Bone Loss In Shoulder Arthroplasty Syllabus
2015-02-17
: Pdf Bone Loss In Shoulder Arthroplasty Syllabus Bone_Loss_in_Shoulder_Arthroplasty_Syllabus 2 2015 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 54
1
Carl J. Basamania, MD, FACS
The PolyClinic and
Swedish Orthopaedic Institute
Seattle, Washington
B2 Glenoid Bone Loss and
Shoulder Arthroplasty:
Bone Grafts and Augmented
Glenoid Components
Presenter Disclosure Information
B2 Glenoid Bone Loss and Shoulder Arthroplasty:
Bone Grafts and Augmented Glenoid Components
Carl J. Basamania, MD, FACS
Disclosure Information
The following relationships exist:
DePuy/Johnson and Johnson: Consultant, Royalties
Biomet: Consultant, Royalties
Sonoma Orthopaedics: Consultant, Royalties
Invuity: Consultant, Stock Options
BioPoly: Consultant, Stock Options
Nothing of value received for this presentation
No “off label” use of any products
Glenoid Bone Loss in Osteoarthritis
•OA is the most common indication for TSA
•At least 75% of patients have some
posterior bone loss resulting in increased
glenoid retroversion
•In patients with severe OA, mean glenoid
version of 11° retroversion (range 2°
anteversion to 32° retroversion)
•Freidman, et al, JBJS, 1997
2
General Rules
•Bone loss must be addressed
•Glenoid rim erosion encompassing greater
than 25% to 30% of the articular surface
requires grafting
•Correct glenoid retroversion to < 10
degrees
–ideally < 6 degrees
Options for Management of
Posterior Glenoid Bone Loss in OA
•Ream the high side to correct version
•Use a bone graft to correct version
•Use a custom implant to correct version
•Reverse total shoulder arthroplasty
Place the humeral component in anatomic version
Problems with Eccentric Reaming
•The maximum amount of
retroversion that can be
corrected with eccentric
reaming is 15 degrees
–Warner, et al, JSES,
2007;16:843–848
•Medialization of joint line
•Cuff weakness
•Creates smaller glenoid
•Can result in significant
head/glenoid mismatch
3
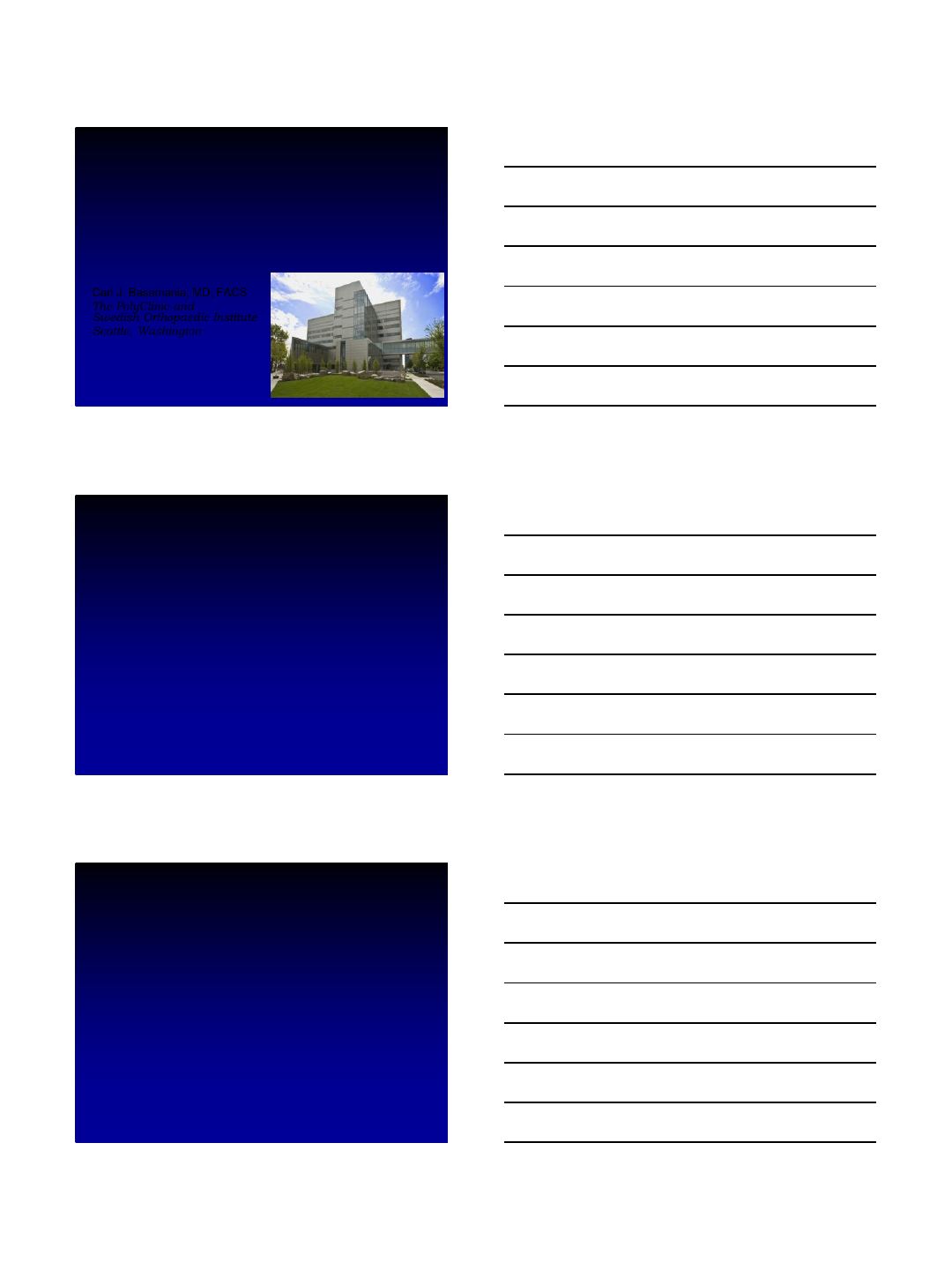
Glenoid with Posterior
Erosion
Bone
Graft
Bone Grafting
•Restores the
original glenoid
plane
•Malunion, non-
union, and
increased surgical
time
•10 fold higher
failure rate than
normal TSA
Cuomo, F., Checroun, A. “Avoiding Pitfalls and Complications in Total
