HSS Grand Rounds Complex Cases January 2018 | Volume 7, Issue 1 215f7b6c 8f80 4c91 9c48 13724c8cd0f1
2018-06-11
: Pdf 215F7B6C-8F80-4C91-9C48-13724C8Cd0F1 215f7b6c-8f80-4c91-9c48-13724c8cd0f1 6 2018 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 18

Grand Rounds from HSS
MANAGEMENT OF COMPLEX CASES
The Complex Joint Reconstruction Center (CJRC) was established
at Hospital for Special Surgery in January 2017 to treat the most
challenging cases in joint reconstruction. Since then, over 500
patients have been treated, with multidisciplinary input from expert revision joint-
replacement surgeons and specialists from imaging, biomechanics, infectious disease,
pathology, and basic science. Currently, 13 member surgeons have a dedicated clinical
and research interest in this complex area of arthroplasty, and a registry has been
created to closely monitor patient outcomes. Data from the registry are helping us
determine mechanisms of failure and possible preventive strategies based on basic
science and biomechanical research. Prospective outcome analysis will also aid us in
improving algorithmic approaches to complex joint disorders.
The cases presented in this issue demonstrate 3 of the most challenging problems
of acetabular bone loss, with solutions that ensure hip stability and proper implant
selection. The authors—Christopher Jones, MD, PhD, and Peter K. Sculco, MD, in
Case 1; Jason L. Blevins, MD, and Alexander S. McLawhorn, MD, MBA, in Case 2; and
Colin Y. L. Woon, MD, Peter H. Sun, MS, and Michael B. Cross, MD, in Case 3—have
clearly dened the need for thorough evaluation of anatomical deciencies through
the use of advanced imaging and 3-dimensional modeling, which provide the key to
preparation for surgery. Biomechanical consultation is also crucial in aiding anatomic
restoration through the use of augmentation, bone grafting, and customized implants.
These authors are experts in the treatment of such complex cases, including the
potentially catastrophic complications that can arise during their management.
Together, these 3 cases reinforce the need for a focused center such as the Complex
Joint Reconstruction Center.
We invite you to view our archives at hss.edu/complexcases and to send us your
feedback at complexcases@hss.edu.
From the Director
Complex Joint Reconstruction Center
Thomas P. Sculco, MD
AUTHORS
Michael B. Cross, MD
Assistant Attending Orthopaedic Surgeon
Hospital for Special Surgery
Assistant Professor of Orthopaedic Surgery
Weill Cornell Medicine
Alexander S. McLawhorn, MD, MBA
Assistant Attending Orthopaedic Surgeon
Hospital for Special Surgery
Assistant Professor of Orthopaedic Surgery
Weill Cornell Medicine
Peter K. Sculco, MD
Assistant Attending Orthopaedic Surgeon
Hospital for Special Surgery
Assistant Professor of Orthopaedic Surgery
Weill Cornell Medicine
COAUTHORS
Jason L. Blevins, MD
Orthopaedic Surgery Resident
Hospital for Special Surgery
Christopher W. Jones, MD, PhD
Orthopaedic Surgery Fellow
Complex Joint Reconstruction Center
Hospital for Special Surgery
Peter H. Sun, MS
Design Engineer
Hospital for Special Surgery
Colin Y. L. Woon, MD
Orthopaedic Surgery Fellow
Adult Reconstruction & Joint Replacement
Hospital for Special Surgery
In This Issue
Case 1
Dealing with
Major Bone
Decits in
Revision Total
Hip Arthroplasty
Case 2
Treatment of
Acetabular
Bone Loss with
Dual-Mobility
Cup-in-Cup
Construct
Case 3
Revision Custom
Acetabular Biange
Implant for Large
Acetabular Defects
After Failed
Custom Triange
Thomas P. Sculco, MD
Director, HSS Complex Joint Reconstruction Center
Surgeon-in-Chief Emeritus
January 2018 | Volume 7 Issue 1
ORTHOPAEDIC SURGERY

January 2018 | Volume 7 Issue 1
1 | Grand Rounds
Case Report A 59-year-old woman presented
with a 3-year history of progressively worsen-
ing right buttock and groin pain radiating to
her knee and requiring opioid analgesia. Born
with bilateral developmental dysplasia of the
hip (DDH) and congenital talipes equinovarus,
the patient underwent primary right total hip
arthroplasty (THA) at age 34 in 1983 and left
THA in 1984. She required multiple revisions
of both hips. Her most recent right THA
revision in 2005 was complicated by infection
requiring a 2-stage reconstruction with antibi-
otic spacer prior to reimplantation.
Signicant medical history included hyper-
tension, anxiety and depression, peripheral
neuropathy, osteoporosis, and 30 pack-
years of smoking. The patient required
crutches from childhood due to DDH and a
right foot drop for which she had not worn
an ankle-foot orthosis. She was wheelchair
dependent due to worsening pain.
