There’s No Such Thing As A SpO2 Simulator 6001759A There Is Sp O2 W
2015-05-08
: Pdf 6001759A There-Is-No-Such-Thing-As-A-Spo2-Simulator W 6001759A_There-is-no-such-thing-as-a-SpO2-simulator_w 04 2015 x7mag uploads wp-content
Open the PDF directly: View PDF ![]() .
.
Page Count: 3
There’s no such thing
as a SpO2 simulator
Why a primary calibration reference does not exist
and how to properly measure SpO2 accuracy
White Paper
One of the most essential elements in medical
equipment maintenance is functional testing, or in
other words, verifying the competence of a device
by applying it to another device that mimics the
physiological signal of interest.
For the majority of devices, this simulation is
a direct analog of the clinical signal. Simulators
for the electrocardiograph (ECG) or for an electro-
encephalogram (EEG) provide voltage waveforms
that mimic those parameters. Simulators for
non-invasive blood pressure provide a pneumatic
pressure signal identical to the blood pressure
waveform found in an artery. Invasive blood pres-
sure, temperature, and cardiac output simulators
produce varying patterns of resistance or imped-
ance to mimic the output of a strain gauge or a
thermistor.
Simulation of oxygen saturation in humans,
however, presents a challenge. A pulse oxim-
eter uses two wavelengths of light: a red signal,
which is partially absorbed by non-oxygenated
hemoglobin, and an infra-red (IR) signal, which is
partially absorbed by oxygenated hemoglobin in
the patient’s arterial blood.
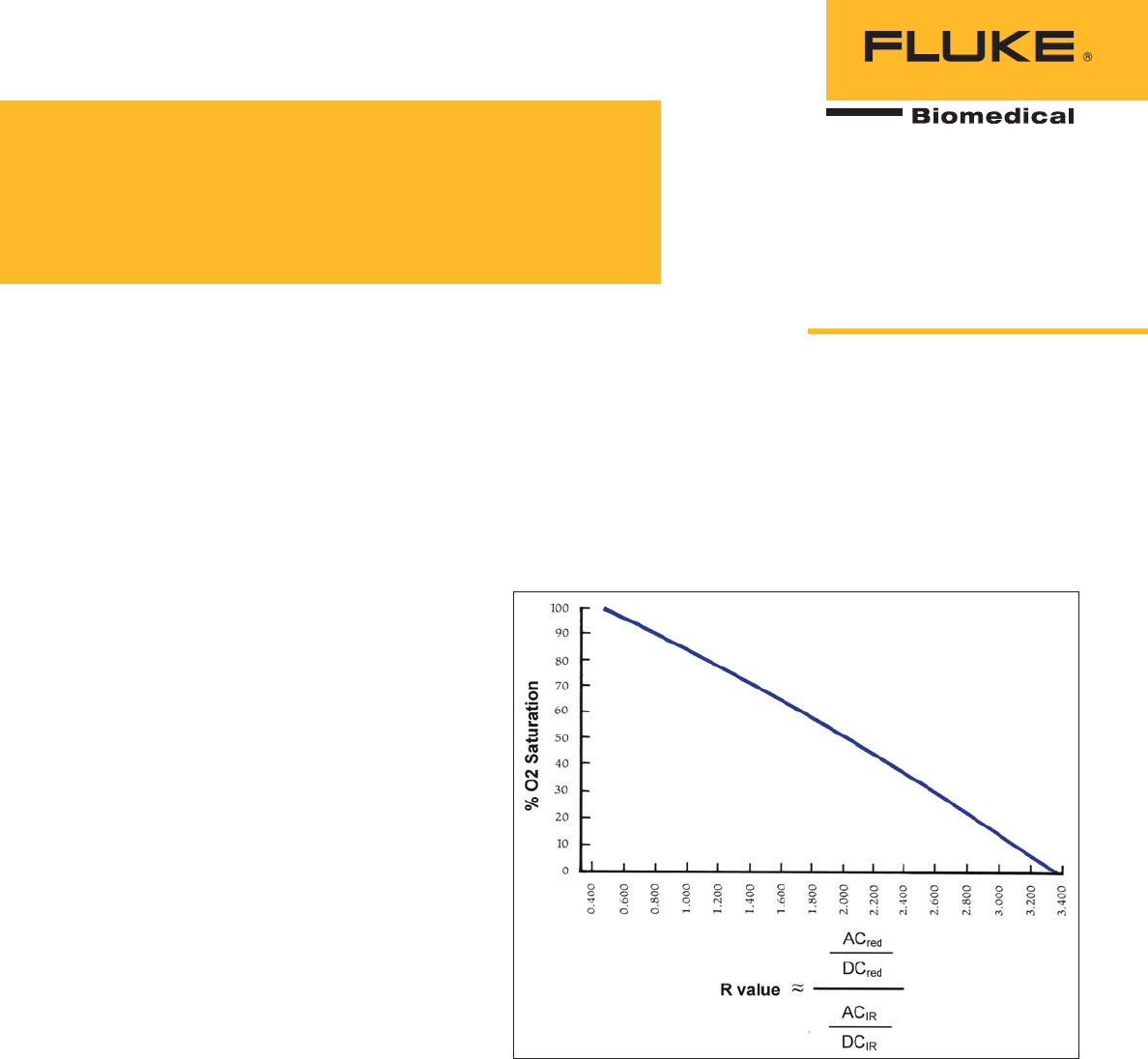
At any level of oxygen saturation, the ratio of the
pulsatile and non-pulsatile signals is derived for
both wavelengths. The red ratio is then divided
by the IR ratio (a “ratio of ratios”) to produce a
value (R) which correlates with the known oxygen
saturation value to produce an “R-curve” unique
to each manufacturer. At any value of R, the moni-
tor’s firmware “looks-up” and displays the percent
oxygen saturation. Since the absorption waveform
is pulsatile, the monitor also derives and displays
the pulse rate.
