A6c5fa7a 169d 492c B13e 6764b9f95f32
2017-02-07
: Pdf A6C5Fa7A-169D-492C-B13E-6764B9F95F32 a6c5fa7a-169d-492c-b13e-6764b9f95f32 2 2017 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 40
2/7/2017
1
www.prismsports.org
PRiSM Presents:
Management of Adolescent
Shoulder Instability
7 February 2017
VuMedi Webinar
Moderator:
Matthew R. Schmitz, M.D.
Pediatric Sports Medicine and
Young Adult Hip Preservation
San Antonio Military Medical Center
www.prismsports.org
Carlin Senter, MD, FACP
•Associate Professor
•Primary Care Sports Medicine
•University of California San
Francisco
•Co-Director UCSF Sports
Concussion Program
•Head Team Physician SF
Deltas
www.prismsports.org
Dele Kammen, MD
•Pediatric Radiologist
•UCSF Benioff Children’s
Oakland
•Harvard Medical School
•UPenn Radiology Resiency
•UCSF Peds Radiology
Fellowship
2/7/2017
2
www.prismsports.org
Michelle Cappello, PT, MSPT, SCS
•Masters in PT from Boston
University
•Board Certified Sports
Clinical Specialist
•American Physical Therapy
Association
•Soccer player, coach, mom
www.prismsports.org
Dr Nirav K. Pandya
•Assistant Professor,
Orthopaedic Surgery, UCSF
•Director of Pediatric Sports
Medicine, UCSF Benioff
Childrens’ Hospitals
•Undergrad: Univ of Chicago
•Med School: Univ of Chicago
•Residency: Penn
•Fellowship: Rady Children’s
San Diego
www.prismsports.org
Brett Burton –Bio
•Education:
–University of Nebraska-Lincoln
(Athletic Training)
–University of Nebraska Medical Center
(Physical Therapy)
–St. Luke’s Sports Medicine
(Physical Therapy Residency)
•Experience:
–Worked closely with the University of
Nebraska Baseball Team
–Trained at the Andrews Institute, Athletes’
Performance (currently EXOS), and the
Mayo Clinic
–Currently serves as physical therapist at
Northwest Nazarene University and treats
several adolescent patients in outpatient
clinical setting at St. Luke’s Rehab in Idaho
2/7/2017
3
PRiSM is a multidisciplinary society
focused on research in pediatric
sports medicine.
Features of PRiSM membership:
•Guiding new research by joining
a Research Interest Group
•Leadership development
through board and committee
participation
•Registration discounts to the
Annual Meeting
•Access to Clinical Orthopaedics
and Related Research, PRiSM's
official journal
2/7/2017
1
www.prismsports.org
Adolescent Shoulder Instability:
Patient Presentation
Carlin Senter, MD
Associate Professor
Primary Care Sports Medicine
UCSF Medicine and Orthopaedics
February 7, 2017
www.prismsports.org
Epidemiology
•Shoulder is most commonly dislocated joint in
the body
–1-2% of the population
•90-95% of shoulder dislocations are anterior
•20% of shoulder dislocations occur in patients
under 20 years of age.
•Mechanism = fall on outstretched arm or
collision, especially when arm is abducted and
externally rotated
www.prismsports.org
Shoulder anatomy:
Bony stability
2/7/2017
2
www.prismsports.org
Injured structures
•Anterior dislocation
–Failure of anterior inferior glenohumeral ligaments
–+/- axillary nerve injury
