MergedFile 1e519cc5 Af50 400e B1d4 4289df5645b6
2017-10-02
: Pdf 1E519Cc5-Af50-400E-B1D4-4289Df5645B6 1e519cc5-af50-400e-b1d4-4289df5645b6 10 2017 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 36
9/27/2017
1
The Problem of Relapse in Myeloma
PARAMESWARAN HARI
Medical College of Wisconsin
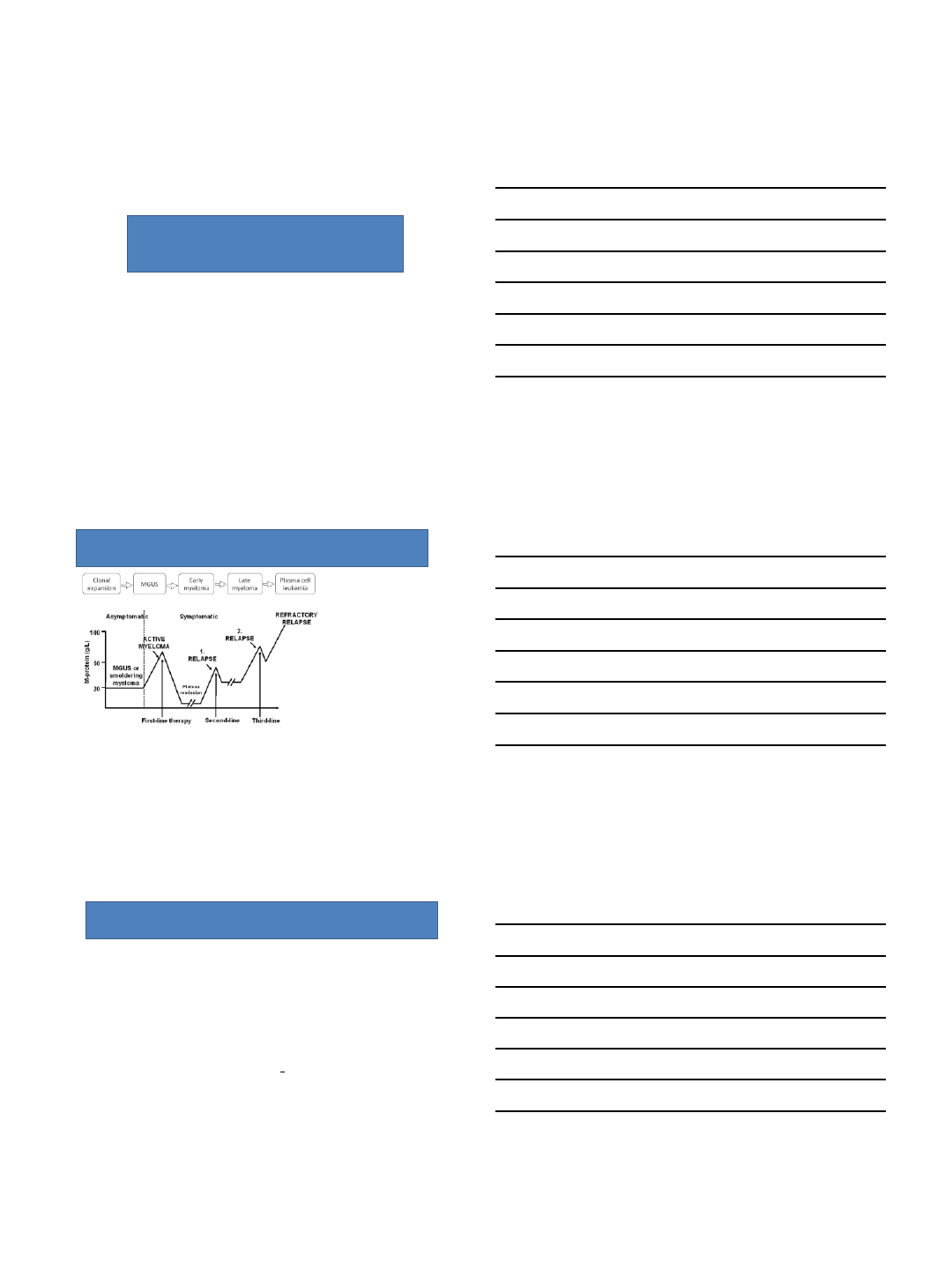
Relapse is the hallmark of multiple myeloma
•Definitions
•Relapse from CR / Biochemical
Progression / Clinical Relapse
•Biological Correlates
•Choosing when to treat
•Risk Stratification of Relapse
Definitions- Relapse
•From CR
•Mainly used for clinical trials
•Reappearance of serum or urine M-protein by immunofixation or electrophoresis or
abnormal FLC ratio
•Development of ≥5% plasma cells in BM
•Any other sign of progression (ie, new plasmacytoma, lytic bone lesion, or
hypercalcemia)
•Clinical relapse
•New CRAB findings
•New plasmacytomas or bone lesions (fractures do not necessarily count)
•Increasing size of existing plasmacytomas (>50%)
•Hyperviscosity related to paraprotein
Kumar et al, Lancet Oncol, 2017
9/27/2017
2
Definitions- Progression
•Increase of 25% from lowest confirmed response value in one or more of:
–Serum M-protein (absolute increase must be ≥0.5 g/dL)
–Serum M-protein increase ≥1 g/dL, if the lowest M component was ≥5 g/dL
–Urine M-protein (absolute increase must be ≥200 mg/24 h)
–Light chain disease: the difference between involved and uninvolved FLC levels
(absolute increase must be >10 mg/dL)
•Non-secretory: 25% increase in bone marrow plasma-cell percentage irrespective of
baseline status (absolute increase must be ≥10%)
•Appearance of a new lesion(s), ≥50% increase from nadir
•≥50% increase in circulating plasma cells (minimum of 200 cells per μL) if this is the only
measure of disease
Kumar et al, Lancet Oncol, 2017
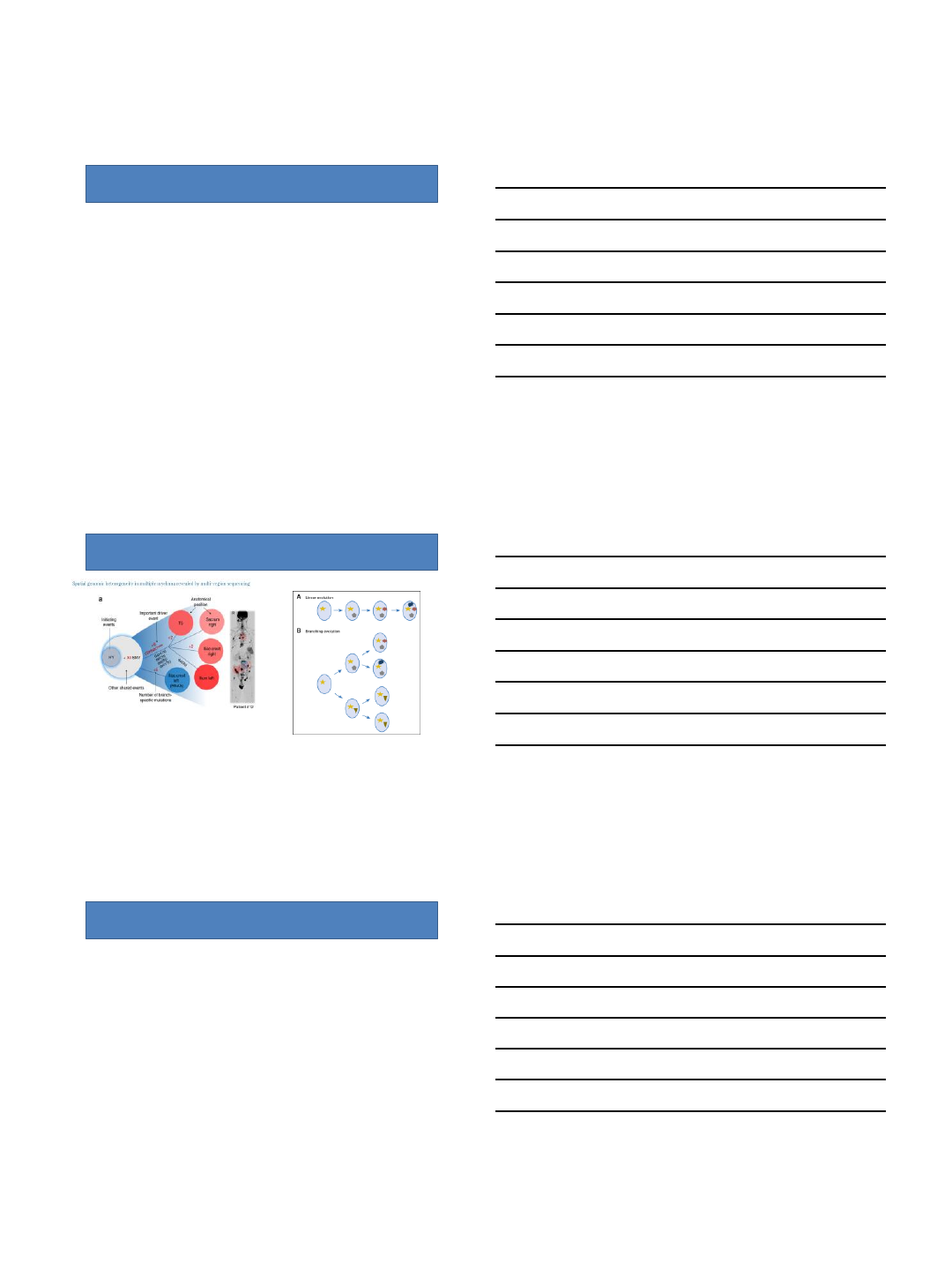
Multiclonal disease with spatial and temporal
heterogeneity
•Acquired genomic events with progression
Rasche L et al Nature Communications 8, Article number: 268(2017)
Case presentation
•62 YO M with standard risk MM dx’d in 1/2013
–Received RVD x 3nCR
–Auto-HCT with melphalan 200 in 6/2013sCR
–Maintenance lenalidomide started in 9/2013
•On routine bloodwork 4/2017 SPEP shows reappearance of M protein at
0.1 g/dL
Now what??
9/27/2017
3
Importance of full re-staging at suspected
relapse/progression
•History- determine co-morbidities
•Physical- determine PS
•Labs –including PB flow for PCs
•Bone marrow, including FISH, cytogenetics, +/- GEP
–Determine new clones
–Risk stratification
–Possibly help with clinical decision making (BCMA, 11:14)
•Imaging- beware of EMD
–PET/CT
–PET/MRI
Dingli et al, Mayo Clin Proc, 2017
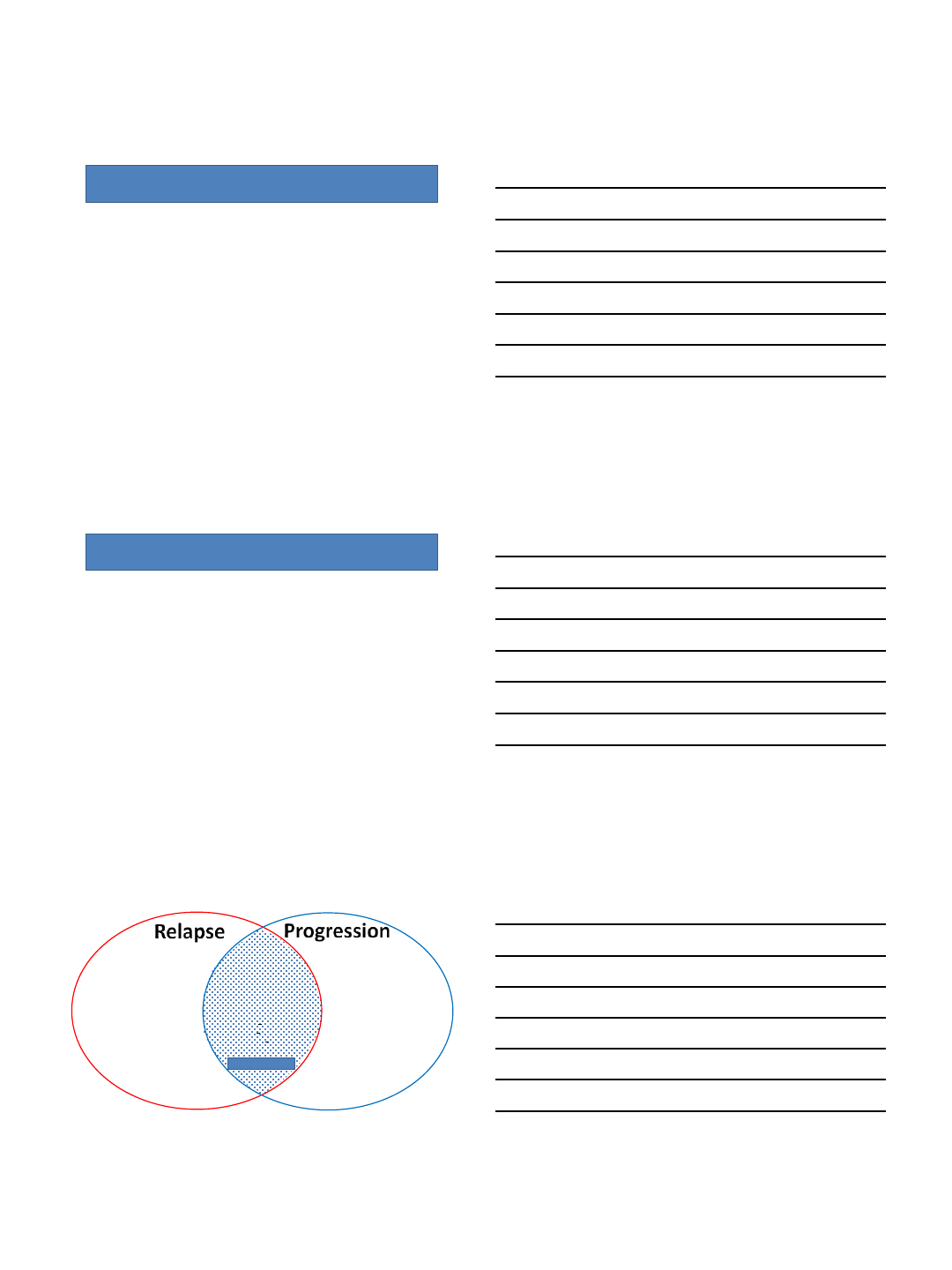
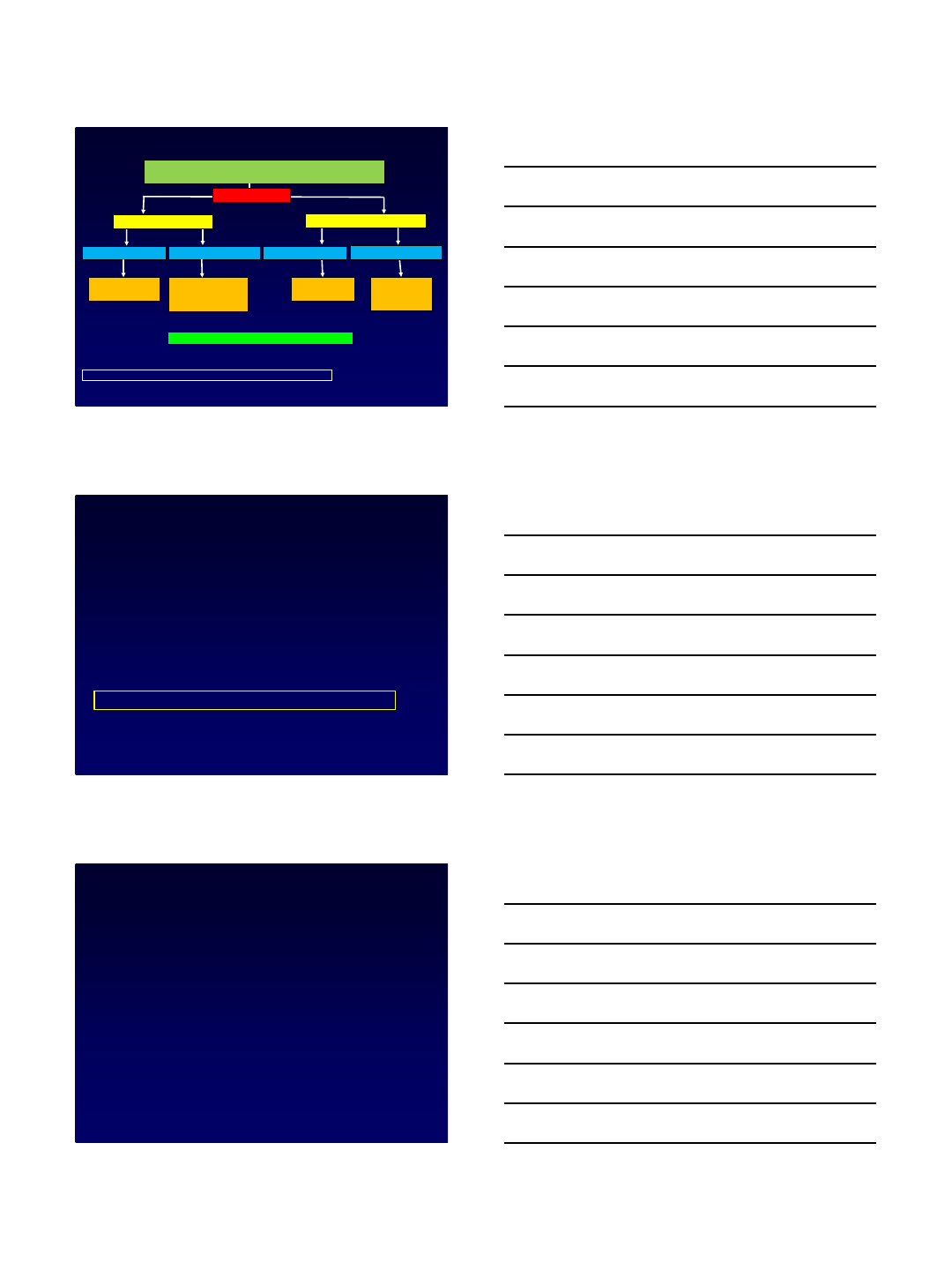
Loss of CR or Never CR or Sustained CR
Hoering A et al Blood. 2009 Aug 13; 114(7): 1299–1305.
