A2b93dff E83a 4115 A9fa 03a3be46e05f
2017-01-30
: Pdf A2B93Dff-E83A-4115-A9Fa-03A3Be46E05F a2b93dff-e83a-4115-a9fa-03a3be46e05f 1 2017 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 30
1/30/2017
1
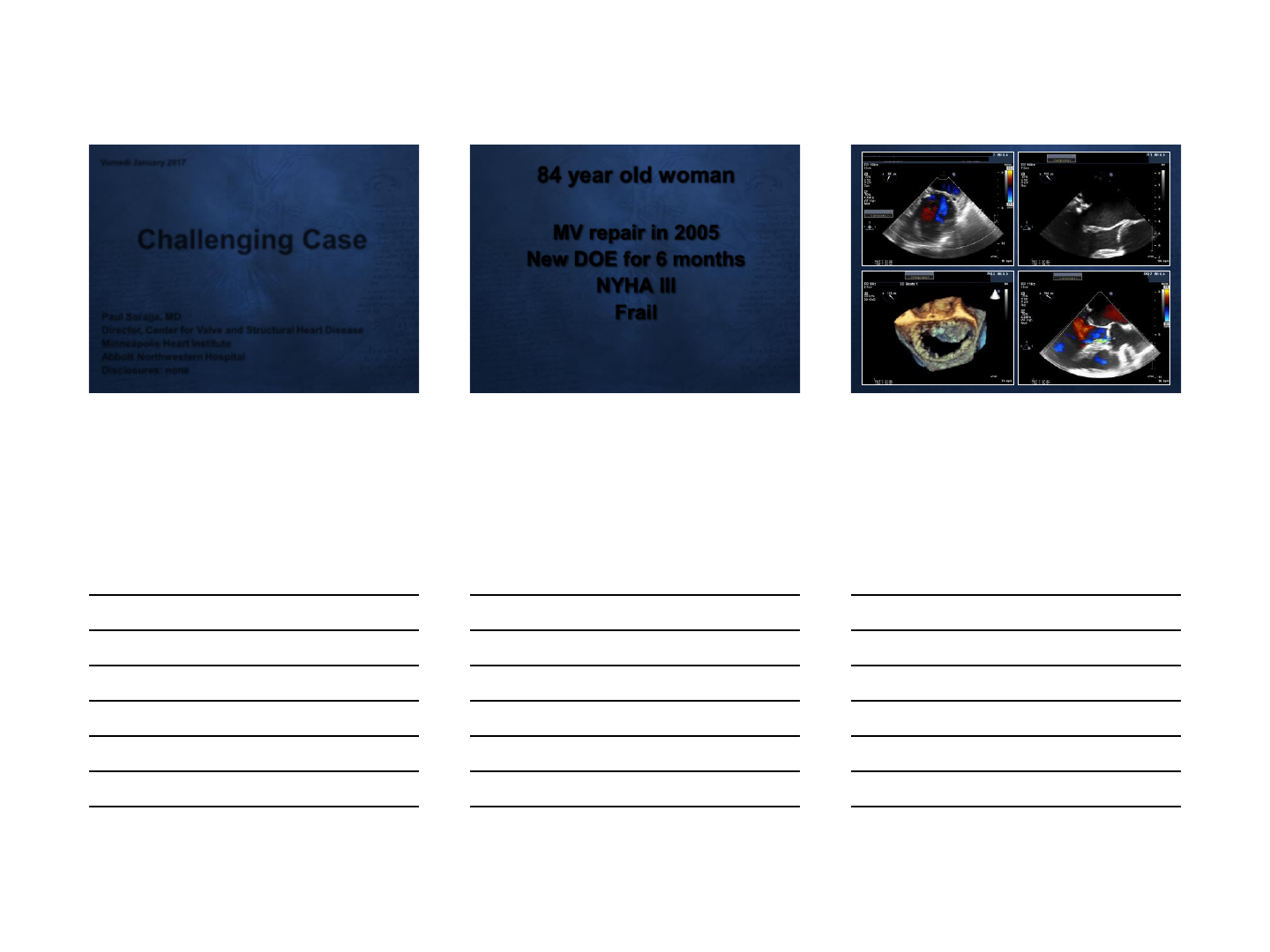
Challenging Case
Paul Sorajja, MD
Director, Center for Valve and Structural Heart Disease
Minneapolis Heart Institute
Abbott Northwestern Hospital
Disclosures: none
Vumedi January 2017
84 year old woman
MV repair in 2005
New DOE for 6 months
NYHA III
Frail
1/30/2017
2
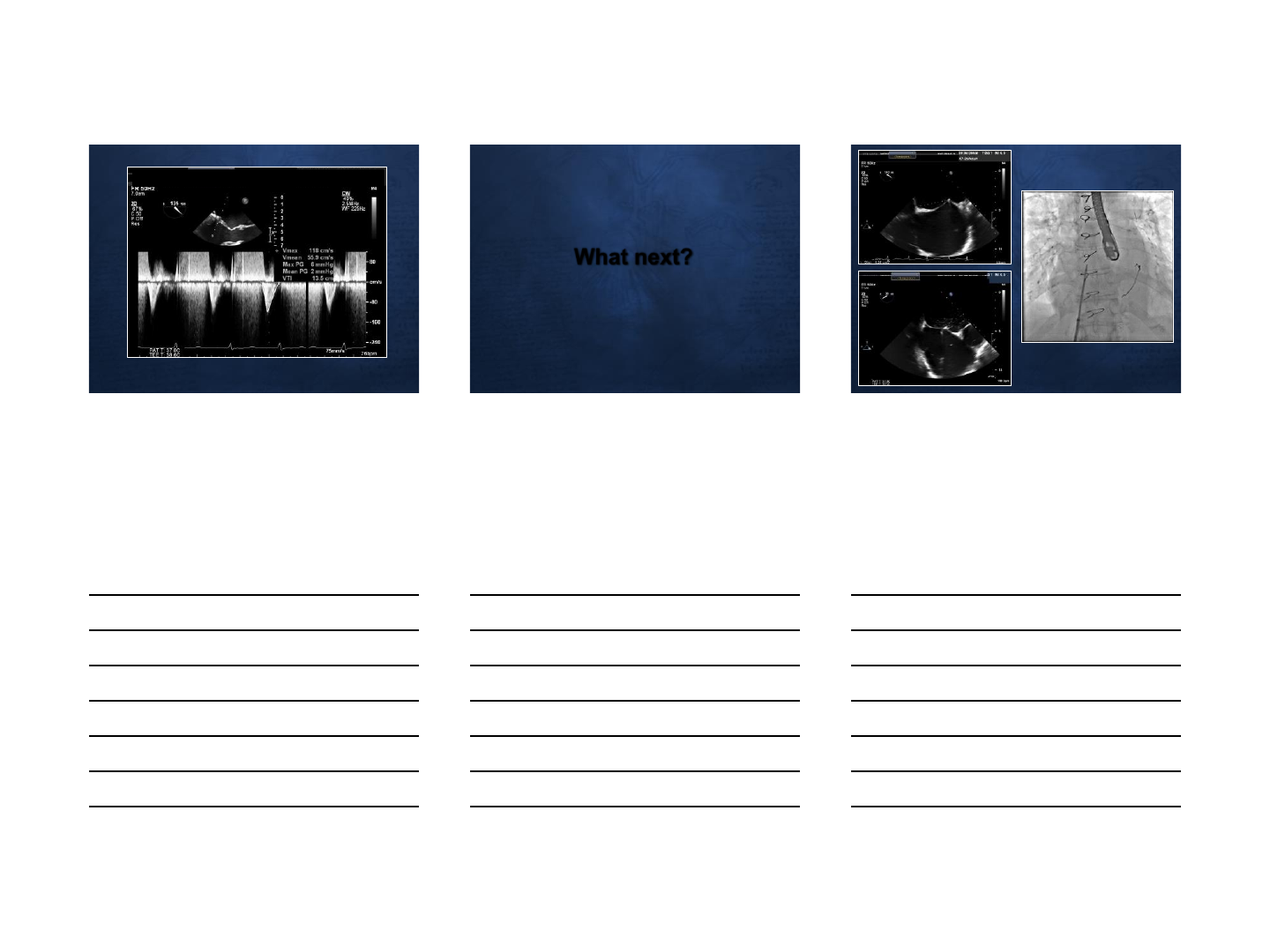
What next?
1/30/2017
3
1/30/2017
4
1/30/2017
1
Itsik Ben-Dor ,MD
Augusto Pichard ,MD
MedstarWashington Hospital Center.