https://posna.org/Physician-Education/Study-Guide/Shoulder-Dislocation-Instability.
Accessed January 29, 2017.
www.prismsports.org
Traumatic Instability
•T –Traumatic
•U –Unidirectional
•B –Bankart Lesion
•S –Surgical
www.prismsports.org
Multidirectional Instability
•A –Atraumatic
•M –Multidirectional
•B –Bilateral
•R - Rehab, rehab, rehab
•I –Inferior Capsular
Shift
2/7/2017
3
www.prismsports.org
Shoulder dislocation:
History
•Trauma vs atraumatic
•Past history of dislocation or subluxation
•Age at time of first dislocation
www.prismsports.org
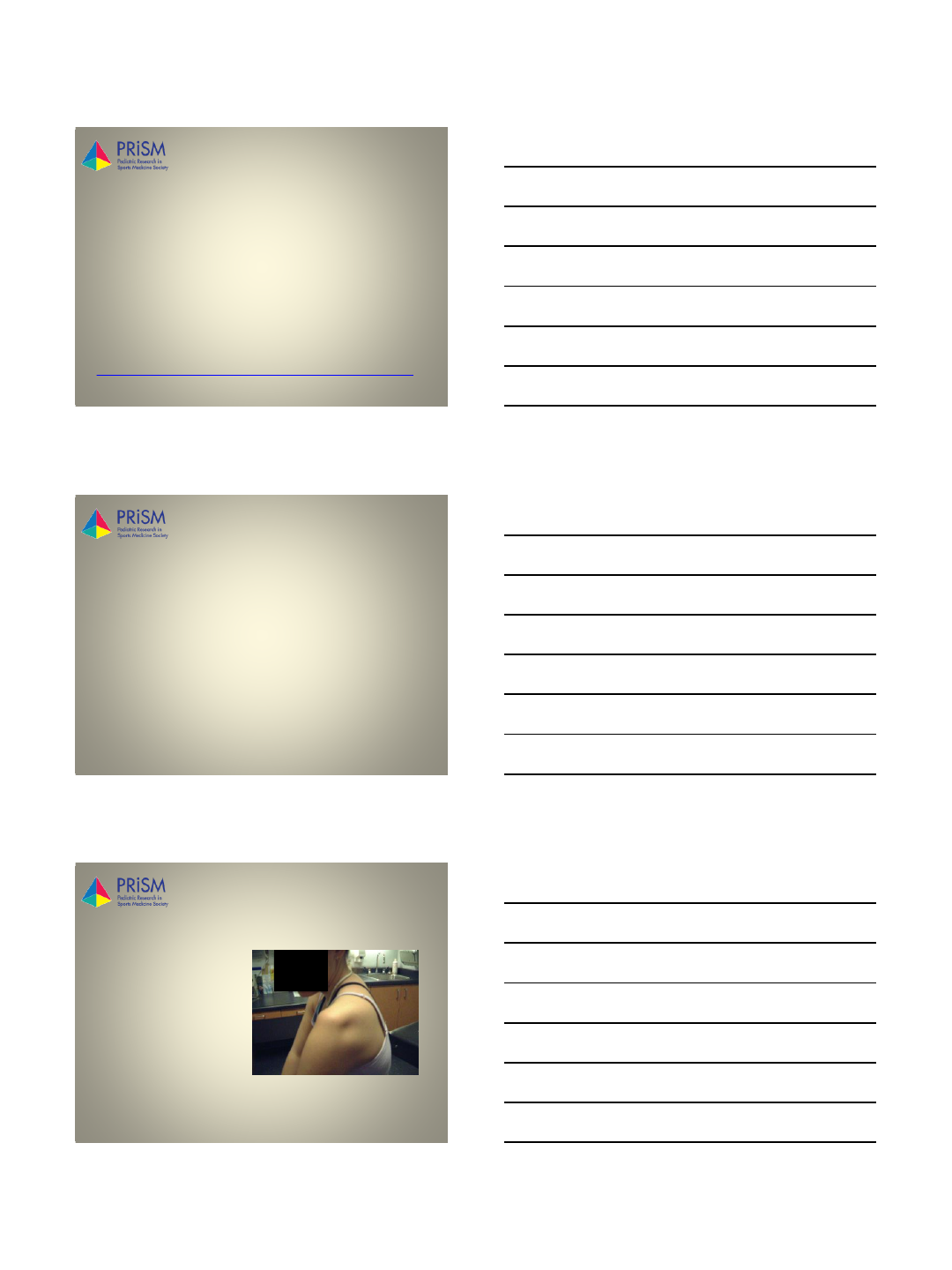
Anterior shoulder
dislocation: Acute exam
•Athlete will use other arm
to hold affected arm
•Flat appearance of deltoid
•Humeral head palpable
anteriorly, below coracoid
•Neurovascular status
–Axillary nerve in particular
•Sensation lateral shoulder
•Contraction deltoid muscle
www.prismsports.org
Anterior shoulder
dislocation: Full exam
•Inspection
•Palpation
•Range of Motion
•Neurovascular
2/7/2017
4
www.prismsports.org
Anterior shoulder
dislocation: Special tests
•Load and shift
–Patient supine
–Shoulder abducted 45
degrees in plane of
scapula, 30 degrees of
flexion, neutral rotation
–Axial force with examining
hand centering humeral
head in glenoid fossa
–Other hand applies
anterior force to check
translation
www.prismsports.org
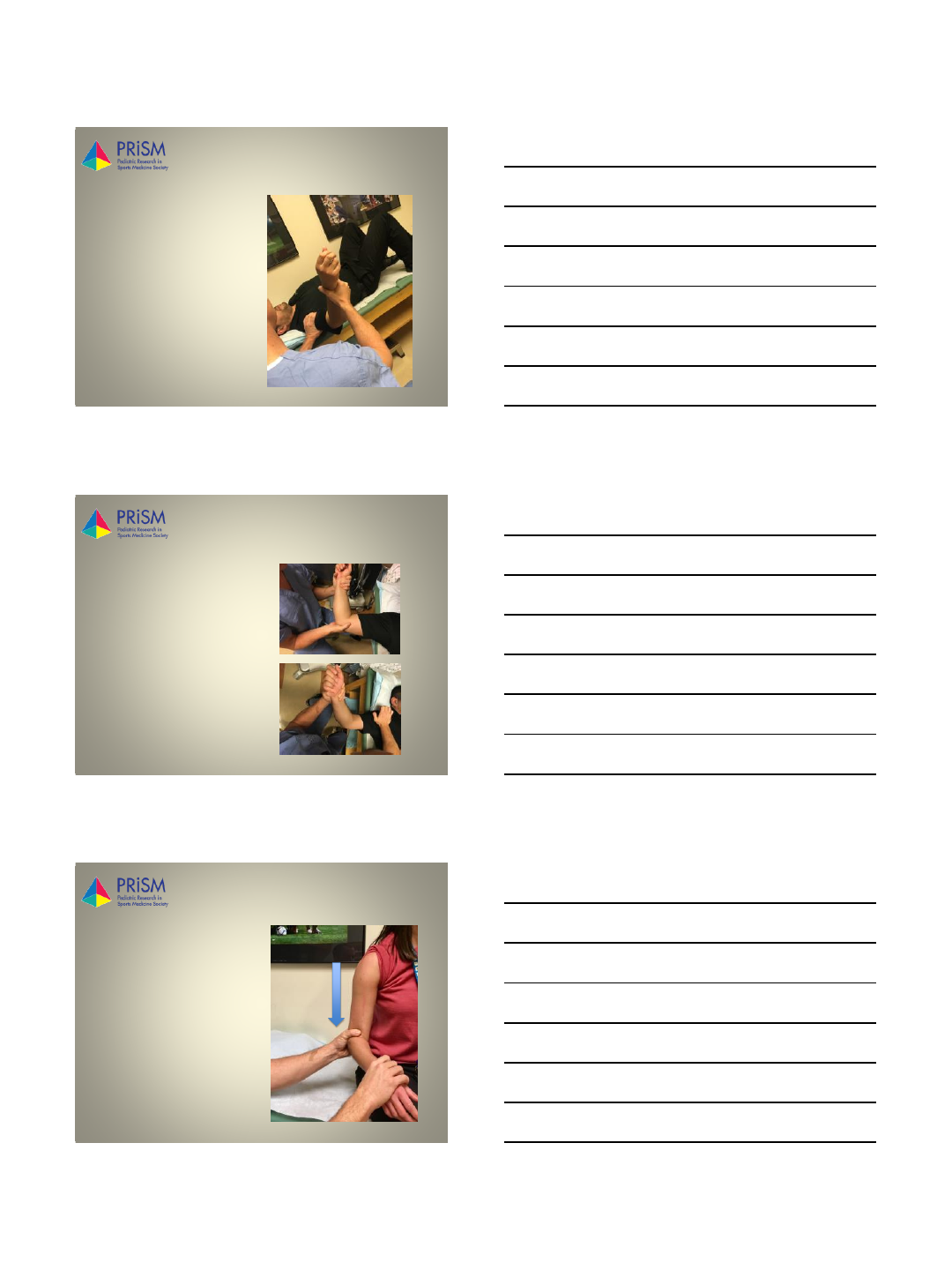
Anterior shoulder
dislocation: Special tests
•Apprehension test
–Patient is supine
–Affected arm in abduction,
extension and external
rotation
–Apply gentle anterior
translation on proximal
humerus apprehension
•Relocation test
–Apply posteriorly directed
force instability is
relieved
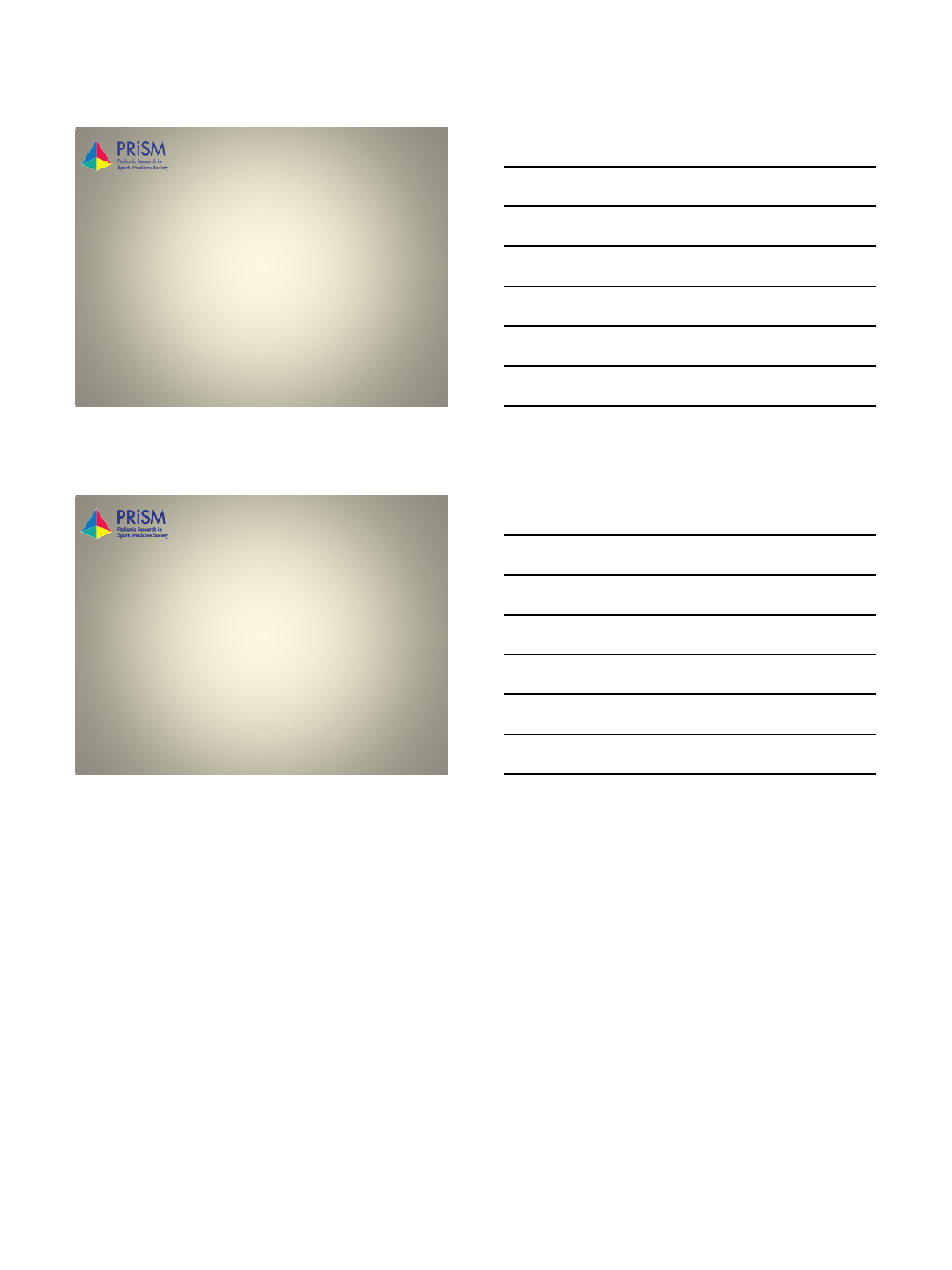
www.prismsports.org Instability: Sulcus Sign
•Inferior instability
•Arm relaxed in
neutral position
•Arm pulled
downward at elbow
•Positive test is a
visible sulcus at
infra-acromial area
–Compare to
contralateral side
2/7/2017
5
www.prismsports.org
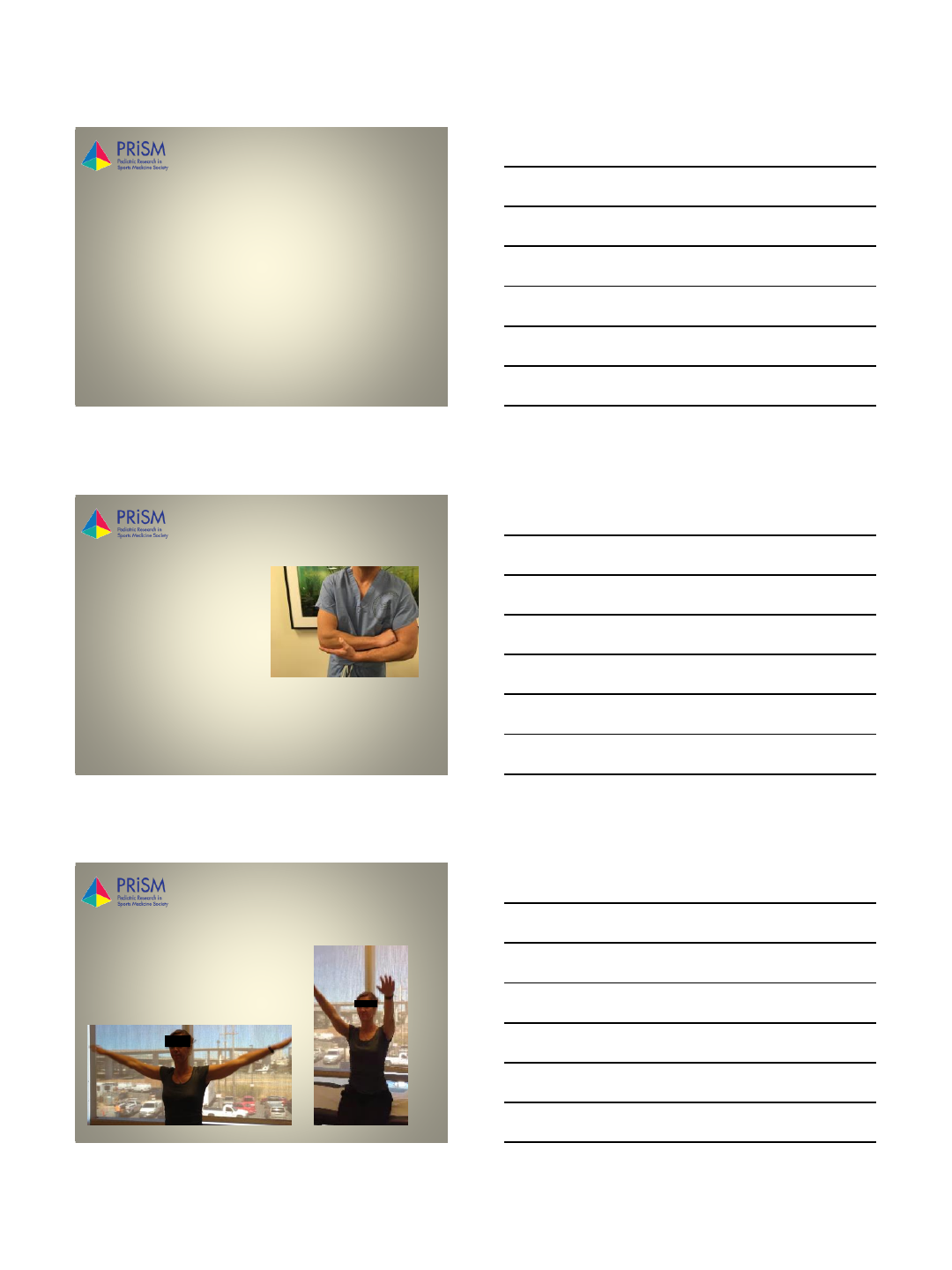
Anterior shoulder
dislocation, recurrent
•Beighton score for joint hypermobility
–Passively dorsiflex 5th MCP joint by at least 90°
–Oppose thumb to the volar aspect of the ipsilateral
forearm
–Hyperextend elbow by at least 10°
–Hyperextend kne by at least 10°
–Place hands flat on floor without bending knees
•1 point for each maneauver (R and L side)
•4 or more points generalized joint
hypermobility
www.prismsports.org
Thank you!
1
1
Imaging of Glenohumeral Instability in
the Adolescent Patient
Dele Kammen MD
bkammen@mail.cho.org
Department of Diagnostic Imaging
2/7/17
2
Disclosure
Advisory Board on Hypophosphatasia
Alexion Pharmaceuticals, Inc.
3
Goals
Imaging acute traumatic shoulder dislocation
Imaging chronic instability with repeated dislocation
Diagnostic Imaging
Characterize extent of structural damage
Show osseous and soft tissue abnormalities
Guide surgical planning
Choice of stabilization procedure
2
4
Imaging Modalities
Radiographs
MRI
MR arthrography
•Direct