Shoulder Arthroplasty. Orthop Clin North Am. 1998; 518.
Severe Glenoid Erosion
Use of a Bone Graft
•Greater than 1
cm.
•Bone graft
–Humeral head
–Iliac crest graft
•Screw fixation
•Avoid cement
wedges
4
5
Bone loss with Reverse TSA
•Bone loss
–Glenoid
•Reaming
•Cancellous grafting
Use of a RTSA
•Problems:
–In my experience, most of the posterior
erosion cases are in active males
–What do you do with a younger (<70) male
with an intact rotator cuff who wants to remain
as active as possible?
6
Can you use an augmented
glenoid?
Glenoid with
Posterior Erosion
Augmented Glenoid
•No medialization
•No implant
undersizing
•No need to bone
graft
•Re-establishes
normal joint line
•Returns cuff to
normal tension
Design Rationale
•Addresses posterior glenoid
erosion
–Walch Type B2
•Same peg fixation design as the
Anchor Peg Glenoid
–Central fluted interference fit peg
–Two inferior pegs
–One superior peg
•Novel instrumentation
–Accurate placement, orientation,
and precise bone preparation
7
13°
Design Rationale (cont.)
•Spherical anterior backside
•Conical posterior backside (13 degree
angle)
–Design effectively counteracts posterior
loading
Optimal Augmented Design
•Question:
–Is there an
optimal design
that counteracts
or minimizes the
deforming forces
on the glenoid
component?
Iannotti, et al, JSES, 2013, 22, 1530-1536
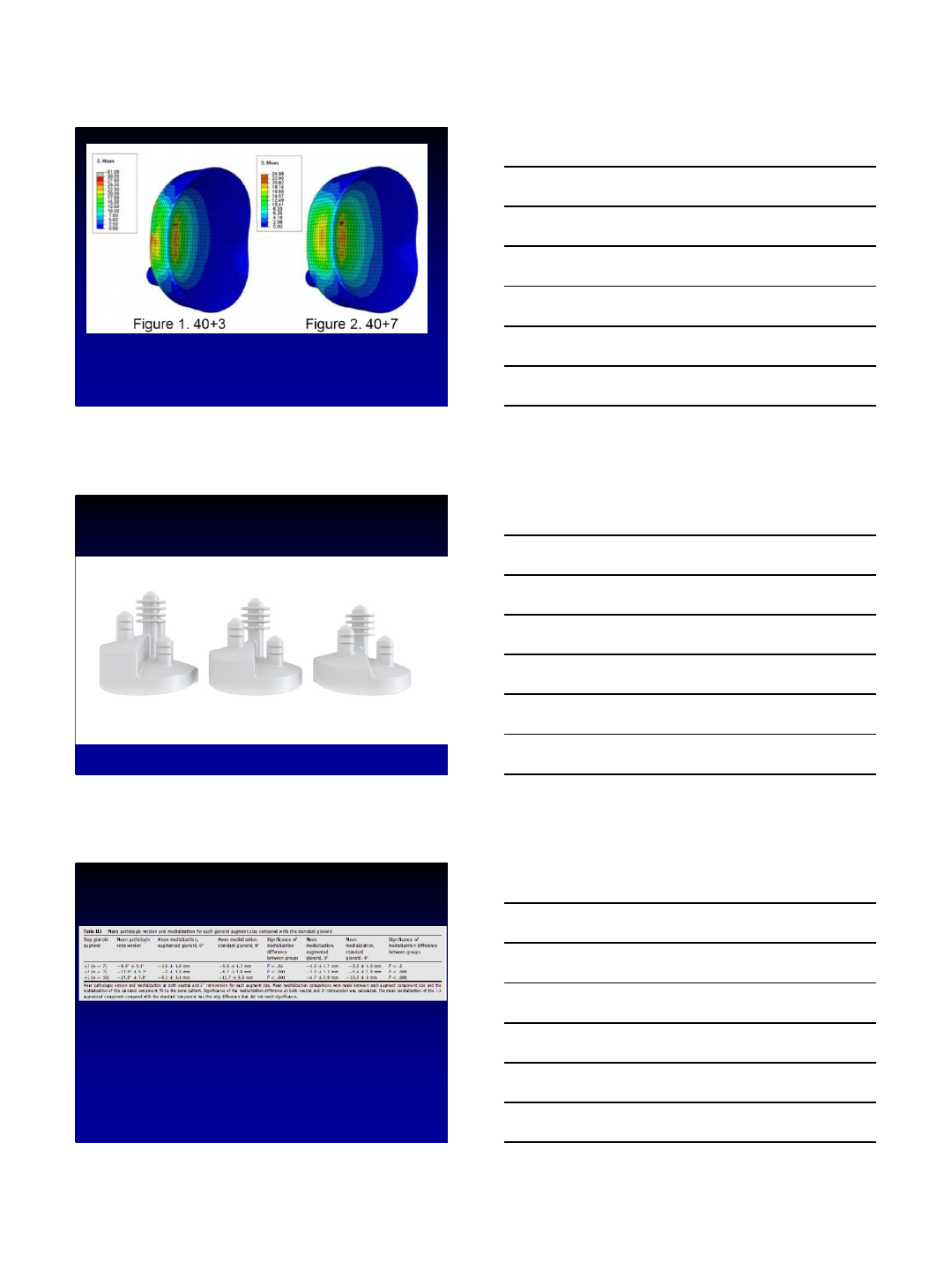
Optimal Augmented Design
• The “stepped”
design was the
only design that
showed no
increase in lift off of
the component
compared to a
standard glenoid
Iannotti, et al, JSES, 2013, 22, 1530-1536
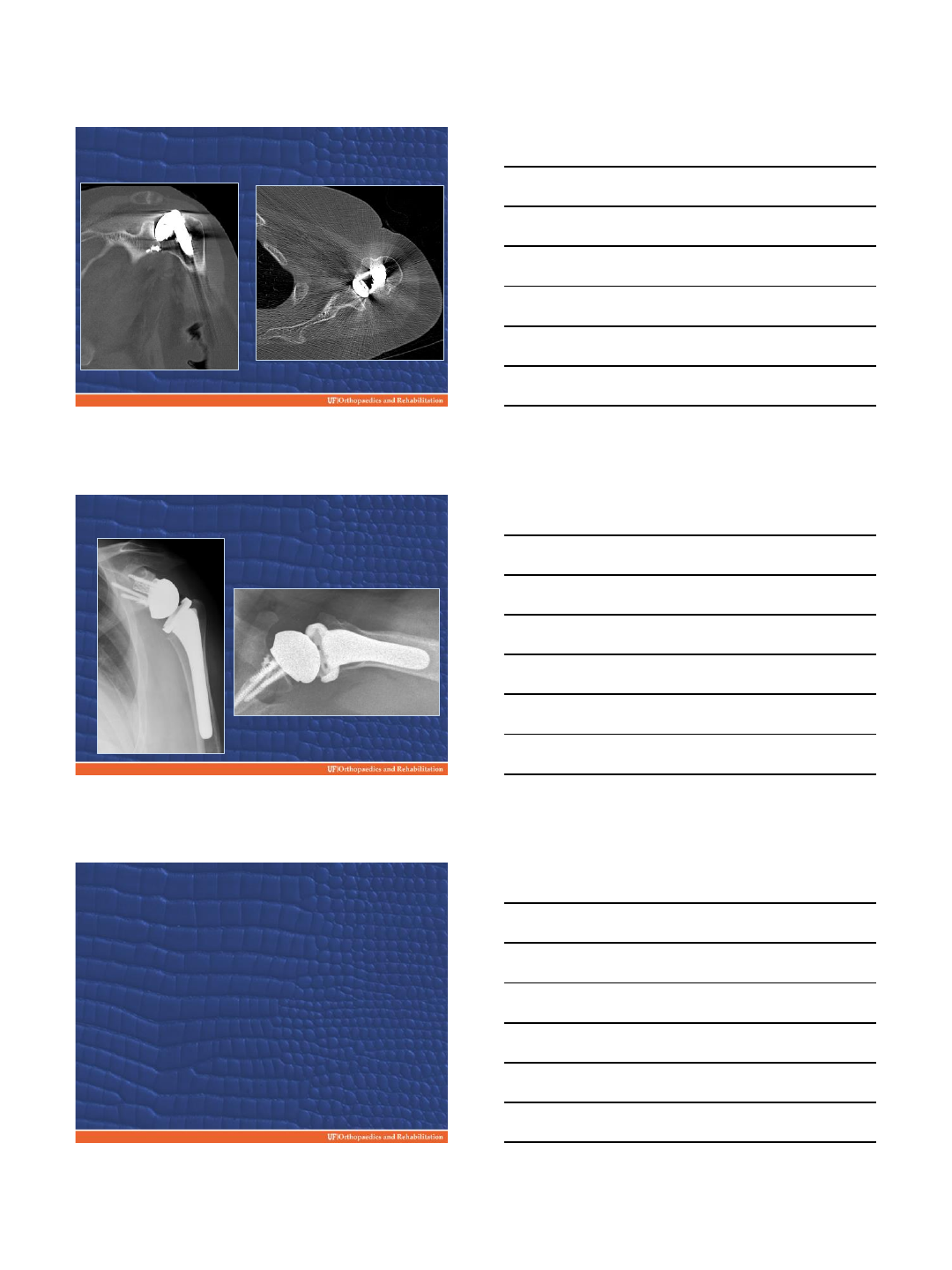
8
Size Range
+7mm +5mm +3mm
Amount of Possible Correction
Augmented glenoids allowed correction up to
27.9 degrees (±7.9 degrees) with no significant
medialization
Sabesan, et al, JSES, 2014, 23, 964-973
9
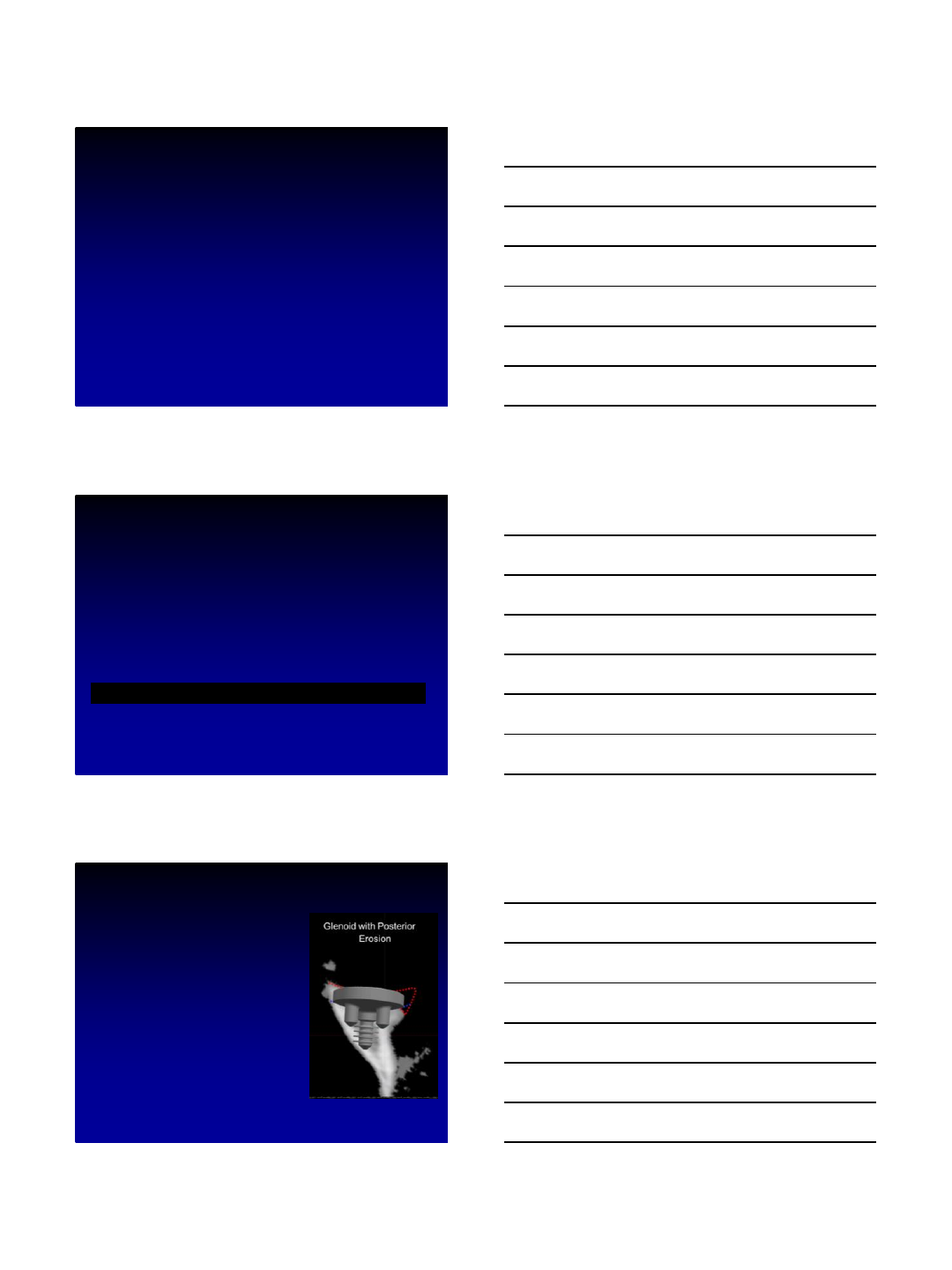
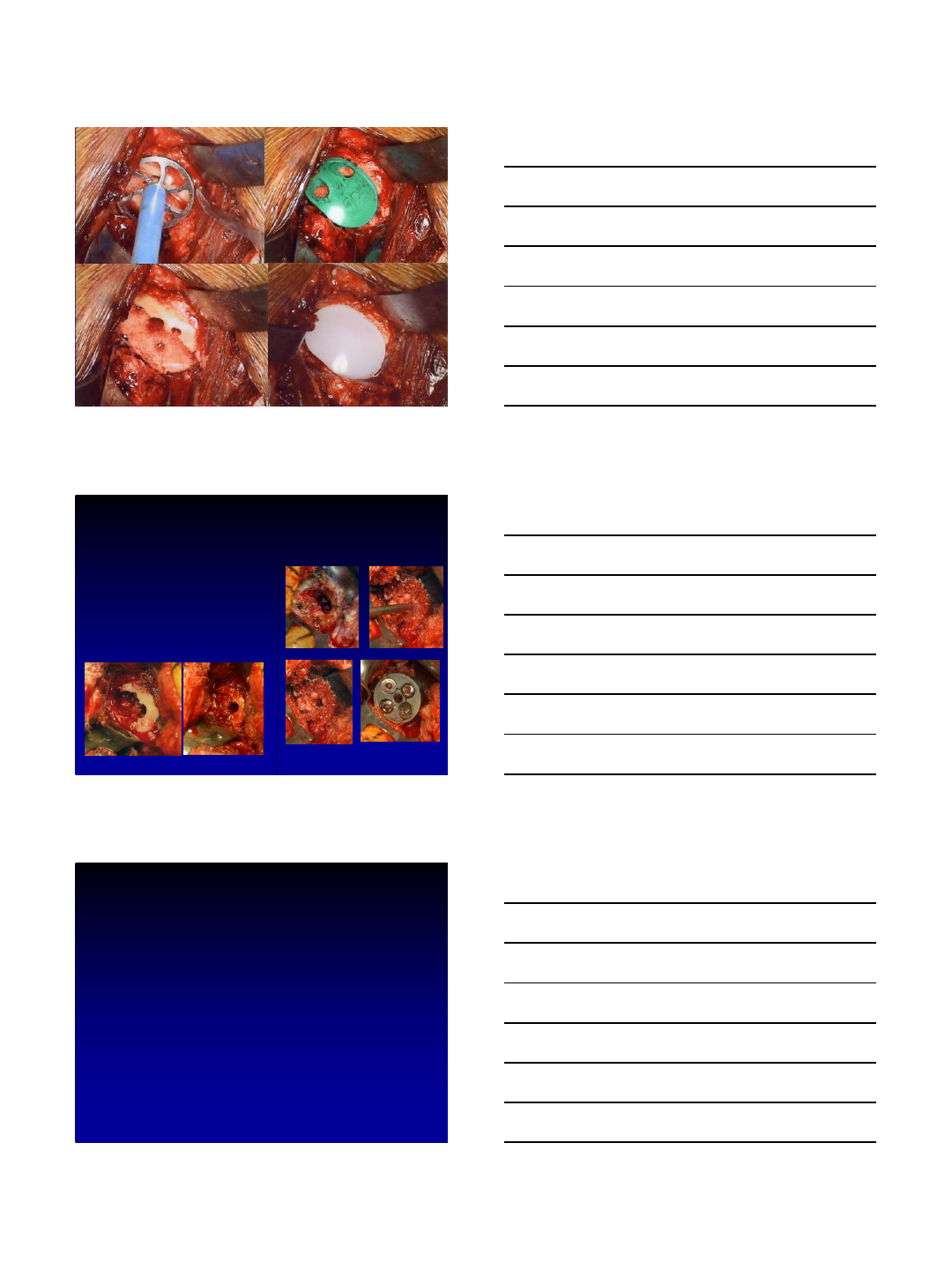
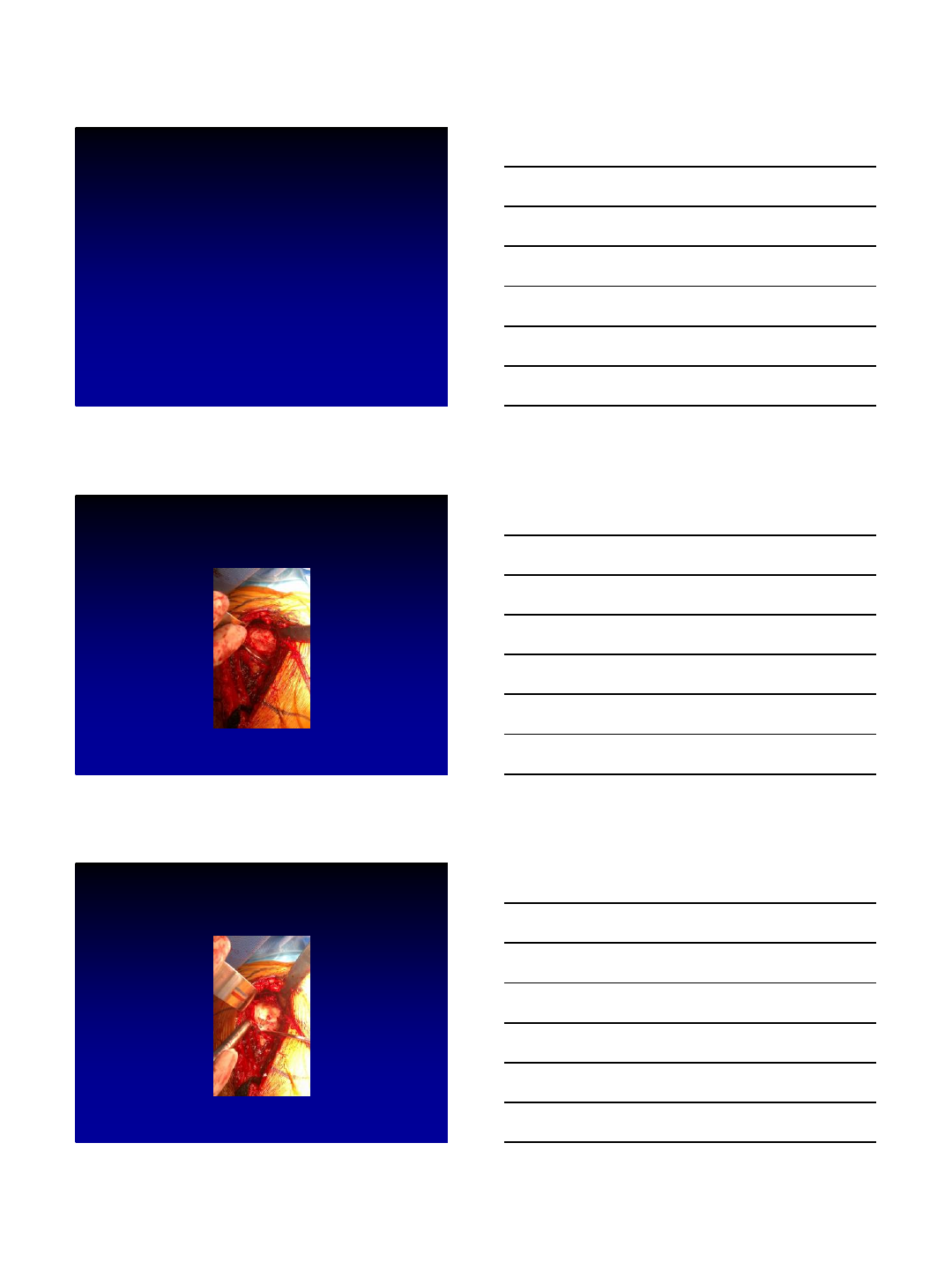
Surgical Technique
Glenoid Exposure
Walch B2
Anterior Reaming
10
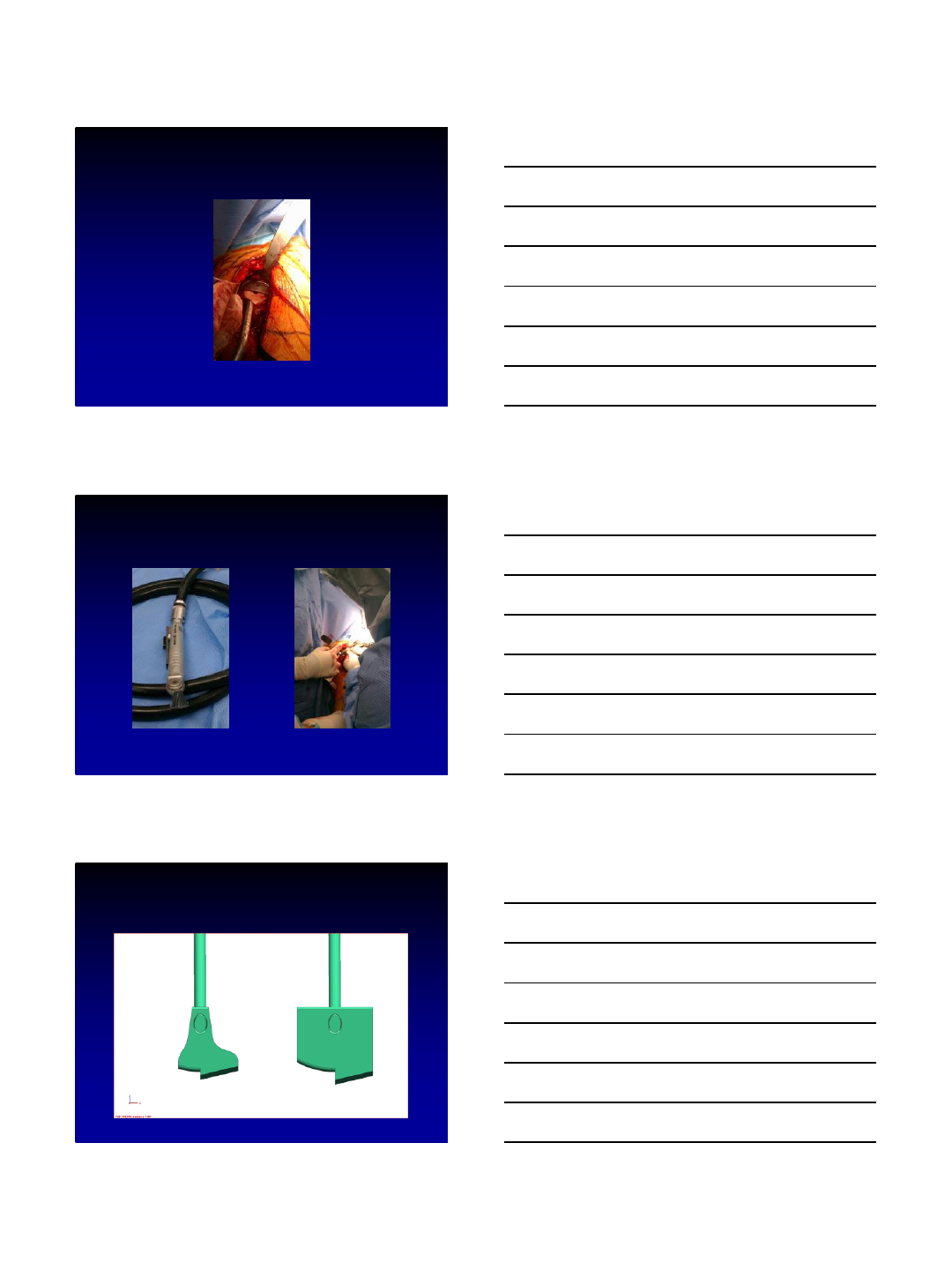
Posterior Guide
Oscillating Rasp
Glenoid “Hoes”
11
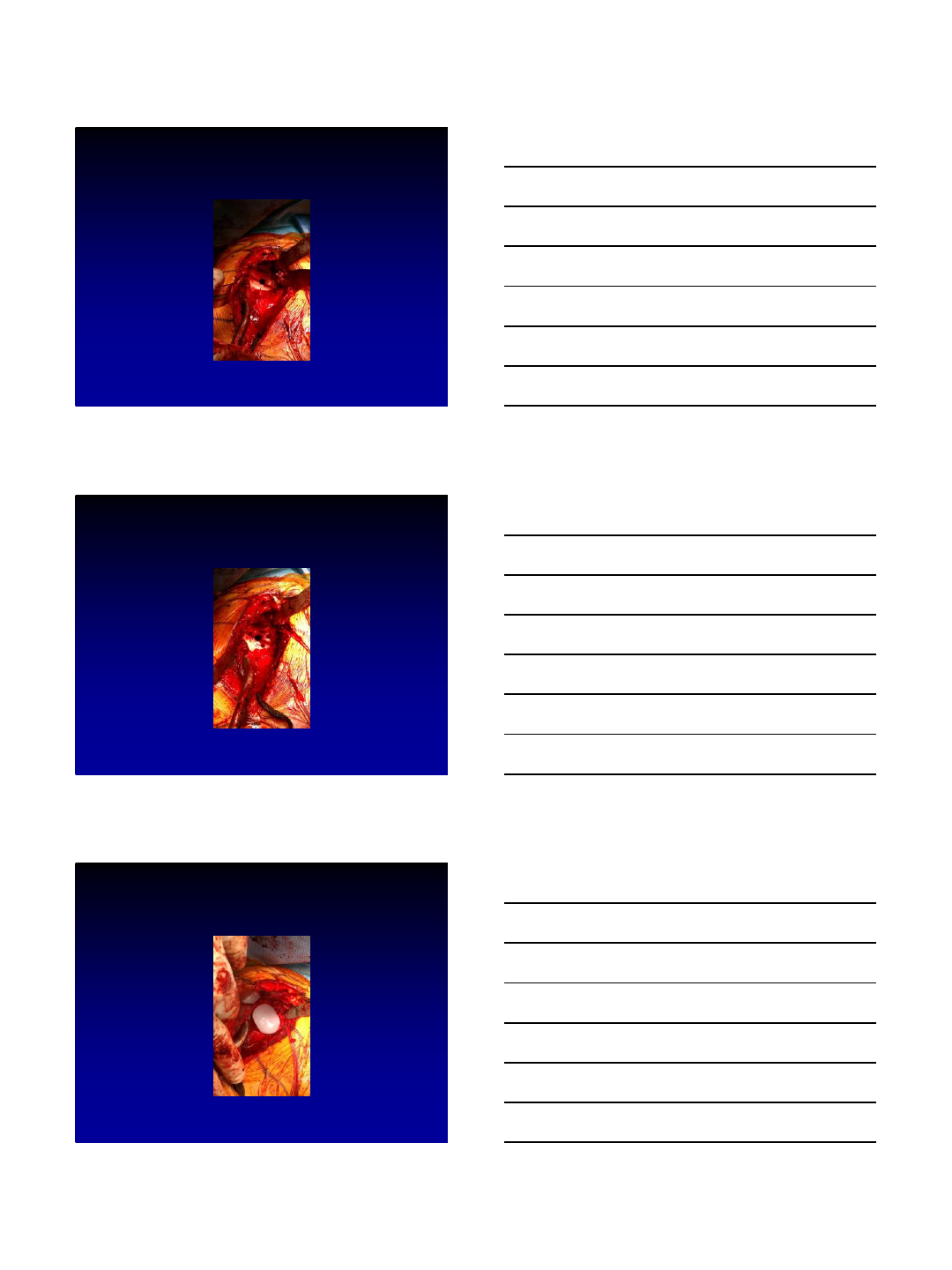
Posterior Step
Peripheral Drill Holes
Final Implant
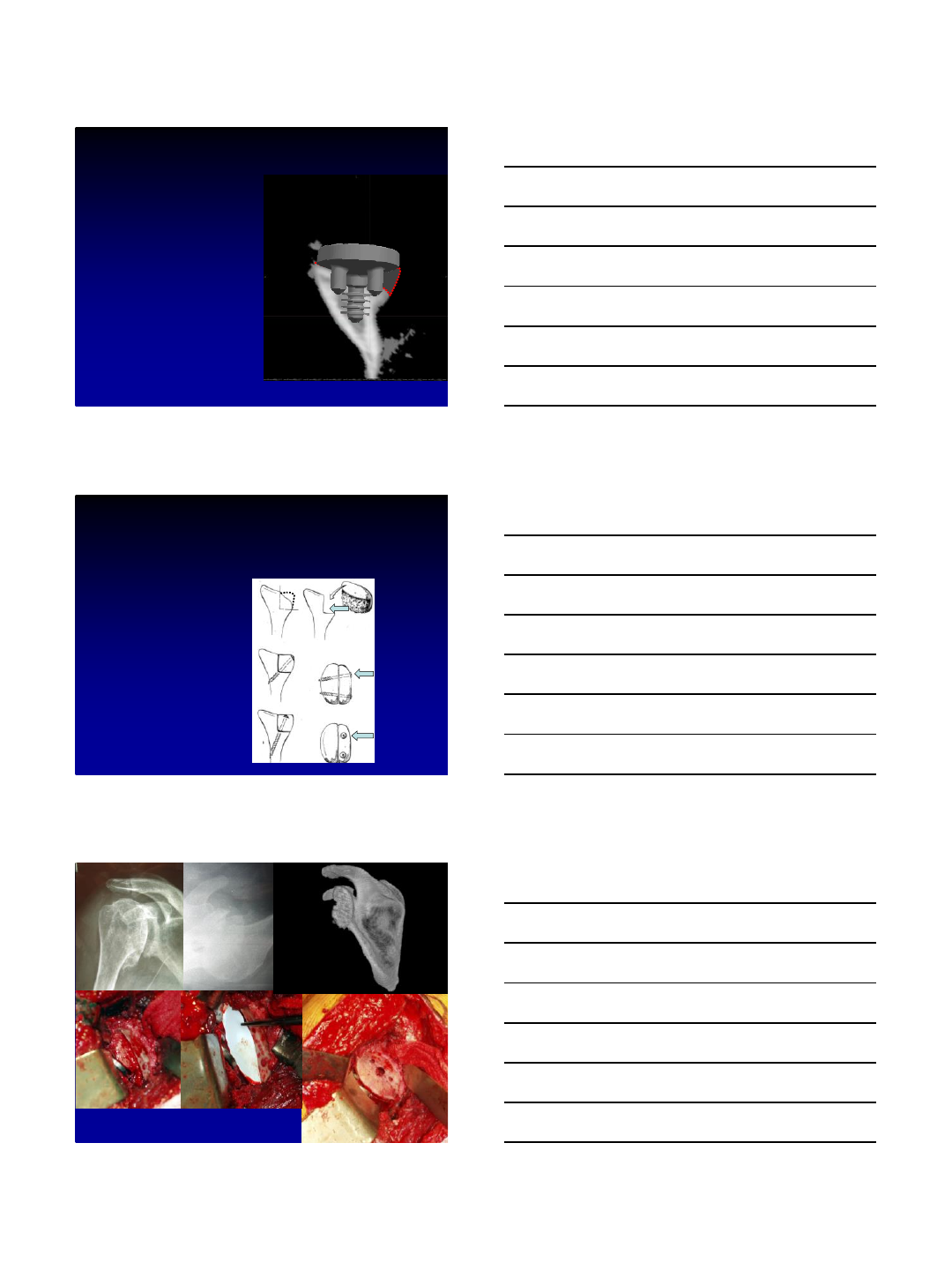
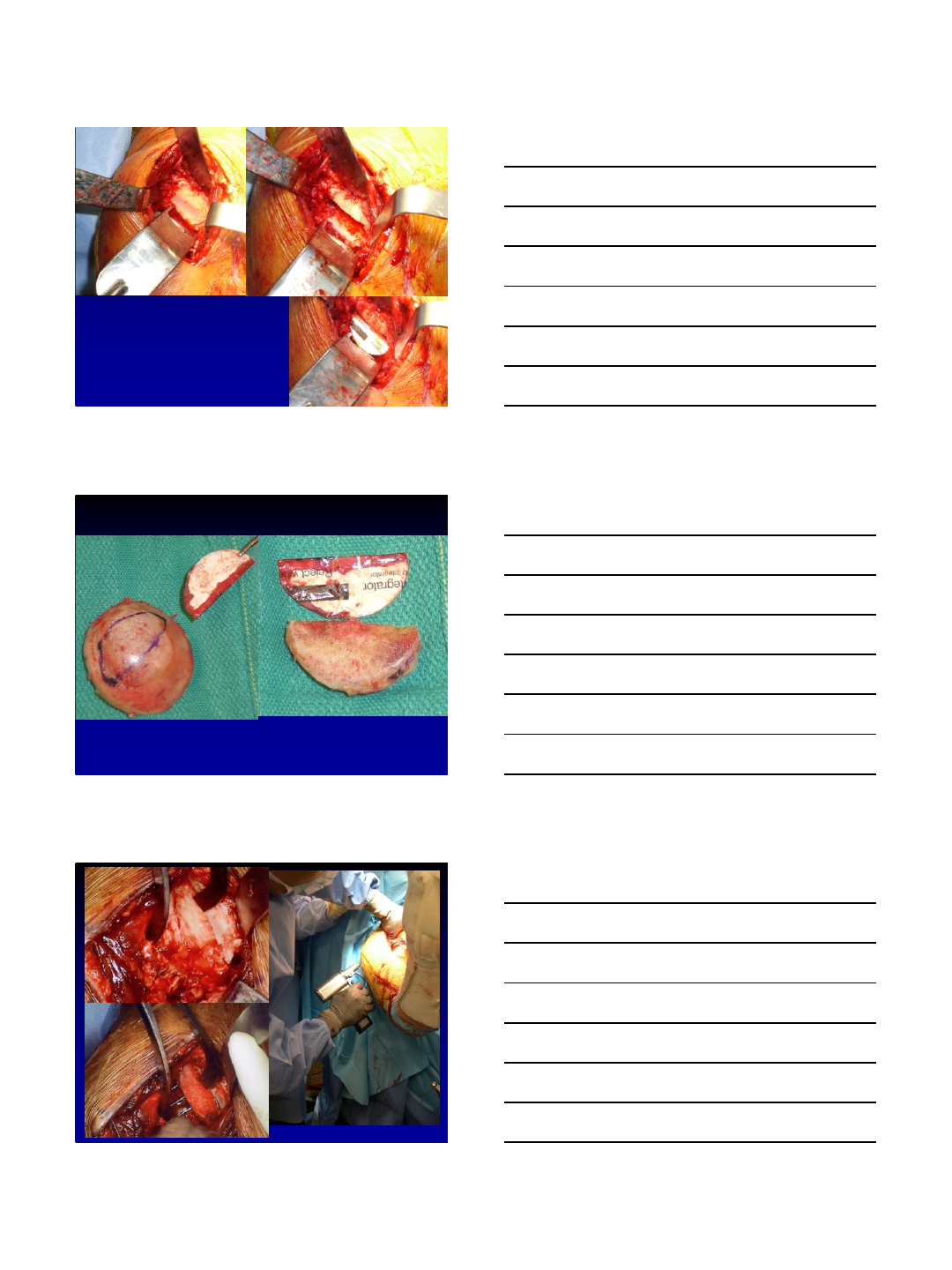
12
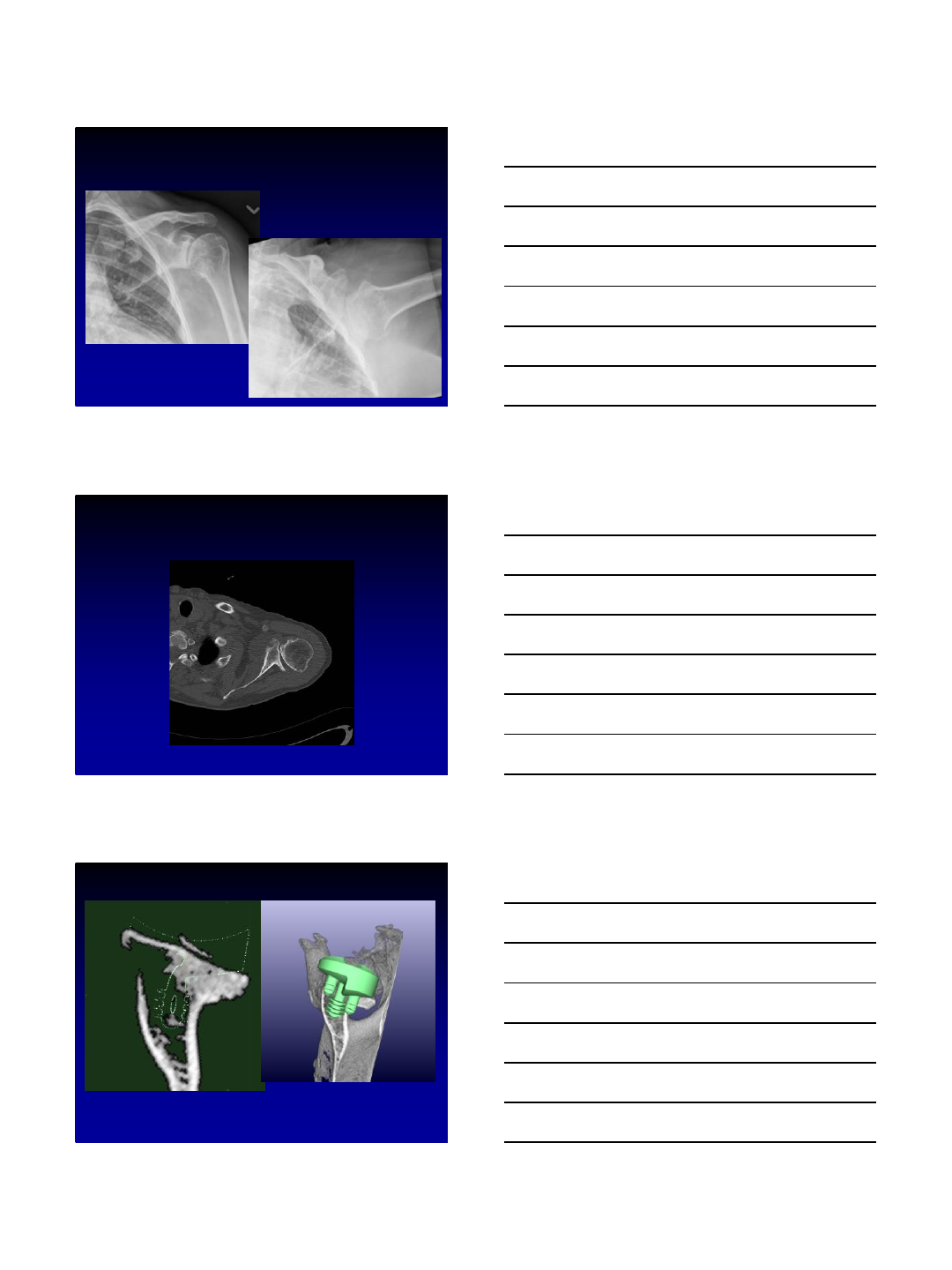
