9 14 16 PRISM Syllabus
2016-09-14
: Pdf 9 14 16 Prism Syllabus 9_14_16_PRISM_Syllabus 9 2016 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 23
9/13/2016
1
Management of Adolescent ACL Injuries:
Treatment Outside of the Operating
Room:
Prevention
Christin Zwolski, PT, DPT, OCS
Cincinnati Children’s Hospital Medical Center
No Disclosures
Christin Zwolski, PT, DPT, OCS
Cincinnati Children’s Hospital Medical Center
How To Prevent an ACL Injury?
Neuromuscular
Training (NMT)
•Plyometric training
•Biomechanical
technique training
•Strength training
•Balance training
•Core stability training
9/13/2016
2
AAOS
Management of ACL Injuries CPG
AAOS
Management of ACL Injuries CPG
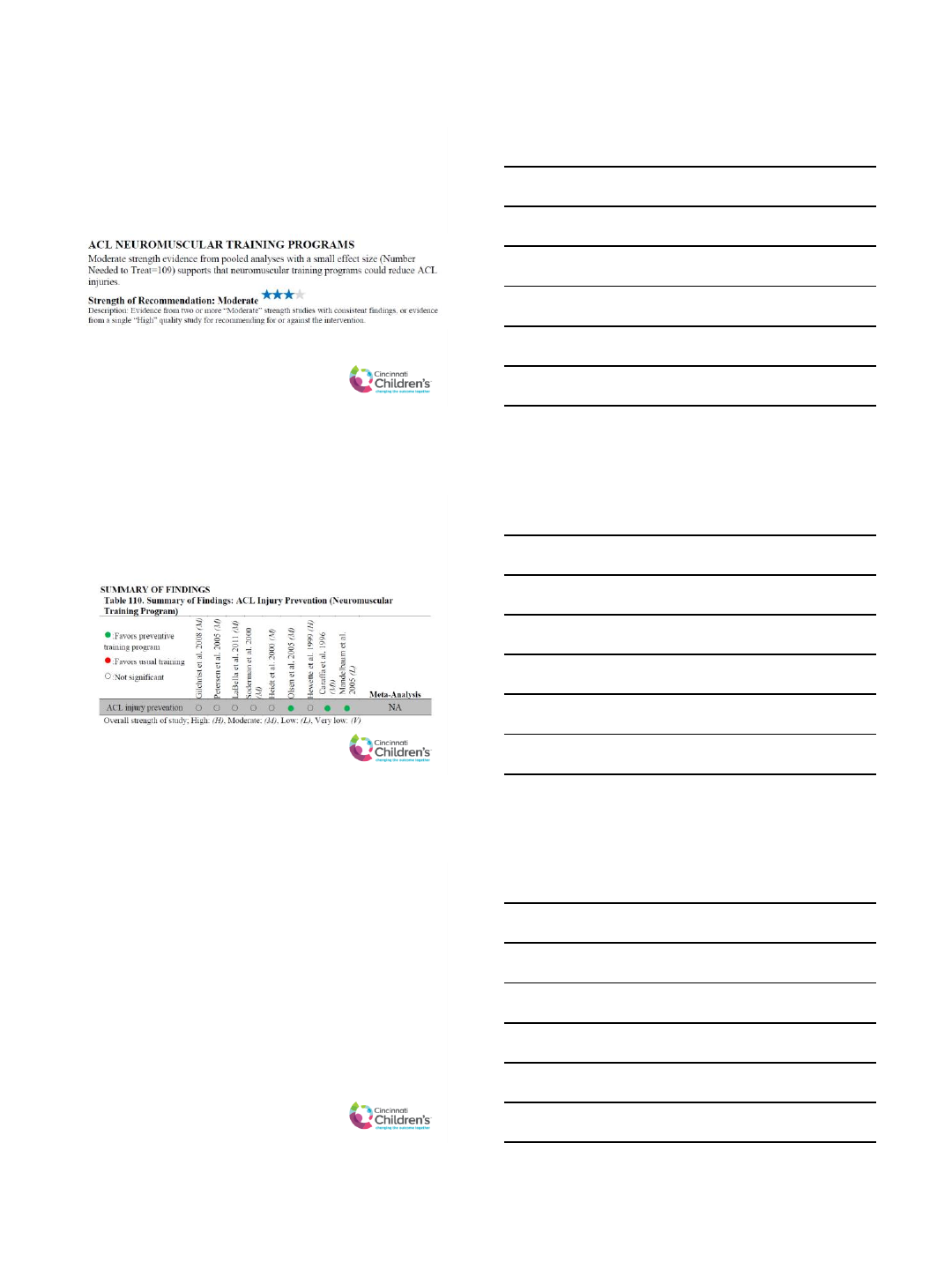
Studies that Favor NMT
Olsen et al. 2005 (M)
Caraffa et al. 1996 (M)
Mandelbaum et al. 2005 (L)
Overall strength of study:
M=moderate
L=low
•NMT warm-up
programs
•All demonstrate
significant reduction in
ACL injuries after
training
9/13/2016
3
Studies Found Not Signifigant
Gilchrist et al. 2008 (M)
Petersen et al. 2005 (M)