•Indirect
CT
5
Radiographs
Obtained following acute dislocation
Routine series
•AP internal and external rotation
•Scapular Y view
•Axillary view
Post-reduction films
•Evaluate for fractures
•Residual malalignment
6
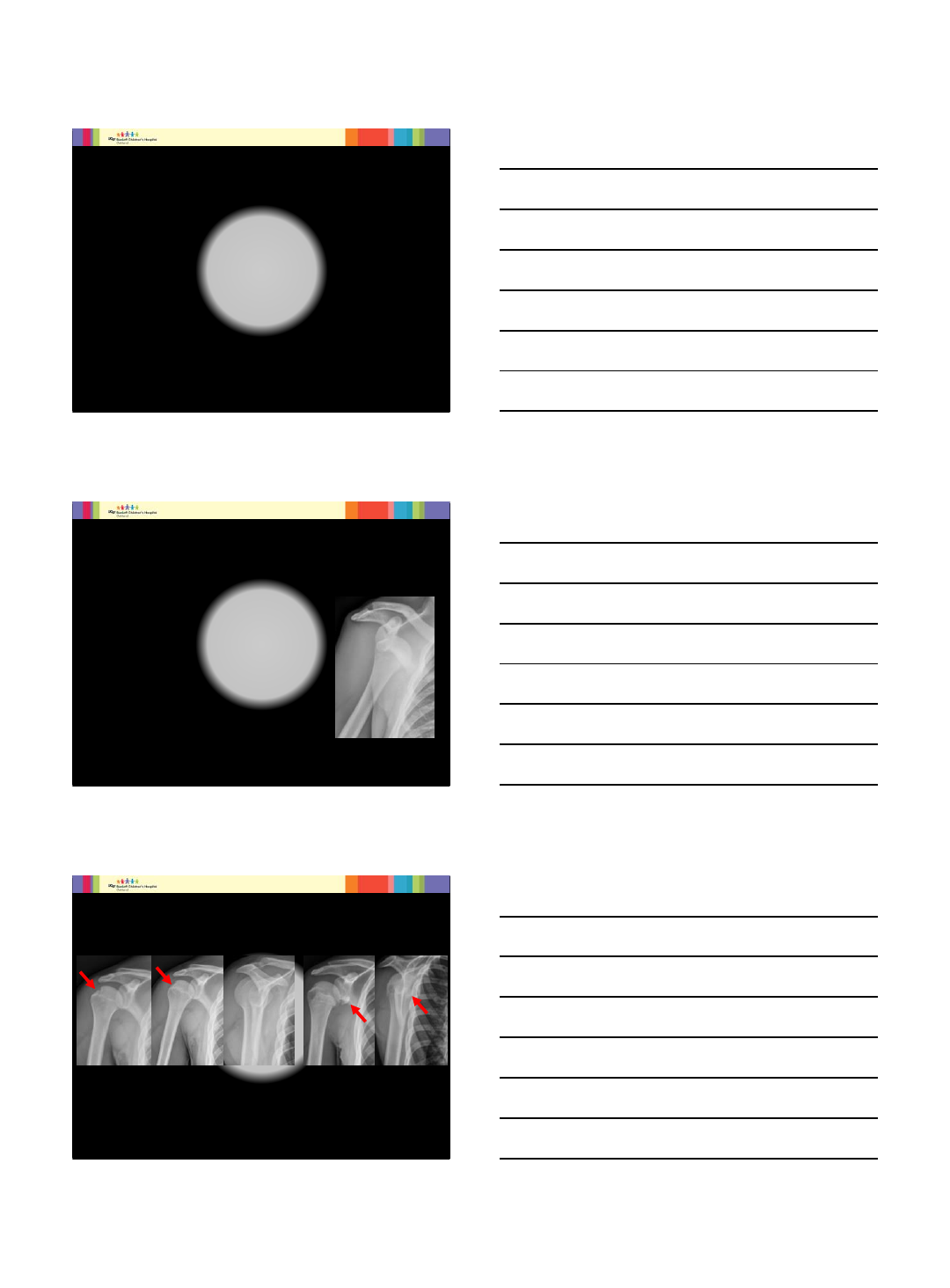
Radiographs
Hills-Sachs Bankart
External Rotation Internal Rotation Y-view External Rotation Y-view
Patient 1 Patient 2
3
7
MRI
Acute setting
•Joint effusion or hemarthrosis
•MR arthrogram not necessary
•Mechanism evident by edema pattern
s
Conventional MRI
Axial T2 FS
8
Standard MRI Technique
3T
Axial
T2 FS
PD
Sagittal
T2 FS
T2
Coronal
T2 FS
T1
TE/TR
T2 60/3000
PD 30/3000
T1 15/600
9
Axial T2 FS Axial PD
14 year old football player with 5 repeated traumatic dislocations
4
10
Sagittal T2 FS Sagittal T2
14 year old football player with 5 repeated traumatic dislocations
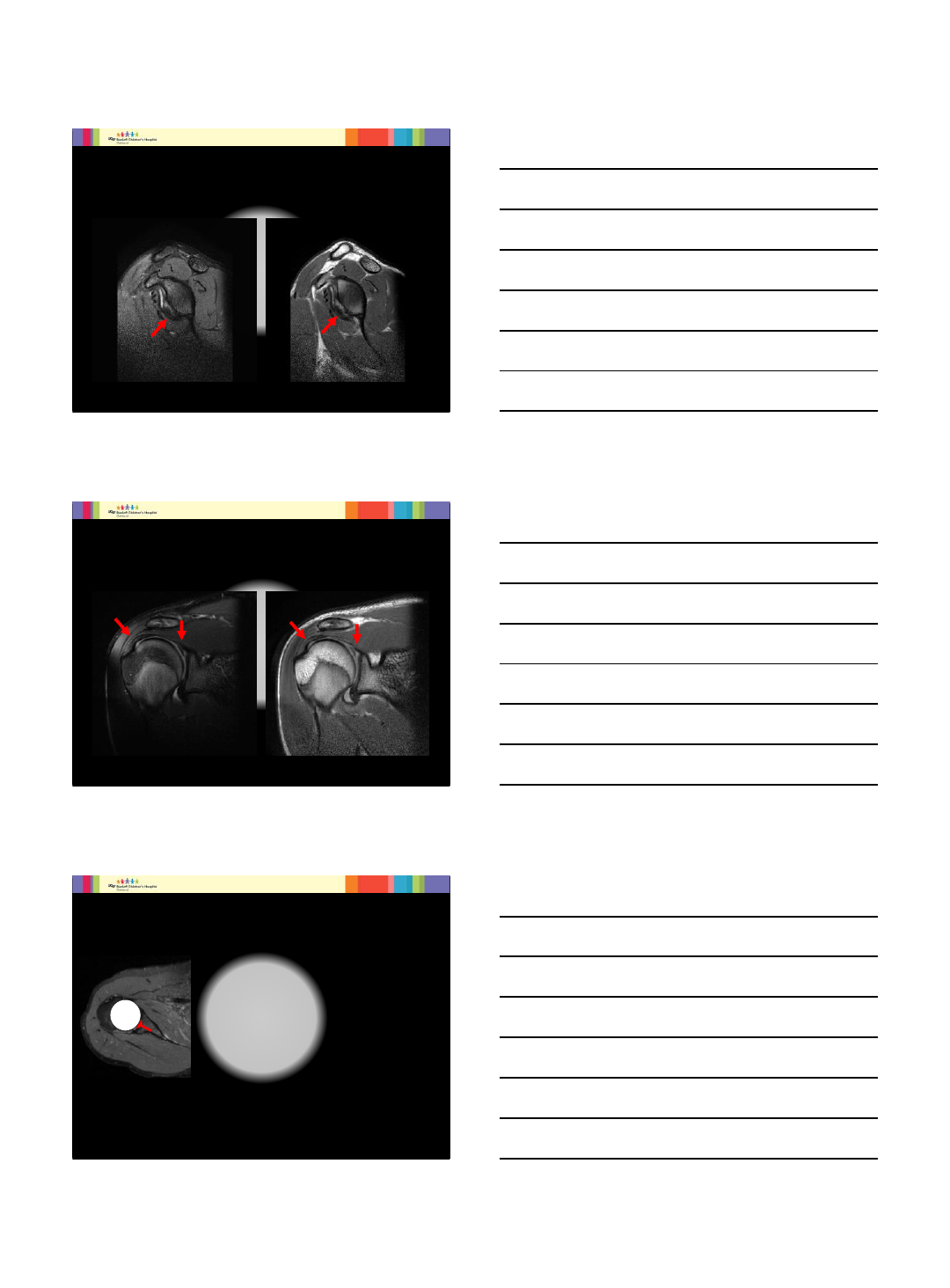
11
Coronal T2 FS Coronal PD
Osseous Bankart
SLAP tear
Rotator cuff tendinosis
14 year old football player with 5 repeated traumatic dislocations
12
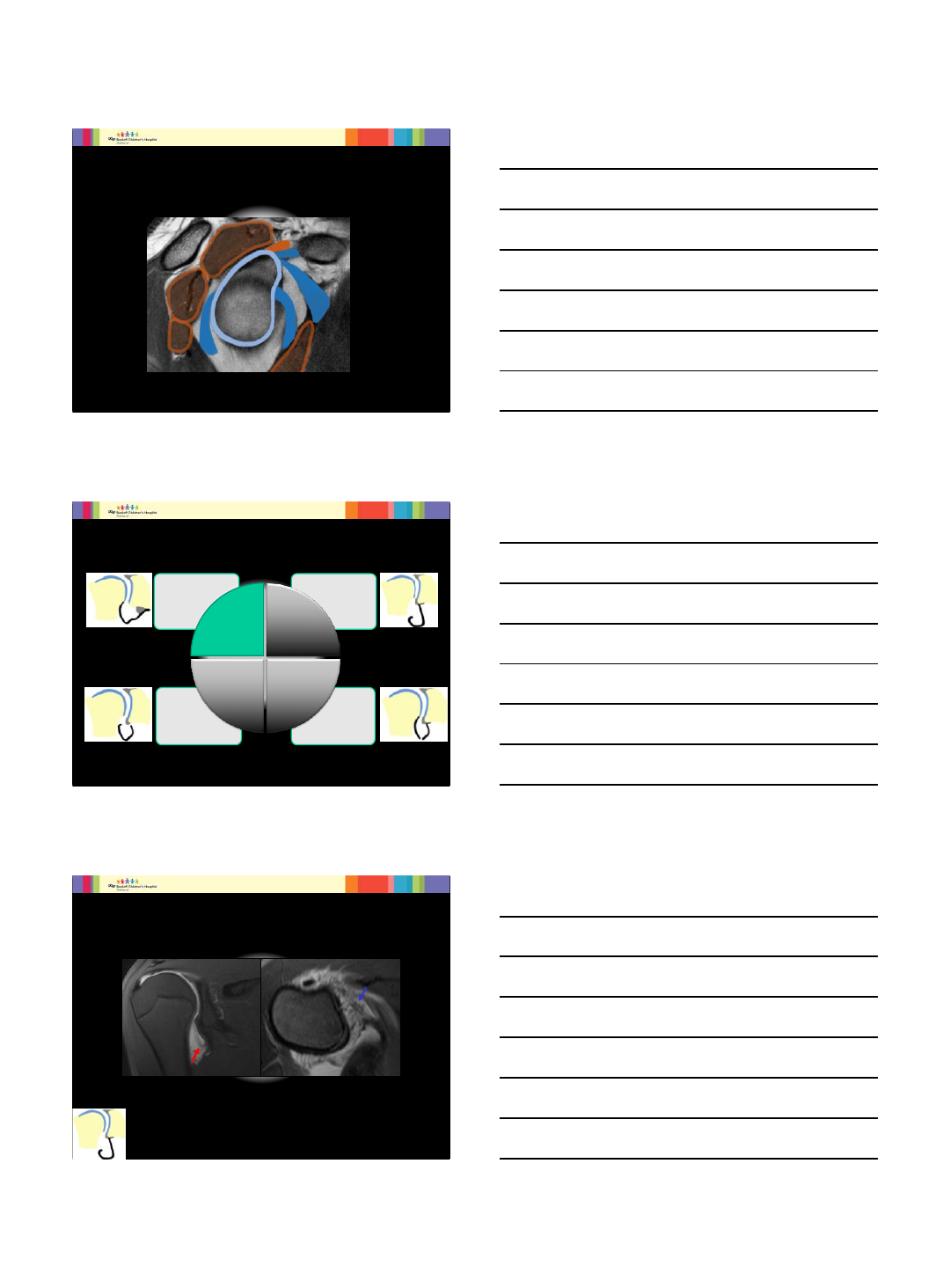
Glenohumeral Joint Anatomy
Like a golf ball on a tee
The greatest range of motion of any joint
Vulnerable to instability
Dynamic and static stabilizers
5
13
Stabilizers of the Glenohumeral Joint
Infraspinatus
MGHL
Supraspinatus
Subscapularis
Teres minor
Biceps tendon
SGHL
IGHL
Glenoid and
Labrum
14
Inferior labroligamentous Injuries
•Tear
•Sprain
•Floating
AIGHL
•HAGL
•BHAGL
•Bankart
•Perthes
•ALPSA
•GLAD Glenoid
Failure
75%
Humeral
Failure
15%
Capsular
Failure
Humeral
and
Glenoid
Failure
15
Patient with prior anterior shoulder dislocation
Courtesy of Dr. Diego Jaramillo, Miami Children’s Hospital
MR Arthrogram T1 FS
Humeral Avulsion Glenohumeral Ligament HAGL
6
16
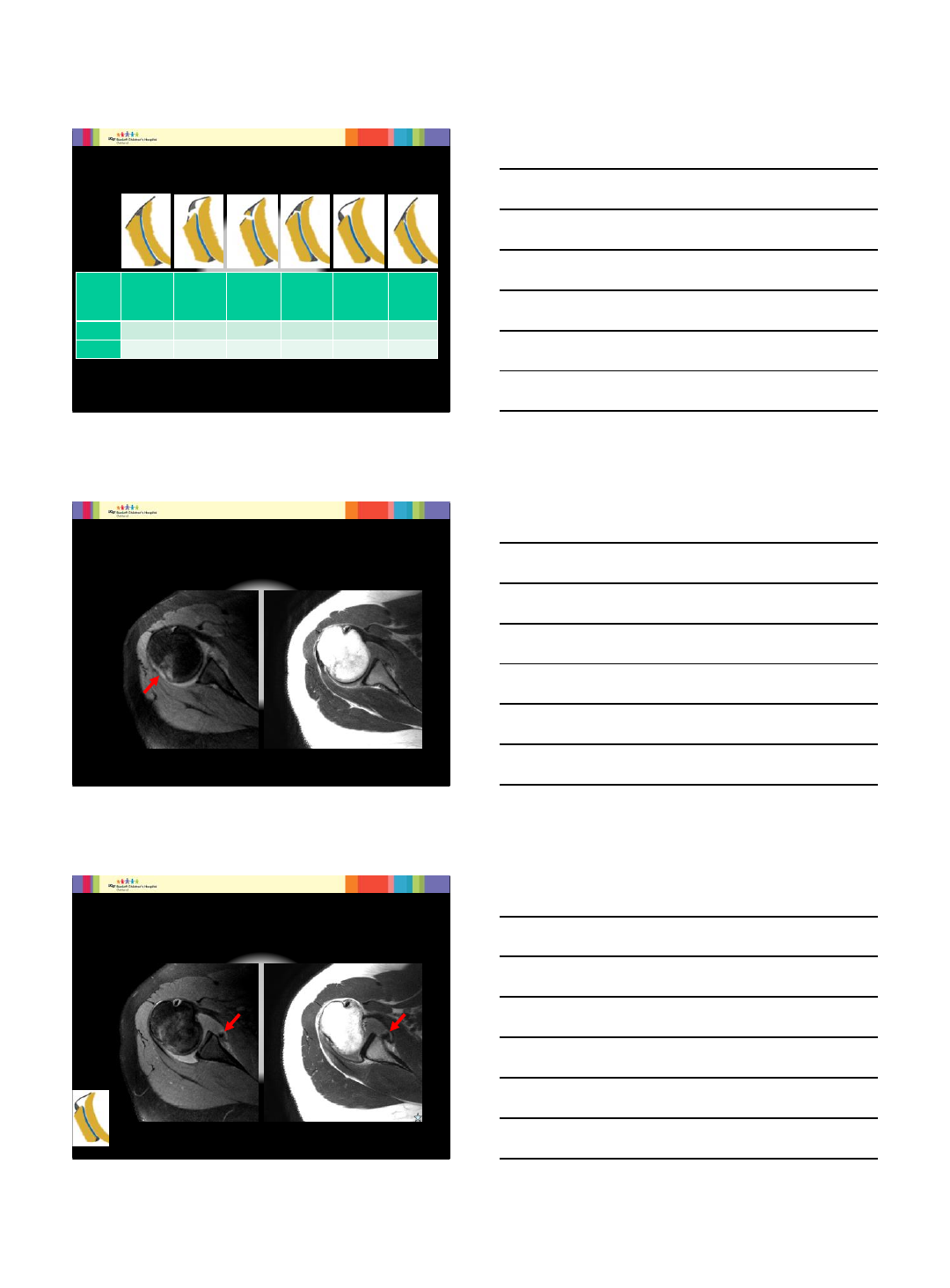
Capsulo-Labral Lesions
Lesion Normal Soft Tissue
Bankart Osseous Bankart Perthes
A
nterior
L
abroligamentous
P
eriosteal
S
leeve
A
vulsion
ALPSA
G
leno-
L
abral
A
rticular
D
isruption
GLAD
Periosteum Normal Stripped and
Torn Torn Stripped Stripped Mildly Stripped
Labrum Normal Displaced Displaced Nondisplaced Medially
Displaced Nondisplaced
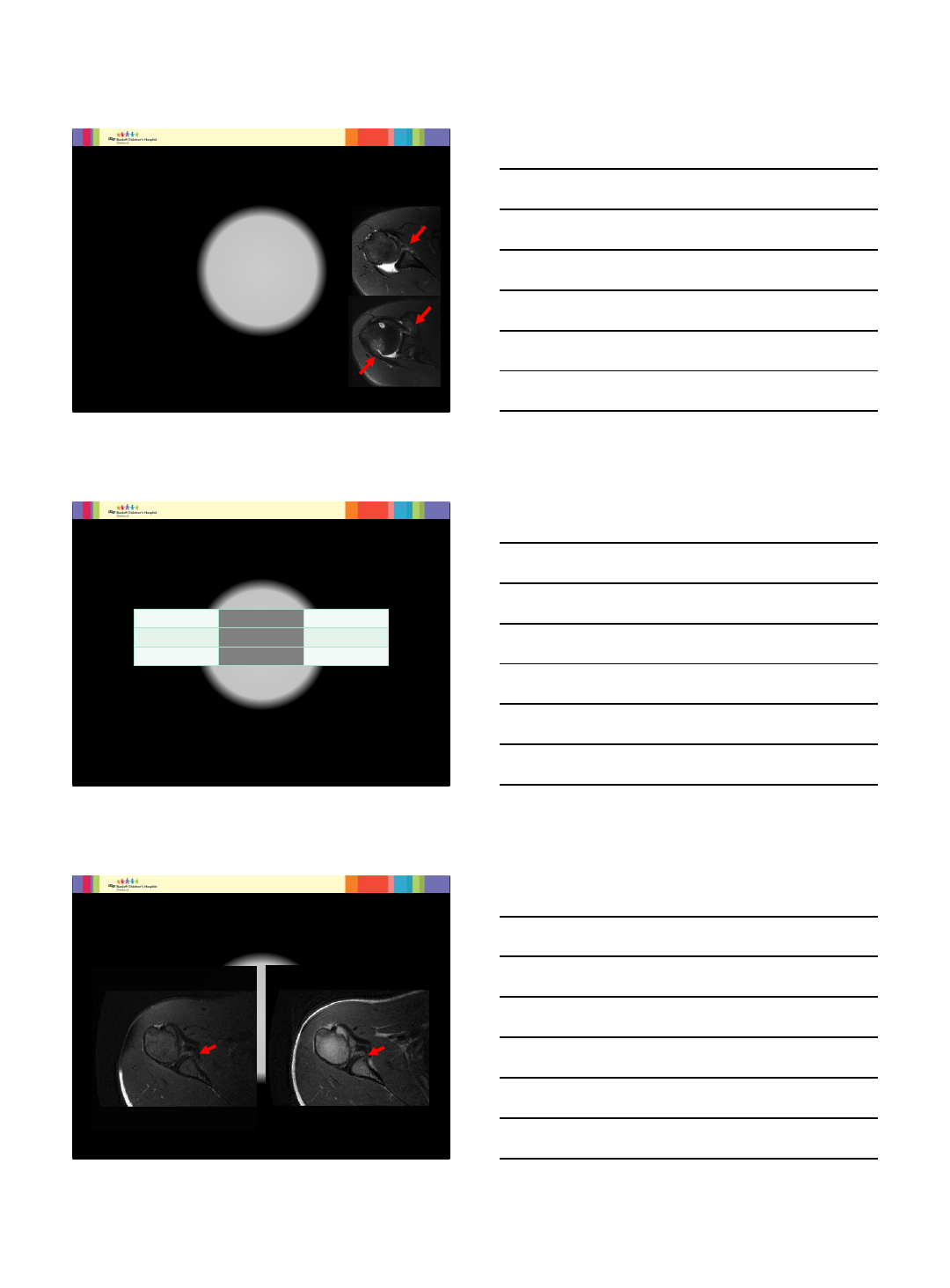
17
•Axial T2 FS •Axial T2
17 year old female with 5 episodes of anterior shoulder dislocation
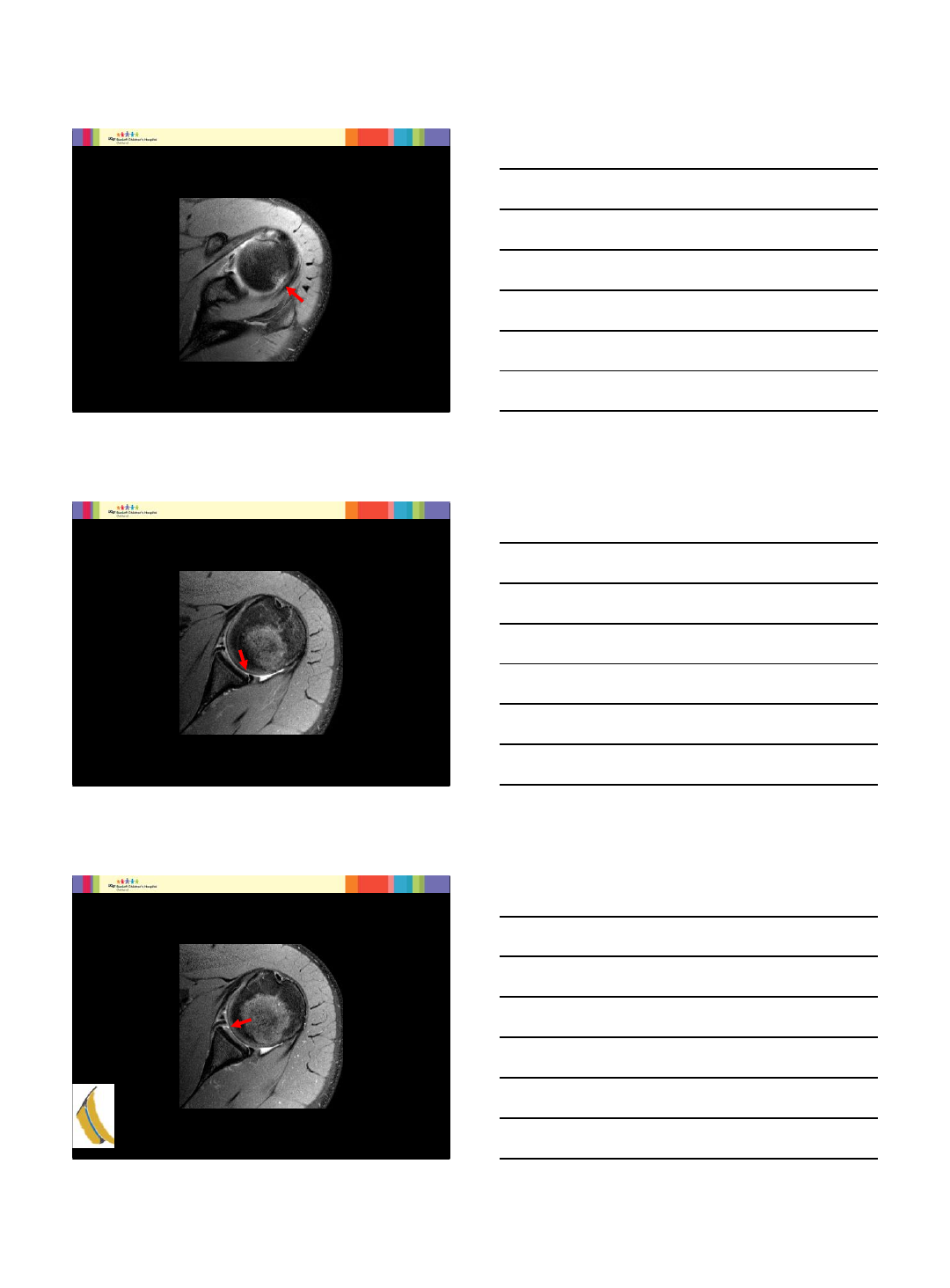
18
•Axial T2 FS •Axial T2
Anterior Labroligamentous Periosteal Sleeve Avulsion ALPSA
17 year old female with 5 episodes of anterior shoulder dislocation
7
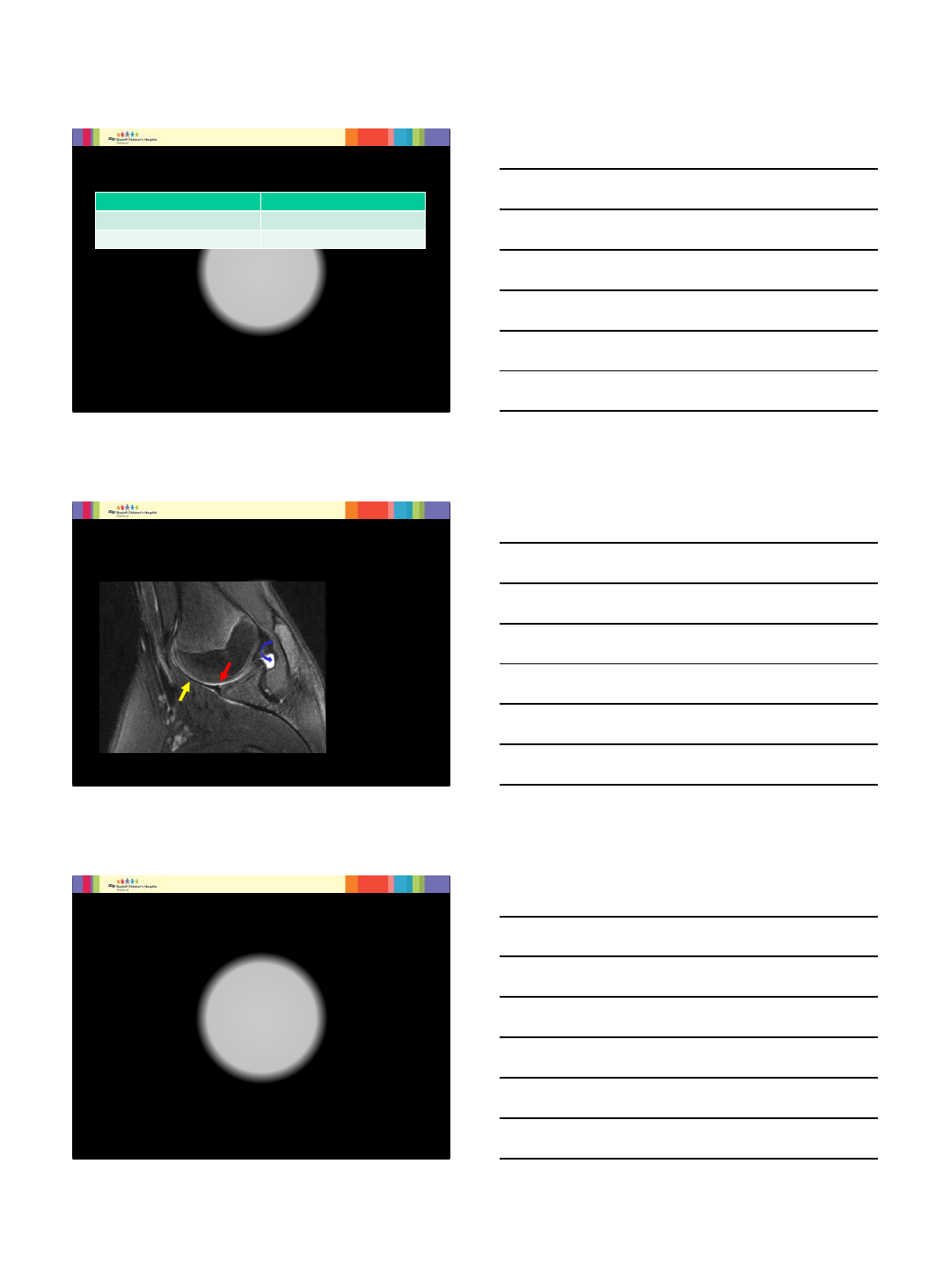
19
17 year old football player s/p several traumatic dislocations
Axial T2 FS
20
Axial T2 FS
21
Axial T2 FS
GlenoLabral Articular Disruption GLAD
8
22
MR Arthrogram
Direct Indirect
Arthrogram with dilute gadolinium solution IV injection of gadolinium
Joint Distension Does not distend joint
ABduction External Rotation (ABER)
Provocative positioning maneuvers
23
Abduction External Rotation (ABER)
Place anterior band of
IGHL under tension
Labral tear at
attachment site of IGHL
