ACL Imaging Syllabus
2014-02-26
: Pdf Acl Imaging Syllabus ACL_Imaging_Syllabus 2 2014 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 51
- Can flexible Reamers Improve Access to the Femoral Insertion Site ACL Imaging & Reconstruction Webinar 2014 Mark E. Steiner, MD New England Baptist Hospital Boston
- Disclosures
- Failures of ACL Reconstruction
- One vs Two Bundle ACL SB = DB with AM Drilling (not with TT Drilling)
- Biomechanics of Anatomic SB vs DB – Ho, Arthroscopy ‘09
- SB Centered (Anatomic) in ACL Footprint = DB
- Anatomic Transtibial Drilling Tibial or Femoral Tunnels have to be compromised
- Does it Matter if the Tibial or Femoral tunnel is Compromised
- Trying to Find an Anatomic ACL View of the Notch Varies
- Problem with Clock Face Too much variability
- Finding the ACL Footprint Intercondylar and bifurcate Ridges
- Measurements to the ACL Center at 90° flexion
- Flexible Reamers = Reconstruction in 90° Flexion
- AM Aimer at Height of ACL → Point just deep to ACL
- Enlarge Pilot Hole with the Awl
- Aimer Placed Through AM Portal Pin Positioned in Starter Hole
- Guidepin Placement
- Advance Flexible Reamer Over Pin
- Tunnels ≈ 40 mm Length
- Tunnel low at 90° = Tunnel posterior at 20°
- Nitinol Pin Creates a Straight Tunnel
- Interference Screw Fixation with Flexible Screwdriver at 90°
- Biomechanics of Aperture vs Suspensory Fixation
- Anatomic Nonimpinging Graft
- Keep It Anatomic
2/25/2014
1
Anatomy of the ACL
Dr. Freddie H. Fu
Distinguished Service Professor
David Silver Professor and Chairman
Department of Orthopaedic Surgery
University of Pittsburgh
Head Team Physician
University of Pittsburgh Athletic Department
VuMedi Webinar
February 26, 2014
Disclosures
Freddie H. Fu, MD, DSc (Hon), DPs (Hon)
None
University of Pittsburgh Department of
Orthopaedic Surgery
Royalties and Stock Options: None
Consulting Income: None
Research and Educational Support: Smith & Nephew
Other Support: Department of Orthopaedic Surgery of the University of Pittsburgh
receives funding from Arthrocare, Synthes, Stryker, Johnson & Johnson,
DePuy, DonJoy, Breg, Omeros, Biomet, Mitek
“Whenever you are having anatomy
sessions, pay particular attention,
because orthopaedics is all anatomy,
plus a little bit of common sense.”
Anatomy is the Basis of
Orthopaedic Surgery
J. Hughston
Fracture Fixation
2/25/2014
2
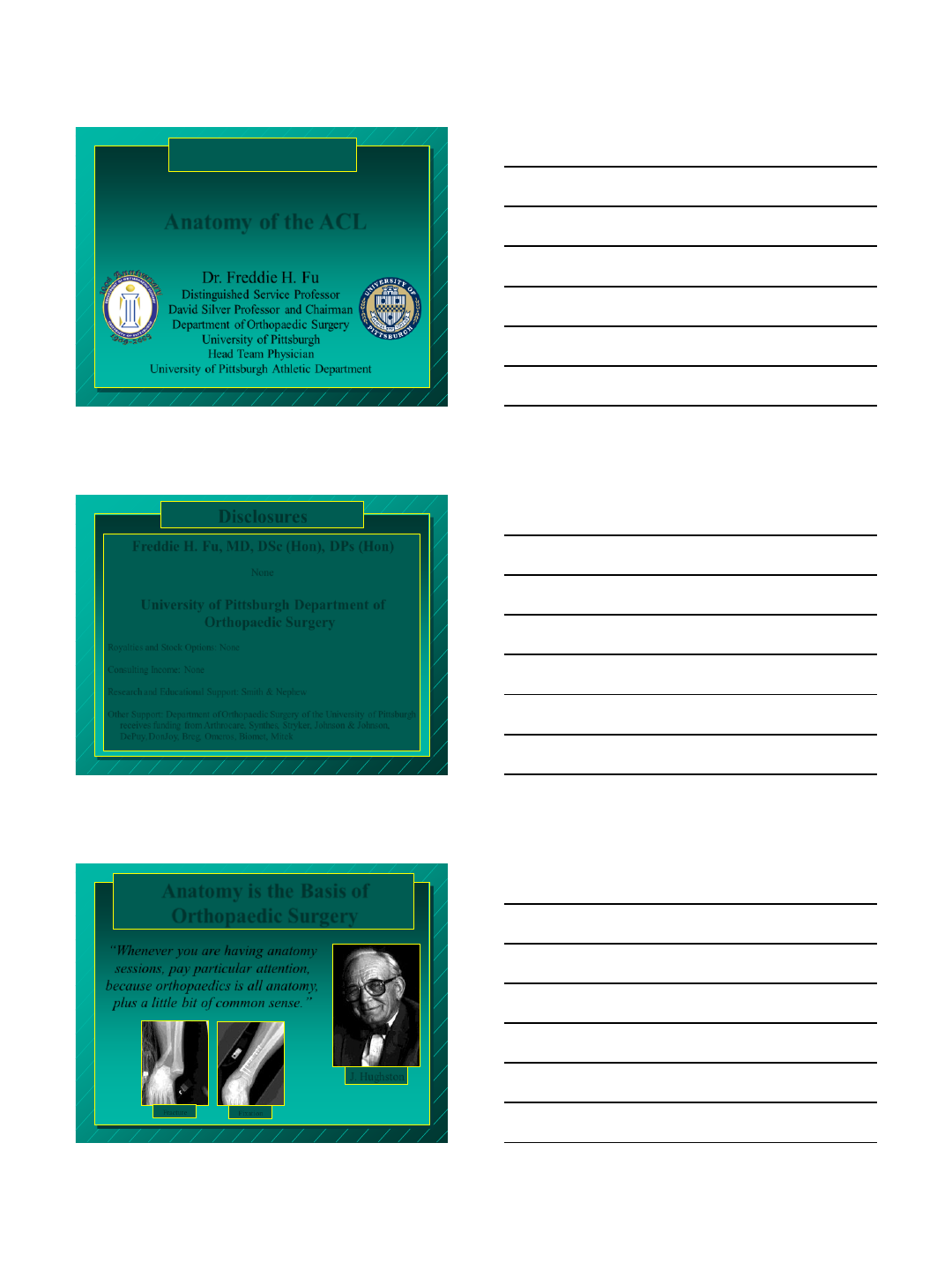
Anatomy of the ACL
Fetus
AM PL
microscopic
view
AM PL
AM PL
LFC
AM PL
LFC
AM
PL
Human Arthroscopic
AM
PL
Casagranda, Towers, Fu, et al, Am J Roent 2009
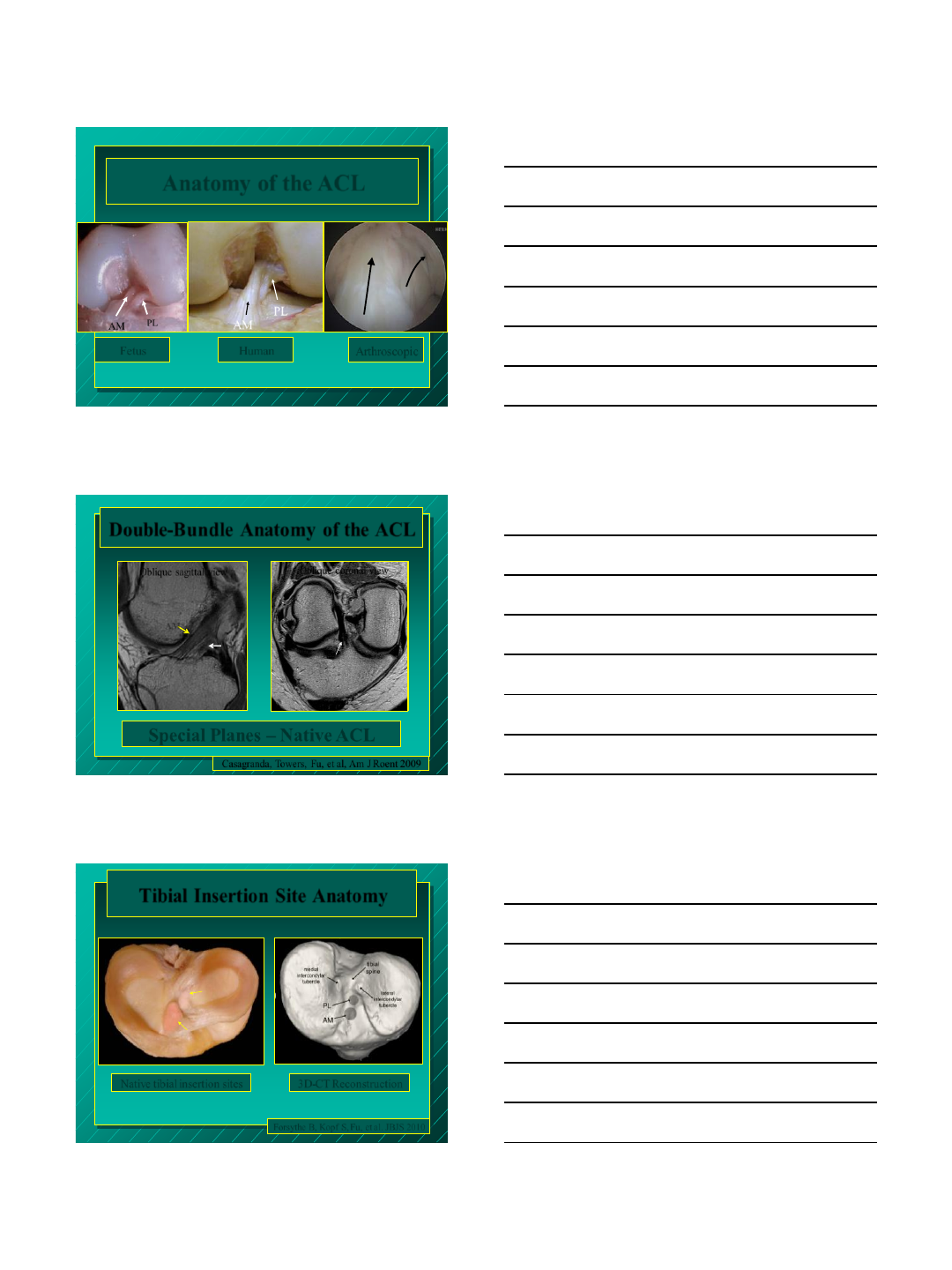
Special Planes – Native ACL
Oblique sagittal view
Double-Bundle Anatomy of the ACL
Oblique coronal view
AM
Oblique coronal view
PL
PL
AM
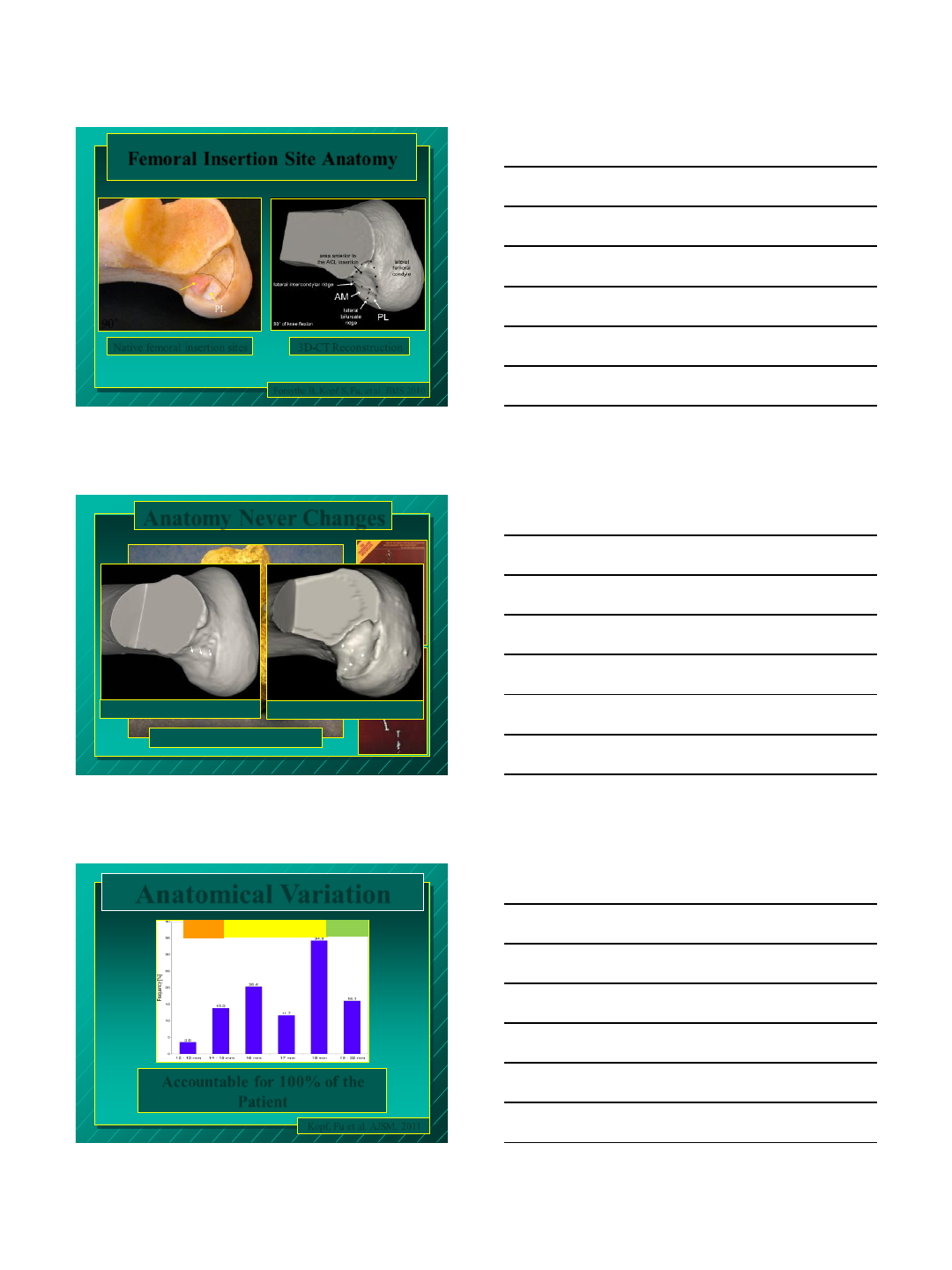
Tibial Insertion Site Anatomy
Native tibial insertion sites 3D-CT Reconstruction
Forsythe B, Kopf S, Fu, et al. JBJS 2010
2/25/2014
3
PL
AM
90°
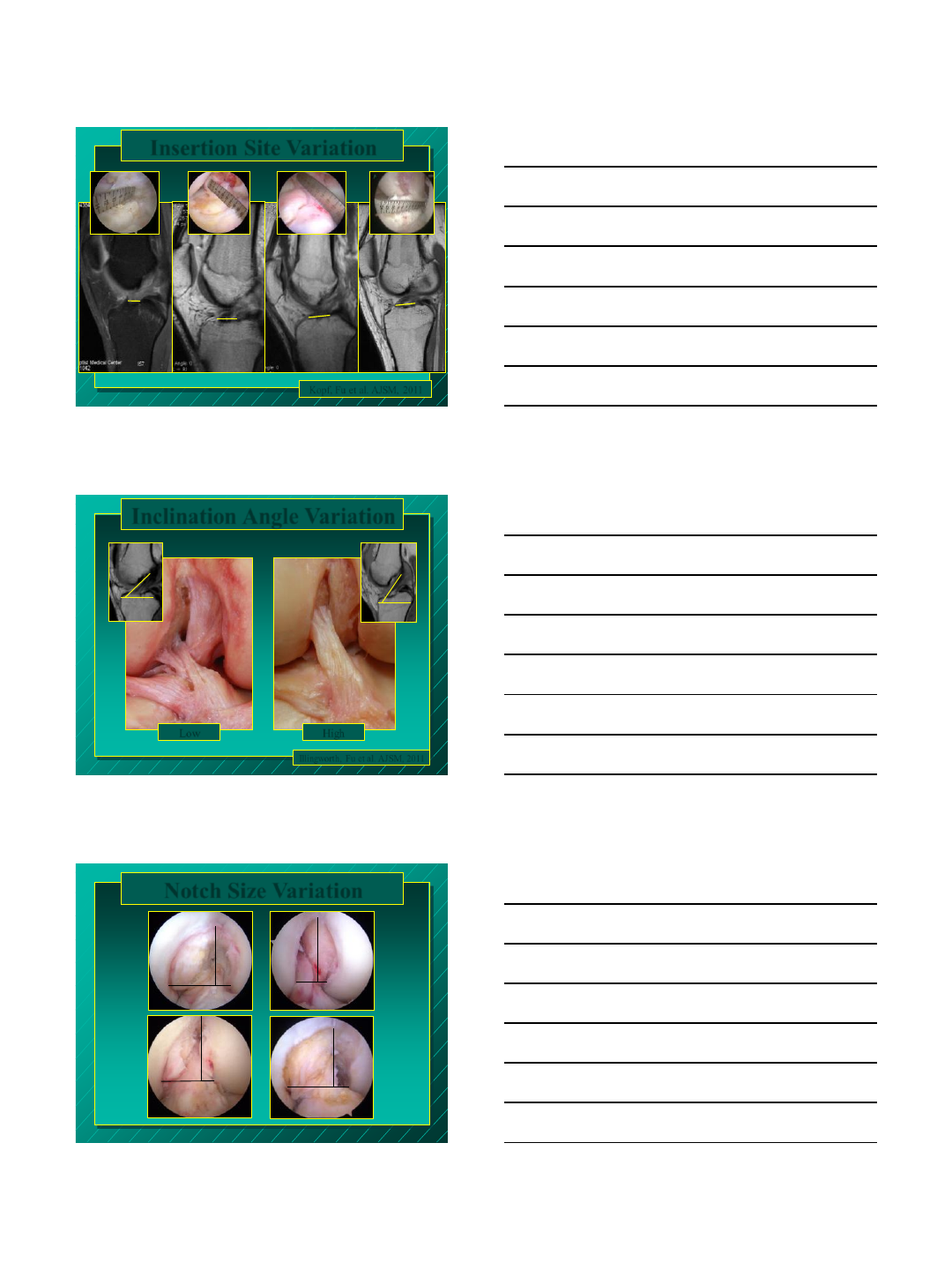
Femoral Insertion Site Anatomy
Forsythe B, Kopf S, Fu, et al. JBJS 2010
Native femoral insertion sites 3D-CT Reconstruction
Lucy (3.2 Million years old) Modern Human
Lucy (3.2 Million years old)
Anatomy Never Changes
Anatomical Variation
14-18 SB or DB
<14 SB >18 DB
Kopf, Fu et al. AJSM, 2011
Accountable for 100% of the
Patient
2/25/2014
4
13 mm 24 mm
Insertion Site Variation
Kopf, Fu et al. AJSM, 2011
20 mm
16 mm
Illingworth, Fu et al. AJSM, 2011
Inclination Angle Variation
Low
43°
High
55°
Notch Size Variation
24 mm
16 mm
10 mm
22 mm
14 mm
20 mm
22 mm
11 mm
2/25/2014
5
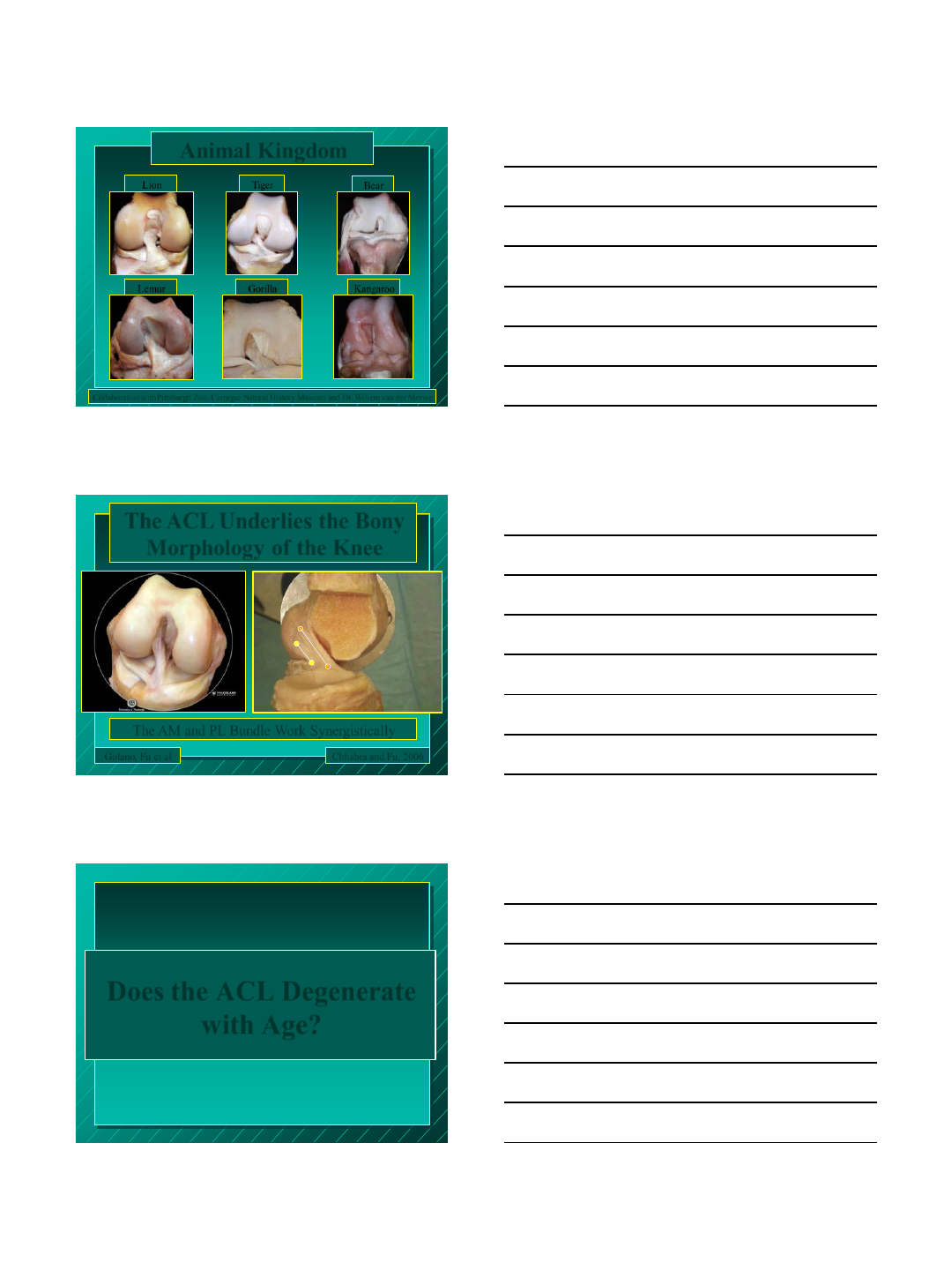
Lemur Kangaroo
Bear
Tiger
Gorilla
Animal Kingdom
Collaboration with Pittsburgh Zoo, Carnegie Natural History Museum and Dr. Willem van der Merwe
Lion
The ACL Underlies the Bony
Morphology of the Knee
AM
PL
Chhabra and Fu, 2006 Golano, Fu et al
The AM and PL Bundle Work Synergistically
Does the ACL Degenerate
with Age?
