5 2 16 Convatec Risk Mitigation
2016-05-02
: Pdf 5 2 16 Convatec Risk Mitigation 5_2_16_Convatec_Risk_Mitigation 5 2016 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 29
1
Reducing Surgical Site Infection
in Cardiac Surgery
Scott Schubach, MD
Chairman, Dept. of Thoracic & Cardiovascular Surgery
Winthrop University Hospital
Associate Professor, Surgery
Stony Brook School of Medicine
Presentation sponsored by ConvaTec
Introduction
Curriculum Vitae
Education:
–Medical degree from Baylor College of Medicine
–Trained in general surgery at Dartmouth Hitchcock
Medical Center
–Trained in cardiac surgery at University of Pittsburgh
Physician at Winthrop University Hospital since
1991
Chairman of Dept. of Thoracic & Cardiovascular
Surgery since 2001
Introduction
Winthrop University Hospital
Teaching hospital
Affiliate of SUNY Stony
Brook
Located in Mineola, NY
520 open heart procedures
done annually by group of 4
surgeons
2
Surgical Site Infections (SSI)
Defined by CDC
At or near operative site
Occurs in post-op period
Reportable if it occurs within 30
days post-op
Three major sources
Patient
Healthcare Team
OR environment
Most common pathogens for
sternal wound infections1
Staph aureus
Staph epidermis
1Singh, K et al, Overview and Management of Sternal Wound Infection, Seminars in Plastic Surgery, Volume 25, Number 1 2011
SSIs: Scope of the Problem
Surgical wound infections
MOST common infection
in surgical patients
Common nosocomial
infection
Associated with substantial
morbidity and mortality1
–60% more likely ICU admit
–2x increase in mortality
during perioperative period
post-op LOS1
treatment costs1
1Banbury, MK, Experience in prevention of sternal wound infections in nasal carriers of Staphylococcus aureus, Surgery, 2003
Nov
SSIs: Scope of the Problem
Cardiac Surgery
Annual US procedural
volume:
–>600,000 cardiac procedures1
–395,000 CABG procedures2
3.5% infection rate post-
CABG procedures3
Cost to treat mediastinitis
estimated to be $40,000 -
$50,0003
1Elgharably H, et al. First Evidence of Sternal Wound Biofilm Following Cardiac Surgery, PLoS One, 2013 Aug 1;8(8),
2http://www.cdc.gov/nchs/fastats/insurg.htm, 3http://www.infectioncontroltoday.com/articles/2008/03/cabg-infections-are-
costly-and-dangerous-staffs-m.aspx
3
Sternal Wound Infections (SWI)
Risk Factors
Obesity
Renal insufficiency
Diabetes
COPD
Peripheral Vascular Disease
Existing pre-op infection
Steroid use
Malnutrition
Sternal Wound Infections
Incidence of Sternal Wound Infection (SWI): 1-8%1
SWI mortality rates reaching 40%1
Treatment requires:1
–Prolonged antibiotic courses
–Repeated surgical interventions
–Longer hospital stay
Can occur in any procedure requiring median
sternotomy
1Elgharably H, et al. First Evidence of Sternal Wound Biofilm Following Cardiac Surgery, PLoS One, 2013 Aug 1;8(8)
Deep Sternal Wound Infections
Increased hospital LOS > 2 full weeks compared
to any other post-op complication1
Associated with other complications such as:1
–Prolonged ventilation
–Bleeding
–Renal failure
–Atrial fibrillation
–Increased rates of stroke
–Need for inotropic or mechanical cardiac
support
1Atkins, Z, Wolfe, W, Sternal Wound Complications following Cardiac Surgery, www.intechopen.com
4
Reimbursement Challenges
No CMS reimbursement for treatment of:
SSI, mediastinitis, following Coronary
Artery Bypass Graft (CABG)
SSI following Cardiac Implantable
Electronic Device (CIED)
http://www.cms.gov/HospitalAcqCond
State Reporting of SSI’s
Government Oversight and Physician Data
Tracking
Twenty one (21)states require hospitals to report
surgical site infection, 14 states so far have posted
the information publicly
Report and data available to public- CA, OR, WA,
CO, IL, MO, PA, OH, SC, NJ, NY, MA, VT And
NH
http://www.ama-assn.org/amednews/2012/04/02/prsb0402.htm
Winthrop Story
Task force formed to reduce
incidence of SWI
Increased Sternal Wound Infection rate
Infection rate is state and patient reportable
Hospitals do not get paid for Sternal Wound
Infection readmissions
5
Evaluated Current Practices
Operating room team’s sterile technique
Hand washing technique
Room ventilation
Instrument sterilization
Operating room traffic
Baseline SWI Prevention
Strategy
Adherence to core pre-operative antibiotic
protocols
–Administer antibiotics within 1 hour of
incision (2 hours for Vancomycin)
Approach to SWI Prevention
Address all potential sources of infection:
Pre-operative Preparation
Operating Room Environment
Operating Room Team
Post-operative Care of Patient and Wounds
Patient Co-morbidities
6
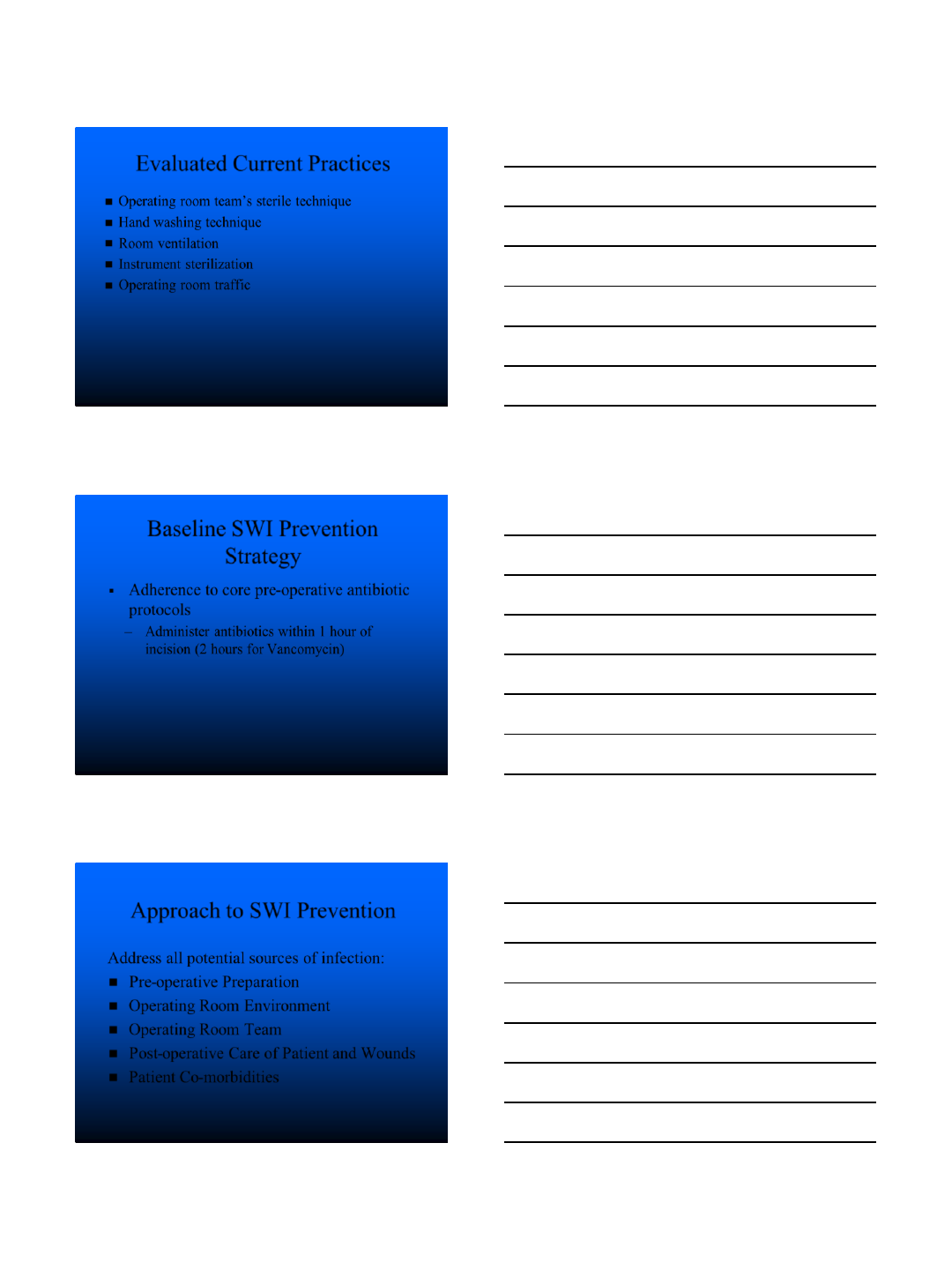