Outlines undersurface of
Infraspinatus tendon
24
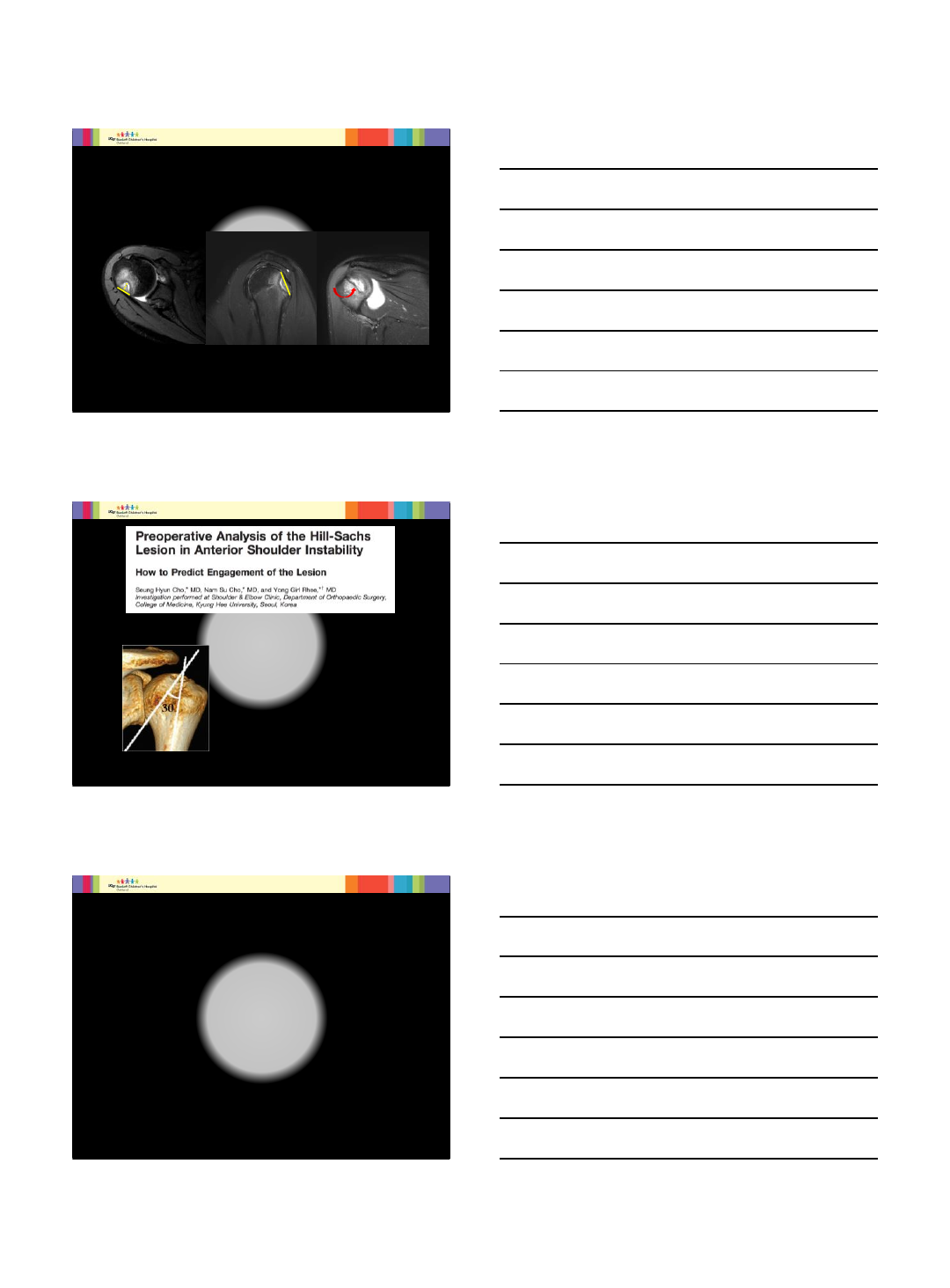
Pre-operative Planning
MDCT or MRI with volume rendering
•Quantify Glenoid deficiency
•Measure Hills-Sachs
9
25
Axial T2 FS Sagittal T2 FS Coronal T2 FS
16 year old girl with shoulder instability and multiple dislocations
26
The American Journal of Sports Medicine, Vol. 39, No. 11, 2011 DOI: 10.1177/0363546511398644
Engaging Hills-Sachs vs nonengaging
•More horizontally oriented to shaft
26˚vs 14˚
•Engaging lesions -larger width
and depth
27
No gold standard for quantification of Hill-Sachs defects
Classifications based on size, depth, location
No correlation between various classifications
No treatment algorithm based on classifications
10
28
16 year old who experienced his first shoulder dislocation 1 year
prior while playing football and has had multiple dislocations since.
Courtesy of Dr. Mimi Lin, Washington Radiologist Medical Group
29
Critical Area for Glenoid Deficiency is 25%
Defect greater than 25% glenoid width would
need bone grafting (Burkhart, De Beer)
Burkhart SS, Debeer JF, Tehrany AM, et al (2002) Quantifying glenoid bone loss arthroscopically in shoulder instability.
Arthroscopy 18:488-491.
Normal
Glenoid Significant
Bone Loss
30
Contact area of humerus on glenoid = glenoid track for critical ROM
Width of track is 84% glenoid width
Bankart lesions decreases width of tract
If medial margin of Hills-Sachs defect is more medial than glenoid
tract, standard stabilization are unlikely to stabilize the shoulder
11
31
Good agreement between 4 observers about % glenoid bone loss
Poor agreement assessing Hills-Sachs defect
Poor reliability of the glenoid track classification
Method
•71 patients with anterior
inferior shoulder instability
•4 Reviewers
Goal
Assess reproducibility of
characterizing bipolar bone
loss and treatment
32
Summary
In the acute setting radiographs
MRI and MR arthrography
•Osseous and soft tissue abnormalities
CT and MRI with 3D reformations
•Characterize and measure glenoid deficiency
and Hill-Sachs lesions for preoperative
planning
33
THANK YOU!!!
Imaging of Glenohumeral Instability in
the Adolescent Patient
2/7/2017
1
www.prismsports.org
Traumatic Anterior Shoulder Instability:
Rehabilitation Through Return to Play
Michelle Cappello, PT, MSPT, SCS
USCF Benioff Children’s Hospitals
Sports Medicine Center for Young Athletes
February 7th, 2017
www.prismsports.org Objectives
•Review conservative management for primary
TASI
•Review evidence based return to sport criteria
for traumatic anterior shoulder instability (TASI)
www.prismsports.org
Traumatic Anterior Shoulder
Instability (TASI)
•Treatment of first time traumatic GH dislocators will be
different from that of a patient with atraumatic
instability. Micro vs. Macro
•A gradual graded advancement of ROM and exercise
progression will be required, based on the degree of the
acute injury
•Goals remain the same; dynamically stabilize the
inherently unstable glenohumeral joint.