2/25/2014
6
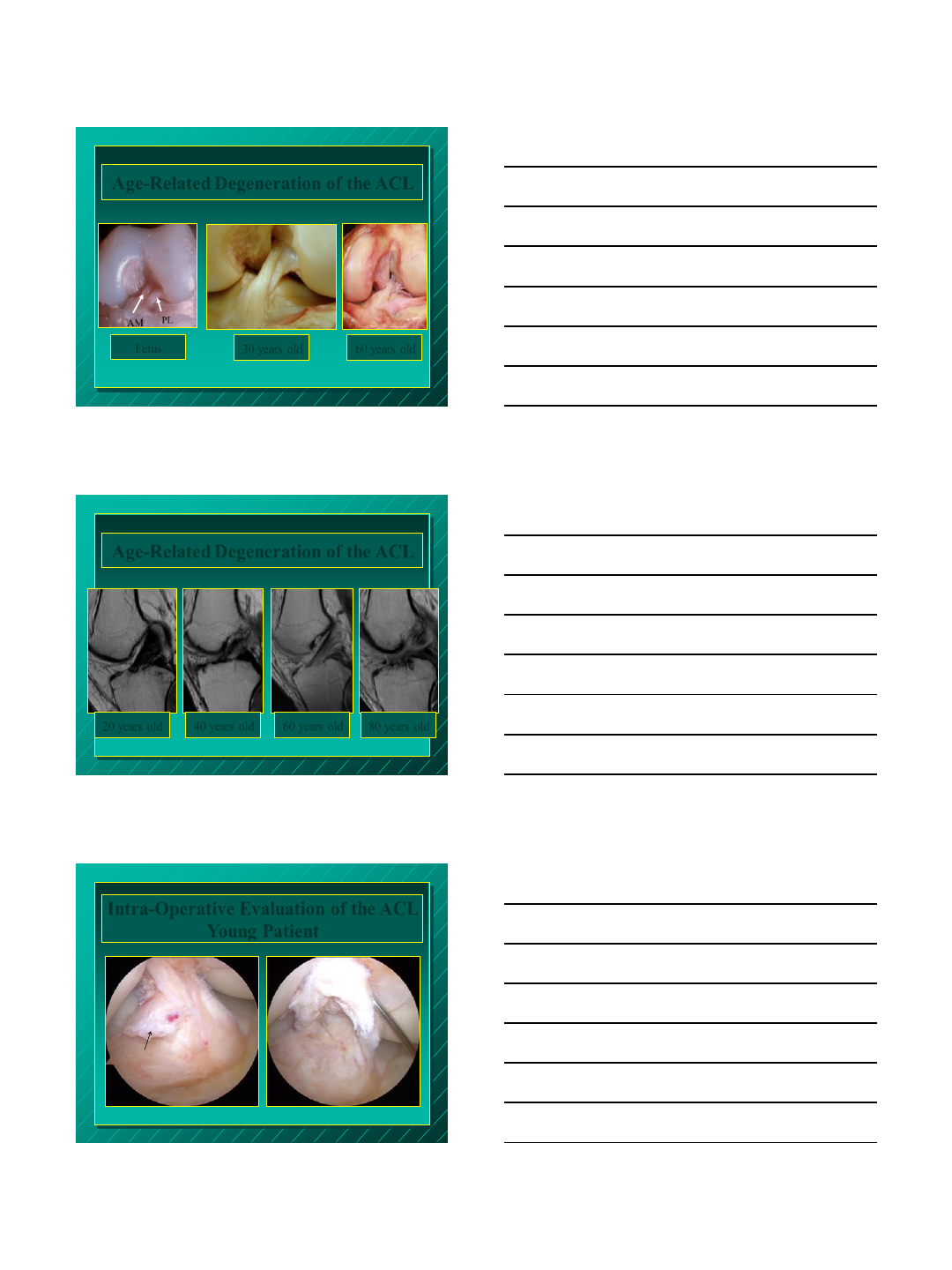
Age-Related Degeneration of the ACL
Fetus 60 years old
AM PL
microscopic
view
30 years old
Age-Related Degeneration of the ACL
20 years old 40 years old 60 years old 80 years old
Intra-Operative Evaluation of the ACL
Young Patient
PL
AM
AM
PL
2/25/2014
7
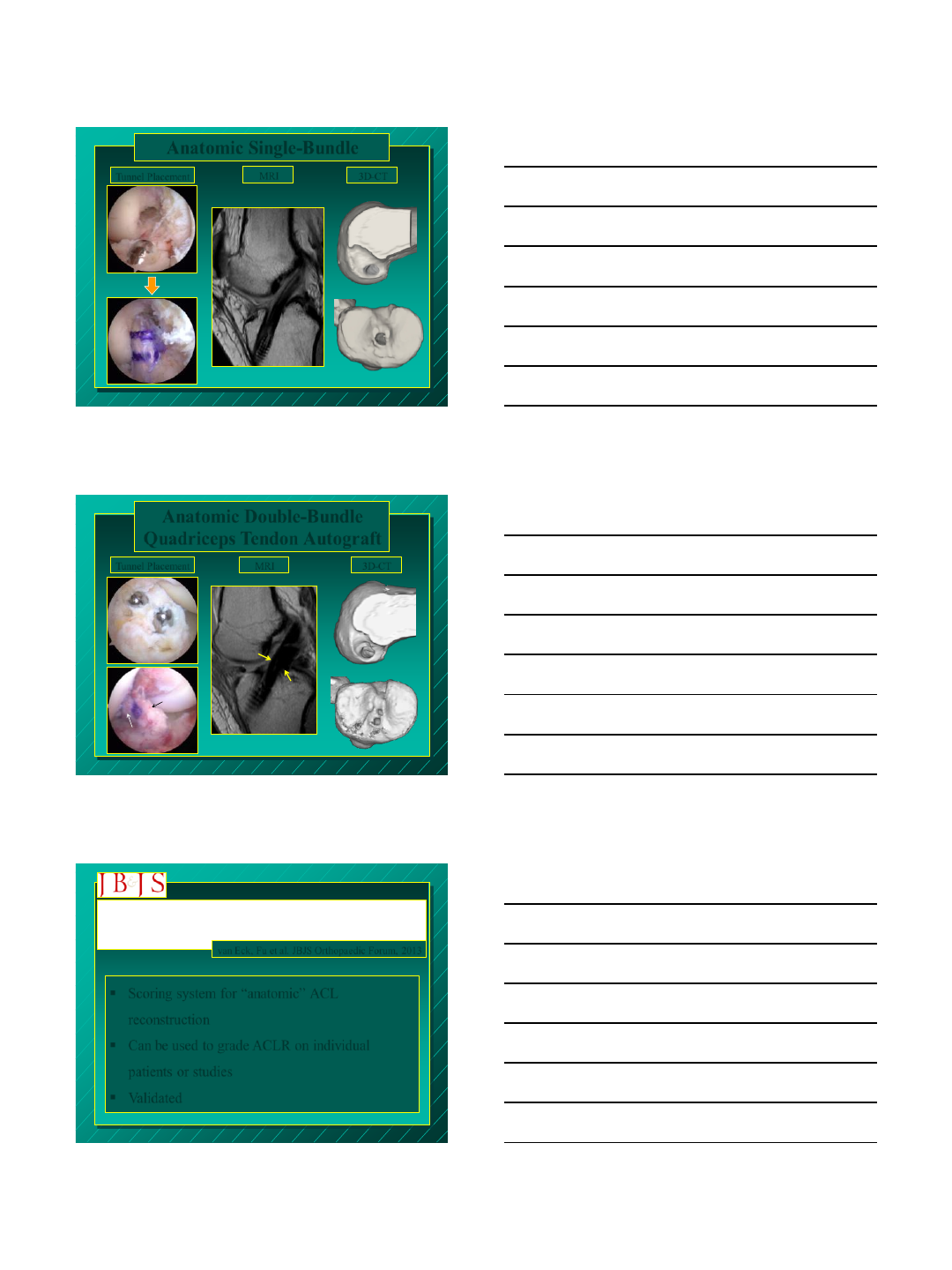
Anatomic Single-Bundle
MRI
Tunnel Placement 3D-CT
68%
63%
Anatomic Double-Bundle
Quadriceps Tendon Autograft
MRI Tunnel Placement 3D-CT
AM
PL
AM
PL
63%
55%
Evidence to Support the Interpretation and Use of the
Anatomic Anterior Cruciate Ligament Reconstruction
Checklist van Eck, Fu et al. JBJS Orthopaedic Forum, 2013
Scoring system for “anatomic” ACL
reconstruction
Can be used to grade ACLR on individual
patients or studies
Validated
2/25/2014
8
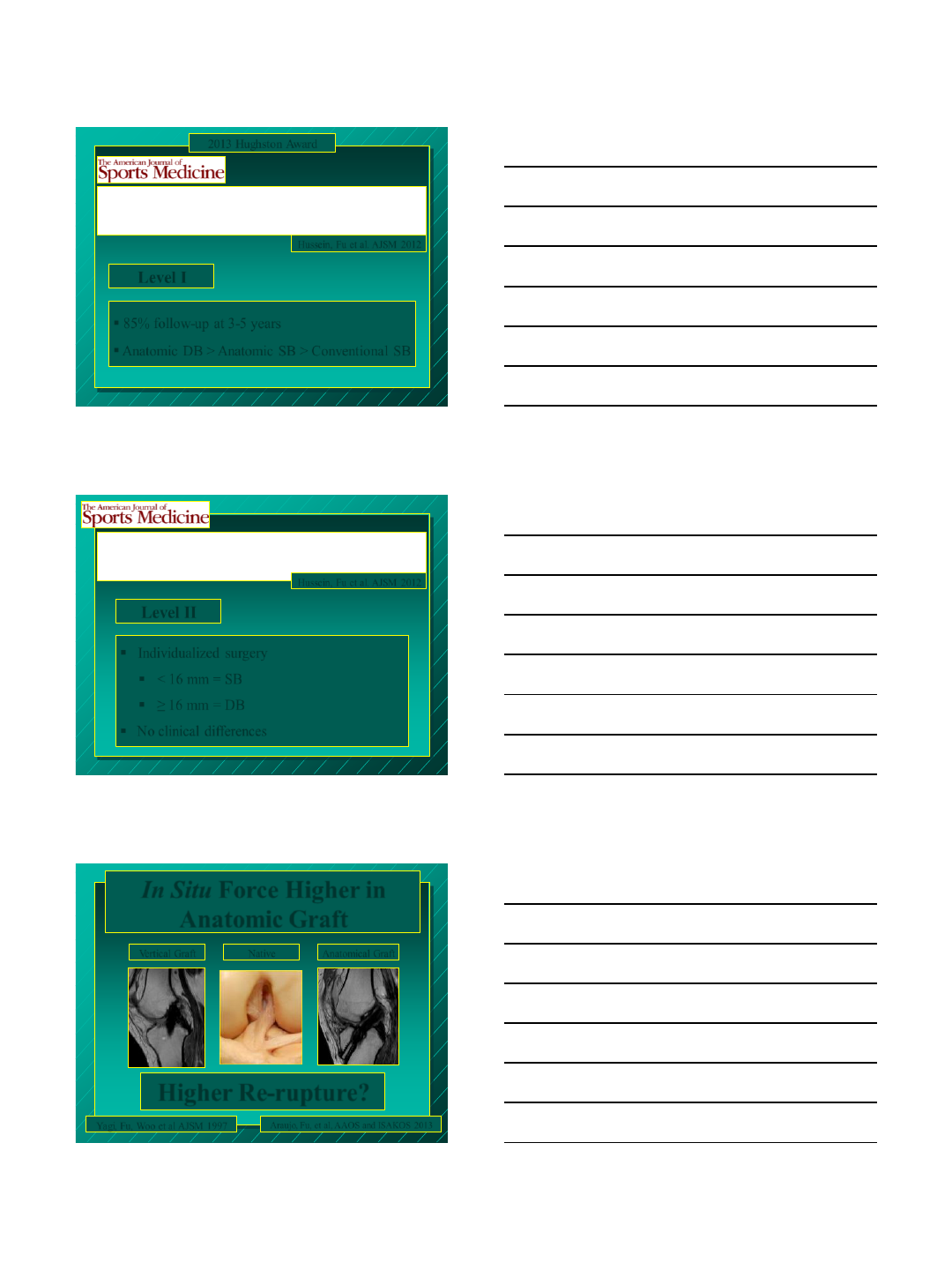
Level I
Prospective randomized Clinical Evaluation of Conventional
Single-Bundle, Anatomic Single-Bundle, and Anatomic
Double-Bundle Anterior Cruciate Ligament Reconstruction
Hussein, Fu et al. AJSM 2012
85% follow-up at 3-5 years
Anatomic DB > Anatomic SB > Conventional SB
2013 Hughston Award
Individualized Anterior Cruciate Ligament Surgery: A
Prospective Study Comparing Anatomic Single- and Double-
Bundle Reconstruction. Hussein, Fu et al. AJSM 2012
Level II
Individualized surgery
< 16 mm = SB
≥ 16 mm = DB
No clinical differences
In Situ Force Higher in
Anatomic Graft
Araujo, Fu, et al, AAOS and ISAKOS 2013
Anatomical Graft Vertical Graft Native
Higher Re-rupture?
