Ankle Fractures Syllabus
2014-10-21
: Pdf Ankle Fractures Syllabus Ankle_Fractures_Syllabus 10 2014 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 96
10/21/2014
1
Ankle Fractures: Controversies & Challenges
Assessment of injury, classification
Ashish Shah, MD
Assistant Professor Orthopaedics
[Foot & Ankle]
University of Alabama, Birmingham , AL USA.
Disclosure
Consultant
-Arthrex
-Tornier
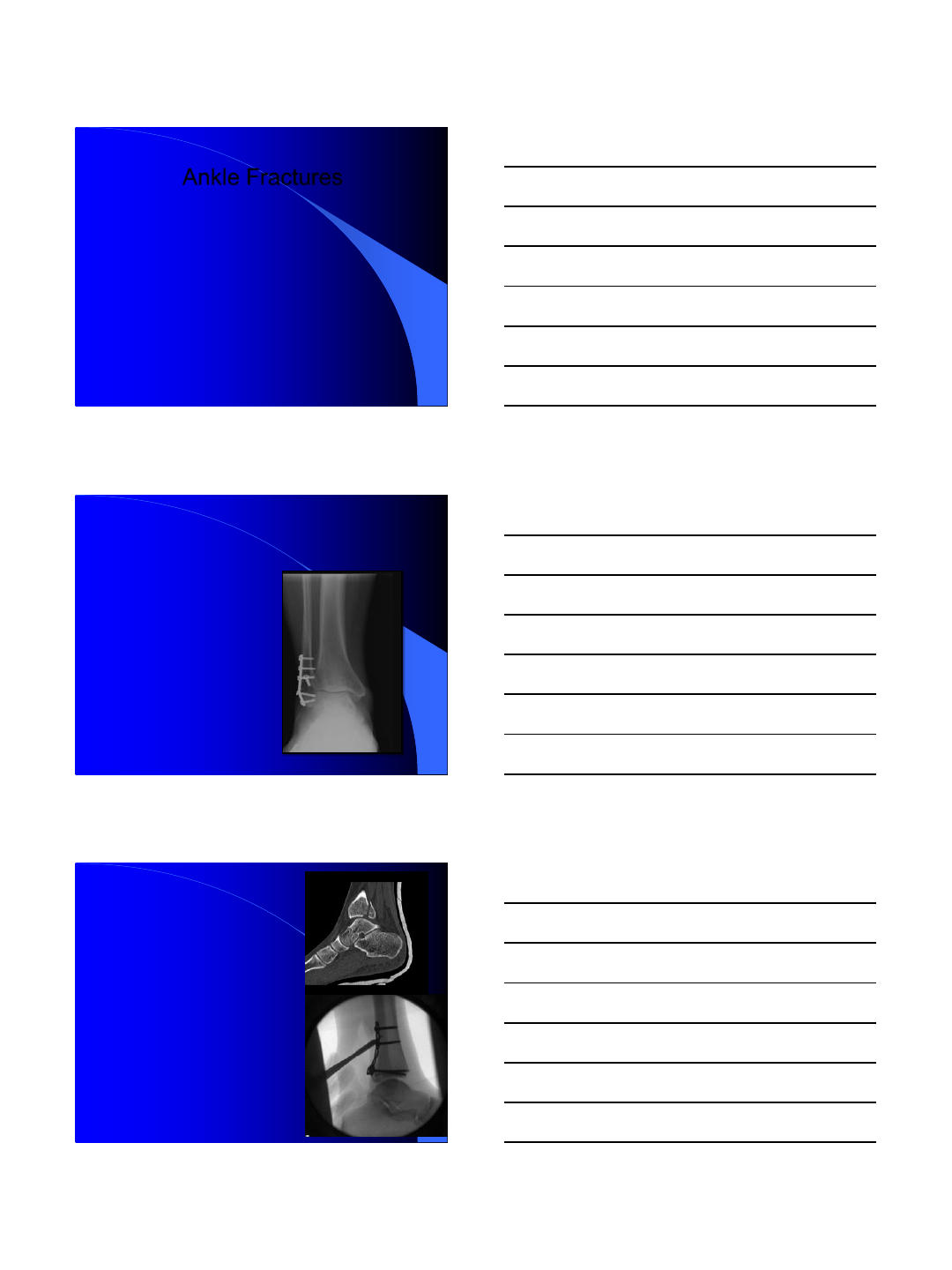
-Ankle fractures
involve a spectrum
of injury patterns
from simple to
complex, such that
these injuries are
not always “just an
ankle fracture.
10/21/2014
2
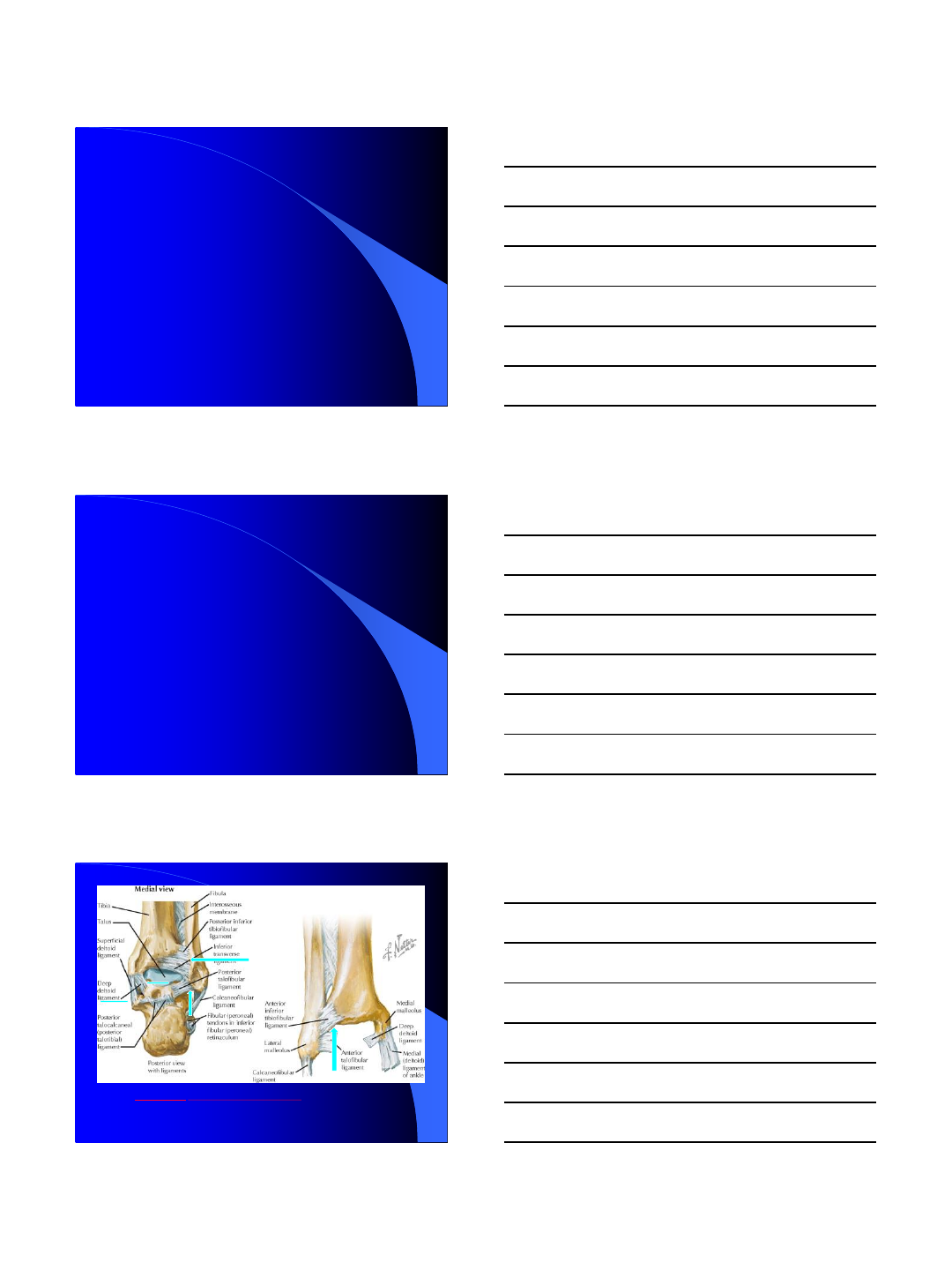
Case 1
-58 year old WM
comes with 2 weeks
history of trivial
trauma.
-Presentation in the
clinic walking without
any support.
-Pain level 2/10
-Is it normal???
-Am I missing something here??
Case 2
-38 year old WM fell in
the backyard and got
ankle fracture.
-Came to the ER
walking with pain
level 1/10.
-Doesn’t sound
Normal??
Case 3
-47 year old female
with ORIF ankle
fracture [1 year ago],
still complaining about
7/10 pain with
ambulation.
-Fracture seems to be
healed but what next??
10/21/2014
3
Ankle Fractures
-Why Should I worry about ankle fractures?
-1 mm of lateral translation of the talus
reduced surface contact area in the ankle
joint by 42%; lateral translation of 2mm by
64%.
Ramsey P.L., Hamilton W.: J Bone Joint Surg Am 1976; 58: 356-357
2 mm of shortening or
lateral shift of the
fibula, or external
rotation > 5 degrees,
increases contact forces
in the ankle joint leads
to early ankle arthritis.
-Thordarson D.B., Motamed S.,et al
J Bone Joint Surg Am 1997; 79:
1809-1815
-Significant loss of
tibiotalar contact with
posterior malleolar
fractures involving
greater than 33% of
the joint surface.
-Hartford JM et al. CORR 1995; 320: pp. 182-
187
10/21/2014
4
The ankle joint is subject to enormous forces across
a relatively small surface area of contact, with up to
1.5 times body weight with gait and greater than 5.5
times body weight with more strenuous activity.
-Lets recall our basic Anatomy structures in
the next couple of slides.
Jon C. Thompson Netter’s Concise Orthopaedic Anatomy, CHAPTER 10, 337-383
10/21/2014
5
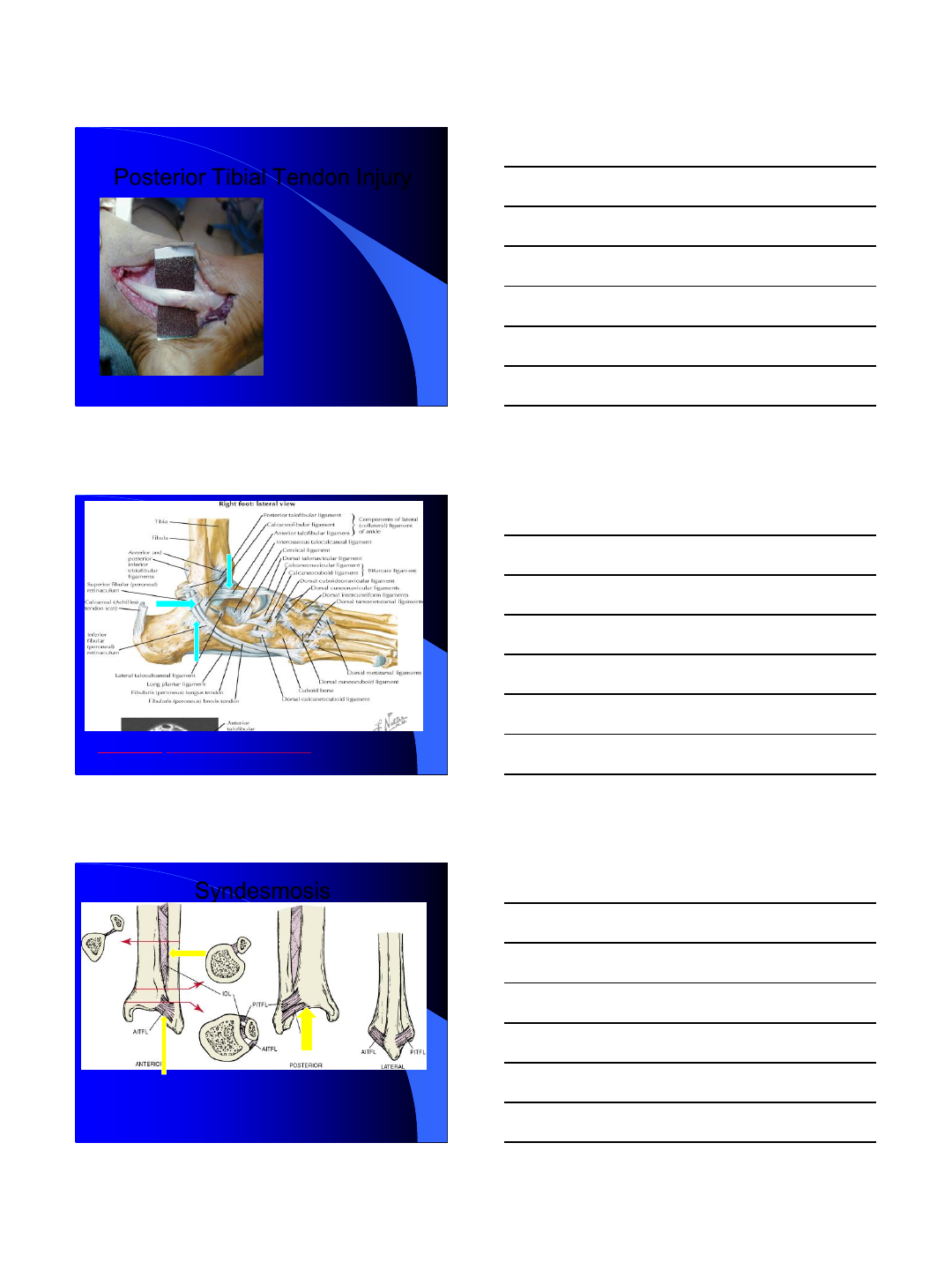
Posterior Tibial Tendon Injury
-During Injury
-Irritation secondary
to Tension Bend
wiring/screws
-Progressive tear
and flattening of
foot.
Jon C. Thompson Netter’s Concise Orthopaedic Anatomy, CHAPTER 10, 337-383
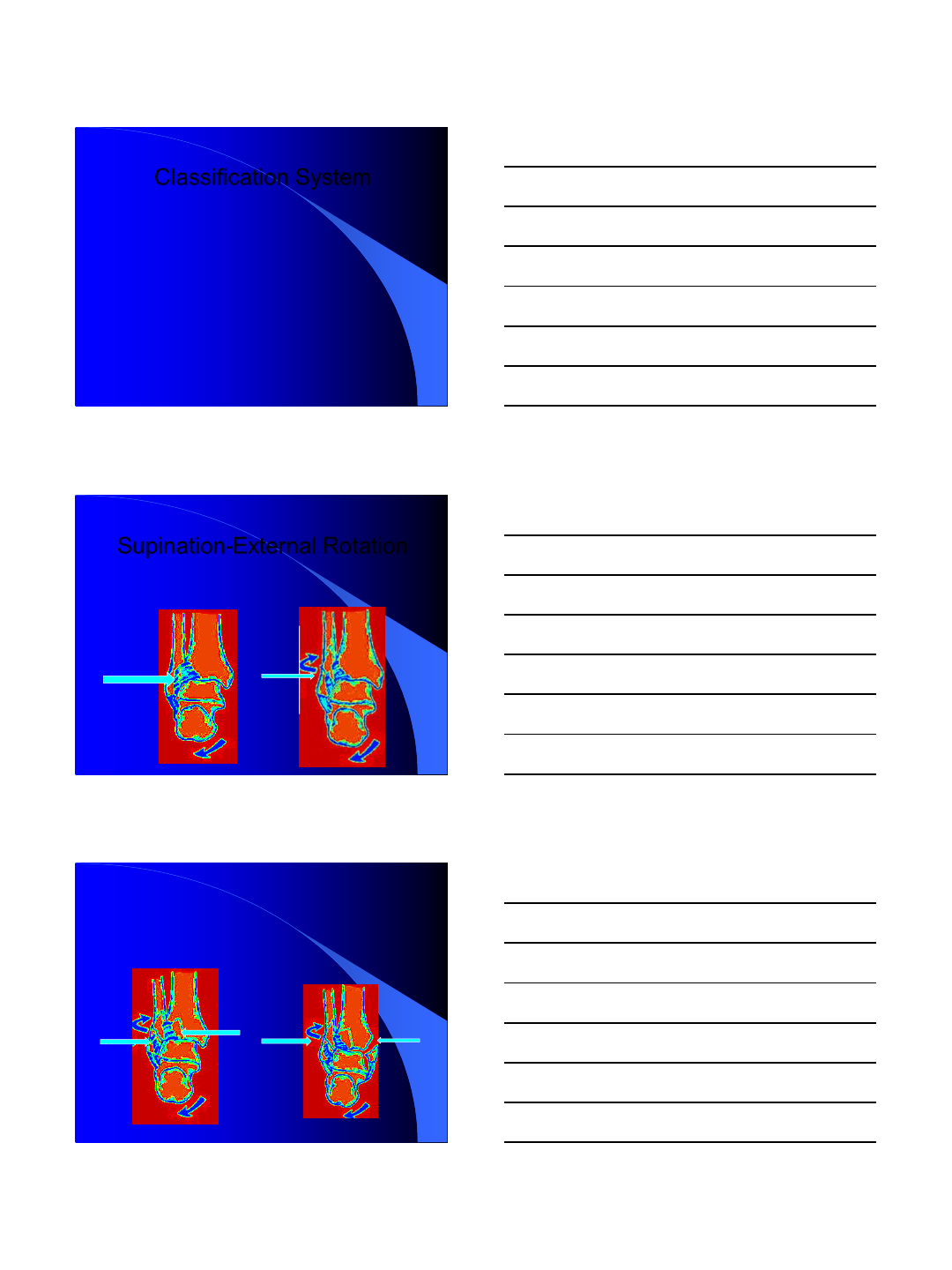
Syndesmosis
Carr JB, Trafton PG Skeletal trauma: fractures, dislocations, ligamentous injuries, 2nd ed,, 1998, WB Saunders
10/21/2014
6
Classification System
-The two most commonly used classification systems are the Lauge-Hansen and Danis-
Weber ( [AO] Müller) systems.
-The Lauge-Hansen system is based on the suspected injury mechanism. Fractures are
categorized by a combination of foot position and direction of force.
Lauge-Hansen N: Arch Surg 1948; 56: pp. 259-317
-The Danis-Weber system is based on the level of the fibula fracture and is divided into
three types. This system is easier to remember and has more relevance to operative
decision making.
Weber BG: Die Verletzungen des oberen Sprunggelenkes
-Mast and Teipner first combined these in 1980
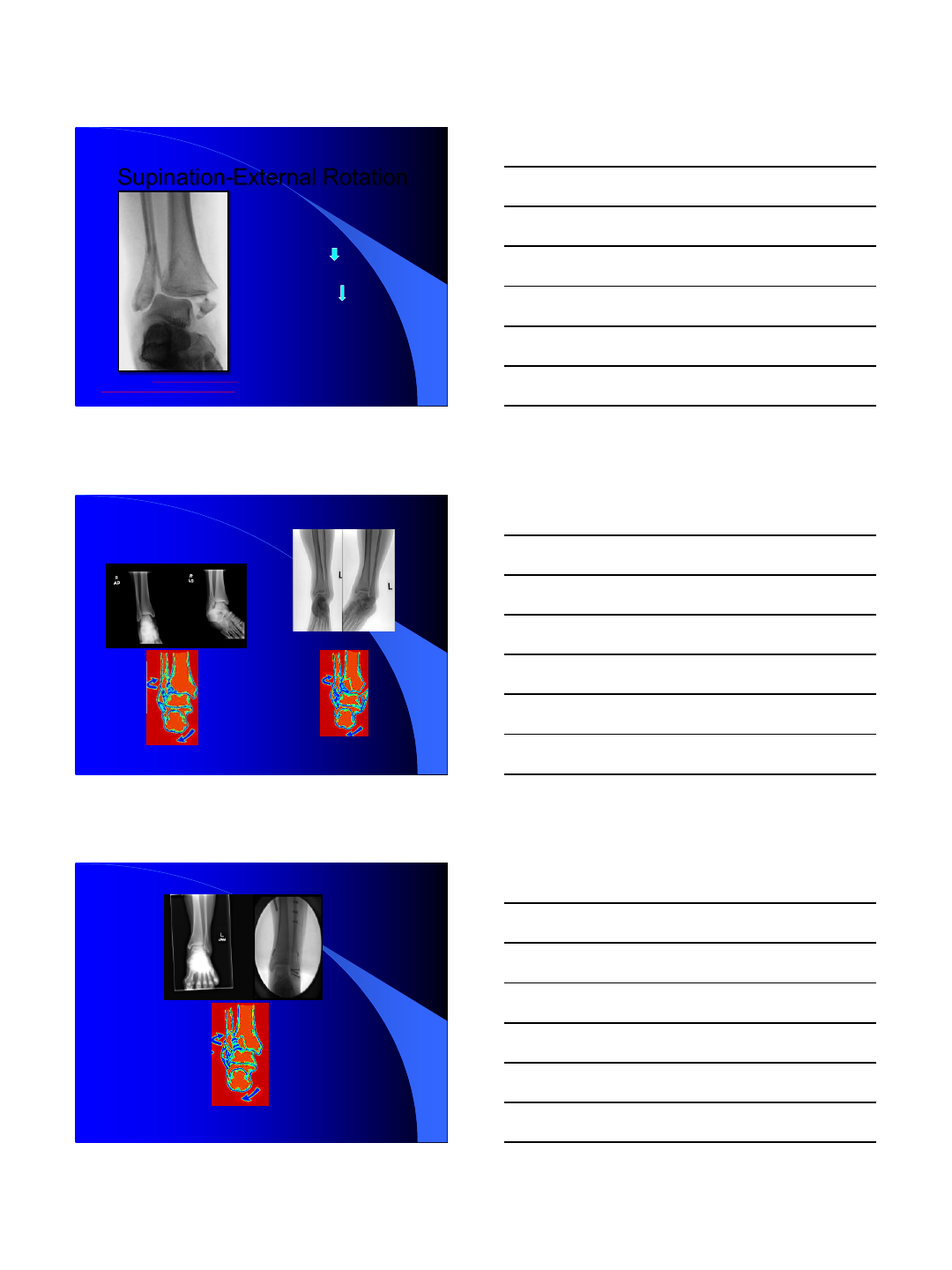
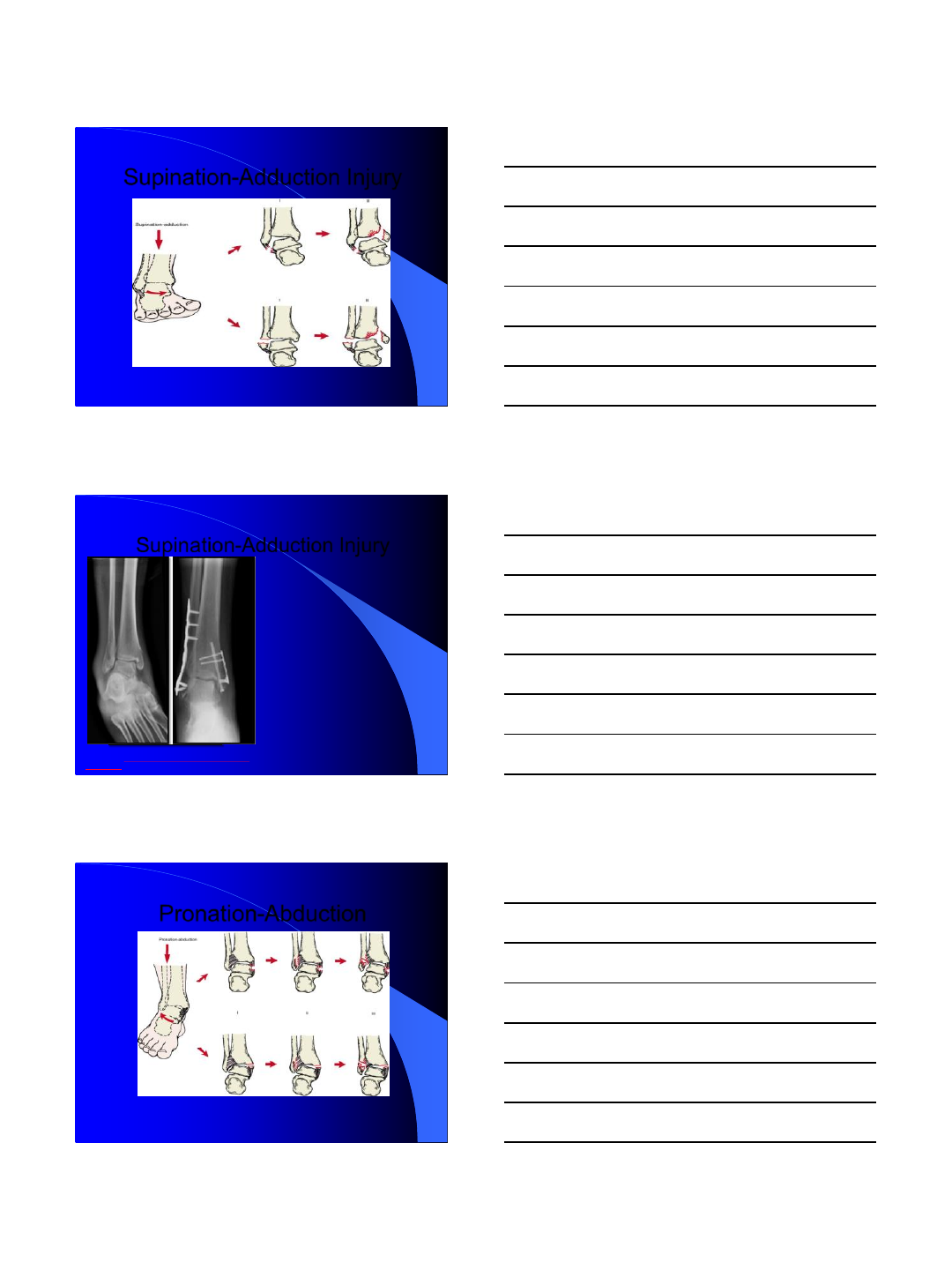
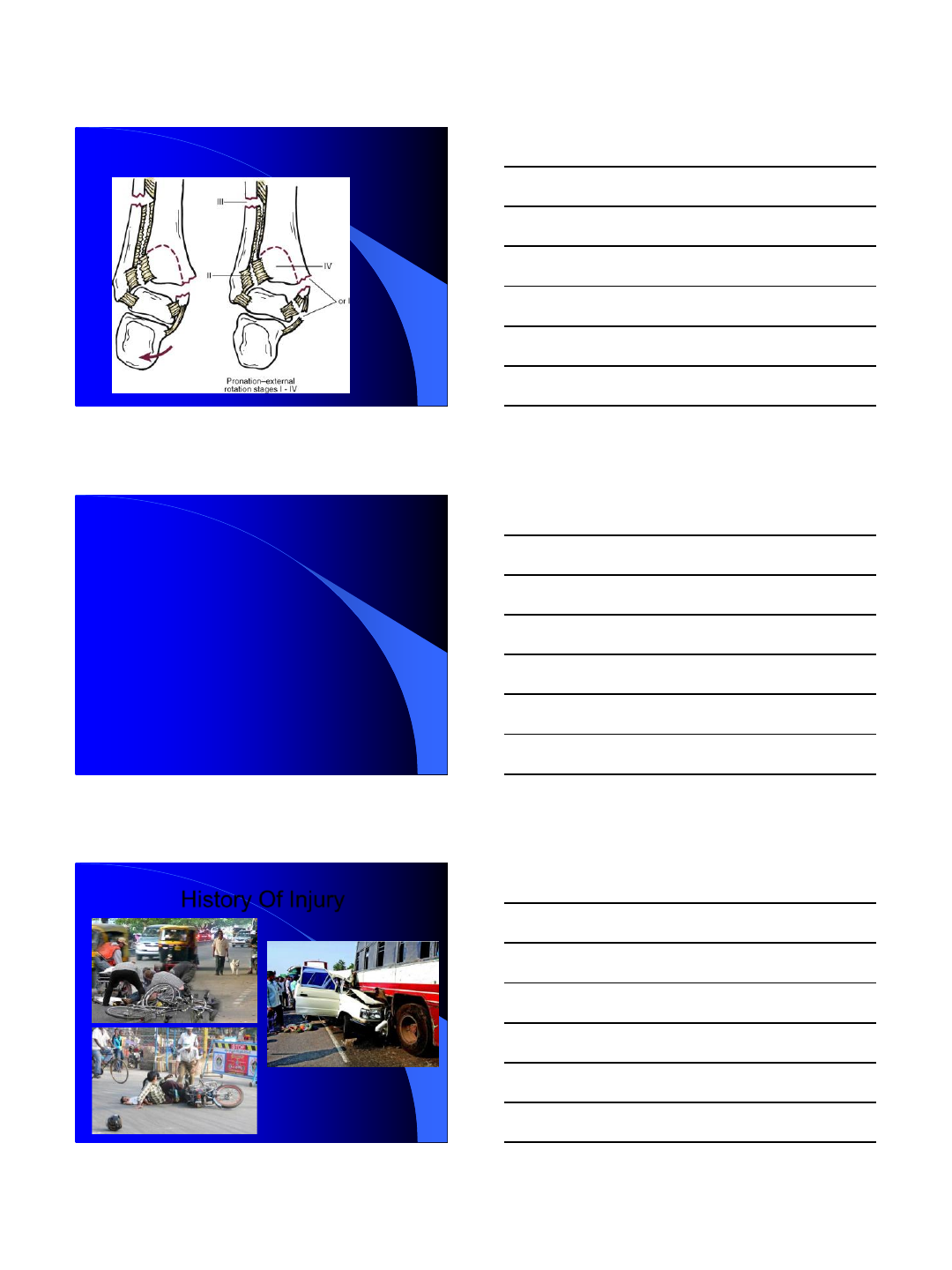
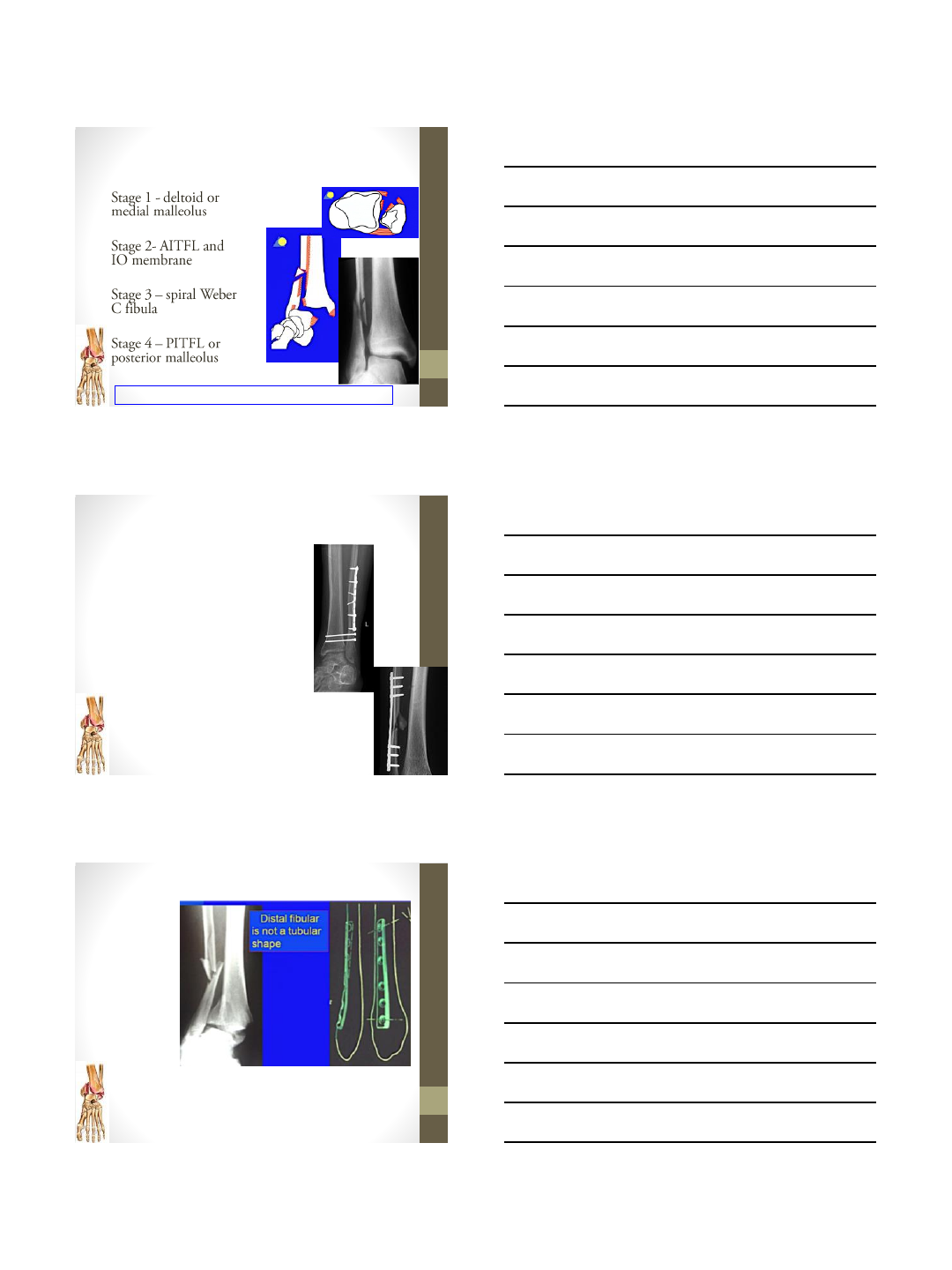
Supination-External Rotation
-SER I failure of the anterior-
inferior tibiofibular ligament
(AITFL)
SER II a spiral oblique fibula fracture at or just
above the ankle mortise
SER III failure of the posterior-inferior
tibiofibular ligament (PITFL) or posterior
malleolus fracture
SER IV tension failure of the deep deltoid
ligament or transverse avulsion fracture of
the medial malleolus
10/21/2014
7
Supination-External Rotation
-Medial tenderness, swelling, and
ecchymosis are poor predictors of
deltoid incompetence.
-If no medial widening stess
radiographs
-Gravity/External Rotation stress
-If stable be placed in a
prefabricated fracture boot and
allowed to weight-bear to
tolerance; repeat weight-bearing
radiographs are obtained 5–7 days
later.
Michael Clare Foot and Ankle Clinics of
North America 01/2009; 13(4):593-610.
SER II a spiral oblique fibula fracture at or just
above the ankle mortise
SER IV tension failure of the deep deltoid ligament or
transverse avulsion fracture of the medial malleolus
SER III failure of the posterior-inferior tibiofibular ligament (PITFL) or posterior malleolus fracture
10/21/2014
8
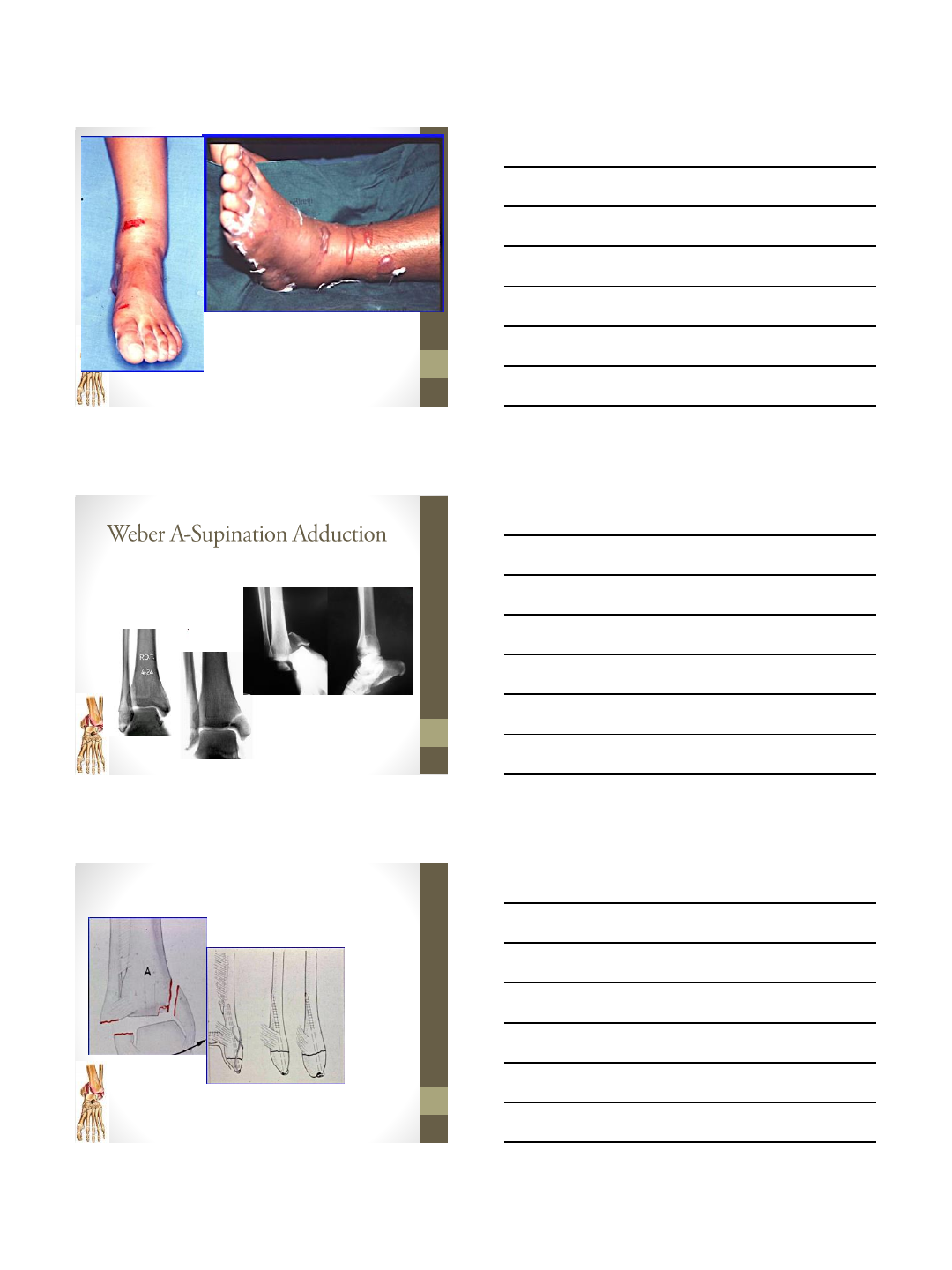
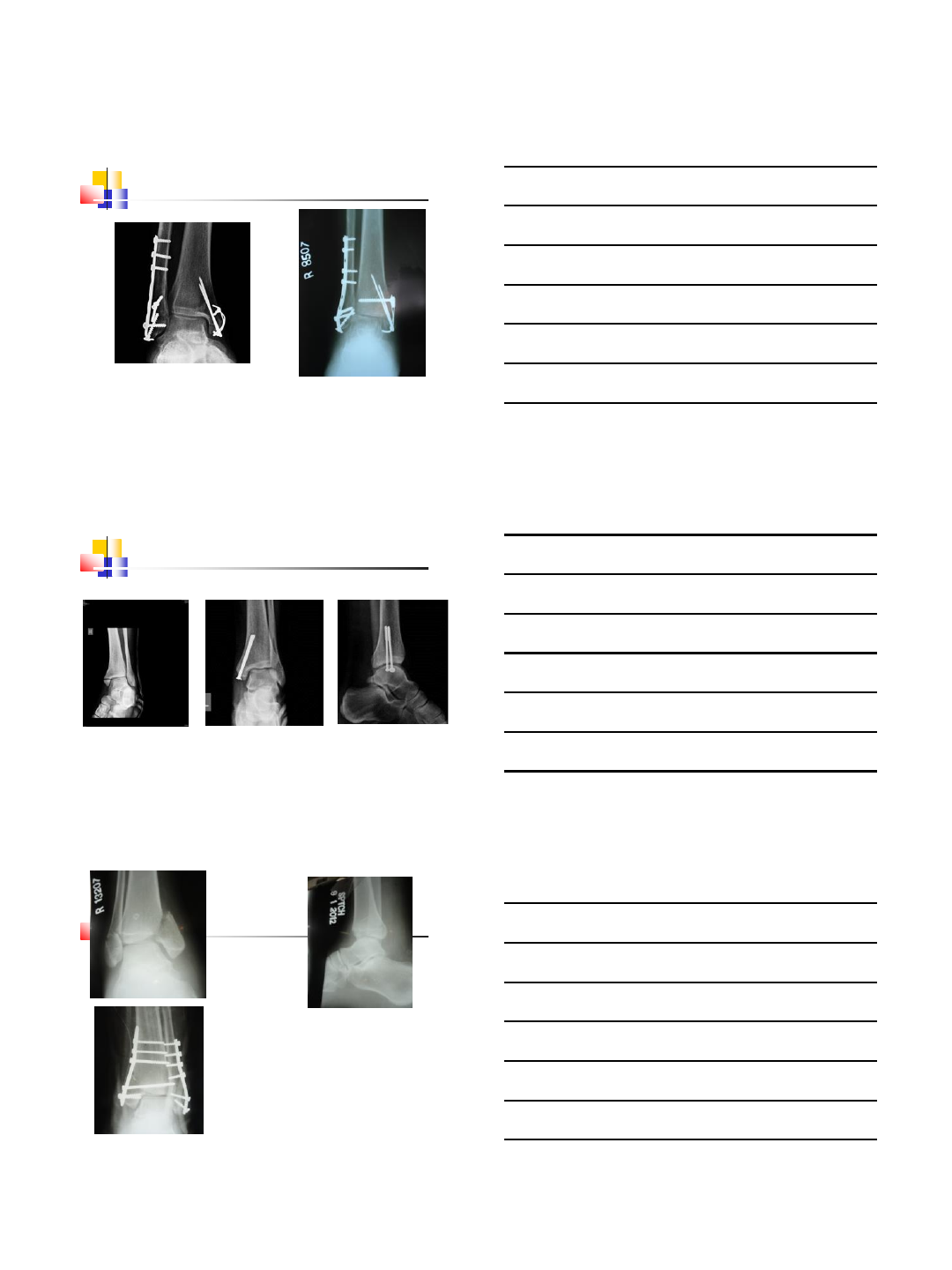
Supination-Adduction Injury
Lauge –Hansen Supination-Adduction Injury
Supination-Adduction Injury
-10%–20% of ankle fractures
-Avulsion fracture of lateral
malleolus/lateral ligament
injury
&
-vertical shear fracture of Medial
Malleolous .
