Acl Syllabus
Acl Syllabus acl_syllabus acl_syllabus 3 2013 pdf 258413772373414384
2013-02-24
: Pdf Acl Syllabus acl_syllabus 2 2013 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 46

8/20/2012
1
8 min
Avoiding Complications
with the Transtibial
Technique
Stephen M. Howell, MD
Professor Mechanical Engineering
Member of Biomedical Graduate Group
University of California at Davis
Sacramento, CA
Conflict of Interest
•Consultant and receive royalties
from Biomet Sports Medicine
•Co-founder of OtisMed and designer
of kinematically aligned TKA
•Consultant for Stryker
•Share guidelines for placing the tibial
and femoral tunnels in the sagittal and
coronal plane that avoids
complications with the transtibial
technique
Objective

8/20/2012
2
Placement of Tibial Tunnel
in the Sagittal Plane
•Applies to both the
transtibial and AM
portal techniques
•Tibial tunnel must
be just posterior to
intercondylar roof
•Anterior placement
causes loss of
extension and
instability from roof
impingement
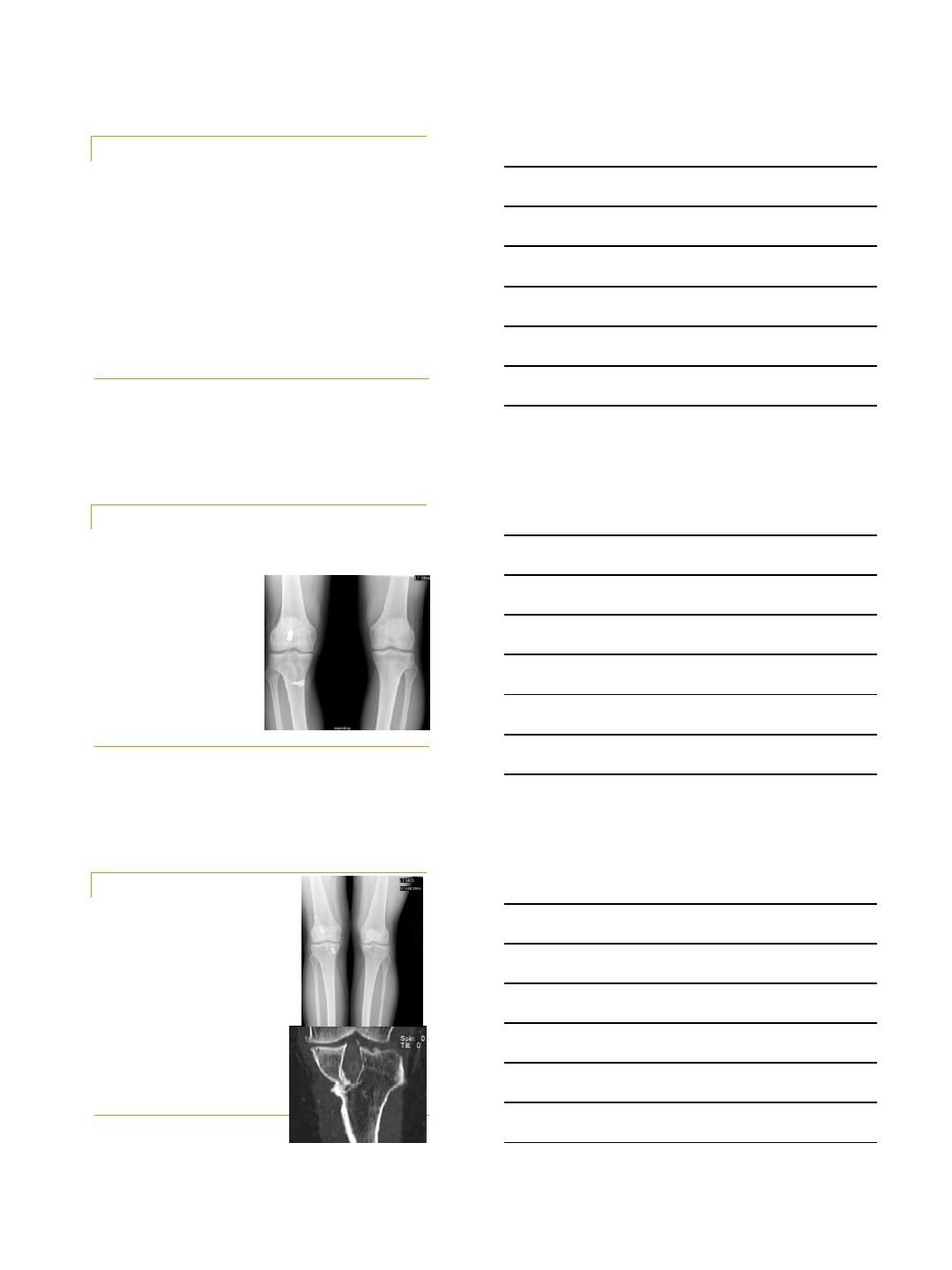
Place Tibial Tunnel ‘Just’ Posterior to
Intercondylar Roof in Extended Knee
Customize the AP Location of the
Tibial Tunnel
•Applies to both the
transtibial and AM
portal techniques
•An ‘average
placement’ results
in ‘average results’
and a higher
failure rate
•Howell, AJSM, 1995

8/20/2012
3
Placement of Tibial
Tunnel in the Coronal
Plane
•Applies to both the
transtibial and AM portal
techniques
•Tunnel should be
between tibial spines
•Medial placement
causes PCL
impingement and loss
of flexion and instability
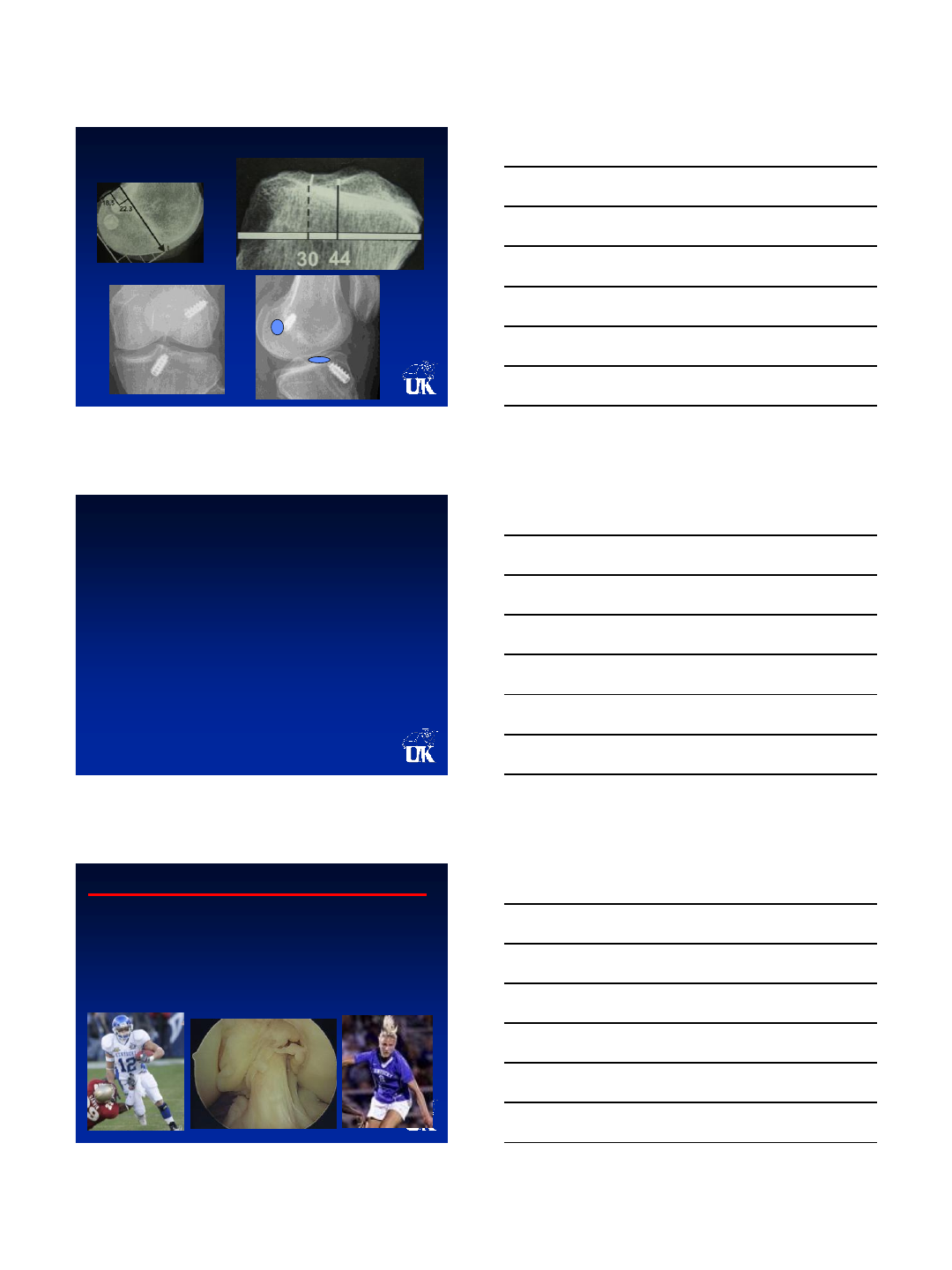
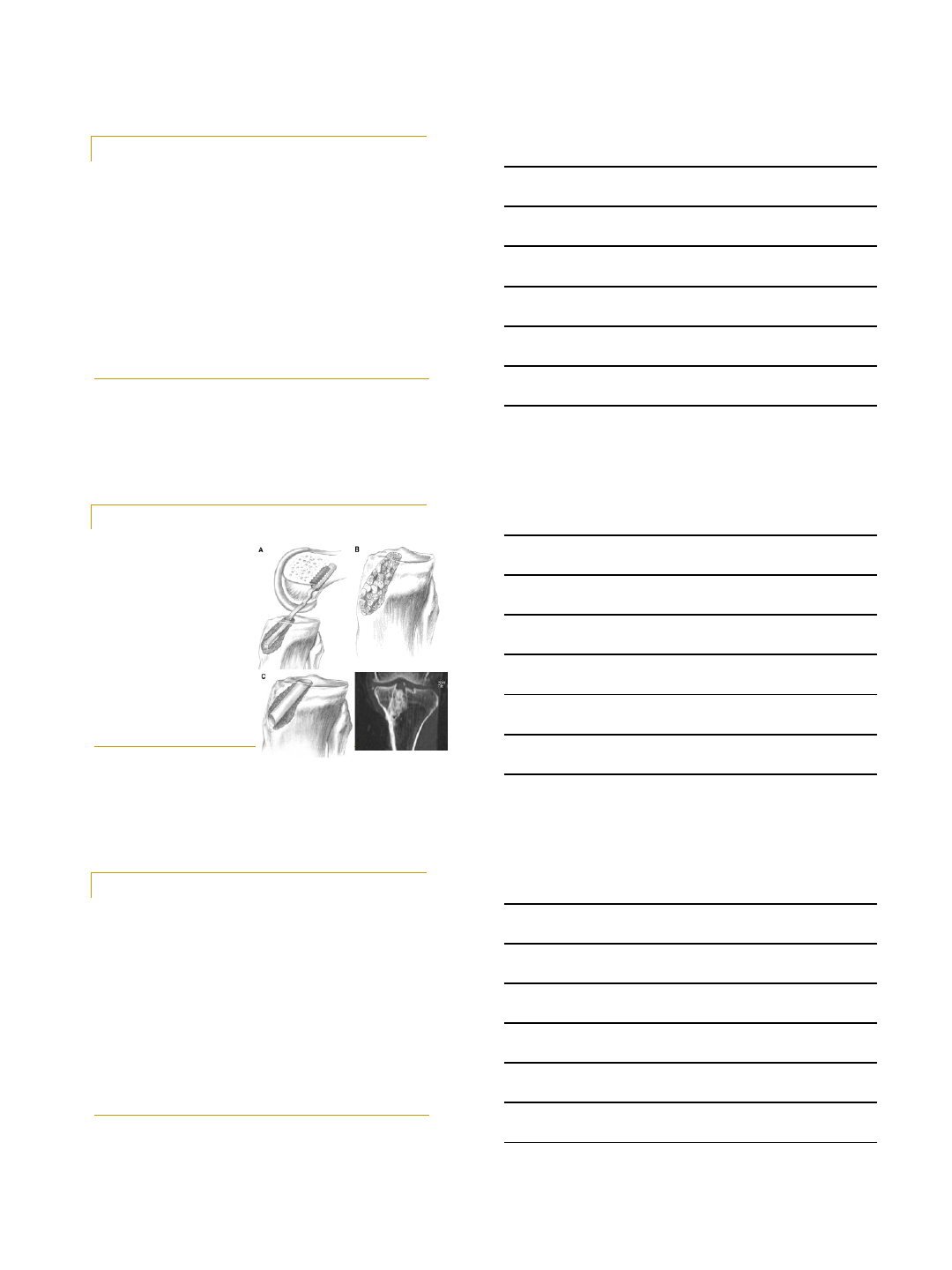
Place Tibial Tunnel Between Tibial
Spines and Through Tip of Lateral Spine
Romano, AJSM, 1993
•Places femoral
tunnel HALF-WAY
down side-wall
minimizing loss of
flexion and instability
from PCL
impingement
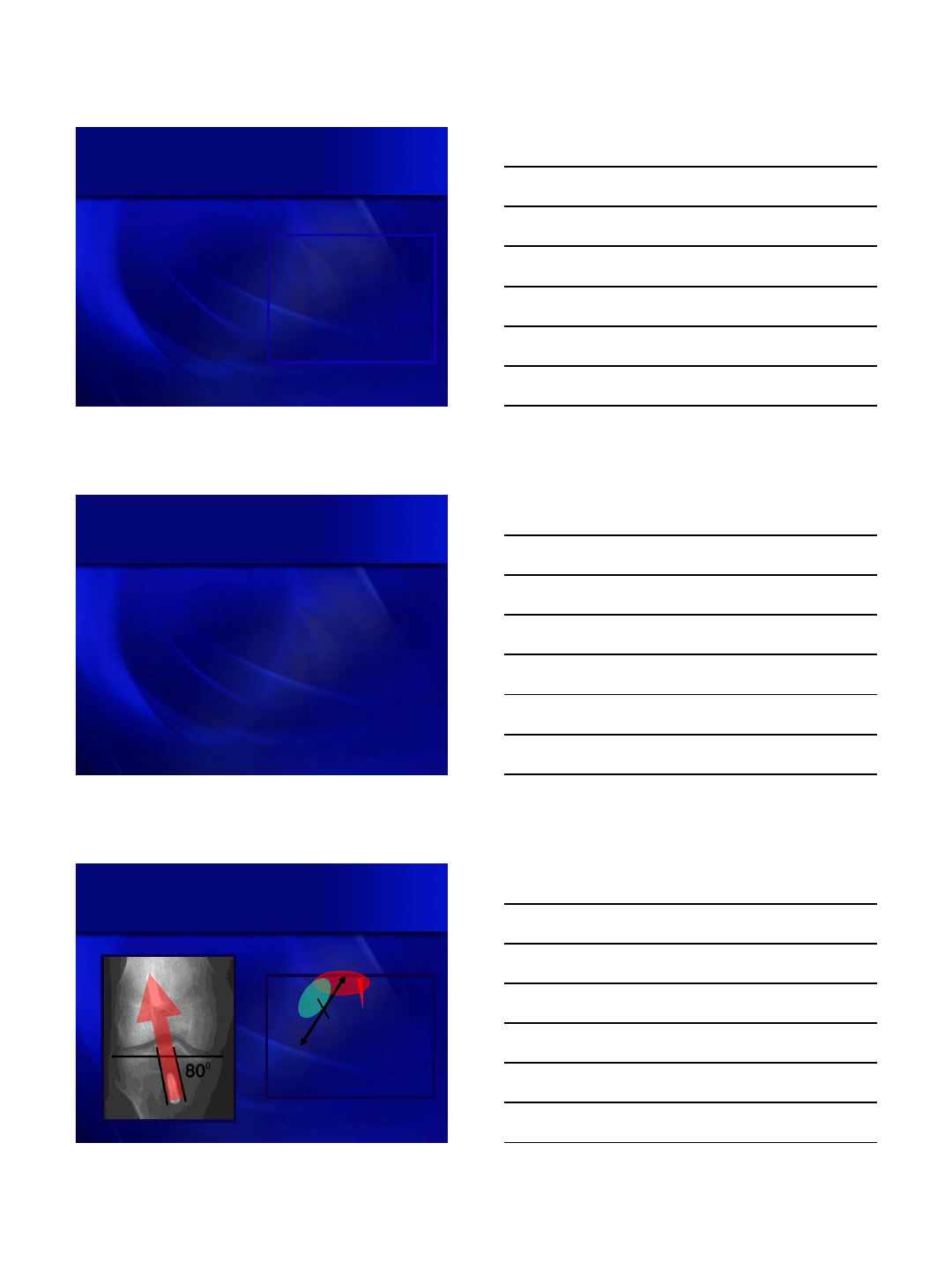
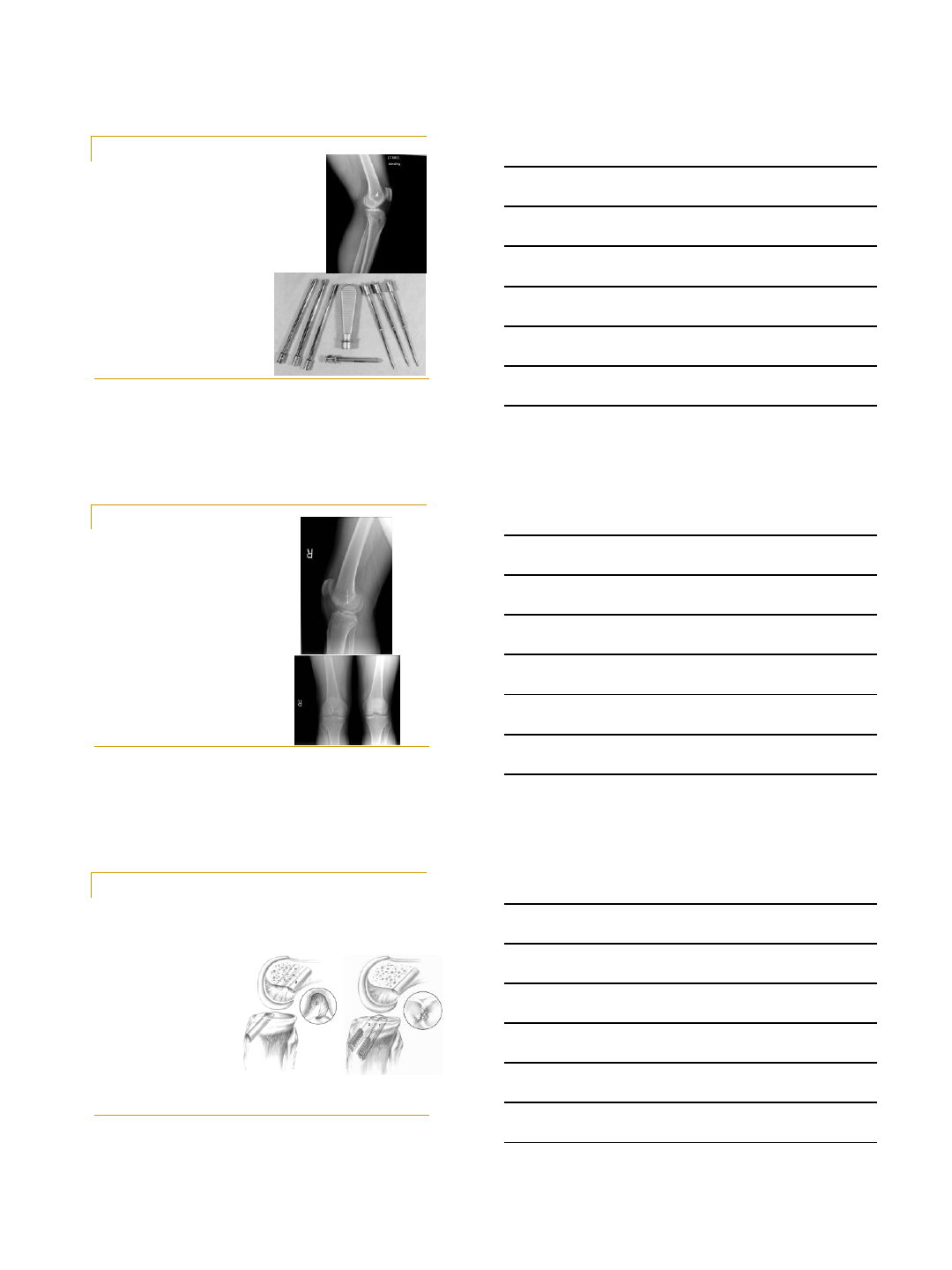
For Transtibial Technique, Set the
Tibial Tunnel at an Angle of 60-650
•Simmons, Howell, Hull, JBJS, 2003
60-65
8/20/2012
4
QuickTime™ and a
Sorens on Video 3 decompres sor
are needed to see this picture.
