MergedFile 6dd9d1f7 63f2 47c3 9e31 Fc6543b64a5d
2018-05-08
: Pdf 6Dd9D1F7-63F2-47C3-9E31-Fc6543B64A5D 6dd9d1f7-63f2-47c3-9e31-fc6543b64a5d 5 2018 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 25
5/7/2018
1
Immune Based Treatment Options
in Lymphoma: CAR-t cells
Leo I. Gordon, MD, FACP
•We are entering a new era in treatment for lymphomas
•CAR T-cell therapy may represent one of the more effective
immunotherapeutic options
•Challenges
•Time to manufacture
•Patient selection and toxicity management
•integration with or replacement of existing modalities (chemotherapy, small
molecule inhibitors, autologous vs allogeneic stem transplant)
•cost
•CAR T-cell therapy likely to alter how we treat DLBCL
Summary
5/7/2018
2
The Case for Cancer Cellular Therapy
Presented By Carl June at 2016 ASCO Annual Meeting
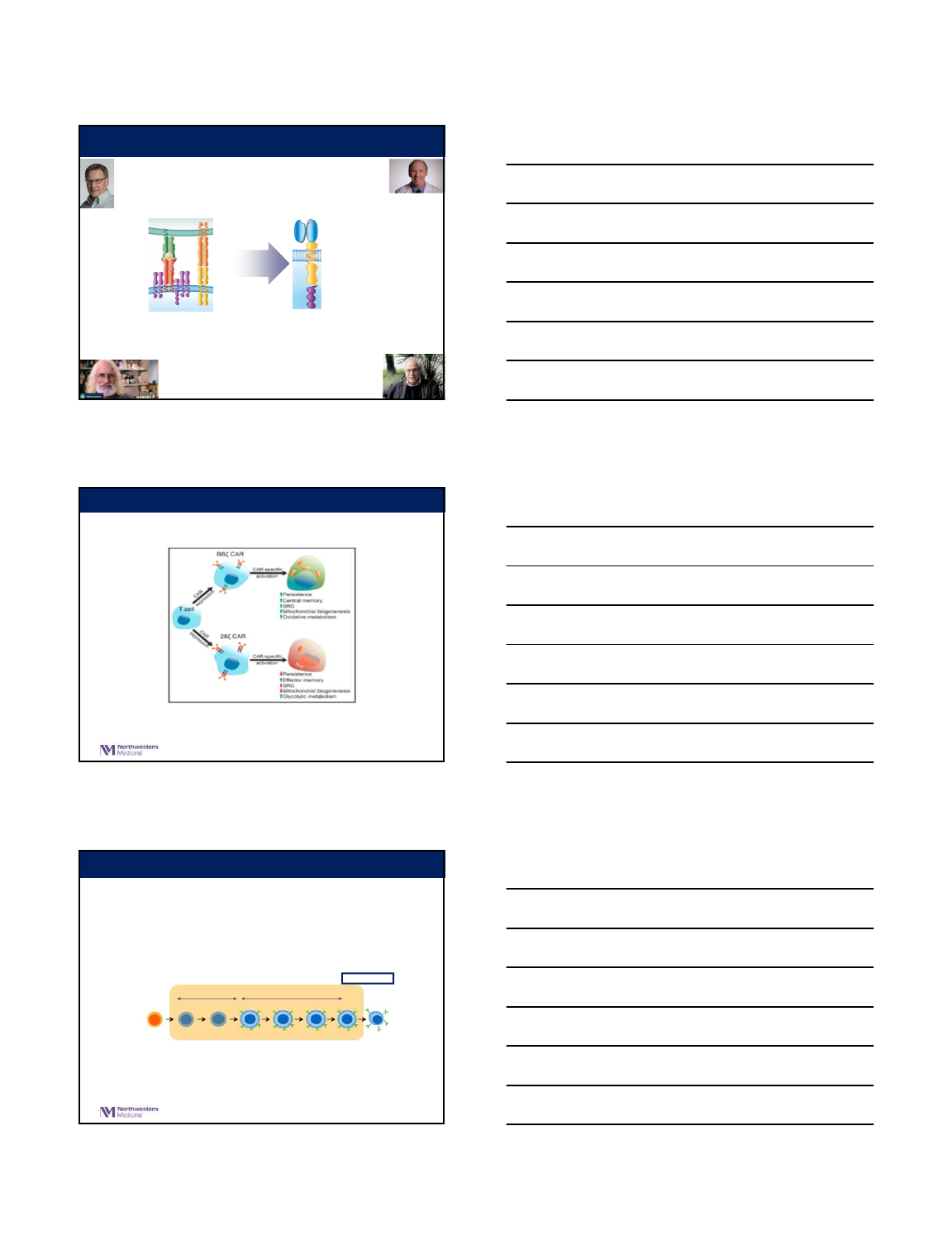
Graft vs. Leukemia/Lymphoma:
The case for allogeneic transplant
•Presence of GvHD reduces the
likelihood of recurrence in
leukemia patients who had an
allogeneic transplant.
•Provided rationale for “mini”
transplants to take advantage of
GvL effect without high dose
chemotherapy
5/7/2018
3
scFv: recognize tumor
surface proteins
Costimulatory Signal 2:
CD28 or 4-1BB or OX40
Essential Signal 1:
CD3z
APC
CD28
CD28
L
pMHC
TCR
CD3
z
T Cell Receptor Chimeric Antigen Receptor
CAR T cells are genetically altered to express CAR on the cell surface.
T Cell
Activation Independent of MHC
Limited to cell surface proteins
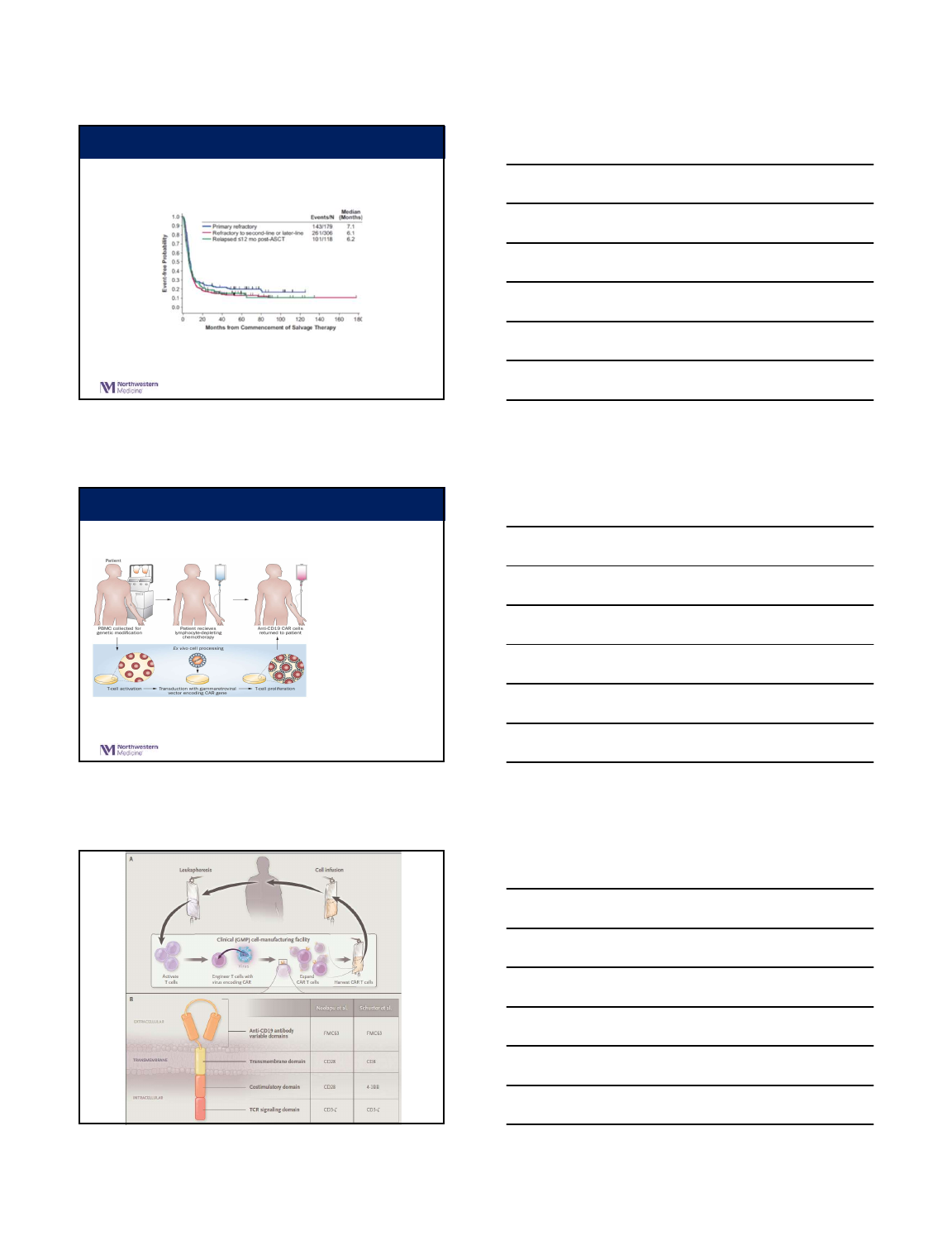
CAR Design: Critical Elements
CAR Construct: CD28 vs 4-1BB
Kalawekar at el, 2016
CAR Construct: Antigen Selection
•
CD19 expression is generally restricted to B cells and B cell
precursors1
•
CD19 is not expressed on hematopoietic stem cells or other tissue
•
CD19 is expressed by most B-cell malignancies
•
CLL, B-ALL, DLBCL, FL, MCL
Image adapted from JanewayCA, Travers P, Walport M, et al. Immunobiology. 5th ed. New York, NY: Garland Science; 2001:221-293;
ScheuermannRH, et al. Leuk Lymphoma. 1995;18:385-397; and Feldman M, Marini JC. Cell cooperation in the antibody response. In: Roitt
I, Brostoff J, Male D, eds. Immunology. 6th ed. Maryland Heights, Missouri: Mosby;2001:131-146.
Pro-B Pre-B Activated
B cell
Hematopoietic
stem cell
Memory
B cell
(IgG, IgA)
Plasma
cell
(IgG)
Immature
(IgM)
Mature
(IgM, IgD)
CD19 expression
B cell lymphomas
and leukemias
