2 9 16 Epicardial Mapping And Ablation Techniques To Control Ventricular Tachycardia Syllabus
2016-02-09
: Pdf 2 9 16 Epicardial Mapping And Ablation Techniques To Control Ventricular Tachycardia Syllabus 2_9_16_Epicardial_Mapping_and_Ablation_Techniques_to_Control_Ventricular_Tachycardia_Syllabus 2 2016 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 29
2/8/2016
1
HOW TO DECIDE ON AN INITIAL APPROACH: ENDO, EPI, OR BOTH?
Noel G. Boyle MD PhD, Jason Bradfield MD,
Kalyanam Shivkumar, MD PhD
UN IVE RSI TY O F C ALI FORN IA, LO S A NGEL ES
UC LA
BERKELEY • DAVIS • IRVINE • LOS ANGELES • RIVERSIDE • SAN DIEGO • SAN FRANCISCO SANTA BARBARA • SANTA CRUZ
Cardiac Arrhythmia Center
Neurocardiology Research Center of Excellence
Interventional Cardiovascular Programs
The mission of the UCLA Cardiac Arrhythmia Center is to
generate new knowledge in the field of cardiac electrophysiology
and cardiovascular therapeutics
Cardiac Arrhythmia Center
DISCLOSURES: University of California (UCLA campus) has patents
developed by my group in the areas of catheter technology, embolism
prevention technology, minimally invasive methods for cardiac
interventions, cardiac neural diagnostics and therapeutics
2/8/2016
2
When to go epicardial
•General concepts
•ECG criteria
•Etiology & Imaging criteria
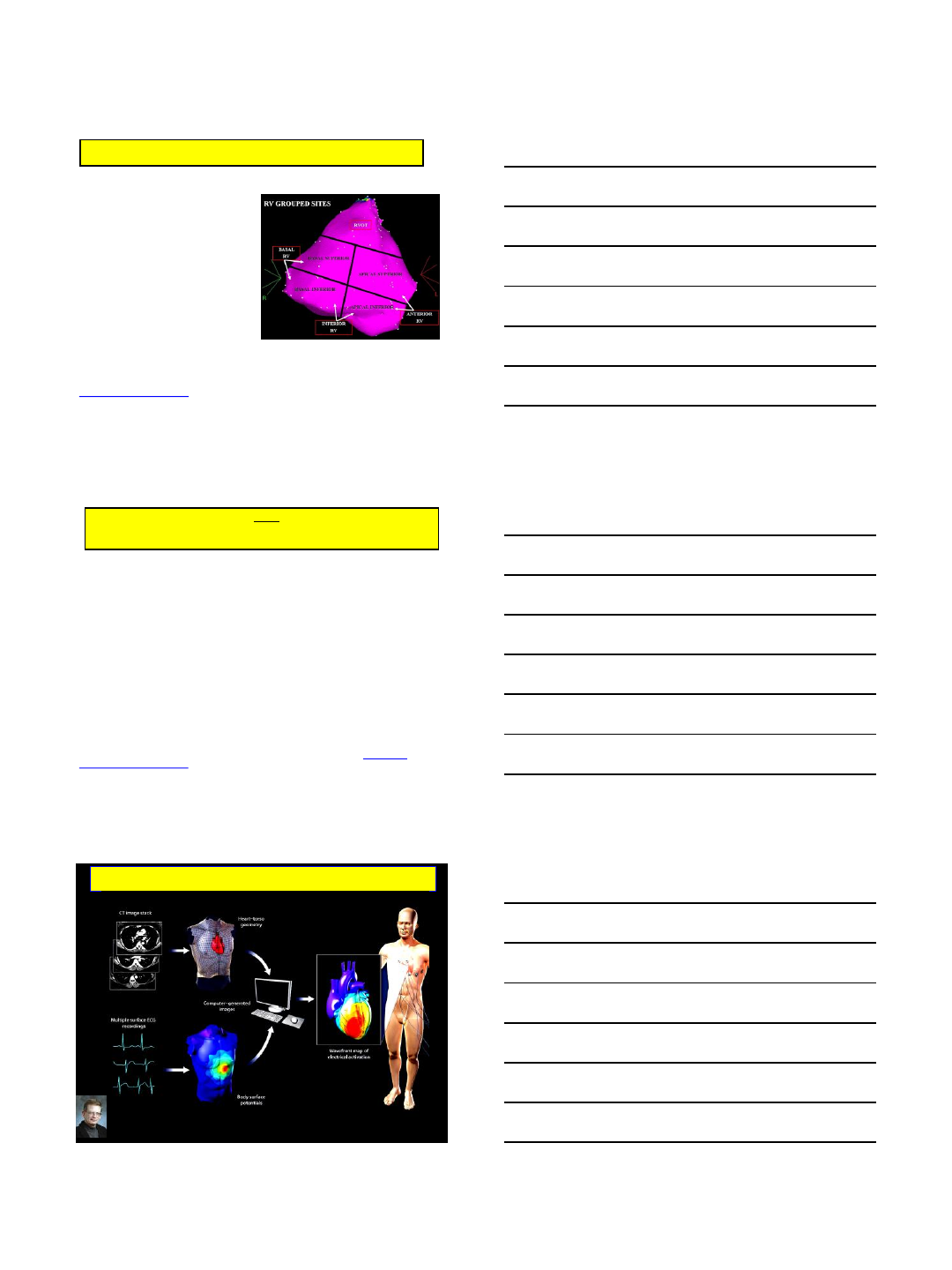
Anterior Access:
Lateral Tricuspid annulus
Anterior Right Ventricle
Inferior/Posterior/Lateral
Access areas
Lateral mitral annulus
LAA
LV ant and lat wall
Posterior left atrium (via
oblique sinus)
Diaphragmatic surfaces of
RV and LV
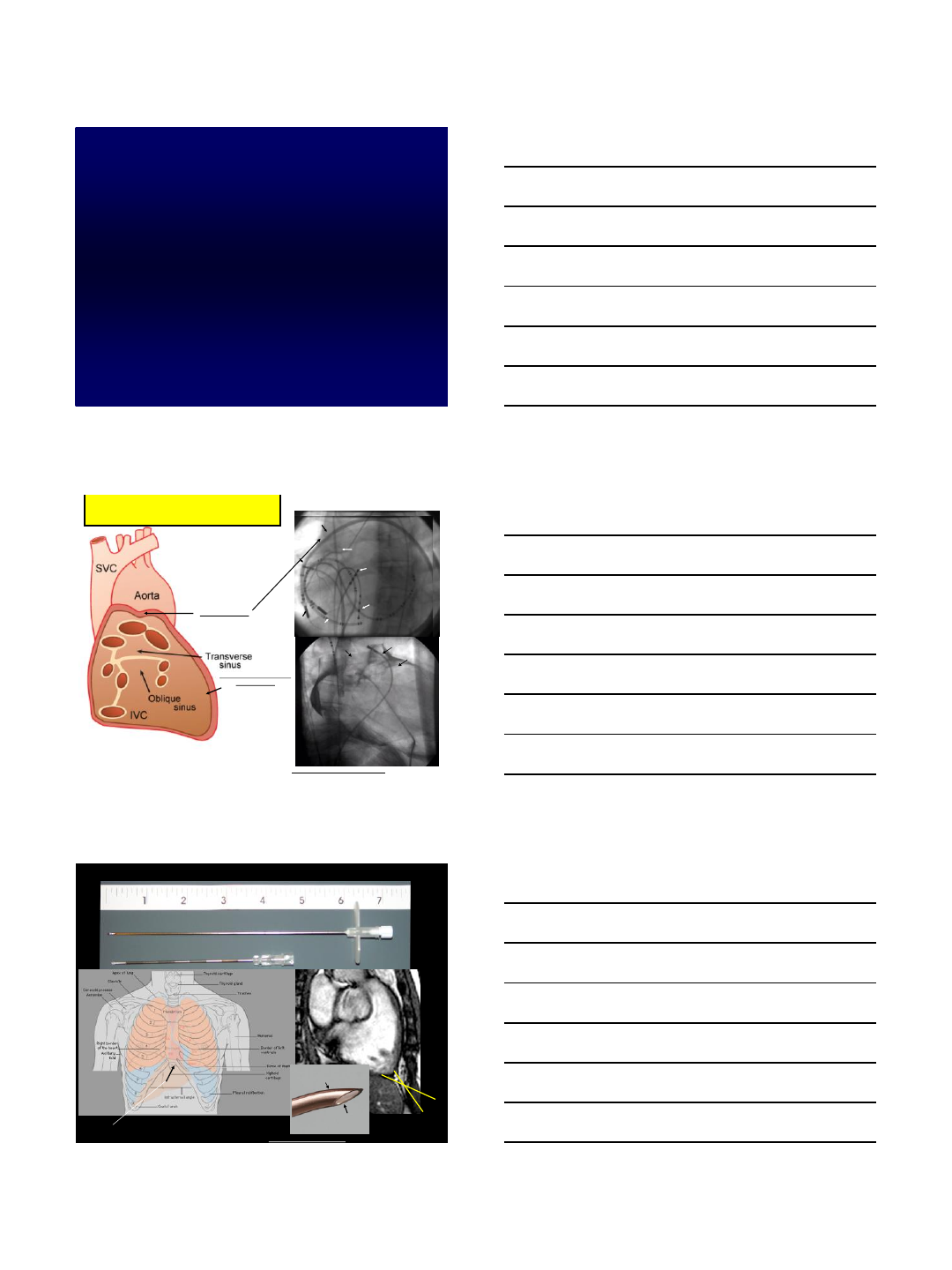
SCHEMATIC OF PERICARDIAL SINUSES AND
ACCESS TO VARIOUS EPICARDIAL REGIONS VIA
THE PERICARDIAL SPACE
PAAorta
LAA
C
PA
LIPV
LSPV
RIPV
RSPV
SVC
Aorta
A
EPI
ENDO RV
HIS
CS
HRA RCA
Halo
Sheath in Transverse
Sinus
EPI
ENDO RV
HIS
CS
HRA RCA
Halo
Sheath in front of
Great Arteries
B
Boyle NG & Shivkumar K: Epicardial Interventions in Electrophysiology Circulation 2012 ;126:1752-1769
Anterior
Inferior
Direction of Needle Entry
EPICARDIAL ACCESS NEEDLES AND LANDMARKS FOR NEEDLE ENTRY
RV
Liver
Curved end faces Heart
Open end away from Heart
toward right inferior quadrant 3-6
O'clock viewed from caudal view
Boyle NG & Shivkumar K: Epicardial Interventions in Electrophysiology 2012 Circulation 2012 ;126:1752-1769
2/8/2016
3
Dangers of Pericardial Access
•RV perforation
•Pericardial bleeding
•Liver Injury
•Abdominal Bleeding
•Entry into left pleural space
epicardial/intramural
hematoma RV perforation Liver entry
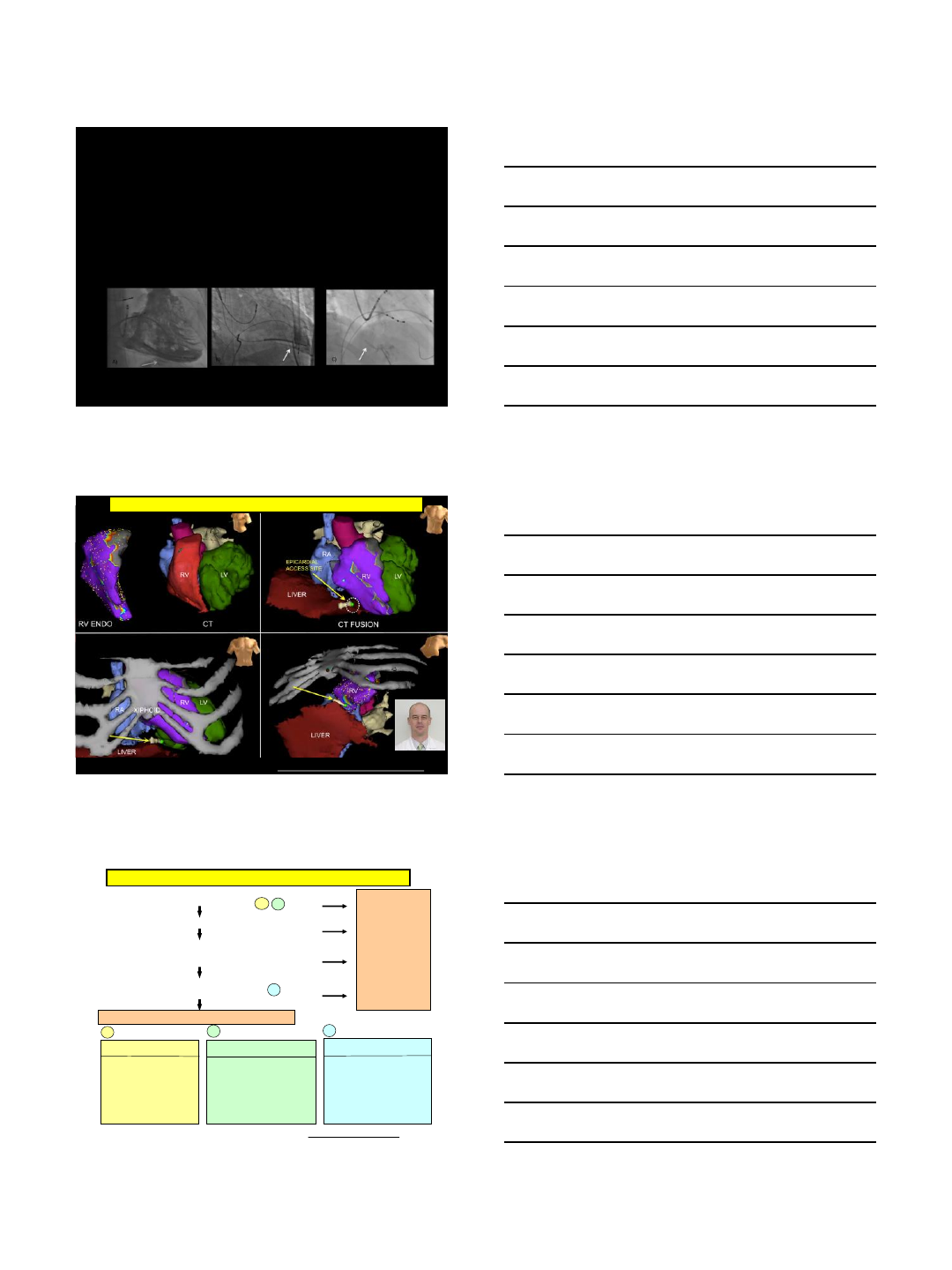
ELECTROANATOMIC MAPPING AIDED EPICARDIAL ACCESS
Bradfield J, Tung R, Vaseghi M, Moriarty JM, Boyle NG, Buch E, Mandapati R, Shivkumar K. Our Approach To Minimize Risk Of Epicardial Access:
Standard Techniques With The Addition Of Electroanatomic Mapping Guidance. Journal of Cardiovascular Electrophysiology 2013 (in press)
1. ECG suggest Epicardial VT exit site
2. Prior unsuccessful Endocardial Ablation
3. Define SCAR location with CE imaging:
4. Consider likelihood of Epicardial circuit
for Underlying Substrate:
Sub epicardial or mid-myocardial scar
Perform Endocardial Mapping and Ablation first
ECG Criteria (Berruezo et al Circ 2004)
1) Pseudo-delta >34 ms
2) IDT (V2) >85 ms
3) Shortest RS complex
>121 ms
4) ORS duration >211 ms
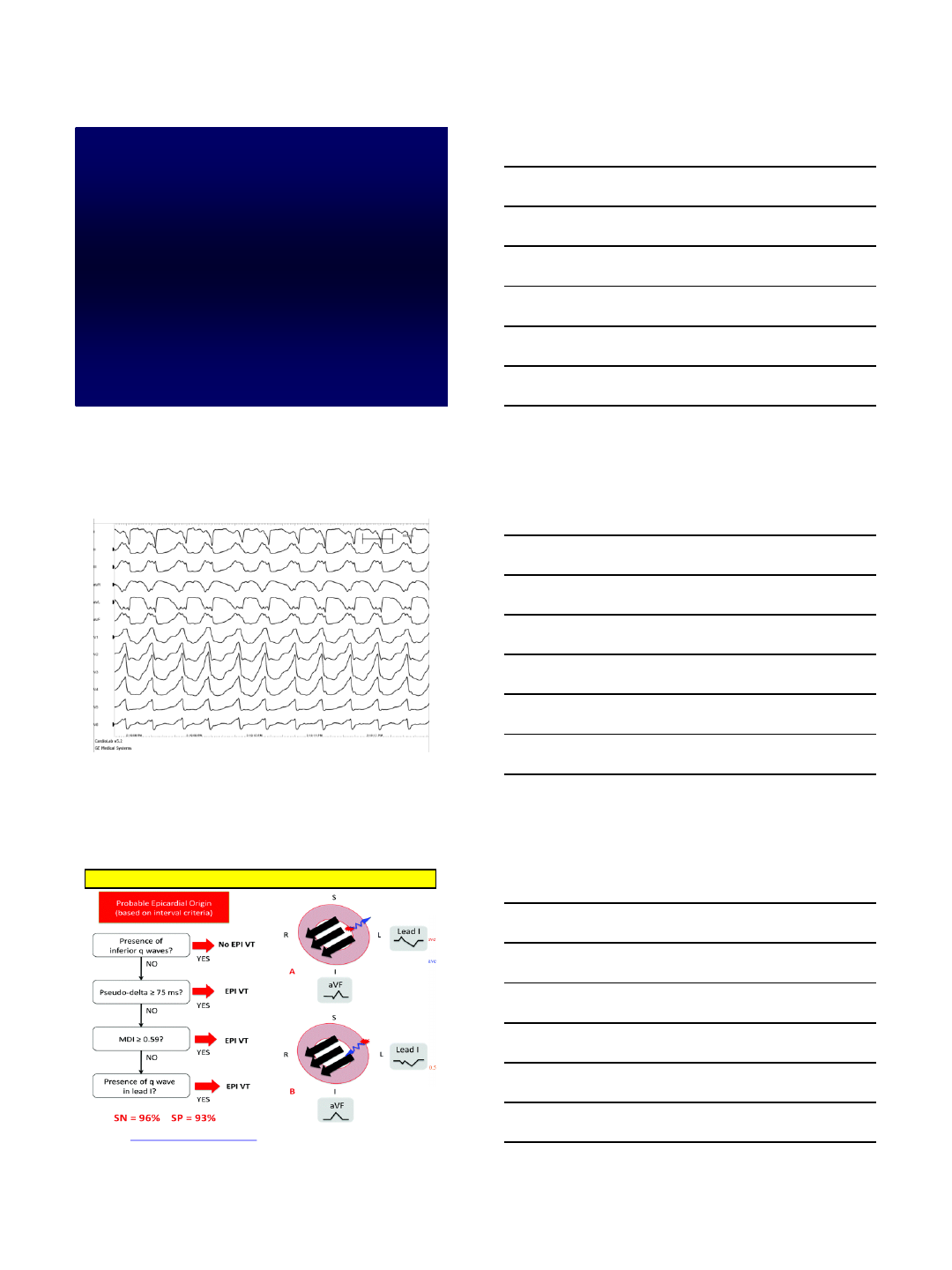
1) Absence of inferior Q wave
2) Pseudodelta ≥75 ms
3) MDI >0.59
4) Presence of Q wave in lead I
Probability of Epicardial
Focus (Sacher F et al JACC 2010)
Normal
ICM
NICM
ARVC
Other CM
ECG Criteria for NICM (Valles E Circ AE 2010)
6%
16%
35%
41%
18%
Consider
obtaining
Epicardial
Access for
Mapping
(and
Ablation)
NO
NO
NO
LOW
YES
YES
YES
HIGH
AB
C
ABC
Approach to Assessing Need for Epicardial Access/Ablation
Boyle NG & Shivkumar K: Epicardial Interventions in Electrophysiology, Circulation 2012;126:1752-1769
2/8/2016
4
When to go epicardial
•General concepts
•ECG criteria
•Etiology & Imaging criteria
1) Absence of inferior Q wave
2) pseudo-delta ≥75 ms
3) MDI >0.59
4) Presence of Q wave in
lead I
ECG CRITERIA FOR NON ISCHEMIC CARDIOMYOPATHY
Valles E, Bazan V, Marchlinski FE. Ecg criteria to identify epicardial ventricular tachycardia in nonischemic
cardiomyopathy. Circ Arrhythm Electrophysiol. 2010;3:63-71
2/8/2016
5
1) pseudo-delta >34 ms
2) intrinsicoid deflection
time (v2) >85 ms
3) shortest RS complex >121
ms
4) QRS duration >211 ms
Bazan V, Bala R, Garcia FC, Sussman JS, Gerstenfeld EP, Dixit S, Callans DJ, Zado E, Marchlinski FE.
Twelve-lead ECG features to identify ventricular tachycardia arisingfrom the epicardial right ventricle.
Heart Rhythm. 2006;3:1132-1139
TWELVE-LEAD ECG FEATURES TO IDENTIFY VENTRICULAR
TACHYCARDIA ARISING FROM THE EPICARDIAL RIGHT VENTRICLE
•Pseudodelta wave (PdW)
•Intrinsicoid deflection time (IDT)
•Shortest RS complex (SRS)
•QRS duration (QRSd)
•Maximum deflection index (MDI)
•Q or q wave in lead I (QWL1)
•Absence of q waves in inferior leads aVR/aVL ratio
QRS CHARACTERISTICS FAIL TO RELIABLY IDENTIFY
VENTRICULAR TACHYCARDIAS THAT REQUIRE EPICARDIAL
ABLATION IN ISCHEMIC HEART DISEASE
Martinek M, Stevenson WG, Inada K, Tokuda M, Tedrow UB. QRS characteristics fail to reliably identify
ventricular tachycardias that require epicardial ablation in ischemic heart disease. J Cardiovasc
Electrophysiol. 2012;23:188-193
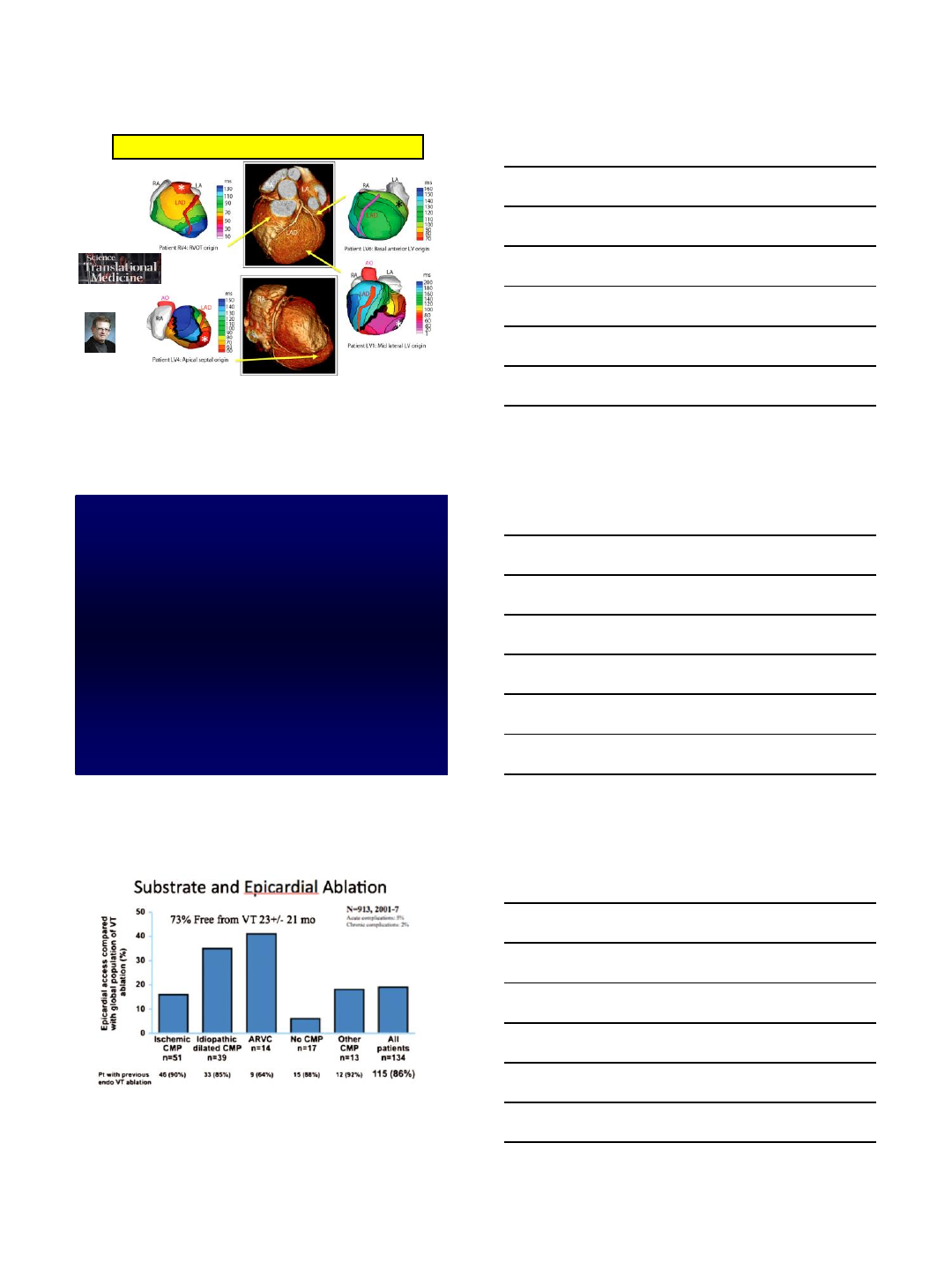
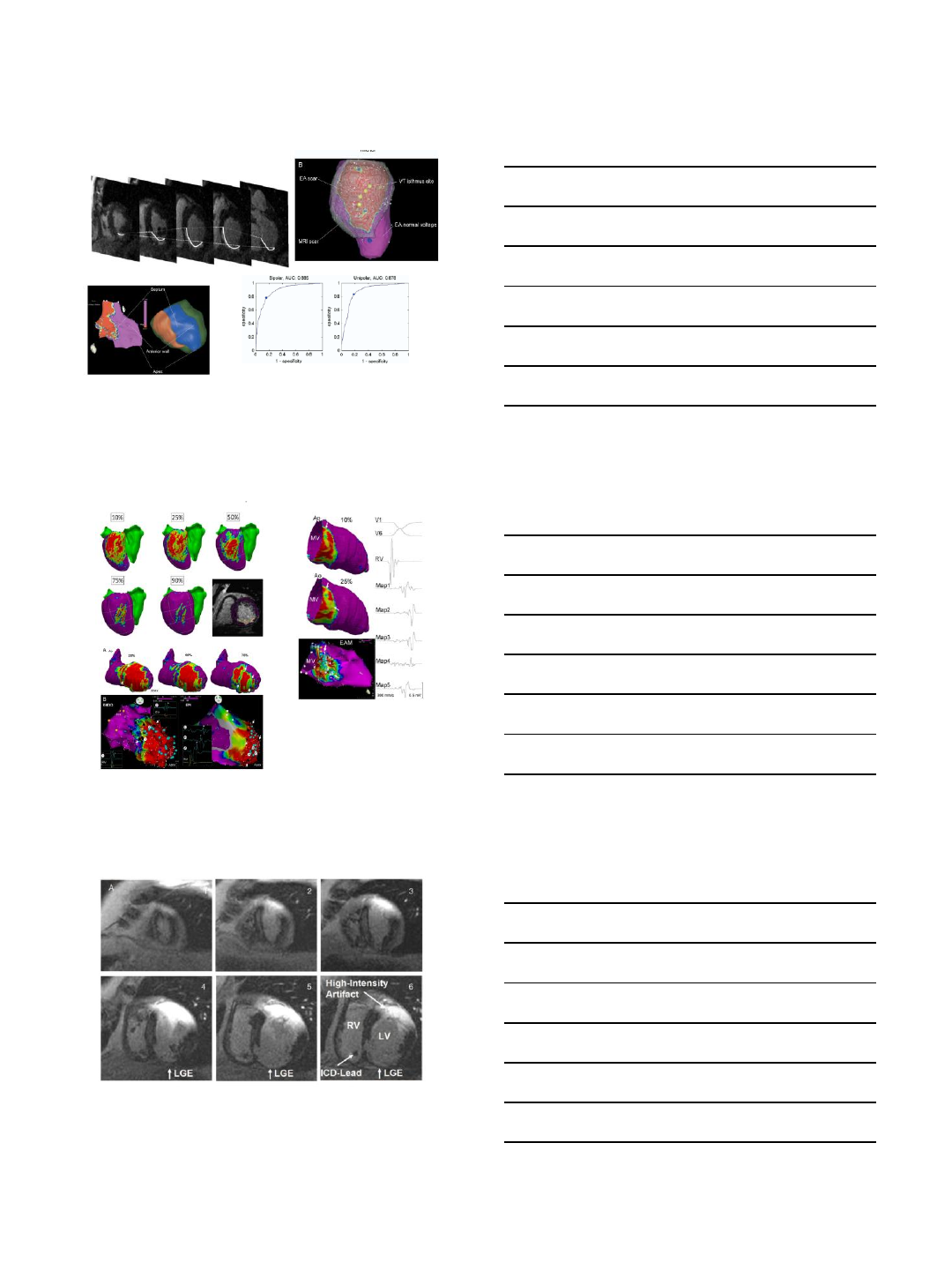
ECGI: Surface ECG combined with CT imaging to produce 3D
maps of electrical activity on the surface of the human heart.