Yagi, Fu, Woo et al AJSM 1997
2/25/2014
9
Transtibial ACL Femoral Tunnel Preparation
Increases Odds of Repeat Ipsilateral Knee Surgery
Duffee, MOON Group, Kaeding et al JBJS 2013
Repeat Ipsilateral Knee Surgery
2.5x higher with TT drilling than
AM drilling
Anatomic ACL Reconstruction
Rehabilitation Should Be
Modified Accordingly
Return to Sports
Functional Testing Healing?
3 months
6 months
Time zero
1 year
2/25/2014
10
See the Big Picture!
Anatomy Biology
Proprioception Rehabilitation
Biomechanics Kinematics
Thank You!
University of Pittsburgh
Cathedral of Learning
2/24/2014
1
This speaker receives
royalties from
Smith and Nephew
Medial Portal
For
ACL Reconstruction
William G. Clancy, Jr., MD, PhD (Hon)
Medial Portal
Very
distinct advantages
over a
lateral portal
2/24/2014
2
Medial Portal
Why?
Medial Portal
1. More obliquity of the approach angle to
the LFC
2. Less flexion needed
3. Better visualization of the Bifuricate
Ridge and posterior edge of the LFC
4. Seldom need to perform a notchplasty
5. More accurate tibial tunnel
Medial Portal
To achieve these benefits
need to create
a superior medial portal
for
arthroscopic visualization
2/24/2014
3
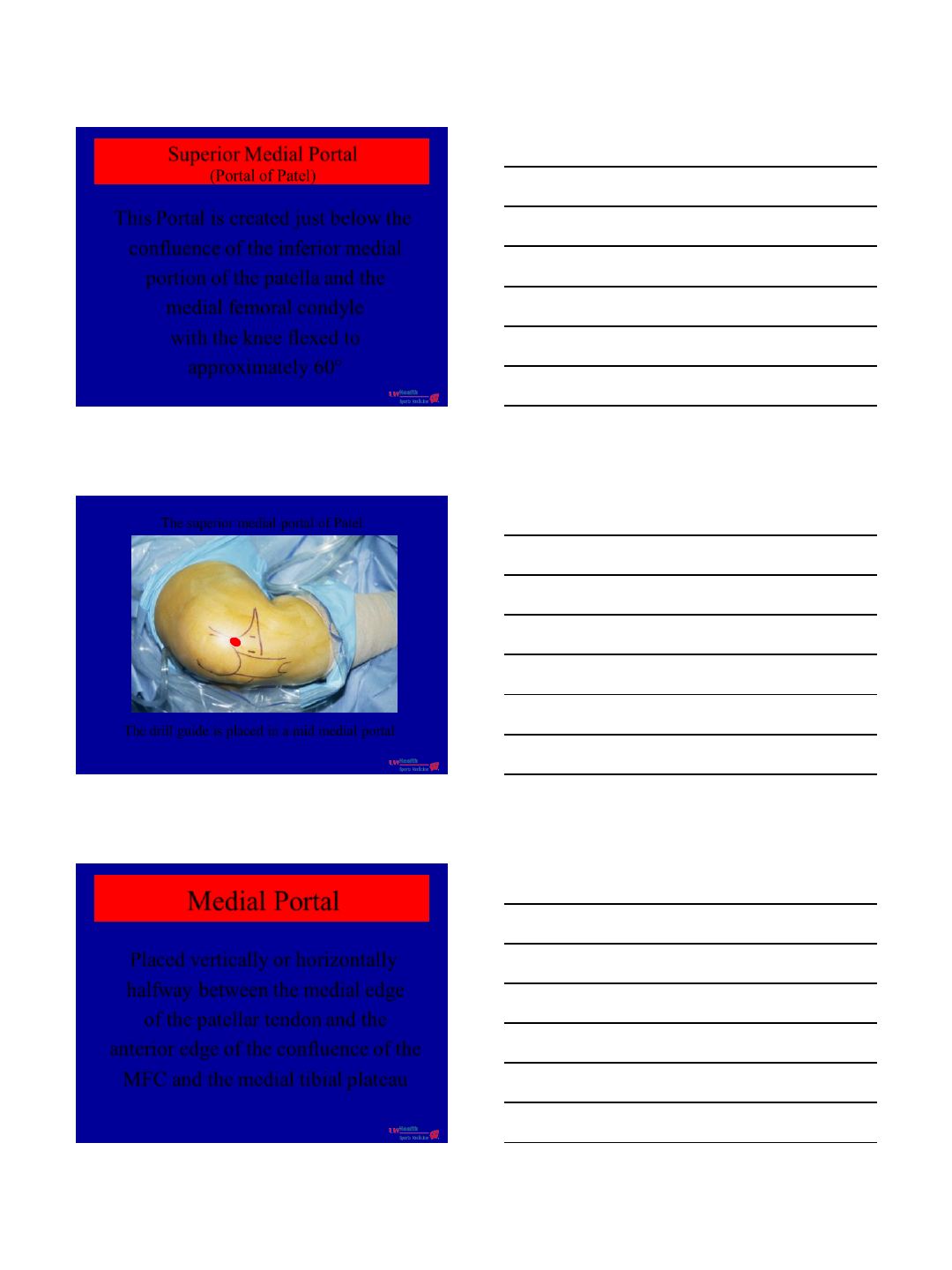
Superior Medial Portal
(Portal of Patel)
This Portal is created just below the
confluence of the inferior medial
portion of the patella and the
medial femoral condyle
with the knee flexed to
approximately 60°
