MergedFile 8dfccaf6 3eaf 4453 809b 3198b646f0eb
2017-11-21
: Pdf 8Dfccaf6-3Eaf-4453-809B-3198B646F0Eb 8dfccaf6-3eaf-4453-809b-3198b646f0eb 11 2017 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 36
11/21/2017
1
Hypertension:
Guidelines and Updates
William C. Cushman, MD
Professor, Preventive Medicine, Medicine, Physiology
University of Tennessee Health Science Center
Chief, Preventive Medicine, Memphis VA Medical Center
Memphis, Tennessee
Hypertension 2017: Where are We Now?
VuMedi Webinar, November 21, 2017
Presenter Disclosure Information
William C. Cushman, MD, FACP, FASH, FAHA
FINANCIAL DISCLOSURE:
Institutional Grant: Lilly
Uncompensated Consulting: Takeda, Novartis
I was a member of JNCs 7 & 8, but not the 2017 ACC/AHA HTN Guidelines
The content does not necessarily represent the official views of the SPRINT
or ACCORD Steering Committees, the NIH, the VA, or the U.S. government
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/
APhA/ASH/ASPC/NMA/PCNA
Guideline for the Prevention, Detection, Evaluation, and
Management of High Blood Pressure in Adults
© American College of Cardiology Foundation and American Heart Association, Inc.
11/21/2017
2
Publication Information
This slide set is adapted from the 2017
ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/ NMA/PCNA Guideline for the
Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults
Published on November 13, 2017, available at: Hypertension and Journal of the
American College of Cardiology.
The full-text guidelines are also available on the following websites: AHA
(professional.heart.org) and ACC (www.acc.org)
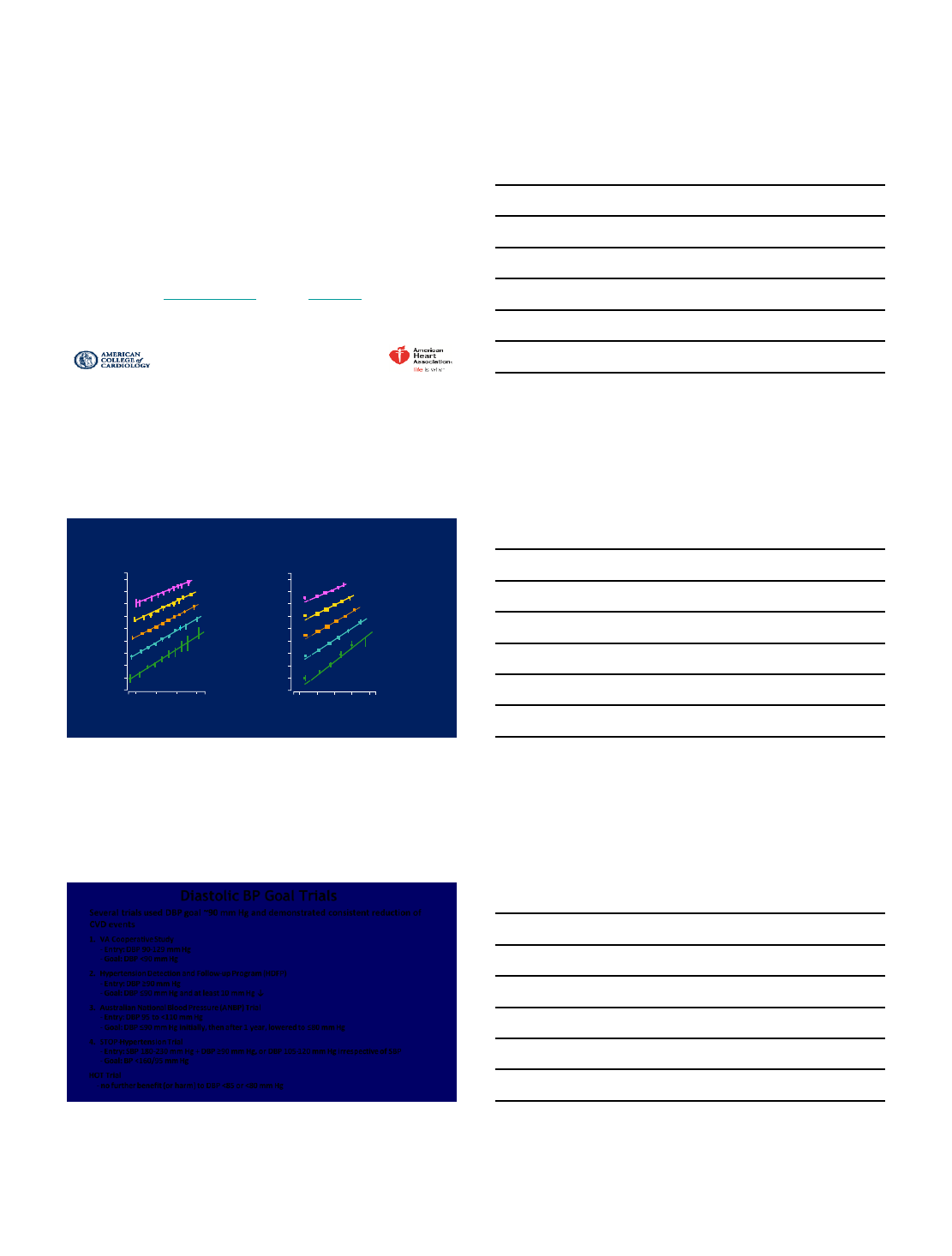
Blood Pressure (BP) and Cardiovascular Disease (CVD) Risk
Systolic Blood Pressure (SBP)
40-49 years
50-59 years
60-69 years
70-79 years
80-89 years
Age at risk:
IHD Mortality
(Floating Absolute Risk and 95% CI)
256
128
64
32
16
8
4
2
1
120 140 160 180
Usual SBP (mm Hg)
Di astolic Blood Pressure (DBP)
IHD Mortality
(Floating Absolute Risk and 95% CI)
256
128
64
32
16
8
4
2
1
70 80 90 100 110
Usual DBP (mm Hg)
Age at risk:
40-49 years
50-59 years
60-69 years
70-79 years
80-89 years
Lewington et al. Lancet. 2002;360:1903-1913.
Diastolic BP Goal Trials
Several trials used DBP goal ~90 mm Hg and demonstrated consistent reduction of
CVD events
1. VA Cooperative Study
- Entry: DBP 90-129 mm Hg
- Goal: DBP <90 mm Hg
2. Hypertension Detection and Follow-up Program (HDFP)
-Entry: DBP ≥90 mm Hg
- Goal: DBP ≤90 mm Hg and at least 10 mm Hg ↓
3. Australian National Blood Pressure (ANBP) Trial
- Entry: DBP 95 to <110 mm Hg
- Goal: DBP ≤90 mm Hg initially, then after 1 year, lowered to ≤80 mm Hg
4. STOP-Hypertension Trial
- Entry: SBP 180-230 mm Hg + DBP ≥90 mm Hg, or DBP 105-120 mm Hg irrespective of SBP
- Goal: BP <160/95 mm Hg
HOT Trial
- no further benefit (or harm) to DBP <85 or <80 mm Hg
11/21/2017
3
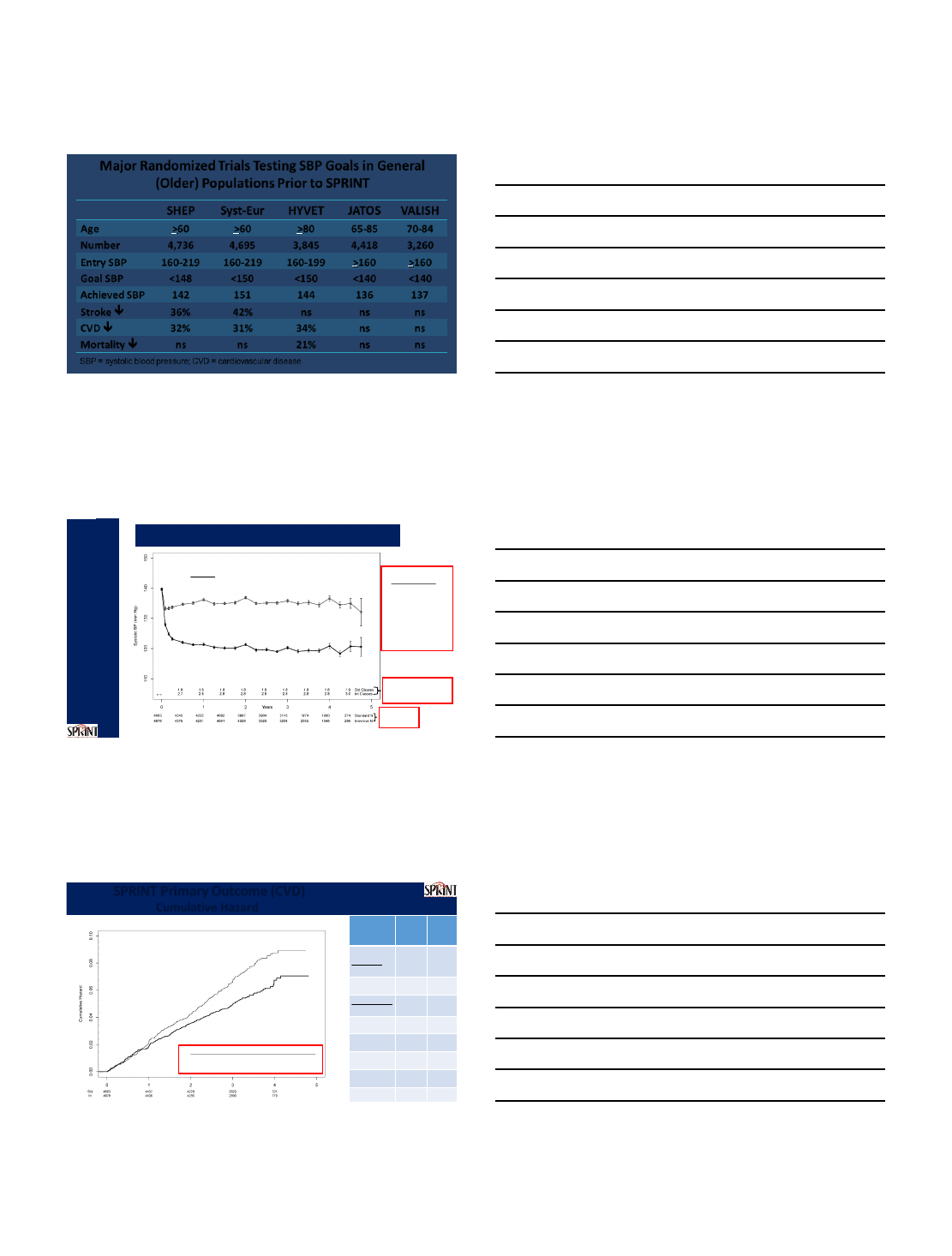
Major Randomized Trials Testing SBP Goals in General
(Older) Populations Prior to SPRINT
SHEP Syst-Eur HYVET JATOS VALISH
Age >60 >60 >80 65-85 70-84
Number 4,736 4,695 3,845 4,418 3,260
Entry SBP 160-219 160-219 160-199 >160 >160
Goal SBP <148 <150 <150 <140 <140
Achieved SBP 142 151 144 136 137
Stroke 36% 42% ns ns ns
CVD 32% 31% 34% ns ns
Mortality ns ns 21% ns ns
SBP = systolic blood pressure; CVD = cardiovascular disease
Systolic BP Intervention Trial (SPRINT)
Mean SBP
136.2 mm Hg
Mean SBP
121.4 mm Hg
Average SBP
(During Follow-up)
Standard: 134.6 mm Hg
Delta: 13.5 mm Hg
Intensive: 121.5 mm Hg
Average number of
antihypertensive
medications
Number of
participants
Standard
Intensive
Year 1
SBP goal <140 mm Hg
SBP goal <120 mm Hg
Number of
Participants
Hazard Ratio = 0.75 (95% CI: 0.64 to 0.89)
Standard
Intensive
(243 events)
During Trial (median follow-up = 3.26 years)
Number Needed to Treat (NNT)
to prevent a primary outcome = 61
SPRINT Primary Outcome (CVD)
Cumulative Hazard
(319 events)
The SPRINT Research Group. N Engl J Med. 2015;373:2103-16
Hazard
Ratio
P value
Primary
Outcome
0.75
<0.001
Components
All
MI
0.83
0.19
Non
-MI ACS
1.00
0.99
All Stroke
0.89
0.50
All HF
0.62
0.002
CVD Death
0.57
0.005
25% reduction
P<0.001
11/21/2017
4
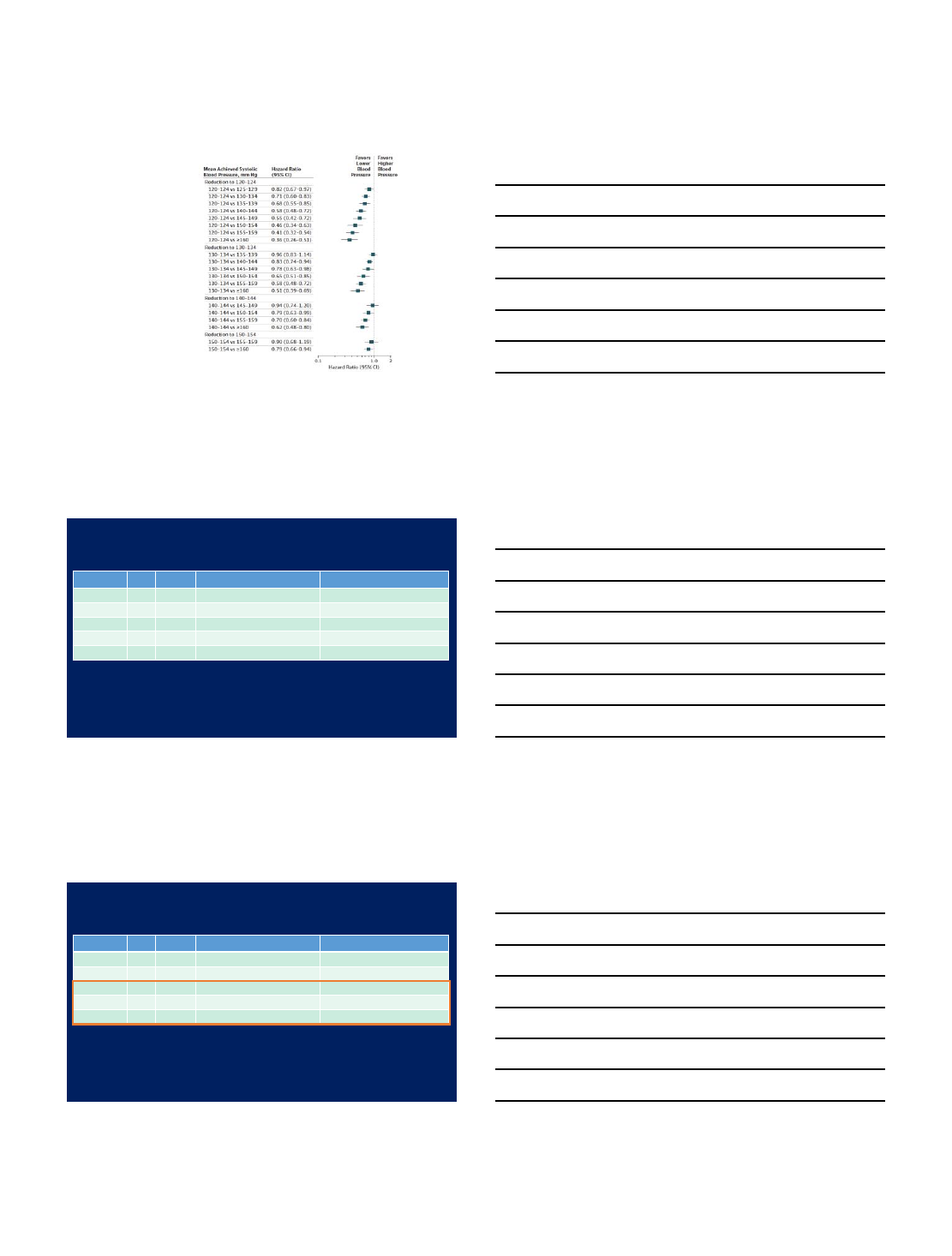
Hazard ratios and 95%CIs
for major CVD associated
with more intensive
reductions in SBP
Bundy JD, et al. JAMA Cardiol.
