THE KNEE SOCIETY | VIRTUAL FELLOWSHIP 49eaf96e Aae7 479f 8f01 2b681767c867
2018-01-10
: Pdf 49Eaf96E-Aae7-479F-8F01-2B681767C867 49eaf96e-aae7-479f-8f01-2b681767c867 1 2018 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 63

THE KNEE SOCIETY | VIRTUAL FELLOWSHIP
Robotics in Knee Arthroplasty
Presented by:
Jess H. Lonner, MD
Rothman Institute
Philadelphia, PA
DISCLOSURES
Royalties
Zimmer Biomet, Smith and Nephew
Consultant
Zimmer Biomet, Smith and Nephew
Speaker’s bureau
Zimmer Biomet, Smith and Nephew
Publishers:
Saunders, Lippincott Williams Wilkins, Springer
Shareholder:
Blue Belt Technologies, CD Diagnostics
ROBOTS IN INDUSTRY
Efficient
Economical
Exacting
BILL GATES
“Robotics industry today is where the PC industry was
30 years ago.”**
**(Especially healthcare)
Bill Gates, Scientific American 2007
EXPERIENCE WITH ORTHOPAEDIC ROBOTS
Initial skepticism
Early adopters showed value
Alignment
Soft tissue balance
Recovery
Blood loss
Safety (semi-autonomous)
Increased utilization with pricing improvements
Lonner JH. Operative Techniques in Orthopaedics 2015
STORY OF ROBOTICS IN KNEE ARTHROPLASTY
Study in patterns that define technological progress and innovation, in general
Newer companies/technologies
Declining capital and maintenance costs
Smaller space requirements
Broadening access
Increased utilization
Expanding applications
Lonner JH. Operative Techniques in Orthopaedics 2015
STAKEHOLDERS WILL INFLUENCE FURTHER GROWTH OF
ROBOTICS

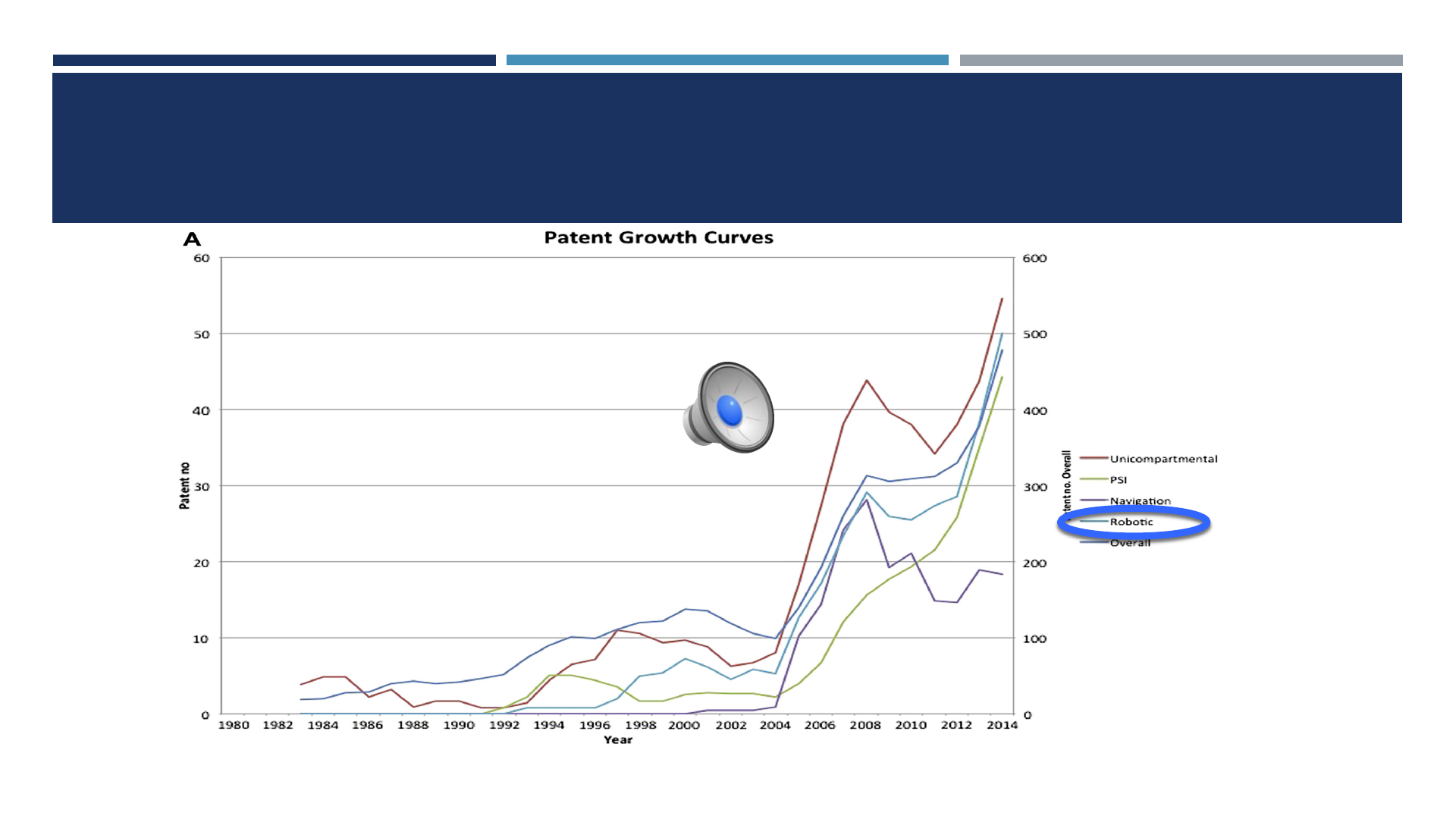
PATENTS AS A SURROGATE INDICATOR OF INNOVATION
Dalton DM et al. J Arthroplasty 2016

KEY DISTINCTION IN ORTHOPAEDIC
ROBOTICS
Autonomous- robot operates independently
TCat (formerly Robodoc)–iThink Surgical
FDA approved for THA
Not FDA approved for TKA
Semi-autonomous- surgeon guided; haptic or speed/exposure constraint
Mako (Stryker)
FDA approved for THA, UKA, PFA, TKA
Navio (Smith and Nephew)
FDA approved for UKA, PFA, TKA
OmniBot (Omni)
FDA approved for TKA
COMPLICATIONS WITH AUTONOMOUS
SYSTEMS
Complications THA
Soft tissue injuries, over-resection
Severe abductor injuries/sciatic nerve injuries
18% revision due to instability (vs 4% control)
Aborted cases TKA
8% soft tissue injury
Honl et al JBJS 2003
Chun et al J Arthrop 2011

ADVANCEMENT OF SEMI-AUTONOMOUS ROBOTIC SYSTEMS
Safety and avoidance of soft tissue complications has been key distinction
ROBOTICS FOR TKA?
Unclear need for “precise” alignment
Potential roles:
Optimizing soft tissue balance?
Bicruciate retaining TKA?
Access, balance
Facilitating efficiencies?
Reducing instrument storage/sterilization needs/costs?
Applicable for ASC’s

ROBOTICS FOR UKA?
94% survivorship at 10-15 yrs in hands of high volume
surgeons…
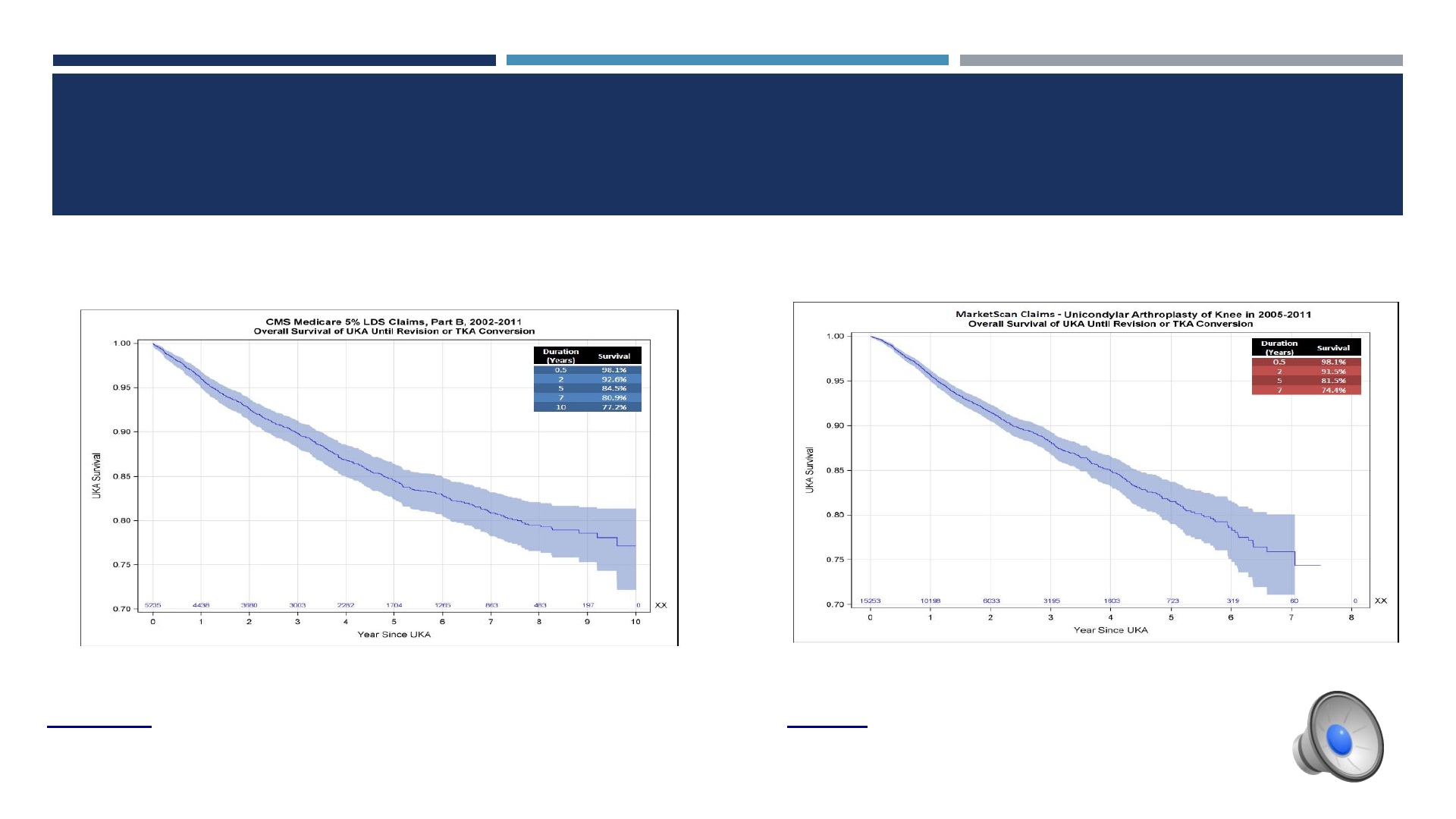
…BUT
> Age 65 < Age 65
10-yr survivorship 77% 7-yr survivorship 74%
Ong, Kurtz, Hansen, Lonner AAHKS 2014
WHAT IMPACTS THE RESULTS OF UKA?
Pathology/Disease
Patient selection
Component design
Polyethylene quality
Surgeon experience/volume
Accuracy of implantation
Soft tissue balance
MALALIGNMENT PREDISPOSES TO FAILURE
Coronal malalignment of tibial component >3° varus
Mechanical limb varus >8°
Posterior tibial slope >7°
Collier /Engh et al. J Arthroplasty 2006;
Hernigou JBJS 2004; Chatellard Orthop
Traumatol Surg Res 2013
UKA MALALIGNMENT > IN MIS THAN OPEN WITH STANDARD
INSTRUMENTATION
Greater inaccuracy in tibial component alignment and limb alignment
Fisher DA et al. (J Arthrop 2003)
Hamilton WG et al. (J Arthrop 2006)
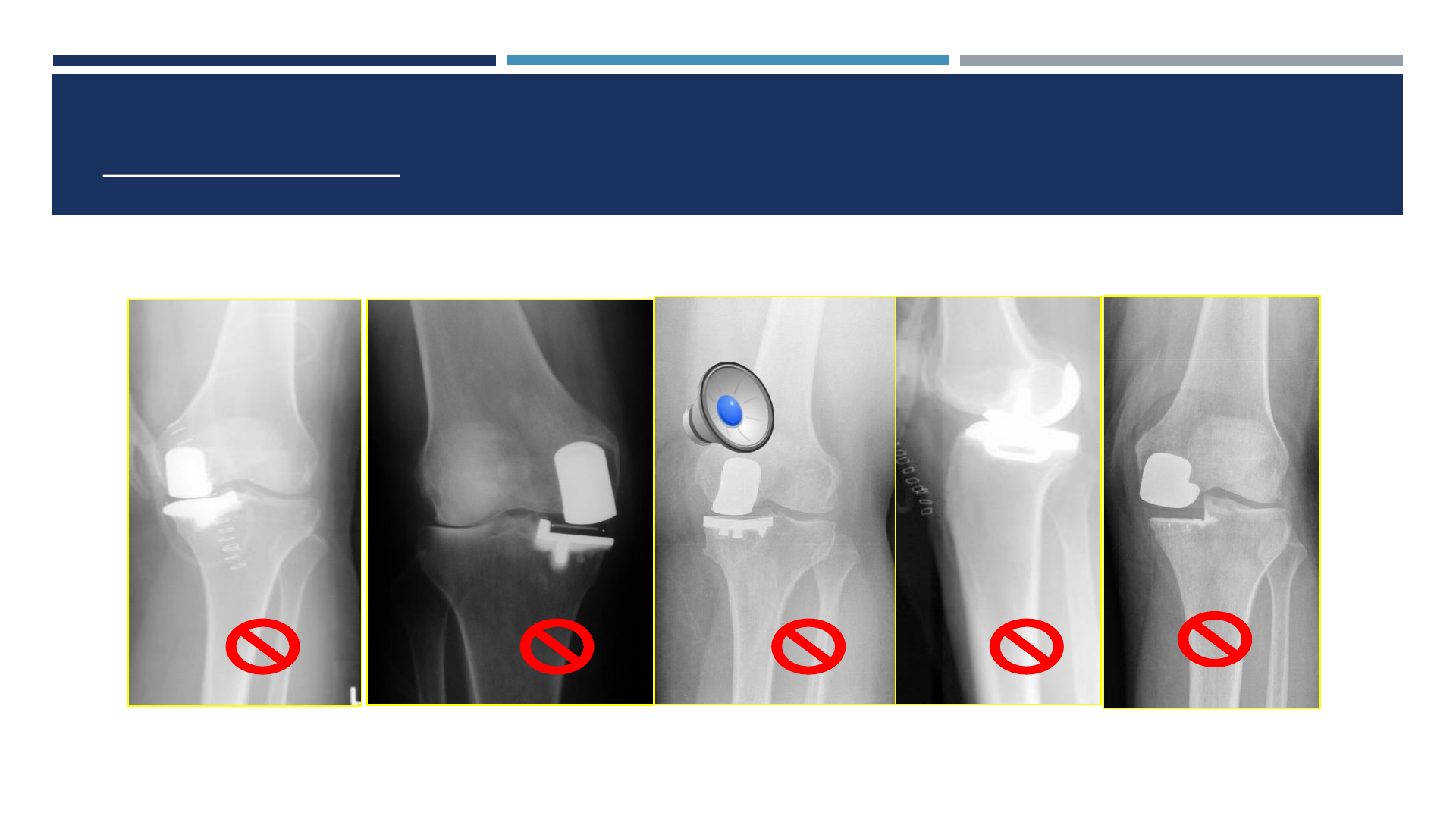
OUTLIERS IN ALIGNMENT IN UKA WITH
CONVENTIONAL METHODS
40-60% of cases are malaligned beyond 2° of plan
Keene G et al JBJS Br 2006;
Cobb J et al JBJS Br 2006
RATIONALE OF ROBOTICS FOR UKA
Simplify the procedure
Reduce the amount of instrumentation
Eliminate surgical steps
Enhance accuracy
Bone preparation/component alignment
Soft tissue balance
Improve clinical results
Lonner JH. American Journal of Orthopedics 2009
SEMI-AUTONOMOUS ROBOTICS IN KNEE
ARTHROPLASTY IN U.S.