Operation Room Environment
Limit traffic in and out of OR
Operating Room Team
1. Stopped using Avagard gel and returned to
practice of scrubbing hands
2. Change gloves more frequently
3. Educated entire team on sterile field
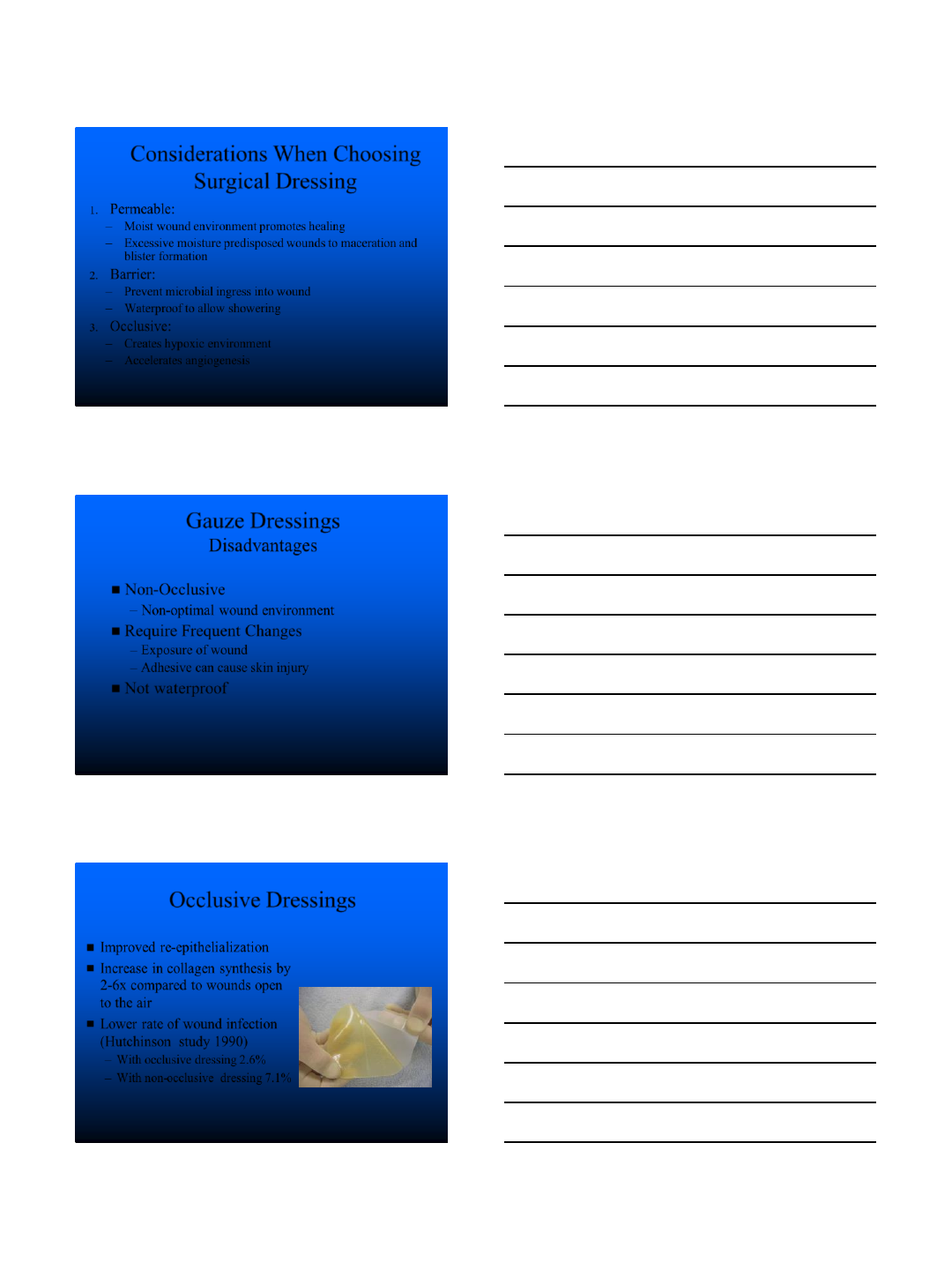
Patient
1. Use chlorhexidine to cleanse the
skin
2. Apply occlusive dressing,
AQUACEL®Ag Surgical, in
operating room
3. Dressing left on for 5 days,
removed prior to discharge
4. Emphasize at discharge patients
can wash over incision with soap
and water
7
Considerations When Choosing
Surgical Dressing
1. Permeable:
–Moist wound environment promotes healing
–Excessive moisture predisposed wounds to maceration and
blister formation
2. Barrier:
–Prevent microbial ingress into wound
–Waterproof to allow showering
3. Occlusive:
–Creates hypoxic environment
–Accelerates angiogenesis
National Institute for Health and Clinical Excellence.
Surgical Site Infection Guideline.
Gauze Dressings
Disadvantages
Non-Occlusive
–Non-optimal wound environment
Require Frequent Changes
–Exposure of wound
–Adhesive can cause skin injury
Not waterproof
Occlusive Dressings
Improved re-epithelialization
Increase in collagen synthesis by
2-6x compared to wounds open
to the air
Lower rate of wound infection
(Hutchinson study 1990)
–With occlusive dressing 2.6%
–With non-occlusive dressing 7.1%
Patel C, Surgical Wound Infections. Current Treatment in Infectious Diseases. 2000;2:147-153. Michie D. Influence of
Occlusive and Impregnated Dressings on Incisional Healing: Ann Plastic Surg. 1994. Hulten L. Dressings for Surgical
Wounds. Am J Surg. 1994. .Xi et al Wound Repair, 2000. Hutchinson, JJ, McGuckin, M, Occlusive dressings: A
microbiologic and clinical review, American Journal of Infection Control, Aug 1990
8
AQUACEL®Ag Surgical Dressing
Advantages
Barrier to pathogen transmission1
Microbicidal effects of silver ion2
Dressing may be left in place up to
7 days
–Less potential hospital exposure of
wound
–Less potential for pain associated
with dressing changes
Patient satisfaction
–Immediate showering
1 Nelson Laboratories Report, Viral Penetration ASTM Method F1671, Procedure Number :ST0062 Rev07, Protocol Detail Sheet No.
200902139 Rev 1, Laboratory no. 483744, 7th August 2009
2Jones SA, Bowler PG, Walker M, Parsons D. Controlling wound bioburden with a novel silver-containing Hydrofiber dressing. Wound
Repair Regen. 2004;12(3):288-294.
Basic component is cellulose
Carboxymethylation* process alters the absorption capacity
Hydrofiber®technology allows for fluid to be absorbed directly into
the fibers
A bond is formed with the absorbed fluid to hold it within the fiber
1Waring MJ, Parsons D. Physico-chemical characterisation of carboxymethylated spun cellulose fibres. Biomaterials. 2001;22:903-912.
*Carboxymethylation: addition of sodium carboxymethyl
Cellulose fragment
Advanced Dressings
Hydrofiber®Technology
AQUACEL® Ag
Broad-spectrum Antimicrobial Activity
Jones SA, Bowler PG, Walker M, Parsons D. Controlling wound bioburden with a novel silver-containing Hydrofiber®dressing.
Would Repair Regen. 2004;12:288-294.
Aerobic Bacteria
Staphylococcus aureus (NCTC 8532)
Staphylococcus aureus (clinical isolate)
Pseudomonas aeruginosa (clinical isolate, x2 strains)
Enterobacter cloacae (clinical isolate)
Streptococcus pyogenes (clinical isolate)
Klebsiella pnuemoniae (clinical isolate, x3 strains)
Enterococcus faecalis (clinical isolate)
Escherichia coli (NCIMB 8545)
Escherichia coli (NCIMB 10544)
Acinetobacter baumannii (NCIMB 9214
Anerobic Bacteria
Bacteroides fragilis (clinical isolate)
Peptostreptococcus anaerobius (clinical isolate)
Clostridium ramosum (clinical isolate)
Clostridium clostridioforme (clinical isolate)
Clostridium cadaveris (clinical isolate)
Clostridium perfringens (clinical isolate)
Tissierella praeacute (clinical isolate)
Antibiotic-resistant Bacteria
MRSA (NCTC 10442)
MRSA (NCTC 12232)
MRSA (clinical isolate, x8 strains)
VRE (NCTC 12201)
VRE (clinical isolate, x2 strains)
Serratia marcescens (clinical isolate)
Pseudomonas aeruginosa (NTC 8506)
Yeasts
Candida albicans (NCPF 3179)
Candida albicans (NCPF 3265)

9
Hydrofiber®Ag Dressing
Bacterial Sequestration & Bactericidal Activity
Newman GR, Walker M, Hobot J, Bowler P. Biomaterials. 2006;27(7):1129-1139.
T = 20 mins
T = 60 mins
T = 2-3 mins
T = 40 mins
Green = Alive
Red = Dead
T = Time in minutes
Confocal microscopy of Pseudomonas
aeruginosa on hydrated Hydrofiber®Ag
dressing fiber
Dressing Change
Technique
Stretching of hydrocolloid portion (like stretching
“taffy”) allows gentle adhesive release from skin.