-Association with medial Tibial
plafond impaction injury.
Michael Clare Foot and Ankle Clinics of North America 01/2009;
13(4):593-610.
Pronation-Abduction
Lauge –Hansen Pronation-Abduction injury

10/21/2014
9
Pronation-Abduction
-Transverse avulsion fracture of the
medial malleolus.
-(II) failure of the AITFL and PITFL
-(III) a transverse fibula fracture at or
above the ankle mortise with
communution.
-Check for syndesmois Integrity.
-Lateral Tibial Plafond should be
inspected for any impaction.
-Mast J.:. In Müller M.E., Allgöwer M.,
-Manual of internal fixation. New York: Springer-
Verlag, 1991,
Michael Clare Foot and Ankle
Clinics of North America 01/2009;
13(4):593-610.
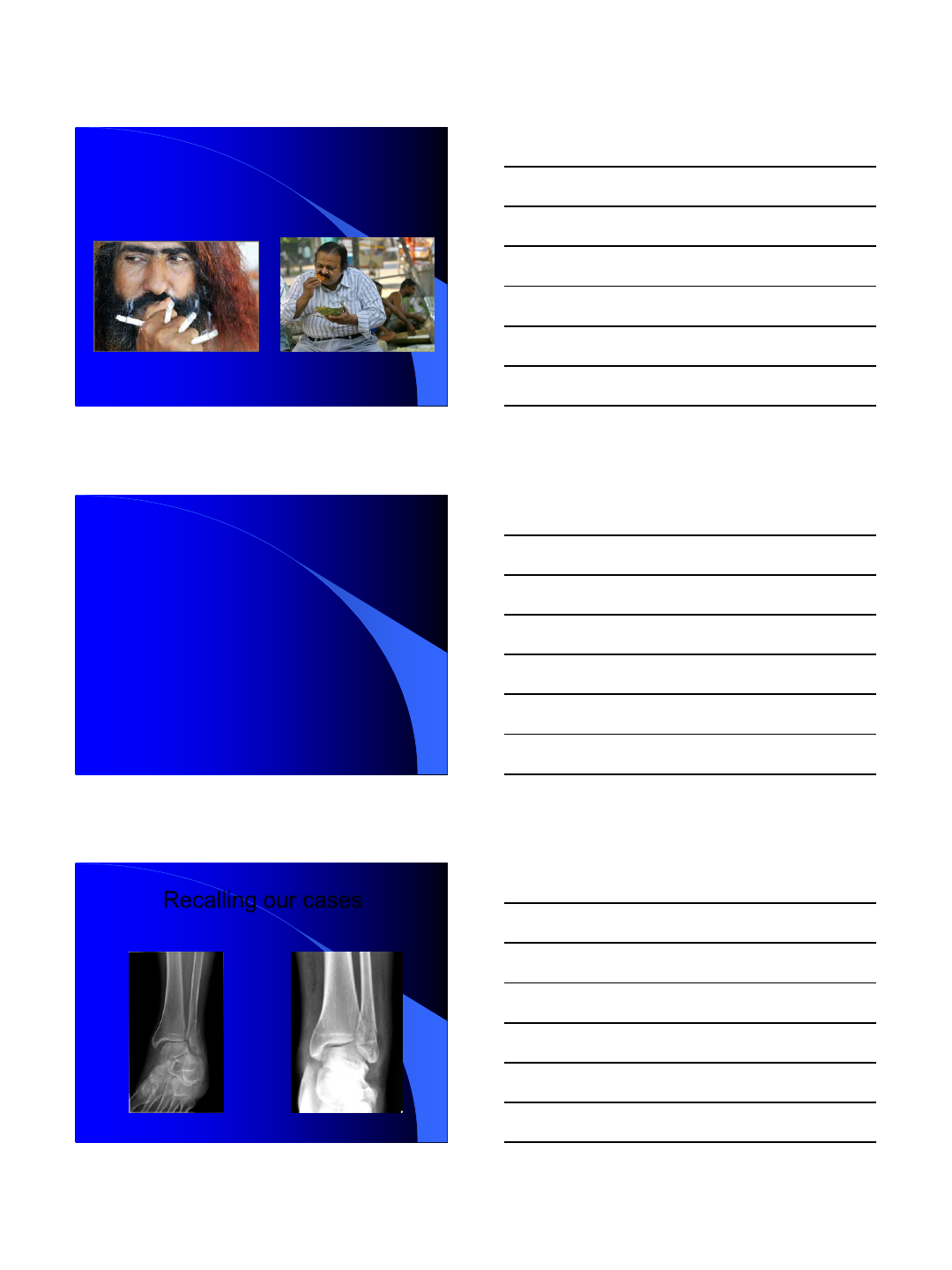
Lauge –Hansen Pronation-External Rotation injury
Pronation-External Rotation
-(I) Tension failure of the deep deltoid
ligament or transverse avulsion fracture
of the medial malleolus
-(II) failure of the AITFL
-(III) a spiral oblique fibula fracture
above the ankle mortise
-(IV) failure of the PITFL or posterior
malleolus fracture
-Commonly associated with instability
of the syndesmosis.
Michael Clare
Foot and Ankle
Clinics of North
America
01/2009;
13(4):593-610.
10/21/2014
10
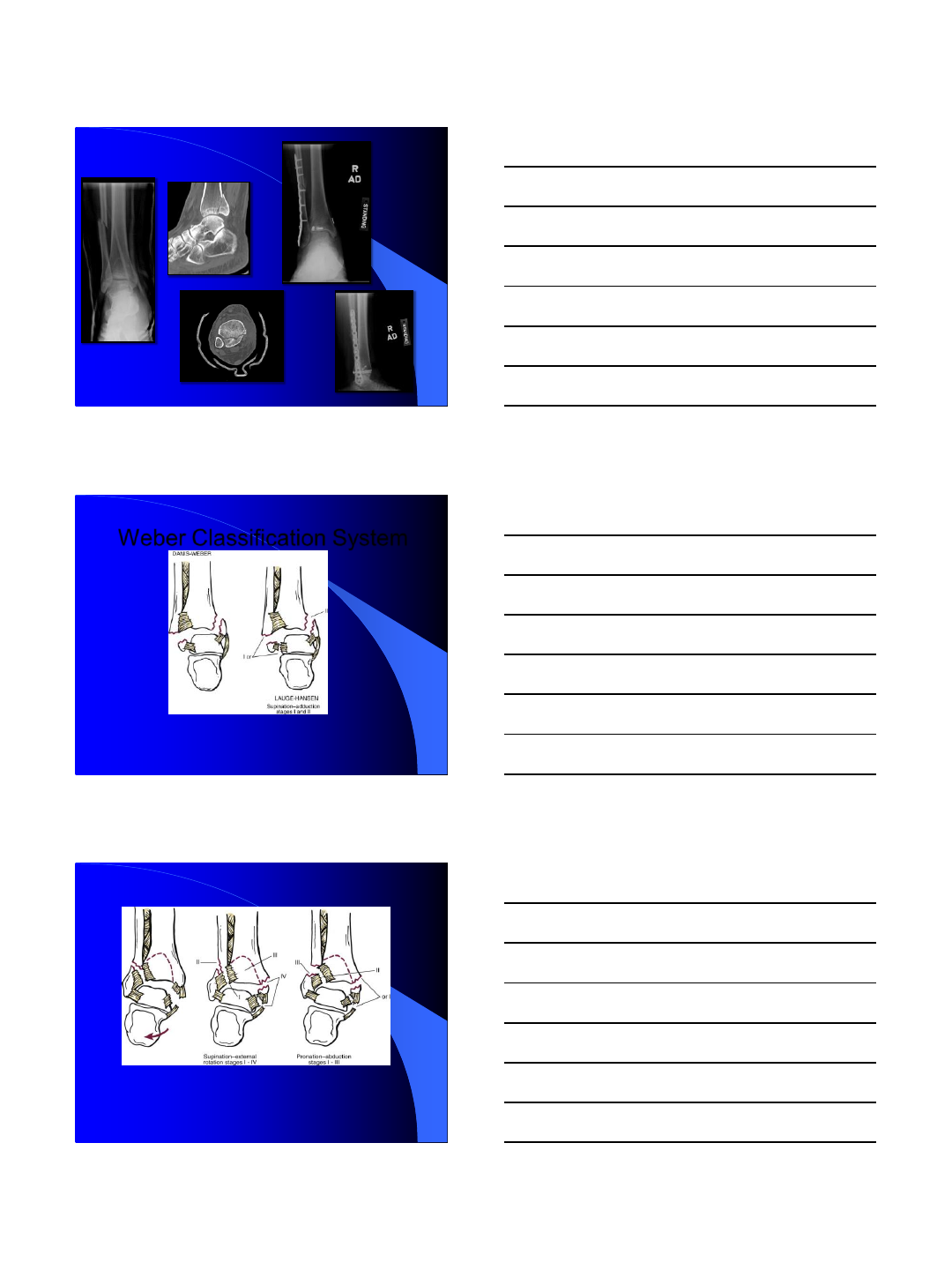
Weber Classification System
Carr JB, Trafton PG: Jupiter JB, Levine AM, Trafton PG, editors:
Skeletal trauma: fractures, dislocations, ligamentous injuries, 2nd ed,
1998.
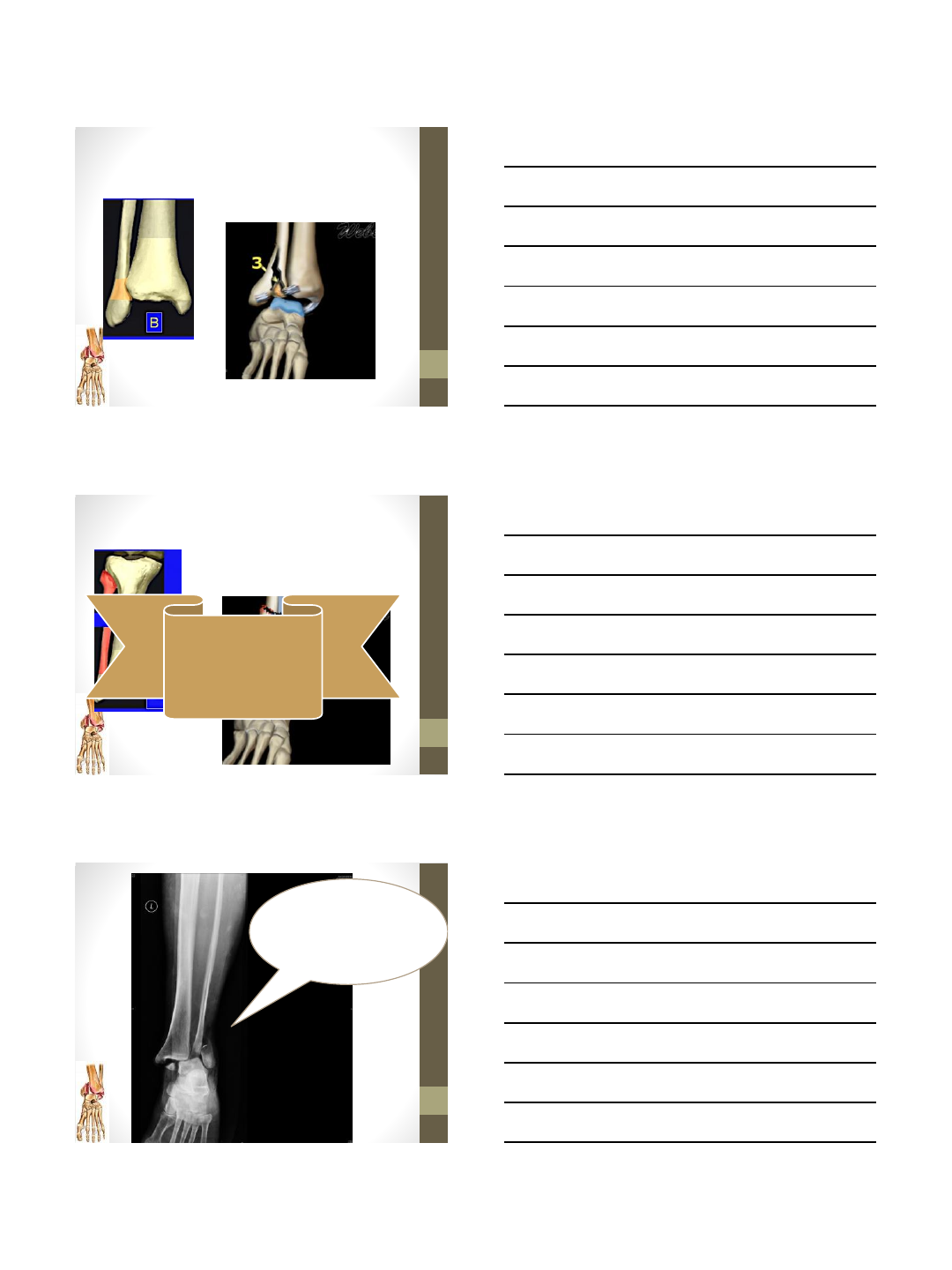
Type A:
Infrasyndesmotic
Injury
Carr JB, Trafton PG: Jupiter JB, Levine AM, Trafton PG, editors:
Skeletal trauma: fractures, dislocations, ligamentous injuries, 2nd ed,
1998.
Type B: Transsyndesmotic Injury
10/21/2014
11
Carr JB, Trafton PG: Jupiter JB, Levine AM, Trafton PG, editors: Skeletal trauma:
fractures, dislocations, ligamentous injuries, 2nd ed, 1998.
Type C:
Suprasyndesmotic
Injury
Assessment of the
Injury
History Of Injury
10/21/2014
12
Smoking Diabetes
History of primary Rx.
Level of Pain
Past Medical History :
Cardiac Disease.
Neuropathy ??: Diabetes, Alcohol, Thyroid,
Nerve Injury/Neuromascular Disorder
Recalling our cases
Case 1 Case 2
Alcoholic Neuropathy Diabetic Neuropathy

10/21/2014
13
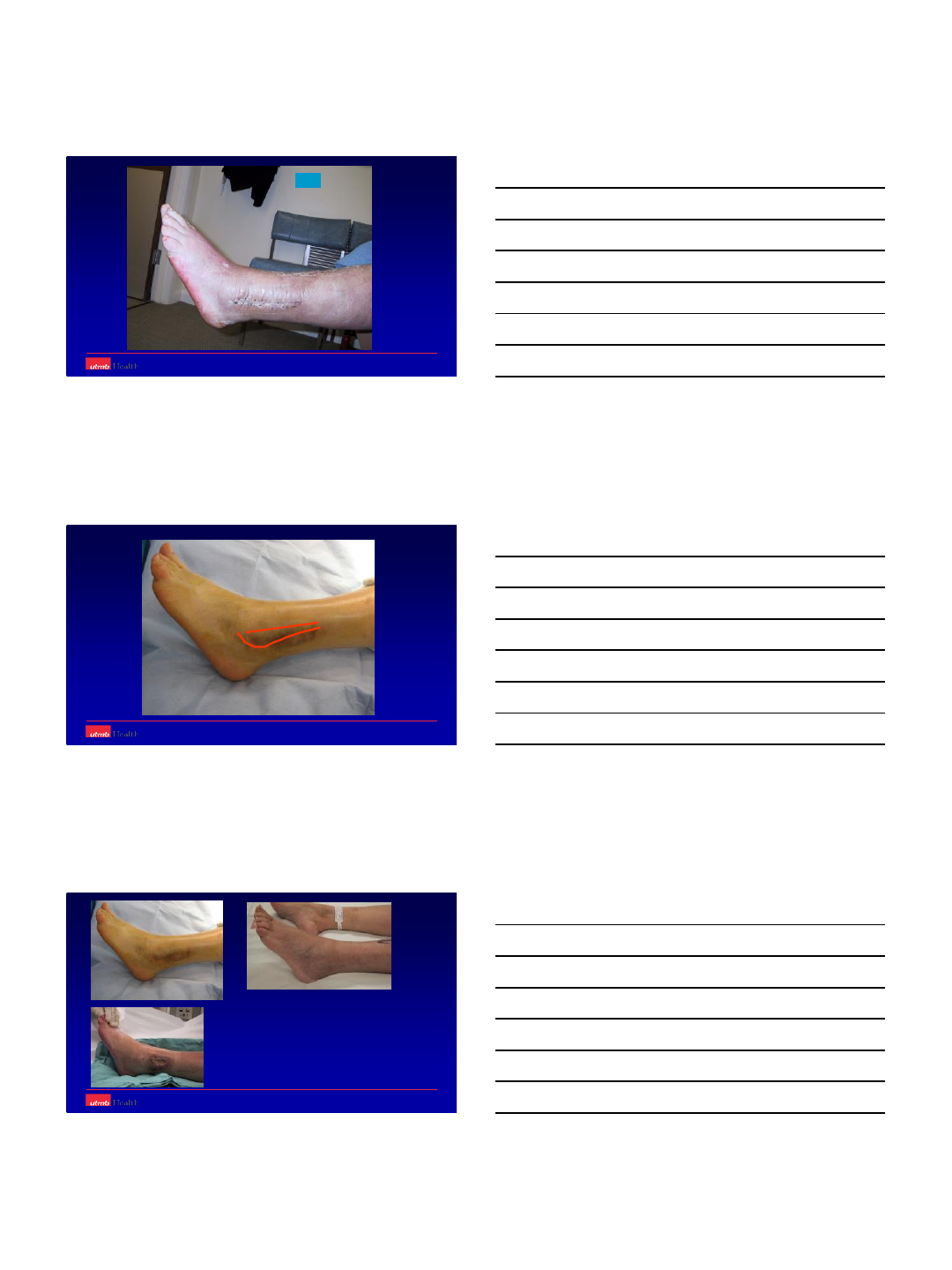
Evaluation of the Patient
-Skin Condition.
-Vascularity/ Capillary
Refill
-R/o Compartment
Syndrome.
-Check nerve status on
the uninjured leg.
-Wrinkle Sign??
Stable Fracture
-Immobilization in AO
splint.
-Elevation.
-Surgery in 10-14 days.
-surgical treatment for an ankle
fracture [except irreducible
dislocation/open fracture] is
certainly not an emergency and can
therefore be completed as an
elective procedure in 10-14 days.
10/21/2014
14
Unstable Fracture/Fracture
Dislocation.
-Attempt Close reduction &
splinting followed by re-xray.
-If unreduced take in the OR for
closed reduction & Ex-Fix
Application vs Definitive
Fixation.
-If open fracture/ poor skin
condition. –Closed Reduction-
External Fixator &
Debridement
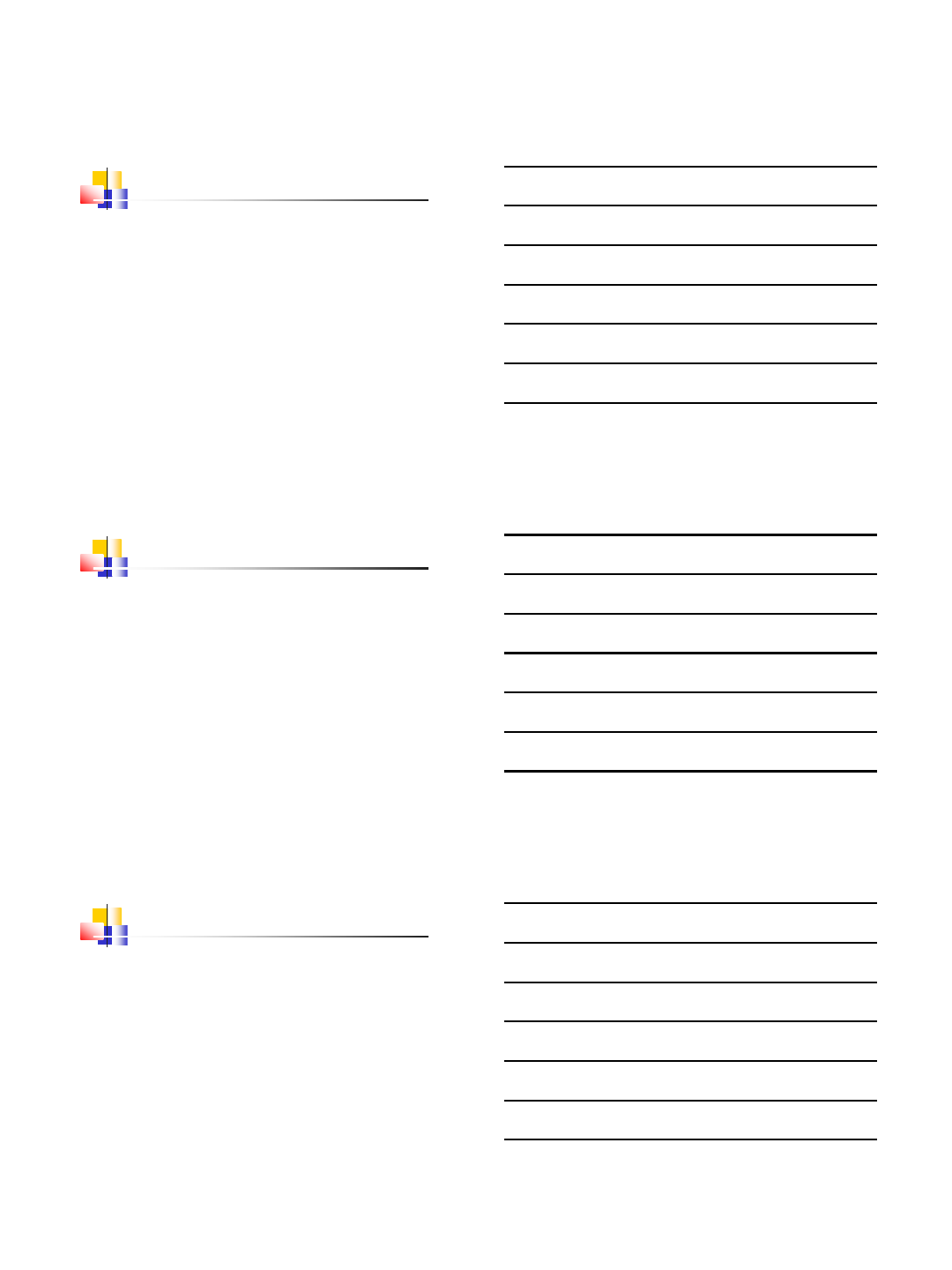
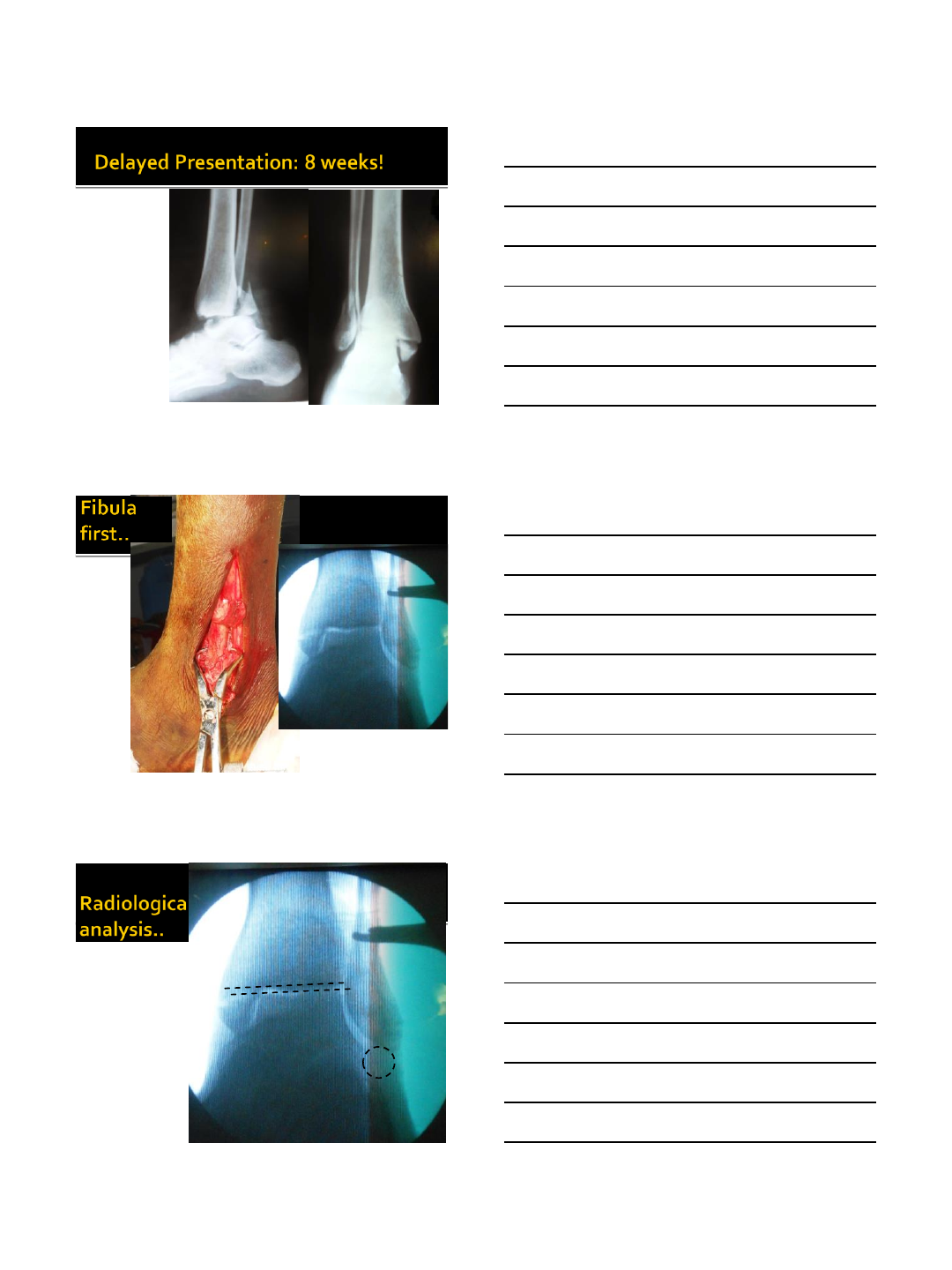
Presentation in the
clinic at 3 weeks of
injury[in the splint]
without any reduction.
Reduction
Attempted in the
cast-room.
Patient was
taken to the
OR on the
same day
for the
ORIF
Radiographic Evaluation
-Xrays
3 views [AP/ Mortise/ Lateral view of the
injured and opposite ankle].
Knee xrays if suspicious about maisonneuve
injury.
-CT Scan
10/21/2014
15
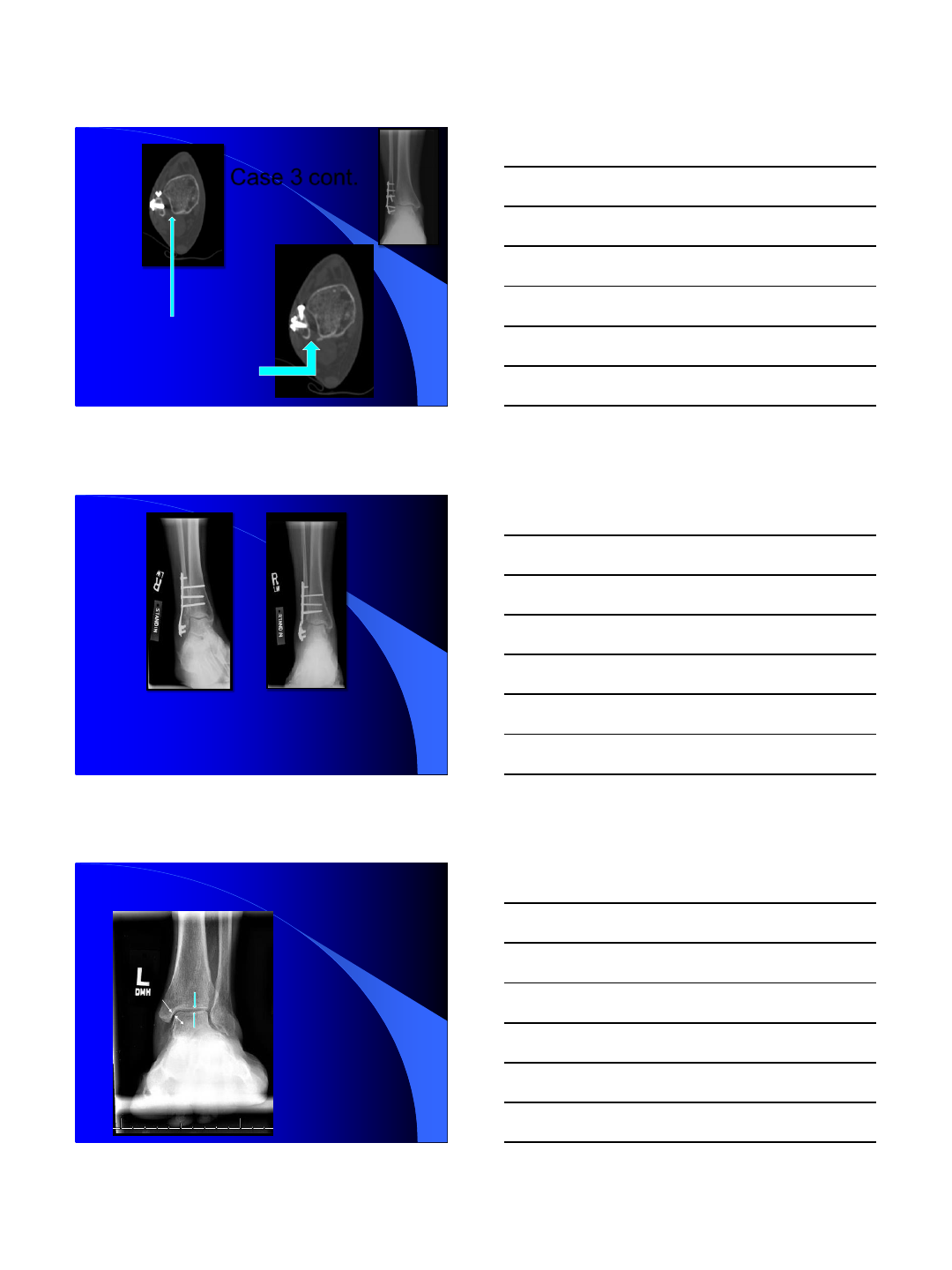
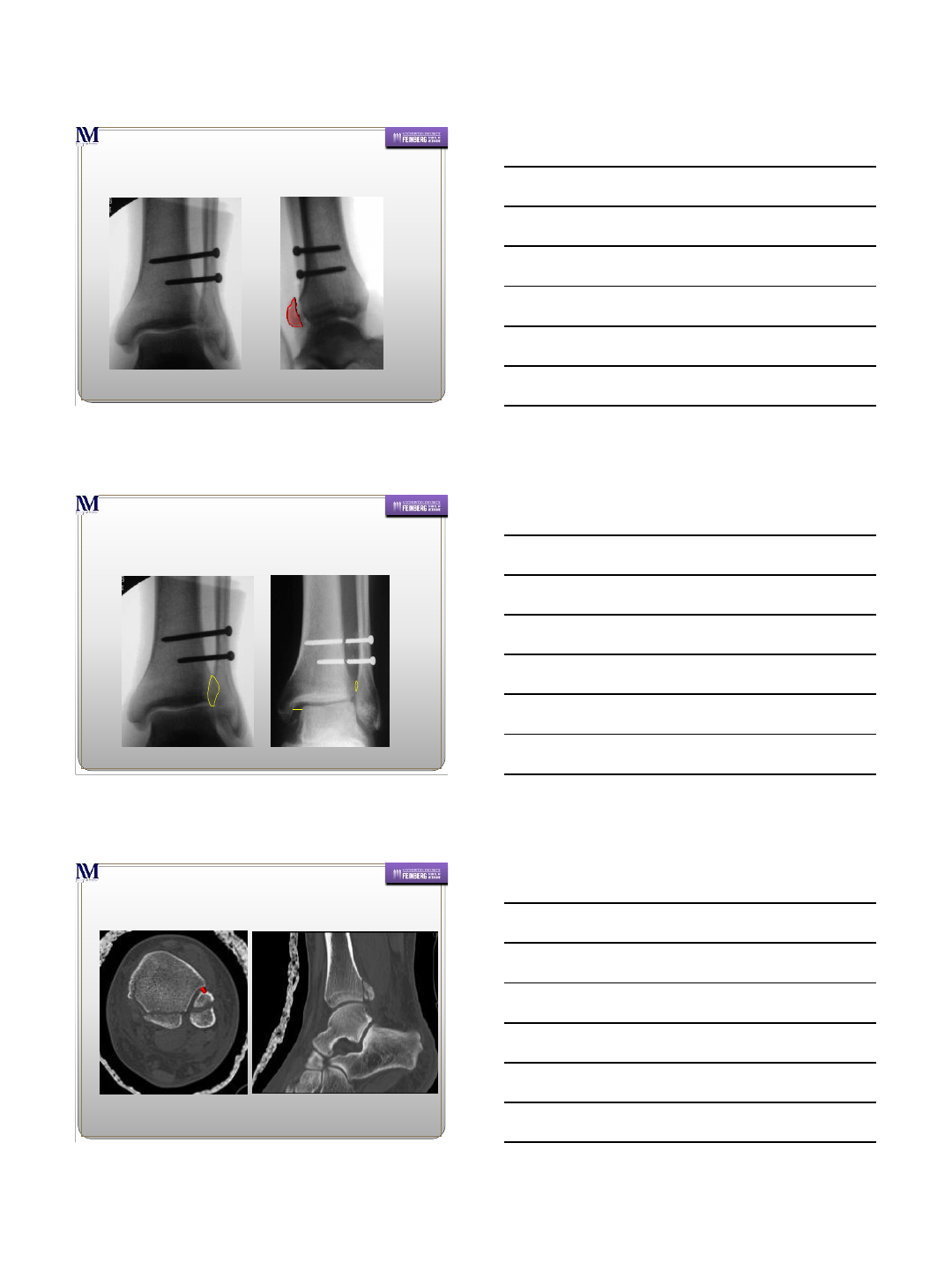
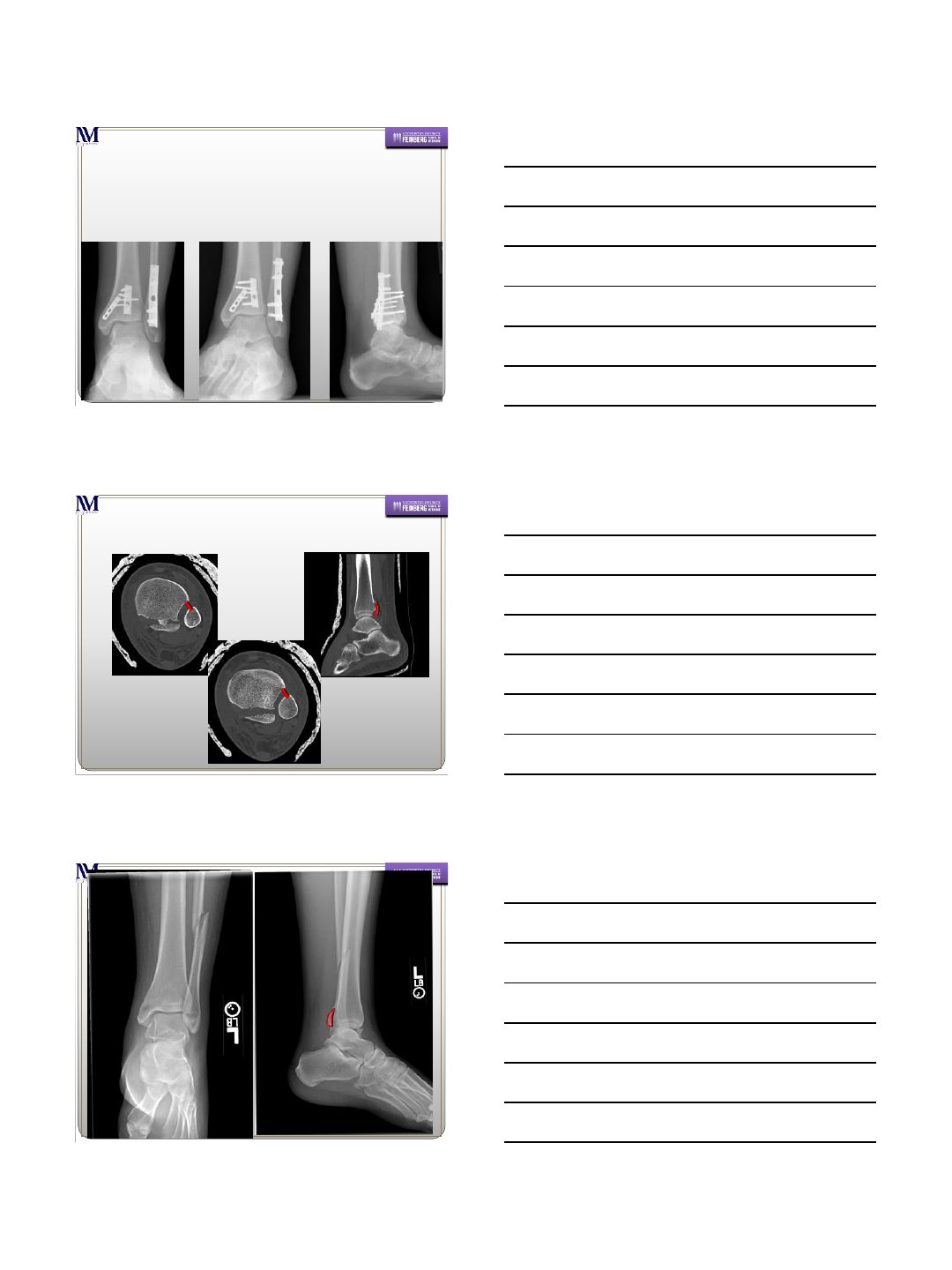
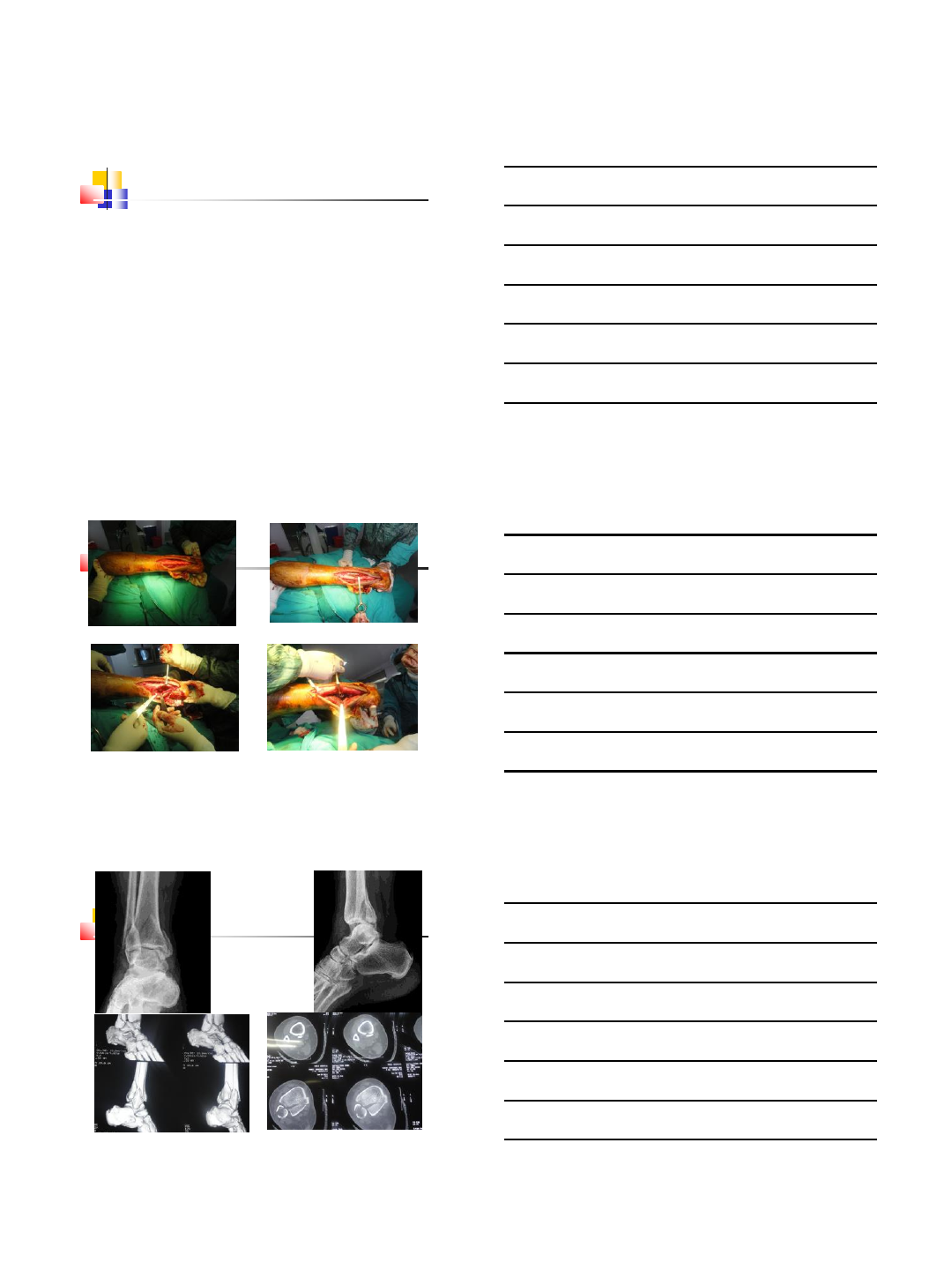
Failed to Identify
the syndesmotic
injury.