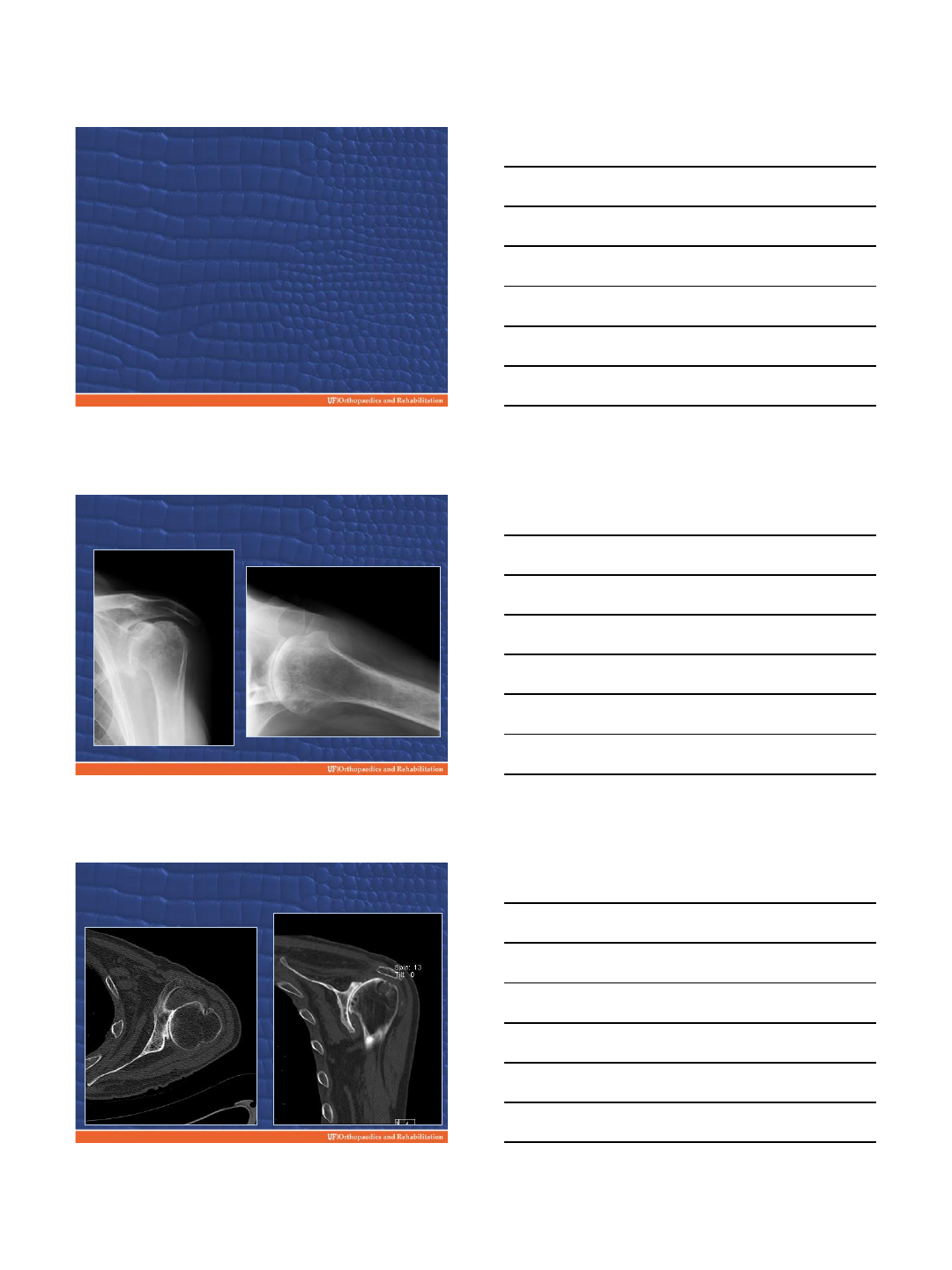
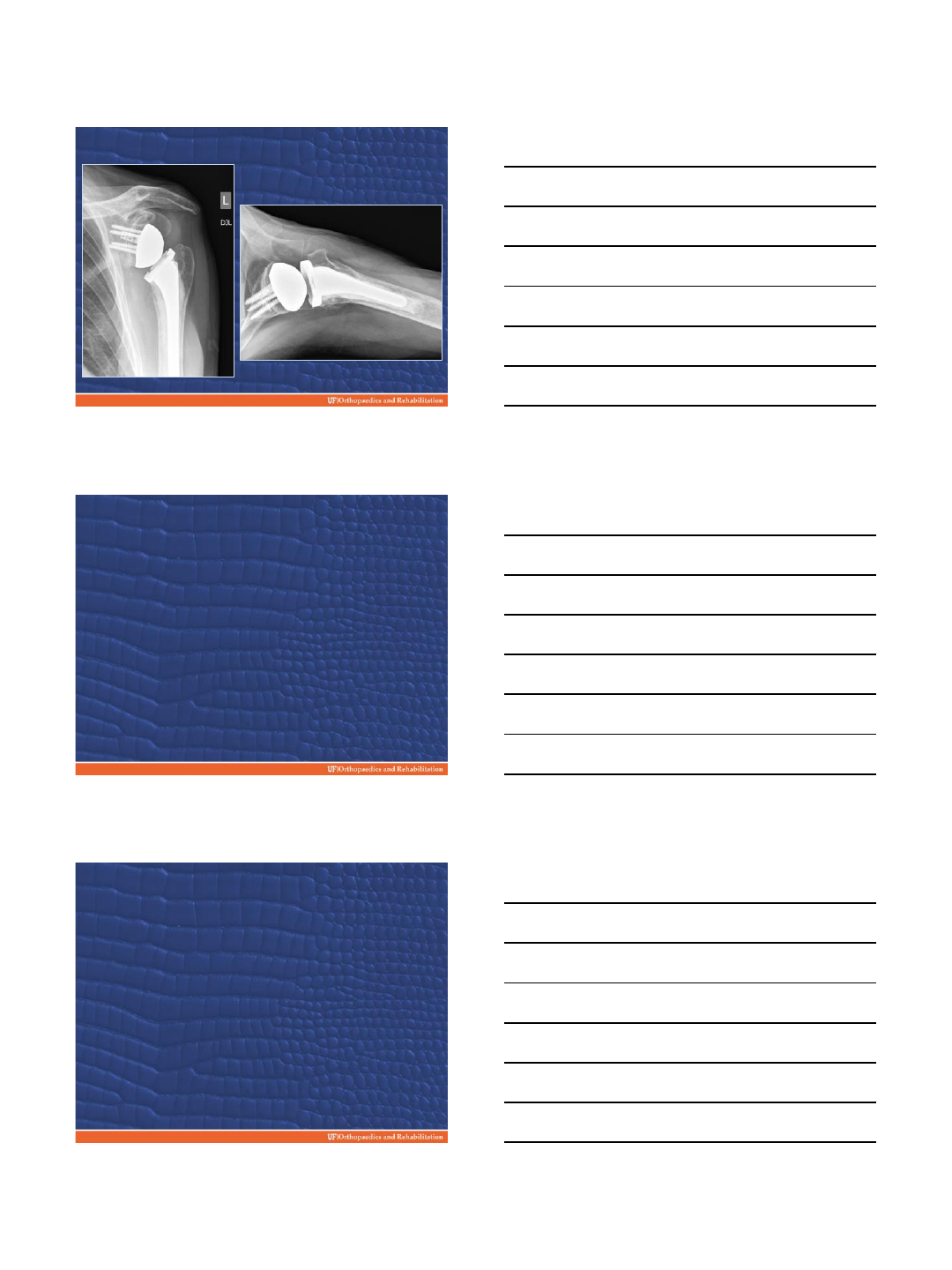
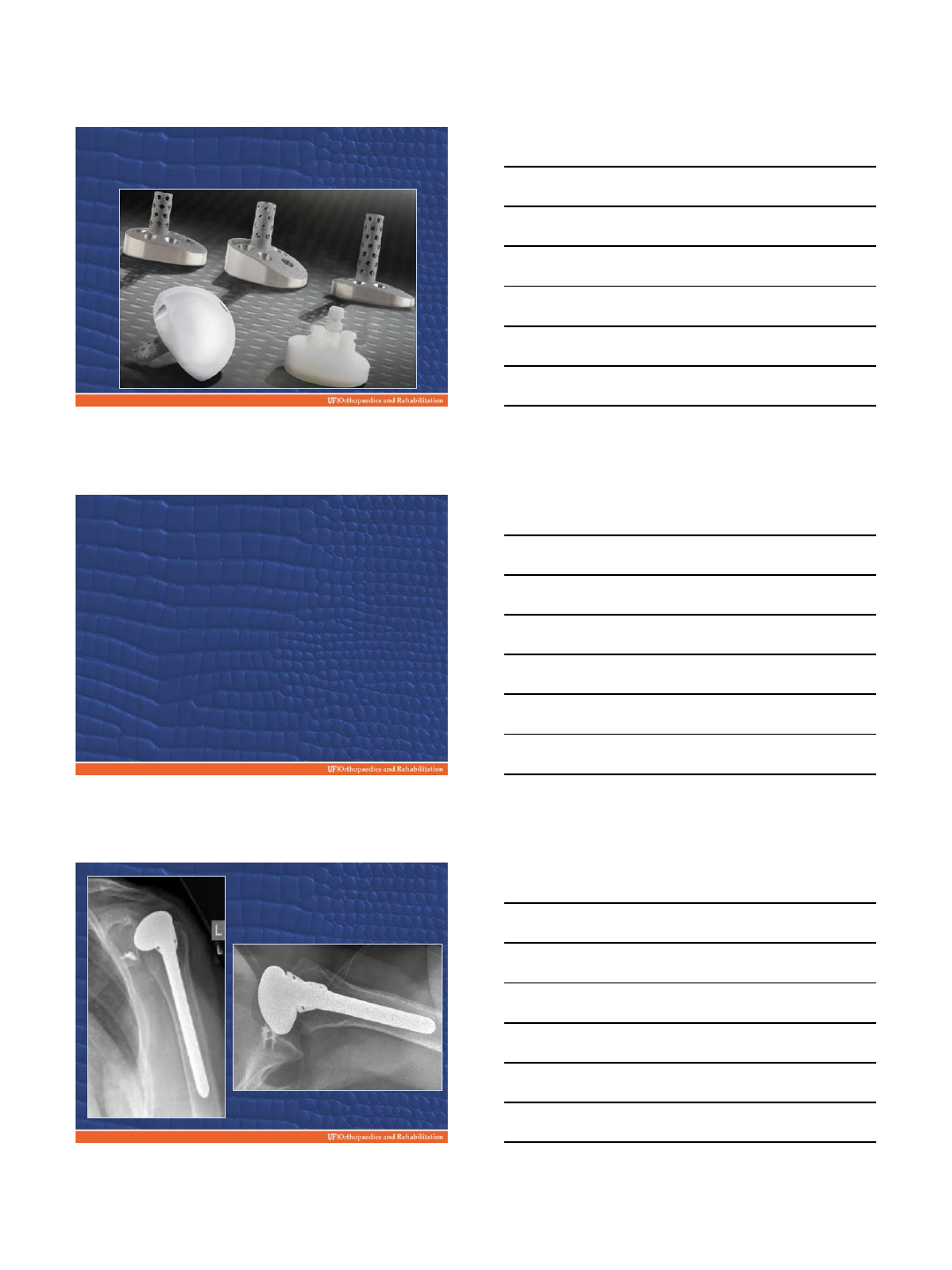
Case Example:
60 year old female
Posterior glenoid erosion
13
Thanks!
2/16/2015
1
HOW TO DEAL
WITH B2-B3 GLENOID ?
Vumedi Webinar Feb 17, 2015
Disclosure
- Royalties: TORNIER
- Equity: IMASCAP
- Board of the French
Orthopedic Society
J Arthroplasty 1999
2/16/2015
2
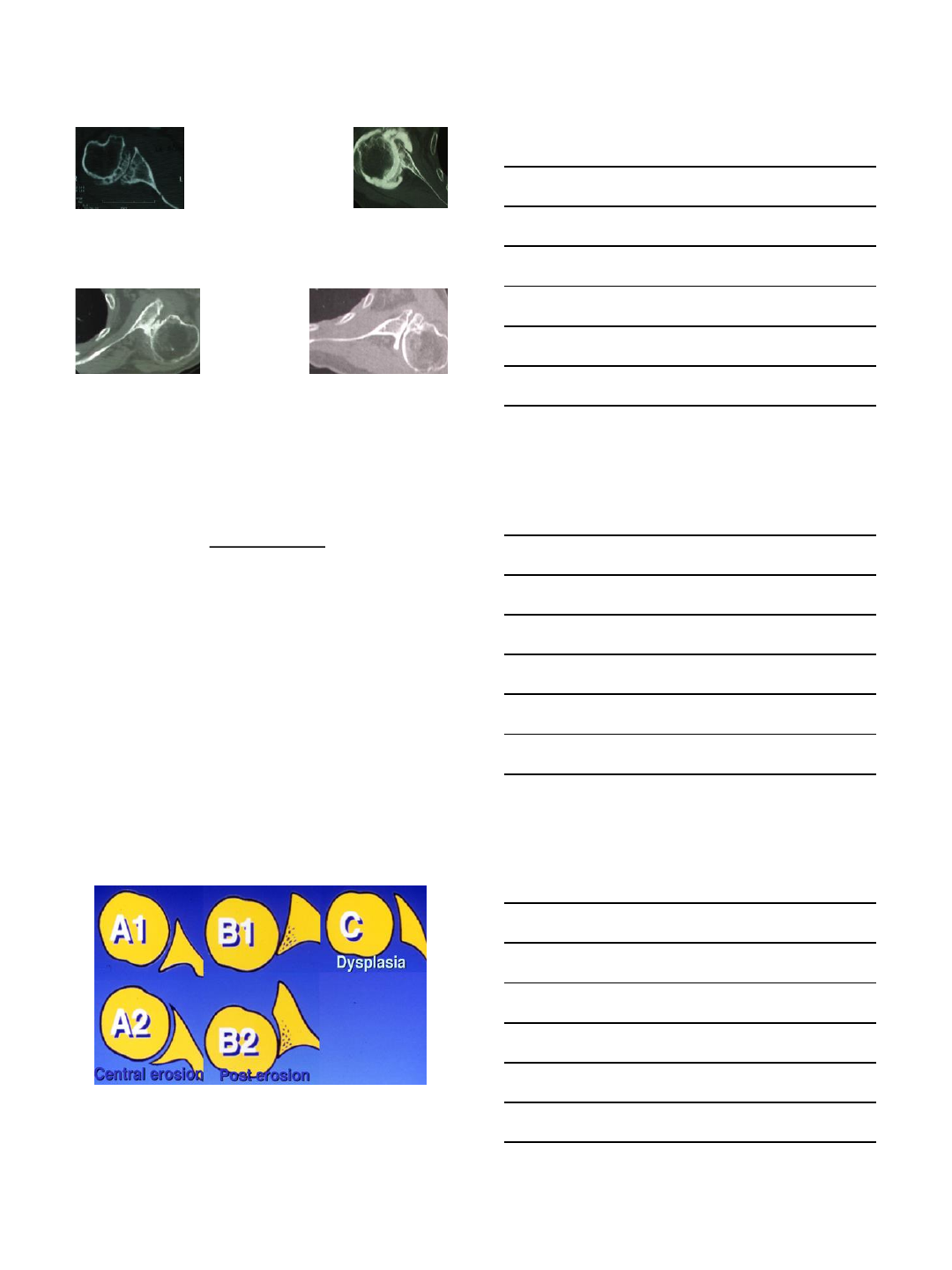
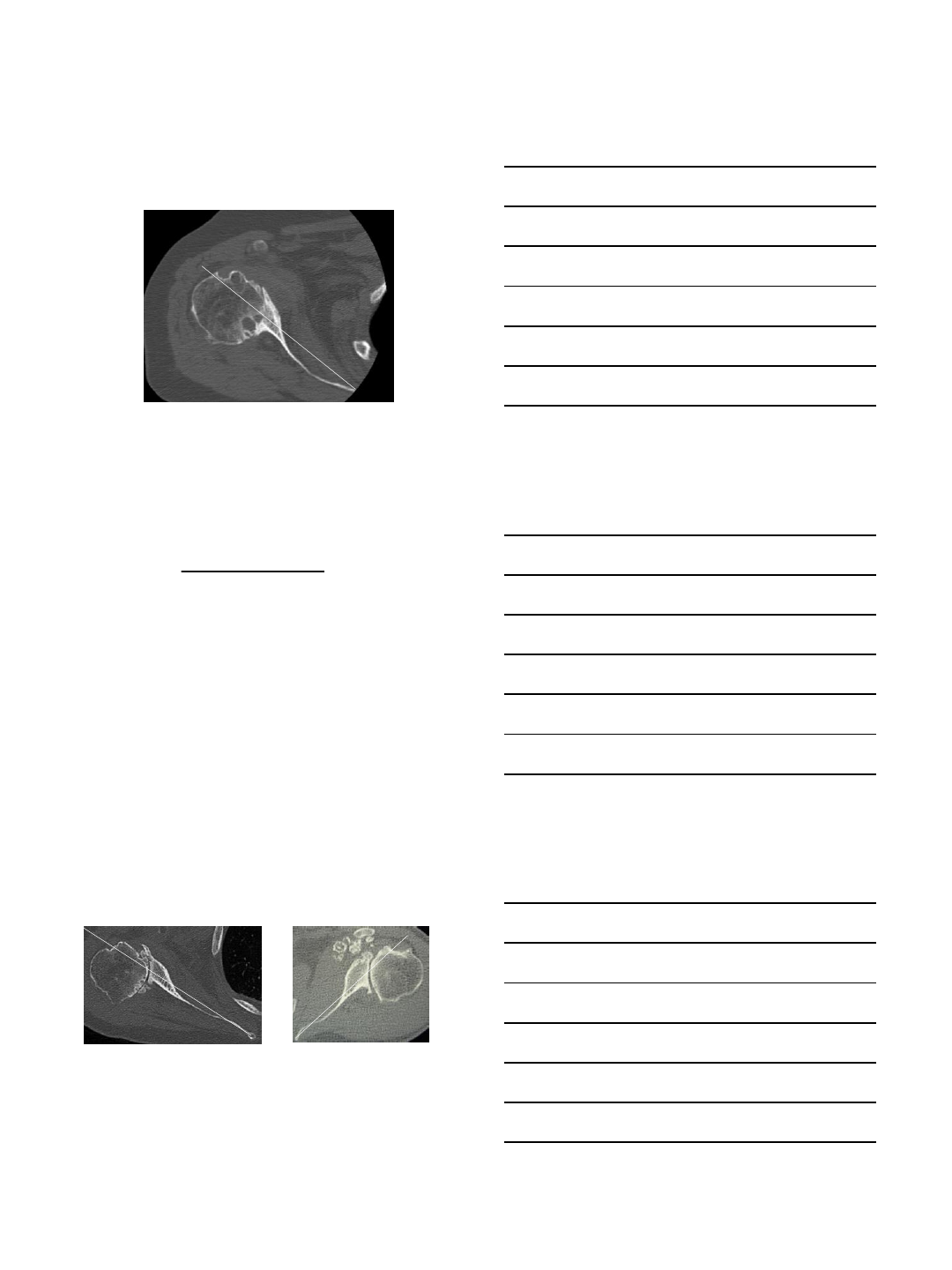
« This classification is not accurate & reliable »
(Scalise & Iannotti)
Pb with degree of retroversion
Type C (dysplasia) is > 25°
Type B2 (2ary erosion) can also be > 25°
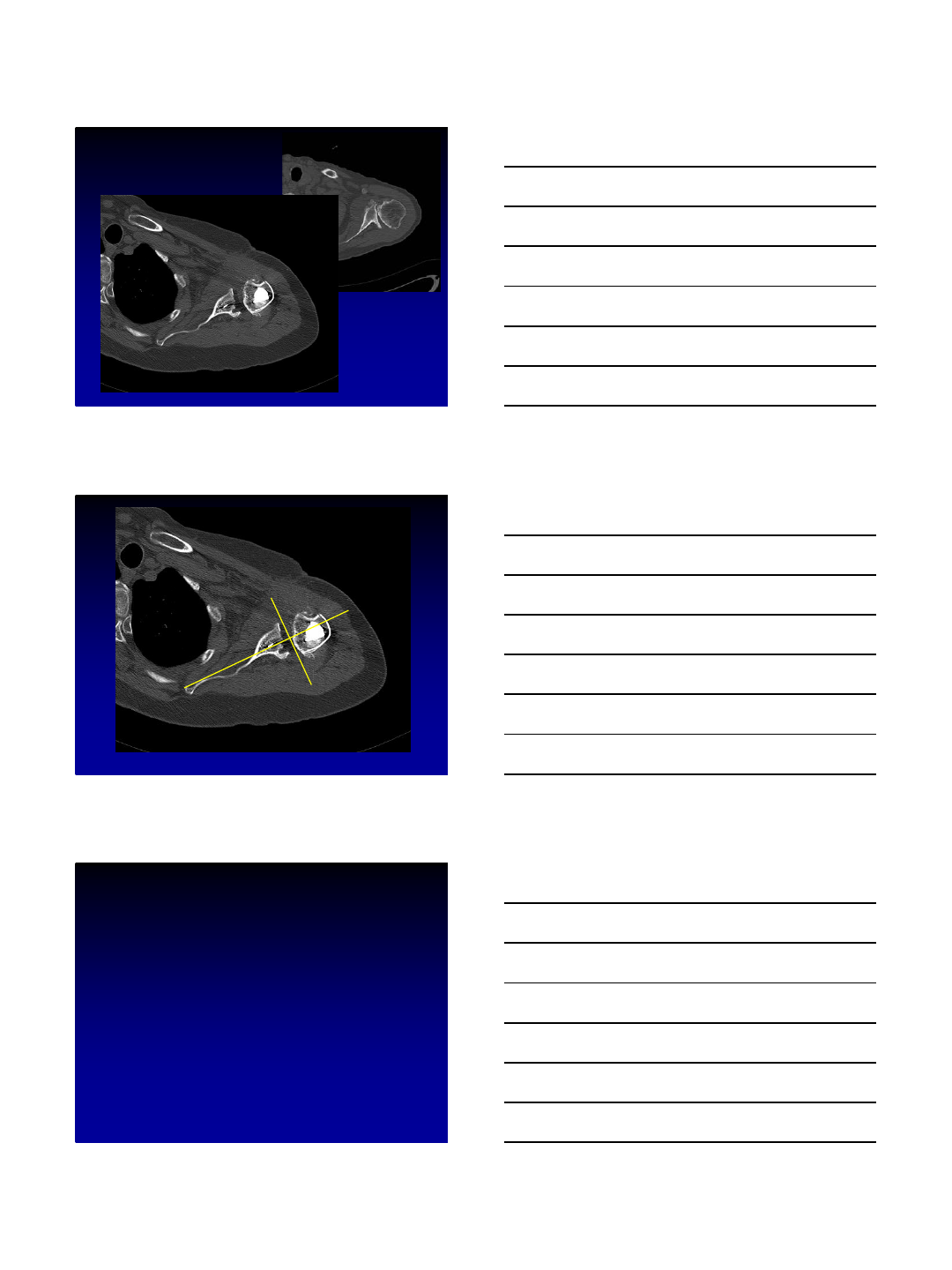
B2 glenoid is the consequence of
1/ static posterior subluxation of the HH
2/ secondary erosion of the posterior part of the glenoid
Need to have the proof of
secondary posterior wear
•see the paleo glenoid
• subluxation of the HH
( degrees of retroversion is not part of the diagnostic: 15 to 60
°
…)
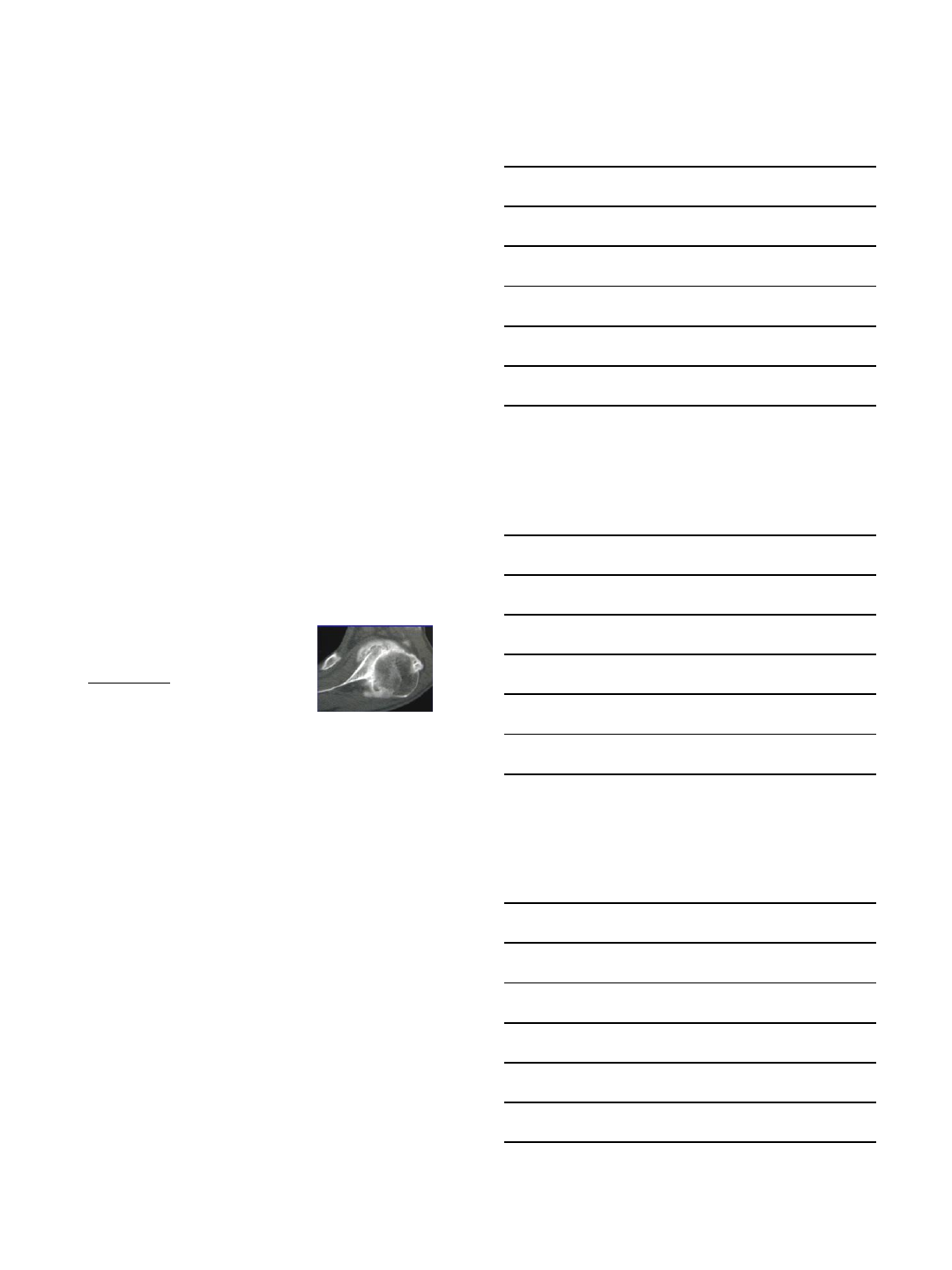
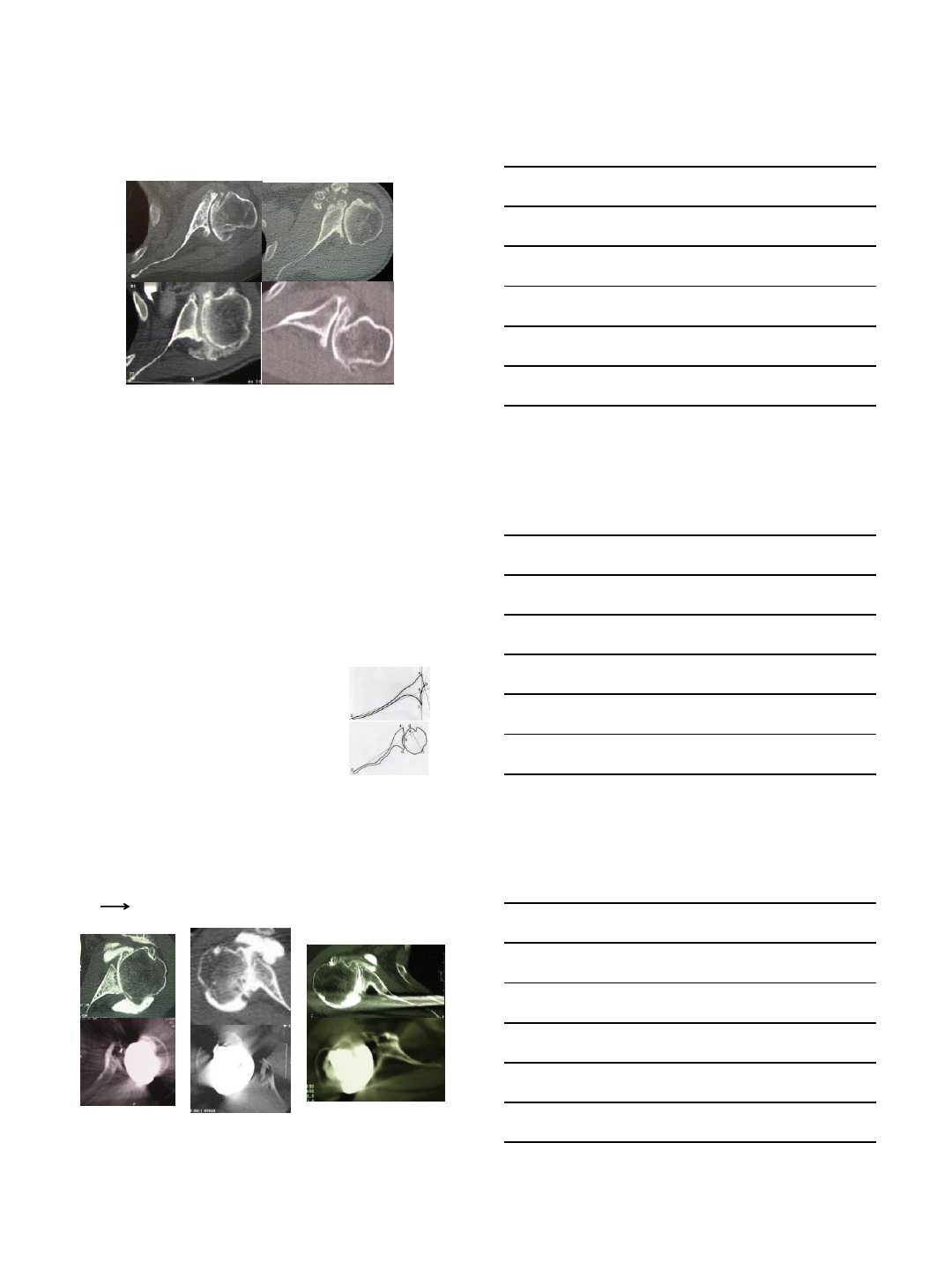
B2 and A2 are sometimes confused
if the paleo glenoid is absent
Paleo glenoid not always visible
•level of the cut
• osteophytes’ anterior reconstruction
• severe erosion and minimal subluxation
concentric or eccentric glenoid…
2/16/2015
3
Same patient at
2 ≠ levels
B2
A2
1/ level of the cut
may change the
glenoid shape
Biconcave
Concentric
1997
1995
2013
1999
B1
B2 C
B2
2/ osteophyte’s anterior reconstruction
Biconcave becomes concentric…
Osteophyte’s anterior reconstruction
Eccentric glenoid becomes a concentric one !
2/16/2015
4
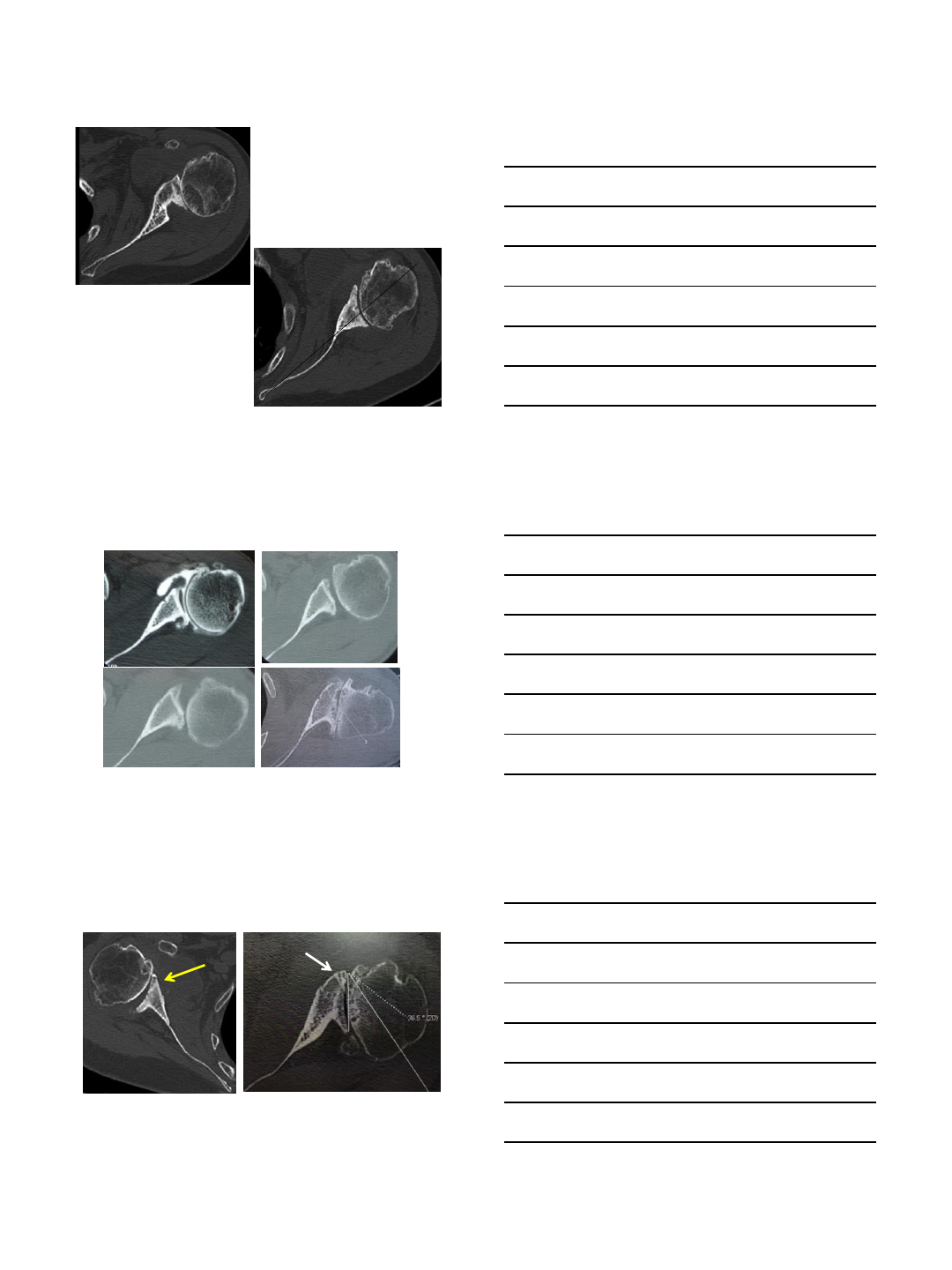
3/ Severe erosion –minimal subluxation
concentric glenoid but severe RV
Introduction of
B3 glenoid
- No paleo-glenoid (concentric glenoid,
no biconcavity)
- Glenoid erosion & retroversion > 15°
- Posterior subluxation of the HH > 70%
B3 Glenoid
HH subluxation > 70%
Retroversion > 15°
No paleo-glenoid
Concentric glenoid
2/16/2015
5
Types B2 - B3 How to address ?
B2 and anatomic TSA 1992-2007
92 cases - 77m f-up
(Eccentric reaming, bone graft, post capsulorraphy, hum antev.)
- 66.3% sastisfied or very satisf.
- 16.3 % Revisions
- 20.6% glenoid loosening
Intermed. glenoid RV > 27°= 50% complic
Sublux / scapula > 80% = 50% complic