CR achieved and Lost
Never CR
•Re-appearance of
M protein/BJ
•Reappearance of
5% PCs in BM
•New CRAB event
•New plasmacytoma
•New hyperviscosity
•25% increase in M
protein/BJ/ FLD difference
•10% increase in BM
•50% increase in
plasmacytoma
•50% increase in circulating
PCs
Measured Measured
Clinically relevant
9/27/2017
4
Making your decision
•Immediate treatment for relapse
•Closer follow-up
•Regular follow-up
Indications for treatment
•Clinical relapse (CRAB or plasmacytomas)
•Significant biochemical progression without clinical relapse
•Doubling of the M-component in two consecutive measurements separated by 2
months with the reference value of 5 g/L, (=0.5 g/dL) or
•In two consecutive measurements any of the following increases:
–the absolute levels of serum M protein by ≥10 g/L (=1.0g/dL), or
–an increase of urine M protein by ≥500 mg per 24 hours, or
–an increase of involved FLC level by ≥20 mg/dL (= 200 mg/L) (plus an abnormal FLC
ratio) or 25% increase (whichever is greater)
Ludwig et al, The Oncologist, 2014
•Re-appearance of
M protein/BJ
•Reappearance of
5% PCs in BM
•New CRAB event
•New plasmacytoma
•New hyperviscosity
•50% increase in
plasmacytoma
•25% increase in M
protein/BJ/ FLD difference
•10% increase in BM
•50% increase in
plasmacytoma
•50% increase in circulating
PCs
•Doubling of M protein or
increase by >1 g/dL
•Increase in > 500 mg/24 H BJ
•Increase in LC > 200 mg/L
•Circulating plasma cells
Treatment Indicated
9/27/2017
5
Dingli et al, Mayo Clin Proc, 2017
When to treat if only biochemical
relapse/progression
•Aggressive clinical disease at diagnosis
•Short treatment-free interval/ suboptimal response to previous
treatment line
•Imminent risk for organ dysfunction (pts with previous light chain-
induced renal impairment)
•Unfavorable cytogenetics (t(4;14) or del17p)
Ludwig et al, Oncologist, 2014
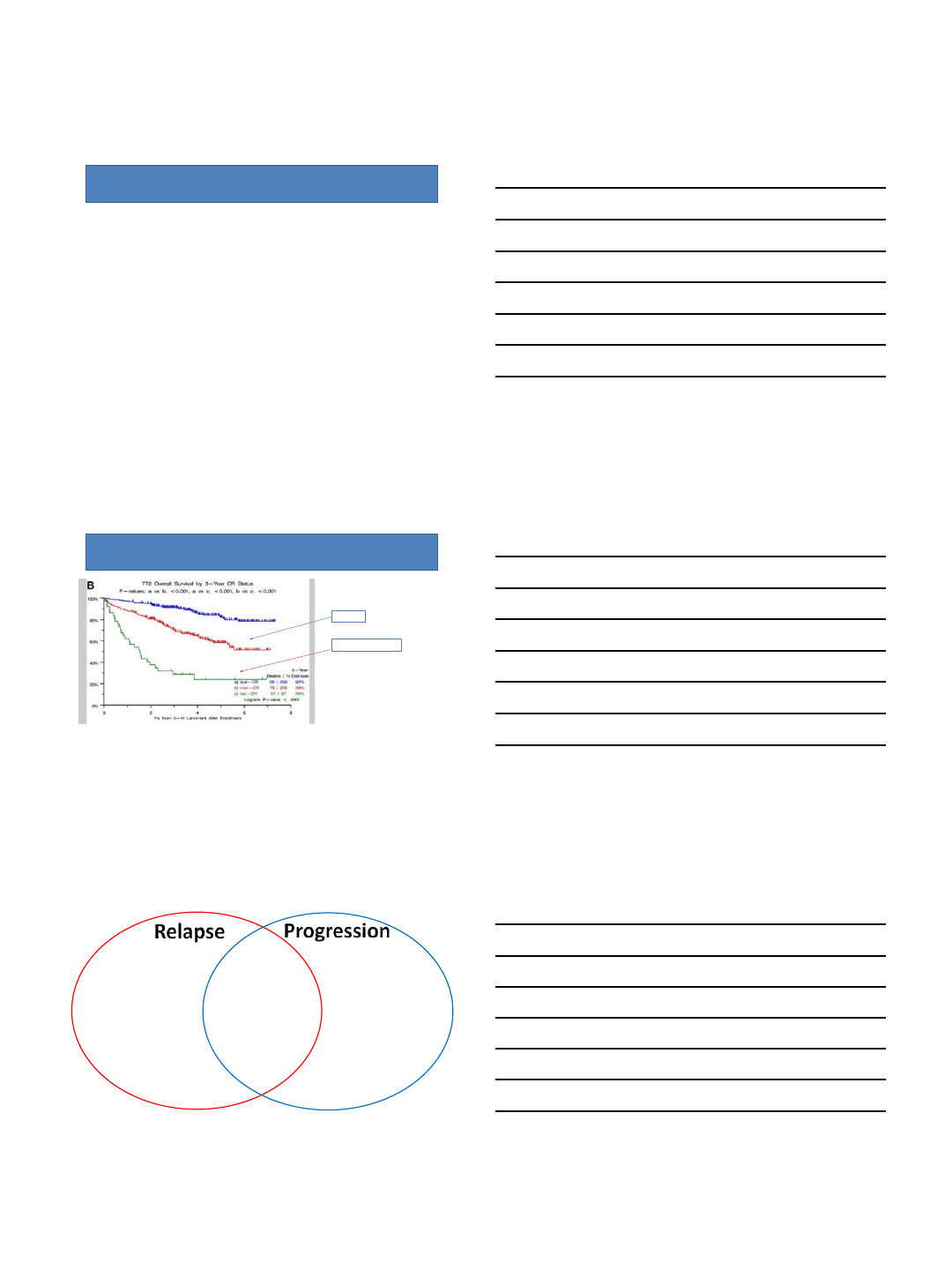
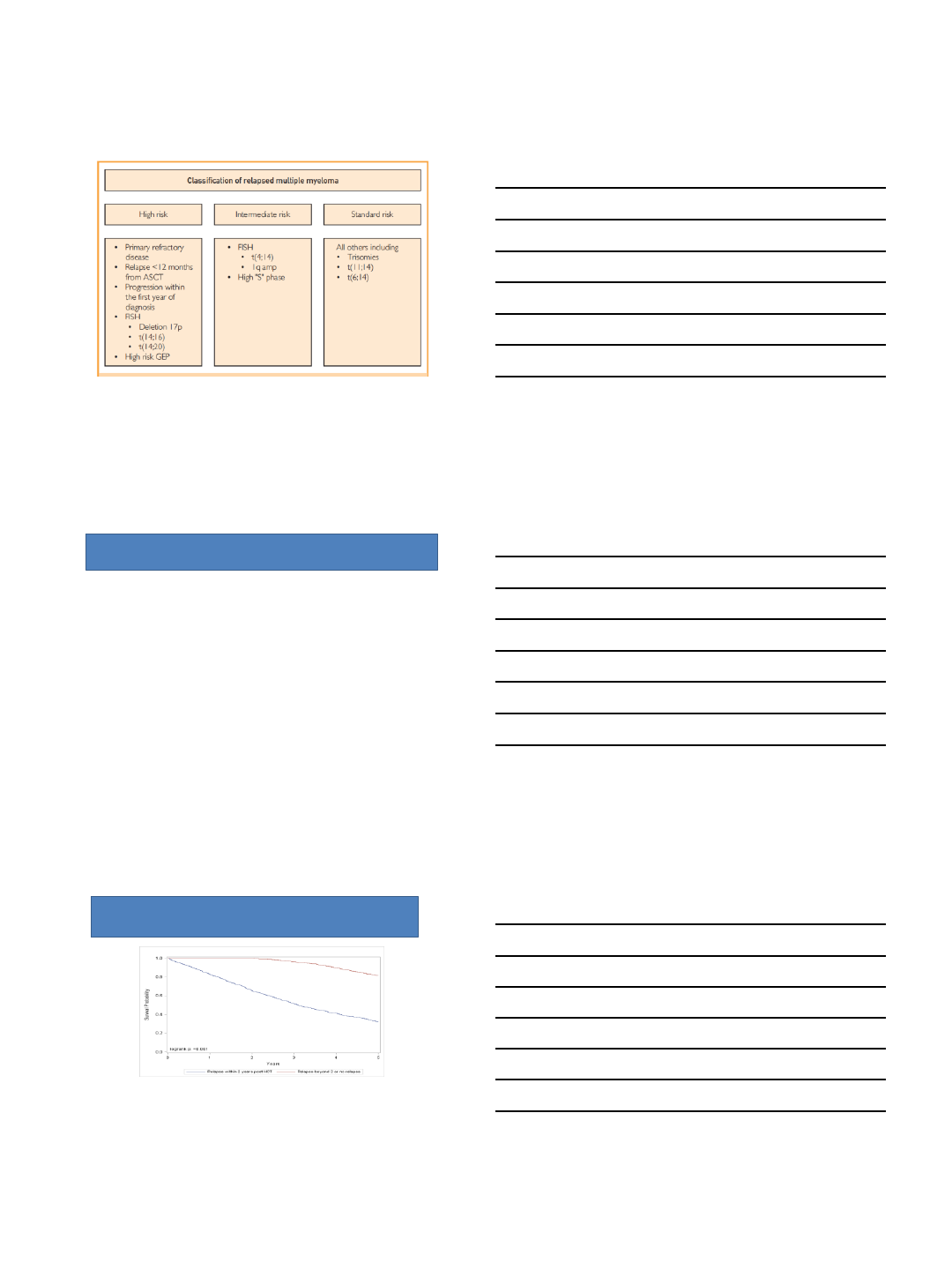
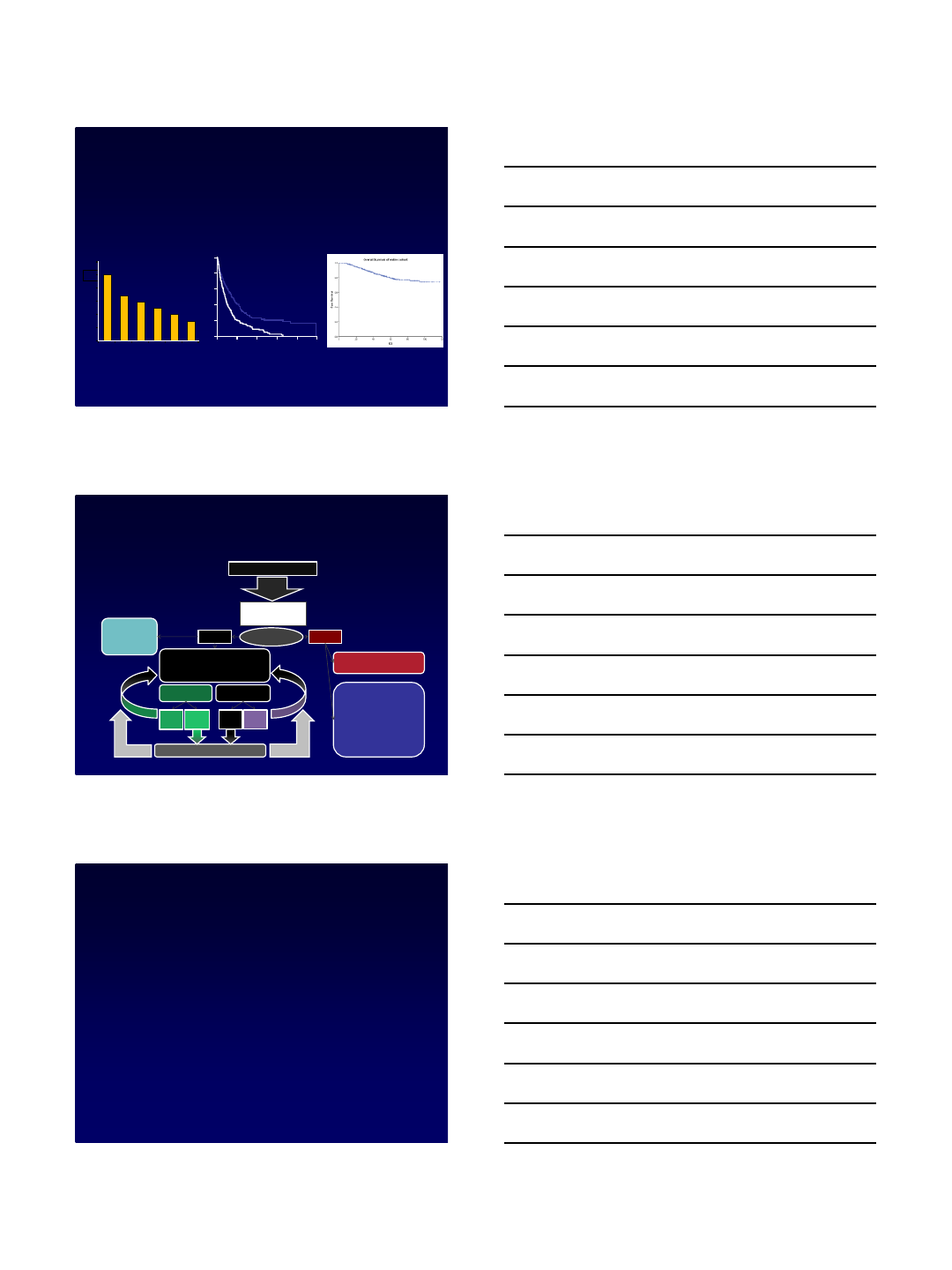
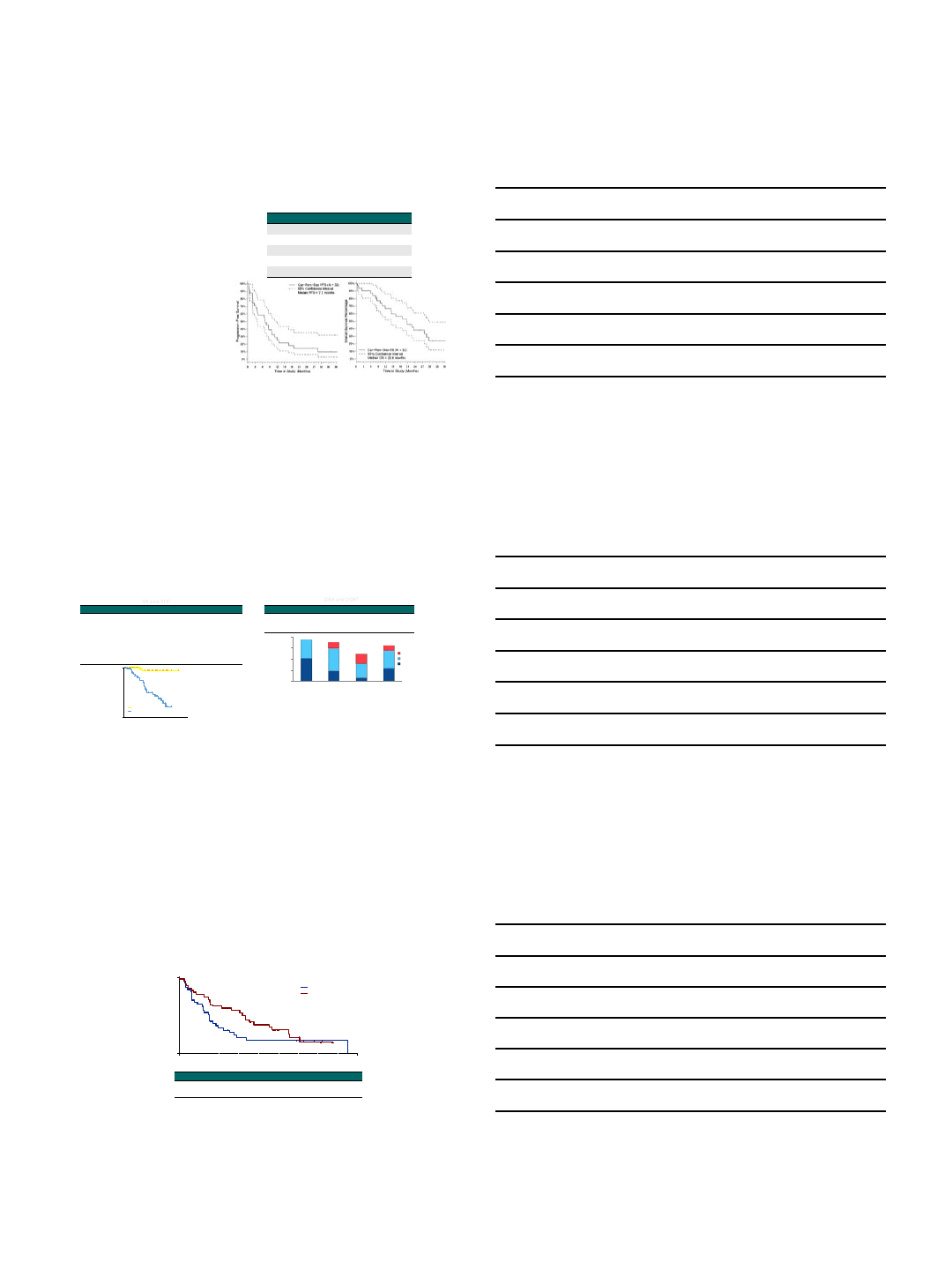
Natural History of early relapse after transplant
Kumar S et al Tandem BMT meetings 2017
15
No relapse by 2 years:
5-year OS 80%
Relapse by 2 years:
5-year OS 32%
9/27/2017
6
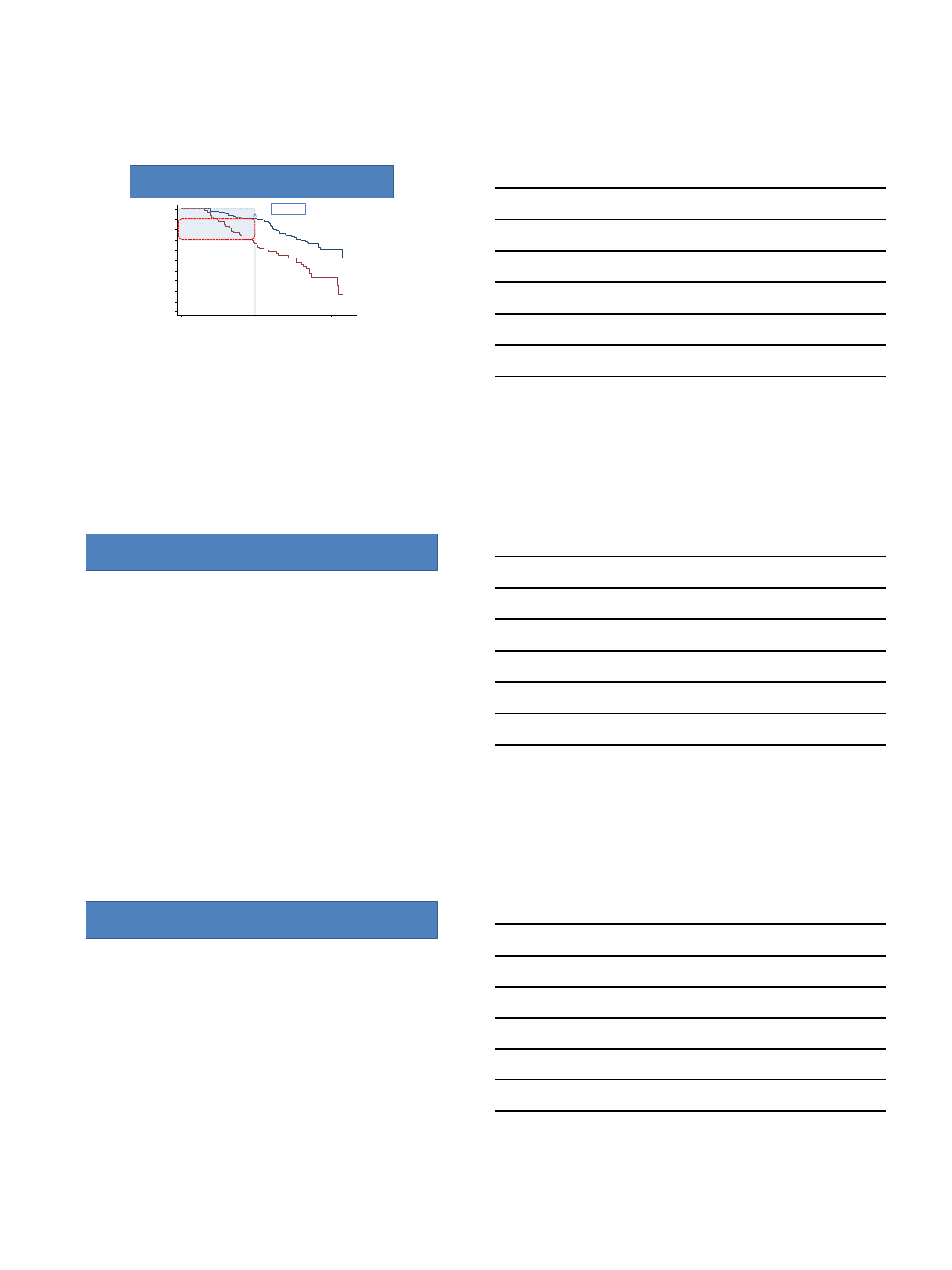
How many pts relapse early?
P<0.001
0
10
20
30
40
50
60
70
80
90
100
Patients (%)
172 166 151 86 17MRD neg 65 57 43 30 4MRD pos
N at risk
012 24 36 48
Months of follow-up
MRD pos
MRD neg
IFM 2009
30% of MRD Pos
10% of MRD Neg
Attal M et al NEJM 2017
Back to the case…
•62 YO M with standard risk MM dx’d in 1/2013
–Received RVD x 3nCR
–Auto-HCT with melphalan 200 in 6/2013sCR
–Maintenance lenalidomide started in 9/2013
•On routine bloodwork 4/2017 SPEP shows reappearance of M protein at 0.1
g/dL
•BM: 5% involvement by plasma cells, normal cytogenetics/FISH
•PET/CT negative
•Followed q3 months with labs
•10/2013 M protein = 0.7
•11/2013 M protein = 1.1
Gray areas
•On maintenance with an M protein rise 0.20.6
–Should we treat earlier if the patient is already on maintenance?
•High-risk patients with increasing light chains, but not quite at
progression
•Persistently PET avid plasmacytomas
•True biochemical progression but questionable performance status
9/27/2017
7
Next Talks
•Choosing a regimen at relapse
–Early Relapse
–Refractory Relapse
•Options for the multirelapsed and refractory
patient
–Immunotherapy
–Clinical Trials of Newer Novel Agents
10/1/2017
1
Early Relapse: Choosing Among Different
Second Line Regimens
Ajay K. Nooka, MD, MPH, FACP
Associate Professor
Department of Hematology and Medical Oncology
Winship Cancer Institute of Emory University
Atlanta, Georgia
Disclosures
➢Advisory board: Celgene, Amgen, Novartis, Spectrum,
Pharmaceuticals and Adaptive technologies
2
Clinical Vignette
72-year-old female with diagnosis of standard risk myeloma
(hyperdiploidy on FISH studies) received induction therapy with RVd
regimen. She underwent upfront transplant and achieved stringent
CR. She opted not to go for maintenance therapy, and was monitored
closely. Four years from her transplant, she started showing
evidence of biochemical progression, and now she is anemic.
