4 20 16 Radial Intervention Syllabus
2016-04-20
: Pdf 4 20 16 Radial Intervention Syllabus 4_20_16_Radial_Intervention_Syllabus 4 2016 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 70
4/20/2016
1
@MountSinaiIR
Radial Approach:
Concepts and Technique
Aaron M. Fischman MD
Icahn School of Medicine at Mount Sinai
Mount Sinai Health System
New York, NY
@MountSinaiIR
Disclosures
Advisory Board: Terumo Interventional Systems, Embolx, Inc.
Consultant: Terumo, Celonova Biosciences, Neuwave Medical, Surefire
Medical
Speaker: Terumo, Merit Medical, Surefire Medical
Research Support: BTG, Merit Medical, Surefire Medical
I AM A RADIALIST!
@MountSinaiIR
Why Radial?
Fewer vascular complications
Greater patient satisfaction
Immediate ambulation
Procedure cost savings
Long term cost savings?
Less pain and anesthesia?
LESS INVASIVE!
Bertrand et al. Comparison of transradial and femoral approaches for percutaneous coronary interventions: a systematic review and hierarchical Bayesian meta-analysis. American heart journal. Apr 2012;163(4):632-
648.
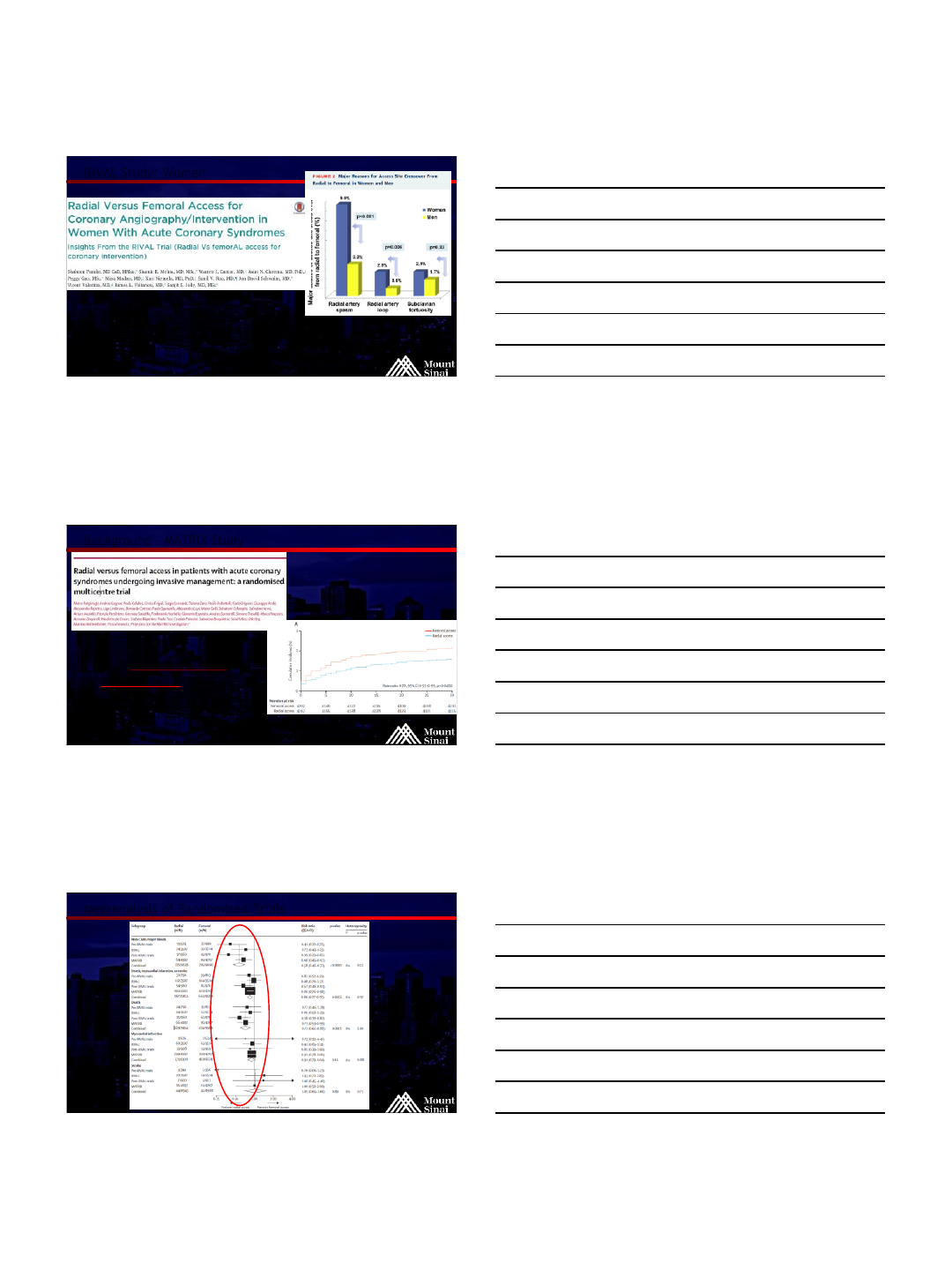
Romagnoli E, Biondi-Zoccai G, Sc iahbasi A, et al. Radial versus femoral randomized investigation in ST-segment elevation acute coronary syndrome: the RIFLE-STEACS (Radial Versus Femoral Randomized
Investigation in ST-Elevation Acute Coronary Syndrome) study. J ournal of the American College of Cardiology. Dec 18 2012;60(24):2481- 2489.
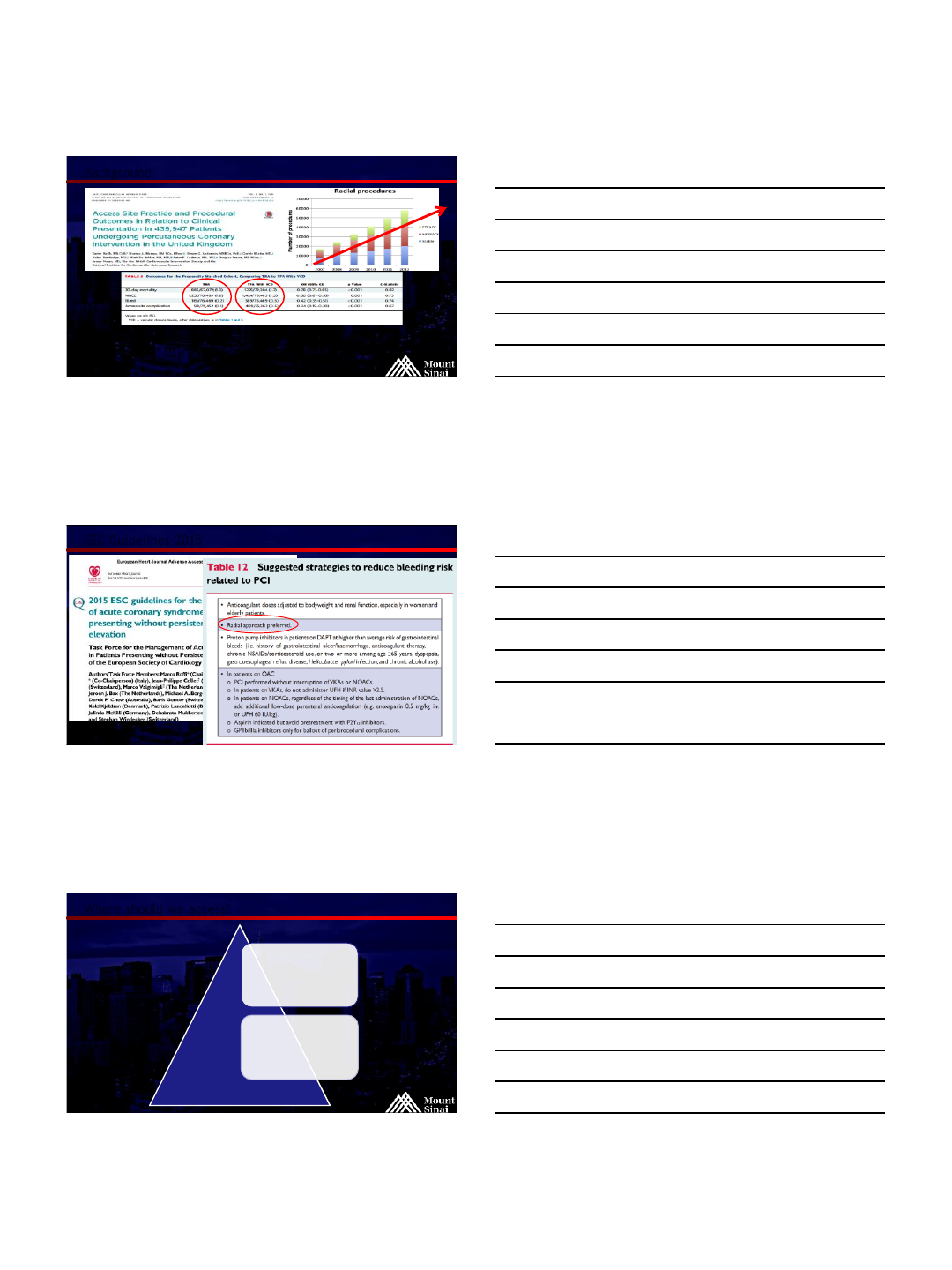
Mehta et al. Effects of Radial Versus Femoral Artery Access in Patients With Acute Coronary Syndromes With or Without ST-Segment Elevation. Journal of the American College of Cardiology. 10/12 2012.
Cooper CJ, El-Shiekh RA, Cohen DJ, et al. Effect of transradial access on quality of life and cost of cardiac catheterization: A randomized comparison. American heart journal. 09/01 1999;138(3 Pt 1):7-7.
4/20/2016
2
@MountSinaiIR
Background
1953 –femoral artery access
Sven Seldinger
1989 –first diagnostic angiogram via radial artery
Dr. Lucien Campeau
1992 –first angioplasty via radial artery
Dr. Ferdinand Kiemeneij -the "father of transradial
intervention”
1993 –first coronary stent via radial artery
Dr. Ferdinand Kiemeneij
@MountSinaiIR
Background
@MountSinaiIR
Background –RIVAL Study
Over 7000 patients randomized
Reduced cardiac mortality in STEMI patients
Metha et al. Radial vs. Femoral Artery Access in STEMI, JACC Vol. 60, 24: 2012
4/20/2016
3
@MountSinaiIR
RIVAL Study: Women
Women higher risk of vascular complication, radial safer than femoral
Women have more benefit with TRA than men, but more crossover
86% preferred radial over femoral
Pandie et al. JACC: Interventions, April 2015
@MountSinaiIR
Background –MATRIX Study
8404 patients randomized
Reduced all-cause mortality
and major bleeding in ACS patients
Valgimigli et al. Radial vs. femoral access in patients with ACS undergoing invasive management: a randomized multicenter trial. The Lan cet,
March 2015
@MountSinaiIR
Metaanalysis of Randomized Trials
4/20/2016
4
@MountSinaiIR
Background
“TRA is superior to … should be considered the preferred access site for percutaneous coronary
intervention.”
Ratib K, Mamas MA, Anderson SG, et al. Access Site Practice and Procedural Outcomes in Relation to Clinical Presentation in 439,947
Patients Undergoing Percutaneous Coronary Intervention in the United Kingdom. J Am Coll Cardiol Intv. 2015;8(1_PA):20-29.
@MountSinaiIR
ESC Guidelines 2015
@MountSinaiIR
Where should we access?
FEMORAL
BRACHIAL
4/20/2016
5
@MountSinaiIR
Where should we access?
RADIAL
FEMORAL
BRACHIAL
@MountSinaiIR
Where should we access?
RADIAL
FEMORAL
@MountSinaiIR
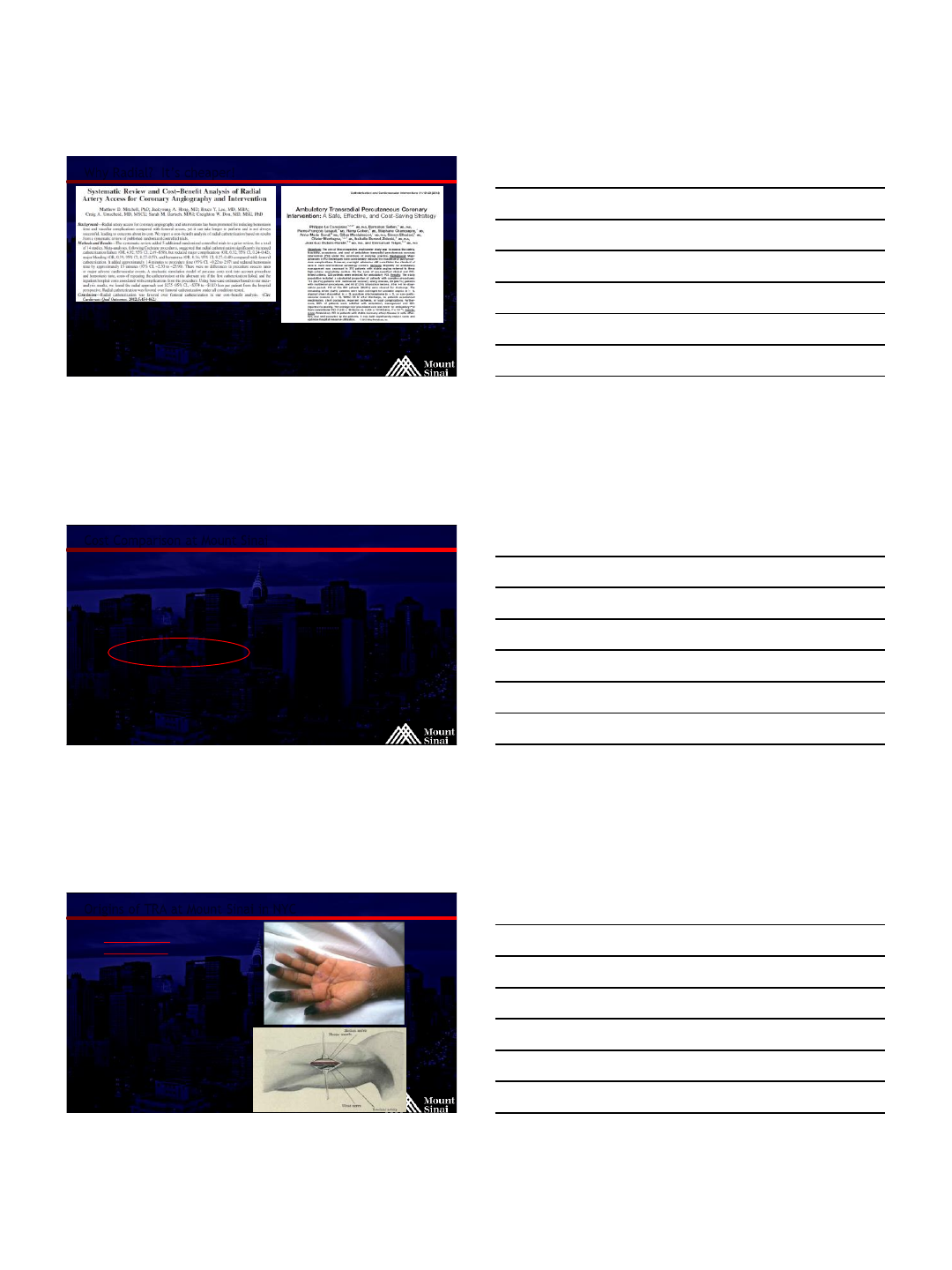
Why Radial? –It hurts less!
4/20/2016
6
@MountSinaiIR
Why Radial? –Recovery is easier
Leave recovery room sooner
@MountSinaiIR
Recovery Room
@MountSinaiIR
Radial Lounge
4/20/2016
7
@MountSinaiIR
Why Radial? It’s cheaper!
@MountSinaiIR
Cost Comparison at Mount Sinai
5F standard sheath
19g needle
5F Sos 80cm
Closure Device
Approx. $230
5F Glidesheath
Microneedle
5F glide cobra 100cm
(or 110 Sarah radial)
TR Band
Estimated direct cost savings in 26 months –$80,000
Indirect costs were not measured
RADIALFEMORAL
Approx. $130
Fischman et al. Scientific Sessions Abstract, SIR 2013. April 17, 2013
@MountSinaiIR
Origins of TRA at Mount Sinai in NYC
Brachial access
complications!
Neuropathy
Brachial hematoma
with arm injury
Extended hospital
stay
4/20/2016
8
@MountSinaiIR
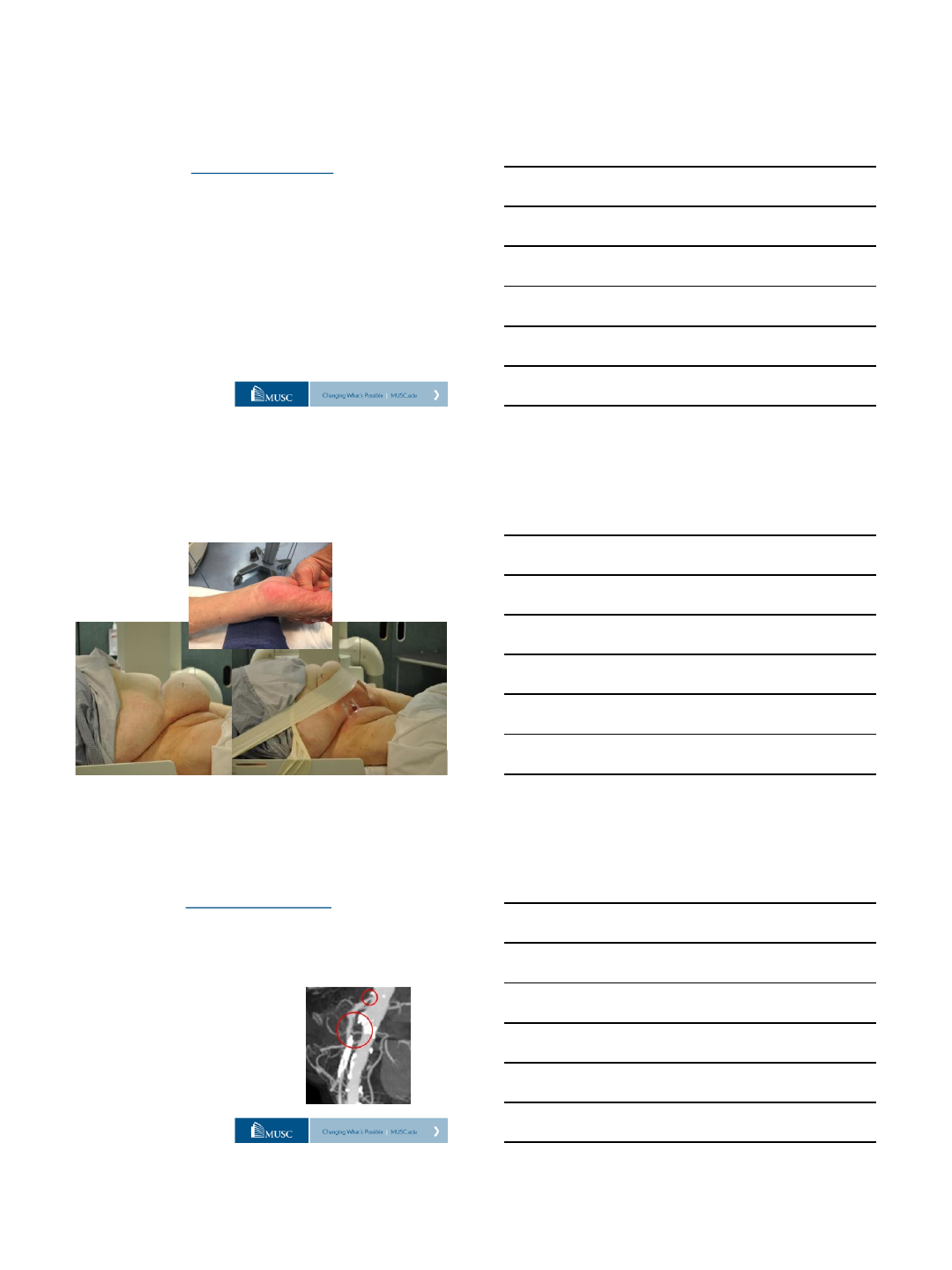
Femoral Access is easy until it is not…….
@MountSinaiIR
Rest pain after TACE –Angioseal
@MountSinaiIR
Adoption of TR Technique in USA
2013: 1 in 6 coronary PCI is TR
2015: 1 in 4 coronary PCI is TR
estimated
Alfonso, Cohen, Cardiac Interventions Today, June 2014
4/20/2016
9
@MountSinaiIR
TRA in IR
Classic IR
Textbook
Published
Sept 2013
What is going
on here????
@MountSinaiIR
Background
177 cases via the radial artery
July 1999 to October 2002
65/70 patients (92.9%) replied that they would request
transradial approach next time
J Clin Gastroenterol 2003;37:412–417
@MountSinaiIR
Early experience: TACE –What did we learn?
100cm is not long
enough in 20% of cases
Glide cobra is “too
floppy”
Sarah/Jacky needs to
be on the shelf!!!
Need longer
microcatheters
4/20/2016
10
@MountSinaiIR
Advantages of TR Approach
Obese patients
Patients with groin sensitivity
No closure device
Less bleeding complications
Immediate ambulation
@MountSinaiIR
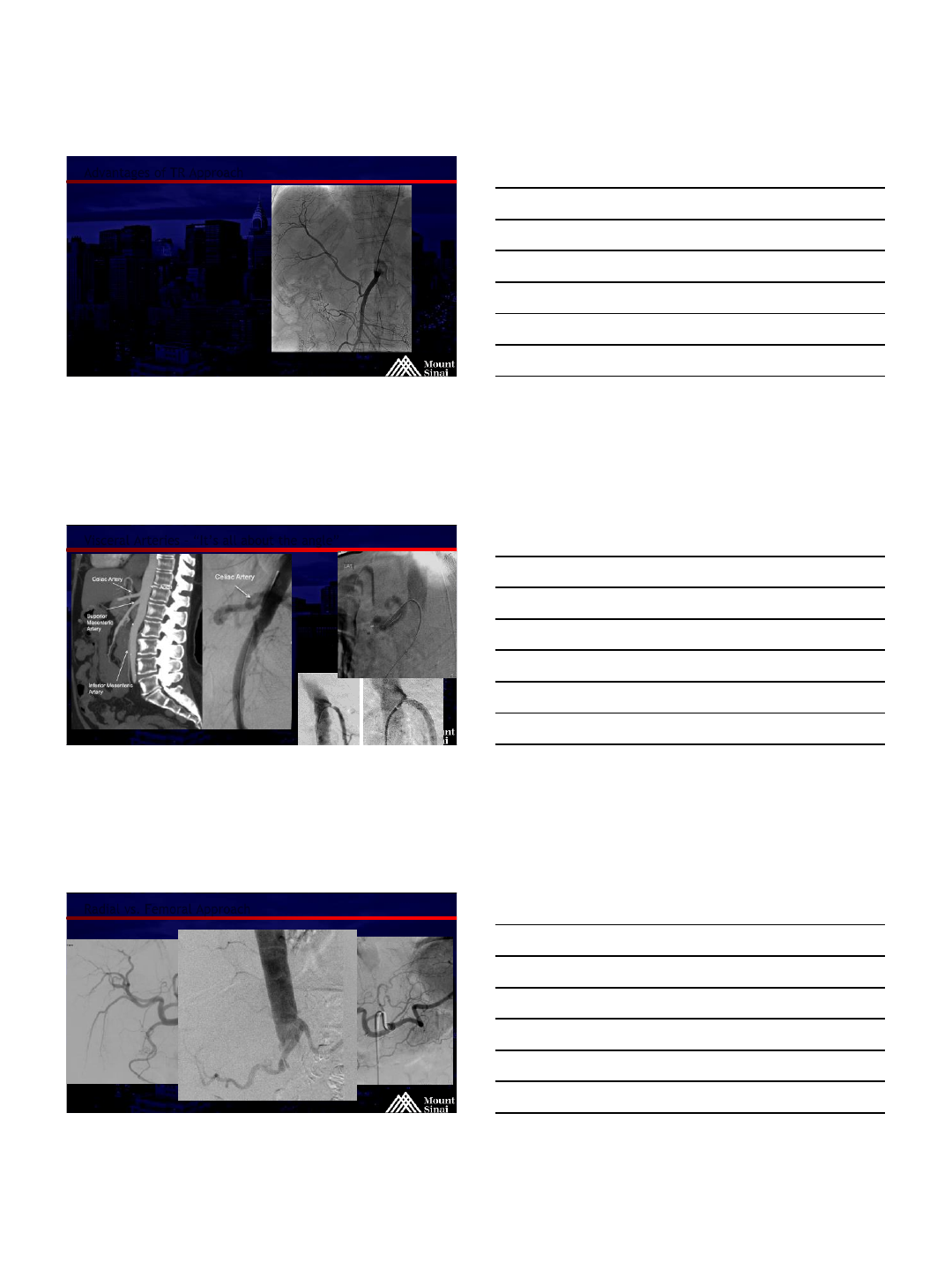
Visceral Arteries – “It’s all about the angle”
@MountSinaiIR
Radial vs. Femoral Approach
4/20/2016
11
@MountSinaiIR
Disadvantages of TR Approach
Arterial size, spasm
Anatomic variants
Severe tortuosity
Cone Beam CT is more difficult,
but not impossible!