Static posterior subluxation recurs
glenoid loosening (rocking horse )
5y 9y
13y
Case 1 Case 2 Case 3
2/16/2015
6
81% females
Mean age: 74.1 yo (66-82 )
17 dominant shoulders (63%)
Exclusion criteria
Rotator cuff tear (2 tendons or more), Cuff tear arthropathy, Post traumatic arthritis
Rheumatoid arthritis, Revision arthroplasty, previous surgery
B2 and Reverse SA 1998-2009
27 cases –54 m f-up
Reverse Prosthesis ( 2 stages)
Structural bone graft (1 stage)
2/16/2015
7
Results
Preop. Postop. p value
Pain 4 14 < 0.0001
Activity 7.9 18.5 < 0.0001
Mobility 14.2 35.1 < 0.0001
Strength 4.5 8.7 < 0.0001
Total 30.6 76.3 < 0.0001
93 % Satisfied or very Satisfied, 7 % Disappointed
Results: Range of Motion
Preop. Postop. p value
AFE 89°152°< 0.0001
RE1 A 3°27°< 0.0001
IR Buttocks T12 < 0.0001
SSV 81.7%
Radiographic results
All the graft but one healed, no glenoid RLL
•Scapular notching: 10 cases (37%)
Grade 1: 6, Grade 2: 4, Grades 3 & 4: 0
•Humerus Radiolucent lines: 2 (8.3%)
Humerus zone 1: 1, zone 7: 1
2/16/2015
8
Current indications for Reverse
in B2-B3 glenoid
•Subluxation HH / scapula
> 80%
•Failure to implant correctly a PE glenoid
- Glenoid RetroVersion > 10°
- Glenoid reaming > ½ suchond bone surf
- Seating < 80%
Thank you !
2/16/2015
1
Tom R. Norris MD
VuMedi Webinar:
Bone Loss in Shoulder Arthroplasty
February 17, 2015
Tricortical Iliac Crest Bone Grafts
COI Disclosure
•Tom R. Norris, MD
Tornier, Inc.
Consultant, stock, royalties, designer, fellowship
support
Disclosure information on AAOS website and
updated 4x/y
Glenoid Bone Loss
•Salvaging a failed shoulder
arthroplasty with glenoid
bone loss is a technically
challenging procedure.
•Iliac crest can allow for
successful one stage
reconstruction of the
glenoid vault in cases of
massive glenoid bone loss.
2/16/2015
2
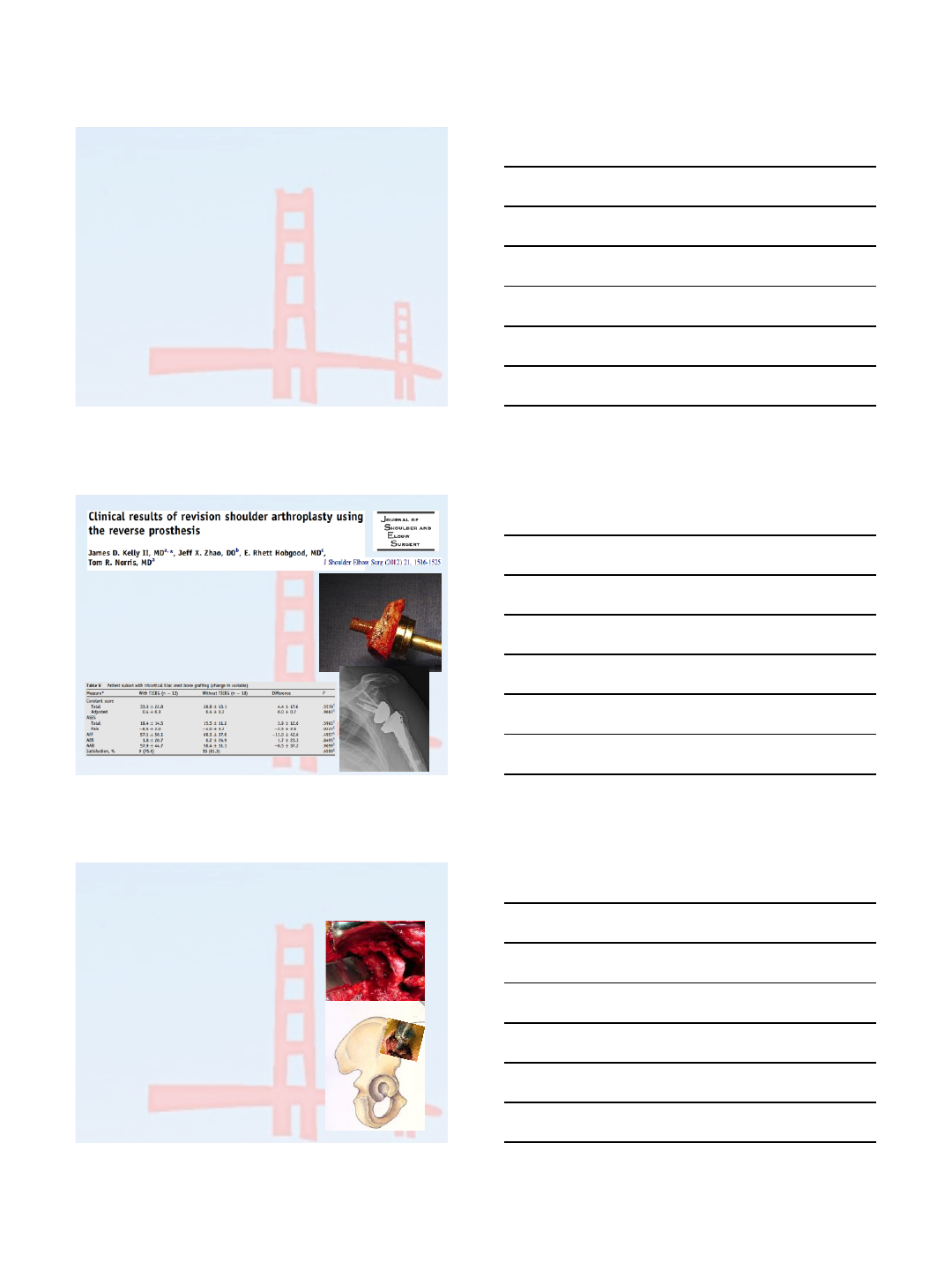
Tricortial iliac crest bone graft for massive
glenoid bone loss during revision shoulder
arthroplasty 2yr follow up
Mark A. Schrumpf MD,
Tom R. Norris MD
ICSES 2013 Nagoya, Japan
Methods
•Database search was performed of a single surgeon’s case
log from ‘05-’10
•Patients who underwent reconstruction of the glenoid
vault in a single stage revision surgery were identified
•All patients were revised to a reverse shoulder prosthesis.
