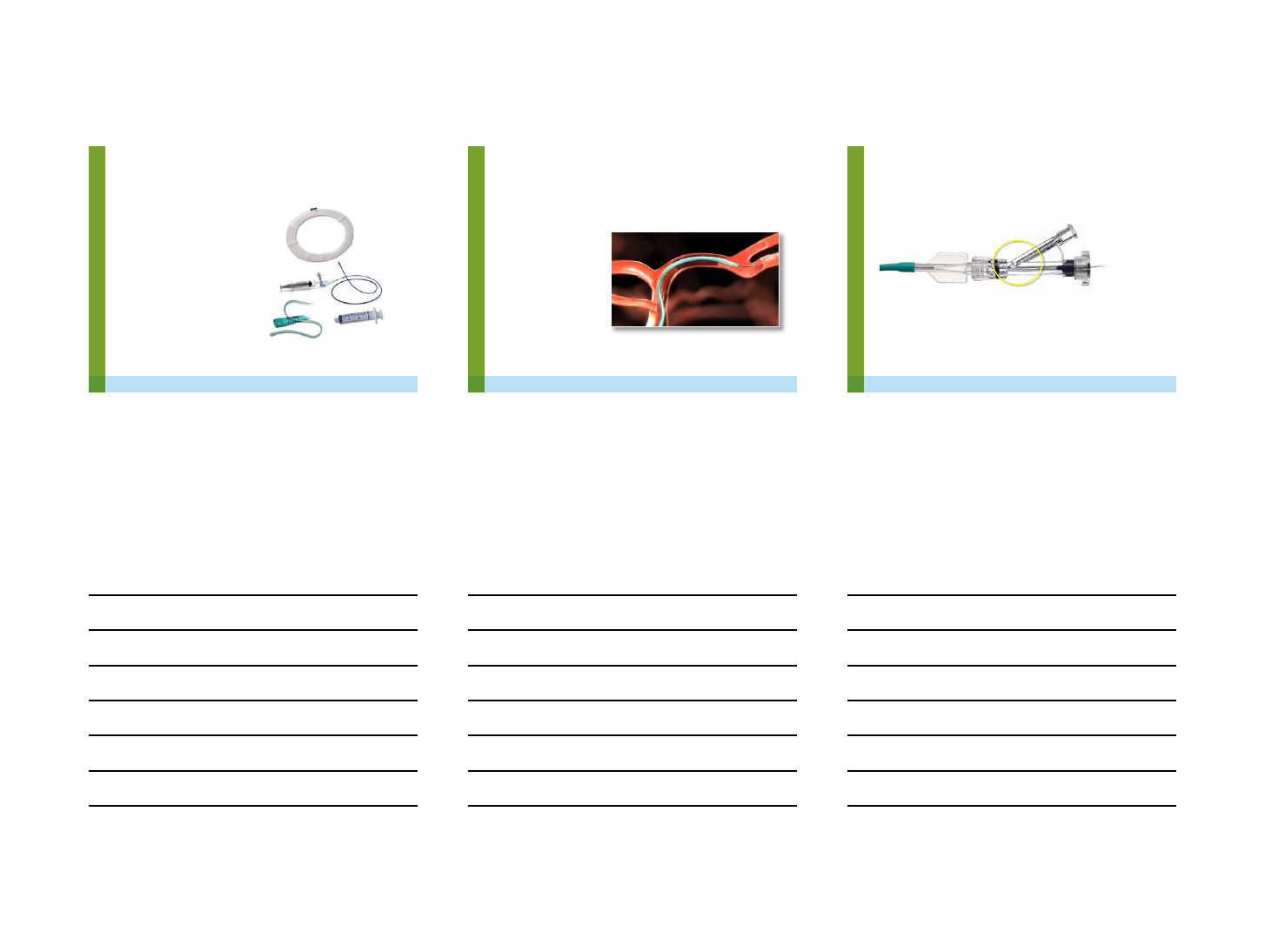
Access Issues
•CTA done in emergency room
-aortic arch (type 1, 2, 3)
-carotid/ vertebral tortousity
-Ca2+/atherosclerotic plaque
•Access –common femoral, direct carotid, radial access
-puncture access site under U/S
Micropuncture kit
19G single wall with 0.035 glide / Amplatz
-8/9F sheath (24 cm / 13 cm) CFA/carotid access
-radial limited 6F female/ ?7F male
-right radial (RVA, LCCA), left radial (LVA, RCCA)

12/8/2015
2
3 |
Carotid/Vertebral Access
•Which Carotid Access Technique?