•Master the “Thrower’s Paradox”; Shoulder loose enough
to throw yet stable enough to prevent injury (Wilk AJSM
2002)
2/7/2017
2
www.prismsports.org
Rehabilitation Overview
•Reduce acute pain & inflammation
•Restore motion and soft tissue mobility
•Emphasize strength balance
•Enhance dynamic humeral head control
•Integrate kinetic chain
•Return to Sports Specific Activity/PLF
www.prismsports.org
TASI Goals of Rehab
OUTCOME MEASURES
•Patient Reported
•Shoulder ROM
•Movement Segment Strength
•Functional Testing: Ybalance, SL squat,
CKCUET, OH Squat, Seated shot put
•Sports Specific training to competition
www.prismsports.org
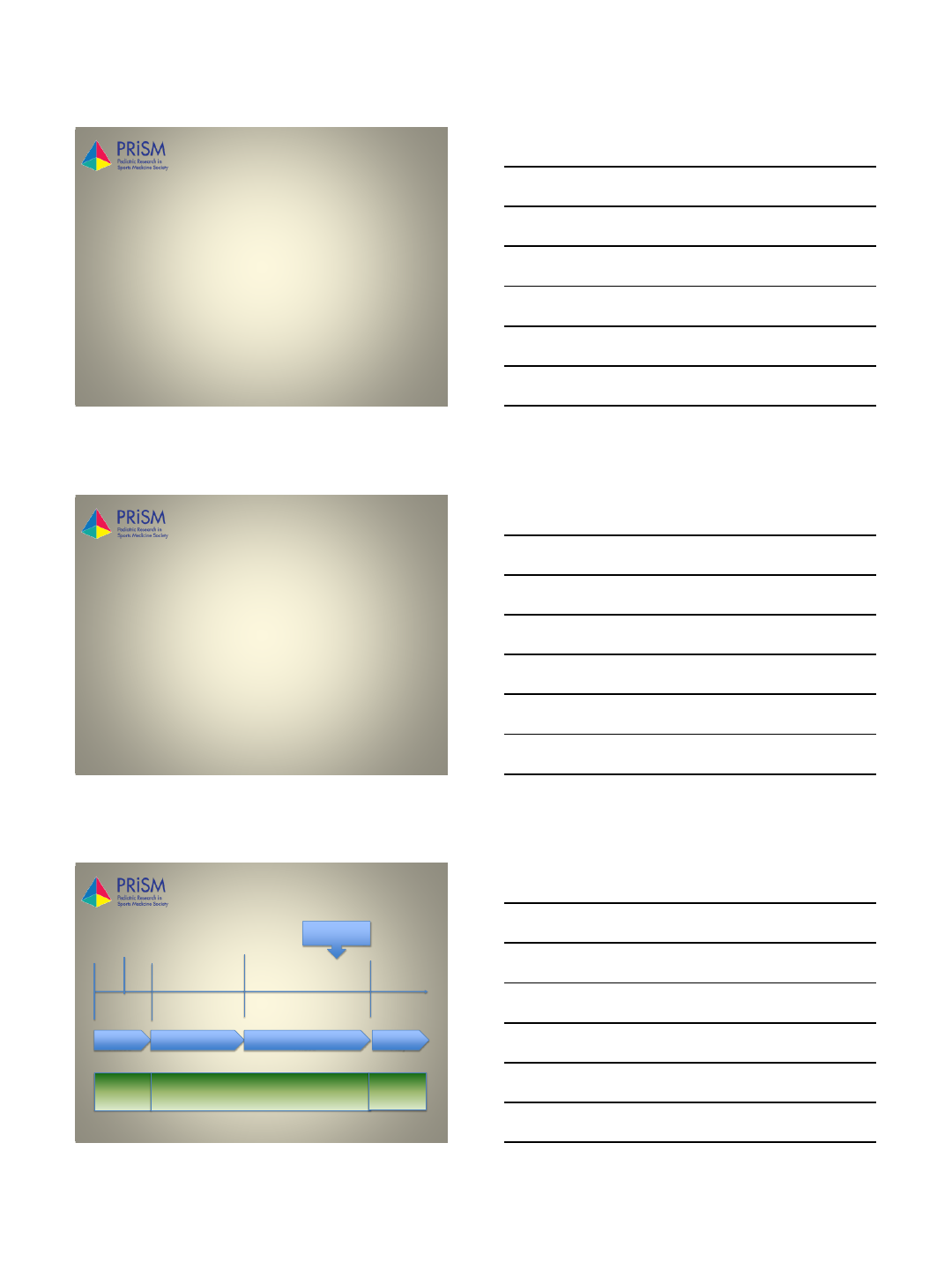
Rehabilitation Timeline
8 weeks +4 weeks
Injury 2 weeks
Sling
Brace PT Day 3-4
Initiate Return
to Sport Testing
Acute
Phase Intermediate Phase Advanced Strengthening
Phase
Return to
Play
DX Specific Pain Management >> Functional Progression Athlete
Specific
2/7/2017
3
www.prismsports.org
Acute Phase
Goals: Protect the injured, healing capsular & labral
structures
1. Abstain from Sport 2+ weeks (control stresses)
–Sling for comfort, no evidence on duration,
inconclusive ER vs. IR of shoulder position
2. Diminish pain & inflammation
3. Reestablish pain –free ROM, Do not push range
4. Delay muscle atrophy & reestablish voluntary
muscle activity
www.prismsports.org
Intermediate Phase
Goals:
1. Improve strength
1. Rotator cuff anterior and posterior
2. Scapular “stabilizers” – incl. serratus anterior
3. Core for energy transfer
2. Normalization of shoulder girdle motion and
arthorkinematics, manual therapy for tissue mobility
3. Enhancing dynamic stabilization of cuff and scapular
muscles & neuromuscular control with upper extremity
activities
–BALANCE net force ant/post/distraction of humoral head
–3-4% decrease in RTC strength results in loss of dynamic
stability (Reinhold, Sports Health 2010)
www.prismsports.org
The Adolescent Shoulder:
Linking development into the plan
of care
CORE:
•Group of muscles that form a cylinder around your waist
TA,RA, IO, EO
Paraspinals
Diaphragm
Pelvic Floor
Hip Muscles
Thoracolumbar Fascia
•Optimum production, transfer, and control of force delivered to the
terminal segment
•Core provides 65% force production, 85% force attenuation
•Glut Max 100% MVIC stride to late cocking phase, Glut Med 40%
•Poor Single leg squat associated with posterior chain weakness
which is underdeveloped in pre/adolescents (Wilk PMR 2016)
Oliver JSCR 2010 &
2015
2/7/2017
4
www.prismsports.org
The Adolescent Shoulder:
Linking Core into the plan of care
www.prismsports.org
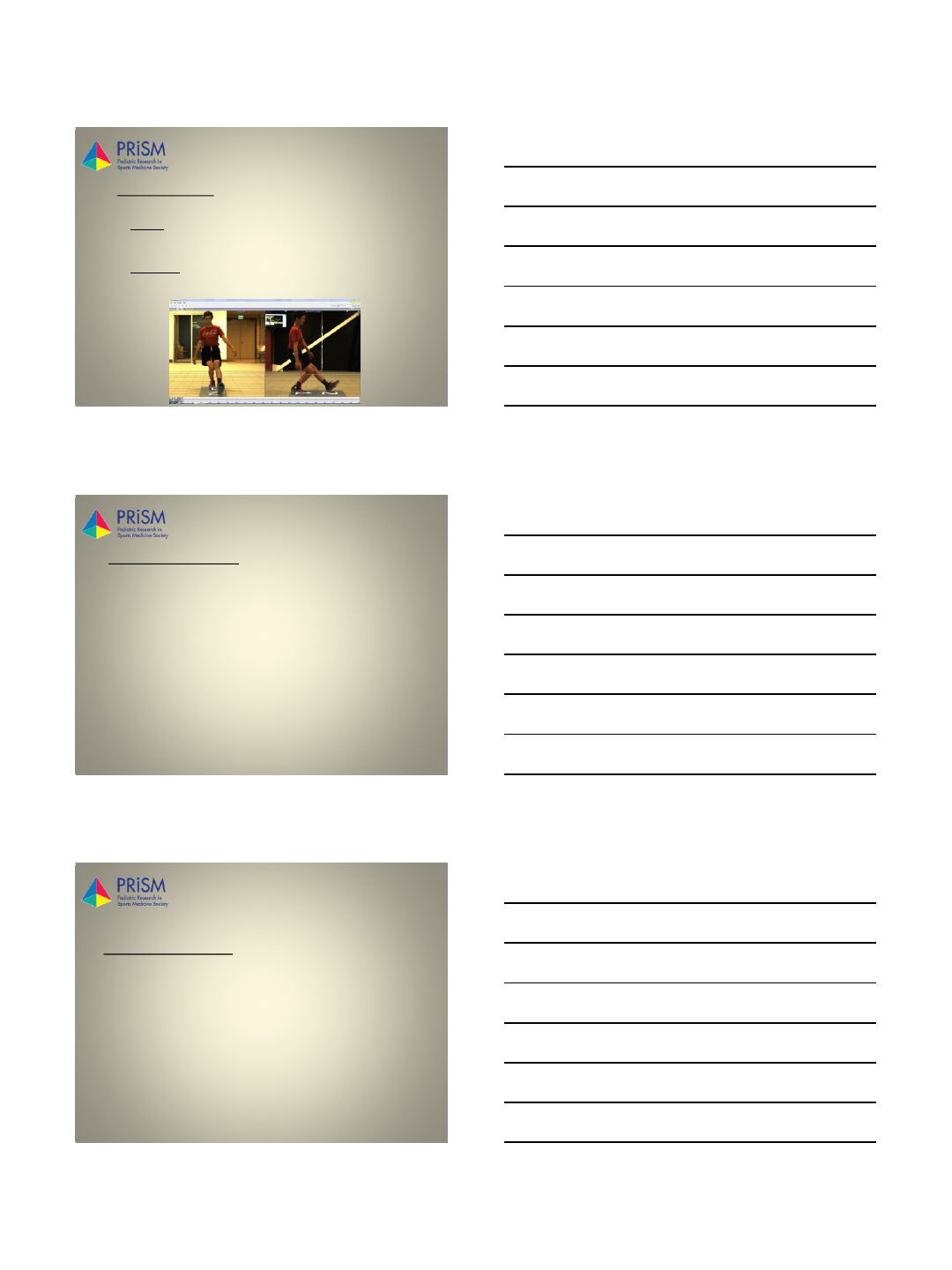
The Adolescent Shoulder: Linking UE & LE
www.prismsports.org
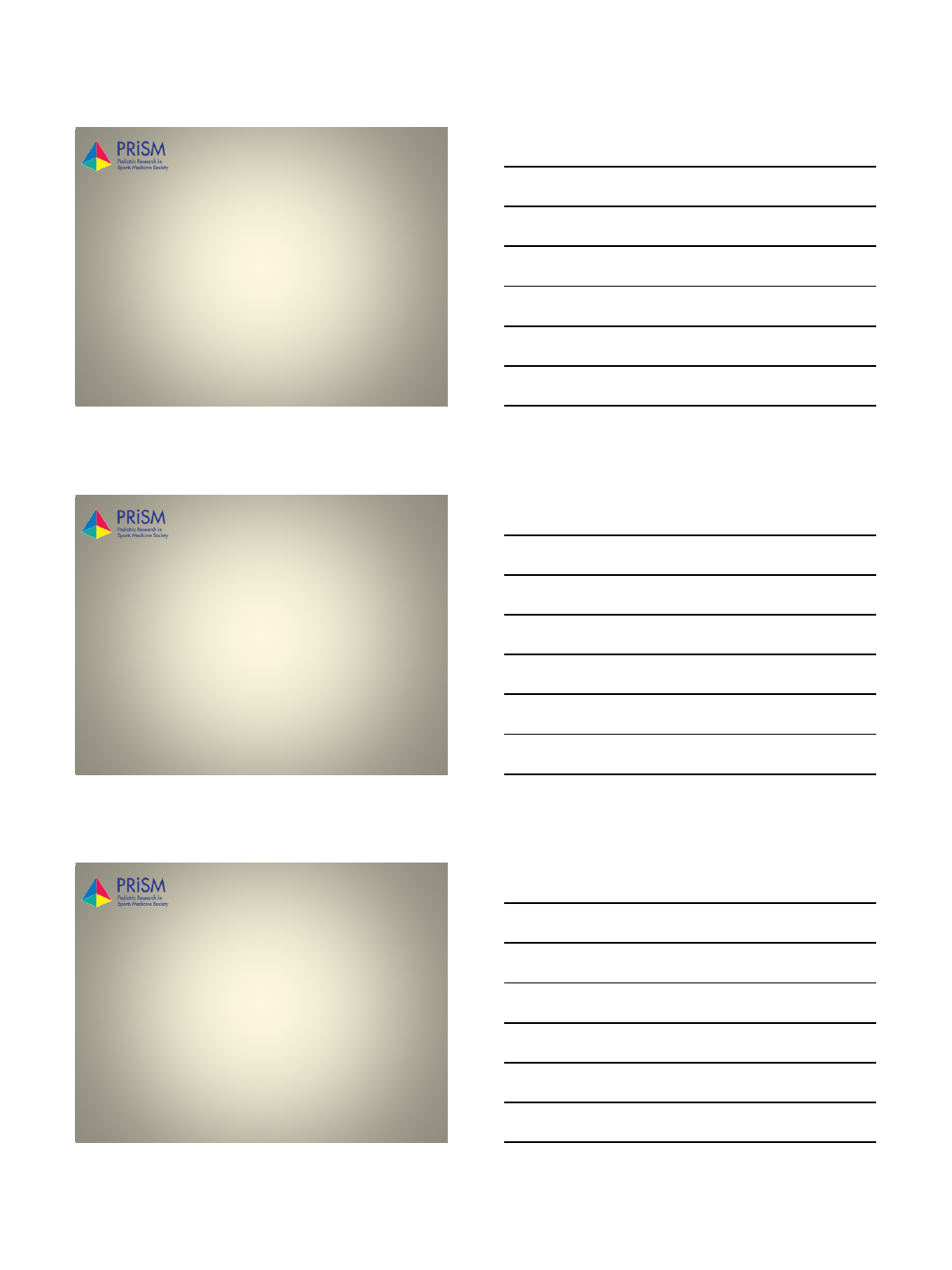
The Adolescent Shoulder: Exercises Examples
Linking UE & LE
2/7/2017
5
www.prismsports.org
Advanced Strengthening
Phase
Goal: improve strength, power, endurance,
MOTOR CONTROL, enhance dynamic stabilizers
of the GH joint and Scapula.