Physical examination revealed multiple well-
healed right hip incisions, groin and buttock
pain with hip motion, and a positive log-roll
test. Range of motion was from full exten-
sion to exion, 100°; internal rotation, 30°;
external rotation, 70°; abduction, 45°; and
adduction, 20°. Right hip abduction power
was signicantly diminished (2/5). Neuro-
vascular examination demonstrated a right
foot drop with 2/5 power in the common
peroneal nerve distribution. Trendelenburg
and Stincheld tests were positive. The right
leg was 1 cm shorter than the left.
Baseline white blood cell count was normal,
but inammatory markers were moderately
elevated (erythrocyte sedimentation rate,
47 mm/hr; C-reactive protein, 6.7 mg/L).
Bilateral hip joint uoroscopy-guided aspira-
tions did not indicate recurrent infection.
Radiographs demonstrated a hybrid right
THA, with femoral stem cement mantle
fracture, metal debris, and periacetabular
radiolucency in all Charnley zones (Fig. 1A).
Computed tomographic (CT) reconstruc-
tion revealed complex bony defects and
a Paprosky IIIA acetabular defect and a
Paprosky IIIA-IIIB femoral defect [1] (Fig. 1B).
Further preoperative evaluation included
3-dimensional computer models of the
pelvis to visualize bone defects and virtual
removal of the existing prosthesis (Fig. 2).
The patient underwent single-stage revision
right THA. Intraoperatively, the fascia lata,
iliotibial band, and hip abductor muscula-
ture were found to be grossly decient due
to previous surgery and adverse reaction
to metallosis. After encountering severe
anterior cortical bone loss in addition to
gluteal deciency, the surgeon decided to
change from a posterior to an anterolateral
approach in order to utilize the anterior bony
defect as a modied Wagner osteotomy [2].
An extended trochanteric osteotomy was
required for prosthesis removal and cement
extraction. Reconstruction was performed
with an uncemented highly porous trabecu-
lar metal (TM) cup, superolateral TM
acetabular augment, long modular tapered
uncemented stem, and dual mobility articu-
lation (Fig. 3). Results of intraoperative
tissue histopathology were consistent with
metallosis and polyethylene debris–induced