You suggest that the following second line regimen delivers the best
depth of response (≥VGPR) based on the data from available
lenalidomide based phase III studies:
1. Elotuzumab with lenalidomide and dexamethasone
2. Daratumumab with lenalidomide and dexamethasone
3. Ixazomib with lenalidomide and dexamethasone
4. Carfilzomib with lenalidomide and dexamethasone
10/1/2017
2
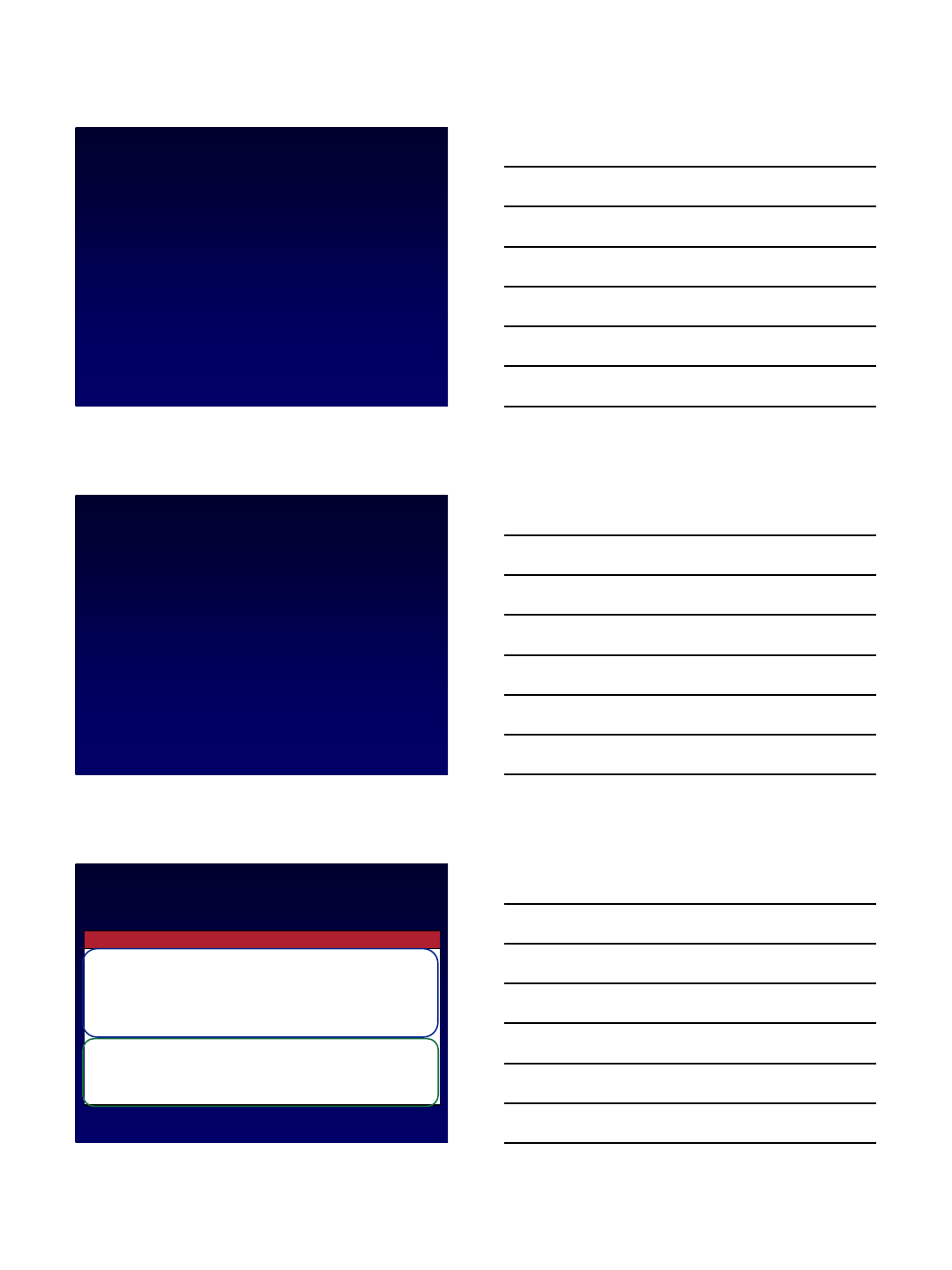
Why is it important to choose the best second
line regimen?
1. Kumar SK, et al. Mayo Clin Proc. 2004;79:867-874.
2. Kumar SK, et al. Leukemia. 2012;26:149-157.
3. Nooka A, et al. institutional data, unpublished.
Pts (%)
1
0
0
8
0
6
0
4
0
0
2
0
012 24 36 48 60
Mos
OS
EFS
Events, n/N
170/286
217/286
Median, Mos
(Range)
9 (7-11)
5 (4-6)
1
2
1
0
8
6
0
2
Firs
tSecond Third Fourth Fifth Sixth
Treatment Regimen
Median Response Duration (Mos)
4
Response Duration With
Increasing Treatment[1]
Survival Outcomes[2]
Response duration in refractory myeloma
Survival Outcomes at Emory[3]
Mos
Relapsed myeloma: previously treated myeloma that progresses in the absence
of any therapy and requires the initiation of salvage therapy.
*
Consider
clinical
trial
Prior
SCT
Transplant eligible; has good PS
•Primary refractory- SCT
•Relapsed/refractory- SCT
Transplant ineligible
-If patient has previous ly responded to
the therapy, tolerated and relapsed at
leas t 6 months after prior drug
exposure
•repeat prior therapy
- Otherwise, cons ider
•*Bortezomib ±Dexamethasone
•*Bortezomib + PLD
•*Lenalidomide + Dexamethasone
•RVD, VTD, CFZ, CRD, VCD, RCD,
DCEP, DT-PACE±V, Cytoxan, Pd,
T
Relapse within first 12
months
-Newer combination
strategies CRD, CPD,
RVD or clinical trial
-Allogeneic transplant
clinical protocol
Symptomatic relapse
Yes No
Relapse with
maintenance therapy
after SCT
Relapse without
maintenance therapy
after SCT
Factors to consider
•Treatment related factors
•Disease related factors
•Patient related factors
Subsequent
relapse
SCT2
Relapse
withi n 36
months
Relapse
beyond 36
months
Relapse
beyond
18-24
months
Relapse
withi n
18-24
months
Subsequent
relapse
Subsequent
relapse
Subsequent
relapse
Relapse beyond the first 12 months
*Bortezomib ±Dexamethasone
*Lenalidomide + Dexamethasone
*Bortezomib ±PLD
RVD, VTD, CFZ, CRD, VCD, RCD, DCEP±V, DT-
PACE±V, Cytoxan, Pd, Td
Nooka, et al. Blood. 2015;125(20):3085-99.
Treatment Options for Relapsed and Refractory
Myeloma (RRMM)
5
Factors to Consider to for Treatment Selection a
Relapse: Disease related Factors
➢Nature of relapse
➢indolent vs aggressive
➢Risk stratification
➢Genetics of initial and relapsed marrow
➢Disease burden
➢High vs low
➢R-ISS staging
➢1 vs 2-3
1. Nooka AK, et al. Blood. 2015;125:3085-3099.
2. Palumbo A, et al. N Engl J Med. 2011;364:1046-1060.
3. Palumbo A, et al. Blood. 2011;118:4519-4529.
4. Orlowski RZ, Lonial S. Clin Cancer Res. 2016;22:5443.
10/1/2017
3
Factors to Consider to for Treatment Selection a
Relapse: Treatment related Factors
➢Previous therapy
➢Pts with PD receiving IMiDs, PIs, or cytotoxic doublet/triplet therapies can
benefit from next-generation regimens
➢Avoid agents of previous regimen-related toxicity
➢Maintenance therapy
➢Regimen-related toxicity
➢Toxicity profile should be considered in light of pt comorbidities
➢Neuropathy: consider neuropathy sparing durgs (avoid bortezomib,
thalidomide)
➢Cardiac issues (uncontrolled HTN, CHF): careful consideration of
carfilzomib
➢COPD: monoclonal antibodies with caution (daratumumab)
➢DVT/PE: use anticoagulation with IMiDs
➢Depth and duration of previous response, tumor burden at relapse
➢Retreatment with previous therapies an option if pt had previous response to
the treatment, acceptable tolerance, and relapse occurred at least 6 mos
after previous exposure
1. Nooka AK, et al. Blood. 2015;125:3085-3099.
2. Palumbo A, et al. N Engl J Med. 2011;364:1046-1060.
3. Palumbo A, et al. Blood. 2011;118:4519-4529.
Factors to Consider to for Treatment Selection a
Relapse: Patient related Factors
➢Renal insufficiency: disease related or due to comorbidities
(hypertension, vascular disease, diabetes, nephrotoxicity)[1]
➢Hepatic impairment common in pts with RRMM[1]
➢Comorbidities and fraility[1]
➢Treatment decisions complicated in elderly
➢↑ toxicity due to ↓ organ function, physiologic reserve
➢European Myeloma Network vulnerability assessment algorithm
anticipates regimen-related toxicities and assists individualizing
therapy with least potential for interruption[2,3]
➢Patient preferences
➢Convenience, ease of travel, insurance and other social factors
1. Nooka AK, et al. Blood. 2015;125:3085-3099.
2. Palumbo A, et al. N Engl J Med. 2011;364:1046-1060.
3. Palumbo A, et al. Blood. 2011;118:4519-4529.
Lenalidomide and Bortezomib-Based Early
Relapse Regimens: PFS and OS
Trial Regimen
PFS (mon)
ORR (%)
VGPR (%) PFS (HR, 95% CI)
OS (HR, 95%
CI
)
ASPIRE
1
N=792
Rd + Carfilzomib 26.3 87.1 69.9 .69 (.57-.83)
P=.0001 .79 (.63-.99)
P=.04
Rd 17.6 66.7 40.4
TOURMALINE
-MM-1
2
N=722
Rd + Ixazomib 20.6 78.3 48.1 .74 (.59-.74)
P=.01 NR
Rd 14.7 71.5 39
ELOQUENT
-23
N=646
Rd + Elotuzumab 19.4 79 33 .70 (.57-.85)
P<.01 .78 (.63-.96)
Rd 14.9 66 28
POLLUX
4
N=569
Rd + Daratumumab
NR 93 75.8 .37 (.28-.50)
P<.0001 .63 (.42-.95)
Rd 18.4 76 44.2
PANORAMA
5
N=768
Vd + Panobinostat 11.99 60.7 28 .63 (.52-.76)
P<.0001 .87 (.69-1.10)
P=.26
Vd 8.08 54.6 16
CASTOR
6
N=498
Vd + Daratumumab
NR 83 59 .39 (.28-.53)
P<.0001 .63 (.42-.96)
Vd 7.2 63 29
ENDEAVOR
7
N=929
Carfilzomib + Dex 18.7 76.7 54 .53 (.44-.65)
P<.0001 .79 (.58-1.08)
P=.06
Vd 9.4 62.3 29
1. Stewart K, et al. N Engl J Med 2015;372:142-52. 2. Moreau P, et al. N Engl J Med 2016; 374:1621-1634.
3. Lonial S, et al. N Engl J Med 2015; 373:621-631. 4. Dimopoulus M, et al. N Engl J Med 2016; 375:1319-1331.
5. San Miguel J, Lancet Oncol 2014; 15: 1195–206. 6. Palumbo A, et al. N Engl J Med 2016; 375:754-766.
7. Dimopoulos M, et al. Lancet Oncol. 2016;17:27-38.
9
10/1/2017
4
FDA Approvals of Novel Agents for Patients with
RRMM
Novel Agent or Regimen
FDA Approval Date
Patient Population
Panobinostat +
bortezomib/dexamethasone
February 23, 2015
•
Patients with ≥2 prior standard therapies,
including bortezomib and an IMiD agent
Carfilzomib +
lenalidomide/dexamethasone
July 27, 2015
•
Patients with relapsed disease who had
received 1-3 prior lines of therapy
Daratumumab
November 16, 2015
•
Patients with at least 3 prior treatments
Ixazomib
+
lenalidomide/dexamethasone
November 20, 2015
•
Patients who had received at least 1 prior
therapy
Elotuzumab
+
lenalidomide/dexamethasone
November 30, 2015
•
Patients with 1-3 prior therapies
Carfilzomib + dexamethasone
January 21, 2016
•
Patients with relapsed disease and 1-3 prior
therapies
Daratumumab +
bortezomib/dexamethasone
November 21,2016
•
Patients who had received at least 1 prior
therapy
Daratumumab +
lenalidomide/dexamethasone
November 21,2016
•
Patients who had received at least 1 prior
therapy
Daratumumab +
pomali
domide/dexamethasone June 16, 2017
•
Patients who had received ≥2 prior standard
therapies, including bortezomib and an IMiD
agent
Orlowski RZ, Lonial S. Clin Cancer Res. 2016;22:5443.
10
Available Regimens in Early Relapse
NCCN Guidelines
Preferred Regimens
Other Regimens
Level 1 Regimens
Doublets
•
Bortezomib/dexamethasone
•
Carfilzomib/dexamethasone
•
Lenalidomide/dexamethasone
Triplets
•
Elotuzumab/lenalidomide/dexamethasone
•
Daratumumab/lenalidomide/dexamethasone
•
Ixazomib/lenalidomide/dexamethasone
•
Carfilzomib/lenalidomide/dexamethasone
•
Daratumumab/bortezomib/dexamethasone
Other
Regimens
•
Repeat primary induction therapy (if relapse at
>6 months)
•
Bortezomib/cyclophosphamide/dexamethasone
•
Bortezomib/lenalidomide/dexamethasone
Level 1 Regimens
•
Bortezomib/liposomal doxorubicin
•
Panobinostat/bortezomib/dexamethasone
Other
PI
-Based
•
Ixazomib/dexamethasone
•
Elotuzumab/bortezomib/dexamethasone
Alkylator
-Based
•
Bendamustine/bortezomib/dexamethasone
•
Bendamustine/lenalidomide/dexamethasone
•
Cyclophosphamide/lenalidomide/dexamethasone
•DCEP (dex/cyclophosphamide/etoposide/cisplatin)
•
DT-PACE (dex/thalidomide/cisplatin/doxorubicin/
cyclophosphamide/etoposide) ± bortezomib (VTD-
PACE)
•
High-dose cyclophosphamide
NCCN Guidelines, Version 3.2017. Accessed August, 2017.
Note: NCCN Guidelines do not break out regimens into separate categories of
early and late relapse
11
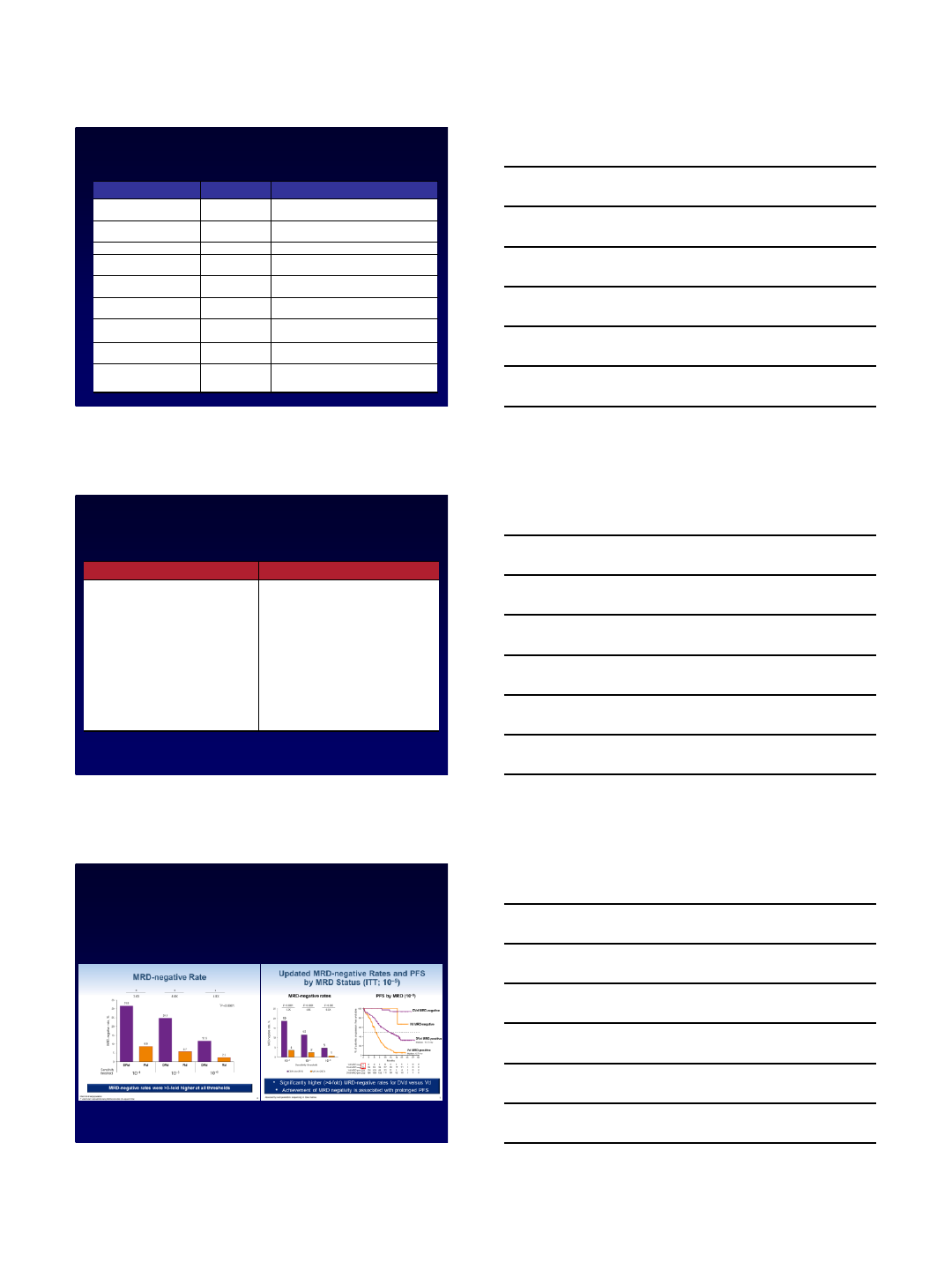
Depth of response
➢MRD negative rate POLLUX MRD negative rates CASTOR
Moreau P, et al. N Engl J Med 2016; 374:1621-1634
Palumbo A, et al. N Engl J Med. 2016;375(17):754-766.
10/1/2017
5
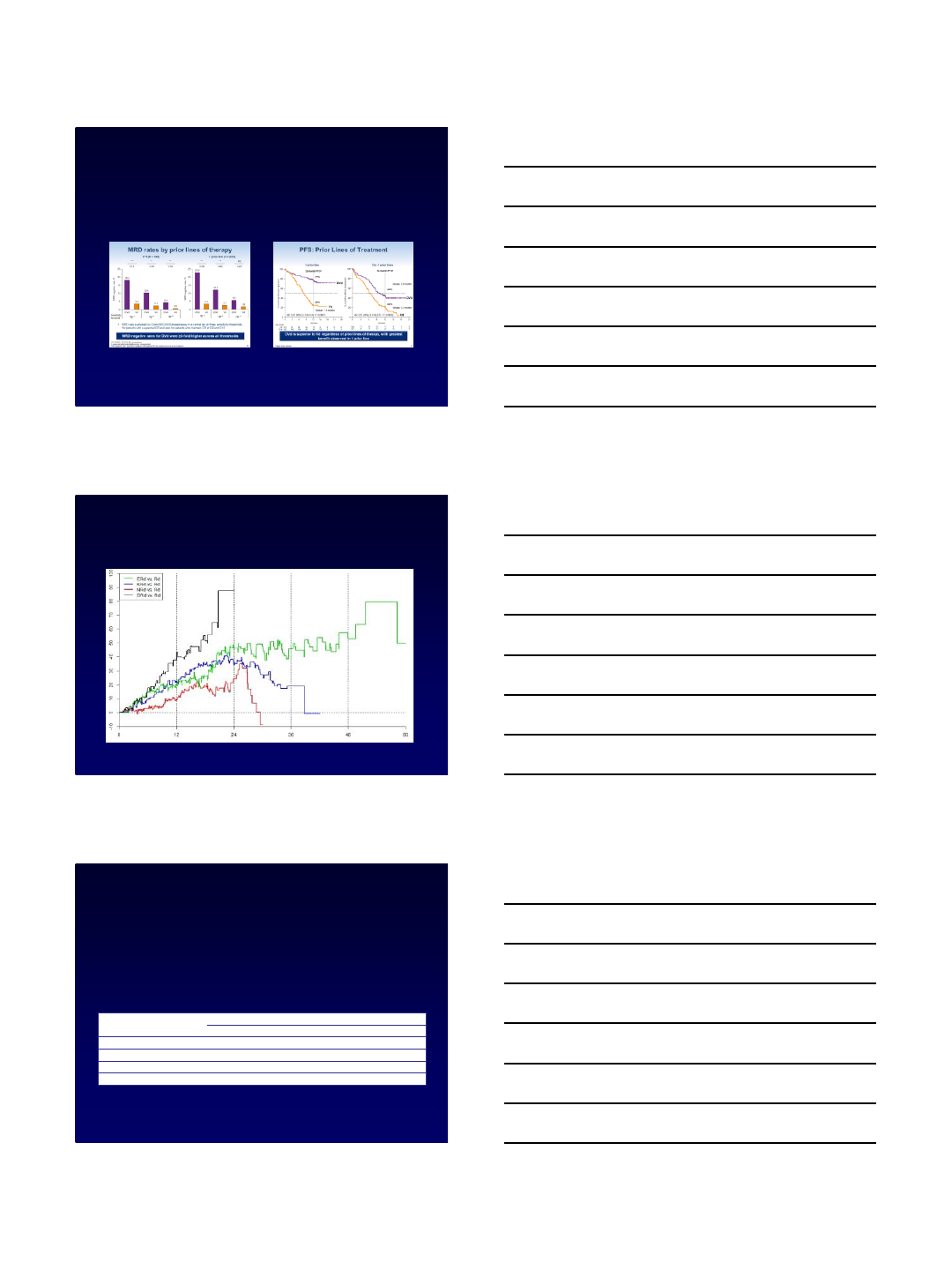
Benefit of antibodies as earlier lines of therapy:
MRD negativity and PFS from CASTOR
MRD –ve rate with DVd as 1st line vs ITT PFS with DVd as 1st line vs 2-3
Mateos MV, et al. Blood. 2016;128: Abstract 1150.