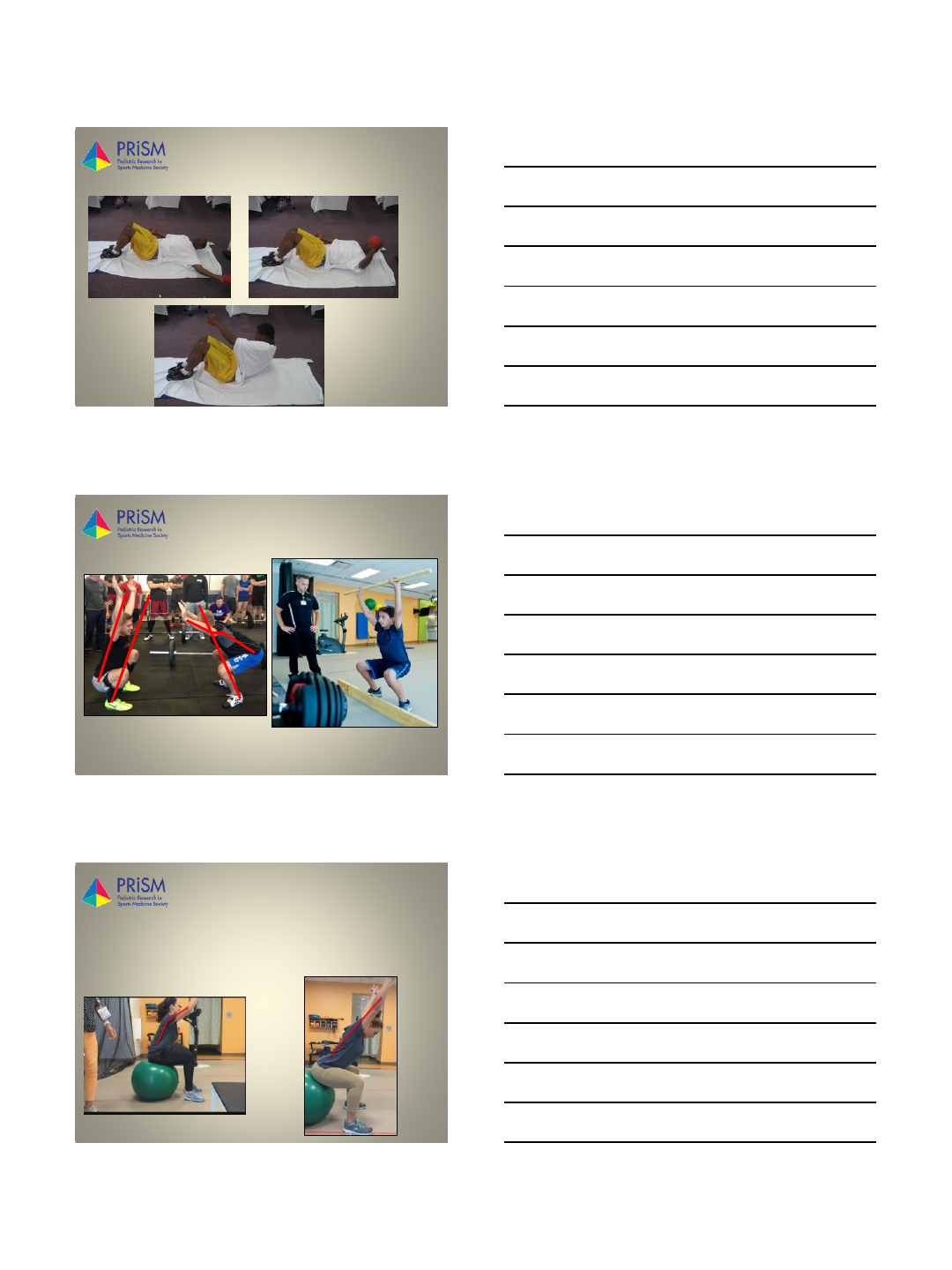
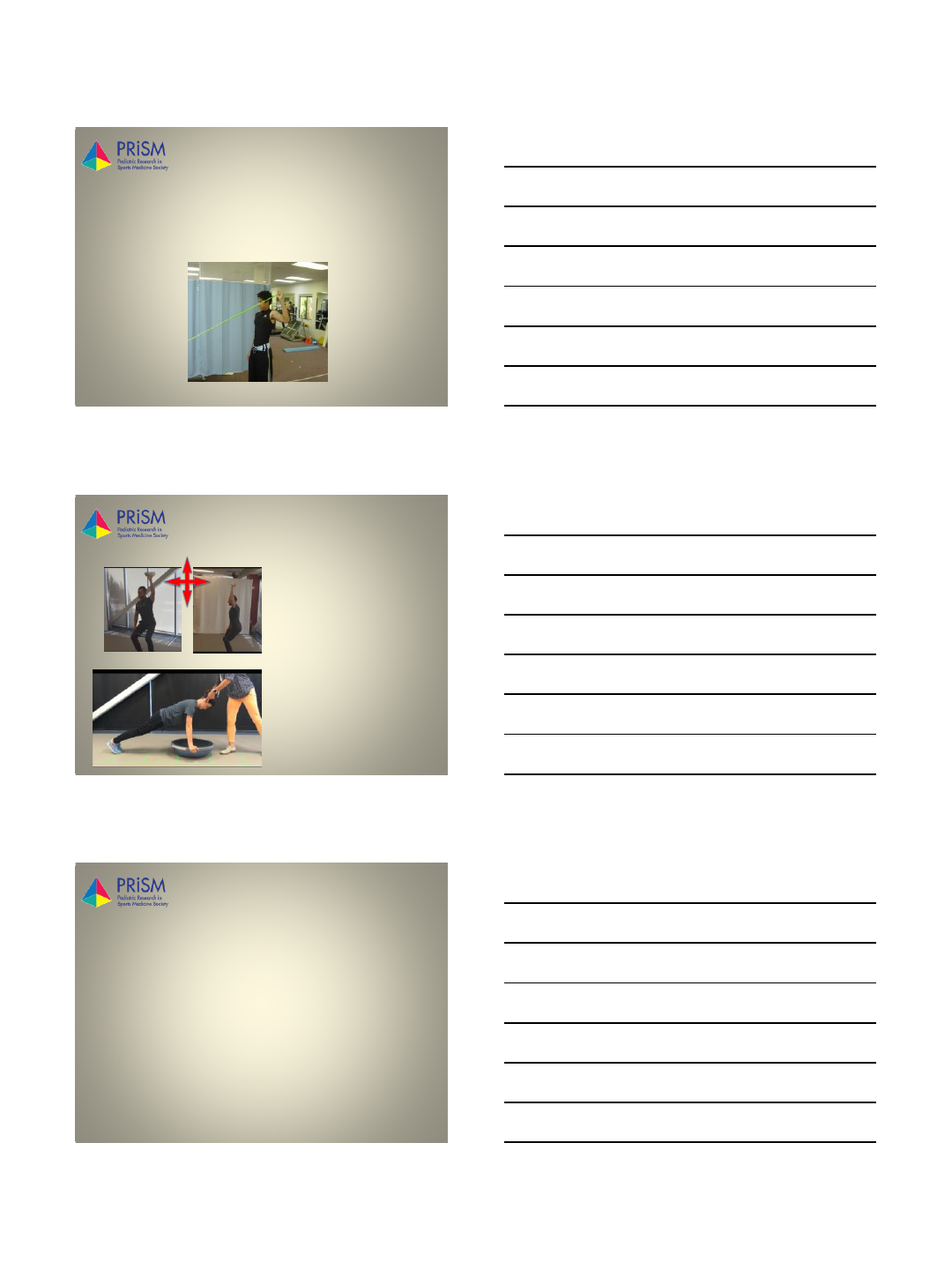
www.prismsports.org
Stabilization
•Rapid torque control
progressing into 90/90
shoulder position
•Closed Kinetic chain for
proprioception training
www.prismsports.org
Return to Play Phase
Goal: Athletes need to be resilient, strong,
technically proficient to robustly maintain proper
motor skill competence within the demands of their
sport
OUTCOME MEASURES
•Patient Reported
•Shoulder ROM
•Movement Segment Strength
•Functional Testing
2/7/2017
6
www.prismsports.org
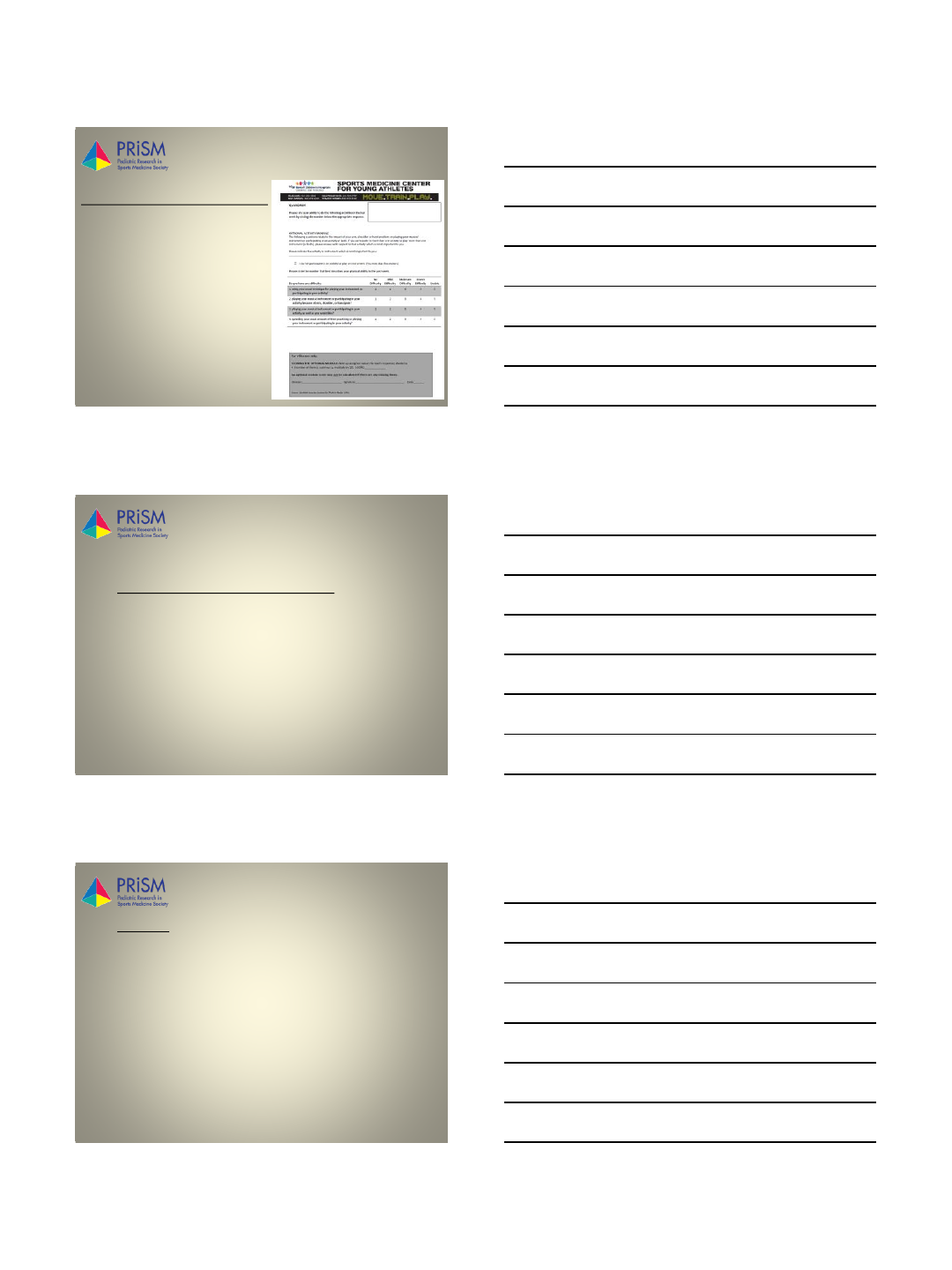
Criteria for Return to Play
1. Patient Reported Outcome Measures
•Quick Dash
•developed by Amer. Society of Ortho
Surgeons
•11 questions, 4 additional with
sports activity module
•goal is < 5 Best possible score = 0
•Kerlan -Jobe Orthopedic Shoulder
and Elbow Score Alberta AJSM 2010
•KJOC > 90% (best possible =
100%)
www.prismsports.org Criteria for Return to Play
2. ROM Shoulder & Posture & Stability Testing
•Demonstrate pain free range of motion with Active shoulder total arc of motion
within 5 degrees of non-throwing side Wilk AJSM 2002. Manske & Ellenbecker IJSM 2005
•Passive shoulder flexion within 5 degrees of non-throwing side Wilk AJSM 2014
•Scapular anterior tilt symmetry within 10 degrees of non-dominant side to
decrease scapular dyskinesia. Kibler et al. JShouderElbow Surg 2002
•Active internal rotation deficit no greater than 20 degrees of non-throwing side
Meister , Keith, et al. AJSM 2005
•Thoracic Kyphosis –no real studies on posture, adult norms = 40°kyphosis
•Demonstrate negative results for shoulder stability with no pain for the
Glenohumeral anterior and posterior drawer with arm elevated to 90 degrees in
scapular plane Sportsfisio 2015 Kevin Wilk, “Return to Play Criteria for the Overhead Athlete.”
www.prismsports.org Criteria for Return to Play
3. Strength
•Dominant side 10% stronger
•Scapular dynamic stabilizers –Endurance test
•Gluteals included
•Isokinetic Strength Testing (to be performed before and after functional testing. Ratio
demands remain the same for both pre and post fatigue) Ratios for isokinetic strength
testing from Wilk et al: AJSM ’93, ‘95
•External Rotation/Internal Rotation ratio 70-76%
•External Rotation/Body Weight ratio 18-23%
•Internal Rotation/Body Weight ratio 26-32%
•Isometric scapular strength for mid trap and lower trapezius within 10% of non-
throwing / dominant side
•Gluteals: Limited studies out there talking about expected/normative strength for hip
musculature. In our practice, we set a goal of 1/3rd the body weight with HHD
2/7/2017
7
www.prismsports.org Criteria for Return to Play
4. Functional Testing
These are the ones we use regularly.
•CKCUEST – Place tape 36” apart with arms in push up position
(hands/toes). Tap across each tape alternately many times as they can in
15 sec. Repeat 3 trials and take average them. >23 touches in 15 seconds
BMC musculoskeletal disorders 2014:
•LE Y balance: Composite score > 92% (Baseball Players Diagnosed With Ulnar
Collateral Ligament Tears Demonstrate Decreased Balance Compared to Healthy
Controls, J. Craig Garrison et al, JOSPT, Oct 2013)
www.prismsports.org Criteria for Return to Play
4. Functional Testing (cont.)
•Perform maximum effort 2 handed chest passes with 8 lb. medicine ball 2
x 20 Sportsfisio 2015 Kevin Wilk
•Perform maximum effort 1 handed “shot-put” throw with 4 lb. medicine
ball 2 x 20 (just need to complete without pain/instability)
•Prone Y endurance test for scapular stabilizers
•Tests fatigue in middle and lower traps.
•Testing performed with 3% of body weight. Metronome set to 60Hz.
•Task failure was defined as: 1. Unable to keep up with metronome, 2.
Demonstration of compensatory strategies, 3. Inability to go above
horizontal each time.
•Only norms available on Football players (26-28 repetitions).
•For OH athlete I would aim for 10% better on dominant side
Pontillo, Marisa, Bryan A. Spinelli, and Brian J. Sennett. "Prediction of in-season shoulder injury from
preseason testing in division I collegiate football players." Sports Health: A Multidisciplinary
Approach (2014): 1941738114523239
www.prismsports.org Criteria for Return to Play
5. Return to Sports
•Begin a specified return to throwing program for
throwing athletes
•Work with a sports specific skills coach
•Build intensity and volume, as well as impact
•Single sports specific task, then add complexities
and reactive drills
•Start with non-contact practice
•Full practice for 2 full weeks
•Competition
2/7/2017
8
www.prismsports.org Summary
1. Return to sports after a shoulder dislocation involves many factors
2. There are ideal criteria that give some guidelines for when to return the athlete to
play, this will be athlete specific, more research need for proven battery of
outcome measures.
3. Timelines for return to play will be athlete specific, and only should occur after
attainment of full strength, motion, stability, and confidence.
4. Fatigue is above all the biggest injury risk, train for dynamic stability / postural
endurance then power/speed
5. Core/Legs provide >65% of power/torque to the UE – “Train the Chain”
2/3/2017
1
www.prismsports.org
Operative Management of
Adolescent Shoulder Instability:
Keys for Success
Dr. Nirav K. Pandya
Assistant Professor of Orthopaedic Surgery
Director of Pediatric Sports Medicine
University of California San Francisco
Nirav.Pandya@ucsf.edu
www.prismsports.org
Disclosures
Consultant - Orthopediatrics
www.prismsports.org
Common Scenario
“So I heard you are the person
who is going to make my
shoulder normal again?”