-Front loading telescopic technique
(Neuron Max, FlowGate, Cook shuttle
sheath)
-Back loading serial stiffening technique
(wire in external carotid then advanced
sheath or guide) (Cello 8F / 6F)
-Remote or Direct access
4 |
5 |
Balloon Guides / Sheaths
•Balloon Guide - Cello 8F(.075in), Cello 6F,
FlowGate 8F (.084in), Merci 8F (>078in)
•Sheath -Cook shuttle sheath (.087in), Neuron Max
(.088in)
12/8/2015
3
6 |
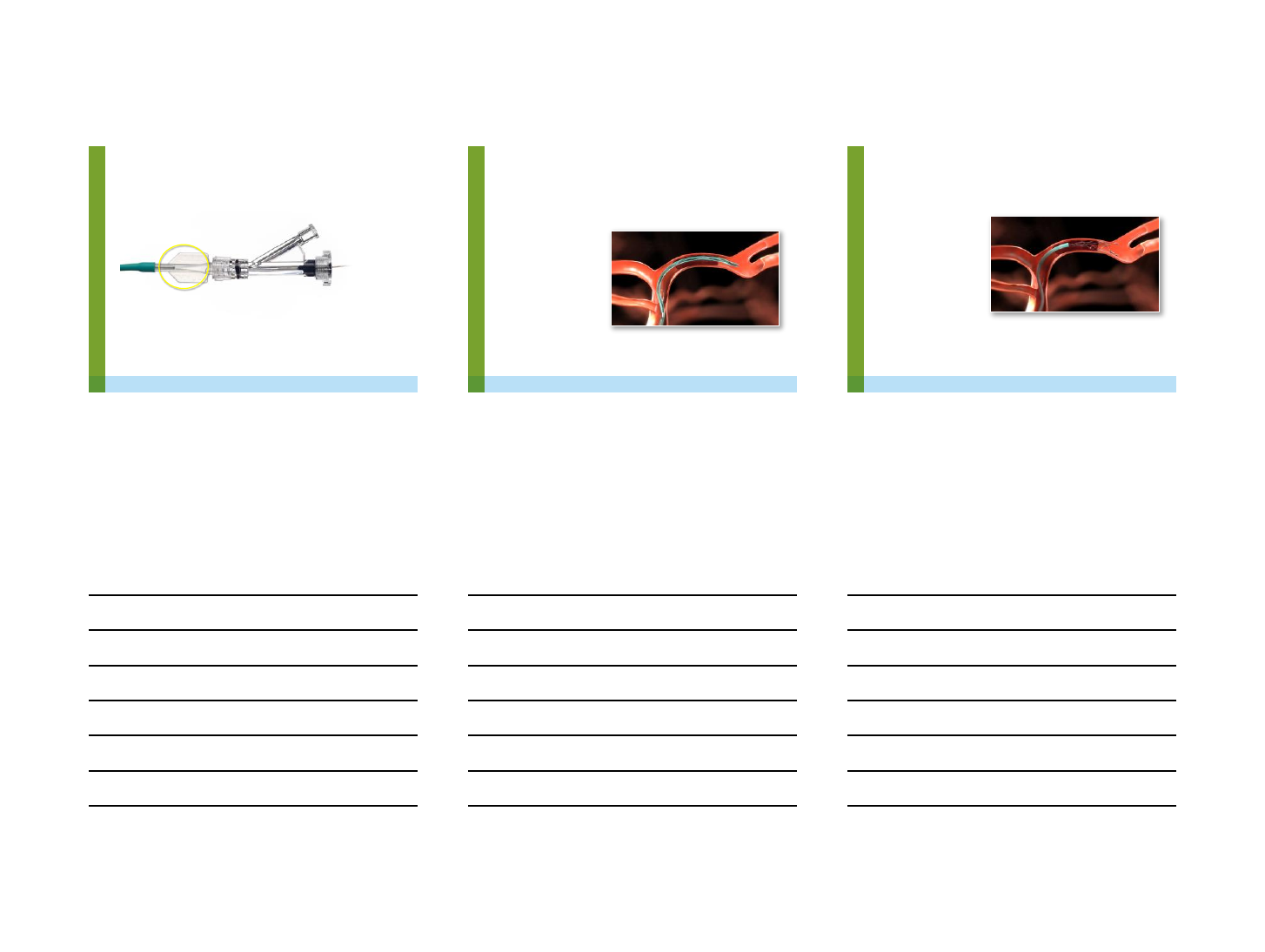
Preparation of Balloon Guide
•Inspect balloon guide
•Attach RHV or Tuohy Borst with Side port to the BGC
•Flush lumen of BGC with heparinised saline
•Insert dilator/catheter through the lumen and flush with HS
•FlowGate - Attach the flow valve, Cello no value
•Attach a 20 ml syringe with 50:50 contrast : saline using a
negative prep
•Inflate the balloon with a 50:50 contrast : saline for flow arrest
during stent retrieval
•During aspiration attached a three way with two 60 ml syringes so
can apply negative aspiration
7 |
Indication Overview
The indication for the Solitaire™FR revascularization device is as follows:
The Solitaire™ FR Revascularization Device is intended to restore blood flow
by removing thrombus from a large intracranial vessel in patients
experiencing ischemic stroke within 8 hours of symptom onset. Patients who
are ineligible for intravenous tissue plasminogen activator (IV t-PA) or who
fail IV t-PA therapy are candidates for treatment.
