Presentation Beyond The Basics Performing Radial STEMI Procedures Dr Sugumaran 040616 TIS 255 04082016
2016-04-12
: Pdf Beyond The Basics Performing Radial Stemi Procedures- Dr Sugumaran 040616 Tis-255-04082016 Beyond_The_Basics_Performing_Radial_STEMI_Procedures-_Dr__Sugumaran_040616_TIS-255-04082016_ 4 2016 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 18
4/10/2016
1
™
Beyond The Basics: Performing Radial
STEMI Procedures
Rajkumar K. Sugumaran, MD
Cardiac Solutions
Phoenix, AZ
TIS-255-04082016
–The opinions expressed by Dr. Sugumaran during
this presentation are his own and do not
necessarily reflect those of Terumo Medical
Corporation. Unattributed data, device selection
and procedural guidance is a matter of physician
preference and opinion derived from Dr.
Sugumaran’s own observations and experiences
and should be treated accordingly.
–All visual representations and other imagery
contained in this presentation are used with
permission from Dr. Sugumaran.
Terumo Medical Corporation Disclaimer
TIS-255-04082016
Why Transradial PCI for STEMI?
Perfusion Test and Patient Prep
Radial Access
Catheter Selection and
Manipulation
Hemostasis
Objective
TIS-255-04082016
4/10/2016
2
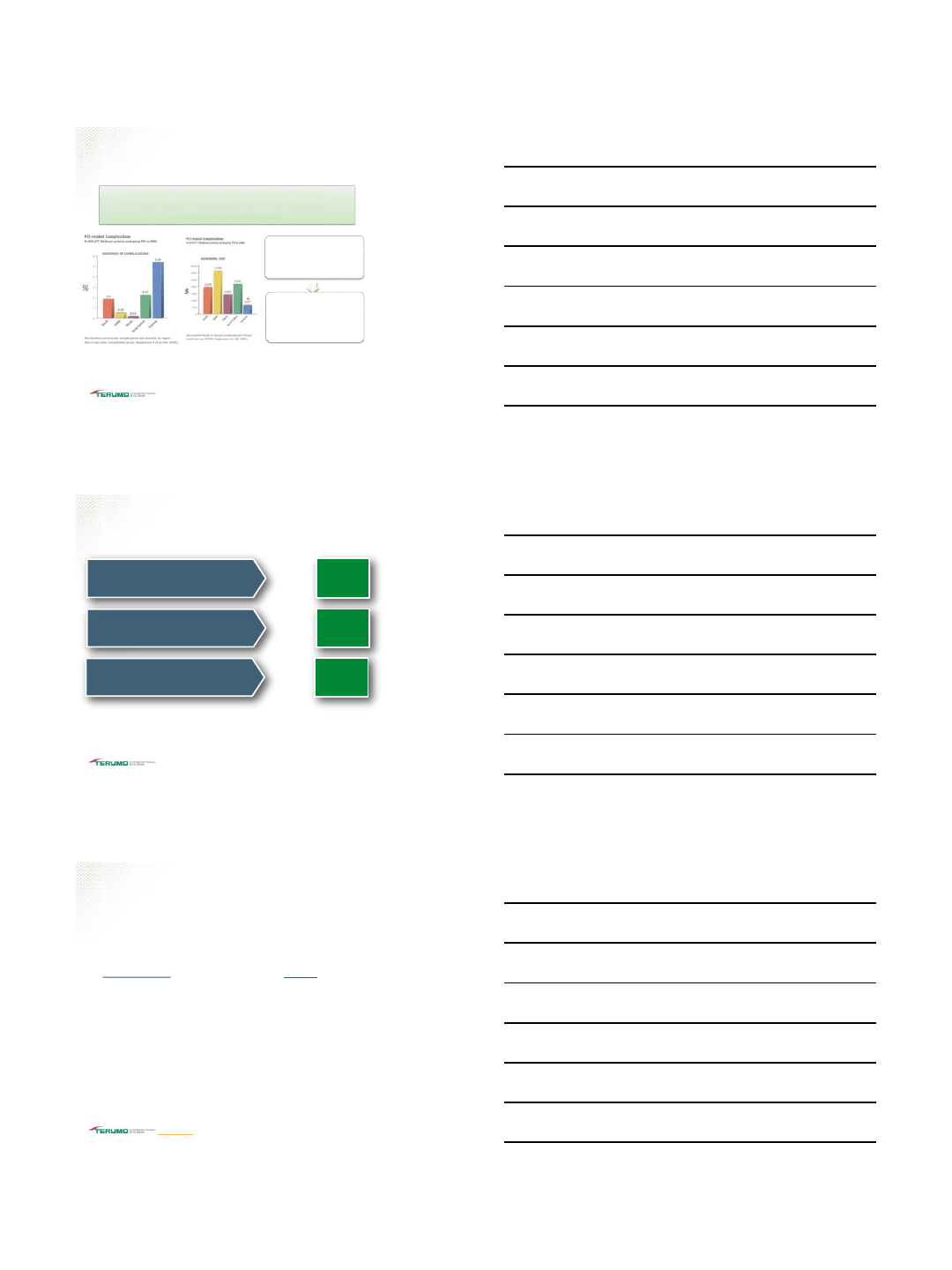
Hospital Resources Consumed in Treating
Complications associated with Percutaneous
Coronary Interventions
For patients with only one
complication, vascular
complications were more
common than all others
combined (4.9% vs 3.3%)
Estimates of the adjusted
incremental hospital costs
of treating any acute
complication varied from
$4k-$33k per patient
Kugelmass A, Cohen D, Brown MD, Simon A, Becker E, and Culler S. American Journal of Cardiology 2006; 97: 322-327
Vascular Access Complications
TIS-255-04082016
Reduction in Bleeding Complications
RIVAL
TRA n = 3507 TFA n =3514
STEMI radial showed 40% Reduction in primary outcome
STEMI/ACS radial showed 63% Reduction in Major Vascular
Complications
MORTAL
Retrospective analysis of 38,872 patients
TRA showed 50% Reduction in Transfusion Rate
TRA reduced 1yr Mortality from 3.9% to 2.8%
RIFLE-STEACS
STEMI TRA (n = 500) vs. TFA (n = 501)
62% Reduction of Access site bleeding complications with TRA
vs. TFA
*The Association Of Arterial Access Site At Angioplasty With Transfusion And Mortality The M.O.R.T.A.L Study: (Mortality benefit of Reduced Transfusion
After PCI via the Arm or Leg); Alex J Chase, Eric B Fretz, William P Warburton, W Peter Klinke, Ronald G Carere
*Effects of Radial Versus Femoral Artery Access in Patients With Acute Coronary Syndromes With or Without ST-Segment Elevation. Shamir R. Mehta, MD,
MSC,* Sanjit S. Jolly, MD, MSC
*Radial Versus Femoral Randomized Investigation in ST-Segment Elevation Acute Coronary Syndrome The RIFLE-STEACS (Radial Versus Femoral
Randomized Inv estigation in ST-Elevation Acute Coronary Syndrome) Study. Enrico Romagnoli, MD, PHD,* Giuseppe Biondi-Zoccai, MD,† Alessandro
Sciahbasi, MD
TIS-255-04082016
Radial Continues to be Supported by Evidence
Minimizing Adverse Haemorrhagic Events by Transradial Access Site and
Systemic Implementation of Angiox (the MATRIX Trial)1
Study Methods
•Randomised, Superiority trial
•8404 Patients, 74 Centers
•Co-primary End Points
•MACE
•NACE
•Secondary End Points
•Individual components of
Composite out comes
•All cause Mortality
•Stroke
•MI
•Bleeding
Results
•Radial garners superior outcomes
•Radial as compared with femoral
access reduces NACE through a
reduction of bleeding and all-cause
mortality
•Co-Primary End Points
•15% relative reduction in MACE
•17% relative reduction in NACE
•Secondary End Points
•28% Reduction in all-cause
mortality
•33% reduction in Bleeding
1J Cardiovasc Transl Res. 20 14 Feb;7(1):101-11. doi: 10.1007/s12265-013-9537-1.
Epub 2014 Jan 7
TIS-255-04082016
4/10/2016
3
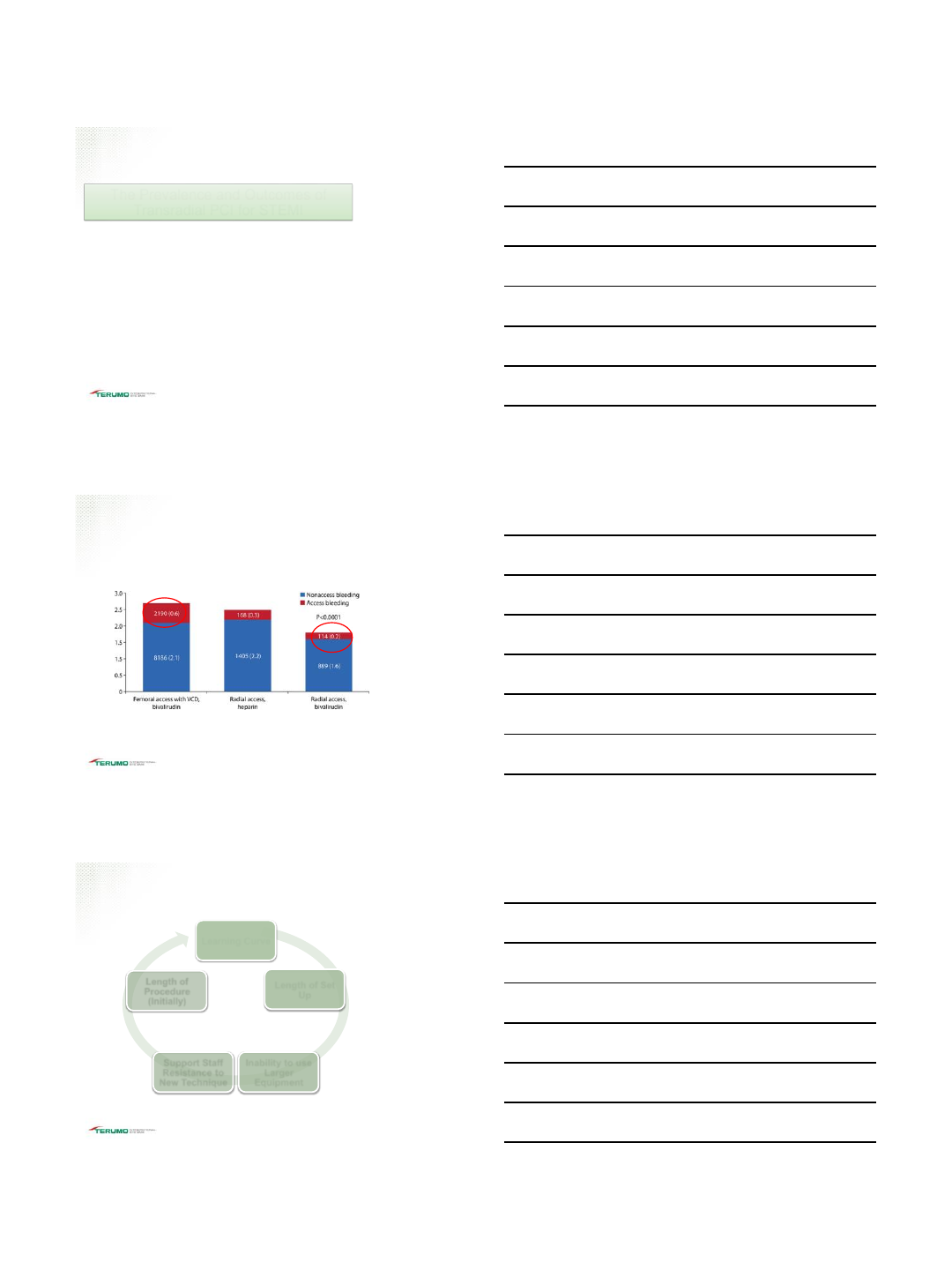
The Prevalence and Outcomes of
Transradial PCI for STEMI
Key Points:
The authors concluded that the wider usage of TRI for STEMI may
significantly improve patient outcomes.