osteolysis. Both histology and extended
cultures conrmed the absence of infection.
The patient’s wound healed well, with no
sign of infection. At 3-month follow-up, she
had progressed to full weight bearing with
crutches, taking tramadol as needed. She
had a range of motion from full extension
to exion of 100°, internal rotation of 20°,
external rotation of 40°, abduction of 30°,
and adduction of 10°. Follow-up radiographs
demonstrated a well-xed implant in excel-
lent alignment, with no change in position
from her immediate postoperative imaging.
Discussion Severe acetabular and femoral
bone loss presents a signicant challenge
to the surgeon performing revision THA.
Complications associated with these
extensive surgeries are signicantly
increased in comparison to primary THA,
with higher rates of dislocation (4% to
8%, respectively) and prosthetic joint
infection (8% to 10%, respectively) [3].
Numerous strategies exist to address bone
deciencies. Acetabular reconstruction
options include the use of cages, cup/cage
combinations, custom ange acetabular
components, and acetabular augmentation
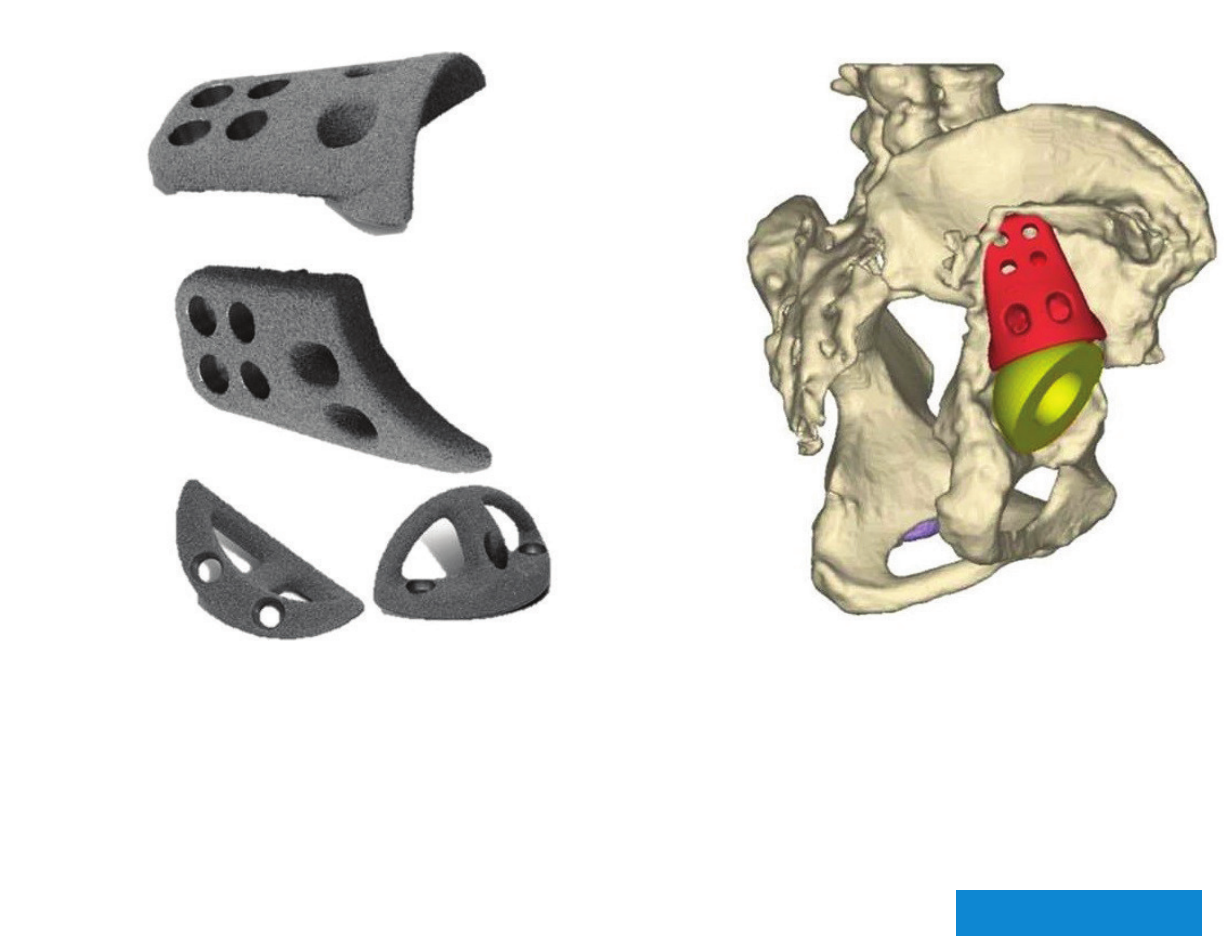
with a TM prosthesis (Fig. 4).
Continued on page 4
Case 1 Case presented by Christopher W. Jones, MD, PhD, and Peter K. Sculco, MD
Dealing with Major Bone Decits in Revision Total Hip Arthroplasty
Fig. 1: (A) Preoperative radiograph demonstrating
a hybrid right THA, with femoral stem cement
mantle fracture, metallic debris, and periacetabular
radiolucency in all Charnley zones.
(B) CT reconstruction revealing complex bony defects
and a Paprosky IIIA acetabular defect and a Paprosky
IIIA/IIIB femoral defect.
Fig. 3: (A) Postoperative radiograph showing right hip
reconstruction with an uncemented highly porous TM
cup, superolateral TM acetabular augment, and long
modular tapered uncemented stem.
(B) Intraoperative photo showing dual mobility
articulation.
Fig. 4: (A) Custom ange acetabular components.
(B) Acetabular augmentation with TM prosthesis.
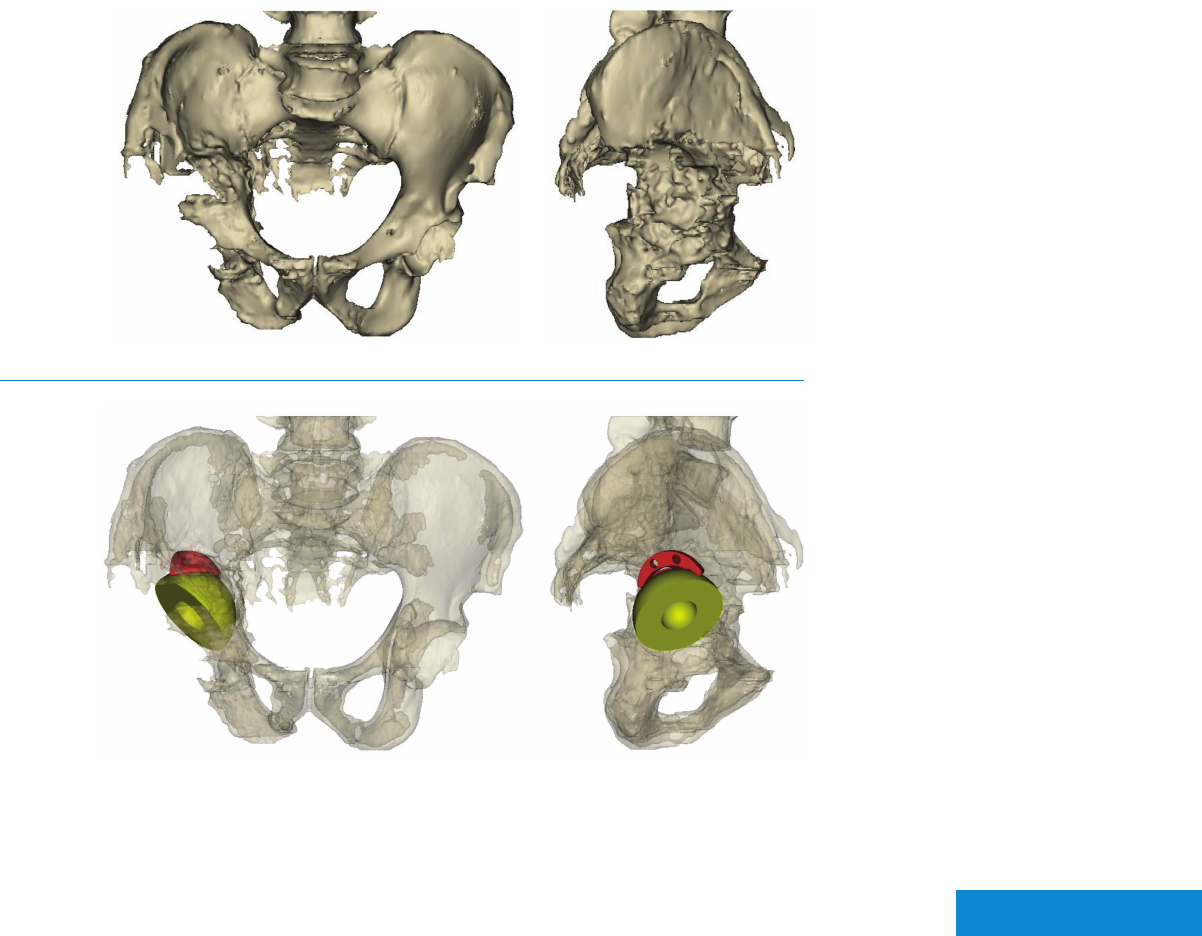
Fig. 2: Computer model of the pelvis showing
(A) bone defects and (B) virtual removal of the
existing prosthesis.