Where does the “R-curve” come from?
Before market introduction, all prototype oxygen
saturation monitors must be validated using in
vivo testing as specified in Standard 80601-2-61
(2011) of the International Standards Organization
(ISO). In a controlled desaturation study, volunteer
subjects breathe a sequence of gas mixtures of
decreasing oxygen content while connected to the
prototype monitor. Arterial blood samples are taken
from the subjects, and the saturation is measured
by a co-oximeter in a clinical laboratory. As shown
in Figure 1, the R-value derived in the monitor is
plotted against each saturation value.
Dennis J. McMahon, CBET-R
Figure 1. Example of an R-curve, correlating O2 saturation with the R value.
The resulting R-curve is then integrated into
the firmware of the monitor. The ISO standard
prescribes the number of subjects, the saturation
range, the laboratory analysis method, motion
conditions, and varied perfusion levels. This vali-
dation method is also stipulated in the pre-market
protocols of many regulatory agencies, such as
the U.S. Food and Drug Administration’s 510(k)
guidelines.

2 Fluke Biomedical There’s no such thing as a SpO2 simulator
Why a primary calibration reference
does not exist
Because pulse oximeters use the manufacturer-
specific R-curve to derive and display saturation,
we will never find a calibration pot or any other
means to adjust the device against a primary refer-
ence. The only currently accepted primary reference
is the in vivo study described above. Theoretically,
a true simulator of oxygen saturation would require
a pulsatile fluid loop which contains a hemoglobin-
like substance transporting oxygen in various
proportions. This theoretical simulator would need
to vary the rate and volume of the fluid pulsations
to mimic the pulse rates and perfusion levels, as
well as provide several levels of optical transmis-
sion to represent various tissue densities. Motion
artifact and interference from ambient lighting
would also be needed. And to be marketable, the
simulator would have to deal with the differences in
the various manufacturer R-curves. This hypotheti-
cal test device would be impractical as a bench-top,
production model. There are no simulators that in-
dependently verify the accuracy of a pulse oximeter.
How to properly measure SpO2
accuracy
Annex FF of ISO Standard 80601-2-61 makes clear
distinctions between the terms “simulator”, “cali-
brator”, and “functional tester”. A calibrator would
be a high-accuracy simulator, capable of electronic
signals or optical responses identical to a human
subject. By definition, a calibrator would also have
to have accuracy much greater than the device
under test, which is already typically 2 percent.
Another annex of the standard requires the
instruction manuals of pulse oximeter equipment
to state that functional testers cannot in general
be used to measure SpO2 accuracy. Rather than
being “primary standards” (or “gold standards”)
against which all monitors are calibrated, current
pulse oximeter testers are “transfer standards”
i.e. they are a reference of comparison validated
against a another standard established previously.
The U.S. FDA carefully defines this as “substantial
equivalence” in its pre-market guidelines.
Since the introduction of the first commercial
pulse oximeter in 1977, the objective performance
verification of these monitors has been elusive.
Healthcare technology personnel should bear in
mind that a SpO2 tester is a secondary standard
which transfers equivalence from prior devices
that have been validated before. The verb “simu-
late” means “to present a false appearance of”,
while the verb “emulate” means “to try to equal or
excel”. Other biomedical equipment testers may be
simulators, but SpO2 testers are, at best, emulators;
they only approximate the physiology of a human
subject.