TRI patients were also significantly less likely to have vascular
complications than the femoral PCI population.
TRI was associated with a lower risk of bleeding and in-hospital
mortality while there was no difference in procedural success.
Transradial PCI for STEMI
Baklanov DV, Kaltenbach LA, Marso SP et al. J Am Coll Cardiol. 2013 Jan 2 9;61(4):420-6
TIS-255-04082016
Baklanov D V et al. Circ Cardiovasc Interv. 2013;6:347-353
This figure demonstrates the rate of percutaneous coronary intervention-associated
bleeding in 501,017 patients grouped by vascular access and anticoagulation.
Transradial and Bivalrudin
TIS-255-04082016
Common Hurdles with Transradial PCI for STEMI
Learning Curve
Length of Set
Up
Inability to use
Larger
Equipment
Support Staff
Resistance to
New Technique
Length of
Procedure
(Initially)
TIS-255-04082016
4/10/2016
4
Transradial Advantages
Benefits of radial access for all patients, especially STEMI
When to start performing radial STEMI?
Why to perform radial STEMI?
Discussing with your Cath Lab Staff in advance of radial
STEMI case
TIS-255-04082016
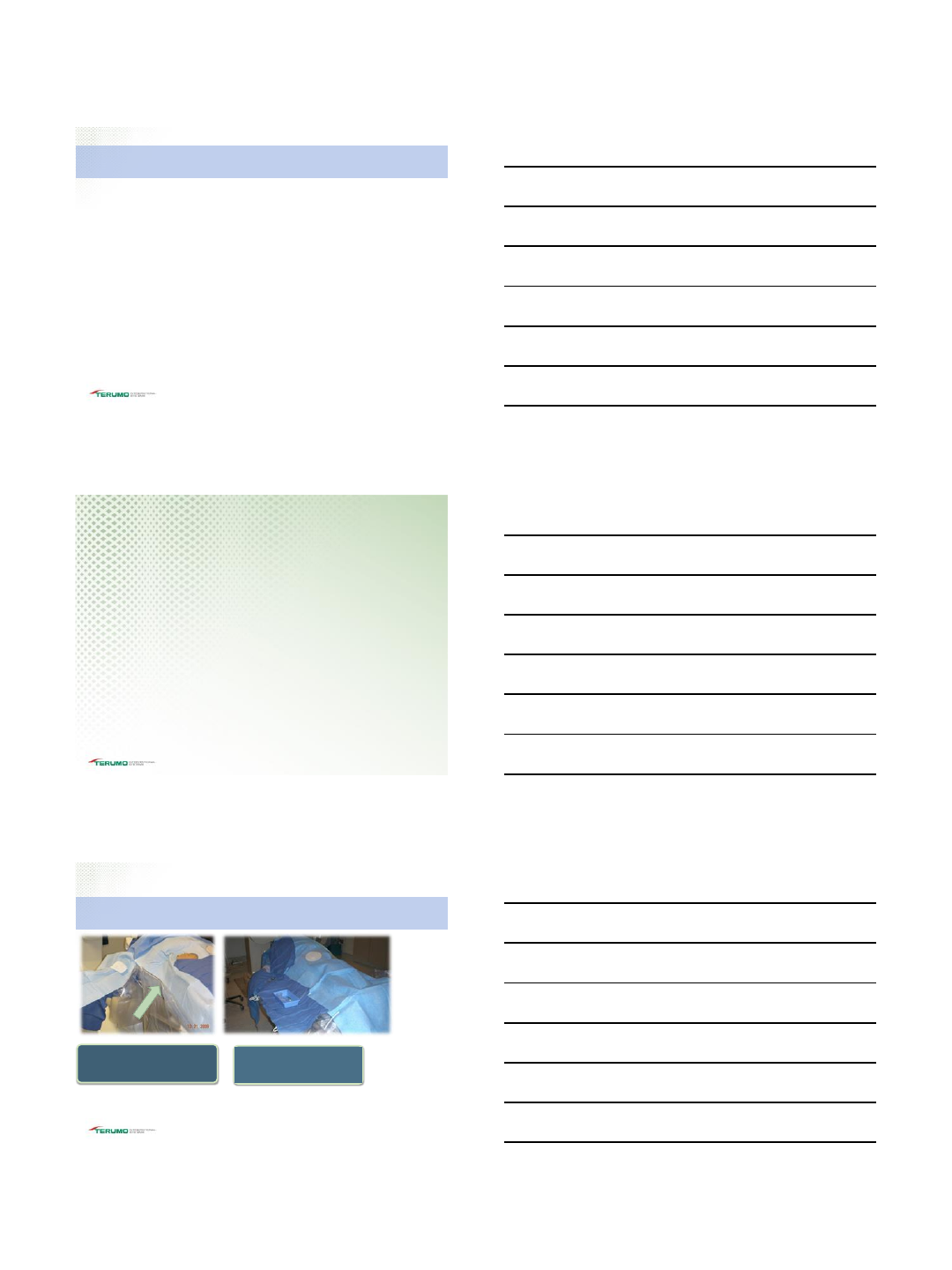
Room Set-up and Prep
TIS-255-04082016
©2014 TERUMO MEDICAL CORPORATION
©2014 TERUMO MEDICAL CORPORATION
Room Set up –Right Radial
Some physicians will access radial artery
with arm at 90 degrees. Once sheath is
inserted and secured, bring right arm in
near right groin site
Other physicians works in same plane
as wrist with equipment easily
accessible
TIS-255-04082016
4/10/2016
5
Begin with the
arm adducted
90 degrees
To work from the
patient’s right, use
pillows, straps or
blankets to elevate
arm
Assess position for
patient comfort and
compliance prior to
prepping site
©2014 TERUMO MEDICAL
CORPORATION
©2014 TERUMO MEDICAL CORPORATION
©2014 TERUMO MEDICAL CORPORATION
Room Set up –Left Radial
TIS-255-04082016
Access the left radial with arm
positioned at 90 degrees to
patient
Position the arm near
patient’s left groin if working
from the patient’s right
©2014 TERUMO MEDICAL CORPORATION
©2014 TERUMO MEDICAL CORPORATION ©2014 TERUMO MEDICAL CORPORATION
Room Set up –Left Radial
TIS-255-04082016
Shave and prep medial to lateral; from
the mid forearm to the mid palm
Shave the upper arm if RHC is to be
performed
Consider shave and or Prep femoral
access site.
Femoral access can prove useful for emergent
access of the femoral artery or vein
Room Set up –Considerations
TIS-255-04082016
4/10/2016
6
Administering Heparin to Avoid RAO
Key Points:
No statistical difference between intra-arterial and
systemic heparin administration in regards to RAO.
500 consecutive patients
Early RAO 5.6% (ia) vs. 6% (systemic)
Late RAO 4% (ia) vs 3.2% (systemic)
Comparison of the Effect of Intra-Arterial Versus
Intravenous Heparin on Radial Artery Occlusion After
Transradial Catheterization
Samir Pancholy: Volume 104, Issue 8, Pages 1083-1085 (15 October 2009)
TIS-255-04082016
Radial Artery Spasm
Vascular Trauma
(Access)
Friction as a result of
catheter movement
or sheath removal Patient Anxiety
The vessel grips
onto the
catheter/sheath
Difficulty of
advancement or
removal
Gives great pain to
the patient if the
system is forced out
What Happens
Reasons
Radial Artery Spasm occurs in 2%-6% of patients
Patel’s Atlas of Transradial Intervention, The Basics and Be yond © 2012 by Tejas Patel
TIS-255-04082016
Additional vasodilators if needed
Gentle Sedation
Spasmolotic Cocktail (Nitroglycerin 200-400mcg, Verapamil 2.5-
5mg). Consider alternate vasodilators/antispasmodic.