QuickTime™ and a
Photo - JPEG decompressor
are needed to see this picture.
Consider Using a Tibial Guide That
References the Intercondylar Roof
•Insert guide
•Extend knee
•Align rod parallel to
joint line and
perpendicular to
tibia, which sets
tunnel at 65 degrees
Placement of Femoral
Tunnel
in the Coronal Plane
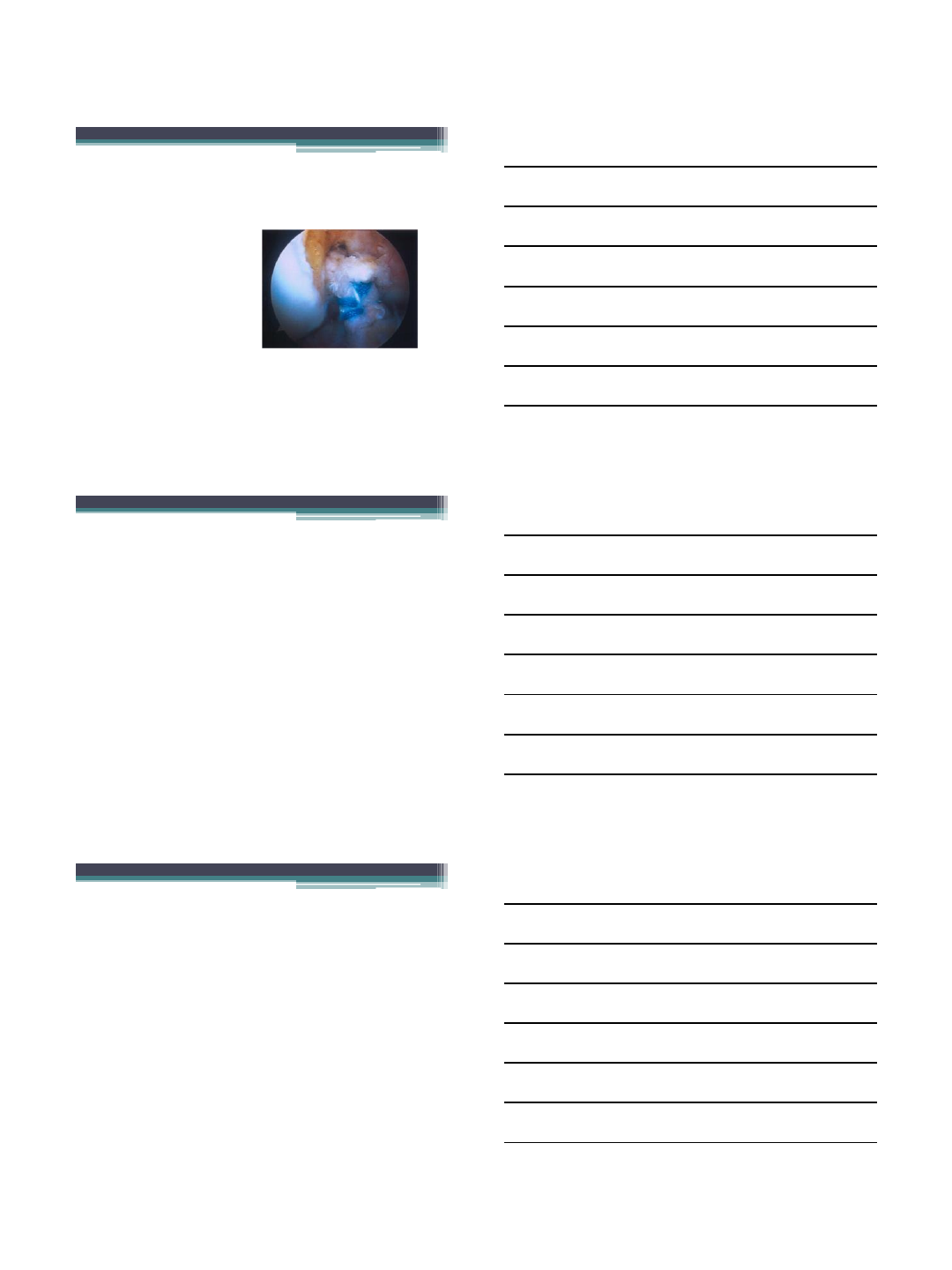
Place the Femoral Tunnel Without
PCL Impingement
QuickTime™ and a
Sorens on Video 3 decompres sor
are needed to see this picture.
50%
50%
View from Transpatellar Tendon Portal

8/20/2012
5
QuickTime™ and a
H.264 decompressor
are needed to see this picture.
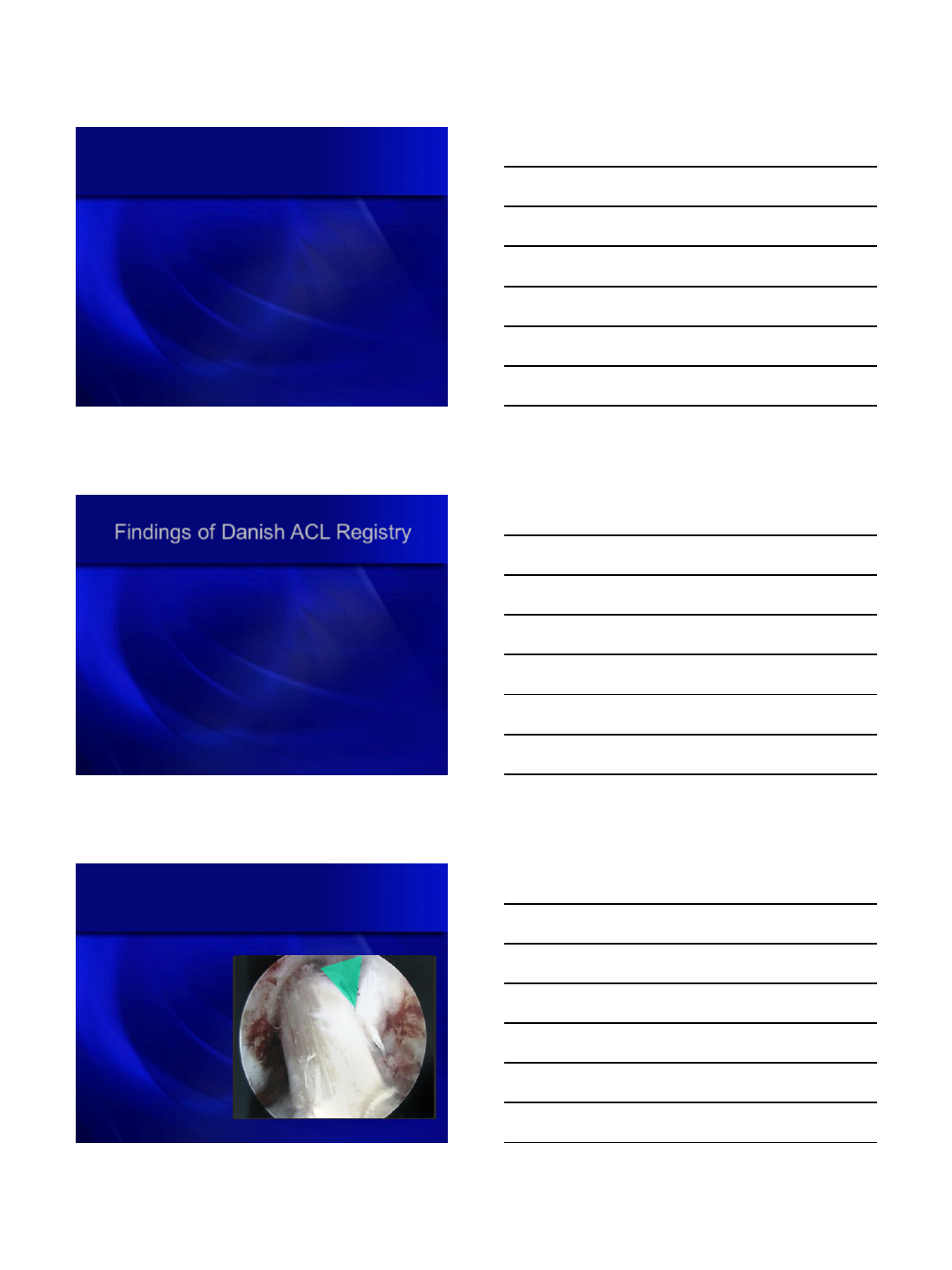
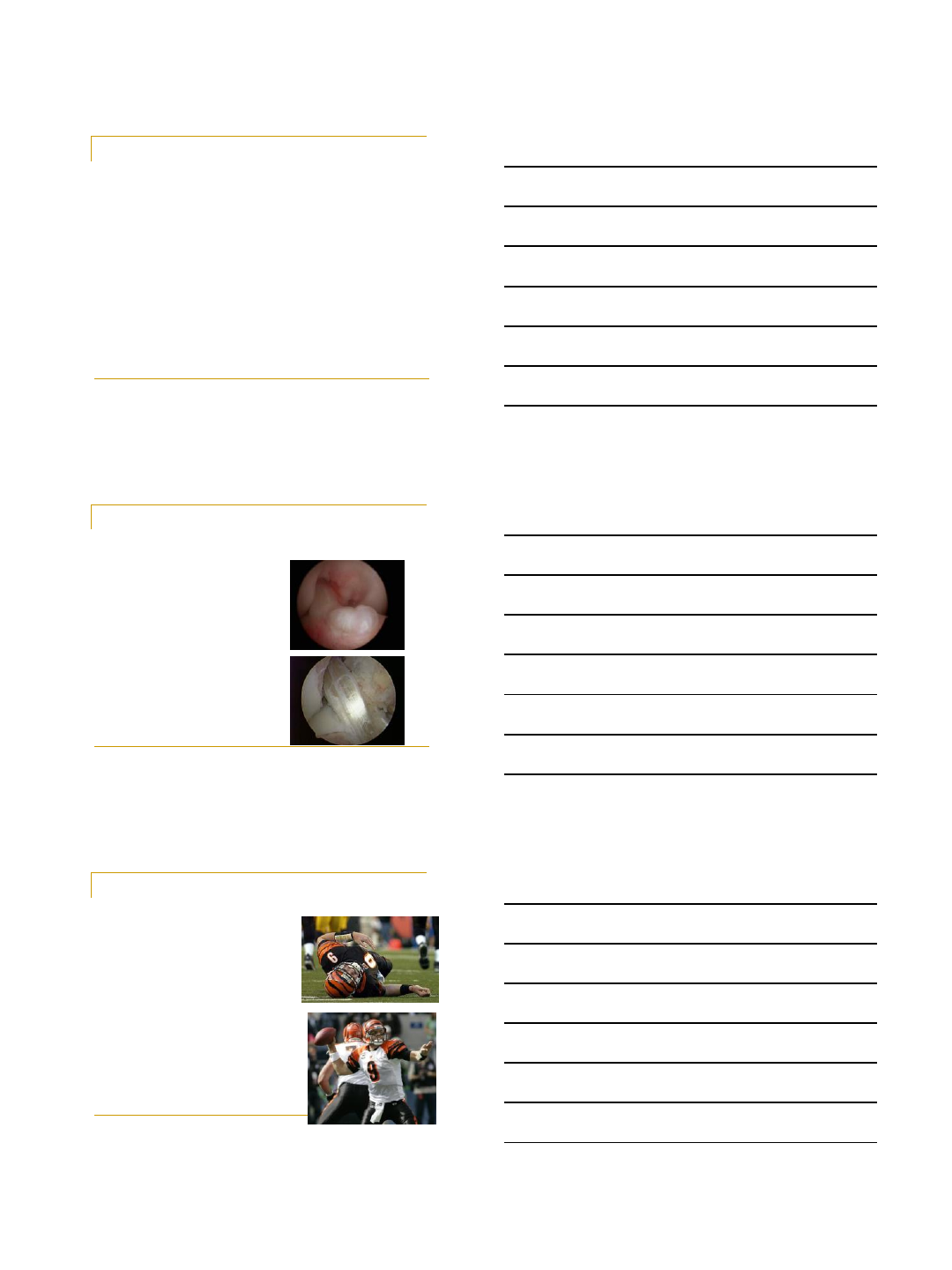
Perform a Wallplasty in Most Knees
•Assess width of
notch with a probe
that matches width of
the ACL graft
•Remove portion of
lateral femoral
condyle from apex of
notch to bottom
QuickTime™ and a
H.264 decompressor
are needed to see this picture.
View from Transpatellar Tendon Portal
QuickTime™ and a
Sorens on Video 3 decompres sor
are needed to see this picture.
QuickTime™ and a
Photo - JPEG decompressor
are needed to see this picture.