•Data was collected in a prospective fashion for ASES,
Constant, WOOS, SANE and patient satisfaction.
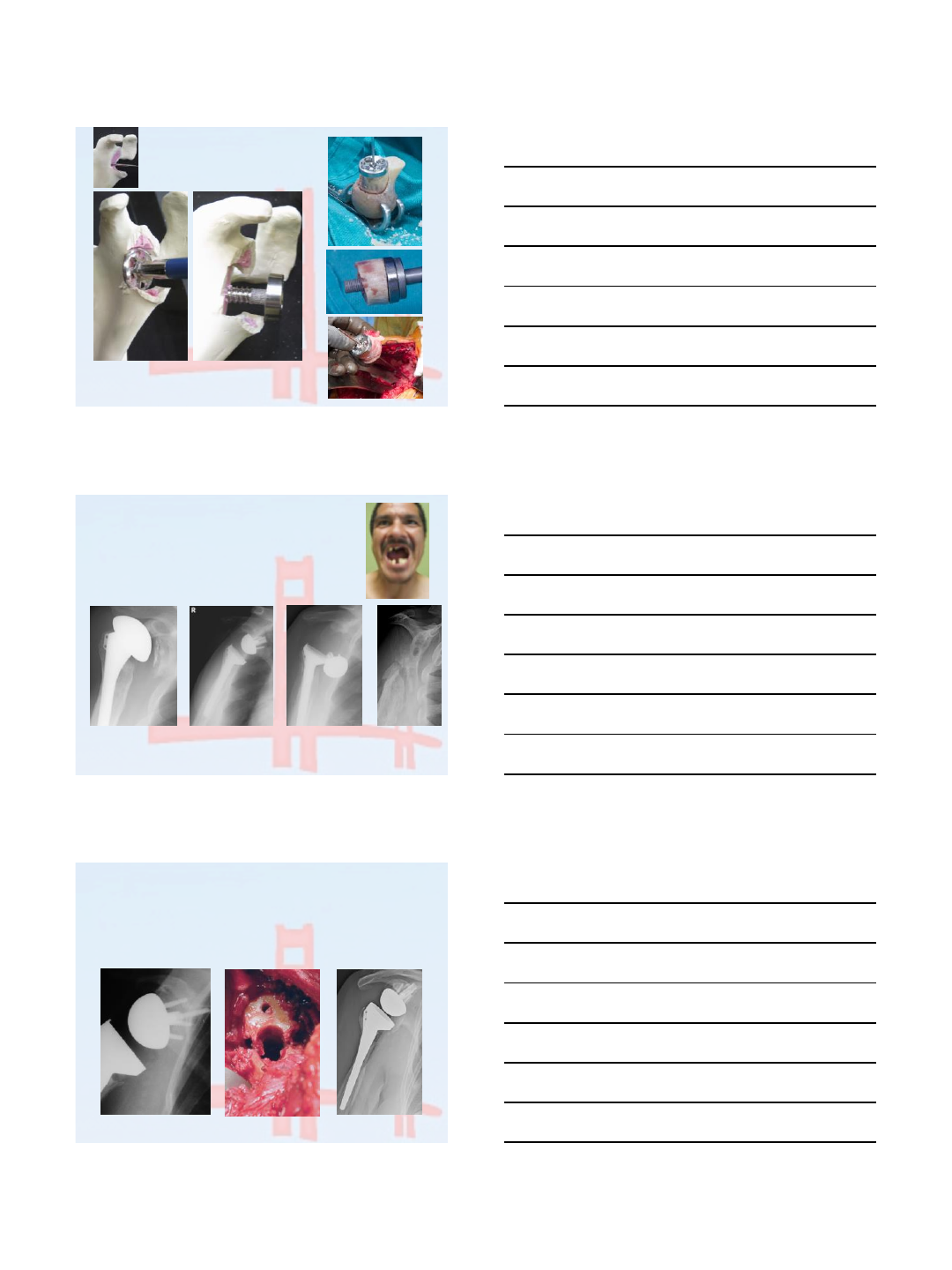
Reconstruction Technique
•Deltopectoral approach used to
retrieve all failed implants
•Recipient glenoid was freed of
any soft tissue while taking care
to protect bone stock
•Iliac crest was prepared in-situ
and baseplate implanted in graft
•Graft cut free of pelvis and fixed
to scapula with baseplate screws

2/16/2015
3
TICBG
Results
•23 shoulders were treated in 21 patients
•Average clinical follow up of 27 months
•Patient had undergone an average of 3 prior
open shoulder surgeries (max 15, min 1).
Clinical scores
•ASES scores improved from 62.9 to 68.3
(p=0.07)
•Constant improved from 37.0 to 44.2 (p=0.07)
•SANE improved from 32.7 to 41.7 (p=0.36)
•WOOS scores changed from 62.2 to 48.2
(p=0.02)
•Patient satisfaction levels improved by 16.3%
(p=0.03)
2/16/2015
4
Range of motion
•Range of motion improved in all directions
except active external rotation.
•AFF increased from 87° to 105° (p=0.06)
•AAB increased from 76° to 103° (p=0.01)
•Internal rotation also improved from between
the buttocks and lumbosacral junction to
between the lumbosacral junction and L3.
•Active external rotation decreased only
slightly from 20° to 17° (p=0.65)
Results –graft healing
•14 of 23 grafts
healed
completely, an
additional 3 had
partial
incorporation of
the crest graft.
•There were only
6 frank graft
failures
Complications/Reoperations
•Unfortunately , 11 of the 23 (48%) shoulders required re-
operation and removal of some or all of their glenoid
components during the follow up period.
–3 of the shoulder were revised for base-plate loosing
–2 for fracture of the glenoid following low energy trauma
–3 for infection
–1 for graft non-union
–1 for graft fracture
–1 for glenosphere baseplate disassociation.
•Three patients had humeral complications with fractures of
the shaft around the humeral stem necessitating
intervention highlighting the complex nature of this group
of patients.
2/16/2015
5
Discussion
•This is a complicated and heterogeneous group of
patients for whom glenoid bone loss is only one of the
challenges faced in restoring shoulder function.
•The overall all cause reoperation rate was high (48%)
•14/23 (61%) of the bone grafts healed completely to
the native scapula and an additional 3 had some
incorporation for a total of 74% adequate graft
healing. This procedure represents a viable option for
single stage revision for massive glenoid defects.
•12 ICBG (12/30 RSA in study)
•Average F/U 34 mo.
•FOS, AFF, AAB significantly increased
–Adj Constant: 24.3-64.6
–ASES: 54.8-71.8
–AFF: 42.0-105.7
–AAB: 39.4-97.7
1st Conclusions
•This procedure represents a viable
option for single stage revision for
massive glenoid defects.
•While this is a complex and difficult
group of patients to treat owing to
bone loss and multiple prior
operations, significant and durable
improvements in satisfaction, range
of motion and functional scores can
be obtained by using iliac crest to
reconstruct the glenoid.
2/16/2015
6
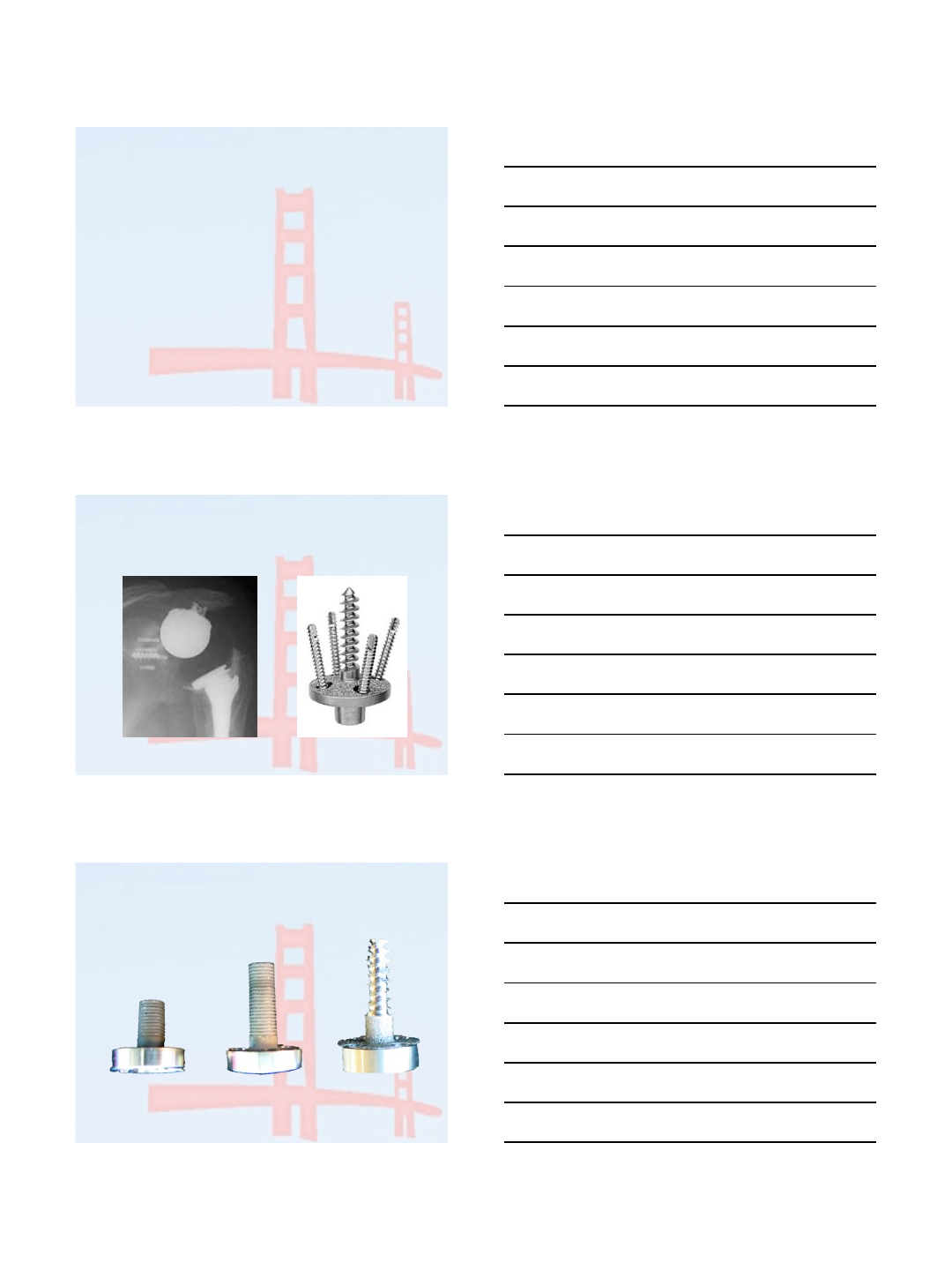
How to improve results?
•Base plate options
•Glenoid anatomy may determine 1 or 2-stage
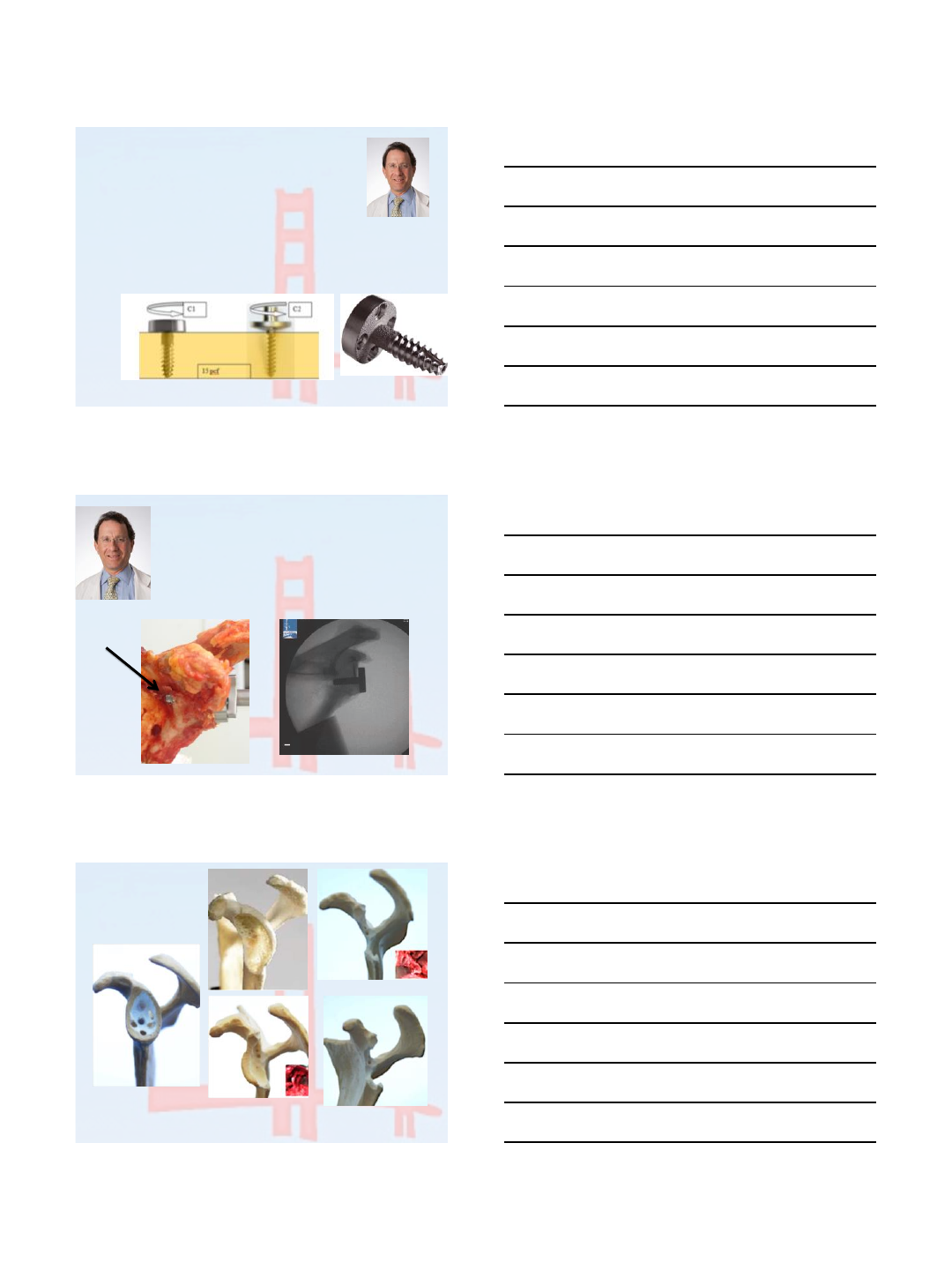
Design advances
Ingrowth, locking screws
Mark 1 design
Long post base plate to engage native
scapula with bone grafts
SPBP LPBP
THREADED or SCREW-IN BP
25-50 mm screw length
2/16/2015
7
Base plate advances
–Base plate designs-one or multi-piece
–Fixation to native scapula with grafts
–Textures or ingrowth coatings
–Threaded BP 10-18x torque/compression
–Length options for bi-cortical fixation and grafts
Threaded Post Baseplate
•Fixation achieved at base of glenoid vault
Base plate low in the glenoid
Bicortical
GBL
1
2A
2B
TYPE 3
Norris TR, Abdus-Salaam S. Lessons learned from the Hylamer experience & technical salvage for
glenoid reconstruction. In: Walch G, Boileau P, Mole D, Favard L, Levigne C, Sirveaux F, editors.
Shoulder concepts 2010: the glenoid. Montpellier: Sauramps Medical; 2010. p. 265-78. ISBN 978-
2840232735.