Use of Smaller sheaths and catheters
Use of Hydrophilic sheath to reduce friction
Patel’s Atlas of Transradial Intervention, The Basics and Be yond © 2012 by Tejas Patel
Radial Artery Spasm Prevention
TIS-255-04082016
4/10/2016
7
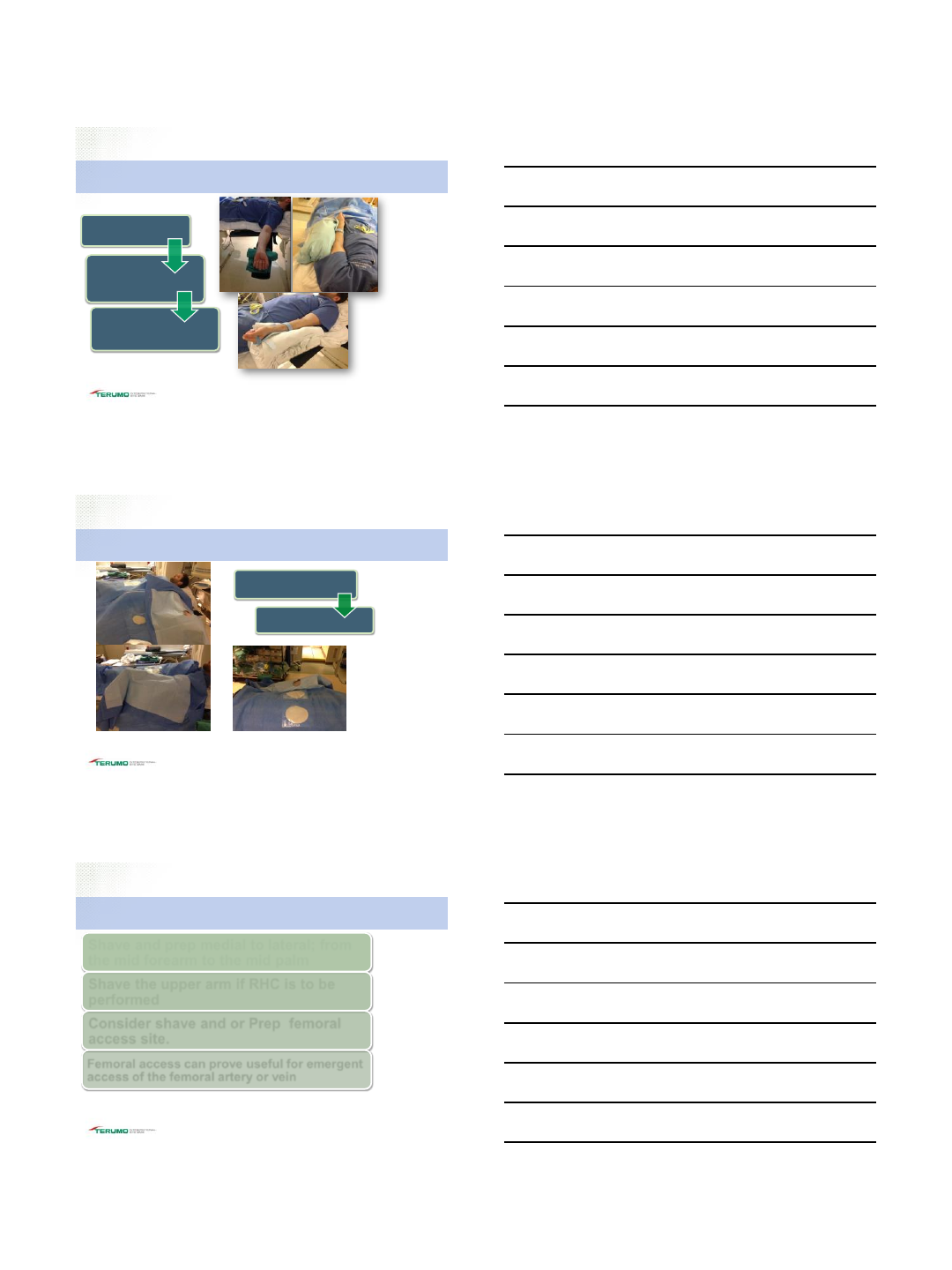
Antispasmotic Cocktail
Verapamil is a very acidic drug. To reduce burning effect, Physician should
consider diluting cocktail with the patient’s blood in a 10-20mL syringe.
Other substitutions would be Nicardipene or Cardene
©2014 TERUMO MEDICAL CORPORATION
TIS-255-04082016
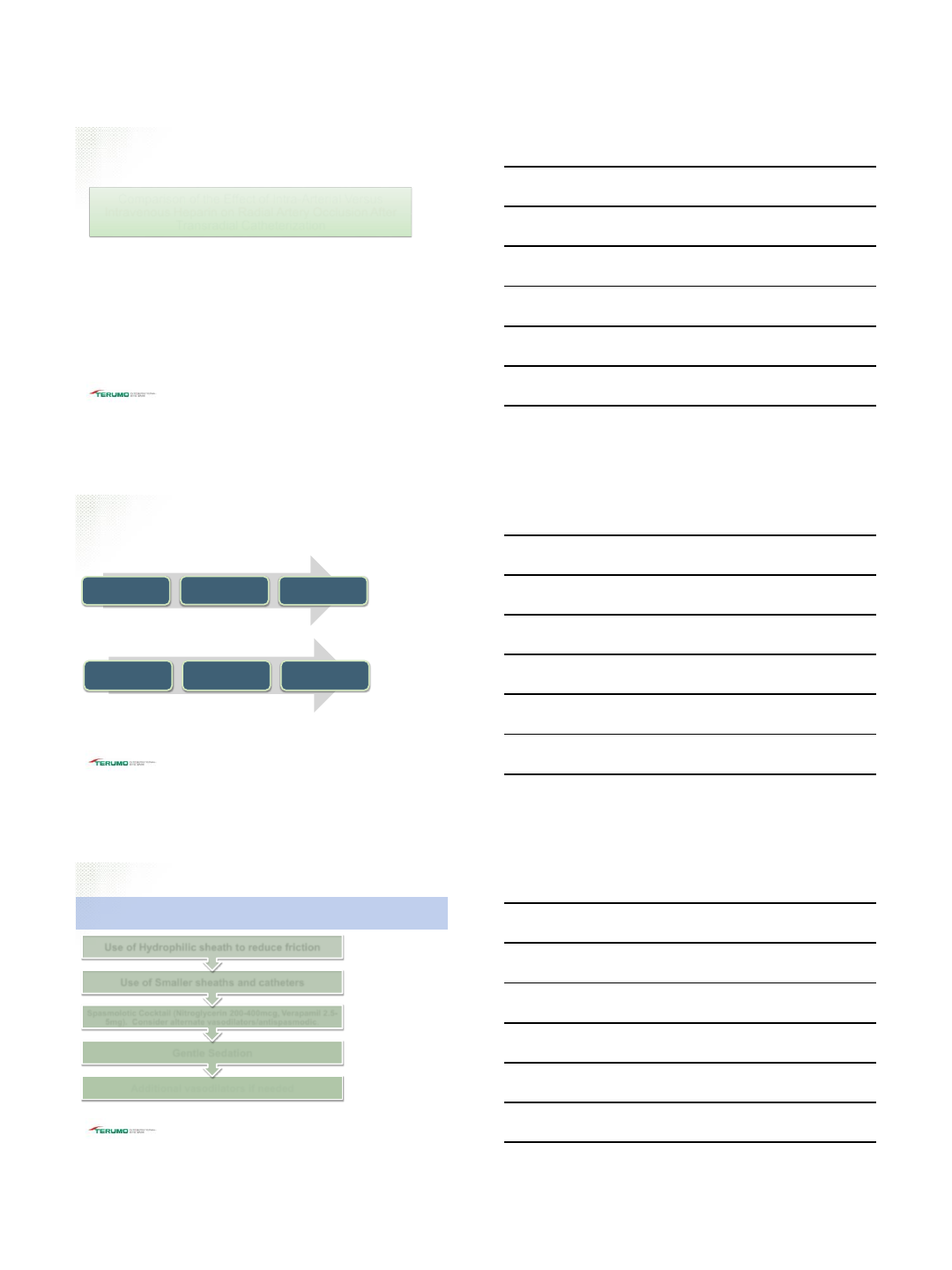
OPTITORQUE™
Coronary diagnostic catheter
Available in 5 Fr and 6 Fr catheter
sizes
Radial shapes are designed to
eliminate catheter swaps
Shaft with 2-ply stainless steel braid
designed for 1-to-1 torque and
accurate placement
Large lumen for high contrast flow