Skin traction is avoided
AQUACEL®Ag Surgical Dressing
CLINICAL RESULTS
10
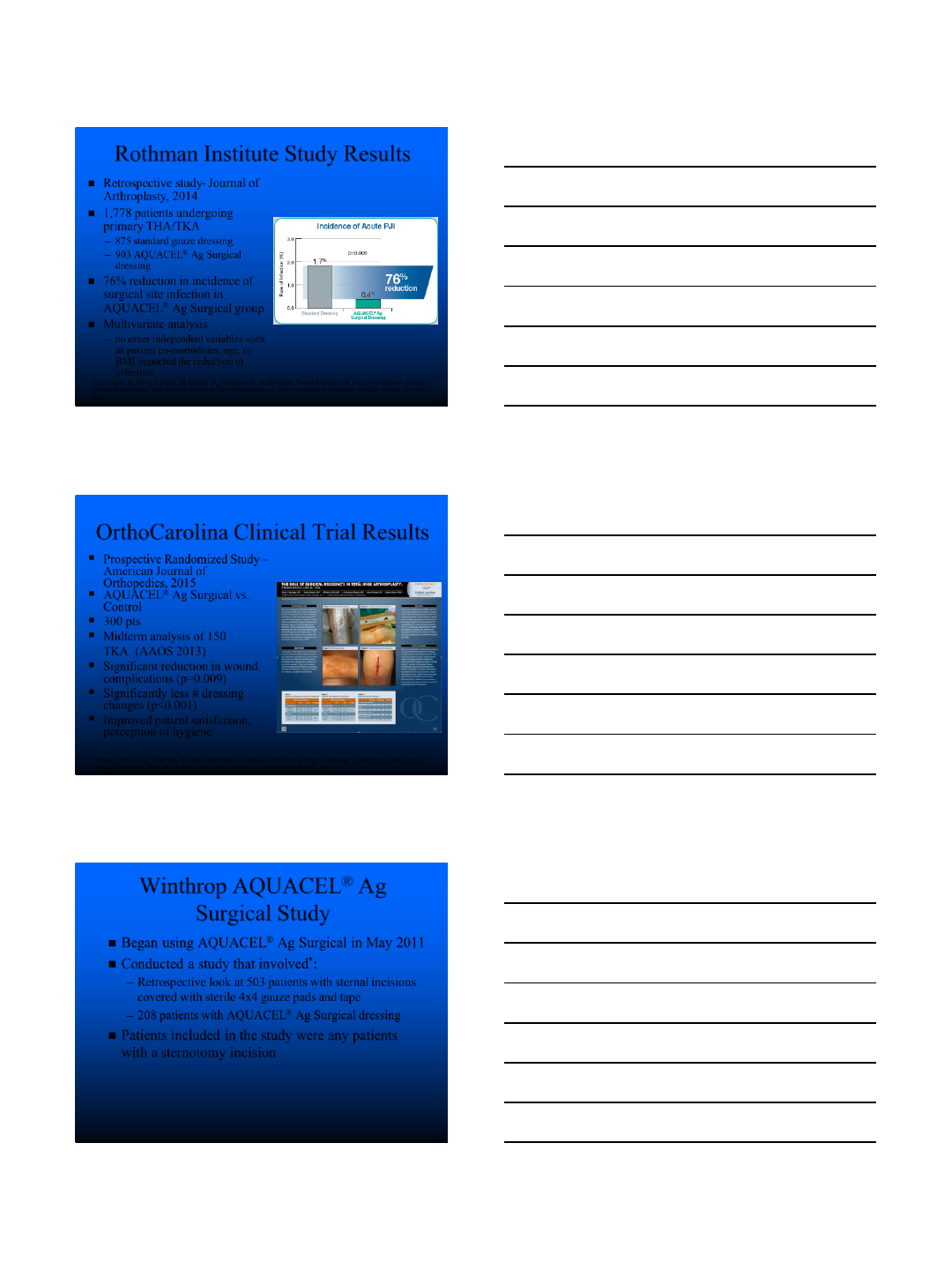
Retrospective study- Journal of
Arthroplasty, 2014
1,778 patients undergoing
primary THA/TKA
–875 standard gauze dressing
–903 AQUACEL®Ag Surgical
dressing
76% reduction in incidence of
surgical site infection in
AQUACEL®Ag Surgical group
Multivariate analysis
–no other independent variables such
as patient co-morbidities, age, or
BMI impacted the reduction in
infection
Rothman Institute Study Results
Cai J, Karam JA, Parvizi J, Smith EB, Sharkey PF. The Aquacel® Ag Hydrofiber Wound Dressing with Ionic Silver Reduces the Rate
of Acute Periprosthetic Joint Infection Following Total Joint Arthroplasty., Poster presented at 22nd annual AAHKS meeting, Nov 2-4,
2012.
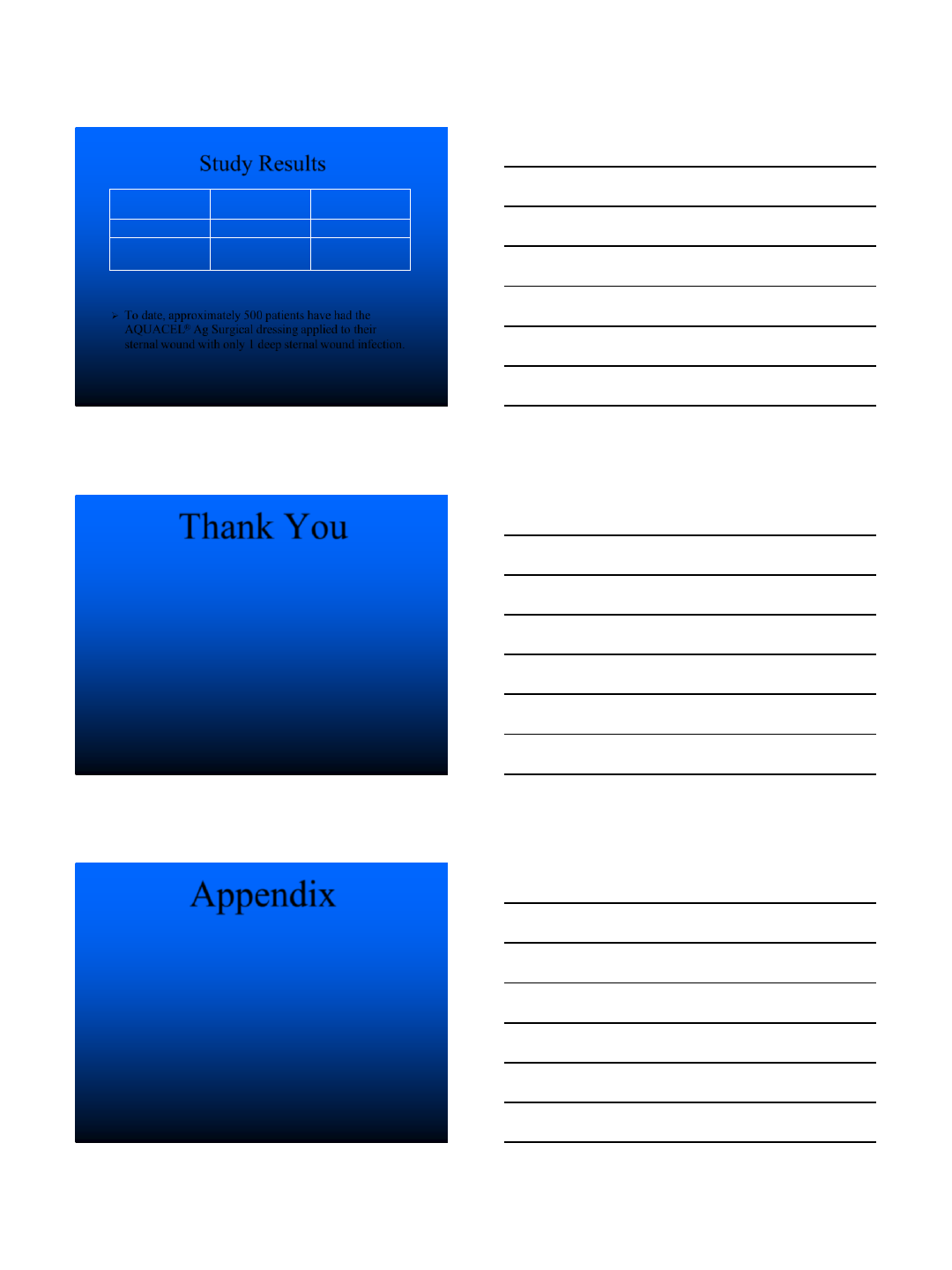
OrthoCarolina Clinical Trial Results
Prospective Randomized Study –
American Journal of
Orthopedics, 2015
AQUACEL®Ag Surgical vs.
Control
300 pts
Midterm analysis of 150
TKA (AAOS 2013)
Significant reduction in wound
complications (p=0.009)
Significantly less # dressing
changes (p<0.001)
Improved patient satisfaction,
perception of hygiene
Springer, BD, Beaver, W, Griffin, W, Mason, JB, Dennos, A, Odum, S. The Role of Surgical Dressings in Total Knee Arthroplasty: A
Randomized Clinical Trial, Poster presented at 2013 AAOS annual meeting; March 19-23, 2013.
Winthrop AQUACEL®Ag
Surgical Study
Began using AQUACEL®Ag Surgical in May 2011
Conducted a study that involved*:
–Retrospective look at 503 patients with sternal incisions
covered with sterile 4x4 gauze pads and tape
–208 patients with AQUACEL®Ag Surgical dressing
Patients included in the study were any patients
with a sternotomy incision
*Data not yet submitted for publication
11
Study Results
To date, approximately 500 patients have had the
AQUACEL®Ag Surgical dressing applied to their
sternal wound with only 1 deep sternal wound infection.
Dressing
Type
# of Deep
SWI
%
of Deep SWI
Gauze and Tape
17
3.4%
AQUACEL
® Ag
Surgical
0
0%
Thank You
Appendix
12
AQUACEL®Ag SURGICAL
Dressing
Polyurethane film provides
waterproof viral and bacterial
barrier *3
Patented Hydrofiber®Technology
absorbs and locks in fluid,
including harmful bacteria.*2
Unique construction enhances
extensibility and flexibility
Skin-friendly hydrocolloid
technology flexes with the
skin during body movement1,3
*As demonstrated in vitro
1Nelson Laboratories Report, Viral Penetration ASTM Method F1671, Procedure Number :ST0062 Rev07, Protocol Detail Sheet No.