8 |
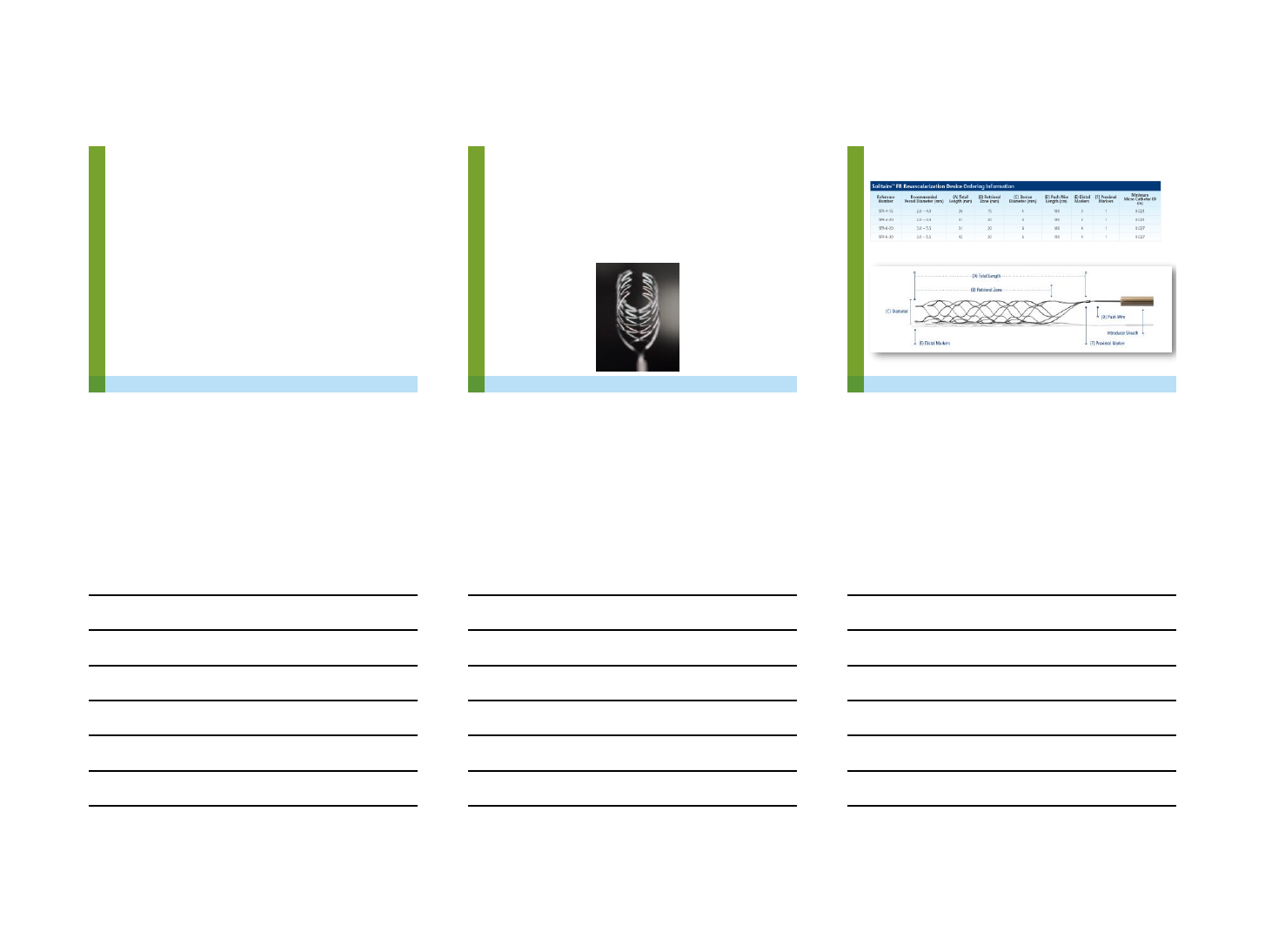
Solitaire™FR Revascularization Device Overview
12/8/2015
4
9 |
Procedural Overview
Procedure Components
1. Solitaire™FR revascularization device
2. Guide Catheter
(8F Balloon Guide Catheter
Recommended –1.90mm ID)
3. Microcatheter (Rebar®catheter 18/27)
4. Aspiration Syringe (60cc)
5. 014" Guidewire
Solitaire™ FR revascularization device procedural steps taken from IFU. For complete instructions for use please see IFU.
10 |
Procedural Overview
Position the microcatheter
Advance the microcatheter
distal to the thrombus position
so that when the Solitaire™FR
revascularization device is fully
deployed, it will extend beyond
both ends of the thrombus.
Solitaire™ FR revascularization device procedural steps taken from IFU. For complete instructions for use please see IFU.
11 |
Procedural Overview
Flush the introducer sheath
Insert the introducer sheath partially into the RHV, tighten the RHV and verify that
fluid exits the proximal end of the sheath.
Solitaire™ FR revascularization device procedural steps taken from IFU. For complete instructions for use please s ee IFU.
12/8/2015
5
12 |
Procedural Overview
Introduce the Solitaire™ FR Device into the microcatheter
Loosen the RHV. Advance the introducer sheath into the microcatheter hub until
firmly seated. Tighten the RHV and advance the Solitaire™FR revascularization
device into the microcatheter. Once the flexible portion of the push wire has entered
the micro catheter shaft, remove the sheath.
Solitaire™ FR revascularization device procedural steps taken from IFU. For complete instructions for use please see IFU.
13 |
Procedural Overview
Deliver the Solitaire™ FR Device
Continue to advance the
Solitaire™FR until its distal
radiopaque markers reach the
end of the properly positioned
microcatheter.
WARNING: IF EXCESSIVE RESIST ANCE IS ENCOUNTERED DURING THE DELIVERY OF THE SOLITAIRE™ FR REVASCULARIZATION
DEVICE, DISCONTINUE THE DELIVERY AND IDENTIFY THE CAUSE OF THE RESISTANCE. ADVANCEMENT OF THE SOLITAIRE™FR
REVASCULARIZATON DEVICE AGAINST RESISTANCE MAY RESULT IN DEVICE DAMAGE AND/OR PATIENT INJURY.
Solitaire™ FR revascularization device procedural steps taken from IFU. For complete instructions for use please see IFU.