preB-ALL
5/7/2018
4
Refractory DLBCL, n=636; ORR 26%, CR 7%; median OS 6.3 months
SCHOLAR-1 – Poor outcomes in R/R DLBCL
Crump et al., Blood 2017
Kochenderfe r, J. N. & Rosenberg, S. A. (2013) Treating B -cell cancer with T c ells expressing anti-CD19 chimeric antigen recep tors.
Nat. Rev. Clin. Oncol. doi:10.103 8/nrclinonc.2013.46
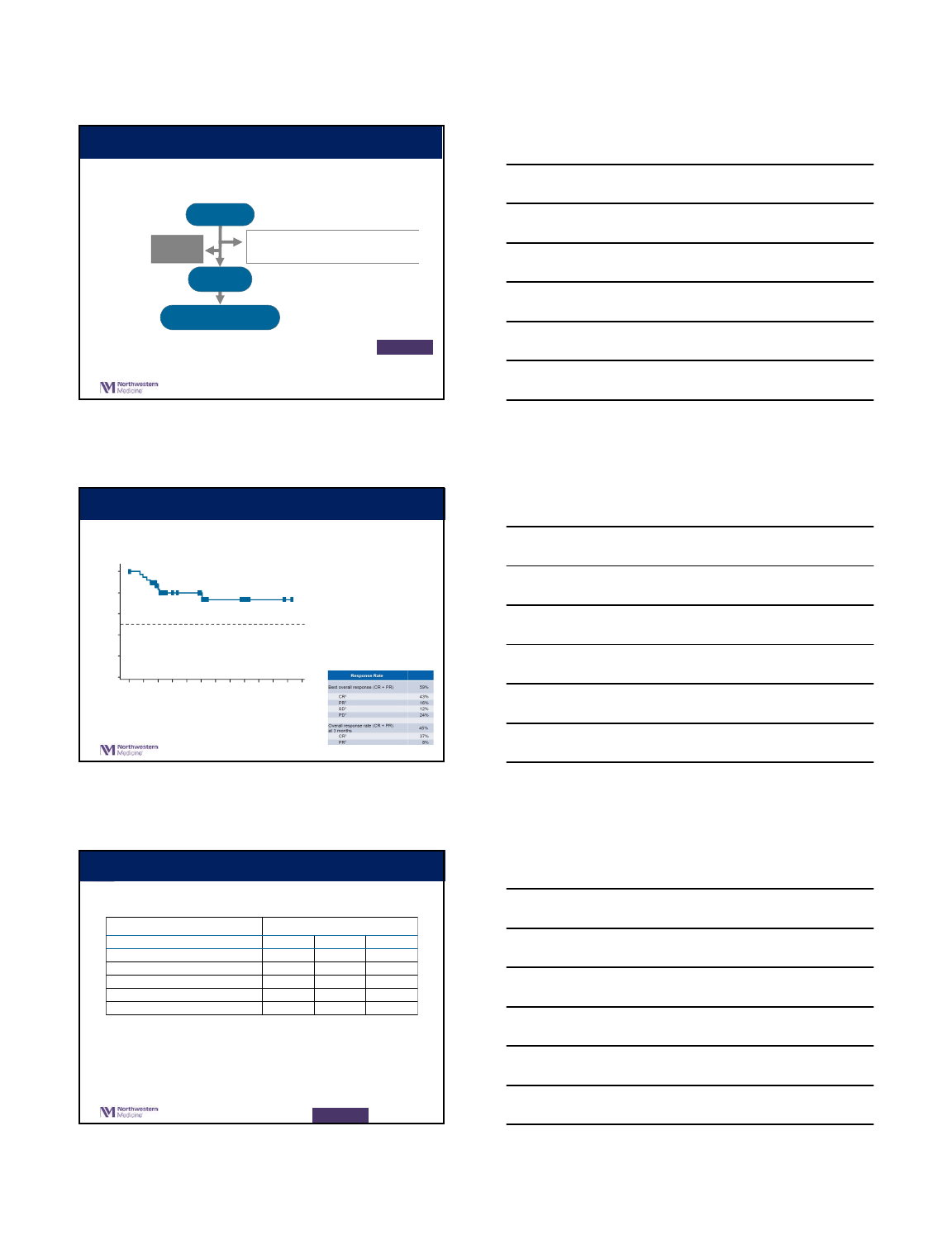
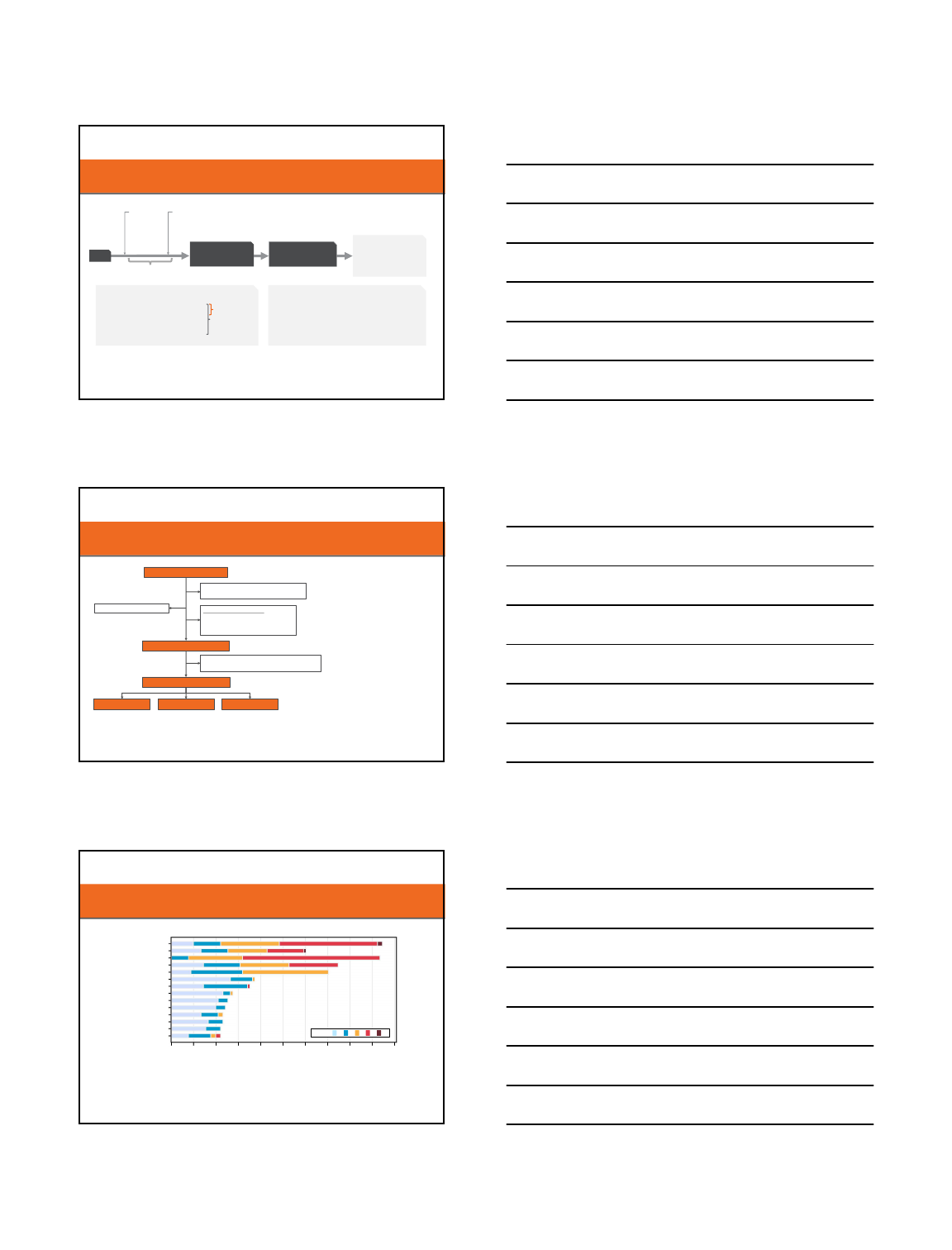
CAR T manufacturing and administration
*
large range on timing
for processing
5/7/2018
5
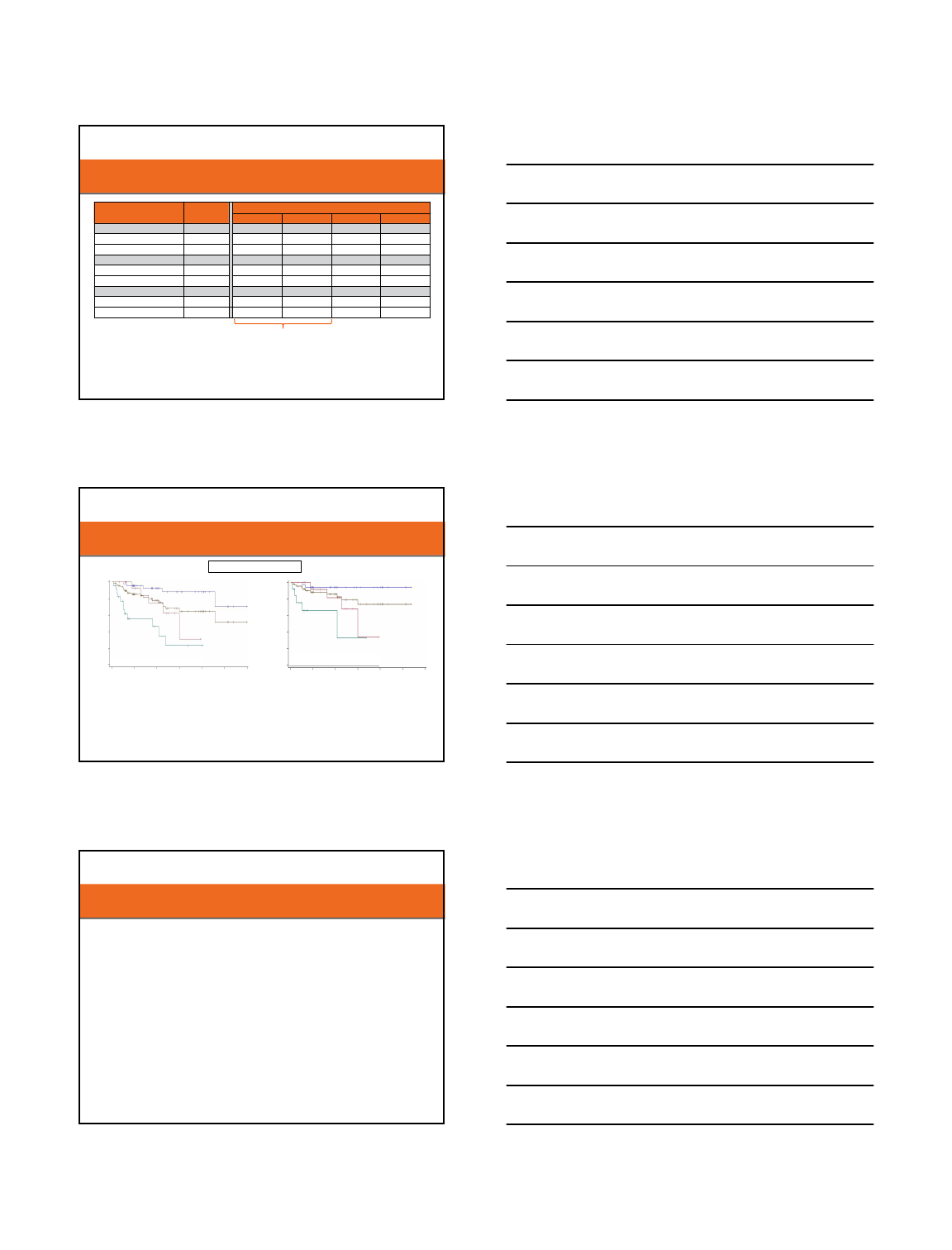
JULIET: Study Status
(Data cut March 2017)
Discontinued before infusion
Total = 43
Inability to manufacture n = 9
Patient-status related
a
n = 34
Enrolled
n = 147
Infused
n = 99
Enrollment began July 2015
Pending
infusion
n = 5
Evaluable for response
n = 81
a
Death (n = 16); physician decision (n = 12); subject decision (n = 3); adverse event (n = 2); protocol deviation (n = 1).
ASH 2017
Schuster SJ, et al. Blood. 2017; 130(23):[abstract 577].
Approval date 12/2017 M-CTL-1176725
13
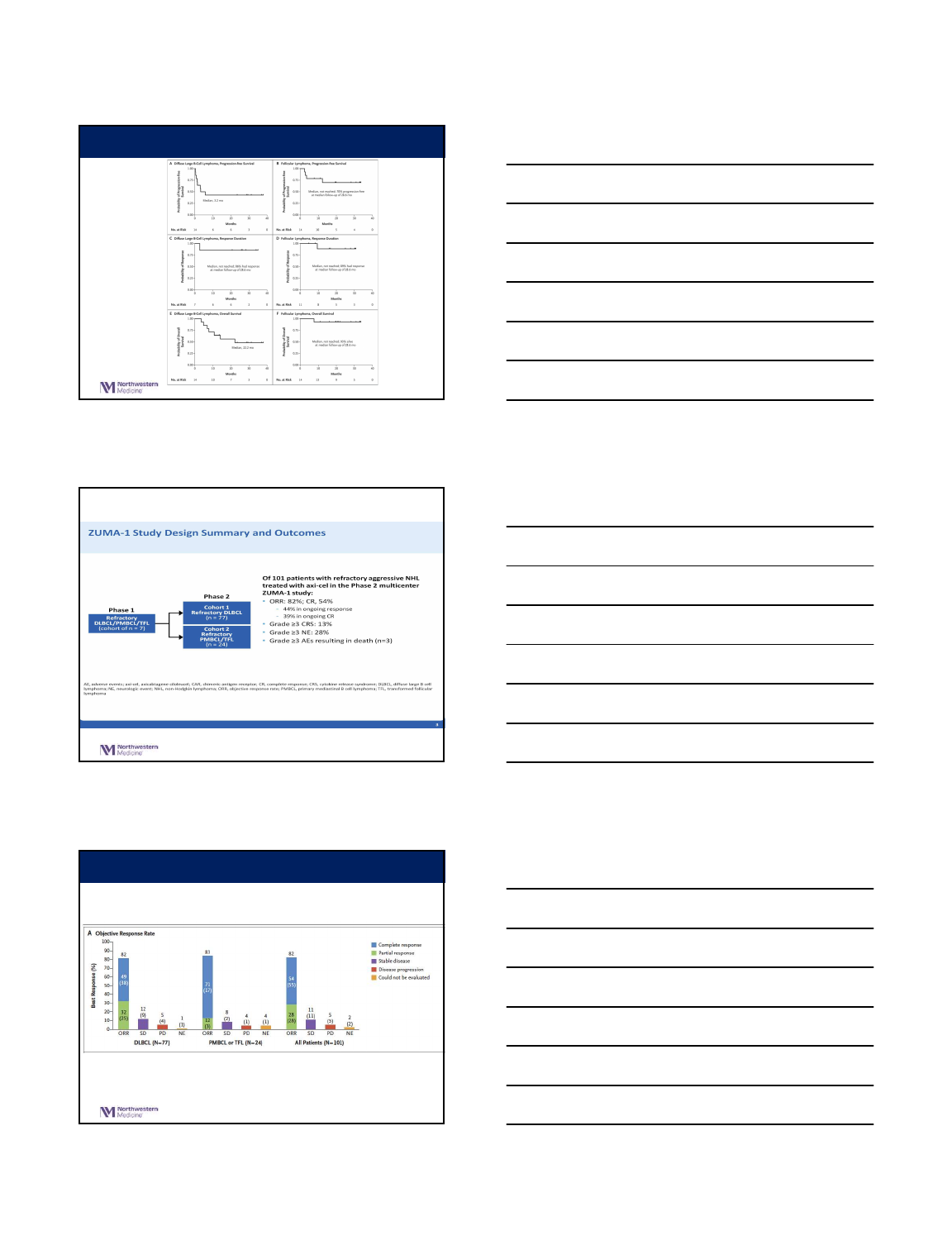
Duration of Response, 74% Relapse-free at 6 Months
•Median DOR and OS not
reached
• Most patients achieving CR
at month 3 have remained in
CR
• No patients proceeded to
transplant while in response
CR, complete response; DOR, duration of response; OS, overall response.
Efficacy analysis set = All patients who received a tisagenlecleucel infusion at least 3
months prior to data-cut date.
Patients still at risk
Probabilty of Relapse Free (%)
Time From Onset of Response (months)
100
80
60
40
20
0
2 3 4 5 7 8 9 10 11 1210 6
01225913161825 936n = 43
ASH 2017
Schuster SJ, et al. Blood. 2017; 130(23):[abstract 577].
Approval date 12/2017 M-CTL-1176725
14
JULIET: Adverse Events of Special Interest
•No deaths attributed to tisagenlecleucel, CRS or cerebral edema
•26 (26%) patients were infused as outpatients
•20/26 (77%) patients remained outpatient for ≥ 3 days after infusion
a
Occurring within 8 weeks of tisagenlecleucel infusion.
b
Cytokine release syndrome was graded using the Penn scale.
c
At day 28.
(N = 99)
AESI
a
All grade, % Grade 3, % Grade 4, %
Cytokine release syndrome
b
58 15 8
Neurological events 21 8 4
Prolonged cytopenia
c
36 15 12
Infections 34 18 2
Febrile neutropenia 13 11 2
AESI, adverse events of special interest.
ASH 2017
Schuster SJ, et al. Blood. 2017; 130(23):[abstract 577].