Virtual planning
Bone resection
Component sizing
Implant alignment
Soft tissue balancing
1ST GENERATION SYSTEM
Image based CT planning and computer guidance
Balance & alignment
Implant positioning and sizing
Intraop virtual gap balancing
Bone prep with 6 mm burr attached to robotic arm
1ST GENERATION SEMI-AUTONOMOUS
ROBOTIC ARM FOR UKA:
Haptic constraint
Efficient
Accurate
Safe
Image-based (preop CT scan)
DOWNSIDES OF 1ST GENERATION SEMI-AUTONOMOUS
ROBOTIC SYSTEM
Capital expense
Preop CT scan
Additional expense
Denials common; high copays; bundled payments
Hospitals “eat cost”
Time/Inconvenience
Radiation exposure
2ND GENERATION SEMI-AUTONOMOUS ROBOTIC SYSTEMS:
Image-free (No CT scan)
Intraop registration/mapping/planning
Intraop gap balancing
Burr Speed/Exposure control
Cost favorable
35% being used in ASC’s for UKA
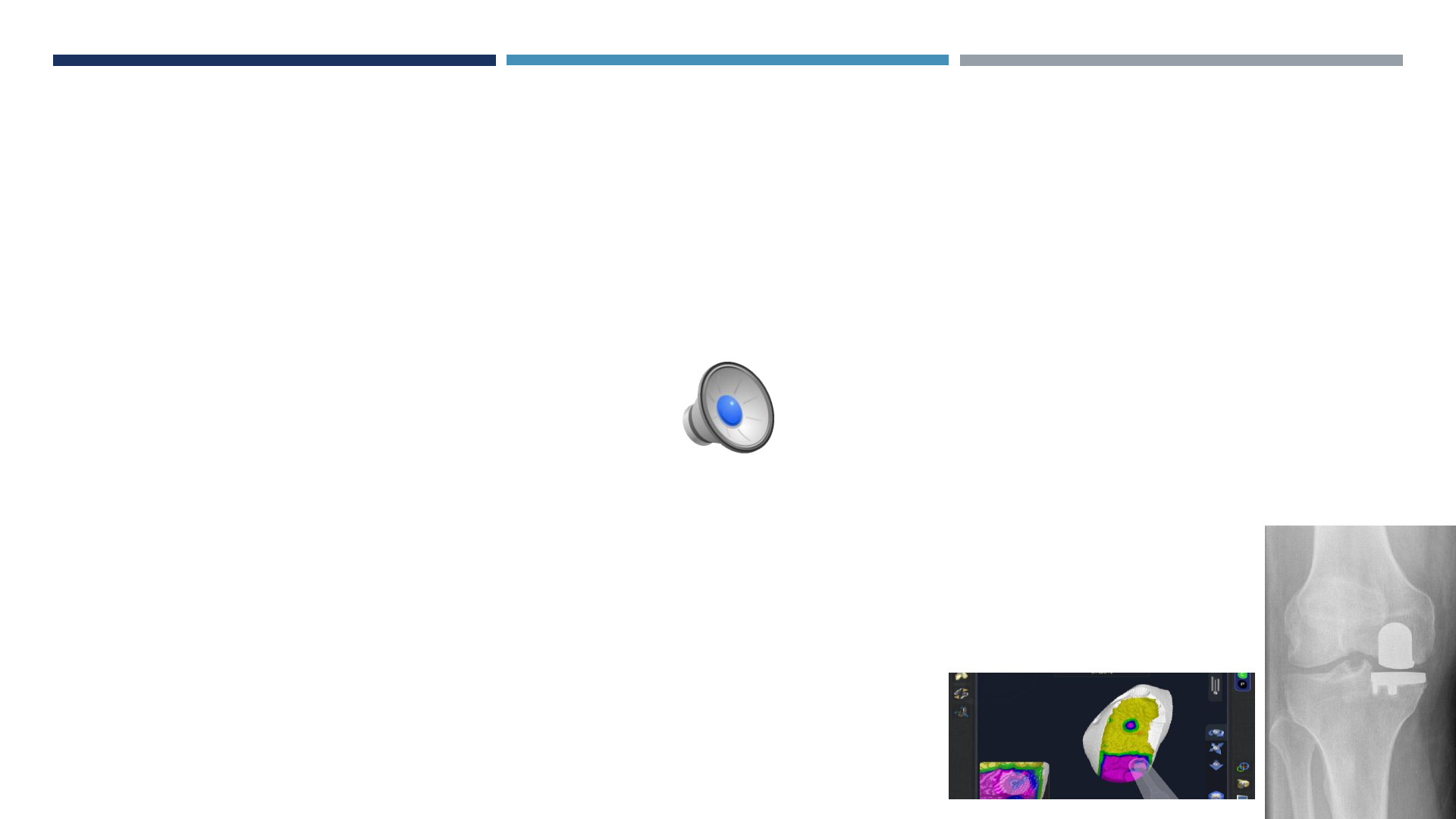
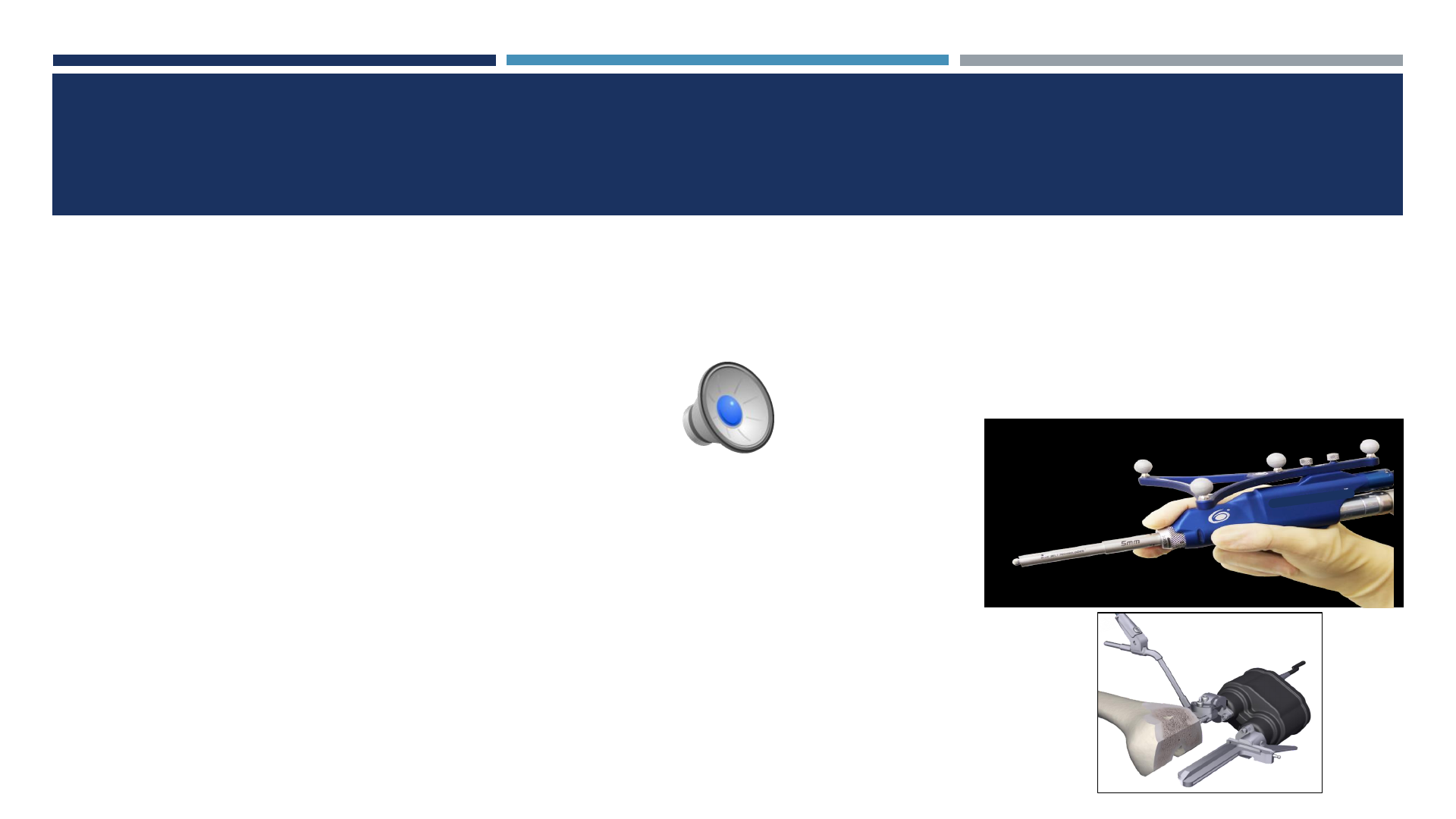
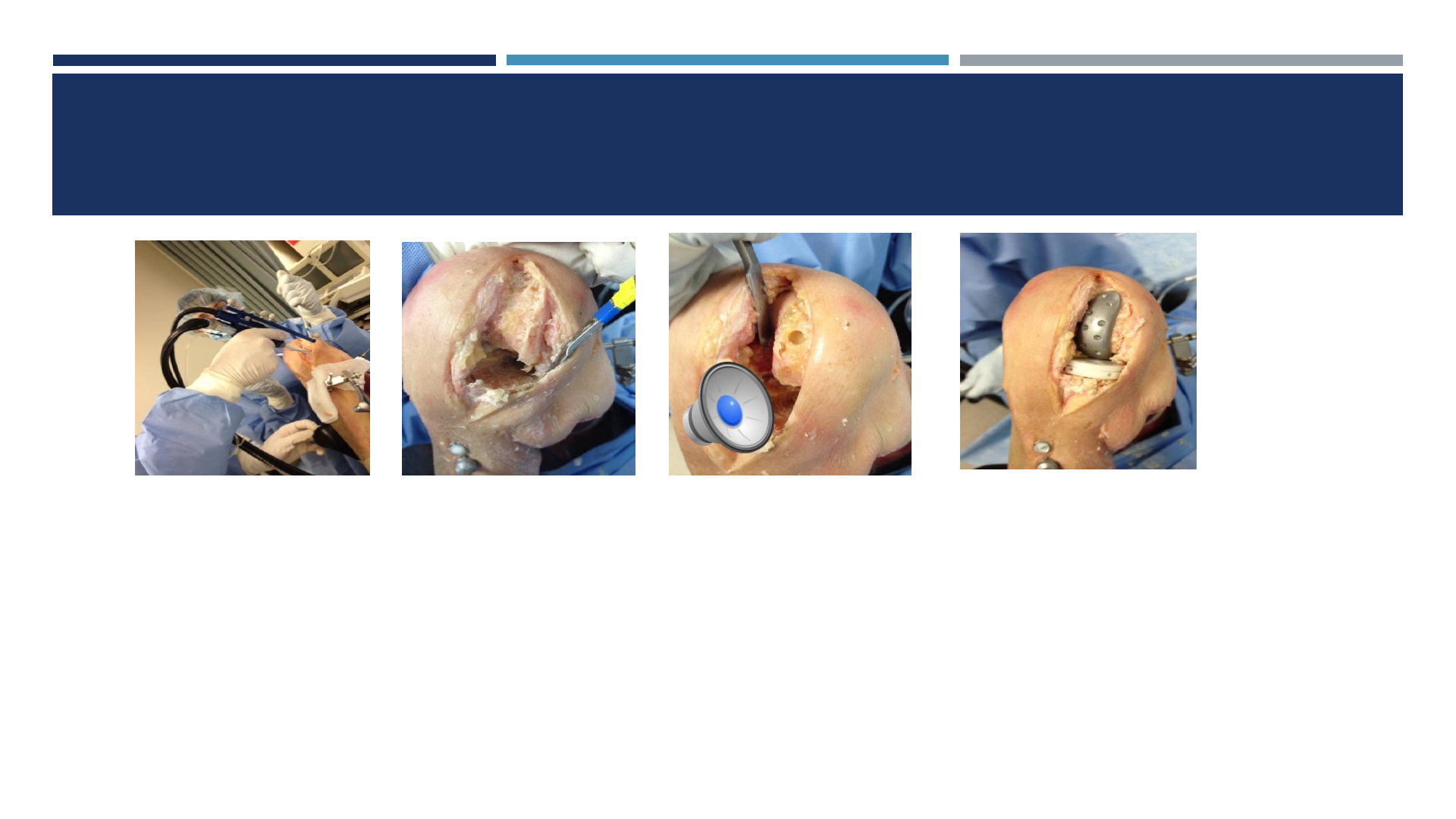
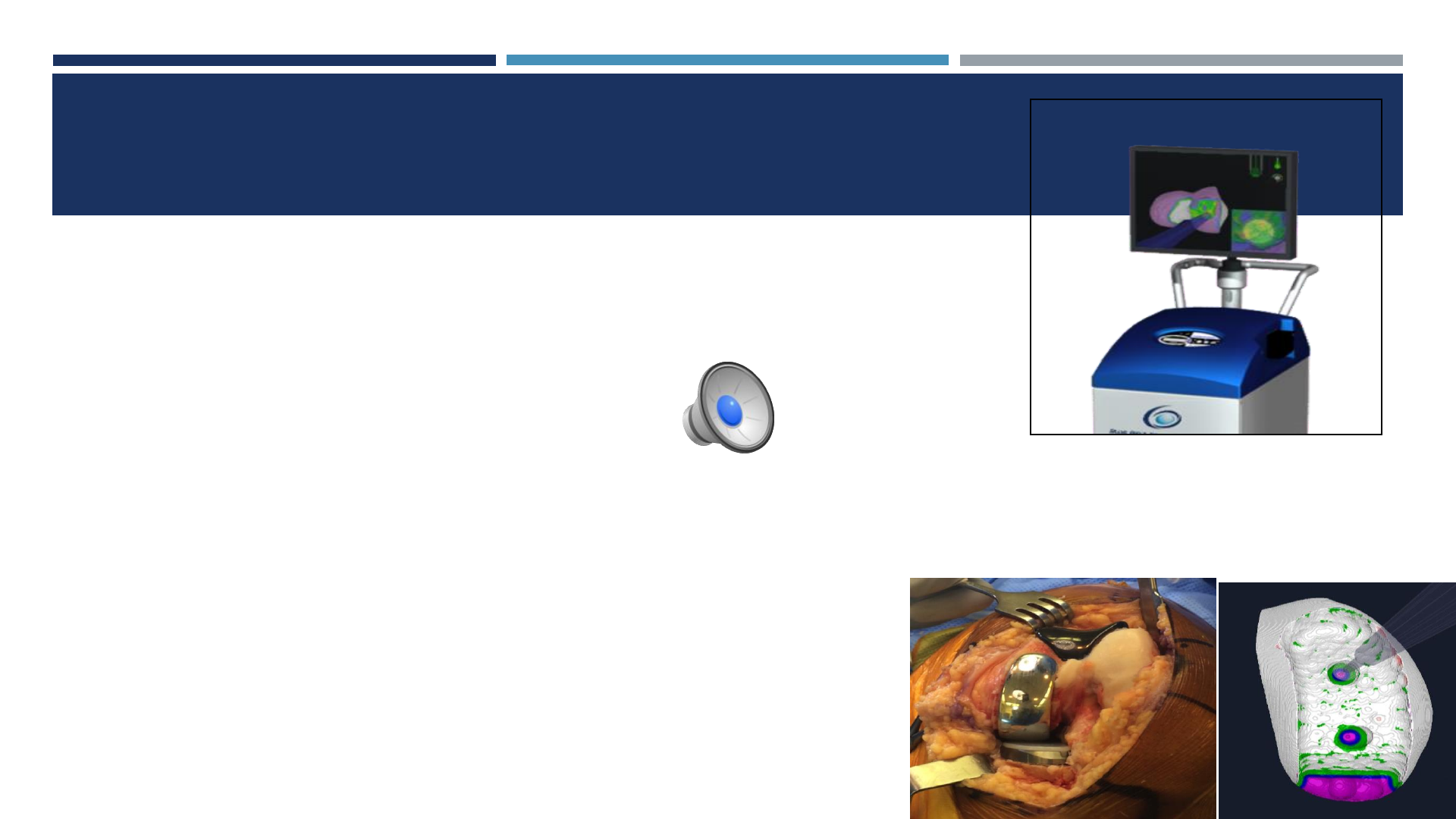
SURGICAL TECHNIQUES

IMAGE FREE SYSTEM: SURFACE MAPPING
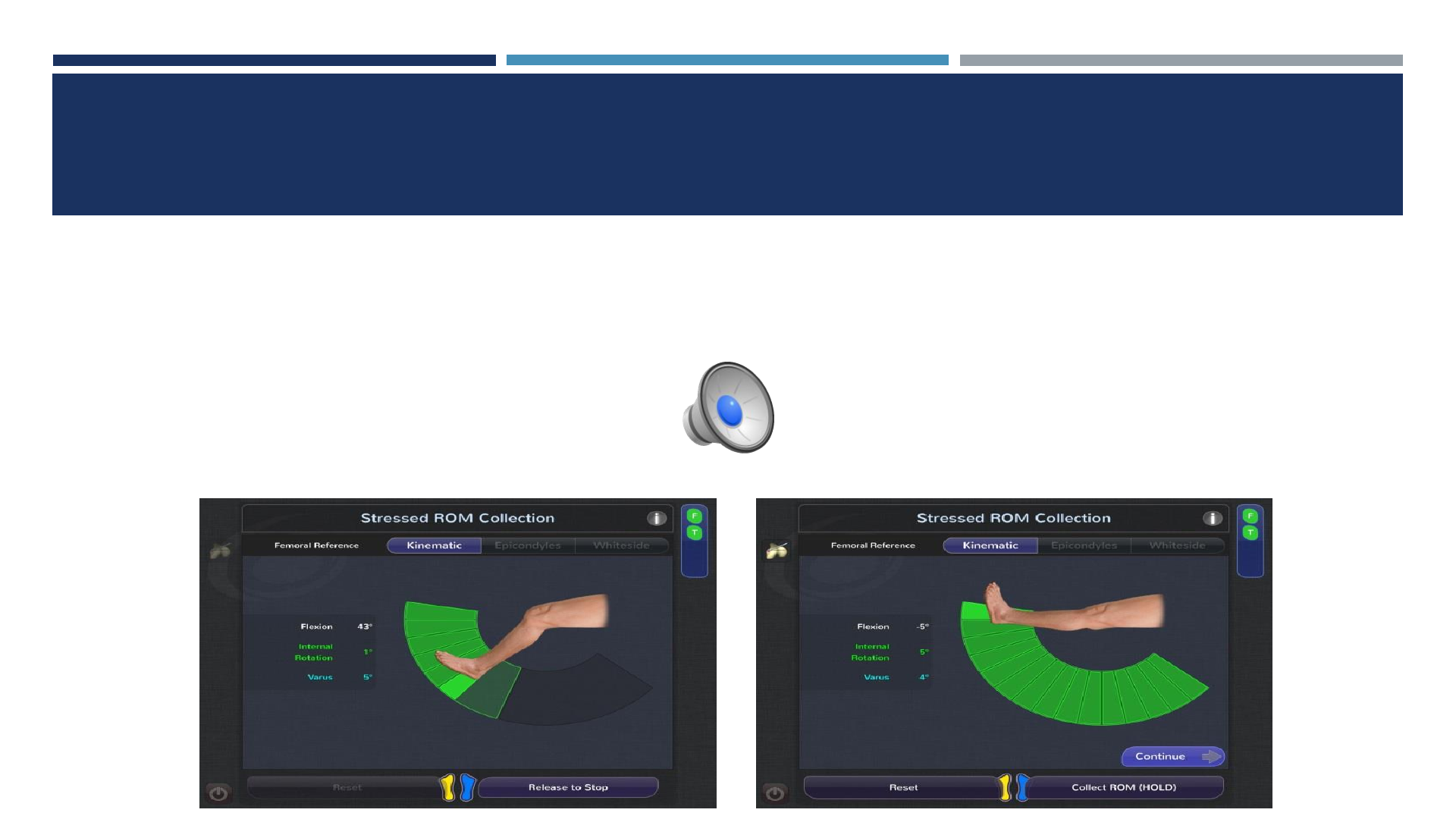
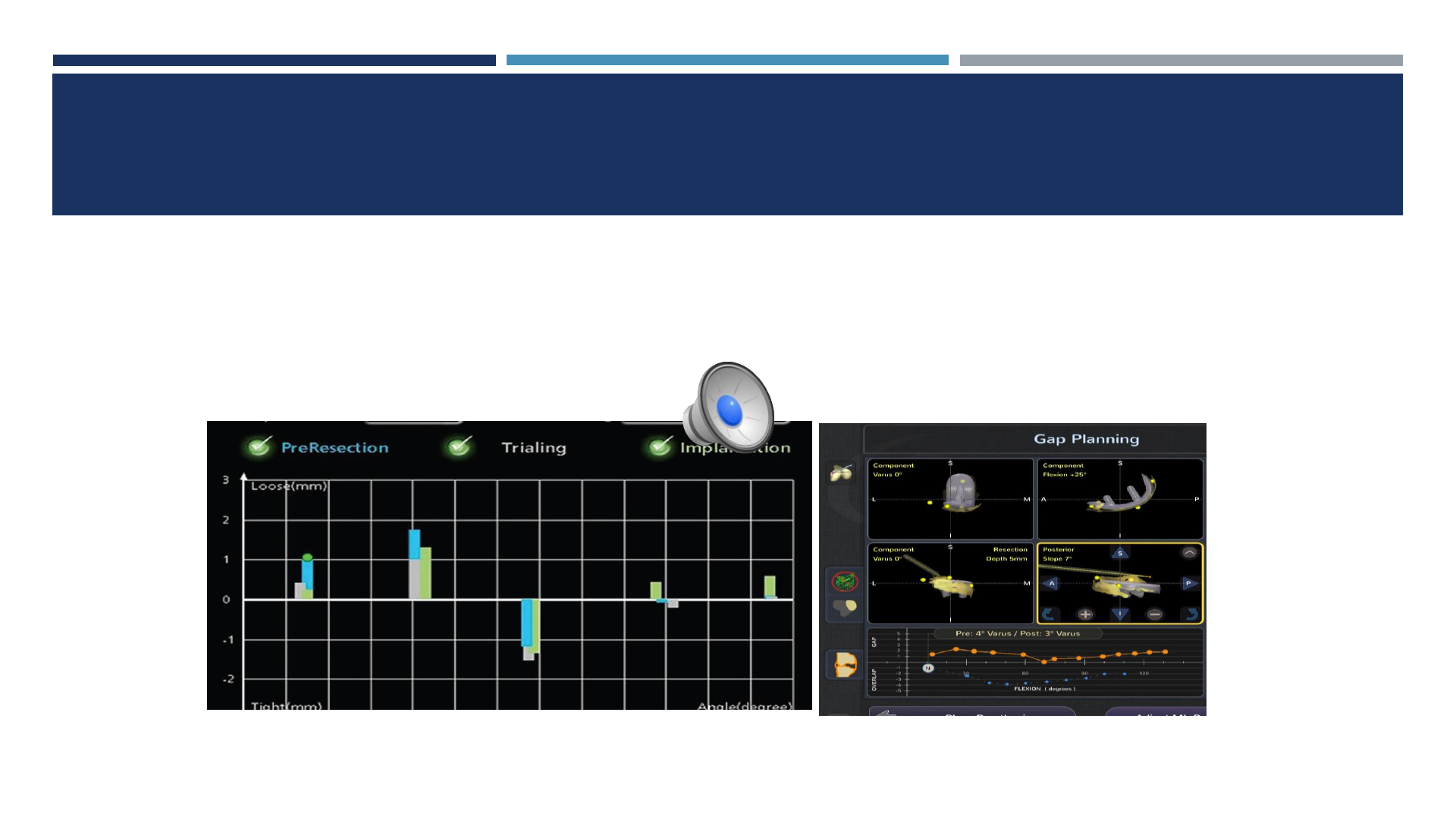
DYNAMIC INTRAOP GAP BALANCING
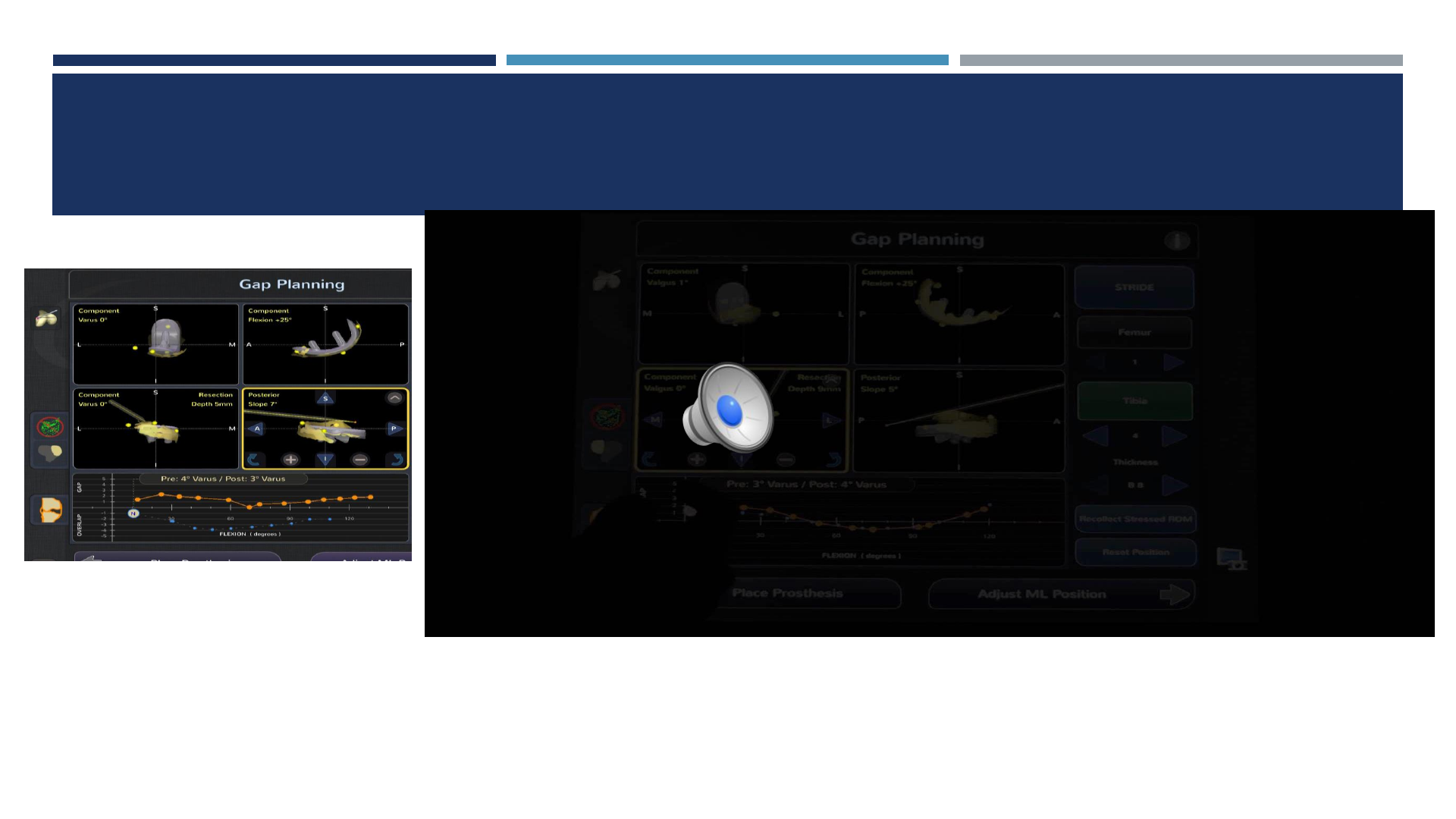
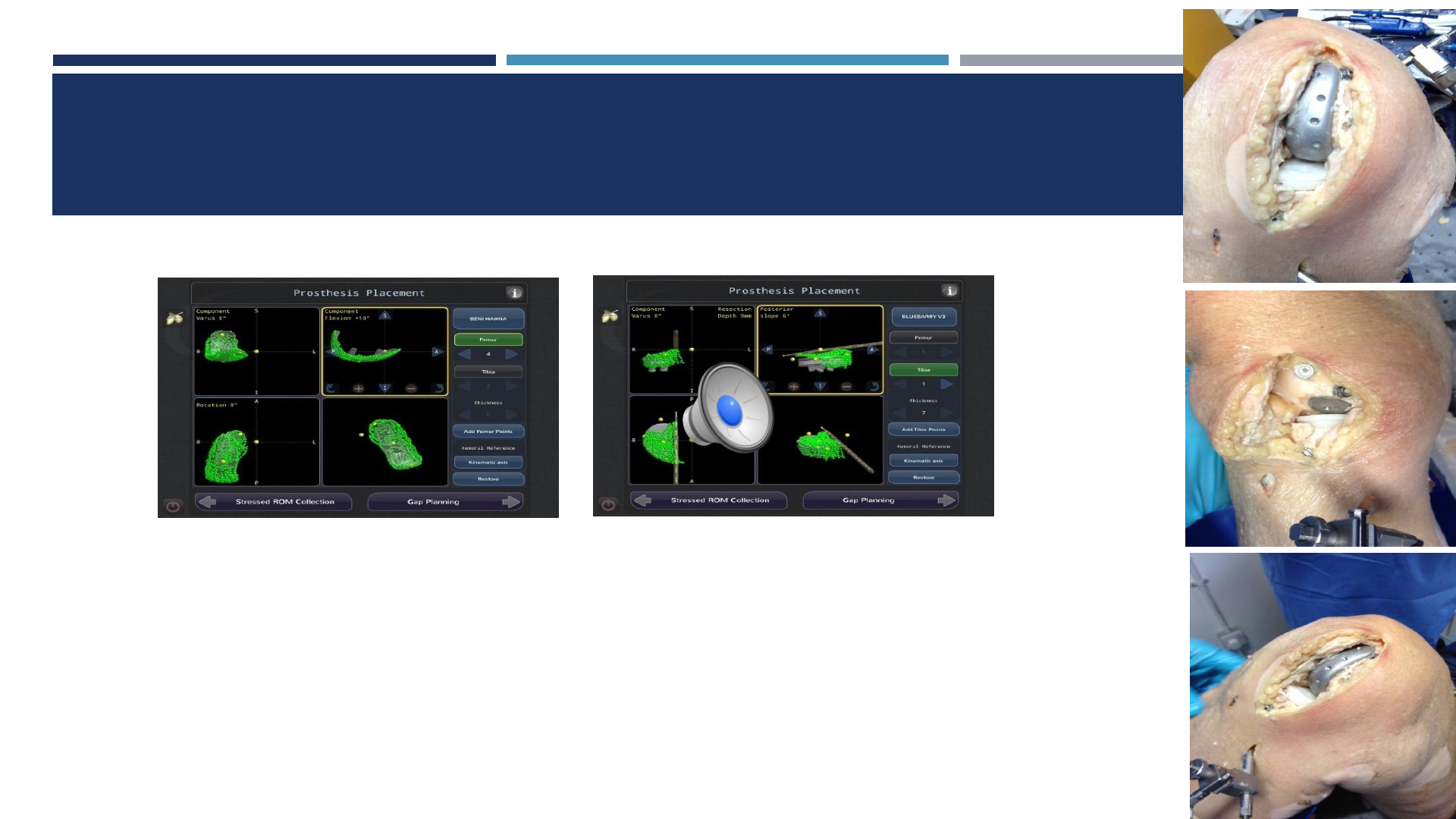
SELECTION OF IMPLANT SIZE/POSITION AND
VIRTUAL GAP BALANCE
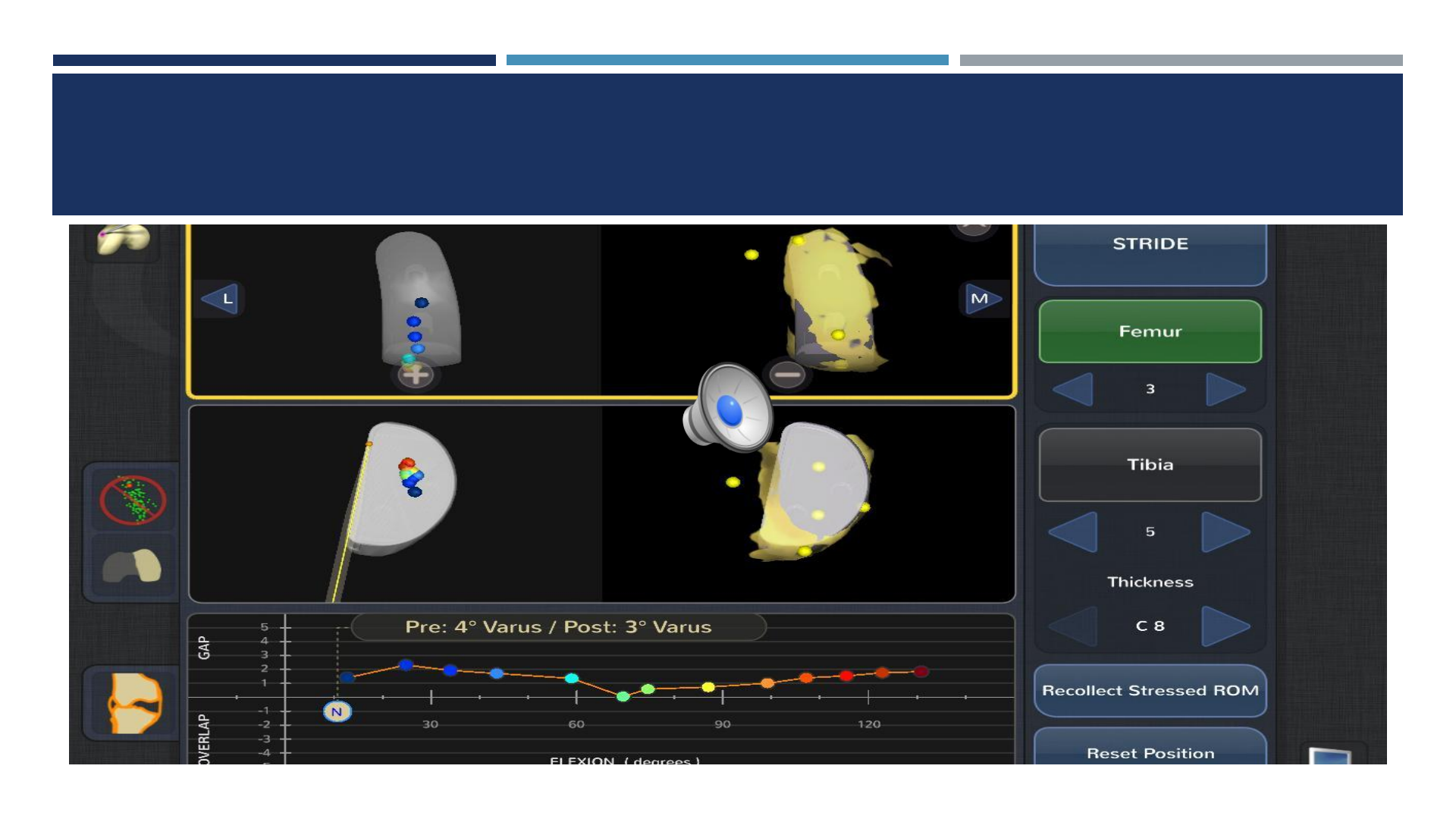
VIRTUAL TRACKING OF FEMUR ON TIBIA
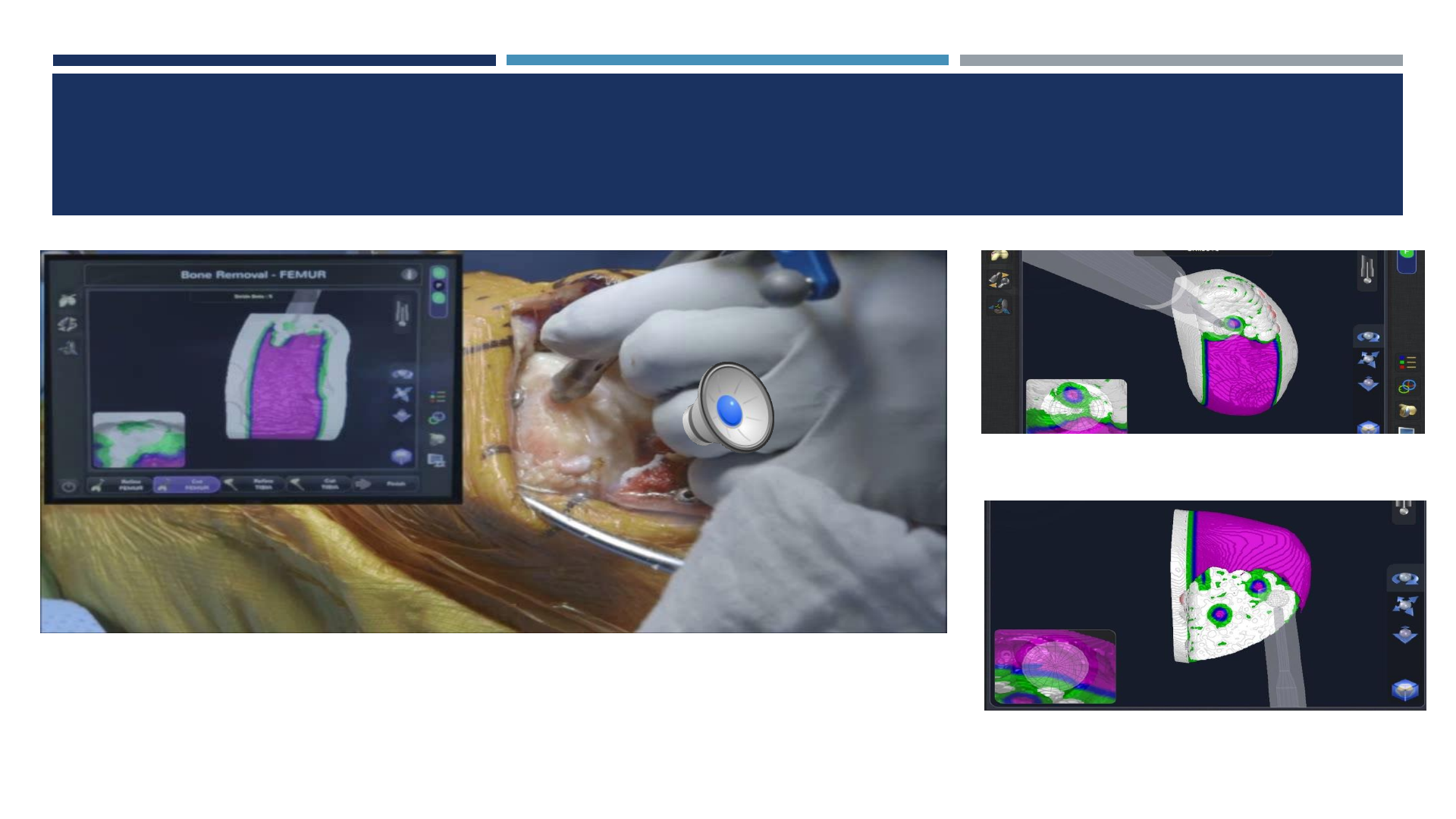
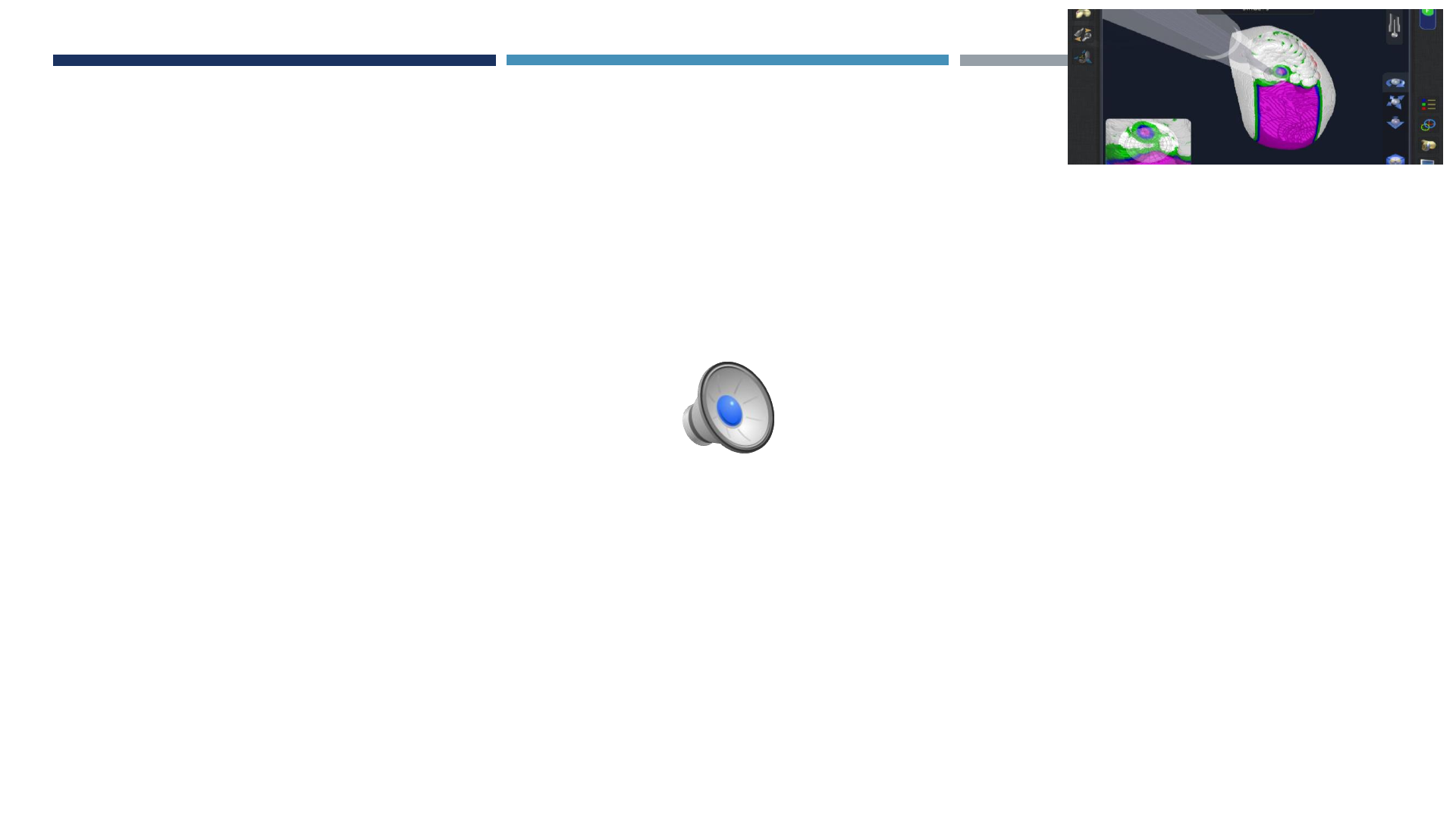
TECHNIQUE: BONE PREPARATION
PREPARED SURFACE

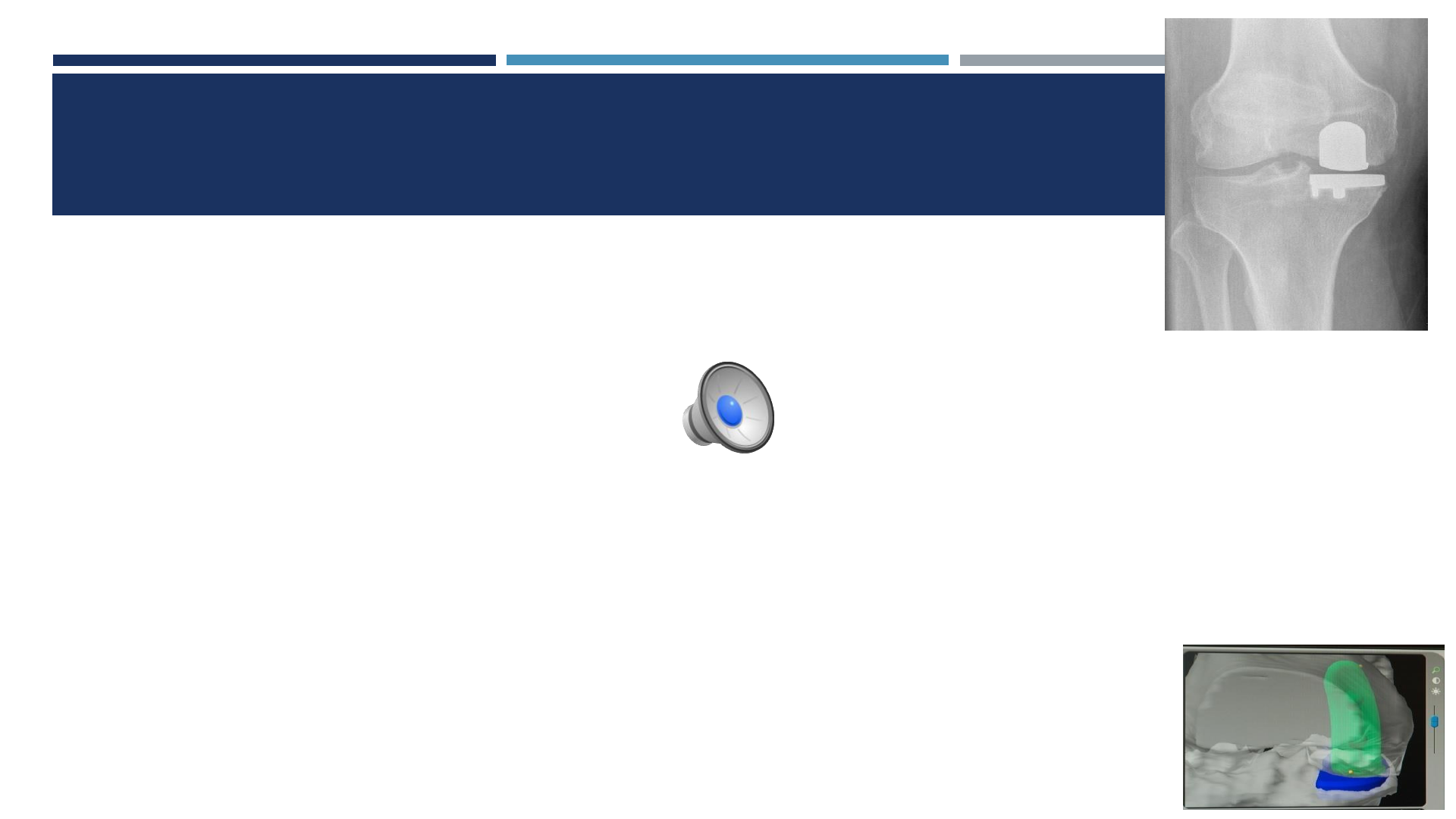
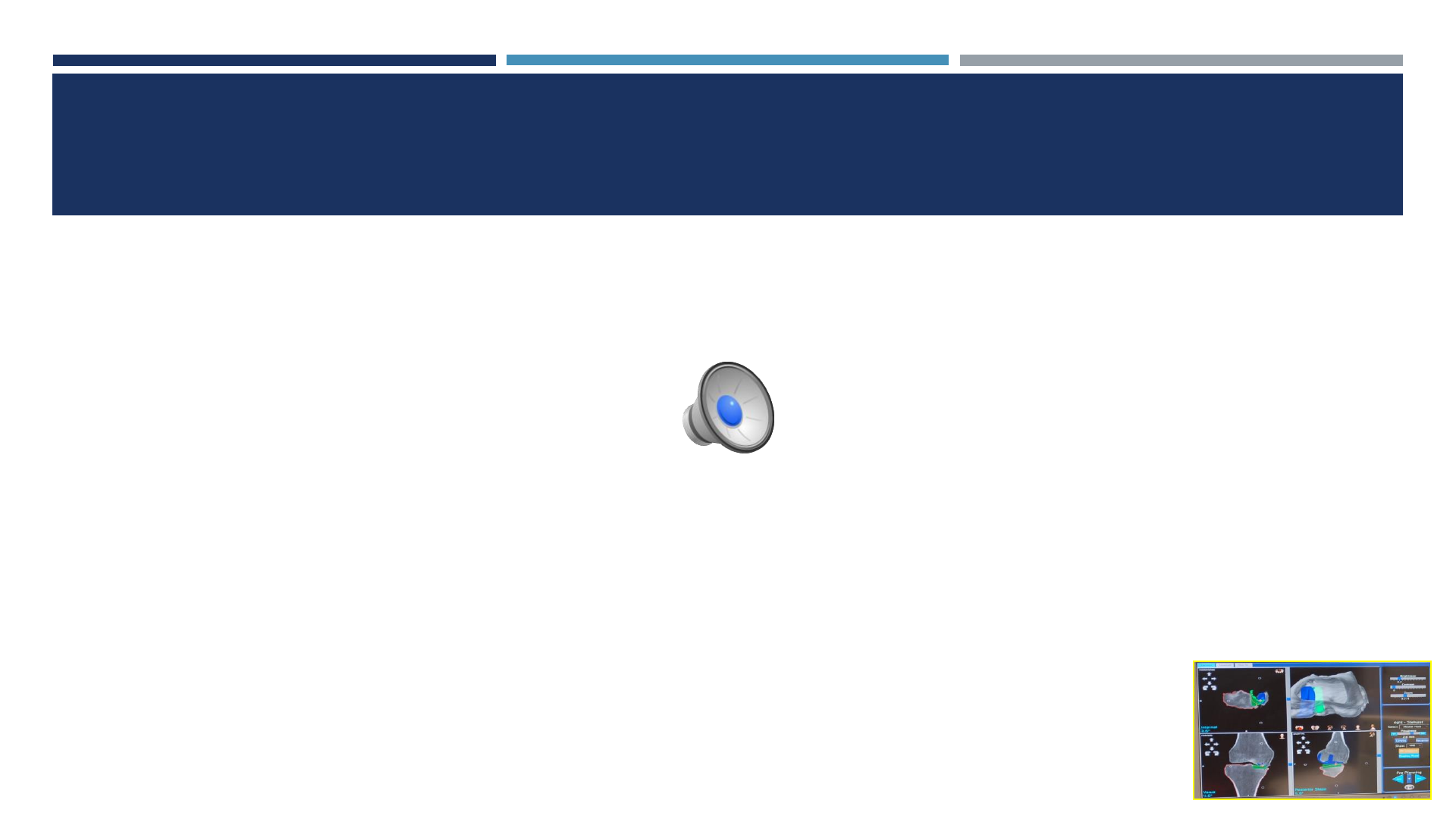
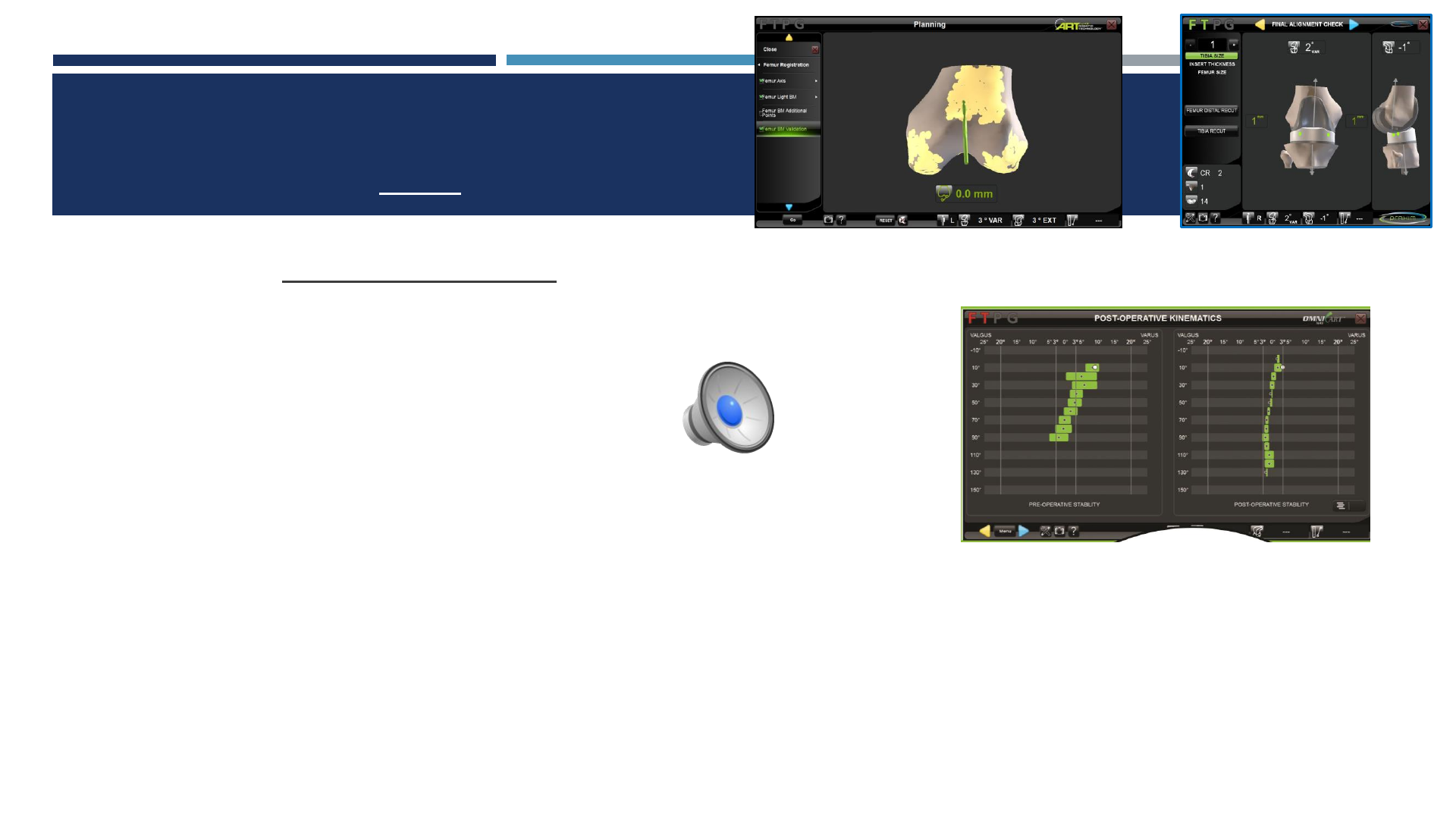