14 |
Procedural Overview
Positioning and Deployment
To deploy the Solitaire™FR
revascularization device, fix the
push wire to maintain position of
the device and carefully
withdraw the microcatheter in
the proximal direction.
To ensure full deployment, the
microcatheter must be proximal
to the proximal radiopaque
marker on the Solitaire™FR
revascularization device. The
usable length of the deployed
Solitaire™device should extend
beyond each side of the
thrombus.
Solitaire™ FR revascularization device procedural steps taken from IFU. For complete instructions for use please s ee IFU.

12/8/2015
6
15 |
Procedural Overview
Prior to retrieval
Reposition the micro catheter
to cover the proximal zone
(proximal 3-4mm) of the
Solitaire™ FR revascularization
device. Lock the RHV onto the
Solitaire™ FR device pushwire.
Wait for 5 minutes to let stent
incorporate into thrombus
Solitaire™ FR revascularization device procedural steps taken from IFU. For complete instructions for use please see IFU.
16 |
Procedural Overview
Recovery
•Prior to retrieval, inflate the balloon in the balloon guide catheter, if a balloon
guide catheter has been selected.
•Do not perform more than three (3) recovery attempts in the same vessel.
•Do not use each Solitaire™FR revascularization device for more than two (2)
thrombus recoveries.
Solitaire™ FR revascularization device procedural steps taken from IFU. For complete instructions for use please see IFU.