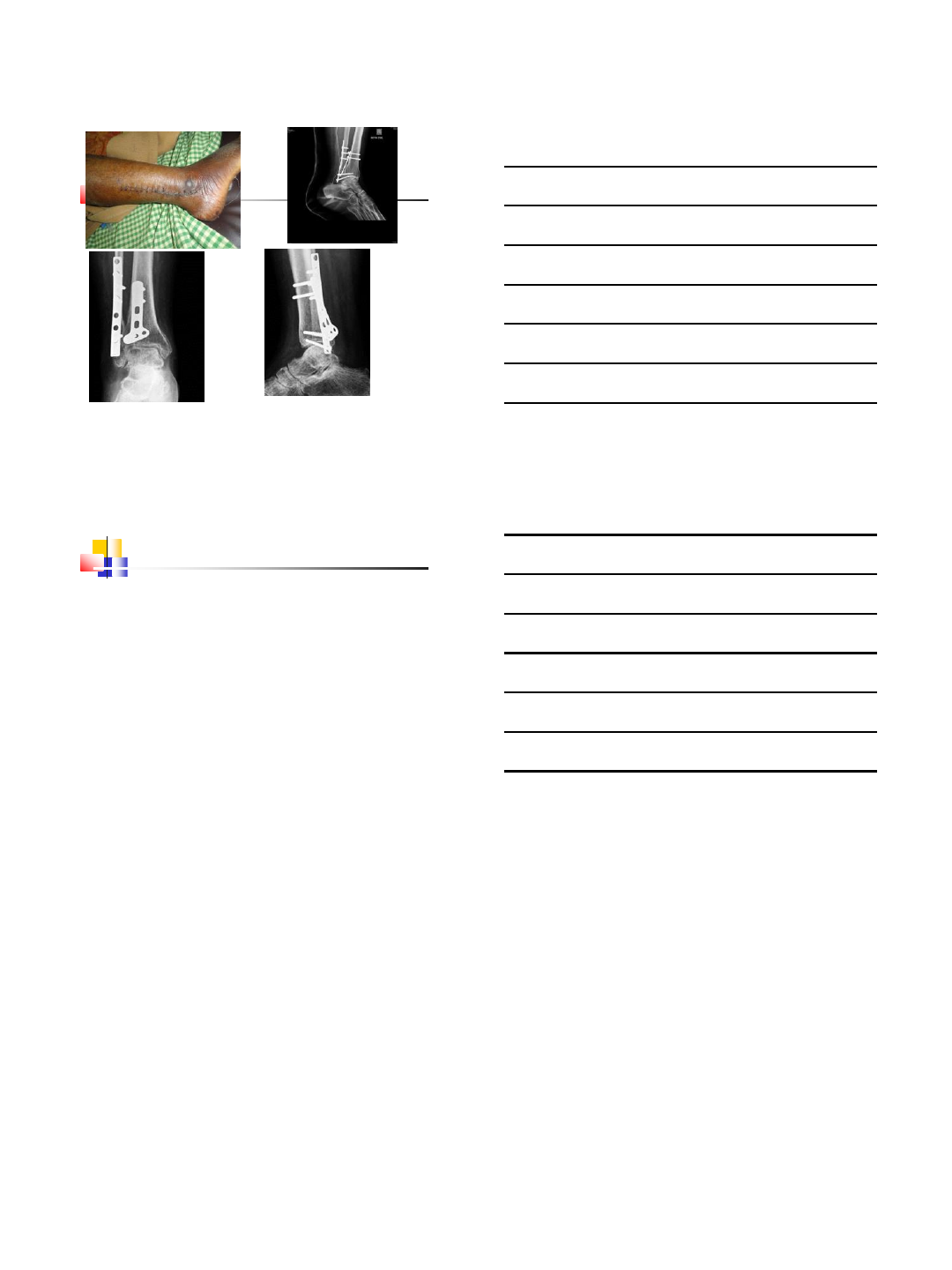
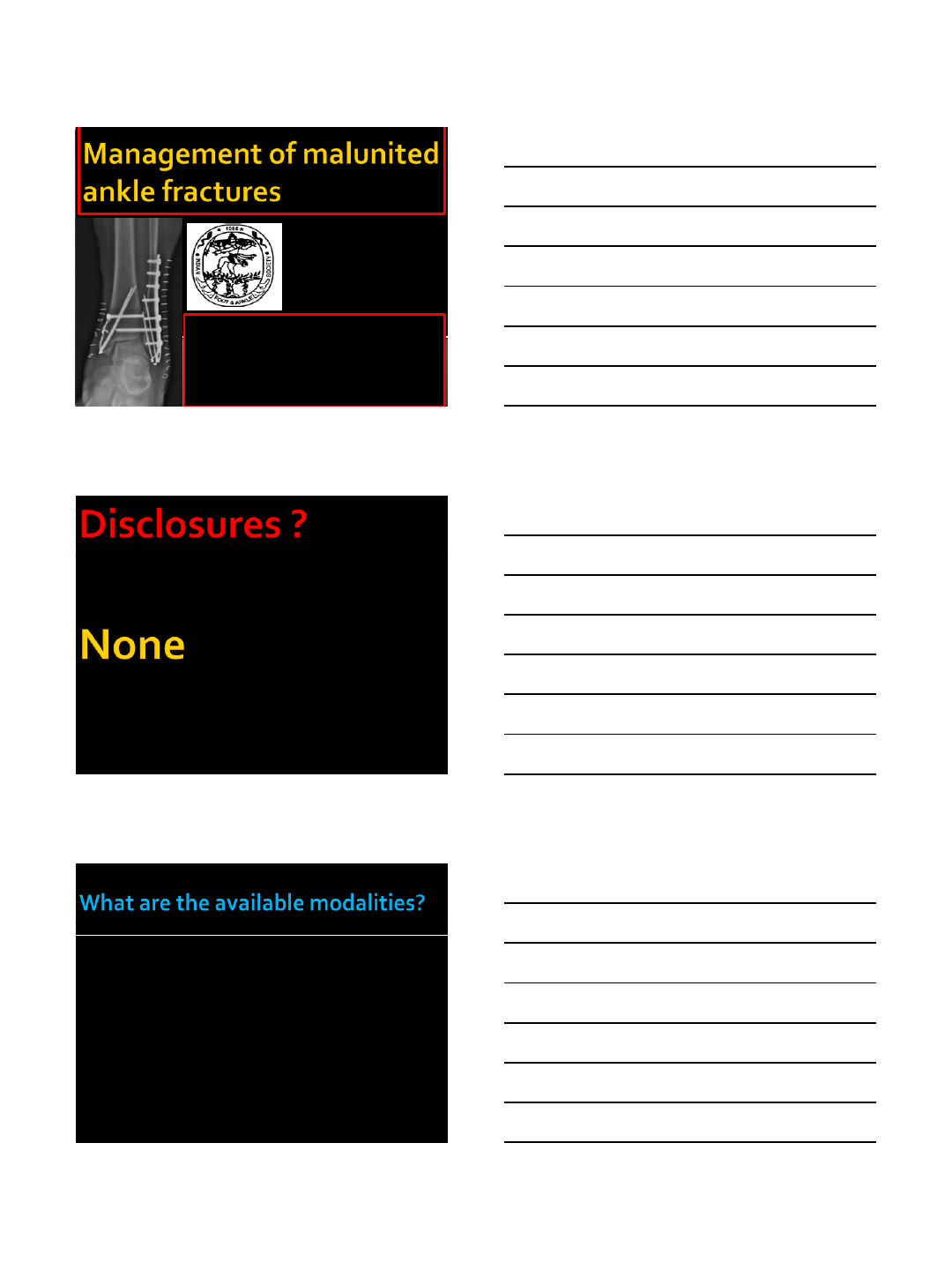
Case 3 cont.
Fibular Osteotomy,
Syndesmotic Fusion.
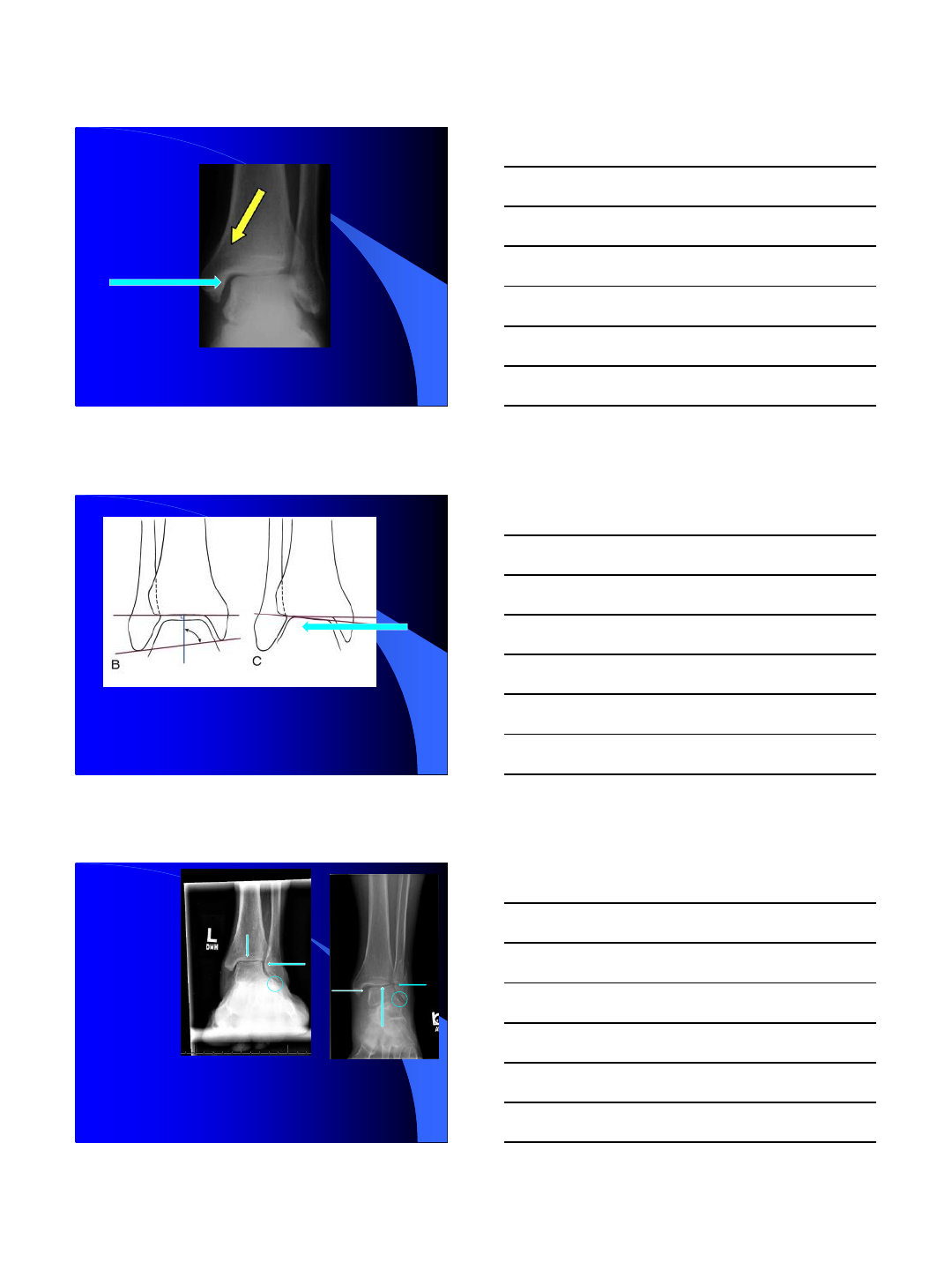
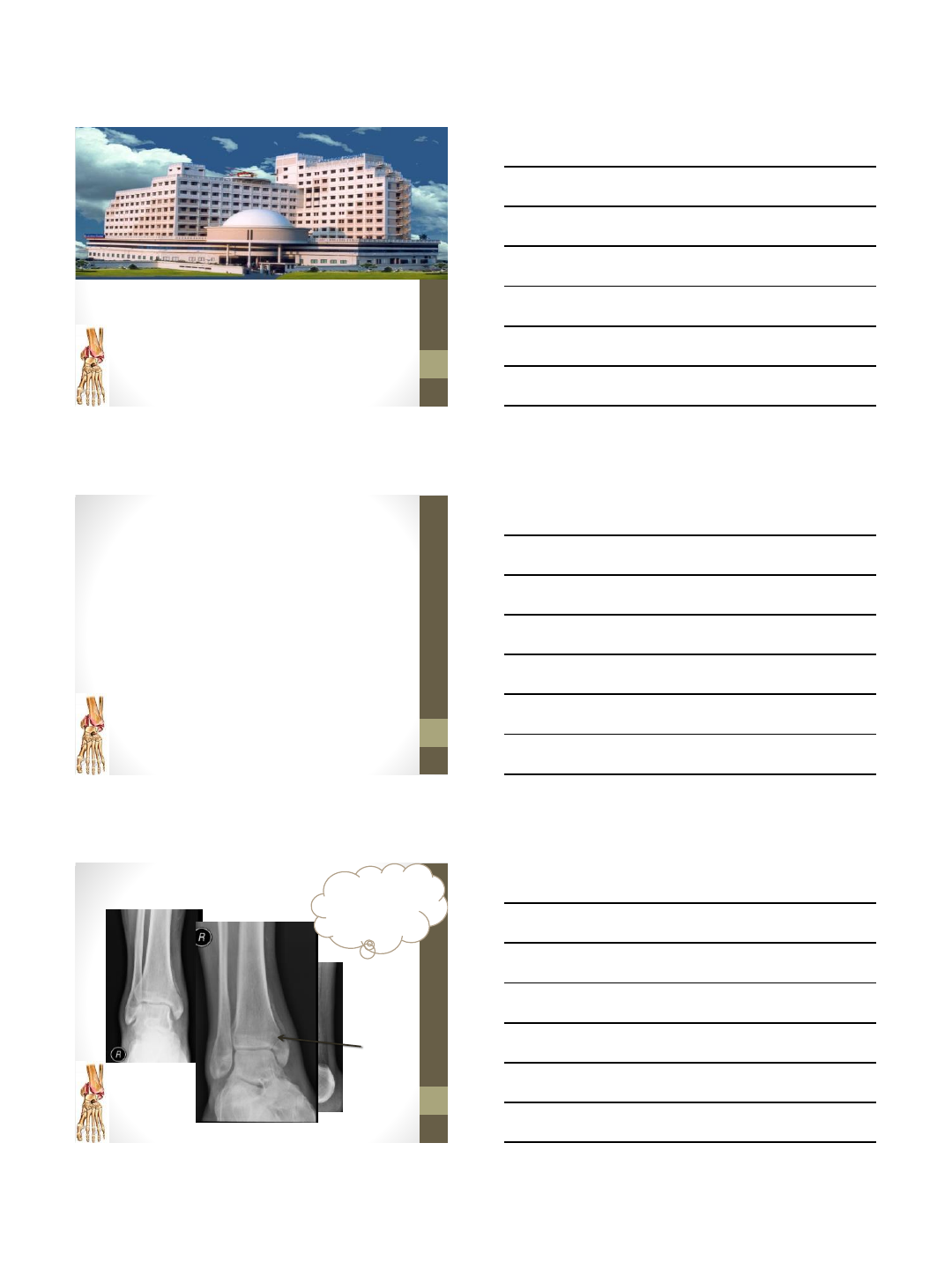
The medial clear space on mortise
views should be less than 4 mm.
The superior joint space within
2 mm medially of its width
laterally. The joint space should
be relatively symmetric.
10/21/2014
16
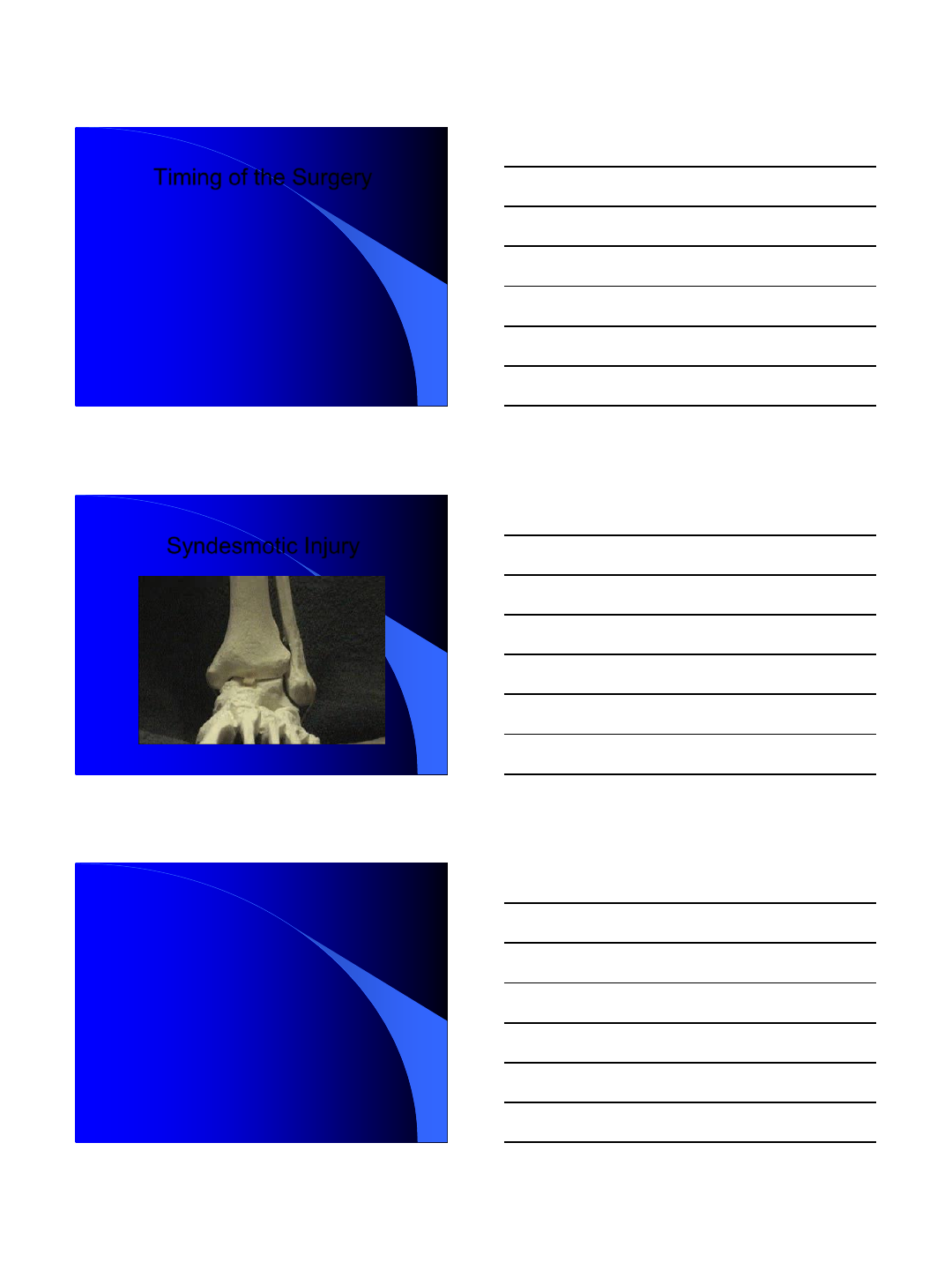
Medial Clear Space > 4mm
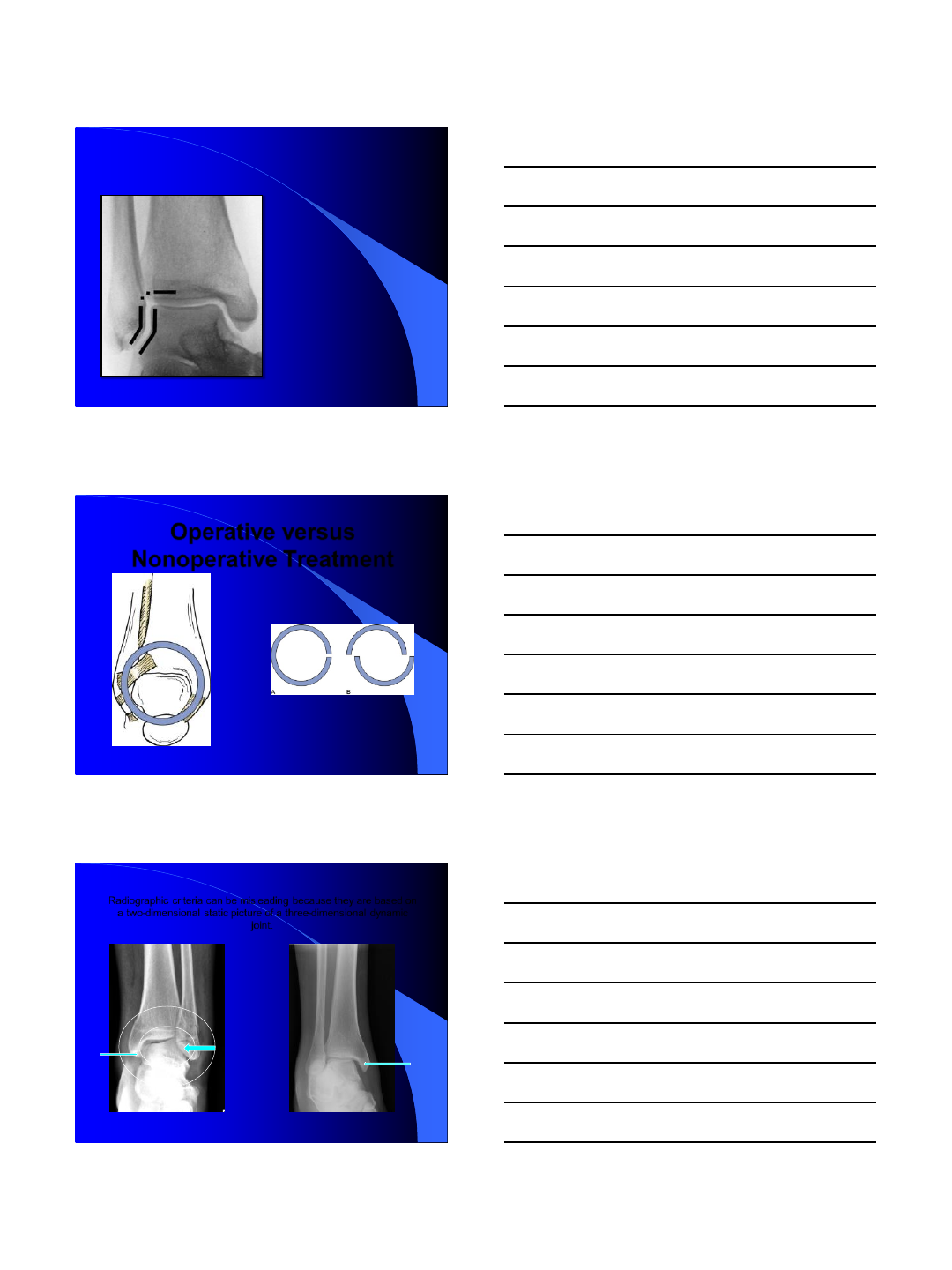
The talocrural angle is 83 degrees ± 4 degrees and normally within 2 degrees of
the opposite ankle.
The talar
tilt angle
(<2 mm).
Mann’s Surgery of the Foot and Ankle. Walling, Art, et al Pages 2003-2040
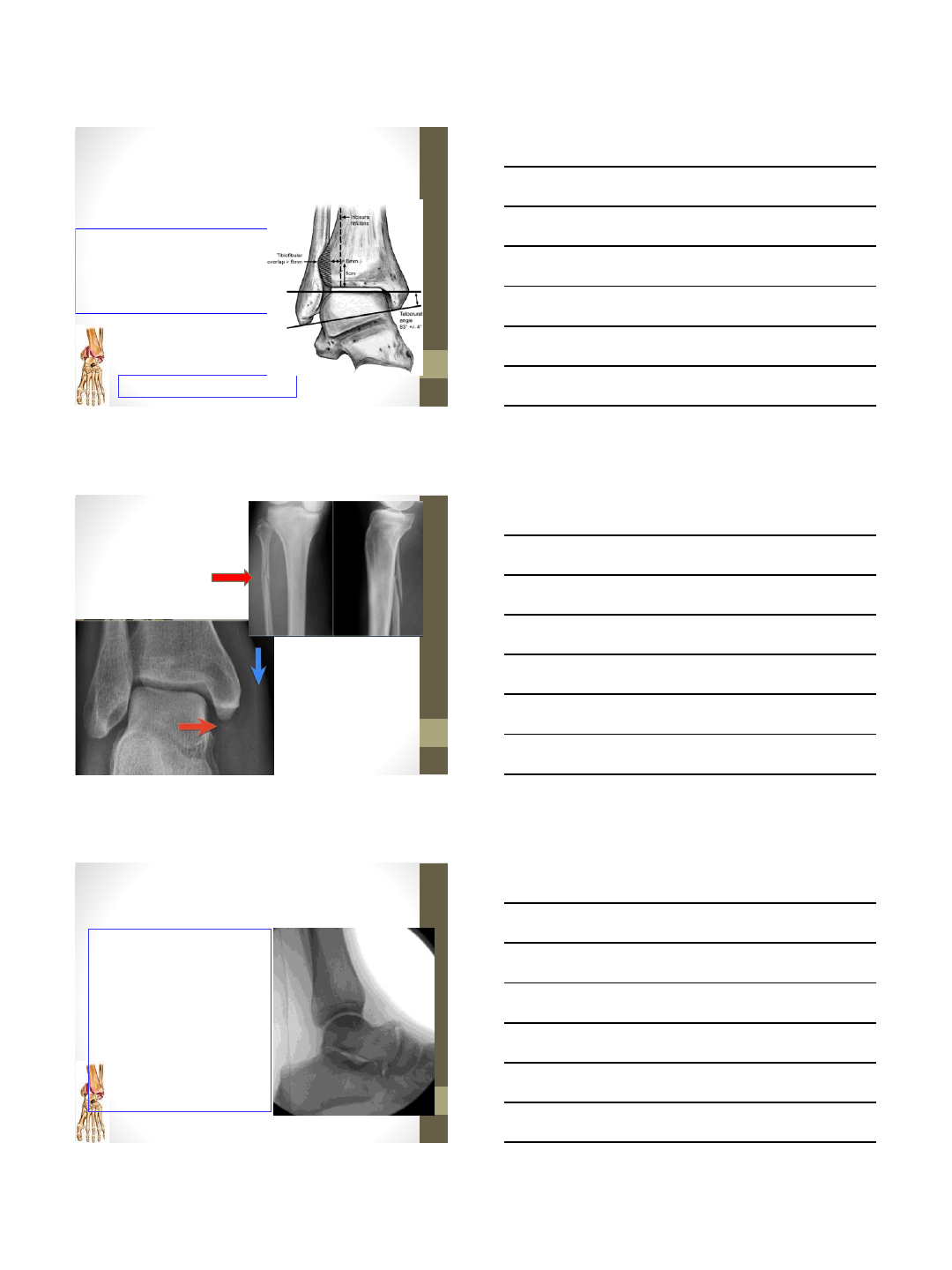
1Parallel joint space.
2, Spike of fibula pointing to the level of the subchondral bone of the tibia.
3, Unbroken curve between the lateral talar articular surface and recess of the distal
fibula. The subchondral bone that forms the Shenton line should be intact.
Weber BG, Simpson LA: Corrective lengthening osteotomy of the fibula. Clin
Orthop Relat Res 199:61-67, 1985.)
A
10/21/2014
17
-Shenton’s line.
-Fibular Length and
Rotation
-Restoration of fibular
length and rotation is
critical in
reestablishing a stable
ankle mortise, and can
be assessed with xray
“Shenton’s line”
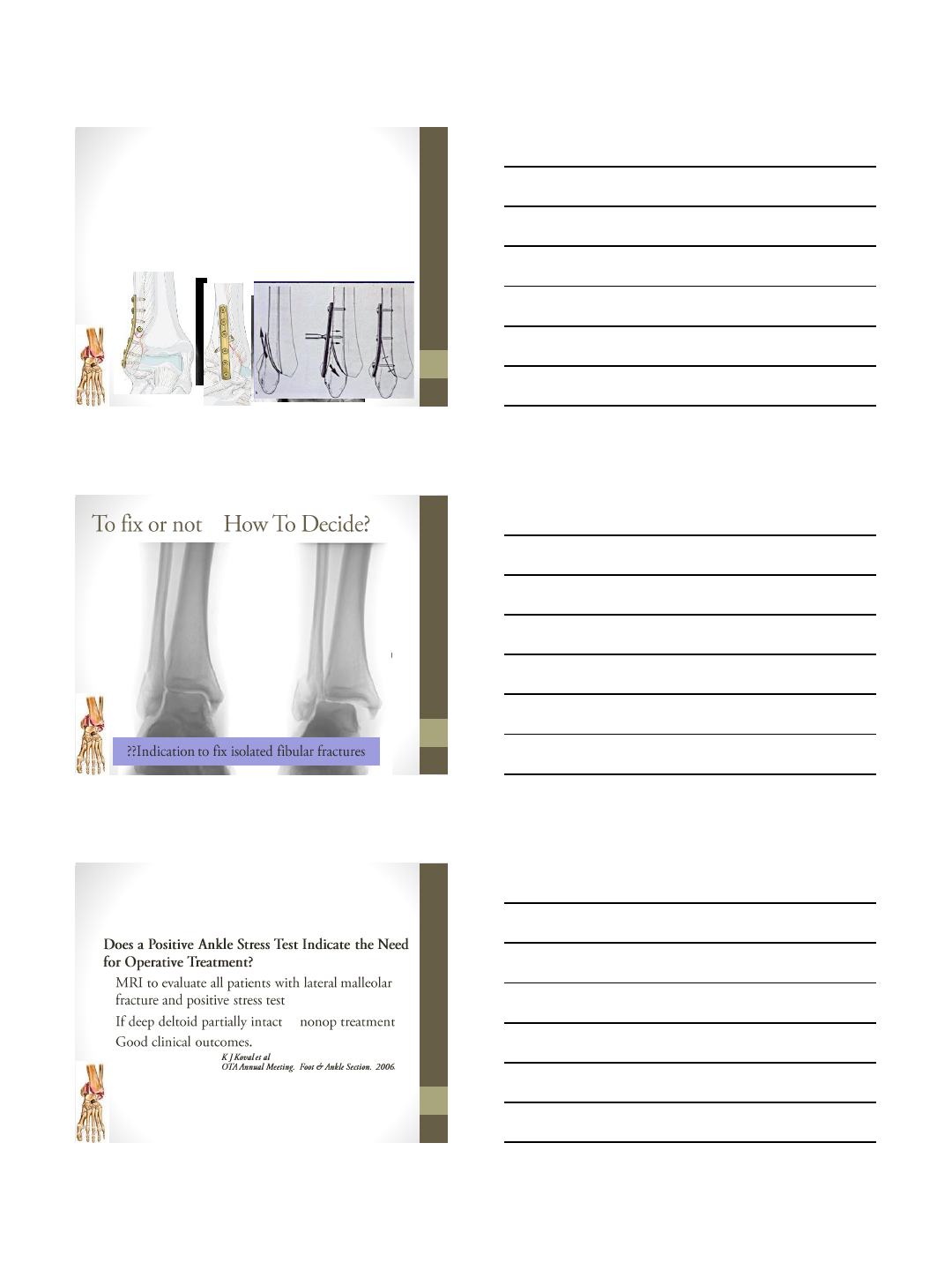
Operative versus
Nonoperative Treatment
Single Break: Stable
Double Break: Unstable
Neer CS: Injuries of the ankle joint:
evaluation. Conn State Med J 1953; 17: pp.
580
Mann’s Surgery of the Foot and Ankle.
Walling, Art et al. Pages 2003-2040
Radiographic criteria can be misleading because they are based on
a two-dimensional static picture of a three-dimensional dynamic
joint.
10/21/2014
18
Timing of the Surgery
-Abrasions should be cleansed and dressed. when practical, within a few hours if
abrasions are present. After 12 to 24 hours, deep or dirty abrasions can contraindicate
surgery until they have resolved
-Early closed reduction and elevation with a compressive dressing and splinting are
important in preventing edema and the development of fracture blisters.
-Fracture blisters adjacent to planned skin incisions do not appear to cause wound
problems unless they are blood filled.
Giordano CP et al. CORR 1994; 307: pp. 214-221
-In the presence of intradermal edema (peau d'orange), marked subcutaneous edema, or
fracture blisters : Delay until wrinkle sign, epithelialization of the abrasion.
Syndesmotic Injury
-Thank You.
10/21/2014
1
Modalities of treatment
in
Ankle injuries
Dr. Rajesh Simon
Consultant, Lakeshore Hospital,
Kochi, Kerala
DISCLOSURE
•I have no financial interest, affiliation or any other
relation ship for any commercial product or any
disclosure to be made.
Roentgenogram
Mortise view
At least 3 views
10/21/2014
2
Evaluation: Radiographic
Antero-posterior View
•Tibiofibular overlap > 6mm
•Talar tilt
•Talocrural angle:83⁰ +/-4
? Comparison Radiograph
Supra
syndesmotic
injury
Evaluation: Radiographic
Lateral View
•Posterior Malleolus
•Talar subluxation
•Distal fibular translation &/or
angulation
•Syndesmotic relationship
•Associated or occult injuries
•Lateral process talus
•Posterior process talus
•Anterior process calcaneus
10/21/2014
3
Evaluation: Radiographic
Other Imaging Modalities
•Stress Views
•Gravity
•Manual
•CT
•Articular involvement
•Posterior malleolus
•MRI
•Ligament and tendon
injury
•Talar dome lesions
•Syndesmosis injuries
Understand the patho-anatomy of
the Fracture before treatment.
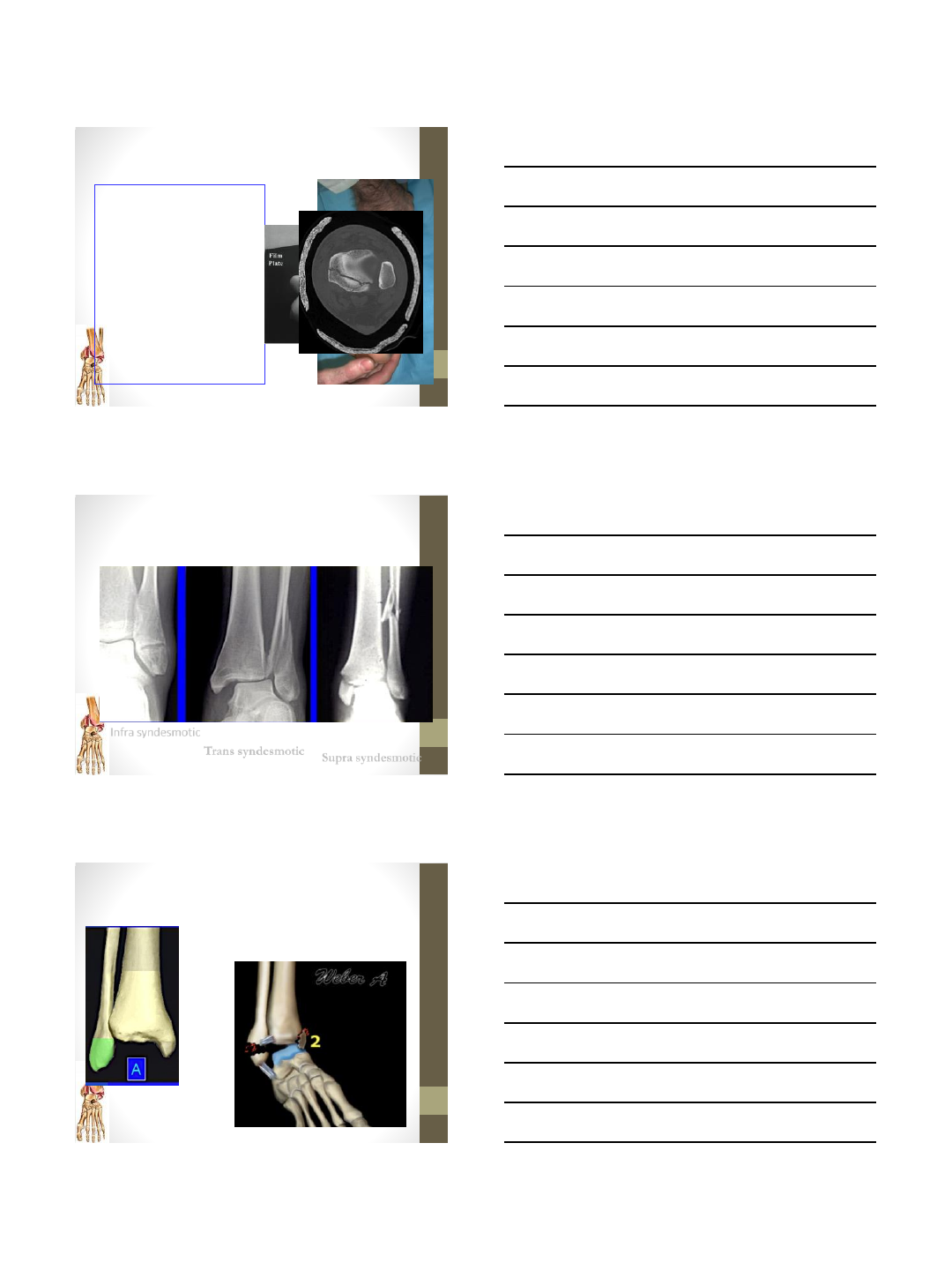
Infra syndesmotic
Trans syndesmotic Supra syndesmotic
AO DanisWeber classification
Infrasyndesmotic
Supination Adduction
10/21/2014
4
AO DanisWeber classification
Transsyndesmotic
Supination External
rotation
AO DanisWeber classification
Suprasyndesmotic
pronation external
rotation
Understanding the injury
helps in reversing the injury
and helps to achieve closed
temporary reduction
Immediate reduction
necessary
10/21/2014
5
•Splintage in situ slab
•Anatomical integrity of ankle
•Correct length of fibula
•Exact position of fibula in fibular notch
•Integrity of syndesmotic ligaments
Success of treatment
1 mm lateral talar displacement reduces
tibiotalar contact surface up to 46 %
Ramsey and Hamilton JBJS 1976
2mm of
shortening or
lateral shift
increases
contact forces
OA ankle
Definitive treatment
Decision Making
Understanding the fracture stability
Fibular fractures
1. With a stable ankle mortise usually heals
uneventfully.