Relative Benefit of PFS: Possibility of delivering
therapy over long term
Betts K, et al. haematologica. 2017;102: Abstract E1300.
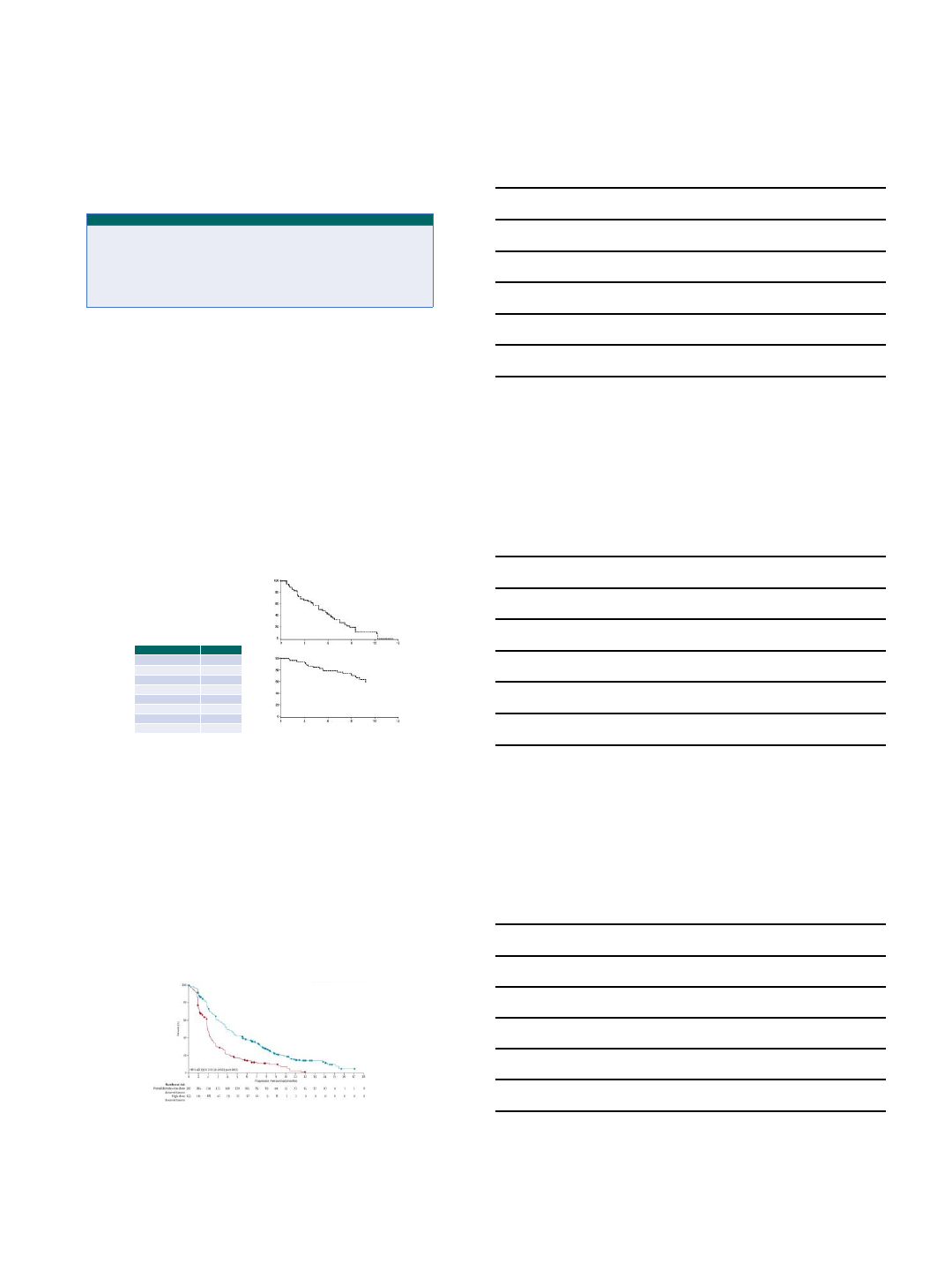
Salvage ASCT in the Relapsed Setting
➢Data from Mayo Clinic Transplant Center suggests that ASCT2 appears safe and effective
treatment for relapsed MM (N = 98)
➢ORR: 86%; median PFS: 10.3 mos; median OS: 33 mos
➢Rate of TRM: 4%, suggesting a favorable benefit-to-risk ratio
➢Shorter TTP after ASCT1 predicts shorter OS post–ASCT2
Gonsalves WI, et al. Bone Marrow Transplant. 2013;48:568-573.
TTP After ASCT1 Median From ASCT2, Mos (Range)
PFS OS
< 12 mos 5.6 (3-8) 12.6 (4-23)
< 18 mos
7.1 (6-8) 19.4 (10-42)
< 24 mos
7.3 (6-10) 22.7 (13-62)
< 36 mos
7.6 (7-12) 30.5 (19-62)
10/1/2017
6
Early relapse (1-3 prior lines of therapy)
-Len maintenance
+Len maintenance
- IRd
- ERd -DRd
-KRd
- ERd
- DPd
- KPd
*increase dose of lenalidomide to 25 mg
-DRd
- DVd
- KPd
Clinical trials
Emory Approach to Early Relapse
-Len maintenance
+Len maintenance
Indolent relapse Aggressive relapse/high risk
Car/Pan as second salvage if IMID used
Clinical Vignette
72-year-old female with diagnosis of standard risk myeloma
(hyperdiploidy on FISH studies) received induction therapy with RVd
regimen. She underwent upfront transplant and achieved stringent
CR. She opted not to go for maintenance therapy, and was monitored
closely. Four years from her transplant, she started showing
evidence of biochemical progression, and now she is anemic.
You suggest that the following second line regimen delivers the best
depth of response (≥VGPR) based on the data from available
lenalidomide based phase III studies:
1. Elotuzumab with lenalidomide and dexamethasone
2. Daratumumab with lenalidomide and dexamethasone
3. Ixazomib with lenalidomide and dexamethasone
4. Carfilzomib with lenalidomide and dexamethasone
Conclusions
➢Novel agents in combination can achieve prolonged
responses even in relapsed disease
➢Depth of response is key even in relapsed disease
➢There are many right ways to treat patients with multiple
myeloma in relapse
➢There are also wrong ways to do it, know your options
➢Regimen with good tolerability, and efficacy (monoclonal antibodies)
➢Despite major advances and newer options, a few
challenges that we face today are
‒how to sequence the available regimens?
‒how to personalize therapy to derive the maximize benefit (eg:
biomarkers)?
‒how to tailor therapy to minimize toxicity yet retain efficacy
10/1/2017
7
Questions??
anooka@emory.edu
10/1/2017
1
Approach to the Patient with Refractory and
Multiply Relapsed Multiple Myeloma
Peter Voorhees, M.D.
Member, Plasma Cell Disorders Program
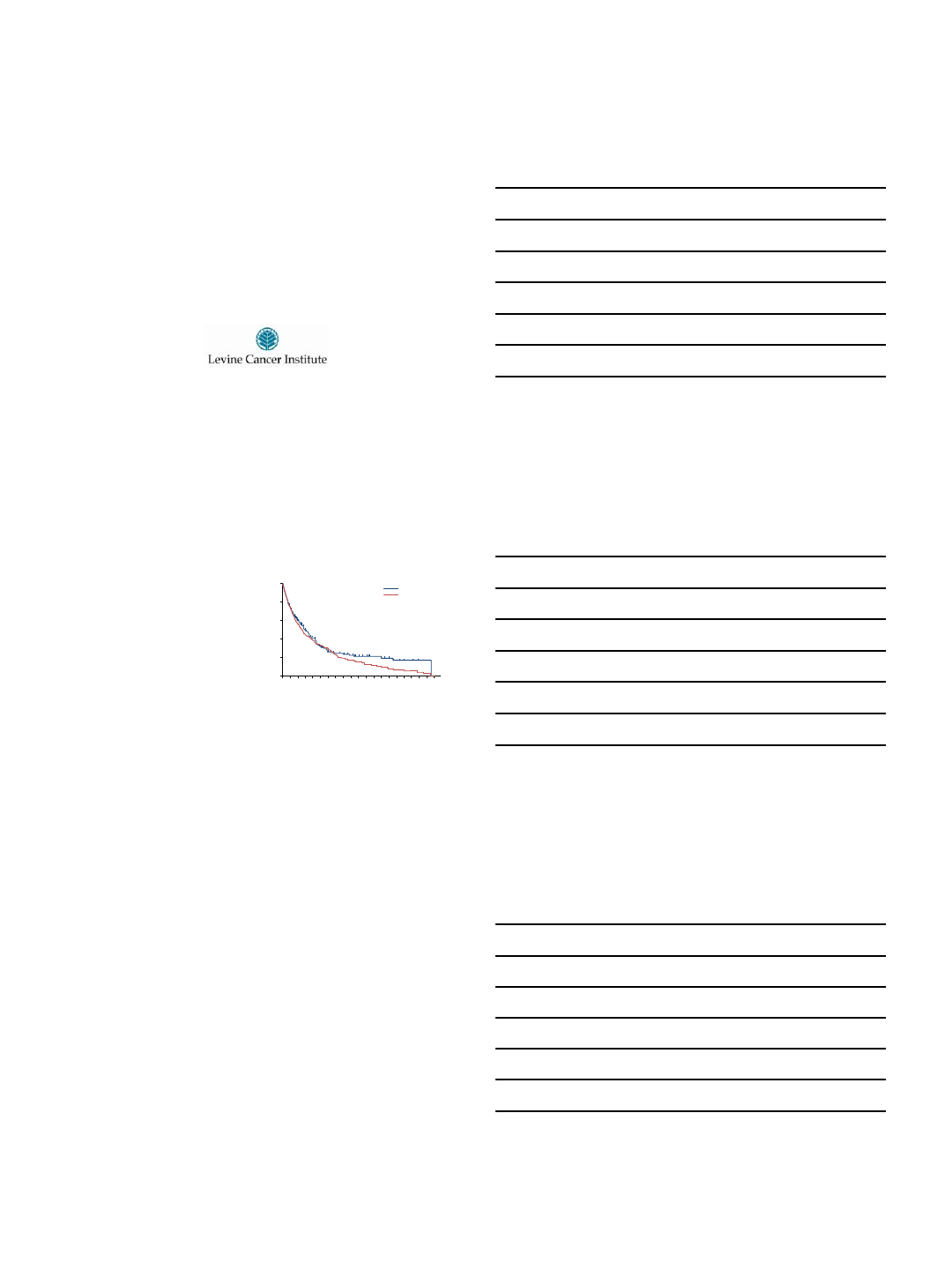
Relapsed/Refractory Disease : Outcomes
•Despite the introduction of IMiDs and PIs,
most patients relapse and outcomes are poor
in relapsed or refractory patients1
•Median OS of 9 months in patients
refractory to bortezomib and ≥1 IMiD1
•Median OS of 8 months in patients with
relapsed or refractory MM who were
double refractory or had relapsed after
≥3 prior lines of therapy, including
pomalidomide and carfilzomib2
1.Kumar SK, et al. Leukemia. 2012;26(1):149-157.
2.Usmani S, et al. Oncologist. 2016. doi:10.1634/theoncologist.2016-0104.
Patients alive, %
Time, months
Kumar SK, et al. 2012.
0
20
40
60
100
80
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54 57 60
Usmani S, et al. 2016.
MM, multiple myeloma; IMiD, immunomodulatory drug; PI, proteasome
inhibitor; OS, overall survival.
Outline
•Available Therapeutic Regimens for later relapse
•General Principles to Guide Therapy Decisions
•Treatment of Later Relapse / Progression (≥2 prior lines of therapy
and/or lenalidomide/bortezomib refractory)
•Emerging therapeutics
•Conclusions
10/1/2017
2
Available Regimens in Late Relapse: NCCN Guidelines
Preferred Regimens
Other Regimens
Late Relapse (≥2 prior lines or
len/bort
refractory)
Level 1 Regimens
Doublets
•
Pomalidomide/dexamethasone
Other Regimens
•
Pomalidomide/bortezomib/dexamethasone
•
Pomalidomide/carfilzomib/dexamethasone
•Pomalidomide/daratumumab/dexamethasone
•
Daratumumab
Late
Relapse (≥2 prior lines or len/bort refractory)
•
Panobinostat/bortezomib/dexamethasone
•
Panobinostat/carfilzomib
•
Pomalidomide/cyclophosphamide/dexamethasone
•
DCEP (dex/cyclophosphamide/etoposide/cisplatin)
•
DT-PACE (dex/thalidomide/cisplatin/doxorubicin/
cyclophosphamide/etoposide) ± bortezomib (VTD-PACE)
•
High-dose cyclophosphamide
NCCN Guidelines, Version 3.2017, accessed August, 2017.
Note: NCCN Guidelines do not break out regimens into separate categories of early and late relapse
PANORAMA-2: A Phase 2 Study of Bortezomib,
Dexamethasone and Panobinostat
Response Category
%
ORR (≥PR)
34.5
CBR (≥MR)
52.7
CR 0.0
nCR 1.8
PR 32.7
MR 18.2
SD 36.4
PD 5.5
Progression-free Survival
Overall Survival
Time (months)
Time (months)
Median PFS: 5.4 mos
Median OS: Not reached
(Median F/U: 8.3 mos)
•55 pts with relapsed and bortezomib-refractory
multiple myeloma (54 prior lenalidomide tx)
•Median prior regimens: 4 (2 –11)
•Median time since diagnosis: 54.8 mos (7.5 –
263.6)
•21-day cycle. Bort 1.3 mg/m2IV D1, 4, 8, 11 (D1,
8 for cycle 9+); Dex 20 mg day of and after bort;
Pano/Placebo 3x/week for the first 2 weeks of
the cycle.
Richardson PG et al. Blood 2013;122:2331-7.
Pomalidomide-Dex vs Dex for
Relapsed/Refractory Multiple Myeloma
•Randomized, phase III study of Pom-Dex vs Dex in relapsed/refractory myeloma
•Baseline characteristics: 1) Median number of prior therapies = 5; 2) Len and bort refractory 75%
•ORR: 31% vs. 10%
•Median PFS 4.0 vs. 1.9 mos
•Median OS: 12.7 vs. 8.1 mos
Pom-Dex
Dex
Miguel JS, et al. Lancet Oncol. 2013;14:1055-1066.
10/1/2017
3
Carfilzomib, Pomalidomide and Dexamethasone for
Relapsed/Refractory Multiple Myeloma
•MTD in phase I: 4-week cycle.
CFZ 27 mg/m2D1, 2, 8, 9, 15, 16;
Pom 4 mg D1-21;
Dex 40 mg D1, 8, 15, 22
•Median lines of therapy: 6 (2–12)
•Len-refractory: 100%
•Bortezomib-refractory: 93.5%
Best Overall Response N=32
VGPR 16%
PR 34%
MR 16%
SD 25%
PD 9%
Median PFS 7.2 months, Median
OS 20.6 months
Shah JJ, et al. Blood. 2015;261:2284-2290.
Phase 1/2 Trial: Pomalidomide, Bortezomib and
Dexamethasone
Time (months)
100
80
40
20
0
60
Success (%)
012 24 30
618
OS
PFS
OS and PFS1
1. Lacy MQ, et al. Blood. 2014;124 (suppl, abstr 304). 2. Richardson PG, et al. Blood. 2015;124 (suppl, abstr 3036).
Median follow-up: 12 months N = 47
Response rate, n (%) 40 (85)
Median OS
Event free at 6 months (%)
Event free at 12 months (%)
NA
100
95
Median PFS, months 10.7 (95% CI 9.4–18.5)
Median DoR, months 13.7 (95% CI 8.5–16.8)
Median 2 prior lines
Prior lenalidomide 100%, prior bortezomib 57%
Refractory to immediate prior line 28%
Median follow-up: 12 months N = 34
Response rate, n (%) 22 (65)
Median DoR, months 7.4 (95% CI 4.4–9.6)
Median 2 prior lines
Prior lenalidomide 100%, prior bortezomib 97%
42 20 824
33
40
25
32
10
17
9
0
20
40
60
80
sCR/CR
VGPR
PR
Escalation
(n = 12)
MTD With
IV BORT
(n = 10)
Total
(N = 34)
MTD With
SC BORT
(n = 12)
Median TTR,
mos (95% CI)
Median DOR,
mos (95% CI)
1.1
(0.7-5.1)a
5.8
(1.2-10.1)
1.4
(0.9-3.2)a
7.4
(4.1-NE)
0.8
(0.7-1.0)a
NE
(3.2-NE)
1.0
(0.7-5.1)
7.4
(4.4-9.6)
OR R and DOR2
8
Phase 1/2 Trial: Pomalidomide, Cyclophosphamide and
Dexamethasone
Median PFS: 9.5 vs 4.4 months (P= .1078)
Median OSa: not reached vs 16.8 months (P= .1308)
•Median number of prior therapies 4
•Must have been refractory to lenalidomide
•Refractory to bortezomib 71%
Proportion
Progression-free survival (months)
1.0
0.8
0.6
0.4
0.2
0.0
Arm N Event Censored Median (95% CI)
POM-LoDEX 36 30 (83%) 6 (17%) 4.4 (2.3, 6.0)
POM-LoDEX + cyclo 34 26 (76%) 8 (24%) 9.5 (4.6, 13.6)
0 3 6 9 12 15 18 21 24 27
POM-LoDEX
POM-LoDEX + cyclo
Log-rank p = 0.1078
Baz R, et al. B lood. 2016;127(21):2561-8. 9
10/1/2017
4
18%
10%
1%
2%
0
5
10
15
20
25
30
35
16 mg/kg
ORR, %
PR VGPR CR sCR
•Median OS: 19.9 months
3%
CR or
better 13%
VGPR or
better
N = 148
Daratumumab as Monotherapy for
Relapsed/Refractory Multiple Myeloma
Progression-Free Survival
Usmani S, et al. Blood. 2016;128:37-44.
Pomalidomide, Dexamethasone and
Daratumumab for Relapsed/Refractory MM
Median OS = 17.5 months (85% CI 13.3 –NE)
Chari, A, et al. Blood 2017;130:974-81.
Median number of prior lines of therapy: 4 (range 1 –13), 71% PI and IMiD refractory, 25% with high risk CGs
Of 17 pts in ≥CR, 35%, 29% and 6% were MRD- at
thresholds of 10-4, 10-5 and 10-6, respectively Median PFS in high risk CG disease
(N=22): 3.9 months (95% CI 2.3 –NE)
Analysis of Daratumumab, Pomalidomide and
Dexamethasone in Relapsed/Refractory Multiple Myeloma
Best Response
Dara and Pom
Naive
(n = 19)
Dara and/or Pom
Refractory
(n = 22)
Dara and Pom
Refractory
(n = 12)
ORR, n % 17 (89.0) 9 (40.9) 4 (33.3)
sCR, n % 7 (36.8) 0 0
CR, n % 1 (5.3) 0 0
VGPR, n % 3 (15.8) 1 (4.5) 1 (8.3)
PR, n % 8 (42.1) 8 (36.4) 3 (25.0)
MR/SD, n % 1 (5.3) 9 (40.9) 6 (50.0)
PD, n % 1 (5.3) 4 (18.2) 2 (16.7)
Median cycles of tx,
n (range) 15 (1-23) 3 (1-8) 3 (1-8)
Nooka AK, et al. Blood. 2016;128:492. 12
10/1/2017
5
Efficacy, Mos All Cohorts
(N = 41)
Dara and Pom Naive
(n = 19)
Dara and Pom
Refractory (n = 12)
Median PFS 7 NR 3
Median follow-up 16 17 8
PFS Dara/Pom/Dex: All Cohorts
Cumulative Survival
1.0
0.8
0.6
0.4
0.2
00 6 12 18 24
Mos
PFS Dara/Pom/Dex: SD or
Better vs No Response
Cumulative Survival
1.0
0.8
0.6
0.4
0.2
00 6 12 18 24
Mos
No response
≥ SD
PFS Dara/Pom/Dex: Cohort 3 SD
or Better vs No Response
Cumulative Survival
1.0
0.8
0.6
0.4
0.2
00 6 12 18 24
Mos
No response
≥ SD
Nooka AK, et al. Blood. 2016;128:492.