17 |
Procedural Overview
Recovery
Retrieve the Solitaire™ FR revascularization device and the micro catheter as a unit
into the guiding catheter under constant aspiration. Continue to aspirate on the
guiding catheter until there is good flow reversal.
Remove the Solitaire™ FR revascularization device out of the distal end of the micro
catheter in order not to damage the device. If additional flow restoration attempts are
desired with the same device clean the device with saline solution. Do not use
solvents or autoclave.
Solitaire™ FR revascularization device procedural steps taken from IFU. For complete instructions for use please s ee IFU.
12/8/2015
7
18 |
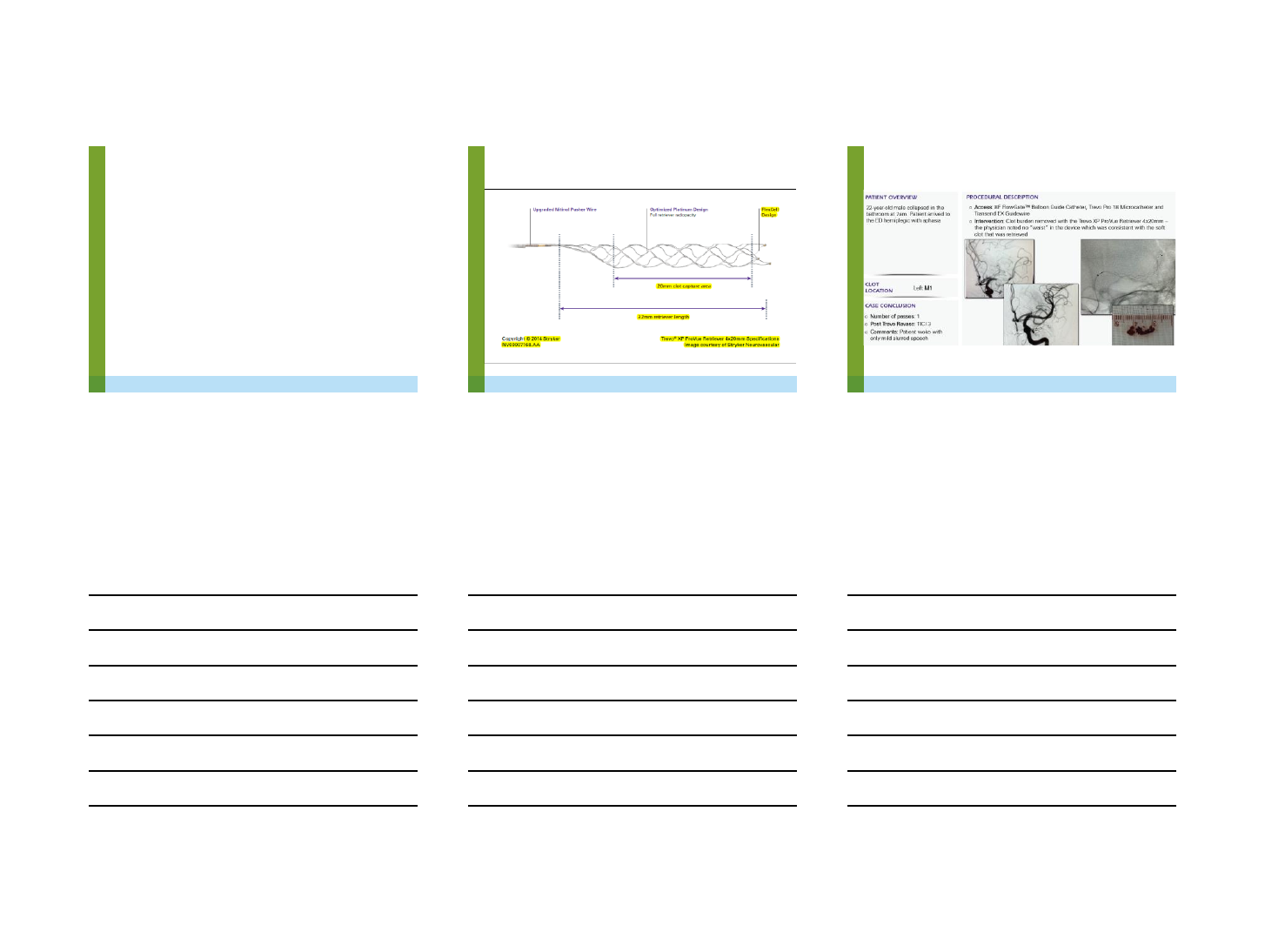
Trevo® XP Pro Retriever
Sizes
–6 mm x 25 mm - Excelsior XT-27 microcatheter
–4 mm x 20 mm - Trevo Pro 18
–3 mm x 20 mm –Trevo Pro 14, Trevo Pro 18
19 |
Trevo® XP Pro Retriever
20 |
12/8/2015
8
21 |
22 |
ADAPT / Solumbra
•ADAPT
-place large bore suction catheter at the face
of the thrombus, then turn on pump
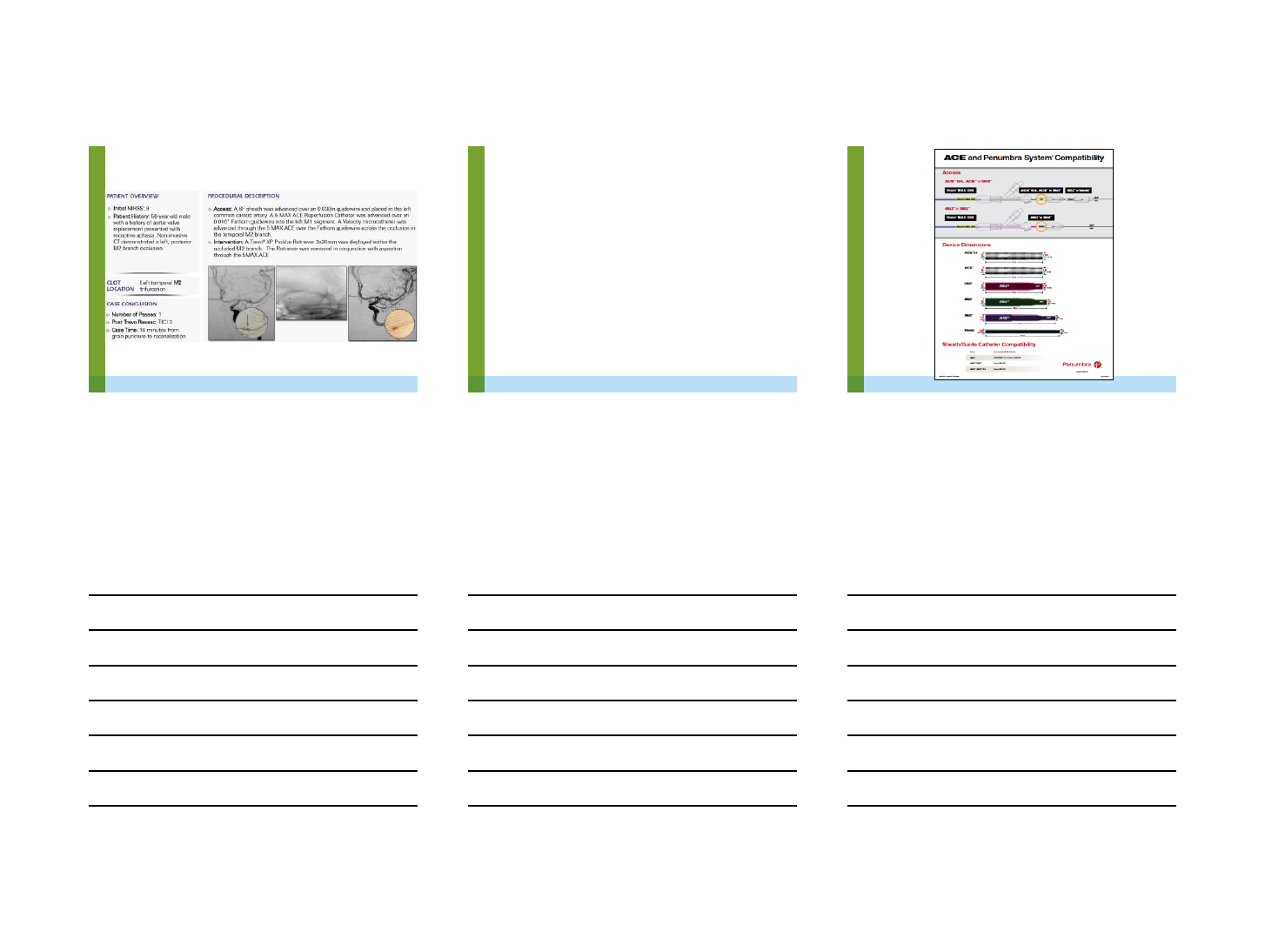
•Solumbra
-place 8 Fr guide catheter into the cervical
ICA, then 5 MAX /ACE catheter into M1
segment, advance a microcatheter distal to
the thrombus, deploy the stent retriever within
the thrombus and then remove the
microcatheter, under local aspiration remove
the 5 MAX/ACE catheter with the stent