@MountSinaiIR
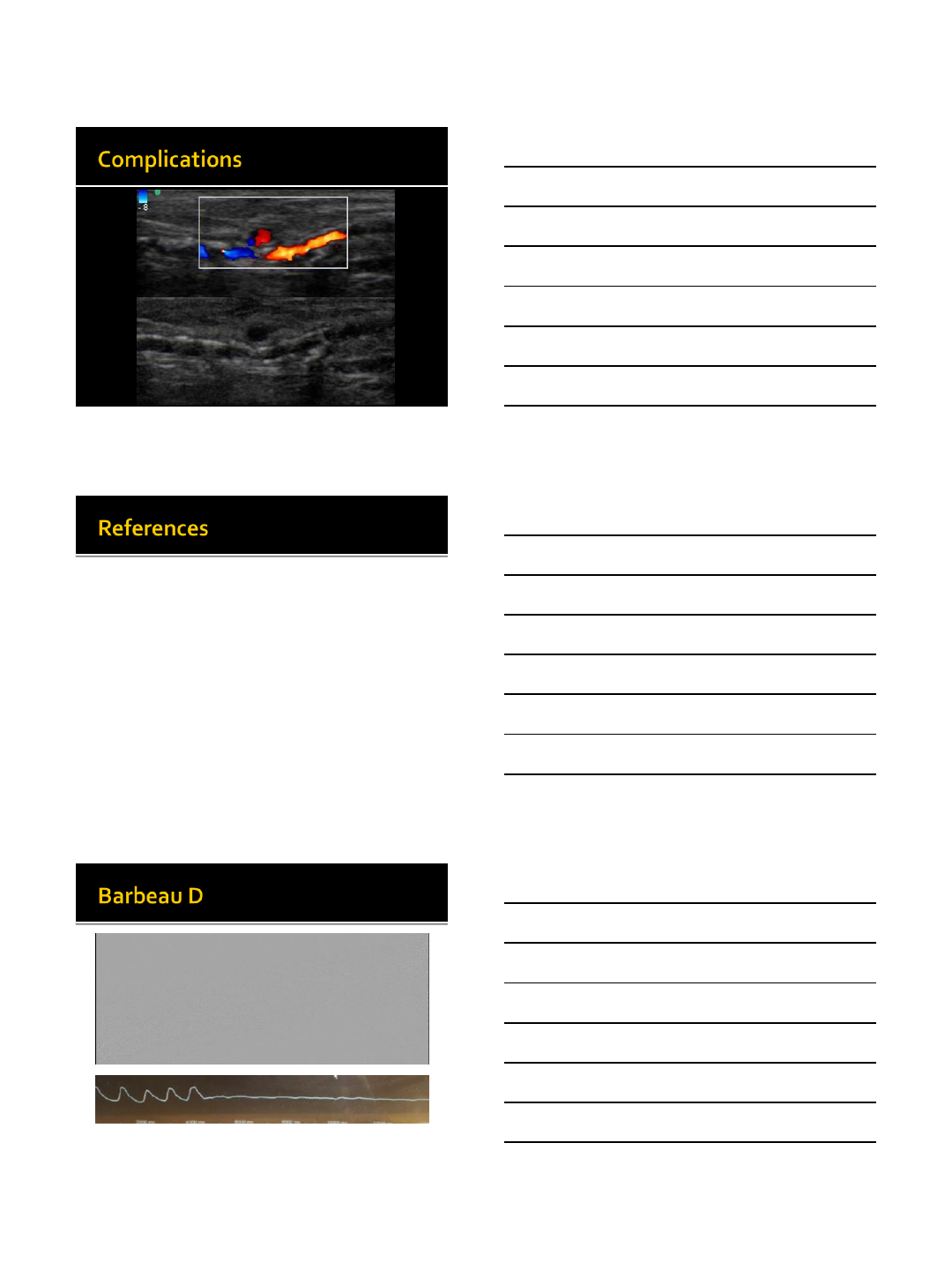
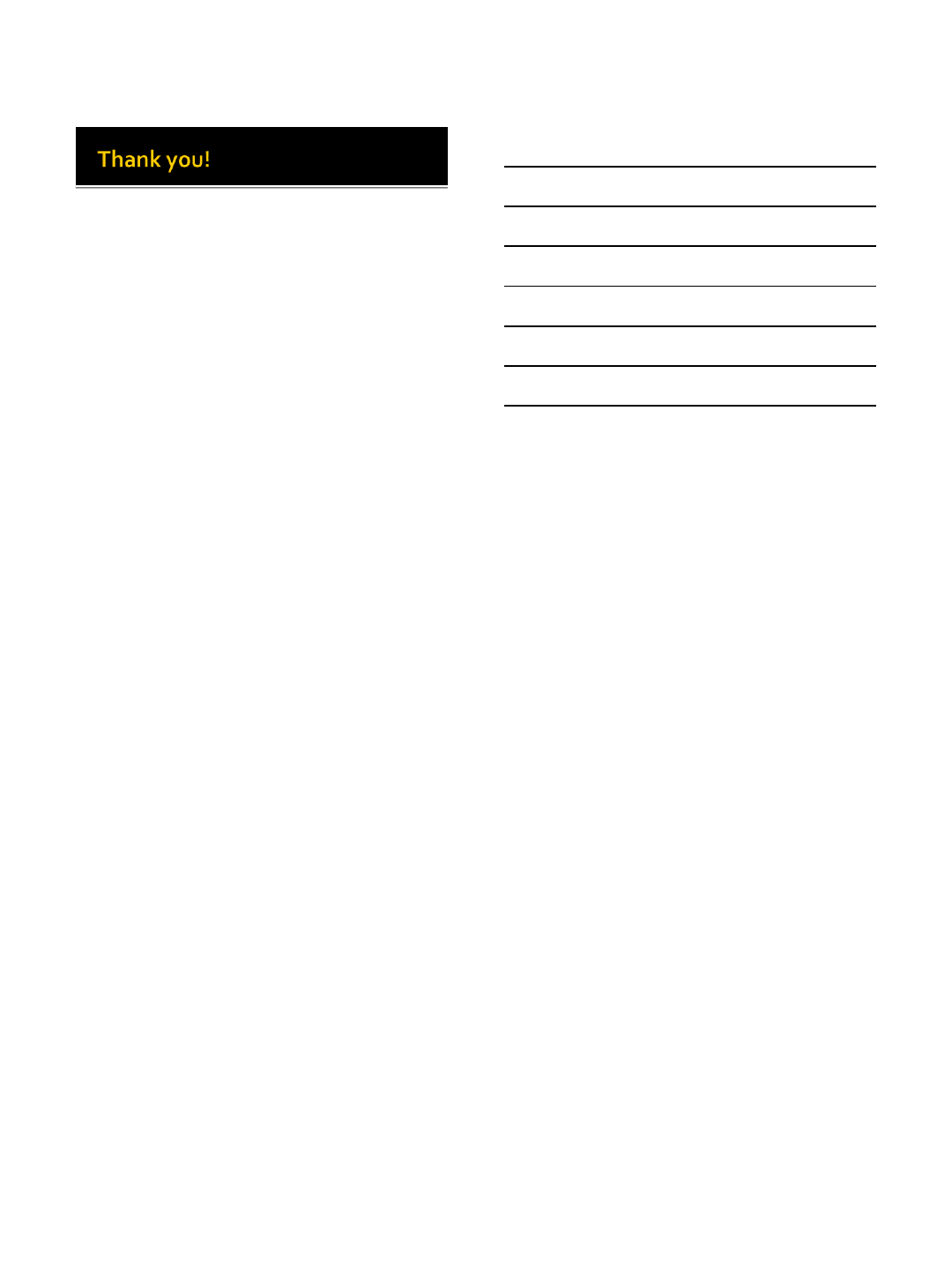
Potential Complications
Hematoma
Radial artery spasm
Pseudoaneurysm
AV fistulas
Vessel perforation
Dissection
Radial arteritis –forearm pain with normal pulse
Treated with NSAIDS or steroids
Compartment syndrome –rare
Radial artery occlusion (1-3%) –asymptomatic
Stroke risk?
@MountSinaiIR
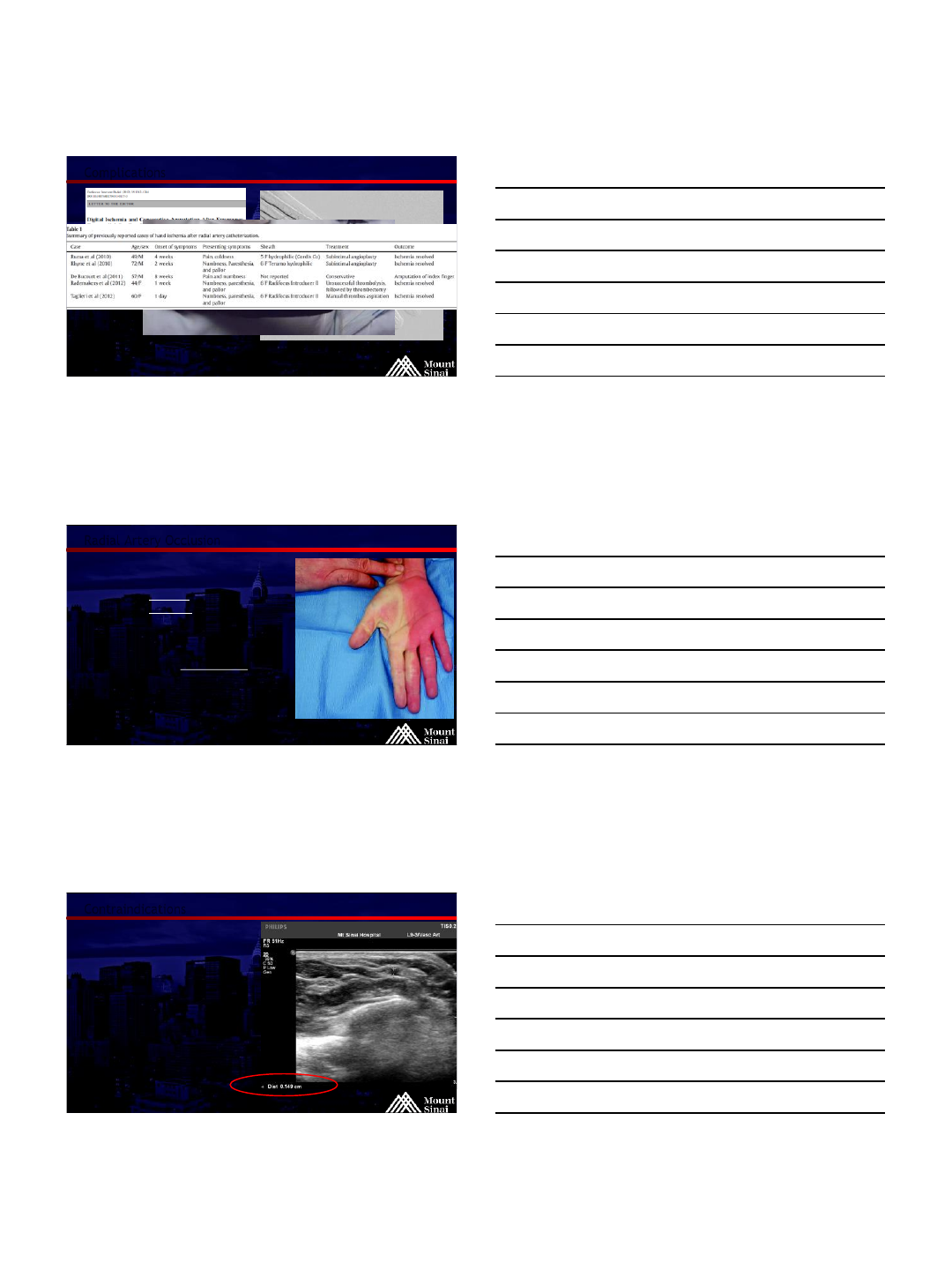
Stroke Risk
Metaanalysis of over 11,000 patients
TF vs TR in cardiology
No difference
Anecdotal in IR –Close to 4000 cases
in the US
None reported
Use good judgement
Patient selection
Consider how often you form femoral
catheters in the arch
Int J Cardiol. 2013 Oct 15;168(6):5234-8. Epub 2013 Aug 14.
Meta-analysis of stroke after transradial versus transfemoral artery catheterization.
Patel VG1,Brayton KM,Kumbhani DJ,Banerjee S,Brilakis ES.
4/20/2016
12
@MountSinaiIR
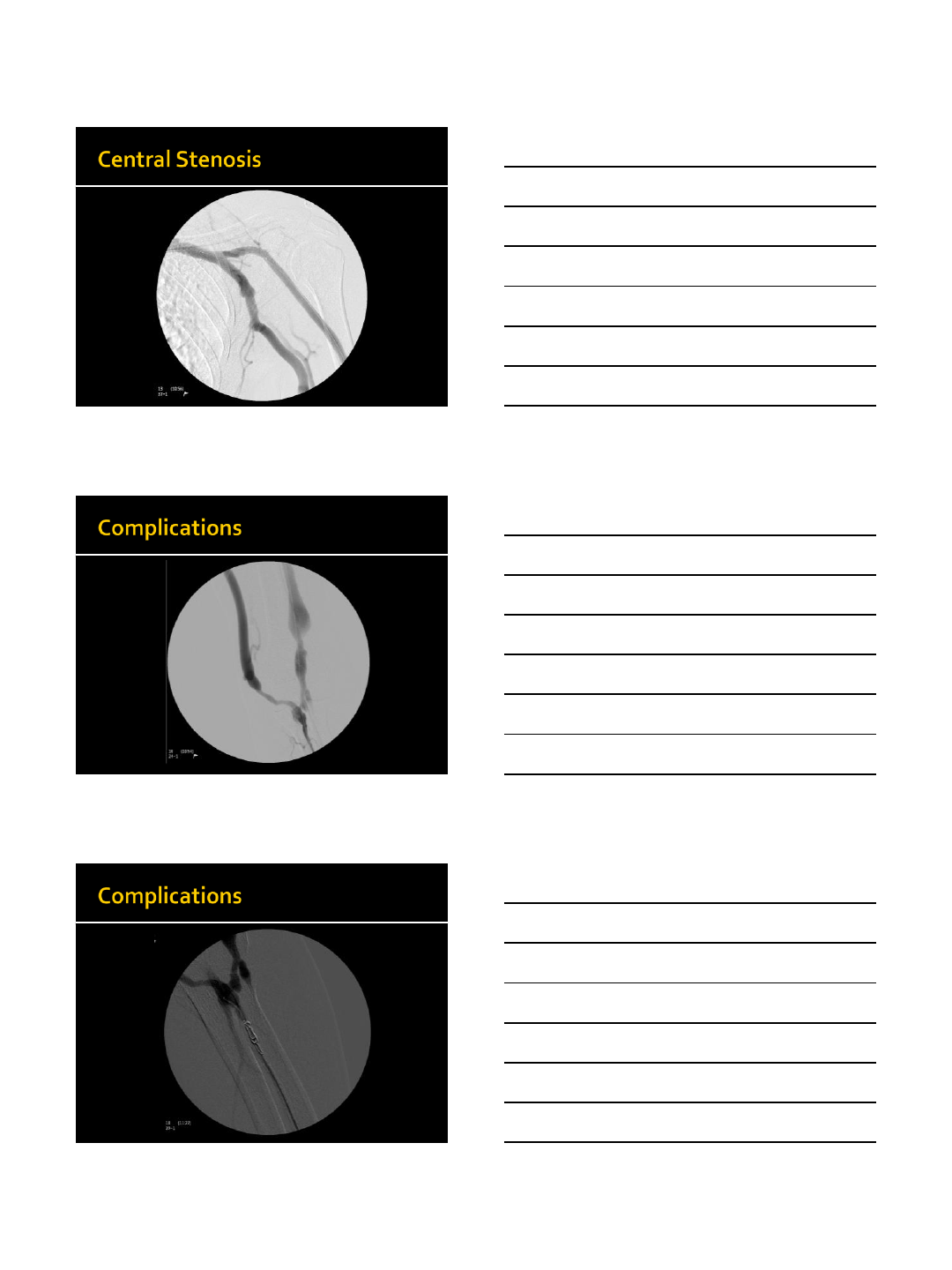
Complications
Need to do
Barbeau test!
@MountSinaiIR
Radial Artery Occlusion
Asymptomatic in Barbeau A-C
More common in women
Incidence increases with sheath size
Incidence decreases with radial artery size
Can be accessed thru occlusion
Technical expertise minimizes
Some people use anticoagulation to treat,
but not really evidence based ????
@MountSinaiIR
Contraindications