Approval date 12/2017 M-CTL-1176725
15
5/7/2018
6
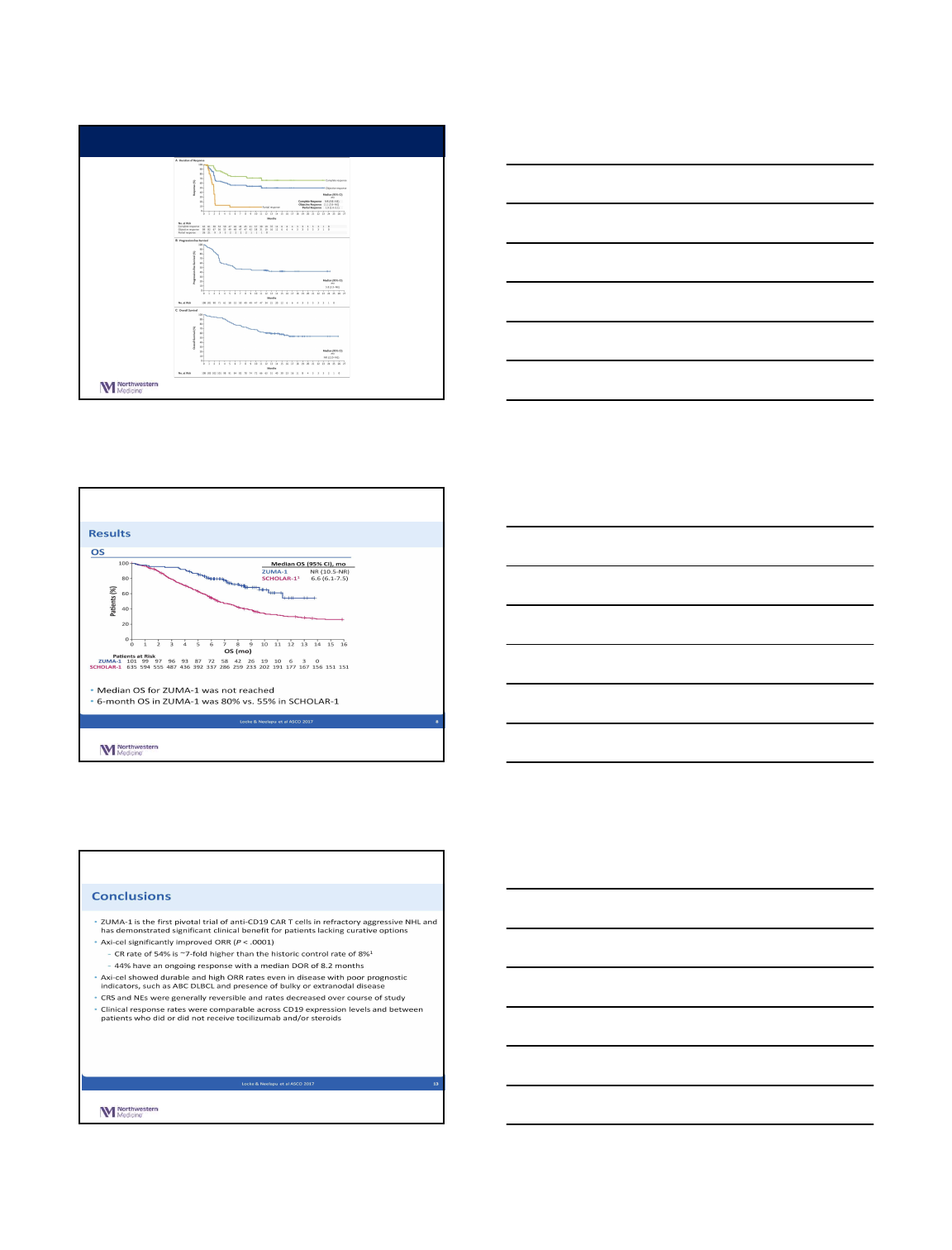
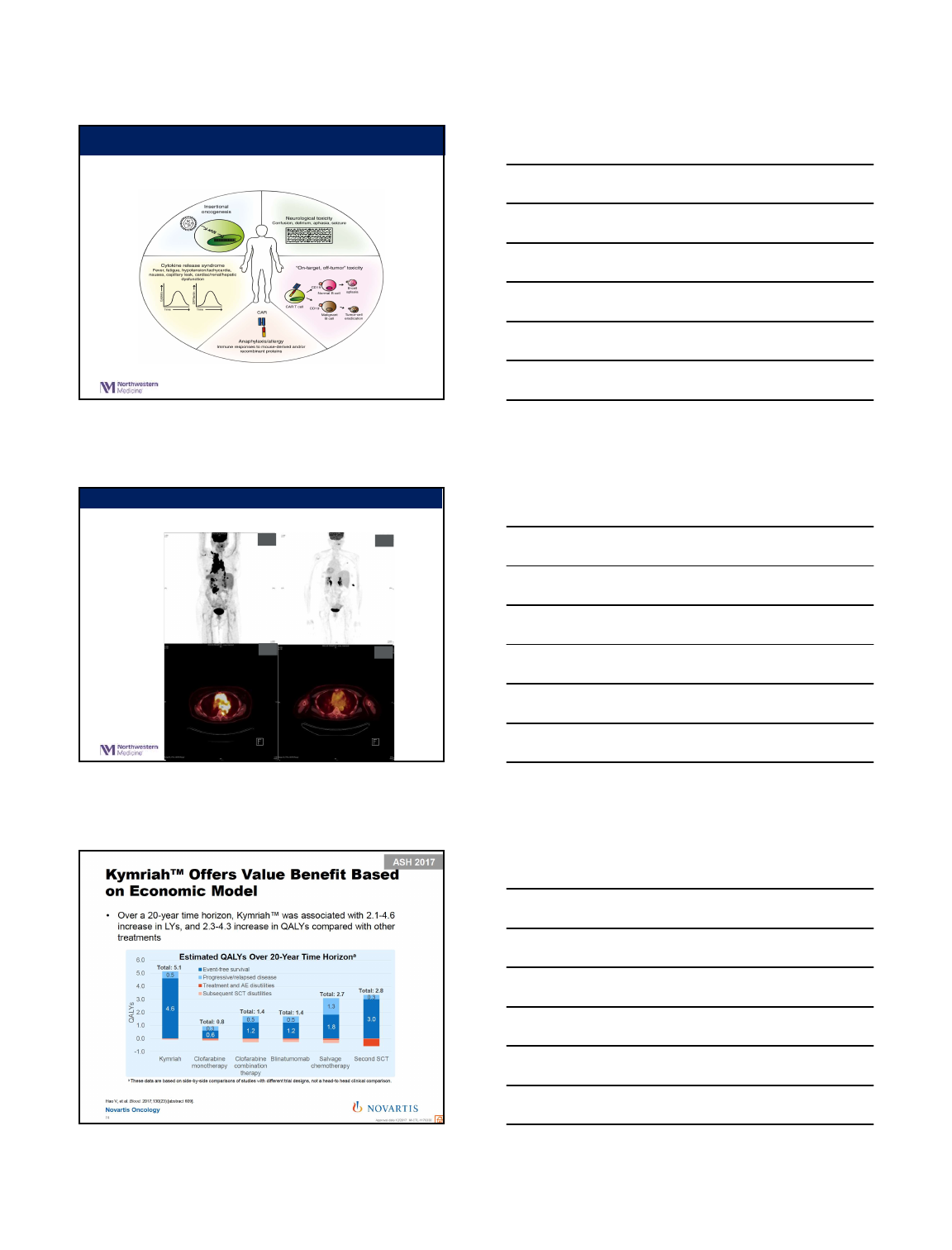
Schuster SJ et al. N EnglJ Med 2017. DOI: 10.1056/NEJMoa1708566
Progression-free Survival, Response Duration, and Overall Survival.
Presented by:
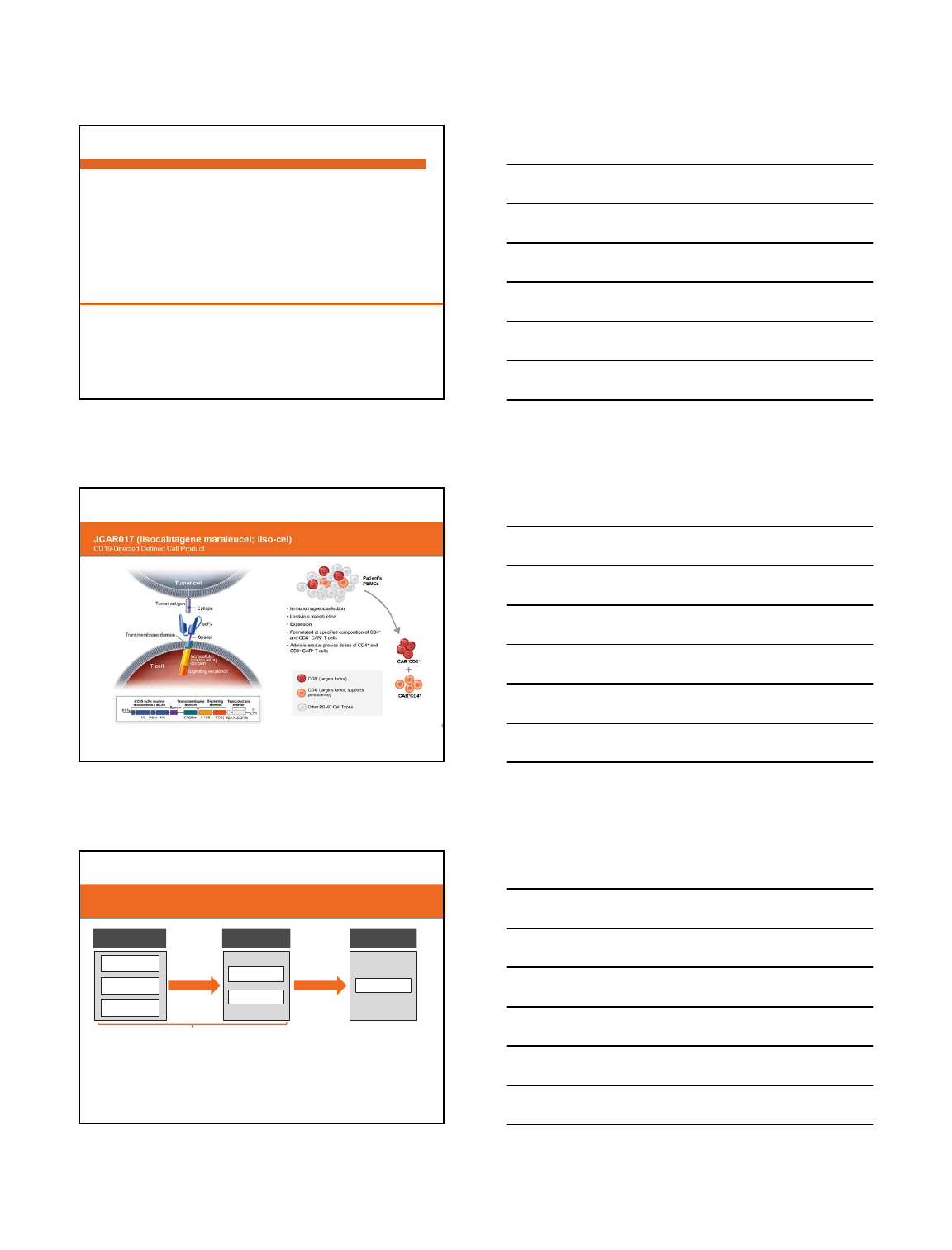
Objective Response Rate among the 101 Treated Patients.
NeelapuSS et al. N EnglJ Med 2017. DOI: 10.1056/NEJMoa1707447
5/7/2018
7
NeelapuSS et al. N EnglJ Med 2017. DOI: 10.1056/NEJMoa1707447
Kaplan–Meier Estimates of the Duration of Response, Progression-
free
Survival, and Overall Survival.
Presented by:
5/7/2018
8
High CR Rates in Relapsed/Refractory Aggressive B-NHL
Treated With the CD19-Directed CAR T Cell Product JCAR017
(TRANSCEND NHL 001; NCT02631044)
Jeremy S. Abramson,
1
M. Lia Palomba,
2
Leo I. Gordon,
3
Matthew Lunning,
4
Jon Arnason,
5
Michael
Wang,
6
Andres Forero-Torres,
7
Tina Albertson,
8
Claire Sutherland,
8
Benhuai Xie,
8
Jacob Garcia,
8
Tanya Siddiqi
9
1
Massachusetts General Hospital Cancer Center, Boston, MA;
2
Memorial Sloan Kettering Cancer Center, New York, NY;
3
Northwestern University Robert H. Lurie Comprehensive Cancer Center, Chicago, IL;
4
University of Nebraska Medical Center, Omaha, NE;
5
Beth Israel Deaconess Medical Center, Boston, MA;
6
University of Texas MD Anderson Cancer Center, Houston, TX;
7
University of Alabama at Birmingham,
Birmingham, AL;
8
Juno Therapeutics, Seattle, WA;
9
City of Hope National Medical Center, Duarte, CA
High Durable CR Rates in R/R Aggressive B-NHL Treated with
JCAR017 (lisocabtagene maraleucel; liso-cel) (TRANSCEND NHL 001):
Defined Composition CD19-Directed CAR T Cell Product Allows for
Dose Finding and Definition of Pivotal Cohort
Jeremy S. Abramson,
1
M. Lia Palomba,
2
Leo I. Gordon,
3
Matthew Lunning,
4
Jon Arnason,
5
Michael Wang,
6
Andres Forero-
Torres,
7
David Maloney,
8
Tina Albertson,
9
Jacob Garcia,
9
Daniel Li,
9
Benhuai Xie,
9
Tanya Siddiqi
10
1
Massachusetts General Hospital Cancer Center, Boston, MA;
2
Memorial Sloan Kettering Cancer Center, New York, NY;
3
Northwestern University Robert H. Lurie
Comprehensive Cancer Center, Chicago, IL;
4
University of Nebraska Medical Center, Omaha, NE;
5
Beth Israel Deaconess Medical Center, Boston, MA;
6
University of
Texas MD Anderson Cancer Center, Houston, TX;
7
University of Alabama at Birmingham, Birmingham, AL;
8
Fred Hutchinson Cancer Research Center, Seattle, WA;
9
Juno Therapeutics, Seattle, WA;
10
City of Hope National Medical Center, Duarte, CA
Multicenter, Seamless Design Pivotal Trial
(TRANSCEND NHL 001; NCT02631044)
a
Disease-specific Dose Findi ng and Dose Expansion cohorts enro lled [DLBCL and MCL].
b
Administered on Day 1.
c
Administered on Day 1 and Day 14.
d
DLBCL FULL cohort: DLBC L, NOS de novo and transform ed from any indolent lymphoma, ECOG 0-2.
e
DLBCL CORE cohort: DLBCL, NOS de novo and transformed fr om FL, ECOG 0-1, high grade B-cell lymphoma.
Dose
Recommendation
by Steering
Committee
Dose Finding
a
(DF) Cohorts
5 × 10
7
cells (DL1),
single dose (S)
b
5 × 10
7
cells (DL1),
double dose (D)
c
1 × 10
8
cells (DL2),
single dose (S)
b
DL1S
DL2S
Dose Expansion
a
(DE) Cohorts
Pivotal DLBCL
Cohort
DL2S
Data will be presented from DF and DE DLBCL cohorts
• 91 patients treated (FULL)
d
• 67 patients treated in identified pivotal patient population (CORE)
e
Enrollment ongoing for
pivotal patient population
4
5/7/2018
9
Screen
TRANSCEND NHL 001 (NCT02631044)
FLU, fludarabine; CY, cyclopho sphamide.
a
Therapy for disease contr ol allowed.
b
ECOG 2 and prior allogenei c HSCT excluded from pivot al cohort.
Lymphodepletion
FLU 30 mg/m2and
CY 300 mg/m2x 3d
FOLLOW-UP
Initial: 12 months
On-study: 24 months
Long-term: up to 15 years after last
JCAR017 treatment
ENROLLMENT COHORTS
§DLBCL after 2 lines of therapy:
–DLBCL, NOS (de novo or transformed FL)
–High grade B-cell lymphoma (double/triple hit)
–DLBCL transformed from CLL or MZL
–PMBCL
–FL3B
§MCL after 1 line of therapy
Pivotal
population
(CORE)
PATIENT ELIGIBILITY
§Prior SCT allowed
b
§Secondary CNS involvement allowed
§ECOG 0-2
b
§No minimum absolute lymphocyte count requirement for apheresis
Liso-cel Manufacturing
a
Enrollment &
Apheresis
PET-positive
disease reconfirmed
JCAR017 (liso-cel)
2-7 days
after FLU/CY
All
enrolled
DLBCL
population
(FULL)
5
CONSORT Diagram: DLBCL Cohort
§Product available for
98% (126/128) of
patients apheresed in
DLBCL cohort
§Six MCL subjects treated
thus far with JCAR017 at
DL1S
§Five patients treated in
outpatient setting as of
October 9 data
snapshot
a
JCAR017-Treated (n=108)
DL1S (n = 45) DL1D (n = 6) DL2S (n = 40)
Leukapheresed (n = 140)
Awaiting product (n=10)
Withdrew before manufacturing (n = 2)
• Received JCAR017, not yet evaluable (n = 6)
• Received nonconforming JCAR017 (n = 11)a
Product unavailable (n = 2) Product available (n = 18)
• Awaiting treatment (n = 4)
• Withdrew (n = 4)
• PD or died (n = 10)
Data as of October 9, 2017
Safety-Evaluable (n=91)
6
a
For further details, see Maloney et al (abstract 1552).
TEAEs and Lab Abnormalities in DLBCL Cohort (FULL, N=91)
TEAE, treatment-emergent adverse event.
a
Data for 5 patients with M CL treated with conforming pro duct at DL1 with at least 28 days of follow-up are not reported.
b
One grade 5 AE of septic shock, unrelated to JCAR017, occurred in the setting of disease progression.
c
One grade 5 AE of diffuse alveola r damage, investigator assessed as related to fludarabine, cyclophosp hamide, and JCAR017, occurred on day 23 in a patient who r efused mechanical ventilation for progressive
respiratory failure while neutropen ic on growth factors and broad-sp ectrum antibiotics and antifungals .
d
Laboratory abnormalities.
TEAEs and Laboratory Abnormalities Occurring in ≥ 20% of Patients
a
Any TEAE
b,c
Fatigue
Decreased appetite
Any related TEAE
c
Nausea
Constipation
Diarrhea
Cytokine release syndrome
0 10 20 30 40 50 60 70 80 90 100
Percentage of Patients
Neutropenia
d
Anemia
d
Thrombocytopenia
d
Hypotension
Dizziness
Headache
Grade 1 2 3 4 5
8
Data as of October 9, 2017
5/7/2018
10
High Rates of Response in FULL DLBCL Population
Homogeneous Patient Population Moving Forward in Pivotal Cohort
FULL By B-NHL Subtype
DLBCL, NOS tFL tCLL/MZL FL3B/PMBCL
BOR, n
a
88 57 19 10 2
ORR, % (95% CI) 74 (63, 83) 74 (60, 85) 84 (60, 97) 50 (19, 81) 100 (16, 100)
CR, % (95% CI) 52 (41, 63) 51 (37, 64) 63 (38, 84) 30 (7, 65) 100 (16, 100)
≥ 3-mo f/u, n
b
72 46 15 9 2
3-mo ORR, % (95% CI) 53 (41, 65) 54 (39, 69) 67 (38, 88) 22 (3, 60) 50 (1, 99)
3-mo CR, % (95% CI) 44 (33, 57) 43 (29, 59) 60 (32, 84) 22 (3, 60) 50 (1, 99)
≥ 6-mo f/u, n
c
54 37 10 6 2
6-mo ORR, % (95% CI) 35 (23, 49) 35 (20, 53) 50 (19, 81) 0 (0, 46) 50 (1, 99)
6-mo CR, % (95% CI) 31 (20, 46) 32 (18, 50) 40 (12, 74) 0 (0, 46) 50 (1, 99)
BOR, best overall response; NOS, not otherwise specified.