“Can I go back and play 6
weeks after surgery?”
“I will never dislocate out again
right?”
“Are you going to do the
surgery with a laser?”
2/3/2017
2
www.prismsports.org
Common Scenario
www.prismsports.org
Key Point
Studies cite up to a 30% re-dislocation rate
with arthroscopic treatment in this age group
PREPARE PATIENTS EARLY
www.prismsports.org
Key H and P
•Sport: collision vs. non-collision
•Sport: throwing / swimming
•Hand dominance
•Number of prior dislocations
•Force needed to dislocate and re-locate
•In-season vs. out-of-season
•Ligamentous laxity
•Expectations
2/3/2017
3
www.prismsports.org
Key H and P
Remember to differentiate atraumatic instability
from traumatic instability
www.prismsports.org What Can I Do?
Open
vs.
Arthroscopic
www.prismsports.org How Do I Decide?
It’s not just
about
throwing some
anchors in and
fixing the
labrum!
2/3/2017
4
www.prismsports.org How Do I Decide?
•I am searching for evidence that I need to
do more than just an arthroscopic labral
repair
•History = collision sports, number of
dislocations, compliance?
•Imaging!!!
www.prismsports.org What’s In My Tool Box?
•Arthroscopic labral repair
•Arthroscopic remplissage
•Open labral repair
•Open Latarjet
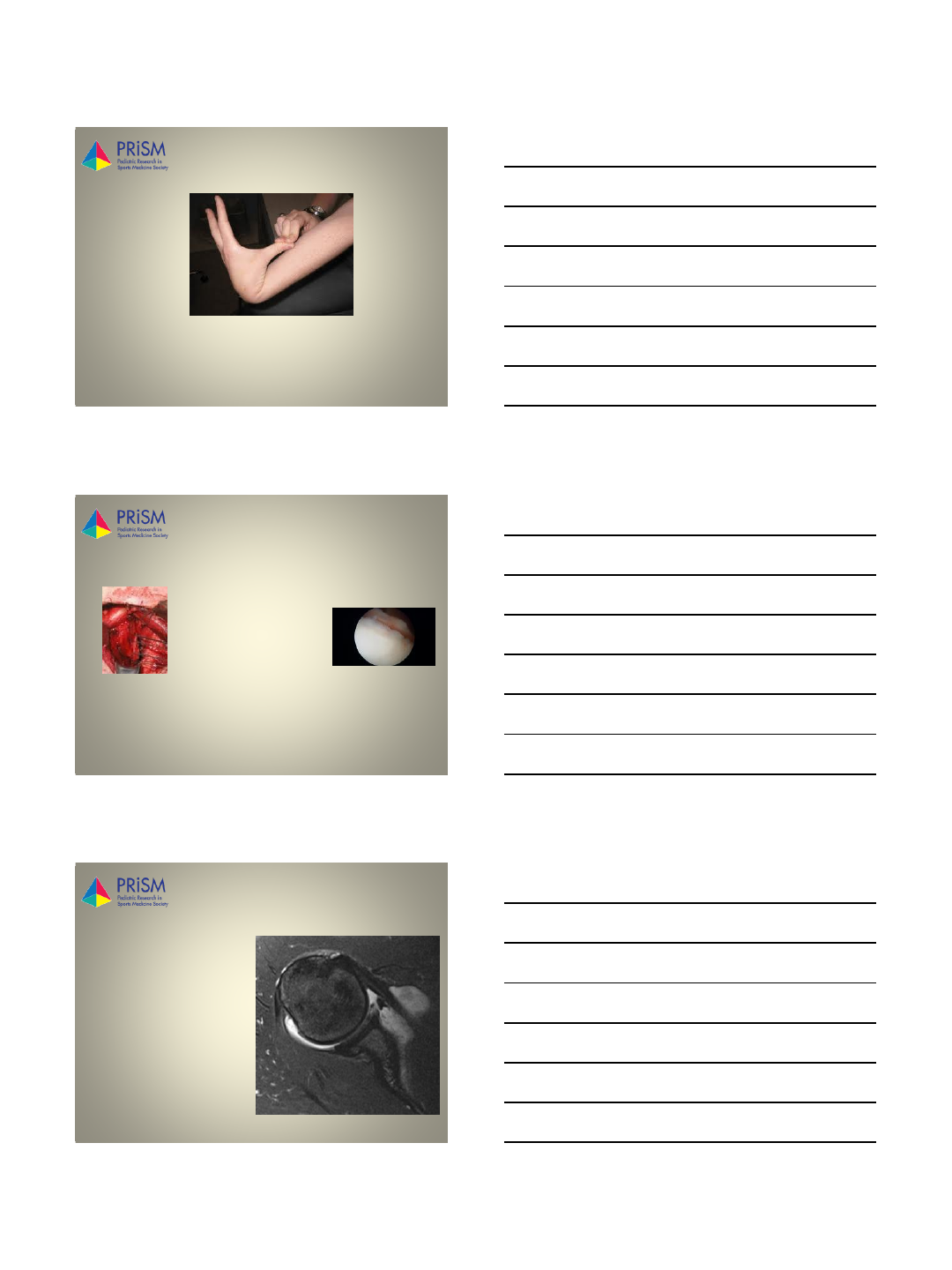
www.prismsports.org Pearl #1
Collision athlete /
extreme athlete =
consider open
repair
2/3/2017
5
www.prismsports.org Pearl #2
On –Track
vs.
Off –Track
www.prismsports.org
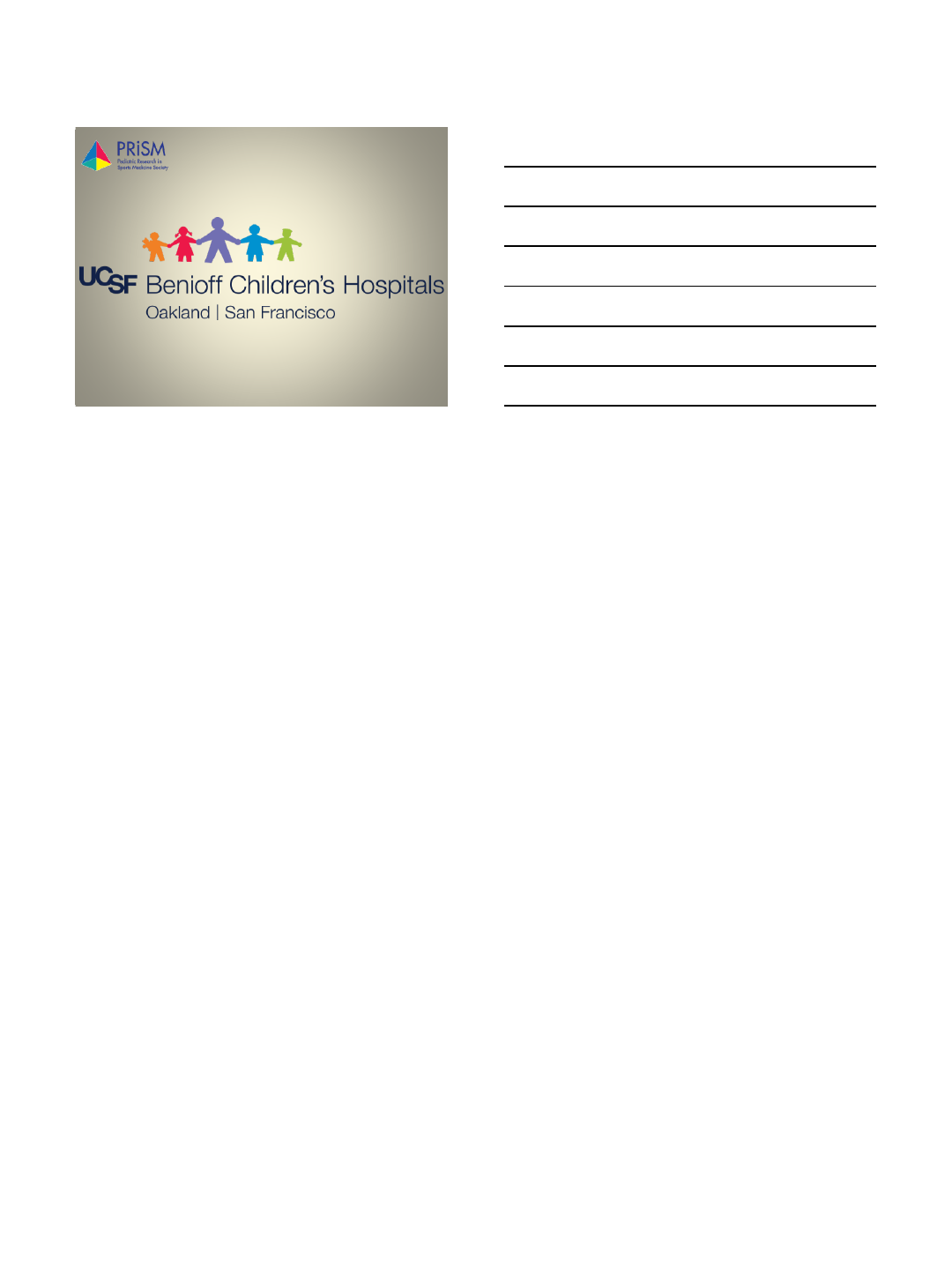
Pearl #2
Engaging Hill
Sach’s
= >
Remplissage
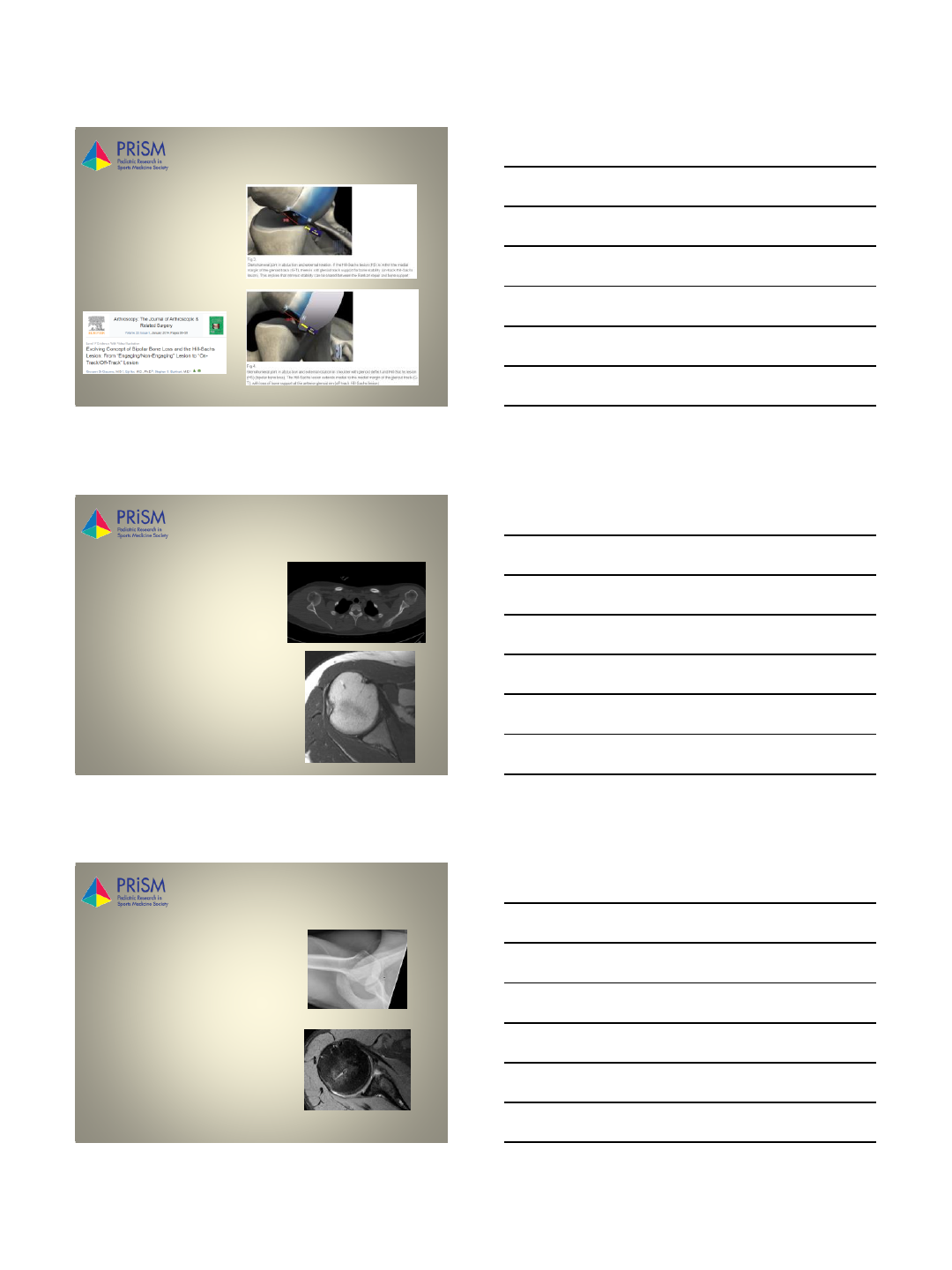
www.prismsports.org Pearl #3
Glenoid Bone
Loss > 25%
=
Open Latarjet
2/3/2017
6
www.prismsports.org What’s In My Tool Box?
•Arthroscopic labral repair
•Arthroscopic remplissage
•Engaging / off-track Hill-Sach’s
•Open labral repair
•Collision / extreme athlete
•Open Latarjet
•> 25% bone loss
www.prismsports.org Labral Repair Keys
•Beach chair vs. lateral
•Mobilize labrum!
• Knotless vs. standard (dealer’s choice)
•Get down low (5:30 – 6:00 o’clock)
•Grab capsule AND labrum AND advance tissue
• Don’t be an anchor animal (space out)
www.prismsports.org Remplissage Keys
•Engaging /
Off-Track
•Prepare bed
•Pass sutures
before
performing
anterior
stabilization

2/3/2017
7
www.prismsports.org Post-Op
•Not worried about stiffness
•Worried about compliance!!
www.prismsports.org What’s The Data??
•17 studies comprising 654 total shoulder instability events
•Patients grouped non-operative vs operative treatment
•Primary non-operative group was more likely to have recurrence compared to
the primary operative group (OR=13.41; 99% CI 3.60 to 49.93, p<0.001)
•The rate of recurrence in patients aged <14 years was high (44.44%)
•For RTP, there is evidence that RTP rates were higher for primary operative
patients (95.3%) versus primary non-operative (41.3%, Z=6.12, p<0.001) and
secondary operative patients (77.6%, Z=2.66, p=0.008).
www.prismsports.org What’s The Data??
•21% re-dislocation rate
•18.75% re-dislocation rate
2/3/2017
8
www.prismsports.org What’s The Data??
•25% re-dislocation rate
www.prismsports.org What’s The Data??