Radial artery too small < 2mm
Larger sheath needed (greater than 7F)
AV fistula / dialysis patient
Severe aortic tortuosity
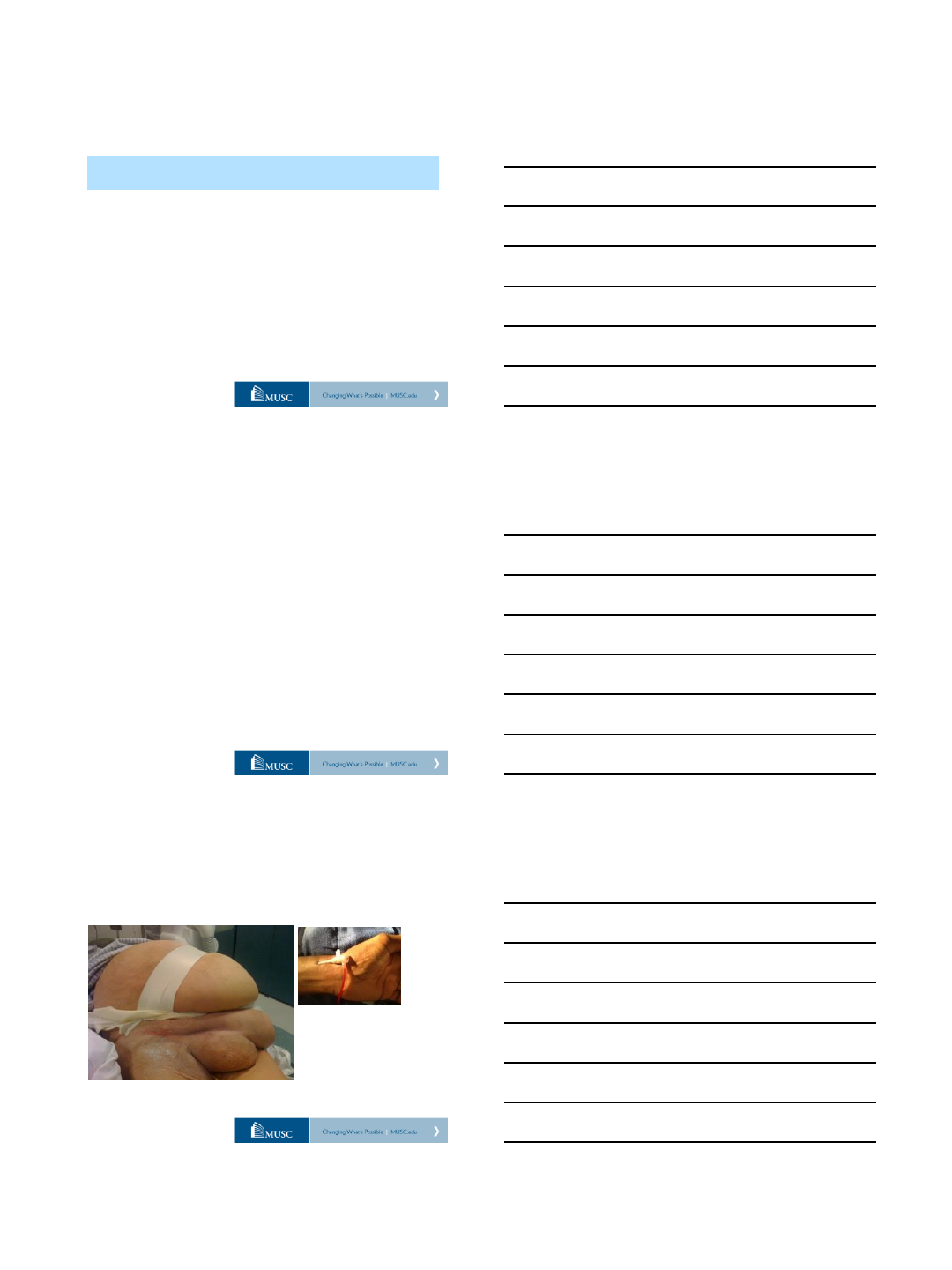
Barbeau D waveform
4/20/2016
13
@MountSinaiIR
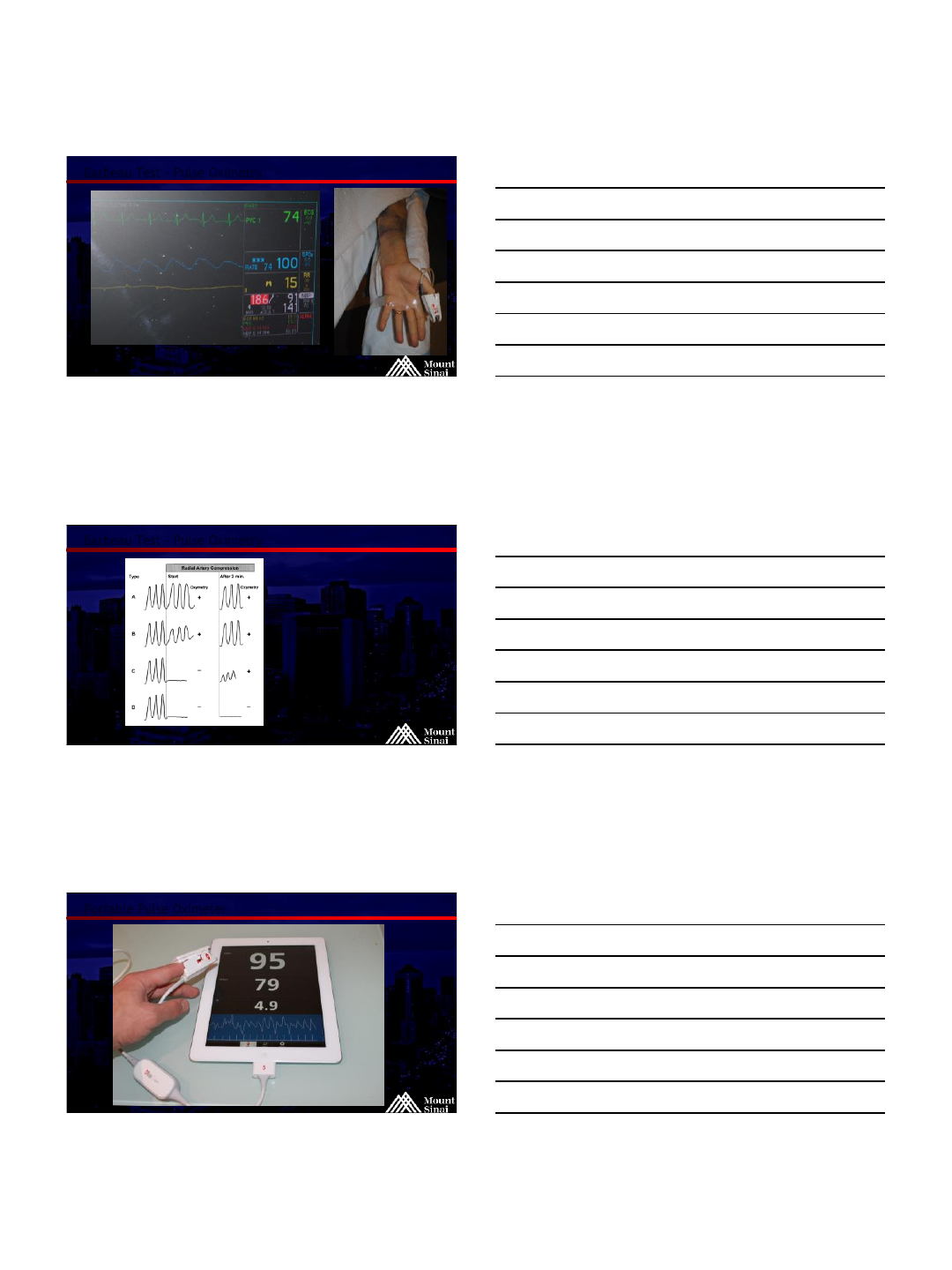
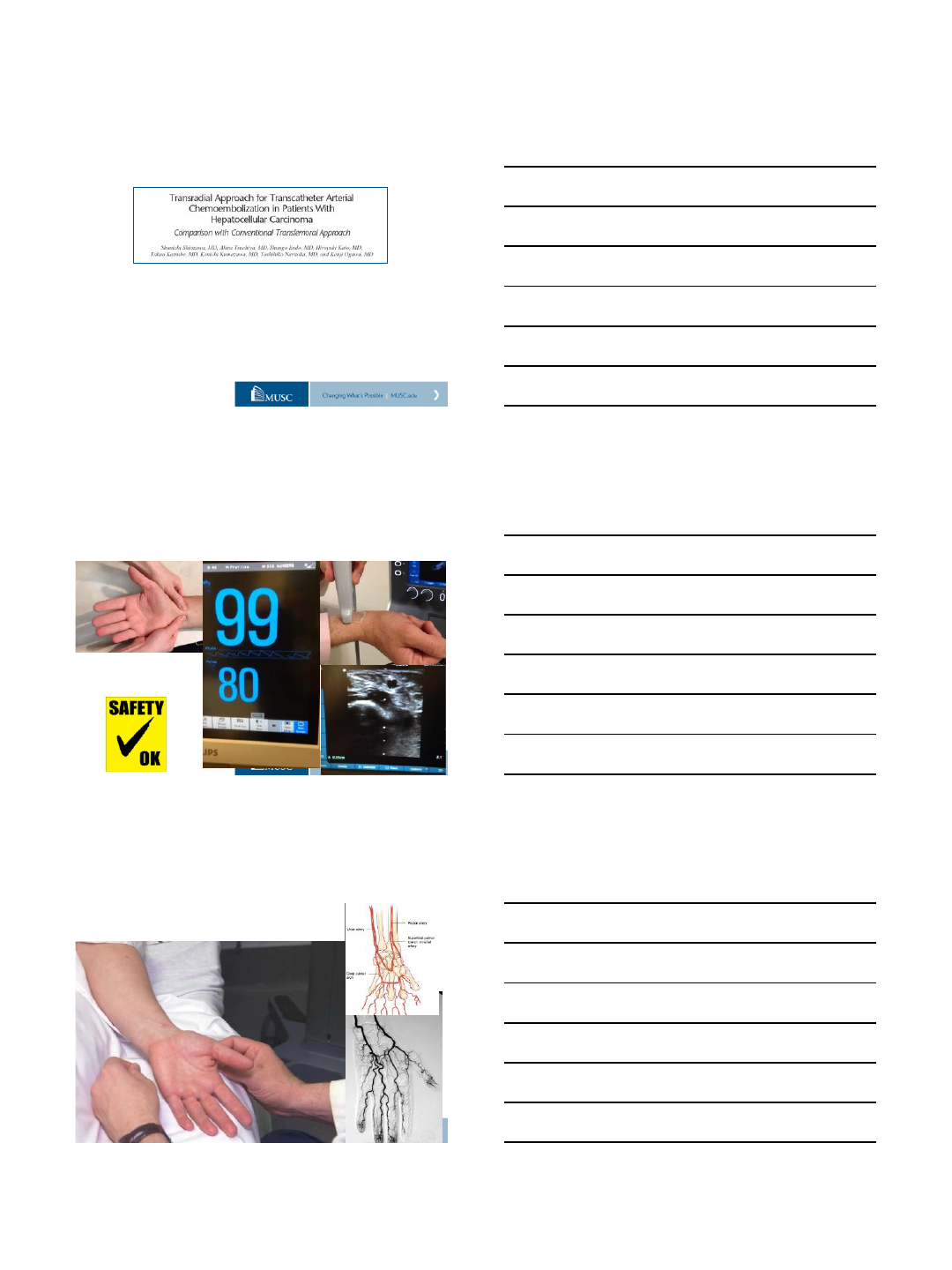
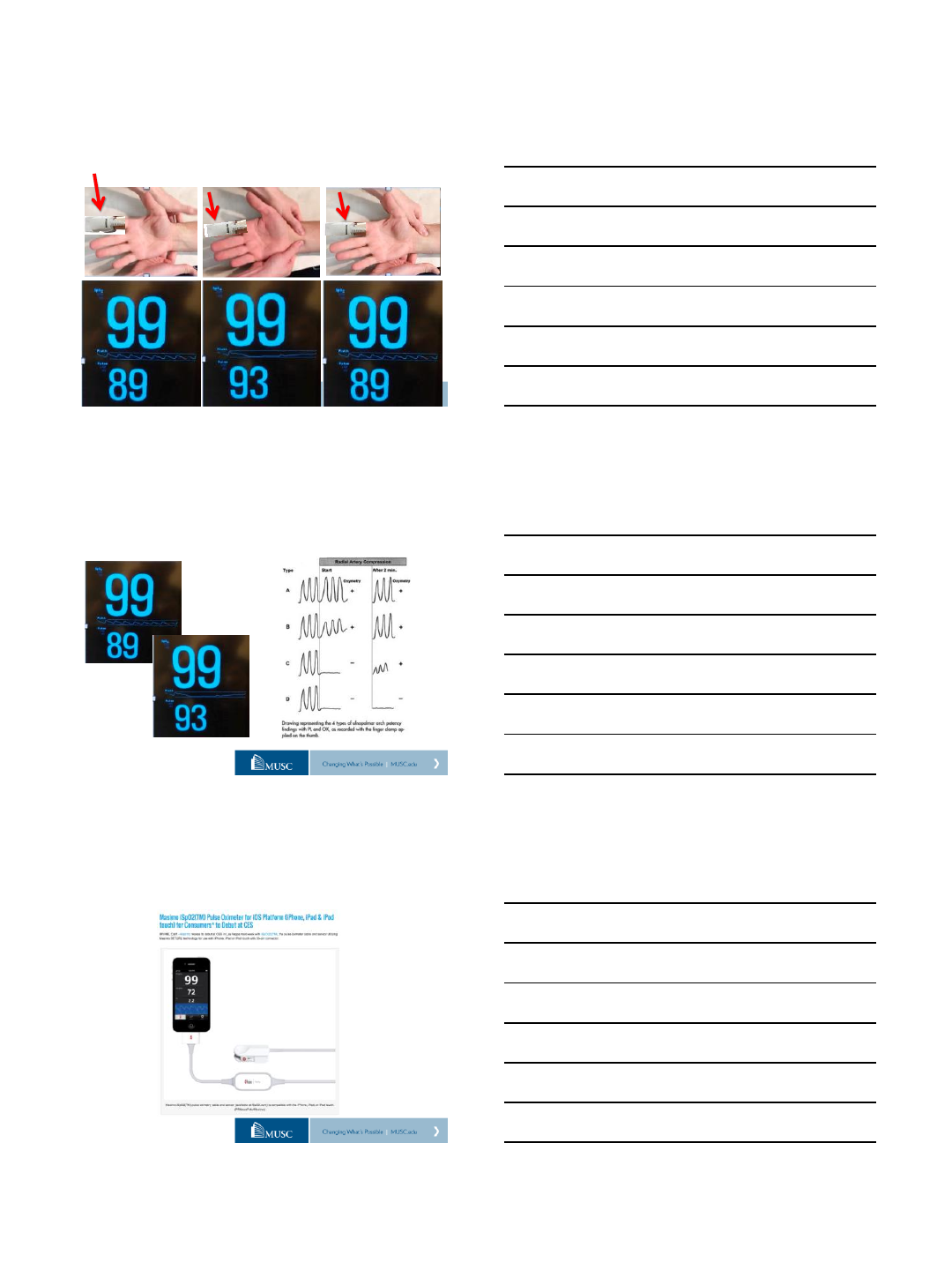
Barbeau Test –Pulse Oximetry
@MountSinaiIR
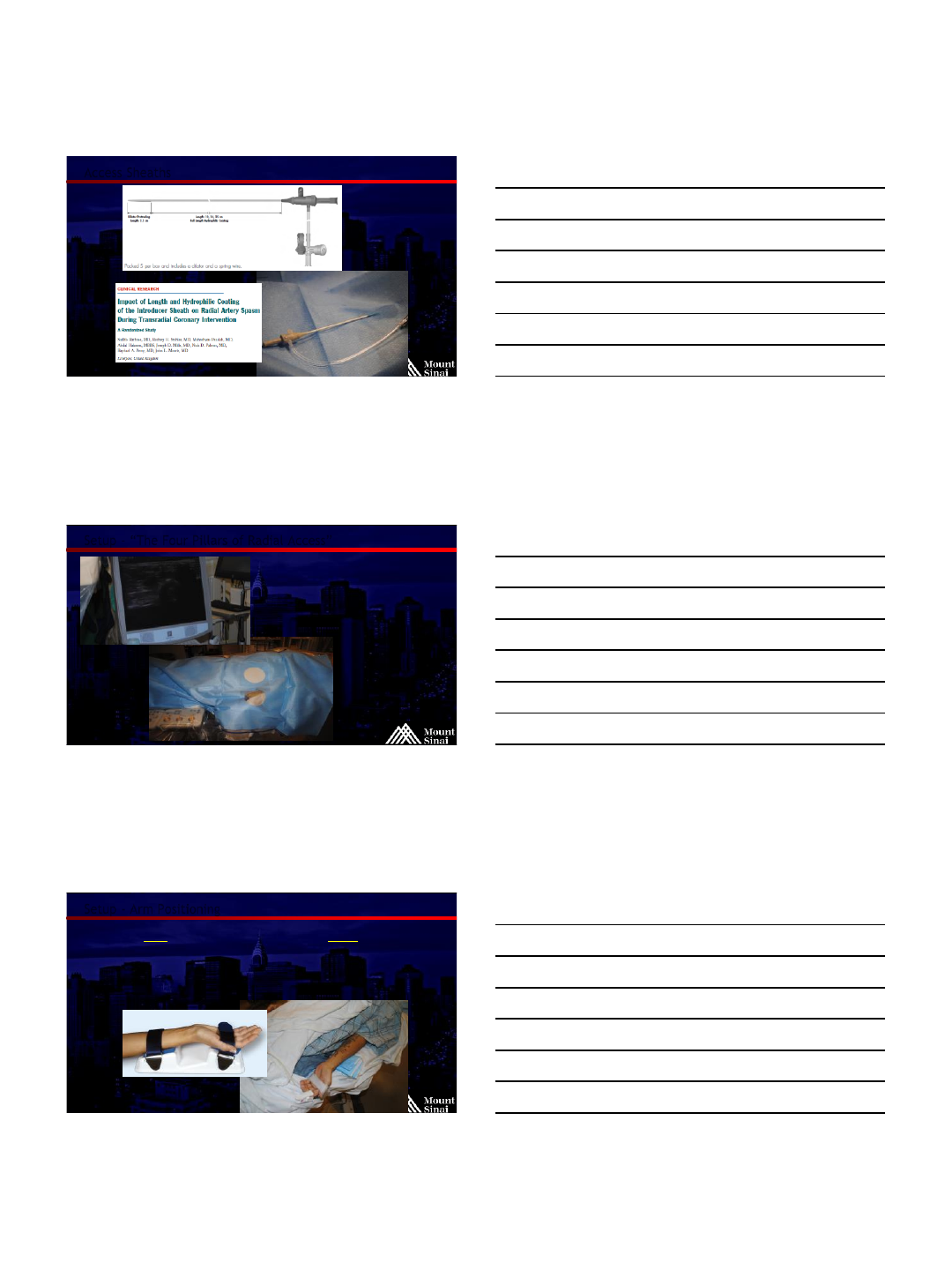
Barbeau Test –Pulse Oximetry
Barbeau et al. Am Heart J 2004;147:489–93
No damping of pulse tracing
immediately after radial artery
compression –15%
Damping of pulse tracing –75%
Loss of pulse tracing followed
by recovery of pulse tracing
within 2 minutes –5%
Loss of pulse tracing without
recovery within 2 minutes - 5%
@MountSinaiIR
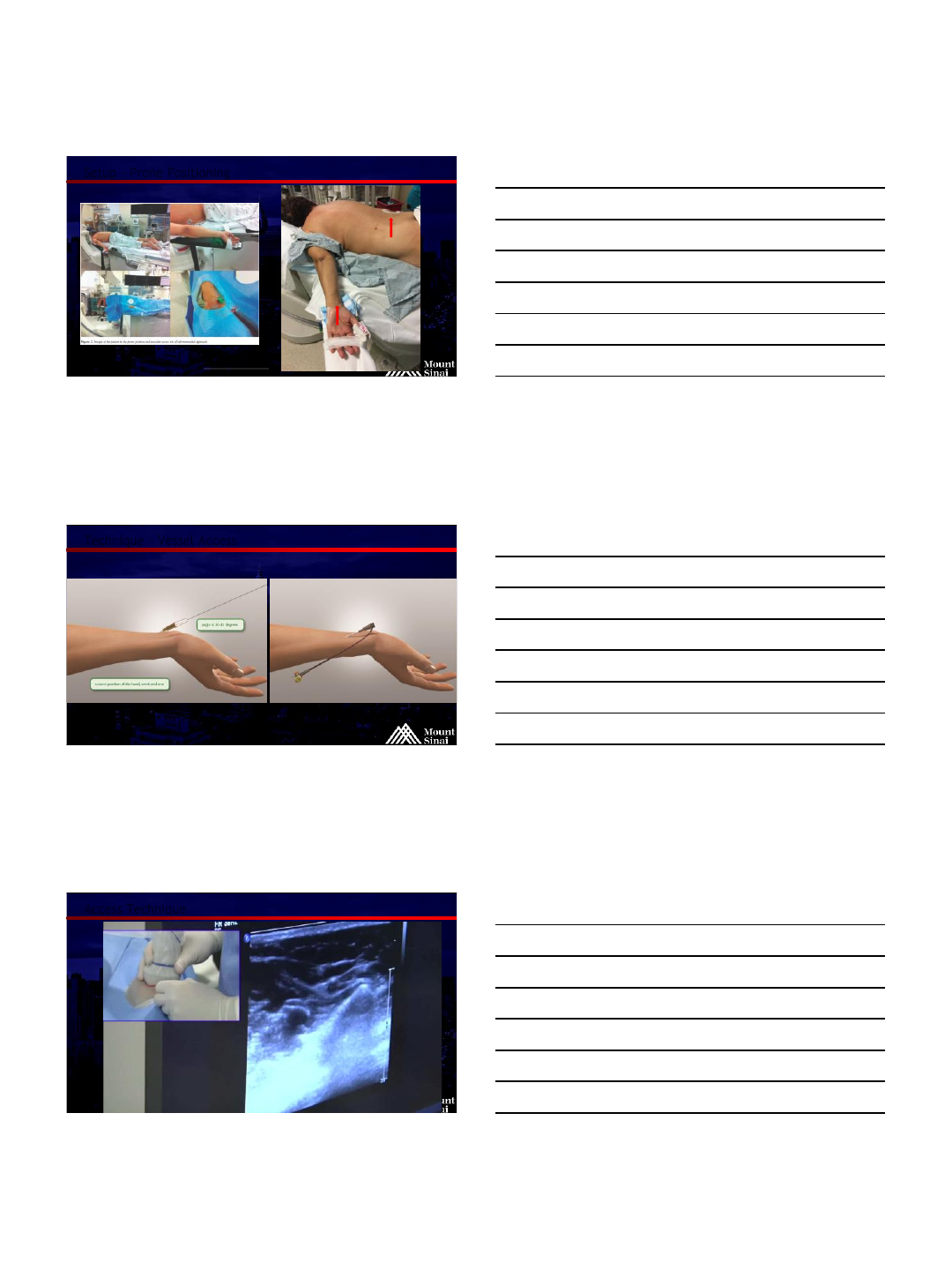
Portable Pulse Oximeter

4/20/2016
14
@MountSinaiIR
Outpatient Office Visits
@MountSinaiIR
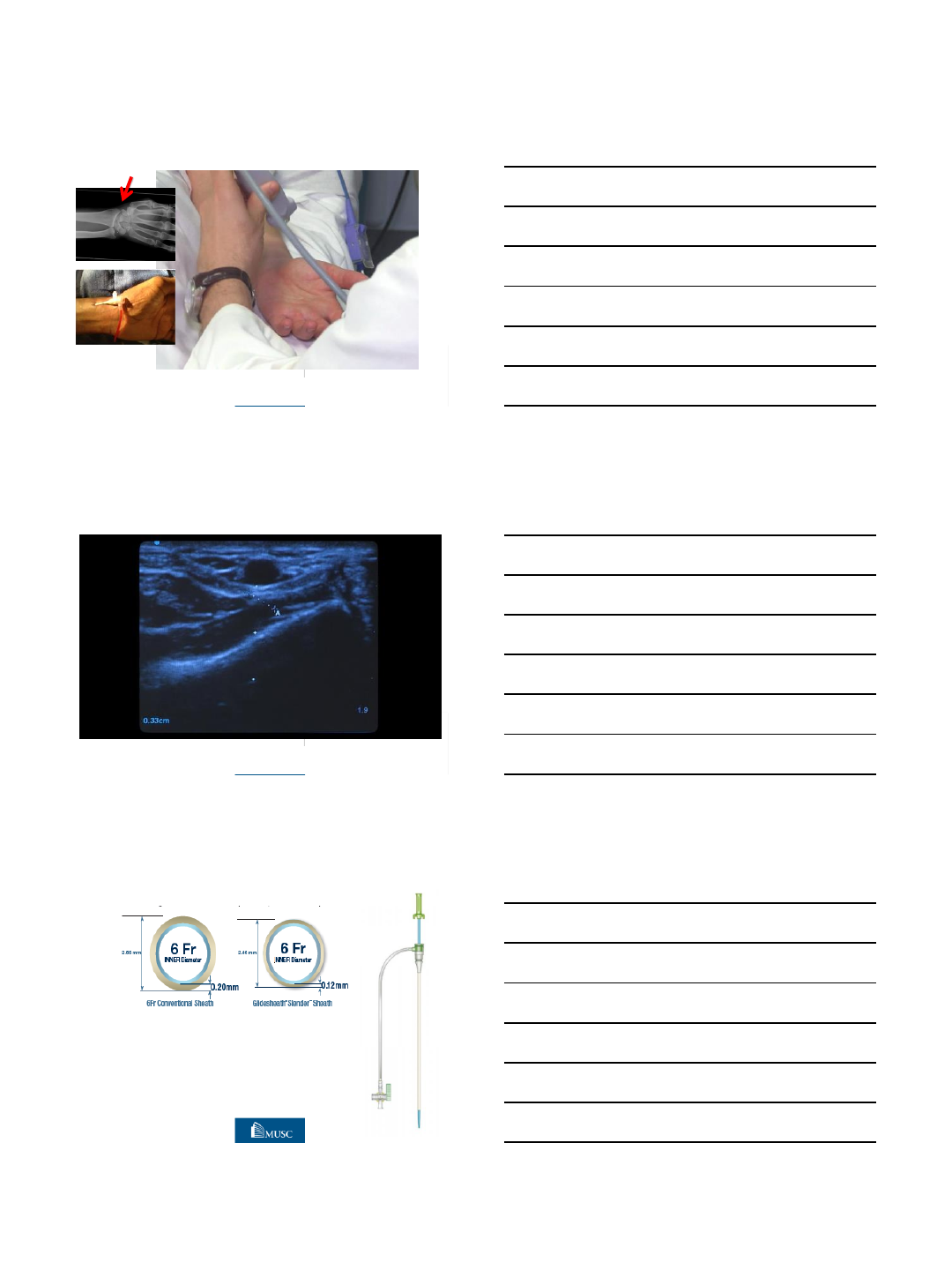
Radial Artery
US studies demonstrate mean diameter of 2.6mm
Range (2.2 to 3.4 mm)
Outer diameter of 6F sheath - 2.6 mm
Outer diameter of 7F sheath –3.1 mm
Outer diameter of 6F Glidesheath slender –2.4 mm
@MountSinaiIR
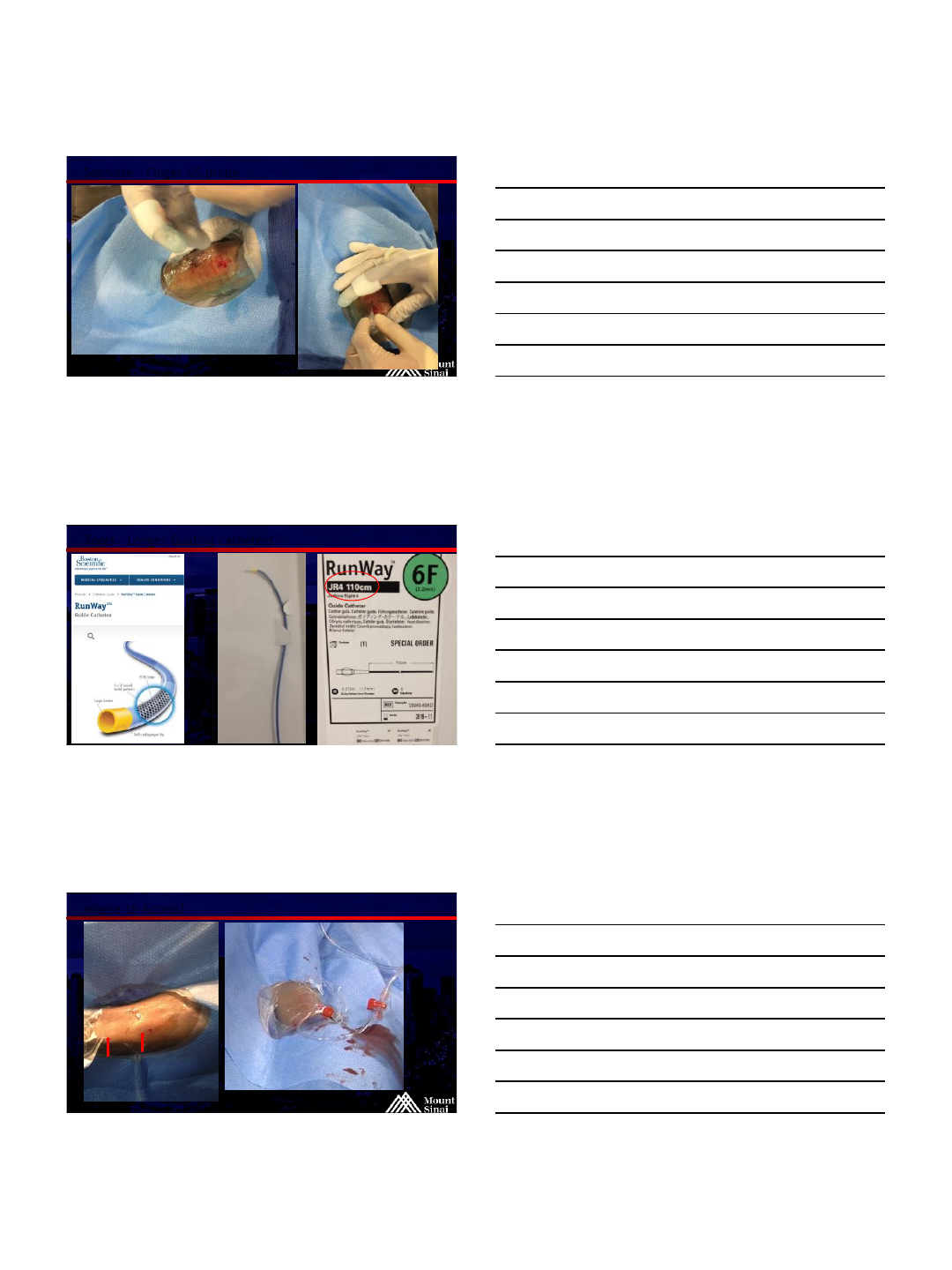
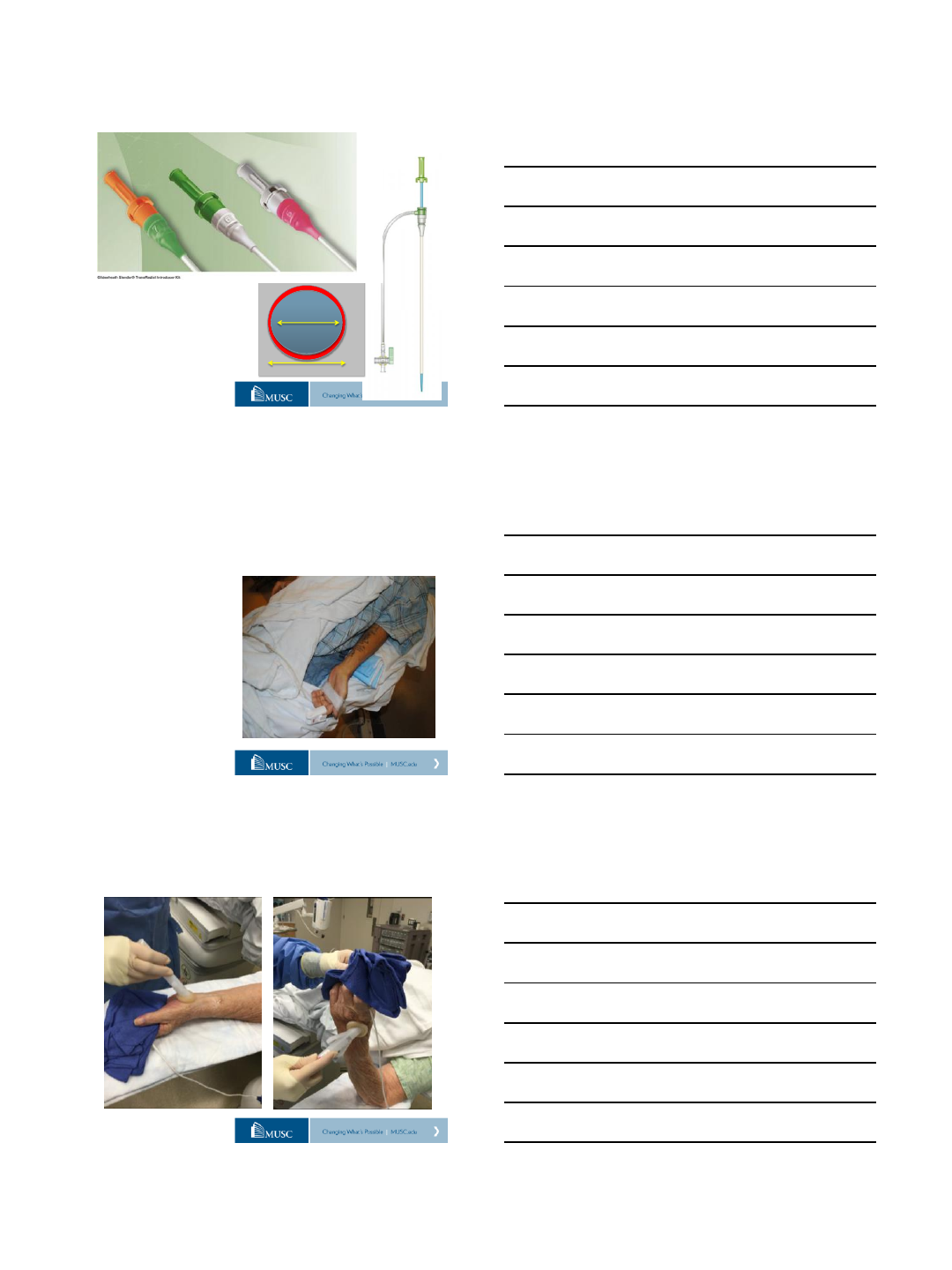
New Sheath Technology
Q4 2013
Thin walled sheath
4-7F sheath size
Allows 1F downsizing!