Washington, DC
TAVR in bicuspid Aortic
valve
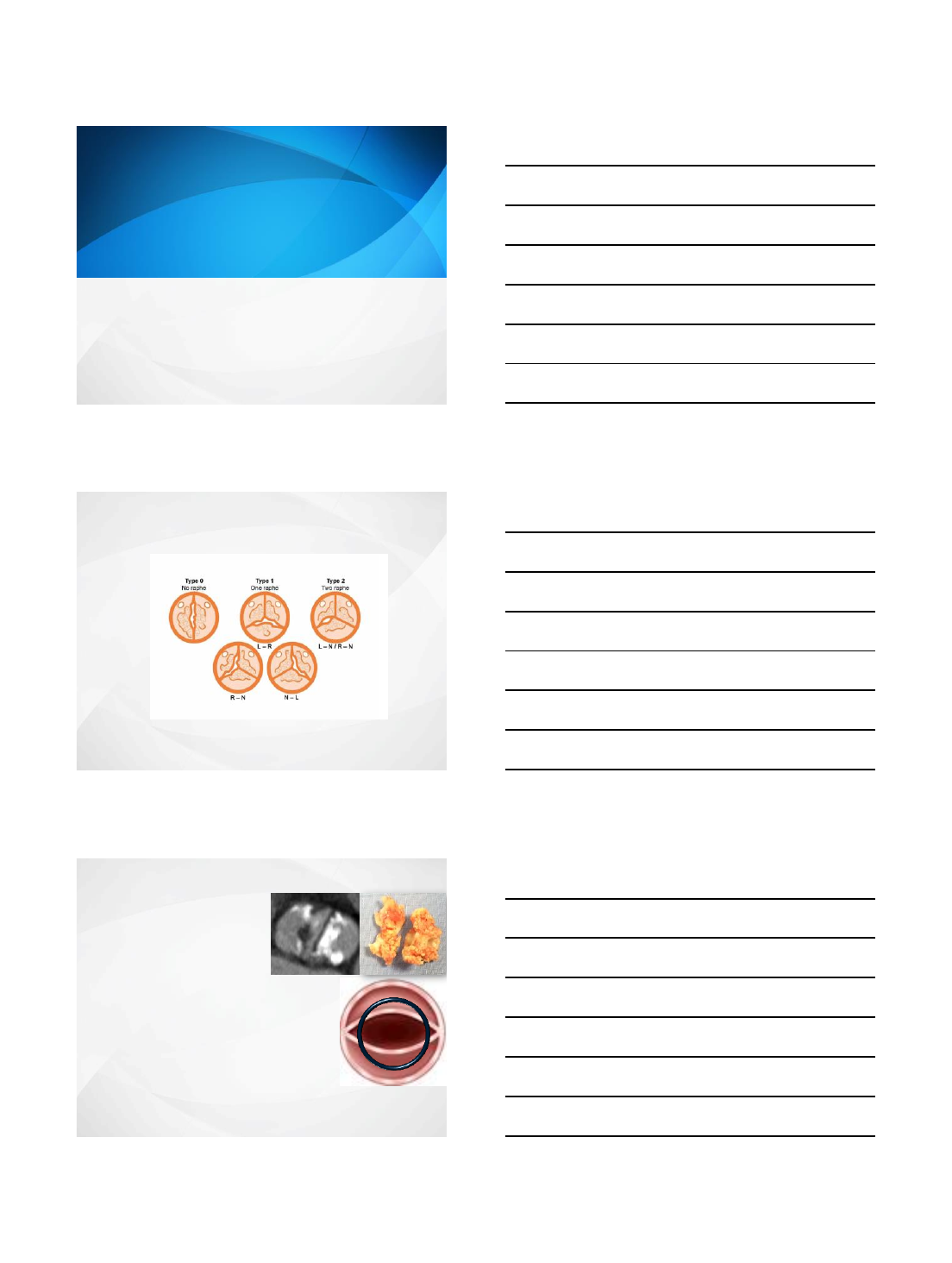
Classification of Bicuspid Valves
Sievers et at. J Thorac Cardiovasc Surg 2007;133:1226-33.
71%
88% 5%
15% 3%
7%
Potential Problems in Bicuspids
Often heavily calcified
Incomplete valve expansion
Paravalvar leak
Annulus rupture
Coronary obstruction
Higer rate of pacemaker
Frequently associated with
ascending aortic aneurysm
Risk of rupture/dissection
Oval shaped valve area
Risk of paravalvar leak
Sizing is difficult
Long-term durability of the TAVI valve?
For these reasons bicuspid valves had been
excluded from all randomized trials
1/30/2017
2
Valve size in bicuspid valves
Avoid oversizing
Risk of rupture
Larger self-expanding valves have less radial force
Usually it is safe to undersize
Very large annuli may still be
suitable for TAVI due to higher
degree of calcification
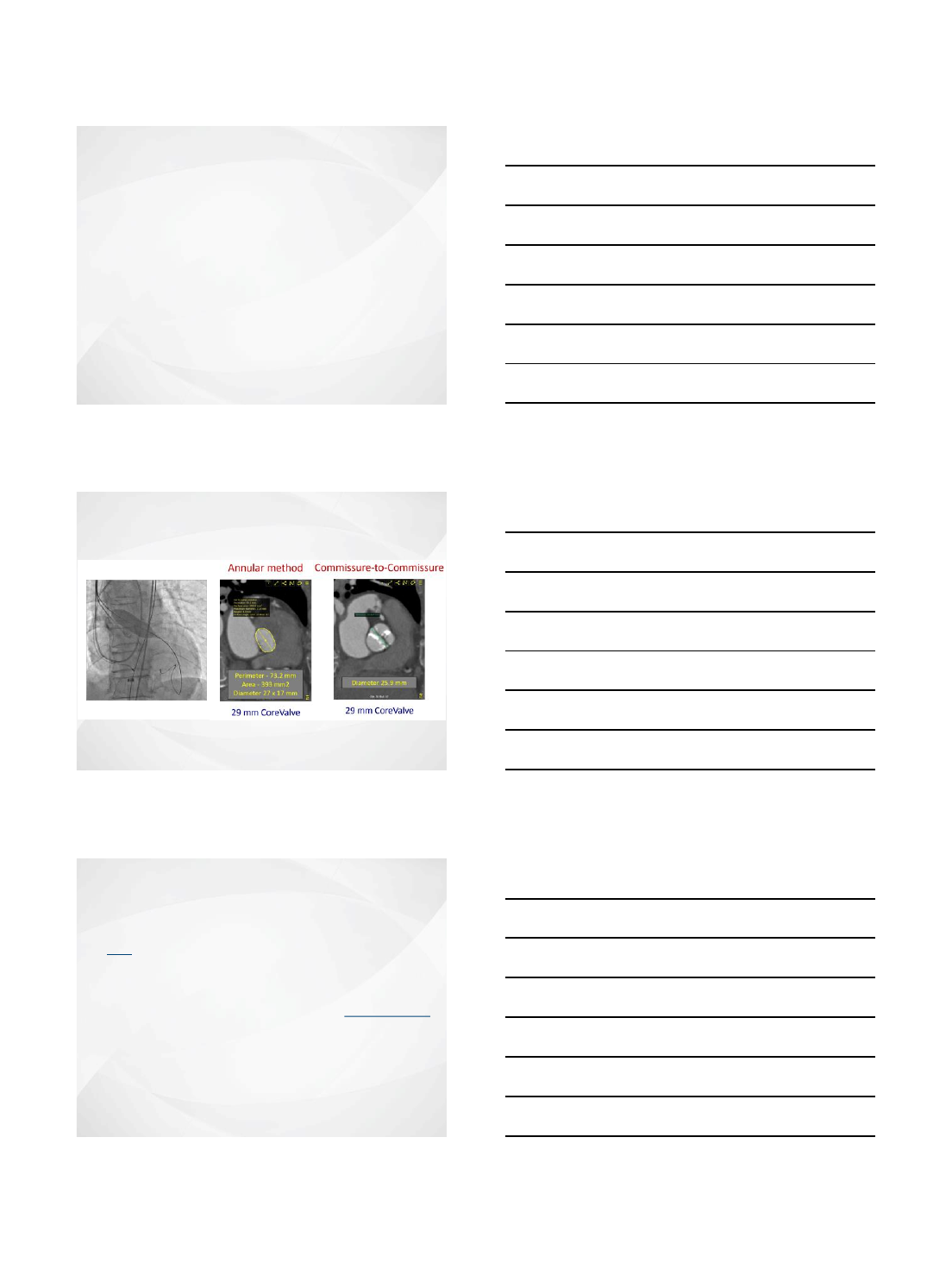
Sizing
Balloon sizing
29 mm Core Valve
Case History
•81 year-old woman with presents with progressive SOB and
leg edema
•
PMH:
•Atrial fibrillation s/p retinal embolus on Eliqius
•DVT
Echo :
EF 20-25%
AVA 0.5cm2 v2 6.3m/sec, mean gradient 106mmHg
Mild to moderate AR
BAV (2 months before) –Maxi 22mm AVA 0.25 to 0.52 cm2
Mean gradient 100 to 43mmHg
STS score: 2.4%
1/30/2017
3
Date of ECHO
01.27.2016 (post BAV)
LVEF (20%)
*
45% Aortic Valve Area (< 1.0cm2)
*
0.7
Mean Aortic Gradient (
40mmHg)
*
44 Aortic Valve Area Index (
<
0.6cm2/m2)
*
0.41
Peak Velocity (4.0 m/sec)
*
4.2
RV Size and Function
Normal size,
borderline reduced
systolic function
Estimated Systolic
Pulmonary Pressure (mmHg)
36
Other Valvular Findings
Mild MR, trace AR; mild TR
Native Coronary and Graft
Findings LM 30%; LAD 10%; LCX = 10%; RCA=10%
Echo
Bicuspid valve
Which Valve would you choose ?