•6 studies, 167 patients
•5.4 % re-dislocation rate
•Low complication rate
•No significant loss of shoulder motion
www.prismsports.org Key Summary
•High repeat dislocation rate in this population
•Assess activity level and expectations
•Know your tools: arthroscopic, open, remplissage, Latarjet
•Engaging / off-track = remplissage; glenoid loss > 25% =
Latarjet
•Start low, shift capsule-labrum arthroscopically
•Be prepared to do a remplissage if necessary
•Post-op = compliance, compliance, compliance
2/3/2017
9
www.prismsports.org Thank You
2/7/2017
1
www.prismsports.org
Postoperative Management and
Return to Play for Adolescent
Shoulder Instability
Brett Burton, PT, DPT, SCS, ATC, CSCS
St. Luke’s Sports Medicine
burtonbr@slhs.org
February 7, 2017
www.prismsports.org
Disclosure
•There are no relevant financial relationships to disclose.
www.prismsports.org
Postoperative Management
•Guiding Principles1
–Communication with surgeon is imperative
–Understand the surgery
•Know all structures involved
–Understand structures to be protected, how they are
stressed, and healing rates
–Impart appropriate levels of stress to the tissue
•Absolute ROM, controlled submaximal loading, and dynamic stability
–Management of initial immobilization and understanding
rate of ROM progression
stressprotection
2/7/2017
2
www.prismsports.org
Postoperative Management
•Rehabilitation Overview - approximate timelines2
–Weeks 0-6: Immobilization in sling
–Weeks 2-4: PROM at graded intervals; isometric exercise
•Screen trunk and lower extremity (mobility, stability, and strength)
and address limitations3
–Weeks 4-8: Basic strengthening exercise
–Weeks 5-6: Begin AROM
–Weeks 8-12: Advanced
strengthening and plyometrics
–Week 16: Return to play
testing performed
–Week 24: Contact and
overhead sports begin
www.prismsports.org
Return to Play
–Pain free movement
–Range of motion established
•Minimize glenohumeral internal
rotational deficit (GIRD) and total
range of motion (TROM) deficits4,5
•Consider specific surgery
•Loss of motion does increase risk of
shoulder or elbow injury6,7
–Strong and pain free manual
muscle testing
•Test throwers in 90/90 position
•Weakness of supraspinatus is also
related to increased risk of injury8,9
Foundational
Criteria
Advanced
Criteria
Advanced
Criteria Under
Fatigue
www.prismsports.org
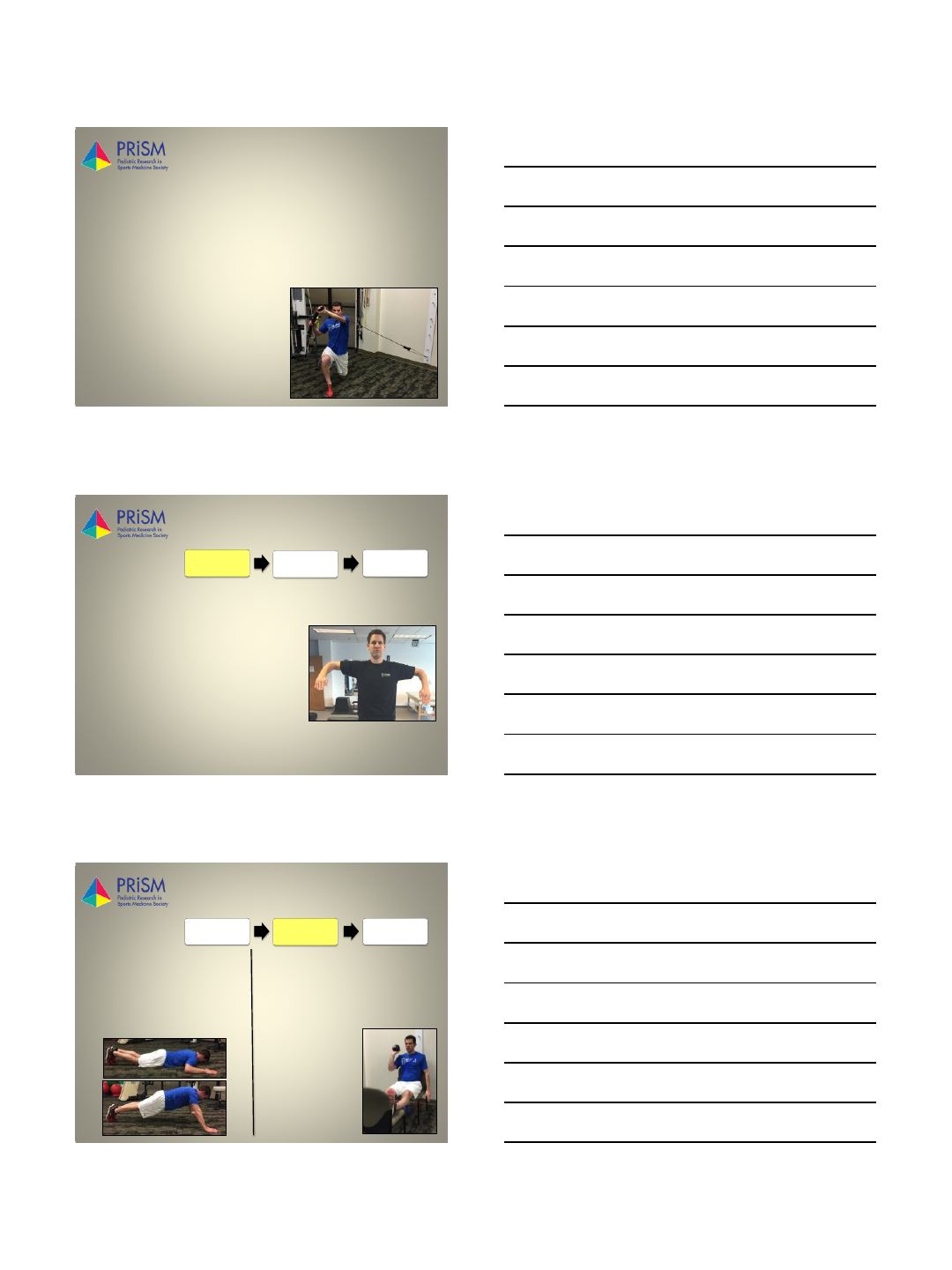
Return to Play
Trunk Stability Push Up10 Single Arm Seated Shot-Put11
•Assesses trunk stability in sagittal
plane while performing bilateral,
closed chained, upper extremity
movement
•Desired score: 2/3
•Utilizes a 6 lb. medicine ball to
assess unilateral, open chained,
upper extremity power
movement
•Desired score:
< 10% difference
between extremities
Foundational
Criteria
Advanced
Criteria
Advanced
Criteria Under
Fatigue
2/7/2017
3
www.prismsports.org
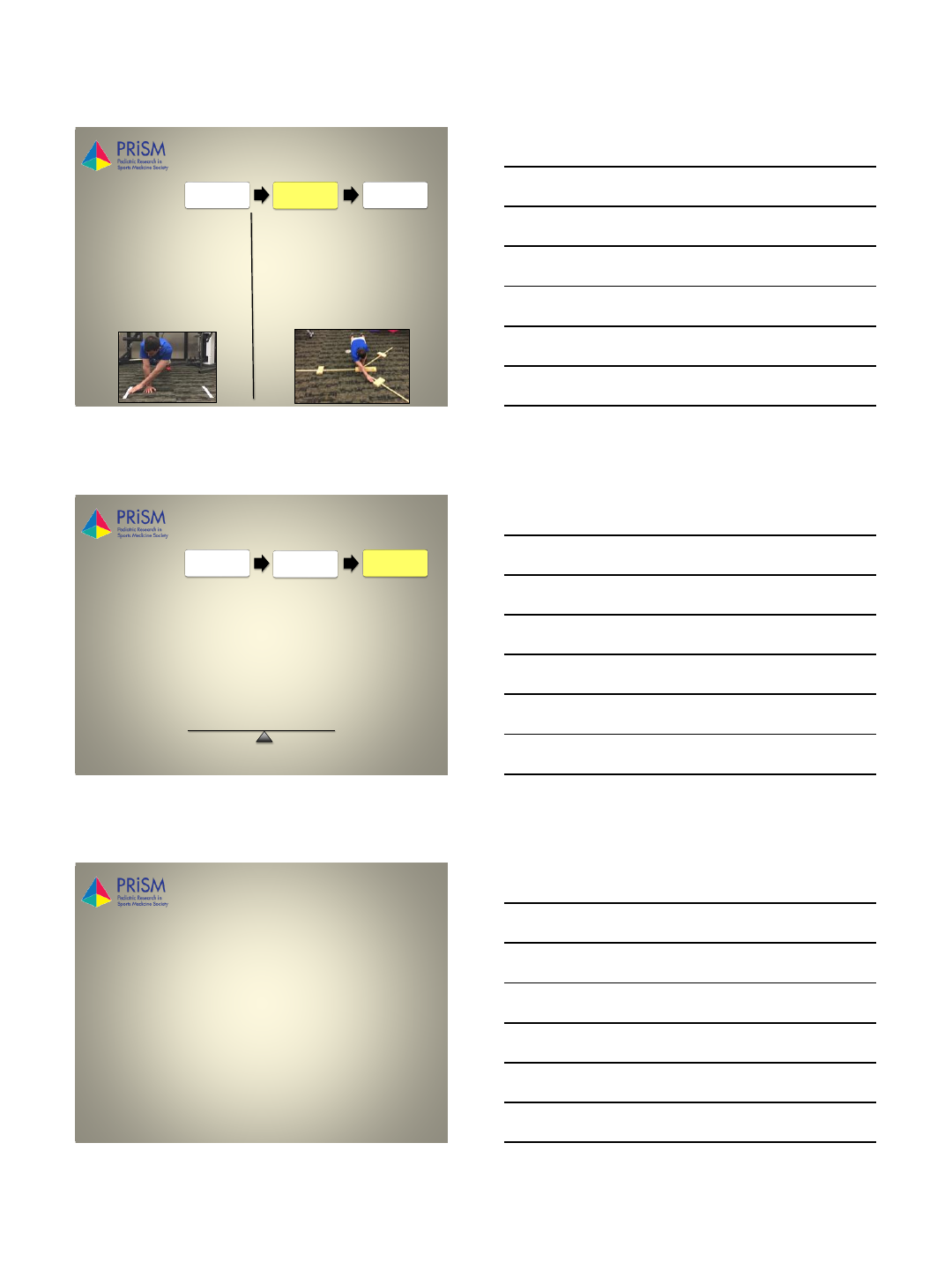
Return to Play
Closed Kinetic Chain Upper
Extremity Stability Test
(CKCUEST)12,13
Upper Quarter Y-Balance
Test (UQ-YBT)12
•Assesses power, speed, and
stability while performing
bilateral, closed chained, upper
extremity movement
•Desired score: minimum of 21
touches, see sport specific norms
•Assesses unilateral stability,
proprioception, and mobility of
thoracic spine, scapula, and upper
extremity
•Desired score: Composite score of
> 80% and < 4 cm reach
difference between extremities
Foundational
Criteria
Advanced
Criteria
Advanced
Criteria Under
Fatigue
www.prismsports.org
Return to Play
•Why re-test while fatigued?
–It’s a better simulation of upper extremity performance
during sport
–Fatigue impacts joint position and sensorimotor system14,15
–Fatigue should show symmetrical decrease in performance
–Asymmetrical decrease may indicate greater compensation
and increased injury risk during play
Foundational
Criteria
Advanced
Criteria
Advanced
Criteria Under
Fatigue
mobility
stability
www.prismsports.org
References
1. Gaunt BW, Shaffer MA, Sauers EL, Michener LA, McCluskey III, GM, Thigpen CA. The American Society of
Shoulder and Elbow Thearpists’ Consensus Rehabilitation Guideline for Arthroscopic Anterior Capsulolabral
Repair of the Shoulder. J Orthop Sports Phys Ther. 2010; 40: 155-168.
2. Milewski MD, Nissen CW. Pediatric and Adolescent Shoulder Instability. Clin Sports Med. 2013; 32: 761-779.
3. Laudner L, Wong R, Onuki T, Lynall R, Meister K. The relationship between clinically measured hip rotational
motion and shoulder biomechanics during the pitching motion. J Sci Med Sport. 2015; 18: 581-584.
4. Shanley E, Rauh MJ, Michener LA, Ellenbecker TS, Garrison JC, Thigpen CA. Shoulder range of motion
measures as risk factors for shoulder and elbow injuries in high school softball and baseball players. Am J
Sports Med. 2011; 39: 2997-2006.
5. Wilk KE, Macrina LC, Fleisig GS, et al. Correlation of glenohumeral internal rotation deficit and total rotational
motion to shoulder injuries in professional baseball players. Am J Sports Med. 2013; 39(2):329-335.
6. Wilk KE, Lacrina LC, Fleisig GS, et al. Deficits in glenohumeral range of motion increase risk of elbow injury in
professional baseball pitchers: A prospective study. Am J Sports Med. 2014; 20: 1-7.
7. Wilk KE, Macrina LC, Fleisig GS, et al. Deficits in glenohumeral passive range of motion increase risk of
shoulder injury in professional baseball pitchers: A prospective study. Am J Sports Med. 2015; 43: 2379-2385.
8. Byram IR, Bushnell BD, Dugger K, Charron K, Harrell FE, Noonan TJ. Preseason shoulder strength
measurements in professional baseball pitchers: Identifying players at risk for injury. Am J Sports Med. 2010;
38: 1375-1382.
2/7/2017
4
www.prismsports.org
References
9. Tyler TF, Mullaney MJ, Mirabella MR, Nicholas SJ, McHugh MP. Risk factors for shoulder and elbow injuries in
high school baseball pitchers: The role of preseason strength and range of motion. Am J Sports Med. 2014;
42: 1993-1999.
10. Cook G, Burton L, Hoogenboom BJ, Voight M. Functional Movement Screening: The Use of Fundamental
Movements as an Assessment of Function –Part 2. Int J Sports Phys Therapy. 2014; 9: 549-563.
11. Negrete RJ, Hanney WJ, Kolber MJ, et al. Reliability, Minimal Detectable Change, and Normative Values for
Test of Upper Extremity Function and Power. J Strength and Cond Res. 2010; 24: 3318-3325.
12. Taylor JB, Wright AA, Smoliga JM, DePew T, Hegedus EJ. Upper extremity physical performance tests in
collegiate athletes. J Sport Rehabil. 2016; 25: 146-154.
13. Pontillo M, Spinelli BA, Sennett BJ. Prediction of In-Season Shoulder Injury From Preseason Testing in Division
I Collegiate Football Players. Sports Health. 2014; 6: 497-503.
14. Tripp BL, Yochem EM, Uhl TL. Functional Fatigue and Upper Extremity Sensorimotor System Acuity in
Baseball Athletes. J Athl Train. 2007; 42: 90-98.
15. Grantham WJ, Byram IR, Meadows MC, Ahmad CS. The Impact of Fatigue on the Kinematics of Collegiate
Baseball Pitchers. Orthop J of Sports Med. 2014; 2: 1-10.