4/20/2016
15
@MountSinaiIR
Access Sheaths
@MountSinaiIR
Setup – “The Four Pillars of Radial Access”
Micropuncture
US guidance
Hydrophilic sheath
Antispasmodic
“cocktail”
@MountSinaiIR
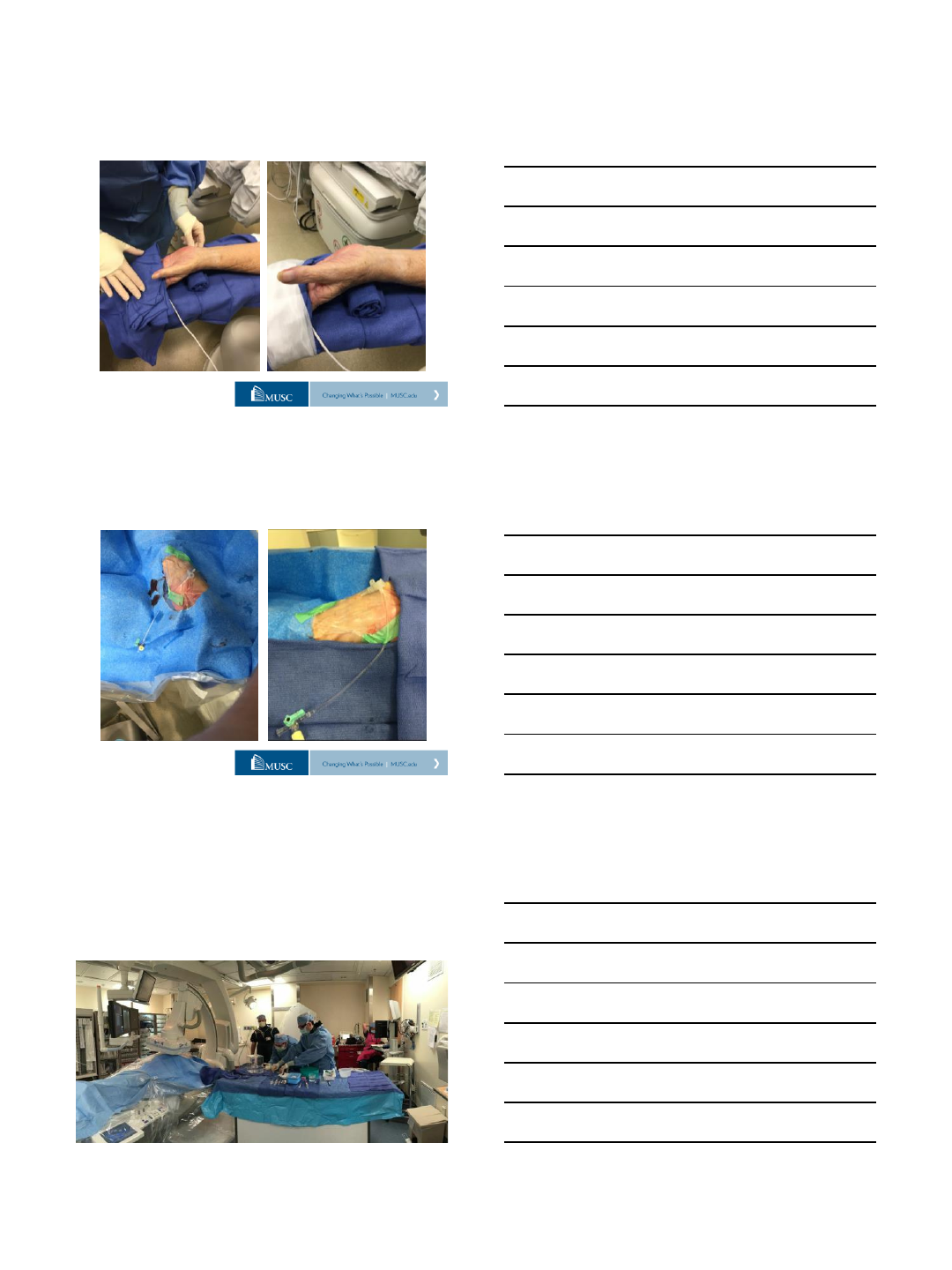
Setup - Arm Positioning
Left wrist used for all interventions below
diaphragm
Prop arm above left groin
Use towel roll and arm board if necessary
4/20/2016
16
@MountSinaiIR
Setup –Prone Positioning
Kwon, S. W., et al. (2012). "Prone position coronary angiography due to intractable back pain: another
merit of transradial approach compared to transfemoral approach." J Invasive Cardiol 24(11): 605-607
@MountSinaiIR
Technique –Vessel Access
@MountSinaiIR
Access Technique
4/20/2016
17
@MountSinaiIR
Sonivate –Finger US probe
@MountSinaiIR
Tools –Longer Guiding catheters
@MountSinaiIR
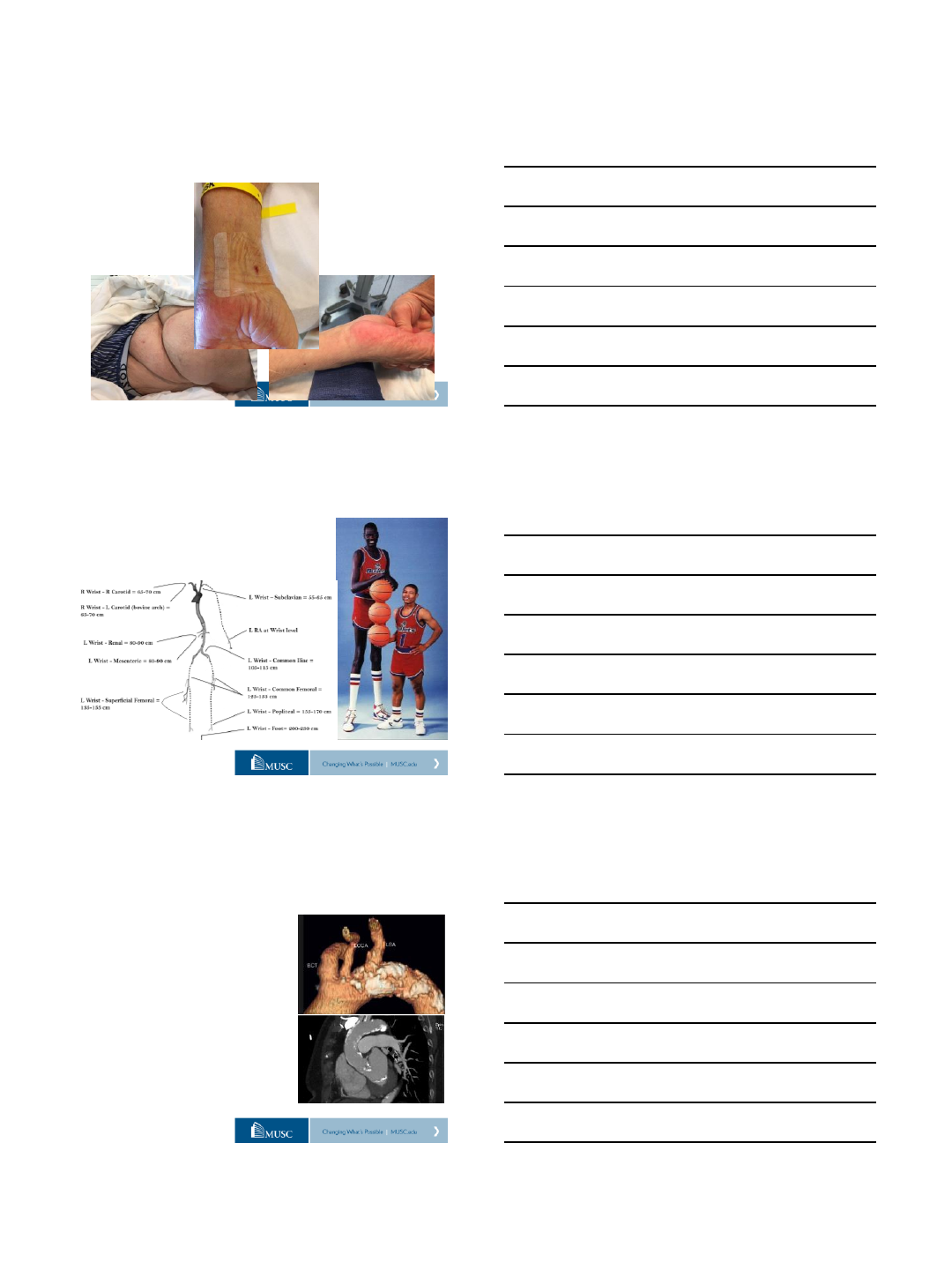
Where to Access?
4/20/2016
18
@MountSinaiIR
PRE-DILATE Protocol
40mg of lidocaine cream (EMLA)
PLUS
30mg of nitroglycerin ointment
@MountSinaiIR
PRE-DILATE Protocol
@MountSinaiIR
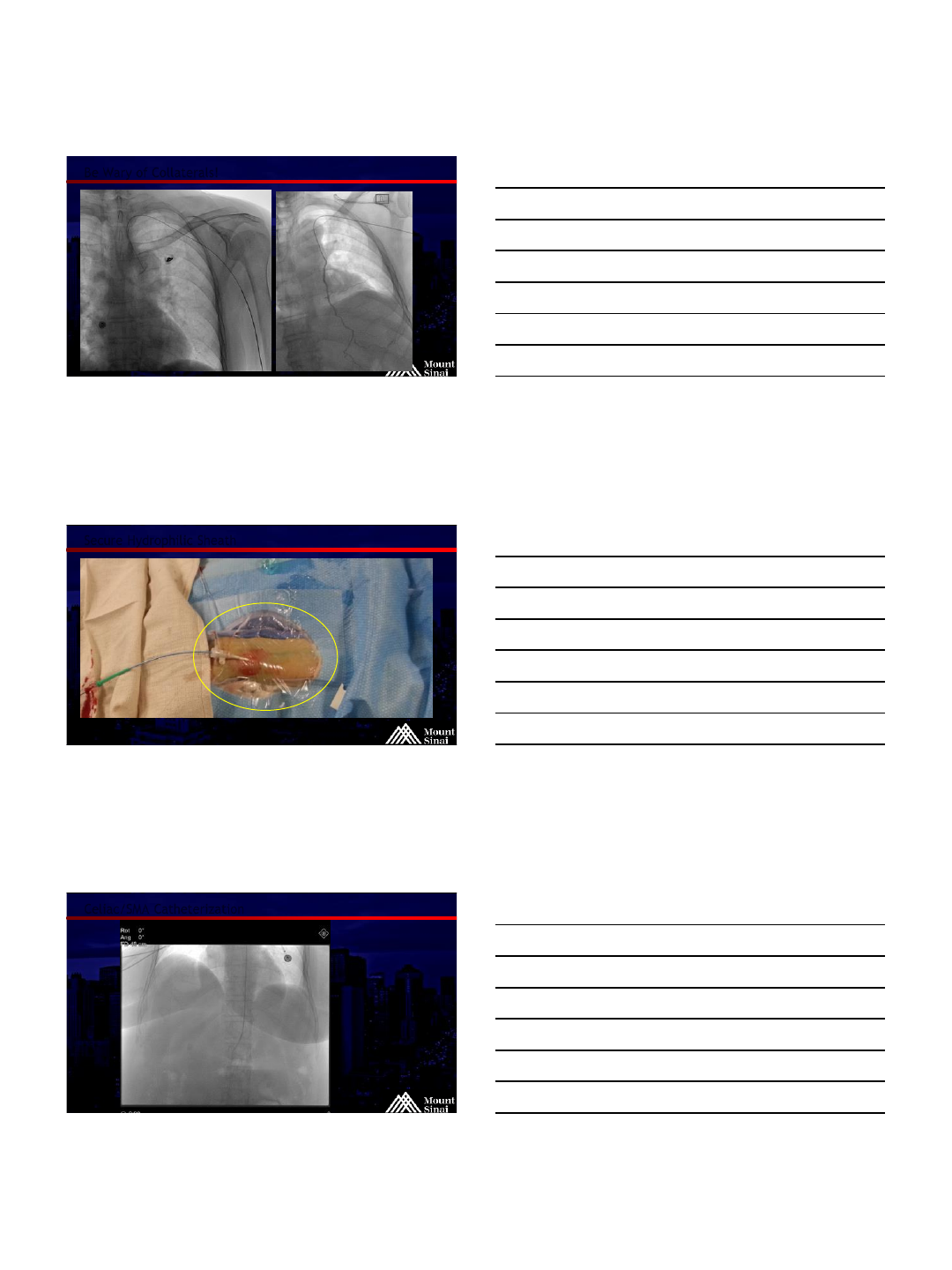
Navigating the Descending Aorta
Reverse Curve
Cobra
Sarah/Jacky
Use an .016 wire to
“flop down”
4/20/2016
19
@MountSinaiIR
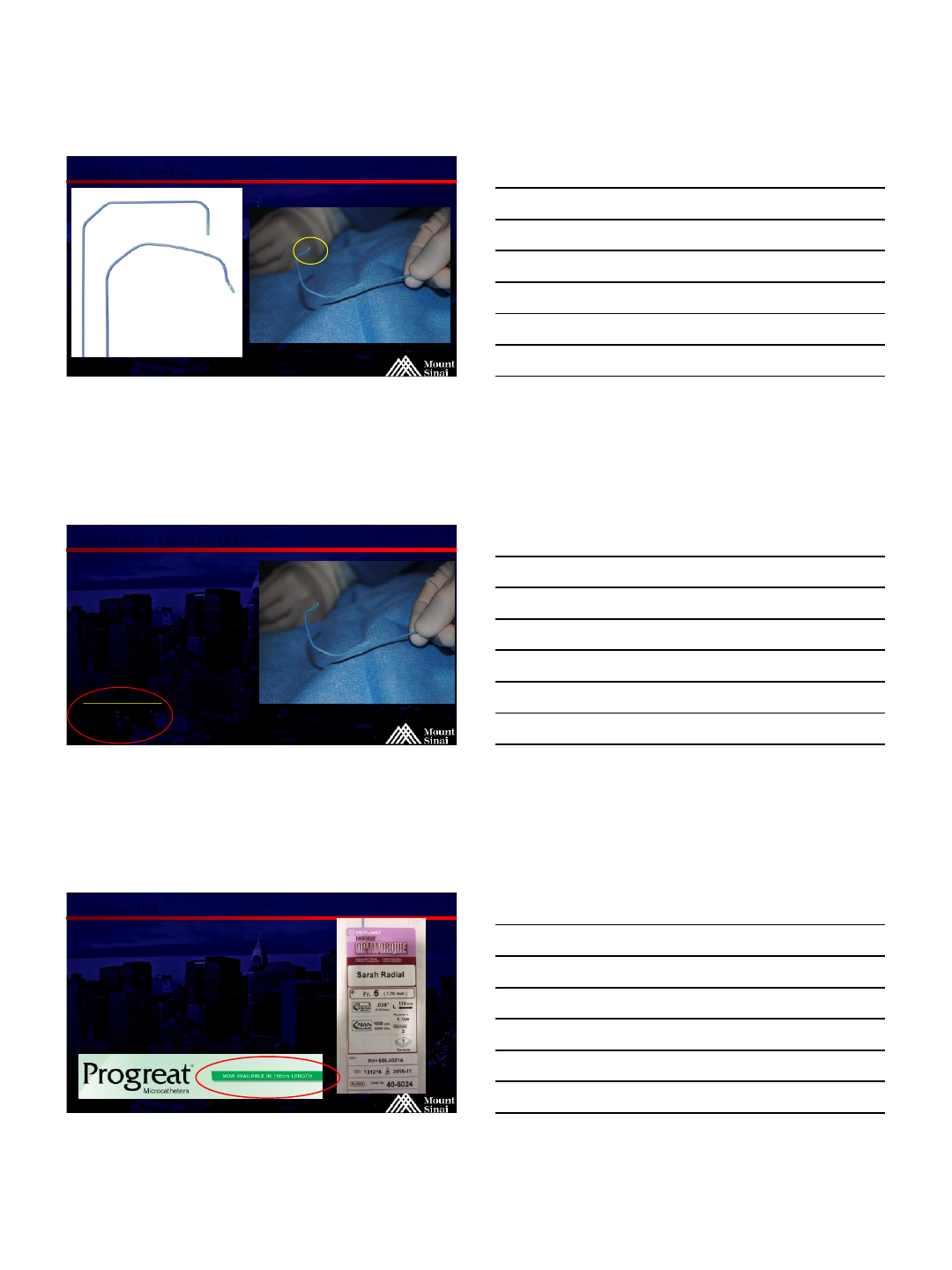
Navigating the Descending Aorta - Sarah
@MountSinaiIR
Navigating the Descending Aorta –Reverse Curve, Pigtail
@MountSinaiIR
Navigating the Descending Aorta - Microwire
4/20/2016
20
@MountSinaiIR
Be Wary of Collaterals!
@MountSinaiIR
Secure Hydrophilic Sheath
@MountSinaiIR
Celiac/SMA Catheterization
4/20/2016
21
@MountSinaiIR
Catheter Selection
@MountSinaiIR
Technique - Catheters Used
5F Sarah Radial 110cm (Terumo)
5F Cobra 100cm (Terumo)
5F Jacky Radial 110cm (Terumo)
4F Aqua 125cm (Cordis)
4F Cobra 100cm (Cordis)
5F Envoy 100 Guidecath (Cordis)
5F JR4 100cm (Cordis)
5F MPA 100cm (Cordis)
5F Bern 120cm (Penumbra)
5F Sherpa AL1 Guide (Medtronic)
5F Sherpa HS1 Guide (Medtronic)
5F Launcher Guide (Medtronic)
Other shapes (Champ, MP1, RDC, MAC, IMA, SCR, SCL)
Longest Lengths in our lab:
Guiding sheath: 110cm
Guiding catheter: 125cm
Diagnostic catheter: 150cm
@MountSinaiIR
Toolbox Tips
110 cm ideal length for visceral arteries
110 Optitorque PIGTAIL is awesome!
Microcatheters should be 150cm, not 130 cm
Glidesheath Slender
Extra “cocktail” for spasm or small arteries
Ultrasound the arm to look for radial loops?
Don’t be afraid to go ulnar if the radial is
small
4/20/2016
22
@MountSinaiIR
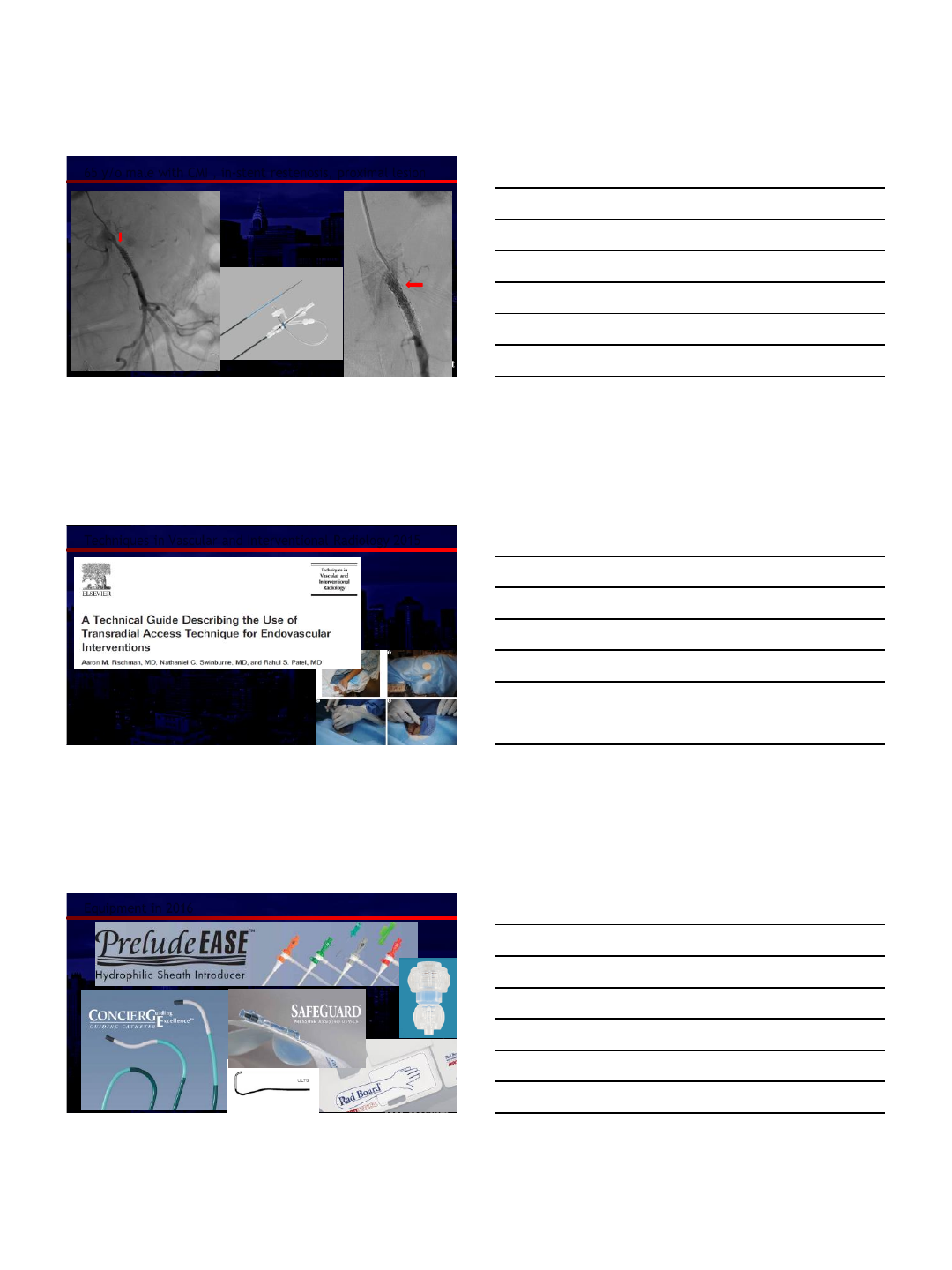
65 y/o male with CMI , in-stent restenosis, proximal lesion
ICAST Covered
Stent
6F Cook Sheath
90 cm, 110 cm
@MountSinaiIR
Techniques in Vascular and Interventional Radiology 2015
@MountSinaiIR
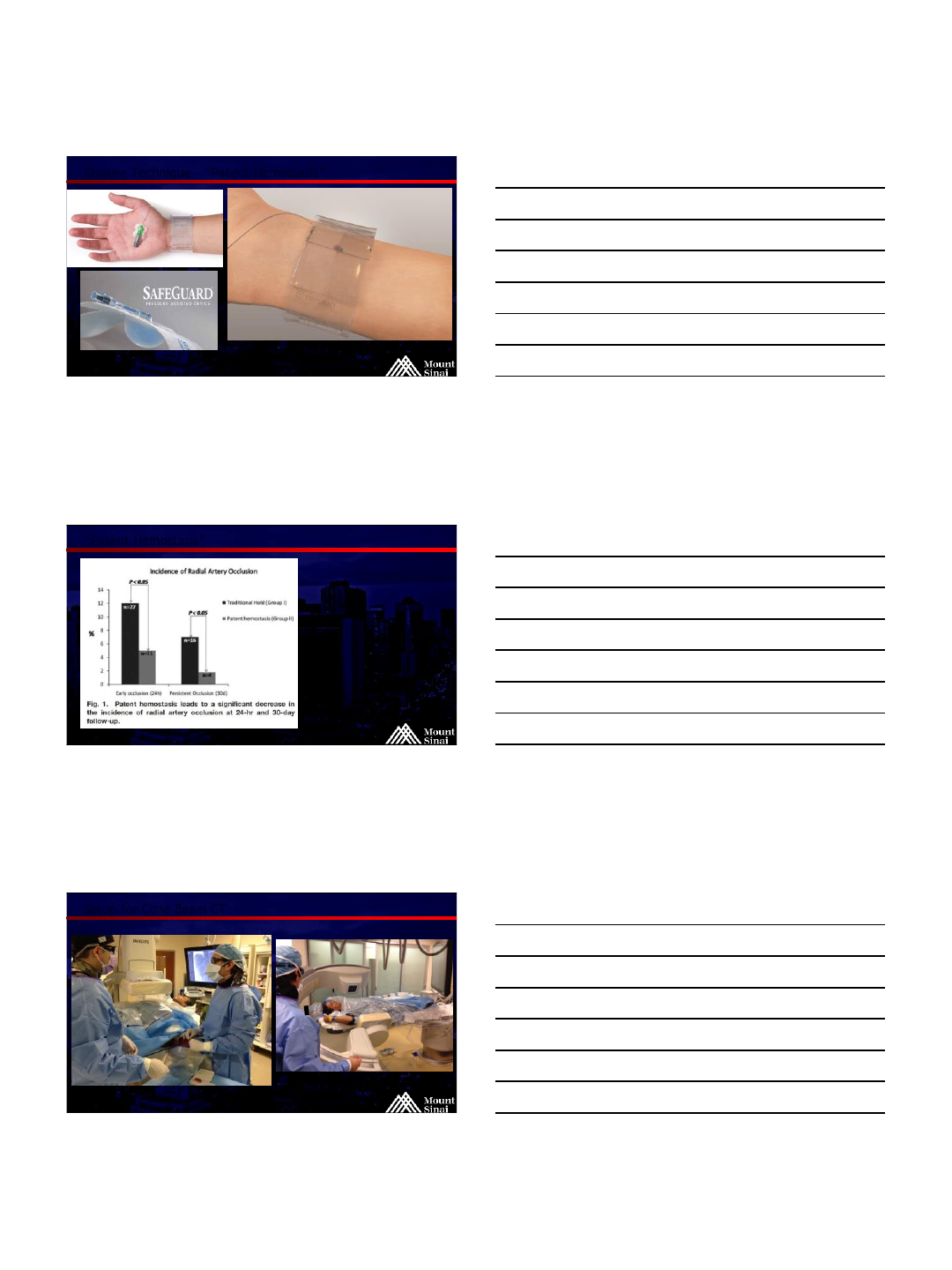
Equipment in 2016
4/20/2016
23
@MountSinaiIR
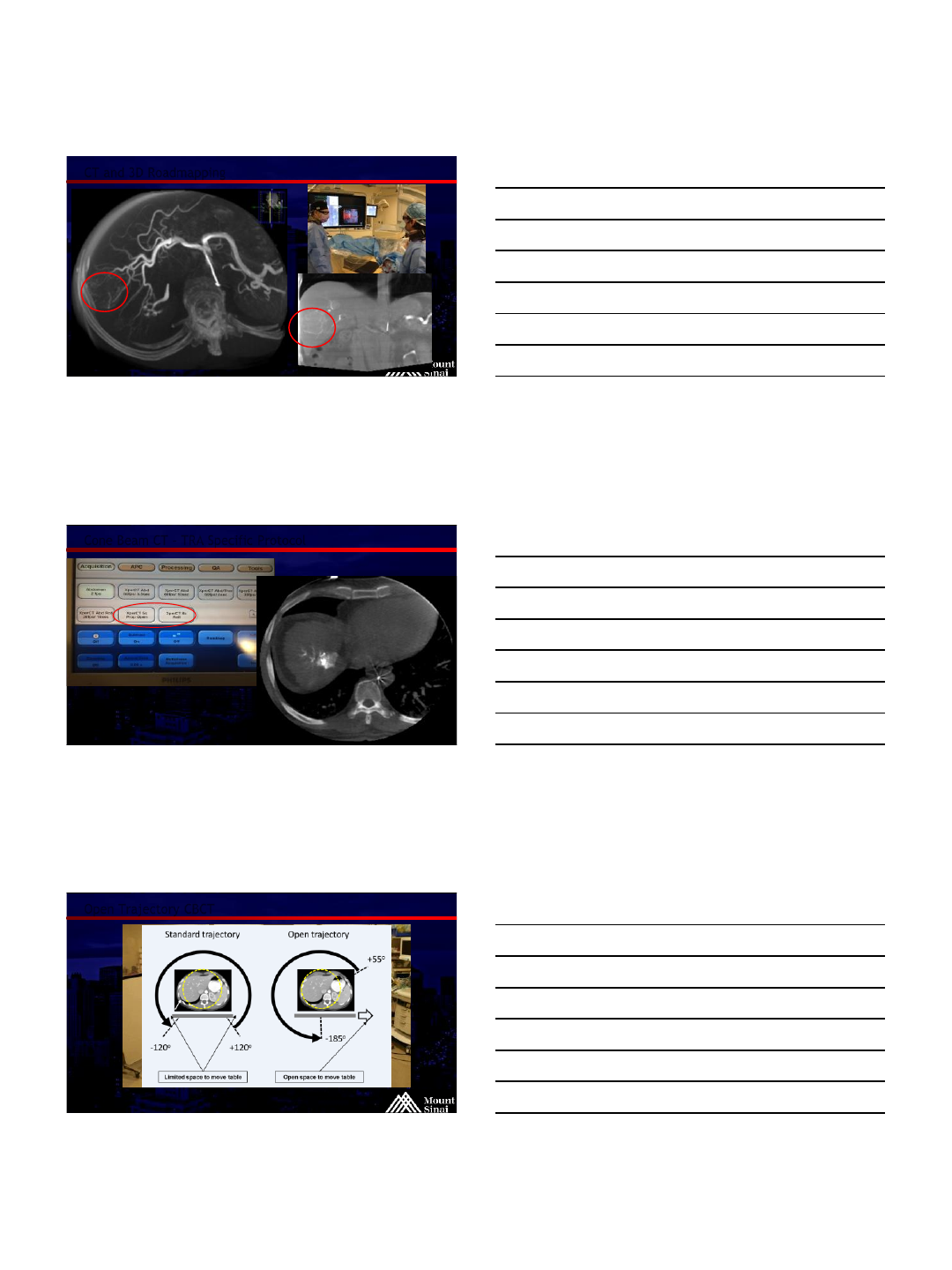
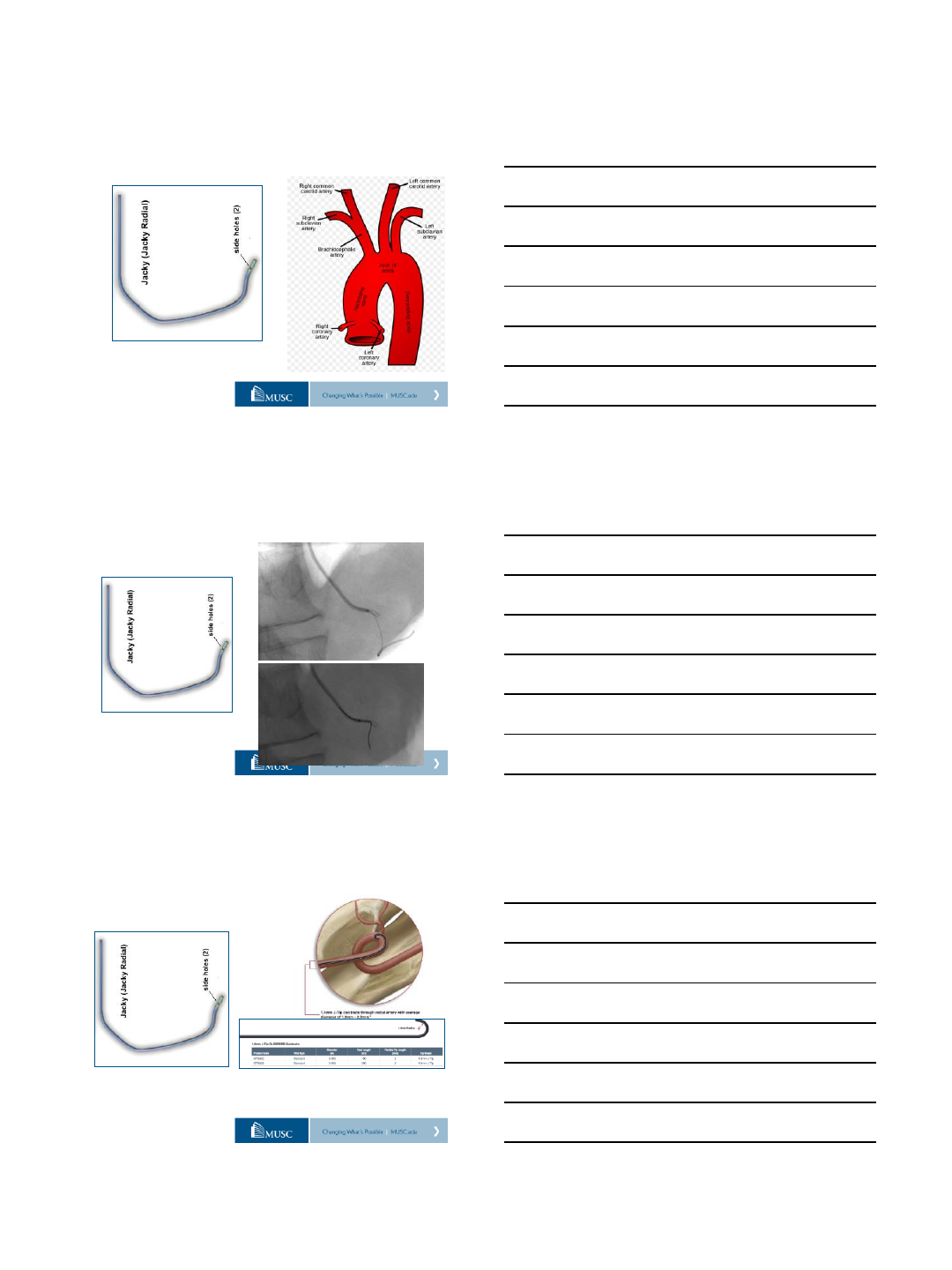
Radial Loop
@MountSinaiIR
Radial Loop – “.016 wire technique”
.016 Microwire
@MountSinaiIR
Brachial Loop
Be Careful!