LaBella et al. 2011 (M)
Soderman et al. 2000 (M)
Heidt et al. 2000 (M)
Hewett et al. 1999 (H)
Overall strength of study:
M=moderate
H=high
•All suggest NMT can be
preventative
•Lack large number of
exposures
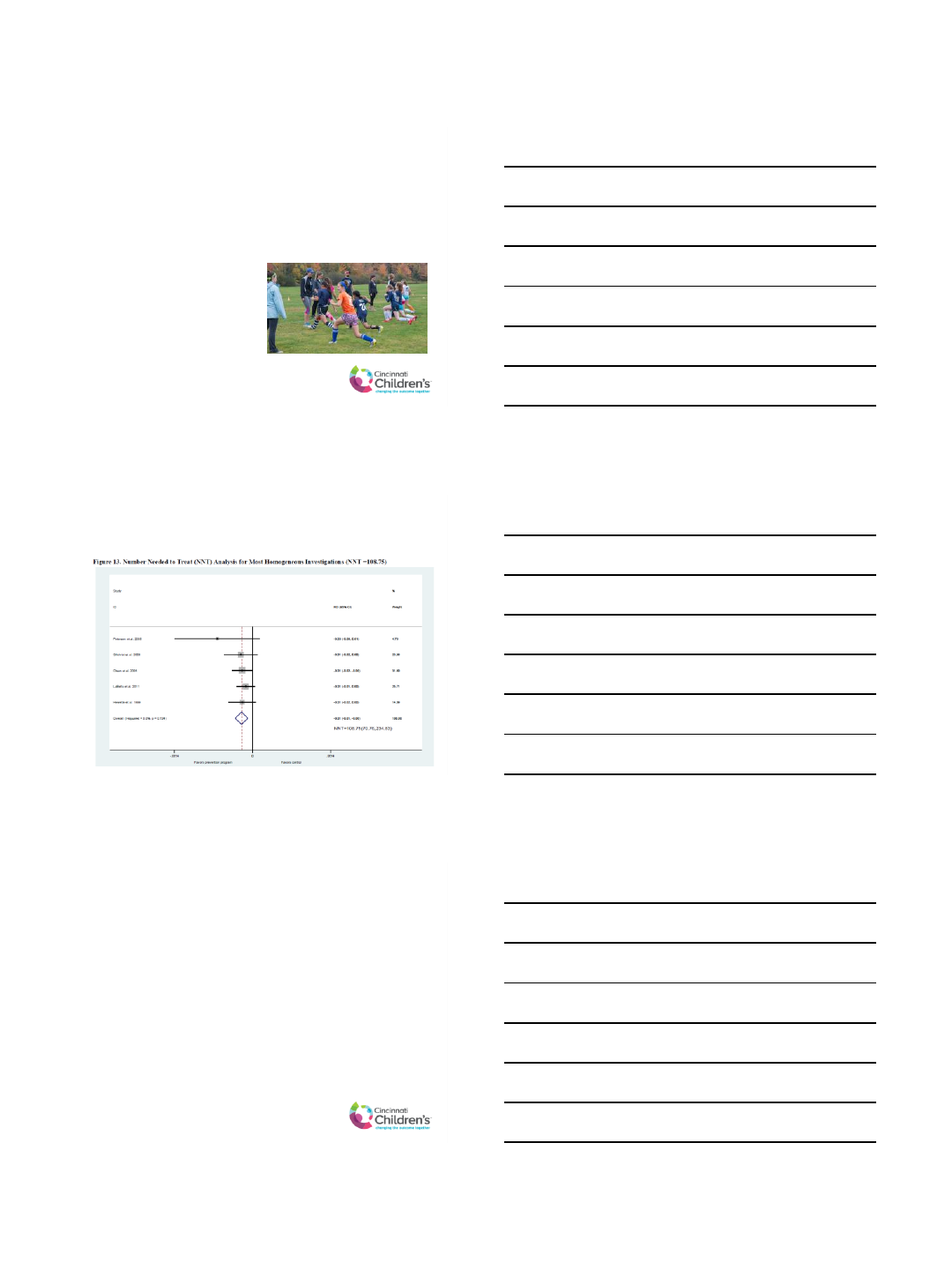
Small Effect Size (AAOS CPG)
•NNT = 109
More Recent Evidence…
•72% reduction in ACL injury rates in girls <18 years
old vs. 16% risk reduction for those ≥18 years old
(LaBella et al. 2014)
•Meta-analysis of Level 1 RCTs of soccer players:
NMT has protective effect (Grimm et al. 2014)
•Neuromuscular and proprioceptive prevention
programs reduce ACL injuries by 50.7% (Donnell-Fink et
al. 2016)
9/13/2016
4
Most Effective NMT Programs
•Duration: minimum of 6 weeks
•Frequency: >1x/week
•Comprehensive (with strength training)
•Combined pre- and in-season training
•Short bursts of activity
•Real-time Feedback with external-focus instructional
strategies
•Timing: Early pubertal maturation
Benjaminse et al. 2015, Ford et al. 2015, Sugimoto et al. 2015, Hewett et al. 2006
Bonus!