2017;2:775-81
42 trials, n=144,220
Most of the trials included
significant numbers of participants
with diabetes mellitus
Changes in BP Categories from JNC7 to
the New Guideline
SBP DBP JNC7 2017 ACC/AHA
<120 and <80 Normal BP Normal BP
120–129 and <80 Prehypertension Elevated BP
130–139 or 80–89 Prehypertension Stage 1 hypertension
140–159 or 90-99 Stage 1 hypertension Stage 2 hypertension
≥160 or ≥100 Stage 2 hypertension Stage 2 hypertension
The categorization of BP should be based on the average of ≥ 2 readings on ≥ 2 occasions following a
standardized protocol.
Adults with SBP and DBP in two categories are designated into the higher category.
Changes in BP Categories from JNC7 to
the New Guideline
SBP DBP JNC7 2017 ACC/AHA
<120 and <80 Normal BP Normal BP
120–129 and <80 Prehypertension Elevated BP
130–139 or 80–89 Prehypertension Stage 1 hypertension
140–159 or 90-99 Stage 1 hypertension Stage 2 hypertension
≥160 or ≥100 Stage 2 hypertension Stage 2 hypertension
The 2017 ACC/AHA guideline definition of hypertension:
SBP ≥ 130 mm Hg or
DBP ≥ 80 mm Hg
11/21/2017
5
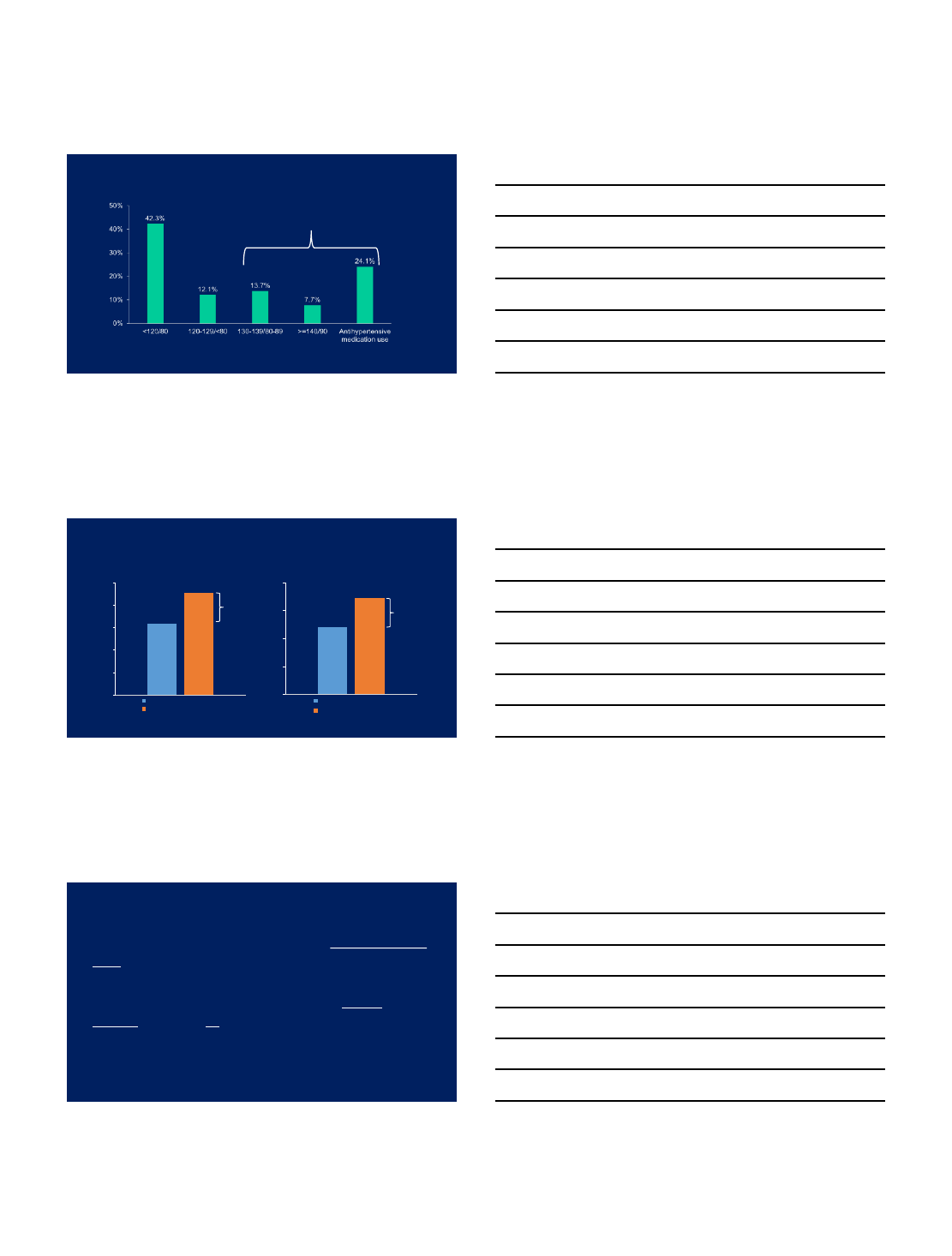
Distribution of US adults into BP Categories –
NHANES 2011-2014
Prevalence of hypertension: 45.6%
Muntner et. al., Journal of the American College of Cardiology 2017 (in press)
Muntner, et. al., Circulation 2017 (in press)
Normal BP Elevated BP
31.9%
45.6%
0%
10%
20%
30%
40%
50%
JNC7 guideline
2017 ACC/AHA guideline
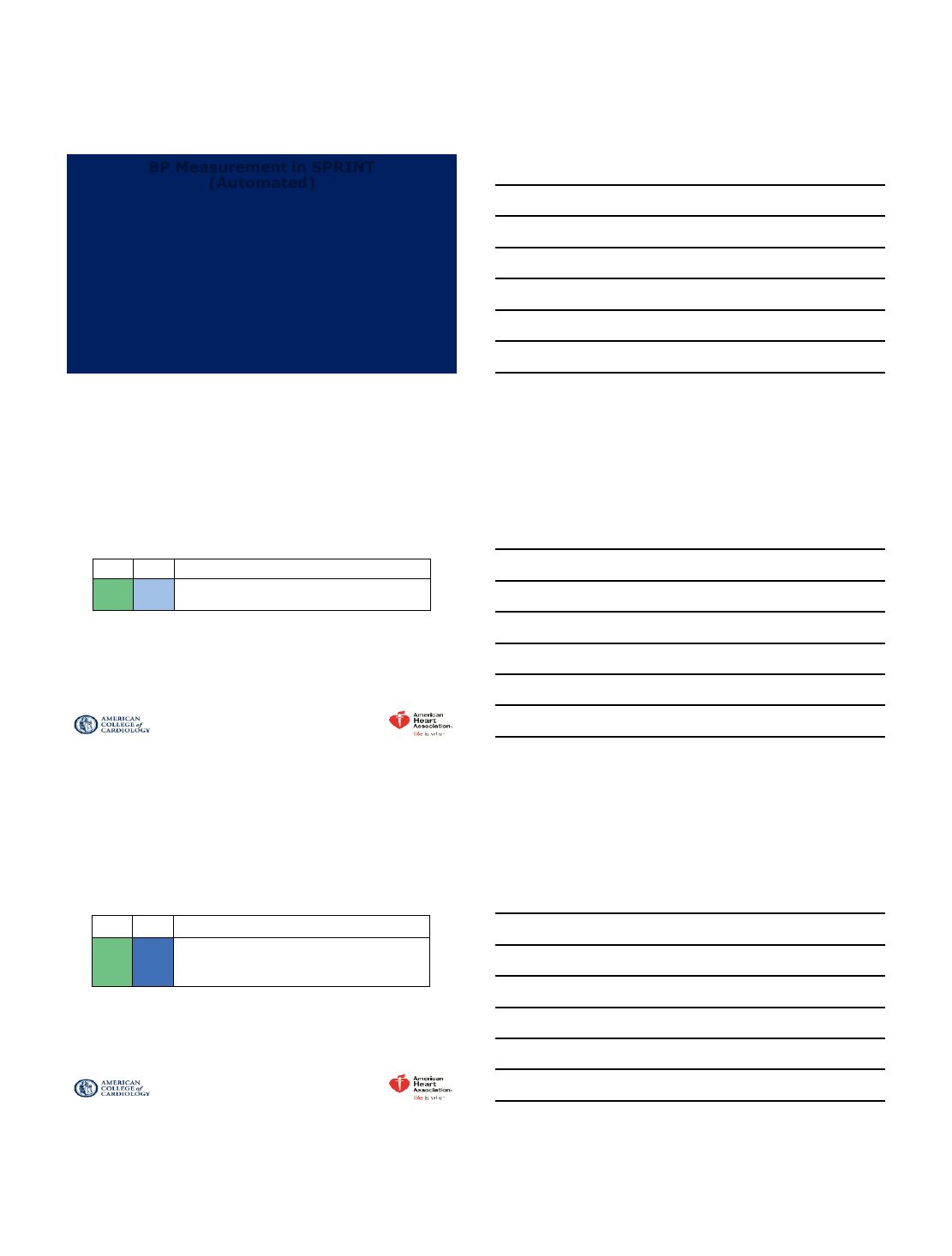
Prevalence of Hypertension –
2017 ACC/AHA and JN7 Guidelines
72.2
103.3
0
30
60
90
120
JNC7 guideline
2017 ACC/AHA guideline
Prevalence of hypertension, % Number of US adults with hypertension, millions
Muntner et. al., Journal of the American College of Cardiology 2017 (in press)
Muntner, et. al., Circulation 2017 (in press)
13.7% 31.1, M
BP Measurement Methodology in SPRINT
•Similar to what has been used in virtually all HTN outcome
trials defining the recommended BP thresholds and goals
in guidelines.
•Similar to what has been recommended for clinical
practice by virtually all HTN guidelines around the world
for decades, including all JNCs, ASH/ISH, VA/DoD,
ESH/ESC, UK/NICE, Canadian/CHEP, Australian, ...
11/21/2017
6
BP Measurement in SPRINT
(Automated)
•Visit BP was the average of 3 seated office BP measurements
obtained using an automated measurement device: Omron
907XL.
•Appropriate cuff size was determined by arm circumference.
•Participant was seated with back supported and arm bared and
supported at heart level.
•Device was set to delay 5 minutes and then take/average 3 BP
measurements, during which time participant refrained from
talking. Cushman, et al. Hypertension. 2016;67:263-5
Accurate Measurement of BP in the Office
COR LOE Recommendation for Accurate Measurement of BP in the Office
IC-EO
For diagnosis and management of high BP, proper methods are
recommended for accurate measurement and documentation of BP.
Out-of-Office and Self-Monitoring of BP
COR LOE Recommendation for Out-of-Office and Self-Monitoring of BP
IASR
Out
-of-office BP measurements are recommended to confirm the
diagnosis of hypertension and for titration of BP
-lowering medication,
in conjunction with telehealth counseling or clinical interventions.
SR indicates systematic review.
11/21/2017
7
BP Treatment Threshold and the Use of CVD Risk Estimation to Guide Drug Treatment of
Hypertension
COR LOE Recommendations for BP Treatment Threshold and Use of Risk Estimation* to
Guide Drug Treatment of Hypertension
I
SBP: A Use of BP-lowering medications is recommended for secondary prevention of
recurrent CVD events in patients with clinical CVD and an average SBP of 130 mm
Hg or higher or an average DBP of 80 mm Hg or higher, and for primary prevention in
adults with an estimated 10-year ASCVD risk of 10% or higher and an average SBP
130 mm Hg or higher or an average DBP 80 mm Hg or higher.
DBP:
C-EO
I C-LD
Use of BP-lowering medication is recommended for primary prevention of CVD in
adults with no history of CVD and with an estimated 10-year ASCVD risk <10% and an
SBP of 140 mm Hg or higher or a DBP of 90 mm Hg or higher.
*ACC/AHA Pooled Cohort Equations (http://tools.acc.org/ASCVD-Risk-Estimator/) to
estimate 10-year risk of atherosclerotic CVD (ASCVD).
http://tools.acc.org/ASCVD-Risk-Estimator/
ACC/AHA POOLED COHORT EQUATIONS
To estimate the 10-year risk of atherosclerotic CVD
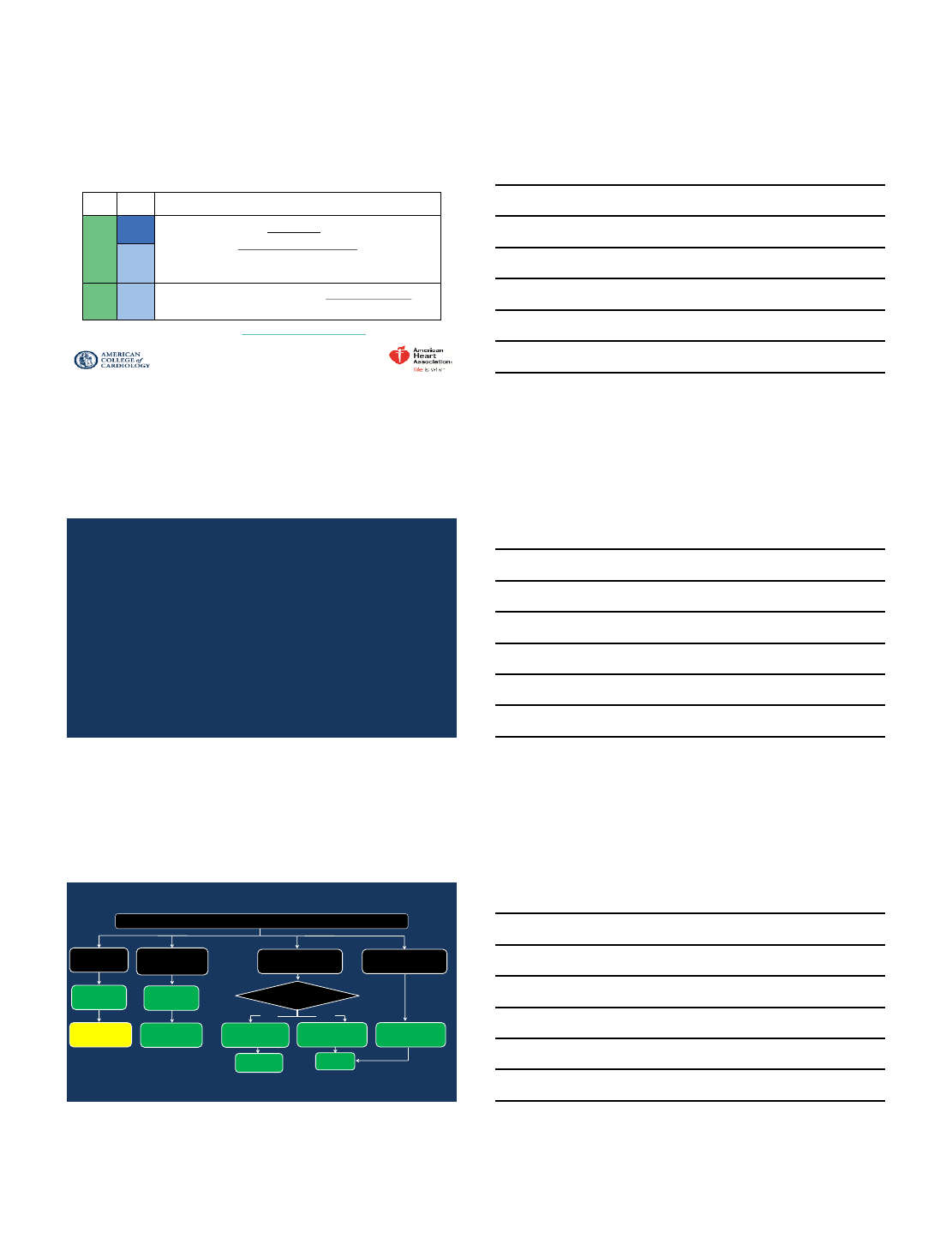
BP thresholds and recommendations for treatment and follow-up
Normal BP
(BP <120/80
mm Hg)
Elevated BP
(BP 120-129/<80
mm Hg)
Stage 1 Hypertension
(BP 130-139/80-89 mm Hg) Stage 2 Hypertension
(BP >140/90 mm Hg)
BP THRESHOLDS AND RECOMMENDATIONS
FOR TREATMENT AND FOLLOW UP
Reassess in 1 y
(Class IIa)
Reassess in
3-6 mo
(Class I)
Non-pharmacologic
therapy
(Class I)
Non-pharmacologic therapy
and BP lowering medication
(Class I)
Reassess in 1
mo
(Class 1)
Promote optimal
lifestyle habits
(Class I)
Non-pharm-acologic
therapy
(Class I)
Clinical CVD or estimated
10 y ASCVD risk ≥ 10%
Yes
No
Non-pharmacologic therapy
and BP lowering medication
(Class I)
Reassess in
3-6 mo
(Class I)
11/21/2017
8
Thank you!