2/16/2015
8
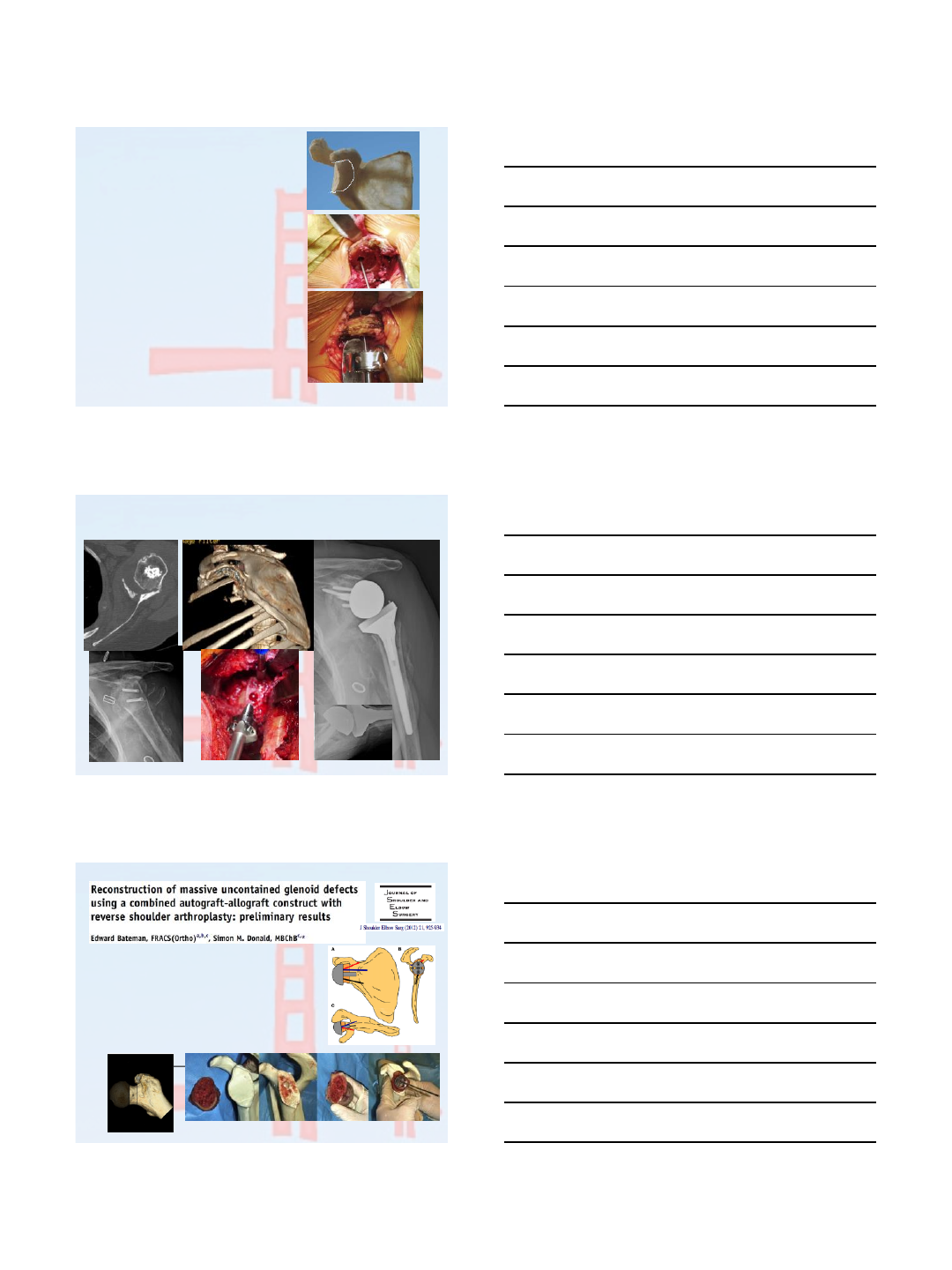
Global Glenoid loss
(GBL type 3)
•Sideways TICBG
•Structural allograft
–Femoral head, neck or
shaft
–Humeral head when
using proximal humeral
combined graft
–BMP
–Consider staging
TICBG—2-stage reconstruction with threaded baseplate
Stage 1-TICBG Stage2 RSA
Absent
glenoid
•Autograft-allograft composite
•5 patients
•Preliminary results show
incorporation of the graft in all
pts
•no infections
2/16/2015
9
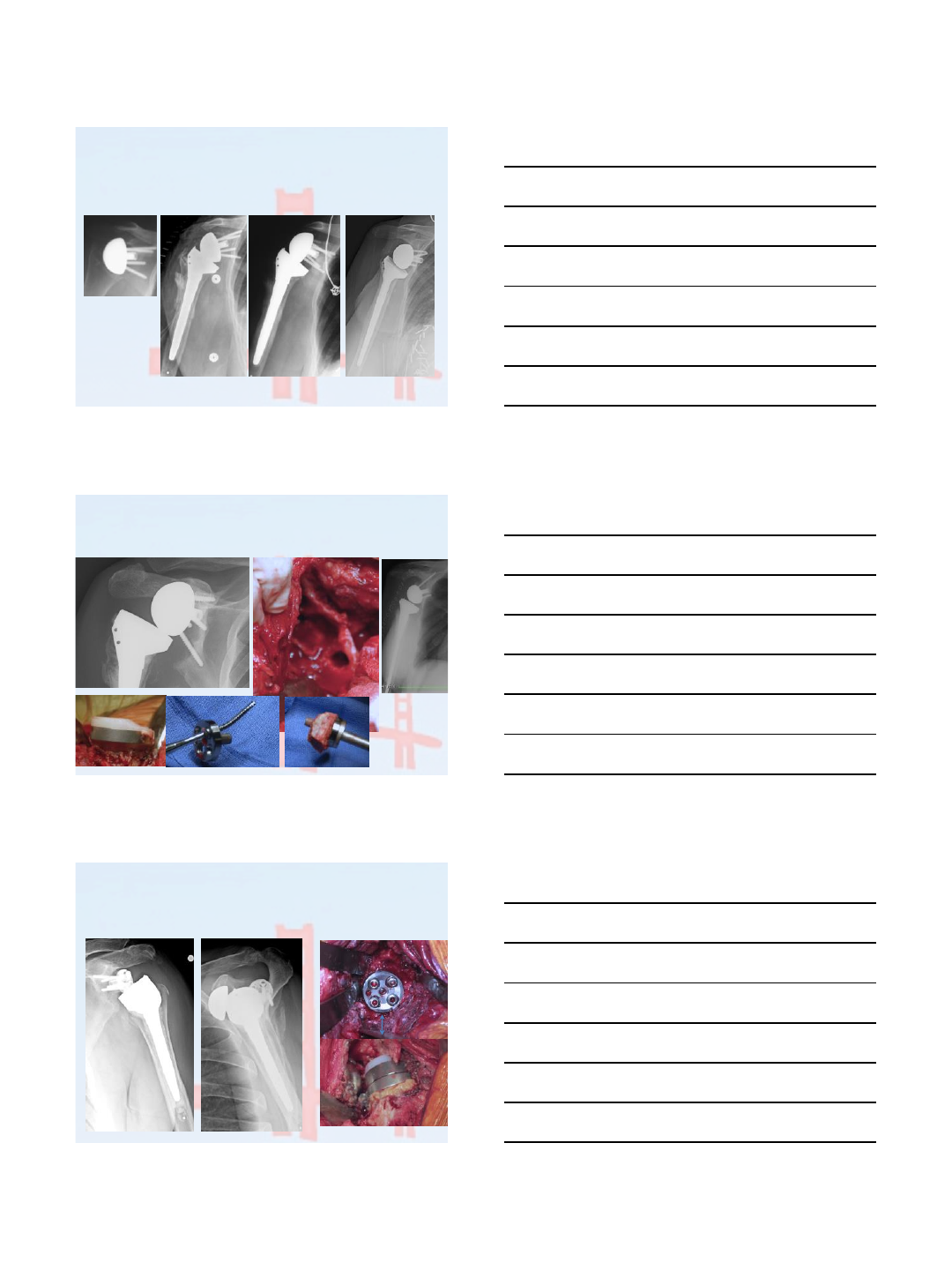
Global GBL
TSAR-RSA-Sepsis GSL-Resection
Balandran-3ops
GL, RCT in TSA 2y RSA
Bone resorption
SEPSIS
Cause for sepsis
resection
2 y
2 y
GSL
Burns 11 ops
Allograft chips GBG
Short post BP
Scapula fx
Op 8
TSAR-RSA1-GBG allograft chips, SPBP
RSAR-TICBG fracture-NU
RSAR2-subside upwards-HO inferior-instability
RSAR3-PH allograft, FNA to glenoid to
lateralize
2/16/2015
10
Scapula fx reaming-Staged RSA
SPBP LPBP-stable
Goldkrause 5 ops
GSLStaged
Early RSAs: placed mid glenoid
Impingement, osteolysis, notch, instability, GSL
GBL2B
Goldman-10ops
GBL 2B
Reposition
LPBP lower
TICBG
TICBG
Metalosis
osteolysis
Malposition high, levers out
dissociation Inferior glenoid levers
out poly
Mangan 3ops
2/16/2015
11
GS Dissociation-malposition BP high
TICBG, lower BP, GS lateralized
Mangan 3ops
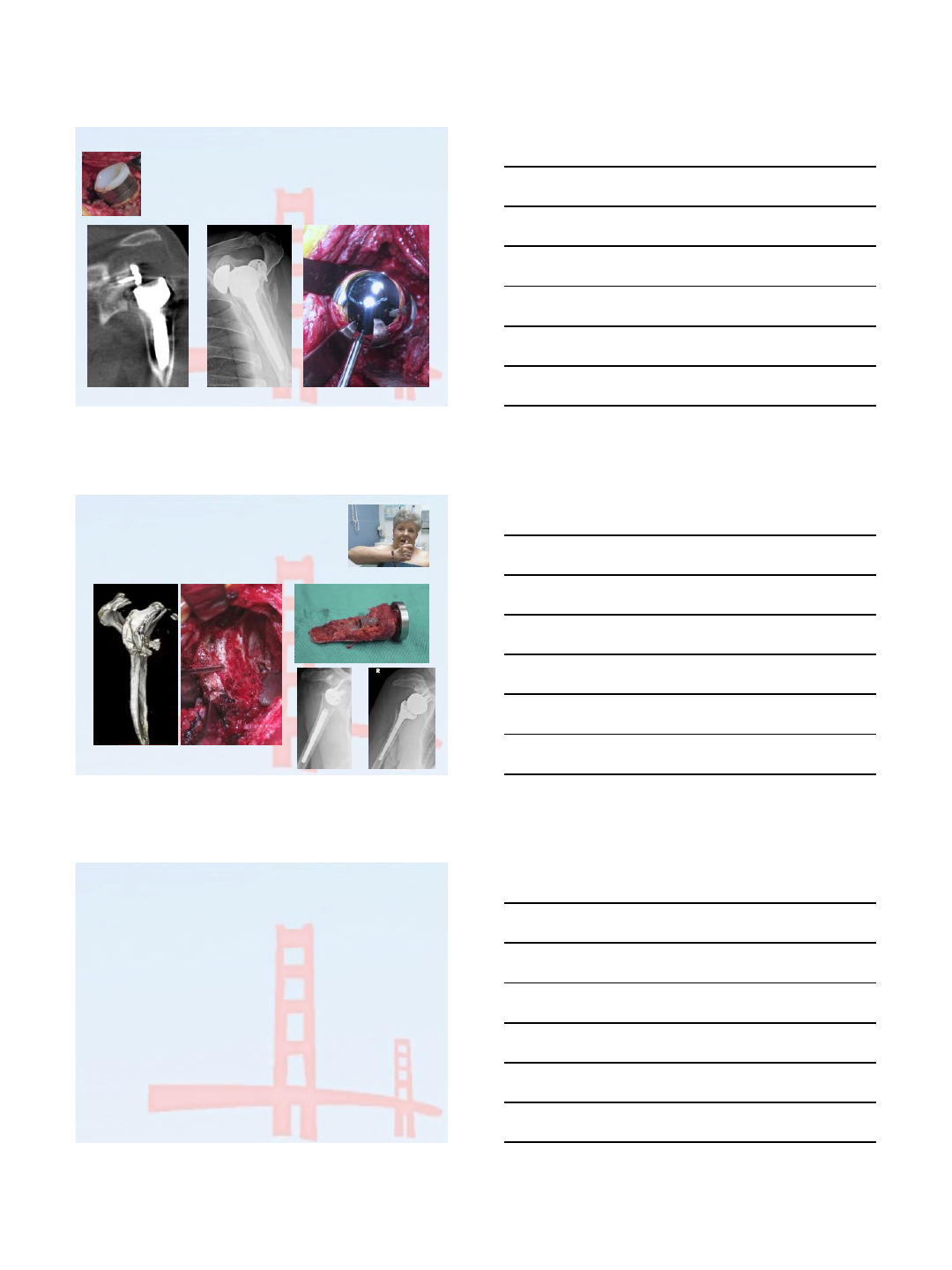
Traumatic GSL in BIORSA
Staged reconstruction for GBL
Ant Fx dislocation-BIORSA
GSL-new fall 2-Stage TICBG
digiroloma-3ops
Conclusions
•Tricortical Iliac Crest Grafts offer a good option
for reconstructing glenoid bone loss in
revision arthroplasty
•Advances on base plate technology with long
posts and screws to engage the native scapula
will improve our outcomes.
•Scapular bone loss plays an important role in
whether the cases can be done in 1 or 2-
stages

1
The Use of Cancellous Bone Graft Harvested
from the Humeral Head (BIORSA Technique)
to Address Glenoid Deficiency:
A CT-Scan Study
Nice - France
Pascal Boileau, Nicolas Morin-Salvo, Gregory Moineau,
Thomas D’Ollonne, Patrick Gendre, Charles Bessière
Disclosure
Pascal Boileau –Royalties - Tornier
Preliminary study good results
for glenoid without bone deficiency !
CORR 2011
42 patients / 42 BIORSA
FU mean : 28 Months (24-40)
100% graft incorporated
No glenoid loosening
19% scapular notching
Excellent mobility
No instability
2
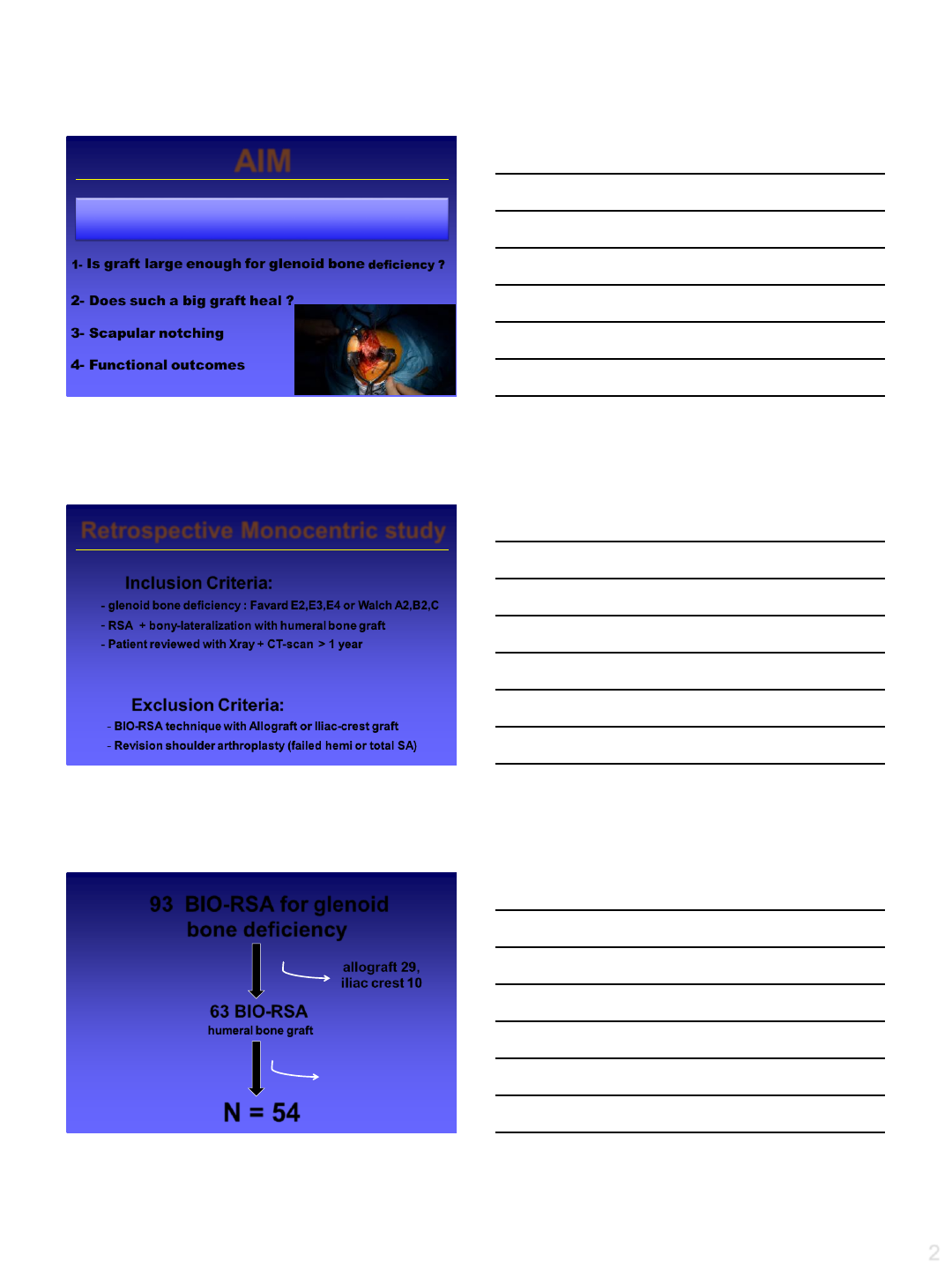
AIM
1- Is graft large enough for glenoid bone deficiency ?
2- Does such a big graft heal ?
3- Scapular notching
4- Functional outcomes
to report the results of the use of BioRSA
technique to address glenoid deficiency
Retrospective Monocentric study
Inclusion Criteria:
-glenoid bone deficiency : Favard E2,E3,E4 or Walch A2,B2,C
-RSA + bony-lateralization with humeral bone graft
-Patient reviewed with Xray + CT-scan > 1 year
Exclusion Criteria:
-BIO-RSA technique with Allograft or Iliac-crest graft
-Revision shoulder arthroplasty (failed hemi or total SA)
2 died
7 lost FU < 1y
93 BIO-RSA for glenoid
bone deficiency
63 BIO-RSA
humeral bone graft
allograft 29,
iliac crest 10
2006 to 2013
N = 54
3
BIO-RSA for Glenoid
Deficiency (n = 54)
Women 70% -73 years [52-85]
-Cuff tears arthropathy CTA (31)
-Osteoarthritis OA (13)
-Osteoarthritis post-instability OA post-inst (2)
-Rheumatoid arthritis RA (6)
- Fracture Sequelae SF (2)
•FU mean : 33 m [12-81]
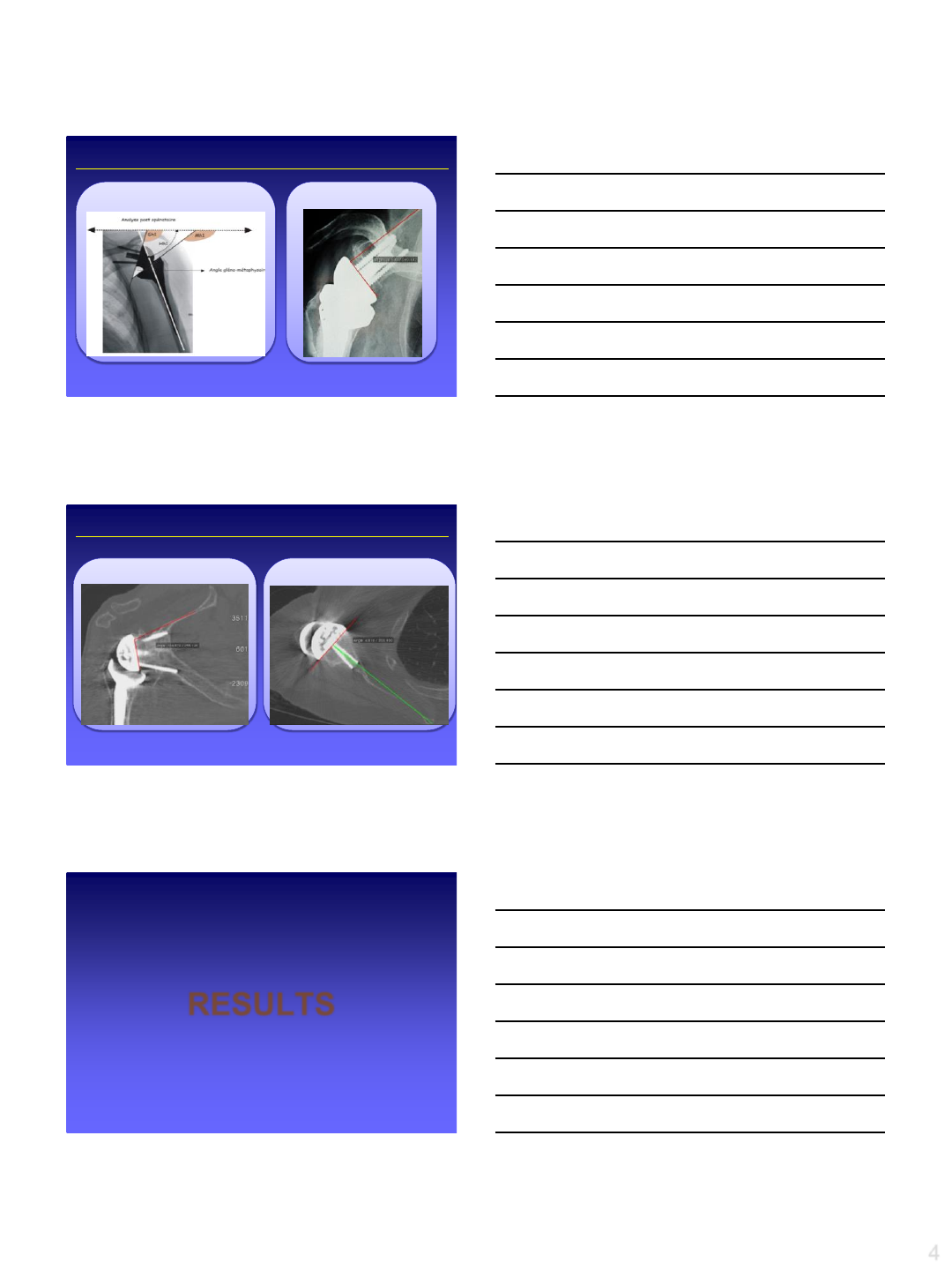
Glenoid Deficiency
Horizontal Plane (WALCH) A2,B2,C
A2 = 8 B2 = 15 C= 7
Glenoid Deficiency
Vertical Plane (FAVARD) E2,E3,E4
E4 = 3E3 = 21E2 = 15
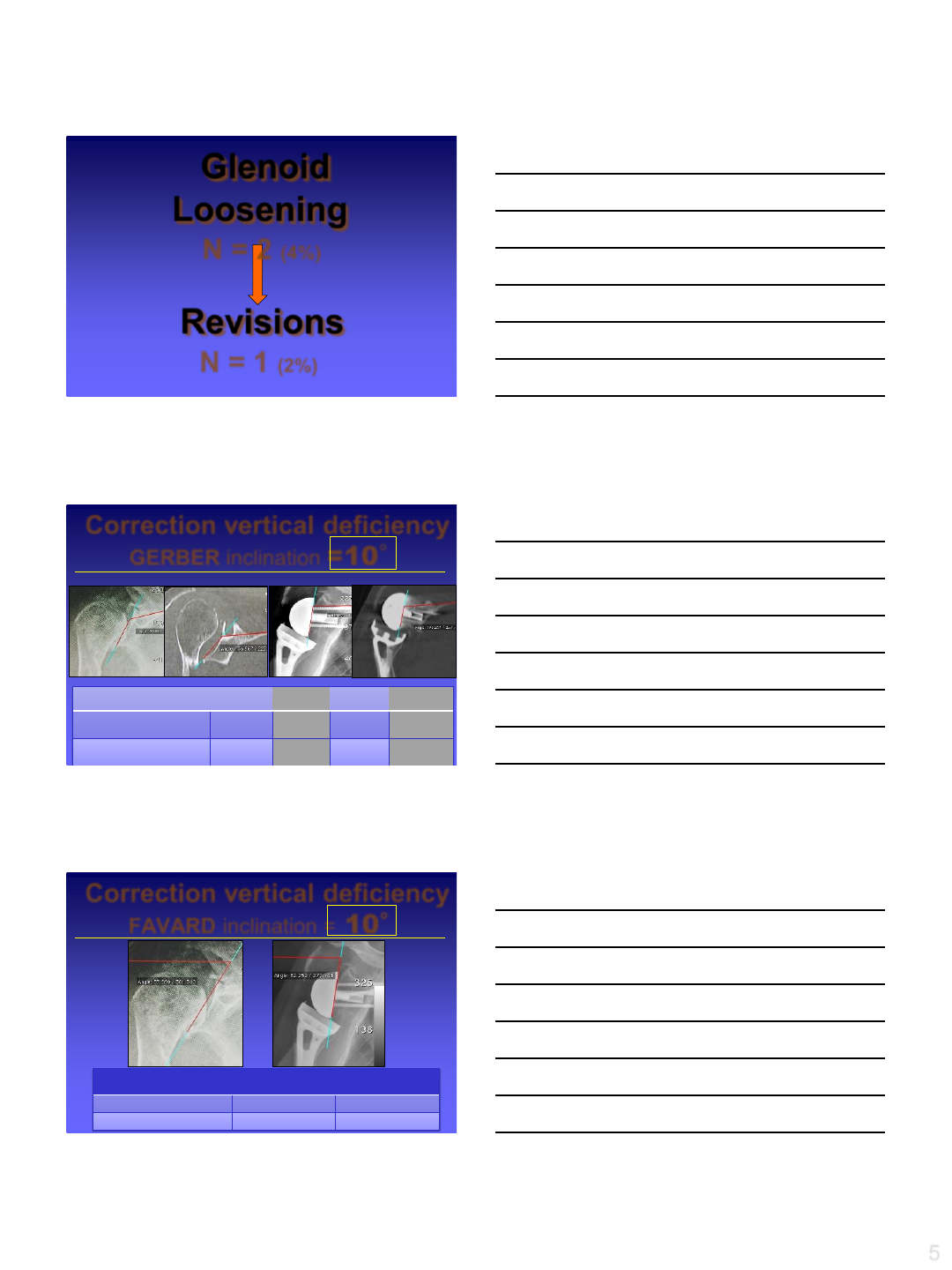
4
GERBER inclination
FAVARD inclination
1) Falaise, Lévigne, Favard, OTSR 2011 : scapular notching in reverse shoulder arthroplasty: influence of
glenometaphyseal angle
2) Maurer, Gerber, et al. JSES 2012 : assessment of glenoid inclination in routine clinical xray and ct-scan;
Radiographic Measurement of Glenoid Inclination
FRIEDMAN versionGERBER inclination
1) Maurer, Gerber, et al : assessment of glenoid inclination in routine clinical xray and ct-scan; JESE 2012
2) Friedman, et al : the use of computized tomography in the measurement of glenoid version; JBJS Am 1992
2D-CT-Scan Measurement of Glenoid Inclination & Version
MPR mode (Multi Planar Reconstruction)
RESULTS
5
Glenoid
Loosening
N = 2 (4%)
Revisions
N = 1 (2%)
Correction vertical deficiency
GERBER inclination =10°
incl. pre-op
Rx
incl.
