MergedFile 36916b3e 66e3 4839 9a38 916878b5e634
2018-04-24
: Pdf 36916B3E-66E3-4839-9A38-916878B5E634 36916b3e-66e3-4839-9a38-916878b5e634 4 2018 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 39
4/24/2018
1
TKI Resistance in Chronic
Myeloid Leukemia
Updates and Challenges in the
Management of Chronic Myeloid Leukemia
April 19, 2018
Michael Deininger MD PhD
Disclosures
Paid Advisory
Board
Paid
Consultant
Research
Funding
Ariad yes no no
Blueprint yes no no
Galena Biopharma yes no no
Incyte yes yes no
Novartis Pharma yes yes yes
Pfizer, Inc. yes yes yes
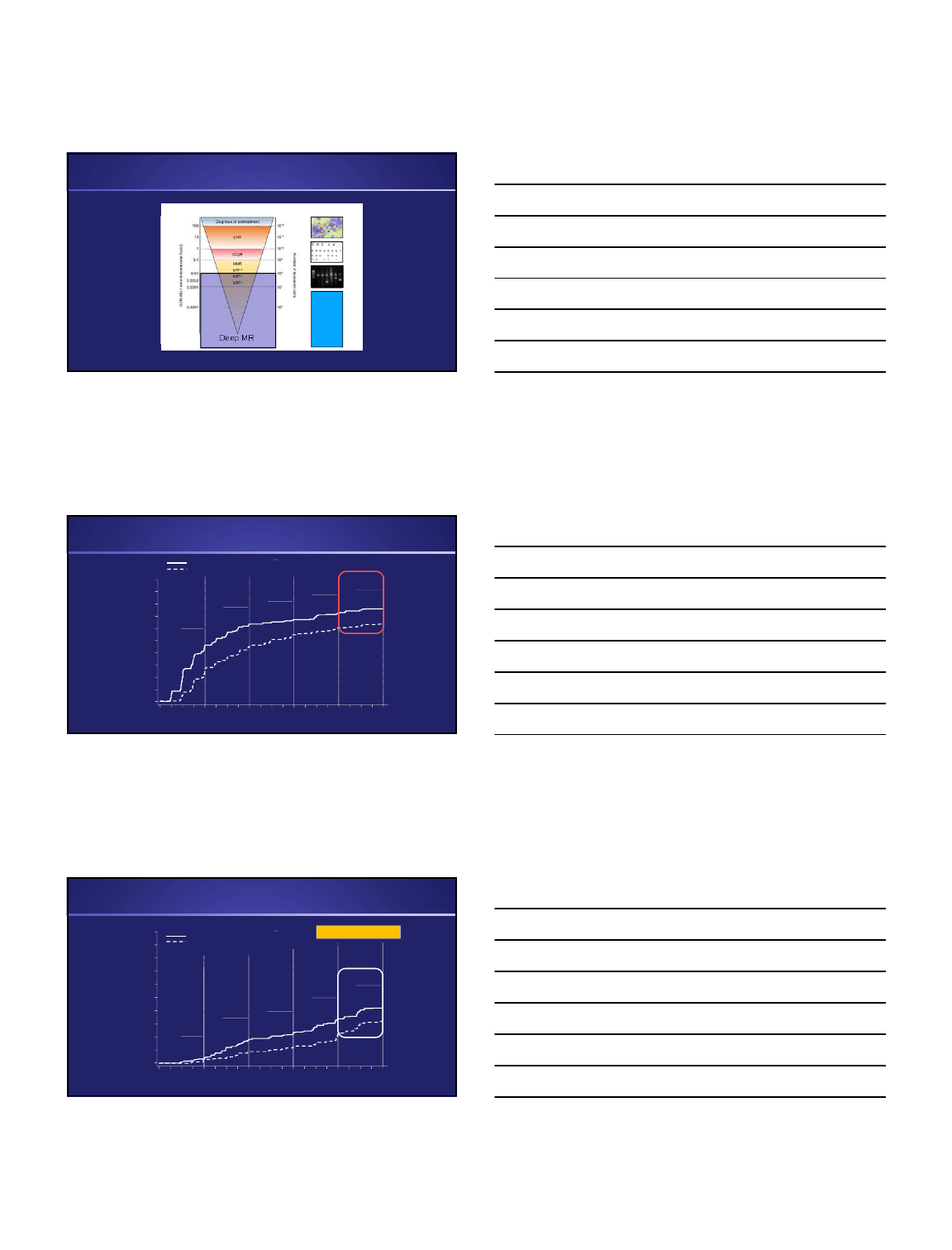
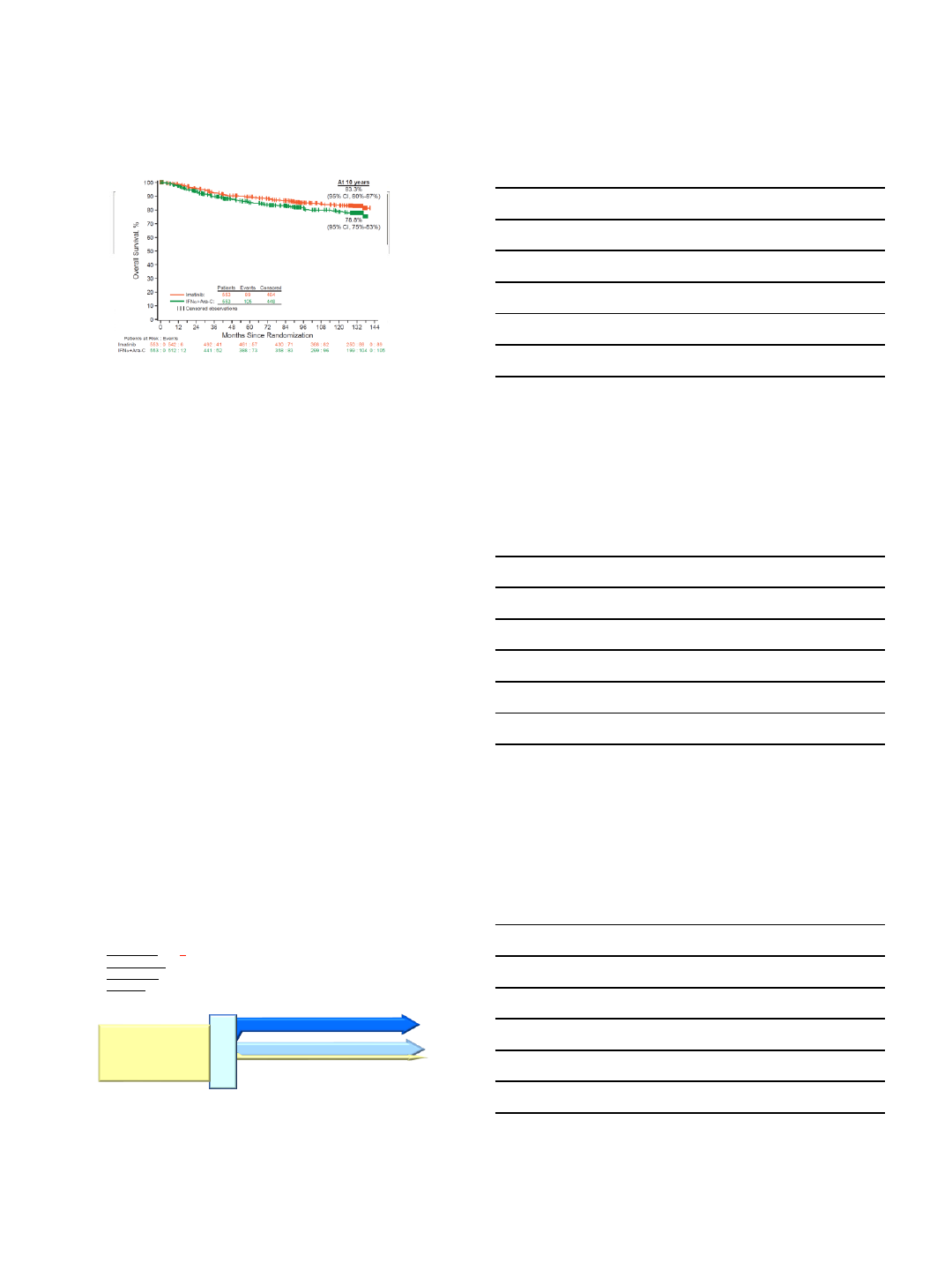
IRIS Study: 10-year Follow-up
Hochhaus et al, NEJM 2017
4/24/2018
2
2G TKIs vs Imatinib in Treatment-Naïve CP-CML
Imatinib 400 mg QD (N = 260)
Dasatinib 100 mg QD (N = 259)
DASISION
R
A
N
D
O
M
I
Z
E
Imatinib 400 mg QD (N = 283)
Nilotinib 300mg BID (N = 282)
R
A
N
D
O
M
I
Z
E
Nilotinib 400mg BID (N = 281)
Imatinib 400 mg QD (N = 241)
Bosutinib 400 mg QD (N = 246)
R
A
N
D
O
M
I
Z
E
ENESTnd BFORE
Saglio et al. NEJM 2017; Kantarjian et al. NEJM 2010; Cortes et al. JCO 2017
Imatinib
400 mg QD
(n = 283)
Nilotinib
300 mg BID
(n = 282)
Nilotinib
400 mg BID
(n = 281)
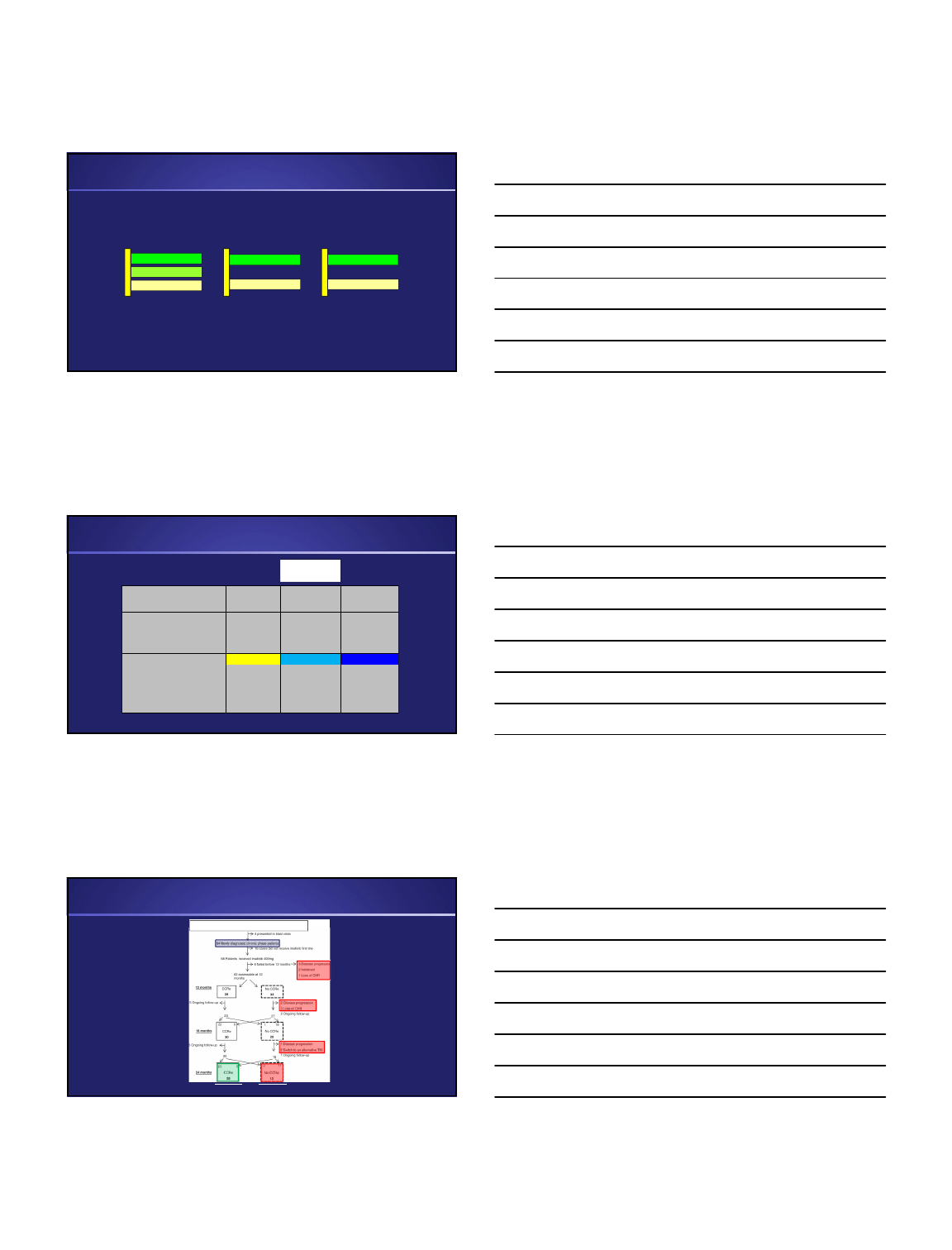
Estimated 5-year PFS, % 91.1 92.0 95.3
Progressions and deaths, n 23 22 11
Hazard ratio (95% CI) — 0.92 (0.51-1.65) 0.46 (0.23-0.95)
Pvalue .77 .03
Estimated 5-year OS, % 91.6 93.6 96.0
Total deaths, n 21 18 10
Deaths in patients with
advanced CML, n
b
15 6 4
Hazard ratio (95% CI) — 0.84 (0.45-1.58) 0.46 (0.22-0.98)
Pvalue — .58 .04
No Difference in Overall Survival – ENESTns as an Example
Approved
frontline dose
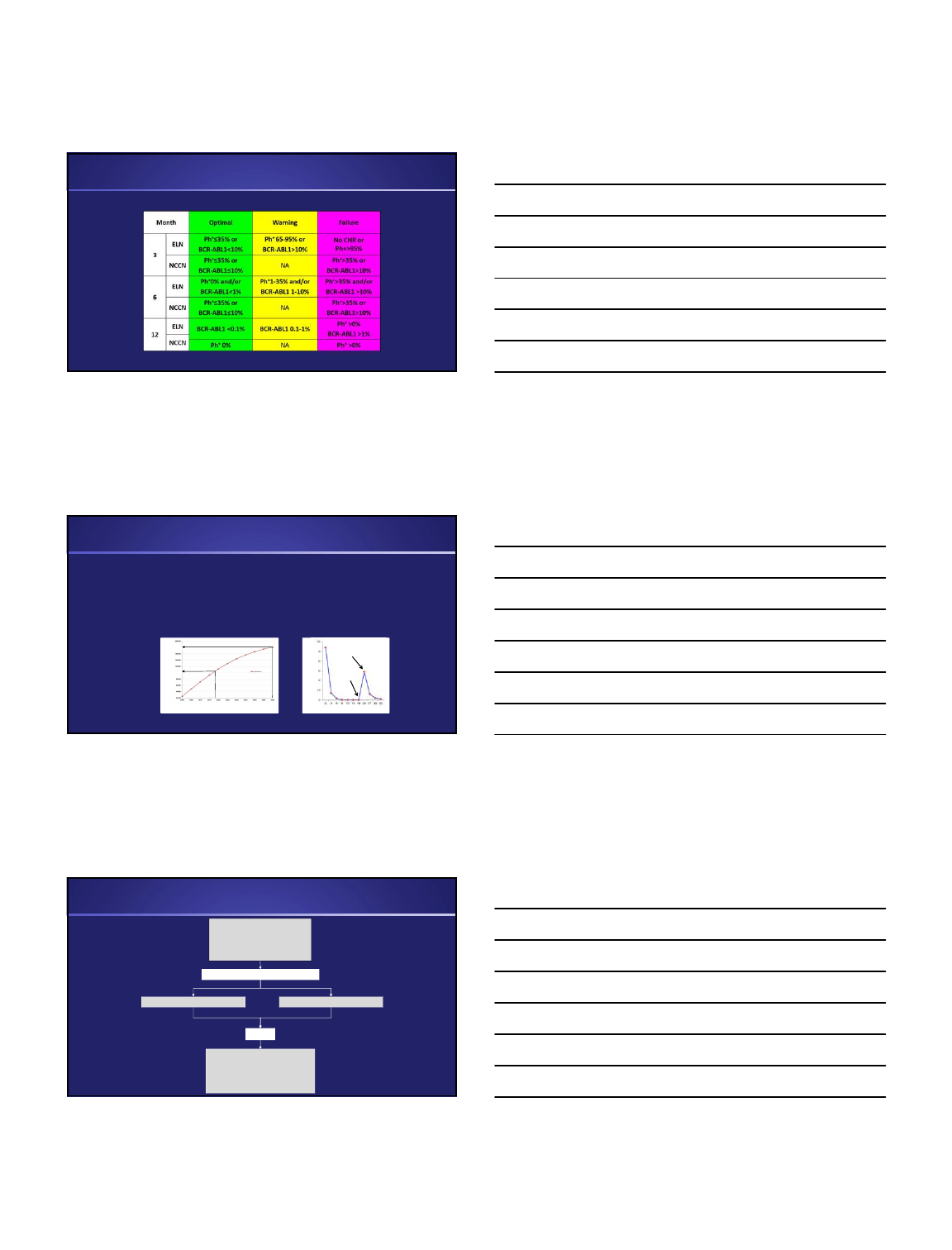
The Community Experience: High Rate of Imatinib Failure
Lucas et al, BJH 2008 27
28
88 newly diagnosed patients in NW UK
4/24/2018
3
Disease Burden & Monitoring on the
International Scale (IS)
?
Deep MR
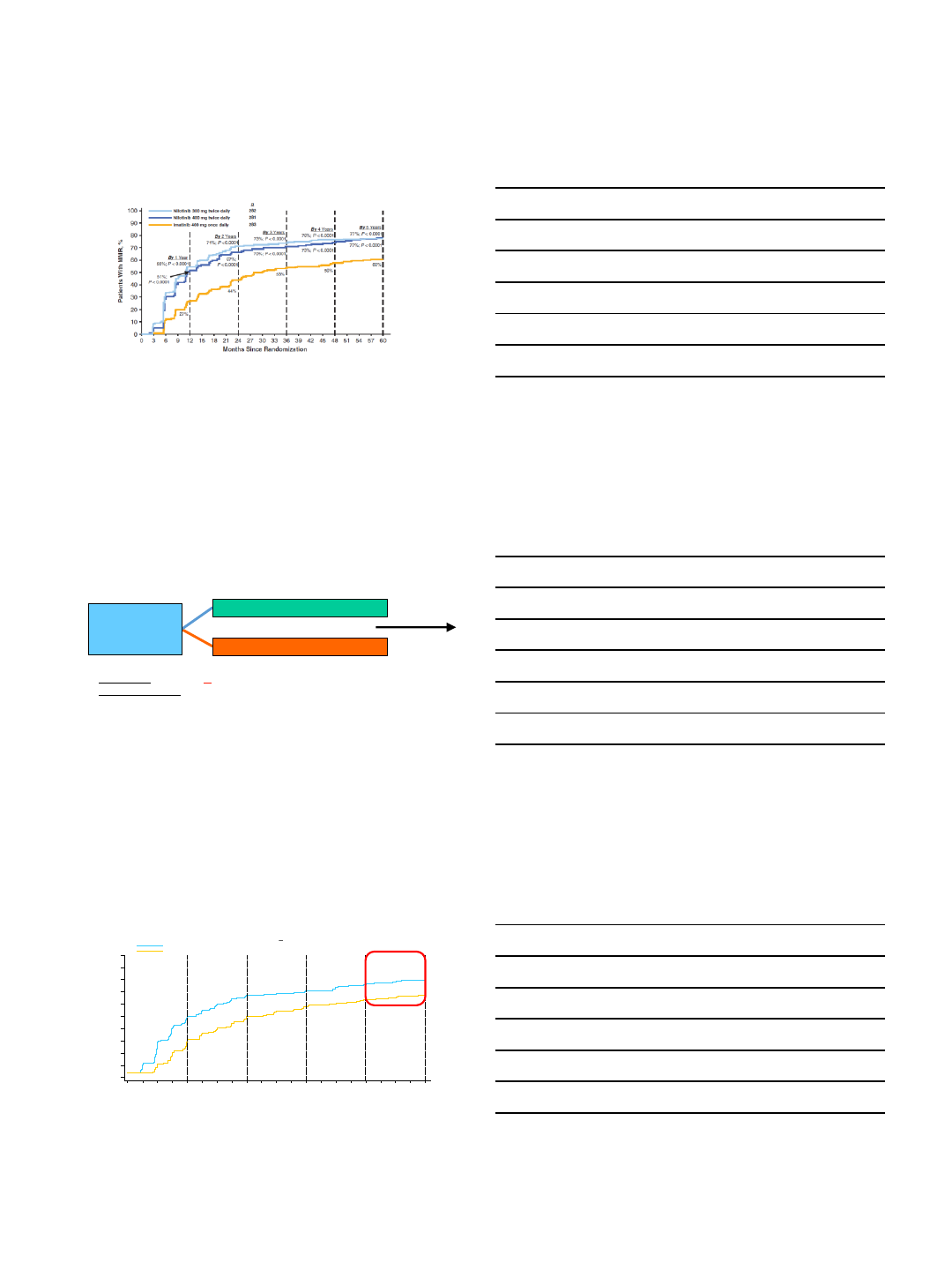
DASISION: Cumulative Incidence of MMR
0 6 12 18 24 30 36 42 48 54 60
100
90
80
70
60
50
40
30
20
10
0
Months Since Randomization
% With MMR
Dasatinib 100 mg QD
N
Imatinib 400 mg QD 260
259
By 1 year
By 2 years
By 3 years
By 4 years By 5 years
28%
46%
55%
60%
64%
46%
64%
67%
73% 76%
p=.0022
Cortes JC, et al. Blood. 2014
NIL 300 BID 77%
DASISION: Cumulative Incidence of MR
4.5
0 6 12 18 24 30 36 42 48 54 60
100
90
80
70
60
50
40
30
20
10
0
By 1 year
By 2 years
By 3 years
By 4 years
By 5 years
3%
8% 13%
23%
33%
5%
19%
24%
34%
42%
Months Since Randomization
% With MR
4.5
Dasatinib 100 mg QD
Imatinib 400 mg QD
N
259
260
p=.0251
NIL 300 BID 54%
Cortes JC, et al. Blood. 2014
4/24/2018
4
Therapeutic Milestones NCCN vs. ELN
Baccarani et al. Blood. 2013;122(6):872-84. Radich et al. J Natl Compr Canc Netw. 2014;12(11):1590-610
Failure with 1
st
line TKI imatinib ~10% on studies
Failure with 1
st
line dasatinib/Nilotinib/bosutinib* ~5% on studies
2G TKIs have long-term toxicities
Treatment free remission limited to minority
Challenges Remain
Stopped
therapy
Restarted
therapy
% BCR-ABL1 (IS)
Months
Cases in the US
181000
2018
2050
* Limited follow-up with the new initial dose of 400mg daily
105000
Year
Failure to reach milestones
Loss of CHR
Loss of CCyR
Confirmed loss of MMR
CCA/Ph
+
Complete diagnostic workup
Physical exam
Bone marrow aspirate/biopsy
Karyotyping
BCR-ABL1 mutation screen
No
Recognizing TKI Failure
Do not rush to conclusions!