The superior medial portal of Patel
The drill guide is placed in a mid medial portal
Medial Portal
Placed vertically or horizontally
halfway between the medial edge
of the patellar tendon and the
anterior edge of the confluence of the
MFC and the medial tibial plateau
2/24/2014
4
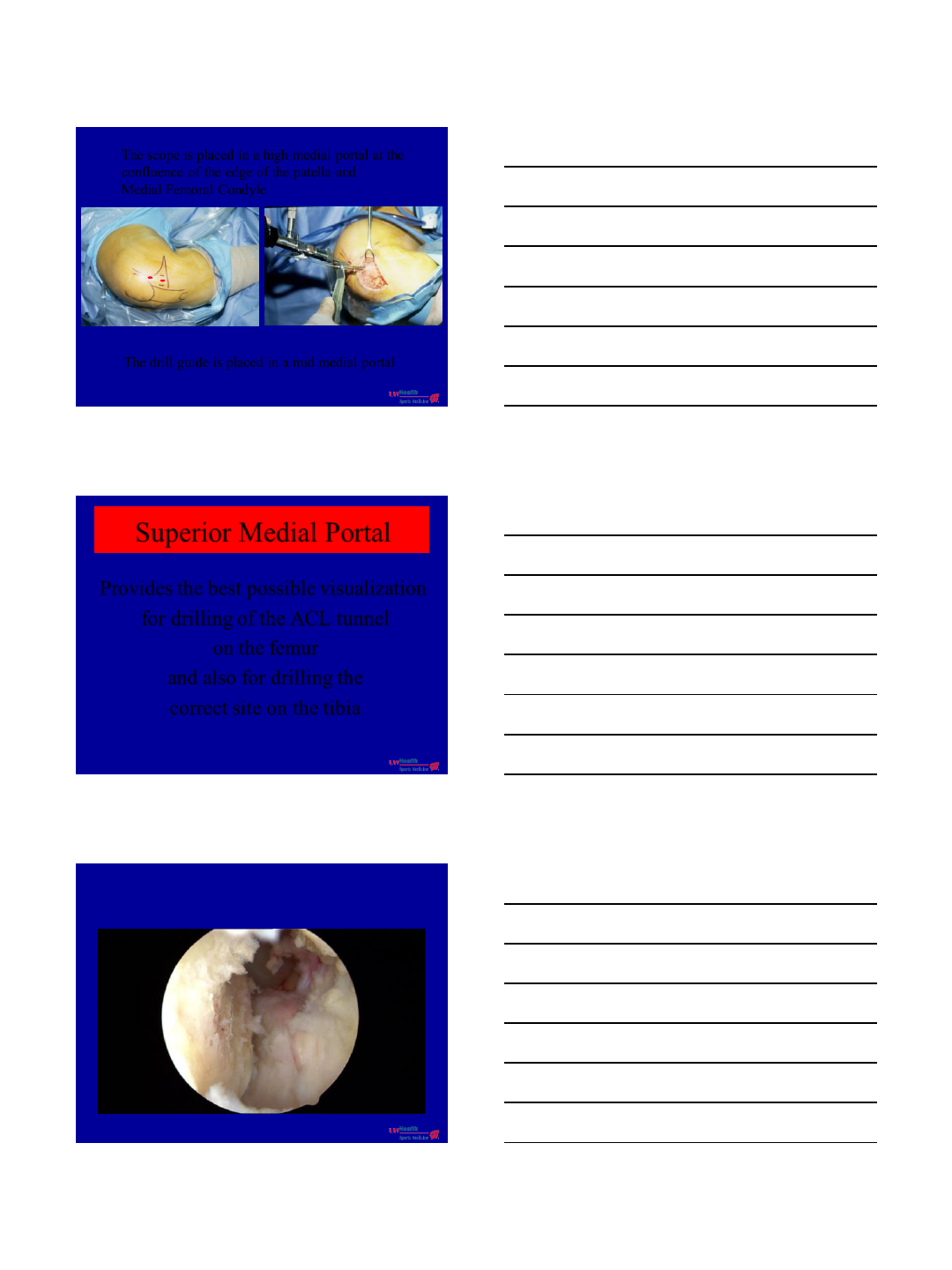
The scope is placed in a high medial portal at the
confluence of the edge of the patella and
Medial Femoral Condyle
The drill guide is placed in a mid medial portal
Superior Medial Portal
Provides the best possible visualization
for drilling of the ACL tunnel
on the femur
and also for drilling the
correct site on the tibia
2/24/2014
5
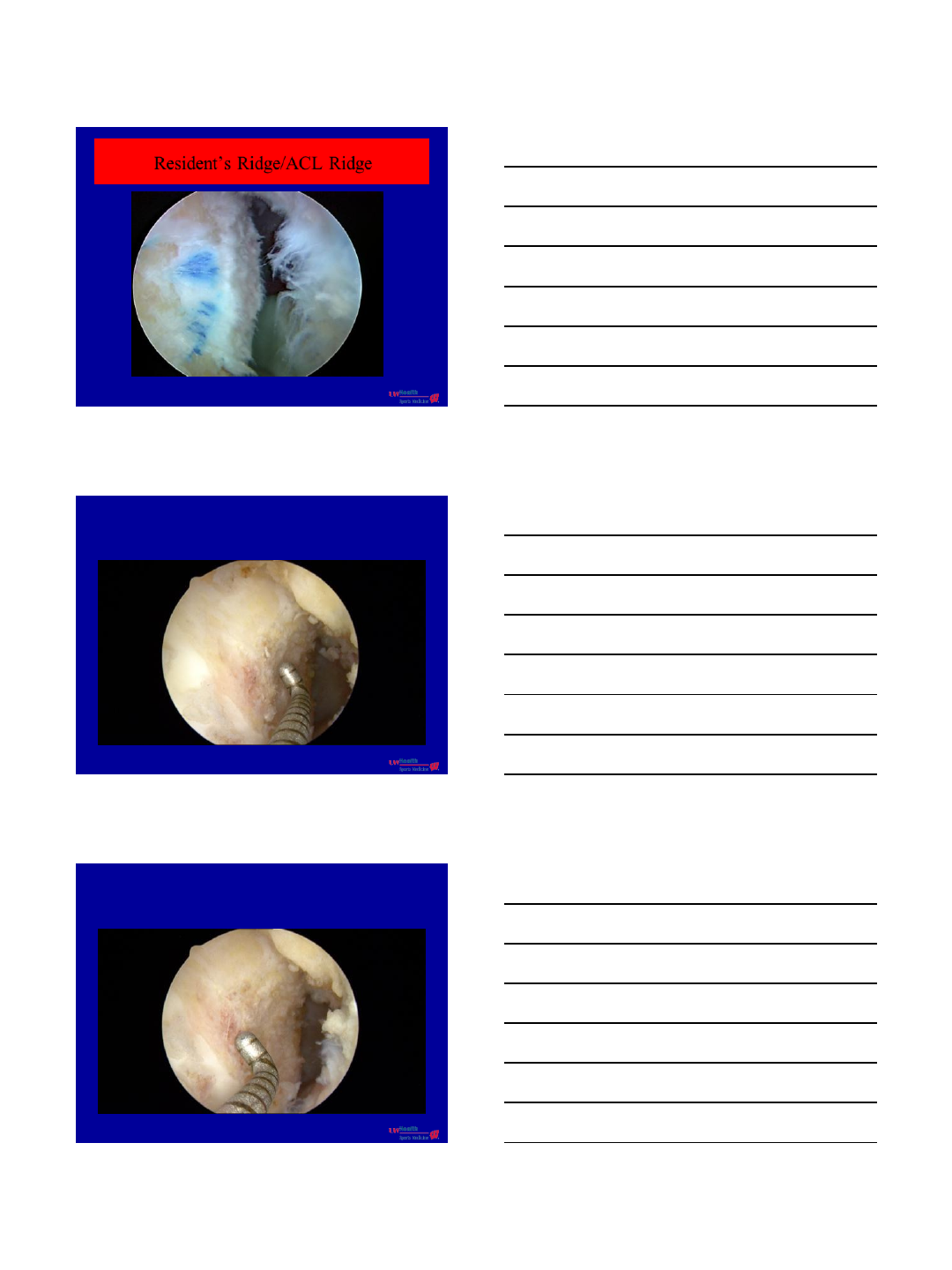
Resident’s Ridge/ACL Ridge
2/24/2014
6
2/24/2014
7
Superior Medial Portal
The distance between the
arthroscope placed through
a lateral or medial portal for
visualizing tibial k-wire placement
is extremely short making it difficult
for accurate k-wire placement
2/24/2014
8
Superior Medial Portal
Evaluating many x-rays and MRI
on ACL reconstructions,
I find that in greater than 75%
of these the tibial tunnel is
placed too far posterior
Normal ACL Transtibial ACL
2/24/2014
9
Superior Medial Portal
The posterior wall of the
tibial tunnel should
abut the base of the tibial spine
and should not enter it
2/24/2014
10
Superior Medial Portal
This portal allows for an
axial or downward view
of the tibial spine and both the
medial and lateral tubercles and