Shivkumar K , Narayan SM Science Transl Med 2011;3:98fs2-98fs2
2/8/2016
6
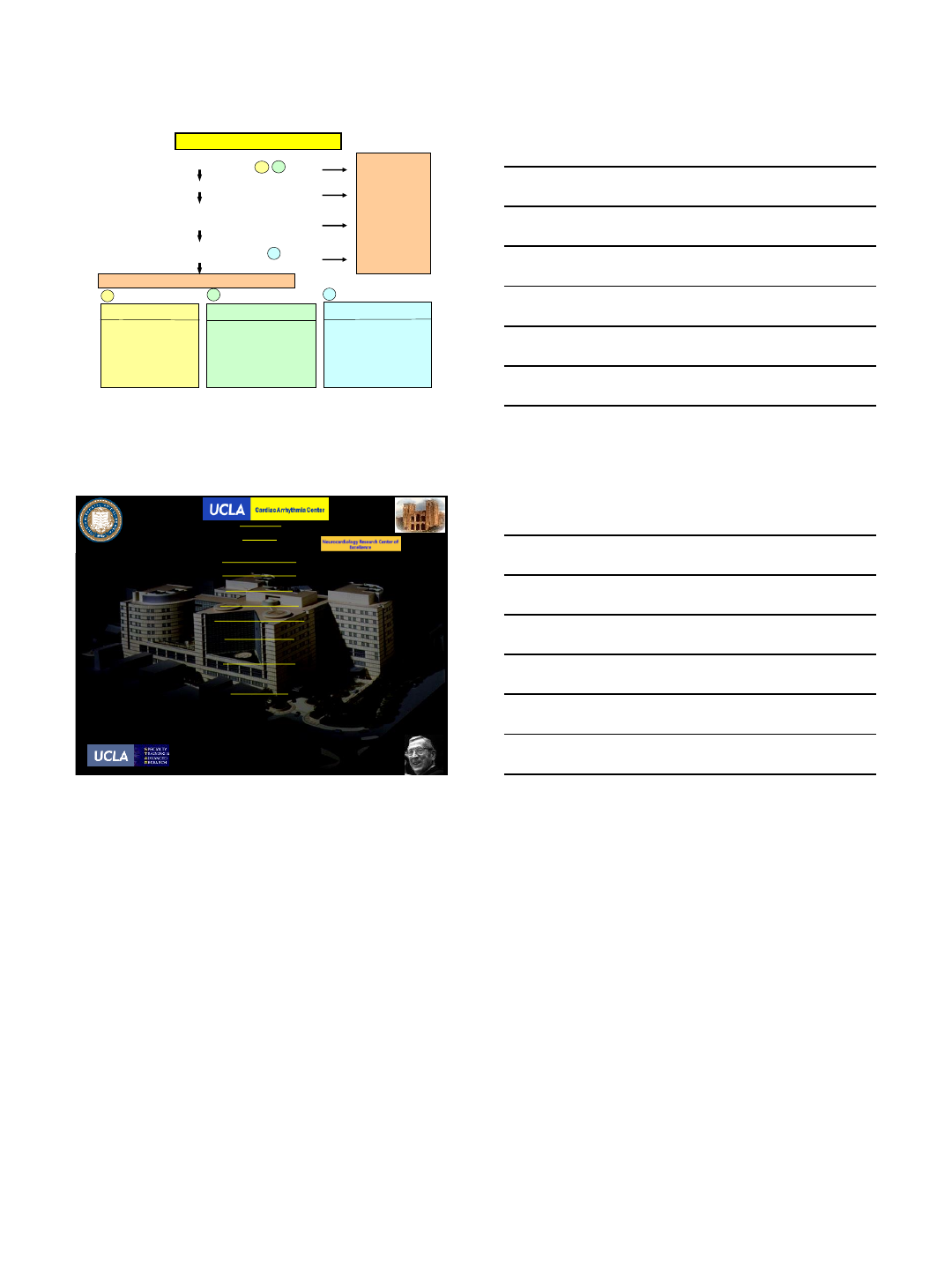
ECGI ISOCHRONE MAPS FOR LOCALIZATION OF VT SITE OF
ORIGIN
Wang Y, Cuculich PS, Zhang J, Desouza KA, Vijayakumar R, Chen J, Faddis MN, Lindsay BD, Smith
TW, Rudy Y. Noninvasive Electroanatomic Mapping of Human Ventricular Arrhythmias with
Electrocardiographic Imaging. Science Translational Medicine. 2011 3(98):98ra84.
When to go epicardial
•General concepts
•ECG criteria
•Etiology & Imaging criteria
Sacher F, Roberts-Thomson K, Maury P, Tedrow U, Nault I, Steven D, Hocini M, Koplan B, Leroux L,
Derval N, Seiler J, Wright MJ, Epstein L, Haissaguerre M, Jais P, Stevenson WG. Epicardial ventricular
tachycardia ablation a multicenter safety study. J Am Coll Cardiol. 2010;55:2366-2372
2/8/2016
7
1. ECG suggest Epicardial VT exit site
2. Prior unsuccessful Endocardial Ablation
3. Define SCAR location with CE imaging:
4. Consider likelihood of Epicardial circuit
for Underlying Substrate:
Sub epicardial or mid-myocardial scar
Perform Endocardial Mapping and Ablation first
ECG Criteria (Berruezo et al Circ 2004)
1) Pseudo-delta >34 ms
2) IDT (V2) >85 ms
3) Shortest RS complex
>121 ms
4) ORS duration >211 ms
1) Absence of inferior Q wave
2) Pseudodelta ≥75 ms
3) MDI >0.59
4) Presence of Q wave in lead I
Probability of Epicardial
Focus (Sacher F et al JACC 2010)
Normal
ICM
NICM
ARVC
Other CM
ECG Criteria for NICM (Valles E Circ AE 2010)
6%
16%
35%
41%
18%
Consider
obtaining
Epicardial
Access for
Mapping
(and
Ablation)
NO
NO
NO
LOW
YES
YES
YES
HIGH
AB
C
ABC
SUMMARY: EPI, ENDO or BOTH
Boyle NG & Shivkumar K: Epicardial Interventions in Electrophysiology, Circulation 2012;126:1752-1769
Cardiomyopathy & Transplantation:
Gregg C. Fonarow MD
Tamara Horwich MD
Daniel Cruz MD
Arnold Baas MD
Mario Deng MD
Ali Nsair MD
ACHD:
Ravi Mandapati MD
Jamil Aboulhosn MD
Pamela Miner RN NP
Cardiac Surgery:
Hillel Laks MD
Murray Kwon MD
Richard Shemin MD
Peyman Benharash MD
Curtis Hunter MD
Jeffrey L. Ardell PhD, Dir
J. Andrew Armour MD PhD
John Tompkins PhD
Eileen So BS
EP Nurse Practitioners:
Shelly Cote RN MN NP
Jean Gima RN MN NP
Geraldine Pavez RN MN NP
Research Administration:
Julie M. Sorg RN MSN
Radiology:
J. Paul Finn MD PhD
Stephen J. Kee MD
John Moriarty MD
Stefan Ruehm MD
Administrative:
Susana Morales
Carmen Mora BS
Julie Ramirez BS
Health System:
Laura Brandsen-Yost MSHA
Erick Ascencio CVT
Center Director
Kalyanam Shivkumar MD PhD
Co-Directors
Noel G. Boyle MD PhD
Aman Mahajan MD PhD
Specialized Program for AF
Eric F. Buch MD, MS, Dir
Specialized Program for VT
Jason Bradfield, MD, Dir
Implanted Devices Clinic
Osamu Fujimura MD, Dir
Cardiac EP, UCLA Olive View
Carlos Macias, MD Dir
Clinical & Translational Research
Marmar Vaseghi MD MS, Dir
West Los Angeles-VAMC:
Zenaida Feliciano MD, Dir
Malcolm Bersohn MD
Janet Han MD
Electrophysiology Faculty:
Olujimi A. Ajijola MD PhD
Carlos Macias MD
Ravi Mandapati MD
EP Fellows/trainees:
Jonathan Hoffman MD
Houman Khakpour MD
Yuliya Krokhaleva MD
Tadanobu Irie MD PhD
Una Buckley MD
David Hamon MD
Pradeep Rajendran BS (MSTP/PhD)
Ray Chui BS (MCIP/PhD)
Echocardiography:
Barbara Natterson MD
Aman Mahajan MD PhD
Cardiac Anesthesia:
Komal Patel MD
Jonathan Ho MD
Coach John R. Wooden
1910-2010
2/8/2016
1
Outcomes of Combined Epicardial
and Endocardial Ablation
Srinivas Dukkipati, MD
Director, Electrophysiology Lab
Icahn School of Medicine at Mount Sinai
New York, NY
Scar-Related VT
LV RV
RF
LV RV
•Coronary artery territory
•Subendocardial or transmural
•Epicardial scar present in ~10%1
Dilated Cardiomyopathy
1Verma A et al. JCE 2005;16:465-71
2Liuba I et al. Heart Rhythm 2014;11:755-62
Myocardial Infarction
•Mid-myocardial & epicardial, patchy
or longitudinal striae
•Scar progression over time2
•Basal –perivalvular3
•Anteroseptal & inferolateral scar
location in 89% of those with VT4
d’Avila A et al.
Heart Rhythm 2006
3HH et al. Circulation 2003; 108:704-10
4Piers S et al. Circ EP 2013;6:875-83
Disclosures
•Biosense Webster –Research Grant
2/8/2016
2
Post-MI: Endo–Epicardial
Homogenization
Di Biase L et al –JACC 2012;60:132-41
•100% non-inducibility achieved in both groups
81%
51%
DCM: Endocardial Ablation
Hsai HH et al –Circ 2003; 108:704-10
•19 pts with DCM and MMVT
–Basal (peri-mitral) scar in ALL
–Endocardial scar <25% of LV
–Of 57 VTs, 88% of induced VTs
were from basal scar
•After ablation, 14/19 (74%) were
non-inducible
•After 22
±
12 months, only 5 pts
(23%) were alive without VT
recurrence
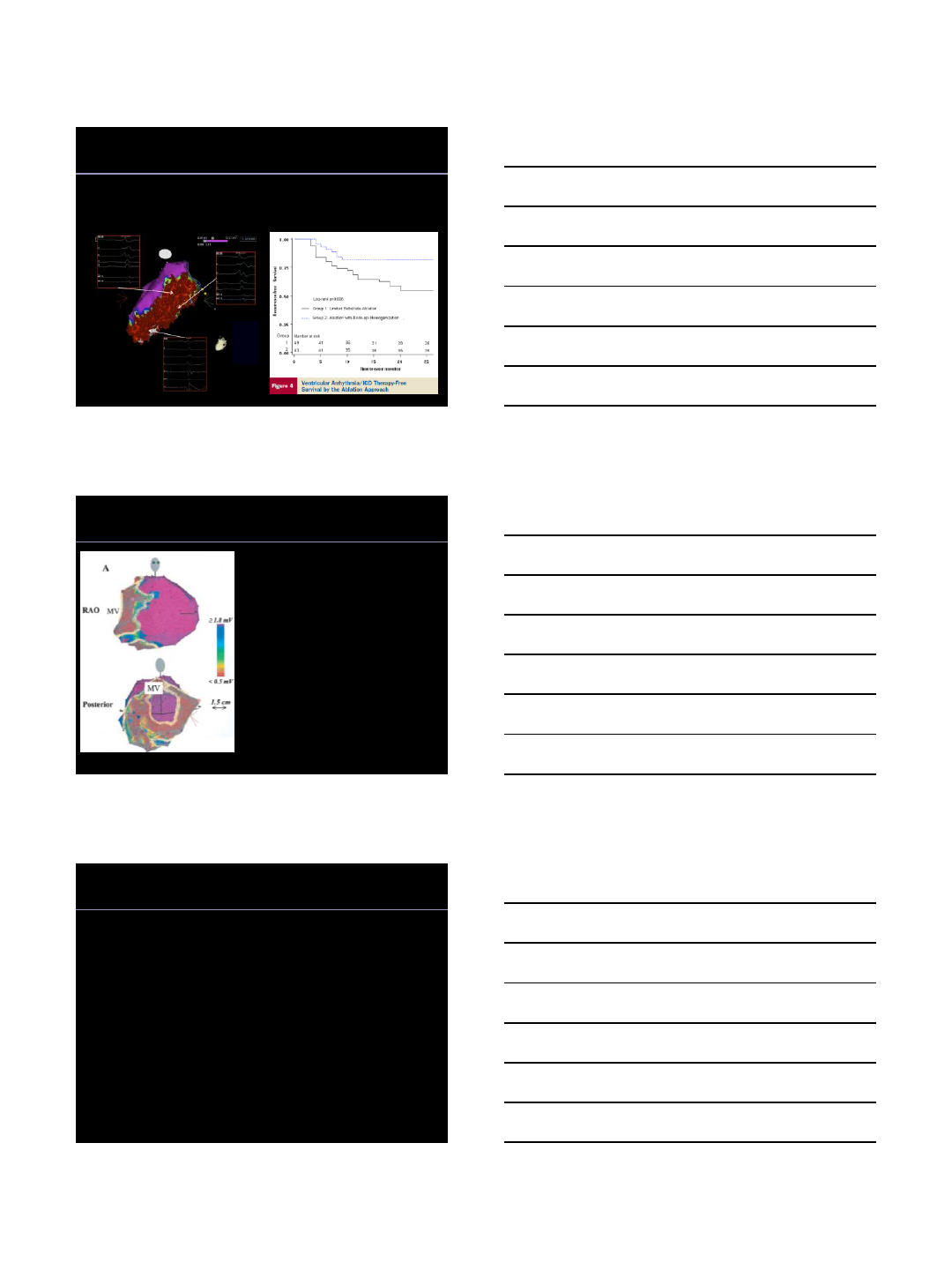
DCM –Epicardial Scar
Cano O et al –JACC 2009; 54:799-808.