Analysis of Daratumumab, Pomalidomide and
Dexamethasone in Relapsed/Refractory Multiple Myeloma
General Treatment Principles
•Overlap between early and late relapse treatment choices
•An early or late relapse regimen may be appropriate as 2nd –4th line therapy
(1 –3 prior lines) depending on the circumstances
•The role of doublets and monotherapy is limited
•Several novel triplets now available with good toxicity profiles
•Consider in the more frail, heavily pretreated patients
•Prior treatment toxicity, disease resistance patterns and co-
morbidities figure particularly prominently into the decision making
process for these patients
•Assess for the presence of t(11;14)
•Always think about a clinical trial
PABST: The Blue Ribbon Approach to Therapy
Decisions for Previously Treated Multiple Myeloma
•Past medical history
•What co-morbidities will impact tolerability
of therapy?
•Adverse events
•What toxicities were experienced with prior
therapy?
•Biochemical vs clinical
relapse/progression
•Standard vs high-risk disease biology
•Treatment history
•Is the disease resistant to specific drug
classes?
10/1/2017
6
Biochemical vs Clinical Progression
•Biochemical progression:
•Progression of disease based on M
protein parameter increase only
•Timing of therapy institution /
escalation dependent on numerous
factors
•Pace of progression
•Original clinical presentation
•Standard vs high-risk disease biology
•Patient / physician comfort level
•Clinical relapse:
•“Direct indicators of increasing
disease and/or end organ dysfunction
(CRAB features) related to the
underlying clonal plasma-cell
proliferative disorder”
•Mandates immediate institution /
escalation of therapy
IMWG Consensus Criteria for Response in MM
Biochemical Progression Clinical Relapse
↑ of ≥25%
from nadir response value in
one or more of the following:
1)
Serum M protein (absolute increase
≥0.5 g/dL, ≥1 g/dL if nadir ≥5 g/dL)
2)
Urine M protein (absolute increase
≥200 mg/24 hours)
3)
Measurable by serum FLC testing
only: difference between involved
and uninvolved FLCs (absolute
increase ≥10 mg/dL)
4)
Non-secretory: bone marrow PC %
(absolute increase ≥10%)
1)
Development of new soft tissue
plasmacytomas or bone lesions
(osteoporotic fractures do not
constitute progression)
2)
Definite increase in the size of
existing plasmacytomas or bone
lesions. A definite increase is defined
as a 50% (and >=1 cm) increase as
measured serially by the SPD§§
of the
measurable les ion
3)
Hypercalcaemia (>11 mg/dL);
4)
Decrease in haemoglobin of >=2 g/dL
not related to therapy or other non-
myeloma-related conditions
5)
Rise in serum creatinine by 2 mg/dL
or more from the start of the therapy
and attributable to myeloma
6)
Hyperviscosity related to serum
paraprotein
≥50% increase
in circulating plasma cells
(minimum 200 cells /
uL) if this is the only
disease measure available
Kumar S et al. Lancet Oncol 2016;17:328-46
Standard vs High-Risk Disease Biology: IMWG
Consensus on Risk Stratification
High-Risk Standard-Risk Low-Risk
Parameters
ISS II/III and t(4;14) or
del(17p13)
Others ISS I/II and absence of
t(4;14), del(17p13) and
+1q21 and age <55
% of Patients
20% 60% 20%
Median OS
2 years 7 years >10 years
•Other factors: Gene expression profile, LDH. circulating plasma cells, response to prior therapy
Chng WJ et al. Leukemia 2014;28:269-77
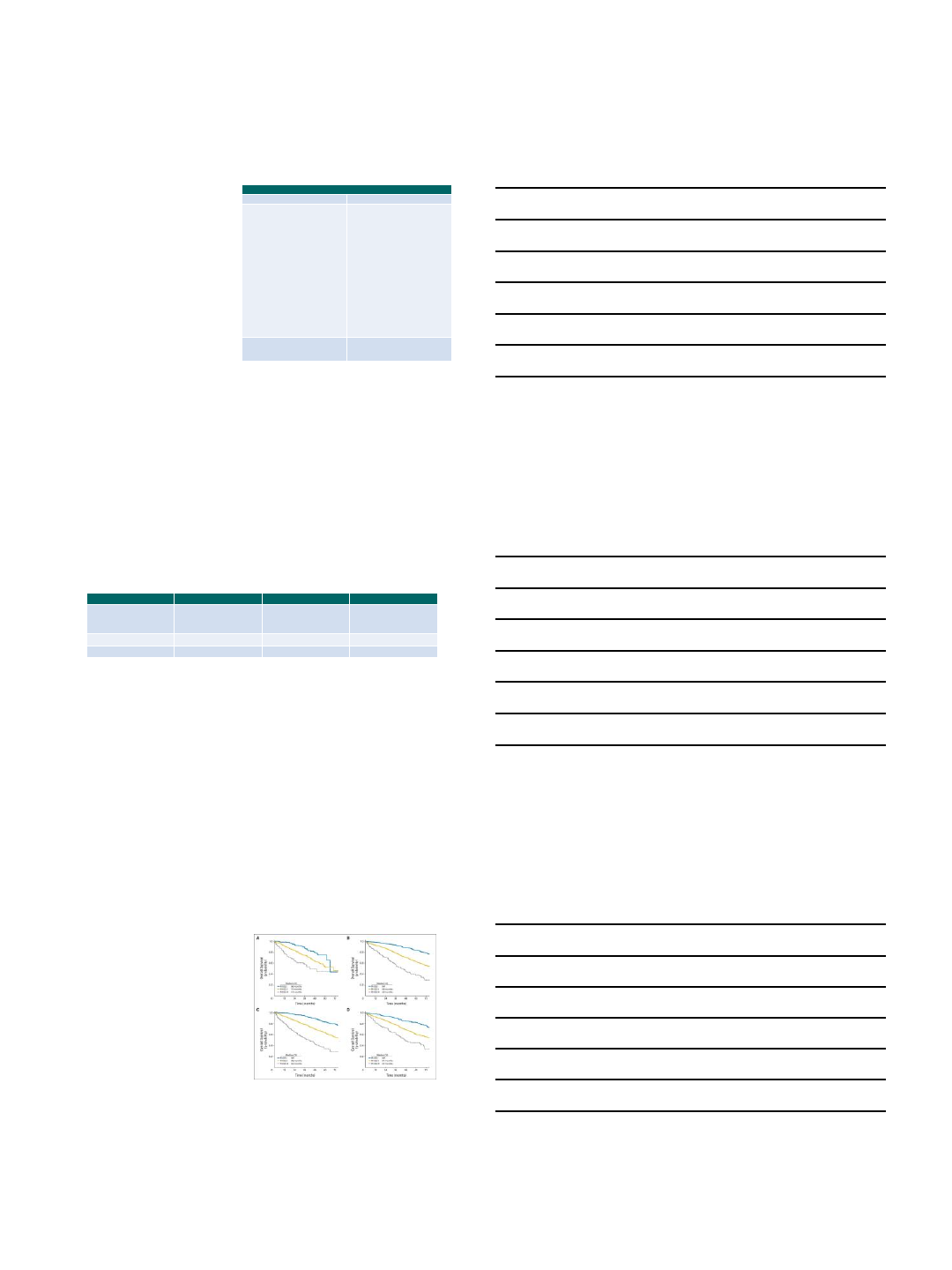
Revised International Staging System
R-ISS stage 1: normal LDH, no high risk
cytogenetic abnormality (CA)*, ISS stage 1
disease
R-ISS stage 2: not stage 1 or 3
R-ISS stage 3: ISS stage 3 disease PLUS
high LDH OR high risk CA
Palumbo et al. JCO 2015;33:2863-2869
*High risk CA = del(17p)
and/or t(4;14) and/or t(14;16)
Transplant-Based Tx
Non Transplant-Based Tx
IMiD-Based Tx Bortezomib-Based Tx

10/1/2017
7
Treatment History
•What regimen(s) has the patient had in earlier lines of therapy?
•Is the disease refractory to a specific treatment?
•Refractory per the IMWG guidelines: disease progression on or within 60 days of the last dose of
therapy
•Lack of response (stable disease) with prior therapy has been included in the definition of refractory in some studies
•Carfilzomib has activity in bortezomib-refractory disease but the reverse has not been well studied
•Pomalidomide has activity in lenalidomide-refractory disease but the reverse has not been well studied
•If refractory, did the patient have disease progression on standard dosing, reduced dosing
due to prior toxicity or maintenance dosing?
•If dose reduced for toxicity, what were the toxicities, and how could they be better managed?
•For patients on maintenance, it is common practice to optimize therapy prior to changing to a non-
cross resistant regimen.
•Increase the dose of lenalidomide and reincorporate dexamethasone for a patient with progression on lenalidomide
maintenance. A 3rd agent is often included in such a scenario (e.g. elotuzumab) but patients with lenalidomide-
refractory disease were not allowed to participate in the ELOQUENT-1 study and the additional impact of this
maneuver has not been well studied
Treatment Choice Algorithm
•First Step
•Review resistance pattern with prior therapy
•Determine biochemical vs clinical relapse
•Assess standard vs high risk disease
•High risk FISH: del(1p), gain 1q, t(4;14), t(14;16), t(14;20), del(17p)
•High LDH, circulating plasma cells, plasma cell leukemia, extramedullary disease
•Second Step
•Refine choice based on co-morbidities and tolerability of previously used drug
classes
Disease Progression (≥2 prior lines of
therapy)
Disease Progression on
Maintenance
Disease Progression on
Standard Dose Therapy
Len/Bort Refractory
Escalate to standard
dose, add back dex
Clinical RelapseBiochemical Progression
or Early Clinical Relapse
with Minimal Morbidity
Biochemical Progression
or Clinical Relapse
+ Pom Ref + CFZ Ref Quad Ref
Len/Bort Ref only
Standard Risk
- KPd
- DPd
-Kd
-Pd
- CyPD
- Dara
High Risk / Clin
Relapse
- KPd
- DPd
Standard or
High Risk
-Kd
- KCyD
- Dara
- DPd
- Vtx-based**
Standard or
High Risk
- DPd
- CyPd
-Pd
- Dara
- Vtx-based**
Standard or
High Risk
- Dara
- DPd*
- Pano-based tx
- Alkylator-
based therapy
if not resistant
- Vtx-based**
Vtx = venetoclax
*Only if disease resistant to prior pom-dex and dara in separate lines of therapy. **If + for t(11;14) (off label use)
10/1/2017
8
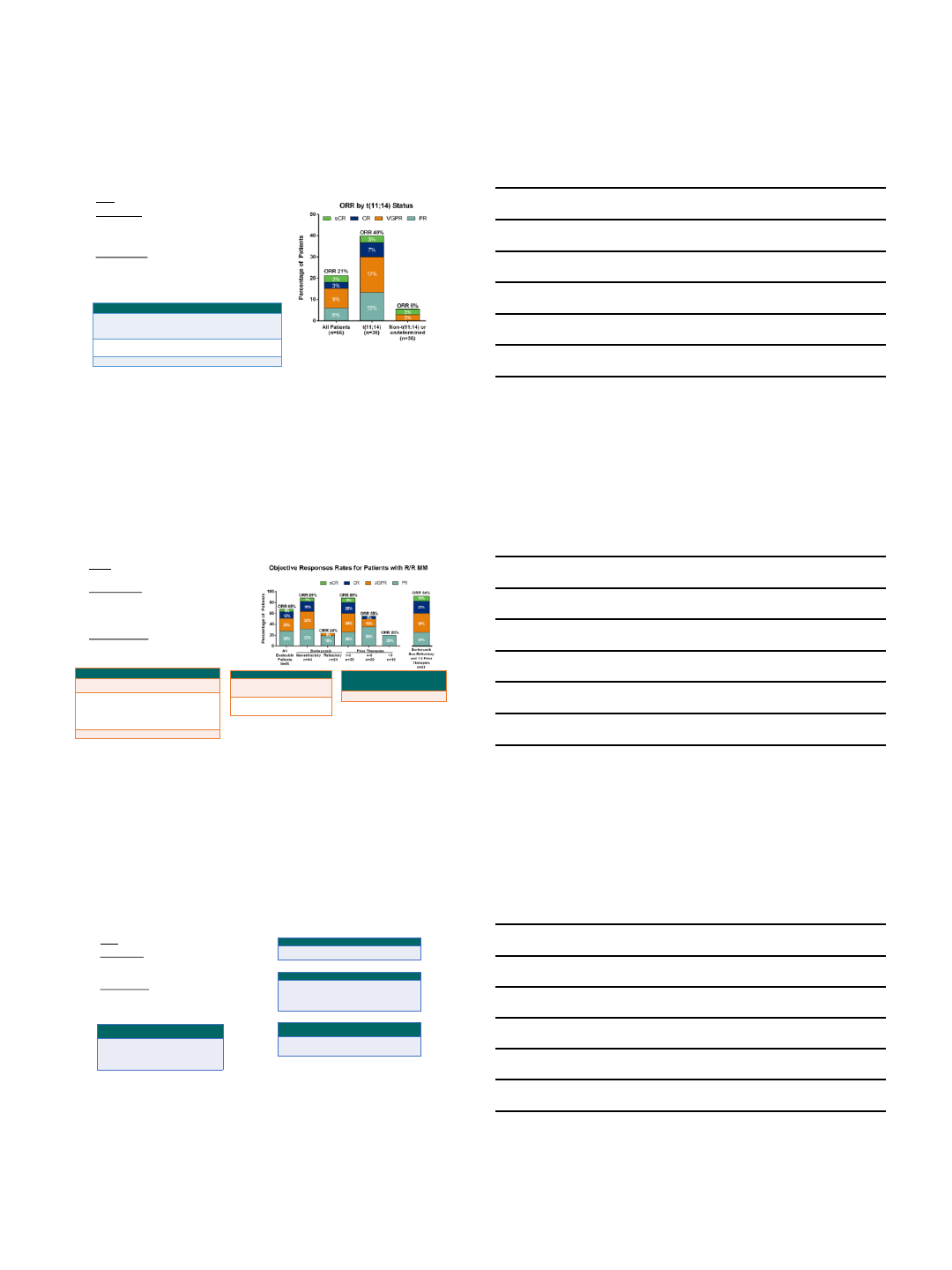
Venetoclax Monotherapy (N=66)
Design: Phase I, open label, study of venetoclax monotherapy
Study Population: RRMM
•Median age: 63 yrs
•ISS stage II/III: 62%
•Median prior therapies: 5 (1-5)
•Prior BTZ: 94% (70% ref)
•Prior REV: 94% (77% ref)
Dosing & Schedule:
VEN: initial 2 week lead in period with weekly dose-escalation
•Final doses: daily at 300 mg, 600 mg, 900 mg, or 1200 mg
•Patients who progressed could receive VEN + dex and remain on study
Safety, n (%)
Venetoclax
Gr 3/4 (≥10%)
Thrombocytopenia (26%), neutropenia (20%),
lymphopenia (15%), anemia (14%), and
decreased white blood cells (12%)
SAEs
≥2 pts
Pneumonia (n=5), sepsis (3), pain, pyrexia,
cough, and hypotension (2 each)
Deaths
8 (all considered unrelated to VEN)
•Median time on VEN: 2.5 mo (0.2-23); 26% received VEN +
dex for a median of 1.4 mo (0.1-11)
Kumar S, et al. ASH 2016. Abstract 488.
Venetoclax + Vd (N=66)
Design: Phase Ib, open label, dose escalation study of
venetoclax + Vd
Study Population: RRMM
•Median age: 64 yrs
•ISS stage II/III: 59%
•Median prior therapies: 3 (1-13)
•Prior BTZ: 32% ref
•Prior REV: 56% ref
Dosing & Schedule:
VEN: daily, 50 mg –1200 mg dose escalation
•RP2D: 800 mg qd
Vd: Dose and schedule not reported
Moreau P, et al. ASH 2016. Abstract 975.
Safety, n (%)
Venetoclax
Gr 3/4 (≥10%)
Thrombocytopenia (29%), anemia (15%)
and neutropenia (14%)
SAEs
≥2 pts
Febrile neutropenia, thrombocytopenia,
cardiac failure, pyrexia, influenza, lower
respiratory tract infection, pneumonia,
sepsis, acute kidney injury, respiratory
failure, embolism, and hypotension
1 DLT: lower abdominal pain (1200 mg Ven)
Deaths
5 (4=PD, 1=RSV infection)
•Discontinuations: 43 (65%), PD
(33), AE (5), withdrawn consent
(2), not specified (3)
Efficacy
All 1-3 Priors
DOR
8.8 mo V non-ref: 10.6 mo
V naïve: 15.8 mo
TTP
8.6 mo V non-ref: 11.3 mo
V naïve: 17.1 mo
Efficacy
With
t(11;14)
Without
t(11;14)
ORR
78% 66%
STORM: Selinexor + Dex (N=79)
Design: Phase II study of Sd
Study Population: RRMM
•48 pts refractory to REV, POM, V, K (Quad)
•33 pts refractory to above + anti-CD38 mAbs
(Penta)
Dosing & Schedule:
S: 80 mg BIW for 6 or 8 doses of a 28 d cycle
D: 20 mg BIW
Median age: 68 yrs
Efficacy
All Quad Penta
ORR
CBR
21%
32%
21%
29%
20%
37%
Vogl DT, et al. ASH 2016. Abstract 491.
Safety, n (%)
Gr 3/4 (≥10%)
All patients
Thrombocytopenia
Neutropenia
Anemia
Fatigue
Hyponatremia
58
21
25
14
20
•Most quad patients (83%) received 6 doses/cycle; penta patients (65%) received 8
dose s/cycle
Efficacy
All Responders Non-
responders
mOS
PFS
DOR
9.3 mo
2.1 mo
NR (>11 mo)
5 mo
5.7 mo
Efficacy
ORR, n (%)
Standard Risk
High
Risk
(17p13)
t(14;16)
t(4;14)
4 (17)
6 (33)
3 (38)
1 (100)
2 (50)
10/1/2017
9
PAVO: SC Daratumumab (N=41)
Design: Ph Ib, open label, multicenter, dose-escalation study
of SC Dara with rHuPH20 (Dara-PH20)
Study Population: N=41
• ≥2 prior lines of therapy
•Prior therapy included an IMiD and a PI
Dose & Schedule:
D (cohort 1): 1200 mg in 60 mL over 20 min (n=8)
D (cohort 2): 1800 mg in 90 mL over 30 min (n=33)
Dara-PH20 was infused via a syringe pump in rotating areas
on the abdomen in 4-week treatment cycles: QW for 8 weeks,
Q2W for 16 weeks, and Q4W thereafter
Efficacy
1200 mg 1800 mg
ORR
25% 41%
Usmani S, et al. ASH 2016. Abstract 1149.