allows for a more correct tibial tunnel
2/24/2014
11
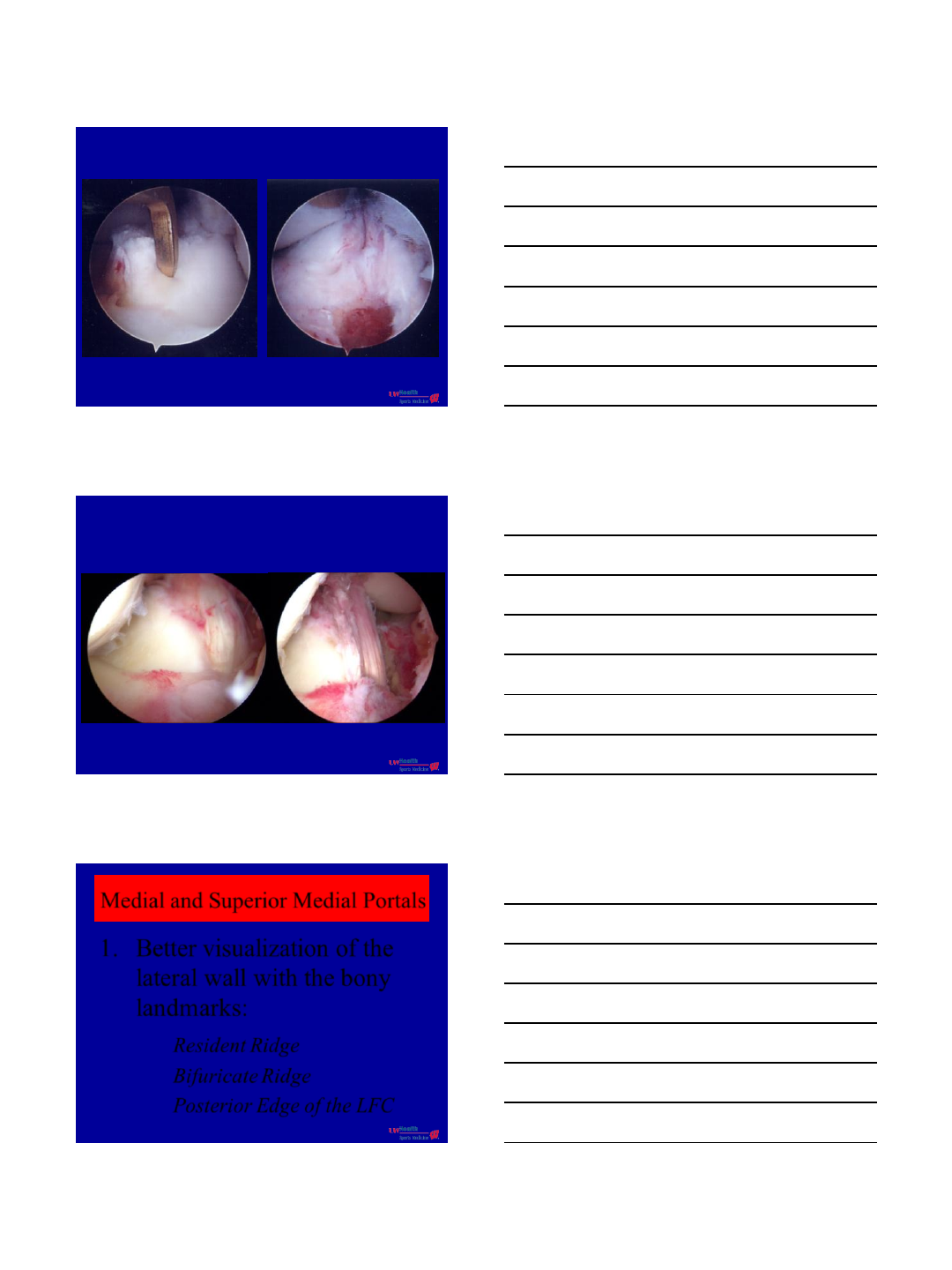
Medial and Superior Medial Portals
1. Better visualization of the
lateral wall with the bony
landmarks:
Resident Ridge
Bifuricate Ridge
Posterior Edge of the LFC
2/24/2014
12
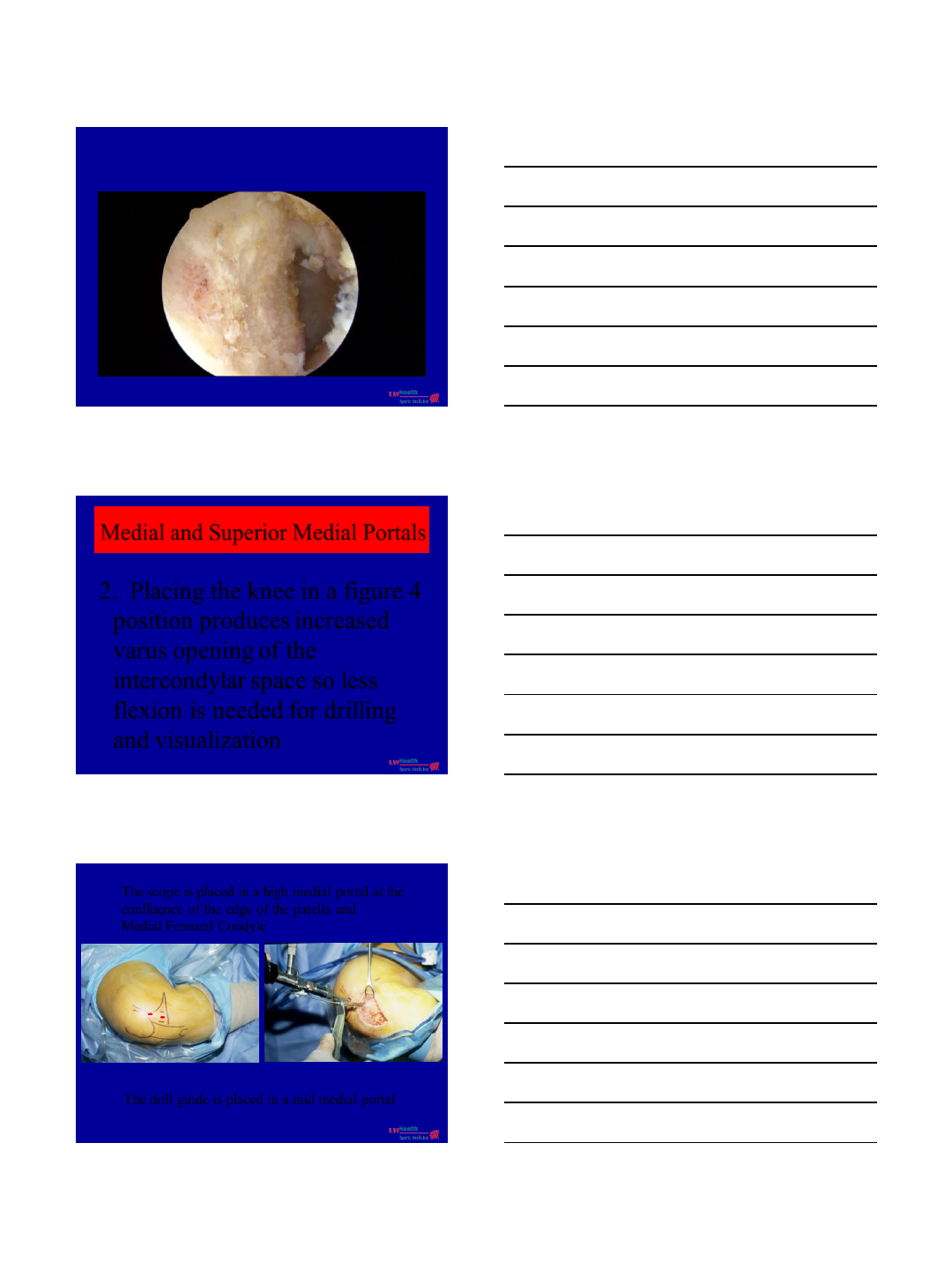
Medial and Superior Medial Portals
2. Placing the knee in a figure 4
position produces increased
varus opening of the
intercondylar space so less
flexion is needed for drilling
and visualization
The scope is placed in a high medial portal at the
confluence of the edge of the patella and
Medial Femoral Condyle
The drill guide is placed in a mid medial portal
2/24/2014
13
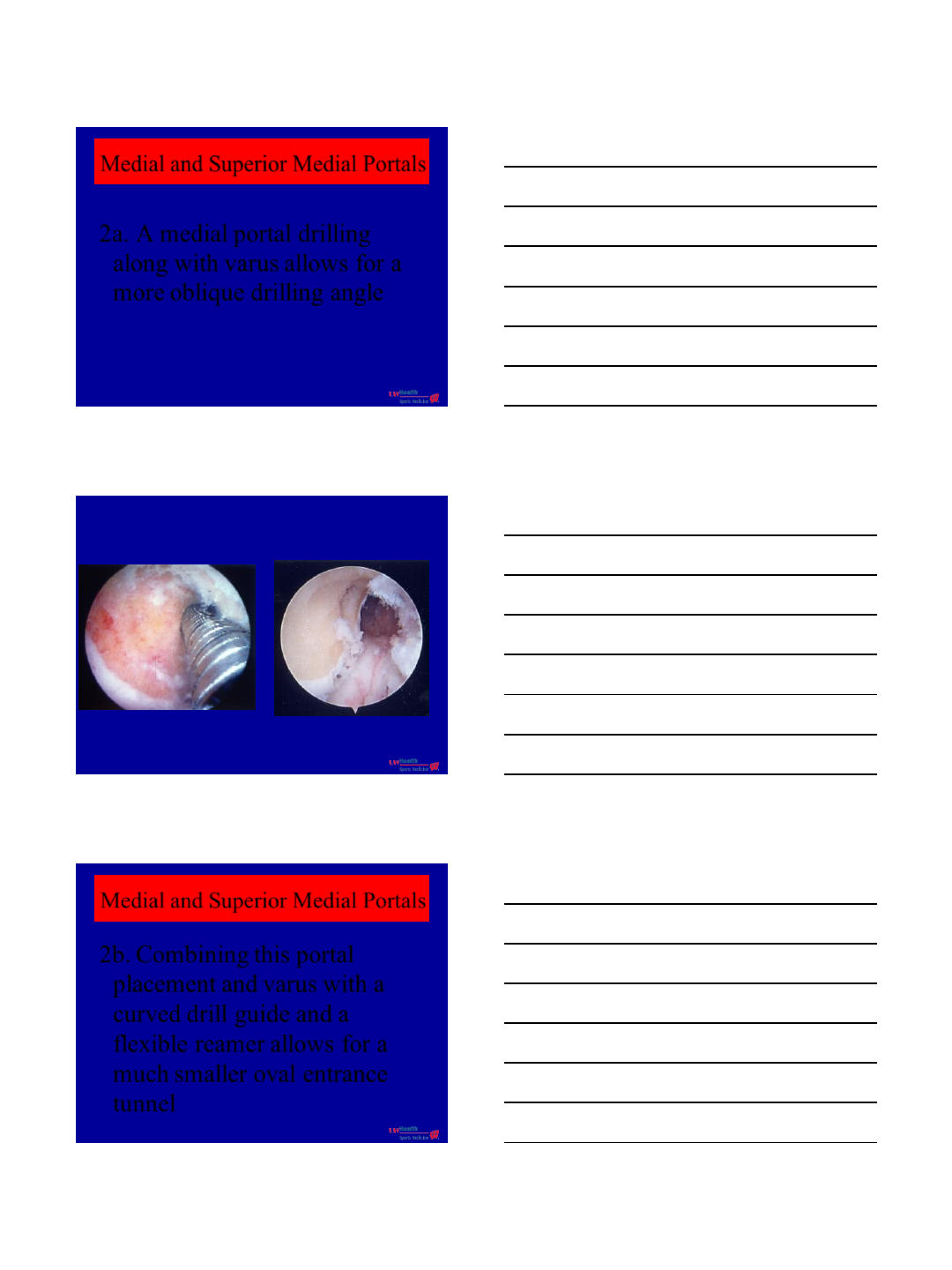
Medial and Superior Medial Portals
2a. A medial portal drilling
along with varus allows for a
more oblique drilling angle
Medial and Superior Medial Portals
2b. Combining this portal
placement and varus with a
curved drill guide and a
flexible reamer allows for a
much smaller oval entrance
tunnel
2/24/2014
14
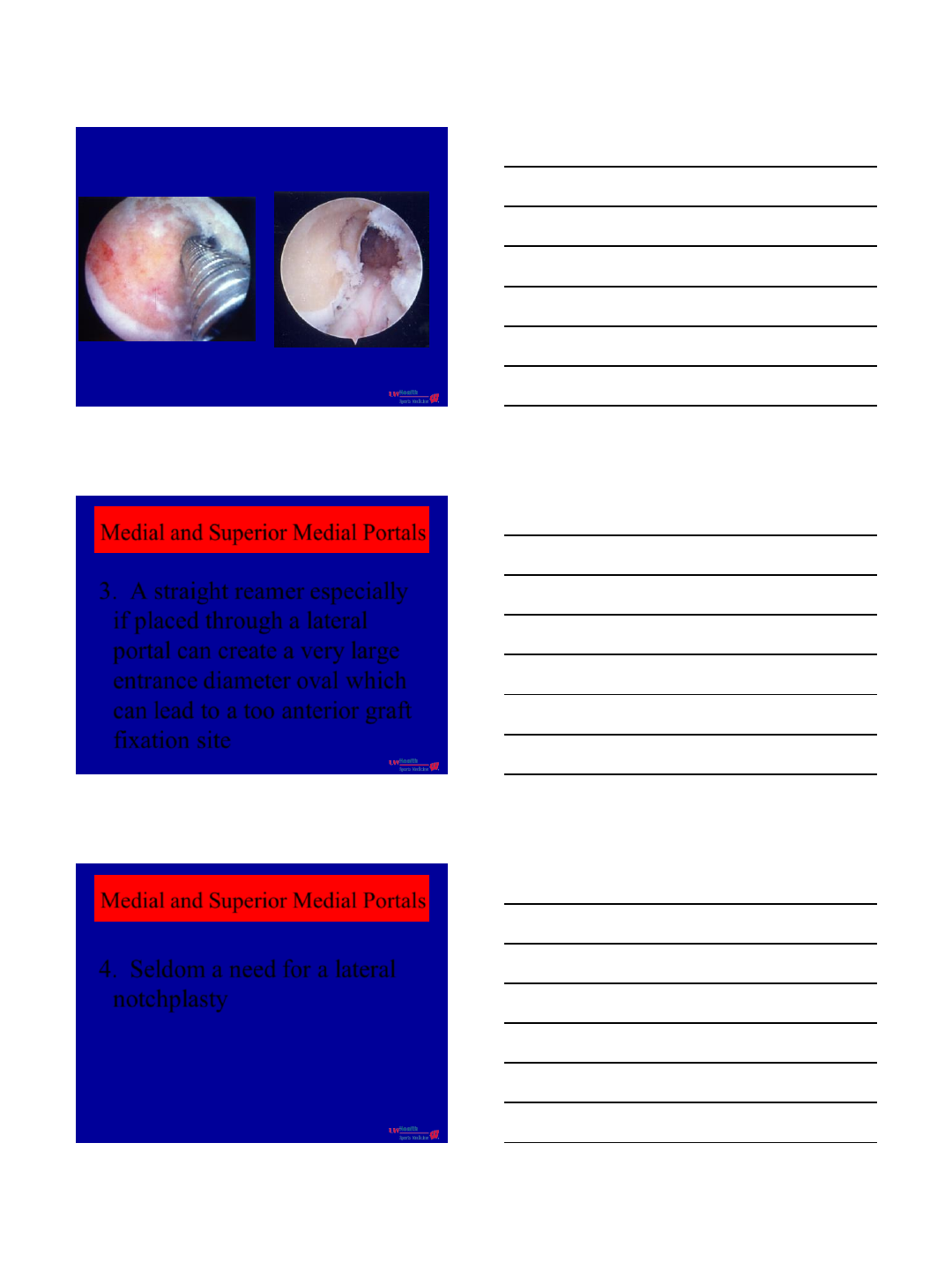
Medial and Superior Medial Portals
3. A straight reamer especially
if placed through a lateral
portal can create a very large
entrance diameter oval which
can lead to a too anterior graft
fixation site
Medial and Superior Medial Portals
4. Seldom a need for a lateral
notchplasty
2/24/2014
15
Lateral Wall Notchplasty
If too much bone is
taken away from the LFC