A B
A B
A B
A B
View enlarged case images

January 2018 | Volume 7 Issue 1
2 | Grand Rounds
Case Report A 57-year-old man presented
with worsening mechanical right hip pain
and limb length discrepancy after multiple
hip surgeries. He was injured in a motorcycle
accident at age 32 and underwent open
reduction and internal xation of a right
acetabular fracture. He subsequently
developed post-traumatic arthritis and
underwent conversion to a total hip
arthroplasty (THA). He underwent 4 revision
THA procedures, most recently 9 years
prior. He required crutches for ambulation.
He denied infectious symptoms. He was an
active smoker but was otherwise healthy.
On examination, the patient had a well-healed
incision over the right hip and a painful limp.
Clinical limb-length measurement revealed
3-cm shortening of the right leg, with normal
lower-extremity sensation, normal distal
power, and 4/5 right hip abductor strength.
Right hip radiographs revealed a long-stem
uncemented femoral component and a
loose acetabular component with broken
screws and extensive osteolysis (Fig. 1).
Laboratory testing was signicant for
elevated inammatory markers including
serum white blood cell (WBC) count of 13.9/
nL, erythrocyte sedimentation rate of 9 mm/
hr, and C-reactive protein level of 4.3 mg/dL.
Aspiration of the right hip yielded 100 cc of
clear uid with a synovial WBC count of 0/
nL and negative cultures. Additional imaging
included a computed tomography (CT) scan
to assess bone stock and for preoperative
planning (Fig. 2).
A revision THA was performed through a
posterior approach. Chronic nonunion of
the greater trochanter was encountered
and preserved within a digastric muscle
sleeve, consisting of the gluteus medius
proximally and the vastus lateralis distally.
Loose hardware was removed along with
metal debris deposited in the surrounding
soft tissues. Intraoperative aspiration,
frozen section, and cultures were negative
for infection. The femoral component was
stable and left in place. The acetabular
component was grossly loose and easily
removed. Acetabular and iliac bone loss was
consistent with a Paprosky IIIa acetabulum
[1]. The posterior–superior defect and
acetabulum were prepared. The trabecular
metal buttress was implanted as a posterior
column buttress corresponding with
preoperative planning. A 74-mm trabecular
metal revision shell was impacted into
appropriate position using computer-
assisted navigation and secured with
screws. Bone cement was applied to unitize
the trabecular metal components, and a
60-mm dual mobility shell was cemented
within the jumbo cup. A +10-mm femoral
head was mated with the appropriate
mobile polyethylene and reduced with good
stability throughout a range of motion.
Discharged home on postoperative day 2,
the patient recovered without complication
and was restricted to 20-lb foot-at weight
bearing with crutches for 6 weeks. He
progressed to 50% (partial) weight bearing
at 6 weeks and full weight bearing at 3
months after surgery. He reported no hip
pain, minimal limp, and resolution of his limb
length discrepancy.
Discussion Revision acetabular surgery
presents a challenge to achieving stable
xation and reducing the chance of
instability. Paprosky IIIa acetabular defects
can be treated with a trabecular metal
augment and trabecular metal shell. Jenkins
et al. recently reported a retrospective
review of 85 hips treated with this type
of construct with 97% survivorship at 10
years [2]. Cementing a liner within a well-
xed cup has been described by Beaulé
et al. with a 78% 5-year survival rate and
a 22% dislocation rate [3]. Increased
instability after revision hip surgery is a
commonly encountered complication [4].