Atraumatic soft tip
Designed to provide greater visibility
around the ostium and lower contrast
pressure from the end hole
©2014 TERUMO MEDICAL CORPORATION
TIS-255-04082016
•Provides multiple points of contact against the contralateral
wall
•Ikari left offers versatility –for use in LCA and RCA
•Optimal STEMI guide cath to reduce DTB
HEARTRAIL™ Guide Catheters
©2014 TERUMO MEDICAL CORPORATION
TIS-255-04082016
4/10/2016
8
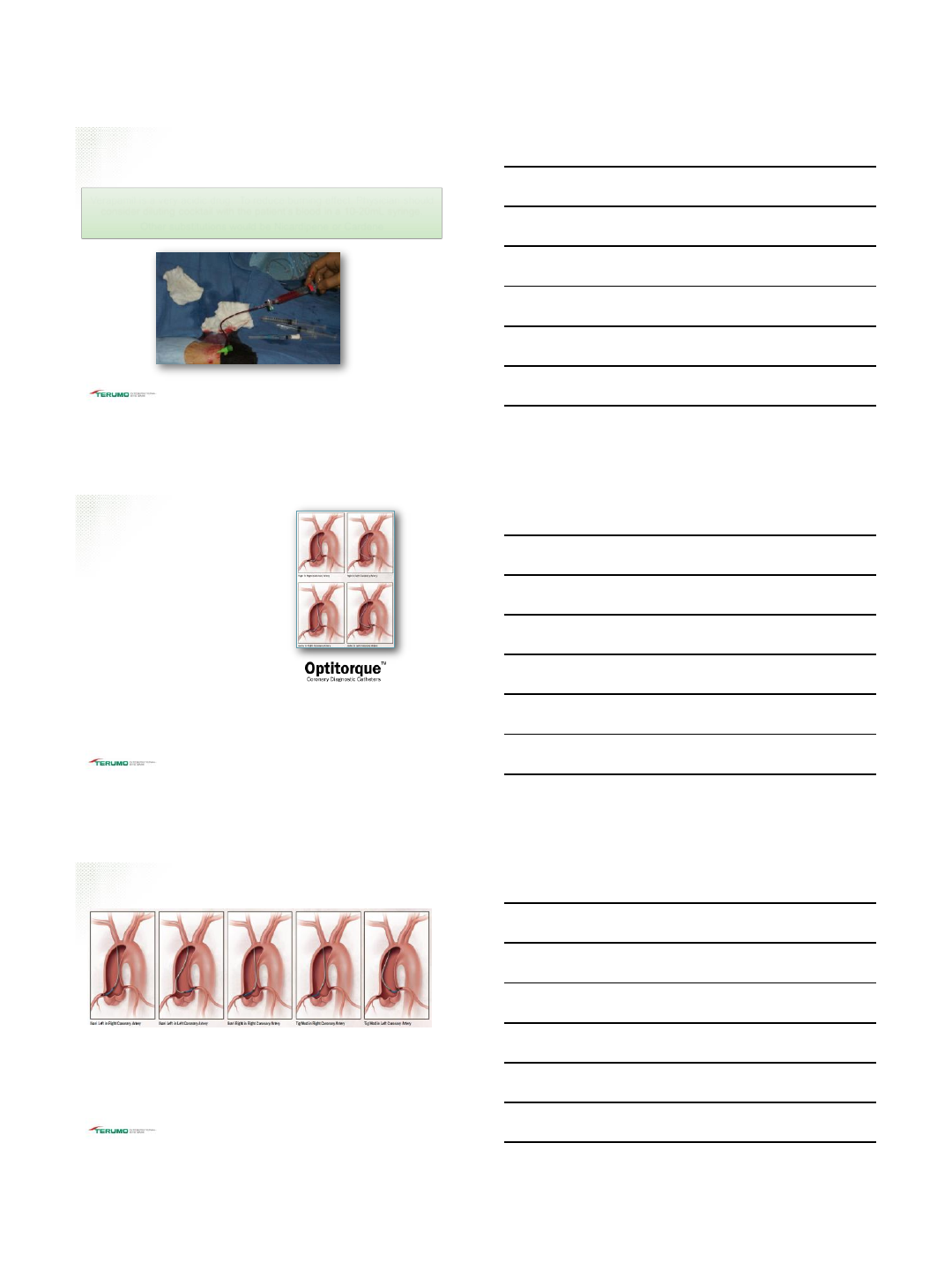
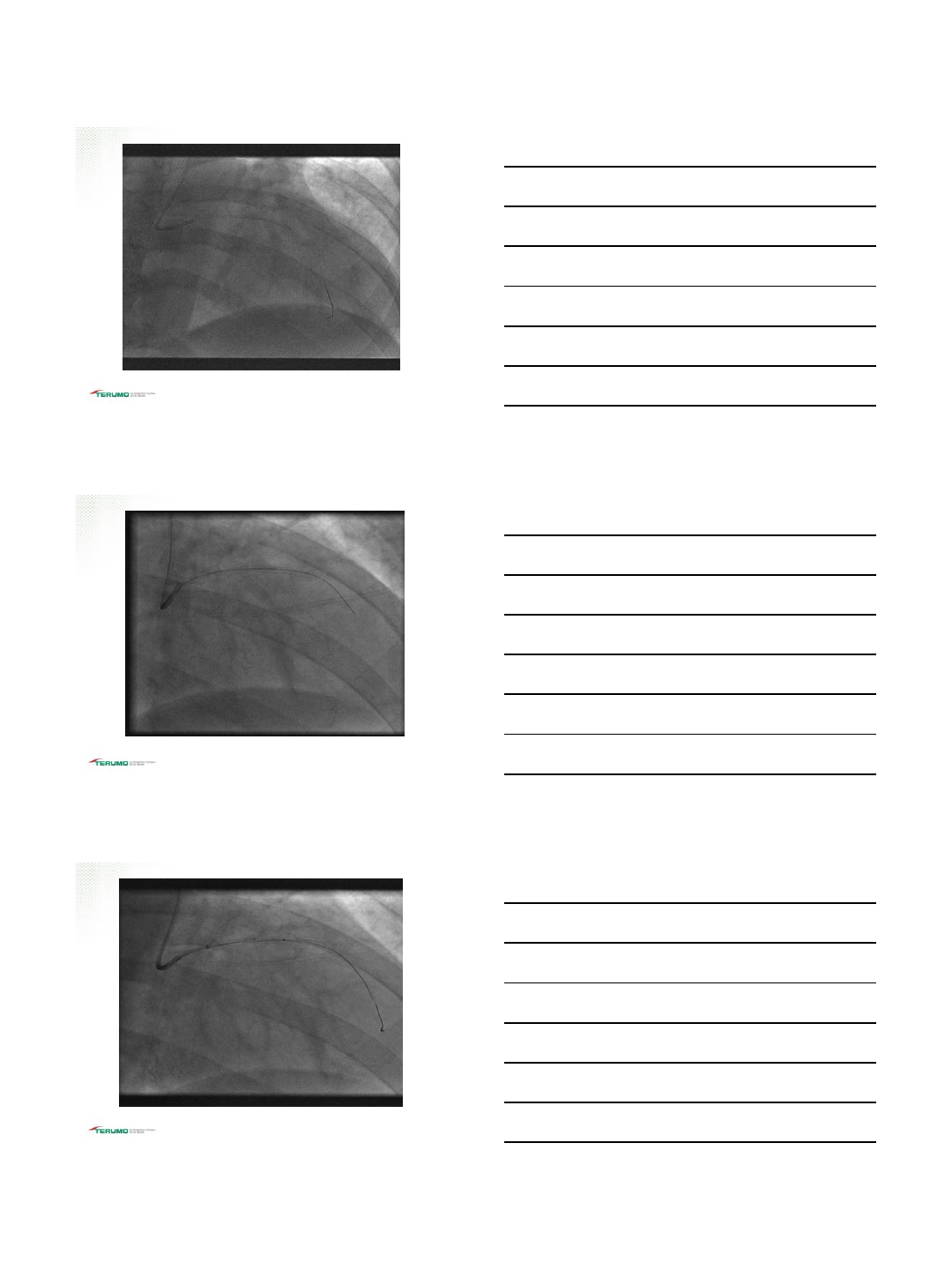
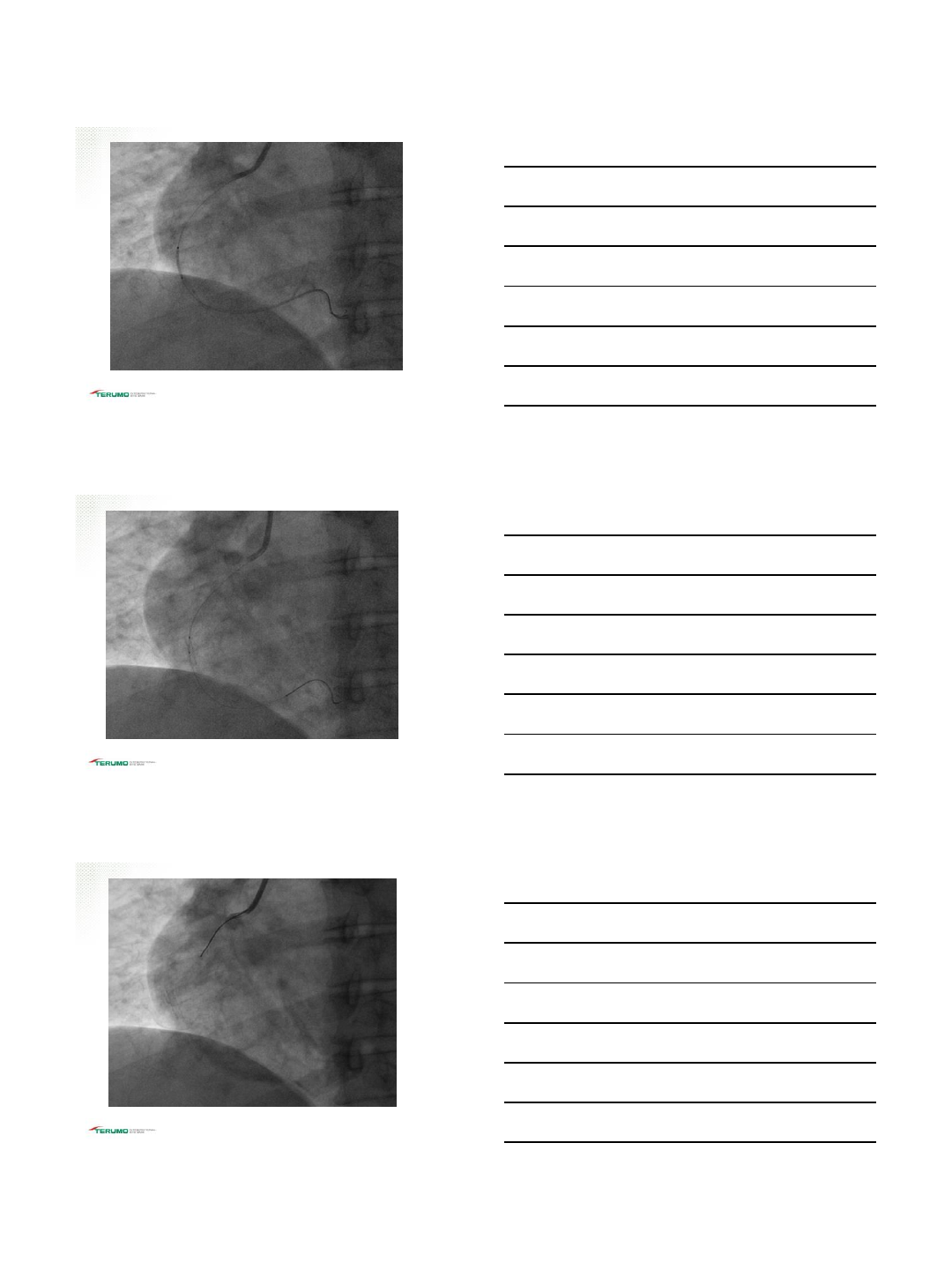
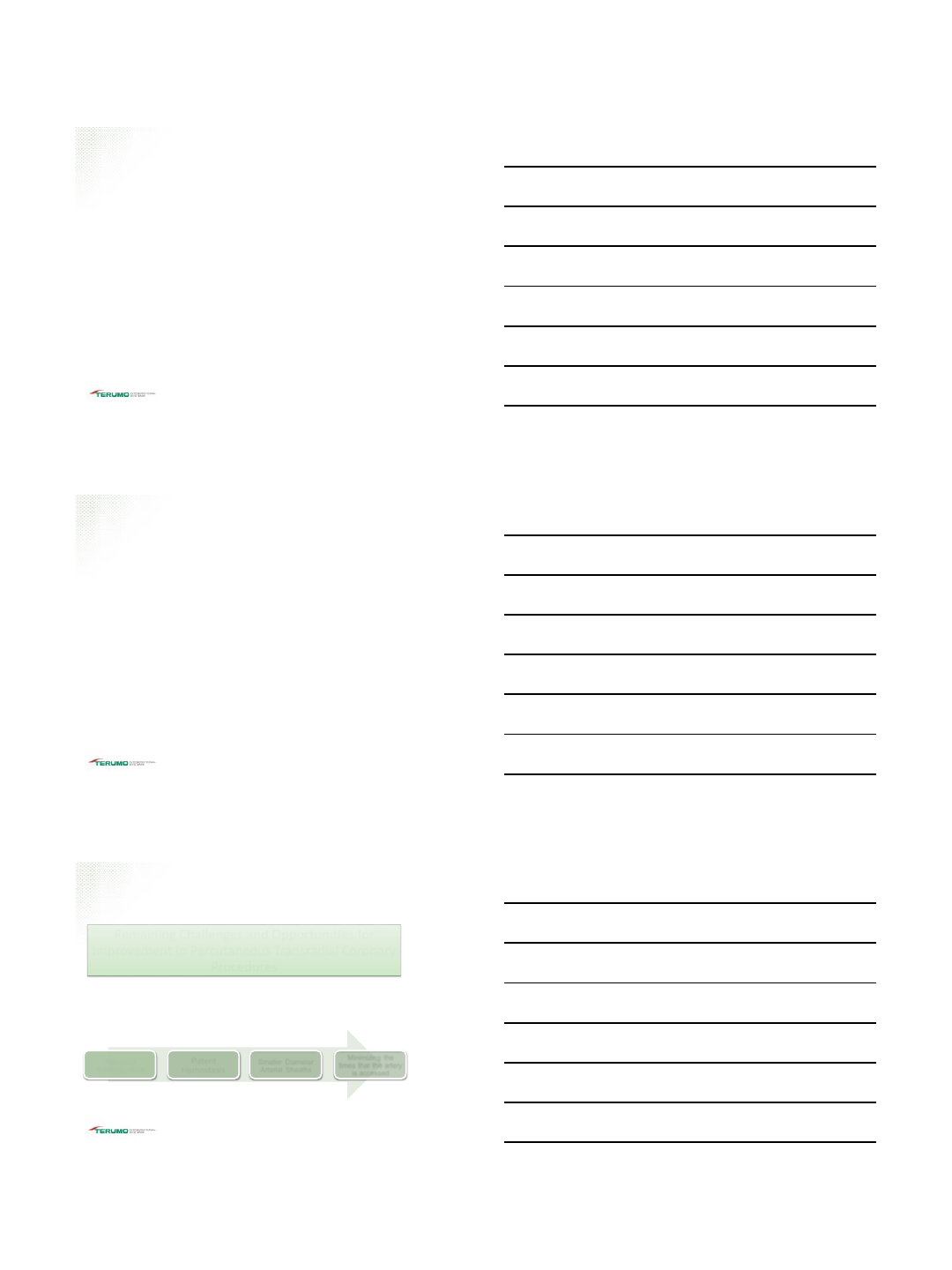
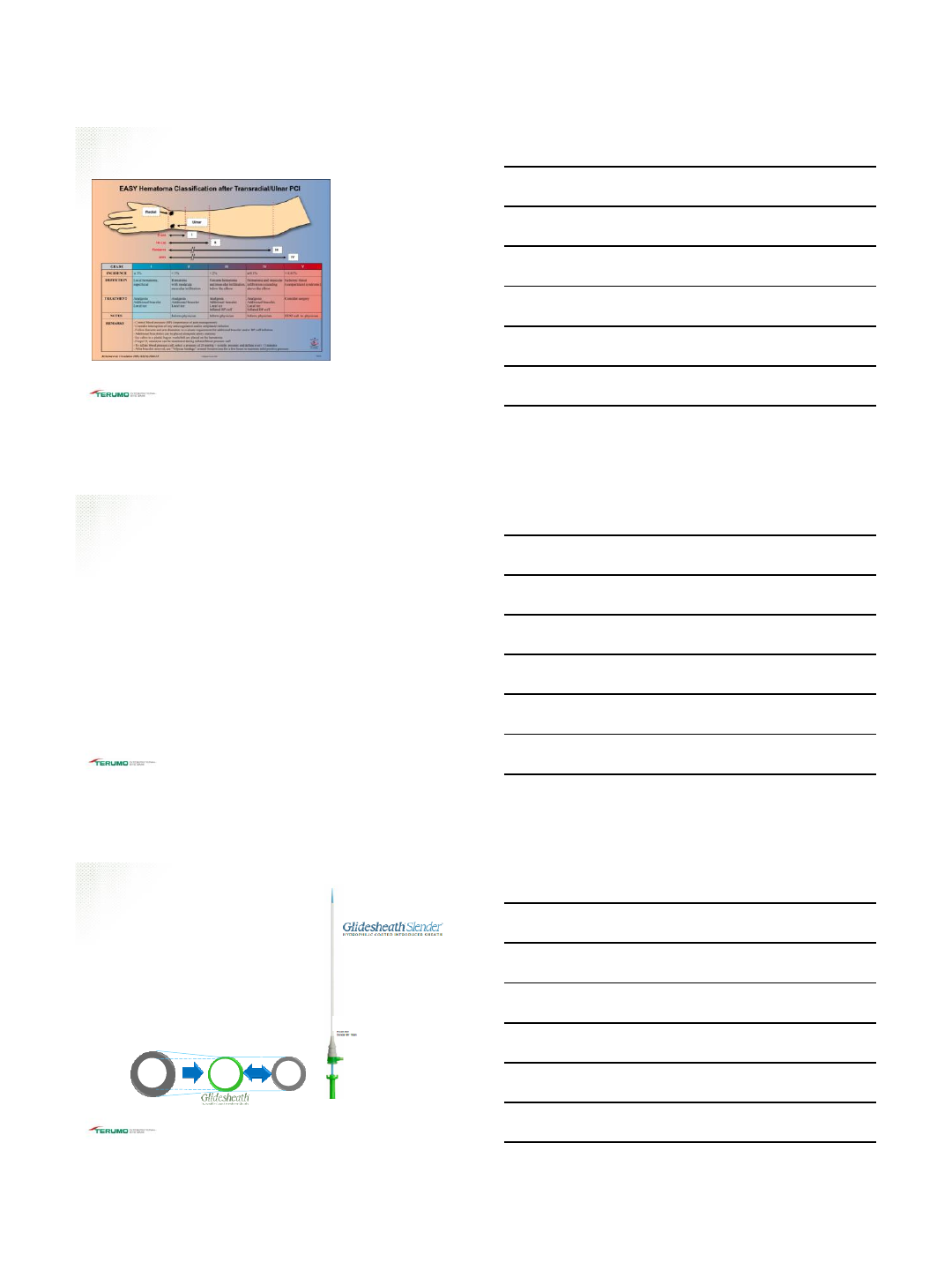
CASE 1
57 y/o morbidly obese WF with a h/o CAD s/p Anterior
MI LAD stents 2014, HTN and HLD presented to hospital
for worsening chest pain. Troponin 0.28
TIS-255-04082016
TIG 4.0
CATHETER