All pulse oximeter testers currently on the
market require the user to select the monitor
manufacturer, or groups of manufacturers, in order
to accommodate the manufacturer’s R-curves. In
addition to saturation and pulse rate, most testers
offer user-selectable values of pulse amplitude,
tissue transmittance, arrhythmias, motion artifact,
and interference from power line frequencies.
Many models also have pre-set combinations of
clinically normal and abnormal values, and may
allow the user to define custom values. All testers
use either an electronic or optical interface with
the unit under test. Some models offer both modes.
Electronic testers apply an electrical signal to the
monitor through its sensor cable, without inclusion
of the sensor. The user-selected electrical signal
mimics various values of saturation and other vari-
ables. These units offer the option of testing the
sensor (presumed to be a finger sensor) by verify-
ing the continuity of the red and infrared LED’s
and that of the photodiode. Some models also test
to confirm the photodiode’s correct response to the
two light signals.
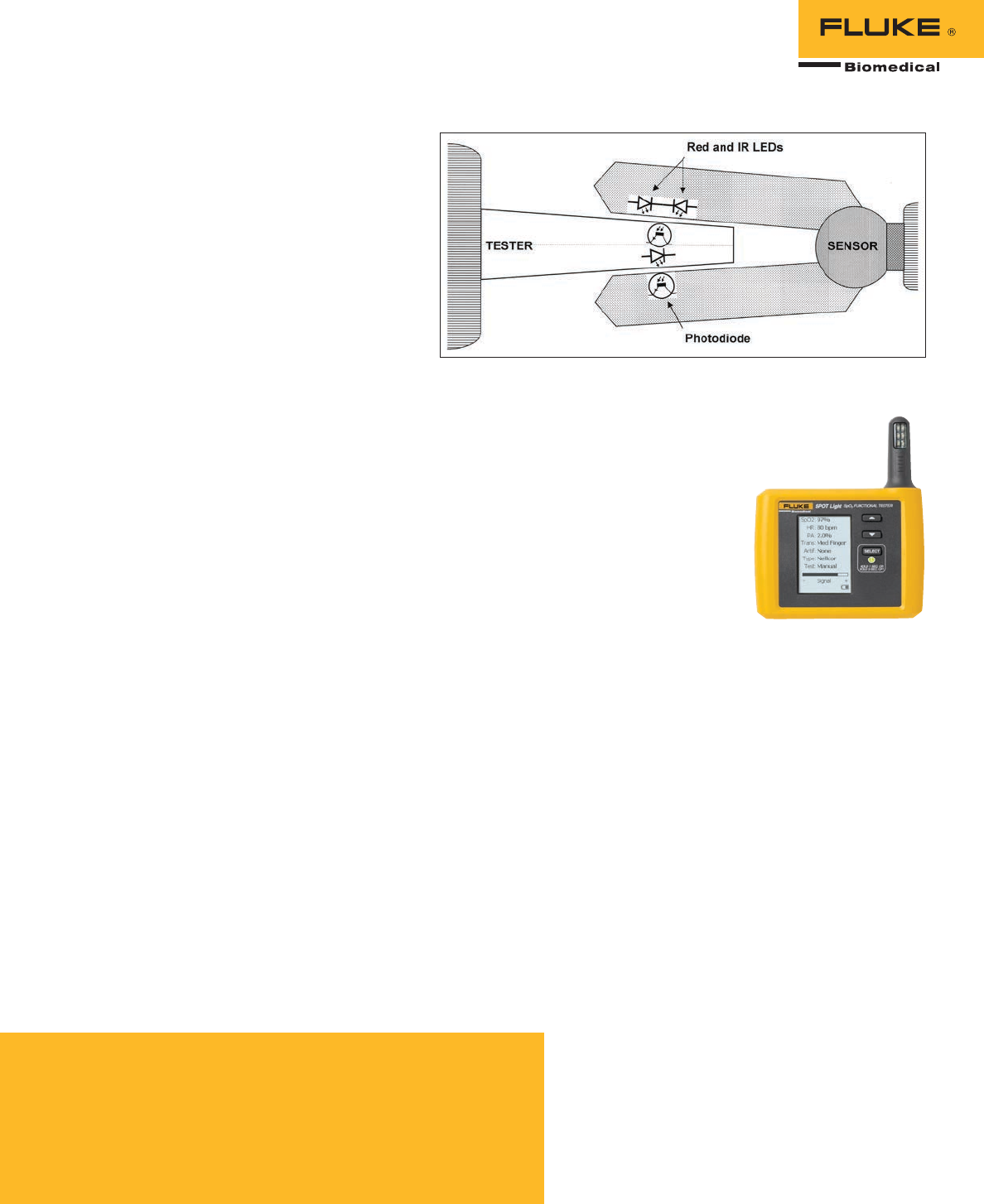
In contrast to the electronic interface, optical
testers provide a physical digit or “artificial finger”
that includes a mechanical and/or opto-electronic
element which allows variable transmission of the
two light signals. (Figure 2.)