Severe spasm can compromise
flow to the hand
Watch the pulse oximeter
4/20/2016
24
@MountSinaiIR
Closure Technique – “Patent Hemostasis”
@MountSinaiIR
“Patent Hemostasis”
Maintain “non-
occlusive pressure!
Should be able to feel
a distal RA Pulse
Samir Pancholy, et al Catheterization and Cardiovascular Interventions 72:335–340 (2008)
@MountSinaiIR
Setup for Cone Beam CT
4/20/2016
25
@MountSinaiIR
CT and 3D Roadmapping
@MountSinaiIR
Cone Beam CT –TRA Specific Protocol
@MountSinaiIR
Open Trajectory CBCT
Courtesy of Philips
4/20/2016
26
@MountSinaiIR
What can’t we do?
SFA and below
Stent and balloon systems
Brachial artery occlusions
400, 500 cm wires?
Extra table? Extra fellows to
hold wires?
@MountSinaiIR
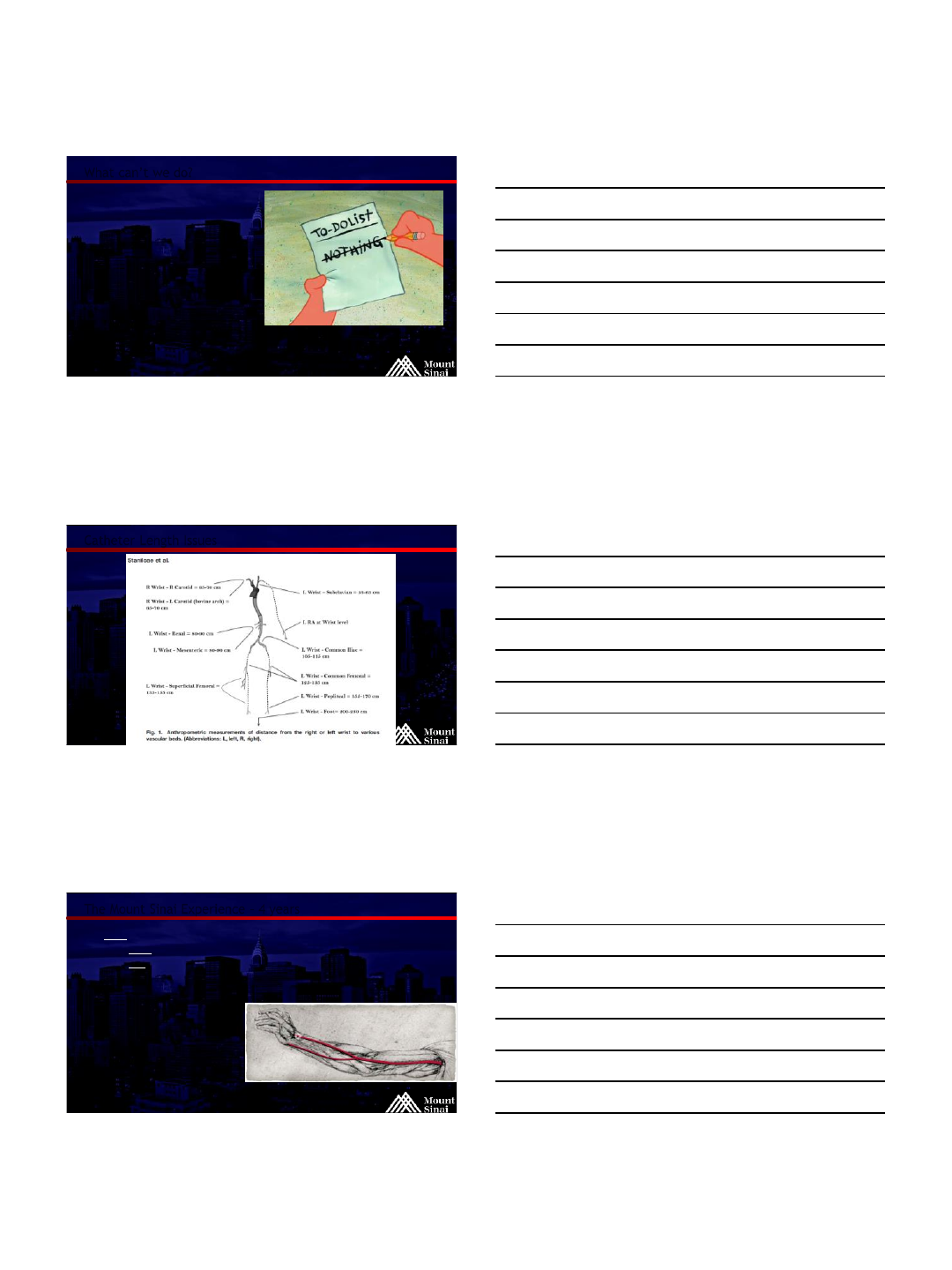
Catheter Length Issues
@MountSinaiIR
The Mount Sinai Experience –4 years
2000 TR interventions since April 2012
Over 1500 Liver Directed Therapies
Over 180 Uterine Fibroid Embolizations
Overwhelming Patient Satisfaction
>90 % Patient preference for TR over TF
Very low complication rate
Repeat interventions common
4/20/2016
27
@MountSinaiIR
Adverse Events –Overall 0.3%
Minor Complications:
22 Grade I access site hematomas
(2.2%)
4 Grade II access site hematomas
(0.4%)
11 cases of RAO (1.1%)
3 Cases requiring TFA crossover
All asymptomatic
Most reaccessed for repeat
procedure
5 cases of RA Thrombosis (.5%)
1 Case requiring TFA Crossover
3 Radial Arteritis (0.3%)
2 extended bleeding (0.2%)
TR band used 12-24 hrs
2 mild hand pain/weakness (.2%)
2 Severe Vasospasm (.2%)
1 Case Requiring TFA Crossover
3 microperforation of branch vessel
(0.3%)
Causing pain <= 24 hours
Major Complications:
1 Large hematoma (0.1%)
TFA Crossover required
1 radial artery pseudoaneurysm (0.1%)
Treated with thrombin
injection
1 seizure (possibly verapamil?) (0.1%)
No additional Adverse Events at 30 days
Fischman et al. Scientific Sessions Abstract, SIR 2013. April 17, 2013
Fischman et al. AIM- RADIAL2013. September 2013
Posham et al. JVIR 2015, in press
Featured Abstract, Scientific Sessions, SIR 2015
@MountSinaiIR
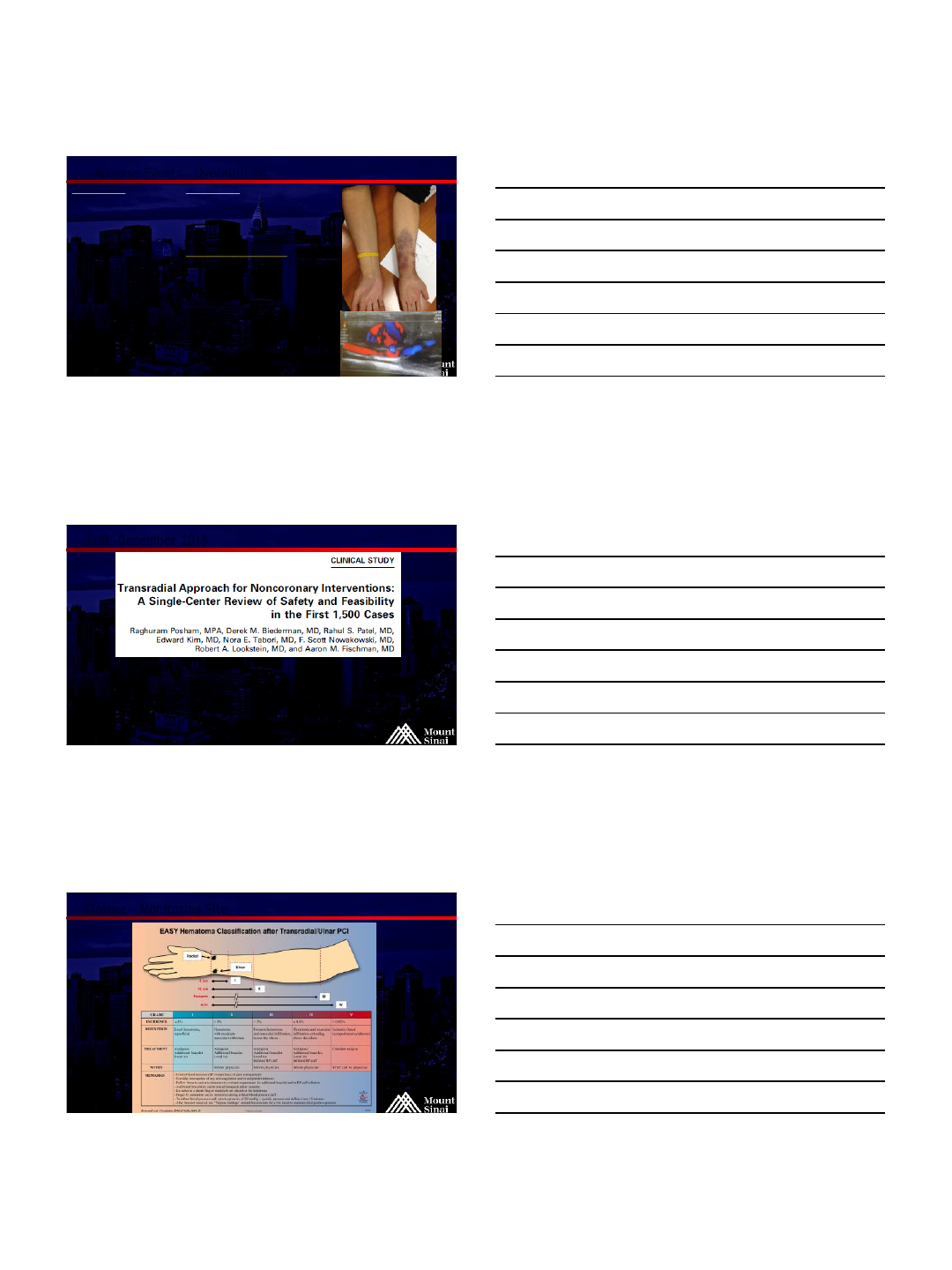
JVIR -December 2015
1,531 procedures in 946 patients
98.2% technical success
0.13% Major Complications (1 PSA, 1 seizure)
2.4% minor complications (hematoma, RAO , arm pain, spasm)
1.8% Crossover rate
Posham R, Biederman DM, Patel RS, Kim E, Tabori NE, Nowakowski FS, Lookstein RA, Fischman AM. Transradial Approach for Noncoronary
Interventions: A Single-Center Review of Safety and Feasibility in the First 1,500 Cases. J Vasc Interv Radiol 2015: Dec 16. Epub. PMID 26706186.
@MountSinaiIR
Closure –Monitoring Site
4/20/2016
28
@MountSinaiIR
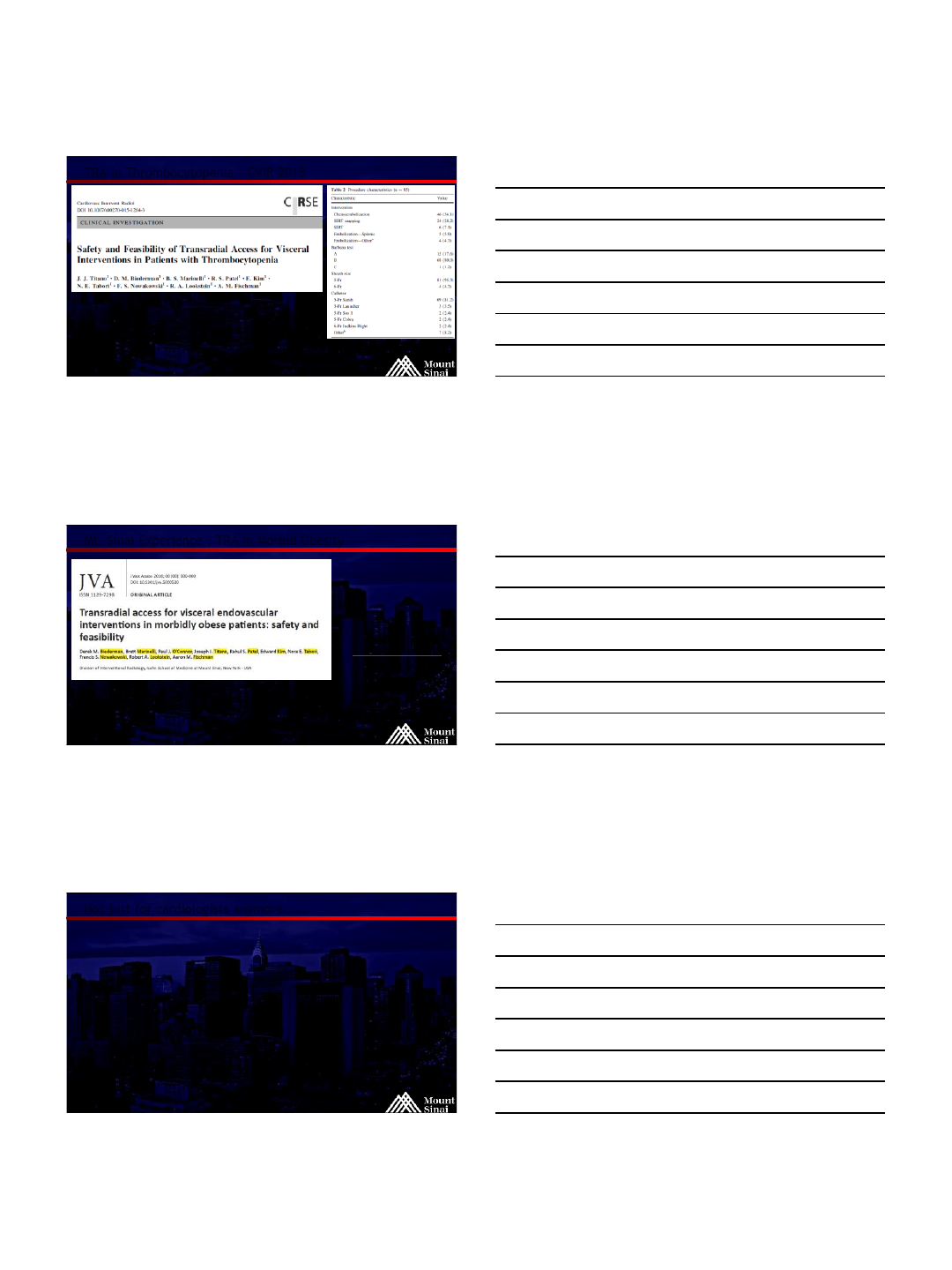
TRA in Thrombocytopenia –CVIR 2015
Titano JJ, Biederman DM, Marinelli BS, Patel RS, Kim E, Tabori NE, Nowakowski FS, Lookstein RA, Fischman AM. Safety and Feasibility of Transradial
Access for Visceral Interventions in Patients with Thrombocytopenia. Cardiovasc Intervent Radiol 2015: Dec 22. Epub. PMID 26696230.
85 procedures in 64 patients with plts <50,000
97.6% TS
No major AEs
5.9% minor access site hematoma
27.1% platelet transfusions
@MountSinaiIR
Mt. Sinai Experience : TRA in Morbid Obesity
22 interventions
17 patients
Median BMI 42.7
100% tech. success
NO complications
@MountSinaiIR
Not just for cardiologists anymore…….
Partial splenic embolization
Renal embolization
Renal angioplasty/stenting
Iliac artery stenting
Mesenteric angioplasty/stenting,
IVUS
Internal Iliac artery embolization
Uterine artery embolization
Carotid artery stenting
RCC met to shoulder –embolization
Dialysis intervention
Gastric Embolization
Prostate Embolization
Hand AVM Embo
Type I Endoleak
Trauma
GI Bleeding (Lower and Upper
Transplant Renal Interventions
Vertebral Interventions
4/20/2016
29
@MountSinaiIR
Where are we headed in 2016 and beyond?
Randomized studies specific
to IR (particularly in
Interventional Oncology)
Quality of life surveys
(IPAD and SMS)
Training courses/CME for IR
Catheter and Guide design
underway…..
Glue Embolization of
bleeding renal mass
@MountSinaiIR
Final Thoughts
Patients request radial approach!
IR trainees benefit greatly from learning radial techniques
Most catheters are designed for femoral approach
Partnership with industry is critical
Training programs
Catheter and equipment development
New procedures lend well to TR
THE TIME IS NOW!