1.Balloon expandable
2. Self expandable
1/30/2017
4
1/30/2017
5
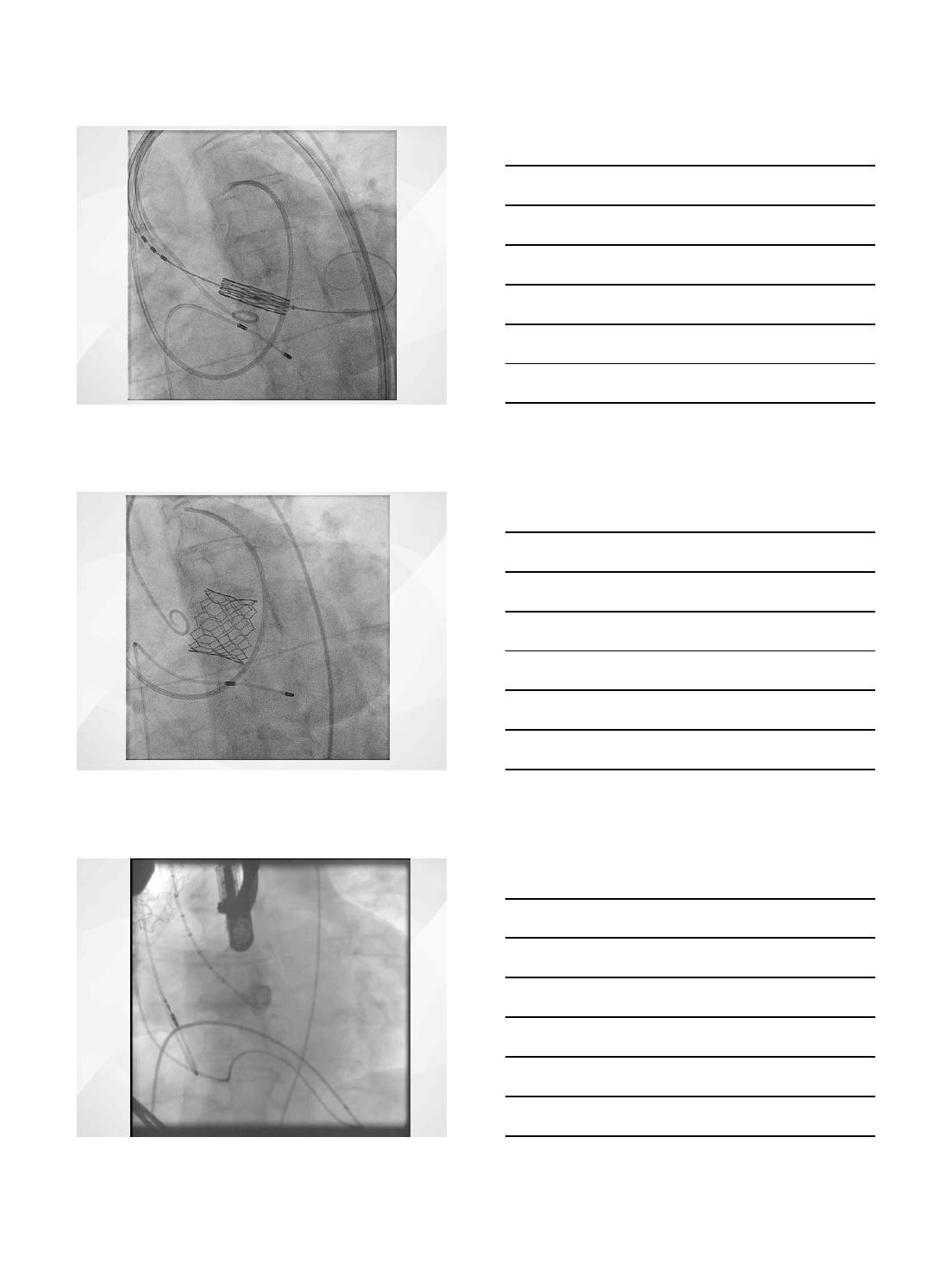
Annulus by CT
Measure
Short Annulus Diameter
25.1
mm
Long
Annulus Diameter
30.0
mm
Annular Perimeter
85.3
mm
Annular Area
581.1
mm
2
Derived diameter (perimeter/area)
27.2/27.2
mm/mm
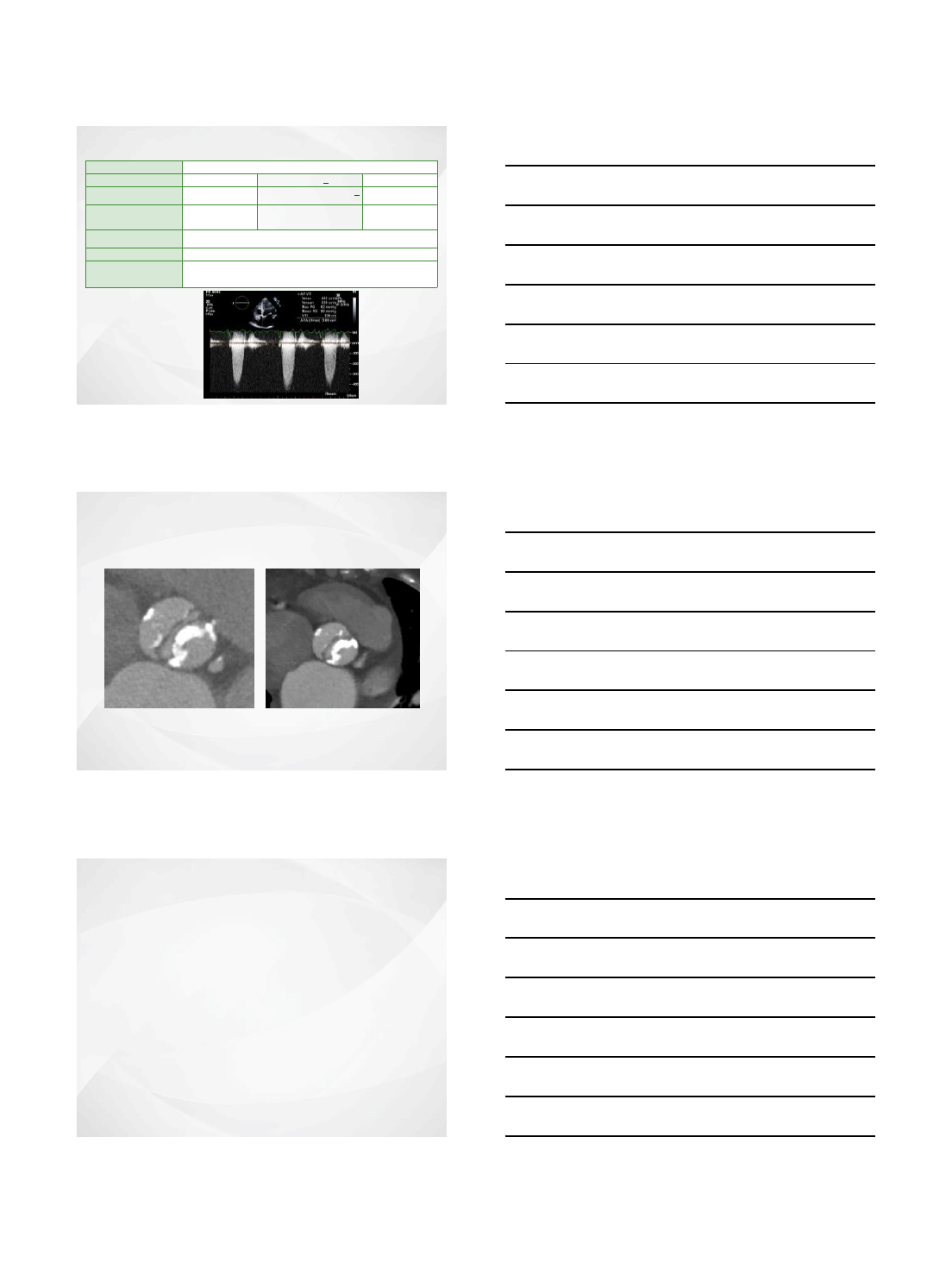
CT Analysis
Aortic Root by CT
Measure
Sinus
of Valsalva Diameter
37.7(L)x30.5(R)
x33.2(N)mm
STJ
Diameter
32.5x35.4mm
Sinus
Height
24.1(L)x21.5(R)x24.0(N)mm
Left Coronary
Height
13.2mm
Right Coronary Height
15.7mm
Aorta
39.1x40.3mm
Angle
44
°
CT Analysis
Right Left
CIA
8.7 10.4
EIA
6.6 7.5
CFA
6.8 7.1
Access
1/30/2017
6
•Right femoral two perclose
•Temporary pacer
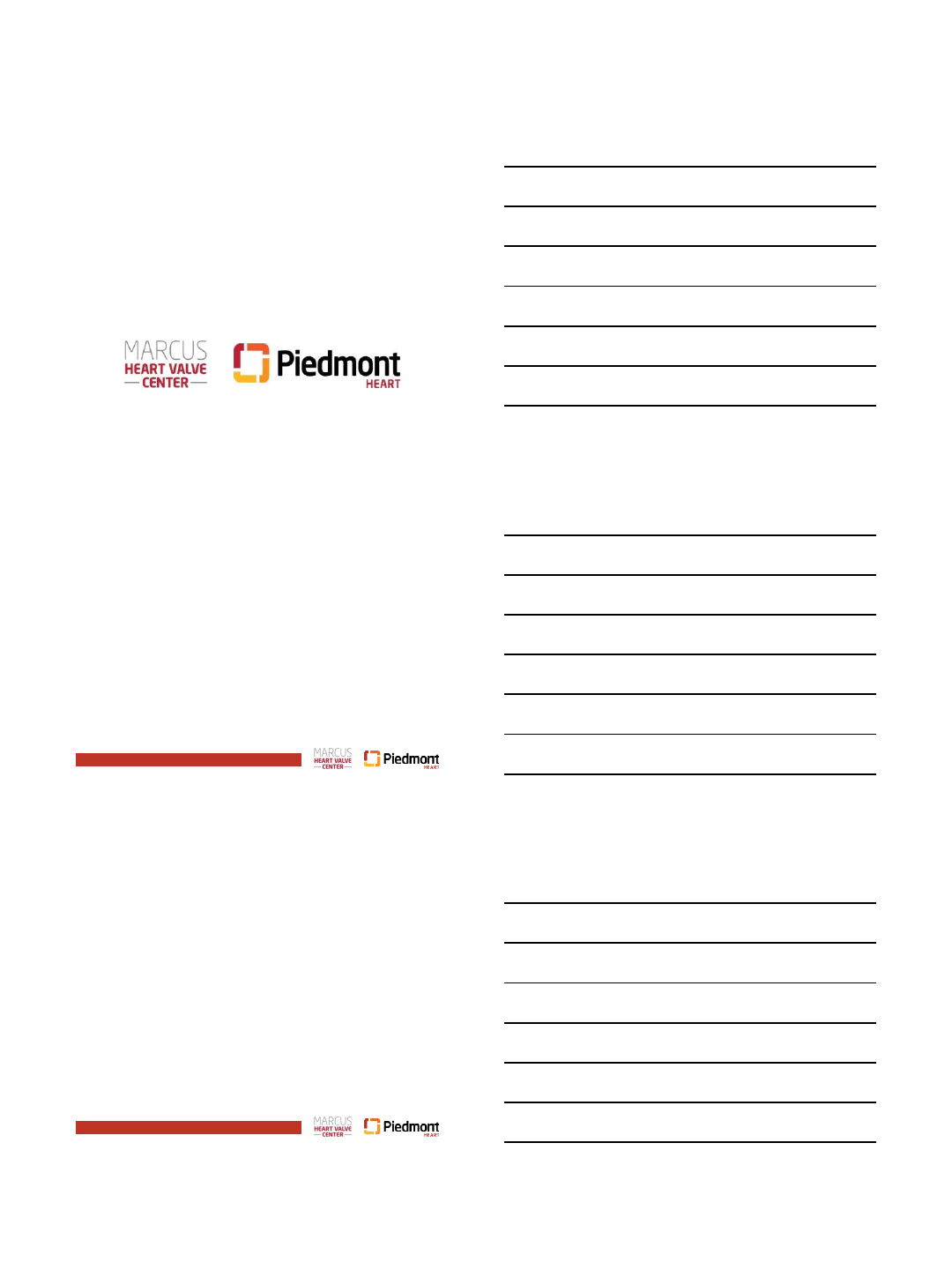
Procedure
Maxi 20/4
BAV
Procedure
31 mm core valve
Procedure
1/30/2017
7
Procedure
True balloon 22mm
Echo post valve
Mild to moderate AR
Hospital course
•LBBB –EP study –CAVB with infra-his
conduction block
•Pacemaker day 3
•Echo at 2 days: moderate AR
•Home day 5
1/30/2017
8
Post discharge
•Shortness of breath with minimal activity
•TTE and TEE
Echo Variable (TTE)
Measure
Peak
Velocity
2.2
m/se
c
Mean
Gradient
11
mmH
g
Calculated AVA
n/a
cm
2
Severity of AR
Severe
Severity of MR
Mild
Ejection Fraction
55-
60
%
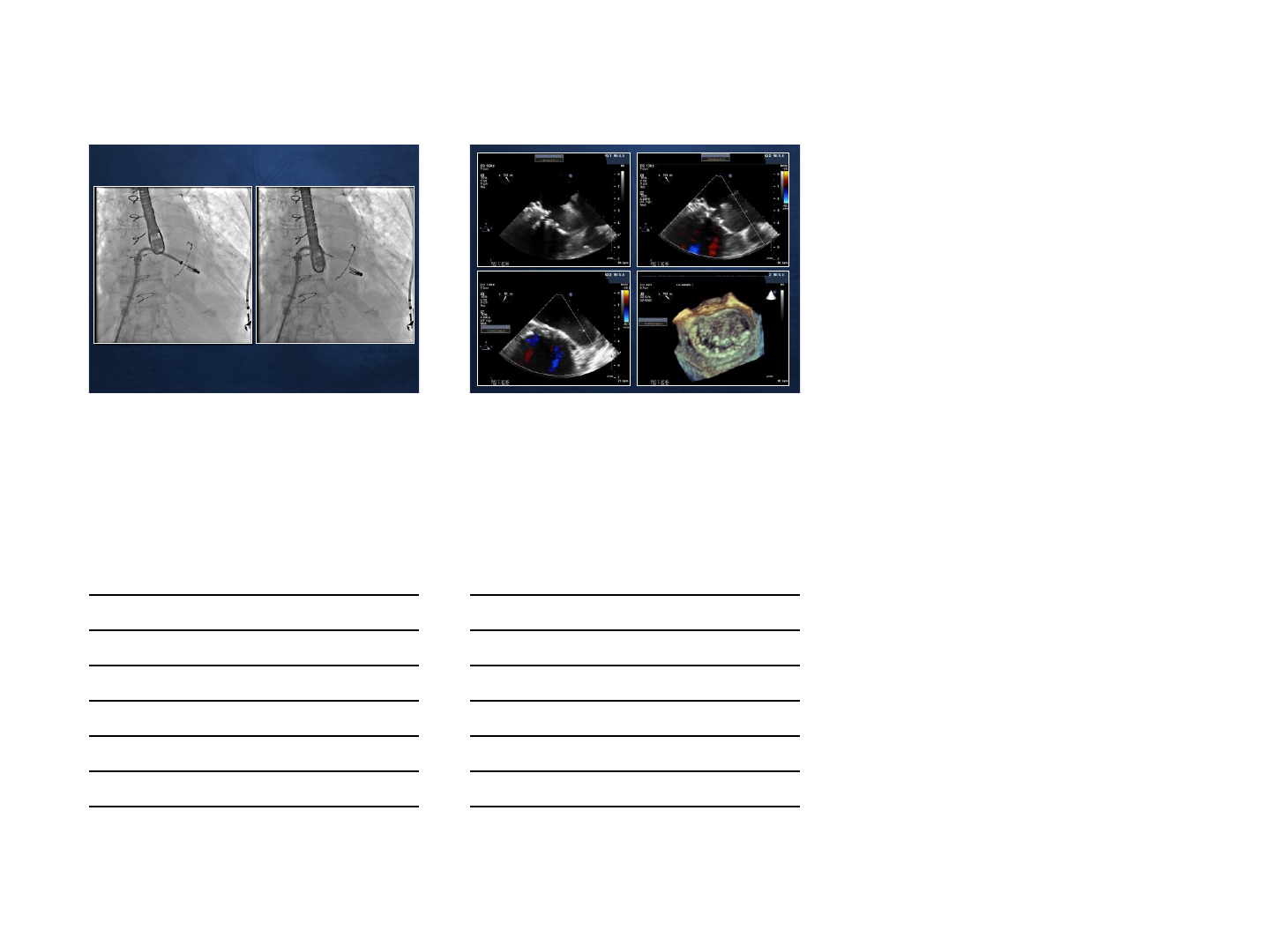
2
paravalvular
leaks: the larger leak in the
non
-coronary cusp and the smaller is
more anterior.
Reversal of flow in the descending and