Participation in NMT can lead to improved sports
performance:
•LE and abdominal strength
•Vertical jump height
•Estimated maximal aerobic power
•Speed
•Agility
•Isokinetic strength
•Balance
Noyes et al. 2012, DiStefano et al. 2010
Cost-Effective Analysis
Swart et al. 2014:
On average, the implementation of a universal
training program would…
•Save $100 per player per season
•Reduce the incidence of ACL injury from 3% to 1.1%
per season
9/13/2016
5
What happens after one NMT
session?
Root et al. 2016:
•Landing technique improves (LESS)
•Does not impair sport performance (vertical jump,
long jump, shuttle run)
Limitations of NMT Research
•Lack of high-strength, double-blind RCTs
•Low generalizability (i.e. study populations)
•Heterogenous protocols
•Lack of compliance
Future NMT Research
•Multi-site studies using standardized NMT program
•Larger sample sizes of high-risk athletes
•Optimization of protocols
•Improved delivery
9/13/2016
6
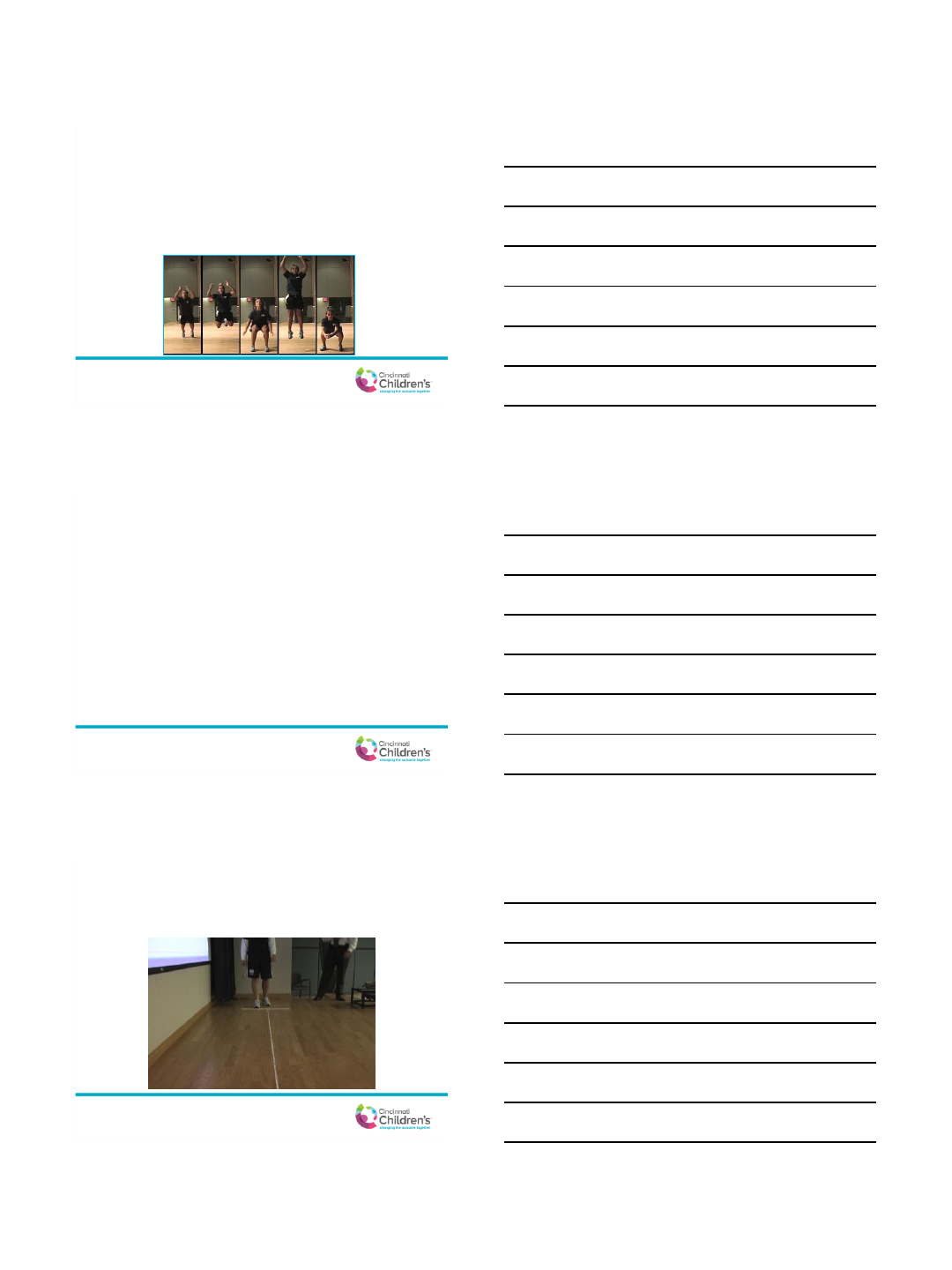
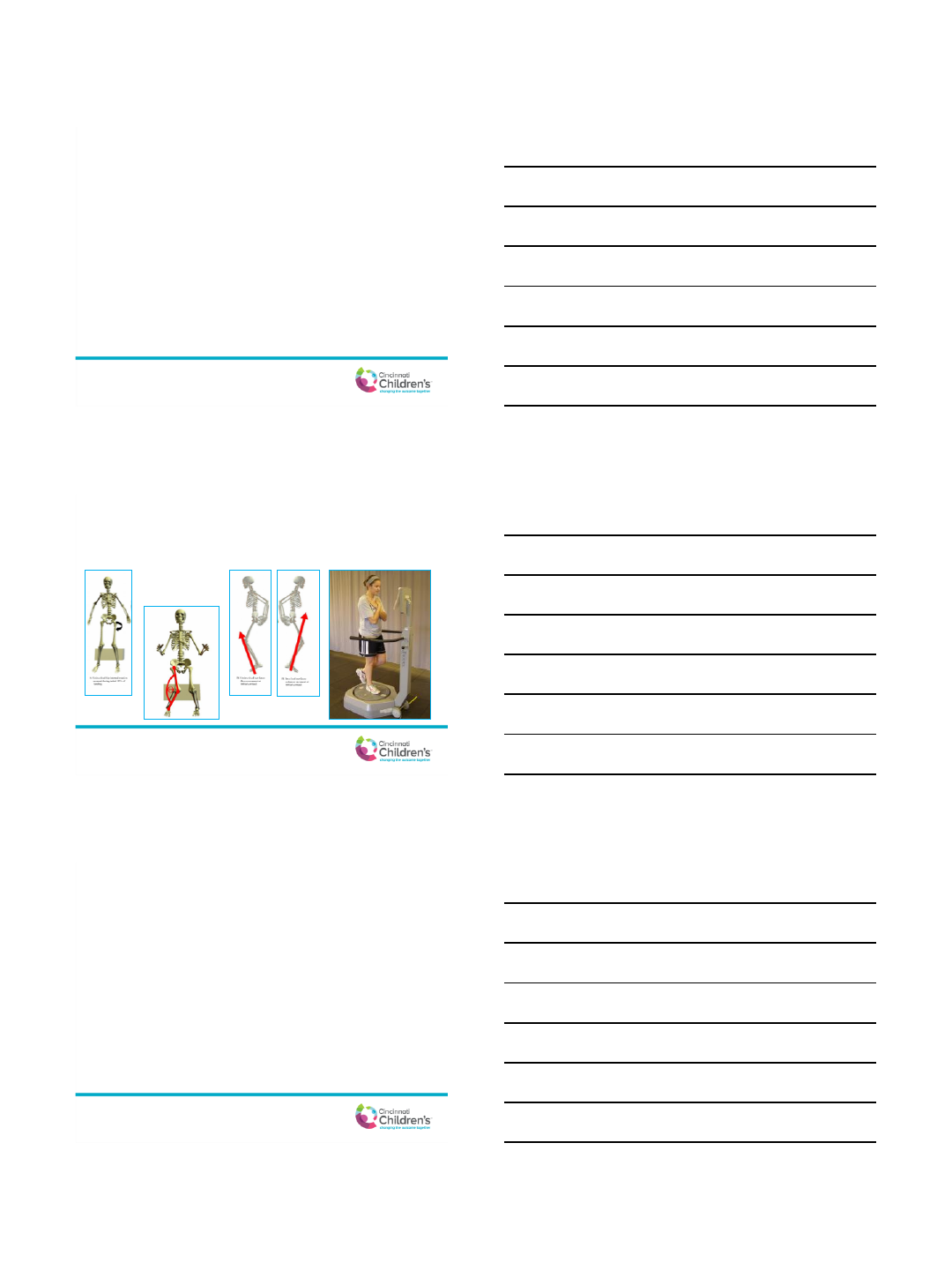
Risk Assessment
•Tuck Jump (Myer et. al 2008)
•Drop Vertical Jump (DL and SL)
(Redler et al. 2016)
•Landing Error Scoring System
(LESS) (Padua et al. 2015)
ACL Injury Prevention Programs
•Prevent Injury and
Enhance Performance
(PEP)
•Knee Ligament Injury
Prevention (KLIP)
•FIFA 11+
•FIFA 11+ Kids
•Sportsmetrics
Thank You!