Homogeneous CORE patient population
identified and will move forward in pivotal trial
10
a
Includes patients with event of PD, d eath, or 28-day restaging scan s. Two patients did not have restagin g scans available.
b
The denominator is nu mber of patients who received JC AR017 ≥ 3 months ago, prior t o data snapshot date, with an efficac y assessment at month 3 or pr ior assessment of PD or death.
c
The denominator is number of patien ts who received JCAR017 ≥ 6 months ago, prior to data snapsh ot date, with an efficacy assessm ent at month 6 or prior assessment o f PD or death. Data as of October 9, 2017
Overall Survival (OS)
Early OS Encouraging in High-Risk DLBCL Patient Population
14
Data as of October 9, 2017
100
80
60
40
20
0
30 6 9 12 15 18
PR 16 11 8 2 0
All 965 39 30 15 3 0
CR 936 26 20 12 3 0
Non-
responder
13 2 2 1 0
Overall Survival (months)
% Survival
At Risk
Median F/U=6.2 months
All : NR (NR, NR); 86% (73, 93)
CR : NR (NR, NR); 94% (78, 98)
PR : 9.0 mos (4.9, NR); 81% (44, 95)
Nonresponders: 6.2 mos (0.6, NR); 66% (33, 86)
CORE
PR 19 12 8 2 0
All 1388 53 37 20 4 0
CR 1246 35 25 16 4 0
Overall Survival (months)
At Risk
Non-
responder
23 6 4 2 1 0
100
80
60
40
20
0
30 6 9 12 15 18
% Survival
CR : NR (13.7, NR); 92% (78, 98)
PR : 9.0 mos (3.8, NR); 75% (40, 91)
Nonresponders: 5.4 mos (1.5, NR); 46% (21, 68)
FULL
Median F/U=6.2 months
All : NR (9.0, NR); 78% (66, 86)
mOS (95% CI); 6 mo OS (95% CI)
mOS, median OS; mos, mo nths.
TRANSCEND NHL 001: Conclusions
§JCAR017 (lisocabtagene maraleucel; liso-cel), a CD19-directed CAR T cell product with defined
composition, shows potent and durable responses in poor-prognosis patients with R/R aggressive NHL
§The pivotal cohort has begun enrollment in the CORE population based on encouraging durable
response rate at dose level 2
–74% ORR and 68% CR rate at 3 months and 50% CR at 6 months
–Across dose levels, 80% of patients in CR at 3 months remain in response at month 6 and 92% of patients in CR
at 6 months remain in response
§Liso-cel toxicities have been manageable at all dose levels tested with a favorable safety profile that
may enable outpatient administration
–Low rates of severe CRS (1%) and NT (12%)
–Evaluation of outpatient administration is ongoing in pivotal cohort (Maloney et al, abstract 1552)
§Optimized, commercial-ready liso-cel defined cell product being utilized for pivotal cohort with expected
apheresis to product release < 21 days
15
5/7/2018
11
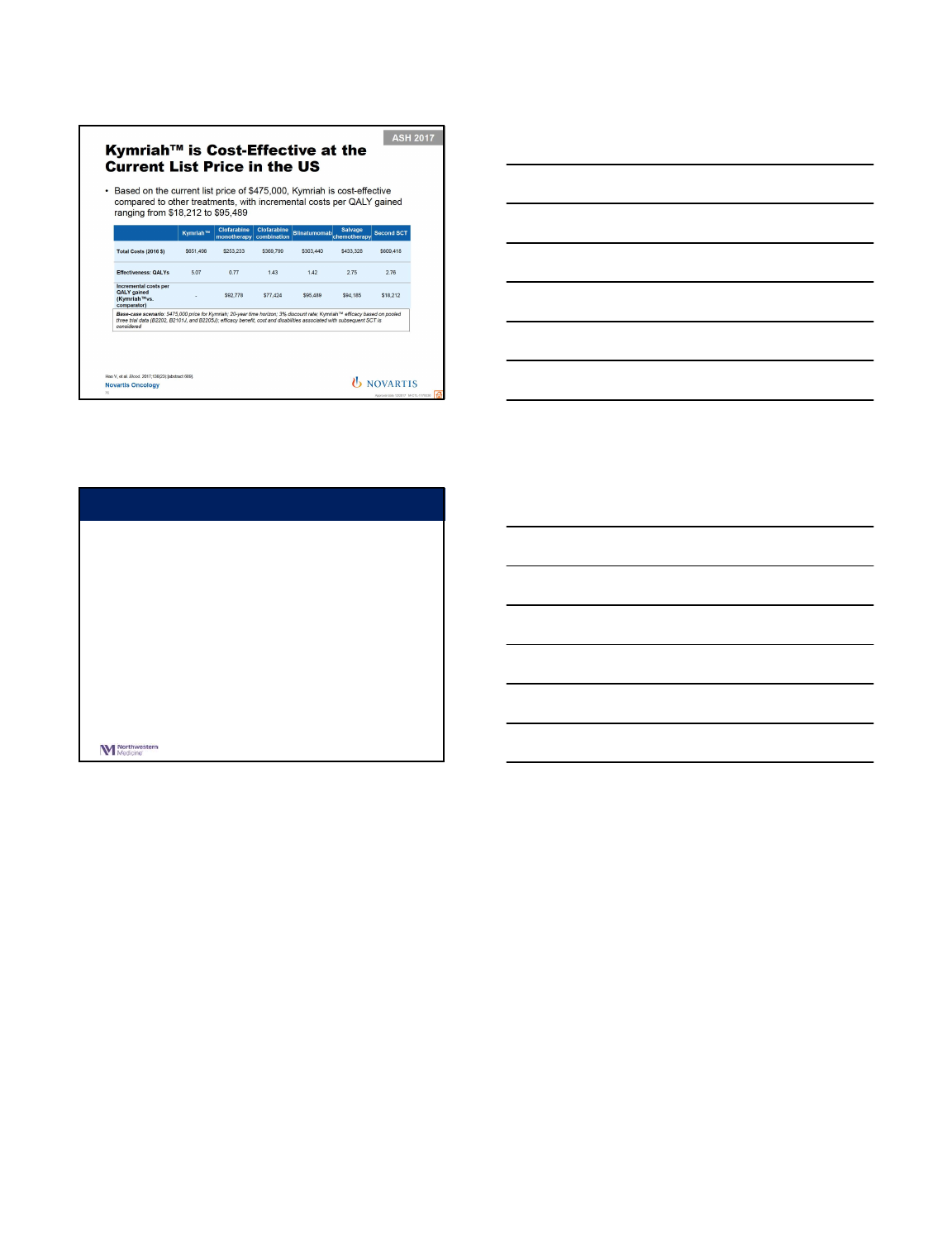
Challice L Bonifant, published online
20 April 2016. doi:10.1038/mto.2016.11
CAR T Toxicities
BASELINE Day +30
DLBCL AFTER CAR-T THERAPY
5/7/2018
12
•We are entering a new era in treatment for lymphomas
•CAR T-cell therapy may represent one of the more effective
immunotherapeutic options
•Challenges
•Time to manufacture
•Patient selection and toxicity management
•integration with or replacement of existing modalities (chemotherapy, small
molecule inhibitors, autologous vs allogeneic stem transplant)
•cost
•CAR T-cell therapy likely to alter how we treat DLBCL
Summary
5/8/2018
1
Treatment of Newly Diagnosed DLBCL in 2018
John Pagel, M.D., Ph.D.
Chief of Hematologic Malignancies
Director of Hematopoietic Stem Cell Transplantation Program
CENTER FOR BLOOD DISORDERS AND STEM CELL TRANSPLANTATION
SWEDISH CANCER INSTITUTE
COI
•Consultant for Pharmacyclics and Gilead Sciences
WHO Classification of Aggressive B- Cell Lymphoid Neoplasms 2008 v
2016
2016
D
iffuse large B-cell lymphoma (DLBCL),N OS
−
REQUIRED Germinal Center DLBLC
−
REQUIRED ABC DLBCL
−
Tcell/histiocyte-rich large B-cell lymphoma
−
Primary DLBCLof the CNS
−
Primary cutaneous DLBCL, legtype
−
EBV positive DLBCL, NOS
−
EBV+ Mucocutaneous ulcer
DL
BCL associated with chronic inflammation
L
ymphomatoid granulomatosis
P
rimary mediastinal (thymic) large B-cell lymphoma
In
travascular large B-cell lymphoma
A
LK positive large B-cell lymphoma
Pl
asmablastic lymphoma
P
rimary effusion lymphoma
HHV8 positive DLBCL, NOS
Hi
gh grade B-cell lymphoma, with MYC and BCL2 and/or BCL6 rearrangements
High
grade B-cell lymphoma, NOS
B
-celllymphoma, unclassifiable, with features intermediate between DLBCL
a
nd classical Hodgkin lymphoma
Swerdlow et al. Blood (2016) http://dx.doi.org/10.1182/blood-2016-01-643569 *Excluding Precursor Neoplasms
2008
D
iffuse large B-cell lymphoma (DLBCL), NOS
−
OPTIONAL Germinal Center/Activated B cell
−
Tcell/histiocyte-rich large B-cell lymphoma
−
Primary DLBCLof the CNS
−
Primary cutaneous DLBCL, legtype
−
EBV positive DLBCL, NOS
−
EBV+ Mucocutaneous ulcer
DL
BCL associated with chronic inflammation
L
ymphomatoid granulomatosis
P
rimary mediastinal (thymic) large B-cell lymphoma
In
travascular large B-cell lymphoma
A
LK positive large B-cell lymphoma
Pl
asmablastic lymphoma
P
rimary effusion lymphoma
Large B
-cell lymphoma arising in HHV8-associated multicentric Castleman Dis
High
grade B-cell lymphoma, NOS
5/8/2018
2
Coiffier et al. ASCO 2007.Abstract 8009.
International Standard of Care: R-CHOP
Rituximab 375 mg/m2 day 1
Cyclophosphamide 750 mg/m2 day 1
Doxorubicin 50 mg/m2 day 1
Vincristine 1.4 mg/m2 day 1 (2 mg max)
Prednisone 40 mg/m2 (or 100 mg) daily x 5
Age > 60 Pegfilgrastim 6 mg subcut day 2
Original Gela LNH 98-5 confirmed in multiple studies
GOYA R-CHOP v G-CHOP for DLBCL: Study design
•Statistical assumption for primary endpoint: G-CHOP v R-CHOP HR = 0.75
•Number of CHOP cycles pre-planned in advance for all pts at each site
•Stratification factors: number of CHOP cycles, IPI, geographic region
•§Confirmatory endpoint
•Exploratory endpoint: PFS by cell of origin
Primary endpoint
Secondary
and other endpoints
•
PFS (INV-assessed)
•
PFS (IRC-assessed)§
•
OS, EFS, DFS, DoR, TTNT
•
CR/ORR at EOI (+/− FDG-PET)
•
Safety
Previously untreated DLBCL
Age ≥18 years
IPI 2 or IPI 1 (not age) or IPI 0
with bulky disease 7.5cm
ECOG PS ≤2
Target enrolment: 1400
G-CHOP (N=706)
G1000mg C1 D1/8/15 and C2–8 D1
CHOP 6 or 8 cycles every 21 d ays
R-CHOP (N=712)
R 375mg/m2C1–8 D1
CHOP 6 or 8 cycles every 21 da ys
Randomized 1:1
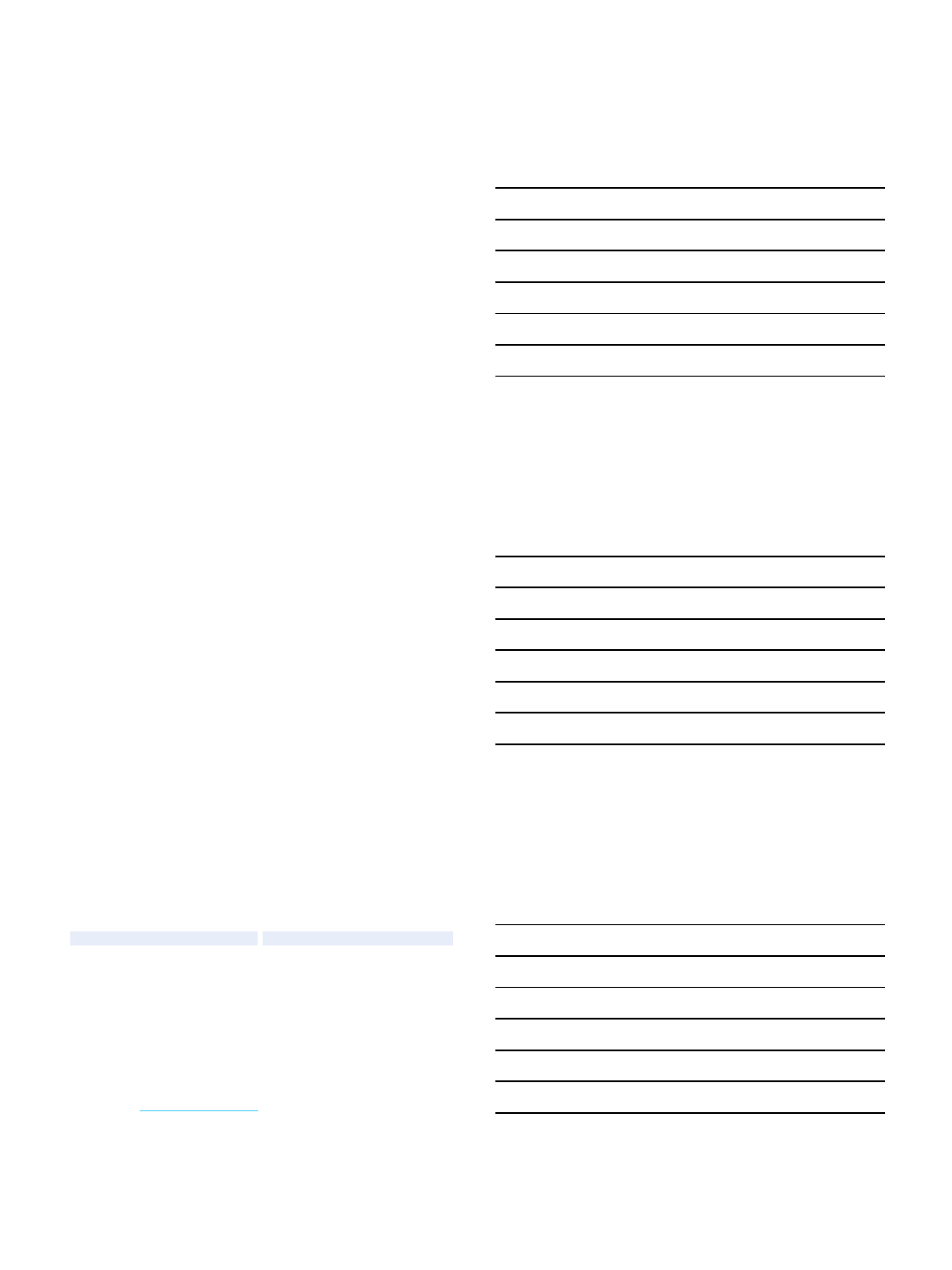
Vitolo U, et al. ASH 2016 Abstract 470
GOYA: Investigator-assessed PFS and OS
*Stratified analysis; stratification factors: IPI score, number of
planned chemotherapy cycles. Median follow-up: 29 months
R-
CHOP,
n=712
G-
CHOP,
n=706
Pts with event, n (%)
215 (30.2)
201 (28.5)
1
-yr PFS, % 79.8 81.6
2
-yr PFS, % 71.3 73.4
3
-yr PFS, % 66.9 69.6
HR (95%
CI), p-value* 0.92 (0.76, 1.11),
p=0.3868
Vitolo U, et al. ASH 2016 Abstract 470
No. of patient s at risk
R-CHOP
G-CHOP
712
706
616
622
527
540
488
502
413
425
227
240
142
158
96
102
41
39
6
2
R-CHOP (n=712)
G-CHO P (n=706)
6 12 18 24 30 36 42 48 54
Time (months)
60
Probability
1.0
0.8
0.6
0.4
0.2
0
0
No. of patients at risk
R-CHOP
G-CHOP
712
706
663
659
617
616
586
582
540
552
319
316
190
201
138
138
71
67
9
8
R-CHOP (n=712)
G-CHOP (n=706)
Probability
1.0
0.8
0.6
0.4
0.2
0
0 6 12 18 24 30 36 42 48 54
Time (months)
60
PFS OS
R-
CHOP,
n=712
G-
CHOP,
n=706
Pts with event, n (%)
126 (17.7) 126 (17.8)
1
-yr OS, % 89.9 90.7
2
-yr OS, % 83.7 83.9
3
-yr OS, % 81.4 81.2
HR (95%
CI), p-value* 1.00 (0.78, 1.28),
p=0.9982

5/8/2018
3
Dose-Adjusted (DA)-EPOCH-R
•Dosed every 21 days if ANC > 1/μL and PLTS > 100KμL
•Dose-adjusted based on ANC nadir:
–>500/μL, increase cytotoxic drugs by 20%
–<500/μL for 1-3 days, no change
–<500/μL for >3 days or FN, decrease cytotoxic drugs by 20%
Wilson, J Clin Oncol 2008 26: 2717-2724; Lunning et al. SHO, abstract
Drug
Dose
Rituximab
375 mg/m
2day 1 IVPB
Doxorubicin
10 mg/m
2/day x 4 by CI
Vincristine
0.4 mg/m
2/day x 4 by CI
Etoposide
50 mg/m
2/day x 4 by CI
Cyclophosphamide
750 mg/m
2day 5 IVBP
Prednisone
60 mg/m
2BID days 1-5 oral
Filgrastim
*
Weight
-adjusted dose starting day 5 until ANC > 5000/μL
*Data from MSKCC showed identical rate of dose-adjustment with filgrastim or
pegfilgrastim
Wilson W H et al. Haematologica 2012;97:758-765
CALGB 59910: Multi-Center DA-EPOCH-R, Outcomes
CALGB 50303: DA-EPOCH-R vs RCHOP21
•OBJECTIVES:
–Primary
•EFS untreated de novo DLBCL treated with RCHOP vs DA-R-EPOCH
•Determine molecular predictors of outcome (using molecular profiling) in patients treated with these regimens.