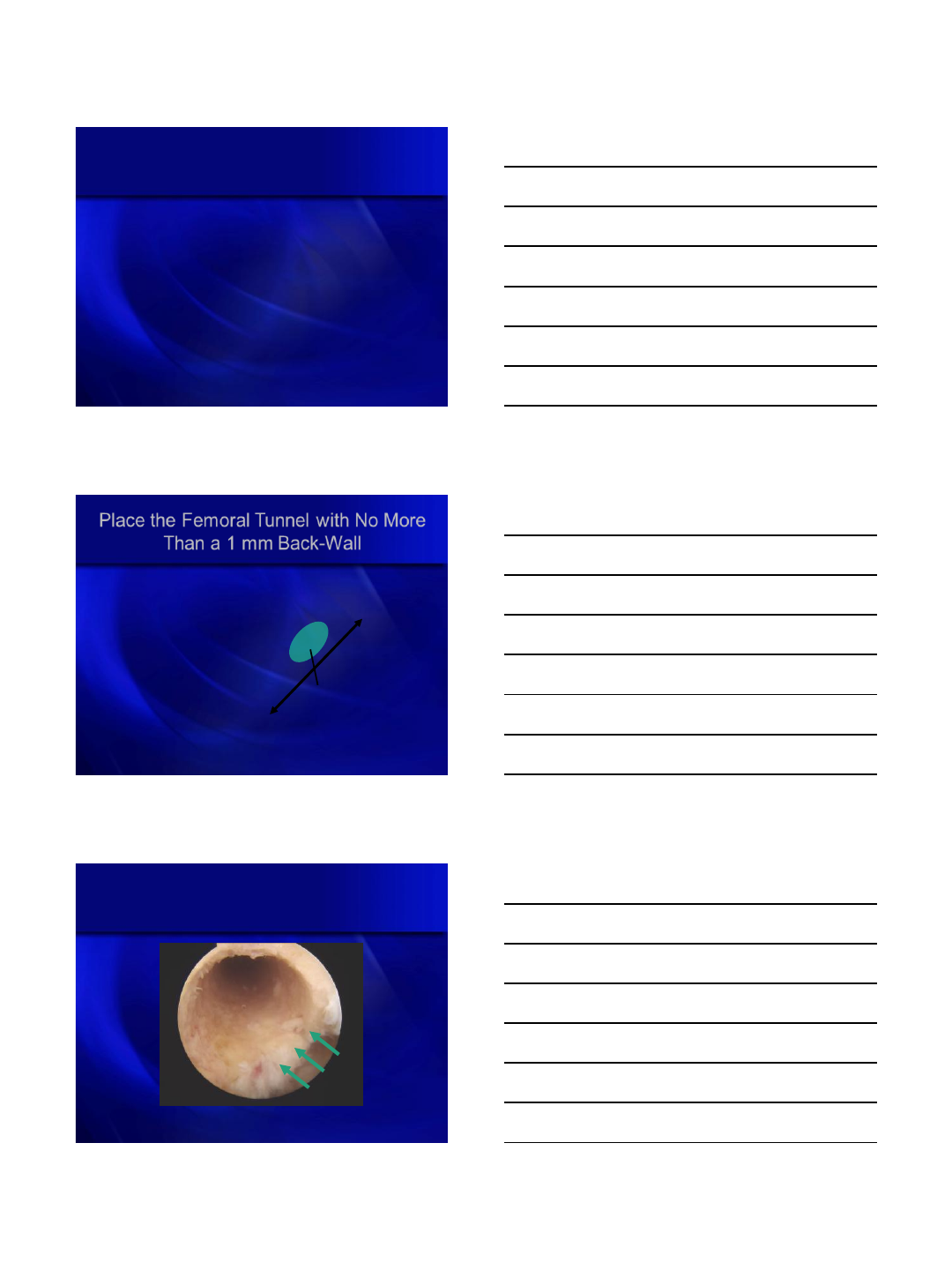
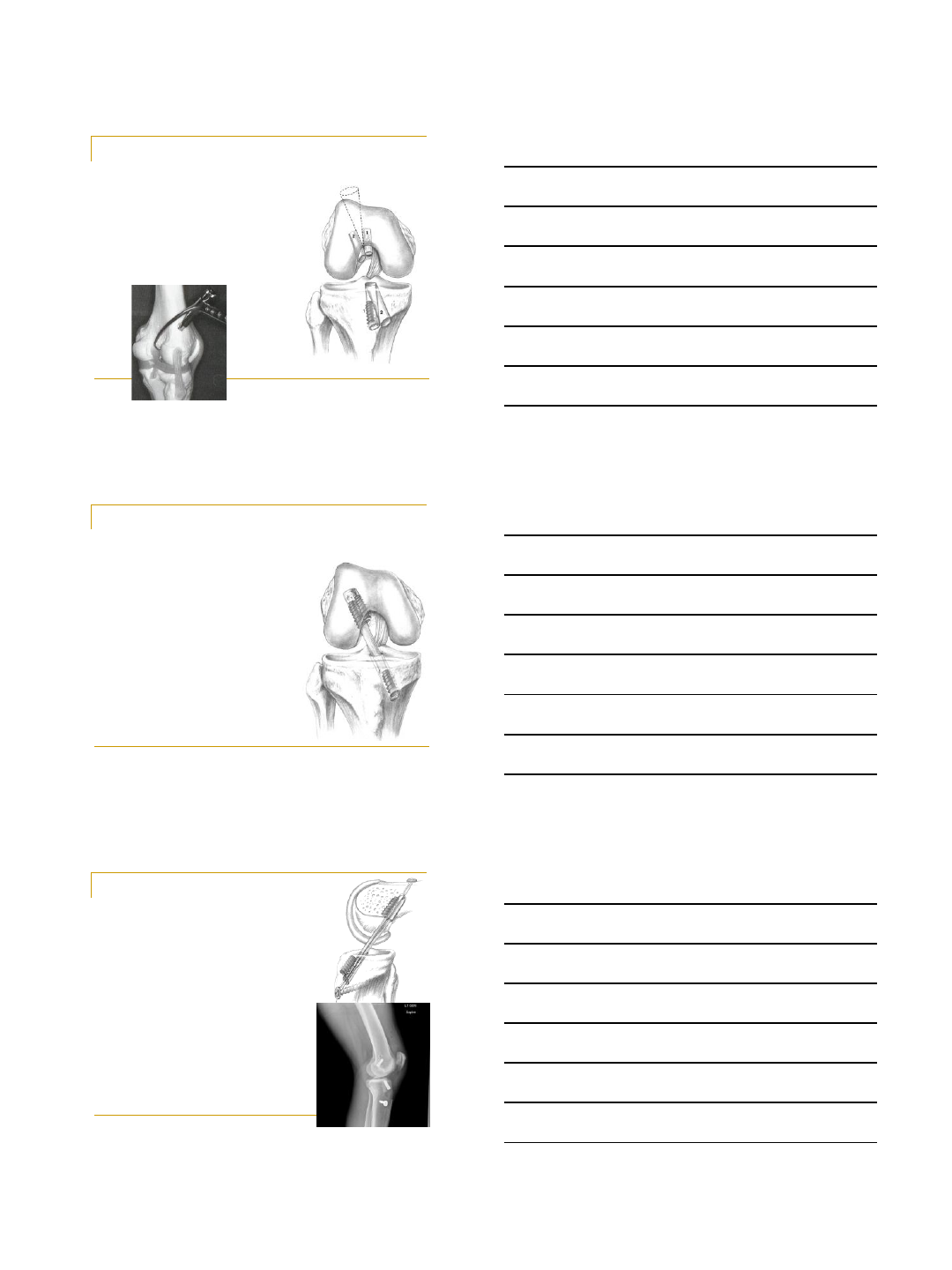
Place Femoral Tunnel NO MORE
than Half-Way Down Side-Wall
•Widen notch & avoid
placement close to
the PCL
•Insert, hook, & rotate
aimer away from PCL
•Moves femoral
tunnel down side
wall
50%
50%
View from Transpatellar Tendon Portal
QuickTime™ and a
Sorens on Video 3 decom pressor
are needed to see this picture.
QuickTime™ and a
Photo - JPEG decompressor
are needed to see this picture.
Photograph the ‘Triangle’ Documenting
there is No PCL Impingement
View from Transpatellar Tendon Portal
8/20/2012
6
Placement of Femoral
Tunnel
in the Sagittal Plane
•Applies to both the
transtibial and AM
portal techniques
•Consider an over-
the-top femoral
aimer with an
offset no more
than 1 mm
Place the Femoral Tunnel with No More
Than a 1 mm Back-Wall
QuickTime™ and a
H.264 decompressor
are needed to see this picture.
View from Transpatellar Tendon Portal
50%
50%
QuickTime™ and a
Sorens on Video 3 decom pressor
are needed to see this picture.
QuickTime™ and a
Photo - JPEG decompressor
are needed to see this picture.
Photograph the 1mm Backwall
Documenting the Femoral Tunnel is
Posterior
View from Transpatellar Tendon Portal
1 mm
8/20/2012
7
Summary
Findings of Danish ACL Registry
•Anteromedial technique has a 2 times greater risk of
revision compared to transtibial technique
•KSSTA, Star Paper, 2012
1 mm
Arthroscopically Document Femoral
Tunnel is Well-Positioned
•Photograph ‘triangle’
showing no PCL
impingement
•Photograph 1mm
back-wall showing
posterior femoral
tunnel
8/20/2012
8
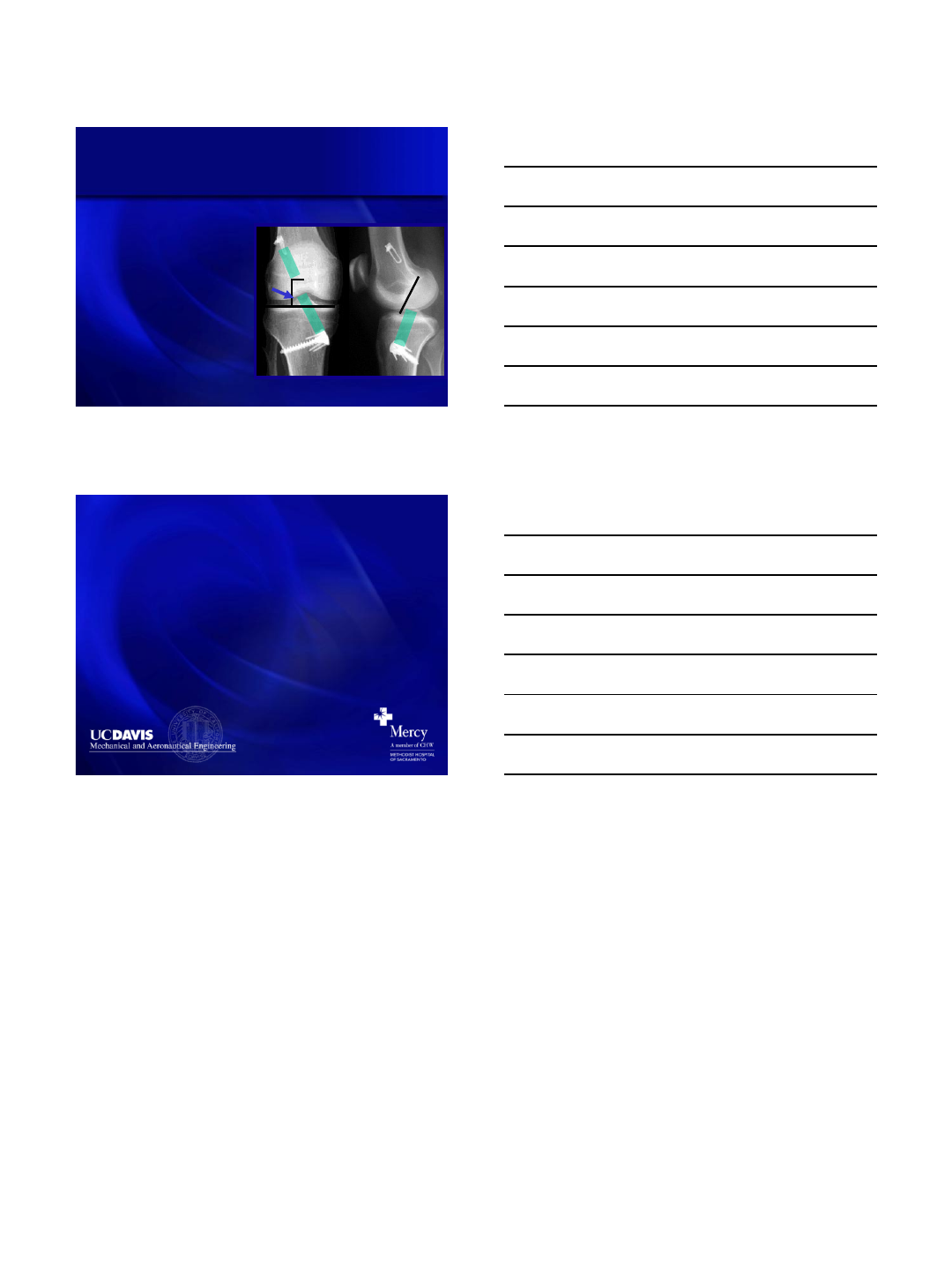
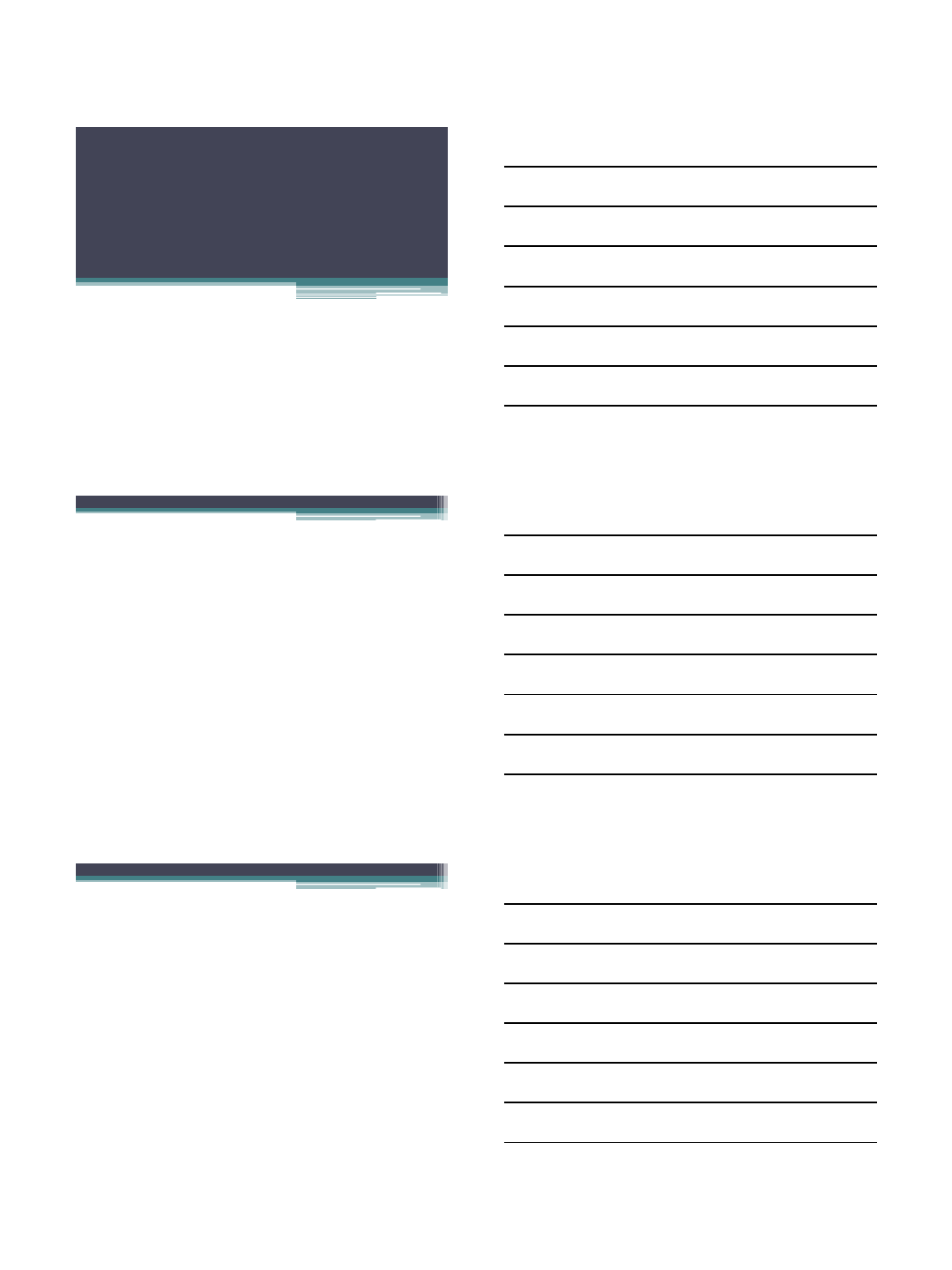
Radiographically Document Tibial and
Femoral Tunnels are Well-Positioned
•Coronal plane
•Widen notch
•Place tibial tunnel
through tip of lateral
spine
•Angle 60-650 (TT
technique)
•Sagittal plane
•Posterior to
intercondylar roof
•Parallel to
intercondylar roof (TT
technique)
60-65
Thank You!
ACL Surgery: Medial Portal
Pearls and Pitfalls
Darren L. Johnson, M.D.
Professor and Chairman
Department of Orthopedic Surgery
Medical Director of Sports Medicine
University of Kentucky School of Medicine
Disclosure
•Consultant: Smith-Nephew Endoscopy
–Royalties: Instrument development
•Institution: Research/Education
–Smith-Nephew Endoscopy
–DJO Orthopaedics
Clinical experience
•19 years: Academic
•100% sports practice
•KNEE/SHOULDER
•450 cases/yr
•175-200 ACL/YR
•25-30+ REVISION
ACL
•20 COMBINED
PCL/MCL/FCL
•Acute/Chronic
•Fellowship:3 fellows
Reproducing Anatomy
“Whenever you are having your
anatomy sessions, pay particular
attention, because orthopaedics is
all anatomy, plus a little bit of
common sense.”
J. Hughston
ACL Technique
Secret of Success
•Perhaps the most
important factor for
ACL Reconstruction
in 2012 is surgical
technique!
–Anatomic ACL
Reconstruction!
Forsythe B, Kopf S, Wong A, Martins C, Anderst W, Tashman S,
Fu F. J Bone Joint Surg Am. 2010;92:1418-1426.
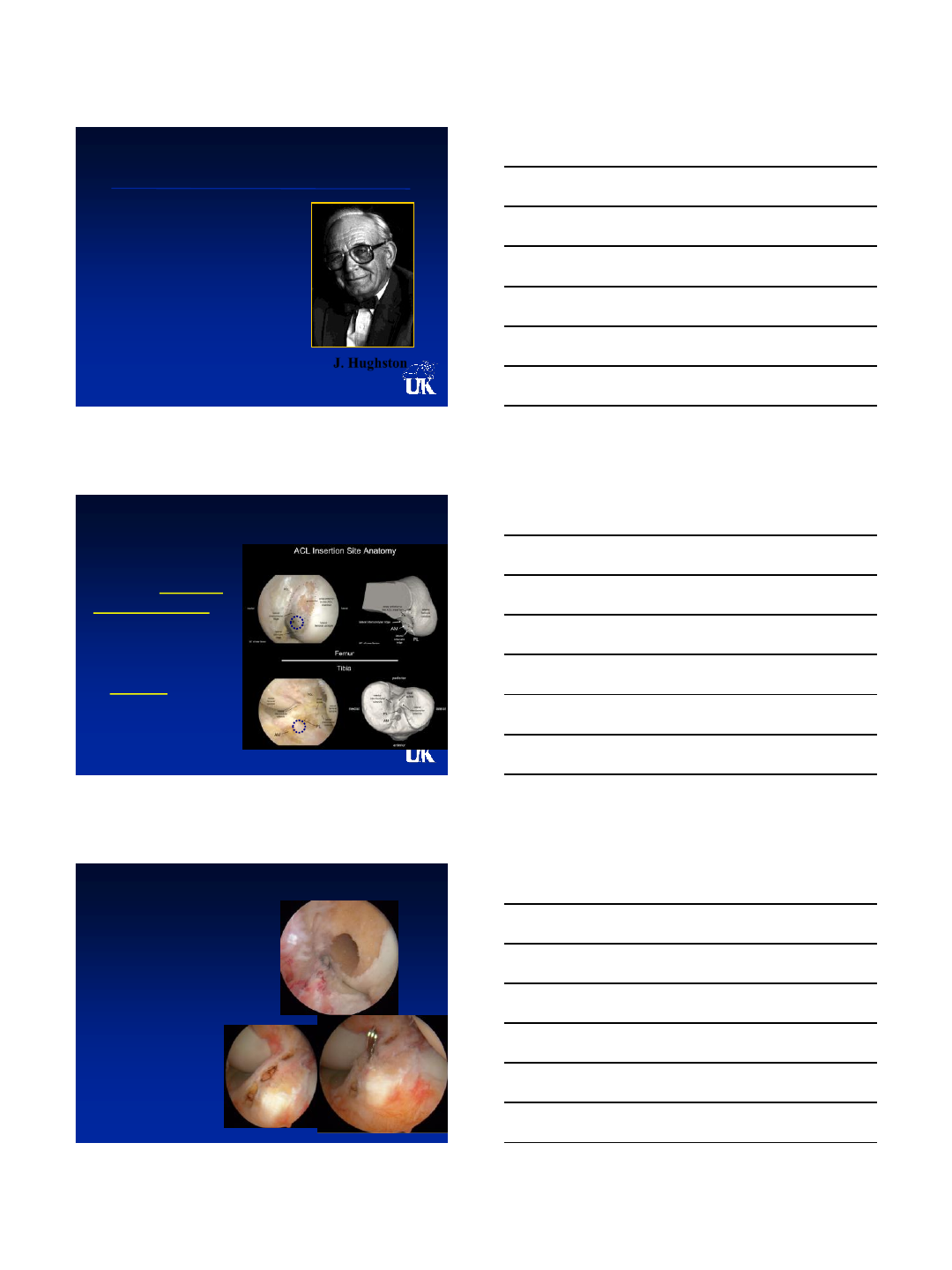
Why Medial Portal drilling??