@MountSinaiIR
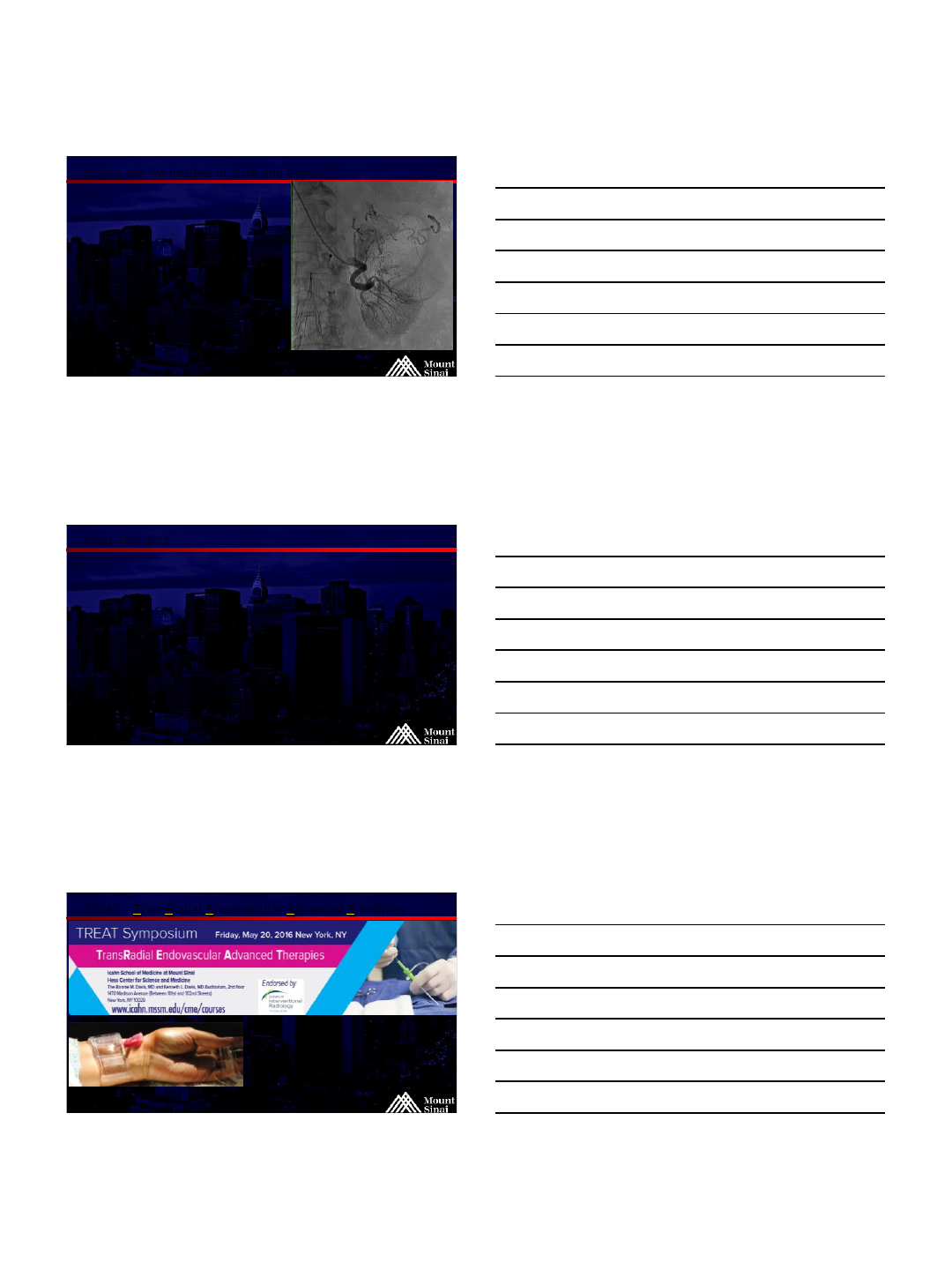
TREAT –TransRadial Endovascular Advanced Therapies
CME Course –2nd annual
“First Ever” in IR
May 2016
Live Cases
Dedicated to TRA
Embolization
Course Directors: Aaron Fischman MD, Rahul Patel, MD
4/11/2016
1
Transradial Approach
for Mesenteric
Interventions
Dr Darren Klass MBChB MD MRCS FRCR FRCPC
Clinical Assistant Professor
University of British Columbia
Overview:
LA mixture
100mcg GTN
9mL 1% Lidocaine
10mL syringe
Inject along length of RA under
Palpation for length of needle (4cm)
Tumescent anaesthesia
Single wall 60 degree puncture
No skin nick
LA mixture
100mcg GTN
9mL 1% Lidocaine
10mL syringe
Inject along length of RA under
Palpation for length of needle (4cm)
Tumescent anaesthesia
Single wall 60 degree puncture
No skin nick
Sheath and cocktail injection
Insert radial sheath
Inject antispasmodic
Flush sheath and connect to
infuser
US evaluation of RA
or 2mL angiogram
Insert catheter
preloaded with
wire
4/11/2016
2
Anti-spasmodic cocktail
Hemodilute
with aspirated
blood to 20mL
and slowly
reinject
2000IU
Heparin
200mcg
GTN
2.5mg
Verapamil
‘’
▣5fr Sheath workhorse
▣6fr for specific indication
□Radial spasm
□Small target vessel
▣7fr
□Avoid unless procedure
dictates –advanced cases
Sheath
Selection
Advanced
cases:
Technical considerations
Room Set up
Issues around hemodynamics
4/11/2016
3
Approach to advanced cases:
▣Assess anatomy carefully
□Origins of vessels
□Tortuosity
□Distance to target
▣Inventory
□Longer delivery systems
□120cm minimum
□Wire lengths
□Monorail vs OTW
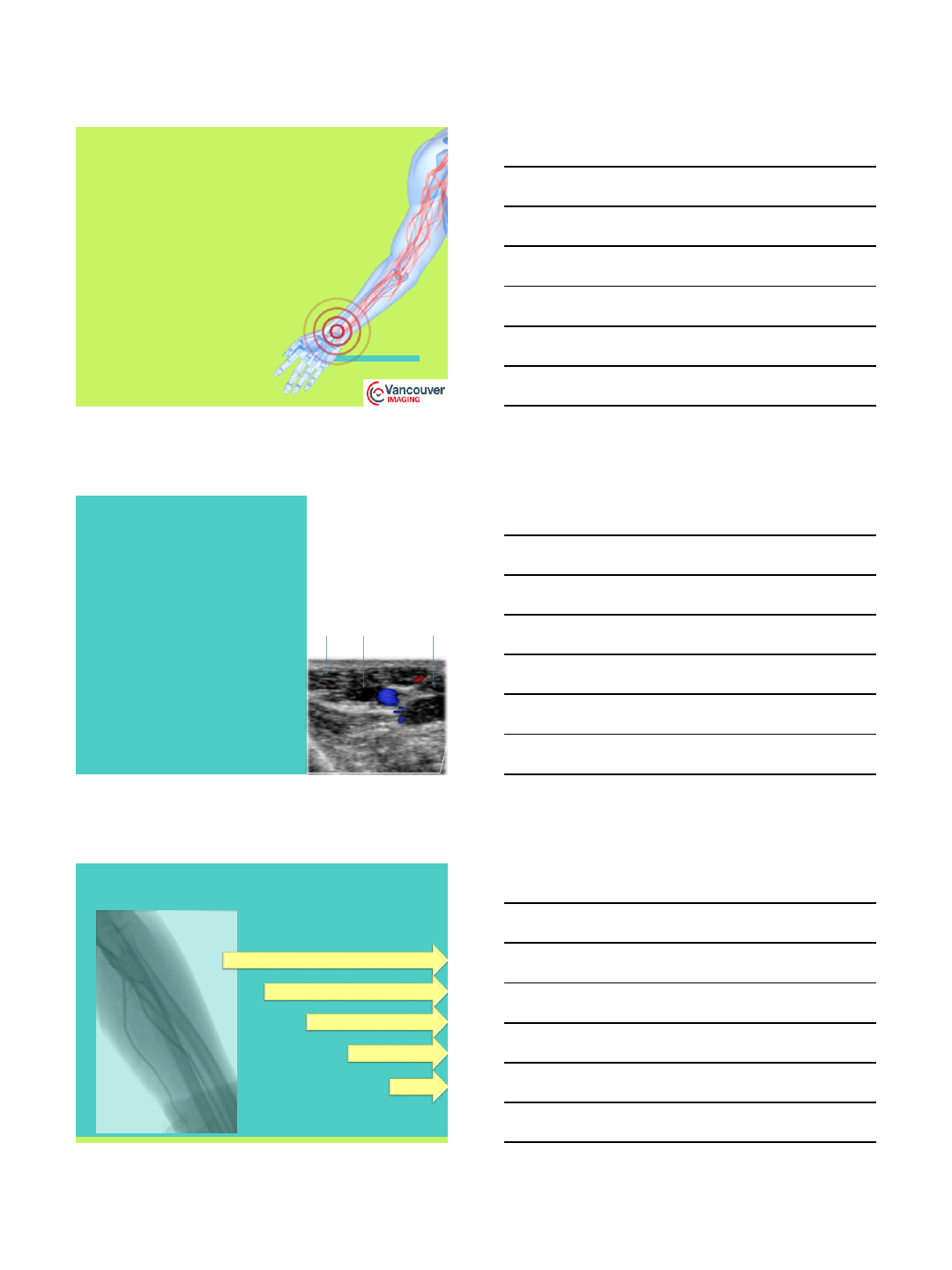
Access:
Decide on sheath size prior to puncture
Assess size of the RA
Decide whether the vessel can accommodate sheath
Guide catheter vs Sheathless guidecath
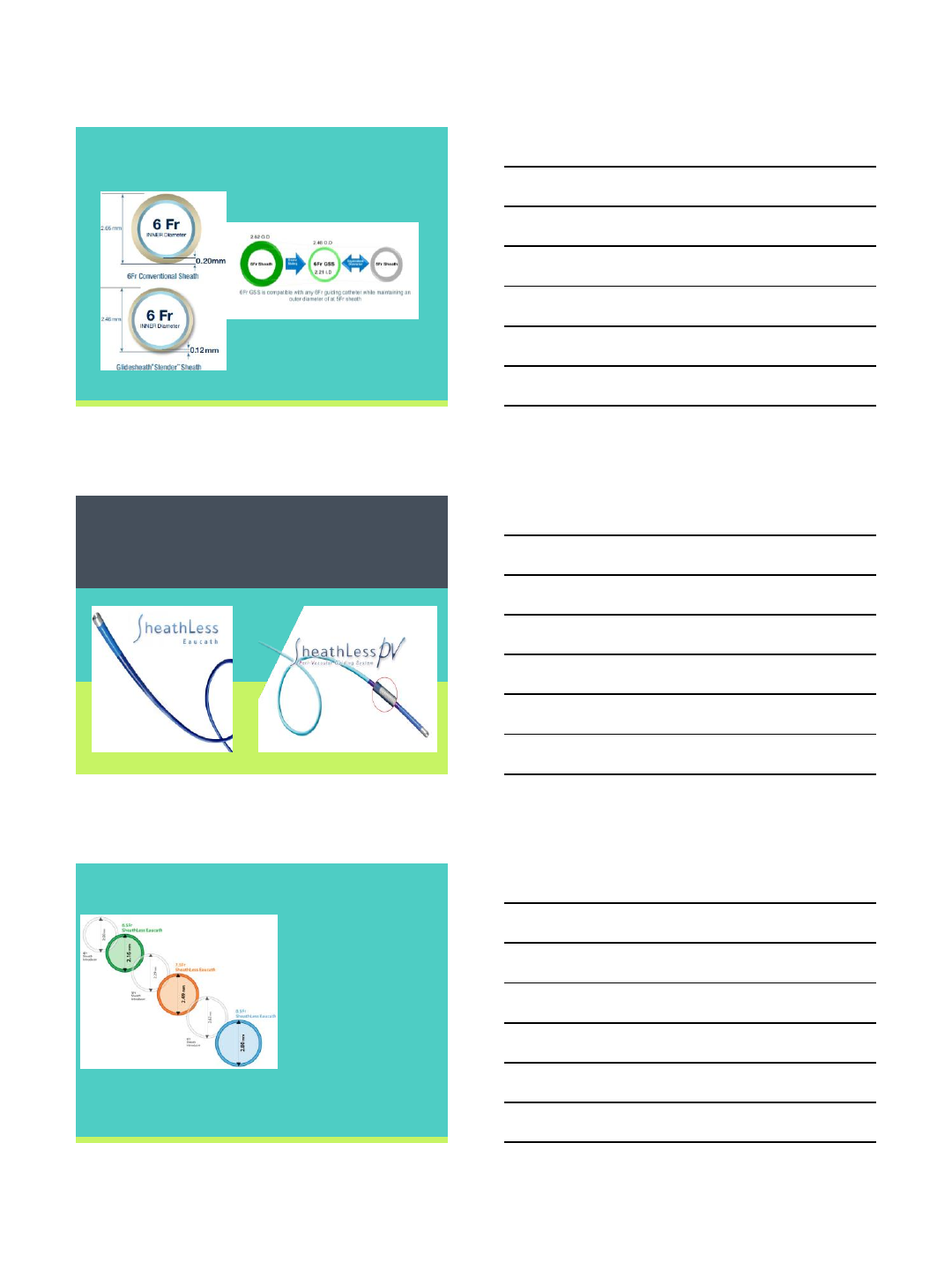
RA size and sheath compatibility
RA size 10mm proximal to styloid (n=250)
3.1 ± 0.6 mm in men
2.8 ± 0.6 mm in women11
Ext diameter 6-F sheath is 2.52 mm
86% men and 63% of woman suitable for 6Fr sheath
Sheathless guide - outer diameter 1.5 F smaller than
the analogous sheath capable of accommodating a
guide catheter of the same caliber.
Saito S et al Catheter Cardiovasc Interv. 1999;46:173-178.
4/11/2016
4
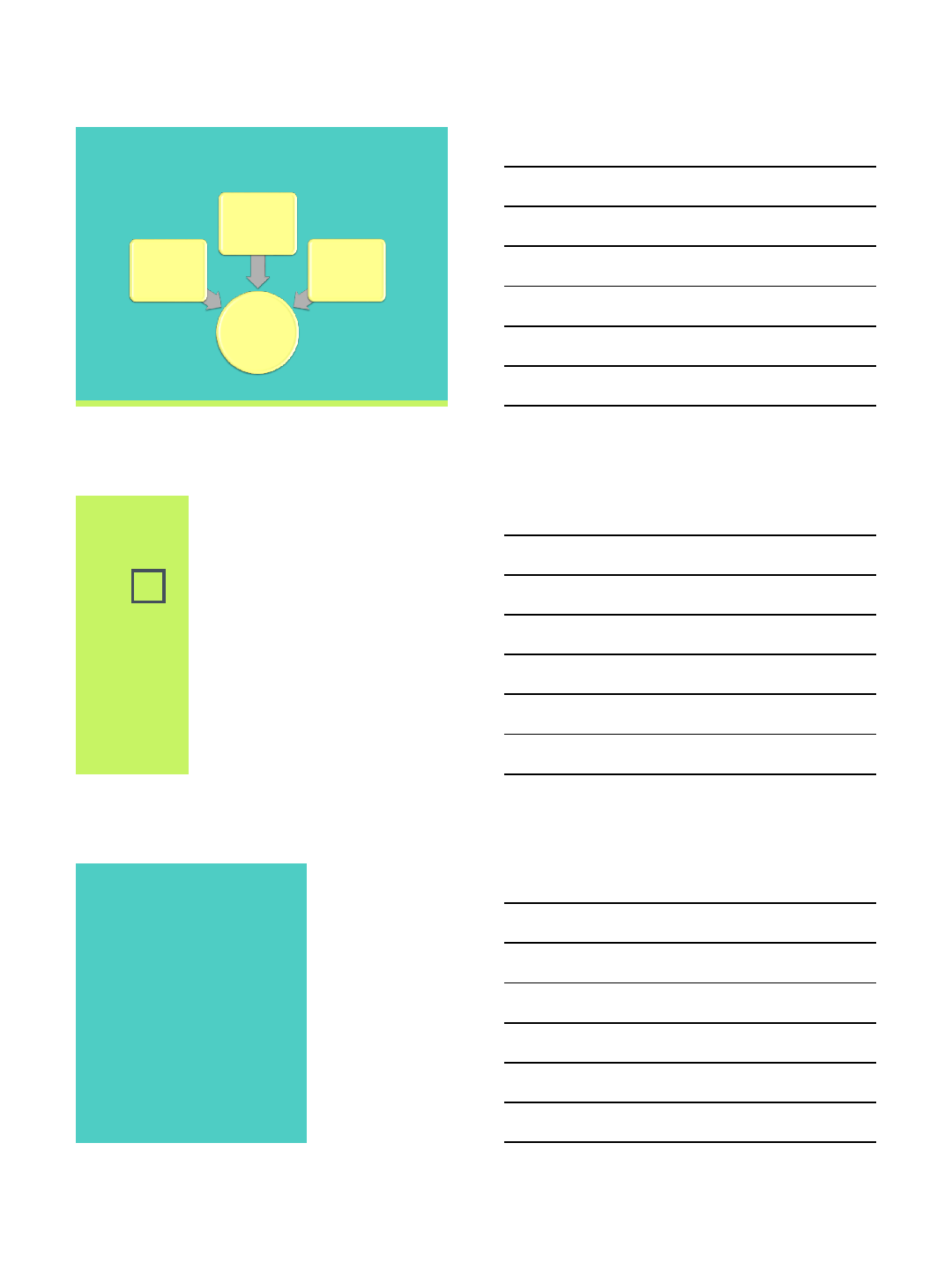
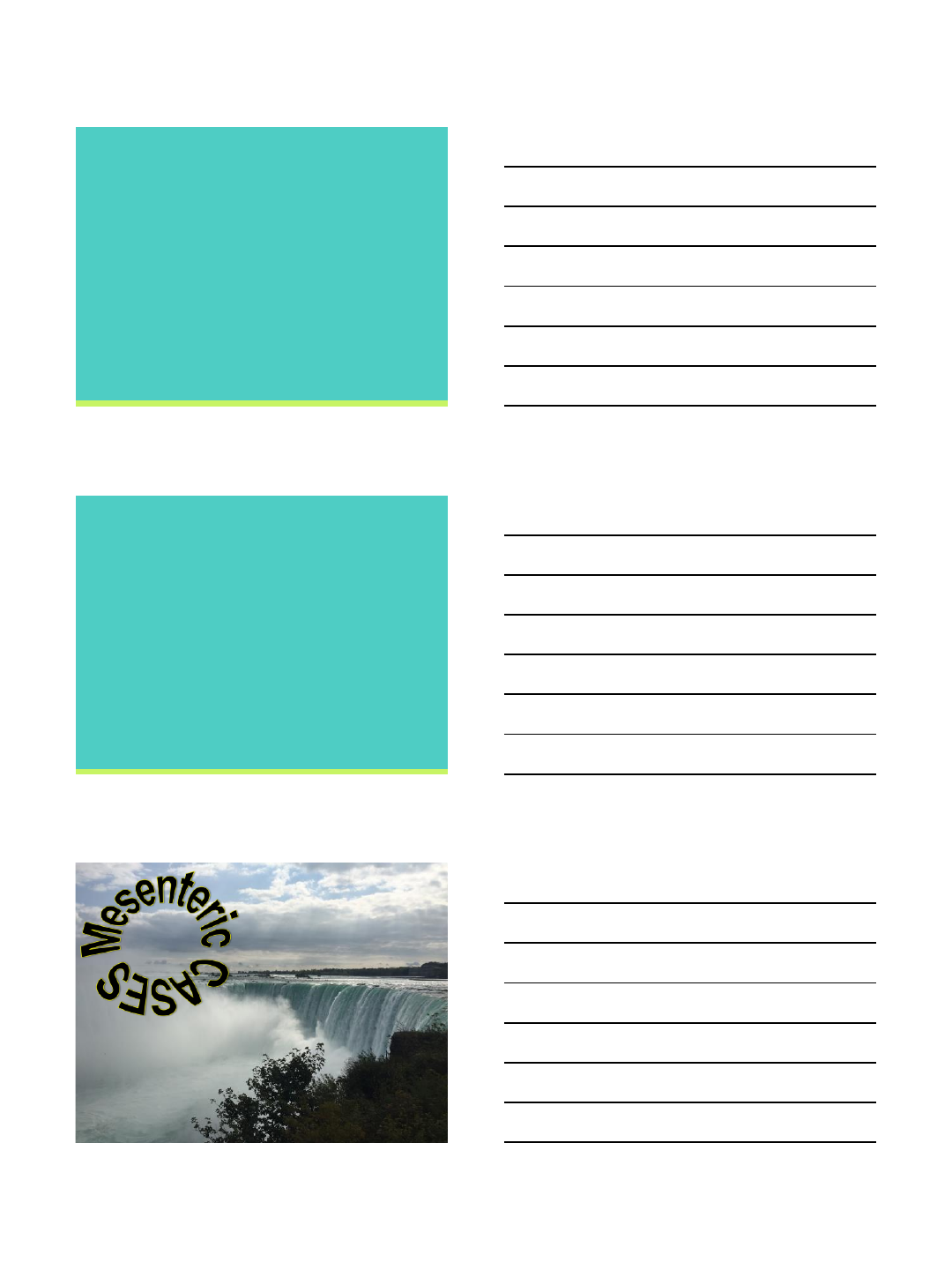
Terumo Slender
Asahi Sheathless Guidecath
Eaucath (100cm) Sheathless PV (120cm)
Sheathless Guidecath
Ability to deliver balloon
mounted stents
Saves repeated exchanges
along the RA
Allows for easy cannulation
of visceral vessels
Y90 administration
Needs a hemostatic valve
FLO 30
HVA 100
4/11/2016
5
Advanced cases:
▣Once you have decided the case requires a larger
bore sheath, change the cocktail when inserting the
sheath.
Hemodilute
with aspirated
blood to 20mL
and slowly
reinject
5000IU
Heparin
200mcg
GTN
2.5mg
Verapamil
Technique for sheathless
guidecath insertion
Insert 5Fr
sheath
Cocktail
125cm
catheter into
upper AA
Stiff
exchange
wire 260mm
Remove 5Fr
sheath
Insert
Sheathless
guide
4/11/2016
6
Creating a
platform:
Guide
catheters
Need sheath 1 Fr size larger
7Fr guide catheter
8Fr sheath
8Fr guide catheter (2.7mm OD)
6Fr sheath (2.62mm OD)
Concierge Guidecath
▣100cm - limited
▣Multiple shapes
▣Ult 1/2/3
▣JR4
▣AR3
▣0.057” ID
▣Surefire
▣Snare
Guide catheters
4/11/2016
7
Technical considerations:
▣Guide catheters are stiffer than diagnostic.
▣More torque
▣Stable in vessels
▣Sheathless guide
□Use 5Fr catheter to cannulate target vessel and
advance sheathless guide over catheter and wire.
Sheathless PV:
▣125cm base catheter will be too short.
▣Lose length on HVA and hub
▣150cm catheter base.
□Stent and balloon delivery lengths.