–Secondary
•Compare ORR and OS
•Compare the toxicity of these regimens in these patients.
•Correlate the clinical parameters (i.e., toxicity, response, survival outcomes, and laboratory results) with molecular
profiling in patients treated with these regimens.
•Determine the use of molecular profiling for pathological diagnosis
•PET/CT parameters as potential biomarker, predictive value of interim PET, reproducibility and standardization of PET/CT
DA-EPOCH-R
R-CHOP
DeNovo DLBCL
No discordant
disease
CS IIX-IV
DeNovo DLBCL
No discordant
disease
CS IIX-IV
R
A
N
D
O
M
I
Z
E
n= 478 patients (239 per treatment arm)
Wilson et al. ASH 2016, Abstract 489
5/8/2018
4
Arm
N
Events
3 Y (95% CI) 5 Y (95% CI)
R
-CHOP 233 64 0.81 (0.75-0.85) 0.69 (0.62-
0.75)
DA
-EPOCH-R 232 70 0.79 (0.73-
0.84)
0.66
(0.59-
0.72)
Wilson et al. ASH 2016, Abstract 489
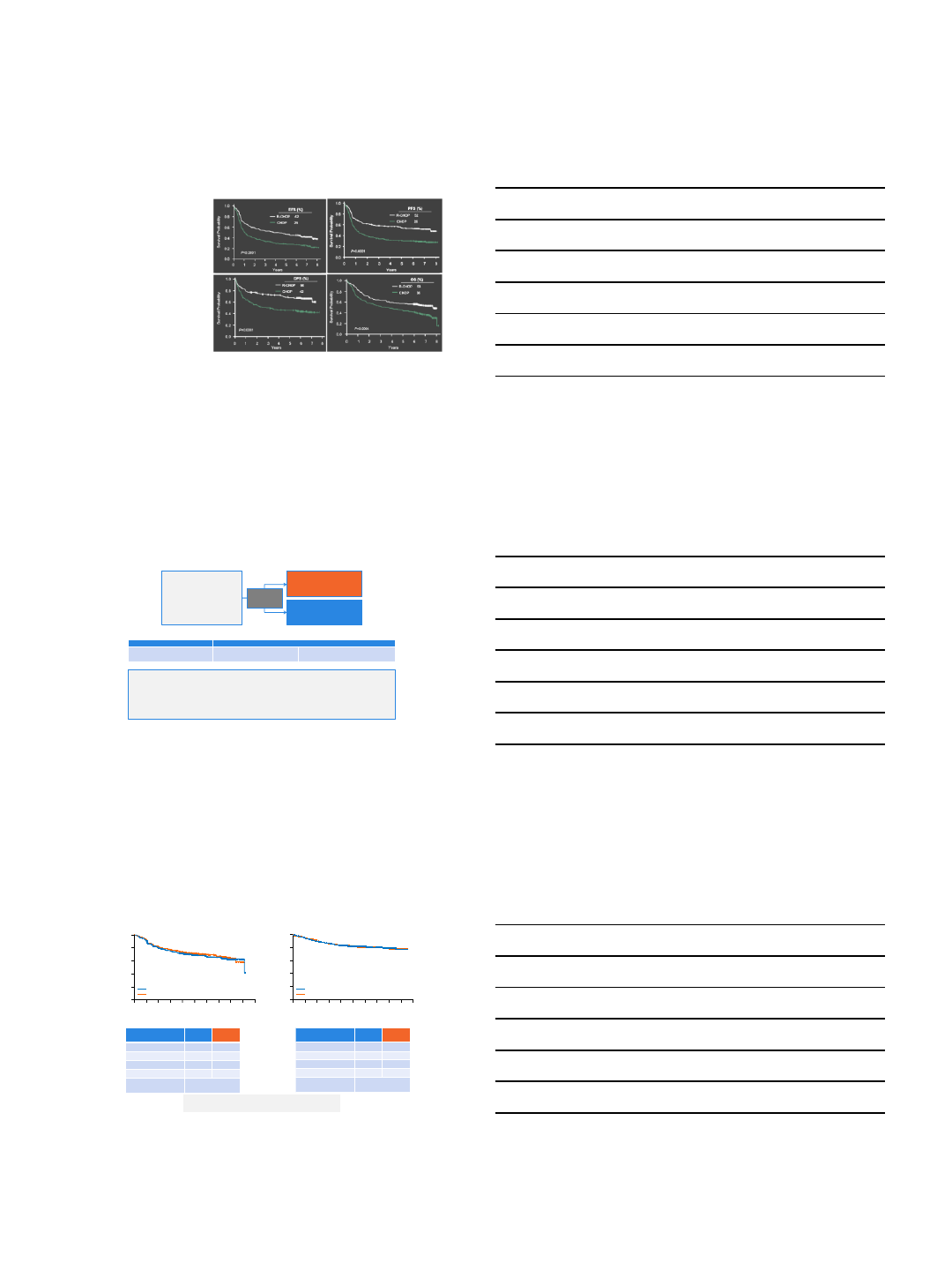
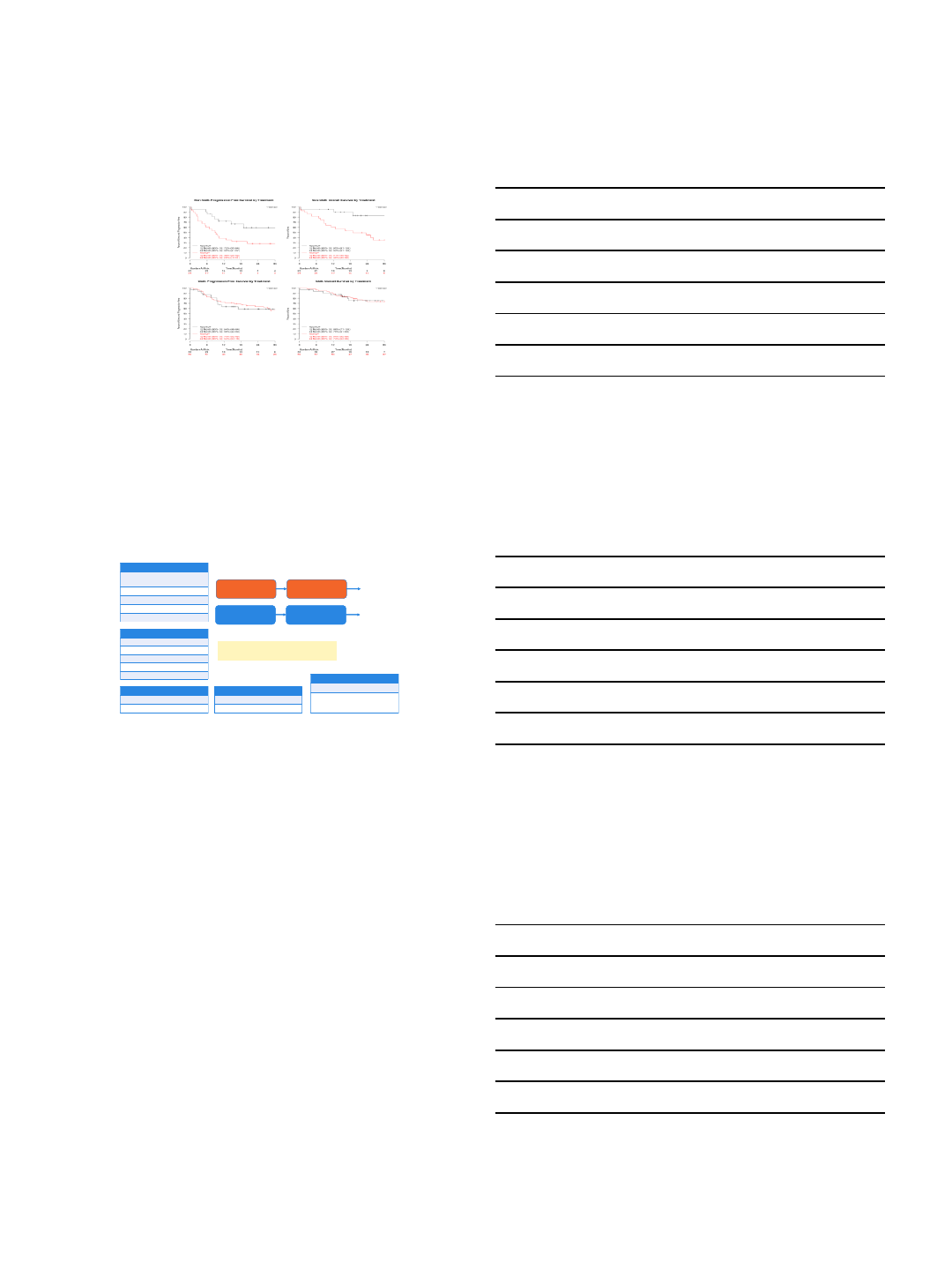
CALGB 50303: Event-Free and Overall Survival
Arm
N
Events
3 Y (95% CI) 5 Y (95% CI)
R
-CHOP 233 44
0.85 (0.80
-0.89) 0.80 (0.74-
0.85)
DA
-EPOCH-R 232 50
0.85 (0.79
-
0.89)
0.76 (0.70-
0.71)
Years from Study Entry
Probability event free
0 1 2 3 4 5
0.0 0.2 0.4 0.6 0.8
R-CHOP
DA-EPOCH-R
HR=1.14 (0.82-1.61)
p = 0.4386
PFS
Years from Study Entry
Survival Probability
0 1 2 3 4 5
0.0 0.2 0.4 0.6 0. 8
R-CHOP
DA-EPOCH-R
HR=1.18 (0.79-1.77)
p = 0.42
OS
Additional analyses pending including outcome by COO, DH and DE
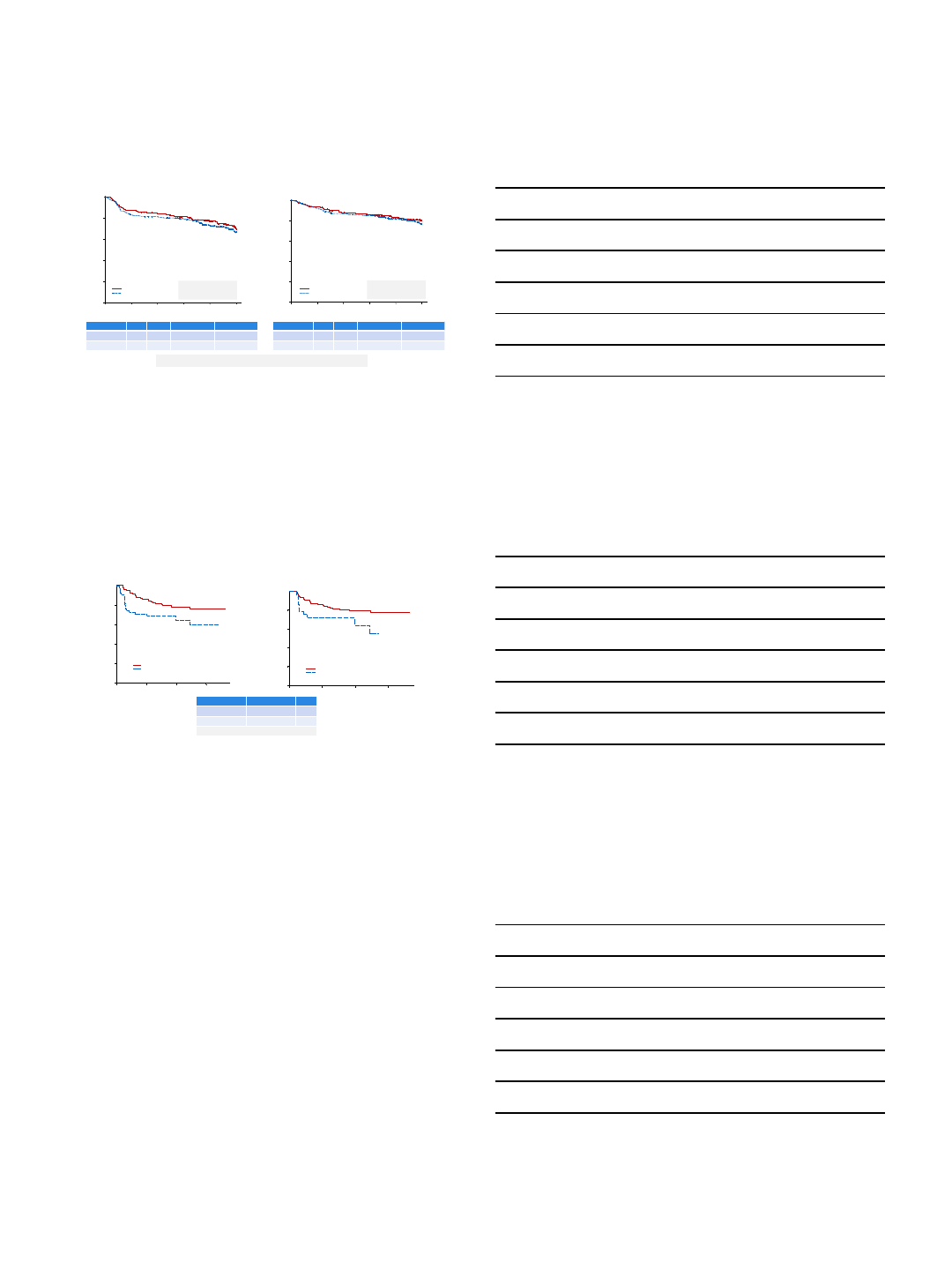
CALG 50303: PET Sub-study n=171
Interim
Post Cycle 2
Years from Study Entry
Probability event free
0 2 4 6
0.0 0.2 0.4 0.6 0.8
PET-negative
PET-positive
N= 104
N= 55
Events= 23
Events= 19
p-value= 0.0339
EOT
Post Cycle 6
Years from Study Entry
Probability event free
0 2 4 6
0.0 0.2 0.4 0.6 0.8
PET-negative
PET-positive
N= 121
N= 29
Events= 25
Events= 10
p-value= 0.0567
PET neg = Deauville 1-3
Schoder, H, Menton, France 2016; Wilson et al. ASH 2016, Abstract 489
Timing of PET
3 year EFS
p
Interim
81% (
-) vs 69% (+) 0.034
End
of treatment
80% (
-) vs 72% (+) 0.057
Treatment arms combined for analysis
Methods for determination of COO
•Gene Expression Profiling on fresh tissue
–‘The gold standard’
–Not practically applicable in clinical practice
•Immunohistochemistry
–Widely available
–Reproducibility may be difficult
–Many assays (Hans, Choi, Muris, Natkurman, Tally)
–Lack of correlation with GEP in many studies
•GEP of formalin-fixed paraffin-embedded (FFPE) tissue
–Multiple platforms
–Hybrid capture/fluorescent reporter emerging as a widely validated assay
5/8/2018
5
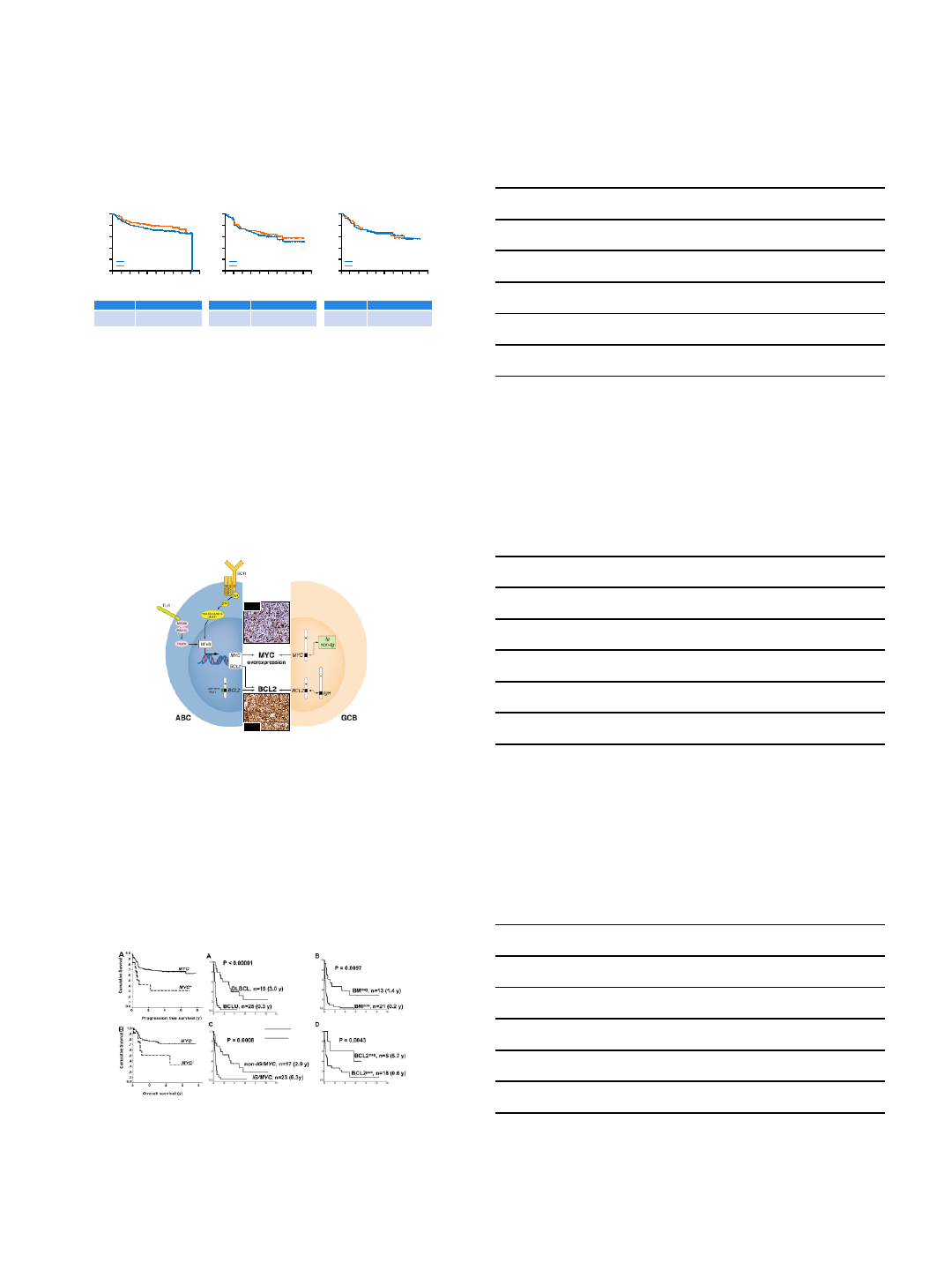
GOYA: COO is prognostic
*Exploratory analysis; COO classification available in 933 pts; missing COO classifications due to: restricted
Chinese export license, n=252; CD20+ DLBCL not confirmed, n=102; missing/inadequate tissue, n=131; PFS
HR=0.82 (0.64, 1.04) in pts with COO classification; PFS HR=1.18 (0.85, 1.64) in pts without COO classification
†Unstratified analysis
Vitolo U, et al. ASH 2016 Abstract 470
HR (95%
CI)†0.72 (0.50, 1.01)
3
-yr PFS 71% vs 79%,
R-CHOP vs G-CHOP
HR (95%
CI)†0.86 (0.57, 1.29)
3
-yr PFS 58% vs 61%,
R-CHOP vs G-CHOP