•Anatomy:100% fill
of tunnel within
native footprint
•Independent tibial
tunnel placement
•Size of opening is
accurate: not oval
P
L
SB
A
M
SB
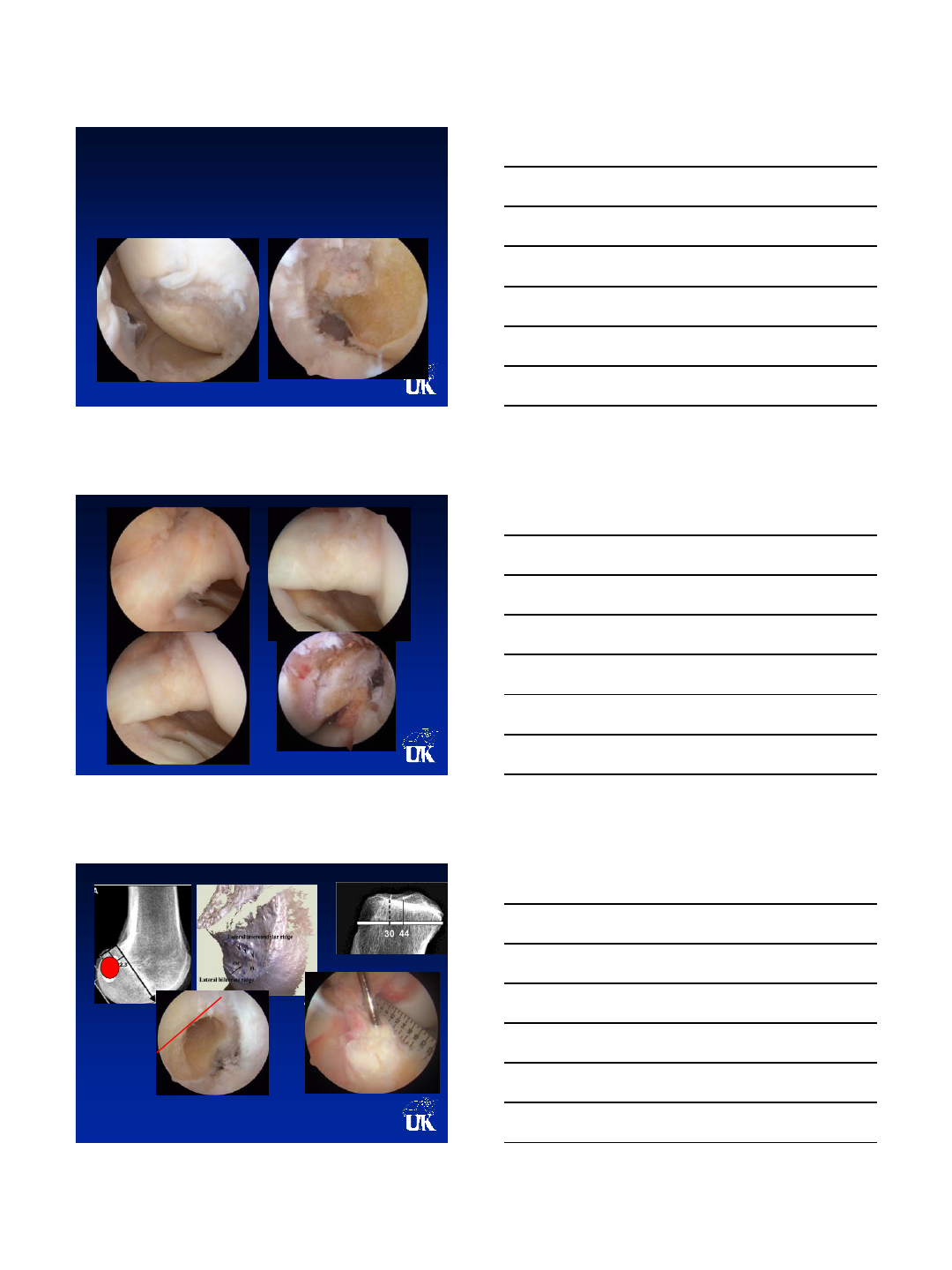
Pitfalls of MP drilling
•Damage to MFC
•Short femoral tunnel
•Posterior blow-out
Zantop T, Wellman M, Fu FH, Petersen W. Tunnel Positioning of Anteromedial and Posterolateral
Bundles in Anatomic Anterior Cruciate Ligament Reconstruction: Anatomic and Radiographic
Findings. Am J Sports Med. 2008; 36:65-72.
Anatomic ACL Reconstruction
90
°
Patient Setup is Critical
•Patient Set up for
Hyperflexion in
Arthroscopic Leg
Holder
•Note Flexion of Hip
Which Allows Knee
Hyperflexion
Portal Placement is Critical
•MUST Include
Accessory
Anteromedial Portal
For Drilling and
Fixation of Femoral
Tunnels
High “Tight” Anterolateral
Low “Tight” Anteromedial
Accessory Anteromedial
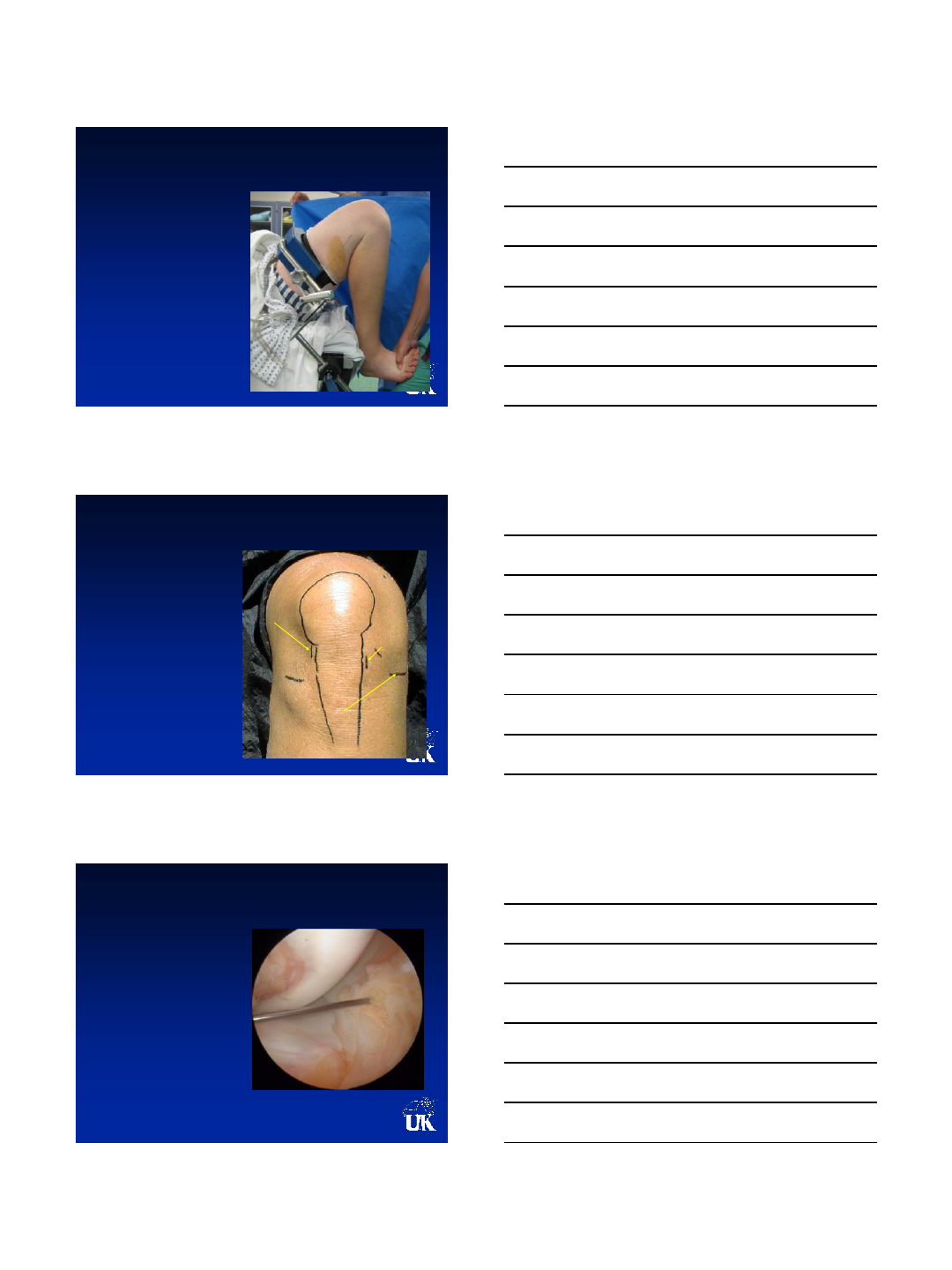
Accessory Far Medial Portal
•Create Under Direct
Visualization of
Spinal Needle
•Just Over Medial
Meniscus
•Horizontal Allows
Side-to-Side
Movement for
Drilling and Pins
•Drill is
perpendicular to
wall: round tunnel
not oval!

Drilling femoral tunnel
•130º Flexion
•Guide Pin and
Drilling From
Accessory Medial
Portal
•View From mid
portal
•Direction
determines tunnel
length: 32-40mm
•Aim proximal to FCL
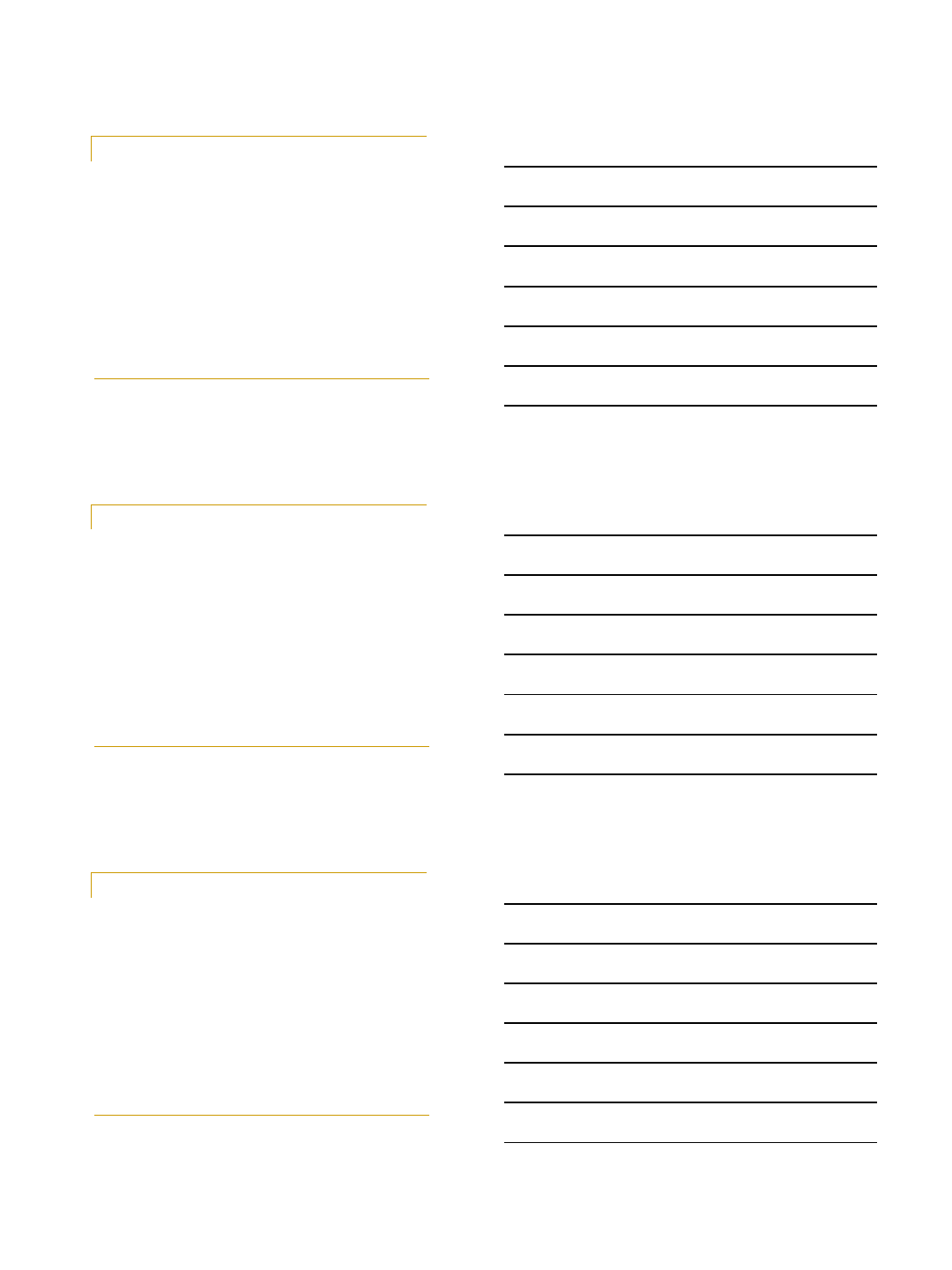
Femoral Tunnel
X-ray Anatomic SB
Video Clip
Future of ACL Surgery
We will individualized the surgery/rehab/RTP to
the athlete, injury pattern, unique patients
anatomy/pathologic kinematics. Not all
athletes with an ACL injury will have the same
operation/rehabilitation timeline/RTP
THANK YOU
8/16/2012
1
Central Quadriceps Free Tendon
Reconstruction of the ACL
John P. Fulkerson
Orthopedic Associates of Hartford
Clinical Professor of Orthopedic Surgery
University of Connecticut School of Medicine
Farmington, Connecticut
•The author is president of the Patellofemoral
Foundation that receives undirected grant
support from Smith and Nephew and DJO
Why use quadriceps free
tendon for ACL reconstruction?
•Easy Access, low morbidity harvest
•Less pain and quicker rehab than other
autografts (Joseph et al)
•Preserve hamstrings-no loss of power in flexion
•No added risk of patella fracture
•Strong graft
•Possible simultaneous harvest
•No evidence of anterior knee pain at long term
follow up (DeAngelis, Cote and Fulkerson)
8/16/2012
2
Original Descriptions-Quad tendon
with bone
Marshall, Blauth, Staubli
•Quad tendon in continuity with patellar
tendon: Clin Orthop 143: 97-106, 1979.
•Quad tendon with bone: Unfallheilkunde 87:
45-51, 1984
First published description of quad
tendon without bone for ACLR 1998
•Isolated Quad
tendon without
bone: Techniques
in Orthopedics
13(4): 367-374,
1998.
• Op Tech Sports
Med 7:195-200,
1999.