•Part 2 of the study will examine the RP2D of Dara-PH20 vs IV Dara monotherapy
•1800 mg was selected as the RP2D
Safety
Gr 3/4
Fatigue (2 pts), influenza, hypertension,
dyspnea, and tumor lysis syndrome
ONLY SEEN IN 1200 MG DOSE
IRR
(most Gr 1/2)
Chills, fever, rigors, vomiting, itching, edema of
the tongue, non-cardiac chest pain, and
wheezing; all occurred at 1st
infusion and were
controlled with treatment
NO GRADE 3 IRR SEEN IN 1800 MG DOSE
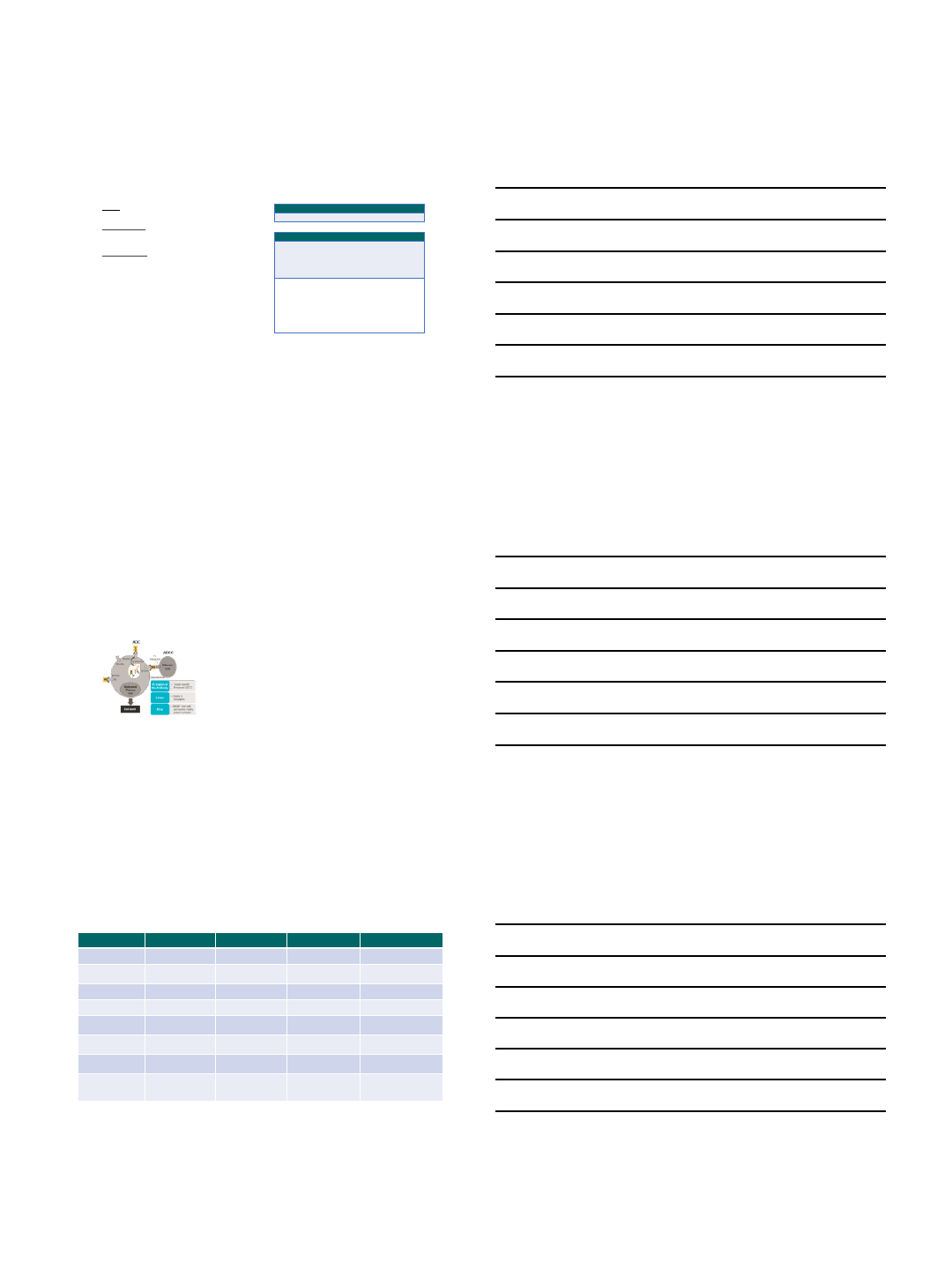
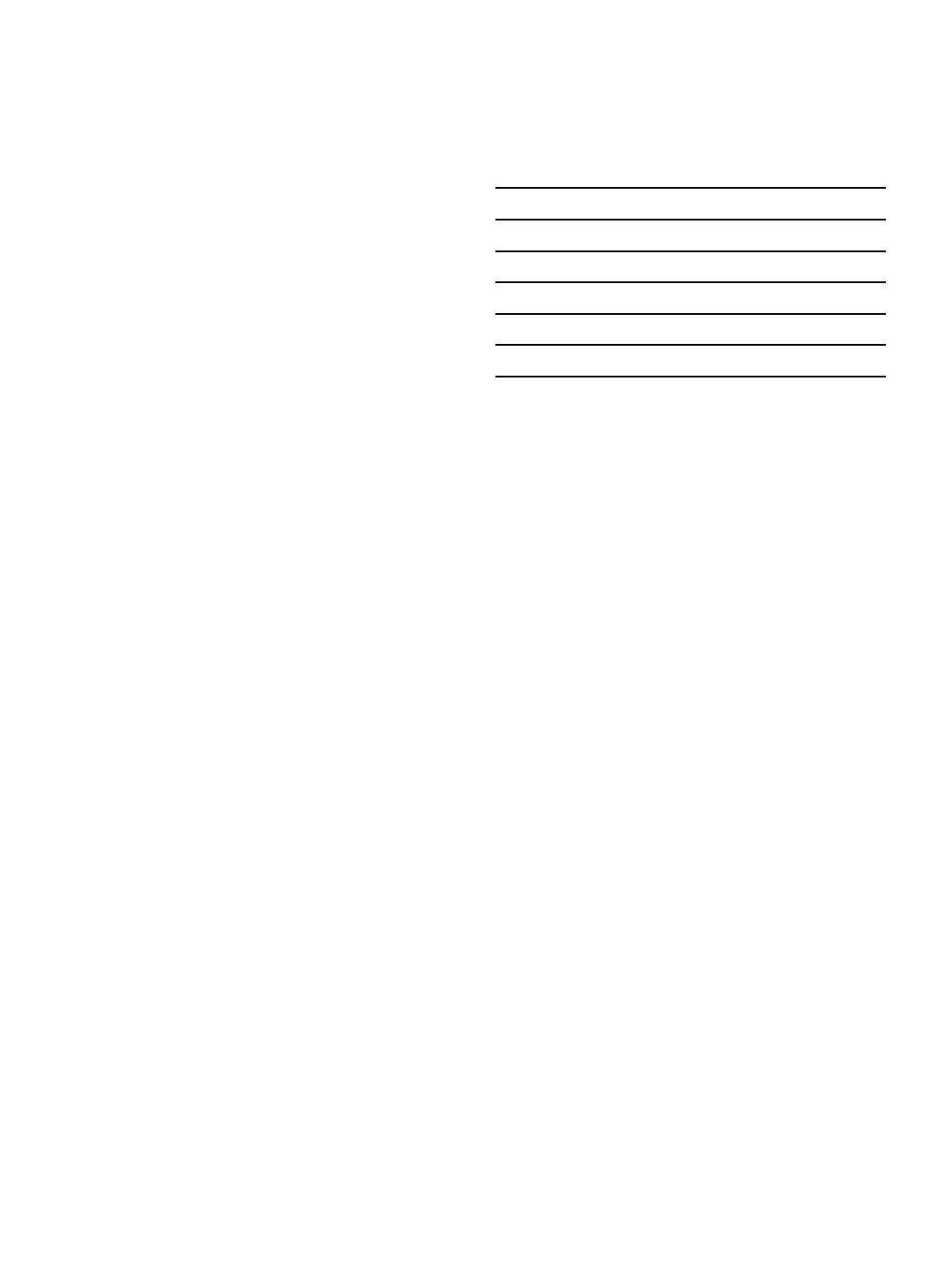
First in Human Study with GSK2857916,
An Antibody Drug Conjugated to Microtubule-disrupting
Agent Directed Against B-cell Maturation Antigen (n=30)
–BCMA expression is restricted to B cells at later stages
of differentiation and is requisite for the survival of long
lived plasma cells
–BCMA is broadly expressed at variable levels on
malignant plasma cells
Cohen A, et al. ASH 2016.
–GSK2857916 was well tolerated with no DLTs up to 4.6
mg/kg q3w; MTD was not reached
–AEs were manageable with ocular toxicity emerging as
the most frequent reason for dose modifications
–Hematologic toxicities such as thrombocytopenia and
anemia are expected in the disease under study
–66.7% ORR including a stringent CR observed at
higher doses of GSK2857916 in this refractory
population
–3.4 mg/kg was selected as the dose to investigate
in the expansion phase of the study based on the
totality of the data from Part 1
–Pharmacodynamic and correlative analyses are
ongoing
B-cell Maturation Antigen (BCMA)-specific chimeric antigen receptor T
cells (CART-BCMA) for MM
Anti-BCMA CAR Bb2121 LCAR-B38M CART-BCMA
Group/Company NCI Bluebird/Celgene/NCI Nanjing Legend Biotech Novartis/UPenn
Binder/co-stimulatory
signaling
Murine/CD3 & CD28 Murine/CD3 & 41-BB Murine/CD3 & 41-BB Fullay human/CD3 & 41-BB
Transfection Gamma-retroviral Lentiviral Lentiviral Lentiviral
Trial ID NCT02215967 NCT02658929 NCT03090659 NCT02546167
BCMA expression
required?
Yes Yes Yes No
Median prior lines of
therapy
7 7 3 9
Latest efficacy 1 CR (relapsed), 7 PRs
in 16 patients
4 CRs, 12 PRs in 18
patients
15 CRs and 13 PRs in 35
patients
1 CR, 3 PRs in 9 patients
Safety summary Substantial but
reversible
1 death,
cardiopulmonary
arrest (unrelated)
Transient CRS 1 death –progressive
disease/candidaemia
10/1/2017
10
Conclusions
•There are many right ways to treat patients with multiple myeloma in relapse
•There are also wrong ways to do it
•As long as you have a PABST (review PMHx, adverse events, biochemical vs
clinical relapse, standard vs high-risk disease, treatment history), you will come to
a good answer for your patient
•Use your local/regional Myeloma Specialists as a resource when questions arise
about risk status, when to change treatment in biochemical relapse, optimal
therapy when the preferred regimens may not be good options
•Always consider a clinical trial, especially in increasingly refractory and / or high
risk disease. We have gotten better at treating this disease but have a long ways
to go!
9/28/2017
1
2017 Trends in MM Rx:
Restoring Immune Function
•Immunomodulatory drugs, other small molecules
(eg, HDACi’s)
•Monoclonal antibodies
•Checkpoint inhibitors
•Vaccines
•Cellular therapies
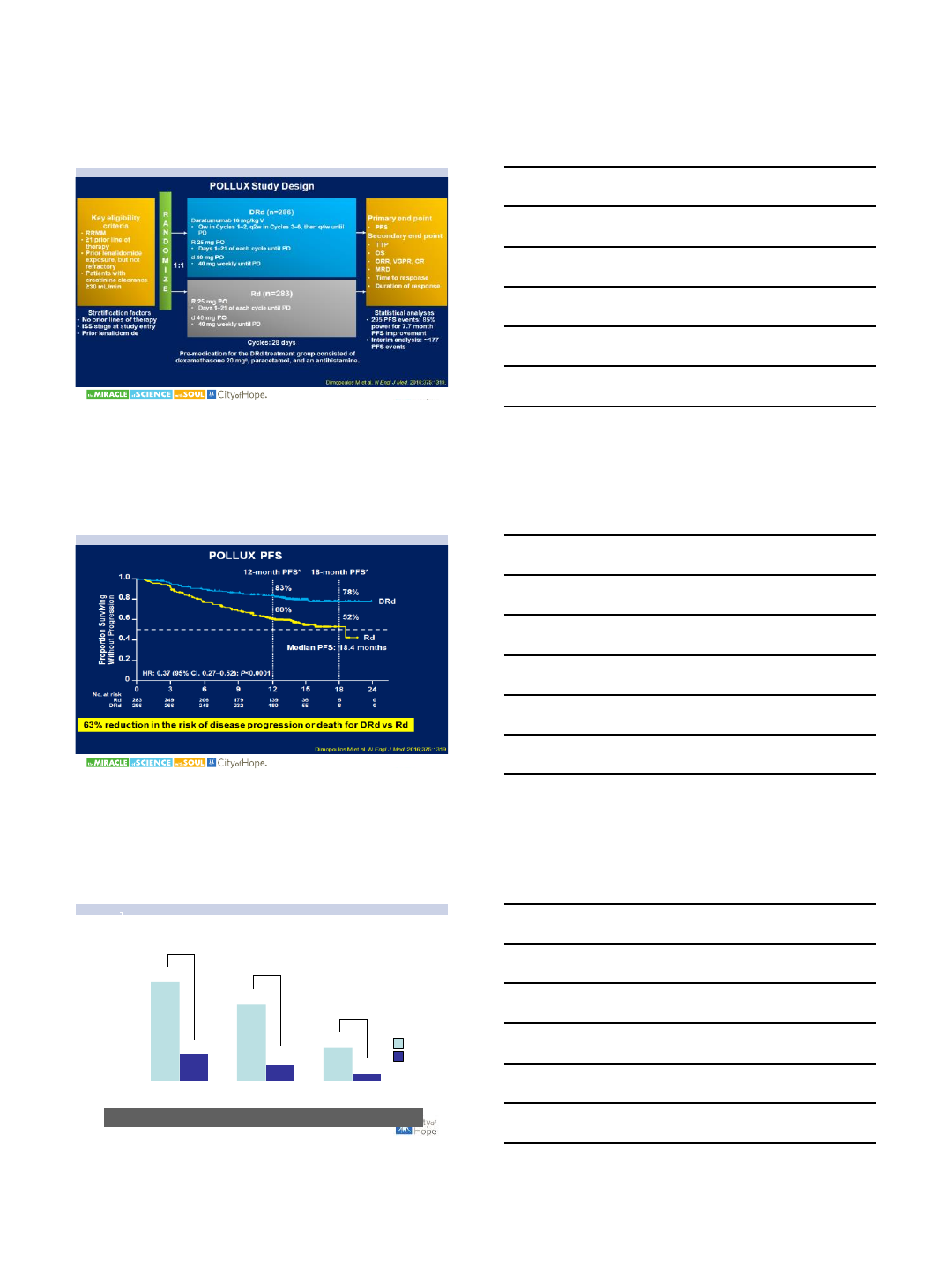
Monoclonal Antibodies Kill MM
Through Multiple Mechanisms
Rd (n = 325)
LEN: 25 mg, d1–21
DEX: 40 mg, d1, 8, 15, 22
28-day cycles until progression
N=646
RRMM
1–3 prior lines
Not LEN-refractory
ERd (n = 321)
ELO: 10 mg/kg, d1, 8, 15, 22
(cycles 1–2); d1, 15 (cycles ≥ 3);
LEN: 25 mg, d1–21
DEX: weekly equivalent, 40 mg
28-day cycles until progression
•Primary end points: PFS, ORR
•Secondary end points: OS, DoR, QoL, safety
ELOQUENT 2:
Elotuzumab-Rd (ERd) vs Rd
Lonial S et al. N Engl J Med. 2015;373:621.
9/28/2017
2
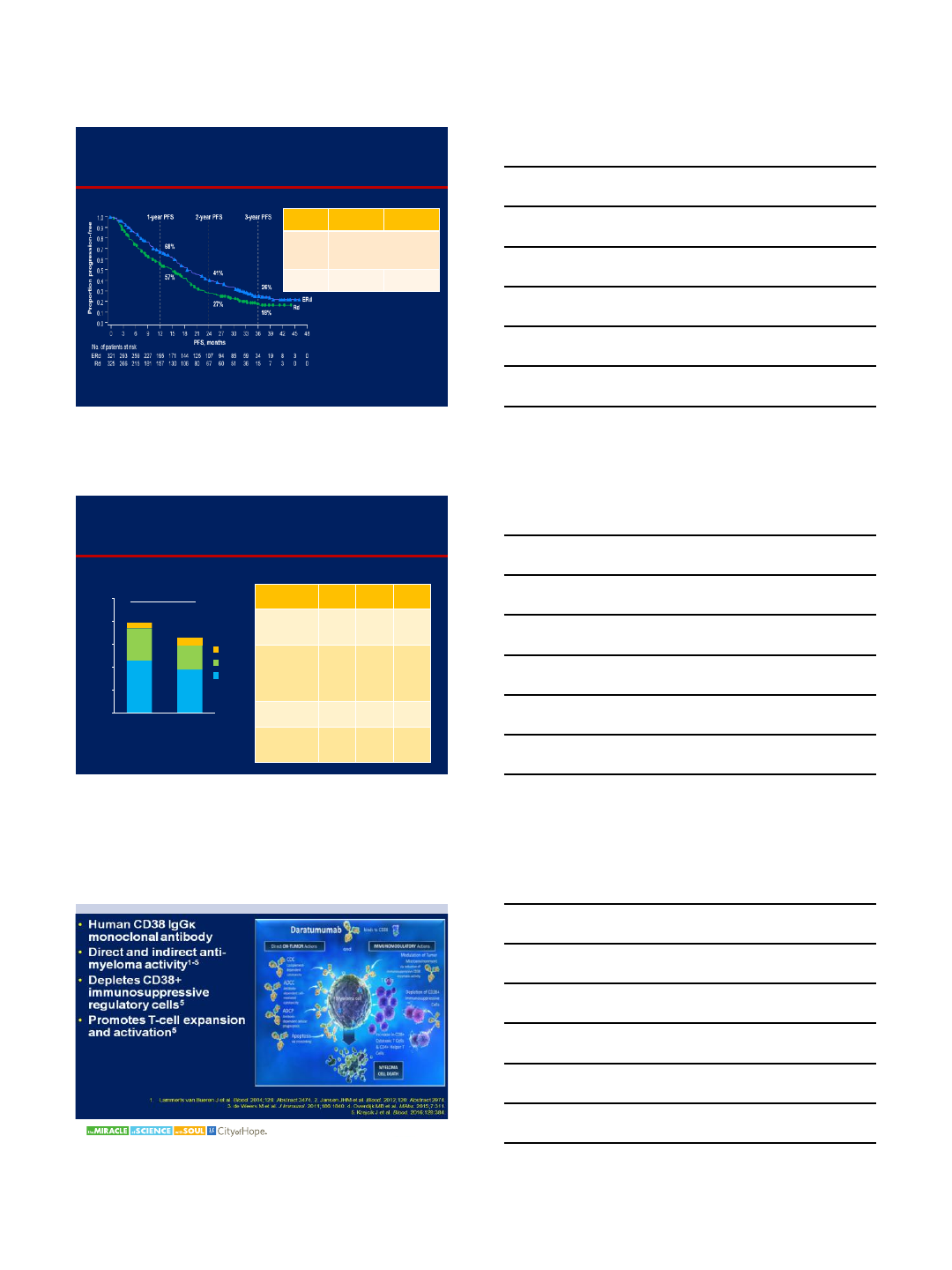
ELOQUENT-2: ERd vs Rd
Progression-Free Survival
Dimopoulos MA et al. Blood. 2015;126: Abstract 28.
ERd
(n=321) Rd
(n=325)
Median
PFS, mos
(95% CI)
19.4
(16.6−22.2) 14.9
(12.1−17.2)
HR=0.73
(95% CI 0.60−0.89;
P
=0.0014)
3
-yr PFS,
%
26 18
CR
VGPR
PR
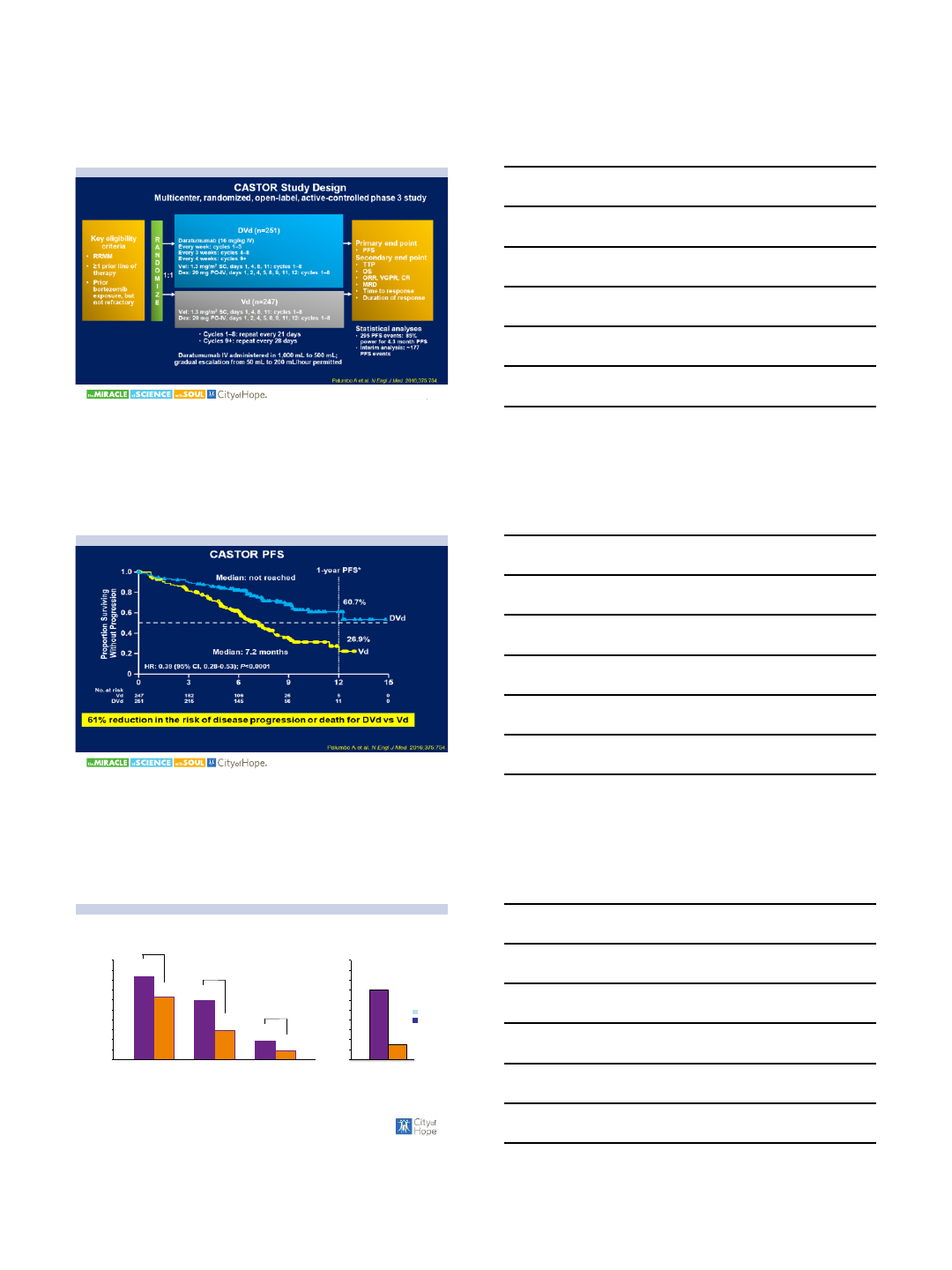
ELOQUENT-2: ERd vs Rd
Efficacy
*Values may not sum due to rounding.