Thus, articulations with enhanced stability,
such as dual-mobility constructs and fully
constrained liners, should be strongly
considered for use in revision THA. A fully
constrained liner was not used in this case,
as it may have a higher risk of failure in
patients of younger age and with higher
activity levels [5]. The use of a dual-mobility
cup has been shown to reduce dislocation
rates after revision THA [6]. In the current
case, the cup-in-cup construct using (1) the
trabecular metal cup and augment and (2)
a dual-mobility bearing couple maximized
the probability of biological xation and
minimized the risk of postoperative
instability, respectively. ■
Continued on page 4
Case 2 Case presented by Jason L. Blevins, MD, and Alexander S. McLawhorn, MD, MBA
Treatment of Acetabular Bone Loss with Dual-Mobility
Cup-in-Cup Construct
Fig. 3: Intraoperative photo of nal acetabular
reconstruction.
Fig. 4: Postoperative right hip radiographs: A) antero
posterior view; B) cross-table lateral view.
A B
Fig. 1: Preoperative Judet radiographs of the right hip
showing acetabular and iliac bone loss with broken
hardware and evidence of loose acetabular component.
Fig. 2: A) Anteroposterior and lateral CT
3-dimensional reconstructions of pelvis used for
preoperative planning revealing Paprosky IIIa
acetabular defect and B) Anteroposterior and lateral
reconstructions showing planned orientation of
trabecular metal buttress and shell.
A
B
View enlarged case images

January 2018 | Volume 7 Issue 1
3 | Grand Rounds
Case Report A 55-year-old woman present-
ed with worsening left groin and lateral hip
pain for 2 months that was aggravated by
weight bearing and shifting of body weight,
particularly in bed. She also noted “noises”
coming from her hip with activity. Her
medical history included juvenile rheuma-
toid arthritis requiring multiple orthopaedic
surgeries, as well as hypothyroidism and
chronic bilateral foot drop. She was not
taking disease-modifying antirheumatic
drugs (DMARDs), biologics, or steroids for
rheumatic disease.
The patient had bilateral total hip arthro-
plasty (THA) at age 13 and had subsequently
undergone multiple revision hip procedures.
Her most recent left hip surgery, 7 years
prior, was revision using a custom triange
acetabular component and a modular
tapered femoral component.
At baseline, the patient was conned to a
wheelchair, using her lower limbs for trans-
fers. She wore ankle-foot orthotics on both
lower extremities. On physical examination,
she was 4 ft., 10 in. tall and weighed 148 lbs.
(body mass index, 30.9). She had 0° to
90° of active exion in both hips; muscle
strength of 4/5 for hip exion and extension
and knee extension and exion; and ankle
and great toe dorsiexion strength of 0/5.
Serial radiographs revealed a failed left
acetabular triange component with loos-
ening of the ischial and ilial anges (Fig. 1).
Computed tomographic (CT) imaging
showed radiolucency medial to the acetab-
ular component along with displacement
of the ischial portion of the left triange,
suggestive of loosening (Fig. 2). Tests for
infection including erythrocyte sedimenta-
tion rate, C-reactive protein level, and hip
aspiration were negative.
The patient underwent revision left THA with
a custom biange acetabular component. To
reduce the risk of early prosthetic loosening,
initial xation was enhanced by cement
injected into ischial screw holes prior to
screw placement (Fig. 3). With distalizing
and medializing of the acetabular compo-
nent the hip could not be reduced, but stable
reduction was achieved by shortening the
proximal body of the modular tapered stem.
Preoperative planning using 3-dimensional
reconstructions and computer modeling—
in collaboration with the HSS Biomechanics
Department—allowed shortening of the
femoral component to be anticipated.
Intraoperatively, it was necessary to elevate
the sciatic nerve, which was encased in scar
tissue adhering to the posterior ischium.
Postoperative radiographs showed accu-
rate placement of the acetabular compo-
nent (Fig. 4). The patient was toe-touch
weight bearing for 6 weeks after surgery;
weight bearing was increased gradually
over several months. Eight months after
surgery she uses a walker, weight bearing
as tolerated, for short distances and has no
pain in her hip.
Discussion A biange or triange acetabular
component is a customizable implant option
for Paprosky IIIA-IIIB defects [1-4]. These
custom components for large acetabular
defects are rigid (unlike traditional cages)
and have the potential for biologic ongrowth;
a plasma-sprayed porous coating with
a hydroxyapatite layer promotes bone
ongrowth. The implant can address large
amounts of bone loss while providing
immediate xation using multiple screws.
When a previous custom triange acetabu-
lar implant has failed, leaving large acetabu-
lar defects, the surgeon must determine
the reasons for failure so as to increase the
chance of success of the next implant. In
this case, contributing factors included poor
existing bone stock, the small number of
screws used in the ischial and ilial anges,
the older screw design (closely spaced
shallow threads leading to reduced screw
pullout strength), and failure to medialize
the cup as much as possible to improve hip
biomechanics.