200902139, Rev 1, Laboratory no. 483744, 7th August 2009, 2Walker M, Hobot JA, Newman GR, Bowler PG. Scanning electron
microscopic examination of bacterial immobilisation in a carboxymethylcellulose (Aquacel) and alginate dressings. Biomaterials. 2003;
24:883-890.8. 3WHRI 3264 Laboratory Test Comparison of AQUACEL® Surgical Dressing ‘New Design’and the
Jubilee Method of Dressing Surgical Wounds . 7th Oct 2009
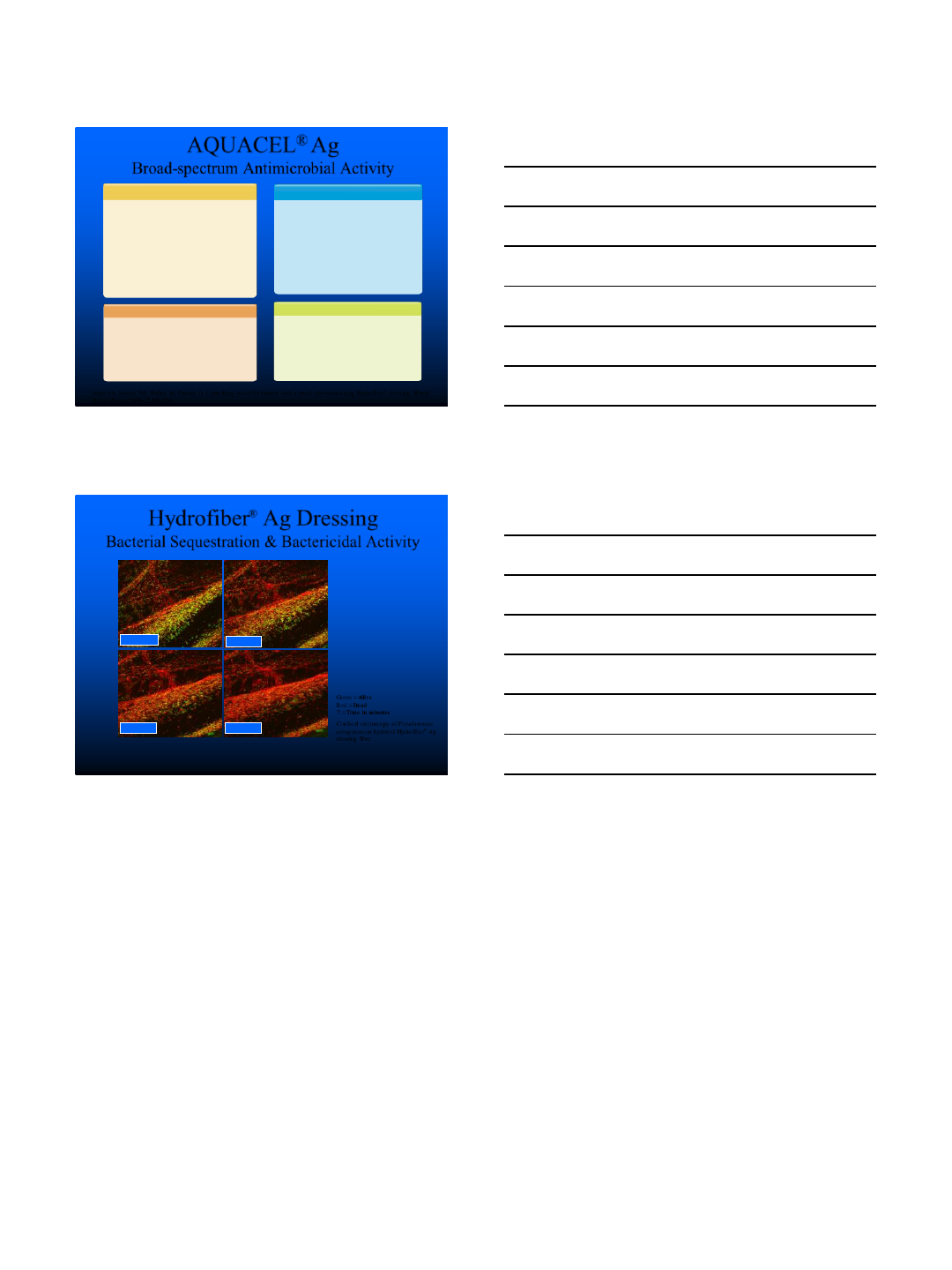
Locks in fluid*1
Sequesters bacteria2,3
Traps harmful enzymes*4,5
Hydrofiber®dressing Alginate dressing Gauze dressing
1Waring MJ, Parsons D. Biomaterials. 2001;22:903-912;
2Walker M, Hobot JA, Newman GR, Bowler PG. Biomaterials. 2003;24(5):883-890;
3Newman GR, Walker M, Hobot J, Bowler P. Biomaterials. 2006;27(7):1129-1139;
4Hoekstra MJ, Hermans MHE, Richters CD, Dutrieux RP. J Wound Care. 2002;11(2):113-117;
5Walker M, Bowler PG, Cochrane CA. Ostomy Wound Manage. 2007;53(9):18-25.
Dressing With Hydrofiber®Technology *
*as demonstrated in vitro
Sequestration test: a simple experiment using fluids of different colors to demonstrate the ability of dressings to lock in fluid
Hydrofiber®Technology w/ Ionic Silver
AQUACEL®Ag Dressing
Reduction in bioburden to
reduce risk of infection is key
to optimal wound healing 1
Ionic silver (Ag) has broad
spectrum antimicrobial activity2
Hydrofiber®Ag dressing more
effective at killing bacteria in
vitro on simulated wounds with
uneven contours than a
nanocrystalline silver-
containing dressing 4
1Bowler PG, Cochrane CA. Ostomy Wound Manage. 2003:49(8)(suppl):S2-S5;
2Maillard J, Denyer SP. London: MEP Ltd, 2006:7-10.;
3Bowler PG, Jones SA, Walker M, Parsons D. J Burn Care Rehabil. 2004;25:192-196;
4Jones S, Bowler PG, Walker M. Wounds. 2005;17(9):263-270.
13
AQUACEL® Ag
Broad-spectrum Antimicrobial Activity
Jones SA, Bowler PG, Walker M, Parsons D. Controlling wound bioburden with a novel silver-containing Hydrofiber®dressing. Would
Repair Regen. 2004;12:288-294.
Aerobic Bacteria
Staphylococcus aureus (NCTC 8532)
Staphylococcus aureus (clinical isolate)
Pseudomonas aeruginosa (clinical isolate, x2 strains)
Enterobacter cloacae (clinical isolate)
Streptococcus pyogenes (clinical isolate)
Klebsiella pnuemoniae (clinical isolate, x3 strains)
Enterococcus faecalis (clinical isolate)
Escherichia coli (NCIMB 8545)
Escherichia coli (NCIMB 10544)
Acinetobacter baumannii (NCIMB 9214
Anerobic Bacteria
Bacteroides fragilis (clinical isolate)
Peptostreptococcus anaerobius (clinical isolate)
Clostridium ramosum (clinical isolate)
Clostridium clostridioforme (clinical isolate)
Clostridium cadaveris (clinical isolate)
Clostridium perfringens (clinical isolate)
Tissierella praeacute (clinical isolate)
Antibiotic-resistant Bacteria
MRSA (NCTC 10442)
MRSA (NCTC 12232)
MRSA (clinical isolate, x8 strains)
VRE (NCTC 12201)
VRE (clinical isolate, x2 strains)
Serratia marcescens (clinical isolate)
Pseudomonas aeruginosa (NTC 8506)
Yeasts
Candida albicans (NCPF 3179)
Candida albicans (NCPF 3265)
Hydrofiber®Ag Dressing
Bacterial Sequestration & Bactericidal Activity
Newman GR, Walker M, Hobot J, Bowler P. Biomaterials. 2006;27(7):1129-1139.
T = 20 mins
T = 60 mins
T = 2-3 mins
T = 40 mins
Green = Alive
Red = Dead
T = Time in minutes
Confocal microscopy of Pseudomonas
aeruginosa on hydrated Hydrofiber®Ag
dressing fiber
5/2/2016
1
Incidence & Burden of Infections
Following Cardiac Surgery
Gorav Ailawadi, MD
Chief, Adult Cardiac Surgery
University of Virginia
May 2, 2016
Disclosures
•Convatec
•Abbott Vascular
•St. Jude
•Edwards
•Mitralign
•Atricure
Outline
•Overview of Major Infections Following
Cardiac Surgery
–Incidence
–Cost
•DSWI
•Pneumonia
5/2/2016
2
Hospital Acquired Infections
•1.7 million individuals acquire HAI
•Leads to 100,000 deaths annually
•Results in additional $6.5 billion additional
health care expenditures
Perencevich EN, Pittet D. JAMA 2009; 301: 1285-7.