retriever as a unit into the guide catheter
23 |Copyright © 2015 Penumbra, Inc. All rights reserved. 9097 Rev. B USA 05/15 23
12/8/2015
9
24 |
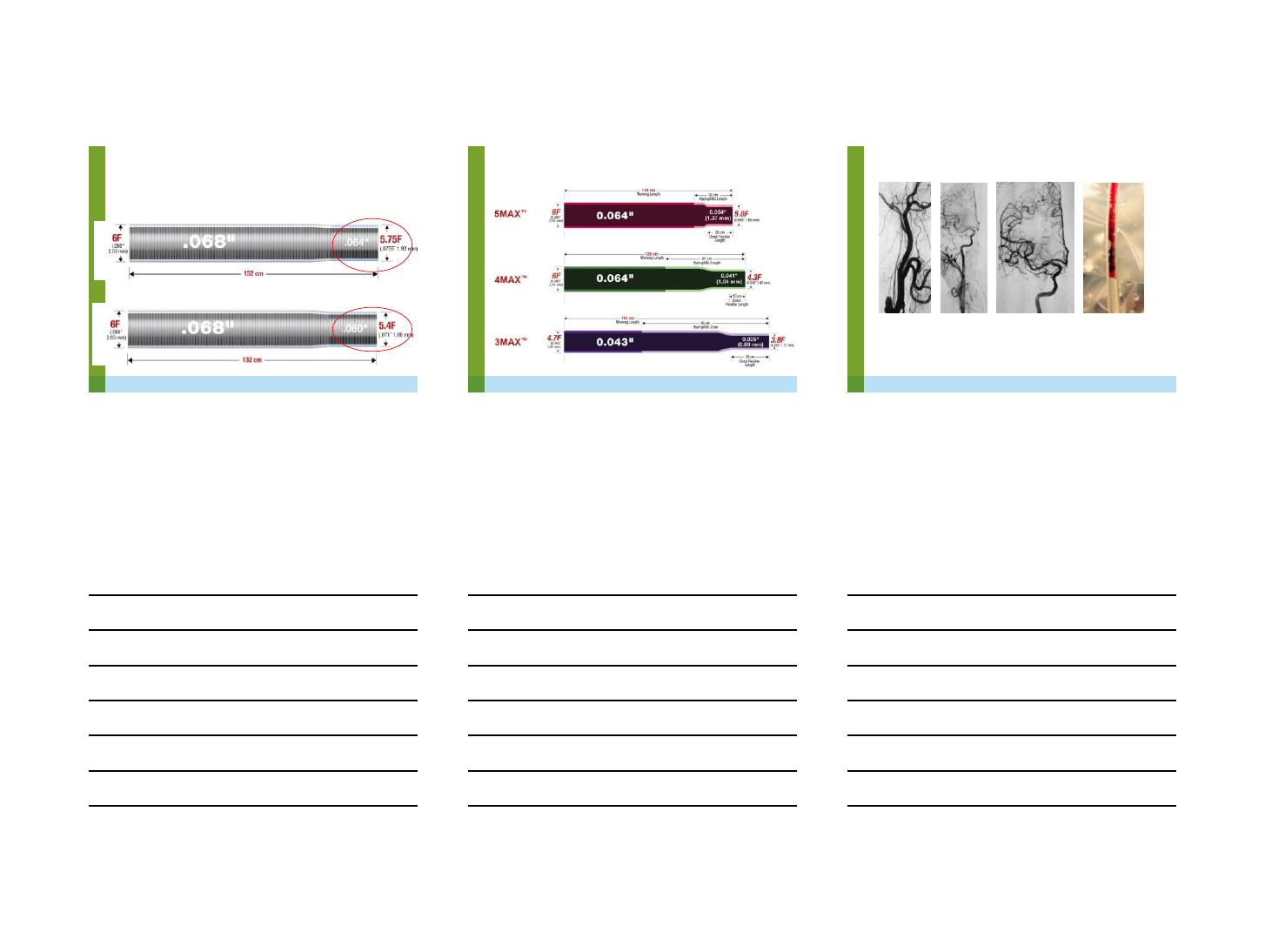
ACE™Dimensions
ACE™64
ACE
Copyright © 2015 Penumbra, Inc. All rights reserved. 9097 Rev. B USA 05/15 24
25 |
MAX™Dimensions
Copyright © 2015 Penumbra, Inc. All rights reserved. 9097 Rev. B USA 05/15 25
26 |
•Baseline NIHSS = 18
•1 revascularization attempt
•TICI 3
•NIHSS at 24 hours = 0
With the courtesy of Dr. Murcia, San Sebastian, Spain
Copyright © 2015 Penumbra, Inc. All rights reserved. 9097 Rev. B USA 05/15 26
ADAPT Technique
12/6/2015
1
Training Standards, Credentials,
and Education for Intra-arterial
Catheter-directed Treatment of
Acute
Ischemic Stroke
David Sacks, MD
The Reading Health System
Dec 2015
Disclosures
•No conflicts of interest
•Intracranial drugs are off label
IA Stroke Issues
•Benefits of IA stroke care
•Risk/benefit very dependent on pt
selection, physician skills, infrastructure
•Hospital desire to keep stroke pts
•Need for IA manpower (24x7)
•Hirsch et al JNIS 2009
•Interest in IA from several specialties
•Problems with current training

12/6/2015
2
Training paradigms
•ABR certified
–Exclusive, what is the training provided?
•Fellowship
–Exclusive, what is the training?
•Case experience
–Must check outcomes
–Do outcomes meet benchmarks?
–What benchmarks
•What should you know, do you know, and can
you do?