CT-BASED SYSTEM: PREOP PLANNING
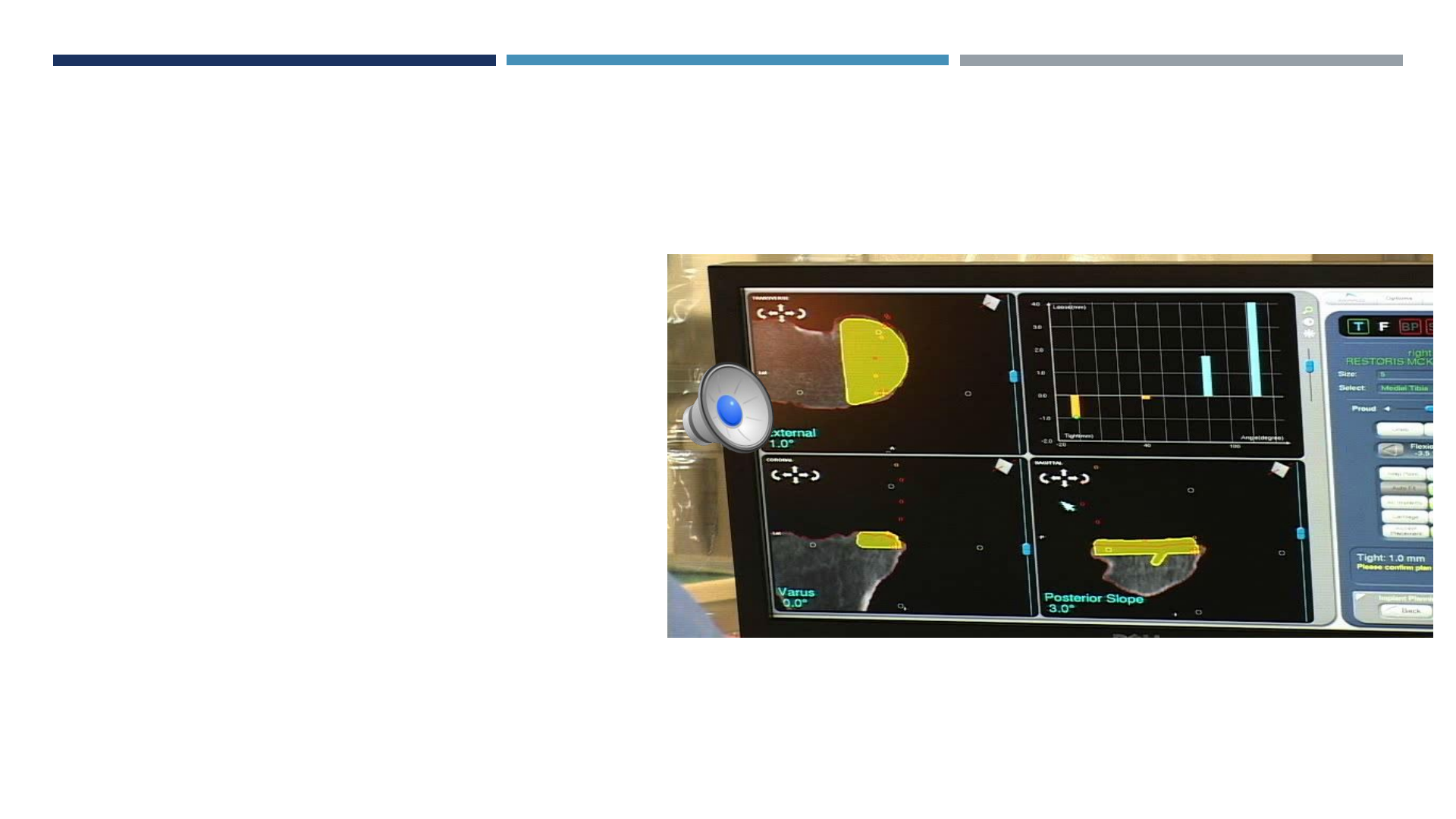
IMAGE-BASED SYSTEM: DYNAMIC SOFT-TISSUE GAP BALANCING
Remove osteophytes
Tension MCL/LCL
Capture tissue tension through
ROM
Adjust prn
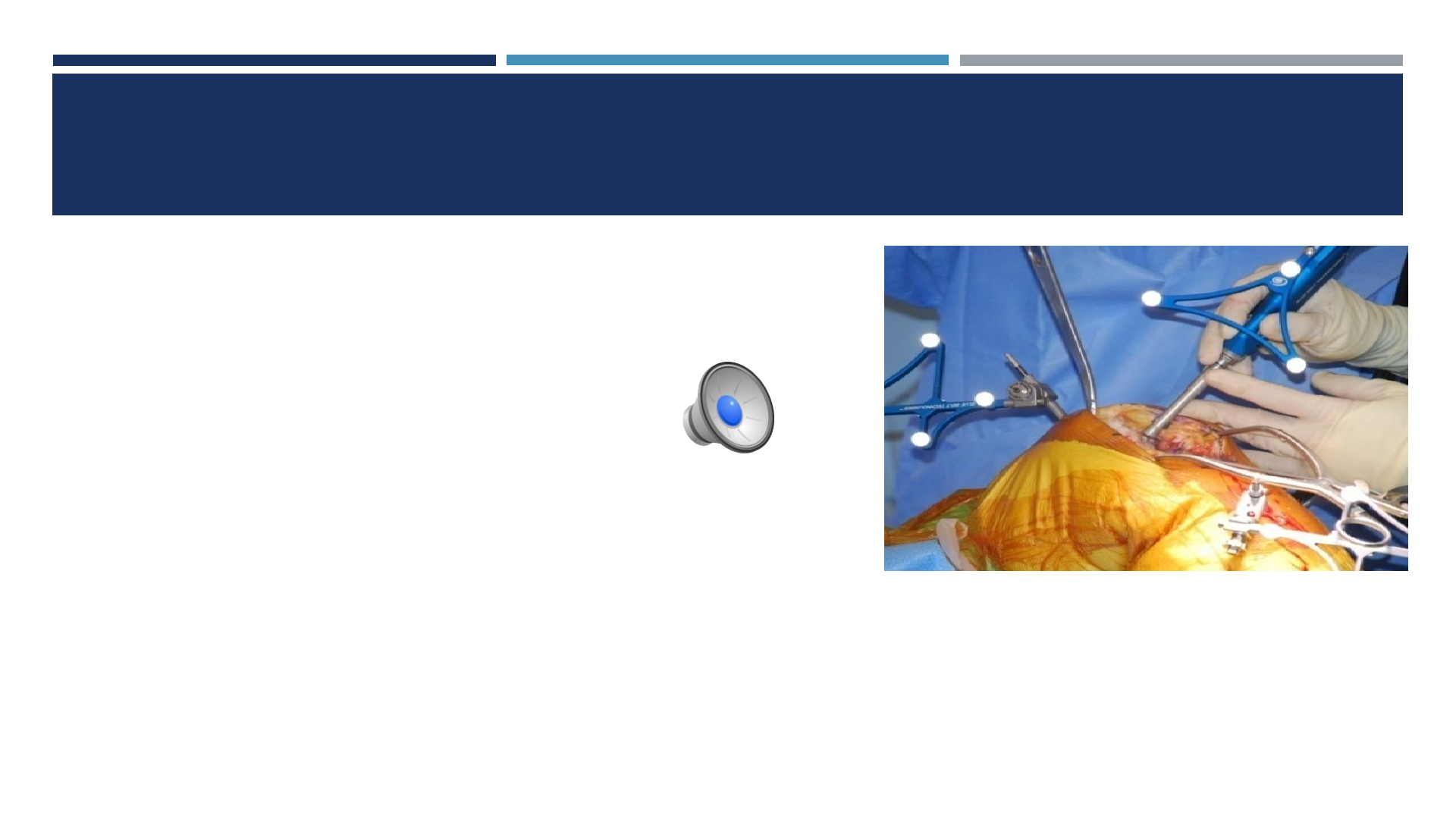
IMAGE BASED SYSTEM: HAPTIC CONSTRAINT
Bone resection volume based upon planned component
placement and size

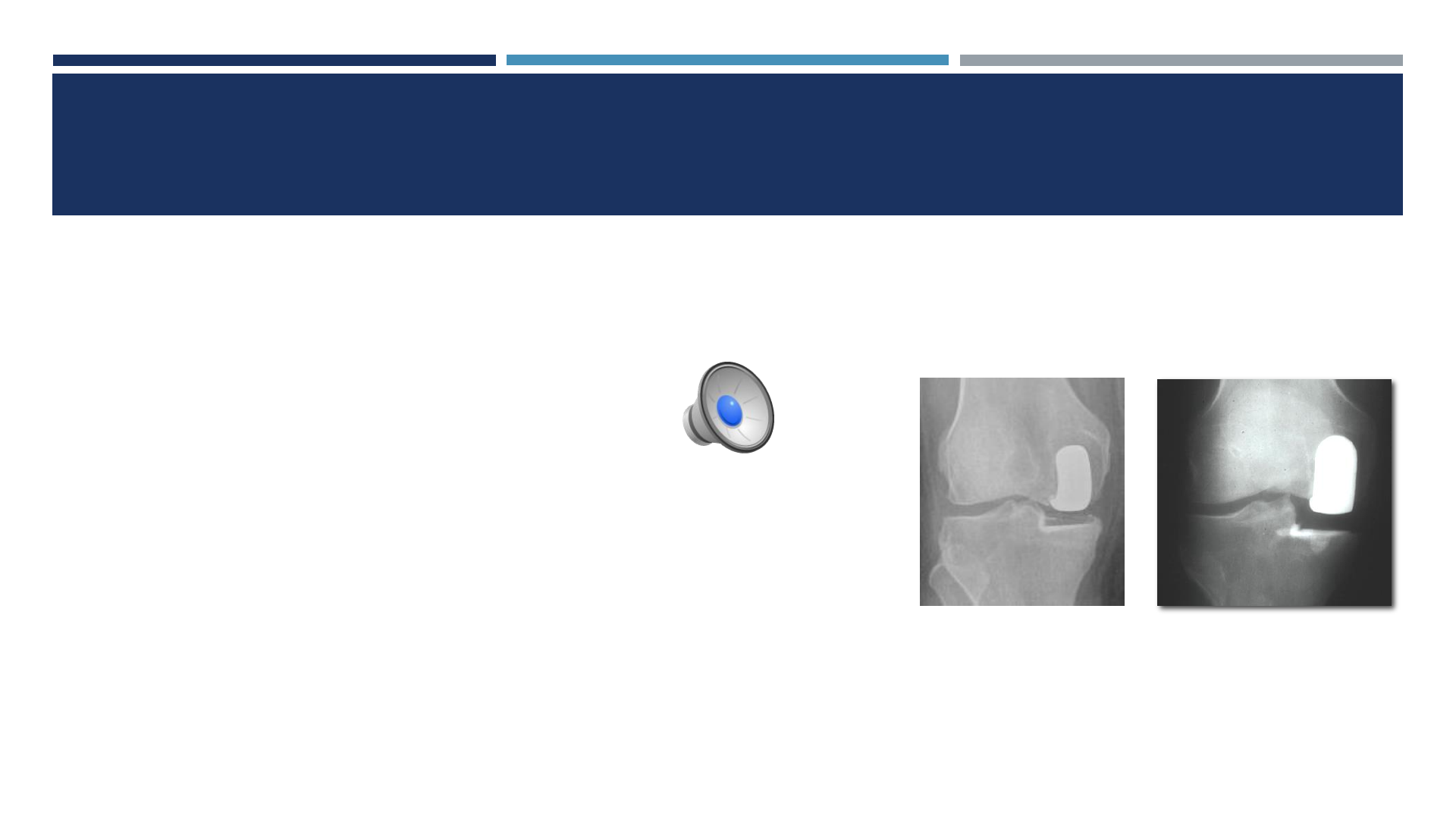
IMAGE-BASED SYSTEM: ASSESSING ACCURACY
OF IMPLANT POSITION
DATA???
KEY STUDIES
Accuracy of bone preparation
Pre-clinical (cadaveric specimens) and clinical studies
Comparison of intraoperative plan for limb alignment with postop limb alignment
Clinical (navigated measures)
Accuracy of tibial component alignment and volumetric bone preservation
Radiographic
Learning Curve
Safety