TIS-255-04082016
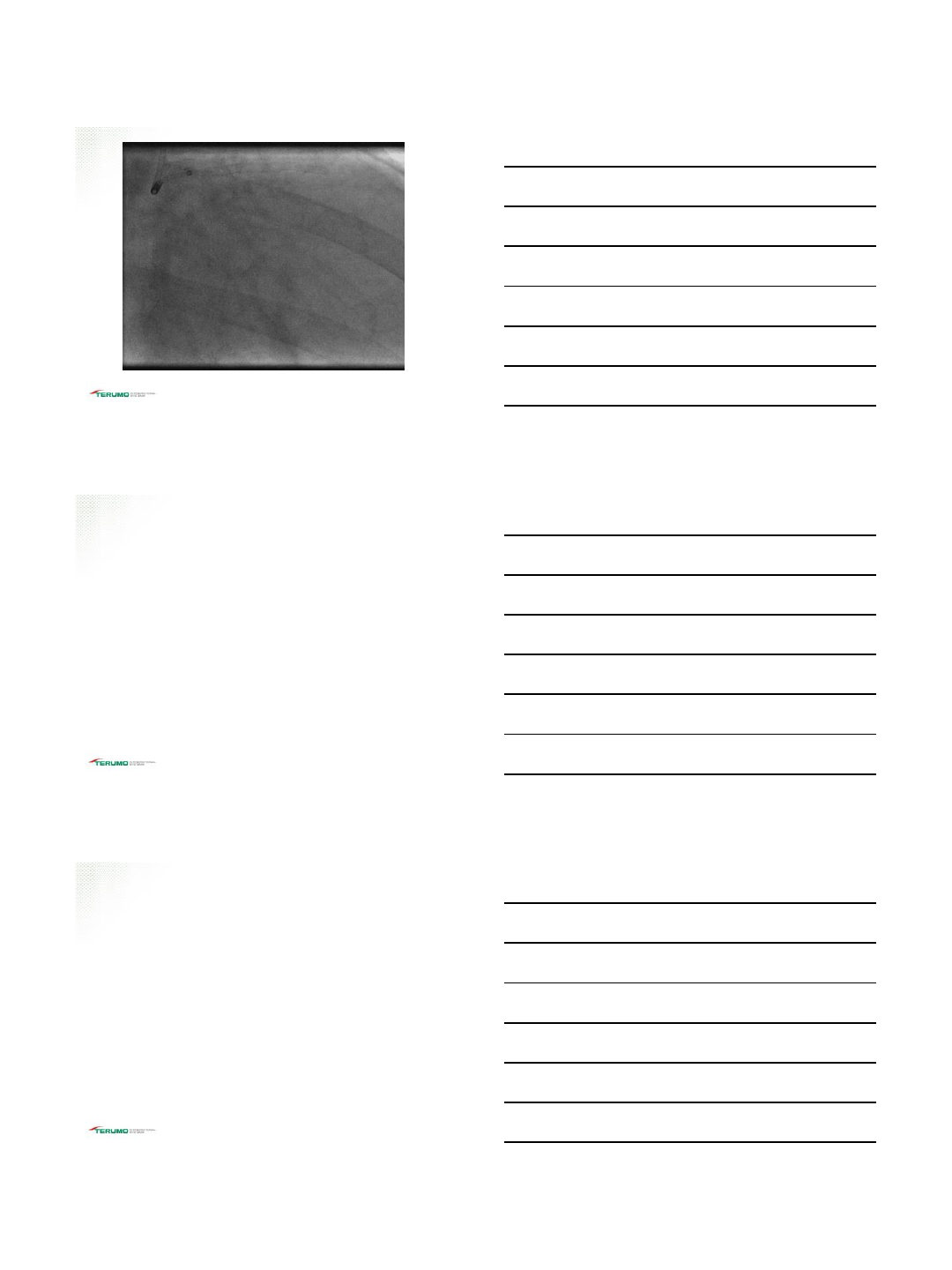
IKARI 3.5 L
GUIDE
RUNTHROUGH®
NS Coronary
Guidewire
TIS-255-04082016
4/10/2016
9
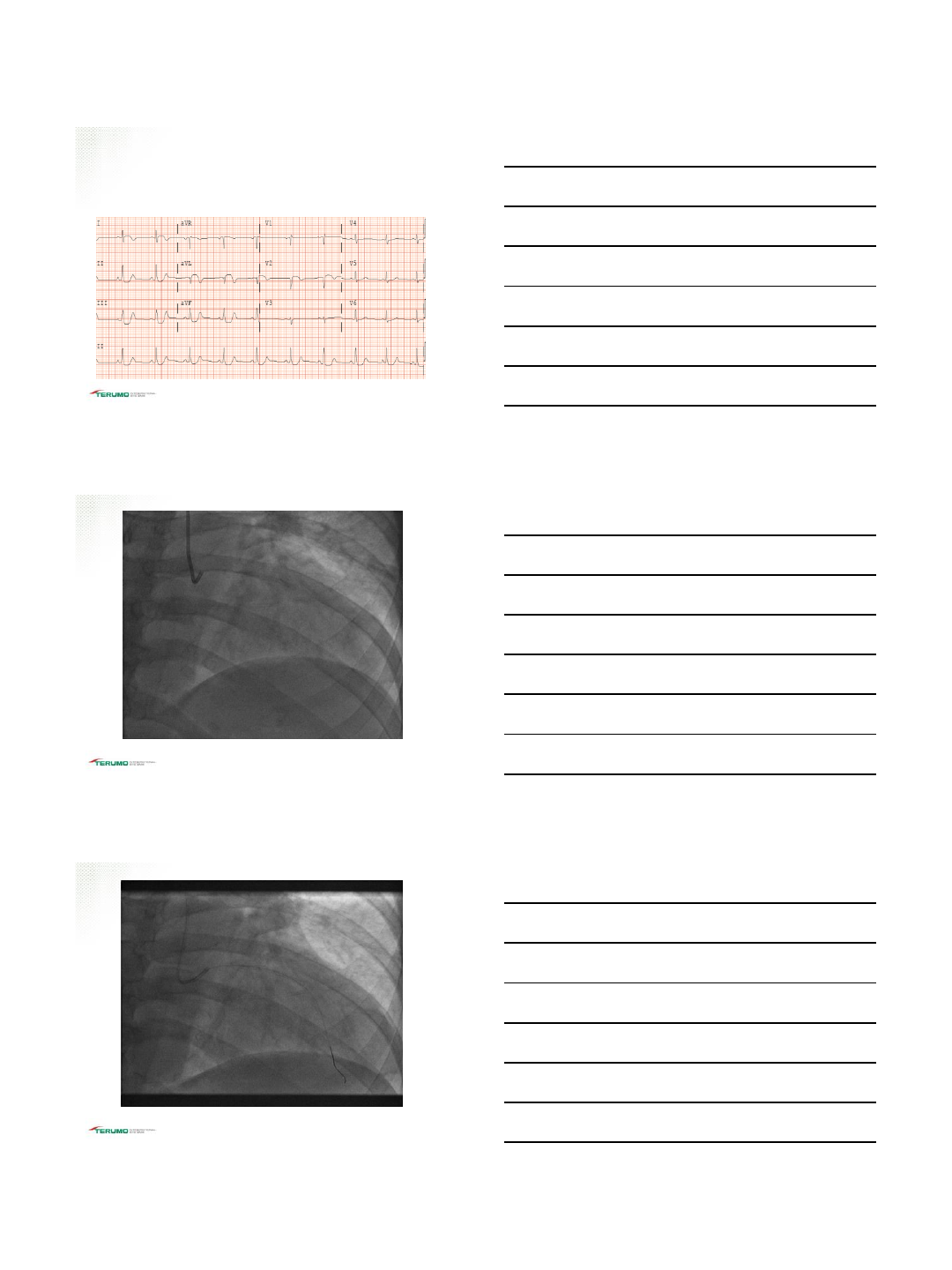
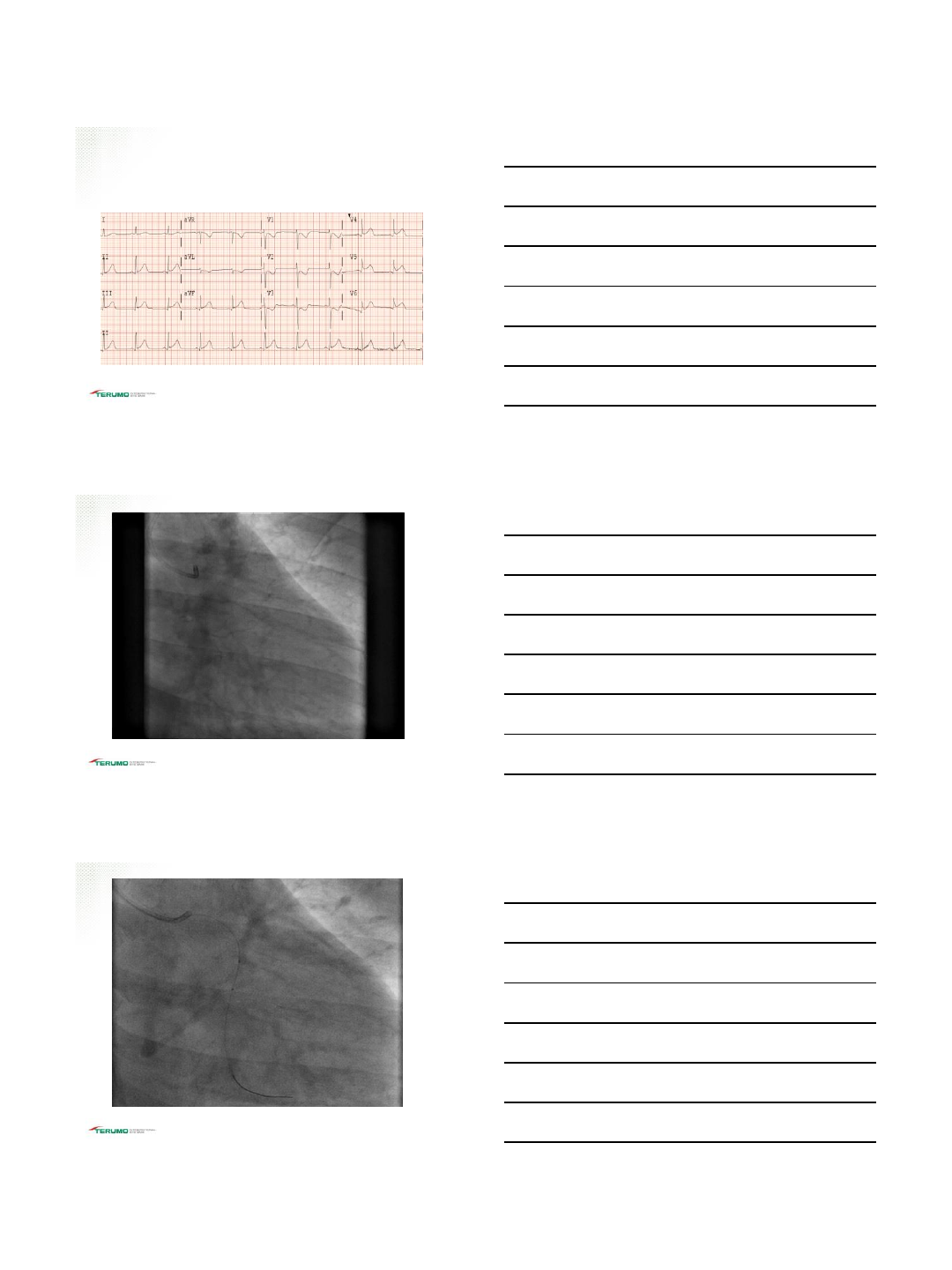
ASPIRATION
THROMBECTOMY
TIS-255-04082016
TIS-255-04082016
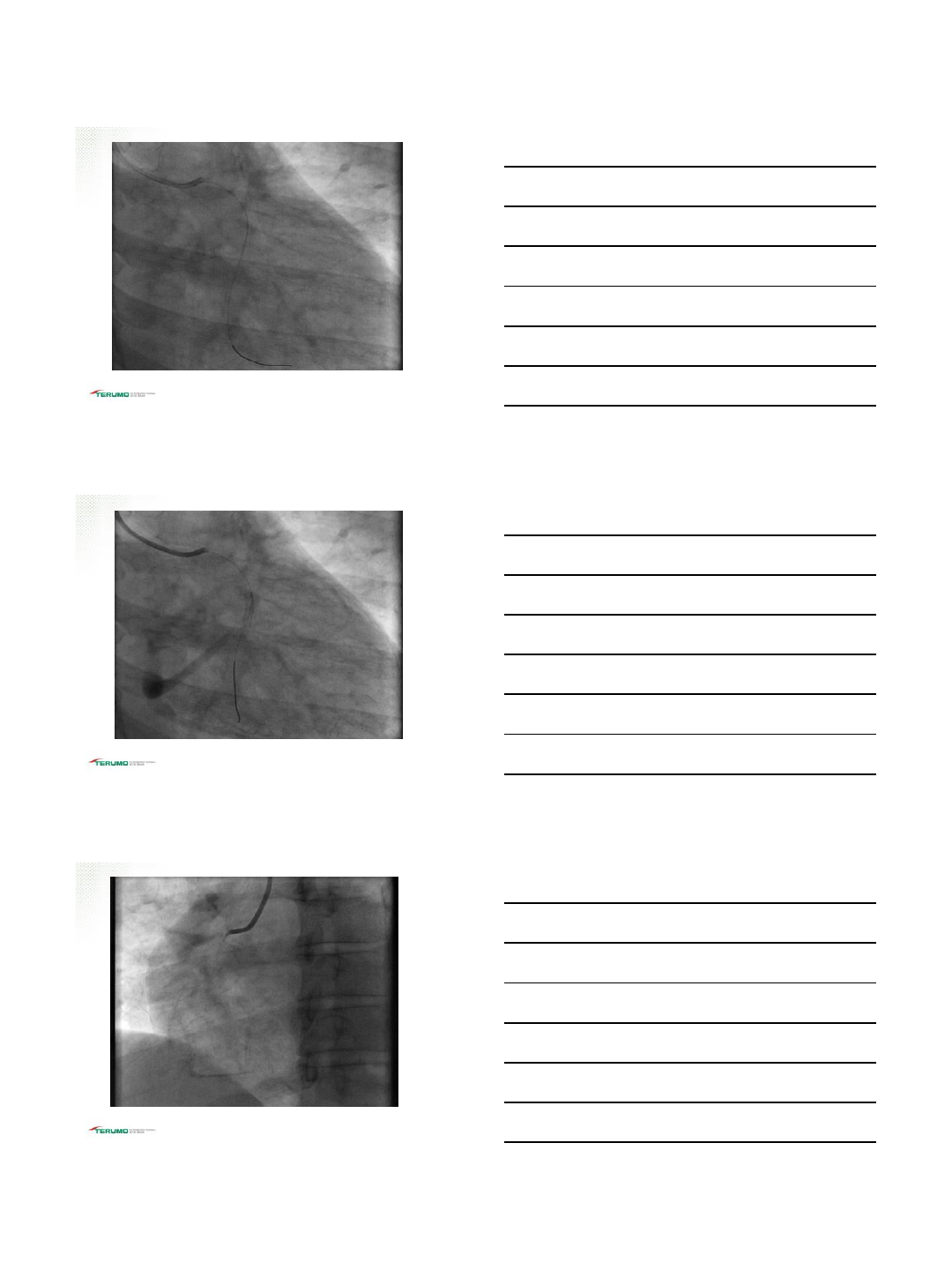
EXTRA SUPPORT
WITH 6F
GUIDELINER
TIS-255-04082016
4/10/2016
10
TIS-255-04082016
POLLING QUESTION
Which is the strongest independent predictor for radial
artery spasm?
A. Female gender
B. Diabetes
C. Hypertension
D. Small radial artery diameter
E. Unsuccessful access at first attempt
TIS-255-04082016
Answer
D. Small radial artery diameter
TIS-255-04082016
4/10/2016
11
CASE 2
48 y/o Hispanic female with a h/o Diabetes mellitus,
HTN, and HLD developed shortness of breath and
crushing chest pain after dinner. Troponin 0.20