abdominal aorta consistent with severe
paravalvular leak.
TEE one month post
Next step ?
•Para valvular closure device
•Valve in valve core or Edwards
•Surgery
1/30/2017
9
Annulus by CT
Measure
Short Annulus Diameter
25.1
mm
Long
Annulus Diameter
30.0
mm
Annular Perimeter
85.3
mm
Annular Area
581.1
mm
2
Oversizing
11.9
%
S3
Procedure
29mm S3 Edwards
Procedure
1/30/2017
10
Procedure
No AR
Hospital course
Day one post procedure mild chest pain
Cardiac enzyme –troponin 14 →35 →43 stable
Hospital course
Day one post procedure mild chest pain
1/30/2017
11
Hospital course
Discussion with CV surgery for CABG or PCI
More than 24 hours post infarct
Medical treatment
Discharge day 5 after the procedure
1/30/2017
12
Asymmetric anatomy
Annulus-orifice “mismatch”
Incomplete apposition
Paravalvular leak
Annular rupture
Aggressive
post-dilation
Incorrect valve
sizing
Valve-in-valve
Challenges for TAVI in BAV
Non-circular &
inadequate
expansion
Impaired
valve
durability
Migration
Conclusions
TAVI in bicuspid valves is feasible but may be
technically more difficult.
Results are comparable to those tricuspid valves.
Paravalvular leaks may be more frequent.
Pacemaker may be more frequent.
Oversizing of the valve should be avoided.
Balloon sizing may be better than CT sizing.
Supra-annular sizing better than balloon sizing.
Patients with large annulus may still be suitable
for TAVI if the valve is bicuspid
Better results can be expected with newer
valves.