then containment for
side to side sheer is lost
Lateral Wall Notchplasty
Lateral to medial sheer
has been shown to increase poly wear
in total knees and the loss of
containment by a large notchplasty
could lead to increased
cartilage surface wear
2/24/2014
16
Notchplasty
Too much notchplasty at the
femoral insertional area will
place the graft too lateral
Small Intercondylar Notch
One technique does not fit all!
Even a flexible reamer system in a
narrowed notch or small knee
cannot always achieve
correct tunnel placement.
A rear entry system should be utilized for
correct placement.
University of Wisconsin
Thank You
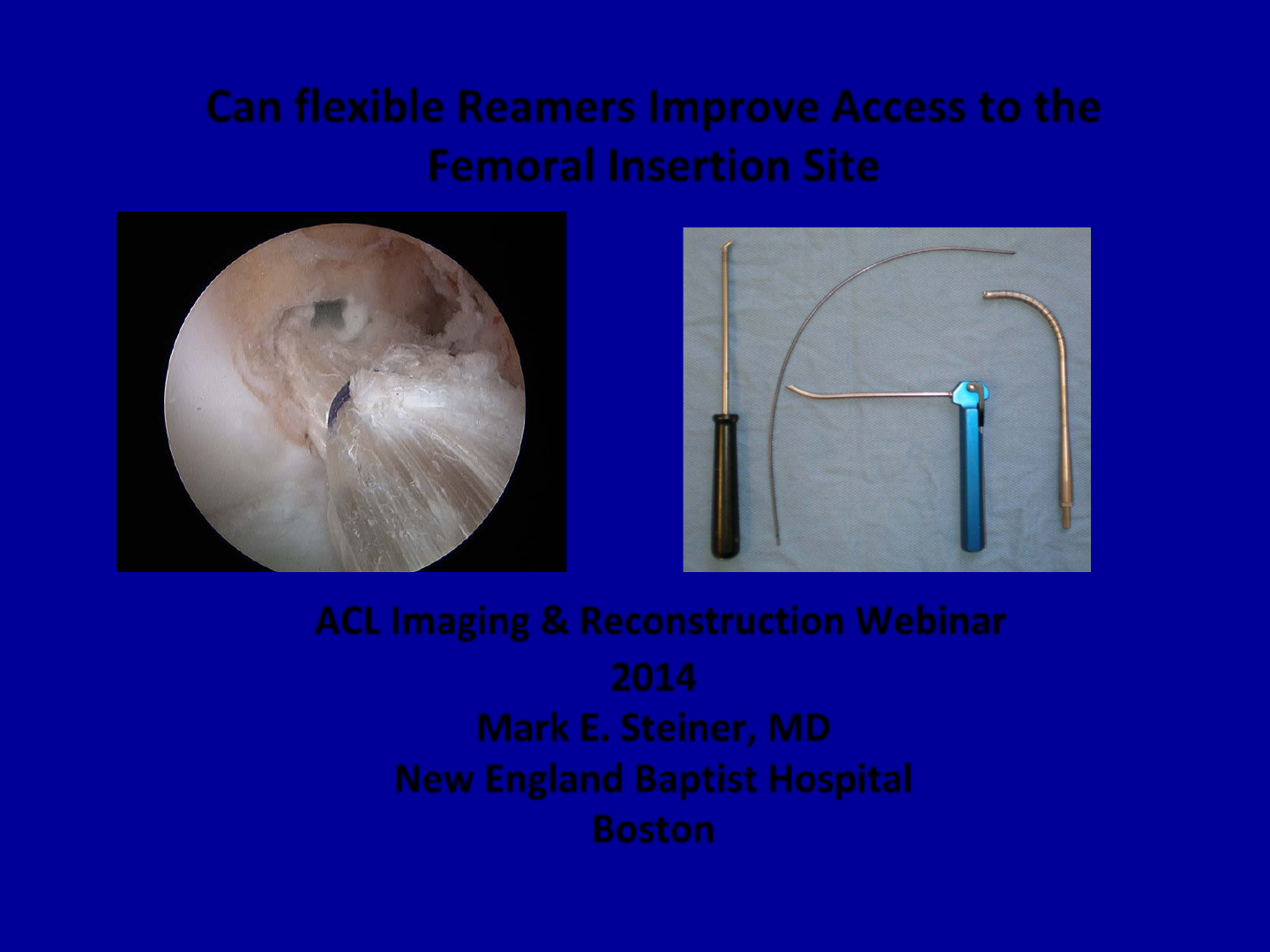
Can flexible Reamers Improve Access to the
Femoral Insertion Site
ACL Imaging & Reconstruction Webinar
2014
Mark E. Steiner, MD
New England Baptist Hospital
Boston
Disclosures
•Consulting and Royalties Stryker
•Fellowship Support Arthrex
Don Joy
Mitek
Smith & Nephew
Con Med
•Research Support Don Joy
Stryker
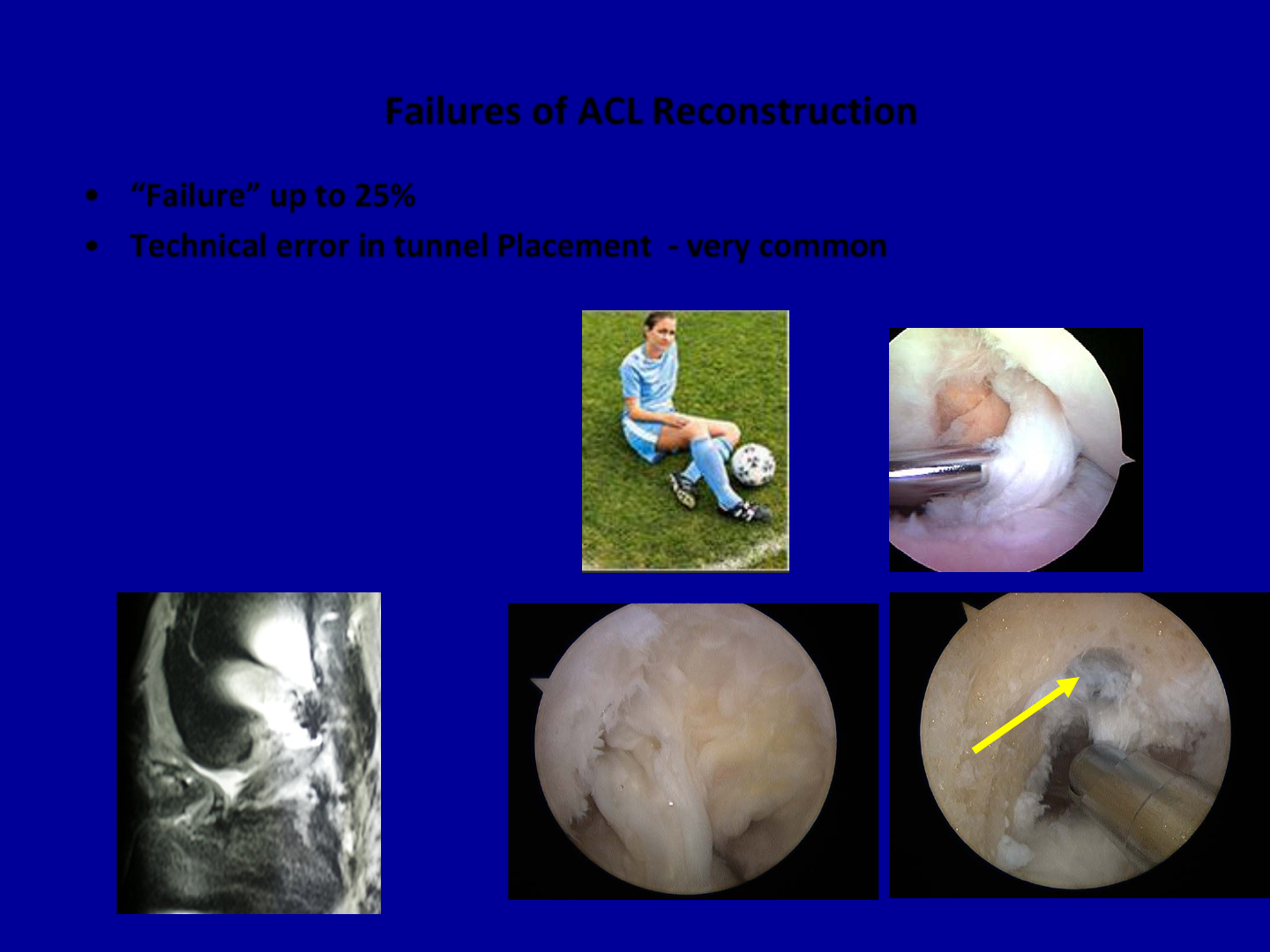
Failures of ACL Reconstruction
•“Failure” up to 25%
•Technical error in tunnel Placement - very common
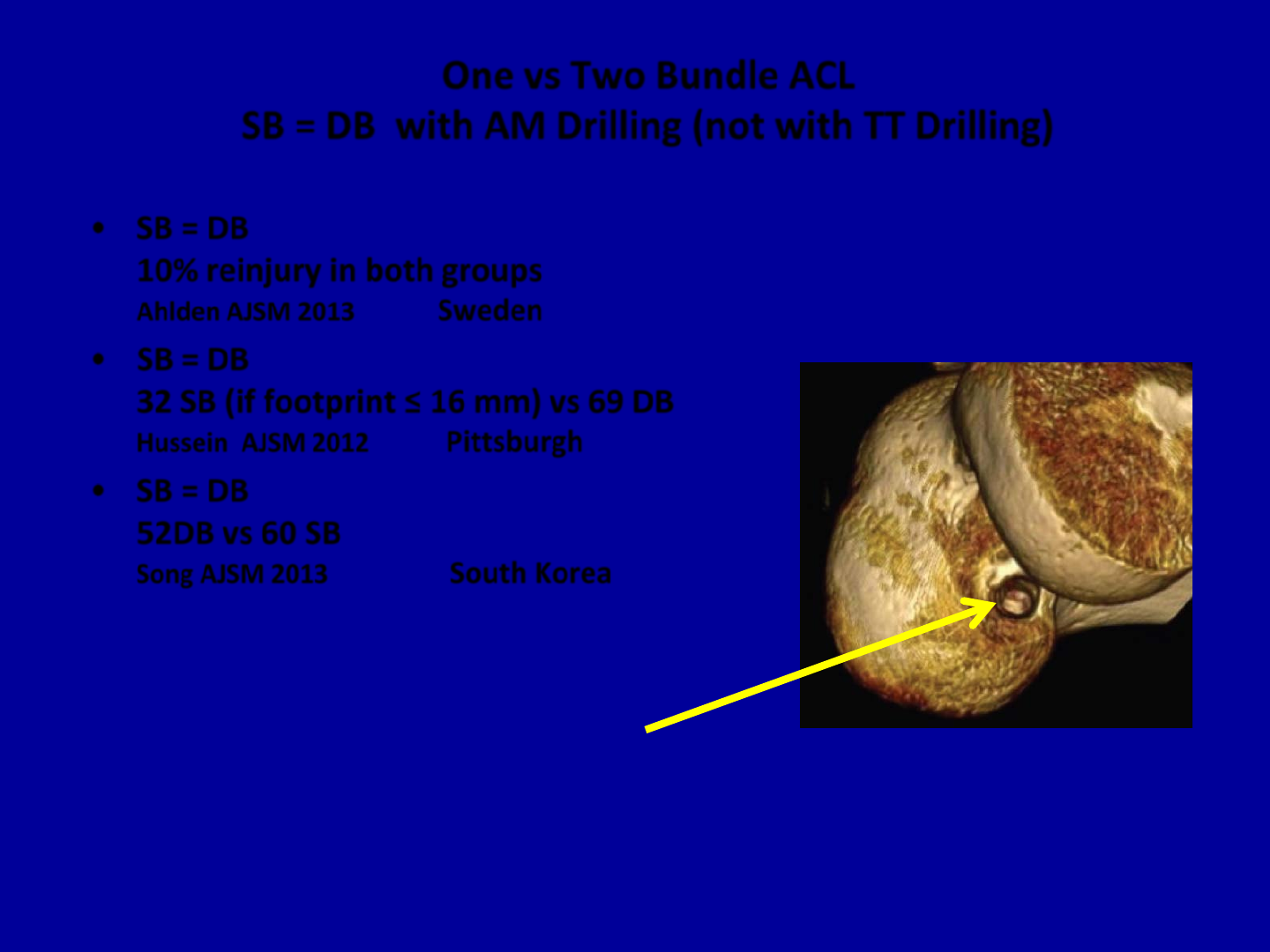
One vs Two Bundle ACL
SB = DB with AM Drilling (not with TT Drilling)
•SB = DB
10% reinjury in both groups
Ahlden AJSM 2013 Sweden
•SB = DB
32 SB (if footprint ≤ 16 mm) vs 69 DB
Hussein AJSM 2012 Pittsburgh
•SB = DB
52DB vs 60 SB
Song AJSM 2013 South Korea