•22 pts with DCM and failed prior endocardial ablation
(n=20) or VT suggestive of epicardial origin (n=2)
•Combined epicardial/endocardial mapping was performed
•Scar Location
Epicardial scar in 18 pts (82%) –basal LV/lateral wall
Endocardial scar in 12 pts (54%) –basal LV
•Scar Area
Epicardial = 55.3 ±33.5 cm2
Endocardial = 22.9 ±32.4 cm2(p < 0.01)
•F/U 18 ±7 months
71% free of VT
2/8/2016
3
Cano O et al. JACC 2009;54:799-808
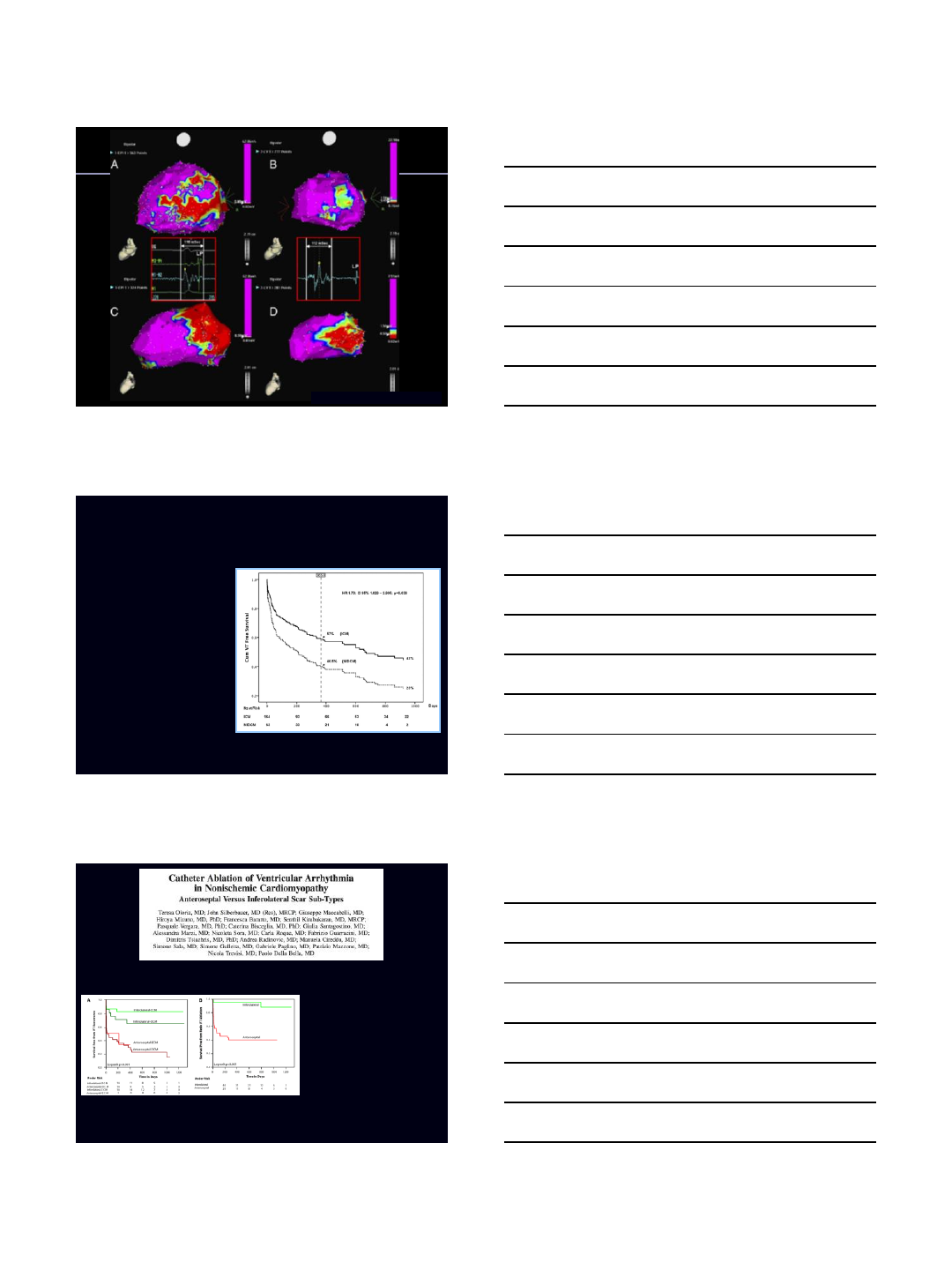
Single Procedure VT-free Survival:
ICM vs. NICM
VT-free Survival at 1 year:
ICM = 57%,
NICM = 40.5%
Results From the Prospective
Heart Centre of Leipzig VT
(HELP-VT) Study
Dinov B et al –
Circulation 2014;129:728-36
•224 pts. (ICM 164, NICM 63)
•Epicardial ablation:
ICM 1.2%
NICM 30.8%
•Acute procedural success (non-
inducibility of VT):
ICM 77.4%
NICM 66.7%
VT-free Survival at 1 year:
ICM = 57%,
NICM = 40.5%
ECM: early CM
DCM: LVEF<45%, mod-severe LV dilatation
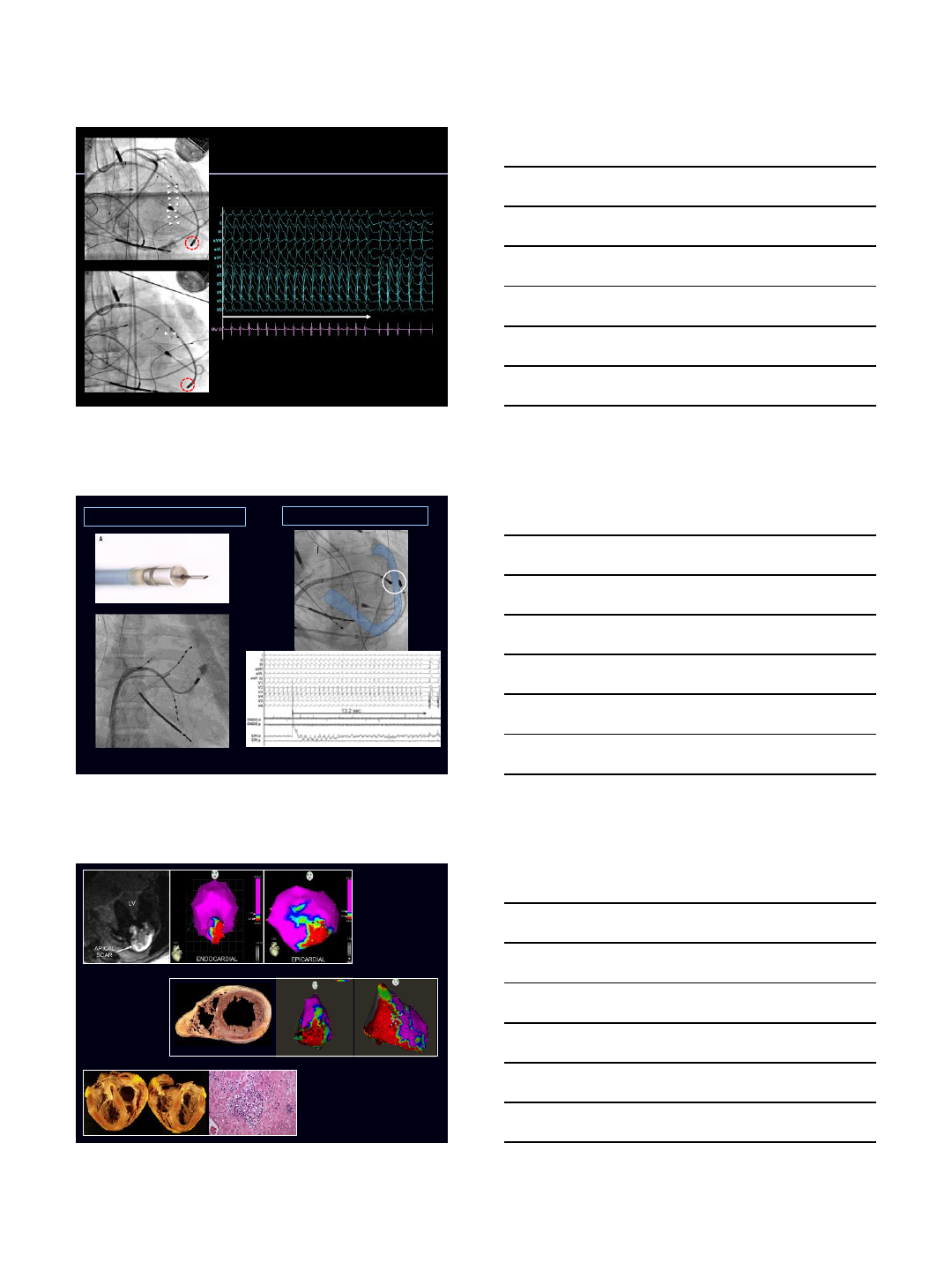
•87 pts. with NICM and VT:
Anteroseptal scar 44
inferolateral 43
•Presence of anteroseptal scar
was associated with a HR 5.5
(p<0.001) for VT recurrence
Circ EP 2014;7:414-23
2/8/2016
4
Transcoronary
Ethanol Ablation
VT Termination
Sapp J L et al. Circ 2013;128:2289-2295 Koruth JS et al. Heart Rhythm 2012;9:1932-41
INFUSION NEEDLE ABLATION BIPOLAR RFA
RV ENDOCARDIAL EPICARDIAL
RV