2. With an unstable ankle mortise heal with significant
functional problems…because instability allows for
talar shift.
10/21/2014
6
Disaster to operate
TIMING
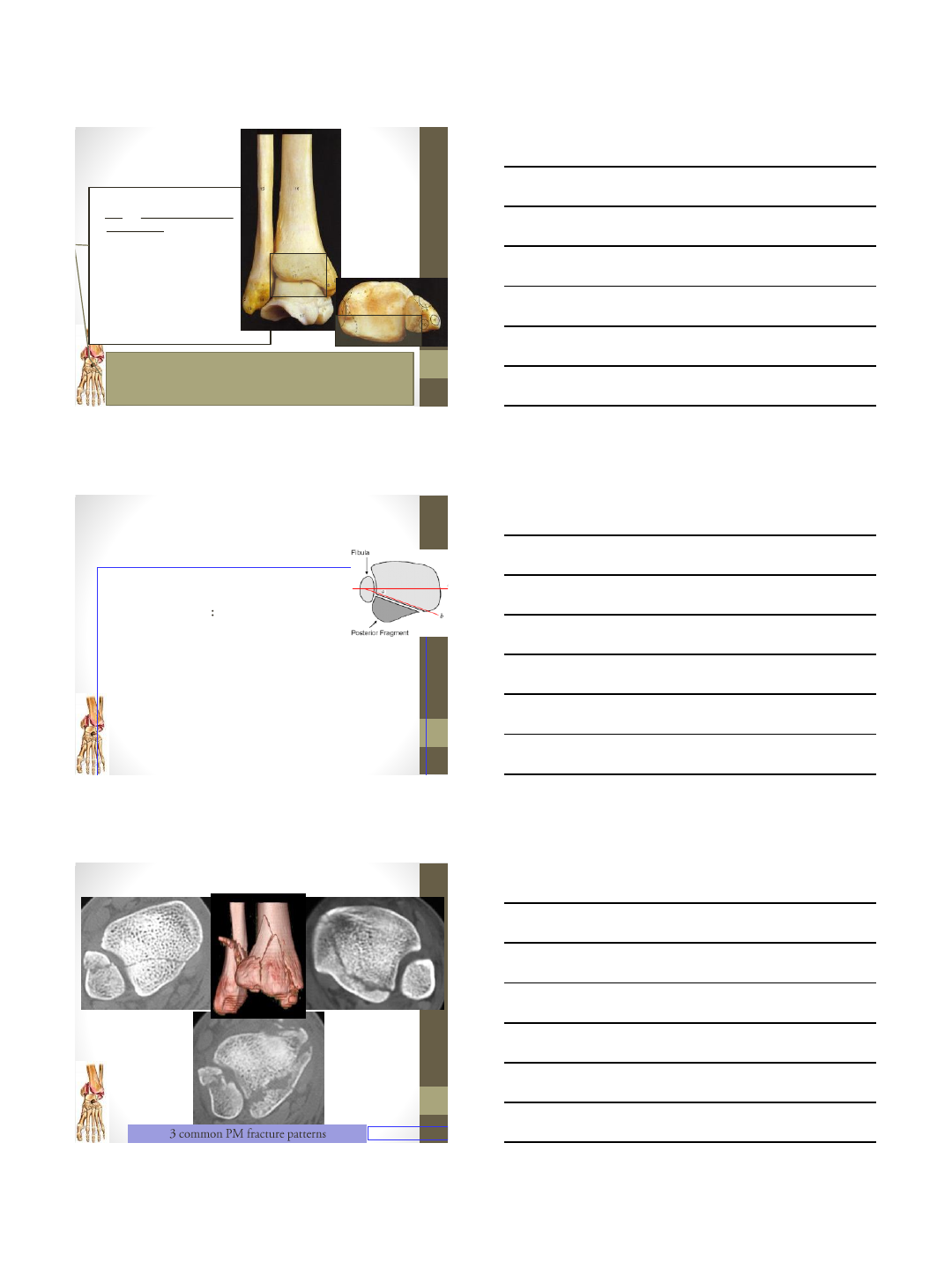
Lateral malleolus
TBW
Cancellous screw
10/21/2014
7
•Type of fixation depend on size of medial malleolus
•Standard fixation is two 4mm cancellous screws
•TBW for small fragments
Medial malleolus
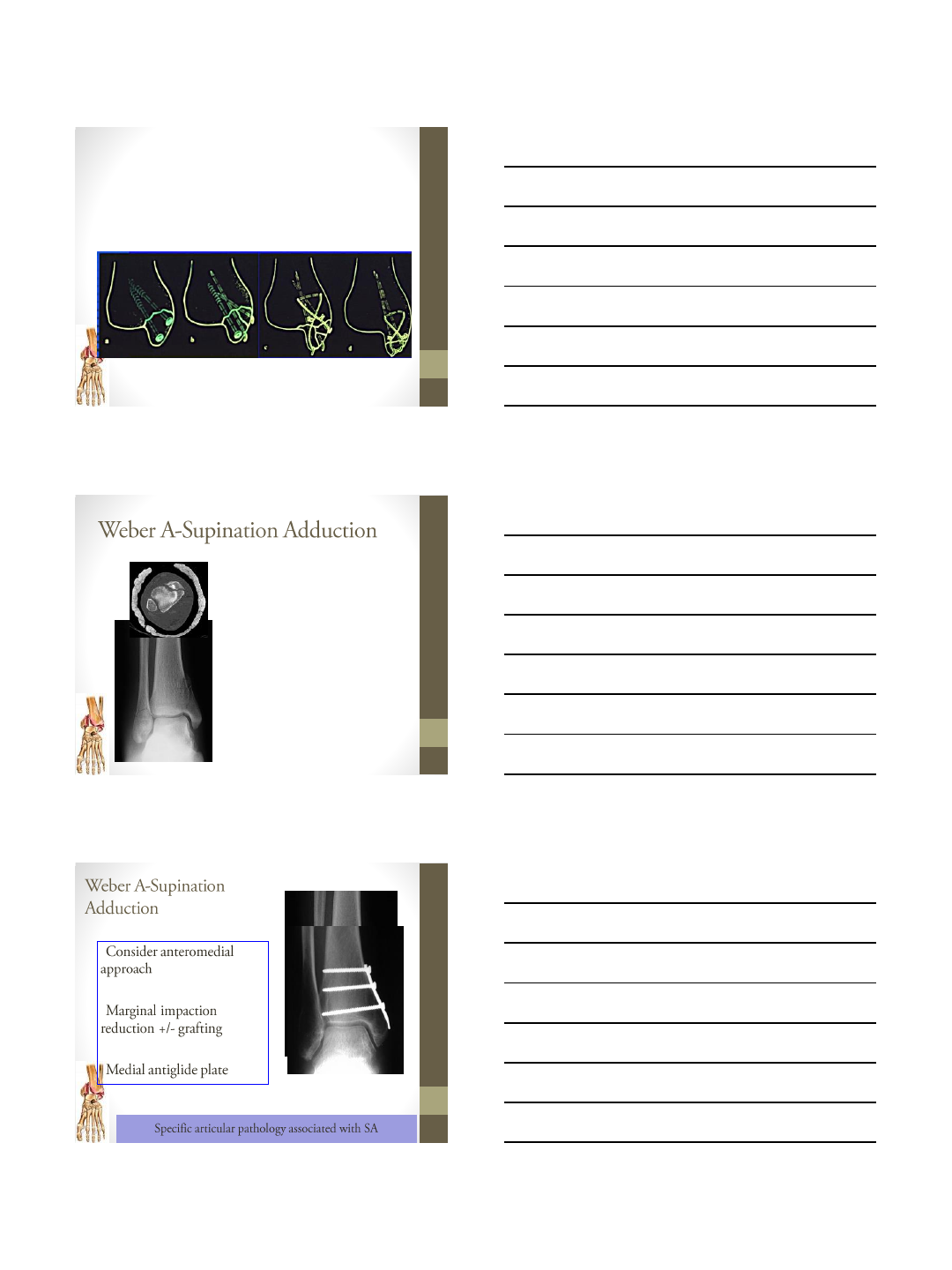
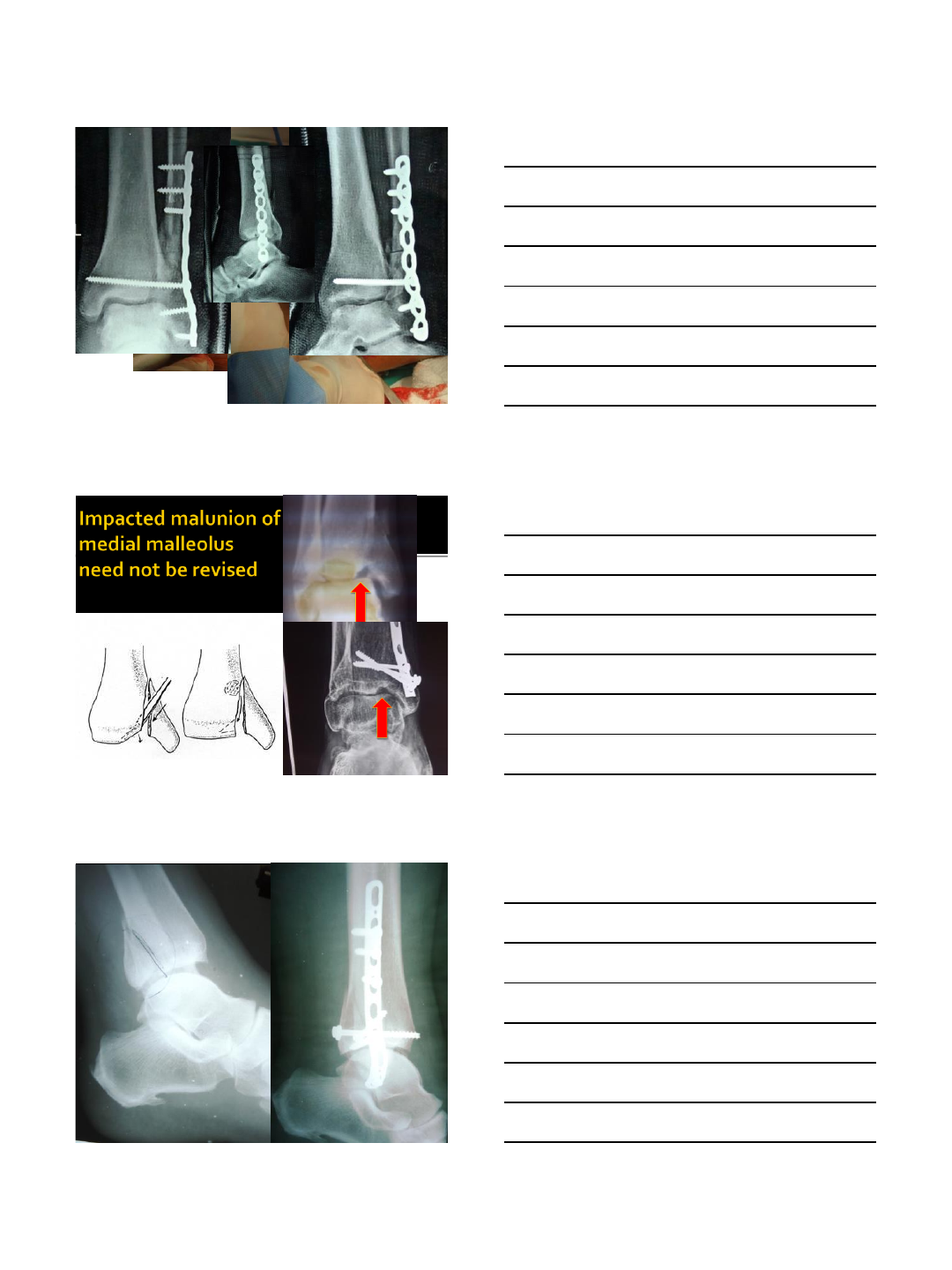
•Medial injury: vertical shear
type medial malleolar
fracture
•BEWARE OF IMPACTION
•
•
•
10/21/2014
8
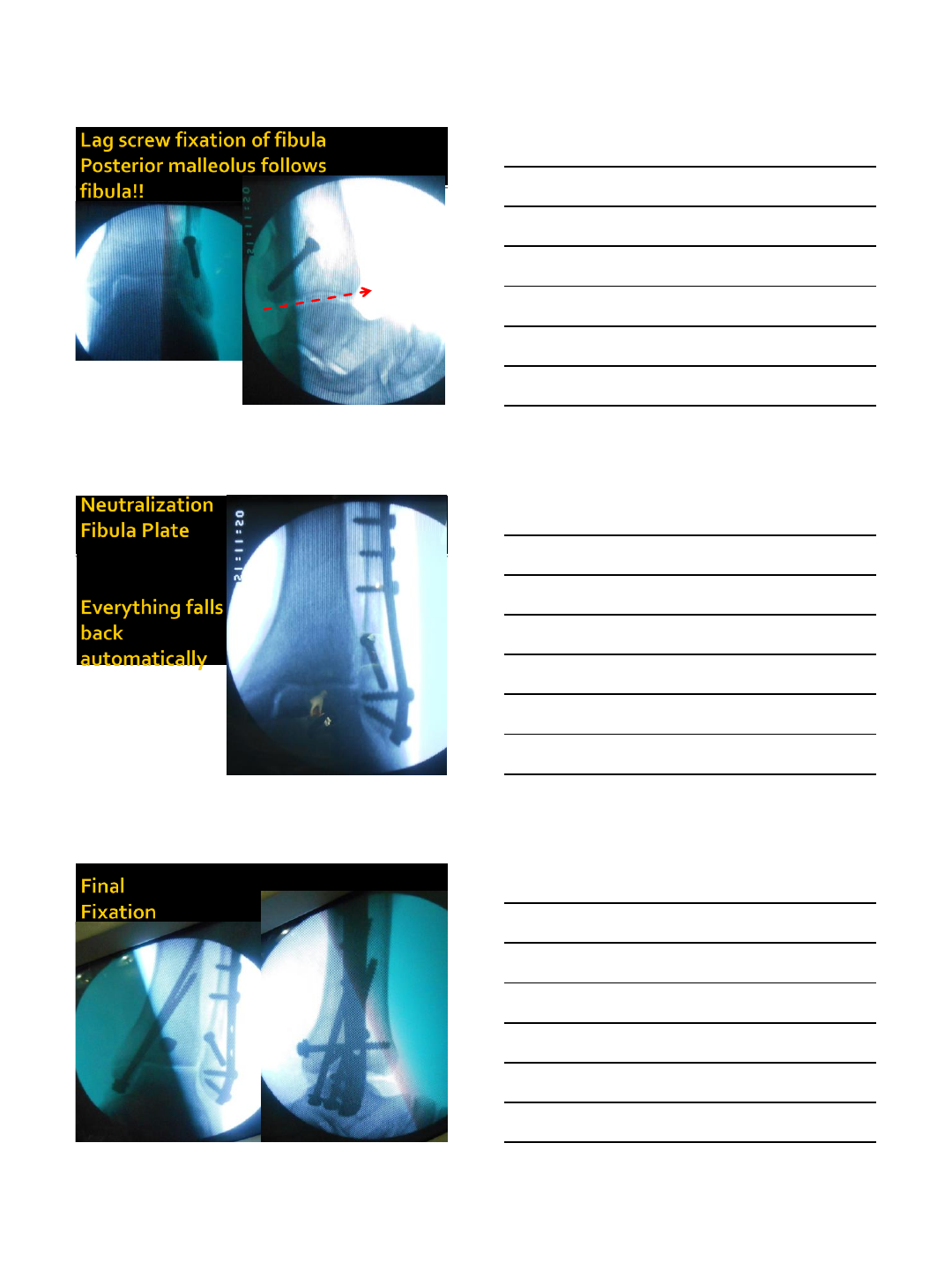
•Unstable fractures
•Reduction of fibula = reduction of joint
Weber B ( Supination External Rotation)
Lag screw and
neutralisation plate Antiglide plate and lag
screw
Options
Hanging
Mortise
view
Decision Making
•
•
•
•
Base your decision to operate on your findings and the risk:benefit
ratio in isolated fibular fracture Weber 2/ SER types
10/21/2014
9
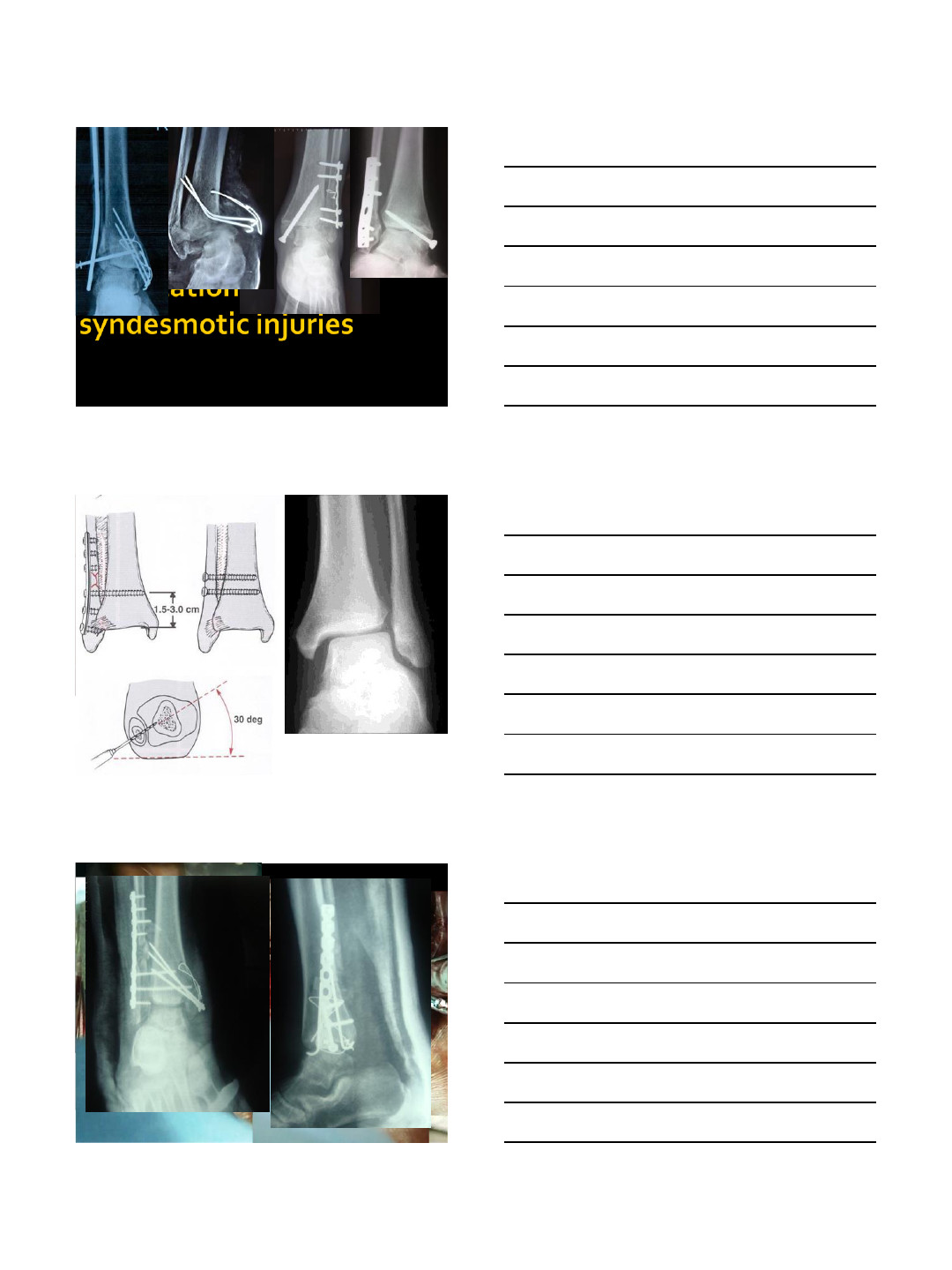
Type C (Pronation External Rotation )
•
•
•
•
HIGHLY UNSTABLE…SYNDESMOTIC INJURY COMMON
Type C (Pronation External Rotation )
•Final Objective
Restore:
•Fibular length and rotation
•Ankle mortise
•Syndesmotic stability
•Options
•Lag screw and neutralization plate
•Compression plating
•Bridge plating
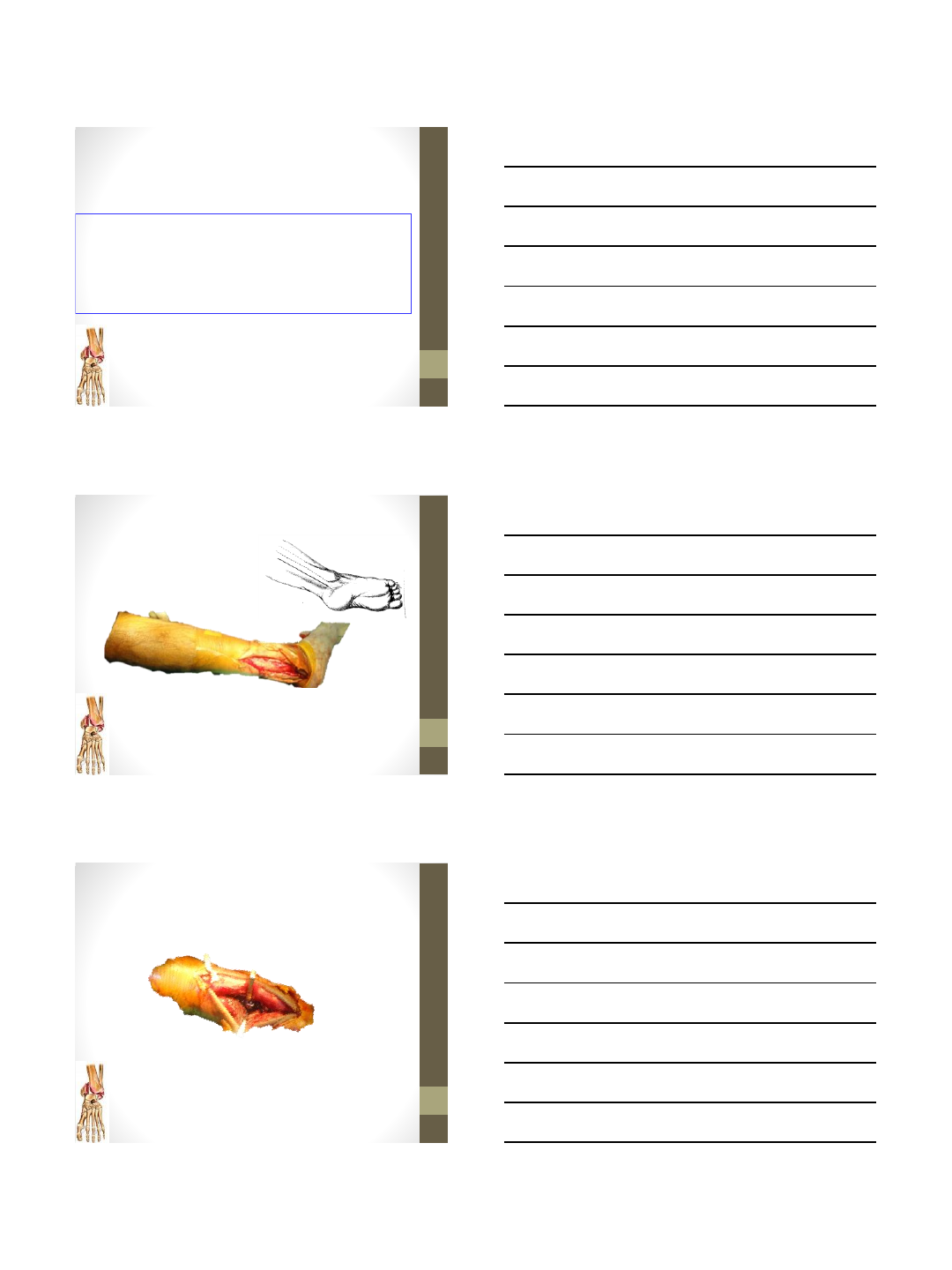
1/3rd tubular plate usually recommended
LCP in osteoprotic comminutions
Plate should be twisted –Mal rotation
Remember
10/21/2014
10
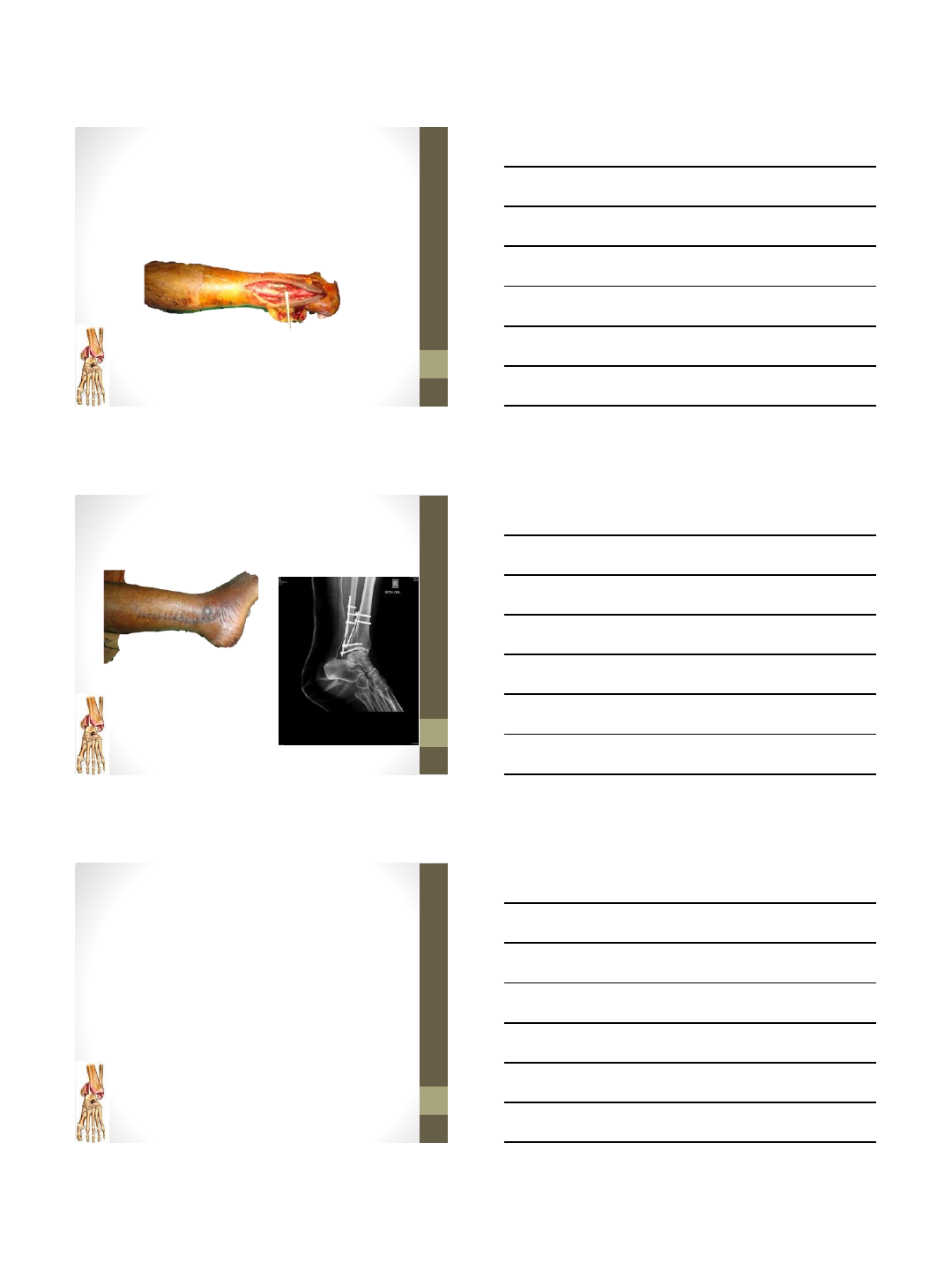
Posterior malleolus
Hartford’s experiment
Size Decrease tibio talar
contact area
•25% 4%
•33% 13%
•50% 22%
Hartford et al 1995 Tibiotalar contact area: contribution of posterior
malleolus and deltoid ligament CORR, 320, 182-7
Posterior Malleolus Fractures:
Radiographic Evaluation
•Indication for fixation: > 25% joint surface on
lateral view
•Fracture pattern
•Variable
•Difficult to assess on standard lateral radiograph
•Fracture orientation not purely in coronal plane
•Larger laterally than medially & obliquely oriented
Suggested X-rays
•External rotation lateral view [Decoster FAI 2000]
•CT scan [Haraguchi JBJS 2006]
Posterior Malleolus Fracture
Haraguchi et al. JBJS 2006
Type I- posterolateral oblique type Type II- medial extension type
Type III- small shell type
67%19%
14%
10/21/2014
11
Posterior Malleolus Fractures:
Indications for Fixation
•Stability
•Posterior translation of talus
•ER of talus [syndesmotic widening]
•A step off or gap more than 2-3mm after
reduction of the lateral and medial fragments
Incision
Post mall fixation-
Between Peronei and FHL
10/21/2014
12
Fibula fixation Ant to Peronei
Post op
Thanks Dr. Sunil/ Dr. Sarang
Take home message
•Understand the patho anatomy and treat
accordingly
•Ankle instability is key indication for surgery
•Regain Length and alignment of fibula
•Assess the Posterior malleolus and Syndesmosis
•Know surgical technique and proper implant
10/21/2014
13
10/21/2014
1
Anish R. Kadakia MD
Assistant Professor
Northwestern University
Department of Orthopedic Surgery
The Syndesmosis "What, When, and How"
Historic radiographic criteria
•Radiographic evaluation of the tibiofibular
syndesmosis
Harper & Keller Foot Ankle 1989
–Radiographs taken of 12 mounted fresh cadaver
lower extremity specimens
– “Normal” radiographic criteria reported
•Tibiofibular clear space (AP & mortise views) < 6 mm
•Tibiofibular overlap (mortise view) > 1 mm
Materials & methods
1415 consecutive pts aged 18 –65 with complete series of ankle
radiographs evaluated at University of Michigan’s foot &
ankle clinic
(Shah AS, Kadakia AR et. al. Foot Ankle Int. 2012)
392 pts (218 F, 174 M) with normal ankle radiographs included
83 sets of bilateral normal radiographs compared
10/21/2014
2
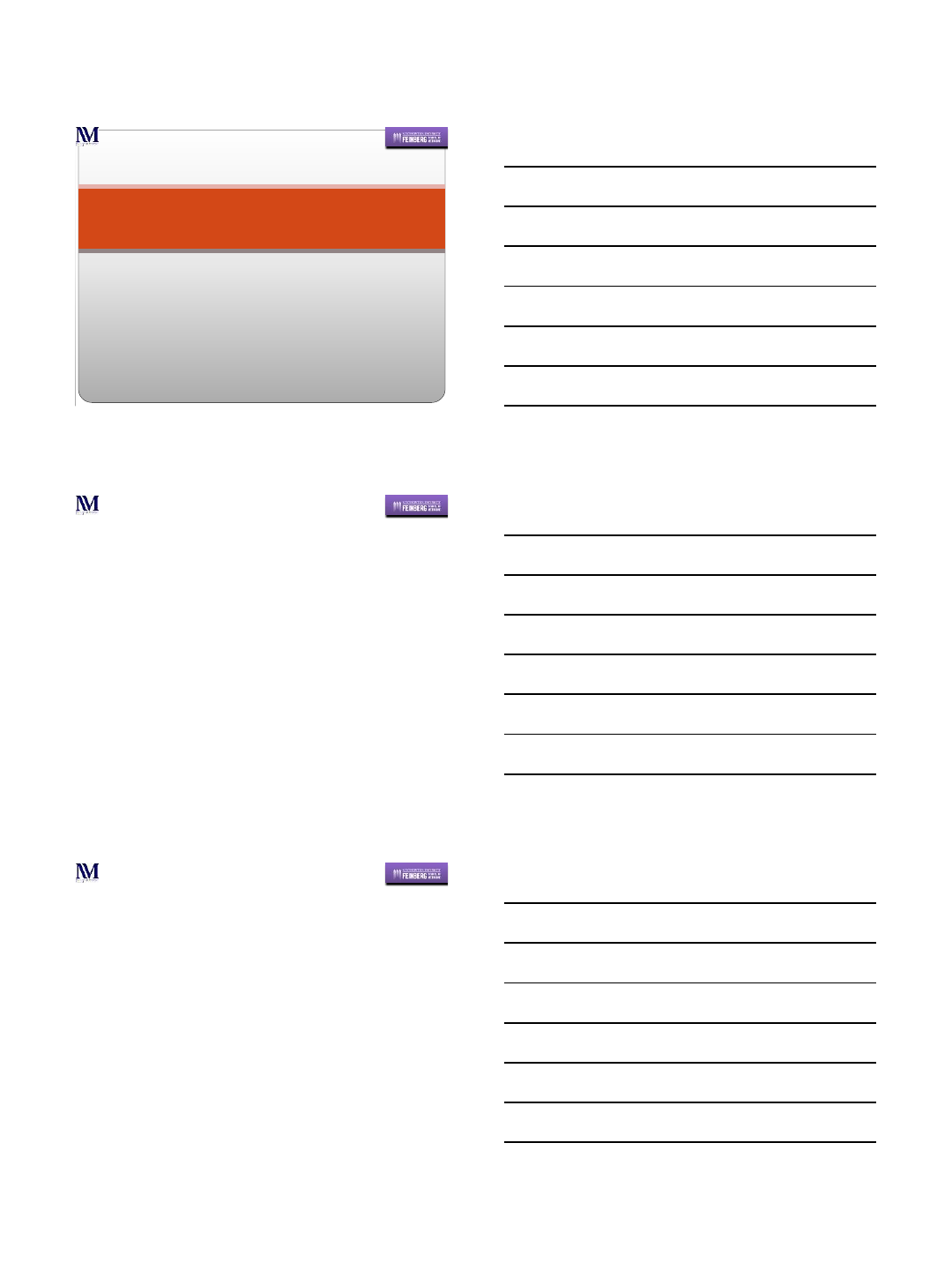
Tibiofibular overlap (mortise)
4.9% pts < 0 mm
7.7% pts < 1 mm
0
20
40
60
80
100
120
< 0 0 - 1 1.1 - 2 2.1 - 3 3.1 - 4 4.1 - 5 5.1 - 6 6.1 - 7 7.1 - 8 > 8
Tibiofibular Overlap (Mortise), mm
Number of Patients
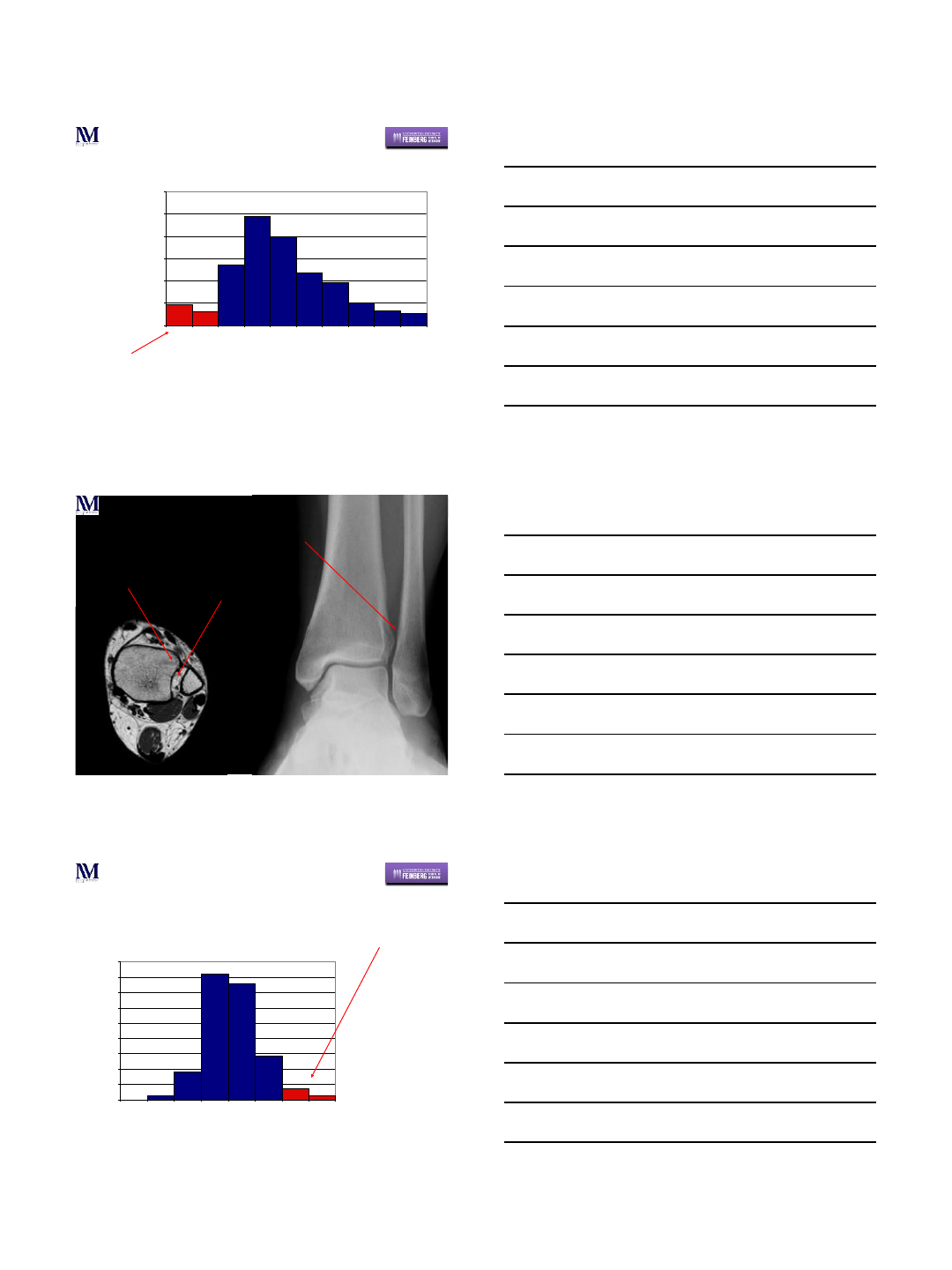
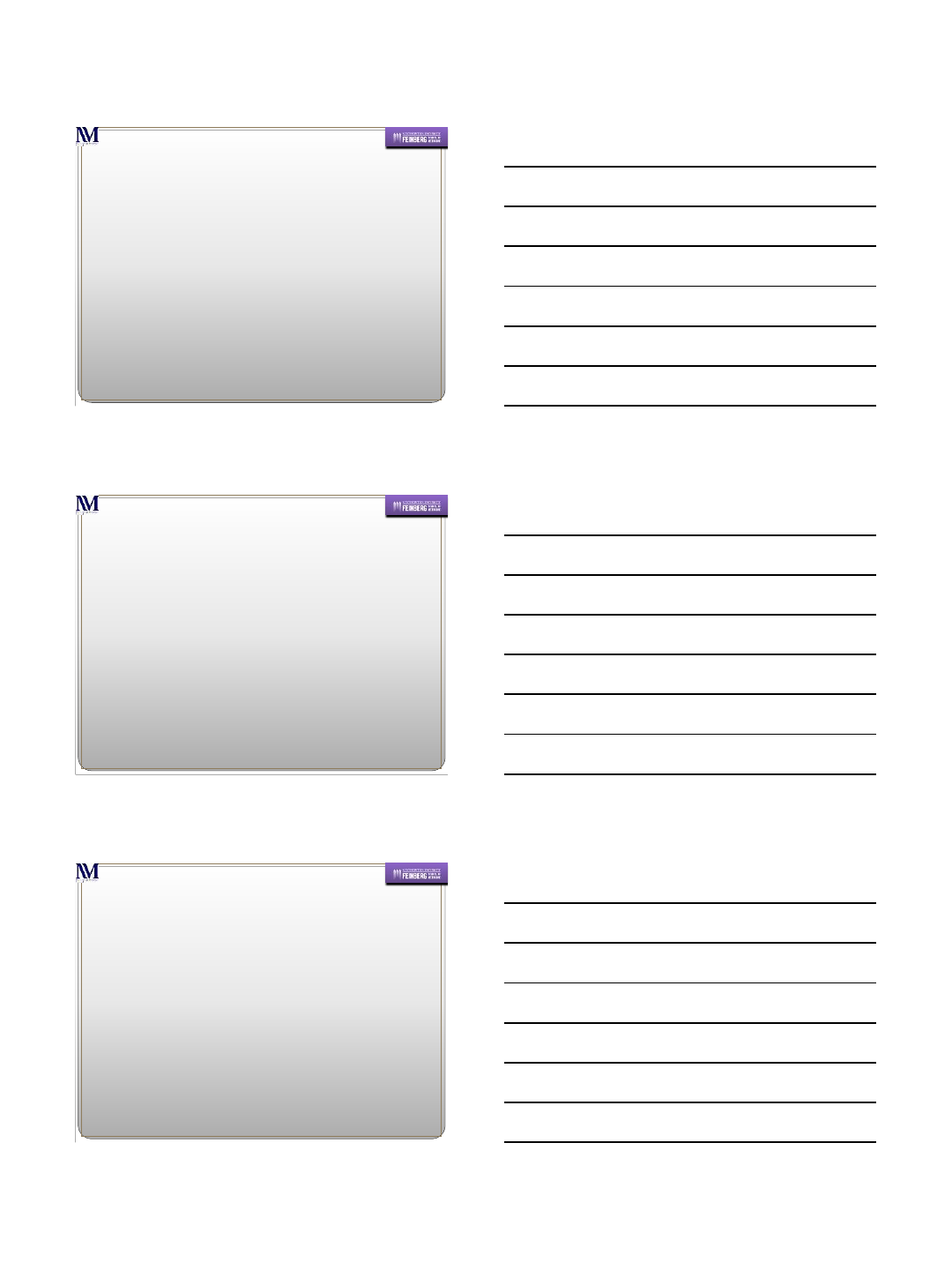
Example
34 yo F
L talonavicular ganglion
Diminutive anterior
tibial tubercle Rectangular-shaped
syndesmosis
Lack of overlap
0
20
40
60
80
100
120
140
160
180
0.0 - 1 1.1 - 2 2.1 - 3 3.1 - 4 4.1 - 5 5.1 - 6 6.1 - 7 7.1 - 8
Tibiofibular Clear Space (Mortise), mm
Number of Patients
Tibiofibular clear space (mortise)
4.3% pts > 6 mm
10/21/2014
3
Comparison radiographs
•In our series, mortise tibiofibular clear space is
the most useful measurement when
comparing to contralateral radiographs
–75% of contralateral radiographs within 1 mm
–95% of contralateral radiographs within 2 mm
•Measure of tibiofibular clear space relatively
independent of ankle rotation
Pneumaticos et al Foot Ankle Int 2002
When should we fix it?