Christy Zwolski, PT, DPT, OCS
Christin.Zwolski@cchmc.org
9/13/2016
1
Management of
Adolescent ACL Injuries:
Work-up
Attending Physician, Primary Care Sports Medicine
Department of Pediatric Orthopedic Surgery
The Children’s Hospital of Philadelphia
•ACL rupture is typically caused by rotation/translation of
the knee with foot planted; often non-contact
•Physical Exam:
•Effusion and decreased ROM common
•Lachman and/or anterior drawer: increased anterior translation of tibia
•Lachman is very sensitive and specific
•Pivot shift
•KT-1000
9/13/2016
2
•Should be done at initial assessment
•Utility: rule out fractures, evaluate physes
•Obtain 4 views: AP, lateral, tunnel, sunrise
•Associated fractures may include:
•Segond fx: lateral tibial condyle avulsion
•Lateral femoral condyle impaction
•Tibial spine avulsion
•In practice, insurance likely requires radiographs prior to
advanced imaging
Segond fracture
•Sensitivity and specificity generally 95+%
•A number of articles describe similar accuracy for
clinical evaluation
•MRI is most useful for confirming the diagnosis and
defining associated injuries
•In practice it is necessary prior to surgical
intervention
9/13/2016
3
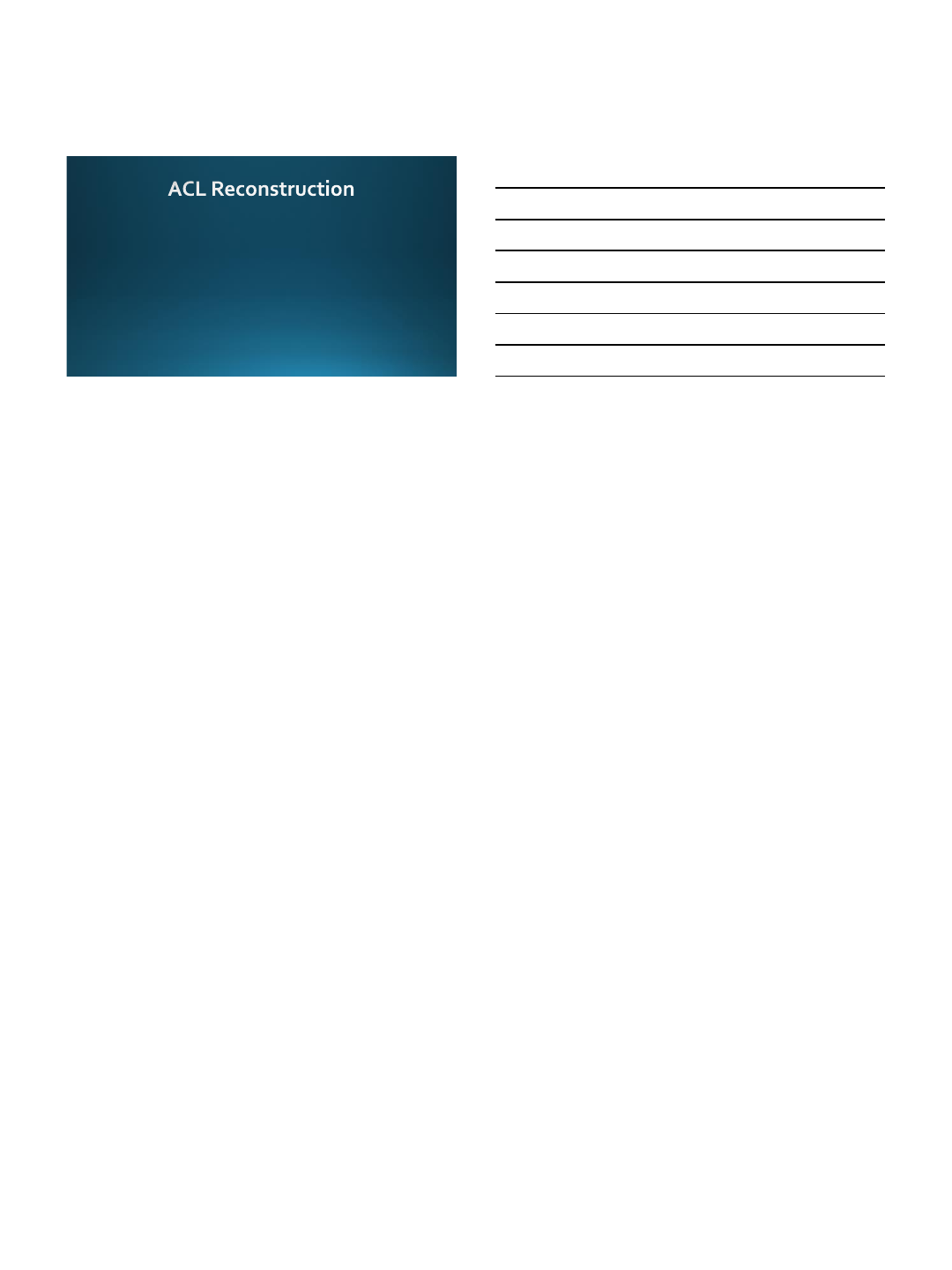
•ACL may appear thick with increased intra-substance
signal on T2 images
•May see complete rupture with lack of fiber continuity, or
possible avulsion type rupture
•Bone bruise pattern: posterior lateral tibial plateau and
lateral femoral condyle
•Assess for associated injuries: menisci, articular cartilage
MRI: ACL rupture
•Starts from the time we suspect ACL tear clinically
•Discuss the importance of attaining normal knee motion
and maintaining quad strength pre-operatively
•May need pre-op physical therapy
•Protection: brace, crutches, weight bearing status?