Quad tendon strength
•The Central Quad
Tendon is thicker than
the patellar tendon
•9 vs 4.8 mm thick
•Staubli has shown
comparable strength
•Partial thickness (7mm)
harvest is preferable
•No rupture or problem
with quad tendon in 17
year experience using
CQT for ACLR
8/16/2012
3
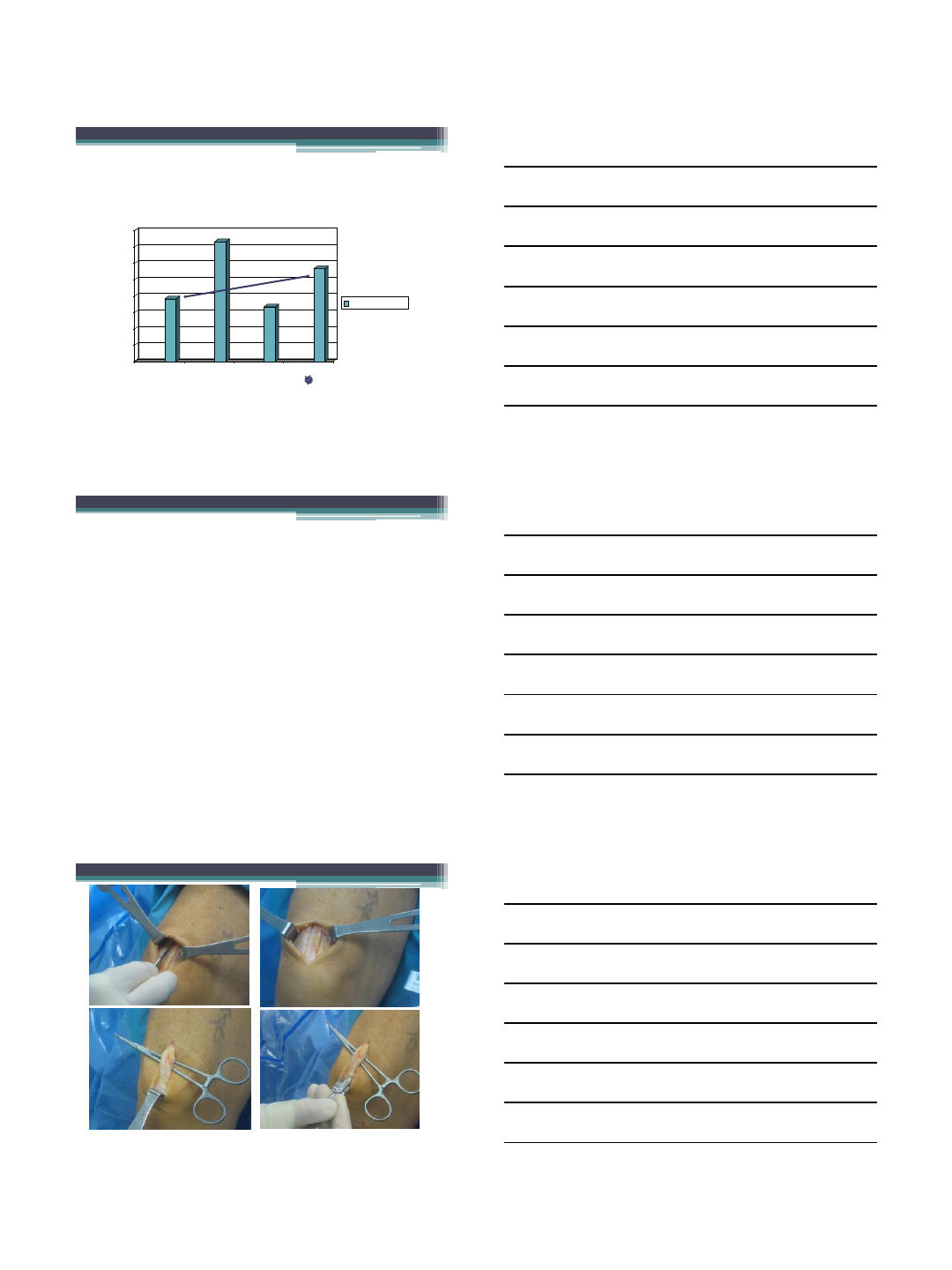
Quad tendon is stronger after CQFT
harvest than PT before
harvest(Mazzocca)
0
500
1000
1500
2000
2500
3000
3500
4000
Intact PT Intact QT harvestPT harvestQT
3-D Column 3
Newtons to failure
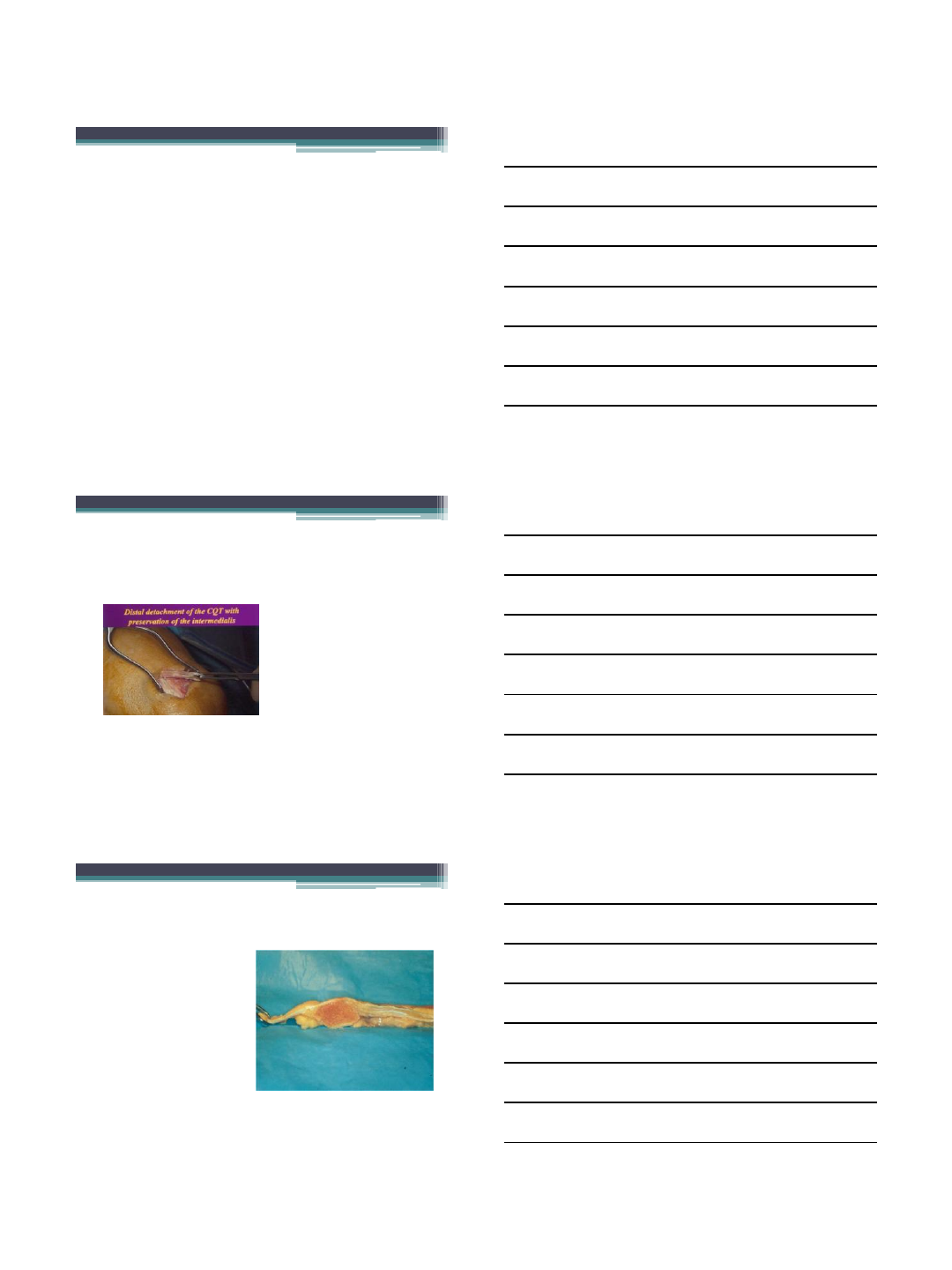
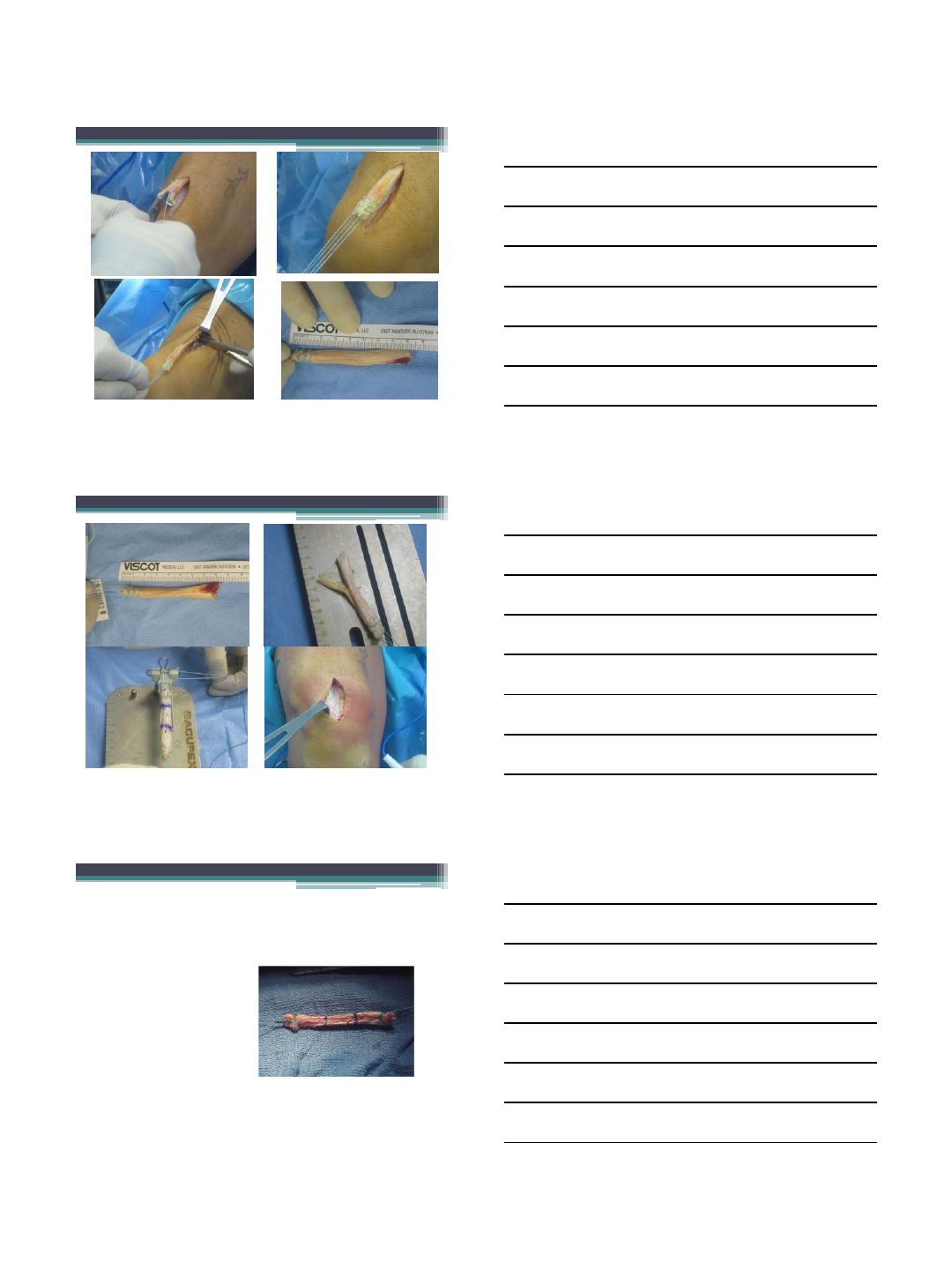
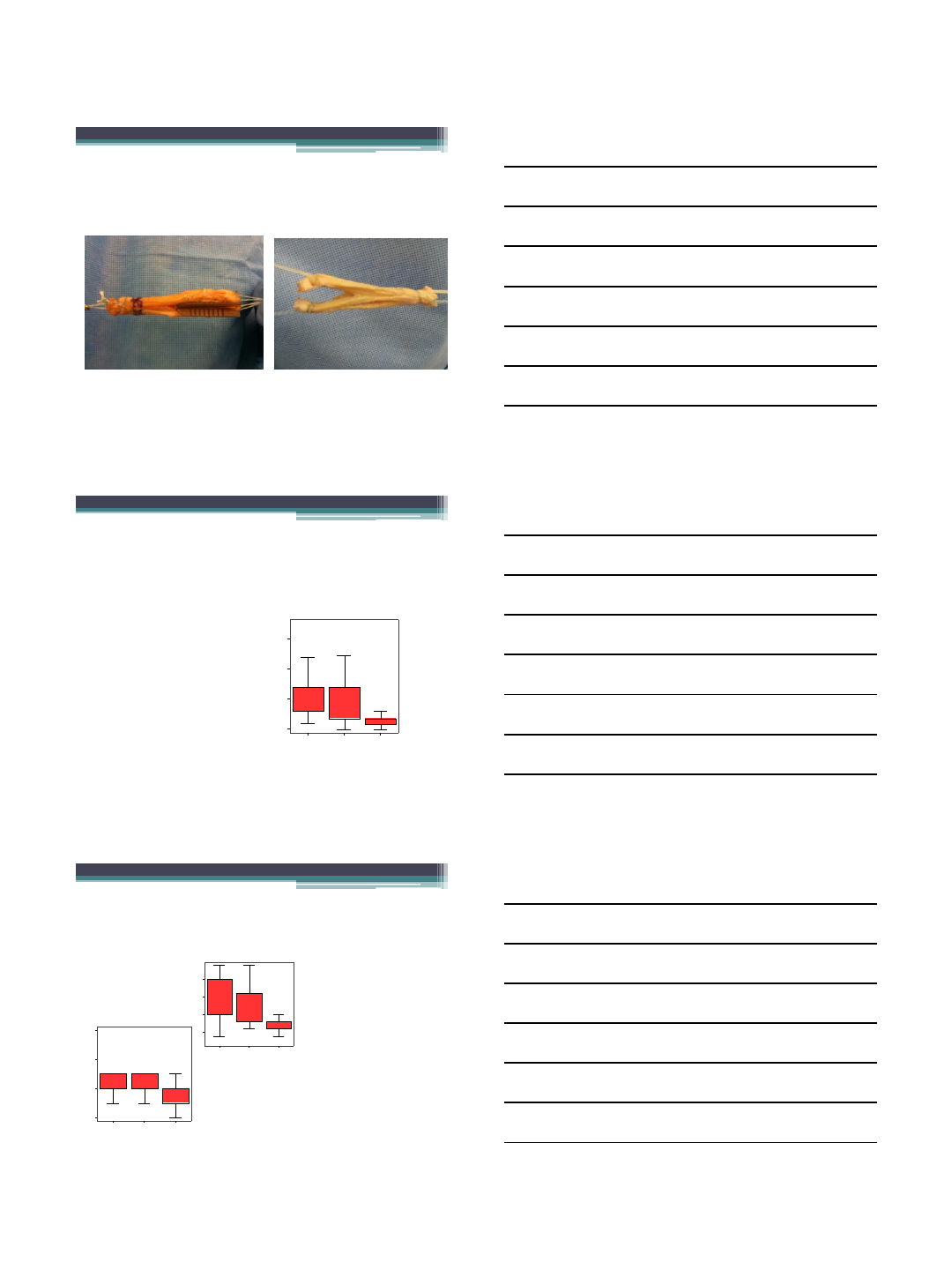
Release under direct vision
•Pull tendon distally and release
•At least 7 cm from distal end
•Then whip stitch the second end
8/16/2012
4
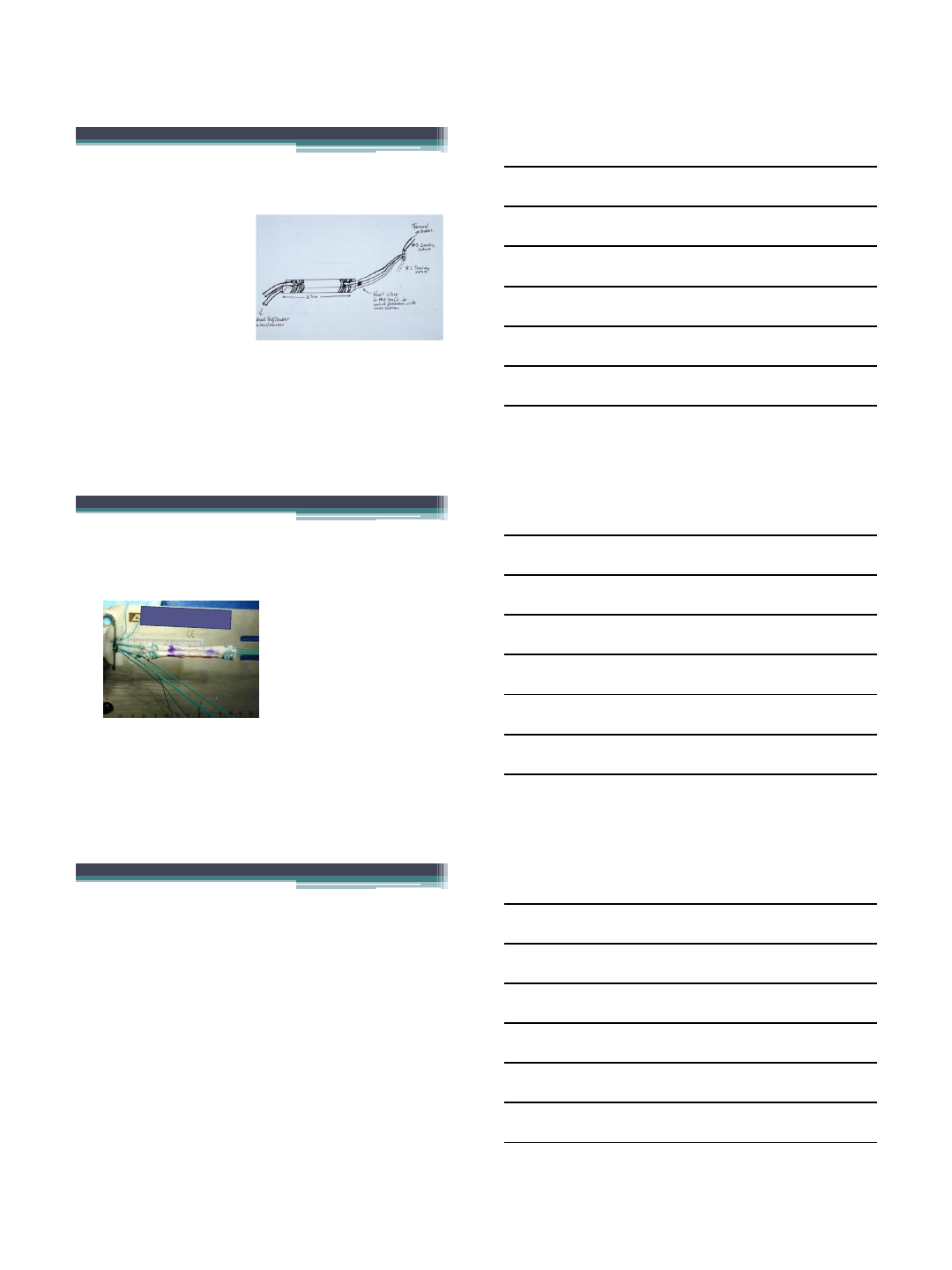
CQFT GRAFT
•2-2.5 cm in each
tunnel
•Bone disk option on
femoral end to meet
screw tip
•#5 nonabsorbable
suture whip stitches
•7 cm long graft or
longer
8/16/2012
5
The endobutton works well with
CQFT
•Our experience with
endobutton fixation has
been very successful.
•With four strands of
ultrabraid or fiberwire,
fixation is extremely
secure.