Positions on IA stroke training
•SNIS
–Investigational, difficult, need ESN fellowship,
transport pt to regional center
•Meyers et al. J NeuroInterv Surg 2009
•Heck JNIS 2011
•SIR
–Not investigational, difficult, can train committed
and skilled interventionist, treat patient locally
•Connors et al. JVIR 2009
•Sacks and Connors commentary JVIR 2009
•Sacks JNIS 2011
Evidence
•Not Class 1: RCT, case series, registries
•Local anecdotes
•INSTOR results
•Case series by IR, IC
•Belisle et al. JVIR 2009;20:327-333
•Fjetland et al. Cardiovasc Interv Radiol 2012;35:1029-
1035
•Burkart et al. JVIR 2013;24:1267-1272
•Sanak et al. JVIR 2013;24:1273-1279
•Htyte et al. Cath Cardiovasc Interv 2015;85:1043-1050
•Goktekin et al. Eurointervention 2014;10:876
12/6/2015
3
SIR IA Stroke Training
JVIR Dec 2009
•Cognitive and Clinical
•Imaging
•Technical
•Stroke specific experience
•Facility
•Exam
Cognitive
1. Understanding of and certification in assessing the
NIHSS
2. 6 months ACGME formal neuroscience training
including neuroanatomy, neuropathology,
neurovascular imaging, hemodynamics
3. Stroke specific training in clinical presentation of
stroke and associated vascular territories
4. Training in stroke specific exams for stroke mimics
and conversion reactions
5. Ability to evaluate imaging criteria for appropriate
patients for acute stroke treatment
Cognitive
6. Ability to differentiate acute ischemic lesions as
compared to chronic lesions and/or tumors, etc.
7. Ability to differentiate TIA from acute infarct
8. Ability to recognize etiology of TIA and acute stroke,
including stenosis and embolus
9. Knowledge of cerebrovascular hemodynamics as it
relates to perfusion imaging, and clinical presentation
10. Knowledge of pharmacological agents used for acute
stroke therapy
11. Understanding peri-procedural and post-procedural
hemodynamics and implications for appropriate patient
care
12/6/2015
4
Brain Imaging
1. Interpretation of 200 CT and 50 CTA
2. Interpretation of 200 MRI and 50 MRA
3. Interpretation of 25 CT/MR perfusion
4. Interpretation of 200 cerebral arteriograms
What about a Team Approach
•Clinical is done by neurologist
•Imaging is done by dx radiologist
•Patient selection is done by neurologist
•Procedure is done by interventionist
–No need for neuro skills (IR, IC)
–No need for imaging skills (IC)
Is this model good enough???
If so, discard the SIR training and INR fellowship
Technical
1. Hands on equipment experience
2. Arteriography performance
a. 100 cerebral (bilateral carotid and at least single-
vessel vertebrobasilar injections)
OR
50 cerebral and 150 non cerebral
AND
b. 30 selective microcatheter procedures including 5
ICA/ECA
12/6/2015
5
IA Stroke Specific
•5 proctored
–in person
OR
–electronically/telephonically
•What does this mean?
Facility
1. Primary stroke center or equivalent
2. Quality assurance program specifically assessing
stroke patients, acute stroke treatments, and
clinical outcomes
3. Facility support for submission of all cases to a
national stroke registry for interventional stroke
therapy
•Commitment of facility
•Education
•National QA
Are these Standards
Restrictive?
YES
–This is not like hepatic embo for an exanguinating
trauma patient
–Stroke pts may improve spontaneously or may be
harmed by attempted revasc
–You need to know how to select and treat patients
–Dirty Harry
NO
The standards define your competence
12/6/2015
6
Problems with this Training
Model
1. Is it all really necessary? Obsolete?
What about the team approach?
2. There are few cerebral angios to do.
3. Who will proctor, how?
4. Local hospitals want it, want me to do
it, and if not me, who?
5. Where can I learn?
6. Who offers a test?
QA
•Locally
–90 day clinical outcomes
–Times from sx onset to ER, CT/MRI, IR,
treatment
–Multisociety QA benchmarks
•Nationally
–INSTOR registry
–Need to revise training?
Multisociety QA
Sacks et al. JVIR 2013;24:151-163
•Door to puncture < 2 hrs (75%)
•Puncture to start of revasc < 45 mins (50%)
•Recanalization (60%)
•SICH < 12%
•90 day good outcomes > 30%
•Cases submitted to registry (100%)
•Submitted for publication
•May be adopted for accreditation
12/6/2015
7
IA Stroke Courses
•SIR Vancouver 1 day add on to meeting
•SIR ? Stand alone meeting
–Course prep prior to meeting
•CIRSE annual meeting
•ICCA Prague 2016
(www.iccaonline.org)
What do I really Think?