pre-
op
Ct-Scan
incl. post
-
op
Rx
incl. post-
op
Ct-Scan
Total
series (n = 54) 106.4°
(71;142)
104.9°
(68;139)
96.1°
(70;122)
95.9°
(71;121°)
Favard
E2, E3 (n=39) 111°
(95;142)
112.1°
(96;138)
97.6°
(70;122)
97.3°
(71;121)
27 m post-op
27 m post-op
(ns)
(ns)(ns)
(ns)
Correction vertical deficiency
FAVARD inclination = 10°
incl. pre-op
Rx
incl. post-op
Rx
Total
series (n = 54) 88.1°(54;117) 98.1°(64;129)
Favard
E2, E3 (n=39) 82°(54;106) 93.5°(68;118)
27 m post-op
(p=0.003)
(p=0.001)
6
Correction horizontal deficiency
= 10°
version pre-op version post-op
Total
series (n = 54) -12.1°(-49;+15) -4.7°(-32;+21)
Walch
B2, C (n=30) -21.1°(-49;0) -10.6°(-32;+4)
asymetric
graft
33m post-op
(p=0.08)
(p=0.06)
52/54 Graft incorporated (96%)
3m Post-op 18m Post-op
GRAFT HEALING
FU mean : 33m [12-81]
12m Post-op
52/54 Graft incorporated (96%)
GRAFT HEALING
(CT-scan) FU mean : 33m [12-81]
46 m post-opE3 / C
combined
7
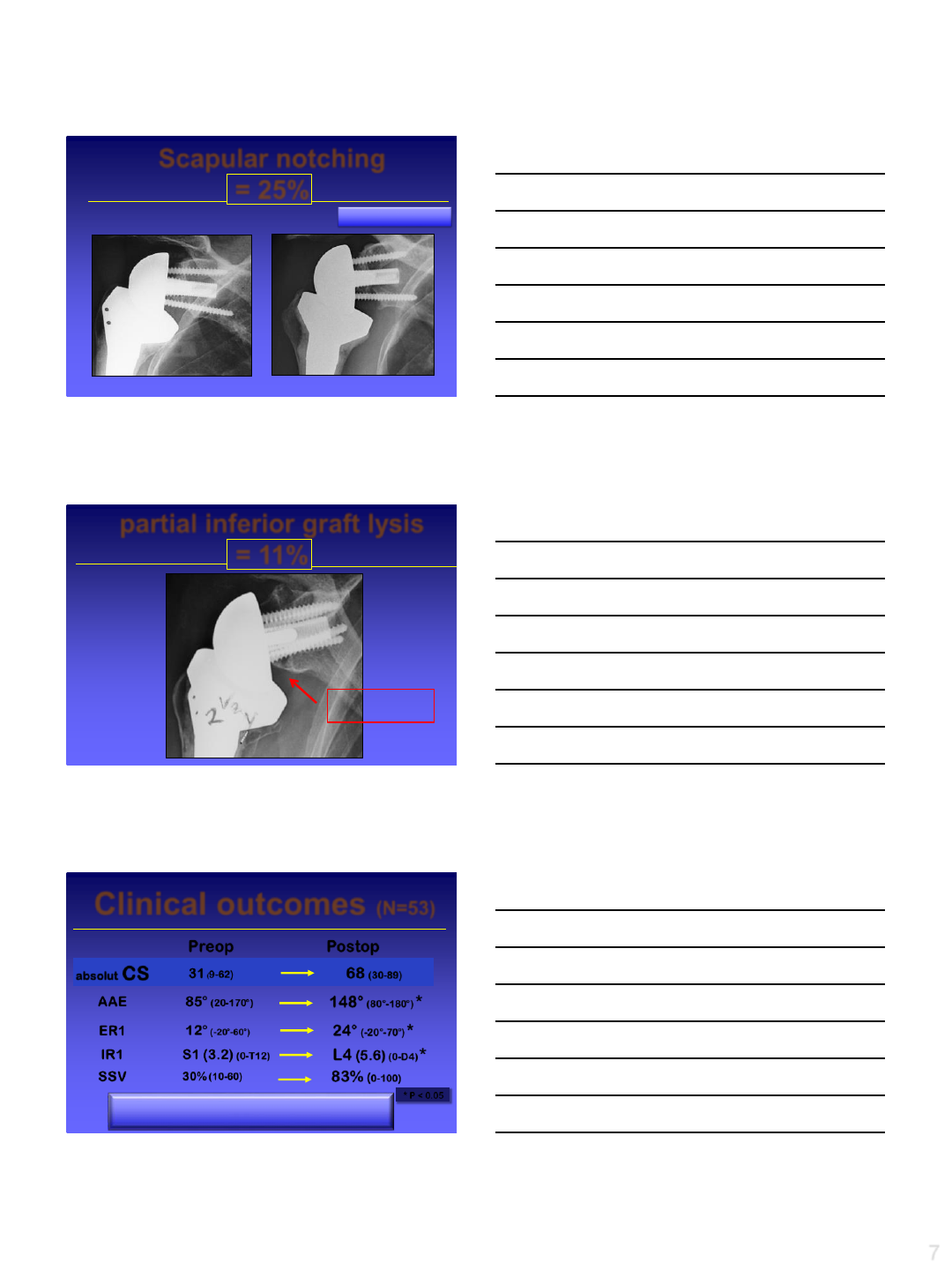
Scapular notching
= 25%
64m Post-Op
67m Post-Op
(NONE NOTCH GRADE 4)
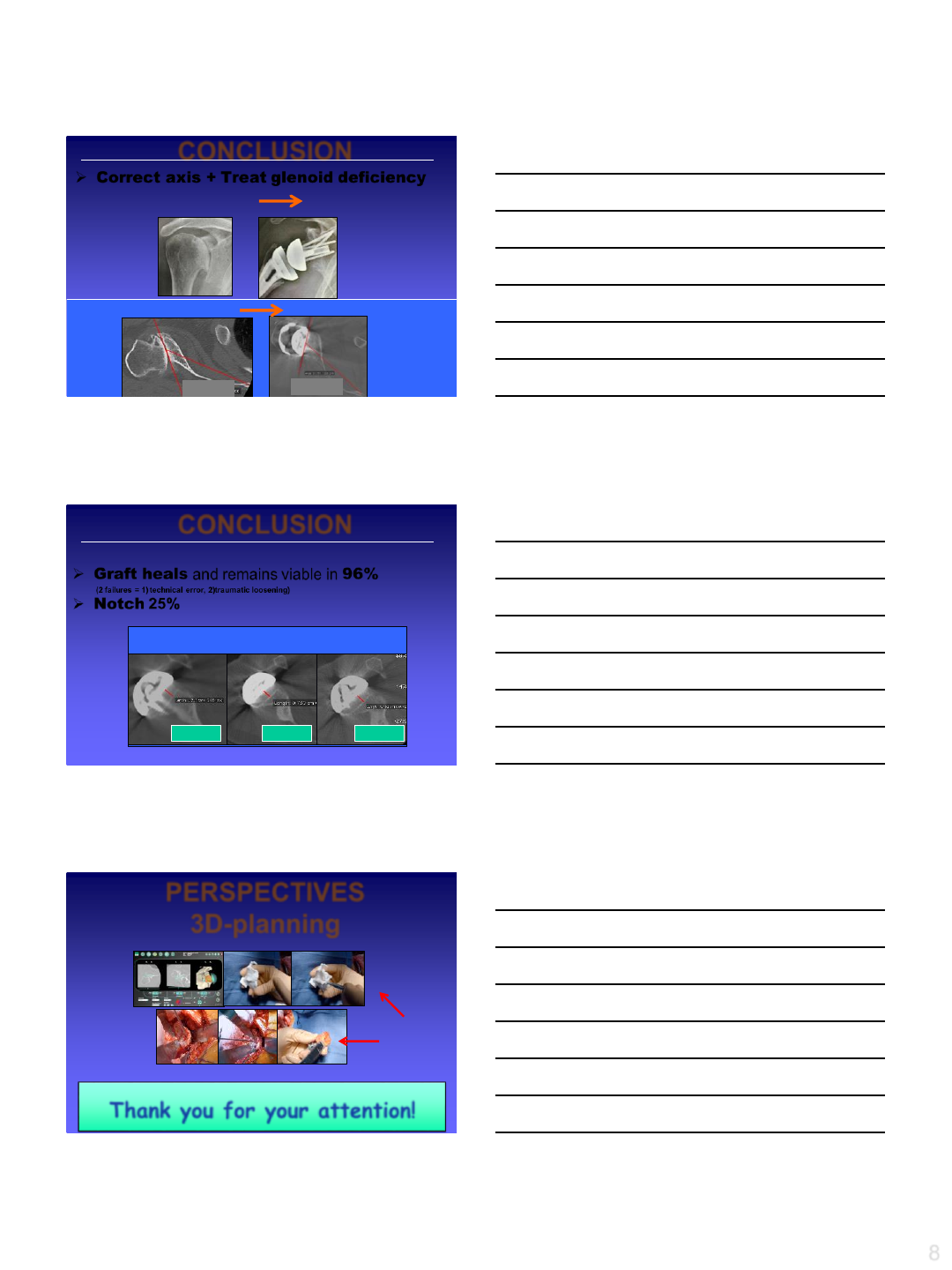
partial inferior graft lysis
= 11%
24m Post-Op
GRAFT
HEALED
partial inferior lysis
(remodelling)
NO INSTABILITY
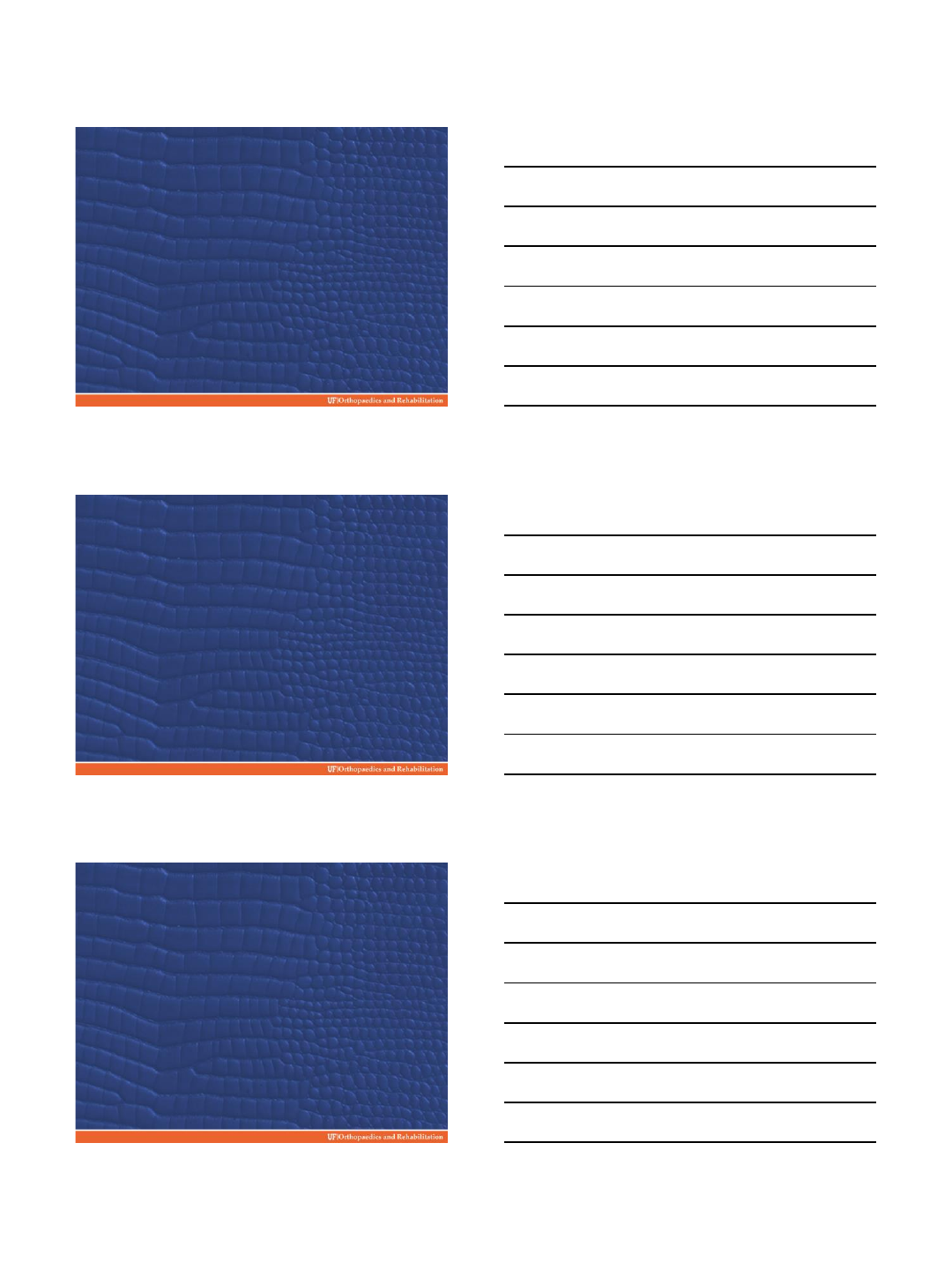
Clinical outcomes (N=53)
Preop Postop
absolut CS 31(9-62) 68 (30-89)
AAE 85°(20-170°)148°(80°-180°) *
ER1 12°(-20°-60°)24°(-20°-70°) *
IR1 S1 (3.2) (0-T12) L4 (5.6) (0-D4) *
SSV 30% (10-60) 83% (0-100)
* P < 0.05
8
45°30°
Correct axis + Treat glenoid deficiency
inclination -10°
Version +10°
CONCLUSION
Graft heals and remains viable in 96%
(2 failures = 1) technical error, 2)traumatic loosening)
Notch 25%
CONCLUSION
GRAFT HEALING
6m post-op 2y post-op 5y post-op
PERSPECTIVES
3D-planning
Thank you for your attention!
cut-guide & graft
dimension
personalized
2/16/2015
1
Reverse TSA - How to
Handle Glenoid Bone Loss
Thomas W. Wright MD
University of Florida
Department of Orthopaedics
Disclosure
•Design Surgeon for Exactech
–Institutional research support
–Royalties
Introduction Glenoid Wear - RTSA
•Reaming solutions
•Bone graft Solutions
•Metal solutions
•Early Outcomes
2/16/2015
2
Glenoid Bone Loss - Reaming
•Ream to correct deformity
–Give up valuable subchondral
bone
–Correct only about 15 degrees
–Glenoid shrinks
Eccentric Reaming
Issues w/ eccentric reaming:
•Insufficient bone stock
•Implant downsizing
•Peg Perforation
•Implant loosening loss subchondral
support
How much can I correct it?
2/16/2015
3
Glenoid Bone Loss - Grafting
•Bone Graft defect
–Humeral head autograft if present
–Allograft or autograft iliac crest
–Technically demanding
–Graft needs to heal
–Use extended post
Cases Humeral Head Autograft
2/16/2015
4
Glenoid Bone Loss –Metal Solutions
•Metal soutions
–Posterior augment
–Superior augment
–Posterior –superior augment
–Lateralized glenosphere
Hypothesis
•Severe Glenoid Wear
treated metal augments
will have comparable
outcomes RTSA patients
with normal glenoid
2/16/2015
5
Metal Solutions Augmented
Baseplates
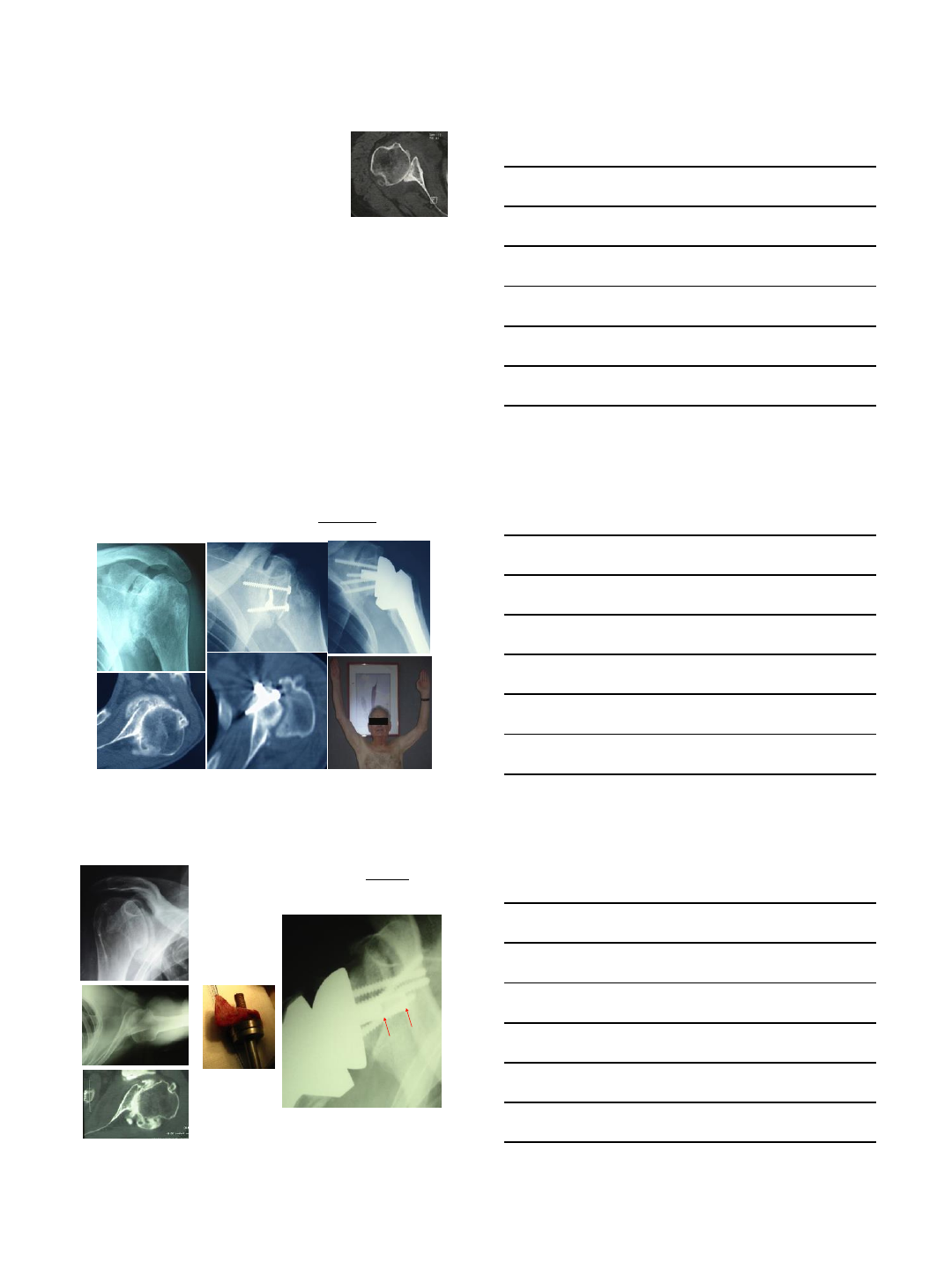