Non-compliance or drug interaction? Laboratory error or imprecision?
4/24/2018
5
Mechanisms of TKI Resistance
BCR-ABL
Reactivation?
Yes No
Factors Influencing Selection of Salvage Therapy
Disease phase
BCR-ABL1 mutation analysis
Previous TKI exposure and response(s)
Past medical history
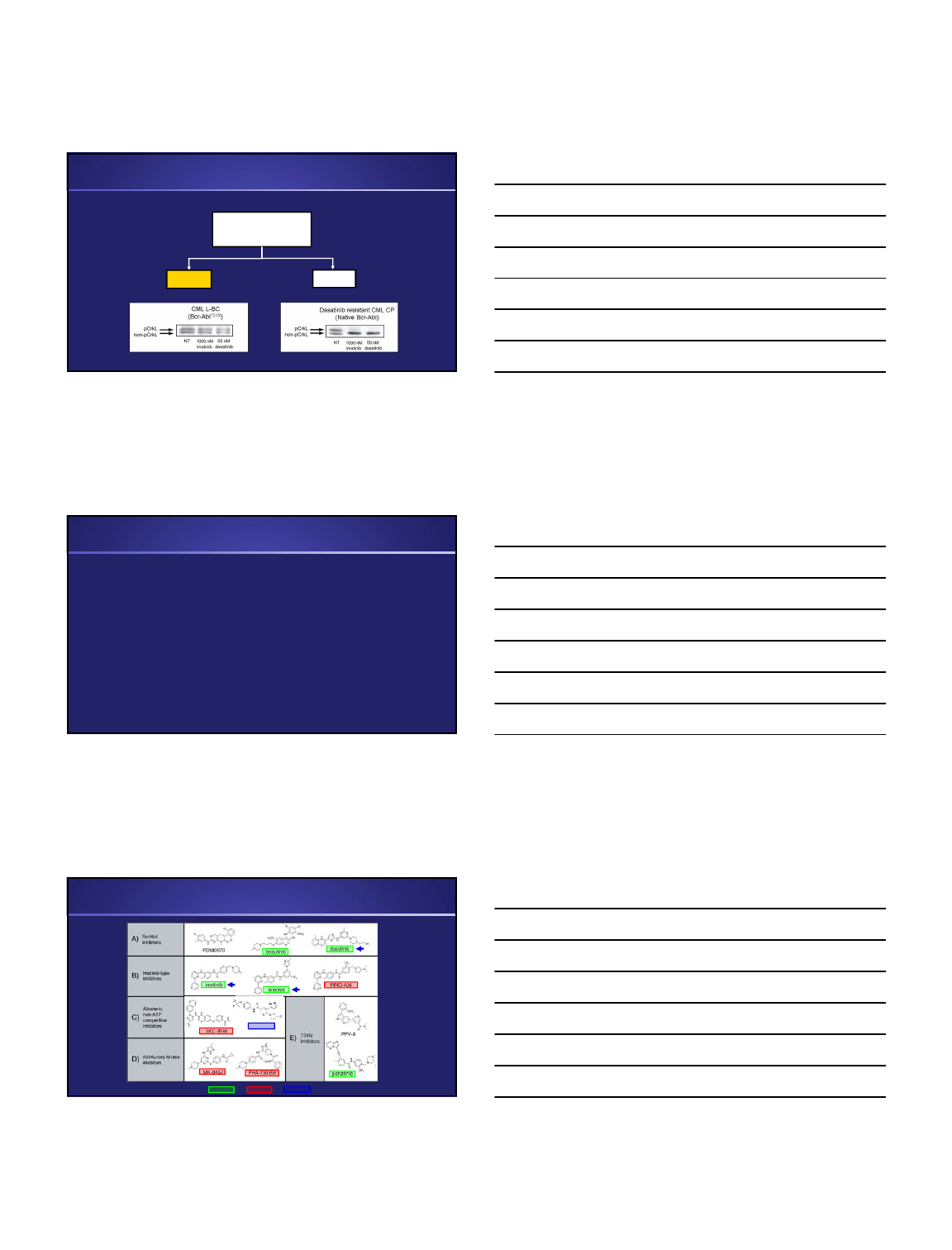
ABL1 Kinase Inhibitors
ponatinib
approved failed in trials
DCC-2036 asciminib
4/24/2018
6
Resistance Due to BCR-ABL1 Point Mutations
Relatively resistant
Completely resistant
Single
BCR-ABL1
Mutants
Imatinib
Nilotinib
Bosutinib
Dasatinib
Ponatinib*
TKI Resistance
* FDA-approved 12/2012
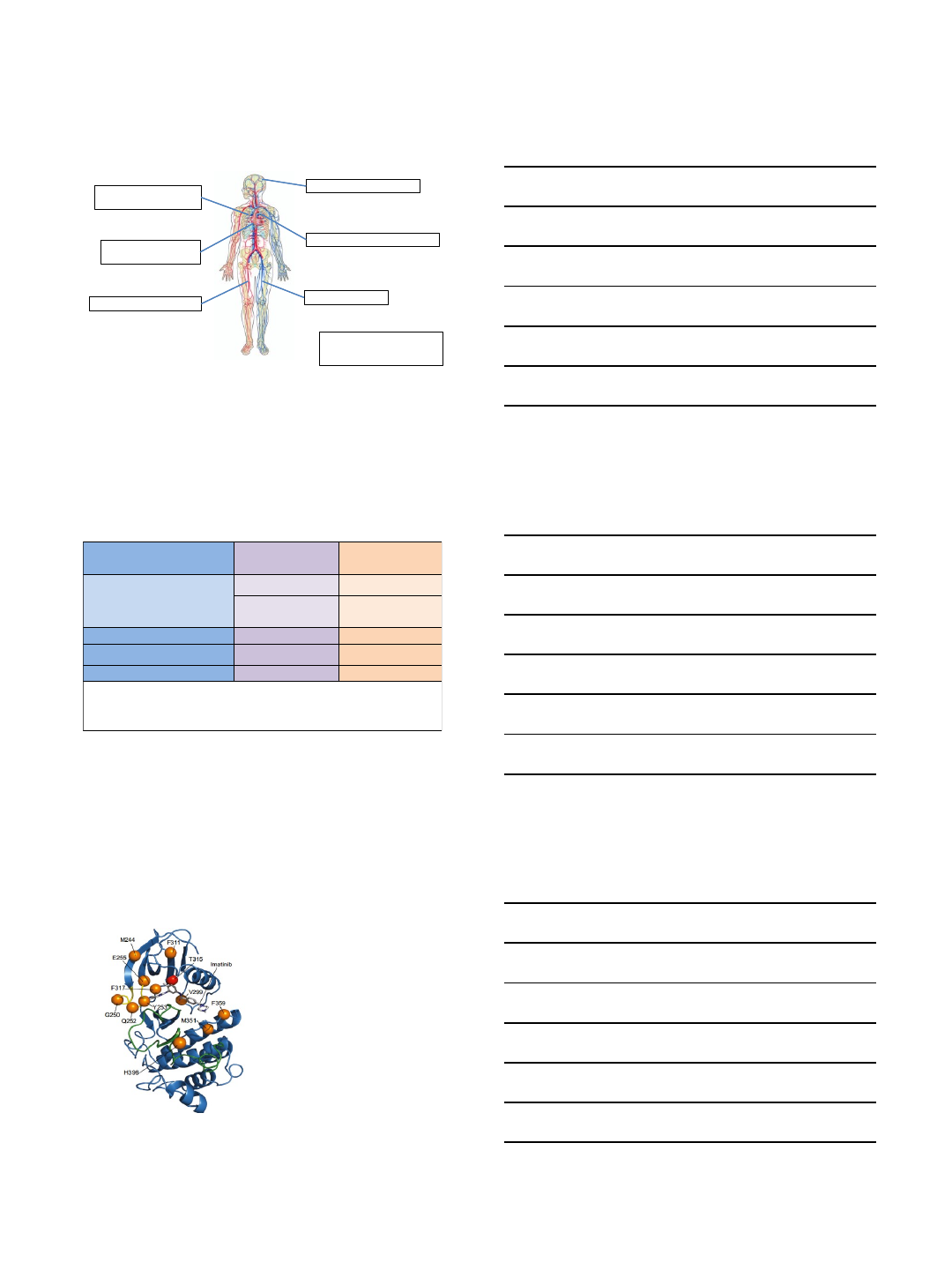
T315I
O
’
Hare et al. Cancer Cell 2009.
Past Medical History Impacts Therapy Selection
IM NIL DAS BOS PON
Diabetes
POAD
CHF
Prolonged QT
PHT
GI Bleeding
IBS
Pancreatitis
Impaired LF
Thrombembolism
Few absolute contraindications
Many better or worse picks
Clinical judgment crucial
Problems Potential
Somewhat elevated
Elevated
Typically contraindicated
Low
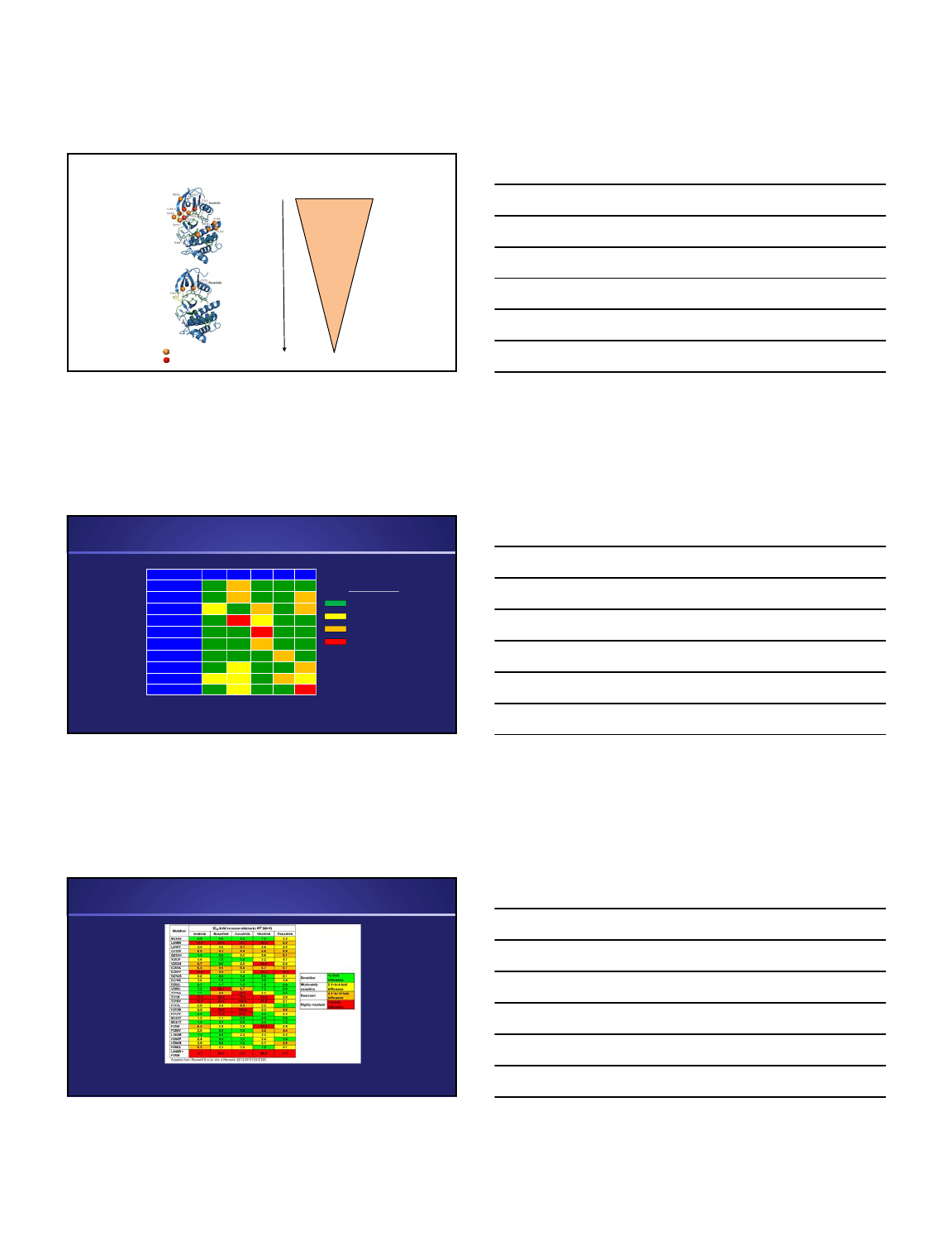
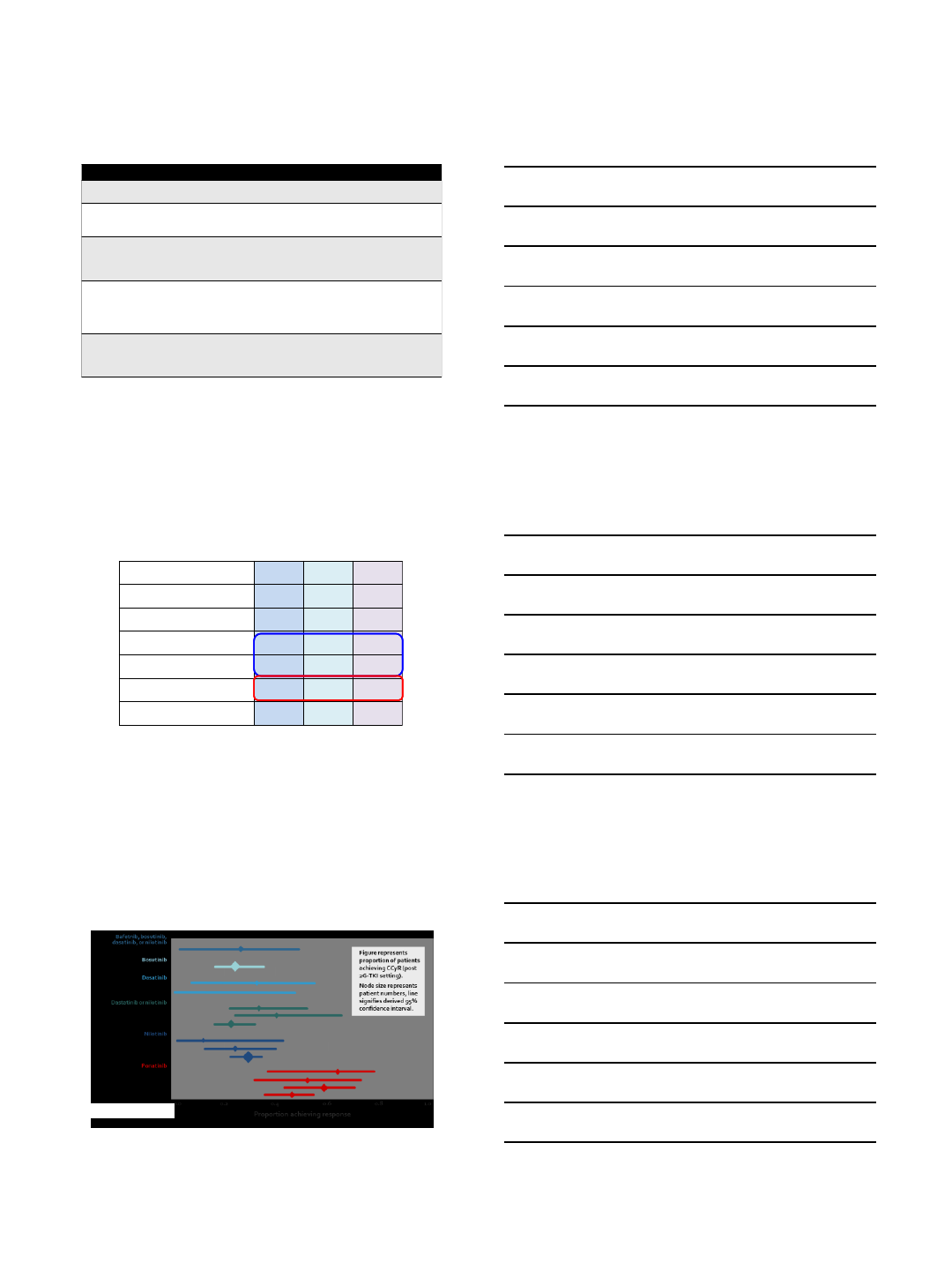
Relative Activity Profile of Various TKIs in Imatinib-Resistant Mutants
Eiring et al. Genome Biol. 2014;15(9):461
But: In vitro sensitivity is imperfect correlate of in vivo efficacy.