•Consider the emotional impacts
•Know some timelines for your surgeons
9/13/2016
4
•Graft choice depends on several factors
•Patient age, skeletal maturity
•Surgeon experience
•In adolescents the most common options are
autograft hamstrings or cadaver graft
•Hamstrings obtained from ipsilateral knee
9/13/2016
1
Management of Adolescent ACL
Injuries: Treatment Outside of
the Operating Room
Post Operative Physical Therapy
Kyle Sela, PT, DPT, SCS, OCS
PT Sports Medicine Coordinator, St. Luke’s Health System
Boise, ID
Disclosures
•None to report
AAOS Guidelines
•Bottom Line Up Front
•Moderate evidence to support the following post-operative physical therapy
guidelines
•Accelerated vs non-accelerated rehab programs
•Unrestricted and immediate range of motion (ROM) vs delayed
•Immediate weight bearing vs delayed
•Early, but limited range during open kinetic chain (OKC) exercises vs delayed and full
motion
•Early closed kinetic chain (CKC) exercises vs delayed
9/13/2016
2
Accelerated vs Nonaccelerated
•Recommendations based off of 2 studies (Beynnon 2005, 2011)
•BTB Grafts were used for all subjects
•Non-adolescent populations: 18-50 years of age
•Randomized into 2 groups
•Accelerated program progressed subjects over 19 weeks
•Exercises thought to produce increased sheer on the graft were initiated earlier
•Nonaccelerated program lasted 32 weeks
•Followed out to 24 months
•Results
•No differences in almost all outcome measures
•Knee laxity, activity level, pain, ADLs, quality of life, articular cartilage biomarkers
•Increased quad strength in accelerated group at 3 month follow up only
•1 re-tear (6 months out, nonaccelerated group)
•Aggressive vs nonaggressive hamstring autograft (Christensen 2013)
•No difference between groups (only followed to 24 weeks)
Unrestricted and Immediate Extension ROM
•Early active extension after anterior cruciate ligament reconstruction
does not result in increased laxity of the knee. (Isberg 2006)
•22 BTB Subjects
•Randomized into 2 groups
•Full passive or active extension immediately vs delayed
•Follow up at 6 months and 2 years
•Results
•No difference between groups in any outcome measure
•Laxity
•Self reported scores
•Hop testing
Early but limited motion during OKC strengthening
•OKC in restricted range 90-45° shown to be safe (Fleming 2005, Escamilla
1998)
•Early OKC exercises in hamstring autograft may increase laxity (Heinji 2007)
•Early vs late start of OKC in both BTB and HS ACLR (4 groups)
•Early hamstring group demonstrated significantly increased AP laxity
•No other differences between groups were found (strength, pain, function)
•Best time to implement safe OKC exercises? (Fukuda 2013)
•Early start (4 weeks) vs Late start (12 weeks)
•Restricted motion at knee extension machine from 45-90
•Results
•No difference in knee joint laxity
•Earlier group had quicker return of quad strength
•No difference in function
9/13/2016
3
Future Research in Post-Op Therapy
•Shift focus from differences in early rehab to later rehab guidance
•Identify optimal return to play, duty or work measures and benchmarks to guide rehab
•Improve long term tracking of ACLR patients
•What is re-tear or contralateral tear rate in specific populations
•Better describe those who re-tear vs those who don’t
•Repeat functional testing in “graduates” to identify regression
•Is there sufficient evidence to support Neuromuscular Electrical Stimulation
(NMES)?
•Seems promising in ACLR and other post-op populations (Erlandson 2014)
•Rehab trends to keep an eye on in the literature
•Blood Flow Restriction Training (BFR)
•Force plates for training and evaluation
References
•Beynnon, B. D., Uh, B. S., Johnson, R. J., Abate, J. A., Nichols, C. E., Fleming, B. C., ... & Roos, H. (2005). Rehabilitation After Anterior
Cruciate Ligament Reconstruction A Prospective, Randomized, Double-Blind Comparison of Programs Administered Over 2 Different
Time Intervals. The American journal of sports medicine,33(3), 347-359.