HR (95%
CI)†1.02 (0.60, 1.75)
3
-yr PFS 64% vs 62%
R-CHOP vs G-CHOP
GCB ABC Unclassified
No. of patients at risk
R-CHOP
G-CHOP
269
271
234
246
200
217
191
207
166
178
94
113
64
75
46
50
19
22
2
1
Time (months)
0 6 12 18 24 30 36 42 48 54 60
0
0.2
0.4
0.6
0.8
1.0
Probability
No. of patients at risk
R-CHOP
G-CHOP
118
125
101
106
84
90
77
84
65
79
36
42
21
31
15
17
5
8
1
1
Time (months)
0 6 12 18 24 30 36 42 48 54 60
0
0.2
0.4
0.6
0.8
1.0
Probability
No. of patients at risk
R-CHOP
G-CHOP
75
75
65
63
54
57
52
51
43
43
36
28
25
17
15
10
6
3
1
Time (months)
0 6 12 18 24 30 36 42 48 54 60
0
0.2
0.4
0.6
0.8
1.0
Probability
R-CHOP (n=269)
G-CHOP (n=271)
R-CHOP (n=118)
G-CHOP (n=125)
R-CHOP (n=75)
G-CHOP (n=75)
Double-Hit B-cell Lymphomas
Mottock & Gascoyne, CCR 2014
MYC
BCL2
Expression of MYC
and BCL2 is a
consequence of the
biology of ABC
DLBCL
Translocation of BCL2
and/or BCL6 is seen in
a subset of GC DLBCL;
simultaneous
translocation of MYC
is seen in ~6% of cases
of GC DLBCL.
Reclassified in WHO as
HGBCL with
rearrangement of MYC
and BCL2 and/or BCL6
“Double Hit”BCL2/MYC TranslocatedMYC+ DLBCL
Savage KJ et al. Blood 2009; Johnson NA et al. Blood 2009
R-CHOP
treated
MYC Translocation in DLBCL Associated with Poor Outcomes
with CHOP-based Therapy
5/8/2018
6
DA-EPOCH-R for DLBCL with translocation of MYC and BCL2 and/or BCL6
Characteristic
Number
52
Median age
61 y (29
-80)
IPI Score
0-2
3-5
35%
65%
Histology
DLBCL
BCL
-U
86%
14%
BCL2 translocated
by FISH
14/31*
*31 of 52 tested
Progression-Free Survival of DH Case (n=14)*
0
10
20
30
40
50
60
70
80
90
100
6 12 18 36 42 48 54
*
Months
Proportion
Progression free
24 30
*Cases were censored if they were transplanted;
number censored for transplant NOT REPORTED
Dunleavy, ASH 2015
Adam M. Petrich et al. Blood 2014;124:2354-2361
Impact of induction regimen and SCT on outcomes in DH lymphoma: a multicenter
retrospective analysis
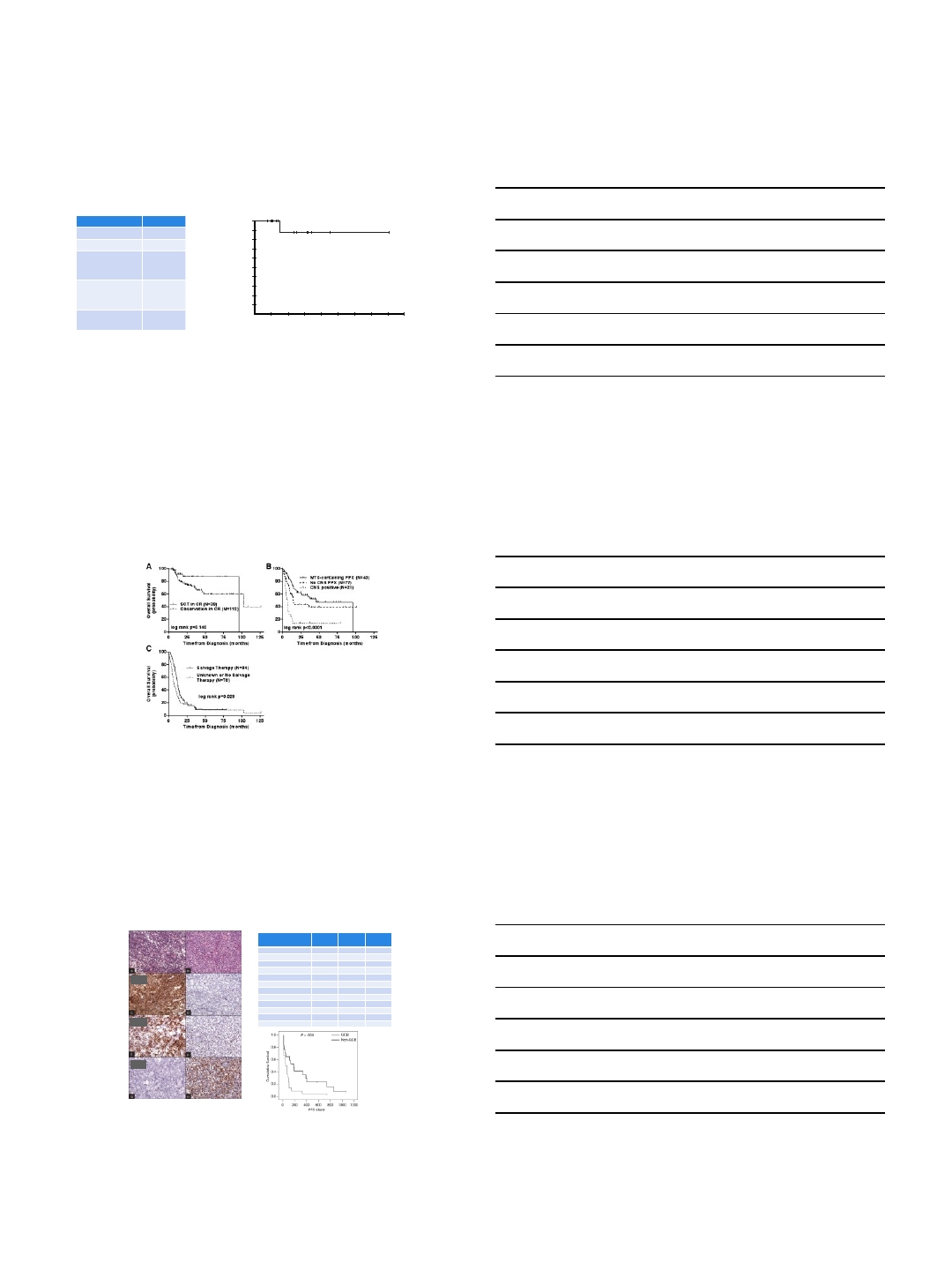
Lenalidomide for DLBCL: Impact of Cell of Origin
CD10
BCL6
IRF4
All GCB Non-GCB
Lenalidomide cycles
Median (Range) 2 (1-35) 2 (1-21) 4 (1-35)
Response
CR 6 (15.0) 1 (4.3) 5 (29.4)
PR 5 (12.5) 1 (4.3) 4 (23.5)
SD 7 (17.5) 7 (30. 4) 0
PD 21 (52.5) 14 (60.9) 7 (41.2)
Unknown 1 (2.5) 0 1 (5.9)
ORR (CR + PR)
11 (27.5) 2 (8.7) 9 (52.9)
PFS, mo
Median 2.6 1.7 6.2
95% CI 0.9-4.2 0.3-3.1 2.9-9.6
Hernandez-Ilizaliturri et al, Cancer 2011 117:5058
5/8/2018
7
Mayo Series: Outcomes for RL-CHOP v R-CHOP Case Match Control by
Cell of Origin
Nowakowski et al. ASH 2012, ASCO 2014
Non-GC DLBCL
GC DLBCL
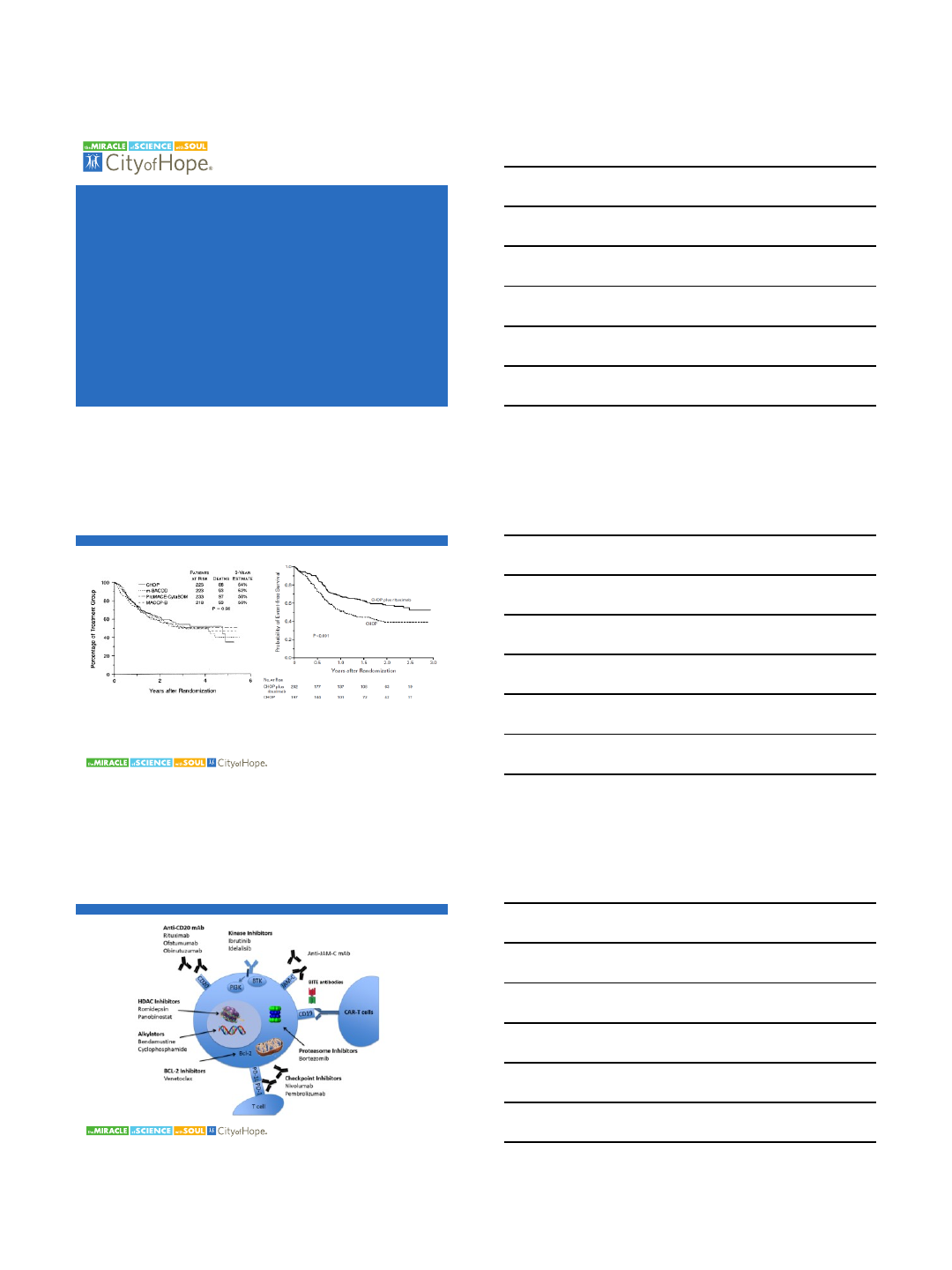
ROBUST (NCT02285062): Lenalidomide Plus R-CHOP Chemotherapy (R2-CHOP) Versus Placebo Plus R-
CHOP Chemotherapy in Subjects With Untreated ABC-DLBCL, Phase 3, double-blind, placebo-
controlled
Inclusion
DLBCL, ABC-type, untreated
COO by Lymph2Cx
Measurable disease by CT/MRI
ECOG 0-2
Age 18-80
IPI ≥2
Evaluation
Interim evaluation after cycle 4
EOT (6 cycles) FDG
-PET
Clinical Endpoints
Primary: Progression-free survival
Secondary: OS, CRR, Duration of CR,
TTNT, ORR, QOL
Sample Size/Statistical Plan
Sample size: 560
90% to detect increase in PFS of 60%
Double-blind, placebo
controlled