1. Absolute values are not reliable given the variability noted.
2. Use contralateral mortise radiograph for comparison, side-
to-side difference in tibiofibular clear space of 2 mm
suggests syndesmotic disruption.
3. Overlap does not guarantee an intact syndesmosis!
4. If Normal ankle has 8mm of overlap and injured ankle has
4mm of overlap => INJURY
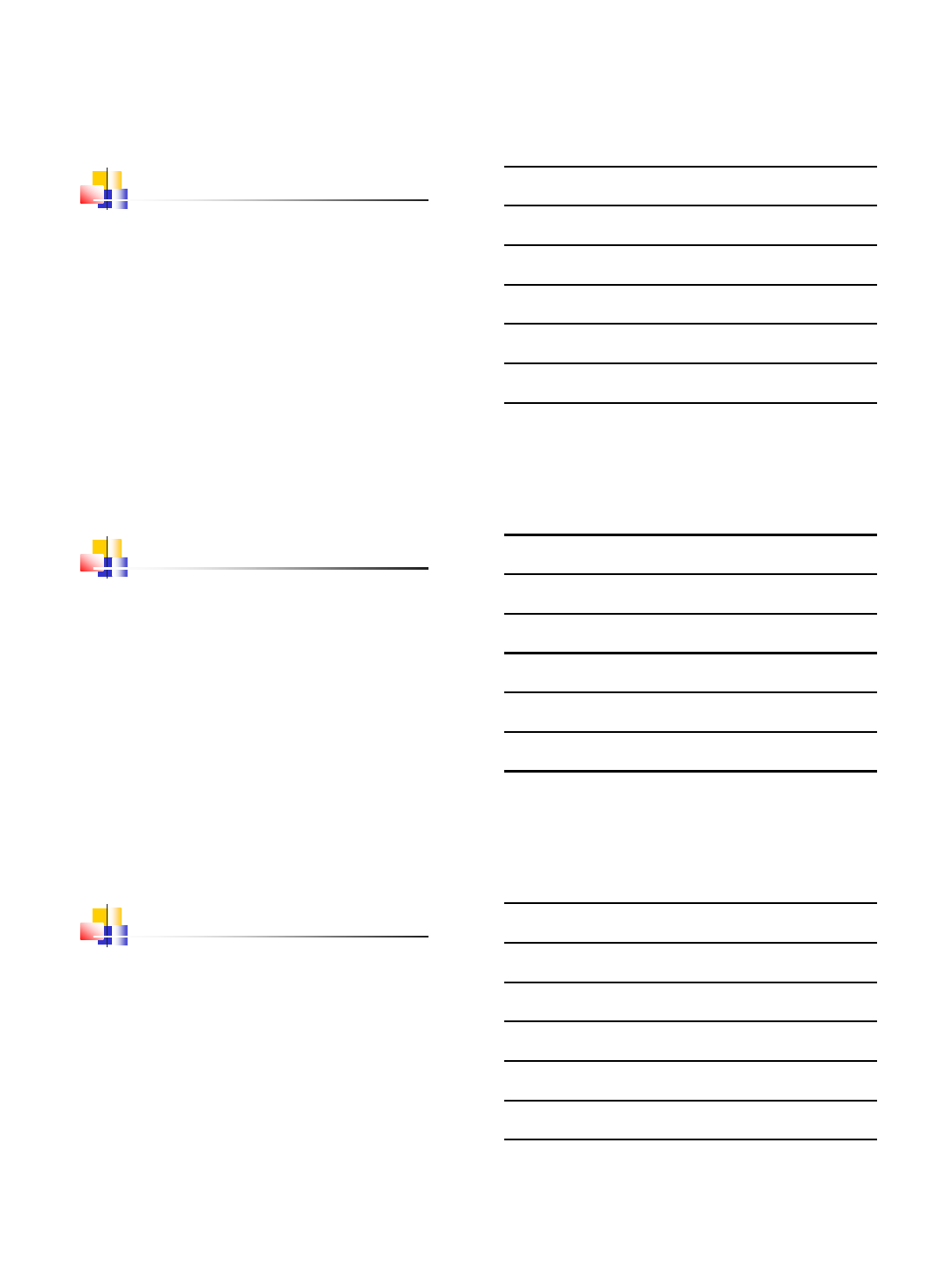
Mal-reduced PL fragment =
Malreduced syndesmosis
10/21/2014
4
Syndesmotic Fixation w/ Mal
reduced Post Mall
(Moore et al. Foot Ankle Int. 2006)
79 days PO
ORIF Post Mall can be enough
10/21/2014
5
Final PO
Rarely –require additional
ORIF syndesmosis
10/21/2014
6
1 year PO
Logical Protocol
2mm Side to Side Difference
Medial Clear Space Widening with Prox
fibular Fracture
Medial Clear Space widening w/o
Fibular Fx
Medial Clear Space widening after ORIF
fibula
MRI confirmation of Syndesmotic Injury
Posterior Malleolus Fracture
Obtain CT or MRI to assess displacement
Anatomic => Can ORIF syndesmosis alone
Displaced => ORIF Posterior malleolus
Anterior Tib/Fib wide => ORIF Posterior
Malleolus AND Syndesmosis
10/21/2014
7
HOW?
Old Controversies
3.5mm or 4.5mm?
No biomechanical advantage of the 4.5mm screw
(Thompson MC and Gesink DS, Foot Ankle Int. 2000)
3 or 4 cortices?
No significant difference in outcome at a mean f/u of 8.4 years
(Wikeroy AK. J Orthop Trauma. 2010)
No significant difference in outcome at a mean f/u of 150 days
(Moore JA. Foot Ankle Int. 2006)
Hardware Removal?
No clinical superiority noted with removal of HWR
New Controveries
Plate and Screws
May decrease risk of fibular fracture
Plate and Locked Screws
May decrease mal-reduction as screws cannot “drive” the fibula
into a mal-reduced position
Plate with 1 screw and 1 Suture button
Suture button may allow superior reduction as cannot “drive”
the fibula
Suture button may “back-up” screw fixation
NO Data to support these claims
10/21/2014
8
Suture Button Fixation
Why?
Eliminate need for hardware removal?
May allow more physiologic movement –theoretically
conducive toward soft tissue healing.
Excessive motion however –is detrimental
Sagittal Plane Relevance
Fibula is more unstable in the sagittal plane after
sectioning of the syndemosis
(Candal-Couto JJ. et. al. Injury, 2004)
Sectioned the AITFT/IOL/PITFL
Hook test performed in both planes
Mean Displacement
oCoronal –1.5mm
oSagittal –8.8mm
Additional sectioning of Deltoid
Mean Displacement
oCoronal –3.2mm
oSagittal –11.7mm
Sagittal Plane Relevance
Biomechanical evaluation
(Klitzman R. et. al. Foot Ankle Int. 2010)
Single suture button vs. single tri-cortical screw
Increased motion of the fibula in the sagittal plane with the
suture button compared to intact
NOT restoring the primary instability pattern
Fibula will follow the posterior malleolus and leads to mal-
reduction when considering this as a uni-planar injury.
May appear closed on the AP
However, can be posterior subluxated.
10/21/2014
9
What about 2 Suture Buttons?
Biomechanical Comparison
(Soin SP et. al. Foot Ankle Int. 2009)
2 diverging suture buttons
Single 3.5mm screw
NO Difference in the fibular movement in any plane.
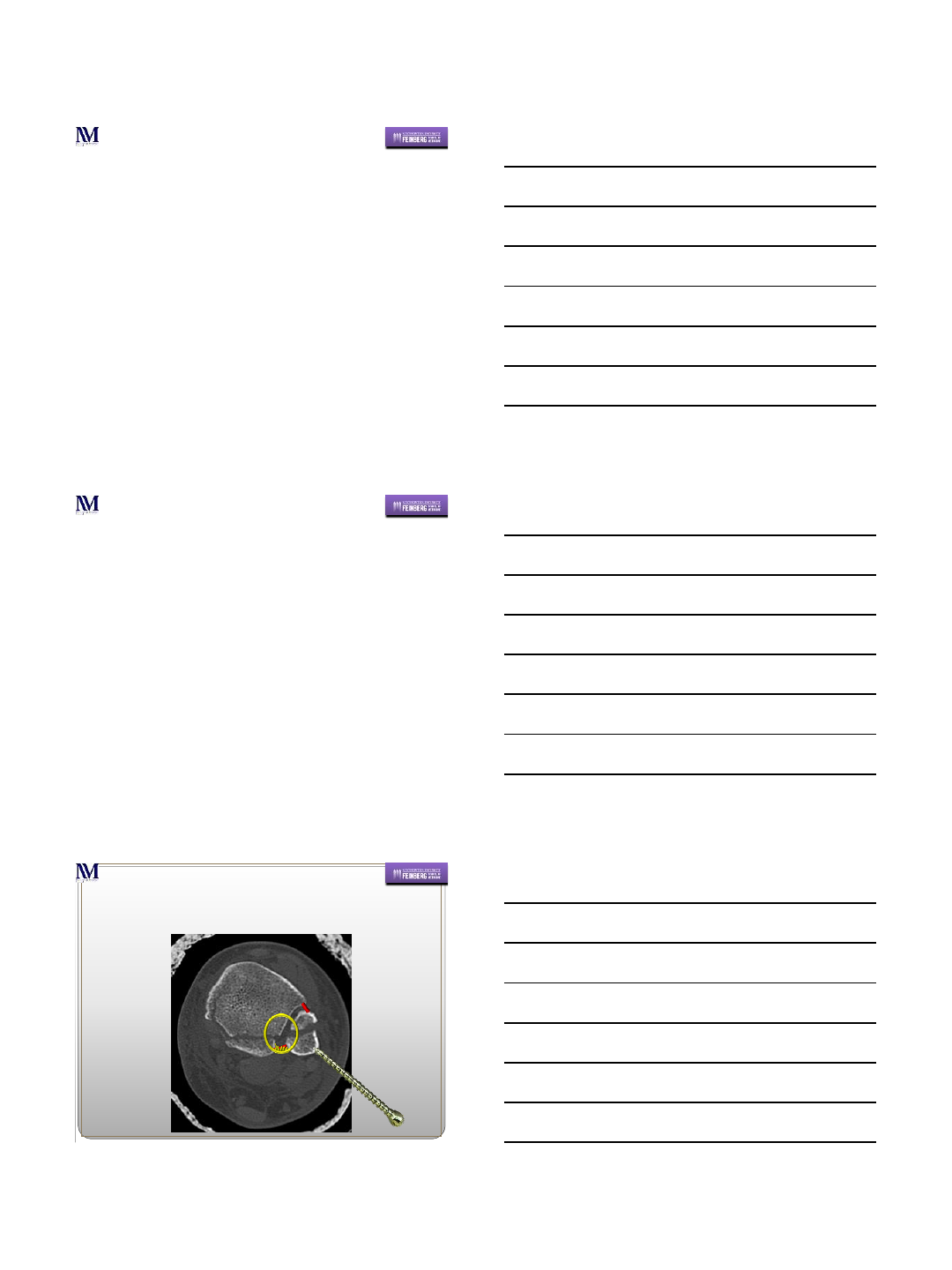
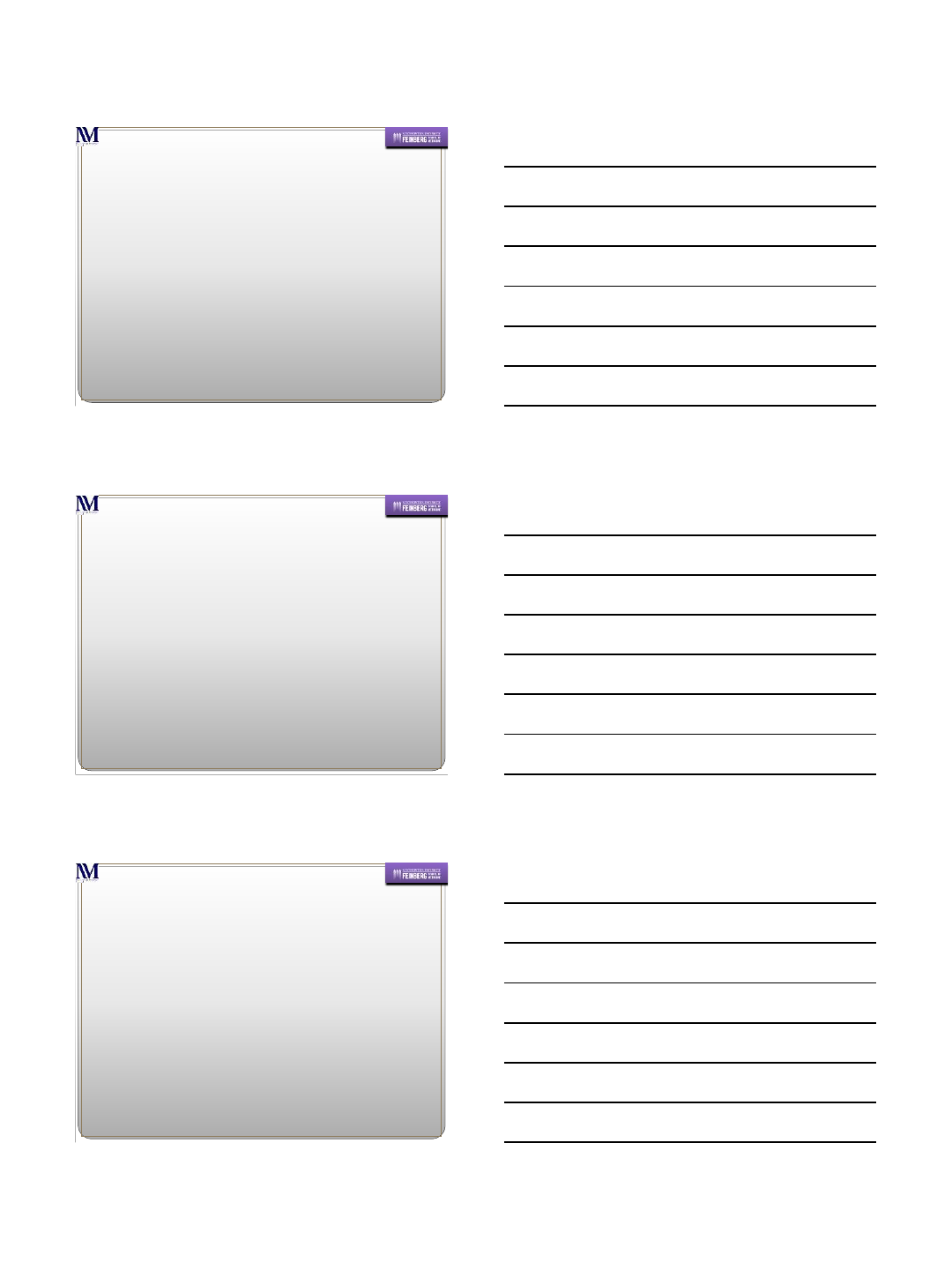
Reduction –Most Critical Aspect
Where do I apply the clamp?
Anatomic axis of the syndesmosis
Lateral Malleolar Ridge
Central point of the medial tibial cortex
1cm Proximal to the joint
Reduction
10/21/2014
10
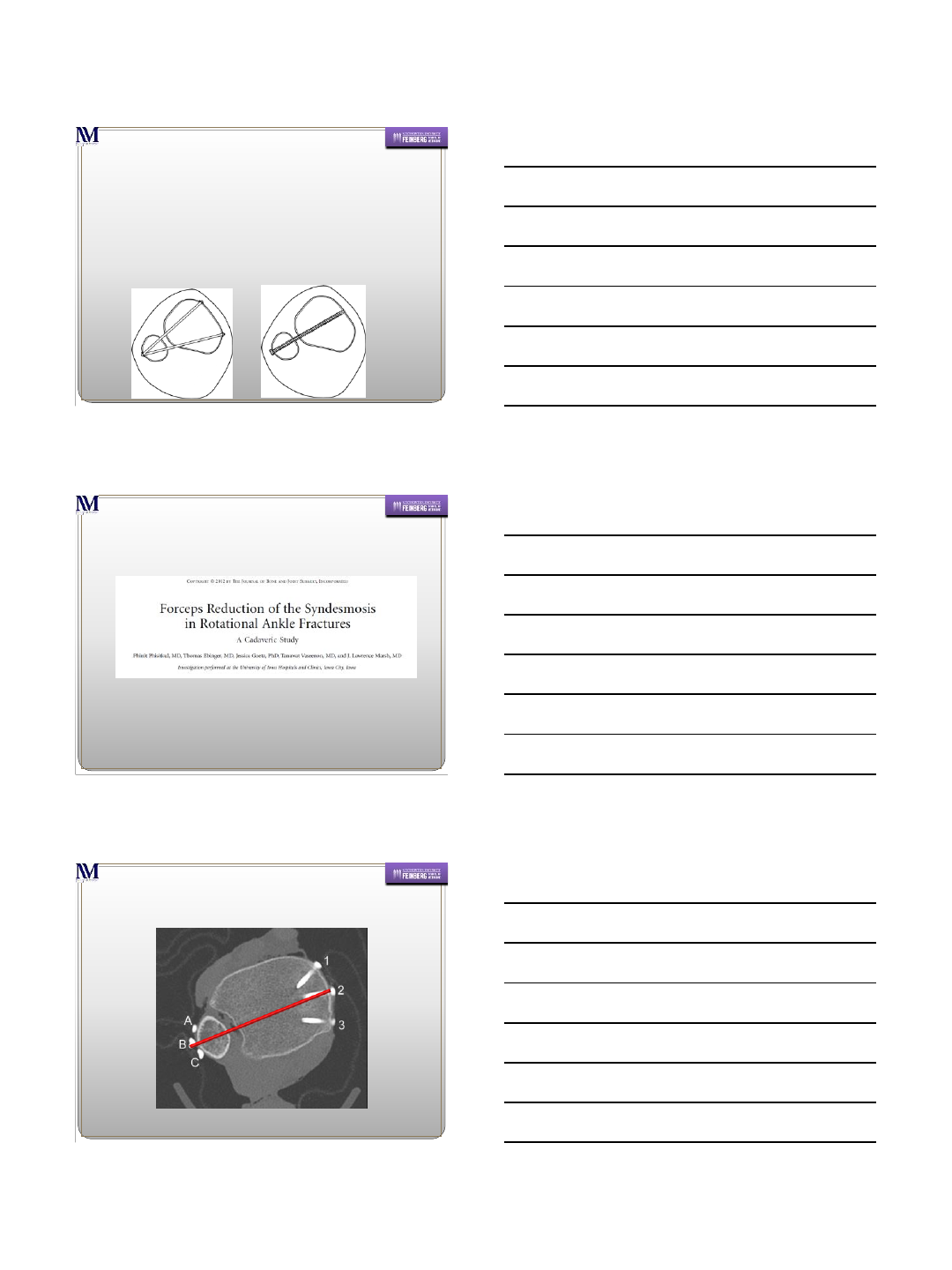
Reduction
Oblique placement will lead to malreduction
Adding PM fracture made things
worse for A3
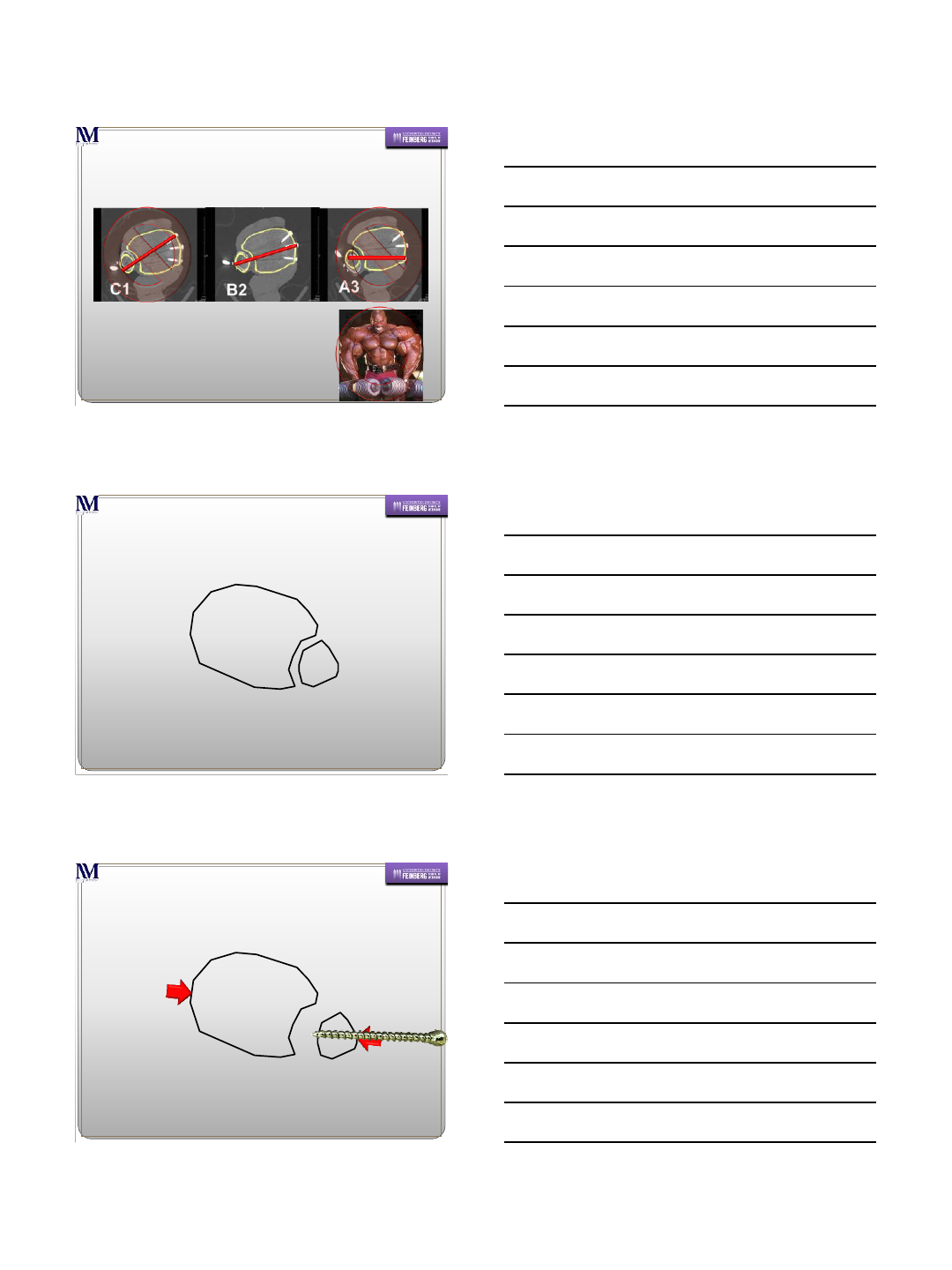
Do NOT have to “crush” it.
Over-compression of the articular
surface can occur.
Why this can lead to malreduction
Posterior Lip Intact
Slight malrotation may “self correct” s/p HWR
10/21/2014
11
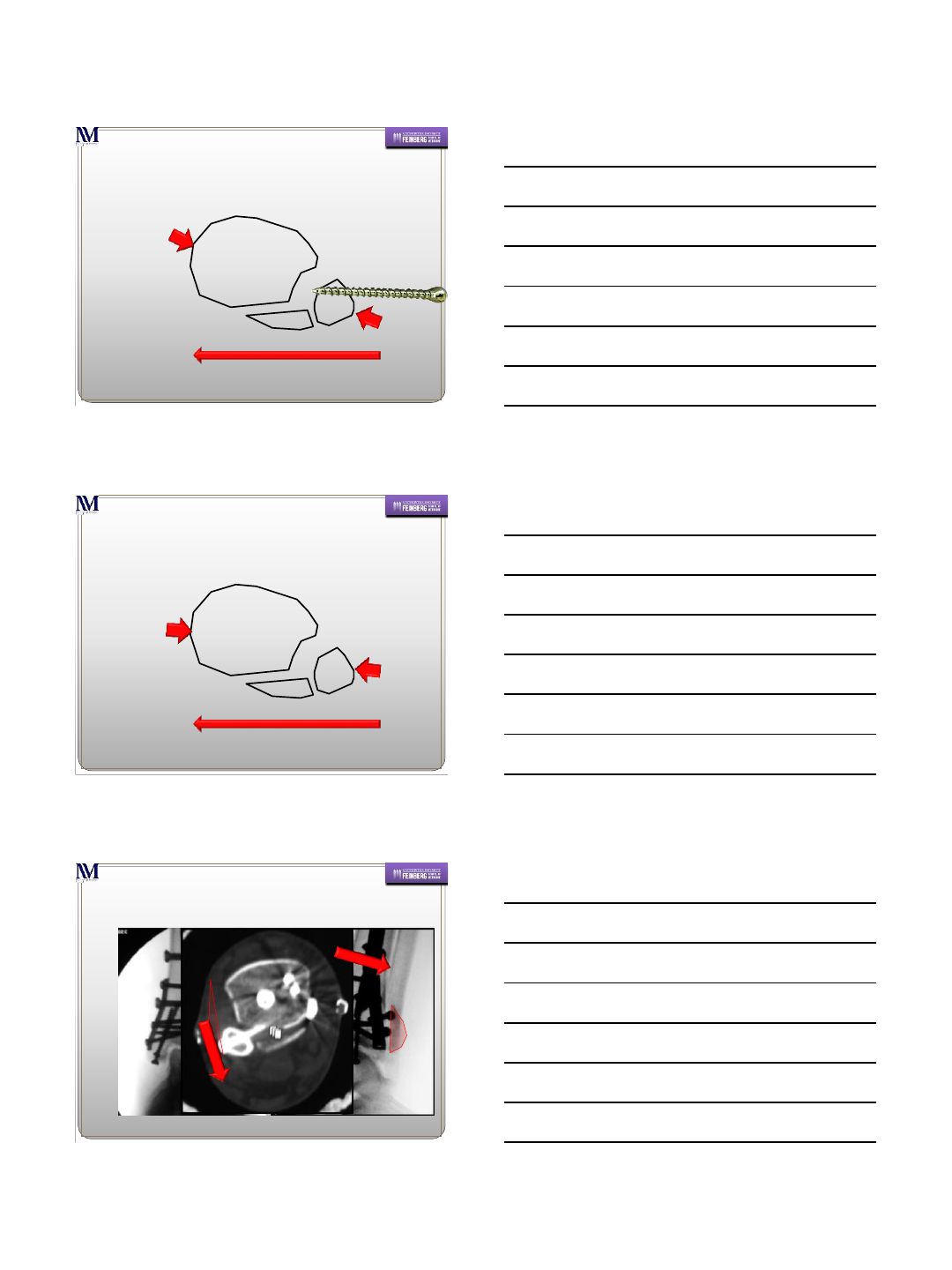
Poster Mall Fx + Sagittal Instability
= Bad News
Poster Mall Fx + Sagittal Instability
+ Bad Clamp = Worse
Slightly “over-reduced” –
(Will NOT correct s/p HWR)
(Miller AN, et. Al. Foot Ankle Int. 2009)
10/21/2014
12
Summary
How?
No clearly superior method
Critical Points
Location –Approximately 2cm above plafond
Superior stability compared to 3.5cm above plafond
Minimize risk of placement within the tib-fib joint.
May risk injury to peroneal artery –clinical relevance unknown
Reduction is critical –open and observe reduction if
needed. (Unfortunately, still risk of malreduction)
If screw –no smaller than 3.5mm
If suture button –utilize 2 in diverging fashion.
Single suture button allows more motion than normal
My preferred method
With Fibular ORIF
Single 3.5mm tri-cortical screw with quad-cortical drill hole
Without Fibular ORIF
4 hole plate with 2 central holes for syndesmotic screw
2 3.5mm screws
PO protocol
NWB 6 weeks
WBAT in CAM walker weeks 6-12
WBAT in ASO weeks 12 until HWR (weeks 16-20)
Screws may break
Thank You
1
Posteriorly Unstable & Osteoporotic
Ankle Fractures
Prof. V. K. Panchbhavi MD, FACS
Chief Division of Foot & Ankle Surgery
Director Foot & Ankle Fellowship Program
University of Texas Medical Branch
Galveston, Texas, USA
Department of Orthopedic Surgery and Rehabilitation
Disclosures
Consultant
–Stryker / SBi
Editor-in-Chief
–Techniques in Foot & Ankle Surgery - LWW
Editorial Board / Reviewer
–FAI /JBJS / CORR / Orthopaedia.com / FootEducation.com
Research Funds
–Arthrex and Wright Medical –2008/9
Department of Orthopedic Surgery and Rehabilitation
Objectives
What is different ?
Do standard methods of stabilization work?
What are special concerns ?
2
Posteriorly Unstable Ankle Fractures
Instability
Instability
SAD SER
Spiral
What is the mechanism, direction of forces ?
“Hyperplantarflexion”
Oblique fracture plane
3
In which direction is this ankle fracture most unstable ?
Instability
4
5
Department of Orthopedic Surgery and Rehabilitation
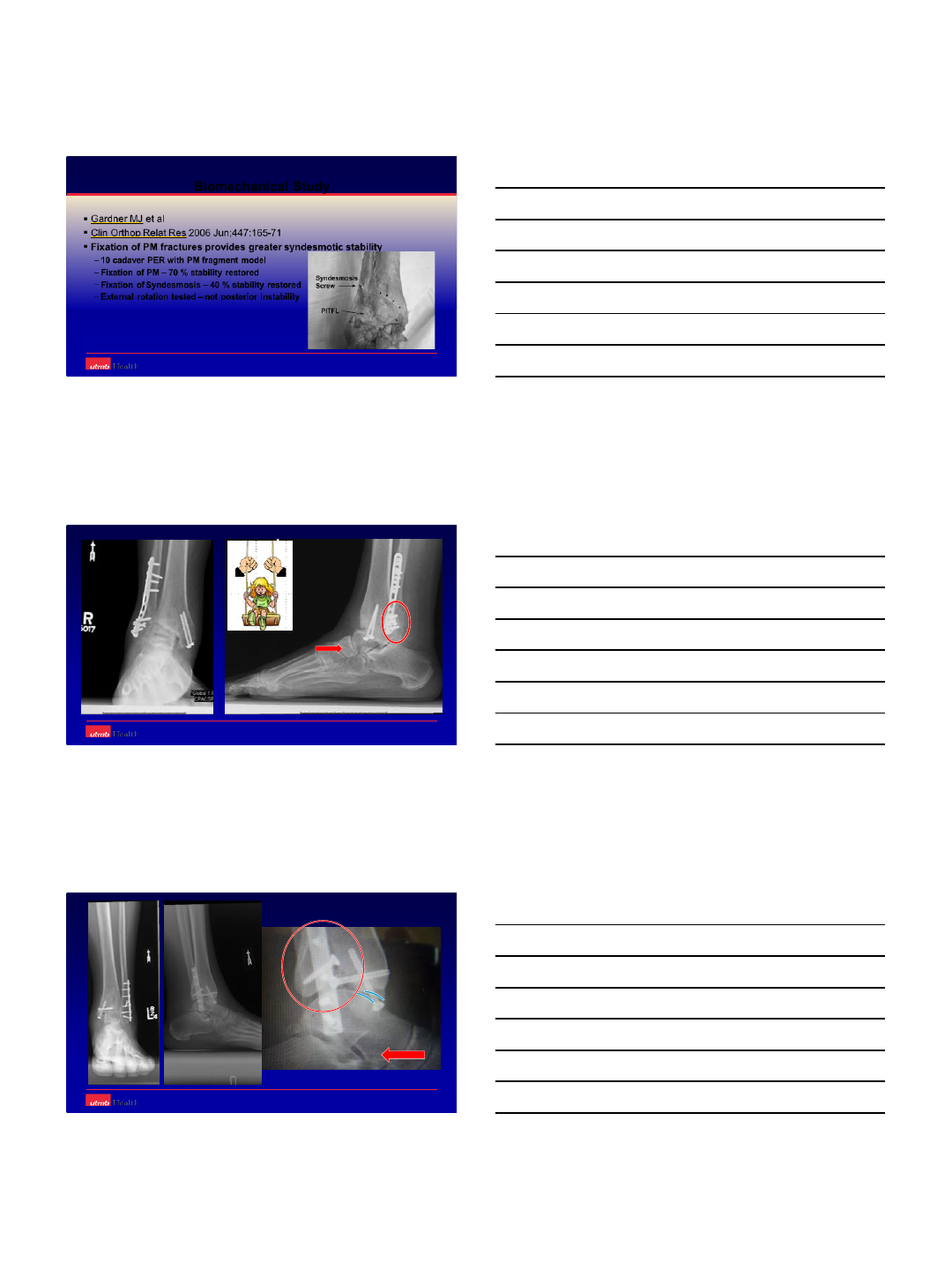
Biomechanical Study
Gardner MJ et al
Clin Orthop Relat Res 2006 Jun;447:165-71
Fixation of PM fractures provides greater syndesmotic stability
–10 cadaver PER with PM fragment model
–Fixation of PM –70 % stability restored
–Fixation of Syndesmosis –40 % stability restored
–External rotation tested –not posterior instability
6
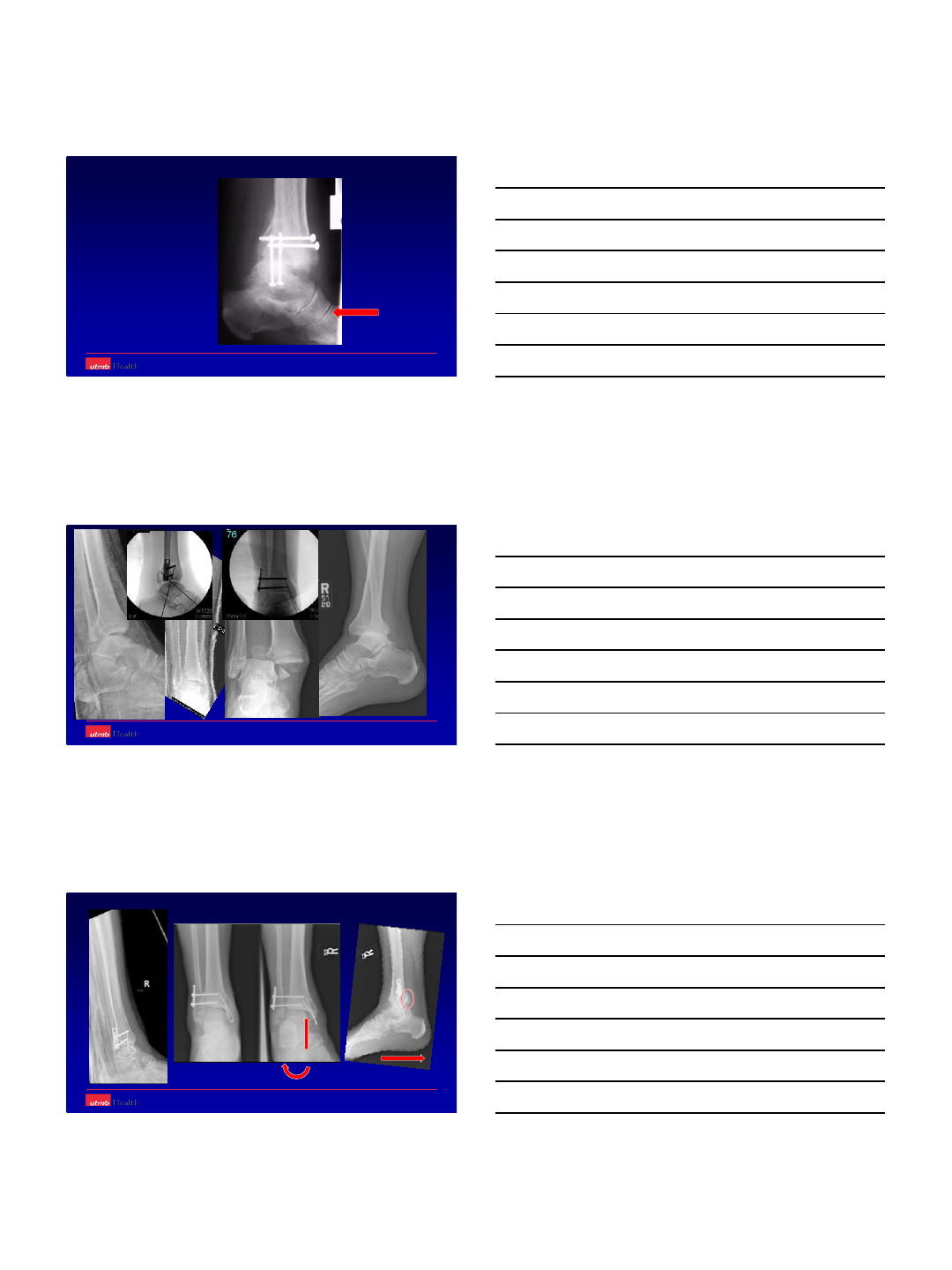
PER
Small size PM
7
Size does not matter
Instability does !!
as does the direction and plane of instability !!