•Short tunnel with
anatomic femoral
fixation and “bungee
cord” effect has not
been noted
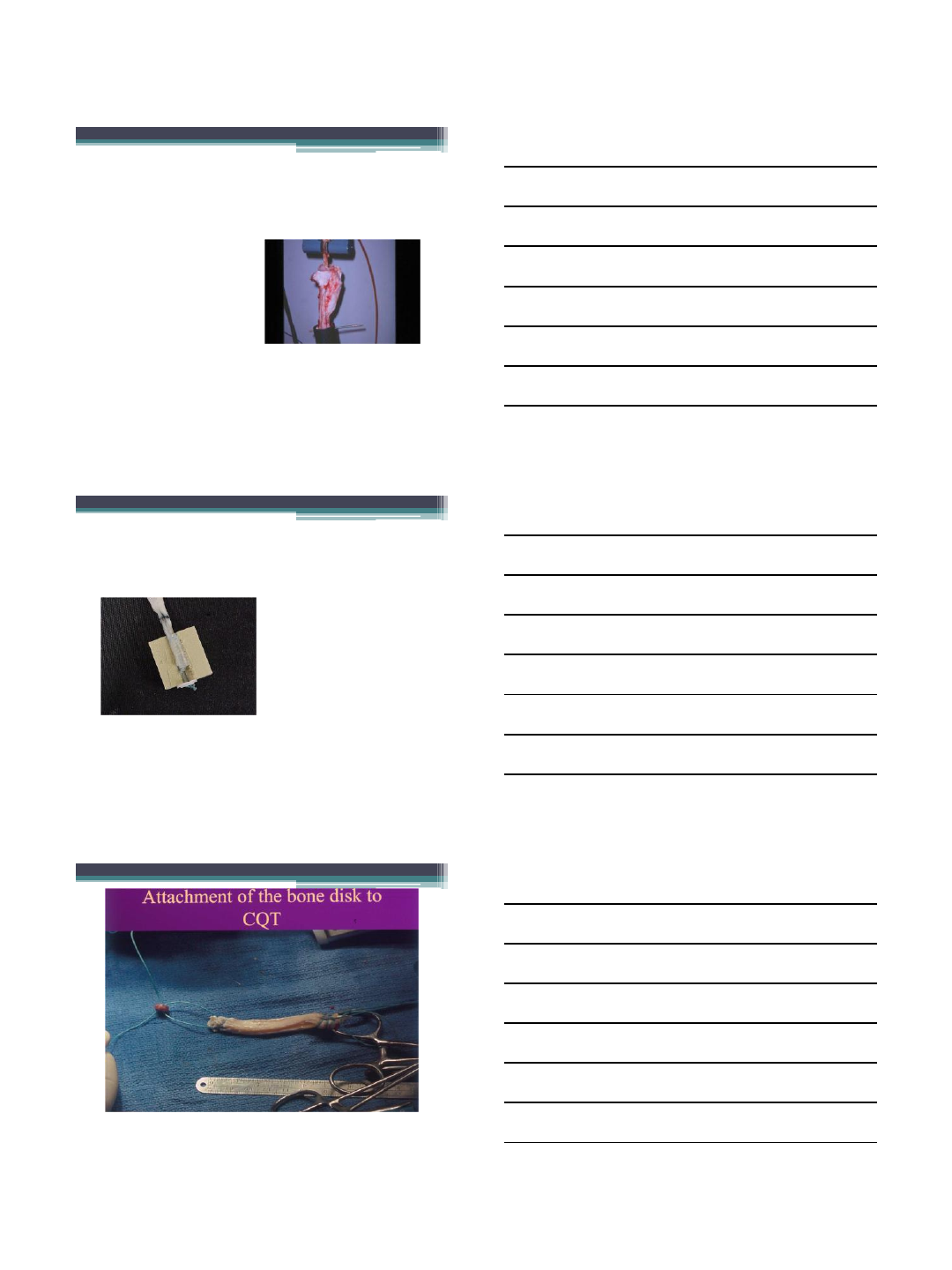
Preparation
•# 5 whip stitches (4
strands) each end.
Currently use
Ultrabraid
•Endo button
•Play
Video
8/16/2012
6
MTS Testing of CQFT Fixation using
biointerference screw
•With Compression
and Anchor
fixation, using
bioabsorbable screw in
a”stuffed”tunnel one
size smaller than the
screw, there is <1mm of
slippage after 2500
cyclical loads of 150
Newtons (Nagarkatti,
Jan/Feb 2001 AJSM)
Load to failure-soft tissue screw
with button anchor
•Note graft tearing
beyond screw (density
matched foam bone)
•Button reduces slippage
to very low level
•Illustration courtesy of
Patrick Kwok, M.D.
This is an option, but I do not currently use this technique
8/16/2012
7
CQFT advanced into femoral socket
•Graft should be snug
in the socket such
that passage will
require a firm pull
and probe
assistance
•Ultrabraid, #5
ethibond or
fiberwire sutures
My preference
•Endobutton with Ultrabraid (4 strands) whip
stitched on femoral end
•With or without biointerference screw femoral
side
•Recessed biointerference screw or button on the
tibial side
We can say with confidence that you do
not need to take a bone block from the
patella any more than you need to take
bone with a hamstring graft
8/16/2012
8
Double bundle options with quad free
tendon
Quad tendon has intermedius and rectus components
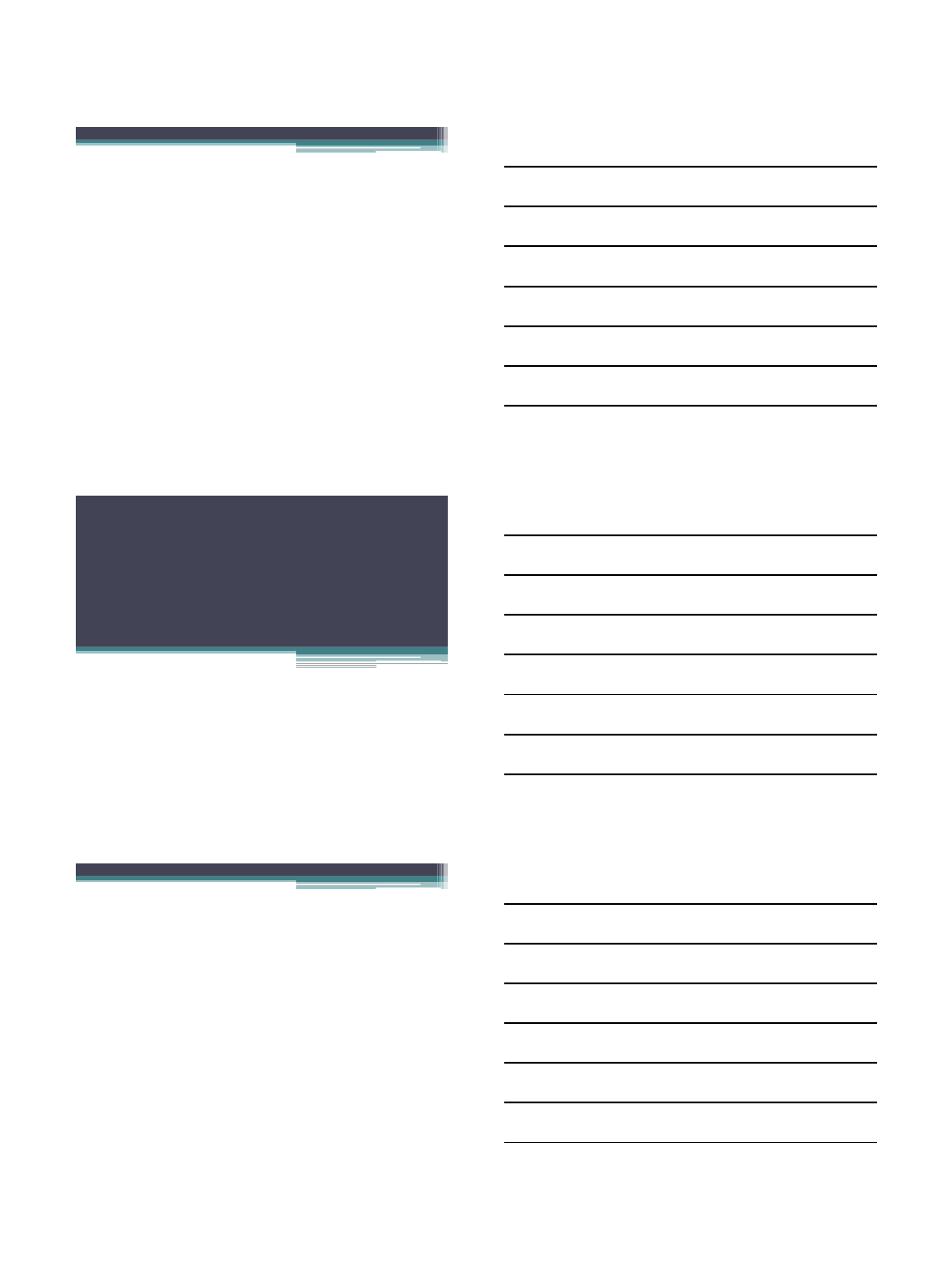
Post operative pain medication after
ACLR comparing BTB, hamstrings,
and CQFT
•Perhaps most
striking of all is the
consistently
diminished pain
medication
requirements of
CQFT reconstructed
patients (Joseph,
2000)
Days to zero pain meds by graft types
BT B Hamstrng Quad Td n
Graft type
0
20
40
60
Meds(days)
n=25 n=21 n=18
Restoration of ROM after CQFT ACLR
compared to BTB and hamstring
Weeks to full extension by graft types
BTB Hamst rng QuadTd n
Graft type
2.5
5.0
7.5
10.0
Full Ext
n=25 n=21 n=18
•Mick Joseph
(independent PT)
studied BTB,
hamstring, and
CQFT ACLR
prospectively and
found more rapid
return of ROM in
CQFT patients
Weeks to 120 P-Flex by graft types
BTB Hamst rng QuadT dn
Graft type
3
5
7
9
120 Flex
n=25 n=21 n=18
8/16/2012
9
CQFT data >2 years
•DeAngelis et al. Clinics in Sports Med 26(4), October
2007. 66 month mean f/u (24-105). Five patients
with known graft failure out of 154 patients >2 years.
Using Noyes’ criteria of arthrometric success up to 5
mm side-side, 94% success at > 1 year (86% <3mm).
Single leg hop quotient 0.96
•>90% return to pre-injury athletic activity
•Two NCAA national champions after CQFT ACLR-
lacrosse (Univ of Virginia) and gymnastics (Univ of
Michigan)
•No anterior knee pain or motion loss >2 yrs (Cote)
•Walter Shelton is reporting similar results with quad
free tendon ACL reconstruction (Arthroscopy, 2010).
No anterior knee pain or loss of
motion at follow up >2 years!
\