•Beynnon, B. D., Johnson, R. J., Naud, S., Fleming, B. C., Abate, J. A., Brattbakk, B., & Nichols, C. E. (2011). Accelerated Versus
Nonaccelerated Rehabilitation After Anterior Cruciate Ligament Reconstruction A Prospective, Randomized, Double-Blind Investigation
Evaluating Knee Joint Laxity Using Roentgen Stereophotogrammetric Analysis. The American journal of sports medicine,39(12), 2536-
2548.
•Christensen, J. C., Goldfine, L. R., & West, H. S. (2013). The effects of early aggressive rehabilitation on outcomes after anterior cruciate
ligament reconstruction using autologous hamstring tendon: a randomized clinical trial. J Sport Rehabil,22(3), 191-201.
•Erlandson, A. K., & Lauber, C. A. (2014). Neuromuscular electrical stimulation compared to exercise alone for regaining strength in
patients post anterior cruciate ligament surgery: A critically appraised topic. Journal of Athletic Medicine• Volume,2(3).
•Fleming, B. C., Oksendahl, H., & Beynnon, B. D. (2005). Open-or closed-kinetic chain exercises after anterior cruciate ligament
reconstruction?.Exercise and sport sciences reviews,33(3), 134-140.
•Fukuda, T. Y., Fingerhut, D., Moreira, V. C., Camarini, P. M. F., Scodeller, N. F., Duarte, A., ... & Bryk, F. F. (2013). Open Kinetic Chain
Exercises in a Restricted Range of Motion After Anterior Cruciate Ligament Reconstruction A Randomized Controlled Clinical Trial. The
American journal of sports medicine,41(4), 788-794.
•Heijne, A., & Werner, S. (2007). Early versus late start of open kinetic chain quadriceps exercises after ACL reconstruction with patellar
tendon or hamstring grafts: a prospective randomized outcome study. Knee Surgery, Sports Traumatology, Arthroscopy,15(4), 402-
414.
•Isberg, J., Faxén, E., Brandsson, S., Eriksson, B. I., Kärrholm, J., & Karlsson, J. (2006). Early active extension after anterior cruciate
ligament reconstruction does not result in increased laxity of the knee. Knee surgery, sports traumatology, arthroscopy,14(11), 1108-
1115.
9/12/2016
1
Management of Adolescent
ACL Injuries: Bracing
Opal Griffin, LAT, ATC
St. Luke’s Health System, Boise ID
Sports Medicine: Outreach Athletic Training
Disclosers:
Presenter: Opal Griffin, LAT, ATC
With respect to the following presentation, there has been no relevant (direct
or indirect) financial relationship between the party listed above (and/or
spouse/partner) and any for-profit company in the past 24 months which
could be considered a conflict of interest.
All images that are included are for clarification purposes only, not a
suggestion of the “best brace” or the type that was specifically tested.
Prophylactic Bracing:
Ortho Guidelines from the AAOS (5, 6)
Limited evidence supports Preventative braces might not be prescribed
Studies showed no reductions in ACL injuries with Bracing
Only tested American HS and Collegiate FB players.
Future Research
Would this be different in other papulations?
Female Soccer has the highest rate of ACL injury per the AAOS
Greater population size?
Younger population?
9/12/2016
2
Postoperative Functional Bracing:
Ortho Guidelines from the AAOS (1, 2, 3)
Moderate evidence does not support routine use
not proven effective when compared to neoprene knee sleeve and no
bracing.
Routine use cannot be supported
There was lack of efficacy following ACL reconstruction..
Types of Braces Studied (examples)
Functional Bracing Neoprene sleeve
Postoperative Functional Bracing:
2015 Review published in Sports Health (4)
Anterior Cruciate Ligament Reconstruction Rehabilitation: MOON Guidelines
Postoperative bracing did NOT improve: pain, swelling, range of
motion or safety
“Eleven studies… no study demonstrated a clinically significant or
relevant improvement in safety, range of motion including
extension, or other outcome measures.7,15,19,25,27,31,36,43,47,50,57,67”
Supported by 17 studies that the MOON group considered to be level 1
or 2 evidence
9/12/2016
3
Postoperative Bracing: Exception
Meniscal Injury with about half of
all ACL injuries. Per the AAOS.
Meniscal repair requires support
post surgically.
References:
Functional knee braces after ACLR
1. Birmingham TB, Bryant DM, Giffin JR et al. A randomized controlled trial
comparing the effectiveness of functional knee brace and neoprene sleeve use
after anterior cruciate ligament reconstruction. Am J Sports Med 2008;36:648-
655.
2. McDevitt ER, Taylor DC, Miller MD et al. Functional bracing after anterior
cruciate ligament reconstruction: a prospective, randomized, multicenter study.
Am J Sports Med 2004;32:1887-1892.
3. Risberg MA, Holm I, Steen H, Eriksson J, Ekeland A. The effect of knee bracing
after anterior cruciate ligament reconstruction. A prospective, randomized
study with two years' follow-up. Am J Sports Med 1999;27:76-83.