Posteriorly unstable PER
Oblique fracture plane
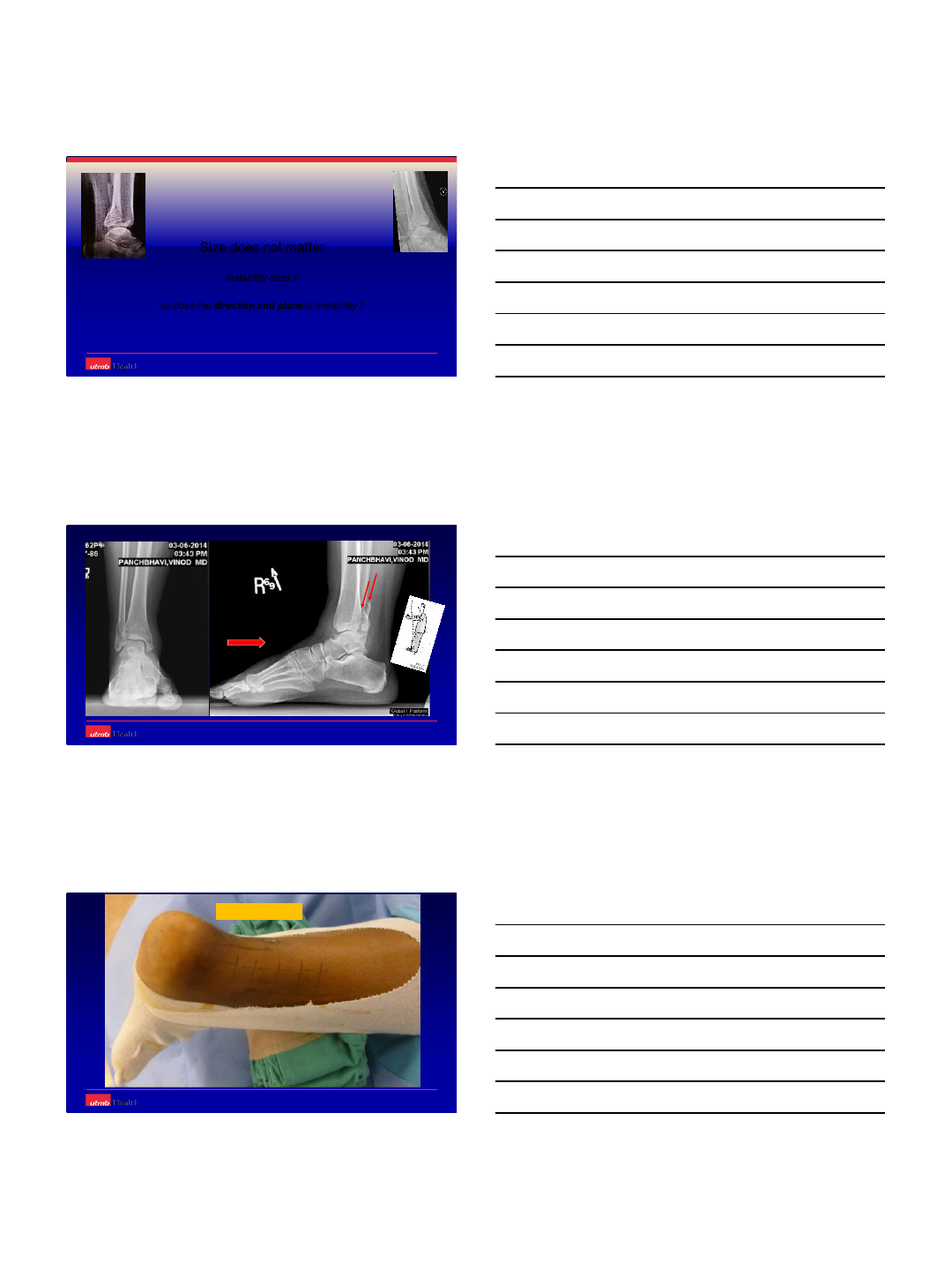
Posteriorly unstable
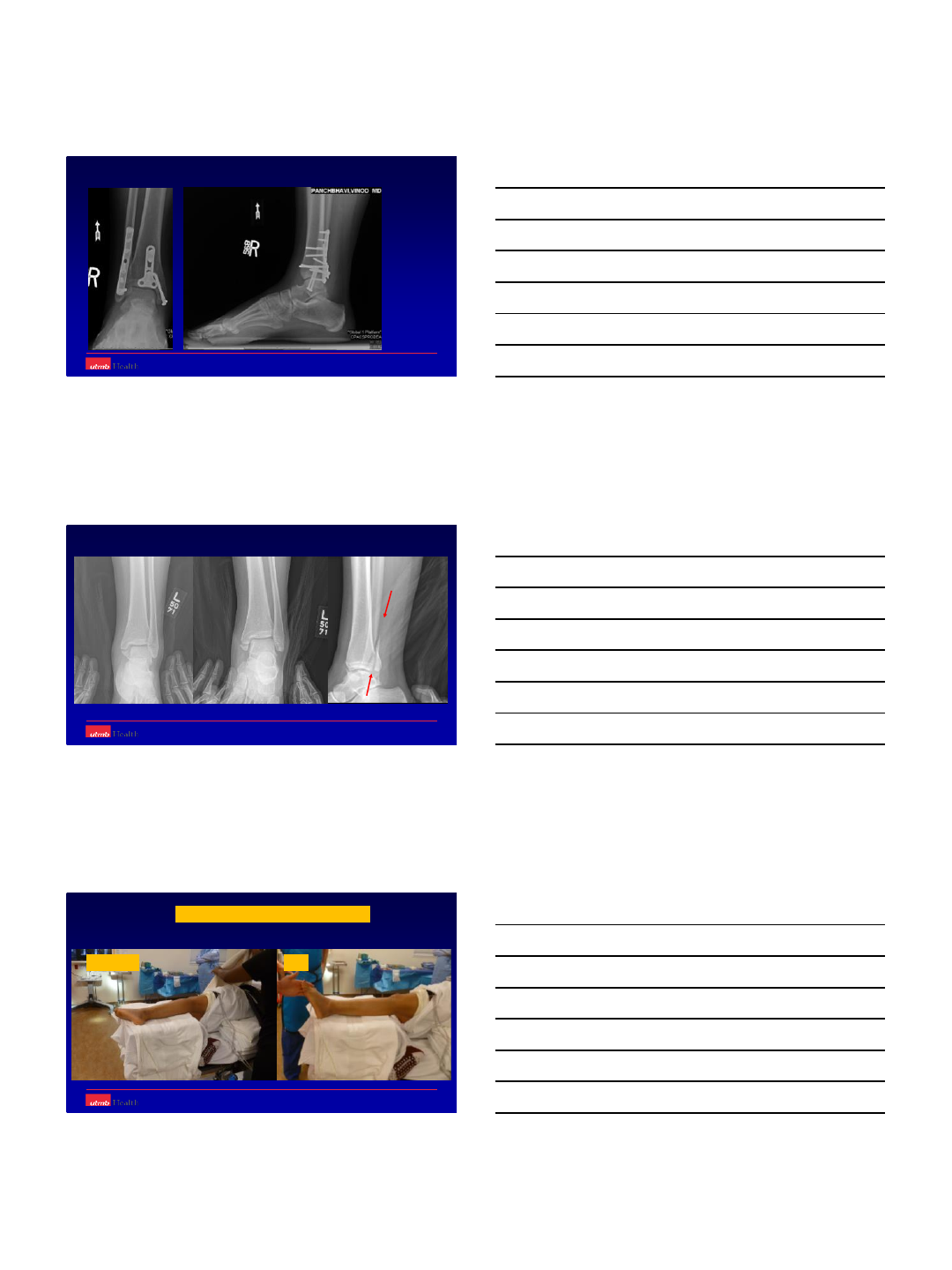
Prone position
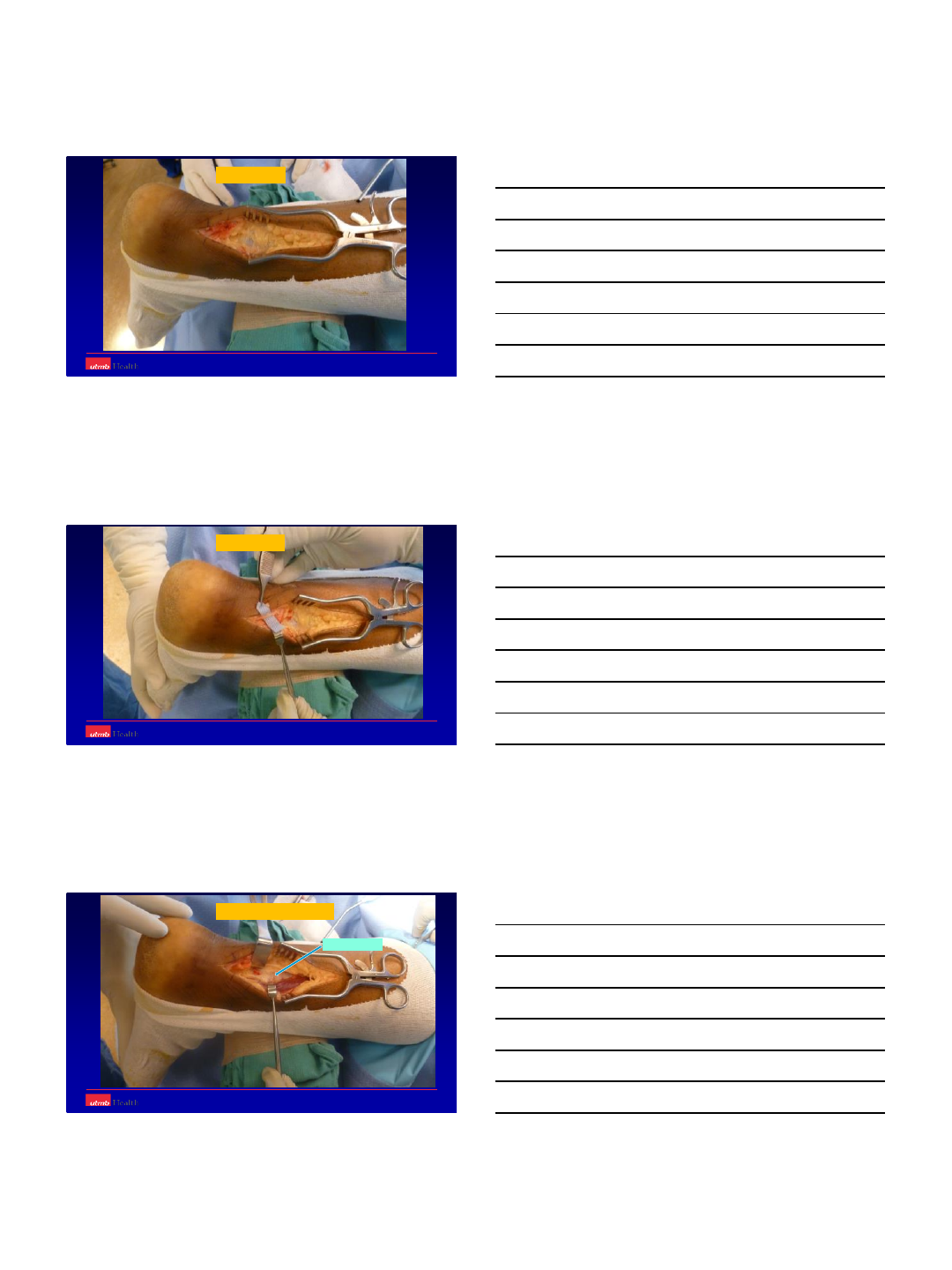
8
Deep fascia
Sural nerve
Peroneals retracted
Fascia over FHL
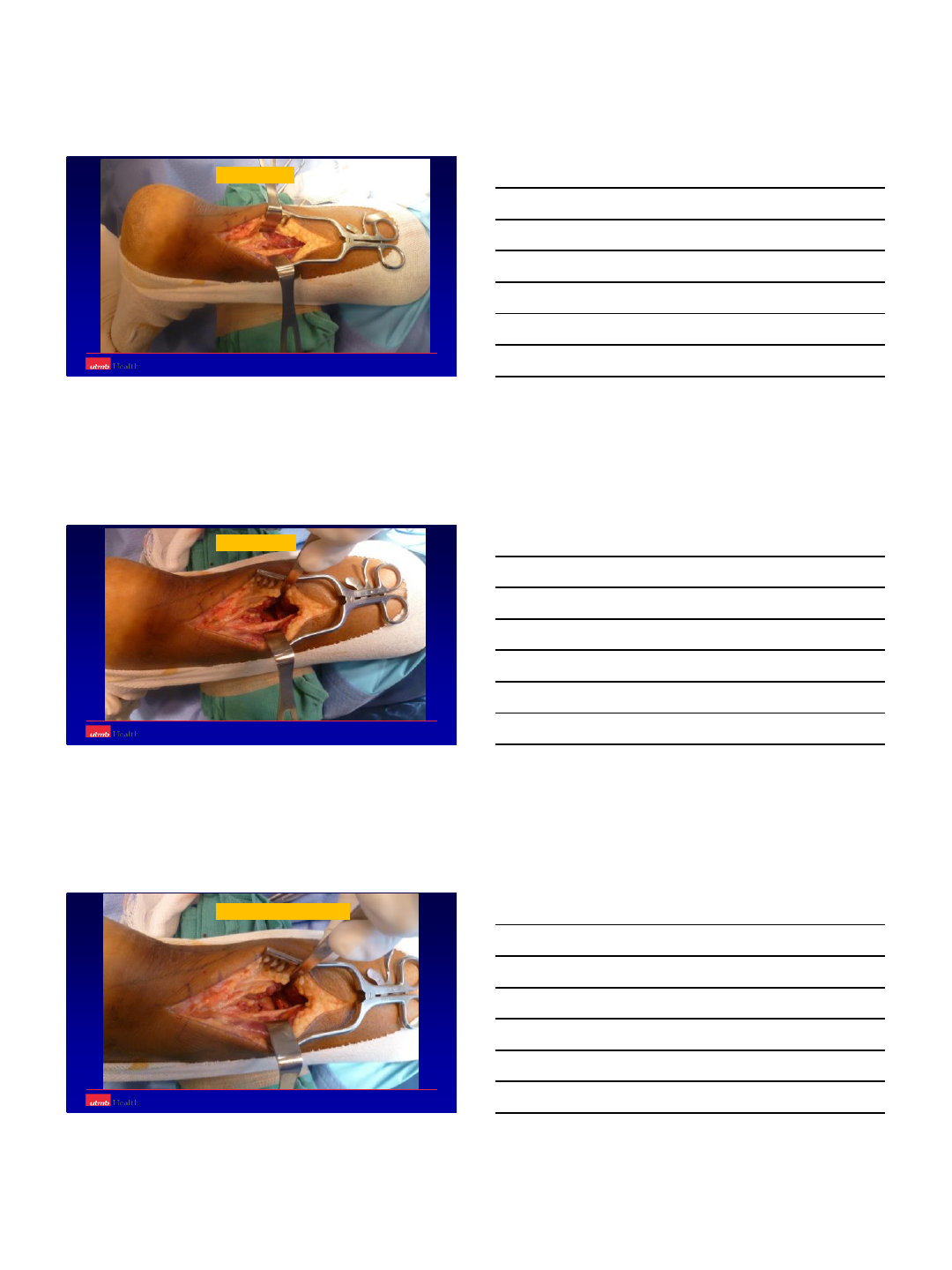
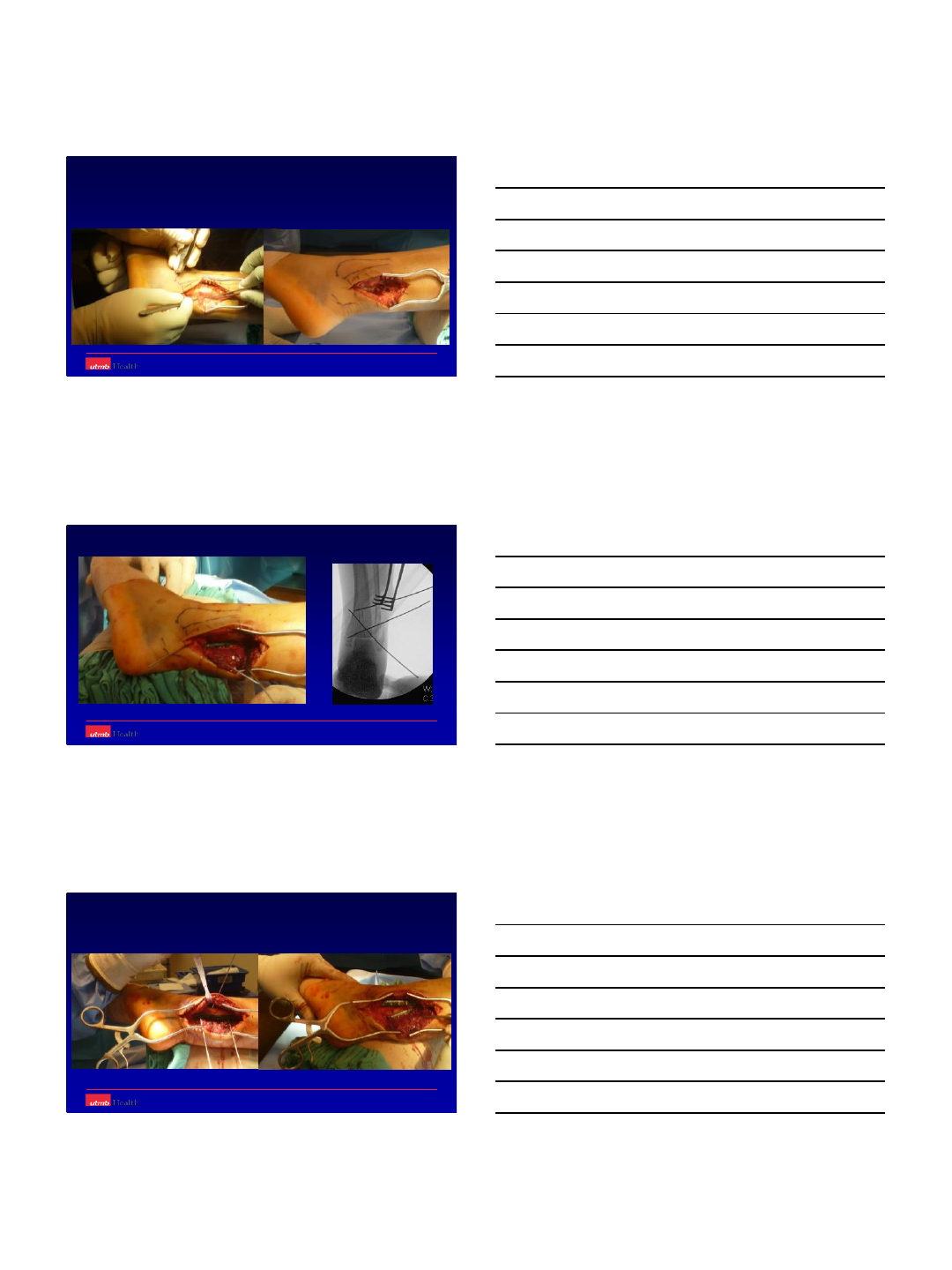
9
FHL exposed
FHL retracted
Fracture & PM exposed
10
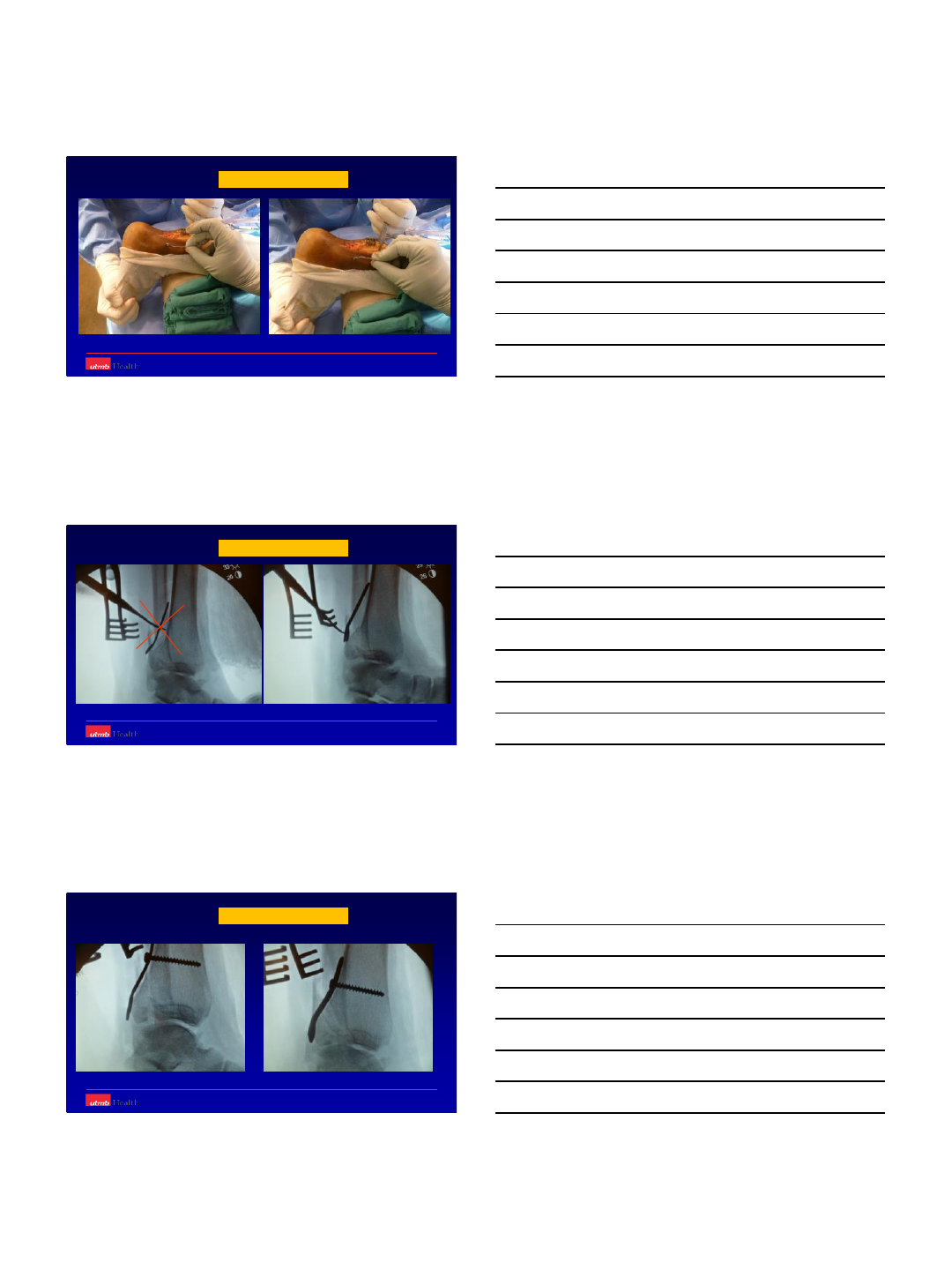
Buttress plate contour
Buttress plate contour
Don’t follow the curve
Buttress plate contour
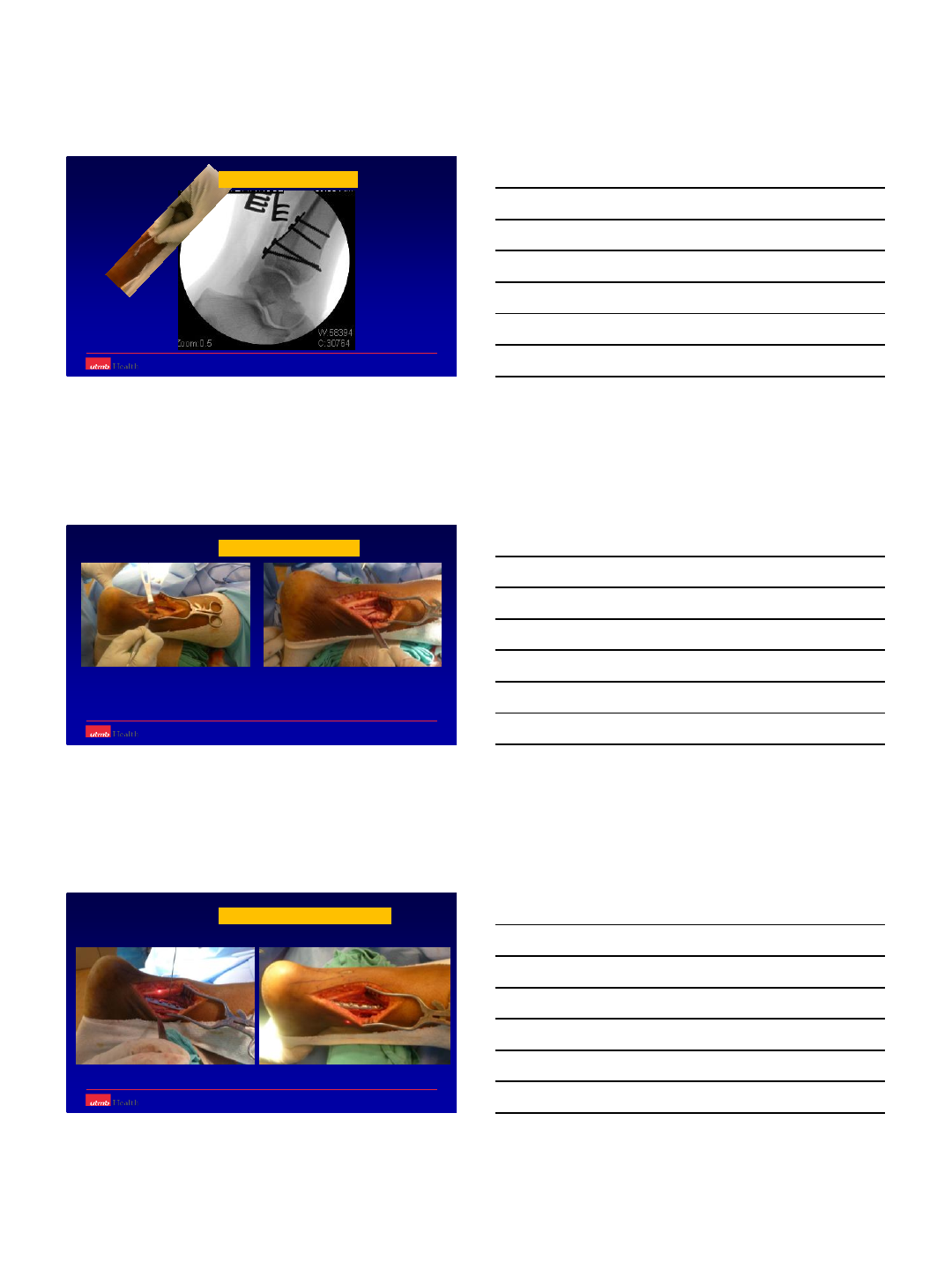
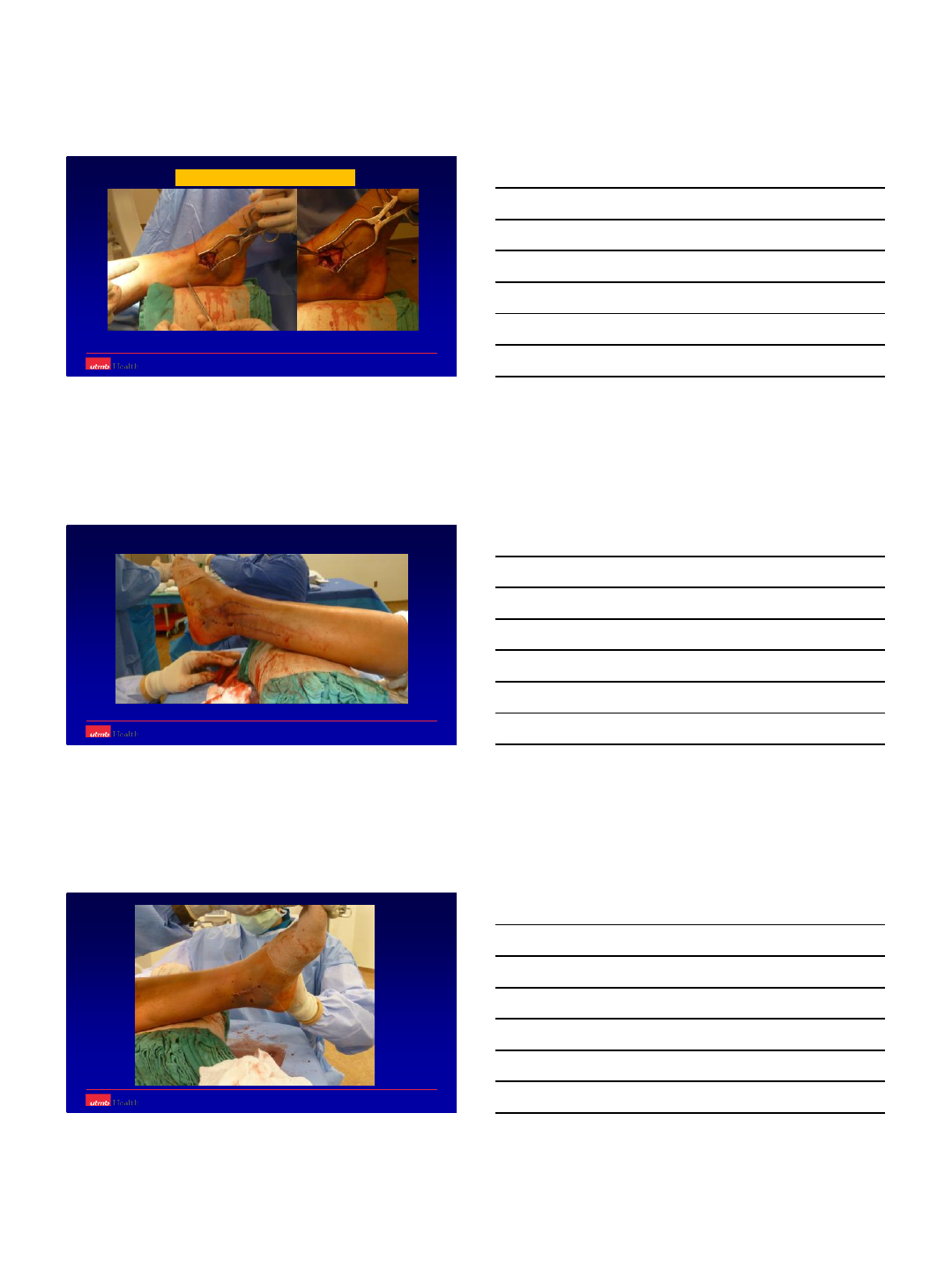
11
Get a ‘true’ lateral image
Fibular fracture exposed
Fracture reduction and Plating
12
PM unobstructed by fibular plate
Prone position easier for PM / LM
Prone position ‘strange’ for MM
13
Oblique fracture plane
Sloppy lateral with platform for leg
PM + LM MM
14
15
Position not so ‘strange’ for MM
16
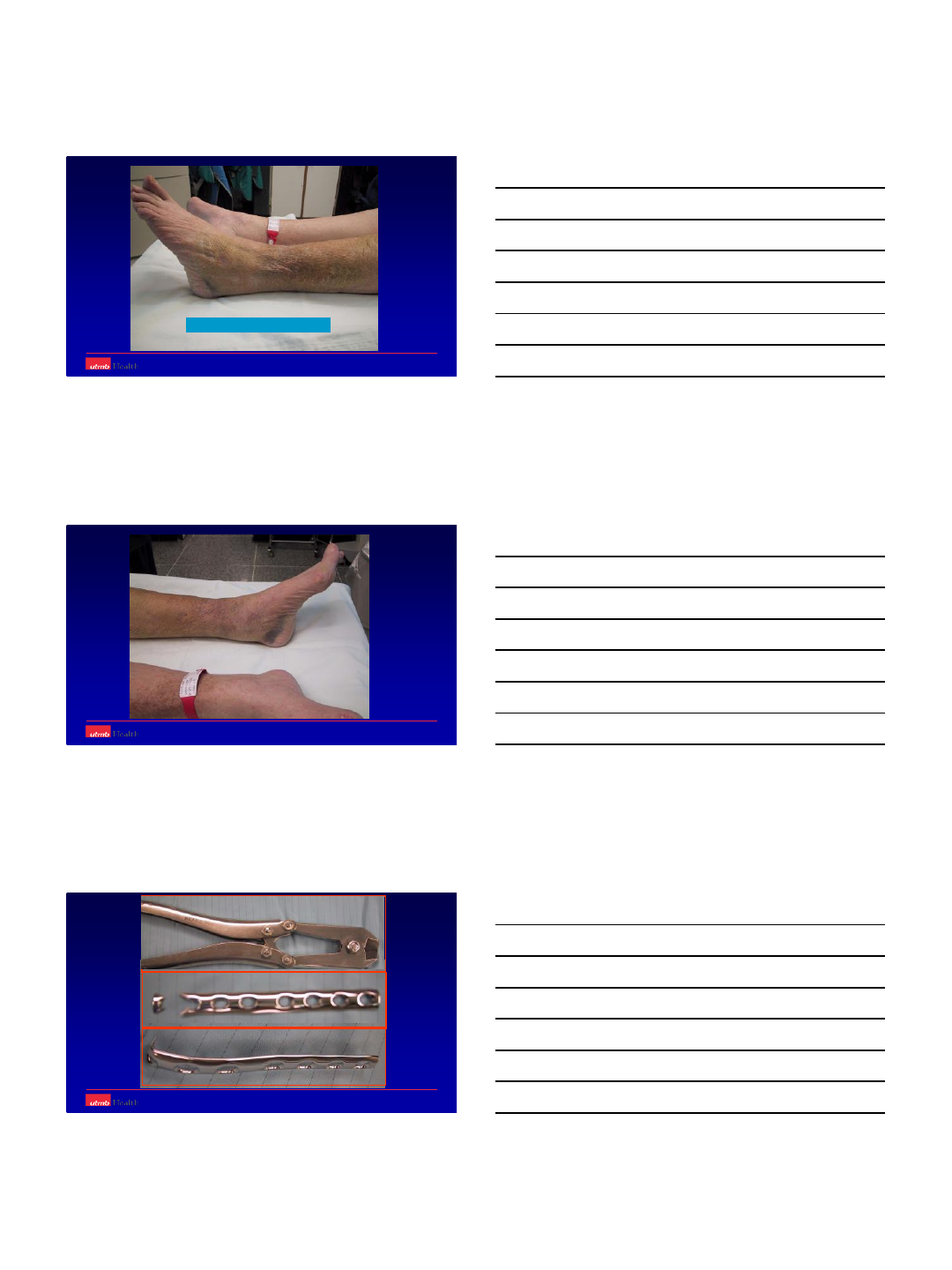
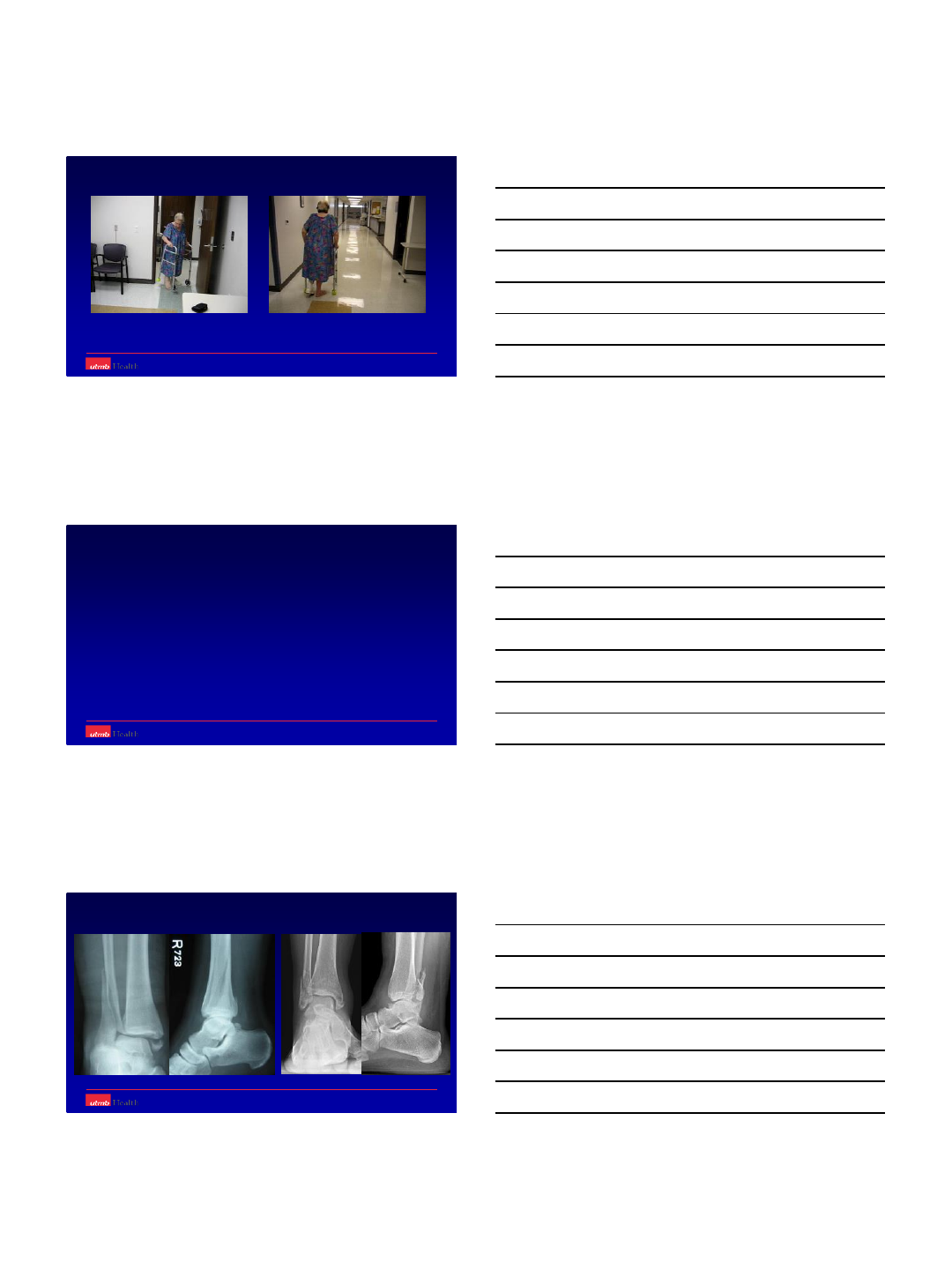
Osteoporotic Ankle Fractures
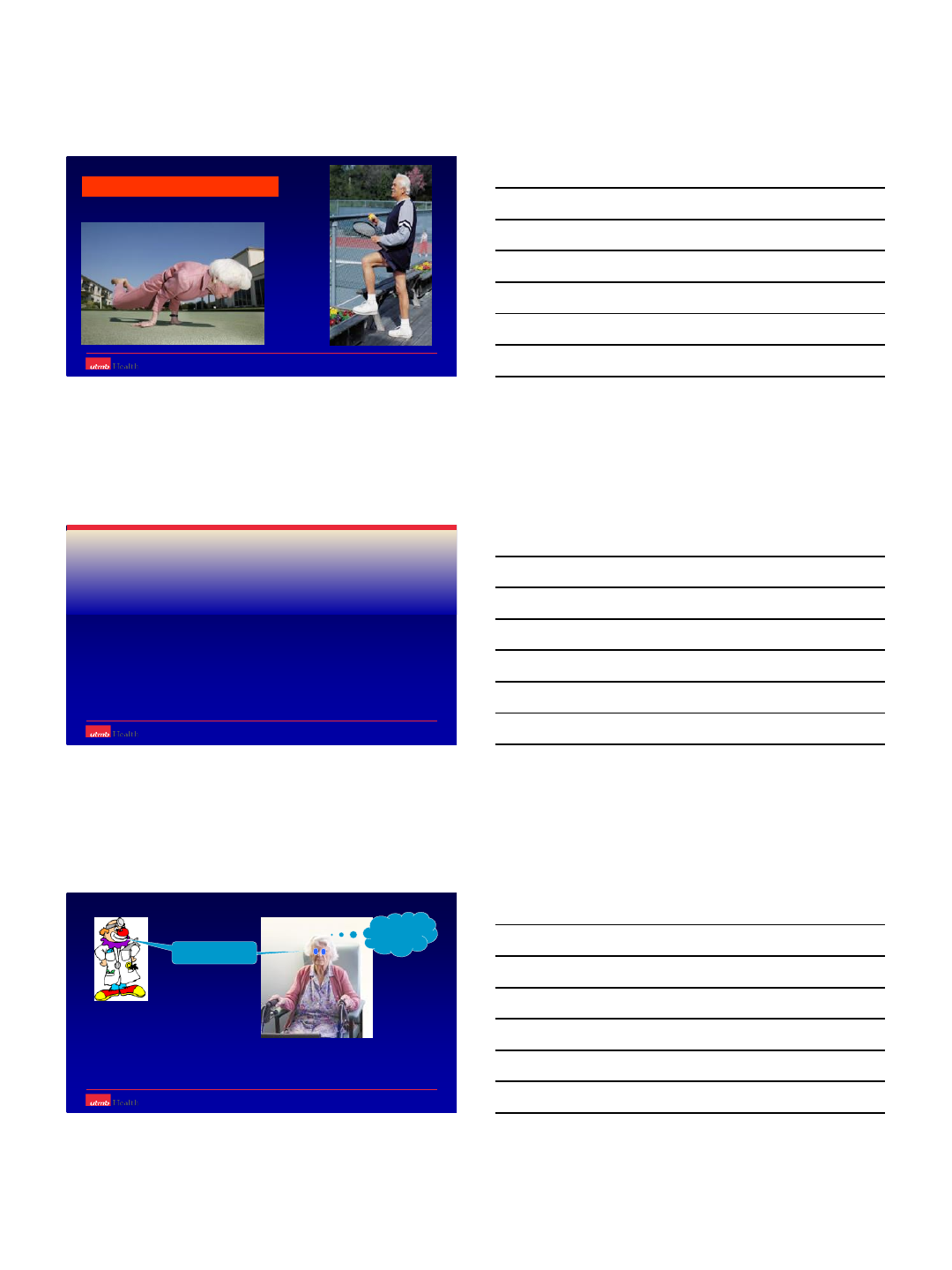
17
Living longer and more active
What are the special issues ?