Radiation avoidance by using image-free systems (eliminating preop CT scans)
Survivorship and satisfaction
TIBIAL ALIGNMENT -- UKA
Initial 31 robotic UKA’s with Haptic, CT-based robotic system
Matched group of preceding 27 conventional UKA
Height, weight, ROM, alignment
Study parameter: Tibial alignment
(Lonner, John, Conditt CORR 2009)
TIBIAL ALIGNMENT -- UKA
Variance: 2.6x greater with manual techniques (p<0.05)
RMS error: 3.4(manual) vs. 1.8(robot)
Coronal alignment –Avg error:
Manual: 2.7 +/- 2.1more varus
Robot: 0.2 +/-1.8 (p<0.0001)
(Lonner, John, Conditt CORR 2009)
ACCURACY OF COMPONENT POSITIONING IN UKA:
SEMI-AUTONOMOUS ROBOT VS. CONVENTIONAL
Prospective RCT, 120 patients
62 robotic UKA (Robotic)
58 conventional (Conventional)
Component alignment and position determined by CT scan
Coronal, sagittal and axial positioning
Bell SW et al. J Bone Joint Surg. 2016
ACCURACY OF COMPONENT POSITIONING IN UKA:
SEMI-AUTONOMOUS ROBOT VS. CONVENTIONAL
Robotic assistance had:
significantly lower component median implantation errors in all 3 component
parameters (p<0.01)
Significantly fewer outliers >2° of target positions
Bell SW et al. J Bone Joint Surg. 2016
PRE-CLINICAL ACCURACY
25 cadaveric specimens
Image-free semi-autonomous system (2nd Generation robot)
Medial UKA
3 surgeons
Lonner, Smith, Picard, Hamlin - Clin Orthop 2014
ANALYSIS METHOD
Preop plan
Postop analysis
Optical probe inserted into implant divots
Surface positions mapped
Postop position compared to plan
Lonner, Smith, Picard, Hamlin - Clin Orthop 2014
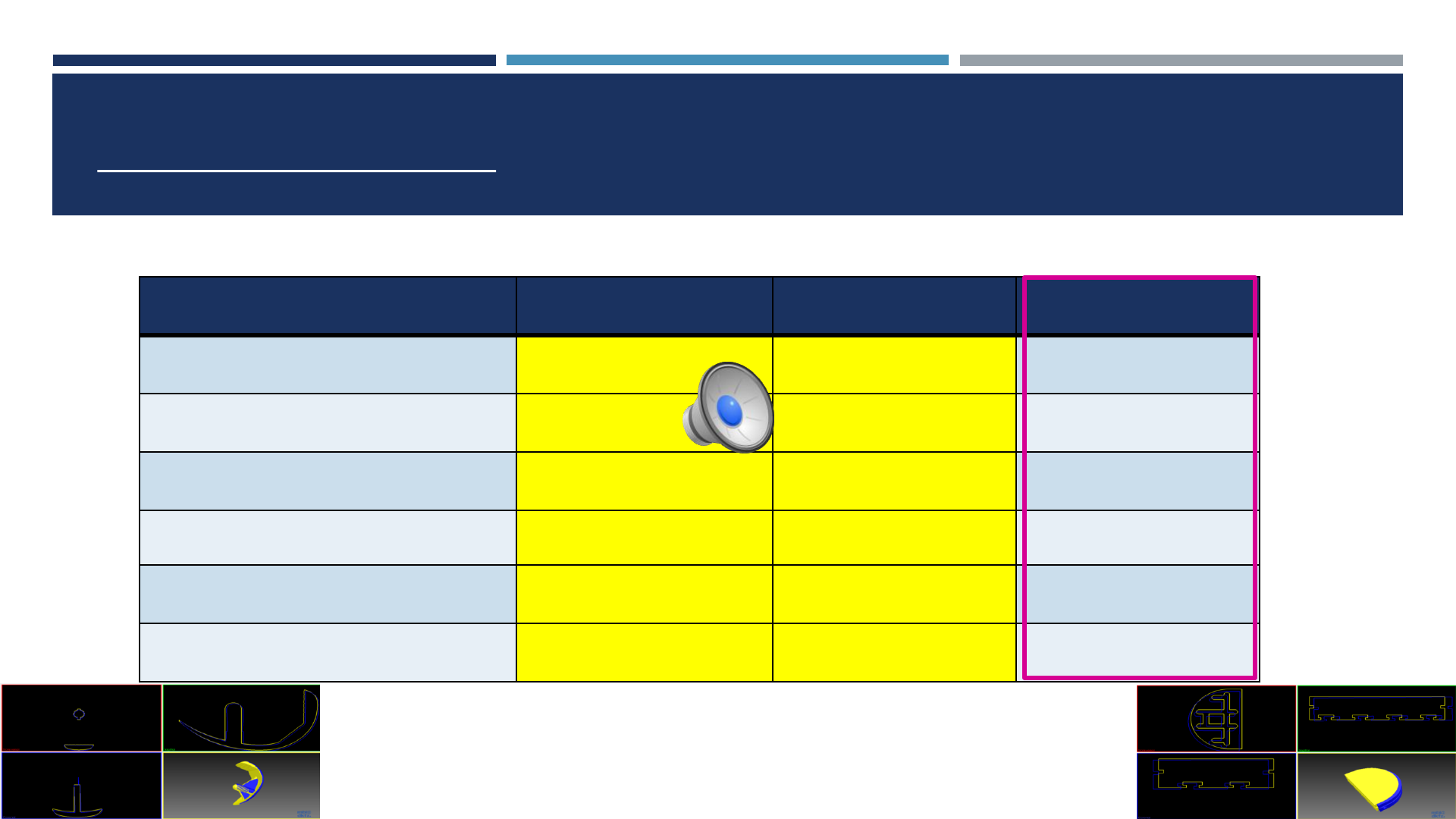
ALIGNMENT:
SEMI-AUTONOMOUS ROBOTS VS. MANUAL