4/11/2016
8
4/11/2016
9
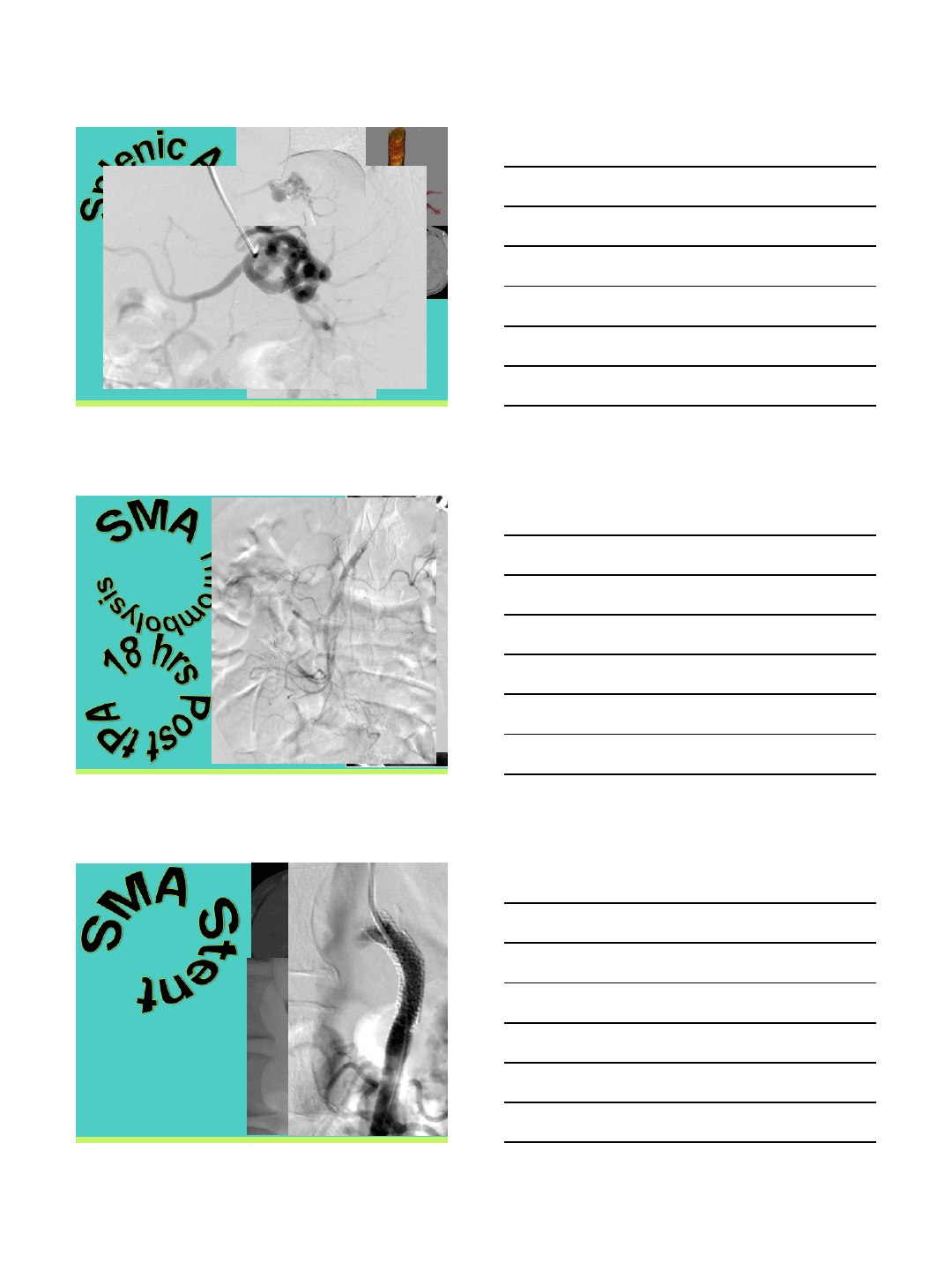
TECHNICAL:
Neuron guidecath 6Fr 110cm
Penumbra suction thrombectory system
Abciximab 0.25mg/KG
Balloon angioplasty of kink in splenic artery
600mg loading dose Clopidogrel po
0.125mcg/kg/min for 60 mins post procedure
Transradial Approach
for Mesenteric
Interventions
Dr Darren Klass MBChB MD MRCS FRCR FRCPC
Clinical Assistant Professor
University of British Columbia
4/12/2016
1
Amish Patel MD
Interventional Institute
Holy Name Medical Center
Teaneck, NJ
None
Understand the data regarding transradial
dialysis access interventions
Become familiar with tools
Become familiar with common clinical
scenarios and complications
4/12/2016
2
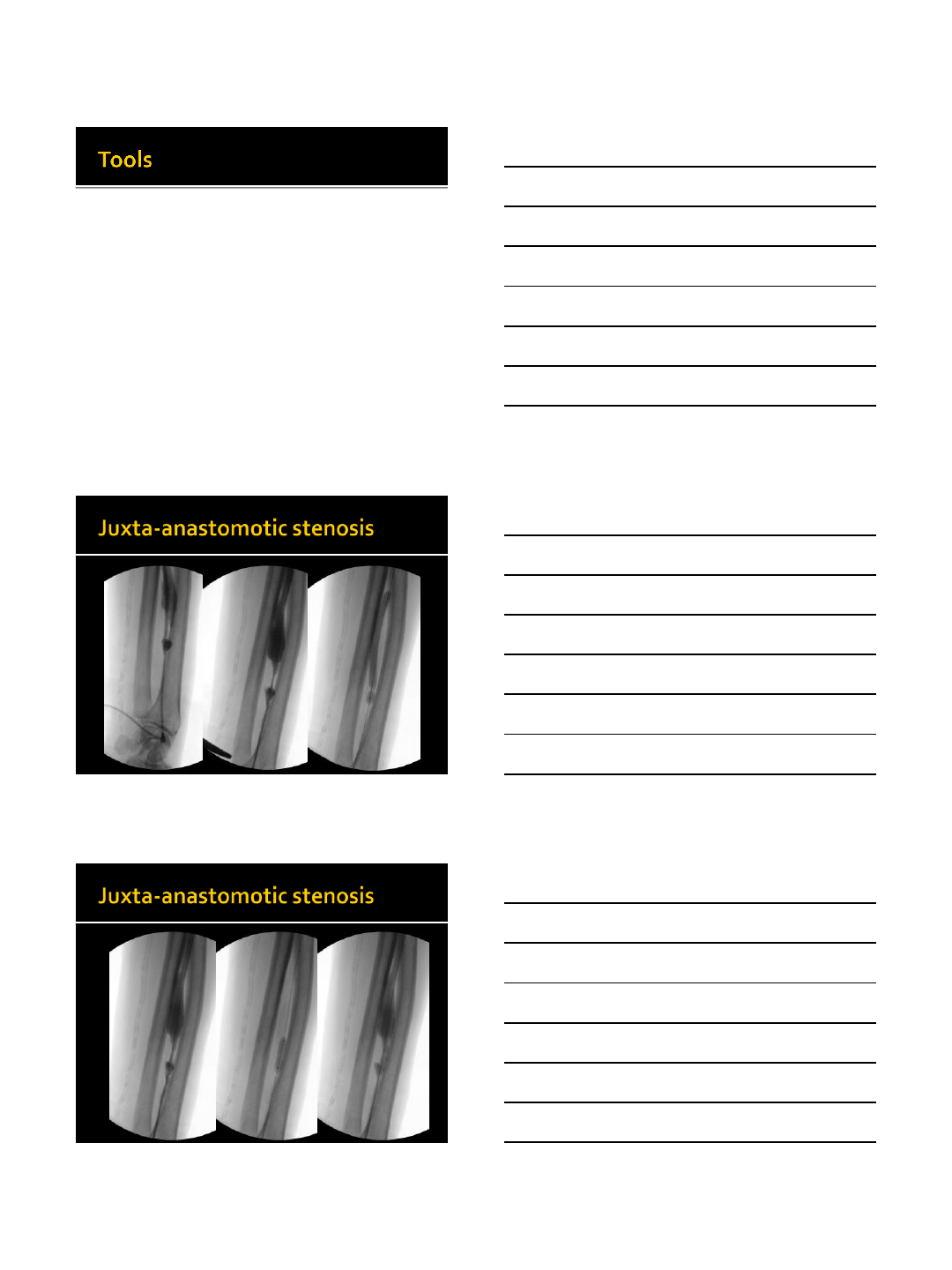
Seminal paper
11 patients
Mix of stenoses and occlusions
100% success
Safe and feasible
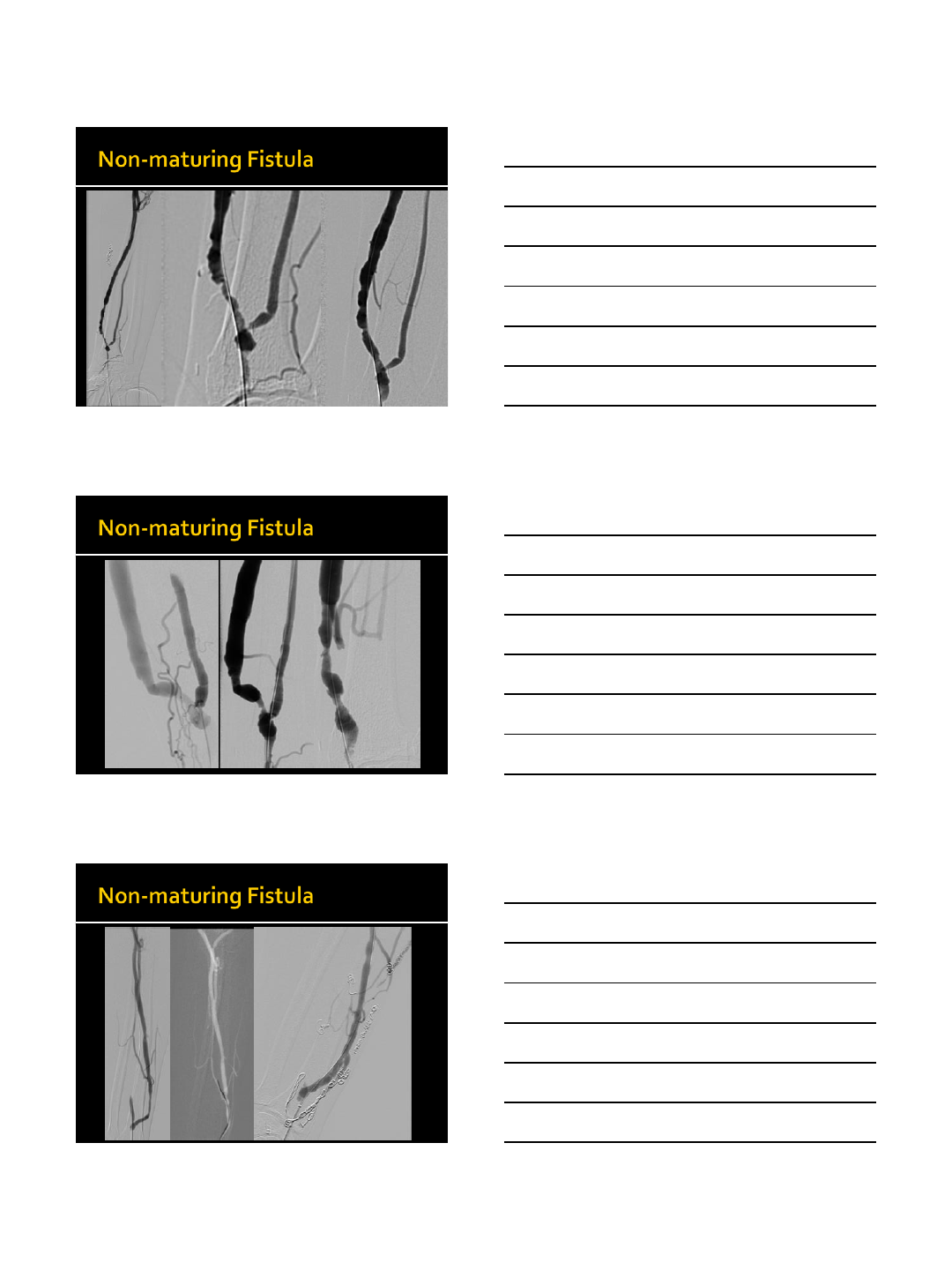
48 patients
Occluded fistulae
Balloon thrombectomy, Arrow-Trerotola,
AngioJet
96% success
154 procedures in 131 patients
52 (33.8%) totally occluded AVF
Excluding those, 99% success
3-m and 1-yr patency similar to direct
puncture
4/12/2016
3
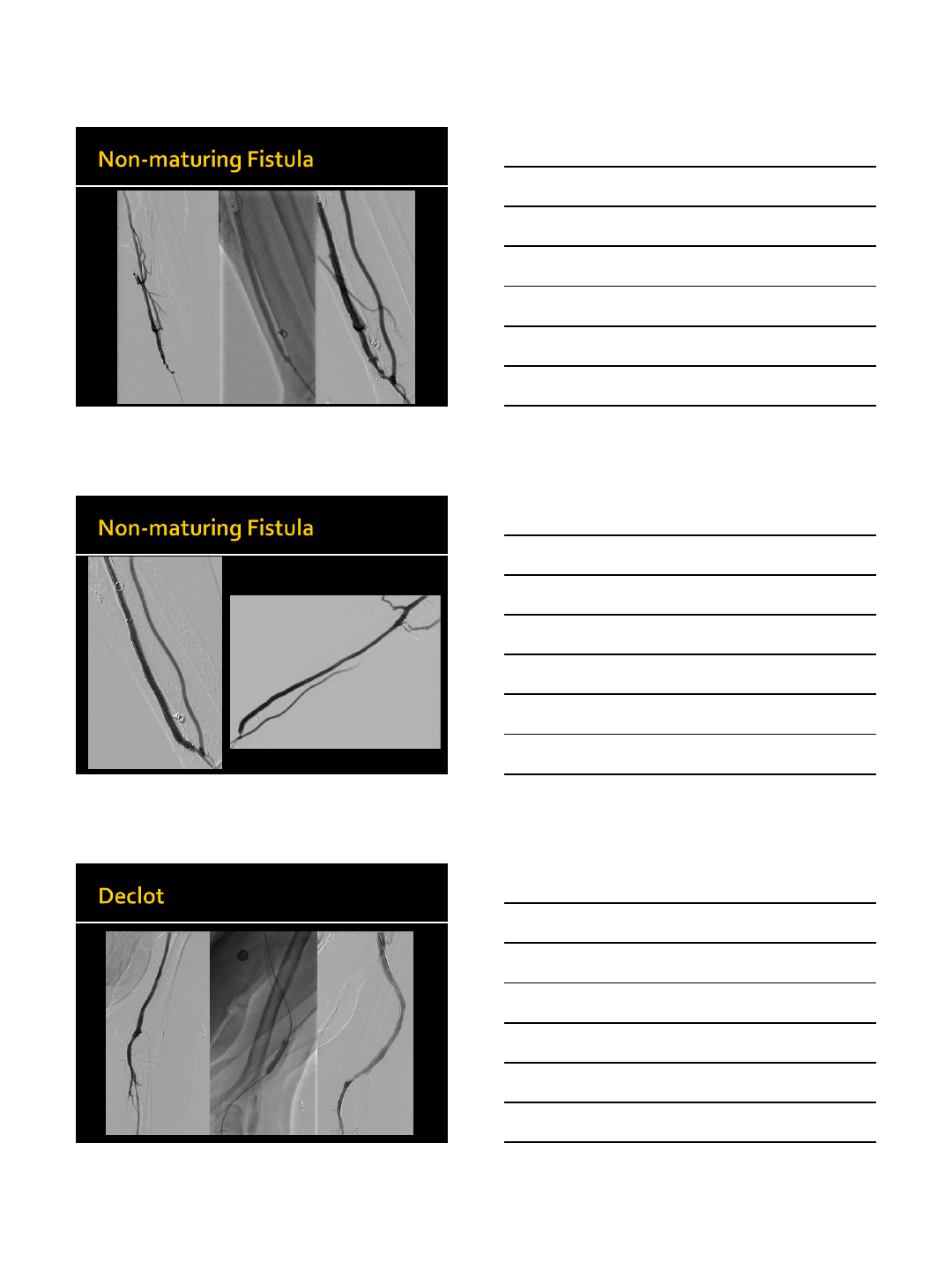
50 procedures
88% success
Could not cross lesion most failures
1, 3, 6, 12-m and 1-yr patency similar to direct
puncture
7 procedures in 5 patients
Thrombosed upper arm grafts
100% success
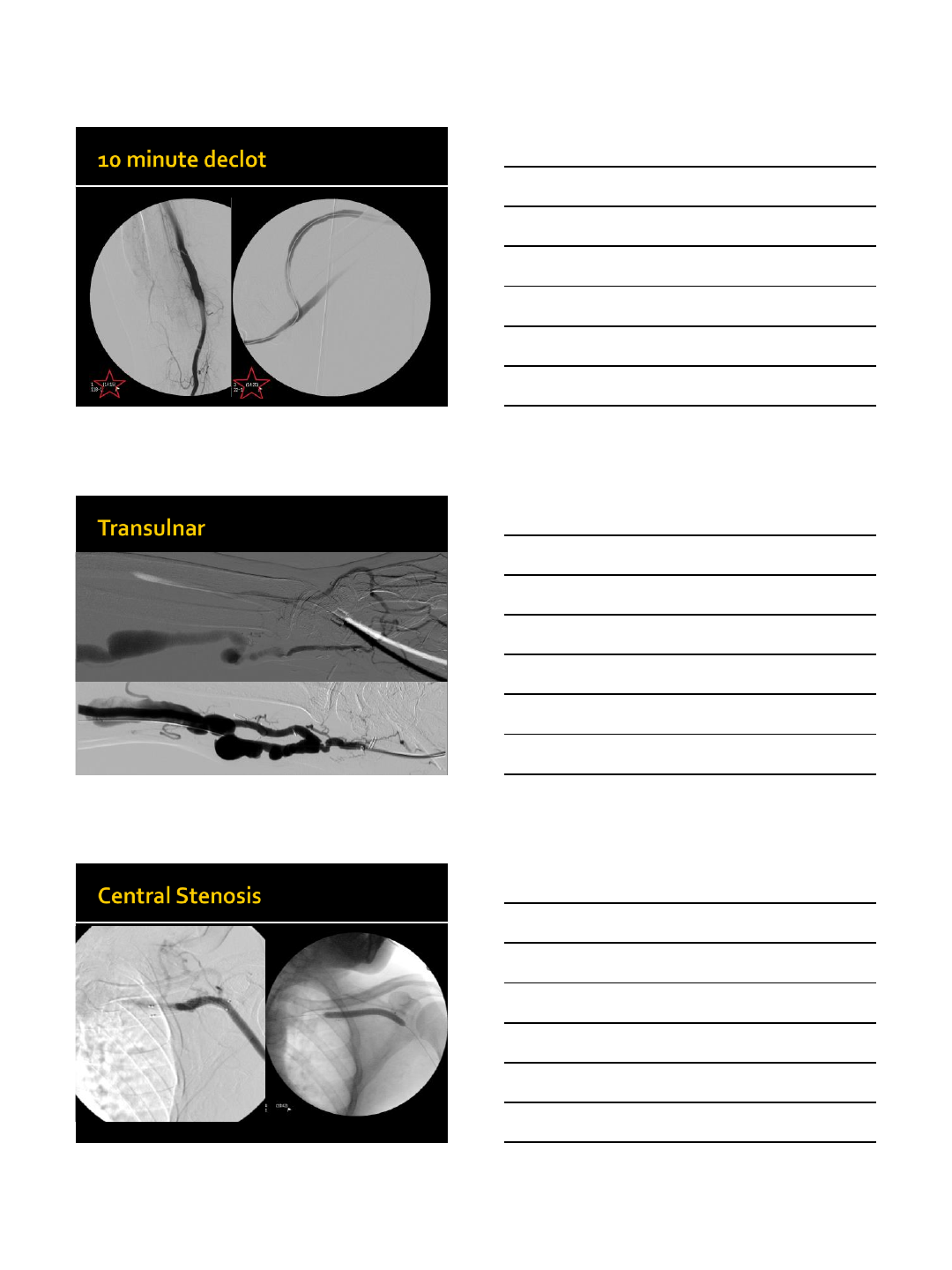
ADVANTAGES
Single puncture
Able to treat lesions at
artery site, anastomosis
site, or multiple sites
Hemodynamic
monitoring to gauge
immediate success
No fistula compression
High clinical success rate
DISADVANTAGES
Puncture technique may
be complex and
demanding
More potential for
complications with
repeated procedures
Only small balloons can
be accommodated
Easy to achieve
hemostasis
4/12/2016
4
Glidesheath (Terumo)
4 Fr and 6 Fr Slender
0.018” PTA Balloon
Sterling (Boston Scientific)
Advance 18LP (Cook)
Fox or Armada Balloon (Abbott)
4/12/2016
5
4/12/2016
6
4/12/2016
7
4/12/2016
8
4/12/2016
9
Kawarada O. Transradial Intervention for Native Fistula
Failure. Catheterization and Cardiovascular Interventions
(2006) 68:513–520.
Wu CC. Radial artery approach for endovascular salvage of
occluded autogenous radial-cephalic fistulae. Nephrol Dial
Transplant (2009) 24: 2497–2502.
Chen SM. Outcomes of Interventions Via a Transradial
Approach for Dysfunctional Brescia-Cimino Fistulas.
Cardiovasc Intervent Radiol (2009) 32:952–959.
Le L. Transradial approach for percutaneous intervention
of malfunctioning arteriovenous accesses. J Vasc Surg (2015)
61:747-53.
4/12/2016
10
amishpatelmd@gmail.com
4/13/2016
1
Marcelo Guimaraes, MD FSIR
Division of Vascular Interventional Radiology
Associate Professor of Radiology and Surgery
Medical University of South Carolina
Transradial Approach for
Hepatic Interventions
VuMedi Webinar
Radial Approach for Visceral Interventions
Disclosure
Consultant
-Terumo Interventional Systems
-Cook Medical
Patents holder
- Cook Medical
Why Radial access?
Courtesy of Marcelo Guimaraes, MUSC
4/13/2016
2
Why radial access for visceral interventions?
Patient’s perspective
Immediate ambulation
Greater patient satisfaction
Shorten length of stay
Fewer access site complications (bleeding)
Mobility is allowed: nausea/vomiting
chronic back pain
access to the restroom
Why radial access?
“Pressure Hemostasis” concept
Borderline coagulopathy in liver disease
> INR, < platelets
Favorable anatomy for
catheterization from above
Why radial access for visceral interventions?
Technical perspective
4/13/2016
3
Supplies cost savings (no closure device)
Quicker turn-over of recovery beds
Optimization of the recovery area space
Why radial access for visceral interventions?
Work-flow/business perspective
Cost Analysis
MUSC
RADIAL
~ $120/case
Supplies (only) savings/year: $ 48-60K
FEMORAL
COAGULOPATHY ?
MANY PATIENTS HAVE COAGULOPATHY FROM LIVER DISEASE
Hypersplenism
Thrombocytopenia 16K, 4 packs…. 22K.??
4/13/2016
4
Coagulopathy ?
Radial access. When?
Suitable for everyone?
Radial access. When?
Suitable for everyone?
Patients > 70 years
History of stroke
Calcified Aortic arch
4/13/2016
5
Background
177 cases via the radial artery
›July 1999 to October 2002
65/70 patients (92.9%) replied that they would
request transradial approach next time
J Clin Gastroenterol 2003;37:412–417
Physical exam:
Allen’s test
Work-up in clinic
Safety check - Eligibility for TRI access
Physical exam: Allen’s test
Edgar Van Nuys Allen, American physician, 1893-1986
Safety check - Eligibility for TRI access
4/13/2016
6
Barbeau’s test Barbeau GR, et al. Am Heart J. 2004;147:489-493.
Safety check - Eligibility for TRI access
TIS-936-09182015
Barbeau’s test Barbeau GR, et al. Am Heart J. 2004;147:489-493.
Safety check - Eligibility for TRI access
EVALUATION FOR ELIGIBILITY ANYWHERE…
4/13/2016
7
Patency and Radial artery > 2.0mm (AP diameter): good for 5-Fr sheath
* Female, smoker
Safety check - Eligibility for RAVI access
Radial artery US exam –2 objectives
Radial artery > 2.0mm (AP diameter): good for 5-Fr sheath
* Female, smoker
Safety check - Eligibility for RAVI access
Radial artery US exam
New Sheath Technology
Glidesheath Slender™
Introduce like a 5-Fr
Use as a 6-Fr
1-Fr reduction in outer diameter
Thin walled sheath
4/13/2016
8
New Sheath Technology
Glidesheath Slender™
4/5 Fr, 5/6 Fr , 6/7 Fr
Outer diameter (O.D.)
Inner diameter (I.O.)
O.D.
I.O.
Radial access step-by-step
3 alternatives for left arm positioning:
Crossing the pelvis
Left side of the body
90 degrees abduction
4/13/2016
9
Radial access step-by-step
Table, arm set up
Arm positioning in 90 degrees abduction
TIS-936-09182015
4/13/2016
10
Radiation safety
•> Distance from the radiation source
•Shield: between the operator and patient/radiation source
4/13/2016
11
RADIAL ACCESS –ALL SET UP?
Check the BP. IV bolus
of saline?
Devices handy
Arm positioned correctly. Hand palm gently taped
Material for radial access
Ultrasound
Material for radial access
Micropuncture kit
Introducer sheath
Needle
0.021”wire
Shorter needle:
- standard needle
-“jelco”
4/13/2016
12
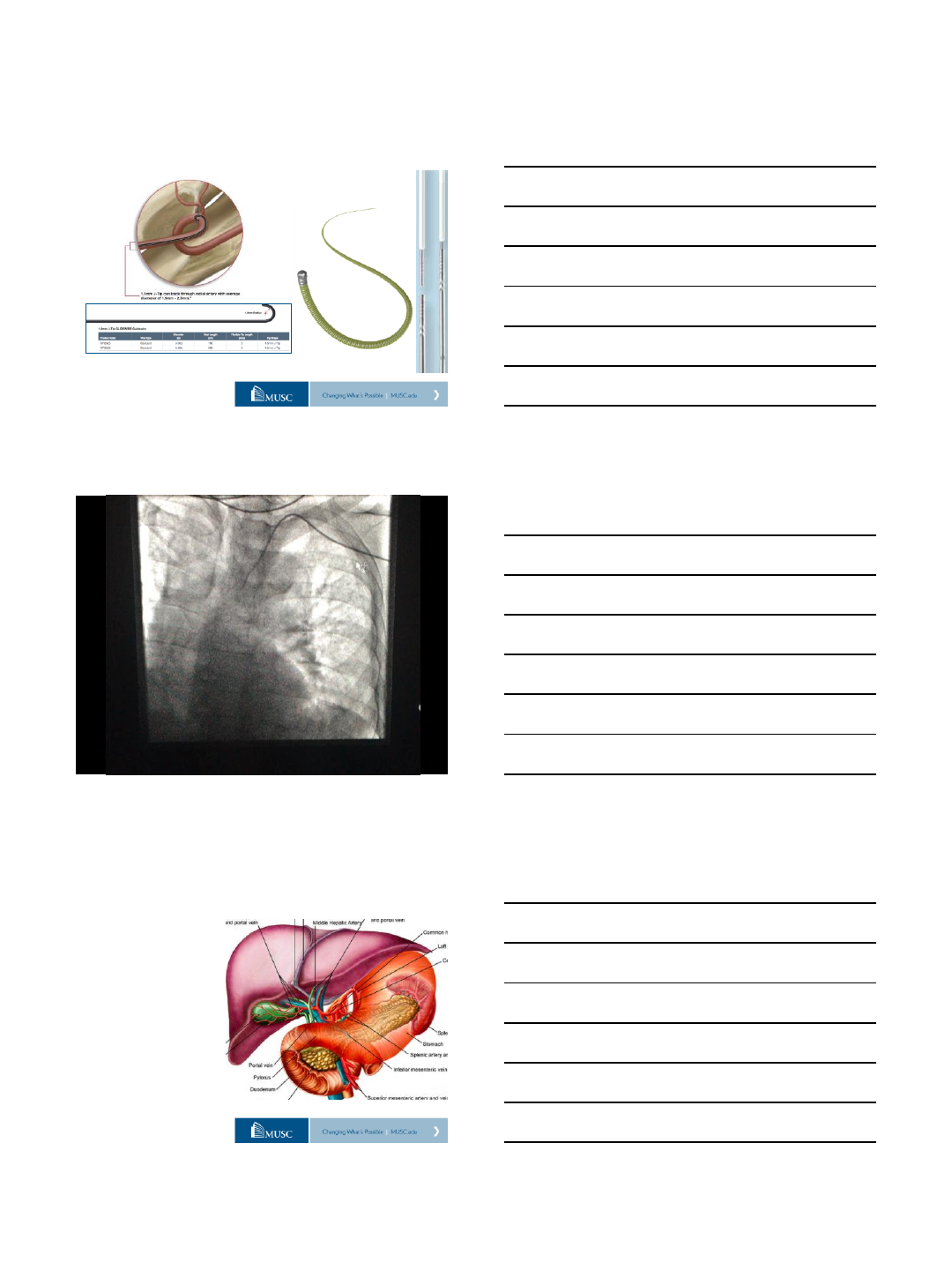
TERUMO INTERVENTIONAL SYSTEMS
Material for TR visceral interventions
Ultrasound
Micropuncture kit
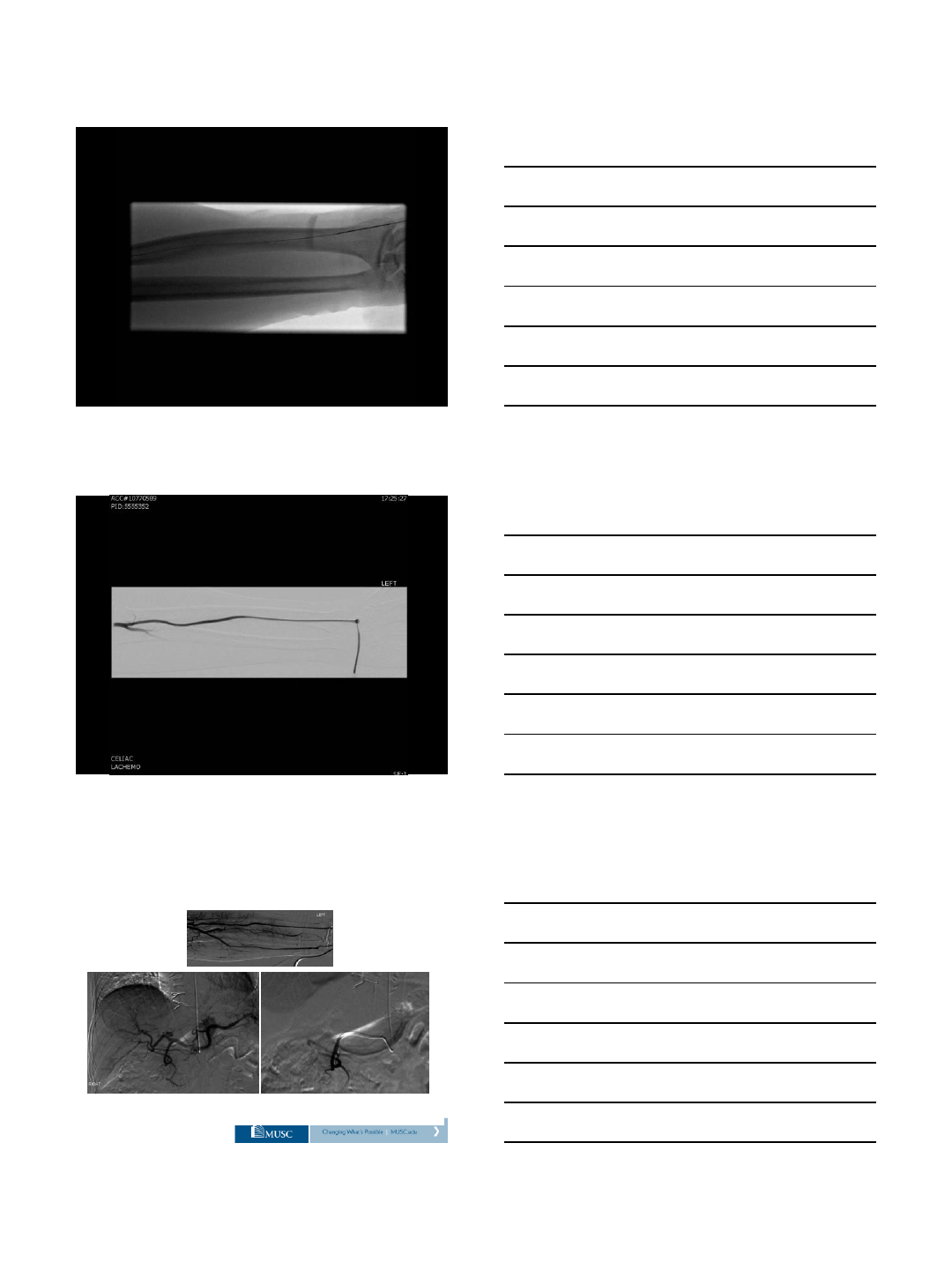
Radial sheath 5-Fr (4-Fr)
Jacky catheter 5-Fr 110cm
1.5 mm J GLIDEWIRE 0.035”
Progreat Microcatheter 2.8 Fr, 130 cm
Progreat 150 cm + Advantage microwire 0.018”180cm
TIS-936-09182015
Heparin:
IV Bolus + additional doses as needed
(3-4,000 units, 1,000 units in 30 min)
Vasodilator: via radial sheath (beginning / end of the case)
Nitroglycerine, 200 ug each time
Medications
VASOSPASM AND THROMBOSIS PREVENTION
Hand warmer? Nitro paste?
Radial arteriogram
after vasodilator:
•Hand injection
•5-6 cc
•Forceful hand injection
•Catheter at the level
of the brachial?