46 38
28
21
4
7
0
20
40
60
80
100
ERd Rd
Patients (%)
ORR 79%a
ORR 66%*
n=321 n=325
P<0.001 ERd
(n=321) Rd
(n=325) HR;
Pvalue
Median
PFS,
months219.4 14.9 0.73;
0.0014
Median
TTNT,
months233 21
0.62
(95%
CI
0.50–
0.77)
Median OS,
months243.7 39.6 0.77;
0.0257
Median
DoR,
months120.7 16.7 NR
Responses1
1. Lonial S et al. N Engl J Med. 2015;373:621-31.
2. Dimopoulos MA et al. Blood. 2015;126: Abstract 28.
Daratumumab: Mechanism of Action
9/28/2017
3
Phase 3 Randomized Controlled Study of DVd vs Vd
in Pts With Relapsed or Refractory MM: CASTOR
Phase 3 Randomized Controlled Study of DVd vs Vd
in Pts With Relapsed or Refractory MM: CASTOR
Overall Response Ratea
aResponse-evaluable population.
P <0.0001
83
63 59
29
19
9
0
10
20
30
40
50
60
70
80
90
100
Response rate, %
ORR ≥VGPR
P <0.0001
P = 0.0012 DVd
Vd
14
3
0
2
4
6
8
10
12
14
16
18
20
%
MRD-neg (10-4)≥CR
11
9/28/2017
4
Phase 3 Randomized Controlled Study of DRd vs Rd
in Pts With Relapsed or Refractory MM: POLLUX
Phase 3 Randomized Controlled Study of DRd vs Rd
in Pts With Relapsed or Refractory MM: POLLUX
12
MRD-negative Rate
DRd
Rd
0
5
10
15
20
25
30
35
40
45
50
MRD-negative rate (%)
MRD-neg (10-4) MRD-neg (10-5)MRD-neg (10-6)
30%
8%
P <0.0001
23%
5%
P <0.0001
10%
2%
P <0.0001
Response-evaluable set. Assessed by next g eneratio n sequenci ng in bone marrow.
Significantly higher MRD-negative rates for DRd vs Rd
9/28/2017
5
Daratumumab in High-Risk Patients
Rationale for DARA + POM-D
14
•In a randomized, Phase 3 study, pomalidomide plus low-dose
dexamethasone (POM-D) in patients relapsed from or refractory to
previous treatment with bortezomib or lenalidomide1 resulted in the
following:
–ORR = 31%
–Median PFS of 4.0 months
–Median OS of 12.7 months
•Pomalidomide increases CD38 expression in a time and dose-
dependent fashion in multiple myeloma cells2
1. San Mi guel J, et al. Lancet Oncol. 2013;1 4(11)1055-1066.
2. Boxha mmer R, et al. Presented at 51st American Socie ty of Clinical Oncolog y (ASCO)
Annu al Meeti ng; May 29 -June 2, 2015; Chicago, IL. Abstract 8588.
MMY1001: DARA + POM-D Arm
Treat 6 patients with DARA + POM-D
If ≤1 patient has DLTs
Enroll 6 additional patients
Expand up to 88 patients
Eligibility criteria
•Refractory to last line of therapy
• ≥2 prior lines of therapy,
including 2 consecutive cycles
of lenalidomide and bortezomib
•Pomalidomide naïve
•ECOG score ≤2
•Absolute neutrophil count
≥1.0×109/L, and platelet count
≥75×109/L for patients with
<50% plasma cells (>50×109/L,
otherwise)
•Calculated creatinine clearance
≥45 mL/min/1.73 m2
15
DARA* IV 16 mg/kg +
Pomalidomide 4 mg (Days 1-21) +
Dexamethasone 40 mg QW
Open-label, multicenter, six-arm, Phase 1b
study
(28-day cycles)
*QW for Cycles 1-2, Q2W for Cycles 3-6, and Q4W beyond.
9/28/2017
6
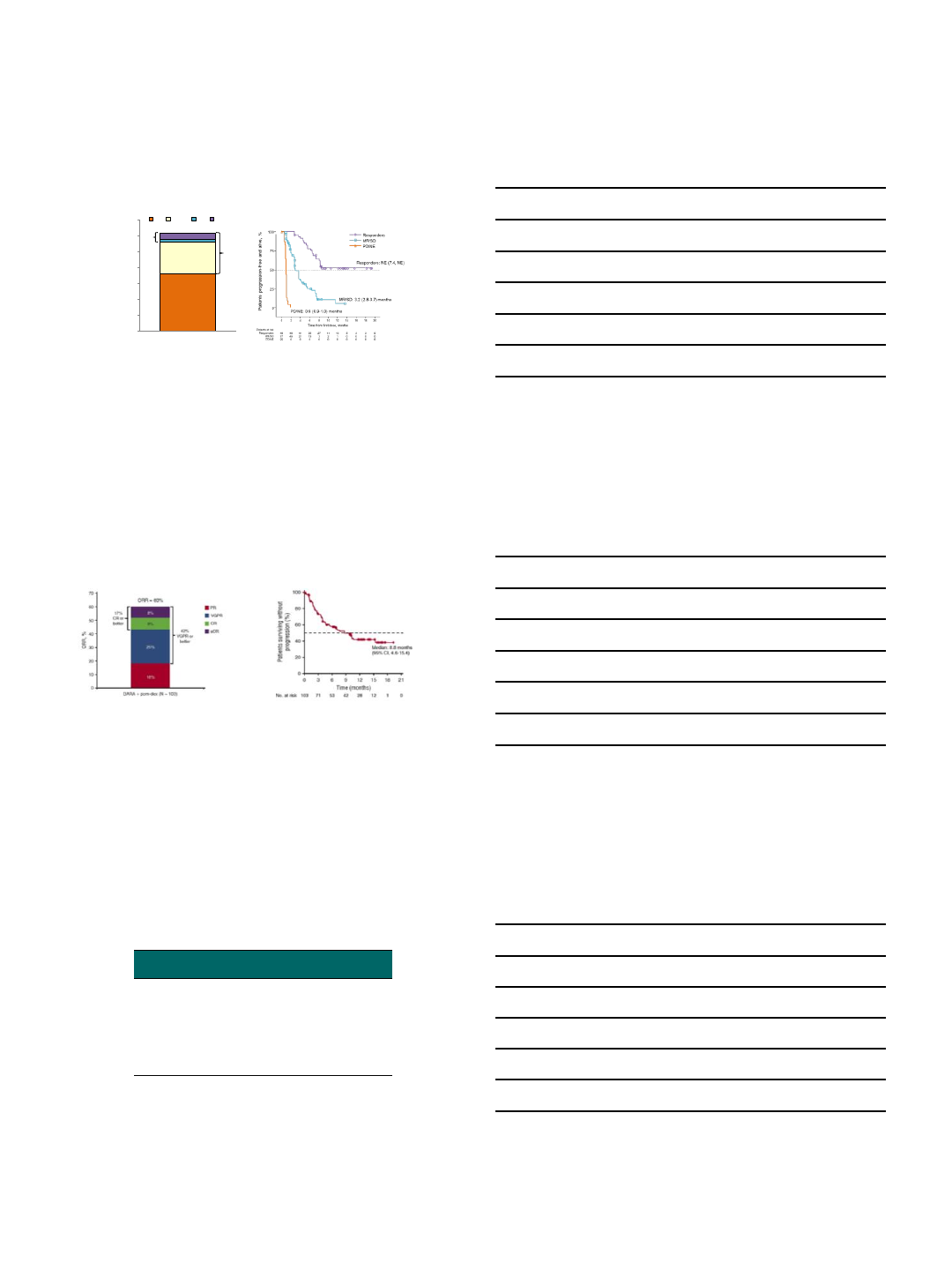
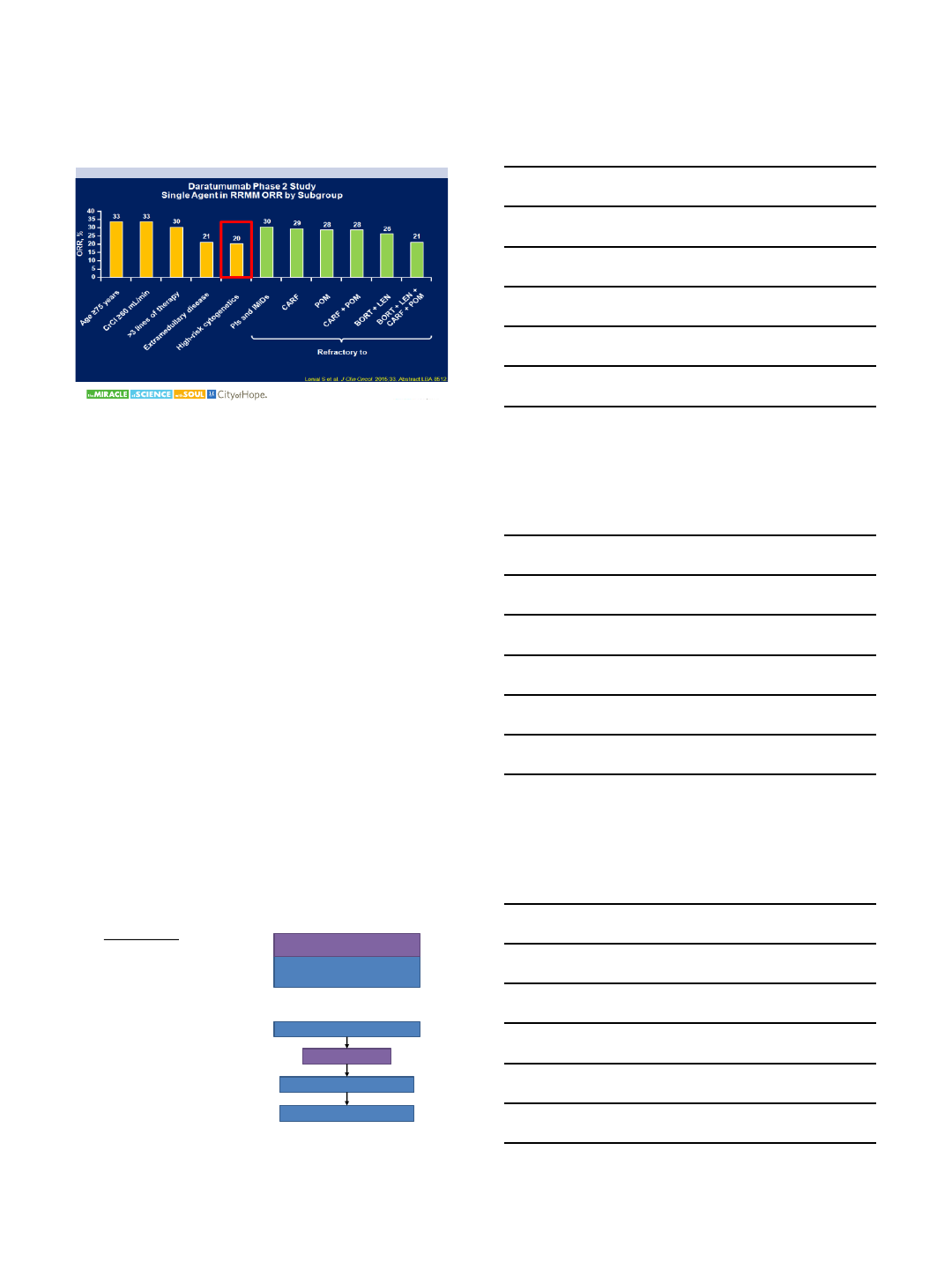
Overall Response Rate:
DARA + POM-D
•ORR = 71%
•ORR in double-refractory patients = 67%
•Clinical benefit rate (ORR + minimal response) = 73%
DARA + POM-D
(N = 75)
n (%) 95% CI
Overall response rate
(
sCR+CR+VGPR+PR) 53 (71) 59.0-80.6
Best response
sCR
CR
VGPR
PR
MR
SD
PD
4 (5)
3 (4)
25 (33)
21 (28)
2 (3)
17 (23)
3 (4)
1.5-13.1
0.8-11.2
22.9-45.2
18.2-39.6
0.3-9.3
13.8-33.8
0.8-11.2
VGPR
or better (sCR+CR+VGPR
)
32 (43) 31.3-54.6
CR
or better (sCR+CR) 7 (9) 3.8-18.3
ORR = 71%
16
43%
VGPR or
better
9%
CR or
better
28%
33%
4%
5%
0
10
20
30
40
50
60
70
80
16 mg/kg
ORR, %
PR VGPR CR sCR
N = 75
Progression-free Survival at 6 Months:
DARA + POM-D
17
0
Patients progression-free and alive, %
2 6
Time from first dose, months
0
20
60
80
100
4
40
Patients at risk 98 67 39 19
6-month PFS rate = 66% (95% CI, 52.3-75.9)
•Median follow-up of 4.2 months
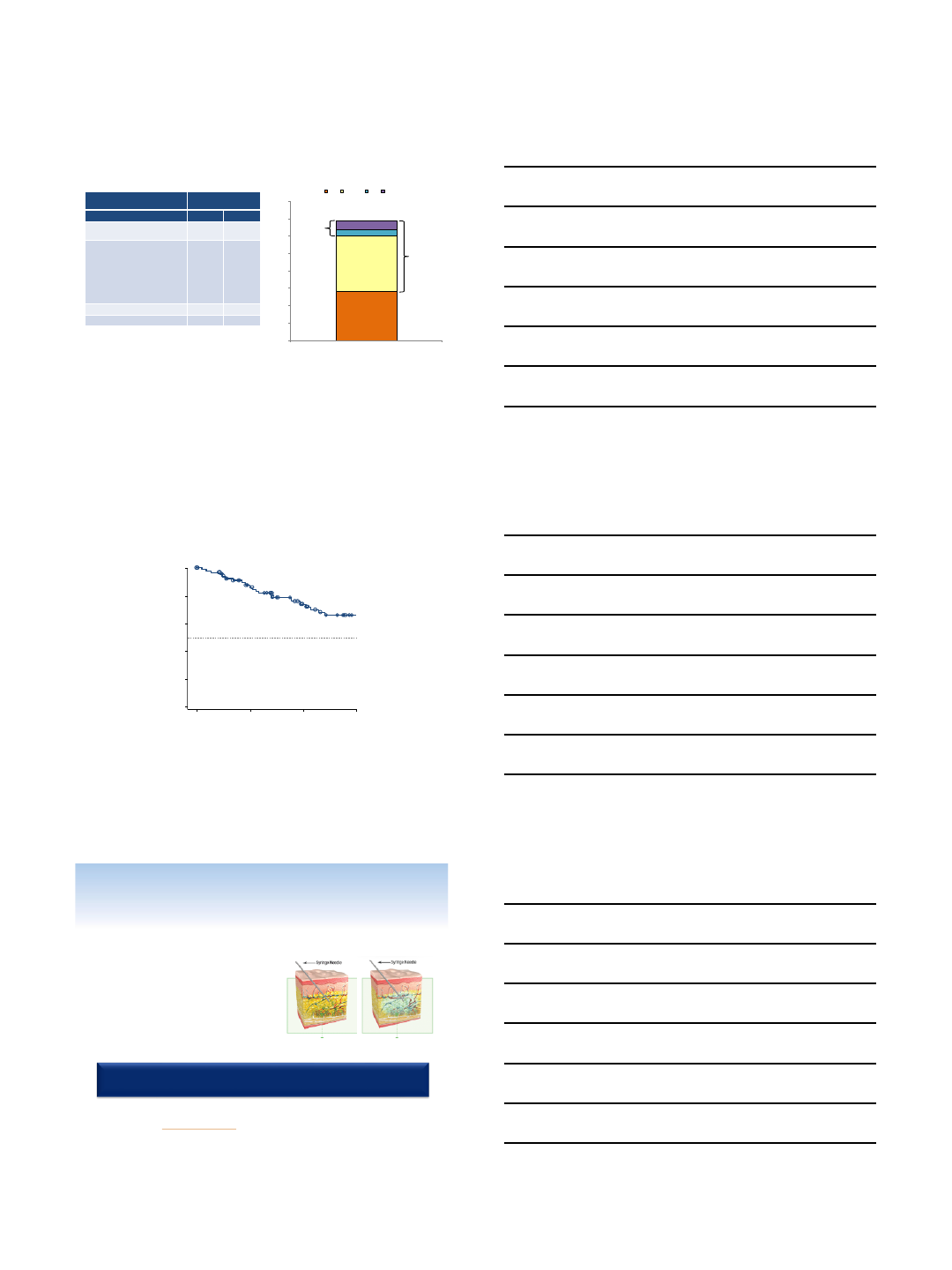
Coming Soon?;Recombinant
Human Hyaluronidase
▪ENHANZE™ platform of recombinant
human hyaluronidase (rHuPH20)
temporarily breaks down the hyaluronan
barrier, allowing rapid absorption of
injected drugs1
▪Herceptin SC®and MabThera SC®are
approved in Europe as co-formulate
products with rHuPH202,3
–Dosing time is 5 to 8 minutes with SC
versus 0.5 to 6 hours with IV4-6
18
1. Halozyme Therapeutics. Mechanism of action for Hylenex recombinant
(hyaluronidase human injection). www.hylenex.com/mechanism-of-action.
Accessed 11/8/2016.
2. European Medicines Agency. Herceptin: EPAR –product information. 2016
3. European Medicines Agency. MabThera: EPAR –product information. 2016.
4. Ismael G, et al. Lancet Oncology. 2012;13(9):869-878.
5. Shpilberg O, et al. Br J Cancer. 2013;109(6):1556-1561.
6. De Cock E, et al. Plos One. 2016;11(6):e0157957.
Schematic of rHuPH201
Aim: To determine the safety, pharmacokinetics, and efficacy of
DARA as SC administration
9/28/2017
7
Key eligibility criteria
•RRMM with measurable disease
• ≥2 prior lines of treatment
•Not received anti-CD38 therapy
PAVO: Study Design
Phase 1b, open-label, multicenter, dose-finding, proof of concept study
19
RRMM, relapsed or refractory multiple myeloma; QW, weekly; Q2W, every 2 weeks; Q4W, every 4 weeks; Ctrough, trough concentration; ORR, overall response rate; CR, complete response;
PK, pharmacokinetic.
aGroup 2 comprises 4 distinct cohorts, each treated with DARA 1,800 mg and rHuPH20 45,000 U. Ctrough on Cycle 3/Day 1 in Group 1 supported dose selection for Group 2. The study
evaluation team reviewed safety after Cycle 1 and PK after Cycle 3/Day 1 for each group.
bAdminis tered 1 hour prior to infusion.