CTSN
•Supported by U01 HL088942
Cardiothoracic Surgical Trials Network
(CTSN)
•Funding Agencies:
•National Heart, Lung, and Blood Institute
•National Institute of Neurological Disorders and
Stroke
•Canadian Institutes for Health Research
5/2/2016
3
Investigators
•Data Coordinating Center: InCHOIR
•Montefiore –Einstein
•Emory University
•Duke University
•Hôpital Laval
•University of Virginia Health System
•Montreal Heart Institute
•University of Pennsylvania
•Columbia University Medical Center
•Cleveland Clinic Foundation
•University of Maryland
•Brigham and Women's Hospital
•Sacré-Cœur de Montréal
•Ohio State University Medical
Center
•East Carolina Heart Institute
•Wellstar / Kennestone
•Baylor Research Institute
•University of Southern California
•St. Michael’s Hospital
•Toronto General Hospital
•Mission Hospital
•NIH Heart Center at Suburban
Hospital
•Inova Heart & Vascular Institute
•University of Alberta Hospital
•Centre Hospitalier de l'Université de
Montréal
•Sunnybrook Health Sciences Centre
•Aarhus University
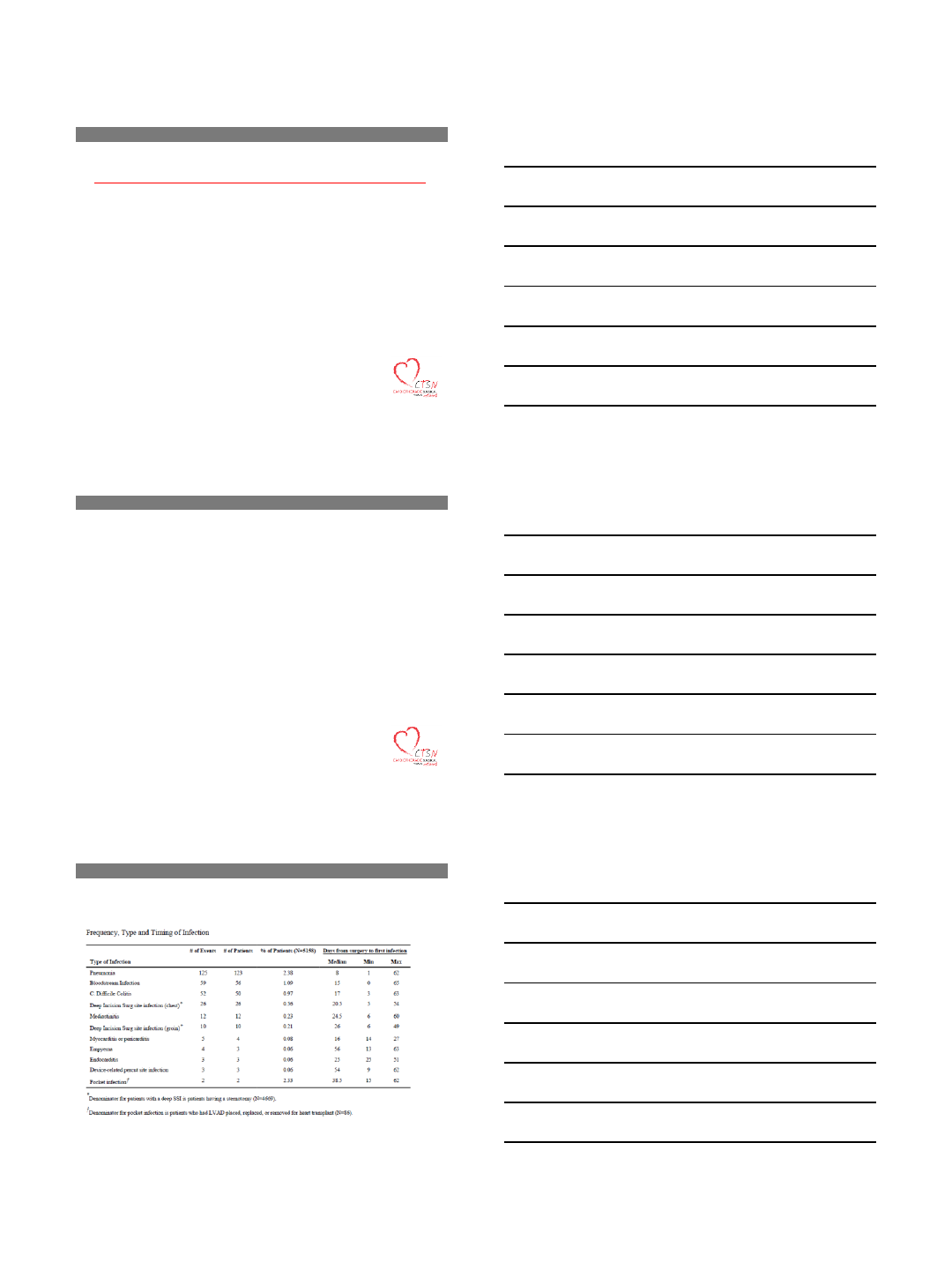
Methods
•5,158 patients prospectively enrolled at 10 core
CTSN sites
•Infections identified and adjudicated up to 65
days after index surgery
•4.6% (237 patients) experienced major infection
•SSI (sternum or secondary site), mediastinitis,
infectious pericarditis, endocarditis, cardiac device