11/21/2017
1
BP Targets in Patients with and without
Chronic Kidney Disease.
Clive Rosendorff, MD, PhD, DScMed,
FACC, FAHA, FRCP.
Professor of Medicine (Cardiology), Icahn School of
Medicine at Mount Sinai, New York, NY, USA
and
James J. Peters VA Medical Center, Bronx, NY, USA
Hypertension 2017: Where are we now?
Disclosures
I was a member of the SPRINT Intervention Committee
I have no other disclosures relating to the subject
matter of this presentation.
Lower Is Better:
12.7 million person years
IHD Rates by SBP, DBP, and Age
SBP DBP
IHD Mortality
(Floating Absolute Risk, 95% CI)
256
128
64
32
16
8
4
2
1
120 140 160 180
Usual SBP (mm Hg)
256
128
64
32
16
8
4
2
1
70 80 90 100 110
Usual DBP (mm Hg)
IHD = ischemic heart disease; CI = confidence interval.
Lewington et al. Lancet. 2002;360:1903-1913.
40–49
50–59
60–69
70–79
80–89
Age at Risk (y)
11/21/2017
2
Impact of Pre-Hypertension on CV Risk
Lower Blood Pressure is Better
Normal BP: < 120/80 mm Hg; Pre-hypertension: 120–139 or 80–89 mm Hg.
Vasan RS et al. N Engl J Med. 2001;345:1291-1297.
Cumulative
Incidence of CV
Events(%)
Normal BP
(< 120/80)
Years
Cumulative
Incidence of CV
Events (%)
130-139 or 85-89
120-129 or 80-84
10
16
12
8
6
4
2
0
14 Men
Normal BP
(< 120/80)
130–139 or 85–89
120-129 0r 80-84
12
10
8
6
4
2
0
Women
02 4 6 8 10 12
Sipahi I et al. J Am Coll Cardiol. 2006;48:833-838.
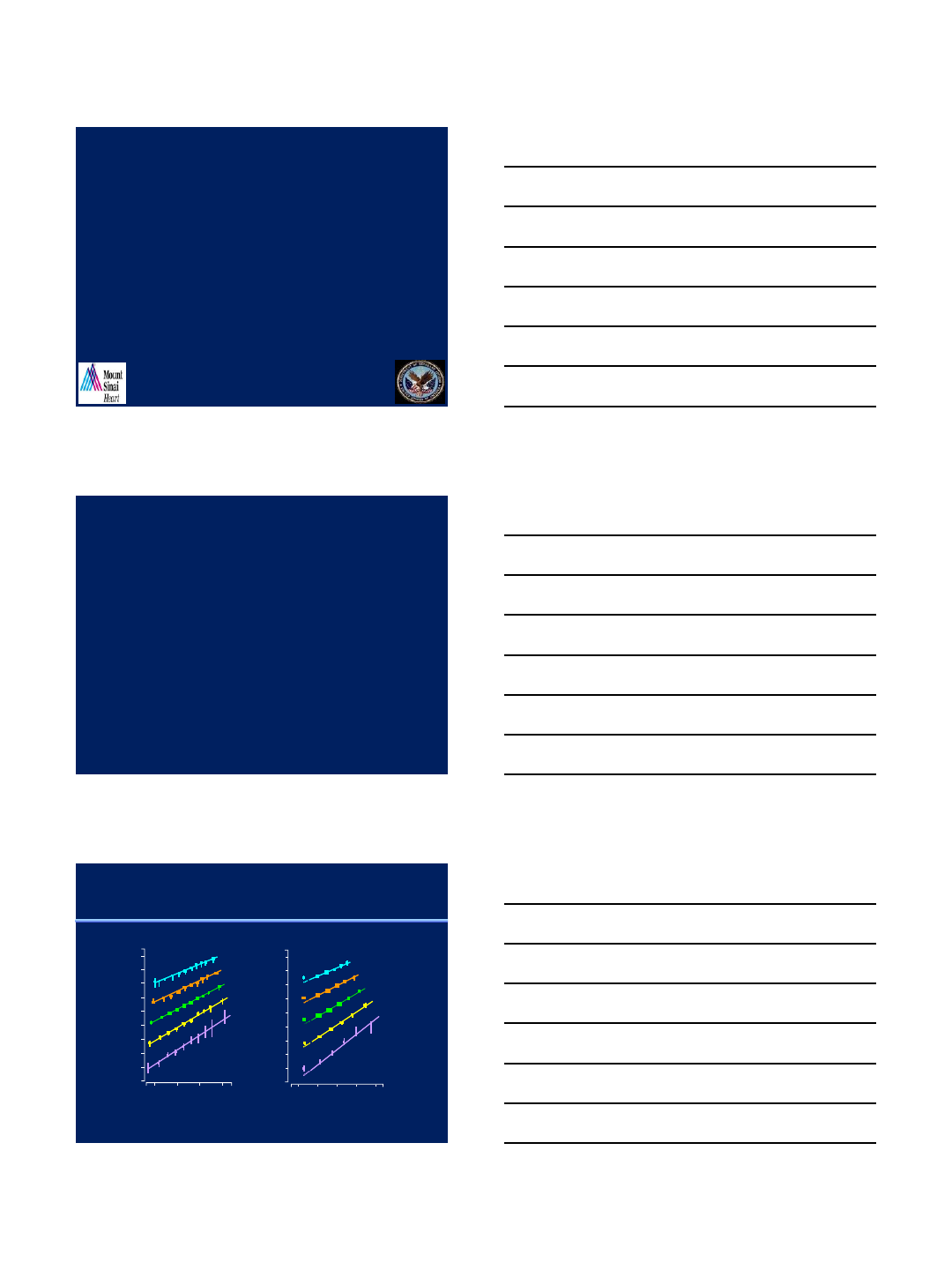
Progression Rate of Coronary Artery Disease
According to JNC 7 BP Categories
Δin Atheroma Volume (mm3)
JNC 7 Categories
Normal Prehypertension Hypertension
<120/80 120-139/80-89 ≥140/90
-
-
-
-
-
-
-
-
-
-
-
P<.001 by ANCOVA
P<.001
P=.039
P=.01
30
25
20
15
10
5
0
–5
–10
–15
–20
500
400
300
200
0
100 150 2000
S.B.P. (mmHg)
Total
Organ
Blood
Flow
(ml/min)
P1
Rosendorff, In “Hypertension, A Companion to Braunwald’s Heart Disease”
Ed. Black & Elliott, Elsevier 2013; 253-261
11/21/2017
3
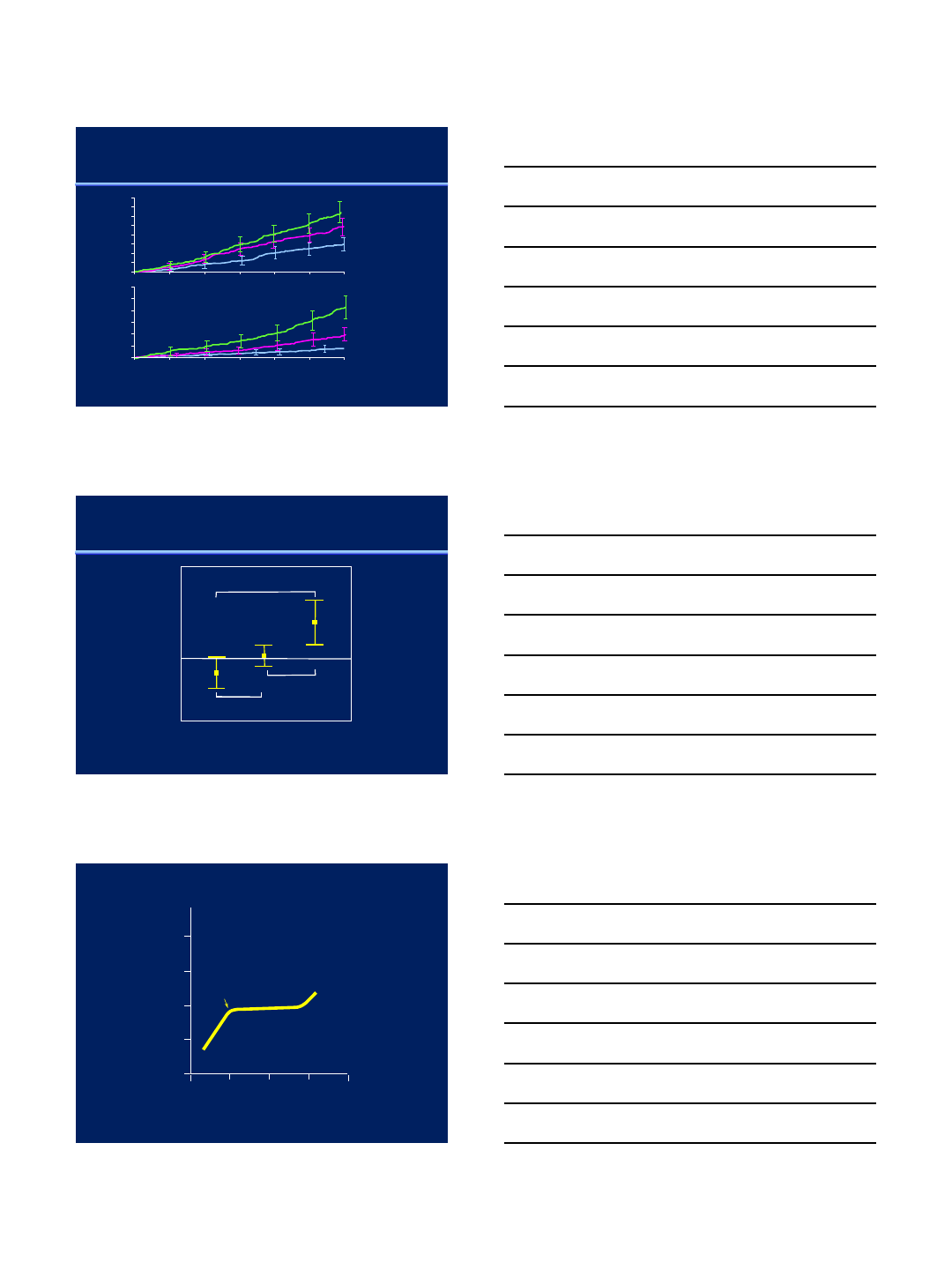
Achieved B.P. and the Rate of Decline in Renal Function.
Khosla et al. Med Clin N Am 2009;93:697-715
Selected Baseline Characteristics of the SPRINT Population
CHARACTERISTIC INTENSIVE
TREATMENT (N=4678) STANDARD
TREATMENT (N=4683)
Criterion for increased CV risk –no. (%)
Age ≥75 yr 1317 (28.2) 1319 (28.2)
Chronic kidney
disease 1330 (28.4) 1316 (28.1)
Cardiovascular
disease 940 (20.1) 937 (20)
Framingham
R.S.≥15%
2870 (61.4) 2867 (61.2)
Estimated GFR –ml/min/1.73m2
All 71.8±20.7 71.7±20.5
eGFR ≥60 81.3±15.5 81.1±15.5
eGFR <60 47.8±9.5 47.9±9.5
11/21/2017
4
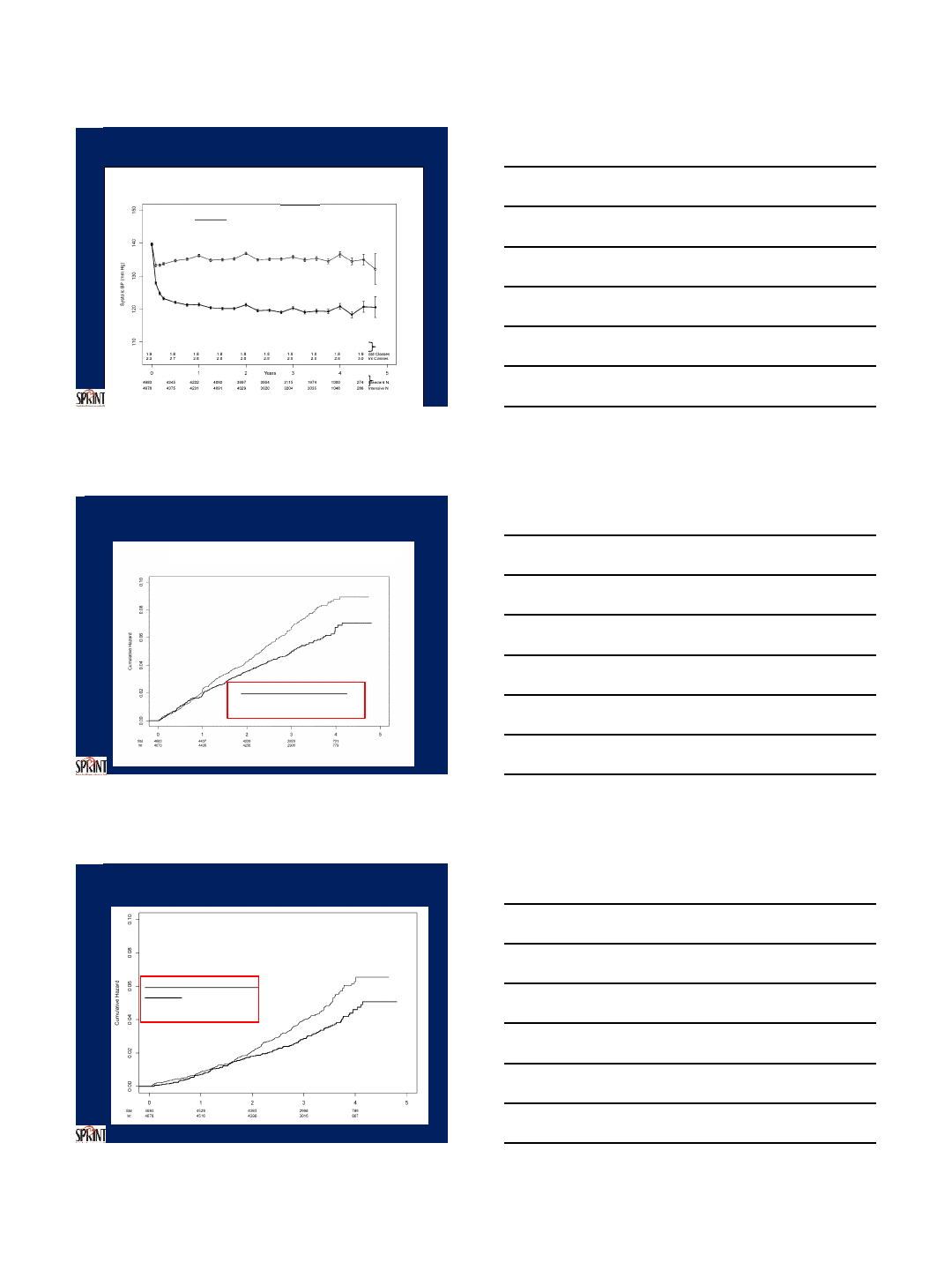
Systolic BP During Follow-up
Mean SBP
136.2 mm Hg
Mean SBP
121.4 mm Hg
Standard
Intensive
Year 1
Number of
Participants
Hazard Ratio = 0.75 (95% CI: 0.64 to 0.89)
Standard
Intensive
(243 events)
Median follow-up = 3.26 years)
Number Needed to Treat (NNT) to
prevent a primary outcome = 61
SPRINT Primary Outcome
MI, ACS, stroke, HF, CV death
(319 events)
Include NNT
SPRINT -All-cause Mortality
Cumulative Hazard
Hazard Ratio = 0.73 (95% CI: 0.60 to 0.90)