Dubrey SW et al. Prog Cardiovasc Dis 2010;52:336-46
AP Burke - http://emedicine.medscape.com
HCM
ARVC
Cardiac
Sarcoidosis
2/8/2016
5
•22 pts with HCM & drug
refractory VT undergoing
catheter ablation
•Epicardial RFA in 13 pts
(59%)
•Acute procedural success: 86%
•At 20 ±9 months –73% VT
free
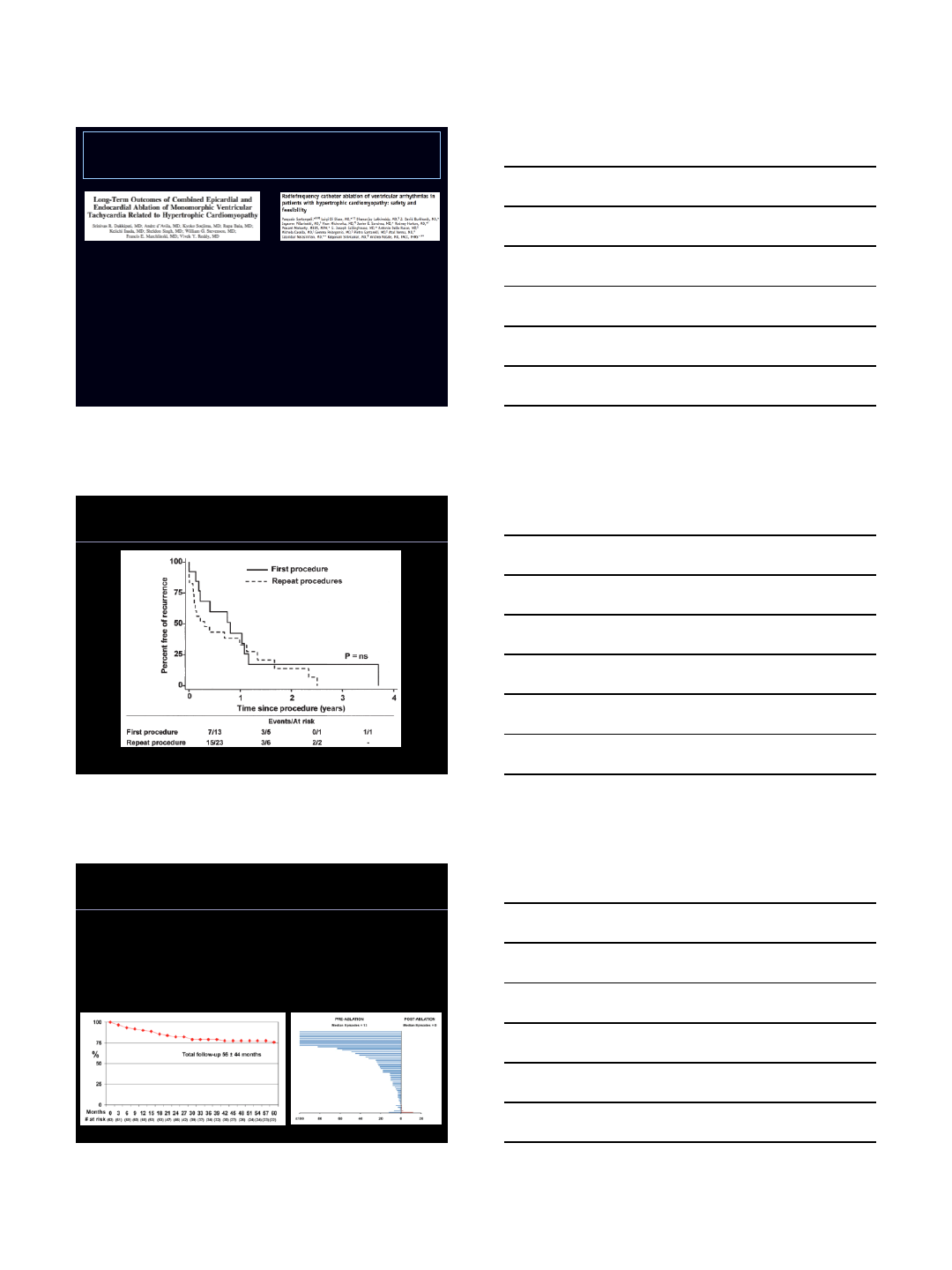
•10 pts. with HCM & drug refractory
VT undergoing combined
epicardial-endocardial ablation
•Epicardial scar present in 8/10
(80%)
•Acute procedural success: 89%
•At 37 ±17 months –78% VT free
Hypertrophic Cardiomyopathy
Circ EP 2011;4:185-194 Heart Rhythm 2010;7:1036-42
Dalal et al JACC 50:432, 2007
ARVC-VT: Endocardial Ablation
ARVC-VT: Combined Endocardial &
Epicardial Ablation
Santangeli P et al –Circ EP 2015;8:1413-21
•62 pts. with ARVC-VT undergoing endocardial ±epicardial ablation
•Follow-up 56 ±44 months
Freedom from Ventricular Arrhythmias VT Frequency
71%
2/8/2016
6
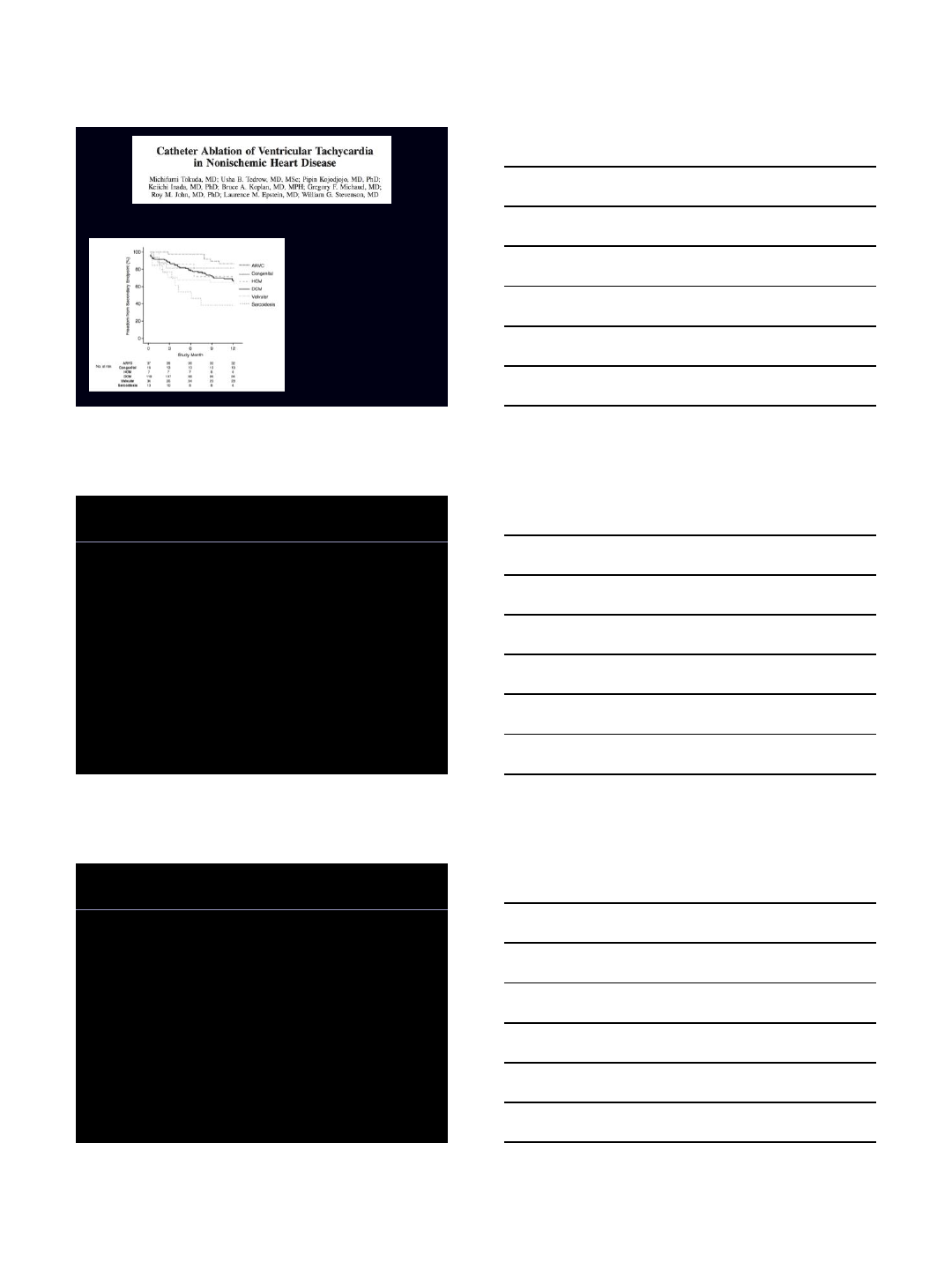
VT-free Survival at 1 year:
ICM = 57%,
NICM = 40.5%
Circ EP 2012;5:992-1000
•224 pts. with NICM and VT:
•Epicardial ablation:
•DCM 29%
•ARVC 30%
•Sarcoidosis 15%
•HCM 43%
•Congenital 6%
•Valvular 3%
•Secondary endpoint: freedom
from death, transplantation, VT
hospitalization
Final Thoughts
•Unlike in ischemic VT, scar in other substrates is NOT
predominantly limited to the sub-endocardium
•Epicardial scar present in:
ICM ~10%
other substrates ≥ 30%
•An endocardial ±epicardial ablation approach
best results in ICM and ARVC
suboptimal results in DCM (inferolateral scar better than
anteroseptal scar) and Cardiac Sarcoidosis
•Better mapping and ablation technologies are necessary
to improve outcomes
2/8/2016
1
Role of Imaging Techniques in
Catheter Ablation of Ventricular
Tachycardia
Amin Al-Ahmad, MD, FACC, FHRS, CCDS
Texas Cardiac Arrhythmia Institute
Austin, Texas
Disclosures
•Medtronic
•St Jude Medical
•Boston Scientific
•Biosense
•Apama Medical
•Khalila Medical
Introduction
•Pathophysiology of VT in complex
•Interplay between substrate, triggers
•Understanding the substrate is helpful in
targeting VT
•Imaging during procedures to guide in
ablation and prevent compliactions
2/8/2016
2
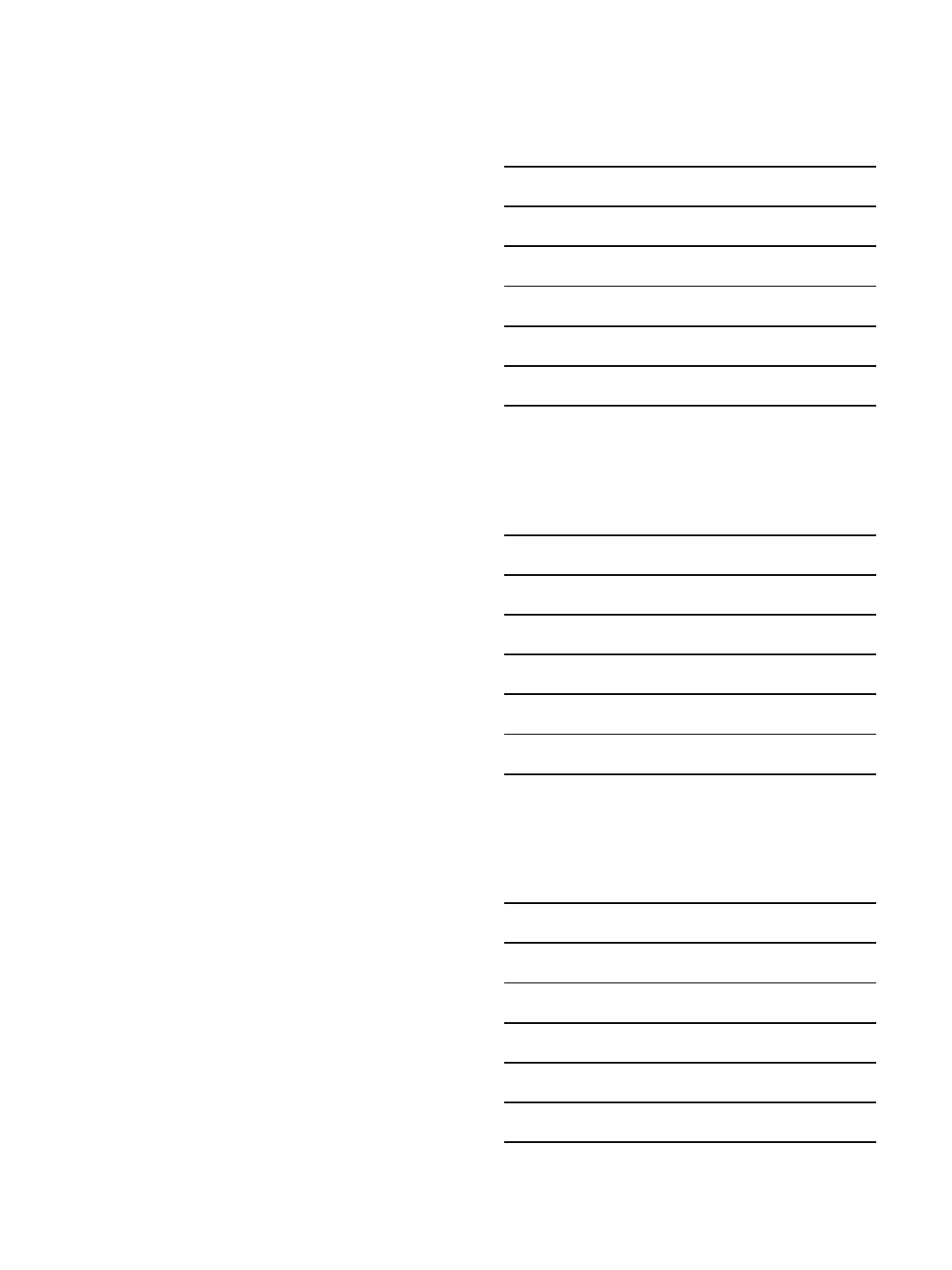
Pre-Procedural Imaging
•Nuclear
–Perfusion
–Viability
–Innervation
•MRI
–Late enhancement
•CT scan/Rotational Fluoroscopy
Rijnierse et al. JNC 2015
2/8/2016
3
Rijnierse et al. JNC 2015
Perez-David JACC 2011
Perez-David JACC 2011
2/8/2016
4
Desjardins et al. HR 2009
Fernandez-Armenta et al. Circ A&E 2013
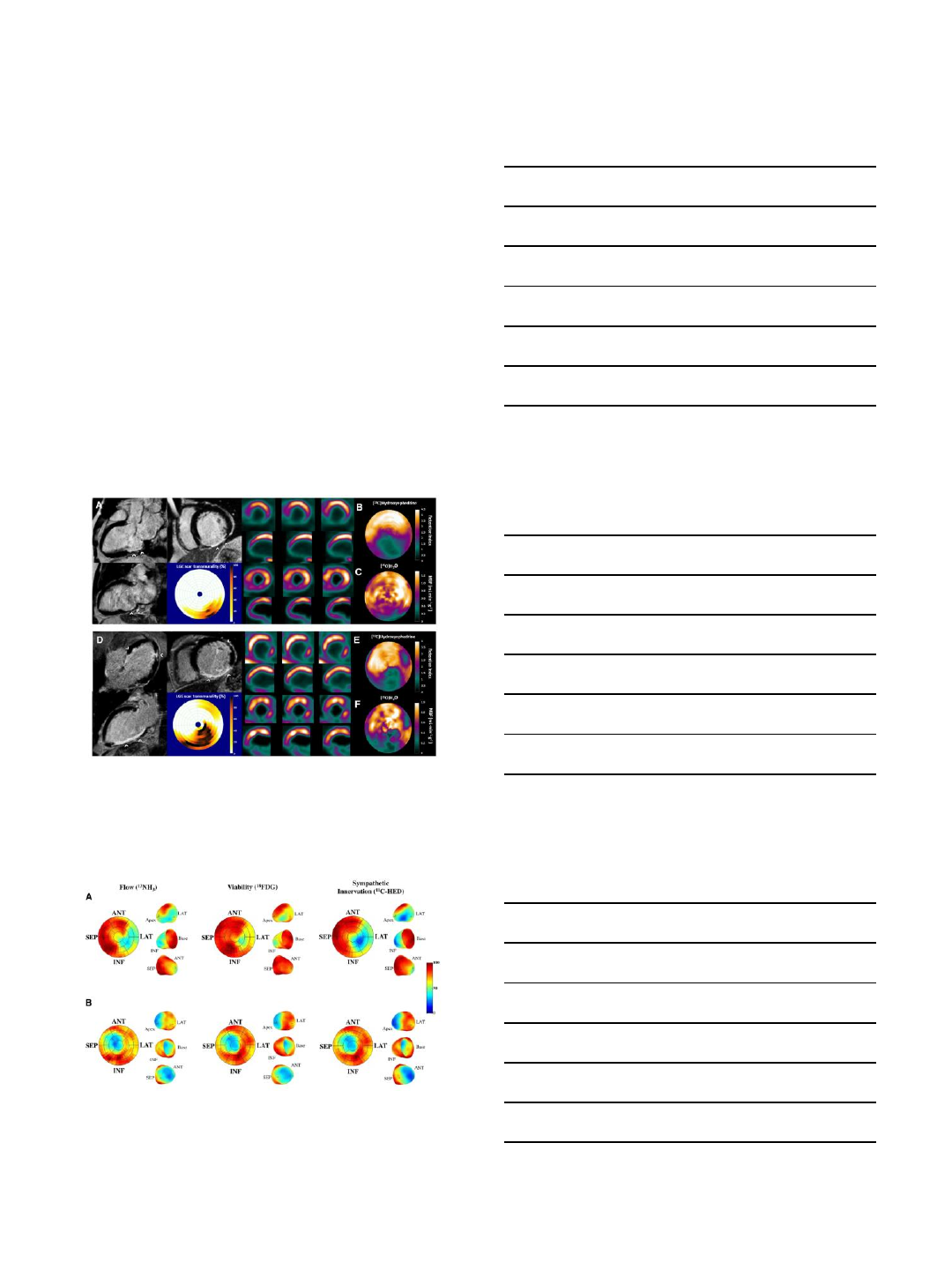
Dickfeld et al. Circ A&E 2011
2/8/2016
5
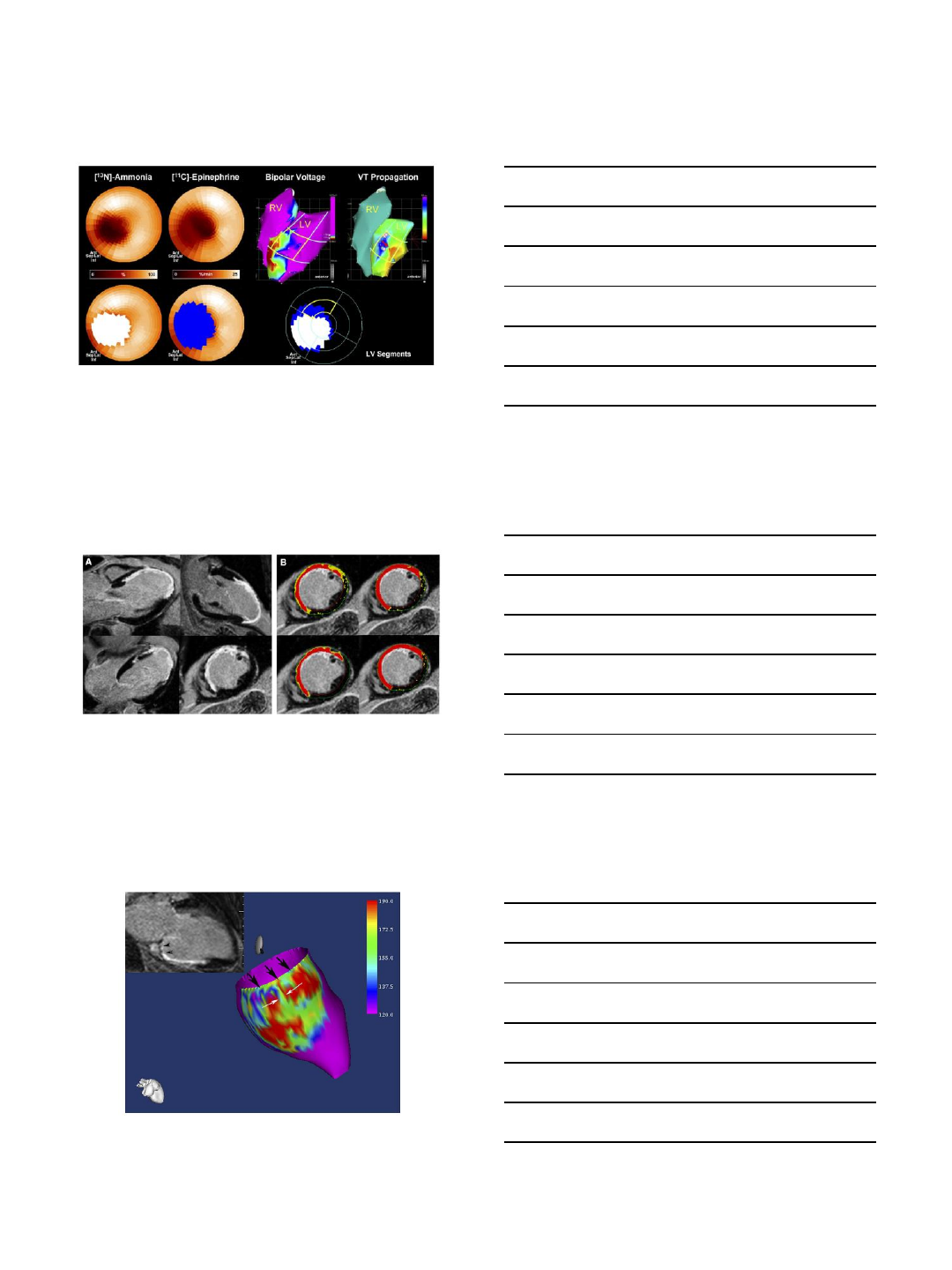
Komatsu et al. Circ A&E 2013
Cochet et al. JCE 2013
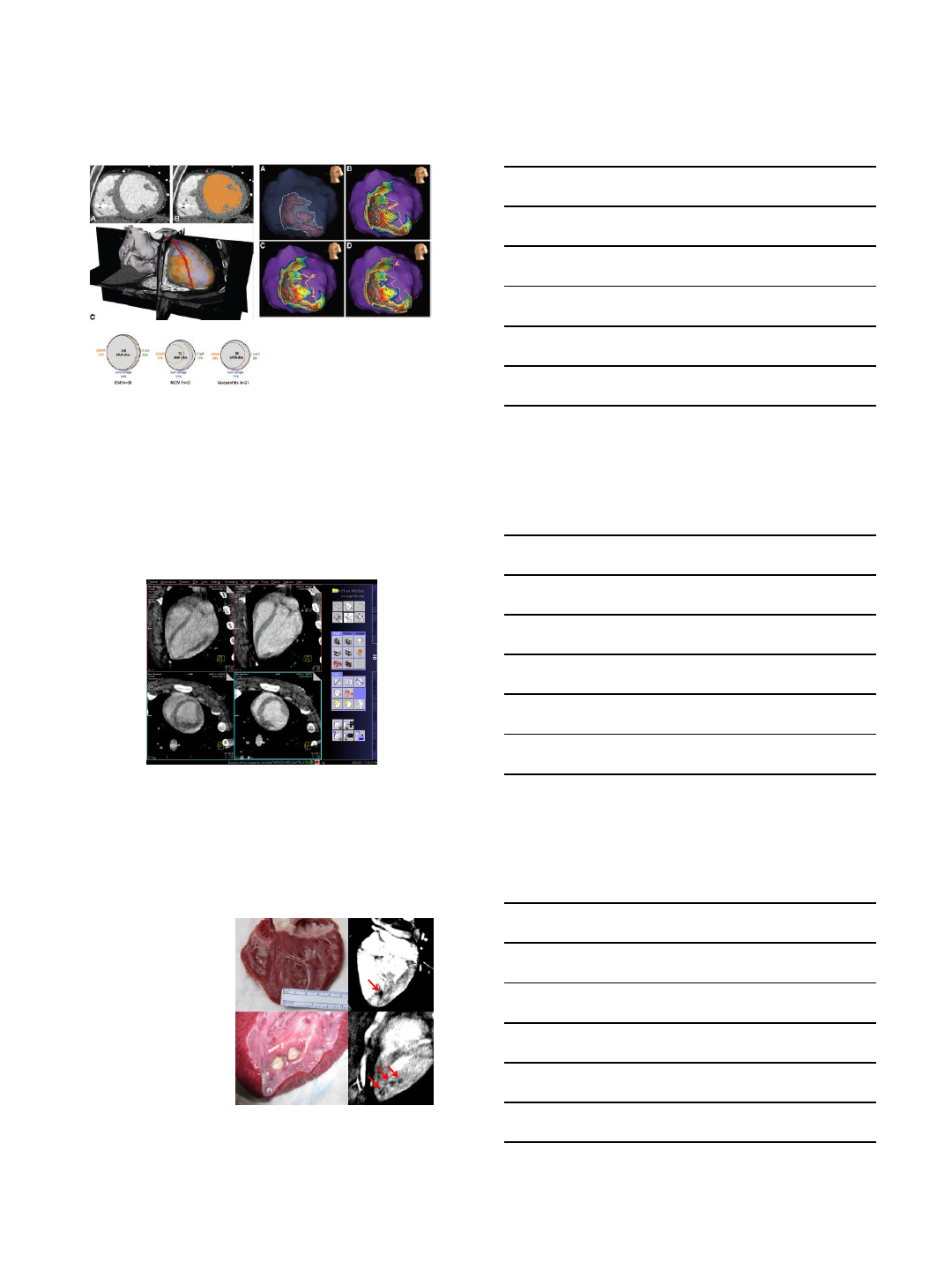
CT Scan- Wall thinning