4/24/2018
7
1. Line therapy
Imatinib
Dasatinib
Nilotinib
Dasatinib
Nilotinib
Bosutinib
Ponatinib
2. Line therapy 3. Line therapy
Dasatinib
Nilotinib
Ponatinib
Bosutinib
Omacetaxine
T315I
70%
Treatment History and Salvage Therapy – Likelihood of CCyR
1. Line therapy
Imatinib
Dasatinib
Nilotinib
Dasatinib
Nilotinib
Bosutinib
Ponatinib
2. Line therapy 3. Line therapy
Dasatinib
Nilotinib
Ponatinib
Bosutinib
Omacetaxine
20%
20%
50-
70%
10%
Treatment History and Salvage Therapy – Likelihood of CCyR
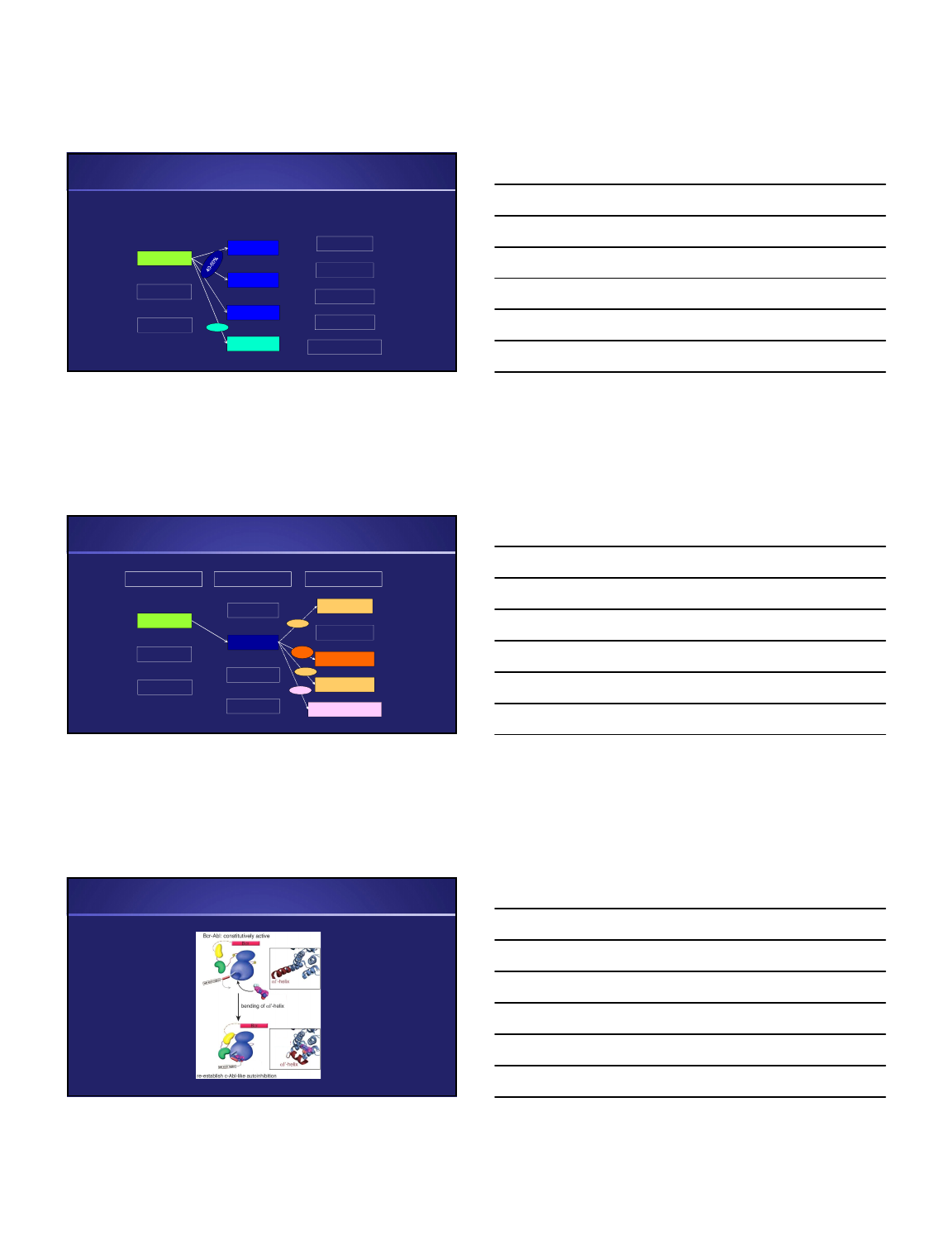
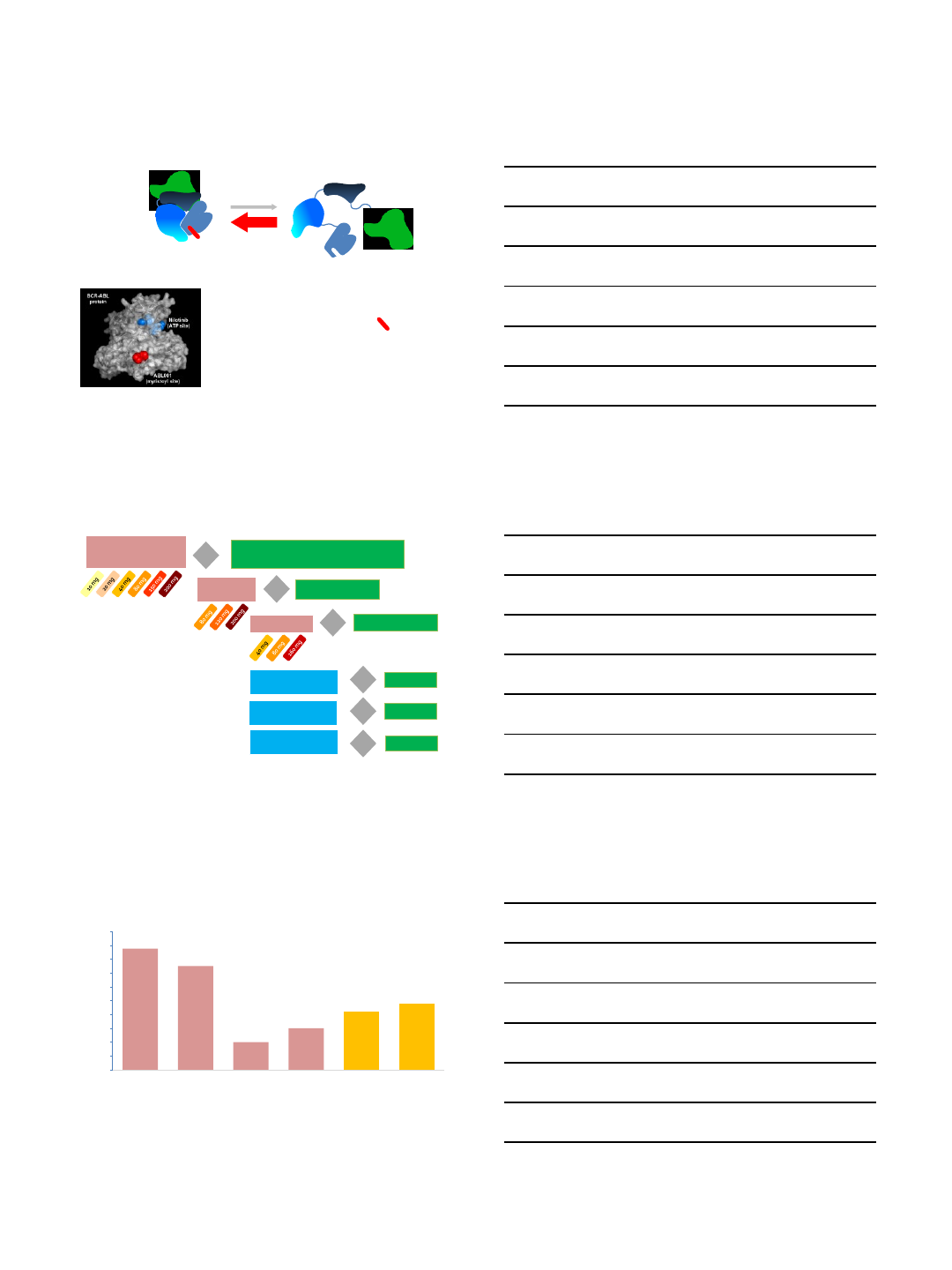
Hantschel O. Haematologica. 2012;97:195-97
Binders at the Myristoylation Site Allosterically Enforce Autoinhibition

4/24/2018
8
Asciminib: Allosteric BCR-ABL1 Inhibition
Binds with high affinity to the myristoyl pocket of ABL1 kinase to
mimic the native myristate ligand
Ba/F3 BCR-ABL1 IC
50
: ~3 nM
Demonstrates an extremely selective kinase profile
Currently in Phase 1/2
Wylie et al. Nature. 2017;543(7647):733-737
Activity of Asciminib in Comparison with Catalytic Site TKIs
Wylie et al. Nature. 2017;543(7647):733-737
Myristate
pocket
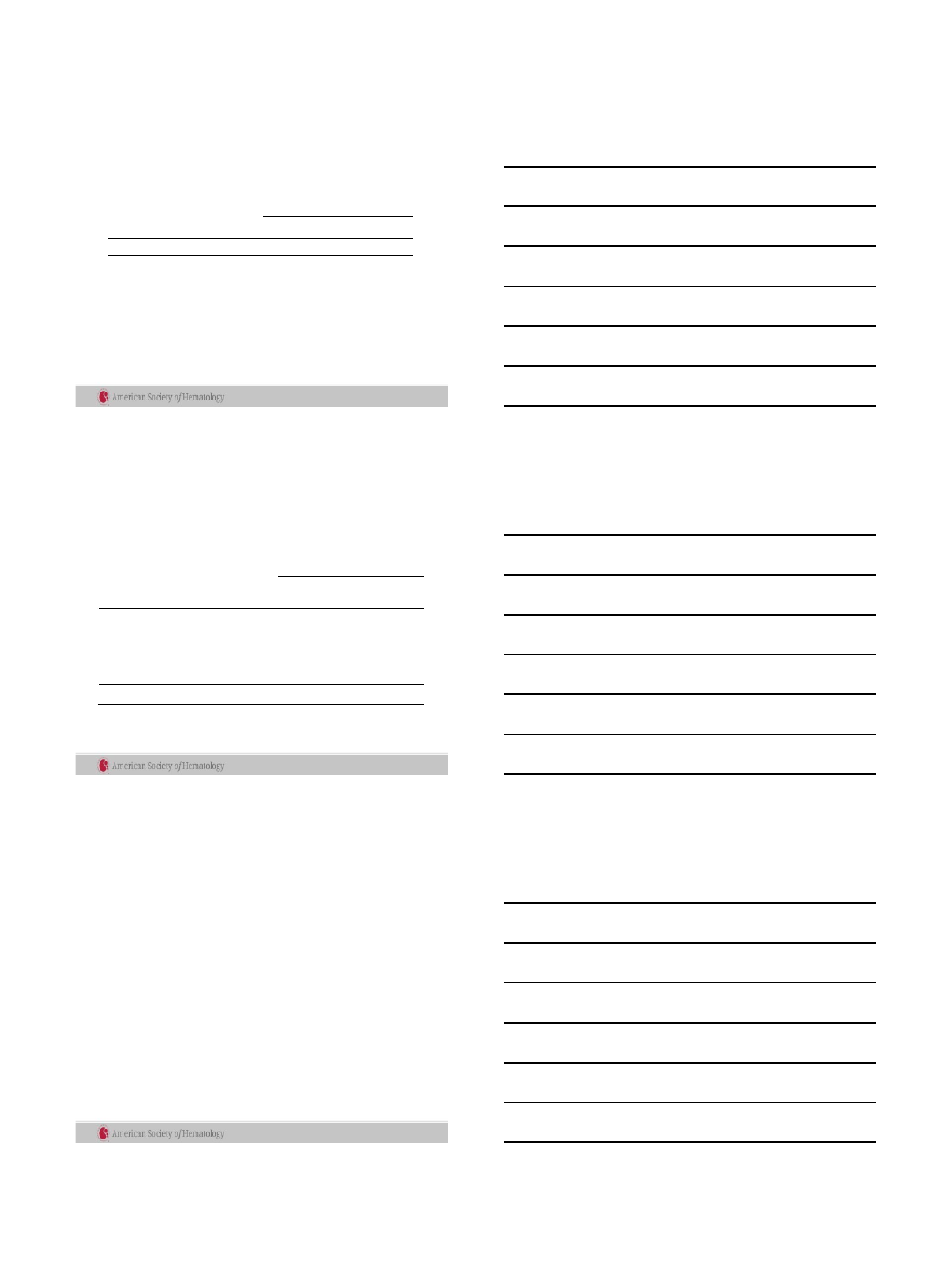
Responses in Patients With CML Treated With Single-Agent BID ABL001
With ≥ 3 Months Exposure on Study
0
10
20
30
40
50
60
70
80
90
100
Hematologic
Disease
(CHR relapse)
Cytogenetic
Disease
(> 35% Ph+) (> 0.1% IS)
Patients With Response, %
CHR:
88%
(14/16)
CCyR:
75%
(9/12)
MMR:
20%
(10/50)
MMR:
42%
(16/38)
(> 0.1% IS)
Disease Status at Baseline
(≤ 10% IS) (≤ 10% IS)
≥ 1-log
reduction:
30%
(10/33)
≥ 1-log
reduction:
48%
(12/25)
Hematologic
Response
Within 6 mo
Molecular Response
Within 6 mo
a,b
Molecular Response
Within 12 mo
b,c
Molecular Disease Molecular Disease
Cytogenetic
Response
Within 6 mo
a
Hughes et al. ASH 2016, abstract # 625
4/24/2018
9
Other BCR-ABL1 Inhibitors of Potential Interest
Radotinib
Chemically almost identical to nilotinib
Similar activity
Approved in South Korea
carbon in nilotinib
K0706
Structure unpublished
Active against BCR-ABL1
T315I
Phase 1/2 study in refractory CML is ongoing (Sponsor: Sun
Pharmaceuticals)
Axitinib
Main targets VEGFR1-3; KIT; PDGFR
Approved for RCC
Selective activity against BCR-ABL1
T315I
vs. native BCR-ABL1
(Pemovska et al. Nature 2015; Zabriskie et al. Leukemia 2015)
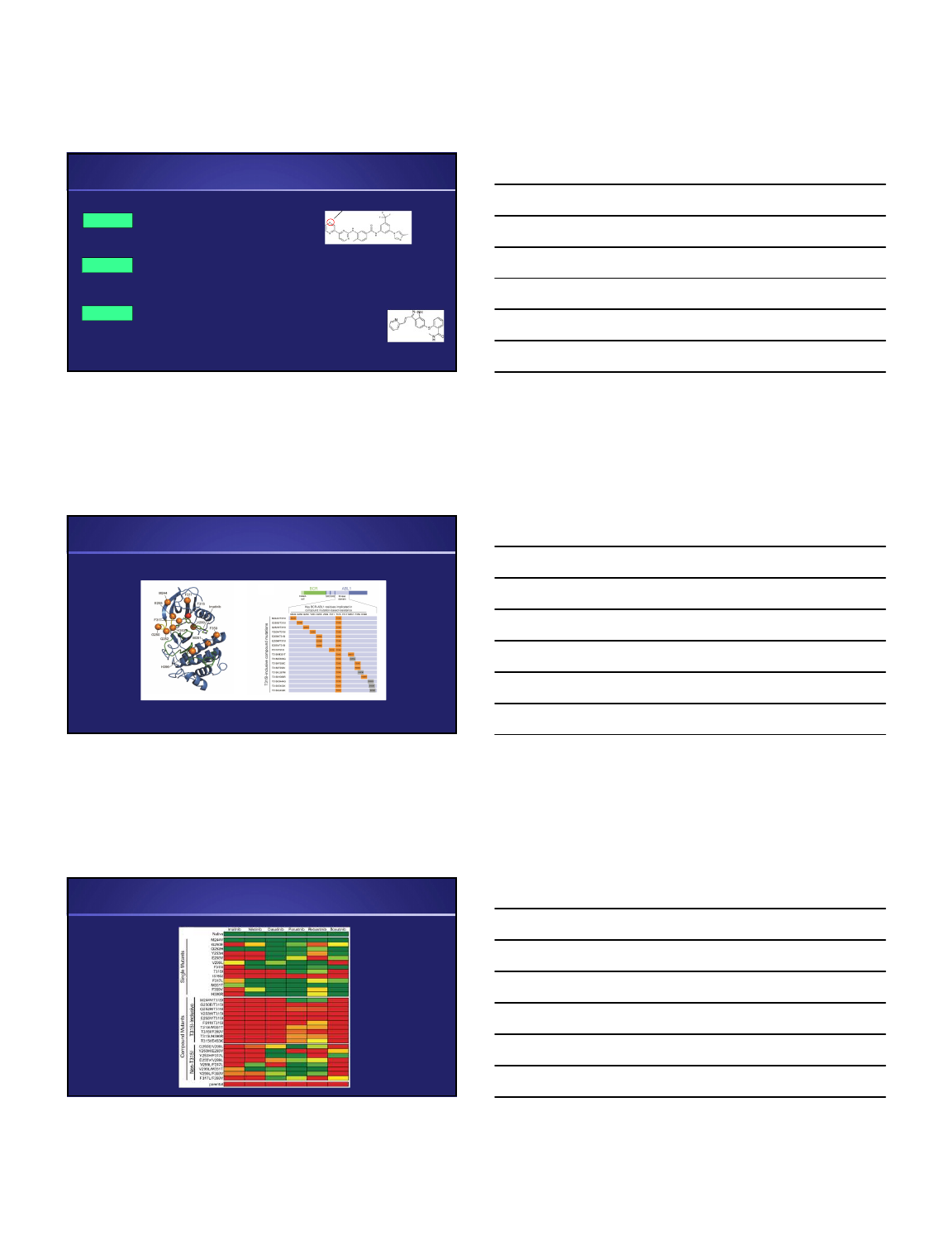
T315I-Inclusive Compound Mutations Confer
Universal TKI Resistance
Zabriskie et al. Cancer Cell 2014
Cellular BCR-ABL1 TKI Sensitivity
Zabriskie et al. Cancer Cell 2014
4/24/2018
10
Rationalizing Resistance due to E255V/T315I
Zabriskie et al. Cancer Cell 2014
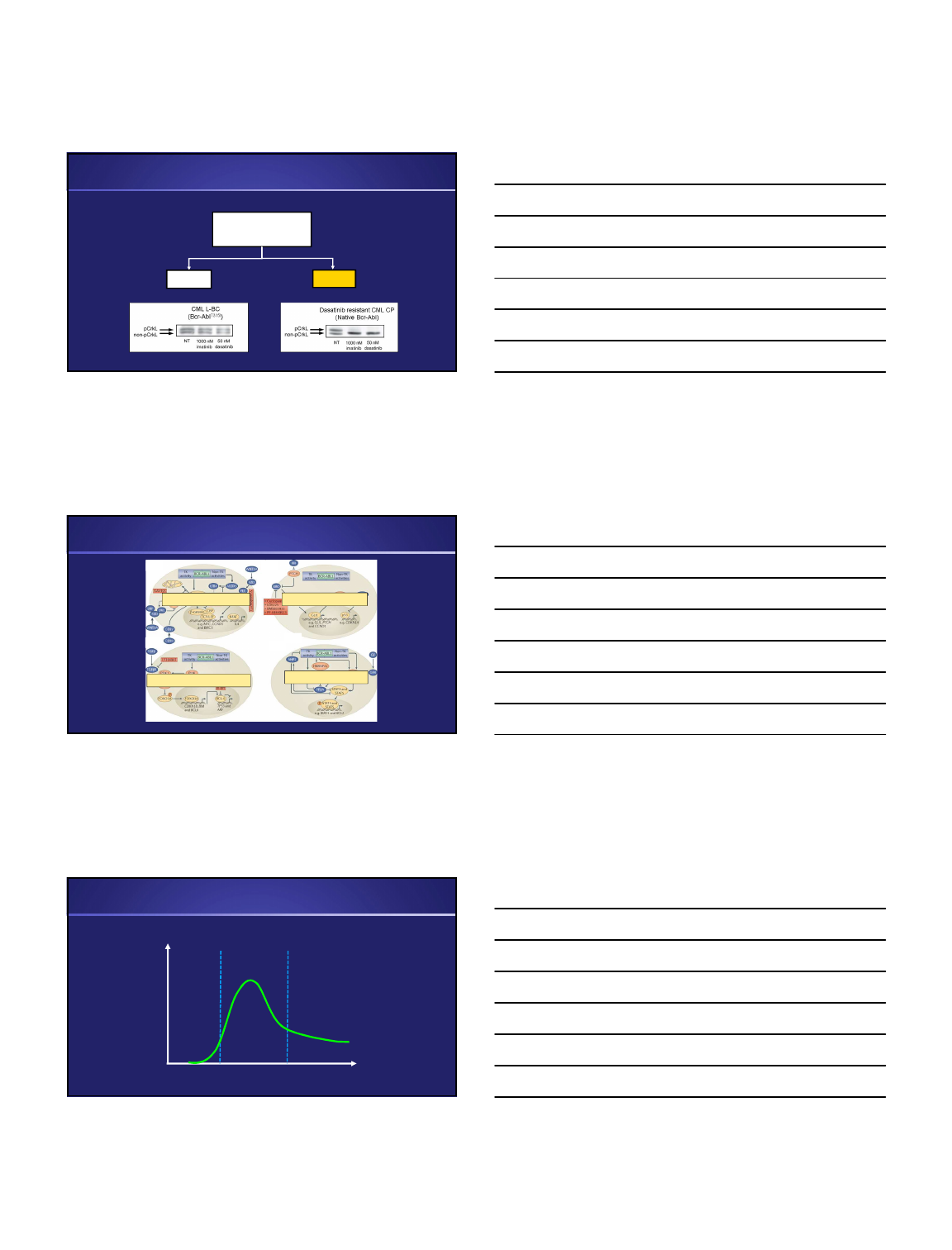
Efficacy of Ascminib alone and in Combination with Nilotinib
WT
M244V
G250E
Q252H
Y253H
E255V
V299L
F311I
T315I
F317L
M351T
H396R
1
10
100
1000
10000
100000
ABL001 IC50 [nM]
Single Mutants
O’Hare T, Zabriskie M, Deininger M, unpublished
Efficacy Against Single
BCR-ABL1 Mutants
Efficacy in Combination
with Nilotinib
A
BL001
0
2000
4000
6000
8000
10000
12000
ABL001 IC50 [nM]
Nilotinib
N
ilotinib + 250 nM ABL001
0
1000
2000
3000
4000
5000
Nilotinib IC50 [nM]
Y253H/E255VENU-based Mutagenesis Assay
Nilo Nilo+ABL001
ABL001
Nilotinib
Nilotinib + 250 nM ABL001
0
2000
4000
6000
8000
10000
12000
Nilotinib IC50 [nM]
ABL001
0
400
800
1200
1600
2000
ABL001 IC50 [nM]
E255V/T315I
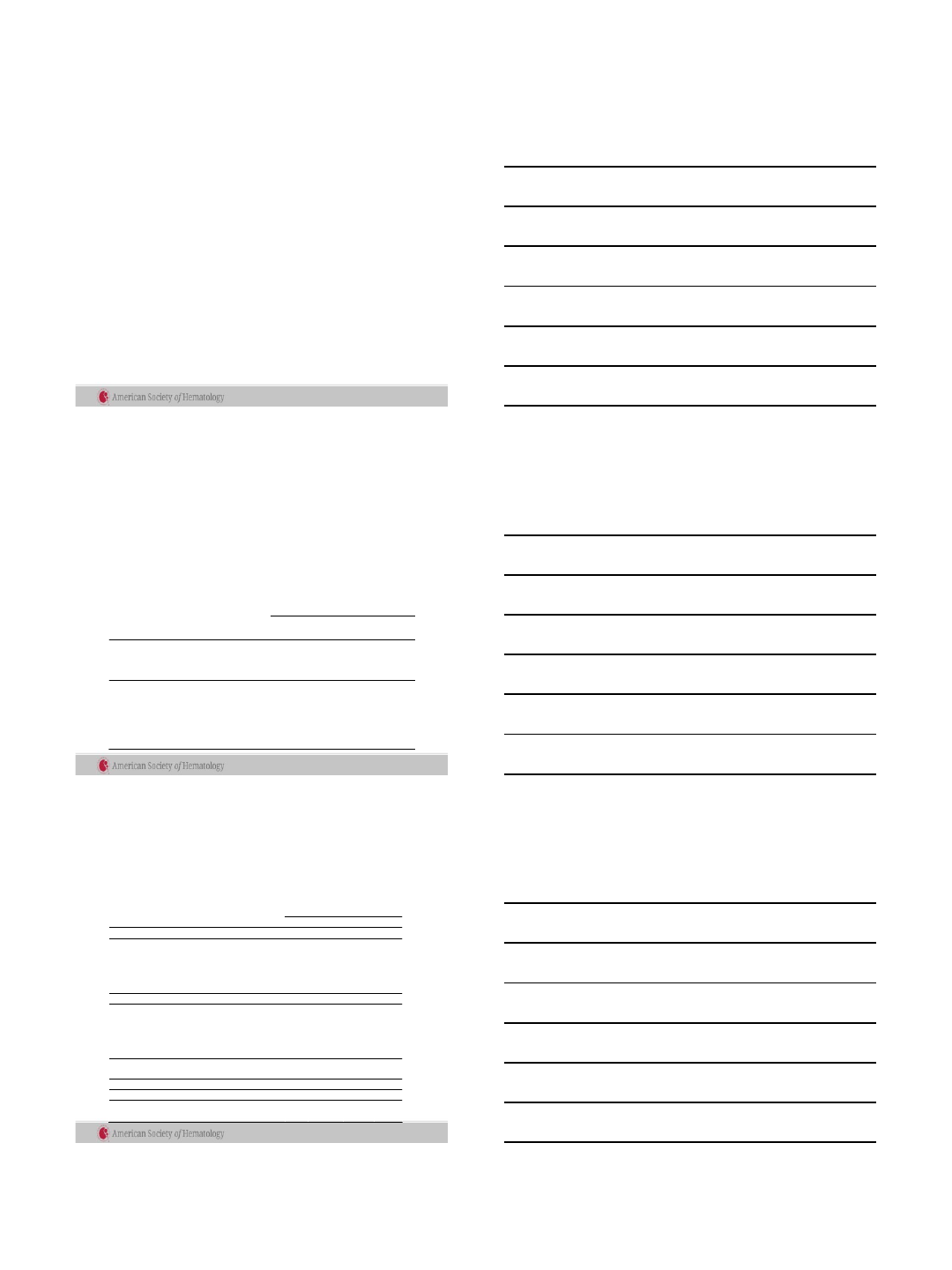
How far can we get with BCR-ABL1 Inhibition? Responses to Ponatinib 45mg
vs. Imatinib 400mg Daily (EPIC Trial)
Cave: Low numbers at 9, 12 months due to
study closure
Imatinib Ponatinib
Lipton et al. Lancet Oncol. 2016. 17(5):612-21
44
43
33
9
Nilotinib 300mg BID (ENESTnd)
Ponatinib:
Potent
Very long on-target time
Long half-life
Vascular toxicity
4/24/2018
11
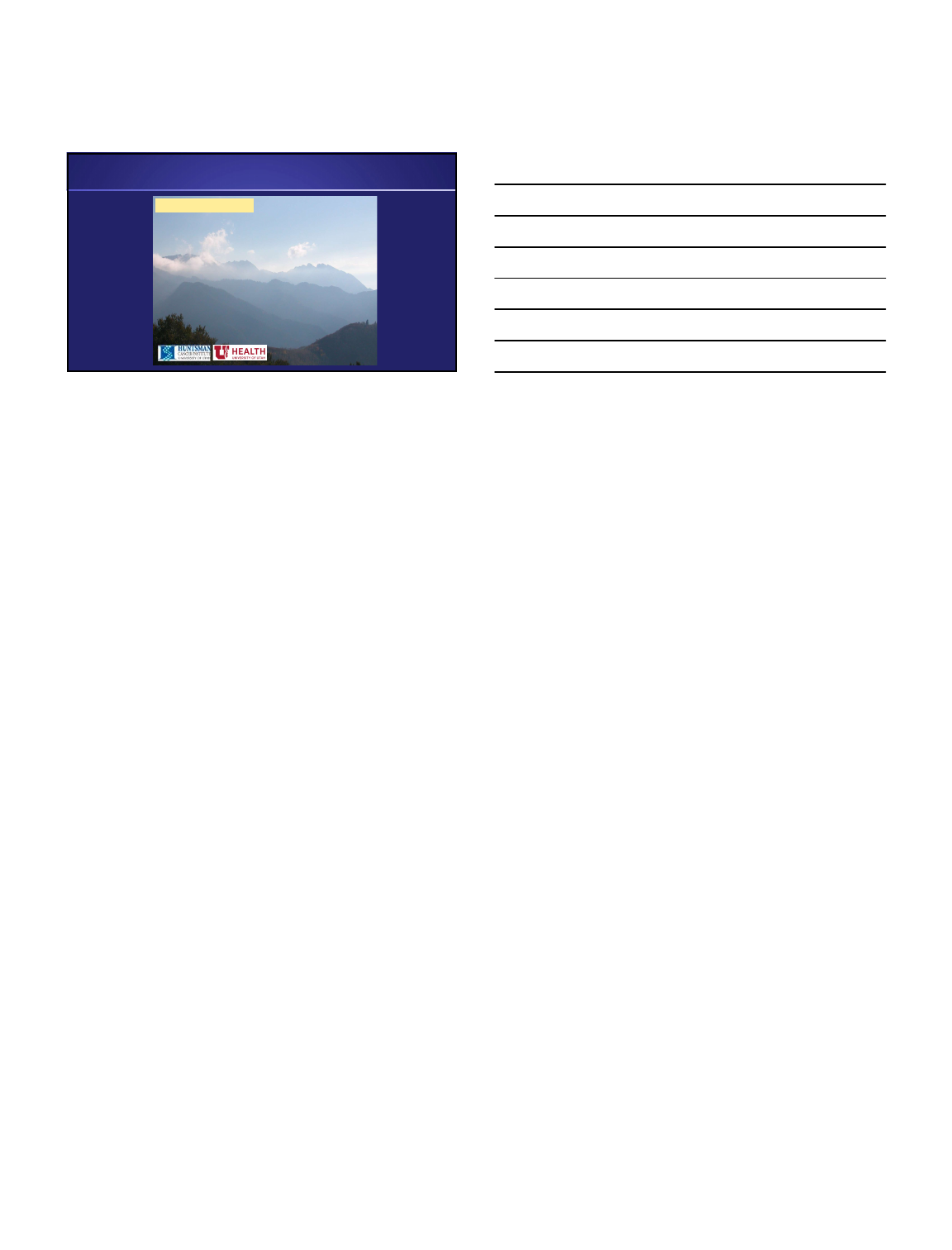
Mechanisms of TKI Resistance
BCR-ABL
Reactivation?
Yes No
O’Hare, Zabriskie, Eiring, Deininger, Nat Rev Canc 2012
Wnt/b-catenin Hedgehog
PI3K/AKT/FOXO3A/BCL6 JAK/STAT/PP2A
Alternative Survival Pathways in CML LSC
Instead of a Summary: How CML Works
BCR-ABL1 Dependence
Chronic Phase Blast PhaseMRD
Progression
4/24/2018
12
Acknowledgments
Tony Pomicter
Will Heaton
Phillip Clair
Anya Senina
Jonathan Ahmann
Anna Eiring
Dongqing Yan
Matt Zabriskie
Anca Franzini
Srinivas Tantravahi
Ami Patel
Funding Source
The Leukemia & Lymphoma Society
NIH/NCI
Aspire Mechanism
V Foundation
Deininger/O’Hare Lab
4/24/2018
1
Michael J. Mauro, MD
Leader, Myeloproliferative Neoplasms Program
Memorial Sloan Kettering Cancer Center, New York, NY
Multi-drug Resistant and Intolerant CML:
What to do?
Five Things
•What are we aiming for and what trips us up
•Approaching the ‘failing patient’: why?
mutations, adherence, other?
•ABL001
•PF-114
•K0706
International Standard
(IS) qPCR
10%
1%
0.1%
0.01%
0.0032%
Early Molecular Response:
<10% or 1-log (10x) drop from
starting level
Complete Cytogenetic Response:
<1% or 2-log (100x) drop
Major Molecular Response:
<0.1% or 3-log (1000x) drop
4-log drop (<0.01%)
4.5 log drop, ‘MR4.5’,
Complete Molecular Remission:
<0.0032%; below the level of
detection for standard labs
Early Molecular Response
Complete Cytogenetic Response
Major Molecular Response
MR4
MR5-6?
MR4.5
‘CMR’
Early Molecular Response
Complete Cytogenetic Response
Major Molecular Response
MR4
MR4.5
‘CMR’
eligible for
‘treatment free remission’
trials
‘Shrinking the iceberg’: response expectations
Plainly stated:
1. PCR at diagnosis = very important, like a timing chip when you run a race (where did you start?)
2. Early response at 3mo should be ‘on track’, 10x lower than start, ~10% (if you start ~100%)
3. Complete cytogenetic response (~1% on the PCR scale; 100x lower) is very important and protective
4. Major molecular response (MMR, ~0.1% on the PCR scale; 1000x lower) adds further protection
5. Deep Molecular remission: aiming for 0.01% or lower (10,000x lower than start) and staying that way
4/24/2018
2
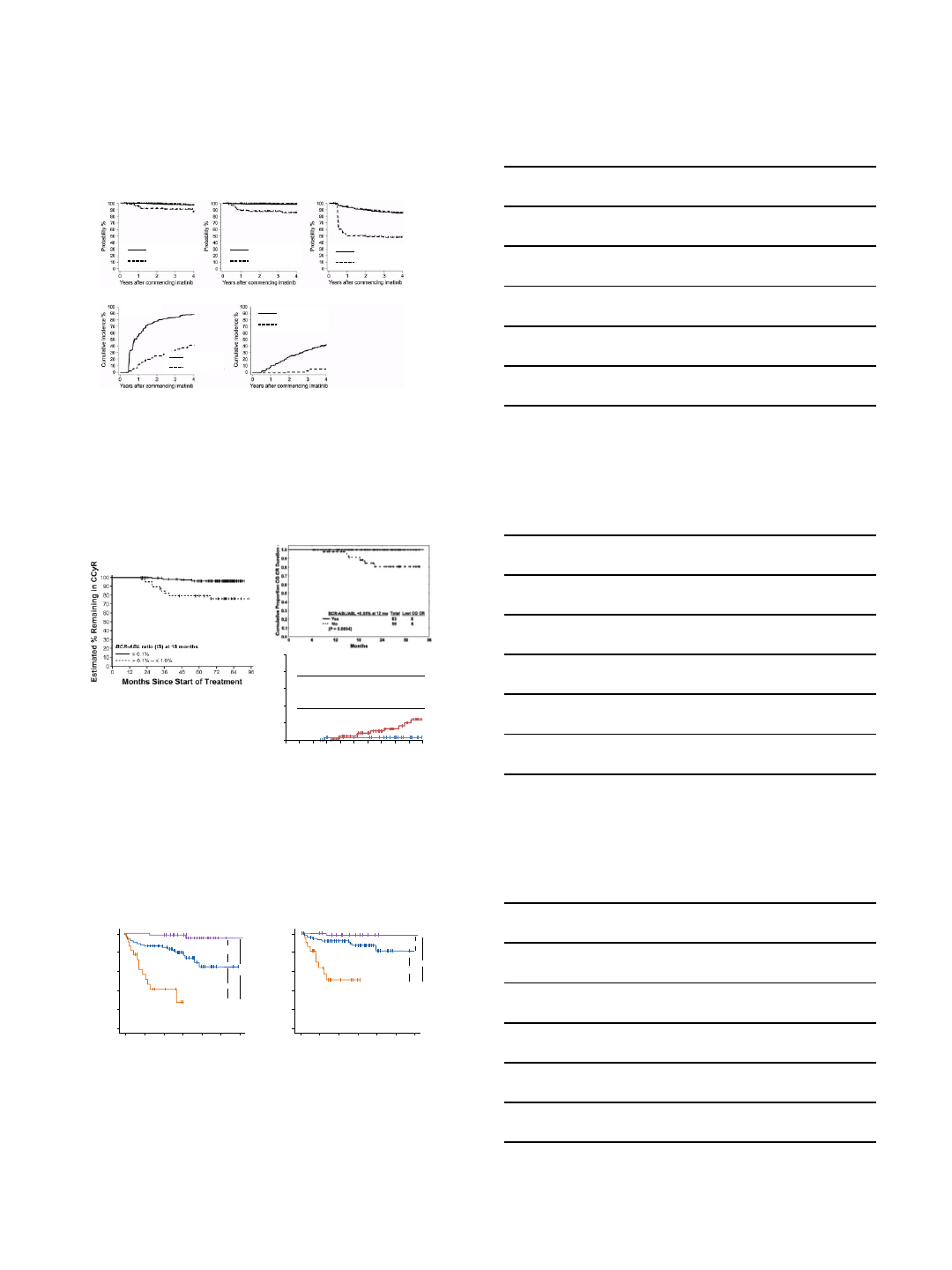
Branford S et al. Blood 2014;124:511-518
Overall Survival Progression-Free Survival Failure-Free Survival
Major Molecular Response Complete Molecular Response
≤ 10%
> 10%
≤ 10%
> 10%
≤ 10%
> 10%
≤ 10%
> 10%
≤ 10%
> 10%
Impact of BCR-ABL values ≤10% @ 3 months
Value of MMR in prolonging remission
Response at
12 months n Loss of CCyR
CCyR without MMR 95 24%
CCyR plus MMR 32 3%
Months Since Start of Imatinib Therapy
Loss of CCyR (%)
P = 0.04
0
20
40
60
80
100
0 6 12 18 24 30 36 42 48 54 60
Hughes T, et al. Blood 2010; 116(19):3758-65; Cortes J et al. Clin Cancer Res 2005;11:3425-3432; Marin D, et al. Blood 2008; 112(12):4437-44
Aside from being a launching point for ‘TFR’ trials,
does ‘CMR’ add value for CML patients?
23 11 5 1 0 0 0
92 81 60 33 10 3 0
65 63 53 35 15 3 2
CCvR+MMR-
CCvR+MMR+CMR-
CCvR+MMR+CMR+
Number at risk
23 11 5 1 0 0 0
92 81 60 33 10 3 0
65 63 53 35 15 3 2
CCvR+MMR-
CCvR+MMR+CMR-
CCvR+MMR+CMR+
Number at risk
p= 0.00124
p< 0.0001
p< 0.0001
1.0
0.8
0.6
0.4
0.2
0.0
020 40 60 80 100 120
Follow-up (Months)
Event Free Survival
EFS
CCyR+MMR+CMR+
CCyR+MMR+CMR-
CCyR+MMR-
p= 0.0335
p< 0.0001
p< 0.0001
1.0
0.8
0.6
0.4
0.2
0.0
020 40 60 80 100 120
Follow-up (Months)
Failure Free Survival
FFS
CCyR+MMR+CMR+
CCyR+MMR+CMR-
CCyR+MMR-
EFS = event-free survival; FFS = failure-free survival.
CMR Defined as undetectable BCR-ABL with a sensitivity of at least 4.7 logs on 2 consecutive analyses at least 2 months apart.
Etienne G et al. Haematologica 2014;99:458-464
4/24/2018
3
Choosing your tools: comparing TKI toxicity in CML
Issue
Imatinib
Nilotinib
Dasatinib
Bosutinib
Ponatinib
Dosing
QD/BID, with
food
BID,
without
food (2h)
QD, w/ or
w/o food
QD,
with
food
QD, w/ or
w/o food
Long term
safety
Most
extensive
Extensive;
Emerging
toxicity
Extensive;
Emerging
toxicity
Extensive,
No emerging
toxicity
More limited but
increasing;
Emerging toxicity
Heme
toxicity
intermediate
least
Most
severe;
ASA
-like
effect;
lymphocytosis
~
dasatinb in
2
nd, 3rd line;
~
nilotinib in
1
st line
thrombocytopenia
ASA
-like effect
Non
-
Heme
toxicity
Edema, GI
effects,
Phos
lipase, bili,
chol, glu
Black box: QT
prolongation;
screening req’d
Pleural
/
pericardial
effusions
Diarrhea;
transaminitis
lipase, pancreatitis;
rash; hypertension;
Black box:
vascular
occlusion, heart failure,
and hepatotoxicity
Emerging
toxicities
early
question re:
CHF; ?late
renal effects
Vascular
events (ICVE,
IHD, PAD)
PAH
(pulmonary
arterial
hypertension)
?
Mild renal
effects
Vascular events (ICVE,
IHD, PAD, VTE)
Post-Imatinib:
2nd Generation TKIs offer similar benefits
Dasatinib Bosutinib Nilotinib
Months follow-up >24 Median of 24 >24
Complete Hematologic Response 89% 86% 77%
Major Cytogenetic Response 59% 54% 56%
Complete Cytogenetic Response 44% 41% 41%
2-year Progression Free Survival 80% 79% 64%
2-year Overall Survival 91% 92% 87%
Shah et al. Haematologica 2010; 95: 232-40, Kantarjian et al. Blood 2011; 117: 1141-45; Cortes et al. Blood 2011; 118; 4567-76
3rd line therapy:
Switch to alternate 2nd gen agent versus ponatinib?
Lipton J, et al. ASH 2013. Abstract 4010.
4/24/2018
4
Kantarjian, et al. Blood. 2012;119:1981-1987.
The most significant ‘late effects’:
CML TKI Associated Cardiovascular Adverse Effects
10
Cerebrovascular Disease
Coronary Heart Disease
Myocardial Infarction
Pulmonary Arterial Hypertension
Venous Thrombosis
Peripheral Arterial Disease
Cardiomyopathy
Congestive Heart Failure
Morbidity and mortality; ? Effect on survival observations in front-line studies?
? Delay/deferral of advantageous therapy both in front-line and salvage
Cardiomyocyte Injury?
Endothelial Dysfunction?
Atherosclerosis?
Endothelial Dysfunction?
Atherosclerosis?
Endothelial Dysfunction?
Atherosclerosis?
Endothelial Dysfunction?
Platelet dysfunction?
Prothrombotic state?