During Trial (median follow-up =
3.26 years)
Number Needed to Treat
(NNT) to Prevent a death = 90
Standard
(210 deaths)
Intensive
(155 deaths)
11/21/2017
5
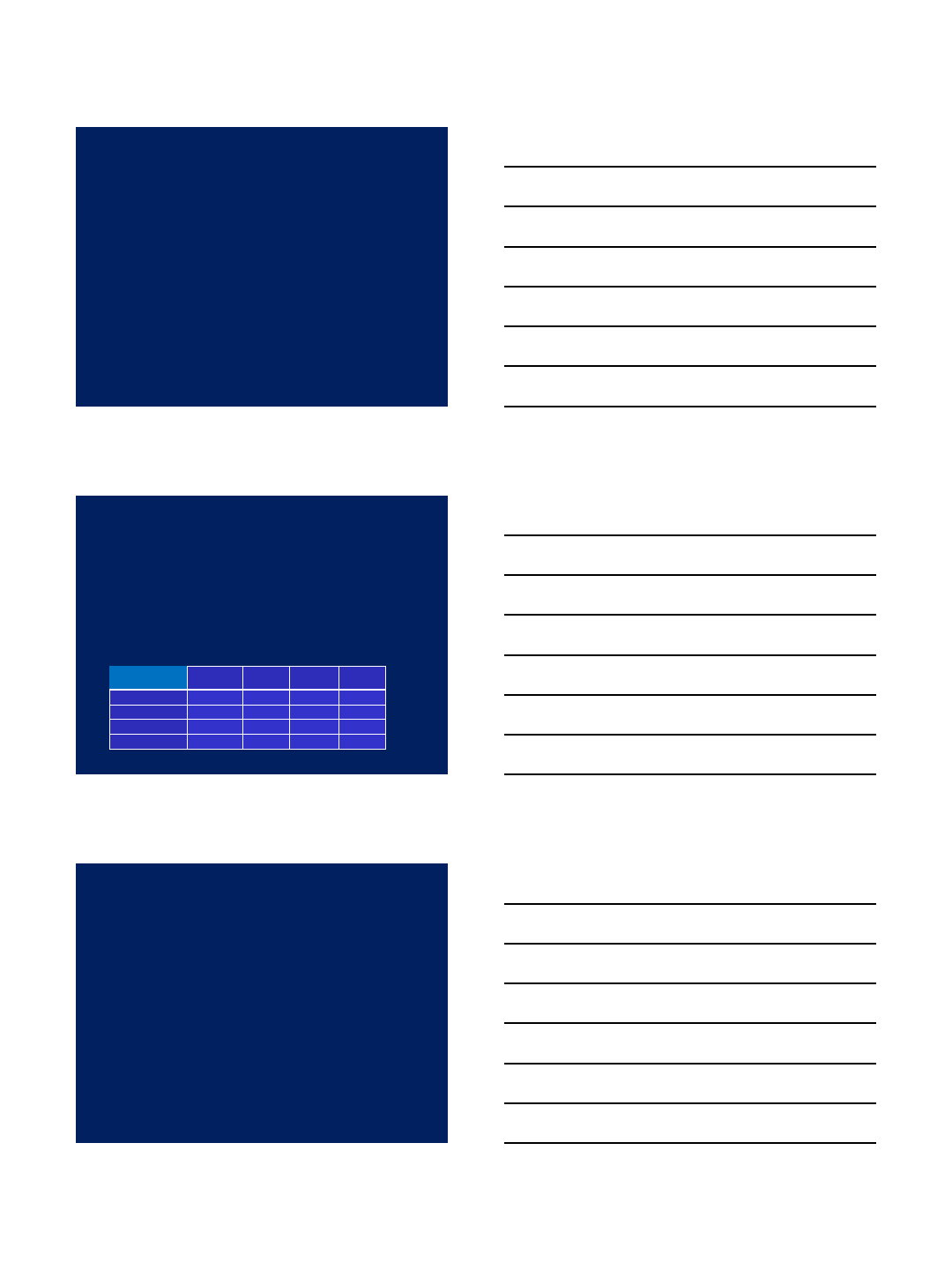
SPRINT Primary Outcome and its Components
Event Rates and Hazard Ratios
Intensive
Standard
No. of
Events
Rate,
%/year
No. of
Events
Rate,
%/year
HR (95% CI)
P value
Primary Outcome
243
1.65
319
2.19
0.75 (0.64,
0.89)
<0.001
All MI
97
0.65
116
0.78
0.83 (0.64,
1.09)
0.19
Non
-MI ACS
40
0.27
40
0.27
1.00
(0.64,
1.55)
0.99
All Stroke
62
0.41
70
0.47
0.89 (0.63,
1.25)
0.50
All HF
62
0.41
100
0.67
0.62 (0.45,
0.84)
0.002
CVD Death
37
0.25
65
0.43
0.57 (0.38,
0.85)
0.005
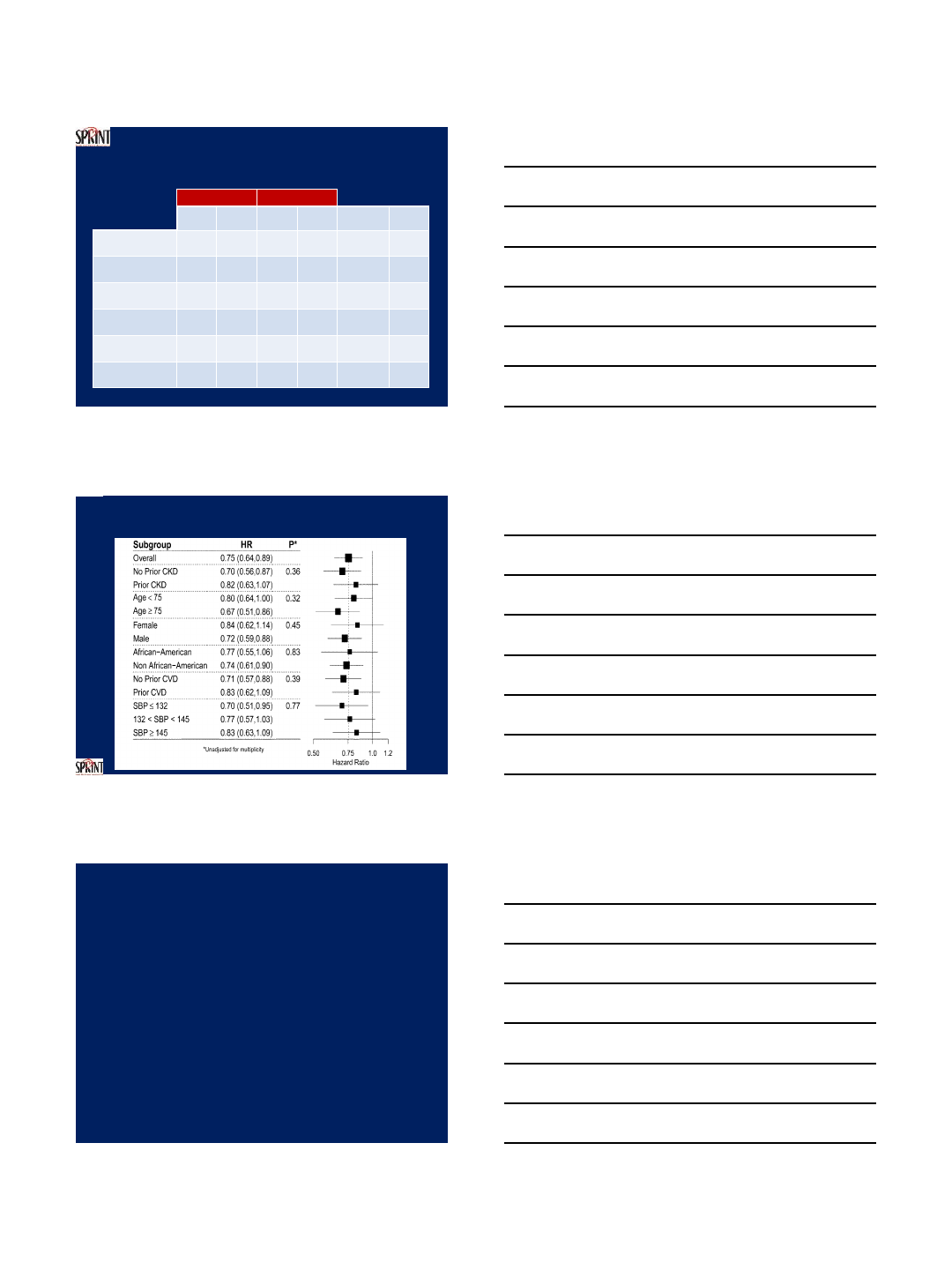
Primary Outcome Experience in the Six Pre-specified
Subgroups of Interest
*Treatment by subgroup interaction
It is a fool who is blown about
with every wind of criticism
Samuel Johnson 1709-1784
CRITICISMS
1. Unacceptable incidence of adverse events
2. “I would not apply these findings to my elderly, frail patients”
3. The absolute risk reduction is small
4. No benefit in preventing stroke
5. We do not measure blood pressure with the same care as in SPRINT
11/21/2017
6
It is a fool who is blown about
with every wind of criticism
Samuel Johnson 1709-1784
CRITICISMS
1. Unacceptable incidence of adverse events
2. “I would not apply these findings to my elderly, frail patients”
3. The absolute risk reduction is small
4. No benefit in preventing stroke
5. We do not measure blood pressure with the same care as in SPRINT
Adverse Events
1.Patients without CKD at Baseline: ≥30% reduction in
eGFR:
Standard: 0.35%/y
Intensive: 1.21%/y P<0.001 (?RAS blockers)
2. Other
Intensive
%Standard
%HR P
Hypotension 2.4 1.4 1.67 0.001
Syncope 2.3 1.7 1.33 0.05
Hyponatremia 3.8 2.1 1.76 <0.001
Hypokalemia 2.4 1.6 1.50 0.006
It is a fool who is blown about
with every wind of criticism
Samuel Johnson 1709-1784
CRITICISMS
1. Unacceptable incidence of adverse events
2. “I would not apply these findings to my elderly, frail patients”
3. The absolute risk reduction is small
4. No benefit in preventing stroke
5. We do not measure blood pressure with the same care as in SPRINT
11/21/2017
7
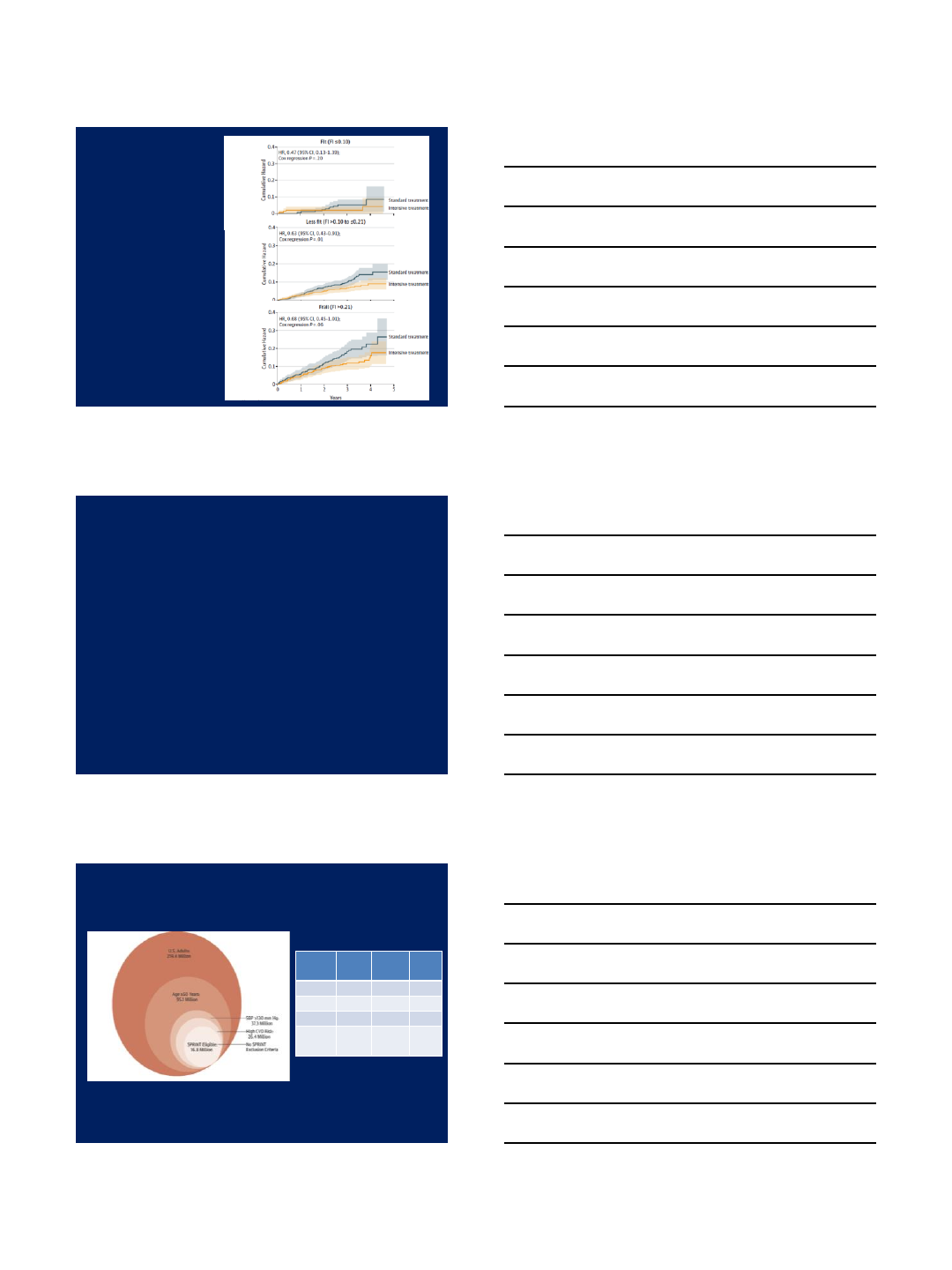
SPRINT
Primary Outcome
in Subjects >75 years,
by Baseline Frailty Status
Williamson et al.
JAMA 2016,
doi:10.1001/jama.2016.7050
It is a fool who is blown about
with every wind of criticism
Samuel Johnson 1709-1784
CRITICISMS
1. Unacceptable incidence of adverse events
2. “I would not apply these findings to my elderly, frail patients”
3. The absolute risk reduction is small
4. No benefit in preventing stroke
5. We do not measure blood pressure with the same care as in SPRINT
Generalizability of SPRINT Results to the U.S. Adult Population, and
Potential Impact on Outcomes.
Bress et al. J Am Coll Cardiol. 2016;67(5):463-472.
CV
Events
%/y
Mortality
%/y
Stroke
%/y
Standard
2.19 1.40 0.47
Intensive
1.65 1.03 0.41
Difference
0.54 0.37 0.06
Fewer
events
p.a.