Group 1 (n = 8)
DARA: 1,200 mg
rHuPH20: 30,000 U
Group 2a(n = 45)
DARA: 1,800 mg
rHuPH20: 45,000 U
Dosing schedule
▪Approved schedule for IV
▪1 Cycle = 28 days
Infusion time
▪1,200 mg: 20-min infusion (60 mL)
▪1,800 mg: 30-min infusion (90 mL)
Pre-b/post-infusion medication
▪Acetaminophen,
diphenhydramine, montelukast,
and methylprednisolone
Primary endpoints
•Ctrough of DARA at
Cycle 3/Day 1
•Safety
Secondary endpoints
•ORR
•CR
•Duration of response
•Time to response
IRRs
20
1,200 mg
n = 8
1,800 mg
n = 45
IRR, % (n)
13 (1) 24 (11)
Chills 13 (1) 9(4)
Pyrexia 0(0) 9(4)
Pruritus 0(0) 4(2)
Dyspnea 13 (1) 0(0)
Flushing 0(0) 2(1)
Hypertension 0(0) 2(1)
Hypotension 0(0) 2(1)
Nausea 0(0) 2(1)
Non-cardiac chest
pain
13 (1) 0(0)
Oropharyngeal pain 0(0) 2(1)
Paresthesia 0(0) 2(1)
Rash 0(0) 2(1)
Sinus headache 0(0) 2(1)
Tongue edema 0(0) 2(1)
Vomiting 0(0) 2(1)
Wheezing 0(0) 2(1)
▪All IRRs in the 1,800-mg
group were grade 1 or 2
▪One grade 3 IRR of dyspnea
in the 1,200-mg group
▪No grade 4 IRRs were
observed
▪All IRRs occurred during or
within 4 hours of the first
infusion
▪No IRRs occurred during
subsequent infusions in
either group
▪Abdominal wall SC injections
were well tolerated
Low IRR incidence and severity with DARA SC
Immune Checkpoint Inhibitors in MM
9/28/2017
8
Immune Checkpoint Inhibitors for
Relapsed/Refractory Multiple Myeloma
Pneumonitis
Type Trial Patient Types Study
Phase Site(s)
CAR T
CART-19 for multiple myeloma
Relapsed/ refractory
1University of
Pennsylvania
Safety study of CAR-
modified T cells
targeting NKG2D-ligands
Relapsed/ refractory
1Dana-Farber
Cancer Institute
Study of T cells targeting B-cell
maturation antigen (BCMA) for
previously treated multiple myeloma
Relapsed/ refractory
1
National Cancer
Institute
University of
Pennsylvania
MILs
Tadalafil and lenalidomide
maintenance with or without activated
marrow infiltrating lymphocytes (MILs)
in high-risk myeloma
Newly diagnosed;
relapsed (without
prior ASCT) 2Sidney Kimmel
Comprehensive
Cancer Center
Adoptive immunotherapy with
activated marrow-infiltrating
lymphocytes and cyclophosphamide
graft-versus-
host disease prophylaxis
in patients with relapse of hematologic
malignancies after allogeneic
hematopoietic cell transplantation
Relapsed/ refractory
1Sidney Kimmel
Comprehensive
Cancer Center
Affinity-
enhanced
T cells
Engineered autologous T cells
expressing an affinity-
enhanced TCR
specific for NY-ESO-1 and LAGE-1
Relapsed/
refractory 1/2 City of Hope
University of
Maryland
DLI CD3/CD28 activated Id-KLH primed
autologous lymphocytes Post-transplant 2 University of
Pennsylvania
9/28/2017
9
Myeloma CAR Therapy
•Which Target:
–CD19, CD138, CD38, CD56, kappa, Lewis Y, CD44v6, CS1 (SLAMF7),
BCMA
•Many questions remain about CAR design:
–Optimal costimulatory domains
–Optimal vector
–Optimal dose and schedule
–Need for chemotherapy
–Perhaps “cocktails” of multiple CARs or CARs + chemotherapy will be
required for best outcomes
Which Target: BCMA
Multiple myeloma cells
expressing BCMA
(brown color = BCMA protein)
B cell maturation antigen (BCMA)
▪A member of the TNF receptor
superfamily
▪Expression is largely restricted to
plasma cells and mature B cells
▪Not detectable in any other normal
tissues
▪Expressed nearly universally on multiple
myeloma cells
▪Anti-MM efficacy validated in initial
studies11. Ali et al., Blood 2016 128: 1688. Cohen et al.,
ASH 2016, abstract 1147
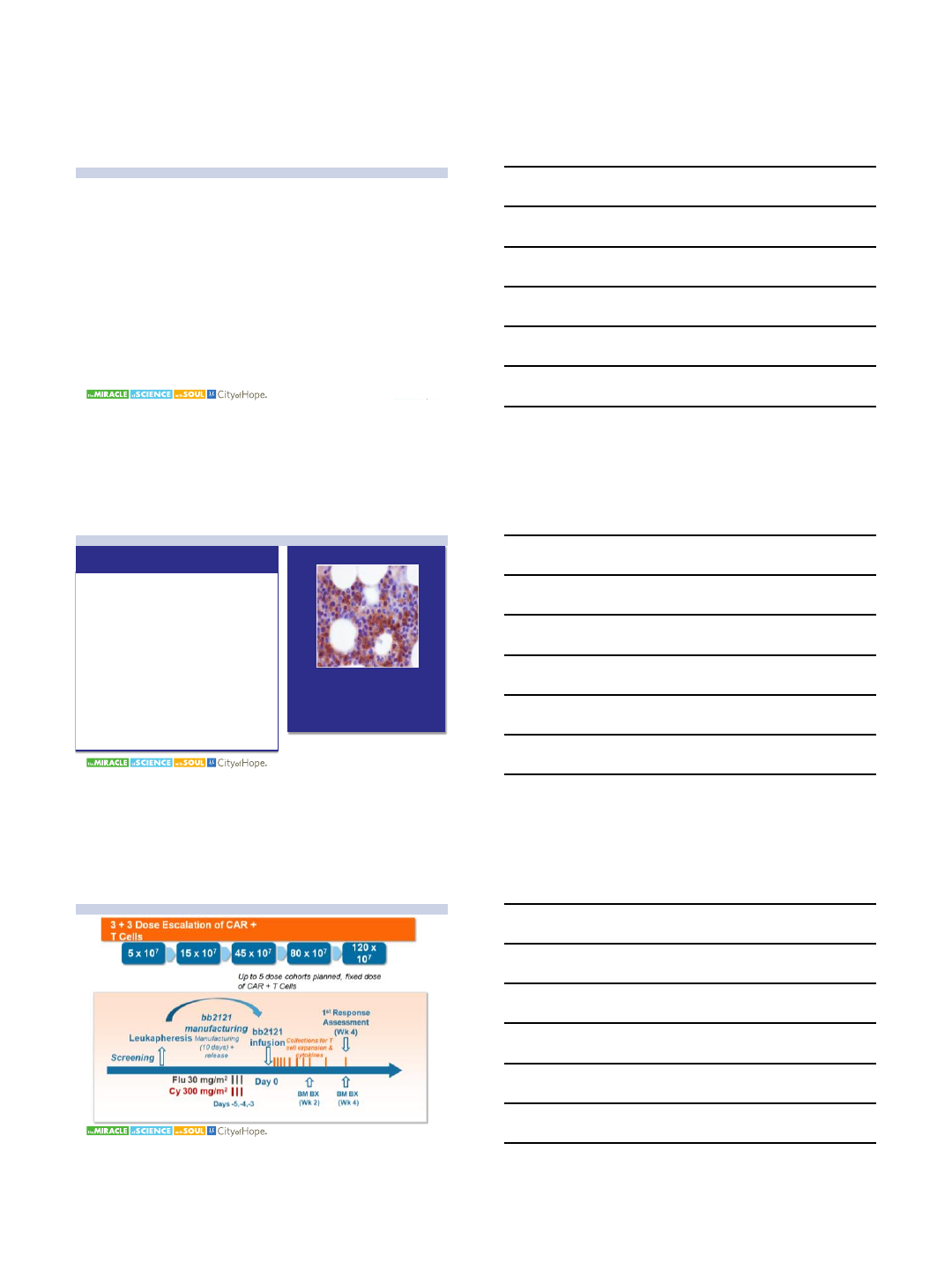
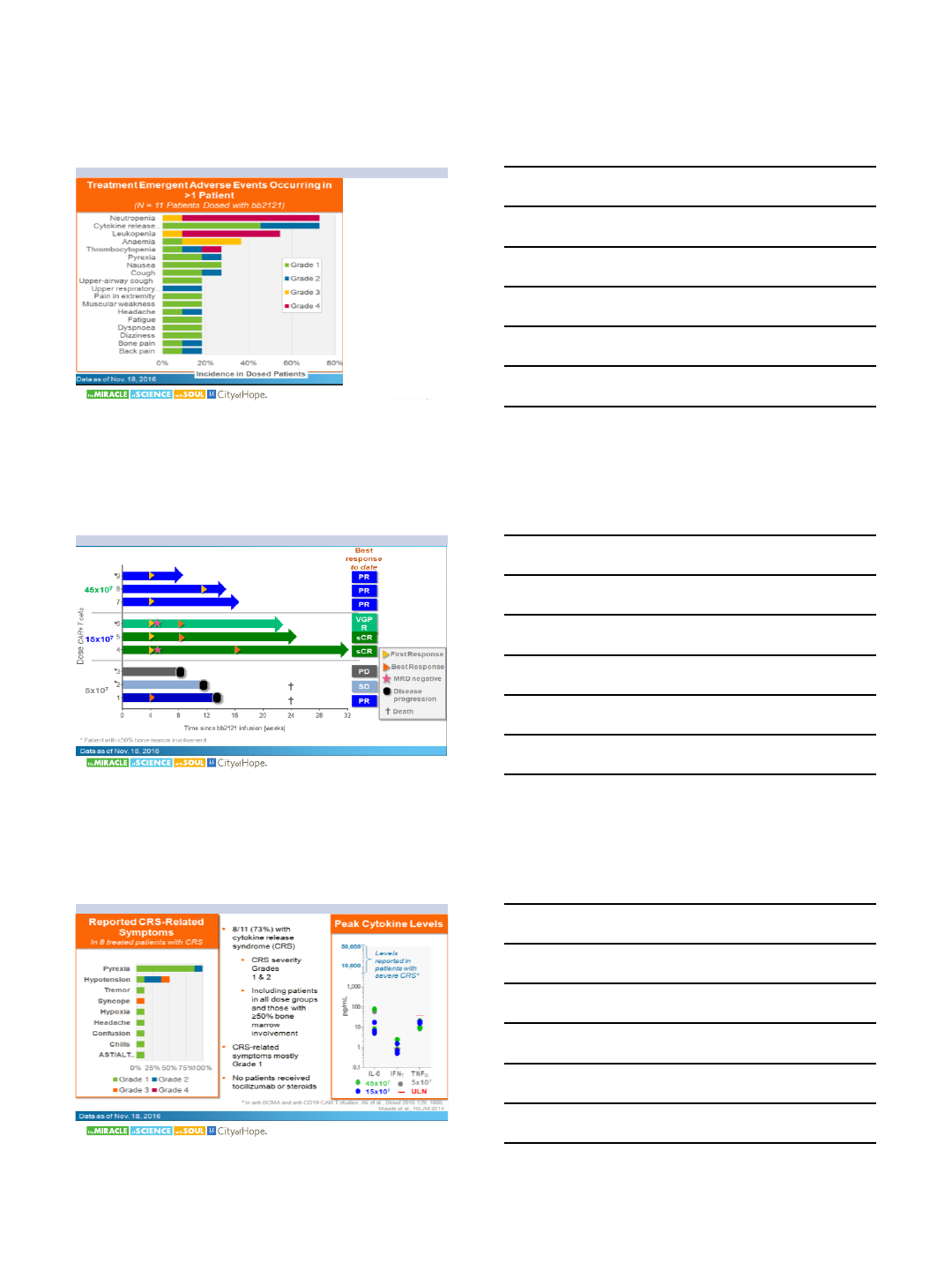
CRB-401 Study Design
9/28/2017
10
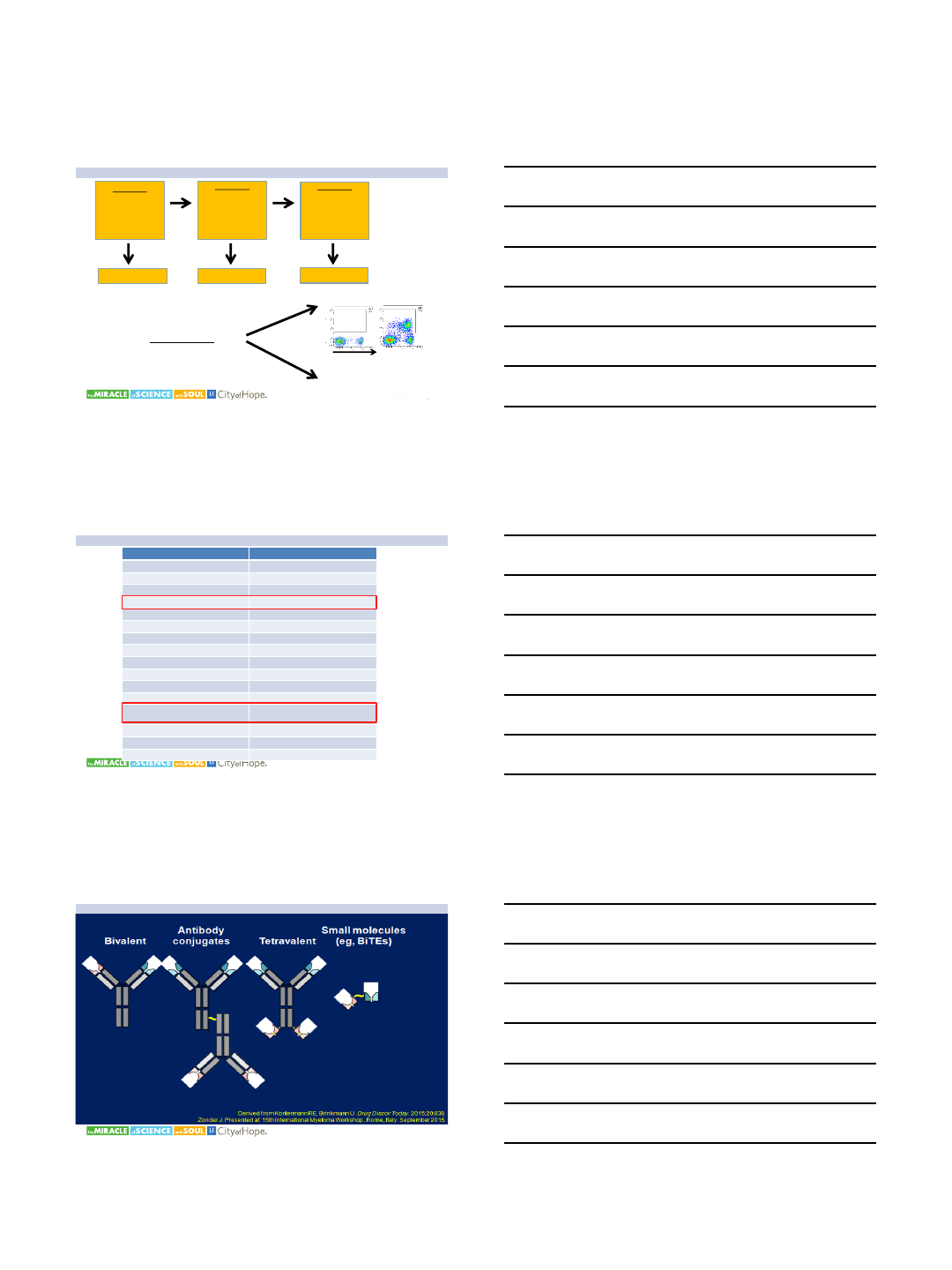
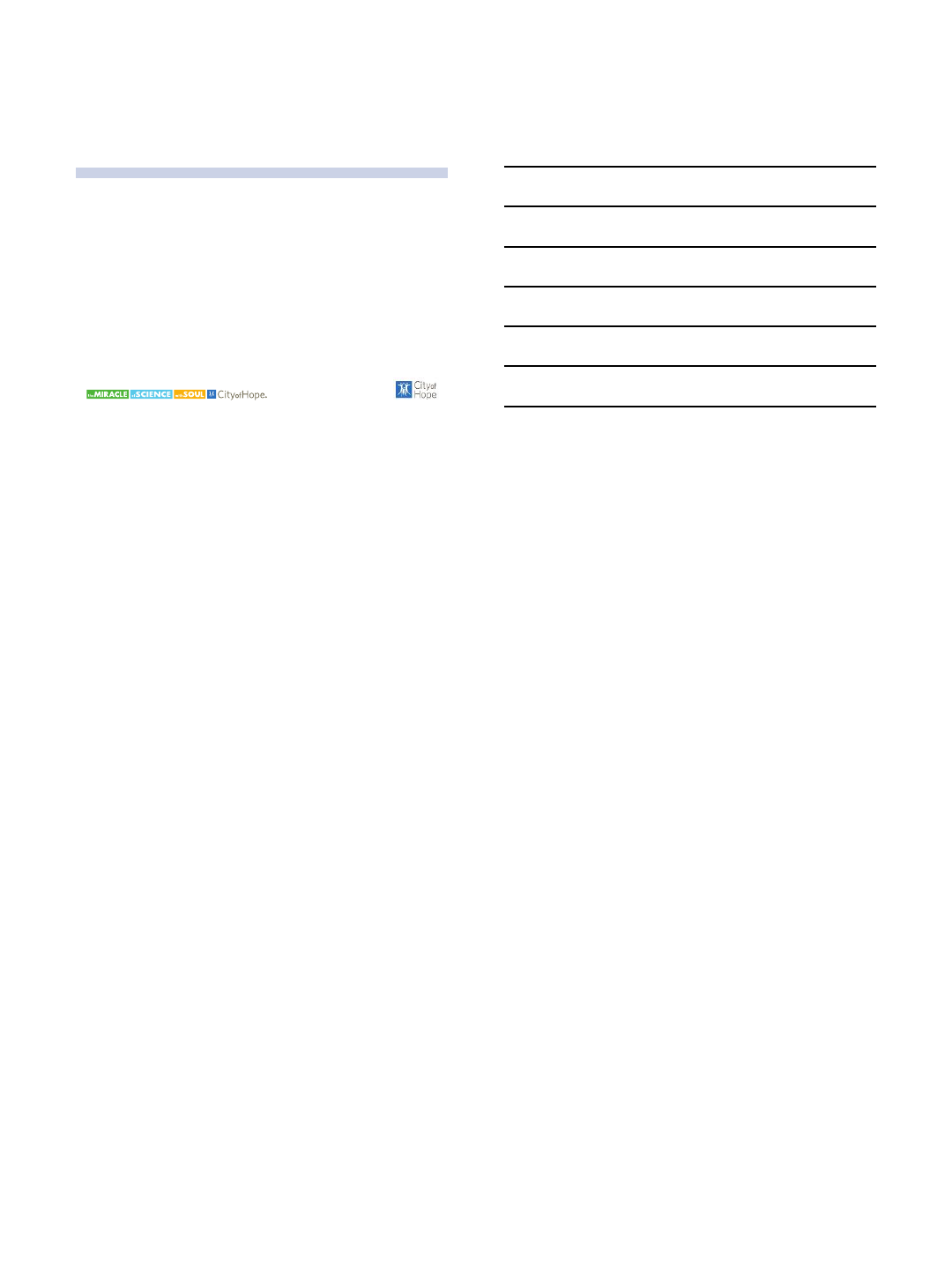
▪No DLTs to date
▪Cytopenias related
to fludarabine/
cyclophosphamide
lymphodepletion,
as expected
▪No ≥ Grade 3
cytokine release
syndrome or
neurotoxicity
Adverse Events Generally Mild, No ≥ Grade 3
CRS* or Neurotoxicity
*CRS uniformly graded according
to Lee et al., Blood 2014;124:188-
195
Best Response and Time Since bb2121 Infusion
Cytokine Release Syndrome Summary
9/28/2017
11
UPENN; BCMA CAR TRIAL
•Primary objective
–Safety
•Secondary
–Feasibility
–Efficacy (response rates, PFS, OS, MRD)
•Exploratory:
–CART-BCMA expansion, persistence, phenotype
–Impact on normal B cell and PC compartments
–BCMA expression pre- and post-treatment
–Cytokine/chemokine levels
–Soluble BCMA, BAFF, APRIL levels
–Assess for anti-CAR immune responses
–Impact on tumor microenvironment
Cohort 1
1 - 5 x 108
CAR+ T cells
(n=3-6)
Cohort 2
Cytox 1.5 g/m2
+
1 - 5 x 107
CAR+ T cells
(n=3-6)
Cohort 3
Cytox 1.5 g/m2
+
1 - 5 x 108
CAR+ T cells
(n=3-6)
Up to n=9 Up to n=9 Up to n=9
4 week
delay
between
subjects
CD8
BCMA-CAR
Pre Day 7
2) qPCR
1) Flow
Patient characteristics –Cohort 1 (n=9)
Characteristic Median (range) or %
Age 57 (44 –70)
Gender 67% male; 33% female
Isotype IgG (33%), IgA (44%), LC (22%)
Prior lines of therapy 9 (4-11)
Lenalidomide
100% (refractory: 78%)
Bortezomib
100% (refr: 89%)
Pomalidomide
100% (refr: 89%)
Carfilzomib
100% (refr: 89%)
Autologous SCT
78%
Cyclophosphamide
100% (refr: 67%)
Daratumumab
44% (refr: 44%)
Anti-
PD1
33% (refr: 33%)
High-risk genetics
-17p or TP53
mutation
100%
67%
Extramedullary dz 33%
% BM plasma cells 80 (15 –95)
Day 0 absolute CD3 258/µL (117 –1354)
Bi-Specific Antibody (bsAb) Constructs
9/28/2017
12
Conclusions
•Immunotherapy is an active strategy for myeloma
therapy
•Optimal targets for immunotherapy remain under
study