•Fatigue
•Musculoskeletal Sx / Cramping
•Exercise-Induced Symptoms
Other:
Omacetaxine for CML After Failure of ≥2 TKIs
Response, % CP
N=81
AP
N=41
Primary endpoint(s)
Major Cytogenetic
Response: 20%
Major Hematologic
Response: 27%
Complete Cytogenetic
Response: 10%
Complete
Hematologic
Response: 24%
Median duration, months 17.7 9
Median Progression Free
Survival, months 9.6 4.7
Median Overall Survival, months 33.9 16
•11 patients (9 chronic phase, 2 accelerated phase) ongoing response
•Median 35 cycles over median 39 months
•Median response duration:
•14 months for chronic phase, 24 months for accelerated phase
Kantarjian. Blood 120: abst 2767; 2012
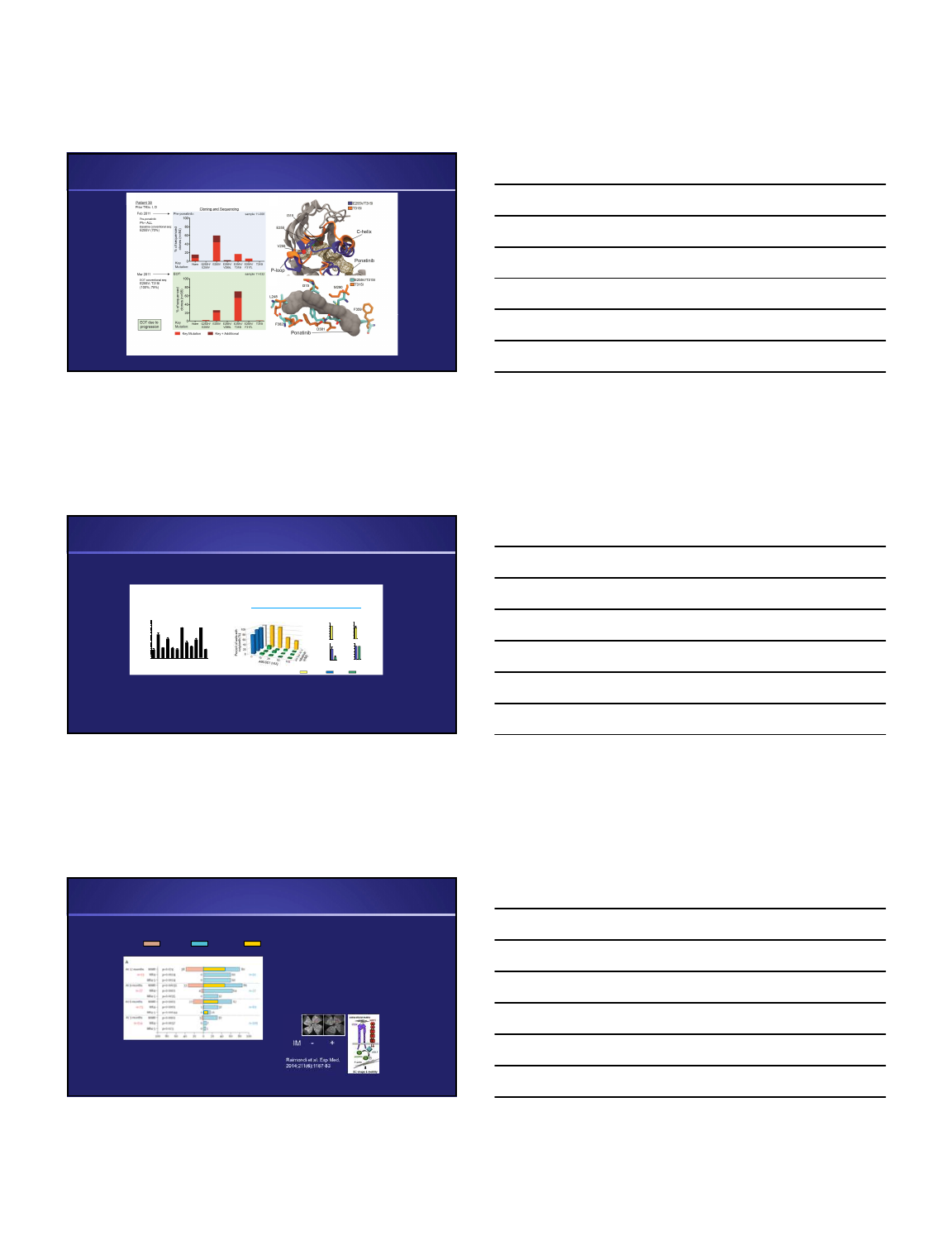
Resistance to TKIs: point mutations
•>100 mutations described
in imatinib and subsequent
generation TKI treated
patients; only a handful
(~10) account for the vast
majority (~85%) of
clinically observed
mutations
•Single and compound
mutations are found in the
same subset of 12 key
positions
4/24/2018
5
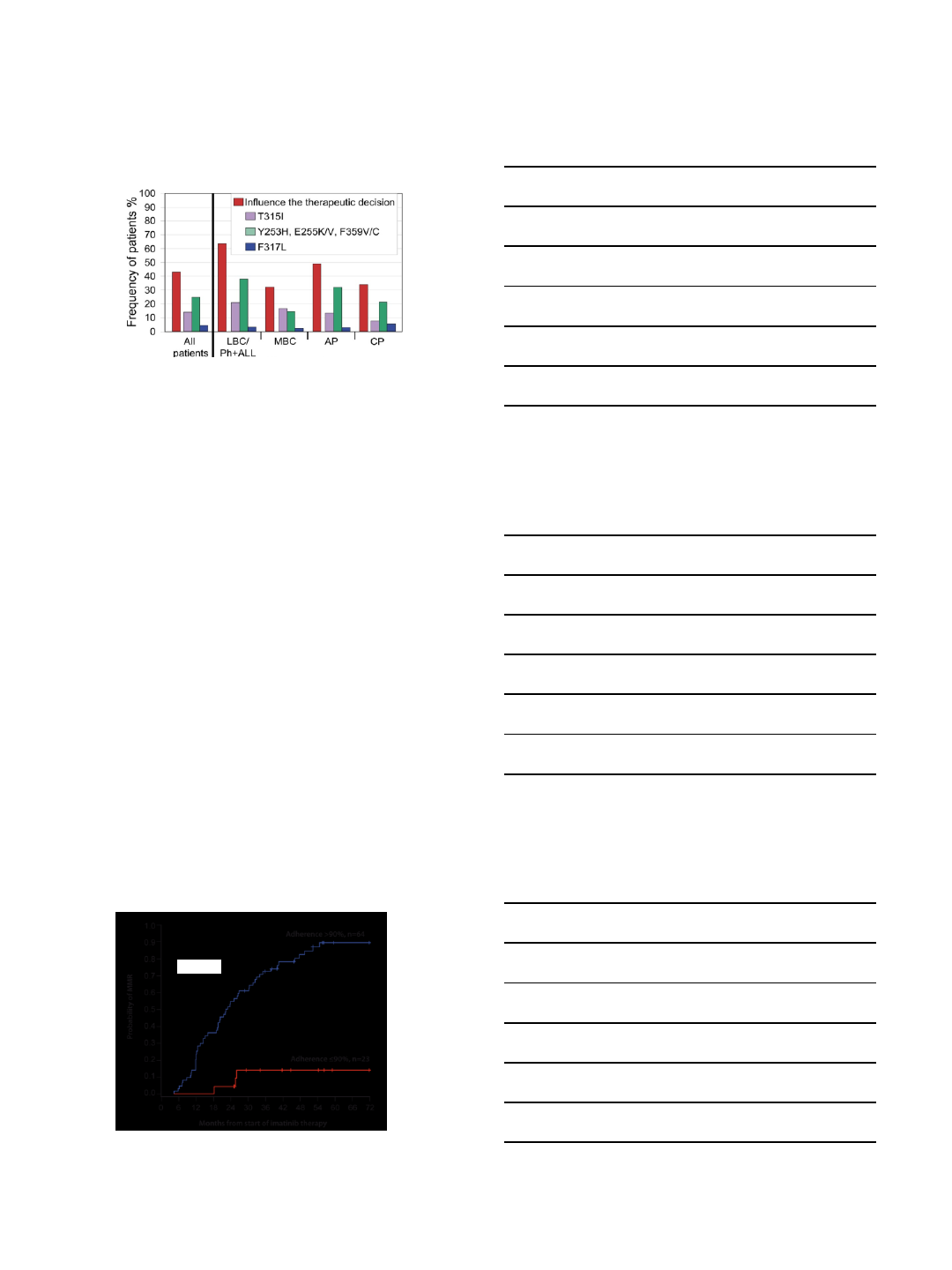
Likelihood mutation testing will influence TKI choice
Branford S et al, Blood 2009
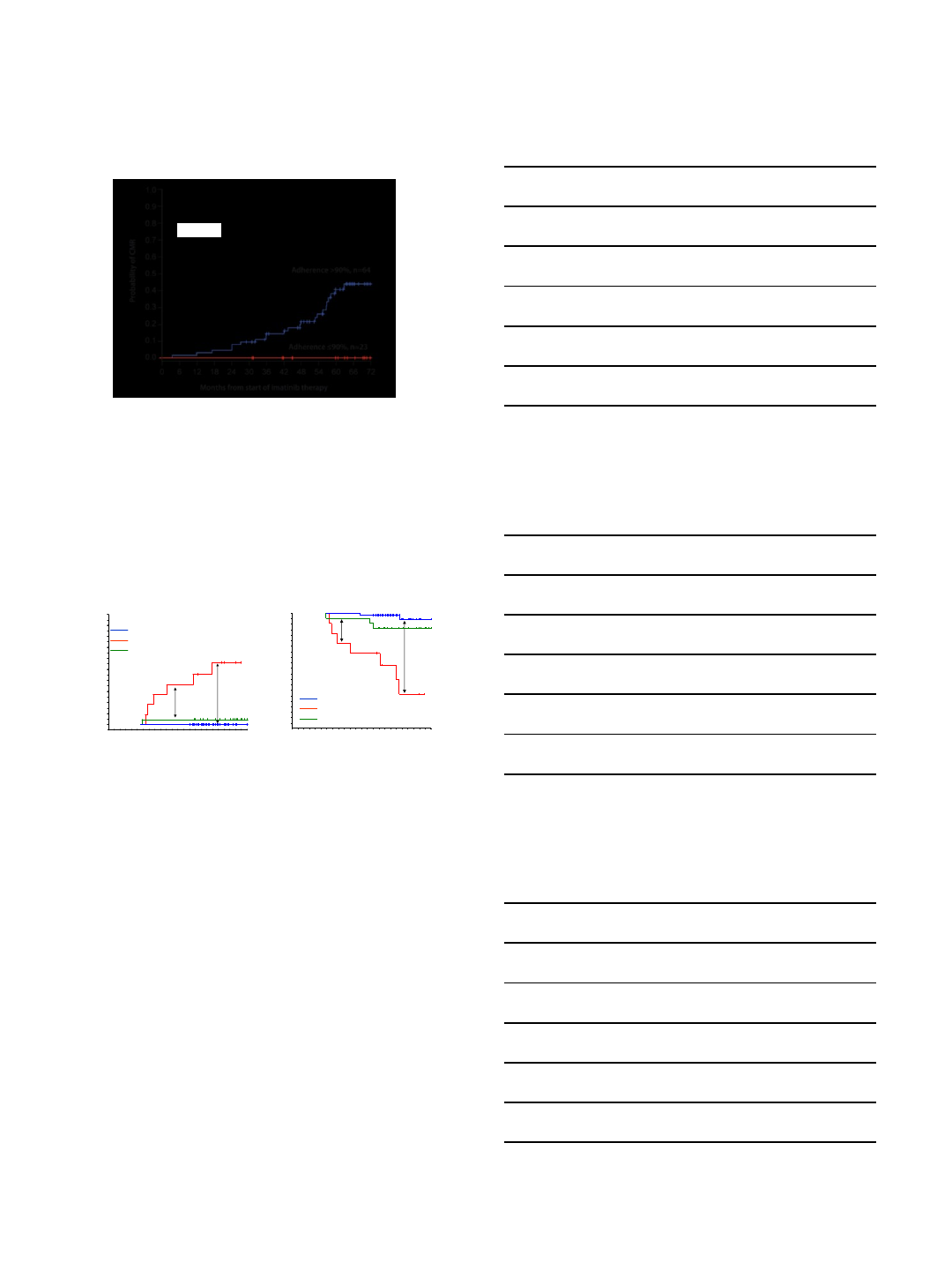
Adherence
Marin D, et al. J Clin Oncol 2010; 28(14): 2381–2388.
6-year probability of MMR according to
the measured adherence rate
p<0.001
4/24/2018
6
Marin D, et al. J Clin Oncol 2010; 28(14): 2381–2388.
6-year probability of CMR according to
the measured adherence rate
p=0.002
Probability of imatinib failure
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
Months from enrolment
0
0.0
2418126
p<0.0001
CCyR, no MMR, Adherence Rate ≤85%, n=11
MMR, n=53
CCyR, no MMR, Adherence Rate >85%, n=23
p=0.003
p<0.0001
Cumulate incidence of loss of CCyR
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
Months from enrolment
0
0.0
2418126
p<0.0001
CCyR, no MMR, Adherence Rate ≤85%, n=11
MMR, n=53
CCyR, no MMR, Adherence Rate >85%, n=23
p=0.0009
p<0.0001
Adherence and the achievement of MMR are the
only independent predictors for outcome
Marin D, et al. J Clin Oncol 2010; 28(14): 2381–2388.
Practical approach to a patient with resistance
(or intolerance +/- resistance)
•First, determine what the
disease state requires
–disease phase
–prior TKI exposure
–mutational status
•T315I unique
•Select mutations may
support role of specific
2nd generation TKIs
•Predictive potential
imprecise
•‘iceberg’ phenomenon
•More detailed assays not
routinely incorporated
(deep sequencing, etc)
•Next, balance therapy risk
and toxicity potential with
known comorbidities
–are there true
‘contraindications’?
–does risk outweigh benefit
expected from therapy?
–can risk be mitigated or
anticipated?
–enlist the patient’s insight,
trust, and awareness
4/24/2018
7
What is the role of allografting in CML?
Status
TKIs
Transplant
Accelerated
or Blast
transformation has
occurred
Interim
treatment to
best response/minimal
residual disease
ASAP
Imatinib failure in chronic
phase, T315I (+)
Ponatinib with caution,
ABL001 (experimental)
If no response to
Ponatinib
/ABL001
Imatinib failure in chronic
phase without clonal
evolution, mutations,
good
response
Long
-term second line
TKIs
Third line post second
TKI failure or beyond
IM failure in chronic
phase
with clonal
evolution, mutations,
poor response
Interim
treatment to
best response
Second
line, taken
case by case
Older
age (≥65 – 70) post
imatinib
failure
Long
-term second line
TKIs
May
forgo allo
SCT for
many yrs of QOL
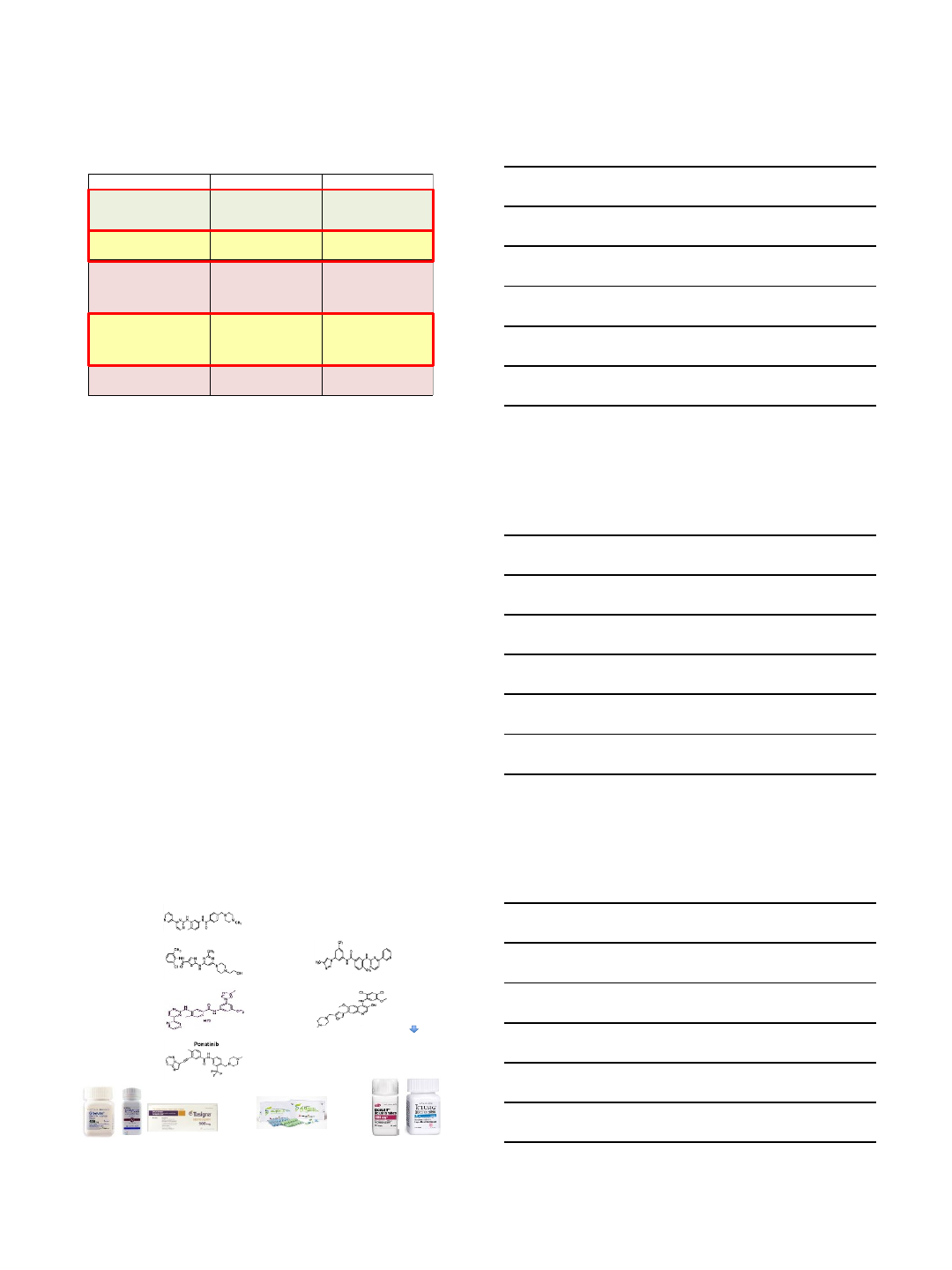
New Agents:
ABL001, PF-114, K0706
At present, five oral, small molecular kinase inhibitors approved in
the US for Ph+ Leukemia: a ‘spoil of riches’; more on the way?
1st Gen. TKI
2nd Gen. TKIs
3rd Gen. TKI
Others: K0706; PF-114
2001
Novartis
(1st line)
2007/2010
BMS
(1st, 2nd line)
2012/2015
IL-YANG:
(1st, 2nd line)
2012
Pfizer
(2nd/3rd line)
2012
Ariad
(2nd?/3rd line)
2007/2010
Novartis
(1st, 2nd line)
Radotinib (IY5511)
Imatinib (STI571)
Dasatinib (BMS354825) Nilotinib (AMN107)
Bosutinib (SKI606)
Ponatinib (AP24534)
2017:
1st/2nd/3rd line
4th Gen. TKI (allosteric):
ABL001
South Korea
only
4/24/2018
8
SH2
SH3
BCR
ACTIVE
4th generation TKI ABL001 Allosterically Inhibits
BCR-ABL1 Kinase Activity
Kinase
ABL001
t(9;22)
BCR
SH2
SH2
SH3
Kinase
INACTIVE
ABL001
Ottmann et al, ASH 2015 Abstract #138
•Developed to gain greater
BCR-ABL1 inhibition, with
activity against BCR-ABL1
mutations conferring
resistance to TKIs
•Potential to combine with
TKIs for greater
pharmacological control of
BCR-ABL1
Dose Escalation
Bayesian Logistic Regression
CML—completed
ABL001, po, BID
Dose Expansion
CML (20 mg, 40 mg)–completed
T315I mutation (150 mg)–ongoing
Dose Escalation
Ph+ ALL/CML-BP
Combo Dose Escalation
CML
ABL001+nilotinib
MTD
RDE
Expansion
Dose Expansion
Ph+ ALL/CML-BP
Combo Dose Escalation
CML
ABL001+imatinib
Expansion
Combo Dose Escalation
CML
ABL001+dasatinib
Expansion
Dose Escalation
CML
ABL001, po, QD
Dose Expansion
CML
MTD
RDE
MTD
RDE
MTD
RDE
MTD
RDE
MTD
RDE
ABL001X2101: Study Design
A multicenter, phase 1, first-in-human study
•Primary outcome: estimation of MTD/RDE
•Secondary outcomes: safety, tolerability,
preliminary anti-CML activity,
pharmacodynamics, pharmacokinetic
profile
ALL, acute lymphocytic leukemia; BID, twice daily; BP, blast phase;
CML, chronic myeloid leukemia; MTD, maximum tolerated dose;
Ph+, Philadelphia chromosome-positive; po, peroral; QD, once
daily; RDE, recommended dose for expansion
Hughes TP, et al. Blood. 2016; 128 (22): [abstract 625].
47 of 77 (61%) patients with
CML treated with single-
agent ABL001 BID were
resistant to their last TKI
Responses in Patients With CML Treated With Single-Agent
BID ABL001 With ≥3 Months Exposure on Study
0
10
20
30
40
50
60
70
80
90
100
Hematologic
Disease
(CHR relapse)
Cytogenetic
Disease
(>35% Ph+) (>0.1% IS)
Patients With Response, %
CHR:
88%
(14/16)
CCyR:
75%
(9/12)
MMR:
20%
(10/50)
MMR:
42%
(16/38)
(>0.1% IS)
Disease Status at Baseline
CCyR, complete cytogenetic response; CHR, complete hematologic response; IS, International Scale; MMR, major molecular response; mo, months
aPatients had ≥6 months of treatment exposure or achieved response within 6 months
bBCR-ABL1IS reduction achieved
cPatients had ≥12 months of treatment exposure or achieved response within 12 months
(≤10% IS) (≤10% IS)
≥1-log
reduction:
30%
(10/33)
≥1-log
reduction:
48%
(12/25)
Hematologic
Response
Within 6 mo
Molecular Response
Within 6 moa,b
Molecular Response
Within 12 mob,c
Molecular Disease Molecular Disease
Cytogenetic
Response
Within 6 moa
Hughes TP, et al. Blood. 2016; 128 (22): [abstract 625].