The surgical team employed several
engineering and surgical principles to
enhance xation while addressing the exist-
ing defect: (1) 7 screws were placed in the
ilium, the largest bony contact point; (2) 5
ischial screws were placed, including a long
“homerun” screw (Fig. 3), which reduces
the risk of ischial lift o (the most common
mode of failure from posterior–superior
Case 3 Case presented by Colin Y. L. Woon, MD, Peter H. Sun, MS, and Michael B. Cross, MD
Revision Custom Acetabular Biange Implant for Large Acetabular
Defects After Failed Custom Triange
Continued on page 4
Fig. 2: Comparative 3-dimensional reformatted CT
images showing a shift in ischial position from 2010
(shown in red) to 2017 (shown in gray), suggestive of
loosening.
Fig. 3: Biange construction demonstrating ilial
screws, ischial screws (including long homerun
screw), dome screw, and obturator hook.
7 Ilial Screws
Obturator Hook
5 Ischial Screws
1 Dome Screw
(Non-Locking Screw)
*Possible Intraoperative
Adjustment of Orientation
54mm Cup
Fig. 4: Postoperative images: A) immediate
postoperative image of the left hip; B) planned
position compared with actual position, showing < 4
mm discrepancy.
A B
Fig. 1: Serial radiographs showing progressive
loosening of left triange implant: A) immediate
postoperative; B) 4 years later; C) 7 years later.
A
B C
View enlarged case images

January 2018 | Volume 7 Issue 1
4 | Grand Rounds
Trabecular metal (tantalum) is a highly
porous bioinert metal ideal for complex
arthroplasty applications, providing
initial stability through an extremely
high co-ecient of friction. Rapid bony
ingrowth and nal stability is facilitated
by the implant’s high surface area. A TM
acetabular implant, augmented with a
superior and lateral buttress, enables
acetabular reconstruction providing strong
mechanical support and secure biological
ingrowth surface. TM augments used to
treat acetabular defects have demonstrated
consistent improvement in patient-reported
outcome measures and a low rate of
complications [3-5].
In this case, preoperative computer
modelling and a 3-dimensional printed
solid model gave the surgeon extensive
information on the intricate pattern of bone
loss and the ideal component position.
Thus, the surgeon could decide how to work
with very limited bone stock, particularly in
the medial and posterior acetabular regions.
This case demonstrates the principles
integral to success in revision THA,
including multidisciplinary preoperative
planning, selection of a prosthesis that
provides initial and long-term xation when
faced with extensive bone loss, and an
ability to change the surgical approach to
accommodate unexpected ndings. ■
REFERENCES:
1. Paprosky WG, Perona PG, Lawrence JM. Acetabular
defect classication and surgical reconstruction in
revision arthroplasty: a 6-year follow-up evaluation.
J Arthroplasty.1994;9(1):33–44. doi:10.1016/0883-
5403(94)90135-X.
2. Wagner H. Revision prosthesis for the hip joint in
severe bone loss. Orthopade. 1987;16(4):295–300.
3. Van Kleunen JP, Lee GC, Lementowski PW, Nelson
CL, Garino JP. Acetabular revisions using trabecular
metal cups and augments. J Arthroplasty. 2009;24(6
Suppl):64–68. doi:10.1016/j.arth.2009.02.001.
4. Siegmeth A, Duncan CP, Masri BA, Kim WY, Garbuz
DS. Modular tantalum augments for acetabular
defects in revision hip arthroplasty. Clin Orthop Relat
Res. 2009;467(1):199–205. doi:10.1007/s11999-
008-0549-0.
5. Abolghasemian M, Tangsataporn S, Sternheim A,
Backstein D, Sar O, Gross AE. Combined trabecular
metal acetabular shell and augment for acetabular
revision with substantial bone loss: a mid-term
review. Bone Joint J. 2013;95-B(2):166–172.
doi:10.1302/0301-620X.95B2.30608.
Case 1 Continued Case 2 Continued Case 3 Continued
REFERENCES:
1. Paprosky WG, Perona PG, Lawrence JM. Acetabular
defect classication and surgical reconstruction in
revision arthroplasty. J Arthroplasty. 1994;9(1):33–
44. doi:10.1016/0883-5403(94)90135-X.
2. Jenkins DR, Odland AN, Sierra RJ, Hanssen AD,
Lewallen DG. Minimum ve-year outcomes with
porous tantalum acetabular cup and augment
construct in complex revision total hip arthroplasty.
J Bone Joint Surg Am. 2017;99(10):e49. doi:10.2106/
JBJS.16.00125.
3. Beaulé PE, Ebramzadeh E, Le Du M, Prasad
R, Amstutz HC. Cementing a liner into a stable
cementless acetabular shell: the double-socket
technique. J Bone Joint Surg Am. 2004;86-
A(5):929–34.
4. Wetters NG, Murray TG, Moric M, Sporer SM,
Paprosky WG, Valle Della CJ. Risk factors for
dislocation after revision total hip arthroplasty. Clin
Orthop Relat Res. 2013;471(2):410–6. doi:10.1007/
s11999-012-2561-7.