90,700 62,200
10,100
11/21/2017
8
It is a fool who is blown about
with every wind of criticism
Samuel Johnson 1709-1784
CRITICISMS
1. Unacceptable incidence of adverse events
2. “I would not apply these findings to my elderly, frail patients”
3. The absolute risk reduction is small
4. No benefit in preventing stroke
5. We do not measure blood pressure with the same care as in SPRINT
Patients with Events (%)
0
5
10
15
20
Years Post-Randomization
0 1 2 3 4 5 6 7 8
Patients with Events (%)
0
5
10
15
20
Years Post-Randomization
0 1 2 3 4 5 6 7 8
Nonfatal Stroke Total Stroke
HR = 0.63
95% CI (0.41-0.96)
P=0.03
HR = 0.59
95% CI (0.39-0.89)
P=0.01
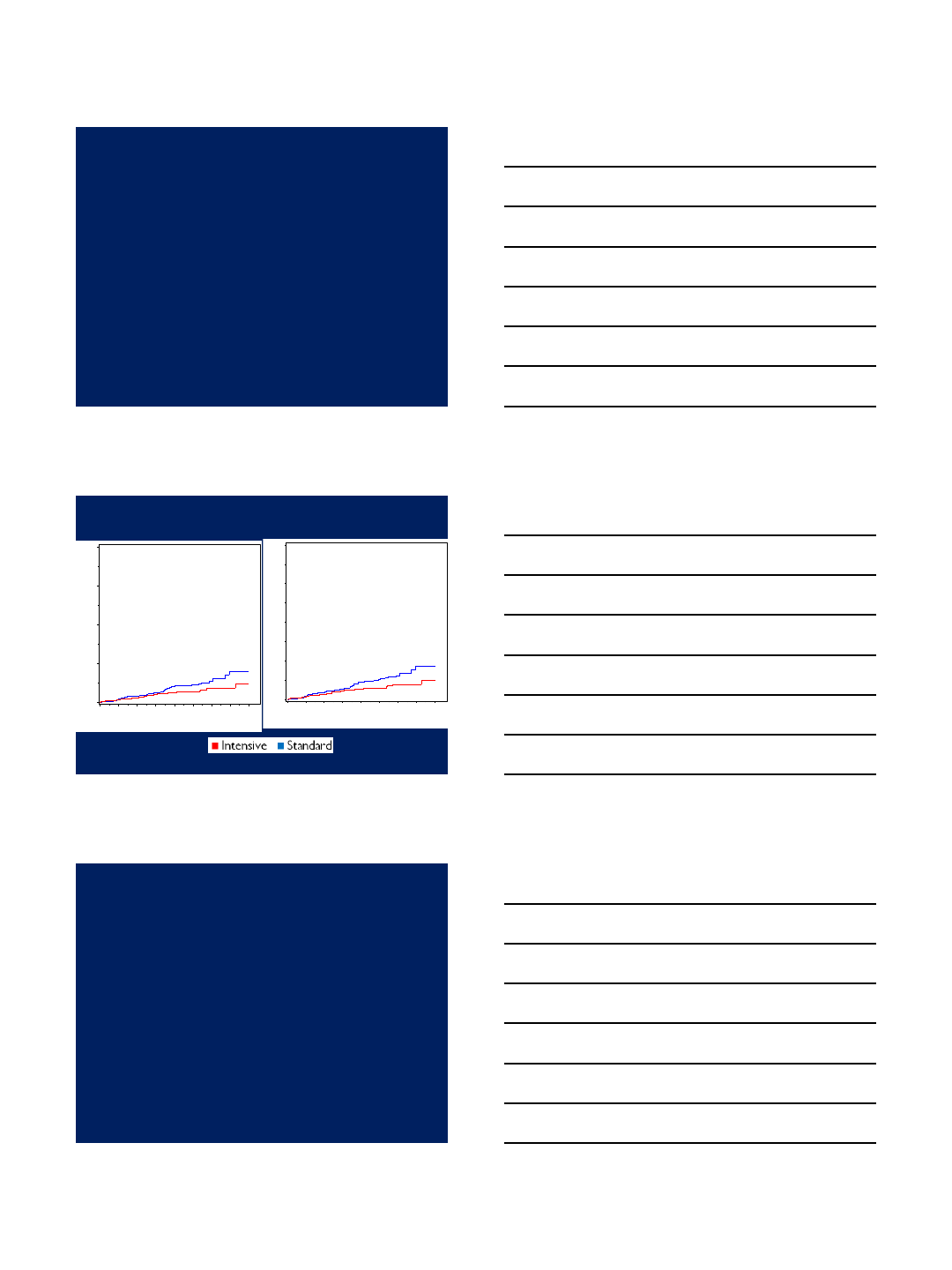
ACCORD - STROKE
Why were Stroke Outcomes in ACCORD and
SPRINT Different?
An Hypotheses
ACCORD stroke K-M curves started to diverge at about 3.5
years. SPRINT was stopped before that (median follow-up
3.26 years). The SPRINT 11% RRR for stroke might have
increased to significant levels with more time.
11/21/2017
9
It is a fool who is blown about
with every wind of criticism
Samuel Johnson 1709-1784
CRITICISMS
1. Unacceptable incidence of adverse events
2. “I would not apply these findings to my elderly, frail patients”
3. The absolute risk reduction is small
4. No benefit in preventing stroke
5. We do not usually measure blood pressure with the same care as in
SPRINT.
“The doctor will now measure your blood pressure”
BP MEASUREMENT
1. Patient sits in a quiet room for
5 minutes.
2. Automated BP measurement
system.
3. Mean of 3 measurements.
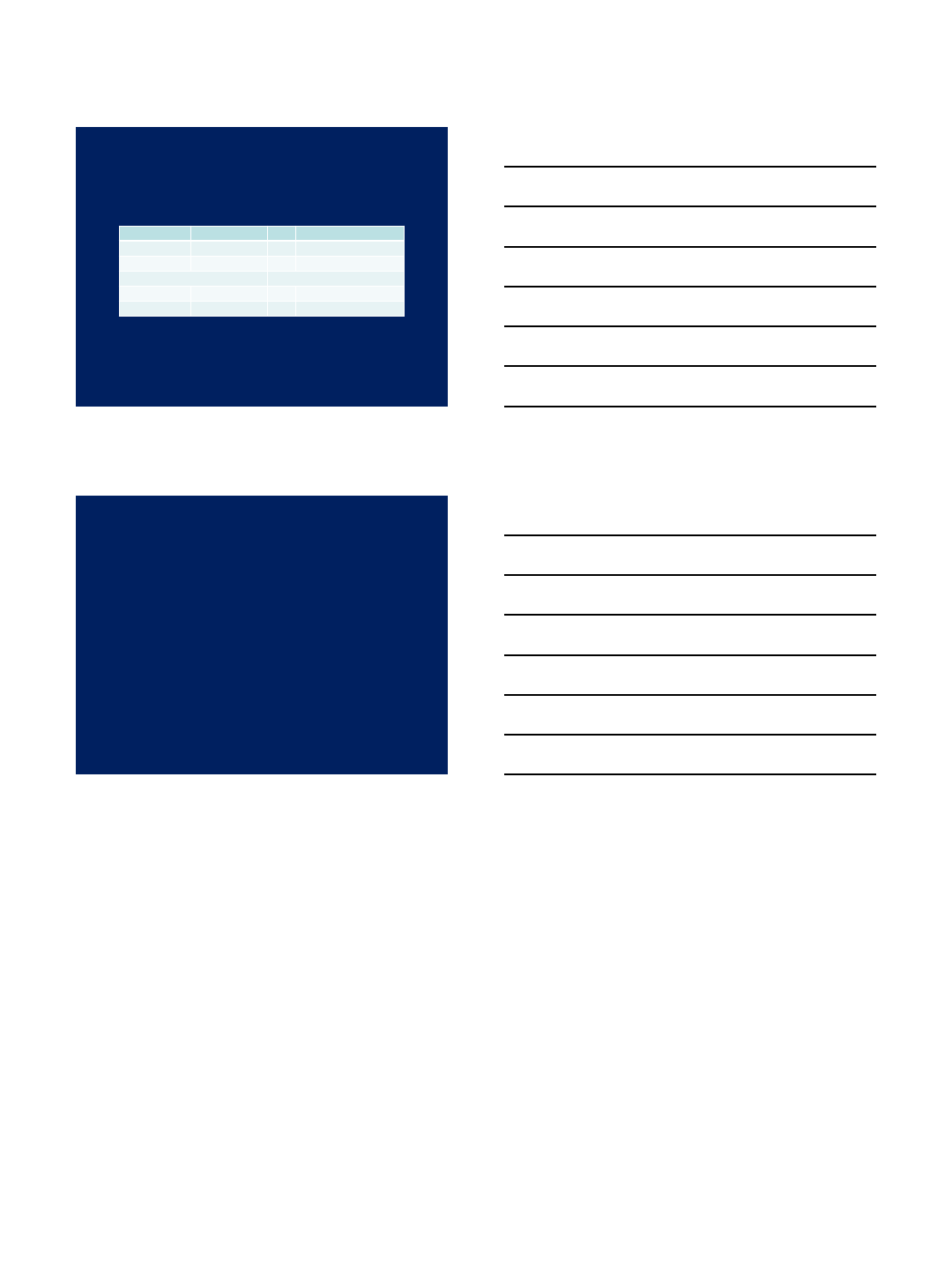
11/21/2017
10
Categories of BP in Adults
BP Category
SBP
DBP
Normal
<120
mm Hg
and
<80 mm Hg
Elevated
120
-129 mm Hg
and
<80 mm Hg
Hypertension
Stage 1
130
-139 mm Hg
or
80
-89 mm Hg
Stage 2
≥140 mm Hg
or
≥90 mm Hg
Whelton PK et al. 2017 High Blood Pressure Clinical Practice Guideline
Summary
•The 130/80 mm Hg cutoff for the diagnosis of hypertension and
for the goal of anti-hypertensive treatment is reasonable.
•However, physicians should be aware that a SBP target of
<120 mm Hg has been shown to reduce cardiovascular events
and mortality.
• BP is a continuous variable, so “lower is better”, as long as
patients are carefully monitored for symptoms or signs of
intolerance.
•Management should, therefore, be individualized.
1
Non-Pharmacological Treatment
of Hypertension
Marcos Rothstein, MD
Professor of Medicine
Department of Medicine ~ Division of Nephrology
Medicine
Nephrology
“Haemastaticks”
(1733)
Stephen Hales
(1677-1761)
Medicine
Nephrology
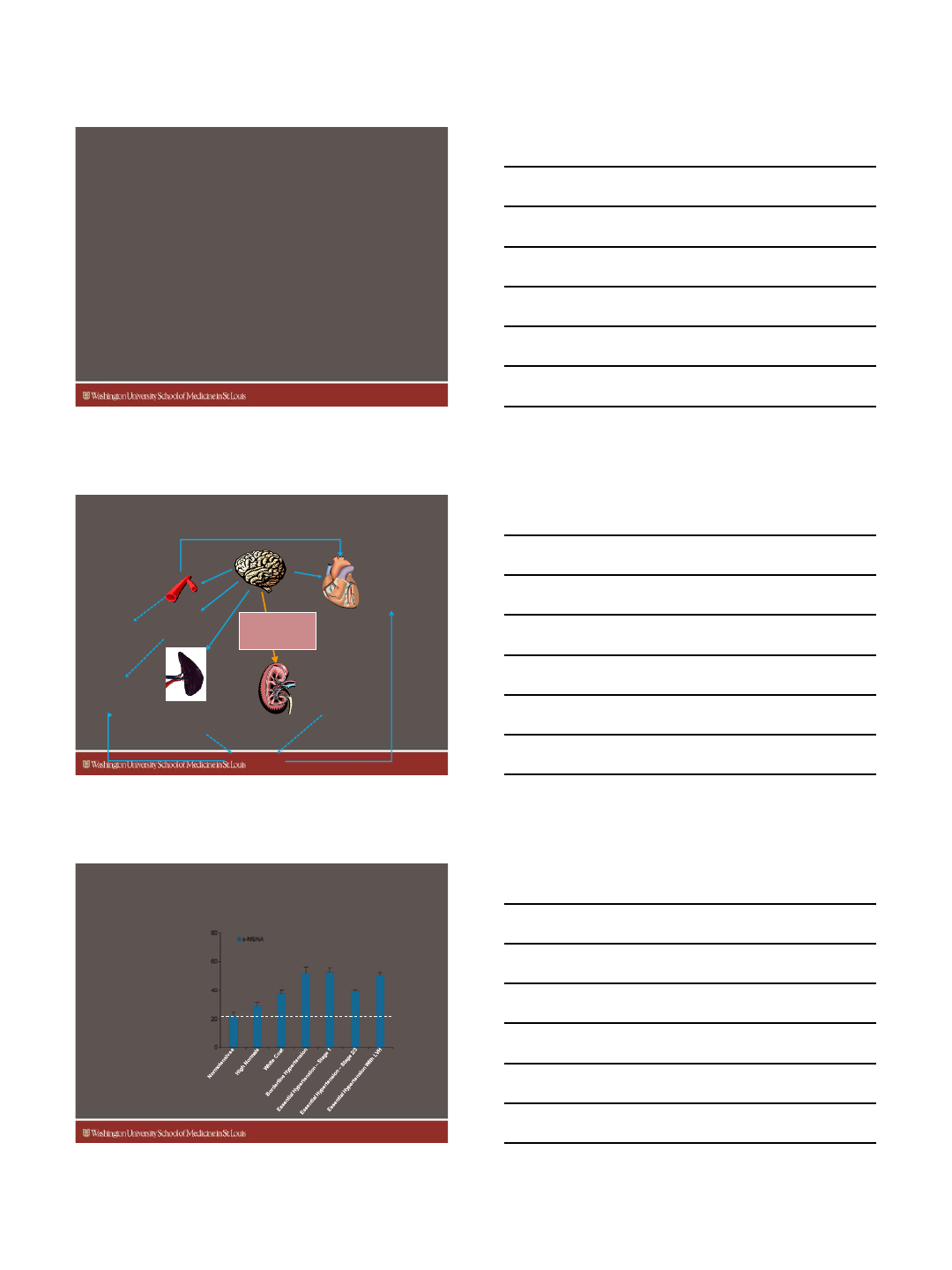
Failure of Current Multidrug Approach
to Successfully Treat Hypertension
Kearney PM, et al. J Hypertens. 2004; 22:11-19.
Percentage of Patients (%)
53%
41% 34%
29%
61%
50%
16%
Hypertension Control in Treated Hypertensive Patients
2
Medicine
Nephrology
Forms of Human HTN with
Neurogenic Component
•Essential HTN
•Obesity-renal HTN
•Renal HTN
•HTN associated with
obstructive sleep apnea
•Preeclampsia
Medicine
Nephrology
Hypertrophy
↑ Arrhythmia
↑ Oxygen
Consumption
Vasoconstriction
Insulin
Resistance
Consequences of Chronic Elevated
Central Sympathetic Drive
Renal
Sympathetic
Efferent Nerves
↑ Renin Release
↑ Sodium Retention
↓ Renal Blood Flow
Dyspnea,
Sleep
Disturbances
↑ pCO2
Sensitivity
Recruitment of
Splanchnic venous
Blood pools
Congestion
Medicine
Nephrology
Central Sympathetic Drive in
Hypertension
s-MSNA=single-unit efferent sympathetic nerve activity.
LVH=left ventricular hypertrophy.
*P<0 .05 Compared with borderline hypertension.
†P<0.05 Compared with white coat hypertension.
‡P<0.05 Compared with nor mal pressure.
§P<0 .05 Compared with high -normal pressure.
¶P<0 .05 Compared with essential hypertension–stage 1.
#P<0 .05 Compared with essential hypertension–stage 2/3.
Adapt ed from Smith P, et al. Am J Hyp ertens. 2004; 17:217-2 22.