Low blood counts and pancreas enzyme elevation are
main side effects of higher intensity seen to date
13.3% and 37.5% achieved MMR by 6 and 12 months
29.4% and 42.9% achieved ≥1-log reduction by 6 and 12 mo
8 of 10 (80%) patients with >35% Ph+ achieved CCyR by 6
mo
4/24/2018
9
CABL001A2301 (Planned): Study Design
A phase 3, Multicenter, Open-label, Randomized
Study of ABL001 Versus Bosutinib
2:1
Randomization
CML CP patients (N =
222 planned),
previously treated
with ≥ 2 ATP binding
TKIs
ABL001
40 mg BID
Lack of response
Failure/Intolerance
Bosutinib
500 mg QD
Lack of response
Failure/Intolerance
Survival follow-up
•Primary endpoints: Major Molecular Response (MMR) rate at 24 weeks
•Key secondary endpoint: MMR rate at 96 weeks
BID, twice daily; CML, chronic myeloid leukemia; CP, chronic phase; QD, once
daily; TKI, tyrosine kinase inhibitor
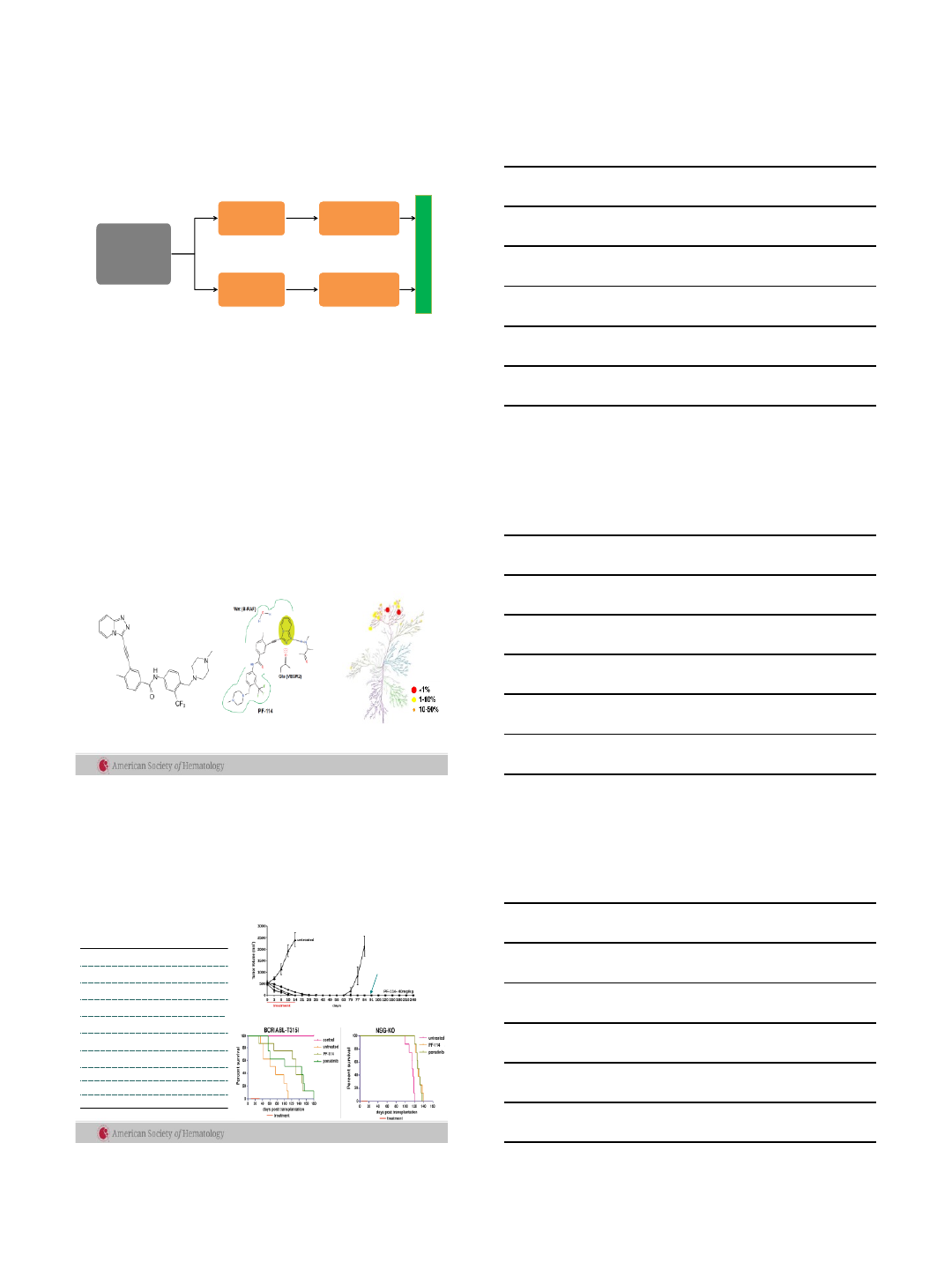
PF-114 phase 1 study
PF-114 –Novel 3rd Generation Inhibitor of Bcr-Abl
PF-114 PF-114 kinase inhibition
profile (100 nM)
•PF-114: 3rd generation Abl inhibitor, close structural analog of ponatinib
•PF-114 rationally designed to avoid inhibition of numerous off-target
kinases and potentially avoid life-threatening side effects
Structure-inspired disruption of
off-target interactions with
kinases like VEGFR2 and B-Raf
Cortes J et al, ASH 2017
PF-114 phase 1 study
Pre-clinical Characterization of PF-114
•Cytotoxicity to Ph+ ALL PDLTC and BaF3 cells
with native BCR/ABL and mutant variants
Cell line Bcr-Abl
variant
IC50,
nM*
PDLTC, VB p210 15
PDLTC, PH P185 3
PDLTC, CM p210 7
PDLTC, KW p185 5
PDLTC, DW p185 7
PDLTC, BV p185 3
PDLTC, KO p185, T315I 75
BaF3 p185, Y253F 25
BaF3 p185, E255K 25
BaF3 p185, F317L 100
*Medical Clinic of Ghoethe University, Frankfurt, Germany
•Xenograft K562 CML cell line model
AUC 15uM*h
Ponatinib
Dose 25 mg/kg
AUC 24uM*h
PF-114
Dose 40 mg/kg
AUC 15uM*h
Orthotopic murine BaF3 cell
model of T315I+ CML
NSG Mice iv xenograft of human
T315I Ph+ALL
Cortes J et al, ASH 2017
4/24/2018
10
PF-114 phase 1 study
Phase 1 Study Design and Outcome Measures
•Design
–3+3 dose escalation till MTD (DLT during 1-st 28-day cycle)
–Expanded cohorts (10-15 pts each) at ≤MTD; total enrollment ~44 pts
•Eligibility
–CML CP or CML AP patients who failed ≥2 TKIs, or intolerant of TKIs, or with
T315I
•Primary endpoints
–DLT(s) during 1-st 28-day cycle
–MTD
•Secondary endpoints
–Incidence of AEs
–PK
–Rates of hematologic, cytogenetic, molecular responses
•Exploratory endpoints
–Pharmacodynamic response (p-CrkL/CrkL)
–Pharmacogenetic relations (response across BCR/ABL mutant forms)
Cortes J et al, ASH 2017
PF-114 phase 1 study
Preliminary Analysis of Safety:
Hematologic Adverse Drug Reactions
n of patients with
adverse drug
reactions
Gr 1
Gr 2
Gr 3
Gr 4
Blood and lymphatic system
disorders
4/24
1/24
3/24
neutropenia
2 1 2
thrombocytopenia
2 2
anemia
1
Cortes J et al, ASH 2017
PF-114 phase 1 study
n of patients
with adverse drug reactions
Gr 1
Gr 2Gr 3
Gr
4
Skin and subcutaneous tissue disorders
18/24
13/24 4/24
psoriasiform
skin lesions 13 10 3
dry skin
5 1
itching
2 1
rash
1 1 1
hyperemia
1 1
Gastrointestinal disorders
7/24
1/24
diarrhea
6 1
abdominal
pain 2
nausea
1
stomatitis
1
pain
in the right hypochondrium 1
General disorders and administration site
conditions
1/24
fever
1
Nervous system disorders
2/24
dizziness
1
headache
1
Cortes J et al, ASH 2017
Non-Heme AEs
4/24/2018
11
PF-114 phase 1 study
n of patients with
adverse drug reactions
Gr 1
Gr
2Gr 3
Gr 4
Investigations
4/24
2/24
hypophosphatemia
1
increase of cholesterol
1 1
increase of LDL
1
decrease
of HDL 1
increase
of ALT 1
increase of AST
1
increased
level of creatinine 1
Cortes J et al, ASH 2017
Biochemical AEs
PF-114 phase 1 study
Preliminary Analysis of Efficacy of PF-114
Phase of
CML
BCR/ABL
mutation
status
Total number
of patients
Rate of CHR
Rate of
MCyR
%
n
*/N** %
n
*/N
***
Chronic T315I 940 2/5 80 4/5
All 21 36 4/11 40 4/10
Acceleration
T315I 100/1 00/1
All 250 1/2 00/2
Blast T315I 1100 1/1 00/1
n*- number of patients who achieved response during treatment
N** - number of patients evaluable for hematologic response assessment: were not in CHR at enrollment
N*** - number of patients evaluable for cytogenetic response assessment: were not in MCyR at enrollment and completed at least 3 cycles
Cortes J et al, ASH 2017
PF-114 phase 1 study
Conclusions
•PF-114 mesylate exhibits anti-leukemia activity in a heavily
pretreated CML patients including those with T315I
mutation
•MTD has not been reached
–50, 100, 200, 400, 500 mg dose cohorts have been studied
–600 mg cohort is currently being studied
•A single DLT of grade 3 erythematous rash observed
•No cardiovascular events have been observed
•A Phase 2 multicenter international study is planned for
2018
Cortes J et al, ASH 2017
4/24/2018
12
K0706: Program
K0706: as an efficacious, tolerable and safer treatment alternative for Chronic
Myeloid Leukemia or Ph+ Acute Lymphoid Leukemia patients who have failed ≥ 2
lines of therapies and/or ineligible due to comorbidities which limit the
administration of other TKIs
K0706: equipotent to Ponatinib in CML cellular* & in vivo efficacy assays with
limited potential for off-target effects based on the long term toxicity studies
K0706: Novel BCR-ABL tyrosine
kinase inhibitors for treatment of
Chronic Myeloid Leukemia (CML)
Courtesy of Sun Pharma / personal communication
SUN-K0706: Preclinical Data Summary
0
500
1000
1500
2000
2500
3000
1 4 6 8 1012151821 1 3 4 7 101417222428313539424549525459
Tumor volume (mm3)
Days post treatment initiation
K0706 (10 mg/kg, o.d., 21 days)
Ponatinib (10 mg/kg, o.d., 21
days)
Vehicle
Kinases
IC
50
(nM)
IC50
SUN-
K706
Ponatini
b
Abl
0.9 0.7
Abl(T315I)
8 2
Abl (M351T)
0.8 0.3
Abl (Q252H)
0.8 0.4
Abl
(Y253F) 1 0.3
In vitro In vivo
Effective against the wild type
and mutation bearing CML cell lines
Caused tumor regression in an imatinib-
resistant xenograft model
Courtesy of Sun Pharma / personal communication
K0706:Long-term monitoring of K562
xenograft growth
0
500
1000
1500
2000
2500
3000
3500
1 4 6 8 10 12 15 18 21 24 28 32 35 38 43 45 49 52 56 60 63 66 70 74 77 80
Tumor volume (mm3)
Days after treatment initiation
K0706 (1 mg/kg, p.o., o.d., 21 days) K0706 (3 mg/kg, p.o., o.d., 21 days)
Imatinib (150 mg/kg, p.o., o.d., 21 days) Ponatinib (3 mg/kg, p.o., o.d., 21 days)
Placebo (p.o., o.d., 21 days) K0706 (10 mg/kg, p.o., o.d., 21 days)
K0706: Demonstrates comparable long term tumour control with Ponatinib
Courtesy of Sun Pharma / personal communication
4/24/2018
13
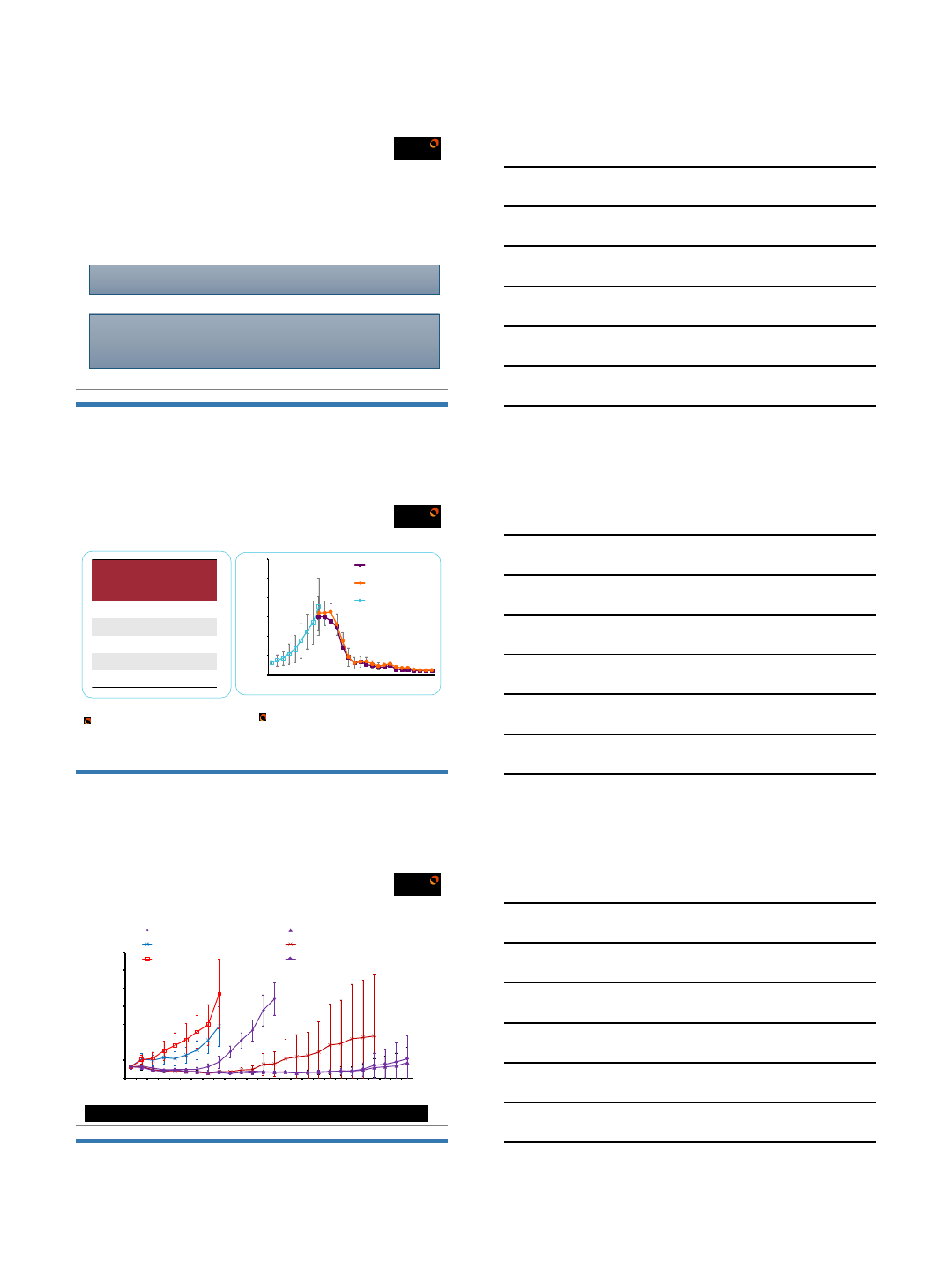
Part B: Subject Profile & Disposition
0%
5%
10%
15%
20%
25%
30%
35%
40%
India France Korea Belgium USA
36%
9%
27%
18%
9%
% Country wise enrolment
81%
18%
Native BCR-
ABL
BCR-ABL
Mutation
1 Subject: T315I mutation
1 Subject: F359V mutation
1 Subject: T315I mutation status
under investigation
Male
64%
Female
36%
Cohort/Dose level
Disposition of
Subject 12 mg 24 mg 48mg 66mg All Subjects
Subjects enrolled (N)
1 1 6 3 11
Received study medication (N)
1 1 6 3 11
Subjects completing Cycle 1 (N)
1 1 5 2 10
No
of Cycles completed Cycle 9 Cycle 5 Cycle 3 Cycle 1 NA
Subjects discontinued (N
)Nil Nil 1 (SAE) 1 (SAE)
Courtesy of Sun Pharma / personal communication
Toxicity: ICH in BP patient, tenosynovitis with successful rechallenge
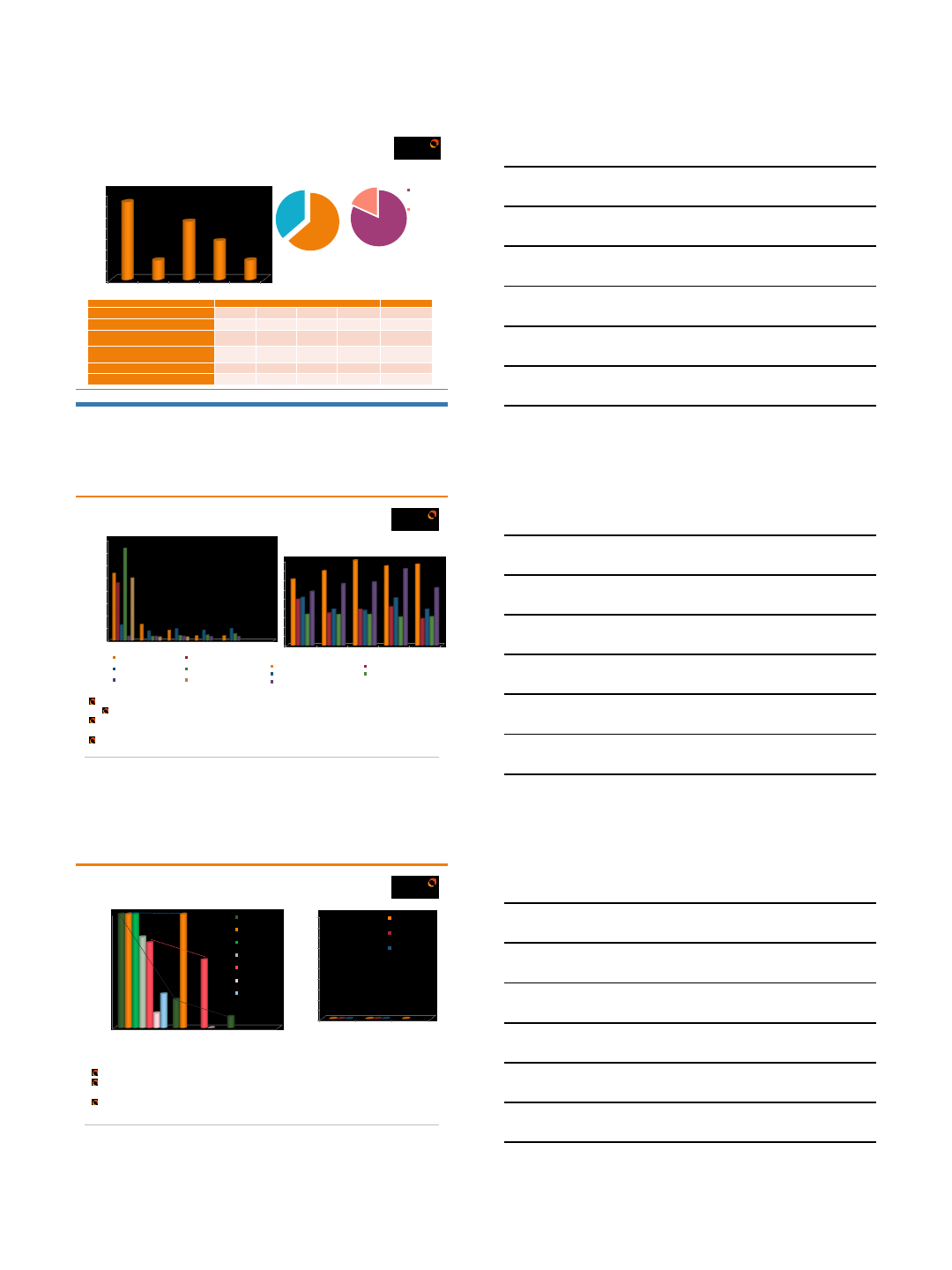
Efficacy
Hematological response
38
SPARC Presentation Confidential
9/11 Subjects demonstrated complete hematological response by end of Cycle 1
3/11 Achieved; 6/11 Maintained
Transient self-limiting grade 1 /2 neutropenia associated with study drug was observed in 2/11
subjects
This was self-limiting and recovered by end of Cycle 1 without intervention
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
Screening C1D8 C1D15 C122 C1D28
Cells/mL
35600501 (Refractory) 35600503 (Refractory)
35600102 (Refractory) 5600101 (Intolerant)
25000201 (Refractory) 41000103 (Refractory)
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
Screening C1D8 C1D15 C122 C1D28
35600101 (Intolerant) 41000101 (Intolerant)
5600201 (Intolerant) 25000201 (Refractory)
84000201 (Intolerant and Refractory)
Cells/mL
Subjects: Study entry : Loss of
haematological response
Subjects: Study entry in Haematological response
Courtesy of Sun Pharma / personal communication
Efficacy
Cytogenetic response
SPARC Presentation Confidential
Cytogenetic response data in maturing process
Subject with loss of cytogenetic response transition: Partial cytogenetic response & evolving
cytogenetic response
Subjects with complete cytogenetic response: Maintained cytogenetic response
*: Not applicable; Subject discontinued from study
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Screening C3D28 C6D28
35600501
5600101
41000102
41000103
35600102
35600503
25000201
% Philadelphia Cell Positivity
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Screening C3D28 C6D28
35600101
5600201
41000101
% Philadelphia Cell Positivity
Subjects: Study entry :Loss of cytogenetic response Subjects: Study entry: Complete cytogenetic
response
*
Courtesy of Sun Pharma / personal communication
4/24/2018
14
In CP and AP CML, No Early Gain in Overall Survival with SCT vs Ponatinib
*P-value <0.05. OS = overall survival; IQR = interquartile range; NR = not reached. FE. Nicolini et al., ASH 2015 Abst. #480; Blood, submitted
Conclusions
•CML is highly treatable; ‘functional cure’ appears feasible
•Generic imatinib is here; more TKIs still in development
•Early response increasingly predictive of long term success
•Resistance based in mutations can drive treatment choice but is likely
quite complex; Novel agents in study (ABL001)
•Second /third line therapy effective, needs to be carefully chosen
(risk/benefit of ponatinib vs other alternatives)
•SCT still needed as an option
•New options/new drugs on the horizon
Many TKIs
Response
Remission
Cure?
Many TKIs
Response
Remission
Cure?
= Long,
Happy,
Healthy
Life!
= Long,
Happy,
Healthy
Life!
Thank you for your attention!