Annulus by CT
Measure
Short Annulus Diameter
24.0
mm
Long
Annulus Diameter
31.0
mm
Annular Perimeter
89.0
mm
Annular Area
621.0
mm
2
Oversizing
3
%
CT Analysis (1/6/2017)
S3

1/30/2017
13
Aortic Root by CT
Measure
Sinus
of Valsalva Diameter
(L)35x(R)32
x(N)37mm
Sinotubular
Junction Diameter
31x32mm
Sinus
Height
(L)21x(R)20x(N)25mm
Left Coronary
Height
19mm
Right Coronary Height
15mm
Aorta
35x37mm
Angle
53
°
CT Analysis (1/6/2017)
1/30/2017
14
1/30/2017
1
Preemptive Alcohol Septal
Ablation in Prevention of
LVOT Obstruction for TMVR
Christopher U. Meduri, MD MPH
Co-Director Marcus Heart Valve Center
Piedmont Heart Institute
Atlanta, GA
Page 2
Disclosures
Affiliation Company
●Proctor/Speaker/Advisory Board ●Boston Scientific
●Proctor/Speaker/Consultant/Grant ●Medtronic
●Proctor/Grant ●Edwards
•Proctor/Consultant ●Mitralign
Will be discussing the use of THV for off-label uses
Page 3
M.K.
•76 y/o woman with severe PVD, LM disease, severe
AS and severe MS with MAC with NYHA III
symptoms
1/30/2017
2
Page 4
M.K.
•76 y/o woman with severe PVD, LMT disease,
severe AS and severe MS with MAC with NYHA III
symptoms
•Extreme risk because of porcelain aorta
Page 5
Baseline Angio
Page 6
Coronary Stenting
1/30/2017
3
Page 7
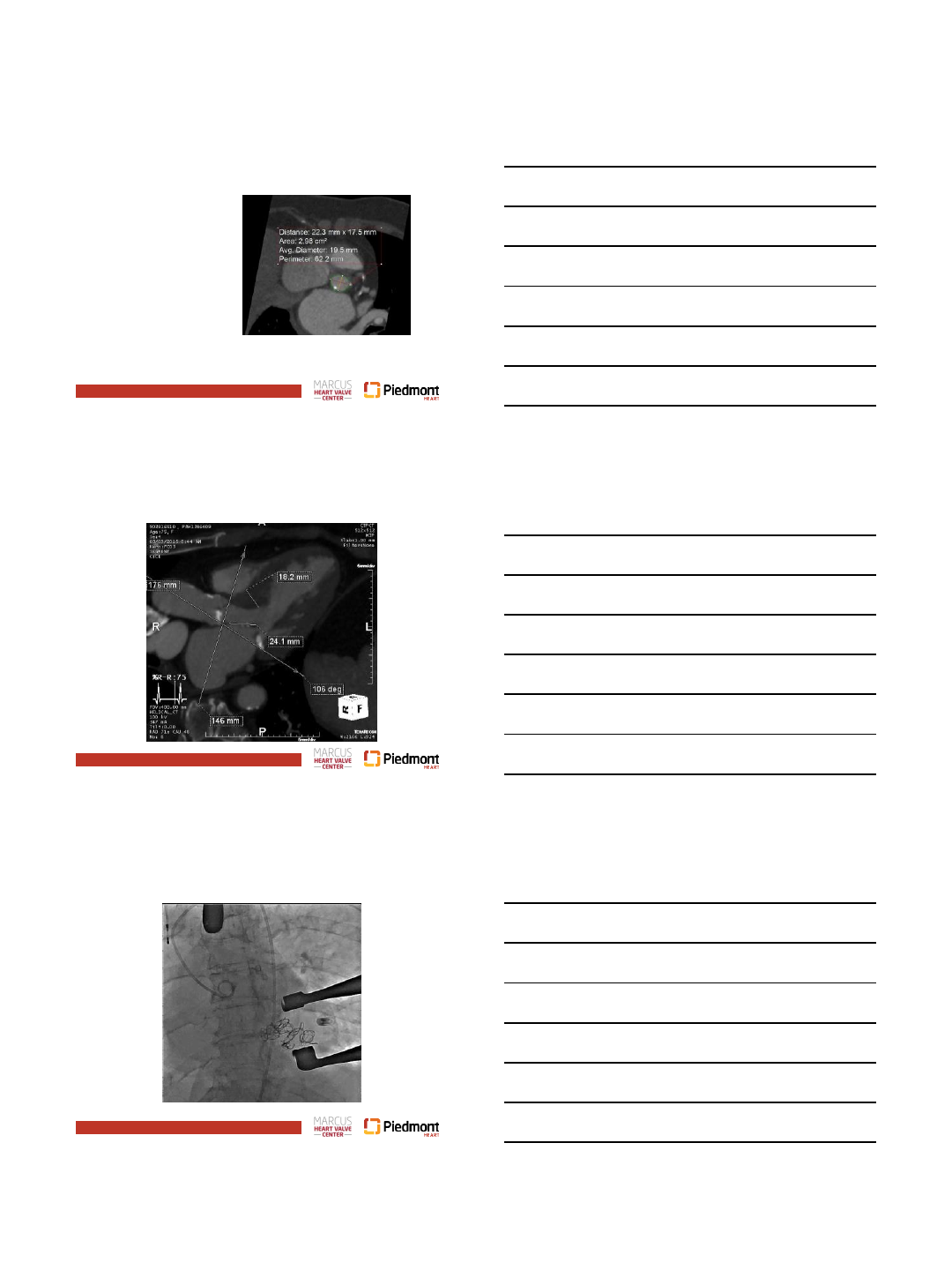
TAVR Planning
•Normal LV/RV
function
•Aortic velocity = 4.1
meters/sec
•Aortic annulus area
= 309 mm2
•Area derived
annulus = 19.8 mm
•Ileofemorals = 4.0 –
4.5 cm
Page 8
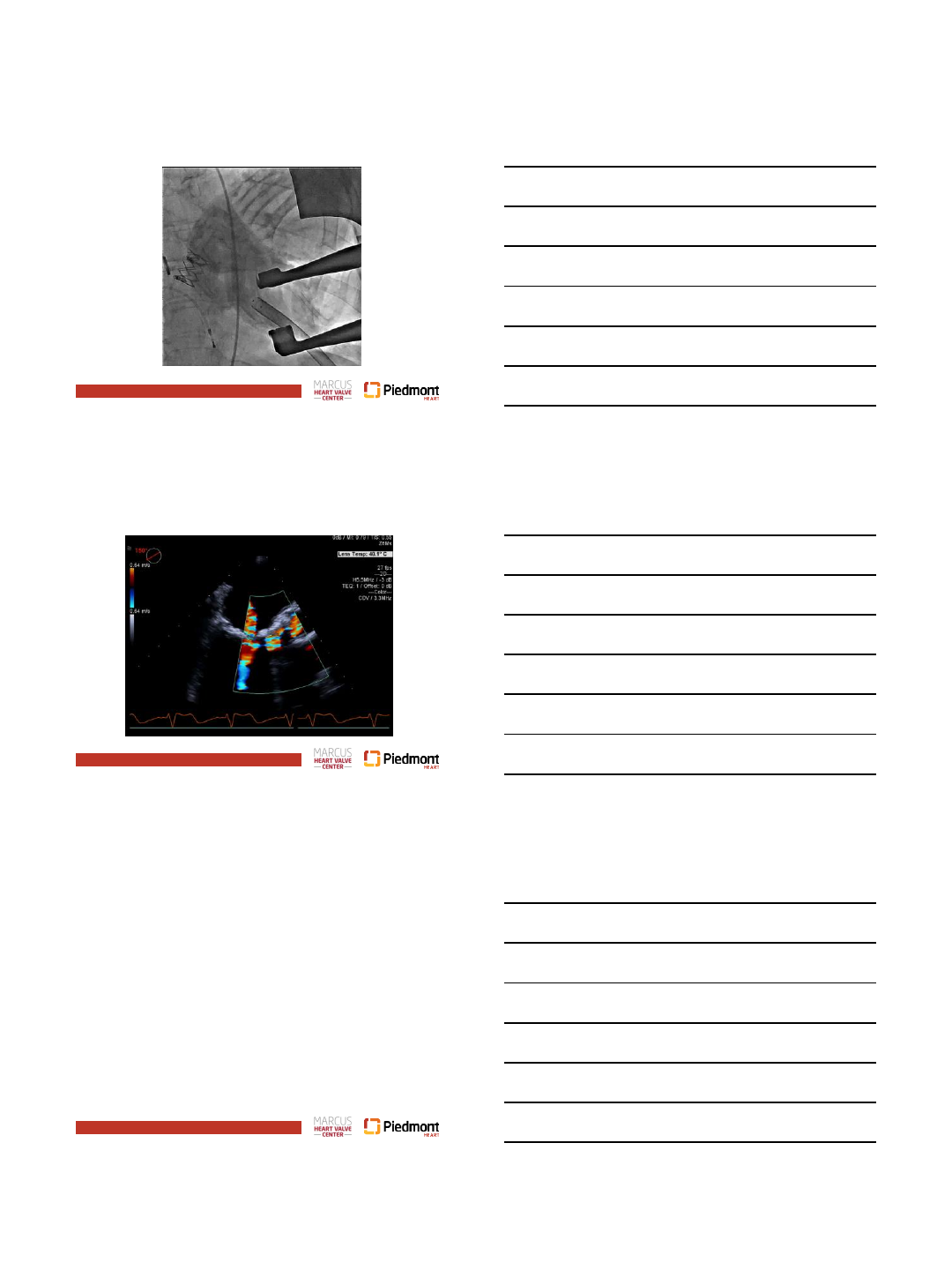
Do We Treat Mitral Stenosis?