TIS-255-04082016
IKARI 3.5 L
GUIDE,
RUNTHROUGH®
NS Coronary
Guidewire
TIS-255-04082016
TIS-255-04082016
4/10/2016
12
TIS-255-04082016
DES 3.0X16
TIS-255-04082016
IKARI 3.5 L GUIDE
TIS-255-04082016
4/10/2016
13
IKARI 3.5 L
GUIDE
RUNTHROUGH®
NS Coronary
Guidewire
PRIMARY
STENTING
DES 2.5 X12
TIS-255-04082016
3.0 X10 NC POST
DILATION
TIS-255-04082016
TIS-255-04082016
4/10/2016
14
POLLING QUESTION
Which of the following is a predictor of RAO ( Radial
arterial occlusion)?
A. Female gender
B. Length of procedure
C. Lack of blood flow during compression D. Insufficient
anticoagulation
E. Ratio of artery diameter/ diameter of sheath < 1
F. All of the above
TIS-255-04082016
Answer
F. All of the above
TIS-255-04082016
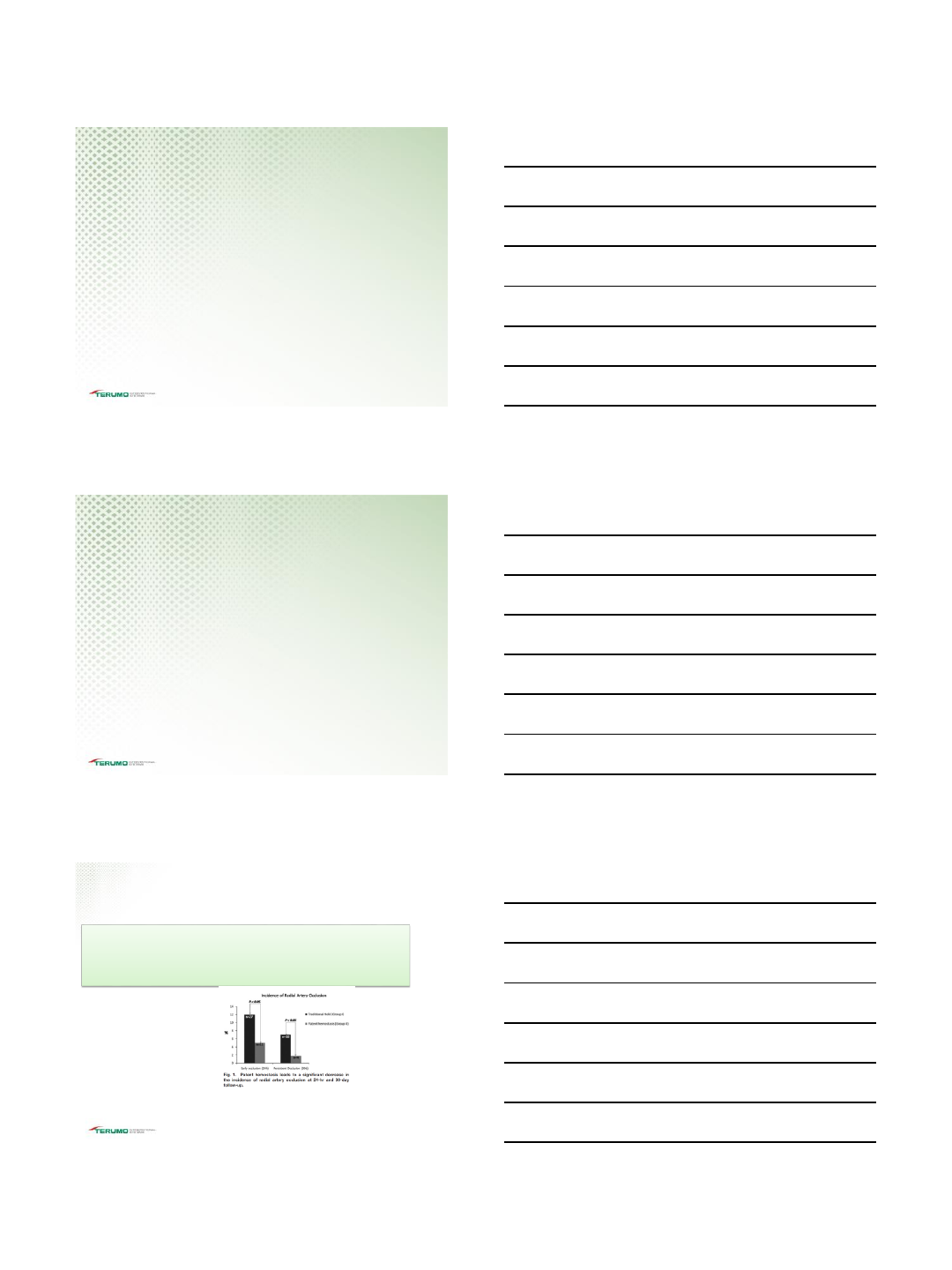
Radial Artery Occlusion (RAO)
Remaining Challenges and Opportunities for
Improvement in Percutaneous Transradial Coronary
Procedures
Key Points:
•The authors grouped strategies aimed at minimizing the risk of arterial occlusion into three
categories: Proven to Reduce Risk, May Reduce Risk, or Not Shown to Reduce Risk.
• The Four “Proven to Reduce Risk” strategies were:
Adequate
Anticoagulation Patent
Hemostasis Smaller Diameter
Arterial Sheaths
Minimizing the
times that the artery
is accessed
Rao SV, Bernat I, Bertrand OF. Eur Heart J. 2012 Oct; 33(20)2521-6
TIS-255-04082016
4/10/2016
15
Complications
While rare, complications
from Transradial Access
can occur.
TIS-255-04082016
RAO Dosing Considerations
•The current Society for Cardiac Angiography and Interventions best
practice guidelines suggest a heparin dose of 50 units/kg (up to a 5,000-
unit maximum dose) for a radial diagnostic procedure.