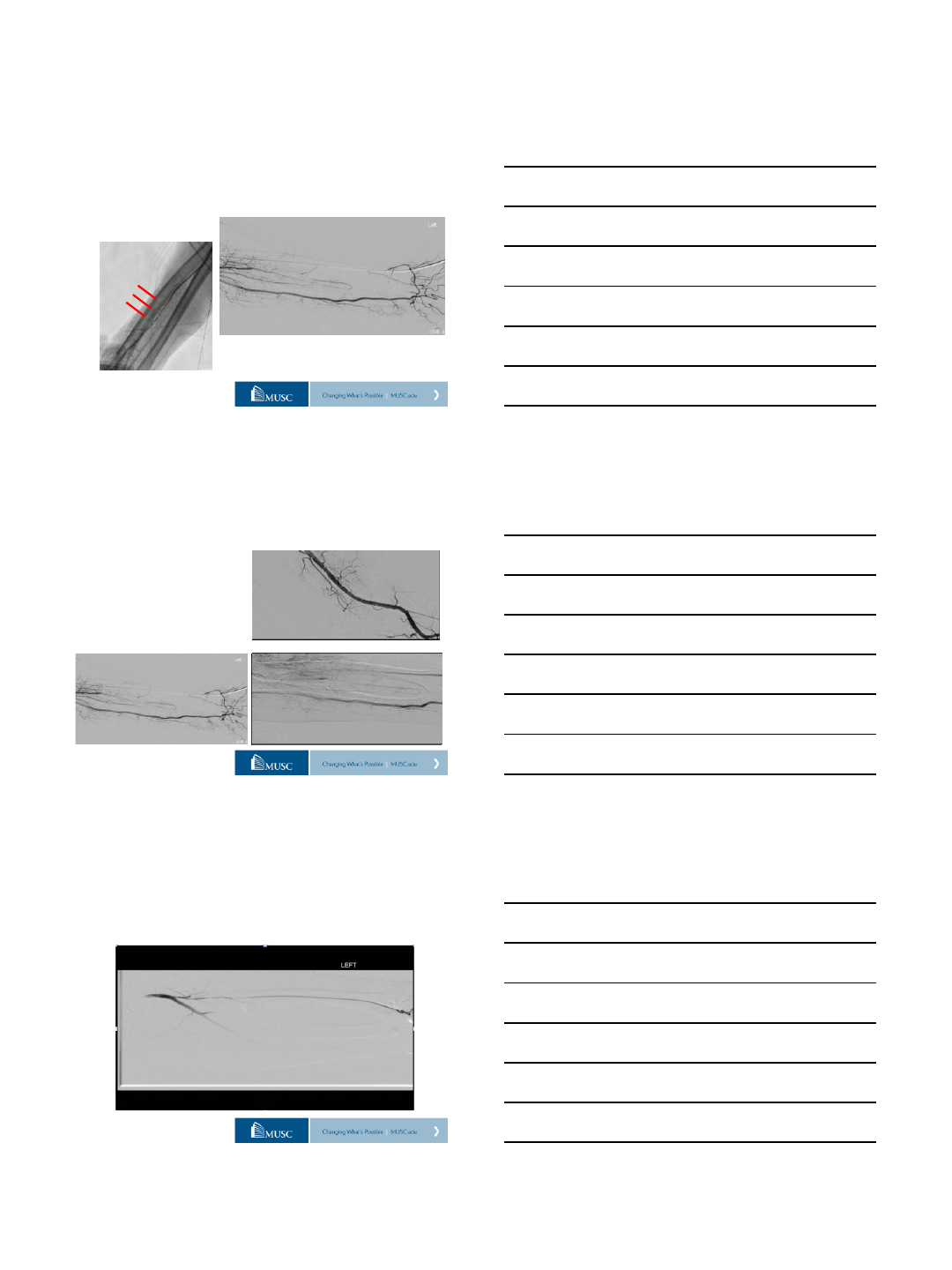
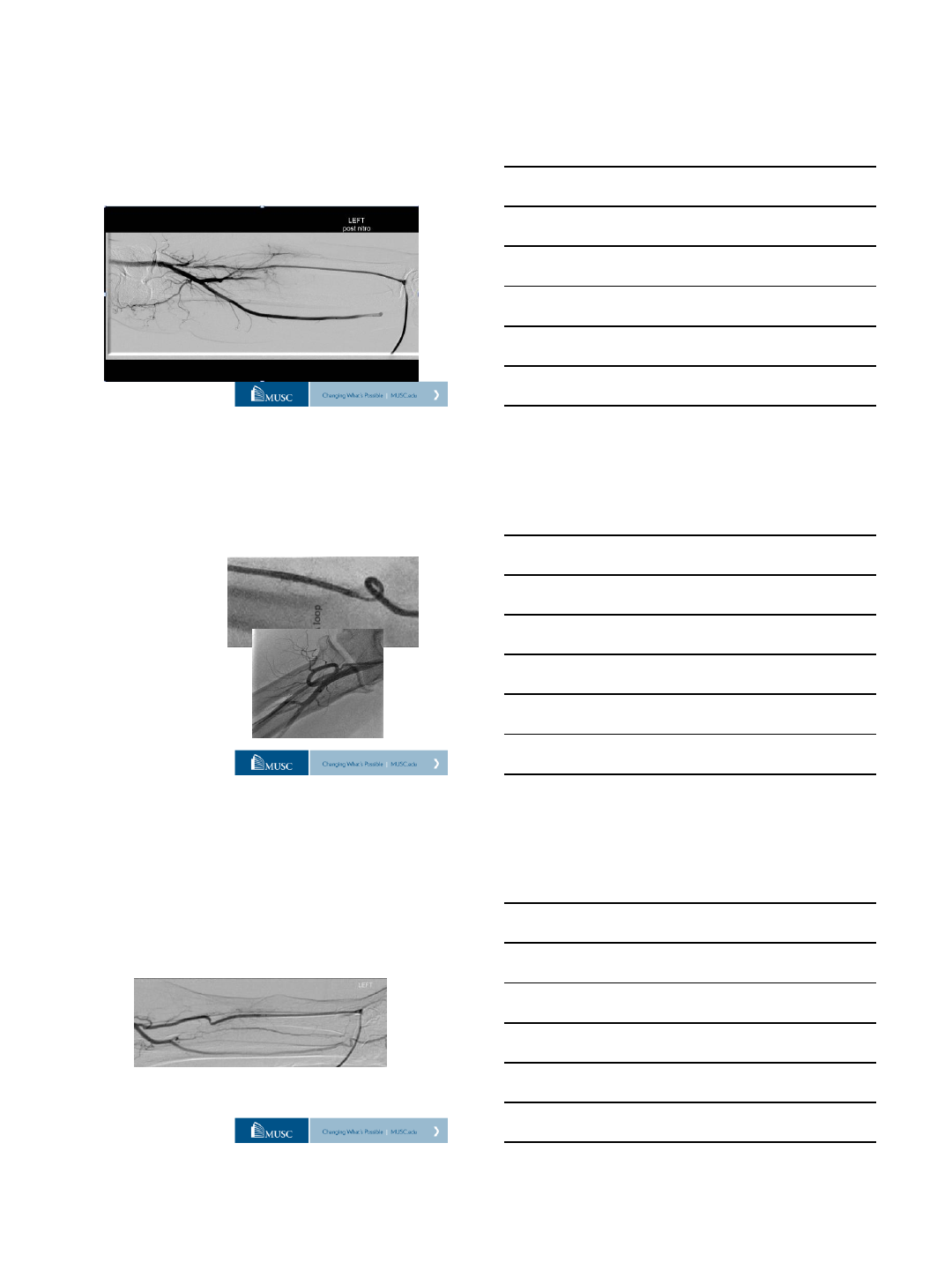
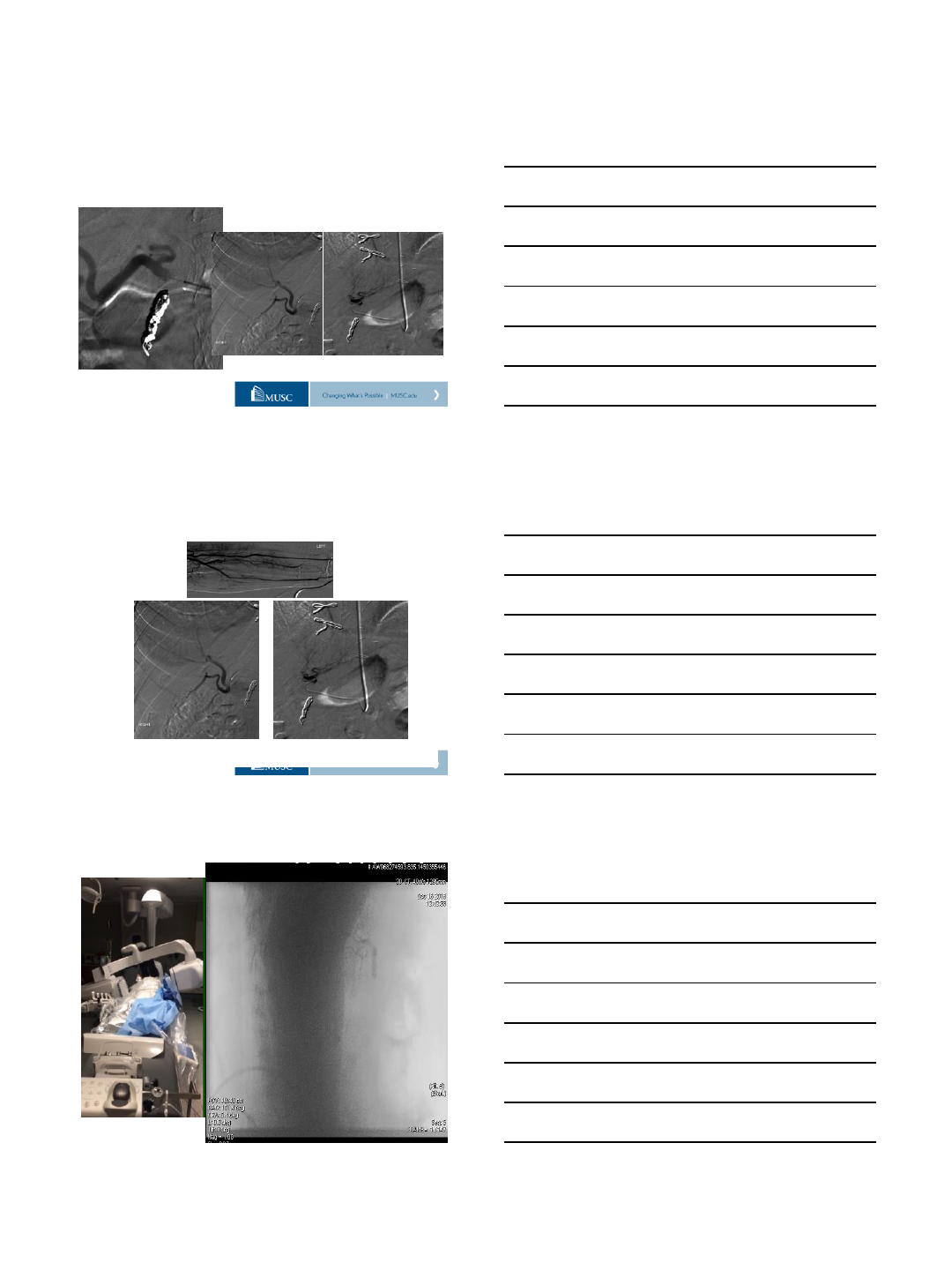
Importance of forearm angiograms at
the beginning and and of the case
4/13/2016
13
Importance of forearm angiograms at
the beginning and and of the case
Arterial size, spasm
Anatomic variants
Severe tortuosity
No flow in the introducer
sheath. Now what?
Advance a microcatheter
proximally and inject
Nitroglycerin at the level of
Brachial artery.
Importance of forearm angiograms at
the beginning and and of the case
Resistance encountered during the aspiration of the
sheath lateral check flow. Gentle hand injection...
Importance of forearm angiograms at
the beginning and and of the case
4/13/2016
14
Nitroglycerin injection through the sheath…
Importance of forearm angiograms at
the beginning and and of the case
•Variations of the
anatomy
•Difficult anatomy
Importance of forearm angiograms at
the beginning and and of the case
Tips & Tricks
Difficulty to advance the guidewire
towards the shoulder?
4/13/2016
15
SMOOTH RIDE TO THE DESCENDING AORTA…
5-Fr Jacky or Sarah diagnostic catheters
SMOOTH RIDE TO THE DESCENDING AORTA…
5-Fr Jacky catheter
SMOOTH RIDE TO THE DESCENDING AORTA…
0.035”1.5m J-tip GLIDEWIRE
5 Fr Jacky catheter
4/13/2016
16
SMOOTH RIDE TO THE DESCENDING AORTA…
0.035”1.5mm Hydrophilic wire 0.035”Wholey wire
$ 39.70 $ 50.33
TRI - liver directed therapies
Bland embolization
Chemoembolization
Radioembolization
4/13/2016
17
Y –90 Work-up, Infusion of MAA Tc 99
Coil Embolization of GDA,
R gastric art.
Infusion of MAA Tc 99
Devices: 5 Fr Jacky catheter
Progreat 2.8 Fr, 130 cm with pre-loaded wire
TIS-936-09182015
4/13/2016
18
Y –90 Work-up, Infusion of MAA Tc 99
Infusion of MAA Tc 99 (simulator)
SPECT nuclear medicine exam
Embolization of GDA, R gastric
arteries
7 days later…
Radio-embolization: Y –90 Infusion
Devices: 5 Fr Jacky catheter
Progreat 2.8 Fr, 130 cm with pre-loaded wire
TIS-936-09182015
4/13/2016
19
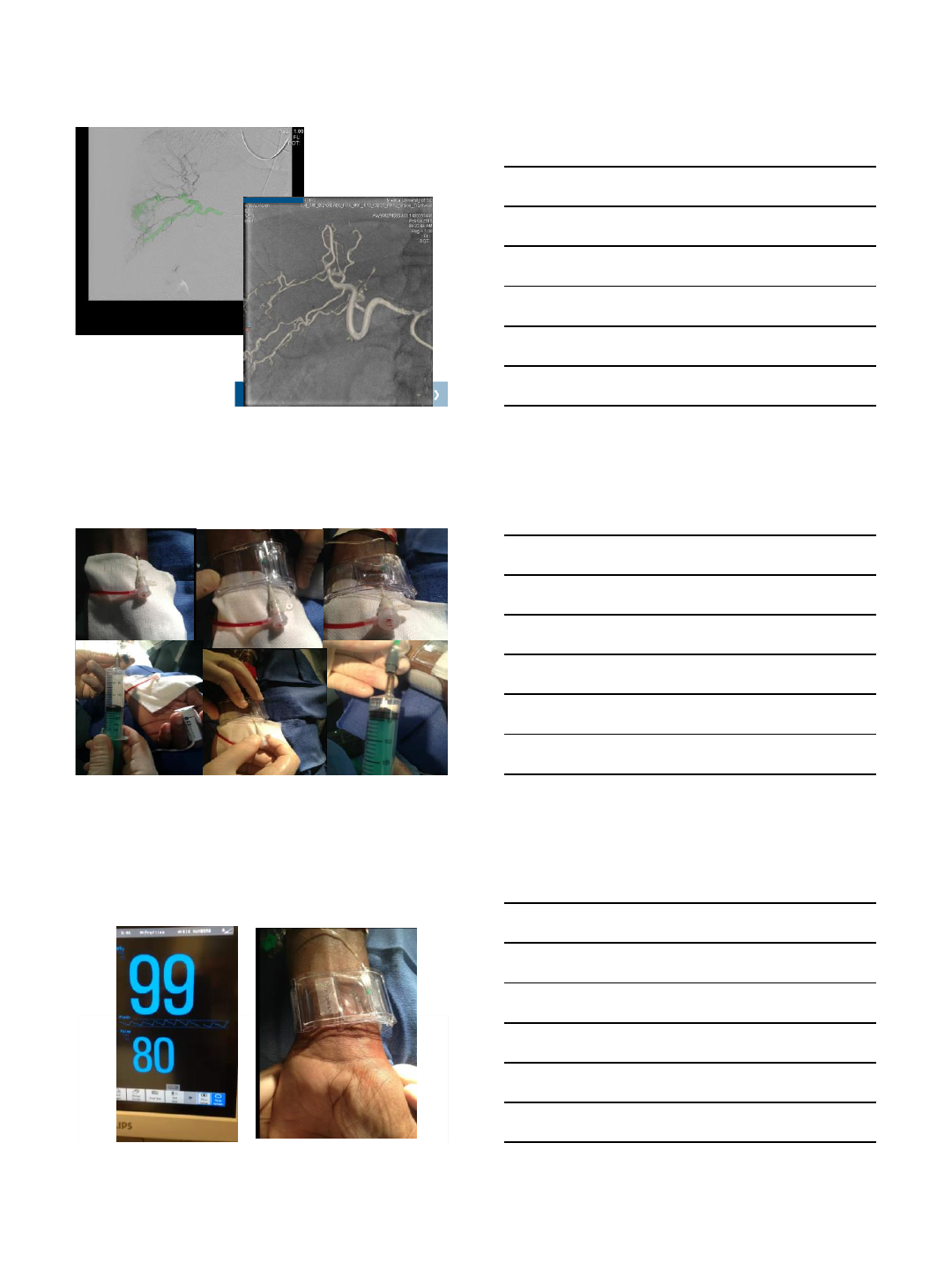
Case
Inject 15 cc of air in the TB
band. Keep connection tight Remove the sheath slowly
Radial sheath removal: Patent Hemostasis concept
Have extra 5 cc of air ready
to be injected while sheath
is removed TIS-936-09182015
Patent hemostasis Patent Hemostasis concept
4/13/2016
20
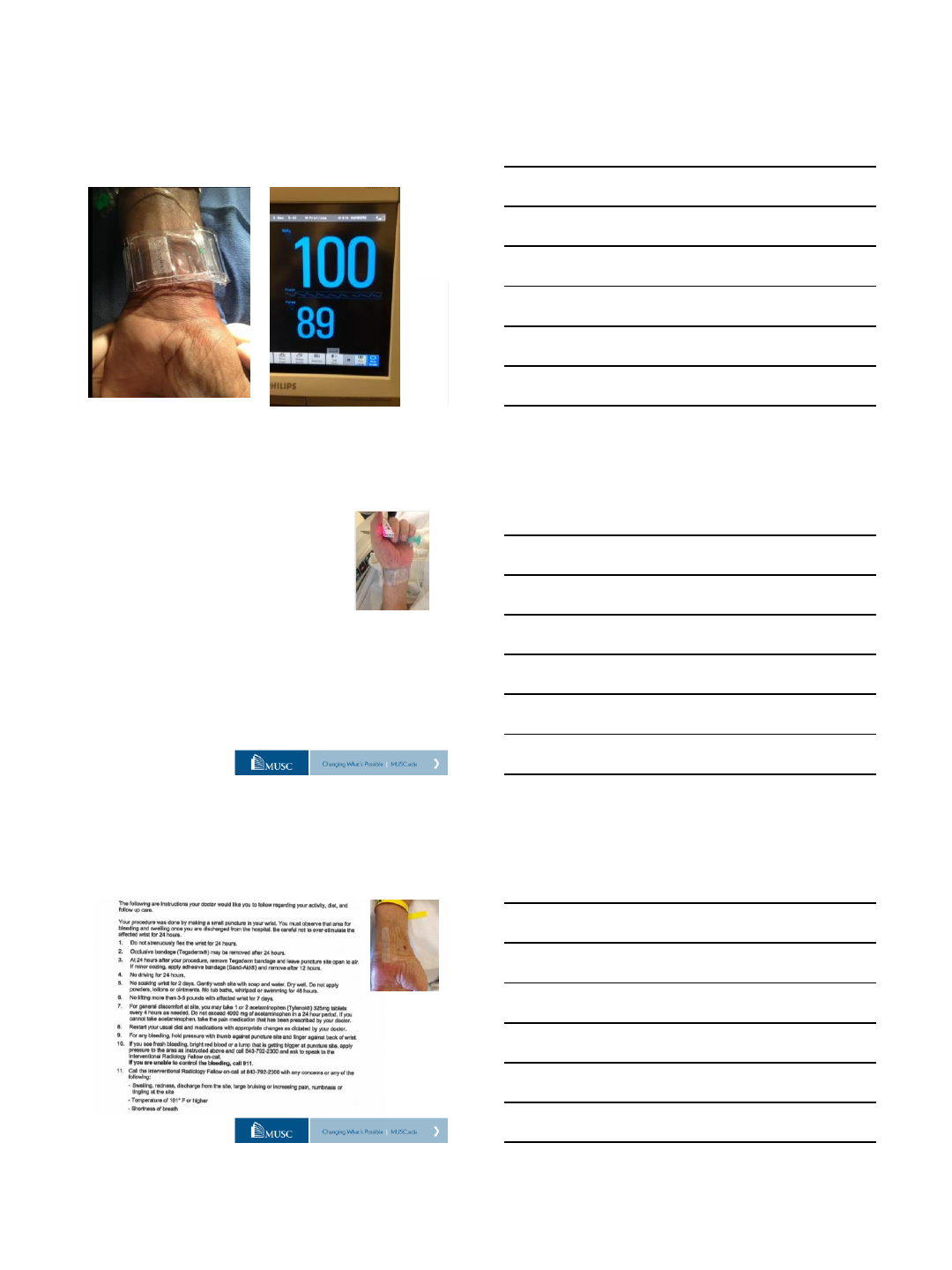
Radial sheath removal
Low Pressure Hemostasis to maintain flow through the artery
Inadequate O2 wave?
Deflate 0.5-1cc at the time
Check O2 pulse
MUSC - Nursing Protocols
5-Fr : patient is discharged in 2h
Observation for 1 h
Within the 2nd hour: deflation of 3-4 cc every 15’
Full deflation should be completed in 1 h
Observation, reinflate as needed
Alternative: deflation within the 1 h.
MUSC –DISCHARGE INSTRUCTIONS
4/13/2016
21
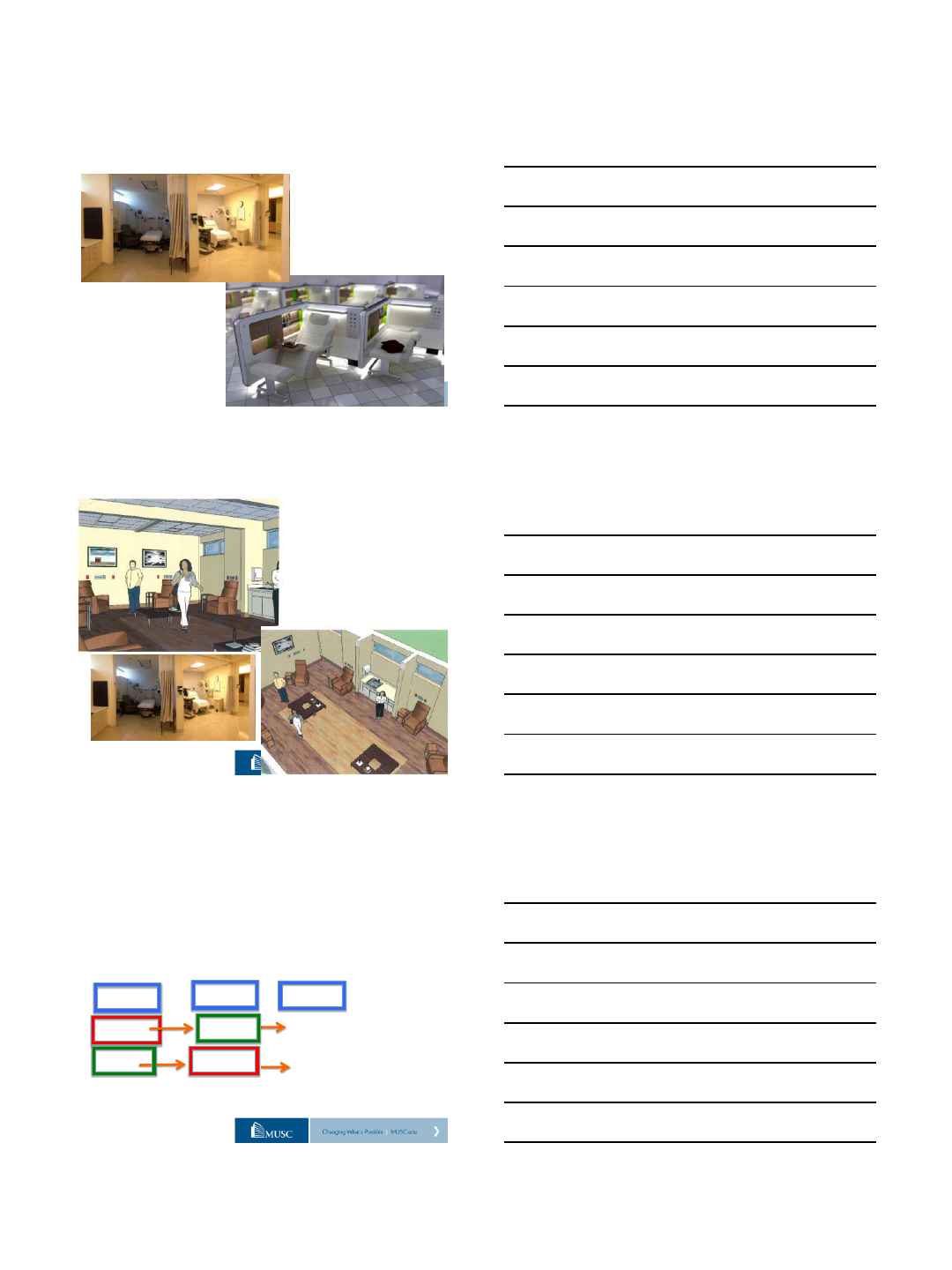
PATIENT’S SATISFACTION…
•Discharge in 1.5 - 2 h
•Comfortable environment
•Radial lounge: optimization
- space
- human resources
Radial lounge
MUSC
ACCESS Trial –MUSC/USA
TACE under Radial vs Femoral artery access
Prospective and Randomized Clinical trial
Study design (3 procedures):
TACE #1 TACE #2 TACE #3
FEMORAL RADIAL PATIENT’S
RADIAL FEMORAL SELECTION
4/13/2016
22
Transradial Interventions Course
Med University of South Carolina
Charleston / SC
guimarae@musc.edu
Radial Access Training Program