Aorto-Mitral
Angle 106
degrees
Septal Bulge
1.8cm
Page 9
23 mm Sapien XT
1/30/2017
4
Page 10
23 mm Sapien XT
Page 11
23 mm Sapien XT
Page 12
Recurrent Dyspnea 6 months later
•23 Sapien XT gradients = 27/15 mmHg (post
procedure = 28/17 mmHg)
•No aortic regurgitation
1/30/2017
5
Page 13
Re-assessment of Mitral Valve
Page 14
Re-assessment of Mitral Valve
Page 15
Re-assessment of Mitral Valve
1/30/2017
6
Page 16
Severe MAC
Page 17
Risk Factors for LVOT Obstruction
Page 18
Severely Hypertrophied Basal Septum
1/30/2017
7
Page 19
Aorto-Mitral Images
Page 20
Proceed?
•Very high risk of LVOT obstruction
•No potential surgical bailout for patient if worse
•Must be confident in result and have ability to
remove if needed
•Plan for septal ablation and request compassionate
use Lotus in MAC from FDA
Page 21
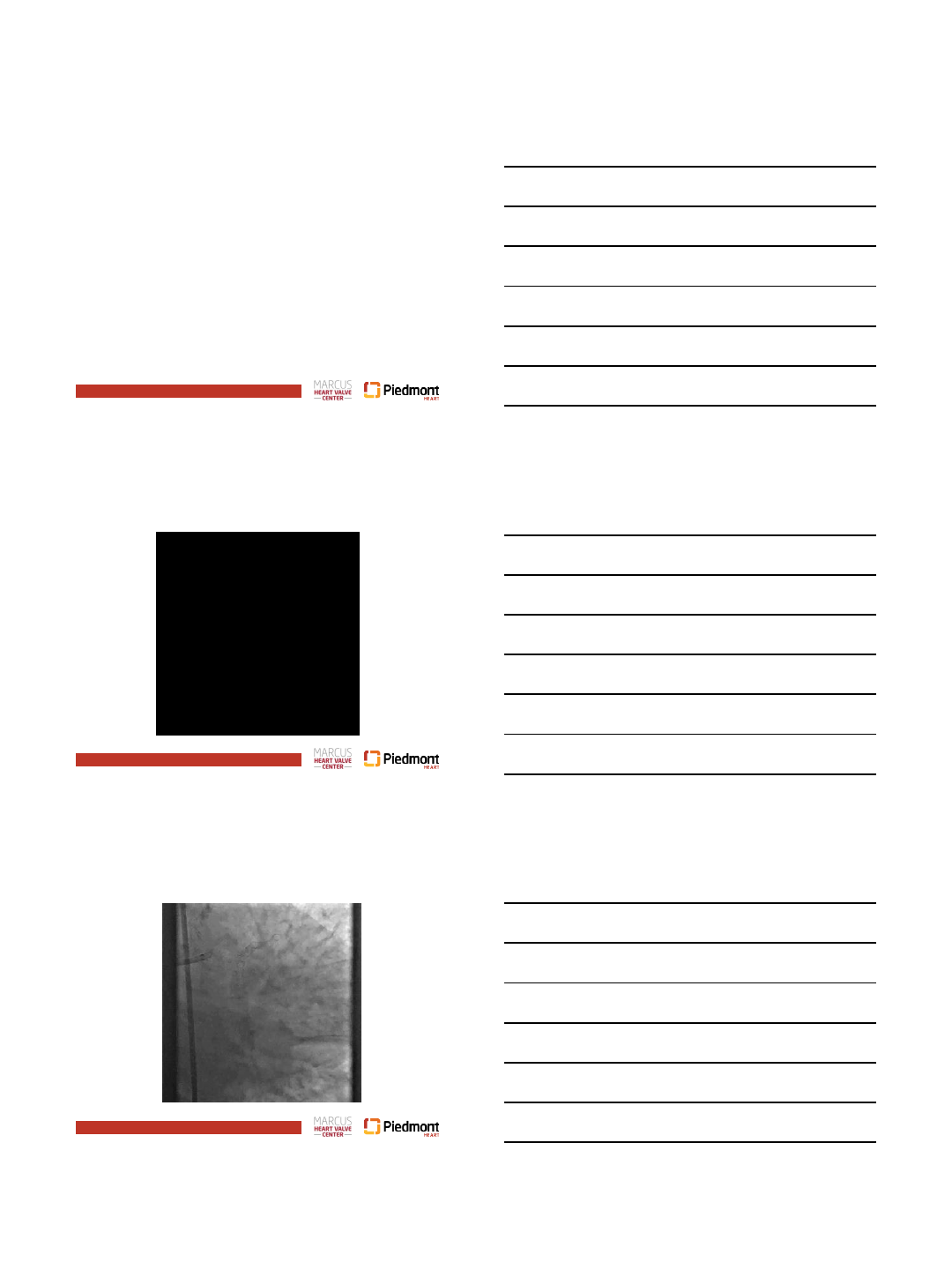
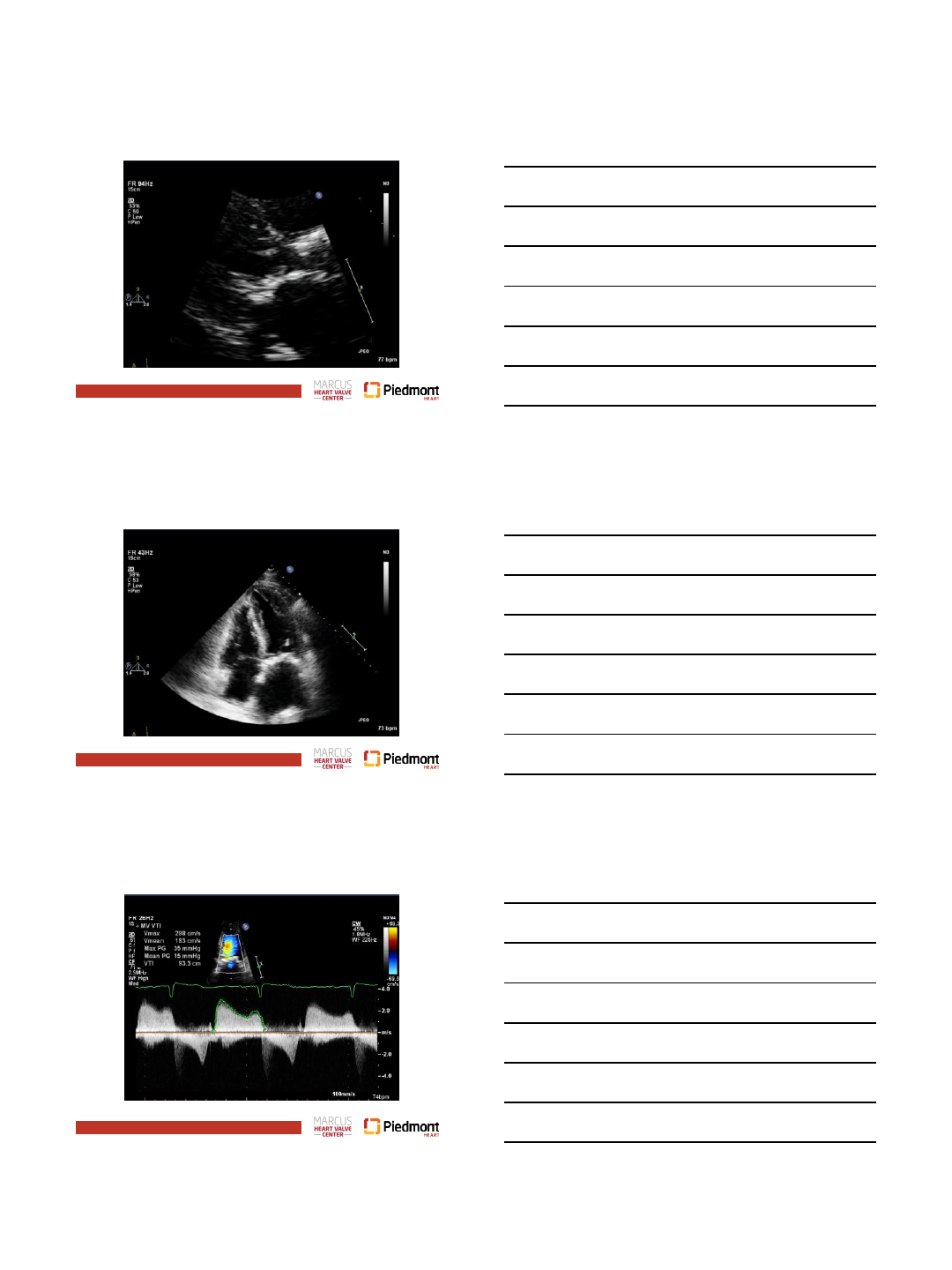
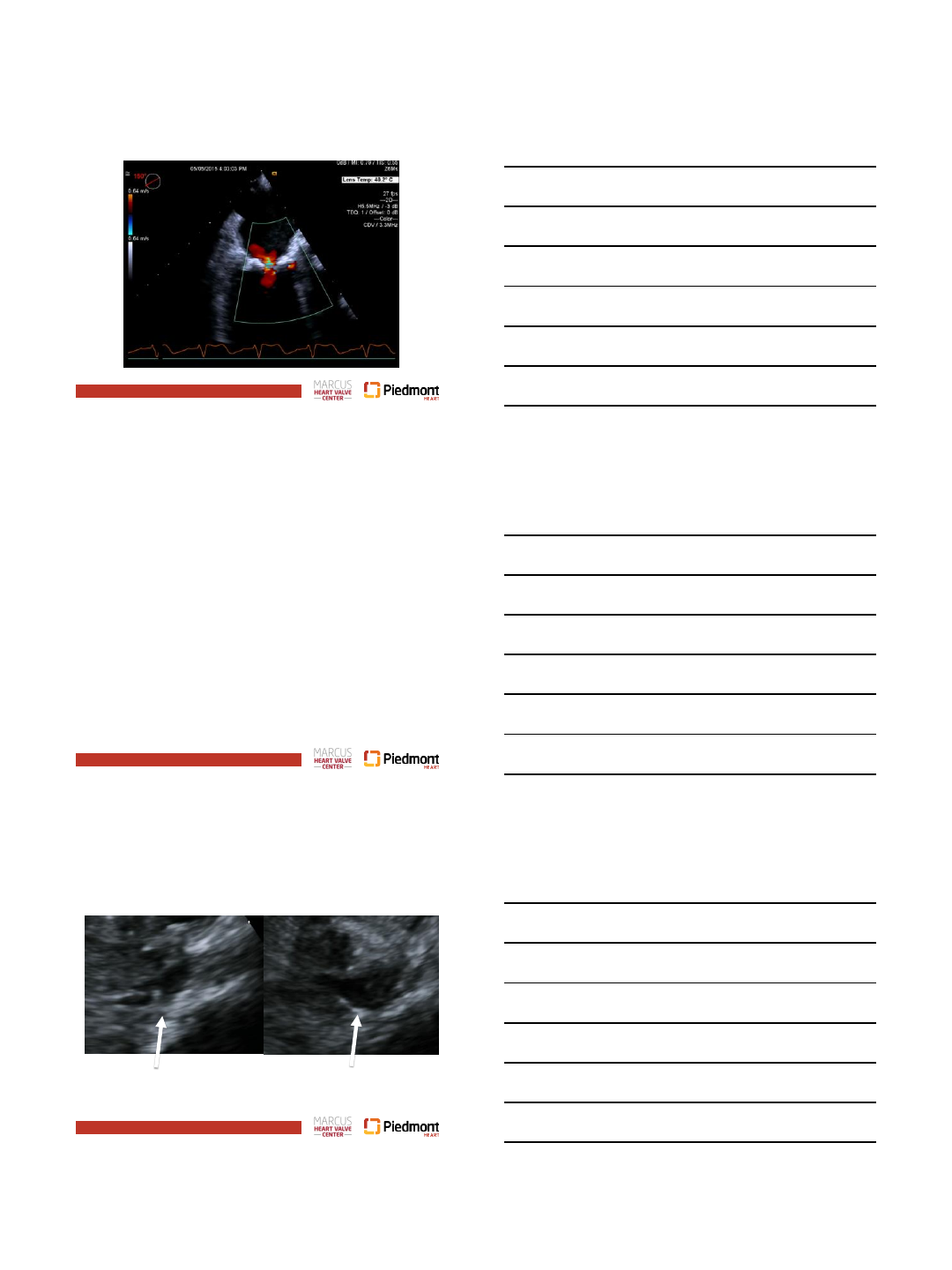
Alcohol Septal Ablation
LVOT Pre-Ablation LVOT Post-Ablation

1/30/2017
8
Page 22
Page 23
Pre Procedure
Page 24
1/30/2017
9