Questions?
maurom@mskcc.org
212-639-3107
4/24/2018
1
Upfront Treatment Strategies for Patients
with CML
Daniel J. DeAngelo, MD, PhD
Adult Leukemia Program
Dana-Farber Cancer Institute
Brigham and Women’s Hospital
Associate Professor of Medicine
Harvard Medical School
Boston, MA
2017 Master Class Course
Presenter Disclosure Information
The following relationships exist related to this
presentation:
•Dr. Daniel DeAngelo has served as a consultant for Amgen, Celgene,
Incyte, Novartis, Pfizer, Shire and Takeda Pharmaceuticals
•I have also received research funding from Glycomimetics and Blueprint
Pharmaceuticals
Off-Label/Investigational Discussion
In accordance with CME policy, faculty have been asked to disclose discussion of
unlabeled or unapproved use(s) of drugs or devices during the course of their
presentations.
CML: Management in the Era of Multiple Tyrosine Kinase Inhibitors
4/24/2018
2
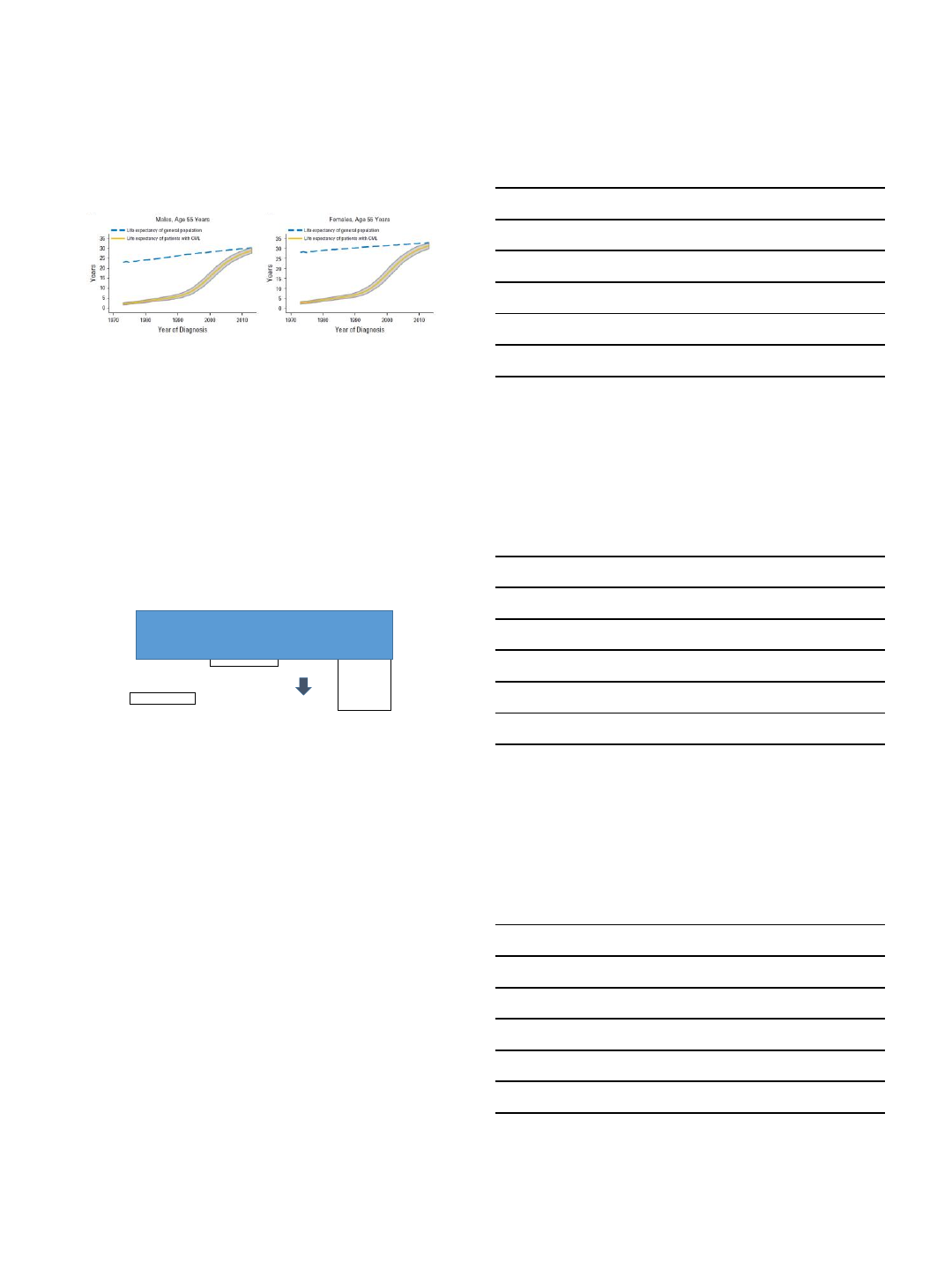
Life Expectancy of Patients with CML Approaches
the General Population
Bower et al., J Clin Oncol 2016 34: 2851-7.
CML Current Status: 2018
Imatinib
Nilotinib
Dasatinib
Bosutinib
Ponatinib
Refractory response
Suboptimal response
Relapse
Intolerance
SCT
Nilotinib
Dasatinib
Bosutinib
Refractory
response
Suboptimal
response
Relapse
Intolerance
T315I
Other: Omacetaxine
Generic imatinib finally here!
What Can We Expect From
Front-line Imatinib in CP CML?
IRIS Trial Data
4/24/2018
3
MMR
A Hochhaus, RA Larson, F Guilhot, et al. New Engl J Med 2017 376: 917-27.
•There are consistent data from multiple studies
demonstrating that patients who have very rapid
responses with any TKI have excellent long term
outcomes and that some patients with slower responses
fare more poorly.
• Responses are faster with “second” generation TKIs
ENESTnd: Nilotinib vs Imatinib in Newly Diagnosed
Chronic Phase CML
•Primary endpoint: MMR at 12 mos, defined as ≤ 0.1% BCR-ABL(/ABL ratio) on International Scale
•Secondary endpoint: CCyR by 12 mos
•Other endpoints: time/duration of MMR and CCyR; EFS, PFS, time to AP/BP, OS
•Stratificationby Sokal risk
Imatinib 400 QD (n = 283)
Nilotinib 300 BID (n = 282)
R
A
N
D
O
M
I
Z
E
Nilotinib 400 BID (n = 281)
Newly Diagnosed
CML-CP
(N = 846)
217 centers;
35 countries
Saglio G, et al. N Engl J Med. 2010;362(24):2251-2259.
4/24/2018
4
ENESTnd: Cumulative Incidence of MMR
a
Pvalues are nominal.
bFor each arm, the curve stops at the latest time point at which a patient first achieved MMR. Hochhous A, et al. Leukemia. 2016: 1044-1054.
Dasatinib vs Imatinib in Treatment-naive CML:
DASISION
•Primary endpoint: Confirmed CCyR by 12 months
•Secondary/other endpoints: Rates of CCyR and MMR; times to confirmed CCyR, CCyR and MMR; time in confirmed
CCyR and CCyR; PFS; overall survival
Follow-up
5 years
Randomized*
Imatinib 400 mg QD (n = 260)
Dasatinib 100 mg QD (n = 259)
N = 519
108 centers
26 countries
*Stratified by Hasford risk score
Kantarjian H, et al. N Engl J Med. 2010;362(24):2260-2270.
DASISION: Cumulative MMR Rates Over Time
Months Since Randomization
% With MMR
Dasatinib 100 mg QD
N
Imatinib 400 mg QD 260
259
By 1 year
By 2 years
By 3 years
By 4 years
By 5 years
28%
46%
55%
60%
64%
46%
64% 67%
73% 76%
0 6 12 18 24 30 36 42 48 54 60
100
90
80
70
60
50
40
30
20
10
0
p=0.0022
Cortes et al. J Clinic Oncol 2016: 2333-2340
4/24/2018
5
BFORE Study Design:
First-line Bosutinib vs Imatinib in CML
▪BFORE (NCT02130557) is an ongoing (expected
duration 5 years), multinational, randomized, open-
label, two-arm, phase 3 study
▪Prespecified primary endpoint:
−MMR at 12 months in the mITT population
▪mITT population: Ph+ patients with
e13a2/e14a2 transcripts, excluding Ph−
patients and those with unknown Ph status
and/or BCR-ABL transcript type*
−Bosutinib: n=246
−Imatinib: n=241
▪Current analysis based on ≥18 months of
follow-up†
•* 12 Ph‒patients (ie, 0 o f ≥10–99 metaphases at baseline; n=6 in each arm), 8 patients with atypical transcripts (n=3 in bosutinib arm; n=5 in imatinib arm), and 31 patients with unknown Ph status (n=13 in bosutinib arm; n=18 in imatinib arm
[includes 2 p atients also listed as having atypical transcripts]).
•† All Pv alues, ex cept MMR at 1 2 months a nd CCy R by 12 months in the mITT population, are for descriptive purposes only; no adjustments for multiple comparisons.
•CCyR=complete cytogenetic respo nse; CML =chronic myeloid leukemia; C P=chronic phase; ECOG PS=Eastern Cooperative Oncology Group performance status; mITT=modified intent-to-trea t; MMR=major molecular response; Ph=Philadelphia
chromosome
Eligibility
•≥18 years of age
•New molecular diagnosis
of BCR-ABL1+ (Ph+ or Ph−)
CP CML
•ECOG PS 0 or 1
•No prior medical treatment
for CML
Stratification
•Sokal risk group
•Geographic region
1:1
N=536
Imatinib
400 mg once daily
(n=268; 3 not treated)
Bosutinib
400 mg once daily
(n=268)
Gambacorti-Passerini et al., ASH 2017, abstract #896
Cumulative Incidence of Response
(mITT Population)
BFORE: First-line Bosutinib vs Imatinib in CML
* 18-mo nth data shown; data after 72 weeks subject to change to due to incomp lete follow-up.
† Gray’s test P-value.
CI=confidence interval; CM L=chronic myeloid leukem ia; CCyR=complete cytogenetic respo nse; HR=hazard ra tio; m ITT=m odified intent-to-treat; M MR=majo r molecular response
Cumulative Incidence of
MMR*
Probability of MMR (%)
HR=1.36 (95% CI: 1.09–1.69); P=0.0079†
Weeks
012 24 36 48 60 72 84
100
80
40
60
20
0
Patients at risk, n
246 232 206 119 94 75 58 39
Bosutinib
241 235 204 151 116 87 62 38Imatinib
Bosutinib
Imatinib
Cumulative Incidence of
CCyR*
Probability of CCyR (%)
100
80
40
60
20
0
Weeks
012 24 36 48 60 72 84
HR=1.33 (95% CI: 1.10–1.62); P=0.0049†
Patients at risk, n
246 229 121 50 20 8 5 2
Bosutinib
241 229 149 70 40 20 12 2Imatinib
Bosutinib
Imatinib
Gambacorti-Passerini et al., ASH 2017, abstract #896
BUT….
•NO SURVIVAL ADVANTAGE with nilotinib,
dasatinib or bosutinib in randomized trials
•Only about 60-65% of patients remain on their
initial drug
•And then there are the toxicities…
4/24/2018
6
LONGER TERM FOLLOW-UP OF SECOND and
THIRD GENERATION TKIs
•Dasatinib - late pleural effusions, pulmonary
hypertension; T/NK cells
•Nilotinib –hyperglycemia, peripheral arterial
occlusive disease, other arterial thromboses
•Bosutinib –less information; diarrhea and
transaminitis
•Ponatinib - MAJOR arterial thrombotic issues
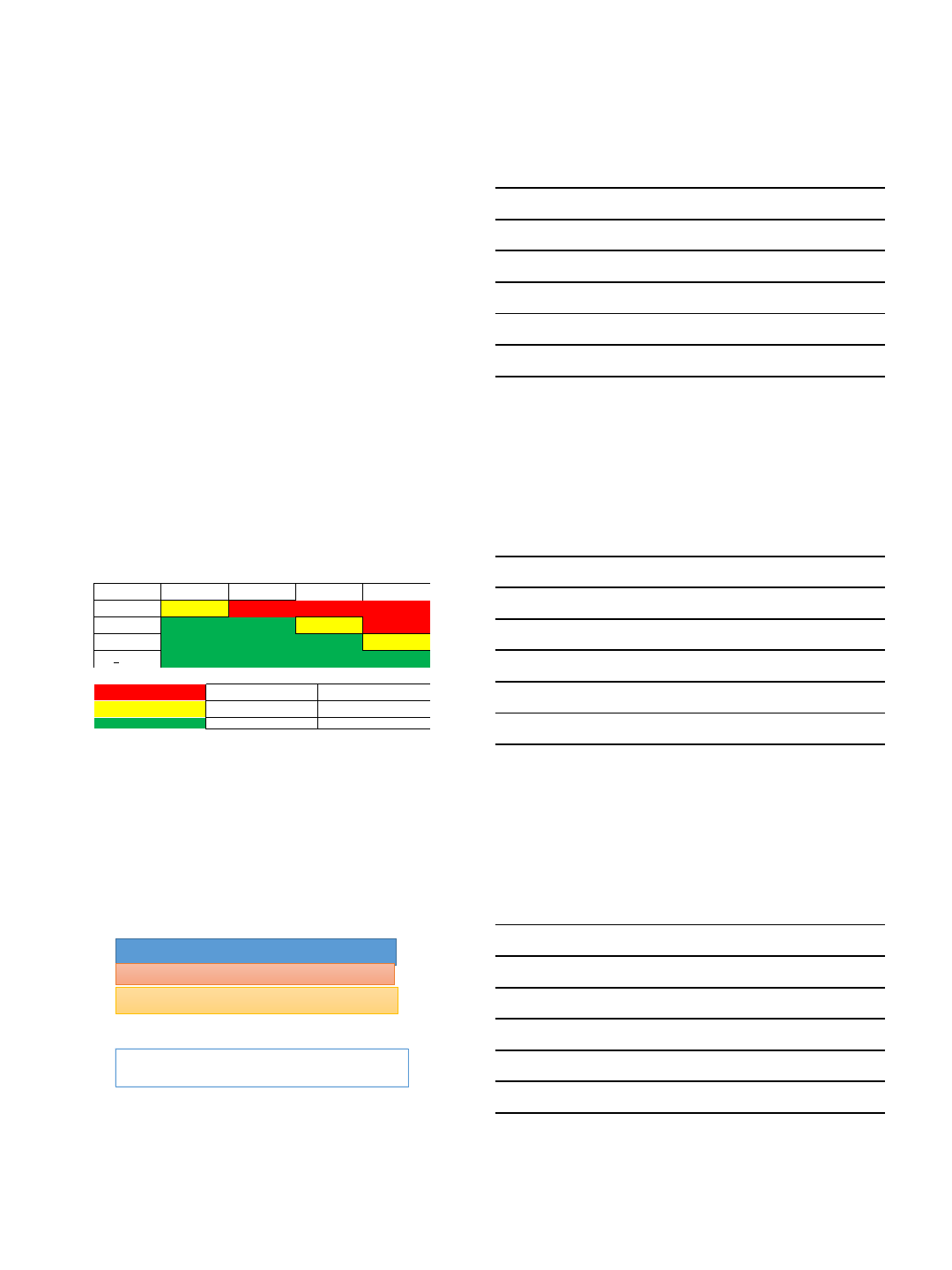
CML Molecular Response Milestones
BCR-ABL1 (IS) 3 months 6 months 12 months > 12 months
> 10% YELLOW RED
1% - 10%
GREEN
YELLOW RED
0.1% - 1% GREEN YELLOW
< 0.1% GREEN
Clinical Considerations Treatment options
RED
Evaluate compliance
and drug interactions
Mutation testing
Switch to alternate TKI
Consider
screen for HSCT
YELLOW
Same as above
Consider
switch to alternate TKI or continue
(may increase dose of imatinib to 800 mg)
GREEN
Monitor response and toxicity
Continue same TKI
NCCN 2017 Guidelines
CML Monitoring Frequency
NCCN Guidelines 2017; Mahon et al., Lancet Oncol 2010; 11: 1029–35
The 3 month QRT-PCR may be uniquely important in defining long
term outcome!
If these criteria aren’t met (primary resistance, ~15% on imatinib):
check for ABL TKD mutation and switch therapy
Repeat marrow exams are not necessary once CCyR achieved (check
at 6 months and 6 months thereafter prn) (PB FISH also reasonable)
Check QPCR q 3 months x 3yrs, then q 3-6 months thereafter or if increase by 1 log
after MMR achieved, then repeat in 1-3 months
When to check for ABL TKD mutation and switch therapy:
loss of response (heme or cytog relapse) or disease progression to AP/BP
confirmed 1 log increase in bcr-abl1 transcript and loss of MMR
4/24/2018
7
CML Response Definitions, Monitoring and Milestones
Jabbour E, et al. Cancer. 2007;109(11):2171-2181.
Marin D, et al (European LeukemiaNet) Blood 2008;112(12):4437-4444.
Marin D et al J Clin Oncol 2012; 30(3):232-8.
Response Type Response Definition When It Should be
Achieved
Complete hematologic
response (CHR) Normalization of blood counts;
resolution of disease signs and symptoms <1-3 months
Initial Molecular response Reduction in BCR-ABL transcript levels in peripheral blood
by ≥ 1 log, or BCR-ABL/ABL ratio reduced to ≤ 10 % IS <3 months
Major cytogenetic response
(MCyR) ≤ 35% Ph+ cells <6 months
Complete cytogenetic
response (CCyR) 0% Ph+ cells <12 months
Major molecular response
(MMR) Reduction in BCR-ABL transcript levels in peripheral blood
by ≥ 3 log, or BCR-ABL/ABL ratio reduced to ≤ 0.1% IS <12 - 18 months
Complete molecular
response (CMR) Reduction in BCR-ABL transcript levels in peripheral blood
by ≥ 4.5 log, or undetectable BCR-ABL/ABL transcript ??
ABCDE Steps to Reduce CV Risk in Patients
with CML
•A
•Awareness of CV risks and signs
•Aspirin in appropriate patients
•Ankle-brachial Index (ABI) at baseline and f/u
•B
•Blood pressure control
•C
•Cigarette/tobacco cessation
•Cholesterol monitoring and treatment
•D
•Diabetes mellitus monitoring and treatment
•Diet and weight control
•E
•Exercise
Moslehi and Deininger, J Clin. Oncol 2015 33: 4210-8
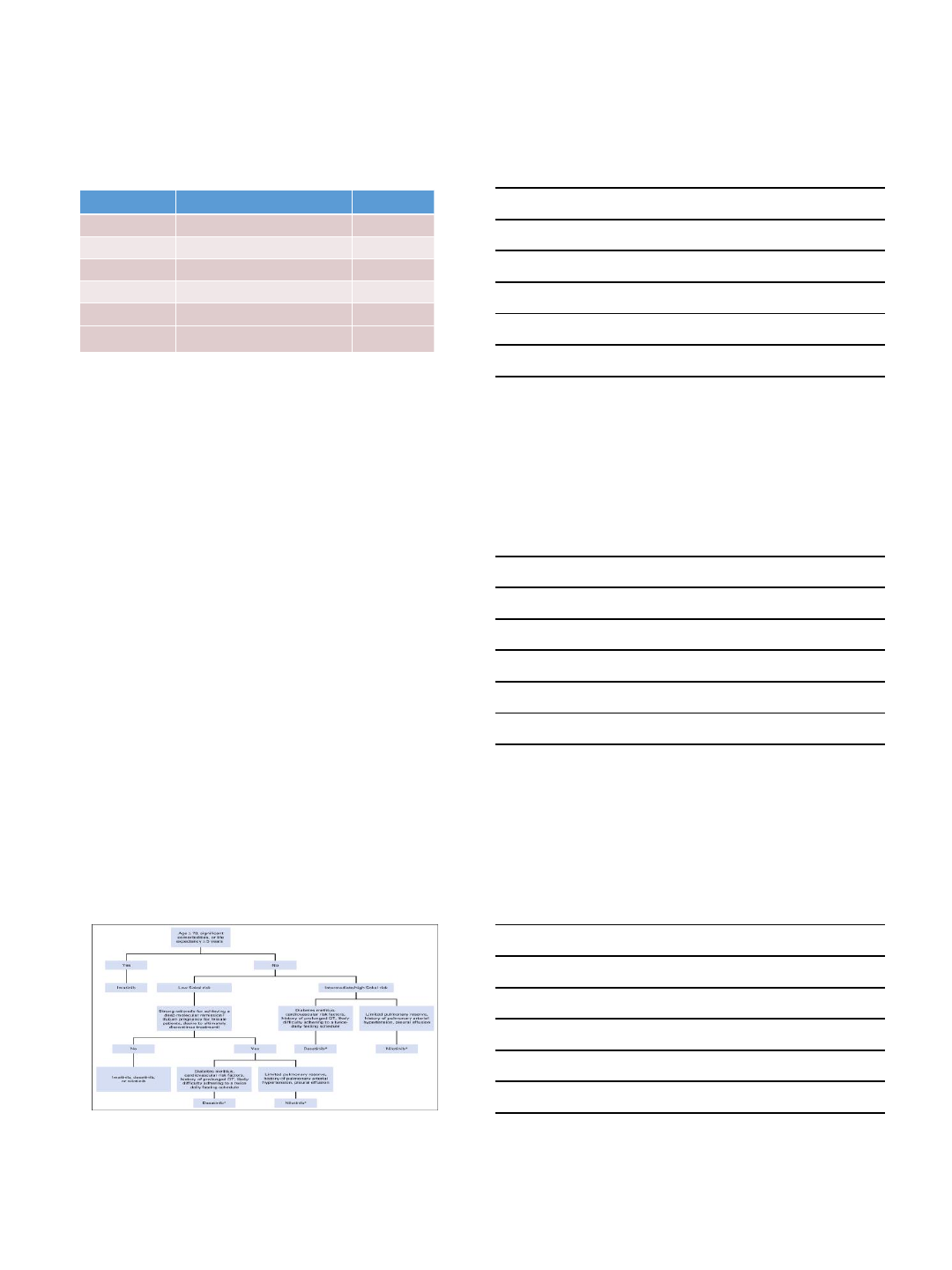
Algorithm for Frontline TKI Therapy in CML
Neil P. Shah; JCO 2018, 36, 220-224
Bosutinib offers a third 2nd Gen choice
4/24/2018
8
Chronic Myeloid Leukemia: Conclusions
•Chronic Myeloid Leukemia
•Generic imatinib finally here
•First line imatinib vs nilotinib vs dasatinib vs bosutinib?