Anatomic Femoral Tunnel
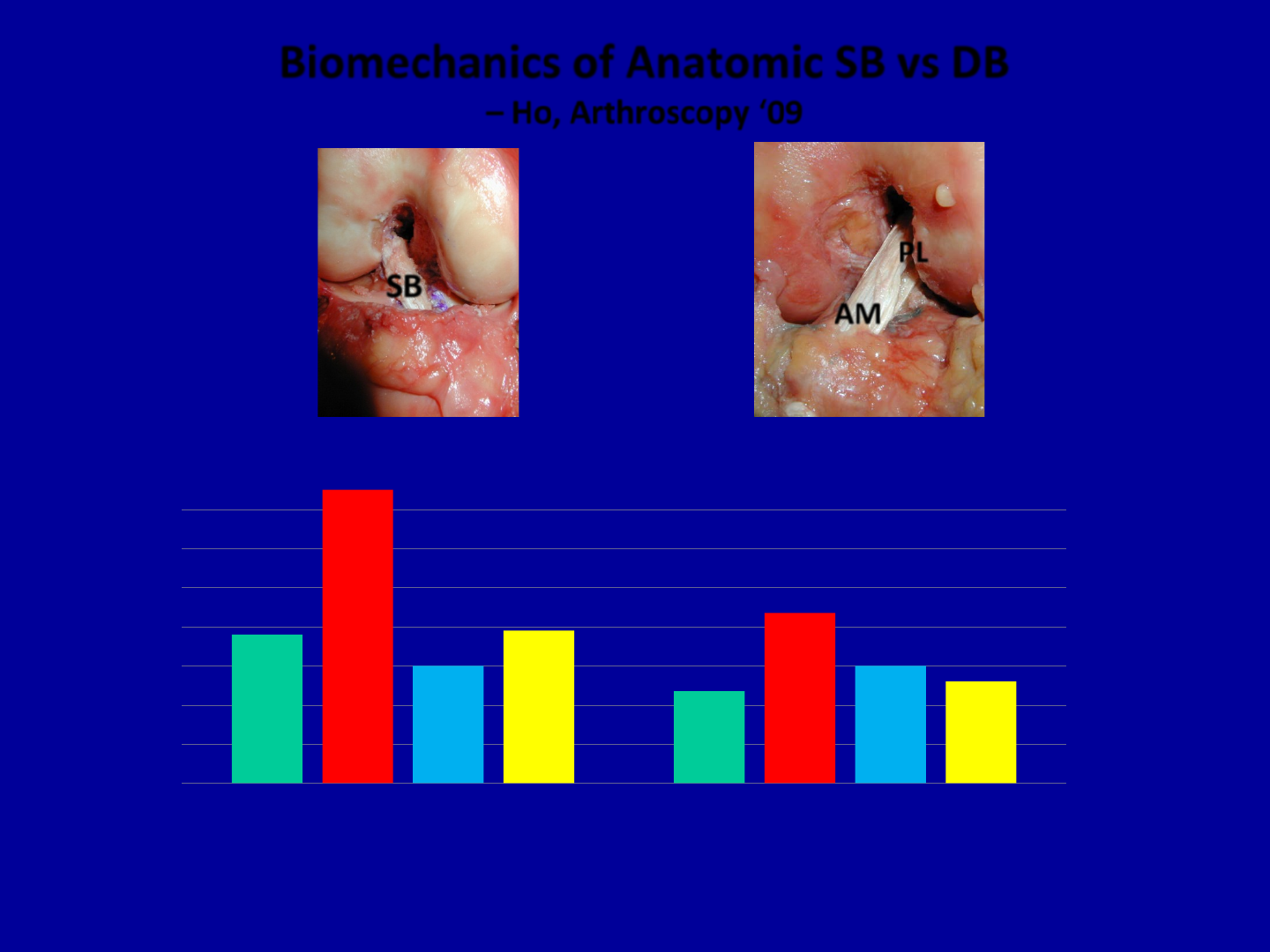
Biomechanics of Anatomic SB vs DB
– Ho, Arthroscopy ‘09
NL NL cut cut SB SB DB DB
30°
60°
Anterior Translation
4 mm
8 mm
12 mm
AM
PL
SB
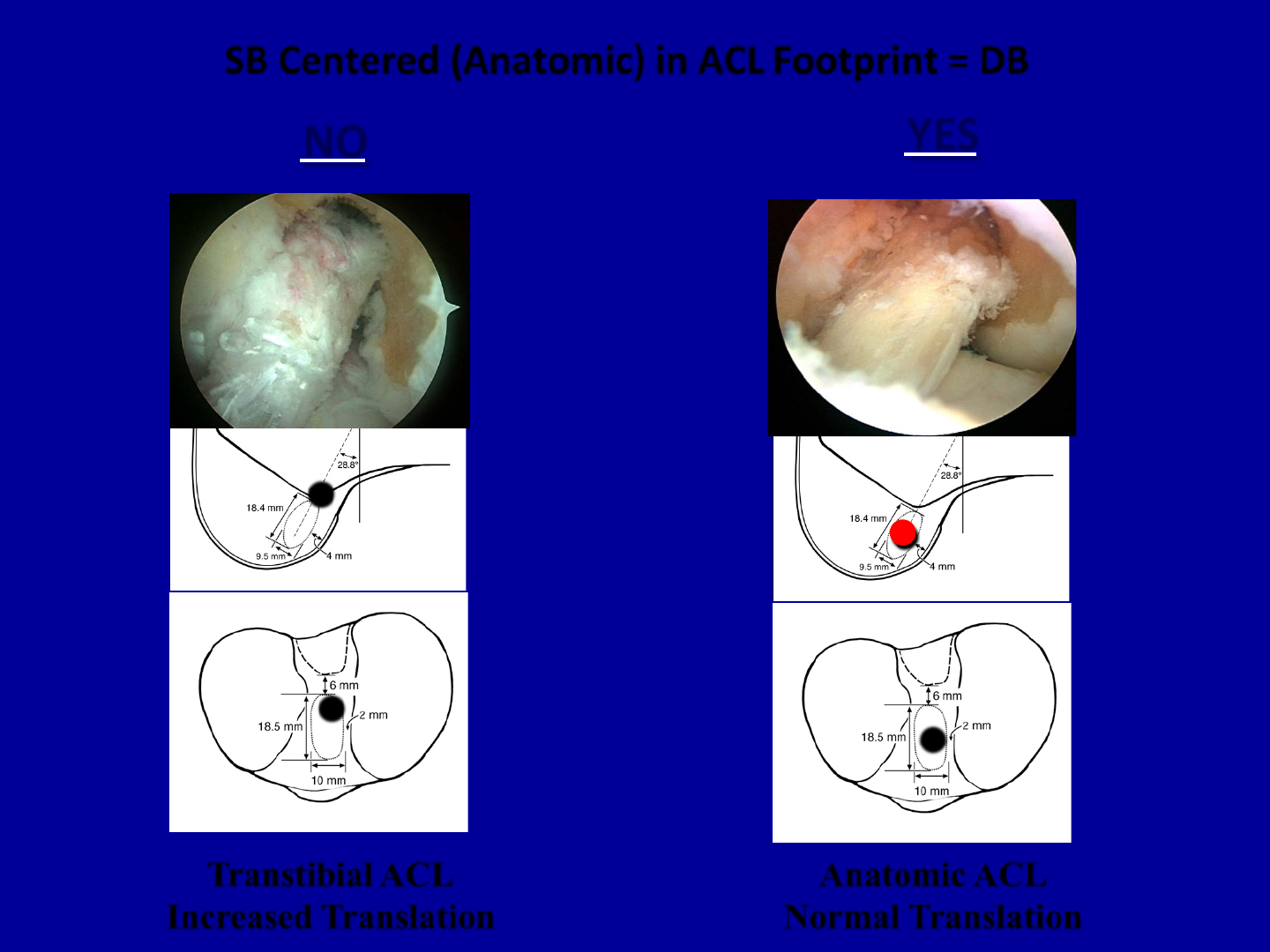
SB Centered (Anatomic) in ACL Footprint = DB
•
•
•
Transtibial ACL
Increased Translation Anatomic ACL
Normal Translation
NO YES

Anatomic Transtibial Drilling
Tibial or Femoral Tunnels have to be compromised
Drilling under Tibial Plateau Failed Vertical Tunnel
Anatomic Tibial Tunnel Places a Vertical Femoral Tunnel
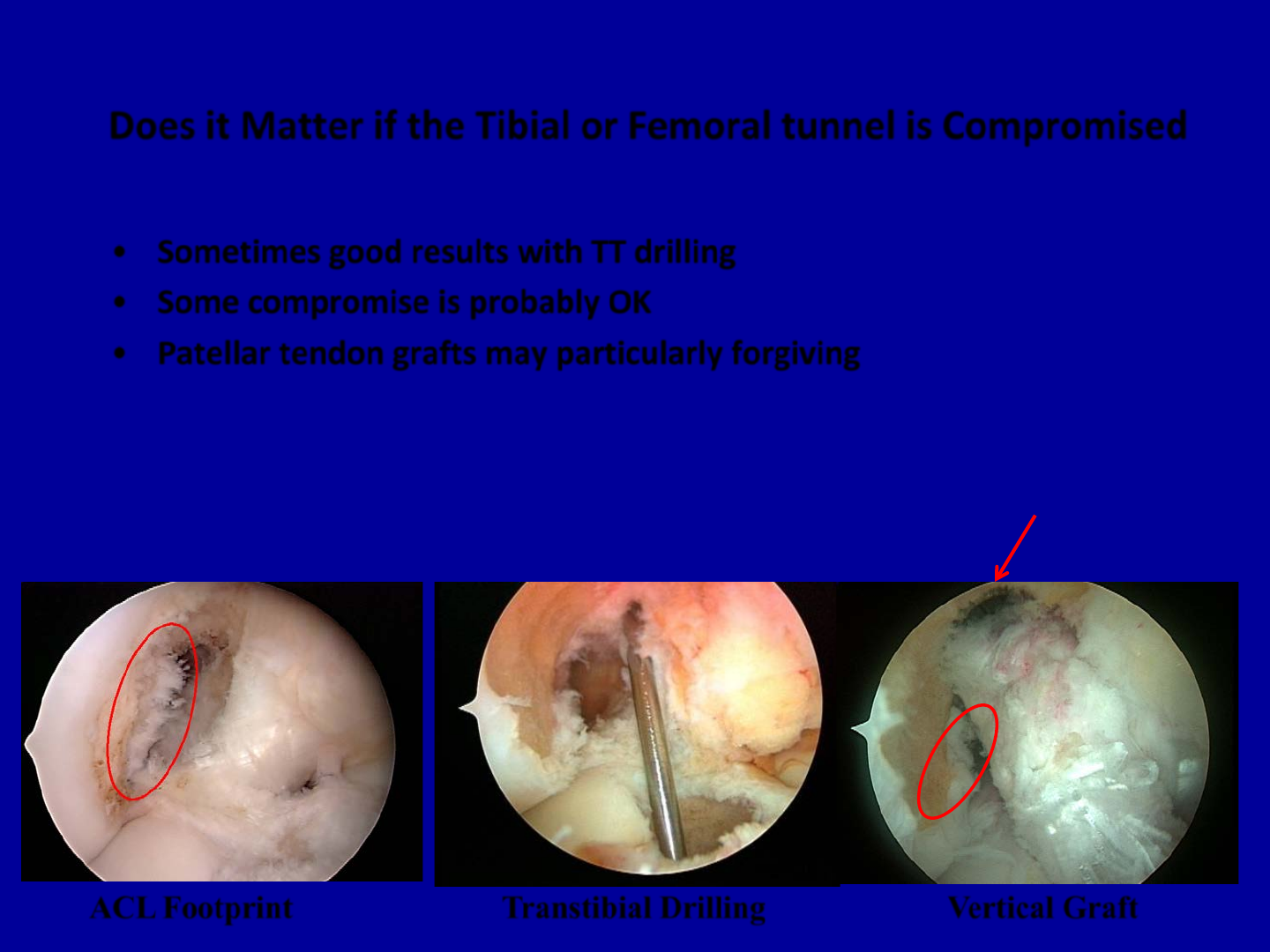
Does it Matter if the Tibial or Femoral tunnel is Compromised
•Sometimes good results with TT drilling
•Some compromise is probably OK
•Patellar tendon grafts may particularly forgiving
Transtibial Drilling ACL Footprint Vertical Graft
Bone plug rotated
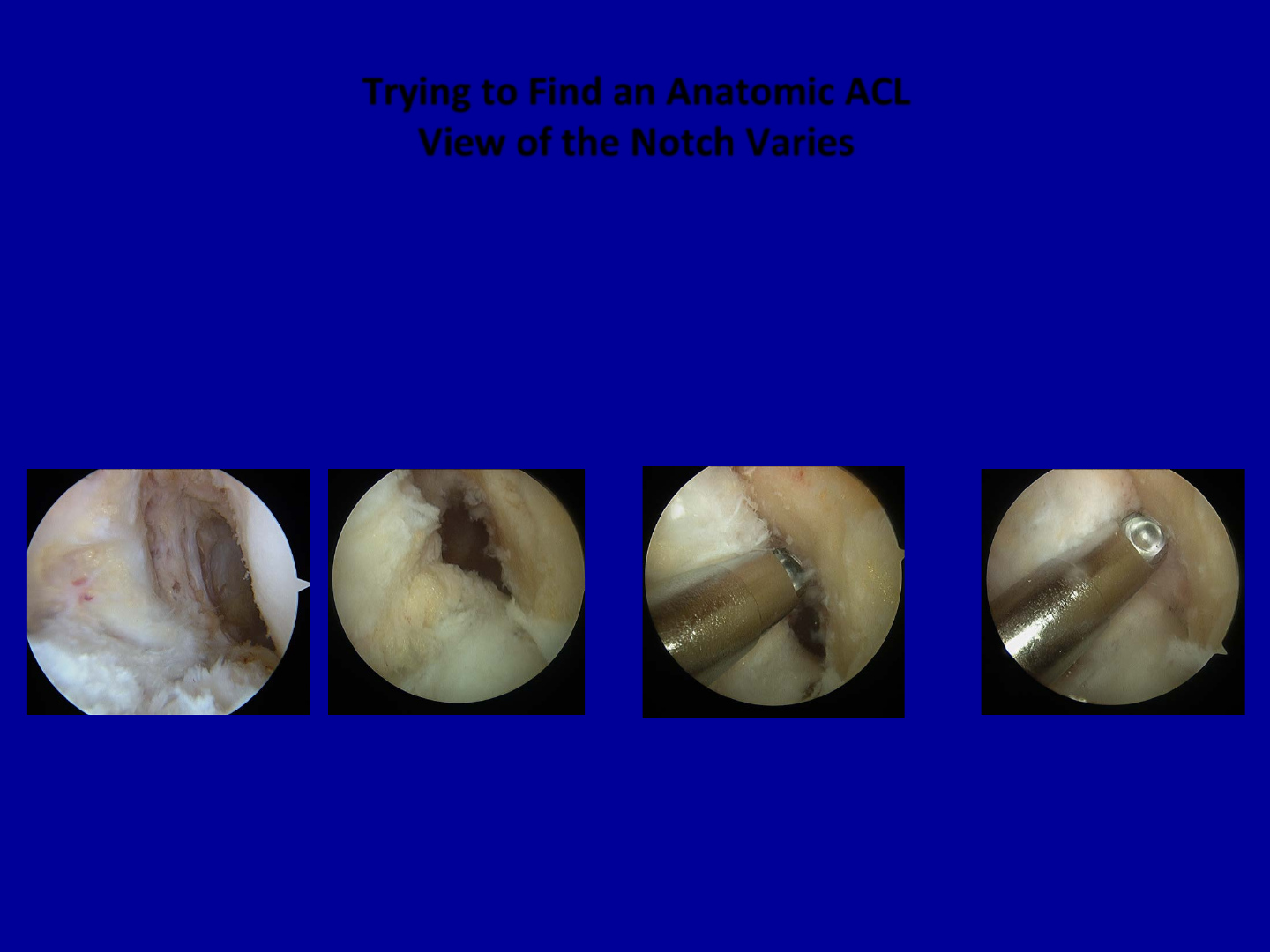
Trying to Find an Anatomic ACL
View of the Notch Varies
90° 110° 125°
•Best view at 55°
•Changes with flexion
•Posterior “closes” with flexion
•Portal changes perspective
55°
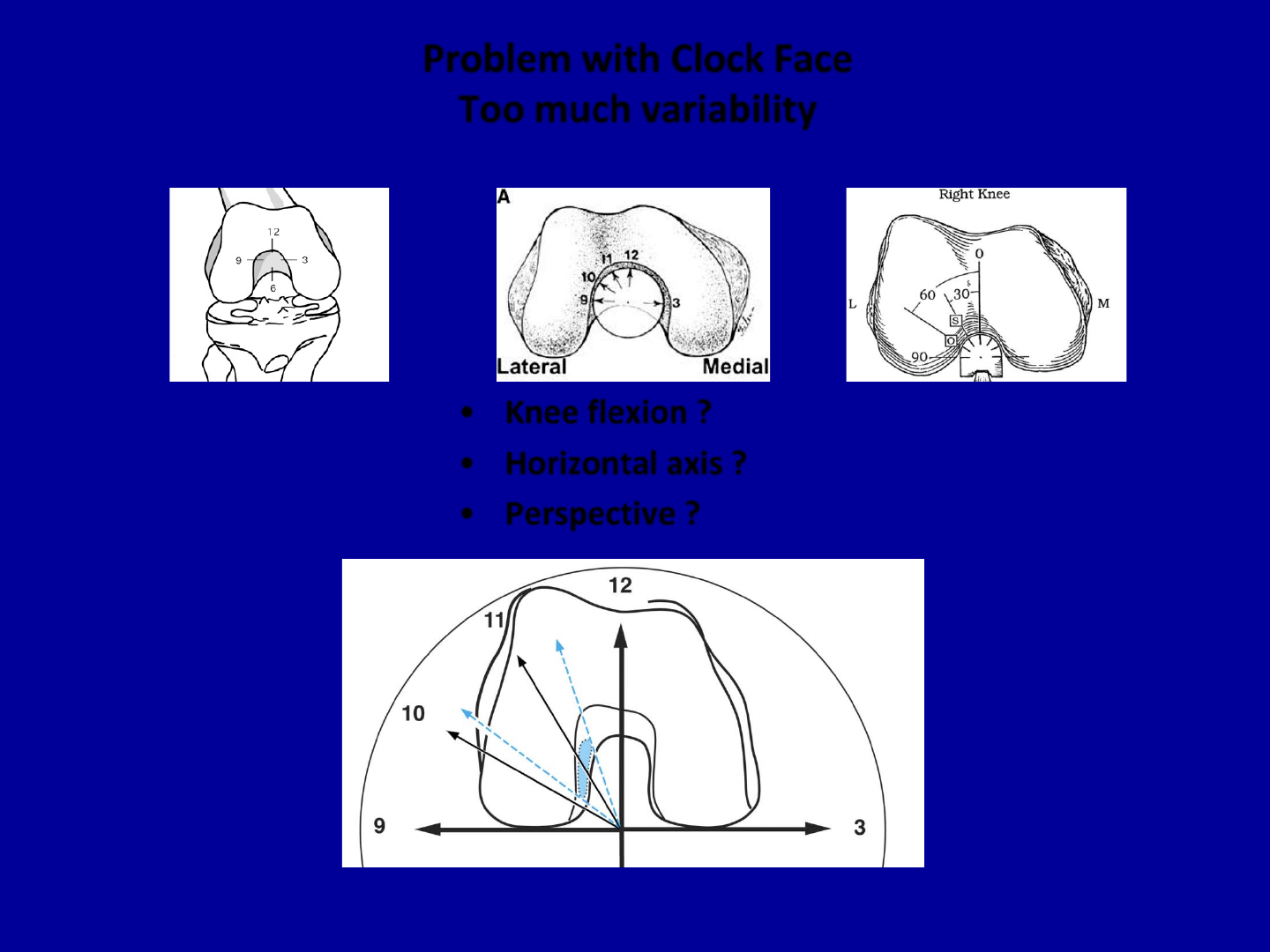
Problem with Clock Face
Too much variability
•Knee flexion ?
•Horizontal axis ?
•Perspective ?
Heming AJSM 2007
IKDC Pittsburgh Duke
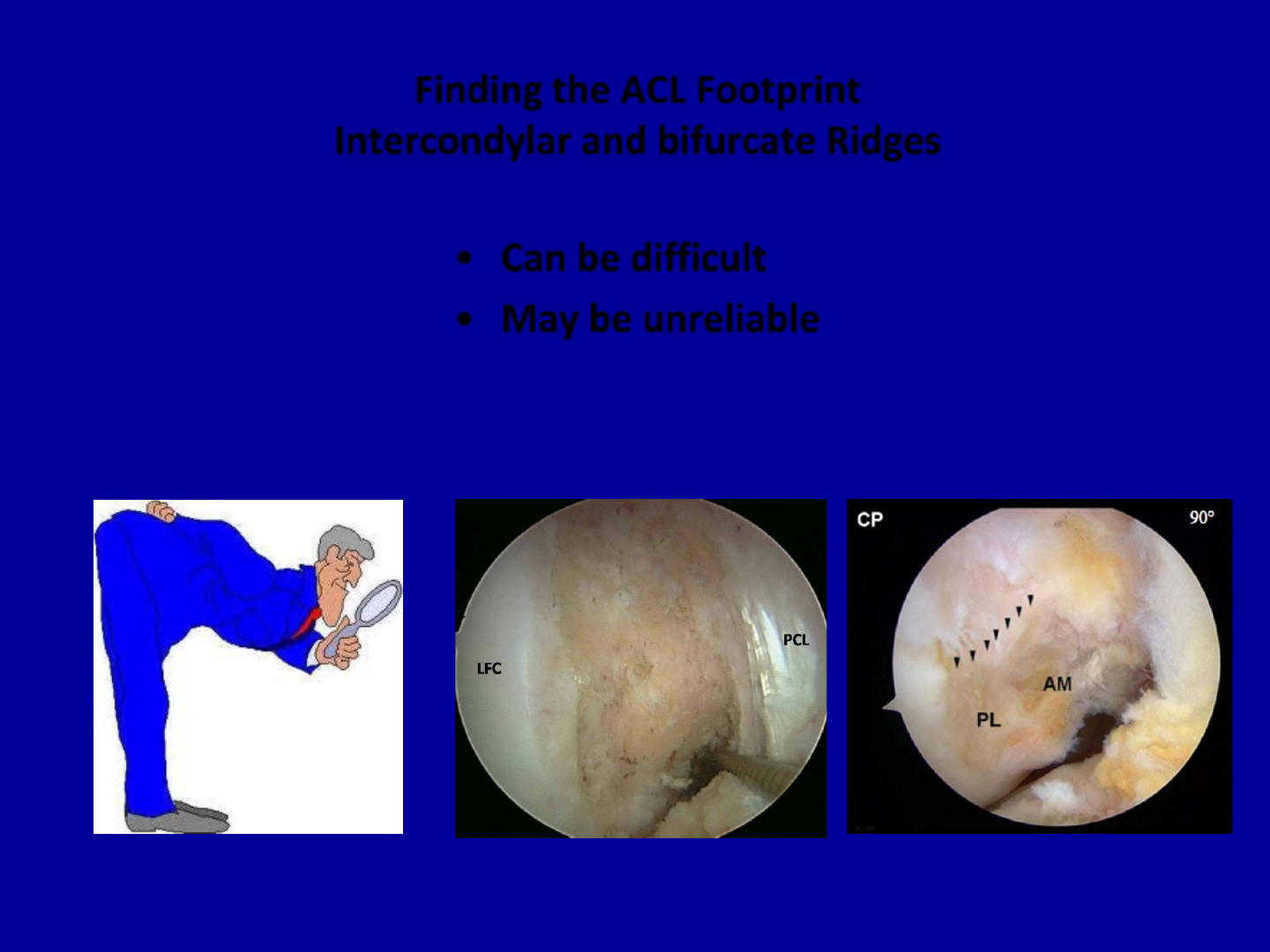
Finding the ACL Footprint
Intercondylar and bifurcate Ridges
•Can be difficult
•May be unreliable
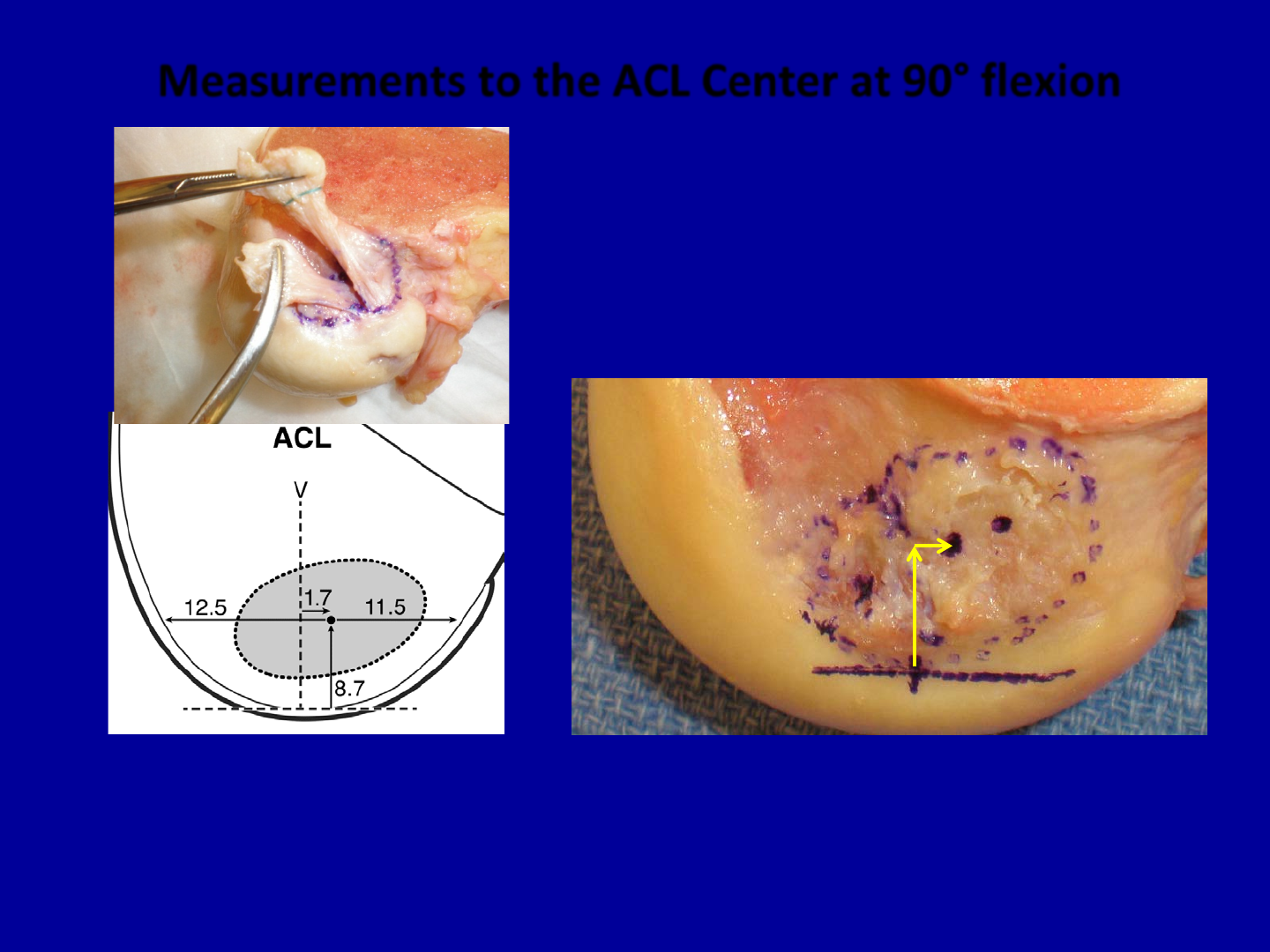