RMS Error Image-Free CT-Based Manual
Flex/Ext (°)1.6 2.1 4.1
Varus/Valgus (°)2.3 2.1 6.0
Int/Ext (°)1.7 3.0 6.3
Prox/Dist (mm) 1.3 1.0 2.8
Ant/Post (mm) 1.3 1.6 2.4
Med/Lat (mm) 0.9 1.0 1.6
Dunbar et al J Arthrop 2012
Jenny J Arthrop 2002
Lonner et al CORR 2014
2.6x less variability than manual techniques (p<0.05)
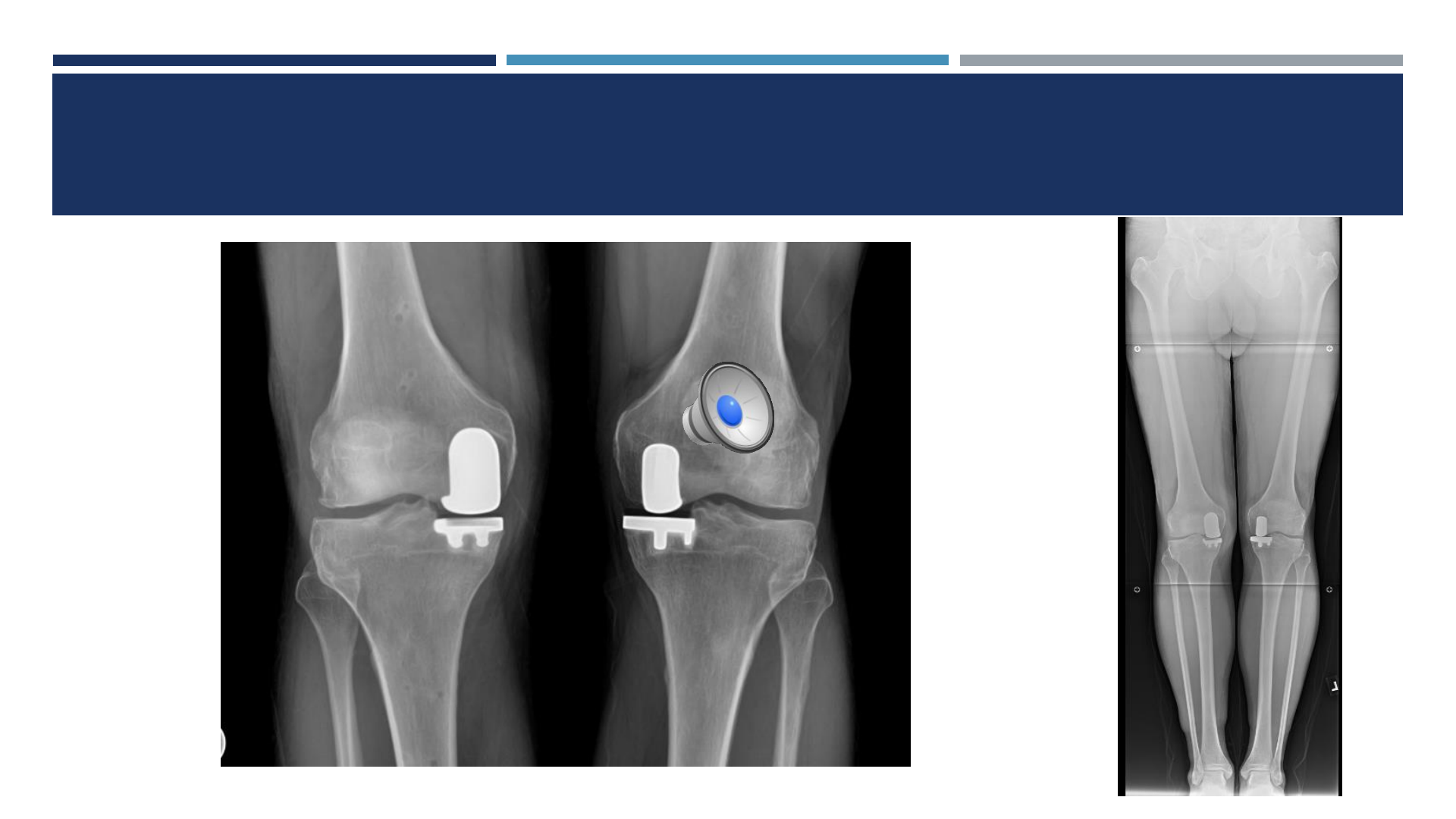
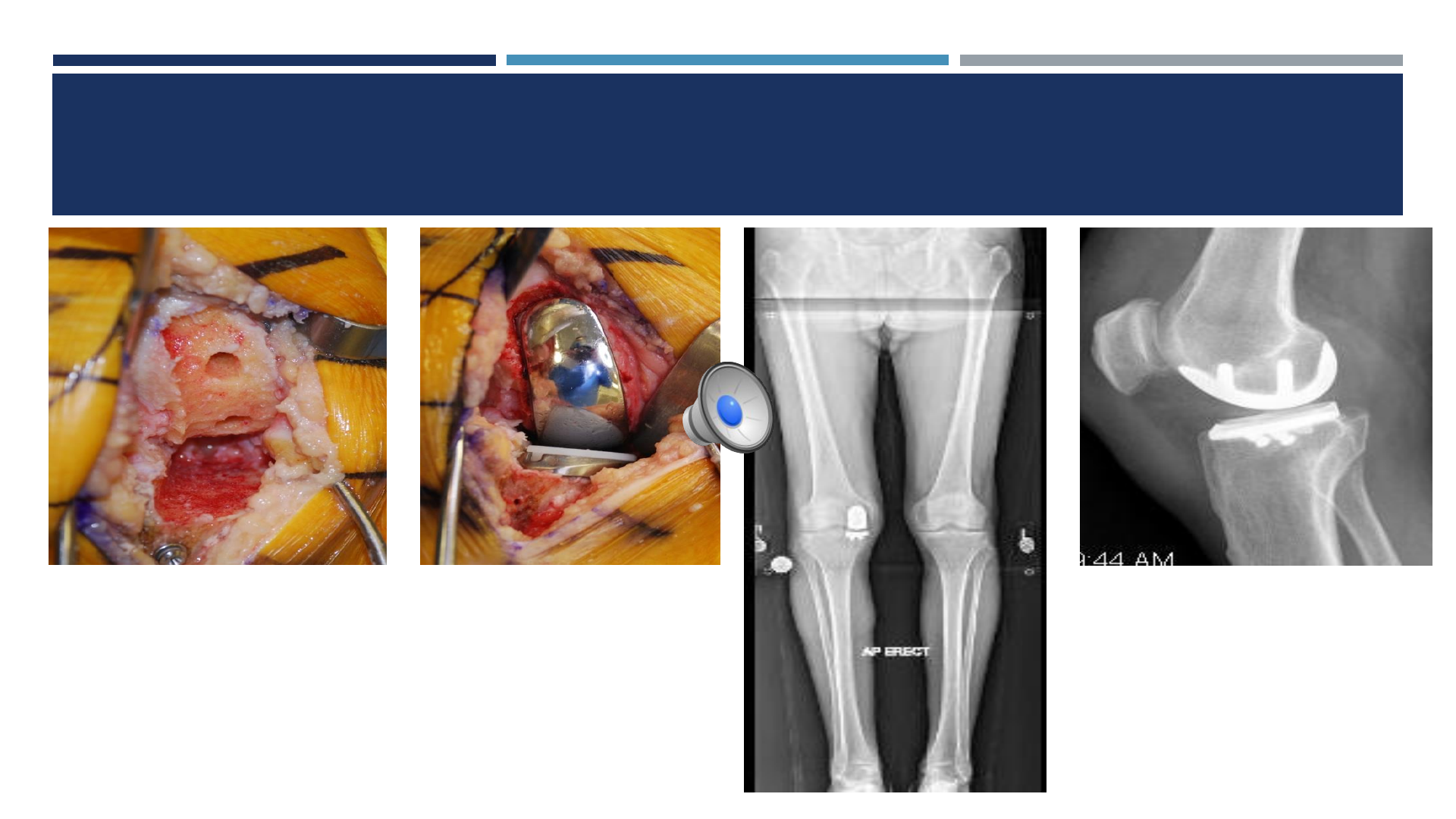
ALIGNMENT: NO APPARENT DIFFERENCE -- CT-BASED VS IMAGE-FREE
ROBOTIC SYSTEMS
6 wks post Image- free 6 yrs post CT-based
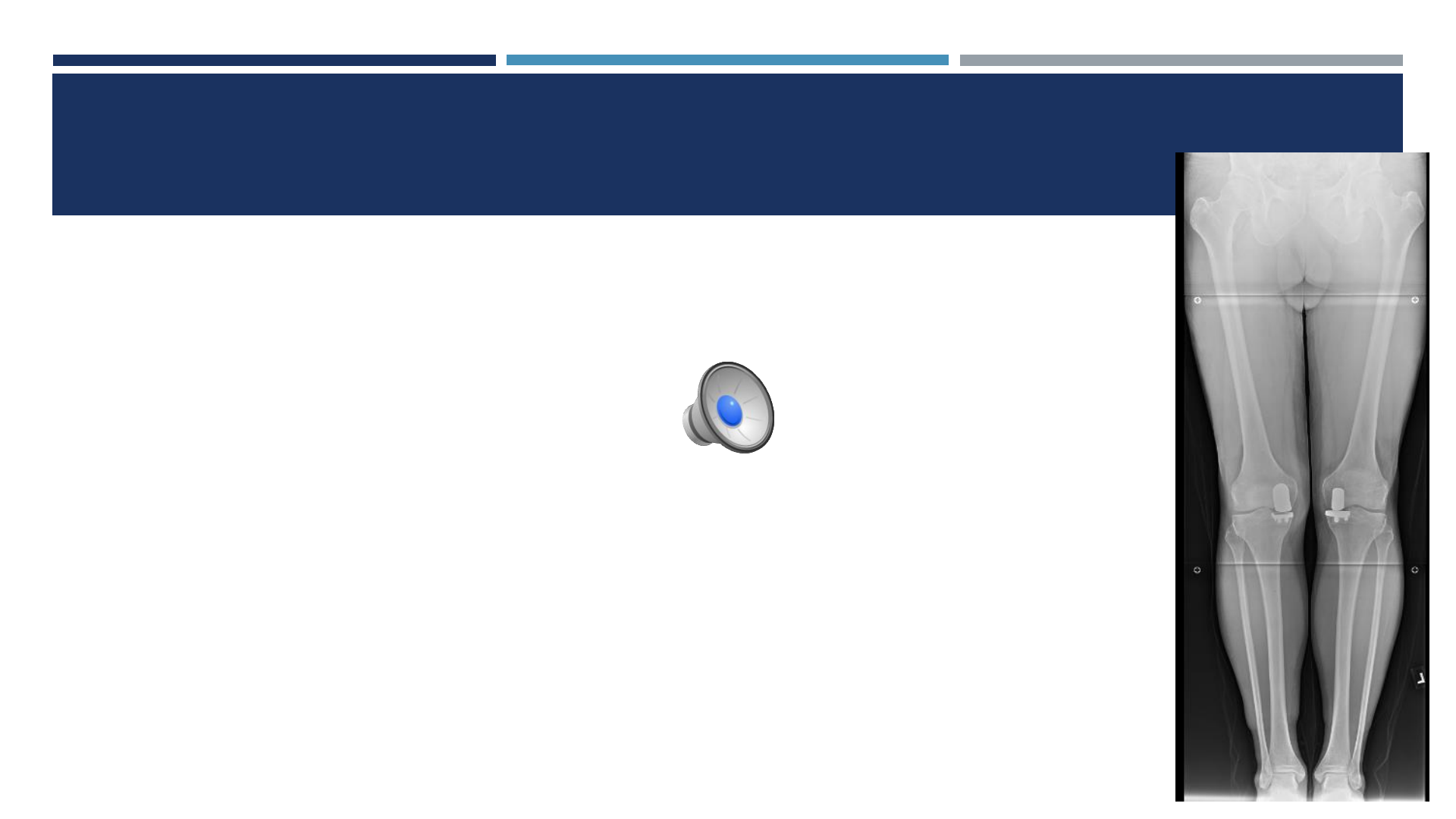
PLANNED VERSUS ACHIEVED LIMB ALIGNMENT
65 cases, image-free robotic system
Multiple surgeons
Postop limb alignment ≤1°from plan 92% (60/65)
F Picard, A Gregori, J Bellemans, J Lonner, J Smith, D Gonzales, A Simone, B
Jaramaz –CAOS July 2014
TIBIAL RESECTION (ROBOTIC VS.