infection, pneumonia, C Diff colitis
Frequency, Type and Timing of Infection
5/2/2016
4
Organism Type
Organism Type
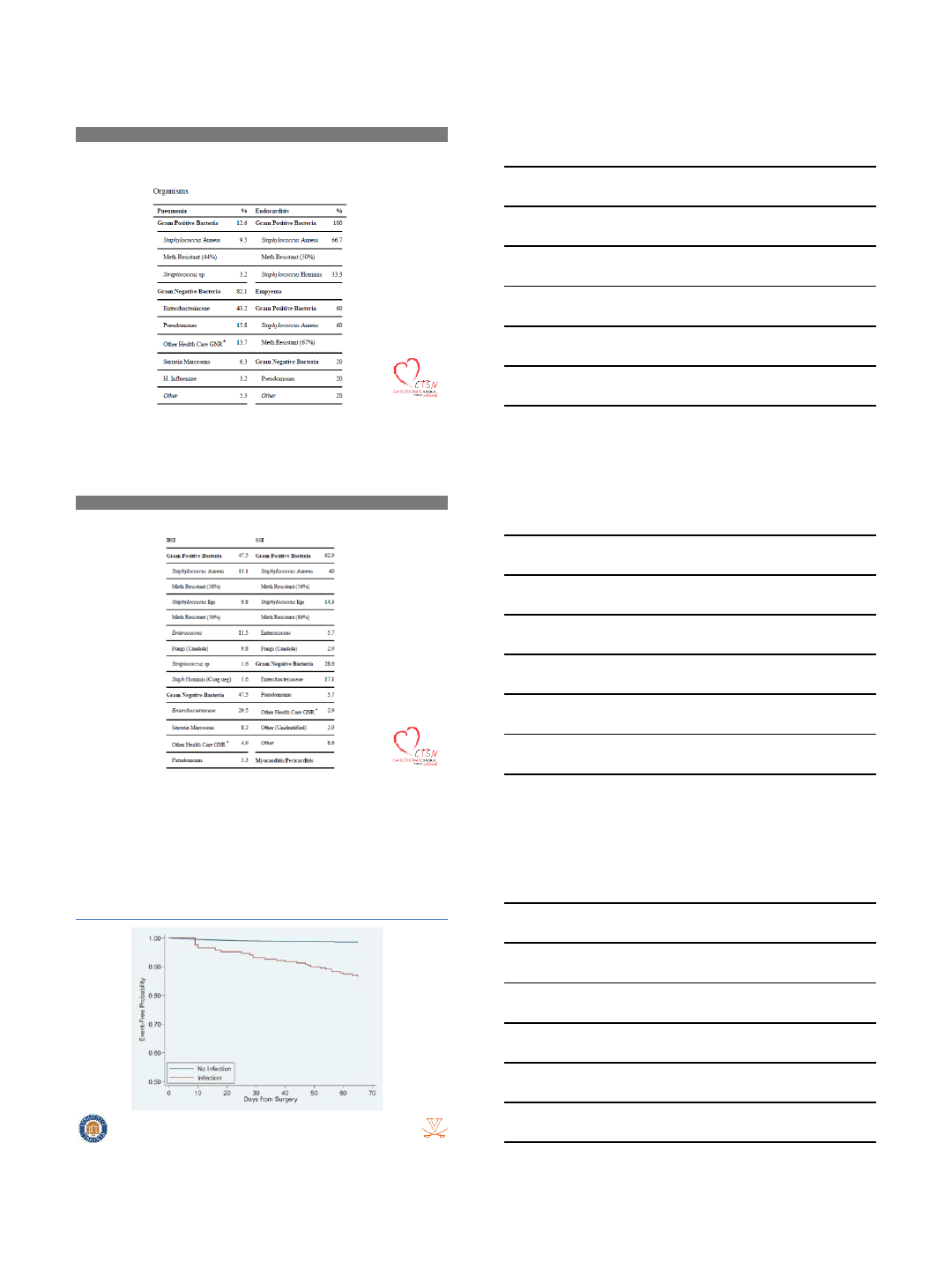
Survival Impact of Major Infection
Gelijns AC, et al. J Am Coll Cardiol. 64(4):372-81, 2014.
5/2/2016
5
•Site of infection N, % Incidence
•Bacteremia 9 (30%) 5.23%
•Sternotomy site infection 8 (26.7%) 4.65%
•Infection of vascular catheters 5 (16.7%) 2.90%
•Pneumonia 4 (13.3%)2.32%
•Mediastinitis 1 (3.3%) 0.58%
•Urinary tract infection 1 (3.3%) 0.58%
•Total 30 (100%) 17.42%
Sites of Infection
Lola, et. Al Journal of Cardiothoracic Surgery2011 6:151
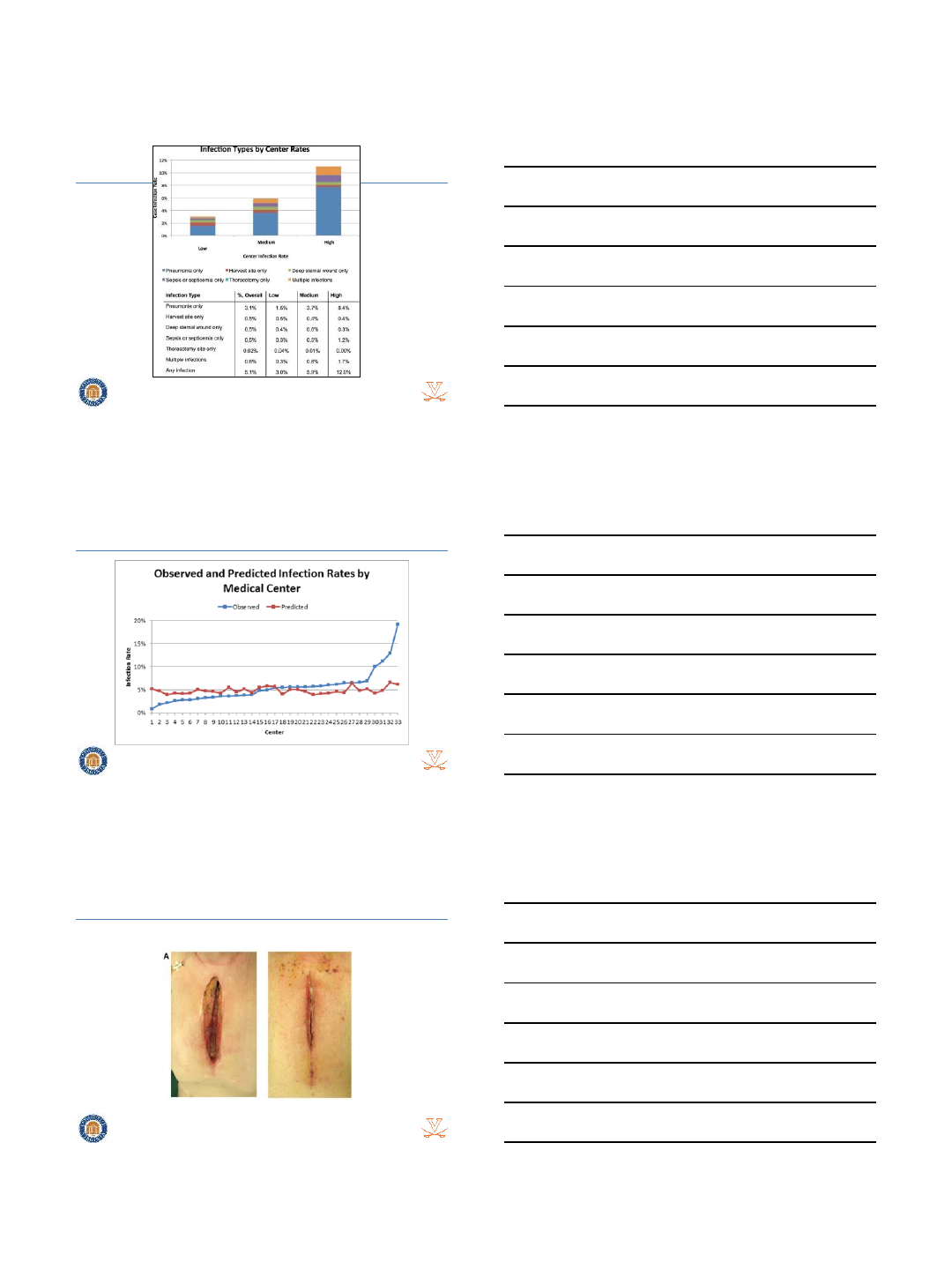
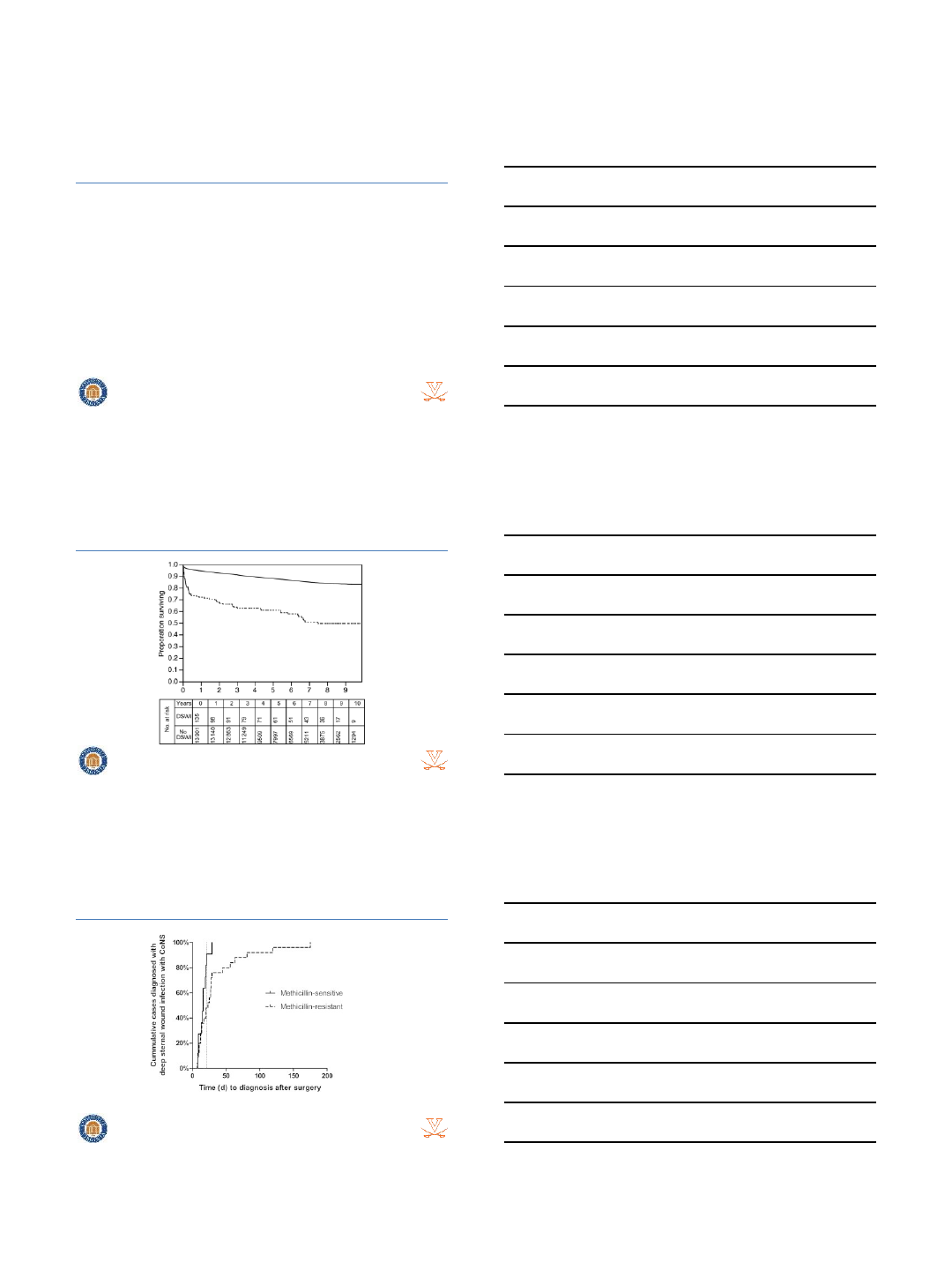
Cost of Infection
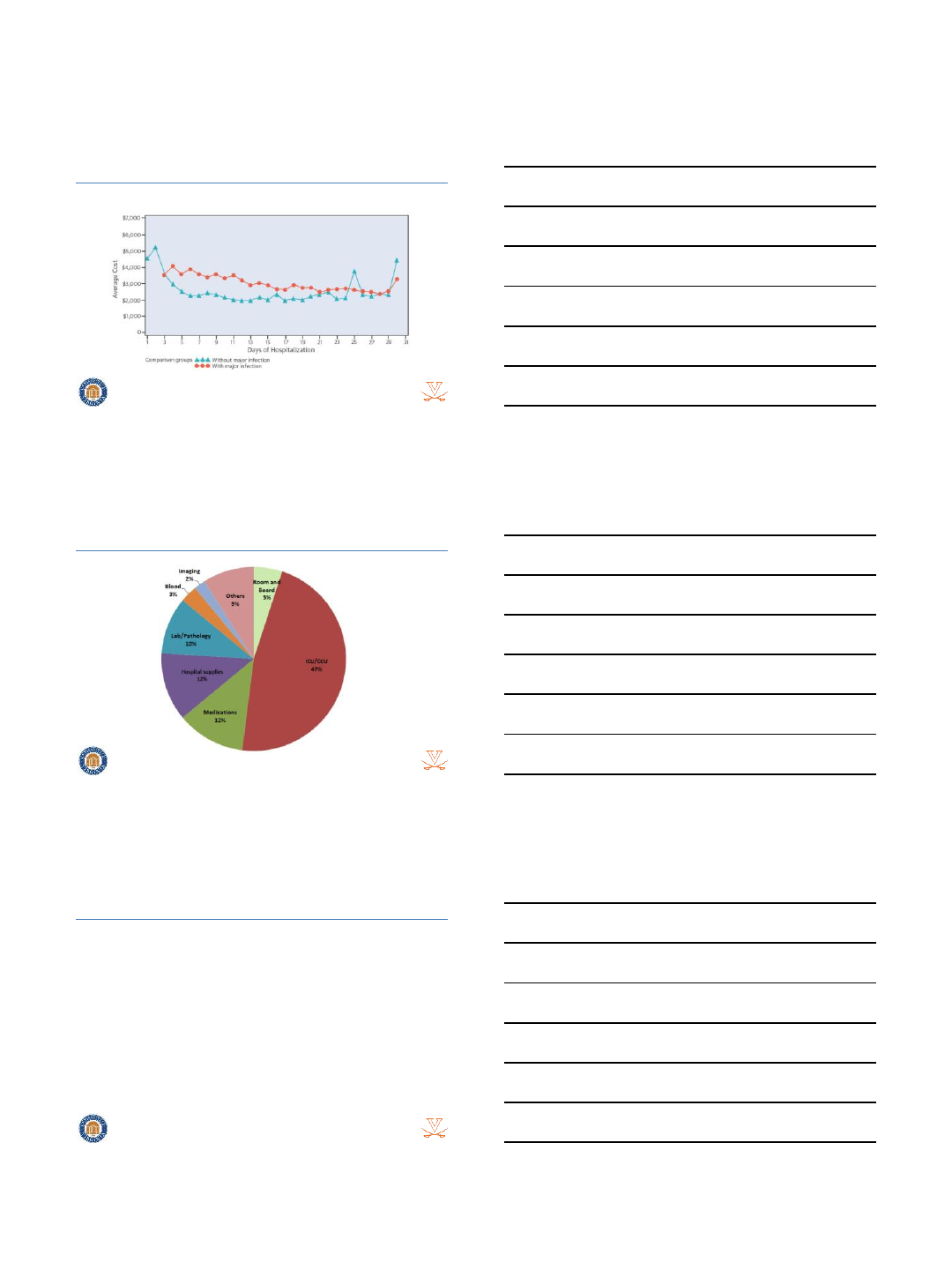
5/2/2016
6
Average Cost Per Day With Infection
Incremental Costs By Type
Center Variability in Infection
5/2/2016
7
Circ Cardiovasc Qual Outcomes. 2014 Jul; 7(4): 567–573
Survival Impact of Infection
Circ Cardiovasc Qual Outcomes. 2014 Jul; 7(4): 567–573
DSWI
5/2/2016
8
DSWI Incidence and Impact
•Incidence ranges: 0.5% -6.8%
•In hospital Mortality: 7-35%
•1 year survivors of DSWI: 15% survival
disadvantage
•10 yr survival after CABG:
–Without DSWI: 70%
–With DSWI: 39%!
Cotogni P, et al. World J Crit Care Med. 4(4), 2015.
Survival Impact of DSWI
Bilal H, et al. Interact Cardiovasc Thorac Surg. 2013 17(3):479-484.