Image of LV scar- Rotational
Fluoroscopy
Day 0 Day 30
•29 RF ablation
lesions were
created and
visualized
•All lesions
exhibited a
perfusion defect
•24 lesions
(83%) had a
peripheral
enhancing ring
Visualization of RF Lesions--Rotational
Fluoroscopy
Girard E, Al-Ahmad A. et al. JACC Imaging 4(3): 259-268, 2011
2/8/2016
6
Procedural Imaging
•ICE
–2D
–3D
•Fluoroscopy registration tools
ICE for VT
•Placement of the ICE catheter in the RA or RV
or pericardium allows visualization of the left
ventricle
–Structures:
•papillary muscle
•false tendon
•valves
•coronary arteries
2/8/2016
7
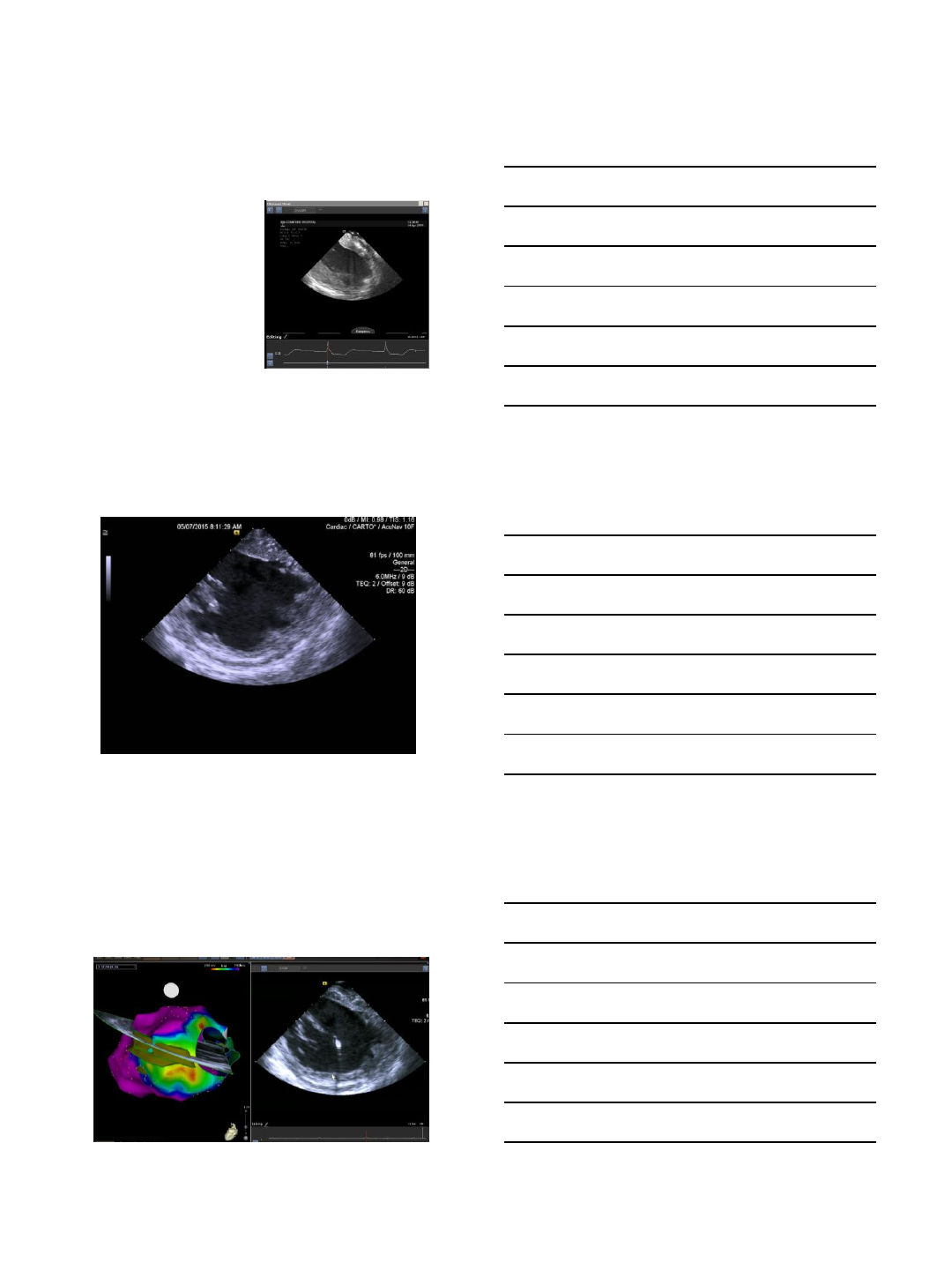
3D Reconstructed Images
2/8/2016
8
Vaseghi et al, HeartRhythm 2006
2/8/2016
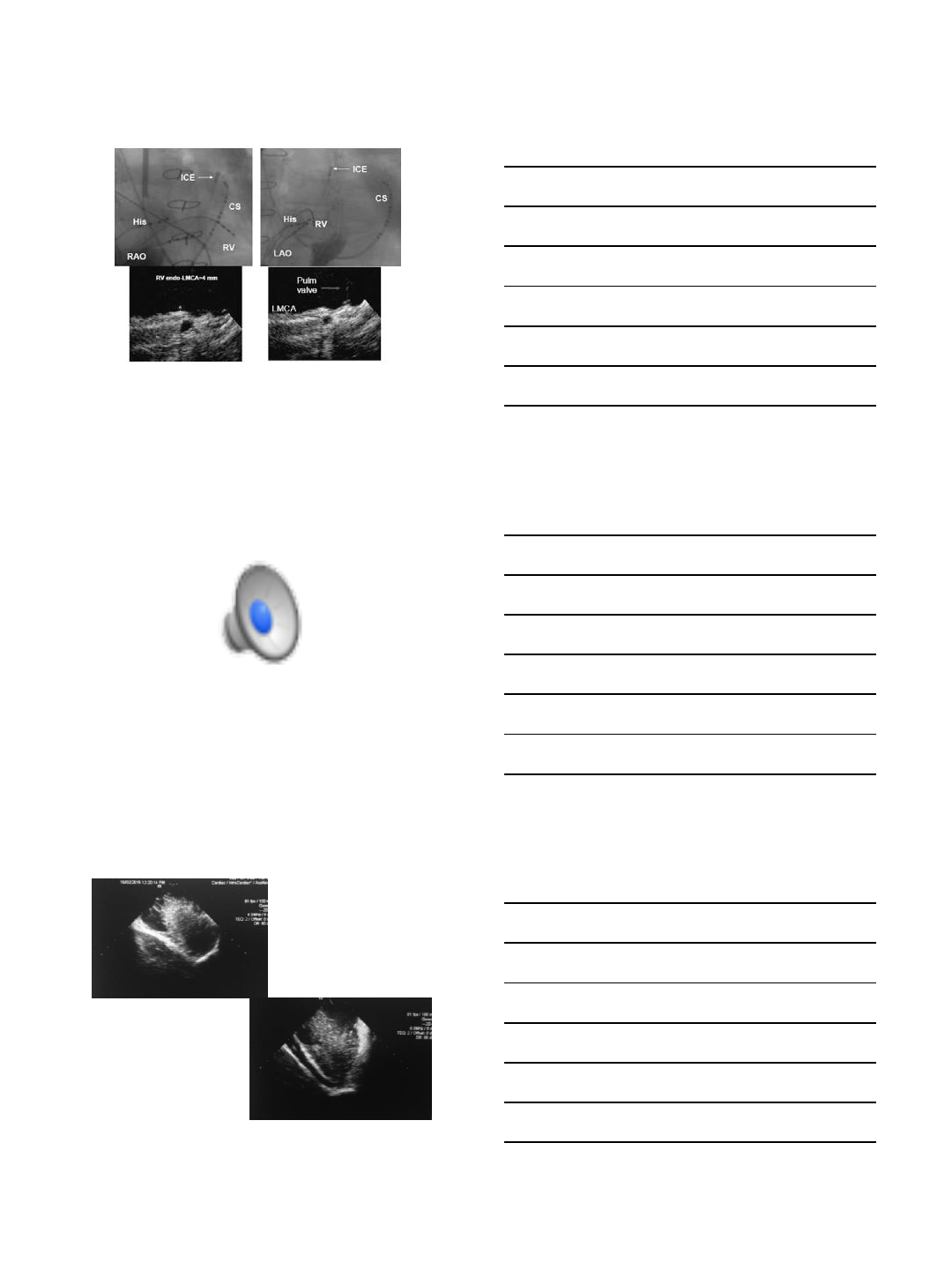
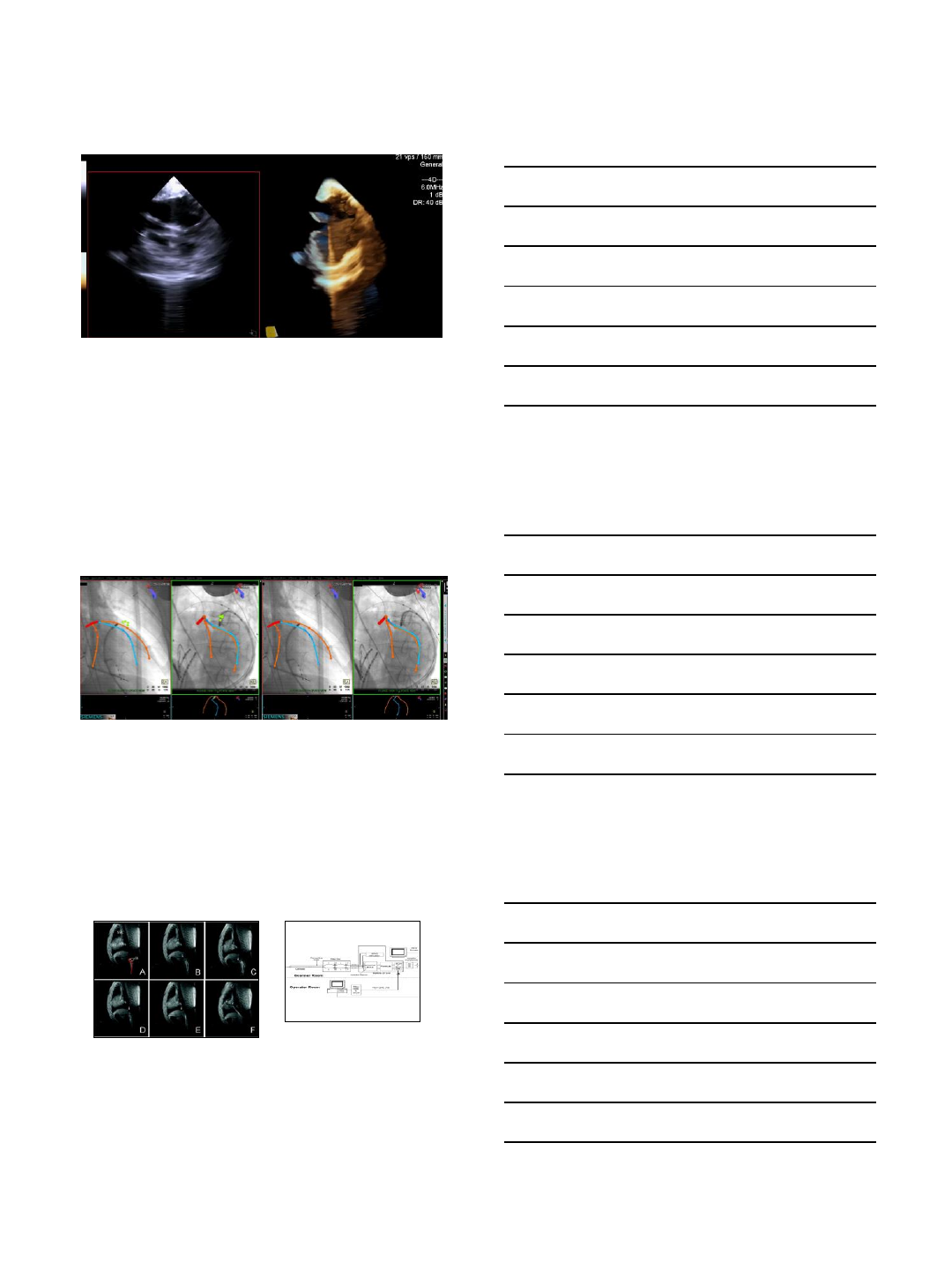
9
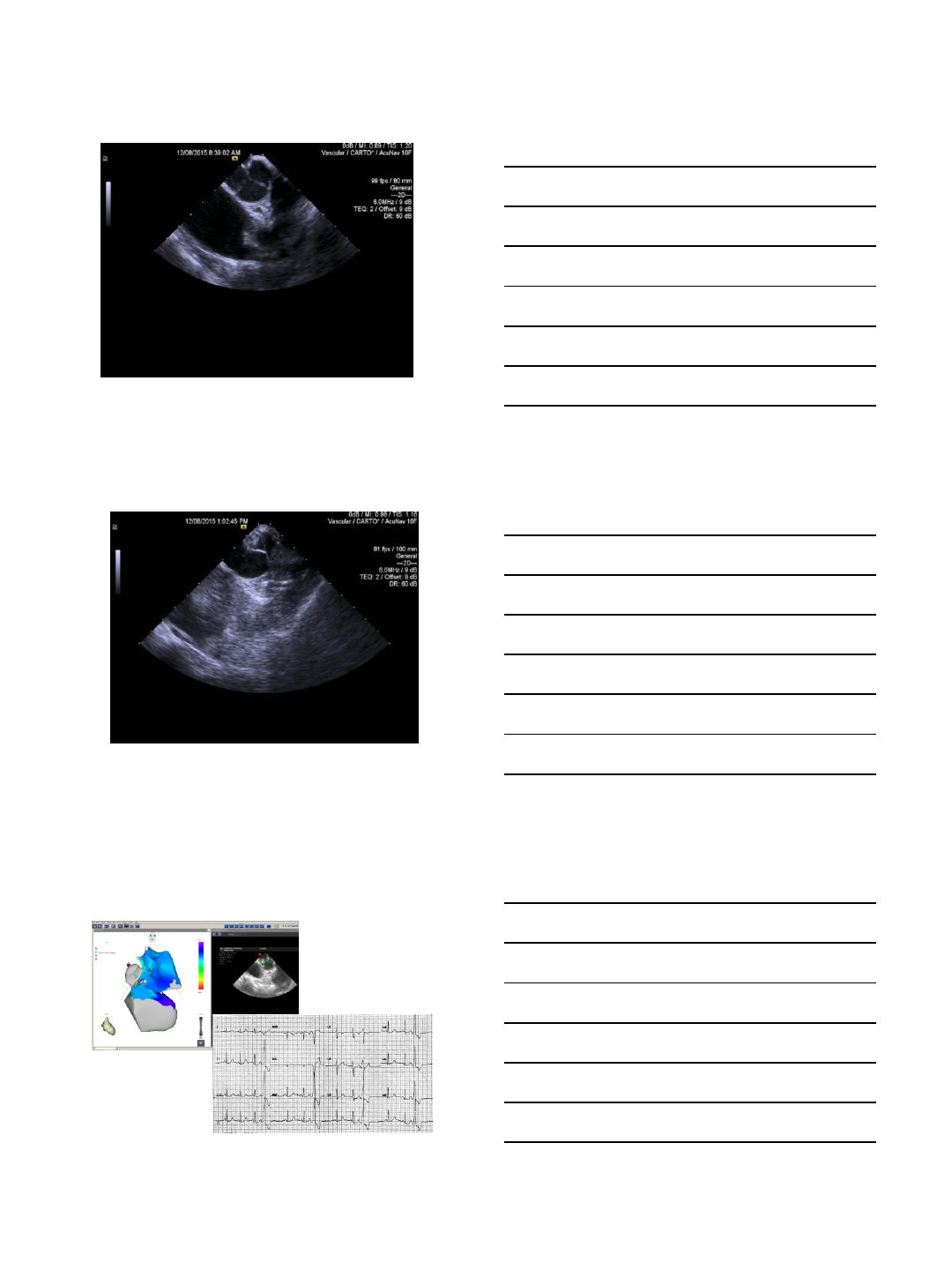
ICE for VT
•Visualization of areas
of wall thinning or wall
motion abnormalities
Epicardial Scar
Unipolar voltage ICE Image
2/8/2016
10
Epicardial VT
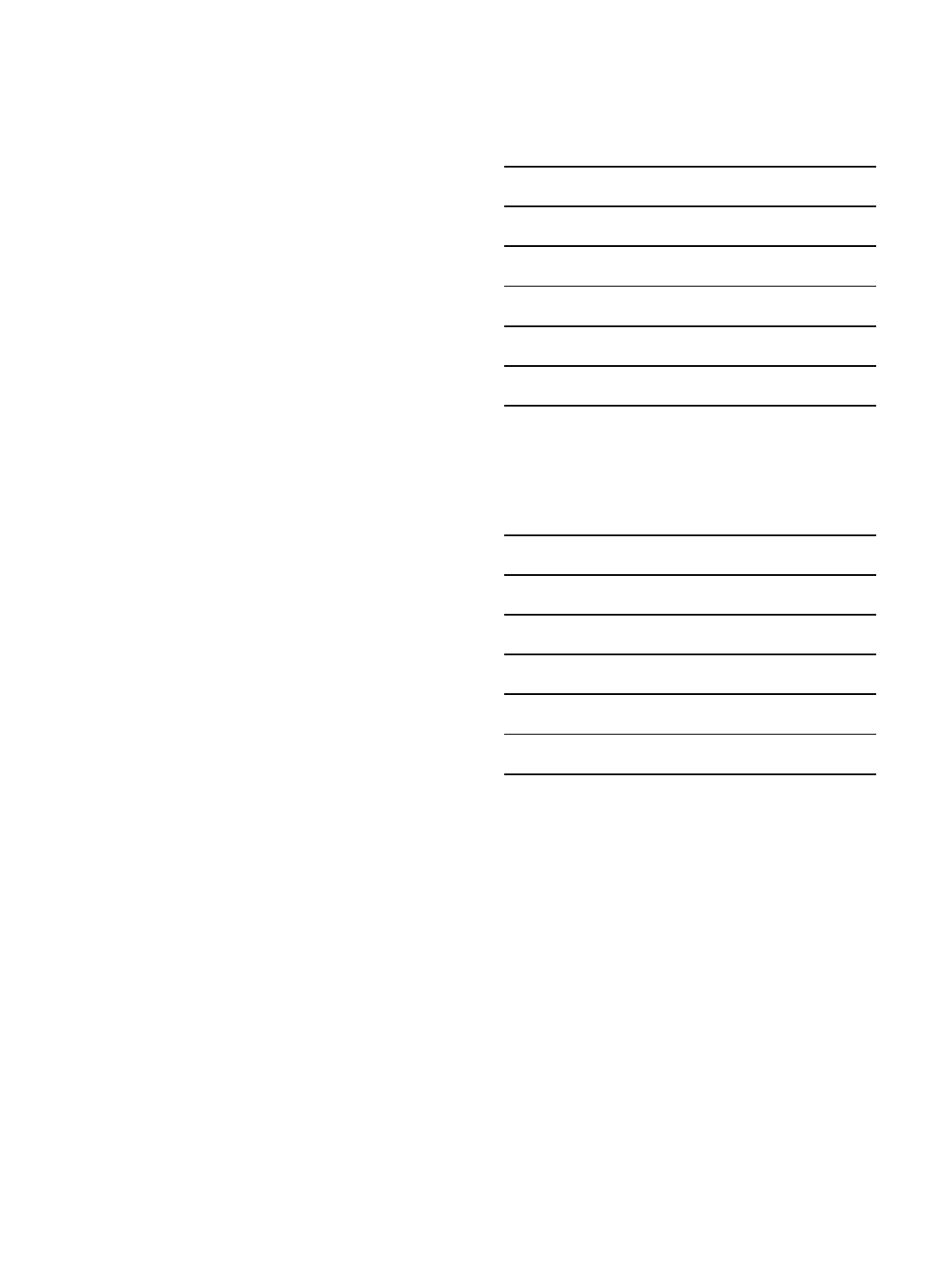
Interventional MRI
Nazarian S, et al. Circulation. 2008
Real-time guidance of a passive catheter to the His bundle position in the
canine model. A, Catheter bipolar electrodes (Bi) are shown in the inferior
vena cava. B, The catheter is advanced, with tip (arrow) entering hepatic
vein. C, Catheter buckling as a result of advancement into a hepatic vein.