Conclusions regarding CQFT
•Very favorable results at average f/u>5 years
(DeAngelis, 2007)
•No ROM loss or anterior knee pain in our f/u.
•Residual strength of quad tendon after harvest is
greater than patella tendon before harvest.
•Well suited for double bundle ACLR
•Less post op pain and risk than other autografts
•Least morbid of the autograft alternatives with
comparable long term results. Therefore, quad tendon
without bone is our first choice autograft for all ACLR
patients
Revision ACL Reconstruction
-Causes-
VuMedi Webinar
Avoiding Complications and
Revision ACL Reconstruction
Dr. Freddie H. Fu
Distinguished Service Professor
David Silver Professor and Chairman
Department of Orthopaedic Surgery
University of Pittsburgh
Head Team Physician
University of Pittsburgh Athletic Department
Anatomic ACL Reconstruction is the
functional restoration of the ACL to its
native dimensions, collagen
orientation, and insertion sites.
Individualized Anatomic
ACL Reconstruction
http://www.vumedi.com
van Eck, Fu et al. Arthroscopy, 2010
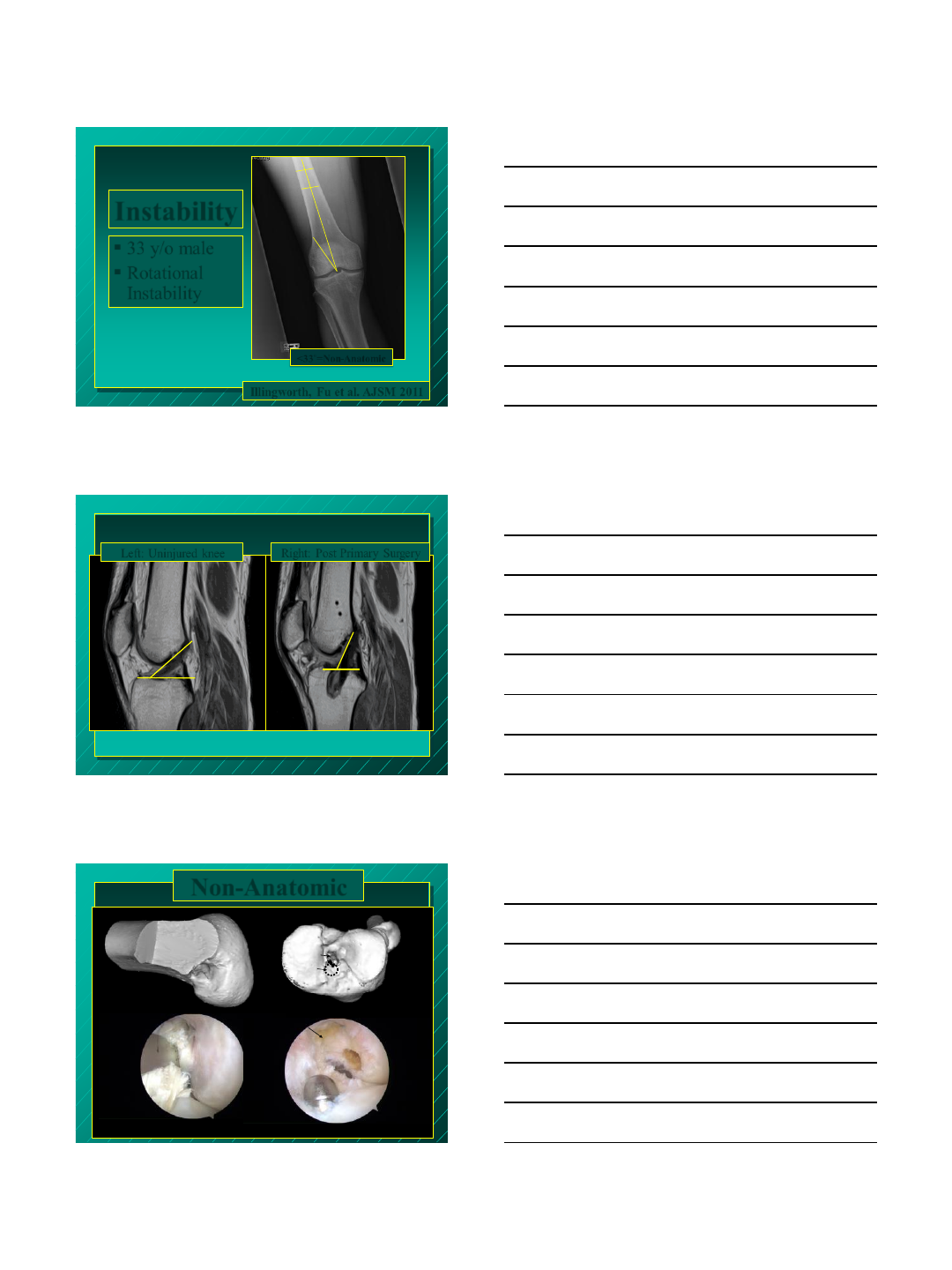
33 y/o male
Rotational
Instability
Instability
8°
Illingworth, Fu et al. AJSM 2011
<33˚=Non-Anatomic
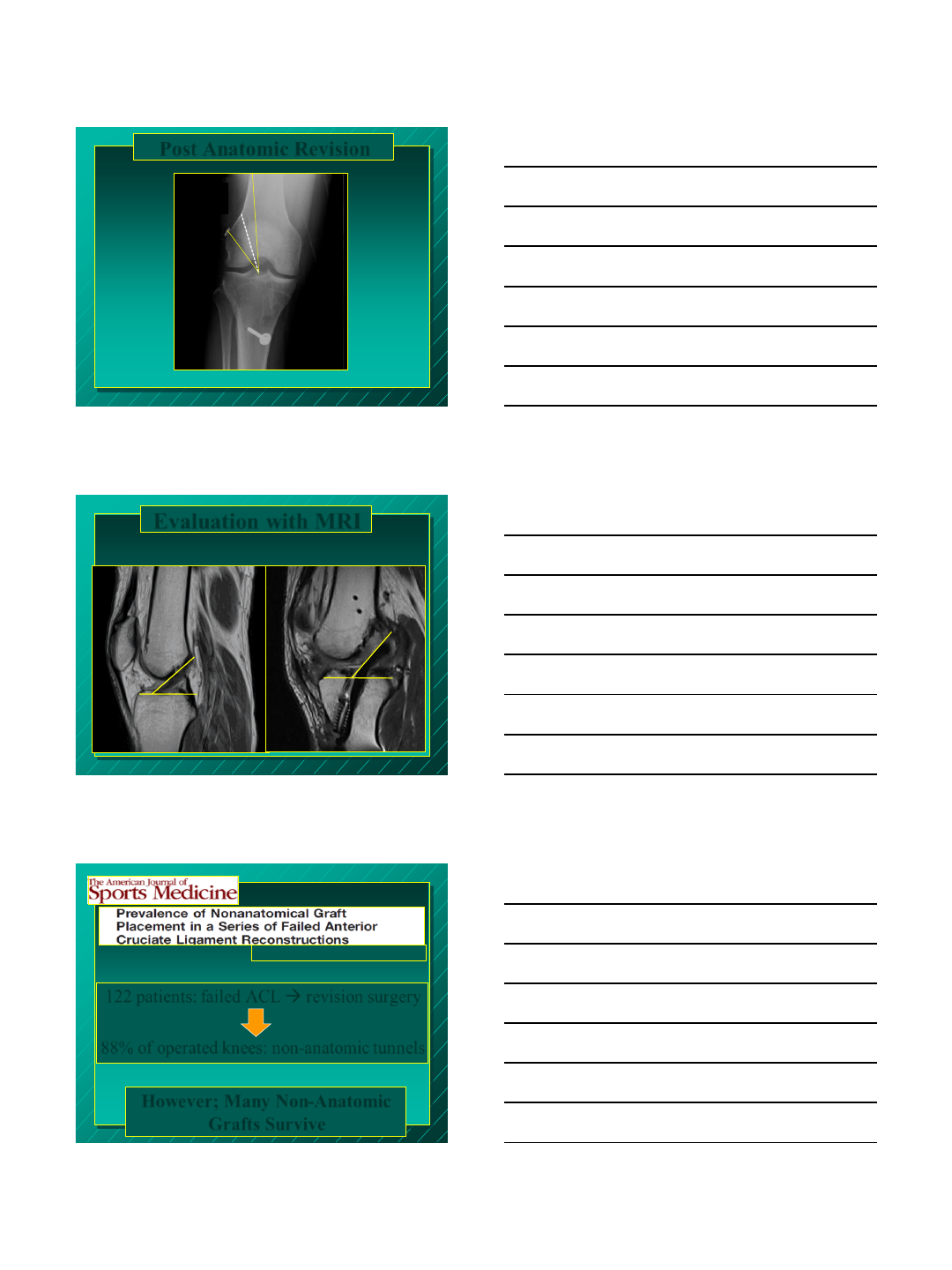
Right: Post Primary Surgery
77.8°
45.3°
Left: Uninjured knee
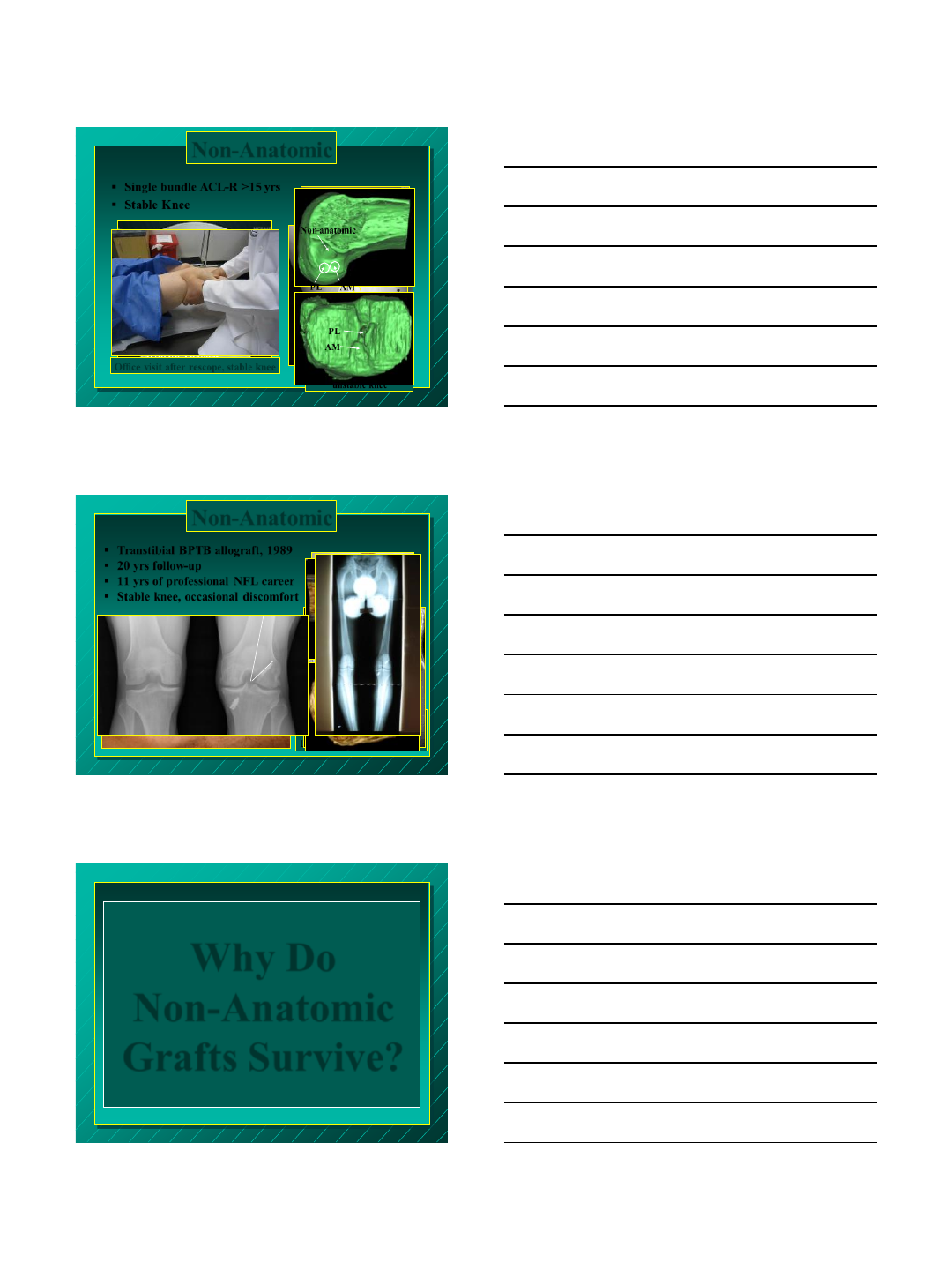
Non-Anatomic
PL
Old
Tunnel
PL
AM
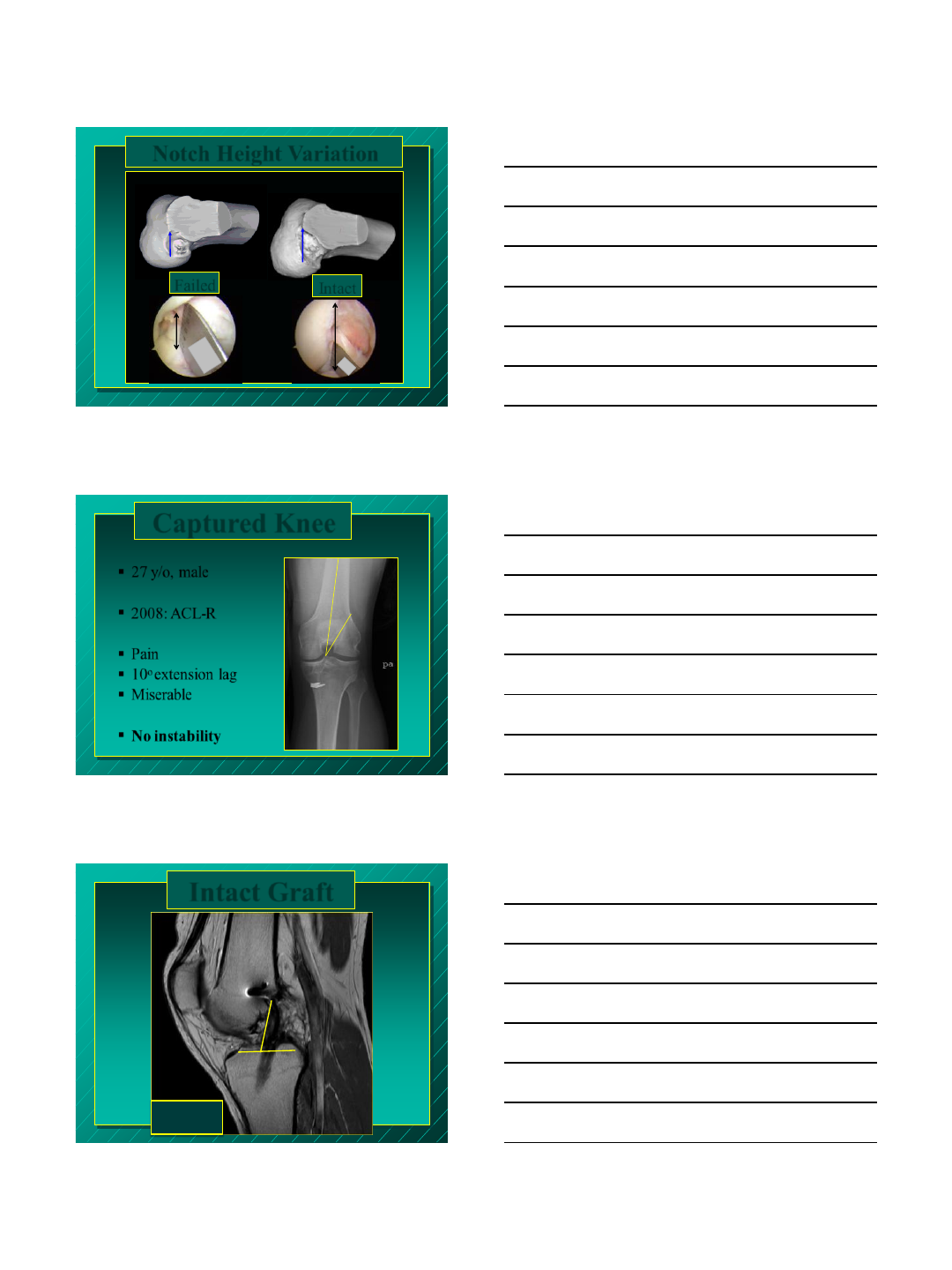
Post Anatomic Revision
49°
New Tunnel
Old Tunnel
Evaluation with MRI
Left: Uninjured knee Right: Post Anatomic Revision
46 °
45.3°
122 patients: failed ACL revision surgery
88% of operated knees: non-anatomic tunnels
Marchant, Noyes et al. AJSM Oct. 2010
However; Many Non-Anatomic
Grafts Survive
PL
Non-anatomic
AM
Office exam: stable knee
Under anesthesia:
unstable knee
Single bundle ACL-R >15 yrs
Stable Knee
10°
arthritic changes
Non-anatomic
AM
PL 90
°
PL
AM
Office visit after rescope, stable knee
Non-Anatomic
Transtibial BPTB allograft, 1989
20 yrs follow-up
11 yrs of professional NFL career
Stable knee, occasional discomfort
Post-OP 1989
ROM:
Right (operative): 7 to 137
Left: -2 to 142
PL
AM
AM
PL
Non-anatomic position
90º
33º
Arthritic changes Left: 4° Varus
Right: 8.5° Varus
Non-Anatomic
Why Do
Non-Anatomic
Grafts Survive?
Notch Size Variation Notch Height Variation
10mm
11mm
25mm
Notch Width (9-21mm)
Notch Height (10-28mm)
11mm
11mm
25mm
11mm 25mm
Failed Intact
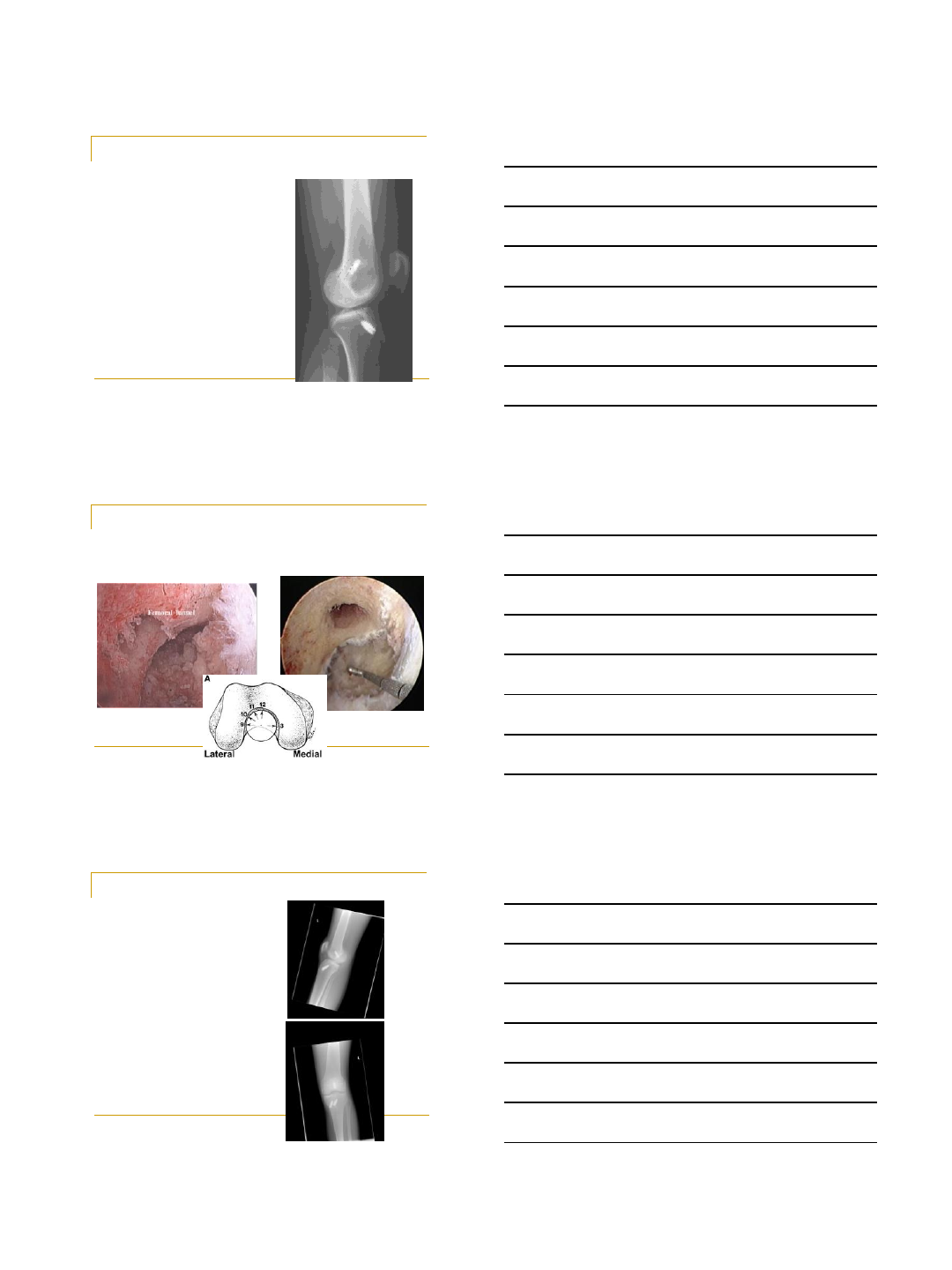
27 y/o, male
2008: ACL-R
Pain
10o extension lag
Miserable
No instability
Captured Knee
20
72°
Average
43˚ - 57˚
Intact Graft

Non-Anatomic
Intact Graft Non-Anatomic
5 Days Post Op
17
53
Relieved Patient
Increased Extension
We Have To Eliminate
Non-Anatomic ACL
Reconstruction as a Risk
Factor For Osteoarthritis

What Did We Tell Our
Patients?
95% Success Rate
Back to Activity in 6 Months
Criteria to Return to
Sports
Full Range of Motion
Quadriceps-Strength
Graft-Healing?