Randomization 1:1
Exclusion
Lymphoma other than DLBCL
HIV, HBV, HCV active infections
LVEF <45%
Peripheral neuropathy, grade ≥2
Other malignancies < 5 years disease free
Study Start Date: January 2015
Estimated Study Completion Date: September 2022
Estimated Primary Completion Date: June 2018
Placebo +
R-CHOP × 4
Placebo +
R-CHOP × 4
Lenalidomide +
R-CHOP × 4
Lenalidomide +
R-CHOP × 4
Placebo +
R-CHOP × 2
Placebo +
R-CHOP × 2
Lenalidomide +
R-CHOP × 2
Lenalidomide +
R-CHOP × 2
⇑
Interim Evaluation
NR off study
⇑
EOT Evaluation
IWG 2007 with
Deauville PET
Conclusions
•DLBCL should always be approached with curative intent
–The majority of patients will be cured with R-CHOP
–R-CHOP remains the standard of care for de novo DLBCL in most situations
–DA-R-EPOCH is a reasonable alternative with OS ~80% at 5 years
•No difference in EFS and OS
–G-CHOP does not appear to be better than R-CHOP for newly diagnosed DLBCL
•Not all DLBCL are created equally
–GCB versus non-GCB
•Data is limited for GCB versus non-GCB
•MYC alteration and Double Hit DLBCL remain challenging
•Many novel agents and approaches are in development and warrant further investigation
5/7/2018
1
Click to edit Master Presentation Date
NOVEL TREATMENTS OF DIFFUSE
LARGE B-CELL LYMPHOMA
Jasmine Zain, M.D.
Director, T-Cell Lymphoma Program
City of Hope National Medical Center
Fisher RI et al. N Engl J Med 1993;328:1002-1006.Coiffier B, et al. NEJM. 2002.
NO NEW FDA-APPROVED AGENTS SINCE RITUXIMAB!
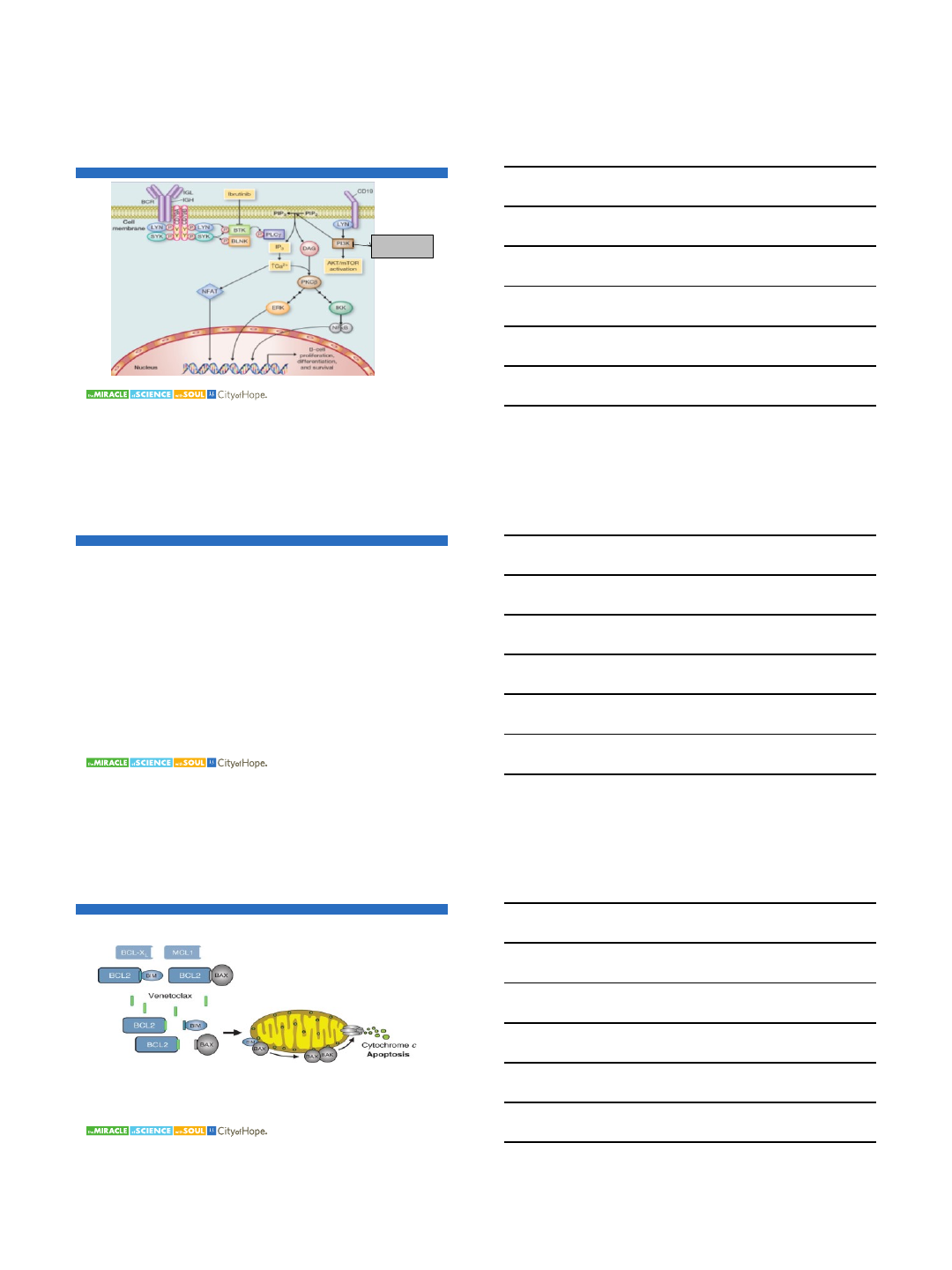
POTENTIAL TARGETS FOR TREATING B-CELL MALIGNANCIES
5/7/2018
2
•Immune modifiers -
Lenalidomide
•Molecualar targets- Ibrutinib,
Venetoclax, Idelalisib
•Antibodies and antibody drug
conjugates –anti CD37
•Blinotumumab and other
bispecific antibodies
•Immune-check point inhibitors
•Microenvoirnment targets- Anti
CD47
•Epigenetic agents
BROAD CATEGORIES FOR TARGETED AGENTS FOR DLBCL
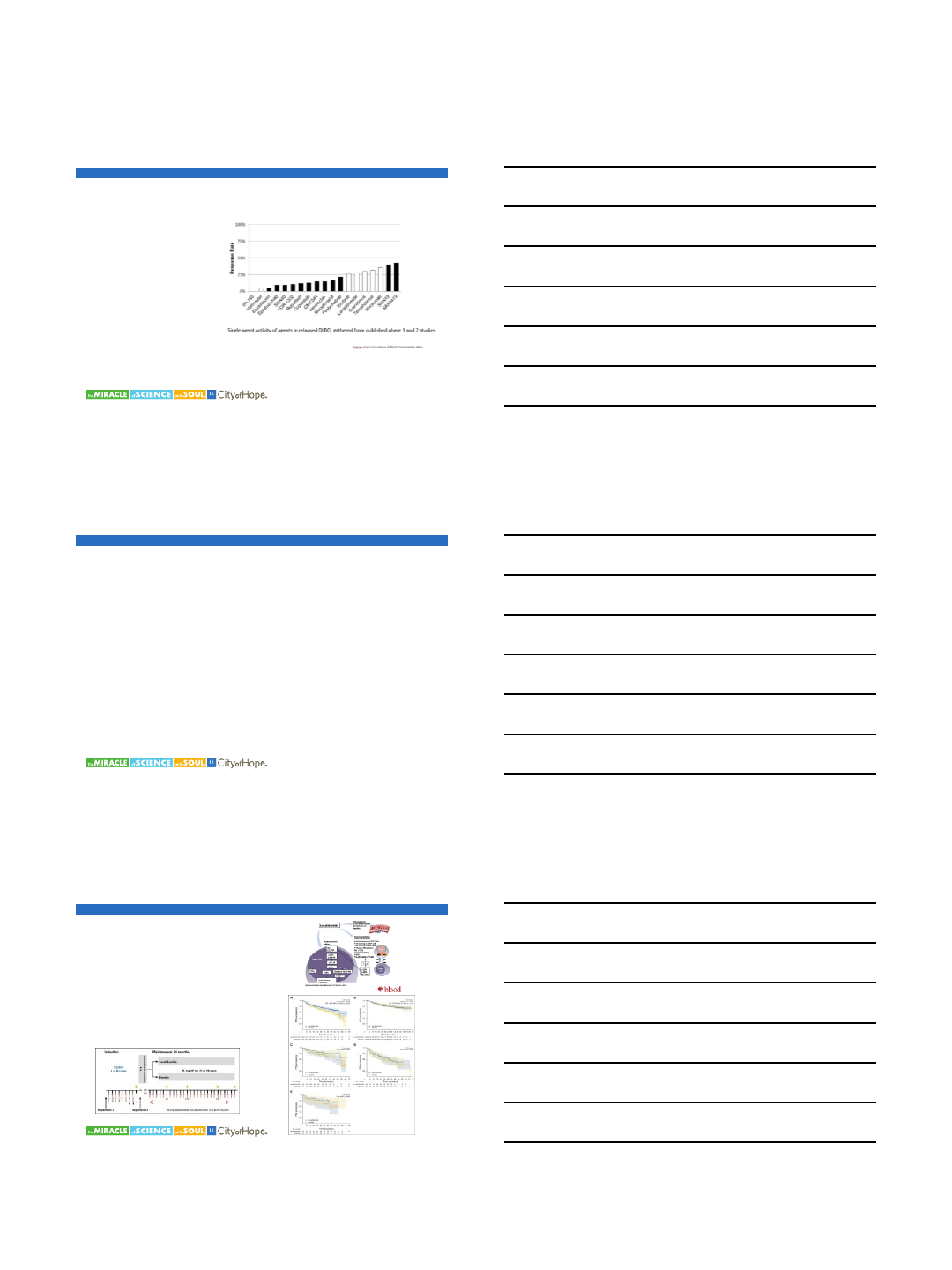
IMPROVE ON R-CHOP?
•HDAC inhibitors = no
•Bortezomib = no
•Next up:
–Lenalidomide (immunomodulator)
–Polatuzumab vedotin (anti-CD79b ADC)
–Venetoclax (BCL2 inhibitor)
–SGN-CD19A (anti-CD19 ADC)
Lenalidomide has an ORR of 19% and 28% in RR.
Witzig, et al. Zinzani, et al. 2008.
More effective in non-GCB subtype- ORR 53% vs
9%. Hernandez, et al. Cancer. 2011.
Tested in combination with Rituximab, RICE and as
maintenance post transplant. Feldman, et al. 2014.
Lenalidomide maintenance vs placebo in elderly
patients after RCHOP. PFS was not reached in the
Len arm vs 58.9 months in the placebo arm. Diff was
notable in the GCB subtype. Thieblemont, et al. Blood. 2017.
LENALIDOMIDE
5/7/2018
3
TARGETED TERAPIES –PI3K INHIBITORS
Idealisib, TGR-
1202, copanlisib
B-cell
Herrera AF and Jacobsen EJ. CCR. 2014.
IBRUTINIB
•Selective and irreversible inhibitor of BTK
•Modest clinical activity in DLBCL as a single agent - 23% seen mostly
in the ABC-subtype.
•Phase 1b/2 study of Ibrutinib plus lenalidomide and Rituximab is
underway. Preliminary results show a RR of 44%.
•RCHOP vs RCHOP+ibrutinib for non-GCB subtype of DLBCL.
•Most common side effects are rash and diarrhea.
Konopleva M, et al. Cancer Discovery. 2016.