Baseline activity
(normotensives)
*
†
*
†
‡
*
†
‡
§*
‡
§
¶
†
‡
§
#
Sympathetic Activity per Minute
Sympathetic
drive is elevated
in multiple types
of hypertension

3
Medicine
Nephrology
Kidneys
↓ HR ↑Vasodilation
↓Stiffness
↑Diuresis
↓Renin
secretion
Carotid Baroreceptor Stimulation
Heart Vessels
Brain
Autonomic Nervous System
Inhibited Sympathetic Activity
Enhanced Parasympathetic Activity
Baroreflex Activation Therapy (BAT)
Continuously Modulates the Autonomic Nervous System
Medicine
Nephrology
The CVRx Rheos System
Programming
System
Baroreflex Activation
Leads
Implantable Pulse
Generator
Medicine
Nephrology
BP Pre/Post Implant
SBP DBP MAP HR Device RX
Pre 202 ±21 108 ±9134 ±11 79 ±7NA
6 Mths 153 ±15 80 ±13 101 ±13 64 ±8Amps = 8
Freq = 30 pps
Width = 480
8 Yrs* 130 ±10 70 ±690 ±668 ±5Amps = 7
Freq = 50 pps
Width = 120
*Drug Rx –Maxide 75/50 mgs QD
St. Louis Patient #2
4
Medicine
Nephrology
Change in Antihypertensive
Therapeutic Index Over Time
1 Year 2 Years 3 Years
*p value = 0.05
**p value < 0.001
*
**
Medicine
Nephrology
Moving Forward:
Miniaturization to Reduce Procedure Invasiveness
1st Generation Lead
New Generation Lead
Medicine
Nephrology
5
Medicine
Nephrology
Medicine
Nephrology
Medicine
Nephrology
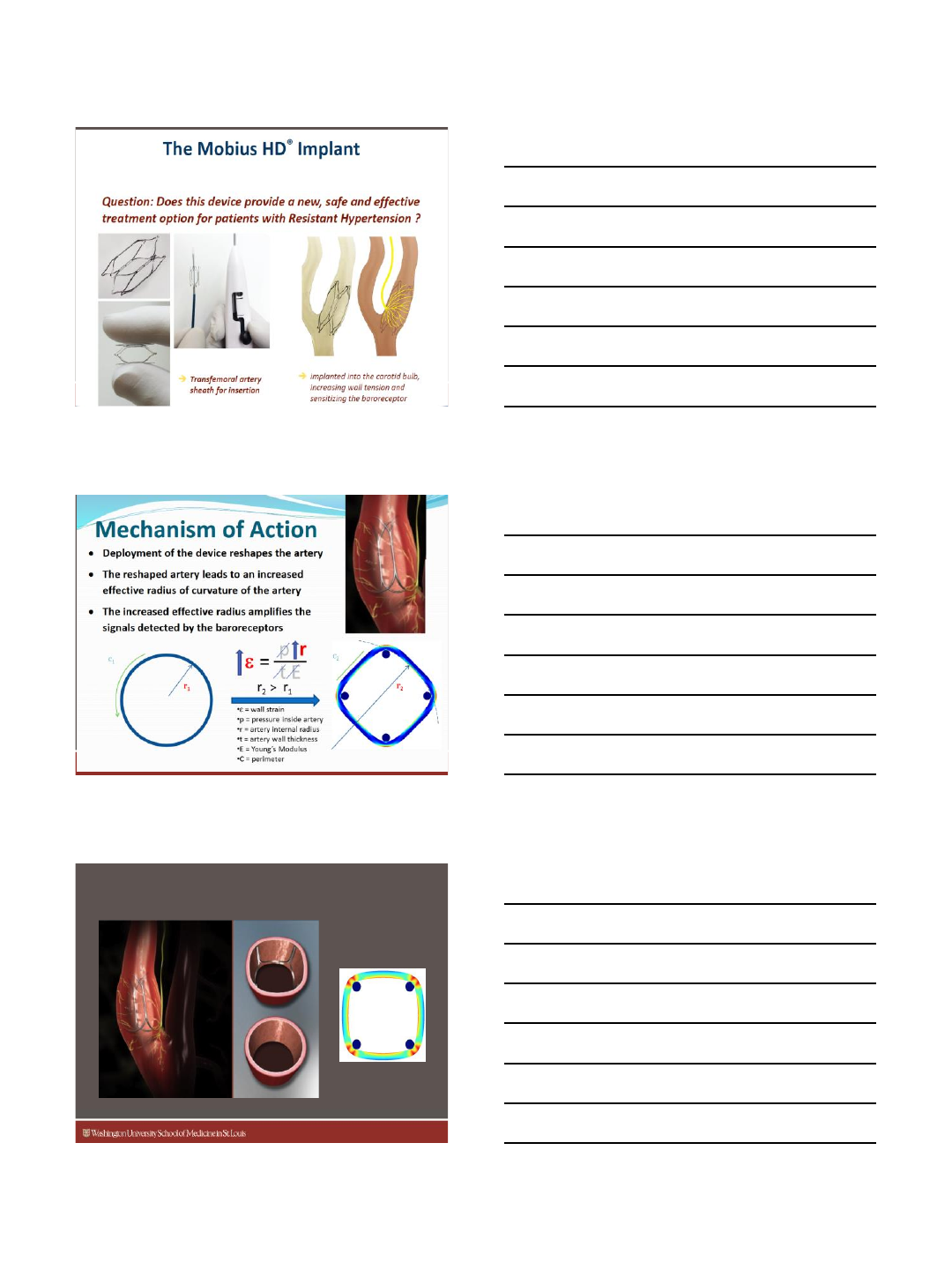
Vascular Dynamics Mobius Device
6
Medicine
Nephrology
Medicine
Nephrology
Renal Nerves as a Therapeutic Target
Medicine
Nephrology
Techniques
RFA
US
Cryoblation
Pharmacological sympathetic blockade
Internal
Non-Invasive
7
Medicine
Nephrology
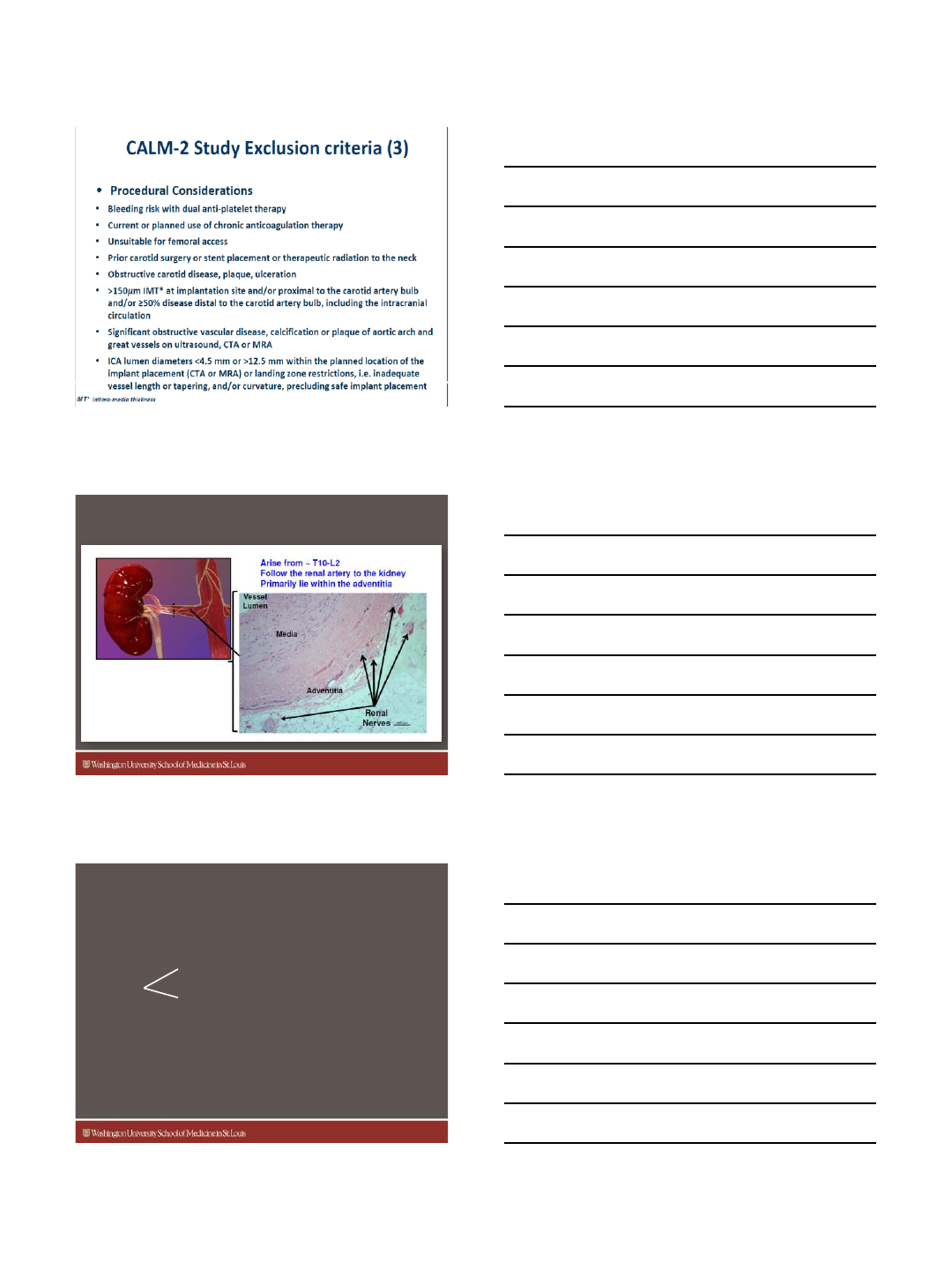
Denervation Catheter Designs
Medicine
Nephrology
Staged Clinical Evaluation
First-in-Man ✓
Series of Pilot studies ✓
Symplicity HTN-2 ✓
EU/AU Randomized Clinical Trial
Symplicity HTN-1
USA
Symplicity HTN-3
US Randomized Clinical Trial
EU/AU
Other Areas of Research:
Insulin Resistance, HF/Cardiorenal,
Sleep Apnea, More
Symplicity HTN-1 Investigators. Hypertension. 2011;57:911-917.
Medicine
Nephrology
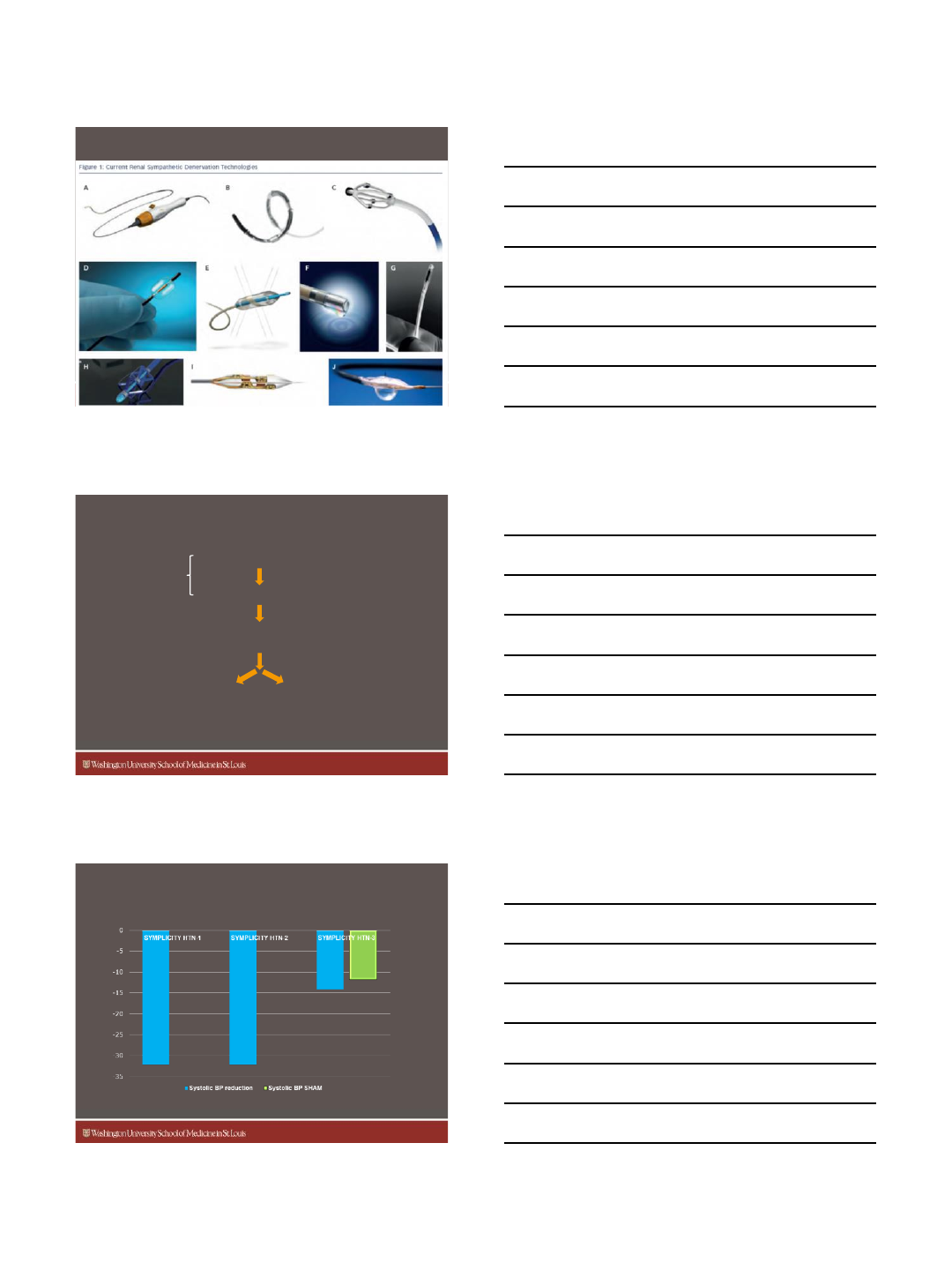
BP Lowering Effect of
SYMPLICITY HTN trials
Symplicity HTN-1 Investigators. Hypertension. 2011;57:911-917; Symplicity HTN-2 Investigators. Lancet.
2010;376:1903-1909 ; Bhatt DL, Kandzari DE, O’Neill WW, et al...Bakris GL. N Engl J Med 2014;370:1393-1401
.
BP change
(mmHg)
8
Medicine
Nephrology
What Does This Mean?