This type tests the entire monitor system (sensor,
cable, and monitor) at once, which can save time
when performance testing many units. As with the
electronic types, these enable the user to select a
range of values of saturation and other variables
3 Fluke Biomedical There’s no such thing as a SpO2 simulator
and pre-sets, depending on the manufacturer.
One vendor offers a set of calibrated fingers, or
artificial digits with integrated dyes to allow
transmission of light corresponding to a specific
saturation.
Currently marketed SpO2 testers offer a variety
of functions, and the equipment technician must
decide how thoroughly to test. Most SpO2 moni-
tors will be accurate at clinically “normal” values,
but equipment technicians must detect when the
monitor gives inaccurate values in the abnormal
range, where clinicians must decide on clinical
corrective action.
One widely promoted tester provides five pre-
set combinations of saturation value, pulse rate,
and pulse amplitude, where a unit like the SPOT
Light SpO2 functional tester by Fluke Biomedical
enables independent selection of eight differ-
ent saturations and pulse rates, three levels of
light transmission, and the option of artifact from
respiration and line frequencies. The SPOT Light
also offers a selection of R-curves for eight differ-
ent manufacturers, where another unit offers only
three R-curves to cover all makers. With optical
testers, precise positioning of the sensor probe
on the digit can be problematic. Most units give
an indication if the probe is placed incorrectly
on the digit, but there is no indication of maxi-
mized signal strength. The SPOT Light includes
an on-screen signal quality indicator to enable
optimal placement of the probe, assuring consis-
tent readings. The SPOT Light sets up in seconds
to send SpO2 saturation, heart rate, perfusion,
transmission, artifact noise, and eight different
manufactures custom R-curves to a pulse oximeter
or patient monitor.
Figure 2. Testing finger using an LED and photodiode to interact with an
SpO2 sensor.
About the ProSim SPOT Light
SpO2 functional tester
Featuring an exclusive ergonomic
design, the ProSim SPOT Light is the first
comprehensive SpO2 functional tester
to come in a handheld and easy-to-use
device. SPOT Light is lightweight and
flexible with three custom presets spe-
cially-designed to make it the fastest and
easiest-to-use device on the market today
for pulse oximeter functional testing.
A helpful LCD display and three simple buttons
make it effortless to rapidly change parameters
and view each signal output sent to the pulse
oximeter at a glance. An interchangeable, long-life
battery ensures uninterrupted all-day operation
without need to connect to a power supply.
To learn more about the SPOT Light SpO2 Func-
tional Tester Pulse Oximeter Analyzer, click here
or visit www.flukebiomedical.com.
Fluke Biomedical.
Better products. More choices. One company.
Fluke Biomedical
6045 Cochran Road
Cleveland, OH 44139-3303 U.S.A.
For more information, contact us at:
(800) 850-4608 or Fax (440) 349-2307
Email: sales@flukebiomedical.com
Web access: www.flukebiomedical.com
©2013 Fluke Biomedical. Specifications subject
to change without notice. Printed in U.S.A.
12/2013 6001759A_EN
Modification of this document is not permitted
without written permission from Fluke Corporation.
About the author
Dennis J. McMahon, CBET-R, is a biomedical equipment technician with
over forty years of medical technology experience. After earning a degree
in Chemistry in the late ‘60s, he worked as an anesthesia technician at
Harborview Medical Center until 1977. He certified as a biomedical
technician in 1983, and attended service schools for a variety of clinical
technology over the following three decades. Dennis currently instructs at
North Seattle Community College and serves as the Education Chair for the
Washington State Biomedical Association (WSBA).
References
• Chan, A: Biomedical Device Technology 2008. C Thomas - Publisher
• FDA Guidance for Industry and FDA Staff: Pulse Oximeters – Premarket
Notification Submissions [510k]
• International Standards Organization, Standard 80601-2-61 (2011): Medical
electrical equipment - Particular requirements for the basic safety and
essential performance of pulse oximeter equipment
• Severinghaus, J: Takuo Aoyagi: Discovery of Pulse Oximetry
Anesth Analg 2007; 105 S1-4