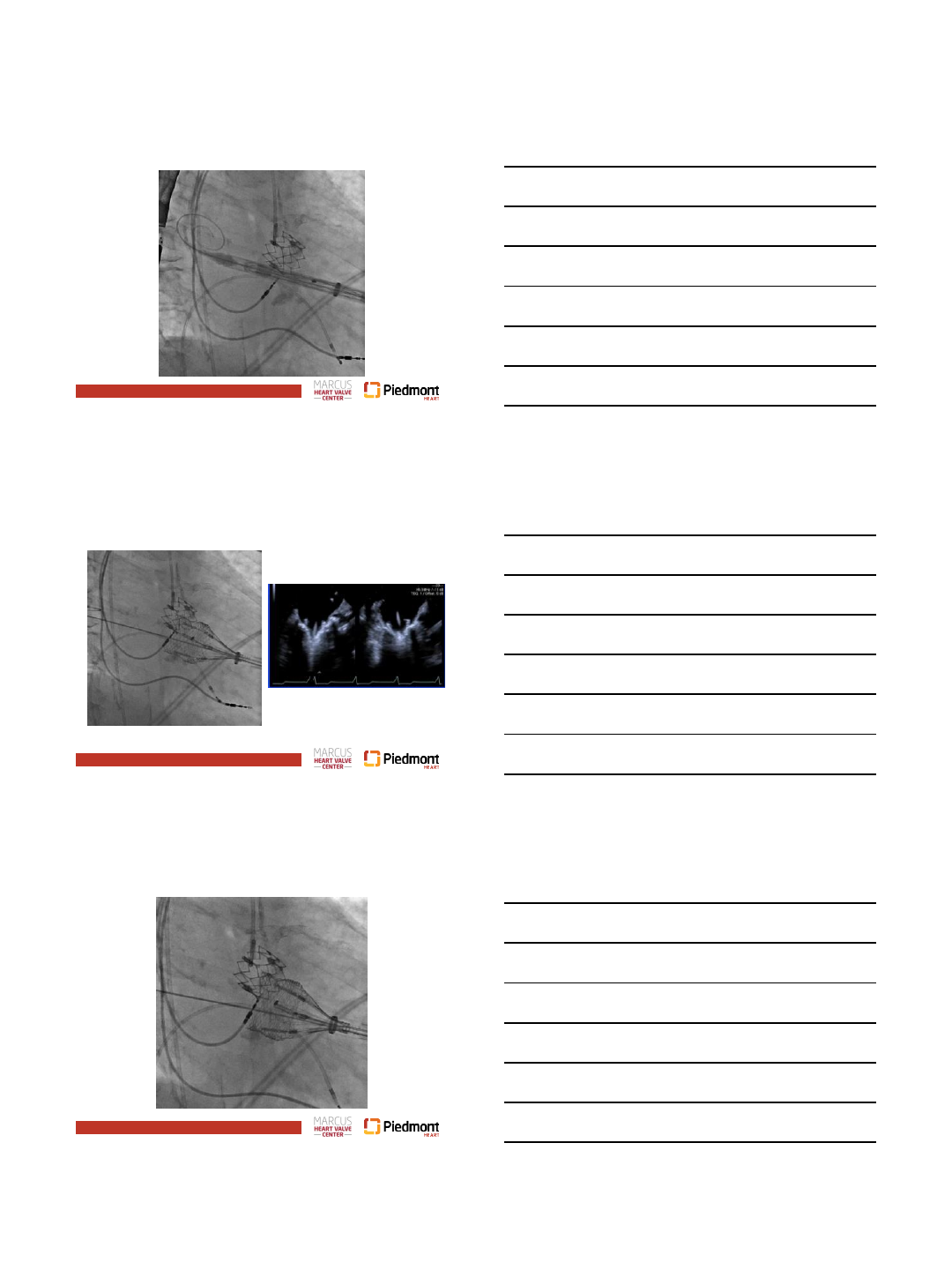
Page 25
Page 26
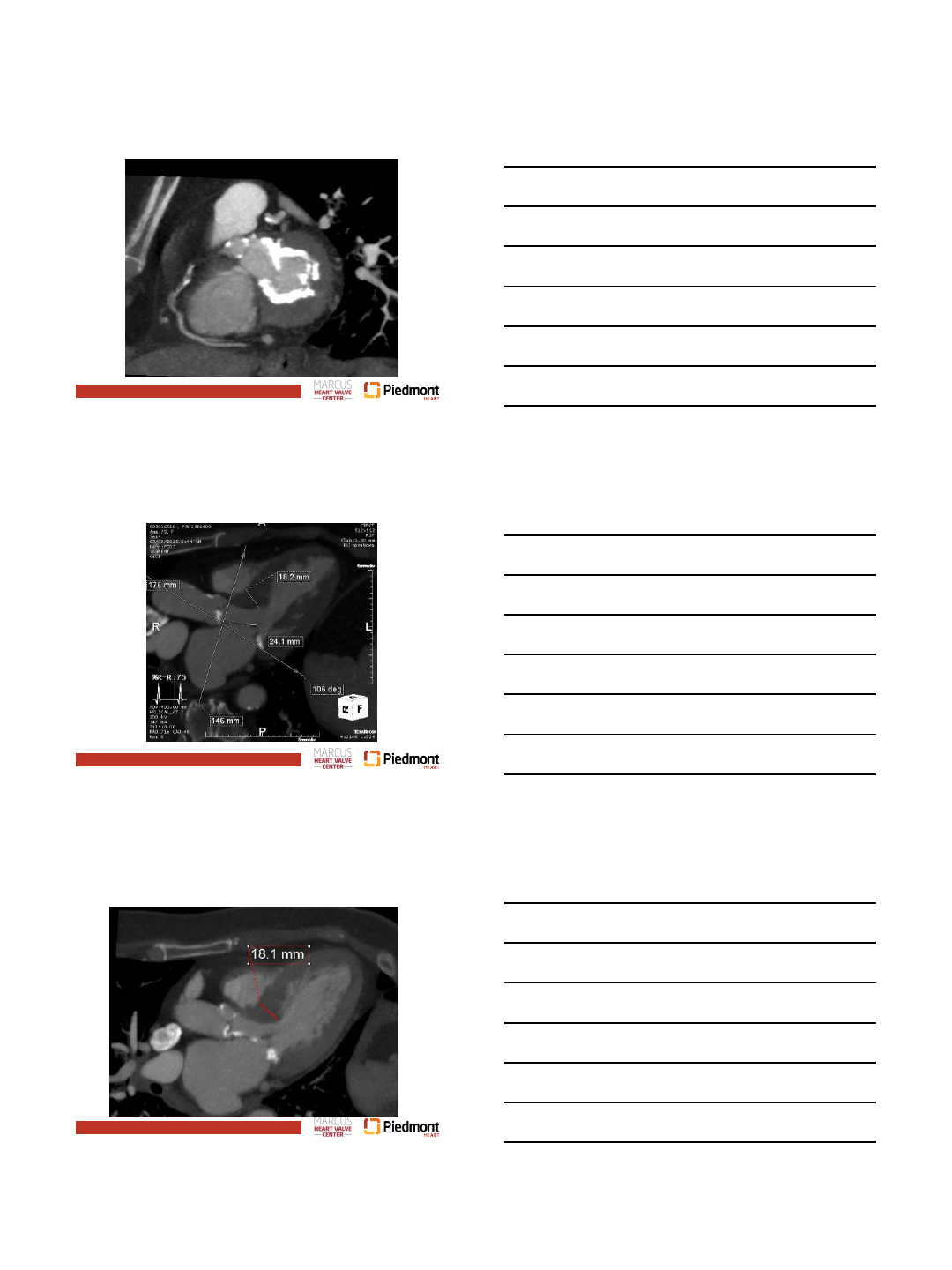
TEE Guidance of Implant Depth
Page 27
1/30/2017
10
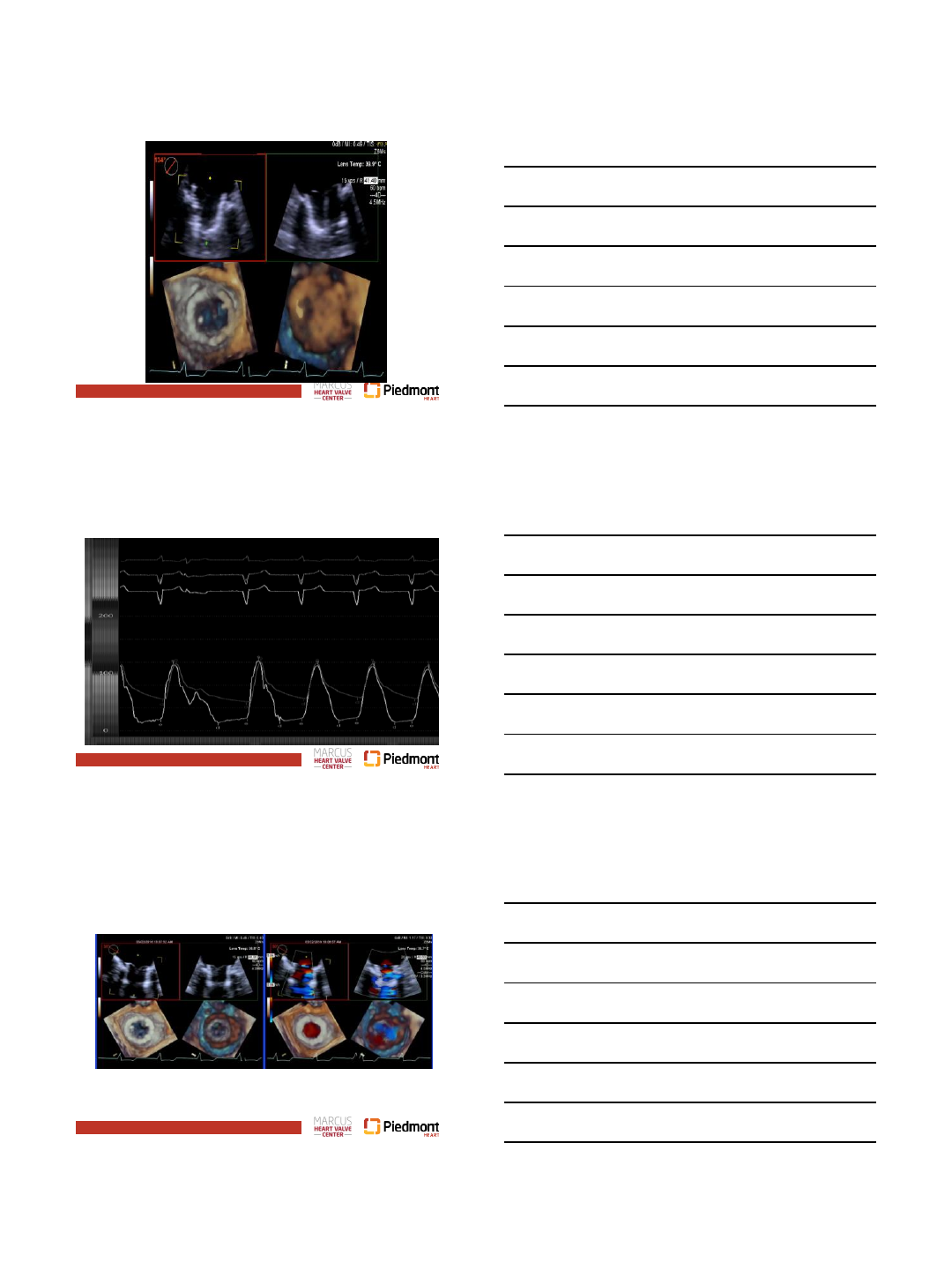
Page 28
Page 29
No LVOT Gradient
Page 30
Post Procedure
1/30/2017
11
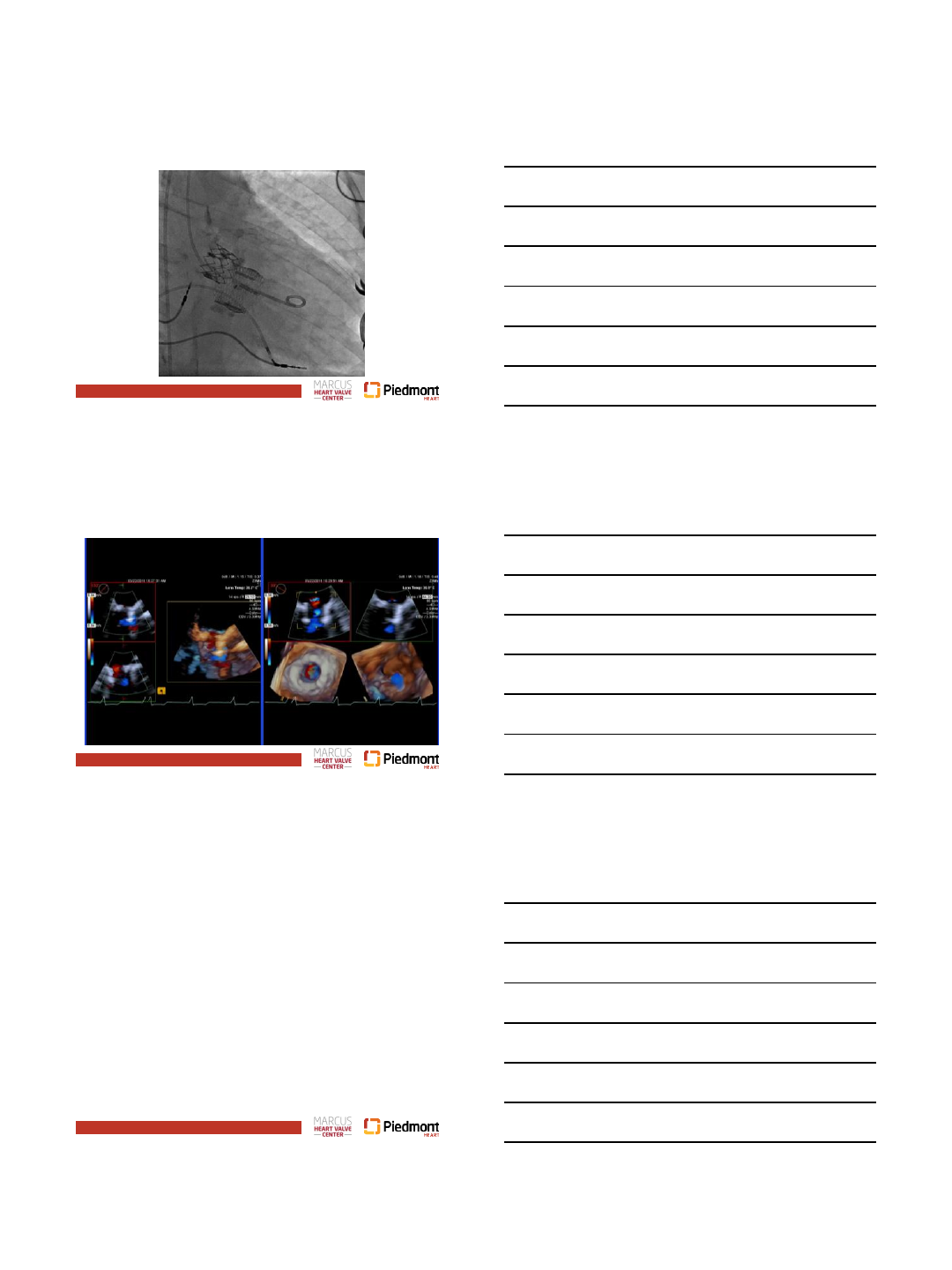
Page 31
No MR/PVL
Page 32
Page 33
Post-Procedure
•Extubated on table
• Within 6 hours walking laps around CVICU saying, “I
feel like a new person”
•Discharge POD 2
•Walked 2.5 miles without stopping within 1 week of
procedure!