5. Noble PC, Durrani SK, Usrey MM, Mathis KB,
Bardakos NV. Constrained cups appear incapable of
meeting the demands of revision THA. Clin Orthop
Relat Res. 2012;470(7):1907–16. doi:10.1007/s11999-
011-2212-4.
6. Philippot R, Adam P, Reckhaus M, Delangle F, Verdot
FX, Curvale G, et al. Prevention of dislocation in total
hip revision surgery using a dual mobility design.
Orthop Traumatol Surg Res. 2009;95(6):407–13.
doi:10.1016/j.otsr.2009.04.016.
directed forces of an adducted hip); (3)
a long dome screw was placed along the
sciatic buttress (Fig. 3); (4) a biange design
with only 2 points of bone contact is easier
to seat than a traditional triange implant;
an obturator hook that adds an extra point
of xation against ischial lifto to a biange
construct can also be used, considered in
this case but not required; (5) safe implant
placement requires a large posterolateral
exposure and identication of the sciatic
nerve; and (6) purposely medializing the hip
center reduces shear forces, reducing the
risk of late implant failure [5].
Medializing the implant is necessary as the
constrained liner eectively lateralizes the
hip center by up to 3 mm. As seen in our case,
shortening of the modular femoral compo-
nent may be necessary for subsequent joint
reduction in multiply revised individuals with
a high hip center and large amounts of scar
tissue. This case also highlights the impor-
tance of the multidisciplinary approach that
is often necessary for these complex cases. ■
REFERENCES:
1. Sheth NP, Nelson CL, Springer BD, Fehring TK,
Paprosky WG. Acetabular bone loss in revision total
hip arthroplasty: evaluation and management. J Am
Acad Orthop Surg. 2013;21(3):128-139. doi:10.5435/
JAAOS-21-03-128.
2. Abdel MP, Trousdale RT, Berry DJ. Pelvic discontinuity
associated with total hip arthroplasty: evaluation and
management. J Am Acad Orthop Surg. 2017;25(5): 330-
338. doi:10.5435/JAAOS-D-15-00260.
3. Berasi CCt, Berend KR, Adams JB, Ruh EL, Lombardi
AV, Jr. Are custom triange acetabular components
eective for reconstruction of catastrophic bone
loss? Clin Orthop Relat Res. 2015; 473(2):528-535.
doi:10.1007/s11999-014-3969-z.
4. Buckup J, Salinas EA, Valle AG, Boettner F. Treatment of
large acetabular defects: a surgical technique utilizing
impaction grafting into a metallic mesh. HSS J. 2013;
9(3):242-246. doi:10.1007/s11420-013-9350-z.
5. Barlow BT, Oi KK, Lee YY, Carli AV, Choi DS, Bostrom
MP. Outcomes of custom ange acetabular compo-
nents in revision total hip arthroplasty and predictors
of failure. J Arthroplasty. 2016;31(5):1057-1064. doi:
10.1016/j.arth.2015.11.016.

Grand Rounds January 2018
Follow us on:
All rights reserved. ©2018 Hospital for Special Surgery
Grand Rounds from HSS MANAGEMENT OF COMPLEX CASES
Editorial Board
EDITOR
Edward C. Jones, MD, MA
Assistant Attending Orthopaedic Surgeon
Hospital for Special Surgery
Assistant Professor of Orthopaedic Surgery
Weill Cornell Medicine
BOARD
Todd J. Albert, MD
Surgeon-in-Chief and Medical Director
Korein-Wilson Professor of Orthopaedic Surgery
Hospital for Special Surgery
Chairman and Professor of Orthopaedic Surgery
Weill Cornell Medicine
Friedrich Boettner, MD
Associate Attending Orthopaedic Surgeon
Hospital for Special Surgery
Associate Professor of Clinical
Orthopaedic Surgery
Weill Cornell Medicine
Alexander P. Hughes, MD
Assistant Attending Orthopaedic Surgeon
Hospital for Special Surgery
Assistant Professor of Orthopaedic Surgery
Weill Cornell Medicine
Robert G. Marx, MD, MSc, FRCSC
Attending Orthopaedic Surgeon
Hospital for Special Surgery
Professor of Orthopaedic Surgery
and Public Health
Weill Cornell Medicine
Helene Pavlov, MD, FACR
Radiologist-in-Chief Emeritus
Department of Radiology and Imaging
Hospital for Special Surgery
Professor of Radiology
Professor of Radiology in Orthopaedic Surgery
Weill Cornell Medicine
Laura Robbins, DSW
Senior Vice President
Global & Academic Aairs
Hospital for Special Surgery
Associate Professor
Graduate School of Medical Sciences
Clinical Epidemiology and
Health Services Research
Weill Cornell Medicine
Joy Jacobson
Managing Editor, HSS Journal
Education & Academic Aairs
Hospital for Special Surgery
DESIGN/PRODUCTION
Marcia Ennis
Senior Creative Director
Education Marketing & Digital Communications
Randy Hawke
Associate Director
Education Marketing & Digital Communications
Joyce Thomas
Assistant Designer
Education Marketing & Digital Communications
Now Available
Featured Online CME Oerings
The eld of musculoskeletal medicine is highly dynamic
and rapidly changing. These modules are designed to help
orthopaedic professionals remain informed of current issues
aecting musculoskeletal medicine.