Don’t bear weight
You must be
kidding !!
Co morbidities
–Poor balance / Dementia
–Diabetes, PVD
Poor soft tissue envelope
Poor bone quality
18
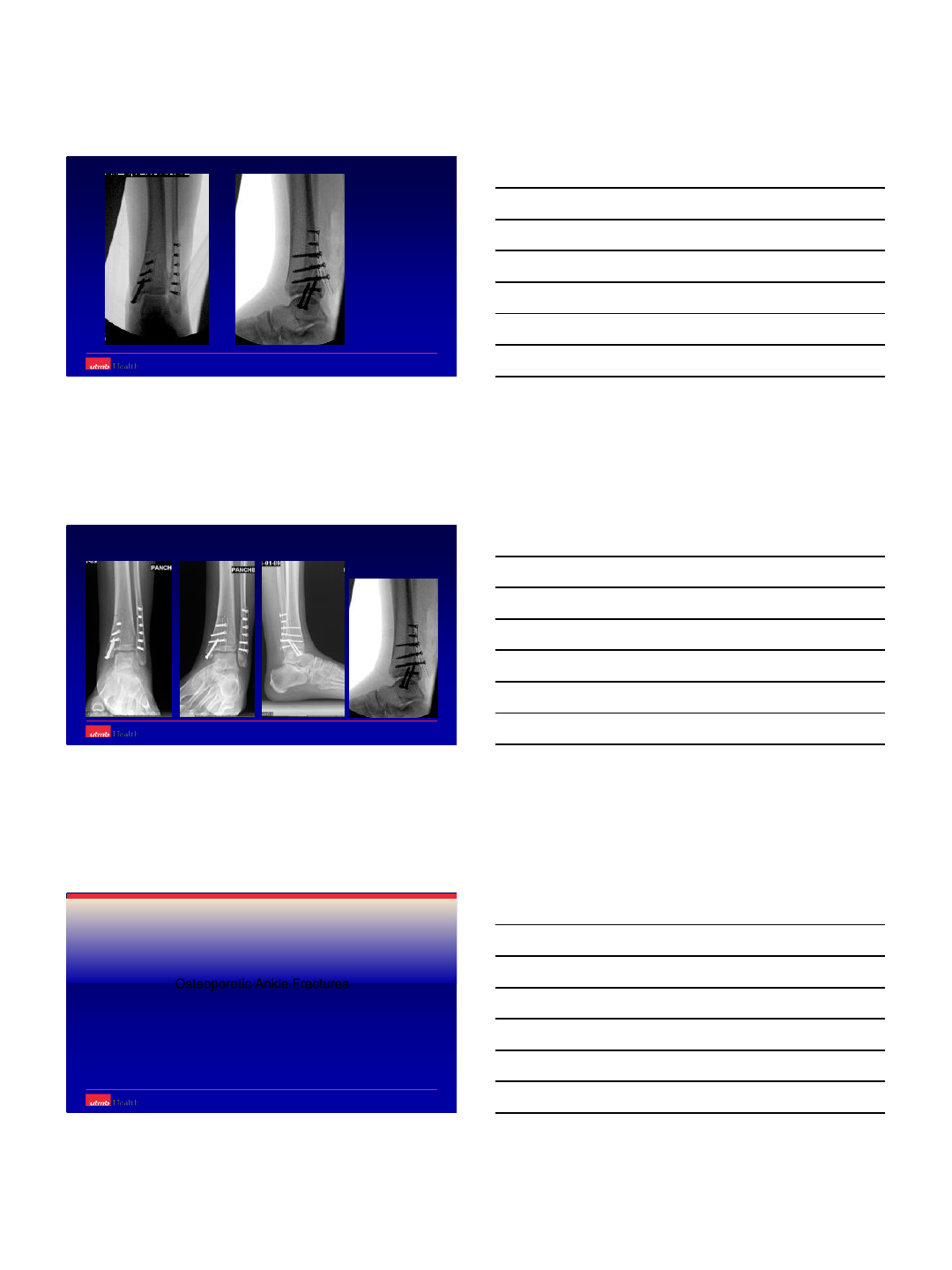
88 yr F Walked unaided before ---- now stays home and manages few steps with frame
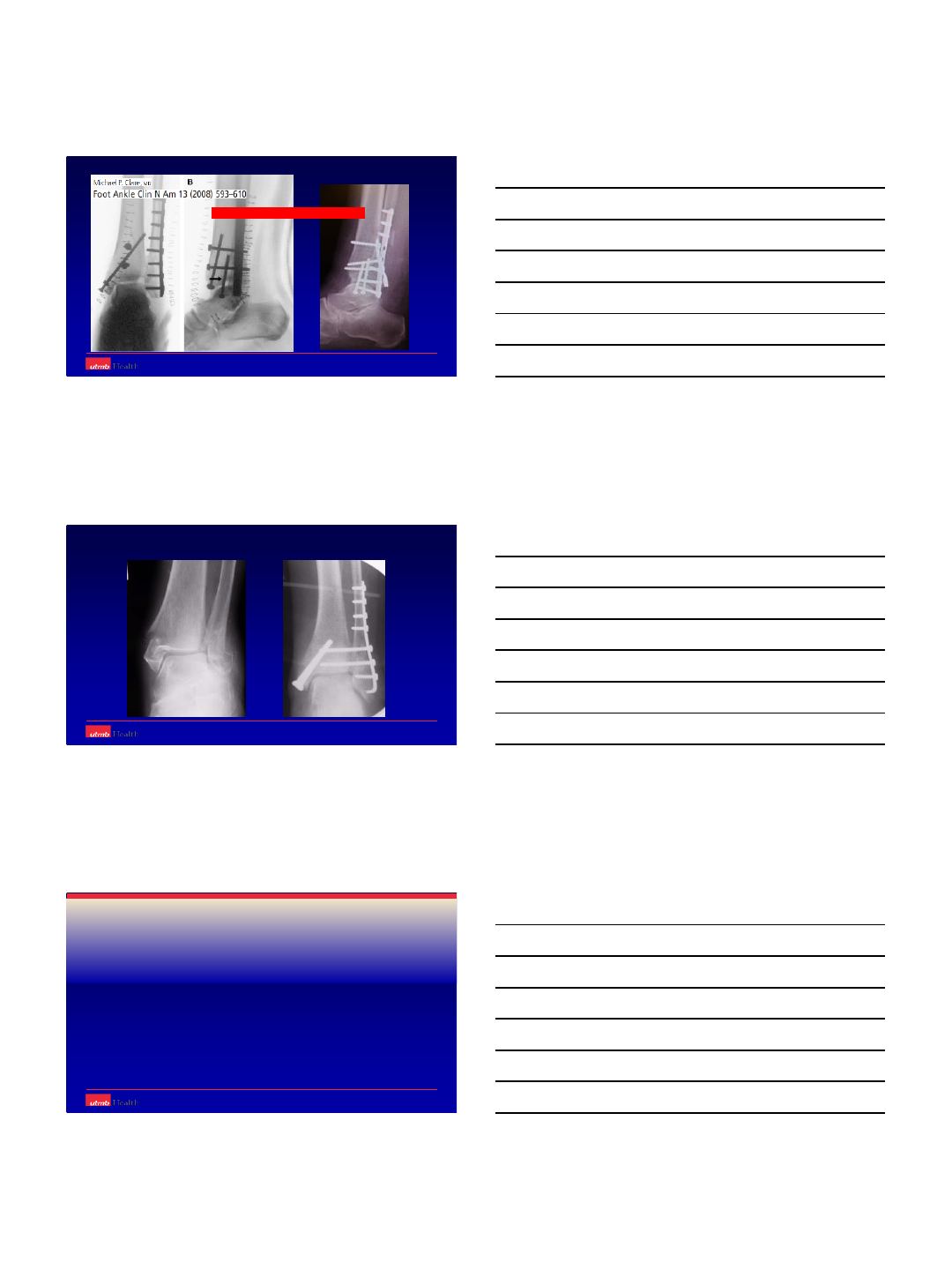
12 Wks.
Cast Rx can fail
ORIF Rx can fail too
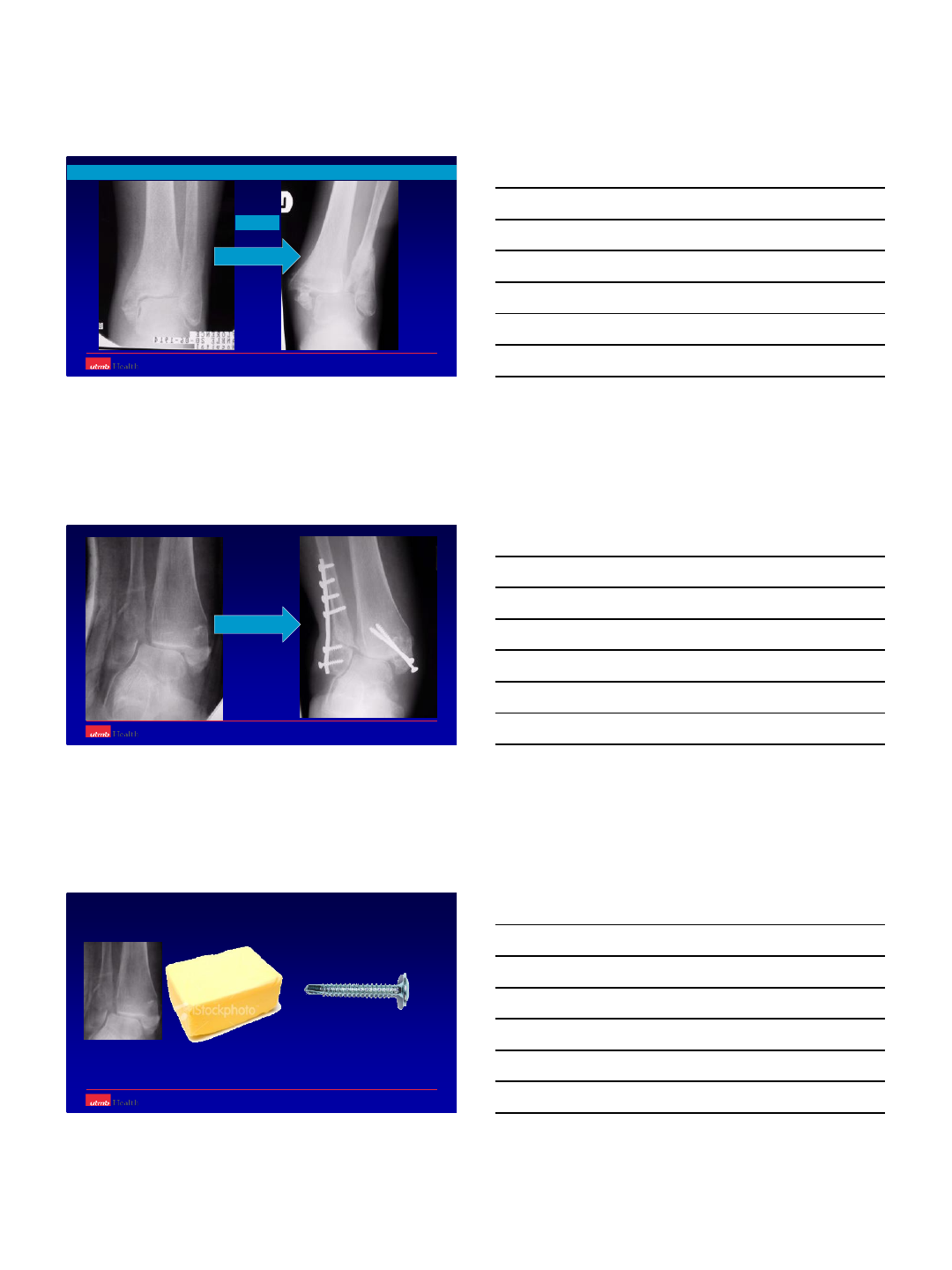
19
ORIF –standard fixation
What should we do different ??
–can fail
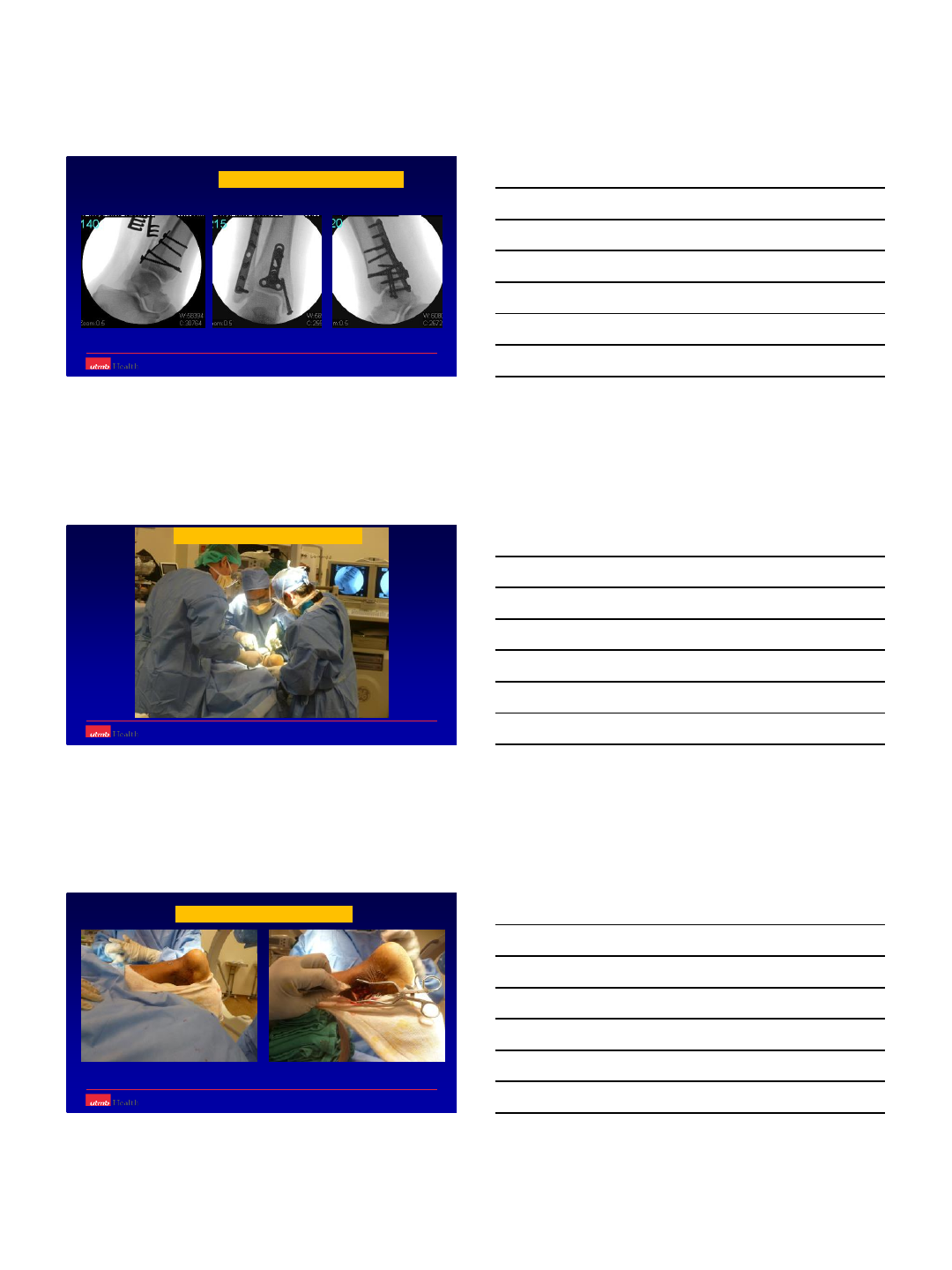
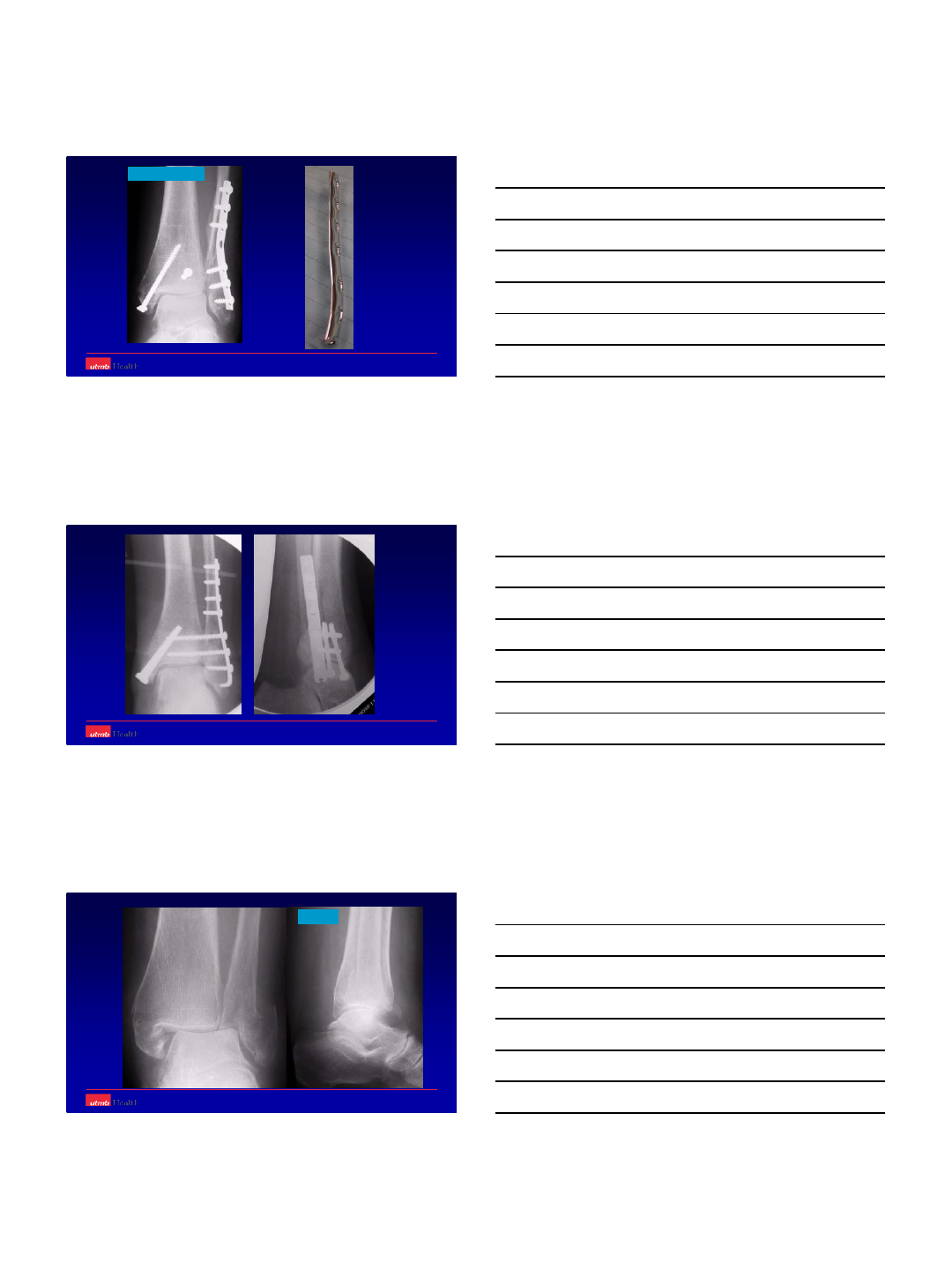
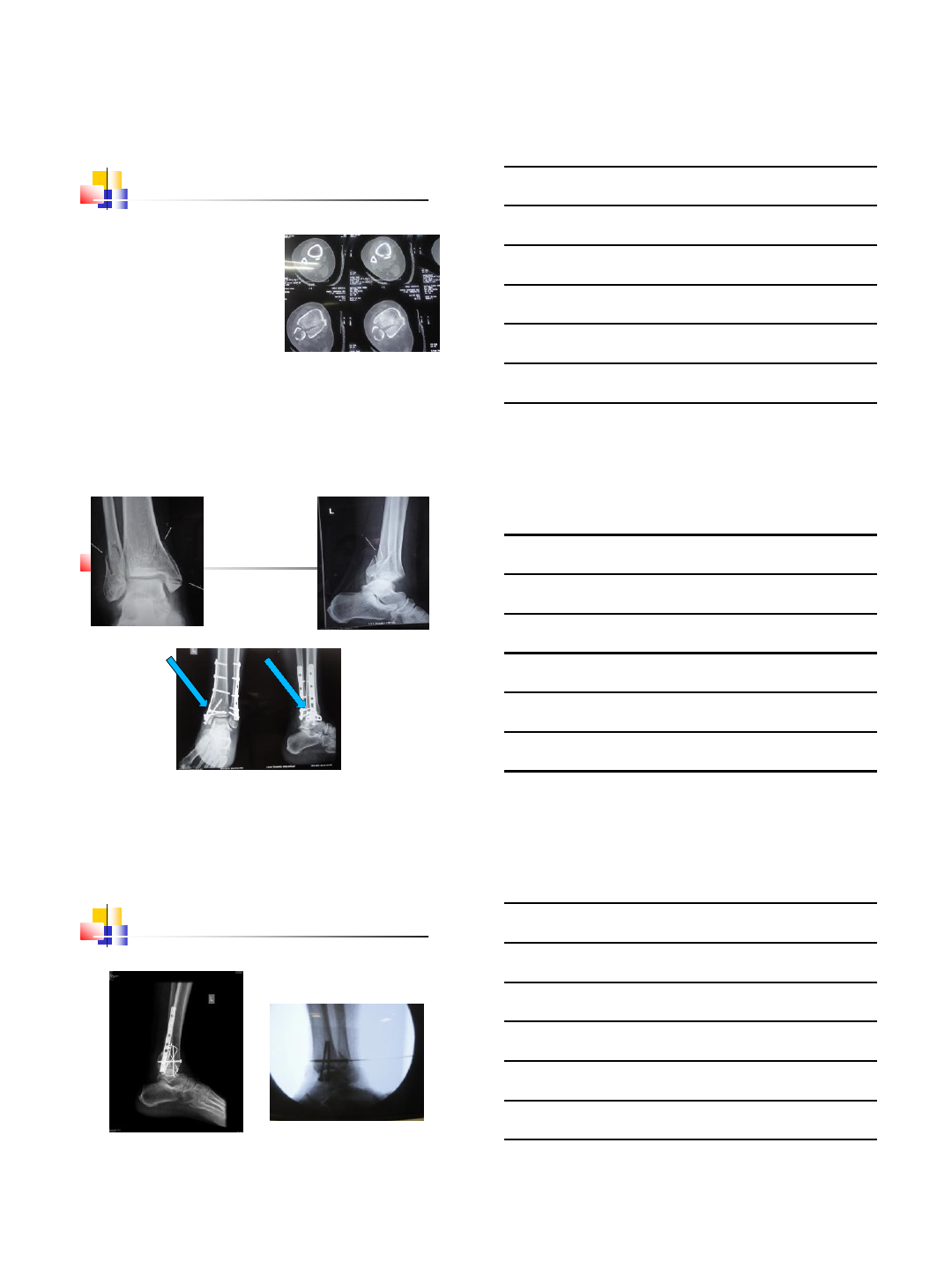
Augmented ORIF
Hook Plate and Tibia-Pro-Fibula Screws
80 Yr F - Fit and active
20
‘Wrinkle ready’ for ORIF at 2 wks.
21
The ‘wrong’ bend
The
‘Right’
Curves
21-11-02
76 yrs. F16-03-02
22
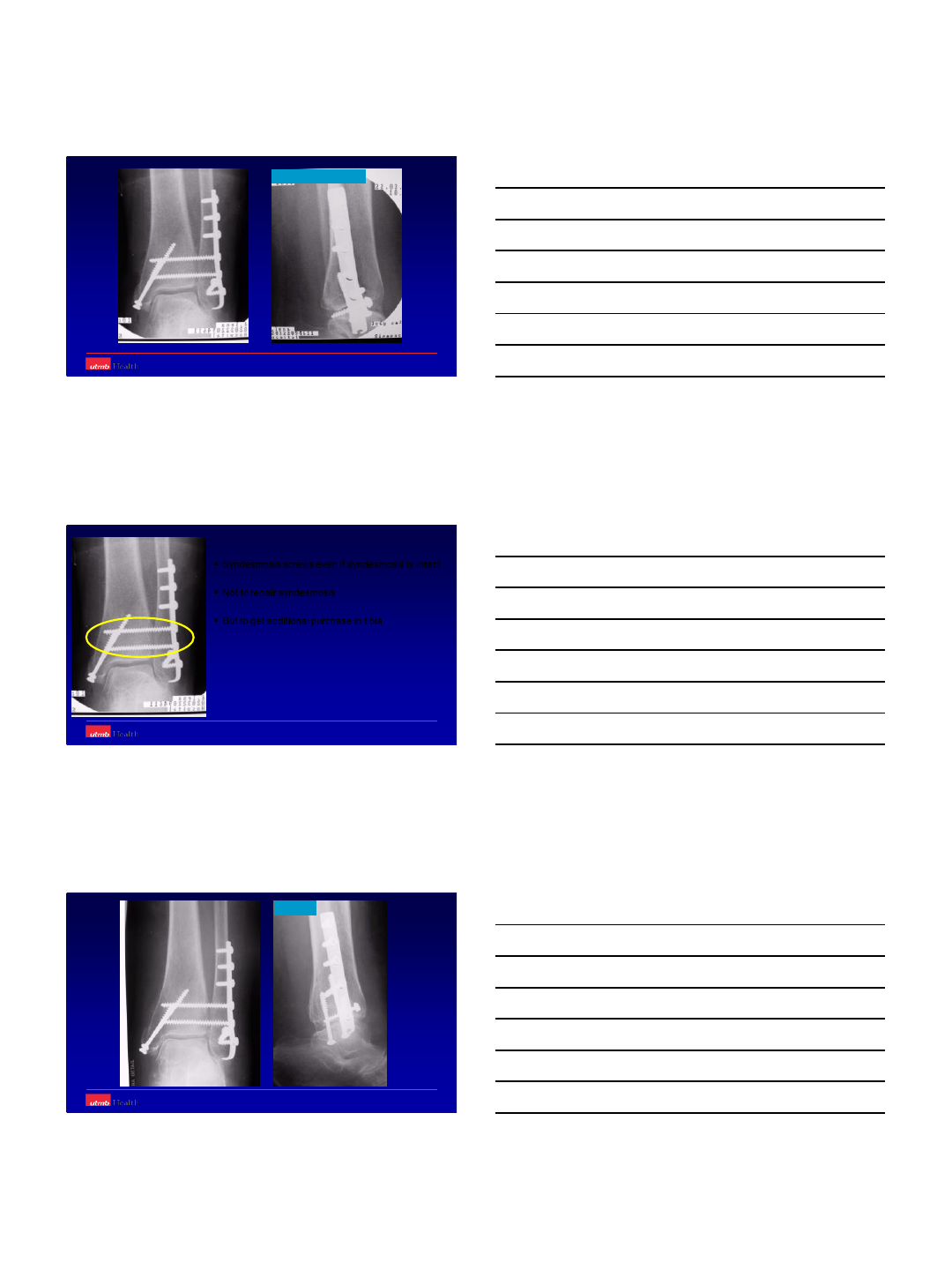
22-03-02 Intraoperative images
22-03-02
Syndesmosis screws even if syndesmosis is intact
Not to repair syndesmosis
But to get additional purchase in tibia
3 months
11-06-03
23
6 wk
Avoid SC dissection
Avoid creating flaps
Longer incision better
Avoid self retainers
24
Standard
Tx HP+TPFS
Tx
n = 15 16
Malunion 1 0
Wound
breakdown 20
AOFAS 57 » 83 55 » 81
Olerud
Molander 37 » 43 42 » 50
N=31 (55-90) Av –71 years
FU –18 months
Panchbhavi VK, Mody MG, Mason WT:
Combination of Hook Plate and Tibia Pro-Fibular Screw Fixation of
Osteoporotic Ankle Fracture. Foot Ankle Int. 26(7) 510- 515: 2005
How stable should be the fixation??
Enough to allow the elderly bear full weight
25
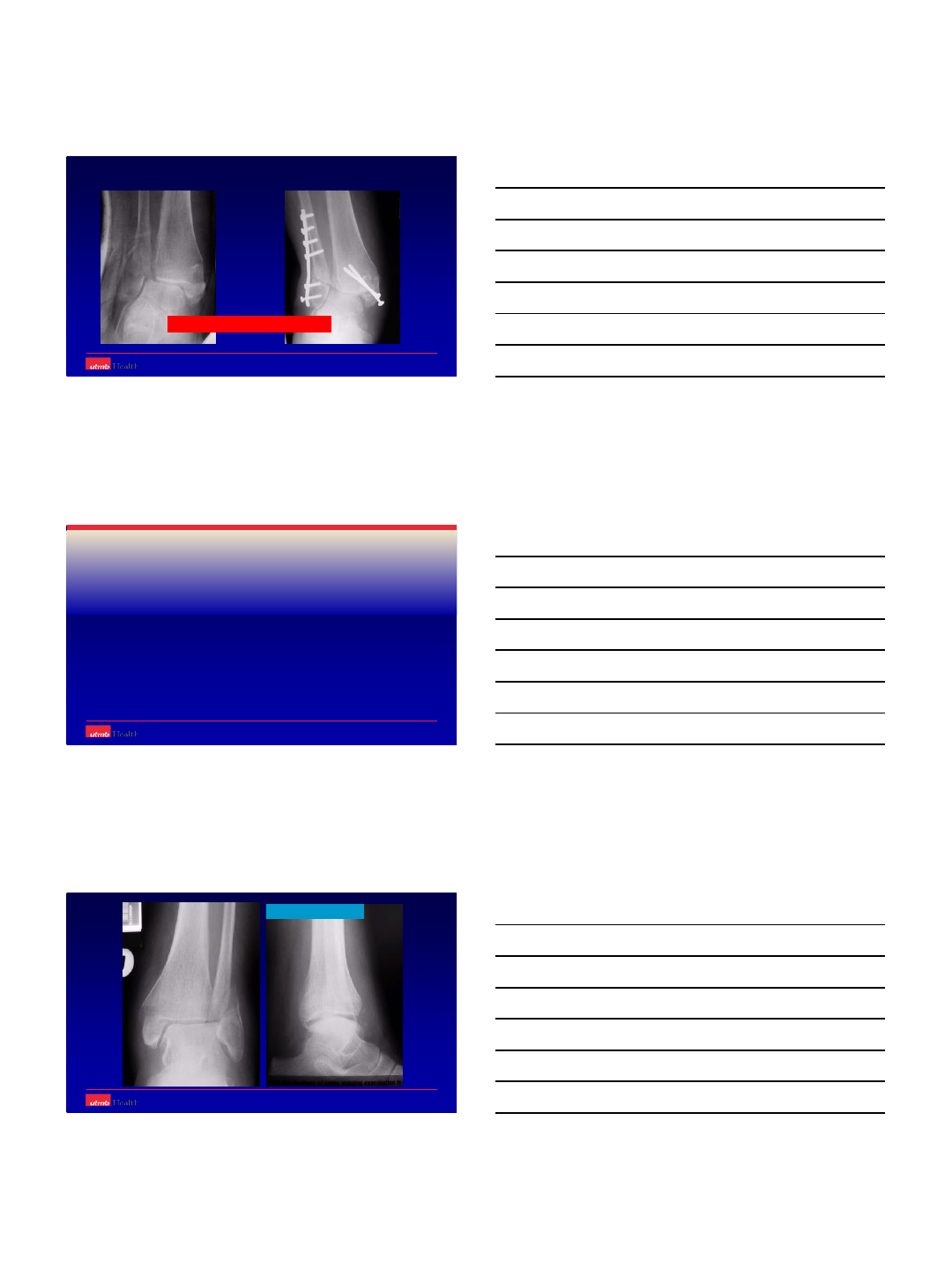
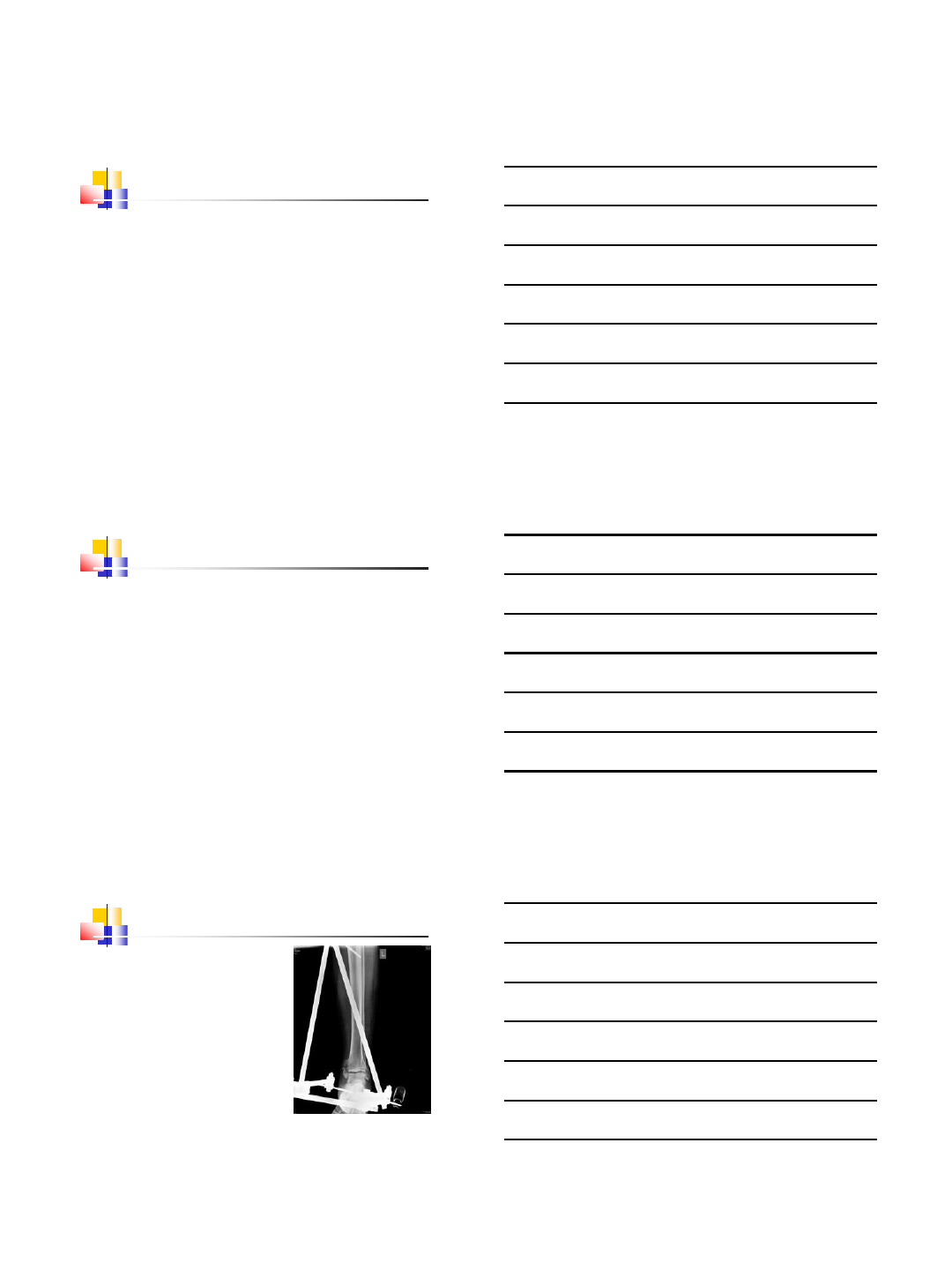
What next ??
Can we augment bone ??