•Renal Denervation does not work
•Wrong mouse trap
Next generation RF devices
Chemical
Ultrasound
•Wrong population of pt’s
Too extreme
Medicine
Nephrology
Simplicity HTN3: Exploring an Unexpected
Result
•Inadequate operator technique
•Misunderstood renal nerve anatomy
•Suboptimal catheter design
Medicine
Nephrology
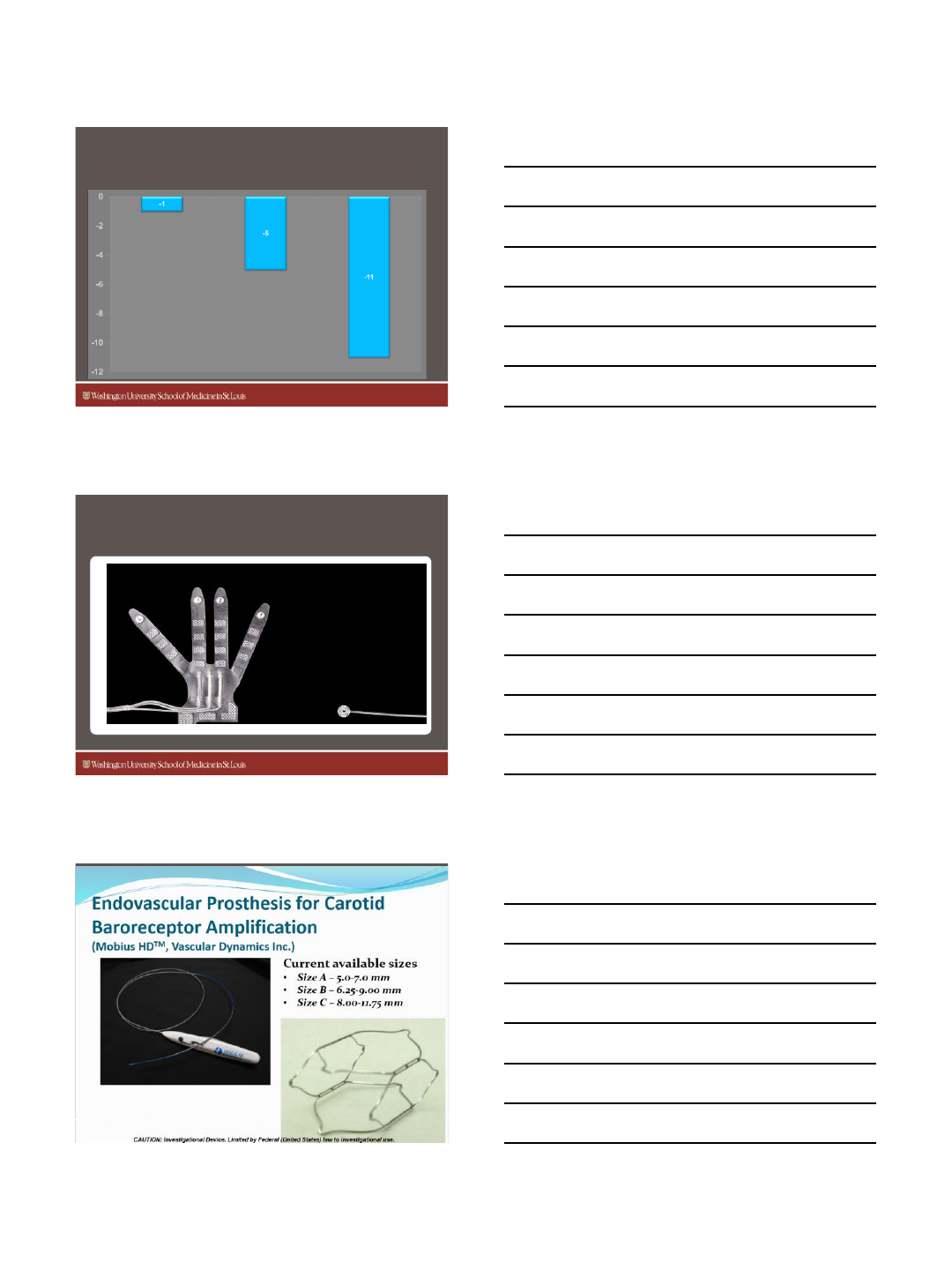
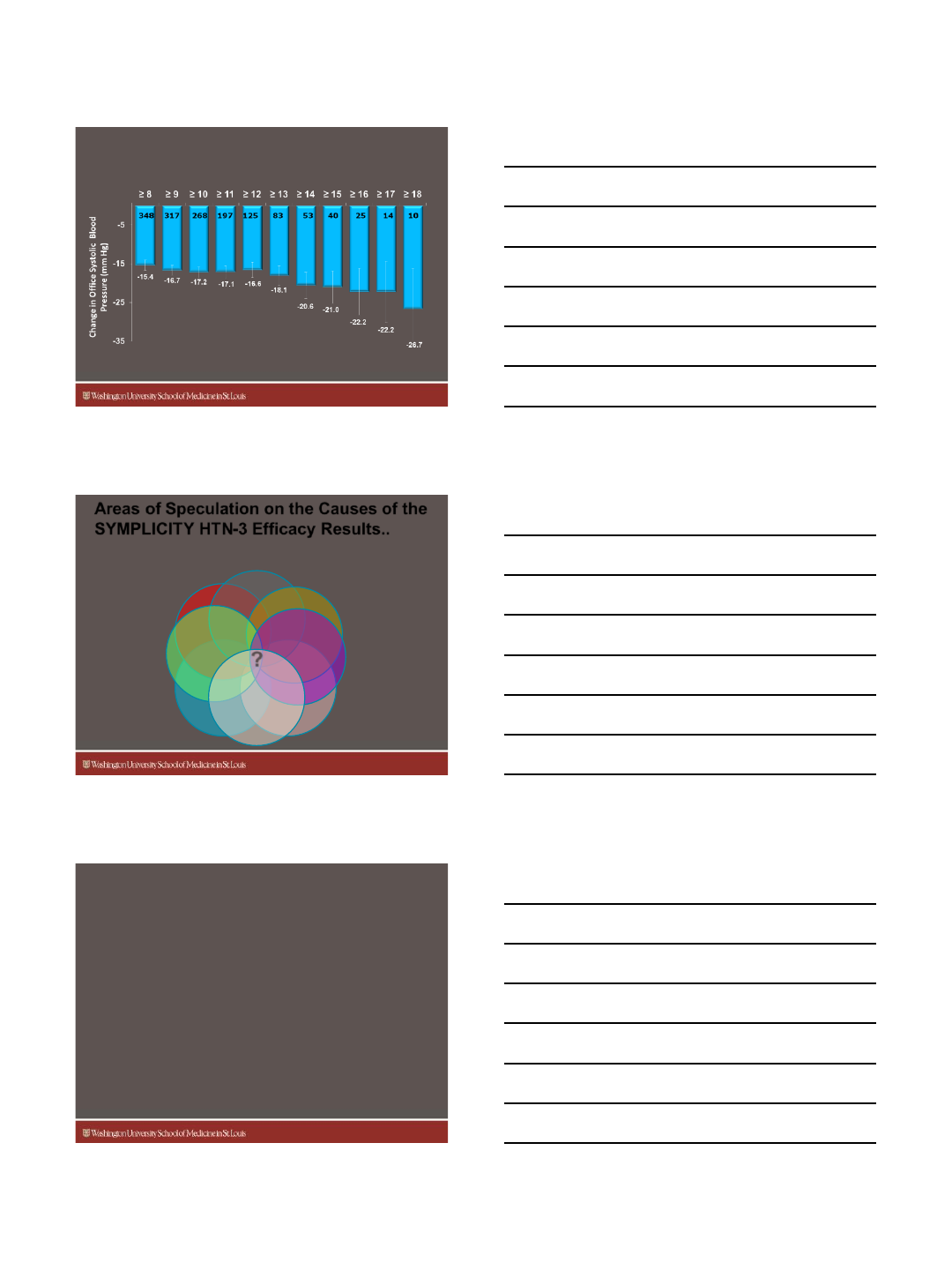
Inferior Anterior Superior Posterior
Procedural Variability
Correlation with # of ablations
Correlation with 4-quadrant ablation pattern
Cross-
section of
artery 4-quadrant ablation pattern
9
Medicine
Nephrology
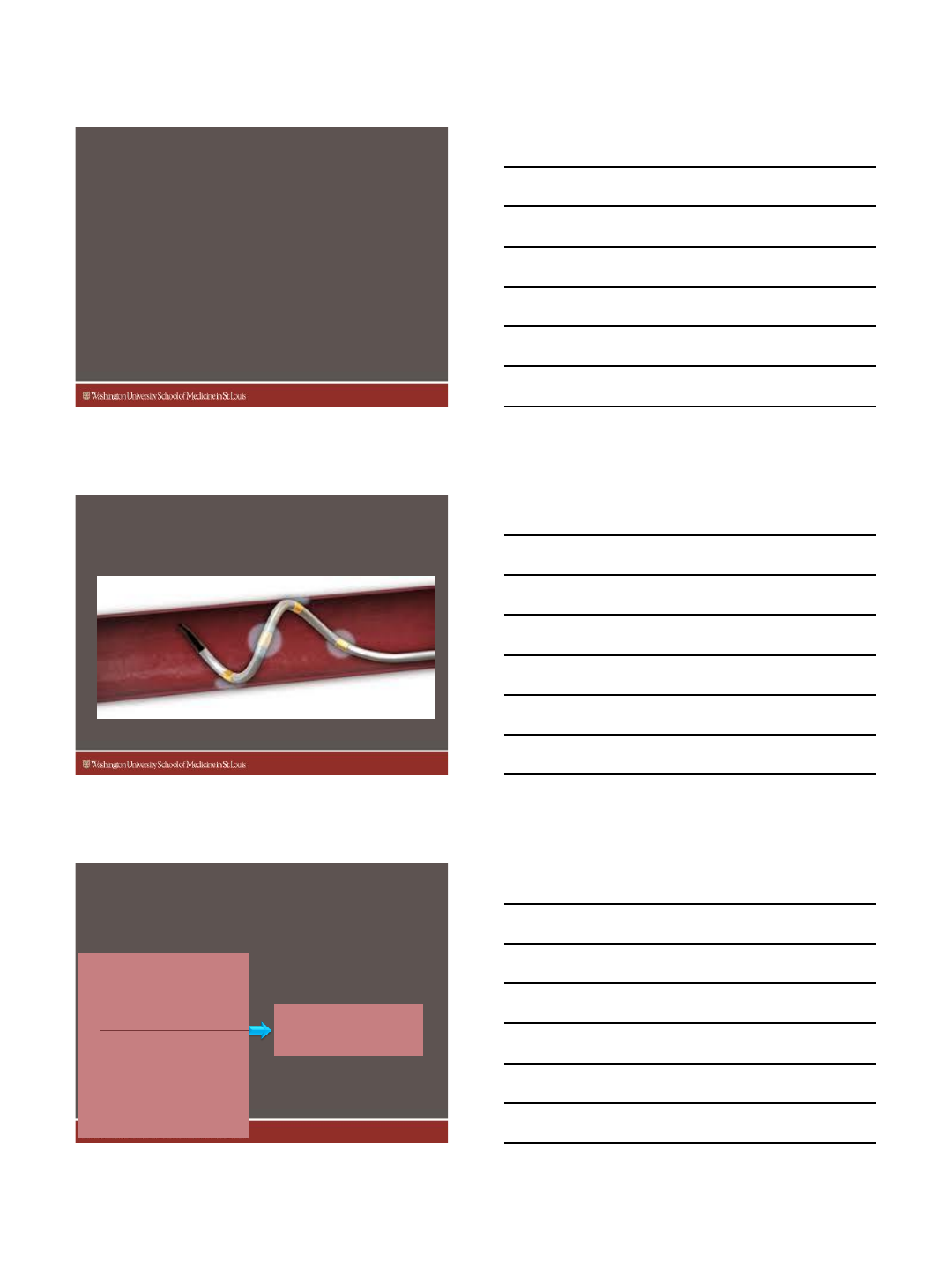
Baseline SBP
(mm Hg) 180 180 180 181 181 180 182 183 186 188 185
Error bars =
±
1 SE
Relationship Between SBP Changes and Number of
Ablations Attempted for Denervation Group at 6 Months
Number of ablations remains significant after adjustment for baseline blood pressure
n
Medicine
Nephrology
Areas of Speculation on the Causes of the
SYMPLICITY HTN-3 Efficacy Results..
Hawthorne
Effect Placebo Effect
Patient
Demographics
Heterogeneity of U.S.
Operator Experience
Trial Design/
Conduct
?
Medication
Changes or
Adherence
Catheter
Design
?
RTM S. Salmon, CRT 2014
Medicine
Nephrology
Ongoing Studies
Recruiting Patients
https://clinicaltrials.gov/ct2/results?term=renal+denervation&pg=2
•SPYRAL HTN-ON MED Study
•SPYRAL HTN-OFF MED Study
•Renal Sympathetic Denervation in Metabolic Syndrome
(Metabolic Syndrome Study)
•Renal Denervation Using the Vessix Renal Denervation System
for the Treatment of Hypertension (REDUCE HTN:REINFORCE)
•TrAnsCatHeter Intravascular Ultrasound Energy deliVery for
rEnal Denervation (ACHIEVE)
10
Medicine
Nephrology
Ongoing Studies
Recruiting Patients
https://clinicaltrials.gov/ct2/results?term=renal+denervation&pg=2
•Renal Denervation using the KONA External Ultrasound device
•Renal Denervation in Patients with Chronic Heart Failure and
Resynchronization therapy
•Renal Denervation in Patients with Heart Failure Secondary to Chagas
Disease
•Renal Denervation in Patients with Heart Failure and Severe Left
Ventricular Dysfunction
•A Feasibility Study to Evaluate the Effect of Concomitant Renal
Denervation and Cardiac Ablation on AF Recurrence
•Renal Denervation in Patients Undergoing VT Ablation: Combined
Renal Denervation and VT Ablation vs Simply VT Ablation
Medicine
Nephrology
Medtronic Spyral Catheter
Medicine
Nephrology
SPYRAL HTN
Global Clinical Trial Program
SPYRAL HTN Pivotal
•Based on OFF/ON trial results
•Cost Effectiveness Data/QOL to
be measured
First Phase Includes
Two Parallel Trials
20 Sites Globally
Second Phase
SPYRAL HTN-OFF MED
•100 patients
•Sham RCT (1:1)
•Main body and branch ablation
•No specific medication requirement
•Focus on ABPM change at 3 months
•QOL data to be measured
SPYRAL HTN-ON MED
•100 patients
•Sham RCT (1:1)
•Main body and branch ablation
•No max tolerated dose
•Focus on ABPM change at 3 months
•QOL data to be measured
11
Medicine
Nephrology
Adventitial Delivery Targets the Renal
Sympathetic Nerves
The Bullfrog Micro-
Infusion Catheter
•Uses common balloon-
inflation techniques (2 atm)
•Allows targeted deliver to
renal sympathetic nerve
sheath
•FDA 510(k)-cleared for
delivery to the vessel wall and
perivascular area
Medicine
Nephrology
Paradise: Ultrasound Technology for
Renal Denervation
•Cool –to protect the renal
artery –from the inside
•Heat –to ablate the renal
nerves –on the outside
Ultrasonic Heating Paradise Thermal Profile
Paradise RDN System Objective
Cool 0-1mm
Ablate 1-6mm
Paradise Technology Modeling
Water Cooling
Paradise Thermal Profile Objective:
Protect Renal Arteries & Ablate Renal Nerves
Medicine
Nephrology
Kona Medical Surround Sound® HTN Therapy
Non-Invasive Renal Denervation
Imaging and therapy
ultrasound positioned
beneath patient
External ultrasound energy
guided by ultrasound
image and motion tracking
Focused ultrasound energy
administered in treatment
“pattern” to ablate nerves
located outside of artery
Energy field
surrounds artery,
ablates renal nerves
1
53 4
Ultrasound imaging
used to identify renal
artery
2
Note: Kona Surround Sound Hypertension Therapy is investigational and not approved for sale
12
Medicine
Nephrology
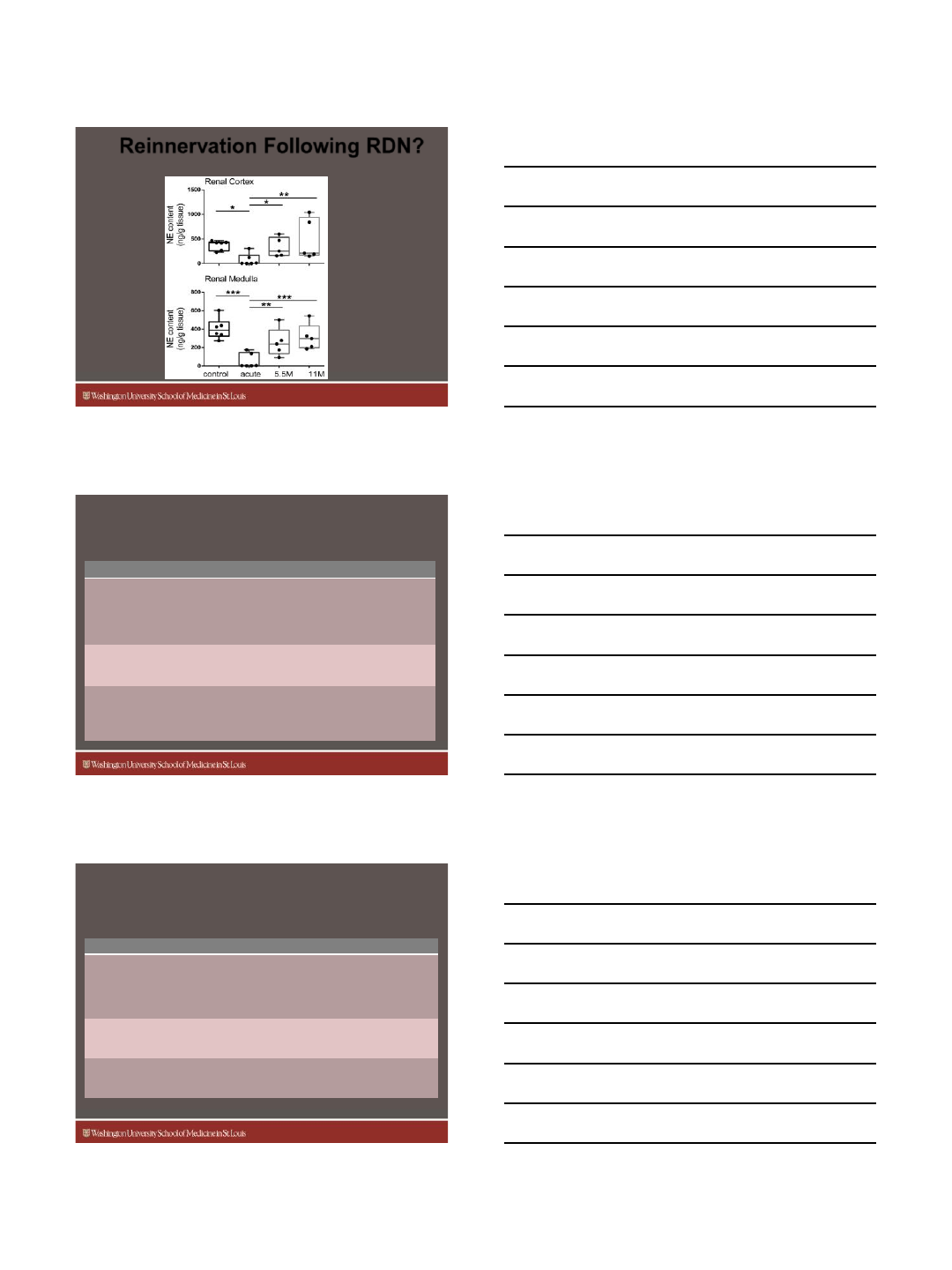
Reinnervation Following RDN?