D, The catheter tip is withdrawn into the inferior vena cava. E, The
catheter tip is advanced beyond the hepatic vein branch in the inferior
vena cava. F, The catheter tip is advanced to the tricuspid annulus. SVC
indicates superior vena cava; L, liver; RV, right ventricle; and RA, right
atrium.
2/8/2016
11
Conclusions
•Pre-procedural imaging is helpful in gaining
insight into stuructural and functional
substrate for VT
•CT and MRI correlate well with EA mapping
•Intra-cardiac ultrasound is valuable during VT
ablation for identifying substrate, catheter
location and preventing complications
Thank You
2/2/2016
1
Epicardial Mapping and Ablation Techniques:
How to Prevent and Manage Complications
Mathew D. Hutchinson, MD
Associate Professor of Medicine
University of Pennsylvania
Disclosures
Within the past 12 months, I have received modest
financial support from the following entities:
1. Medtronic- lecture honoraria
2. Biosense Webster- advisory panel
3. Abiomed- lecture honoraria
Perioperative
considerations
•Patient selection
–Habitus
–Prior surgery, pericarditis
•Hematologic issues
–Anticoagulation management
–Blood products
•Equipment
–Access-related
–Coronary angiography
–Phrenic protection
•Surgical backup
N Acute Chronic
Sacher
et al.
156
5.1% 1.9%
Tung et
al.
109
8.8% NR
Della Bella
et al.
218
2.3% 1.8%
Piers et al.
29 7% 3%
Sacher et al. J Am CollCardiol 2010; 55:2366-72
Tung et al. Heart Rhythm 2013; 10:490-498
Della Bella et al. CircArrhythm Electrophysiol 2011; 4:653-9
Piers et al. CircArrhythm Electrophysiol 2013; 6:513-521
Pericardial access complications
2/2/2016
2
Anatomy of the approach
RV LV
Liver
RV
LV
Larrey’s
Space
Catheter
Anterior
Flat Lateral
Tricks and tips
1. Needle techniques
2. Define cardiac border
3. Use ICE, contrast
4. Don’t panic with RV perf
5. Confirm guidewire position
6. Maintain sheath hygiene
AP
RAO 30º LAO 40º
Apex
LV
RV
LAO 50º
RV
LV
Access-related
complications
•Superficial vessels
•Abdominal viscera
•Cardiac chambers
•Epicardial vessels
Inferior
Phrenic A
Anterior
Phrenic N
Superior
Epigastric
Internal
Thoracic
Musculo-
phrenic
Rectus
Abdominus
L Pleural
Cavity
RV LV
Ross et al. Heart Rhythm 2011; 8:318-21
2/2/2016
3
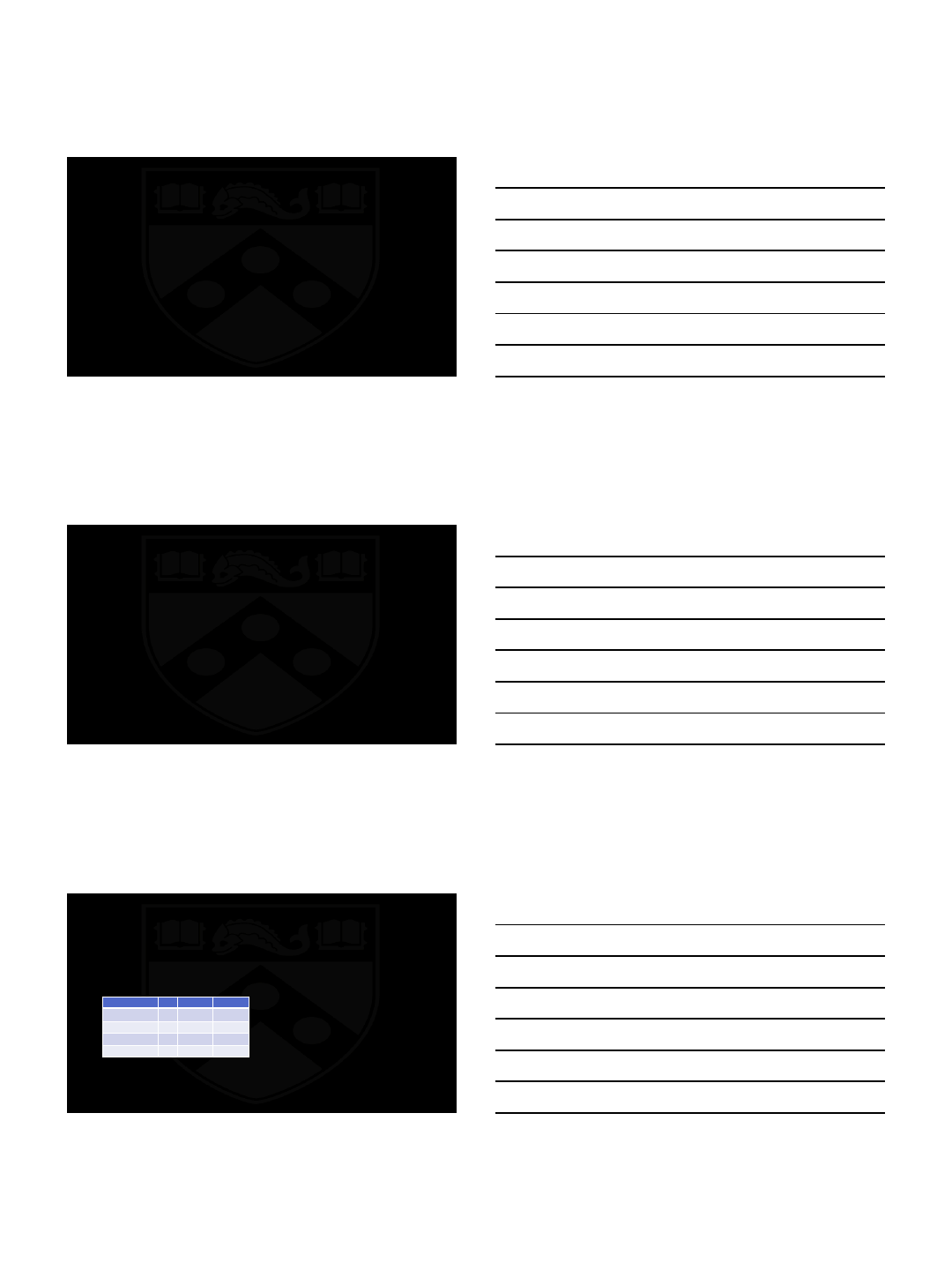
Approach-specific complications
Anterior: In-and-out RV
perforation Posterior: Liver laceration
Koruth et al. Heart Rhythm 2011; 8:1652-7
Ablation-related coronary injury
•Presentation
•Acute occlusion, spasm
•Chronic stenosis
•Likelihood of vessel injury:
•Proximity to vessel (<2mm)
•Internal diameter (<1.8mm)
•Energy source (RF>cryo)
Intimal hyperplasia
D’Avila et al. PACE 2002; 25:1488-92
Lustgarten et al. Heart Rhythm 2005; 2:82-90
Hypotension
during RF
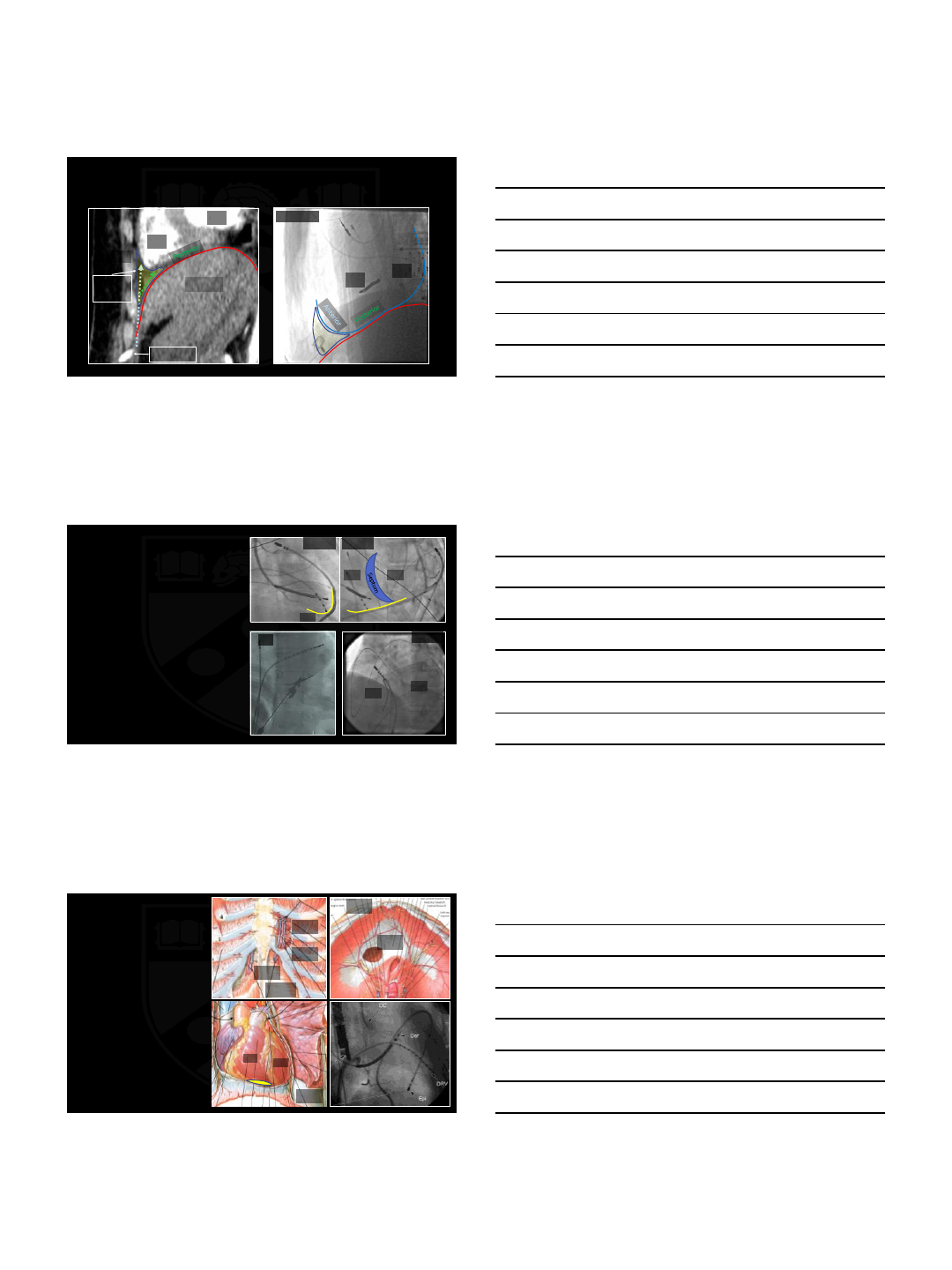
Phrenic nerve protection
Phrenic capture at 20mA
Diaphragm
Fan et al. Heart Rhythm 2009 6(1): 59-64
LV
•Double pericardial access required
•Consider steerable sheath
•Position ablator between LV and balloon
•Alternative air +/- fluid- increased DFT
Diaphragm
LV
B
Non-compliant balloon 18x40
LV
B
2/2/2016
4
Re-access after pericarditis/cardiac surgery
•28 pts; 4-9% total epi procedures
•Acute success 17/28
•100% with adhesions (anterior
post surgical)
•Blunt dissection required for
mapping; deflectable sheath
•Complications: ~10% (no deaths)
Sosa et al. J Interv Card Electr 2004; 10:281-288
Roberts-Thompson et al. J Cardiovasc Electrophysiol 2010; 21:406-411
Tschabrunn et al. Heart Rhythm 2013; 10:165-169
Summary- Epi access complications
•Relatively high complication rate
•Adequate planning and equipment is essential to success
•Complications specific to timing and approach
•Develop a specific technique, but modify it as required
Thank You!
2/2/2016
5