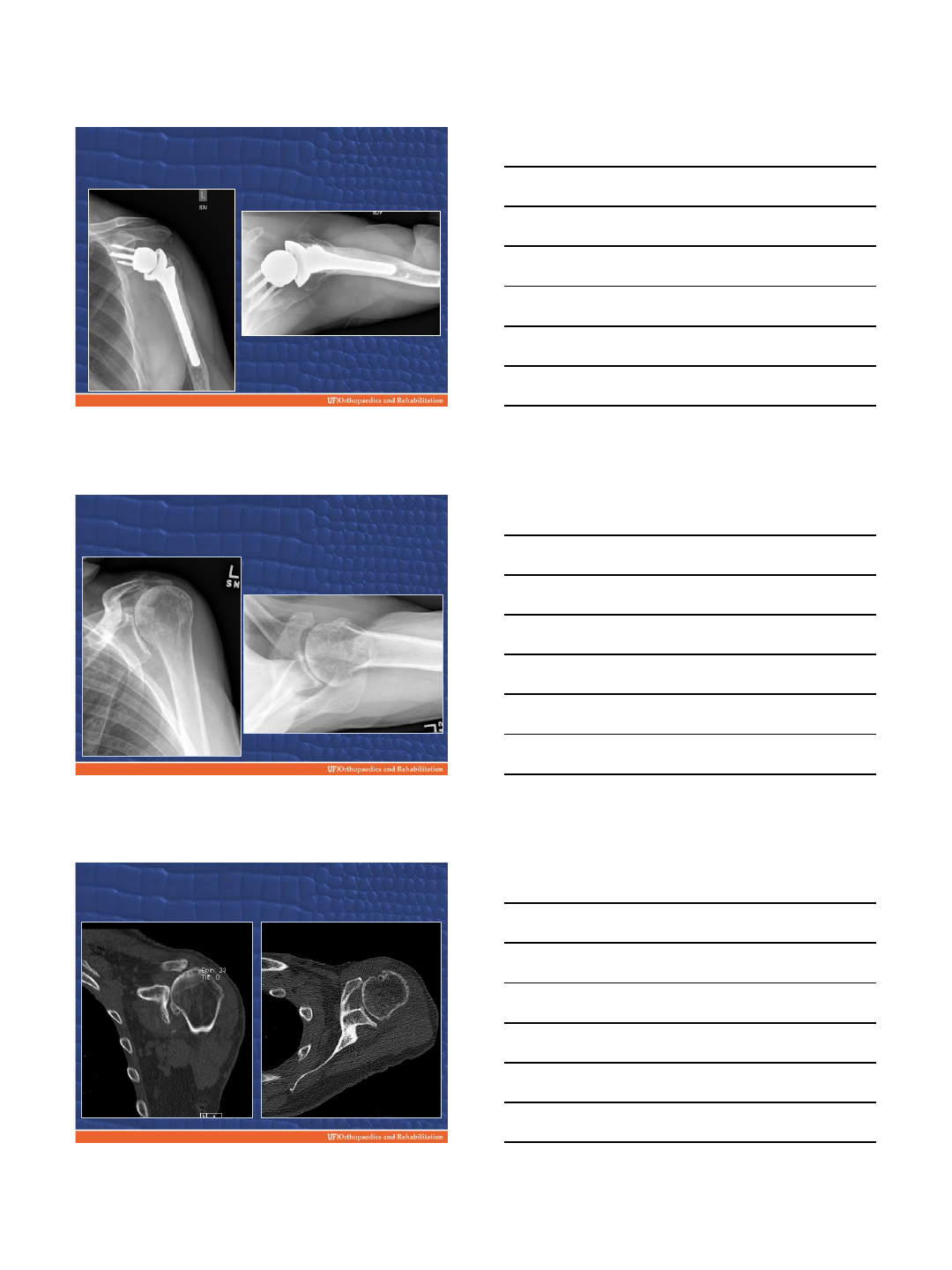
Case –Augmentation with Metal
•60 failed hemi
•Previous surgery for instability
•Pain/ bad function
2/16/2015
6
Superior Augmented Baseplate
Superior Augmented Baseplate
•29 Patients
–20 primary
–9 revision
•Age - 70
•Average F/U –18 months
•Complication –1 dislocation
2/16/2015
7
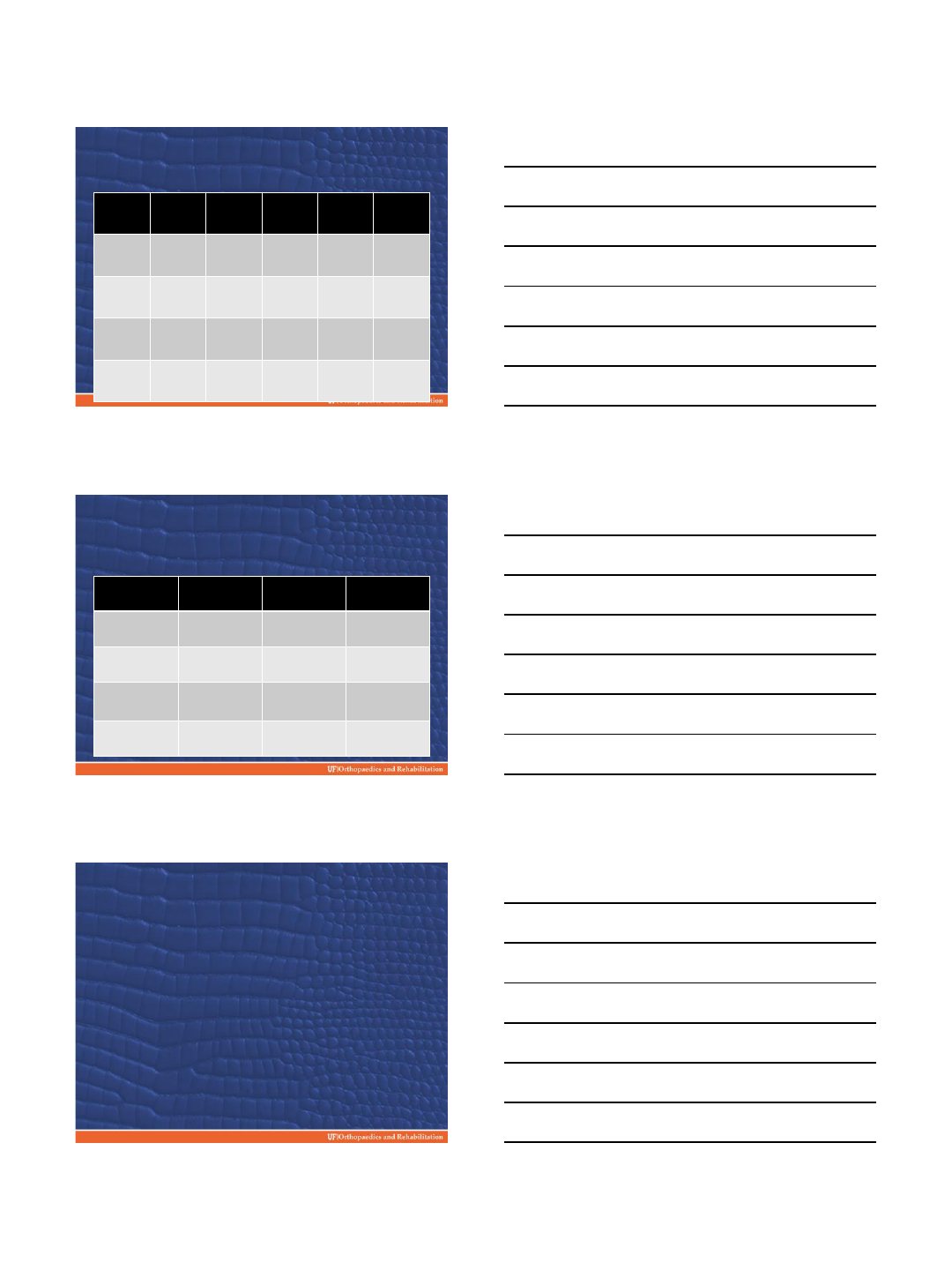
Superior Augmented Baseplate
SPADI
100
SST
ASES
UCLA
Constant
Nrl
Pre op
69
4
33
13
33
Final
F/U
32
8
71
28
67
Change
-37
good
+4
+38
+15
+34
Control 2
year
22
9
79
29
76
Superior Augmented Objective
Outcomes
Active
elevation
Active
External Rot
Active Internal
Rot
Preop
75
17
S2
Post Op
116
28
L3
Improvement
+41
+11
+5 anatomic
segments
Control
127
27
L3
Augmentation Metal-Lateralized
•Lateral Center of Rotation
Implant
–Encore –32std and 32-4
–Exactech –lateralized
glenosphere
–Others
2/16/2015
8
Lateral Center Of Rotation
Lateralized Glenosphere
Medial Wear
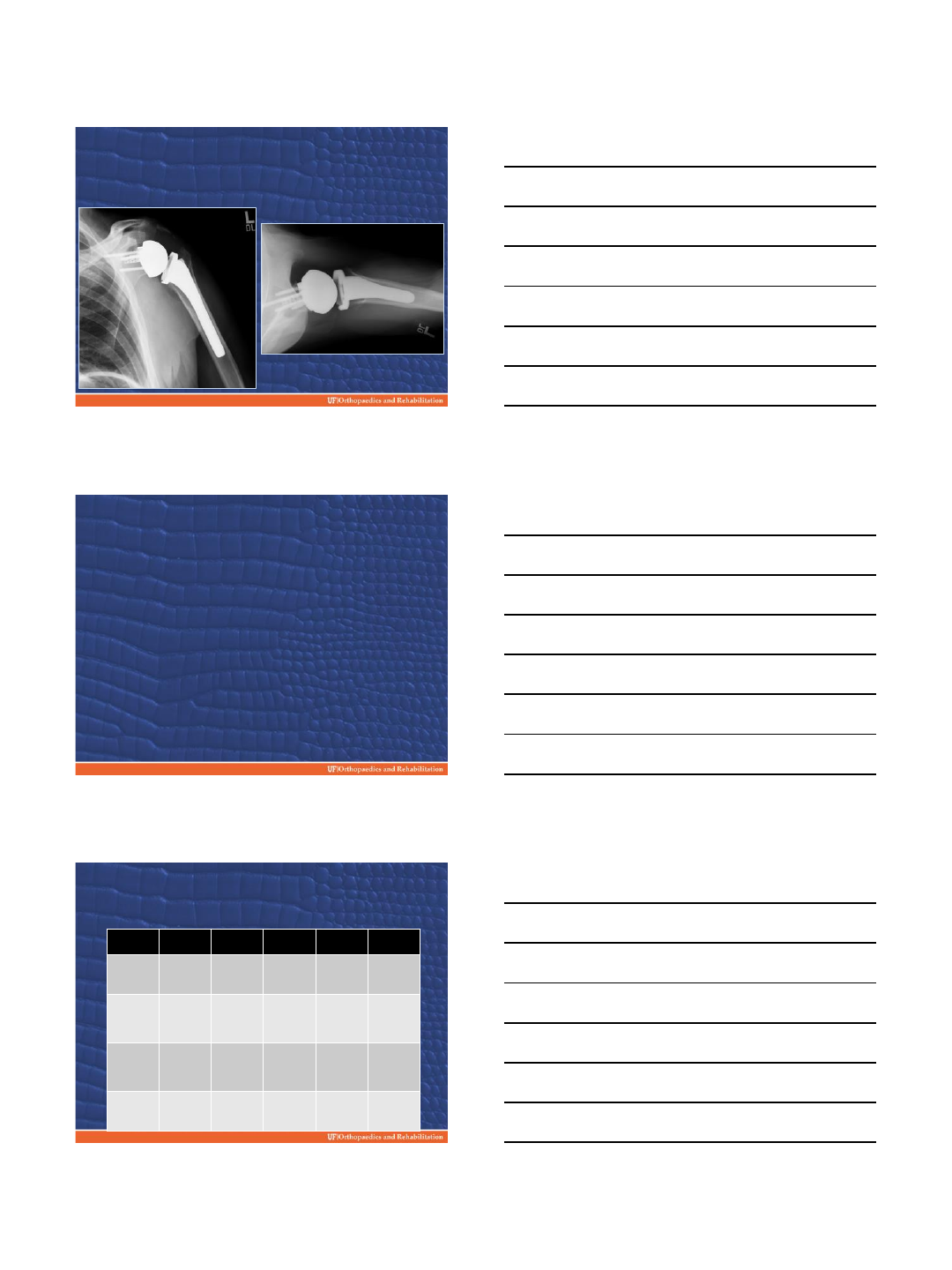
2/16/2015
9
Superior Augment/Lateralized
Glenosphere
Lateralized Glenosphere
•N=29
•Age –67
•Follow-up Ave –8 months
•One dislocation
Lateralized Glenosphere Functional
Outcomes
SPADI 100
SST
ASES
UCLA
Constant
Nrl
Pre Op
75
3
30
11
28
Final
F/U
34
8
70
27
59
Improvem
ent
-41
Good
+5
+40
+16
+31
Control 1
year
30
9
70
27
67
2/16/2015
10
Lateralized Glenosphere Objective
Active
Elevation
Active
External Rot
Active Internal
Rot
Pre
Op
61
12
S2
Final
F/U
97
19
L5
Improvem
ent
+36
+7
+2
anatomic
Seg
Control 1
yr
118
23
L4
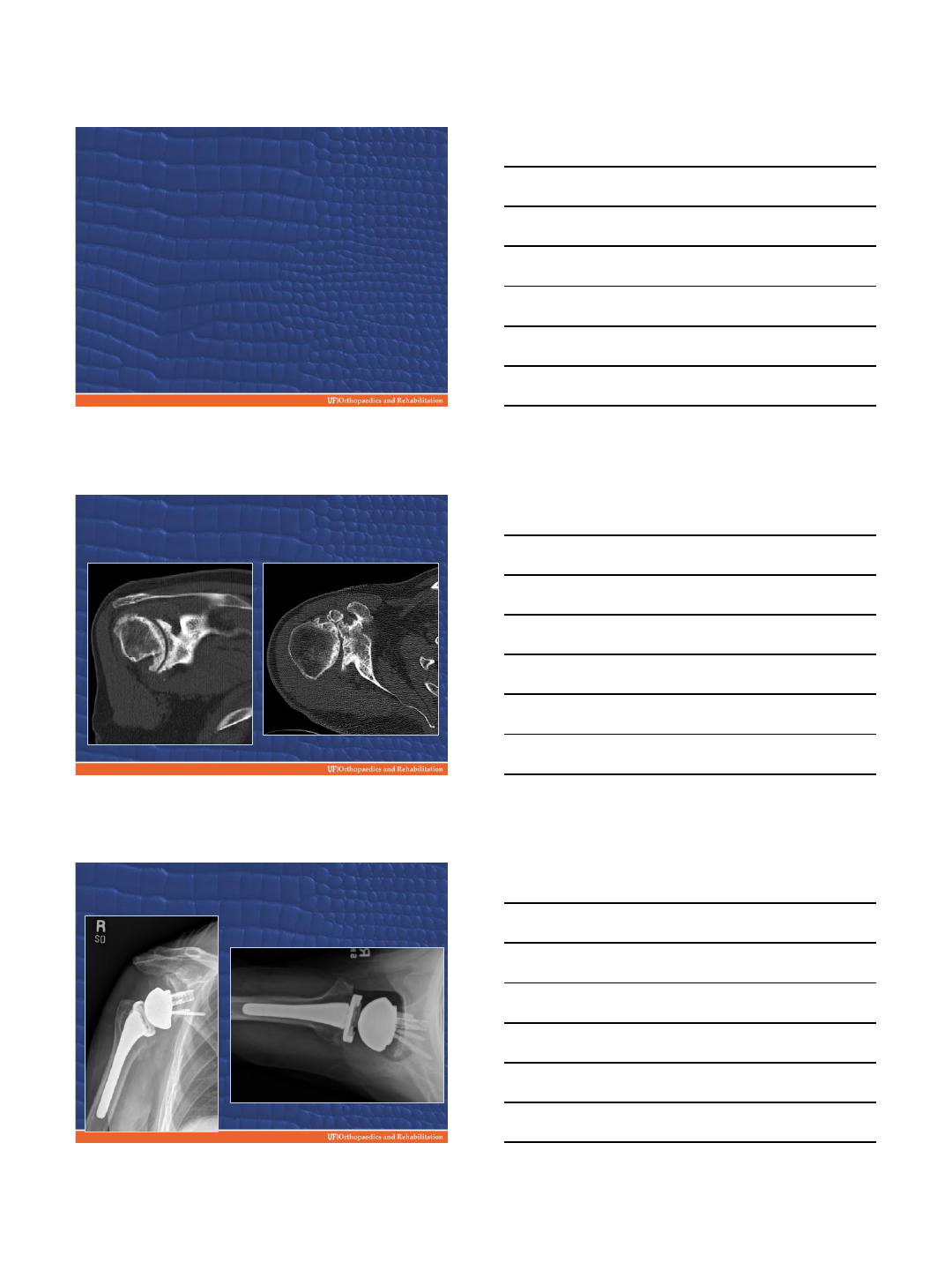
Posterior Wear
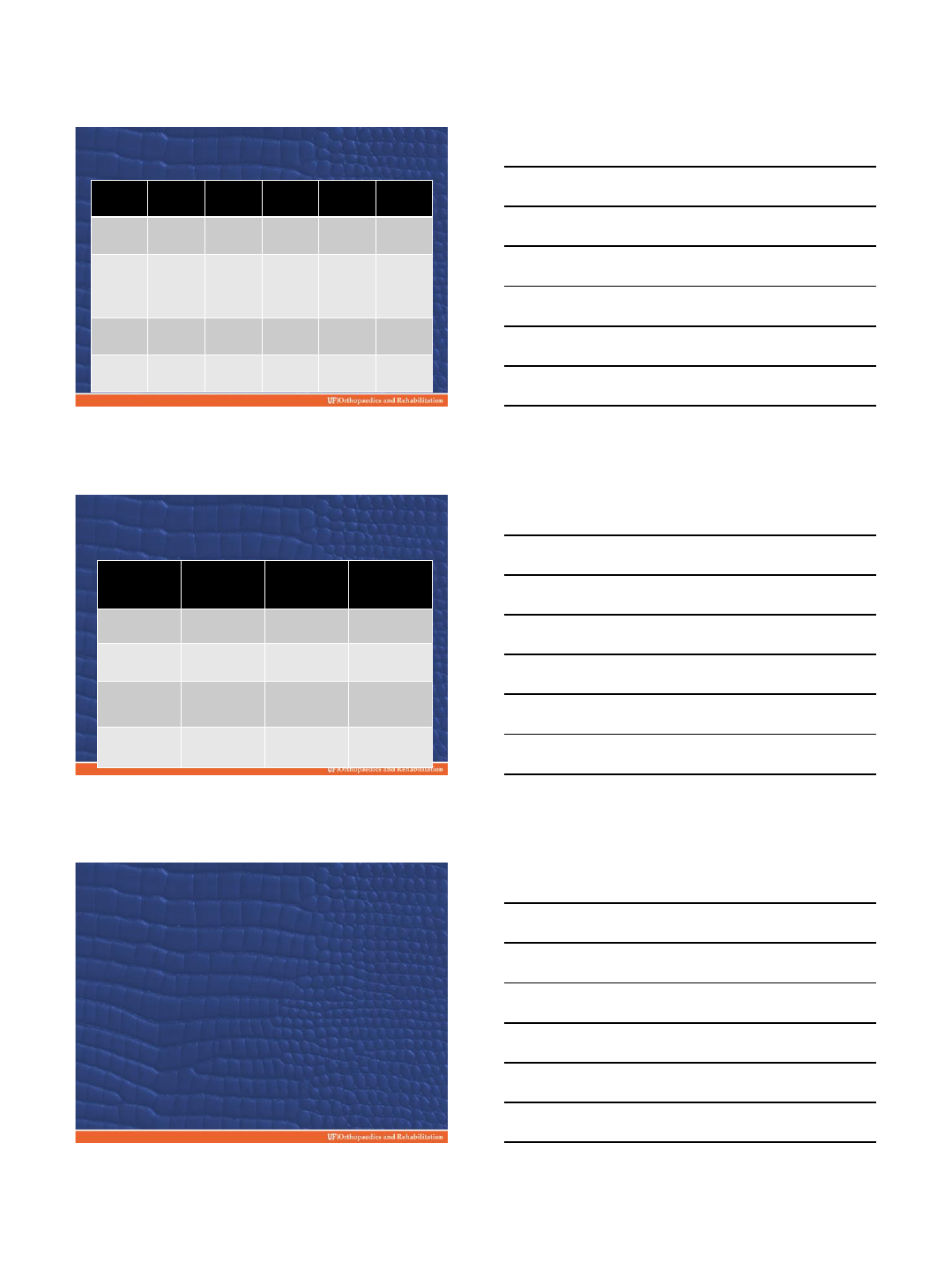
Posterior Augmented Baseplate
2/16/2015
11
Posterior Augmented Baseplate
•N=42
•Age –71
•Follow-up Average –12 months
•Complications –1 intraop
tuberosity fx
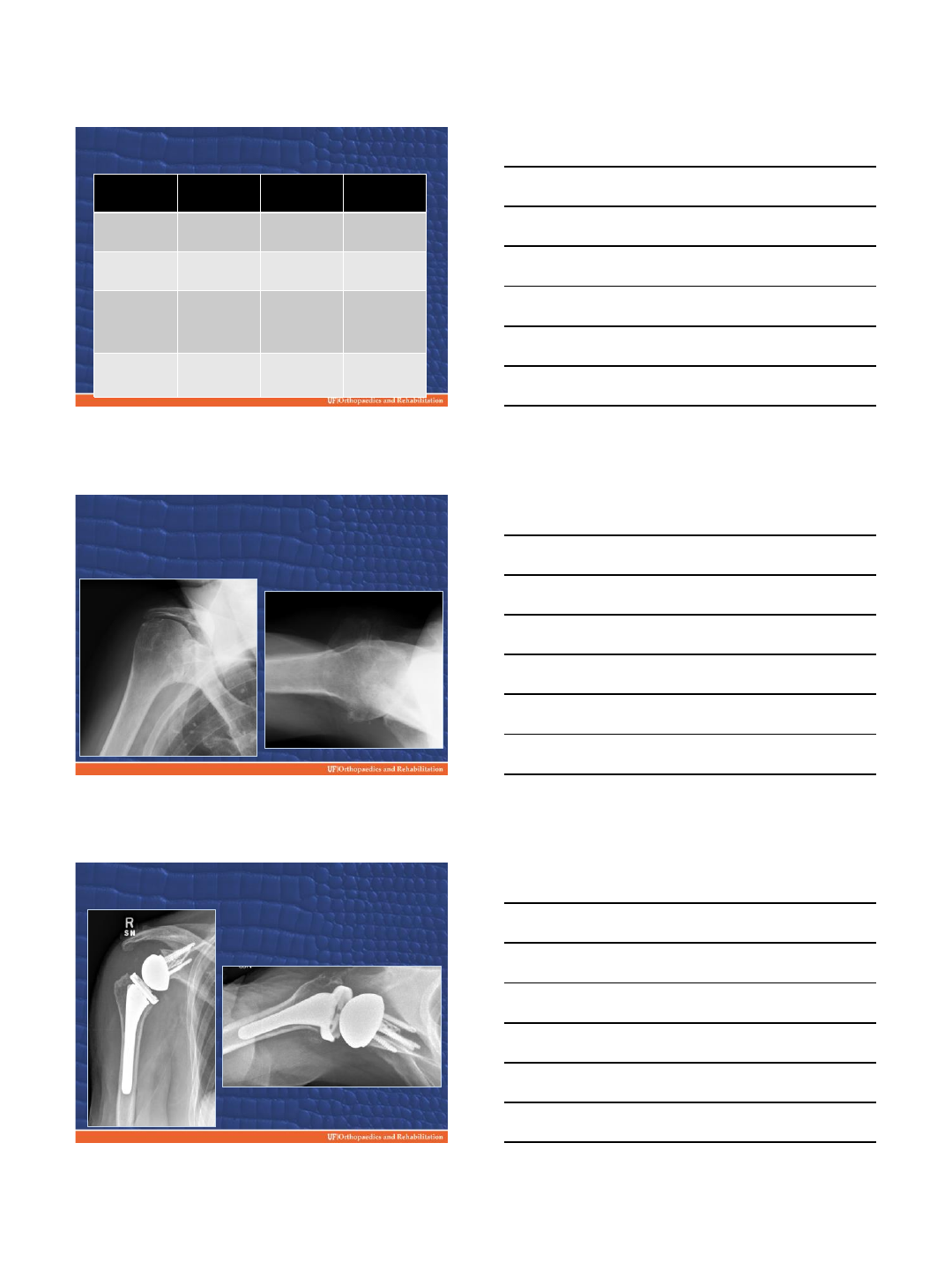
Functional Outcomes Posterior
Augmented
SPADI 100
SST
ASES
UCLA
Constant Nrl
Pre
Op
58
4
43
15
44
Post Op
19
10
81
30
74
Improvement
-39
Good
+6
+38
+15
+30
Control 1
yr
30
9
70
27
67
Objective Outcomes Posterior
Augmented
Active Elevation
Active External
Rot
Active Internal
Rot
Preop
87
18
S2
Final F/U
127
26
L3
Change
+40
+8
+4
Anatomic
Seg
Control 1
yr
118
23
L4
2/16/2015
12
Posterior Superior Augment
•Severe glenoid wear
•Previously only treatment –
bone grafting
•Posterior superior wear
patterns –common in CTA
•N=5 only 6 months average f/u
Posterior Superior Augment
Posterior Superior Augment
2/16/2015
13
Posterior Superior Augment
Functional Outcomes
SPADI 100
SST
ASES
UCLA
Constant Nrl
Preop
65
5
46
13
38
Final
follow
–
up 6
months
29
8
75
27
57
Change
36
3
29
14
19
Control 6
months
34
8
68
26
61
Posterior Superior Augment
Outcomes
Active
elevation
Active
External
Rotation
Active Internal
Rotation
Preop
62
16
S%
Final Follow
-
up
101
35
S1
Change
39
19
4
Control 6
months
111
21
L5
Conclusion Ugly Glenoid
•Be Aware
•Know the solutions
•Solutions are in evolution
•Can make a big difference with patient
–Pain
–Function
–Durability implant
•Based on Short term f/u metal
augments are a viable solution
2/16/2015
14