Augmenting bone with CaSO4 + CaPO4
26
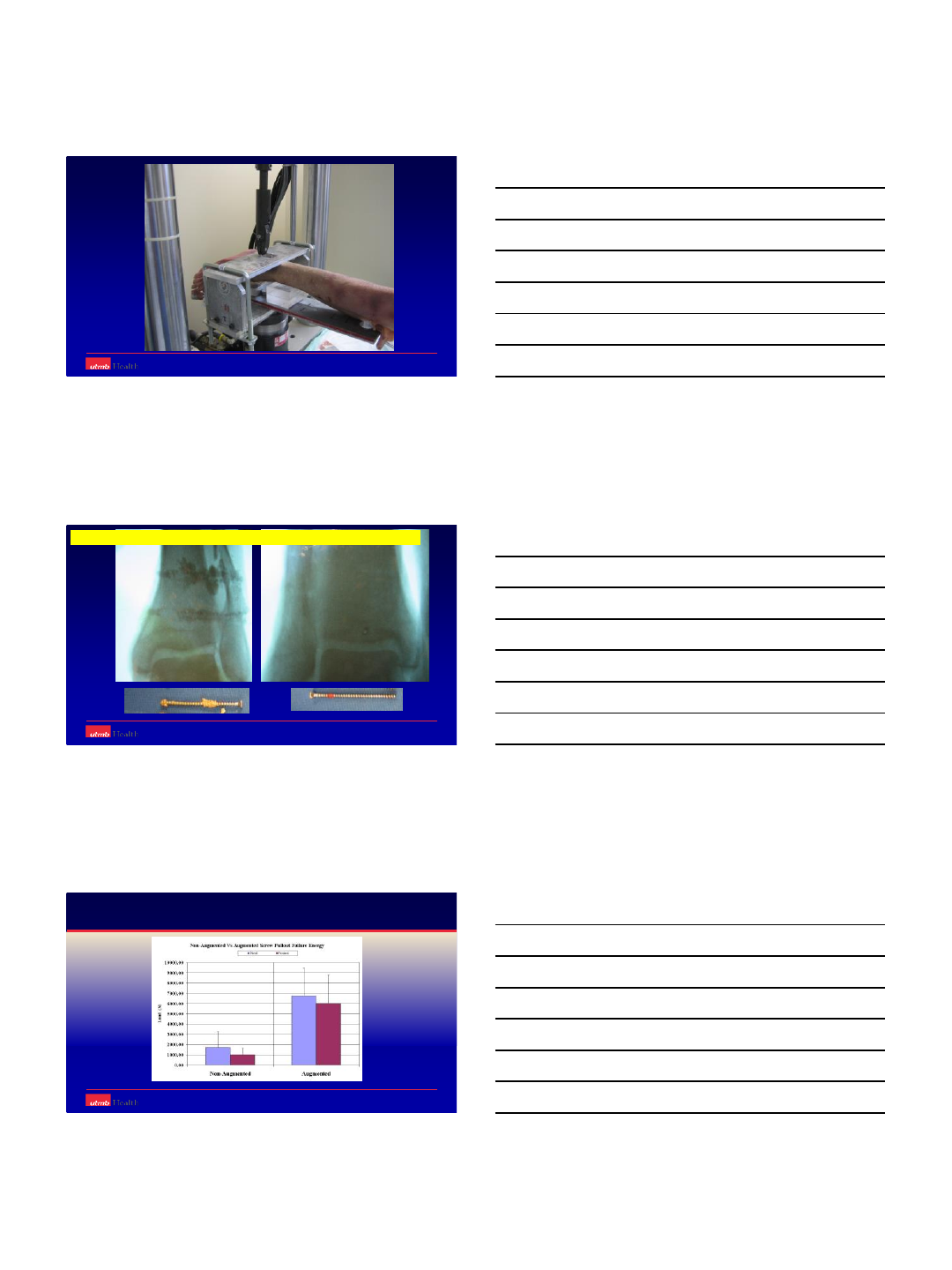
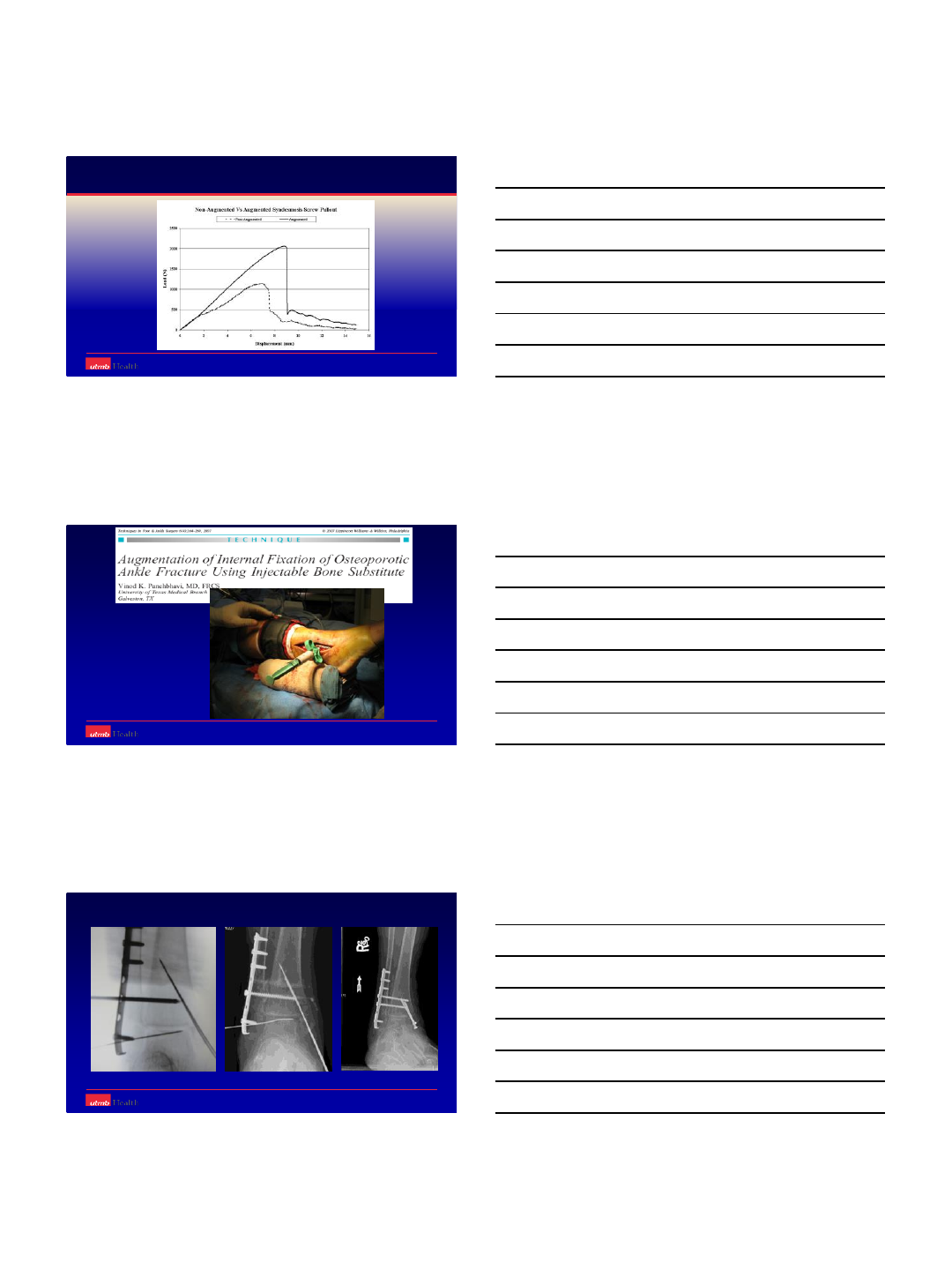
Augmented with CaS04+CaP04
Screws pull out shatters bone……………………..leaves bone almost intact
Department of Orthopedic Surgery and Rehabilitation
Panchbhavi VK, Valluraupalli S, Morris R, Patterson R:
The Use of Calcium Sulphate and Calcium Phosphate Composite Graft to
Augment Screw Purchase in Osteoporotic Ankles Foot Ankle Int. 29(6) 2008
27
Department of Orthopedic Surgery and Rehabilitation
Panchbhavi VK, Valluraupalli S, Morris R, Patterson R:
The Use of Calcium & Calcium Phosphate Composite Graft to Augment Screw Purchase in Osteoporotic Ankles
Foot Ankle Int. 29(6) 2008
28
Summarizing…Principles
Study the fracture plane and direction of instability
Spiral Oblique
29
A-P instability requires stable butress fixation
Osteoporotic fractures require augmented fixation
Thank You
10/16/2014
1
Emerging Truth from
Controversies
Dr Sampat S Dumbre Patil
Noble Hospital, Magarpatta,
Pune, Maharashtra, India.
Controversies in ankle fractures
Timing of fixation.
Use of tourniquet.
Med malleolar fixation
Posterior malleolar fixation.
Timing of Surgery.
Dictated by soft
tissue condition
Joint spanning
fixator helps
Wait for skin
wrinkles to appear
10/16/2014
2
International Orthopaedics
March 2013, Volume 37, Issue 3, pp 489-494
The timing of ankle fracture surgery and the effect on infectious complications; A
case series and systematic review of the literature
A delay in surgery is associated with
significant rise in infectious wound
complications
These fractures should preferably be treated
within 24 hours
Timing
Reduce deformity as early as possible
Span –Scan –Plan
Fix within 24 hrs. or wait for a week
Consider mechanism of injury
Blisters
No conclusive data to help management
Early surgical intervention prevents blister
formation
Blisters allowed to resolve prior to surgery
10/16/2014
3
Tourniquet
Concern in PVD and DM
Increase in pain and swelling after use of
tourniquet
ROM restored early in non tourniquet group
Konrad G et al - clinic orthop relat res. 2005 apr.
Clin Orthop Relat Res. 2005 Apr;(433):189-94.
Tourniquets may increase postoperative swelling and pain after internal
fixation of ankle fractures.
Konrad G, Markmiller M, Lenich A, Mayr E, Rüter A
Level 1 (randomized controlled trial).
Increased postop swelling & pain
Better ROM
Recommended not using a tourniquet
Rational Sequence of Fixation in
Trimalleolar Fractures
Posterior malleolar fixation
Medial exploration and fixation
Restoration of fibular length
Assessment of mortise stability
10/16/2014
4
Zhongguo Gu Shang. 2008 Apr;21(4):300-1.
[Surgical treatment of pronation and supination external rotation trimalleolar
fractures].
[Article in Chinese]
Xu YQ1, Zhan BL, He FX, Wei HD.
ORIF started with posterior,
then medial and lateral malleolus
and lastly the distal tibiofibular syndesmosis
fixation in a sequence
Rational sequence of fixation in
trimalleolar fractures.
Sequence depends on mechanism of injury
and comminution
Achieving fibula length is helpful
If fibula is comminuted - medial malleolus can
be reduced first
Fixation of fibula
Infrasyndesmotic- Screw / TBW / Plating
Transsyndesmotic- Plate / Screw /TBW
Suprasyndesmotic - Plating
10/16/2014
5
Fibula fixation with nail- or plate?
Fibular Fracture Fixation
Anti-glide Plate / Lateral plate
Plate on post aspect
Peroneal tendon
irritation
Low profile
Lateral Malleolus Fixation with
Deltoid Ligament Repair
Deltoid ligament does not require routine
exploration or repair
Explored if:
- Difficultly in reduction of fibular fracture
- Interposition of ligament, periosteum, PT
tendon
10/16/2014
6
J Orthop Trauma. 2014 Sep 2. [Epub ahead of print]
Deltoid Ligament Repair vs. Syndesmotic Fixation in Bimalleolar
Equivalent Ankle Fractures.
Jones CR1, Nunley JA 2nd
Conclusion
Repairing deltoid vs. repairing syndesmosis
Subjective, functional and radiological
outcomes are comparable
Strategies Trauma Limb Reconstr. 2012 Aug;7(2):73-85. doi:
10.1007/s11751-012-0140-9. Epub 2012 Jul 6.
The diagnosis and treatment of deltoid ligament lesions in
supination-external rotation ankle fractures: a review.
Stufkens SA1, van den Bekerom MP, Knupp M, Hintermann B, van
Dijk CN.
There is no evidence found for suturing but
exploration is thought to be beneficial in case of
interposition of medial structures.
Medial Malleolar Fixation
Tension Band Wiring
One screw, one k wire
Two screws
Plate
10/16/2014
7
Int Orthop. 2014 Jan;38(1):83-8. doi: 10.1007/s00264-013-2168-y.
Epub 2013 Nov 20.
A comprehensive analysis of patients with malreduced ankle
fractures undergoing re-operation.
Ovaska MT1, Mäkinen TJ, Madanat R, Kiljunen V, Lindahl J.
Fixation of an associated medial malleolar fracture with
other than two parallel screws were also associated
with re-operation.
Injury. 2014 Sep;45(9):1365-7. doi: 10.1016/j.injury.2014.05.031. Epub
2014 Jul 3.
A clinical evaluation of alternative fixation techniques for medial malleolus
fractures.
Barnes H1, Cannada LK2, Watson JT1.
The headless compression screw is a beneficial alternative
to the conventional methods of medial malleolus fixation
Foot Ankle Int. 2014 May;35(5):471-7. doi: 10.1177/1071100714524553. Epub
2014 Feb 13.
Comparison of surgical techniques of 111 medial malleolar fractures classified
by fracture geometry.
Ebraheim NA1, Ludwig T, Weston JT, Carroll T, Liu J
•Transverse #s - TBW and lag screws- similar rates of
union. TBW - less revision surgery / fewer
complications
•Oblique fractures- effectively treated with lag screws
•Vertical #s - superior outcomes with buttress plating
10/16/2014
8
Medial Malleolar Fixation - TBW
TBW loop thr. bone TBW loop around post screw
Medial Malleolar Fixation - 2 Screws
Buttress plate required for
large fragment with vertical fracture
10/16/2014
9
Bone Joint J. 2013 Dec;95-B(12):1662-6. doi: 10.1302/0301-620X.95B12.30498.
Screw fixation of medial malleolar fractures: a cadaveric biomechanical study
challenging the current AO philosophy.
Parker L1, Garlick N, McCarthy I, Grechenig S, Grechenig W, Smitham P
Better fixation with
3.0 mm partially threaded or
4.5 mm fully threaded screws
engage the physeal scar
Traditionally partially threaded screws are
recommended for medial malleolar fixation
Posterior Malleolar Fixation
Indications for fixation
Post fragment >25%.
Persistent subluxation of joint
Better to fix posterior malleolus for syndesmotic
stability and articular congruency.
Posterior Malleolus Fixation
When a posterior malleolar fracture is
present, we recommend anatomic
reconstruction, regardless of the size of the
fracture fragment, to recreate the incisura;
this obviates the need for syndesmotic
screws
Clin Orthop Relat Res. 2010 April; 468(4): 1129–1135.
10/16/2014
10
Post Malleolus
Posterolateral fragment
(Volkmann's triangle)
attached to fibula -
Reduction of fibular
fracture helps
Separate screw fixation for medial malleolus
Posterior Malleolus Fixation
Anterior to Posterior Posterior to Anterior
10/16/2014
11
Chin Med J (Engl). 2013 Oct;126(20):3972-7.
Advances and disputes of posterior malleolus fracture.
Fu S1, Zou ZY, Mei G, Jin D.
•Direct posterior malleolus fixation is suitable to
stabilize syndesmotic injury.
•Direct reduction and buttress plate fixation of
posterior malleolus fracture through the
posterolateral approach.
Incision Fibula plating Ant to peronei
Posterior malleolus exposure Plating posterior malleolus
Posterolateral approach for posterior malleolus
Case study
10/16/2014
12
Conclusion
Timing –dictated by soft tissues
Use of tourniquet –concerns in PVD & DM
Medial exploration if soft tissues impinge
Posterior malleolus - anatomic reconstruction
10/21/2014
1
Dr.Rajiv Shah
Foot & Ankle Surgeon
President, IFAS
India
Revision fixation
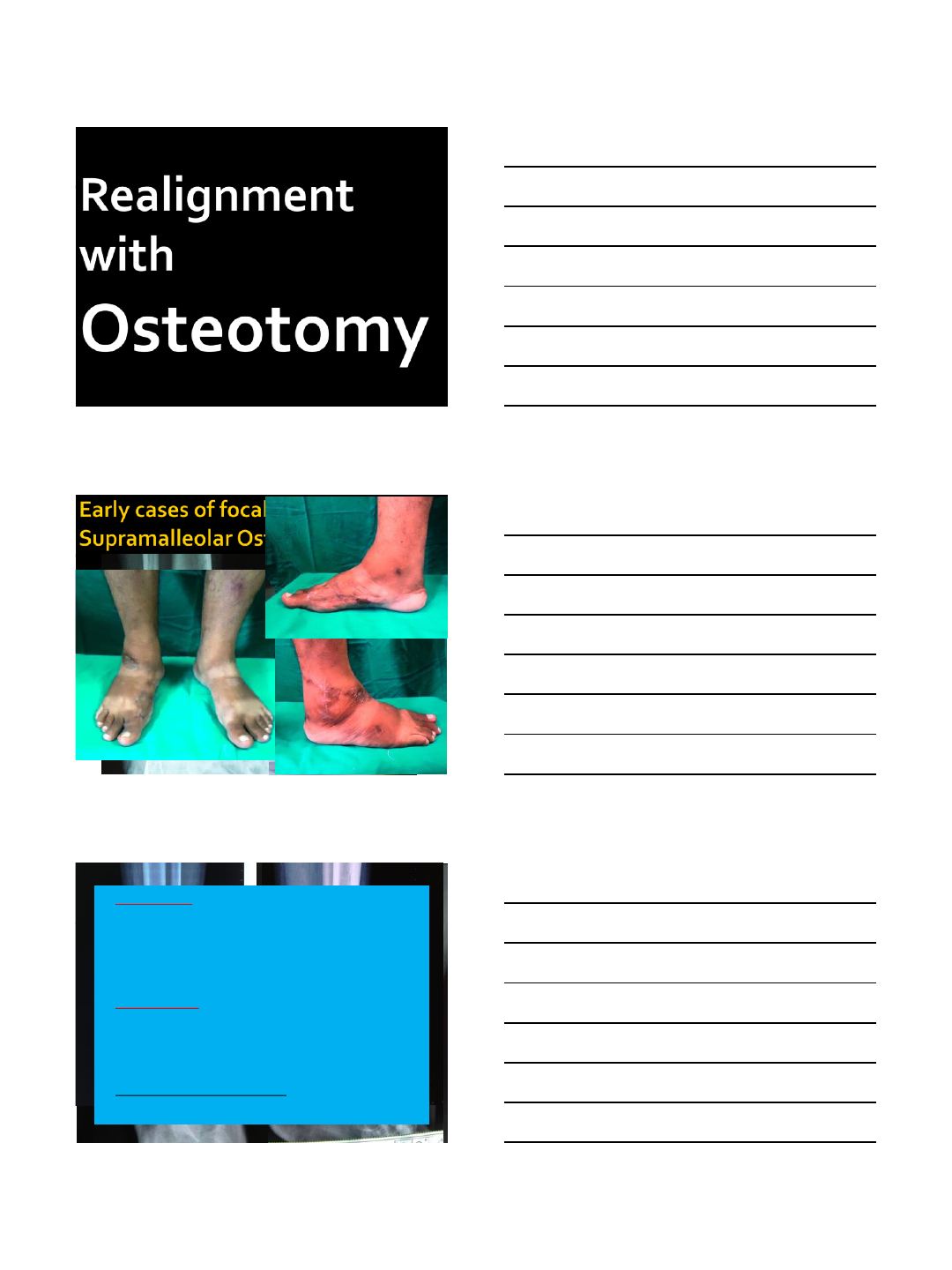
Realignment with osteotomy
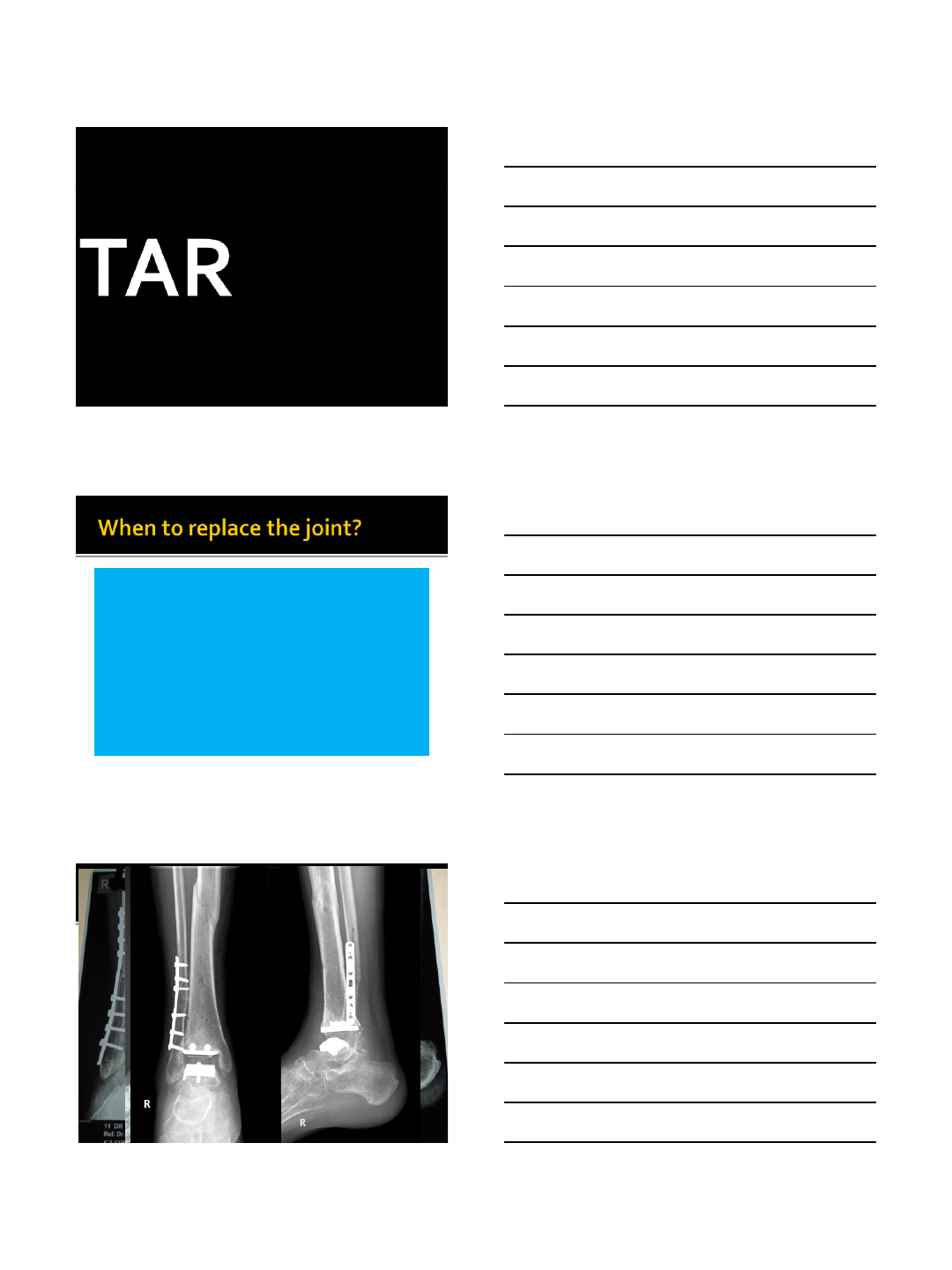
Ankle replacement
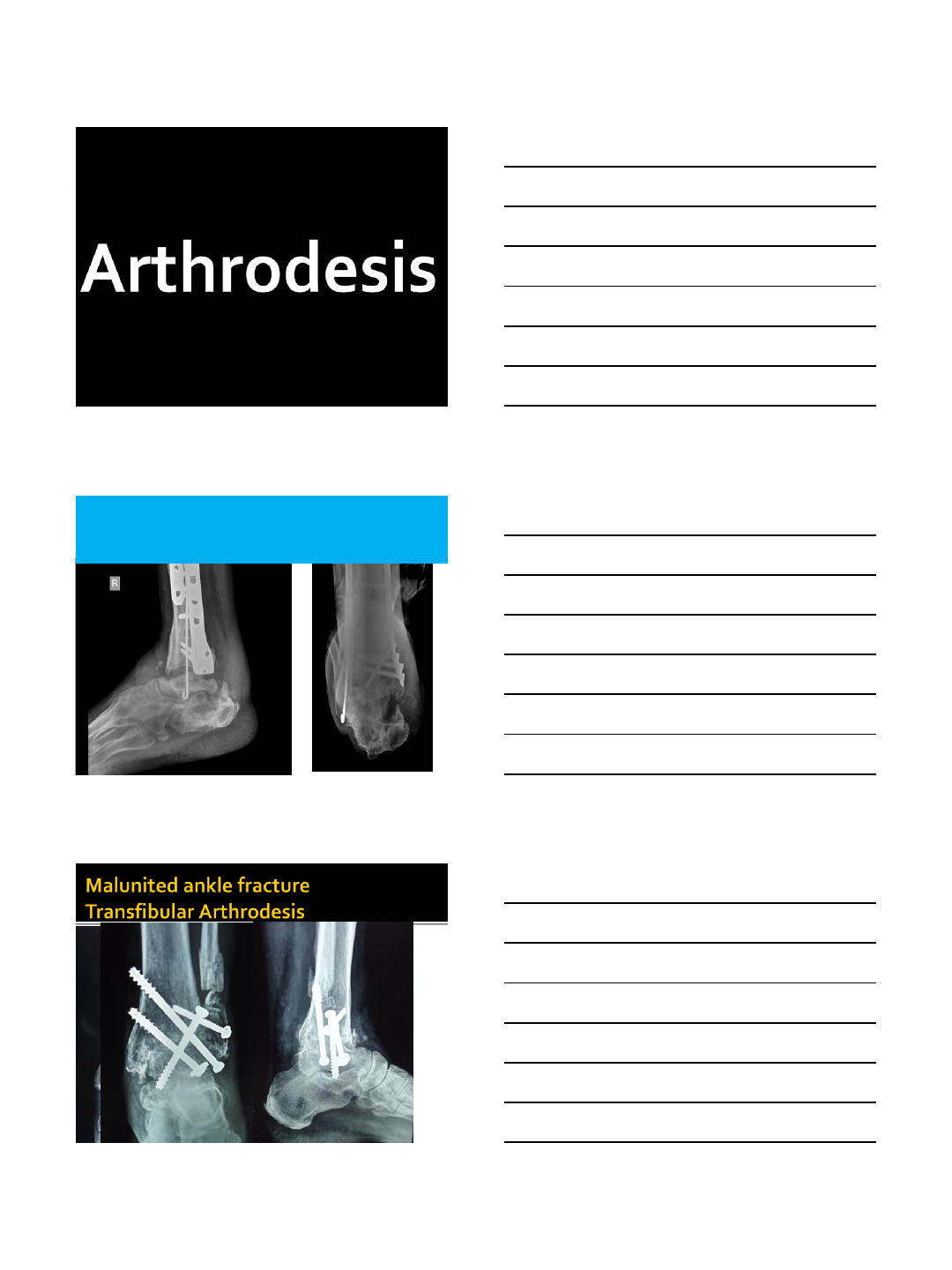
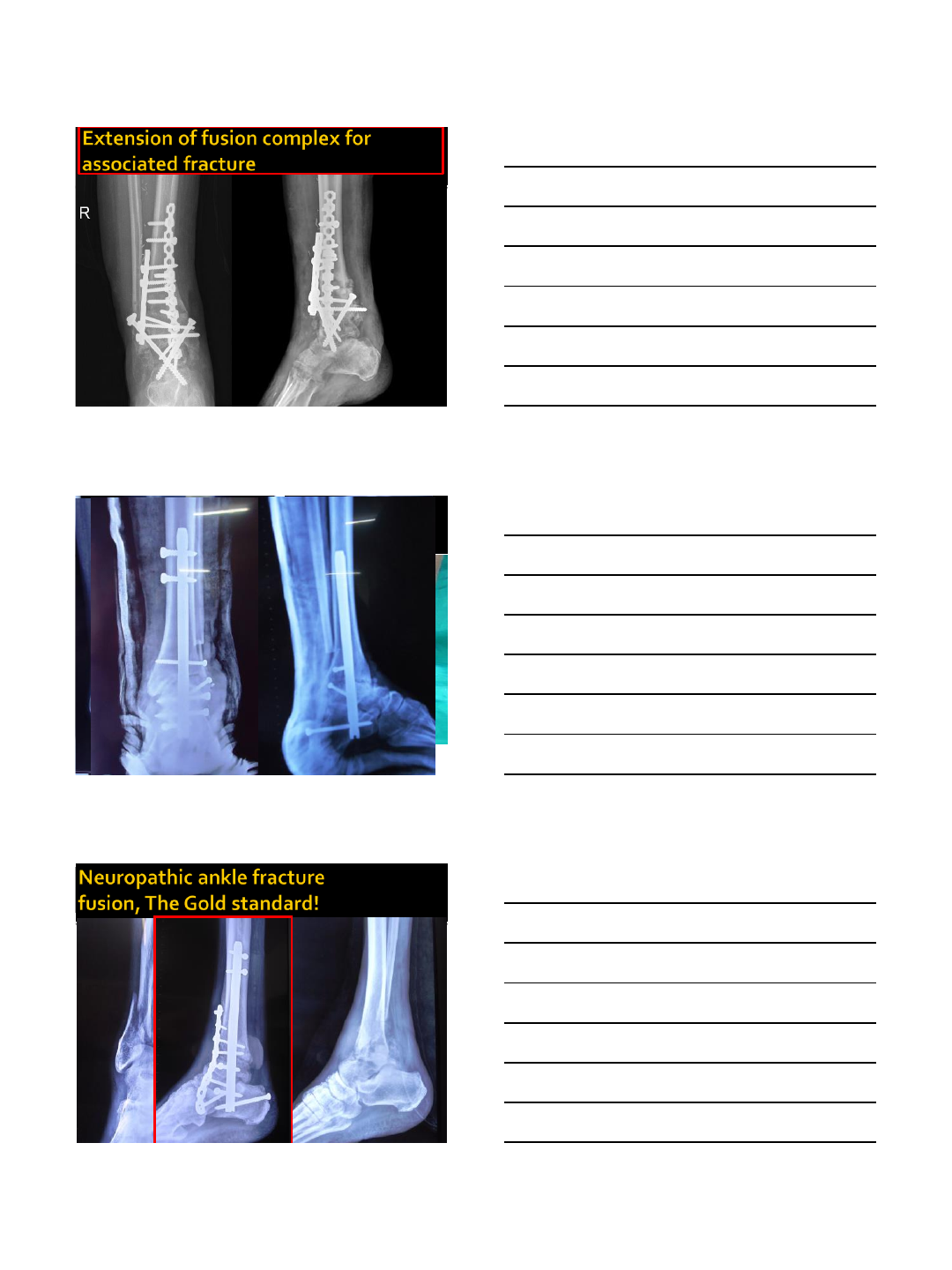
Fusion = ankle arthrodesis
10/21/2014
2
Duration may not matter!
While there is no optimal time to perform
reconstructions the fact is that…
Patients continue to
improve up to 7 years
post reconstruction!
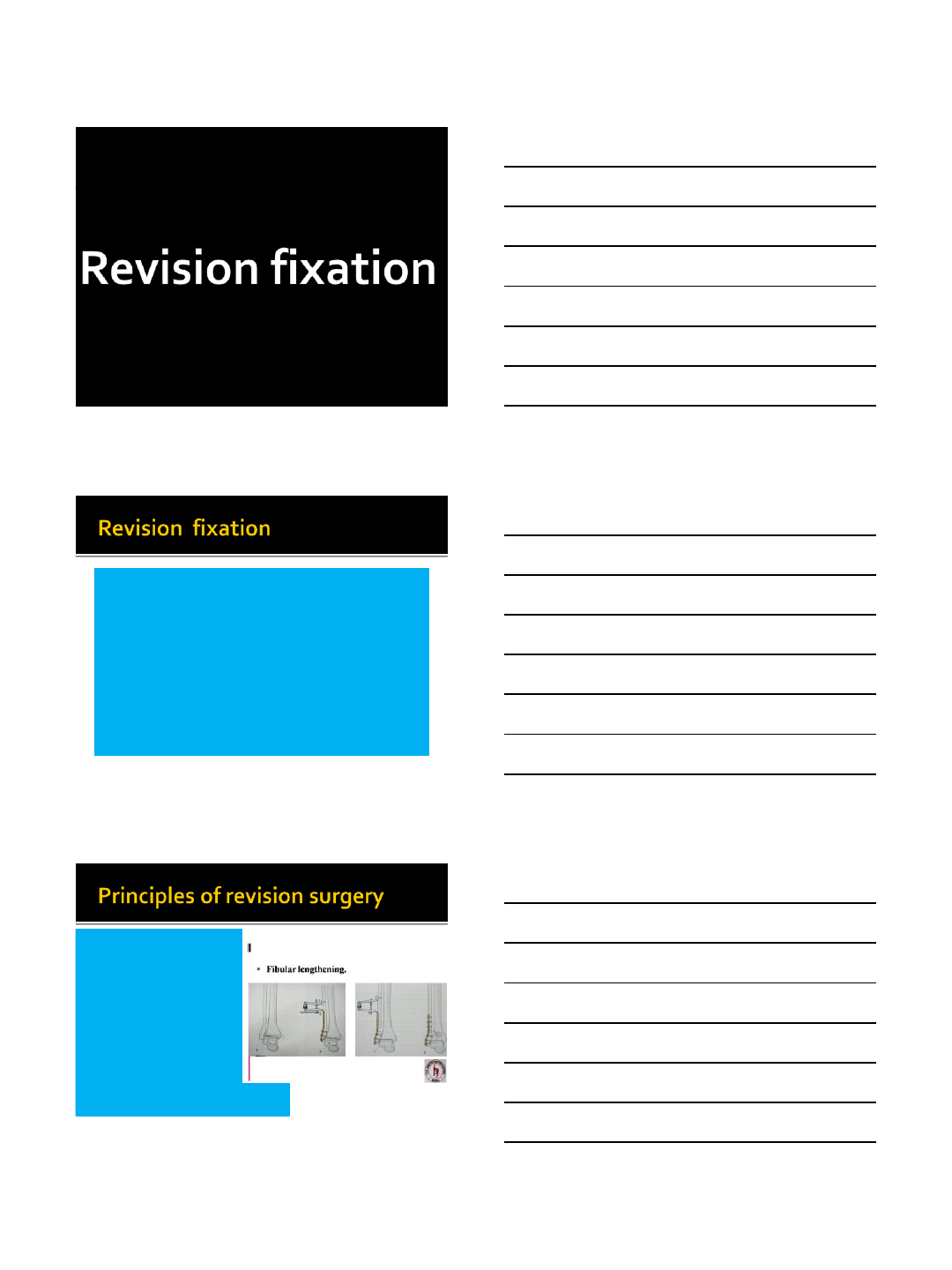
Fibular lengthening
Correction of talar tilt
Fixation of medial
malleolus
Syndesmotic fixation
Ligament
reconstruction
Releases
Arthroscopy
10/21/2014
3
7
8
9
10/21/2014
4
10
11
12
10/21/2014
5
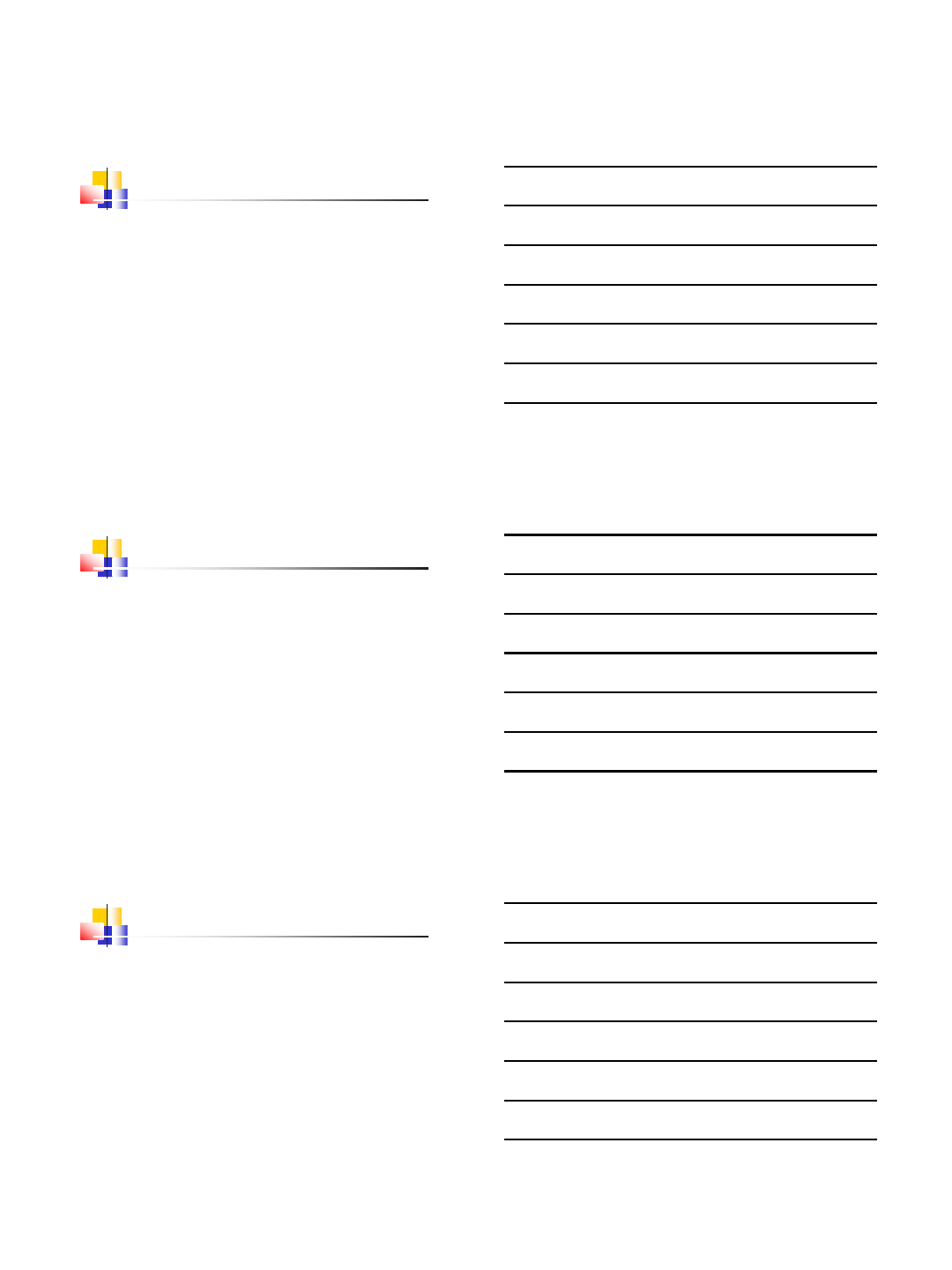
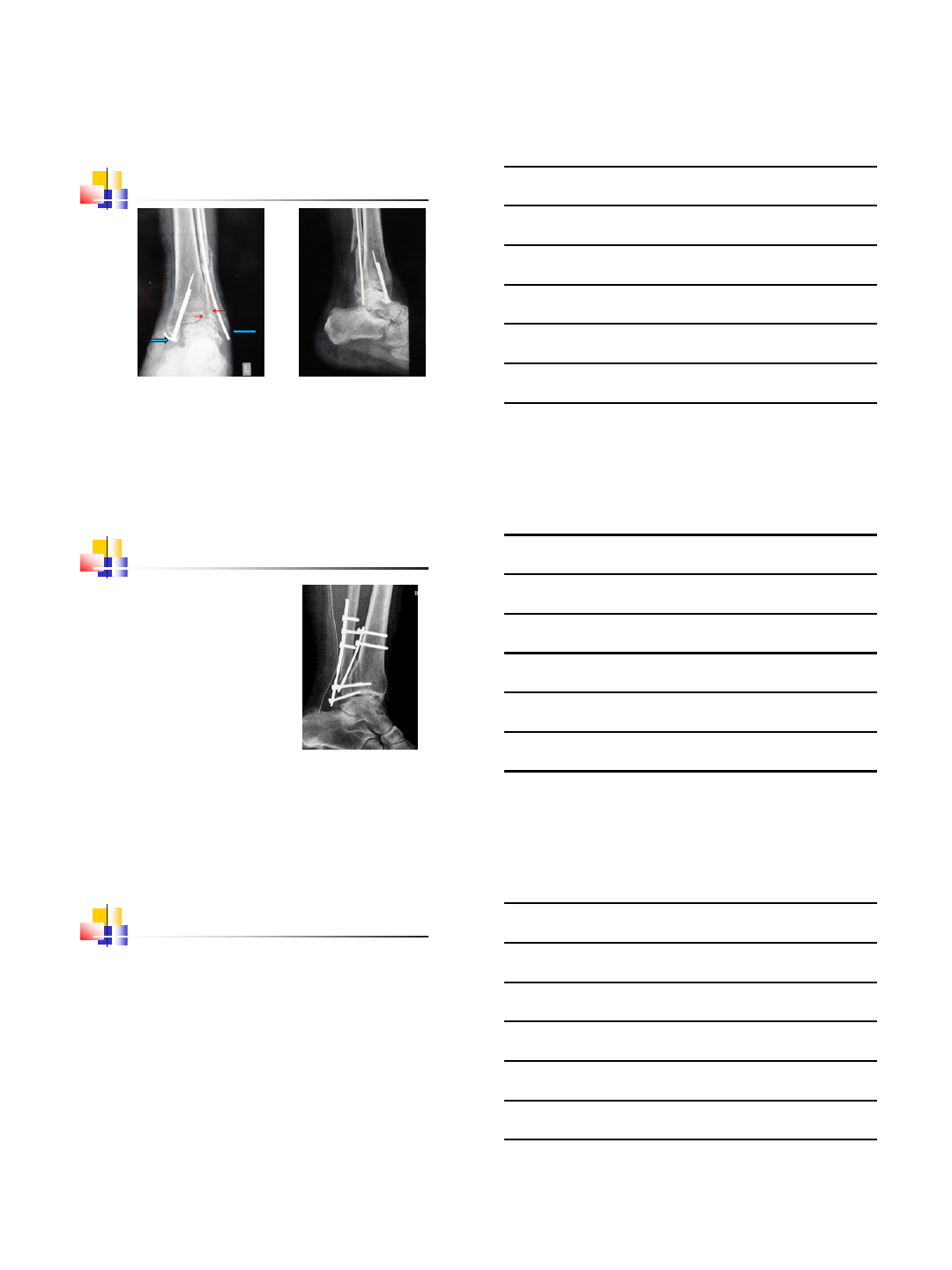
13
Malreduced
ankle,
syndesmosis
widened, fibula
rotated
10/21/2014
6
10/21/2014
7
20
21
Varus ankle:
Medial open wedge supramalleolar
Lateral close wedge supramalleolar
Lateral displacement hindfoot osteotomy
Valgus ankle:
MCO if mild valgus
Medial close wedge supramalleolar
Lateral open wedge supramalleolar
+/-Ligament reconstruction
10/21/2014
8
There is minimal deformity
No infection
No neuropathy
No vascular compromise
No AVN
Good soft tissue envelope
24
10/21/2014
9
26
Fusion –young patient with global arthritis, gross
deformities, infection, neuropathy, gross
instability & bone loss
27
10/21/2014
10
28
30
10/21/2014
11
Age &
activity
Young &
active
Revision
TAR over
Fusion
Old &
sedentary
Fusion
Orthosis
Arthritis &
deformity
Minimal
Osteotomy
TAR
Global with
deformity Fusion
10/21/2014
12
Infection
diabetes
Fusion
Revision
fixation??
Coronal plane
malunion
malunion in valgus
Leave it alone
Sagital plane
malunion
malunion in varus
Revise
36