SINGLE AGENT
RESPOSNE RATE IN R/R
DLBCL WAS 18%
BCL-2 INHIBITION - VENETOCLAX
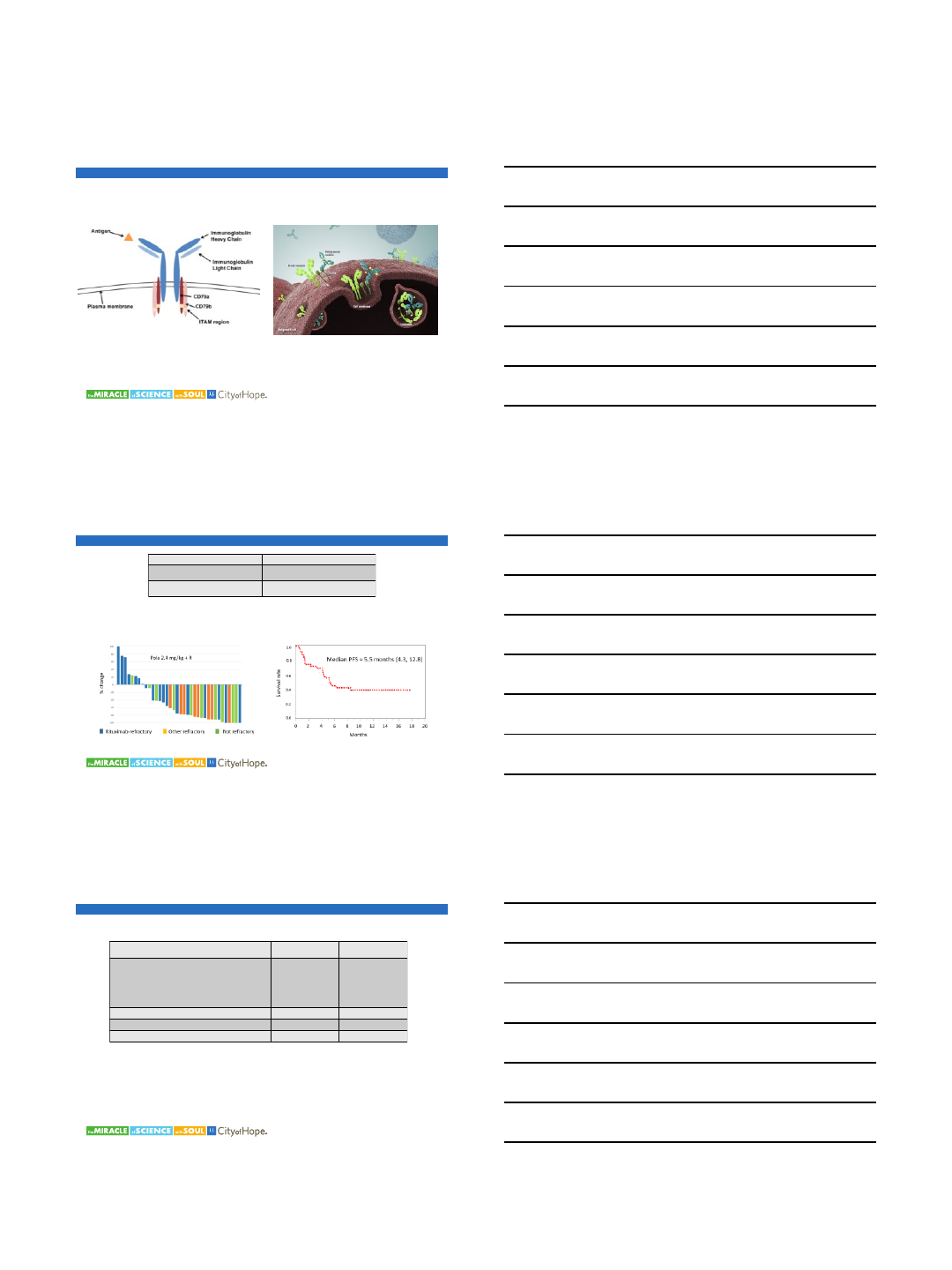
5/7/2018
4
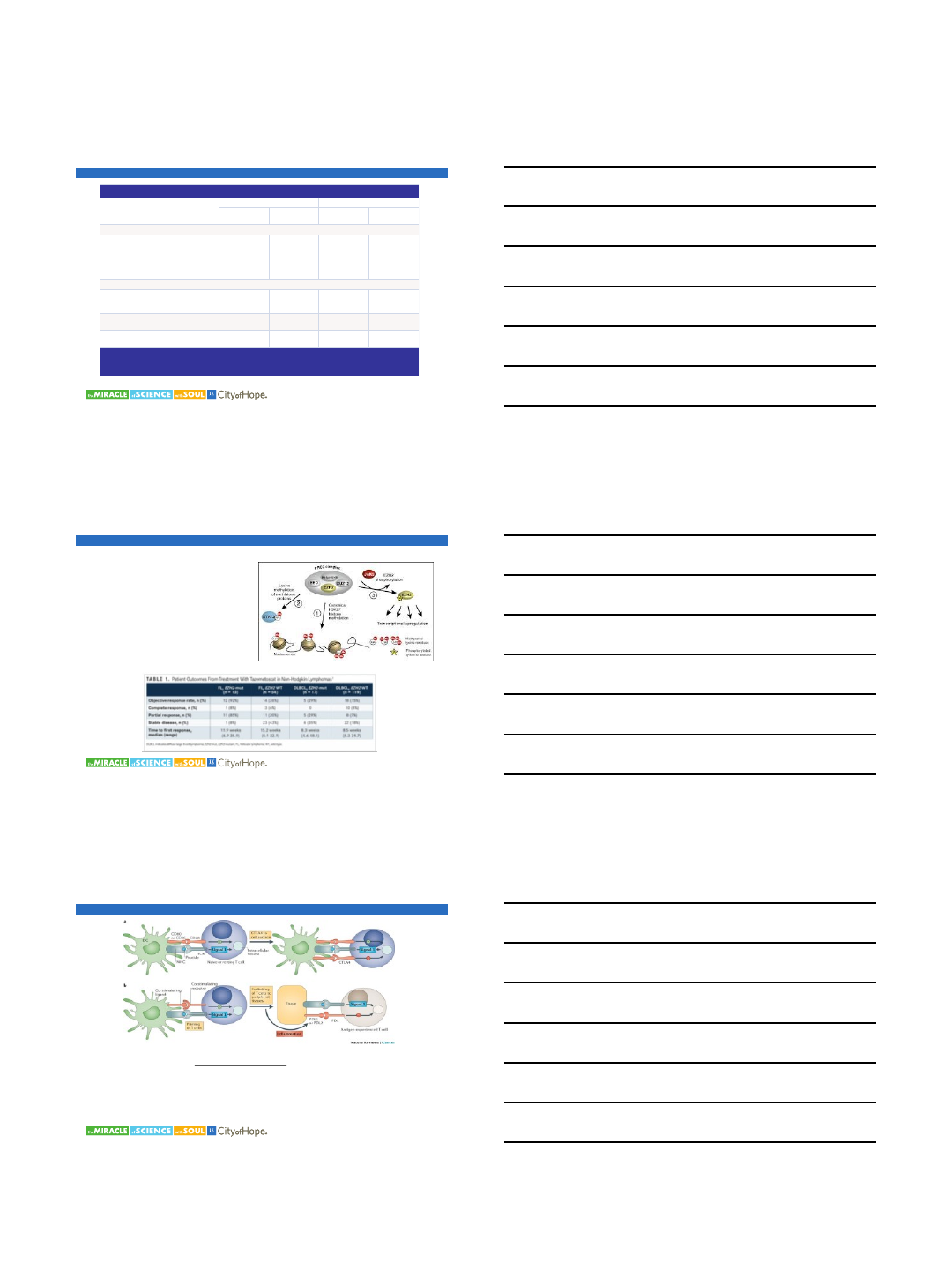
POLATUZUMAB VEDOTIN- ADC TARGETS CD79B CONJUGATED TO MMAE
POLATUZUMAB VEDOTIN IN R/R DLBCL
Treatment Regimen Best Overall Response
Pola 1.8–2.4 mg/kg 51%1
Pola 1.8–2.4 mg/kg + rituximab 56%2
Morschhauser F, et al. Blood 2014; 124:4457.
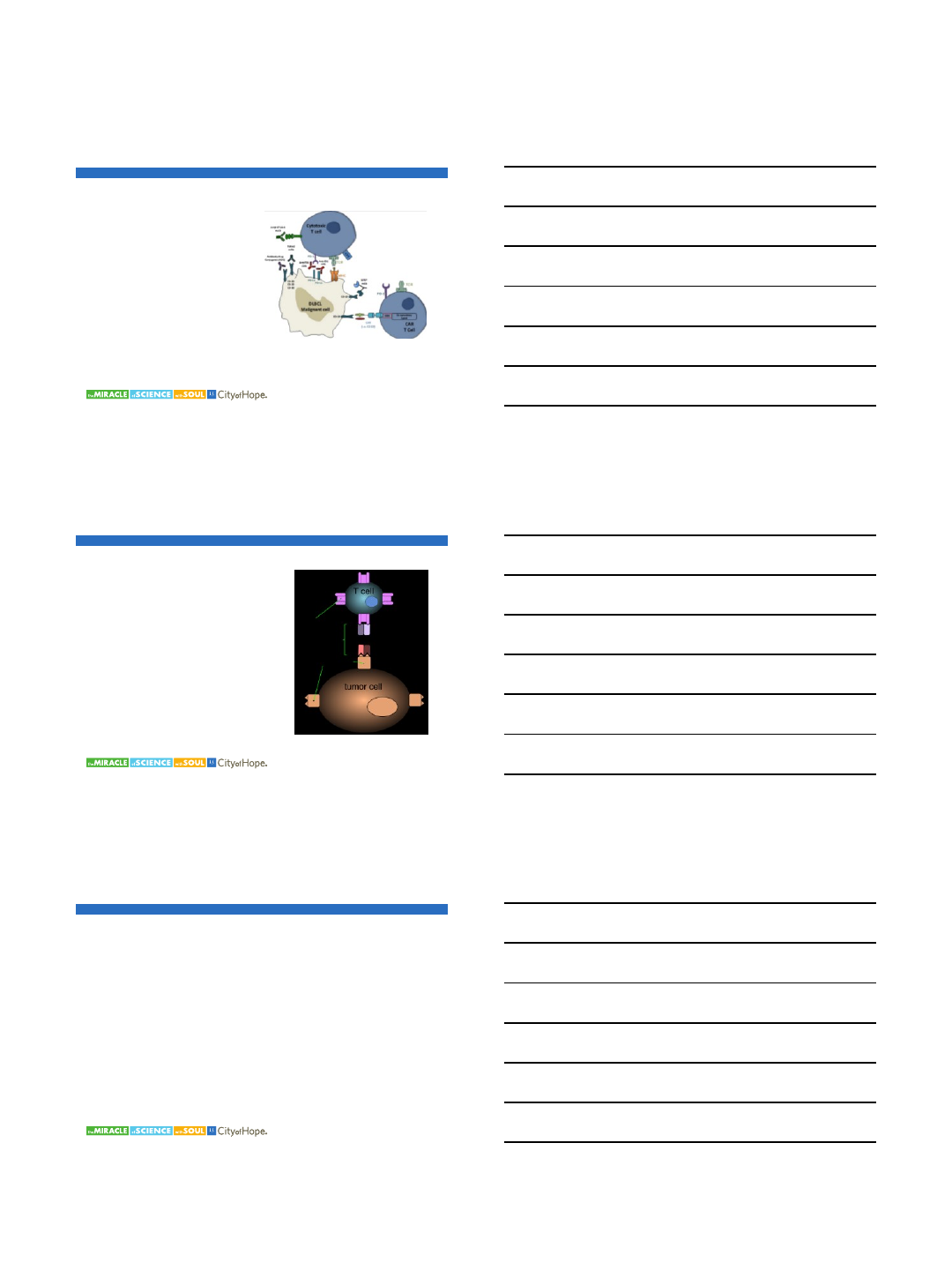
R/R DLBCL from the ROMULUS trial: pola + rituximab:
Best SPD Change from Baseline Progression-Free Survival
Palanca-Wessels MCA, et al. Lancet Oncol 2015; 16: 704-15.
FL
(N=35)
DLBCL
(N=43)
Objective response, n (%)
Complete Response
[90% CI]
Partial Response
[90% CI]
24 (69)
11 (31)
[19–47]
13 (37)
[24–52]
17 (40)
9 (21)
[11–34]
8 (19)
[10–31]
Stable disease, n (%) 4 (11) 0
Progressive disease, n (%) 1(3) 18 (42)
Unable to evaluate, n (%) 6 (17)b8 (19)c
aPatients who received ≥1 dose of study treatment; assessment per Lugano Criteria (Cheson 2014)
bNo Pola dose due to IRR from G, taken off-study (n=2); no PET assessment (n=2); taken off -study due to neutropenia before assessment (n=1); fatal pneumonia
before assessment (n=1)
cDied before assessment (n=1); PD not by PET (n=4); not assessed due to hospitalization / taken of f study (n=2);
W/D consent / not dosed (n=1)
Data Cut-Off: 26 JUL 2016
Download this presentation: http://tago.ca/TPHI
POLATUZUMAB VEDOTIN PLUS OBINUTUZUMAB
5/7/2018
5
POLA + R/G-BENDAMUSTINE
Investigator-Assessed Response by PET/CTa
FL DLBCL
Pola + BR
(n=6)
Pola + BG
(n=26)
Pola + BR
(n=6)
Pola + BG
(n=27)
Best Objective Response
ORR, n (%)
CR
PR
SD
PD
UE
6 (100)
4 (67)
2 (33)
0
0
0
23 (89)
17 (65)
6 (23)
0
1 (4)
2 (8)
3 (50)
2 (33)
1 (17)
0
2(33)
1 (17)
16 (60)
11 (41)
5 (19)
2 (7)
6 (22)
3 (11)
Objective Response at End of Treatment
ORR, n (%)
CR
PR
5 (83)
4 (67)
1 (17)
21 (81)
17 (65)
4 (15)
3 (50)
2 (33)
1 (17)
10 (37)
9 (33)
1 (4)
Median duration of response, mo (range)b16.1
(3.8–16.3)
NR
(15.2–20.6)
NR
(0.03–14.5)
NR
(0.03–15.7)
Median PFS, mo
(range)b
18.4
(7.2–18.9)
NR
(1.4–17.1)
NR
(1.5–22.7)
5.4
(0.03–17.6)
aModified Lugano 2014 response criteria: for CR, repeat bone marrow biopsy required to confirm clearance of bone marrow if involved at
screening. bKaplan-Meier method; range data are at clinical data cut-off.
CT, computed tomography; ORR, objective response rate; PD, progressive disease; PET, positron emission tomography; PFS,
progression-free survival; PR, partial response; SD, stable disease; UE, unable to evaluate.
EZH2 - INHIBITORS
Enhancer of zeste homolog 2 (EZH2)
results in methylation of the histone H3-
associated with gene repression
EZH2 activating mutations and
overexpression is seen in cancers, GCB
type of DLBCL not ABC subtype
EZH2 inhibitor Tazemostat is in clinical
trials- first in class inhibitor of mutated and
wild type EZH2.
Initial trials showed promising activity in B-
cell lymphomas.
CHECKPOINT INHIBITION: PD-1 PATHWAY
Pardoll DM. Nature Reviews Cancer. 12, 252-264 (April 2012).
Effects of PD-L1 binding:
Inhibits T-cell activation
Inhibits cytokine production
Decreased cytolytic activity of CD4+ and CD8+ cells
5/7/2018
6
CHECK POINT INHIBITORS IN DLBCL
•CTLA-4 AND PD-1 are being
targeted.
•CT-011 (pidilizumab) in post
ASCT- 16 mo PFS 72% including
high risk patients. Armand, et al.
2013.
•Nivolumab- ORR 36% Lesokin, et al.
2016.
•Pembrolizumab- in trials –
encouraging rates in PMBCL and
CNS.
•Combinations with other
therapies especially CAR-T.
Juarez-Salcedo, et al. 2017.
BISPECIFIC ANTIBODIES
Phase II study of single agent bispecific
engager (BiTE®) antibody
Blinatumomab–ORR was 43% including
19% CRs. Viardot, et al. 2016.
Trials ongoing with lenalidmide and
alternative strategies of administration
(subcutaneous) using Blinatumomab,
lenalidmide.
Other targets –CD 20 bispecific engager
antibodies- encouraging RR and do not
require CD19.
CONCLUSION
•Many promising strategies to treat RR DLBCL
•Combination therapies are likely to win
•Attempts to improve upon RCHOP continue especially for double hit
and ABC subtypes