Booth et al, Hypertension 2015
NE content in sheep following RDN and at 5.5 and 11 months
Medicine
Nephrology
Indications for Renal Denervation
Looking to the Future
Indication Comment
1. Treatment-resistant hypertension
(TRH)
•Poorly defined condition
•TRUE TRH is rare
•Inconsistent evidence that RDN
is better than drugs
•Improved RDN studies ongoing
2. Patients with poor drug compliance
•Improved in long-term BP
control could justify RDN
intervention
3. Systolic HTN in the elderly
•Sympathetic NS is a factor
•Responds well to drugs
•Question about ablation energy
across atherosclerotic vessels
Medicine
Nephrology
Indications for Renal Denervation
Looking to the Future
Indication Comment
4. Hypertension in young adults
•High sympathetic NS is a hallmark
•Early evidence for LVH, arterial
stiffness, etc
•RDN could potentially improve life-
long natural history of HTN
5. Hypertension related to CKD •Early evidence the RDN may
reduce rate of decline
6. Atrial fibrillation and heart failure •These are being studied
independent of hypertension
13
Medicine
Nephrology
Adapted from Physiology; Berne & Levy
Neuro-Hormonal HTNStructural HTN
Structural verses Neuro Hormonal
Hypertension
Medicine
Nephrology
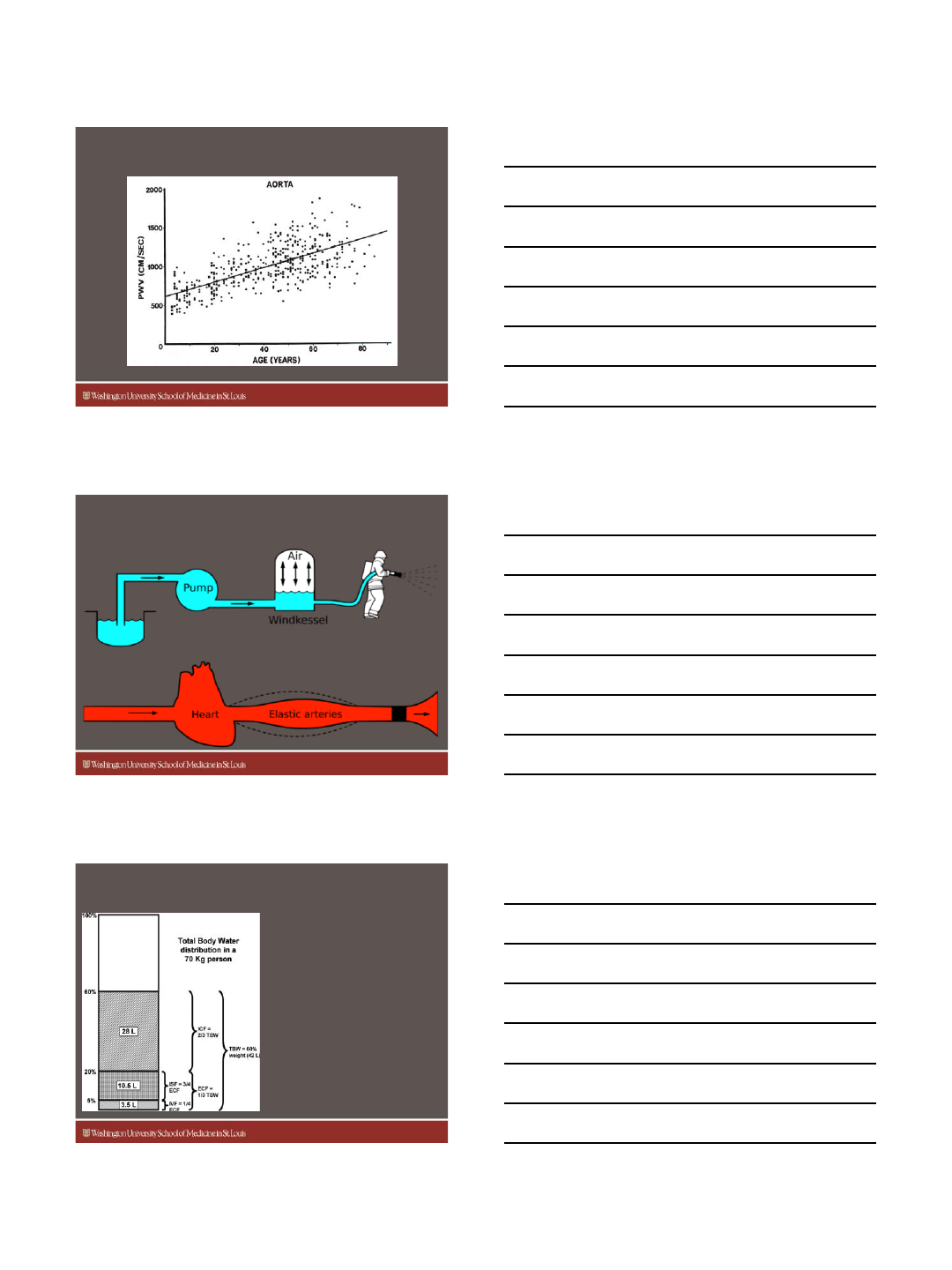
Elastic Fibers are Terminally Differentiated
After the age of 50, HTN is principally Structural
Burt. Hypertension 1995;25:313
Age
Systolic BP
Diastolic BP
Medicine
Nephrology
Renal Sympathetic Activity
Declines with Age
Esler et.al., J Cardiovasc Pharmacol, 1986
14
Medicine
Nephrology
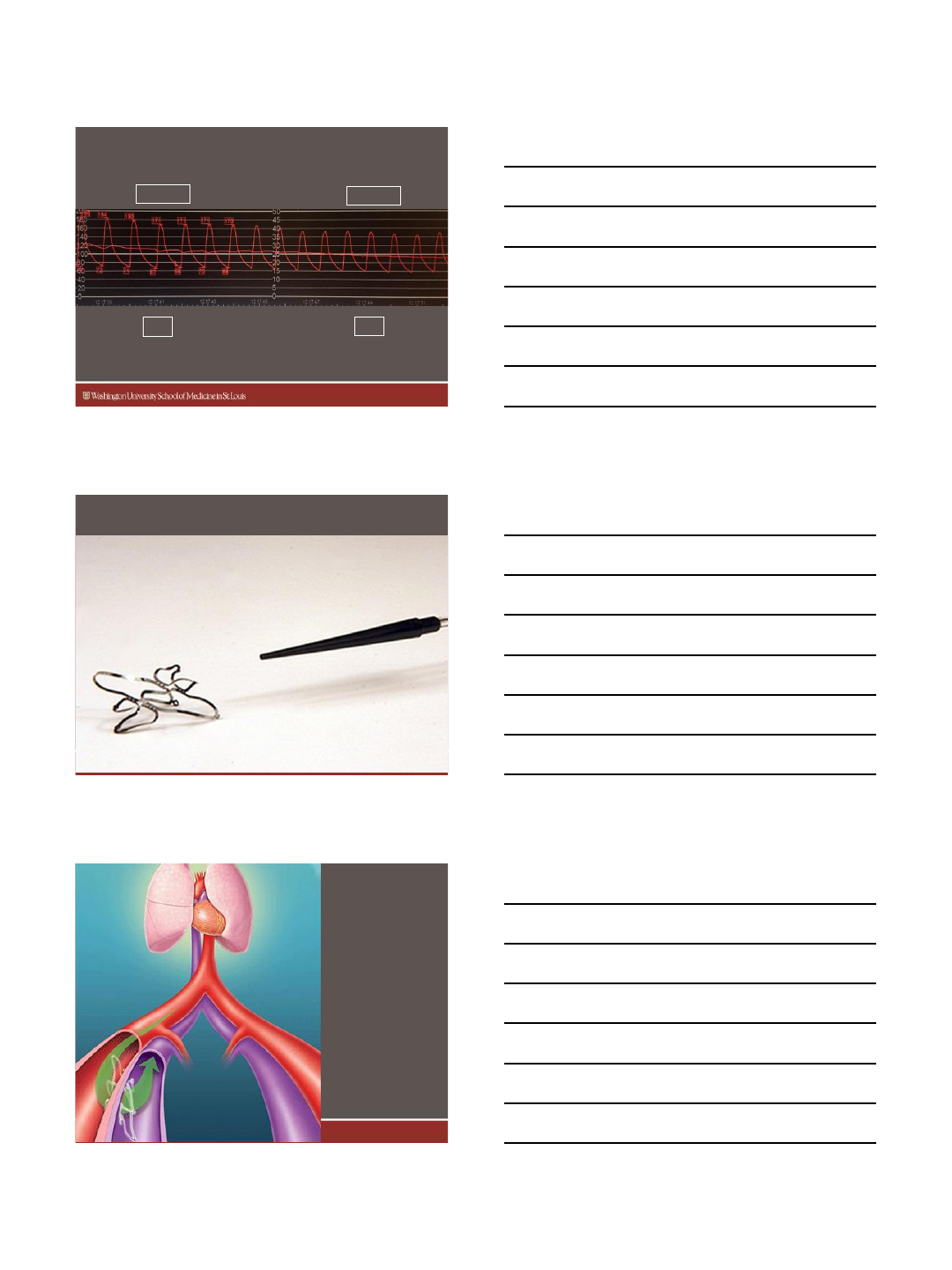
Loss of Aortic Elasticity Increases
Pulse Wave Velocity
Avolio et al; Circ:1983
Medicine
Nephrology
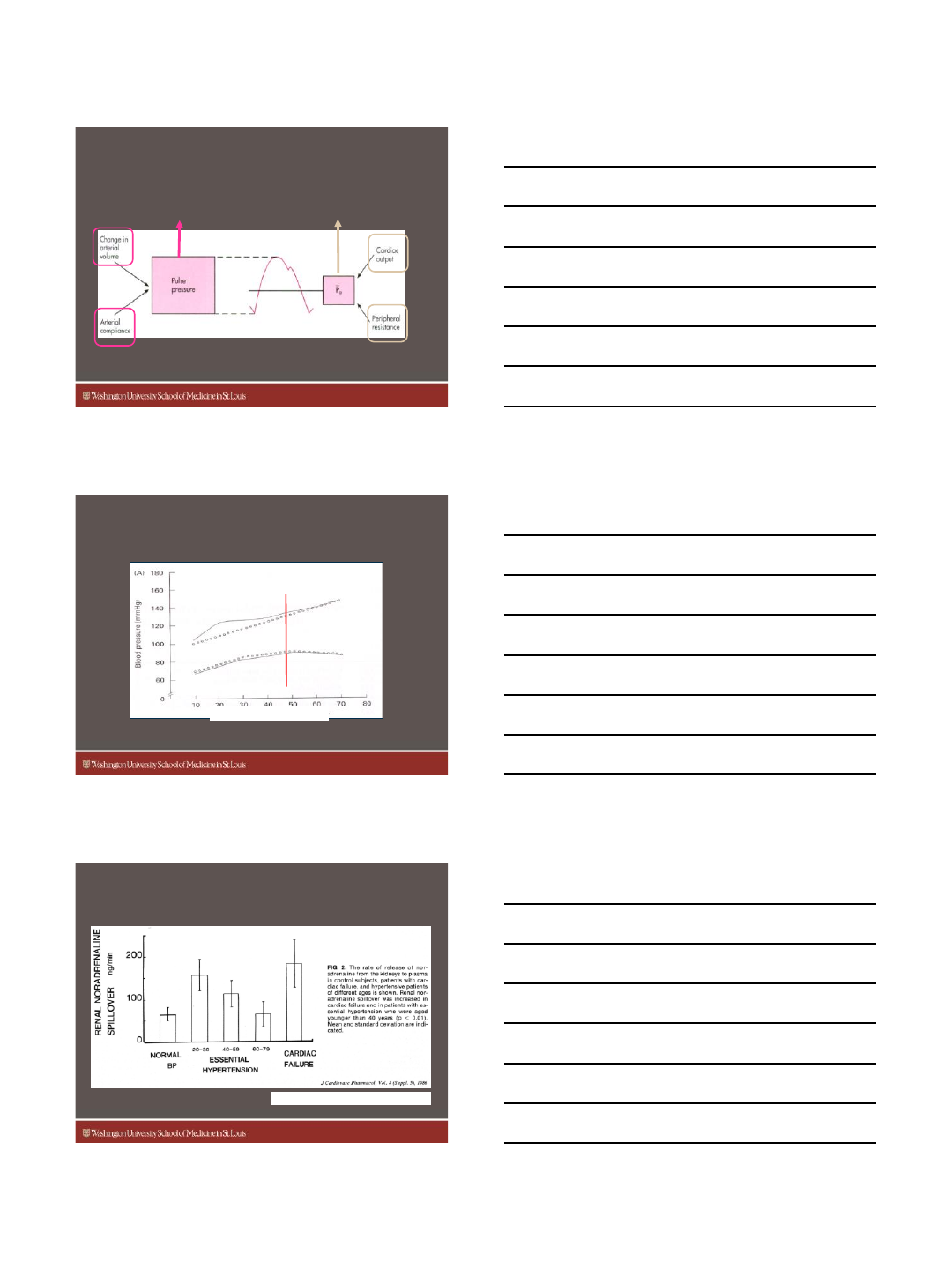
The aorta is meant to buffer each heart beat
The Windkessel Function of the Aorta
Medicine
Nephrology
Reduction of Arterial Volume
with Diuretics
adapted by Cevasco M and Dunlap ME
2.4% of total body water is arterial
(42l water in a 70kg adult);
To reduce effective arterial
volume by 1 liter, a diuretic must
remove 25% circulating volume;
Restoring Windkessel with
diuretics inherently activates RAA
and is associated with systemic AE.
15
Medicine
Nephrology
Mechanical solutions for structural hypertension:
Immediate BP reduction (-28/-15 mmHg)
150-153
Systolic BP
Diastolic BP ~60
186-180
~72
( mmHg )
( mmHg )
Eliminates the possibility of placebo, sham or Hawthorne effects
Medicine
Nephrology
ROX Coupler Device
Medicine
Nephrology
ROX
Coupler
Device
16
Medicine
Nephrology
Systolic BP
Diastolic BP
Randomized RH-02: Change in Office BP
p-values 3, 6, 9 and 12m < 0.0001; 24m <
0.015
AV Coupler Group Control Group
3 Mo
n=42 6 Mo
n=42 9 Mo
n=38 12 Mo
n=38 24 Mo
n=9 3 Mo
n=33 6 Mo
n=34
Statistically significant at all points
Medicine
Nephrology
Valencia Technologies Patent US 8805512 B1
Electroceutical
(eCoin)
Medicine
Nephrology
eCoin for the Rx of HTN
17
Medicine
Nephrology
Median Nerve Stimulation
•Activates somatic afferent nerve fibers in the
BP control centers of the brain:
•Arcuate and periventricular nuclei of the
hypothalamus
•Ventrolateral periaqueductal gray in the midbrain
•Nucleus tractus solitary
•Caudal ventral lateral medulla
This stimulation will release opioids, GABA and
cause sustained inhibition of sympathetic premotor
neurons, responsible for vasoconstriction
Tjen-A-Looi SC, Li P, et al. AJP, 2007:293(6):H3627-H3635
Medicine
Nephrology
Median Nerve Stimulation
•30 minute stimulation will release prolonged
transcriptional precursors such as mRNA
preproenkephalin (PPE) for over 72 hrs.
•Long-term effects are seen between 4-8 wks
•Proposed scheme: 30 min sessions weekly at
5-10 pulses/sec.
Li M, Tjen-A-Looi SC, et al. Autonomic Neuroscience 2012:170(0):30-35
Medicine
Nephrology
18
Medicine
Nephrology
Summary
•Resistant Hypertension is a “Rule-Out”
Diagnosis
•Poor Drug and Diet Adherence and High
Sodium Intake are most common causes
•Device Therapy is still evolving and moving
forward