4. Wright R, Haas, A, Anderson, J et al. and MOON Group. Anterior Cruciate
Ligament Reconstruction Rehabilitation: MOON Guidelines. Sports Health
2015;7:239-243.
Prophylactic knee bracing
5. Sitler M, Ryan J, Hopkinson W et al. The efficacy of a prophylactic knee brace
to reduce knee injuries in football. A prospective, randomized study at West
Point. Am J Sports Med 1990;18:310-315.
6. Deppen RJ, Landfried MJ. Efficacy of prophylactic knee bracing in high school
football players. J Orthop Sports Phys Ther 1994;20:243-246.
Questions…
Thank you for joini ng us!
9/13/2016
1
Return to Sport after ACL
Reconstruction: How
Objective is your Decision?
Mark V. Paterno PT, PhD, MBA, SCS
Coordinator of Orthopaedic and Sports Physical Therapy
Acting Scientific Director
Division of Occupational Therapy and Physical Therapy
Associate Professor, Division of Sports Medicine
Cincinnati Children’s
Cincinnati, OH
Objectives
1. Review current evidence regarding RTS after ACL
reconstruction
2. Discuss current criteria used to determine
readiness to RTS.
3. Identify potential opportunities to improve RTS
decision making in this population
9/13/2016
2
CLINICAL QUESTION:
When is it safe to return to sports (RTS)
after ACL Reconstruction?
1. What is “safe”?
2. What are the functional demands of the sport?
RTS: When is it safe?
1. Incidence of 2nd ACL injury after ACLR and RTS
Ipsilateral Graft Re-tear (Wright et al JBJS 2011)
Contralateral ACL Injury (Wright et al JBJS 2011)
2. Incidence of Secondary Injury after ACLR and RTS
3. Incidence of Osteoarthritis after ACLR and RTS
50-100% of patients develop OA after ACL injury
Lohmander et al 2004
9/13/2016
3
RTS: When are you able to return
to your prior level of function?
What factors are necessary to insure success:
•Strength
•Balance/Postural Stability
•Mechanical Stability/Functional Stability
•Power
•Endurance
•Agility
•Etc….
ACL Return to Sport: Systematic
Review
Kvist J. “Rehabilitation Following Anterior Cruciate
Ligament Injury: Current Recommendations for
Sports Participation.” Sports Med 2004: 34(4): 269-
280.
34 articles between 1998-2003
ACL Return to Sport: Systematic
Review- Kvist Sports Med 2004
Outline of criteria reported:
•13/34 assessed isokinetic strength
•25/34 used jump testing
•14/34 reported some clinical criteria (i.e.
ROM, knee stability etc.)
•4/34 had no assessment of strength or
performance
9/13/2016
4
ACL Return to Sport: Systematic
Review- Barber-Westin et al 2011
Systematic Review (n=264)
•40% : no criteria
•13% : objective criteria
Current Return to Sport Measures
1. Time from surgery
2. Strength
3. Knee Laxity
4. Functional Performance
Testing
Single Hop X-Hop Triple Hop Timed Hop
Current Return to Sport Measures
“…low correlations between various hop test scores
and self-reported measures of function may
indicate that neither of these methods can stand
alone as an adequate assessment of knee
function.”
Fitzgerald GK et al
“Hop Tests as Predictors of Dynamic Knee Stability”
JOSPT 2001
9/13/2016
5
Return to Sport Assessment:
What are we missing?
1. Patient reported outcomes
2. Assessment of movement quality
3. Patient readiness to return to activity
RTS: Patient Reported Outcomes
1. Patient Reported Quality of Life Measure
2. Region Specific Assessment
•IKDC: Zwolski et al AJSM 2015
•KOOS: Wasserstein et al Osteo Cart 2015 (MOON Data)
•Others
RTS: Assessment of Movement
Quality
9/13/2016
6
RTS: Assessment of Movement
Quality
“Biomechanical Measures during Landing and
Postural Stability Predict Second Anterior Cruciate
Ligament Injury after ACL Reconstruction and
Return to Sport”
Paterno et al AJSM 2010
RTS: Predictors of 2nd ACL Injury
Paterno et al AJSM 2010
RTS: Patient Readiness to RTS
1. Fear of Reinjury/Lack of Confidence
•Lentz et al JOSPT 2012: Athletes who RTS had lower level
of kinesiophobia
•Lentz et al AJSM 2015: Athletes who did not RTS due to
fear of reinjury was older, lower quad strength and
lower IKDC
2. Other Factors
9/13/2016
7
Summary
1. Limited evidence exists regarding RTS decision
making after ACLR
2. Current criteria used to determine readiness to
RTS may not identify those at high risk for injury
or likely to maintain pre-injury level of function
3. Future work needs to better identify critical
factors to use to determine readiness to safely
return to sport
Thank you!!
Mark V. Paterno PT, PhD, MBA, SCS
Cincinnati Children’s
mark.Paterno@cchmc.org
@mvpaternopt