Timing of DSWI
5/2/2016
9
Pneumonia
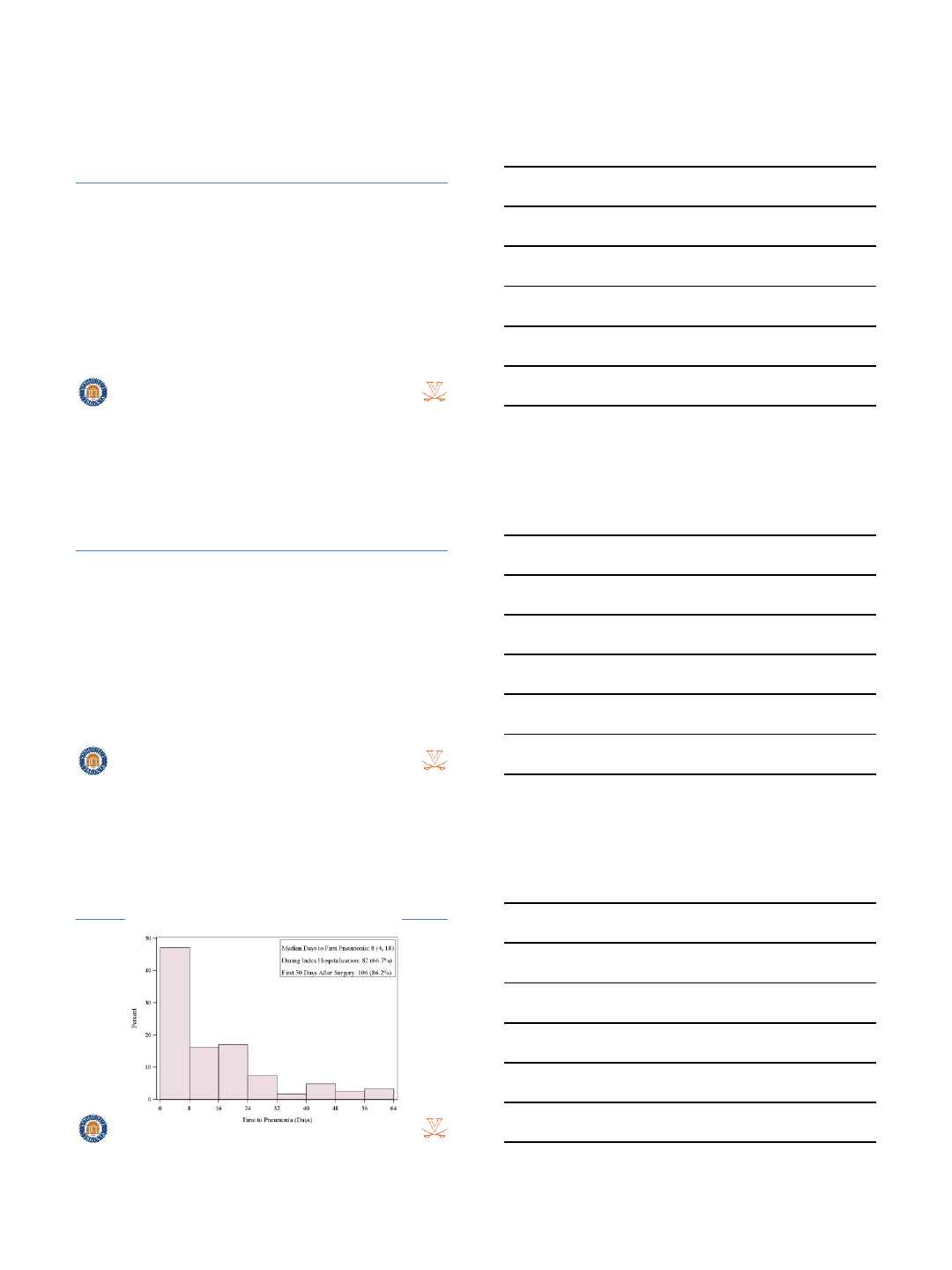
CTSN: Pneumonia
•2.4% (123 of 5,158 patients)
•40% of all major infections
•67% diagnosed during index hospitalization
•86% diagnosed within 30 days
–14% developed pneumonia after 1st month
Time to Pneumonia
5/2/2016
10
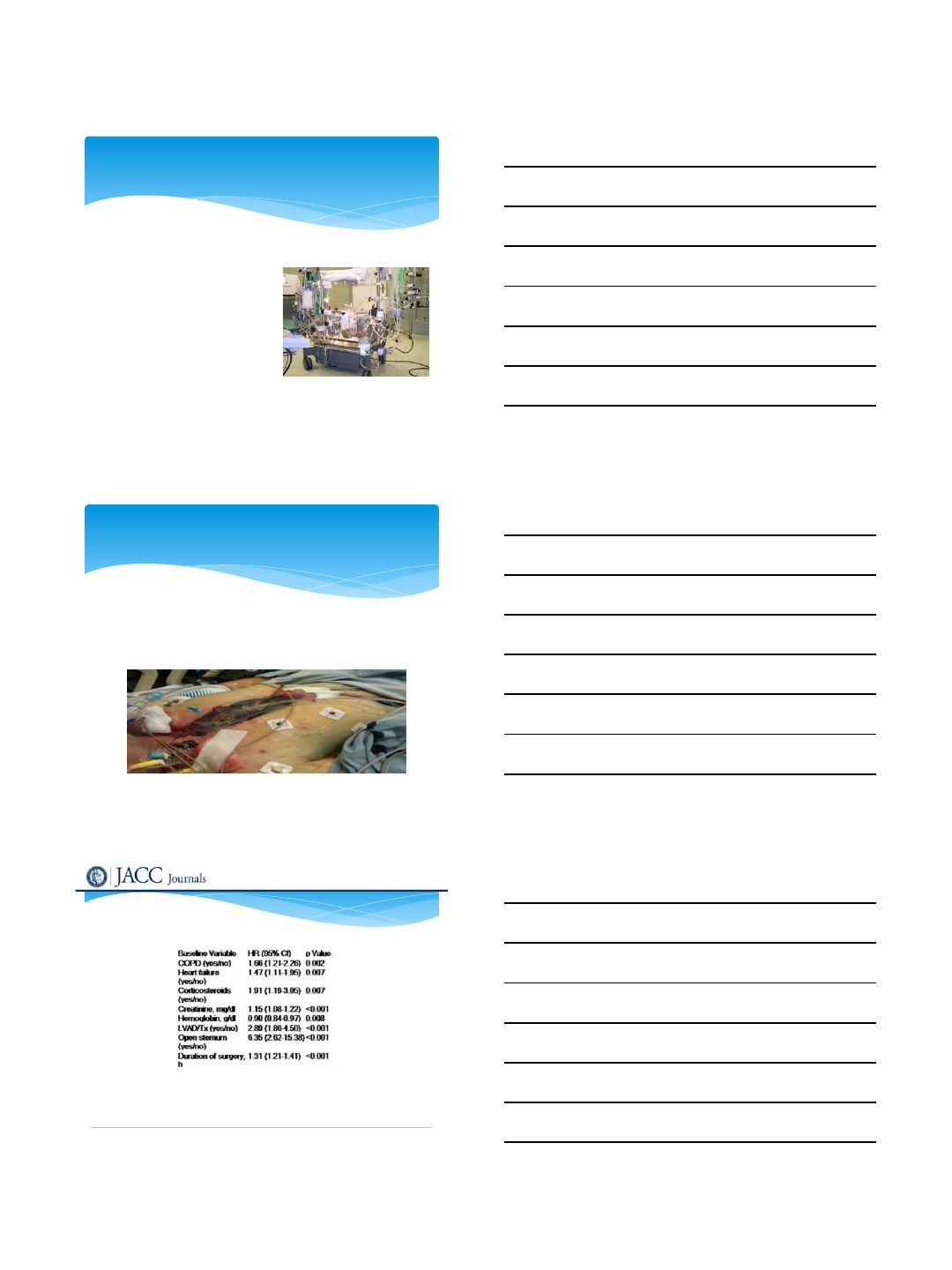
Impact of Pneumonia on Mortality
Variable
HR (95% CI) P Value
Pneumonia
8.89 (5.02, 15.75) <0.001
Age (year)
1.03 (1.01, 1.05) <0.001
Male
0.60 (0.39, 0.91) 0.02
Diabetes
*(yes/no) 1.57 (1.03, 2.41) 0.04
Heart Failure (yes/no)
1.86 (1.24, 2.80) 0.003
Creatinine, mg/dL
1.17 (1.06, 1.30) 0.002
Hemoglobin, g/dL
0.85 (0.75, 0.95) 0.005
Conclusions
•Increasing patient comorbidities
•Surgical infections still prevalent
•Significant financial burden of infections
•Significant mortality effect from infections
Conclusions
•Increasing patient comorbidities
•Surgical infections still prevalent
•Significant financial burden of infections
•Significant mortality effect from infections
•No consensus on Best Management!
5/2/2016
1
Risk Factors of Infections After
Cardiac Surgery
Justin Sambol MD FACS
Chief, Division of Cardiothoracic Surgery
Rutgers-New Jersey Medical School
Consultant for ConVatec
No other disclosures
Disclosures
Infection following cardiac surgery associated with
significant cost
Increases hospital LOS
Increases Morbidity
Increases need for further surgery
Increases mortality
Infections Following Cardiac Surgery
5/2/2016
2
Pneumonia
Surgical Site Infections
Superficial Sternal Wound Infections
Deep Sternal Wound Infections
Saphenectomy Site
Septicemia
Types of Infections After Cardiac
Surgery
Preoperative Factors
Intraoperative Events
Postoperative Course
Why do Infections Occur?
Age >70
Obesity with BMI >30 kg/m2
Immunosuppression
COPD
Diabetes (NIDDM as well as IDDM)
Renal Insufficiency
Critical preoperative status (infections,
sepsis, cardiogenic shock)
Preoperative Risk Factors
5/2/2016
3
Prolonged operative time
Prolonged bypass time
Use of Bilateral Internal
Mammary Artery
Intraoperative use of blood
products
Intraoperative Risk Factors
Prolonged mechanical ventilation
Vasopressor support
Need for transfusions
Reoperation for bleeding (data is variable)
Postoperative Risk Factors
Date of download: 4/12/2016 Copyright © The American College of Cardiology. All rights reserved.