■ Special Considerations in Pediatric Patella Instability
■ MPFL Reconstruction: Have We Found the Holy Grail
■ Epidemiology of Lumbar Spine Disorders in Athletes
■ Is There a Role for Interventional Spine Procedures?
■ Controlled Substances Education Program
(CME/3 hour training)
New Surgical Videos
■ Scapholunate Ligament Repair*
■ Pathomechanics of the SLAC Wrist:
The Importance of the Midcarpal Joint*
■ Distal Femur Osteotomy to Correct Knock-knee Deformity*
*Non-accredited modules
Hospital for Special Surgery holds
Accreditation with Commendation, the
highest level of recognition oered by
the Accreditation Council for Continuing
Medical Education (ACCME).
For more information, visit hss.edu/eAcademy.
HSS Journal, The Musculoskeletal Journal of Hospital for Special Surgery, is devoting an
upcoming issue to articles representing multidisciplinary perspectives on opioid use and
misuse, safe prescribing, and pain management.
For more information on submitting, go to hss.edu/hss-journal-submission-information or
contact Joy Jacobson, Managing Editor, at jacobsonj@hss.edu or 6 46.797. 8 5 09.
The Opioid Crisis and Safe Pain Management in Musculoskeletal Health
A Special Issue of HSS Journal®
Guest Editor: Seth Waldman, MD, Department of Anesthesiology, Hospital for Special Surgery
Deadline: June 1, 2018
Call for
Manuscripts

January 2018 | Volume 7 Issue 1
Grand Rounds | CASE 1
Dealing with Major Bone Decits in Revision Total Hip Arthroplasty
Figure 1: (A) Preoperative radiograph demonstrating a hybrid right THA, with femoral stem cement mantle
fracture, metallic debris, and periacetabular radiolucency in all Charnley zones.
(B) CT reconstruction revealing complex bony defects and a Paprosky IIIA acetabular defect and a Paprosky
IIIA/IIIB femoral defect.
A B
Return to Case


January 2018 | Volume 7 Issue 1
Grand Rounds | CASE 1
Dealing with Major Bone Decits in Revision Total Hip Arthroplasty
Figure 3: (A) Postoperative radiograph showing right hip reconstruction with an uncemented highly porous
TM cup, superolateral TM acetabular augment, and long modular tapered uncemented stem.
(B) Intraoperative photo showing dual mobility articulation.
A B
Return to Case

January 2018 | Volume 7 Issue 1
Grand Rounds | CASE 2
Treating of Acetabular Bone Loss with Dual-Mobility Cup-in-Cup Construct
Figure 1: Preoperative Judet radiographs of the right hip showing acetabular and iliac bone loss with broken
hardware and evidence of loose acetabular component.
Return to Case
January 2018 | Volume 7 Issue 1
Grand Rounds | CASE 2
Treating of Acetabular Bone Loss with Dual-Mobility Cup-in-Cup Construct
Figure 2: A) Anteroposterior
and lateral CT 3-dimensional
reconstructions of pelvis used
for preoperative planning
revealing Paprosky IIIa
acetabular defect and
B) Anteroposterior and lateral
reconstructions showing
planned orientation of
trabecular metal buttress
and shell.
A
B
Return to Case



January 2018 | Volume 7 Issue 1
Grand Rounds | CASE 3
Revision Custom Acetabular Biange Implant for Large Acetabular
Defects After Failed Custom Triange
Figure 1: Serial radiographs showing progressive loosening of left triange implant: A) immediate
postoperative; B) 4 years later; C) 7 years later.
AB
C
Return to Case

January 2018 | Volume 7 Issue 1
Grand Rounds | CASE 3
Revision Custom Acetabular Biange Implant for Large Acetabular
Defects After Failed Custom Triange
Figure 2: Comparative 3-dimensional reformatted CT images showing a shift in ischial position from 2010
(shown in red) to 2017 (shown in gray), suggestive of loosening.
Return to Case

January 2018 | Volume 7 Issue 1
Grand Rounds | CASE 3
Revision Custom Acetabular Biange Implant for Large Acetabular
Defects After Failed Custom Triange
Figure 3: Biange construction demonstrating ilial screws, ischial screws (including long homerun screw),
dome screw, and obturator hook.
7 Ilial Screws
Obturator Hook
5 Ischial Screws
1 Dome Screw
(Non-Locking Screw)
*Possible Intraoperative
Adjustment of Orientation
54mm Cup
Return to Case

January 2018 | Volume 7 Issue 1
Grand Rounds | CASE 3
Revision Custom Acetabular Biange Implant for Large Acetabular
Defects After Failed Custom Triange
Figure 4: Postoperative images: A) immediate postoperative image of the left hip; B) planned position
compared with actual position, showing < 4 mm discrepancy.
A B
Return to Case