Measurements to the ACL Center at 90° flexion
•8.5 mm up lateral wall
•1.5 mm deep to a vertical line from low point
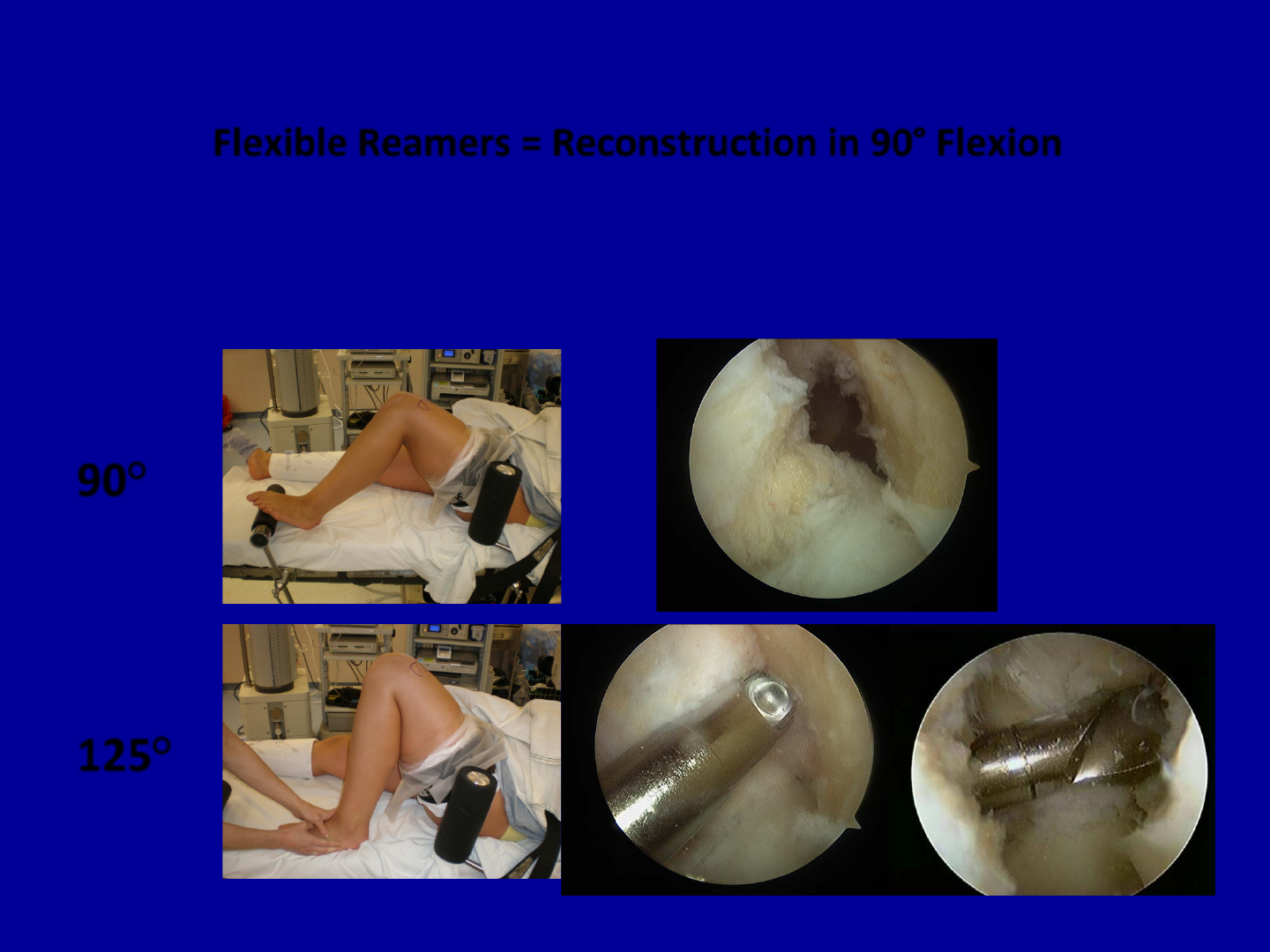
Flexible Reamers = Reconstruction in 90° Flexion
90°
125°
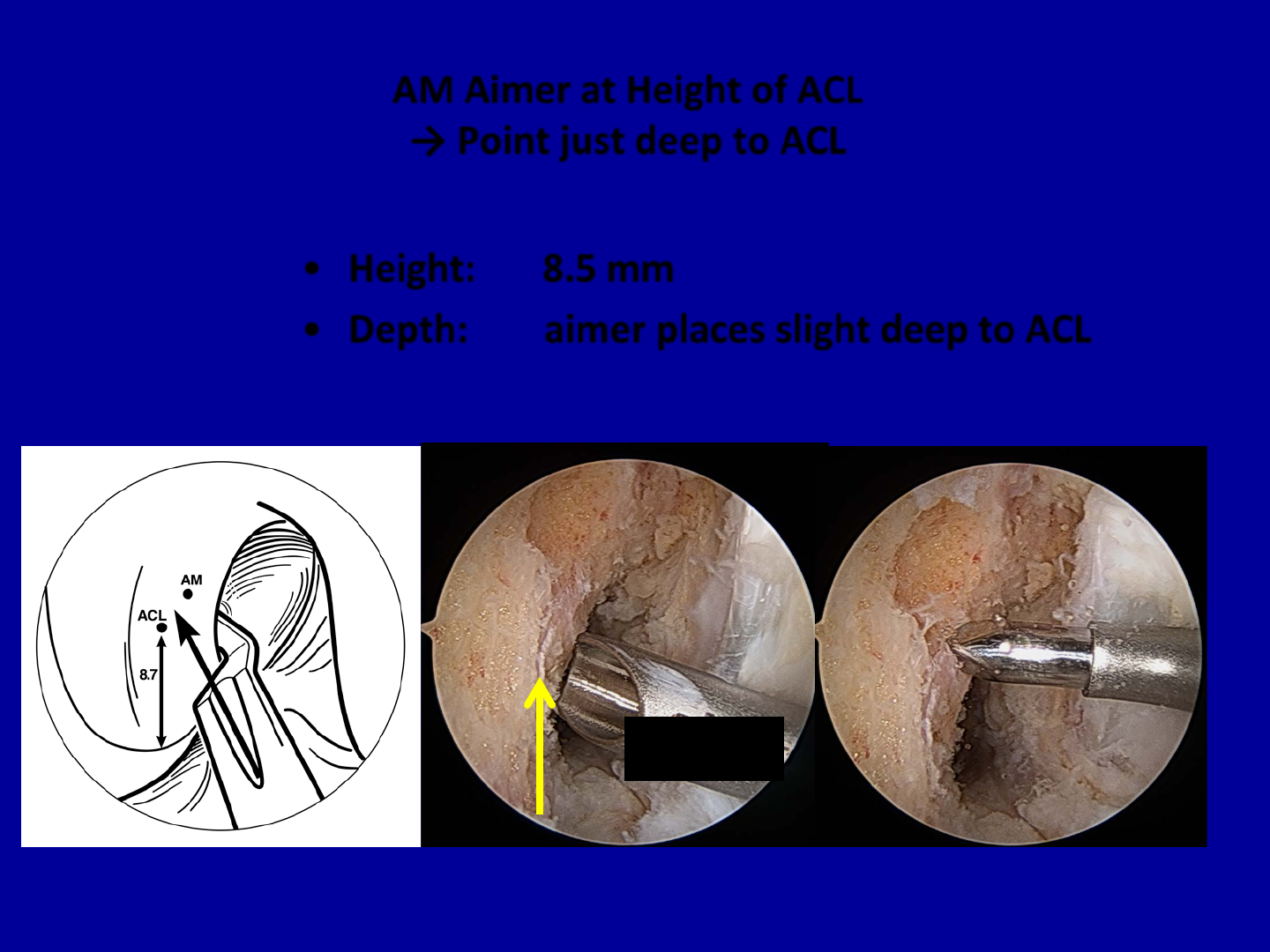
AM Aimer at Height of ACL
→ Point just deep to ACL
•Height: 8.5 mm
•Depth: aimer places slight deep to ACL
8.5 mm
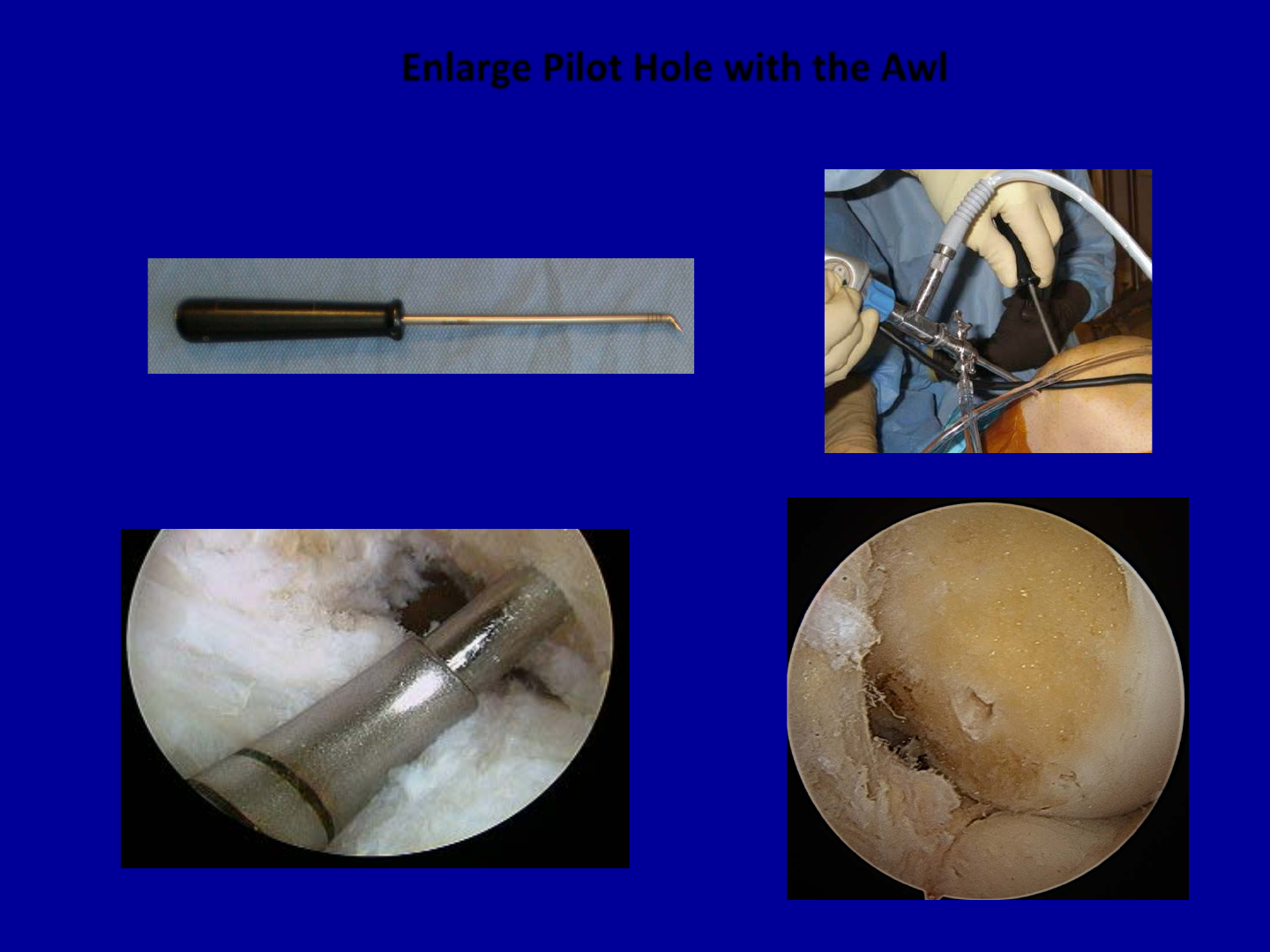
Enlarge Pilot Hole with the Awl

Aimer Placed Through AM Portal
Pin Positioned in Starter Hole

Guidepin Placement
•Pin Exits in safe zone on lateral thigh

Advance Flexible Reamer Over Pin
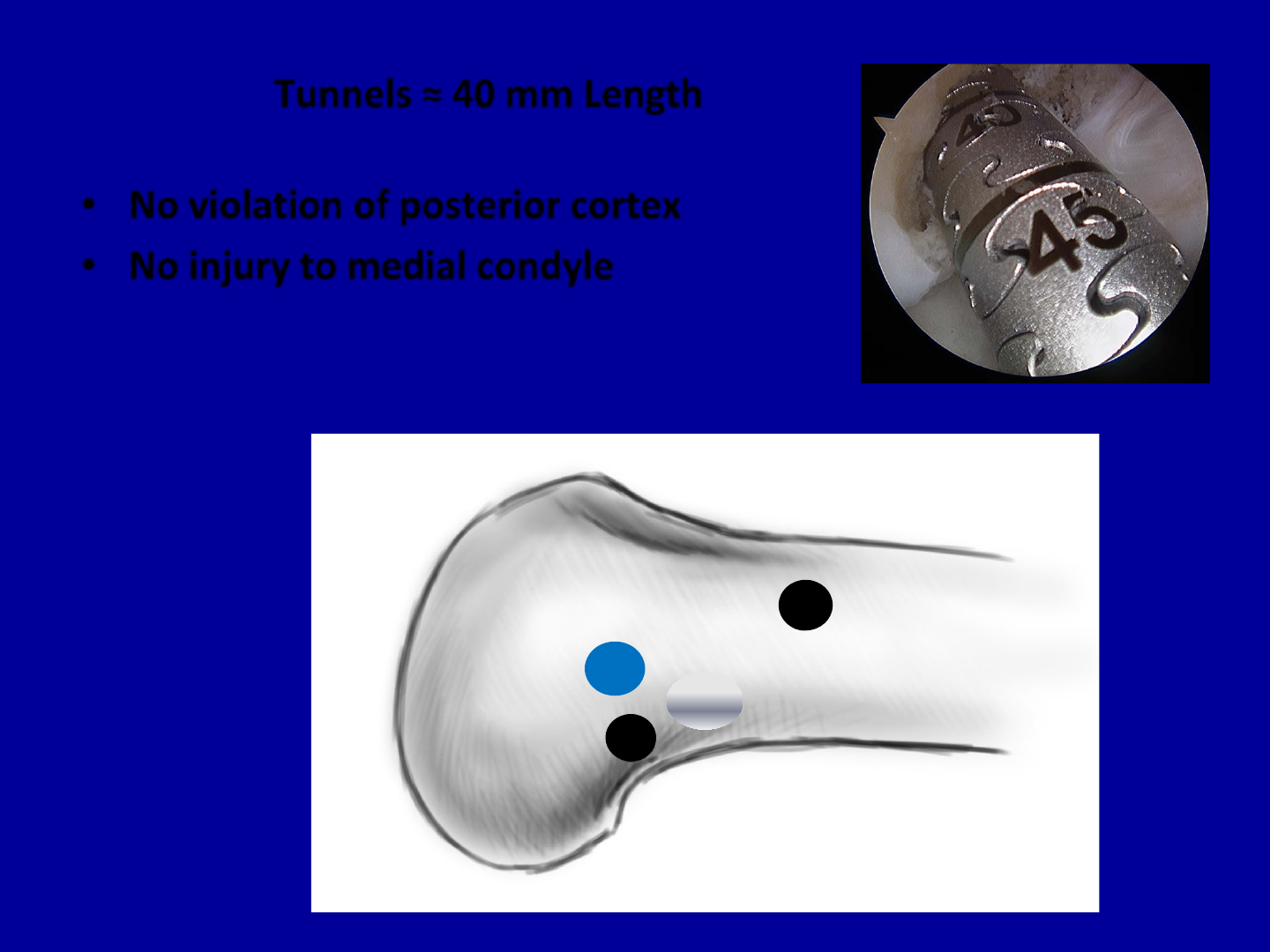
Tunnels ≈ 40 mm Length
•No violation of posterior cortex
•No injury to medial condyle
54mm
42mm
32 mm
TT
AM Rigid
AM Flexible
Arthroscopy ‘12
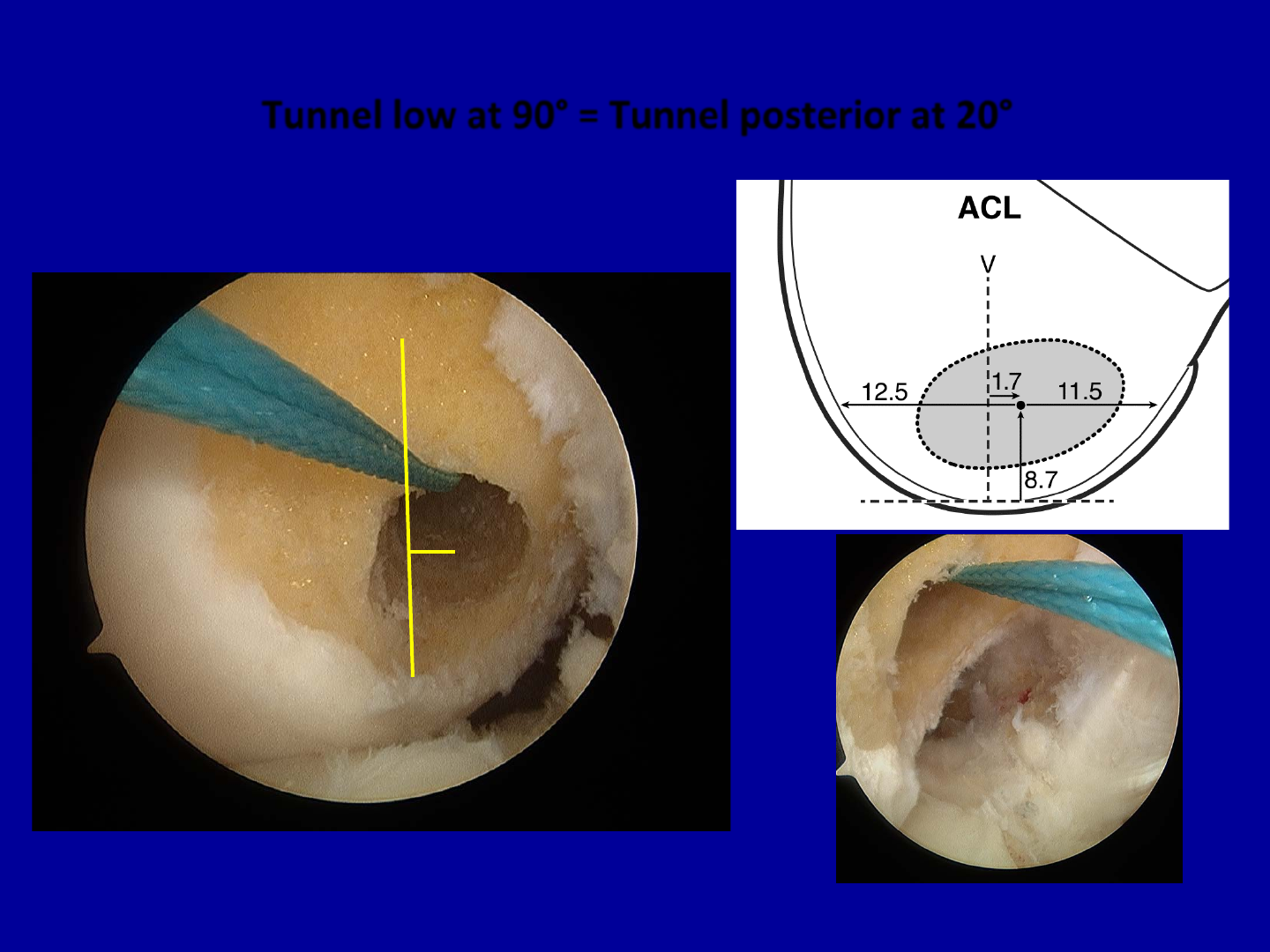
Tunnel low at 90° = Tunnel posterior at 20°
V
90°
extended
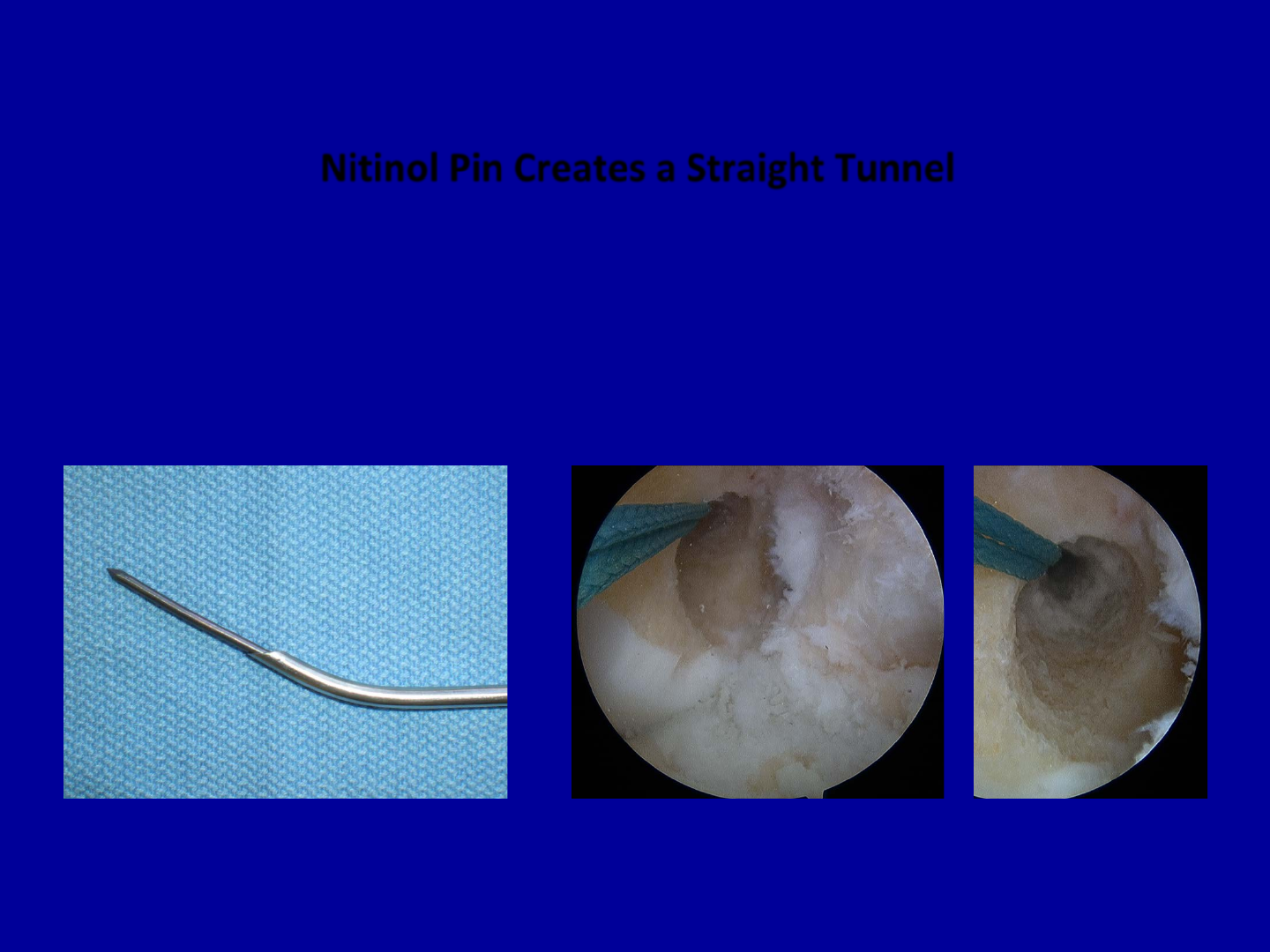
Nitinol Pin Creates a Straight Tunnel
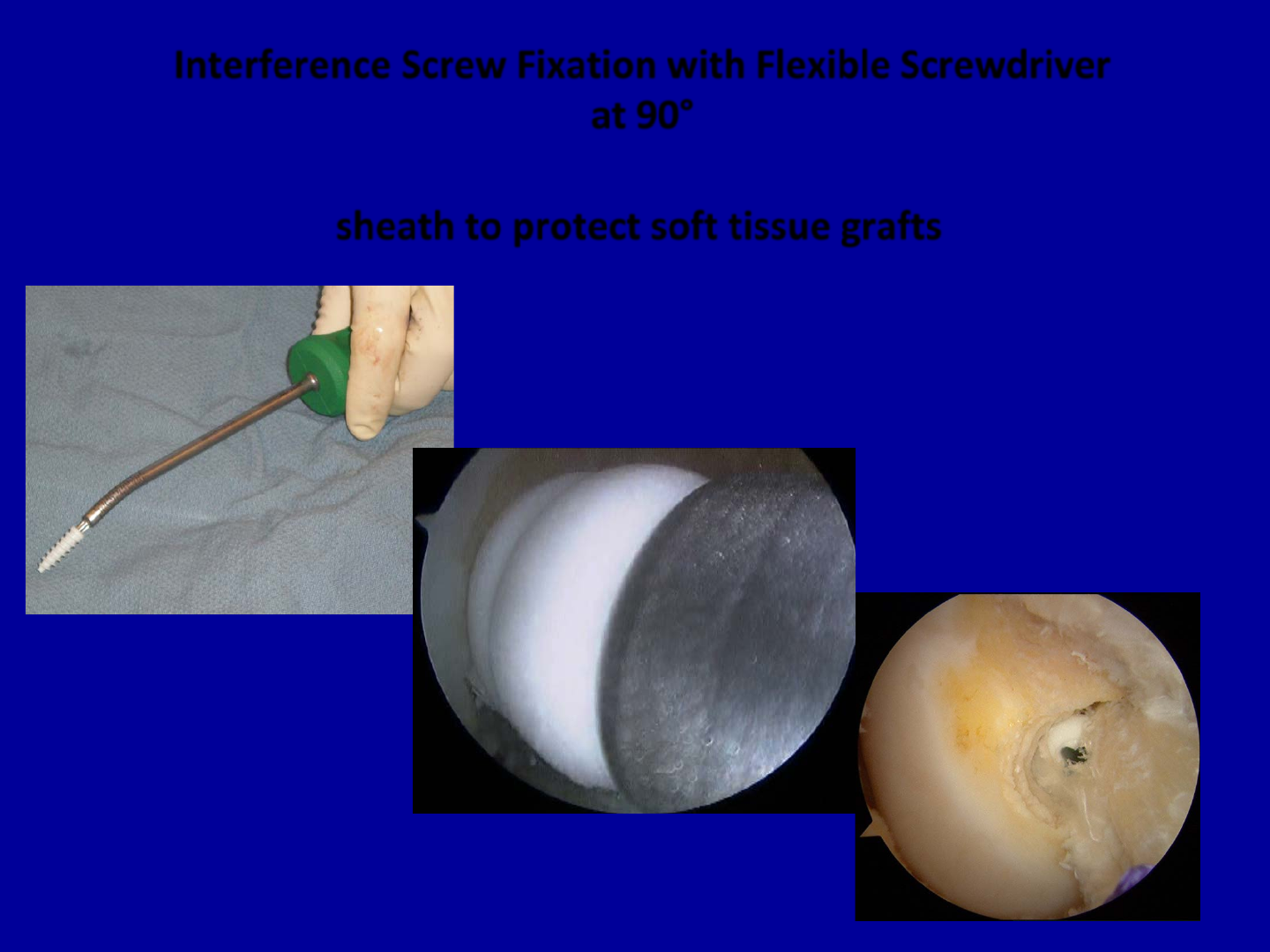
Interference Screw Fixation with Flexible Screwdriver
at 90°
sheath to protect soft tissue grafts
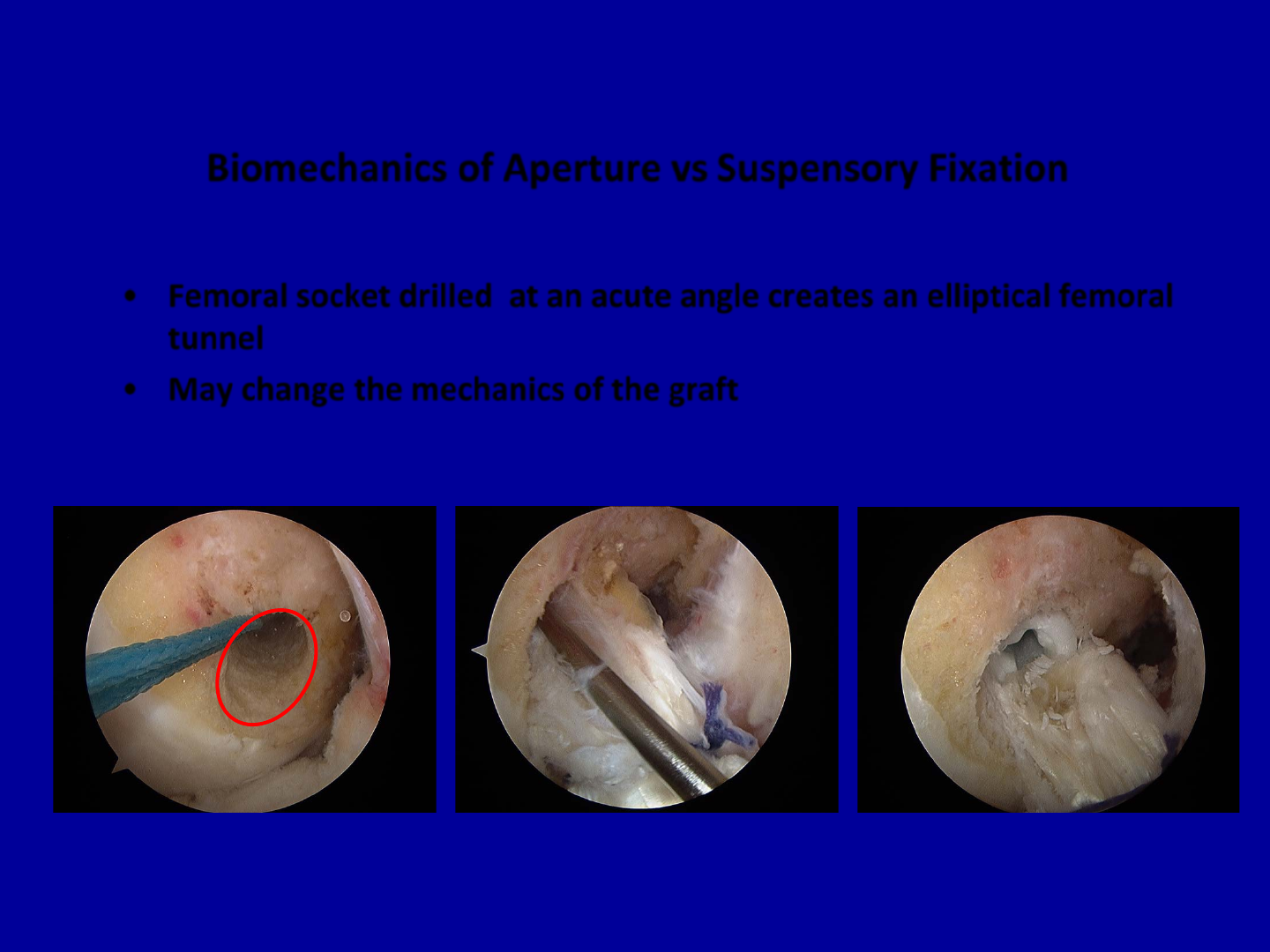
Biomechanics of Aperture vs Suspensory Fixation
•Femoral socket drilled at an acute angle creates an elliptical femoral
tunnel
•May change the mechanics of the graft
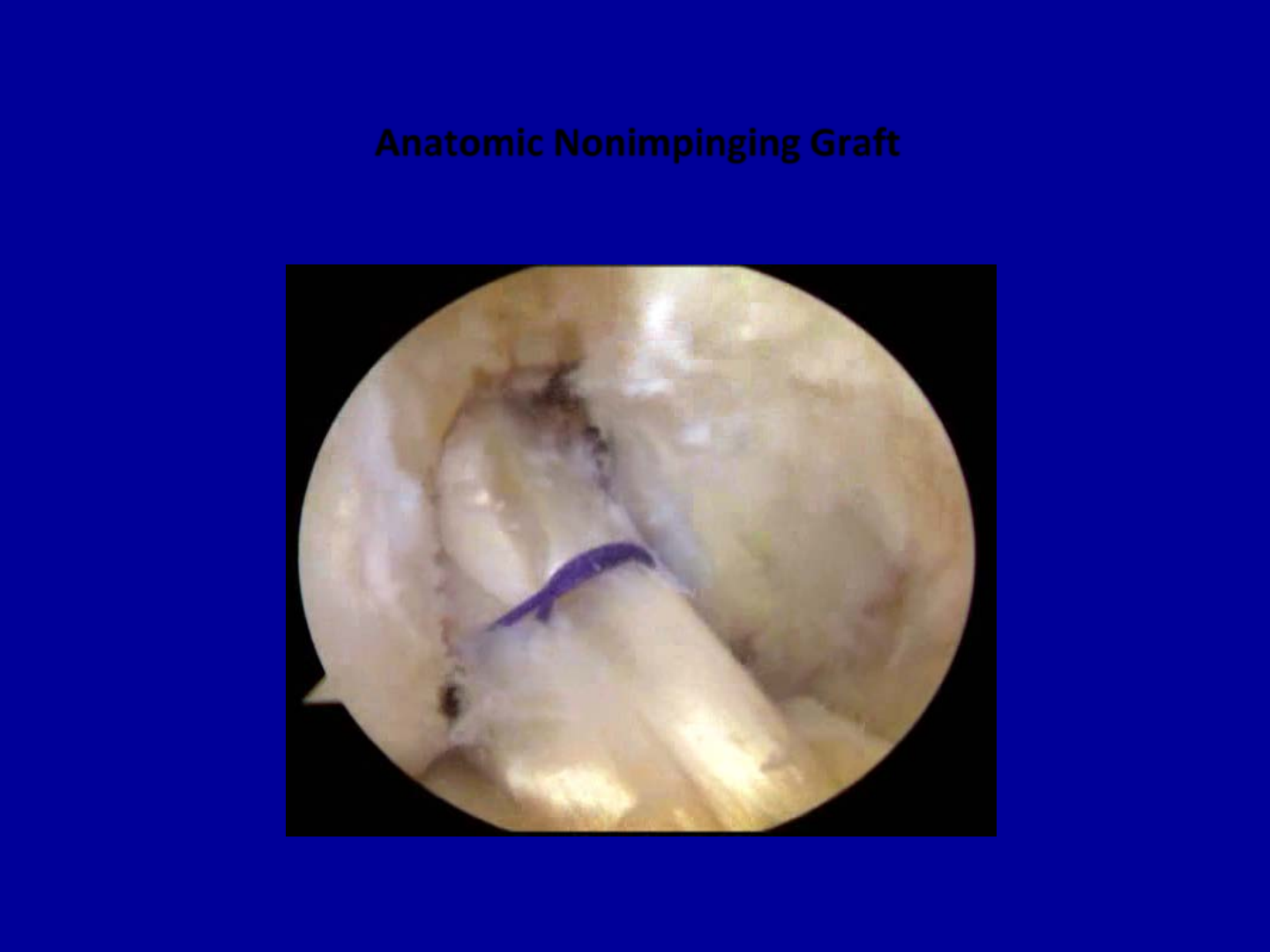
Anatomic Nonimpinging Graft
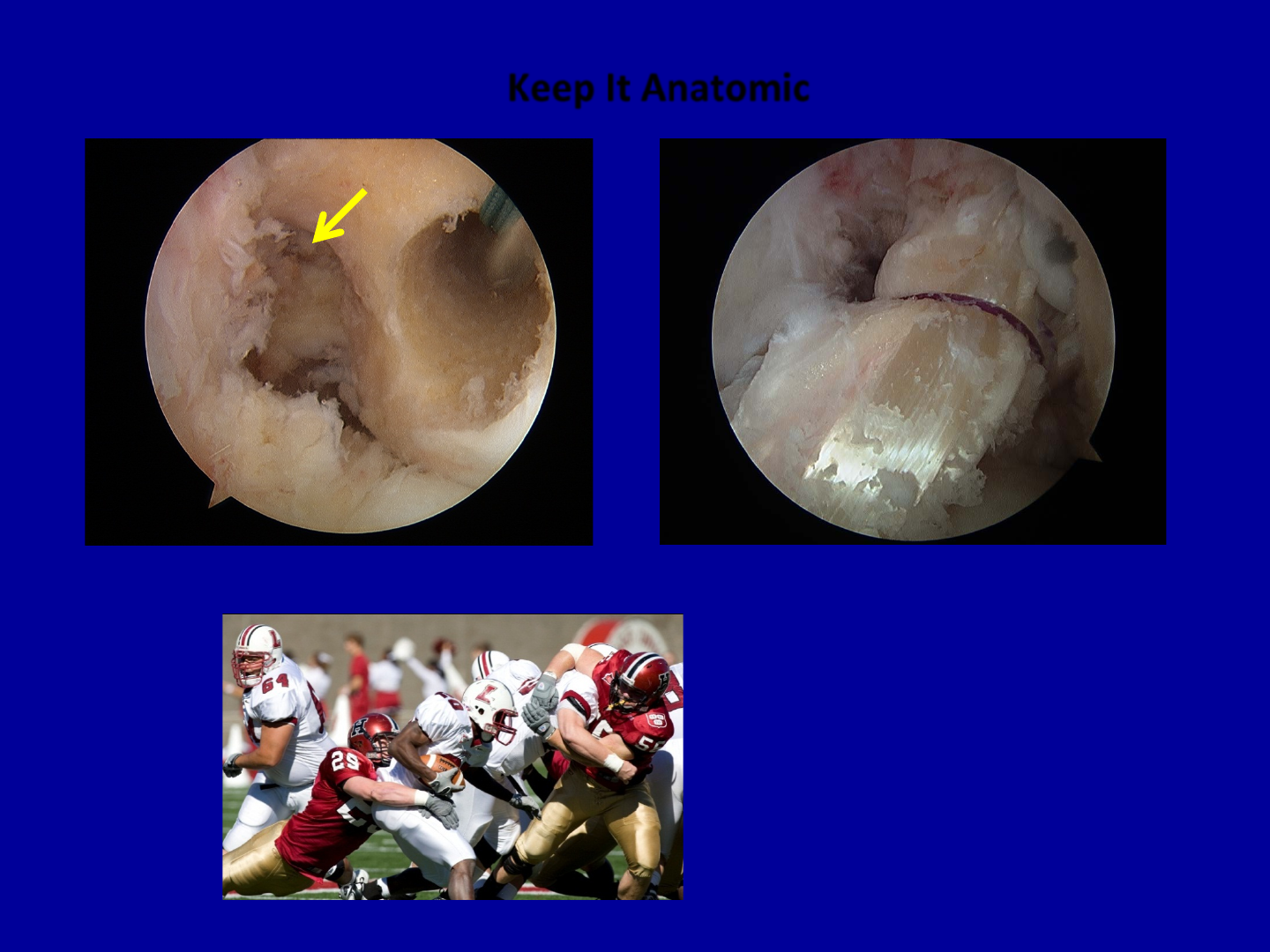
Keep It Anatomic
Old
Thank you