Return to Sports
6 Months Post-op:
Went Back to
Practice
MRI:
Immature Graft
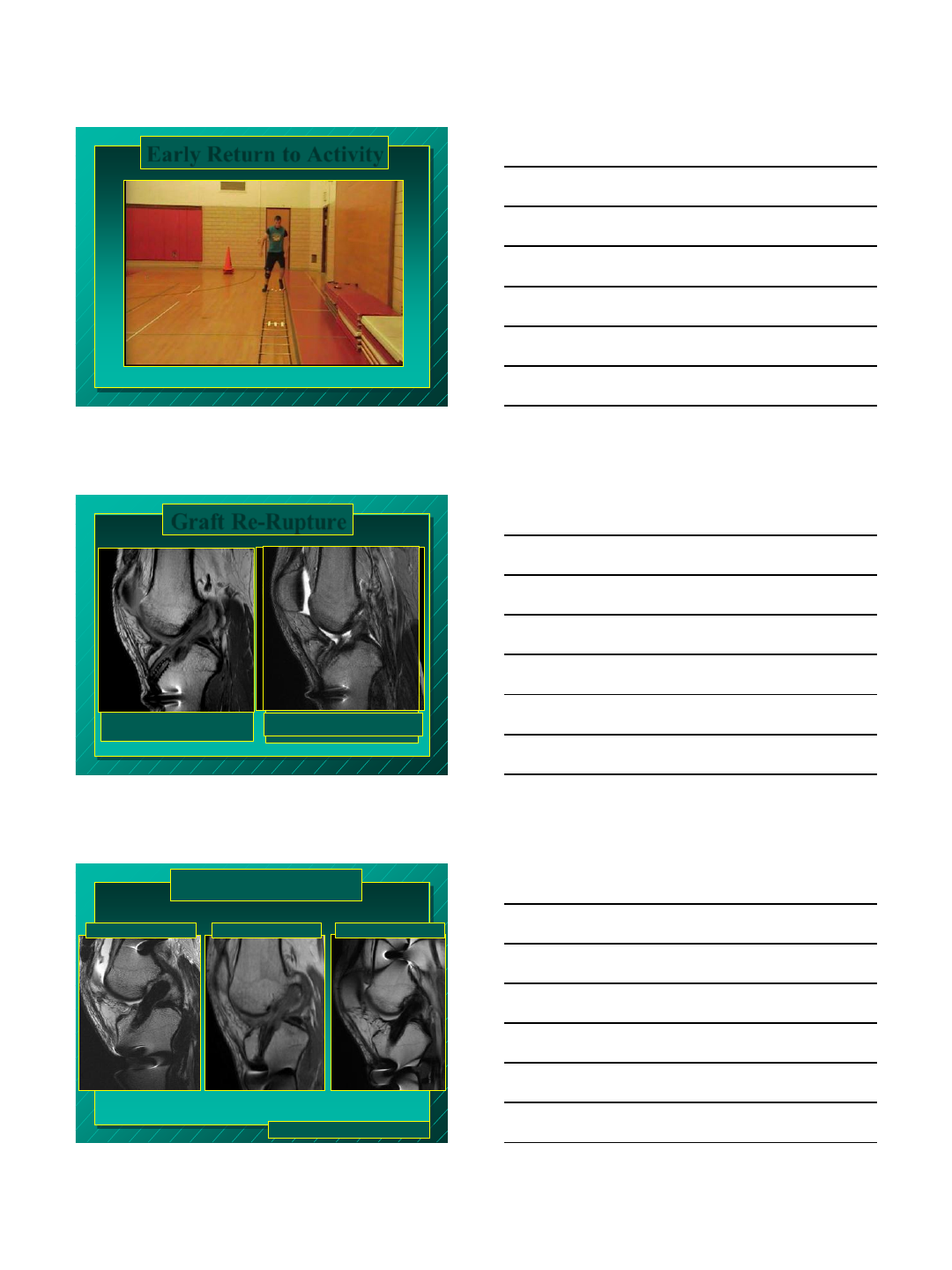
Early Return to Activity
AM
PL
4 yr post ACL-R
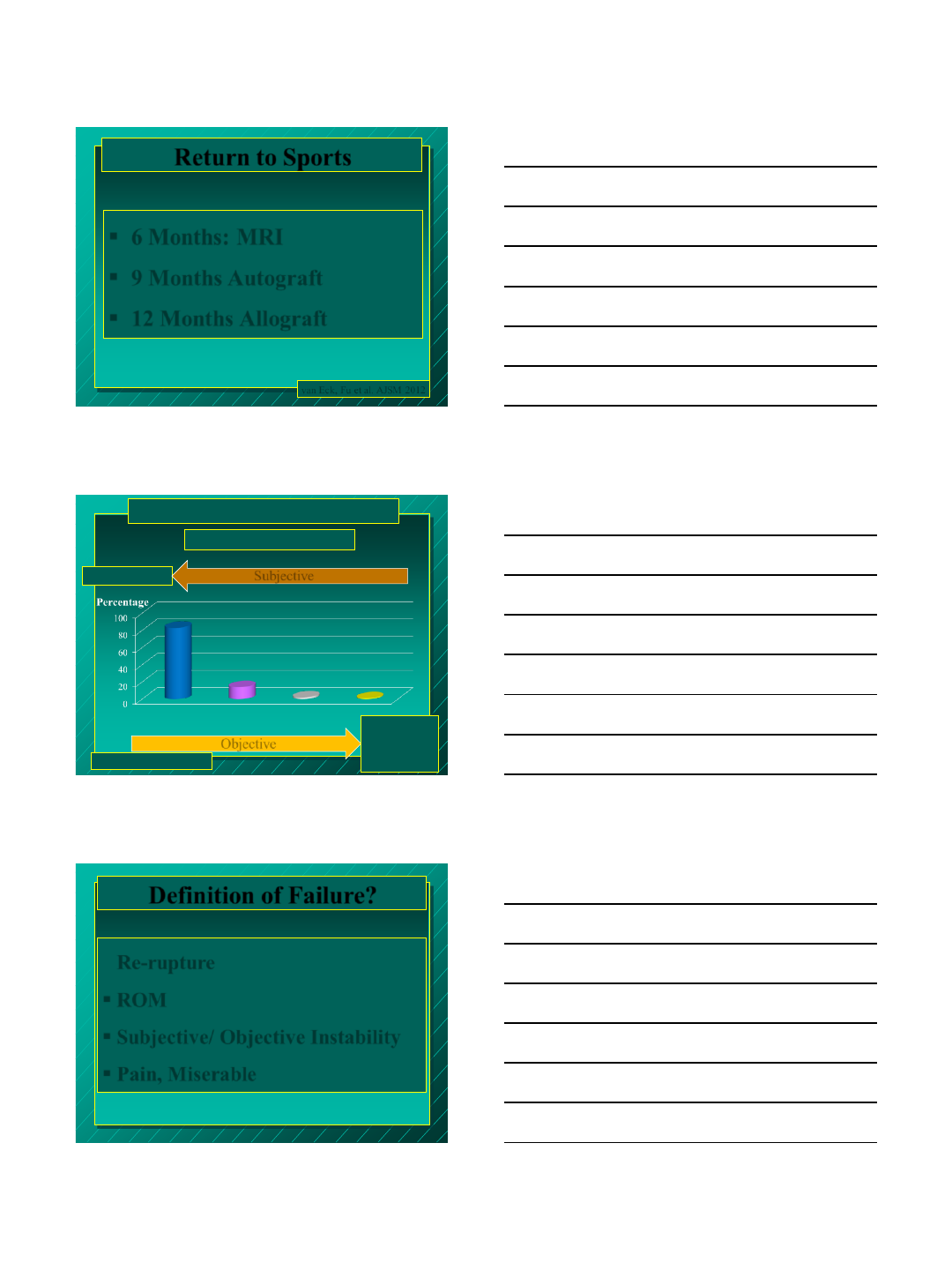
Healed Graft
Graft Re-Rupture
Re-rupture
4 months post ACL reconstruction
Unhealed Graft
Miyawaki, Fu et al. Ongoing Study
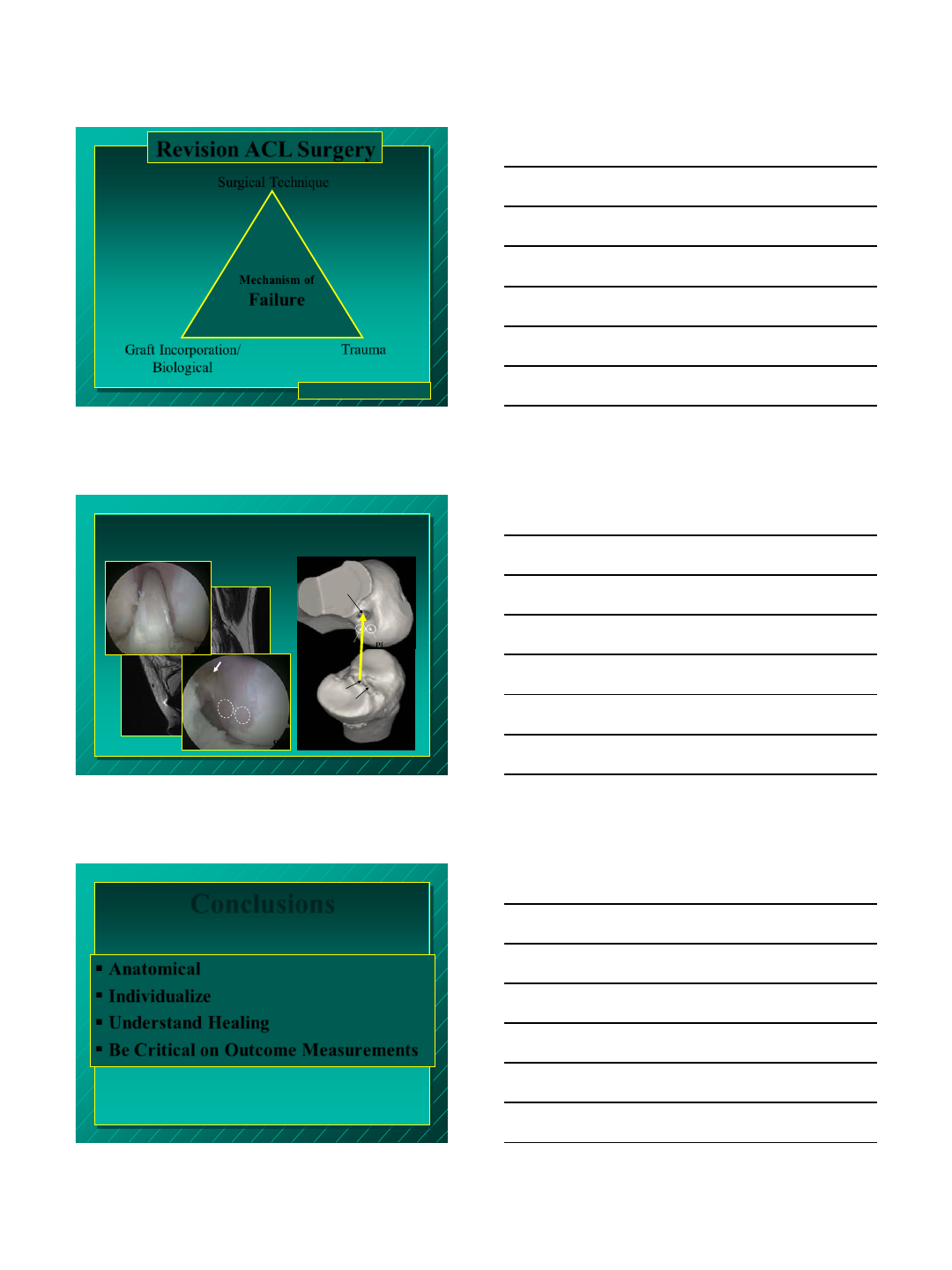
Time Zero 24 months
Graft Healing
6 months
Return to Sports
6 Months: MRI
9 Months Autograft
12 Months Allograft
van Eck, Fu et al. AJSM 2012
How Do We Measure Success?
Survey amongst 215 surgeons
Orthopaedics Today, 2011
Patient feels stable
and satisfied Negative pivot shift
on exam KT-1000 < 3mm
difference Follow-up observation
Objective
83
14 2 1
•3T MRI
•3D CT
•Biomarkers
•RSA
•Return to Sports
Subjective
Definition of Failure?
Re-rupture
ROM
Subjective/ Objective Instability
Pain, Miserable
Graft Incorporation/
Biological
Trauma
Surgical Technique
Mechanism of
Failure
Revision ACL Surgery
Harner, Fu et al. AAOS 1994
AM PL
90°
PL
High AM
AM
Tunnel mismatch
Failure of Graft Incorporation after Non-
Anatomic Tunnel Placement
90º
PL
AM
90º
Conclusions
Anatomical
Individualize
Understand Healing
Be Critical on Outcome Measurements

Thank You!
1
1
Revision ACL Reconstruction
David R. McAllister, MD
Associate Team Physician
UCLA Athletic Department
Chief, Sports Medicine Service
Professor
Department of Orthopaedic Surgery
David Geffen School of Medicine at UCLA
Los Angeles, CA
USA
2
Disclosure
Member of Medical Board of Trustees and
Consultant to MTF
3
Outline
Epidemiology
Causes of Failure
Pre-operative evaluation
Surgical considerations
Clinical Results
2
4
Demographics
250,000 ACL
reconstructions per year
performed in United States
Annual incidence of ACL
tears in the US is 1 in 3000
Americans
Average age: 26
70% occur as result of
indirect contact
Annual Cost is > 2 Billion
dollars
Graft failure rate is ~8%
5
Goals of Revision ACL Surgery
Provide stable joint
Preserve Meniscus
Maintain full ROM
Return to sport, work, daily
activities
? Chondroprotective
? Prevent osteoarthritis
6
Success
Functional stability
Relief of Symptoms
Return to pre-injury level of activity
Objective outcomes:
Lachman, anterior drawer, pivot shift tests,
KT 1000
Kocher et al. AJSM 2004
Pivot shift is the only test shown to correlate
with subjective satisfaction
3
7
Recurrent Instability
Early failure (<6months)
Surgical technical error
Failure of graft incorporation
Diagnostic error
Incorrect or aggressive rehab
Premature return to sport
Late failure ( > 1 year )
Significant re-injury
Delayed return to sport
8
MARS Study
460 patients (57% men; median age, 26 years).
Mode of failure as deemed by the revising surgeon:
traumatic (32%)
technical (24%-majority femoral tunnel malposition)
biologic (7%)
combination (37%)
infection (<1%)
Graft choice for revision ACL reconstruction was
45% autograft, 54% allograft, and more than 1%
both allograft and autograft.
Meniscus and/or chondral damage was found in
90% of patients.
Wright et al, AJSM 2010
9
Surgical Technique
Most avoidable cause of graft failure
Technical Errors:
Non-anatomic tunnel placement
Inadequate notchplasty
Inadequate graft fixation
Improper graft tensioning
Improper graft selection
Failure to address secondary stabilizers
4
10
Anatomic Tunnel Placement
Many ACL graft failures are
caused by tunnel mal-
position
Aberrant tunnel placement
can lead to:
Loss of knee ROM
Graft impingement
Stretch-out and Laxity
11
Femoral Tunnel 12
9
12
9
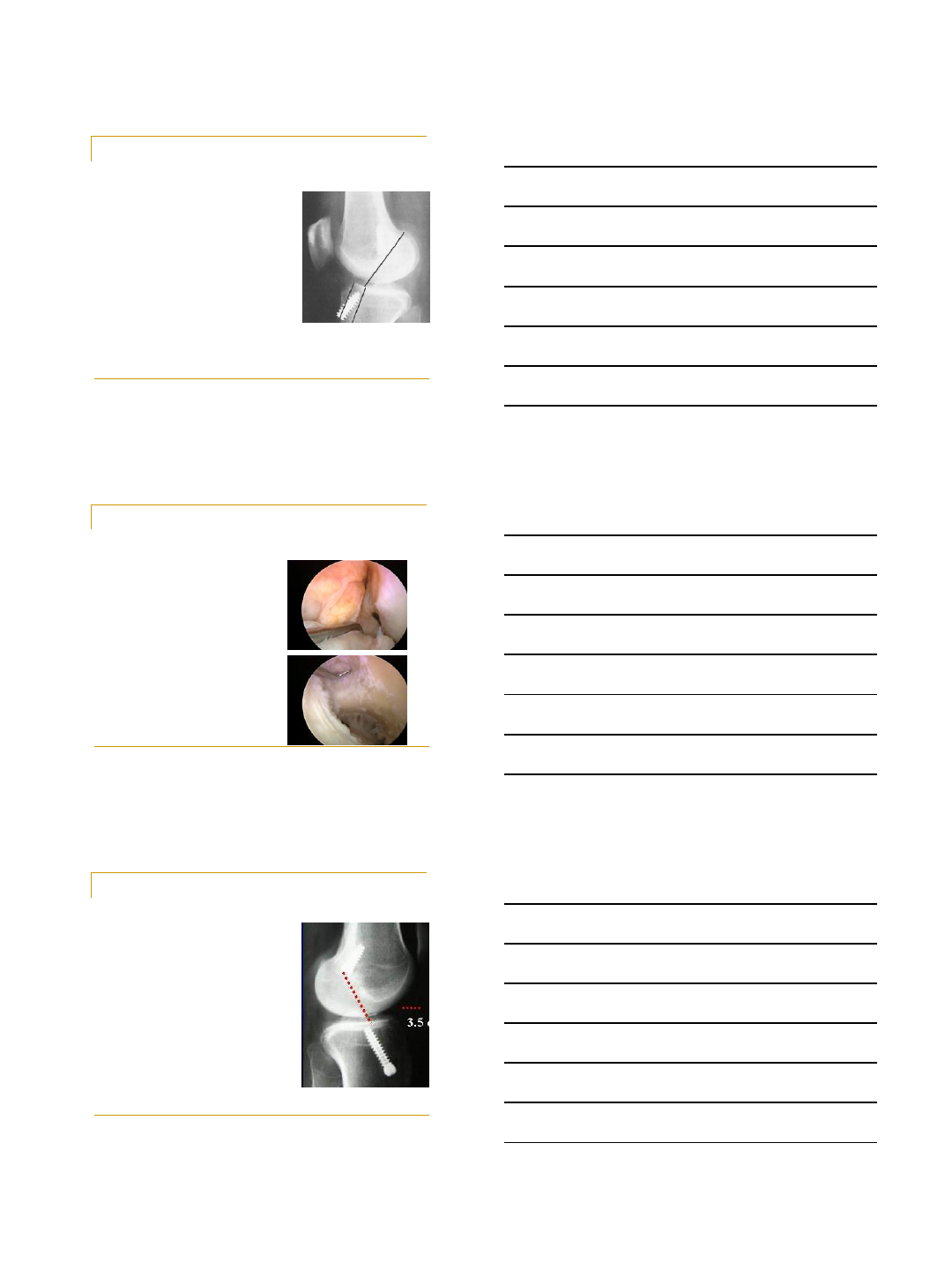
Femoral Tunnel Placement
Oblique Vertical
12
Femoral Tunnel Placement
Too Anterior
A common error
Tight in flexion
Lax in extension
Loss of flexion or stetch-
out of graft
Too Vertical
May not provide enough
rotational stability
5
13
Aberrent Tibial Tunnel Placement
Too Anterior
Notch impingement
Too Posterior
PCL impingement
14
Inadequate Notchplasty
ACL graft often larger than
native ACL
Need clearance between graft
and roof of notch
Notch large enough to
accommodate full ROM
Inadequate notchplasty
Impingement in extension
loss of extension
Can lead to graft attrition
Formation of “cyclops” lesion
15
Graft Fixation
Tibial fixation is weak point
Less bone density
Dual Photon Absorptometry (DEXA)
of the tibial metaphysis less bone
density than femoral metaphysis.
Angle of force
Line of force on graft directly in line
with tibial tunnel
Line of force on graft oblique to
femoral tunnel in WB
6
16
Graft Incorporation
Biologic failure may occur from:
Loosening within tunnel before bony ingrowth
Delayed remodeling of allografts
Avascularity caused by over tensioning of graft
Avascularity from allografts
Allograft immunologic response
Infection
17
Pre-operative Evaluation
Etiology of failure
Is there symptomatic
instability?
Whether or not a patient
is a candidate for revision
18
Radiographs
X-rays: AP, lateral, 45° PA weight
bearing view
Arthritis
Size and position of previous tunnels
Previous hardware
Notch architecture
Alignment
CT
Bone tunnel enlargement
MRI
Bone tunnel enlargement
Graft integrity
Associated injuries
7
19
Surgical Considerations
Staging
Graft selection
Hardware removal
Notchplasty
Bone tunnel placement
Graft fixation
Rehabilitation
20
Staging
Tunnel expansion
Bone grafting as a separate
procedure required less than
10% of cases in MARS series
Wright et al, AJSM 2010
Loss of motion
Limb mal-alignment
21
Graft Selection
Auto vs Allograft
Allograft
Advantages
Shorter operative time
Smaller incisions
Avoid donor site morbidity
No size limitation (for large tunnel diameters can use a large bone plug)
Disadvantages
May play role in failure
Longer incorporation times
Immunologic reaction
Higher cost
Disease transmission
Radiation kills viruses but required dosage alters graft integrity
8
22
Surgical Considerations
Hardware removal
Remove only when necessary
Commercially available revision set
may be helpful
Use fluoroscopy, if necessary
Avoid stripping screw head
Knee flexion angle should be the
same as when screw was inserted
Notchplasty
As necessary
23
Tunnel Placement
The most important and
challenging hurdle
Anatomic vs non-
anatomic
Tunnel widening or no
tunnel widening
24
Tunnel Placement
Non anatomic tunnels
Drill new anatomic tunnels
Leave old hardware in place
9
25
Tunnel Placement
Anatomic or near anatomic
Remove old hardware
Redirect anatomic tunnel
Two incision technique, AM
portal, etc.
26
Tunnel Placement
Tunnel widening
Staged bone grafting
Stacked interference screws
Larger bone plugs
Bone Dowels
27
Graft Fixation
Secure graft fixation is
critical
May re-enforce primary
fixation
Post and washer
Staple
Endobutton
Stacked interference
screws
10
28
Revision ACL results
Diamantopoulos et al. AJSM 2008
107 pt with 73 month f/u
Avg Lysholm score was 88.5
62/107 had normal or near normal results on IKDC
Battaglia et al. AJSM 2007
63 pt with 72 month f/u
71% good to excellent results
59% returned to sports
25% required additional surgery
O’Neil et al. AJSM 2004
48 revision ACL with f/u of 90 months
73% had normal or near normal scores on IKDC
6% failure rate
225 primary ACL
92% had normal or near normal scores on IKDC
7% failure rate
29
Comparative Studies
Ahn et al. AJSM 2008
56 revision vs 117 primary
reconstructions
Variety of grafts used (hamstring
autografts, BTB allograft, Achilles
allograft)
No difference in laxity
Lysholm score 63 vs 93
IKDC score 85% A/B vs 95% A/B
No differences between grafts used
30
Summary
Revision ACL reconstruction will continue
to be a growing problem
Identify the cause of failure
Identify the appropriate candidate for
reconstructions
Need meticulous pre-operative planning
Inform patients on appropriate
expectations
{kind=link}