1. IR can do an excellent job treating strokes
2. Training needs are between the SIR
standards and the “Team” approach
3. The facility is every bit as critical as the
interventional physician
4. Not every hospital should offer IA
Offering this care badly but locally is worse than a transfer
5. Hospitals will do what they want, and they
may want you
6. QA QA QA QA QA QA

12/2/2015
1
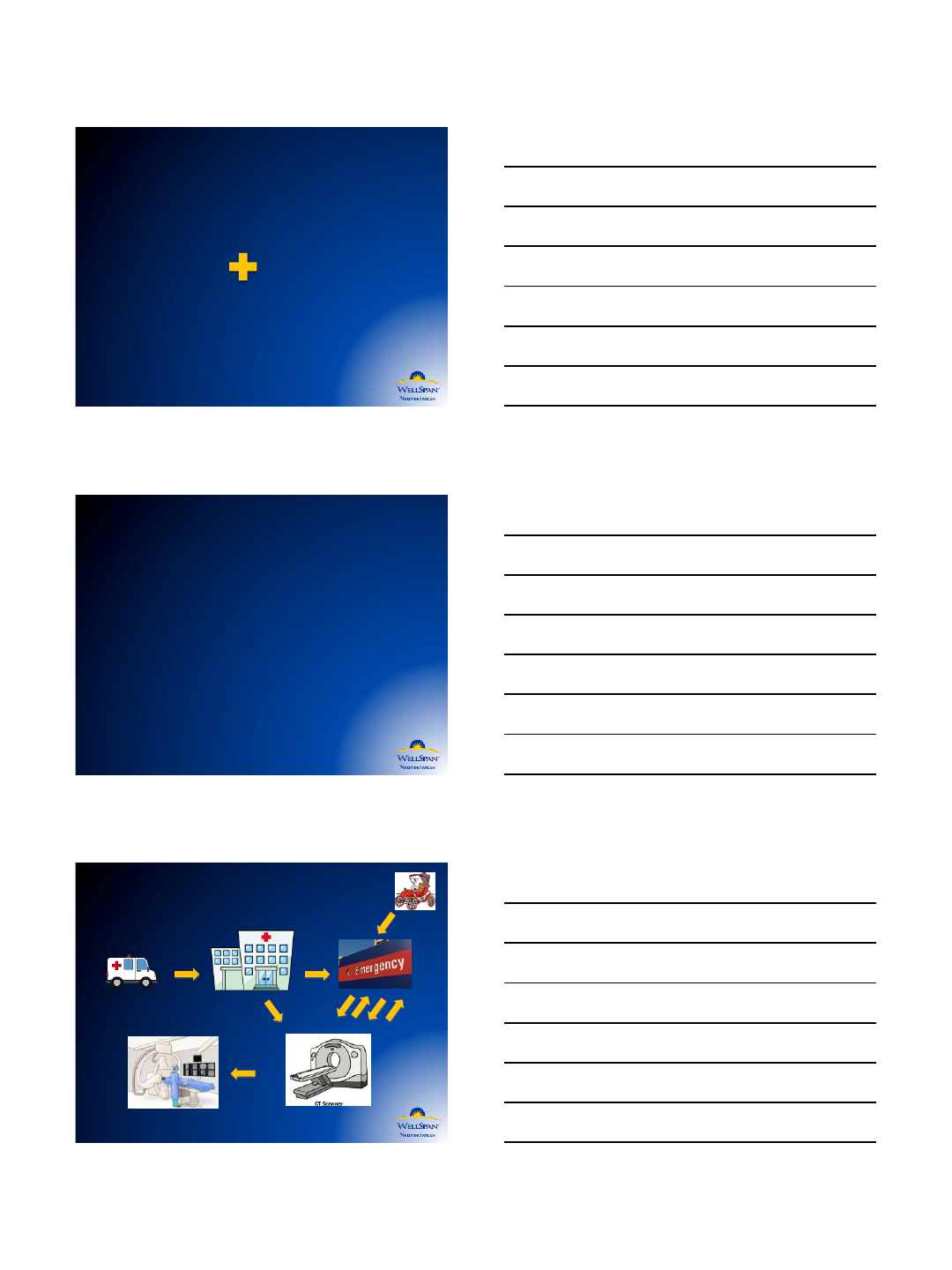
An Algorithm for Treating
the Acute Stroke Patient:
Door to Lab Protocol
Martin G Radvany, MD, FSIR
Chief, Endovascular Surgical Neuroradiology
York Hospital, York PA
Disclosures
•Stryker –Medical Advisory Board
“Time
is
Brain”
The typical patient loses 1.9
million neurons each minute in
which stroke is untreated.
Saver, Stroke 2006
12/2/2015
2
Time is
Brain Imaging
Improving Patient Selection
MR CLEAN
REVASCAT
EXTEND-IA
SWIFT PRIME
ESCAPE
THRACE
THERAPY
Indications for IA Stroke Therapy
(Class I; Level of Evidence A). (New recommendation):
a. Prestroke mRS score 0 to 1
b. Acute ischemic stroke receiving intravenous r-tPA within 4.5 hours
of onset according to guidelines from professional medical
societies
c. Causative occlusion of the internal carotid artery or proximal MCA
(M1)
d. Age ≥18 years
e. NIHSS score of ≥6
f. ASPECTS of ≥6
g. Treatment can be initiated (groin puncture) within 6 hours of
symptom onset
2015 AHA/ASA Stroke Guideline
Stroke Patient Flow
12/2/2015
3
Optimizing Door to Lab Time
•Pre-Hospital Assessment
–NIHSS
–LAMS (L.A. Motor Scale)
–RACE (Rapid Arterial oCclusion Evaluation)
•Stroke Protocol
–Alert ED/Stroke/Interventional Teams
–EMS vs POV
•Rapid Assessment with Imaging
–Point of care Renal Function Testing
•Prompt Treatment for patients with LVO
Facilitate patient care and movement
•Have designated transport monitoring
equipment ready
•Have a designated health care provider
accompany patient from the time they
enter hospital
–They get TPA in ED
–They go for intervention
Thank you!
Martin Radvany
mradvany@wellspan.org
12/2/2015
4