•How to choose? Imatinib a very reasonable choice for elderly and low-risk patients
•Late side effects important (CV for nilotinib; pleural effusions for dasatinib)
•Compliance still most important
•Need to minimize CV risk factors
•Need to better understand the “ultimate” goal of therapy
•Cytogenetic remission vs. major molecular response vs complete molecular
remission?
Questions & Answers
?
4/24/2018
1
Are we ready for treatment discontinuation?
Javier Pinilla-Ibarz MD, PhD
Senior Member
Malignant Hematology Department
H. Lee Moffitt Cancer Center
Disclosures
•Consulting: Novartis, Pfizer and Takeda.
•Speaker Bureau: Takeda.
Why consider stopping?
•TKI therapy is associated with reduced QOL
•High cost to patient and society
•Potential for long term toxicity
–Cardiovascular
–Pulmonary
–Thyroid dysfunction
•Children and adolescents:
–Substantial growth abnormalities
–Effect on pregnancy/fertility
4/24/2018
2
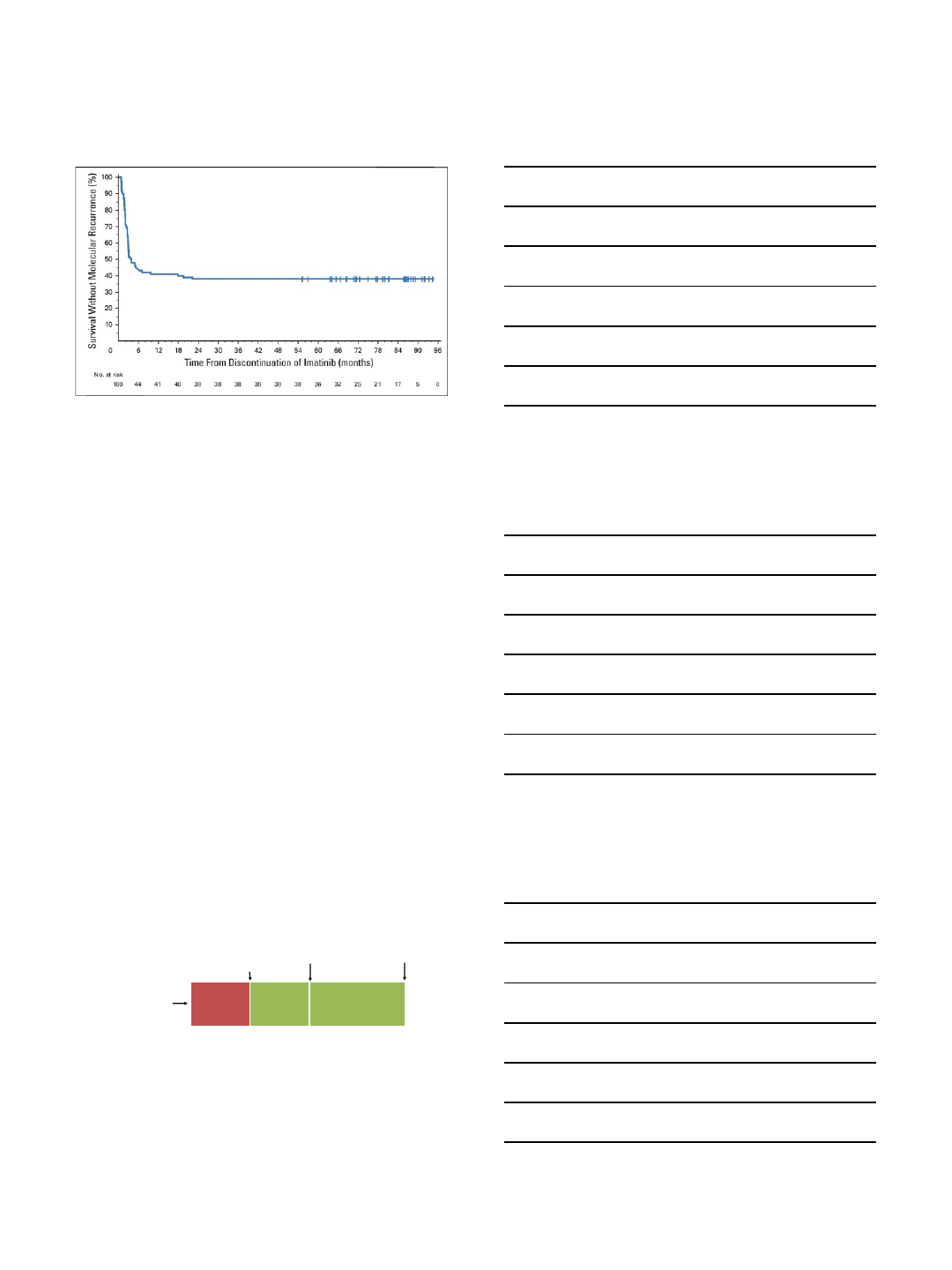
Long Term Follow Up From STIM
Etienne G. Journal of Clinical Oncology 35, no. 3 (January 2017) 298-305
•Median Follow Up: 77 months
•n=100
•38% Treatment Free Remission
•61% relapsed: 80% in months 1-3, 15% in months 4-7
•Median time to molecular relapse: 2.5 months
Multivariate Analysis From STIM
•Two factors predictive of molecular relapse
1. High-risk Sokal score at diagnosis
•HR 2.22
•95% CI 1.11-4.42
•P=0.024
2. Imatinib duration < 58.8 months prior to
discontinuation
•HR 0.54
•95% CI 0.32-0.92
•P=0.024
Etienne G. Journal of Clinical Oncology 35, no. 3 (January 2017) 298-305
EURO-SKI: Study Design
Sauselle S, et al. ASH 2017. Abstract 313.
CML pts receiving
TKI for ≥ 3 yrs with
deep MR* for ≥ 1 yr
and no history of TKI
failure (N = 755*)
Screening
(≤ 6 W ks)
MR4confirmation†
Follow-Up
RQ-PCR Q4W,
then Q6W
Follow-Up
RQ-PCR Q3M
TKI
Cessation
Yr 1 Yr 3
*In primary analysis of 868 preregistered pts.
†MR4, defined as detectable BCR-ABL ≤ 0.01%, or undetectable BCR-ABL in samples with ≥ 10,000 ABL or ≥ 24,000
GUS transcripts, respectively.
Primary endpoint: molecular recurrence
(BCR-ABL > 0.1%, ie, loss of MMR)
•Largest TFR study to date
•Goal was to establish criteria for TKI discontinuation
4/24/2018
3
EURO-SKI: Molecular
Recurrence-Free Survival
Month Pts at Risk, n MRFS, % (95% CI)
6457 61 (58-65)
12 396 55 (51-58)
18 333 52 (49-56)
24 219 50 (47-54)
36 31 47 (43-51)
Sauselle S, et al. ASH 2017. Abstract 313.
EURO-SKI: Conclusions
•Study defined stopping criteria for TKI
cessation in CML patients who achieve
durable deep MR
•Preferred cutoffs for 6-mo probability of MMR
loss
–TKI duration: 5.8 yrs
–MR4duration: 3.1 yrs
•Probability of TFR increased almost linearly
per each additional year of first-line imatinib
and duration of MR4
Sauselle S, et al. ASH 2017. Abstract 313.
ENESTfreedom
Enrollment and Inclusion Criteria
Total enrollment n=215
Minimum treatment duration
required prior to discontinuation
≥3 years frontline nilotinib
Minimum response required prior to
discontinuation
Sustained MR4.5 for at least 1 year
RQ-PCR
(standardized to the IS)
every 12 weeks
•Adults with CML-CP
•b2a2 and/or b3a2 transcripts
•≥ 2 y frontline nilotinib
•MR4.5 at screening
(central laboratory)
TFR Phase
(192 weeks)
Reinitiation
Phase
Loss of MMR
(molecular
relapse)
Enroll
N = 215
Sustained Deep
Molecular Response
Consolidation
Phase
(52 weeks)
RQ-PCR (standardized to the IS)
every 4 weeks for 48 weeks, every 6
weeks for 48 weeks, and then every
12 weeks
Study Design
Hochhaus A. ASCO Annual Meeting 2016. Abstract #7001
•37.9% of nilotinib 300mg BID treated patients on ENESTnd met the
inclusion criteria for attempting TFR on ENESTfreedom
Treatment was nilotinib 300mg BID in all treatment phases
4/24/2018
4
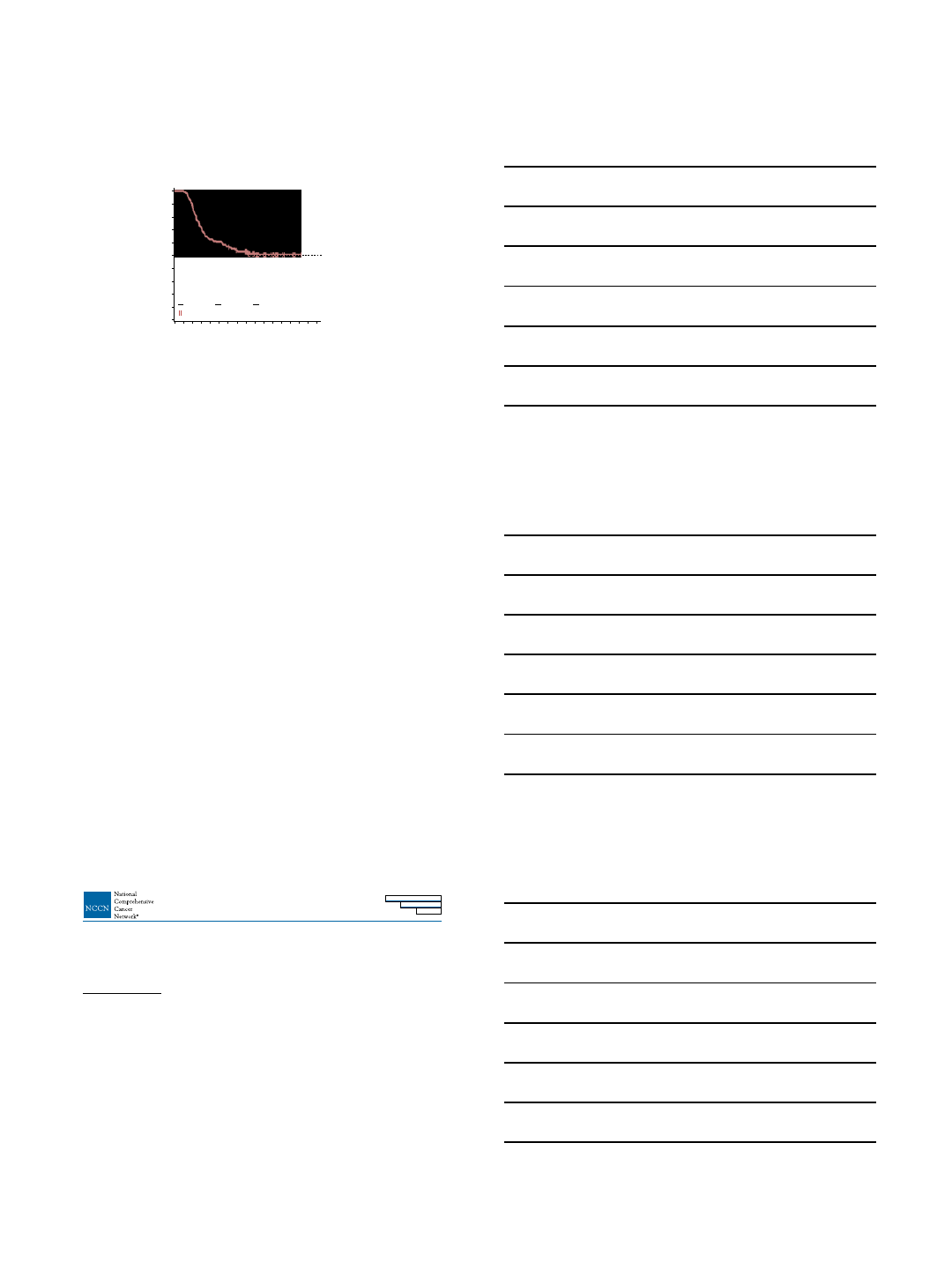
Primary Endpoint and Treatment-Free Survival
Kaplan-Meier Estimated Treatment-Free Survivala
aDefined as the time from the start of TFR until the earliest of any of the following: loss of MMR, reinitiation of nilotinib for any reason, progression to
accelerated phase/blast crisis, or death due to any cause.
Treatment-Free Survival, %
100
90
80
70
60
50
40
30
20
10
0
Time Since TFR, weeks
72 968460480362412
0:911:9112:9138:9190:89190:0
At Risk : Events
108:81120:70165:25
Pts Evt Cen
190 91 99
Censored observations
Hochhaus A. ASCO Annual Meeting 2016. Abstract #7001
•190 patients
entered the TFR
phase
•51.6% of patients
(95% CI, 44.1-
58.9%) remained
in TFR after 48
weeks
TKI Withdrawal Syndrome
–Diffuse musculoskeletal pain and joint pain
–Occurs in approximately 30% of patients after
stopping TKIs
–Median duration 6 months
Lee et al. Haematologica. 2016 Jun;101(6):717-23.
Richter et al. J Clin Oncol. 2014;32(25):2821–2823.
CML-E
DISCONTINUATION OF TKI THERAPY1
Criteria for TKI Discontinuation
•
A ge ≥ 18 years .
• Chronic phase CML. No prior history of accelerated or blast phase CML.
•
O n ap p ro v ed T K I therap y (im atin ib , d as atin ib , n ilo tin ib , b o s u tin ib , o r p o n atin ib ) fo r at leas t three years .
•
P rio r ev id en c e o f q u an tifia
b
l e
BCR-ABL1 transcript.
•
S tab le m o lecu lar res p o n s e (M R 4 ;
BCR-ABL1
≥ 0.01% IS ) fo r ≥ 2 years , as d o c u m en ted o n at leas t fo u r tes ts , p erfo rm ed at leas t three m o n ths ap art.
• Access to a reliable qPCR test with a sensitivity of detection
at leas t M R 4 .5 (B C R -A B L 1 ≥ 0.003 2 % IS )
and provides results within 2 weeks.
• Monthly molecular monitoring for one year, then every 6 weeks for the second year, and every 12 weeks thereafter
(in d efini tel y)
is recommended
fo r p atien ts w ho rem ain in M M R (M R 3 ;
BCR-ABL1
≥
0.1% IS) after discontinuation of TKI therapy.
• Prompt resumption of TKI within 4 weeks of a loss of MMR with molecular monitoring every 4 weeks until MMR is re-established, then every 12
weeks thereafter
is reco m m en d ed in d efin
i
tel y for pat ien t s
who have reinitiated TKI therapy after a loss of MMR. For those who fail to achieve
MMR after three months of TKI resumption, BCR-ABL1 kinase domain mutation testing should be performed, and monthly molecular monitoring
should be continued for another six months.
•
C o n s u ltatio n w ith a C M L S p ec ialty C en ter to rev iew the ap p ro p riaten es s fo r T K I d is c o n tin uatio n an d p o ten tial ris ks an d b en efit
s
of treat me n t
discontinuation, including TKI withdrawal syndrome.
• Reporting of the following to a member of the NCCN CML panel is strongly encouraged:
A n y s ign ific
a
n t ad v er s e ev en t be l iev ed to be rel at ed to treat me n t d is c o n tin uatio n .
Progression to accelerated or blast phase CML at any time.
Failure to regain MMR after three months following treatment reinitiation.
• Discontinuation of TKI therapy appears to be safe in select CML patients.
• Clinical studies that have evaluated the s afety and effic
a
cy of TKI discontinuation have employed strict eligibility criteria and have mandated
more frequent molecular monitoring than typically recommended for patients on TKI therapy.
• Some patients have experienced signific
a
nt adverse events that are believed to be due to TKI discontinuation.
• Discontinuation of TKI therapy should only be performed in consenting patients after a thorough discussion of the potential risks and
benefit
s
.
• Outside of a clinical trial, TKI discontinuation should be considered only if ALL of the criteria included in the list below are met.
1See full prescribing information for nilotinib: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/022068s026lbl.pdf
Version 4.2018, 01/24/18 © National Comprehensive Cancer Network, Inc. 2018, All rights reserved. The NCCN Evidence BlocksTM, NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.
NCCN Guidelines Version 4.2018
Chronic Myeloid Leukemia
NCCN Evidence BlocksTM
NCCN Guidelines Index
Table of Contents
Discussion
Note: For more information regarding the categories and defin
i
tions us ed for the NCCN Evidence Blocks tm
, see page EB-1.
All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
4/24/2018
5
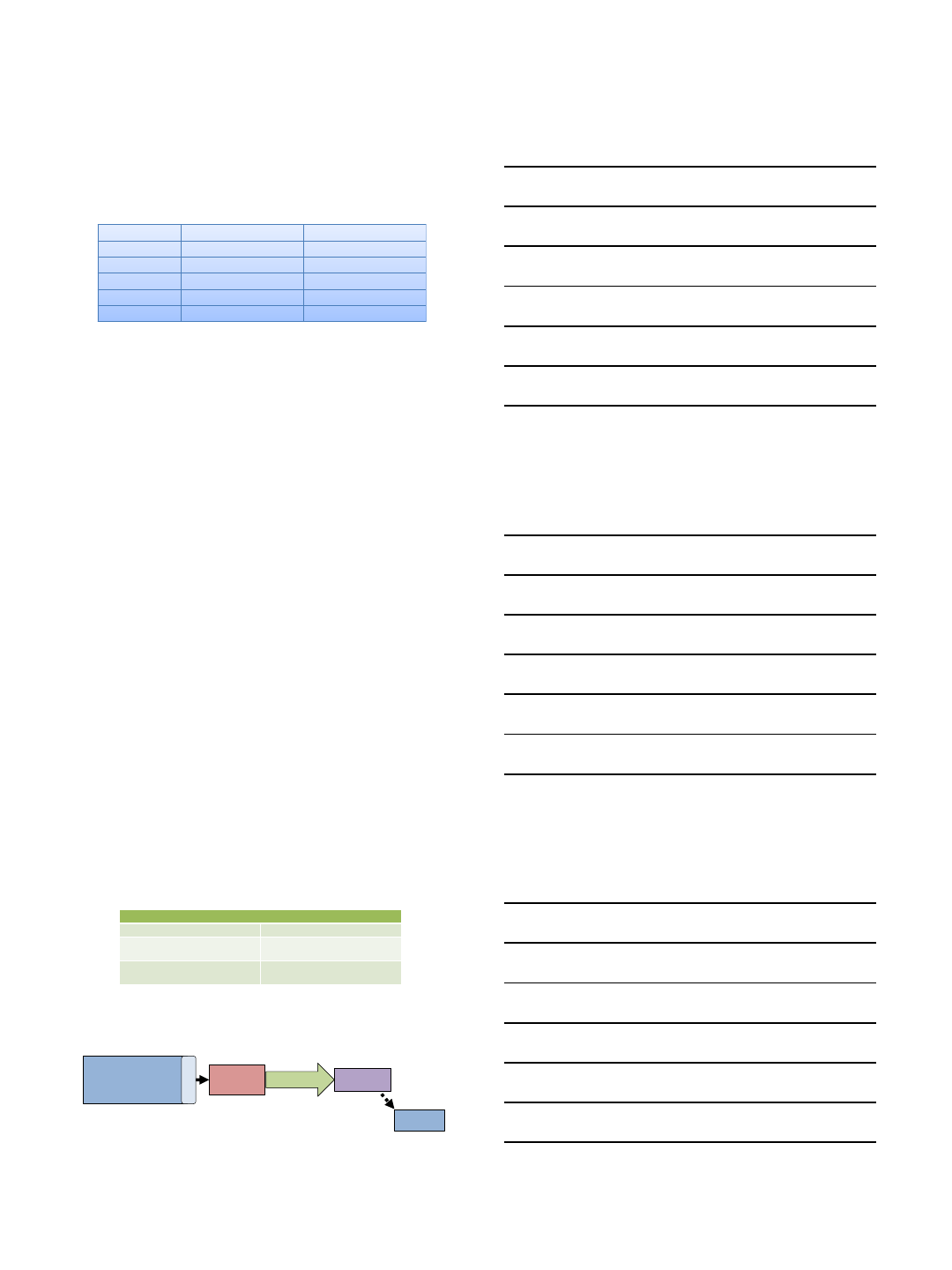
Is Stopping TKI Realistic?
50% achieve MR4 or MR 4.5
50% restart TKI
70-80% of newly diagnosed patients
with CML will need long term TKI
therapy
Atallah et al EHA iCMLf 2017
Conclusions
•Most patients with chronic phase CML will
do well with current therapy
•Stopping TKIs is ready for prime time
–A select group of patients
–With proper monitoring
•Multi-team approach is a key component to
the success and safety of TFR