From: Management Practices and Major Infections After Cardiac Surgery
J Am Coll Cardiol. 2014;64(4):372-381. doi:10.1016/j.jacc.2014.04.052
Baseline and Procedure Characteristics Associated With Infection
Table Title:
5/2/2016
4
Optimization of blood glucose (HbA1C < 8.0%)
Reduce Obesity (BMI <30 kg/m2)
Cessation of Cigarette Smoking
Optimization of COPD
Avoid operative time > 7 hours
CPB time <180 min
Optimize postoperative cardiac output
Minimize bleeding and postoperative transfusion
Mitigation of Risk Factors
Sajja LR, International Journal of Surgery 16 (2015) 171-178
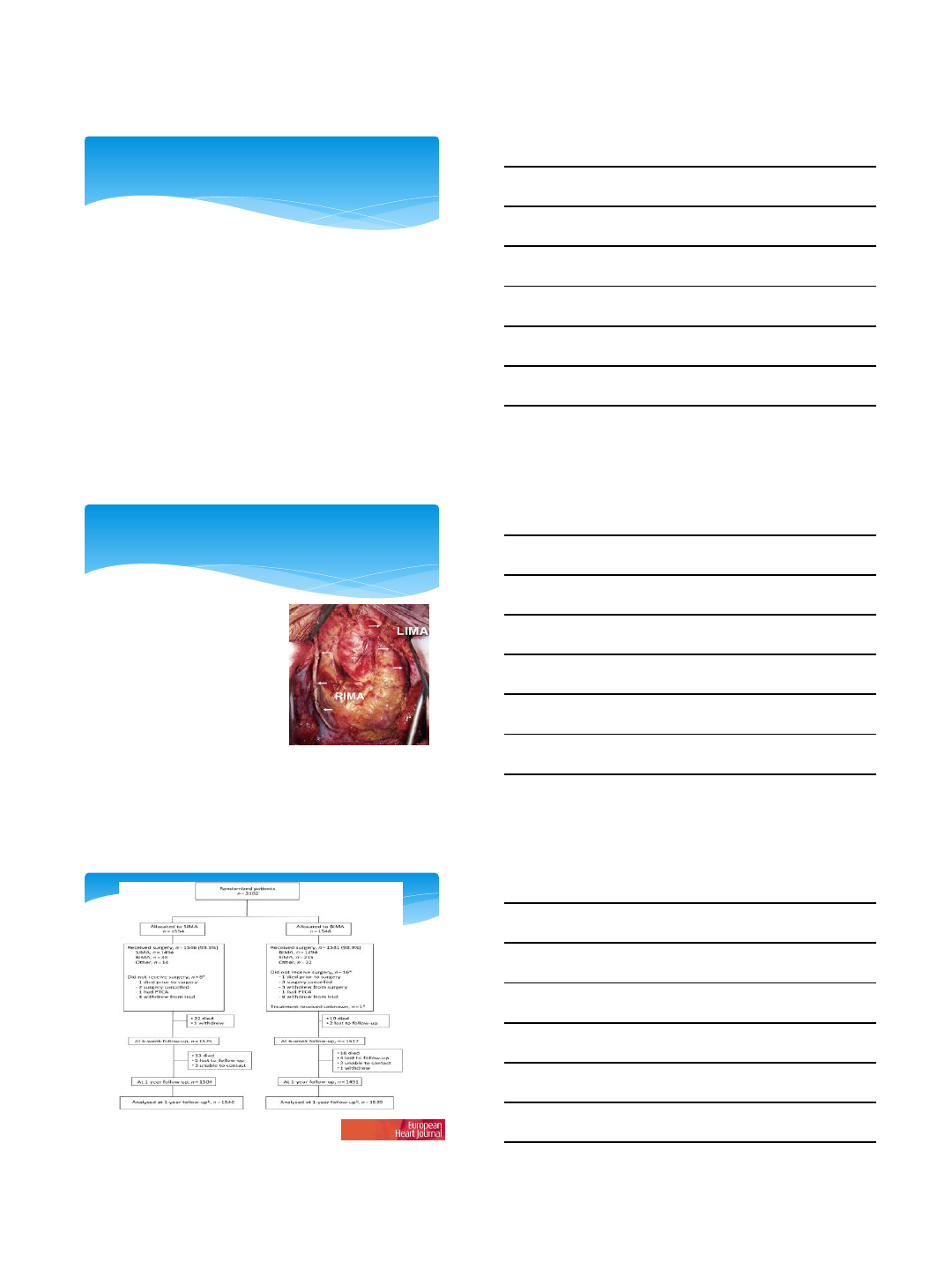
The use of Bilateral Internal
Mammary Artery (BIMA)
requires special
consideration
Emerging data that BIMA
improves survival following
CABG
Increased risk of Deep
Sternal Wound Infection???
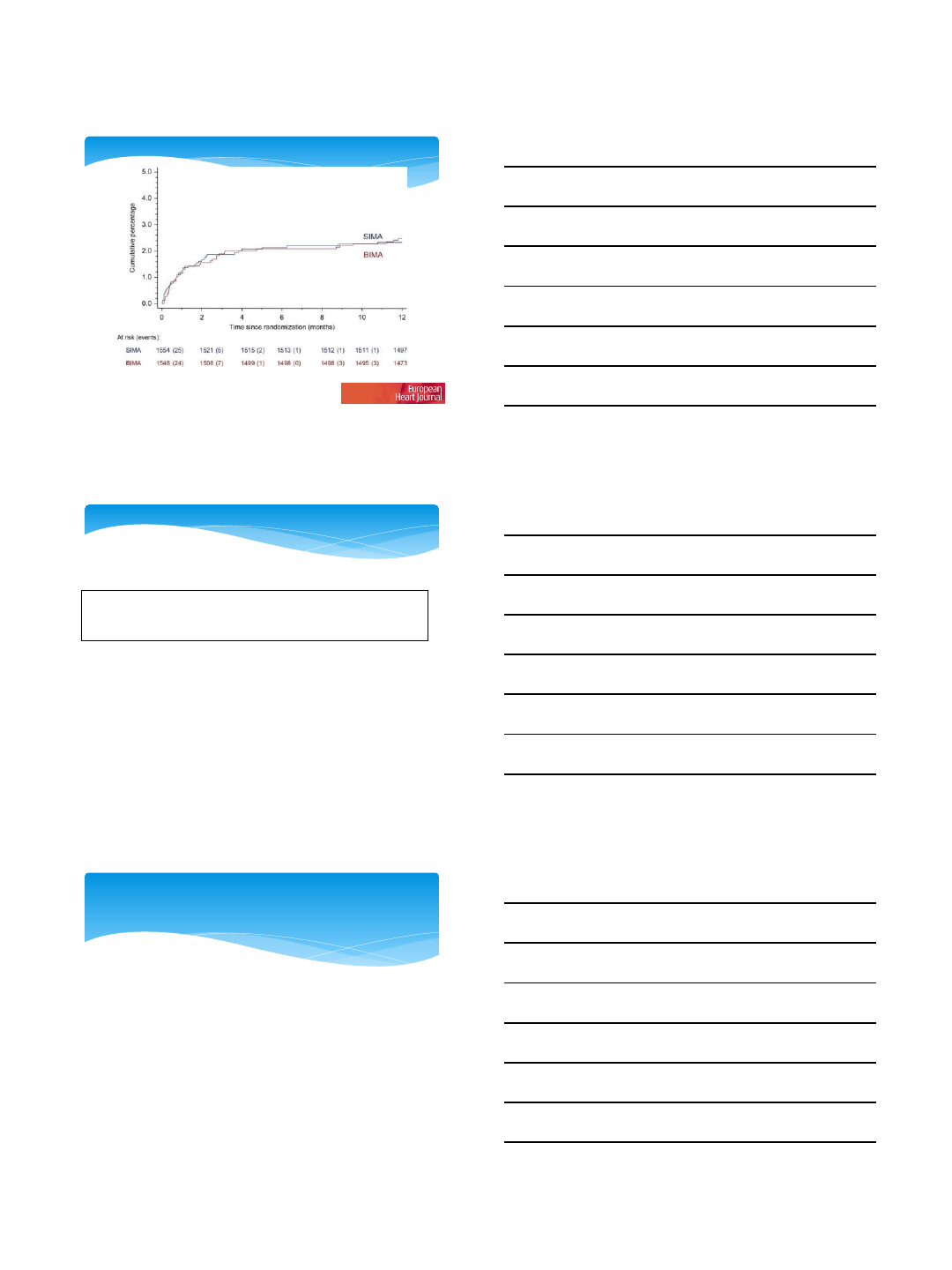
Bilateral Internal Mammary Artery
David P. Taggart et al. Eur Heart J 2010;31:2470-2481
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author
2010. For permissions please email: journals.permissions@oxfordjournals.org
5/2/2016
5
Survival to 1 year.
David P. Taggart et al. Eur Heart J 2010;31:2470-2481
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author
2010. For permissions please email: journals.permissions@oxfordjournals.org
Table 3
Adverse event data by randomized group
SIMA (n= 1552) BIMA (n= 1542) Relative risk (95% CI)
Sternal wound reconstruction 9 (0.6%) 29 (1.9%) 3.24 (1.54–6.83)
No history of diabetes 4 15
Insulin-dependent diabetes 2 5
Non-insulin-dependent diabetes 3 9
MI event at 30 days 23 (1.5%) 22 (1.4%) 0.96 (0.54–1.72)
CVA event at 30 days 19 (1.2%) 15 (1.0%) 0.79 (0.40–1.56)
Revascularization at 30 days 6 (0.4%) 11 (0.7%) 1.85 (0.68–4.98)
MI event at 1 year 31 (2.0%) 30 (2.0%) 0.97 (0.59–1.60)
CVA event at 1 year 28 (1.8%) 23 (1.5%) 0.83 (0.48–
1.43)
Revascularization at 1 year 20 (1.3%) 27 (1.8%) 1.36 (0.77–2.41)
Infections following cardiac surgery increase cost,
morbidity and mortality
Risks of Infection are multifactorial
Mitigation of these risks, when possible, can
significantly reduce the sequeli of these infection
The benefits of the use of BIMA should be carefully
weighed against the added risk of infection
Conclusion