•Prophet Study used anticoagulation protocol of 50 units/kg to a maximum
dose of 5000 Units
Rao SV, Tremmel JA, Gilchrist IC, et al. Best practices for transradial angiography and intervention: a consensus statement from the society for cardiovascular
angiography and intervention’s transradial working group. Catheter Cardiovasc Interv. 2014;83:228-236
Pancholy S, Coppola J, Patel T, Roke-Thomas M. Comment in Catheter Cardiovasc Interv. 2008 Sep 1;72(3):341-2
TIS-255-04082016
GLIDESHEATH®SLENDER™
Introducer Sheaths
The smallest 6 Fr sheath on the market
Take advantage of compatibility with 6 Fr devices
Perform diagnostic and interventional procedures
without upsizing to a larger sheath
Incorporates Terumo Glide Technology™ for ease
of insertion and removal
Equivalent
Diameter
6 Fr
6 Fr Sheath 5 Fr Sheath
Equivalent
Lumen
6 Fr Glidesheath Slender is compatible with 6 Fr guiding catheter
while maintaining outer diameter of current 5 Fr sheath
©2014 TERUMO MEDICAL CORPORATION
TIS-255-04082016
4/10/2016
16
Catheter Selection & Manipulation
TIS-255-04082016
Radial Hemostasis
TIS-255-04082016
Radial Hemostasis
Prevention of Radial Artery Occlusion –Patent
Hemostasis Evaluation Trial (PROPHET Study)
A Randomized Comparison of Traditional Versus Patency
Documented Hemostasis after Transradial Catheterization
Pancholy S, et al Catheterization and Cardiovascular Interventions 72:335-340 2008
Conclusion
Patent hemostasis is successful
in significantly lowering the
incidence of radial artery
occlusion after TRA, without
compromising hemostatic efficacy
TIS-255-04082016
4/10/2016
17
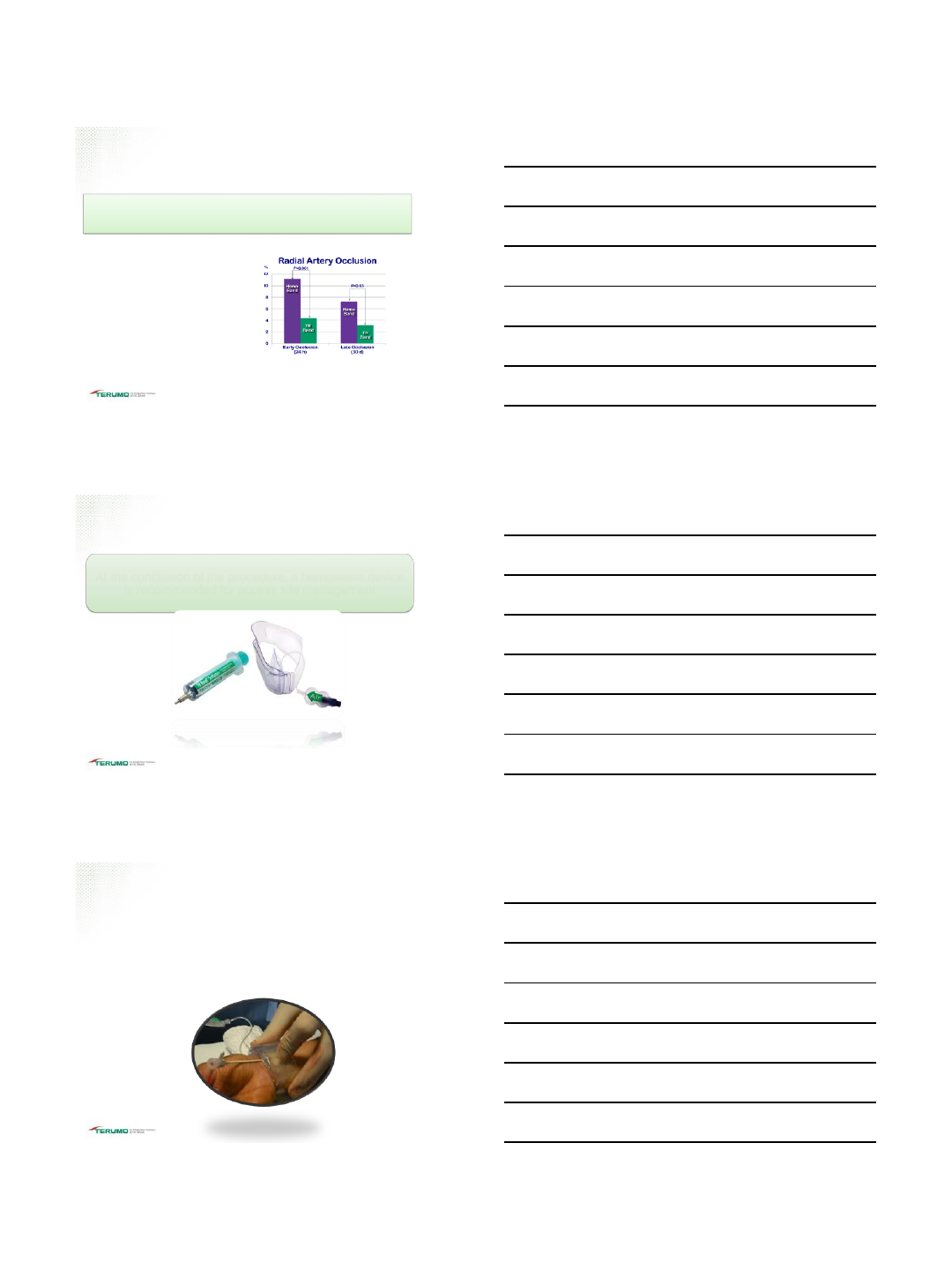
Radial Hemostasis
Conclusion
•TR BAND®Radial Compression
Device provides equivalent
hemostatic efficacy and a lower
incidence of radial artery occlusion
after transradial catheterization
compared to the HemoBand.
•A device with a lower incidence of
this complication is desirable over
other available choices.
Impact of Two Different Hemostatic Devices on Radial
Artery Outcomes after Transradial Catheterization
Pancholy S. J Inv asive Cardiol 2009 Mar;21(3):101-4
TIS-255-04082016
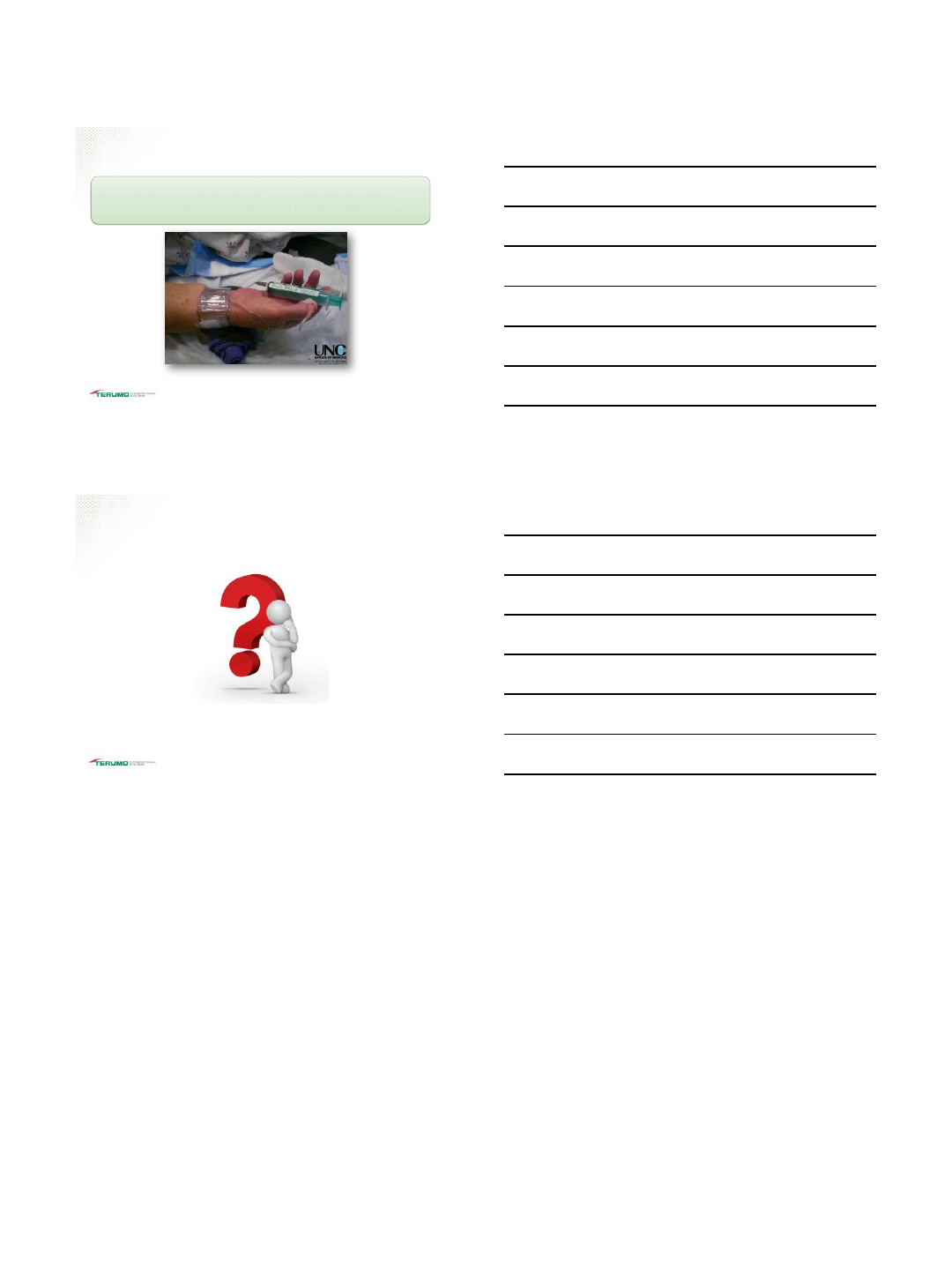
Radial Hemostasis
At the conclusion of the procedure, a hemostasis device
is recommended for access site management
TIS-255-04082016
•Important to understand the “Patent” hemostasis technique.
•Close attention to placement of the TR BAND®Radial
Compression Device
•Monitor duration of compression
©2014 TERUMO MEDICAL CORPORATION
Radial Hemostasis
TIS-255-04082016
4/10/2016
18
Radial Hemostasis
Once hemostasis is achieved transport the patient with the inflation
syringe attached either to the patients chart or taped to the patient.
TIS-255-04082016
Thank you! Questions?
TIS-255-04082016