CONVENTIONAL)
Industry Data
27,989 conventional UKA’s
8421 semi-autonomous robotic UKA’s
Studied variable: tibial poly thickness
Implications for revision to TKA
Complexity, need for augments/stems
Ponzio DY, Lonner JH. Am J Orthop 2016
8 mm 10 mm
Robotic Conventional
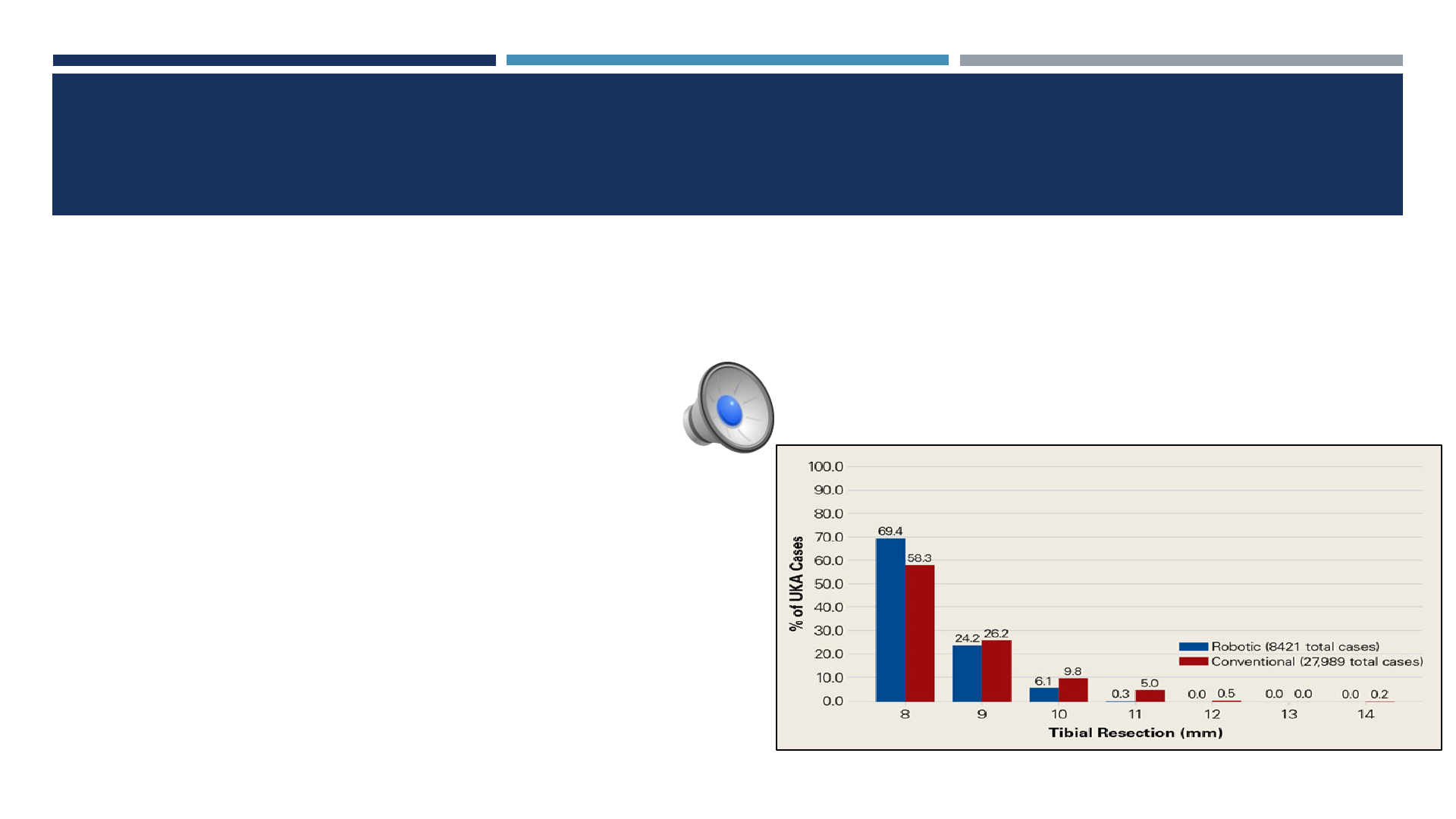
TIBIAL RESECTION (POLY SIZES)
8-mm and 9-mm polyethylene inserts
Robotic group: 93.6%
Conventional group: 84.5% (P< .0001).
Aggressive tibial resection, requiring tibial inserts ≥10 mm
Robotic group: 6.4%
Conventional group: 15.5%
Tibial inserts >11 mm
Robotic group: 0.3%
Conventional group: 5.7%
No differences between 2 semi-autonomous robots
Ponzio DY, Lonner JH. Am J Orthop 2016
LEARNING CURVE
Eleven novice users (2nd generation image-free system)
Precision achieved immediately
Mean of 8 procedures to reach a steady state surgical time
(95% confidence interval 6-11)
Avg. steady state surgical time 45 minutes (range 37-55 minutes)
A Gregori, F Picard, J Lonner, R Marquez, J Smith, A Simone, B Jaramaz - CAOS Abstract 2014
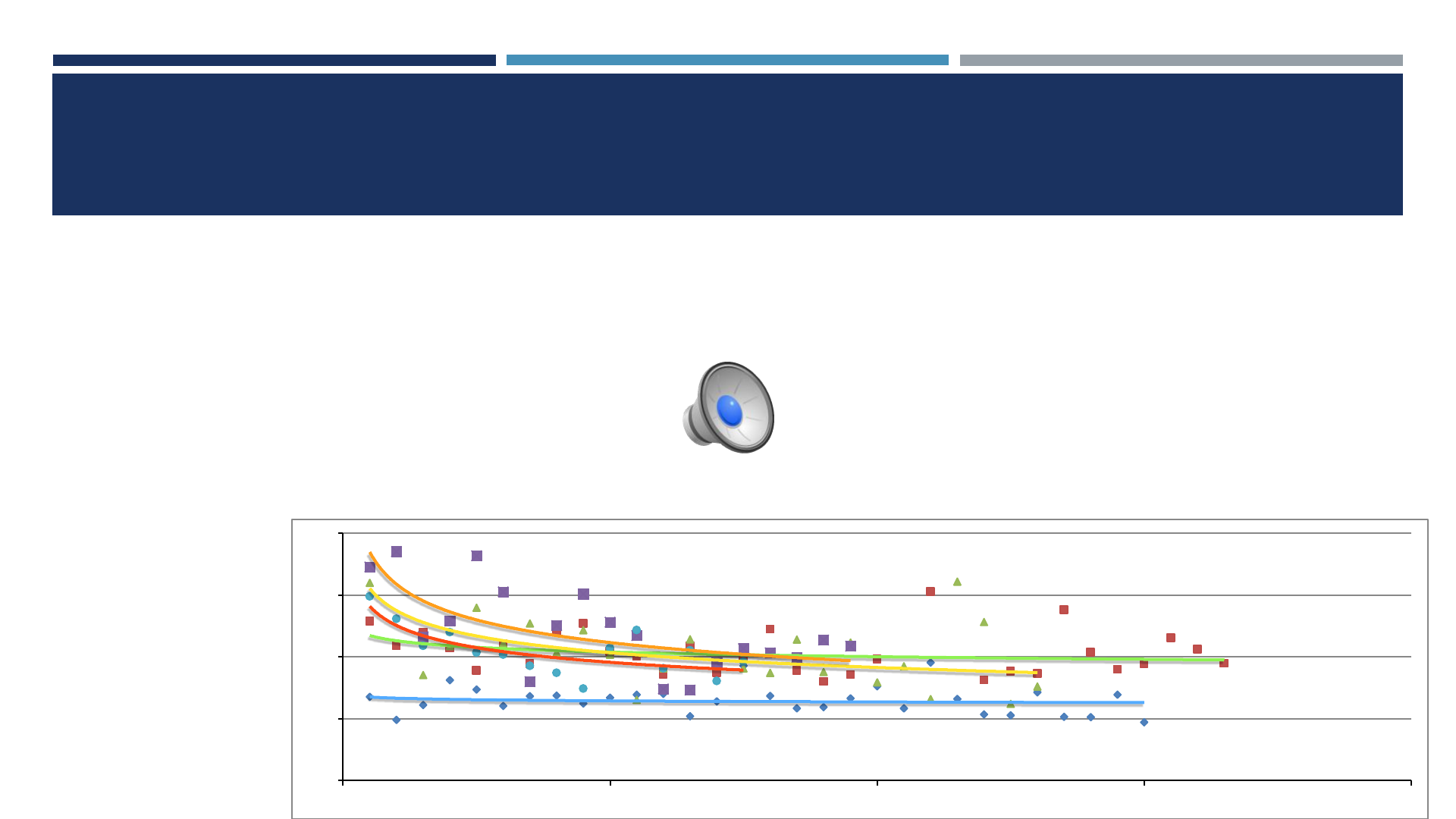
LEARNING CURVE
Greatest improvement in “Cutting Phase”:
Average improvement from 42 to 24 minutes.
Least improvement in “Anatomic Registration” and “Implant Planning”:
Average improvement from 14 minutes to 6 minutes.
The mean steady state surgical time for all surgeons was 45 minutes (SE 4.3, p<0.001).
0.
27.5
55.
82.5
110.
010 20 30 40
Surgical Time (mins)
Surgical Case Number
Learning curve
GAP BALANCING
•Final ligament balance after implantation accurate within
0.53 mm compared to dynamic plan
Plate JF et al Advances in Orthopedics 2013
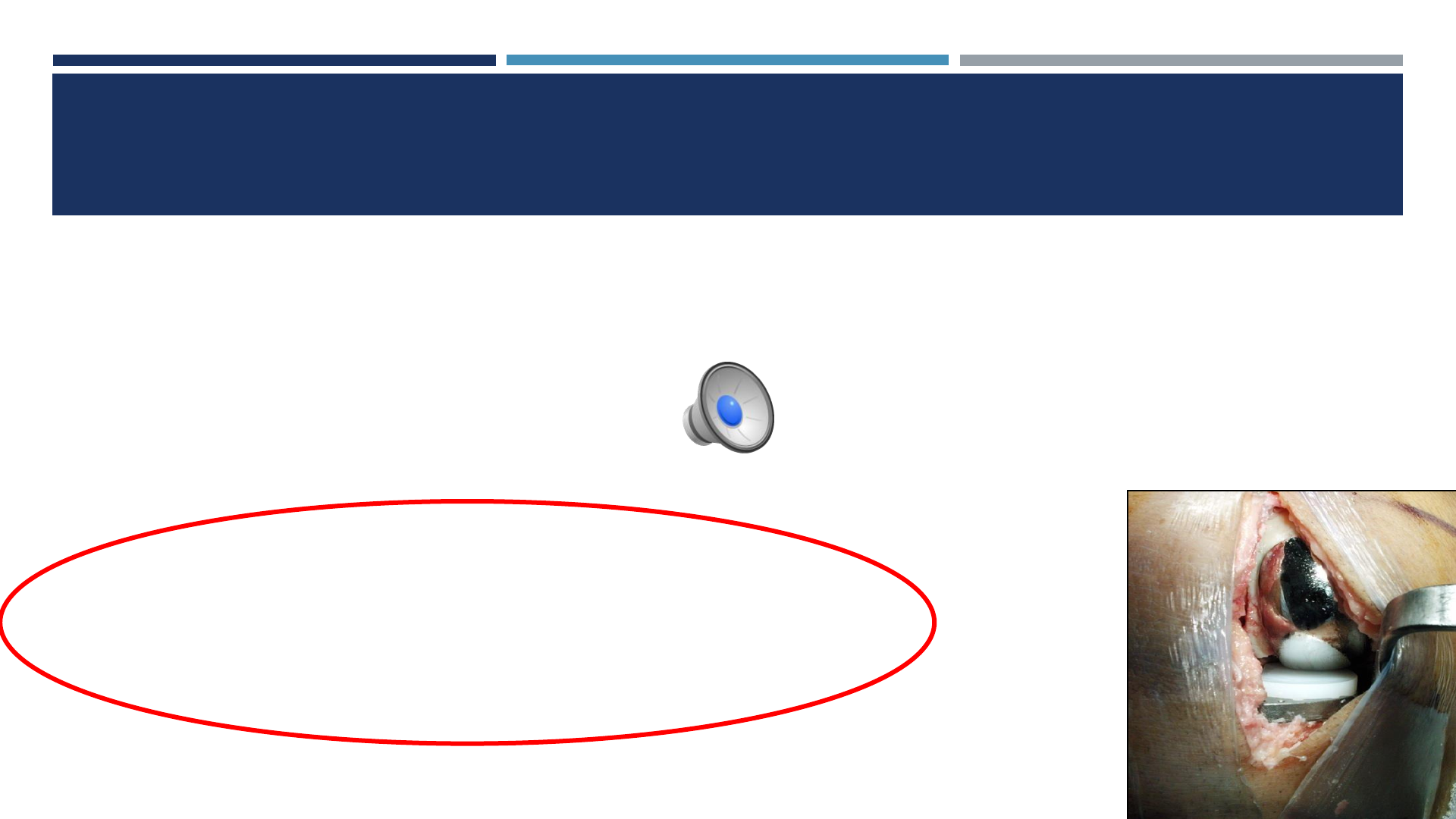
SAFETY: SEMI-AUTONOMOUS ROBOTIC SYSTEMS
Initial 1010 cases
Single surgeon (JHL)
No robot-related soft tissue complications
RADIATION FROM
PREOP CT SCANS
236 scans 2011-2013
1st generation image-based system
ED of radiation from LE CT scan:
4.8 +/- 3.0 mSv
25% had add’l CT scans (est cumulative ED of 6-103 mSv)
Note: 10 mSv increases risk of fatal cancer by 1 in 2000
Ponzio DY, Lonner JH. J Arthroplasty 2015
SURVIVORSHIP AND SATISFACTION
909 consecutive semi-autonomous robotic UKA’s
6 surgeons
FB metal-backed implant
Follow up: mean 30 mos [range, 22-52 mos]
Survivorship: 98.8% (96% if non-responders failed)
92% satisfied in patients without revision
COPYRIGHT © 2016 THE KNEE SOCIETY
Pearle AD et al. Knee 2017
ROBOTICS FOR TKA?
100 TKA’s
50 conventional
50 autonomous robotic-assisted (currently not approved for use in U.S.)
Mechanical axis outliers >3°:
Robotic: 0%
Conventional: 24%
No differences in ROM or function scores
Song EK, Bargar WL et al. Clin Orthop 2013
ROBOTICS FOR TKA?
Prospective RCT
60 TKA’s
29 conventional
31 autonomous robotic-assisted (currently not approved for use in U.S.)
Mechanical axis outliers >3°:
Robotic: 0%
Conventional: 19% (p=0.05)
Joint line outliers (>5mm):
Robotic: 3.2%
Conventional: 20% (p=0.05)
Liow MHL et al. J Arthrop 2014
ROBOTICS FOR TKA
Image-free semi-autonomous system (FDA approved)
108 initial cases
Radiographic alignment data:
Mechanical axis within 3°: 91%*
Tibial component alignment within 3°: 99%
Femoral axis alignment within 3°: 99%
COPYRIGHT © 2016 THE KNEE SOCIETY Koenig JA, Plaskos C. Influence of Pre-Operative Deformity on
Surgical Accuracy and Time in Robotic-Assisted TKA. Bone Joint
J 2013;95-B (S-28) 62
* Unpublished data suggests improved
mechanical alignment with new kinematic
balancing algorithm
CONCLUSION: ROBOTICS
Image-free vs CT based
Autonomous vs. semi-autonomous
Cost favorable?
ASC-feasible?
Expanding applications
UKA, PFA, BiKA
THA, TKA
Etc, etc.
CONCLUSION:
ROBOTICS
Semi-autonomous systems:
Accurate bone preparation, implant position, soft
tissue gap balance
Safe
Further study needed to determine:
Functional outcomes
Impact on late results/durability
CONCLUSION: ROBOT
Medicine is prime for a “disruption”
Growing influence of smart technologies in knee arthroplasty
Robotics fits into that paradigm
Exponential utilization and development
Stay tuned…
THANK YOU.
